Embed Size (px)
Citation preview

Assoc. Prof. Mária Pallayová, MD, [email protected]
Department of Human Physiology, UPJŠ LF
April 28, 2020 (12th week – Summer Semester 2019/2020)
Reproductive Physiology
Human Physiology Course

Introduction
One of nature's primary goals is perpetuation of the
species. All living organisms must reproduce in some
manner.
Function of the reproductive system is to produce offspring.
Puberty is the age at which the reproductive organs mature
sufficiently to allow reproduction.
Reproductive organs of both the male and female produce
sex cells called gametes.
A combination of the female gamete (ovum) and male
gamete (sperm) is called fertilization.

Sex vs. Gender
Sex - refers to biological characteristics that distinguish
female from male. The distinction may be made on the
basis of chromosomes, gonads, internal and external
morphology, and hormonal status.
Gender - gender identification - refers to the concept
held by the individual (or by those raising the individual)
that the individual is male, female, or ambivalent.

The Male Reproductive
System
♂

The organs of the male reproductive system consist of the
testes and the accessory organs (scrotal sac + penis +
accessory glands).
Pathway of spermatozoa:
– Epididymis
– Ductus deferens (Vas deferens)
– Ejaculatory duct
the male reproductive role is to produce viable sperm, and
to deliver the sperm to the female reproductive system
Male Organs of Reproduction

Male Organs of Reproduction
Testes
– Produce sperm and secrete testosterone causing the
appearance of secondary sexual characteristics
(facial and body hair, deepened voice, increased
muscle mass, thickening of the bones)
Epididymis
– A tube on the surface of each testis that stores the
sperm while they mature
Penis
– Semen and urine are excreted

Seminal vesicles
– Active secretory gland
– Contributes ~60% total volume of semen
– Secretions contain fructose, prostaglandins, fibrinogen
Prostate gland
– Secretes slightly acidic prostate fluid
Bulbourethral glands/COWPER’S GLANDS
– Secrete and add a thick alkaline mucus to the semen
that acts as a lubricant during sexual excitement
Male accessory glands

The primary and secondary
sexual characteristics

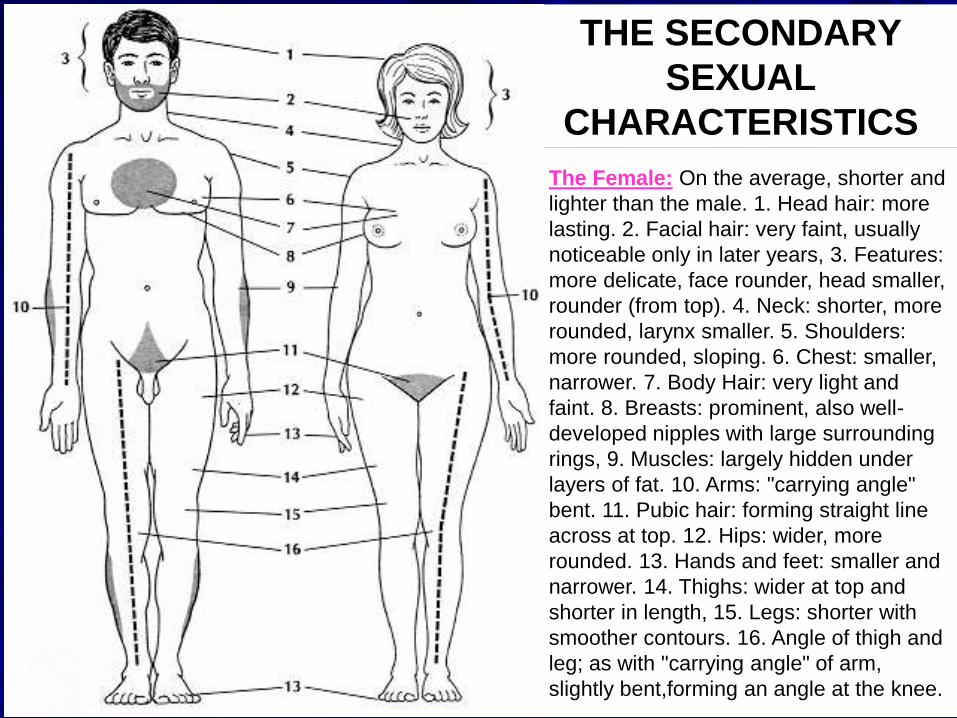
THE SECONDARY
SEXUAL
CHARACTERISTICS
The Male: On the average, taller and
heavier than the female. 1. Head hair: may
fall out with age. 2. Facial hair: grows
throughout adult life. 3, Features: more
pronounced, face longer, head (front to
back) longer. 4. Neck: thicker, longer,
larynx one-third larger. 5. Shoulders:
broader, squarer. 6. Chest: larger in every
dimension. 7. Body hair: more evident,
especially on chest and arms. 8. Breasts:
rudimentary in size. 9. Muscles: bigger,
more obvious. 10. Arms: longer, thicker,
"carrying angle" straight. 11. Pubic hair:
growing up to a point, forming triangle. 12.
Hips: narrower. 13. Hands and feet: larger,
fingers and toes stronger and blunter. 14.
Thighs: more cylindrical with bulge of
muscles. 15. Legs: longer, bulging calves.
16. Angle of thigh and leg; as with
"carrying angle" of arm, forming straight
line, thigh to ankle.
THE SECONDARY
SEXUAL
CHARACTERISTICS
The Female: On the average, shorter and
lighter than the male. 1. Head hair: more
lasting. 2. Facial hair: very faint, usually
noticeable only in later years, 3. Features:
more delicate, face rounder, head smaller,
rounder (from top). 4. Neck: shorter, more
rounded, larynx smaller. 5. Shoulders:
more rounded, sloping. 6. Chest: smaller,
narrower. 7. Body Hair: very light and
faint. 8. Breasts: prominent, also well-
developed nipples with large surrounding
rings, 9. Muscles: largely hidden under
layers of fat. 10. Arms: "carrying angle"
bent. 11. Pubic hair: forming straight line
across at top. 12. Hips: wider, more
rounded. 13. Hands and feet: smaller and
narrower. 14. Thighs: wider at top and
shorter in length, 15. Legs: shorter with
smoother contours. 16. Angle of thigh and
leg; as with "carrying angle" of arm,
slightly bent,forming an angle at the knee.

