Embed Size (px)
Citation preview
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Quantitative MRI of the prefrontal cortex and executive function in patientswith temporal lobe epilepsy
Simon Sean Keller a,*, Gus Baker b, Joseph John Downes c, Neil Roberts d
a Magnetic Resonance and Image Analysis Research Centre (MARIARC), University of Liverpool, Pembroke Place, Liverpool L69 3BX, UKb Walton Centre for Neurology and Neurosurgery, Liverpool, UKc Department of Psychology, University of Liverpool, Liverpool, UKd Clinical Research Imaging Centre (CRIC), Queen’s Medical Research Institute (QMRI), University of Edinburgh, Edinburgh, UK
a r t i c l e i n f o
Article history:Received 21 November 2008Revised 4 March 2009Accepted 5 March 2009Available online 11 April 2009
Keywords:EpilepsyExecutive functionHippocampusPrefrontal cortexQuantitative MRI
a b s t r a c t
We investigated the relationship between prefrontal cortex (PFC) and hippocampal volume and executivefunctioning in patients with temporal lobe epilepsy (TLE). Prefrontal volume and hippocampal volumewere studied using stereology in conjunction with point counting and voxel-based morphometry onMR images. Executive functioning was assessed using tests routinely incorporated into presurgical neu-ropsychological evaluation. Relative to 30 healthy controls, 43 patients (26 left, 17 right) with TLE hadvolume atrophy of the ipsilateral hippocampus and bilateral dorsal PFC. Performance on the workingmemory index of the Wechsler Memory Scale was positively correlated with the volume of all prefrontalregions, and the Controlled Oral Word Association Test with the left dorsal PFC, whole left PFC, and lefthippocampus. Stroop Color–Word Interference performance was not related to volume of dorsal PFC. The‘‘extratemporal neuropsychological profile” frequently observed in patients with TLE may be due toextended damage to brain regions remote from the epileptogenic focus. In particular, volume atrophyof the dorsal PFC may account for deficits in executive functioning.
� 2009 Elsevier Inc. All rights reserved.
1. Introduction
Many patients with temporal lobe epilepsy (TLE) experienceneurocognitive disturbances classically not associated with tempo-ral lobe function. Some patients are impaired on tasks that requirefrontal lobe processing in a similar way to patients with frontallobe epilepsy [1]. As hippocampal sclerosis is the most commonneuropathological correlate of TLE, it has been suggested that hip-pocampal pathology may be the primary cause of executive dys-function in this patient group. For example, Giovagnoli [1]reported deficits on the Wisconsin Card Sorting Test (WCST), whichrelies largely on frontal lobe processing, in patients with medialTLE and hippocampal sclerosis, but not in patients with lateralTLE and no hippocampal abnormalities. This is supported by anearlier study that found that patients with TLE with unilateral hip-pocampal sclerosis performed more poorly than patients withfrontal lobe or temporal lobe neocortical lesions on the same task[2]. However, other studies have failed to find a relationship be-tween hippocampal sclerosis and measures of frontal lobe functionin patients with TLE [3–6]. Although recent MRI studies have dem-onstrated that patients with TLE may have atrophy of prefrontalcortex relative to healthy controls [7–9], no work to date has pro-
spectively examined the relationship between prefrontal volumeand executive functioning in patients with TLE.
During presurgical evaluation for medically intractable TLE, allpatients undergo baseline neuropsychological assessment to deter-mine their current cognitive and affective status and to predictpostsurgical neurocognitive outcome. The neuropsychological bat-tery used at the Walton Centre for Neurology and Neurosurgery(WCNN) in Liverpool includes assessment of executive functioningusing a combination of the Stroop Color–Word Interference task[10], the Controlled Oral Word Association Test (COWAT) [11],and the working memory index of the Wechsler Memory ScaleThird Edition (WMS-III) [12]. The present study sought to investi-gate whether performance on the aforementioned neuropsycho-logical tasks of executive functioning are preferentially related tothe structure of the PFC or hippocampus in patients with TLE.
The present study used two complementary quantitative mag-netic resonance (MR) image analysis techniques to investigatethe neuroanatomical correlates of executive function in patientswith TLE: stereological region-of-interest analysis and whole-brainvoxel-based morphometry (VBM). Stereological analysis providedunbiased volume estimation of the left and right dorsal and ventralPFC, hippocampus, and cerebral hemispheres, and VBM quantifiedgray matter concentration (GMC) over the entire brain. There weretwo primary objectives of the present study. First, we sought toinvestigate whether patients with unilateral TLE have volume
1525-5050/$ - see front matter � 2009 Elsevier Inc. All rights reserved.doi:10.1016/j.yebeh.2009.03.005
* Corresponding author. Fax: 0151 7945635.E-mail address: [email protected] (S.S. Keller).
Epilepsy & Behavior 15 (2009) 186–195
Contents lists available at ScienceDirect
Epilepsy & Behavior
journal homepage: www.elsevier .com/locate /yebeh
Author's personal copy
alterations of prefrontal cortical subfields relative to healthy con-trols, and whether particular volume alterations are dependenton the hemispheric side of seizure onset. Previous VBM studieshad shown that patients with unilateral left or right TLE haveGMC reduction of right [7] or bilateral [8] dorsal PFC relative tohealthy controls. These findings have not been replicated usingquantitative MRI region-of-interest analyses. Second, we soughtto investigate the relationship between executive functioningusing three neuropsychological tasks, and prefrontal and hippo-campal volume using stereological analysis and VBM, in patientswith TLE. We hypothesized that dorsal prefrontal volume, andnot hippocampal volume, would be associated with executivefunctioning in patients with TLE, based on previous work demon-strating the importance of dorsal prefrontal cortex for executivefunctions [13–17].
2. Methods
2.1. Participants
Thirty neurologically and psychiatrically healthy individualswere studied as a control population (see Table 1 for information).Forty-three nonconsecutive patients with medically intractableunilateral TLE undergoing presurgical evaluation were retrospec-tively selected from a large clinical database of patients. Each pa-tient had complete archives of demographic information; clinicalhistory; electroclinical information; volumetric data on the hippo-campus, amygdala, temporal lobe, and cerebral hemisphere; hip-pocampal relaxometry; and an accessible three-dimensional T1-weighted MR image for quantitative analysis of the prefrontal cor-tex. Temporal lobe seizure onset was determined using noninva-sive electroencephalogram (EEG) recordings and invasiveforamen ovale recordings in conjunction with video telemetrywhen EEG recordings were nonlocalizing, together with other rou-tine presurgical evaluation techniques (baseline neuropsychologi-cal evaluation, diagnostic MRI, and Wada testing). Of the 43patients, 26 had unilateral left TLE and 17 had unilateral rightTLE (Table 1).
2.2. Neuropsychological evaluation
All patients underwent full neuropsychological assessment aspart of their consideration for the epilepsy surgery program atWCNN, which included tests of intellectual functioning, memoryfunctioning, attention and concentration, language, executive func-tioning, and mood [18]. For the present study, data from the StroopColor–Word interference test, WMS-III, and COWAT were ana-lyzed. In the present investigation, Stroop scores were availablefor all 43 patients, the working memory component of WMS-III
for 23 patients (7 with right TLE), and the COWAT for 22 patients(6 with right TLE).
