Embed Size (px)
Citation preview

Renal Vascu lar I n t e r v e n t i o n s
John H. Rundback and Joshua L. Weintraub
R ENAL ARTERY STENOSIS (RAS) second- ary to atherosclerosis or fibromuscular dys-
plasia (FMD) is the most common origin of secondary hypertension. In young individuals, es- pecially women, fibrodysplastic RAS has long been recognized as an infrequent but correctable cause of hypertension, in older patients, athero- sclerotic (or atheromatous) RAS (ARAS), a man- ifestation of systemic atherosclerosis, is an increas- ingly recognized reason for renal insufficiency, t-3 As the median age of the United States population rises, 4 the prevalence of atherosclerotic RAS is increasing. This has resulted in recent dramatic increases in the use of renal artery angioplasty and stenting (Murphy T, personal communication)) Between 1996 and 2001, the annual volume of renal artery interventions billed to Medicare in- creased 242%, with an annual increase in renal artery stenting of 364%. Over the same time period, renal artery bypass surgery declined by 45% from 4,040 to 2,260 procedures annually, reflecting an increased trend toward percutaneous minimally invasive interventions for RAS (T Mur- phy, personal comanunication).
NATURAL HISTORY OF RAS
Atherosclerotic disease accounts for two thirds of cases of RAS. Approximately one third of lesions are bilateral, and 75% are ostial (variably defined but usually considered to be within 5 mm of the aortic lumen). As early as 1968, Meaney et al 5 and Wollenweber et al 6 in 2 separate reports noted that ARAS is often an anatomically progres- sive process. Meaney described interval worsening of ARAS in 36% of 39 patients followed for a mean 27 monthsfl whereas Wollenweber reported a somewhat higher 60% rate of disease progression in 30 patients followed for 28 months. More contemporary series have reproduced these earlier results. Becket et al 8 found that nearly 50% of lesions having a greater than 75% initial stenosis
From the New York Presbyterian Hospital, College of Phy- sicians and Surgeons of Columbia University, New York, NK
Address reprint requests to John H. Rundback, MD, FSIR, New York Presbyterian Hospital, New York, NY 10032.
Copyright 2002, Elsevier Science (USA). All rights reserved. 0037-198X/02/3704-0008535.00/0 do# l O.l O53/sroe.2002.35481
developed progressive stenosis or occlusion over a 13-month period. Tollefson and Ernst 9 performed sequential aortograms on 48 patients and found disease progression in 53%, with 7 arteries (all with initial stenosis >80%) developing occlusion. Schreiber and colleagues 1° reported a mean angio- graphic follow-up of 52 months on 85 patients with ARAS, with clinical follow-up out to 87 months. During that period of time, 44% of lesions pro- gressed and 16% occluded. Progressive ARAS was associated with decreasing renal size and function but not with hypertension control. Finally, in a prospective study using renal duplex sonography over a mean of 32 months, Zierler et aP 1 found the cumulative incidence of ARAS progression from <60% to -->60% to be 48% at 3 years, with a cumulative rate of occlusion (for arteries initially greater then 60% stenosed) to be 7% at 3 years. Only 8% of patients with initially normal renal arteries developed a >60% stenosis during this same interval.
There has been limited data regarding the impact of ARAS on renal size and function. In their study, Wollenweber et al 6 described functional deteriora- tion in 19%. Schreiber et allo noted decreasing renal size and function in 70% and 54% of their patients, respectively. In a 2-year follow-up of 54 patients with ARAS initially greater than 60%, Strandness ~2 reported an average decrease in renal length of 1.9 cm. The estimated risk of loss of more than 1 cm (approximately 30% of renal mass) was 19% at 1 year. In a retrospective evaluation of renal function deterioration, Connolly et a113 noted that the risk of eventual dialysis correlated with the initial angiographic pattern of disease. They found the 2-year, actuarial hemodialysis-free survival to be 97% for patients with unilateral stenosis, 82% for bilateral stenosis, and 45% with unilateral renal artery occlusion and contralateral stenosis or oc- clusion. ~3 In a prospective evaluation of renal function in patients with ARAS, Dean et a114 serially followed renal function in 41 patients over a range of 6 to 78 months. Forty-one percent eventually required surgical revascularization, ei- ther for progressive excretory dysfunction (present in 46%) or renal atrophy (>10% loss of renal length, present in 37%). Similar to other investi- gators, acceptable blood pressure control was noted in nearly all cases. Unfortunately, although
312 Seminars in Roentgenology, Vol 37, No 4 (October), 2002: pp 312-326

RENAL VASCULAR iNTERVENTIONS 313
Fig 1. Percutaneous transluminal renal angioplasty. A 43- year-old woman presented with new onset hypertension unre- sponsive to 3 medications. (A) Flush aortogram shows fibro- muscular dysplasia (medial fibroplasia) involving the distal right renal artery. (B) Selective angiography shows the classic "string of beads" appearance. (C) Post-PTRA image shows marked improvement in the angiogram, The patient's hyper- tension resolved.
these data clearly suggest both anatomic and func- tional progression in many patients with athero- sclerotic RAS, there remain no reliable predictors of disease progression on a case-to-case basis.
FMD consists of several histologic subtypes, with medial fibroplasia being the most common. This lesion is characterized by fibrous replacement of the vascular media resulting in alternating areas of arterial constriction and poststenotic dilatation, the classic "string of beads" appearance. Although almost one third of medial fibroplastic lesions will progress, occlusion is uncommon, and there gen- erally is no change in renal size or function until late in the disease. ~5 Conversely, other forms of FMD, including perimedial fibroplasia and intimal hyperplasia, invariably result in progressive renal artery obstruction and renal atrophy. Although angiographic distinction of the different forms of FMD is important, all types respond well to per- cutaneous transluminal angioplasty, limiting the clinical importance of this differentiation (Fig 1).
PREVALENCE OF ARAS
In patients undergoing angiography for periph- eral vascular disease (PVD), ARAS is present in 14% to 44% (Table 1)] 6-23 with bilateral disease present in approximately 20% to 29% of cases. 24-26 Among patients being evaluated for PVD, ARAS is more prevalent in patients with hypertension. Eyler et a116 evaluated the renal arteries in 500 patients undergoing peripheral angiography. In this series, ARAS was present in 62% of hypertensive patients compared with 32% of normotensive pa-
Table 1. Prevalence of RAS in Patients With PVD
Author Year n %RAS
Eyler et al TM 1962 500 44 Dustan et aH 7 1984 111 35 Bonomo et a118 1988 300 15 Priollet et a119 1990 99 14 Salmon and Brown 2° 1990 374 31 Choudri et a121 1990 100 42 Olin et a122 1990 395 44 Totals 1879 35

314 RUNDBACK AND WEINTRAUB
tients. ARAS has been similarly correlated with coronary and carotid atherosclerosis. 27,a8 Harding et a129 found significant ARAS in 15% of 1,235 patients undergoing cardiac catheterization, and Uzu et a125 discovered ARAS in 39% of Japanese men with a history of hypertension and myocardial infarction. In hypertensive patients undergoing car- diac catheterization, preexistent azotemia has been identified as a predictor of ARAS. 3° In another study of 201 patients receiving lower extremity arteriography, coronary artery disease was the only clinical predictor of renal artery stenosis, a3 The presence of RAS may also signify an increased risk of cardiovascular events. In 1 series of 86 patients ~ver the age of 70 presenting with New York Heart Association class II to IV heart failure, 34% were found to have stenosis of at least 50% involving at least 1 renal artery. 3~
Atheromatous RAS is also highly prevalent in patients with renal insufficiency, and when be- lieved to be the etiology for the renal disease is Lermed ischemic nephropathy. In a prospective evaluation of 21 azotemic patients (serum Cr -> 2.0 mg/dL) older than 45 years old, O'Neil et all found RAS in 14%. The presence of RAS was associated with a more rapid decline in renal function and ~ignificantly more extrarenal atherosclerosis. Renal artery stenosis is also an increasing cause of end-stage renal disease (ESRD) requiring renal replacement therapy. Appel et al 2 noted that 10 of 45 (22%) ESRD patients had renovascular disease ?n duplex sonography, and in an audit of patients presenting to a renal unit at the Royal Free Hospi- tal in the United Kingdom, atherosclerotic reno- vascular disease was the cause for renal failure in 14% of patients over the age of 50. 3 Furthermore, patients with ESRD resulting from RAS appear to nave the worst prognosis of any dialysis patient group. Mailloux et a132 noted that these patients .~ad only a 27-month median survival, with a 5-year survival of 18%, corresponding to an ap-
proximately 30% per year mortality. Renovascular ESRD also poses a tremendous economic burden. According to the 2001 USRDS, 33 there were 80,128 incident ESRD patients in 1999, with an average cost of $36,600 per annum. 34 If 14% of these patients have a renovascular cause of ESRD, then this amounts to a fiscal responsibility of $410.5 million dollars per year in the United States alone.
