Embed Size (px)
Citation preview

REVIEW
Psychosis Following TraumaticBrain Injury
Rachel A. Batty ,1,2,3 Susan L. Rossell,1,2 Andrew J.P. Francis,3 and Jennie Ponsford4,5
1 Brain and Psychological Sciences Research Centre (BPsyC), Faculty of Life and Social Sciences,Swinburne University of Technology, Melbourne VIC 3122, Australia2 Cognitive Neuropsychiatry Laboratory, Monash-Alfred Psychiatry Research Centre (MAPrc), The AlfredHospital and Central Clinical School Monash University, Melbourne, VIC 3004, Australia3 School of Health Science, Psychology and Disability, RMIT University, Bundoora, VIC 3083, Australia4 School of Psychology and Psychiatry, Monash University, Clayton, VIC, 3800, Australia5 Monash-Epworth Rehabilitation Research Centre, Epworth Hospital, Richmond, VIC 3121, Australia
Psychosis following traumatic brain injury (PFTBI) has received modest empiricalinvestigation, and is subsequently poorly understood, identified and treated. Thecurrent article reports on consistencies in PFTBI phenomenology according tothe existing peer-reviewed literature. The potential for psychotic symptoms postTBI, aetiological propositions, prevalence, significance of onset latency and injuryseverity, clinical and cognitive neuropsychological presentation and injury local-isation/neuroimaging data are reviewed. Substantial methodological limitationsassociated with the majority of publications informing this work are also dis-cussed. Despite controversies in the literature, psychosis following TBI appears tobe three times more prevalent than psychotic disorders in the general population,and comparable in presentation to other idiopathic psychotic spectrum disorders,including schizophrenia.
Keywords: traumatic brain injury, psychosis, schizophrenia, review
It has been estimated that up to 10% of traumat-ically brain injured (TBI) patients go on to expe-rience symptoms of psychosis (Achte, Hillbom,& Aalberg, 1969; Davison & Bagley, 1969;Fujii & Ahmed, 2001; Fujii, Ahmed, & Hishinuma,2004), with a range spanning from 1.35% (medianestimate provided by Davison & Bagley, 1969) to9.2% (Fujii et al., 2004). These patients suffer aclinically complex dual diagnosis that is often ac-companied by substantial distress and disability.Both the effect of TBI on new psychotic symp-toms and the phenomenology of psychosis fol-lowing TBI remain controversial. For instance, al-though cause-and-effect has not been established,‘Psychotic Disorder Due to Traumatic Brain In-jury (PDTBI)’ has been used previously to referto dually diagnosed patients (e.g., Fujii & Ahmed,2002a; Fujii et al., 2004).
In line with existing evidence, the currentarticle refers instead to ‘Psychosis Following Trau-
Address for correspondence: Rachel Batty, Neuroimaging Facility, Brain and Psychological Sciences ResearchCentre, PO Box 218, Hawthorn, VIC, 3122, Australia. E-mail: [email protected]
matic Brain Injury (PFTBI)’. It was the intentionof this review to identify consistencies in PFTBIphenomenology from peer-reviewed publicationsof the highest quality. This is an important first stepin elucidating the nature of PFTBI. A number ofperspectives germane to PFTBI phenomenologyare reviewed, including: the potential for psychoticsymptoms post TBI, aetiological propositions,prevalence, the significance of onset latency andinjury severity, clinical presentation, cognitiveneuropsychological profile, and neuroimaging andlocalisation data. Finally, a discussion devotedto the shortcomings of this literature highlightsimportant methodological limitations likely toexplain phenomenological inconsistencies.
Method of Literature ReviewElectronic searches of the PUBMED, psycINFOand the National Center for Biotechnology
BRAIN IMPAIRMENT page 1 of 21 c© The Authors 2013 doi: 10.1017/BrImp.2013.10 1

RACHEL A. BATTY ET AL.
Information (NCBI) databases were conductedbiannually between March 2009 and July 2012with the keywords psychosis and traumatic braininjury, schizophrenia and traumatic brain injury,delusion and traumatic brain injury, or halluci-nation and traumatic brain injury. Fifty-two ini-tial publications were found, of which 26 wereconsidered relevant to the review. Additional cita-tions from review articles were retrieved, includ-ing earlier publications not found by the databasesearchers, and work that had covered psychoticsyndromes under psychiatric sequelae post TBI.
Peer-reviewed articles reporting on a selectionof case histories were favoured where available,and duplicates were removed. Two large literaturereviews were included: the first from Davison andBagley (1969), because their work represented anovel and influential study at the time of publica-tion; and the second from Corcoran and Malaspina(2007), because their review describes data fromthe subsequent four decades. A stand-alone epi-demiological study was included because, whilethe use of standardised diagnostic criteria is com-promised, this methodology affords a large samplesize (i.e., N = 5034; Silver, Kramer, Greenwald, &Weissman, 2001). By contrast, work from Buck-ley et al. (1993) provided valuable neuroimagingdata and standardised clinical assessments of a se-lect group of cases where the development of psy-chotic symptoms clearly followed cerebral trauma(i.e., N = 5). The remaining studies were chosenfor review on the basis that they made a contri-bution to one or more of the domains of interest,and were not already covered by existing reviewssummarised in this work.
Defining PsychosisPsychotic symptoms are generally categorised aspositive, negative and cognitive. These includedelusions, hallucinations, disorganised languageand behaviour, poverty of speech, emotion and/ormotivation, and impairments in executive function,memory and insight (American Psychological As-sociation (APA), 1994, 2000; Andreasen & Olsen,1982; Henry & Crawford, 2004; Kay, Fiszbein,& Opler, 1987; Liddle, 1987). To meet DSM-IV(APA, 2000) criteria for schizophrenia, any twosymptoms must be present for a significant part of1 month, continue for at least 6 months, and inter-fere with personal hygiene, occupational function-ing or social interaction. Cases of psychosis (Burg,McGuire, Burright, & Donovick, 1996; Koponenet al., 2002, 2006), schizophrenia (Fujii et al., 2004;Malaspina et al., 2001; Silver et al., 2001), and iso-lated symptoms such as hallucinations (Stewart &Brennan, 2005) and delusions (Butler, 2000;
Feinberg, Eaton, Roane, & Giacino, 1999) havebeen identified in the PFTBI literature to date.
The Potential for Psychosis Post TBICohorts at RiskTBI and psychotic disorders share risk factors thatmay help to explain dual diagnosis in some cases.Male gender, substance use and abuse, and/or ex-isting psychiatric sequelae are highly correlatedwith both head injury and psychosis. Young malesinjured in road-traffic accidents show the high-est rates of TBI (Bruns Jr & Hauser, 2003), anda higher incidence of psychosis has been estab-lished in young, but not middle-aged or elderly,males (Abel, Drake, & Goldstein, 2010; Jablenskyet al., 1992; McGrath, Saha, Chant, & Welham,2008). Higher-than-average rates of substance use,especially alcohol and cannabis abuse, and otherpsychopathologies, such as comorbid mood andanxiety disorders, are also shared by both co-horts (Gould, Ponsford, Schonberger, & Johnston,2011; Hartley, Haddock, & Barrowclough, 2012;Ponsford, Draper, & Schonberger, 2008; Rossler,Hengartner, Angst, & Ajdacic-Gross, 2012; West,2011; Westermeyer, 2006; Wisdom, Manuel, &Drake, 2011).
Increased Vulnerability as a Consequenceof the TBIPost-traumatic amnesia (PTA) follows emergencefrom coma in the majority of TBI cases. This state,in which there is confusion and disorientation,impaired new learning and generalised cognitivedisturbance, is frequently associated with the de-velopment of symptoms that may be interpretedas psychosis, such as delusions and hallucinations(Snow & Ponsford, 2012). Although these gener-ally resolve with emergence from PTA, there ispotential for this condition to be labelled a psy-chosis, especially in cases where this continues forweeks or months, as it may in cases of very severeTBI. This would account for some reported casesof PFTBI.
Continuing cognitive and behavioural impair-ments and their impact on functional outcomesfollowing TBI may also mediate the develop-ment of psychotic symptoms. Cognitive impair-ments are most common in the domains of at-tention, information processing speed, workingmemory, new learning and memory, and execu-tive functions (Beauchamp et al., 2011; Lezak,1979; Ponsford & Kinsella, 1992, Rios, Perianez,& Munoz-Cespedes, 2004). Reduced behaviouralcontrol, with irritability, aggression, impulsivity,
2
PSYCHOSIS FOLLOWING TRAUMATIC BRAIN INJURY
disinhibition and/or lack of initiative is also com-mon, as is a lack of awareness of these changes(Ponsford, Sloan, & Snow, 2012). These impair-ments affect the injured individual’s capacity foremployment or study, leisure activities, and socialand personal relationships, creating increasing de-pendency on family and social isolation.
Similar cognitive and behavioural dysfunctionis documented in psychotic disorders, during theprodromal phase and post onset. Neurocognitivedeficits are well established across domains oflanguage and memory, processing speed, atten-tion and executive function (Broome et al., 2010;Evans, Chua, McKenna, & Wilson, 1997; Henry &Crawford, 2004; Joshua & Rossell, 2009; Rossell& David, 2006). Behavioural changes are also ap-parent, especially in disinhibition and amotivation(Gard, Fisher, Garrett, Genevsky, & Vinogradov,2009; Hughes, Fulham, Johnston, & Michie, 2012;Medalia & Brekke, 2010; Nakagami, Hoe, &Brekke, 2010), and psychosocial problems arecommon, including emotion perception, commu-nication and self-care. As in TBI, these typi-cally result in social isolation (Goreishizadeh,Mohagheghi, Farhang, & Alizadeh, 2012;Nakagami et al., 2010; Switaj et al., 2012).
Psychiatric IllnessCognitive and behavioural changes of this kindresult in long-term psychological stress post in-jury. Significant emotional distress, pre-injury sub-stance abuse and post-injury psychosocial stres-sors, may constitute further risks for psychiatricillness (Kim et al., 2007; Ponsford et al., 2008).Indeed, numerous studies have documented ele-vated rates of psychiatric disorder following TBI(Gould et al., 2011; Hoofien, Gilboa, Vakil, &Donovick, 2001; Koponen et al., 2002; Whelan-Goodinson, Ponsford, Johnston, & Grant, 2009).These may be as high as 70% prevalence ofboth depression and anxiety post injury (Kimet al., 2007; Lewis, 1942), although some stud-ies have reported much lower rates (e.g., Anson &Ponsford, 2006; Hiott & Labbate, 2002; Jorgeet al., 2004; Rutherford, Merrett, & McDonald,1977). A recent prospective study showed that45.8% of participants without any psychiatric his-tory developed a post-injury psychiatric disorder(Gould et al., 2011). However, the rates of psy-chotic disorders in this study were not higher thanthose in a comparison sample from the general pop-ulation. Nevertheless, psychiatric illness, depres-sion and anxiety, in particular, have recently beenassociated with the development of psychosis, es-pecially in cases with comorbid substance misuse(Hartley et al., 2012).
Structural and Functional CerebralAbnormalitiesBrain regions and associated circuitry implicatedin the neurogenesis of psychotic symptoms over-lap substantially with those commonly affectedby TBI (McAllister & Ferrell, 2002; Rao &Lyketsos, 2003). Due to the internal structure ofthe skull, the frontal lobe (posterior base) and tem-poral lobe (anterior pole) have an especially in-creased vulnerability to traumatic injury, as doesthe hippocampal formation, with added vulnera-bility due to the mechanical force of the blow, in-tracranial pressure and/or hypoxia (Bigler, 2007;DeKosky, Kochanek, Clark, Ciallella, & Dixon,1998; Gennarelli & Graham, 1998; McAllister &Ferrell, 2002). Similarly, fronto-temporal pathol-ogy and hippocampal dysfunction are implicatedin the neurogenesis and persistence of psychoticsymptoms (Bachus & Kleinman, 1996; Borgwardtet al., 2007; Ellison-Wright, Glahn, Laird, Thelen,& Bullmore, 2008; Friston, Liddle, Frith, Hirsch,& Frackowiak, 1992; Zierhut et al., 2013). Hip-pocampal dysfunction has been demonstrated dur-ing language and memory encoding in schizophre-nia (Jessen et al., 2003; Zierhut et al., 2010), withrecent evidence suggesting that hippocampal mor-phology may further underlie positive symptomssuch as hallucinations and delusions (Csernanskyet al., 2002; Zierhut et al., 2013).
