Embed Size (px)
Citation preview

© 2015 International Journal of Nutrition, Pharmacology, Neurological Diseases | Published by Wolters Kluwer - Medknow118
Recent advances in pharmacological management of substance use disorders
Diwakar Sharma, Sujita Kumar Kar
ABSTRACT
Pharmacological management is an important pillar in the treatment of substance use disorders. Decades back, researchers were struggling to find specific pharmacological agents for management of different substance use disorders. However, in the past two decades many effective pharmacological interventions have been discovered, approved, and recommended by several international management guidelines. In recent years, many novel pharmacological agents have been introduced or are in different phases of trial. This review focuses on the current understanding about different pharmacotherapeutic options and recent advances in the management of substance use disorders.
Key words: Novel pharmacological agents, pharmacological management, substance use disorder
Department of Psychiatry, King George’s Medical University, Lucknow, Uttar Pradesh, India
Address for correspondence: Dr. Sujita Kumar Kar, Department of Psychiatry, King George’s Medical University, Lucknow - 226 003, Uttar Pradesh, India. E-mail: [email protected]
INTRODUCTION
The management of substance use disorder includes both pharmacological and nonpharmacological interventions. There was slow growth in the pharmacotherapeutic modalities of intervention for substance use disorder till the early part of the 1990s, but over the last two decades there has been remarkable growth in this area.[1] Despite the growth in pharmacological management, the available treatment options fall short of addressing the needs for management of all substance use disorders. Specific pharmacological management is still not available for psychoactive substances such as cocaine, amphetamine and other stimulants, inhalants, and even cannabis. However, research is still ongoing with regard to designing specific pharmacological interventions for these substances. This review focuses on current understanding about different pharmacotherapeutic
options and recent advances in the management of substance use disorders.
CURRENT UNDERSTANDING IN THE MANAGEMENT OF COMMON SUBSTANCE USE DISORDERS
AlcoholAlcohol hangover is a common withdrawal phenomenon characterized by headache, nausea, diarrhea, tremor, and irritability, leading to noticeable impairment.[2] Hangover usually results from physiological changes mediated by dehydration, hormonal imbalance, and chemokine dysregulation.[2] In an earlier study it was found that prophylactic use of the prostaglandin inhibitor (or nonsteroidal anti‑inflammatory drug, i.e. NSAID) tolfenamic acid
How to cite this article: Sharma D, Kar SK. Recent advances in pharmacological management of substance use disorders. Int J Nutr Pharmacol Neurol Dis 2015;5:118-27.
Received: 30-06-2015, Accepted: 17-07-2015
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
Review Ar t ic le
Access this article onlineQuick Response Code:
Website:
www.ijnpnd.com
DOI:
10.4103/2231-0738.167505
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]

Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4 119
reduced the severity of hangover symptoms.[3] Over three decades, beliefs have changed little. As per current evidences, rehydration and treatment with NSAIDs causes improvement in alcohol hangover symptoms.[2] Supplementation with vitamin B6 (pyridoxine) is also found to be helpful.[2]
Benzodiazepines are commonly used for the management of alcohol withdrawal symptoms.[4,5] Benzodiazepines not only control the withdrawal symptoms but also prevent seizure and progression to delirium tremens.[4,6] Long-acting benzodiazepines such as diazepam and chlordiazepoxide are preferred for management of all forms of alcohol withdrawal-related symptoms including delirium tremens, provided that the liver function test is normal.[7] In states of compromised liver function and for the elderly, long-acting benzodiazepines are to be avoided and short-acting benzodiazepines such as oxazepam and lorazepam may be used.[5,7] Different types of regimen such as symptom-triggered regimen, loading-dose (front-loading) regimen, and fixed-dose regimen are used for managing symptoms of withdrawal.[5,7] Dexmedetomidine, an alpha-2 adrenergic agonist is found to be effective in the management of delirium tremens where benzodiazepine-related oversedation is a concern, particularly in elderly patients.[5]
In clinical studies, disulfiram, acamprosate, and naltrexone were found to have modest effect sizes.[8] The opioid antagonist naltrexone plays an important role in the management of alcohol dependence.[9,10] It reduces the number of drinks, decreases the chance of relapse as well as increases abstinence.[9] Another opioid receptor antagonist, nalmefene, has been approved recently for alcohol dependence.[8] In severe hepatic dysfunction, naltrexone needs to be avoided.[11] Patients on naltrexone should undergo regular evaluation of their liver function tests.[11] Most patients taking naltrexone tolerate it well, but some may develop side effects such as nausea, vomiting, headache, dizziness, fatigue, or insomnia.[11]
Acamprosate decreases the calcium influx through voltage-sensitive calcium channels, and normalizes the gamma-aminobutyric acid (GABA) and glutamate balance in the brain; however, it does not have any action mediated through the opioid pathway.[9,12] Due to lack of affinity for the opioid pathway, addition of agents acting through the opioid pathway (e.g., naltrexone) can be more beneficial.[12] It can be safely given in patients with hepatic impairment. Some patients using acamprosate
may experience side effects. The most common side effects are gastrointestinal (nausea, vomiting, diarrhea, abdominal pain). Some may experience headache, drowsiness, and even dermatological lesions. Acamprosate needs to be avoided in patients with known hypersensitivity, pregnancy, lactation, renal impairment, and extreme young/old age.[11]
Disulfiram was the first medication to get United States Food and Drug Administration (USFDA) approval for use in cases of alcohol dependence in 1948.[13] Disulfiram is suitable for clients remaining adherent to therapy and having good motivation.[9,14] Disulfiram acts by inhibiting the enzyme aldehyde dehydrogenase; when consumed along with alcohol, acetyldehyde accumulation occurs due to enzymatic inhibition, resulting in unpleasant disulfiram/ethanol reaction.[14,15] The effect of disulfiram on alcohol metabolism starts within 2 hours of its ingestion.[11] Ingestion of alcohol by a patient who is already taking disulfiram results in unpleasant reaction characterized by cardiorespiratory difficulty (palpitation, tachycardia, hypotension, hyperventilation, chest pain, choking sensation, etc.), tremulousness, ataxia, headache, visual difficulties, flushing, and nausea and vomiting.[11] Common side effects of disulfiram are gastrointestinal (dyspepsia, nausea, abnormal taste); however, patients also develop side effects such as hepatitis, neurological impairment (peripheral neuropathy), and dermatological and psychiatric problems (psychosis). Use of disulfiram should be avoided in cases with underlying cardiac diseases (coronary artery disease, cardiomyopathy, arrhythmia, congestive cardiac failure), renal failure, stroke, pregnancy, and/or psychosis.[11]
