Embed Size (px)
Citation preview

Eur, J. Epidemiol. 0392-2990
December I985, p. 235-256 VoI. 1, No. 4
' S RECENT ADVANCES IN C H L A M Y D I A 7 I R A C H O M A T I ~
S. LAD,ANY and I. SAROV'
Virology Unit Faculty of Health Sciences Ben Gurion University of the Negev POB 653, Beer Sheva 84105 . Israel
Key words: ( ' h lamyd ia t rachomat i s - Plasmid chlamydial 'infections - C. tra- chomat is , diagnosis.
Chlamydia trachomatis is an obligate intracellular energy parasitic bacterium with a genome of 660 X 106 daltons, possessing a plasmid and unique life cycle which includes the differentiation of the infective elementary body to a replicative reticulate body.
C. trachomatis is the etiological agent of trachoma, which affects approximately 500 milli~on people in developing countries. Recently it became evident that in industri.alised Western nations ,certain strains of C. trachomatis are the most common cause of sexually transmitted infections such as non-gonoccocal urethritis, cervicitis, endometritis, sMpingitis and subsequent ectopic pregnancies or infertility, perihepa~it:is, neonatal conjunctivitis and pneumonia, adult conjunctivitis and epididymitis. Since C. trachomatis infections are often asymptomatic, widespread screening of sexually active young people is needed in order to initiate early antibiotic treatment which may prevent serious complications such as ectopic pregnancies and infertility. Development of sensitive and simple techniques for mass screening for detection of C,hlamydia in excreti:ons as well as techniques for detection of specific markers of chronic in~ernal infections (such as Chlamydia specific IgA antibodies) is of great importance.
Classi f icat ion
Chlamydiae are obligate intracel.lular bacte- ria which parasitize the host cell for nutr ients and energy (175). They undergo a complex and unique developmental cycle (6, 108), with two main s t ruc tures : the smaller (300 nm in diameter) e lementary body (EB) which is the infectious particle, and the larger (1000 nm in diameter) reticulate body (RB) which is .engaged in intra- cellular multiplication. For many years Chlamyd ia t rachomat i s has been known as the causative agent o,f t rachoma. More recently, it has been reco,g- nized as a c o m m o n cause of sexually t ransmit ted infections. Already at the onset of the century, Halbers taedter and von Prowazek observed in- clusions of the t rachoma agent in infected conjunc- tival scrapings (68). These authors classified the chl,amydiae as ,, chlamydozoans ,~. Due to their s,ize (the EB being the size of the largest viruses) and to their obligatory intracellular paras,itism,
Corresponding author.
chlamydiae were later classified as viruses (228). Since chlamydiae contain both RNA and DNA, contain r ibosomes (165, 207) and mult iply by binary fission, they were finally recognized as bacteria (reviewed in 175, 228). Because of the unique developmental cycle of chlamidiae, a spe- cial o rder has been ,established consisting of one family - Chlamydiaceae , one genus - Chlamy- dia, and two species - Chlal~ydia t rachomat i s and Chlamydia psi t taci (145, 199). The 'two spe- cies are different,iated on the basis of sulfon- amide susceptibility and of the presence of gly- cogen-containing inclusions that stain with iodi- ne: C. trachol~zatis is suscept.ible to Sulfonamide .and is iodine positive, while C. psi t taci .is Sulfon- amide resistant and iodine negative ,(174)..C. psi t taci comprises a large number of serotypes, with major differences between the mammal ian and the avian types (175). As for C. t rachomat ls , three biovars have been defined: lymphogranu- loma venereum (LGV), t r achoma ( t rachoma, hu-
235
Ladany S. and Sarov I. Eur. J. Epidemiol,
m a n oculogenital infections and all o ther h u m a n isolates except LGV) and mouse pneumoni t i s agent (130). On the basis of the mic ro immuno- f luorescence test C. trachomatis isolates of hu- m a n or igin are classified into 15 serotypes (62), types A, B, Ba and C being associa ted main ly w,ith endemic blinding t r achoma, types D through K main ly wi th sexually t r ansmi t t ed infections, and types L1, L.~ and L3 wi.th LGV.
Life Cycle
Chlamydia l infect ion is ini t iated by the at- t a chmen t of the EB to a host cell, fol lowed by endocytos is (14, 108, 175, 228). The m e c h a n i s m o,f this endocytos is is unclear . Chlamydiae were found, by Byrne and Moulder (20), to enter non- profess ional phagocytes ten to one hundred t imes fas te r than Escherichia coli and polys tyrene la- tex sphers , implying a parasi te-specif ic mecha- nism. Phagocytosis of ch lamydiae was b rough t abou t by the in terac t ion .of hea t labile paras i te surface ligands wi th e lements of the host cell surface. Ward and Murray (229) observed on e lec t ron mic rographs tha t chlamydial ingest ion involved m o v e m e n t of the hos,t cell m e m b r a n e , leading to in ter ior iza t ion in tight, endocytic vac- uoles. Endocytos is was marked ly inhibi ted by inhibi tors of hos t cell mic ro f i l amen t funct ion or of host cell micro tubules , bu t was not i,nhib'ited by inh~ibitors of receptor -media te endocytosis . The au thors concluded tha t the i r findings were consis tent wi th a mic rof i l ament -dependen t zip- per m e c h a n i s m of endocytosis . On the o the r hand, S/5derlund and Kih l s t r6m .(190) found tha t inter- nal izat ion of ch lamydiae into McCoy cells was inhibi ted by inhibi tors of recep tor -media ted endo- Cytosis, and suggested a const i tut ive cellular pro- ces,s such as recep tor -media ted endocytosis .
Throughou t their in t racel lular life, chlamy- diae r emain in :an inclusion fo rmed by the cell m e m b r a n e of the host cell, no phagolysosomal fusion (P-LF) occurr ing (52). In contrast , chla- mydiae ,inactivated by hea t o r neutra l ized by an- t i se rum were shown to be phagoeyt ized al~d to appea r in lysosomes, indicat ing tha t an intrin- sic p r o p e r t y of the chlamydial s t ruc tu re p reven ts the usual host lysosornal response (52). Based on the findings of Levy and Moulder (105) tha t i sola ted EB cell walls of C. psittaci associa ted wi th L cells in essential ly the same m a n n e r as did the intact cells, E issenberg et al (44), applying severM approaches , showed tha t isolated EB .en- velop.es pers i s t in host phagosomes in the ab- sence of P-LF. For example, t r ansmiss ion elec- l r on mic roscopy of mac rophages whose lysoso- mes were m a r k e d wi th fer r i t in revealed the per- s istence o.f individual envelopes in phagosomes devoid of ferri t in, yet EB envelopes hea ted to 56~C for 15 minutes were consis tent ly found ,in
l i ~ l ~ oleni~llao y bealy
W t
Q ~ mflullR
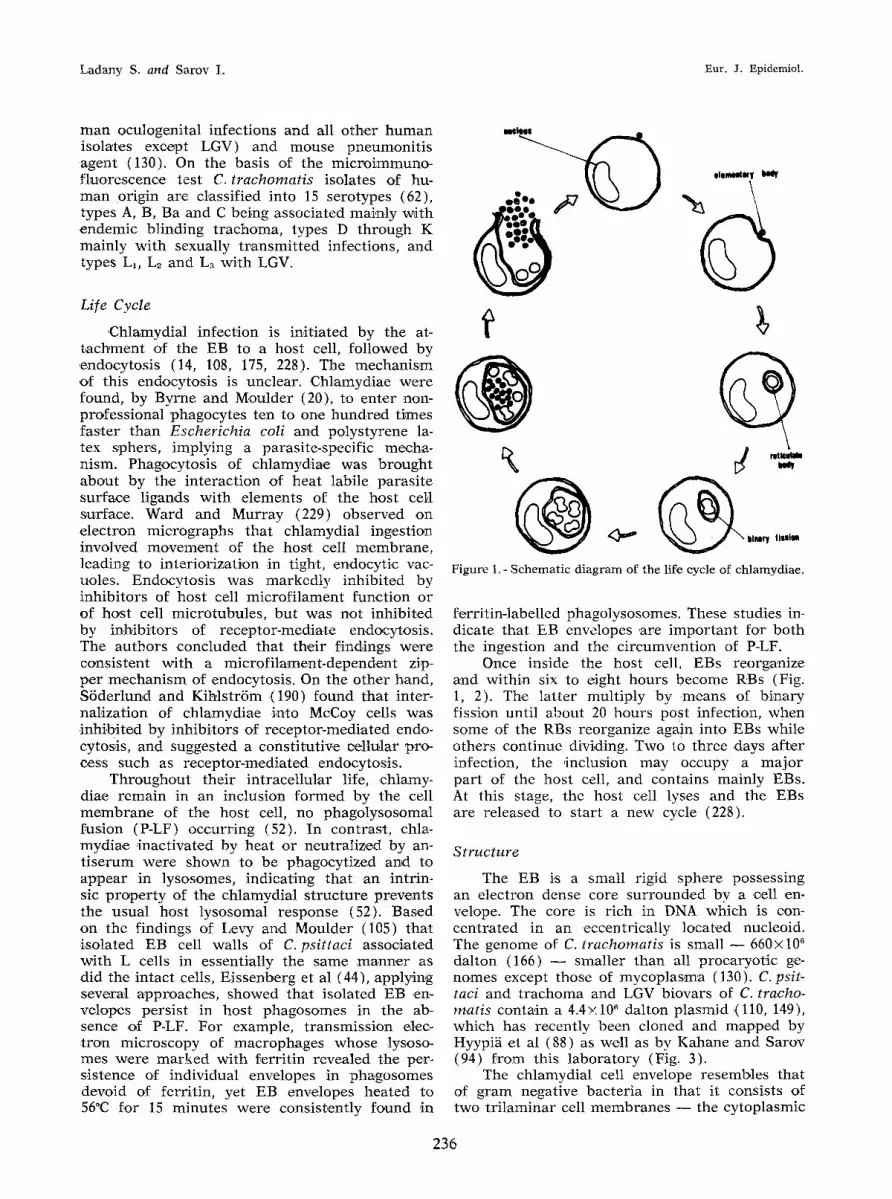
Figure 1.- Schematic diagram of the life cycle of chlamydiae.
f.erritin-labelled phagolysosomes. These studies in- dicate that EB envelopes .are impor t an t for bo th the ingestion and the c i rcumvent ion of P-LF.
Once inside the host cell. EBs reorganize and within six to eight hours become RBs (Fig. 1, 2). The la t ter mul t ip ly by .means of b inary fission until about 20 hours PoSt infection, when some of the RBs reorganize again into EBs while others .continue dividing. Two to three ,days a f te r infection, the inclus'ion may occupy a m a j o r pa r t of the host cell, and contains mainly EBs. At this stage, the host cell lyses and the EBs are released to s tar t a new cycle (228).
Structure
The EB i.s a small rigid sphere possessing an e lect ron dense core su r rounded by a cell en. velope. The core is r ich in DNA which is con- centrat.ed in an eccentr ical ly located nucteoid. The genome of C. trachornatis is small - - 660;(106 dalton (166) - - smal ler than all pro.caryotic g.e- nornes except those o.f mycoplas,ma (130). C. psit- taci .and t r a c h o m a and LGV biovars of C. tracho- matis contain a 4.4>: 106 dal ton p lasmid .(110, 149), which has recent ly been cloned and m a p p e d by Hyypig et al (88) as well as by Kahane and Sarov (94) f rom this labo.ratory (Fig. 3).
The chlamydial cell envelope resembles that of g r am negative bac te r ia in that it consists of two t r i l aminar cell m e m b r a n e s - - the cy toplasmic
236

