Embed Size (px)
Citation preview

Law and Human Behavior, Vol. 22, No. 1, 1998
Psychopathy and Recidivism Among Female Inmates
Randall T. Salekin,1 Richard Rogers,1 Karen L. Ustad,2 andKenneth W. Sewell1
Despite a plethora of studies investigating psychopathy among male offenders, little isknown about the applicability of this construct to female populations. Research hasshown that prevalence rate, symptom presentation, and diagnostic comorbidity differfor females as compared to males. The current study is the first to examine therelationship between psychopathy and recidivism among women. Recidivism data ona sample of 78 female inmates were examined at a 1-year interval in relation to thePsychopathy Checklist-Revised (PCL-R), inclusion criteria for the Antisocial PersonalityDisorder Diagnosis from the Personality Disorder Examination (PDE), and selectedscales from the Personality Assessment Inventory (PAI; Antisocial and Aggressionscales). The egocentricity subscale of the PAI, Factor 1 of the PCL-R, and the verbalaggression subscale of the PAI were the best predictors of future recidivism. Specificdifferences emerged between male and female offenders when comparing the presentdata with previous studies of male psychopaths.
A converging body of research has demonstrated that psychopathy is a predictorof recidivism in male offenders. Salekin, Rogers, and Sewell (1996) performed ameta-analysis of 18 studies that utilized versions of the Psychopathy Checklist (PCL,Hare, 1985; PCL-R, Hare, 1991; PCL-SV, Hart, Cox, & Hare, 1995) with men andfound that the measure was a moderately good predictor of recidivism (Cohen's d= .55). Moreover, previous studies investigating the psychopathy-recidivism rela-tionship in men have shown that psychopaths are likely to recidivate within thefirst year upon their release (Hart, Kropp, & Hare, 1988; Serin, Peters, & Barbaree,1991). While the psychopathy-recidivism relationship has been extensively re-searched with men, this relationship remains uninvestigated in female populations.
It is necessary to highlight that researchers and clinicians have not alwaysagreed upon the defining features of the syndrome (Lilienfeld, 1994; Lykken, 1995;Rogers, Duncan, Lynett, & Sewell, 1994). Although considerable theoretical andempirical attention has focused on understanding the psychopathic personality, a
1University of North Texas. Please address correspondence to Randall T. Salekin, who is now at YaleUniversity, 425 George St., New Haven, CT 06511.
2Yale Univeristy.
109
0147-7307/98/0200-109$15.00/l © 1998 American Psychology-Law Society/Division 41 of the American Psychological Association

110 Salekin, Rogers, Ustad, and Sewell
debate continues on whether the construct is primarily behaviorally based or per-sonality based (Lilienfeld, 1994). Perhaps the most influential conceptualization ofpsychopathy was provided by Cleckley (1941) who described psychopaths primarilyby personality traits (e.g., superficiality and grandiosity) or their absence (e.g., lackof empathy and remorse).
Historically, Antisocial Personality Disorder (APD) has been used synony-mously with the term psychopathy. However, Serin (1996) argued that the APDcriteria fail to distinguish (a) the callous, remorseless psychopath from other anti-social individuals, and (b) does not address affective and interpersonal processes(e.g., shallow affect and manipulation) that are necessary for a diagnosis of psy-chopathy. This assertion is not completely accurate, given that APD criteria includeboth manipulativeness and remorselessness; nonetheless, APD is more heavilyweighted with behavioral criteria than is psychopathy. In contrast, Hare (1985, 1991)has incorporated both personality and behavioral criteria equally in his measure ofpsychopathy, combining the early theories of Cleckley (1941) and Robins (1966).Differing conceptualizations of the syndrome underscore the importance of inves-tigating female psychopathy/APD from a number of theoretical perspectives.
Research on psychopathy and APD suggests that there are differences betweenmen and women in regard to these disorders. Most notably, psychopathy is lessprevalent in women than in men. Moreover, psychopathy appears to be sympto-matically different in women than men. Finally, research has shown that there ismore overlap between antisocial personality disorders/psychopathy and other dis-orders (e.g., depression, anxiety, and histrionic personality disorder) in women thanin men. These three gender differences are described briefly below.
Prevalence of Psychopathy in Female Populations
Salekin, Rogers, and Sewell (1997) examined psychopathy in female offendersin a jail setting and found that the overall prevalence rate was lower in women(15.5%) than what is typically reported for men (25% to 30%; Hare, 1985, 1991).In an early study on psychopathy,3 Robins (1966) reported that girls were less likelyto have been seen at a child guidance clinic for conduct problems than were boys,and were also less likely to be diagnosed as psychopathic in adulthood. Specifically,only 12% of girls with behavioral problems were later diagnosed as psychopathicin comparison to 50% of boys.
Other researchers have found similar gender differences for psychopathy. Forinstance, Zagon and Jackson (1994) found significantly lower total scores on theSelf Report Psychopathy (SRP) measure for female than male college students.
3Although Robins (1966) uses the term "sociopathy" throughout her book, she refers to it as beingsynonymous with psychopathy. Her diagnosis of sociopathy included a "failure to conform to societalnorms" in at least five of the following areas: (a) work history, (b) financial dependency, (c) arrests,(d) marital history, (e) alcohol abuse, (f) school history including truancy, (g) impulsiveness, (h) sexualbehavior, (i) "wild" adolescence, (j) vagrancy, (k) belligerency, (1) maintenance of social relationships,(m) lack of guilt, (n) somatic complaints, (o) poor Armed Forces performance, (p) pathological lying,(q) drug use, and (r) suicide attempts.
Female Psychopathy and Recidivism 111
This difference was apparent for both personality traits and socially deviant behav-ior. Similarly, Forth, Brown, Hart, and Hare (1996) found psychopathy scores (PCL-SV) to be significantly lower in female university students than in male universitystudents. Neary (1990) concluded that PCL-R scores were generally lower in bothAfrican American and Anglo American women in a prison population than thosetypically reported in studies of men. More recently, Rutherford, Cacciola, Alterman,and McKay (1996) found considerably lower average PCL-R total scores for femalemethadone patients (M = 13.8; SD = 7.0) than for male methadone patients (M= 17.9; SD = 7.6). Gender differences in the prevalence of psychopathy are con-sistent with research findings for APD (see Kass, Spitzer, & Williams, 1983; Reich,1987). According to Mulder, Wells, Joyce, and Bushnell (1994), "No matter howantisocial behavior has been conceptualized, men have consistently been found tobe antisocial more often than women, regardless of age, race, or socioculturalstatus" (p. 279).
Gender differences also have been observed in childhood disorders related toadulthood APD/psychopathy. For instance, the reported rate for Conduct Disorderin children ages 4 to 11 was 6.5% for boys and 1.8% for girls. At ages 12 to 16years, the rate was 10.4% for boys and 4.1% for girls (Offord, Adler, & Boyle,1986; Offord, Boyle, & Racine, 1991). In summary, the lower prevalence of psy-chopathy in women has been convincingly demonstrated in the empirical literature.
Gender Differences in Psychopathic Backgrounds and Symptomatology
The backgrounds of individuals with psychopathy and APD appear to be in-fluenced by gender. With regard to background characteristics, Mulder et al. (1994)found that antisocial women were more likely than antisocial men to (a) be chroni-cally unemployed, (b) have high rates of marital separation, and (c) be dependenton social assistance programs. Additionally, these researchers found that antisocialwomen had lower rates of unlawful behavior, were more likely to have relationshipdifficulties, and were more likely to tell lies than their male counterparts.
Other researchers have noted additional gender differences with regard to theclinical presentation of APD/psychopathy. For example, Robins (1966) concludedthat girls diagnosed as psychopathic in adulthood differed from boys by their lateronset of childhood behavioral problems and more frequent sexual misbehavior.Rutherford, Alterman, Cacciola, and Snider (1995) also noted that the violent andaggressive childhood criteria of APD from the DSM-III-R had little relationshipto the assessment of APD in women. In other words, those women who met criteriafor a diagnosis of APD typically did not have violent and aggressive childhood symp-toms. One explanation for these gender differences is developmental differences inonset and presentation. In fact, research is beginning to show that this might bethe case. For example, Silverthorn and Frick (1997) have found that antisocial girlsare less likely than antisocial boys to engage in aggressive acts; rather, antisocialgirls engage in other antisocial acts, such as stealing.