Ondansetron, primarily used as an antiemetic agent, is also found to be effective in cases of alcohol dependence in some clinical trials and plays a promising role in early-onset alcohol dependence.[8,9] A recent study revealed that ondansetron is effective in reducing the number of drinks in patients of alcohol dependence possessing specific genetic characteristics.[16]
The antiepileptic agent topiramate with its antiglutaminergic and GABA-agonistic activities has been found effective in alcohol dependence.[9,17] It reduces cortico–mesolimbic dopamine release, resulting in a decrease in the reward following alcohol intake.[18] Topiramate is effective in heavy drinkers for whom abstinence is the goal.[19] It reduces the number of drinks as well as increases the period of abstinence.[18,19] In a randomized control trial (RCT), topiramate was found to be more effective in controlling
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]

Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4120
the alcohol withdrawal symptoms in comparison to placebo.[18,20] The commonly reported side effects are neurological (sedation, confusion, cognitive impairment, paresthesia/numbness, blurring of vision).[11] Patients also experience reduction in appetite, headache, dizziness, fatigability, and renal side effects.[11]
Baclofen, a GABAB receptor agonist, is also being used in management of alcohol dependence as an off-label agent. It is effective in reducing craving for alcohol as well as withdrawal-related anxiety and increases the period of abstinence. Baclofen can be given even in patients with moderate to severe cirrhosis of liver.[21] Drug-related serious side effects are unlikely, as found in studies.[22]
Another antiepileptic agent gabapentin has been found to improve different parameters of sleep in patients with alcohol dependence,[23,24] though some contradicting results have also been noted in some other studies.[25]
Studies have found a link between the serotonin transporter gene and alcohol dependence, early-onset alcoholism, and heavy drinking.[26] However, contradicting evidences regarding the effectiveness of selective serotonin reuptake inhibitors (SSRIs) in alcohol dependence have been observed.[26]
Trazodone is an antidepressant belonging to the category serotonin antagonist and reuptake inhibitor (SARI) has a role in alcohol and benzodiazepine dependence.[27] It decreases the need of benzodiazepine in management of alcohol dependence; however, it is yet to be approved for use in alcohol and other drug dependence.[27] It is useful as an option for a hypnotic agent in managing substance use disorders.[23,28]
In a Cochrane Database review (2010), it was found that gamma-hydroxybutyric acid (GHB) was effective in controlling the withdrawal symptoms in alcohol dependence.[29] It was found to be superior to naltrexone and disulfiram in maintaining abstinence; however, evidences are lacking regarding its efficacy in comparison to benzodiazepines.[29] The risk associated with GHB is its abuse potential, which is likely to decrease its popularity.[29] Deficiency of vitamins and micronutrients, particularly thiamine, may be a potential risk factor for development of delirium tremens and Wernicke–Korsakoff syndrome in patients with alcohol use disorder. Hence supplementation with a high dose of thiamine along with adequate hydration measures remains the mainstay of treatment of these conditions.
NicotineUnclear neurobiology may be one of the obstacles against the availability of a better drug in the management of nicotine dependence.[30] Recently the focus of management of nicotine dependence has been on three pharmacological agents: Nicotine replacement therapy (NRT), bupropion, and varenicline.[18,31] NRT is a short-term therapy involving the use of nicotine chewing gum, transdermal nicotine patch, nicotine pastilles/lozenges, nicotine nasal spray, or vapor inhaler.[31] Interestingly, this has been effective not only toward nicotine abstinence in those willing to quit but also in reducing the habit size of nicotine use among smokers not willing to quit.[32] Evidence from one meta-analytic study demonstrated that combining a nicotine patch with an oral form of NRT was more effective than a single type of NRT. Additionally, NRTs increase the rate of quitting by 50–70% regardless of the setting or the intensity of additional support provided to the individual. Provision of more intense levels of support is not essential to the success of NRT, although beneficial in facilitating the likelihood of quitting.[33] Smoking cessation is often followed by weight gain, an effect not seen with NRTs, but this does not persist after the termination of treatment.[34,35] The cognitive symptoms associated with nicotine withdrawal also improve with NRT, which is mediated through the modulation of the default network of nicotine addiction.[30]
Bupropion acts by inhibiting the reuptake of the monoamine neurotransmitter dopamine. Its usefulness in addiction is ascribed to its probable effects on dopamine reward pathways or to inhibition of nicotinic acetylcholine receptors. The sustained-release formulation of bupropion is recommended for use in nicotine dependence.[31] Recent research has shown that those smokers who metabolized nicotine faster had relatively better outcome.[36] The combination of bupropion and NRT is a more effective modality than each alone.[12,31]
Tricyclic antidepressant nortriptyline is also effective in reducing craving and withdrawal symptoms in nicotine dependence, and thus improves chances of quitting. The modes of action of bupropion and nortriptyline are independent of their antidepressant effect and they are of similar efficacy to nicotine replacement.[37]
Varenicline is a synthetic partial agonist of the α4β2 nicotinic receptor.[31] In a recent Cochrane review (2012) it had been found to increase the chances of successful
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]

Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4 121
long-term smoking abstinence by two–to–three-fold when compared to pharmacologically unassisted quitting attempts.[38] A prospective cohort study demonstrated that using varenicline with the least professional support for smokers appeared to be more effective than NRT in achieving abstinence.[39] Its main adverse effect is nausea, but it is mostly of mild to moderate intensity and tends to subside over time. There is a need for further trials of the efficacy of varenicline treatment extended beyond 12 weeks according to the current consensus regime.