The Male Reproductive System

The testes (testicles) are paired oval glands that descend
into the scrotum.
At the onset of puberty, the testes produce testosterone
(the male sex hormone).
Testosterone stimulates and promotes the growth of the
secondary sex characteristics in the man.
Epididymis is a comma-shaped organ on the top of the
testicle. It stores and propels the sperm toward the urethra
during ejaculation.
From the epididymis, sperm enters the vas deferens
(ductus deferens) that transports sperm to the urethra.
Male Organs of Reproduction

The reproductive glands in the male serve to produce
fluids that are added to the sperm to form SEMEN.
These secretions are vital for keeping the sperm cells
alive and motile (able to move).
The SPERM are cells that have a tail, head, and neck.
The sperm are produced in the TESTICLES.
The testes produce sperm throughout the life of the
male. (Unlike the female, who are born with all the eggs
they will ever have.)
Male Organs of Reproduction

During its trip toward the outside world, sperm picks up
fluids from the glands. When the sperm and fluid join
together, it is then called SEMEN.
COWPER’S GLANDS add a thick mucus to the semen
that acts as a lubricant during sexual excitement.
The PENIS is the male sex organ that transports the
semen into the vagina. A slightly enlarged region at the
tip of the penis is called the GLANS.
The glans of the penis is covered by a fold of skin called
the PREPUCE or FORESKIN.
Male Organs of Reproduction

The Structure of the Testes

The Epididymis

The D
uctu
s D
efe
rens
an
d A
cce
sso
ry G
lan
ds
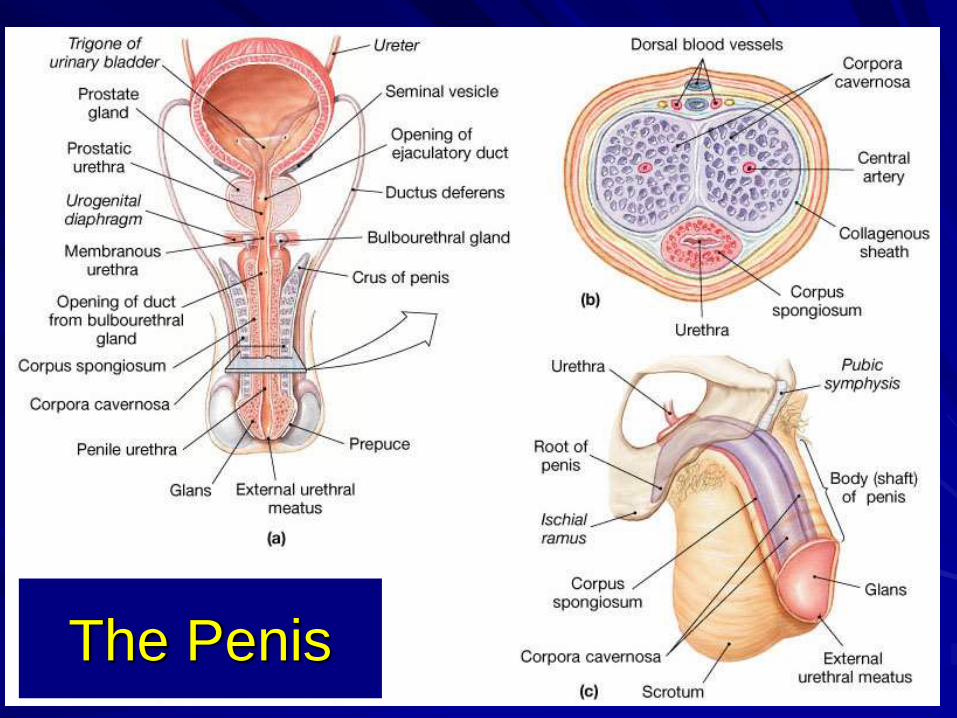
The Penis

