Embed Size (px)
Citation preview

290 The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5
IN PRACTICE
matthew Grissinger, michael J. Gaunt
reducing harm in Patients using insulin
Controlling blood sugars with insulin is an important part of managing hyperglycemia in diabetic patients. However, the literature has shown that the use of insulin has been associated with more medication errors than any other type or class of drug. This article will highlight medication errors that may arise during the use of insulin in the long-term facility and provide risk-reduction recommendations to address the potential for error and patient harm.
Key wordS: Adverse drug event, Blood glucose, Contributing factors, Hypoglycemia, Institute for Safe Medication Practices, Insulin, Medication errors, Risk-reduction strategies, Sliding scale.
aBBreviationS: ADE = Adverse drug event, BG = Blood glucose, ED = Emergency department, ISMP = Institute for Safe Medication Practices, MAR = Medication administration record, NEISS-CADES = National Electronic Injury Surveillance System–Cooperative Adverse Drug Event Surveillance, T1DM = Type 1 diabetes mellitus.
introduction
For many years, the literature has shown that the use of insulin has been associated with more medication errors than any other type or class of
drug. According to the National Diabetes Fact Sheet, from 2011, 25.8 million children and adults in the United States, representing 8.3% of the population, have diabetes. Nearly 30%, or 10.9 million, of individuals 65 years of age and older have diabetes.1
Controlling blood sugars with insulin is essential in the management of hyperglycemia in diabetic patients. Cohen et al. reported in 1998 that 11% of harmful medication errors result from insulin misadministration.2 In 2004, the Pennsylvania Patient Safety Authority (Authority) estab-lished that 25% of all medication errors reported involve high-alert medications, and 16.3% of those events involved insulin products.3 The U.S. Pharmacopeial Convention’s MEDMARX 2008 data report showed that insulin was the leading product involved in harmful medication

The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5 291
errors, representing 16.2% of all harmful medication error reports.4
Budnitz et al. analyzed data from the National Electronic Injury Surveillance System–Cooperative Adverse Drug Event Surveillance (NEISS-CADES) system, a nationally representative, size-stratified, probability sample of hospitals (excluding psychiatric and penal institutions) in the United States and its territories with a minimum of six beds and a 24-hour emergency depart-ment (ED).5 Between January 1, 2004, and December 31, 2005, the researchers found that 9 of the 10 medications that most commonly caused patients 65 years of age and older to visit EDs were in three medication classes (oral anticoagulants or antiplatelet agents, antidiabetic agents, and narrow therapeutic index agents). Together, these three medication classes caused nearly half of all ED visits for adverse drug events (ADEs) but were prescribed in only 9.4% of outpatient visits. other studies of ADEs in older adults have also found that high percentages of ADEs are caused by these medication classes.6-8
According to Budnitz et al., three commonly pre-scribed drugs—warfarin, insulin, and digoxin—accounted for one-third of all ED visits for ADEs. The risk for ED visits for ADEs involving these medications was clinically and statistically significantly higher than medications on the Beers list, which are always considered to be poten-tially inappropriate.5
In a subsequent analysis of NEISS-CADES data from January 1, 2007, through December 31, 2009, Budnitz et al. estimated that nearly 266,000 ED visits and 99,700 hospitalizations for ADEs occurred among patients 65 years of age and older.9 The four most commonly implicated medications were warfarin, insulins, oral anti-platelet agents, and oral hypoglycemic agents. These four medications accounted for approximately two-thirds of the hospitalizations. According to the study authors, nearly all of the hospitalizations caused by warfarin, insulins, or oral hypoglycemic agents involved unintentional overdoses.
Insulin therapy has always required thoughtful man-agement; however, over the last decade, the release of new insulin formulations, insulin delivery devices, and blood glucose (BG) monitors has made this process increasingly complex.10 This complexity introduces vulnerability into the medication-use system, increasing
the risk of medication errors and patient harm.over the years, the Institute for Safe Medication
Practices (ISMP) has gained a great deal of insight into the medication-use system through reports of medica-tion errors and by performing onsite analyses of the medication-use process at various health care organiza-tions. It also has identified weaknesses that are common to many organizations. This system-based philosophy forms the foundation of ISMP’s approach to preventing medica-tion errors.11
The following discussions of contributing factors involved in medication errors associated with the use of insulin have been organized into selected key system elements. System-based causes of medication errors can be directly traced to weaknesses or failures in these key elements (Figure 1).12
The use of insulin has been associated with more medication errors than any other type or class of drug.