Vol. i, 1985 Recent advances in Chlamydia trachomatis
Figure 2.- Chlamydia trachomatis L 2 434 (Bu) in MA-104 cells- a) Elementary body enclosed in cytoplasmic pha- gosome, 6 hrs post infection (pi) (X70,000); b) Inclusion body containing several reticulate bodies, 24 hrs (pi) (X20,O00); c) Inclusion body containing many elementary and reticulate bodies, 48 hrs pi (X20,000). (courtesy of E. Manor, Ben Gurion University, Beer Sheva)
m e m b r a n e and the outer m e m b r a n e (210). Un- like g ram negative bacter ia , no pept idoglycan lay- er co,ul,d b,e seen in .electron microgr.aphs be- tween tile inner and .outer membran.es .of chla- mydiae (22), and no significant amoun t of mura- mic acid could be detected (4,55). Nevertheless , the .development of RBs, their convers ion into EBs, and apparen t ly the synthesis of the tlexago-
Ec0R / \
lH,0d \ ]Eco r / '\ ,, \ EcoRI~ /BamHl ,
Figure 3. - Restriction enzyme cleavage map of the native chlamydial plasmid PDCPB cloned in PBR 322. Thin line represents 7.03 kb chlamydial plasmid sequences; broad line represents PBR sequences. (from Kahane and Sarov, reference 94).
nal subuni ts of the cell envelope (see be low) are inhibi ted by penicillin (121, 122). Moreover , chla- mydiae have penicill in binding pro te ins s imi lar to those of bac te r ia (4). Thes,e findings might suggest the presence of a t ,etrapeptide s t ruc tu re s imilar to the cross-linking te t rapept ide side chain of pep t idoglycan molecules. Caldwell e t :al (22) speculated that the chlamydial t e t r apep t ide may be co.valently bound to a protein, r a the r than to a polysacchar ide . Extensive e lec t ron microscopic s tudies of C. ps i t tac i and C. t rachomat i s EBs (34, 63, 109, 119, 190, 122, 198) revealed a complex arch i tec ture of the cell envelope. The inner sur- face of the outer m e m b r a n e is composed of hex- agonally a r r ayed subun,its abou t 17 n m in diam- eter. Chang et al (34) suggested tha t these subuni ts can be considered as the equivalent o.f the bac ter ia l S-layer.
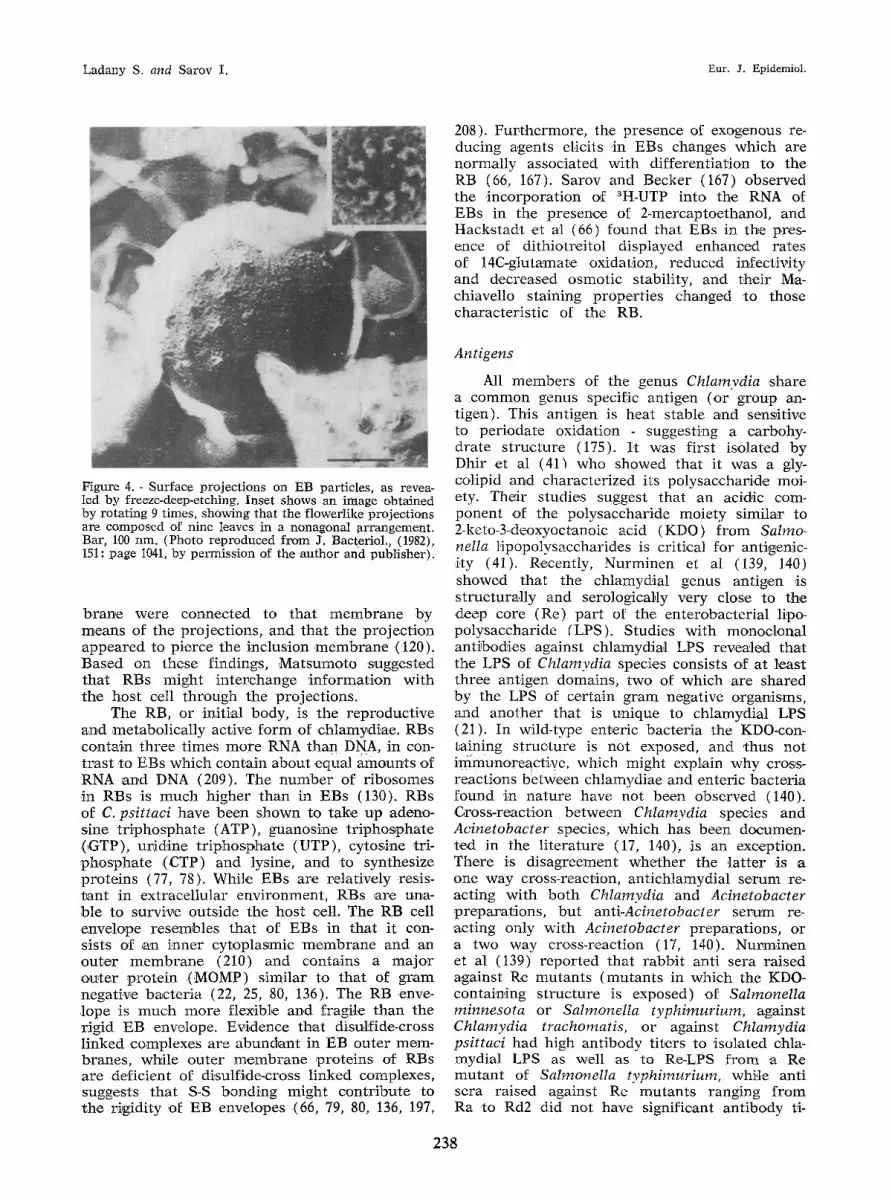
The surface project ions , observed on a sin- gle p a t c h of the EB otlter surface (63, 119, 120), are a s t ruc tu re unique to chlamydiae (,F~g. 4). On the average, there are eighteen pro jec t ions in each patch. The pro jec t ions measu re a b o u t 10 n m in di,ameter, their m a x i m u m length is ap- p rox imate ly 20 rim, and they .are hexagonal ly g rouped wi th a centre to centre spacing of abou t 50 n m ( 1 2 0 ) . One end o'f each p ro jec t ion is connected with the cy toplasmic m e m b r a n e , while the o ther end p ro t rudes th rough a rose t te or flov~erlike s t ruc tu re in the cell wall. Each rose t te is abou t 30 n m ~in diameter , and is composed of ni~ae radial ly a r rayed leaves. The surface pro jec t ions are p resen t in RBs as welt (120). Ma t sumoto observed tha t RBs ad jacent to the inclusion mere-
237
Ladany S. and Sarov I. Eur. J. Epidemiol.
20'8). Fur the rmore , the presence of exogenous re- ducing agents elicits .in EBs changes which are normal ly associa ted with .differentiation to the RB (66, 167). Sarov and Becker (167) .obse rved the incorpora t ion o,f aH-UTP into. the RNA of EBs 'in the p resence of 2-mercaptoethanol , and Hacks t ad t .et al (66) found tha t EBs 'in the p.res- ence of di thiotrei tol displayed enhanced rates o,f 14C-glutamate oxidation, reduced infectivity and decreased osmot ic stability, and their Ma- chiavello staining p roper t i es changed ,to those charac ter i s t ic of the RB.
Figure 4. - Surface projections on EB particles, as revea- led by freeze-deep-etching. Inset shows an image obtained by rotating 9 times, showing that the flowerlike projections are composed of nine leaves in a nonagunal arrangement. Bar, 100 nm. (Photo reproduced from J. Bacteriol., (1982), 151: page 1041, by permission of the author and publisher).
b r ahe were connected to tha t .membrane by means of the project ions , arid tha t the p ro jec t ion appea red to p ierce the inclusion m e m b r a n e .(120). Based on these findings, M a t s u m o t o sugges~e.d tha t RBs might in te rchange in fo rma t ion wi th the host cell th rough the project ions .
The RB, or initial body, is the reproduct ive and metabol ica l ly active f o r m o.f chlamydi,~e. RBs contain t h r e e t imes m o r e RNA than DNA, in .con- t r as t to EBs which contain abou t .equal amoun, ts of RNA and DNA (209). The n u m b e r of r ibosomes in RBs is m u c h higher than in EBs (130). RBs .o,f C. psittaci have been shown to take up ader~o- sine t r i phospha t e (ATP), guanosi,ne t r iphospha te (GTP) , ur id ine t r i phospha te (UTP), cytosine tri- p h o s p h a t e ,(CTP) and lysine, and ,to synthesize pro te ins (77, 78). While EBs are relat ively resis- t an t in ext race l lu lar envi ronment , RBs ,are una- hie to survive outs ide the hos,t cell. The RB cell envelope resembles tha t of EBs in tha t i t con- sists o~f ,an inner cy toplasmic m e m b r a n e and an ou te r m e m b r a n e (210) and contains a m a j o r ou, ter p ro te in .(MOMP) s imilar to tha t of g r am negat ive bac te r i a (22, 25, 80, 136). The RB enve- .lope is m u c h m o r e flexible and fragile than the r igid EB envelope. Evidence tha t disulfide-cross l inked complexes are abundan t in EB outer mem- branes , whi}e ou te r m e m b r a n e p ro te ins of RBs are def ic ient of disulfide.cross l inked complexes, suggests tha t S-S bonding might cont r ibu te to the r igidity of EB envelopes (66, 79, 80, 136, 197,
Antigens
All m e m b e r s of the genus Chiamvdia share a c o m m o n genus specific .antigen (,or g roup an- tigen). This ant igen is heat s table and sensit ive to per ioda te oxidation - suggesting a carbohy- drate s t ruc tu re (175). I t was first isolated by Dhir et al (41) who showed tha t it was a gly- colipid and charac ter ized its polysacchar ide moi- ety. Their studies suggest that ,an acid,ic com- ponent of the polysacchar ide moie ty s imilar to 2-keto-3-deoxyoctanoic acid (KDO) f r o m Salmo- nella f ipopolysacchar ides is criti,cal for anti,genic- ,ity (41). R, ecently, Nurminen et al (139, 140) showed that the chlamydial genus ant igen is s t ruc tura l ly and serologicalcly very close to the deep core (Re) pa r t o.f the en terobac ter ia l lipo- polysacchar ide (LPS). Studies wi th monocl,onal ant ibodies against chlamydiM LPS revealed tha t the LPS of Chlamvdia species consists of at leas~ three antigen domains , two of which are shared by the LPS of cer tain g r am negative organisms, and ano the r that is unique to chlamydial LPS (21). In wild-type enteric bac te r ia the KDO-con- raining s t ruc tu re .is not exposed, and ~hus not immunoreac t ive which might explain why cross- react ions be tween chlamydiae and enteric bac te r ia found in na ture have not been observed (140). ,Gross-reaction b e t w e e n Chlamydia species and Acinetobacter species, which has been documen- ted in the l i te ra ture (17, 140), .is an exception. There is d i sagreement whe the r the l a t t e r is a one way cross-reaction, ant ichlamydia l s e rum re- act ing wi th bo th Chlamydia and Acinetobacter p,reparations, bu t anti-Acinetobacter se rum re- act ing only wi th Acinetobacter prepara t ions , or a two way cross-react ion (17, 140). Nurminen et al (139) r epor t ed tha t rabb i t anti sera ra ised against Re mu tan t s ( m u t a n t s in which the KDO- contain,ing s t ruc ture is exposed) of Salmonella minnesota or Salmonella typhimurium, against Chlamydia trachomatis, or against Chlamydia psittaci had high ant ibody t i lers to isolated ch~a- mydial LPS as well as to Re-LPS f rom ,a Re m u t a n t of Salmonella typhimurium, while anti sera raised against Re mu tan t s ranging f r o m Ra .to Rd2 did not have significant an t ibody ti-
238
Vol. 1, 1985 Recent advances in Chlamydia trachomatis
ters to either chlamydial LPS or the Re-LP~S. These findings were supported by similar data of Caldwell and Hitchcock (21). N urmi~aen et al also found hgh antibody titers against the chla- mydial LPS in sera o,f several patients conva- lescin.g from chtamydial in.fections but not in pooled serum of ten healthy adults (139). Based on their studies, Nurminen et al suggested that Re-LPS from Salmonella species (139) o.r Acine- tobacter LPS (140) could be used as antigen in serological diagnosis of chlamyd,ial infections.
Aside from the LPS-like genus specific anti- gen, ch'lamydiae also have species-subspecies, and s,erotyp,e-specific antigens which are asso- ciat.ed with surface proteins (130). A 155,000 ctalton polypepti.de species speci.f, ic antigen of C. trachomatis was isolated by Caldwell and Kuo (23) from lymphogranuloma venereum strain L2/434/Bu organisms. In studies of select.i.vely radiolab,ell,ed chlamydial surface polypepti,des from several C. trachomatis .serotypes, Salari and Ward (163) identified a 155,000 dalton polypeptide which is probably ident,icai with the 155,000 ,dal- ton s,pecies specific antigen described by CMd- well and Kuo. Salari and Ward also isolated a 118,000 d.alton surface polypeptide, unique to lymphogranuloma venereum strains, and a 29,000 dalton polypeptide which might be :identical to the type-specific ant,i,~en of 30,000 dattons puri- fied by Hourihan et al (.86). The presence of a 60,000 dalton and a 62,000 ,d,alton protein in all 15 laboratory serotype reference strains of C. tra- chomatis was reported by Newhall .et al (135). Antibodies against these proteins were detected in the sera of nearly all culture-positive patients but only rarely in apparently uninfected patients. Catdwell et al (22), applying sodium dodecyl sul- fate-polyacrylamide gel electrophoresis (SD,S- PA- GE) on extrinsically radio-.iodinated whole-cell lys,ates of Chlamydia, identified a 39,500 dalton major auger membrane protein (MOMP) from EBs o,f C. trachomatis serotypes C, E and L> Chla- mydial major envelope proteins of molecular weights ranging from 38,000 daltons to 43,000 dalt.ons were described by other authors as well (e.g. 80, 163). Salari and Ward found that the molecular weight of their polypeptide depended on the serotype. The major polypep,tides isola- ted from serotypes A, B and C, from serotypes D, E, F, G, I and L~, and from types L, and L~ had molecular weights of 39,500 daltons, 38,000 daltons and 42,000 daltons respectively (163). More recently, the MOMP of chlamydial EBs was identified in dimer, tr imer and other mu,lt.inaeric forms which were stabilized by disulfide media- t.ed cross linking (136). Most of the MOMP of RBs was found to be present in envelopes as monomers (79).
Antigen analysis, using antibodies raised in rabbits against isolated chlamydiM polypep~i,des
or murine monoclonal antibodies against C. tra- chomatis, demonstrated that the MOMP of C. trachomatis contains species, subspecies, and perhaps type-specific antigenic domains (25, 196). Fluorescein-labelled monoc,lonal antibodies, which recognize the MOMPs of all 15 serotypes o.f C. trachomatis but do not cross-react with C. psit- taci, have been used to diagnose C. trachomatis infections (137, 206). Purified MOMP has been utilized as antigen for sere.diagnosis of chlamy- di,al pneumonia in infants by enzyme immune- assay (153). However, in an analysis o{ human serological responses to proteins of C. tracho- matis by an immunoelectrophoretic trans,fer meth- od, N.ewhall et al (135) found that the MOMP bound antibodies from all the human s,era tes- ted, regardless of evidence of in, fect'ion. A pos- sib,le explanation of this discrepancy .could be that Newhall's method detects a non-specific epi- tope, which is not exposed in the ,other tech- niques.
The importance of the MOMP in the irffec- tious process was indicated by Ca'ldwell and Perry (24) who showed that the infectivity of C. trachomatis can be neutralized in vitro with angibodies to the MOMP.
CHLAMYDIAL INFECTIONS
LymphogranuIoma venereum or LGV (re- viewed in 65, 174, 180, 217) is a sexually transmitted disease of worldwide distribution. It is most prevalent in tropical and subtropical areas of Africa and Asia (65) and relatively uncommon in industrialized countries. It is li]~ely, though, that in developing and in industrialized countries LGV is both under-reported and mis-diagnosed (180, 216). The causative agent of LGV is more invasive than other strains, and has an affinity for lymphoid tissues rather than for .epithelial cells of mucous membranes (62, 55, 174). The incubation period .is usually three to thirty days (180). The characteristic clinical picture consists .of three stages. During the first stage, a transient .and often imperceptible genital lesion occurs. In the second stage, lymphadenopathy (bub:o) develops, and the thi,rd stage may invo'lve ,late destructive lesions of the lower gastrointestinal tract and other organ systems (143, 174, 180).
Trachoma (reviewed .in 38, 65, 143, 174), one of the most ancient diseases of man, is still a major public health problem in developing corm.tries, particularly in Africa and Asia (38). It is esti- mated that approximately 500 million people are affect,ed by trachoma, with at least two million blind and a much larger number suffering par- tial loss of vision (33). As mentioned before, Halberstaedter and van Prowazek were the first
239