Typical ejaculate = 2-5 ml fluid
– Contains between 20 – 100 million spermatozoa per ml
Seminal fluid
– A distinct ionic and nutritive glandular secretion
Contents of Semen

Testes are formed in abdomen and descend
into scrotum at 7th month of development
Temperature in scrotum is slightly lower than
in body
Spermatogenesis (formation of sperm)
sperm-forming cells
Sertoli cells
interstitial cells-produce testosterone
Process takes about 9-10 weeks

Notes
It takes approximately 65 to 70 days to develop
spermatozoa from the earliest stages of spermatogonia.
Because the production of sperm depends on LH and
FSH, a lack of GnRH (Kallmann’s syndrome) will reduce
the production of LH, FSH, and sperm.
Temperature is important in regulating sperm production.
Optimal sperm production occurs at 2 to 3 degrees C
lower than body temperature.

Testes produce mature spermatozoa
Sperm enter epididymis
– Elongated tubule with head, body and tail regions
– Monitors and adjusts fluid in seminiferous tubules
– Stores and protects spermatozoa
– Facilitates functional maturation of spermatozoa
Male reproductive tract

Seminiferous tubules
– Contain spermatogonia
Stem cells involved in spermatogenesis
– Contain sustentacular cells
Sustain and promote development of sperm
Spermatogenesis

The Seminiferous Tubules

The Seminiferous Tubules

Sp
erm
ato
ge
ne
sis


Spermiogenesis and Spermatozoon Structure

Spermatazoa in testes are not yet capable of fertilization
Epididymis- is actually over 20 feet long!
spermatazoa complete maturation
as they move through epididymis
(about 2 weeks)
Ductus deferens (vas deferens)
Ejaculatory duct

Ejaculatory duct
Sperm
Seminal fluid
secretions from prostate
seminal vesicles
bulbourethral glands (Cowper’s glands)
Activate sperm
Provide nutrients
Contractions help move sperm
Buffers

Control of erection
Hypothalamus (conscious control)
Parasympathetic nerves
neurotransmitter- nitric oxide?
promotes blood flow into penis
(sildenafil-Viagra promotes vasodilation)
Control of emission and ejaculation
sympathetic nerves- muscle contraction

Puberty is the time of life when sexual maturation occurs.
Greatly increased testosterone secretion during puberty
stimulates the growth of the penis and the testes.
Testosterone also brings about and maintains the male
secondary sex characteristics that develop during puberty,
including the growth of a beard, axillary (underarm) hair,
and pubic hair.
Regulation of Male Hormone
Levels

Regulation of Male Hormone
Levels
At the time of puberty, the sex organs mature, and then
changes occur in the physique of males.
The cause of puberty is related to the level of sex
hormones in the body, as regulated by the negative
feedback system.
This feedback system functions long before puberty, but
the level of hormones is low because the hypothalamus is
supersensitive to feedback control.

At the start of puberty, the hypothalamus becomes less
sensitive to feedback control and begins to increase its
production of gonadotropin-releasing hormone, which
stimulates the anterior pituitary to produce the gonadotropic
hormones.
– Two gonadotropic hormones, FSH (follicle-stimulating
hormone) and LH (luteinizing hormone), are named for
their function in females but exist in both sexes,
stimulating the appropriate organs in each.
Regulation of Male Hormone
Levels

Gonadotropic hormones
FSH promotes spermatogenesis in the seminiferous
tubules (targets sustentacular cells to promote
spermatogenesis)
LH promotes androgen (e.g., testosterone) production in
the interstitial cells
LH in males is also called interstitial cell-stimulating
hormone (ICSH)

Regula
tion
of
repro
ductio
n
in th
em
ale

Regulation, hormonal products, and interactions
between Leydig and Sertoli cells. ABP, androgen-
binding protein; E, estradiol; T, testosterone; R, receptor.

Negative Feedback Mechanisms
The hypothalamus, anterior pituitary, and testes are
involved in a negative feedback system.
The system maintains testosterone production at a fairly
constant level.
When the amount of testosterone in the blood rises to a
certain level, it causes the hypothalamus and anterior
pituitary to decrease the secretion of GnRH and LH.
As the level of testosterone begins to fall, the
hypothalamus increases its secretion of GnRH, and the
anterior pituitary increases its secretion of LH; thus,
stimulation of the interstitial cells occurs.

Only minor fluctuations of the testosterone level occur in
the male, and the feedback mechanism in this case acts
to maintain testosterone at a normal level.
A similar feedback mechanism maintains the continuous
production of sperm.
The sustentacular cells in the wall of the seminiferous
tubules produce a hormone called inhibin that blocks
GnRH and FSH secretion when appropriate.
Negative Feedback Mechanisms

Negative feedback
Regulation of testosterone
secretion involves negative
feedback by testosterone
on GnRH and LH.
Regulation of sperm
production involves
negative feedback by
inhibin on GnRH and FSH.