CLINICAL PRESENTATION
Several clinical clues may alert the clinician to the presence of RAS (Table 2). These include sudden onset of hypertension; onset of hyperten- sion before the age of 30 or after 50; and malig- nant, accelerated, or drug-resistant hypertension. Hypertension without a family history in patients who smoke or have systemic atherosclerosis also increases the likelihood of RAS. 35 On physical examination, a characteristic holosystolic flank murmur is associated with RAS in 55% of pa- tients, 36 and more than 30% of patients with advanced Kimmelstiel-Wilson retinopathy will have renovascular hypertension. 37 Mild proteinuria frequently occurs in association with RAS, but severe proteinuria is usually more indicative of underlying intrinsic renal disease, and the degree of albuminuria inversely correlates with renal functional outcomes after revascularization. 38 Hy- pokalemia may also be noted in patients with RAS secondary to aldosterone mediated urinary potas- sium excretion and was present in 15% of patients in the US Cooperative study. 39,4° Finally, a dis- crepancy in size between the 2 kidneys of more than 1.5 cm should prompt an investigation for the presence of RAS.
Renal insufficiency induced by an angiotensin- converting enzyme inhibitor or angiotensin II re- ceptor blocker is a strong indicator of bilateral or solitary RAS, presumably because of reduced glo- merular filtration after inhibition of angiotensin
Table 2. Clinical Features of RAS
History Physical examination Laboratory
Onset <30 or >50 yr old Malignant, accelerated, drug resistant hypertension Smoking Systemic atherosclerosis No family history of hypertension ACE1 or ARB induced renal failure Unexplained or rapidly progressive renal failure Recurrent pulmonary edema
Epigastric bruit Retinopathy Asymmetric renal size
Hypokalemia Mild or absent proteinuria Elevated plasma renin activity
Abbreviations: ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker.

RENAL VASCULAR INTERVENTIONS
Table 3. Anatomical Indications for Renal Revascularization
315
Indicators for PTRA: -> 50% diameter RAS with a translesional pressure gradient of at least 20 mm Hg > 80% diameter RAS, without measuring translesional gradient patent intrarenal arteries without significant or multiple stenosis (ie, viable kidney) target kidney >7 cm in length
Stenosis greater than 70%-80% may be considered for prophylactic intervention (in the absence of clinical indicators) to empirically prevent the progression of the stenosis to occlusion (approximately 5%/yr risk), particularly if the entire renal functional mass is at risk
Indications for renal stenting: Failure to attain a hemodynamically satisfactory result by renal artery angioplasty
>30% diameter residual renal artery stenosis Greater than a 20 mm Hg residual peak systolic pressure gradient Presence of a f low limiting dissection of the renal artery
Restenosis (>50%) of a lesion that was successfully treated by angioplasty in the past, with recurrent clinical symptoms Primary treatment of ostial RAS because of overhanging aortic plaque
II-induced constriction of the efferent renal arte- riole. Similarly, renal failure precipitated by a reduction in blood pressure in response to other classes of antihypertensive medications suggests the presence of RAS, as does any unexplained or sudden deterioration of renal function. Recurrent flash pulmonary edema out of proportion to abnor- malities of left ventricular ejection function is a recognized phenomenon occurring in patients with ARAS and is most likely secondary to intravascu- lar volume expansion and ventricular diastolic dysfunction. In a series of 55 consecutive azotemic patients, Pickering 36 found recurrent pulmonary edema in 25%. Pulmonary edema usually resolves after successful revascularization. 41,42
BACKGROUND AND INDICATIONS FOR PERCUTANEOUS INTERVENTION
Percutaneous transluminal renal angioplasty (PTRA) was first described by Grundzig et a143 in
1974. Although the placement of metallic endo- prostheses to restore arterial patency was envi- sioned by Dotter and Judkins 44 in 1964, it was more than 2 decades later that Palmaz et al45 first reported the use of metal stents for the treatment of RAS. Initial clinical series in Europe by Kuhn et a146 and Joffre et a l , 47 a s well as the early results of the US multicenter trial, 48 established renal artery stenting (PTRS) as an important treatment adjunct in patients failing balloon angioplasty alone. Since that time, PTRA and PTRS have become widely accepted as a first-line therapy for many patients suffering from symptomatic RAS.
Ideally, patients being considered for renal re- vascularization should have both anatomic (mor- phologic) and clinical criteria for intervention (Ta- bles 3 and 4). In approaching these patients, the decision to pursue revascularization is often diffi- cult, and several questions need to be considered.
Is revascularization possible and safe? Bilateral
Table 4. Clinical Indications for Renal Revascularization
Hypertension (88-91) accelerated hypertension-sudden worsening of previously controlled hypertension refractory hypertension-hypertension resistant to treatment with at least 3 medications of different classes including a diuretic malignant hypertension-hypertension with coexistent evidence of end-organ damage, including left ventricular hypertrophy,
congestive heart failure, visual or neurological disturbance, and/or advanced (grade IV) retinopathy hypertension with a unilateral small kidney hypertension with intolerance to medication
Renal salvage sudden unexplained worsening of renal function 1921 impairment of renal function secondary to antihypertensive treatment, particularly with an angiotensin converting enzyme
inhibitor or angiotensin II receptor blocker (93,94) renal dysfunction not attributable to another cause
Cardiac disturbance syndromes recurrent flash pulmonary edema out of proportion to left ventricular impairment (95-97) unstable angina in the setting of significant RAS
Medication flexibility clinical need to use ACEI or ARB (ie, for treatment of proteinuria or cardiac dysfunction) that would be otherwise
contraindicated due to risk of inducing renal failure intolerance to antihypertensive medications

316 RUNDBACK AND WEINTRAUB
iliac/femoral occlusions or severe aortic athero- sclerosis are relative contraindications to interven- tion, with the latter likely to be associated with a greater risk of cholesterol or atheroembolism. Al- though certain renal artery lesions are better treated from an axillary or brachial approach, this is accompanied by higher puncture site-related and upper extremity neurologic complications. In pa- tients with equivocal stenoses or in patients at an unusually high risk of atheroembolism because of an aortic aneurysm or marked aortic irregularity, a determination of renal vein renins (RVR) may be considered, and a positive study is highly predic- tive of a beneficial response to revascularization. 49 In patients with azotemia, the size of the kidney to be revascularized should be evaluated. Kidneys less than 7 cm in length do not usually warrant revascularization, 5° particularly if nonfunctional on a radionuclide renal scan, having markedly increased echogenicity and cortical thinning on ultrasonography, or associated with progressive advanced azotemia (serum creatinine > 4.0 rag/ dL). The condition of the intrarenal vessels on arteriography may also preclude intervention. Hy- pertensive patients with an atrophic kidney should have RVRs determined and treated either with catheter-directed ablation 51 or surgical nephrec- tomy if the RVR lateralizes to the affected side.
What are the reasons for treatment? As noted in table 3, there are many different reasons for per- forming renal revascularization. The importance of treatment must be weighed against potential risks. Angioplasty or stenting of an incidentally discov- ered <80% diameter RAS without a good clinical indicator is rarely warranted. In contradistinction, because of the documented high risk of occlusion in untreated lesions exceeding 80%, 52,53 prophy- lactic revascularization can be justified in this setting, particularly if the entire renal mass is jeopardized by renal ischemia. This strategy may allow intervention at an earlier stage before the development of a more technically challenging higher-grade stenosis or occlusion and before ir- reversible critical loss of functional renal paren- chyma. 54
When treating azotemic patients, what it the risk of progressive renal insufficiency with and without intervention? Chabova et a155 in a recent study found that only 9% of patients with renal insuffi- ciency followed for 3 years progressed to renal replacement theory, with a higher rate of progres-
sire azotemia in individuals with bilateral disease. This relatively low risk of clinical disease progres- sion, particularly in mildly azotemic patients with only unilateral disease, needs to be considered before undertaking revascularization. Although several reports support the concept that better stabilization of renal function is seen after revas- cularization in patients with more mild levels of renal dysfunction, 56-5s it is not clear whether this is because of intervention or inherent to the natural history of the disease. Furthermore, no thresholds for this effect have been defined, and it remains to be determined whether there is an impact of revascularization on overall dialysis-free survival in azotemic patients. Finally, even with the use of renal protective agents 59,6° and alternative contrast agents, intervention has an approximately 2% to 5% risk of aggravating renal dysfunction.
TECHNIQUE OF RENAL ANGIOPLASTY AND STENTING
When performing renal interventions, careful preintervention planning is necessary to assure the highest possible technical success. The best route for crossing the lesion should be carefully as- sessed. Arteries with a sharp caudal angulation from the aorta are often best approached from the axillary or brachial artery (Fig 2). For mild or equivocal lesions, translesional pressure measure- ments should be performed to confirm the hemo- dynamic significance before intervention.