Ladany S. and Sarov I. Eur. J. Epidemiol.
to associate Chtamydia with t r a c h o m a (68). Tra- c h o m a is a chronic kera toconjunct iv i t i s charac- ter ized by follicles and scarr ing o,f the pa lpebra l eonjunct iva, as well .as pannus , kerat i t i s and Scarring of the co rnea (38). The pathogenesis of bl inding t r a c h o m a is dependent upon the in- te rac t ion .or the combined effects of C. tracho- mat is infect ion and secondary bac ter ia l patho- gens (175). Endemic t r a c h o m a is associ,ated wi,th a low s t anda rd of living and low sociohygienic levels (143). T ransmiss ion is frown pe r son to person, and in endemic areas whote famil ies ~re ~ffect,ed (174). The ra te of infect ion is espe- cially high among chil,dren. Active infect ion dis- appea r s usual ly by the age of ten to fifteen, but visual loss may occur 15 to 20 or more years la ter (174).
OCULOGENITAL INFECTIONS
Mate genital infect ions
(Reviewed 'in 56, 61, 65, 141-143, 176, 192,211,216) Genital t r ac t infect ions in men were f irst
l inked to ChIamydia by Lindner, who found typical ch lamydia l inclusions in u re th ra l epithelial cells of men wi th ~ongonococcal ure thr i f i s ( 143 ).
Nongonococcal urethri t is (NGU) is a very c o m m o n f o r m of urethriti .s in men. According to an e s t ima te of the ~, Centers for Disease Con- t rol ,>, NGU occurs in the USA twice as of ten as gonococcal u re thr i t i s (216). In o ther wes te rn in- dlastrialized countr ies the incidence of NGU ~s high ,as well (142). C. trachomatis is t,h,e m a j o r i~denfifiable cause of NGU. I t ca, n be isola ted f r o m approx ima te ly 30-50% of NGU pat ients , f r o m 20-30% of gonor rhoea pat ients , bu,t f r o m only 0-7% of heal thy controls (60, 65, 90, 174, 183, 216). Fu r the rmore , C. trachomatis has been isola ted f rom 60% of female sex pa r t ne r s of men wi th ch lamydia l NGU, but in only 10% o,f part- ners wi th non.chlamyd,ial NGU (142). Ureapla- sma urealy t icum has been suggested as ,a caus- at ive ,agent of nonchlamydia l NGU (142, 174). The incubat ion per iod of NGU is cons idered ,to be one ,t.o th ree weeks, bu t symptomles s infect ions m a y occur .(142). S y m p t o m s include var$ous de- grees .of dysur ia and /or u re th ra l discharge, ur- gency o r f requency of ur inat ion, mea ta l or ure- th ra l i r r i t a t ion (50). Clear clinical differentia- t ion be tween gonococcal ure thr i t i s and NGU is .probably not poss ible (175), nor is clinical di,f- fe rent ia t ion be tween ch tamydia l and nonchlamy- dia l NGU (142, 183).
Postgonococcal urethri t is (PGU) is defined as pe rs i s ten t u re th ra l infect ion in pat ients wi th negat ive cul tures for Neisseria gonorrhoeae, fol- lowing t r e a t m e n t of .gonococcal urethr i t i s . I t is
believed to be a resul t of mixed infect io~s of Neisseria gonorrhoeae and one or more agents of NGU the t r ea tmen t of which has been ,effec- tive against Neisseria gonorrhoeae, but not against the o ther agent (142). In var ious studies, C. tra- chomatis has been recovered f r o m .about 40-80% of PGU pat ients (60, 90, 216).
Epididymit is . - Acute epididymit is is one of the compl ica t ions of NGU, occurr ing in up to 3% of NGU pat ients (73, 96). I t is a serious com- pl icat ion which m a y lead to infertili ty. C. tra- chomatis is a m a j o r cause of epididymit is in men unde r 35 years of age (10, 182). The etiologic role of C. trachomatis has been ,demonstra ted by isolat ion of the mic robe f rom epi,didymal ,aspi- ra te (10, 182).
Prostatitis. - According to Paavonen (143), pros ta t i t i s m a y accompany NGU in up to 20% of pat ients . Prosta t i t i s is, however , not well de- f ined (143, 216) and the etiologic role o,f C. tra- chomatis in its var ious fo rms ,(acute, chronic bacter ia l and chronic abacter ia l ) has not been fully es tabl ished (100, 116, 142, 201, 216). Evi- dence against an etiologic role of C. trachomatis in pros ta t i t i s was p resen ted by MSrdh et al (116) who isola ted C. trachomatis f r o m the u r e th r a of only one 53 pat ients wi th non acute pros- tati t is and f rom none of 28 specimens of pro,s- tatic fluid f rom the same patients. Serological evidence of chlamydial infect ion was found in seven pat ients , bu t the present ing s y m p t o m s of these pat ients suggested NGU ra the r than pros- tariffs. There are o ther studies which s.uggest the C: trachomatis may be a 6ausative agent of p ros t a t i t i s . For example , Krauss et al (100) iso- lated C. trachomatis as sole agent .from ure th ra l swabs af ter pros ta t ic massage in 43 (18.5%) of 233 pa t ien ts wi th non acute prostat i t is , and in 5 (7.7%) of 65 control pe r sons ; chlamydial IgA :antibodies were found by Suominen et al (201) in the semen of 51.5% of inferti le m e n having a s y m p t o m a t i c chronic pros ta t i t i s as c o m p a r e d to 23.2% ( p < 0 . 0 1 ) o f ferti le men and 26.9% (p<0.05) of in~ertil,e men wi thout signs of chronic pros- tatitis. The fat ter s tudy indicates tha t C. tracho- marls m a y inter fere wi th fert i l i ty in men.
Female genital infections
(Reviewed in 45, 65, 72, 141, 1.43, 174, 176, 204, 211, 216, 232, 233)
Cervicitis is the mos t c o m m o n chlamydi'al int~ection of the female genital t rac t (33). The f irst isolation of C. trachomatis f rom the ~fe- male genital t rac t was f rom the cervix of a m o t h e r of a newborn infant suffer ing f rom .inclusion conjunct ivi t is (91). S.ince then, C. trachomatis has been isolated f r o m the cervix of cervieifis pa-
240
Vol. l, 1985 Recent advances in Chlamydia trachomatis
tients in many laboratories. In various studies the isolation rate of C. trachomatis f r om women with mucopuru len t en,doceraricitis ranged between 34% and 63%, as c.ompared to 3-5% f rom unselect- ed non pregnant women (204). C. trachomatis could also be isolated f rom exper imental chlamy- dial .infections of the cervix in animals ('89). In biopsy speci,mens f rom the cervix of women wi.th cervi.citis, intracel lular chlamydiM inclusions can be identif ied by light and electron microscopy (232). The prevalence of chlamydial cervicitis var- ies in different populat ions, and there are high risk g r o u p s . T h u s in women atten.d,ing veneral dis- ease cl.inics, the isolation rates of C. trachomatis f rom the .cervix have ranged between 12% and 37% (232).
Relatively high frequencies of C. trachomat is cervical infection have been found in female adolescents 8-10% ,in non pregnant (51, 58) and 37% in pregnant (7 l ) adolescents. ,Cervici,tis is often symptomless (141, 143, 176). Thus Oriel (141) repor ted that 63% of chlamydia] eervicitis pat ients in his depar tment , a t tended for con- tact tracing action ra ther than for investigation of symptoms. The commones t symptom of chla- mydial ce.rvicitis is vaginal discharge (141). Other symptoms are dysuria, u r inary frequency, and dull pelvic pain (72, 141, 232).
The major dangers of chlamydial cervici,t~is are : a) the agent is f requentIy t ransmi t ted to male contacts and to the newborn, and b) the infection might :spread to the fallopian tube and cause salpingitis and subsequent infertit.i'ty (176, 216). Diagnosis of chlamydial .cervicitis, bo th clinicMly apparen t as well as asymptomatic , and appropr ia te t rea tment , .are therefore 'of great importance.
Endometr i t i s . - Recent studies indicate tha t endometr i t i s may be caused by Chlamydia. G u n ~ et al (64) cul tured C. trachornatis f rom endo- metriaI tissne of a woman with non-puerperal endometr i t i s , whose cervical cul ture was nega- tive and whose serum IgG and IgM t}ters to C. trachomatis were elevated. Miirdh et al (115) and Sweet et al (204) isolated C. trachomatis f rom the endomet r ium of women who had symp- toms of salpingitis. It was sug, gested that C. t rachomatis ascends f rom the cervix and spreads through the endomet r ium to the fallopian tubes (115).
Salpingitis. - Recent investigations have bean centered on the role of C. trachomatis in acute and ,chro,ni,c salpir~gitis which mLght lead to in- fertility. C. trachornatis was isolated f rom fal- lopian tube specimens of pat ients with acute salpingitis by Eilard et .al in 1976 (43), and short ly a f te rwards by M~rdh et al .(117). Moller et a'l (125) produced acute salpingitis in grivet monkeys by inoculation of a C. t rachomat is strMn isolated f rom the fMtopian tubes of a pafie~at
with acute salpingitis. During the ,course of the infecti,on the animals responded with a s,i,gnif- icant increase in serum IgG and IgM antibodies to C. trachomatis. Mgrdh et al (114) found that chlamydial ant ibody t.iters in paired sera f rom 60 consecutive patients with a.cu,te salpingiti,s cor- related with the severity of the tubal inflamma- tion (as shown by laparoscopy) and the dura- tion of the lower abdominal pain before atten- dance. In this study, evidence was brought , by cul ture and/or serological tests, that acute sal- pingitis .in Lund, Sweden, is associated with con- cur ren t genital chlamydial infection in 58% .of pat~ients, whereas gonococcal in.fection and My. coplasma hominis occur in 8% and 12% res.pec- tively. In two serological studies in the United States, a significant rise in IgG and/or IgM anti- bodies against C. tracho.matis was demons t ra ted in 20-23% of cases of acute salpingit,is (46, 203).
The prevalence rate of C. trachornatis serum IgG ( t i t e r >--64) and IgA ( t i ter ~16) antibodies, as de termined in this labora tory by a singte ,an- tigen (Lx) indirect immunoperoxidase assay (Ipa- zyme Cblamydia, Saw'on Diagnostics Ltd., Beer Sheva), was significantly higher in salpingitis pat ients (67% for IgG and 37% for IgA) than in controls (23% for IgG and 4% for !gA) ; the prev- alence rate o.f elevated C. trachomatis serum IgG (__>128) and IgA (->32) ant ibody ti ters was also significantly higher in the salpingitis pa- tients (57% for IgG and 20°,5 for IgA) than in controls (8% for IgG and 2% for IgA) (I51).
Of par t icu lar interest is the presence of chla- mydia IgA antibodies in serum of 4°,5 of arppar- ent ty healthy women. Are these women suffer- ing f rom a silent (subclinical) active chlamydial infection? Salpingi'tis may be caused by a va,riety of organisms, such as Neisseria gonorrhoeae, C. tracho~natis and Mycoptasma horninis, the rel- ative impor tance of which seems to vary in d~i,f- ferent populat ions (204, 233).
A s tudy by Westergaard et al (231) indicates that the presence of C. trachomatis in the cer- vical canal in asymptomat ic women at the t ime of induced abor t ion increases the risk of po.st- abortal salpingitis. This was suppor ted by the observat ion of Moiler et al (124) that adminis- t rat ion of antibiotics effective against ChIamydia to C. trachomatis positive women pr io r m the operat ion, reduced the f requency of salpingitis significantly. Some epidemiologic studies .indi- cated that the use of in t rauter ine contracept ive devices increases (47, 56, 184) and the use o.f oral contracept ives decreases (184) the risk of contract ing salpingitis. Fur thermore , in a s tudy of 546 women with a first episode of salpingitis, .the degree of inf lammation of the fallopian tubes, .as seen during laparoscopy, was much mild- er in oraI contracept ive users than in non-users (202).
241

Ladany S. and Sarov I. Eur. J. Epidemiol.
In a recent article Washington et al (230) stress tha t a l though there is an apparen t effect of oral contraceptives against gonococcal and markedly symptomat ic pelvic in f lammatory di- sease (PID), this should not be generalized to all forms of PID. According to these authors , oral contracept ives may in fact increase the in- cidence of chlamydial PID.
Acute perihepati t is is ,an . inflammatory reac- tion of the liver capsule and the per i toneum of the abdominal wall adjacent to the liver (113). The disease is usually associated with acute ,sal- pingitis and re fe r red to as the Curtis-Fitz-Hugh syndrome. In 1980, Wolmer-H,anssen et al (236) repor ted three cases of laparosco~ically verified perihepat i t is with cul tural ( f rom the cervix) a n d / o r serological evidence of C. trachoma- tis infection. Since then, several o ther cul tura l and serological studies have indicated ,that C. trachoma- tis is f requent ly associated with acute perihepa- t'itis (13, 113). C. trachomatis has also been iso- lated ,from the liver capsule (237) and f rom perito- neal fluid (103) in perihepati t is .
Consequences of female genital infections
Inferti l i ty. - Evidence that chlamydial salpin- gitis can cause infert i l i ty comes f rom second-look laparoscopies about six months af ter 1,aparoscopi- cally verif ied and proven .chlamydial ,salpingitis. The second laparoscopy revealed closed faltopia~a tubes i'n two of eleven cases (238). Moreover, Hen- ry-Suchet et al (82) have shown that C. tracho- matis could be isolated f rom a significant per- centage of abdominal cultures in women wi th no clinical evidence o f PID, suffering f rom me- chan,ical steril i ty due to tubal obs t ruct ion or adhesions, suggesting that C. trachomatis causes silent salpingitis which results in i,nfertil~ty. In a recent study, we have fo~and that only 10% of inferti le women with abnormal hysterosalpin- gography recalled having s'alpingitis - i n d i c a t i n g that most infections were asymptomat ic (171). A correla t ion between the presence of anti- bodies ,to C. trachomatis and mechanical ,in,fertilily was found in various serological studies (35, 56, 92, 126, 128, 152, 171).
Ef fec t on pregnancy outcome. - In a prospec- tive s tudy o,f morbid i ty associated with C. tra- chomat is infections during pregnancy, Mart in et al (118) have shown that for women with ante- pa r tum chlamydial infection the mean d~rat ion of gestat ion was significantly shor te r than for noninfected women, and sti l lbirth or neonatal death occurred in 66% of infected women com- pared with 3.4% of the control group. However, the number of pat ients in this s tudy was small, o ther Lpossible infectious causes of p rematur i ty or perinatal morta l i ty were not sought, and
pathological studies were incomplete. Several o ther studies (71, 75, 214) did not indicate that cervical chlamydial infection alone ,had an adverse ,effect on pregnancy outcome. However, one of the studies (75) suggests that IgM-seroposit:ive C. tra- chomat i s4nfec ted women may be at " increased risk for a low-birth-weight infant and p rema tu re rup ture of membranes .
,Cervical neoplasia. - Several recent studies suggest an association between cervical chlamy- dial infection and cervical neoplasia. C. tracho- marls was isolated significantly more f requent ly f rom cervices of women with cervical intraepi- thelial neoplasia and invasive cervical cancer than f rom cervices of control subjects (72). Cervical intraepithelial neoplasia was more c o m m o n in chlamydial than in non-chlamydial cervieitis (144) and ,in women who were seroposit ive than in women who were seronegative .for antibodies to C. trachomatis (28). In cervical secret~ions, lo- cal IgA antibodies to C. trachomatis were found in 100% of pat ients with invasive cervical cancer, 61% of pat ients with .cervical intraepithelial neo- plasia, 39% of pat ients with cervicitis and 12% of controls (95). Significantly, higher serum an- t ibody t i ters to C. trachomatis were found in women with cervical neop.lasia than ,in control subjects (72). A s t ronger association with cer- vical neoplasia for serum chlamydial antibodies than for Herpes s implex virus type 2 anti,bodies was found (178). There are several repor ts on ~improvement of premal ignant cervical abno~mal- i,ties, following tetracycline t rea tment (72).
Neonatal infections (Reviewed ii{ 1, 8, 9, 84, 174, 215)
It has been es t imated that f rom 25% to 70% of mothers with chlamydial cervioitis t r ansmi t the infect ion to their infants (32, 54, 70, 81, 204, 215). Thus the incidence of .neonatal chlamydial infect ion is a funct ion of the prevalence of chla- mydial cervicitis among pregnant women. The la t ter has ranged, in various studies, f rom 2% to 30% (204), the higher rates prevail ing .among lower socio-economic groups. Eighteen to 50% of exposed infants develop conjunctivitis, 15%-20% devel,op nasopharyngeal infection, and 3%-18% develop pneumonia (1). Vaginal and recta l in- fect.ions have been documented as wetl, and there is suggestive evidence that chlamydiae are prob- ably responsible for some cases of bronchiolit is , early recur ren t otitis media and gast.roenteritis ( 176, 181 ).
Inclusion conjunct iv i t is of the newborn ( ICN ) or inclusion b lennor rhea is a mucopuru len t con- junctivit is which develops 5 to 14 days af te r b i r th (174). Untreated, it usually lasts several weeks, wi thout compromising sight, bu t some
242

gol. I, 1983 Recent advances in Chlamydia trachomatis
infants develope micropannus and conjunctivi t is scarring (84, 176). Already in 1909, Halberstaed- ter .and von Prowazek found in t racytoplasmic !n.clusions, similar to those produced by t rachoma, in conju,nctival scrapings of infants with non- gonococcal conjunctivi t is and in scrapings ,from the ure thra l orifice of their mothers (69). These in- vestigators also showed that genital secretions f rom a mo the r of an infant with ICN caused a similar disease when inoculated into a baboon or monkey (1). That neonatal infect ion is usually re la ted to passage through an infected b i r th canal {174) has since been conf i rmed 'in many epidemiologieal studies in which no infect ion of infants f rom seronegati,ve mothers has been re- por ted (1) ; infect ion i.n infants delivered by caesarean section was very rare (1, 57, 101), and chtamydial diseases developed in infants during the first four months of life (1, 84).
Chlamydial pneumonia is a very common pneumonia in infants (204). The usual age of onset ranges f rom two weeks to 4 months (176) and 'is p receded by ICN i:n half of the cases (204). That C. trachomatis can cause pneumonia in neo- nates ,exposed during passage through an infec- ted b i r th canal was first suggested in 1975 by Schach te r et al (179). These au thors observed an :infant born to a mothe r with chl.amydial cervicitis. The infant developed ICN, and while on topical chemotherapy for I.CN, .developed pneu- monia. Chlamydiae were recovered f rom .his spu- tum at a t ime when conjunctival specimens were sterile. In 1977, Beem and Saxon (7) demon- strat.ed a,n association between C. trachomatis and a distinctive pneumonia syndrome in in,fants. The pneumonia was character ized by a chronic afe- brile course, diffuse lung involvement, elevated serum ~i,mmunogl.obulins G and M, tachypnea and a distinctive staccato cough. Nasopharyngeal C. trachomatis was found in 18 of 20 infants with the ,pneumonia syndrome, and t i ters of IgG anti- bodies to C. trachomatis were si,gni, f.icant.ly ele- vated in all of them. A~e .rut diagnosis was typ- ically 6 weeks. The etiology of C. trachomatis .in this syndrome was la ter conf i rmed by isola- tion ,of Chlamvdia f rom lung biopsies =of infants with chlamydi'aI pneumonia (3, 53), thorough se- rological evidence (153, 177, 220), in epidemic- logic stud.ies (54, 70, 76), and in studies of .animal models (74). Isolat ion of C. trachomatis f rom the nasopharynx is not sufficient to establish chla- mydial .etiology in infant pneumonia since there are many cases of nasopharyngeal in~fection with ,C. trachomatis without involvemen.t of the lower respi 'ratory t ract ( l , 84). Detect,ion of specific I,gM ,antibodies to C. trachomatis may be the method of choice in diagnosing chlamydial pneu- monia in infants (177). '
Adult chlamydial ophthalmia (paratrachoma)
( reviewed in 159, 223)
Adult chlamydial ophthalmia is generally caused by C. trachomatis serovars D through K and usually results f rom acc.iden,tal t ransfer of infec- ted genital discharge to the eye, but a few cases of eye :to eye t ransmiss ion have been descri,bed (223). The venereal na ture of chlamydiat ,eye di- sease was demonst,rated by Ronners tam et al (160), who observed a much higher f requency o,f genital chlamydial infection among patients with chl~my- dim ,eye infection, than in the average popu,lation. The most common form of adult chlamydial oph- thalm=ia is inclusion conjunctivit is , which presents as an acute or chronic follicular conju,r~cti,vitis (223). Recently, Wishart et al (234) found cul tural an.d/or serological evidence for C. trachomatis ~n- fection in 9% of 140 consecut ive acute conjuncti- vitis patients, Infect ion caused by herpes simplex virus and by adenovirus were diagnosed in 21% and 8% respectively. The authors stress the impor- tance of labo,ra~ory differential diagnosis of acute .conjunctivitis which enabled correct management for the diagnosed patients and discharge of pa- tients in whom C. trachomatis, adenovirus a.n,d herpes simplex virus were excluded as possible causes of infection.
Respiratory tract infection in adulls
C. trachomatis has been known since 1977 (7) to cause pneumonia in infants born to cervi- ral ly infected mothers . Over the last 5 years, evi- dence has been accumulated that it is also asso- ciated with pharyngit is (98), pneumonia (99, 200, 205) and exacerbat ion of chronic bronchi t is ,(205) in adults. C. trachomatis has also been isolated f rom the lower respi ra tory t rac t of pat ients wi th a wide spec t rum of resp i ra tory infections (205). One s tudy of pat ients with atypical pnet~monias of unclear etiology showed tha t between 21% and 32% had serological evidence of C. trachomatis infection (99). Recently, mediast inal lymphadeni- tis as well as pneumonia were repor ted in labora- tory staff who were in contact with L~ or L2 sero- var of C. trachomatis (11). In a recent s tudy in our la~boratory (146) four cases of lower .respira- tory infection caused by C. trachomatis were ob- served. Three of them had clin.i,cal and radio- logical findings of atypical pneumonia , while one had an acute exacerbat ion .o.f chronic .obstructive pu lmonary disease. No.ne of the patients had signs .of .ocular or genitourina,ry infections. All pa- t,ients had specific IgM, IgA and IgG antibodies to C. trachomatis during the acute infection, and were seronegative for C. psittaci. No speci,fic clini- cal or radiological pat terns were found. Two o.f the patients with pneumonia were labora tory staff who
243