The Stroop task was administered as described in the StroopNeuropsychological Screening Test Manual [19]. Both stages of theStroop task were administered using standardized applications,but only data from the second (color–word) interference taskwas used for analysis. For both tasks, performance was measuredeither as the time taken to complete the parts of the test or asthe number of words read (or colors reported) in 2 minutes. Anyerrors were subtracted from the total score. Scoring on the second(color–word) task was used to assess frontal lobe functioning, as itis this test that provides the interference. Although only the color–word task is used for interpretation, both tasks should always beadministered, as the first (color task) has a priming effect on thedegree of interference in the second task [19].
The WMS-III [12] provides measures of numerous componentsof memory function, including visual and auditory immediate anddelayed recall and recognition. In the present study, only data fromthe working memory component, which are obtained from twoparticular subtests (letter number sequencing and spatial span),were analyzed. For the former, participants were orally presentedwith an intermixed set of letters and numbers, and were instructedto overtly recall each number and letter in ascending sequential or-der (e.g., ‘‘2 B 4 F 7 J”). For the spatial span task, participants firstobserved the examiner tap a sequence of numbered blocks, andwere then required to tap the same sequence, which increased inlength with each trial. Scoring was based on the number of correcttrials. Further information on the exact scoring method is availablein Wechsler [12].
The COWAT is an overt verbal fluency task that required eachparticipant to orally generate as many words as possible beginningwith the letters F, A, and S. A response time of 1 minute was givenfor each letter, and participants were instructed not to generatenouns (e.g., France or Adam) or repeat words with alternative end-ings (e.g., eat and eating). The scoring system was based on the to-tal number of words correctly generated. Further information onthe scoring system is available in Spreen and Strauss [20].
2.3. MRI
2.3.1. AcquisitionT1-weighted images were obtained for all subjects using a 1.5-T
SIGNA whole-body MRI system (GE Medical Systems, Milwaukee,WI, USA). A spoiled gradient echo (SPGR) pulse sequence(TE = 9 ms, TR = 34 ms, flip angle = 30�) produced 124 coronal T1-weighted images with a FOV of 20 cm. Acquired images were ofvoxel size 0.781 � 0.781 � 1.6 mm. Acquisition time was 13 min56 s for a 1 NEX scan.
2.4. Stereology
The Cavalieri method of modern design stereology in conjunc-tion with point counting [21] was used to estimate the volume ofthe prefrontal cortical subfields, hippocampi, and cerebral hemi-spheres of all subjects. In the Cavalieri method, volume is directlyestimated from equidistant and parallel MR images of the brainwith a uniform random starting position. A second level of sam-pling is required to estimate the section area from each image byapplying point counting. The mathematical justification and imple-mentation of the methodology are simple, and it can be applied tostructures of arbitrary shape [22]. This technique has been widelyapplied to reliably estimate brain compartment volume in a time-effective manner [7,8,22–30]. Stereology has been shown to be atleast as precise as tracing and thresholding volumetry techniquesand substantially more time efficient [25].
Table 1Demographic information for all participants and clinical information for patientsstudied in the present investigation.
Controls Left TLE Right TLE
N 30 26 17Age 43.8 (11.7) 32.0 (8.7) 33.4 (9.4)Gender (%)Male 36.7 46.2 23.5Female 63.3 53.8 76.5Handedness (%)Right 100 92.3 100Left 0 7.7 0Age at onset of epilepsy — 8.8 (8.3) 11.56 (8.6)Duration of epilepsy (years) — 24.2 (12.7) 23.2 (12.0)
Note. Values are means (SD), unless otherwise indicated.
S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195 187

Author's personal copy
2.4.1. Prefrontal cortexVolume estimation of the left and right dorsal and ventral pre-
frontal cortical subfields using stereology was based on the princi-ples of a previous study [23]. All three-dimensional T1-weightedimages were realigned perpendicular to the bicommissural planeusing BrainVoyager software (R. Goebel, Brain Innovation,www.BrainVoyager.com) running on a PC workstation (DellDimension, Pentium II 400, Windows XP), and the 256 �256 � 124 acquired voxels of side 0.781 � 0.781 � 1.6 mm wereinterpolated to cubic voxels of side 1.0 mm. The left and right dor-sal and ventral prefrontal cortical subfields were manually demar-cated using BrainVoyager. Two demarcations were marked on eachimage: First, to demarcate dorsal prefrontal cortex (DPFC) fromventral prefrontal cortex (VPFC), a marker was placed on the axialsection where the anterior commissure and posterior commissurecould be simultaneously visualized. Second, a marker was placedon a coronal image at the level of the genu of the corpus callosum,which served as the caudal border of the DPFC. Most of the pointcounting was guided by the markers placed using BrainVoyager.This is particularly true for the DPFC. Posterior regions of the VPFCare not demarcated by the markers, and require visualization ofanatomy to delineate VPFC from adjacent subcortical anatomy.At midline, a boundary between medial prefrontal brain tissueand cerebrospinal fluid (CSF) is clearly visible for the majority ofcases. When the cortical border with the CSF is obscured in themidline slices of the image, the anteroventral-most tip of the cor-pus callosum guided the posterior cortical boundary. Laterally, theboundary followed the anteriormost portion of the caudate nu-cleus. More laterally, the boundary was demarcated by the anteriorbranch of the Sylvian fissure. These anatomical features were visu-alized by the rater during point counting. Fig. 1 illustrates pointcounting for volume estimation of DPFC and VPFC.
Volume estimation of the left and right DFPC and VPFC wasachieved through sampling a series of equally spaced sagittal MRimages, beginning with a random starting position, using Easymea-
sure software [24]. Each image was overlain with a test systemcomprising a regular array of test points, and the number of pointslying within the transect through each prefrontal region was re-corded. Separation between test points on the square grid usedfor point counting was 0.8 cm (i.e., 8 pixels) for the DPFC and0.7 cm (i.e., 7 pixels) for the VPFC. Slice interval was 0.4 cm (everyfour MR sections). Unbiased estimates of transect area were ob-tained by multiplying the total number of points recorded by thearea corresponding to each test point (e.g., 0.8 � 0.4 = 0.32 cm2
for DPFC). An unbiased estimate of volume was obtained as thesum of the estimated areas of the structure transects on consecu-tive systematic sections multiplied by the distance between sec-tions. Approximately 150–200 points were recorded on 10 to 15systematic random sections per structure (left/right/DPFC/VPFC).Sectioning and point counting intensities were optimized toachieve a coefficient of error on the Cavalieri volume estimatesof below 5% [21]. An inter-/intrarater reliability study was carriedout by three raters who estimated prefrontal volumes. Intraclasscorrelation coefficients were calculated and were greater than 0.9.
