Embed Size (px)
Citation preview
ISSN: 0970-5333
VOL. 28 | Issue 3 | September-December 2014
INDIAN Journal of
PAINPAINPAIN
Indian Society for Study of Pain
Ind
ian Jo
urn
al of P
ain • V
olume 28 • Issue 3 • S
eptem
ber-D
ecemb
er 2014 • Pages 125-***
www.indianjpain.org
184 Indian Journal of Pain | September-December 2014 | Vol 28 | Issue 3
Post traumatic pain: ?CRPS
IntroductionPain is defined by the International Association for the Study of Pain (IASP) as an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.
Pain elicited by injury and activation of nociceptors is called ‘acute pain’ and is one of the most common reasons for seeking medical help.
Chronic pain maybe elicited by injury or disease but is likely to get perpetuated by factors that are pathogenetically and physically remote from the originating cause.
The World Health Organization (WHO) estimates that 4.8 billion people (79% of the world’s population) have inadequate access to treatment for moderate to severe pain.[1] The pain treatment for children is assumed to be even worse than for adults. Reports in literature emphasize the prevalence of pain in children:1. Chronic pain aff ects 25% of children, 8% of these have
intense and frequent pain.[2]
Access this article online
Quick Response Code:Website: www.indianjpain.org
DOI: 10.4103/0970-5333.138458
ABSTRACTAlthough there is an increased awareness of and treatment of acute pain in infants and children, the lack of awareness on various chronic and persistent pains in children often leads to physicians/pediatricians pursuing an endless search for the underlying etiology of the discomfort. Continued lab investigations are undertaken for the sake of “completeness” to search for a biological explanation for the pain. The author would like to present this case report where there was no obvious cause for the pain found on investigations. The child was treated for neuropathic pain with complete recovery. Though complex regional pain syndrome (CRPS) was suspected, the diffi culty in establishing a diagnosis, convincing caregivers and compliance to pharmacotherapy are the major challenges in the pediatric pain patients.
Key words: Caregivers, investigations, neuropathic pain, pediatric pain, post-trauma pain
Kritika Doshi1-5
1Joint Secretary, ISSP-Mumbai, 2Managing Committee Member-AMC (Association of Medical Consultants), 3Convener, Anti Noise Pollution Cell of AMC, 4Dr Doshi’s Pain Relief Centre, Thane, 5Consultant in Pain-Bethany, Jupiter Hospitals, Thane, Maharashtra, India
2. Another report shows-out of the 57% of children with recurrent pain, 6% will have chronic pain[3,4]
3. Statistics in Canada from 12-17 yrs old children report 2% of boys and 6% girls report chronic pain[5]
4. Huguet & Miro have reported the Pain related disability to be 5%[6]
Assessing pain in children is challenging. Some of the various factors compounding the problem are:1. Adult pain measures cannot be applied to preverbal
and young children2. They are dependent on adult caregivers to interpret
their behavior and other signs that they have pain3. Fear and anxiety complicate the assessment of pain as
they may have the fear of “injections” and underreport their pain.
Pediatricians as the primary physicians need to ask, assess and measure pain because untreated pain can have long-term deleterious eff ects. Pain can cause limitations in activity, psychological problems as well as contribute to disability-hence, recurrent and chronic pains have an impact not only on the child but also on their families!
Children who seek treatment for their pain represent the group of patients experiencing the worst impairment.[7]
Case Report
Address for correspondence:Dr. Kritika Doshi,
104, Rohini, Tarangan II, Thane - 400 606, Maharashtra, India.E-mail: [email protected]
Doshi: Post traumatic pain: ?CRPS
Indian Journal of Pain | September-December 2014 | Vol 28 | Issue 3 185
Persistent pain also aff ects the emotional status of children -they are less cheerful and more depressed compared to children without pain[8]
As Pain practioners, we need to prevent progression of pain to chronicity not only on humanitarian grounds but also as evidence suggests to prevent long-term neurophysiological changes[9] as well as immunological changes.[10]
Chronic pain also has negative eff ects on family life:1. increased fi nancial burden- direct cost of hospitalization,
doctors’ fees2. Indirect costs due to time taken off work, transportation
etc.
This case represents the usual challenge to the Clinician where no obvious pathophysiologic source of pain can be identifi ed.
Konijenberg[11] highlighted this problem where the child continues to suffer; parents are frustrated by lack of diagnosis and investigations do not off er any solution.