Pharmacologic adjuncts are important for pre- venting procedure-related complications. Patients should be adequately hydrated. If PTRA or stent- ing is anticipated, acetylsalicylic acid (81 mg) is given beginning the day of the procedure. Heparin sulfate should be administered to provide full anticoagulation before crossing the renal artery stenosis (as a 3,000-10,000 U initial bolus) as well as periodically during continued catheter and de- vice manipulation (as an additional bolus of 1000 U/h). If available, measuring the activated clotting time is useful to assure adequate levels of antico- agulation. The use of protamine sulfate to reverse heparinization after the procedure should be avoided because this may risk hypotension and acute stent thrombosis. Once the lesion is crossed, intra-arterial nitroglycerin should be liberally de- livered through the catheter in 100 to 200 /xg aliquots to prevent wire and catheter-induced va- sospasm. Intra-arterial verapamil (1-2.5 mg) is

RENAL VASCULAR INTERVENTIONS 317
very effective for treating spasm resistant to nitro- glycerin but should be used with caution in patients with first-degree heart block.
Angioplasty is performed using well-established techniques, s Although only the basic concepts will be mentioned in this article, technical tricks for performing complex renal stent cases have been described61(Fig 3). Once a stenosis is identified by aortography, the lesion is carefully and atraumati- cally crossed by using a floppy-tipped guidewire and appropriately shaped shepherds crook or co- bra-shaped catheter. Depending on the balloon or stent system used, exchange is then made for a stiffer wire to facilitate subsequent catheter manip- ulations. The shortest possible balloon with a
Fig 2. Access site for renal intervention. (A) The right renal artery shows a sharp caudal angulation from the aorta. This was approached from a brachial access site. The left renal artery has a transverse orientation and is best approached from a femoral access. (B) The left renal artery stent has been deployed. A balloon expandable stent is positioned from a brachial approach over the right renal artery stenosis. {C) Postangioplasty and stenting views shows the marked caudal angulation of the right stent and the transverse postioning of the left renal artery stent.
diameter equal to the normal width of the target renal artery is positioned across the stenosis and slowly inflated, with care taken to avoid balloon sliding that may risk dissection. After deflation, the balloon is removed while maintaining guidewire position across the treated site. Completion angiog- raphy is performed by a guiding catheter or sheath, or more rarely, using a pigtail catheter introduced parallel to the guidewire or from a different vas- cular access site. If there is a satisfactory angio- graphic appearance and no residual transstenotic gradient, the guidewire is carefully removed.
Despite the use of stents in the renal arteries for more than 10 years, trials are still underway to obtain approval by the US Food and Drug Admin-
318 RUNDBACK AND WEINTRAUB
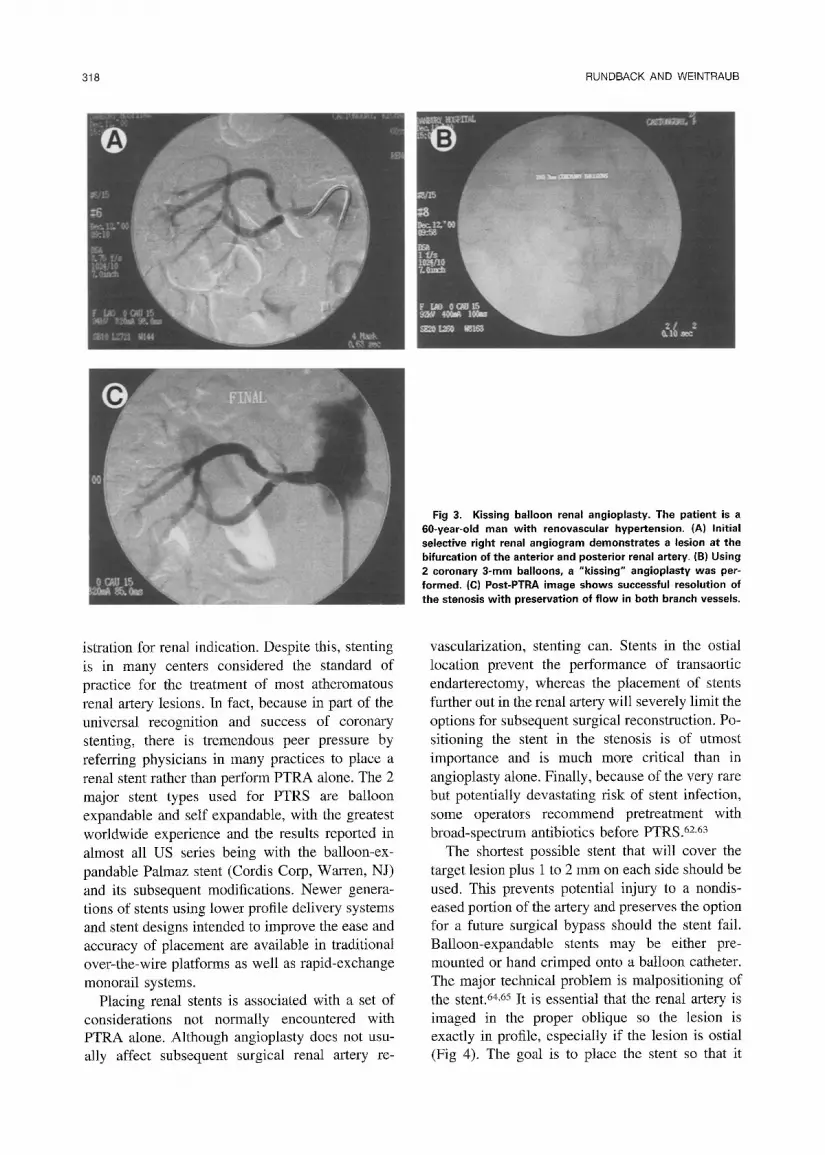
Fig 3. Kissing balloon renal angioplasty. The patient is a 60-year-old man with renovascular hypertension. (A) Initial selective right renal angiogram demonstrates a lesion at the bifurcation of the anterior and posterior renal artery, (B) Using 2 coronary 3-mm balloons, a "kissing" angioplasty was per- formed. (C) Post-PTRA image shows successful resolution of the stenosis with preservation of flow in both branch vessels.
istration for renal indication. Despite this, stenting is in many centers considered the standard of practice for the treatment of most atheromatous renal artery lesions. In fact, because in part of the universal recognition and success of coronary stenting, there is tremendous peer pressure by referring physicians in many practices to place a renal stent rather than perform PTRA alone. The 2 major stent types used for PTRS are balloon expandable and self expandable, with the greatest worldwide experience and the results reported in almost all US series being with the balloon-ex- pandable Palmaz stent (Cordis Corp, Warren, NJ) and its subsequent modifications. Newer genera- tions of stents using lower profile delivery systems and stent designs intended to improve the ease and accuracy of placement are available in traditional over-the-wire platforms as well as rapid-exchange monorail systems.
Placing renal stents is associated with a set of considerations not normally encountered with PTRA alone. Although angioplasty does not usu- ally affect subsequent surgical renal artery re-
vascularization, stenting can. Stents in the ostial location prevent the performance of transaortic endarterectomy, whereas the placement of stents further out in the renal artery will severely limit the options for subsequent surgical reconstruction. Po- sitioning the stent in the stenosis is of utmost importance and is much more critical than in angioplasty alone. Finally, because of the very rare but potentially devastating risk of stent infection, some operators recommend pretreatment with broad-spectrum antibiotics before PTRS. 6z63
The shortest possible stent that will cover the target lesion plus 1 to 2 mm on each side should be used. This prevents potential injury to a nondis- eased portion of the artery and preserves the option for a future surgical bypass should the stent fail. Balloon-expandable stents may be either pre- mounted or hand crimped onto a balloon catheter. The major technical problem is malpositioning of the stent. 64,65 It is essential that the renal artery is imaged in the proper oblique so the lesion is exactly in profile, especially if the lesion is ostial (Fig 4). The goal is to place the stent so that it

RENAL VASCULAR INTERVENTIONS 319
Fig 4. Profiling. It is important to image the renal arteries in the proper obliquity, especially for an ostial lesion. (A) The right renal artery is often best imaged from a straight anterior- posterior image. (B) The left renal usually arises obliquely from the aorta. This is best visualized with a 20 ° to 40 ° left anterior oblique image. (C) Computed tomograpy image after stenting shows the angle of origins of the renal arteries from the aorta. (D) Oblique view on angiography show the marked shortening of the right renal stent when viewed in the left anterior oblique (LAO). The right renal ostium is best visualized in anterior- posterior or right anterior oblique (RAO).
covers the lesion and extends 1 to 2 mm past it on both sides; for ostial lesions, the proximal end should extend 1 to 2 mm into the aorta to ensure that it covers the ostium adequately. As with angioplasty alone, the completion angiogram after stenting should be performed with a technique that preserves wire position across the stenosis to facil- itate repeated interventions including further stent dilatation or placement of additional stents. This also decreases complications by obviating the need to recross the lesion in the event of a dissection or other vessel injury.