2.4.2. HippocampusQuantitative MRI measures of the volume of the hippocampus
using the Cavalieri method of modern design stereology in combi-nation with point counting were available in the context of the pre-surgical evaluation program, and the methods of hippocampalstereology have been described in detail elsewhere [7,8,25–27].For analysis, the three-dimensional T1-weighted MR images weretransferred to ANALYZE (Mayo Foundation, Rochester, MN, USA)on a SPARC 10 workstation (SUN Microsystems, Santa Clara, CA,USA), and the 256 � 256 � 124 acquired voxels of side0.781 � 0.781 � 1.6 mm were linearly interpolated to 256 �256 � 256 cubic voxels of side 0.781 mm. Image sections werereformatted perpendicular to the long axis of the hippocampusto provide optimal visualization of medial temporal lobe struc-tures. The direction of reformatting was adjusted so that the brain
Fig. 1. Point counting for stereology in medial (left) to lateral (right) regions of the dorsal (top) and ventral (bottom) prefrontal cortex.
188 S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195

Author's personal copy
appeared symmetrical on the reformatted sections. The hippocam-pus as defined in the present study comprised hippocampus prop-er, dentate gyrus, ambient gyrus, subiculum, fimbria, alveus, andhippocampal vertical digitations. We excluded the uncus and cho-roid plexus. The posteriormost section of the hippocampus was de-fined as the section on which the lateral ventricles divide intofrontal and temporal horns. On the anteriormost section, the hip-pocampus was differentiated from the amygdala by visualizationof the alveus and typically additionally by a region of CSF superiorto the alveus.
Volume estimation was achieved by sampling a series of equallyspaced MR images, beginning with a random starting position.Each image was overlain with a test system comprising a regulararray of test points, and the number of points lying within eachtransect through the hippocampus was recorded. Separation be-tween test points on the square grid used for point counting was0.234 cm (i.e., 3 pixels) and slice interval was also 0.234 cm forthe hippocampus. Unbiased estimates of transect area were ob-tained by multiplying the total number of points recorded by thearea corresponding to each test point (i.e., 0.234 �0.234 = 0.0548 cm2). An unbiased estimate of structure volumewas obtained as the sum of the estimated areas of the structuretransects on consecutive systematic sections multiplied by the dis-tance between sections. Approximately 150 points were recordedon 10 to 15 systematic random sections. Intraclass correlationcoefficients were calculated and were greater than 0.9 in intra-and interrater reliability studies, as previously reported [7,8,26,27].
2.4.3. Cerebral hemispheresAs neuropsychological–prefrontal correlations could potentially
be due to larger brains in general, we additionally measured thevolume of the left and right cerebral hemispheres to control forthe effects of brain size. The application of stereological methodsto estimate the volume of the cerebral hemispheres has been de-tailed previously [26,27]. Briefly, after image interpolation andreformatting identical to that for hippocampal volume measure-ments, the left and right hemispheres were sampled separatelyon every 15th MR section (i.e., 1.17 cm) using a square grid of 15pixels (i.e., 1.2 cm). Measurements excluded the brainstem andcerebellum. All supratentorial gray matter and white matter wassampled.
2.5. Voxel-based morphometry
Prior to voxel-based statistical analysis, MR images were spa-tially processed using SPM5 (Wellcome Department of CognitiveNeurology, www.fil.ion.ucl.ac.uk), running in Matlab 5.3 (TheMathworks, Natick, MA, USA) on a PC workstation (Dell Dimension,Pentium II 400, Windows XP). Optimized VBM techniques wereperformed as described in our previous studies (automatic seg-mentation, linear and nonlinear (7 � 8 � 7 basis functions) nor-malization, 10-mm smoothing) [9,31,32]. We have previouslyreported that VBM analyses incorporating the modulation stepare less sensitive in detecting frontal lobe effects in patients withTLE [7–9,31,32]. We therefore performed analyses without inclu-sion of the modulation step, and compared findings of GMC withchanges in prefrontal volume estimates obtained using stereology.
2.6. Statistical analysis
2.6.1. StereologyStatistical analyses were administered using SPSS Version 11 for
Windows (SPSS Inc., Chicago, IL, USA). A combination of 3 � 2mixed ANOVAs, one-way ANOVAs, and t tests, in addition to Tu-key’s HSD post hoc testing, were used for comparison of prefrontaland hippocampal morphology between patient groups and con-
trols. Pearson’s coefficient was used for the within-group analysisof association between neuropsychological performance and vol-ume of neuroanatomical structures. Because of the relatively smallsample size, we did not incorporate a stringent correction for mul-tiple comparisons given that such a correction may have obscuredsubtle but significant effects.
2.6.2. Voxel-based morphometryThe spatially processed images were compared between pa-
tients with left TLE, patients with right TLE, and controls on a vox-el-by-voxel basis using the general linear model. Contrasts weredefined to detect whether each voxel of tissue had a greater or les-ser probability of being gray matter between groups. For neuroana-tomical–cognitive relationships, the spatially processed images ofpatients with left TLE and those with right TLE were entered intoa multiple regression model with Stroop, COWAT, and workingmemory performance as covariates of interest. The output for eachcomparison is a statistical parametric map of the t statistic (SPM{t}),which was transformed to a normal distribution (SPM{z}) andthresholded at P < 0.05 (corrected for multiple comparisons). To in-crease the sensitivity of detecting neuroanatomical–cognitive rela-tionships, we used a small volume correction (SVC) on the brainregions of interest, thresholding at P < 0.05. Spherical SVCs of 20and 10 mm were used on prefrontal cortex and hippocampus,respectively.
3. Results
3.1. Neuroanatomical comparisons
3.1.1. StereologyIn controls, mean left and right hippocampal volumes were
found to be 2.5 ml (SD = 0.4) and 2.6 ml (SD = 0.4), respectively.Mean left and right hippocampal volumes in patients with leftTLE were 1.5 ml (SD = 0.3) and 2.5 ml (SD = 0.5), and in patientswith right TLE, 2.4 ml (SD = 0.4) and 1.8 ml (SD = 0.6). A 3 � 2 mixedANOVA revealed a significant main effect of group(F(1, 69) = 12.551, P < 0.001), a significant effect of side of hippo-campus (F(1, 69) = 33.749, P < 0.001), and a significant group � sideinteraction (F(2, 69) = 151.088, P < 0.001). Further investigation ofthe group � side interaction using a one-way ANOVA revealed sig-nificant differences in left (F(2, 71) = 47.93, P < 0.001) and right(F(2, 71) = 13.65, P < 0.001) hippocampal volume between groups,with patients with left TLE having reduced left hippocampal vol-umes (Tukey’s HSD, 0.9732, P < 0.001) and patients with right TLEhaving reduced right hippocampal volumes (Tukey’s HSD, 0.7257,P < 0.001) compared to controls. There were no significant differ-ences in hippocampal volume contralateral to the side of seizureonset between patient groups and controls (P = 0.692 in patientswith left TLE, and P = 0.822 in patients with right TLE).
Table 2 summarizes the descriptive statistics of prefrontal cor-tical subfield volume in controls and patients. Two 3 � 2 ANOVAs
Table 2Mean volumes of left and right ventral and dorsal prefrontal cortex in controls,patients with left TLE, and patients with right TLE.