Hormonal Feedback and the Regulation of
the Male Reproductive Function


Testosterone
The male sex hormone, has many functions.
It is essential for normal development and function of the
sex organs in males (e.g., greatly increased testosterone
secretion at the time of puberty stimulates maturation of
the penis and the testes).

Secondary Sex Characteristics
Testosterone also brings about and maintains the male
secondary sex characteristics, which develop at the
time of puberty and visibly distinguish males from
females.
These characteristics include
– a pattern of male hair growth,
– activity of cutaneous glands,
– pitch of the voice,
– muscle strength.

At puberty, males experience growth of a beard, axillary
hair, and pubic hair (that tapers toward the navel).
A side effect of testosterone activity is baldness. Genes for
baldness are probably inherited by both sexes, but baldness
is seen more often in males because of the presence of
testosterone. This makes baldness a sex-influenced trait.
Testosterone also causes oil and sweat glands in the skin to
secrete, thereby contributing to acne and body odor.
Testosterone

The larynx and vocal cords enlarge, causing the voice to
change.
The “Adam’s apple” is a part of the larynx, and it is
usually more prominent in males than in females.
Testosterone is responsible for the greater muscular
strength of males.
Testosterone

It prompts the larynx and the vocal cords to enlarge, causing
the voice to change.
It is partially responsible for the muscular strength of males.
Testosterone also stimulates oil and sweat glands in the
skin; therefore, it is largely responsible for acne and body
odor. Another side effect of testosterone is baldness.
Genes for baldness are probably inherited by both sexes,
but baldness is seen more often in males because of the
presence of testosterone.
Testosterone

Quiz
The production of estradiol by the testes requires:
(A) Sertoli cell follistatin
(B) LH and Leydig cells
(C) Activin but not LH
(D) Leydig cell, Sertoli cells, LH, and FSH
(E) Leydig cells and FSH
Quiz
The production of estradiol by the testes requires:
(A) Sertoli cell follistatin
(B) LH and Leydig cells
(C) Activin but not LH
(D) Leydig cell, Sertoli cells, LH, and FSH
(E) Leydig cells and FSH

Quiz - Explanation
The production of estradiol by the testes requires Leydig cell,
Sertoli cells, LH, and FSH.
The production of estradiol requires Leydig cells, under the influence
of LH, which stimulates androgen production. The androgen diffuses
to Sertoli cells, which contain aromatase, the enzyme that converts
androgens to estrogens under the influence of FSH.
Follistatin binds activin and would reduce FSH secretion, an essential
component for estradiol production.
Estradiol is not produced by Leydig cells.
Activin would increase the secretion of FSH, which is a necessary
component for estradiol, but other cells and hormones are required.
Similarly, Leydig cells would need LH to stimulate the production of
the androgen precursor of estrogen.
Sertoli cells, under the influence of FSH, are needed to aromatize
androgen from Leydig cells.

In the testes, luteinizing hormone (LH) controls the synthesis
of testosterone by Leydig cells, and follicle-stimulating
hormone (FSH) increases the production of androgen-binding
protein, inhibin, and estrogen by Sertoli cells.
Spermatozoa are produced within the seminiferous tubules of
both testes. Sperm develop from spermatogonia through a
series of developmental stages that include spermatocytes
and spermatids.
The sperm mature and are stored in the epididymis. At the
time of ejaculation, sperm are moved by muscular contrations
of the epididymis and vas deferens through the ejaculatory
ducts into the prostatic urethra. The sperm are finally moved
out of the body through the urethra in the penis.
Key concepts

Key concepts (cont.)
LH and FSH secretion by the anterior pituitary are
controlled by gonadotropin-releasing hormone (GnRH).
Testosterone mainly reduces LH secretion, whereas
inhibin reduces the secretion of FSH. The testicular
hormones complete a negative-feedback loop with the
hypothalamic-pituitary axis.
Androgens have several target organs and have roles in
regulating the development of secondary sex
characteristics, the libido, and sexual behavior.

The most potent natural androgen is
dihydrotestosterone, which is produced from the
precursor, testosterone, by the action of the enzyme
5alpha-reductase.
Male reproductive dysfunction is often due to a lack of
LH and FSH secretion or abnormal testicular
morphology.
Key concepts (cont.)

The Female
Reproductive System
♀

• The female reproductive system is composed of
internal and external organs of reproduction.
• Internal organs of reproduction:
• OVARIES
• FALLOPIAN TUBES
• UTERUS
• VAGINA
• External organs of reproduction
• GENITALIA
Female Organs of Reproduction

Ovaries
The ovaries are located in the pelvic cavity.
The ovaries produce estrogens and progesterone, the
female sex hormones.
The hypothalamus and the pituitary gland control the
hormonal secretions of the ovaries.

Internal Organs of Reproduction
Ovaries are paired glands that produce eggs and hormones
(estrogen and progesterone) for ovulation and pregnancy.
Ovaries store egg cells (oocytes), and mature the stored
eggs until ovulation.
Fallopian tubes (OVIDUCTS = the connection between the
ovary and the uterus) transport the mature ovum from the
ovary to the uterus. Oviducts have FIMBRAE to coax the
ovulated egg into the tube. Once inside the tube, the egg
travels toward the uterus. When sperm is available,
fertilization usually occurs in the oviduct.