COMPLICATIONS AND THEIR PREVENTION
Complications of PTRA and stenting are re- ported to occur in 5% to 10% of patients and include spasm, thrombosis, dissection, and embo- lization. 66,67 The routine use of adjunctive anti- spasmodic medications and heparin helps prevent the first 2 of these problems. Acute occlusion is rare and is usually caused by dissection or throm- bosis. Angiographic distinction of these 2 entities will allow appropriate treatment with stents or thrombolysis, respectively. Frank rupture with ret-
roperitoneal extravasation of contrast requires sur- gical repair, although there is recent experience with the successful use of stent grafts. The PTA balloon or an occlusion balloon should be inflated across the site of rupture until definitive therapy is undertaken. Iced saline can be infused through the catheter to help preserve the kidney while the operating room is readied. If this does not control the hemorrhage a large occlusion balloon can be inflated across the renal origin. In contrast, perfo- ration by only a guide wire is almost always self-sealing, and peripheral perforations that do not stop bleeding can be treated with subsegmental transcatheter occlusion using coils or gel foam.
One of the major potential complications with renal angioplasty is the embolization of cholesterol crystals or atheromatous plaque. Microcholesterol crystal embolization occurs in approximately 1% to 2% of patients and is potentially severe or even fatal. Patients with marked aortic irregularity are at particular risk. Unfortunately, there is no specific treatment for cholesterol crystal embolization. Careful patient and access-site selection and greater operator experience can help minimize the

320 RUNDBACK AND WEINTRAUB
risk, as can the use of soft-tipped catheters and guide wires. Symptomatic distal embolization of dislodged large plaque is rare but may require surgical embolectomy, bypass, or thrombolysis.
Transient contrast-related declines in renal func- tion may be seen in up to 13% of patients under- going renal interventions. 68 The risk factors for renal failure after administration of iodinated con- trast material are well known and include preex- isting renal insufficiency, dehydration, diabetic nephropathy, hyperuricemia, and multiple my- eloma. Fortunately, in patients with normal renal function, the risk of permanent renal impairment is small. Alternative contrast agents including gado- linium and CO 2 are routinely used in patients with marginal renal reserve. In addition, premedication with mucomyst or fenoldopam may decrease the renal toxicity of iodinated contrast material. 59,6°
POSTPROCEDURE CARE
Every patient should be closely monitored after renal intervention. Immediately after procedure patients are well hydrated. Blood pressure, volume status, urine output, and serum creatinine are mon- itored closely. Acute deteriorations of renal func- tion may warrant repeat angiography, further inter- vention, or bypass. Patients are generally advised to take an antiplatelet agent (eg, acetylsalicylic acid 81 mg daily) postprocedurally. Although the use of other antiplatelet medication such as ticlo- pidine, clopidigrel, dipyridamole, and cilostazol have shown clinical promise for preventing pro- gressive vascular stenosis in other vascular beds, 69-7j their role after renal interventions is not yet established. Routine systemic anticoagulation is not used except in patients with known hyper- coagulable states. If the patient has persistent or increasing back or flank pain, arterial rupture or impending rupture as well as total occlusion must be considered, and a computed tomography scan is warranted to look for extravasation around the renal artery and kidney.
TECHNICAL RESULTS OF RENAL ANGIOPLASTY AND STENTING
PTRA has become well established for the treatment of RAS caused by fibromuscular dyspla- sia, with reported rates of technical success ranging from 88% to 100% and hypertensive benefit in 79% to 100%. 72-74 Similarly, excellent immediate- and long-term results can be achieved for PTRA of
nonostial atheromatous RAS, with an overall clin- ical benefit that is often related to such factors as renal size, comorbid medical conditions, and co- existent essential hypertension. 75-84 Despite this, the role of PTRA in treating patients with athero- sclerotic RAS has remained controversial, primar- ily because of the poor technical success and high restenosis rates of PTRA alone for the treatment of ostial lesions in most series. 85-89 Stenting has improved the technical success of PTRA for these eases 9°,91 by providing a scaffold that displaces aortic atheroma. In a prospective randomized trial, Van de Ven and associates 91 reported a primary success rate of 88% for PTRS compared with 57% for PTRA. In ostial lesions, the radial force of the stent counteracts the elastic recoil and geometric remodeling that are significant contributors to both early and late restenoses. 92,93 Furthermore, stents produce a smoother luminal surface that is theo- retically less likely to cause platelet aggregation, smooth muscle cell stimulation, and intimal hyper- plasia (IH). 94,95 For this reason, several investiga- tors have advocated the increasingly common practice of primary stenting of ostial lesions. 68,96,97 In contrast, other investigators, using strictly de- fined criteria for ostial lesions, have noted that a smaller than previously thought proportion of these ostial stenoses are actually because of aortic plaque. 98 Furthermore, although supported by ret- rospective series, it has not been definitively shown that stenting results in improved long-term patency when compared with a perfect response after PTRA alone. 99-1°2 Prospective long-term studies are needed to firmly answer this question.
After stenting, restenosis caused by IH occurs in approximately 16% of treated arteries. ~o3 Since the development of approximately 1 mm of IH cover- ing the stent surface is a normal part of stent healing (Fig 5), the risk of restenosis is geometri- cally related to the initial degree of stent expan- sion. In the US multicenter study, stents dilated to less than 6 mm had nearly double the risk of restenosis. 1°4 A significantly higher rate of reste- nosis was also observed in smokers and in women, whereas the effect of gender was not confirmed in 1 other study. ~°5 Van de Ven et al 9~ reported restenosis in 48% of patients treated by PTRA versus 14% after stent placement, although there were no differences in clinical outcomes between the 2 groups. Of note, even modest levels of restenosis may be an important cause of clinical
RENAL VASCULAR INTERVENTIONS 321
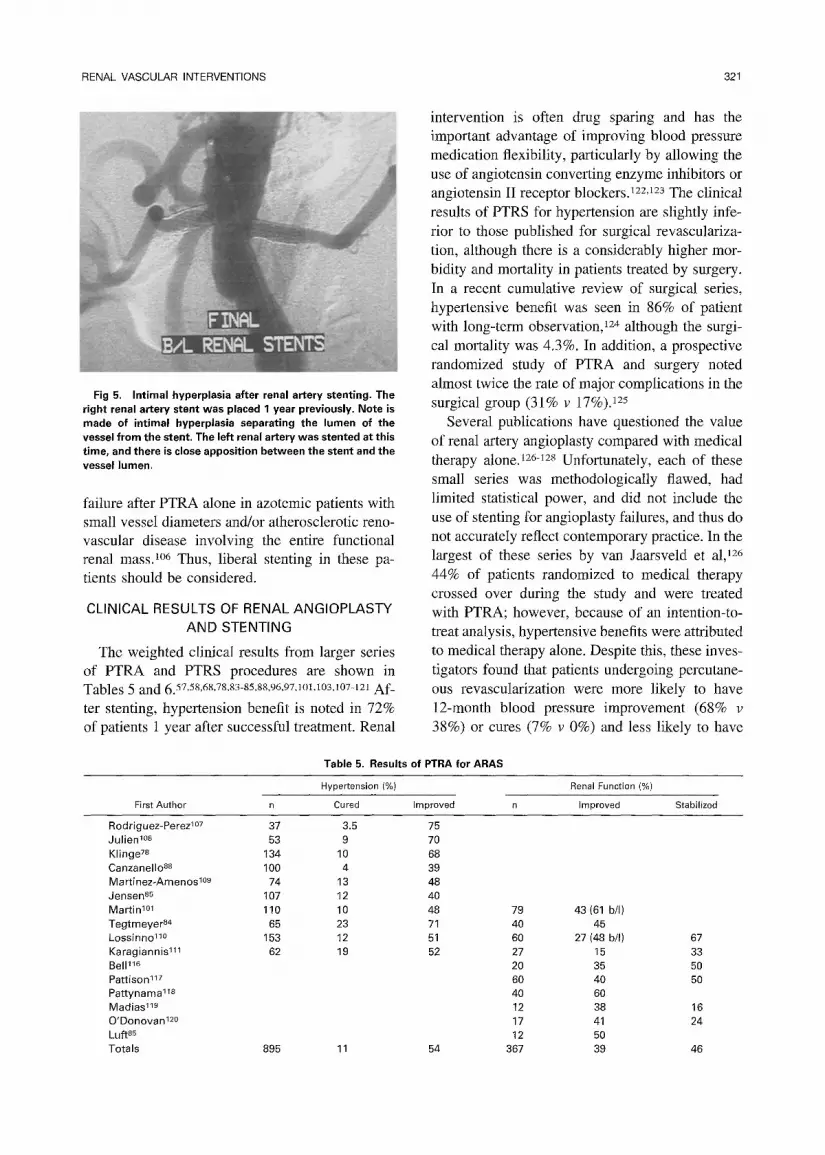
Fig 5. Intimal hyperplasia after renal artery stenting. The right renal artery stent was placed 1 year previously. Note is made of intimal hyperplasia separating the lumen of the vessel from the stent, The left renal artery was stented at this time, and there is close apposition between the stent and the vessel lumen,
failure after PTRA alone in azotemic patients with small vessel diameters and/or atherosclerotic reno- vascular disease involving the entire functional renal massJ °6 Thus, liberal stenting in these pa- tients should be considered.