Cytisine is a naturally occurring α4β2 nicotinic receptor partial agonist isolated from Cytisus laburnum. It is estimated to be both more clinically effective as well as more cost-effective than varenicline. However, there is a lack of head–to–head trials of cytisine and varenicline, making it still difficult to prefer one over the other.[40,41]
Clonidine is an adrenergic agonist that acts through the α2 receptors of the brain. Its sympatholytic property makes it a potent antihypertensive. It is also found to be effective in reducing the withdrawal symptoms and craving resulting from nicotine.[31,42]
The electronic cigarette or e-cigarette (EC) is an electronic device that heats a liquid usually comprised of propylene glycol and glycerol, with or without nicotine, stored in disposable or refillable cartridges or a reservoir, into an aerosol for inhalation. It was found to help smokers unable to stop smoking altogether to reduce their cigarette consumption when compared with placebo ECs and nicotine patches. There have been concerns and reluctance regarding ECs from some health-care providers following a Centers for Disease Control and Prevention (CDC) report that suggested that ECs should be treated with caution as it can act as initiation for the use of conventional cigarettes or other tobacco products.[43] However, recent research has shown its ability to help smokers to stop smoking in the long term when compared with placebo ECs, and allowing ECs to compete with cigarettes in the marketplace might decrease smoking-related morbidity and mortality.[44,45]
OpioidsCurrently, opioid substitution therapy (OST) is the backbone of opioid dependence management. Pharmacological agents prescribed and dosed rationally have been found to decrease opioid withdrawal to a variable extent, reduce illicit drug use, cause minimal euphoria, and decrease adverse consequences resulting from opioid use [e.g., human
immunodeficiency virus (HIV) infection, overdose complications].[46]
Methadone, an asynthetic opioid agonist at the µ-opioid receptor, is effective in producing cross-tolerance and blockade of the effect of externally administered narcotics. It has slow onset of action when taken orally, and its long elimination half-life (24–36 h) allows it to be used as either a maintenance therapy or a detoxification agent. Its effectiveness had been reported to vary in different studies, ranging from as low as 20% to as high as 70%.[47,48]
Availability of methadone as a treatment for opioid dependence varies widely, as some countries allow it to be dispensed freely, while others have banned it. It has the potential risk of QT prolongation and an increased risk of overdose mortality due to respiratory depression. It is the agent of choice at most controlled or government-run clinics with a harm-reduction approach.
Levomethadyl acetate or LAAM, a longer-acting derivative of methadone, allows for thrice-weekly dosing. However, it is no longer in use and has been removed from markets over concerns of cardiac side effects: QT prolongation and torsades de pointes.[49]
Buprenorphine is a high‑affinity partial agonist at the µ-opioid receptor and an antagonist at the κ-opioid receptor. Its ceiling effect on respiratory depression confers a high clinical safety profile and thus a low risk of physical dependence and a long duration of action, and upon discontinuation results in a relatively mild withdrawal syndrome.[50,51] Injection misuse of buprenorphine has called for prescription of the drug in a fixed‑dose combination (4:1) with naloxone. Naloxone being an opioid receptor antagonist precipitates withdrawal symptoms and thus does not produce euphoric effects. The 4:1 ratio had been arrived upon on the basis of results from several clinical studies.[52]
Recent studies suggest that retention with buprenorphine is lower than for methadone, but that buprenorphine may be associated with less drug use. Higher doses of buprenorphine are associated with better retention rates.[53]
Slow-release oral morphine (SROM) is a natural derivative of opium and has also been tried as a maintenance agent. It has been found to be as effective as buprenorphine in controlling withdrawal, and craving, and on quality of life on short-term follow-up.[54]
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]
Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4122
Clonidine reduces withdrawal symptoms such as nausea, vomiting, diarrhea, cramps, and sweating, but does not have much effect on muscle aches, insomnia, distress, or drug craving during an acute withdrawal state. However, it enables the use of an opioid antagonist (e.g., naltrexone) if indicated, immediately after withdrawal symptoms subside.
Naltrexone is an oral, long-acting, opioid antagonist with high affinity to µ-opioid receptors. A daily dose of naltrexone (50 mg) will block the pharmacologic effects of 25 mg intravenous (IV) heroin for as long as 24 h, and increasing the dose extends its duration of action to 48 h with 100 mg and 72 h with 150 mg.[55] Earlier in a Cochrane Database review it had been found to be effective in treating of opioid dependence, but only in a highly motivated subset of the population.[56] However, after all its potential appeal as a medication for maintenance treatment, the clinical utility of naltrexone as a treatment for opioid dependence has been limited.[57] In a recent study it was found that extended-release naltrexone was effective in reducing the depressive symptoms associated with heroin dependence but had no significant effect on anhedonia.[58]
Oral naltrexone with or without psychotherapy was found to be no better than placebo or no pharmacological treatments with regard to the number of participants reincarcerated in treatment, use of the primary substance of abuse, or side effects.[59] Because of low rates of treatment-seeking, poor adherence to treatment, frequent relapse, and major societal consequences associated with opioid dependence, sustained-release technologies for administering the opioid antagonist naltrexone (XR-NTX) in the form of intramuscular injectable or implantable polymers have been explored.[60] Studies so far show that it is a feasible, safe, and effective option for assisting abstinence efforts.[61] Along similar lines, sustained-release formulations of buprenorphine have been developed, in part to address concerns about adherence and diversion, but initial experiments are yet to give results.
In a few countries, diacetylmorphine or heroin is available to treat heroin dependence under strict supervision.[62] Recent evidence demonstrates an added value of heroin prescribed alongside flexible doses of methadone for long-term, treatment-refractory opioid users to reach a decrease in the use of illicit substances, involvement in criminal activity and incarceration, a possible reduction in mortality, and an increase in retention in treatment. Due to the higher rate of serious
adverse events, heroin prescription should remain a treatment for people who are currently failing or have in the past failed maintenance treatment, and it should be provided in clinical settings where proper follow-up is ensured.[63]
CannabisCurrently there are no accepted pharmacological treatment interventions for cannabis use disorders. Severe effects of cannabis intoxication such as anxiety, panic, and psychosis are treated symptomatically with a benzodiazepine or atypical antipsychotic medication. No medication is approved specifically for the treatment of cannabis intoxication. Though in an experimental stage, early researches suggest that fatty acid amide hydrolase (FAAH) inhibitor, which prevents breakdown of endocannabinoids such as anandamide, might offer benefits in the treatment of acute cannabis withdrawal by enhancing brain endocannabinoid activity.[64] The future holds promise in the form of such molecules, although earlier experience with the endocannabinoid receptor antagonist rimonabant met with major adverse effect issues, resulting in its abrupt discontinuation from markets.