Volume (ml)
Controls Left TLE Right TLE
Left VPFC 10.5 (2.8) 9.2 (2.7) 10.4 (3.8)Right VPFC 10.4 (2.5) 9.4 (2.3) 10.8 (3.3)Left DPFC 23.6 (4.6) 21.1 (3.9)a 22.1 (3.3)a
Right DPFC 23.7 (3.7) 21.6 (3.8)a 21.0 (3.5)a
Note. Values are means (SD). VPFC (DPFC), ventral (dorsal) prefrontal cortex.a Significantly different from controls (see main text).
S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195 189

Author's personal copy
were used to analyze VPFC and DPFC volume separately. Resultsindicated no significant group difference (F(1, 70) = 1.72,P = 0.19), left–right asymmetry (F(1, 70) = 0.78, P = 0.38), orgroup � side interaction (F(2, 70) = 0.56, P = 0.57) in VPFC volume.Analysis of DPFC volumes revealed that there was a significantmain effect of group (F(1, 70) = 3.28, P = 0.04), but no significantleft–right asymmetry (F(1, 70) = 0.33, P = 0.57) or side � groupinteraction (F(2, 70) = 1.45, P = 0.24). Further investigation of thesignificant main effect of group on DPFC volume using a one-wayANOVA revealed that significant group differences were restrictedto the right DPFC (F(2, 70) = 3.455, P = 0.03), with possibly a trendin the left DPFC (F(2, 70) = 2.615, P = 0.08). Post hoc investigationusing Tukey’s HSD revealed that right DPFC volumes were reducedin both patient groups relative to controls, and that left DPFC vol-ume was significantly reduced when patients with left and thosewith right TLE were combined relative to controls (F(2, 70) = 3.28,P = 0.04).
3.1.2. Voxel-based morphometryGMC reduction and increase in patients with left and right TLE
relative to controls is illustrated in Fig. 2 (reduction = red-orange,increase = purple-blue). Peak coordinates and statistical signifi-cance levels of all effects are provided in Table 3. In patients withleft TLE, GMC reduction was identified in left hippocampus, leftdorsolateral prefrontal cortex, bilateral dorsomedial prefrontal cor-
tex, and left occipitoparietal cortex. In patients with right TLE, GMCreduction was identified in right hippocampus, right dorsolateralprefrontal cortex, bilateral dorsomedial prefrontal cortex, andmedial parietal cortex (including posterior cingulate gyrus andprecuneus). Areas of GMC increase were identified in bilateralparahippocampal gyrus in patients with left and right TLE relativeto controls. Further areas of GMC increase were identified in rightinsula and left cerebellum in patients with left TLE and in medio-ventral prefrontal cortex in patients with right TLE.
3.2. Neuroanatomical–cognitive relationships
One-way ANOVAs revealed that there was no difference inStroop (F(1, 41) = 0.323, P = 0.573) or WMS III (F(1, 21) = 0.649,P = 0.429) performance between patients with left and right TLE.However, patients with left TLE performed significantly worse onthe COWAT relative to patients with right TLE (F(1, 20) = 9.139,P = 0.007). The only significant correlation found between the threetasks was between performance on the WMS-III and performanceon COWAT in patients with left TLE only (r = 0.551, P = 0.027).
3.2.1. StereologyWhen all patients were pooled, several significant correlations
emerged. First, performance on the working memory componentof the WMS-III was positively correlated with volume of left DPFC
Fig. 2. Results from voxel-based morphometry for group comparison analyses of patients with left and patients with right TLE and controls. Red-orange regions indicate graymatter concentration reduction and blue-purple regions indicate gray matter concentration increase in patients relative to controls. The top rows for each group indicateeffects in prefrontal cortex (PFC), and the bottom rows indicate effects in the medial temporal lobe (MTL). Images are in neurological convention (R = R/L = L). (Forinterpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
190 S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195

Author's personal copy
(r = 0.415, P = 0.049), left VPFC (r = 0.600, P = 0.002), right VPFC(r = 0.507, P = 0.013), whole (i.e., dorsal and ventral) left PFC(r = 0.561, P = 0.005), whole right PFC (r = 0.433, P = 0.039), and to-tal (i.e., left and right) PFC (r = 0.533, P = 0.009). These correlationsare illustrated in Fig. 3. WMS-III performance was not correlatedwith left (P = 0.204) or right (P = 0.915) hippocampal volume. Sec-ond, performance on the COWAT was positively correlated withvolume of the left hippocampus (r = 0.524, P = 0.012), left DPFC(r = 0.426, P = 0.048), and whole left PFC (r = 0.463, P = 0.030). Therelationships between COWAT performance and neuroanatomicalvolume are illustrated in Fig. 4. Finally, Stroop performance wascorrelated only with volume of the left VPFC (r = 0.357,
P = 0.019). All other effects were nonsignificant (P > 0.055). Therewere no correlations between left or right hemisphere volumeand neuropsychological performance when all patients were ana-lyzed together, although there was a trend for relationships be-tween left hemisphere volume and COWAT performance(r = 0.301, P = 0.174) and working memory performance on theWMS-III (r = 0.371, P = 0.081).
When patients were separated according to the side of seizureonset, significant correlations were observed only for the rightTLE group. This was surprising given that neuropsychological scoreswere available for only 17 (Stroop), 7 (WMS-III), and 6 (COWAT) pa-tients with right TLE. In these patients, the working memory
Table 3Results from voxel-based morphometry.
Analysis Contrast Region Voxel cluster SPM{z} Peak coordinates
Patients with left TLE vs controls GMC reduction Bilateral medial PFC, left dorsolateral PFC 8554 5.29b �17 27 59Left occipitoparietal cortex 7428 5.11a �55 �63 33Left hippocampus 1509 5.04a �32 �15 �18
GMC increase Left PHG 2645 5.87c �26 �27 �21Right PHG 2999 5.48b 23 �49 �4Right cerebellum, PHG 2734 4.95a 23 �53 �23Left insula 1635 4.93a �39 �1 10
Patients with right TLE vs controls GMC reduction Medial parietal cortex 3452 5.12a -1 �60 37Bilateral medial PFC 3038 5.11a 8 45 42Right hippocampus 643 5.04a 36 �20 14Left dorsal PFC 1905 5.00a �8 9 65Right dorsolateral PFC 877 4.95a 32 32 43Right parietal cortex 731 4.93a 45 �57 51
GMC increase Bilateral medioventral PFC 2410 5.45b 4 29 �16Bilateral medial PFC 1739 5.33b �10 47 9Right PHG 1437 5.04a 29 �19 28Left PHG, amygdala, hippocampus 1568 4.92a –26 �18 -20
Note. Region, voxel cluster size (spatial extent), significance (SPM{z}), and coordinates of peak effect are indicated. All results are reported at P < 0.05, corrected for multiplecomparisons. GMC, gray matter concentration; PFC, prefrontal cortex; PHG, parahippocampal gyrus.
a Significant at the P < 0.05 level, when corrected for multiple global comparisons.b Significant at the P < 0.025 level, when corrected for multiple global comparisons.c Significant at the P < 0.01 level, when corrected for multiple global comparisons.