Uterus = a muscular pear-shaped, hollow organ located
between the bladder and the rectum. Structure in which
the zygote is implanted following conception. Function is
to nourish and protect the growing fetus until birth.
Cervix = is a term denoting the neck of the uterus and
the extension of it into the top portion of the vagina (for
delivery of a fetus).
Vagina= a muscular tube that extends from the cervix
(neck of the uterus) to the exterior of the body.
Functions: sexual intercourse, receptor of semen,
discharge of menses, and passage for delivery of fetus.
The vagina is lined by mucus. This mucus is a lubricant.
Internal Organs of Reproduction

Female External Organs
The external organs are collectively known as
GENITALIA:
LABIA MAJORA = the larger outer lips of the vagina.
LABIA MINORA = smaller inner lips of the vagina.
CLITORIS = small projection of tissue located between
the labia minora; contains many nerve endings. Similar
to the penis in males.
BARTHOLIN’S GLANDS = for lubrication.
Mammary glands = ducts that secrete milk (lactation)
following pregnancy
Muscular organ
– Mechanical protection
– Nutritional support
– Waste removal for the developing embryo and
fetus
Supported by the broad ligament and 3 pairs
of suspensory ligaments
The uterus

Myometrium – outer muscular layer
Endometrium – a thin, inner, glandular
mucosa
Perimetrium – an incomplete serosa
continuous with the peritoneum
Uterine wall consists of three
layers:

The Uterus

The Uterine Wall

The Uterine Wall

Estrogen and Progesterone
The female sex hormones, estrogens and progesterone,
have many effects on the body. In particular, estrogens
secreted during puberty stimulate the growth of the
uterus and the vagina.
Estrogen is necessary for egg maturation and is largely
responsible for the secondary sex characteristics in
females, including female body hair and fat distribution.
In general, females have a more rounded appearance
than males because of a greater accumulation of fat
beneath the skin.

Also, the pelvic girdle is wider in females than in males,
resulting in a larger pelvic cavity.
Both estrogen and progesterone are required for breast
development and for regulation of the uterine cycle,
which includes monthly menstruation (discharge of blood
and mucosal tissues from the uterus).
Estrogen and Progesterone

Regulation of Female Hormone
Levels
At the time of puberty in females, the hypothalamus
increases its secretion of GnRH, and the anterior
pituitary releases larger amounts of the gonadotropins,
FSH and LH.
These hormones stimulate the ovaries to produce eggs
and elevated estrogen and progesterone levels.


The Hormonal Regulation of Ovarian Activity

Regula
tion
of
the
rep
rod
uctiv
etra
ctin
the
fem
ale

Estrogen and Progesterone
In particular, estrogen stimulates the growth of the uterus
and the vagina.
Estrogen is also necessary for egg maturation and the
onset of the menstrual cycle, as well as for the
development of the secondary sex characteristics in
females.

Secondary Sex Characteristics
These characteristics include the female pattern of body
hair and fat distribution.
In general, females have a more rounded appearance
than males because of a greater accumulation of fat
beneath the skin.
Also, the pelvic girdle enlarges in females so that the
pelvic cavity has a larger relative size compared to that
of males females have wider hips.
Both estrogen and progesterone are required for breast
development.

Control the reproductive cycle
Coordinate the ovarian and uterine cycles
Key hormones include:
– FSH
Stimulates follicular development
– LH
Maintains structure and secretory function of corpus
luteum
– Estrogens
Have multiple functions
– Progesterones
Stimulate endometrial growth and secretion
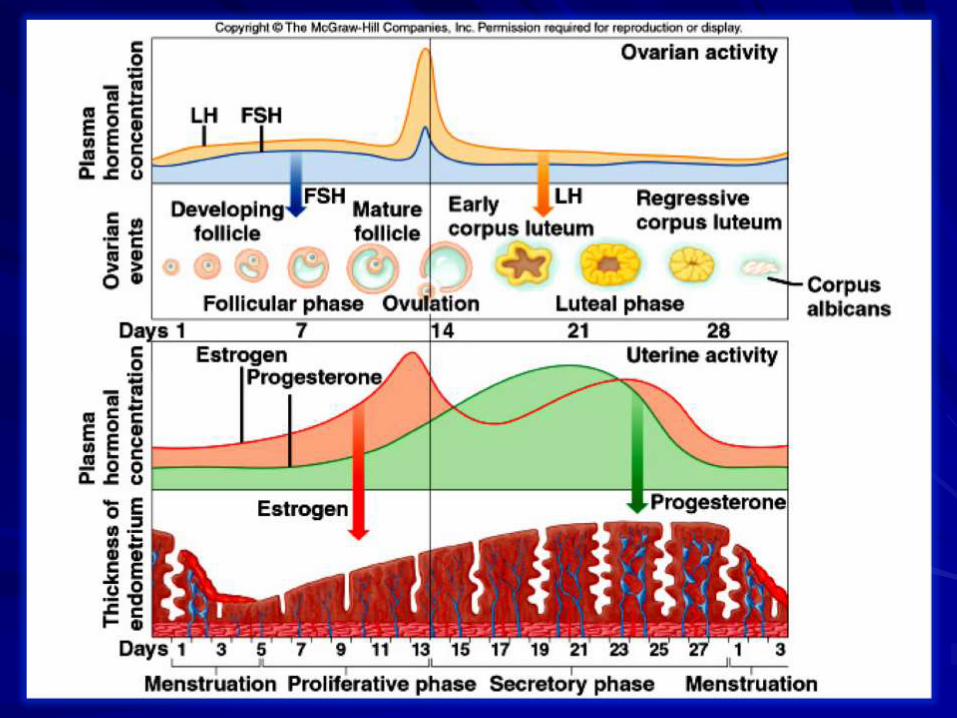
Hormones of the female reproductive cycle

