Embed Size (px)
Citation preview

Psychological Interventions for Involuntary Childlessness
Four empirical studies for evaluation and efficacy of psychological interventions
regarding the mental health and the pregnancy rate among infertile patients
Psychologische Interventionen bei ungewollter Kinderlosigkeit Vier empirische Studien zur Evaluation und Effektivität psychologischer Interventionen auf
das psychische Befinden und die Schwangerschaftschancen bei infertilen Patienten
Inauguraldissertation der Philosophisch-humanwissenschaftlichen Fakultät der Universität
Bern zur Erlangung der Doktorwürde vorgelegt von
Katja, Hämmerli
Weesen
Selbstverlag, Bern, 2009

Von der Philosophisch-humanwissenschaftlichen Fakultät auf Antrag von
Prof. Dr. Hansjörg Znoj (Hauptgutachter) und Prof. Dr. Pasqualina Perrig-Chiello (Zweit-
gutachterin) angenommen
Bern, den 8. Oktober 2009 Der Dekan: Prof. Dr. Roland Seiler
Danksagung
2
Danksagung
Ich danke allen von Herzen, die mich während meiner Arbeit an meiner Dissertation unter-
stützt und dadurch zu deren Entstehung beigetragen haben. Ich danke:
Den Patienten, welche in den Forschungsarbeiten teilgenommen haben. Durch die Ar-
beit mit ihnen konnte ich wertvolle Erfahrungen sammeln und vieles lernen.
Prof. Dr. Hansjörg Znoj, meinem Doktorvater, für seine kompetente Unterstützung und
sein Vertrauen in meine Arbeit. Er hat mir die nötige Freiheit gegeben meine wissenschaftli-
chen Interessen zu verfolgen, mich dabei aber auch mit seiner Erfahrung begleitet.
PD Dr. Jürgen Barth und Dr. Thomas Berger für die fruchtbare Zusammenarbeit und
deren fundierte Unterstützung. Ich konnte sehr viel von ihnen lernen.
Prof. Dr. Pasqualina Perrig-Chiello für ihre wertvolle, konzeptuelle Unterstützung im
Rahmen des SNF-Forschungsprojekts und die Mitbeurteilung meiner Arbeit.
Dem ganzen SNF-Forschungsprojekt-Team, Dr. Salome Burri, lic. phil. Patricia Graf
und PD Dr. med. Dorothea Wunder. Ich bedanke mich für eine gute und angenehme Zusam-
menarbeit.
Dem wissenschaftlichen und klinischen Team des Lehrstuhls für Klinische Psychologie
und Psychotherapie der Universität Bern für den regen Austausch und die angenehme Ar-
beitsatmosphäre.
Meinen Eltern und meiner Schwester, welche mich auf verschiedenste Weise auf dem
Weg bis hierher unterstützt haben.
Meinem Mann, dem ein ganz spezieller Dank gebührt. Ohne ihn wäre vieles nicht (so
einfach) möglich gewesen - von ganzem Herzen danke.
Bern, im Juli 2009 Katja Hämmerli
Zusammenfassung
3
Zusammenfassung
Unerfüllter Kinderwunsch und deren medizinische Behandlung werden von vielen Paaren als
grosse psychische Belastung erlebt. Psychologische Interventionen werden immer häufiger
zur Verbesserung des psychischen Wohlbefindens und allenfalls sogar zur Steigerung der
Schwangerschaftschancen infertiler Patienten eingesetzt – erste empirische Belege weisen auf
eine positive Wirksamkeit hin. Basierend auf diesem Hintergrund war das Ziel dieser Arbeit
die Evaluation und Überprüfung der Wirksamkeit psychologischer Interventionen auf das
psychische Befinden und die Schwangerschaftschancen von infertilen Patienten. Zur Errei-
chung dieses Ziels werden in der aktuellen Dissertationsschrift vier empirische Artikel darge-
stellt. Die vier Artikel wurden in der vorliegenden Umbrella in einen theoretischen Rahmen
eingebettet. Nach einem Einstieg ins Thema Infertilität und der Darstellung der Fragestellun-
gen dieser Dissertation wurden zunächst bestehende infertilitätsspezifische Theorien aufge-
zeigt. Anschliessend wurde das Thema „Infertilität“ in folgende drei psychologische Ansätze
eingebettet, woraus sich jeweils wichtige psychologische Aspekte der Infertilität erklären
liessen: die Konsistenztheorie von Grawe (1998, 2003), zwei Trauermodelle (Phasenmodelle
der Trauer, z. B. Bowlby, 1961, 1980; duales Prozessmodell, Stroebe & Shut, 1999) und das
transaktionale Stressmodell von Lazarus und Folkman (1984). Aus diesen drei unterschiedli-
chen Sichtweisen auf die Infertilität wurden Implikationen für die psychologische Unterstüt-
zung von infertilen Patienten abgeleitet. Abschliessend wurden die Ergebnisse der vier empi-
rischen Artikel in Bezug auf diesen theoretischen Rahmen diskutiert und weiterführende Fra-
gestellungen dargestellt.
Inhaltsverzeichnis
4
Inhaltsverzeichnis
Danksagung............................................................................................................................... 2
Zusammenfassung..................................................................................................................... 3
1. Einleitung .............................................................................................................................. 6
2. Warum ist Kinderkriegen ein wichtiges Motiv? ................................................................. 11
3. Hauptfragestellung und Übersicht der Dissertation ............................................................ 14
4. Theoretischer Rahmen......................................................................................................... 16
4.1 Infertilitätsspezifische Theorien ............................................................................ 16
4.2 Infertilität als Inkonsistenzquelle – individuell unterschiedliche Auswirkungen
der Infertilität......................................................................................................... 17
4.3 Infertilität als (wiederholter) Trauerprozess – eine häufige erlebte Reaktion....... 20
4.4 Verarbeitung der ungewollten Kinderlosigkeit und Umgang damit ..................... 26
5. Implikationen der drei theoretischen Ansatzpunkte für psychologische Interventionen bei
infertilen Patienten .............................................................................................................. 30
6. Vorgelegte Artikel............................................................................................................... 33
6.1 Kurzzusammenfassungen der vier Artikel ............................................................ 33
Artikel 1: What are the issues infertile women are dealing with?: A qualitative approach
Artikel 2: Psychological interventions for infertile patients: A review of existing research
and a new comprehensive approach
Artikel 3: The efficacy of psychological interventions for infertile patients: a meta-
analysis examining mental health and pregnancy rate
Artikel 4: Internet-Based Support for Infertile Patients: A Randomized Controlled
Study
Inhaltsverzeichnis
5
1. Diskussion ............................................................................................................................. 1
1.1 Zusammenfassung der wichtigsten Resultate und Beantwortung der
Hauptfragestellung ........................................................................................... 1
1.2 Integration der Ergebnisse in den theoretischen Rahmen ................................ 3
1.3 Weiterführende Fragestellungen und Projekte ................................................. 6
Literaturverzeichnis................................................................................................................... 9
Abbildungsverzeichnis ............................................................................................................ 22
Anhang
A: Fragebogen des Kinderwunsch Online Coachings (Version: Messzeitpunkt t1 (zu Beginn);
weibliche Version)
B: Feedback-Fragebogen zum Programm des Kinderwunsch Online Coachings
C: Informations- und Anmeldeunterlagen des Kinderwunsch Online Coachings
D: Kodierschema der qualitativen Inhaltsanalyse
E: Review of the manuscript „Internet-Based Support for Infertile Patients: A Randomized
Controlled Study“ from the Journal of Behavioral Medicine
D: Curriculum vitae
Anmerkung: Aus Gründen der Vereinfachung wird in der folgenden Arbeit das Maskulinum verwendet – ge-
meint sind damit aber sowohl Frauen und Männer
Einleitung
6
1. Einleitung
Kinder gebären und eine Familie gründen ist ein zentrales Motiv vieler junger Erwachse-
ner (Erdle, 2008; Lampic, Svanberg, Karlström, & Tydén, 2006). So wünschen sich drei Vier-
tel aller Frauen, die ein Studium beginnen, ein Leben mit Kindern. Erstaunlicherweise haben
aber nur 43% der 30- bis 39-jährigen früheren Studentinnen Kinder (Erdle, 2008). Daraus
ergibt sich die Frage, warum dieser Wunsch nicht verwirklicht wurde.
Ungewollte Kinderlosigkeit ist kein neuzeitliches Problem, sondern ist schon lange be-
kannt (Burns & Covington, 2006). Die Bibel ist eine der frühesten Quellen, worin die Bedeu-
tung von Fruchtbarkeit und Unfruchtbarkeit thematisiert wurde (Atwood & Dobkin, 1992). So
wurde der häufig zitierte Ausdruck „seid fruchtbar und vermehret euch“ als Aufforderung
Nachkommen zu produzieren interpretiert. Anhand der folgenden Stelle wird die psychische
Belastung aufgrund der Unfruchtbarkeit deutlich: „Als Rahel sah, dass sie Jakob keine Kinder
gebar, wurde sie eifersüchtig auf ihre Schwester. Sie sagte zu Jakob: Verschaff’ mir Söhne!
Wenn nicht, sterbe ich.“ (Genesis 30:1-3). Diese frühe Beschreibung der psychischen Aspek-
te der Infertilität lässt sich jedoch in den aktuellen Definitionen der Infertilität nicht finden. So
definiert die Weltgesundheitsorganisation (WHO, 2002) Infertilität als die Unfähigkeit eines
Paares nach einem Jahr regelmässigem ungeschützten Sexualverkehr schwanger zu werden
oder eine Schwangerschaft zu beenden. Weiter kann zwischen Sterilität, der Unfähigkeit
überhaupt schwanger zu werden, und Infertilität, der Unfähigkeit eine Schwangerschaft aus-
tragen zu können, unterschieden werden (Strauss, 2000). Die Begriffe Sterilität und Infertilität
sowie Fruchtbarkeits-, Fertilitätsstörungen und ungewollte Kinderlosigkeit werden heute in
der Literatur häufig synonym gebraucht (Gnoth et al., 2005; Strauss, 2000). In der vorliegen-
den Arbeit werden die Begriffe Infertilität und ungewollte Kinderlosigkeit ebenfalls synonym
verwendet.
Einleitung
7
Das ungewollte Ausbleiben des Kindersegens betrifft immer mehr Paare (Wischmann,
2005). 3 % bis 9 % der Paare mit Kinderwunsch gelten als ungewollt kinderlos, wobei jede
dritte Frau länger als ein Jahr auf eine Schwangerschaft wartet (Helfferich & Küppers-
Chinnow, 1996; Huinink & Brähler, 2000). Die Zahl ungewollt kinderloser Paare hat in den
westlichen Ländern in den letzten Jahren zugenommen und wird auch weiter aufgrund des
ansteigenden Durchschnittsalters der Erstgebärenden zunehmen (Cousineau & Domar, 2007).
Das Alter gilt als wichtigster prognostischer Faktor für eine Schwangerschaft (Michelmann &
Himmel, 2005; Taylor, 2003). So ist die Fruchtbarkeit bei Frauen zwischen 35 und 39 Jahren
nur noch halb so hoch als bei Frauen zwischen 19 und 26 Jahren (Taylor, 2003). Während in
der Schweiz 1975 das Durchschnittsalter der Frauen bei der Erstgeburt noch bei 28 Jahren
lag, ist das Alter der Frauen in den letzten Jahren steigend und lag 2007 bei 30.8 Jahren (Bun-
desamt für Statistik, 2008). Diese Altersverschiebung lässt sich in den meisten westlichen
Ländern beobachten und wird insbesondere durch längere Ausbildungszeiten und einen späte-
ren Eintritt ins Berufsleben der Frauen erklärt (Cousineau & Domar, 2007; Stammer, Verres,
& Wischmann, 2004). Alarmierend ist, dass sich viele junge Menschen der reduzierten
Fruchtbarkeit mit steigendem Alter zu wenig bewusst zu sein scheinen (Bunting & Boivin,
2008; Lansac, 1995; Skoog Svanberg, Lampic, Karlström, & Tydén, 2006). Lampic et al.
(2006) konnten zeigen, dass in einer studentischen Stichprobe mehr als die Hälfte der Frauen
im Alter nach 35 Jahren planten Kinder zu haben. Die Frauen waren sich dabei der Tatsache
ungenügend bewusst, dass in diesem Alter die weibliche Fruchtbarkeit bereits abnehmend ist.
Früher wurde ungewollte Kinderlosigkeit auf dem Hintergrund von Geistern und Religion
erklärt und mit pflanzlichen Heilmitteln, Ritualen und Gebeten behandelt (Johnston, 1963;
Walker, 1983). Mit zunehmendem medizinischem Verständnis im 18. Jahrhundert wurde In-
fertilität stärker als medizinisches Problem anstatt als übernatürliches Ereignis betrachtet. Ein
weiterer wichtiger Meilenstein war die Einführung der Reproduktionsmedizin mit der Geburt
Einleitung
8
von Louise Brown 1978 (dem ersten im Labor per In-Vitro-Fertilisation (IVF) gezeugten
Menschen), welche ganz neue Möglichkeiten für die Paare bot und die Fortpflanzung unab-
hängig vom Geschlechtsverkehr machte (Burns & Covington, 2006). Mit dem medizinischen
Fortschritt wurde die Aufmerksamkeit lange Zeit ausschliesslich auf die medizinischen
Aspekte der Infertilität gelegt, wobei die psychologische Seite der ungewollten Kinderlosig-
keit kaum beachtet wurde.
In den letzten Jahren nahmen immer mehr infertile Paare reproduktionsmedizinische Be-
handlungen in Anspruch (Andersen, Carlsen, & Loft, 2008). Ungefähr die Hälfte aller Paare
weltweit suchen medizinische Hilfe (Boivin, Bunting, Collins, & Nygren, 2007). In der
Schweiz nahm 2007 die Anzahl reproduktionsmedizinischer Behandlungen im Vergleich zum
Vorjahr um 13 Prozent zu (Bundesamt für Statistik, 2008). So wurde 2007 bei 5400 Paaren
eine reproduktionsmedizinische Behandlung durchgeführt. Durch die steigende Inanspruch-
nahme medizinischer Unterstützung hat sich auch die psychische Belastung infertiler Paare
verändert. Im Allgemeinen wird Infertilität von den betroffenen Paaren als eine der schlimm-
sten Krisen in ihrem Leben beschrieben (Freeman, Boxer, Rickels, Tureck, & Mastroianni,
1985; Kerr, Brown, & Balen, 1999). Dennoch ist der Anteil psychopathologisch auffälliger
Personen mit 15 % bis 20 % nicht höher als in der Allgemeinbevölkerung (Strauss, Brähler, &
Kentenich, 2004; Wright, Allard, Lecours, & Sabourin, 1989). Die reproduktionsmedizini-
schen Behandlungen gelten als die stressreichsten Techniken in der Behandlung der Infertili-
tät (Eugster & Vingerhoets, 1999). Daher wurden auch insbesondere während der reproduk-
tionsmedizinischen Behandlung kurzfristig erhöhte Werte in Depressivität, Ängstlichkeit und
Stress gefunden (Eugster & Vingerhoets, 1999; Chen, Chang, Tsai, & Juang, 2004). Neben
der zeitlichen, finanziellen und emotionalen Belastungen durch eine reproduktionsmedizini-
sche Behandlung stellen meist das nicht vorhersagbare Ergebnis und ein negativer Behand-
lungsausgang zusätzlich starke Belastungen dar (Olivius, Friden, Borg, & Bergh, 2004;
Einleitung
9
Verhaak et al., 2007). Die psychische Belastung steigt oft mit der Zahl erfolgloser Behand-
lungszyklen weiter an (Beutel et al., 2000). Die reproduktionsmedizinische Behandlung stellt
für viele Paare eine ergänzende Chance dar den Traum eines eigenen Kindes realisieren zu
können, geht aber auch oftmals mit einer erhöhten psychischen Belastung einher. Dies wider-
spiegeln auch die hohen Abbruchraten bei reproduktionsmedizinischen Behandlungen, wel-
che auf die hohe psychische Belastung durch die medizinische Behandlung zurückgeführt
werden (Smeenk et al., 2004; Verberg et al., 2008).
Zusammenfassend kann gesagt werden, dass durch die starke medizinische Fokussierung
lange Zeit die psychologische Seite ungewollter Kinderlosigkeit vernachlässigt wurde. Dies
scheint auch heute noch teilweise so zu sein, was sich beispielsweise in den fehlenden psy-
chologischen Dimensionen der aktuellen Definitionen der Infertilität zeigt. Durch den repro-
duktionsmedizinischen Fortschritt in den letzten Jahren wurde die Aufmerksamkeit haupt-
sächlich auf die medizinische Seite gerichtet. Gleichzeitig entwickelte sich aber auch parallel
zum medizinischen Fortschritt die psychologische Beratung bei ungewollter Kinderlosigkeit
(Burns & Covington, 2006). Bereits 1930 wurden psychologische Aspekte der Infertilität in
der Literatur beschrieben, jedoch erst in den letzten 30 Jahren etablierte sich die psychologi-
sche Beratung als eigenständiges Aufgabengebiet (Covington, 1995). Historisch betrachtet
war vor 1970 die Aufgabe der Psychologen die der Infertilität zugrunde liegenden psychi-
schen Probleme zu behandeln, um so die Unfruchtbarkeit zu beheben (Greil, 1997). Menning
(1980) war die erste, welche psychische Probleme als Folge der Infertilität und nicht als Ursa-
che dieser bezeichnete. Das Ziel psychologischer Beratung war von dieser Zeit an die Linde-
rung psychischer Belastungen resultierend aus dem unerfüllten Kinderwunsch und deren me-
dizinischen Behandlung (Bresnick & Taymor, 1979).
Psychische Aspekte der Infertilität nehmen immer mehr an Bedeutung zu betrachtet man
beispielsweise die erhöhte psychische Belastung während der reproduktionsmedizinischen
Einleitung
10
Behandlung und die dadurch resultierenden hohen Abbruchraten. Obwohl bis heute im Alltag
die Beachtung psychologischer Aspekte oft noch zu kurz kommt und spezifische psychologi-
sche Angebote bei Infertilität zu wenig verfügbar sind, entwickelt sich die psychologische
Unterstützung immer stärker zu einem wichtigen Bestandteil in der Behandlung infertiler Paa-
re (Wischmann, 2008).
Warum ist Kinderkriegen ein wichtiges Motiv?
11
2. Warum ist Kinderkriegen ein wichtiges Motiv?
In der Vergangenheit stellte die Frage, ob ein Paar Kinder haben wollte, für viele Erwach-
sene eher eine „biologisch determinierte oder kulturell unvermeidliche Anforderung“ dar
(Michaels, 1988, S. 23). Heutzutage ist es in westlichen Ländern eher eine persönliche Ent-
scheidung (Gloger-Tippelt, 2007). Die Qualität des Kinderwunsches hat sich gewandelt von
eher versorgungszentrierten Motiven hin zu persönlichen, sinnstiftenden Motiven (Gauda &
Keller, 1987; Strauss, 1991). Zur Beantwortung der Frage der Bedeutung des Kinderwun-
sches ist es hilfreich einen Blick auf die Entwicklungspsychologie der Lebensspanne (Baltes,
Reese, & Lipsitt, 1980) zu werfen.
Elternschaft wird in der Entwicklungspsychologie als eine Entwicklungsaufgabe des Er-
wachsenenalters gesehen. Entwicklungsaufgaben strukturieren die Lebensspanne als eine
Folge von Herausforderungen, die vom Individuum als persönliche Entwicklungsziele wahr-
genommen werden (Havighurst, 1973). So formulierte Havighurst (1972) in seinem normati-
ven Entwicklungsmodell die Gründung einer Familie als Aufgabe des frühen Erwachsenenal-
ters. Erikson (1988) geht davon aus, dass die Elternschaft zum Gelingen der Entwicklungsstu-
fe der Generativität beitragen kann. Mit dem Begriff „Generativität“ meint Erikson (1988) die
Stiftung und Erziehung der nächsten Generation. Gelingt keine erfolgreiche Auseinanderset-
zung mit dieser Phase, droht Stagnation und damit eine Verarmung der Persönlichkeit.
Diese klassischen Entwicklungsmodelle widersprechen dem heutigen Erkenntnisstand, da
Entwicklungsverläufe nicht mehr als universell, sondern als multidirektional und interindivi-
duell variabel in einer Wechselwirkung zwischen Individuum und Gesellschaft gesehen wer-
den (Faltermaier, Mayring, Saup, & Strehmel, 2002). Dennoch ist der heuristische Wert der
klassischen Entwicklungsmodelle und den daraus formulierten wichtigen Entwicklungsthe-
men zu betonen.
Warum ist Kinderkriegen ein wichtiges Motiv?
12
Trotz der heute stark individualisierten Lebensphase des jungen Erwachsenenalters mit
alternativen Lebensformen (z. B. bewusst gewählte Kinderlosigkeit, nicht eheliche Lebens-
gemeinschaften und Lebensgemeinschaften Homosexueller), gehört die Gründung einer eige-
nen Familie weiterhin zu den häufigen und wichtigsten Lebensschritten im jungen Erwachse-
nenalter (Baltes et al., 1980; Faltermaier et al., 2002). Ungewollte Kinderlosigkeit stellt ein
nicht-normatives Ereignis oder kritisches Lebensereignis dar, welches die Lebensperspektive
einer Person bedrohen und schwer zu bewältigen sein kann. Ist das Lebensziel der Eltern-
schaft bedroht, kommt es gemäss dem Zwei-Prozess-Modell von Brandstätter (2007) meist
zunächst zu vermehrten Anstrengungen dieses Ziel zu erreichen beispielsweise durch die In-
anspruchnahme von medizinischer Hilfe. Führen diese Anstrengungen jedoch nicht zum Ziel,
geht dies mit einer erhöhten psychischen Belastung und dem Risiko für die Entstehung de-
pressiver Störungen einher (Abramson, Seligman, & Teasdale, 1978; Ingram, 1990) – zumin-
dest solange wie das Ziel der Elternschaft aufrechterhalten wird. Nach Brandstätter (2007)
wird diese Situation durch akkomodative Prozesse, der Anpassung resp. Ablösung von Zielen
gelöst. Das Aufgeben oder Anpassen von einem gemeinsamen Lebensentwurf stellt eine
grosse Herausforderung für Paare mit unerfülltem Kinderwunsch dar (Wischmann & Stam-
mer, 2006). Der Umgang mit dem unerfüllten Kinderwunsch kann auch durch das Modell der
selektiven Optimierung mit Kompensation (SOK; Baltes, 1997; Baltes, Lindenberger, &
Staudinger, 1998) erklärt werden, welches erfolgreiche Entwicklung als Maximierung von
Gewinnen und Minimierung von Verlusten ansieht. Der unerfüllte Kinderwunsch kann als
eine verlustbasierte Selektion bezeichnet werden, was die Veränderung oder Aufgabe des
Ziels eigene Kinder zu haben beschreibt. Je nach Anpassung des Ziels werden entsprechende
zielbezogene Mittel zur Optimierung eingesetzt. Ist ein Paar beispielsweise mit der Tatsache
konfrontiert keine eigenen Kinder auf natürlichem Weg haben zu können (Selektion), ent-
schliesst es sich vielleicht mit reproduktionsmedizinischer Hilfe dieses Ziel zu erreichen (Op-
Warum ist Kinderkriegen ein wichtiges Motiv?
13
timierung). Den Verlust eigene Kinder auf natürlichem Weg zu bekommen, kann beispiels-
weise durch vermehrte Konzentration auf berufliche Ziele kompensiert werden (Kompensati-
on).
Kinderlose Paare im mittleren Lebensalter befinden sich in einer speziellen Situation, da
sie einerseits realisieren, dass die Generationenabfolge unterbrochen wurde und andererseits
dass sie das Fehlen von Nachkommen durch ausserfamiliäre Kontakte kompensieren müssen
(Perrig-Chiello & Höpflinger, 2001). Die entwicklungspsychologische Sichtweise bestätigt
somit die Bedeutung der Familie für die individuelle Entwicklung über die Lebensspanne,
aber auch deren Wichtigkeit für die Gesellschaft im Sinne des Generationenvertrags (Perrig-
Chiello, Höpflinger, & Suter, 2008). Aus den genannten Erläuterungen wird die Bedeutung
des unerfüllten Kinderwunsches deutlich, welche häufig eine lange Zeit des mittleren Er-
wachsenenalters prägt. Der unerfüllte Kinderwunsch scheint Auswirkungen auf den gesamten
weiteren Lebensverlauf haben zu können (Onnen-Isemann, 1995, 2000). Bisher ist jedoch
wenig dazu bekannt und es wäre interessant zu überprüfen, welche spezifischen Auswirkun-
gen ungewollte Kinderlosigkeit auf weitere Lebensphasen der betroffenen Paare hat.
Hauptfragestellung und Übersicht der Dissertation
14
3. Hauptfragestellung und Übersicht der Dissertation
Die Hauptfragestellung dieser Dissertationsarbeit betrifft die Überprüfung der Wirksam-
keit psychologischer Interventionen auf das psychische Befinden und die Schwangerschafts-
chancen infertiler Patienten. Ausgehend von dieser Hauptfragestellung ergaben sich weitere
Ziele dieser Arbeit wie die Identifikation relevanter Themen und Anliegen infertiler Frauen
und die Entwicklung zwei neuer Behandlungsansätze, wovon einer bereits evaluiert werden
konnte. Somit beinhaltet diese Dissertationsschrift die qualitative Erfassung spezifischer
Themen infertiler Frauen (Artikel 1), einen allgemeinen Überblick über den Stand der For-
schung zu psychologischen Interventionen bei Infertilität (Artikel 2), die Überprüfung der
Wirksamkeit bisheriger psychologischer Unterstützungen mit Hilfe eines metaanalytischen
Verfahrens (Artikel 3), die Entwicklung einer integrativen, psychologischen face-to-face In-
tervention (Artikel 2) und die Entwicklung und Evaluation des ersten deutschsprachigen in-
ternet-basierten Angebots für infertile Patienten in einer randomisierten Studie (Artikel 4).
Der Aufbau dieser Dissertationsarbeit gliedert sich wie folgt: Ein theoretischer Rahmen
der Infertilität wird dargestellt, indem zunächst die Entwicklung der infertilitätsspezifischen
Theorien aufgezeigt wird. Aufgrund der bisher ungenügenden Integration des aktuellen For-
schungsgebiets in allgemeine psychologische Theorien wird Infertilität in drei psychologische
Ansätze eingebettet, woraus sich jeweils insbesondere ein wichtiger Aspekt der Infertilität
erklären lässt. Anhand des konsistenztheoretischen Modells des psychischen Geschehens
nach Grawe (1998, 2003) wird erklärt, welche individuell unterschiedlichen Auswirkungen
Infertilität auf das psychische Funktionieren haben kann. Eine häufig erlebte Reaktion bei
infertilen Patienten sind Verlustgefühle mit resultierender Trauer, welche anhand von zwei
verschiedenen Modellen der Trauer expliziert werden sollen. Schliesslich wird der individuell
unterschiedliche Umgang mit der ungewollten Kinderlosigkeit gemäss dem transaktionalen
Stressmodells von Lazarus und Folkman (1984) erläutert. Aus diesen drei unterschiedlichen
Hauptfragestellung und Übersicht der Dissertation
15
theoretischen Sichtweisen sollen Implikationen für die psychologische Betreuung infertiler
Patienten abgeleitet werden. Danach werden die vier Artikel dieser Dissertationsarbeit kurz
zusammengefasst dargestellt und deren Ausgangsfragestellungen expliziert. Anschliessend
folgen die einzelnen Artikel, deren wichtigste Resultate in der Diskussion zusammengefasst
werden und darauf basierend wird die Hauptfragestellung beantwortet. Abschliessend werden
die Ergebnisse der Artikel mit dem eingangs aufgestellten theoretischen Rahmen in Zusam-
menhang gebracht und weiterführende Fragestellungen und Projekte dargestellt.
Theoretische Einbettung
16
4. Theoretische Einbettung
4.1 Infertilitätsspezifische Theorien
Historisch gesehen dominierten lange Zeit die ungefähr um 1930 entstandenen psychoge-
nen Infertilitätstheorien (Berg & Wilson, 1991; Wischmann, 2003). Dieser psychosomatisch
medizinische Ansatz ging davon aus, dass Fertilitätsstörungen psychische Ursachen haben
(Greil, 1997; Stanton & Dunkel-Schetter, 1991). Insbesondere psychoanalytisch orientierte
Autoren widmeten sich der Frage nach unbewussten Konflikten und Abwehrmechanismen,
welche eine Schwangerschaft erschweren oder verhindern können (Benedek, 1952; Christie,
1994). Kritisiert wurden diese Forschungsbemühungen besonders im Hinblick darauf, dass
die Aussagen meist auf klinischen Einzelfallstudien bzw. kleinen Patientenzahlen basierten
und ausgehend vom klinischen Eindruck Verallgemeinerungen getroffen wurden (Henning &
Strauss, 2000; Wischmann, 2003). Bisher konnte auch in methodisch sorgfältigen Studien
kein wissenschaftlicher Nachweis für die psychische Verursachung von Infertilität im oben
genannten Sinne erbracht werden (Henning & Strauss, 2000; van Balen, 2002; Wischmann,
2003).
Ausgehend von der Zeit der sexuellen Revolution Ende 1970 kamen durch die Erfahrung
des negativen Einflusses der medizinischen Behandlung auf das psychische Befinden inferti-
ler Patienten die psychologischen Konsequenztheorien auf („psychological sequelae oder
psychological consequences theories“; Greil, 1997; Menning, 1980). Gemäss diesen Theorien
wird psychische Belastung als Folge der Infertilität verstanden und nicht als Ursache. Aber
auch dieser Ansatz war nicht frei von Kritik (Greil, 1997). So wurden die Anwendung eines
medizinischen Modells auf die komplexe psychosoziale Erfahrung der Infertilität und der
Nicht-Einbezug von beeinflussenden sozialen und kulturellen Faktoren auf die Auswirkungen
der Infertilität kritisiert (Greil, 1997). Infertilität wird heute überwiegend als psychosomati-
Theoretische Einbettung
17
sche Einheit verstanden, wobei es bisher kein allgemein anerkanntes und empirisch bestätig-
tes Modell der Infertilität gibt (Wischmann, 2003).
Infertilität wurde bisher wenig in allgemeine psychologische Theorien integriert und empi-
risch überprüft. Wie bereits in der Einleitung dieser Arbeit dargestellt, wurden psychische
Aspekte und die dahinter stehenden psychologischen Mechanismen der Infertilität lange Zeit
stark vernachlässigt. Die Wichtigkeit der Beachtung psychischer Aspekte wird durch empiri-
sche Ergebnisse und den subjektiven Leidensdruck infertiler Paare bestätigt. Die im Folgen-
den dargestellte theoretische Einbettung der Infertilität in drei allgemeine psychologische
Theorien soll zu einem umfassenderen Verständnis psychologischer Mechanismen der Inferti-
lität beitragen. Dazu werden die einzelnen Theorien soweit für das Verständnis notwendig
kurz erläutert und danach wird die Infertilität in die jeweilige Theorie integriert. Diese Inte-
gration wird mit bestehenden empirischen Resultaten der Infertilität ergänzt und mit einer
Diskussion abgeschlossen. Der hier dargestellte theoretische Hintergrund hat nicht den An-
spruch umfassend zu sein oder ein neues theoretisches Modell der Infertilität zu begründen.
Vielmehr werden drei Aspekte der Infertilität - individuelle Auswirkungen der Infertilität,
Trauer als häufige Reaktion der Infertilität und Umgang mit Infertilität - dargestellt, woraus
sich wichtige Implikationen für die psychologische Betreuung infertiler Patienten ergeben.
4.2 Infertilität als Inkonsistenzquelle – individuell unterschiedliche Auswirkungen der Inferti-
lität
Die Konsistenztheorie von Grawe (1998, 2004) wird als grundsätzlich bekannt angenom-
men und daher nur kurz dargestellt. Die Konsistenztheorie geht davon aus, dass der menschli-
che Organismus nach der Übereinstimmung bzw. Vereinbarkeit der gleichzeitig ablaufenden
neuronalen resp. psychischen Prozesse strebt. Die psychischen Prozesse sind darauf ausge-
richtet, die Grundbedürfnisse eines Menschen gleichzeitig möglichst gut zu befriedigen.
Theoretische Einbettung
18
Wenn sich diese verschiedenen nach Bedürfnisbefriedigung strebenden Prozesse nicht zuwi-
derlaufen, sind sie konsistent miteinander. Konsistent ist das psychische Geschehen in dem
Ausmass, in dem die realen Erfahrungen mit den intentionalen Schemata kongruent und die
motivationalen Schemata miteinander konkordant sind. So wird das Erleben und Verhalten
eines Menschen unmittelbar von seinen motivationalen Schemata bestimmt. Motivationale
Schemata beinhalten Ziele (Annäherungs- und Vermeidungsziele) und Mittel, die das Indivi-
duum im Laufe seines Lebens entwickelt hat, um seine Grundbedürfnisse zu befriedigen und
sie vor Verletzungen zu schützen. Grawe (1998) nimmt folgende vier Grundbedürfnisse an:
Bedürfnis nach Orientierung und Kontrolle, Lustgewinn/Unlustvermeidung, Bindungsbedürf-
nis und Bedürfnis nach Selbstwerterhöhung und –schutz. Gibt es eine Nichtübereinstimmung
zwischen den aktivierten motivationalen Zielen und der Wahrnehmungen mit der Umgebung
(Inkongruenz) oder eine Nichtvereinbarkeit zweier oder mehrerer gleichzeitig aktivierter mo-
tivationaler Tendenzen (Diskordanz), entsteht Inkonsistenz. Dauerhaft erhöhte Inkonsistenz
geht mit schlechter Gesundheit und der Ausbildung psychischer Störungen einher (Fries &
Grawe, 2006; Grawe, 2004; Grosse Holtforth & Schneider, 2008).
Bei der Integration der Infertilität in die Konsistenztheorie, kann Infertilität als Quelle von
Inkongruenz aufgefasst werden. Wenn ein Paar wiederholt vergeblich versucht ein Kind zu
bekommen, erlebt es jeden Monat beim Eintreten der Monatsblutung eine Diskrepanz zwi-
schen den motivationalen Zielen und der realen Wahrnehmung. Zudem entsteht Diskordanz
beispielsweise, wenn der Wunsch nach einem Kind auf natürlichem Weg besteht, jedoch nur
mit Hilfe medizinischer Unterstützung möglich ist, was wiederum im Konflikt mit den eige-
nen moralischen Einstellungen stehen kann. Somit können beim unerfüllten Kinderwunsch
mehrere Grundbedürfnisse gleichzeitig verletzt sein: Das Bedürfnis nach Orientierung und
Kontrolle ist dadurch verletzt, weil infertile Paare Kontrollverlust in verschiedenen Bereichen
erleben. Beispielsweise Kontrollverlust der eigenen Sexualität und Fruchtbarkeit, der Ver-
Theoretische Einbettung
19
wirklichung der Ziele im Leben und Erleben von Kontrollverlust bei der Inanspruchnahme
von medizinischer Hilfe (Domar & Seibel, 1997; Mahlstedt, 1985). Infertilität kann auch als
unkontrollierbare Inkongruenz nach Grawe (2004) oder als unkontrollierbarer Stress nach
Huether (2005) bezeichnet werden. So entsteht unkontrollierter Stress resp. Inkongruenz in
Situationen, in welchen die wichtigsten Ziele schwer bedroht oder verletzt sind, ohne dass
man etwas dagegen tun kann. Beim unerfüllten Kinderwunsch ist das Ziel eines eigenen Kin-
des bedroht und die persönliche Beeinflussung dieses Zieles scheint (zunächst) nicht gegeben.
Das Bindungsbedürfnis wird dahingehend verletzt, indem die Geburt eines Kindes und damit
die Gründung einer eigenen Familie in Frage gestellt sind. Viele infertile Paare fühlen sich in
ihrem Umfeld sehr isoliert und allein gelassen (Atwood & Dobkin, 1992). Zudem sehen sich
viele Paare häufig mit unangenehmen Fragen und Kommentaren konfrontiert (Wischmann &
Stammer, 2006). Erstaunlicherweise hat sich die Partnerschaftsqualität empirisch als sehr sta-
bil erwiesen, obschon kurzfristige Verschlechterungen in der Partnerschaftszufriedenheit bei-
spielsweise durch die Belastung einer medizinischen Behandlung möglich sind (Cousineau &
Domar, 2007). In Bezug auf das Bedürfnis nach Selbstwerterhöhung und Selbstwertschutz
konnte gezeigt werden, dass infertile Frauen und Männer im Vergleich zu Personen ohne Fer-
tilitätsstörungen einen tieferen Selbstwert aufweisen (Hammarberg, Fisher, & Wynter, 2008;
Verhaak et al., 2007). Schliesslich ist das Bedürfnis nach Lustgewinn und Unlustvermeidung
bei Infertilität verletzt, wenn infertile Paare frühere Aktivitäten, Hobbies und Kontakte als
wichtige Ressourcen einschränken oder sogar aufgeben, aber auch wenn die psychische Bela-
stung zunimmt (Stammer, Wischmann, & Verres, 2002). Die Art und Weise, wie Personen
mit ihrem unerfüllten Kinderwunsch umgehen, beeinflusst, ob die erlebte Belastung resp. In-
konsistenz weiter anhält oder sogar noch zunimmt. Zudem führt die erlebte Diskrepanz zwi-
schen den aktivierten Grundbedürfnissen und der Unmöglichkeit, diese Bedürfnisse zu be-
friedigen zu einer allgemeinen verstärkten neuronalen Aktivierung, welche auch weitere pro-
Theoretische Einbettung
20
blematische Schemata (z. B. „sei perfekt“ oder „vermeide Kontrollverlust“) aktivieren kann.
Dadurch wird die Inkonsistenz weiter erhöht und Vermeidungsziele stärker ausgeprägt. An-
näherungsziele können immer schlechter verwirklicht werden, was zu einer schlechten Be-
dürfnisbefriedigung führt. Aufgrund der hohen Inkonsistenz können psychische Störungen
entstehen, die als ungünstige Ordnungsmuster dysfunktional bezüglich der Bedürfnisbefriedi-
gung sind (Grawe, 1998, 2004).
Durch dieses Modell kann somit erklärt werden, warum insbesondere während der medizi-
nischen Behandlung gehäuft kurzfristig erhöhte psychische Belastungen berichtet werden
(Boivin & Kentenich, 2002; Haemmerli, Znoj, Stoklas, Wunder, & Perrig-Chiello, 2009d). Es
erklärt aber auch, warum nur ein geringer Teil infertiler Patienten unter klinisch relevanten
Belastungen leidet (Leiblum & Greenfield, 1997; Wischmann, 2006). Da sich infertile Patien-
ten neben dem Kinderwunsch in deren allgemeinen Vulnerabilität, den aktuellen Belastungen
und Anforderungen der gegenwärtigen Lebenssituation unterscheiden, gehen sie auch unter-
schiedlich mit der Inkongruenz „Infertilität“ um. Daraus resultiert, dass die psychischen Aus-
wirkungen durch die Infertilität individuell verschieden sind.
4.3 Infertilität als (wiederholter) Trauerprozess – eine häufig erlebte Reaktion
In der allgemeinen Trauerforschung wird betont, dass Trauer ein sehr komplexer Prozess
ist, welcher von Mensch zu Mensch und in verschiedenen Kulturen individuell unterschied-
lich ist (Cowles & Rodgers, 1991; Stroebe, Hansson, Schut, & Stroebe, 2008; Znoj, 2004).
Trauer an sich ist keine Krankheit und meist ist keine psychologische Unterstützung notwen-
dig. Dennoch sind Verlustereignisse mit einem erhöhten Sterblichkeitsrisiko, einer Verminde-
rung der körperlichen Gesundheit und einer erhöhten Nutzung von Gesundheitsdiensten ver-
bunden (Stroebe, Schut, & Stroebe, 2007). Es gibt zwar keine genormten Trauerreaktionen,
jedoch lassen sich durchaus Grundzüge der Trauerreaktion beschreiben (Znoj, 2004; Znoj &
Theoretische Einbettung
21
Maercker, 2005). So dauert die Trauer meist länger als allgemein angenommen und ist beglei-
tet von unterschiedlichen, intensiven Gefühlen wie Angst, Schuld, Wut und Traurigkeit. Wie
eine Person nach einem Verlust reagiert ist davon abhängig, welche Bedeutung der Verlust
für sie hat (Neimeyer, 2001). Der Begriff „Bedeutung“ wird dabei unterschiedlich interpre-
tiert. Kognitive Stresstheorien meinen mit diesem Begriff den Bewertungsprozess im Umgang
mit dem Verlust und dessen Beziehung zur Bewältigung und Anpassung (Lazarus & Folk-
man, 1984). Aus der Perspektive der Bindungstheorien ist damit die Bedeutung der Bezie-
hung zur verstorbenen Person gemeint, wobei die Trauer universal als Produkt biologisch
determinierter Bindung betrachtet wird (Bowlby, 1980). Bis heute gibt es noch kein allgemein
gültiges Modell in der Trauerforschung (Stroebe, Stroebe, & Hansson, 1993).
Bei der ungewollten Kinderlosigkeit wird einerseits zu Beginn bei der Diagnose ein
schwerer Verlust erlebt, andererseits werden aber auch sukzessive Anhäufungen von Verlust-
erlebnissen über die Zeit beschrieben (Burns & Covington, 2006). So erfährt ein Paar jeden
Monat erneut mit dem Einsetzen der Menstruation ein Gefühl von Trauer – ausgelöst durch
den Verlust der erhofften Schwangerschaft. Die Erfahrung der Infertilität wird oft von den
betroffenen Paaren mit dem Verlust eines nahe stehenden Angehörigen (Domar, Broome,
Zuttermeiser, Seibel, & Friedman, 1992; Kerr et al., 1999) oder mit der Trauer bei einer un-
heilbaren Krankheit oder bei einem Todesfall verglichen (Cooper-Hilbert, 2001; McDaniel,
Hepworth, & Doherty, 1992). Das Verlustgefühl bezieht sich dabei auf mehrere Bereiche:
Selbstwertverlust (durch die Tatsache nicht fähig zu sein schwanger zu werden), Verlust der
Sexualität (durch die veränderte Sexualität oder den Wegfall dieser), Gefühle von Kontroll-
verlust über das eigene Leben und die eigenen Ziele, Verlust der Privatsphäre (aufgrund der
intrusiven medizinischen Behandlung), Verlust von wichtigen Beziehungen, Verlust von Si-
cherheit, Abschied von wichtigen Lebensplänen (eine Familie zu gründen) und der Verlust
Theoretische Einbettung
22
der Hoffnung ein eigenes Kind zu erziehen (Conway & Valentine, 1987; Mahlstedt & John-
son, 1987).
Infertilität ist geprägt von tiefen Verlustgefühlen mit Trauerreaktionen (Kemeter & Fiegl,
1998). Trauer und Depression sind die am meisten genannten emotionalen Reaktionen bei
infertilen Patienten, welche in 77 % der Artikel zitiert wurden, während Angst nur in 40 %
der Artikel erwähnt wurde (Dunkel-Schetter & Lobel, 1991). Gleich wie bei der allgemeinen
Trauer gehen bei der Infertilität verschiedene Gefühle mit der Trauer einher (Burns & Co-
vington, 2006). Das Ausmass der Trauer wird zudem ebenfalls direkt in Beziehung zur Stärke
der Bindung (dem Wunsch nach Elternschaft resp. nach einem Kind) gesetzt (Burns & Co-
vington, 2006). Die Verarbeitung von Verlusten hat eine Wirkung auf die Langzeitanpassung
der Paare und auch auf die zukünftigen Entscheidungen bezüglich der medizinischen Behand-
lung und möglicher Alternativen (Burns & Covington, 2006).
Es werden im Folgenden zwei Modelle aus der Trauerforschung dargestellt, in welche die
Infertilität integriert wird. Als erstes Erklärungsmodell werden die Phasenmodelle der Trauer
erläutert. Mehrere Autoren haben den Trauerprozess untersucht und Phasen der Trauer be-
schrieben (Bowlby, 1980; Glick, Weiss, & Parkes, 1974; Pollock, 1987). Bowlby (1961,
1980) und Parkes (1972; Parkes & Weiss, 1983) waren die ersten, welche folgende vier Pha-
sen des Trauerprozesses beschrieben haben: Schock – Taubheit, Sehnsucht – Suche, Desorga-
nisation – Verzweiflung und Reorganisation. Kübler-Ross (1969) adaptierte die Theorien von
Bowlby (1961, 1980) und Parkes (1972) und beschrieb 5 Stufen: Verleugnung-Abspaltung-
Isolation, Wut, Verhandeln, Depression und Akzeptanz. Trauer ist jedoch kein linearer Pro-
zess mit klar abgrenzbaren Stufen, vielmehr eine Zusammensetzung von überlappenden und
fliessenden Phasen, welche von Person zu Person unterschiedlich sind. Die Phasentheorien
der Trauer wurden bisher kaum untersucht und sind deshalb noch nicht empirisch bestätigt
(Shuchter & Zisook, 1993; Znoj, 2004). In einer ersten empirischen Untersuchung konnten
Theoretische Einbettung
23
gewisse Phasen im Trauerprozess bestätigt werden (Maciejewski, Zhang, Block, & Prigerson,
2007).
Abgesehen davon sind Phasenmodelle heuristisch sehr wertvoll und wurden auch schon
zur Erklärung der Infertilität angewandt. Atwood und Dobkin (1992) definierten vier Phasen
der Trauer beim unerfüllten Kinderwunsch, welche oft mehrfach durchlaufen werden: 1) Un-
glaube und Verleugnung, 2) Angst, Wut und Kontrollverlust, 3) Isolation, Entfremdung,
Schuld, tiefer Selbstwert, Kummer und Depression und 4) Auflösung. Phase 3 wird als die
belastendste Phase im Trauerprozess beschrieben, während dieser auch die meisten Paare
psychologische Unterstützung aufsuchen. Mehrere Parallelen der allgemeinen Phasenmodelle
der Trauer sind zu den oben genannten Phasenmodellen der Infertilität zu erkennen. Dennoch
scheint ein wichtiger Unterschied zu sein, dass beim unerfüllten Kinderwunsch die Trauer erst
dann vollständig aufgelöst und integriert werden kann, wenn das Paar den Kontrollverlust
über die eigene Fruchtbarkeit akzeptiert oder sogar erst wenn es entweder die Elternschaft
erreicht hat oder die Kinderlosigkeit akzeptieren konnte (Unruh & McGrath, 1985; Watkins &
Baldo, 2004). Nicht allen Paaren gelingt jedoch diese Verarbeitung der Trauer vollständig
(Watkins & Baldo, 2004). Unabhängig von der Auflösung der Trauer scheint in gewissen
Lebensphasen der Paare die Trauer über diese Erfahrung wieder aufzutauchen (Unruh &
McGrath, 1985).
Die auch in der Infertilität vorherrschenden psychodynamisch orientierten Phasenmodelle
(z. B. Freud, 1917) fordern die Auflösung der Trauer, damit neue Bindungen und Beziehun-
gen eingegangen werden können. Der Verlust ist dann verarbeitet, wenn das Bestehen einer
emotionalen Bindung zur verstorbenen Person beendet ist, wodurch die Aufnahme einer neu-
en, engen Beziehung möglich wird. Dem gegenüber steht in der allgemeinen Trauerforschung
die Auffassung der „Continuing Bonds“, wobei Beziehungen zur verstorbenen Person fortbe-
stehen können (Rothaupt & Becker, 2007). Der damit verbundene Begriff „Meaning Recon-
Theoretische Einbettung
24
struction“ beschreibt die Aufgabe der Trauer in der Integration des Verlustes in die Lebens-
welt des Trauernden (Neimeyer, 2001). So gibt es insbesondere in der westlichen Welt zwei
konkurrierende Trauerauffassungen: die kontinuierliche Form der Trauer und die Auflösung
der Beziehung zur verstorbenen Person in relativ kurzer Zeit (wenige Monate bis höchstens
wenige Jahre; Znoj, 2004). Bisher wurde beim unerfüllten Kinderwunsch die Auffassung der
Integration des Verlustes in die Lebenswelt der infertilen Paare kaum beachtet. Es ist dem-
nach noch unklar, ob diese Sichtweise sinnvoll ist und welche Implikationen dies für die Be-
ratung infertiler Paare haben könnte.
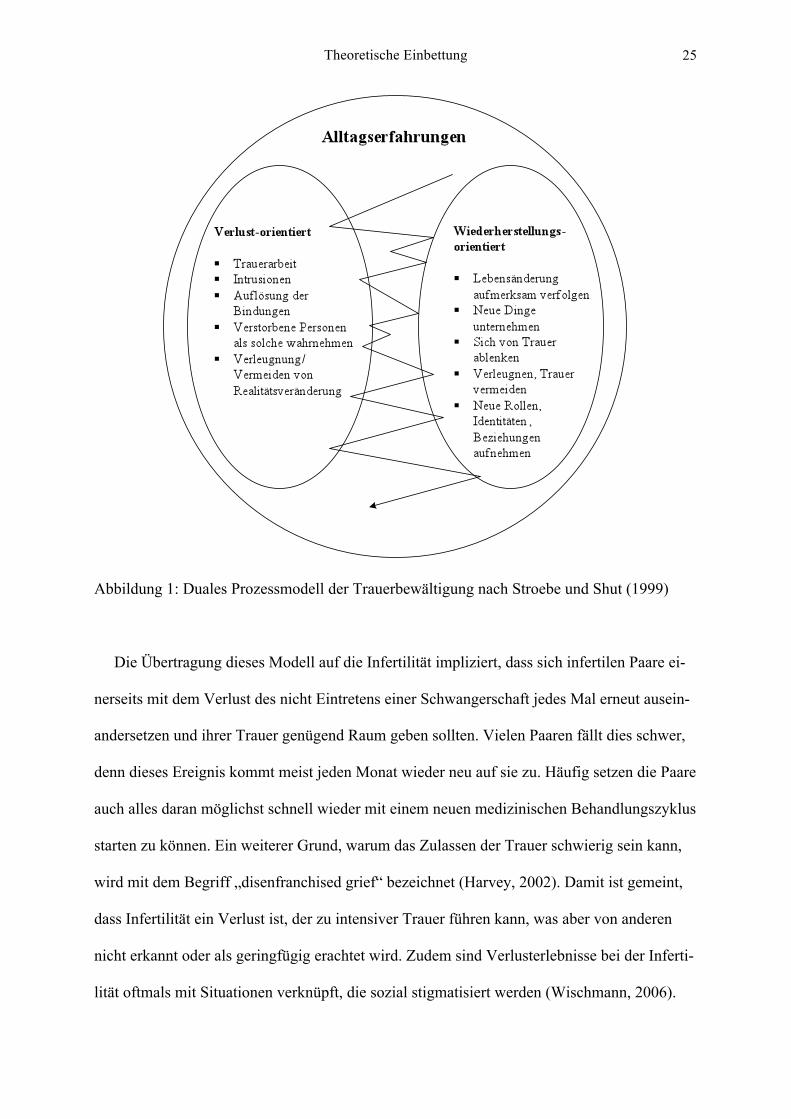
Mit der Darstellung der Infertilität anhand des zweiten Trauermodells soll ein Ausblick in
diese Richtung gemacht werden. Das duale Prozessmodell der Trauer von Stroebe und Shut
(1999; siehe Abbildung 1) integriert die beiden oben genannten Trauerauffassungen als
gleichwertige Sichtweisen und impliziert wichtige Mechanismen der Bewältigung. Die er-
folgreiche Adaptation der Trauer hängt gemäss dem Prozessmodell von der gelungenen Ba-
lance von Trauerarbeit und aktiver Zuwendung zu neuen Aufgaben ab. Damit ist gemeint,
dass durch ein regelmässiges Abwechseln - auch Oszillieren genannt - zwischen der emotio-
nalen und gedanklichen Auseinandersetzung mit dem Verlust und dem Kümmern um Anfor-
derungen und um neue Aufgaben aus der Umwelt eine optimale Verarbeitung der Trauer
möglich ist. Wenn bei der Verarbeitung des Verlustes auch positive Gefühle zugelassen wer-
den können und der Verlust als Chance gesehen werden kann, kann die Verarbeitung des
Verlustes besser und schneller gelingen (Bonanno, 2004; Bonanno & Keltner, 1997).
Theoretische Einbettung
25
Abbildung 1: Duales Prozessmodell der Trauerbewältigung nach Stroebe und Shut (1999)
Die Übertragung dieses Modell auf die Infertilität impliziert, dass sich infertilen Paare ei-
nerseits mit dem Verlust des nicht Eintretens einer Schwangerschaft jedes Mal erneut ausein-
andersetzen und ihrer Trauer genügend Raum geben sollten. Vielen Paaren fällt dies schwer,
denn dieses Ereignis kommt meist jeden Monat wieder neu auf sie zu. Häufig setzen die Paare
auch alles daran möglichst schnell wieder mit einem neuen medizinischen Behandlungszyklus
starten zu können. Ein weiterer Grund, warum das Zulassen der Trauer schwierig sein kann,
wird mit dem Begriff „disenfranchised grief“ bezeichnet (Harvey, 2002). Damit ist gemeint,
dass Infertilität ein Verlust ist, der zu intensiver Trauer führen kann, was aber von anderen
nicht erkannt oder als geringfügig erachtet wird. Zudem sind Verlusterlebnisse bei der Inferti-
lität oftmals mit Situationen verknüpft, die sozial stigmatisiert werden (Wischmann, 2006).
Theoretische Einbettung
26
Da die herkömmliche Unterstützung bei der Verarbeitung oft fehlt, kann bei der Infertilität
der Verlust belastender sein (Harvey, 2002). Das Modell betont andererseits die Wichtigkeit,
dass sich infertile Paare um Ziele und Aufgaben in ihrem Leben neben dem Kinderwunsch
kümmern sollen. Es kommt aber leider häufig vor, dass Paare im Laufe ihrer Kinderwunsch-
zeit wichtige Bereiche in ihrem Leben vernachlässigen oder gar einschränken (Stammer et al.,
2002). Deshalb ist die Beibehaltung der Lebensbereiche neben dem Kinderwunsch als wichti-
ge Ressourcen bedeutsam für die Verarbeitung der Verlusterlebnisse.
4.4 Verarbeitung der ungewollten Kinderlosigkeit und Umgang damit
Stress- und Copingtheorien wurden von verschiedenen Autoren auf die Infertilität übertra-
gen. So wird Infertilität als ein Stressor (oder eine Krise) beschrieben, welcher durch Unvor-
hersagbarkeit, Negativität, Unkontrollierbarkeit und Ambiguität charakterisiert wird (Stanton
& Dunkel-Schetter, 1991; Taylor, 1990; Taymor & Bresnick, 1979). Dabei erleben infertile
Paare die ungewollte Kinderlosigkeit einerseits als Bedrohung (z. B. durch den Verlust der
eigenen Fruchtbarkeit) und andererseits als Gewinn (z. B. durch die Verbesserung der Part-
nerschaftszufriedenheit; Eckert, Sobeslavsky, & Held, 1998; Greil, 1991). Infertilität als
Stressor kann dabei als kontrollierbar (z. B. bezüglich der Entscheidung für oder gegen eine
medizinische Behandlung) und als unkontrollierbar (z. B. schwanger zu werden) erlebt wer-
den. Insbesondere der Umgang mit dieser bedrohenden und unkontrollierbaren Seite der In-
fertilität, analog zur oben genannten Auffassung der Infertilität als unkontrollierte Inkongru-
enz (Grawe, 2004) oder unkontrollierbarer Stress (Huether, 2005), ist eine grosse Herausfor-
derung für infertile Paare. Infertile Paare erleben beispielsweise die Diagnose als einen ein-
zelnen akuten Stressor resp. als zeitlich limitierte Krise. Die meisten infertilen Paare nehmen
die ungewollte Kinderlosigkeit aber als chronischen Stressor wahr, wobei sich über die Zeit
hinweg die emotionale Belastung und die Herausforderungen anhäufen können (Burns & Co-
Theoretische Einbettung
27
vington, 2006). Dabei sind verschiedenen Copingstrategien notwendig, um unabhängig vom
Ergebnis eine erfolgreiche Verarbeitung, Anpassung und Aufrechterhaltung des emotionalen
und partnerschaftlichen Gleichgewichts aufrechtzuerhalten.
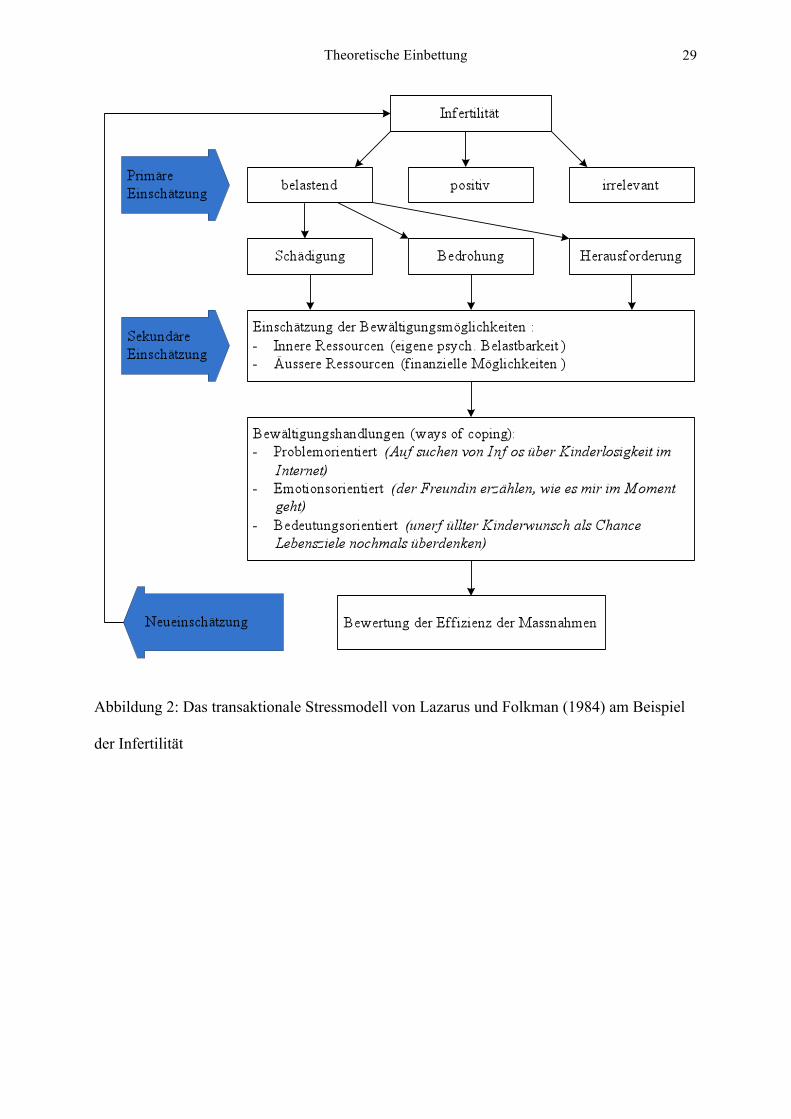
Die Darstellung der Infertilität anhand des transaktionalen Stressmodells (Lazarus &
Folkman, 1984) erklärt, 1) warum Infertilität als unterschiedlich stressvoll erlebt wird, 2) be-
schreibt Faktoren, welche eine Anpassung erleichtern oder verhindern und 3) gibt Hinweise
darauf, wo psychologische Interventionen ansetzen könnten. Es wird aufgrund der breiten
Bekanntheit des transaktionalen Stressmodells darauf verzichtet dieses zu erklären, sondern
direkt Infertilität in das Modell integriert (siehe Abbildung 2). Das Modell geht davon aus,
dass mehrere Bewertungsprozesse darüber entscheiden, ob ein Individuum ein Ereignis als
belastend empfindet und entsprechende Bewältigungshandlungen (Coping) initiiert. Ange-
wandt auf die Infertilität wird zunächst bei der primären Bewertung die ungewollte Kinderlo-
sigkeit danach bewertet, ob sie belastend, positiv oder irrelevant erscheint. Meist erleben die
Paare die Infertilität nach der primären Einschätzung als Belastung. Nun wird in einem näch-
sten unbewussten Bewertungsschritt eingeschätzt, ob der unerfüllte Kinderwunsch als Schä-
digung, Bedrohung oder Herausforderung wahrgenommen wird. Je nachdem wie die Infertili-
tät erlebt wird, werden in der sekundären Bewertung die Bewältigungsmöglichkeiten nach
Vorhandensein der inneren und äusseren Ressourcen eingeschätzt. Eine Stressreaktion wird
nun nur dann ausgelöst, wenn die betroffene Person zum Schluss kommt, dass ihre Bewälti-
gungsmöglichkeiten im Umgang mit der Infertilität ungenügend sind. Lazarus und Folkman
(1984) unterscheiden zwischen zwei Arten von Bewältigungshandlungen: Während das pro-
blemorientierte Coping direkt versucht die stressauslösende Situation zu beeinflussen, wird
das emotionsorientierten Coping vor allem dann eingesetzt, wenn die Person glaubt die Situa-
tion an sich aktuell nicht beeinflussen zu können und deshalb das Ziel die Regulation der
Stressemotionen ist. Im Umgang mit der Infertilität sind beide Bewältigungsarten sehr wirk-
Theoretische Einbettung
28
sam (Stanton, 1991). Problemorientiertes Coping hilft den Paaren Entscheidungen bezüglich
medizinischer Behandlung und alternativen Wegen zu treffen. Da Infertilität oftmals länger
andauert und als unkontrollierbar erlebt wird, ist emotionsorientiertes Coping zur Bewälti-
gung der psychischen Belastung sehr entscheidend. Folkman (1997) hat als eine weitere Be-
wältigungsart das bedeutungsorientierte Coping hinzugefügt, wobei es um eine Neubewer-
tung der Situation geht. Bei der Infertilität könnte dies beispielsweise sein, dass das Paar die
positiven Seiten ihrer ungewollten Kinderlosigkeit sieht. Abschliessend wird aufgrund der
durchgeführten Bewältigungsstrategie eine Neubewertung der Situation gemacht. In der Co-
pingliteratur wurde der Zusammenhang zwischen der Art des Copings und der erlebten Bela-
stung oft bestätigt (Austenfeld & Stanton, 2004). Bei der Infertilität zeigte sich, dass aktiv-
vermeidende Copingstrategien mit einem höheren Stresslevel einhergehen (Schmidt, Holen-
stein, Christensen, & Boivin, 2005). Somit scheinen die Art der Bewertung der Infertilität und
der Umgang damit sehr relevant für das psychische Wohlbefinden zu sein.
Theoretische Einbettung
29
Abbildung 2: Das transaktionale Stressmodell von Lazarus und Folkman (1984) am Beispiel
der Infertilität
Implikationen der drei theoretischen Ansätze für psychologische Interventionen bei infertilen Patienten
30
5. Implikationen der drei theoretischen Ansätze für psychologische Interventionen bei
infertilen Patienten
Psychologische Intervention bei infertilen Patienten sind nicht per se indiziert, sondern
insbesondere dann sinnvoll, wenn die psychische Belastung nicht mehr selber bewältigt wer-
den kann oder auch als Unterstützung in stressreichen Zeiten beispielsweise während einer
medizinischen Behandlung (Boivin, 2003). Verschiedene Ziele und Aufgaben psychologi-
scher Interventionen wurden in der Literatur genannt (Burns & Covington, 2006; Wischmann,
2006). Je nach Situation des infertilen Paares sind unterschiedliche Arten psychologischer
Interventionen notwendig. Verschiedene mögliche Ansatzpunkte abgeleitet von den drei theo-
retischen Modellen sollen im Folgenden diskutiert werden, wobei dabei nicht der Anspruch
an eine umfassende Übersicht zu psychologischen Interventionen bei infertilen Patienten be-
steht.
Die Konsistenztheorie betont genau diese individuelle Sichtweise (Grawe, 1998). Die auf-
grund der Infertilität entstandene Inkongruenz im psychischen Geschehen der Patienten kann
über die Bearbeitung der identifizierten Quellen der Inkongruenz reduziert werden (Grosse
Holtforth & Grawe, 2004). Dabei gilt es individuell zu schauen, in welchen Bereichen aktuell
Belastungen vorliegen und mit welchen Interventionen dabei geholfen werden kann. So kann
es beispielsweise bei einem Paar, welches vor kurzem erfahren hat, dass es auf natürlichem
Weg keine Kinder bekommen kann, angezeigt sein, über Infertilität aufzuklären und Informa-
tionen zu geben. Nicht direkt mit der Infertilität in Zusammenhang stehende Bereiche wie z.
B. Unzufriedenheit bei der Arbeit, sind ebenfalls zu beachten und auch dort soll Unterstüt-
zung angeboten werden. Solche weitere Inkongruenzquellen können zusätzlich dazu beitra-
gen, dass sich die psychische Belastung erhöht. Sehr wichtig sind der Einbezug und die Stär-
kung positiver Lebensbereiche und eigener Ressourcen, da bei der Infertilität und deren medi-
zinischer Behandlung häufig die Problemorientierung überwiegt.
Implikationen der drei theoretischen Ansätze für psychologische Interventionen bei infertilen Patienten
31
In der Arbeit mit infertilen Paaren sollte den wiederholten Verlusterlebnissen begleitet von
Trauerreaktionen besondere Aufmerksamkeit geschenkt werden. Damit ist nicht gemeint, dass
bei jedem Trauerprozess interveniert werden sollte. Aus der allgemeinen Trauerforschung ist
bekannt, dass therapeutische Unterstützung die natürliche Trauerreaktion kaum beeinflussen
kann resp. sogar negative Ergebnisse daraus resultieren können (Znoj, 2004). Der Trauer
während der Infertilität sollte besondere Beachtung geschenkt werden, weil Infertilität zu
starken Trauergefühlen führen kann, welche aber oft zu wenig erkannt und welchen einen zu
geringen Stellwert gegeben wird („disenfranchised grief“; Harvey, 2002). Das Fehlen der
Anerkennung und das ungenügende Verarbeiten der Verluste kann einen negativen Einfluss
auf die längerfristige Anpassung der infertilen Patienten haben (Burns & Covington, 2006).
Es erscheint wichtig die erlebte Trauer der infertilen Paare zu normalisieren und zu validieren
(Daniluk, 2001; Forrest & Gilbert, 1992). Infertile Paare sollten auch dazu ermutigt werden,
die Trauer zuzulassen und sich für deren Verarbeitung genügend Zeit zu nehmen (z. B. nach
einem negativen Schwangerschaftstest nicht gleich wieder mit der nächsten medizinischen
Behandlung zu starten). Während Frauen der Trauer meistens einen emotionaleren Ausdruck
verleihen, drücken Männer ihre Trauer häufig verdeckter und weniger beobachtbar aus (Burns
& Covington, 1999). Das kann dazu führen, dass die Männer zur „vergessenen Trauerge-
meinde“ werden. Deshalb ist es wichtig, den Mann in seiner Trauer gleichwertig zu beachten.
Psychologische Unterstützung ist indiziert, wenn der Trauerprozess nicht durchlaufen werden
kann und jemand in einer Phase des Trauerprozesses feststeckt. Hier ist aber zu beachten, dass
bei Infertilität auch von chronischer Trauer gesprochen wird, welche nach unterschiedlichen
Meinungen von Autoren erst mit der Akzeptanz über den Kontrollverlust der eigenen Frucht-
barkeit (Watkins & Baldo, 2004), dem Erreichen der Elternschaft oder der Akzeptanz der
Kinderlosigkeit aufgelöst werden kann (Burns & Covington, 2006). Im Allgemeinen scheint
sicherlich einerseits die Unterstützung der Akzeptanz des aktuell unerfüllten Kinderwunsches
Implikationen der drei theoretischen Ansätze für psychologische Interventionen bei infertilen Patienten
32
(unabhängig von der Frage, ob eine endgültige Auflösung des Trauerprozesses erst nach Er-
reichung der Elternschaft oder dem Abschied des Kinderwunsches möglich ist) und anderer-
seits die Förderung der Aktivitäten ausserhalb des Kinderwunsches und der Betrachtung al-
ternativer Perspektiven wichtig zu sein (Stammer et al., 2004). Genau diese Balance von
Trauerarbeit und aktiver Zuwendung neuer Aufgaben beschreibt das duale Prozessmodell der
Trauer als Voraussetzung für eine erfolgreiche Adaptation (Stroebe & Shut, 1999). Bei der
psychologischen Unterstützung infertiler Patienten ist demnach darauf zu achten, dass diese
Balance vorhanden ist.
Generell können Paare im Umgang mit der Kinderlosigkeit und deren medizinischen Be-
handlung unterstützt werden. Dabei können verschiedene Arten von Bewältigungsstrategien
je nach Situation günstig sein (Stanton, 1991). Da insbesondere vermeidungsorientiertes Co-
ping mit erhöhtem Stress einhergeht, ist es wichtig diese Bewältigungsstrategien durch andere
zu ersetzen (Schmidt et al., 2005; Terry & Hynes, 1998). Dabei sollte der Tatsache Rechnung
getragen werden, dass Frauen und Männer unterschiedlich mit dem unerfüllten Kinderwunsch
umgehen (Watkins & Baldo, 2004). Den Paaren soll insbesondere geholfen werden, wieder
ein Gefühl von Kontrolle über ihr Leben zu erlangen (Atwood & Dobkin, 1992; Cooper-
Hilbert, 2001). Dabei liegt der entscheidende Weg zur Wiedererlangung der Kontrolle im
Entscheidungsprozess über das eigene Leben. Das Ziel ist, dass das Paar die Kontrolle über
ihre Fruchtbarkeit loslassen kann, aber die Kontrolle über die eigenen Lebensentscheidungen
(z. B. für oder gegen eine nächste medizinische Behandlung) wieder erhält (Daniluk, 2001).
So gelingt es auch Infertilität als Stressor kontrollierbarer und dadurch weniger bedrohlich zu
erleben.
Vorgelegte Artikel
33
6. Vorgelegte Artikel
6.1 Kurzzusammenfassungen der vier Artikel
Im Rahmen dieser Forschungsarbeit sind insgesamt 7 Artikel entstanden, wovon 4 Artikel
in die vorliegende Dissertation eingeschlossen wurden. Im Folgenden soll kurz der jeweilige
Hintergrund und die Fragestellungen der vier Artikel dargestellt werden.
Artikel 1: What are the issues infertile women are dealing with?: A qualitative approach
Trotz der wachsenden Forschung im Bereich psychologischer Interventionen bei infertilen
Patienten ist wenig über die spezifischen Probleme und Anliegen infertiler Patienten bekannt.
Ein genaues Verständnis der Themen infertiler Patienten ist jedoch die Voraussetzung für die
Entwicklung effektiver psychologischer Interventionen. Deshalb versucht dieser Artikel mit
Hilfe einer qualitativen Inhaltsanalyse relevante Themen infertiler Frauen zu identifizieren
und mögliche Beziehungen dieser zum psychischen Befinden herzustellen.
Artikel 2: Psychological interventions for infertile patients: A review of existing research
and a new comprehensive approach
Im zweiten Artikel wird ein systematischer Überblick über das Forschungsthema „psycho-
logische Interventionen bei infertilen Patienten“ gegeben. Ausgehend von dem im ersten Teil
des Artikels gegebenen Überblick, wird die psychologische Gruppenintervention, welche im
Rahmen des Forschungsprojektes des Schweizerischen Nationalfonds (SNF-Nr. 325100 -
11375411) aktuell durchgeführt wird, theoretisch abgeleitet und dargestellt. Erste Resultate
zur Durchführbarkeit der Gruppenintervention sind abschliessend in diesem Artikel präsen-
tiert.
Vorgelegte Artikel
34
Artikel 3: The efficacy of psychological interventions for infertile patients: a meta-
analysis examining mental health and pregnancy rate
Zur Beantwortung der Fragestellung, ob psychologische Interventionen bei infertilen Pati-
enten zur Verbesserung des psychischen Befindens oder sogar zur Steigerung der Schwanger-
schaftsraten führen, wurde eine Metaanalyse gemacht. Ausgangspunkt dafür waren zwei frü-
here Reviews (Boivin, 2003; De Liz & Strauss, 2005), welche insbesondere in Bezug auf die
Schwangerschaftsrate zu unterschiedlichen Resultaten gekommen sind. Deshalb war das Ziel
dieser Metaanalyse durch eine Einschränkung auf methodisch bessere Studien und eine
grössere Anzahl von Studien definitivere Antworten auf die eingangs genannte Frage geben
zu können.
Artikel 4: Internet-Based Support for Infertile Patients: A Randomized Controlled
Study
Ausgehend von den folgenden Gründen wurde ein internet-basiertes Programm für inferti-
le Patienten entwickelt: Während des SNF-Forschungsprojektes gab es immer wieder Rekru-
tierungsschwierigkeiten, wobei die teilnehmenden Paare gleichzeitig die Rückmeldung gaben,
dass es zu wenig psychologische Unterstützungsangebote bei unerfüllten Kinderwunsch ge-
ben würde. Die auch in der Literatur beschriebene geringe Nutzung von psychologischen An-
geboten bei Infertilität kann auf Angst vor Stigmatisierung, Skepsis über die Wirksamkeit
einer solchen Unterstützung und Angst vor emotionaler Destabilisierung zurückgeführt wer-
den (Boivin, Scanlan, & Walker, 1999; Wischmann, 2008). Immer mehr Personen mit uner-
fülltem Kinderwunsch suchen jedoch Austausch und Unterstützung im Internet (Cousineau &
Domar, 2007). Aus der Literatur ist mir bisher nur ein internet-basiertes psychologisches Be-
handlungsprogramm für infertile Patienten bekannt, welches positive Effekte auf das psychi-
Vorgelegte Artikel
35
sche Befinden gezeigt hat (Cousineau et al., 2008). Auf diesem Hintergrund wurde das erste
deutschsprachige internet-basierte Programm – Kinderwunsch Online Coaching
(www.kinderwunsch.online-therapy.ch) – für infertile Patienten entwickelt. Dafür wurde ei-
gens ein Manual geschrieben, Teilnehmer wurden rekrutiert und eine randomisierte kontrol-
lierte Studie durchgeführt. In diesem vierten Artikel wird die Beschreibung und Evaluation
des Programms dargestellt.