drug informationNurses and other health care professionals in the long-term care facility may not have access to the most up-to-date drug information. For example, facilities may not have Internet-based sources of drug information and thus must rely on printed, paper references. Although administration or pharmacy may provide new references on a yearly basis, the nursing staff may also rely on older, familiar references. This may not seem critical to accurate dosing, but drug information is frequently updated to contain new clinical information and products and to cor-rect errors. For instance, Mosby’s Nursing Drug Reference corrected a potentially serious mistake in their publica-tion: the pharmacokinetic properties of insulin aspart (NovoLOG) and insulin glargine (Lantus) were switched.13
Another source of information about drugs for nurses in long-term care facilities is the medication administra-tion record (MAR). But information designed from a pharmacy (i.e., product) point-of-view can actually contribute to medication errors. For example, MAR
292 The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5
reducing harm in PatientS uSing inSulin
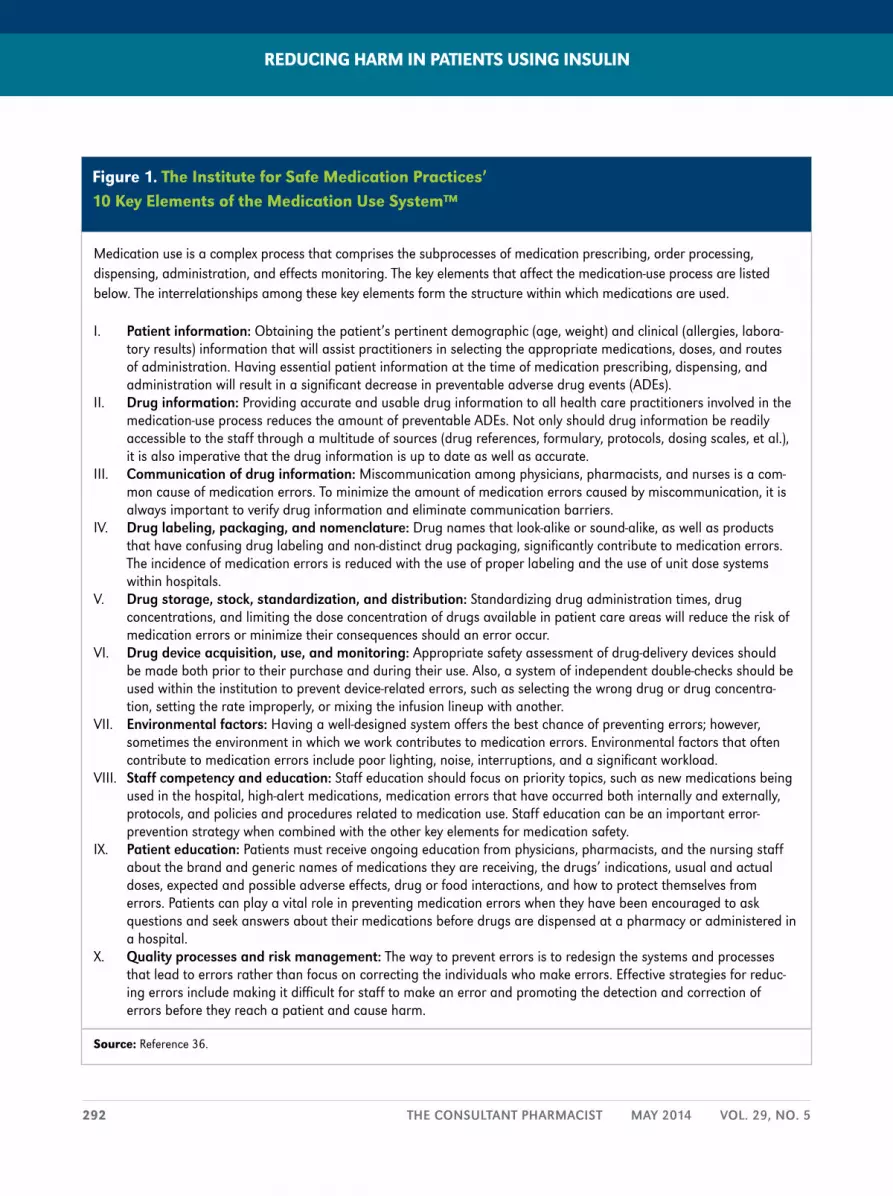
Figure 1. the institute for Safe medication Practices’ 10 Key elements of the medication use System™
Medication use is a complex process that comprises the subprocesses of medication prescribing, order processing, dispensing, administration, and effects monitoring. The key elements that affect the medication-use process are listed below. The interrelationships among these key elements form the structure within which medications are used.
I. Patient information: Obtaining the patient’s pertinent demographic (age, weight) and clinical (allergies, labora-tory results) information that will assist practitioners in selecting the appropriate medications, doses, and routes of administration. Having essential patient information at the time of medication prescribing, dispensing, and administration will result in a significant decrease in preventable adverse drug events (ADEs).
II. Drug information: Providing accurate and usable drug information to all health care practitioners involved in the medication-use process reduces the amount of preventable ADEs. Not only should drug information be readily accessible to the staff through a multitude of sources (drug references, formulary, protocols, dosing scales, et al.), it is also imperative that the drug information is up to date as well as accurate.
III. Communication of drug information: Miscommunication among physicians, pharmacists, and nurses is a com-mon cause of medication errors. To minimize the amount of medication errors caused by miscommunication, it is always important to verify drug information and eliminate communication barriers.
IV. Drug labeling, packaging, and nomenclature: Drug names that look-alike or sound-alike, as well as products that have confusing drug labeling and non-distinct drug packaging, significantly contribute to medication errors. The incidence of medication errors is reduced with the use of proper labeling and the use of unit dose systems within hospitals.
V. Drug storage, stock, standardization, and distribution: Standardizing drug administration times, drug concentrations, and limiting the dose concentration of drugs available in patient care areas will reduce the risk of medication errors or minimize their consequences should an error occur.
VI. Drug device acquisition, use, and monitoring: Appropriate safety assessment of drug-delivery devices should be made both prior to their purchase and during their use. Also, a system of independent double-checks should be used within the institution to prevent device-related errors, such as selecting the wrong drug or drug concentra-tion, setting the rate improperly, or mixing the infusion lineup with another.
VII. environmental factors: Having a well-designed system offers the best chance of preventing errors; however, sometimes the environment in which we work contributes to medication errors. Environmental factors that often contribute to medication errors include poor lighting, noise, interruptions, and a significant workload.
VIII. staff competency and education: Staff education should focus on priority topics, such as new medications being used in the hospital, high-alert medications, medication errors that have occurred both internally and externally, protocols, and policies and procedures related to medication use. Staff education can be an important error-prevention strategy when combined with the other key elements for medication safety.
IX. Patient education: Patients must receive ongoing education from physicians, pharmacists, and the nursing staff about the brand and generic names of medications they are receiving, the drugs’ indications, usual and actual doses, expected and possible adverse effects, drug or food interactions, and how to protect themselves from errors. Patients can play a vital role in preventing medication errors when they have been encouraged to ask questions and seek answers about their medications before drugs are dispensed at a pharmacy or administered in a hospital.