Variable degrees of cerebral atrophy are shownfollowing TBI, the degree and progression ofwhich is not necessarily related to injury severity,and may continue for years following the trauma(Belina & Kovacic, 2011; Ross, 2011; Ross et al.,2012; Tate, Khedraki, Neeley, Ryser, & Bigler,2011). Cortical white and grey matter loss, withreduced medial and middle frontal, medial andsuperior temporal gyri, and dorsolateral prefrontalcortex volumes, is further considered characteristicof schizophrenia (Borgwardt et al., 2007; Fusar-Poli, McGuire, & Borgwardt, 2011; Ho et al.,2003; Mathalon, Sullivan, Lim, & Pferrerbaum,2001; Pantelis et al., 2003; Pridmore & Bowe,2011). These grey matter changes have been shownin ‘at risk’ healthy individuals (Lawrie et al., 1999;Mathalon et al., 2001; Pantelis et al., 2003), iso-lated from the effects of antipsychotics (Pridmore& Bowe, 2011; Steen, Mull, McClure, Hamer, &Lieberman, 2006) and moderated by chronicity(Horn et al., 2010; Mathalon et al., 2001).
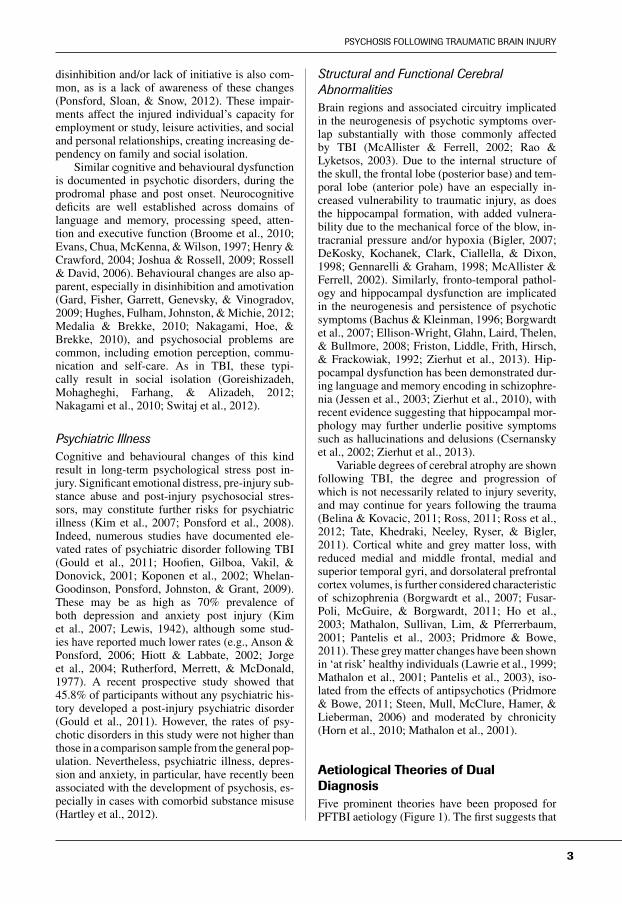
Aetiological Theories of DualDiagnosisFive prominent theories have been proposed forPFTBI aetiology (Figure 1). The first suggests that
3
RACHEL A. BATTY ET AL.
FIGURE 1
Schematic depicting five prominent conceptualisations of the traumatic brain injury and psychosis/schizophreniarelationship.
brain injury activates an existing hereditary sus-ceptibility to schizophrenia (i.e., as the ‘stress’component in stress–diathesis theory (Corcoran &Malaspina, 2007; Kim, 2008)). In the second the-ory the relationship is identical, but allows for thedevelopment of any symptom/s along the contin-uum of psychosis (Corcoran & Malaspina, 2007;Kim, 2008; for review of the continuum see Ver-doux & van Os, 2002). The third proposes that TBIinitiates the development of a unique set of psy-chotic symptoms via a chain reaction of structuraland/or functional changes in the brain (Kim, 2008).In this account, genetic vulnerability is less influ-ential, and current DSM-IV (APA, 1994, 2000)criteria allow for the diagnosis of cases fitting thistype under ‘psychotic disorder due to a generalmedical condition’.
Fourth, a case for ‘reverse causality’ has beenproposed, where the existence of psychosis in-creases the likelihood of trauma (David & Prince,2005; Nielsen, Mortensen, O’Callaghan, Morsa, &Ewald, 2002). This acknowledgement of increasedinjury rates in the psychotic population is not con-fined to head trauma, and does not explain neuro-logical insult prior to the development of psychoticsymptoms. Even so, reverse causality has been pro-posed as an explanation for PFTBI (e.g., David &Prince, 2005), and researchers continue to look torates of injury in schizophrenia for PFTBI preva-lence estimates (e.g., Nielsen et al., 2002). Finally,the potential for a spurious relationship has beennoted, whereby psychosis-proneness increases thelikelihood of both psychosis and trauma. In this ex-planation genetic proneness is a causal mediatingfactor that accounts for the erroneously observedrelationship between brain injury and psychosis(Corcoran & Malaspina, 2007).
The first three models agree that TBI demon-strates causality in the ensuing psychotic symp-
toms, yet differ in their definition of the subse-quent psychosis and, thus, the importance of herita-ble vulnerability. For instance, DSM-IV-diagnosedschizophrenia has established heritability (modelone), which is not necessarily a prerequisite forthe manifestation of psychotic symptoms generally(model two) (Egan et al., 2001; McGuffin, Asher-son, Owen, & Farmer, 1994). However, heritabilityneed not be a requirement of the model, given thatexisting literature has demonstrated PFTBI bothin those with (e.g., AbdelMalik, Husted, Chow, &Bassett, 2003) and without (e.g., Fujii & Ahmed,2001) a heritable predisposition. The hypotheti-cally ‘unique’ symptom profile proposed by thethird model is impractical given that psychotic out-come can only be informed by the thorough stan-dardised clinical and neuropsychological assess-ment of PFTBI cases in the first instance. The factthat more than one theoretical model exists servesas evidence that sufficient empirical research isyet to be published. Further, and as identifiedby the second theoretical model, the past decadeof research has reconceptualised psychosis gen-erally, whereby psychotic thoughts, experiencesand behaviour, exist on a continuum (i.e., a psy-chosis spectrum), rather than as categorical distinc-tions per se (Badcock & Dragovic, 2006; Myin-Germeys, Krabbendam & van Os, 2003; Verdoux& van Os, 2002). In this sense, the proposed cat-egorisation of symptoms in the first model is alsosomewhat theoretically out-dated.
Claims of reverse causality offer an incom-plete, and subsequently inadequate, picture ofdually diagnosed patients. Similarly, a spuriousrelationship relies on the genetic liability (i.e., her-itability) of a patient, and can therefore be dis-counted by existing evidence. Thus, provided therequirement for heritability is removed, the sec-ond theoretical model most accurately reflects the
4
PSYCHOSIS FOLLOWING TRAUMATIC BRAIN INJURY
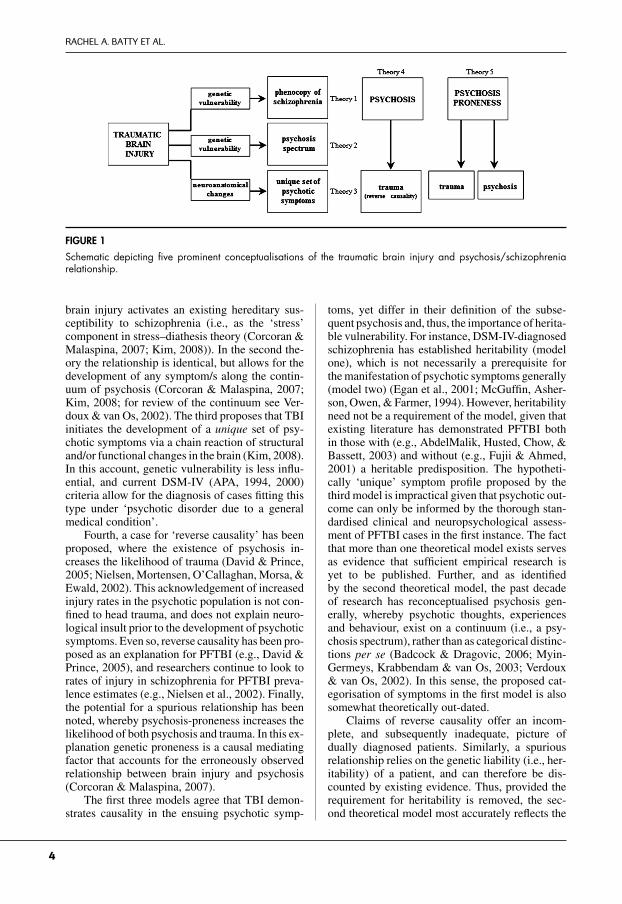
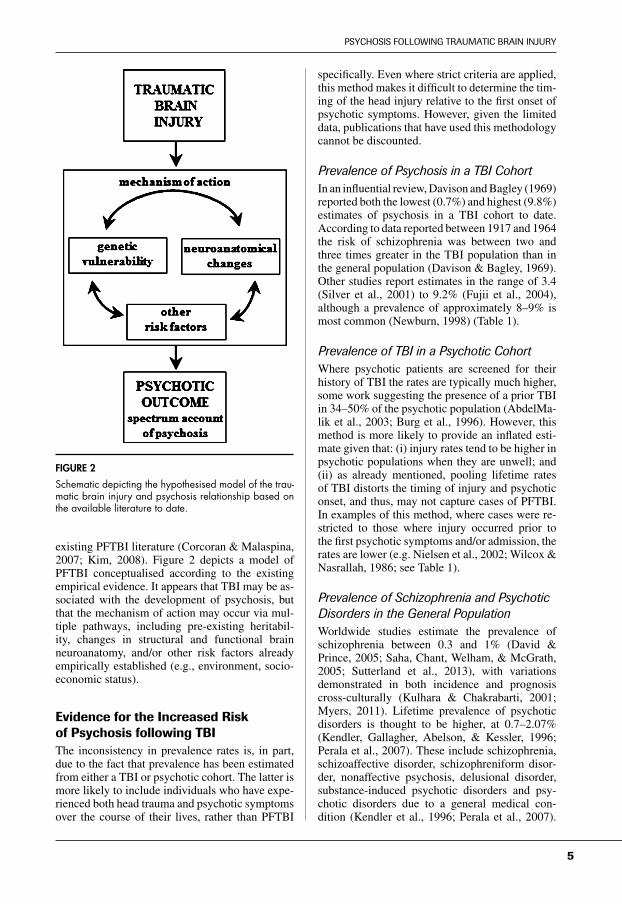
FIGURE 2
Schematic depicting the hypothesised model of the trau-matic brain injury and psychosis relationship based onthe available literature to date.
existing PFTBI literature (Corcoran & Malaspina,2007; Kim, 2008). Figure 2 depicts a model ofPFTBI conceptualised according to the existingempirical evidence. It appears that TBI may be as-sociated with the development of psychosis, butthat the mechanism of action may occur via mul-tiple pathways, including pre-existing heritabil-ity, changes in structural and functional brainneuroanatomy, and/or other risk factors alreadyempirically established (e.g., environment, socio-economic status).
Evidence for the Increased Riskof Psychosis following TBIThe inconsistency in prevalence rates is, in part,due to the fact that prevalence has been estimatedfrom either a TBI or psychotic cohort. The latter ismore likely to include individuals who have expe-rienced both head trauma and psychotic symptomsover the course of their lives, rather than PFTBI
specifically. Even where strict criteria are applied,this method makes it difficult to determine the tim-ing of the head injury relative to the first onset ofpsychotic symptoms. However, given the limiteddata, publications that have used this methodologycannot be discounted.