Artikel 1
Haemmerli, K., Znoj, H., & Berger, T. (submitted). What are the issues in-
fertile women are dealing with?: A qualitative approach.
Running head: Issues important to infertile women
What are the Issues Confronting Infertile Women?
A Qualitative Approach
Katja Haemmerli
University of Bern, Bern, Switzerland
Hansjörg Znoj
University of Bern, Bern, Switzerland
Thomas Berger
University of Bern, Bern, Switzerland
Ms. Katja Haemmerli, University of Bern, Institute of Psychology, Department of Clinical Psychology
and Psychotherapy, Gesellschaftsstrasse 49, 3012 Bern, Switzerland, Tel.: 0041 31 631 45 83, Fax:
0041 31 631 41 55, email: [email protected]
Prof. Dr. Hansjörg Znoj, University of Bern, Institute of Psychology, Department of Clinical Psychol-
ogy and Psychotherapy, Gesellschaftsstrasse 49, 3012 Bern, Switzerland, Tel.: 0041 31 631 45 91,
Fax: 0041 31 631 41 55, email: hansjö[email protected]
Dr. Thomas Berger, University of Bern, Institute of Psychology, Department of Clinical Psychology
and Psychotherapy, Gesellschaftsstrasse 49, 3012 Bern, Switzerland, Fax: 0041 31 631 41 55, email:
Katja Haemmerli, MSc., Ph.D. student at the Department of Clinical Psychology and Psychotherapy
of the University of Bern, Bern, Switzerland

Hansjörg Znoj, is the professor at the Department of Clinical Psychology and Psychotherapy of the
University of Bern, Bern, Switzerland
Thomas Berger, Dr., is a post-doch assistant at the Department of Clinical Psychology and Psycho-
therapy of the University of Bern, Bern, Switzerland

Abstract
Infertility is a stressful experience but little is known about the specific issues infertile women are
dealing with. The aim of the present study is to identify themes important to infertile women and ex-
amine possible associations with mental health levels. Emails of 57 infertile women who participated
in a German-language Internet-based treatment to infertility were analyzed by qualitative content an-
alysis. The themes most important to infertile women were emotions surrounding their wish for a
child, coping with this unfulfilled wish, and medical aspects. Clinically anxious women reported sub-
stantially and significantly more negative and positive emotions than non-anxious women did (Mann-
Whitney U(1)=178; p=0.034). Participants who were both clinically anxious and depressed reported
more negative emotions and substantially fewer positive emotions when compared to participants who
were solely anxious. The themes identified, considered important by infertile women, could be helpful
to health professionals working in fertility treatment.
Key words: counseling, distress, emotions, infertility, Internet, pregnancy, psychological issues, re-
productive medicine, women’s health
Infertility is a stressful experience (Menning, 1980). But what exactly is meant by stressful experi-
ence in this context? What are the key issues confronting infertile patients? Little is known about the
specific themes and burdens affecting infertile patients.
Many psychological studies have focused on the psychological consequences of infertility and its
medical treatment. For instance, the effects of assisted reproductive treatment (ART) have frequently
been discussed in the literature: ARTs are considered the most stressful techniques used to treat infer-
tility (Eugster & Vingerhoets, 1999). Undergoing ART presents a physical and emotional burden as-
sociated with high levels of depressive symptoms, anxiety, and distress (Brkovich & Fisher, 1998;
Chen, Chang, Tsai, & Juang, 2004; Eugster & Vingerhoets, 1999; Greil, 1997). The waiting period
between embryo transfer and pregnancy test as well as the failure of such pregnancy attempts are de-
scribed as presenting great strains for infertile patients (Boivin & Takefman, 1995; Klonoff-Cohen,
Chu, Natarajan, & Sieber, 2001; Verhaak, Smeenk, Nahuis, Kremer, & Braat, 2007). In addition,
stress surrounding infertility may be attributed to any number of specific issues, including prevention
or postponement of an important life goal (having a child), the cyclic nature of treatment, the side
effects of fertility medications, or marital conflicts related to infertility (Mahlstedt, 1985). Neverthe-
less, overall levels of mental distress, anxiety, and depression found among infertile patients do not
appear to differ much from those observed in general populations (Covington & Burns, 2006; Dunkel-
Schetter & Lobel, 1991; Leiblum & Greenfeld, 1997). High levels of mental distress found among
infertile patients are often interpreted as short-term reactions (Chen et al., 2004; Eugster & Vinger-
hoets, 1999; Wischmann, 2005).
Historically, the psychological impact of infertility was first examined using qualitative methods
(Valentine, 1986). Based on initial qualitative findings, numerous quantitative studies followed. These
studies used standard instruments and designs in order to acquire data on the impact of infertility on
individuals’ mental health and on couples’ relationships (Hammerberg, Astbury, & Baker, 2001;
Slade, Emery, & Lieberman, 1997).
In recent years, the importance of qualitative research in this area has once again gained attention
(Green, Galvin, & Home, 2003; Peddie, van Teijlingen, Bhattacharya, 2005; Redshaw, Hockley, &
Davidson, 2007). However, to the best of our knowledge, no qualitative studies have been undertaken
that investigate the psychosocial issues considered important by infertile patients as well as infertile
patients’ responses to these issues. Thus, the aim of the present study was to identify these critical
themes and corresponding patient responses. In addition, we were interested in possible associations
between specific responses to infertility and levels of mental health as measured by standard self-
report questionnaires. The findings of qualitative research supply a richness of detail that is often ab-
sent in quantitative studies and may provide additional insights into the complexity of infertile
women’s psychological reactions and their impact on personal mental health.
Methods
Study design and participants
The data used in this study derive from the Child Wish Online Coaching project (unpublished ob-
servation). This 8-week Internet-based treatment for infertile patients consists of several components,
including a self-help guide based on a cognitive-behavioral approach. In the course of the treatment,
participants also receive assistance and support from a therapist via email. In this way, participants are
encouraged to discuss important issues surrounding their unfulfilled wish for a child with a therapist
online. The emails exchanged between patients and therapists in the context of this project constituted
the data analyzed in the present study.
The study sample was recruited by means of articles in regional newspapers and advertisements in
Swiss and German fertility websites. Data used for the present study were collected between May and
September of 2008. Approval for the study was obtained from the Cantonal Research Ethics Commit-
tee in Bern (Switzerland). The sample consisted of women suffering from primary or secondary infer-
tility for at least 1 year, independent of actual medical treatment. Additional criteria for inclusion
were: not receiving any other psychological treatment for the duration of the study; having access to
the Internet; being at least 18 years of age; and, having written at least 1 email message to the therapist
in the course of the online treatment. A total of 57 women fulfilled these criteria and were included in
the qualitative analysis described here (see Table 1). With respect to age, the sample ranged from 26 to
42 years. In all, 59% of the women were from Switzerland, 40% were from Germany, and 1 woman
was from Austria. The mean duration of participants’ wish for a child was 2.9 years (range 1-7 years),

and 45.6% of the participants had already made use of ART prior to beginning the Online Coaching
treatment. The number of messages sent by participants ranged between 1 and 13 messages, with a
mean of 3.77 (SD = 2.87). On average, the messages contained 732 words (SD = 953.09) and ranged
in length from 6 to 4,911 words.
INSERT TABLE 1 ABOUT HERE.
Qualitative analysis
The messages between patients and therapists were analyzed using qualitative content analysis
(Mayring, 2008). Demanding careful examination and constant comparison on the part of researchers,
qualitative content analysis primarily relies on inductive reasoning to determine emergent categories
and themes from a set of data. Nevertheless, the generation of such categories and themes may also be
influenced by theories, and may therefore also include deductive reasoning.
The qualitative content analysis involved several steps. In step 1, messages related to technological
aspects of the Internet-based treatment were excluded from the analysis. In step 2, 2 members of the
research team began independently generating possible categories from the data using inductive rea-
soning. As is typically done in qualitative content analyses, individual themes detected in the mes-
sages were used as coding units (in most cases paragraphs). While creating the categories, the raters
applied the constant comparative method developed by Glaser and Strauss (1967). They compared text
units assigned to a specific category to those already assigned to that category in order to better under-
stand the category itself and to make differences between it and other categories more explicit. Each
text unit was solely assigned to a single category (i.e., the categories were mutually exclusive). A 3rd
step involved the repeated validation of the coding scheme with the other rater. Coding consistency
was checked via assessment of inter-rater agreement. In an iterative process, problems concerning
coding rules and definitions of categories were discussed and step 2 and 3 were repeated until suffi-
cient coding consistency was achieved. Finally, all messages were coded.
Quantitative measures
The following demographic data were gathered at baseline: age, occupational status, nationality,
education level, duration of wish for a child, previous medical and psychological treatments. For the
purpose of quantitative analysis, we also used the following 2 self-report questionnaires during base-
line assessment:
Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977): The CES-D consists
of 20 items and is used to quantify the severity of depressive symptomatology. Scores range from 0 to
60, with scores of 16 or higher indicating clinical depression (Radloff, 1977). At baseline, internal
consistency of the CES-D in our sample was alpha = 0.93.
State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, & Lushene, 1970): The STAI consists
of 40 items and is used to assess general levels of anxiety. Scores above 33 (STAI-S) or above 35
(STAI-T) indicate clinically significant state or trait anxiety respectively (Spielberger, Gorsuch, &
Lushene, 1970). In our sample, the Cronbach’s alphas at baseline were 0.93 for state anxiety and 0.91
for trait anxiety.
Statistical analysis
The reliability of the qualitative text analysis was evaluated using Cohen’s kappa (Cohen, 1960),
which represents a chance-corrected measure of agreement between 2 raters. In order to calculate the
level of inter-rater reliability using this measure, the 2 raters coded 10% of the data (Wirtz & Caspar,
2002). For the sake of quantitative analysis, non-parametric tests (Spearman rank correlations, Mann-
Whitney U tests) were used, since the frequency of coded themes was not normally distributed.
Results
Inter-rater reliability
In order to analyze the reliability of the coding system, Cohen’s kappa was calculated (see Table
2). The inter-rater reliabilities of the main categories ranged between κ = 0.64 (category: “Pregnant
women, families, children”) and κ = 0.92 (category: “Somatic signs associated with the wish for a
child”). These values indicate good to excellent agreement between the 2 raters.
INSERT TABLE 2 ABOUT HERE.
Important themes emerging from the qualitative data analysis
A total of 213 messages written by 57 infertile women were analyzed. A total of 14 main catego-
ries encompassing 34 subcategories were extracted from these data (see Table 2). The most important
themes that emerged from the qualitative analysis were as follows:
Theme 1: Emotions. In their written messages, the infertile women often described the emotions
they experienced surrounding the unfulfilled wish for a child. Most frequently, they wrote of hopes
and fears: “I really hope we are lucky this time” or “Yesterday, I had to cry because of my fear of a
negative result” are 2 examples. Other important emotions included sadness (“When I got home feel-
ing totally dejected, I received a text message”), stress (“Exercise really helps me deal with stress”),
and enjoyment (“Thanks to my happy anticipation of the next treatment, I’m able to look ahead with a
sense of optimism”). The broad range of additional emotions described in the messages – such as jeal-
ousy, hopelessness, anger, self-pity, gratitude, blame, courage, shame, and disappointment – confirm
that experiencing the unfulfilled wish for a child is a highly emotional life event. Most interestingly,
negative emotions such as fear, sadness, and hopelessness nearly always occurred in combination with
positive counterparts such as hope, gratitude, and enjoyment.
Theme 2: Coping with childlessness. Many participants wrote about their ways of dealing with in-
fertility and their unfulfilled wish for a child. It turned out that the various coping styles described by
Schmidt, Christensen and Holenstein (2005) were very useful in capturing the strategies outlined in
the participants’ messages. These authors adapted the Ways of Coping Questionnaire by Lazarus and
Folkman (1984) to apply to infertile patients, thereby distinguishing 4 coping styles: active-
confronting coping, meaning-based coping, active-avoidance coping, and passive-avoidance coping.
In our study, an example of active-confronting coping included: “We have decided to take a break
from trying to have a child and are going to take a trip somewhere.” An example of meaning-based
coping strategies included: “I try to tell myself that these people can’t do anything to harm my baby.”
Finally, evidence of active-avoidance coping strategies (e.g., “I tried to take my mind off of the situa-
tion”) and passive-avoidance coping strategies (e.g., “I could only sit in the corner and wait for the
result”) were also found in the messages.
Theme 3: Medical aspects. Evidently, the participants in our psychosocial Online Coaching treat-
ment also desired to discuss medical aspects surrounding infertility and its medical treatment. This
category was further subdivided into “Diagnostics,” “Treatment,” and “Financial aspects of medical
treatment.” “My uterus is myomatous” or “Today, I have another one of thousands of pre-exams” are
examples from the subcategory “Diagnostics.” “Yesterday, I had my second embryo transfer” or
“Now, we are in the next treatment cycle” are examples from the subcategory “Treatment.” In addi-
tion, several participants mentioned the financial burden of medical treatments.
Theme 4: Aspects and activities independent of the wish for a child. A considerable number of
messages surrounded activities and aspects of the infertile women’s lives that were not directly related
to their unfulfilled wish for a child. It was possible to reliably divide this category between positive
aspects – based on statements such as “Well, at least we’ve finished our new aquarium and put fish in
it” – and negative aspects, based on statements such as “I’m trying to find a solution for my family so
that my sister can recover.”
Theme 5: Attitude towards the wish for a child. Participants also revealed their manner of thinking
about their unfulfilled wish for a child. Some participants tried to find explanations for their unful-
filled wish for a child (e.g., “Sometimes I wonder if the image I have of my mother somehow pro-
duces a block in me”). Others described an intense, sometimes ruminative focus upon the wish for a
child (e.g., “I can’t think of anything else except our desire to have a child”). Finally, negative (e.g.,
“Sometimes I’m afraid of becoming emotionally numb”) and positive attitudes (e.g., “This experience
has given me the chance to think about many things in my life”) toward the unfulfilled child wish
were revealed.
Other themes that were extracted from the data are presented in Table 2. They included: “Couples’
relationship” (positive and negative statements regarding women’ relationships with their partners);
“General well-being” (e.g. “I’ve improved a lot today”); “Negative results concerning a pregnancy”
(e.g., initiation of menstruation, a miscarriage, a negative pregnancy test, or termination of a preg-
nancy); “Somatic signs associated with the wish for a child” (e.g., bodily sensations linked to the wish
for a child such as premenstrual syndrome); the “Waiting periods” (e.g., waiting for the start of a
treatment or the results of a pregnancy test; and, “Loss of control” (e.g., statements concerning the
impossibility of influencing the outcome of a treatment).
Quantitative results
Frequency of qualitative categories
Table 3 presents the coding frequency for each qualitative category. “Emotions” was the most
prevalent category. Of the 57 female participants, 61.4% verbalized feelings concerning their unful-
filled wish for a child. Hope, anxiety, sadness, stress, and enjoyment were the most commonly ex-
pressed emotions, accounting for 61% of all emotions mentioned. We found a Spearman rank correla-
tion of rho(57) = 0.77 between the frequency of negative and positive emotions mentioned: The more
that a given participant wrote about negative emotions, the more likely it was that that same partici-
pant verbalized positive emotions as well.
With respect to the category “Coping with childlessness,” it was found that 63.2% of the partici-
pants mentioned their way of coping with the unfulfilled wish for a child. Most of the women de-
scribed active-confronting coping strategies (35.1%), followed by meaning-based (28.8%), active-
avoidance (16.2%), and passive-avoidance (12%) coping strategies. A closer inspection of the data
revealed that use of specific coping strategies did not appear stable over time. For instance, a partici-
pant who reported use of active-confronting coping in 1 message might write about meaning-based
coping in another message. In terms of correlations, the association between the 4 coping strategies
ranged between rho(57) = 0.36 and rho(57) = 0.56.
Statements concerning medical aspects were made by more than half of the participants (56.1%).
With respect to this category, a Mann-Whitney U test revealed no significant mean difference between
infertile women receiving medical treatment and women not receiving medical treatment (Mann-
Whitney U(1) = 394; p = 0.920). Among the participants who wrote about medical aspects, 64.3%
discussed medical treatments, 30.5% raised issues related to diagnostics, while 5% mentioned finan-
cial aspects.
A total of 71.9% of the women wrote about themes and activities unrelated to their wish for a child.
About two-thirds of these statements (63.7%) were coded as being positive, while one-third (35.6%)
of them were judged to be negative. More than half of the infertile women (64.4%) wrote about their
attitudes towards their unfulfilled wish for a child. In all, 41.5% of the infertile women reported sub-
jective explanatory models, while 31.9% mentioned an intense, sometimes ruminative focus upon the
wish for a child. Finally, half of the women (50.9%) wrote about their general well-being (59.5% posi-
tive statements; 40.5% negative statements). The remaining categories touched upon were mentioned
by less than 50% of the infertile women (see Table 3).
INSERT TABLE 3 ABOUT HERE.
Socio-demographic characteristics and frequency of categories
We explored differences and relationships between demographic characteristics and the frequency
with which participants wrote about specific themes. No significant rank correlations were found be-
tween the age of the participants and the frequency with which they mentioned any of the themes be-
longing to the established categories. In addition, no significant rank correlations were found between
the duration of participants’ wish for a child and subjects of any of the categories. The only significant
associations that emerged from the data were small and were related to participants’ level of educa-
tion. Participants with a higher level of education tended to write more frequently about themes inde-
pendent of their wish for a child (rho(57) = 0.33, p = 0.012) as well as about waiting periods, such as
when waiting for the results of a pregnancy test (rho(57) = 0.27, p = 0.045). No significant differences
were revealed with respect to the frequency with which particular groupings of participants (e.g., na-
tionality, occupational status, medical treatment, previous psychological treatments) mentioned
themes in a given category. Overall, participants’ demographic characteristics and their history of
medical or psychological treatment did not appear to exert an influence on the issues they raised in
their statements.
Clinical status and frequency of categories
We further examined whether the issues raised by clinically distressed participants could be distin-
guished from the themes discussed by participants that were not clinically depressed or anxious. For
this purpose, 2 groups were created according to the Center for Epidemiologic Studies Depression
Scale (CES-D; Radloff, 1977) and the State-Trait Anxiety Inventory (STAI; Spielberger et al., 1970).
In the CES-D, scores above 15 are considered to reflect clinical depression (Radloff, 1977). Of the 57
participants, 31 exceeded this criterion for clinical depression, while 26 did not. Nonparametric Mann-
Whitney tests revealed no differences between the 2 groups according to any of the categories, with p-
values ranging from 0.06 to 0.96. For instance, although clinically depressed participants mentioned
negative emotions slightly more often than non-depressed participants, this difference was far from
significant, registering a p-value of 0.22.
With regard to the STAI, scores above 33 on the state anxiety scale (STAI-S) and scores above 35
on the trait anxiety scale (STAI-T) indicate clinically significant anxiety (Spielberger et al, 1970). As
there was near-perfect overlap between participants who exceeded the cut-off scores on the STAI-S
and the STAI-T scales, we decided to concentrate solely on the STAI-T scale to distinguish 2 groups.
A total of 44 of the 57 participants exceeded the criteria for clinically significant trait anxiety. This
produced 2 unequal groups, with the non-anxious group on the small side (N=13). Nevertheless, the
clinically anxious group verbalized substantially and significantly more emotions than the non-anxious
group (Mann-Whitney U(1)=178; p=0.034): Interestingly, this applied to both negative and positive
emotions. On average, the frequency with which clinically anxious participants mentioned negative
emotions was 2.93, while the frequency among non-anxious women was 0.77. Further, clinically anx-
ious participants mentioned positive emotions 8 times more often than non-anxious participants (mean
frequency 1.57 vs. 0.17). Further dividing the clinically anxious group into a clinically depressed
group and non-depressed group revealed an interesting dissociation between negative and positive
emotions. We identified 16 participants who were clinically anxious but not clinically depressed. On
average, this subgroup mentioned a negative emotion 2.38 times and a positive emotion 2.50 times.
The 28 participants who were both clinically anxious and clinically depressed reported a negative
emotion 3.25 times and a positive emotion 1.04 times. This means that among clinically anxious pa-

tients, the addition of clinical depression was related to an increase in the number of negative emotions
reported (from 2.38 to 3.25) as well as a decrease in positive emotions (from 2.50 to 1.04).
Discussion
This study provided an opportunity to shed light on the issues confronting infertile women: The 3
most important themes that arose were emotions surrounding the wish for a child, coping with the
wish for a child, and medical aspects. Other important issues included life independent of the wish for
a child, individual attitudes towards the wish for a child, couples’ relationships, and general well-
being. With 1 exception – that of highly educated women mentioning waiting periods and aspects
independent of their wish for a child wish with greater frequency – the themes uncovered in our study
occurred among the infertile women independent of their demographic characteristics or their histories
of medical or psychological treatment. Clinically anxious women mentioned emotions significantly
more often than non-anxious women: negative emotions about 4 times and positive emotions about 8
times more frequently. Further, significantly fewer positive emotions were reported among women
who fulfilled the criteria for both clinical anxiety and depression.
The single most important issue cited by the infertile women was the presence of emotions sur-
rounding the unfulfilled wish for a child. The experience of infertility and its medical treatment are
often described as a rollercoaster ride of emotions (Menning, 1980; Watkins & Baldo, 2004). In our
sample, generally negative emotions like anxiety occurred alongside positive emotions like hope and
enjoyment. This finding confirms that positive and negative emotions are equally present and relevant
among infertile women.
One interesting result of the present study was that infertile women with clinically relevant levels
of anxiety mentioned positive and negative emotions significantly more often than those who did not
suffer from clinically relevant anxiety. In addition, those participants who were both clinically anxious
and depressed exhibited fewer positive and more negative emotions than those who were solely clini-
cally anxious. The present finding of fewer positive and more negative emotions among depressed
participants may be explained by the fact that depression is linked to a decrease in positive emotions
as well as an increase in negative emotions (Gotlib & Hammen, 2002; Greenberg & Watson, 2006).
Findings from neuroscience also support the notion that depression bears a direct link to reductions in
positive emotions (Davidson, Pizzagalli, Nitschke, & Putman, 2002; Grawe, 2007).
Emotion regulation is crucial to general well-being. Psychological problems like anxiety and de-
pression are strongly associated with deficits in emotion regulation (Gross & Levenson, 1997). Inter-
ventions that target emotion-regulation skills may improve the effectiveness of psychotherapeutic
interventions (Berking et al., 2008). Having the ability to identify and label emotions is an important
skill in regulating one’s emotions (Bagby, Parker, & Taylor, 1994; Feldman-Barrett, Gross, Christen-
sen, & Benvenuto, 2001).
The greater frequency of emotions mentioned among clinically distressed women might also be a
result of the Internet-based treatment in which they were participating. The results of a separate
evaluation of the Internet-based treatment itself revealed that it was especially effective for patients
with clinically relevant levels of distress and depression (unpublished observation). As a result, such
participants’ increased expression of emotions can be viewed as an important treatment effect. The
results of the present qualitative study indicate that infertile women, particularly those with clinically
relevant levels of anxiety, bear a great need to communicate their emotions surrounding the unfulfilled
wish for a child. In addition, infertile women must learn to cope with the “ups and downs” of various
emotions, for example, feelings of hope and anxiety (“I don’t know whether to be hopeful or pessimis-
tic”) as well as handle incriminating feelings like jealousy and blame.
Coping with the unfulfilled wish for a child was another relevant theme frequently cited by the
study participants. Infertility is characterized by the following dimensions of stress: unpredictability,
negativity, uncontrollability, and ambiguity (Stanton & Dunkel-Schetter, 1991). In addition, infertility
is often perceived as dichotomous: on the one hand, it is considered harmful (e.g., threatening impor-
tant life goals) and uncontrollable (e.g., attaining conception); on the other hand, it is seen as somehow
beneficial (e.g., strengthening a couple’s marriage) and controllable (e.g., when deciding for medical
treatment) (Stanton, 1991). For the majority of couples, infertility amounts to a chronic stressor due to
associated emotional distress, demanding treatments, and various events that accumulate over an ex-
tended period of time and require different coping strategies in order to successfully adjust, adapt, and
maintain emotional and marital equilibrium regardless of the ultimate outcome (Covington & Burns,
2006; Schmidt et al., 2005). The present results showed that infertile women used active-confronting
and meaning-based coping strategies with the greatest frequency. These 2 coping strategies are often
associated with low fertility problem stress (Berghuis & Stanton, 2002; Schmidt et al., 2005; Terry &
Hynes, 1998). In our sample, active-avoidance and passive-avoidance coping strategies were used
with lesser frequency.
Medical aspects represented the 3rd issue most frequently mentioned by the study participants. Ac-
cording to the present results, many infertile women are concerned with medical treatment and diag-
nostic aspects. Surprisingly – in view of the high costs of medical treatment – financial aspects were
rarely mentioned. The demand for medical services related to infertility is on the rise (Covington &
Burns, 2006). Many infertile couples are subjected to a medical marathon ranging from diagnostic
inquiries to high-tech treatments such as in vitro fertilization (IVF). ARTs are considered particularly
stressful by many infertile patients and can trigger high levels of short-term mental distress (Chen et
al., 2004; Eugster & Vingerhoets, 1999). There is some evidence that distress levels may influence the
outcome of fertility treatments, as well as influence patients’ decisions to continue treatment or not
(Domar, 2006). Psychological interventions have been shown to be effective in improving infertile
patients’ mental health and even in increasing their pregnancy rate (Haemmerli, Znoj, & Barth, 2009).
The issues of importance to infertile women identified in the present study appear to occur inde-
pendent of their psychosocial characteristics. One particular exception was the fact that women with a
higher education level more frequently mentioned aspects of their lives independent of the wish for a
child, in addition to mentioning waiting periods with greater frequency. An explanation for the first
part of this result may be that infertile women with a higher level of education actually have more
going on in their lives independent of their wish for a child – such as career goals or leisure activities –
or simply choose to focus more on such aspects. As for waiting periods: we have no plausible explana-
tion for the result that more highly educated women have a greater need to discuss such waiting peri-
ods.
In addition to the issues identified in the present study, other well-known themes may also bear
great importance to infertile women. For example, sexuality is often an important issue to infertile
women, as infertile couples’ sexual activity is frequently impacted at some point (Wischmann, 2005).
Another theme associated with infertility is the stress that results from others’ reactions to infertility
and communicating with others about infertility in general (Lemmens et al., 2004). Further, adapting
to unintentional childlessness, letting go of the wish for a child, and seeking out alternative life goals
or other parenting options such as adoption all represent emotionally difficult processes (Daniluk,
2001). The relevant themes mentioned by the infertile women in this study are not considered exhaus-
tive. It is important to address infertile women directly regarding the above-mentioned issues, as it is
not always easy for patients to raise such themes independently.
This present study has its limitations. Due to the small sample size, there may be a lack of statisti-
cal power necessary to detect significant relationships between the themes identified and the infertile
women’s mental health levels. We also limited our analysis to infertile women since very few infertile
men participated in the study. Further, the present sample took part in an Internet-based treatment
study and may be not representative of infertile patients in general. Selection bias may be present as
the sample consisted of individuals who had expressed interest in an Internet-based treatment.
Future research should further evaluate the issues of importance to infertile women so as to in-
crease our understanding of their specific problems and needs. The role of emotions among infertile
patients in general, and among highly distressed infertile patients in particular, must be better under-
stood. To date, there has been little research examining gender-specific aspects of infertility or psy-
chological interventions for infertile patients. The issues of importance to infertile men, for example,
were not been captured in the present study. Infertile women and men ought to be analyzed separately
as there appear to be differences between the issues confronting them as groups. Having a precise
understanding of the issues important to infertile patients represents a precondition for providing them
specific and efficient psychological support.
Conclusions
The present qualitative study provides insights into the issues confronting infertile women. The is-
sues identified may be helpful to health professionals working in the area of fertility treatment. In par-
ticular, it appears important that such professionals direct their attention to the emotions experienced
by infertile women. As infertile women confront many different emotions, emotion regulation plays a

central role in their experience of infertility. In cases where infertile women make frequent mention of
their emotions, this may indicate the presence of high levels of anxiety. Infertile women should be
offered support in coping with their emotions. Particularly when providing psychological support to
infertile women with clinically high levels of anxiety and depression, enhancement of positive emo-
tions presents an important goal. Another issue of great importance to infertile women is coping with
the unfulfilled wish for a child in general. Infertile women must be supported in dealing with strains
concerning their childlessness by means of active-confronting and meaning-based coping strategies.
Finally, psychological support should be available to infertile patients at every stage of medical treat-
ment and actively offered to those patients experiencing high levels of distress.
Acknowledgments
The authors wish to thank Isabelle Pfister for her contribution to the qualitative analysis. The pre-
sent study was supported by a grant from the Swiss National Science Foundation, Bern, Switzerland
(grant no. 325100 -11375411).
Author Disclosure Statement
No competing financial interests exist.
References
Bagby, R. M., Parker, J. D., & Taylor, G. J. (1994). The twenty-item Toronto Alexithymia Scale II:
convergent, discriminant, and concurrent validity. Journal of Psychosomatic Research, 38, 33-40.
Berghuis, J. P., & Stanton, A. L. (2002). Adjustment to a dyadic stressor: a longitudinal study of
coping and depressive symptoms in infertile couples over an insemination attempt. Journal of Con-
sulting and Clinical Psychology, 70, 433-438.
Berking, M., Wupperman, P., Reichardt, A., Pejic, T., Dippel, A., & Znoj, H. (2008). Emotion-
regulation skills as a treatment target in psychotherapy. Behaviour Research and Therapy, 46, 1230-
1237.
Boivin, J., & Takefman, J. E. (1995). Stress level across stages of in vitro fertilization in subse-
quently pregnant and nonpregnant women. Fertility and Sterility, 64, 802-810.
Brkovich, A. M., & Fisher, W. A. (1998). Psychological distress and infertility: forty years of re-
search. Journal of Psychosomatic Obstetrics and Gynaecology, 19, 218-228.
Chen, T. H., Chang, S. P., Tsai, C. F., & Juang, K. D. (2004). Prevalence of depressive and anxiety
disorders in assisted reproductive technique clinic. Human Reproduction, 17, 2313-2318.
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological
Measurement, 20, 37-46.
Covington, S., & Burns, L. H. (2006). Infertility Counseling: A Comprehensive Handbook for Cli-
nicians (2th. ed.). New York: Cambridge University Press.
Daniluk, J. C. (2001). Reconstructing their lives: A longitudinal, qualitative analysis of the transi-
tion to biological childlessness for infertile couples. Journal of Counseling and Development, 79, 439-
449.
Davidson, R. J., Pizzagalli, D., Nitschke, J. B., & Putman, K. (2002). Depression: Perspectives
from Affective Neuroscience. Annual Review of Psychology, 53, 545-574.
Domar, A. D. (2006). Psychological stress and infertility. In B. D. Rose (Ed.), Up To Date. Welles-
ley, MA.
Dunkel-Schetter, C., & Lobel, M. (1991). Psychological reactions to infertility. In A. L. Stanton &
C. Dunkel-Schetter (Eds.), Infertility: Perspectives from Stress and Coping Research (pp. 29-57). New
York, London: Plenum Press.
Eugster, A., & Vingerhoets, A. J. (1999). Psychological aspects of in vitro fertilization: a review.
Social Science & Medicine, 48, 575-589.
Feldman-Barrett, L., Gross, J. J., Christensen, T. C., & Benvenuto, M. (2001). Knowing what
you’re feeling and knowing what to do about it: mapping the relation between emotion differentiation
and emotion regulation. Cognition & Emotion, 15, 713-724.
Glaser, B. G., & Strauss, A. (1967). Discovery of Grounded Theory. Strategies for Qualitative Re-
search. Sociology Press.
Gotlib, I, H., & Hammen, C. L. (2002). Handbook of Depression. New York: Guilford Press.
Grawe, K. (2007). Neuropsychotherapy: How the Neurosciences Inform Effective Psychotherapy.
Routledge.
Greil, A. L. (1997). Infertility and psychological distress: a critical review of the literature. Social
Science & Medicine, 45, 1679-1704.
Green, D., Galvin, H., & Horne, B. (2003). The psycho-social impact of infertility on young male
cancer survivors: a qualitative investigation. Psychooncology, 12, 141-152.
Greenberg, L. S., & Watson, J. C. (2006). Emotion-Focused Therapy for Depression. Washington,
D.C.: American Psychological Association.
Gross, J. J., & Levenson, R. W. (1997). Hidding feelings: The acute effects of inhibiting
negative and positive emotion. Journal of Abnormal Psychology, 106, 95-103.
Hammerberg, K., Astbury, J., & Baker, H. W. B. (2001). Women’s experience of IVF: a follow-up
study. Human Reproduction, 16, 374-383.
Haemmerli, K., Znoj, H., & Barth, J. (2009). The Efficacy of Psychological Interventions for Infer-
tile Patients: A Meta-analysis Examining Mental Health and Pregnancy Rate. Human Reproduction
Update, 15, 279-295.