Ladany S. and Sarov I. Eur. I. Epidemiol,
were e~posed to L2 (434 Bu) s erovar of C. tracho- matis.
The source o,f t ransmiss ion in adult pat ients is speculative, and passage f rom the eyes to ~he uppe r respi, r a to ry t rac t via drainage, orogenital sexual pract ices (98, 99) and inhalat ion .of aero- solised organisms (11) have been suggested. Data collected uet i l now shows no characteris.fi,c clin- ical pa t t e rn of C. trachomatis resp~irato.ry infec- tions. One study also shows great variabili ty in radiological features, a l though a character is t ic pa t t e rn of s treaky mult i lobar infi l t rates is de- scribed <42).
Other chlamydial iniections
Results of serological studies point towards an association between C. trachomatis and ,, sex- ually acquired reactive ar thr i t is ,, ( S A R A ) i n c l - uding R, eiter 's syndrome. The presence of ant,i- chlamydial antibodies was significantly more fre- quent and the mean ti ters were si,gr~ificantly higher in SARA patients than in rheumat ic and heal thy controls (2, 97, 240). Chlamydiae were recovered f rom 35% o,f SARA pat ients ; this iso- lation ra te is similar to that f rom men wi th NGU (2, 97). C. trachomatis may also be involved in barth.olinitis and urethr i t i s in the female (72, 141, 204), proct i t is (132), ankylosing spondylit is (40), endocardi t is (222), myocardi t i s (157), m,e- ningoencephali t is (133), chronic liver disease with ascites (185), mult iple sclerosis (148) an, d diar- rhea ,(19).
Epidemiology of chlamydial infection in children
Whi}e the horizontal sexual t ransmiss ion and the vert ical per inata l t ransmiss ion of C. tracho- matis are well established, little is known about the .epidemiology of chlamydial infectio~ns in ,child- hood. In several serologic stu&i,es of children f rom infants to 15 years of age, a progressive increase in the prevalence of serum ant ibodies to C. trachomatis has been observed (12, 138, 164). The clinical s,ignificance of this age re- ~ated r ise in seroposit ivi ty as well as the routes of t ransmiss ion of C. trachoma~is in chfl.dlmod are unknown. Recently, Ringel et al (157) report- ed serological evidence for C. trachomatis myo- cardit is in a 9 year old girl. Burney ,et al (18) de te rmined antibodies against C. trachomatis as well as antibodies against an atypical chlamydial agent (IOL-207). In this study, evidence o,f infec- t ion with C. trachornatis was confined to chil- d ren under the age of seven years. In contrast , infect ion with ChIamydia IOL-207 was rare be- fore the age of five years and thereaf te r became increasingly common wi th increasing age. The authors suggest that .the mode of t ransmiss ion of the two ,agents is different and that ChIamydia
IOL-207 may be t ransmi t ted at school. Thus the progressive increase in seroposit ivi ty to C. tracho- matis dur ing childhood, observed by o ther au- thors may ,perhaps be due to cross react ion with Chlamydia IOL-207.
TREATMENT
Trea tment of chlamydial infections is revie- wed in several recent articles (15, 16), and the Centers fo r Disease Control have i.ssued treat- ment guidelines for sexually t ransmi t ted ,diseases, including C. trachomatis infections (27). The tetra- cyclines are usually the drugs of choice 5or chla- ,mydial infections. Ery th romyc in is r ecommended for p regnant women, infants, young chi ldren .and other pat ients in whom tetracyclines are co~tra- ir~dicated or not tolerated. Since ,it takes 48 to 72 hours for chlamydia to complete a ,cycle of infect ion, and since mos t ant imicrobials do not pene t ra te cells well, mult iple dose regimens are required (15). In uncompl ica ted gen~ital in~ections at least 7 days of t r ea tmen t are recommended. The t rea tment per iod should be extended ,to 10 days for epididymitis and salpingitis and to two to three weeks for neonatal infections. Topical ther- apy for neonatal inclusion conjunct ivi t is is not re- liable, and systemic therapy is needed (15). As C. trachomatis commonly occurs s imultaneously with gonococcal infections, pat ients harbour ing N. go- norrhoeae should be tested for the presence of C. trachomatis infect ion :and given appropr ia te treat- ment (27, 36, 191).
LABORATORY DIAGNOSIS
OF CHLAMYDIAL INFECTIONS
(Reviewed in 49, 143, 158, 174, 220)
Three methods are applied in the labora tory d~agnosis of chlamydial infect ions: direct demon- s t ra t ion .of chlamydiae in clinical specitmens, iso- lat ion o,f chlamydiae in cell culture, and serology, each baying its advantages :and pitfalls, and none being applicable to all chlamydial i,n.fections.
Direct demonstrat ion in clinical specimens. - Prior to the development of cell cul ture tech- niques for .isolation of chlamydiae, the demo.nstra- t ion of chlamydial inclusions in conjunctival scrapings or genital t rac t specimens was the only me thod available for the .diagnosis of chlamy- dial :infections (174). The th ree most commonly used st,aining techniques were Giemsa, iodSne and f luorescent antibody. Giemsa staining was tra- diction.ally the me thod of choice for conjunctival scrapings; f luorescent ant ibody staining is the most sensitive; and iodine stainiaag (which de- t,ects only C. trachomatis and not C. psittaci in-
244

Vol. 1, 198~ Recent advances in Chlatnydia trachomaus
clusions) the least sensitive p rocedure ,(158). Despite its relatively low sensitivity, C*iemsa is still useful in areas of byperendemic t rachoma ( 158, 174).
Isolation. - Since chlamydiae are intracellular parasites, *heir isolation requires cell cul ture tech- niques. Gordon and Quan (59) were the first to describe a cell cul ture technique for the rout ine iso- lation of C. trachomatis f rom clinical specimens, and the principles of their method are the basis of isolation procedures developed since (39, 49, 158). Many cell lines are susceptible to infection with chlamydiae, those most widely used are McCoy, HeLa 229 and BHK-21 (158). In order to reduce competi t ion with the parasite, host cell m.onolayers are e i ther i r radia ted or treat- ed with an ant imetabol i te such as 5-iodo-2-deoxyu- ridine .or cycloheximide (39).
Sampling, t r anspor t and storage of speci- mens must be pe r fo rmed with great care in .or- der to obtain optimal results. The involved ana- tomic site mus t be appropr ia te ly sampled, cul- ture of discharges is inadequate, and .an adequate sample of epithelial cells must be obta ined ,(204).
Isolat ion of C. trachornatis serotypes A th.ro~agh K requires centr i fugat ion of the clinical specimen onto the monolayer (49, 59). Following an .incu- bation period of 24-72 hours, monol.ayers are stained and examined under the microscope for the presence of inclusions. Iodine, Gi.emsa ,and im- munof luorescence are most commonly used for staining (158).
Mohammed and Hillary (123) recent ly used toluidine blue staining to detect C. trachomatis inclusions in cul tures f rom ctinical specimens. This method is easier and faster to pe r fo rm than Giemsa staining and was fcu,nd by the .authors to be more sensitive than iodine staining .in bo th McCoy and HeLa 229 cell cultures. In McCoy cel.l cul tures its sensitivity was equal to that of Giemsa staining. Recently, immunof luorescent staini,ng with monoclonal antibodies has been de- scribed (195, 243) and its sensitivity has been repor ted to exceed that of iodine (193, 243) and Giemsa staining (195). The sensitivity of chlamy- dial cul ture techniques is unknown (204). Scha- chter and Grossman est imated that in NGU or cerv4citis the sensitivity of cul ture techniques is 70-80% and for o ther conditions (except neo- natal conjunct ivi t is) less than that (176).
Serology. - The most commonly used assays for antibodies to chlamydia are complement fixa- tion (CF) and microimmunof luorescence . The CF test was first used to detect ant ibodies to cklamydiae by Bedson in 1935, who applied it for the diagnosis of psittacosis (5). The test i.s still used to diagnose LGV and psittacosis, but its sensitivity is insufficient for the detect ion of antibodies in oculogenital infections. Since the
CF test detects antibodies against the acidic li- popolysacchar ide antigen common to all mem- bers of the genus Chlamydia (41), it does not .distin- guish between infections caused by C. trachoma- tis and C. psittaci.
The neveer indirect micro immunof luorescence (M1F) test, originally developed by Wang and Grayston in 1970 (225) to serotype C. trachomatis strains, has since been widely used for detect ion of antibodies in pat ients ' serum and local secre- tions (220). EBs serve as antigen, and anti- bodies against type specific surface proteins are detected. The test can therefore different iate be- tween antibodies produced against C. trachomatis and C. psittaci (220). Originally each sample was tested separately against EBs of each s.erotype, a laborious and expensive procedure . Effor ts to simplify the test have i.nvolved the use of pooled antigens (219, 227) or a single broadly l~eacting antigen, usually L2, which has been est imated to cover 95.5% of the C. trachomatis antibodies de- tected in the original MIF test (213). Yong et al used purif ied RBs of immunotype C/TW-3/OT as a single antigen for a MIF test (241). The authors found that the RB anligen had a sensi- tivity similar to that of the EB antigen in detec- ting antibodies in endocervical secretions and in serum, but was genus-specific ra the r than type-specific. Wang and Grayston (226), however, repor ted the RB MIF test to be tess sensitive than the EB test, especially for IgM. Richmond and Caul (155) have developed a single antigen indirect immunof luorescence test which employs C. trachomatis serotype E infected cells as the antigen. Subsequently, Saikku and Paavonen (161) used C. trachomatis serotype L_~ for their 'im- munof luorescence test. These assays are genus specific like the CF test, but of higher sensitivi,ty ,(220).
A simple indirect immunoperoxidase anti- body assay (IPA) which utilizes air dried ,infected cells has been developed in this labora tory (67). We have adapted this system for the detect ion of C. trachomatis specific serum IgG (30), I.gA and IgM (171) antibodies using cells infected with C. tracho~7eatis serotype L>
Other immunoassay techniques described for detect ion of antibodies against Chlamydia ,include the enzyme linked immunosorben t as- say (ELISA) (29, 48, 104, 107, 112, 162, 189) and the rad io immunoassay (RIA) (212). For most of these assays, antigens are prepared f rom sero- type L.~ strain and are ei ther whole EBs (29), whole RBs (162) or extracted genus specific sol- uble antigen (48). These assays have been applied to detect antichlamydial IgG (29, !04, 112, 162, 189, 212) and IgA (31, 212) in serum, as well as IgA in local secretions (188, 212). ELISA and RIA are generally acknowledged to be highly sen- sitive, and are suited for large scale assays, as
245

Ladany S. and Sarov I. Eur. J. Epidemiol.
they lend themselves to au tomat ion . They require, however , special equipment . All the indirect immunoass .ays descr ibed here are more sensit ive than the CF test, and unl ike the la t ter have the potenti.al of detect ing dif ferent immunoglobu l in classes (e.g., IgG, IgA and IgM).
Current problems
C. trachomatis poses a challenge to m o d e r n medicine, bo th in unders t and ing the host~agent re la t ionship and in finding ways of prevent ion, diagnosis and therapy. Prob lems awai t ing eluci- daft.on include :
What is the molecular basis of the differen- t i a t i o n o f E B s t.o RBs .and vice versa? A recent s tudy by H a c k s t a d t et al (66) on the effect of exogenous reducing agents on pur i f ied EBs provides some in fo rmat ion on the early stages of dif..ferentia- tion. Results of this s tudy imply tha t reduct ive cleavage of disulfide bonds of the MOMP is an ear ly .event in the convers ion of EBs to RBs, which in tu rn leads to increased permeabi l i ty of the chlamydial outer m e m b r a n e . The mecha- n ism of the reduct ion and the m a n n e r of partic- ipat ion of the host cell in its ini t iat ion are not known. Current knowledge of the m e c h a n i s m of p revent ion o.f P-LF, which enables ch lamydiae to survive in the host i le env i ronment of the host cell is l imited. Although res is tance to P-LF is not unique to chlamydiae, and has been observed in Toxoplasma gondii (93), Leishmania (106) and Legionella pneumophiIa (85) as well, i~s m e c h a n i s m i.s not unders tood. Recently, Zeichner (244) found small di,fferences of ,phagosome mem- b rane pro te ins be tween m a c r o p h a g e phagosomes containing infect ious C. psittaci and those conta i - ning heat inac t iva ted C. psittaci. I t is possible tha t dur ing the stage of creat ing a phagosome, infec- t ious ch lamydiae induce selection of specific phagosorne m e m b r a n e componen t s which signals for avoidance of P-LF.
Cellular and humo,ral i m m u n e responses to chlamyd, ial in,fecfions 'and the role they p lay in res is tance to reinfection, in resolut ion of on- going .infection, and in the deve lopment ,of severe i n f l a m m m o r y disease are poorly unders tood. Recently, it has been shown tha t ,potymorpho- nuc lear leukocytes have the abil i ty to inact ivate ch lamydiae (242, 245). I t has also been demon- s t ra ted tha t genus-specific chlamydial antigens can be detected on host cell m e m b r a n e s (156). Nevertheless, , cytotoxici ty towards Chlamydia in- fected ta rge t cells could not be detected (147, 154). Fur the r studies are requi red to u n d e r s t a n d the significance o,f these findings regarding cell med ia ted and humora l immun i ty to chlamydiae.
Is there a la tent f o r m of C. trachomatis in- fect ion in vivo? Pers is tent chlarnydi.al infect ion in .cell cul ture can be achieved by various pro-
cedures. As for in vivo pers i s ten t infection, per- sons who have left t r achoma-endemic .areas and who have not had active disease since cMldhood may develop acute t r a c h o m a in their sixties or seventies (174). Moreover, C. trachomatis lung in- fection can be reac t iva ted in mice by immun.o- suppress ive the rapy wi th cor t i sone (239). Whe- ther pers i s ten t infection actually occurs in m a n and to wha t extent is difficult to assess, pa r t ly because of the p rob lem of dist inguishing be tween pers is tent , chronic inapparent , and r ecu r ren t infection. I f pers is tent infection occurs in vivo, what is the na tu re o,f the ,chlamydia .organism in the do rman t stage? Is it an RB, an EB, or a specific .cryptic form, as suggested by Moulder .et al (131)?
Do antibiot ics such as the tetracycl ines which effect clinical cure, eradicate chlamydiae? Could se,me ch lamydiae s~rvive such t r ea tmen t and cause pers is tent or chronic inap,parent infection? Is .damage to the inclusion m e m b r a n e or inhi- bitio,n o.f its fo rma t ion needed for comple te erad- ication o,f chlamydiae? This speculat ion is sup- por t ed by resul ts of a recent s tudy ,from our l abora to ry (186) on the ,~-interferon media ted inhibi t ion of chlamydial g rowth in cell culture. Low doses o,f in te r fe ron influenced the .extent o,f m a t u r a t i o n of RBs to EBs, causing par t ia l :and reversib.le inhibition. However , high in ter feron concent ra t ions inhibi ted inclusion fo rma t ion .and resul ted in comple te and i r revers ible restrict,ion of chlamydial growth.
What is the extent of nonsexual t ransmiss ion of chlamydial infection in adults and in chi ldren? Do clinical mani fes ta t ions such as ophthalmia , r e sp i ra to ry t rac t infections and myocardi t i s play an impor t an t role in the epidemiology of chla- mydia l infections?
What is the cont r ibut ion of chlamydial infec- tion to fai lure of in vitro fert i l ization ( IVF)? Re- cently, Moss and Steptoe (129) ra ised the p.ossi- bility of a link be tween chlamydial infect ion in bo th husband and wife and loss of ova fo.llowing IVF. Anti-chlamydial therapy to bo th p a r m e r s was fol lowed by successful ovum implan ta t ion and uneventful pregnancy. As chtamydial infect ion is a c o m m o n cause of tubal obst ruct ion, m a n y w o m e n requir ing IVF may h a r b o u r C. tracho- marls in their genital t ract , wi th an adverse effect on implan ted pregnancies. Fu r the rmore , chlamy- dia have been shown to adhere to spe rma tozoa (235), and to survive during c ryopreserva t ion (187). Couples should therefore b.e t,est,ed for C. trachomatis infection pr ior to IVF.
What is the na ture of the associat ion of C. trachomatis with cervical neoplasia (150)? Is C. trachomatis a p r i m a r y fac tor in the deve lopment of cervical cancer? I f so, are the neoplast ic changes the resul ts of a direct e f f e c t .of C. trachomatis or are they pe rhaps caused by react ive oxidizing
246