Among the drugs studied so far, the one with the most clinical potential in reducing cannabis withdrawal has been dronabinol, which is a synthetic formulation of trans-Δ9-tetrahydrocannabinol (THC), the primary psychoactive component in cannabis.[65] It has shown promising efficacy in several human laboratory studies and open‑label case series, at doses up to 90 mg/day in three divided doses, with minimal side effects.[66] But at the same time it did not improve rates of abstinence in controlled trials, though it significantly improved treatment retention.[67]
Neurotransmitter modulation strategy has been utilized in managing cannabis dependence in order to reduce the reinforcing effects of and craving for cannabis. Drugs utilized as an off-label use in this strategy are entacapone, N-acetylcysteine (NAC), atomoxetine, buspirone, and divalproex. Initial research so far is in favor of buspirone and entacapone over those other drugs.[66] Recently, cannabinoid replacement therapy (CRT) has been used in patients with cannabis use disorder to manage the withdrawal symptoms.[68,69] It is used in the form of buccal spray, which contains a combination of THC and cannabidiol.[68] Allsop et al., 2014 in an RCT found that CRT is effective in controlling cannabis withdrawal symptoms significantly, besides reducing craving and depressive symptoms.[69]
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]

Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4 123
StimulantsAs per the current research evidences, no pharmacological agent has been found to be effective in the management of stimulant dependence.[70,71] In recent years, the effectiveness of dopamine agonists, antidepressants and disulfiram has been studied in trials on cocaine dependence; however, the outcome was not convincing.[70,71] Early findings of some open-label trials and RCTs have been promising about the efficacy of modafinil (a drug recommended for the treatment of narcolepsy) and propranolol, but the result needs replication in a larger population.[12,72] It has also been suggested that dopamine releasers such as modafinil may be more effective for cocaine dependence than for methamphetamine dependence, where a dopamine reuptake inhibitor such as bupropion is more effective.[73] In the particular case of methamphetamine or “crystal meth” dependence, drugs such as methylphenidate that block catecholamine reuptake from and increase catecholamine release into the synapse have been found to be effective to some extent. As immediate-release oral methylphenidate has more potential for abuse, sustained-release methylphenidate had been studied and found effective in reducing its use and associated cravings and depressive symptoms.[74] According to Elkashef et al. 2012, topiramate reduces the amount and relapse rates in those methamphetamine addicts who were already abstinent but does not ensure abstinence itself.[75]
Cholinesterase inhibitors such as rivastigmine have been explored as an option for treatment of methylamphetamine dependence with some encouraging results.[76] Likewise, naltrexone appears to be a highly promising medication for amphetamine dependence.[77] Serotonergic agents such as SSRIs, mirtazapine, and ondansetron have been also explored, but convincing data is still required before their recommendation for clinical use.[78] Research is already exploring the avenues of other molecules such as varenicline, NAC, and the phosphodiesterase inhibitor ibudilast.[79,80]
InhalantsNo medication has been found to be able to reverse acute inhalant intoxication or help in managing dependence or withdrawal symptoms. Management of inhalant intoxication and withdrawal is largely along conservative lines.[81] There is little research literature concerning treatment needs and successful treatment modalities specific to inhalant users so far.
BenzodiazepinesAs of now, no pharmacotherapy is registered for the treatment of benzodiazepine dependence or withdrawal. However, there is an increasing interest in the GABAA benzodiazepine receptor antagonist flumazenil.[82]
Major indications for the use of flumazenil have been in the management of suspected benzodiazepine overdose, and the reversal of benzodiazepine sedative effects associated with general anesthesia or diagnostic or therapeutic procedures.[83] Oral bioavailability and the very short half‑life of flumazenil potentially limit its free use in clinical settings and also its usefulness for the prevention of long-term withdrawal symptoms. It has been underutilized as an agent to manage persistent or reemerging withdrawal symptoms following cessation of long-term benzodiazepine use.[84]
Recent studies using bolus or continuous, IV, and subcutaneous mode of administration have shown the likely efficacy for flumazenil in the management of acute benzodiazepine withdrawal.[85] The main problems associated with the use of this drug are high relapse rates, higher risk of seizure, and cardiac complications, which highlights the need for RCTs.
RECENT ADVANCES IN THE MANAGEMENT OF SUBSTANCE USE DISORDERS
