Embed Size (px)
Citation preview

12/08/22 1
Revenue Cycle Management

12/08/22 2
Here’s What You’ll Learn
Introduction to Revenue Cycle Concept Zero to Zero Departments & Functions Process Key Definition & Metrics
Market Conditions Impact to Revenue Cycle
Modern Day Bounty Hunters Charity Care Future with Health Care Reform

12/08/22 312/08/22 3
What is Revenue Cycle? All the administrative and clinical functions, processes, and software applications that contribute and manage the registration, charging, billing, payment and collections tasks associated with a patient encounter.
Revenue Cycle is the process that begins when a patient comes into the system and includes all those activities that have occurred in order to have a zero balance
In other words, think… Zero to Zero!

“Hospitals exist in a very uncertain time. Reimbursement risk runs high, and receiving payments from patients is not guaranteed. The ability to capture lost revenue and improve the ability to forecast actual revenue received to the budget is necessary for hospitals' and other service providers' survival and vitality.”
Source: Wall Street 2010
Importance of Revenue CycleAnd You…

REGU
LATI
ONS
PROCESS
CULTURE
TOOLS
PEOPLE
The Revenue “Cycle”
BILLING
CDMP
SCHEDULING
REGISTRATIONINSURANCE
VERIFICATION
FINANCIALCOUNSELING
CASE MGMT/QUR
CDM/CHARGECAPTUREMEDICAL
RECORDS
CUSTOMER SERVICE
THIRD PARTYFOLLOW- UP
SELF PAYCOLLECTIONS
PROGRAMADMINISTRATI
ON
CASH POSTING
POSTPAYMENT REVIEW
TECHNOLOGY
CUSTOMER
EXPECTATIONS
PAYO
RS
POINT OF SERVICE
COLLECTIONS
DENIALS MANAGEMENT
FINANCIAL CLEARANCE

Patient Access
DocumentationOf
ServicesBilling Receivables
Management Customer Service
Hospital
Scheduling
Registration
Pre-Registration
Eligibility &Verification
FinancialCounseling
CareDelivery
PatientDischarge
Transcription
ChargeMaster
Coding/CDMP
ChargeCapture
PaymentPosting
ClaimsEditor
CustomerInquiries
BillReconciliation
ContractualAdjustments
LegalCollections
IssueResolution
SecondaryBilling
Bad Debt/Write OffsPatient
Statements
Process Flow by Department
LateCharges
UtilizationManagement
DischargePlanning
CaseManagement
ClaimsSubmission Follow-Up
Appeals/Denial Mgmt
Feedback

12/08/22 7
Patient Access
The “Front Door” to the hospital and the first step in the revenue cycle process for the majority of patients.
The important functions and information gathered in Access include: Scheduling services (surgery not included) Verifying of Insurance Obtaining Authorizations and certifications Gathering patient demographics and insurance information Pre-Services/Point of Service collections Identifying the referring physician Informing the patient on instructions for the date of service, referral
process, etc. Informing patient of referral process Financial Counseling Medicaid Eligibility/Charity Care Responsible for 50% of claims data

12/08/22 8
Health Information Management (HIM)
Health information management (HIM) is the practice of maintenance and care of health records by traditional and electronic means in hospitals, physician's office clinics, health departments, health insurance companies, and other facilities that provide health care
The important functions and information gathered in HIM include: Providing and Managing Transcription Services Coding services documented by Physicians
CPT codes (procedures) ICD-9 (diagnosis) HCPC (supplies, drugs, etc.) ASC Codes
Ensure Codes accurately reflect patient services Acts as a Liaison between all areas Serves as Subject Matter Experts in HIPAA, Documentation and Coding Educates, presents, and trains on opportunities to improve
Case Mix Index (CMI) Oversees and responds to Defense Audits Manages storage and retrieval of medical records Implementation of Electronic Health Record System Building the Compliant Documentation Management Program (CDMP)