Case ReportA 10 years, male child weighing 26 kg, a 5th std student was referred by to the Pain Clinic by the Rheumatologist for severe left lower limb pain refractory to analgesics.
The child had a fall while training for “long jump” when he fell on his back. He presented 2 days after fall to the pediatrician with h/o pain in left hip joint with diffi culty in walking.
Patient was hospitalized in view of severe pain for further investigations and treatment.• Past history included h/o allergic cough, surgery for
congenital hydrocoele at 8 years of age.
• Routine investigations showed: • Hb= 13.9 g/dl, CBC= 8,530/cumm, ESR= 07mm/hr,
Urine R= wnl , CPK = 101U/L (26–192), • SGOT = 43U/l , Sr Ca++ = 10 mg/dl, Sr Phos= 5.8 mg/
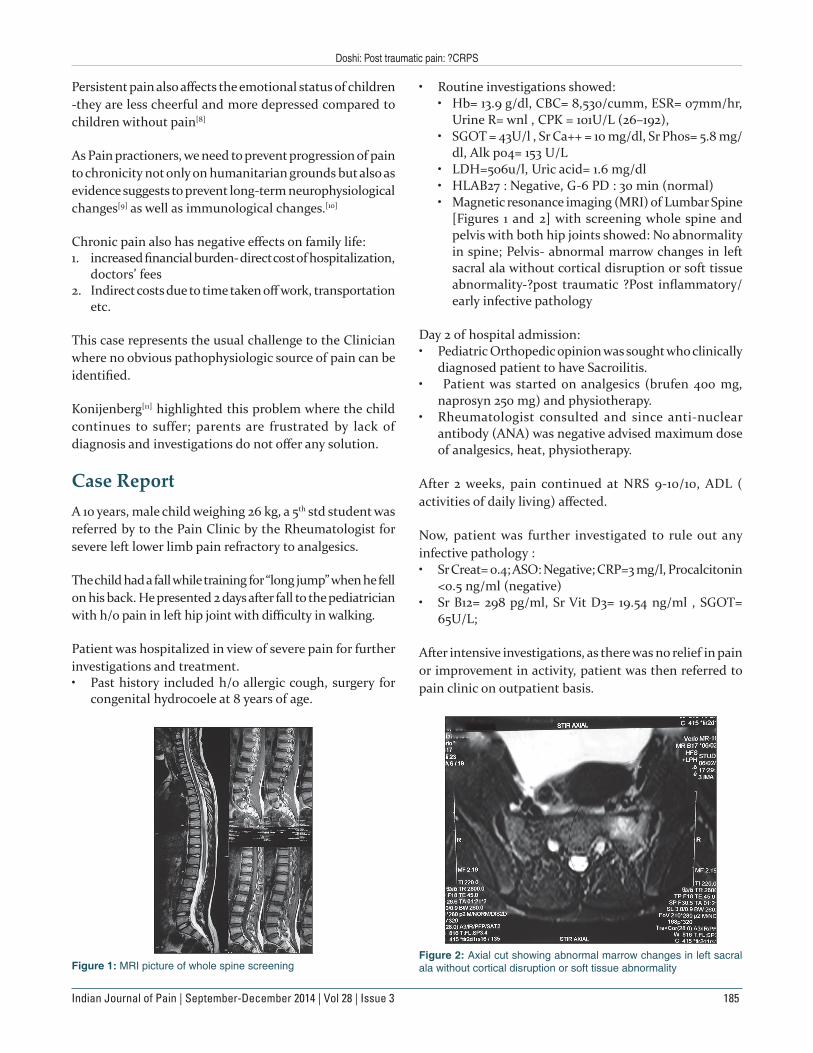
dl, Alk po4= 153 U/L • LDH=506u/l, Uric acid= 1.6 mg/dl • HLAB27 : Negative, G-6 PD : 30 min (normal) • Magnetic resonance imaging (MRI) of Lumbar Spine
[Figures 1 and 2] with screening whole spine and pelvis with both hip joints showed: No abnormality in spine; Pelvis- abnormal marrow changes in left sacral ala without cortical disruption or soft tissue abnormality-?post traumatic ?Post infl ammatory/ early infective pathology
Day 2 of hospital admission:• Pediatric Orthopedic opinion was sought who clinically
diagnosed patient to have Sacroilitis.• Patient was started on analgesics (brufen 400 mg,
naprosyn 250 mg) and physiotherapy. • Rheumatologist consulted and since anti-nuclear
antibody (ANA) was negative advised maximum dose of analgesics, heat, physiotherapy.