In the development of craving for alcohol, several neurobiological mechanisms such as the hypothalamo–adrenal axis and metabolic pathway involving leptin are found to be involved, which can be potential targets of pharmacological intervention.[86] Recent evidences suggest the potential role of topiramate in the management of withdrawal symptoms of cocaine dependence in addition to its role in alcohol dependence.[87] The combination of topiramate and cognitive behavioral therapy (CBT) may be helpful in cases of comorbid alcohol and cocaine dependence.[87] The antiepileptic levetiracetam was also tested in alcohol dependence in clinical trials but was found to be ineffective.[8] Prazosin, an alpha-1 receptor antagonist is undergoing clinical trials for use in alcohol dependence.[8] Varenicline, an approved agent in cases of nicotine dependence is also undergoing alcohol dependence clinical trials, but the results are so far mixed and further studies are required to prove its efficacy against alcohol dependence.[8] Current researches also focus on the field of pharmacogenetics, and it has been found that
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]
Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4124
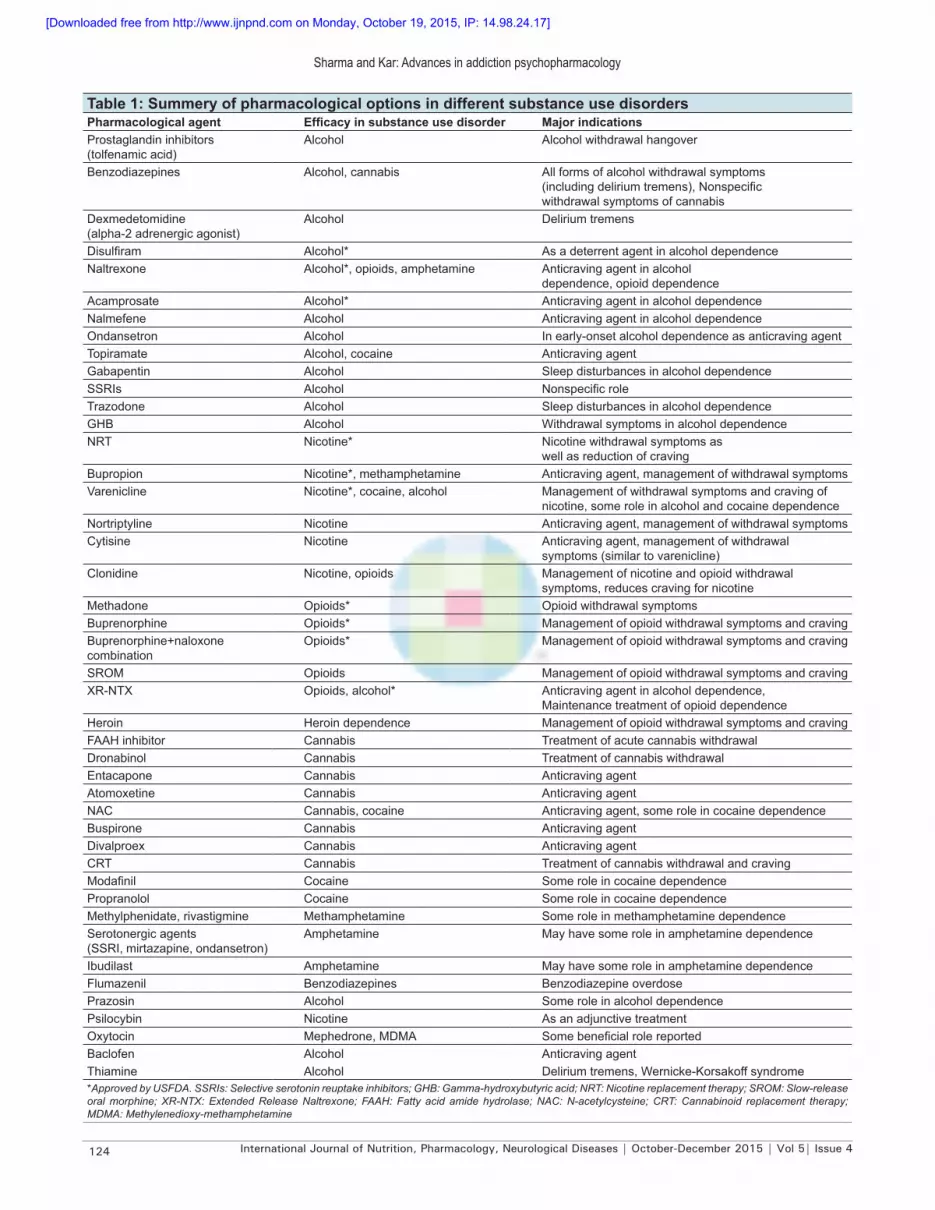
Table 1: Summery of pharmacological options in different substance use disordersPharmacological agent Efficacy in substance use disorder Major indicationsProstaglandin inhibitors (tolfenamic acid)
Alcohol Alcohol withdrawal hangover
Benzodiazepines Alcohol, cannabis All forms of alcohol withdrawal symptoms (including delirium tremens), Nonspecific withdrawal symptoms of cannabis
Dexmedetomidine (alpha-2 adrenergic agonist)
Alcohol Delirium tremens
Disulfiram Alcohol* As a deterrent agent in alcohol dependenceNaltrexone Alcohol*, opioids, amphetamine Anticraving agent in alcohol
dependence, opioid dependenceAcamprosate Alcohol* Anticraving agent in alcohol dependenceNalmefene Alcohol Anticraving agent in alcohol dependenceOndansetron Alcohol In early-onset alcohol dependence as anticraving agentTopiramate Alcohol, cocaine Anticraving agentGabapentin Alcohol Sleep disturbances in alcohol dependenceSSRIs Alcohol Nonspecific roleTrazodone Alcohol Sleep disturbances in alcohol dependenceGHB Alcohol Withdrawal symptoms in alcohol dependenceNRT Nicotine* Nicotine withdrawal symptoms as
well as reduction of cravingBupropion Nicotine*, methamphetamine Anticraving agent, management of withdrawal symptomsVarenicline Nicotine*, cocaine, alcohol Management of withdrawal symptoms and craving of
nicotine, some role in alcohol and cocaine dependenceNortriptyline Nicotine Anticraving agent, management of withdrawal symptomsCytisine Nicotine Anticraving agent, management of withdrawal
symptoms (similar to varenicline)Clonidine Nicotine, opioids Management of nicotine and opioid withdrawal
symptoms, reduces craving for nicotineMethadone Opioids* Opioid withdrawal symptomsBuprenorphine Opioids* Management of opioid withdrawal symptoms and cravingBuprenorphine+naloxone combination
Opioids* Management of opioid withdrawal symptoms and craving
SROM Opioids Management of opioid withdrawal symptoms and cravingXR-NTX Opioids, alcohol* Anticraving agent in alcohol dependence,
Maintenance treatment of opioid dependenceHeroin Heroin dependence Management of opioid withdrawal symptoms and cravingFAAH inhibitor Cannabis Treatment of acute cannabis withdrawalDronabinol Cannabis Treatment of cannabis withdrawalEntacapone Cannabis Anticraving agentAtomoxetine Cannabis Anticraving agentNAC Cannabis, cocaine Anticraving agent, some role in cocaine dependenceBuspirone Cannabis Anticraving agentDivalproex Cannabis Anticraving agentCRT Cannabis Treatment of cannabis withdrawal and cravingModafinil Cocaine Some role in cocaine dependencePropranolol Cocaine Some role in cocaine dependenceMethylphenidate, rivastigmine Methamphetamine Some role in methamphetamine dependenceSerotonergic agents (SSRI, mirtazapine, ondansetron)
Amphetamine May have some role in amphetamine dependence
Ibudilast Amphetamine May have some role in amphetamine dependenceFlumazenil Benzodiazepines Benzodiazepine overdosePrazosin Alcohol Some role in alcohol dependencePsilocybin Nicotine As an adjunctive treatmentOxytocin Mephedrone, MDMA Some beneficial role reportedBaclofen Alcohol Anticraving agentThiamine Alcohol Delirium tremens, Wernicke-Korsakoff syndrome*Approved by USFDA. SSRIs: Selective serotonin reuptake inhibitors; GHB: Gamma-hydroxybutyric acid; NRT: Nicotine replacement therapy; SROM: Slow-release oral morphine; XR-NTX: Extended Release Naltrexone; FAAH: Fatty acid amide hydrolase; NAC: N-acetylcysteine; CRT: Cannabinoid replacement therapy; MDMA: Methylenedioxy-methamphetamine
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]

Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4 125
the presence of a specific gene increases treatment responsiveness to a particular pharmacotherapy modality. A single-nucleotide polymorphism in the exon of OPMR1 gene (rs1799971) and the gene encoding for dopamine receptor (subtype D4), i.e. DRD4, are associated with good response to naltrexone.[88] Similarly, the gene SLC6A4, which is related to serotonin transport, is associated with good response to ondansetron in cases of alcohol dependence.[88]
Recent literature has mentioned psilocybin as a potentially efficacious adjunct to the current smoking-cessation treatment modality, but it requires further research before application in clinical settings.[89] The hormone oxytocin is also being explored as an option in addiction psychiatry, especially for mephedrone, 3,4-methylenedioxy-methamphetamine (MDMA), etc.[90] Table 1, above summerizes the role of different pharmacological agents in substance use disorders.