12/08/22 9
Patient Financial Services (PFS) Patient Financial Services is the “cash machine” of the hospital. The important functions and information gathered in PFS include:
Charge Master/Revenue Integrity Billing Overseeing Claims Edits to ensure “Clean Claim Submissions” Employing tools to ensure accuracy in charge capture Follow-Up with Insurance companies
Appeals Denials Un-paid Claims
Customer Service Collections Cash Posting Subject Matter Experts
Government Billing Commercial and Managed Care Billing
Employs and Oversees systems and vendors to enhance Services provided to patients Revenue Cost to Collect

12/08/22 10
Charge Master A comprehensive listing of hospital charges The Revenue Integrity team are a critical component to billing
compliance and charge capture and is often considered the "life blood" to a Hospital's Revenue Cycle by touching almost every department within the facility. Standardization of charge master Department level review of all processes and charges with
management staff to ensure all billable charges are represented on the CDM
CDM reviews and updates to ensure compliance for all payors Market pricing, transparency and defensibility strategies Revenue cycle system mapping to ensure charge capture and
compliant billing Acuity-based charging methodology development and implementation Maintenance strategies, controls and tools for maintaining an accurate
and compliant CDM Educational and training tools
12/08/22 11
The Importance of Charge Capture A key part of the Revenue Cycle but does not report to Revenue Cycle “Bill what you do” – the process where services provided are entered
into the system; charges and expected reimbursements are calculated The important functions and information gathered in Charge Processing
include: Keyers and coders enter data automatically from a charge master
or manually input Claims Manager software scrubs entries for correctness Problems sent to department work file for processing or corrections Reconciliation performed to insure all entries received and entered
into the system Accuracy of service and charge Appropriate edits to scrub data Charge entered timely for prompt payment Daily Charge Logs Reviewed

Process Flow: For Real?

Process Flow Overview

Required Billing Elements - Where do they come from?50% - Patient Access, Registration 15% - Charge Entry Areas15% - Medical Records 20% - Billing
Patient Demographic Data Patients last name, first name, and middle initial Patient address Birth date Male (M) or Female (F) Marital Status Admission date or start of care date
Encounter Specific Hour patient was admitted for inpatient or outpatient care Occurrence Codes Code indicating the priority of admission--1 indicates emergency; 2 urgent;
3 elective; 4 newborn; and 9 information not available. Code indicating the source of admission or outpatient service Provider has patient signature on file permitting release of data (Y or N) Principal Diagnostic Coding (ICD-9-CM code) Admitting Diagnostic Coding (ICD-9-CM code)
Insurance Information The name and number identifying each payer that payment is expected Assignment of benefits (Y) yes; (N) no The name of the patient or insured individual Relationship of the insured (person having insurance) to the patient Insured’s identification number assigned by the payer organization The group name/plan through which the insurance coverage is provided The insurance group number Employment status code Employer’s name and address
Required Elements:
Revenue Cycle – Where Does the Information Come From?

12/08/22 15
Access: Metrics
Registration accuracy rate Denials
No Authorization Not Eligible
Telephone Statistics Hold Times Abandonment Rates Other
Point of Service Collections “Red Flags” – Incorrect Claim Demographics

12/08/22 16
HIM: Metrics Discharges Not Final Billed (DNFB) Turnaround Times
Dictation/Transcription Record Requests & TAT CDMP
Queries Rate Response Rate Agreement Rate
RAC Audits & Timeliness Responses

12/08/22 17
PFS: Metrics Cash Expected Reports Days in A/R Aging Analysis by Payer Unbilled Accounts Receivable Late Charge Postings by Service Area Claim Denial Volumes / Amounts / Types Bad Debt / Bad Debt Recovery Levels Cost to Collect

Top Issues Influencing Health Care Industry
Record spending on health information technology Significant changes in benefit plan design, plan pricing and the health
plan landscape New risks and opportunities may emerge as payment models shift from
fee-for-service to new models that focus on performance, health outcomes and shared cost savings
Health organizations may feel the trickle down effect of decreased utilization by price sensitive consumers.
A further uptick in merger and acquisition activity to share administrative burdens and IT investments, gain market share and fill strategic gaps.
Pharmaceutical companies see an opportunity to increase their visibility with consumers, influence health outcomes and reduce healthcare costs while increasing revenue using digital strategies and technology.
The use of mobile health and wireless technologies by all health organizations is expected to continue to surge.
Source: PwC 2010 18

Source: OHA 2010 19
Revenue StreamWhere the Money Comes from...