X. Quality processes and risk management: The way to prevent errors is to redesign the systems and processes that lead to errors rather than focus on correcting the individuals who make errors. Effective strategies for reduc-ing errors include making it difficult for staff to make an error and promoting the detection and correction of errors before they reach a patient and cause harm.
Source: Reference 36.

The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5 293
entries often prominently display the concentration of insulin vials. This can be seen in Figure 2, in which the MAR displays the concentration of insulin aspart (i.e., 100 UNIT/M) rather than the patient-specific dose on the top line. one case reported to the Authority stated that a printed medication list from a previous facility indicated “Lantus 100 units/mL 15 units once a day subcutaneously at 8 pm.” The nurse reconciling the patient’s medications misread the patient’s dose as 100 units. An order for “Lantus 100 units SQ at hs” [subcutaneous at bedtime] was telephoned in by the physician, and a nurse administered the medication as ordered.14
In addition, prescriber and pharmacy order-entry computer systems thought to be designed to detect unsafe orders may not be up to the task. These systems, although helpful in detecting some unsafe orders, including many drug-drug interactions, may not catch all errors involving over- or underdoses of insulin.15
The potential for tremendous variety in the medications prescribed, dispensed, and administered in long-term care facilities introduces complexity and risk into the medication-use system. Given all the drug products on the market, it is impossible for health care practitioners to be familiar with and knowledgeable of each product. When health care practitioners are unfamil-iar with a drug, they are less likely to identify and catch an error before it reaches the patient. A formulary process could provide long-term care facilities with the opportu-nity to proactively address medication errors, which, by its very nature, reduces the chances for medication errors by limiting the number of drugs (i.e., limiting the variety of insulin products within facilities) per indication.
communication of drug informationThe Diabetes Control and Complications Trial, a prospective, randomized controlled trial of intensive versus standard glycemic control involving patients in an acute care setting, with relatively recently diagnosed type 1 diabetes mellitus (T1DM), showed that improved glycemic control is associated with significantly decreased rates of microvascular (retinopathy and nephropathy) as well as neuropathic complications.16 This led to the
recommendation that T1DM be treated by using multiple insulin injections (three to four injections per day of basal and prandial insulin) as well as by matching the dose of prandial insulin to carbohydrate intake, premeal blood glucose, and anticipated activity.
However, the use of multiple-dose injections of insulin throughout the day can add complexity to controlling a patient’s blood glucose. For example, correction doses, sometimes referred to as “coverage” or erroneously as “sliding scales,” are used to adjust glucose levels around mealtimes. organizations often do not standardize the dosing of insulin ranges for meals and have multiple algo-rithms for correction doses, such that a facility may have “low-dose,” “medium-dose,” and “high-dose” algorithms that require the nursing staff to obtain and document each patient’s BG reading, determine the patient’s ordered algorithm, and then select the proper dose based on the BG reading.
(It should be noted that while the phrase “sliding scale” may be used in place of “correction dose” or “coverage,” sliding-scale insulin regimens used alone are ineffective and potentially harmful. When using subcutaneous insulin
Figure 2. example of Prominent display of Product concentration on a medication adminstration record
Source: Institute for Safe Medication Practices.

296 The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5
injection therapy, scheduled or standing insulin regimens should be the standard of care).17-20
Another problem with coverage orders is how they are displayed on a MAR, where the entire block reserved to list the directions for the administration of insulin is filled with a variety of numbers, relating to both the BG ranges and the dosing ranges (Figure 2). In fact, in an analysis of 2,685 event reports to the Authority that mentioned medication errors involving the use of insulin products, the predominant theme of wrong-dose events involved the dosing of insulin based on a range of BG values with a corresponding coverage dose, determined by a patient’s BG reading.14
one problem often seen with coverage orders is the clarity of handwritten orders from physicians, a particular problem when an organization does not have a standard-ized, preprinted, or computerized protocol or form to order insulin, including the type of coverage (e.g., low, high). Adding to the complexity of these orders are the multiple values often used for multiple ranges of blood sugars. Problems have also occurred when shortcuts are taken when writing these types of orders for insulin. For example, orders have been written stating doses of insulin as “6+1” or “6+2” instead of writing out “7” or “8” (Figure 3).