There has been recent enthusiasm regarding the development of “vaccines” in addiction pharmacotherapy. Structurally these vaccines are abused-drug–related micromolecular compounds, linked to a large immunogenic protein, which results in the generation of an antigen-specific, immunoglobulin G (IgG)-mediated antibody response upon introduction of the drug in future. Current research in addiction immunotherapy is focused on developing vaccines or antibodies for managing dependence on addictive agents such as cocaine, nicotine, opioids, and methamphetamine.[91]
CONCLUSION
The morbidity, mortality, and psychosocial burden associated with substance use disorders are enormous. Developing effective management strategies for substance use disorders is very important for reducing the burden of substance use on both the individual and society. Despite the growing number of pharmacological options during the last two decades, targeted and effective interventions are still lacking in adequacy. In addition, there is still no convincing pharmacotherapy that exists for managing disorders related to the use of cannabis, inhalants, cocaine, etc. Thus, further research and resources are still required for exploring the same. Advances in our understanding of underlying neurobiological phenomena in these disorders have just begun to provide glimpses of exciting future avenues where novel treatments await to be unearthed.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES
1. Kranzler HR, Amin H, Modesto‑Lowe V, Oncken C. Pharmacologic treatments for drug and alcohol dependence. Psychiatr Clin North Am 1999;22:401‑23.
2. Wiese JG, Shlipak MG, Browner WS. The alcohol hangover. Ann Intern Med 2000;132:897‑902.
3. Kaivola S, Parantainen J, Osterman T, Timonen H. Hangover headache and prostaglandins: Prophylactic treatment with tolfenamic acid. Cephalalgia 1983;3:31‑6.
4. Amato L, Minozzi S, Vecchi S, Davoli M. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev 2010;CD005063.
5. Sehgal V, Bajwa SJ, Consalvo JA, Bajaj A, Sehgal R. Delirium tremens in the elderly: Emerging role of dexmedetomidine. Int J Nutr Pharmacol Neurol Dis 2015;5:89‑94.
6. AmatoL,MinozziS,DavoliM.Efficacyandsafetyofpharmacologicalinterventions for the treatment of the Alcohol Withdrawal Syndrome. Cochrane Database Syst Rev 2011;CD008537.
7. Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines in Psychiatry. 11th ed. UK: Wiley‑Blackwell; 2012. p. 356‑72.
8. Müller CA, Geisel O, Banas R, Heinz A. Current pharmacological treatment approaches for alcohol dependence. Expert Opin Pharmacother 2014;15:471‑81.
9. Castro LA, Baltieri DA. The pharmacologic treatment of the alcohol dependence. Rev Bras Psiquiatr 2004;26(Suppl 1):S43‑6.
10. Modesto‑Lowe V, Van Kirk J. Clinical uses of naltrexone: A review of the evidence. Exp Clin Psychopharmacol 2002;10:213‑27.
11. Grover S, Bhateja G, Basu D. Pharmacoprophylaxis of alcohol dependence: Review and update Part I: Pharmacology. Indian J Psychiatry 2007;49:19‑25.
12. O’Brien CP. Anticraving medications for relapse prevention: A possible new class of psychoactive medications. Am J Psychiatry 2005;162:1423‑31.
13. Zindel LR, Kranzler HR. Pharmacotherapy of alcohol use disorders: Seventy‑five years of progress. J StudAlcoholDrugsSuppl 2014;75(Suppl 17):79‑88.
14. SkinnerMD,LahmekP,PhamH,AubinHJ.Disulfiramefficacyinthe treatment of alcohol dependence: A meta‑analysis. PLoS One 2014;9:e87366.
15. Swift RM. Drug therapy for alcohol dependence. N Engl J Med 1999;340:1482‑90.
16. Kenna GA, Zywiak WH, Swift RM, McGeary JE, Clifford JS, Shoaff JR, et al. Ondansetron reduces naturalistic drinking in nontreatment‑seeking alcohol‑dependent individuals with the LL 5’‑HTTLPR genotype: A laboratory study. Alcohol Clin Exp Res 2014;38:1567‑74.
17. Cohen J, Dervaux A, Laqueille X. Topiramate in substance‑related and addictive disorders. Presse Med 2014;43:892‑901.
18. Shinn AK, Greenfield SF. Topiramate in the treatment of substance‑related disorders: A critical review of the literature. J Clin Psychiatry 2010;71:634‑48.
19. Kranzler HR, Covault J, Feinn R, Armeli S, Tennen H, Arias AJ, et al. Topiramate treatment for heavy drinkers: Moderation by a GRIK1 polymorphism. Am J Psychiatry 2014;171:445‑52.
20. Krupitsky EM, Rudenko AA, Burakov AM, Slavina TY, Grinenko AA, PittmanB,et al.Antiglutamatergicstrategiesforethanoldetoxification:Comparison with placebo and diazepam. Alcohol Clin Exp Res 2007;31:604‑11.
21. MuzykAJ,RivelliSK,GagliardiJP.Definingtheroleofbaclofenforthe treatment of alcohol dependence: A systematic review of the evidence. CNS Drugs 2012;26:69‑78.
22. Müller CA, Geisel O, Pelz P, Higl V, Krüger J, Stickel A, et al. High‑dose baclofen for the treatment of alcohol dependence (BACLAD study): A randomized, placebo‑controlled trial. Eur Neuropsychopharmacol
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]

Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4126
2015. [Epub ahead of print]23. Kolla BP, Mansukhani MP, Schneekloth T. Pharmacological treatment
of insomnia in alcohol recovery: A systematic review. Alcohol Alcohol 2011;46:578‑85.
24. Karam‑Hage M, Brower KJ. Open pilot study of gabapentin versus trazodone to treat insomnia in alcoholic outpatients. Psychiatry Clin Neurosci 2003;57:542‑4.
25. Myrick H, Malcolm R, Randall PK, Boyle E, Anton RF, Becker HC, et al. A double‑blind trial of gabapentin versus lorazepam in the treatment of alcohol withdrawal. Alcohol Clin Exp Res 2009;33:1582‑8.
26. Atigari OV, Kelly AM, Jabeen Q, Healy D. New onset alcohol dependence linked to treatment with selective serotonin reuptake inhibitors. Int J Risk Saf Med 2013;25:105‑9.
27. Funk S. Pharmacological treatment in alcohol‑, drug‑ and benzodiazepine‑dependentpatients‑the significanceof trazodone.Neuropsychopharmacol Hung 2013;15:85‑93.
28. Bossini L, Casolaro I, Koukouna D, Cecchini F, Fagiolini A. Off‑labelusesof trazodone:A review.ExpertOpinPharmacother2012;13:1707‑17.
29. Leone MA, Vigna‑Taglianti F, Avanzi G, Brambilla R, Faggiano F. Gamma‑hydroxybutyrate (GHB) for treatment of alcohol withdrawal and prevention of relapses. Cochrane Database Syst Rev 2010;CD006266.
30. Menossi HS, Goudriaan AE, de Azevedo‑Marques Périco C, Nicastri S, de Andrade AG, D’Elia G, et al. Neural bases of pharmacological treatment of nicotine dependence‑insights from functional brain imaging: A systematic review. CNS Drugs 2013;27:921‑41.