Vol. 1, 1985 Recent advances in Chlamydia trachomatis
species p roduced by ch lamydia ac t ivated poty- morph.onuclear leukocytes (245)? An i m p o r t a n t object ive for fu ture research is the deve lopment o,f vaccines against C. trachomatis infections. Vac- cines against t r achoma have been tested in bo th non-human p r imates and in humans . In so,me stud- i,es immuniza t ion induced a shor t Hved pro tec t ion but in .others it was fol lowed by hypersenMtivfity and increased severi ty of disease (11,127). Recently molecular genetic approaches have been utilized to p repa re defined chlamydial ant igens in an Esche- riehia coli expression sys tem (134, 194). Perhaps, in the future, such molecu la r cloning techniques will enable the p repa ra t ion of chlamydial anti- gens which induce protec t ive immun i ty and do not cont r ibu te to pathogenesis .
Genital chlamydial infections, in. females as well as in males, are often a s y m p t o m a t i c (61, 141, 143, 171, 176, 192). Ear ly detect ion of these infections is of real value since effective treat- ments exist which might prevent C. trachomatis f rom reaching and damaging the uppe r genital tract, and might minimize t ransmiss ion o.f the agent to sexual pa r tne r s and to newborns . Screen- ing and t rea t ing o.f consor ts is of great impor- tance as well. Thus the need for s imple an,d rapid diagnostic ,tests, which are feasible for popula- tion screening, cannot be overemphasized.
Isola t ion and identif icat ion of ch lamydia in cell cul ture is highly specific, bu t expensive and t ime consuming, and it cannot be p e r f o r m e d in every labora tory . Several new approaches t.o de- tect ion of chlamydial antigen in clinical s,peci- mens have been repor ted . These include ,direct immunof luorescence staining of smears using mo- noclonal ant ibodies and monoclonal antibody- based ELISAs (26, 206). These methods are of the same order of sensit ivity and specificity as isolat ion in cell cul ture (26, 206), bu t ~re much s impler and are rapid.
Recently, Hyypifi et al (87) and Kahan,e and Sa- rov (94) r epor ted the detect ion of Chlamydia by DNA hybridizat ion with a native chlamydial pl,as- mid probe, All 15 serotypes of C. trachomatis could be detected, wi th a sensit ivity of 10-100 pg DNA (87) and 1-5 pg DNA (94). These assays seem promising, but techniques are still too cumber- some and t ime consuming for rout ine diagnostic purposes . One o.f the p rob lems in using d.etection of ch lamydiae as a s t andard diagnostic tes.t is the fact that C. tracornatis cannot be isolated ,in internal infections such as salpingitis, unless invasive pro- cedures a re applied. In such cases, the availabil- ity of serologic ma rke r s of chlamydi,al infect ion is of special impor tance . Techniques for detect ion of ant ibodies in se rum or secret ions are usual ly simple, relat ively inexpensive, :and compat ib le wi th process ing large n u m b e r s o,f samples. The pos- sibility that elevated se rum ti tres of specific IgG ant ibodies m a y serve as a m a r k e r for early de-
tect ion of active C. trachomatis infect ion has been indicated in a n u m b e r of studies (37, 83, 92, 102, 114, 128, 171, 221, 224). Par t icular ly elevated anti C. trachomatis IgG ti tres were found in diseases such as salpingitis, mechanica l infertili ty, perihe- pati t is and pneumoni t i s (37, 75, 83, 102, 114, 151, 153, 171, 203, 221, 224). Considerable evidence is being 'accumulated that se rum specific IgA anti- body may be a potent ia l m a r k e r for detect ion o,f active viral and ch lamydia l infection (167-169, 172, 173, 218) and reviewed by Sarov et al (170).
Recent studies have shown a significantly higher prevalence rate of C. trachomatis specific s e rum IgA ant ibodies in pat ients wi th C. tracho- matis isolation-posit ive NGU, in women with sal- p'ingitis and in inferti le women, when compared respect ively with ma tched controls (31,171). I~n the case of salpingitiS, we have recent ly demon- s t ra ted by an indirect immunope rox idase assay that chlamydia-specif ic s e r u m IgA ant ibodies could serve as a poten'tial m a r k e r for active C. tracho- rnatis infect ion (151). A thorough analysis of the pers is tence of se rum IgA ant ibodies to Chl.amy- dia is requi red to evaluate whe the r :detection of specific IgA ant ibodies by the indirect immuno- peroxi,dase assay has the potent ia l for sero,di- agnosis of chlamydial infection in a singl,e :serum sample, We are present ly examining prospect ively the .possibility that serial se rum examinat ions for C. trachornatis IgG and IgA ant ibodie s may be of value in moni tor ing t r ea tmen t wit.h doxy- cvcline hvdrochlor ide in salpingitis pat ients .
Acknowledgements
This review was supported in part by the Middle East Eye Research Institute (MEERI).
Our special thanks are extended to Dr. Maureen Friedman and Dr. Avi Porat, of the Faculty of Health Sciences, Ben Gurion University of the Negev, and to Dr. Peter Csango, from Kristiansand, Norway, for their enlightening remarks. We also thank Yona Aloni for the preparation of Fig. 1, and Mrs. Deborah Cohen for her invaluable assistance in the prepara- tion and editing of the manuscript.
247
Ladany S. and Sarov I. Eur. J. Epidemiol.
R E F E R E N C E S
I. Alexander E.R. and Harrison R. (1983): Role of Chlamydia trachomatis in perinatal infection. - Rev. Infect. Dis., 5: 713-7'19.
2. Amor B.A. (1983): Chlamydia :and Reiter's syn- d rome. - Brit. J. Rheumatol., 22 (suppl. 2): 156-160.
3. Arth C., yon Schmid t B., Grossman M. and Scha- chter J. (1978): Chlamvdia p n e u m o n i t i s . - J. Pe- diatr., 93: 447449.
4. Barbour A.G., Amano K.-I. Hacks tadt T., Perry L. and CaldwelI H.D. (1982): Chlamydia tracho- matis has penicil l in-binding proteins bu t not de- tectable muramic acid. - J. Bacteriol., 15I: 420-428.
5. Bedson S.P. (1935): Complement-fixation reac- tion in the diagnosis of human psittacosis. - Lancet, 2: 1277-1280.
6. Bedson S.P. and Bland J.Q.W. (1932): A morpho- logical study of psittacosis virus with the de- scription of a developmental cycle. - Br. J. Exp. Pathol., 13: 461-466.
7. Beem M.O. and Saxon E.M. (1977): Respiratory tract colonization and a distinctive pneumoni,a syndrome in infants infected with Chlamydia trachomatis. - N. Engl. J. Med., 296: 306-310. :
8. Beem M.O. and Saxon E.M. (1982): Chlamydia trachomatis infections of infants. In: Chlamydia Infections,, M~irdh P.-A., Holmes K.K., Oriel J,D., Piot P. and Schachter J. (eds). - Elsevier Bio- medical Press, Amsterdam, p. 199-212.
9. Bell T.A. (1985): Chlamydia trachomatis, Myco- p lasma hominis, and Ureaplasma ureaty t icum infections in infants. - Seres. in Perinatol., 9: 29-37.
10. Berger R.E., Alexander E.R., Harni~ch ].P., Paul- sen C.A., Monda G.D., Ansell J. and Holmes K.K. (1979): Etiology, manifes ta t ions and therapy of acute epididymitis: Prospective study of 50 cases. - J. Urol., 121: 750-754.
11. Bernste in D.I.. Hubbard T., Wenman W.M., Hol- mes K.K., Liebhaber H., Schachter J., Barnes R. and Lovetr M.A. (1984): Mediastinal and supra- clavicular lymphadenit is and pneumon'i t is due to Chlamydia trachomatis serovars L and L,. - New Engl. J. Med., 31l: 1543-1546.
12. Black S.B., Grossman M., Cles L. and Schachter Y.~ (1981)i Serologic evidence of chlamydial infec- t ion in children. - J. Pediat., 98 (1): 65-67. :
13. Bolton J.P. and Darougar S. (1983): PerihePati- t i s . - Br. Med. Bull., 39: 159-]62.
14. Bose S.K. and Smi th G.B. (1984): Positive co- operativity in the ad,herence between elementary bodies of Chlamydia trachomatis strain UW-31 and HeLa cells. - F E M S Microbiol. Letters, 23: 55-58.
15. B o w i e W.R. (1982): In vitro and in vivo efficacy of ant imicrobials against Chlamydia trachoma- tis. - Infect., lO(suppl. 1): $46-$52.
16. Bowie W.R. (1984): Epidemiology and therapy of Chlamydia trachomatis infections. - Drugs, 27: 459-468.
17. ~ Brade H. and Brunner H. (1980): Detection of chlamydial inclusion bodies with ant isera to Acinetobacter calcoaceticus subspecies anitratus by indirect immunofluorescence. - Infect., 8: 215-216.
18. Burney P., Forsey T., Darougar S., S i t tampalam Y., Booth P. and Chamberlain R. (1984): The epidemiology of chlamydial infections in child- hood: A serological investigation. - Internat . J. Epidemiol., 13: 491-495.
19. Butler T., Bennish M., Schachter ]. and StoIl B.]. (1985): Serological evidence for chlamydial in- fection in patients with acute diarrhoea. - Trans. Roy. Soc. Trop. Med. Hyg., 79: 4243.
20. Byrne G.I. and Moulder ].W. (1978): Parasite specified phagocytosis of ChIamydia psi t taci and ChIamydia trachomatis by L and HeLa cells. - Infect. Immun. , 19: 598-606.
21. Caldwell H.D. and Hitchcoock P.J. (1984): Mono- clonal ant ibody against a genus-specific antigen of Chlamydia species: Location of the epitope on chlamydial lipopolysaccharide. - Infect. Im- mun., 44: 306-314.
22. Caldwell H.D., Kromhout J. and Schqchter J. (1981): Purification and part ial characterization of the major outer membrane protein of Chla- mydia trachomatis. - Infect. Immun. , 31: 1i61-1176.
23. Caldwell H.D. and Kuo C.-C. (1977): Purif icat ion of a Chlamydia trachomatis - specific antigen by im- munoadsorp t ion with monospecific antibody. - J. Immunol. , 118: 437-441.
24. CaldwelI H.D. and Perry L.J. ( 1982): Neutral izat ion of Chlamydia trachomatis infectivity with anti- bodies to the major outer membrane p ro te in . - Infect. Immun. , 38:745-754
25. Caldwell H.D. and Schach~er J. (1982): Antigenic ;analysis of the major outer membrane protein of Chlamydia spp. - Infect. Immun. . 3.5." 1024-1031.
26~ Caul E.O. and Paul. I.D. (1985): Monoclona] anti- body based ELISA for detecting ChIamydia tra- chomatis. - Lancet. 1: 279.
27. Centers for Disease Control. (1983): Sexually trans- mit ted diseases: t rea tment guidelines... Rev. Infect. D i s . ) (suppl.): $729-$746.
28. CeveninL R.. Costa S., Rumpianes i F.. Donati M.. Guerra B.. Diana R. and Antonini N.P. (1981): Cytological and histopathological abnormali t ies of the cervix in genital Chlamydia trachomatis infections. - Br. J. Vener. Dis., 57:334-337
29. Cevenini R., Donati M. and Rumpianes i F. (1981): Elementary bodies as single ant,igen in a micro-
248