Fig. 3. Significant positive correlations between performance on the working memory index of the WMS-III (raw scores) and (A) left DPFC, (B) left VPFC, (C) right VPFC, (D)whole left PFC, (E) whole right PFC, and (F) entire PFC in all patients. All significant correlations stand when the outlier is removed from analyses.
S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195 191

Author's personal copy
component of the WMS-III was positively correlated with the vol-ume of the left VPFC (r = 0.790, P = 0.035), whole right PFC(r = 0.786, P = 0.036), and total PFC (r = 0.786, P = 0.036); COWATperformance was correlated with volume of the left DPFC(r = 0.840, P = 0.036) and whole right PFC (r = 0.839, P = 0.037);and Stroop performance was correlated with volume of the leftVPFC (r = 0.495, P = 0.043). No hippocampal volume–neuropsycho-logical performance correlations existed. There were no correla-tions between left or right hemisphere volume andneuropsychological performance when patients were analyzed sep-arately according to the side of seizure onset.
3.2.2. Voxel-based morphometryNo GMC–cognitive relationships were observed using whole-
brain correction for multiple comparisons or small volume correc-tions on the prefrontal cortex or hippocampus when patientgroups were analyzed separately or together.
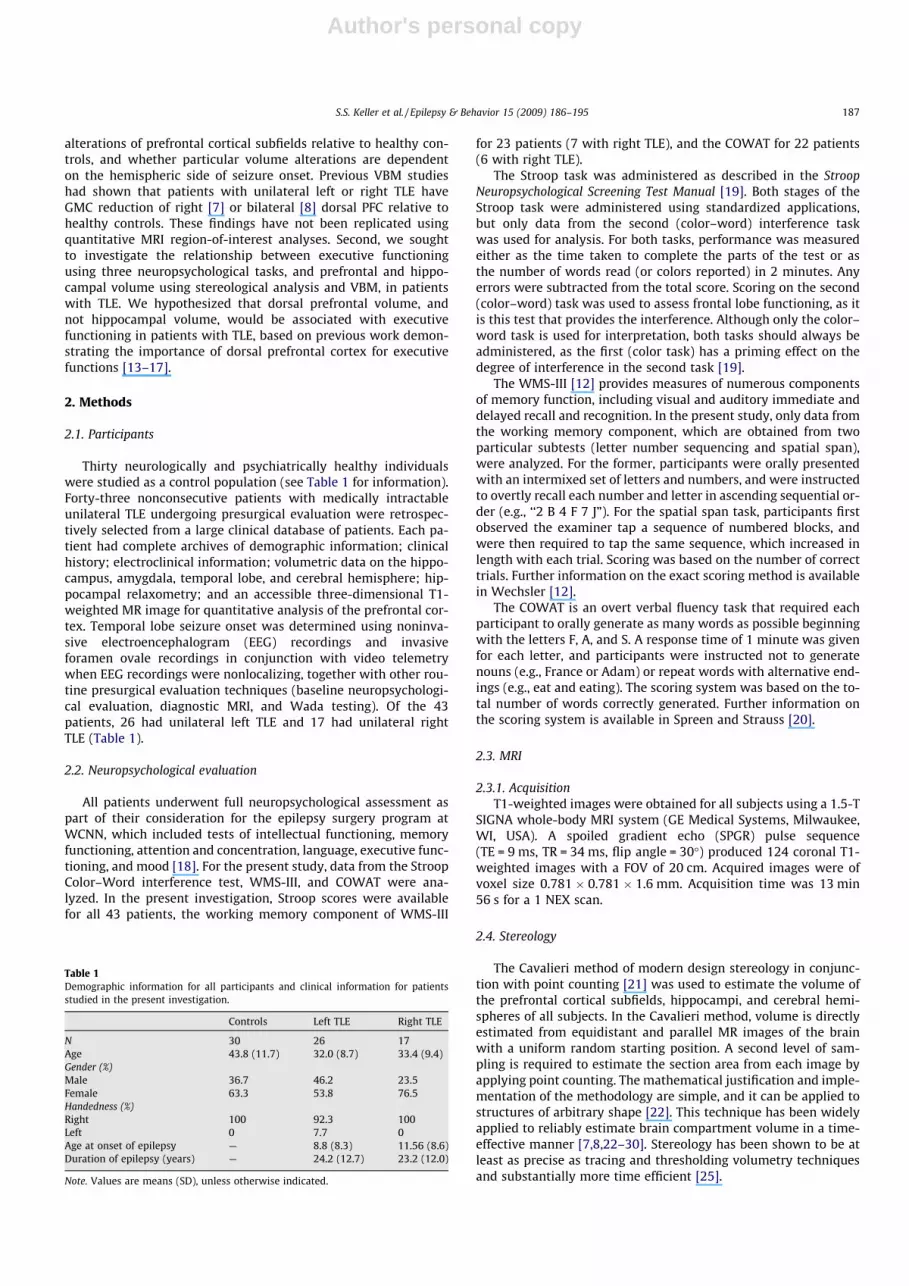
Fig. 5 schematically illustrates the significant findings of thepresent study.
4. Discussion
There were two primary objectives of the present study. First,we sought to investigate whether patients with unilateral TLE havevolume alterations of prefrontal cortical subfields relative tohealthy controls, and whether particular volume alterations aredependent on the side of seizure onset. We found that patientswith unilateral left and right TLE had significant volume reductionof right DPFC relative to controls, and significant volume reductionof left DPFC was obtained only when patients with left and thosewith right TLE were pooled in a single analysis. No differences were
observed in VPFC. These results were obtained using both stereol-ogy and VBM, as was volume reduction of the hippocampus ipsilat-eral to the side of seizure onset. Second, we sought to investigatethe relationships between the volumes of prefrontal cortical sub-fields and hippocampus and neuropsychological performance onthe executive measures. We found that performance on (1) theworking memory index of WMS-III was positively correlated withthe volume of all prefrontal cortical regions other than right DPFC,(2) COWAT performance was positively correlated with left DPFC,whole left PFC, and left hippocampal volumes, and (3) Stroop per-formance was positively correlated with left VPFC volume. No sig-nificant correlations were observed between neuropsychologicalperformance and whole cerebral hemisphere volume, and withhippocampal volume when patients were separated according tothe side of seizure onset. We discuss the neurocognitive implica-tions of these results after highlighting pertinent methodologicalissues.
4.1. Methodological issues
There are few studies that have assessed the morphology of theprefrontal cortex in patients with TLE. Those that have analyzedprefrontal structure have employed VBM techniques to studywhole-brain morphology (see Keller and Roberts [9] for a review).Some of these studies have reported prefrontal gray matter reduc-tion in patients with TLE relative to controls. Discrepancies be-tween studies may relate to differences in VBM techniqueemployed or the sample of patients with TLE studied (e.g., whetherpatients were classified according to electroclinical information,hippocampal volume, or psychometric information). To our knowl-edge, the present study is the first to prospectively focus on the
Fig. 4. Significant positive correlations between performance on the COWAT (raw scores) and (A) left DPFC, (B) whole left PFC, and (C) left hippocampus in all patients.