31. Douaihy AB, Kelly TM, Sullivan C. Medications for substance use disorders. Soc Work Public Health 2013;28:264‑78.
32. Jain R, Majumder P, Gupta T. Pharmacological intervention of nicotine dependence. Biomed Res Int 2013;2013:278392.
33. Stead LF, Perera R, Bullen C, Mant D, Hartmann‑Boyce J, Cahill K, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 2012;11:CD000146.
34. AubinHJ,FarleyA,LycettD,LahmekP,AveyardP.Weightgaininsmokersafterquittingcigarettes:Meta‑analysis.BMJ2012;345:e4439.
35. FarleyAC,HajekP,LycettD,AveyardP.Interventionsforpreventingweight gain after smoking cessation. Cochrane Database Syst Rev 2012;1:CD006219.
36. PattersonF,SchnollRA,WileytoEP,PintoA,EpsteinLH,ShieldsPG,et al. Toward personalized therapy for smoking cessation: A randomized placebo‑controlled trial of bupropion. Clin Pharmacol Ther 2008;84:320‑5.
37. Hughes JR, Stead LF, Hartmann‑Boyce J, Cahill K, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev 2014;1:CD000031.
38. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev 2012;4:CD006103.
39. KotzD,BrownJ,WestR.Prospectivecohortstudyoftheeffectivenessof varenicline versus nicotine replacement therapy for smoking cessation in the “real world”. BMC Public Health 2014;14:1163.
40. Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: An overview and network meta‑analysis. Cochrane Database Syst Rev 2013;5:CD009329.
41. Leaviss J, Sullivan W, Ren S, Everson‑Hock E, Stevenson M, Stevens JW, et al.Whatistheclinicaleffectivenessandcost‑effectivenessofcytisinecompared with varenicline for smoking cessation? A systematic review and economic evaluation. Health Technol Assess 2014;18:1‑120.
42. GourlaySG,SteadLF,BenowitzNL.Clonidineforsmokingcessation.Cochrane Database Syst Rev 2004:CD000058.
43. More than a quarter‑million youth who had never smoked a cigarette used e‑cigarettes in 2013. Center for Disease Control. PressRelease.August25,2014.Availablefrom:http://www.cdc.gov/media/releases/2014/p0825‑e‑cigarettes.html.2014.[Lastaccessedon2015 Feb 14].
44. McRobbie H, Bullen C, Hartmann‑Boyce J, Hajek P. Electronic cigarettesforsmokingcessationandreduction.CochraneDatabaseSyst Rev 2014;12:CD010216.
45. HajekP,EtterJF,BenowitzN,EissenbergT,McRobbieH.Electroniccigarettes:Reviewofuse, content, safety, effects on smokers andpotentialforharmandbenefit.Addiction2014;109:1801‑10.
46. Metzger DS, Woody GE, O’Brien CP. Drug treatment as HIV prevention: A research update. J Acquire Immune Defic Syndr 2010;55(Suppl 1):S32‑6.
47. Fudala PJ, Bridge TP, Herbert S, Williford WO, Chiang CN, Jones K, et al.Buprenorphine/NaloxoneCollaborativeStudyGroup.Office‑basedtreatmentofopiateaddictionwithasublingual‑tabletformulation of buprenorphine and naloxone. N Engl J Med 2003;349:949‑58.
48. Hser YI, Saxon AJ, Huang D, Hasson A, Thomas C, Hillhouse M, et al. Treatmentretentionamongpatientsrandomizedtobuprenorphine/naloxone compared to methadone in a multi‑site trial. Addiction 2014;109:79‑87.
49. Wieneke H, Conrads H, Wolstein J, Breuckmann F, Gastpar M, Erbel R, et al. Levo‑alpha‑acetylmethadol (LAAM) induced QTc‑prolongation‑results from a controlled clinical trial. Eur J Med Res 2009;14:7‑12.
50. Teoh SK, Mello NK, Mendelson JH, Kuehnle J, Gastfriend DR, Rhoades E, et al. Buprenorphine effects on morphine‑ and cocaine‑induced subjective responses by drug‑dependent men. J Clin Psychopharmacol 1994;14:15‑27.
51. FudalaPJ,JaffeJH,DaxEM,JohnsonRE.Useofbuprenorphineinthetreatmentofopioidaddiction.II.Physiologicandbehavioraleffectsofdaily and alternate‑day administration and abrupt withdrawal. Clin Pharmacol Ther 1990;47:525‑34.
52. Mendelson J, Jones RT, Welm S, Brown J, Batki SL. Buprenorphine and naloxone interactions in methadone maintenance patients. Biol Psychiatry 1997;41:1095‑101.
53. Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev 2014;2:CD002207.
54. Rao R, Ambekar A, Yadav S, Sethi H, Dhawan A. Slow‑release oral morphine as a maintenance agent in opioid dependence syndrome: An exploratory study from India. J Subst Use 2012;17:294‑300.
55. Rawson RA, McCann MJ, Hasson AJ, Ling W. Addiction pharmacotherapy 2000: New options, new challenges. J Psychoactive Drugs 2000;32:371‑8.
56. Kirchmayer U, Davoli M, Verster A. Naltrexone maintenance treatment for opioid dependence. Cochrane Database Syst Rev 2003;CD001333.
57. Warner EA, Kosten TR, O’Connor PG. Pharmacotherapy for opioid and cocaine abuse. Med Clin North Am 1997;81:909‑25.
58. Zaaijer ER, van Dijk L, de Bruin K, Goudriaan AE, Lammers LA, Koeter MW, et al.Effectof extended‑releasenaltrexoneon striataldopamine transporter availability, depression and anhedonia in heroin‑dependent patients. Psychopharmacology (Berl) 2015;232:2597‑607.
59. Minozzi S, Amato L, Vecchi S, Davoli M, Kirchmayer U, Verster A. Oral naltrexone maintenance treatment for opioid dependence. Cochrane Database of Syst Rev 2011;CD001333.
60. Krupitsky E, Nunes EV, Ling W, Illeperuma A, Gastfriend DR, Silverman BL. Injectable extended‑release naltrexone for opioid dependence: A double‑blind, placebo‑controlled, multicentre randomised trial. Lancet 2011;377:1506‑13.
61. Kunøe N, Lobmaier P, Ngo H, Hulse G. Injectable and implantable sustained release naltrexone in the treatment of opioid addiction. Br J Clin Pharmacol 2014;77:264‑71.
62. Blanken P, Hendriks VM, Koeter MW, van Ree JM, van den Brink W. Craving and illicit heroin use among patients in heroin‑assisted treatment. Drug Alcohol Depend 2012;120:74‑80.