Klonoff-Cohen, H., Chu, E., Natarajan, L., & Sieber, W. (2001). A prospective study of stress
among women undergoing in vitro fertilization or gamete intrafallopian transfer. Fertility and Sterility,
76, 675-687.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer.
Leiblum, S. R., & Greenfeld, D. A. (1997). The course of infertility: immediate and long-term reac-
tions. In S. Leiblum (Ed.), Infertility: Psychological Issues and Counselling Strategies (pp. 83-102).
New York, John Wiley & Sons.
Lemmens, G. M. D., Vervaeke, M., Enzlin, P., Bakelants, E., Vanderschueren, D., D’Hooghe, T. et
al. (2004). Coping with infertility: a body-mind group intervention programme for infertile couples.
Human Reproduction, 19, 1917-1923.
Mahlstedt, P. P. (1985). The psychological component of infertility. Fertility and Sterility, 42, 335-
346.
Mayring, P. (2008). Qualitative Inhaltsanalyse. Grundlagen und Techniken [Qualitative content
analysis. Basics and techniques.] (10th ed.). Weinheim, Basel: Beltz Verlag.
Menning, B. E. (1980). The emotional needs of infertile couples. Fertility and Sterility, 34, 313-
319.
Peddie, V. L., van Teijlingen, E., & Bhattacharya, S. (2005). A qualitative study of women’s deci-
sion-making at the end of IVF treatment. Human Reproduction, 20, 1944-1951.
Radloff, L. S. (1977). The CES-D Scale. A Self-Report Depression Scale for Research in the Gen-
eral Population. Applied Psychological Measurement, 1, 385-401.
Redshaw, M., Hockley, C., & Davidson, L. L. (2007). A qualitative study of the experience of
treatment for infertility among women who successfully became pregnant. Human Reproduction, 22,
295-304.
Schmidt, L., Christensen, U., & Holstein, B. E. (2005). The social epidemiology of coping with in-
fertility. Human Reproduction, 20, 1044-1052.
Slade, P., Emery, J., & Lieberman, B. A. (1997). A prospective, longitudinal study of emotions and
relationships in in-vitro fertilization treatment. Human Reproduction, 12, 183-190.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1970). Manual for the State-Trait Anxiety In-
ventory. Palo Alto, CA, USA: Consulting Psychological Press.
Stanton, A. L. (1991). Cognitive appraisals, coping processes, and adjustment to infertility. In A. L.
Stanton & C. Dunkel-Schetter (Eds.), Infertility: Perspectives from Stress and Coping Research (pp.
87-108). New York: Plenum Press.
Stanton, A. L., & Dunkel-Schetter, C. (1991). Psychological adjustment to infertility. In A. L.
Stanton & C. Dunkel-Schetter (Eds.), Infertility: Perspectives from Stress and Coping Research (pp.
3-16). New York: Plenum Press.
Terry, D. J., & Hynes, G. J. (1998). Adjustment to a Low-Control Situation: Reexamining the Role
of Coping Responses. Journal of Personality and Social Psychology, 74, 1078-1092.
Valentine, D. P. (1986). Psychological impact of infertility: identifying issues and needs. Social
Work in Health Care, 11, 61-69.
Verhaak, C. M., Smeenk, J. M. J., Nahuis, M. J., Kremer, J. A. M., & Braat, D. D. M. (2007).
Long-term psychological adjustment to IVF/ICSI treatment in women. Human Reproduction, 22, 305-
308.
Watkins, K. J., & Baldo, T. D. (2004). The infertility experience: Biopsychosocial effects and sug-
gestions for counselors. Journal of Counseling and Development, 82, 394–420.
Wirtz, M., & Caspar, F. (2002). Beurteilerübereinstimmung und Beurteilerreliabilität [Rater
agreement and rater reliability]. Göttingen: Hogrefe.
Wischmann, T. (2005). Psychosocial aspects of fertility disorders. Urologe, A 44, 185-94.
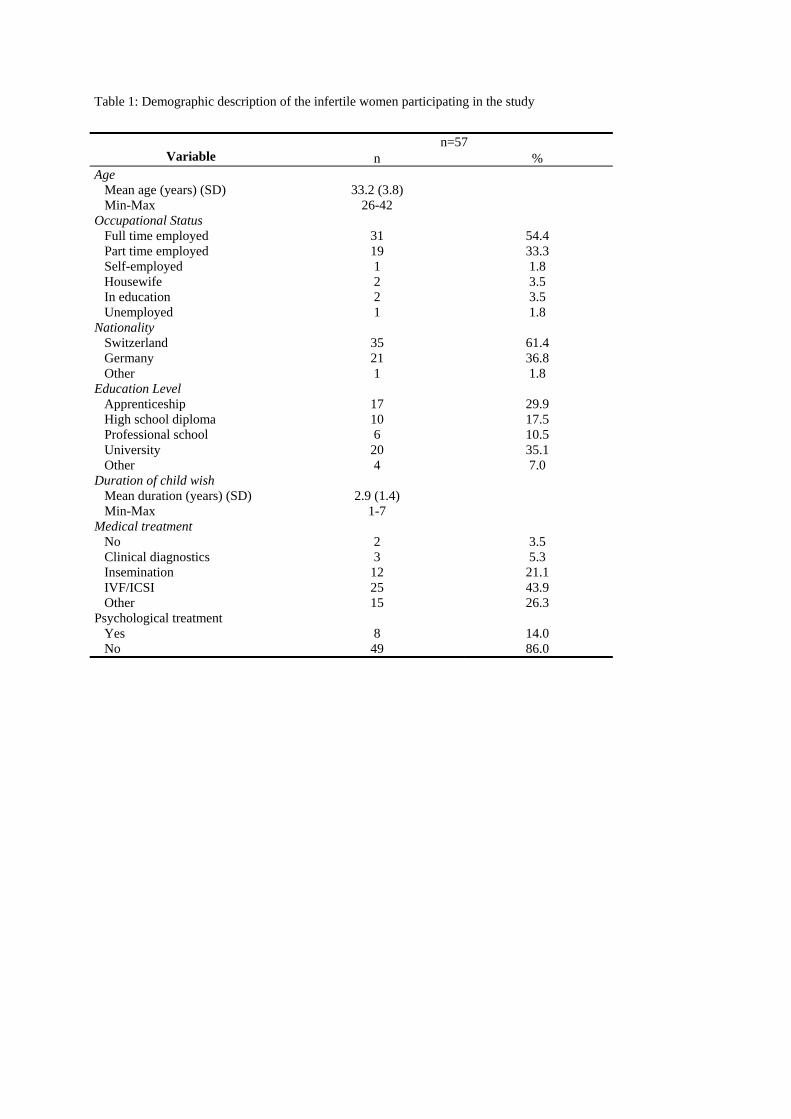
Table 1: Demographic description of the infertile women participating in the study
n=57 Variable n %
Age Mean age (years) (SD) 33.2 (3.8) Min-Max 26-42 Occupational Status Full time employed 31 54.4 Part time employed 19 33.3 Self-employed 1 1.8 Housewife 2 3.5 In education 2 3.5 Unemployed Nationality
1 1.8
Switzerland 35 61.4 Germany 21 36.8 Other Education Level
1 1.8
Apprenticeship High school diploma Professional school University Other
17 10 6
20 4
29.9 17.5 10.5 35.1 7.0
Duration of child wish Mean duration (years) (SD) Min-Max Medical treatment No Clinical diagnostics Insemination IVF/ICSI Other Psychological treatment Yes No
2.9 (1.4) 1-7
2 3
12 25 15
8
49
3.5 5.3
21.1 43.9 26.3
14.0 86.0
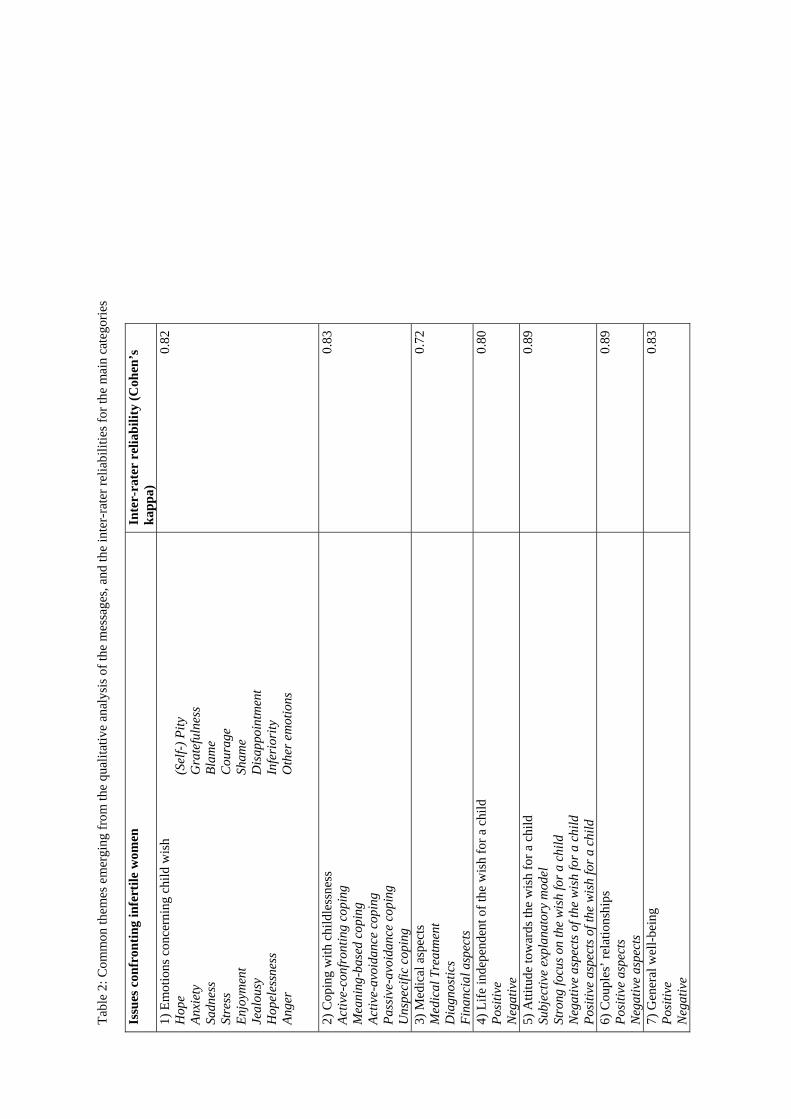
Tabl
e 2:
Com
mon
them
es e
mer
ging
from
the
qual
itativ
e an
alys
is o
f the
mes
sage
s, an
d th
e in
ter-
rate
r rel
iabi
litie
s for
the
mai
n ca
tego
ries
Issu
es c
onfr
ontin
g in
fert
ile w
omen
In
ter-
rate
r re
liabi
lity
(Coh
en’s
ka
ppa)
1)
Em
otio
ns c
once
rnin
g ch
ild w
ish
Hop
e An
xiet
y Sa
dnes
s St
ress
En
joym
ent
Jeal
ousy
H
opel
essn
ess
Ange
r
(Sel
f-) P
ity
Gra
tefu
lnes
s Bl
ame
Cou
rage
Sh
ame
Dis
appo
intm
ent
Infe
rior
ity
Oth
er e
mot
ions
0.82
2) C
opin
g w
ith c
hild
less
ness
Ac
tive-
conf
ront
ing
copi
ng
Mea
ning
-bas
ed c
opin
g Ac
tive-
avoi
danc
e co
ping
Pa
ssiv
e-av
oida
nce
copi
ng
Uns
peci
fic c
opin
g
0.83
3) M
edic
al a
spec
ts
Med
ical
Tre
atm
ent
Dia
gnos
tics
Fina
ncia
l asp
ects
0.72
4) L
ife in
depe
nden
t of t
he w
ish
for a
chi
ld
Posi
tive
Neg
ativ
e
0.80
5) A
ttitu
de to
war
ds th
e w
ish
for a
chi
ld
Subj
ectiv
e ex
plan
ator
y m
odel
St
rong
focu
s on
the
wis
h fo
r a c
hild
N
egat
ive
aspe
cts o
f the
wis
h fo
r a c
hild
Po
sitiv
e as
pect
s of t
he w
ish
for a
chi
ld
0.89
6) C
oupl
es’ r
elat
ions
hips
Po
sitiv
e as
pect
s N
egat
ive
aspe
cts
0.89
7) G
ener
al w
ell-b
eing
Po
sitiv
e N
egat
ive
0.83
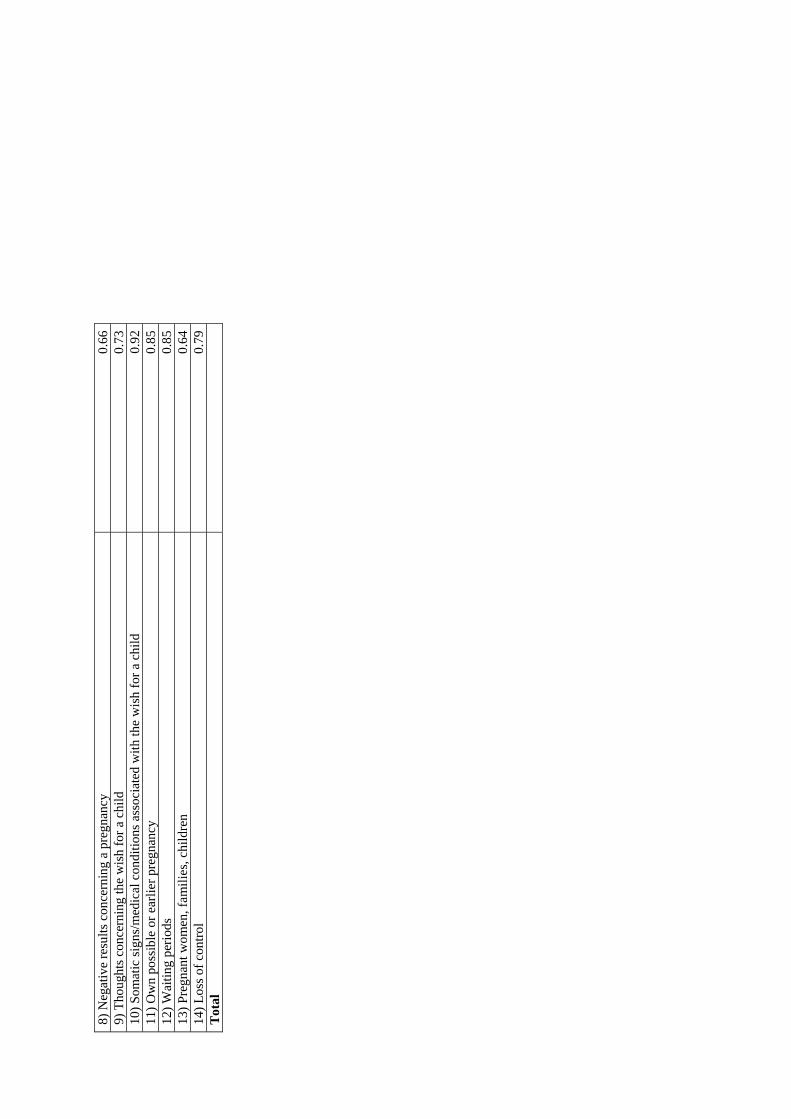
8) N
egat
ive
resu
lts c
once
rnin
g a
preg
nanc
y 0.
66
9) T
houg
hts c
once
rnin
g th
e w
ish
for a
chi
ld
0.73
10
) Som
atic
sign
s/m
edic
al c
ondi
tions
ass
ocia
ted
with
the
wis
h fo
r a c
hild
0.
92
11) O
wn
poss
ible
or e
arlie
r pre
gnan
cy
0.85
12
) Wai
ting
perio
ds
0.85
13
) Pre
gnan
t wom
en, f
amili
es, c
hild
ren
0.64
14
) Los
s of c
ontro
l 0.
79
Tot
al
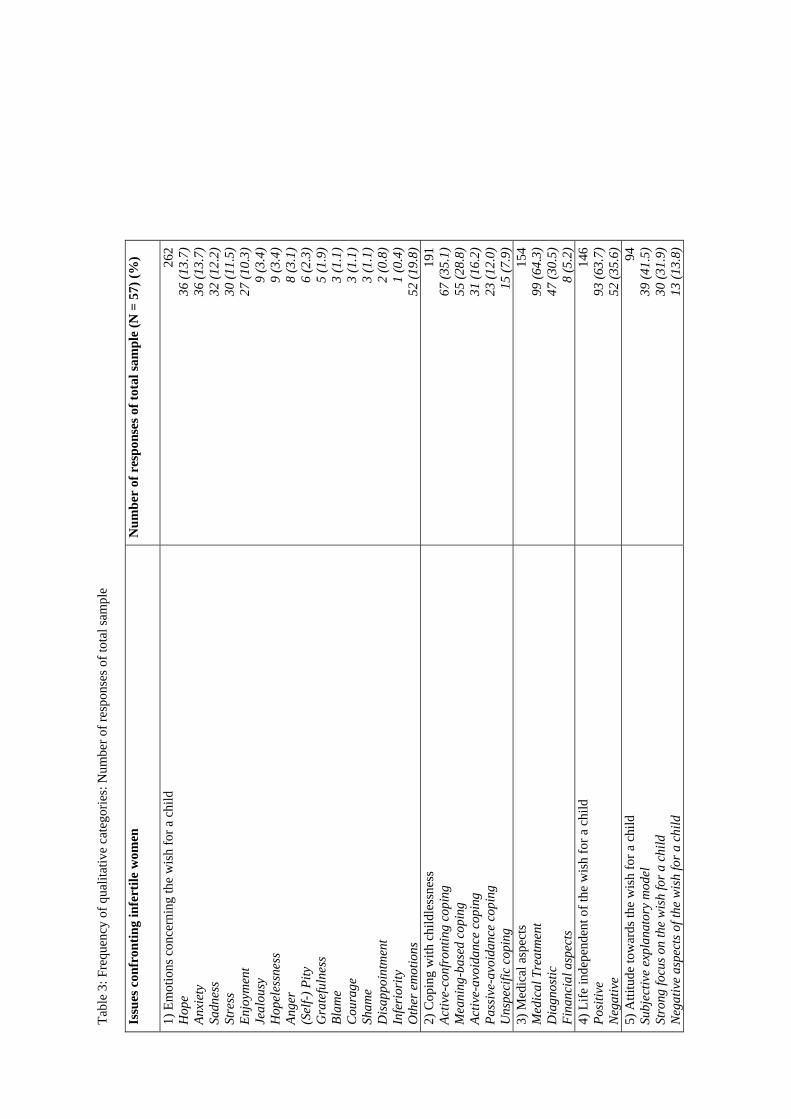
Tabl
e 3:
Fre
quen
cy o
f qua
litat
ive
cate
gorie
s: N
umbe
r of r
espo
nses
of t
otal
sam
ple
Issu
es c
onfr
ontin
g in
fert
ile w
omen
N
umbe
r of
res
pons
es o
f tot
al sa
mpl
e (N
= 5
7) (%
)
1) E
mot
ions
con
cern
ing
the
wis
h fo
r a c
hild
H
ope
Anxi
ety
Sadn
ess
Stre
ss
Enjo
ymen
t Je
alou
sy
Hop
eles
snes
s An
ger
(Sel
f-) P
ity
Gra
tefu
lnes
s Bl
ame
Cou
rage
Sh
ame
Dis
appo
intm
ent
Infe
rior
ity
Oth
er e
mot
ions
262
36 (1
3.7)
36 (1
3.7)
32 (1
2.2)
30 (1
1.5)
27 (1
0.3)
9 (3
.4)
9 (3
.4)
8 (3
.1)
6 (2
.3)
5 (1
.9)
3 (1
.1)
3 (1
.1)
3 (1
.1)
2 (0
.8)
1 (0
.4)
52 (1
9.8)
2)
Cop
ing
with
chi
ldle
ssne
ss
Activ
e-co
nfro
ntin
g co
ping
M
eani
ng-b
ased
cop
ing
Activ
e-av
oida
nce
copi
ng
Pass
ive-
avoi
danc
e co
ping
U
nspe
cific
cop
ing
191
67 (3
5.1)
55 (2
8.8)
31 (1
6.2)
23
(12.
0)15
(7.9
) 3)
Med
ical
asp
ects
M
edic
al T
reat
men
t D
iagn
ostic
Fi
nanc
ial a
spec
ts
154
99 (6
4.3)
47 (3
0.5)
8 (5
.2)
4) L
ife in
depe
nden
t of t
he w
ish
for a
chi
ld
Posi
tive
Neg
ativ
e
146
93 (6
3.7)
52 (3
5.6)
5)
Atti
tude
tow
ards
the
wis
h fo
r a c
hild
Su
bjec
tive
expl
anat
ory
mod
el
Stro
ng fo
cus o
n th
e w
ish
for a
chi
ld
Neg
ativ
e as
pect
s of t
he w
ish
for a
chi
ld
94
39 (4
1.5)
30 (3
1.9)
13 (1
3.8)
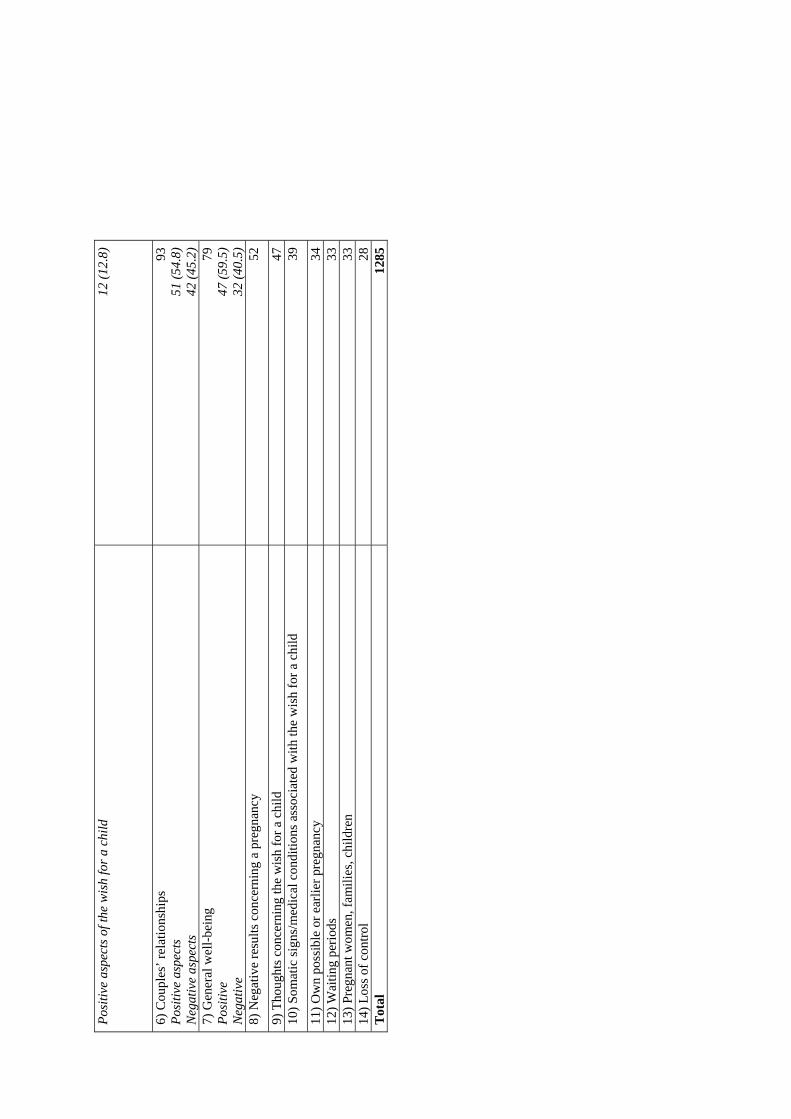
Posi
tive
aspe
cts o
f the
wis
h fo
r a c
hild
12
(12.
8)
6) C
oupl
es’ r
elat
ions
hips
Po
sitiv
e as
pect
s N
egat
ive
aspe
cts
93
51 (5
4.8)
42 (4
5.2)
7)
Gen
eral
wel
l-bei
ng
Posi
tive
Neg
ativ
e
79
47 (5
9.5)
32 (4
0.5)
8)
Neg
ativ
e re
sults
con
cern
ing
a pr
egna
ncy
52
9) T
houg
hts c
once
rnin
g th
e w
ish
for a
chi
ld
47
10) S
omat
ic si
gns/
med
ical
con
ditio
ns a
ssoc
iate
d w
ith th
e w
ish
for a
chi
ld
39
11) O
wn
poss
ible
or e
arlie
r pre
gnan
cy
34
12) W
aitin
g pe
riods
33
13
) Pre
gnan
t wom
en, f
amili
es, c
hild
ren
33
14) L
oss o
f con
trol
28
Tot
al
1285
Artikel 2
Haemmerli, K., Znoj, H., Burri, S., Graf, P., Wunder, D., & Perrig-Chiello,
P. (2008). Psychological interventions for infertile patients: A review of ex-
isting research and a new comprehensive approach. Counselling and
Psychotherapy Research, 8, 246-252.
RESEARCH ARTICLE
Psychological interventions for infertile patients: A review ofexisting research and a new comprehensive approach
KATJA HAEMMERLI*1, HANSJOERG ZNOJ1, SALOME BURRI1, PATRICIA GRAF1,DOROTHEA WUNDER2, & PASQUALINA PERRIG-CHIELLO3
1Institute of Psychology, Department of Clinical Psychology and Psychotherapy, University of Bern, Switzerland,2Department of Obstetrics and Gynaecology, Inselspital Bern, University Hospital and University of Bern, Switzerland,and 3Institute of Psychology, Department of Developmental Psychology, University of Bern, Switzerland
AbstractThe usefulness of psychological support for infertile patients has been highlighted in the literature over the past number ofyears. This article provides a review of existing research on psychological interventions for infertile patients, and presents theFertility Group Intervention as an example of the application of existing research. There is clear empirical evidence of high levelsof depressive symptoms, anxiety, and distress among infertile patients undergoing assisted reproductive treatment (ART).Infertile patients need and require increased psychological support. Various studies indicate the efficacy of psychologicalinterventions for infertile patients with respect to their mental health and, in part, pregnancy rates. However, many suchstudies exhibit methodological problems. Therefore, in future research, additional studies of high-quality design are needed toachieve more definitive answers on the efficacy and indication of psychological interventions for infertile patients. Currently,the Fertility Group Intervention represents a comprehensive therapeutic approach integrating established empirical andtheoretical approaches with the aim of helping infertile patients ! particularly those undergoing ART ! cope with distressrelated to their infertility and medical treatment. This article further outlines the therapeutic background and structures,treatment goals, practical implications, and feasibility of the Fertility Group Intervention.
Keywords: Assisted reproductive treatment, counselling, infertility intervention, psychotherapy
Introduction
The majority of couples affected by infertility describethe experience as one of the most shattering events oftheir lives (Brkovich & Fisher, 1998; Burns & Coving-ton, 2006). Infertility is a common problem aroundthe world, and is clearly defined as a disease (WorldHealth Organisation (WHO), 1992). The prevalence ofinfertility varies throughout the world from less than5% to over 30% in certain regions, while its incidenceis increasing in general (WHO, 2003).
The emotional effects of both infertility and itsmedical treatment are well documented. The largemajority of studies indicate high levels of mentaldistress among infertile patients (Chen, Chang, Tsai,& Juang, 2004; Eugster & Vingerhoets, 1999; Wisch-mann, 2005). Some researchers suggest that elevatedanxiety and depression may actually lower pregnancyrates (Klonoff-Cohen, Chu, Natarajan, & Sieber, 2001;Smeenk et al., 2001). However, others find no evidencefor a relationship between women’s mental health andtheir likelihood of becoming pregnant following re-productive medical treatment (Anderheim, Holter,Bergh, & Moller, 2005; Boivin & Takefman, 1995).
In general, while the majority of information andsupport available to infertile patients focuses on themedical and technical aspects of treatment, manyinfertile patients may actually require more psycholo-gical help from medical centres (Sundby, Olson, &Schei, 1994). About 50% of infertile patients end upsearching for infertility information online, and ex-press finding the Internet helpful for both gatheringinformation and sharing their experience with others(Himmel, Meyer, Kochlen, & Michelmann, 2005;Kahlor & Mackert, in press).
The present article provides a review of the existingresearch on psychological interventions for infertilepatients. It offers an overview of established psycho-logical interventions and highlights some of theirspecific key elements. In addition, the efficacy andindication of psychological interventions for infertilepatients are discussed. Finally, the Fertility GroupIntervention is presented as an application of theexisting theoretical and empirical literature described,and its therapeutic foundations and structures, treat-ment goals, practical implications, and feasibility areoutlined.
*Corresponding author. E-mail: [email protected]
Counselling and Psychotherapy Research, December 2008; 8(4): 246!252
1473-3145 (print)/1746-1405 (online) – 2008 British Association for Counselling and PsychotherapyDOI: 10.1080/14733140802292895
Downloaded By: [Haemmerli, Katja] At: 10:16 17 November 2008
Psychological interventions for infertilepatients: a review of the existing research
Multi-factorial conditional model of fertility disorders
Several theoretical models of fertility disorders exist.Nowadays, many authors reject the psychodynamic-oriented model (the ‘psychogenic’ hypothesis) ofinfertility (Greil, 1997). Menning (1980) first describedinfertility as a complex life crisis and indicated thatpsychological distress is a consequence of infertilityrather than a cause of infertility. Today infertility isprimarily viewed as a psychosomatic whole (Wisch-mann, 2003). Fertility disorders are explained using amulti-factorial conditional model, where infertility isviewed as a consequence not only of physiologicalconditions ! such as hormonal changes, inflamma-tions, or semen quantity ! but also of psychologicalconditions ! such as the experience of stress, e.g.marital discord and social constraints (Bents, 1991;Burns & Covington, 2006; Cousineau & Domar,2007). Since infertility is an unplanned and unex-plained stressor, couples typically lack the knowledgeand coping strategies necessary to adequately man-age infertility stress (Peterson, Pirritano, Christensen,& Schmidt, 2008). As a result, individual coping andemotion regulation strategies represent importantfactors influencing the mental distress caused byinfertility. Thus, psychological factors must also betaken into account when treating infertile patients.
Overview of psychological interventions
Various types of psychological interventions alreadyexist for infertile patients. Individually, these interven-tions focus on specific therapeutic approaches such aspsychodynamic/-analytic interventions (e.g. Sarrell &DeCherney, 1985), mind/body-orientated relaxation(e.g. Levitas et al., 2006), cognitive-behaviouraltherapies (e.g. Noorbala et al., 2008), education(e.g. Chan, Ng, Chan, Ho, & Chan, 2006), and onlinecounselling interventions (Cousineau et al., 2008).They are offered in a variety of settings (i.e. individual,couple or group) usually to infertile patients under-going medical treatment, but also to patients notreceiving any medical treatment. The duration ofpsychological interventions for infertile patientsranges from 1 to 32 sessions. In the following, someof the important elements of such psychologicalinterventions for infertile patients are individuallydiscussed.
Educational and supportive intervention: basicassumptions. It is well known that psychologicalsupport can minimise both adverse physiological andpsychological side effects (Redd, Montgomery, &DuHamel, 2001) among those undergoing treatmentfor certain medical conditions, such as cancer. Groupinterventions emphasising education and skills train-ing, and supportive interventions, have been proveneffective in producing positive changes in mental
health (Boivin, 2003; McNaughton-Cassill, Bostwick,Arthur, Robinson, & Neal, 2002).
Educational elements in psychological interventionsfor infertile patients function to convey informationabout medical treatment and the interaction betweenphysiological and psychological conditions, and toprovide patients with the skills to deal with infertility.Infertile patients are taught communication andemotion regulation skills as well as stress reductiontechniques, such as relaxation exercises. Supportiveelements are employed in several interventions, suchas emotional expression and support as well asdiscussion of thoughts and feelings surroundinginfertility. Of central importance is the exchange ofideas between participants dealing with the sameproblems, and flexible responses to their needs.
Group and couple format. Groups provide opportu-nities for peer support, new learning, personal insight,and stress reduction (Fiedler, 2005). In a groupformat, the following curative group factors (whichdo not arise in individual therapy) are important(Grawe, 1980): cohesion, openness, trust, and atti-tude towards work. These factors are central tosupporting the individual’s therapeutic progress. Re-search on the effectiveness of groups has revealedcapacity for positive impact in areas such as sense ofbelonging, education, and having the strength tomove on (Lentner & Glazer, 1991). While a meta-analysis by de Liz and Strauss (2005) found group andindividual therapies to be equally effective, Boivin(2003) suggests that group therapies may provideadditional benefits due to the following: they enableinfertile patients to share their experiences and theyencourage solidarity, both of which represent copingstrategies.
In Switzerland in 2007, 47% of infertility caseswere attributed to male factors, 17% were attributedto female factors, 23% were attributed to bothpartners, and 9% remained unclear (for 4% therewas no information or other factors; Swiss FederalOffice of Statistics, 2007). Several studies haveindicated that men, too, are affected psychologicallyby infertility (e.g. Carmeli & Birbaum-Carmeli, 1994).Within couples, one partner’s coping patterns tend toimpact the personal, social, and marital distress levelof the other partner (Peterson et al., 2008). Thecouples approach to infertility therapy may addressmarital adjustment and sexual satisfaction, usingtherapy to facilitate communication between maritalpartners (Eunpu, 1995). Boivin (2003) has reported ofmen and women benefiting equally from counselling.It is therefore important that both partners take partin infertility interventions.
Duration and open access. In a meta-analysis byHoward, Kopta, Krause and Orlinsky (1986), 53% ofthe patients in psychotherapy exhibited improvementsafter eight sessions. Psychological interventions forinfertile patients should last between 6 and 12
Psychological interventions for infertile patients 247
Downloaded By: [Haemmerli, Katja] At: 10:16 17 November 2008
sessions as longer interventions demonstrate betteroutcomes (Boivin, 2003). In clinical practice, the opengroup format is often used. In an open group, thetherapeutic approach must be accommodated topatients’ individual needs (Grawe, 1980). Curativegroup factors can also be achieved in open groupformats (Fluckiger, Regli, & Grawe, 2005).
Intervention for patients receiving assistedreproductive treatment. Assisted reproductive treat-ments (ART) ! including in vitro fertilisation (IVF) andintracytoplasmatic sperm injection (ICSI) ! are oftenconsidered the most stressful techniques used to treatinfertility (Eugster & Vingerhoets, 1999). Unpredict-able outcomes and failed attempts at fertilisationpresent strong risks for feelings of anxiety, depression,and distress (Verhaak et al., 2007). Therefore, psy-chological support should also focus on adjustment tothe possibility of treatment failure and continuedchildlessness.
Relaxation exercises. Relaxation exercises, such asguided imagery and progressive muscle relaxation(e.g. Bongartz & Bongartz, 2000; Jacobson, 1938;Lazarus, 1984) are a common element in psychologi-cal interventions for infertile patients. Relaxationexercises are known to be effective in the treatmentof diverse patient groups (Grawe, Donati, & Bernauer,1994). In infertility treatment, relaxation training ispart of a psychophysiological approach. The goal ofthese interventions is to modify physiological re-sponses to stress, including acute and prolongedneurochemical, hormonal, and neuroanatomicalchanges (Burns & Covington, 2006). The reducedarousal of the autonomic and sympathetic nervoussystems that can result from relaxation exercises mayin turn enhance fertility (Reading, 1991). Severalstudies examining interventions that included relaxa-tion training with infertile patients have reportedpositive effects on mental health (Chan et al., 2006;Schmidt, Tjørnhøj-Thomsen, Boivin, & Nyboe Ander-sen, 2005) and even on pregnancy rates (Domar et al.,2000; Levitas et al., 2006).
Efficacy and indication of psychologicalinterventions
Many studies have investigated the efficacy of psy-chological interventions for infertile patients withrespect to mental health and pregnancy rate; psycho-logical interventions have been shown to positivelyaffect the former and, to a certain extent, the latter(Boivin, 2003; de Liz & Strauss, 2005; Haemmerli,Znoj, & Barth, submitted). While there are varioustypes of psychological interventions available toinfertile patients, it often remains unclear what theirindividual specific objectives are. Future research mustseek to evaluate who benefits from which type ofpsychological intervention, and at which point in timea given intervention should be indicated.
Compared with the costs associated with medicaltreatment, psychological interventions are cost-effi-cient to implement. Indeed, psychological supportought to be made available to infertile patients at anypoint in time during their medical treatment (Wisch-mann, 2005), as well as for infertile patients who arenot undergoing any medical treatment whatsoever(Haemmerli et al., submitted). Finally, psychologicalinterventions are absolutely mandatory for infertilepatients who have mental disorders (Cousineau &Domar, 2007; Wischmann, 2005).
Application: the Fertility GroupIntervention
Content of the Fertility Group Intervention
The Fertility Group Intervention represents an applica-tion of the various elements discussed above. Fewattempts have been made to integrate such diversetherapeutic approaches. Therefore, the Fertility GroupIntervention seeks to fill this gap by integratingestablished empirical and theoretical approaches toinfertility in one therapeutic programme.
The Fertility Group Intervention is a combination ofclarification and mastery techniques, based primarilyon principles of cognitive behavioural therapy (e.g.Fliegel, Groeger, Kunzel, Schulte, & Sorgatz, 1998),clarification-orientated therapy (e.g. Sachse, 2003),and system therapy (e.g. Stammer, Verres, & Wisch-mann, 2004). The principal goal of the Fertility GroupIntervention is to improve infertile patients’ mentalhealth and quality of life, not primarily to increasetheir pregnancy rate. The intervention follows princi-ples ! described below ! that are well established asbeing important factors in the treatment of infertilepatients (e.g. Bents, 1991; Stammer et al., 2004).
Specifically, the primary characteristics of the Ferti-lity Group Intervention are: (1) a structured group/couple setting; (2) a combination of educational andsupportive therapeutic elements; (3) a series of 10therapeutic sessions, differing in their content, carriedout in an open group format; and (4) relaxationexercises, which are integral.
The intervention is being developed as part of thestandard care for infertile patients receiving assistedreproductive treatment (ART) at the Fertility Centre ofthe University Hospital of Bern, Switzerland. Theintervention consists of 10 sessions organised accord-ing to 10 thematic blocks (see description of groupsessions). The sessions are held weekly and last 120minutes each. Infertile patients may enter the inter-vention group at any time.
Organisation of the group and description of thegroup sessions
Infertile patients from the Fertility Centre of theUniversity Hospital of Bern (Switzerland), who fulfilthe following inclusion criteria, are invited to partici-pate in the educational, supportive intervention: (1)
248 K. Haemmerli et al.
Downloaded By: [Haemmerli, Katja] At: 10:16 17 November 2008

those able to provide written consent for studyparticipation and IVF/ICSI treatment; (2) not currentlyreceiving psychological treatment; (3) indicated forIVF/ICSI treatment ! suffering from primary or sec-ondary infertility; and (4) of reproductive age (max-imum 42 years). IVF specialists from the FertilityCentre are charged with patient recruitment. Thepsychological intervention is considered part of pa-tients’ medical treatment and begins three to fiveweeks before the start of the ART. Participation in theintervention is optional and based on self-referral,since mandatory interventions may induce suspiciousor defensive behaviour in some patients (Boivin,Scanlan, & Walker, 1999). It is recommended thatboth partners take part in the intervention, but it isalso possible for only one partner to participate.
Each infertile patient receives 10 2-hour groupsessions, held evenings on a weekly basis at theUniversity of Bern, Switzerland, outpatient clinic. Twotrained psychologists conduct each session. Groupsizes range from 6 to 12 participants. The FertilityGroup Intervention consists of 10 thematically differ-ing group sessions. All of the themes are relevant toinfertile patients.
Although all of the sessions have the same basicstructure, each week introduces a different topic.Every session begins with two relaxation exercises: arapid progressive muscle relaxation and guided ima-gery. Following this, each patient’s course of medicaltreatment since the previous session and their currentwell-being are discussed in an opening round. Newparticipants are welcomed and asked to introducethemselves.
Next, the particular evening’s topic is introduced,proceeded by a segment of psychological education,including a short theoretical segment, and groupdiscussions. Every session is punctuated by a shortbreak. Each evening’s specific topic is observed for theentire duration of the session. Every session ends withan attempt to extract the most important points fromthe meeting and a short closing round of discussion.The individual topics covered in each session aredescribed below. The manual and additional informa-tion about the Fertility Group Intervention can beacquired by contacting the first author of this article.
Session 1: Emotions ! acceptance and tolerance.Emotion regulation is crucial to general well-being.Psychological problems are strongly associated withdeficits in emotion regulation (Gross & Levenson,1997). Infertility and its medical treatment are stress-ful experiences and can result in different emotionalreactions. High levels of negative emotions maydecrease couples’ conception rates.
Session 2: The wish for a child ! where is the previouslife?. Infertile patients often intensively pursue thegoal of having their own child. They invest a greatdeal of time, money, and emotion in their attempts tofulfil their wish for a child. Couples frequentlydisregard activities, hobbies, and contacts; these are,
however, important resources (Stammer, Wischmann,& Verres, 2002). In fact, the optimal use of suchresources is particularly important during such adifficult time.
Session 3: Coping with stress due to the reactions ofothers ! communication with outsiders. Infertilepatients are often confronted with questions andadvice from others (Wischmann & Stammer, 2006).These comments can be painful for couples. Anotherimportant issue is handling information and commu-nication surrounding infertility in the workplace.Medical treatment for infertility is associated with anenormous and unpredictable investment of time,which can in turn affect patients’ professional lives.
Session 4: Enjoy life and feel good. In times of highburden, pleasure and enjoyment are often ignored.However, it is precisely in such situations that theability to enjoy things gains in importance (Koppen-hofer, 2004). During enjoyable experiences, neuro-transmitters like dopamine, endorphins, andserotonin are released that in turn positively affectone’s mood and well-being.
Session 5: Attitude towards medical treatment. In-fertile couples experience different emotions concern-ing their medical treatment, such as hope and eageranticipation, but also fear and uncertainty (Burns &Covington, 2006). The optimal organisation of thetreatment course and the establishment of a positiveattitude towards treatment are very important.
Session 6: Self-esteem strengthening. In stressfulsituations, people are often self-destructive. Feelingsof blame may arise, eliciting additional stress reactionsin the body. Finding a constructive way of coping withdifferent situations becomes more difficult, and avicious cycle emerges. Self-reproach is often foundamong infertile patients. Feelings of self-reproach,such as not being a complete woman or being a badgenitor, are very destructive. It is very helpful tocultivate a caring and self-supporting attitude towardsoneself (Gilbert & Irons, 2004).
Session 7: Meaning of the wish for a child. To achievea comprehensive self-understanding, it is important tounderstand how one’s wish for a child has developedand changed over time (Stammer et al., 2004).Discussion about how life with a child will be canhelp establish patients’ wishes and fears. Individualclarification of wishes through imagery can lead to amore positive experience of medical treatment, whichcan otherwise be a rather passive and often alienatingexperience.
Session 8: Disappointment and hope. The success ratefor assisted reproductive treatments in Switzerland iscurrently about 24.3% (IVF: 22.9%; ICSI: 24.6%) perinitiated cycle (FIVNAT-CH, 2007). The thought of notgetting pregnant is unpleasant and painful; therefore,
Psychological interventions for infertile patients 249
Downloaded By: [Haemmerli, Katja] At: 10:16 17 November 2008

couples attempt to suppress it out of their conscious-ness. Such efforts are often ineffective since feelingsarise that elicit gradual physiological changes andbecause the responsible cerebral centres are notdeliberately manageable. Thus, the thoughts re-emerge and increase internal strains. It is thereforeimportant to face such thoughts and the negativeemotions associated with them. This enhances pa-tients’ sense of control and their chances of coping.As adaptation to unintentional childlessness is anemotionally difficult process, it is also important todiscuss other parenting options like adoption as wellas future goals independent of the wish for a child(Daniluk, 2001).
Session 9: Waiting period. The phase betweenembryo transfer and pregnancy test is often describedas one of the most stressful times (Boivin & Takefman,1995; Klonoff-Cohen et al., 2001). Therefore, it isimportant to discuss with couples how they want todeal with this period.
Session 10: We are the champions!. A couple’spartnership is a significant resource, one of whichthey may no longer be aware. The unfulfilled wish fora child and medical treatment represent great bur-dens on a couple’s partnership (Wischmann, 2005). Awell functioning partnership can be a source of powerand support.
Feasibility of the Fertility Group Intervention
Different factors confirm the usefulness and accep-tance of the Fertility Group Intervention. A pilot study(Haemmerli et al., submitted) investigated 62 infertilepatients undergoing treatment at the Fertility Centreof the University Hospital of Bern, Switzerland. Thestudy’s results revealed that a high proportion of theinfertile patients had depressive symptoms. More than40% scored above the threshold for mild depressionand 26% exhibited clinically relevant depressivesymptoms. The Fertility Group Intervention was devel-oped on the basis of these results and the need formore psychological help expressed on the part ofinfertile patients.
An evaluation of the intervention’s efficacy iscurrently underway at the Fertility Centre. To date,the fourth intervention cycle has been completed with18 couples. The usefulness and acceptance of theintervention would appear to be confirmed by thefact that only one couple out of the total 18 has optedto drop out. According to the participants’ descrip-tions of their experiences, the psychological interven-tion provides many benefits and offers them helpfulstrategies for dealing with their infertility. All groupmembers maintain private contact outside the coursecontext. The psychologists themselves describe theintervention programme as very feasible. The inter-vention addresses the issue of infertility and fulfils theneeds of the infertile patients.
In comparison to the costs of assisted reproductivetreatments, the psychological intervention is verycost-efficient, representing only a small fraction ofthe cost of medical treatment. The interventionprogramme outlined above can be readily adopted,transferred, and implemented elsewhere provided it isconducted in an adequate course setting by trainedpsychologists. The Fertility Group Intervention appearsto be a useful and feasible option for infertile patients.
Conclusions
This article has reviewed the existing research onpsychological interventions for infertile patients.Based on the needs expressed by infertile patientsfor more psychological help, the Fertility GroupIntervention has been presented as an integrative,theoretical, and empirical approach to infertilitytherapy. In light of the evidence of psychologicalinterventions’ efficacy in connection with infertilepatients’ mental health and pregnancy rate, psycho-logical interventions should be integrated into thetreatment of such patients. Future research ought tofocus on discovering the best setting for thesepsychological interventions, as well as how they arebest implemented.
Acknowledgements
This study was carried out with support from theSwiss National Science Foundation (grant no. 325100-11375411).
Biographical notes
Katja Haemmerli: Research assistant, University ofBern, Department of Clinical Psychology and Psy-chotherapy; Psychotherapist in education (Master ofAdvanced Studies in Psychotherapy).Hansjoerg Znoj: Professor for Clinical Psychologyand Psychotherapy, University of Bern. Habilitation in2001; Professor for Clinical Psychology at the Uni-versity of Bern since 2006. Grants and honours: SwissNational Foundation (SNF) personal grant recipientfrom 1993 to 1996; recipient of SNF grants toresearch coping with spinal cord injury, coping amongtraumatised Bosnian refugees, and infertility. Recipi-ent of grants from Oncosuisse, SUVA. Researchinterests: Psychotherapy process research; copingand regulation of emotion following traumatisinglife events; clinical psychology; health psychology;bereavement.Salome Burri: Psychotherapist, University of Bern,Department of Clinical Psychology and Psychother-apy; Supervisor of Master of Advanced Studies inPsychotherapy.Patricia Graf: Psychotherapist, University of Bern,Department of Clinical Psychology and Psychother-apy.Dorothea Wunder: Assistant Medical Director andHead of the Fertility Centre of the University Hospital
250 K. Haemmerli et al.
Downloaded By: [Haemmerli, Katja] At: 10:16 17 November 2008
of Bern. Research interests: reproductive medicineand gynaecological endocrinology. Swiss NationalFoundation (SNF) grant recipient together with Prof.Znoj and Prof. Perrig-Chiello to investigate the impactof psychological support for patients whose wish for achild remains unfulfilled.Pasqualina Perrig-Chiello: Professor for Devel-opmental Psychology, University of Bern. She is acertified systemic family therapist. Her research andteaching topics focus on individual differences in well-being, health, and family relations across the span oflife. She chairs a national research programme onchildhood, youth, and intergenerational relations andis a member of the Swiss National Research Council.
References
Anderheim, L., Holter, H., Bergh, C., & Moller, A. (2005). Doespsychological stress affect the outcome of in vitro fertilization?Human Reproduction, 20, 2969!2975.
Bents, H. (1991). Verhaltenstherapeutische Paartherapie bei Kin-derwunschpatienten. [Behavioural couple therapy for child wishpatients.]. In E. Brahler & A. Myer (Eds.), PsychologischeProbleme in der Reproduktionsmedizin. Jahrbuch der Medizi-nischen Psychologie (pp. 144!155). Berlin: Springer.
Boivin, J. (2003). A review of psychosocial interventions in infertility.Social Science and Medicine, 57, 2325!2341.
Boivin, J., & Takefman, J. E. (1995). Stress level across stages of invitro fertilization in subsequently pregnant and nonpregnantwomen. Fertility and Sterility, 64, 802!810.
Boivin, J., Scanlan, L.C., & Walker, S.M. (1999). Why are infertilepatients not using psychosocial counselling? Human Reproduc-tion, 14, 1384!1391.
Bongartz, W., & Bongartz, B. (2000). Hypnosetherapie (2. Aufl.)[Hypnosis therapy (2nd ed.)]. Gottingen: Hogrefe.
Brkovich, A.M., & Fisher, W.A. (1998). Psychological distress andinfertility: forty years of research. Journal of PsychosomaticObstetrics and Gynaecology, 19, 218!228.
Burns, L.H., & Covington, S.H. (2006). Infertility counseling. Acomprehensive handbook for clinicians (2nd ed). Cambridge:Cambridge University Press.
Carmeli, Y.S., & Birbaum-Carmeli, D. (1994). The predicament ofmasculinity: towards understanding the male experience ofinfertility treatments. Sex Roles, 30, 663!677.
Chan, C.H.Y., Ng, E.H.Y., Chan, C.L.W., Ho, P.C., & Chan, T.H.Y.(2006). Effectiveness of psychosocial group intervention forreducing anxiety in women undergoing in vitro fertilization: arandomized controlled study. Fertility and Sterility, 85, 339!346.
Chen, T.-H., Chang, S.-P., Tsai, C.-F., & Juang, K.-D. (2004).Prevalence of depressive and anxiety disorders in an assistedreproductive technique clinic. Human Reproduction, 19, 2313!2318.
Cousineau, T.M., & Domar, A.D. (2007). Psychological impact ofinfertility. Best Practice & Research Clinical Obstetrics andGynaecology, 21, 293!308.
Cousineau, T.M., Green, T.C., Corsini, E., Seibring, A., Showstack,M.T., Applegarth, L., et al. (2008). Online psychoeducationalsupport for infertile women: a randomized controlled trial.Human Reproducation, 23, 554!566.
Daniluk, J.C. (2001). Reconstructing their lives: a longitudinal,qualitative analysis of the transition to biological childlessnessfor infertile couples. Journal of Counselling and Development,79, 439!449.
De Liz, T.M., & Strauss, B. (2005). Differential efficacy of group andindividual/couple psychotherapy with infertile patients. HumanReproduction, 20, 1324!1332.
Domar, A.D., Clapp, D., Slawsby, E.A., Dusek, J., Kessel, B., &Freizinger, M. (2000). Impact of group psychological interven-tions on pregnancy rates in infertile women. Fertility and Sterility,73, 805!811.
Eunpu, D.L. (1995). The impact of infertility and treatment guide-lines for couples therapy. The American Journal of FamilyTherapy, 23, 115!128.
Eugster, A., & Vingerhoets, A.J. (1999). Psychological aspects of invitro fertilization: a review. Social Science and Medicine, 48,575!589.
Fiedler, P. (2005). Verhaltenstherapie in Gruppen (2. Aufl.) [Beha-vioural therapy in groups (2nd ed.)]. Weinheim: Beltz.
FIVNAT-CH (2007). Annual report 2005. Retrieved 15 November2007 from http://www.sgrm.org/49638/49773.html.
Fliegel, S., Groeger, W.M., Kunzel, R., Schulte, D., & Sorgatz, H.(1998). Verhaltenstherapeutische Standardmethoden (4. Aufl.)[Standard methods of behavioural therapy (4th ed.)]. Weinheim:Psychologie Verlags Union.
Fluckiger, C., Regli, D., & Grawe, K. (2005). Allgemeine Psychother-apie im Gruppensetting: Das Zusammenspiel von gruppen- undinterventionsspezifischen Wirkfaktoren. [General psychotherapyin group setting: the interaction of group and interventionspecific curative factors]. Gruppenpsychotherapie und Gruppen-dynamik, 41, 306!322.
Gilbert, P., & Irons, C. (2004). A pilot exploration of the use ofcompassionate images in a group of self-critical people. Memory,12, 507!516.
Grawe, K. (1980). Einleitung [Introduction]. In K. Grawe (Ed.),Verhaltenstherapie in Gruppen (pp. 9!26). Munchen: Urban &Schwarzenberg.
Grawe, K., Donati, R., & Bernauer, F. (1994). Entspannungsverfah-ren [Relaxation techniques]. In K. Grawe, R. Donati & F. Bernauer(Eds.), Psychotherapie im Wandel. Von der Konfession zurProfession (pp. 579!626). Gottingen: Hogrefe.
Greil, A.L. (1997). Infertility and psychological distress: a criticalreview of the literature. Social Science and Medicine, 45, 1679!1704.
Gross, J.J., & Levenson, R.W. (1997). Hidding feelings: the acuteeffects of inhibiting negative and positive emotion. Journal ofAbnormal Psychology, 106, 95!103.
Haemmerli, K., Znoj, H., & Barth, J. (under review). The efficacy ofpsychological interventions for infertile patients: a systematicreview and meta-analysis examining mental health and preg-nancy rate. Manuscript submitted for publication.
Himmel, W., Meyer, J., Kochlen, M.M., & Michelmann, H.W.(2005). Information needs and visitors’ experience of an internetexpert forum on infertility. Journal of Medical Internet Research,7, e20.
Howard, H.I., Kopta, S.M., Krause, M.S., & Orlinsky, D.E. (1986).The dose!effect relationship in psychotherapy. American Psy-chologist, 41, 159!164.
Jacobson, E. (1938). Progressive relaxation: a physiological andclinical investigation of muscular states and their significance inpsychology and medical practice. Chicago: The University ofChicago Press.
Kahlor, L., & Mackert, M. (in press). Perceptions of infertilityinformation and support sources among female patients whoaccess the Internet. Fertility and Sterility.
Klonoff-Cohen, H., Chu, E., Natarajan, L., & Sieber, W. (2001). Aprospective study of stress among women undergoing in vitrofertilization or gamete intrafallopian transfer. Fertility andSterility, 76, 675!687.
Koppenhofer, E. (2004). Kleine Schule des Geniessens [Little schoolof enjoy]. Lengerich: Pabst Science Publishers.
Lazarus, A.A. (1984). In the mind’s eye: the power of imagery forpersonal enrichment. New York: Guildford Press.
Lentner, E., & Glazer, G. (1991). Infertile couples’ perceptions ofinfertility support-group participation. Health Care for WomenInternational, 12, 317!330.
Levitas, E., Parmet, A., Lunenfeld, E., Bentov, Y., Burstein, E., Friger,M., et al. (2006). Impact of hypnosis during embryo transfer onthe outcome of in vitro fertilization!embryo transfer: a case-control study. Fertility and Sterility, 85, 1404!1408.
McNaughton-Cassill, M.E., Bostwick, J.M., Arthur, N.J., Robinson,R.D., & Neal, G.S. (2002). Efficacy of brief couples supportgroups developed to manage the stress of in vitro fertilizationtreatment. Mayo Clinic Proceeding, 77, 1060!1066.
Psychological interventions for infertile patients 251
Downloaded By: [Haemmerli, Katja] At: 10:16 17 November 2008

Menning, B.E. (1980). The emotional needs of infertile couples.Fertility and Sterility, 34, 313!319.
Noorbala, A.A., Ramazanzadeh, F., Malekafzali, H., Abedinia, N.,Forooshani, A.R., Shariat, M., et al. (2008). Effects of apsychological intervention on depression in infertile couples.International Journal of Gynecology and Obstetrics, 101, 248!252.
Peterson, B.D., Pirritano, M., Christensen, U., & Schmidt, L. (2008).The impact of partner coping in couples experiencing infertility.Human Reproducation, 23, 1128!1137.
Reading, A. (1991). Psychological intervention and infertility. In A.Stanton & C. Dunkel-Schetter (Eds.), Infertility: perspectives fromstress and coping research (pp. 183!196). New York: Plenum.
Redd, W.H., Montgomery, G.H., & DuHamel, K.N. (2001). Beha-vioral intervention for cancer treatment side effects. Journal ofthe National Cancer Institute, 93, 810!823.
Sachse, R. (2003). Klarungsorientierte Psychotherapie [Clarification-orientated psychotherapy]. Gottingen: Hogrefe.
Sarrel, P.M., & DeCherney, A.H. (1985). Psychotherapeutic inter-vention for treatment of couples with secondary infertility.Fertility and Sterility, 43, 897!900.
Schmidt, L., Tjørnhøj-Thomsen, T., Boivin, J., & Nyboe Andersen, A.(2005). Evaluation of a communication and stress managementtraining programme for infertile couples. Patient Education andCounseling, 59, 252!262.
Smeenk, J.M., Verhaak, C.M., Eugster, A., van Minnen, A., Zielhuis,G.A., & Braat, D.D. (2001). The effect of anxiety and depressionon the outcome of in-vitro fertilization. Human Reproduction,16, 1420!1423.
Stammer, H., Wischmann, T., & Verres, R. (2002). Counselling andcouple therapy for infertile couples. Family Process, 41, 111!122.
Stammer, H., Verres, R., & Wischmann, T. (2004). Paarberatungund -therapie bei unerfulltem Kinderwunsch [Couple counsellingand psychotherapy for unfulfilled child wish]. Gottingen: Ho-grefe.
Sundby, J., Olsen, A., & Schei, B. (1994). Quality of care forinfertility patients. An evaluation of a plan for a hospitalinvestigation. Scandinavian Journal of Social Medicine, 22,139!144.
Swiss Federal Office of Statistics (2007). 2006 nahmen 5000 Paareeine Behandlung zur medizinisch unterstutzten Fortpflanzung inAnspruch. Retrieved 30 November 2007 from http://www.bfs.admin.ch/portal/de/tools/search.simple.html.
Verhaak, C.M., Smeenk, J.M.J., Evers, A.W.M., Kremer, J.A.M.,Kraaimaat, F.W., & Braat, D.D.M. (2007). Women’s emotionaladjustment to IVF: a systematic review of 25 years of research.Human Reproduction Update, 13, 27!36.
Wischmann, T. (2003). Psychogenic infertility ! myths and facts.Journal of Assisted Reproduction and Genetics, 20, 485!494.
Wischmann, T. (2005). Psychosocial aspects of fertility disorders.Urologe, A, 44, 185!194.
Wischmann, T., & Stammer, H. (2006). Der Traum vom eigenenKind [The dream of the own child]. Stuttgart: Kohlhammer.
World Health Organization . (1992). International statistical classi-fication of diseases and related health problems. Geneva: WHO.
World Health Organization . (2003). Progress report in reproductivehealth research, No. 23. Geneva: WHO.
252 K. Haemmerli et al.
Downloaded By: [Haemmerli, Katja] At: 10:16 17 November 2008

Artikel 3
Haemmerli, K., Znoj, H., & Barth, J. (2009). The Efficacy of Psychological
Interventions for Infertile Patients: A Meta-analysis Examining Mental
Health and Pregnancy Rate. Human Reproduction Update, 15, 279-295.
...........................................................................................................................
The efficacy of psychologicalinterventions for infertile patients: ameta-analysis examining mentalhealth and pregnancy rateKatja Hammerli1,3, Hansjorg Znoj1, and Jurgen Barth2
1Institute of Psychology, Department of Clinical Psychology and Psychotherapy, University of Bern, Switzerland 2Institute of Social undPreventive Medicine (ISPM), Division of Social and Behavioural Health Research, University of Bern, Switzerland
3Correspondence address. E-mail: [email protected]
table of contents
† Introduction† Methods† Results
Description of controlled studiesEfficacy of psychological interventions
† Discussion† Supplementary data
background: Psychological interventions for infertile patients seek to improvemental health and increase pregnancy rates. The aim of thepresent meta-analysis was to examine if psychological interventions improve mental health and pregnancy rate among infertile patients. Thus,controlled studies were pooled investigating psychological interventions following the introduction of assisted reproductive treatments (ART).
methods: The databases of Medline, PsycINFO, PSYNDEX, Web of Science and the Cochrane Library were searched to identify relevantarticles published between 1978 and 2007 (384 articles). Included were prospective intervention studies on infertile patients (women and men)receiving psychological interventions independent of actual medical treatment. The outcome measures were mental health and pregnancy rate.A total of 21 controlled studies were ultimately included in a meta-analysis comparing the efficacy of psychological interventions. Effect sizes (ES)were calculated for psychological measures and risk ratios (RR) for pregnancy rate.
results: The findings from controlled studies indicated no significant effect for psychological interventions regarding mental health(depression: ES 0.02, 99%CI:20.19, 0.24; anxiety: ES 0.16, 99%CI:20.10, 0.42; mental distress: ES 0.08, 99%CI:20.10, 0.51). Nevertheless,there was evidence for the positive impact of psychological interventions on pregnancy rates (RR 1.42, 99% CI: 1.02, 1.96). Concerning preg-nancy rates, significant effects for psychological interventions were only found for couples not receiving ART.
conclusions: Despite the absence of clinical effects onmental health measures, psychological interventions were found to improve somepatients’ chances of becoming pregnant. Psychological interventions represent an attractive treatment option, in particular, for infertile patientswho are not receiving medical treatment.
Key words: assisted reproductive treatment / infertility / meta-analysis / psychological intervention / pregnancy
IntroductionCouples often describe the experience of infertility as a critical, signifi-cant life event bearing emotional challenges (Menning, 1980; Freemanet al., 1985; Dunkel-Schetter and Lobel, 1991). Nevertheless, on
balance, infertile patients do not differ from the general populationwith respect to short-term (Wright et al., 1989; Dunkel-Schetterand Lobel, 1991; Leiblum and Greenfield, 1997; Covington andBurns, 2006) or long-term (Strauss et al., 2004) levels of mental dis-tress, anxiety and depression.
& The Author 2009. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved.For Permissions, please email: [email protected]
Human Reproduction Update, Vol.1, No.1 pp. 1–17, 2009doi:10.1093/humupd/dmp002
Human Reproduction Update Advance Access published February 5, 2009

In addition to the evidence of encouraging long-term adaptationprocesses among infertile couples, there is clear empirical evidencethat assisted reproductive treatments (ART) have a negative short-term influence on the mental distress levels of such couples. Inseveral studies, infertile patients undergoing ART reported highlevels of depressive symptoms, anxiety and distress (Greil, 1997; Brko-vich and Fisher, 1998; Eugster and Vingerhoets, 1999; Chen et al.,2004). Higher levels of anxiety and depression were also foundamong infertile women not receiving ART when compared with arepresentative sample of the German population (Wischmann et al.,2001b).
In some studies, high levels of depressive symptoms, anxiety anddistress have been associated with reduced chances of becoming preg-nant during ART (Demyttenaere et al., 1992, 1998; Thiering et al.,1993; Facchinetti et al., 1997; Klonoff-Cohen et al., 2001; Smeenket al., 2001). Other authors have failed to find a relationshipbetween women’s mental distress and their chances of becomingpregnant during ART (Visser et al., 1994; Boivin and Takefman,1995; Harlow et al., 1996; Slade et al., 1997). Systematic reviews(Eugster and Vingerhoets, 1999; Klonoff-Cohen, 2005; Homan et al.,2007) have summarized these controversial findings and concludedthat psychosocial factors like psychosocial distress, ineffective copingstrategies, anxiety and depression may possibly lower one’s chancesof becoming pregnant.
Two major goals of psychological interventions for infertile patientsare to improve their mental health and increase their pregnancy rate.Two previously published reviews sought to examine the efficacy ofsuch psychological interventions with respect to the mental healthand pregnancy rate of infertile patients.
In a first narrative review, Boivin (2003) examined whether specificpsychological interventions are more efficacious than usual care.According to her review, mixed results were obtained for the efficacyof psychological interventions with respect to anxiety and depressionamong infertile patients. Positive study results were found more fre-quently in connection with anxiety (8 of 13 analyses, 61.5%) than inconnection with depressive symptoms (5 of 13 analyses, 38.4%). Noclear effect was found for psychological interventions with respectto interpersonal functioning (3 of 11 analyses, 27.3%); however,infertility-specific stress was reduced in all studies (six of six analyses,100%) and target behaviour (e.g. sexual behaviour) was also modifiedin 10 of 10 analyses (100%). No clear efficacy for psychological inter-ventions was reported for pregnancy rates following treatment; threeof eight analyses reported an increased pregnancy rate 6–18 monthsafter the psychological intervention.
In a second review, de Liz and Strauss (2005) conducted ameta-analysis of the comparative efficacy of psychological interven-tions in group settings versus those in individual or couples settings.The studies they included assessed anxiety (N ! 10), depressivesymptoms (N ! 10) and pregnancy rate (N ! 16). It is important tonote that pre–post effect sizes (ES) were calculated for psychologicalmeasures without taking into account the study design, i.e. no com-parisons to control groups were reported by the authors. Withrespect to anxiety, their results pointed to the efficacy of psychother-apeutic strategies labelled both as individual or couples psychotherapy(significant ES 0.17, 95% CI: 0.05, 0.29) and those labelled as grouptherapy (significant ES 0.36, 95% CI: 0.24, 0.48) in a pre–post com-parison. They also report of a weak pre–post intervention effect on
depressive symptoms for individual or couples psychotherapy (ES0.12, 95% CI: 0.002, 0.24) and group therapy (ES 0.19, 95% CI:0.07, 0.31). However, the review’s most interesting result was itsreport of a higher conception rate among patients following a psy-chotherapeutic intervention. The mean pregnancy rate for patientswho received psychotherapy preceding or accompanying their treat-ment for infertility was 45% (18 studies), whereas only 14% of thepatients in control groups (six studies) became pregnant.
These two initial reviews came to divergent conclusions regardingthe resulting pregnancy rate; and, in the case of de Liz and Strauss(2005), this was a very prominent result of the study. While de Lizand Strauss (2005) reported an enhanced pregnancy rate from con-trolled and uncontrolled studies, Boivin (2003) came to a more cau-tious interpretation from eight controlled studies of highermethodological quality. In order to arrive at a valid conclusion, it isessential to compare the resultant pregnancy rates solely from con-trolled studies. Otherwise, researchers risk ignoring factors contribut-ing to the pregnancy rate that should have been controlled for.Therefore, it is possible that de Liz and Strauss’ study overestimatesthe efficacy of psychological interventions for infertile patients inregard to pregnancy rate.
The present meta-analysis sought to provide more definitiveanswers regarding the efficacy of psychological interventions for infer-tile patients by limiting its analysis to controlled investigations and byintegrating those relevant studies published recently.
The following research questions were examined:
(i) Do psychological interventions improve mental health (anxiety,depression, mental distress, interpersonal functioning andinfertility-specific stress) in patients with infertility?
(ii) Are psychological interventions effective in increasing the preg-nancy rate among infertile couples?
(iii) Do study and patient characteristics (sex, duration of interven-tion, ART and randomization) alter the efficacy of the psychologi-cal interventions studied?
Methods
Inclusion and exclusion criteriaThe inclusion criteria for the studies were: (i) study participants had to beinfertile women and men independent of actual medical treatment; (ii)prospective study designs; (iii) participants must have received a psycho-logical intervention (e.g. counselling, cognitive-behavioural therapy, edu-cational interventions, relaxation, psychodynamic/-analyticinterventions); and (iv) the study had to report on one outcomemeasure at minimum (mental health, interpersonal functioning, infertility-specific stress or pregnancy rate).The included studies drew from both published and unpublished
sources, and the literature search was limited to the timeframe from1978 to 2007. The year 1978 was selected as a lower limit since thatyear marked the first time a child was born as a result of in vitro fertilization(IVF), greatly altering medical treatment of infertility from then on. Owingto the introduction of such medical treatments, the period prior to 1978simply is not comparable with the period following. Finally, studies of anylanguage or cultural background were considered eligible for inclusion.Case reports, unsystematic narratives, expert opinions, magazines, news-paper articles and commentaries were excluded.
2 Hammerli et al.

DesignFor the meta-analysis, studies were included that employed a controlgroup design independent of their type of allocation (randomized or non-randomized). These studies were used to compare post-intervention effi-cacy of the psychological intervention.
Participants and definition of infertilityThe study participants were women and men suffering from infertility,independent of the actual medical treatment used to treat their infertility.Different definitions and classifications of infertility exist, and stem eitherfrom the World Health Organization (WHO) or organizations like theEuropean Society of Human Reproduction and Embryology (ESHRE) orfrom the authors of primary studies themselves. For clinical purposes,the gold standard definition of infertility is ‘the inability of a couple toachieve conception or to bring a pregnancy to term after a year ofregular, unprotected sexual intercourse’ (WHO, 2002). Nevertheless, acut-off value of 2 years is used in many epidemiological studies (WHO,1975). In addition to these dichotomous classifications, there are alsograded classification systems of infertility in use, with grading rangingfrom fertile to infertile based on the duration of one’s unfulfilled wishfor a child and clinical characteristics (Gnoth et al., 2005; Habbemaet al., 2004). Since there is no clear, accepted definition utilized by every-one, the present meta-analysis included any studies using a sample labelledas infertile according to any of the above-mentioned definitions.
InterventionsFor the purposes of the present meta-analysis, a psychological interventionwas defined as a face-to-face intervention: (i) designed to influencepsychological functioning; (ii) based on a psychological theory and (iii)incorporating psychological strategies through interaction. The psychologi-cal interventions could be provided in a variety of settings (i.e. individual,couple or group; inpatient or outpatient).
Control group conditionsThe control group participants did not receive a psychological interven-tion. They were either on waiting lists or received routine care. Themeta-analysis also included two studies that reported of patients whodeclined the intervention, as long as such patients constituted ,50% ofthe total sample of the control group (Ellenberg and Koren, 1982;Strauss et al., 2002).
Outcome measuresThe outcome measures were psychological dimensions as well as theresultant pregnancy rate. The psychological dimensions compriseddepressive symptoms, anxiety, mental distress, interpersonal functioningand infertility-specific stress. These dimensions were all assessedthrough the use of self-report questionnaires. Pregnancy rate wasdefined as evidence of pregnancy according to clinical or ultrasound par-ameters (ultrasound visualization of a gestational sac; Zegers-Hochschildet al., 2006). The resultant pregnancy rate was assessed either by patients’self-reports or according to the reports of their clinicians.
Literature search and data sourcesA systematic approach was used to identify relevant studies. The followingdatabases were searched for relevant studies published between 1978 and2007: MEDLINE (U.S. National Library of Medicine, 1978 to April 2007),PsycINFO (American Psychological Association, 1978 to January–March2007), PSYNDEX (German database of the Center for Psychological Infor-mation and Documentation at the University of Trier, Germany 1978 to
January–March 2007), Web of Science (Social Sciences Citation Index,1978 to April 2007) and the Cochrane Library (1978 to Issue 1, 2007).When performing the search, two primary concepts were combinedwith ‘and’. The two primary search concepts were: (i) ‘infertil*’, ‘fertilitydisorder/treatment/problems’, ‘sterility’, ‘IVF’, ‘ICSI’, ‘involuntary child-lessness’, ‘ET’, ‘assisted reproduction’ and (ii) ‘psychotherap*’, ‘CBT’,‘psychological intervention’, ‘psychoeducation’, ‘hypnosis’, ‘autogenictraining’, ‘behavioural therapy’ (see the Supplementary Appendix fordetailed information on the literature search). All results were downloadedand stored in the reference database program EndNote 10. The databasesearch resulted in 384 references.A total of eight reviews were found as a result of this initial search.
Next, the eight reviews were manually checked for further study citations.In addition, the congress abstracts of ESHRE (European Society of HumanReproduction, 2002 to 2006) and ASRM (American Society for Reproduc-tive Medicine, 2002 to 2006) were searched for unpublished studies, andthe authors of these studies were contacted. In sum, five authors of con-trolled studies were contacted for additional information: all of themresponded. As a result of the manual search, 13 additional referenceswere included in the meta-analysis.
Study selection and data extractionThe initial literature search of databases yielded 384 references. Next, 307references were excluded based on their titles or abstracts. In anadditional step, 49 references were excluded on the basis of their con-tents. In the end, 21 studies (culled from the database search plus fromthe manual search) published in 26 papers were included in themeta-analysis. A total of 356 references were ultimately excluded andcoded according to their reason for exclusion (see Supplementary Appen-dix). The respective reasons for exclusion were: (i) the study was not anempirical investigation (n ! 253); (ii) the study did not report on a psycho-logical intervention (n ! 77); (iii) due to the characteristics of the study’ssample (no infertile persons, n ! 14); (iv) excluded as review (n ! 8)and (v) due to the absence of an evaluation of the psychological interven-tion (n ! 4).In order to conduct a reliability analysis of the selection process (i.e.
study inclusion or exclusion), the first author and another trainedperson independently rated 80 publications on the basis of their titleand abstract. Their percentage of agreement and the inter-ratterreliabilities (kappa) were as follows: study excluded ! 93% (kappa !0.84); study included based on title and/or abstract ! 99% (0.94);excluded as review ! 99% (0.66) and unclear ! 93% (NA). The percen-tage agreement (inter-rater reliabilities) for the exclusion criteria wereas follows: no psychological intervention ! 96% (0.89); no evaluation ofthe intervention ! 99% (NA); incorrect sample ! 99% (0.66);non-empirical report or case reports ! 96% (0.92). These numbers indi-cate excellent reliability of study selection.The present meta-analysis included 21 studies that utilized a control
group. An additional 14 studies were found that only reported results ofan uncontrolled design; they were excluded from the meta-analysis.Finally, six studies with a controlled design were treated as uncontrolledstudies and excluded from the meta-analysis due to one of the followingreasons: no face-to-face intervention (Cousineau et al., 2006), dropoutof control group (Clark et al., 1995, 1998; Galletly et al., 1996b), fertilecontrol group (O’Moore et al., 1983) or insufficient data (Takefmanet al., 1990; Melamed et al., 2005).
Data extractionThe first author and one other trained person independently rated all data ofthe included studies. Both reviewers coded each study in a paper/pencilcodebook. Following this initial coding, differences between the two
Psychological interventions for infertile patients 3