Researchers have observed gender differences in the factor structure of thePCL-R. Harpur, Hare, and Hakstian (1989) and Hare, Harpur, Hakstian, Forth,

112 Salekin, Rogers, Ustad, and Sewell
Hart, and Newman (1990) found the following two-factor model for male popula-tions: F1 is characterized by selfish, callous, and remorseless use of others and F2
is characterized by chronically unstable, antisocial, and socially deviant lifestyles(Hare, 1991). Salekin et al. (1997) found a somewhat different two-factor structurefor female offenders: F1 was characterized by lack of empathy/guilt, interpersonaldeception, sensation seeking, and proneness to boredom and F2 was characterizedby early behavioral problems, promiscuity, and adult antisocial behavior. The pri-mary differences in the factor structure are delineated below. First, for the femalesample, F1 included the items "proneness to boredom" and "sensation seeking,"while F2 included the item which addresses "promiscuous sexual behavior." Second,for F2, only four of Hare et al.'s nine loadings were replicated across genders. Third,there was substantially more item overlap in the female sample than has been foundfor men (i.e., poor behavioral control, lack of realistic goals, and impulsivity loadedon both factors). Fourth, three items failed to load above .40 in the female sample(i.e., failure to accept responsibility, many short- term relationships, and revocationof conditional release). Last, several items loaded in the reverse direction in thefemale sample (i.e., proneness to boredom, impulsivity, and irresponsibility). In gen-eral, the Salekin et al. factor structure loosely resembled the Hare et al. factorstructure in that it was primarily personality and behaviorally based, although F2was not as clearly defined.
Other research has indicated that certain PCL-R items may not be directlyapplicable to women. Rutherford et al. (1996) found that three items on the PCL-Rwere weakly related to total psychopathy scores for women. Specifically, juveniledelinquency, grandiosity, and failure to accept responsibility for one's own actionsaccounted for very little of the variance in total PCL-R scores (each item accountedfor approximately 4% of the variance). In a similar vein, Strachan, Williamson, andHare (1990) discovered two PCL-R items that were not well suited to women (i.e.,revocation of conditional release and juvenile delinquency), despite similar totalPCL-R scores between men and women.
Comorbidity of Women Psychopathy
Mulder et al. (1994) reported that antisocial women have higher rates thanantisocial men of suicidal behavior and comorbid disorders, such as depression andanxiety. Similarly, Lilienfeld, Van Valkenburg, Larntz, and Akiskal (1986) found thatfemale psychopathy may have substantial overlap with two other disorders: soma-tization and histrionic personality disorder. Cloninger and Guze (1970a, b) gatheredevidence suggesting that sociopathy and hysteria may be related (i.e., concordanceof 32.5%). Robins (1966) also found that adolescent girls in treatment for antisocialbehaviors were later diagnosed as adult hysterics. Clearly, further research is neededto better understand the comorbidity of women with psychopathic characteristics.
From the aforementioned findings, female psychopaths differ from male psy-chopaths in three substantive ways: (a) prevalence, (b) background and symptompattern, and (c) diagnostic comorbidity. Given that there is a mounting body of

Female Psychopathy and Recidivism 113
evidence suggesting gender differences in psychopaths, we were interested in ex-amining the generalizabilty of the psychopathy-recidivism relation to women.
PSYCHOPATHY AND PREDICTIVE VALIDITY
To validate the construct of psychopathy, researchers have often utilized exter-nal criteria. Such criteria have included behaviors that infringe on the rights ofothers: (a) recidivism, (b) institutional infractions, (c) physical aggression, and (d)verbal aggression. This type of validation is based on the notion that psychopathicindividuals are more likely to engage in criminal behavior due to an interpersonalstyle that involves deceit, manipulation, and disregard for the rights of others. Hareand Hart's (1993) conclusion is representative of this notion: "Given the charac-teristics of psychopathy listed in the PCL-R, it comes as no surprise that the dis-order is implicated in a disproportionate amount of serious repetitive crime andviolence" (p. 106). Due to the importance placed on identifying predictors of per-sistent criminality, recidivism has been the most widely researched external crite-rion. As mentioned previously, a moderate relationship between recidivism andpsychopathy in men has been established.
A critical question that remains unanswered is the relationship of psychopathyto recidivism among women. Understanding this relationship constitutes a necessarystep in the validation of psychopathy among women. If psychopathy measures areable to show adequate predictive validity in women, then their use in forensic set-tings would be warranted and could contribute substantially to dangerousness/riskassessments. On the other hand, if their predictive validity is only modest, then thisinformation is also important given that inaccurate classifications/predictions couldlead to serious ramifications for the examinee (e.g., not being given the opportunityfor parole).
The purpose of the present study is to investigate the psychopathy-recidivismrelation in female offenders and to examine whether its direction and magnitudeis similar to that found in male offenders. To address this issue, we examined theeffectiveness of two psychopathy measures and an APD scale in the prediction ofrecidivism. As such, a goal of the study was to examine the relative effectivenessof these three scales as they relate to recidivism in female offenders. We also hy-pothesized that the aggressivity scale of the PAI would be predictive of recidivismin female inmates. Thus, we included this scale and its subscales in our analyses.
METHOD
Participants
The sample consisted of 78 female inmates at the Tarrant County Jail in FortWorth, Texas. The participants had a mean age of 30.57 years (SD = 7.69) withan average of 11.24 years (SD = 1.81) of education. The racial composition of thesample was 49 (62.8%) Anglo Americans, 22 (28.2%) African Americans, 6 (7.7%)

114 Salekin, Rogers, Ustad, and Sewell
Hispanic Americans, and 1 (1.3%) Native American. The sample was ethnicallycomparable to the overall inmate composition of Tarrant County Jail. Both adju-dicated offenders and those with trials pending were evaluated. The sample utilizedin this study consisted of a portion (78 of 103) of the inmates that were evaluatedoriginally in the Salekin et al. (1997) study. The 25 inmates who were sentencedto prison or otherwise institutionalized were not included, given that they did nothave an opportunity to recidivate.
Instruments
Personality Assessment Inventory.
The PAI is a 344-item multiscale inventory of adult psychopathology that in-cludes four validity scales, 11 clinical scales, five treatment scales, and two inter-personal scales (Morey, 1991). The PAI was advantageous for the current studyover other self-report measures for the following reasons: (a) its antisocial scalehas a contemporary theoretical base, and it provides (b) easy reading comprehen-sion, (c) gradations of item responses on a 4-point scale, (d) relatively brief ad-ministration time, and (e) nonoverlapping clinical scales. The PAI has also beenshown to have good psychometric properties (Morey, 1991, 1996).
The Antisocial scale (ANT) of the PAI is unique in that it has a more con-temporary theoretical base for psychopathy than do other multiscale self-report in-ventories. The scale's theoretical underpinnings stem from the work of Cleckley(1941), Robins (1966), and Harpur et al. (1989). The ANT scale is composed of atotal of 24 items that make up three subscales tapping different components of thesyndrome. Two facets, Egocentricity (ANT-E; 8 items) and Stimulus seeking (ANT-S; 8 items), represent personality aspects of the psychopathic character. ANT-E in-cludes the hallmark characteristics of pathological egocentricity and narcissism,while ANT-S addresses the tendencies to seek excitement and thrills as well as lowboredom tolerance. A third facet, Antisocial Behaviors (ANT-A; 8 items), representsa construct similar to the conduct problems addressed by the DSM definition ofAPD.
The PAI ANT scale, at least preliminarily, appears to be a reliable and validmeasure of psychopathy. With regard to the reliability of the measure, Morey (1991)found Cronbach alpha values were high for both genders (i.e., women = .81; men= .84). The test-retest reliability for the entire sample was high at .89. Validitystudies have shown the PAI ANT scale to be a valid measure of psychopathy(Morey, 1991). As with other measures of psychopathy (e.g., the PCL-R), the PAIANT scale correlated moderately with MMPI scales 4 and 9 (rs = .34 and .44,respectively). Moreover, Morey found that the ANT scale was highly related to theSelf Report Psychopathy measure (r = .82).
The Aggression scale of the PAI taps characteristics and attitudes related toanger, hostility, and aggression. This also includes a history of aggression (bothphysical and verbal) and attitudes conducive to aggressive behavior. The AGG scale(18 items) is composed of three subscales: Aggressive Attitude (AGG-A, 6 items),

Female Psychopathy and Recidivism 115
Verbal Aggression (AGG-V 6 items), and Physical Aggression (AGG-P, 6 items).AGG-A includes such characteristics as being easily angered and poor anger man-agement. AGG-V includes characteristics such as not being intimidated by confron-tation and being critical or insulting of others with little provocation. AGG-Pincludes items related to physical displays of anger, including physical fights, dam-age to property, and threats of violence.