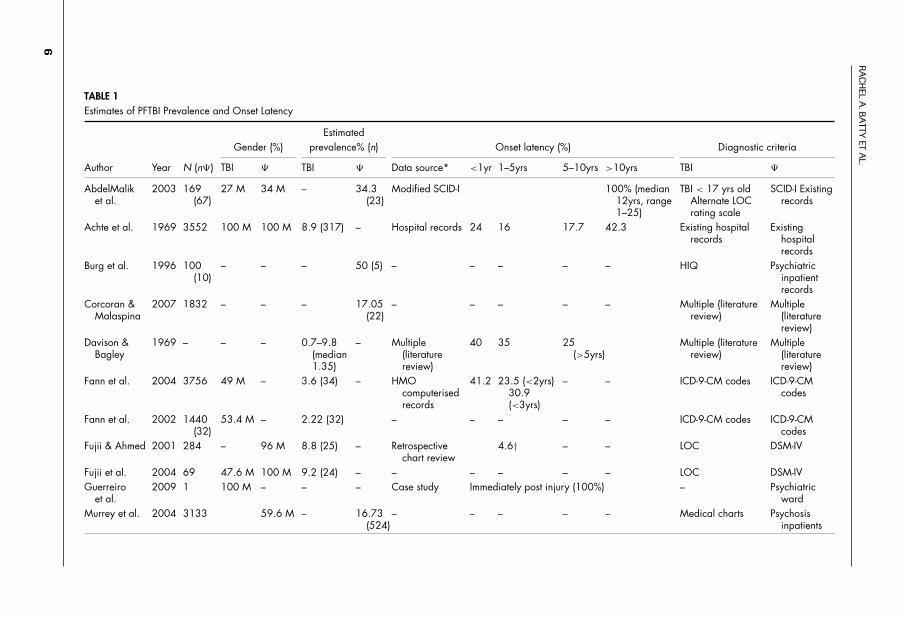
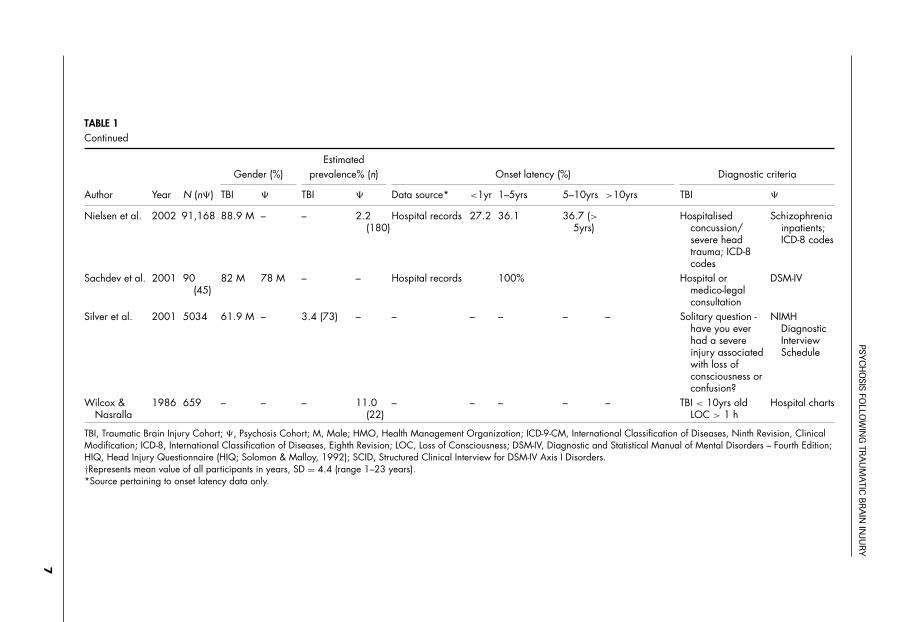
Prevalence of Psychosis in a TBI CohortIn an influential review, Davison and Bagley (1969)reported both the lowest (0.7%) and highest (9.8%)estimates of psychosis in a TBI cohort to date.According to data reported between 1917 and 1964the risk of schizophrenia was between two andthree times greater in the TBI population than inthe general population (Davison & Bagley, 1969).Other studies report estimates in the range of 3.4(Silver et al., 2001) to 9.2% (Fujii et al., 2004),although a prevalence of approximately 8–9% ismost common (Newburn, 1998) (Table 1).
Prevalence of TBI in a Psychotic CohortWhere psychotic patients are screened for theirhistory of TBI the rates are typically much higher,some work suggesting the presence of a prior TBIin 34–50% of the psychotic population (AbdelMa-lik et al., 2003; Burg et al., 1996). However, thismethod is more likely to provide an inflated esti-mate given that: (i) injury rates tend to be higher inpsychotic populations when they are unwell; and(ii) as already mentioned, pooling lifetime ratesof TBI distorts the timing of injury and psychoticonset, and thus, may not capture cases of PFTBI.In examples of this method, where cases were re-stricted to those where injury occurred prior tothe first psychotic symptoms and/or admission, therates are lower (e.g. Nielsen et al., 2002; Wilcox &Nasrallah, 1986; see Table 1).
Prevalence of Schizophrenia and PsychoticDisorders in the General PopulationWorldwide studies estimate the prevalence ofschizophrenia between 0.3 and 1% (David &Prince, 2005; Saha, Chant, Welham, & McGrath,2005; Sutterland et al., 2013), with variationsdemonstrated in both incidence and prognosiscross-culturally (Kulhara & Chakrabarti, 2001;Myers, 2011). Lifetime prevalence of psychoticdisorders is thought to be higher, at 0.7–2.07%(Kendler, Gallagher, Abelson, & Kessler, 1996;Perala et al., 2007). These include schizophrenia,schizoaffective disorder, schizophreniform disor-der, nonaffective psychosis, delusional disorder,substance-induced psychotic disorders and psy-chotic disorders due to a general medical con-dition (Kendler et al., 1996; Perala et al., 2007).
5
RA
CH
ELA
.BA
TTYET
AL.
TABLE 1Estimates of PFTBI Prevalence and Onset Latency
EstimatedGender (%) prevalence% (n) Onset latency (%) Diagnostic criteria
Author Year N (n�) TBI � TBI � Data source* <1yr 1–5yrs 5–10yrs >10yrs TBI �
AbdelMaliket al.
2003 169(67)
27 M 34 M – 34.3(23)
Modified SCID-I 100% (median12yrs, range1–25)
TBI < 17 yrs oldAlternate LOCrating scale
SCID-I Existingrecords
Achte et al. 1969 3552 100 M 100 M 8.9 (317) – Hospital records 24 16 17.7 42.3 Existing hospitalrecords
Existinghospitalrecords
Burg et al. 1996 100(10)
– – – 50 (5) – – – – – HIQ Psychiatricinpatientrecords
Corcoran &Malaspina
2007 1832 – – – 17.05(22)
– – – – – Multiple (literaturereview)
Multiple(literaturereview)
Davison &Bagley
1969 – – – 0.7–9.8(median1.35)
– Multiple(literaturereview)
40 35 25(>5yrs)
Multiple (literaturereview)
Multiple(literaturereview)
Fann et al. 2004 3756 49 M – 3.6 (34) – HMOcomputerisedrecords
41.2 23.5 (<2yrs)30.9(<3yrs)
– – ICD-9-CM codes ICD-9-CMcodes
Fann et al. 2002 1440(32)
53.4 M – 2.22 (32) – – – – – ICD-9-CM codes ICD-9-CMcodes
Fujii & Ahmed 2001 284 – 96 M 8.8 (25) – Retrospectivechart review
4.6† – – LOC DSM-IV
Fujii et al. 2004 69 47.6 M 100 M 9.2 (24) – – – – – – LOC DSM-IVGuerreiro
et al.2009 1 100 M – – – Case study Immediately post injury (100%) – Psychiatric
wardMurrey et al. 2004 3133 59.6 M – 16.73
(524)– – – – – Medical charts Psychosis
inpatients
6
PSYC
HO
SISFO
LLOW
ING
TRA
UM
ATIC
BR
AIN
INJU
RY
TABLE 1Continued
EstimatedGender (%) prevalence% (n) Onset latency (%) Diagnostic criteria
Author Year N (n�) TBI � TBI � Data source* <1yr 1–5yrs 5–10yrs >10yrs TBI �
Nielsen et al. 2002 91,168 88.9 M – – 2.2(180)
Hospital records 27.2 36.1 36.7 (>5yrs)
Hospitalisedconcussion/severe headtrauma; ICD-8codes
Schizophreniainpatients;ICD-8 codes
Sachdev et al. 2001 90(45)
82 M 78 M – – Hospital records 100% Hospital ormedico-legalconsultation
DSM-IV
Silver et al. 2001 5034 61.9 M – 3.4 (73) – – – – – – Solitary question -have you everhad a severeinjury associatedwith loss ofconsciousness orconfusion?
NIMHDiagnosticInterviewSchedule
Wilcox &Nasralla
1986 659 – – – 11.0(22)
– – – – – TBI < 10yrs oldLOC > 1 h
Hospital charts
TBI, Traumatic Brain Injury Cohort; �, Psychosis Cohort; M, Male; HMO, Health Management Organization; ICD-9-CM, International Classification of Diseases, Ninth Revision, ClinicalModification; ICD-8, International Classification of Diseases, Eighth Revision; LOC, Loss of Consciousness; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders – Fourth Edition;HIQ, Head Injury Questionnaire (HIQ; Solomon & Malloy, 1992); SCID, Structured Clinical Interview for DSM-IV Axis I Disorders.†Represents mean value of all participants in years, SD = 4.4 (range 1–23 years).*Source pertaining to onset latency data only.
7

RACHEL A. BATTY ET AL.
Thus, even at the highest rates of lifetime preva-lence, it appears that psychotic disorders occur ata much greater frequency following TBI than inthe general population. With reference to the high-est estimates taken from a TBI cohort (i.e., 9.2%,Fujii et al., 2004) and those of psychotic disordersin the general population (i.e., 2.07%, Perala et al.,2007), psychosis following TBI may occur at a rateat least three times that of the general population.
Onset LatencyThe details of studies reviewed for estimates ofonset latency are contained in Table 1 alongsidethe prevalence estimates. Temporal information re-lated to the injury and onset of psychotic symptomsis not always collected (e.g., Silver et al., 2001),and the source of reported data is often unknown(e.g., Davison & Bagley, 1969). Yet, this informa-tion is imperative in the establishment of causalfactors associated with the emerging psychosisand, indeed, an accurate diagnosis of PFTBI. With-out it, the direction of the PFTBI relationship (i.e.,whether the TBI occurred before or after the emer-gence of psychotic symptoms), and the durationof the time period in between (i.e., onset latency)remain unclear.
These limitations may at least partially explainwhy the literature reporting onset latency is incon-sistent. Rates of onset occur with similar frequencyacross time bands; between 40 and 50%1 duringthe first year (Davison & Bagley, 1969; Fann et al.,2004), 1–5 years (Fujii & Ahmed, 2001; Nielsenet al., 2002; Sachdev, Smith, & Cathcart, 2001),5–10 years (Achte et al., 1969; Davison & Bagley,1969; Nielsen et al., 2002), and greater than 10years post TBI (Achte et al., 1969; Bamrah &Johnson, 1991). If these rates are presumed ac-curate, one must conclude that: (i) there is no reli-able onset latency post TBI; and/or (ii) variabilitymay reflect the influence of factors unrelated tothe injury, such as, for example, familial support,environmental stressors and resilience.2 Fujii andAhmed (2002b) reported that a shorter time lagbetween injury and psychotic onset was evidentin cases with mild, relative to severe, brain in-jury. However, it should be noted that the majority1 Reflects the mean rate (%) collapsed across studies for
each latency band.2 Socio-environmental factors, resilience characteristics
and social/familial support have demonstrated influ-ence in the onset of psychotic symptoms in proneindividuals, and improved treatment outcome (e.g.,Albert et al., 2011; Bourque, van der Ven, Fusar-Poli, & Malla, 2012; Must, Janka, & Horvath, 2011;Smieskova, Fusar-Poli, Riecher-Rossler, & Borgwardt,2012).
of the cases they reviewed had unspecified injuryseverity, with their final assessment drawn from 22moderate–severe cases, and only seven mild cases.
The Significance of Injury SeverityThe development of psychotic symptoms is furtherlikely to be mediated by the specific injury; sever-ity, lesion location, the directional force of the blowand/or rapid head movement, and internal sec-ondary injury such as swelling, bleeding and apop-totic and necrotic cell death (Raghupathi, 2004;Rink et al., 1995). Indeed, altered neuronal apop-tosis has been linked to the progressive loss of greymatter associated with psychotic onset (Glantz,Gilmore, Lieberman, & Jarskog, 2006). A hand-ful of findings have suggested that greater injuryseverity may be associated with an increased riskof post-injury psychosis (Fujii & Ahmed, 2002b;Hillbom, 1960; Sachdev et al., 2001). For instance,Sachdev et al. (2001) found that injury severitydetermined according to the duration of loss ofconsciousness predicted PFTBI (although no othermeasures of injury severity reached significance).However, conflicting findings have also been pub-lished. In fact, Fujii and Ahmed (2001) found thattheir nonpsychotic TBI cohort showed relativelymore moderate to severe injuries. In line with theirlater work reporting a shorter time lag before psy-chotic onset for cases with mild brain injury (Fujii& Ahmed, 2002b), greater severity may not neces-sarily be associated with greater risk.