63. Ferri M, Davoli M, Perucci CA. Heroin maintenance for chronic heroin‑dependent individuals. Cochrane Database Syst Rev 2011;CD003410.
64. Clapper JR, Mangieri RA, Piomelli D. The endocannabinoid system as a target for the treatment of cannabis dependence. Neuropharmacology 2009;56(Suppl 1):235‑43.
65. Vandrey R, Haney M. Pharmacotherapy for cannabis dependence: How close are we? CNS Drugs 2009;23:543‑53.
66. Levin FR, Kleber HD. Use of dronabinol for cannabis dependence: Two case reports and review. Am J Addict 2008;17:161‑4.
67. Levin FR, Mariani JJ, Brooks DJ, Pavlicova M, Cheng W, Nunes EV. Dronabinol for the treatment of cannabis dependence: A randomized, double‑blind, placebo‑controlled trial. Drug Alcohol Depend 2011;116:142‑50.
68. Allsop DJ, Lintzeris N, Copeland J, Dunlop A, McGregor IS. Cannabinoid replacement therapy (CRT): Nabiximols (Sativex) as a novel treatment for cannabis withdrawal. Clin Pharmacol Ther 2015;97:571‑4.
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]

Sharma and Kar: Advances in addiction psychopharmacology
International Journal of Nutrition, Pharmacology, Neurological Diseases | October-December 2015 | Vol 5| Issue 4 127
69. Allsop DJ, Copeland J, Lintzeris N, Dunlop AJ, Montebello M, Sadler C, et al. Nabiximols as an agonist replacement therapy during cannabis withdrawal: A randomized clinical trial. JAMA Psychiatry 2014;71:281‑91.
70. Amato L, Minozzi S, Pani PP, Solimini R, Vecchi S, Zuccaro P, et al. Dopamine agonists for the treatment of cocaine dependence. Cochrane Database Syst Rev 2011;CD003352.
71. PaniPP,TroguE,VaccaR,AmatoL,VecchiS,DavoliM.Disulfiramfor the treatment of cocaine dependence. Cochrane Database Syst Rev 2010:CD007024.
72. Kampman KM, Volpicelli JR, Mulvaney F, Alterman AI, Cornish J, Gariti P, et al.Effectivenessofpropranololforcocainedependencetreatment may depend on cocaine withdrawal symptom severity. Drug Alcohol Depend 2002;63:69‑78.
73. Stoops WW, Rush CR. Agonist replacement for stimulant dependence: A review of clinical research. Curr Pharm Des 2013;19:7026‑35.
74. Rezaei F, Emami M, Zahed S, Morabbi MJ, Farahzadi M, Akhondzadeh S. Sustained‑release methylphenidate in methamphetamine dependence treatment: A double‑blind and placebo‑controlled trial. Daru 2015;23:2.
75. Elkashef A, Kahn R, Yu E, Iturriaga E, Li SH, Anderson A, et al. Topiramate for the treatment of methamphetamine addiction: A multi‑center placebo‑controlled trial. Addiction 2012;107:1297‑306.
76. De La Garza R 2nd, Newton TF, Haile CN, Yoon JH, Nerumalla CS, Mahoney JJ 3rd, et al. Rivastigmine reduces “Likely to use methamphetamine” in methamphetamine‑dependent volunteers. Prog Neuropsychopharmacol Biol Psychiatry 2012;37:141‑6.
77. Karila L, Weinstein A, Aubin HJ, Benyamina A, Reynaud M, Batki SL. Pharmacological approaches to methamphetamine dependence: A focused review. Br J Clin Pharmacol 2010;69:578‑92.
78. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine‑type stimulant dependence: An update. Drug Alcohol Rev 2013;32:449‑60.
79. Newman AH, Blaylock BL, Nader MA, Bergman J, Sibley DR, Skolnick P. Medication discovery for addiction: Translating the dopamine D3 receptor hypothesis. Biochem Pharmacol 2012;84:882‑90.
80. PlebaniJG,LynchKG,YuQ,PettinatiHM,O’BrienCP,KampmanKM.Results of an initial clinical trial of varenicline for the treatment of cocaine dependence. Drug Alcohol Depend 2012;121:163‑6.
81. WilliamsJF,StorckM;AmericanAcademyofPediatricsCommitteeonSubstanceAbuse;AmericanAcademyofPediatricsCommitteeon Native American Child Health. Inhalant abuse. Pediatrics 2007;119:1009‑17.
82. NuttD,Lingford‑HughesA.Addiction:Theclinical interface.Br JPharmacol 2008;154:397‑405.
83. ThomsonJS,DonaldC,LewinK.Useofflumazenilinbenzodiazepineoverdose. Emerg Med J 2006;23:162.
84. SaxonL,HjemdahlP,HiltunenAJ,BorgS.Effectsofflumazenilinthetreatment of benzodiazepine withdrawal‑‑a double‑blind pilot study. Psychopharmacology (Berl) 1997;131:153‑60.
85. Hulse G, O’Neil G, Morris N, Bennett K, Norman A, Hood S. Withdrawal and psychological sequelae, and patient satisfaction associatedwithsubcutaneousflumazenilinfusionforthemanagementof benzodiazepine withdrawal: A case series. J Psychopharmacol 2013;27:222‑7.
86. Hillemacher T, Kornhuber J, Bleich S. Neurobiological mechanisms and pharmacological treatment options for alcohol craving. Fortschr Neurol Psychiatr 2007;75:26‑32.
87. KampmanKM,PettinatiHM,LynchKG,SprattK,WierzbickiMR,O’Brien CP. A double‑blind, placebo‑controlled trial of topiramate for the treatment of comorbid cocaine and alcohol dependence. Drug Alcohol Depend 2013;133:94‑9.
88. Arias AJ, Sewell RA. Pharmacogenetically driven treatments for alcoholism: Are we there yet? CNS Drugs 2012;26:461‑76.
89. JohnsonMW,Garcia‑RomeuA,CosimanoMP,GriffithsRR.Pilotstudy of the5‑HT2AR agonist psilocybin in the treatment of tobacco addiction. J Psychopharmacol 2014;28:983‑92.
90. McGregor IS, Bowen MT. Breaking the loop: Oxytocin as a potential treatment for drug addiction. Horm Behav 2012;61:331‑9.
91. Shen XY, Orson FM, Kosten TR. Vaccines against drug abuse. Clin Pharmacol Ther 2012;91:60‑70.
[Downloaded free from http://www.ijnpnd.com on Monday, October 19, 2015, IP: 14.98.24.17]





