CLINICAL RESULTS OF RENAL ANGIOPLASTY AND STENTING
The weighted clinical results from larger series of PTRA and PTRS procedures are shown in Tables 5 and 6. 57,58,68,78,83-85,88,96,97,101,103,107-121 Af-
ter stenting, hypertension benefit is noted in 72% of patients 1 year after successful treatment. Renal
intervention is often drug sparing and has the important advantage of improving blood pressure medication flexibility, particularly by allowing the use of angiotensin converting enzyme inhibitors or angiotensin II receptor blockers, t22,123 The clinical results of PTRS for hypertension are slightly infe- rior to those published for surgical revasculariza- tion, although there is a considerably higher mor- bidity and mortality in patients treated by surgery. In a recent cumulative review of surgical series, hypertensive benefit was seen in 86% of patient with long-term observation, 124 although the surgi- cal mortality was 4.3%. In addition, a prospective randomized study of PTRA and surgery noted almost twice the rate of major complications in the surgical group (31% v 17%). 125
Several publications have questioned the value of renal artery angioplasty compared with medical therapy alone. 126-~28 Unfortunately, each of these small series was methodologically flawed, had limited statistical power, and did not include the use of stenting for angioplasty failures, and thus do not accurately reflect contemporary practice. In the largest of these series by van Jaarsveld et al, 126 44% of patients randomized to medical therapy crossed over during the study and were treated with PTRA; however, because of an intention-to- treat analysis, hypertensive benefits were attributed to medical therapy alone. Despite this, these inves- tigators found that patients undergoing percutane- ous revascularization were more likely to have 12-month blood pressure improvement (68% v 38%) or cures (7% v 0%) and less likely to have
Table 5. Results of PTRA for ARAS
First Author
Hypertension (%)
Cured Improved
Renal Function (%)
Improved Stabilized
Rodriguez-Perez I°7 37 3.5 75 Julien 1°8 53 9 70 Klinge 78 134 10 68 Canzanello a8 100 4 39 Martinez-Amenos 1°9 74 13 48 Jensen 85 107 12 40 Martin TM 110 10 48 Tegtmeyer 84 65 23 71 Lossinno 11° 153 12 51 Karagiannis TM 62 19 52 Belp16 Pattison 117 Pattynama ~8 Madias 1~9 O'Donovan 120 Luft85 Totals 895 11 54
79 43(61 b/I) 40 45 60 27(48 b/I) 67 27 15 33 20 35 50 60 40 50 40 60 12 38 16 17 41 24 12 50
367 39 46
322 RUNDBACK AND WEINTRAUB
Table 6, Contemporary Results of Larger Series of Renal Stenting
Hypertension (%) Renal Function (%}
First Author n Cured Improved n Improved Stabilized
lannone 97
White aa
Bium 103
Tuttle 112
Oorros 6s
Henry 113 184 19 Rocha-Singh TM 127 6 Rodriguez-Lopez 115 108 11 Siablis l~e 62 62 Totals 937 9
54 4 35 22 36 46 I00 76 44 22 78 68 16 62 20 100
129 2 53 97 13 105 1 42 106 33(U/L)
38(b/L) 61 48 29 50 71 28 57 32 100
8 0 100 63 448 26 60
76
33 (U/L) 42 (b/L) 67 59
blood pressure deterioration (9% v 33%) or pro- gression to renal artery occlusion (0% v 16%).
Renal intervention has clinical benefit in the majority of patients treated for ischemic nephrop- athy, particularly for slowing the decline in renal function. 129-131 Patients in whom there is rapid decline in function before intervention have the greatest chance of renal improvement.132-J 34 Over- all benefit is noted in close to 90% of patients and is directly related to the pretreatment glomerular filtration rate. In a large multicenter registry com- prising 1,058 successful stent insertions, patients having higher initial creatinine levels (>2.0 rag/ dL) were more likely to stabilize than to improve renal function# 8 Using life-table analysis, Rund- back et aW report noted stabilization or improve- ment in renal function at l-year follow-up in 84% of patients whose initial serum creatinine was 1.5 to 2.0 mg/dL compared with only 38% when the serum creatinine exceeded 3.0 mg/dL. 57 Unilateral PTRS appears to provide equivalent clinical bene- fit to bilateral revascularization, although most investigators recommend bilateral intervention if it is technically feasible and both kidneys are of reasonable size. 57,136 The coexistence of diabetes mellitus does not adversely affect clinical out- comes. 137
The usefulness of renal revascularization in patients with recurrent episodes of flash pulmonary edema has been described. 41,4ml39 Bloch et a141 treated 25 patients with a history of congestive heart failure. At a mean follow-up of 18 months, 77% of patients receiving bilateral stents and 33% treated by unilateral PTRS had no recurrence of pulmonary edema. 4~ Khosla et al~39 have also noted renal artery stenting to be beneficial in patients with unstable angina. 137 In their small experience, 9 of 12 (75%) patients undergoing both
PTRS and coronary angioplasty had sustained improvement in angina compared with 4 of 6 (67%) patients treated by PTRS alone.
COST-EFFECTIVENESS OF PTRS
PTRA and PTRS are cost-effective in compari- son to surgery. Weibull et a1125 prospectively studied 58 nondiabetic patients randomized to either PTRA (n = 29) or surgical revascularization (SR, n = 29). No stents were used in this series. Even though 31% of the PTRA ultimately required SR (17% because of technical failure of PTRA alone), PTRA was still 12% less expensive. More recently, Xue et al ~4° reported a retrospective cost analysis of PTRA, stenting, and bypass surgery at a single tertiary care center. At 1-year follow-up, equivalent clinical outcomes were seen in all 3 patient groups, although the complication rates were significantly higher in the patients treated by surgery. Predominantly because of higher proce- dural costs and longer hospital stays, SR costs almost 7 times more than PTRS and nearly 15 times the cost of PTRA. These data further support the role of PTRA and PTRS as the initial treatment in patients with symptomatic RAS.
CONCLUSION
Percutaneous renal revascularization has been practiced for 25 years. PTRA and PTRS allow successful and durable renal revascularization in nearly all cases and provide a favorable clinical outcome for the majority of treated patients. How- ever, several important areas of further investiga- tion are necessary. There is still controversy con- cerning the effect of renal revascularization on cardiovascular events, dialysis-free survival, and overall mortality. 13,68,141 Studies are under way to answer these questions (Cooper C, personal corn-

RENAL VASCULAR INTERVENTIONS 323
munication). t42 N e w genera t ions of vascular s tents
and embol iza t ion pro tec t ion devices need to be
tes ted for their re la t ive ease o f use and cl inical
efficacy. The role o f drug-e lu t ing stents, wh ich
have s h o w n great p romise in other arterial beds , 143
needs to be evaluated. E m e r g i n g b iochemica l
markers o f R A S represen t in t r iguing resea rch tools
to bet ter unders tand renovascu la r pa thophys io l -
ogy 144J45 and prov ide the theoret ic potent ia l o f
predic t ing the r e sponse to revascular izat ion. Fi-
nally, r a n d o m i z e d prospec t ive trials are necessary
to def ine the proper pat ient select ion, l ong- t e rm
outcomes , and bes t me t h o d s of t rea tment for pa-
t ients wi th renovascu la r disease.