After 2 weeks, pain continued at NRS 9-10/10, ADL ( activities of daily living) aff ected.
Now, patient was further investigated to rule out any infective pathology :• Sr Creat= 0.4; ASO: Negative; CRP=3 mg/l, Procalcitonin
<0.5 ng/ml (negative)• Sr B12= 298 pg/ml, Sr Vit D3= 19.54 ng/ml , SGOT=
65U/L;
After intensive investigations, as there was no relief in pain or improvement in activity, patient was then referred to pain clinic on outpatient basis.
Figure 1: MRI picture of whole spine screeningFigure 2: Axial cut showing abnormal marrow changes in left sacral ala without cortical disruption or soft tissue abnormality
Doshi: Post traumatic pain: ?CRPS
186 Indian Journal of Pain | September-December 2014 | Vol 28 | Issue 3
In pain clinicPatient was seen 2 weeks after fall. Child presented with limping gait, inability to bear weight on left leg. Pain was NRS 10. He had been absent from school since the fall (for 15 days).
Child was in severe pain according to mother- though child appeared comfortable while sitting; mother said he was constantly groaning in his sleep.
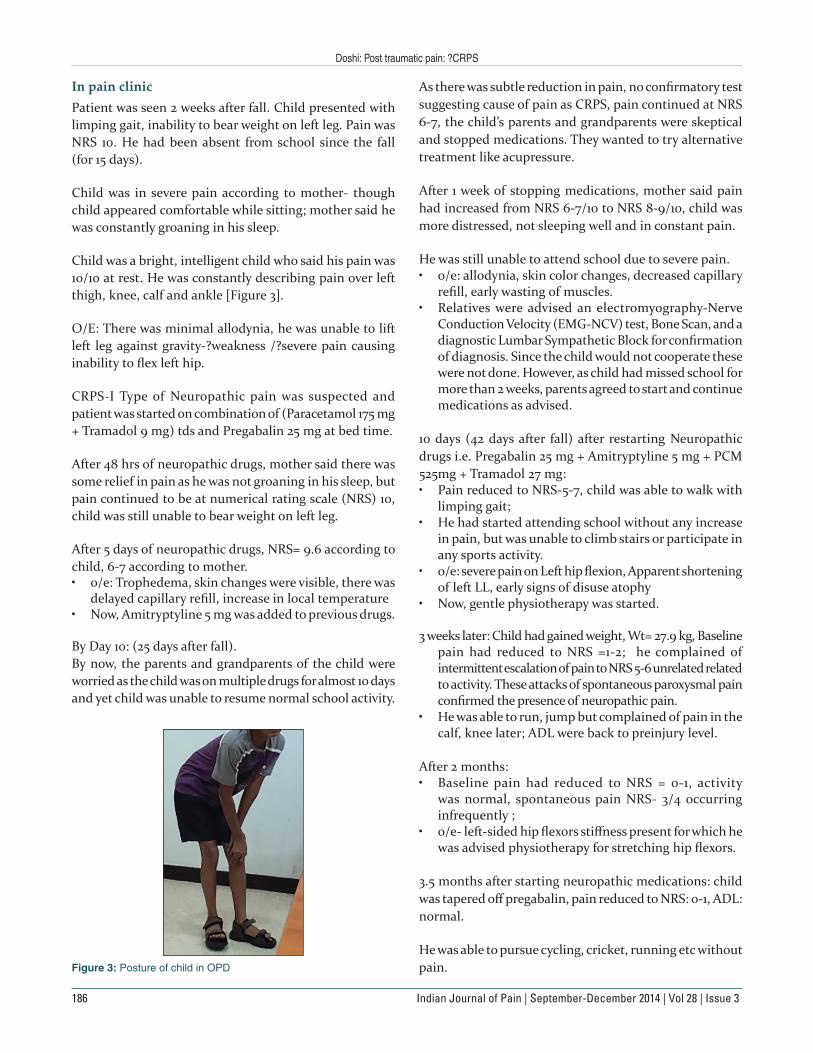
Child was a bright, intelligent child who said his pain was 10/10 at rest. He was constantly describing pain over left thigh, knee, calf and ankle [Figure 3].