Morey (1991) found the reliabilty of the aggression scale to be high for bothwomen and men (alphas = .82 and .87, respectively). Test-retest reliability was alsohigh at .81 for the entire sample. Validity data showed that the Aggression scalewas moderately correlated with Wiggins content scales on the MMPI (Morey, 1991).Specifically, the AGG scale correlated positively with authority problems (r =.27),hostility (r = .62), and poor morale (r = .36). Morey (1991) also found that theAGG scale was highly correlated (r = .83) with the NEO Personality Inventory(NEO-PI; Costa & McCrae, 1985) hostility facet.
Psychopathy Checklist—Revised.
The PCL-R is a semi-structured interview that assesses two correlated factorsof psychopathy (Hare, 1991). The first factor (F1) reflects personality characteristics,such as callousness, lack of remorse, pathological lying, and manipulativeness.Meloy (1992) has referred to this factor as reflecting "aggressive narcissism." Thesecond factor (F2) reflects behavioral characteristics such as boredom, impulsive-ness, criminal versatility, and poor parole risk. The PCL-R consists of 20 items thatare assessed on the basis of a person's lifetime functioning. A 3-point scale measuresthe degree to which the personality/behavior of the individual matches the itemdescription: 0 = no; 1 = maybe4; 2 = yes. The item ratings are then summed andprovide a global score that is intended to be indicative of an individual's level ofpsychopathy (Hare, 1991).
The PCL-R has been found to be a reliable and valid measure of psychopathywith male inmates (Hare, 1991). Interrater reliabilities are high, with intraclasscorrelations (ICC) of .83. With regard to internal consistency, Hare has reportedCronbach alphas ranging from .83 to .91. Convergent validity data show that thePCL-R is moderately related to MMPI scales 4 and 9 (rs = .25 and .27, respec-tively). The PCL-R was moderately correlated with the Self Report Psychopathymeasure (r = .54). Using a sample of female substance abuse patients, Rutherford,Alterman, and Cacciola (1996a; see also Rutherford et al, 1996b) found similarresults for internal consistency: Cronbach's alpha was .84 for methadone patientsand .83 for cocaine patients. Recent studies examining the construct of psychopathyin women have shown the PCL-R to have good convergent and discriminant validity(Rutherford et al., 1996; Salekin et al., 1997). Previous studies have indicated thatboth factors are related to recidivism in men (e.g., Serb, 1996). Two studies have
4This rating system, which utilizes "maybe," lacks specificity and may lead to differing prevalence ratesas well as misclassifications. We suggest that the midscore be indicative of the target having thepersonality trait or behavioral characteristic at a "subclinical level" or "to some degree."

116 Salekin, Rogers, Ustad, and Sewell
shown that F2 items are more related to recidivism (Barbaree, Seto, Serin, Amos,& Preston, 1994; Harpur et al., 1989) and one study (Serin, 1996) has indicatedthat F1 is more related to violent recidivism than F2, but that both factors are pre-dictive of general recidivism.
Personality Disorder Examination.
The PDE (Loranger, 1988; Loranger, Susman, Oldham, & Russakoff, 1987) isa semi-structured interview for the assessment of personality disorders. Interviewerstypically make several standardized inquiries for each criterion. The PDE allowsfor both categorical and dimensional scoring. The Antisocial scale of the PDE (A-PDE) is composed of DSM-III-R criteria for Antisocial Personality Disorder. A-PDE measures a pattern of irresponsible and antisocial behavior from childhoodor early adolescence into adulthood. With regard to childhood criteria, the A-PDEmeasures lying, truancy, stealing, vandalism, initiating fights, running away fromhome, and physical cruelty. In terms of adult criteria, the A-PDE measures suchcharacteristics as failure to honor financial obligations, failure to plan ahead andfunction as a responsible parent, and an inability to sustain consistent work behav-ior. In addition, A-PDE assesses lack of remorse, manipulativeness, adult physicalfighting, and recklessness without regard for personal safety (e.g., frequently drivingwhile intoxicated).
In general, the PDE has been found to be a reliable and valid measure ofpersonality disorders (Rogers, 1995). The PDE has evidenced high ICCs spanningfrom .81 to .97. Validation studies have also shown the PDE to have good conver-gent validity with various personality measures including the Personality DiagnosticQuestionnaire-Revised and the Structured Clinical Interview for DSM-III-R Per-sonality Disorders (Rogers, 1995).
Procedure
Inmates were approached by a researcher and asked to participate in the study.In accordance with the University of North Texas and Tarrant County Jail EthicalReview Board guidelines, participants provided written, informed consent. Inter-views were conducted by an advanced doctoral student in clinical psychology whohad completed a course in structured interviewing and who had attended a work-shop on the Psychopathy Checklist-Revised. The inmates were typically evaluatedin a 3- to 4-hour session with several breaks. Inmates were administered the threepsychopathy/APD measures prior to their release: the PAI, the PCL-R, and thePDE. All psychological measures were administered individually in their entiretyand according to standard instructions. For the purposes of this study, we focusedupon the Antisocial scale (ANT) of the PAI, the PCL-R, and the Antisocial scaleof the Personality Disorder Examination (A-PDE). Because aggression is thoughtto be related to psychopathy, the PAI Aggression (AGG) scales were also examinedto determine their relation to recidivism among women.

Female Psychopathy and Recidivism 117
Recidivism data were collected a minimum of 12 months from the originaltime of assessment (range from 12 to 16 months; median = 14 months). Recidivismdata were gathered from the Tarrant County Jail computer system, which keepscurrent records of the performance of inmates from the time of their release. Thissystem accesses arrest, detention, and incarceration of all offenders for correctionaland law enforcement facilities throughout the state of Texas. Female offenders whohad been sentenced to prison or transferred out of state were excluded from thepresent study resulting in a sample size of 78. One limitation of the data base isthat it does not record criminal offenses committed in other states.
RESULTS
Prevalence
The sample had a mean PAI ANT T-score of 64.05 (SD = 15.62), a meanPCL-R score of 17.86 (SD = 8.48), and a mean A-PDE score of 18.87 (SD =8.65). Psychopathy classifications were based on recommended cutoff scores. Forthe PAI, a T-score of 80 classified 11 (14.1%) of the participants as psychopathic.When the PCL-R was utilized, women with a score >29 were classified as psycho-pathic. Prevalence of psychopathy on the PCL-R was 12.9% (n = 10). With thePDE, participants who had four or more adult symptoms and three or more child-hood symptoms were diagnosed as having APD. Utilizing this cutoff score, 40(51.3%) of the women were diagnosed as having APD. Differences in prevalencerates between psychopathy measures and the PDE Antisocial Scale may be relatedto the low cutoff score for APD. That is, APD requires that an individual have atleast three childhood symptoms and greater than three adult APD symptoms. Thisbenchmark differs substantially from the PCL-R, which requires that an individuallyfully meet 15 of the 20 items or have a greater proportion of partial scores to beconsidered a psychopath.
Relations Between Psychopathy and Recidivism
The overall recidivism rate for the entire sample was 41%. Representativecharges during the 14-month follow-up period included theft, delivery of a con-trolled substance with intent to sell, fraud, and, to a lesser extent, assault andother violent acts. Table 1 presents point biserial correlation coefficients betweenthe Psychopathy Checklist-Revised total and factor scores, the Personality As-sessment Inventory Antisocial and Aggression scales, the APD scale of the Per-sonality Disorder Examination, and recidivism. When investigating totalpsychopathy measures, only the Antisocial scale of the PAI was related to recidi-vism to a significant degree (r = .26). Subscales of psychopathy measures thatwere related to recidivism included the F1 scale of the PCL-R (r = .26) and theANT-E scale of the PAI (r = .27). Scales that were theoretically related to thepsychopathy construct also were found to be associated with recidivism. Specifi-

118 Salekin, Rogers, Ustad, and Sewell
Table 1. Correlations Between Psychopathy Scales and Recidivism: A 14-Month Follow-up withFemale Offenders (N = 78)
Scales
PCL-RF1
F2ANTANT-EANT-AANT-SAGGA-PDE
F1
.85**
F2
.92**
.60**
ANT
.51**
.34*
.53**
ANT-E
.46**
.31*
.46**
.88**
ANT-A
.41**
.30*
.42**
.87**
.62**
ANT-S
.47**
.29*
.51**
.91**
.73**
.67**
AGG A-PDE
.44** .64**
.33*
.44**
.74**
.61**
.64**
.70**
.40**
.71**
.73**
.54**
.69**
.68**
.65**
Recidivism
.20
.26*
.14
.26*
.27*
.20
.20
.29*
.18Note. PCL-R = Psychopathy Checklist-Revised; F1 = Factor 1 of the PCL-R; F2 = Factor 2 of thePCL-R; ANT = the Antisocial Scale of the Personality Assessment Inventory; ANT-E = Egocentricitysubscale; ANT-A = Antisocial behaviors; ANT-S = Stimulus seeking; AGG = Aggression Scale of thePersonality Assessment Inventory; A-PDE = Antisocial Scale of the Personality Disorder Examination.