reviewers were solved in discussion, giving rise to a final joint coding. Thecalculation of ES and the calculation of standard errors of effect measureswere performed through a double data extraction procedure (K.H. and J.B.).
Effect size calculation and data analysisAll the outcome measures were assessed post-intervention or at follow-up(FU) (ranging from 1 to 12 months). ES for interval data were calculatedthrough comparisons between groups independent of their baselinevalue. Only one ES was calculated per individual study. If data fromthree groups were available stemming from one study (two different inter-vention groups plus one control group), one ES was calculated for theentire study through a collective comparison of the effects registered byits treatment groups versus the control conditions (McQueeney et al.,1997; Domar et al., 2000a, b; Wischmann et al., 2001a, b, 2002;Strauss et al., 2002; Emery et al., 2003, 2006). If data from female andmale participants were available, they were included separately in themeta-analysis and used for subgroup analysis.ES for interval data were calculated from mean and standard deviation
using Wilson’s (2001) ES calculator. In one study (Tuschen-Caffier et al.,1999), where solely median data were reported, the ES was calculatedusing the approach developed by Hozo et al. (2005). An ES of !0.20 to0.50 indicates a low effect; !0.50 to 0.80 indicates a medium effectand !0.80 indicates a large effect (Cohen, 1977) between groups. ES .0 indicate a beneficial effect for the given psychological intervention. Thestandard error of ES was separately computed in an Excel sheet accordingto the formula provided by Lipsey and Wilson (2001). ES differences werecomputed according to Altman and Bland (2003).Data on the number of pregnancies following the intervention were
compared with the number of pregnancies in the control group using rela-tive risks. Since missing data are highly relevant when measuring the effi-cacy of interventions, the pregnancy rate was calculated using anintention to treat (ITT) analysis or, if the data were not sufficient, fromFU data only. According to the ITT model, patients were classified aschildless if they were not reached at FU. The FU model was restrictedto information stemming from subjects with FU information available. Rela-tive risks of the pregnancy rate were calculated (Rosenthal et al., 2000), i.e.a relative risk larger than 1 indicates a higher pregnancy rate for the inter-vention group versus usual care and vice versa.Data analysis was carried out using Review Manager 5.0 (2007). The
main analysis focused on outcome measures through a comparison ofintervention and control groups. All subgroup analyses followed pre-specified hypotheses of confounders of efficacy. For the pooling of intervaldata, the standardized mean procedure was chosen since the outcomemeasures differed between studies. For the pooling of the relative risk,the Mantel–Haenszel approach (Hauck, 1989) was used. A randomeffect model for pooling the studies was employed in all outcomes dueto the anticipated heterogeneity of the primary studies. The 99% CI wasused since multiple hypotheses were tested. The CIs represent 99%ranges, which indicate a statistically significant effect when zero (0)values are excluded from the ES measures or values of 1 are excludedfrom the relative risks.Heterogeneity between the studies was assessed by examining forest
plots of trials, by calculating a chi-square heterogeneity test and throughI2 statistics. The chi-squared value is used to test for statistically significantheterogeneity between trials and indicates heterogeneity if statistical sig-nificance is found. In addition, higher I2 values indicate greater variabilitybetween trials than would be expected due to chance alone (range 0–100%; Higgins et al., 2003). Higgins et al. (2003) propose as heterogeneityindicators I2 values of 25% for low heterogeneity, 50% for moderate het-erogeneity and 75% for high heterogeneity. As publication bias might bepresent, data were analysed from each outcome in funnel plots in order
to spot unexpected study results. The results of the funnel plots are avail-able via the Internet.
Results
Description of studiesA total of 21 studies were included in the meta-analysis of controlledstudies (Table I; the included studies are marked in the reference list).Exactly 1420 persons were assigned to the intervention group and3342 persons were assigned to the control group. Of the totalnumber of studies, 11 were carried out in Europe (three inGermany, two in Italy and one each in the UK, the Netherlands, Swit-zerland, Israel, the Czech Republic and Denmark), 5 were from theUS, 3 were from China and 2 were from Canada. The majority ofthe studies were published in English (n ! 19), whereas one studywas written in German and another in Chinese. Further, 10 of thestudies reported on patients receiving ART (IVF/intracytoplasmicsperm injection: ICSI) for infertility, whereas 8 of the studies investi-gated patients not receiving IVF/ICSI (i.e. receiving other medicaltreatments like intrauterine sperm insemination). Finally, three of thestudies reported on patients who received mixed treatments. In themajority of the studies, patients were referred by their general prac-titioner or by fertility clinics. In some of the studies, patients wererecruited by newspaper advertisements, from adoption waiting listsor from psychiatric services. The mean duration of infertility was 3.8years (1.5–5.9). The mean age of the intervention group participantswas 32.7 (27–36.5), whereas the mean age of the control group par-ticipants was 32.9 (27–38.5). A total of seven studies included womenonly; seven studies included men and women and seven studiestreated couples only. Randomized allocation was used in 12 of thestudies, whereas 9 of the studies used non-randomized allocation.
The following psychosocial outcomes were reported (number ofstudies): depression (12), anxiety (12), mental distress (8), interperso-nal functioning (5) and infertility-specific stress (5). Pregnancy rateswere reported in 14 of the studies. Most of the studies assessedother dimensions as well (e.g. self-efficacy, implantation rate, intensityof the wish for a child) not covered by the dimensions listed above(14). The time point of assessment following the intervention variedstrongly from 30 min on up to 3 years. Most of the studies measuredoutcomes between 4 weeks and 6 months after the psychologicalintervention.
The intervention strategies employed included counselling(Connolly et al., 1993; Wischmann et al., 2001a, b, 2002;McNaughton-Cassill et al., 2002; Strauss et al., 2002; Emery et al.,2003, 2006; De Klerk et al., 2005; Zhen et al., 2005), cognitive-behavioural therapies (Stewart et al., 1992; Liswood, 1995; Domaret al., 2000a, b; Facchinetti et al., 2004; Tarabusi et al., 2004), edu-cation (McQueeney et al., 1997; Tuschen-Caffier et al., 1999;Shu-Hsin, 2003; Chan et al., 2006), mind/body orientated relaxation(Rezabek et al., 2003; Levitas et al., 2006), psychodynamic/-analytic(Ellenberg and Koren, 1982; Sarrel and DeCherney, 1985) andmixed interventions (Schmidt et al., 2005). The total duration of theinterventions varied between 1–5 h (8), 6–12 h (8), 13–25 h (3)and .25 h (1). The number of sessions was comparable with thetotal duration: 1–5 sessions (8), 6–12 sessions (10) and 13–32 ses-sions (1). In 11 of the studies, patients in the control group did not
4 Hammerli et al.
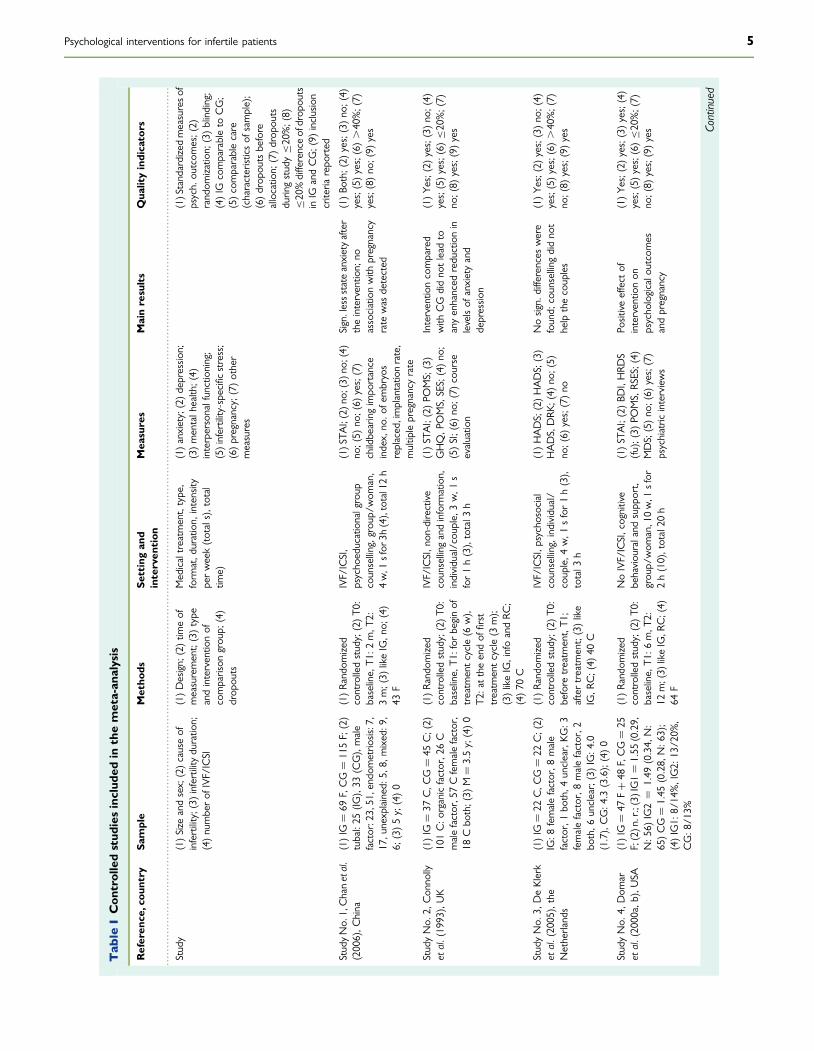
........................................................................................................................................................................................................................................................
Tab
leICon
trolledstud
iesinclud
edin
themeta-an
alysis
Referen
ce,cou
ntry
Sample
Metho
dsSe
ttingan
dinterven
tion
Mea
sures
Mainresults
Qua
lityindicators
Study
(1)Size
andsex;
(2)causeof
infertility;(3)infertility
duratio
n;(4)numberof
IVF/ICSI
(1)Design;
(2)tim
eof
measurement;(3)type
andinterventio
nof
comparison
grou
p;(4)
drop
outs
Medicaltreatm
ent,type,
form
at,d
uration,
intensity
perweek(totals),total
time)
(1)anxiety;(2)d
epression;
(3)mentalhealth;(4)
interpersonalfunctioning;
(5)infertility-specific
stress;
(6)pregnancy;(7)other
measures
(1)Standardizedmeasureso
fpsych.
outcom
es;(2)
random
izatio
n;(3)blinding;
(4)IG
comparableto
CG;
(5)comparablecare
(characteristicsof
sample);
(6)drop
outsbefore
allocatio
n;(7)drop
outs
durin
gstudy"20%;(8)
"20%differenceofdrop
outs
inIG
andCG;(9)
inclusion
criteria
repo
rted
StudyNo.1,Chanetal.
(2006),C
hina
(1)IG
!69
F,CG!
115F;(2)
tubal:25
(IG),33
(CG),male
factor:23,51,endom
etrio
sis:7,
17,u
nexplained:5
,8,m
ixed:9
,6;
(3)5y;(4)0
(1)Ra
ndom
ized
controlledstudy;(2)T0
:baseline,
T1:2
m,T
2:3m;(3)
likeIG,n
o;(4)
43F
IVF/ICSI,
psycho
educationalgroup
counsellin
g,grou
p/wom
an,
4w,1
sfor
3h(4),total12h
(1)S
TAI;(2)n
o;(3)n
o;(4)
no;(5)
no;(6)
yes;(7)
childbearingimpo
rtance
index,
no.o
fembryos
replaced,implantatio
nrate,
multip
lepregnancyrate
Sign.lessstate
anxietyafter
theinterventio
n;no
associationwith
pregnancy
rate
was
detected
(1)Bo
th;(2)
yes;(3)no
;(4)
yes;(5)yes;(6).40%;(7)
yes;(8)no
;(9)
yes
StudyNo.
2,Con
nolly
etal.(1993),UK
(1)IG
!37
C,C
G!
45C;(2)
101C:o
rganicfactor,2
6C
malefactor,57Cfemalefactor,
18Cbo
th;(3)
M!
3.5y;(4)0
(1)Ra
ndom
ized
controlledstudy;(2)T0
:baseline,
T1:for
beginof
treatm
entcycle(6
w),
T2:attheendof
first
treatm
entcycle(3
m);
(3)likeIG,infoandRC
;(4)70
C
IVF/ICSI,n
on-dire
ctive
counsellin
gandinform
ation,
individual/cou
ple,
3w,1
sfor1h(3),total3
h
(1)ST
AI;(2)PO
MS;(3)
GHQ,P
OMS,SES;(4)no
;(5)SI;(6)
no;(7)
course
evaluatio
n
Interventio
ncompared
with
CG
didno
tlead
toanyenhanced
reductionin
levelsof
anxietyand
depressio
n
(1)Ye
s;(2)yes;(3)no
;(4)
yes;(5)yes;(6)"20%;(7)
no;(8)
yes;(9)yes
StudyNo.
3,DeKlerk
etal.(2005),the
Netherlands
(1)IG
!22
C,C
G!
22C;(2)
IG:8
femalefactor,8
male
factor,1
both,4
unclear,KG
:3femalefactor,8
malefactor,2
both,6
unclear;(3)IG:4
.0(1.7),CG:4
.3(3.6);(4)0
(1)Ra
ndom
ized
controlledstudy;(2)T0
:before
treatm
ent,T1
;aftertreatm
ent;(3)like
IG,R
C;(4)
40C
IVF/ICSI,p
sychosocial
counsellin
g,individual/
couple,4
w,1
sfor1h(3),
total3
h
(1)HADS;(2)HADS;(3)
HADS,DRK
;(4)
no;(5)
no;(6)
yes;(7)no
Nosign.
differences
were
found;
counsellin
gdidno
thelp
thecouples
(1)Ye
s;(2)yes;(3)no
;(4)
yes;(5)yes;(6).40%;(7)
no;(8)
yes;(9)yes
StudyNo.
4,Dom
aret
al.(2000a,b),U
SA(1)IG!
47F#
48F,CG!
25F;(2)n
.r.;(3)IG1!
1.55
(0.29,
N:5
6)IG2!
1.49
(0.34,
N:
65)CG!
1.45
(0.28,
N:6
3);
(4)IG1:
8/14%,IG2:
13/2
0%,
CG:8
/13%
(1)Ra
ndom
ized
controlledstudy;(2)T0
:baseline,
T1:6
m,T
2:12
m;(3)
likeIG,R
C;(4)
64F
NoIVF/ICSI,cognitive
behaviou
raland
supp
ort,
grou
p/wom
an,10w,1
sfor
2h(10),total20
h
(1)ST
AI;(2)BD
I,HRD
S(fu);(3)
POMS,RS
ES;(4)
MDS;(5)no
;(6)
yes;(7)
psychiatric
interviews
Positiveeffect
ofinterventio
non
psycho
logicalo
utcomes
andpregnancy
(1)Ye
s;(2)yes;(3)yes;(4)
yes;(5)yes;(6)"20%;(7)
no;(8)
yes;(9)yes Co
ntinued
Psychological interventions for infertile patients 5
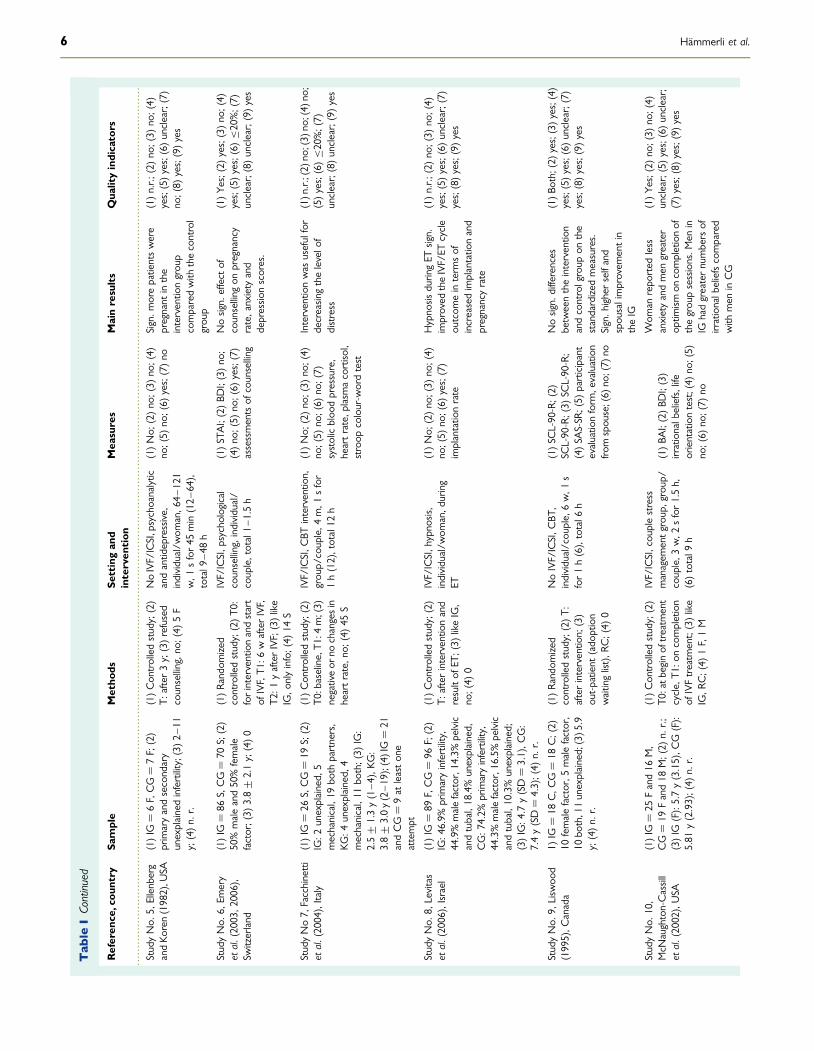
........................................................................................................................................................................................................................................................
Tab
leIContinued
Referen
ce,cou
ntry
Sample
Metho
dsSe
ttingan
dinterven
tion
Mea
sures
Mainresults
Qua
lityindicators
StudyNo.
5,Ellenberg
andKo
ren(1982),U
SA(1)IG
!6F,CG!
7F;(2)
primaryandsecondary
unexplainedinfertility;(3)2
–11
y;(4)n.
r.
(1)Con
trolledstudy;(2)
T:after3y;(3)refused
counsellin
g,no
;(4)
5F
NoIVF/ICSI,psychoanalytic
andantid
epressive,
individual/w
oman,6
4–121
w,1
sfor45
min(12–6
4),
total9
–48
h
(1)No;
(2)no
;(3)
no;(4)
no;(5)
no;(6)
yes;(7)no
Sign.m
orepatientswere
pregnant
inthe
interventio
ngrou
pcomparedwith
thecontrol
grou
p
(1)n.r.;
(2)no
;(3)
no;(4)
yes;(5)yes;(6)unclear;(7)
no;(8)
yes;(9)yes
StudyNo.
6,Em
ery
etal.(2003,2
006),
Switzerland
(1)IG
!86
S,CG!
70S;(2)
50%maleand50%female
factor;(3)
3.8+
2.1y;(4)0
(1)Ra
ndom
ized
controlledstudy;(2)T0
:forinterventio
nandstart
ofIVF,T1
:6wafterIVF,
T2:1
yafterIVF;(3)like
IG,o
nlyinfo;(4)
14S
IVF/ICSI,p
sychological
counsellin
g,individual/
couple,total1–1
.5h
(1)ST
AI;(2)BD
I;(3)no
;(4)no
;(5)
no;(6)
yes;(7)
assessmentsof
counsellin
g
Nosign.
effect
ofcounsellin
gon
pregnancy
rate,anxiety
and
depressio
nscores.
(1)Ye
s;(2)yes;(3)no
;(4)
yes;(5)yes;(6)"20%;(7)
unclear;(8)unclear;(9)yes
StudyNo7,
Facchinetti
etal.(2004),Italy
(1)IG
!26
S,CG!
19S;(2)
IG:2
unexplained,
5mechanical,19
both
partners,
KG:4
unexplained,
4mechanical,11
both;(3)
IG:
2.5+
1.3y(1–4
),KG
:3.8+
3.0y(2–19);(4)IG!
21andCG!
9at
leaston
eattempt
(1)Con
trolledstudy;(2)
T0:baseline,T1
:4m;(3)
negativeor
nochangesin
heartrate,n
o;(4)45
S
IVF/ICSI,C
BTinterventio
n,grou
p/couple,4
m,1
sfor
1h(12),total12
h
(1)No;
(2)no
;(3)
no;(4)
no;(5)
no;(6)
no;(7)
systolicbloo
dpressure,
heartrate,p
lasm
acortiso
l,stroop
colour-w
ordtest
Interventio
nwas
usefulfor
decreasin
gthelevelo
fdistress
(1)n
.r.;(2)
no;(3)
no;(4)
no;
(5)yes;(6)"20%;(7)
unclear;(8)unclear;(9)yes
StudyNo.
8,Levitas
etal.(2006),Israel
(1)IG
!89
F,CG!
96F;(2)
IG:4
6.9%
primaryinfertility,
44.9%malefactor,14.3%
pelvic
andtubal,18.4%unexplained,
CG:7
4.2%
primaryinfertility,
44.3%malefactor,16.5%
pelvic
andtubal,10.3%unexplained;
(3)IG:4
.7y(SD!
3.1),C
G:
7.4y(SD!
4.3);(4)
n.r.
(1)Con
trolledstudy;(2)
T:afterinterventio
nand
resultof
ET;(3)
likeIG,
no;(4)
0
IVF/ICSI,h
ypno
sis,
individual/w
oman,d
uring
ET
(1)No;
(2)no
;(3)
no;(4)
no;(5)
no;(6)
yes;(7)
implantatio
nrate
Hypno
sisdurin
gET
sign.
improved
theIVF/ET
cycle
outcom
einterm
sof
increasedimplantatio
nand
pregnancyrate
(1)n.r.;
(2)no
;(3)
no;(4)
yes;(5)yes;(6)unclear;(7)
yes;(8)yes;(9)yes
StudyNo.
9,Lisw
ood
(1995),C
anada
1)IG
!18
C,C
G!
18C;(2)
10femalefactor,5
malefactor,
10bo
th,11unexplained;(3)5
.9y;(4)n.
r.
(1)Ra
ndom
ized
controlledstudy;(2)T:
afterinterventio
n;(3)
out-patient
(ado
ption
waitinglist),R
C;(4)
0
NoIVF/ICSI,C
BT,
individual/cou
ple,
6w,1
sfor1h(6),total6
h
(1)SC
L-90-R;(2)
SCL-90-R;(3)
SCL-90-R;
(4)SA
S-SR
;(5)
participant
evaluatio
nform
,evaluation
from
spou
se;(6)
no;(7)
no
Nosign.
differences
betw
eentheinterventio
nandcontrolgroup
onthe
standardize
dmeasures.
Sign.h
igherselfand
spou
salimprovem
entin
theIG
(1)B
oth;
(2)yes;(3)yes;(4)
yes;(5)yes;(6)unclear;(7)
yes;(8)yes;(9)yes
StudyNo.
10,
McN
aughton-Cassill
etal.(2002),USA
(1)IG
!25
Fand16
M,
CG!
19Fand18
M;(2)
n.r.;
(3)IG
(F):5.7y(3.15),C
G(F):
5.81
y(2.93);(4)
n.r.
(1)Con
trolledstudy;(2)
T0:atb
eginof
treatm
ent
cycle,T1
:oncompletion
ofIVFtreatm
ent;(3)like
IG,R
C;(4)
1F,1M
IVF/ICSI,cou
plestress
managem
entgrou
p,grou
p/couple,3
w,2
sfor1.5h,
(6)total9
h
(1)BA
I;(2)BD
I;(3)
irrationalb
eliefs,life
orientationtest;(4)
no;(5)
no;(6)
no;(7)
no
Wom
anrepo
rted
less
anxietyandmen
greater
optim
ismon
completionof
thegrou
psessions.M
enin
IGhadgreaternumbers
ofirrationalb
eliefscompared
with
men
inCG
(1)Ye
s;(2)no
;(3)
no;(4)
unclear;(5)yes;(6)unclear;
(7)yes;(8)yes;(9)yes
6 Hammerli et al.
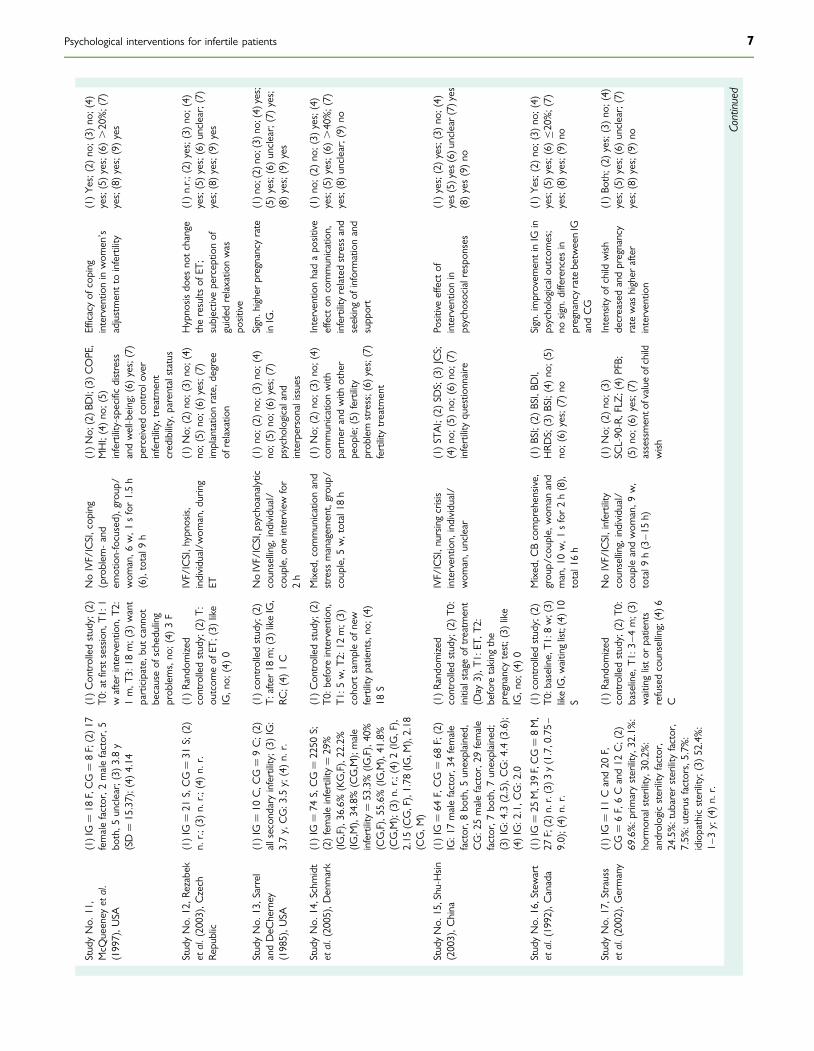
StudyNo.
11,
McQ
ueeney
etal.
(1997),U
SA
(1)IG!
18F,CG!
8F;(2)1
7femalefactor,2
malefactor,5
both,5
unclear;(3)3.8y
(SD!
15.37);(4)
4.14
(1)Con
trolledstudy;(2)
T0:atfi
rstsessio
n,T1
:1wafterinterventio
n,T2
:1m,T
3:18
m;(3)
want
participate,
butcannot
becauseof
scheduling
prob
lems,no
;(4)
3F
NoIVF/ICSI,cop
ing
(problem
-and
emotion-focused),group/
wom
an,6
w,1
sfor1.5h
(6),total9
h
(1)N
o;(2)B
DI;(3)C
OPE,
MHI;(4)no
;(5)
infertility-specificdistress
andwell-b
eing;(6)
yes;(7)
perceivedcontrolo
ver
infertility,treatm
ent
credibility,parentalstatus
Efficacyof
coping
interventio
ninwom
en’s
adjustmentto
infertility
(1)Ye
s;(2)no
;(3)
no;(4)
yes;(5)yes;(6).20%;(7)
yes;(8)yes;(9)yes
StudyNo.
12,R
ezabek
etal.(2003),Czech
Republic
(1)IG
!21
S,CG!
31S;(2)
n.r.;
(3)n.
r.;(4)n.
r.(1)Ra
ndom
ized
controlledstudy;(2)T:
outcom
eof
ET;(3)
like
IG,n
o;(4)0
IVF/ICSI,h
ypno
sis,
individual/w
oman,d
uring
ET
(1)No;
(2)no
;(3)
no;(4)
no;(5)
no;(6)
yes;(7)
implantatio
nrate,d
egree
ofrelaxatio
n
Hypno
sisdo
esno
tchange
theresults
ofET
;subjectiveperceptio
nof
guided
relaxatio
nwas
positive
(1)n.r.;
(2)yes;(3)no
;(4)
yes;(5)yes;(6)unclear;(7)
yes;(8)yes;(9)yes
StudyNo.
13,Sarrel
andDeC
herney
(1985),U
SA
(1)IG
!10
C,C
G!
9C;(2)
allsecon
dary
infertility;(3)IG:
3.7y,CG:3
.5y;(4)n.
r.
(1)controlledstudy;(2)
T:after18
m;(3)
likeIG,
RC;(4)
1C
NoIVF/ICSI,psychoanalytic
counsellin
g,individual/
couple,o
neinterview
for
2h
(1)no
;(2)
no;(3)
no;(4)
no;(5)
no;(6)
yes;(7)
psycho
logicaland
interpersonalissues
Sign.higherpregnancyrate
inIG.
(1)n
o;(2)n
o;(3)n
o;(4)yes;
(5)yes;(6)unclear;(7)yes;
(8)yes;(9)yes
StudyNo.
14,Schmidt
etal.(2005),Denmark
(1)IG
!74
S,CG!
2250
S;(2)femaleinfertility!
29%
(IG,F),36.6%(KG,F),22.2%
(IG,M
),34.8%(C
G,M
);male
infertility!
53.3%(IG
,F),40%
(CG,F),55.6%(IG
,M),41.8%
(CG,M
);(3)n.
r.;(4)2(IG
,F),
2.15
(CG,F),1.78
(IG,M
),2.18
(CG,M
)
(1)Con
trolledstudy;(2)
T0:b
eforeinterventio
n,T1
:5w,T
2:12
m;(3)
coho
rtsampleof
new
fertilitypatients,no
;(4)
18S
Mixed,com
municationand
stress
managem
ent,grou
p/couple,5
w,total18
h
(1)No;
(2)no
;(3)
no;(4)
communicationwith
partnerandwith
other
peop
le;(5)
fertility
prob
lem
stress;(6)
yes;(7)
fertilitytreatm
ent
Interventio
nhadapo
sitive
effect
oncommunication,
infertilityrelatedstress
and
seekingof
inform
ationand
supp
ort
(1)no
;(2)
no;(3)
yes;(4)
yes;(5)yes;(6).40%;(7)
yes;(8)unclear;(9)no
StudyNo.
15,Shu-H
sin(2003),C
hina
(1)IG
!64
F,CG!
68F;(2)
IG:1
7malefactor,3
4female
factor,8
both,5
unexplained,
CG:2
5malefactor,2
9female
factor,7
both,7
unexplained;
(3)IG:4
.3(2.5),CG:4
.4(3.6);
(4)IG:2
.1,C
G:2
.0
(1)Ra
ndom
ized
controlledstudy;(2)T0
:initialstageof
treatm
ent
(Day
3),T
1:ET
,T2:
before
taking
the
pregnancytest;(3)
like
IG,n
o;(4)0
IVF/ICSI,n
ursin
gcrisis
interventio
n,individual/
wom
an,u
nclear
(1)ST
AI;(2)SD
S;(3)JCS;
(4)no
;(5)
no;(6)
no;(7)
infertilityquestio
nnaire
Positiveeffect
ofinterventio
nin
psycho
socialrespon
ses
(1)yes;(2)yes;(3)no
;(4)
yes(5)
yes(6)
unclear(7)
yes
(8)yes(9)no
StudyNo.
16,Stewart
etal.(1992),Canada
(1)IG!
25M,39F,CG!
8M,
27F;(2)n
.r.(3)
3y(1.7,0.75–
9.0);(4)
n.r.
(1)controlledstudy;(2)
T0:baseline,T1
:8w;(3)
likeIG,w
aitinglist;(4)1
0S
Mixed,C
Bcomprehensive,
grou
p/couple,w
oman
and
man,1
0w,1
sfor2h(8),
total16h
(1)BSI;(2)BSI,BD
I,HRD
S;(3)BSI;(4)no
;(5)
no;(6)
yes;(7)no
Sign.improvem
entinIG
inpsycho
logicalo
utcomes;
nosign.
differences
inpregnancyratebetw
eenIG
andCG
(1)Ye
s;(2)no
;(3)
no;(4)
yes;(5)yes;(6)"20%;(7)
yes;(8)yes;(9)no
StudyNo.
17,Strauss
etal.(2002),Germany
(1)IG
!11
Cand20
F,CG!
6F,6Cand12
C;(2)
69.6%:p
rimarysterility,32.1%:
horm
onalsterility,30.2%:
andrologicsterilityfactor,
24.5%:tubarer
sterilityfactor,
7.5%
:uterusfactors,5.7%
:idiopathicsterility;(3)52.4%:
1–3
y;(4)n.
r.
(1)Ra
ndom
ized
controlledstudy;(2)T0
:baseline,
T1:3
–4m;(3)
waitinglistor
patients
refusedcounsellin
g;(4)6
C
NoIVF/ICSI,infertility
counsellin
g,individual/
coupleandwom
an,9
w,
total9
h(3–1
5h)
(1)No;
(2)no
;(3)
SCL-90-R,FLZ
;(4)
PFB;
(5)no
;(6)
yes;(7)
assessmento
fvalue
ofchild
wish
Intensity
ofchild
wish
decreasedandpregnancy
rate
was
higher
after
interventio
n
(1)Bo
th;(2)
yes;(3)no
;(4)
yes;(5)yes;(6)unclear;(7)
yes;(8)yes;(9)no
Continued
Psychological interventions for infertile patients 7
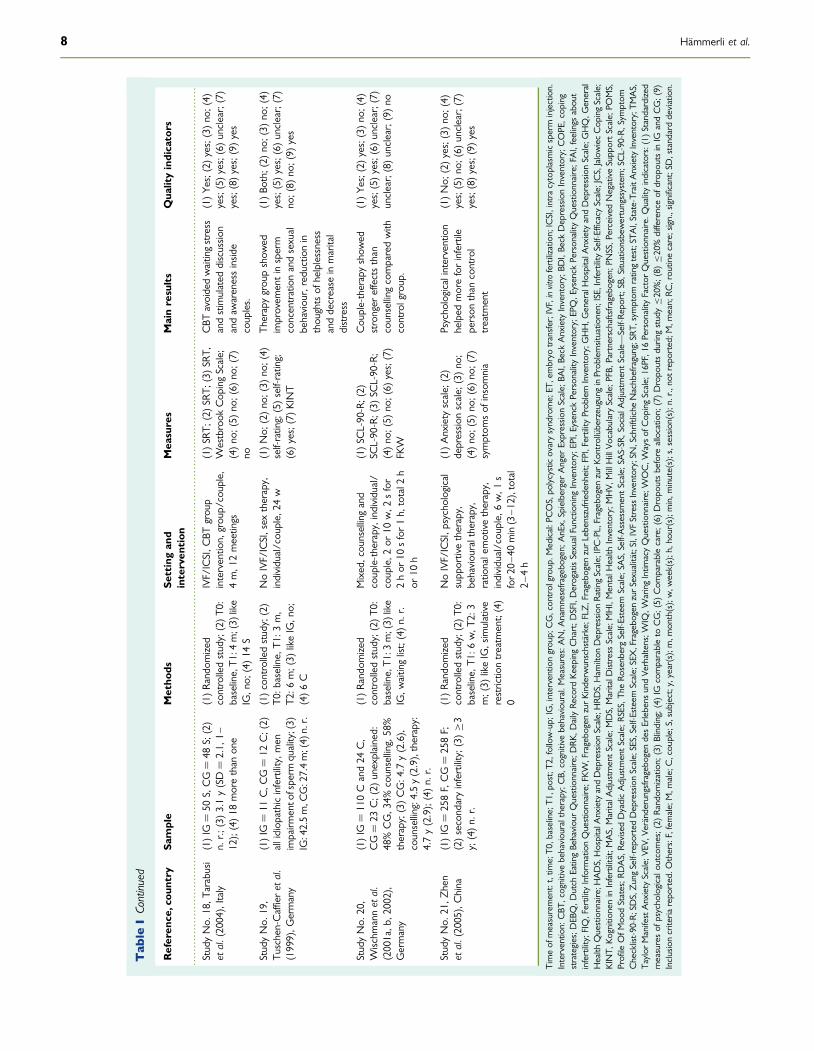
........................................................................................................................................................................................................................................................
Tab
leIContinued
Referen
ce,cou
ntry
Sample
Metho
dsSe
ttingan
dinterven
tion
Mea
sures
Mainresults
Qua
lityindicators
StudyNo.
18,T
arabusi
etal.(2004),Italy
(1)IG
!50
S,CG!
48S;(2)
n.r.;
(3)3.1y(SD!
2.1,
1–12);(4)18
morethan
one
(1)Ra
ndom
ized
controlledstudy;(2)T0
:baseline,T1
:4m;(3)
like
IG,n
o;(4)14
S
IVF/ICSI,C
BTgrou
pinterventio
n,grou
p/couple,
4m,1
2meetings
(1)SR
T;(2)SR
T;(3)SR
T,W
estbrook
Cop
ingScale;
(4)no
;(5)
no;(6)
no;(7)
no
CBT
avoidedwaitingstress
andstimulated
discussio
nandaw
arenessinsid
ecouples.
(1)Ye
s;(2)yes;(3)no
;(4)
yes;(5)yes;(6)unclear;(7)
yes;(8)yes;(9)yes
StudyNo.
19,
Tuschen-Caffieret
al.
(1999),G
ermany
(1)IG
!11
C,C
G!
12C;(2)
allidiop
athicinfertility,men
impairm
ento
fsperm
quality;(3)
IG:42.5m,C
G:27.4m;(4)
n.r.
(1)controlledstudy;(2)
T0:b
aseline,
T1:3
m,
T2:6
m;(3)
likeIG,n
o;(4)6C
NoIVF/ICSI,sex
therapy,
individual/cou
ple,
24w
(1)No;
(2)no
;(3)
no;(4)
self-rating;(5)self-rating;
(6)yes;(7)KINT
Therapygrou
pshow
edimprovem
entinsperm
concentrationandsexual
behaviou
r,reductionin
thou
ghtsof
helplessness
anddecrease
inmarital
distress
(1)Bo
th;(2)
no;(3)
no;(4)
yes;(5)yes;(6)unclear;(7)
no;(8)
no;(9)
yes
StudyNo.
20,
Wischm
annet
al.
(2001a,b
,2002),
Germany
(1)IG
!110Cand24
C,
CG!
23C;(2)
unexplained:
48%CG,3
4%counsellin
g,58%
therapy;(3)CG:4
.7y(2.6),
counsellin
g:4.5y(2.9),therapy:
4.7y(2.9);(4)n.
r.
(1)Ra
ndom
ized
controlledstudy;(2)T0
:baseline,T1
:3m;(3)
like
IG,w
aitinglist;(4)n.
r.
Mixed,cou
nsellingand
couple-therapy,individual/
couple,2
or10
w,2
sfor
2hor
10sfor1h,
total2
hor
10h
(1)SC
L-90-R;(2)
SCL-90-R;(3)
SCL-90-R;
(4)no
;(5)
no;(6)
yes;(7)
FKW
Cou
ple-therapyshow
edstronger
effectsthan
counsellin
gcomparedwith
controlgroup.
(1)Ye
s;(2)yes;(3)no
;(4)
yes;(5)yes;(6)unclear;(7)
unclear;(8)unclear;(9)no
StudyNo.
21,Z
hen
etal.(2005),China
(1)IG
!258F,CG!
258F;
(2)secondaryinfertility;(3)!3
y;(4)n.
r.
(1)Ra
ndom
ized
controlledstudy;(2)T0
:baseline,
T1:6
w,T
2:3
m;(3)
likeIG,simulative
restrictio
ntreatm
ent;(4)
0
NoIVF/ICSI,p
sychological
supp
ortivetherapy,
behaviou
raltherapy,
ratio
nalemotivetherapy,
individual/cou
ple,
6w,1
sfor2
0–40
min(3–1
2),total
2–4
h
(1)Anxiety
scale;
(2)
depressio
nscale;
(3)no
;(4)no
;(5)
no;(6)
no;(7)
symptom
sof
insomnia
Psycho
logicalintervention
helped
moreforinfertile
person
than
control
treatm
ent
(1)No;
(2)yes;(3)no
;(4)
yes;(5)no
;(6)
unclear;(7)
yes;(8)yes;(9)yes
Timeof
measurement:t,tim
e;T0
,baseline;T1
,post;T2
,follow-up;
IG,interventiongrou
p;CG,con
trolgrou
p.Medical:P
COS,po
lycysticovarysynd
rome;ET
,embryo
transfer;IVF
,invitrofertilization;
ICSI,intra
cytoplasmicsperm
injection.
Interventio
n:CBT
,cognitivebehaviou
raltherapy;C
B,cognitive
behaviou
ral.Measures:AN,A
namnesefra
gebo
gen;
AnEx,
SpielbergerAnger
Expressio
nScale;
BAI,Be
ckAnxiety
Inventory;BD
I,Be
ckDepressionInventory;COPE,cop
ing
strategies;D
EBQ,D
utch
EatingBe
haviou
rQuestionnaire;D
RK,D
ailyRe
cord
KeepingChart;D
SFI,DerogatisSexualFunctio
ning
Inventory;EPI,EysenckPerson
ality
Inventory;EPQ,E
ysenck
Person
ality
Questionnaire;FAI,feelings
abou
tinfertility;FIQ,Fertility
Inform
ationQuestionnaire;FKW
,Fragebo
genzurKinderwunschstarke;FLZ,Fragebo
genzurLebenszufriedenheit;
FPI,FertilityProb
lem
Inventory;GHH,G
eneralHospitalA
nxietyandDepressionScale;GHQ,G
eneral
Health
Questionnaire;H
ADS,HospitalA
nxietyandDepressionScale;HRD
S,Ham
ilton
DepressionRa
tingScale;IPC-PL,Fragebogen
zurK
ontrolluberzeugung
inProb
lemsituatio
nen;ISE,InfertilitySelf-EfficacyScale;JCS,JalowiecCop
ingScale;
KINT,
Kognition
eninInfertilitat;M
AS,MaritalA
djustm
entScale;
MDS,MaritalD
istress
Scale;
MHI,MentalH
ealth
Inventory;MHV,
MillHillVo
cabulary
Scale;
PFB,
Partnerschaftsfra
gebo
gen;
PNSS,P
erceived
NegativeSupp
ortScale;
POMS,
ProfileOfM
oodStates;R
DAS,Re
visedDyadicAdjustm
entScale;
RSES,T
heRo
senbergSelf-Esteem
Scale;
SAS,Self-Assessm
entScale;
SAS-SR
,SocialA
djustm
entScale—
Self-Re
port;SB,
Situationsbewertungssystem;SCL-90-R,S
ymptom
Checklist-90-R;SDS,ZungSelf-repo
rted
DepressionScale;SES,Self-Esteem
Scale;SEX,Fragebo
genzurSexualitat;SI,IVF
Stress
Inventory;SN
,SchriftlicheNachbefragung;SRT
,sym
ptom
ratingtest;STA
I,State-TraitA
nxietyInventory;TM
AS,
Taylor
ManifestAnxiety
Scale;VE
V,Ve
randerungsfra
gebo
gendesErlebens
undVe
rhaltens;W
IQ,W
aringIntim
acyQuestionnaire;W
OC,W
aysof
Cop
ingScale;16PF,1
6Person
ality
Factor
Questionnaire.Q
ualityindicators:(1)
Standardize
dmeasuresof
psycho
logicalo
utcomes;(2)
Random
izatio
n;(3)Blinding;(4)
IGcomparableto
CG;(5)
Com
parablecare;(6)
Dropo
utsbefore
allocatio
n;(7)Dropo
utsdurin
gstudy"20%;(8)
"20%differenceof
drop
outsinIG
andCG;(9)
Inclusioncriteria
repo
rted.O
thers:F,female;M,m
ale;C,cou
ple;S,subject;y,year(s);m,m
onth(s);w,w
eek(s);h,hou
r(s);m
in,m
inute(s);s,sessio
n(s);n
.r.,no
treported;
M,m
ean;RC
,rou
tinecare;sign.,significant;SD
,standarddeviation.
8 Hammerli et al.
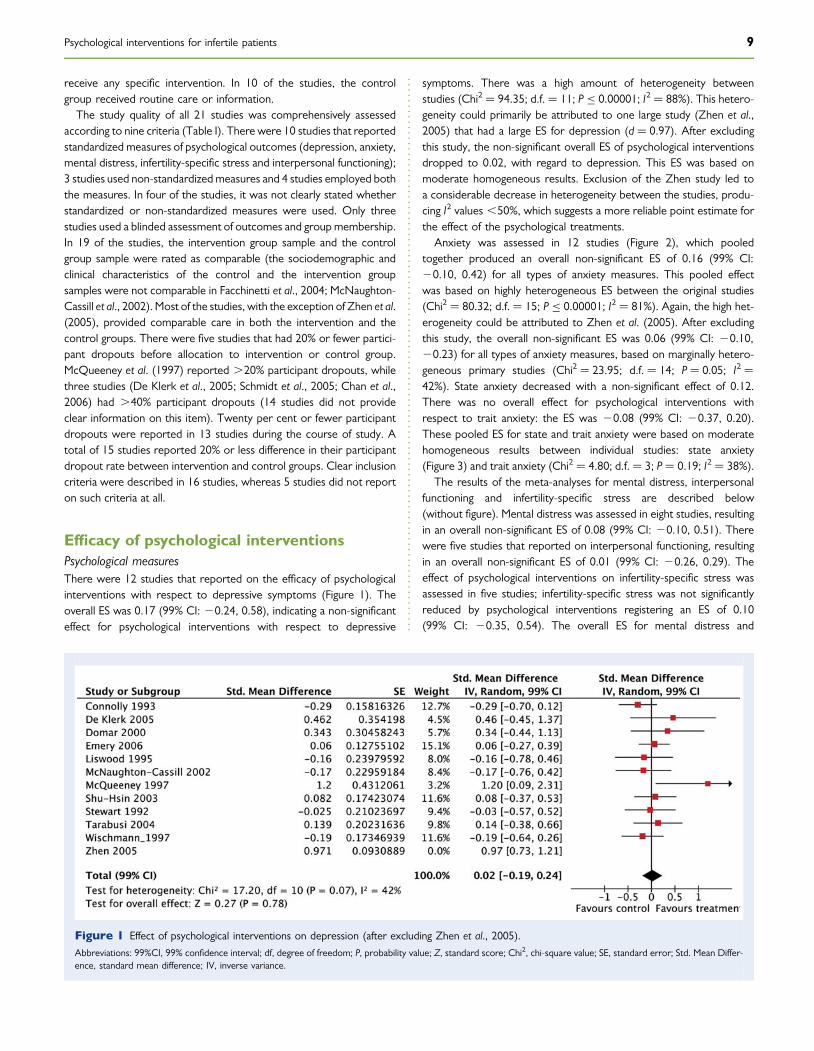
receive any specific intervention. In 10 of the studies, the controlgroup received routine care or information.
The study quality of all 21 studies was comprehensively assessedaccording to nine criteria (Table I). There were 10 studies that reportedstandardized measures of psychological outcomes (depression, anxiety,mental distress, infertility-specific stress and interpersonal functioning);3 studies used non-standardizedmeasures and 4 studies employed boththe measures. In four of the studies, it was not clearly stated whetherstandardized or non-standardized measures were used. Only threestudies used a blinded assessment of outcomes and groupmembership.In 19 of the studies, the intervention group sample and the controlgroup sample were rated as comparable (the sociodemographic andclinical characteristics of the control and the intervention groupsamples were not comparable in Facchinetti et al., 2004; McNaughton-Cassill et al., 2002). Most of the studies, with the exception of Zhen et al.(2005), provided comparable care in both the intervention and thecontrol groups. There were five studies that had 20% or fewer partici-pant dropouts before allocation to intervention or control group.McQueeney et al. (1997) reported .20% participant dropouts, whilethree studies (De Klerk et al., 2005; Schmidt et al., 2005; Chan et al.,2006) had .40% participant dropouts (14 studies did not provideclear information on this item). Twenty per cent or fewer participantdropouts were reported in 13 studies during the course of study. Atotal of 15 studies reported 20% or less difference in their participantdropout rate between intervention and control groups. Clear inclusioncriteria were described in 16 studies, whereas 5 studies did not reporton such criteria at all.
Efficacy of psychological interventionsPsychological measuresThere were 12 studies that reported on the efficacy of psychologicalinterventions with respect to depressive symptoms (Figure 1). Theoverall ES was 0.17 (99% CI: 20.24, 0.58), indicating a non-significanteffect for psychological interventions with respect to depressive
symptoms. There was a high amount of heterogeneity betweenstudies (Chi2 ! 94.35; d.f. ! 11; P " 0.00001; I2 ! 88%). This hetero-geneity could primarily be attributed to one large study (Zhen et al.,2005) that had a large ES for depression (d ! 0.97). After excludingthis study, the non-significant overall ES of psychological interventionsdropped to 0.02, with regard to depression. This ES was based onmoderate homogeneous results. Exclusion of the Zhen study led toa considerable decrease in heterogeneity between the studies, produ-cing I2 values ,50%, which suggests a more reliable point estimate forthe effect of the psychological treatments.
Anxiety was assessed in 12 studies (Figure 2), which pooledtogether produced an overall non-significant ES of 0.16 (99% CI:20.10, 0.42) for all types of anxiety measures. This pooled effectwas based on highly heterogeneous ES between the original studies(Chi2 ! 80.32; d.f. ! 15; P " 0.00001; I2 ! 81%). Again, the high het-erogeneity could be attributed to Zhen et al. (2005). After excludingthis study, the overall non-significant ES was 0.06 (99% CI: 20.10,20.23) for all types of anxiety measures, based on marginally hetero-geneous primary studies (Chi2 ! 23.95; d.f. ! 14; P ! 0.05; I2 !42%). State anxiety decreased with a non-significant effect of 0.12.There was no overall effect for psychological interventions withrespect to trait anxiety: the ES was 20.08 (99% CI: 20.37, 0.20).These pooled ES for state and trait anxiety were based on moderatehomogeneous results between individual studies: state anxiety(Figure 3) and trait anxiety (Chi2 ! 4.80; d.f. ! 3; P ! 0.19; I2 ! 38%).
The results of the meta-analyses for mental distress, interpersonalfunctioning and infertility-specific stress are described below(without figure). Mental distress was assessed in eight studies, resultingin an overall non-significant ES of 0.08 (99% CI: 20.10, 0.51). Therewere five studies that reported on interpersonal functioning, resultingin an overall non-significant ES of 0.01 (99% CI: 20.26, 0.29). Theeffect of psychological interventions on infertility-specific stress wasassessed in five studies; infertility-specific stress was not significantlyreduced by psychological interventions registering an ES of 0.10(99% CI: 20.35, 0.54). The overall ES for mental distress and
Figure 1 Effect of psychological interventions on depression (after excluding Zhen et al., 2005).Abbreviations: 99%CI, 99% confidence interval; df, degree of freedom; P, probability value; Z, standard score; Chi2, chi-square value; SE, standard error; Std. Mean Differ-ence, standard mean difference; IV, inverse variance.
Psychological interventions for infertile patients 9
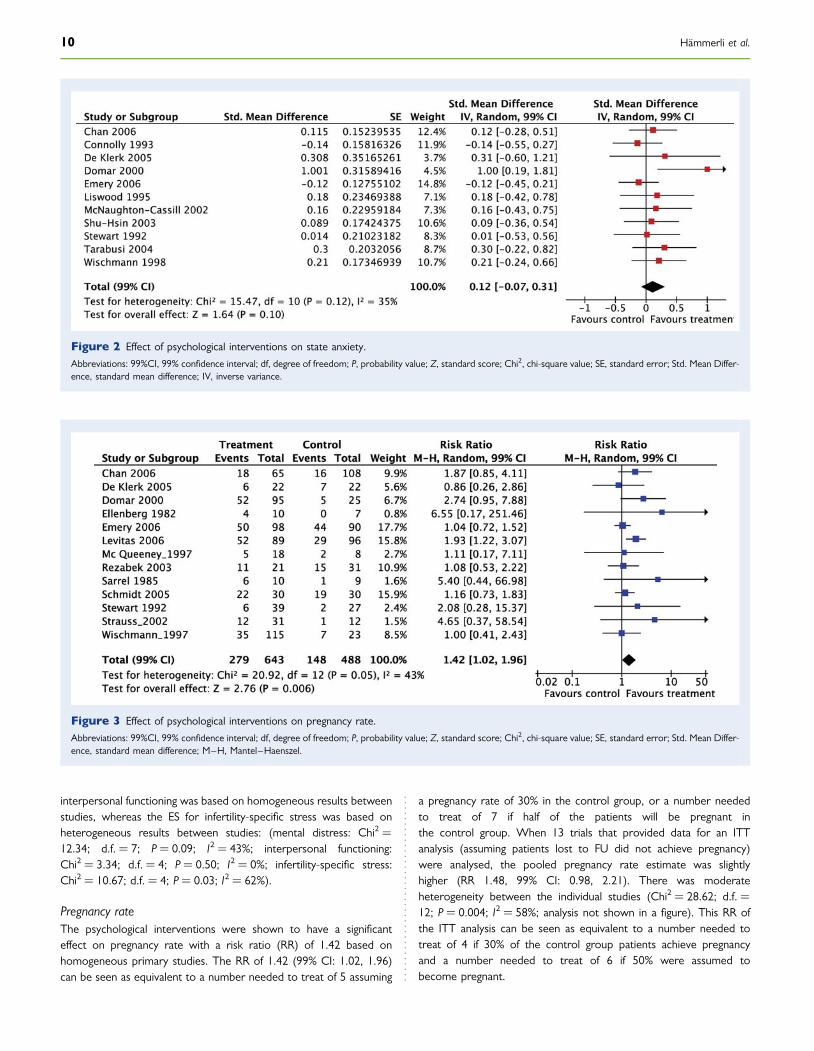
interpersonal functioning was based on homogeneous results betweenstudies, whereas the ES for infertility-specific stress was based onheterogeneous results between studies: (mental distress: Chi2 !12.34; d.f. ! 7; P ! 0.09; I2 ! 43%; interpersonal functioning:Chi2 ! 3.34; d.f. ! 4; P ! 0.50; I2 ! 0%; infertility-specific stress:Chi2 ! 10.67; d.f. ! 4; P ! 0.03; I2 ! 62%).
Pregnancy rateThe psychological interventions were shown to have a significanteffect on pregnancy rate with a risk ratio (RR) of 1.42 based onhomogeneous primary studies. The RR of 1.42 (99% CI: 1.02, 1.96)can be seen as equivalent to a number needed to treat of 5 assuming
a pregnancy rate of 30% in the control group, or a number neededto treat of 7 if half of the patients will be pregnant inthe control group. When 13 trials that provided data for an ITTanalysis (assuming patients lost to FU did not achieve pregnancy)were analysed, the pooled pregnancy rate estimate was slightlyhigher (RR 1.48, 99% CI: 0.98, 2.21). There was moderateheterogeneity between the individual studies (Chi2 ! 28.62; d.f. !12; P ! 0.004; I2 ! 58%; analysis not shown in a figure). This RR ofthe ITT analysis can be seen as equivalent to a number needed totreat of 4 if 30% of the control group patients achieve pregnancyand a number needed to treat of 6 if 50% were assumed tobecome pregnant.
Figure 2 Effect of psychological interventions on state anxiety.Abbreviations: 99%CI, 99% confidence interval; df, degree of freedom; P, probability value; Z, standard score; Chi2, chi-square value; SE, standard error; Std. Mean Differ-ence, standard mean difference; IV, inverse variance.
Figure 3 Effect of psychological interventions on pregnancy rate.Abbreviations: 99%CI, 99% confidence interval; df, degree of freedom; P, probability value; Z, standard score; Chi2, chi-square value; SE, standard error; Std. Mean Differ-ence, standard mean difference; M–H, Mantel–Haenszel.
10 Hammerli et al.

Subgroup analysisA subgroup analysis for sex, duration of intervention, ART and ran-domization was performed to analyse variables moderating theeffect of psychological interventions between the studies (Table II).No significant effects on psychological outcomes were found in separ-ate analyses among women and men following psychological interven-tions. Further, no significant ES difference for psychological measureswas found between women and men.
A second subgroup analysis was performed that looked at inter-vention duration (Table II). Longer psychological interventions (sixor more sessions) demonstrated ES statistically comparable withthose of shorter interventions (five or fewer sessions) for allpsychological outcomes (e.g. state anxiety: d ! 0.28 versus d !0.07; mental distress: d ! 0.26 versus d ! 0.09). Out of six psycho-logical outcome measures assessed, only one ES difference wasfound which was significant—that of anxiety (P ! 0.007)—andpointed to a benefit of longer interventions. With respect to preg-nancy rate, longer psychological interventions (FU data only: RR1.87; P ! 0.07) were not significantly more effective than shorterinterventions (FU data only: RR 1.33; P ! 0.05). Regarding preg-nancy rate, the overall ES of long interventions was based onhomogeneous original studies, whereas the estimates for shortpsychological interventions were based on the nearly homogeneousES of the original studies.
A third subgroup analysis was performed looking at medicaltreatment type. The studies were grouped according to the criteriaof whether the women underwent assisted reproductive treatmentor not (ART: IVF/ICSI versus no IVF/ICSI; Table II). Regardingpsychological outcomes, no significant overall ES was found forpsychological interventions in those studies where patients did notreceive IVF/ICSI treatment. However, with respect to pregnancyrate, psychological interventions were significantly effective (FUdata only: RR 2.73; ITT: RR 4.06) only in cases where patientswere not treated with IVF/ICSI than those treated with IVF/ICSI(FU data only: RR 1.34; ITT: RR 1.29). Both estimates ofnon-IVF/ICSI treated patients were based on the highly homo-geneous ES of the original studies. There was a large differencebetween IVF/ICSI and no IVF/ICSI in the RR of the pregnancyrate at FU (RR 1.39) and the RR of the pregnancy rate resultingfrom the ITT analysis (RR 2.77). However, the ES differenceswere not statistically significant different for pregnancy rate in FUstudies (P ! 0.19) and for ITT analysis (P ! 0.09).
A further subgroup analysis was conducted on those studies thatused randomization for their allocation of patients (Table II). Con-ducting a conservative estimate using randomized controlled studiesrevealed no significant overall ES with respect to any psychologicaloutcomes. Non-randomized studies also failed to display anysignificant overall ES. Non-randomized studies indicated slightlyhigher overall effects of psychological interventions with regard toone’s chances of becoming pregnant (FU data only: RR 1.63;ITT: RR 1.65) versus randomized studies (FU data only: RR 1.31;ITT: RR 1.38). With the exception of infertility-specific distress(P ! 0.002), no significant ES differences were found withrespect to any psychological outcomes. The ES differences werenot significant for pregnancy FU (P ! 0.36) and for ITT analysis(P ! 0.40).
Exploration of publication biasUse of a funnel plot revealed markedly symmetrical results withrespect to interpersonal functioning and infertility-specific stress.Unsymmetrical results were found with respect to depression,anxiety, state anxiety, trait anxiety, mental distress and pregnancy.The latter results can be interpreted as a hint of possible publicationbias, as smaller studies that did not demonstrate efficacy might nothave been published.
DiscussionThe results of this meta-analysis of psychological interventions forpatients suffering from infertility do not indicate their overall efficacywith respect to mental health. However, some evidence was foundfor the efficacy of psychological interventions in achieving pregnancy.With respect to mental health, the findings of this meta-analysis onefficacy stand in contrast to the results of Boivin (2003) and de Lizand Strauss (2005); however, its findings pointing to an increased preg-nancy rate due to psychological interventions are in line with the twoprevious reviews. The differences in results concerning mental healthmay be attributed to the present meta-analysis’ strict criteria forinclusion (controlled studies only) versus those of other reviews,which encompass mixed study designs, including pre–post compari-son studies.
As the present results indicate no significant effects in general forpsychological interventions in connection with mental health, theyrun somewhat counter to research results in other areas of beha-vioural medicine where efficacy has been shown. However, it isimportant to note that in behavioural medicine psychological interven-tions for distressed patients have proven less effective than interven-tions for patients with mental disorders only. Psychologicalinterventions have only demonstrated small effects among patientswith somatic illnesses: type 1 diabetes patients have improvedthrough psychological intervention registering an ES of 0.26 (Winkleyet al., 2006); patients with lower back pain have displayed non-significantly reduced depressive symptoms registering an ES of 0.34(Hoffman et al., 2007); depressed coronary heart disease patientshave improved through psychological or psychopharmacological inter-vention registering ES ranging from 0.30 to 0.35 (Lesperance et al.,2007). Further, it is important to note that, contrary to some of thetypes of patient groups described above, patients with infertility gen-erally exhibit good mental health (Dunkel-Schetter and Lobel, 1991;Eugster and Vingerhoets, 1999; Wischmann, 2005). There is alsogeneral agreement among researchers that high levels of depressivesymptoms, anxiety and distress among infertile patients are possiblyonly short-term reactions to infertility and its treatment medically.This could lead to a floor effect for psychological interventions. Thesmall ES of psychological interventions for infertile patients mightalso be explained by emotional adjustment processes, which arepresent in patients not receiving psychological interventions as well.
As mentioned, the present results also indicate that psychologicalinterventions may be effective in increasing couples’ pregnancy rate.However, this result only provides answers regarding the averageeffect of psychological interventions on pregnancy rate. The positiveeffect on pregnancy must be interpreted cautiously since highereffects were found in non-randomized studies (trend) and a clear
Psychological interventions for infertile patients 11
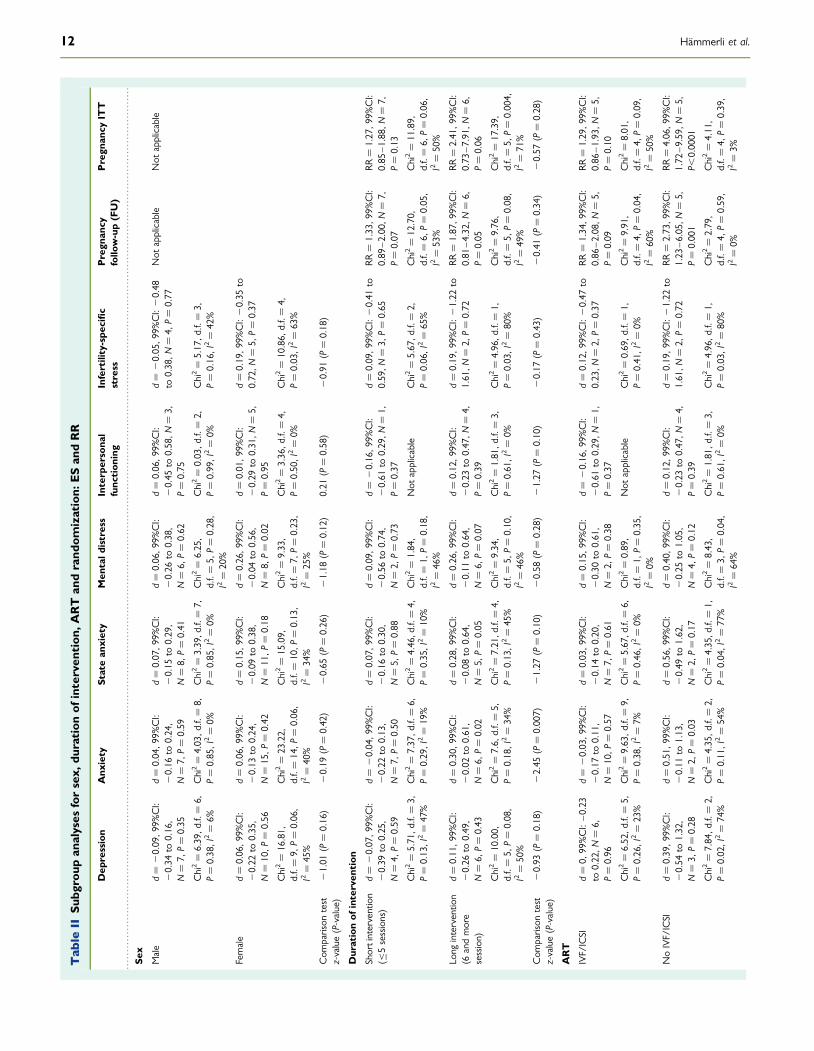
..........................................................................................................................................................................................................................................................
Tab
leII
Subg
roup
analyses
forsex,
duration
ofinterven
tion
,ART
andrand
omization:
ESan
dRR
Dep
ression
Anx
iety
Statean
xiety
Men
tald
istress
Interp
ersona
lfunc
tion
ing
Infertility-spe
cific
stress
Pregn
ancy
follo
w-up(FU)
Pregn
ancy
ITT
Sex
Male
d!
20.09,9
9%CI:
20.34
to0.16,
N!
7,P!
0.35
d!
0.04,9
9%CI:
20.16
to0.24,
N!
7,P!
0.59
d!
0.07,9
9%CI:
20.15
to0.29,
N!
8,P!
0.41
d!
0.06,9
9%CI:
20.26
to0.38,
N!
6,P!
0.62
d!
0.06,9
9%CI:
20.45
to0.58,N
!3,
P!
0.75
d!
20.05,9
9%CI:20.48
to0.38,N
!4,
P!
0.77
Not
applicable
Not
applicable
Chi2!
6.39,d
.f.!
6,P!
0.38,I
2!
6%Chi2!
4.03,d
.f.!
8,P!
0.85,I
2!
0%Chi2!
3.39,d
.f.!
7,P!
0.85,I
2!
0%Chi2!
6.25,
d.f.!
5,P!
0.28,
I2!
20%
Chi2!
0.03,d
.f.!
2,P!
0.99,I
2!
0%Chi2!
5.17,d
.f.!
3,P!
0.16,I
2!
42%
Female
d!
0.06,9
9%CI:
20.22
to0.35,
N!
10,P
!0.56
d!
0.06,9
9%CI:
20.13
to0.24,
N!
15,P
!0.42
d!
0.15,9
9%CI:
20.09
to0.38,
N!
11,P
!0.18
d!
0.26,9
9%CI:
20.04
to0.56,
N!
8,P!
0.02
d!
0.01,9
9%CI:
20.29
to0.31,N
!5,
P!
0.95
d!
0.19,9
9%CI:20.35
to0.72,N
!5,
P!
0.37
Chi2!
16.81,
d.f.!
9,P!
0.06,
I2!
45%
Chi2!
23.22,
d.f.!
14,P
!0.06,
I2!
40%
Chi2!
15.09,
d.f.!
10,P
!0.13,
I2!
34%
Chi2!
9.33,
d.f.!
7,P!
0.23,
I2!
25%
Chi2!
3.36,d
.f.!
4,P!
0.50,I
2!
0%Chi2!
10.86,
d.f.!
4,P!
0.03,I
2!
63%
Com
parison
test
z-value(P-value)
21.01
(P!
0.16)
20.19
(P!
0.42)
20.65
(P!
0.26)
21.18
(P!
0.12)
0.21
(P!
0.58)
20.91
(P!
0.18)
Durationof
interven
tion
Shortintervention
("5sessions)
d!
20.07,9
9%CI:
20.39
to0.25,
N!
4,P!
0.59
d!
20.04,9
9%CI:
20.22
to0.13,
N!
7,P!
0.50
d!
0.07,9
9%CI:
20.16
to0.30,
N!
5,P!
0.88
d!
0.09,9
9%CI:
20.56
to0.74,
N!
2,P!
0.73
d!
20.16,9
9%CI:
20.61
to0.29,N
!1,
P!
0.37
d!
0.09,9
9%CI:20.41
to0.59,N
!3,
P!
0.65
RR!
1.33,9
9%CI:
0.89
–2.00,N
!7,
P!
0.07
RR!
1.27,9
9%CI:
0.85
–1.88,
N!
7,P!
0.13
Chi2!
5.71,d
.f.!
3,P!
0.13,I
2!
47%
Chi2!
7.37,d
.f.!
6,P!
0.29,I
2!
19%
Chi2!
4.46,d
.f.!
4,P!
0.35,I
2!
10%
Chi2!
1.84,
d.f.!
1,P!
0.18,
I2!
46%
Not
applicable
Chi2!
5.67,d
.f.!
2,P!
0.06,I
2!
65%
Chi2!
12.70,
d.f.!
6,P!
0.05,
I2!
53%
Chi2!
11.89,
d.f.!
6,P!
0.06,
I2!
50%
Long
interventio
n(6
andmore
session)
d!
0.11,9
9%CI:
20.26
to0.49,
N!
6,P!
0.43
d!
0.30,9
9%CI:
20.02
to0.61,
N!
6,P!
0.02
d!
0.28,9
9%CI:
20.08
to0.64,
N!
5,P!
0.05
d!
0.26,9
9%CI:
20.11
to0.64,
N!
6,P!
0.07
d!
0.12,9
9%CI:
20.23
to0.47,N
!4,
P!
0.39
d!
0.19,9
9%CI:21.22
to1.61,N
!2,
P!
0.72
RR!
1.87,9
9%CI:
0.81
–4.32,N
!6,
P!
0.05
RR!
2.41,9
9%CI:
0.73
–7.91,
N!
6,P!
0.06
Chi2!
10.00,
d.f.!
5,P!
0.08,
I2!
50%
Chi2!
7.6,
d.f.!
5,P!
0.18,I
2!
34%
Chi2!
7.21,d
.f.!
4,P!
0.13,I
2!
45%
Chi2!
9.34,
d.f.!
5,P!
0.10,
I2!
46%
Chi2!
1.81,d
.f.!
3,P!
0.61,I
2!
0%Chi2!
4.96,d
.f.!
1,P!
0.03,I
2!
80%
Chi2!
9.76,
d.f.!
5,P!
0.08,
I2!
49%
Chi2!
17.39,
d.f.!
5,P!
0.004,
I2!
71%
Com
parison
test
z-value(P-value)
20.93
(P!
0.18)
22.45
(P!
0.007)
21.27
(P!
0.10)
20.58
(P!
0.28)
21.27
(P!
0.10)
20.17
(P!
0.43)
20.41
(P!
0.34)
20.57
(P!
0.28)
ART
IVF/ICSI
d!
0,99%CI:–0.23
to0.22,N
!6,
P!
0.96
d!
20.03,9
9%CI:
20.17
to0.11,
N!
10,P
!0.57
d!
0.03,9
9%CI:
20.14
to0.20,
N!
7,P!
0.61
d!
0.15,9
9%CI:
20.30
to0.61,
N!
2,P!
0.38
d!
20.16,9
9%CI:
20.61
to0.29,N
!1,
P!
0.37
d!
0.12,9
9%CI:20.47
to0.23,N
!2,
P!
0.37
RR!
1.34,9
9%CI:
0.86
–2.08,N
!5,
P!
0.09
RR!
1.29,9
9%CI:
0.86
–1.93,
N!
5,P!
0.10
Chi2!
6.52,d
.f.!
5,P!
0.26,I
2!
23%
Chi2!
9.63,d
.f.!
9,P!
0.38,I
2!
7%Chi2!
5.67,d
.f.!
6,P!
0.46,I
2!
0%Chi2!
0.89,
d.f.!
1,P!
0.35,
I2!
0%
Not
applicable
Chi2!
0.69,d
.f.!
1,P!
0.41,I
2!
0%Chi2!
9.91,
d.f.!
4,P!
0.04,
I2!
60%
Chi2!
8.01,
d.f.!
4,P!
0.09,
I2!
50%
NoIVF/ICSI
d!
0.39,9
9%CI:
20.54
to1.32,
N!
3,P!
0.28
d!
0.51,9
9%CI:
20.11
to1.13,
N!
2,P!
0.03
d!
0.56,9
9%CI:
20.49
to1.62,
N!
2,P!
0.17
d!
0.40,9
9%CI:
20.25
to1.05,
N!
4,P!
0.12
d!
0.12,9
9%CI:
20.23
to0.47,N
!4,
P!
0.39
d!
0.19,9
9%CI:21.22
to1.61,N
!2,
P!
0.72
RR!
2.73,9
9%CI:
1.23
–6.05,N
!5,
P!
0.001
RR!
4.06,9
9%CI:
1.72
–9.59,
N!
5,P,
0.0001
Chi2!
7.84,d
.f.!
2,P!
0.02,I
2!
74%
Chi2!
4.35,d
.f.!
2,P!
0.11,I
2!
54%
Chi2!
4.35,d
.f.!
1,P!
0.04,I
2!
77%
Chi2!
8.43,
d.f.!
3,P!
0.04,
I2!
64%
Chi2!
1.81,d
.f.!
3,P!
0.61,I
2!
0%Chi2!
4.96,d
.f.!
1,P!
0.03,I
2!
80%
Chi2!
2.79,
d.f.!
4,P!
0.59,
I2!
0%
Chi2!
4.11,
d.f.!
4,P!
0.39,
I2!
3%
12 Hammerli et al.
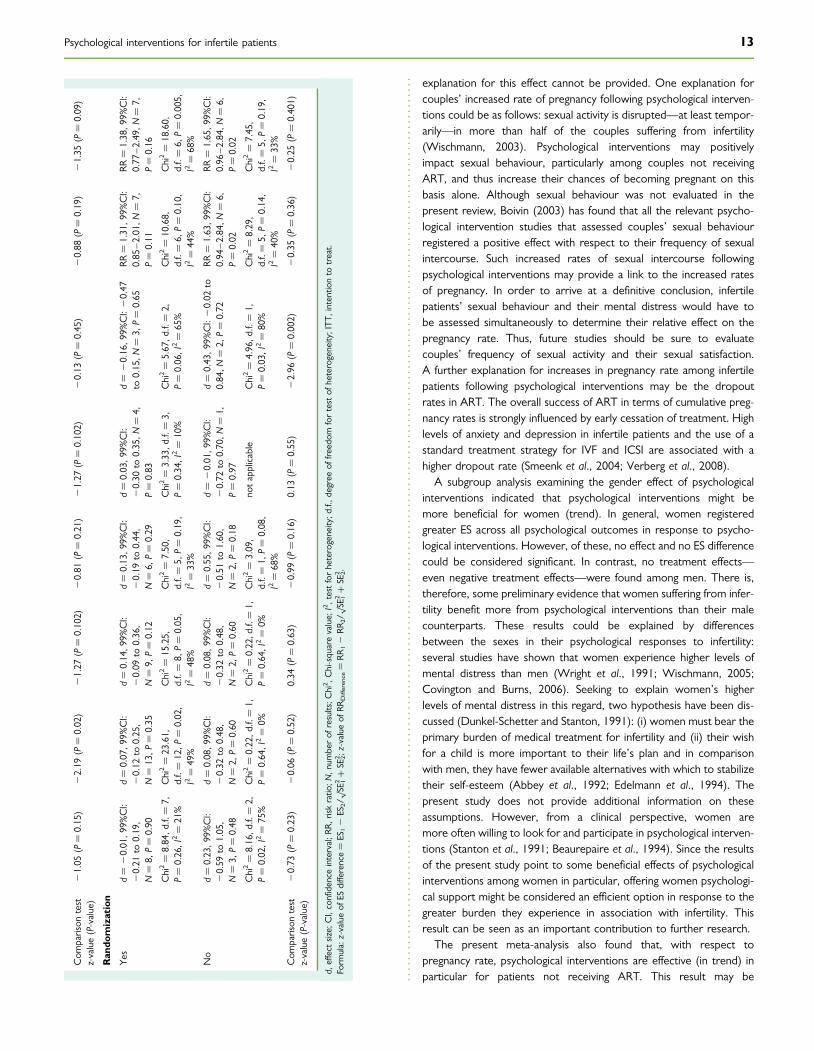
explanation for this effect cannot be provided. One explanation forcouples’ increased rate of pregnancy following psychological interven-tions could be as follows: sexual activity is disrupted—at least tempor-arily—in more than half of the couples suffering from infertility(Wischmann, 2003). Psychological interventions may positivelyimpact sexual behaviour, particularly among couples not receivingART, and thus increase their chances of becoming pregnant on thisbasis alone. Although sexual behaviour was not evaluated in thepresent review, Boivin (2003) has found that all the relevant psycho-logical intervention studies that assessed couples’ sexual behaviourregistered a positive effect with respect to their frequency of sexualintercourse. Such increased rates of sexual intercourse followingpsychological interventions may provide a link to the increased ratesof pregnancy. In order to arrive at a definitive conclusion, infertilepatients’ sexual behaviour and their mental distress would have tobe assessed simultaneously to determine their relative effect on thepregnancy rate. Thus, future studies should be sure to evaluatecouples’ frequency of sexual activity and their sexual satisfaction.A further explanation for increases in pregnancy rate among infertilepatients following psychological interventions may be the dropoutrates in ART. The overall success of ART in terms of cumulative preg-nancy rates is strongly influenced by early cessation of treatment. Highlevels of anxiety and depression in infertile patients and the use of astandard treatment strategy for IVF and ICSI are associated with ahigher dropout rate (Smeenk et al., 2004; Verberg et al., 2008).
A subgroup analysis examining the gender effect of psychologicalinterventions indicated that psychological interventions might bemore beneficial for women (trend). In general, women registeredgreater ES across all psychological outcomes in response to psycho-logical interventions. However, of these, no effect and no ES differencecould be considered significant. In contrast, no treatment effects—even negative treatment effects—were found among men. There is,therefore, some preliminary evidence that women suffering from infer-tility benefit more from psychological interventions than their malecounterparts. These results could be explained by differencesbetween the sexes in their psychological responses to infertility:several studies have shown that women experience higher levels ofmental distress than men (Wright et al., 1991; Wischmann, 2005;Covington and Burns, 2006). Seeking to explain women’s higherlevels of mental distress in this regard, two hypothesis have been dis-cussed (Dunkel-Schetter and Stanton, 1991): (i) women must bear theprimary burden of medical treatment for infertility and (ii) their wishfor a child is more important to their life’s plan and in comparisonwith men, they have fewer available alternatives with which to stabilizetheir self-esteem (Abbey et al., 1992; Edelmann et al., 1994). Thepresent study does not provide additional information on theseassumptions. However, from a clinical perspective, women aremore often willing to look for and participate in psychological interven-tions (Stanton et al., 1991; Beaurepaire et al., 1994). Since the resultsof the present study point to some beneficial effects of psychologicalinterventions among women in particular, offering women psychologi-cal support might be considered an efficient option in response to thegreater burden they experience in association with infertility. Thisresult can be seen as an important contribution to further research.
The present meta-analysis also found that, with respect topregnancy rate, psychological interventions are effective (in trend) inparticular for patients not receiving ART. This result may be
Com
parison
test
z-value(P-value)
21.05
(P!
0.15)
22.19
(P!
0.02)
21.27
(P!
0.102)
20.81
(P!
0.21)
21.27
(P!
0.102)
20.13
(P!
0.45)
20.88
(P!
0.19)
21.35
(P!
0.09)
Ran
domization
Yes
d!
20.01,9
9%CI:
20.21
to0.19,
N!
8,P!
0.90
d!
0.07,9
9%CI:
20.12
to0.25,
N!
13,P
!0.35
d!
0.14,9
9%CI:
20.09
to0.36,
N!
9,P!
0.12
d!
0.13,9
9%CI:
20.19
to0.44,
N!
6,P!
0.29
d!
0.03,9
9%CI:
20.30
to0.35,N
!4,
P!
0.83
d!
20.16,9
9%CI:20.47
to0.15,N
!3,
P!
0.65
RR!
1.31,9
9%CI:
0.85
–2.01,N
!7,
P!
0.11
RR!
1.38,9
9%CI:
0.77
–2.49,
N!
7,P!
0.16
Chi2!
8.84,d
.f.!
7,P!
0.26,I
2!
21%
Chi2!
23.61,
d.f.!
12,P
!0.02,
I2!
49%
Chi2!
15.25,
d.f.!
8,P!
0.05,
I2!
48%
Chi2!
7.50,
d.f.!
5,P!
0.19,
I2!
33%
Chi2!
3.33,d
.f.!
3,P!
0.34,I
2!
10%
Chi2!
5.67,d
.f.!
2,P!
0.06,I
2!
65%
Chi2!
10.68,
d.f.!
6,P!
0.10,
I2!
44%
Chi2!
18.60,
d.f.!
6,P!
0.005,
I2!
68%
No
d!
0.23,9
9%CI:
20.59
to1.05,
N!
3,P!
0.48
d!
0.08,9
9%CI:
20.32
to0.48,
N!
2,P!
0.60
d!
0.08,9
9%CI:
20.32
to0.48,
N!
2,P!
0.60
d!
0.55,9
9%CI:
20.51
to1.60,
N!
2,P!
0.18
d!
20.01,9
9%CI:
20.72
to0.70,N
!1,
P!
0.97
d!
0.43,9
9%CI:20.02
to0.84,N
!2,
P!
0.72
RR!
1.63,9
9%CI:
0.94
–2.84,N
!6,
P!
0.02
RR!
1.65,9
9%CI:
0.96
–2.84,
N!
6,P!
0.02
Chi2!
8.16,d
.f.!
2,P!
0.02,I
2!
75%
Chi2!
0.22,d
.f.!
1,P!
0.64,I
2!
0%Chi2!
0.22,d
.f.!
1,P!
0.64,I
2!
0%Chi2!
3.09,
d.f.!
1,P!
0.08,
I2!
68%
notapplicable
Chi2!
4.96,d
.f.!
1,P!
0.03,I
2!
80%
Chi2!
8.29,
d.f.!
5,P!
0.14,
I2!
40%
Chi2!
7.45,
d.f.!
5,P!
0.19,
I2!
33%
Com
parison
test
z-value(P-value)
20.73
(P!
0.23)
20.06
(P!
0.52)
0.34
(P!
0.63)
20.99
(P!
0.16)
0.13
(P!
0.55)
22.96
(P!
0.002)
20.35
(P!
0.36)
20.25
(P!
0.401)
d,effect
size;
CI,confidenceinterval;R
R,riskratio
;N,n
umberof
results;C
hi2 ,Chi-squarevalue;
I2,testforheterogeneity;d
.f.,d
egreeof
freedom
fortestof
heterogeneity;ITT
,intentio
nto
treat.
Form
ula:z-valueof
ESdifference!
ES12
ES2/p S
E 12#
SE22 ;z-valueof
RRDifference!
RR12
RR2/p S
E 12#
SE22 .
Psychological interventions for infertile patients 13