O/E: There was minimal allodynia, he was unable to lift left leg against gravity-?weakness /?severe pain causing inability to fl ex left hip.
CRPS-I Type of Neuropathic pain was suspected and patient was started on combination of (Paracetamol 175 mg + Tramadol 9 mg) tds and Pregabalin 25 mg at bed time.
After 48 hrs of neuropathic drugs, mother said there was some relief in pain as he was not groaning in his sleep, but pain continued to be at numerical rating scale (NRS) 10, child was still unable to bear weight on left leg.
After 5 days of neuropathic drugs, NRS= 9.6 according to child, 6-7 according to mother.• o/e: Trophedema, skin changes were visible, there was
delayed capillary refi ll, increase in local temperature • Now, Amitryptyline 5 mg was added to previous drugs.
By Day 10: (25 days after fall).By now, the parents and grandparents of the child were worried as the child was on multiple drugs for almost 10 days and yet child was unable to resume normal school activity.
As there was subtle reduction in pain, no confi rmatory test suggesting cause of pain as CRPS, pain continued at NRS 6-7, the child’s parents and grandparents were skeptical and stopped medications. They wanted to try alternative treatment like acupressure.
After 1 week of stopping medications, mother said pain had increased from NRS 6-7/10 to NRS 8-9/10, child was more distressed, not sleeping well and in constant pain.
He was still unable to attend school due to severe pain.• o/e: allodynia, skin color changes, decreased capillary
refi ll, early wasting of muscles.• Relatives were advised an electromyography-Nerve
Conduction Velocity (EMG-NCV) test, Bone Scan, and a diagnostic Lumbar Sympathetic Block for confi rmation of diagnosis. Since the child would not cooperate these were not done. However, as child had missed school for more than 2 weeks, parents agreed to start and continue medications as advised.
10 days (42 days after fall) after restarting Neuropathic drugs i.e. Pregabalin 25 mg + Amitryptyline 5 mg + PCM 525mg + Tramadol 27 mg:• Pain reduced to NRS-5-7, child was able to walk with
limping gait; • He had started attending school without any increase
in pain, but was unable to climb stairs or participate in any sports activity.
• o/e: severe pain on Left hip fl exion, Apparent shortening of left LL, early signs of disuse atophy
• Now, gentle physiotherapy was started.
3 weeks later: Child had gained weight, Wt= 27.9 kg, Baseline pain had reduced to NRS =1-2; he complained of intermittent escalation of pain to NRS 5-6 unrelated related to activity. These attacks of spontaneous paroxysmal pain confi rmed the presence of neuropathic pain.
• He was able to run, jump but complained of pain in the calf, knee later; ADL were back to preinjury level.
After 2 months: • Baseline pain had reduced to NRS = 0-1, activity
was normal, spontaneous pain NRS- 3/4 occurring infrequently ;
• o/e- left-sided hip fl exors stiff ness present for which he was advised physiotherapy for stretching hip fl exors.
3.5 months after starting neuropathic medications: child was tapered off pregabalin, pain reduced to NRS: 0-1, ADL: normal.
He was able to pursue cycling, cricket, running etc without pain.Figure 3: Posture of child in OPD

Doshi: Post traumatic pain: ?CRPS
Indian Journal of Pain | September-December 2014 | Vol 28 | Issue 3 187
4 months after starting amitryptyline, it was tapered and stopped.
Night dose of PCM + Tramadol (175 mg + 9 mg) were continued for 3 more weeks and stopped.
5 months later, child was back to complete activity including athletics training with no residual deficit, weakness.
DiscussionWhen the child presented, he had pain in the left L4 dermatomal distribution-this did not correlate with MRI findings of abnormal marrow changes in left sacral ala without cortical disruption or soft tissue abnormality.
Clinically, there was apparent limb length discrepancy.
When the child had the fall, there was probably a blunt injury to the left hip fl exors mainly psoas major with lumbar plexus irritation. The MRI had evidence of abnormal marrow changes in sacral ala- the psoas tendon and lumbar plexus are in anatomic proximity.
The nerve irritation or edema could cause pain that the child was experiencing and this would explain his response to neuropathic drugs and complete recovery from symptoms.
Long-term consequences of recurrent and chronic pain can have an impact not only on the child but also on their families. Pain can cause limitations in activity, psychological problems as well as contribute to disability.