*p < .05; **p < .01.
cally, AGG of the PAI was correlated (r =.29) with recidivism. Of the AGGsubscales, verbal aggression and aggressive attitude were most highly related (rs= .29 and .25, respectively).
Accuracy of Psychopathy for Predicting Recidivism in Female Offenders
Using the cutoff scores suggested for the psychopathy instruments (see Table2), we examined their classification accuracy with regard to sensitivity, specificity,positive predictive power (PPP), and negative predictive power (NPP). In the caseof this study, sensitivity is the proportion of inmates who recidivate that obtain ascore above the cutoff score on a psychopathy measure. Specificity is the proportionof inmates who do not recidivate that obtain normal range scores (below cutoff)on a psychopathy measure. PPP is the likelihood that a person above the cutoffon a psychopathy measure actually recidivated. Negative predictive power, on theother hand, is the likelihood that a person with a normal score on a psychopathymeasure (below cutoff) does not recidivate (Glaros & Kline, 1988). For the PAIANT scale, sensitivity was .04, specificity was .82, PPP was .14, and NPP was .51.When utilizing the PCL-R, sensitivity was .11, specificity was .91, PPP was .50, andNPP was .55. Finally, when using the PDE, sensitivity was .73, specificity was .17,PPP was .36, and NPP was .50. Overall, classification accuracy for the psychopathy-recidivism relation was poor for all measures using standard cutoff scores. The PCL-R performed moderately better than both the PAI and the PDE.
Receiver Operating Characteristic Curves Applied to thePsychopathy-Recidivism Relationship
Utilizing receiver operating characteristic (ROC) curves, we further assessedthe accuracy of predictions of recidivism based on the range of psychopathy scores.
Female Psychopathy and Recidivism 119
Table 2. Classification Accuracy of the Psychopathy Measures forPrediction of Recidivism for a 14-Month Period (N = 78)
Measure
PAIPCL-RA-PDE
Cutoff
>80>29>3a
Sens
.04
.11
.73
Spec
.82
.91
.17
PPP
.14
.50
.36
NPP
.51
.55
.50Note: PAI = the Antisocial Scale on the PAI; PCL-R = thePsychopathy Checklist; A-PDE = the Antisocial Scale on thePersonality Disorder Examination. Sens = sensitivity; Spec =specificity; PPP = positive predictive power; NPP = negativepredictive power.
"For a diagnosis of APD the individual must also have met thecriterion of more than 2 conduct problems.
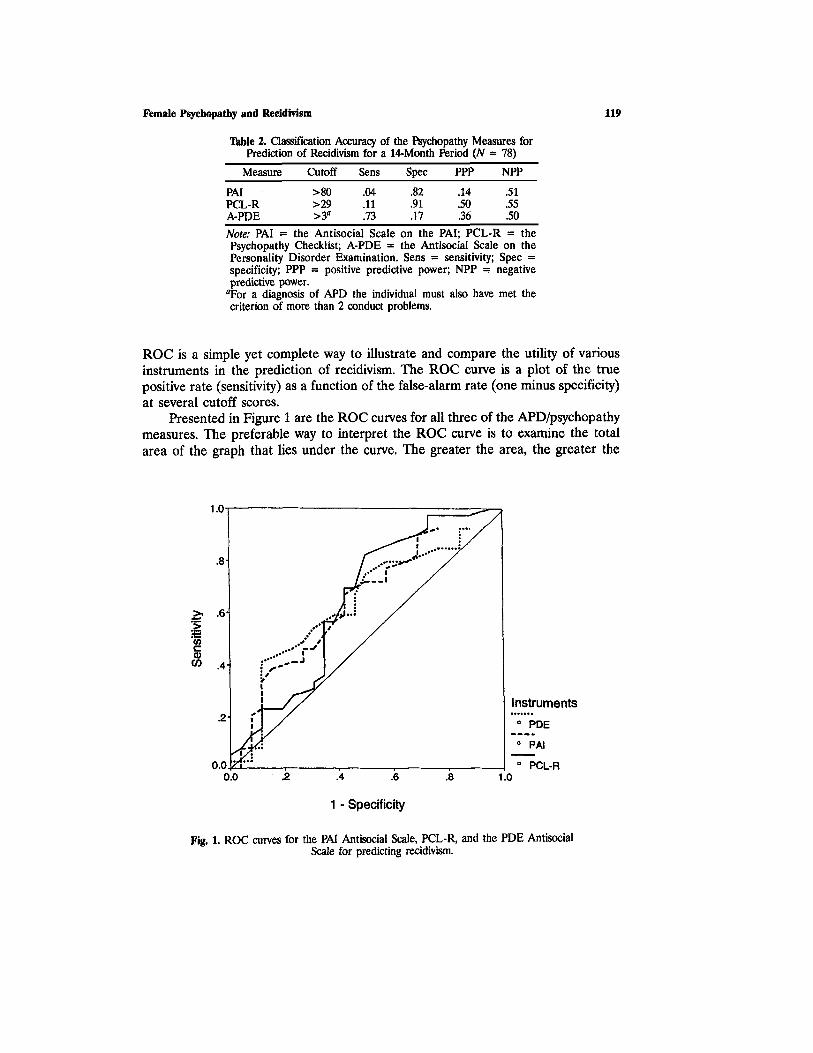
ROC is a simple yet complete way to illustrate and compare the utility of variousinstruments in the prediction of recidivism. The ROC curve is a plot of the truepositive rate (sensitivity) as a function of the false-alarm rate (one minus specificity)at several cutoff scores.
Presented in Figure 1 are the ROC curves for all three of the APD/psychopathymeasures. The preferable way to interpret the ROC curve is to examine the totalarea of the graph that lies under the curve. The greater the area, the greater the
Fig. 1. ROC curves for the PAI Antisocial Scale, PCL-R, and the PDE AntisocialScale for predicting recidivism.
120 Salekin, Rogers, Ustad, and Sewell
Table 3. Predictions of Recidivism: Discriminant Analyses Utilizing theDifferent Psychopathy Measures (N = 78)
Measure
ANT-E*ANT-SANT-A
PCL-F1*PCL-F2
AGG-V*AGG-AAGG-P
Canonicalcorrelation
.26
.25
.29
Wilks'lambda
.94*
.94*
.91*
HR
61
63
61
Sens
.75
.71
.71
Spec
.50
.56
.53
PPP
.55
.57
.56
NPP
.71
.70
.69
Note. ANT = the Antisocial Scale of the Personality Assessment Inventory;PCL-R = the Psychopathy Checklist-Revised. AGG = the Aggression Scaleof the Personality Assessment Inventory. HR = hit rate; Sens = sensitivity;Spec = specificity; PPP = positive predictive power; NPP = negativepredictive power.
*p < .05.
difference at each point between true-positive and false-alarm rates. The greaterthe difference, the more effective the instrument is at predicting recidivism. For allthree psychopathy instruments, the predictability of recidivism was found to be mod-erate. Specifically the areas under the curves were .64, .64, and .59 for the ANTscale, the PCL-R, and the PDE, respectively.
Odds ratios (OR) for each of the curves were also calculated to facilitate inthe interpretation of these results. Odds ratios are a measure of effect size and arecalculated by using the formula OR = (TP x TN)/(FP x FN), where TP = truepositive, TN = true negative, FP = false positive, and FN = false negative. Oddsratios are well suited for 2 x 2 dichotomous data (Fleiss, 1994) because of theirstraightforward interpretation. For example, an odds ratio of 2 can be understoodas indicating that the criterion group (i.e., psychopaths) is twice as likely to possessthe criterion characteristic (i.e., recidivism) as the comparison group (i.e., nonpsy-chopaths). A large effect size is an odds ratio of 2.5 or greater (Douglas & Hart,1996; Fleiss, Williams, & Dubro, 1986). For the current study, odds ratios of 1.03,1.06, and 1.00 were produced for the ANT scale, the PCL-R, and the PDE, re-spectively.