Vol. 1, 1985 Recent advances in Chlamydia trachomatis
ELISA test for Chlamydia trachomatis anti- bodies. - Microbiol., 4: 347-351.
30. Cevenini R., Rumpianesi F., Donati M. and Sarov I. (1983): A rapid immunoperoxidase assay for the detection of specific IgG antibodies to Chla- mydia trachomatis. - J. Clin. Pathol., 36: 353-356.
31. Cevenini R., Sarov I., Rumpianesi F., Donati M., Melega C., Varotti C. and La Placa M. (1984): Serum specific IgA ant ibody to Chlamydia tra- chomatis in pat ients with chlamydial infections, detected by ELISA and an immunofluorescence test. - J. Clin. Patbol., 37: 686-691.
32. Chandler J.W., Alexander E.R., Pheiffer T.A., Wang S.-P., Holmes K.K and English M. (1977): Ophthal- mia n eona torum associated with maternal chla- mydial infections. - Tr. Am. Acad. OphthaI. Otol., 83: OP302-OP308.
33. Chandler R. and Dawson M.D. (1982): Review of eye infections with Chlamydia trachomatis. - In: Chlamydial Infections, MSrdh P.-A., Holmes K.K., Oriel J.D., Piot P. and Schachter J. (eds). Elsevier Biomedical Press, Amsterdam, p. 71-81.
34. Chang J.J., Leonard K., Arad T., Pitt T., Zhang Y.X. and Zhang I.H. (1982): S t ructura l studies of the outer envelope of Chlamydia trachomatis by electron microscopy. - J. Mol. Biol., 161: 579-590.
35. Conway D., Glazener C.M.A., CaM E.O., Hodgson J., Hull M.G.R., Clarke S.K.R. and Stirrat G.M. (1984): Chlamydial serology in fertile and infer- tile women. - Lancet, 1: 191-193.
36. Csango P.A., Sah,eson A., Gundersen T., Jagars G. and Bjerk O. (1984): Treatment of acute gono- coccal urethri t is in men with s~multaneous infection with ChIamydia trachomatis. - Br. J. Vener. Dis., 60: 95-98.
37. Darougar S., Forsey T., Wood J.J., Bolton J.P. and Allan A. (1981): Chlamydia and the Curtis- Fitz-Hugh syndrome. - Brit. J. Vener. Dis., 57: 391-394.
38. Darougar S. and Jones B.R. (1983): Trachoma. - Brit. Med. Bull. 39 (2): 117-122.
39. Darougar S. and Treharne J.D. (1982): Cell cul- ture for the isolation of C. traehomatis - a review. In: Chlamydial Infections, M~irdh P.-A., Holmes K.K., Oriel J.D., Piot P. and Schachter J. (eds). - Elsevier Biomedical Press, Amsterdam, p. 265-274.
40. Delbarre F. and Amor B. (1976): Ankylosing spondylitis and Reiter 's syndrome: Genetic and microbial studies. In: Infections and Immunology in t~he Rheumat ic Diseases, Dumonde, D,C. (ed). Blackwell Scientific Publications, Oxford, p. 159- 163.
41. Dhir S.P., Hakomori S., Kenny G.E. and Grayston J.T. (1972): Immunochemica l studies on chlamy- dial group ant igen (presence of a 2-keto-3-deoxy- carbohydrate as i m m u n o d o m i n a n t group). - J. Im- munol., 109: 1t6-122.
42. Edelman R.B., Harm L.E. and Simon M. (1984): Chlamydia trachomatis pneumonia in adults: ra- diographic appearance. - Radiol., 152: 279-282.
43. Eilard T., Brorsson J.-E., Hamark B. and Forss- man L. (1976): Isolat ion of chlamydia in acute salpingitis. - Scand. J. Infect. Dis., 9 (suppl.): 82-84.
44. Eissenberg L.G., Wyrick P.B., Davis C.H. and Rumpp J.W. (1983): Chlamydia psittaci elemen- tary body envelope: ingestion and inhibi t ion of pbagolysosome fusion. - Infect. Immun. , 40: 741-751o
45. Elkabetz A. and Sarov I. (1984): Genital Chla- mydia t,rachomatis infections in the female. - Ha~refuah, 106: 469-472.
46. Eschenbach D.A., Buchanan T.M., Pollock H.M., Forsyth P.S. et al. (1975): Polymicrobial etiology of acute pelvic inf lammatory disease. - N. Engl. J. Med., 293: 166-171.
47. Eschenbach D.A., Harnisch ].P. and Holmes K.K. (1977): Pathogenesis of acute pelvic inf lamma- tory disease: role of contraception and other risk factors. - Am. J. Obstet. Gyneco,l., 128: 838-850.
48. Evans R.T. and Taylor-Robinson D. (1982): De- velopment and evaluation of an enzyme linked immunosorben t assay (ELISA), using chlamydial group ant igen to detect antibodies to Chlamy- dia trachomatis. - ~. Clin. Patho1., 35: 1122-1128.
49. Evans R.T. and Woodland R.M. (1983): Detection of chlamydiae by isolation and direct examina- tion. - Brit. Med. BuIl., 39: 181-186.
50. Felman Y.M.. Mehil M.A. and Nikitas J.A. (1981): Nongonococcal uret'hritis. A clinical review. - J. Am. Med. Assoc., 245: 381-386.
5:1. Fraser ].J., Rettig P.]. and Kaplan D.W. (1983): Prevalence of cervical Chtamydia trachomatis and Neisseria gonorrhoeae in female adolescents. - Pediat., 7l: 333-336.
52. Friis R.R. (1972): In teract ion of L cells and Chla- mydia psittaci: entry of the parasite and host responses to its development. - J. Bacteriol., 110: 706-721.
53. Frommell G.T., Bruhn F.W. and Schwartzman J.D. (1977): Isolat ion of Chlamydia traehomatis from infant lung tissue. - N. Engl. J. Med., 296: 1150~1152.
54. Frommell G.T, Rothenberg R., Wang S.-P., Mc- intosh K., WintersgiIl C., Allaman 1. and Orr I. (1979): Chlamydial infections of mothers and their infants. - J. Pediat., 9.5: 28-32.
55. Garnett A.J., Harrison M.Y. and Manire G.P. (I974): A search for the bacterial mucopeptide component , muramic acid in Chlamydia. - 3. Gen. Microbiol., 80: 315-318.
56. Gibson M., Gump D., Ashikaga T. and Hall B. (1984): Pat terns of adnexal in f lammatory da- mage: Chlamydia, the in t rau ter ine device, and
249

Ladany S. and Sarov I. Eur. J. Epidemiol.
h i s to ry of pelvic i n f l ammato ry disease. - Ferfil . Steril. , 41: 47-52.
57. Givner L., Rennels M., Woodward C. and Huang S. (1981): Chtamydia trachomatis infect ion in infant del ivered by cesarean section. Pediat. , 68: 420-421.
58. Golden N., Hammerschlag M., Neuhoff S. and Gteyzer A. (1984): Prevalence of Chlamydia tra- comatis cervical infect ion in female adolescents . - Am. J. Dis. Child., 138: 562-564.
59. Gordon F.B. and Quan A.L. (1965): I so la t ion of the t r achoma agent in cell culture. - Proc. Soc. Exp. Biol. Med., 118: 354-359.
60. Gracea E., Botez D., Costantinescu S., Vizitiu 0., Georgescu-Braita M., Lazar M. and Panoiu L. (1983): Geni ta l MycopIasmas and Chlamydiae in men ure thr i t i s . - Arch. Roum. Path. :Exp. Micro- biol., 42: 25-30. !!
61, Grant J.B.F., Brooman P.J.C., Chov~,dhury S.D., Sequeira P. and BIacklock N.J. (19~85): The cl~i- nical p resen ta t ion of ChIamydia trachomatis in a serological pract ice . - Br. J. Urol., 57: 218-221.
62. Grayston J.T. and Wang S.-P. (1975): New know- ledge of ch lamydiae and the diseases they cause. - J. Infect . Dis., 132: 87-105.
63. Gregory W.W., Gardner M., Byrne G.1. and Moul- der J.W. (1979): Arrays of hemispher ic projec- t ions on ChIamydia psittaci and Chlamydia tra- chomatis observed by scanning e lec t ron micro- scopy. - J. Bacteriol. , 138: 241-244.
64. Gump D.W., Dickstein S. and Gibson M. (1981): Endomet r i t i s re la ted to Chlamydia trachomatis infection. - Annales. Int . Med., 95: 61-63.
65. Guze P.A., Bayer A,S., Anthony B.F., TilIman D.B. and Bills R. (1981): Spec t rum of h u m a n ohlamy- dial in fec t ions . - West. J. Med., 135: 208-225.
66. Hackstadt T., Todd W.J. and Catdwell H.D. (t985): Disulfide-me&iated in terac t ions of the c.hlamy- dial malior ou te r m e m b r a n e pro te in : role in the d i f ferent ia t ion of chlamydiae . - J. Bacter iol., 161: 25-34.
67. Haikin H., Leventon-Kriss S. and Sarov L (t979): Ant ibody to var icel la zos ter v i rus induced mem- b rane antigen: immunoperox~dase assay wi th a i r d r i ed ta rge t cells. - J. Infect. Dis., 140: 61)1-604.
68. Halberstaedter L. and yon Prowazek S. (1907): Zur Atiologie des Trachoms. - Dtsch. Med. Wschr., 32: 1285-1287.
69. Halberstaedter L. and yon Prowazek S. (1909): Ueber Chlamydozoen Befunde bei Blennorrhoea neona to rum non gonorrhcrica. Berlin. Klin. Wschr., 41: 1839-1840.
70. Hammerschlag M.R., Anderka M., Semine D.Z., McComb D. and McCormaek W.M. (1979): Pro- spect ive s tudy of ma te rna l and infant i le infect ion wi th Chlamydia trachomatis. - Ped~at., 64: 142-148.
71. Hardy P.H., Hardy J.B., Nell E.E., Graham D.A., Spence M.R. and Rosenbaurn R.C. (1984): Preva- lence of six sexually t r ansmi t t ed disease agents among pregnant inner-city adolescents and preg- nancy outcome. - Lancet, 2: 333-337.
72. Hare M.J., Mrcog M.A. and Thin R.N. (1983): Chla- mydiaI infection of the lower genital t rac t of women. - Brit. Med. Bull., 39: 138-144.
73. Harnisch J.P.. Berger R.E. and Alexander E.R. (1977): Aetiology of acute epididymit is . - Lancet, 1: 819-821.
74. Harrison H.R., Alexander E.R. arid Chiang W.-T. (1979): Exper imen ta l nasopharyngi t i s and pneu- monia caused by Chlamydia trachomatis in infant baboons: His topathologic compar i son wit,h a case in a human infant. - J. Infect. Dis., 139: 141-146.
75. Harrison H.R., Alexander E.R., Weinstein L., Lewis M., Nash M. and Sire D.A. (1983): Cerv4cal Chla- mydia trachomatis and mycop lasmal infections in pregnancy. Epidemiology and outcomes. - J. Amer. Med. Assoc., 250: 1721-1727.
76. Harrison H.R., English M.G., Lee C.K. and Alexan- der E.R. (1978): Chlamydia trachomatis infant pneumoni t i s : compar i son with matched controls and o ther infant pneumoni t is . - N. Engl. J. Med., 298: 702-708.
77. Hatch T.P. (1982): Host free activi t ies of Chla- mydia. In: Chlamydial Infect ions, MSrdh P.-A., Holmes K.K., Oriel J.D., Piot P. and Scthachter J. (eds). Elsevier Biomedical Press, Amsterdam, p. 25-28.
78. Hatch T.P., AI-Hossainy E. and Sitverman J.A. (1982): Adenine nucleot ide and lysine t r anspo r t in ChIamydia psittaci. - J. Bacteriol. , 150: 662-670.
79. Hatch T.P., Allan I and Pearce J.H. (1984): Struc- tura l and polypept ide differences be tween enve- lopes of infective and reproduc t ive life cycle forms of Chlamydia spp. - J. BacterioI. , 157: 13-20.
80. Hatch T.P., Vance D.W. and AI-Hossainy E. (198,1): Ident i f ica t ion of a m a j o r envelope pro te in in ChIamydia spp. - J. Bacteriol. , 146: 426-429.
81. Heggie A.D., Lumicao G.G., Stuart L.A. and Gryves M.T. (1981): Chlamydia trachomatis in- flections in mothers and infants. - Am. J. Dis. Child., 135: 507-511.
82. Henry-Suchet J., Catalan F., Loffredo V., Serfaty D., Siboulet A., Peral Y., Sanson M.J., Debache C., Pigeau F., Coppin R., DeBrux J. and Poynard T. (1980): Microbiology of specimens ob ta ined by laparoscopy from controls and f rom pat ien ts wi th pelvic i n f l ammato ry disease or infer t i l i ty wi th tubal obs t ruct ion: ChIamydia trachomatis and Ureaplasma ureatyticum. - Am. J. O b s t e t . Gynecol., 138: 1022-1025.
83. Henry-Suchet H., Catalan F., Paris X. and Lof- fredo V. (1982): Ant ibody t.iter to ChIarnydia trachomatis in acute salpingit is and obs t ruc t ive
250

Vol. 1, 198J Recent advances in Chlartzydia trachomatis
s~erilities. In: Chlamydia Infections, M~irdh P.-A., Holmes K.K., Oriel J.D., Plot P. and Schachter J. (eds). Elsevier Biomedical Press, Amsterdam, p. 183-187.
84. Hobson D. and Rees E. (1983): Chlamydial in- fections in neonates and older children. - Brit. Med. Bull., 39: 128-132.
85. Horowitz M.A. (1983): The Legionnaires ' disease bacter ium (Legionella pneumophila) inhibits pha- gosome-lysosome fusion in h u m a n monocytes. - J. Exp. Med., 158: 2108-2126.
86. Hourihan J.T., Rota T.R. and McDonald A.B. (1980): Isolation and purif icat ion of a type-specific anti- gen from Chlamydia trachomatis propagated in cell culture using molecular shift chromatogra- phy . - J. Immunol . , 124: 2399-2404.
87. Hyypiii T., JaIava A., Larsen S.H., Terho P. and Hukkanen V. (1985): Detection of Chlamydia tra- chomatis in clinical specimens by nucleic acid spot hybridization. - o r. Gen. MicrobioL, 131: 975- 978.
88. Hyypiii T., Larsen S.H., Stahlberg T. and Terho P. (1984): Analysis and detection of chlamydial DNA.- J. Gen. Microbiol., 130: 3159-3164.
89. Ito J.[., Harrison H.R., Alexander E.R. and Billings L.J. (1984): Es tabl i shment of genital t ract infection in the CF-1 mouse by intravaginal inoculat ion of a human oculogenital isolate of Chlamydia trocho- marls. - J. Infect. Dis., 150: 577-582.
90. Jahn G., Jenish A. and Blenk H. (1983): Gonor- rhoeic urethr i t is - frequently a mixed infection with Chlamydia and Mycoplasma: results of tests on 143 males with acute gonorrhoea. - Dtsch. ivied. Wschr., 108: 896-901.
91. Jones B.R., Collier L.H. and Smith C.H. (1959): Isolat ion of virus from inclusion blennorhea. - Lancet, 1: 902-905.
92. Jones B.R., Ardery B.R., Hui S.L. and CIeary R.E. (1982): Correlation between serum ant ichlamydial antibodies and tubal factor as a cause of infertil- ity. - Fert,il. Steril., 38: 553-558.
93. Jones T.C. and Hirsch J.G. (1972): The interact ion between Toxoplasrna gondii and mammal i an cells. II. The absence of lysosomal fusion with phagocy- tic vacuoles containing living parasites. - J. Exp. Med., 136: 1,173-1194.
94. Kahane S. and Sarov L (1985): Detection of chla- mydia by DNA hybridizat ion with a native chla- mydial plasmid probe. Submit ted for publication.
95. Kalimo K., Terho P., Honkonen E., Griinroos M. and HaIonen P. (1981): ChIamydia trachornatis and herpes simplex virus IgA antibodies in cer- vical secretions of pat ients with cervicM atypia. - Br. J. Obstet. Gynaecol., 88: 1130-1134.
96. Kau[man R.D. and Wiesner P.J. (1974): Nonspe- cific urethrit is . - N. Engl. J. Med., 291: 1175-1177.
97. Keat A., Thomas B.J. and Taylor-Robinson D. (1983): Chlamydial infection in the aetiology of arthritis. - Br. Med. Bull., 39: 169-174.
98. Komaroff A.L., Aronson M.D., Pass T.M., Ervin C.T., Branch W.T. and Schachter J. (1983): Sero- logic evidence of chlamydial and mycoplasmal pharyngit is in adults. - Science, 222: 927-929.
99. Komaroff A.L., Aronson M.D. and Schachter J. (1981): Chlamydia trachomatis infection in adults with community-acquired pneumonia. - J. Amer. Med. Assoc., 245: 1319-1322.
i00. Krauss H., Schie[er H.G., Weidner W., Arens M. and Ebner H. (1983): Significance of Chlamydia trachomatis in ,Abac te r ia l , , prostatit is. - Zbl. Bakt. Hyg., I. Abt. Orig., A254: 541-551.
101. La Scolea L.J., Paroski J.S., Burzynski L. and Faden H.S. (1984): Chlamydia trachomatis infec- tion in infants delivered by cesarean section. - Clin. Pediat., 23: 118-120.
102. Leinonen M., Saikku P., Nurminen M., Wahlstr6m E., Puolakkainen M. and MSkelii P.H. (1983): Antibody response to purified chlamydial com- ponents in various chlamydial infections. First European Congress of Clinical Microbiology, Bo- logna, Abstract No. 309.
103. Le Marchand P. and Goudeau A. (1984): Isolat ion of Chlamydia trachomatis from peri toneal fluid in perihepatitis. - Brit. Med. J., 289: 470.
104. Levy N.J. and McCormack W.M. (1982): Detection of serum ant ibody to chlamydia with ELISA. In: Chlamydial Infections, MSrdh P.-A., Holmes K.K., Oriel J.D., Plot P. and Schachter J. (eds). Elsevier Biomedical Press, Amsterdam, p. 341-344.
105. Levy N.J. and Moulder J.W. (1982): At tachment of cell wails of Chlamydia psittaci to mouse fi- broblasts (L cells) .- Infect. Immun. , 37: 1059-1065.
106. Lewis D.H. and Peters W. (1977): The resistance of int racel lular Leishmania parasites to digestion by lysosomal enzymes. - Ann. Trop. Med. Parasitol., 71: 295-312.
107. Lewis V.J., Tracker W.L. and Mitchell S.H. (1977): Enzyme-linked immunosorben t assay for chlamy- dial antibodies. - J. Clin. MicrobioL 6: 507-510.
108. Litwin J. (1959): The psittacosis group of orga- nisms. - J. Infect. Dis., 105: 129-160.
109. Louis C., Nicolas G., Eb F., Lefebvre J.-F. and Orfila J. (1980): Modification of the envelope of Chlamydia psittaci during its developmental cycle freeze-fracture study of complementary replicas. - J. Bacteriol., 141: 868-875.
110. Lowett M., Kuo C.-C., Holmes K.K. and Falkow S. (1980): Plasmids of the genus Chlamydia. In: Current Chemotherapy and Infectious Diseases, vol. 2, Nelson J.D. and Grassi C. (eds). Ameri- can Society for Microbiology, Washington D.C., p. 1250-1252.
251