Problems with handwritten orders for insulin go beyond the coverage orders discussed above and include the use of dangerous abbreviations or dose expressions and other shortcuts. The use of the letter “U” to abbrevi-ate “unit” has been known to contribute to medication errors, and has been discussed for several decades.21 The abbreviation “U” has been confused for the numeral “0” and “4,” resulting in 10-fold overdoses in some cases. one example reported to the Authority involved a patient who erroneously received 50 units of HumaLOG (insulin lispro recombinant) on two occasions and was later found in respiratory distress that progressed to cardiopulmonary arrest. He remained on mechanical ventilation until he died a week later.22
Although writing out the complete word “units” is the recommended alternative to using the abbreviation “U,” be aware that 10-fold overdoses may still occur when
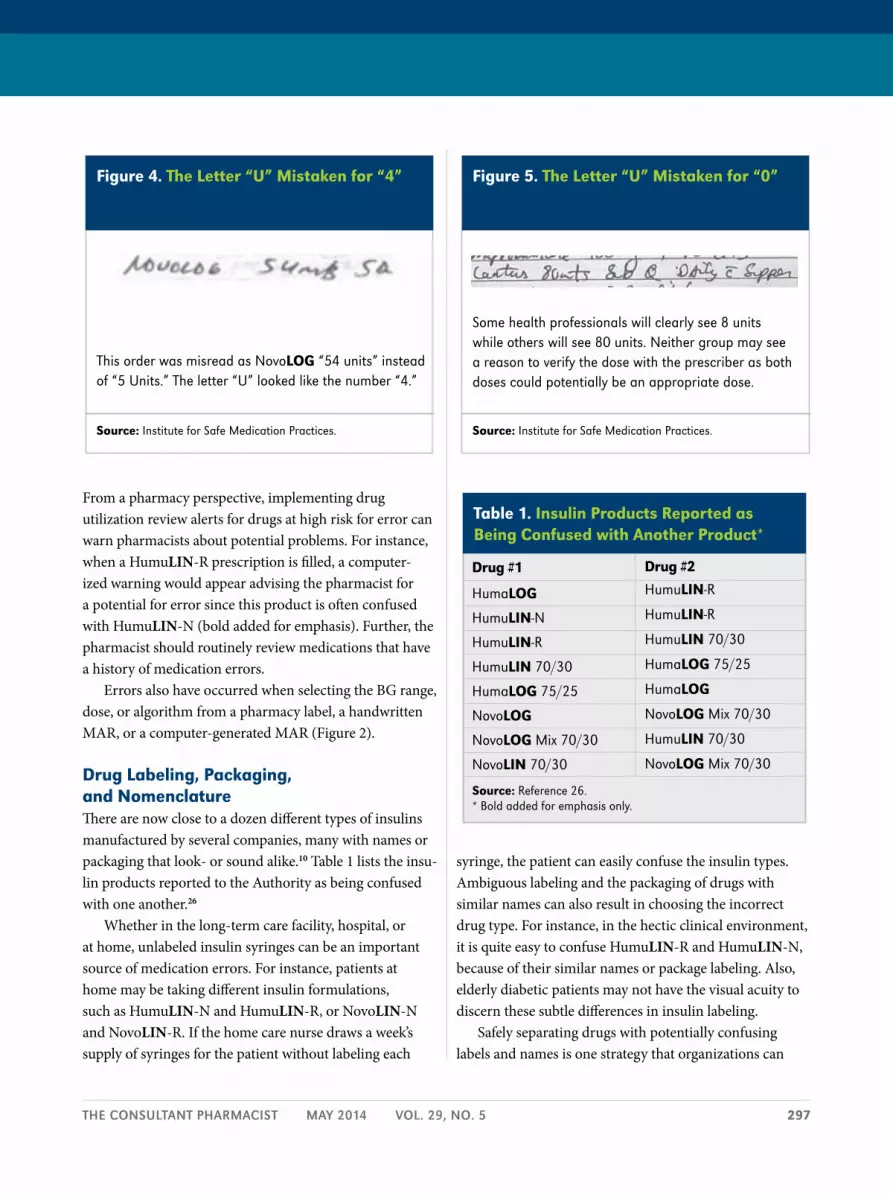
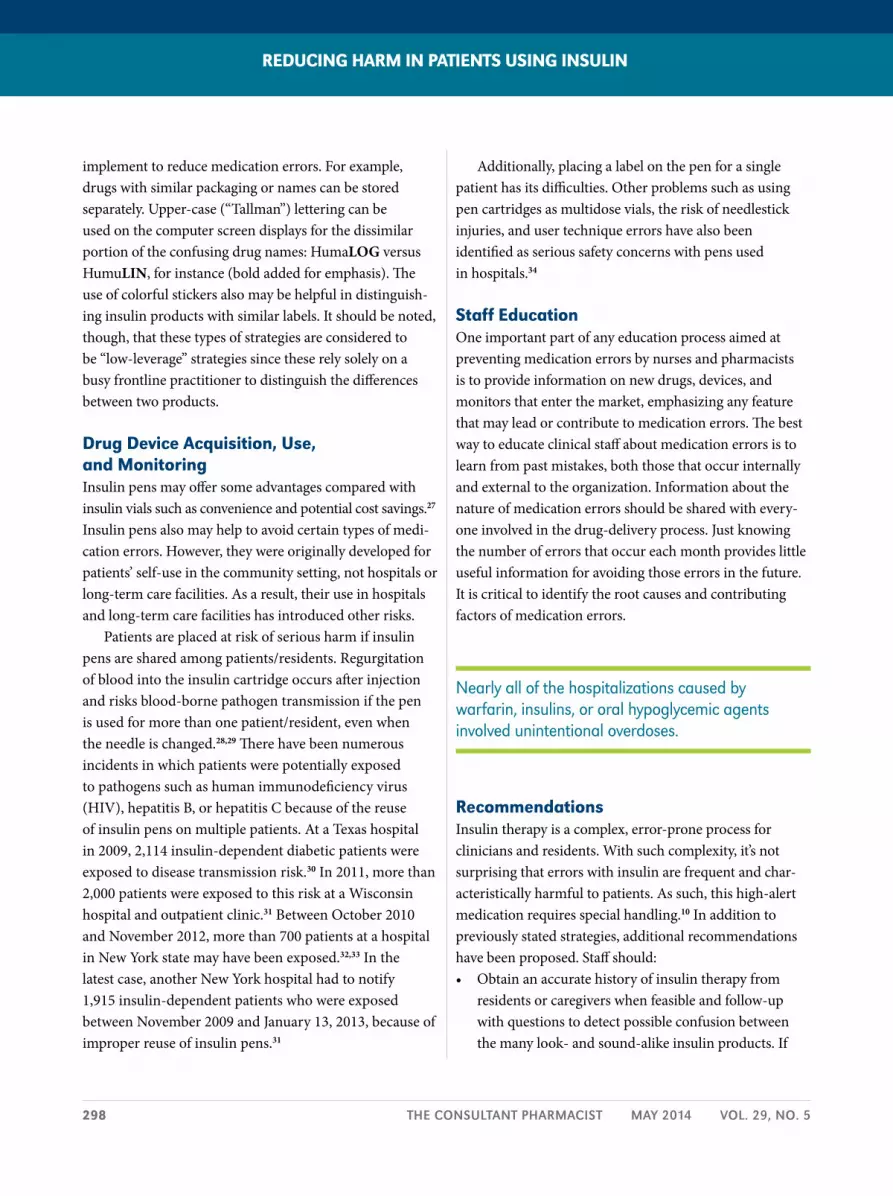
writing the word “unit(s),” particularly when there is inadequate white space between the dose number and the word or the “u” portion of “units” is separated from the rest of the word. one example reported to ISMP involved a handwritten order that was misread as NovoLOG “54 units” instead of the intended “5 Units” (Figure 4).23 The word “Units” had been written out, but the letter “U” looked like the number “4,” and the remaining part of the word “nits” was read as “units.” The mistake was made by three practitioners who either dispensed or administered the medication. The patient received the large dose of insu-lin and required treatment for severe hypoglycemia. This error occurred despite the prescriber’s avoidance of the abbreviation “U” for units. In Figure 5, does the order call for 8 units or 80 units of Lantus? A pharmacist was able to prevent a potential error because he had access to patient information from a previous admission, during which that patient had been receiving 8 units of Lantus, not 80 units.24
The use of standardized drug-ordering protocols and order forms can overcome some of these barriers. Minimizing the use of verbal prescription orders and nonstandard symbols, such as slash marks that can be read as a number, also can reduce the likelihood for misinter-pretation and error.25
once these complex orders have been written, prob-lems have occurred when transcribing the orders to MARs or entering them into computerized order-entry systems.