confounded by the duration of infertility and the duration of theinterventions. The mean duration of infertility among patients receivingART was !4.8 years; among patients not receiving ART, the meanduration of infertility was !3.5 years. ART are conducted after a com-prehensive diagnostic exploration, once it has been decided that apatient’s fertility disorder will not respond to other medical treat-ments. In addition, the present analysis revealed that patients receivingART participated in psychological interventions that were markedlyshorter in duration, averaging 3.6 sessions (1–12 sessions), whencompared with the psychological interventions visited by patientsnot receiving ART, which averaged 9.8 sessions (2–20 sessions).Boivin (2003) reported that psychological interventions of a longerduration—between 6 and 12 weeks—are more effective. Theresults of the present study appear to point in the same direction.In a subgroup analysis examining the duration of the interventions,higher ES were found for longer interventions (six or more sessions);however, only one of the ES differences between longer and shorterinterventions could be labelled significant. Short interventions didnot display any effects even negative effects on infertile patients’mental health. From the perspective of clinicians, it does not appearpromising to offer psychological treatments of five or fewer sessions.
Owing to the dearth of relevant studies available, a subgroup analy-sis focussing on the types of psychological interventions was not con-ducted in the present meta-analysis. The studies included in thepresent meta-analysis can be organized into six groups according tothe intervention strategies (see description) they employed. Asthere were no more than six studies for any one treatment strategyand because the studies did not all assess the same outcomemeasures, the present meta-analysis could not provide any infor-mation concerning the individual efficacy of different types of interven-tions for infertile patients.
There are several limitations suggested for the present study results.The database EMBASE was not included in the literature search, as theresearch team did not have free access to this electronic resource;since achievement of a comprehensive literature search is a prerequi-site of systematic reviews, additional sources were explored manually.Further, the funnel plots point to possible publication bias. It is poss-ible that other smaller, relevant studies that failed to prove an effectfor psychological interventions simply have not been published. Thepresent findings are also limited by the fact that only 12 randomizedcontrolled trials were found as a result of the literature searchversus 9 studies that employed a non-randomized method of allo-cation. There was considerable heterogeneity between studies withrespect to certain outcomes. The heterogeneity of the Zhen et al.(2005) might be explained by its very specific study sample (insomniapatients with secondary infertility) and possible hidden methodologicalproblems (suggested by its 100% return rate out of more than 506patients). The studies also differed strongly with respect to the timepoint at which assessment occurred, ranging from 4 weeks to 6months post-intervention. The present study does not provide anyinformation on whether patients differing in cause and duration ofinfertility may benefit more or less from psychological interventions.Several of the effects discussed were only non-significant trends (e.g.greater benefits in women or in infertile patients not receiving ART)and therefore not that reliable. As a result, there is an urgent needfor more and controlled evaluation studies. The results of thepresent meta-analysis can only provide answers regarding the
average efficacy of psychological interventions for infertile patientswith respect to mental health and pregnancy rates.
Recommendations for future researchThe present meta-analysis investigated the efficacy of psychologicalinterventions for infertile patients in connection with their mentalhealth and pregnancy rates. One explanation for the small overall ESof such interventions on psychological outcomes could be the factthat infertile patients do not receive individualized psychological inter-ventions. This lack of differentiated indication of psychological inter-ventions to specific patients may lower the effects of the treatment(Roth and Fonagy, 2004). Future research should vary the specificobjectives of different types of psychological interventions, namelythe setting (single, couple or group), the type (e.g. psychotherapy,counselling and education) and the intensity (frequency and duration)of the intervention in randomized trials. Further, gender and the levelof mental distress are important covariates in observational studieswhen trying to arrive at conclusions regarding the differential effectof psychological treatments in specific populations. Study results arestill inconclusive regarding the best setting for psychological interven-tions aimed at infertile patients. Although De Liz and Strauss (2005)have found group and individual/couple interventions to be similarlyeffective, Boivin (2003) reports of group interventions being moreeffective. Future research should also further examine the gender-specific effects of psychological interventions for infertile patients.To date, the effect of including women’s partners in treatment hasnot been adequately examined. Women and men ought to be ana-lysed separately as there appear to be important differences in theirprocessing of fertility-related information. Further, infertility patients’level of mental distress often varies according to the phase of infertilityin which they find themselves. Therefore, patients’ phase of infertilitymust also be taken into account. While there are several relevantnotions of mental distress used in the literature (mental distress, dis-tress caused by infertility, infertility-specific distress), there is still noclear accepted definition of mental distress used in connection withinfertility. Adequate measures for infertility-specific mental distress(e.g. the intensity of one’s wish for a child, cognitions about infertility)must be established in order to meaningfully examine the efficacy ofrelevant psychological interventions. Additionally, the dose–responserelationship needs to be assessed further by focusing on the durationand intensity of psychological interventions. Overall, there are meth-odological flaws present in some primary studies. It is imperativethat future research studies employ high-quality research design andthat their results be presented in a clear, unequivocal manner inorder to achieve more definitive conclusions regarding the efficacyof psychological interventions for infertile patients.
Clinical implicationsPsychological interventions should be integrated in the treatment ofinfertility as the present study indicates that psychological interventionsare somewhat effective in increasing pregnancy rates. However, withrespect to mental health, the efficacy of psychological interventionsfor infertile patients could not be verified. Nevertheless, the presentstudy provides some hints that psychological interventions which lastlonger—i.e. interventions with a duration of six or more sessions—may have a greater effect on infertile patients’ mental health and
14 Hammerli et al.
pregnancy rates. Finally, the present study indicates that psychologicalinterventions are effective in increasing the pregnancy rates in particu-lar among patients not receiving ART.
ConclusionsThe findings of the present study provide some evidence in support ofintegrating psychological interventions as an early treatment strategyfor infertile patients. Psychological interventions appear to increaseinfertile women’s chances of becoming pregnant—in particular thosewho are not receiving ART. On the basis of the results, psychologicalinterventions are beneficial for infertile patients, but more randomizedcontrolled trials are needed.
Supplementary dataSupplementary data are available at http://humupd.oxfordjournals.org.
AcknowledgementsThe authors extend their deepest thanks to all the researchers whoprovided them with additional information on their studies. Theauthors also wish to thank Anu Lannen, Martin Grosse Holtforth, Mat-thias Berking, Sven Tholen and Michelle Cattin for their valuable com-ments on earlier versions of the manuscript.
Conflict of interest: none declared.
FundingThe present study was supported by a grant from the Swiss NationalScience Foundation (grant no. 325100-11375411).
References*References marked with an asterisk were included as controlled studies inthe meta-analysis. oReferences marked with a point were excluded asuncontrolled studies or excluded controlled studies of the meta-analysis.
Abbey A, Halman LJ, Andrews FM. Psychosocial treatment anddemographic predictors of the stress associated with infertility. FertilSteril 1992;57:122–128.
Altman DG, Bland JM. Interaction revisited: the difference between twoestimates. Br Med J 2003;326:219.
Beaurepaire J, Jones M, Thiering P, Saunders D, Tennant C. Psychosocialadjustment to infertility and its treatment: male and female responsesat different stages of IVF/ET treatment. J Psychosom Res 1994;38:229–240.
oBentsH.VerhaltenstherapeutischePaartherapiebeiKinderwunschpatienten.In: Brahler E, Myer A (eds). Psychologische Probleme in derReproduktionsmedizin. Jahrbuch der Medizinischen Psychologie, Vol. 5. Berlin:Springer, 1991, 144–155.
Boivin J. A review of psychosocial interventions in infertility. Soc Sci Med2003;57:2325–2341.
Boivin J, Takefman JE. Stress level across stages of in vitro fertilization insubsequently pregnant and nonpregnant women. Fertil Steril 1995;64:802–810.
oBrandt KH, Zech H. Effects of short-term psychotherapy on the successof an in vitro fertilization/embryo transfer program. Wien MedWochenschr 1991;141:17–19.
oBrandt K, Zech H. Results of a prognosis study of in vitro fertilization afterbrief psychotherapy. Geburtshilfe Frauenheilkd 1992;52:297–300.
oBresnick ER. A holistic approach to the treatment of the crisis ofinfertility. J Marital Fam Ther 1981;7:181–188.
oBresnick E, Taymor ML. The role of counseling in infertility. Fertil Steril1979;32:154–156.
Brkovich AM, Fisher WA. Psychological distress and infertility: forty yearsof research. J Psychosom Obstet Gynaecol 1998;19:218–228.
*Chan CHY, Ng EHY, Chan CLW, Ho PC, Chan THY. Effectiveness ofpsychosocial group intervention for reducing anxiety in womenundergoing in vitro fertilization: a randomized controlled study. FertilSteril 2006;85:339–346.
Chen TH, Chang SP, Tsai CF, Juang KD. Prevalence of depressive andanxiety disorders in assisted reproductive technique clinic. HumReprod 2004;17:2313–2318.
oChristie G, Morgan A. Individual and group psychotherapy with infertilecouples. Int J Group Psychother 2000;50:237–250.
oChristie G, Morgan A. Individual therapy, group therapy and co-therapywork with infertile couples. Aust J Psychother 2006;25:83–103.
oClark AM, Ledger W, Galletly C, Tomlinson L, Blaney F, Wang X,Norman RJ. Weight loss results in significant improvement inpregnancy and ovulation rates in anovulatory obese women. HumReprod 1995;10:2705–2712.
oClark AM, Thornley B, Tomlinson L, Galletley C, Norman RJ. Weight lossin obese infertile women results in improvement in reproductiveoutcome for all forms of fertility treatment. Hum Reprod 1998;13:1502–1505.
Cochrane Collaboration: Review Manager 5.0. www.cc-ims.net/RevMan(4 September 2007, date last accessed).
Cohen J. Statistical Power Analysis for the Behavioral Sciences, revised edn.New York: Academic Press, 1977.
oConnolly KJ, Edelmann RJ, Bartlett H, Cooke ID, Lenton E, Pike S. Anevaluation of counselling for couples undergoing treatment for in-vitrofertilization. Hum Reprod 1993;8:1332–1338.
oCousineau TM, Corsini EA, Green TC, Barnard MT, Seibring A. Arandomized-controlled study of an online infertility psychoeducationalprogram. In: Abstracts of the 62nd Annual meeting of the ASRM, NewOrleans, LA, 2006 Abstract O-130. Fertil Steril.
Covington S, Burns LH. Infertility Counseling: A Comprehensive Handbook forClinicians, 2nd edn. New York, NY: Cambridge University Press, 2006.
*De Klerk C, Hunfeld JAM, Duivenvoorden HJ, den Outer MA, Fauser B,Passchier J, Macklon NS. Effectiveness of a psychosocial counsellingintervention for first-time IVF couples: a randomized controlled trial.Hum Reprod 2005;20:1333–1338.
De Liz TM, Strauss B. Differential efficacy of group and individual/couplepsychotherapy with infertile patients. Hum Reprod 2005;20:1324–1332.
Demyttenaere K, Nijs P, Evers-Kiebooms G, Koninckx PR. Coping and theineffectiveness of coping influence the outcome of in vitro fertilizationthrough stress responses. Psychoneuroendocrinology 1992;17:655–665.
Demyttenaere K, Bonte L, Gheldof M, Vervaeke M, Meuleman C,Vanderschuerem D, D’Hooghe T. Coping style and depression levelinfluence outcome in in vitro fertilization. Fertil Steril 1998;69:1026–1033.
oDomar AD, Seibel MM, Benson H. The mind/body program forinfertility: a new behavioral treatment approach for women withinfertility. Fertil Steril 1990;53:246–249.
oDomar AD, Zuttermeister PC, Seibel M, Benson H. Psychologicalimprovement in infertile women after behavioral treatment: areplication. Fertil Steril 1992;58:144–147.
oDomar AD, Friedman R, Zuttermeister PC. Distress and conception ininfertile women: a complementary approach. J Am Med Womens Assoc1999;54:196–198.
Psychological interventions for infertile patients 15
*Domar AD, Clapp D, Slawsby E, Kessel B, Orav J, Freizinger M. Theimpact of group psychological interventions on distress in infertilewomen. Health Psychol 2000a;19:568–575.
*Domar AD, Clapp D, Slawsby EA, Dusek J, Kessel B, Freizinger M. Impactof group psychological interventions on pregnancy rates in infertilewomen. Fertil Steril 2000b;73:805–811.
Dunkel-Schetter C, Lobel M. Psychological reactions to infertility. In:Stanton AL, Dunkel-Schetter C (eds). Infertility: Perspectives from Stressand Coping Research. London, New York: Plenum Press, 1991, 29–57.
Dunkel-Schetter C, Stanton AL. Psychological adjustment to infertility. In:Stanton AL, Dunkel-Schetter C (eds). Infertility: Perspectives from Stressand Coping Research. London, New York: Plenum Press, 1991,197–222.
Edelmann RJ, Humphrey M, Owens DJ. The meaning of parenthood andcouples’ reactions to male infertility. Br J Med Psychol 1994;67:291–299.
*Ellenberg J, Koren Z. Infertility and depression. Int J Fertil 1982;27:219–223.
*Emery M, Beran M-D, Darwiche J, Oppizzi L, Joris V, Capel R, Guex P,Germond M. Results from a prospective, randomized, controlledstudy evaluating the acceptability and effects of routine pre-IVFcounselling. Hum Reprod 2003;18:2647–2653.
*Emery M, Joris V, Beran M-D, Darwiche J, Capel R, Guex P, Germond M.Prospective study of pre-IVF counselling: one-year follow-up. J ReprodMed Endocrinol 2006;1:77–78.
Eugster A, Vingerhoets AJ. Psychological aspects of in vitro fertilization: areview. Soc Sci Med 1999;48:575–589.
Facchinetti F, Matteo ML, Artini GP, Volpe A, Genazzani AR. An increasedvulnerability to stress is associated with poor outcome of in vitrofertilization-embryo transfer treatment. Fertil Steril 1997;67:309–314.
*Facchinetti F, Tarabusi M, Volpe A. Cognitive-behavioral treatmentdecreases cardiovascular and neuroendocrine reaction to stress inwomen waiting for assisted reproduction. Psychoneuroendocrinology2004;29:132–173.
Freeman EW, Boxer AS, Rickels K et al. Psychological evaluation andsupport in a program of in vitro fertilization and embryo transfer.Fertil Steril 1985;43:48–53.
oGalletly C, Clark A, Tomlinson L, Blaney F. Improved pregnancy rates forobese, infertile women following a group treatment program: an openpilot study. Gen Hosp Psychiatry 1996a;18:192–195.
oGalletly C, Clark A, Tomlinson L, Blaney F. A group program for obese,infertile women: weight loss and improved psychological health.J Psychosom Obstet Gynaecol 1996b;17:125–128.
Gnoth C, Godehardt E, Frank-Herrmann P, Friol K, Tigges J, Freundl G.Definition and prevalence of subfertility and infertility. Hum Reprod2005;20:1144–1147.
Greil AL. Infertility and psychological distress: a critical review of theliterature. Soc Sci Med 1997;45:1679–1704.
Habbema JDF, Collins J, Leridon H, Evers JLh, Lunefeld B, te Velde ER.Towards less confusing terminology in reproductive medicine: aproposal. Hum Reprod 2004;19:1497–1501.
Harlow CR, Fahy UM, Talbot WM, Wardle PG, Hull MG. Stress andstress-related hormones during in-vitro fertilization treatment. HumReprod 1996;11:274–279.
Hauck WW. Odds ratio inference from stratified samples. Commun StatA-Theor 1989;18:767–800.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistencyin meta-analyses. Br Med J 2003;327:557–560.
Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis ofpsychological interventions for chronic low back pain. Health Psychol2007;26:1–9.
oHolzle C, Brandt U, Lutkenhaus R, Wirtz M. Solution-focused counselingfor involuntarily childless couples. In: Strauss B (ed). Involuntary
Childlessness: Psychological Assessment, Counseling, and Psychotherapy.Ashland, OH: Hogrefe and Huber Publishers, 2002, 105–126.
Homan AC, Davies M, Norman R. The impact of lifestyle factors onreproductive performance in the general population and thoseundergoing infertility treatment: a review. Hum Reprod Update 2007;11:1–15.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance fromthe median, range, and the size of sample. BMC Med Res Methodol2005;5:1–10.
oKemeter P, Fiegl J. Das psychosomatisch orientierte Gesprach imRahmen der Sterilitatsbehandlung - eine Quantifizierung derGesprachsschwerpunkte und der therapeutischen Strategien. J FertilReprod 1999;9:23–31.
Klonoff-Cohen H. Female and male lifestyle habits and IVF: what is knownand unknown. Hum Reprod Update 2005;11:179–203.
Klonoff-Cohen H, Chu E, Natarajan L, Sieber W. A prospective study ofstress among women undergoing in vitro fertilization or gameteintrafallopian transfer. Fertil Steril 2001;76:675–687.
Leiblum SR, Greenfield DA. The course of infertility: immediate andlong-term reactions. In: Leiblum S (ed). Infertility: PsychologicalIssues and Counselling Strategies. New York: John Wiley & Sons, 1997,83–102.
Lesperance F, Frasure-Smith N, Koszycki D, Laliberte M-A, van Zyl LT,Baker B, Swenson JR, Ghatavi K, Abramson BL, Dorian P et al. Effectsof citalopram and interpersonal psychotherapy on depression inpatients with coronary artery disease: the Canadian CardiacRandomized Evaluation of Antidepressant and Psychotherapy Efficacy(CREATE) trial. JAMA 2007;297:367–379.
*Levitas E, Parmet A, Lunenfeld E, Bentov Y, Burstein E, Friger M,Potashnik G. Impact of hypnosis during embryo transfer on theoutcome of in vitro fertilization-embryo transfer: a case–controlstudy. Fertil Steril 2006;85:1404–1408.
Lipsey MW, Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA: Sage,2001.
*Liswood MP. Treating the crisis of infertility: a cognitive-behavioralapproach. Dissertation Abstracts International Section A: Humanitiesand Social Sciences 55(12-A) 1995.
oMcNaughton-Cassill ME, Bostwick JM, Vanscoy SE, Arthur NJ,Hickman TN, Robinson RD, Neal GS. Development of brief stressmanagement support groups for couples undergoing in vitrofertilization treatment. Fertil Steril 2000;74:87–93.
*McNaughton-Cassill ME, Bostwick JM, Arthur NJ, Robinson RD, Neal GS.Efficacy of brief couples support groups developed to manage the stressof in vitro fertilization treatment. Mayo Clin Proc 2002;77:1060–1066.
*McQueeney DA, Stanton AL, Sigmon S. Efficacy of emotion-focused andproblem-focused group therapies for women with fertility problems.J Behav Med 1997;20:313–331.
oMelamed RM, Bonetti TC, Pasqualotto FF, Locambo-Freitas CV,Iaconelli A, Borges E. Previous counseling to assisted reproductiontreatment does bring the couples to reality. In: Abstracts of the 61stAnnual meeting of the ASRM, Montreal, Canada, 2005. Abstract P-669.Fertil Steril.
Menning BE. The emotional needs of infertile couples. Fertil Steril 1980;34:313–319.
oO’Moore AM, O’Moore RR, Harrison RF, Murphy G, Carruthers ME.Psychosomatic aspects in idiopathic infertility: effects of treatmentwith autogenic training. J Psychosom Res 1983;27:145–151.
oPengelly P, Inglis M, Cudmore L. Infertility: couples’ experiences and theuse of counselling in treatment centres. Psychodyn Couns 1995;1:507–524.
*Rezabek K, Vichova V, Pavelkova J, Zivny J. Hypnosis during embryotransfer does not ameliorate IVF results. In: Abstracts of the 19th AnnualMeeting of ESHRE, Madrid, Spain, 2003. Abstract P-403. Hum Repro.
16 Hammerli et al.
Rosenthal R, Rosnow RL, Rubin DB. Contrasts and Effect Sizes in BehavioralResearch: A Correlational Approach. New York, NY: Cambridge UniversityPress, 2000.
Roth A, Fonagy P. What Works for Whom? A Critical Review of PsychotherapyResearch, 2nd edn. New York, NY: Guilford Press, 2004.
*Sarrel PM, DeCherney AH. Psychotherapeutic intervention for treatmentof couples with secondary infertility. Fertil Steril 1985;43:897–900.
*Schmidt L, Tjornhoj-Thomsen T, Boivin J, Nyboe Andersen A. Evaluationof a communication and stress management training programme forinfertile couples Patient. Educ Couns 2005;59:252–262.
*Shu-Hsin L. Effects of using a nursing crisis intervention program onpsychosocial responses and coping strategies of infertile womenduring in vitro fertilization. J Nurs Res 2003;11:197–208.
Slade P, Emery J, Lieberman BA. A prospective, longitudinal study ofemotions and relationships in in-vitro fertilization treatment. HumReprod 1997;12:183–190.
Smeenk JM, Verhaak CM, Eugster A, van Minnen A, Zielhuis GA,Braat DD. The effect of anxiety and depression on the outcome ofin-vitro fertilization. Hum Reprod 2001;16:1420–1423.
Smeenk JM, Verhaak CM, Stolwijk AM, Kremer JA, Braat DD. Reasons fordropout in an in vitro fertilization/intracytoplasmic sperm injectionprogram. Fertil Steril 2004;81:262–268.
Stanton AL, Tennen H, Affleck G, Mendola R. Cognitive appraisal andadjustment to infertility. Women Health 1991;17:1–15.
*Stewart DE, Boydell KM, McCarthy K, Swerdlyk S, Redmond C,Cohrs W. A prospective study of the effectiveness of briefprofessionally-led support groups for infertility patients. Int J PsychiatryMed 1992;22:173–182.
*Strauss B, Hepp U, Stading G, Mettler L. Focal counseling for women andcouples with an unfulfilled desire for a child: a three-step model. In:Strauss B (ed). Involuntary Childlessness: Psychological Assessment,Counseling, and Psychotherapy. Ashland, OH: Hogrefe and HuberPublishers, 2002, 79–103.
Strauss B, Brahler E, Kentenich H. Fertilitatsstorungen - psychosomatischorientierte Diagnostik und Therapie. Stuttgart: Schattauer, 2004.
oTakefman J, BrenderW, Boivin J, Tulandi T. Sexual and emotional adjustmentof couples undergoing infertility investigation and the effectiveness ofpreparatory information. J Psychosom Obstet Gynaecol 1990;11:275–290.
*Tarabusi M, Volpe A, Facchinetti E. Psychological group supportattenuates distress of waiting in couples scheduled for assistedreproduction. J Psychosom Obstet Gynaecol 2004;25:273–279.
Thiering P, Beaurepaire J, Jones M, Saunders D, Tennant C. Mood state asa predictor of treatment outcome after in-vitro fertilization-embryotransfer technology (IVF/ET). J Psychosom Res 1993;37:481–491.
Tuschen-Caffier B, Florin I, KrauseW, PookM.Cognitive-behavioral therapyfor idiopathic infertile couples. Psychother Psychosom 1999;68:15–21.
Verberg MFG, Eijkemans MJC, Heijnen EMEW, Broekmans FJ, de Klerk C,Fauser BCJM, Macklon NS. Why do couples drop-out from
IVF treatment? A prospective cohort study. Hum Reprod 2008;23:2050–2055.
Visser AP, Haan G, Zalmstra H, Wouters I. Psychosocial aspects of in vitrofertilization. J Psychosom Obstet Gynaecol 1994;15:35–43.
Wilson DB. Effect size determination program. University of Maryland,College Park, 2001. http://mason.gmu.edu/~dwilsonb/ma.html.
Winkley K, Landau S, Eisler I, Ismail K. Psychological interventions toimprove glycaemic control in patients with type 1 diabetes: systematicreview and meta-analysis of randomised controlled trials. Br Med J2006;333:65.
Wischmann T. Psychogenic infertility—myths and facts. J Assist ReprodGenet 2003;20:485–494.
Wischmann T. Psychosocial aspects of fertility disorders. Urologe A 2005;44:185–194.
*Wischmann T, Stammer H, Scherg H, Gerhard I, Strowitzki T, Verres R.Evaluation of the psychological effects of counselling and couple-therapywith infertile couples. Paper presented at the 17th Annual Meeting ofthe European Society for Human Reproduction and Embryology. HumReprod 2001a;16:198.
*Wischmann T, Stammer H, Scherg H, Gerhard I, Verres R. Psychologicalcharacteristics of infertile couples: a study of the “Heidelberg FertilityConsultation Service”. Hum Reprod 2001b;16:1753–1761.
*Wischmann T, Stammer H, Scherg H, Gerhard I, Verres R. Couplecounselling and therapy for the unfulfilled desire for a child: thetwo-step approach of the “Heidelberg Infertility Consultation”. In:Strauss B (ed). Involuntary Childlessness: Psychological Assessment,Counseling, and Psychotherapy. Ashland, OH: Hogrefe and HuberPublishers, 2002, 127–150.
World Health Organization. The epidemiology of infertility: report of aWHO Scientific Group. WHO, Geneva, 1975.
World Health Organization. Current practices and controversies inassisted reproduction. Report of meeting on “Medical, Ethical andSocial Aspects of Assisted Reproduction”, 17–21 September 2001.WHO Headquarters, Geneva, Switzerland, 2002.
Wright J, Allard M, Lecours A, Sabourin S. Psychosocial distress andinfertility: A review of controlled research. Int J Fertil 1989;34:126–142.
Wright J, Duchesne C, Sabourin S, Bissonnette F, Benoit J, Girard Y.Psychosocial distress and infertility: men and women responddifferently. Fertil Steril 1991;55:100–108.
Zegers-Hochschild F, Nygren K-G, Adamson GD, de Mouzon J,Lancaster P, Mansour R, Sullivan E. The ICMART glossary on ARTterminology. Hum Reprod 2006;21:1968–1970.
Zhen XH, Xie H, Xu X. Psychotherapy intervention for the insomniastatus in patients with secondary infertility. Zhongguo Linchuang Kangfu2005;9:33–35.
Submitted on January 9, 2008; resubmitted on December 16, 2008; accepted onJanuary 3, 2009
Psychological interventions for infertile patients 17
Artikel 4
Haemmerli, K., Znoj, H., & Berger, T. (revised). Internet-based support for
infertile patients: a randomised controlled trial.

Running title: Child Wish Online Coaching
Internet-Based Support for Infertile Patients: A Randomized Controlled Study
K. Haemmerli1*, H. Znoj1 and T. Berger1
1Institute of Psychology, Department of Clinical Psychology and Psychotherapy, University
of Bern, Switzerland
23. April 2009
Corresponding Author:
*University of Bern, Institute of Psychology, Department of Clinical Psychology and Psycho-
therapy, Gesellschaftsstrasse 49, 3012 Bern, Switzerland, Tel.: 0041 31 631 45 83, Fax: 0041
31 631 41 55, email: [email protected]

Abstract
This study aimed to evaluate the efficacy and patient acceptance of the first German-
language Internet-based treatment for infertile patients. Infertile patients (N = 124) were ran-
domly assigned to either an eight-week Internet-based cognitive-behavioral treatment, or to a
waiting-list control group. Participants were assessed at treatment start, post-treatment, and at
a five-month follow-up. Outcome measures included mental health and pregnancy rate. Re-
sults showed greater effects in the intervention group compared to the control group, but dif-
ferences between the groups were not statistically significant (range of Cohen’s d = 0.16 to d
= 0.38). Subgroup analysis revealed that the intervention was significantly effective for clini-
cally distressed and depressed participants (overall within- and between-group effect sizes,
Cohen’s d = 0.98 and 0.52). No effects were found regarding pregnancy rate. The treatment
was assessed as positive or very positive by 80% of the participants. The findings of the pres-
ent study and the high demand for such support confirm that internet-based interventions are a
promising approach.
Key words: Infertility, Internet-based treatment, Mental Health, Assisted Reproduction, Cog-
nitive behavior therapy
Introduction
Infertility and its medical treatment are very stressful. Several studies have reported high
levels of mental distress among infertile patients (Chen et al., 2004; Eugster and Vingerhoets,
1999; Wischmann, 2005). Psychological interventions have proven effective for infertile pa-
tients in improving mental health and increasing pregnancy rates (Boivin, 2003; De Liz and
Strauss, 2005; Haemmerli et al., 2009). However, psychological support is rarely offered until
medical treatment is sought (Cousineau and Domar, 2007). While assisted reproductive
treatments (ART) are often considered to be the most stressful way of treating infertility
(Eugster and Vingerhoets, 1999), efficacy of psychological interventions, particularly in im-
proving pregnancy rates among infertile patients not receiving ART was reported (Haemmerli
et al., 2009). Offering psychological interventions in advance of fertilization treatments may
reduce the number of treatment cycles patients require to achieve pregnancy (Campagne,
2006). Provision of psychological support could reduce the high dropout rate from medical
treatment on the part of infertile patients with high levels of distress (Verberg et al., 2008).
Despite the overwhelming opinion of researchers and practitioners as to the importance
and potential benefits of psychological interventions for infertility patients, very few such
patients actually take advantage of psychological support when it is made available to them
(Boivin et al., 1999;Wischmann, 2005). The low utilization of psychological interventions
may be attributed to fears of stigmatization surrounding acceptance of such support, to skepti-
cism regarding efficacy, and to fears of emotional destabilization (Wischmann, 2008). Since
less distressed infertile patients often cope successfully with the strains of infertility on their
own, psychological interventions should be offered to patients suffering from high levels of
distress (Boivin et al., 1999).
An increasing number of infertile patients look to printed materials or surf the World Wide
Web for information and support (Cousineau and Domar, 2007). The Internet, which offers
the possibility of anonymous communication, is often considered less stigmatizing than face-
to-face psychological support. A vast amount of information about infertility and numerous
self-help forums exist on the World Wide Web. More than half of all infertile patients seek
out fertility-related information on the Internet, and many of them consider the information
available and the opportunity for anonymous exchange to be of help (Himmel et al., 2005;
Kahlor and Mackert, 2009). However, studies evaluating the quality of fertility clinic websites
have concluded that they are often inadequate (Huang et al., 2005; Okamura et al., 2002).
To the best of our knowledge, only one Internet-based psychological treatment program
for infertile patients has been evaluated to date (Cousineau et al., 2008). This brief (60- to 90-
minute) educative, stress-management program was shown to decrease infertility-specific
distress and increase self-efficacy among infertile women undergoing medical treatment. The
Child Wish Online Coaching evaluated in the present study is the first Internet-based German
language treatment. It consists of cognitive-behavioral interventions for both infertile women
and men. To date, only a handful of studies have examined mental health among infertile
men, but these have shown that infertile men also suffer from high levels of mental distress
(Cousineau and Domar, 2007). The Child Wish Online Coaching program may be provided to
infertile patients independent of the current medical treatment they receive.
The main purpose of the randomized controlled trial described here was to examine the
efficacy of Online Coaching with regards to mental health (depression, anxiety, and infertil-
ity-specific distress) and pregnancy rate by comparing an intervention group with a waiting-
list control group. Another aim was to evaluate the efficacy of the Online Coaching in particu-
lar for patients with clinically relevant levels of distress or depression. Our trial included both
highly and minimally distressed and depressed patients. We further examined if the effects
found in the intervention group were still present at a five-month follow-up, and, for explora-
tory purposes, we evaluated the responses of participants in the waiting-list control group
once they received the treatment themselves. The final aim of the study was to examine pa-
tients’ overall acceptance and usage of the Child Wish Online Coaching program.
Methods
Participant eligibility and recruitment
Participants were recruited through the University of Bern, Switzerland, by means of arti-
cles in regional newspapers and advertisements in Swiss and German fertility websites. Ap-
proval for the study was obtained from the Cantonal Research Ethics Committee of Bern,
Switzerland. Recruitment took place between March 2008 and May 2008. Informed consent
was obtained in writing from all participants.
Individuals were eligible to participate in the study if they met the following criteria for
inclusion: a) women and men suffering from primary or secondary infertility for at least one
year; b) not undergoing any other psychological treatment for the duration of the study; c)
bearing access to a computer with an Internet connection; and, d) at least 18 years of age. Our
website provided general information about infertility and its medical treatment as well as an
outline of the study and the criteria for participation. This information was accessible to any-
one. After registering participants, mailings were sent out via the postal service that contained
further information about the study, copies of the documents confirming informed consent,
and the various baseline questionnaires. Following a final check of eligibility, participants
received a login name and password in order to enter the secured client zone and begin with
the treatment. Over the course of the entire recruitment and intervention process, contact with
the patients was limited to email contact, with no face-to-face contact occurring at any point.
Procedure
124 participants met all the inclusion criteria and were randomized to the treatment group
(n = 60) or waiting-list control group (n = 64) using an online randomization program (Ran-
domization.com, 2008). A total of 124 participants were regarded as providing sufficient
power for later statistical analyses. Figure I presents participant flow through the study. If
couples registered for Online Coaching, both partners were assigned to the same group. After
eight weeks, the intervention and the waiting-list control group completed another assess-
ment, and the waiting list control group began with the treatment. A total of 14 people (five in
the treatment group and nine in the control group) dropped out between pre- and post-
assessment and failed to complete post-assessment questionnaires (11.3%). Of the five par-
ticipants in the treatment group who did not complete post-assessment questionnaires, one
participant indicated having no time and four participants did not provide with any reason. In
the control group: six participants became pregnant during the waiting period; one participant
wanted to start the Online Coaching program at a later date; one woman’s partner fell ill; and
one participant no longer wanted to participate following randomization. According to an
intention-to-treat paradigm, we set the post-test data for the non-completers at their baseline
pre-test level.
The intervention group was assessed once more at a five-month follow-up, three months
after the post-assessment. 80% (n = 48) of the 60 participants in the treatment condition re-
turned follow-up questionnaires. The control group also completed a post-assessment after
receiving the eight-week treatment. After receiving treatment, 11 participants of the control
group did not complete the questionnaire: five participants got pregnant in the course of On-
line Coaching; two no longer wished to take part in the study; and, four remaining participants
dropped out due to differing preconceptions of Online Coaching, family illness, or unknown
reasons.
On average, each of the 52 intervention group participants who filled out the post-
treatment measures completed approximately 79% of the Online Coaching program. Of these,
half completed the entire self-help guide (14 sessions), 15 (28.8%) completed 50% or more,
11 (21%) completed less than 50%, and one participant (1.9%) only completed the first ses-
sion. As for the control group, the 41 participants who filled out the post-treatment measures
completed, on average, approximately 72% of the program. In the control group, 44% of the
participants completed the entire self-help guide, 13 (31.7%) completed 50% or more, and 10
(24.4%) completed less than 50%.
Please insert Figure I approximately here
Intervention
The Child Wish Online Coaching program’s goal is to improve the mental health of the
infertile patients who participate, not solely or primarily to increase their pregnancy rate. The
intervention consists of an eight-week Internet-based program encompassing an interactive
self-help guide, a module for patients to establish regular text-based contact with a therapist, a
continuous monitoring and feedback system examining patients’ responses, as well as col-
laborative elements and forums that offer participants the opportunity to share their experi-
ences with other patients. We employ SSL (Secure Sockets Layer) encryption to secure all
Internet-based communication and participants are identified using anonymous login names
and passwords.
The content of the self-help guide is primarily based on principles of cognitive behavioral
therapy and well-established treatment topics for infertile patients (e.g. Bents, 1991), and is
further supplemented with clarification-oriented therapy techniques (e.g. Sachse, 2003) and
system therapy (e.g. Stammer et al., 2004). The Child Wish Online Coaching program con-
sists of a total of 108 web pages divided into 13 sessions.
In the first session, participants are advised to clarify their motives, hopes, and fears con-
cerning their wish for a child as well as any unrealistic expectations they might have (e.g.
Stammer et al., 2004). The goal of the second session of the intervention program is for pa-
tients to analyze their own stress and to better understand what contributes to it. In session
three, participants are taught different ways of coping with stress and learn new strategies for
coping with stress in everyday life (Kaluza, 2004). Several studies have indicated a positive
effect of relaxation exercises on mental distress (e.g. Chan et al., 2006) and on pregnancy rate
(e.g. Levitas et al., 2006). In the fourth session, progressive muscle relaxation (PMR; Jacob-
son, 1938) is introduced as a further strategy for reducing stress. Infertility and its medical
treatment are often described as an emotional rollercoaster. In session five, participants re-
ceive various information and strategies for coping with stressful feelings. The goal of the
sixth session is for patients to learn how to better handle unpleasant reactions and comments
from those around them, and how to identify an appropriate policy on sharing information
about their infertility with others (Wischmann and Stammer, 2006). Goals of session seven
include encouraging patients to pay closer attention to what they enjoy and to integrate it
more frequently into everyday life. The goal of the eighth session is for couples to achieve an
understanding of their differences and to find ways of realizing the needs of both partners
(Wischmann and Stammer, 2006). The ninth session focuses on participants’ lives before try-
ing to conceive a child. Once the period of intensive effort towards having a child begins,
earlier positive activities and contacts can often go neglected and should be reactivated. In
session 10, participants are encouraged to clarify their anxieties and fears surrounding medi-
cal treatment and to consider the possibility of having a positive experience with such treat-
ment (Covington and Burns, 2006). Session 11 targets realizing the strengths inherent to each
couple’s relationship as well as future projects they might share independent of their wish for
a child. The period of waiting between embryo transfer, pregnancy test, and result is often
described as the most stressful (Boivin and Takefman, 1995; Klonoff-Cohen et al., 2001). In
session 12, participants receive tips on to how to organize the periods of waiting and how to
handle a negative pregnancy test. The aims of session 13 include establishing effective self-
support and strengthening self-esteem.
Each web page and each session builds upon the previous, and users only gain access to
the next site once they have completed all the previous sites and tasks. However, since many
tasks and exercises are repeated, working through the self-help guide is not simply a matter of
sequential progression. A final section following session 13 focuses on repetition. It empha-
sizes the importance of practice and involves repeating the exercises and tasks introduced in
previous sessions.
At the end of every session (with the exception of sessions two and 13), participants have
the opportunity to share their experiences with other participants in the context of forums. In
addition, throughout the course of the program, participants are given the option of anony-
mously publishing their own responses regarding the history of their wish for a child, their
stress models, and their ways of coping with stress. Such collaborative elements take full ad-
vantage of the medium provided by the Internet, and may represent promising new ways of
realizing therapeutic factors associated with group therapy in an individual setting (Berger
and Caspar, 2008).
Child Wish Online Coaching is a treatment that involves minimal contact with therapists.
When patients log into the program for the first time, they are redirected to the contact mod-
ule, where they are introduced to a therapist and informed that they may contact this therapist
at any time. These therapists respond to patients within two days of receiving their queries. In
addition, these therapists are instructed to write brief, motivational messages to the patients
once a week. In our trial, the mean number of messages written by patients was 4.2 (Min: 0;
Max: 19), with individual messages averaging 156 words in length.
Therapists
The therapists involved in the study included, on the one hand, a psychologist bearing a
master’s degree in clinical psychology and, on the other hand, two postgraduate students of
psychology (three women in total): The former therapist, who has combined a postgraduate
course of studies in clinical psychology together with psychotherapy and is highly experi-
enced in treating infertile patients, trained and supervised the latter two therapists before and
during the trial.
Measures
All the outcome measures assessed at baseline, at post-treatment (two months after base-
line), and at five-month follow-up were collected using paper-and-pencil questionnaires. The
following basic demographic information was collected at baseline: age, gender, citizenship,
native language, education level, living arrangement, marital status, duration of wish for a
child, previous infertility-related medical treatment, and history of psychological treatment.
Two and five months later, demographic information was again collected with regards to
medical treatment, supplementary psychological support, and pregnancy status.
The principal psychological outcome measures used included the Center for Epidemi-
ologic Studies Depression Scale (CES-D; Hautzinger et al., 1988; Radloff, 1977) and the
State-Trait Anxiety Inventory (STAI; Spielberger et al., 1970). Participants’ resultant preg-
nancy rate was also assessed. The CES-D quantifies the severity of depressive symptomatol-
ogy and consists of 20 items. Scores range from 0 to 60, with scores of 16 or higher reflecting
clinical depression (Hautzinger et al., 1988). At baseline, the internal consistency of the CES-
D for our sample was alpha=0.92. The STAI assesses general levels of anxiety and consists of
40 items. Scores above 33 (STAI-S) and above 35 (STAI-T) indicate clinically significant
state and trait anxiety respectively (Spielberger et al., 1970). At baseline, the Cronbach’s al-
pha for our sample was 0.94 for state anxiety and 0.89 for trait anxiety. Pregnancy rate was
defined as evidence of pregnancy according to clinical or ultrasound parameters (ultrasound
visualization of a gestational sac; Zegers-Hochschild et al., 2006) and was assessed per pa-
tients’ self-reports. We also included the Infertility Distress Scale (IBS; Pook and Krause,
2002). The IBS is an 11-item validated questionnaire that assesses infertile patients’ level of
mental distress stemming from infertility. Here are some examples of items: “How upset were
you the last time you learned, despite your hopes, that you had not become pregnant?”; “How
upsetting is your unfulfilled wish for a child at present?”; “How much distress do you cur-
rently experience at work?”; “How much distress do you currently experience in your rela-
tionship (aside from problems related to your unfulfilled wish for a child)?” IBS scores
ranged from 0 (none at all) to 4 (very intense). It was determined that a cut-off score of 21
indicated a clinically relevant level of distress (Pook and Krause, 2002). In our sample, Cron-
bach’s alpha was 0.73 at baseline.
After finishing the treatment program, all participants were also asked to respond to a
questionnaire assessing their level of acceptance of the treatment program (intervention group
at post-assessment and control group at post-treatment). The research team developed the
questionnaire on the basis of existing questionnaires used to assess acceptance of Internet
interventions. It consisted of 20 items and asked participants to respond on a 5-point Likert
scale (1=not at all; 5=completely) to a series of questions surrounding their overall satisfac-
tion with content, helpfulness, and Internet or program-related technical problems.
Statistical analysis
Group differences in demographic data, pre-test measures, and acceptance of treatment
were analyzed using t-tests (two-tailed) and chi-square tests. Pre-post changes in outcome
measures were analyzed using repeated measures analyses of variance. Post-follow-up
changes within the intervention group and pre-post changes within the control group were
evaluated using dependent t-tests (two-tailed). All calculations of within- and between-group
effect sizes (Cohen’s d) were based on the pooled standard deviation. Group differences in
pregnancy rates were analyzed by calculating relative risks (RR; Rosenthal et al., 2000): A
relative risk larger than 1 indicates a higher pregnancy rate for the intervention group versus
the control group. For the eight-week assessment, analyses were performed on an intention-
to-treat basis. We calculated our results on a last observation carried forward basis (LOCF),
replacing missing post-treatment values with pre-treatment values.
Results
Sample characteristics
Table I shows a summary of the demographic characteristics at baseline arranged accord-
ing to group. The majority of participants were female (83.1%). Participants ranged between
22 and 45 years of age, with an average age of 33.5. The sample comprised 81 participants
from Switzerland, 38 from Germany, and five participants from other countries (two from
France, one from Austria, one from the US, and one from the Netherlands). The mean dura-
tion of participants’ wish for a child was 3.1 years (range 1-10 years), while 63.7% of the par-
ticipants had made use of medical treatment before beginning with the Online Coaching
treatment. Independent sample t-tests and chi-square tests revealed no significant differences
between the participants in the intervention group and the control group with respect to
demographic characteristics or any of the main outcome measures recorded at baseline. Infer-
tile patients receiving medical treatment (N = 76) displayed significantly higher levels of in-
fertility-specific distress at baseline (t(117) = 3.2, p = 0.002) in comparison to infertile pa-
tients not receiving any medical treatment (N = 43). At baseline, our sample as whole dis-
played high levels of mental distress across all measures: infertility-specific distress (M
=24.97; SD = 4.5), depression (M = 17.03; SD = 10.7), state anxiety (M = 43.34; SD =
11.76), and trait anxiety (M = 43.32; SD = 9.66).
Please insert Table I approximately here
Main outcomes
Table II shows the results for all outcome measures, including change scores with 95%
confidence intervals and effect sizes. Although mean change scores were higher in the inter-
vention group in comparison to the control group across all dimensions measured, repeated
measures analysis of variance revealed that none of the group-time interactions were signifi-
cant (IBS: F(1,116) = 2.75; P = 0.10, CES-D: F(1,117) = 1.99; P = 0.16, STAI-S: F(1,117) =
0.008; P = 0.93, STAI-T: F(1/117) = 0.01; P = 0.92). The corresponding between-group effect
sizes (Cohen’s d) were 0.16 for the IBS, 0.34 for the CES-D, 0.38 for the STAI-S, and 0.34
for the STAI-T. Within-group effect sizes for the intervention group were 0.78 for the IBS,
0.49 for the CES-D, 0.46 for the STAI-S, and 0.37 for the STAI-T. For the control group, the
within-group effect sizes were 0.41 for the IBS, 0.26 for the CES-D, 0.40 for the STAI-S, and
0.39 for the STAI-T. In a post-post comparison between intervention and control group (inde-
pendent t-test), significant mean differences were found for depression (CES-D: t(113) = -2.2,
P = 0.03), state anxiety (STAI-S: t(113) = -2.6, P = 0.01), and trait anxiety (STAI-T: t(113) =
-2.3, P = 0.02). No significant mean difference was found for infertility-specific distress be-
tween the two groups (IBS: t(112) = -1.4, P = 0.15).
In order to check for potential confounding factors due to medical treatments, medical
status was analyzed as a between-group factor. This analysis revealed that medical treatments
did not affect patients’ outcome (e.g., no significant main effect of interaction with medical
treatment was found).
Please insert Table II approximately here
Subgroup analysis
An additional analysis was conducted on participants who exceeded the cut-off scores for
the IBS and the CES-D at pre-treatment, reflecting clinically relevant distress levels and clini-
cally relevant levels of depression. The rationale of this subgroup analysis was that only par-
ticipants with clinically relevant pre-treatment levels of distress or depression could benefit
from an intervention targeting psychological problems. Twenty-one participants in the inter-
vention group and 28 participants in the control group were found who exceeded both a score
of 20 on the IBS and a score of 15 on the CES-D (Hautzinger et al., 1988; Pook and Krause,
2002). Table III shows the results of the outcome measures for this subgroup. Repeated meas-
ures analysis resulted in highly significant interactions with respect to the CES-D
(F(1,47)=8.82, P < 0.01), however no significant interactions were found in connection with
the other measures (IBS: F(1,47)=1.41; P=0.24, STAI-S: F(1,47)=0.42; P=0.52, STAI-T:
F(1,47)=0.02, P=0.9).
The corresponding between-group effect sizes were 0.67 for the CES-D, 0.20 for the IBS,
0.82 for the STAI-S, and 0.37 for the STAI-T. In this subgroup, within-group effect sizes of
1.55 (CES-D), 0.98 (IBS), 0.83 (STAI-S), and 0.55 (STAI-T) were found in the intervention
group.
Please insert Table III approximately here
The effect of delayed treatment in the control group and results at follow-up
We examined the impact of receiving delayed treatment among members of the control
group as well as the maintenance of treatment effects among members of the intervention
group at the five-month follow-up. In the control group, a dependent t-test revealed signifi-
cant mean differences indicating a positive effect of the intervention across all mental health
measures between the assessment which followed the eight-week waiting period and the as-
sessment after receiving the online treatment (see Table II: CES-D: t(40)=2.0, P=0.049;
STAI-S: t(40)=2.1, P=0.045; STAI-T: t(40)=3.0, P=0.005; IBS: t(40)=4.0,P<.001). A sub-
group analysis of highly distressed and depressed patients produced the same type of results
(see Table III).
As for the intervention group, analysis of the five-month follow-up data revealed that the
participants maintained the effects of their treatment for the entire period. While the im-
provements among participants were significant between pre- and post-assessment (see Table
II: CES-D: t(52)=2.8, P=0.007; STAI-S: t(52)=3.1, P=0.003; STAI-T: t(52)=3.4, P=0.001;
IBS: t(51)=5.7,P<0.001), no significant effects were found between post-assessment and fol-
low-up (CES-D: t(45)=-1.2, P=0.237; STAI-S: t(47)=-1.6, P=0.119; STAI-T: t(47)=-0.994,
P=0.325; IBS: t(45)=1.3,P=0.207).
Effects of treatment on pregnancy rates
The post-treatment assessment (two months after baseline) revealed no significant effect
for Online Coaching on pregnancy rate when comparing the intervention to the control group
(intention to treat: RR 0.79, 95%CI:0.19,3.30). At this point, three women (7%) had become
pregnant in the treatment group while four women (9.1%) had become pregnant in the control
group. No additional comparison between the groups was possible at the five-month follow-
up since the control group had begun receiving the treatment following their waiting period,
and no separate follow-up assessment was performed for the control group. As for the inter-
vention group, 15 women (31%) became pregnant between the post-treatment assessment and
the follow-up assessment.
Adherence and sessions completed
The average number of sessions completed (out of 13 sessions in total) by the intervention
group participants was 10.5 (SD = 4.3), while the participants in the control group completed
an average of 10.1 (SD = 4.6) sessions. About 46% of all participants completed every ses-
sion. The number of sessions completed did not correlate with pre-, post- or follow-up treat-
ment scores for any of the outcome measures (all Spearman’s rho < 0.1; all ps > 0.5).
Acceptance of the treatment
Table IV summarizes evaluative data from the participant feedback questionnaire as to
participant satisfaction and their assessment of the usefulness of the Child Wish Online
Coaching program. Average levels of participant satisfaction were high. The mean of the total
evaluation of the program was 4.0 (SD = 0.75) out of a maximum of 5, indicating a positive
overall assessment of Online Coaching among participants. Subgroup analysis according to
gender revealed a much more positive assessment of Online Coaching among females when
compared to males. Female participants: expressed greater appreciation for the Online Coach-
ing program (t(94) = 2.442, p < 0.05); found Online Coaching significantly more beneficial
(t(94) = 2.667, p < 0.01); were more satisfied (t(94) = 3.006, p < 0.01); found Online Coach-
ing more appropriate to the difficulties they faced (t(94) = 3.949, p < 0.01); found that it re-
duced their difficulties more frequently; (t(94) = 2.697, p < 0.01); were more likely to par-
ticipate again (t(94) = 3.385, p < 0.01); and, wished to spend more time with Online Coaching
and receive weekly feedback from the therapists (t(94) = 2.691, p < 0.01). Male participants,
by comparison, were significantly less satisfied with the Online Coaching program (t(94) =
3.300, p < 0.01). However, these results are based on only 13 male participants.
Please insert Table IV approximately here
Discussion
This study investigated the efficacy and patient acceptance of the first German-language
Internet-based treatment for infertile patients. The results of our randomized controlled trial
revealed greater effects in the intervention group compared to the control group for all mental
health outcome measures, though the differences between the groups were not statistically
significant. Between-group effect sizes ranged between d = 0.16 for the Infertility Distress
Scale (IBS) and d = 0.38 for the state subscale of the State-Trait Anxiety Inventory (STAI).
One of the main reasons for failing to find significant results at post-assessment may be the
lack of statistical power to detect small to medium effect sizes. Another reason has to do with
the small to moderate within-group improvements that were observed in the waiting-list con-
trol group across all measures and therefore attenuated between-group differences. While the
presence of such effects in the control group highlight the importance of controlling treatment
condition for time and assessment effects—e.g., by controlling for the regression-to-the-
mean—some of the improvements found in the control group may be related to the fact that
control group members knew they would participate in the treatment following a waiting pe-
riod, and may therefore have experienced positive effects due to their anticipation of this
treatment. Another explanation for the improvements in the control group may be that the
control group members used other online information and support during the waiting phase.
Nevertheless, the effect sizes found in our trial are similar to the effect sizes that were
found for the first web-based support program for infertile women (d = 0.24 to d = 0.47;
Cousineau et al., 2008). Further, if one compares the effect sizes observed in our trial with the
efficacy found for face-to-face psychological interventions for infertile patients, the efficacy
of Online Coaching is comparable or even higher. De Liz and Strauss (2005), for example,
conducted a meta-analysis comparing the efficacy of psychological interventions in group
settings to those in individual or couples settings. They found effect sizes for anxiety and de-
pression ranging between d = 0.12 and d = 0.36 in all groups. Another recent meta-analysis
(Haemmerli et al., 2009) revealed even lower effects for psychological interventions with
respect to mental health, with effect sizes ranging between d = 0.01 and d = 0.10. Therefore,
the results of the present study lend further support to the idea that Internet-delivered inter-
ventions entailing minimal therapist contact represent a promising new treatment approach for
a wide range of psychological and health problems, including the problems faced by infertile
patients. Indeed, recent meta-analyses and systematic reviews reveal that moderate to strong
effects are observed post-treatment in Internet delivered-interventions (Barak et al., 2008;
Cuijpers et al., 2008; Williams et al., 2007). Of special interest with respect to the present
study is the finding that, overall, much higher effects are observed in Internet-based interven-
tions in connection with problems that are more psychological in nature, such as anxiety dis-
orders and depression, as opposed to problems that are primarily physiological or somatic in
nature, such as recurrent headache or tinnitus (Barak et al., 2008). Average effect sizes found
in connection with somatic problems—perhaps a good comparison to infertile patients’ condi-
tion—equal d = 0.27: This number lies in between the effect sizes found in our own trial (Ba-
rak et al., 2008).
This brings us to another problem inherent to our analysis of the sample as a whole. A
treatment targeting psychological problems can only be expected to work if those participat-
ing in the treatment suffer from psychological problems. In our trial, we included both pa-
tients with high and patients with low levels of distress and depression. If, however, we limit
our analysis to participants suffering from clinically relevant levels of distress and depression
at pre-treatment, medium to large between-group effects for measures of depression (CES-D:
d = 0.67) are revealed, as are large between-group effects for measures of state anxiety
(STAI-S: d = 0.82). In addition, within-group effect sizes for this subsample of highly dis-
tressed and depressed participants were medium to large for all psychological measures (CES-
D: d = 1.55; IBS: d = 0.98; STAI-S: d = 0.83; STAI-T: d = 0.55). While the between-group
differences were highly significant with regard to depression (CES-D), no other significant
effects were found with respect to other outcome measures. Nevertheless, particularly in the
case of a small subsample such as this, the dearth of significant effects may again be attrib-
uted to problems of statistical power.
One possible lesson to be learned from these results is that, for research purposes, only
participants exceeding cut-off scores at pre-treatment should be included in future studies. On
the other hand, our data reveal that participants who were not highly distressed or depressed
were also highly satisfied with the treatment and found it useful. It is possible that outcome
effects were not found among participants with low levels of distress because outcome meas-
ures were restricted to the assessment of symptoms. If measures of well-being or general
functioning had been included, it may have been possible to find treatment effects among
those displaying low symptomatological impairment. The very high effect sizes found for
depression may be explained by the fact that the Child Wish Online Coaching program targets
depressive symptoms in particular. Examples of the intervention’s depression-specific treat-
ment content include its psychoeducative elements, its lessons on modifying negative cogni-
tions, and its elements promoting behavioral activation.
The study’s follow-up results revealed that intervention participants were able to maintain
their improvements over a period of five months. Significant improvements were also ob-
served for all mental health outcomes among participants in the control group once they re-
ceived the treatment (both the entire sample and the subsample of highly distressed partici-
pants). Taken together, such results clearly support the efficacy of Child Wish Online Coach-
ing for infertile patients.
The results of the present study showed no effect for Online Coaching on the pregnancy
rates of infertile women. In general, studies are still inconclusive on the efficacy of psycho-
logical interventions with respect to pregnancy rates. Increased pregnancy rates have been
reported in two meta-analyses (De Liz and Strauss, 2005; Haemmerli et al., 2009), while an-
other review (Boivin, 2003) found no such effect on infertile women’s chances of becoming
pregnant. One simple explanation for our results is that the time between the pre- and post-
assessments (eight weeks) may have been too short to reasonably expect any effect on the
pregnancy variable. Other studies reporting of increased pregnancy rates following psycho-
logical interventions have assessed pregnancy rates after a year or longer (Domar et al., 2000;
McQueeney et al., 1997). The present study is also clearly limited by the fact that the control
group received the treatment following a waiting period, eliminating the possibility of com-
paring pregnancy rates at follow-up. In the intervention group, 31% of the female participants
became pregnant between the post-assessment and the follow-up assessment. All in all, fur-
ther research is warranted that examines the possible effects of Internet-based psychological
interventions on the pregnancy rates of infertile women when assessed approximately one
year later after baseline.
At baseline, our sample displayed high levels of mental distress. The mean for the total
sample exceeded cut-off scores of clinical relevancy with respect to levels of depression,
anxiety, and infertility-specific distress. Indeed, most studies report increased rates of depres-
sive symptoms among infertile women, with rates of mild to moderate clinical depression
ranging from 8% to 54% (Cuijpers et al., 2008). Further, most (Fassino et al., 2002; Matsu-
bayashi et al., 2001) studies, though not all (Emery et al., 2003; Gulseren et al., 2006), have
found a higher prevalence of depressive symptoms among infertile patients when compared to
fertile control groups. In addition, several studies have reported that levels of anxiety are often
elevated in infertile patients (Covington and Burns, 2006). With a mean value of 24.97 at
baseline, our sample displayed a high level of infertility-specific distress when compared with
the standard mean value, 16.05 (SD = 6.6), of a comparison group of andrology clinic patients
(Pook and Krause, 2002). Assisted reproductive treatments (ART) are often described as the
most stressful techniques used to treat infertility, and there is clear empirical evidence that
infertile patients undergoing ART in particular display high levels of mental distress
(Brkovich and Fisher, 1998; Chen et al., 2004; Eugster and Vingerhoets, 1999). The present
study included both infertile patients receiving various medical treatments as well as patients
not receiving any medical treatment. In our sample, infertile patients receiving medical treat-
ment displayed significantly higher levels of infertility-specific distress at baseline in com-
parison to infertile patients not receiving medical treatment. Thus, the sample’s heterogeneity
with respect to medical treatment may have lowered the effects found for Online Coaching in
regards to mental health.
Finally, the present study examined participants’ acceptance and usage of Online Coach-
ing. Most participants (80%) assessed their experience with Online Coaching as positive or
very positive. Further, the majority of participants (64.5%) described themselves as fully or
very familiar with use of the Internet, with 90.6% of them reporting that they could not have
benefited more from Online Coaching had their computer literacy been better. However, re-
sults showed that men were more critical and less satisfied with Online Coaching than were
women. This might be explained by two factors: First, in several infertility studies, higher
levels of mental distress were found in women than men (Covington and Burns, 2006;
Wischmann, 2005; Wright et al., 1991). Similarly, in our sample, only three of 21 men re-
ported high levels of mental distress. Thus, men’s good relative level of mental health, indi-
cating lower psychological strain, may lead them to benefit less from Online Coaching by
comparison to women. The second important factor is that women are more often willing to
look for and participate in psychological interventions (Boivin, 2003), a point that was further
confirmed by the present study (women: N = 103; men: N = 21). Out of 20 participating cou-
ples, men were responsible for the couple’s registration in only five cases, while one man
participated in the intervention without his partner. Several men reported participating for the
sake of their partner. Thus, it is possible that the male participants were generally less moti-
vated than their female counterparts. Finally, it is still generally unclear whether women and
men benefit equally from psychological interventions (Boivin, 2003; Haemmerli et al., 2009).
There are several limitations suggested for our study. Our sample was not representative of
typical infertile patients who seek traditional face-to-face support. The participants in our
sample displayed lower durations of infertility, reported higher levels of distress, and were
better educated than the general population (Haemmerli et al., 2009; Verhaak et al., 2007).
Furthermore, selection bias could be present as the sample was composed of individuals who
had expressed interest in our Internet-based treatment. Such factors limit our ability to gener-
alize the results. A further limitation is presented by the fact that we did not differentiate
medical treatment types. Such differentiation could be important because assisted reproduc-
tive treatments have been shown to be the most stressful forms of treatments for infertility,
causing higher levels of mental distress among affected patients. Such patients often describe
the phase between embryo transfer and pregnancy test as a particularly stressful period
(Boivin and Takefman, 1995; Klonoff-Cohen et al., 2001). Unfortunately, in our study, it was
not possible to control for the various phases of medical treatment. In addition, information on
the cause of participants’ infertility was not collected. The time between pre- and follow-up-
assessment—five months—may also have been too short to detect long-term effects on men-
tal health. The intervention and the control group completed approximately 79% and 72% of
the Online Coaching program. The main reason of not completing the whole program of the
participant was that the duration of 8 weeks was too short. Therefore it would be important to
extend the duration of the Online Coaching. Further, the present study likely did not have
enough statistical power to test moderators. Only 17% of the total sample was composed of
men. To date, there has been little research into the gender-specific effects of infertility or
psychological interventions for infertile patients. In the future, women and men should be
analyzed separately as there appear to be potential differences in their processing of fertility-
related information. Due to the dearth of male participants in our study, it was not possible to
examine what additional benefits might be presented by both partners taking part in such In-
ternet-based interventions. A couples-based approach to infertility therapy can address addi-
tional important aspects such as marital adjustment and sexual satisfaction, using therapy to
facilitate communication between marital partners (Eunpu, 1995).
Overall, the positive effects of Online Coaching on infertile patients’ mental health are
promising. A strength of our study was the high rate of participation. The demand for this
type of online support is clearly evidenced by the registration of 165 participants in three
months. Further, the study showed that infertile patients experiencing lower levels of mental
distress were nevertheless also interested in this type of psychological support and were very
satisfied with Online Coaching. Infertile patients may find Internet-based interventions less
stigmatizing and more accessible than face-to-face interventions. Additionally Internet-based
treatments may be more cost-effective than face-to-face inventions, and represent a small
fraction of the costs associated with typical medical treatments. As a next step, the practicabil-
ity and the effectiveness of the Online Coaching in routine clinical practice has to be verified.