Ladany S. and Sarov I. Eur. J. Epidemiol.
111. MacDonald A.B., McComb D. and Howard L. (1984): I m m u n e response of owi monkeys to topical vaccinat ion with i r radiated ChIamydia trachomatis. - J. Infect. Dis., 149: 439-442.
112. Mahony J.B., Schachter J. and Chernesky M.A. (1983): Detection of ant ichlamydial immunoglob- u l in G and M antibodies by enzyme-linked im- rrmnosorbent assay. - J. Clin. Microbiol., 18: 270-275.
113. Miirdh P.-A. and Hanssen P.W. (1982): Three no- vel manifes ta t ions of Chlamydia trachomatis in- fection-endometritis, perihepati t is and meningo- encephal i t i s . - Infect. 10 (suppl. 1): $57-$60.
lt14. Miirdh P.-A., Lind I., Svensson L., Westr6m L. and Moller B.R. (1981): Antibodies to Clamydia trachomatis, Mycoplasma hominis, and Neisse- ria gonorrhoeae in sera f rom patients with acu- te salpingitis. - Br. J. Vener. Dis., 57: 125-129.
115. Miirdh P.-A. Moiler B.R., Ingerslev H.J. Ni~ssler E. Westr6m L. and Wolner-Hanssen P. (198,1): Er~dometritis caused by Chlamydia trachomatis. - Br. J. Vener. Dis., 57: 191-195.
116. Miirdh P.-A., Ripa K.T., Colleen S., Treharne J.D. a n d Darougar S. (1978): Role of Ch!amydia tra-
chomatis in non-acute prostati t is . - Brit. J. Vener. Dis., 54: 330-334.
117. Miirdh P.-A., Ripa K.T., Svensson L. and Westr6m L. (1977): Chlamydia trachomatis in pat ients with acute salpingitis. - N. Engl. J. Med., 296: 1377-1379.
118. Martin D.H., Koutsky L., Eschenbach D.A., Da- ling J.R., Alexander E.R., Benedetti J.K. and Hol- mes K.K. (1982): Prematur i ty and per inatai mor- tal i ty in pregnancies complicated by materna l Chlamydia trachomatis infections. - J. Amer. Med. Assoc., 247: 1585-1588.
119. Matsumoto A. (1982): Surface project ions of Chla- mydia ps~ttaci elementary bodies as revealed by freeze-deep-etching. - J. Bacteriol., 151: 1040-1042.
120. Matsumoto A. (1982): Morphology of Chlamydia psittaci elementary bodies as revealed by electron microscopy. - Kawasaki Med. J., 8: 149-157.
121. Matsumoto A. and Manire G.P. (1970): Electron microscopic observat ions on the effects of per~i- eillin on the morphology of ChIamydia psittaci. - J. Bacteriol., 101: 278-285.
122. Matsumoto A. and Manire G.P. (1970): Electron microscopic observat ions on the fine struct~ure of cell wails of Chlamydia psittaci. - J. Bacteriol., 104: 1332-1337.
123. Mohammed N.R.S. and Hillary I.B. (1984): De- tection of Chlamydia trachomatis inclusions in McCoy and HeLa-229 cells: an al ternative stai- ning technique using toluidine blue. - J. Clin. Pathol., 37: 682-685.
124. Moiler B.R., Ahrons S., Laurin J. and Miirdh P.-A. (1982): Pelvic infect ion after elective abort ion
associated with Chlamydia trachomatis. - Obstet. Gynecol., 59: 210-213.
125. Moiler B.R., Freundt E.A. and M~irdh P.-A. (1980): Experimental pelvic inf lammatory disease pro- voked by Chlamydia t rachomatis and Mycoplasma hominis in grivet monkeys. - Amer. J. Obstet. Gynecol.. 138: 990-995.
126. Moiler B.R., Taylor-Robinson D., Furr P.M., To[t B. and Allen J. (1985): Serological evidence that chlamydiae and mycoplasmas are involved in in- fertility of women. - J. Repro& Fert., 73: 237-240.
127. Monnickendam M.A. and Pearce J.H. (1983): Im- mune response and chlamydial infection. - Brit. Med. Bull., 39: 187-193.
128. Moore D.E., Foy H.M., DaIing J.R., Grayston J.T., Spadony L.R., Wang S.-P., Kuo C.-C. and Eschen- bach D.A. (1982): Increased frequency of serum antibodies to ChIamydia trachomatis in inferti l i ty due to distal tubal disease. - Lancet, 2: 574-577.
129. Moss T.R. and Steptoe P.C. (1984): Chtamydia trachomatis: importance in in vitro fertilization. - J. Roy Soc. Med., 77: 70-72.
130. Moulder ].W. (1984): Looking at chlamydiae with- out looking at their hosts. - ASM News, 50: 353- 362
131. Moulder J.W., Levy N.J. and Schulman L.P. (~1980): Persistent infection of mouse fibroblasts (L ceils) with Chlamydia psittaci: evidence for a cryptic chlamydial form. - Infect. Immun. , 30: 874-88.3.
132. Munday P.E. and Taylor-Robinson D. (1983): Chla- mydiai infection in proctitis and Crohn's disease. - Br. Med. Bull., 39: 155-158.
133. Myhre E.B. and Miirdh P.-A. (1982): Unusual ma- nifestations of Chlamydia trachomatis infections. - Scan& J. Infect. Dis., 32 (suppl.): 122-125.
134. Nano F.E. and CatdwelI H.D. (1985): Expression of ~he chlamydial genus-specific lipopolysaccha- ride epitope in Escherichia coll. - Science,, 228: 742-744.
135. NewhalI VW.J., Batteiger B. and Jones R.B. ('1982): Analysis of the huma n serological re- sponse to proteins of Chlamydia trachomatis. - Infect. Immun. , 38: 1181-1189.
136. NewhalI VW.J. and Jones R.B. (1983): Disul- fide-linked oligomers of the major outer mem-
b r a n e protein of Chtamydiae. - J. Bacteriol., 154: 998q001.
137. Nowinski R.C., Tam M.R., Goldstein L.C., Stong L., Kuo C.-C., Corey L., S tamm W.E. Handsfield H.H., Knapp J.S. and Holmes K.K. (1983): Mono- clonai antibodies for diagnosis of infectious di- seases in humans. - Soence, 219: 537-644.
138. Numazaki K., Chiba S., Nakata S., Yamanaka 7". and Nakao 7. (1984): Prevalence of antibodies to Chlamydia trachomatis in Japanese persons determined by microimmunofluorescence using
252

Vol. 1, 1985 Recent advances in Chlamydia trachomatis
re t icu la te bodies as single antigen. - Pediat. In- fect. Dis., 3: 105-109.
139. Nurminen M., Leinonen M., Saikku P. and M//- kelii P.H. (1983): The genus-specific ant igen of Chlamydia: resemblance to the l ipopolysaccha- r ide of enter ic bacter ia . - Science, 220: 1279-1281.
140. Nurminen M., Wahlstr6m E., Kleemola M., Lei- nonen M., Saikku P. and Miikelii P.H. (1984): Im- munological ly re la ted ke todeoxyoctona te - contain- ing s t ruc tures in ChIamydia trachomatis, Re mu- tants of Salmonella species and Acinetobacter calcoaceticus vat. anitratus. Infect. Immun. , 44: 609-613.
141. Oriel J.D. (1982): Epidemiology of genital chla- m y d i a l infections. Infect., 10 (suppl. 1)): $32-$39.
142. Oriel J.D. and Ridgway G.L. (1983): Genital in- fection in men. - Brit. Med. Bull., 39: 133-137.
143. Paavonen J. (1979): Chlamydial infections. - Med. Biol., 57: 152-164.
144. Paavonen Y., Brunham R., Kiviat N.. Stevens C., Kuo C.-C., S t a m m W.E. and Holmes K.K. (1982): Cervicitis - etiologic, cl inical and h is topathologic findings. In: Chlamydial Infections, MSrdh P.-A., Holmes K.K., Oriel J.D., Piot P. and Schach te r J. (eds). Elsevier Biomedical Press, Amste rdam, p. 141-145.
145. Page L.A. (1968): Proposal for the recogni t ion of two species in the genus Chlamydia Jones, Rake, and Stearns , 1945. - Int. J. Syst. Bacteriol. , 18: 51-66.
146. Paran H., Heimer D. and Sarov I. (1985): Sero- logical, cl inical and radiological f indings in adul t s wi th b roncho-pu lmonary infections caused by Chlan~ydia trachomatis. - Submi t t ed for publi- cation.
147. Pavia C.S. and Schachter J. (1983): Fai lure ~o detect cel l -mediated cytotoxici ty against ChIamy- dia trachomatis infected cells. - Infect. Immun. , 39: 1271-1274.
148. Perlmutter L.J. and Darvish M. (1983): Possible re la t ionship of ch lamydia to mul t ip le sclerosis. - Med. Hypoth. , 12" 95-98.
149. Peterson E.M. and De La Maza L.M. (1983): Cha- rac ter iza t ion of Chlamydia DNA by res t r i c t ion and endonuclease cleavage. - Infect . Immun. , 41: 604-608.
150. Piura B., Sarov B. and Sarov I. (1985): Genital ch lamydia l infect ion and cervical cancer. - Am. J. Obstet, Gyneco]., 152: 363.
151. Piura B., Sarov I., Sarov B., Kleinman D., Chaim W. and Insler V. (1985): Se rum IgG and IgA spe- cific for Chlamydia trachomatis in salpingi t is pat ients as de te rmined by immunoperox idase as- s a y . - Eur. J. Epidemiol. , 1 (2): 110-116.
152. Punnonen R., Terho P., Nikkanen V. and Meur- man D. (1979): Chlamydial serology in infer t i le
women by immunof luorescence . - Ferti l . Steril. , 31: 656-659.
153. Puolakkainen M., Saikku P., Leinonen M., Nur- minen M., Viiiiniinen P. and Miikelii P. (1984): Chlamydial pneumoni t i s and its serodiagnosis in infants. - J. Infect. Dis., 149: 598-604.
154. Qvigstad E. and Hirschberg H. (1984): Lack of cel l -mediated cytotoxici ty towards Chlamydi a tra- chomatis infected ta rge t cells in humans . - Acta Path. Microbiol . Immunol . Scan& Sect. C., 92: 153-159.
155. Richmond S.J. and CaM E.O. (1975): F luorescent an t ibody studies in ch lamydia l infections. - J. Clin Microbiol. , 1: 345-352.
156. Richmond S.J. and Stirting P. (1981): Localiza- t ion of ch lamydia l group ant igen in McCoy cell monolayers infected with Chlamydia trachomatis or Chlamydia psittaci. - Infect. Immun. , 34: 561-570.
157. Ringel R.E., Brenner J.[., Rennels M.B., I-Iuang S.-W., Wang S.-P., Grayston J.T. and Berman M.A. (1982): Serologic evidence for Chlamydia tra- ohomatis myocardi t i s . - Pediat., 70: 54-56.
158. Ripa K.T. (1982): Microbiological diagnosis of Chlamydia trachomatis infection. - Infect., 10 (suppl. 1): S19-$24.
159. Rgnnerstam R. and Persson K. (1982): Chlamy- dial eye infection in adults . - Scand. J. Infect . Dis., 32 (suppl. 1): 111-115.
160. Ri~nnerstam R., Persson K., Hansson H. and Ren- marker K. (1985): Prevalence of ch lamydia l eye infection in pat ients a t tending an eye clinic, a VD clinic, and in heal thy persons. - Br. J. Ophthal- mol., 69: 385-388.
161. Saikku P. and Paavonen J. (1978): Single-antigen immunof luorescence test of ch lamydia l anti- bodies. - J. Clin. Microbiol., 8: 119-122.
162. Saikku P., Paavonen Y., giiiiniinen P. and gaheri A. (1983): Solid-phase enzyme immunoassay for ch lamydia l ant ibodies. - J. Clin. Microbiol. , 17: 22-27.
163. Salari S.H. and Ward M.E. (1981): Polypept ide composi t ion of Chlamydia trachomatis. - J. Gen. Microbiol. , I2.3: 197-207.
164. San Yoaquin V.H., Rett ig P.J., Newton J.Y. and Marks M.L (1982): Prevalence of ch lamydia l an- t ibodies in children. - Amer. J. Dis. Child., 136: 425427.
165. Sarov I. and Becker Y. (1968): RNA in the ele- men ta ry bodies of t r achoma agent. - Nature, 217: 849-852.
166. Sarov I. and Becke t Y. (1969): Trachoma agent DNA. - J. Mol. Biol., 42: 581-589.
167. Sarov I. and Becker Y. (1971): Deoxyribonucleic acid-dependent r ibonucleic acid po lymerase activ- i ty in purif ied t r a c h o m a e lementary bodies: ef- fect of s o d i u m chlor ide on r ibonucle ic acid tran- script ion. - J. Bacteriol. , 107: 593-598.
253
Ladany S. and Sarov I. Eur. J. Epidemiol.
168. Sarov 1., Friedman M., Levy E., Pascal L., Aymard M., Bosshard S., Chardonnet Y. and Revillard J.P. (1984): Detection of recurrent cytomegalo- virus infection in renaI- transplant patients. - I. Infect. Dis., 149: 277.
169. Sarov I. and Haikin H. (19~3): H u m a n cytome- galovirus specific IgA antibodies detected by im- munoperoxidase assay in serum of pat ients with cytomegalovirus infections. - J. Virol. Meth., 6: 161-169.
170. Sarov 1., Insler V., Sarov B., Cevenini R., Rum- pianesi F., Donati M., Kleinman D., Piura B., Lie- berman J., K immel N., Friedman M. and La PIaca M. (1984): Specific serum IgA antibodies in the diagnosis of active viral and chlamydial infec- tions. In: New Horizons in Microbiology, Sanna A. and Morace G. (eds). Elsevier Biornedical Press, Amsterdam, p. 157-168.
171. Sarov l., Kleinman D., Cevenini R., Holcberg G., Potashnik G., Sarov B. and Insler V. (1985): Spe- cific IgG and IgA antibodies to Chlamydia tra- chomatis in infertile women. - Int . J. Fertil., 22: in press.
i72. Sarov I., Levy E., Aymard M., Chardonnet Y., Bosshard S., Revitlard J.P., Friedman M., Nord E., Greiff M. and Haikin H. (1982): Detection of virus-specific IgA antibodies in serum of kid- ney t ransplant with recurrent cytomegalovirus infection by enzymeimmuno and radioimmuno- assay techniques. - Clin. Exp. Immunol . , 48: 321-328.
173. Sarov I., Siqueira-Linhares M., Chardonnet Y., Levy E., Aymard M., Bosshard S., Nord E. and ReviIIard J.P. (1981): Detection of specific IgA antibodies in serum of kidney t ransplant patients with recurrent cytomegalovirus infection. - In- tervirol., 15: 228-234.
174. Schachter J. (1978): Chlamydial infections. - New Engl. J. Med., 298: 428-435, 490-495, 540-549.
175. Schachter J. and CaldweIl H.D. (1980): Chlamy- diae. - Ann. Rev. Microbiol., 34: 285-309.
176. Schachter J. and Grossman M. (,1981): Chlamy- dial infections. - Ann. Rev. Med., 32: 45-61.
177. Schachter J., Grossman M. and Azimi P.H. 0982): Serolog-y of Chlamydia trachomatis in infants. - J. Infect. Dis., 146: 530-535.
178. Schachter .r., Hill E.C., King E.B., Heilbron D.C., Ray R.M., Margolis A.J. and Greenwood S.A. (1982): ChIamydia trachomatis and cervical neo- plasia. - J. Amer. Med. Assoc., 248: 2134-2138.
179. Schachter 1., Lure L., Gooding C.A. and Ostler B. (1975): Pneumoni t is following inclusion blennor- rhea. - J. Pediat., 87: 779-780.
180. Schachter J. and Osoba A.O. (1983): Lympho- granuloma venereum. - Brit. Med. Bull., 39: 151-154.
181. Schaefer C., Harrison H.R., Boyce W.B. and Lewis M. (1985): Illnesses in infants born to worn-
en with Chlamydia trachomatis infection. Amer. J. Dis. Child., 139: 127-133.
182. ScheibeI J.H., Andersen J.T., Brandenkof f P., Geer- dsen J.P., Bay-Nielson A., Schultz B.A. and Wal- ter S. (1983): Chlamydia trachomatis in acute epididymitis. - Scand. J. UroL Nephrol., 17: 47-50.
183. Scieux C., Colimon R., Mazeron M.C., Ronco E., Cahuzac P. and Perot Y. (1983): Uretrites et cervicites non gonococciques. - La Presse Med., 12: 1523-1526.
184. Senayake P. and Kramer D.G. (1980): Contra- ception and the etiology of pelvic inf lammatory disease: new perspectives. - Am. J. Obstet. Gyne- col., 138: 852-860.
185. Shabot J.M., Roark G.D. and Truant A.L. (1983): Chlamydia trachomatis in Ibe ascitic fluid of pat ients with chronic liver disease. - Amer. I. Gastroenterol., 78: 29,1-294.
186. Shemer Y. and Sarov f. (1985): Inhibi t ion of growth of Chtamydia trachomatis by huma n gam- ma interferon. - Infect. Immun. , 48 (2): 592-596.
187. Sherman J.K. and Jordan G.W. (1985): Cryosur- vival of Chtamydia trachomatis during cryopre- servation of human spermatozoa. - Ferfil. Steril., 43: 664-666.
188. Skaug K., Otnaess A.-B. Orstavik I. and Jerve F. (1982): Chlamydial secretory IgA antibodies in huma n milk. - Act Path. Microbiol. Immunol . Scand. Sect. C., 90: 21-25.
189. Skaug K., Vik I.S.S., Qvigstad E., Ulstrup J.C. and Jerve F. (1982): Chlamydial serum IgG anti- bodies with acute salpingitis measured by enzyme- l inked immunosorben t assays, - Act. Path. Mi- cobiol. Immunol . Scand. Sect.'C., 90: 67-71.
190. SiSderIund G. and Kihlstr6m E. (1983): Effect of methylamine and monodansylcadaver ine on the susceptibili ty of McCoy cells to ChIamydia trachomatis infection. - Infect. Immun. , 40: 534-541.
191. S t a m m W.E., Guinan M.E., Johnson C., Starcher T., Hohnes K.K. and McCormaclc W.M. (1984): Effect of t rea tment regimens for Neisseria go- norrhoeae on simultaneous infection with Chla- mydia trachomatis. - N. Engl. 3. Med., 310: 545-549.
192. S t a m m W.E., Koutsky LA., Benedett i J.K., lour- den J.L., Brunham R.C. and Holmes K.K. (1984): Chlamydia trachomatis urethral infections in men. - Ann. Intern. Med., 100: 47-51.
193. S t a m m W.E., Tam M., Koester M. and Cles L. (1983): Detection of Chlamydia trachomatis in McCoy cell cultures with fluorescein-conjugated mono,clona! an t ibod ie s . - J. Clin. Microbiol., 17: 666-668.
194. Stephens R.S., Kuo C.-C., Newpor t G. and Aga- bian N. (1985): Molecular cloning and expres- sion of Chlamydia trachomatis major outer mem- brane protein antigens in Escherichia coll. - In- fect. Immun. , 47: 713-718.
254