192 S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195
Author's personal copy
structure of the prefrontal cortex in patients with TLE. Prefrontalvolumetry is not routinely performed during presurgical MRI eval-uation for patients being considered for temporal lobe resection, asmultimodal invasive (e.g., ictal foramen ovale or depth electroderecordings in combination with video telemetry) and noninvasive(e.g., interictal surface EEG recordings) investigations specificallyindicate a temporal lobe seizure focus. However, quantitative anal-ysis of prefrontal volume may be important in understanding whymany patients with TLE show evidence of an ‘‘extratemporal lobe”neuropsychological profile. The findings obtained in the presentstudy are consistent with our previous work indicating volume lossof right DPFC regardless of the side of TLE [7], and volume loss ofthe left and right DPFC when patients with left and those with rightTLE are combined [8]. However, interpretations of extratemporalTLE effects in combined samples of patients with left and rightTLE should be treated with caution, given that previous work hasshown that such effects may be different according to the side ofseizure onset [7–9,29]. Furthermore, we are reluctant to speculateon the differences in cognitive–neuroanatomical relationships be-tween patients with left and those with right TLE based on the datapresented in this article, given the relatively small sample of pa-tients with right TLE in particular. Our finding that patients withleft TLE scored significantly more poorly on the COWAT relativeto those with right TLE is consistent with the well-known languagedeficits observed in left-sided patients due to damage to the lan-guage-dominant hemisphere.
Stereological analysis of prefrontal cortical subfields and VBManalysis of GMC were consistent in the identification of prefrontalchanges in patients with TLE. A discrepancy may have been ex-pected between results as there were fundamental differences inthe regions of brain morphology being assessed between the two
techniques. Analysis of prefrontal structure using stereology quan-tifies regional compartment volume of gray and white matter to-gether, whereas VBM analyzes regional distribution of only graymatter. Nevertheless, both techniques indicated that (1) DPFC ispreferentially reduced in volume in patients with TLE, (2) the mor-phology of VPFC does not differ from healthy controls, and (3) hip-pocampal volume reduction is observed only on the side ipsilateralto seizure onset, thus providing further evidence for the consis-tency between hippocampal stereology and hippocampal GMCusing VBM [7,8]. It is, however, important to note that althoughVBM and stereology revealed excellent agreement when compari-sons were made between patients and controls, the correlationsobserved between stereologically derived volumes and neuropsy-chological performance were not replicated using VBM.
Although we advocate the potential significance of subtle fron-tal lobe abnormalities causing executive dysfunction in patientswith TLE, we are cautious in the interpretation of the results pre-sented in this study for two reasons. First, we did not obtain neu-ropsychology performance in controls, as this was beyond thescope of the original investigation for which the control MR imageswere acquired, unlike patient neuropsychological performance,which is routinely assessed during presurgical evaluation. We weretherefore unable to compare control and patient neuropsychologi-cal performance in this study. However, the neuropsychologicalprofiles of patients were consistent with previously published co-horts of surgical patients with reduced functioning across a num-ber of key domains including learning and memory, attentionand concentration, and higher executive functioning [18]. We wereunable to confidently ascribe cognitive–neuroanatomical correla-tions to the pathology associated with TLE, given that the samerelationships were not assessed in our controls. Previous work
Fig. 5. Schematic illustration of the main results of the present study. Colors correspond to side of hemisphere and subregion: left dorsal PFC (light blue), left ventral PFC (darkblue), left hippocampus (purple), right dorsal PFC (light yellow), right ventral PFC (dark yellow), right hippocampus (orange). The significant differences/correlations for theseregions are provided in the text underneath highlighted in the corresponding brain region. Nonitalicized text indicates neuroanatomical comparisons between patients andcontrols. Italicized text indicates neuroanatomical–cognitive correlations in patients. �Finding replicated using stereology and voxel-based morphometry. Note the lack ofhippocampal–cognitive correlations. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195 193

Author's personal copy
has indicated that prefrontal volume is related to performance onneuropsychological tasks of executive functioning [33–36]. In par-ticular, normal age-related atrophy of the PFC is inversely corre-lated with increased errors on tasks of executive function [33–35]. However, the patients in our study were younger than the con-trols, so we were confident that any prefrontal changes in mor-phology were not due to normal brain maturation. Second, wewere studying a relatively small sample of patients with TLE (i.e.,n < 100), and as such, we did not incorporate a correction for multi-ple correlations given that the stringent correction may have ob-scured subtle, but biologically significant, cognitive–neuroanatomical correlations. We therefore suggest that theseanalyses are replicated in large samples of patients with availablepsychometric and MRI data incorporating the stringent correctionfor multiple comparisons.
4.2. Neurocognitive Implications
Previous work has speculated that volume changes in the PFCmay be related to executive dysfunction in patients with TLE[7,8]. Abnormalities of frontostriatal cortex are the candidate etiol-ogy of executive dysfunction as these brain regions are intimatelyassociated with executive functions [13–17]. Human lesion andfunctional neuroimaging studies provide evidence of a widespreadnetwork of cortical and subcortical regions involved in executivefunctions, including dorsolateral prefrontal cortex, medial prefron-tal cortex, anterior cingulate gyrus, temporal neocortex, parietalcortex, and basal ganglia (e.g., [37–47]). It is conceivable that dis-ruption to any region of this network could potentially causeimpairments in executive functions. Although we have providedstrong support for the theory that impaired executive functioningmay be due to atrophy of the PFC in patients with TLE, it will beimportant to consider the relationship between neuropsychologi-cal performance and structure of the basal ganglia in particular, gi-ven how the PFC and basal ganglia interact in cognitive processingand the previous documentation of abnormalities of the basal gan-glia in TLE [9,48].
Results observed in the present study are also in keeping withprevious research suggesting that hippocampal sclerosis is not nec-essarily a predictor of executive dysfunction in patients with TLE [3–6]. We failed to observe correlations between hippocampal volumeand Stroop or working memory (WMS-III) performance in the entiregroup of patients or when patients were separated according to theside of seizure onset. There was also no relationship between COW-AT performance and hippocampal volume when patients with leftand those with right TLE were treated separately. However, therewas a significant positive correlation between COWAT performanceand left hippocampal volume when patients with left and those withright TLE were combined. This represented the only hippocampal–cognitive correlate in the present study, and is consistent with a pre-vious study that reported a relationship between verbal fluency andleft hippocampal volume in patients with TLE [49].