The results of our study confirm the promise of using Internet-based support to meet the
treatment needs of infertile patients.
Funding
The present study was supported by a grant from the Swiss National Science Foundation
(grant no. 325100 -11375411).
References
Barak, A., Hen, L., Boniel-Nissim, M., & Shapira, N. (2008). A comprehensive review and a
meta-analysis of the effectiveness of internet-based psychotherapeutic interventions. Journal
of Technology in Human Services, 26, 109-160.
Bents, H. (1991). Verhaltenstherapeutische Paartherapie bei Kinderwunschpatienten. In E.
Brähler & A. Myer (Eds.), Psychologische Probleme in der Reproduktionsmedizin. Jahrbuch
der Medizinischen Psychologie (pp.144-155). Berlin: Springer.
Berger, T., & Caspar, F. (2008). Von anderen patienten lernen: Konsequenzen neuer entwick-
lungen im internet für webbasierte, psychotherapeutische angebote. Psychotherapeut, 53,
130-137.
Boivin, J. (2003). A review of psychosocial interventions in infertility. Social science &
medicine, 57, 2325-2341.
Boivin, J., & Takefman, J. E. (1995). Stress level across stages of in vitro fertilization in sub-
sequently pregnant and nonpregnant women. Fertility and Sterility, 64, 802-810.
Boivin, J., Scanlan, L. C., & Walker, S. M. (1999). Why are infertile patients not using psy-
chosocial counselling? Human Reproduction, 14, 1384-1391.
Brkovich, A. M., & Fisher, W. A. (1998). Psychological distress and infertility: forty years of
research. Journal of Psychosomatic Obstetrics and Gynecology, 19, 218-228.
Campagne, D. M. (2006). Should fertilization treatment start with reducing stress? Human
Reproduction, 21, 1651-1658.
Chan, C. H. Y., Ng, E. H. Y., Chan, C. L. W., Ho, P. C., & Chan, T. H. Y. (2006). Effective-
ness of psychosocial group intervention for reducing anxiety in women undergoing in vitro
fertilization: a randomized controlled study. Fertility and Sterility, 85, 339-346.
Chen, T. H., Chang, S. P., Tsai, C. F., & Juang, K. D. (2004). Prevalence of depressive and
anxiety disorders in assisted reproductive technique clinic. Human Reproduction, 17, 2313-
2318.
Cousineau, T. M., & Domar, A. D. (2007). Psychological impact of infertility. Best practice
& research. Clinical obstetrics & gynaecology, 21, 293-308.
Cousineau, T. M., Green, T. C., Corsini, E. A., Seibring, M. T. S., Showstack, M. T., Apple-
garth, L., Davidson, M., & Perloe, M. (2008). Online psychoeducational support for infertile
women: a randomized controlled trial. Human Reproduction, 23, 554-566.
Covington, S. H., & Burns, L. H. (2006). Infertility Counseling. A Comprehensive Handbook
for Clinicians (Second Edition). Cambridge: University Press.
Cuijpers, P., van Straten, A., & Andersson, G. (2008). Internet-administered cognitive behav-
ior therapy for health problems: a systematic review. Journal of Behavioral Medicine, 31,
169-177.
De Liz, T. M., & Strauss, B. (2005). Differential efficacy of group and individual/couple psy-
chotherapy with infertile patients. Human Reproduction, 20, 1324-1332.
Domar, A. D., Clapp, D., Slawsby, E. A., Dusek, J., Kessel, B., & Freizinger, M. (2000). Im-
pact of group psychological interventions on pregnancy rates in infertile women. Fertility and
Sterility, 73, 805-811.
Emery, M., Béran, M. D., Darwiche, J., Oppizzi, L., Joris, V., Capel, R., Guex, P., & Ger-
mond, M. (2003). Results from a prospective, randomized, controlled study evaluating the
acceptability and effects of routine pre-IVF counselling. Human Reproduction, 18, 2647-
2653.
Eunpu, D. L. (1995). The impact of infertility and treatment guidelines for couples therapy.
The American Journal of Family Therapy, 23, 115-128.
Eugster, A., & Vingerhoets, A. J. (1999). Psychological aspects of in vitro fertilization: a re-
view. Social Science & Medicine, 48, 575-589.
Fassino, S., Piero, A., Boggio, S., Piccioni, V., & Garzaro, L. (2002). Anxiety, depression and
anger suppression in infertile couples: a controlled study. Human Reproduction, 17, 2986-
2994.
Gulseren, L., Cetinay, P., Tokatlioglu, B., Sarikaya, O. O., Gulseren, S., & Kurt, S. (2006).
Depression and anxiety levels in infertile Turkish women. Journal of Reproductive Medicine,
51, 421-426.
Haemmerli, K., Znoj, H., & Barth, J. (2009). The Efficacy of Psychological Interventions for
Infertile Patients: A Meta-analysis Examining Mental Health and Pregnancy Rate. Human
Reproduction Update, 15, 279-295.
Hautzinger, M. (1988). Die CES-D Skala. Ein Depressionsinstrument für Untersuchungen in
der Allgemeinbevölkerung. Diagnostica, 34, 167-173.
Himmel, W., Meyer, J., Kochen, M. M., & Michelmann, H. W. (2005). Information needs and
visitors’ experience of an internet expert forum on infertility. Journal of Medical Internet Re-
search, 7, e20.
Huang, J., Discepola, F., Al-Fozan, H., & Tulandi, T. (2005). Quality of fertility clinic web-
sites. Fertility and Sterility, 83, 538-544.
Jacobson, E. (1938). Progressive relaxation: A physiological and clinical investigation of
muscular states and their significance in psychology and medical practice. Chicago: The
University of Chicago Press.
Kahlor, L., & Mackert, M. (2009). Perceptions of infertility information and support sources
among female patients who access the Internet. Fertility and Sterility, 91, 83-90.
Kaluza, G. (2004). Stressbewältigung – Trainingsmanual zur psychologischen Gesundheits-
förderng. Berlin: Springer Verlag.
Klonoff-Cohen, H., Chu, E., Natarajan, L., & Sieber, W. (2001). A prospective study of stress
among women undergoing in vitro fertilization or gamete intrafallopian transfer. Fertility and
Sterility, 76, 675-687.
Levitas, E., Parmet, A., Lunenfeld, E., Bentov, Y., Burstein, E., Friger, M., & Potashnik, G.
(2006). Impact of hypnosis during embryo transfer on the outcome of in vitro fertilization-
embryo transfer: a case-control study. Fertility and Sterility, 85, 1404-1408.
Matsubayashi, H., Hosaka, F., Izumi, S., Suzuki, T., & Makino, T. (2001). Emotional distress
of infertile women in Japan. Human Reproduction, 16, 966-999.
McQueeney, D. A., Stanton, A. L., & Sigmon, S. (1997). Efficacy of emotion-focused and
problem-focused group therapies for women with fertility problems. Journal of Behavioral
Medicine, 3, 313-331.
Okamura, K., Bernstein, J., & Fidler, A. (2002). Assessing the quality of infertility resources
on the world wide web: tools to guide clients through the maze of fact and fiction. Journal of
Midwifery & Women’s Health, 47, 264-268.
Pook, M., & Krause, W. (2002). Ein Fragebogen zur infertilitätsbedingen Belastung. Repro-
duktionsmedizin, 18, 327-332.
Radloff, L. S. (1997). The CES-D Scale. A Self-Report Depression Scale for Research in the
General Population. Applied Psychological Measurement, 1, 385-401.
Randomization.com. (2008, March 22). Retrieved March 1, 2008, from
http://www.randomization.com
Rosenthal, R., Rosnow, R. L., & Rubin, D. B. (2000). Contrasts and Effect Sizes in Behav-
ioral Research: A Correlational Approach. New York, NY: Cambridge University Press.
Sachse, R. (2003). Klärungsorientierte Psychotherapie. Göttingen: Hogrefe.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1970). Manual for the State-Trait Anxi-
ety Inventory. Palo Alto, USA, CA: Consulting Psychological Press.
Stammer, H., Verres, R., & Wischmann, T. (2004). Paarberatung und –therapie bei unerfüll-
tem Kinderwunsch. Göttingen: Hogrefe.
Verberg, M. F. G., Eijkemans, M. J. C., Heijnen, E. M. E. W., Broekmans, F. J., de Klerk, C.,
Fauser, B. C. J. M., & Macklon, N. S. (2008). Why do couples drop-out from IVF treatment?
A prospective cohort study. Human Reproduction, 23, 2050-2055.
Verhaak, C. M., Smeenk, J. M. J., Nahuis, M. J., Kremer, J. A. M., & Braat, D. D. M. (2007).
Long-term psychological adjustment to IVF/ICSI treatment in women. Human Reproduction,
22, 305-308.
Williams, K. E., Marsh, W. K., & Rasgon, N. L. (2007). Mood disorders and fertility in
women: a critical review of the literature and implications for future research. Human Repro-
duction Update, 13, 607-616.
Wischmann, T. (2005). Psychosocial aspects of fertility disorders. Urologe, A44, 185-194.
Wischmann, T. (2008). Implications of psychosocial support in infertility – a critical ap-
praisal. Journal of Psychosomatic Obstetrics and Gynecology, 29, 83-90.
Wischmann, T., & Stammer, H. (2006). Der Traum vom eigenen Kind. Psychologische Hilfen
bei unerfülltem Kinderwunsch (Third Edition). Stuttgart: Kohlhammer.
Wright, J., Duchesne, C., Sabourin, S., Bissonnette, F., Benoit, J., & Girard, Y. (1991). Psy-
chosocial distress and infertility: men and women respond differently. Fertility and Sterility,
55, 100-108.
Zegers-Hochschild, F., Nygren, K. G., Adamson, G. D., de Mouzon, J., Lancaster, P., Man-
sour, R., & Sullivan, E. (2006). The ICMART glossary on ART terminology. Human Repro-
duction, 21, 1968-1970.
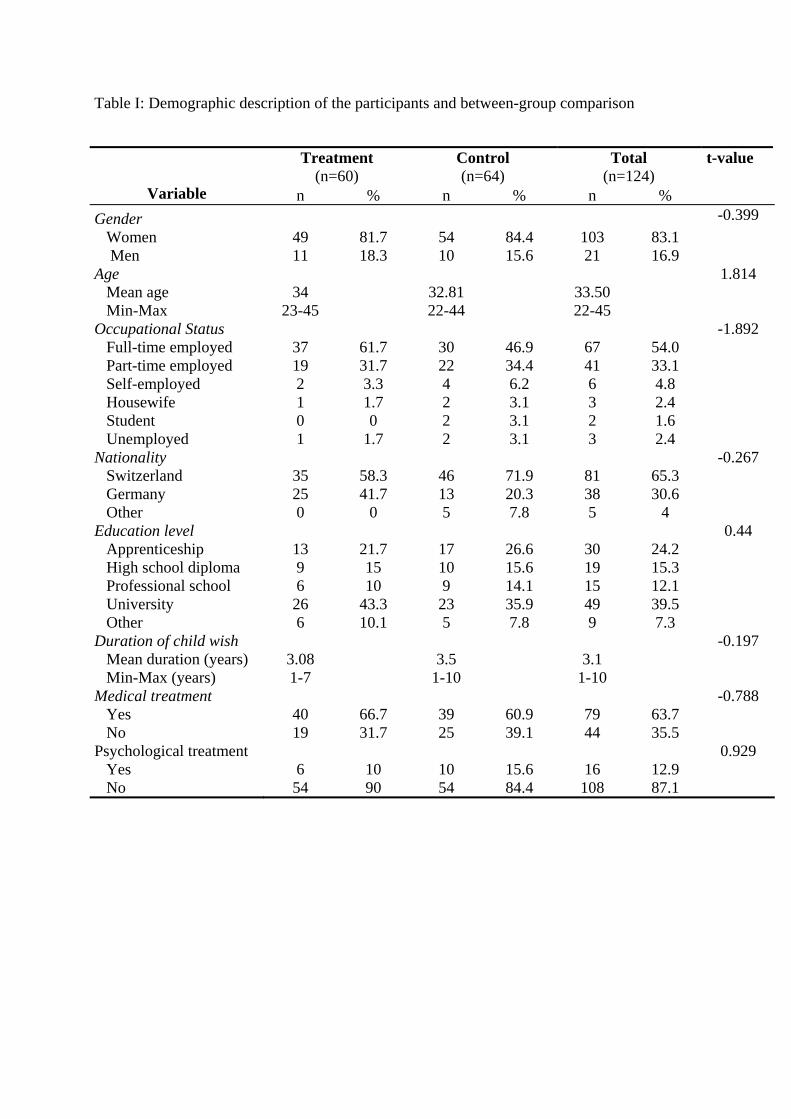
Table I: Demographic description of the participants and between-group comparison
Treatment (n=60)
Control (n=64)
Total (n=124)
t-value
Variable n % n % n % Gender -0.399 Women 49 81.7 54 84.4 103 83.1 Men 11 18.3 10 15.6 21 16.9 Age 1.814 Mean age 34 32.81 33.50 Min-Max 23-45 22-44 22-45 Occupational Status -1.892 Full-time employed 37 61.7 30 46.9 67 54.0 Part-time employed 19 31.7 22 34.4 41 33.1 Self-employed 2 3.3 4 6.2 6 4.8 Housewife 1 1.7 2 3.1 3 2.4 Student 0 0 2 3.1 2 1.6 Unemployed Nationality
1 1.7 2 3.1 3 2.4 -0.267
Switzerland 35 58.3 46 71.9 81 65.3 Germany 25 41.7 13 20.3 38 30.6 Other Education level
0 0 5 7.8 5 4
0.44
Apprenticeship High school diploma Professional school University Other
13 9 6 26 6
21.7 15 10
43.3 10.1
17 10 9 23 5
26.6 15.6 14.1 35.9 7.8
30 19 15 49 9
24.2 15.3 12.1 39.5 7.3
Duration of child wish -0.197 Mean duration (years) Min-Max (years) Medical treatment Yes No Psychological treatment Yes No
3.08 1-7
40 19 6 54
66.7 31.7
10 90
3.5 1-10
39 25
10 54
60.9 39.1
15.6 84.4
3.1 1-10
79 44
16 108
63.7 35.5
12.9 87.1
-0.788
0.929
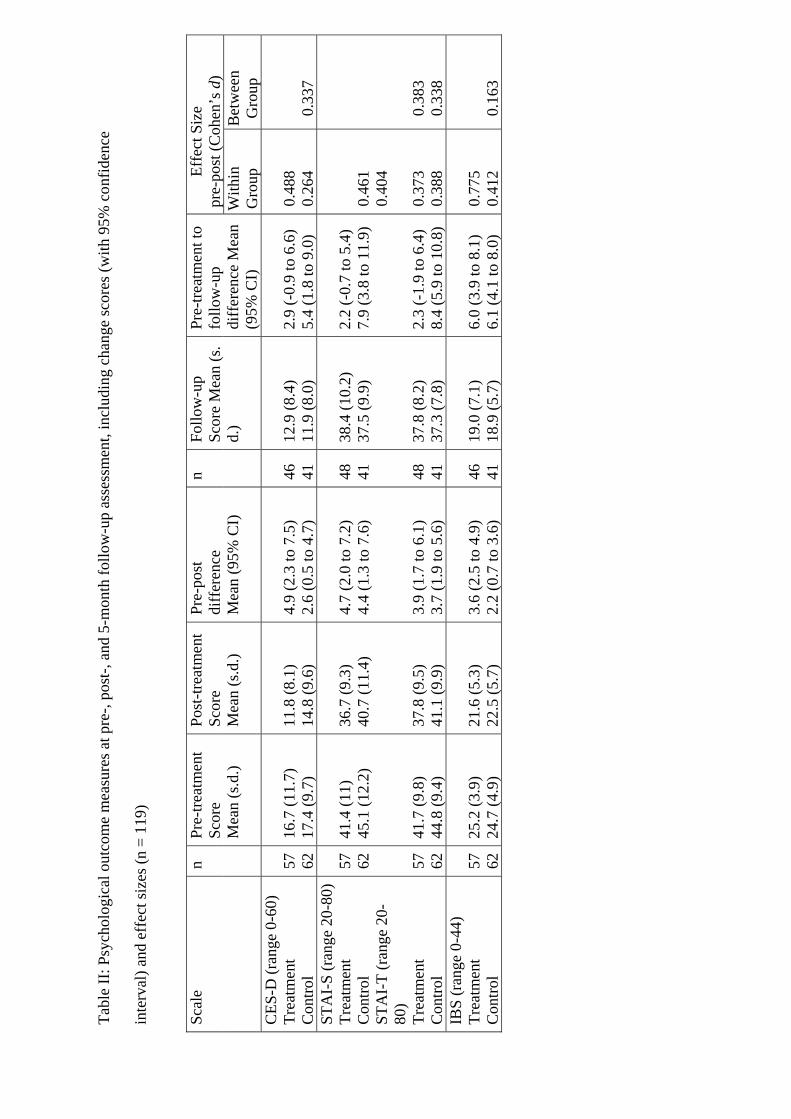
Tabl
e II
: Psy
chol
ogic
al o
utco
me
mea
sure
s at p
re-,
post
-, an
d 5-
mon
th fo
llow
-up
asse
ssm
ent,
incl
udin
g ch
ange
scor
es (w
ith 9
5% c
onfid
ence
inte
rval
) and
eff
ect s
izes
(n =
119
)
Ef
fect
Siz
e
pre-
post
(Coh
en’s
d)
Scal
e n
Pre-
treat
men
t Sc
ore
M
ean
(s.d
.)
Post
-trea
tmen
t Sc
ore
Mea
n (s
.d.)
Pre-
post
di
ffer
ence
M
ean
(95%
CI)
n Fo
llow
-up
Scor
e M
ean
(s.
d.)
Pre-
treat
men
t to
follo
w-u
p di
ffer
ence
Mea
n (9
5% C
I)
With
in
Gro
up
Bet
wee
n G
roup
C
ES-D
(ran
ge 0
-60)
Tr
eatm
ent
Con
trol
57
62
16.7
(11.
7)
17.4
(9.7
)
11.8
(8.1
) 14
.8 (9
.6)
4.9
(2.3
to 7
.5)
2.6
(0.5
to 4
.7)
46
41
12.9
(8.4
) 11
.9 (8
.0)
2.9
(-0.
9 to
6.6
) 5.
4 (1
.8 to
9.0
)
0.
488
0.26
4
0.
337
STA
I-S
(ran
ge 2
0-80
) Tr
eatm
ent
Con
trol
STA
I-T
(ran
ge 2
0-80
) Tr
eatm
ent
Con
trol
57
62
57
62
41.4
(11)
45
.1 (1
2.2)
41
.7 (9
.8)
44.8
(9.4
)
36.7
(9.3
) 40
.7 (1
1.4)
37
.8 (9
.5)
41.1
(9.9
)
4.7
(2.0
to 7
.2)
4.4
(1.3
to 7
.6)
3.9
(1.7
to 6
.1)
3.7
(1.9
to 5
.6)
48
41
48
41
38.4
(10.
2)
37.5
(9.9
) 37
.8 (8
.2)
37.3
(7.8
)
2.2
(-0.
7 to
5.4
) 7.
9 (3
.8 to
11.
9)
2.3
(-1.
9 to
6.4
) 8.
4 (5
.9 to
10.
8)
0.46
1 0.
404
0.37
3 0.
388
0.38
3 0.
338
IBS
(ran
ge 0
-44)
Tr
eatm
ent
Con
trol
57
62
25.2
(3.9
) 24
.7 (4
.9)
21.6
(5.3
) 22
.5 (5
.7)
3.6
(2.5
to 4
.9)
2.2
(0.7
to 3
.6)
46
41
19.0
(7.1
) 18
.9 (5
.7)
6.0
(3.9
to 8
.1)
6.1
(4.1
to 8
.0)
0.77
5 0.
412
0.
163
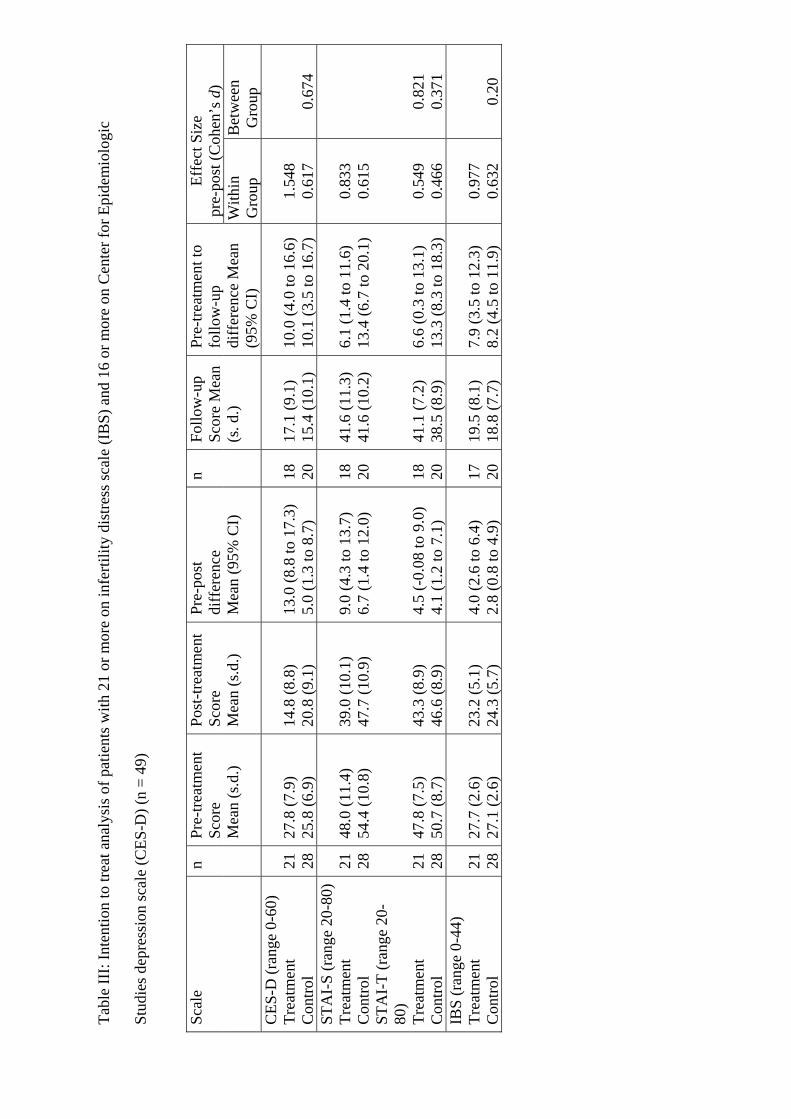
Ta
ble
III:
Inte
ntio
n to
trea
t ana
lysi
s of p
atie
nts w
ith 2
1 or
mor
e on
infe
rtilit
y di
stre
ss sc
ale
(IB
S) a
nd 1
6 or
mor
e on
Cen
ter f
or E
pide
mio
logi
c
Stud
ies d
epre
ssio
n sc
ale
(CES
-D) (
n =
49)
Ef
fect
Siz
e pr
e-po
st (C
ohen
’s d
) Sc
ale
n Pr
e-tre
atm
ent
Scor
e
Mea
n (s
.d.)
Post
-trea
tmen
t Sc
ore
Mea
n (s
.d.)
Pre-
post
di
ffer
ence
M
ean
(95%
CI)
n Fo
llow
-up
Scor
e M
ean
(s. d
.)
Pre-
treat
men
t to
follo
w-u
p di
ffer
ence
Mea
n (9
5% C
I)
With
in
Gro
up
Bet
wee
n G
roup
C
ES-D
(ran
ge 0
-60)
Tr
eatm
ent
Con
trol
21
28
27.8
(7.9
) 25
.8 (6
.9)
14.8
(8.8
) 20
.8 (9
.1)
13.0
(8.8
to 1
7.3)
5.
0 (1
.3 to
8.7
)
18
20
17.1
(9.1
) 15
.4 (1
0.1)
10.0
(4.0
to 1
6.6)
10
.1 (3
.5 to
16.
7)
1.
548
0.61
7
0.
674
STA
I-S
(ran
ge 2
0-80
) Tr
eatm
ent
Con
trol
STA
I-T
(ran
ge 2
0-80
) Tr
eatm
ent
Con
trol
21
28
21
28
48.0
(11.
4)
54.4
(10.
8)
47.8
(7.5
) 50
.7 (8
.7)
39.0
(10.
1)
47.7
(10.
9)
43.3
(8.9
) 46
.6 (8
.9)
9.0
(4.3
to 1
3.7)
6.
7 (1
.4 to
12.
0)
4.5
(-0.
08 to
9.0
) 4.
1 (1
.2 to
7.1
)
18
20
18
20
41.6
(11.
3)
41.6
(10.
2)
41.1
(7.2
) 38
.5 (8
.9)
6.1
(1.4
to 1
1.6)
13
.4 (6
.7 to
20.
1)
6.6
(0.3
to 1
3.1)
13
.3 (8
.3 to
18.
3)
0.
833
0.61
5 0.
549
0.46
6
0.82
1 0.
371
IBS
(ran
ge 0
-44)
Tr
eatm
ent
Con
trol
21
28
27.7
(2.6
) 27
.1 (2
.6)
23.2
(5.1
) 24
.3 (5
.7)
4.0
(2.6
to 6
.4)
2.8
(0.8
to 4
.9)
17
20
19.5
(8.1
) 18
.8 (7
.7)
7.9
(3.5
to 1
2.3)
8.
2 (4
.5 to
11.
9)
0.
977
0.63
2
0.
20
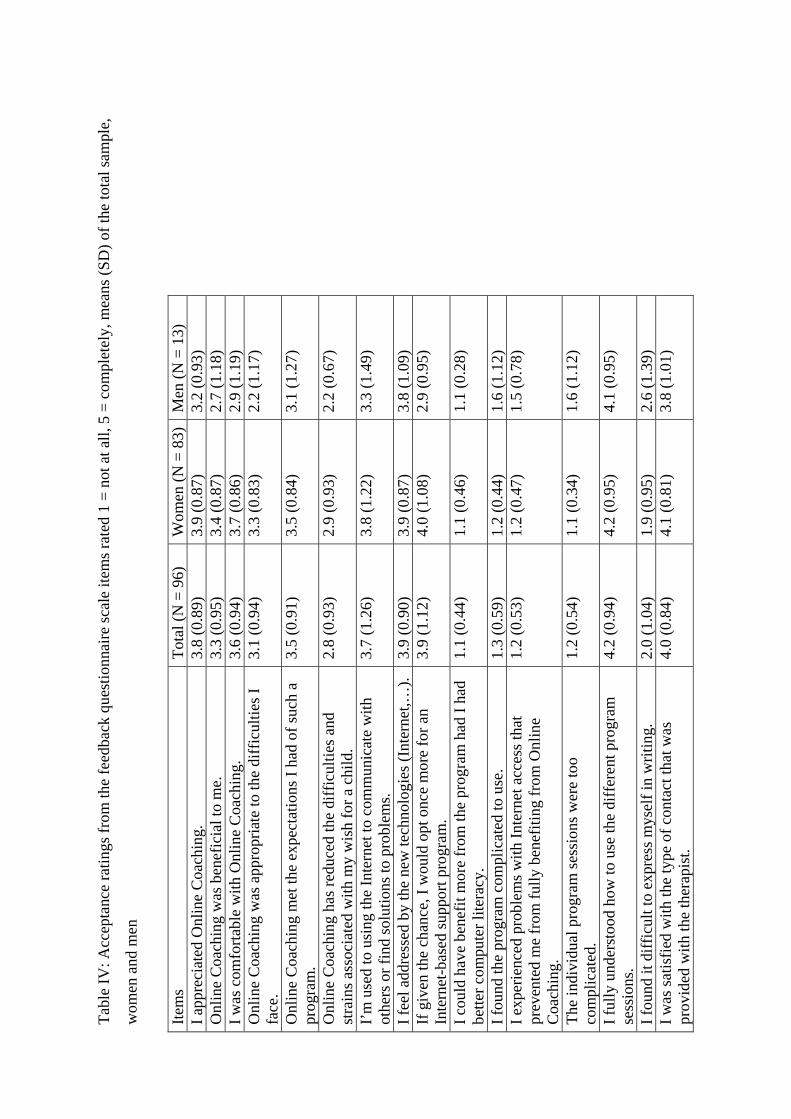
Tabl
e IV
: Acc
epta
nce
ratin
gs fr
om th
e fe
edba
ck q
uest
ionn
aire
scal
e ite
ms r
ated
1 =
not
at a
ll, 5
= c
ompl
etel
y, m
eans
(SD
) of t
he to
tal s
ampl
e,
wom
en a
nd m
en
Item
s To
tal (
N =
96)
W
omen
(N =
83)
Men
(N =
13)
I a
ppre
ciat
ed O
nlin
e C
oach
ing.
3.
8 (0
.89)
3.
9 (0
.87)
3.
2 (0
.93)
O
nlin
e C
oach
ing
was
ben
efic
ial t
o m
e.
3.3
(0.9
5)
3.4
(0.8
7)
2.7
(1.1
8)
I was
com
forta
ble
with
Onl
ine
Coa
chin
g.
3.6
(0.9
4)
3.7
(0.8
6)
2.9
(1.1
9)
Onl
ine
Coa
chin
g w
as a
ppro
pria
te to
the
diff
icul
ties I
fa
ce.
3.1
(0.9
4)
3.3
(0.8
3)
2.2
(1.1
7)
Onl
ine
Coa
chin
g m
et th
e ex
pect
atio
ns I
had
of su
ch a
pr
ogra
m.
3.5
(0.9
1)
3.5
(0.8
4)
3.1
(1.2
7)
Onl
ine
Coa
chin
g ha
s red
uced
the
diff
icul
ties a
nd
stra
ins a
ssoc
iate
d w
ith m
y w
ish
for a
chi
ld.
2.8
(0.9
3)
2.9
(0.9
3)
2.2
(0.6
7)
I’m
use
d to
usi
ng th
e In
tern
et to
com
mun
icat
e w
ith
othe
rs o
r fin
d so
lutio
ns to
pro
blem
s. 3.
7 (1
.26)
3.
8 (1
.22)
3.
3 (1
.49)
I fee
l add
ress
ed b
y th
e ne
w te
chno
logi
es (I
nter
net,…
). 3.
9 (0
.90)
3.
9 (0
.87)
3.
8 (1
.09)
If
giv
en th
e ch
ance
, I w
ould
opt
onc
e m
ore
for a
n In
tern
et-b
ased
supp
ort p
rogr
am.
3.9
(1.1
2)
4.0
(1.0
8)
2.9
(0.9
5)
I cou
ld h
ave
bene
fit m
ore
from
the
prog
ram
had
I ha
d be
tter c
ompu
ter l
itera
cy.
1.1
(0.4
4)
1.1
(0.4
6)
1.1
(0.2
8)
I fou
nd th
e pr
ogra
m c
ompl
icat
ed to
use
. 1.
3 (0
.59)
1.
2 (0
.44)
1.
6 (1
.12)
I e
xper
ienc
ed p
robl
ems w
ith In
tern
et a
cces
s tha
t pr
even
ted
me
from
fully
ben
efiti
ng fr
om O
nlin
e C
oach
ing.
1.2
(0.5
3)
1.2
(0.4
7)
1.5
(0.7
8)
The
indi
vidu
al p
rogr
am se
ssio
ns w
ere
too
com
plic
ated
. 1.
2 (0
.54)
1.
1 (0
.34)
1.
6 (1
.12)
I ful
ly u
nder
stoo
d ho
w to
use
the
diff
eren
t pro
gram
se
ssio
ns.
4.2
(0.9
4)
4.2
(0.9
5)
4.1
(0.9
5)
I fou
nd it
diff
icul
t to
expr
ess m
ysel
f in
writ
ing.
2.
0 (1
.04)
1.
9 (0
.95)
2.
6 (1
.39)
I w
as sa
tisfie
d w
ith th
e ty
pe o
f con
tact
that
was
pr
ovid
ed w
ith th
e th
erap
ist.
4.
0 (0
.84)
4.
1 (0
.81)
3.
8 (1
.01)
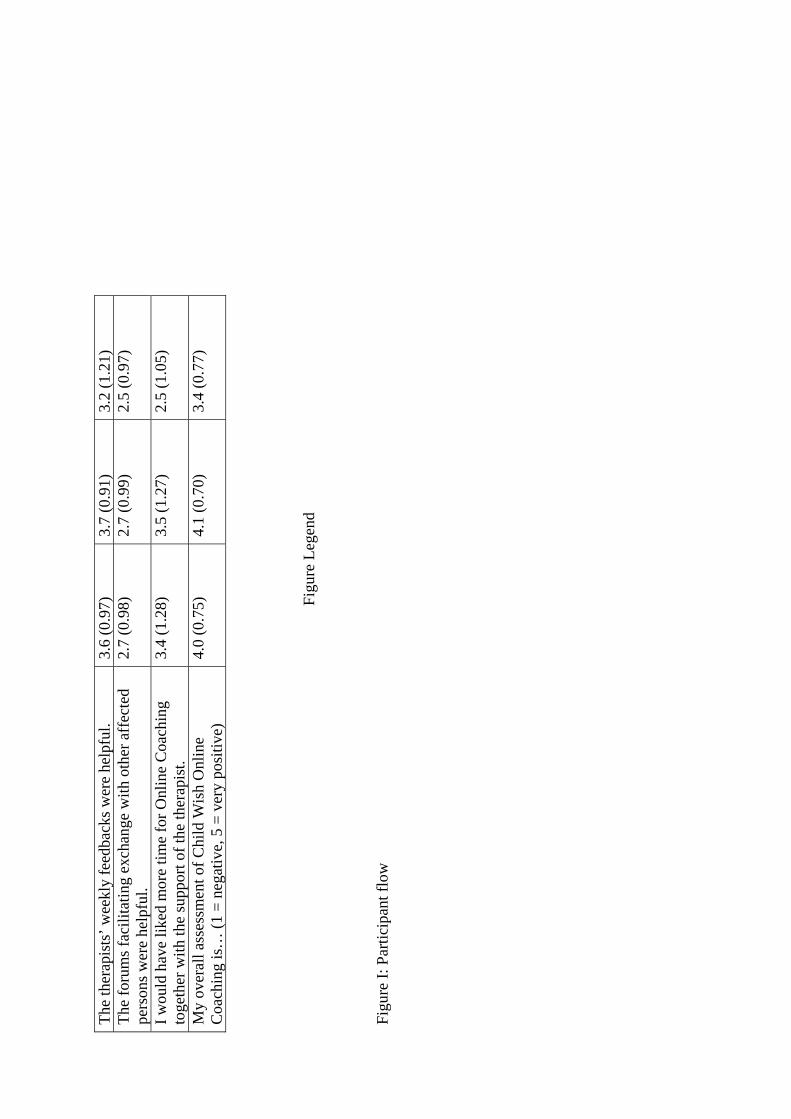
Th
e th
erap
ists
’ wee
kly
feed
back
s wer
e he
lpfu
l. 3.
6 (0
.97)
3.
7 (0
.91)
3.
2 (1
.21)
Th
e fo
rum
s fac
ilita
ting
exch
ange
with
oth
er a
ffec
ted
pers
ons w
ere
help
ful.
2.7
(0.9
8)
2.7
(0.9
9)
2.5
(0.9
7)
I wou
ld h
ave
liked
mor
e tim
e fo
r Onl
ine
Coa
chin
g to
geth
er w
ith th
e su
ppor
t of t
he th
erap
ist.
3.4
(1.2
8)
3.5
(1.2
7)
2.5
(1.0
5)
My
over
all a
sses
smen
t of C
hild
Wis
h O
nlin
e C
oach
ing
is…
(1 =
neg
ativ
e, 5
= v
ery
posi
tive)
4.
0 (0
.75)
4.
1 (0
.70)
3.
4 (0
.77)
Figu
re L
egen
d
Figu
re I:
Par
ticip
ant f
low
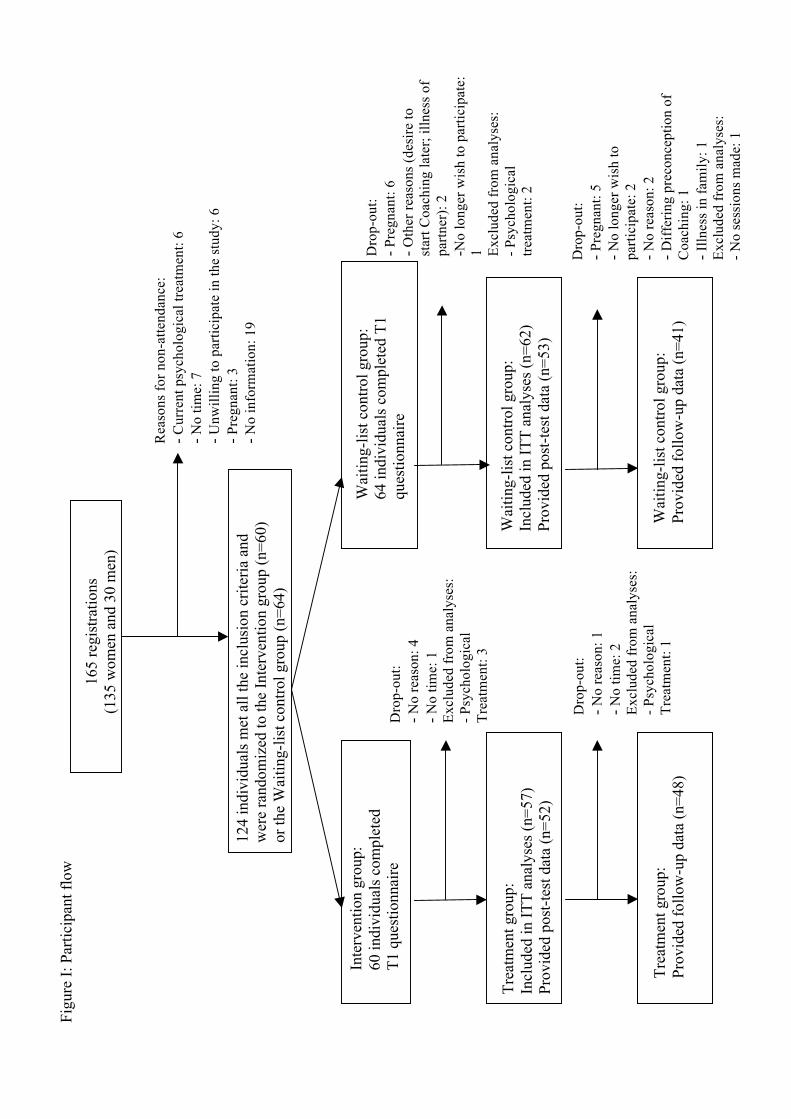
Figu
re I:
Par
ticip
ant f
low
165
regi
stra
tions
(1
35 w
omen
and
30
men
)
12
4 in
divi
dual
s met
all
the
incl
usio
n cr
iteria
and
w
ere
rand
omiz
ed to
the
Inte
rven
tion
grou
p (n
=60)
or
the
Wai
ting-
list c
ontro
l gro
up (n
=64)
Rea
sons
for n
on-a
ttend
ance
: - C
urre
nt p
sych
olog
ical
trea
tmen
t: 6
- No
time:
7
- Unw
illin
g to
par
ticip
ate
in th
e st
udy:
6
- Pre
gnan
t: 3
- No
info
rmat
ion:
19
Inte
rven
tion
grou
p:
60 in
divi
dual
s com
plet
ed
T1 q
uest
ionn
aire
Wai
ting-
list c
ontro
l gro
up:
64 in
divi
dual
s com
plet
ed T
1
ques
tionn
aire
Dro
p-ou
t: - N
o re
ason
: 4
- No
time:
1
Excl
uded
from
ana
lyse
s:
- Psy
chol
ogic
al
Trea
tmen
t: 3
Tr
eatm
ent:
3
Dro
p-ou
t: - P
regn
ant:
6 - O
ther
reas
ons (
desi
re to
st
art C
oach
ing
late
r; ill
ness
of
partn
er):
2
-No
long
er w
ish
to p
artic
ipat
e:
1 Excl
uded
from
ana
lyse
s:
- Psy
chol
ogic
al
treat
men
t: 2
Trea
tmen
t gro
up:
Incl
uded
in IT
T an
alys
es (n
=57)
Pr
ovid
ed p
ost-t
est d
ata
(n=5
2)
Wai
ting-
list c
ontro
l gro
up:
Incl
uded
in IT
T an
alys
es (n
=62)
Pr
ovid
ed p
ost-t
est d
ata
(n=5
3)
Tr
eatm
ent g
roup
: Pr
ovid
ed fo
llow
-up
data
(n=4
8)
Wai
ting-
list c
ontro
l gro
up:
Prov
ided
follo
w-u
p da
ta (n
=41)
Dro
p-ou
t: - N
o re
ason
: 1
- No
time:
2
Excl
uded
from
ana
lyse
s:
- Psy
chol
ogic
al
Trea
tmen
t: 1
Dro
p-ou
t: - P
regn
ant:
5 - N
o lo
nger
wis
h to
pa
rtici
pate
: 2
- No
reas
on: 2
- D
iffer
ing
prec
once
ptio
n of
C
oach
ing:
1
- Illn
ess i
n fa
mily
: 1
Excl
uded
from
ana
lyse
s:
- No
sess
ions
mad
e: 1
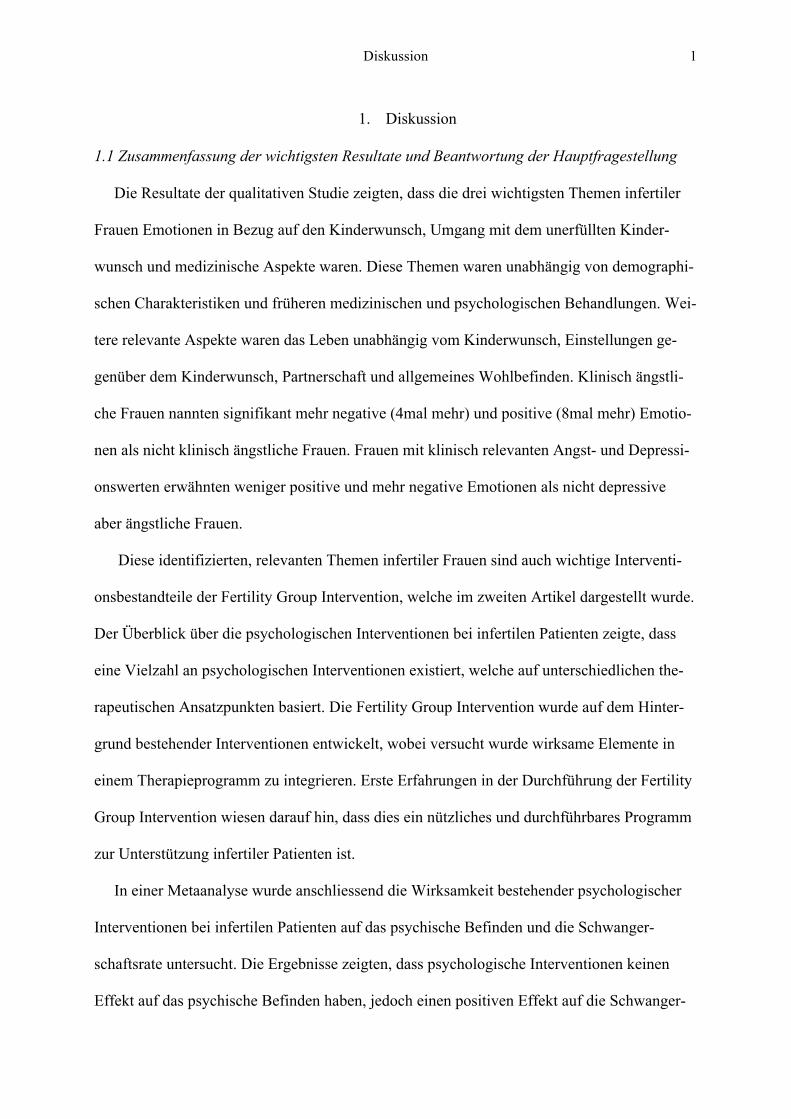
Diskussion
1
1. Diskussion
1.1 Zusammenfassung der wichtigsten Resultate und Beantwortung der Hauptfragestellung
Die Resultate der qualitativen Studie zeigten, dass die drei wichtigsten Themen infertiler
Frauen Emotionen in Bezug auf den Kinderwunsch, Umgang mit dem unerfüllten Kinder-
wunsch und medizinische Aspekte waren. Diese Themen waren unabhängig von demographi-
schen Charakteristiken und früheren medizinischen und psychologischen Behandlungen. Wei-
tere relevante Aspekte waren das Leben unabhängig vom Kinderwunsch, Einstellungen ge-
genüber dem Kinderwunsch, Partnerschaft und allgemeines Wohlbefinden. Klinisch ängstli-
che Frauen nannten signifikant mehr negative (4mal mehr) und positive (8mal mehr) Emotio-
nen als nicht klinisch ängstliche Frauen. Frauen mit klinisch relevanten Angst- und Depressi-
onswerten erwähnten weniger positive und mehr negative Emotionen als nicht depressive
aber ängstliche Frauen.
Diese identifizierten, relevanten Themen infertiler Frauen sind auch wichtige Interventi-
onsbestandteile der Fertility Group Intervention, welche im zweiten Artikel dargestellt wurde.
Der Überblick über die psychologischen Interventionen bei infertilen Patienten zeigte, dass
eine Vielzahl an psychologischen Interventionen existiert, welche auf unterschiedlichen the-
rapeutischen Ansatzpunkten basiert. Die Fertility Group Intervention wurde auf dem Hinter-
grund bestehender Interventionen entwickelt, wobei versucht wurde wirksame Elemente in
einem Therapieprogramm zu integrieren. Erste Erfahrungen in der Durchführung der Fertility
Group Intervention wiesen darauf hin, dass dies ein nützliches und durchführbares Programm
zur Unterstützung infertiler Patienten ist.
In einer Metaanalyse wurde anschliessend die Wirksamkeit bestehender psychologischer
Interventionen bei infertilen Patienten auf das psychische Befinden und die Schwanger-
schaftsrate untersucht. Die Ergebnisse zeigten, dass psychologische Interventionen keinen
Effekt auf das psychische Befinden haben, jedoch einen positiven Effekt auf die Schwanger-
Diskussion
2
schaftschancen. Insbesondere bei infertilen Patienten, welche nicht in reproduktionsmedizini-
scher Behandlung sind im Vergleich zu Patienten unter reproduktionsmedizinischer Behand-
lung, wurde eine Verbesserung der Schwangerschaftsrate durch psychologische Unterstüt-
zung gefunden.
Im vierten Artikel wurde die Wirksamkeit und Akzeptanz des ersten deutschsprachigen
internet-basierten Programms evaluiert. Die Ergebnisse zeigten, dass das Online Coaching
insbesondere auf das psychische Befinden klinisch belasteter infertiler Patienten wirksam
war. Die mittlere Effektstärke des Online Coachings auf das psychische Befinden zwischen
der Interventions- und Kontrollgruppe lag bei 0.52 (von ES 0.20 bis ES 0.82; Cohen, 1977).
Diese Verbesserungen im psychischen Befinden wurden über einen Zeitraum von drei Mona-
ten aufrechterhalten. Es wurden keine Effekte auf die Schwangerschaftschancen gefunden.
Das Online Coaching wurde von 80 % der Teilnehmer positiv oder sehr positiv bewertet. Die
hohe Nachfrage von 165 Anmeldungen innerhalb von drei Monaten widerspiegelt das grosse
Interesse an einem solchen Angebot.
Zur Beantwortung der Hauptfragestellung dieser Dissertation, ob psychologische Interven-
tionen für infertile Patienten zur Verbesserung des psychischen Befindens und der Schwan-
gerschaftschancen wirksam sind: Ausgehend von der durchgeführten Metaanalyse haben psy-
chologische Interventionen keinen Effekt auf das psychische Befinden infertiler Patienten,
können aber die Schwangerschaftschancen verbessern. Obschon sich bei der Metaanalyse ein
positiver Effekt auf die Schwangerschaftsrate gezeigt hat, konnte dieser beim internet-
basierten Programm nicht gefunden werden. Der Hauptgrund dafür war sicherlich die zu kur-
ze Dauer zwischen den Messzeitpunkte für die Entstehung einer Schwangerschaft. Weitere
Forschung ist notwendig um den Einfluss durch psychologische Interventionen auf die
Schwangerschaftschancen infertiler Paare zu klären. Das Ergebnis in Bezug auf das psychi-
sche Befinden steht im Kontrast zu den Resultaten von zwei früheren Reviews (Boivin, 2003;
Diskussion
3
de Liz & Strauss, 2005), welche beide einen positiven Effekt auf das psychische Befinden
infertiler Patienten gefunden haben. Die Evaluation der internet-basierten Intervention zeigte
nur bei klinisch belasteten Patienten positive Effekte auf das psychische Befinden. Dieses
Ergebnis ist ausgehend von der Tatsache gut nachvollziehbar, dass nur bei Personen mit psy-
chischen Problemen überhaupt eine Veränderung durch eine psychologische Intervention,
welche die Verbesserung des psychischen Befindens zum Ziel hat, erwartet werden kann. In
den oben genannten drei Metaanalysen wurde nicht angegeben, wie stark belastet die inferti-
len Patienten zu Beginn waren, was eine wichtige Information gewesen wäre. Der Einfluss
der psychischen Belastung zu Beginn wurde deshalb in der Studie zur Evaluation des Online
Coaching auch analysiert. Basierend auf den bisherigen Ergebnissen kann man zur Schluss-
folgerung kommen, dass nur dann Effekte psychologischer Interventionen auf das psychische
Befinden infertiler Paare zu finden sind, wenn es sich zu Beginn um eine psychisch belastete
Stichprobe gehandelt hat. Dies bedeutet aber nicht, dass psychologische Interventionen bei
nicht oder gering belasteten Personen mit unerfülltem Kinderwunsch nicht sinnvoll sind. Die-
se Aussage wird durch die hohe Akzeptanz und Nachfragen des Online Coachings bestätigt.
1.2 Integration der Ergebnisse in den theoretischen Rahmen
Die folgenden wichtigsten Resultate der vier Artikel sollen nun im Hinblick auf den ein-
gangs dargestellten theoretischen Rahmen diskutiert werden: 1) Emotionen war das am mei-
sten genannte Thema infertiler Frauen, wobei ein Zusammenhang mit dem psychischen Be-
finden gefunden werden konnte (Haemmerli et al., 2009c), 2) psychologische Interventionen
erwiesen sich im Allgemeinen als nicht wirksam in Bezug auf das psychische Befinden, den-
noch wurde bei klinisch belasteten infertilen Patienten ein positiver Effekt gefunden (Haem-
merli et al., 2009a; Haemmerli et al., 2009b), 3) psychologische Interventionen können die
Schwangerschaftschancen infertiler Paare verbessern (Haemmerli et al., 2009a) und 4) eine
Diskussion
4
grosse Nachfrage war beim Online Coaching zu verzeichnen und auch unabhängig von einer
bedeutsamen Verbesserung im psychischen Befinden und in den Schwangerschaftschancen
waren die Teilnehmer mit dem Programm sehr zufrieden.
Infertile Paare erleben wiederholt einen Wechsel von unterschiedlichen Gefühlen, was
häufig als eine Achterbahn von Gefühlen beschrieben wird (Dunkel-Schetter & Lobel, 1991;
Watkins & Baldo, 2004). Bei Verlusterlebnissen mit Trauerreaktionen erleben infertile Paare
ebenfalls eine Vielzahl unterschiedlicher Gefühle (Burns & Covington, 2006). Emotionsregu-
lation ist ein wichtiger Mechanismus zur Konsistenzsicherung und spielt in der Entwicklung,
Aufrechterhaltung und Behandlung psychischer Probleme eine wichtige Rolle (Berking et al.,
2008; Grawe, 2004; Znoj, 2008). Die Ergebnisse des ersten Artikels zeigten, dass Frauen mit
klinisch relevanten Angstwerten mehr negative und mehr positive Emotionen nannten als
nicht klinisch ängstliche Frauen. Das Ausdrücken von Emotionen scheint ein wichtiger Ver-
arbeitungsprozess von infertilen Frauen zu sein, welcher auch mit einer besseren psychischen
Anpassung zusammenhängt (Stanton, 1991). Zudem kann das Ausdrücken von positiven
Emotionen die Verarbeitung der Trauer fördern (Bonanno, 2004). Emotionsorientiertes Co-
ping ist demnach zur Bewältigung der Gefühle im Zusammenhang mit dem unerfüllten Kin-
derwunsch sehr wichtig (Stanton, 1991).
Infertile Patienten sind generell psychopathologisch nicht auffälliger als die Allgemeinbe-
völkerung (Strauss et al., 2004; Wright et al., 1989). Die Anpassung infertiler Patienten an
ihre Situation ist meistens gut und es entstehen keine psychischen Störungen (Bryson, Sykes,
& Traub, 2000; Verhaak et al., 2007). Auch die natürliche Trauerreaktion nach einem Ver-
lusterlebnis analog zur allgemeinen Trauerforschung können infertile Patienten positiv ohne
Unterstützung bewältigen (Znoj, 2004). Auf diesem Hintergrund ist es nicht erstaunlich, dass
kein genereller Effekt von psychologischen Interventionen auf das psychische Befinden infer-
tiler Patienten gefunden wurde. Dennoch gibt es zahlreiche Studien, welche von infertilen
Diskussion
5
Patienten mit erhöhten Werten der psychischen Belastung berichten (Leiblum & Greenfield,
1997; Wischmann et al. 2001). In Abhängigkeit von den eigenen Ressourcen und Bewälti-
gungsstrategien kann die Anpassung an die Infertilität sehr unterschiedlich aussehen (Maha-
jan et al., 2009). So erleben einige Paare die ungewollte Kinderlosigkeit auch als chronischen
Stressor oder chronischen Trauerprozess (Burns & Covington, 2006; Watkins & Baldo,
2004). Deshalb werden psychologische Interventionen oftmals insbesondere bei infertilen
Patienten mit erhöhter psychischer Belastung oder klinisch relevanten Symptomen empfohlen
(Boivin et al., 1999; Cousineau & Domar, 2007).
In der Literatur wurden bisher einige Erklärungen diskutiert, weshalb psychologische In-
terventionen einen positiven Effekt auf die Schwangerschaftsrate infertiler Patienten haben
können: Verbesserung der sexuellen Aktivität (Boivin, 2003; Wischmann, 2003), Verringe-
rung der Abbruchraten während der medizinischen Behandlung (Smeenk et al., 2004; Verberg
et al., 2008) und Reduzierung des psychischen Stresses, welcher einen Einfluss auf biologi-
sche Funktionen haben kann (Cwikel, Gidron, & Sheiner, 2004). Weitere Forschung ist not-
wendig für ein besseres Verständnis der Beeinflussung der Schwangerschaftsraten durch psy-
chologische Interventionen. Es ist aber denkbar, dass unabhängig davon, ob ein Paar klinisch
relevant belastet ist oder nicht, eine psychologische Unterstützung bei der Bewältigung
sexueller Problemen oder bei der Durchführung einer medizinischen Behandlung neben wei-
teren Faktoren wie z. B. dem Alter der Frau einen Einfluss auf die Schwangerschaftschancen
haben kann.
Eine hohe Nachfrage nach dem Angebot einer internet-basierten Unterstützung konnte
verzeichnet werden. Zudem waren die Teilnehmer unabhängig vom Einfluss des Online Coa-
chings auf ihr psychisches Befinden oder ihre Schwangerschaftschancen sehr zufrieden mit
dem Programm. Demnach scheint es analog zu den in der Literatur sehr breit definierten Zie-
len und Aufgaben psychologischer Unterstützung bei infertilen Patienten sinnvoll zu sein die
Diskussion
6
Unterstützung individuell auf die Paare mit unerfülltem Kinderwunsch zuzuschneiden (Co-
vington & Burns, 2006; Stammer et al., 2004; Strauss, 2000). Dieses Vorgehen entspricht
auch dem Verständnis der Konsistenztheorie, wobei das Therapieangebot individuell auf den
Patienten abgestimmt wird (Grawe, 1998). Somit kann abschliessend gesagt werden, dass
individuell angebotene psychologische Unterstützung jederzeit unabhängig von der medizini-
schen Behandlung für infertile Patienten verfügbar und zugänglich sein sollte.
1.3 Weiterführende Fragestellungen und Projekte
Im Folgenden sollen nicht die Empfehlungen an zukünftige Forschung aus den einzelnen
Artikeln wiederholt werden, sondern inhaltlich spannende, weiterführende Fragestellungen
und daraus resultierende neue oder noch laufende Projekte skizziert werden.
Die Rekrutierung der SNF-Studie an der Universitätsfrauenklinik Bern und Basel zur Un-
tersuchung der Wirksamkeit einer psychologischen Gruppenintervention bei infertilen Patien-
ten während der medizinischen Behandlung wird bis Ende 2009 abgeschlossen sein. Danach
werden die Daten ausgewertet und evaluiert. Das Online Coaching als internet-basiertes An-
gebot für infertile Patienten wurde nach der ersten Durchführung bereits verbessert und opti-
miert. So wurden beispielsweise aufgrund der bisherigen Erfahrungen der Inhalt einzelner
Sitzungen aufgrund der Rückmeldungen angepasst, neue Themen wie z. B. Sexualität hinzu-
gefügt, bisherige technische Probleme eliminiert und das Forum für einen besseren Austausch
überarbeitet. Spannende weitere Fragestellungen haben sich aus den ersten Erfahrungen mit
dem Online Coaching ergeben: So wäre es interessant, verschiedene Arten von psychologi-
schen Interventionen als Internetangebot zu vergleichen. Wenig ist bisher zur differentiellen
Indikation von psychologischer Unterstützung bei infertilen Patienten bekannt (Boivin, 2003;
Haemmerli et al., 2009a). Durch die Variation der Art der psychologischen Intervention als
internet-basiertes Angebot könnte man einen ersten Schritt in Richtung der Beantwortung
Diskussion
7
dieser Frage machen. So wäre ein Vergleich des bisherigen Programms mit einer achtsam-
keitsbasierten Intervention sehr spannend. Es gibt verschiedene Ansätze achtsamkeitsbasierter
Therapien (z. B. Achtsamkeitsbasierte Stressreduktion, Kabat-Zinn, 2003; Dialektisch-
Behaviorale Therapie, Linehan, 1993; Akzeptanz und Commitment Therapie, Hayes, Stro-
sahl, & Wilson, 1999), welche sich bei unterschiedlichen psychischen und körperlichen Pro-
blemen als wirksam erwiesen haben (Baer, 2003; Grossmann et al., 2004). Achtsamkeitsba-
sierte Ansätze verstehen unter Heilung nicht das vollständige Verschwinden der Symptome,
sondern eine grundlegende Transformation der Sichtweise der Dinge resp. eine neue Erleb-
nisqualität (Kabat-Zinn, 1990). Kabat-Zinn (1990) entwickelte daraus beispielsweise ein Pro-
gramm in einem verhaltensmedizinischen Setting für Patienten mit diversen chronischen und
stressbedingten Krankheiten. Achtsamkeitsbasierte Ansätze wurden bei Infertilität bisher
kaum angewandt und evaluiert, könnten aber eine viel versprechende Unterstützung oder Er-
gänzung bei der Behandlung infertiler Patienten sein.
Weiter wäre es interessant, ausschliesslich Paare am Online Coaching teilnehmen zu las-
sen, um geschlechtsspezifische Fragestellungen zu klären. Daraus abgeleitet könnte man rele-
vante Themen und Probleme infertiler Männer im Vergleich zu denen bereits identifizierten
Themen der Frauen evaluieren. Zudem könnten paarspezifische Themen wie Sexualität und
Partnerschaftszufriedenheit genauer analysiert werden. Es könnte auch überlegt werden, ob
nur noch infertile Patienten mit einer klinisch relevanten psychischen Belastung in das Pro-
gramm eingeschlossen werden sollten, um überhaupt Veränderungen des psychischen Befin-
dens beobachten zu können. Wichtig wäre auch die Follow-up Messung erst nach ungefähr
sechs Monaten nach Beginn bei der Studie anzusetzen, um einen möglichen Einfluss der psy-
chologischen Intervention auf die Schwangerschaftschancen untersuchen zu können.
Abschliessend kann gesagt werden, dass es aufgrund der hohen Nachfrage und der Zufrieden-
heit mit dem Online Coaching sinnvoll wäre dieses Angebot weiterhin aufrechterhalten zu
Diskussion
8
können. Deshalb wird nun seit April 09 nach der Optimierung des Programms das Online
Coaching neu als Angebot weiterbetrieben. Neu wurde die Dauer des Online Coachings auf
10 Wochen ausgeweitet, der Messzeitpunkt des Follow-up zu einem späteren Zeitpunkt fest-
gesetzt (sechs Monate nach Beginn) und es wird ein Teilnehmerbeitrag von 182 Franken er-
hoben. Dahinter steht insbesondere die Frage, ob es möglich ist das Online Coaching auch
ausserhalb eines Forschungskontextes weiterzuführen. Es ist bekannt, dass viele internet-
basierte Programme für verschiedenste Probleme nach erfolgreicher Evaluation nur schwer in
der Praxis integriert werden konnten. Nun besteht das Angebot des Online Coachings für Per-
sonen mit unerfülltem Kinderwunsch bereits seit einigen Monaten und auch ohne aktive Wer-
bung für das Programm können laufend neue Anmeldungen verzeichnet werden. Internet-
basierte psychologische Interventionen wie das Online Coaching könnten somit ein weiteres
Angebot in der psychologischen Unterstützung infertiler Paare darstellen und somit helfen
Paare mit unerfülltem Kinderwunsch noch besser und umfassender zu begleiten.
Literaturverzeichnis
9
Literaturverzeichnis
Abramson, L. Y., Seligman, M. E. P., & Teasdale, J. D. (1978). Learned helplessness in humans:
Critique and reformulation. Journal of Abnormal Psychology, 87, 49-74.
Andersen, N., Carlsen, E., & Loft, A. (2008). Trends in the use of intracytoplasmatic sperm
injection marked variability between countries. Human Reproduction Update, 14, 593-604.
Atwood, J. D., & Dobkin, S. (1992). Storm clouds are coming: ways to help couples reconstruct the
crisis of infertility. Contemporary Family Therapy, 14, 385-403.
Austenfeld, J. L., & Stanton, A. L. (2004). Coping through emotional approach: a new look at
emotion, coping, and health-related outcomes. Journal of Personality, 72, 1335-1363.
Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical
review. Clinical Psychology: Science and Practice, 10, 125-143.
Baltes, P. B. (1997). On the incomplete architecture of human ontogeny: Selection, optimization,
and compensation as foundation of developmental theory. American Psychologist, 52, 366-
380.
Baltes, P. B., Lindenberger, U., & Staudinger, U. M. (1998). Life-span theory in developmental
psychology. In R. M. Lerner (Ed.), Theoretical models of human development (pp. 1029-
1143). New York: Wiley.
Baltes, P. B., Reese, H. W., & Lipsitt, L. P. (1980) Life-span developmental psychology. Annual
Review of Psychology, 31, 65-110.
Bonanno, G. A. (2004). Loss, Trauma and Human Resilience. American Psychologist, 59, 20-28.
Bonanno, G. A., & Keltner, D. (1997). Facial expressions of emotion and the course of conjugal
bereavement. Journal of Abnormal Psychology, 106, 126-137.
Benedek, T. (1952). Infertility as a psychosomatic defense. Fertility and Sterility, 3, 527-541.
Berg, B. J., & Wilson, J. F. (1991). Psychological functioning across stages of treatment for
infertility. Journal of Behavioral Medicine, 14, 11-26.
Literaturverzeichnis
10
Berking, M., Wupperman, P., Reichardt, A., Pejic, T., Dippel, A., & Znoj, H. (2008). Emotion-
regulation skills as a treatment target in psychotherapy. Behaviour Research and Therapy, 46,
1230-1237.
Beutel, M., Kirchmeyer, P., Weidner, W., Schroeder-Printzen, I., Herrero, J. G., Köhn, F. M., Gips,
H., & Kupfer, J. (2000). Psychische Belastung bei MESA/TESE-Teilnehmern im Vergleich zu
den Partnern von ICSI- und IVF-Teilnehmerinnen. Reproduktionsmedizin, 16, 354-361.
Boivin, J. (2003). A review of psychosocial interventions in infertility. Social Science & Medicine,
57, 2325-2341.
Boivin, J., Bunting, L., Collins, J. A., & Nygren, K. G. (2007). International estimates of infertility
prevalence and treatment-seeking: potential need and demand for infertility medical care. Hu-
man Reproduction, 22, 1506-1512.
Boivin, J., & Kentenich, H. (2002). Guidelines for counseling in infertility. Oxford: Oxford
University Press.
Boivin, J., Scanlan, L. C., & Walker, S. M. (1999). Why are infertile patients not using psychosocial
counselling? Human Reproduction, 14, 1384-1391.
Bowlby, J. (1961). Processes of mourning. International Journal of Psychoanalysis, 42, 317-340.
Bowlby, J. (1980). Attachment and loss: Loss, sadness and depression (Vol. 3). New York: Basic
Books.
Brandtstädter, J. (2007). Hartnäckige Zielverfolgung und flexible Zielanpassung als Entwicklungs-
ressource: Das Modell assimilativer und akkomodativer Prozesse. In J. Brandstädter & U.
Lindenberger (Hrsg.), Entwicklungspsychologie der Lebenspanne (S. 413-445). Stuttgart:
Kohlhammer.
Bresnick, E., & Taymor, M. L. (1979). The role of counseling in infertility. Fertility and Sterility,
32, 154-156.
Literaturverzeichnis
11
Bundesamt für Statistik, BFS (2008, 29. September). Behandlung zur medizinisch unterstützten
Fortpflanzung nahmen 2007 um 13 Prozent. Medienmitteilung Nr. 0350-0809-70, 2007. Re-
trieved February 5, 2009, from
http://www.news.admin.ch/message/index.html?lang=de&msg-id=21703
Bunting, L., & Boivin, J. (2008). Knowledge about infertility risk factors, fertility myths and
illusory benefits of healthy habits in young people. Human Reproduction, 23, 1858-1864.
Bryson, C. A., Sykes, D. H., & Traub, A. I. (2000). In vitro fertilization: a long-term follow-up after
treatment failure. Human Fertility, 3, 214-220.
Burns, L. H., & Covington, S. N. (2006). Psychology of Infertility. In S.N. Covington & L.H. Burns,
(Eds.), Infertility Counselling: A Comprehensive Handbook for Clinicians (2 ed.) (pp. 1-19).
New York: Cambridge University Press.
Chen, T. H., Chang, S. P., Tsai, C. F., & Juang, K. D. (2004). Prevalence of depressive and anxiety
disorders in assisted reproductive technique clinic. Human Reproduction, 17, 2313-2318.
Christie, G. L. (1994). The psychogenic factor in infertility. The Australian and New Zealand
journal of psychiatry, 28, 378-390.
Cohen, J. (1977). Statistical power analysis for the behavioral sciences (revised ed.). New York:
Academic Press.
Conway, P., & Valentine, D. (1987). Reproductive losses and grieving. Journal of Social Work and
Human Sexuality, 6, 43-63.
Cooper-Hilbert, B. (2001). Helping couples through the crisis of infertility. Clinical Update: The
American Association for Marriage and Family Therapy, 3, 1-6.
Cousineau, T. M., & Domar, A. D. (2007). Psychological impact of infertility. Best Practice &
Research Clinical Obstetrics and Gynaecology, 21, 293-308.
Literaturverzeichnis
12
Cousineau, T. M., Green, T. C., Corsini, E. A., Seibring, M. T. S., Showstack, M. T., Applegarth, L.,
Davidson, M., & Perloe, M. (2008). Online psychoeducational support for infertile women: a
randomized controlled trial. Human Reproduction, 23, 554-566.
Covington, S. N. (1995). The role of the mental health professional in reproductive medicine.
Fertility and Sterility, 64, 895-897.
Cowles, K. V., & Rodgers, B. L. (1991). The concept of grief: An foundation for nursing research
and practice. Research in Nursing and Health, 14, 119-127.
Cwikel, J., Gidron, Y., & Sheiner, E. (2004). Psychological interactions with infertility among
women. European journal of obstetrics, gynecology, and reproductive biology, 117, 126-131.
Daniluk, J. C. (2001). Reconstructing their lives: A longitudinal, qualitative analysis of the transition
to biological childlessness for infertile couples. Journal of Counseling & Development, 79,
439-449.
De Liz, T. M., & Strauss, B. (2005). Differential efficacy of group and individual/couple psychothe-
rapy with infertile patients. Human Reproduction, 20, 1324-1332.
Domar, A. D., Broome, A., Zuttermeister, P. C., Seibel, M., & Friedman, R. (1992). The prevalence
and predictability of depression in infertile women. Fertility and Sterility, 58, 1158-1163.
Domar, A. D., & Seibel, M. M. (1997). Emotional aspects of infertility. In M. M. Seibel (ed.),
Infertility: A Comprehensive Text (pp. 29-44). Stamford: Appleton & Lange.
Dunkel-Schetter, C., & Lobel, M. (1991). Psychological reactions to infertility. In A. L. Stanton, &
C. Dunkel-Schetter (Eds.), Infertility: Perspectives from Stress and Coping Research (pp. 29-
57). New York, London: Plenum Press.
Eckert, H., Sobeslavsky, I., & Held, H. J. (1998). Psychische Merkmale bei Paaren mit unerfülltem
Kinderwunsch vor IVF. In E. Brähler & S. Goldschmidt (Hrsg.), Psychosoziale Aspekte von
Fruchtbarkeitsstörungen (S. 27-49). Bern: Huber.
Literaturverzeichnis
13
Erdle, B. (2008). “Kinder ade” – Einige Überlegungen zu sozialen und gesellschaftlichen Ursachen
von Kinderlosigkeit. In D. Kleinschmidt, P. Thorn, & T. Wischmann (Hrsg.), Kinderwunsch
und professionelle Beratung (S. 27-34). Stuttgart: Kohlhammer.
Erikson, E. H. (1988). Der vollständige Lebenszyklus. Frankfurt a.M: Suhrkamp.
Eugster, A., & Vingerhoets, A. J. (1999). Psychological aspects of in vitro fertilization: a review.
Social Sciences and Medicine, 48, 575-589.
Faltermaier, T., Mayring, P., Saup, W., & Strehmel, P. (2002). Entwicklungspsychologie des
Erwachsenenalters. Stuttgart: Kohlhammer.
Folkman, S. (1997). Positive psychological states and coping with severe stress. Social Science &
Medicine, 45, 1207-1221.
Forrest, L., & Gilbert, M. S. (1992). Infertility: An unanticipated and prolonged life crisis. Journal
of Mental Health Counseling, 14, 42-58.
Freeman, E. W., Boxer, A. S., Rickels, K., Tureck, R., & Mastroianni, L. (1985). Psychological
evaluation and support in a program of in vitro fertilization and embryo transfer. Fertility and
Sterility, 43, 48-53.
Freud, S. (1917). Trauer und Melancholie. GW Bd, 10, 427-446.
Fries, A., & Grawe, K. (2006). Inkonsistenz und psychische Gesundheit: Eine Metaanalyse.
Zeitschrift für Psychiatrie, Psychologie und Psychotherapie, 54, 133-148.
Gauda, G., & Keller, H. (1987). Das subjektive Familienkonzept schwangerer Frauen. Zeitschrift für
Entwicklungspsychologie und Pädagogische Psychologie, 19, 32-45.
Glick, I. O., Weiss, R. S., & Parkes, C. M. (1974). The first year of bereavement. New York: Wiley.
Gloger-Tippelt, G. (2007). Familiengründung und Übergang zur Elternschaft. In M. Hasselhorn, &
W. Scheider (Hrsg.), Handbuch der Entwicklungspsychologie (S. 511-521). Göttingen: Hogre-
fe.
Literaturverzeichnis
14
Gnoth, C., Godehardt, E., Frank-Herrmann, P., Friol, K., Tigges, J., & Freundl, G. (2005).
Definition and prevalence of subfertility and infertility. Human Reproduction, 20, 1144-1147.
Grossmann, P., Niemann, L, Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction
and health benefits: A meta-analysis. Journal of Psychosomatic Research, 57, 43-53.
Grawe, K. (1998). Psychologische Therapie. Göttingen: Hogrefe.
Grawe, K. (2003). Neuropsychotherapie. Göttingen: Hogrefe.
Greil, A. L. (1991). Not yet pregnant: Infertile couples in contemporary America. London: Rutgers
University Press.
Greil, A. L. (1997). Infertility and psychological distress: a critical review of the literature. Social
Sciences and Medicine, 45, 1679-1704.
Grosse Holtforth, M., & Grawe, K. (2004). Inkongruenz und Fallkonzeption in der Psychologischen
Therapie. Verhaltenstherapie und Psychosoziale Praxis, 36, 9-21.
Grosse Holtforth, M., & Schneider, W. (2008). Motivation und Motivationskonflikte. In S. Herpertz,
F. Caspar, & C. Mundt (Eds), Störungsorientierte Psychotherapie (S. 191-206). München:
Urban & Fischer.
Haemmerli, K., Znoj, H., & Barth, J. (2009a). The Efficacy of Psychological Interventions for
Infertile Patients: A Meta-analysis Examining Mental Health and Pregnancy Rate. Human
Reproduction Update, 1, 1-17.
Haemmerli, K., Znoj, H., & Berger, T. (2009b). Internet-Based Support for Infertile Patients: A
Randomized Controlled Study. Manuscript revised.
Haemmerli, K., Znoj, H., & Berger, T. (2009c). What are the issues confronting infertile women? A
qualitative approach. Manuscript under review.
Haemmerli, K., Znoj, H., Stoklas, C., Wunder, D., & Perrig-Chiello, P. (2009d). How ist Distress
from Infertility Associated with Depression? Geburtshilfe und Frauenheilkunde, 69, 533-536.
Literaturverzeichnis
15
Hammarberg, K., Fisher, J. R. W., & Wynter K. H. (2008). Psychological and social aspects of
pregancy, childbirth and early parenting after assisted conception: a systematic review. Human
Reproduction Update, 14, 395-414.
Harvey, J. H. (2002). Disenfranchised Grief: New Directions, Challenges, and Strategies for
Practice. Champaign, IL: Research Press.
Havighurst, R. J. (1972). Developmental tasks and education (3th ed.). New York: Longmans,
Green.
Havighurst, R. J. (1973). History of developmental psychology: Socialization and personality
development through the life span. In P. B. Baltes & K. W. Schaie (Eds.), Life-span develop-
mental psychology (pp. 3-24). New York: Academic Press.
Hayes, S. C., Strohsahl, K. D., & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An
Experiental Approach to Behaviour Change. New York: Guilford Press.
Helfferich, C., & Küppers-Chinnow, M. (1996). Verbreitung von und Umgang mit Fertilitätsstörun-
gen. In Bundeszentrale für gesundheitliche Aufklärung, (Hrsg.), Kontrazeption, Konzeption,
Kinder oder keine (S. 113-136). Köln: Bundeszentrale für gesundheitliche Aufklärung.
Henning, K., & Strauss, B. (2000). Psychologische und psychosomatische Aspekte der ungewollten
Kinderlosigkeit: Zum Stand der Forschung. In B. Strauss (Hrsg.), Ungewollte Kinderlosigkeit:
Psychologische Diagnostik, Beratung und Therapie (S. 15-34). Göttingen: Hogrefe.
Huether, G. (2005). Biologie der Angst: Wie aus Stress Gefühle werden (7. Aufl.). Göttingen:
Vandenhoeck & Ruprecht GmbH & Co.
Huinink, J., & Brähler, E. (2000). Die Häufigkeit gewollter und ungewollter Kinderlosigkeit. In E.
Brähler, H. Felder, & B. Strauss (Hrsg.), Fruchtbarkeitsstörungen. Jahrbuch der Medizini-
schen Psychologie, Nr.17 (S. 43-54). Göttingen: Hogrefe.
Ingram, R. E. (1990). Contemporary psychological approaches to depression. New York: Plenum.
Johnston, D. R. (1963). The history of human infertility. Fertility and Sterility, 14, 261-269.
Literaturverzeichnis
16
Kabat-Zinn, J. (1990). Full Catastrophy Living: Using the Wisdom of Your Body and Mind to Face
Stress, Pain and Illness. New York: Delacorte Press.
Kabat-Zinn, J. (2003). Mindfulness-based intervention in context: Past, present and future. Clinical
Psychology: Science and Practice, 10, 144-156.
Kemeter, P., & Fiegl, J. (1998). Adjusting to life when assisted conception fails. Human Reproduc-
tion, 13, 1099-1105.
Kerr, J., Brown, C., & Balen, A. H. (1999). The experiences of couples who have had infertility
treatment in the United Kingdom: results of a survey performed in 1997. Human Reproducti-
on, 14, 934-938.
Kübler-Ross, E. (1969). On death and dying. New York: Springer.
Lampic, C. Svanberg, A. S., Karlstrom P., & Tyden, T. (2006). Fertility awareness, intentions
concerning childbearing, and attitudes towards parenthood among female and male academics.
Human Reproduction, 21, 558-564.
Lansac, J. (1995). Delayed partenting. Is delayed childbearing a good thing? Human Reproduction,
10, 1033-1055.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer.
Leiblum, S. R., & Greenfield, D. (1997). The course of infertility: immediate and long-term
reactions. In S. R. Leiblum (Ed.), Infertility, Psychological Issues and Counseling Strategies
(pp. 83-102). New York: John Wiley & Sons.
Linehan, M. M. (1993). Cognitive-Behavioral Treatment of Borderline Personality Disorder. New
York: Guilford Press.
Maciejewski, P. K., Zhang, B., Block, S. D., & Prigerson, H. G. (2007). An Empirical Examination
of the Stage Theory of Grief. The Journal of the American Medical Association, 297, 716-723.
Literaturverzeichnis
17
Mahajan, N. N., Turnbull, D. A., Davies, M. J., Jindal, U. N., Briggs, N. E., & Taplin, J. E. (2009).
Adjustment to infertility: the role of intrapersonal and interpersonal resources/vulnerabilities.
Human Reproduction, 24, 906-912.
Mahlstedt, P. (1985). The psychological component of infertility. Fertility and Sterility, 43, 335-
346.
Mahlstedt, P., & Johnson, P. (1987). Support to persons experiencing infertility: Family and friends
can help. Journal of Social Work and Human Sexuality, 6, 65-71.
McDaniel, S. H., Hepworth, J., & Doherty, W. (1992). Medical family therapy with couples facing
infertility. The American Journal of Family Therapy, 20, 101-122.
Menning, B. E. (1980). The emotional needs of infertile couples. Fertility and Sterility, 34, 313-319.
Michaels, G. Y. (1988). Motivational factors in the decision and timing of pregnancy. In G. Y.
Michaels & W. A. Goldberg (Eds.), The transition to parenthood: Current theory and re-
search (pp. 23-61). New York: Cambridge University Press.
Michelmann, H., & Himmel, W. (2005). Reproduktionsmedizin in Deutschland – Besonderheiten
und Dilemata. Gesundheitswesen, 67, 605-612.
Neimeyer, R. A. (2001). Meaning Reconstruction & the Experience of Loss. Washington, DC:
American Psychological Association.
Olivius, C., Friden, B., Borg, G., & Bergh, C. (2004). Why do couples discontinue in vitro
fertilization treatment? A cohort study. Fertility and Sterility, 81, 258-261.
Onnen-Isemann, C. (1995). Ungwollte Kinderlosigkeit und moderne Reproduktionsmedizin. In B.
Nauck & C. Onnen-Isemann (Hrsg.), Familie im Brennpunkt von Wissenschaft und Forschung
(S. 473-488). Neuwied: Luchterhand.
Onnen-Isemann, C. (2000). Wenn der Familienbildungsprozess stockt... Eine empirische Studie über
Stress und Coping-Strategien reproduktionsmedizinisch behandelter Partner. Berlin: Springer.
Literaturverzeichnis
18
Parkes, C. M. (1972). Bereavement: Studies of grief in adult life (2nd ed.). New York: International
Universities Press.
Parkes, C. M., & Weiss, R. S. (1983). Recovery from bereavement. New York: Basic Books.
Perrig-Chiello, P., & Höpflinger, F. (2001). Zwischen den Generationen. Zürich: Seismo Verlag.
Perrig-Chiello, P., Höpflinger, F., & Suter, C. (2008). Generationen – Strukturen und Beziehungen.
Zürich: Seismo Verlag.
Pollock, G. H. (1987). The mourning-liberation process in health and disease. Psychiatric Clinics of
North America, 10, 345-354.
Rothaupt, J. W., & Becker, K. (2007). A Literature Review of Western Bereavement Theory: From
Decathecting to Continuing Bonds. The Family Journal: Counseling and Therapy for Couples
and Families, 15, 6-15.
Schmidt, L., Holenstein, B. E., Christensen, U., & Boivin, J. (2005). Communication and coping as
predictors of fertility problem stress: cohort study of 816 participants who did not achieve a
delivery after 12 months of fertility treatment. Human Reproduction, 20, 3248-3256.
Shuchter, S., & Zisook, S. (1993). The course of normal grief. In M. S. Stroebe, W. Stroebe, & R. O.
Hansson (Eds.), Handbook of bereavement: Theory, research and intervention (pp. 23-43).
Cambridge, England: Cambridge University Press.
Skoog Svanberg, A., Lampic, C., Karlström, P. O., & Tydén, T., (2006). Attitudes toward pa-
renthood and awarness of fertility among postgraduate students in Sweden. Gender medicine,
3, 187-195.
Smeenk, J. M., Verhaak, C. M., Stolwijk, A. M., Kremer, J. A., & Braat, D. D. (2004). Reasons for
dropout in an in vitro fertilization/intracytoplasmic sperm injection program Fertility and Ste-
rility, 81, 262-268.
Stammer, H., Verres, R., & Wischmann, T. (2004). Paarberatung und –therapie bei unerfülltem
Kinderwunsch. Göttingen: Hogrefe.
Literaturverzeichnis
19
Stammer, H., Wischmann, T., & Verres, R. (2002). Counselling and couple therapy for infertile
couples. Family Process, 41, 111-122.
Stanton, A. L. (1991). Cognitive Appraisals, Coping Processes, and Adjustment to Infertility. In A.
L. Stanton, & C. Dunkel-Schetter (Eds.), Infertility: Perspectives from Stress and Coping Re-
search (pp. 87-106). New York: Plenum Press.
Stanton, A. L., & Dunkel-Schetter, C. (1991). Psychological adjustment to infertility. In A. L.
Stanton & C. Dunkel-Schetter (Eds.), Infertility: Perspectives from Stress and Coping Re-
search (pp. 3-16). New York: Plenum Press.
Strauss, B. (2000). Ungewollte Kinderlosigkeit: Psychologische Diagnostik, Beratung und Therapie.
Göttingen: Hogrefe.
Strauss, B. (2001). Psychosomatik der Sterilität und der Sterilitätsbehandlung. Stuttgart: Enke.
Strauss, B., Brähler, E., & Kentenich, H. (2004). Fertilitätsstörungen – psychosomatisch orientierte
Diagnostik und Therapie. Stuttgart: Schattauer.
Stroebe, M. S., Hansson, R. O., Schut, H. A., & Stroebe, W. (2008). Handbook of Bereavement
Research and Practice. Advances in Theory and Intervention. Washington, DC: American
Psychological Association.
Stroebe, M. S., & Schut, H. A. (1999). The dual process model of coping with bereavement:
Rationale and description. Death Studies, 23, 197-224.
Stroebe, M. S., Schut, H. A., & Stroebe, W. (2007). Health outcomes of bereavement. Lancet, 370,
1960-1973.
Stroebe, M. S., Stroebe, W., & Hansson, R. O. (1993). Handbook of bereavement: Theory, Research
and Intervention. New York: Cambridge University Press.
Taylor, A. (2003). Extent of the problem. BMJ, 327, 434 - 436.
Taylor, P. J. (1990). When is enough enough? Fertility and Sterility, 54, 772-774.
Taymor, M. L., & Bresnick, E. (1979). Emotional stress and infertility. Infertility, 2, 39-47.
Literaturverzeichnis
20
Terry, D. J., & Hynes, G. J. (1998). Adjustment to a low-control situation: reexamining the role of
coping responses. Journal of Personality and Social Psychology, 74, 1078-1092.
Unruh, A. M., & McGrath, P. J. (1985). The psychology of female infertility: Toward a new
perspective. Health Care for Women International, 6, 369-381.
Van Balen, F. (2002). The psychologization of infertility. In M. C. Inhorn & F. van Balen (eds),
Infertility around the globe (pp. 79-98). Berkeley: University of California press.
Verberg, M. F. G., Eijkemans, M. J. C., Heijnen, E. M. E. W., Broekmans, F. J., de Klerk, C.,
Fauser, B. C. J. M., & Macklon, N. S. (2008). Why do couples drop-out from IVF treatment?
A prospective cohort study. Human Reproduction, 23, 2050-2055.
Verhaak, C. M., Smeenk, J. M., Evers, A. W., Kremer, J. A., Kraaimaat, F. W., & Braat, D. D.
(2007). Women’s emotional adjustment to IVF: a systematic review of 25 years of research.
Human Reproduction Update, 13, 27-36.
Walker, B. G. (1983). The Woman’s Encyclopedia of Myths and Secrets. New York: Harper &
Collins.
Watkins, K. J., & Baldo, T. D. (2004). The Infertility Experience: Biopsychosocial Effects and
Suggestions for Counselors. Journal of Counseling & Development, 82, 394-402.
Wischmann, T. (2003). Psychogene Fertilitätsstörungen. Mythen und Fakten. Gynäkologische
Endokrinologie, 1, 187-196.
Wischmann, T. (2005). Psychosoziale Aspekte bei Fertilitätsstörungen. Urologe, 44, 185-195.
Wischmann, T. (2006). Unerfüllter Kinderwunsch – Stereotype und Fakten. Journal für Reproduk-
tionsmedizin und Endokrinologie, 4, 220-225.
Wischmann, T. (2008). Implications of psychosocial support in infertility – a critical appraisal.
Journal of Psychosomatic Obstetrics & Gynecology, 29, 83-90.
Wischmann, T. & Stammer, H. (2006). Der Traum vom eigenen Kind. Psychologische Hilfen bei
unerfülltem Kinderwunsch (3th ed.). Stuttgart: Kohlhammer.
Literaturverzeichnis
21
Wischmann, T., Stammer, H., Scherg, H., Gerhard, I., & Verres, R. (2001). Psychological character-
istics of infertile couples: a study of the "Heidelberg Fertility Consultation Service". Human
Reproduction, 16, 1753-1761.
Wright, J., Allard, M., Lecours, A., & Sabourin, S. (1989). Psychosocial distress and infertility: a
review of controlled research. International Journal of Fertility, 34, 126-142.
Wright, J., Duchesne, C., Sabourin, S., Bissonnette, F., Benoit, J., & Girard, Y. (1991). Psychoso-
cial distress and infertility: men and women respond differently. Fertility and Sterility, 55,
100-108.
World Health Organization (2002). Current Practices and Controversies in Assisted Reproduction.
Report of meeting on "Medical, Ethical and Social Aspects of Assisted Reproduction" WHO
Headquarters, Geneva, Switzerland, 1721 September 2001.
Znoj, H. (2004). Komplizierte Trauer. Göttingen: Hogrefe.
Znoj, H. (2008). Regulation emotionaler Prozesse in Psychotherapie und Verhaltensmedizin. Bern:
Peter Lang.
Znoj, H., & Maercker, A. (2005). Trauerarbeit und Therapie der komplizierten Trauer. In M.
Linden & M. Hautzinger (Hrsg.), Verhaltenstherapiemanual (S. 401-406). Berlin: Springer.