Menstrual Cycle
Lasts approximately 28 days.
A complex process of hormone secretion and tissue
changes in the uterus.
A mature ovum is released from an ovary on about the
14th day of each cycle.
If the released ovum is not fertilized, the endometrium is
released from the body along with the ovum.
The sloughing of this bloody tissue, or menses, lasts from
3 to 7 days.
The menstrual cycle continues until app. 50 years of age.

Repeating series of changes in the
endometrium
Continues from menarche to menopause
– Menses
Degeneration of the endometrium
Menstruation
– Proliferative phase
Restoration of the endometrium
– Secretory phase
Endometrial glands enlarge and accelerate their rates
of secretion
Uterine cycle

The Uterine Cycle

Menstrual Cycle
a monthly series of events that involve the ovaries and
uterus plus the female sex hormones
is about 28 days long, but it can be as short as 18 days
or as long as 40 days
• Pre-Ovulation Events
• Ovulation
• Post-Ovulation Events
Pre-Ovulation Events
Under the influence of FSH from the anterior pituitary,
several follicles begin developing in the ovary.
Therefore, this period of time (days 1–14) is called the
follicular phase of the ovary.
Although several follicles begin growing, only one follicle
continues developing, and it secretes increasing amounts
of estrogen. This particular follicle becomes more and
more sensitive to FSH and then LH.

Eventually, the very high level of estrogen exerts positive
feedback control over the hypothalamus so that it secretes
ever greater amounts of GnRH.
GnRH induces a surge in FSH and LH secretion by the
pituitary.
The LH level rises to a greater extent than does the FSH
level. Under the influence of so much stimulation,
ovulation occurs.
Pre-Ovulation Events and
Ovulation

While the ovary is experiencing its follicular phase, first
menstruation and then the proliferative phase occur in the
uterus.
During menstruation (days 1–5), a low level of female sex
hormones in the body causes the endometrial tissue to
disintegrate and its blood vessels to rupture.
A flow of blood and tissues, known as the menses, passes
out of the vagina during menstruation, also called the
menstrual period.
Under the influence of estrogen released by the new
follicle, the endometrium thickens and becomes vascular
and glandular. This is the proliferative phase of the uterus,
which ends when ovulation occurs.

Post-Ovulation Events
Under the influence of LH, the ovulated follicle becomes
the corpus luteum.
Therefore, this period of time (days 15–28) is known as
the luteal phase of the ovary.
The corpus luteum secretes progesterone and some
estrogen.
As the blood level of progesterone rises, it exerts
negative feedback control over the anterior pituitary’s
secretion of LH so that the corpus luteum in the ovary
begins to degenerate.
If fertilization of the egg does occur, the corpus luteum
persists for reasons that will be discussed shortly.

Under the influence of progesterone secreted by the
corpus luteum, a secretory phase (days 15–28) begins in
the uterus.
During the secretory phase of the uterus, the
endometrium of the uterus doubles or even triples in
thickness (from 1 mm to 2–3 mm), and the uterine glands
mature, producing a thick, mucoid secretion.
The endometrium is now prepared to receive the pre-
embryo. If implantation of a preembryo does not take
place, the corpus luteum disintegrates, and menstruation
occurs.

If fertilization occurs and is followed by implantation, the
developing placenta produces human chorionic
gonadotropin (HCG), which maintains the corpus
luteum in the ovary until the placenta begins to produce
progesterone and estrogen.
The placental hormones shut down the anterior pituitary
so that no new follicle in the ovaries matures, and they
maintain the endometrium so that the corpus luteum in
the ovary is no longer needed.
Usually, no menstruation occurs during pregnancy.