Discriminant Function Analyses for Determining Recidivism ClassificationAccuracy Based on the PAI and the PCL-R
Three discriminant function analyses were performed to determine whethervarious components of the psychopathy scales or other theoretically related scaleswere useful predictors of recidivism (see Table 3). A discriminant function analysisthat included the PAI antisocial subscales (ANT-E, ANT-S, ANT-A) yielded a Wilks'lambda = .94, x2 (1, 77) = 4.03, p = .05. The overall classification rate was 61.3%,with the ANT-E subscale accounting for most of the variance. Moreover, ANT-E
Female Psychopathy and Recidivism 121
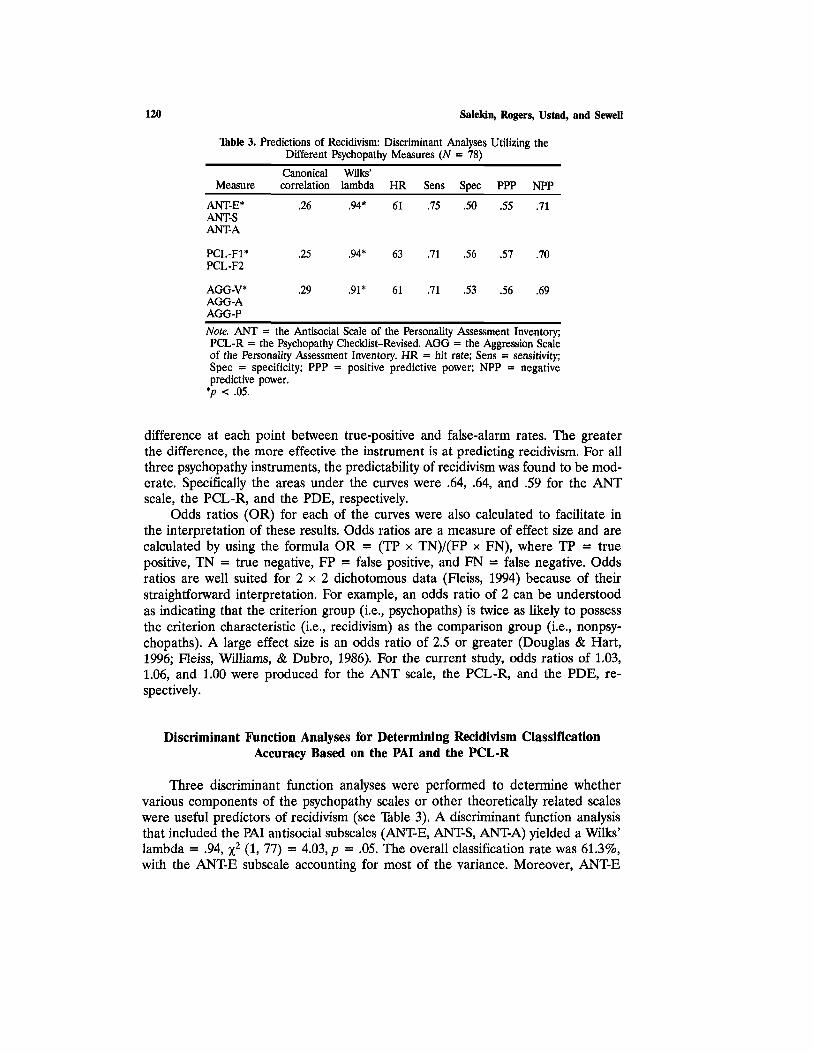
Fig. 2. A comparison of the percentage of psychopaths and nonpsychopaths, based onthe PAI Antisocial Scale, who were not rearrested upon release.
was found to be significantly predictive of recidivism on its own (p < .05). Thepredictor variables for the second discriminant analysis included Factor 1 and Factor2 of the PCL-R. When utilizing these predictors, the discriminant analysis produceda classification accuracy of 62.9% with Wilks' lambda = .94, x2 (1, 77) = 3.72, p= .05. Factor 1 accounted for the most variance in this analysis and was a significantpredictor on its own (p < .05).
Additionally, we performed a discriminant analysis on the Aggression subscales(AGG-A, AGG-P, and AGG-V) of the PAI given that we had hypothesized theirrelation to recidivism in women. A stepwise discriminant analysis yielded a Wilks'lambda = .91, x2 (1, 77) = 5.38, p = .02. The overall classification rate was mod-erate for these predictors, with 61.3% of the individuals being correctly classified.The AGG-V was the only subscale that significantly contributed to the predictionon its own (p < .05). In summary, F1 of the PCL-R, the ANT-E, and the AGG-Vsubscale of the PAI accounted for the most variance in these analyses.
Survival Analyses Based on the PAI, PCL-R, and PDE Psychopathy Measures
Survival analysis is a statistical technique that is well suited for the purpose ofexamining the prediction of recidivism for a given predictor variable. In the presentstudy, survival analyses were used to evaluate the time that it takes for an individualto recidivate and to estimate the rate of occurrence of that event. In addition, we
122 Salekin, Rogers, Ustad, and Sewell
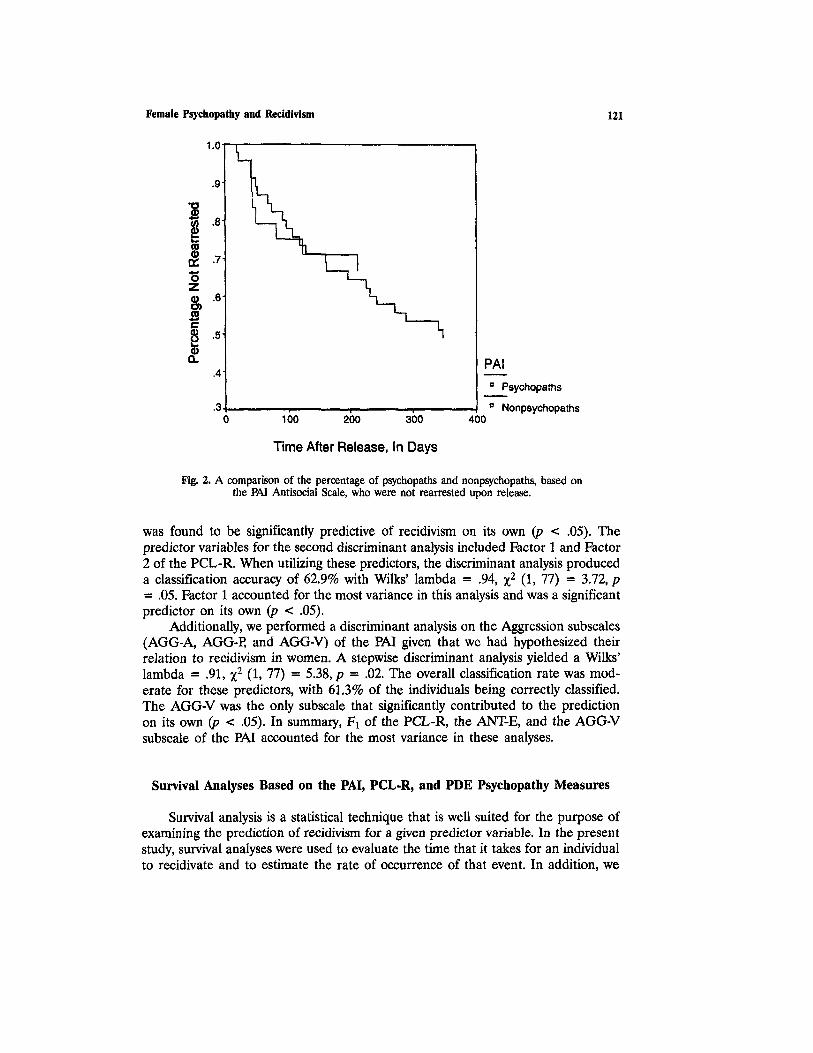
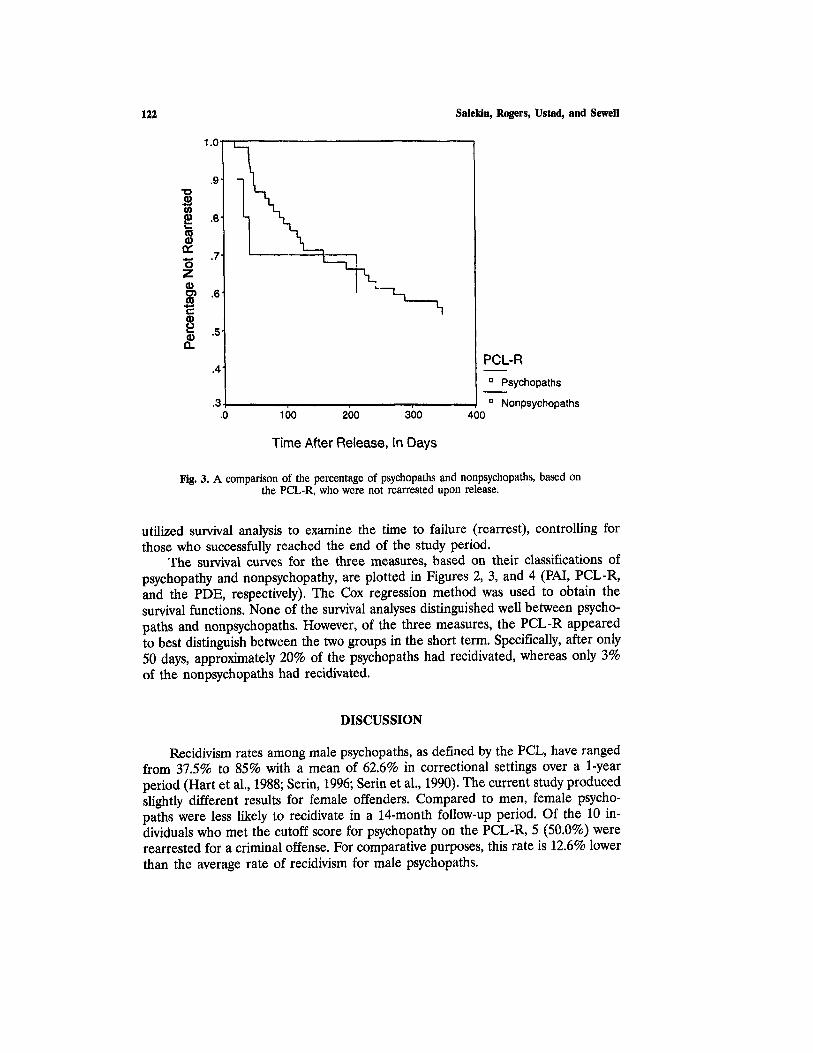
Fig. 3. A comparison of the percentage of psychopaths and nonpsychopaths, based onthe PCL-R, who were not rearrested upon release.
utilized survival analysis to examine the time to failure (rearrest), controlling forthose who successfully reached the end of the study period.
The survival curves for the three measures, based on their classifications ofpsychopathy and nonpsychopathy, are plotted in Figures 2, 3, and 4 (PAI, PCL-R,and the PDE, respectively). The Cox regression method was used to obtain thesurvival functions. None of the survival analyses distinguished well between psycho-paths and nonpsychopaths. However, of the three measures, the PCL-R appearedto best distinguish between the two groups in the short term. Specifically, after only50 days, approximately 20% of the psychopaths had recidivated, whereas only 3%of the nonpsychopaths had recidivated.