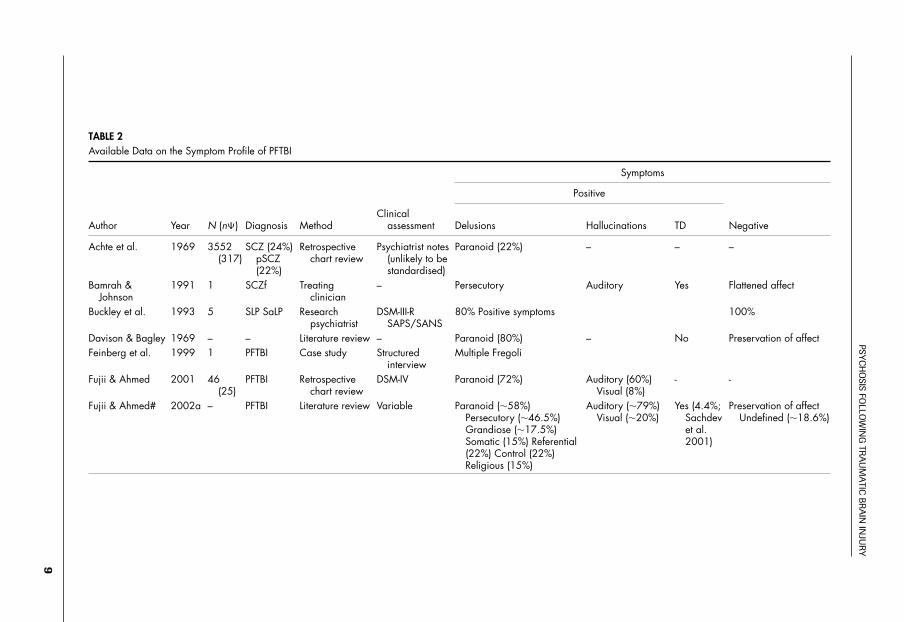
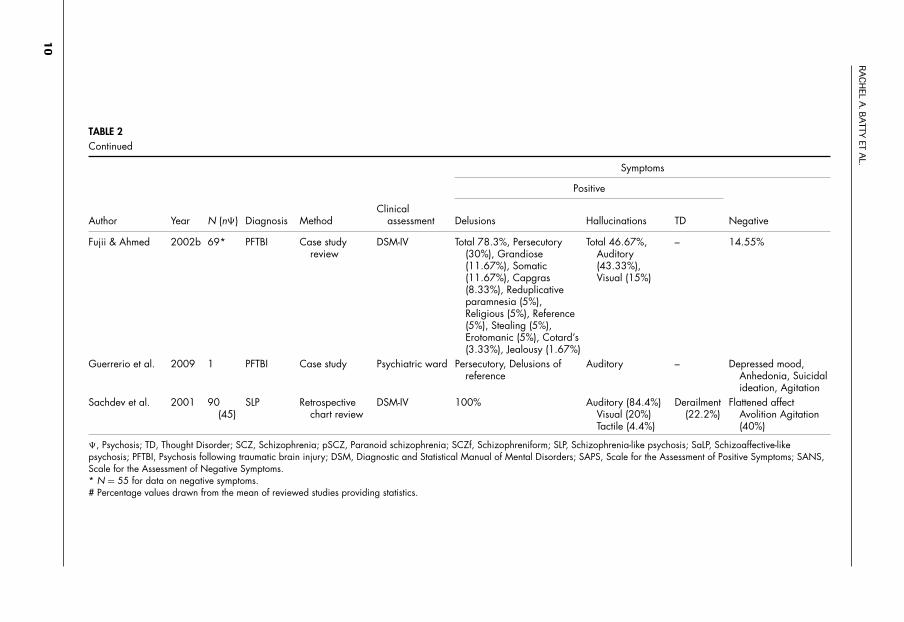
Clinical PresentationA comprehensive and systematic assessment ofthe clinical presentation of PFTBI is yet to bepublished. However, according to the modestclinical data available, all diagnostically salientsymptoms characteristic of schizophrenia havebeen observed in patients with PFTBI (see Ta-ble 2). This includes positive and negative symp-toms, as well as marked cognitive impairment (al-ready defined; APA, 1994). As such, it appears thatPFTBI may be clinically indistinguishable fromschizophrenia.
This is not without controversy. Preliminarywork from Fujii and Ahmed (2002a) highlightedthe ‘absence’ of negative symptoms in PFTBI.Their initial report indicated that three of the sixstudies they reviewed recorded negative pathology(Fujii & Ahmed, 2002a), and a further case studyreview noted that negative symptoms were gener-ally reduced (i.e., 8 of 55, 14.55%; Fujii & Ahmed,2002b). However, seven of the nine publications inthe current review reported negative symptoms inPFTBI at a mean rate of approximately 52% (see
8
PSYC
HO
SISFO
LLOW
ING
TRA
UM
ATIC
BR
AIN
INJU
RY
TABLE 2Available Data on the Symptom Profile of PFTBI
Symptoms
Positive
Author Year N (n�) Diagnosis MethodClinical
assessment Delusions Hallucinations TD Negative
Achte et al. 1969 3552(317)
SCZ (24%)pSCZ(22%)
Retrospectivechart review
Psychiatrist notes(unlikely to bestandardised)
Paranoid (22%) – – –
Bamrah &Johnson
1991 1 SCZf Treatingclinician
– Persecutory Auditory Yes Flattened affect
Buckley et al. 1993 5 SLP SaLP Researchpsychiatrist
DSM-III-RSAPS/SANS
80% Positive symptoms 100%
Davison & Bagley 1969 – – Literature review – Paranoid (80%) – No Preservation of affectFeinberg et al. 1999 1 PFTBI Case study Structured
interviewMultiple Fregoli
Fujii & Ahmed 2001 46(25)
PFTBI Retrospectivechart review
DSM-IV Paranoid (72%) Auditory (60%)Visual (8%)
- -
Fujii & Ahmed# 2002a – PFTBI Literature review Variable Paranoid (∼58%)Persecutory (∼46.5%)Grandiose (∼17.5%)Somatic (15%) Referential(22%) Control (22%)Religious (15%)
Auditory (∼79%)Visual (∼20%)
Yes (4.4%;Sachdevet al.2001)
Preservation of affectUndefined (∼18.6%)
9
RA
CH
ELA
.BA
TTYET
AL.
TABLE 2Continued
Symptoms
Positive
Author Year N (n�) Diagnosis MethodClinical
assessment Delusions Hallucinations TD Negative
Fujii & Ahmed 2002b 69* PFTBI Case studyreview
DSM-IV Total 78.3%, Persecutory(30%), Grandiose(11.67%), Somatic(11.67%), Capgras(8.33%), Reduplicativeparamnesia (5%),Religious (5%), Reference(5%), Stealing (5%),Erotomanic (5%), Cotard’s(3.33%), Jealousy (1.67%)
Total 46.67%,Auditory(43.33%),Visual (15%)
– 14.55%
Guerrerio et al. 2009 1 PFTBI Case study Psychiatric ward Persecutory, Delusions ofreference
Auditory – Depressed mood,Anhedonia, Suicidalideation, Agitation
Sachdev et al. 2001 90(45)
SLP Retrospectivechart review
DSM-IV 100% Auditory (84.4%)Visual (20%)Tactile (4.4%)
Derailment(22.2%)
Flattened affectAvolition Agitation(40%)
�, Psychosis; TD, Thought Disorder; SCZ, Schizophrenia; pSCZ, Paranoid schizophrenia; SCZf, Schizophreniform; SLP, Schizophrenia-like psychosis; SaLP, Schizoaffective-likepsychosis; PFTBI, Psychosis following traumatic brain injury; DSM, Diagnostic and Statistical Manual of Mental Disorders; SAPS, Scale for the Assessment of Positive Symptoms; SANS,Scale for the Assessment of Negative Symptoms.* N = 55 for data on negative symptoms.# Percentage values drawn from the mean of reviewed studies providing statistics.
10
PSYCHOSIS FOLLOWING TRAUMATIC BRAIN INJURY
Table 2). Given that schizophrenia is notoriouslyheterogeneous in its clinical presentation, and neg-ative symptoms are not a requirement for diagnosis(APA, 1994, 2000), there is no definitive evidencefor a profile that is diagnostically distinct fromschizophrenia as it is currently conceptualised.
Another significant gap in the literature is thelack of statistical comparison between clinical pro-files of matched PFTBI and schizophrenia patients.Systematic examination of the clinical presentationof PFTBI using standardised clinical interviews isvital for accurate diagnosis and treatment. Defini-tive conclusions with respect to the clinical pre-sentation of PFTBI, and its likeness to functionalschizophrenia, are thus premature.
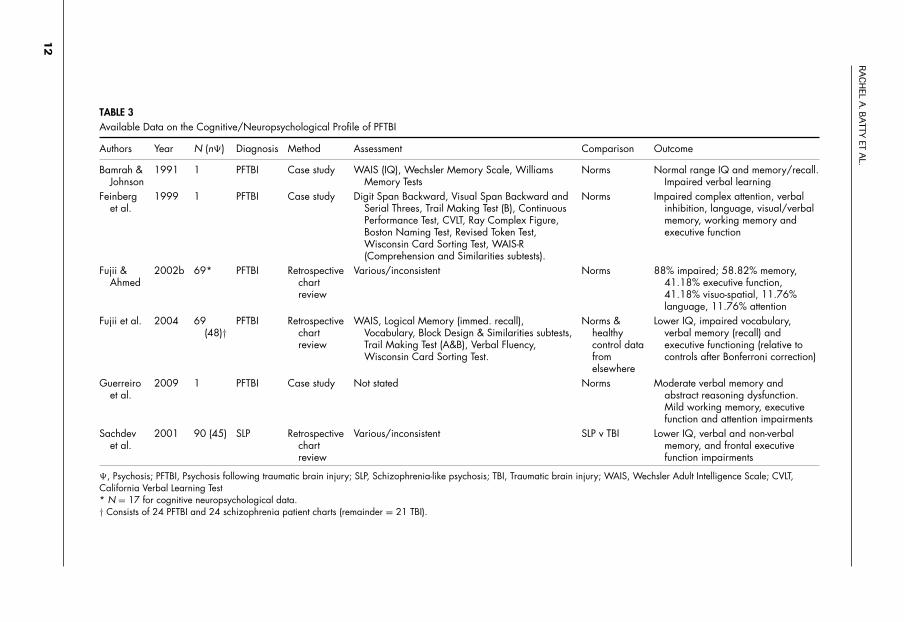
Cognitive Neuropsychological ProfileSimilarly, very little research has detailed the cog-nitive neuropsychological profile of patients withPFTBI. A summary of the available data is con-tained in Table 3. From this work it appears thatsome common deficiencies in language and vo-cabulary (e.g., Fujii & Ahmed, 2002b; Fujii et al.,2004; Sachdev et al., 2001), verbal memory (e.g.,Fujii et al., 2004; Sachdev et al., 2001) and ver-bal learning (e.g., Bamrah & Johnson, 1991) maycharacterise PFTBI. These impairments have beenshown relative both to norms provided by stan-dardised measures (e.g., Bamrah & Johnson, 1991;Fujii et al., 2004) and to matched TBI groups (e.g.,Sachdev et al., 2001). There is also some evidencefor generalised cognitive impairment (e.g., Fujiiet al., 2004; Sachdev et al., 2001).
Neurocognitive impairments of this kind maycontribute to disortions of reality and, especially,the development of delusions, in vulnerable cases.Cognitive models for the formation, content andmaintenance of delusions have been discussed ex-tensively in the literature, usually pertaining to rea-soning and/or attributional biases (Bell, Halligan,& Ellis, 2006; Gilleen & David, 2005), and, morerecently, semantic memory impairment (Rossell,Batty, & Hughes, 2010). A case reported by Pons-ford (2012) presented with temporal lobe damageassociated with slowed verbal processing, and re-lated poor verbal memory. This resulted in themisinterpretation of his social environment and,in the context of social isolation, the developmentof paranoid delusions.
Preliminary evidence has further suggestedthat the presence of psychosis in PFTBI exacer-bates cognitive neuropsychological impairmentsbeyond the effects of the injury (Fujii et al., 2004;Sachdev et al., 2001). Sachdev et al. (2001) re-ported that PFTBI patients had reduced verbal/non-verbal memory and executive function relative to
a TBI control group matched for injury severityand lesion location. Similarly, Fujii et al. (2004)reported reduced performance by PFTBI cases ona range of neuropsychological tests, with the ex-ception of the Trail Making Task (TMT, Forms Aand B; Reitan & Wolfson, 1985) (see Table 3 forthe list of tests reported).3 This was despite milderinjury in the PFTBI patients, compared with TBIpatients, who generally had moderate to severeinjuries. Unfortunately, however, the authors in-spected scores against available norms, instead ofperforming group-wise analyses on these data.