Abbildungsverzeichnis
22
Abbildungsverzeichnis Seite
Abbildung 1: Duales Prozessmodell der Trauerbewältigung nach Stroe-
be und Shut (1999)
25
Abbildung 2: Das transaktionale Stressmodell nach Lazarus und Folk-
man (1984) am Beispiel der Infertilität
29
Anhang

Anhang A Fragebogen des Kinderwunsch Online Coachings (Version: Messzeitpunkt t1 (zu Beginn);
weibliche Version)
W1
Kinderwunsch Online Coaching
Institut für Psychologie Universität Bern
Gefördert durch den Schweizerischen Nationalfonds
(Projekt Nr. 325100 - 11375411) Projektverantwortliche:
Lic. phil. Katja Hämmerli, Prof. Dr. Hansjörg Znoj, Dr. Thomas Berger

Kinderwunsch Online Coaching Woran nehmen Sie teil? Das Kinderwunsch Online Coaching ist ein Projekt des Instituts für Klinische Psychologie und Psychotherapie an der Universität Bern und wird vom Schweizerischen Nationalfond unterstützt. Das Ziel dieser Studie ist die Erforschung der Wirksamkeit eines Online Coaching für Personen mit einem unerfüllten Kinderwunsch. Die Wirksamkeit soll hinsichtlich dem psychischen Befinden und den Chancen auf eine Schwangerschaft untersucht werden. Die Ergebnisse dieser Studie sollen Hinweise darauf geben, ob eine Online Unterstützung für Per-sonen mit unerfülltem Kinderwunsch hilfreich ist und als kostengünstige, flexible Interventi-on in der Praxis angewendet werden soll.
Datenschutz In dieser Studie werden persönliche Daten von Ihnen erfasst. Alle Ihre Angaben werden an-onymisiert und streng vertraulich behandelt. Die anonymisierten Daten sind nur Fachleuten zur wissenschaftlichen Auswertung zugänglich.
Durchführung Füllen Sie die einzelnen Frageblöcke zügig aus. Da es um Einstellungen geht, gibt es keine richtigen oder falschen Antworten. Überlegen Sie nicht lange, was wohl die meisten Leute ankreuzen würden oder welche Antwort den „besten“ Eindruck machen könnte. Wichtig: Kreuzen Sie einfach die Antwort an, die im Moment am besten auf Sie zutrifft.
Bei allfälligen Fragen wenden Sie sich bitte an die folgende Person:
Frau lic. phil. K. Hämmerli : 031 631 45 83
Mit aufrichtigem Dank für Ihre wertvolle Mitarbeit Lic. phil. Katja Hämmerli
Prof. Dr. Hansjörg Znoj Dr. Thomas Berger
1. Angaben zu Ihrer Person Studiennummer: ............
1. Allgemein: Alter:
✎ ....................... Jahre
Nationalität: ❑ CH ❑ D ❑ F ❑ I
❑ andere: ✎ ........................
Muttersprache: ❑ deutsch ❑ französisch ❑ italienisch ❑ andere:
✎ ....................................
2. Ausbildung/ Beruf:
Zur Zeit oder zuletzt ausgeübter Beruf: ✎ ..................................................................................
Erwerbstätigkeit: ❑ nicht berufstätig
❑ arbeitslos ❑ vollzeit erwerbstätig
❑ teilzeit erwerbstätig zu ✎........% ❑ selbständig erwer-bend ❑ Hausfrau
❑ Pension/Altersrente ❑ in Ausbildung ❑ anders: ✎ ...............
Wie hoch ist etwa Ihr monatliches Netto-Einkommen, über das Ihr Haushalt nach Abzug der Steuern, Krankenversicherung und weiteren Sozialabgaben verfügt?
❑ unter 3000 CHF ❑ 3000 – 5000 CHF ❑ 5000 – 7000 CHF ❑ über 7000 CHF
Erreichter Schul- bzw. Stu-dienabschluss:
❑ keiner ❑ Anlehre ❑ Berufslehre ❑ Meisterprüfung ❑ höhere Fachschule ❑ Matura/Lehrerseminar ❑ Universitätsstudium ❑ anderer: ✎ ........................................
3. Wohnsituation: Ich wohne...: ❑ alleine
❑ in Wohngemeinschaft ❑ mit meinem Partner ❑ anderes: ✎................................................ (Mehrfachnennungen möglich)
4. Partnerschaft:
Zivilstand: ❑ ledig ❑ verheiratet ❑ wieder verheiratet
❑ geschieden ❑ verwitwet
5. Kinderwunsch: Seit wann versuchen Sie ein Kind zu bekommen? Seit: ✎ ............................Jahren
Welche Methoden haben Sie bereits ausprobiert, um schwanger zu werden?
Folgende: ✎ .........................................................
.........................................................................................
.........................................................................................
..............................................................(Mehrfachnennu
ngen möglich)
Haben Sie sich bereits einer medizinischen Behandlung (z.B. Insemination, IVF, ICSI) unterzogen?
❑ ja, folgende: ✎
.........................................................
....................................................................................
....................................................................................
....................................................................................
(Mehrfachnennungen möglich)
❑ nein
6. Frühere Behandlungen: Waren Sie schon einmal wegen psychischen Problemen in Be-
handlung?
❑ ja
❑ nein
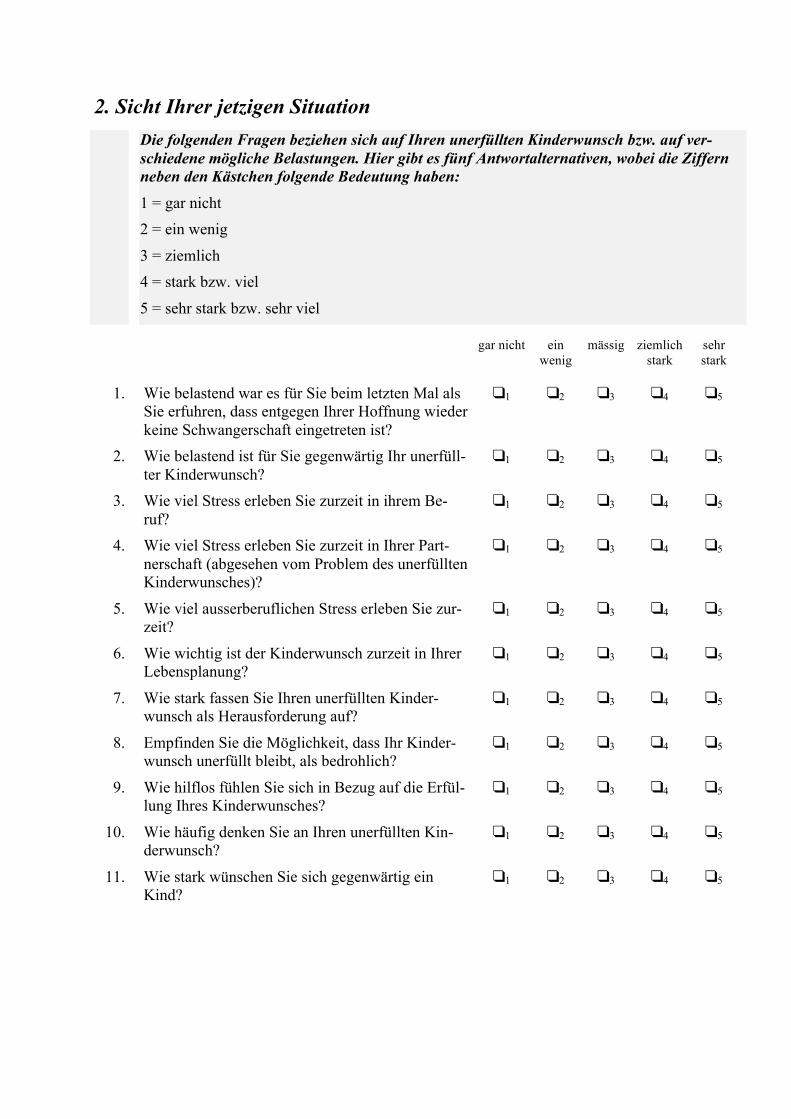
2. Sicht Ihrer jetzigen Situation
Die folgenden Fragen beziehen sich auf Ihren unerfüllten Kinderwunsch bzw. auf ver-schiedene mögliche Belastungen. Hier gibt es fünf Antwortalternativen, wobei die Ziffern neben den Kästchen folgende Bedeutung haben: 1 = gar nicht 2 = ein wenig
3 = ziemlich 4 = stark bzw. viel
5 = sehr stark bzw. sehr viel
gar nicht ein wenig
mässig ziemlich stark
sehr stark
1. Wie belastend war es für Sie beim letzten Mal als Sie erfuhren, dass entgegen Ihrer Hoffnung wieder keine Schwangerschaft eingetreten ist?
1 2 3 4 5
2. Wie belastend ist für Sie gegenwärtig Ihr unerfüll-ter Kinderwunsch?
1 2 3 4 5
3. Wie viel Stress erleben Sie zurzeit in ihrem Be-ruf?
1 2 3 4 5
4. Wie viel Stress erleben Sie zurzeit in Ihrer Part-nerschaft (abgesehen vom Problem des unerfüllten Kinderwunsches)?
1 2 3 4 5
5. Wie viel ausserberuflichen Stress erleben Sie zur-zeit?
1 2 3 4 5
6. Wie wichtig ist der Kinderwunsch zurzeit in Ihrer Lebensplanung?
1 2 3 4 5
7. Wie stark fassen Sie Ihren unerfüllten Kinder-wunsch als Herausforderung auf?
1 2 3 4 5
8. Empfinden Sie die Möglichkeit, dass Ihr Kinder-wunsch unerfüllt bleibt, als bedrohlich?
1 2 3 4 5
9. Wie hilflos fühlen Sie sich in Bezug auf die Erfül-lung Ihres Kinderwunsches?
1 2 3 4 5
10. Wie häufig denken Sie an Ihren unerfüllten Kin-derwunsch?
1 2 3 4 5
11. Wie stark wünschen Sie sich gegenwärtig ein Kind?
1 2 3 4 5
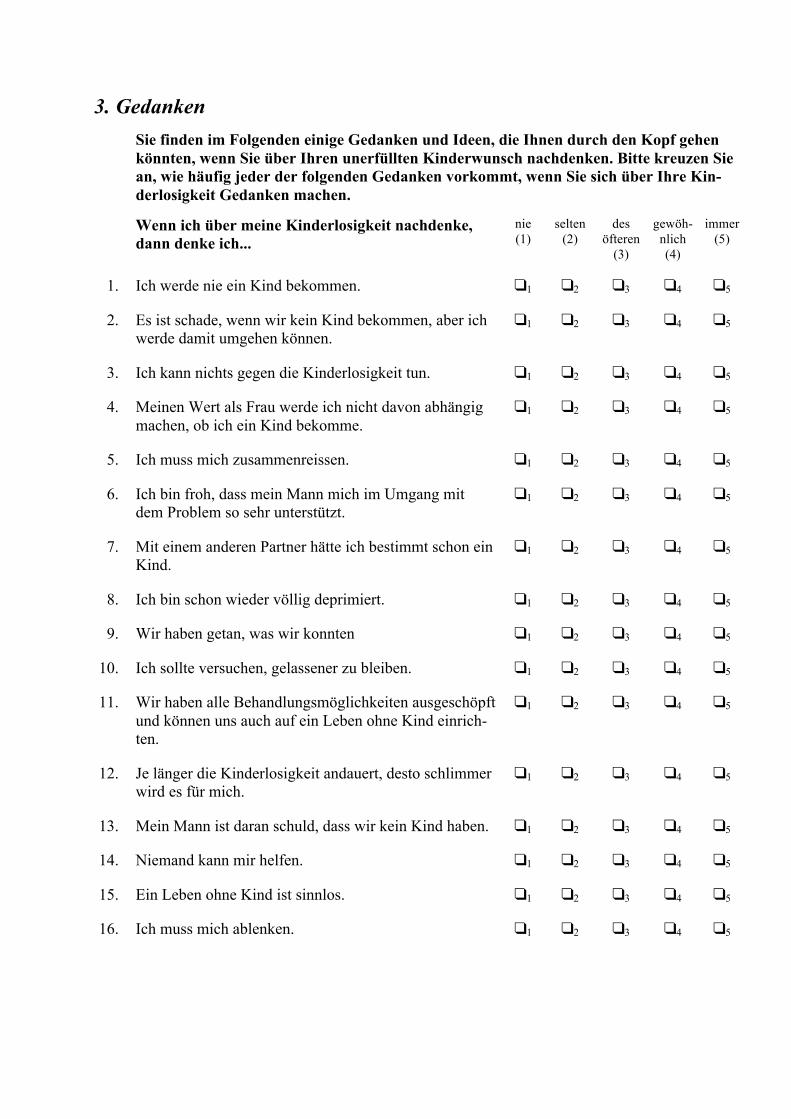
3. Gedanken Sie finden im Folgenden einige Gedanken und Ideen, die Ihnen durch den Kopf gehen
könnten, wenn Sie über Ihren unerfüllten Kinderwunsch nachdenken. Bitte kreuzen Sie an, wie häufig jeder der folgenden Gedanken vorkommt, wenn Sie sich über Ihre Kin-derlosigkeit Gedanken machen.
Wenn ich über meine Kinderlosigkeit nachdenke,
dann denke ich... nie (1)
selten (2)
des öfteren
(3)
gewöh-nlich (4)
immer (5)
1. Ich werde nie ein Kind bekommen. 1 2 3 4 5
2. Es ist schade, wenn wir kein Kind bekommen, aber ich werde damit umgehen können.
1 2 3 4 5
3. Ich kann nichts gegen die Kinderlosigkeit tun. 1 2 3 4 5
4. Meinen Wert als Frau werde ich nicht davon abhängig machen, ob ich ein Kind bekomme.
1 2 3 4 5
5. Ich muss mich zusammenreissen. 1 2 3 4 5
6. Ich bin froh, dass mein Mann mich im Umgang mit dem Problem so sehr unterstützt.
1 2 3 4 5
7. Mit einem anderen Partner hätte ich bestimmt schon ein Kind.
1 2 3 4 5
8. Ich bin schon wieder völlig deprimiert. 1 2 3 4 5
9. Wir haben getan, was wir konnten 1 2 3 4 5
10. Ich sollte versuchen, gelassener zu bleiben. 1 2 3 4 5
11. Wir haben alle Behandlungsmöglichkeiten ausgeschöpft und können uns auch auf ein Leben ohne Kind einrich-ten.
1 2 3 4 5
12. Je länger die Kinderlosigkeit andauert, desto schlimmer wird es für mich.
1 2 3 4 5
13. Mein Mann ist daran schuld, dass wir kein Kind haben. 1 2 3 4 5
14. Niemand kann mir helfen. 1 2 3 4 5
15. Ein Leben ohne Kind ist sinnlos. 1 2 3 4 5
16. Ich muss mich ablenken. 1 2 3 4 5
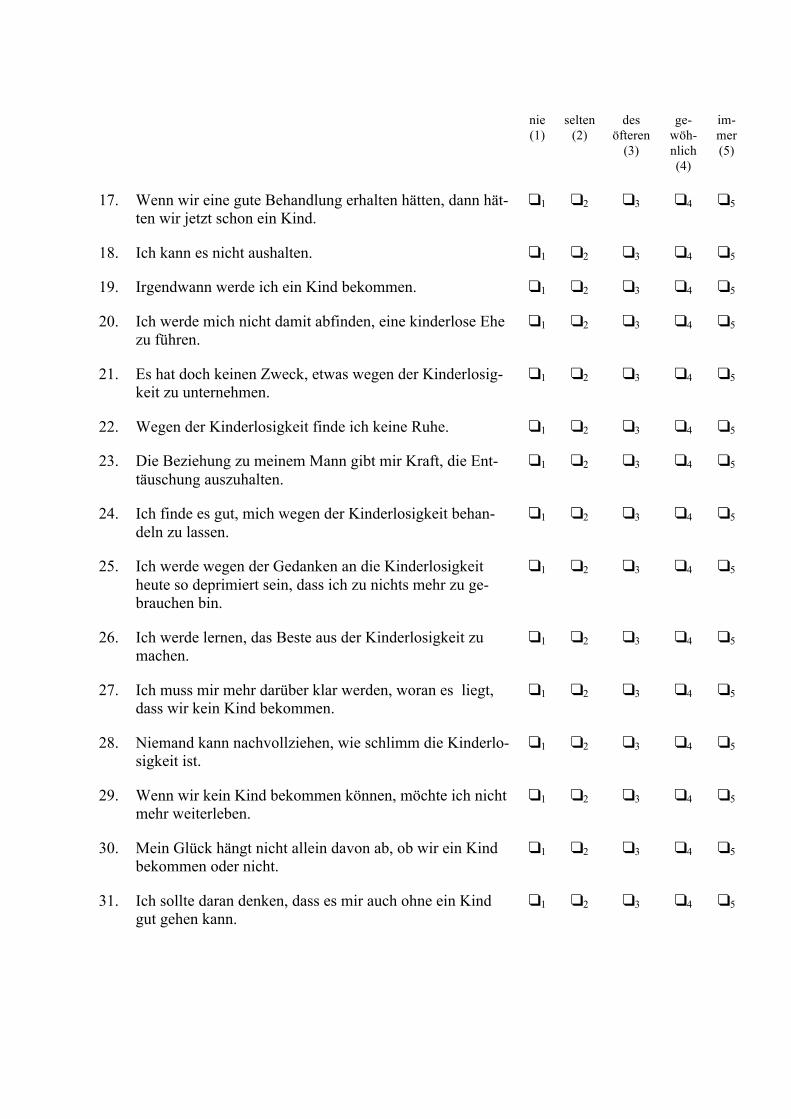
nie
(1) selten
(2) des
öfteren (3)
ge-wöh-nlich (4)
im-mer (5)
17. Wenn wir eine gute Behandlung erhalten hätten, dann hät-
ten wir jetzt schon ein Kind. 1 2 3 4 5
18. Ich kann es nicht aushalten. 1 2 3 4 5
19. Irgendwann werde ich ein Kind bekommen. 1 2 3 4 5
20. Ich werde mich nicht damit abfinden, eine kinderlose Ehe zu führen.
1 2 3 4 5
21. Es hat doch keinen Zweck, etwas wegen der Kinderlosig-keit zu unternehmen.
1 2 3 4 5
22. Wegen der Kinderlosigkeit finde ich keine Ruhe. 1 2 3 4 5
23. Die Beziehung zu meinem Mann gibt mir Kraft, die Ent-täuschung auszuhalten.
1 2 3 4 5
24. Ich finde es gut, mich wegen der Kinderlosigkeit behan-deln zu lassen.
1 2 3 4 5
25. Ich werde wegen der Gedanken an die Kinderlosigkeit heute so deprimiert sein, dass ich zu nichts mehr zu ge-brauchen bin.
1 2 3 4 5
26. Ich werde lernen, das Beste aus der Kinderlosigkeit zu machen.
1 2 3 4 5
27. Ich muss mir mehr darüber klar werden, woran es liegt, dass wir kein Kind bekommen.
1 2 3 4 5
28. Niemand kann nachvollziehen, wie schlimm die Kinderlo-sigkeit ist.
1 2 3 4 5
29. Wenn wir kein Kind bekommen können, möchte ich nicht mehr weiterleben.
1 2 3 4 5
30. Mein Glück hängt nicht allein davon ab, ob wir ein Kind bekommen oder nicht.
1 2 3 4 5
31. Ich sollte daran denken, dass es mir auch ohne ein Kind gut gehen kann.
1 2 3 4 5
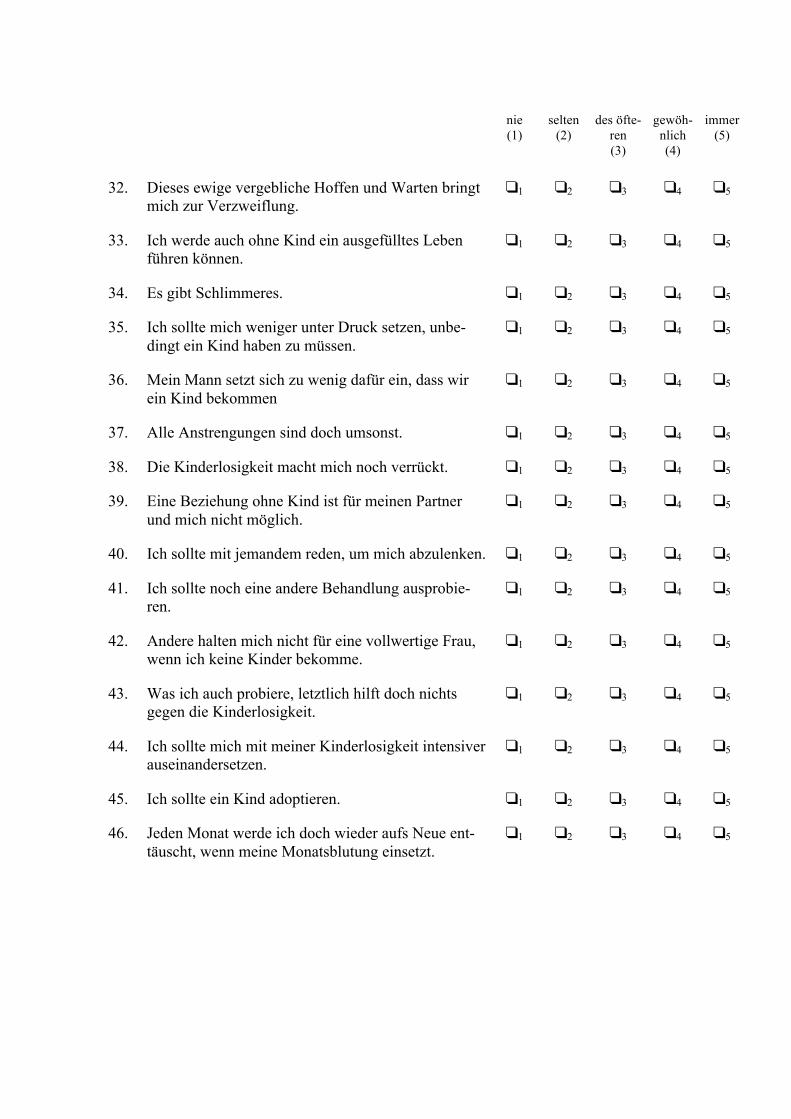
nie
(1) selten
(2) des öfte-
ren (3)
gewöh-nlich (4)
immer (5)
32. Dieses ewige vergebliche Hoffen und Warten bringt mich zur Verzweiflung.
1 2 3 4 5
33. Ich werde auch ohne Kind ein ausgefülltes Leben führen können.
1 2 3 4 5
34. Es gibt Schlimmeres. 1 2 3 4 5
35. Ich sollte mich weniger unter Druck setzen, unbe-dingt ein Kind haben zu müssen.
1 2 3 4 5
36. Mein Mann setzt sich zu wenig dafür ein, dass wir ein Kind bekommen
1 2 3 4 5
37. Alle Anstrengungen sind doch umsonst. 1 2 3 4 5
38. Die Kinderlosigkeit macht mich noch verrückt. 1 2 3 4 5
39. Eine Beziehung ohne Kind ist für meinen Partner und mich nicht möglich.
1 2 3 4 5
40. Ich sollte mit jemandem reden, um mich abzulenken. 1 2 3 4 5
41. Ich sollte noch eine andere Behandlung ausprobie-ren.
1 2 3 4 5
42. Andere halten mich nicht für eine vollwertige Frau, wenn ich keine Kinder bekomme.
1 2 3 4 5
43. Was ich auch probiere, letztlich hilft doch nichts gegen die Kinderlosigkeit.
1 2 3 4 5
44. Ich sollte mich mit meiner Kinderlosigkeit intensiver auseinandersetzen.
1 2 3 4 5
45. Ich sollte ein Kind adoptieren. 1 2 3 4 5
46. Jeden Monat werde ich doch wieder aufs Neue ent-täuscht, wenn meine Monatsblutung einsetzt.
1 2 3 4 5
4. Erlebte Unterstützung Bitte geben Sie an, in welchem Ausmass Sie sich insgesamt von den folgenden Personen,
Personen- und Berufsgruppen in den letzten zwei Monaten unterstützt fühlten. Bitte geben Sie an, wie Sie die Kontakte mit den verschiedenen Personen persönlich erlebten und NICHT, in welchem Ausmass andere Personen tatsächlich Leistungen für Sie erbrachten oder sich bemühten, Ihnen etwas Liebes zu tun. Falls Sie mit einer Person oder einer Berufsgruppe während der letzten zwei Monate gar kei-nen Kontakt hatten, machen Sie bitte ein Kreuz in das Kästchen "kein Kontakt". Kreuzen Sie dieses Kästchen auch dann an, wenn Sie z.B. gar keine Geschwister haben oder wenn die entsprechende Person bereits verstorben ist.
kein
Kontakt nicht unter- stützt
wenig unter- stützt
mittel-mässig
unterstützt
ziemlich unter- stützt
sehr unter- stützt
• Mutter 1 2 3 4 5
• Vater 1 2 3 4 5
• (Ehe-) Partner / (Ehe-) Partnerin
1 2 3 4 5
• Geschwister 1 2 3 4 5
• enge Freunde 1 2 3 4 5
• Bekannte 1 2 3 4 5
• Ärzte 1 2 3 4 5
• Psychologen 1 2 3 4 5
• sonstige: ✎ .................................
1 2 3 4 5
Wie stark fühlen Sie sich insgesamt unterstützt? Bitte tragen Sie den Ort ein, der Ihrer aktuellen Situation am besten entspricht.
allein gelassen
0% 100 %
von allen Seiten unterstützt
5. Umgang mit Schwierigkeiten Im Folgenden wird nach dem Umgang mit schwierigen und unerwarteten Situationen
gefragt. Inwiefern treffen folgende Aussagen auf Sie zu? Folgende Antwortalternativen stehen Ihnen zur Verfügung: (1) stimmt nicht, (2) stimmt kaum, (3) stimmt eher, (4) stimmt genau
stimmt nicht
(1) stimmt kaum
(2)
stimmt eher (3)
stimmt genau
(4)
1. Wenn sich Widerstände auftun, finde ich Mittel und Wege, mich durchzusetzen.
1 2 3 4
2. Die Lösung schwieriger Probleme gelingt mir immer, wenn ich mich darum bemühe.
1 2 3 4
3. Es bereitet mir keine Schwierigkeiten, mei-ne Absichten und Ziele zu verwirklichen.
1 2 3 4
4. In unerwarteten Situationen weiß ich immer, wie ich mich verhalten soll.
1 2 3 4
5. Auch bei überraschenden Ereignissen glau-be ich, daß ich gut mit ihnen zurechtkom-men kann.
1 2 3 4
6. Schwierigkeiten sehe ich gelassen entgegen, weil ich meinen Fähigkeiten immer vertrau-en kann.
1 2 3 4
7. Was auch immer passiert, ich werde schon klarkommen.
1 2 3 4
8. Für jedes Problem kann ich eine Lösung finden.
1 2 3 4
9. Wenn eine neue Sache auf mich zukommt, weiß ich, wie ich damit umgehen kann.
1 2 3 4
10. Wenn ein Problem auftaucht, kann ich es aus eigener Kraft meistern.
1 2 3 4
6. Umgang mit stressvollen Ereignissen Im Folgenden wird beschrieben, wie Menschen auf verschiedene schwierige, stressvolle
oder ärgerliche Situationen reagieren können. Kreuzen Sie bitte an, wie Sie typischerweise reagieren, wenn Sie unter Stress stehen.
Das ist für mich ... sehr unty-
pisch (1)
eher unty-pisch (2)
teils-teils (3)
eher typsich
(4)
sehr typisch
(5) 1. Ich durchdenke zuerst das Problem, bevor ich
etwas unternehme. 1 2 3 4 5
2. Ich werde wütend. 1 2 3 4 5 3. Ich suche den Kontakt mit anderen Menschen. 1 2 3 4 5 4. Ich mache einen Einkaufsbummel. 1 2 3 4 5 5. Ich habe die Befürchtung, dass ich die Situati-
on nicht bewältigen kann. 1 2 3 4 5
6. Ich gehe essen. 1 2 3 4 5 7. Ich erarbeite mir einen Plan und führe ihn auch
aus. 1 2 3 4 5
8. Ich mache mir Vorwürfe, weil ich nicht weiss, was ich machen soll.
1 2 3 4 5
9. Ich denke über die Situation nach und versu-che, aus meinen Fehlern zu lernen.
1 2 3 4 5
10. Ich wünsche mir, ich könnte ungeschehen ma-chen, was passiert ist.
1 2 3 4 5
11. Ich besuche einen Freund/eine Freundin. 1 2 3 4 5 12. Ich versuche, so planmässig und gezielt vorzu-
gehen, dass ich die Situation in den Griff be-komme.
1 2 3 4 5
13. Ich verbringe Zeit mit einem mir nahe stehen-den Menschen.
1 2 3 4 5
14. Ich schaue mir einen Film an. 1 2 3 4 5 15. Ich betätige mich körperlich (z.B. Bewegung,
Sport, körperlich beanspruchende Arbeit). 1 2 3 4 5
16. Normalerweise gelingt es mir, mich innerlich zu beruhigen.
1 2 3 4 5
17. Meistens bekomme ich meine Gefühle ganz gut in den Griff.
1 2 3 4 5
18. Ich reagiere aufbrausend. 1 2 3 4 5 19. Normalerweise kann ich mich ganz gut beherr-
schen. 1 2 3 4 5
7. Beziehungszufriedenheit
Hier ist eine Reihe von Fragen, welche sich auf die Zufriedenheit in der eigenen Part-nerschaft beziehen. Bitte kreuzen Sie die zutreffende Antwortalternative an. Wenn die Antwort unterhalb für Sie zutrifft, dann kreuzen Sie die an, wenn die Antwort unter der Zahl für Sie zutrifft, dann kreuzen Sie die an. Wenn Sie Ihre Antwort irgendwo zwischen und sehen, kreuzen Sie die Zahl an, die Ihrer Beurteilung am besten entspricht. Bitte geben Sie immer nur eine Antwort pro Frage.
1. Wie gut kommt ihr Partner Ihren Bedürfnissen entgegen?
überhaupt nicht
wenig
teils- teils
ziemlich
vollkommen
2. Wie zufrieden sind Sie insgesamt mit Ihrer Beziehung?
sehr unzufrieden
eher unzufrieden
teils- teils
eher zufrieden
sehr zufrieden
3. Wie gut ist Ihre Beziehung verglichen mit anderen?
sehr schlecht
schlecht
durchschnittlich
eher gut
sehr gut
4. Wie oft wünschen Sie sich, diese Beziehung nicht eingegangen zu sein?
niemals
selten
manchmal
oft
sehr oft
5. In welchem Mass hat Ihre Beziehung Ihre ursprünglichen Erwartungen erfüllt?
sehr schlecht
schlecht
durchschnittlich
eher gut
sehr gut
6. Wie sehr lieben Sie Ihren Partner
überhaupt nicht
wenig
teils- teils
ziemlich
vollkommen
7. Wieviele Probleme gibt es in Ihrer Partnerschaft
sehr wenige
wenige
einige
viele
sehr viele
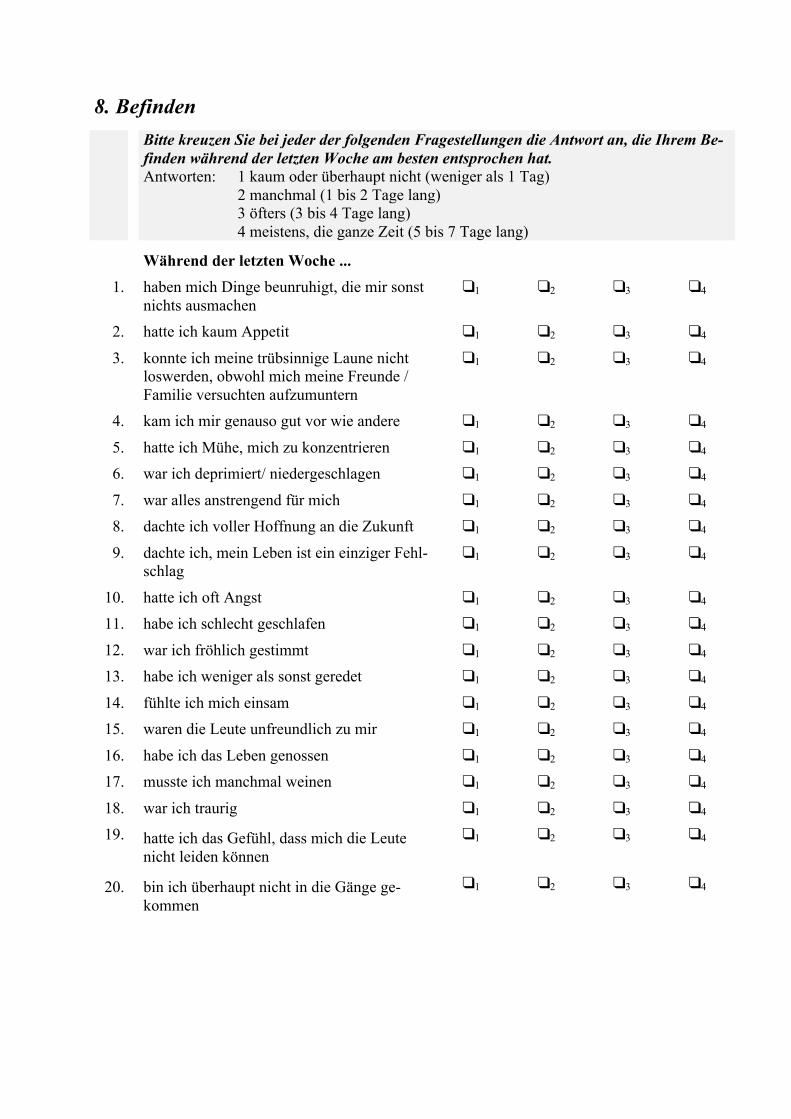
8. Befinden Bitte kreuzen Sie bei jeder der folgenden Fragestellungen die Antwort an, die Ihrem Be-
finden während der letzten Woche am besten entsprochen hat. Antworten: 1 kaum oder überhaupt nicht (weniger als 1 Tag) 2 manchmal (1 bis 2 Tage lang) 3 öfters (3 bis 4 Tage lang) 4 meistens, die ganze Zeit (5 bis 7 Tage lang)
Während der letzten Woche ...
1. haben mich Dinge beunruhigt, die mir sonst nichts ausmachen
1 2 3 4
2. hatte ich kaum Appetit 1 2 3 4
3. konnte ich meine trübsinnige Laune nicht loswerden, obwohl mich meine Freunde / Familie versuchten aufzumuntern
1 2 3 4
4. kam ich mir genauso gut vor wie andere 1 2 3 4
5. hatte ich Mühe, mich zu konzentrieren 1 2 3 4 6. war ich deprimiert/ niedergeschlagen 1 2 3 4
7. war alles anstrengend für mich 1 2 3 4 8. dachte ich voller Hoffnung an die Zukunft 1 2 3 4
9. dachte ich, mein Leben ist ein einziger Fehl-schlag
1 2 3 4
10. hatte ich oft Angst 1 2 3 4 11. habe ich schlecht geschlafen 1 2 3 4
12. war ich fröhlich gestimmt 1 2 3 4 13. habe ich weniger als sonst geredet 1 2 3 4
14. fühlte ich mich einsam 1 2 3 4 15. waren die Leute unfreundlich zu mir 1 2 3 4
16. habe ich das Leben genossen 1 2 3 4 17. musste ich manchmal weinen 1 2 3 4
18. war ich traurig 1 2 3 4 19. hatte ich das Gefühl, dass mich die Leute
nicht leiden können 1 2 3 4
20. bin ich überhaupt nicht in die Gänge ge-kommen
1 2 3 4
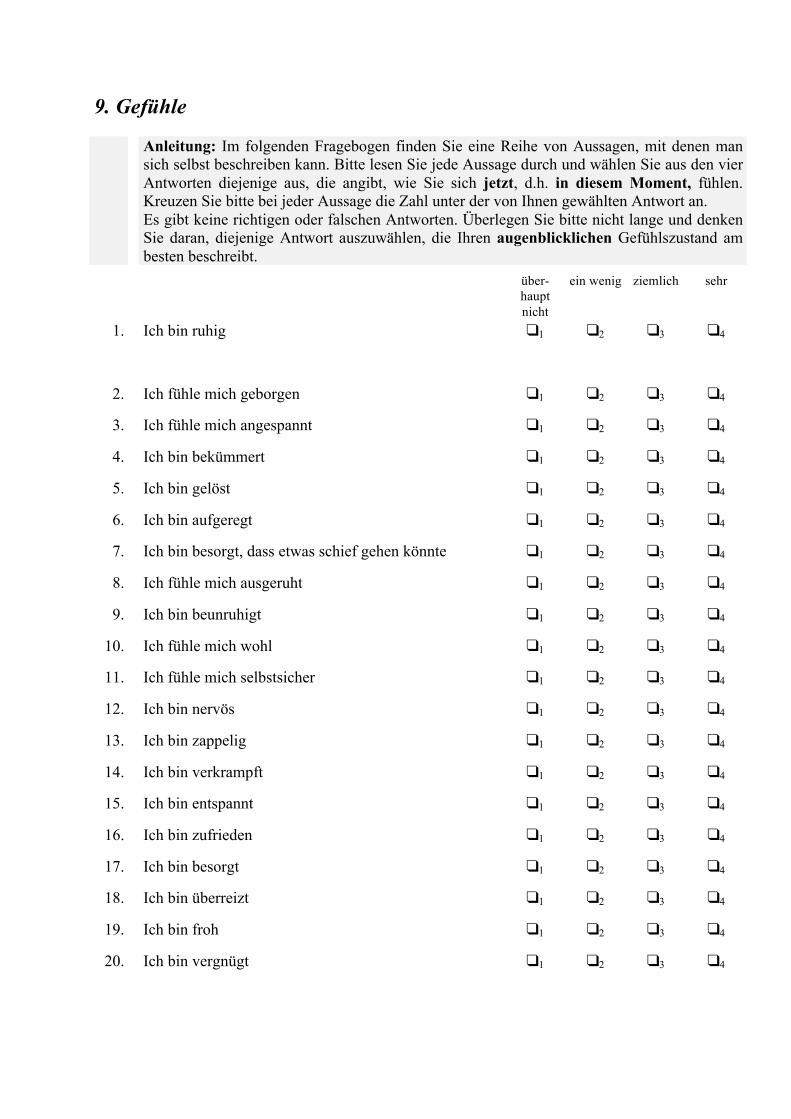
9. Gefühle Anleitung: Im folgenden Fragebogen finden Sie eine Reihe von Aussagen, mit denen man
sich selbst beschreiben kann. Bitte lesen Sie jede Aussage durch und wählen Sie aus den vier Antworten diejenige aus, die angibt, wie Sie sich jetzt, d.h. in diesem Moment, fühlen. Kreuzen Sie bitte bei jeder Aussage die Zahl unter der von Ihnen gewählten Antwort an. Es gibt keine richtigen oder falschen Antworten. Überlegen Sie bitte nicht lange und denken Sie daran, diejenige Antwort auszuwählen, die Ihren augenblicklichen Gefühlszustand am besten beschreibt.
über-haupt nicht
ein wenig ziemlich sehr
1. Ich bin ruhig
1 2 3 4
2. Ich fühle mich geborgen 1 2 3 4
3. Ich fühle mich angespannt 1 2 3 4
4. Ich bin bekümmert 1 2 3 4
5. Ich bin gelöst 1 2 3 4
6. Ich bin aufgeregt 1 2 3 4
7. Ich bin besorgt, dass etwas schief gehen könnte 1 2 3 4
8. Ich fühle mich ausgeruht 1 2 3 4
9. Ich bin beunruhigt 1 2 3 4
10. Ich fühle mich wohl 1 2 3 4
11. Ich fühle mich selbstsicher 1 2 3 4
12. Ich bin nervös 1 2 3 4
13. Ich bin zappelig 1 2 3 4
14. Ich bin verkrampft 1 2 3 4
15. Ich bin entspannt 1 2 3 4
16. Ich bin zufrieden 1 2 3 4
17. Ich bin besorgt 1 2 3 4
18. Ich bin überreizt 1 2 3 4
19. Ich bin froh 1 2 3 4
20. Ich bin vergnügt 1 2 3 4
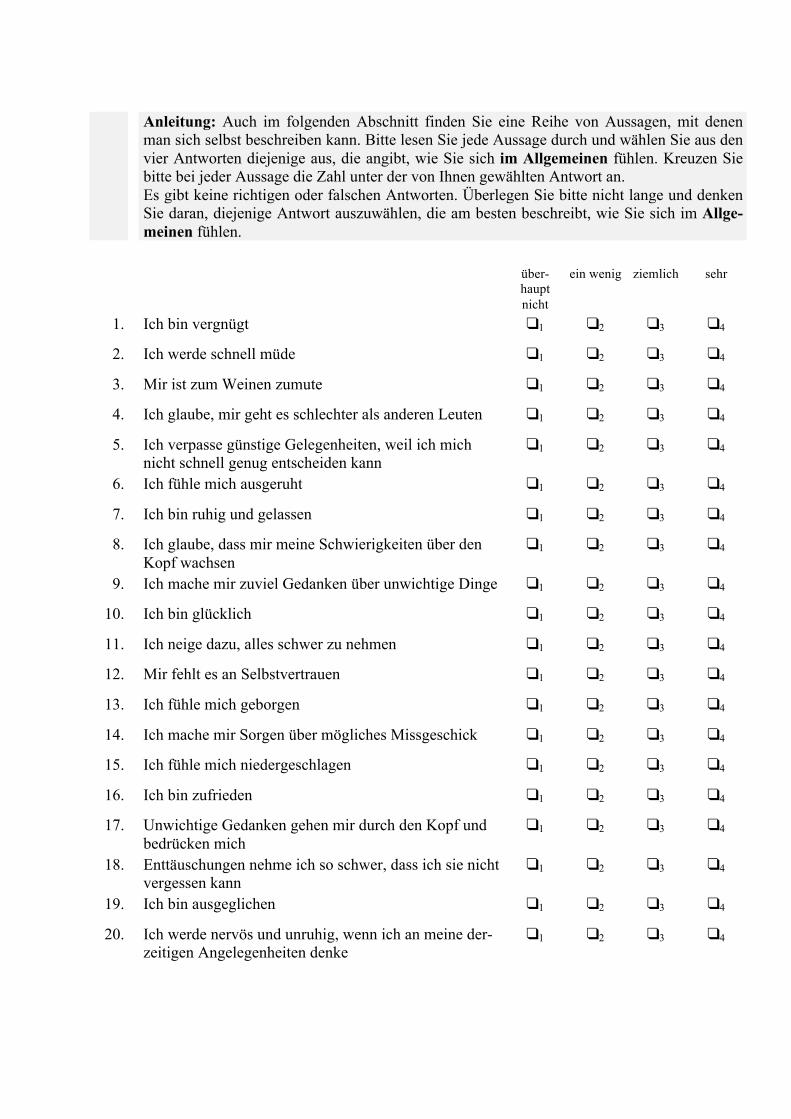
Anleitung: Auch im folgenden Abschnitt finden Sie eine Reihe von Aussagen, mit denen
man sich selbst beschreiben kann. Bitte lesen Sie jede Aussage durch und wählen Sie aus den vier Antworten diejenige aus, die angibt, wie Sie sich im Allgemeinen fühlen. Kreuzen Sie bitte bei jeder Aussage die Zahl unter der von Ihnen gewählten Antwort an. Es gibt keine richtigen oder falschen Antworten. Überlegen Sie bitte nicht lange und denken Sie daran, diejenige Antwort auszuwählen, die am besten beschreibt, wie Sie sich im Allge-meinen fühlen.
über-
haupt nicht
ein wenig ziemlich sehr
1. Ich bin vergnügt 1 2 3 4
2. Ich werde schnell müde 1 2 3 4
3. Mir ist zum Weinen zumute 1 2 3 4
4. Ich glaube, mir geht es schlechter als anderen Leuten 1 2 3 4
5. Ich verpasse günstige Gelegenheiten, weil ich mich nicht schnell genug entscheiden kann
1 2 3 4
6. Ich fühle mich ausgeruht 1 2 3 4
7. Ich bin ruhig und gelassen 1 2 3 4
8. Ich glaube, dass mir meine Schwierigkeiten über den Kopf wachsen
1 2 3 4
9. Ich mache mir zuviel Gedanken über unwichtige Dinge 1 2 3 4
10. Ich bin glücklich 1 2 3 4
11. Ich neige dazu, alles schwer zu nehmen 1 2 3 4
12. Mir fehlt es an Selbstvertrauen 1 2 3 4
13. Ich fühle mich geborgen 1 2 3 4
14. Ich mache mir Sorgen über mögliches Missgeschick 1 2 3 4
15. Ich fühle mich niedergeschlagen 1 2 3 4
16. Ich bin zufrieden 1 2 3 4
17. Unwichtige Gedanken gehen mir durch den Kopf und bedrücken mich
1 2 3 4
18. Enttäuschungen nehme ich so schwer, dass ich sie nicht vergessen kann
1 2 3 4
19. Ich bin ausgeglichen 1 2 3 4
20. Ich werde nervös und unruhig, wenn ich an meine der-zeitigen Angelegenheiten denke
1 2 3 4
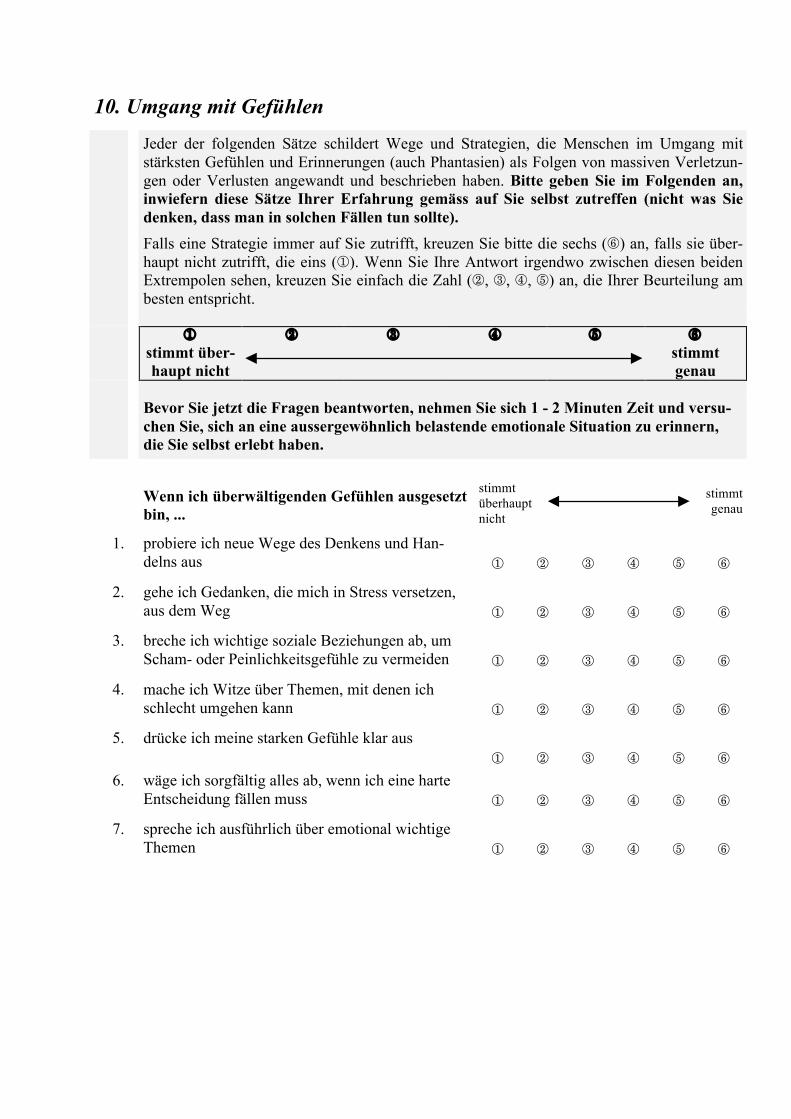
10. Umgang mit Gefühlen
Jeder der folgenden Sätze schildert Wege und Strategien, die Menschen im Umgang mit stärksten Gefühlen und Erinnerungen (auch Phantasien) als Folgen von massiven Verletzun-gen oder Verlusten angewandt und beschrieben haben. Bitte geben Sie im Folgenden an, inwiefern diese Sätze Ihrer Erfahrung gemäss auf Sie selbst zutreffen (nicht was Sie denken, dass man in solchen Fällen tun sollte). Falls eine Strategie immer auf Sie zutrifft, kreuzen Sie bitte die sechs () an, falls sie über-haupt nicht zutrifft, die eins (). Wenn Sie Ihre Antwort irgendwo zwischen diesen beiden Extrempolen sehen, kreuzen Sie einfach die Zahl (, , , ) an, die Ihrer Beurteilung am besten entspricht.
stimmt über-haupt nicht
stimmt genau
Bevor Sie jetzt die Fragen beantworten, nehmen Sie sich 1 - 2 Minuten Zeit und versu-
chen Sie, sich an eine aussergewöhnlich belastende emotionale Situation zu erinnern, die Sie selbst erlebt haben.
Wenn ich überwältigenden Gefühlen ausgesetzt
bin, ...
stimmt überhaupt nicht
stimmt genau
1. probiere ich neue Wege des Denkens und Han-delns aus
2. gehe ich Gedanken, die mich in Stress versetzen, aus dem Weg
3. breche ich wichtige soziale Beziehungen ab, um Scham- oder Peinlichkeitsgefühle zu vermeiden
4. mache ich Witze über Themen, mit denen ich schlecht umgehen kann
5. drücke ich meine starken Gefühle klar aus
6. wäge ich sorgfältig alles ab, wenn ich eine harte Entscheidung fällen muss
7. spreche ich ausführlich über emotional wichtige Themen
Wenn ich überwältigenden Gefühlen ausgesetzt bin, ...
stimmt überhaupt nicht
stimmt genau
8. reagiere ich übertrieben emotional
9. kann ich mich gut entscheiden, ob ich im Moment das Wohl der Gemeinschaft oder meine persönli-chen Bedürfnisse in den Vordergrund stelle
10. bin ich mir meiner Stärken und Schwächen be-wusst und fühle ich mich in den meisten Situatio-nen kompetent
11. weiss ich sowohl, wann ich mir wirklich Sorgen machen muss, als auch wann ich eine Sache auf sich beruhen lassen kann
12. spreche ich, wenn ich mit einem engen Freund / einer engen Freundin zusammen bin, über The-men, die sehr stressvoll für mich sind
13. habe ich die Nase schnell mal voll und breche eine Beziehung / Bekanntschaft ab, wenn mich was ärgert
14. lenke ich mich nach Möglichkeit ab, um schmerz-hafte Gefühle zu vermeiden
15. nehme ich Dinge falsch und verzerrt wahr oder verstehe, was andere meinen, nicht richtig
16. kann ich mich sowohl entspannen als auch harten Einsatz leisten
17. habe ich Beziehungen mit meinen wichtigen Be-zugspersonen, die von gegenseitigem Respekt und von Wertschätzung getragen sind.
18. vermische ich Gedanken und Erinnerungen aus der Vergangenheit mit der Gegenwart und mit Zu-kunftserwartungen
19. arbeite ich hart, gönne mir aber auch genügend Ruhe
Bitte tragen Sie den Ort auf der Linie ein, der meistens für Ihre aktuelle Situation passt.
1) Wie stark fühlen Sie sich durch negative Gefühle belastet?
gar nicht
0 % 100 %
mehr ist nichtmöglich
2) Wie stark sind Ihr Wohlbefinden und Ihre Ausgeglichenheit beeinträchtigt?
gar nicht
0 % 100 %
mehr ist nichtmöglich
Wenn ich überwältigenden Gefühlen ausgesetzt bin, ...
stimmt überhaupt nicht
stimmt genau
20. bin ich ruhelos und beschäftige mich ständig, da-mit keine unangenehmen Gefühle und Gedanken aufkommen
21. muss ich mich selbst und / oder andere ständig beobachten
22. fühle ich mich missverstanden und reagiere des-halb aggressiv auf andere
23. vermeide ich Spannungen, indem ich bestimmten sozialen Ereignissen aus dem Weg gehe
24. habe ich ein gutes Selbstvertrauen
25. entscheide ich sorgfältig, auch wenn die Situation komplex ist
26. kann ich ganz anderer Meinung sein als jemand anderes und dennoch diese Beziehung aufrechter-halten
11. Umsetzen von Zielen Anleitung