Insurance by Percentage Enrolled
20Source: Kaiser Family Foundation 2010

21
Average Health Insurance Premiums and Worker Contributions for Family Coverage, 1999-2009
$4,247
$9,860
$1,543$3,515
1999 2009
Employer Contribution
Worker ContributionNote: The average worker contribution and the average employer contribution may not add to the average total premium due to rounding.
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2009.
$5,791128% Worker
Contribution Increase
131% Premium Increase
$13,375

On the Rise…
Group Health Plan premiums up 9% with expectations of 6% in 2012
High Deductible Health Plans continue to rise
Deductibles and Out of Pockets Increasing 22%
Charity Care, Government Payors Increasing
1.3 Million Uninsured equivalent to the population of Columbus22

12/08/22 23
Adults Living in Poverty

12/08/22 24
Market Conditions State budget issues continue
Traditional Medicaid/Medicaid Managed Care wanting relief More Ohio residents live below the poverty level High Penetration of Self-Insured Employers Shifts of health care costs to Consumers
Increases in Deductibles Increases in Co-Pays But, still coverage offered from employers
Most markets are dominated by few payors Smaller Payors being closed out of the Market Aggressive Managed Care payors
Movements to more complicated contracts

12/08/22 25
Market Conditions Reimbursement Variances
Commercial Payors Continue to Subsidize Government Payors
High Deductible Health Plans Increase Deductibles increasing too
Quality Scores tied to Contract Increases/Consumerism Hospitals Physicians
Multi-Year Contracts with Payors Transparency Growing

12/08/22 26
Charges, Payments, and Cost Charges are the amount the hospital lists as the
price for services. Very few pay this “sticker price.” Payment or Reimbursement is the amount the
hospital actually receives in cash for its services. Private insurers, public insurers, Self Pay and the
uninsured all pay different amounts for the same services. Payment can be either more or less than what it costs the hospital to provide a given service.
Cost is what it actually costs the hospital to provide the services.

12/08/22 2712/08/22 27
Reimbursement Methodologies
Hospitals Percent of Charge Per Diems Case Rate Payment
Diagnosis Related Groups (DRGs)
Medical Severity (MS) DRGs
Globals Ambulatory Patient
Groupings (APGs) Ambulatory Payment
Classifications (APCs) Other
Carve-Outs
Professional Services Fee For Service
discounts Fee Schedules Payment based on
Resource Based Relative Value Based System (RBRVS)
Capitation Withholds Pools
Case Rates

CostGovernment Reimbursement
Charge
Commercial Reimbursement
Subsidies and Payor Mix
Note: Solid lines are status quo; dashes represent future state with costs, reimbursement, and charges shifting.

12/08/22 29

12/08/22 30

Contracted Fee Schedule Match
Source: AMA 2011 National Insurer Report Card 31

12/08/22 32
Administrative Costs
Pre-Authorizations Complex Benefit
Designs Limitations of Network Denials Coordination of Benefits Audits

12/08/22 33
Importance of POS Collections Recent Studies on the “Tipping Point” –
Financial Hardship Limit – found that when the total amount billed to the patient reached 3.5% of the family's gross income, the likelihood of paying the bill dropped dramatically.
Source: TransUnion/NorthShore LIJ Study

12/08/22 34
Modern-Day Bounty Hunters
RAC: Recovery Audit Contractors Medicare
MAC: Medicare Administrative Contractors The new Fiscal Intermediary
MIC: Medicaid Integrity Contractors Medicaid
Managed Care Audits

12/08/22 35
RACs Findings
85%
4%4%6%
2%
Outpatient InpatientSNF OtherRehab
35%
17%8%
40%
Incorrectly CodedOtherNo/Insufficient DocMedically Unnecessary