reducing harm in PatientS uSing inSulin
Figure 3. an ambiguous insulin coverage order
Source: Institute for Safe Medication Practices.
Error-prone abbreviations (e.g., “>”) and dose designations (e.g. “6+1”) increase the risk of error.
The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5 297
From a pharmacy perspective, implementing drug utilization review alerts for drugs at high risk for error can warn pharmacists about potential problems. For instance, when a HumuLIN-R prescription is filled, a computer-ized warning would appear advising the pharmacist for a potential for error since this product is often confused with HumuLIN-N (bold added for emphasis). Further, the pharmacist should routinely review medications that have a history of medication errors.
Errors also have occurred when selecting the BG range, dose, or algorithm from a pharmacy label, a handwritten MAR, or a computer-generated MAR (Figure 2).
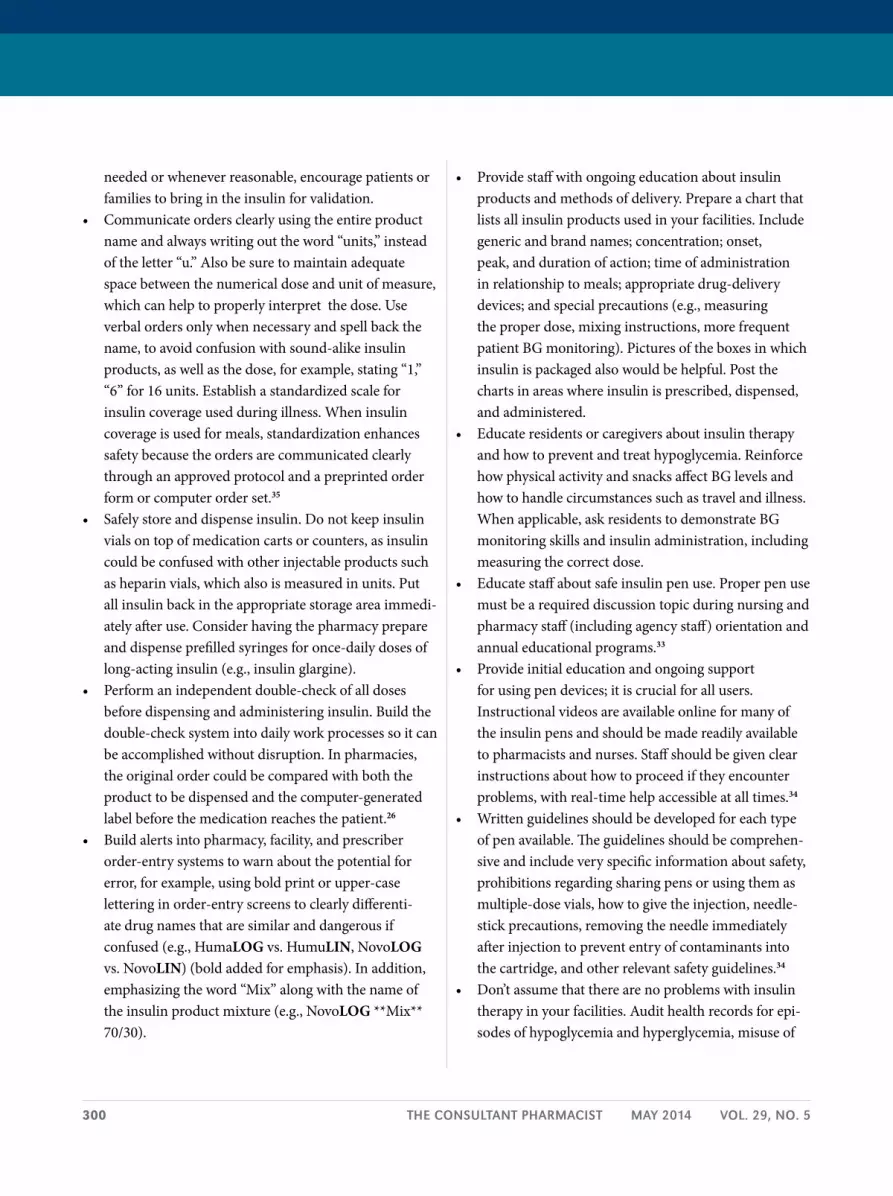
drug labeling, Packaging, and nomenclatureThere are now close to a dozen different types of insulins manufactured by several companies, many with names or packaging that look- or sound alike.10 Table 1 lists the insu-lin products reported to the Authority as being confused with one another.26
Whether in the long-term care facility, hospital, or at home, unlabeled insulin syringes can be an important source of medication errors. For instance, patients at home may be taking different insulin formulations, such as HumuLIN-N and HumuLIN-R, or NovoLIN-N and NovoLIN-R. If the home care nurse draws a week’s supply of syringes for the patient without labeling each
syringe, the patient can easily confuse the insulin types. Ambiguous labeling and the packaging of drugs with similar names can also result in choosing the incorrect drug type. For instance, in the hectic clinical environment, it is quite easy to confuse HumuLIN-R and HumuLIN-N, because of their similar names or package labeling. Also, elderly diabetic patients may not have the visual acuity to discern these subtle differences in insulin labeling.