The work from Sachdev et al. (2001) did, how-ever, report greater left/bilateral temporal, and rightparietal injury in the PFTBI cohort. Although thesedifferences were no longer significant followingBonferroni correction, this may explain reducedverbal memory in some PFTBI patients, given theassociation between verbal memory and the lefttemporal region. However, since Sachdev et al.(2001) are the first authors to have published cog-nitive data on statistically matched patient groups,and lesion location differences did not reach sta-tistical significance, this suggestion is made onlytentatively. By contrast, for instance, the case studypresented by Bamrah and Johnson (1991) alsoshowed deficits in verbal learning in particular,yet the computed tomography (CT) scan of thispatient’s brain indicated a generalised (and espe-cially frontal) atrophy, rather than localised lefthemisphere lesions.4
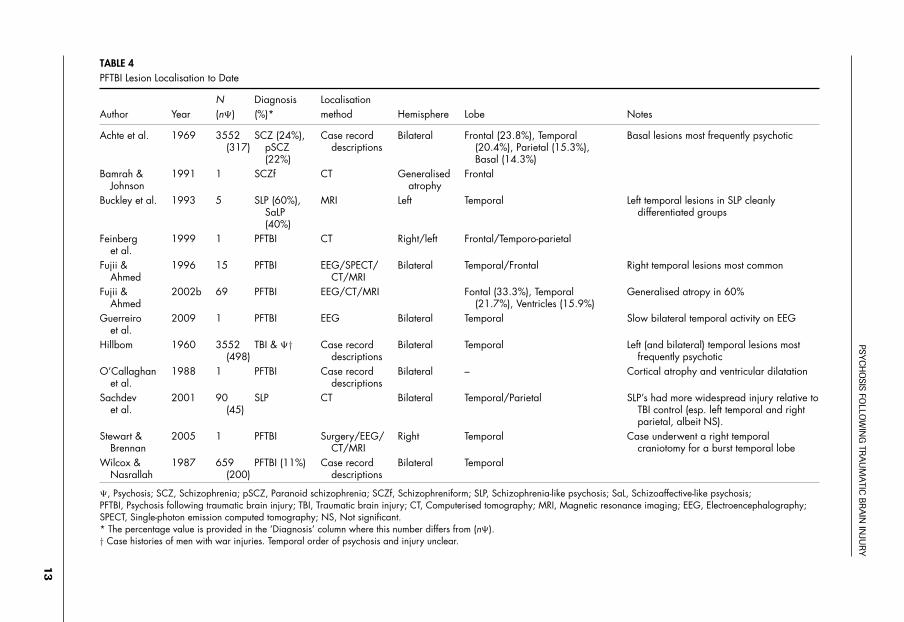
Lesion Localisation and NeuroimagingElectroencephalography (EEG)Table 4 compiles the lesion localisation and neu-roimaging data. Comprehensive empirical event-related potential (ERP) investigations have notbeen published in PFTBI. Existing electroen-cephalograms in dually diagnosed patients havetypically been obtained for diagnostic purposes,where seizures have occurred and/or the extent ofinjury is unclear (Fujii & Ahmed, 1996; Hillbom,1960). Approximately 53% of Hillbom’s (1960)substantial collection of post-war cases (N = 3552)had undergone EEG assessments of this kind, withthe majority of these obtained for patients withmild to moderate brain injuries. Hillbom (1960)
3 The TMT measures executive functions (i.e., process-ing speed, attention and mental switching) particularlysensitive to the effects of brain injury (Ponsford et al.,2008; Senathi-Raja, Ponsford, & Schonberger, 2010).
4 However, the CT scan taken of this patient may nothave revealed the full extent of his injury, and thedamage to his frontal lobe may have been implicatedin his verbal learning and memory impairment.
11
RA
CH
ELA
.BA
TTYET
AL.
TABLE 3Available Data on the Cognitive/Neuropsychological Profile of PFTBI
Authors Year N (n�) Diagnosis Method Assessment Comparison Outcome
Bamrah &Johnson
1991 1 PFTBI Case study WAIS (IQ), Wechsler Memory Scale, WilliamsMemory Tests
Norms Normal range IQ and memory/recall.Impaired verbal learning
Feinberget al.
1999 1 PFTBI Case study Digit Span Backward, Visual Span Backward andSerial Threes, Trail Making Test (B), ContinuousPerformance Test, CVLT, Ray Complex Figure,Boston Naming Test, Revised Token Test,Wisconsin Card Sorting Test, WAIS-R(Comprehension and Similarities subtests).
Norms Impaired complex attention, verbalinhibition, language, visual/verbalmemory, working memory andexecutive function
Fujii &Ahmed
2002b 69* PFTBI Retrospectivechartreview
Various/inconsistent Norms 88% impaired; 58.82% memory,41.18% executive function,41.18% visuo-spatial, 11.76%language, 11.76% attention
Fujii et al. 2004 69(48)†
PFTBI Retrospectivechartreview
WAIS, Logical Memory (immed. recall),Vocabulary, Block Design & Similarities subtests,Trail Making Test (A&B), Verbal Fluency,Wisconsin Card Sorting Test.
Norms &healthycontrol datafromelsewhere
Lower IQ, impaired vocabulary,verbal memory (recall) andexecutive functioning (relative tocontrols after Bonferroni correction)
Guerreiroet al.
2009 1 PFTBI Case study Not stated Norms Moderate verbal memory andabstract reasoning dysfunction.Mild working memory, executivefunction and attention impairments
Sachdevet al.
2001 90 (45) SLP Retrospectivechartreview
Various/inconsistent SLP v TBI Lower IQ, verbal and non-verbalmemory, and frontal executivefunction impairments
�, Psychosis; PFTBI, Psychosis following traumatic brain injury; SLP, Schizophrenia-like psychosis; TBI, Traumatic brain injury; WAIS, Wechsler Adult Intelligence Scale; CVLT,California Verbal Learning Test* N = 17 for cognitive neuropsychological data.† Consists of 24 PFTBI and 24 schizophrenia patient charts (remainder = 21 TBI).
12
PSYC
HO
SISFO
LLOW
ING
TRA
UM
ATIC
BR
AIN
INJU
RY
TABLE 4PFTBI Lesion Localisation to Date
N Diagnosis LocalisationAuthor Year (n�) (%)* method Hemisphere Lobe Notes
Achte et al. 1969 3552(317)
SCZ (24%),pSCZ(22%)
Case recorddescriptions
Bilateral Frontal (23.8%), Temporal(20.4%), Parietal (15.3%),Basal (14.3%)
Basal lesions most frequently psychotic
Bamrah &Johnson
1991 1 SCZf CT Generalisedatrophy
Frontal
Buckley et al. 1993 5 SLP (60%),SaLP(40%)
MRI Left Temporal Left temporal lesions in SLP cleanlydifferentiated groups
Feinberget al.
1999 1 PFTBI CT Right/left Frontal/Temporo-parietal
Fujii &Ahmed
1996 15 PFTBI EEG/SPECT/CT/MRI
Bilateral Temporal/Frontal Right temporal lesions most common
Fujii &Ahmed
2002b 69 PFTBI EEG/CT/MRI Fontal (33.3%), Temporal(21.7%), Ventricles (15.9%)
Generalised atropy in 60%
Guerreiroet al.
2009 1 PFTBI EEG Bilateral Temporal Slow bilateral temporal activity on EEG
Hillbom 1960 3552(498)
TBI & �† Case recorddescriptions
Bilateral Temporal Left (and bilateral) temporal lesions mostfrequently psychotic
O’Callaghanet al.
1988 1 PFTBI Case recorddescriptions
Bilateral – Cortical atrophy and ventricular dilatation
Sachdevet al.
2001 90(45)
SLP CT Bilateral Temporal/Parietal SLP’s had more widespread injury relative toTBI control (esp. left temporal and rightparietal, albeit NS).
Stewart &Brennan
2005 1 PFTBI Surgery/EEG/CT/MRI
Right Temporal Case underwent a right temporalcraniotomy for a burst temporal lobe
Wilcox &Nasrallah
1987 659(200)
PFTBI (11%) Case recorddescriptions
Bilateral Temporal
�, Psychosis; SCZ, Schizophrenia; pSCZ, Paranoid schizophrenia; SCZf, Schizophreniform; SLP, Schizophrenia-like psychosis; SaL, Schizoaffective-like psychosis;PFTBI, Psychosis following traumatic brain injury; TBI, Traumatic brain injury; CT, Computerised tomography; MRI, Magnetic resonance imaging; EEG, Electroencephalography;SPECT, Single-photon emission computed tomography; NS, Not significant.* The percentage value is provided in the ‘Diagnosis’ column where this number differs from (n�).† Case histories of men with war injuries. Temporal order of psychosis and injury unclear.
13

RACHEL A. BATTY ET AL.
did not detail EEG outcome according to casediagnosis and so findings specific to dually diag-nosed PFTBI patients are not available.
The research from Fujii and Ahmed (1996,2002b) has probably been the most informativewith respect to EEG data. In both case history re-views, the authors reported a predominance of tem-poral lobe abnormalities in PFTBI patients (Fujii& Ahmed, 1996, 2002b). A history of seizureswas apparent in the majority of cases (1996), andmore than 70% of the 41 patients in their secondreview (2002b) showed evidence of EEG abnor-malities. The majority of these evidenced slow-ing; however, spiking and dysrhythmia, which arecommon indications of seizure activity, were alsoreported (Ahlskog et al., 1991). Temporal abnor-malities were most common (45.71%), althoughFujii and Ahmed (2002b) also described instancesof frontal (14.29%), parietal (5.71%), occipital(14.29%), central (2.86%) and diffuse (17.14%)impairment, with no hemispheric differences in thesource location of these EEG abnormalities acrosstheir sample. Their work is possibly the first toprovide an indication of the common neurophysi-ological abnormalities in PFTBI.
On the other hand, normal EEG was reportedon two occasions for the patient described by Bam-rah and Johnson (1991), where substantial psychi-atric and psychotic sequelae were experienced overthe patient’s lifetime post TBI. It is unclear howthese data compare statistically with neurophysio-logical function following TBI without psychosis.Slowing, as well as spiking and dysrhythmia duringepileptiform activity, is characteristically shown onEEG scans taken of TBI patients (Hillbom, 1960;Ronne-Engstrom & Winkler, 2006; Wallace,Wagner, Wagner, & McDeavitt, 2001). Focal ab-normalities in the frontal and temporal regions arealso shown most frequently following TBI, and,less commonly, in the parieto-occipital regions(Ronne-Engstrom & Winkler, 2006; Wallace et al.,2001).
Structural NeuroimagingThe magnetic resonance imaging (MRI) and CTdata presented in Table 4 indicate mean PFTBI in-jury localisation rates in the order of 50% frontal,82.5% left temporal, 75% right temporal, 71.8%left parietal, 71.8% right parietal and 14.3% basalinjury. Thus, both left and right frontal and parieto-temporal lesions are most commonly associatedwith PFTBI (Buckley et al., 1993; Fujii & Ahmed,1996, 2002b; Sachdev et al., 2001). Reducedvolume in these regions has been identified inschizophrenia for some time (McAllister & Ferrell,2002). As with EEG, comparisons of injury locali-
sation rates between PFTBI and non-psychotic TBIgroups are lacking, however. Work from Sachdevet al. (2001) may stand alone in this respect, re-porting statistically matched locus of injury acrosstheir groups.5
Existing work, therefore, fails to highlight re-gion(s) associated with an elevated risk for the de-velopment of psychosis post TBI. It is possible thatthe data reflect common injury localisation in TBIgenerally. As previously discussed, this is likely,as frontal and temporal sites have an increasedvulnerability to injury due to the position of thebrain within the skull. The relationship betweenstructural neuroanatomy and psychotic symptomsevidently remains largely unclear. Empirical neu-roimaging data in PFTBI are, overall, extremelylimited, and as with the other aspects of investi-gation in PFTBI, considerable further research isrequired to take the evidence beyond speculation.
Methodological LimitationsSubstantial methodological weaknesses aboundin the PFTBI literature. Intrinsic complexities inthe identification, recruitment and assessment ofPFTBI patients have meant that the available lit-erature is notoriously incomplete. The pooling ofdiscordant, and often unverified, information rep-resents one of the more flawed practices. Chartreview-based studies constitute the majority ofresearch, and tend to draw conclusions aboutphenomenological trends even where substantialamounts of data are missing on measures of inter-est (Burg et al., 1996; Fujii & Ahmed, 2002b).Similarly, critical literature reviews have typi-cally pooled data from studies with incompatiblemethodologies and attempted to draw meaningfulconclusions about PFTBI generally (e.g., Davison& Bagley, 1969). While considerable case-studyreports of both single (e.g., Bamrah & Johnson,1991) and groups of cases (e.g., Rossell et al.,2010) have been published, analyses of these havetheir own empirical shortcomings. For example,the comparability of assessment protocols wheresingle cases are pooled in analysis is questionable,and small-group case studies compromise statis-tical power, making it difficult to draw definitiveconclusions with confidence. Further, injury andsymptom variability across patient groups are of-ten disregarded, despite the influence these mayhave on outcome measures.