3-7 percent of revenue on a variety of community benefit and charity care activities is likely adequate.
An IRS study found that 9 percent of revenue was spent on community benefit.
Nearly 60 percent of the hospitals surveyed provided less than or equal to 5 percent of revenue on uncompensated care
Twenty percent of hospitals surveyed reported total community benefit spending of less than 2 percent of revenue.
Source: Kaiser Daily Health Policy Report Feb 2009
Charity9
8
7
6
5
4
3
2
1

12/08/22 37
Revenue Cycle Management Strategies
A CFO’s Focus on Revenue Cycle
Vendor Management Denials Management Technology Optimization Point of Service Collections Strategic Pricing Contract Management Compliance Documentation/Coding.
Source: Interview with: Vince Schmitz, Senior Vice President & CFO, MultiCare Health System.
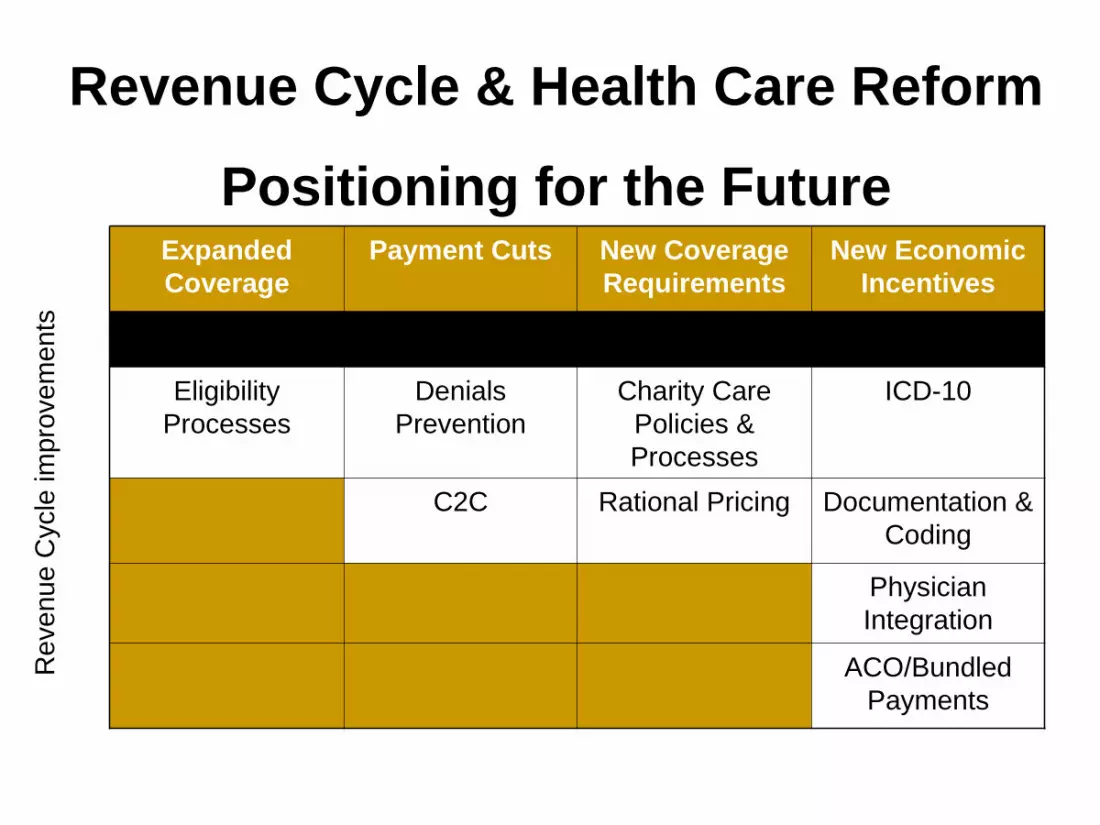
Expanded Coverage
Payment Cuts New Coverage Requirements
New Economic Incentives
Eligibility Processes
Denials Prevention
Charity Care Policies & Processes
ICD-10
C2C Rational Pricing Documentation & Coding
Physician Integration
ACO/Bundled Payments
Revenue Cycle & Health Care Reform
Positioning for the Future
Rev
enue
Cyc
le im
prov
emen
ts

QUESTIONS





