During the menstrual cycle, FSH and LH are released by
the anterior pituitary. FSH promotes the maturation of a
follicle in the ovary. The follicle produces increasing
levels of estrogen, which cause the endometrium to
thicken during the proliferative phase in the uterus. An
LH surge causes ovulation.
After ovulation, LH promotes the development of the
corpus luteum. This structure produces increasing levels
of progesterone, which causes the endometrial lining to
become secretory. Menses due to the breakdown of the
endometrium begins when progesterone production
declines to a low level due to corpus luteum
disintegration.
Menstrual Cycle

Menstrual Cycle

The Hormonal Regulation of the Female Reproductive Cycle

The Hormonal Regulation of the Female Reproductive Cycle



Ovum production
Occurs monthly in ovarian follicles
Part of ovarian cycle
– Follicular phase (preovulatory)
– Luteal phase (postovulatory)
Oogenesis

Oogenesis

Different Stages in the Development
of an Ovum and Follicle

The Ovarian Cycle

The Ovarian Cycle

Key concepts
Pulses of hypothalamic GnRH regulate the secretion of
LH and FSH, which enhance follicular development,
steroidogenesis, ovulation, and formation of the corpus
luteum.
LH and FSH, in coordination with ovarian theca and
granulosa cells, regulate the secretion of follicular
estradiol.
Ovulation occurs as the result of a positive feedback of
follicular estradiol on the hypothalamic-pituitary axis that
induces LH and FSH surges.

Key concepts (cont.)
Follicular development occurs in distinct steps:
primordial, primary, secondary, tertiary, and graafian
follicle stages.
Follicular rupture (ovulation) requires the coordination of
appropriately timed LH and FSH surges that induce
inflammatory reactions in the graafian follicle, leading to
dissolution at midcycle of the follicular wall by several
ovarian enzymes.
Follicular atresia results from the withdrawal of
gonadotropin support.

Key concepts (cont.)
The formation of a functional corpus luteum requires the
presence of an LH surge, adequate numbers of LH
receptors, sufficient granulosa cells, and significant
progesterone secretion.
The uterine cycle is regulated by estradiol and
progesterone, such that estradiol induces proliferation of
the uterine endometrium, whereas progesterone induces
differentiation of the uterine endometrium and the
secretion of distinct products.

Key concepts (cont.)
During puberty, the hypothalamus begins to secrete
increasing quantities of GnRH, which increases LH and
FSH secretion, enhances ovarian function, and leads to
the first ovulation.
Menopause ensues from the loss of numerous oocytes
in the ovary and the subsequent failure of follicular
development and estradiol secretion. LH and FSH levels
rise from the lack of negative feedback by estradiol.

The illustration
summarizes
the eight steps
of fertilization.
ZP, zona
pellucida.
Reproduction is
accomplished
when the egg cell
(female gamete)
is fertilized by the
sperm cell (male
gamete)
Fertilization

Fertilization
The acrosome reaction causes a fusion of the plasma
membrane and the acrosomal membrane of the sperm,
with subsequent release of proteolytic enzymes that help
the sperm enter the ovum.
The zona reaction and pronuclei formation occur after the
sperm has entered the ovum.
Sperm enter the perivitelline space after penetration.
Cumulus expansion assists in movement of the sperm
through the mass of granulosa cells for the sperm to get to
the surface of the zona pellucida.

Development of the placenta
A. Shortly after the blastocyst has
implanted (6 to 7 days after
fertilization), the
syncytiotrophoblast invades
the stroma of the uterus.
B. The invading
syncytiotrophoblast breaks
through into endometrial veins
first, and then later into the
arteries, creating direct
communication between
lacunae and maternal vessels.
In addition, the proliferation of
cytotrophoblasts creates
primary chorionic villi.

Development of the placenta
C. The primary chorionic villus
continues to grow with the
proliferation of
cytotrophoblastic cells. In
addition, mesenchyme from
the extraembryonic coelom
invades the villus, forming the
secondary chorionic villus.
Eventually, these
mesenchymal cells form fetal
capillaries; at this time, the
villus is known as a tertiary
chorionic villus. The lacunae
also enlarge by merging with
one another.

D. With further development, the outer surface of the mature chorionic
villus is covered with a thin layer of syncytiotrophoblast. Under this
are cytotrophoblasts, mesenchyme, and fetal blood vessels. In the
mature placenta, "spiral" arteries from the mother empty directly into
the intervillous space, which is drained by maternal veins.

Pregnancy
Pregnancy results from the union of the ovum and sperm,
usually in the fallopian tube.
Growth of an offspring in the uterus lasts about 280 days (9
months).
The fertilized egg is known as a zygote from the time of
conception to 2 weeks.
It is then considered to be the morula and enters the uterus.
As a blastocyst, it implants in the uterine wall and is
considered to be an embryo through the eighth week.
From 8 weeks to birth, the unborn baby is called a fetus.
During the first 30 days of life, the baby is considered to be
a neonate.