REFERENCES
1. O'Neil EA, Hansen KJ, Canzanello VJ, et al: Prevalence of ischemic nephropathy in patients with renal insufficiency. Am Surg 58:485-490, 1992
2. Appel RG, Bleyer AJ, Reavis S, et ah Renovascular disease in older patients beginning renal replacement therapy. Kid Int 48:171-176, 1995
3. Scoble JE, Sweny P, Stansby G, et al: Patients with atherosclerotic renovascular disease presenting to a renal unit: An audit of outcome. Postrad Med J 69:461-465, 1993
4. Becker GJ, McClenny TE, Kovacs ME, et al: The impor- tance of increasing public and physican awareness of peripheral arterial disease. J Vasc Interv Radiol 13:7-11, 2002
5. Meaney TF, Dustan HP, McCormack LJ: Natural history of renal arterial disease. Radiology 91:881-887, 1968
6. Wollenweber J, Sheps SG, Davis GD: Clinical course of atherosclerotic renovascular disease. Am J Cardiol 21:60-71, 1968
7. Meaney TF, Dustan HP, McCormack LJ: Natural history of renal arterial disease. Radiology 91:881-887, 1968
8. Becker GJ, Katzen BT, Dake MD: Noncoronary angio- plasty. Radiology I70:921-940, 1989
9. Tollefson DFT, Ernst CB: Natural history of atheroscle- rotic renal artery stenosis associated with aortic disease. J Vasc Surg 14:327-331, 1991
10. Schreiber MJ, Pohl MA, Novick AC: The natural history of atherosclerotic and fibrous renal artery disease. Urol Clin North Am 11:383-392, 1984
11. Zierler RE, Bergelin RO, Davidson RC, et al: A pro- spective study of disease progression in patients with athero- sclerotic renal artery disease. Am J Hypertens 9:1055-1061, 1996
12. Strandness DE: Natural history of renal artery stenosis. Am J Kid Dis 24:630-635, 1994
13. Connolly JO, Higgins RM, Walters HL, et al: Presenta- tion, clinical features and outcome in different patterns of atherosclerotic renovascular disease. QJ Med 87:413-421, 1994
14. Dean RH, Kieffer RW, Smithe BM, et al: Renovascular hypertension: Anatomic and renal function changes during drug therapy. Arch Surg 116:1408-1415, 1981
15. Pohl MA, Novick AC: Natural history of atherosclerotic and fibrous renal artery disease: Clinical implications. Am J Kid Dis 5:At20-130, 1985
16. Eyler WR, Clark MD, Garman JE, et al: Angiography of the renal areas including a comparative study of renal arterial stenoses in patients with and without hypertension. Radiology 78:879-891, 1962
17. Dustan HP, Humphries AW, DeWolfe VG, et al: Normal arterial pressure in patients with renal arterial stenosis. JAMA 187:138-142, 1984
18. Bonoma L, DePascale A, Dell'Orso E, et al: Evaluation of the renal arteries with digital angiography in patients with peripheral arteriopathy. Rays 13:49-52, 1988
19. Priollet P, Lazareth I, Maniere-Constantin D, et al: Renal artery stenosis and peripheral vascular diseasse. Lancet 336: 879, 1990
20. Salmon P, Brown NA: Renal artery stenosis and periph- eral vascular disease: Implications for ACE inhibitor therapy. Lancet 336:321, 1990
21. Choudri AH, Cleland JGF, Rowlands PC, et ah Unsus- pected renal artery stenosis in peripheral vascular disease. Br Med J 301:1197-1198, 1990
22. Olin JW, Melia M, Young JR, et al: Prevalence of atherosclerotic renal artery stenosis in patients with atheroscle- rosis elsewhere. Am J Med 88:I46-I51, 1990
23. Swartbol P, Thorvinger BO, Parsson H, et al: Renal artery stenosis in patients with peripheral vascular disease and its correlation to hypertension. A retrospective study. Int Angiol 11:195-199, t992
24. Iglesias JI, Hamburger RJ, Feldman L, et al: The natural history of incidental renal artery stenosis in patients with aortoiliac vascular disease. Am J Med 109:642-647, 2000
25. Uzu T, Inoue T, Fujii T, et al: Prevalence and predictors of renal artery stenosis in patients with myocardial infarction. Am J Kidney Dis 29:733-738, 1997
26. Missouris CG, Belli AM, MacGregor: "Apparent" heart failure: A syndrome caused by renal artery stenoses. Heart 83:152-155, 2000
27. Roberts JC, Moses C, Witldns RH: Autopsy studies in atherosclerosis. I. Distribution and severity of atherosclerosis in patients dying without morphologic evidence of atherosclerotic catastrophe. Circulation 20:511-519, 1959
28. Rossi GP, Rossi A, Zanin L, et al: Excess prevalence of extracranial carotid artery lesions in renovascular hypertension. Am J Hypertens 5:8-15, 1992
29. Harding MB, Smith LR, Himmelstein SI, et al: Renal artery stenosis: Prevalence and associated risk factors in pa- tients undergoing routine cardiac catheterization. J Am Soc Nephrol 2:1608-1616, 1992
30. Rihal CS, Textor SC, Breen JF, et al: Incidental renal artery stenosis among a prospective cohort of hypertensive patients undergoing coronary angiography. Mayo Clin Proc 77:309-316, 2002
31. MacDowall P, Kalra PA, O'Donoghue DJ, et al: Risk of morbidity from renovascular disease in elderly patients with congestive cardiac failure. Lancet 352:13-16, 1998
32. Mallloux LU, Bellucci AG, Mossey RT, et al: Predictors of survival in patients undergoing dialysis. Am J Med 84:855- 862, 1988
33. US Renal Data System, USRDS 200t Annual Data Report: Atlas of End-Stage Renal Disease in the United States,

324 RUNDBACK AND WEINTRAUB
National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2001
34. Friedman EA: End-stage renal disease therapy: An American success story. JAMA 274:1118-1122, 1996
35. Pickering TG: Diagnosis and Evaluation of renovascular hypertension. Circulation 83:I47-I52, 1991
36. Dunnick NR, Sfakianakis GN: Screening for renovascu- lar hypertension. Rad Clin North Am 29:497, 1991
37. Davis BA, Crook JE, Vestal RE, et al: Prevalence of renovascular hypertension in patients with grade III or IV hypertensive retinopathy. N Engl J Med 301:1273-1276, 1979
38. Halimi JM, Ribstein J, DuCailar G, et al: Albuminuria predicts renal functional outcome after intervention in athero- matous renovascular disease. J Hypertens 13:1335-1342, 1995
39. Anderson GH, Blakeman N, Streeten DHP: Prediction of renovascular hypertension: Comparison of clinical diagnostic indices. Am J Hypertens 1:301-304, 1988
40. Simon N, Franklin SS, Bleifer KH, et al: Clinical characteristics of renovascular hypertension. JAMA 220:1209- 1218, 1972
41. Bloch MJ, Trost DW, Picketing TG, et al: Prevention of recurrent pulmonary edema in patients with bilateral renovas cular disease through renal artery stent placement. AJH 12:1-7, 1999
42. Messina LM, Zelenock GB, Yao KA, et al: Renal revascularization for recurrent pulmonary edema in patients with poorly controlled hypertension and renal insufficiency: A distinct subgroup of patients with arteriosclerotic renal artery occlusive disease. J Vasc Surg 15:73-82, 1992
43. Gruntzlg A, Kuhlmann U, Vetter W, et ah Treatment of renovascular hypertension with percutaneous transluminal dila- tation of a renal-artery stenosis. Lancet 1:801-802, 1978
44. Dotter CT, Judkins MP: Transluminal treatment of arteriosclerotic obstruction. Circulation 30:654-670, 1964
45. Palmaz JC, Kopp DT, Hayashi H, et al: Normal and stenotic renal arteries: Experimental balloon-expandable in- traluminal stenting. Radiology 164:705-708, 1987
46. Kuhn FP, Kntkuhn B, Torsello G, et al: Renal artery stenosis: Preliminary results of treatment with the Strecker stent. Radiology 180:367-372, 1991
47. Joffre F, Rousseau H, Bernadet P, et al: Midterm results of renal artery stenting. Cardiovasc Intervent Radiol 15:313- 318, 1992
48. Rees CR, Palmaz JC, Becker GJ, et al: Palmaz stent in atherosclerotic stenoses involving the ostia of the renal arteries: Preliminary report of a multicenter study. Radiology 181:507- 514, 1997
49. Working group on renovascular hypertension, final re- port. Detection, evaluation, and treatment of renovascular hypertension. Arch Intern Med 147:820-829, 1987
50. Novick AC: Options for therapy of ischemic nephropa- thy: Role of angioplasty and surgery. Semin Nephrol 16:53-60, 1996
51. Teigen CL, Mitchell SE, Venbrux AC, et al: Segmental renal artery embolization for treatment of pediatric renovascular hypertension. JVIR 3: I 11-117, 1992
52. Tollefson DFT, Ernst CB: Natural history of atheroscle- rotic renal artery stenosis associated with aortic disease. J Vasc Surg 14:327-331, 1991