DISCUSSION
Recidivism rates among male psychopaths, as defined by the PCL, have rangedfrom 37.5% to 85% with a mean of 62.6% in correctional settings over a 1-yearperiod (Hart et al., 1988; Serin, 1996; Serin et al., 1990). The current study producedslightly different results for female offenders. Compared to men, female psycho-paths were less likely to recidivate in a 14-month follow-up period. Of the 10 in-dividuals who met the cutoff score for psychopathy on the PCL-R, 5 (50.0%) wererearrested for a criminal offense. For comparative purposes, this rate is 12.6% lowerthan the average rate of recidivism for male psychopaths.
Female Psychopathy and Recidivism 123
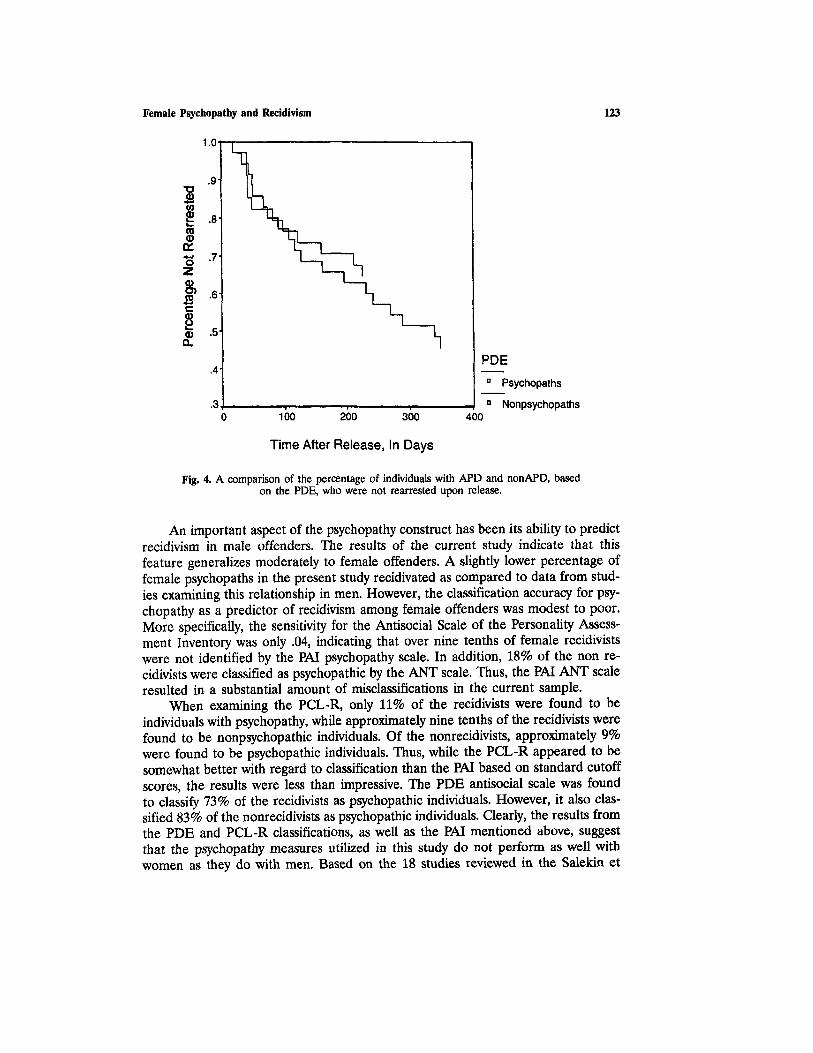
Fig. 4. A comparison of the percentage of individuals with APD and nonAPD, basedon the PDE, who were not rearrested upon release.
An important aspect of the psychopathy construct has been its ability to predictrecidivism in male offenders. The results of the current study indicate that thisfeature generalizes moderately to female offenders. A slightly lower percentage offemale psychopaths in the present study recidivated as compared to data from stud-ies examining this relationship in men. However, the classification accuracy for psy-chopathy as a predictor of recidivism among female offenders was modest to poor.More specifically, the sensitivity for the Antisocial Scale of the Personality Assess-ment Inventory was only .04, indicating that over nine tenths of female recidivistswere not identified by the PAI psychopathy scale. In addition, 18% of the non re-cidivists were classified as psychopathic by the ANT scale. Thus, the PAI ANT scaleresulted in a substantial amount of misclassifications in the current sample.
When examining the PCL-R, only 11% of the recidivists were found to beindividuals with psychopathy, while approximately nine tenths of the recidivists werefound to be nonpsychopathic individuals. Of the nonrecidivists, approximately 9%were found to be psychopathic individuals. Thus, while the PCL-R appeared to besomewhat better with regard to classification than the PAI based on standard cutoffscores, the results were less than impressive. The PDE antisocial scale was foundto classify 73% of the recidivists as psychopathic individuals. However, it also clas-sified 83% of the nonrecidivists as psychopathic individuals. Clearly, the results fromthe PDE and PCL-R classifications, as well as the PAI mentioned above, suggestthat the psychopathy measures utilized in this study do not perform as well withwomen as they do with men. Based on the 18 studies reviewed in the Salekin et

124 Salekin, Rogers, Ustad, and Sewell
al. (1996) meta analysis, the average sensitivity value for PCL in classifying recidi-visists was .37 and the average specificity value was .87.