Safely separating drugs with potentially confusing labels and names is one strategy that organizations can
Figure 4. the letter “u” mistaken for “4”
Source: Institute for Safe Medication Practices.
This order was misread as Novolog “54 units” instead of “5 Units.” The letter “U” looked like the number “4.”
Figure 5. the letter “u” mistaken for “0”
Source: Institute for Safe Medication Practices.
Some health professionals will clearly see 8 units while others will see 80 units. Neither group may see a reason to verify the dose with the prescriber as both doses could potentially be an appropriate dose.
table 1. insulin Products reported as Being confused with another Product*
drug #1
Humalog
Humulin-N
Humulin-R
Humulin 70/30
Humalog 75/25
Novolog
Novolog Mix 70/30
Novolin 70/30
drug #2
Humulin-R
Humulin-R
Humulin 70/30
Humalog 75/25
Humalog
Novolog Mix 70/30
Humulin 70/30
Novolog Mix 70/30
Source: Reference 26. * Bold added for emphasis only.
298 The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5
implement to reduce medication errors. For example, drugs with similar packaging or names can be stored separately. Upper-case (“Tallman”) lettering can be used on the computer screen displays for the dissimilar portion of the confusing drug names: HumaLOG versus HumuLIN, for instance (bold added for emphasis). The use of colorful stickers also may be helpful in distinguish-ing insulin products with similar labels. It should be noted, though, that these types of strategies are considered to be “low-leverage” strategies since these rely solely on a busy frontline practitioner to distinguish the differences between two products.
drug device acquisition, use, and monitoringInsulin pens may offer some advantages compared with insulin vials such as convenience and potential cost savings.27 Insulin pens also may help to avoid certain types of medi-cation errors. However, they were originally developed for patients’ self-use in the community setting, not hospitals or long-term care facilities. As a result, their use in hospitals and long-term care facilities has introduced other risks.
Patients are placed at risk of serious harm if insulin pens are shared among patients/residents. Regurgitation of blood into the insulin cartridge occurs after injection and risks blood-borne pathogen transmission if the pen is used for more than one patient/resident, even when the needle is changed.28,29 There have been numerous incidents in which patients were potentially exposed to pathogens such as human immunodeficiency virus (HIV), hepatitis B, or hepatitis C because of the reuse of insulin pens on multiple patients. At a Texas hospital in 2009, 2,114 insulin-dependent diabetic patients were exposed to disease transmission risk.30 In 2011, more than 2,000 patients were exposed to this risk at a Wisconsin hospital and outpatient clinic.31 Between october 2010 and November 2012, more than 700 patients at a hospital in New York state may have been exposed.32,33 In the latest case, another New York hospital had to notify 1,915 insulin-dependent patients who were exposed between November 2009 and January 13, 2013, because of improper reuse of insulin pens.31
Additionally, placing a label on the pen for a single patient has its difficulties. other problems such as using pen cartridges as multidose vials, the risk of needlestick injuries, and user technique errors have also been identified as serious safety concerns with pens used in hospitals.34
Staff educationone important part of any education process aimed at preventing medication errors by nurses and pharmacists is to provide information on new drugs, devices, and monitors that enter the market, emphasizing any feature that may lead or contribute to medication errors. The best way to educate clinical staff about medication errors is to learn from past mistakes, both those that occur internally and external to the organization. Information about the nature of medication errors should be shared with every-one involved in the drug-delivery process. Just knowing the number of errors that occur each month provides little useful information for avoiding those errors in the future. It is critical to identify the root causes and contributing factors of medication errors.
Nearly all of the hospitalizations caused by warfarin, insulins, or oral hypoglycemic agents involved unintentional overdoses.
recommendationsInsulin therapy is a complex, error-prone process for clinicians and residents. With such complexity, it’s not surprising that errors with insulin are frequent and char-acteristically harmful to patients. As such, this high-alert medication requires special handling.10 In addition to previously stated strategies, additional recommendations have been proposed. Staff should: • Obtainanaccuratehistoryofinsulintherapyfrom
residents or caregivers when feasible and follow-up with questions to detect possible confusion between the many look- and sound-alike insulin products. If
reducing harm in PatientS uSing inSulin
300 The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5
needed or whenever reasonable, encourage patients or families to bring in the insulin for validation.
• Communicateordersclearlyusingtheentireproductname and always writing out the word “units,” instead of the letter “u.” Also be sure to maintain adequate space between the numerical dose and unit of measure, which can help to properly interpret the dose. Use verbal orders only when necessary and spell back the name, to avoid confusion with sound-alike insulin products, as well as the dose, for example, stating “1,” “6” for 16 units. Establish a standardized scale for insulin coverage used during illness. When insulin coverage is used for meals, standardization enhances safety because the orders are communicated clearly through an approved protocol and a preprinted order form or computer order set.35
• Safelystoreanddispenseinsulin.Donotkeepinsulinvials on top of medication carts or counters, as insulin could be confused with other injectable products such as heparin vials, which also is measured in units. Put all insulin back in the appropriate storage area immedi-ately after use. Consider having the pharmacy prepare and dispense prefilled syringes for once-daily doses of long-acting insulin (e.g., insulin glargine).