Even though data presented here support the hypothesis thatprefrontal abnormalities are the likely cause of executive dysfunc-tion, it is difficult to differentiate the impact of prefrontal and hip-pocampal abnormalities on executive function in patients withTLE, given that hippocampal epileptogenic tissue may adversely af-fect the function of frontal lobe regions [50], perhaps interictallymediated via medial temporal lobe–prefrontal cortical connections[17,51]. Invasive EEG investigations in patients with intractableepilepsy have demonstrated preferential propagation of interictalspikes from medial temporal lobe to medial and orbital frontal loberegions [52,53], and ictal activity from the medial temporal lobe toipsilateral frontal lobe regions [54]. Furthermore, previous workhas demonstrated that frontal lobe cognitive impairment is associ-ated with decreased prefrontal glucose metabolism in patients
with TLE using PET [55], and that neonatal lesions to the ventralhippocampus disrupt metabolic properties of pyramidal glutamateneurons in the rodent prefrontal cortex and associated cognition[56]. The suggestion that the effects of electrophysiological disrup-tion to distal extratemporal regions may be a contributing factor toexecutive dysfunction in patients with TLE is supported by a previ-ous study that reported a significant correlation between WCSTperformance and history of secondary generalization of temporallobe seizures [5]. Therefore, it is likely that aberrant hippo-campo-fronto-striatal neurophysiological processes account for atleast part of the executive dysfunction observed in patients withTLE. Results from the present study suggest that neuroanatomicalabnormalities of the PFC may accompany neurophysiologicalabnormalities of the same region in patients with TLE.
If interictal discharges from the pathological medial temporallobe to frontostriatal cortex are the sole cause of executive dys-function in patients with TLE, then it would be expected that im-paired presurgical executive functions would normalize aftersuccessful resective surgery for intractable temporal lobe seizures.Previous studies in this area have reported conflicting results. Her-mann and Seidenberg [4] presented results consistent with thishypothesis. In addition to reporting no relationship between histo-pathological grading of hippocampal sclerosis and presurgicalexecutive function, the authors found that complete cessation ofseizures via resection of temporal lobe epileptogenic cortex leadsto improvement of executive function in patients who were pres-urgically impaired on the WCST. However, Martin et al. [5] re-ported that card sorting ability was not significantly correlatedwith postsurgical seizure status in patients with left and thosewith right TLE, and Seidenberg et al. [57] reported that the numberof WCST perseverative errors was not dependent on postsurgicalseizure outcome in patients with left TLE without hippocampalsclerosis. The data presented in our study are consistent with thoseof Martin et al. [5] and Seidenberg et al. [57] given that we wouldnot expect executive functions to normalize after successful sur-gery for seizure control due to the presence of an underlying struc-tural pathology distal from the epileptogenic cortex (i.e., atrophy ofPFC) that would continue to impair executive functions after tem-poral lobectomy.
5. Conclusions
Using a stereological region-of-interest approach and whole-brain VBM, we have corroborated the findings from previousVBM studies indicating atrophy of the DPFC in patients with TLE.Importantly and for the first time, we provide evidence indicatingthat volume changes in the PFC are correlated with impaired exec-utive functioning. These preliminary data may shed light on whymany patients with focal TLE show evidence of an extratemporalneuropsychological profile.
Acknowledgments
We thank Helen Jones and James Thompson at the Departmentof Psychology, University of Liverpool, for assistance with dataacquisition. We also thank the radiographers, nursing staff, andDr. Enis Cezayirli at MARIARC for their roles in acquisition of pa-tient and control MRI data sets.
References
[1] Giovagnoli A. Relation of sorting impairment to hippocampal damage intemporal lobe epilepsy. Neuropsychologia 2001;39:140–50.
[2] Corcoran R, Upton D. A role for the hippocampus in card sorting? Cortex1993;29:293–304.
[3] Cowey C, Green S. The hippocampus: a ‘working memory’ structure? The effectof hippocampal sclerosis on working memory. Memory 1996;4:19–30.
194 S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195

Author's personal copy
[4] Hermann B, Seidenberg M. Executive system dysfunction in temporal lobeepilepsy: effects of nociferous cortex versus hippocampal pathology. J Clin ExpNeuropsychol 1995;7:809–19.
[5] Martin R, Sawrie S, Gilliam F, et al. Wisconsin Card Sorting performance inpatients with temporal lobe epilepsy: clinical and neuroanatomical correlates.Epilepsia 2000;41:1626–32.
[6] Trenerry M, Westerveld M, Meador K. MRI hippocampal volume andneuropsychology in epilepsy surgery. Magn Res Imaging 1995;13:1125–32.
[7] Keller S, Mackay C, Barrick T, Wieshmann U, Howard M, Roberts N. Voxel basedmorphometric comparison of hippocampal and extrahippocampalabnormalities in patients with left and right hippocampal atrophy.NeuroImage 2002;16:23–31.
[8] Keller S, Denby C, Wieshmann U, Webb J, Roberts N. Voxel-basedmorphometry of grey matter abnormalities in patients with intractabletemporal lobe epilepsy: effects of side of seizure onset and epilepsyduration. J Neurol Neurosurg Psychiatry 2002;73:648–56.
[9] Keller S, Roberts N. Voxel-based morphometry of temporal lobe epilepsy: anintroduction and review of the literature. Epilepsia 2008;49:741–57.
[10] Stroop J. Studies in interference in serial verbal reactions. J Exp Psychol1935;18:643–62.
[11] Benton A, Hamsher K. Multilingual aphasia examination. Iowa City: Universityof Iowa; 1976 [manual revised, 1978].
[12] Wechsler D. The Wechsler memory scale. 3rd ed. San Antonio,TX: Psychological Corp.; 1998.
[13] Goldman-Rakic P. Architecture of the prefrontal cortex and the centralexecutive. In: Grafman J, Holyoak K, Boller F, editors. Structure and functionsof the human prefrontal cortex. Ann NY Acad Sci 1995;769:71-83.
[14] Lombardi W, Andreason P, Sirocco K, et al. Wisconsin Card Sorting Testperformance following head injury: dorsolateral fronto-striatal circuit activitypredicts perseveration. Neurology 1999;21:2–16.
[15] Mentzel H-J, Gaser C, Volz H, et al. Cognitive stimulation with the WisconsinCard Sorting Test: functional MR imaging at 15 T. Radiology 1998;207:399–404.
[16] Miner L, Ostrander M, Sarter M. Effects of ibotenic acid-induced loss ofneurons in the medial prefrontal cortex of rats on behavioural vigilance:evidence for executive dysfunction. J Psychopharmacol 1997;11:169–78.
[17] Passingham R. The frontal lobes and voluntary action. New York: Oxford Univ.Press; 1997.
[18] Moore P, Baker G. The neuropsychological and emotion consequences of livingwith intractable temporal lobe epilepsy: implications for clinical management.Seizure 2002;11:224–30.
[19] Trenerry M, Crosson B, DeBoe J, Leber W. The Stroop neuropsychologicalscreening test. Odessa, TX: Psychological Assessment Resources; 1989.
[20] Spreen O, Strauss E. Compendium of neuropsychological tests: administrationnorms and commentary. 2nd ed. New York: Oxford Univ. Press; 1998.
[21] Roberts N, Puddephat M, McNulty V. The benefit of stereology for quantitativeradiology. Br J Radiol 2000;73:679–97.
[22] García-Fiñana M, Keller S, Roberts N. Confidence intervals for the volume ofbrain structures in Cavalieri sampling with local errors. J Neurosci Methods2009;179:71–7.