5 Although more widespread damage was shown par-ticular to the left temporal and right parietal brain re-gions in PFTBI patients, this did not reach significance(Sachdev et al., 2001).
14

PSYCHOSIS FOLLOWING TRAUMATIC BRAIN INJURY
RecruitmentRecruitment has often been confined to hospital in-patients or chart information taken from inpatientwards, and in one circumstance potential caseswere sought from a list of TBI patients referredfor further neuropsychological testing (Fujii &Ahmed, 2001). Such sources miss mild to moder-ately brain-injured patients who may be experienc-ing psychotic symptoms (Burg et al., 1996; Fujii& Ahmed, 2001; Malaspina et al., 2001), or otherpsychiatric symptoms that may be inadvertentlyconcealing symptoms of psychosis (i.e., symptomsof depression may co-occur with affective flatten-ing; see Fleminger, 2008; Koponen et al., 2002;Mainio et al., 2007 for rates of post-injury depres-sion). On the other hand, long-term PTA may bemisdiagnosed as psychosis following severe TBI.
Investigations across the range of injury sever-ity are warranted, given that the literature hasprovided a number of indications that the de-velopment of psychosis may follow mild headtrauma (Achte et al., 1969; Fujii & Ahmed, 2002b;Fujii et al. 2004). Related to a bias in recruitment,a number of earlier studies reported on service-men/war veterans with penetrating skull injuries(Achte et al., 1969; Corcoran & Malaspina, 2007;David & Prince, 2005; Davison & Bagley, 1969).While these data are valuable because of their ro-bust sample sizes, there are obvious limitations intheir generalisability to other PFTBI populations.Of concern in these populations are inflated rates ofskull-penetrating injuries, and the introduction ofadditional confounding psychopathology that maybe specific to war injuries, such as post-traumaticstress disorder (PTSD).
Clinical ToolsUnstandardised diagnostic criteria have been usedto identify, and rate, both TBI and psychosis (e.g.,Achte et al., 1969). Unsubstantiated cases of self-reported injury are simply not reliable as a basis fordefining the phenomenology of PFTBI (e.g., Silveret al., 2001). Moveover, the use of common classi-fications of TBI (i.e., ICD codes) may only providea broad indication of injury severity. For instance,Nielsen et al. (2002) classified cases broadly underthe category of ‘concussion’ (i.e., ICD code 850).Various methods have been used to define TBIseverity, including the Glasgow Coma Scale (GCS;Teasdale & Jennett, 1974) (e.g., Max et al., 1997),duration of loss of consciousness (Buckley et al.,1993; Hoofien et al., 2001), length of coma, du-ration of post-traumatic amnesia (Koponen et al.,2006) and ICD-10 codes (Fujii & Ahmed, 2002b;Harrison et al., 2006). There is a need for greaterconsistency in the use of injury severity measures
to allow for comparison across studies. Possiblythe most reliable measures of severity are prospec-tively recorded, including the duration of loss ofconsciousness, post-traumatic amnesia and Glas-gow Coma Scale score, where available (Fujii &Ahmed, 2001; Fujii et al., 2004). These are typicalyardsticks in the literature (Buckley et al., 1993;Hoofien et al., 2001), and allow for the most spe-cific determination of injury severity besides neu-roimaging data. Psychotic patients are also morelikely to want to attribute their psychiatric distur-bances to a physical cause, and thus, to report aTBI.
In some cases, diagnoses of psychosis havebeen made from available chart notes alone(Corcoran & Malaspina, 2007; Kim, 2008), or psy-chosis has been labelled grossly without record-ing individual symptom information (e.g., Burget al., 1996; Koponen et al., 2002, 2006). Unsub-stantiated and inconsistent diagnoses are especiallyproblematic in prevalence estimates. Where somestudies have confined their estimates to DSM diag-nostic criteria for schizophrenia (e.g., Fujii et al.,2004; Silver et al., 2001), others have includedcases with one or more psychotic symptoms (e.g.,Achte et al., 1969; Fann et al., 2004). Those us-ing broader definitions of psychosis may havealso included diagnoses not traditionally consid-ered psychotic. For instance, Achte et al. (1969),who estimated a relatively high prevalence of8.9% psychosis in men injured during the Finnishwar, included diagnoses of Korsakoff’s syndrome,‘grave dementia’ and borderline psychotic casesin their estimate. Disparity has also been shownin the concepualisation of the subsequent psy-chotic symptoms; some research has focused onelucidating the potential for schizophrenia (e.g.,AbdelMalik et al., 2003; Corcoran & Malaspina,2007; Kim, 2008; Malaspina et al., 2001; Nielsenet al., 2002), whereas others have conceptualiseda relationship with psychotic symptoms along acontinuum (Buckley et al., 1993; David & Prince,2005; McAllister & Ferrell, 2002; Wilcox & Nas-rallah, 1986).
Further inconsistencies arise in the recordingand assessment of personal and family history ofpsychosis. Research has both: (i) failed to assessthe personal history of psychosis in those present-ing with PFTBI (Burg et al., 1996; Fujii & Ahmed,2002b); and (ii) collapsed groups with and with-out psychoses prior to a TBI in their investiga-tions (Fann et al., 2004). It is essential that theseare reliably recorded and separated in analyses towork toward understanding the nature and/or di-rection of the relationship between psychoses andTBI. Because genetic, especially heritable, liabil-ity in schizophrenia is well established (Kim, 2008;
15

RACHEL A. BATTY ET AL.
Kumar et al., 2010), family history should also bereliably ascertained as a basis for assessing poten-tial aetiological (i.e., genetic) similarities betweenPFTBI and schizophrenia. To date, research hasrelied on retrospective recall, especially when col-lecting data relating to personal and family history(e.g., Burg et al., 1996). This is a particular lim-itation in large community-based prevalence in-vestigations that use questionnaires (Fann et al.,2004; Silver et al., 2001). The risk of unreliablerecall is exacerbated within brain-injured and po-tentially psychotic populations, who are known tohave cognitive deficiencies, particularly in mem-ory (Malaspina et al., 2001; Silver et al., 2001).
ConclusionThe existing PFTBI literature has documented ahandful of consistent findings with regard to thevarious domains reviewed here. Many of the pre-vailing limitations of this work are, at least par-tially, a consequence of inherent difficulties withPFTBI recruitment and assessment. Despite con-troversies surrounding claims of causation, ratesof psychosis following TBI appear to exceed thoseof the general population threefold. Still, this isa relatively small number of patients when con-sidered within the TBI population, explaining theprominence of case-study and retrospective chartor database reviews in the literature. The onset ofpsychotic symptoms, which may be matched inprofile to schizophrenia, can occur any time, fromwithin the first year following injury to more than10 years post injury. Verbal memory impairmentsare relatively common, and a predominance offrontal and temporal injury has been noted. How-ever, these trends are based on extremely limitedwork. It is not yet possible, on the basis of the avail-able evidence, to definitively establish that TBIcauses psychosis. Theorised conceptual models ofthe relationship between TBI and psychosis, andthe phenomenology of PFTBI itself, are prema-ture until comprehensive and standardised investi-gations addressing the methodological confoundsdiscussed in this review are published. Multicen-tre prospective, longitudinal studies of large co-horts including mild, moderate and severe injuries,the assessment of pre-injury psychiatric function,structured clinical diagnostic interviews at regularintervals, cognitive assessment, neuroimaging andgenetic data are required to achieve this.
ReferencesAbel, K.M., Drake, R., & Goldstein, J.M. (2010). Sex
differences in schizophrenia. International Reviewof Psychiatry, 22(5), 417–428.
AbdelMalik, P., Husted, J., Chow, E.W.C., & Bassett,A.S. (2003). Childhood head injury and expres-sion of schizophrenia in multiply affected families.Archives of General Psychiatry, 60(3), 231–236.
Achte, K.A., Hillbom, E., & Aalberg, V. (1969). Psy-choses following war injuries. Acta PsychiatricaScandinavica, 45, 1–18.
Ahlskog, J.E., Mayo Foundation for Medical Educationand Research, & Mayo Clinic Department of Neu-rology. (1991). Clinical examinations in neurology(6th ed.). St. Louis, MO: Mosby Year-Book.
Albert, N., Bertelsen, M., Thorup, A., Petersen, L.,Jeppesen, P., Le Quack, P., . . . Nordentoft, M.(2011). Predictors of recovery from psychosis: Anal-ysis of clinical and social factors associated with re-covery among patients with first-episode psychosisafter 5 years. Schizophrenia Research, 125(2–3),257–256.
American Psychological Association (APA). (1994). Di-agnostic and statistical manual of mental disorders– Fourth Edition (DSM-IV) (4th ed.). Washington,USA: American Psychological Association.
American Psychological Association (APA). (2000). Di-agnostic and statistical manual of mental disorders– fourth edition, test revision (DSM-IV-TR) (4 ed.).Washington, USA: American Psychological Associ-ation.
Andreasen, N.C., & Olsen, S. (1982). Negative v. positiveschizophrenia. Definition and validation. Archives ofGeneral Psychiatry, 39(7), 789–794.
Anson, K., & Ponsford, J. (2006). Coping and emotionaladjustment following traumatic brain injury. Journalof Head Trauma Rehabilitation, 21, 248–259.
Bachus, S.E., & Kleinman, J.E. (1996). The neuropathol-ogy of schizophrenia. Journal of Clinical Psychiatry,11, 72–83.
Badcock, J.C., & Dragovic, M. (2006). Schizotypal per-sonality in mature adults. Personality and IndividualDifferences, 40, 77–85.
Bamrah, J.S., & Johnson, J. (1991). Bipolar affectivedisorder following head injury. British Journal ofPsychiatry, 158, 117–119.
Beauchamp, M., Catroppa, C., Godfrey, C., Morse, S.,Rosenfeld, J.V., & Anderson, V. (2011). Selectivechanges in executive functioning ten years after se-vere childhood traumatic brain injury. Developmen-tal Neuropsychology, 36(5), 578–595.
Belina, S., & Kovacic, S. (2011). CT follow-up and clini-cal outcome in severe traumatic brain injury patients.Collegium Antropologicum, 35(4), 1197–1202.
Bell, V., Halligan, P.W., & Ellis, H.D. (2006). Explainingdelusions: A cognitive perspective. Trends in Cogni-tive Sciences, 10(5), 219–226.
Bigler, E.D. (2007). Anterior and middle cranial fossa intraumatic brain injury: Relevant neuroanatomy andneuropathology in the study of neuropsychologicaloutcome. Neuropsychology, 21(5), 515–531.
Borgwardt, S.J., Riecher-Rossler, A., Dazzan, P., Chitnis,X., Aston, J., Drewe, M., . . . McGuire, P.K. (2007).Regional gray matter volume abnormalities in the
16
PSYCHOSIS FOLLOWING TRAUMATIC BRAIN INJURY
at risk mental state. Biological Psychiatry, 61(10),1148–1156.
Bourque, F., van der Ven, E., Fusar-Poli, P., & Malla,A. (2012). Immigration, social environment and on-set of psychotic disorders. Current PharmaceuticalDesign, 18(4), 518–526.
Broome, M.R., Fusar-Poli, P., Matthiasson, P., Woolley,J.B., Valmaggia, L., Johns, L.C., . . . McGuire, P.K.(2010). Neural correlates of visuospatial workingmemory in the ‘at-risk mental state’. PsychologicalMedicine, 40, 1987–1999.
Bruns, J. Jr, & Hauser, W. (2003). The epidemiology oftraumatic brain injury. A review. Epilepsia, 44(suppl10), 2–10.
Buckley, P., Stack, J.P., Madigan, C., O’Callaghan,E., Larkin, C., Redmond, O., . . . Waddington,J.L. (1993). Magnetic resonance imaging ofschizophrenia-like psychoses associated withcerebral trauma: Clinicopathological correlates.American Journal of Psychiatry, 150(1), 146–148.
Burg, J.S., McGuire, L.M., Burright, R.G., & Donovick,P.J. (1996). Prevalence of traumatic brain injury in aninpatient psychiatric population. Journal of ClinicalPsychology in Medical Settings, 3(3), 243–251.
Butler, P.V. (2000). Diurnal variation in Cotard’s syn-drome (copresent with Capgras delusion) followingtraumatic brain injury. Australian and New ZealandJournal of Psychiatry, 34, 684–687.