• Performanindependentdouble-checkofalldosesbefore dispensing and administering insulin. Build the double-check system into daily work processes so it can be accomplished without disruption. In pharmacies, the original order could be compared with both the product to be dispensed and the computer-generated label before the medication reaches the patient.26
• Buildalertsintopharmacy,facility,andprescriberorder-entry systems to warn about the potential for error, for example, using bold print or upper-case lettering in order-entry screens to clearly differenti-ate drug names that are similar and dangerous if confused (e.g., HumaLOG vs. HumuLIN, NovoLOG vs. NovoLIN) (bold added for emphasis). In addition, emphasizing the word “Mix” along with the name of the insulin product mixture (e.g., NovoLOG **Mix** 70/30).
• Providestaffwithongoingeducationaboutinsulinproducts and methods of delivery. Prepare a chart that lists all insulin products used in your facilities. Include generic and brand names; concentration; onset, peak, and duration of action; time of administration in relationship to meals; appropriate drug-delivery devices; and special precautions (e.g., measuring the proper dose, mixing instructions, more frequent patient BG monitoring). Pictures of the boxes in which insulin is packaged also would be helpful. Post the charts in areas where insulin is prescribed, dispensed, and administered.
• Educateresidentsorcaregiversaboutinsulintherapyand how to prevent and treat hypoglycemia. Reinforce how physical activity and snacks affect BG levels and how to handle circumstances such as travel and illness. When applicable, ask residents to demonstrate BG monitoring skills and insulin administration, including measuring the correct dose.
• Educatestaffaboutsafeinsulinpenuse.Properpenusemust be a required discussion topic during nursing and pharmacy staff (including agency staff) orientation and annual educational programs.33
• Provideinitialeducationandongoingsupportfor using pen devices; it is crucial for all users. Instructional videos are available online for many of the insulin pens and should be made readily available to pharmacists and nurses. Staff should be given clear instructions about how to proceed if they encounter problems, with real-time help accessible at all times.34
• Writtenguidelinesshouldbedevelopedforeachtypeof pen available. The guidelines should be comprehen-sive and include very specific information about safety, prohibitions regarding sharing pens or using them as multiple-dose vials, how to give the injection, needle-stick precautions, removing the needle immediately after injection to prevent entry of contaminants into the cartridge, and other relevant safety guidelines.34
• Don’tassumethattherearenoproblemswithinsulintherapy in your facilities. Audit health records for epi-sodes of hypoglycemia and hyperglycemia, misuse of

The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5 301
the abbreviation “u” in prescriptions, the frequency of verbal insulin orders, and so on. Proactively anticipate and address problems with insulin use in all long-term care settings through the “Failure Mode and Effects Analysis” process and by discussing insulin errors that have happened in other practice sites. Don’t let down your guard with this high-alert medication—even if problems are not obvious today.
conclusionThe management of diabetes remains suboptimal. For many residents with diabetes, intensive therapy is required to achieve the more rigorous goals for glycemic control established by the American Diabetes Association and other organizations to reduce the risks for the serious end-organ complications secondary to this disease. Achieving these goals will remain a daunting task. The initiation of insulin therapy is often delayed, and, because of systemic
problems in the entire drug-delivery process—including confusing drug labeling, unclear physician orders, and insulin self-administration errors—patients with diabetes often receive suboptimal or incorrect insulin treatment.
Reducing errors and maximizing the benefits of insulin therapy will require a concerted effort involving the prescribers, pharmacist, and nursing staff. Key steps must include not only education about the sources of potential medication errors but also effective risk-reduction strate-gies for avoiding those errors in the future. n
Matthew Grissinger, RPh, FISMP, FASCP, is director of error-reporting programs, Institute for Safe Medication Practices, Horsham, Pennsylvania. Michael J. Gaunt, PharmD, is medication safety analyst and editor, ISMP Medication Safety Alert!® Community/Ambulatory Care Edition, Institute for Safe Medication Practices.
Consult Pharm 2014;29:290-302.
© 2014 American Society of Consultant Pharmacists, Inc. All rights reserved.
Doi:10.4140/TCP.n.2014.290.
reducing harm in PatientS uSing inSulin
When health care practitioners are unfamiliar with a drug, they are less likely to identify and catch an error before it reaches the patient.