[23] Cowell P, Sluming V, Wilkinson I, et al. Effects of sex and age on regionalprefrontal brain volume in two human cohorts. Eur J Neurosci2007;25:307–18.
[24] Keller S, Highley R, Sluming V, Rezaie R, Roberts N. Sulcal variability,stereological measurement and asymmetry of Broca’s area on MR images. JAnat 2007;211:534–55.
[25] Keller S, Roberts N. Measurement of brain volume using MRI: software,techniques, choices and prerequisites. J Anthropol Sci 2009;87:127–51.
[26] Mackay C, Roberts N, Mayes A, Downes J, Foster J, Mann D. An exploratorystudy of the relationship between face recognition memory and the volume ofmedial temporal lobe structures in healthy young males. Behav Neurol1998;11:3–20.
[27] Mackay C, Webb J, Eldridge P, Chadwick D, Whitehouse G, Roberts N.Quantitative magnetic resonance imaging in consecutive patients evaluatedfor surgical treatment of temporal lobe epilepsy. Magn Res Imaging2000;18:1187–99.
[28] García-Fiñana M, Cruze-Orive L, Mackay C, Pakkenberg B, Roberts N.Comparison of MR imaging against physical sectioning to estimate thevolume of human cerebral compartments. NeuroImage 2003;18:505–16.
[29] García-Fiñana M, Denby C, Keller S, Wieshmann U, Roberts N. Degree ofhippocampal atrophy is related to the side of seizure onset in temporal lobeepilepsy. AJNR Am J Neuroradiol 2006;27:1046–52.
[30] Salmenperä T, Könönen M, Roberts N, Vanninen R, Pitkänen A, Kälviäinen R.Hippocampal damage in newly diagnosed focal epilepsy: a prospective MRIstudy. Neurology 2005;64:62–8.
[31] Keller S, Wilke M, Wieshmann U, Sluming V, Roberts N. Comparison ofstandard and optimised voxel-based morphometry for analysis of brainchanges associated with temporal lobe epilepsy. NeuroImage2004;73:648–56.
[32] Keller S, Cresswell P, Denby C, et al. Persistent seizures following left temporallobe surgery are associated with posterior and bilateral structural andfunctional brain abnormalities. Epilepsy Res 2007;74:131–9.
[33] Raz N, Gunning-Dixon F, Acker J. Neuroanatomical correlates of cognitiveaging: evidence from structural magnetic resonance imaging.Neuropsychology 1998;12:95–114.
[34] Gunning-Dixon F, Raz N. Neuroanatomical correlates of selected executivefunctions in middle-aged and older adults: a prospective MR study.Neuropsychologia 2003;41:1929–41.
[35] Elderkin-Thompson V, Ballmaier M, Hellemann G, Pham D, Kumar A. Executivefunction and MRI prefrontal volumes among healthy older adults.Neuropsychology 2008;22:626–37.
[36] Schoenemann P, Budinger T, Sarich V, Wang W. Brain size does not predictgeneral cognitive ability within families. PNAS Proc Natl Acad Sci USA2000;97:4932–7.
[37] Banich M, Miham M, Atchley R, et al. fMRI studies of Stroop tasks revealunique roles of anterior and posterior brain systems in attentional selection. JCogn Neurosci 2000;12:988–1000.
[38] Bench C, Frith C, Grasby P, et al. Investigations of the functional anatomy ofattention using the Stroop task. Neuropsychologia 1993;31:907–22.
[39] Bush G, Luu P, Posner M. Cognitive and emotional influences in anteriorcingulate cortex. Trends Cogn Sci 2000;4:215–22.
[40] Bush G, Whalen P, Rosen B, et al. The counting Stroop: an interference taskspecialized for functional neuroimaging—validation study with functionalMRI. Hum Brain Mapp 1998;6:270–82.
[41] Kingma A, Heij W, Fasotti L, Eling P. Stroop interference and disorders ofselective attention. Neuropsychologia 1996;34:273–81.
[42] Leung H-C, Skudlarski P, Gatenby J, Peterson B, Gore J. An event-relatedfunctional MRI study of the Stroop Color Word Interference task. Cereb Cortex2000;10:552–60.
[43] Perret E. The left frontal lobe of man and the suppression of habitual responsesin verbal categorical behaviour. Neuropsychologia 1974;12:323–30.
[44] Peterson B, Skudlarski P, Gatenby C, Zhang H, Anderson A, Gore J. An fMRIstudy of Stroop Word–Color Interference: evidence for cingulate subregionssubserving multiple distributed attentional systems. Biol Psychiatry1999;45:1237–58.
[45] Swick D, Jovanovic J. Anterior cingulate cortex and the Stroop task:neuropsychological evidence for topographic specificity. Neuropsychologia2002;40:1240–53.
[46] Taylor S, Kornblum S, Lauber E, Minoshima S, Koeppe R. Isolation of specificinterference processing in the Stroop task: PET activation studies. NeuroImage1997;6:81–92.
[47] Vendrall P, Junqué C, Pujol J, Jurado M, Molet J, Grafman J. The role ofprefrontal regions in the Stroop task. Neuropsychologia 1995;33:341–52.
[48] Dreifuss S, Vingerhoets F, Lazeyras F, et al. Volumetric measurements ofsubcortical nuclei in patients with temporal lobe epilepsy. Neurology2001;57:1636–41.
[49] Gleissner U, Elger C. The hippocampal contribution to verbal fluency inpatients with temporal lobe epilepsy. Cortex 2001;37:55–63.
[50] Corkin S. Beware of frontal lobe deficits in hippocampal clothing. Trends CognSci 2001;5:321–3.
[51] Barbas H. Connections underlying the synthesis of cognition, memory, andemotion in primate prefrontal cortices. Brain Res Bull 2001;52:319–30.
[52] Kendrick J, Gibbs F. Origin, spread and neurosurgical treatment of thepsychomotor type of seizure discharge. J Neurosurg 1957;14:270–84.
[53] Kendrick J, Gibbs F. Interrelations of medial temporal and orbital frontal areasof man revealed by strychnine spikes. Arch Neurol Psychiatry1958;79:518–24.
[54] Lieb J, Dasheiff R, Engel J. Role of the frontal lobes in the propagation of mesialtemporal lobe seizures. Epilepsia 1991;32:822–37.
[55] Jokeit H, Seitz R, Markowitsch H, Neumann N, Witte O, Ebner A. Prefrontalasymmetric interictal glucose hypometabolism and cognitive impairment inpatients with temporal lobe epilepsy. Brain 1997;120:2283–94.
[56] Lipska B, Aultman J, Verma A, Weinberger D, Moghaddam B. Neonatal damageof the ventral hippocampus impairs working memory in the rat.Neuropsychopharmacology 2002;27:47–54.
[57] Seidenberg M, Herman B, Wyler A, et al. Neuropsychological outcomefollowing anterior temporal lobectomy in patients with and without thesyndrome of mesial temporal lobe epilepsy. Neuropsychology1998;12:303–16.
S.S. Keller et al. / Epilepsy & Behavior 15 (2009) 186–195 195





