Another way of examining the same data was through the use of the ReceiverOperating Characteristic (ROC) curves. The ROC curves show that the PAI andthe PCL-R marginally outperformed the PDE for predicting recidivism, but theirclassification accuracy was modest at best (i.e., areas under the curves were .64 forboth measures). Moreover, odds ratios demonstrated that the psychopathy measuresdid not provide much information beyond chance regarding the prediction of re-cidivism. More specifically, psychopaths were only 1.03 and 1.06 times more likelyto recidivate than nonpsychopaths. Similarly, the results of the survival analysesshowed that it is difficult to distinguish, based on a psychopathy classification, whichindividuals are most likely to recidivate. The exception was the PCL-R, which, inthe very short term, indicated that psychopathic individuals were approximately 10times more likely to recidivate than nonpsychopathic individuals. Overall, the aboveanalyses suggest that classification of recidivists based on psychopathy results in asubstantial amount of false positives and false negatives.
The findings of the current study are meaningful to the conceptualization offemale psychopathy. That is, the lower prevalence of psychopathy in women andthe disparate symptom pattern suggest that psychopathic women are only minimallyat greater risk to recidivate than are nonpsychopathic women. In addition, differ-ences in symptomatology appear to be theoretically important to the psychopathy-recidivism relation for women. Specifically, past research has found that womenwith APD/psychopathy are less aggressive/violent and are less likely to commit othertypes of crimes (Mulder et al., 1994). The findings of the present study augmentthis research by showing that, in general, women are less likely to recidivate thanare men.
Despite poor classification accuracy, a meaningful relationship was found be-tween components of the psychopathy measures and recidivism. Three theoreticallysimilar components of the psychopathy scales were all related to recidivism andalso predicted its occurrence. The Cleckley (1941) criteria that are captured by Fac-tor 1 of the Psychopathy Checklist-Revised and the Egocentricity subscale (ANT-Eof the Antisocial Scale) of the Personality Assessment Inventory showed the greatestpredictive ability along with the verbal aggression subscale (of the Aggression Scale)of the PAI. The constellation of these scales suggests that classic descriptions ofpsychopathy, such as that provided by Cleckley, combined with verbal aggressivitymost appropriately predict recidivism in females.
In contrast, behavioral criteria measured by such scales as the PsychopathyChecklist-Revised (F2) and the Antisocial Behaviors subscale (ANT-A of the Anti-social Scale) of the Personality Assessment Inventory were not predictive of recidi-vism. It appears that a classification of psychopathy characterized by behavioralsymptomatology (i.e., as in DSM-IV) adds little to the prediction of recidivism inthis sample of women. This finding suggests an important gender difference forpsychopathy in that behavioral characteristics (F2) are moderately predictive of gen-eral recidivism in male psychopaths.
Personality traits described by Cleckley (1941) may be especially important tothe assessment of psychopathy and its ability to predict recidivism. In general, it is

Female Psychopathy and Recidivism 125
thought that women are not expected to engage in antisocial behavior, and areactively discouraged from behaving against societal norms (Maccoby, 1986; Silver-thorn & Frick, submitted). Thus, women may experience guilt more often than menfor acting aggressively/violently (Bettencourt & Miller, 1996; Frodi, Macaulay, &Thome, 1977). Silverthorn and Frick (1997) have argued that, because these factorsmay inhibit antisocial behaviors in women, the presence of psychopathic personalitytraits (e.g., lack of remorse and lack of empathy) may be required for women tobreak gender-specific norms in order to engage in a consistent pattern of antisocialbehavior. While we acknowledge this conceptualization as preliminary, the resultsfrom our study provide partial support for this hypothesis.
An important issue regarding psychopathy in women that requires addressingis whether the low prevalence of psychopathy in women is suggestive of a need tolower psychopathy cutoff scores. The classification accuracy data provided in thisstudy suggest that an adjustment in cutoff scores might improve classification ac-curacy; yet, even when a broad range of psychopathy scores was examined, classi-fication accuracy of psychopathy and recidivism showed little improvement. Thatis, identifying female psychopaths for the prediction of recidivism resulted in highfalse-positive and false-negative rates.
In summary, psychopathy appears to be both less pronounced in female of-fenders and less predictive of later recidivism than it is with male offenders. Infemale offenders, personality-based criteria first delineated by Cleckley (1941) ap-pear to be moderately related to recidivism, whereas behavioral criteria do not ap-pear to be effective predictors of recidivism among female offenders. Thisparticularly important finding suggests that female offenders who continue to reof-fend are likely to manifest the traits of callousness and unemotionality. In addition,ROC analysis suggests that adjusting cutoff scores would improve classification ac-curacy only minimally for psychopathic individuals with regard to recidivism. Simplyput, the accuracy of these measures in predicting recidivism suggests that cautionbe used when evaluating female offenders. Clearly, additional research is neededto elucidate the components of psychopathy most predictive of recidivism in women.Examining the patterns in female psychopathy that are indicative of general recidi-vism and dangerousness will be important steps for researchers examining the con-struct of psychopathy in women.
Several limitations of this study indicate the need for additional research. Whilemale psychopaths tend to show moderate rates of recidivism within the first yearof their release, they also continue to recidivate as time elapses, thus increasingtheir overall rate of recidivism. Although the results of the current study show adeparture in recidivism rates within the first year of release from that of previousstudies on male psychopaths, female psychopathy may be more predictive of re-cidivism in the long term. It is likely that more lengthy follow-up periods will pro-vide useful information regarding recidivism rates of female psychopaths.
Future research on female psychopathy also should address the generalizabilityof the recidivism rates found in this study with other female populations. Specifi-cally, research might focus on women who are in prisons rather than jails (or out-patient clinics). While these populations deserve further attention, we contend thatif individuals meet the criteria for psychopathy, they should pose an equal risk of

126 Salekin, Rogers, Ustad, and Sewell
committing crimes regardless of the setting in which they are tested. If there issomething specific to prison psychopaths (or psychopathy in other settings) thatresults in a higher rate of recidivism, researchers need to attend to and elucidatethe criteria that distinguish higher risk psychopaths from lower risk psychopaths invarious settings. Specifically, determining whether differences in recidivism ratesare related to differing constellations of symptoms within the syndrome or whetherdifferences in recidivism rates are related to factors external to the psychopathyconstruct will be paramount. For example, if two inmates receive identical scoreson a psychopathy measure but pose different levels of risk based on their location,then the focus should be on identifying the factors that are related to the differingrisk levels. Further research also should examine the DSM-IV diagnosis of APD.Given that APD has been altered slightly in the latest version of the DSM-IV (con-densed and simplified) and Conduct Disorder criteria have been modified in orderto be more applicable to women, the revised constructs may have changed A-PDE'sability to predict recidivism.
REFERENCES
American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4th ed.).Washington, DC: Author.
Barbaree, H. E., Seto, M. C.t Serin, R. C, Amos, N. L., & Preston, D. L. (1994). Comparisons betweensexual and nonsexual rapist subtypes: Sexual arousal to rape, offense, precursors, and offense char-acteristics. Criminal Justice and Behavior, 21, 95-114.
Bettencourt, B. A., & Miller, N. (1996). Gender differences in aggression as a function of provocation:A meta-analysis. Psychological Bulletin, 119, 422-447.
Cleckley, H. (1941). The mask of sanity. St. Louis; MO: Mosby.Cloninger, C, & Guze, S. (1970a). Female criminals: Their personal, familial and social backgrounds.
Archives of General Psychiatry, 23, 554-558.Cloninger, C., & Guze, S. (1970b). Psychiatric illness and female criminality: The role of sociopathy and
hysteria in the antisocial woman. American Journal of Psychiatry, 127, 303-311.Costa, P. T., & McCrae, R. R. (1985). NEO Personality Inventory: Professional manual. Odessa, FL: Psy-
chological Assessment Resources.Douglas, K., & Hart, S. D. (1996, March). Major mental disorder and violent behavior: A meta-analysis
of study characteristics and substantive factors influencing effect size. Paper presented at the AmericanPsychology-Law Society in Hilton Head, SC.