302 The ConsulTanT PharmaCisT maY 2014 Vol. 29, no. 5
References1. American Diabetes Association. Diabetes Statistics [online]. 2013. Available from http://www.diabetes.org/diabetes-basics/diabetes-statistics/. Accessed July 8, 2013.2. Cohen MR, Proulx SM, Crawford SY. Survey of hospital systems and common serious medication errors. J Healthc Risk Manag 1998;18:16-27.3. Pennsylvania Patient Safety Authority. Focus on high-alert medications. PA PSRS Patient Saf Advis 2004;1:6. Available from http://www.patientsafetyauthority.org/ADVISoRIES/Advisory Library/2004/Sep1(3)/Pages/06.aspx. Accessed June 11, 2013. 4. Hicks RW, Becker SC, Cousin DD, eds. MEDMARX data report. A report on the relationship of drug names and medication errors in response to the Institute of Medicine’s call for action. Rockville, MD: US Pharmacopeial Convention, Inc.; 2008.5. Budnitz DS, Shehab N, Kegler SR et al. Medication use leading to emergency department visits for adverse drug events in older adults. Ann Intern Med 2007;147:755-65.6. Gurwitz JH, Field TS, Harrold LR et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA 2003;289:1107-16.7. Hanlon JT, Schmader KE, Koronkowski MJ et al. Adverse drug events in high risk older outpatients. J Am Geriatr Soc 1997;45:945-8.8. Hanlon JT, Pieper CF, Hajjar ER et al. Incidence and predictors of all and preventable adverse drug reactions in frail elderly persons after hospital stay. J Gerontol A Biol Sci Med Sci 2006;61:511-5.9. Budnitz DS, Lovegrove MC, Shehab N et al. Emergency hospital-izations for adverse drug events in older Americans. N Engl J Med 2011;365:2002-12.10. Institute for Safe Medication Practices. Complexity of insulin therapy has risen sharply in the past decade. ISMP Med Saf Alert Community/Ambulatory Ed 2004;3:1-4.11. Grissinger M. Medication errors in long-term care: part 1. Consult Pharm 2007;22:544-64.12. Cohen MR. Cause of medication errors. Chapter 4. In Cohen MR, ed. Medication Errors. 2nd ed. Washington, DC: American Pharmacists Association; 2007:56-65.13. Institute for Safe Medication Practices. Safety briefs. ISMP Med Saf Alert Acute Care 20023;7:1.14. Pennsylvania Patient Safety Authority. Medication errors with the dosing of insulin: problems across the continuum. Pa Patient Saf Advis 2010;7:9-17. Available from http://www.patientsafetyauthority.org/ADVISoRIES/AdvisoryLibrary/2010/Mar7(1)/Pages/09.aspx. Accessed June 11, 2013.15. Institute for Safe Medication Practices. Safety still compromised by computer weaknesses: comparing 1999 and 2005 pharmacy computer field test results. ISMP Med Saf Alert Acute Care 2005;10:1-3.16. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977–86.17. Queale WS, Seidler AJ, Brancati FL. Glycemic control and sliding scale insulin use in medical inpatients with diabetes mellitus. Arch Intern Med 1997;157:545-52.18. Gearhart JG, Duncan JL 3rd, Replogle WH et al. Efficacy of sliding-scale insulin therapy: a comparison with prospective regimens. Fam Pract Res J 1994;14:313-22.
19. Baldwin D, Villanueva G, McNutt R et al. Eliminating inpatient sliding-scale insulin: a reeducation project with medical house staff. Diabetes Care 2005;28:1008-11.20. Magee MF, Clement S. Subcutaneous insulin therapy in the hospital setting: issues, concerns, and implementation. Endocr Pract 2004;10 Suppl 2:81-8.21. Cohen MR. Medication error reports. Hosp Pharm 1975;10:120.22. Pennsylvania Patient Safety Authority. Abbreviations: a shortcut to medication errors. PA PSRS Patient Safety Advisory 2005;2:19-21. Available from http://www.patientsafetyauthority.org/ADVISoRIES/AdvisoryLibrary/2005/Mar2(1)/Pages/19.aspx. Accessed August 21, 2013.23. Institute for Safe Medication Practices. U looks like 4. ISMP Med Saf Alert Acute Care 2009;14:1-2.24. Institute for Safe Medication Practices. Information from prior admission prevents error. ISMP Med Saf Alert Acute Care 2007;12:1.25. Grissinger M, Kroon L, Penna P. Misadventures in insulin therapy: are your members at risk? J Manag Care Pharm 2003;9:S2-S13.26. Pennsylvania Patient Safety Authority. Complexity of insulin therapy. PA PSRS Patient Saf Advis 2005;2:30-1. Available from http://www.patientsafetyauthority.org/ADVISoRIES/AdvisoryLibrary/2005/jun2(2)/Pages/30.aspx. Accessed July 11, 2013.27. Bazalo G, Weiss RC, Bouchard JR et al. Impact of pen utilization on insulin cost reduction in long-term care facilities. Consult Pharm 2012;27:411-20.28. Sonoki K, Yoshinari M, Iwase M et al. Regurgitation of blood into insulin cartridges in the pen-like injectors. Diabetes Care 2001;24:603. Available from http://care.diabetesjournals.org/cgi/content/full/24/3/603. Accessed August 16, 2013.29. Le Floch JP, Herbreteau C, Lange F et al. Biological material in needles and cartridges after insulin injection with a pen in diabetic patients. Diabetes Care 1998;21:1502-4. Available from http://care.diabetesjournals.org/cgi/reprint/21/9/1502.pdf. Accessed August 16, 2013. 30. Institute for Safe Medication Practices. Hazard alert: reuse of insulin pen for multiple patients risks transmission of bloodborne disease. ISMP Med Saf Alert Acute Care 2009;14:1-2.31. Institute for Safe Medication Practices. ongoing concern about insulin pen reuse shows hospitals need to consider transitioning away from them. ISMP Med Saf Alert Acute Care 2013;18:1-2.32. USA Today. Possible HIV exposure at Buffalo VA hospital. January 14, 2013. Available from http://www.usatoday.com/story/news/nation/2013/01/13/veterans-hospital-hiv/1831705/. Accessed August 16, 2013. 33. Institute for Safe Medication Practices. Insulin pens again used on multiple patients. ISMP Med Saf Alert Acute Care 2013;18:2-3.34. Institute for Safe Medication Practices. Considering insulin pens for routine hospital use? Consider this. ISMP Med Saf Alert Acute Care 2008;13:1-3.35. Institute for Safe Medication Practices. Hmm…let’s think about this. ISMP Med Saf Alert Acute Care 2005;10:1.36. Institute for Safe Medication Practices. Frequently asked questions: 3. What are the “ten key elements” of the medication-use system? Available from http://www.ismp.org/faq.asp#Question_3. Accessed August 13, 2013.





