Labor and Delivery
• Three stages of labor:
– First stage: muscle contractions of the uterus cause
the amniotic sac to rupture and the cervix to open
(dilate) to about 10 cm in diameter allowing passage
of the fetus
– Second stage: delivery of the baby, called parturition
– Third stage: delivery of the afterbirth, or placenta,
which takes place about 15 minutes later

Growth and Development
Growth refers to the changes that can be measured by
changes in height and weight as well as changes in body
proportions
Development describes the stages of change in
psychological and social functioning

The Mammary Glands

A, The breast consists of a series of
secretory lobules, which empty into
ductules. The ductules from 15-20
lobules combine into a duct, which
widens at the ampulla-a small
reservoir. The lactiferous duct
carries the secretions to the outside.
B, The lobule is made up of many
alveoli, the fundamental secretory
units.
C, Each alveolus consists of secretory
epithelial cells (alveolar cells) that
actually secrete the milk, as well as
contractile myoepithelial cells, which
are in turn surrounded by adipose
cells.
D, The alveolar cell secretes the
components of milk via five
pathways.
Cross section of the breasts and milk production

Suckling has four effects:
1.It stimulates sensory
nerves, which carry the
signal from the breast to the
spinal cord where they
synapse with neurons that
carry the signal to the brain.
2.In the arcuate nucleus of
the hypothalamus, the
afferent input from the
nipple inhibits neurons that
release dopamine (DA). DA
normally travels via the
hypothalamic-portal system
to the anterior pituitary
where it inhibits PRL
release by lactotrophs.
Thus, inhibition of DA
release leads to an increase
in PRL release.
Effect of suckling on the release
of PRL, oxytocin, and GnRH

3. In the supraoptic and
paraventricular nuclei of the
hypothalamus, the afferent
input from the nipple triggers
the production and release of
oxytocin in the posterior
pituitary.
4. In the preoptic area and
arcuate nucleus, the afferent
input from the nipple inhibits
GnRH release. GnRH
normally travels via the
hypothalamic-portal system
to the anterior pituitary, where
it stimulates the synthesis
and release of FSH and LH.
Thus, inhibiting GnRH
release inhibits FSH and LH
release, and thereby inhibits
the ovarian cycle.
Effect of suckling on the release
of PRL, oxytocin, and GnRH

Prolactin

Prolactin (cont.)

Prolactin (cont.)

Neural Control of the
Hypothalamic-Pituitary Axis

Menopause
Menopause, the period in a woman’s life during which
the menstrual cycle ceases, is likely to occur between
ages 45 and 55.
The ovaries are no longer responsive to the
gonadotropic hormones produced by the anterior
pituitary, and the ovaries no longer secrete estrogen or
progesterone. At the onset of menopause, the uterine
cycle becomes irregular, but as long as menstruation
occurs, it is still possible for a woman to conceive.
Therefore, a woman is usually not considered to have
completed menopause until menstruation has been
absent for a year.

The hormonal changes during menopause often produce
physical symptoms, such as “hot flashes” (caused by
circulatory irregularities), dizziness, headaches, insomnia,
sleepiness, and depression. These symptoms may be mild
or even absent. If they are severe, medical attention should
be sought.
Women sometimes report an increased sex drive following
menopause. It has been suggested that this may be due to
androgen production by the adrenal cortex.
Menopause

Key concepts
Fertilization of the ovum occurs in the oviduct.
Progesterone and estrogen released from the ovary
prepare the oviduct and uterus for receiving the
developing embryo.
The blastocyst enters the uterus, leaves the surrounding
zona pellucida, and implants into the uterine wall on day
7 of gestation.
Human chorionic gonadotropin (hCG), produced by
trophoblast cells of the developing embryo, activates the
corpus luteum to continue producing progesterone and
estradiol beyond its normal life span to maintain
pregnancy.

Key concepts (cont.)
Shortly after the embryo implants into the uterine wall, a
placenta develops from embryonic and maternal cells and
becomes the major steroid-secreting organ during pregnancy.
Major hormones produced by the fetoplacental unit are
progesterone, estradiol, estriol, hCG, and human placental
lactogen. Elevated estriol levels indicate fetal well-being,
whereas low levels might indicate fetal stress. Human placental
lactogen has a role in preparing the breasts for milk production.
The pregnant woman becomes insulin-resistant during the latter
half of pregnancy in order to conserve maternal glucose
consumption and make glucose available for the developing
fetus.

Key concepts (cont.)
The termination of pregnancy is initiated by strong uterine
contractions induced by oxytocin. Estrogens, relaxin, and
prostaglandins are involved in softening and dilating the
uterine cervix so that the fetus may exit.
Lactogenesis is milk production, which requires prolactin
(PRL), insulin, and glucocorticoids. Galactopoiesis is the
maintenance of an established lactation and requires PRL
and numerous other hormones. Milk ejection is the
process by which stored milk is released; “milk letdown” is
regulated by oxytocin, which contracts the myoepithelial
cells surrounding the alveoli and ejects milk into the ducts.

Key concepts (cont.)
Lactation is associated with the suppression of menstrual
cycles and anovulation due to the inhibitory actions of PRL on
GnRH release and the hypothalamic-pituitary-ovarian axis.
The hypothalamic-pituitary axis becomes activated during the
late prepubertal period, resulting in increased frequency and
amplitude of GnRH pulses, increased LH and FSH secretion,
and increased steroid output by the gonads.
Most disorders of sexual development are caused by
chromosomal or hormonal alterations, which may result in
infertility, sexual dysfunction, or various degrees of
intersexuality (hermaphroditism).





