53. Zierler RE, Bergelin RO, Davidson RC, et al: A pro- spective study of disease progression in patients with athero-
sclerotic renal artery disease. Am J Hypertens 9:1055-1061, 1996
54. Cambria RP, Brewster DC, L'Italien GJ, et al: Renal artery reconstruction for the preservation of renal function. J Vasc Surg 24:371-382, 1996
55. Chabova V, Schirger A, Stanson AW, et al: Outcomes of atherosclerotic renal artery stenosis managed without revascu- larization. Mayo Clin Proc 75:437-444, 2000
56. Dorros G, Jaff M, Jain A, et al: Follow-up of primary Palmaz-Schatz stent placement for atherosclerotic renal artery stenosis. Am J Cardiol 75:1051-1055, 1995
57. Rundback JH, Gray R, Rozenblit G, et al: Renal artery stent placement for the management of ischemic nephropathy. JVIR 9:413-420, 1998
58. Dorros G, Jaff M, Mathiak L, He T, and multicenter registry participants: Multicenter Palmaz stent renal artery stenosis revascularization registry report: Four-year follow-up of 1,058 successful patients. Cathet Cardiovasc Intervent 55: 182-188, 2002
59. Madyoon H, Croushore L, Weaver D, et al: Use of fenoldopam to prevent radiocontrast nephropathy in high-risk patients. Cather Cardiovasc Interv 53:341-345, 2001
60. Tepel M, van der Giet M, Schwarzfeld C, et al: Preven- tion of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med 343:180-184, 2000
61. Rundback JH, Crea G, Rozenblit GN, et al: The difficult renal angioplasty. Cathet Cardiovasc Interv 52:120-126, 2001
62. Latham JA, Irvine A: Infection of endovascular stents: AN uncommon but important complication. Cardiovasc Surg 7:179-182, 1999
63. DeMaioribus CA, Anderson CA, Popham SSG: Mycotic renal artery degeneration and systemic sepsis caused by in- fected renal artery stent. J Vasc Surg 28:547-550, 1998
64. Joffre F, Rousseau H, Bernadet AL, et al: Midterm results of renal artery stenting. Cardiovasc Intervent Radiol 15:313-318, 1992
65. Wihns GE, Peene P, Baert AL, et al: Renal artery stent placement with the use of the Wallstent endoprosthesis. Radi- ology 179:457-462, 1991
66. Beek FJA, Kaatee R, Beutler J, et al: Complications during renal artery stent placement for atherosclerotic ostial stenosis. Cardiovasc Intervent Radiol 20:184-190, 1997
67. Crea GA, Rundback JH, Maddineni S: Managing com- plications of renovascular interventions. Techniq Vasc Inter- vent Rad 2:98-106, 1999
68. Dorros G, Jaff M, Mathiak L, et ah Four-year follow-up of Palmaz-Schatz stent revascularization as treatment for ath- erosclerotic renal artery stenosis. Circulation 98:642-647, 1998
69. Easton JD: Clinical aspects of the use of clopidogrel, a new antiplatelet agent. Semin Thromb Hemost 25:77-82, 1999
70. Tsuchikane E, Fukuhara A, Kobayashi T: Impact of cilostazol on restenosis after percutaneous coronary balloon angioplasty. Circulation 100:21-26, 1999
71. Wheeldon N, Cumberland D: Pharmacologic prevention of acute ischemic complications of coronary angioplasty. Cathet Cardiovasc Diagn 42:249-256, 1997
72. Tegtmeyer CJ, Selby JB, Hartwell GD, et al: Results and complications of angioplasty in fibromuseular disease. Circula- tion 83:1155-1159, 1991
73. Sos TA, Picketing TG, Sniderman K, et al: Percutaneous transluminal renal angioplasty in renovascular hypertension due

RENAL VASCULAR INTERVENTIONS 325
to atheroma or fibromuscular dysplasia. N Engi J Med 309:274, 1983
74. Birrer M, Do DD, Mahler F, Triller J, et al: Treatment of renal artery fibromuscular dysplasia with balloon angioplasty: A prospective follow-up study. Eur J Vasc Endovasc Surg 23:146-152, 2002
75. Greminger P, Steiner A, Schneider E, et al: Cure and improvement of renovascular hypertension after percutaneous translulninal angioplasty of renal artery stenosis. Nephron 51:362, 1989
76. Martin LG, Price RB, Casarella WJ, et al: Percutaneous angioplasty in clinical management of renovascular hyperten- sion: Initial and long-term results. Radiology 155:629, 1985
77. Beebe HG, Chesebro K, Merchant F, et al: Results of renal artery balloon angioplasty limit its indications. J Vasc Surg 8:300-306, 1988
78. Kiinge J, Mali WPTM, Puijlaert CBAJ, et al: Percuta- neous transluminal renal angioplasty: Initial and long-term results. Radiology 171:501-505, 1989
79. Baert AL, Wilms G, Amery A, et al: Percutaneous transluminal renal angioplasty: Initial results and long-term follow-up in 202 patients. Cardiovasc Intervent Radiol 13:22- 26, 1990
80. Bell GM, Reid J, Buist TAS: Percutaneous transluminal angioplasty improves blood pressure and renal function in renovascular hypertension. Quart J Med 63:393-403, 1987
81. Miller GA, Ford KK, Braun SD, et al: Percutaneous transluminal angioplasty versus surgery for renovascular hyper- tension. Am J Roentgenol 144:447, 1985
82. Geyskes GG, Puylaert CBA, Dei HY, et al: Follow-up study of 70 patients with renal artery stenosis treated by percutaneous transluminaI dilatation. Br Med J 287:333, 1983
83. Martin LG, Casarella WJ, Gaylord GM: Azotemia caused by renal artery stenosis: Treatment by percutaneous angioplasty. Am J Roentgenol 150:839-844, 1988
84. Tegtmeyer CJ, Kellum CD, Ayers C: Percutaneous transluminal angioplasty of the renal artery: Results and long- term follow-up. Radiology 153:77-84, 1984
85. Luft FC, Grim CE, Weinberger MH: Intervention in patients with renovascular hypertension and renal insufficiency. J Urol 130:654-656, 1983
86. Weinberger MH, Grim CE, Luft FC, et al: Percutaneous transluminal angioplasty in complicated renal vascular hyper- tension. Nephron 44:51-53, 1986
87. Dean RH, Callis JT, Smith BM, et al: Failed percutane- ous transluminal renal angioplasty: Experience with lesions requiring operative intervention. J Vasc Surg 6:301-307, 1987
88. Canzanello VJ, Millan VG, Spiegel JE, et al: Percutane- ous transluminal renal angioplasty in manament of atheroscle- rotic renovascular hypertension: Results in 100 patients. Hyper- tension 13:163-172, 1989
89. Plouin PF, Dame B, Chatellier G, et al: Restenosis after a first percutaneous transluminal renal angioplasty. Hyperten- sion 21:89-96, 1993
90. Baumgartner I, yon Aesch K, Do DD, et al: Stent placement in ostial and nonostial atherosclerotic renal arterial stenoses: a prospective follow-up study. Radiology 216:498- 505, 2000
91. Van de Ven PJG, Kaatee R, Beutler JJ, et al: Arterial stenting and balloon angioplasty in ostial atherosclerotic reno- vascular disease: A randomised trial. Lancet 353:282-286, 1999
92. Castaneda-Zuniga WR, Formanek A, Tadavarthy M, et al: The mechanism of balloon angioplasty. Radiology 135:565- 571, 1980
93. Post MJ, de Smet BJ, van der Helm Y, et aI: Arterial remodeling after balloon angioplasty or stenting in an athero- sclerotic experimental model. Circulation 96:996-1003, 1997
94. Consigny PM, Cragg AH, Waller BF: Pathophysiology of vascular intervention, in Strandness DE, Van Breda A (eds). Vascular Disease: Surgical and Interventional Therapy. Churchill-Livingstone, New York, 1994
95. Palmaz JC, Tio FO, Schatz RA, et al: Early endotheli- alisation of balloon-expandable stents: Experimental observa- tions. J Intervent Radiol 3:119-124, 1988
96. White CJ, Ramee SR, Collins TJ, et al: Renal artery stent placement: Utility in lesions difficult to treat with balloon angioplasty. J Am Coll Cardiol 30:1445-1450, 1997
97. Iannone LA, Underwood PL, Nath A, et al: Effect of primary balloon expandable renal artery stents on long-term patency, renal function, and blood pressure in hypertensive and renal insufficient patients with renal artery stenosis. Catherizat Cardiovasc Diag 37:243-250, 1996
98. Hoffman O, Carreres T, Sapoval MR, et al: Ostial renal artery stenosis angioplasty: immediate and mid-term anglo- graphic and clinical results. JVIR 9:65-73, 1998
99. Baumgartner I, Triller J, Mahler F: Patency of percuta- neous transluminal renal angioplasty: A prospective sono- graphic study. Kidney Int 51:798-803, 1997