Corcoran, C., & Malaspina, D. (2007). Traumatic braininjury as a risk factor for schizophrenia. Current Psy-chiatry Reviews, 3, 25–32.
Csernansky, J.G., Wang, L., Jones, D., Rastogi-Cruz,D., Posener, J.A., Heydebrand, G., . . . Miller, M.I.(2002). Hippocampal deformities in schizophreniacharacterized by high dimensional brain mapping.American Journal of Psychiatry, 159(12), 2000–2006.
David, A.S., & Prince, M. (2005). Psychosis followinghead injury: A critical review. Journal of Neurology,Neurosurgery and Psychiatry, 76(suppl 1), i53–i60.
Davison, K., & Bagley, C.R. (1969). Schizophrenia-likepsychoses associated with organic disorders of thecentral nervous system: A review of the literature.British Journal of Psychiatry, 114, 113–162.
DeKosky, S.T., Kochanek, P.M., Clark, R.S.B., Ciallella,J.R., & Dixon, C.E. (1998). Secondary injury afterhead trauma: Subacute and long-term mechanisms.Seminars in Clinical Neuropsychiatry, 3(3), 176–185.
Egan, M.F., Hyde, T.M., Bonomo, J.B., Mattay, V.S.,Bigelow, L.B., Goldberg, T.E., . . . Weinbereger,D.R. (2001). Relative risk of neurological signs insiblings of patients with schizophrenia. AmericanJournal of Psychiatry, 158(11), 1827–1834.
Ellison-Wright, I., Glahn, D., Laird, A., Thelen, S.M., &Bullmore, E. (2008). The anatomy of first-episodeand chronic schizophrenia: An anatomical likelihoodestimation meta-analysis. American Journal of Psy-chiatry, 165(8), 1015–1023.
Evans, J. J., Chua, S.E., McKenna, P.J., & Wilson, B.A.(1997). Assessment of the dysexecutive syndrome inschizophrenia. Psychological Medicine, 27(3), 635–646.
Fann, J.R., Burington, B., Leonetti, A., Jaffe, K., Katon,W.J., & Thompson, R.S. (2004). Psychiatric illnessfollowing traumatic brain injury in an adult healthmaintenance organization population. Archives ofGeneral Psychiatry, 61, 53–61.
Fann, J.R., Leonetti, A., Jaffe, K., Katon, W.J.,Cummings, P., & Thompson, R.S. (2002). Psychi-atric illness and subsequent traumatic brain injury:A case control study. Journal of Neurology, Neuro-surgery, and Psychiatry, 72, 615–620.
Feinberg, T.E., Eaton, L.A., Roane, D.M., & Giacino, J.T.(1999). Multiple Fregoli delusions after traumaticbrain injury. Cortex, 35, 373–387.
Fleminger, S. (2008). Long-term psychiatric disordersafter traumatic brain injury. European Journal ofAnaesthesiology, 25(suppl 42), 123–130.
Friston, K.J., Liddle, P.F., Frith, C.D., Hirsch, S.R., &Frackowiak, R.S. (1992). The left medial tempo-ral region and schizophrenia. A PET study. Brain,115(2), 367–382.
Fujii, D., & Ahmed, I. (1996). Psychosis secondaryto traumatic brain injury. Neuropsychiatry, Neu-ropsychology, and Behavioral Neurology, 9, 133–138.
Fujii, D., & Ahmed, I. (2001). Risk factors in psychosissecondary to traumatic brain injury. Journal of Neu-ropsychiatry and Clinical Neurosciences, 13(1), 61–69.
Fujii, D., & Ahmed, I. (2002a). Psychotic disorder fol-lowing traumatic brain injury: A conceptual frame-work. Cognitive Neuropsychiatry, 7(1), 41–62.
Fujii, D., & Ahmed, I. (2002b). Characteristics of psy-chotic disorder due to traumatic brain injury: Ananalysis of case studies in the literature. Journalof Neuropsychiatry and Clinical Neurosciences, 14,130–140.
Fujii, D., Ahmed, I., & Hishinuma, E. (2004). A neu-ropsychological comparison of psychotic disorderfollowing traumatic brain injury, traumatic braininjury without psychotic disorder, and schizophre-nia. Journal of Neuropsychiatry and Clinical Neuro-sciences, 16(3), 306–314.
Fusar-Poli, P., McGuire, S., & Borgwardt, S. (2011).Mapping prodromal psychosis: A critical review ofneuroimaging studies. European Psychiatry, 27(3),181–191.
Gard, D.E., Fisher, M., Garrett, C., Genevsky, A., &Vinogradov, S. (2009). Motivation and its relation-ship to neurocognition, social cognition, and func-tional outcome in schizophrenia. Schizophrenia Re-search, 115(1), 74–81.
Gennarelli, T.A., & Graham, D.I. (1998). Neuropathol-ogy of the head injuries. Seminars in Clinical Neu-ropsychiatry, 3(3), 160–175.
Gilleen, J., & David, A.S. (2005). The cognitive neu-ropsychiatry of delusions: From psychopathology
17
RACHEL A. BATTY ET AL.
to neuropsychology and back again. PsychologicalMedicine, 35, 5–12.
Glantz, L.A., Gilmore, J.H., Lieberman, J.A., & Jarskog,L.F. (2006). Apoptotic mechanisms and the synap-tic pathology of schizophrenia. Schizophrenia Re-search, 81, 47–63.
Goreishizadeh, M.A., Mohagheghi, A., Farhang, S., &Alizadeh, L. (2012). Psychosocial disabilities in pa-tients with schizophrenia. Iranian Journal of PublicHealth, 41(5), 116–121.
Gould, K., Ponsford, J., Schonberger, M., & Johnston, L.(2011). The nature, frequency and course of psychi-atric disorders in the first year after traumatic braininjury, a prospective study. Psychological Medicine,41(10), 2099–2109.
Guerreiro, D.F., Navarro, R., Silva, M., Carvalho, M., &Gois, C. (2009). Psychosis secondary to traumaticbrain injury. Brain Injury, 23(4), 358–361.
Harrison, G., Whitley, E., Rasmussen, F., Lewis, G.,Dalman, C., & Gunnell, D. (2006). Risk ofschizophrenia and other non-affective psychosisamong individuals exposed to head injury: Casecontrol study. Schizophrenia Research, 88(1), 119–126.
Hartley, S., Haddock, G., & Barrowclough, C. (2012).Anxiety and depression and their links with delu-sions and hallucinations in people with a dual diag-nosis of psychosis and substance misuse: A study us-ing data from a randomised control trial. BehaviourResearch and Therapy, 50(1), 65–71.
Henry, J.D., & Crawford, J.R. (2004). A meta-analyticreview of verbal fluency performance in patientswith traumatic brain injury. Neuropsychology, 18(4),621–628.
Hillbom, E. (1960). After-effects of brain injuries. ActaPsychiatrica Neurologica Scandinavica, 142, 1–195.
Hiott, D.W., & Labbate, L. (2002). Anxiety disordersassociated with traumatic brain injuries. NeuroRe-habilitation, 17, 345–355.
Ho, B.C., Andreasen, N.C., Nopoulos, P., Arndt, S., Mag-notta, V., & Flaum, M. (2003). Progressive structuralbrain abnormalities and their relationship to clinicaloutcome: A longitudinal magnetic resonance imag-ing study early in schizophrenia. Archives of GeneralPsychiatry, 60, 585–594.
Hoofien, D., Gilboa, A., Vakil, E., & Donovick, P. J.(2001). Traumatic brain injury (TBI) 10–20 yearslater: A comprehensive outcome study of psychiatricsymptomatology, cognitive abilities and psychoso-cial functioning. Brain Injury, 15(3), 189–209.
Horn, H., Federspiel, A., Wirth, M., Muller, T., Wiest,R., Walter, S., . . . Strik, W. (2010). Gray mattervolume differences specific to formal thought disor-der in schizophrenia. Psychiatry Research, 182(2),183–186.
Hughes, M.E., Fulham, W.R., Johnston, P.J., & Michie,P.T. (2012). Stop-signal response inhibition inschizophrenia: Behavioural, event-related potentialand functional neuroimaging data. Biological Psy-chology, 89(1), 220–231.
Jablensky, A., Sartorius, N., Ernberg, G., Anker, M.,Korten, A., Cooper, J.E., . . . Bertelsen, A. (1992).Schizophrenia: Manifestations, incidence and coursein different cultures. A World Health Organiza-tion ten-country study. Psychological Medicine,20(monogr. suppl.), 1–97.
Jessen, F., Scheef, L., Germeshausen, L., Tawo, Y.,Kockler, M., Kuhn, K.U., . . . Heun, R. (2003).Reduced hippocampal activation during encodingand recognition of words in schizophrenia patients.American Journal of Psychiatry, 106(7), 1305–1312.
Jorge, R.E., Robinson, R.G., Moser, D., Tateno, A.,Crespo-Facorro, B., & Arndt, S.V. (2004). Major de-pression following traumatic brain injury. Archivesof General Psychiatry, 61, 42–50.
Joshua, N., & Rossell, S.L. (2009). Configural face pro-cessing in schizophrenia. Schizophrenia Research,112(1–3), 99–103.
Kay, S.R., Fiszbein, A., & Opler, L.A. (1987). The Pos-itive and Negative Syndrome Scale (PANSS) forschizophrenia. Schizophrenia Bulletin, 13(2), 261–276.
Kendler, K.S., Gallagher, T.J., Abelson, J.M., & Kessler,R.C. (1996). Lifetime prevalence, demographic riskfactors, and diagnostic validity of nonaffective psy-chosis as assessed in a US community sample. TheNational Comorbidity Survey. Archives of GeneralPsychiatry, 53(11), 1022–1031.
Kim, E. (2008). Does traumatic brain injury predisposeindividuals to develop schizophrenia? Current Opin-ion in Psychiatry, 21(3), 286–289.
Kim, E., Lauterbach, E.C., Reeve, A., Arciniegas, D.B.,Coburn, K.L., Mendez, M.F., . . . Coffey, E.C.(2007). Neuropsychiatric complications of traumaticbrain injury: A critical review of the literature (a re-port by the ANPA Committee on Research). Jour-nal of Neuropsychiatry and Clinical Neurosciences,19(2), 106–127.
Koponen, S., Taiminen, T., Kurki, T., Portin, R., Isoniemi,H., Himanen, L., . . . Tenovuo, O. (2006). MRI find-ings and Axis I and II psychiatric disorders after trau-matic brain injury: A 30-year retrospective follow-upstudy. Psychiatry Research: Neuroimaging, 146(3),263–270.
Koponen, S., Taiminen, T., Portin, R., Himanen, L.,Isoniemi, H., Heinonen, H., . . . Tenovuo, O. (2002).Axis I and II psychiatric disorders after traumaticbrain injury: A 30-year follow-up study. AmericanJournal of Psychiatry, 159(8), 1315–1321.
Kulhara, P., & Chakrabarti, S. (2001). Culture andschizophrenia and other psychotic disorders. Psy-chiatrics Clinics of North America, 24(3), 449–464.
Kumar, C.T., Christodoulou, T., Vyas, N.S.,Kyriakopoulos, M., Corrigall, R., Reichenberg, A.,. . . Frangou, S. (2010). Deficits in visual sustainedattention differentiate genetic liability and diseaseexpression for schizophrenia from bipolar disorder.Schizophrenia Research, 124, 1–3.
Lawrie, S.M., Whalley, H., Kestelman, J.N., Abukmeil,S.S., Byrne, M., Hodges, A., . . . Johnstone, E.C.
18
PSYCHOSIS FOLLOWING TRAUMATIC BRAIN INJURY
(1999). Magnetic resonance imaging of brain in peo-ple at high risk of developing schizophrenia. Lancet,353, 30–33.
Lewis, A. (1942). Discussion on differential diagnosisand treatment of post-contusional states. Proceed-ings of the Royal Society of Medicine, 35, 607–614.
Lezak, M.D. (1979). Recovery of memory and learningfunctions following traumatic brain injury. Cortex,15, 63–72.
Liddle, P.F. (1987). The symptoms of chronic schizophre-nia. A re-examination of the positive–negative di-chotomy. British Journal of Psychiatry, 151, 145–151.
Mainio, A., Kyllonen, T., Viilo, K., Hakko, H., Sarkioja,T., & Rasanen, P. (2007). Traumatic brain injury, psy-chiatric disorders and suicide: A population-basedstudy of suicide victims during the years 1988–2004in Northern Finland. Brain Injury, 21(8), 851–855.