The musculoskeletal system is one of the most common sites for pain in children and adolescents. There are few studies reporting on prevalence of CRPS in children. Available data indicate a female to male ratio of 6:1 and more common occurrence in lower than upper extremity.[12]
The differential diagnosis of musculoskeletal pain is vast. If pain is localized and the child is well, the DD includes ‘growing pains’, CRPS, mechanical pain, pauciarticular juvenile idiopathic arthritis (JRA) and spondyloarthropathy. If the child is unwell, infectious arthritis should be considered. If the pain is diff used and the child is unwell - malignancies or autoimmune diseases should be considered. Emerging literature
supports association of chronic musculoskeletal pain with hypermobility. This may be due to central sensitization induced by constant subluxation and slippage.
Konijnenberg and colleagues presented a series of papers in which 17 diff erent pediatricians reviewed the medical records of 134 children with unexplained chronic pain. There was disagreement on diagnostic approach in over a third of the patients and on the primary cause of pain in over half.[11]
When dealing with persistent and chronic pain, the impact of pain on the child’s functioning — school attendance, work quality, mood etc should be given due attention as well as disability — which also needs to be measured.
The WHO treatment Guidelines on Persisting Pain in Children with Medical Illnesses (Geneva 2011) are available on: http://www.who.int/medicines/areas/quality_safety/guide_perspainchild/en/index.html.
References1. Duthey B, Scholten W. Adequacy of opioid analgesic
consumption at country, global and regional level in 2010, its relation to development level and changes compared to 2006. J Pain Symptom Manage 2014;47:283-97.
2. Perquin CW, Hazebroek-Kampschreur AA, Hunfeld JA, Bohnen AM, van Suijlekom-Smit LW, et al. Pain in children and adolescents: A common experience. Pain 2000;87:51-8.
3. van Dijk A, McGrath P, Pickett W, VanDenKerkhof EG. Pain prevalence in nine-to 13-year-old schoolchildren. Pain Res Manage 2006;11:234-40.
4. Stanford EA, Chambers CT, Biesanz JC, Chen E. The frequency, trajectories and predictors of adolescent recurrent pain: A population-based approach. Pain 2008;138:11-21.
5. Ramage-Morin PL, Gilmour H. Chronic pain at ages 12 to 44. Health Rep 2010;21:53-61.
6. Huguet A, Miro J. The severity of chronic pediatric pain: An epidemiological study. J Pain 2008;9:226-36.
7. Hunfeld JA, Perquin CW, Duivenvoorden HJ, Hazebroek-Kampschreur AA, Passchier J, van Suijlekom-Smit LW, et al. Chronic pain and its impact on quality of life in adolescents and their families. J Pediatr Psychol 2001;26:145-53.
8. Langeveld JH, Koot HM, Loonen MC, Hazebroek-Kampschreur AA, Passchier J. A quality of life instrument for adolescents with chronic headache. Cephalgia 1996;16:183-96.
9. Taddio A, Goldbach M, Ipp M, Stevens B, Koren G. Effect of neonatal circumcision on pain responses during vaccination in boys. Lancet 1995;344:291-2.
10. Page GG, Ben-Eliyahu S, Liebeskind JC. The role of LGL/NK cells in surgery-induced promotion of metastasis and its attenuation by morphine. Brain Behav Immun 1994;8:241-50.
11. Konijnenberg AY, DeGraeff-Meeder ER, Kimpen JL, van der Hoeven J, Buitelaar JK, Uiterwaal CS; Pain of Unknown
Doshi: Post traumatic pain: ?CRPS
188 Indian Journal of Pain | September-December 2014 | Vol 28 | Issue 3
charachteristics and follow-up of 75 patients. J Bone Joint Surg 1992;74:910-9.
Origin in Children Study Group. et al. Children with unexplained chronic pain: Do pediatricians agree regarding the diagnostic approach and presumed primary cause? Pediatrics 2004;114:1220-6.
12. Wilder RT, Berde CB, Wolohan M, Vieyra MA, Masek BJ, Micheli LJ. Refl ex sympathetic dystrophyin children. Clinical
How to cite this article: Doshi K. Post traumatic pain: ?CRPS. Indian J Pain 2014;28:184-8.Source of Support: Nil. Confl ict of Interest: None declared.





