Fleiss, J. L. (1994). Measures of effect size for categorical data. In H. Cooper & L. V Hedges (Eds.),The handbook of research synthesis. New York: Russell Sage.
Fleiss, J. L, Williams, J. B. W., & Dubro, A. F. (1986). The logistic regression analysis of psychiatricdata. Journal of Psychiatric Research, 20, 145-209.
Forth, A. E., Brown, S. L., Hart, S. D., & Hare, R. D. (1996). The assessment of psychopathy in maleand female noncriminals: Reliability and validity. Personality and Individual Differences, 20, 531-543.
Frodi, A., Macaulay, J., & Thome, P. R. (1977). Are women always less aggressive than men? A reviewof the experimental literature. Psychological Bulletin, 84, 634-660.
Glaros, A. G., & Kline, R. B. (1988). Understanding the accuracy of tests with cutting scores: Thesensitivity, specificity, and predictive value model. Journal of Clinical Psychology, 44, 1013-1023.
Green, D. M., & Swets, J. A. (1966). Signal detection theory and psychophysics. New York: Wiley.Hare, R. D. (1985a). The Psychopathy Checklist. Unpublished manuscript, University of British Columbia,
Vancouver, BC, Canada.Hare, R. D. (1985b). Comparison of procedures for the assessment of psychopathy. Journal of Consulting
and Clinical Psychology, 53, 7-16.Hare, R. D. (1991). Manual for the Revised Psychopathy Checklist. Toronto, ON, Canada: Multi-Health
Systems.Hare, Harpur, Hakstian, Forth, Hart, & Newman (1990).

Female Psychopathy and Recidivism 127
Hare, R. D., & Hart, S. D. (1993). Psychopathy, mental disorder, and crime. In S. Hodgins (Ed.), Mentaldisorder and crime (pp. 104-115). Newbury Park, CA: Sage.
Harpur, T. J., Hare, R. D., & Hakstian, A. R. (1989). Two factor conceptualization of psychopathy:Construct validity and assessment implications. Psychological Assessment: A Journal of Consultingand Clinical Psychology, 1, 6-17.
Hart, S. D., Cox, D. N., & Hare, R. D. (1994). Manual for the Psychopathy Checklist: Screening Version.Unpublished manuscript, University of British Columbia, Vancouver, BC, Canada.
Hart, S. D., Kropp, P. R., & Hare, R. D. (1988). Performance of male psychopaths following conditionalrelease from prison. Journal of Consulting and Clinical Psychology, 56, 227-232.
Kass, F., Spitzer, R., & Williams, J. (1983). An empirical study of the issue of sex bias in the diagnosticcriteria of DSM-III Axis II personality disorders. American Psychologist, 38, 593-601.
Lilienfeld, S. O. (1994). Conceptual problems in the assessment of psychopathy. Clinical Psychology Re-view, 14, 17-38.
Lilienfeld, S. O., Van Valkenburg, C., Larntz, K., & Akiskal, H. S. (1986). The relationship of histrionicpersonality disorder to antisocial personality and somatization disorders. American Journal of Psy-chiatry, 143, 718-722.
Loranger, A. W. (1988). Personality Disorder Examination (PDE) manual. Yonkers, NY: DV Communi-cations.
Loranger, A. W., Susman, V L., Oldham, J. M., & Russakoff, L. M. (1987). The Personality DisorderExamination: A preliminary report. Journal of Personality Disorders, 1, 1-13.
Lykken, D. T. (1995). The antisocial personalities. Hillsdale, NJ: Lawrence Erlbaum.Maccoby, E. E. (1986). Social groupings in childhood: Their relationship to prosocial and antisocial
behavior in boys and girls. In D. Olweus, J. Block, & M. Radke-Yarrow (Eds.), Development ofantisocial and prosocial behavior: Research, theories, and issues (pp. 263-284). Orlando, FL: AcademicPress.
Meloy, J. R. (1992). Violent attachments. Northvale, NJ: Aronson.Morey, L. C. (1991). Personality Assessment Inventory: A professional manual. Odessa, FL: Psychological
Assessment Resources.Morey, L. C. (1996). An interpretive guide to the Personality Assessment Inventory (PAl). Odessa, FL:
Psychological Assessment Resources.Mulder, R. T., Wells, J. E., Joyce, P. R., & Bushnell, J. A. (1994). Antisocial women. Journal of Personality
Disorders, 8, 279-287.Neary, A. (1990). DSM-III and Psychopathy Checklist assessment of antisocial personality disorder in Black
and White female felons. Unpublished doctoral dissertation, University of Missouri-St. Louis, MO.Offord, D. R., Adler, R. J. M., & Boyle, M. H. (1986). Prevalence and sociodemographic correlates of
conduct disorder. American Journal of Social Psychiatry, 6, 272-278.Offord, D. R., Boyle, M. H., & Racine, Y. A. (1991). The epidemiology of antisocial behavior in child-
hood and adolescence. In D. J. Pepler & K. H. Rubin (Eds.), The development and treatment ofchildhood aggression (pp. 31-54). Hillside, NJ: Lawrence Erlbaum.
Regier, D. A., Myers, J. K., Kramer, M., Robins, L. N., Blazer, D. G., Hough, R. L, Eaton, W. W., &Locke, B. Z. (1984). The NIMH epidemiologic catchment area program: Historical context, majorobjectives, and study population characteristics. Archives of General Psychiatry, 41, 934-941.
Reid, W. H. (1974). The antisocial personality: A review. Hospital and Community Psychiatry, 36, 831-837.Robins, L. N. (1966). Deviant children grown up: A sociological and psychiatric study of sociopathic per-
sonality. Baltimore: Williams and Wilkins.Robins, L. N. (1986). Epidemiology of antisocial personality. In R. Mischels, J. O. Cavenar, A. M. Coo-
per, S. B. Guze, L. L. Judd, G. L. Klerman, & A. J. Solnit (Eds.), Psychiatry, Vol. 3 (Chap. 19, pp.1-14). Philadelphia: Lippincott.
Robins, L. N., Tipp, J., & Przybeck, T. (1991). Antisocial personality. In L. N. Robins & D. A. Regier(Eds.), Psychiatric disorders in America: The epidemiologic catchment area study. New York: FreePress.
Rogers, R. (1995). Diagnostic and structured interviewing: A handbook for psychologists. Odessa, FL: Psy-chological Assessment Resources.
Rogers, R., Duncan, J. C, Lynett, E., & Sewell, K. W. (1994). Prototypical analysis of antisocial per-sonality disorder: DSM-IV and beyond. Law and Human Behavior, 18, 471-483.
Rutherford, M. J., Alterman, A. I., Cacciola, J. S., & Snider, S. C. (1995). Gender differences in diag-nosing antisocial personality disorder in methadone patients. American Journal of Psychiatry, 152,1309-1316.
Rutherford, M. J., Cacciola, J. S., Alterman, A. I., & McKay, (1996). Reliability and validity of therevised psychopathy checklist in women methadone patients. Assessment, 3, 145-156.

128 Salekin, Rogers, Ustad, and Sewell
Salekin, R. T., Rogers, R., & Sewell, K. W. (1996). A review and meta-analysis of the Psychopathy Check-list and Psychopathy Checklist—Revised: Predictive validity of dangerousness. Clinical Psychology:Science and Practice, 3, 203-215.
Salekin, R. T., Rogers, R., & Sewell, K. W. (1997). Construct validity of psychopathy in a female offendersample: A multitrait-multimethod evaluation. Journal of Abnormal Psychology, 106, 576-585.
Serin, R. C. (1996). Violent recidivism in criminal psychopaths. Law and Human Behavior, 20, 207-217.Serin, R. C., Peters, R. D., & Barbaree, H. E. (1990). Predictors of psychopathy and release outcome
in a criminal population. Psychological Assessment: A Journal of Consulting and Clinical Psychology,2, 419-422.
Silverthorn, P, & Frick, P. J. (1997). Developmental pathways to antisocial behavior: The delayed-onsetpathway in girls. Manuscript submitted for publication.
Strachan, K., Williamson, S., & Hare, R. D. (1990). Psychopathy and female offenders. Unpublished study.Department of Psychology, University of British Columbia, Canada.
Zagon, I. K., & Jackson, H. J. (1994). Construct validity of a psychopathy measure. Journal of Personalityand Individual Differences, 17, 125-135.





