Malaspina, D., Goetz, R.R., Friedman, J.H., Kaufmann,C.A., Faraone, S.V., Tsuang, M., . . . Blehar, M.C.(2001). Traumatic brain injury and schizophrenia inmembers of schizophrenia and bipolar disorder pedi-grees. American Journal of Psychiatry, 158, 440–446.
Mathalon, D.H., Sullivan, E.V., Lim, K.O., &Pfefferbaum, A. (2001). Progressive brain volumechanges in the clinical course of schizophrenia inmen: A longitudinal magnetic resonance imagingstudy. Archives of General Psychiatry, 58(2), 148–157.
Max, J.E., Lindgren, S.D., Knutson, C., Pearson, C.S.,Ihrig, D., & Welborn, A. (1997). Child and adoles-cent traumatic brain injury: Psychiatric findings froma paediatric outpatient speciality clinic. Brain Injury,11(10), 699–712.
McAllister, T.W., & Ferrell, R.B. (2002). Evaluation andtreatment of psychosis after traumatic brain injury.NeuroRehabilitation, 17(4), 357–368.
McGrath, J., Saha, S., Chant, D., & Welham, J. (2008).Schizophrenia: A concise overview of incidence,prevalence, and mortality. Epidemiologic Reviews,30, 67–76.
McGuffin, P., Asherson, P., Owen, M., & Farmer, A.(1994). The strength of the genetic effect. Is thereroom for an environmental influence in the aetiologyof schizophrenia? British Journal of Psychiatry, 164,593–599.
Medalia, A., & Brekke, J. (2010). In search of a the-oretical structure for understanding motivation inschizophrenia. Schizophrenia Bulletin, 36(5), 912–918.
Murrey, G.J., Starzinski, D.T., & LeBlanc, A.J. (2004).Base rates of traumatic brain injury history in adultsadmitted to state psychiatric hospitals: A 3-yearstudy. Rehabilitation Psychology, 49(3), 259–261.
Must, A., Janka, Z., & Horvath, S. (2011). Schizophrenia,environment and epigenetics. Neuropsychopharma-cologica Hungarica, 13(4), 211–217.
Myers, N.L. (2011). Update: Schizophrenia across cul-tures. Current Psychiatry Reports, 13(4), 305–311.
Myin-Germeys, I., Krabbendam, L., & van Os, J. (2003).Continuity of psychotic symptoms in the community.Current Opinion in Psychiatry, 16, 443–449.
Nakagami, E., Hoe, M., & Brekke, J.S. (2010). Theprospective relationships among intrinsic motiva-tion, neurocognition, and psychosocial function-ing in schizophrenia. Schizophrenia Bulletin, 36(5),935–948.
Newburn, G. (1998). Psychiatric disorders associatedwith traumatic brain injury. Optimal treatment. CNSDrugs, 9(6), 441–456.
Nielsen, A.S., Mortensen, P.B., O’Callaghan, E., Morsa,O., & Ewald, H. (2002). Is head injury a risk factorfor schizophrenia? Schizophrenia Research, 55(1),93–98.
O’Callaghan, E., Larkin, C., Redmond, O., Stack, J.,Ennis, J.T., & Waddington, J.L. (1988). Early-onsetschizophrenia after teenage head injury. A case re-port with magnetic resonance imaging. British Jour-nal of Psychiatry, 153, 394–396.
Pantelis, C., Velakoulis, D., McGorry, P.D., Wood, S.J.,Suckling, J., Phillips, L., . . . McGuire, P.K. (2003).Neuroanatomical abnormalities before and after on-set of psychosis: A cross-sectional and longitudinalMRI comparison.Lancet, 361(9354), 281–288.
Perala, J., Suvisaari, J., Saarni, S.I., Kuoppasalmi, K.,Isometsa, E., Pirkola, S., . . . Lonngvist, J. (2007).Lifetime prevalence of psychotic and bipolar I dis-orders in a general population. Archives of GeneralPsychiatry, 64(1), 19–28.
Ponsford, J. (2012). Dealing with the impact of TBIon psychological adjustment and relationships. InJ. Ponsford, S. Sloan & P. Snow. (Eds.), Traumaticbrain injury: Rehabilitation for everyday adaptiveliving (pp. 226–262). London, UK: PsychologyPress.
Ponsford, J.L., Draper, K., & Schonberger, M. (2008).Functional outcome 10 years after traumatic brain in-jury: Its relationship with demographic, injury sever-ity, and cognitive and emotional status. Journal of theInternational Neuropsychological Society, 14, 233–242.
Ponsford, J.L., & Kinsella, G. (1992). Attentional deficitsfollowing closed-head injury. Journal of Clinical andExperimental Neuropsychology, 14(5), 822–838.
Ponsford, J.L., Sloan, S., & Snow, P. (2012). Traumaticbrain injury: Rehabilitation for everyday adaptiveliving (2nd ed.). London, UK: Psychology Press.
Pridmore, S., & Bowe, G. (2011). Neuroimaging in thefield of psychoses. Malaysian Journal of MedicalScience, 18(1), 6–11.
Raghupathi, R. (2004). Cell death mechanisms followingtraumatic brain injury. Brain Pathology, 14, 215–222.
Rao, V., & Lyketsos, C.G. (2003). Psychiatric aspects oftraumatic brain injury: New solutions to an old prob-lem. International Review of Psychiatry, 15, 299–301.
Reitan, R.M., & Wolfson, D. (1985). The Halstead–Reitan Neuropsycholgical Test Battery: Therapy and
19
RACHEL A. BATTY ET AL.
clinical interpretation. Tucson, AZ: Neuropsycho-logical Press.
Rink, A., Fung, K., Trojanowski, J.Q., Lee, V.M.Y.,Neugebauer, E., & McIntosh, T.K. (1995). Evidenceof apoptotic cell death after experimental traumaticbrain injury in the rat. American Journal of Pathol-ogy, 147(6), 1575–1583.
Rios, M., Perianez, J.A., & Munoz-Cespedes, J.M.(2004). Attentional control and slowness of infor-mation processing after severe traumatic brain injury.Brain Injury, 18(3), 257–272.
Ronne-Engstrom, E., & Winkler, T. (2006). ContinuousEEG monitoring in patients with traumatic brain in-jury reveals a high incidence of epileptiform activity.Acta Neurologica Scandinavica, 114(1), 47–53.
Ross, D.E. (2011). Review of longitudinal studies of MRIbrain volumetry in patients with traumatic brain in-jury. Brain Injury, 25(13–14), 1271–1278.
Ross, D.E., Ochs, A.L., Seabaugh, J.M., Demark, M.F.,Shrader, C.R., Marwitz, J.H., . . . Havranek, M.D.(2012). Progressive brain atrophy in patients withchronic neuropsychiatric symptoms after mild trau-matic brain injury: A preliminary study. Brain In-jury, 26(12), 1500-1509.
Rossell, S.L., Batty, R.A., & Hughes, L. (2010). Impairedsemantic memory in the formation and maintenanceof delusions post-traumatic brain injury: A new cog-nitive model of delusions. European Archives ofPsychiatry and Clinical Neuroscience, 260(8), 571–581.
Rossell, S.L., & David, A.S. (2006). Are semantic deficitsin schizophrenia due to problems with access or stor-age? Schizophrenia Research, 82(2–3), 121–134.
Rossler, W., Hengartner, M.P., Angst, J., & Ajdacic-Gross, V. (2012). Linking substance use with symp-toms of subclinical psychosis in a community cohortover 30 years. Addiction, 107(6), 1174–1184.
Rutherford, W.H., Merrett, J.D., & McDonald, J.R.(1977). Sequelae of concussion caused by minorhead injuries. Lancet, 309, 1–4.
Sachdev, P., Smith, J.S., & Cathcart, S. (2001).Schizophrenia-like psychosis following traumaticbrain injury: A chart-based descriptive and case con-trol study. Psychological Medicine, 31, 231–239.
Saha, S., Chant, D., Welham, J., & McGrath, J. (2005). Asystematic review of the prevalence of schizophre-nia. PLoS Medicine, 2(5), e141.
Senathi-Raja, D.R., Ponsford, J.L., & Schonberger, M.(2010). Association of age wih long-term psychoso-cial outcome following traumatic brain injury. Jour-nal of Rehabilitation Medicine, 41(8), 666–673.
Silver, J.M., Kramer, R., Greenwald, S., & Weissman, M.(2001). The association between head injuries andpsychiatric disorders: Findings from the New HavenNIMH Epidemiologic Catchment Area Study. BrainInjury, 15(11), 935–945.
Smieskova, R., Fusar-Poli, P., Riecher-Rossler, A., &Borgwardt, S. (2012). Neuroimaging and resiliencefactors: Staging of the at-risk mental state? CurrentPharmaceutical Design, 18(4), 416–421.
Snow, P., & Ponsford, J. (2012). Impairment of con-sciousness. In J. Ponsford, S. Sloan & P. Snow.(Eds.), Traumatic brain injury: Rehabilitation foreveryday adaptive living (pp. 34–65). London, UK:Psychology Press.
Solomon, D.A., & Malloy, P.F. (1992). Alcohol, headinjury, and neuropsychological function. Neuropsy-chology Review, 3(3), 249–280.
Steen, R., Mull, C., McClure, R., Hamer, R., & Lieber-man, J. (2006). Brain volume in first episodeschizophrenia: Systematic review and meta-analysisof magnetic resonance imaging studies. British Jour-nal of Psychiatry, 188, 510–518.
Stewart, B., & Brennan, D.M. (2005). Auditory halluci-nations after right temporal gyri resection. Journalof Neuropsychiatry and Clinical Neurosciences, 17,243–245.
Sutterland, A.L., Dieleman, J., Storosum, J.G., Voor-douw, B.A., Kroon, J., Veldhuis, J., . . . Sturken-boom, M.C. (2013). Annual incidence rate ofschizophrenia and schizophrenia spectrum disordersin a longitudinal population-based cohort study. So-cial Psychiatry and Psychiatric Epidemiology. Ad-vance online publication. doi: 10.1007/s00127-013-0651-9.
Switaj, P., Anczewska, M., Chrostek, A., Sabariego, C.,Cieza, A., & Chatterji, S. (2012). Disability andschizophrenia: A systematic review of experiencedpsychosocial difficulties. BMC Psychiatry, 12, 193–205.
Tate, D.F., Khedraki, R., Neeley, E.S., Ryser, D.K.,& Bigler, E.D. (2011). Cerebral volume loss,cognitive deficit, and neuropsychological perfor-mance: Comparative measures of brain atrophy:II. Traumatic brain injury. Journal of the Inter-national Neuropsychological Society, 17(2), 308–316.
Teasdale, G.M., & Jennett, B. (1974). Assessment ofcoma and impaired consciousness: A practical scale.Lancet, 2, 81–84.
Verdoux, H., & van Os, J. (2002). Psychotic symptoms innon-clinical populations and the continuum of psy-chosis. Schizophrenia Research, 54, 59–65.
Wallace, B.E., Wagner, A.K., Wagner, E.P., & McDeav-itt, J.T. (2001). A history and review of quantitativeelectroencephalography in traumatic brain injury.Journal of Head Trauma Rehabilitation, 16(2), 165–190.
West, S.L. (2011). Substance use among persons withtraumatic brain injury: A review. NeuroRehabilita-tion, 29(1), 1–8.
Westermeyer, J. (2006). Comorbid schizophrenia andsubstance abuse: A review of epidemiology andcourse. American Journal on Additions, 15(5), 345–355.
Whelan-Goodinson, R., Ponsford, J.L., Johnston, L., &Grant, F. (2009). Psychiatric disorders followingtraumatic brain injury: Their nature and frequency.Journal of Head Trauma Rehabilitation, 24(5), 324–332.
20
PSYCHOSIS FOLLOWING TRAUMATIC BRAIN INJURY
Wilcox, J.A., & Nasrallah, H.A. (1986). Childhood headtrauma and psychosis. Psychiatry Research, 21(4),303–306.
Wisdom, J.P., Manuel, J.I., & Drake, R.E. (2011). Sub-stance use disorder among people with first-episodepsychosis: A systematic review of course and treat-ment. Psychiatric Services, 62(9), 1007–1012.
Zierhut, K., Bogerts, B., Schott, B., Fenker, D.,Walter, M., Albrecht, D., . . . Schiltz, K. (2010).
The role of hippocampus dysfunction in defi-cient memory encoding and positive symptoms inschizophrenia. Psychiatry Research, 183(3), 187–194.
Zierhut, K.C., Grabmann, R., Kaufmann, J., Steiner, J.,Bogerts, B., & Schiltz, K. (2013). Hippocampal CA1deformity is related to symptom severity and an-tipsychotic dosage in schizophrenia. Brain, 136(3),804–814.
21





