Vol. 1, 1985 Recent advances in Chlamydia trachomatis
195. Stephens R.S., Kuo C.-C., and Tam M.R. (1982): Sensitivity of immunofluorescence with monoclo- nal antibodies for detection of ChIamydia tra- chomatis inclusions in cell culture. - J. Clin. Mi- crobiol., 16: 4-7.
196. Shephens R.S. Tam M.R., Kuo C.-C., and Nowin- ski R.C. (1982): Monoclonal antibodies to Chla- mydia trachomatis: antibody specificities and an- tigen characterization. - J. Immunol . , 128: 1083-1089.
197. Stirling P., Allan I. and Pearce J.H. (1983): Inter- ference with t ransformat ion of chlamydiae from reproductive to infective body forms by depri- vation of cysteine. - FEMS Microbiol. Lett., 19: 133-136.
198. Stokes G.V. (1978): Surface projections and in- ternal s t ructure of Chlamydia psittaci, - J. Bacte- riol., 133: 1514-1516.
199. Storz J. and Page L.A. (1971): Taxonomy of the chlamydiae: reasons for classifying organisms of the genus Chlamydia, family Chlamydiaceae, in a separate order, Chlamydiales. - Int. J. Syst. Bacteriol., 2!: 332-334.
200. Sundkvist T. and Miirdh P.-A. (1984.): Serological evidence of ChIamydia trachomatis infection in non- immunocompromised adults with pneumo- nia. - J. Infect., 9: 143-147.
201. Suominen .1., GriSnroos M., Terho P. and Wichmann L. (1983): Chronic prostati t is, ChIamydia tracho- marls and infertility. - Int. J. Androl., 6: 405413.
202. Svensson L., Wes tr6m L. and M~irdh P.-A. (1984): Contraceptives and acute salpingitis. - J. Amer. Med. Assoc., 251: 2553-2555.
203. Sweet R.L., Draper D.L., Schachter J., James J., Hadley W.K. anit Brook.~ G.E. (1980): Microbio- logy and pathogenesis of acute salping.itis as determined by laparoscopy: what is the appro- priate site to sample? - Am. J. Obstet. Gynecol., 138: 985-989.
204. Swee t R.L., Schachter J. and Landers D.V. (1983): Chlamydial infections in obstetrics and gyneco- logy. - Clin. Obstet. Gynecol., 26: 143-164.
205. Tack K,J., Peterson P.K, Rasp F.L., O'Leary M., Hanto D., S immons R.L. and Sabath L.D. (1980): Isolation of Chl.amydia trachomatis from the lo- wer respiratory tract of adults. - Lancet, 1: 116-120.
206. Tam M.R., Stature W.E., HandsSield H.H., Ste- phens R. Kuo C.-C., t loImes K.K., Ditzenberger K., Krieger M. and Nowinski R.C. (1984): Cul- ture independent diagnosis of ChIamydia tracho- matis using monoclonal antibodies. - N. Engl. J. Med., 310: 1146-1150.
207. Tamura A. (1967) Isolat ion of r ibosome particles from meningopneumoni t i s organisms. - J. Bacte- riol., 93: 2009-2016.
208. Tamura A. and Manire G.P. (1967): Preparat ion and chemical composit ion of the cell membrane of developmental reticulate forms of meningo- pneumoni t i s organisms.- J. Bacteriol., 94: 1184-1188.
209. Tamura A., Matsumoto A., Higashi N. (1967): Pu- rification and chemical composit ion of ret iculate bodies of the meningopneumoni t i s organisms. - J. Bacteriol., 93: 2003-2008.
210. Tamura A., Matsumoto A., Manire G.P. arid Higa- shi N. (1971): Electron microscope observations on the s t ructure of the envelopes of mature ele- mentary bodies and developmental reticulate for- ms of Chlamydia psittaci. - J. Bacteriol., 105: 335-360.
211. Taylor-Robinson D. and Thomas B.J. (1980): The role of Chlamydia trachomatis in genital t ract and associated diseases. - J. Clin. Pathol., 33: 205-233.
212. Terho P. and Meurman 0. (1981): Chlamydial serum IgG, IgA and local IgA antibodies in patients with genital tract infection measured by solid phase radioimmunoassay. - J. Med. Micro- biol., 14: 77-87.
213. Thomas B.J.. Reeve P. and Oriel J.D. (1976): Sim- plified serological test for antibodies to Chla- mydia trachomatis. - J. Clin. Microbiol., 4: 6-10.
214. Thom.pson S., Lopez B., Wong K.-H., Ramsey C., Thomas J., Reising G., Jenks B., Peacock W., Sanderson M., Goforth S., Zaidi A., Miller R, and Klein L. (1982): A prospective study of chla- mydia and mycoplasma infections during preg- nancy: relation to pregnancy outcome and ma- ternal morbidity. In: Chlamydial Infections, Mgr- dh P.-A. Holmes K.K.. Oriel J.D., Plot P. and Schachter J. (eds). Elsevier Biomedical Press, Amsterdam, p. 155-158.
215. Thompson S.E. and Dretter R.H. (1982): Epide- miology and t rea tment of Chlamydial infections in pregnant women and infants. - Rev. Infect. Dis., 4 (suppl.): $747-$757.
216. Thompson S.E. and Washington A.E. (1983): Epi- demiology of sexually t ransmit ted Chtamydia trachomatis infections. Epidemiol. Rev., 5: 96-123.
217. Thornsteinsson S.B. (1982): Lymphogranuloma venereum: review of clinical manifestat ions, epi- demiology, diagnosis and t reatment . - Scand. J, Infect. Dis., 32 (suppl.): 111-115.
218. Tovi F., Hadar T., Sidi J., Sarov B. and Sarov I. (1985): The significance of specific serum IgA antibodies in the serum in the early diagnosis of z os te r . - J. Infect. Dis., 152-230.
219. Treharne .I.D., Darougar S. and Jones B.R. (1977): Modification of the microimmunofluorescence test to provide a rout ine serodiagnostic test for chlamydial infection. - J. Clin. Pathol., 30: 510-517.
220. Treharne J.D. and Forsey T. (1983): Chlamydiai serology. - Brit. Med. Bull., 39: 194-200.
22l. Treharne J.D., Ripa K.T., Miirdh P.-A., Svensson L. Westrbm L. and Darougar S. (1979): Antibodies to
255
Ladany S. and Sarov I. Eur. J. Epidemiol.
Chlamydia trachomatis in acute salpingitis. - Brit. J. Ven, er. Dis., 55: 26-29.
222. van der Bel-Kahn J.M., Watanakunakorn C., Me- neffe M.G., Long H.D. and Dicter R. (1978): Chla- mydia trachomatis endocarditis. - Amer. Hefirt L, 95: 627-636.
223. Viswalingam N.D., Wishart M.S. and Woodland R.M. (1983): Adult chlamydial oph tha lmia . - Brit. Med. Bul., 39: 123-127.
224. Wang S.-P., Eschenbach D.A. Holmes K.K., Wa- ger G. and Grayston J.T. (1980): Chlamydia tra- chomatis infection in Fitz-Hugh-Curtis syn- drome. - Am. J. Obstet. Gynecol., 138: 1034-1038.
225. Wang S.-P. and Grayston J.T. (1970): Immunolo- gical relat ionship betweeen genital TRIC lym- phogranuloma venereum and related organisms in a new microt i ter indirect ~mmunofluores- cence test. - Am. J. Ophthalmol., 70: 367-374.
226.. Wang S.-P. and Grayston J.T. (1982): M,icro im- munofluorescence ant ibody responses in Chlamy- dia trachomatis infection. In: Chlamydial Infec- tions, M:irdh P.-A. Holmes K.K., Oriel I.D., Plot P. and Schachter J. (eds). Elsevier Biomedical Press, Amsterdam, p. 301-316.
227. Wang S.-P., Grayston .LT., Alexander E.R. and Holmes K.K. (1975): Simplified microimmuno- fluorescence test with t rachoma - lymphogranu- loma v, enereum (Chlamydia trachomatis) anti- gens for use as a screening test for antibody. - J. Clin. Microbiol., 1: 250-255.
228. Ward M.E. (1983): Chlamydial classification, de- velopment and structure. - Brit. Med. Bull., 39: 109-115.
229. Ward M.E. and Murray A. (1984): Control me- chanisms governing the infectivity of Chlamy- dia trachomatis for HeLa cells: mechanisms of endocytosis. - J'. Gen. Mierobiol., 130: 4765A780.
230. Washington A.E., Gore S., Schachter Y. and Swe- et R.L. (1985): Oral contraception, Chlamydia trachomatis infection, and pelvic in f lammatory disease. - .l. Amer. Med. Assoc., 253: 2246-2250.
231. Westergaard L., Philipsen T. and Scheibel J. (1982): Significance of cervical ChIamydia tra- chomatis infection in postabortal pelvic inflam- matory disease. - Obstet. Gynecol., 60: 322-325.
232. Westr6m L. and Miirdh P.-A. (1982): Genital chla- mydial infections in the female. In: Chlamydial Infections, M~irdh P.-A., Holmes K.K. Oa~iel J.J)., Plot P. and Schachter 3. (eds). Elsevier Biomedi- cal Press, Amsterdam, p. 121-139.
233. Westr6m L. and Miirdh P.-A. (1983): Ohlamydial salpingitis - Brit. Med. Bull., 39: !45-150.
234. Wishart P.K., James C., Wishart M.S. and Darou- gar S. (1984): Prevalence of acute conjunctivi t is caused by chlamydia, adenovirus, and herpes simplex virus Jn an ophthalmic casualty depar- tment. - Brit. J. Ophthal., 68: 653-655.
235. Wolner.Hanssen P. and Miirdh P.-A. (1984): In vit,ro tests of the ad~herence of Chlamydia tracho- matis to huma n spermatozoa. - Fertil. Steril., 42: 102-107.
236 Wolner-Hanssen P., Miirdh P.-A. and Westr6m L. (1980): Perihepat i t is and chlamydial sa lpingi t is . - Lancet/ l: 901-903.
237. Wolner-Hanssen P., Svensson L., Westr6m L. and Mardh P.-A. (1982): Isolation of Chtamydia tra- chomatis from the liver capsule in Fitz-Hugh- Curtis syndrome. - N. Engl. J. Med., 306: H3.
238. VoIner-Hanssen P. and westr6m L. (1983): Sec- ond-look laparoscopy after acute s a l p i ng i t i s . - Obstet. Gynecol., 61: 702-704.
239. Yang Y.-S., Kuo C.-C., and Chen W.-J. (1983): Reac- t ivation of Chtamydia trachomatis lung infection in mice by cortisone. - Infect. Immun. , 39: 655-658.
240. Yli-Kerttula U.L, Selander K.K., Terho P.E., Ka- taja J.M. and Vilppula A.H. (1984): The na ture of urogenital involvements in female uro-arthri~ tis with special reference to chlamydial infection.
Clin. Rheumatol., 3: 155-]62.
241. Yong E.C., Chinn J.S., CaldwelI H.D. and Kuo C.-C. (1979): Reticulate bodies as single antigen in Chlamydia trachomatis serology with micro- immunofluorescence. - J. Clin. Microbiol., 10: 35,1-356.
242. Yong E.C., Klebano[f S.J. and Kuo C.-.C. (1982): Toxic effect of huma n polymorphonuclear leu- kocytes on Chlamydia trachomatis. - Infect. Im- mun., 37: 422-426.
243. Zapata M., Chernesky M. and Mahony J. (1984): Indirect immunofluorescence staining of ChIa- mydia trachoma!is inclusions in microcul ture plates with monoclonal antibodies. - J. Clin. Micro- biol., 19: 937-939.
244. Zeichner S.L. (1983): Isolat ion and characteriza- t ion of macrophage phagosomes containi 'ng in- fections and beat-inactivated Chlamydia psittaci: Two phagosomes with different intracel lular be- haviors. - Infect. Immun. , 40: 956-966.
245. Zvillich M. and Sarov I. (1985): In teract ion be- tween huma n polymorphomrclear leukocytes and Chlamydia trachomatis elementary bodies: elec- t ron microscopy and chemiluminescent response. - J. Gen. Microbiol., 131: 2627-2635.
256





