100. Tullis MJ, Zierler E, Glickerman DJ, et al: Results of percutaneous transluminal angioplasty for atherosclerotic renal artery stenosis: A follow-up study of duplex sonography. J Vasc Surg 25:46-54, 1997
101. Martin LG, Cork RD, Kaufman SL: Long-term results of angioplasty in 110 patients with renal artery stenosis. JVIR 3:619-626, 1992
102. Fiala LA, Jackson MR, Gillespie DL, et al: Primary stenting of atherosclerotic renal artery stenosis. Ann Vasc Surg 12:128-133, 1998
103. Blum U, Krumme B, Flugel P, et al: Treatment of ostial renal artery stenoses with vascular endoprostheses after unsuc- cessful balloon angioplasty. N Engl J Med 336:459-465, 1997
104. Rees CR: Stents for atherosclerotic renovascular dis- ease. JVIR 10:689-705, 1999
105. Harjai K, Khosla S, Shaw D, et al: Effect of gender on outcomes following renal artery stent placement for renovascu- lar hypertension. Catbet Cardiovasc Diagn 42:381-386, 1997
106. Rundback JH, Rozenblit GN, Poplausky MP, et al: Balloon angioplasty or stent placement in patients with reno- vascular disease: A retrospective comparison of outcomes. Heart Disease 1:121-125, 1999
107. Rodriguez-Perez JC, Plaza C, Reyes R, ct al: Treatment of renovascular hypertension with percutaneous transluminal angioplasty: Experience in Spain. J Vasc Interv Radiol 5:101- 109, 1994
108. Julien J, Jeunemaitre X, Raynaud A, et al: Influence of age on the outcome of percutaneous angioplasty in atheroma- tous renovascular disease. J Hypertension 7:S 188-S 192, 1989
109. Martinez-Amenos A, Rama H, Sarrias X, et al: Percu- taneous transluminal angioplasty in the treatment of renovas- cular hypertension. J Hum Hypertens 5:97-100, 1991
110. Losinno F, Zuccala A, Busato F, et al: Renal artery angioplasty for renovascular hypertension and preservation of

326 RUNDBACK AND WEINTRAUB
renal function: Long-term angiographic and clinical follow-up. Am J Roentgenol 162:853-857, 1994
111. Karagiannis A, Douma S, Boyiatzis K, et ah Percuta- neous transluminal renal angioplasty in patients with renovas- cular hypertension: Long-term results. Hypertens Res 18:27-3 l, 1995
112. Turtle KR, Chouinard RF, Webber JT, et al: Treatment of atherosclerotic ostial renal artery stenosis with the intravas- cular stent. Am J Kidney Dis 32:611-622, 1998
113. Henry M, Amor M, Henry I, et al: Stents in the treatment of renal artery stenosis: Long-term follow-up. J Endovasc Surg 6:42-51, 1999
114. Rocha-Singh KJ, MishkeI GJ, Katholi RE, et al: Clin- ical predictors of improved long-term blood pressure control after successful stenting of hypertensive patients with obstruc- tive renal artery stenosis. Cathet Cardiovasc Intervent 47:167- 172, 1999
115. Rodriguez-Lopez JA, Werner A, Ray LI, et al: Renal artery stenosis treated with stent deployment: indications, tech- nique, and outcome for 108 patients. J Vasc Surg 29:617-624, 1999
116. Siablis D, Liatsikos EN, Kalogeropoulou K, et al: Metal stents for the management of atherosclerotic renovascular disease. J Endourology 15:993-996, 2001
117. Bell GM, Reid J, Buist TAS: Percntaneous transluminal angioplasty improves blood pressure and renal function in renovascular hypertension. Quart J Med 63:393-403, 1987
118. Pattison JM, Reidy JF, Rafferty MJ, et al: Percutaneous transluminal renal angioplasty in patients with renal failure. Quart J Med 85:883-888, 1992
119. Pattynama PMT, Becker GJ, Brown J, et al: Percuta- neous angioplasty for atherosclerotic renal artery disease: Effect on renal function in azotemic patients. Cardiovasc Intervent Radiol 17:143-146, 1994
120. Madias NE, Kwon OJ, Millan VG: Percutaneous trans- luminal renal angioplasty--A potentially effective treatment for preservation of renal function. Arch Intern Med 142:693-697, I982
121. O'Donovan RM, Gutierrez OH, Izzo JL: Preservation of renal function by percutaneous renal angioplasty in high-risk elderly petients: short-term outcome. Nephron 60:187-192, 1992
122. Isles CG, Robertson S, Hill D: Management of reno- vascular disease: a review of renal artery stenting in ten studies. Quart J Med 92:159-167, 1999
123. Gross CM, Kramer J, Waigand J: Ostial renal artery stem placement for atherosclerotic renal artery- stenosis in patients with coronary artery disease, Catherization Cardiovasc Diag 45:1-8, 1998
124. Rundback JH: Renovascular interventions: Society of Cardiovascular and Inte~wentional Radiology 23rd Annual Sci- entific Meeting Workshop Book. San Francisco, CA, 1998, pp 447-462
125. Weibull H, Berqvist D, Bergentz SE, et al: Percutane- ous transluminal renal angioplasty versus surgical reconstruc- tion of atherosclerotic renal artery stenosis: Prospective ran- domized study. J Vasc Surg 18:841-852, 1993
126. van Jaarsveld BC, Krijnen P, Pieterman H, et al: The effect of balloon angioplasty on hypertension in atherosclerotic renal~artery stenosis. N Engl J Med 342:1007-1014, 2000
127. Webster J, Marshall F, Abdalla, M, et al: Randomised comparison of percutaneous angioplasty vs. continued medical therapy for hypertensive patients with atheromatous renal artery stenosis. J Hum Hypertens 12:329-335, 1998
128. Plouin P-F, Chatellier G, Dame B, et al for the Essai Multicentrique Medicaments vs. Angioplastie (EMMA) Study Group. Blood pressure outcome of angioplasty in atheroscle- rotic renal artery stenosis. Hypertension 31:823-829, 1998
129. Pattynama PMT, Becker GJ, Brown J, et al: Percuta- neous angioplasty for atherosclerotic renal artery disease: Effect on renal function in azotemic patients. Cardiovasc Intervent Radiol 17:143-146, 1994
130. Harden PN, MacLeod MJ, Rodger RSC, et al: Effect of renal artery stenting on progression of renovascular renal failure. Lancet 349:1133-1136, 1997
131. Watson PS, Hadjipetrou P, Cox SV, et al: Effect of renal artery stenting on renal function and size in patients with atherosclerotic renovascular disease. Circulation 102:1671- 1677, 2000
132. Cognet F, Garcier JM, Dranssart M, et al: Percutaneous transluminal renal angioplasb, in atheroma with renal failure: Long term results in 99 patients. Europ Rad 11:2524-2530, 2000
133. Muray S, Martin M, Amoedo ML, et al: Rapid decline in renal function reflects reversibility and predicts the outcome after angioplasty in renal artery stenosis. Am J Kid Dis 39:60-66, 2002
134. Dean RH, Englund R, DuPont WD, et al: Retrieval of renal function by revascularization--Study of preoperative outcome predictors. Ann Surg 202:367-375, 1985
135. Shannon HM, Gillespie IN, Moss JG: Salvage of the solitary kidney by insertion of a renal artery stent. Am J Roentgenol 171:217-222, 1998
136. Zuccala A, Losinno F, Zucchelli A, et al: Renovascular disease in diabetes mellitus: Treatment by percutaneous trans- luminal renal angioplasty. Nephrol Dial Transplant 8:26-29, 1998
137. Khosla S, White C, Collins TJ, et al: Effects of renal artery stent implantation in patients with renovascular hyper- tension presenting with unstable angina or congestive heart failure. Am J Cardiol 80:363-366, 1997
138. Xue F, Bettmann MA, Langdon DR, et al: Outcome and cost comparison of percutaneous transluminal renal angio- plasty, renal arterial stent placement, and renal artery bypass grafting. Radiology 212:378-384, 1999
139. Conlon PJ, Little MA, Pieper K, et al: Severity of renal vascular disease predicts mortality in patients undergoing cor- onary angiography. Kidney Int 60:1490-1497, 2001
140. Zuccala A, Zucchelli P, Campieri C, et al: 3R study renal outcome in renal ischemia: Revascularisation or medical treatment. J Nephrol 13:106-109, 2000
141. Oberhoff M, Herdeg C, Baumbach A, et al: Stent-based antirestenotic coatings (sirolimus/paclitaxeI). Catheter Cardio- vasc Interv 55:404-408, 2002
142. Lerman LO, Nath KA, Rodriguez-Porcel M, et al: Increased oxidative stress in experimental renovascular hyper- tension. Hypertension 37:541-546, 2001
143. Romero JC, Feldstein AE, Rodriguez-PorceI MG, et al: New insights into the pathophysiology of renovascular hyper- tension. Mayo Clin Proc 72:251-260, 1997







![[Atheroembolic renal disease]](https://img.dokumen.tips/doc/110x75/63601031ef4a3767a80c1005/atheroembolic-renal-disease.jpg)





