Sie finden nachstehend eine Liste von unterschiedlich angenehmen und unangenehmen Sachverhalten. Geben Sie bitte an, wie ausreichend Sie die eher angenehmen in der letz-ten Zeit umsetzen können (Teil 1) bzw. wie sehr die eher unangenehmen in der letzten Zeit für Sie zutreffen (Teil 2). Bitte lesen Sie jede Formulierung sorgfältig durch und kreuzen Sie daneben die zutref-fende Einschätzung von 1 bis 5 an. Überlegen Sie nicht erst, welche Antwort "den besten Eindruck" machen könnte, sondern antworten Sie so, wie es auf Sie persönlich zutrifft. Bitte lassen Sie keine Zeile aus!
Teil 1 In der letzten Zeit ... v i e l z u w e n i g v ö l l i g
1. bringe ich Leistung 1 2 3 4 5
2. bin ich unabhängig 1 2 3 4 5
3. glaube ich an mich selbst 1 2 3 4 5
4. habe ich meinen Platz in der Welt 1 2 3 4 5
5. habe ich viele Freunde 1 2 3 4 5
6. kann ich andere beeindrucken 1 2 3 4 5
7. werde ich geachtet und respektiert 1 2 3 4 5
8. gönne ich mir selber etwas 1 2 3 4 5
9. habe ich mich selber unter Kontrolle 1 2 3 4 5
10. lebe ich eine intime Beziehung 1 2 3 4 5
11. verfolge ich breite Interessen 1 2 3 4 5
12. fühle ich mich von anderen beschützt 1 2 3 4 5
13. setze ich mich für Schwächere ein 1 2 3 4 5
14. führe ich ein abwechslungsreiches Leben
1 2 3 4 5
Teil 2 In der letzten Zeit ... v i e l z u w e n i g v ö l l i g
15. bin ich Vorwürfen ausgesetzt
1 2 3 4 5
16. muss ich Schwächen von mir zeigen 1 2 3 4 5
17. kann ich nicht selbst bestimmen 1 2 3 4 5
18. werde ich von anderen nicht akzeptiert 1 2 3 4 5
19. fühle ich mich machtlos 1 2 3 4 5
20. blamiere ich mich 1 2 3 4 5
21. behandle ich andere aggressiv 1 2 3 4 5
22. fühle ich mich von anderen verlassen 1 2 3 4 5
23. genüge ich den Anforderungen nicht 1 2 3 4 5
Bitte tragen Sie den Ort auf der Linie ein, der meistens für Ihre aktuelle Situation passt.
7. Wie stark empfinden Sie Unsicherheit in Ihrer momentanen Lebenssi-
tuation?
gar nicht
0 % 100 %
mehr ist nichtmöglich
12. Rückmeldung War das Ausfüllen des Fragebogens für Sie ... (Zutreffendes bitte ankreuzen)
sehr belastend
ziemlich bela-stend
etwas bela-stend
unent-schieden
etwas entla-stend
ziemlich ent-lastend
sehr entla-stend
- 3 - 2 - 1 0 +1 + 2 + 3
Bemerkungen, bisher unerwähnte für Sie wichtige Themen:
....................................................................................................................................... ....................................................................................................................................... ....................................................................................................................................... ....................................................................................................................................... ....................................................................................................................................... ....................................................................................................................................... ....................................................................................................................................... ....................................................................................................................................... .......................................................................................................................................
Wir danken Ihnen ganz herzlich für Ihre wertvolle Mitarbeit!

Anhang B Feedback-Fragebogen zum Programm des Kinderwunsch Online Coachings
Feedback zum Kinderwunsch Online Coaching
Die folgenden Aussagen beziehen sich auf die Bewertung des Kinderwunsch Online Coa-chings. Hier gibt es fünf Antwortalternativen, wobei die Ziffern neben den Kästchen fol-gende Bedeutung haben: 1 = gar nicht einverstanden 2 = ein wenig einverstanden
3 = ziemlich einverstanden 4 = sehr einverstanden
5 = völlig einverstanden
gar nicht ein wenig
ziemlich sehr völlig
1. Ich habe dieses Coaching geschätzt. 1 2 3 4 5
2. Das Coaching war nützlich für mich. 1 2 3 4 5 3. Ich war zufrieden mit dem Coaching. 1 2 3 4 5
4. Das Coaching war geeignet für meine Schwierig-keiten.
1 2 3 4 5
5. Das Coaching entsprach den Erwartungen, welche ich von einem solchen Programm gehabt habe.
1 2 3 4 5
6. Das Coaching hat meine Schwierigkeiten und Belastungen im Zusammenhang mit dem Kinder-wunsch verringert.
1 2 3 4 5
7. Meine Belastungen durch den Kinderwunsch wurden durch das Coaching längerfristig verrin-gert.
1 2 3 4 5
8. Ich bin gewohnt das Internet zu gebrauchen, um mit anderen zu kommunizieren oder Lösungen für meine Probleme zu suchen.
1 2 3 4 5
9. Ich fühle mich durch die neuen Technologien an-gesprochen (Internet,...).
1 2 3 4 5
10. Rückblickend würde ich mich erneut für eine Un-terstützung per Internet entscheiden.
1 2 3 4 5
11. Ich hätte besser vom Programm profitieren kön-nen, wenn ich bessere Informatikkenntnisse ge-habt hätte.
1 2 3 4 5
gar nicht ein wenig
ziemlich sehr völlig
12. Ich fand die Nutzung des Programmes kompliziert. 1 2 3 4 5 13. Ich hatte Probleme mit meinem Internetzugang,
was mich davon abgehalten hat optimal vom Coa-ching zu profitieren.
1 2 3 4 5
14. Die Sitzungen des Programms waren zu kompli-ziert.
1 2 3 4 5
15. Ich habe die Nutzung der verschiedenen Sitzungen des Programms gut verstanden.
1 2 3 4 5
16. Ich fand es schwierig mich schriftlich auszudrüc-ken.
1 2 3 4 5
17. Ich war zufrieden mit der Art des Kontaktes mit der Therapeutin, welcher mir angeboten wurde.
1 2 3 4 5
18. Die wöchentlichen Feedbacks der Therapeutin waren hilfreich.
1 2 3 4 5
19. Die Foren zum Austausch mit anderen Betroffenen waren sehr hilfreich.
1 2 3 4 5
20.
Ich hätte mir gewünscht, noch mehr Zeit für das Coaching mit der Unterstützung der Therapeutin gehabt zu haben.
1 2 3 4 5
Bitte geben Sie an, wie Ihre Gesamtbewertung auf einer Skala von „sehr negativ“ bis zu „sehr positiv“ fürs Kinderwunsch Online Coaching ist. sehr
negativ negativ eher
positiv positiv sehr
positiv
21. Meine Gesamtbewertung des Kinderwunsch Onli-ne Coaching ist...
1 2 3 4 5
Weitere Bemerkungen: ....................................................................................................................................... ....................................................................................................................................... ....................................................................................................................................... .......................................................................................................................................

Anhang C Informations- und Anmeldeunterlagen des Kinderwunsch Online Coachings
Kinderwunsch Online Coaching: TeilnehmerInnen-Information
INFORMATION Kinderwunsch Online Coaching: Diese Studie ist ein Projekt vom Lehrstuhl für Klinische Psychologie und Psychotherapie an der Universität Bern und wird durch den Schweizerischen Nationalfond unterstützt. Die Studie wird durch Lic. phil. Katja Hämmerli, Prof. Dr. Hansjörg Znoj und Dr. Thomas Berger betreut. Ziel der Studie: Das Ziel der Studie ist es, die Wirksamkeit eines Online Coaching für Personen mit einem uner-füllten Kinderwunsch zu untersuchen. Die Wirksamkeit wird in Bezug auf das psychische Wohl-befinden und die Chancen auf eine Schwangerschaft überprüft. Erste Ergebnisse aus den USA zu Online-Interventionen bei ungewollt kinderlosen Paaren, weisen auf eine sehr gute Wirksamkeit hin. Ablauf der Studie: Das Kinderwunsch Online Coaching dauert 8 Wochen und der Aufwand pro Woche beträgt unge-fähr zwei Stunden. Das Coaching besteht aus verschiedenen thematischen Sitzungen, Austausch mit anderen Betroffenen in Form von Foren und E-Mail-Kontakt mit der Psychologin (K. Häm-merli). Die Sitzungen basieren auf bekannten und wirksamen Prinzipien bei der Behandlung von unerfülltem Kinderwunsch. Eine aktive Teilnahme Ihrerseits am Programm und deren Umsetzung in den Alltag sind notwendig. Während den 8 Wochen werden Sie einige Male von der Therapeu-tin per E-Mail kontaktiert. Sie werden gebeten zu drei Zeitpunkten einen Fragebogen auszufüllen: zu Beginn, nach 8 Wo-chen und nach 5 Monaten. Einteilung in zwei Gruppen: Wenn Sie sich für die Teilnahme an dieser Studie entschlossen haben, werden Sie zufällig in zwei Gruppen aufgeteilt. Durch diese zufällige Einteilung können Verfälschungen, welche die Resultate der Studie verzerren können, vermieden werden.
• Gruppe 1: Sofortiger Beginn mit dem Online Coaching • Gruppe 2: Beginn mit dem Online Coaching nach 2 Monaten
Auswahl der Studienteilnehmer: Personen, welche folgende Kriterien erfüllen, können zur Studie zugelassen werden: - Zugang zu einem PC mit Internetverbindung und E-Mailadresse - Älter als 18 Jahre - Seit mindestens 1 Jahr unter ungewollter Kinderlosigkeit leiden - Nicht bereits in psychotherapeutischer Behandlung sind - Unterzeichnete Einverständniserklärung und Überweisung von 50 Fr. - Motiviert und genügend Zeit die Übungen der Sitzungen zu machen und die Fragebögen auszu-füllen Risiken und Nutzen der Studie: - Risiken: Keine. Es sind keine negativen Effekte bei vergleichbaren Interventionen bekannt. Sie können jederzeit Ihre Teilnahme an der Studie widerrufen.
- Nutzen: Es gibt noch wenige Hinweise auf die Effektivität von Online Coaching bei unerfülltem Kinderwunsch, erste Ergebnisse sprechen jedoch für eine Wirksamkeit. Das Online Coaching kann möglicherweise Ihr Wohlbefinden oder sogar die Schwangerschaftsrate verbessern. Kosten für die Teilnahme: Die Teilnahme am Online Coaching ist gratis. Sie werden zu Beginn der Studie gebeten, 50 Fr. auf ein Konto zu überweisen. Diese 50 Fr. bekommen Sie zurück, wenn Sie die Studie beendet haben (nach dem Ausfüllen des 3. Fragebogens) und auch wenn Sie sich vorher entscheiden, nicht mehr an der Studie teilzunehmen. Die einzige Bedingung die 50 Fr. dann wieder zu bekommen ist, dass Sie alle drei Fragebogen ausfüllen. Das Ziel dieses Vorgehens ist es, dass wir möglichst alle notwendigen Informationen bekommen, um die Wirksamkeit des Coachings zu überprüfen und zu verbessern. Rückzug der Teilnahme: Ihre Teilnahme an dieser Studie ist freiwillig und Sie können sie zu jeder Zeit ohne jegliche Nachteile zurückziehen. Wir bitten Sie bei einem Rückzug Ihrer Teilnahme den dritten Fragebo-gen auszufüllen und uns kurz den Grund für Ihren Rückzug anzugeben. Vertraulichkeit der Angaben: In dieser Studie werden persönliche Angaben von Ihnen erfasst. Die Daten werden anonymisiert und sind nur Fachleuten zur wissenschaftlichen Auswertung zugänglich. Die Vertraulichkeit Ihrer Angaben ist während der ganzen Studie und nach Studienabschluss strikt gewährt. Die für das Programm verwendete Internetseite ist mit der SSL-Verbindung (dieselbe Technik wird von Ban-ken verwendet) gesichert. Sie werden zudem ein Pseudonym benutzen und ein Kennwort für den Zugang zum Programm erhalten. Kontaktperson Bei Fragen bezüglich der Studie wenden Sie sich bitte an die Projektleiterin: Lic. phil. Katja Hämmerli, Lehrstuhl für Klinische Psychologie und Psychotherapie, Universität Bern, Tel. +41 31 631 45 83 oder [email protected]
Kinderwunsch Online Coaching: Anmeldung und Ablauf
Anmeldung und Ablauf
Anmeldung und Ablauf des Kinderwunsch Online Coaching
1) TeilnehmerInnen-Information und Einverständniserklärung genau durchlesen
2) Ausgefüllten ersten Fragebogen und unterzeichnete Einverständniserklärung zurück-
schicken plus 50 Fr. (siehe beigelegter Einzahlungsschein) einzahlen
3) Nach Erhalt der oben aufgeführten Dinge, werden Sie per Mail benachrichtigt in welche
Gruppe Sie zufällig eingeteilt wurden:
Gruppe 1 (sofortiger Beginn des Coachings): Sie erhalten gleich den Benutzername und
das Passwort und können mit dem Coaching starten.
Gruppe 2 (Beginn nach 2 Monaten): Nach zwei Monaten erhalten Sie wie Gruppe 1 den
zweiten Fragebogen zugeschickt. Sobald Sie diesen ausgefüllt zurückgeschickt haben,
bekommen Sie den Benutzername und das Passwort und können mit dem Coaching
starten.
4) Nach zwei Monaten erhalten beiden Gruppen den zweiten Fragebogen. Bitte füllen Sie
diesen aus und senden Sie ihn uns zurück.
5) Nach fünf Monaten erhalten beide Gruppen den letzten Fragebogen. Füllen Sie auch die-
sen ebenfalls aus und schicken Sie ihn uns zurück.
6) Nachdem wir den letzten Fragebogen ausgefüllt erhalten haben, bekommen Sie die 50 Fr.
wieder zurück
Haben Sie noch Fragen?
Bei Fragen bezüglich der Studie können Sie sich gern an die Projektleiterin wenden:
Lic. phil. Katja Hämmerli, Lehrstuhl für Klinische Psychologie und Psychotherapie, Universität
Bern, Tel. +41 31 631 45 83 oder [email protected]
Kinderwunsch Online Coaching : Einverständniserklärung
Einverständniserklärung
- Ich bestätige hiermit, dass ich über die Ziele und den Ablauf der Studie informiert wurde
und die schriftlichen Informationen aufmerksam gelesen und verstanden habe. Meine Fra-
gen im Zusammenhang mit der Teilnahme wurden mir zufrieden stellend beantwortet.
- Ich hatte genügend Zeit, um meine Entscheidung zu treffen.
- Ich wurde über die Risiken und den Nutzen der Studie informiert und bin mir meiner Ver-
pflichtungen bei einer Teilnahme an der Studie bewusst.
- Ich wurde informiert, dass ich jederzeit meine freiwillige Teilnahme an der Studie ohne
jegliche Nachteile zurückziehen kann. Ich habe zur Kenntnis genommen, dass ich die ein-
gezahlten 50 Franken zu Beginn der Studie nach dem Zurücksenden des dritten Fragebo-
gens zurückerhalte.
- Alle meine Angaben werden vertraulich behandelt und die Resultate werden nur zu wis-
senschaftlichen Zwecken verwendet.
- Ich willige in die Publikation der Resultate dieser Studie unter der Bedingung der An-
onymität der Angaben und der Unmöglichkeit einer Identifikation ein.
- Bis zum Abschluss der Studie (nach Abgabe der 3. Fragebogenmessung) werde ich mich
in keine andere psychologische Behandlung begeben.
Der Unterzeichnende akzeptiert die Bedingungen der Studie und nimmt an der Studie teil.
Name, Vorname des Teilnehmers: Name der Studienleiterin:
Hämmerli Katja
Ort, Datum: Ort, Datum :
Bern,
Anhang D Kodierschema der qualitativen Inhaltsanalyse
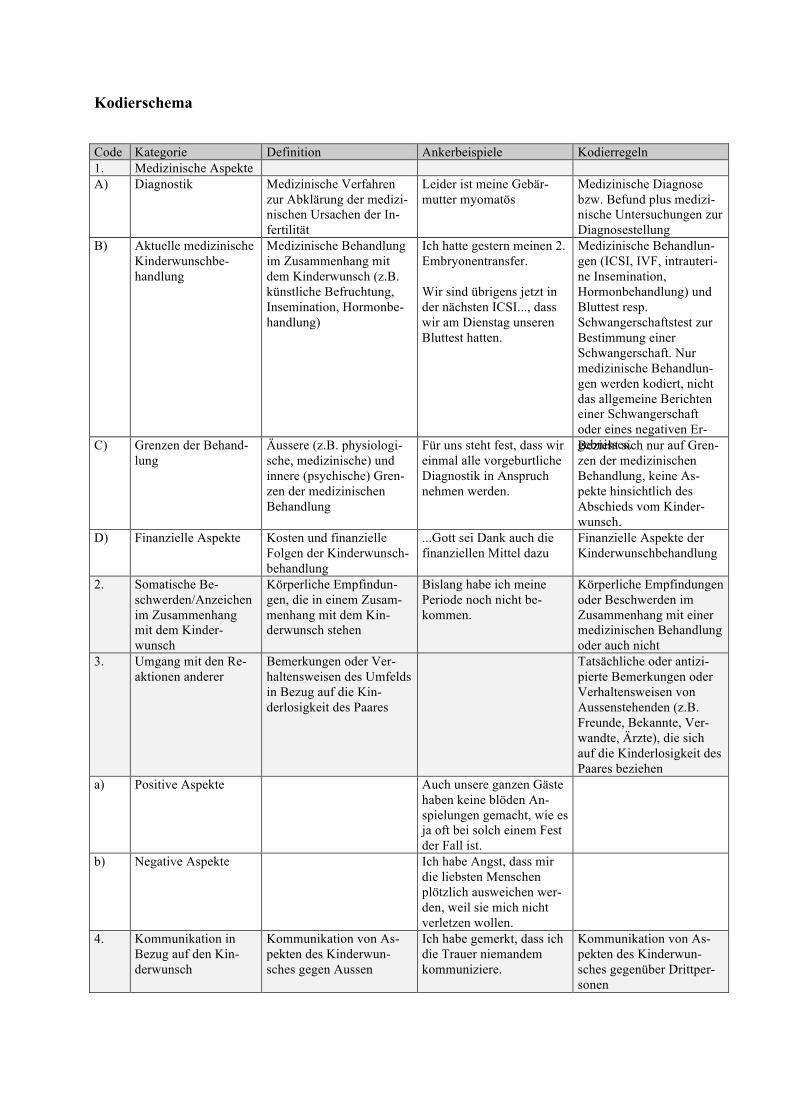
Kodierschema Code Kategorie Definition Ankerbeispiele Kodierregeln 1. Medizinische Aspekte A) Diagnostik Medizinische Verfahren
zur Abklärung der medizi-nischen Ursachen der In-fertilität
Leider ist meine Gebär-mutter myomatös
Medizinische Diagnose bzw. Befund plus medizi-nische Untersuchungen zur Diagnosestellung
B) Aktuelle medizinische Kinderwunschbe-handlung
Medizinische Behandlung im Zusammenhang mit dem Kinderwunsch (z.B. künstliche Befruchtung, Insemination, Hormonbe-handlung)
Ich hatte gestern meinen 2. Embryonentransfer. Wir sind übrigens jetzt in der nächsten ICSI..., dass wir am Dienstag unseren Bluttest hatten.
Medizinische Behandlun-gen (ICSI, IVF, intrauteri-ne Insemination, Hormonbehandlung) und Bluttest resp. Schwangerschaftstest zur Bestimmung einer Schwangerschaft. Nur medizinische Behandlun-gen werden kodiert, nicht das allgemeine Berichten einer Schwangerschaft oder eines negativen Er-gebnisses. C) Grenzen der Behand-
lung Äussere (z.B. physiologi-sche, medizinische) und innere (psychische) Gren-zen der medizinischen Behandlung
Für uns steht fest, dass wir einmal alle vorgeburtliche Diagnostik in Anspruch nehmen werden.
Bezieht sich nur auf Gren-zen der medizinischen Behandlung, keine As-pekte hinsichtlich des Abschieds vom Kinder-wunsch.
D) Finanzielle Aspekte Kosten und finanzielle Folgen der Kinderwunsch-behandlung
...Gott sei Dank auch die finanziellen Mittel dazu
Finanzielle Aspekte der Kinderwunschbehandlung
2. Somatische Be-schwerden/Anzeichen im Zusammenhang mit dem Kinder-wunsch
Körperliche Empfindun-gen, die in einem Zusam-menhang mit dem Kin-derwunsch stehen
Bislang habe ich meine Periode noch nicht be-kommen.
Körperliche Empfindungen oder Beschwerden im Zusammenhang mit einer medizinischen Behandlung oder auch nicht
3. Umgang mit den Re-aktionen anderer
Bemerkungen oder Ver-haltensweisen des Umfelds in Bezug auf die Kin-derlosigkeit des Paares
Tatsächliche oder antizi-pierte Bemerkungen oder Verhaltensweisen von Aussenstehenden (z.B. Freunde, Bekannte, Ver-wandte, Ärzte), die sich auf die Kinderlosigkeit des Paares beziehen
a) Positive Aspekte Auch unsere ganzen Gäste haben keine blöden An-spielungen gemacht, wie es ja oft bei solch einem Fest der Fall ist.
b) Negative Aspekte Ich habe Angst, dass mir die liebsten Menschen plötzlich ausweichen wer-den, weil sie mich nicht verletzen wollen.
4. Kommunikation in Bezug auf den Kin-derwunsch
Kommunikation von As-pekten des Kinderwun-sches gegen Aussen
Ich habe gemerkt, dass ich die Trauer niemandem kommuniziere.
Kommunikation von As-pekten des Kinderwun-sches gegenüber Drittper-sonen
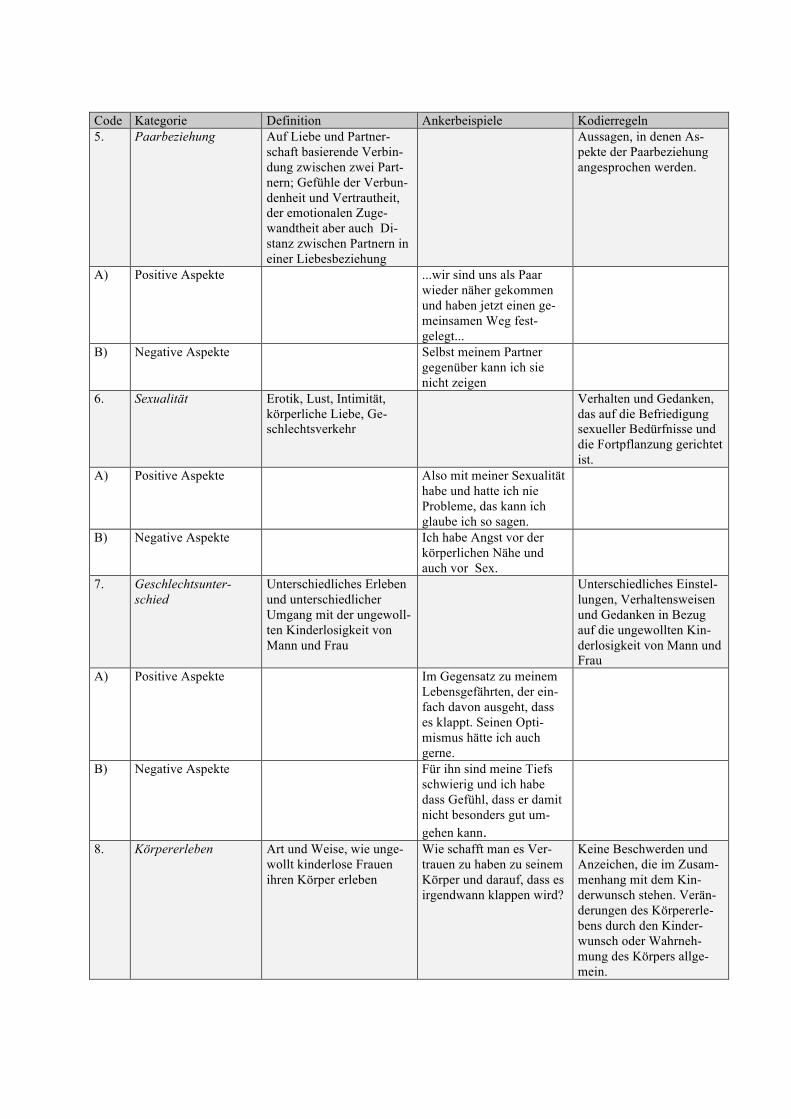
Code Kategorie Definition Ankerbeispiele Kodierregeln 5. Paarbeziehung Auf Liebe und Partner-
schaft basierende Verbin-dung zwischen zwei Part-nern; Gefühle der Verbun-denheit und Vertrautheit, der emotionalen Zuge-wandtheit aber auch Di-stanz zwischen Partnern in einer Liebesbeziehung
Aussagen, in denen As-pekte der Paarbeziehung angesprochen werden.
A) Positive Aspekte ...wir sind uns als Paar wieder näher gekommen und haben jetzt einen ge-meinsamen Weg fest-gelegt...
B) Negative Aspekte Selbst meinem Partner gegenüber kann ich sie nicht zeigen
6. Sexualität Erotik, Lust, Intimität, körperliche Liebe, Ge-schlechtsverkehr
Verhalten und Gedanken, das auf die Befriedigung sexueller Bedürfnisse und die Fortpflanzung gerichtet ist.
A) Positive Aspekte Also mit meiner Sexualität habe und hatte ich nie Probleme, das kann ich glaube ich so sagen.
B) Negative Aspekte Ich habe Angst vor der körperlichen Nähe und auch vor Sex.
7. Geschlechtsunter-schied
Unterschiedliches Erleben und unterschiedlicher Umgang mit der ungewoll-ten Kinderlosigkeit von Mann und Frau
Unterschiedliches Einstel-lungen, Verhaltensweisen und Gedanken in Bezug auf die ungewollten Kin-derlosigkeit von Mann und Frau
A) Positive Aspekte Im Gegensatz zu meinem Lebensgefährten, der ein-fach davon ausgeht, dass es klappt. Seinen Opti-mismus hätte ich auch gerne.
B) Negative Aspekte Für ihn sind meine Tiefs schwierig und ich habe dass Gefühl, dass er damit nicht besonders gut um-gehen kann.
8. Körpererleben Art und Weise, wie unge-wollt kinderlose Frauen ihren Körper erleben
Wie schafft man es Ver-trauen zu haben zu seinem Körper und darauf, dass es irgendwann klappen wird?
Keine Beschwerden und Anzeichen, die im Zusam-menhang mit dem Kin-derwunsch stehen. Verän-derungen des Körpererle-bens durch den Kinder-wunsch oder Wahrneh-mung des Körpers allge-mein.
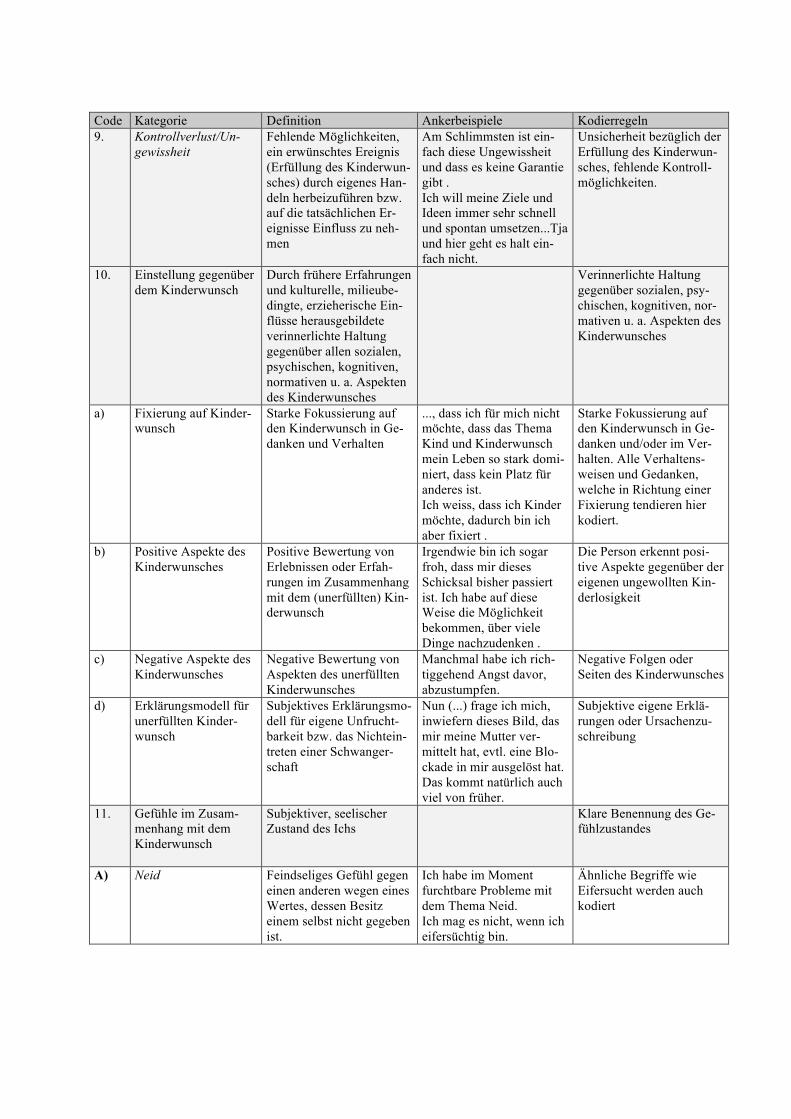
Code Kategorie Definition Ankerbeispiele Kodierregeln 9. Kontrollverlust/Un-
gewissheit Fehlende Möglichkeiten, ein erwünschtes Ereignis (Erfüllung des Kinderwun-sches) durch eigenes Han-deln herbeizuführen bzw. auf die tatsächlichen Er-eignisse Einfluss zu neh-men
Am Schlimmsten ist ein-fach diese Ungewissheit und dass es keine Garantie gibt . Ich will meine Ziele und Ideen immer sehr schnell und spontan umsetzen...Tja und hier geht es halt ein-fach nicht.
Unsicherheit bezüglich der Erfüllung des Kinderwun-sches, fehlende Kontroll-möglichkeiten.
10. Einstellung gegenüber dem Kinderwunsch
Durch frühere Erfahrungen und kulturelle, milieube-dingte, erzieherische Ein-flüsse herausgebildete verinnerlichte Haltung gegenüber allen sozialen, psychischen, kognitiven, normativen u. a. Aspekten des Kinderwunsches
Verinnerlichte Haltung gegenüber sozialen, psy-chischen, kognitiven, nor-mativen u. a. Aspekten des Kinderwunsches
a) Fixierung auf Kinder-wunsch
Starke Fokussierung auf den Kinderwunsch in Ge-danken und Verhalten
..., dass ich für mich nicht möchte, dass das Thema Kind und Kinderwunsch mein Leben so stark domi-niert, dass kein Platz für anderes ist. Ich weiss, dass ich Kinder möchte, dadurch bin ich aber fixiert .
Starke Fokussierung auf den Kinderwunsch in Ge-danken und/oder im Ver-halten. Alle Verhaltens-weisen und Gedanken, welche in Richtung einer Fixierung tendieren hier kodiert.
b) Positive Aspekte des Kinderwunsches
Positive Bewertung von Erlebnissen oder Erfah-rungen im Zusammenhang mit dem (unerfüllten) Kin-derwunsch
Irgendwie bin ich sogar froh, dass mir dieses Schicksal bisher passiert ist. Ich habe auf diese Weise die Möglichkeit bekommen, über viele Dinge nachzudenken .
Die Person erkennt posi-tive Aspekte gegenüber der eigenen ungewollten Kin-derlosigkeit
c) Negative Aspekte des Kinderwunsches
Negative Bewertung von Aspekten des unerfüllten Kinderwunsches
Manchmal habe ich rich-tiggehend Angst davor, abzustumpfen.
Negative Folgen oder Seiten des Kinderwunsches
d) Erklärungsmodell für unerfüllten Kinder-wunsch
Subjektives Erklärungsmo-dell für eigene Unfrucht-barkeit bzw. das Nichtein-treten einer Schwanger-schaft
Nun (...) frage ich mich, inwiefern dieses Bild, das mir meine Mutter ver-mittelt hat, evtl. eine Blo-ckade in mir ausgelöst hat. Das kommt natürlich auch viel von früher.
Subjektive eigene Erklä-rungen oder Ursachenzu-schreibung
11. Gefühle im Zusam-menhang mit dem Kinderwunsch
Subjektiver, seelischer Zustand des Ichs
Klare Benennung des Ge-fühlzustandes
A) Neid Feindseliges Gefühl gegen einen anderen wegen eines Wertes, dessen Besitz einem selbst nicht gegeben ist.
Ich habe im Moment furchtbare Probleme mit dem Thema Neid. Ich mag es nicht, wenn ich eifersüchtig bin.
Ähnliche Begriffe wie Eifersucht werden auch kodiert
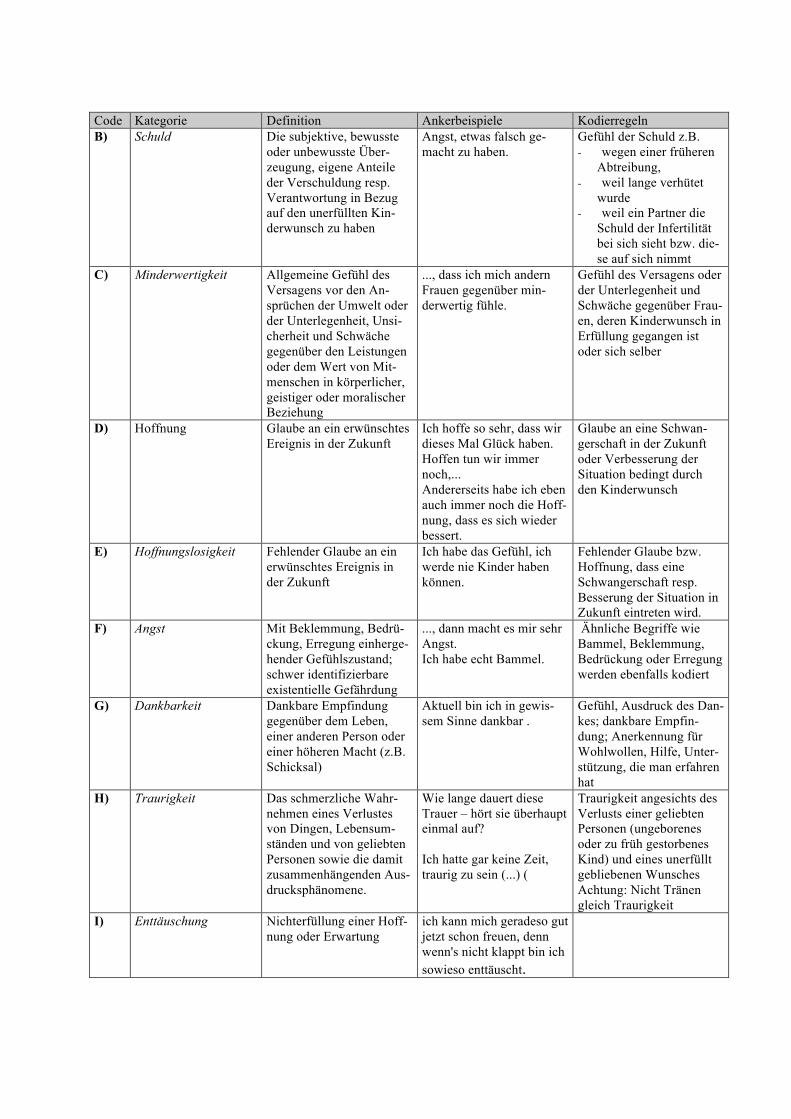
Code Kategorie Definition Ankerbeispiele Kodierregeln B) Schuld Die subjektive, bewusste
oder unbewusste Über-zeugung, eigene Anteile der Verschuldung resp. Verantwortung in Bezug auf den unerfüllten Kin-derwunsch zu haben
Angst, etwas falsch ge-macht zu haben.
Gefühl der Schuld z.B. - wegen einer früheren
Abtreibung, - weil lange verhütet
wurde - weil ein Partner die
Schuld der Infertilität bei sich sieht bzw. die-se auf sich nimmt
C) Minderwertigkeit Allgemeine Gefühl des Versagens vor den An-sprüchen der Umwelt oder der Unterlegenheit, Unsi-cherheit und Schwäche gegenüber den Leistungen oder dem Wert von Mit-menschen in körperlicher, geistiger oder moralischer Beziehung
..., dass ich mich andern Frauen gegenüber min-derwertig fühle.
Gefühl des Versagens oder der Unterlegenheit und Schwäche gegenüber Frau-en, deren Kinderwunsch in Erfüllung gegangen ist oder sich selber
D) Hoffnung Glaube an ein erwünschtes Ereignis in der Zukunft
Ich hoffe so sehr, dass wir dieses Mal Glück haben. Hoffen tun wir immer noch,... Andererseits habe ich eben auch immer noch die Hoff-nung, dass es sich wieder bessert.
Glaube an eine Schwan-gerschaft in der Zukunft oder Verbesserung der Situation bedingt durch den Kinderwunsch
E) Hoffnungslosigkeit Fehlender Glaube an ein erwünschtes Ereignis in der Zukunft
Ich habe das Gefühl, ich werde nie Kinder haben können.
Fehlender Glaube bzw. Hoffnung, dass eine Schwangerschaft resp. Besserung der Situation in Zukunft eintreten wird.
F) Angst Mit Beklemmung, Bedrü-ckung, Erregung einherge-hender Gefühlszustand; schwer identifizierbare existentielle Gefährdung
..., dann macht es mir sehr Angst. Ich habe echt Bammel.
Ähnliche Begriffe wie Bammel, Beklemmung, Bedrückung oder Erregung werden ebenfalls kodiert
G) Dankbarkeit Dankbare Empfindung gegenüber dem Leben, einer anderen Person oder einer höheren Macht (z.B. Schicksal)
Aktuell bin ich in gewis-sem Sinne dankbar .
Gefühl, Ausdruck des Dan-kes; dankbare Empfin-dung; Anerkennung für Wohlwollen, Hilfe, Unter-stützung, die man erfahren hat
H) Traurigkeit Das schmerzliche Wahr-nehmen eines Verlustes von Dingen, Lebensum-ständen und von geliebten Personen sowie die damit zusammenhängenden Aus-drucksphänomene.
Wie lange dauert diese Trauer – hört sie überhaupt einmal auf? Ich hatte gar keine Zeit, traurig zu sein (...) (
Traurigkeit angesichts des Verlusts einer geliebten Personen (ungeborenes oder zu früh gestorbenes Kind) und eines unerfüllt gebliebenen Wunsches Achtung: Nicht Tränen gleich Traurigkeit
I) Enttäuschung Nichterfüllung einer Hoff-nung oder Erwartung
ich kann mich geradeso gut jetzt schon freuen, denn wenn's nicht klappt bin ich sowieso enttäuscht.
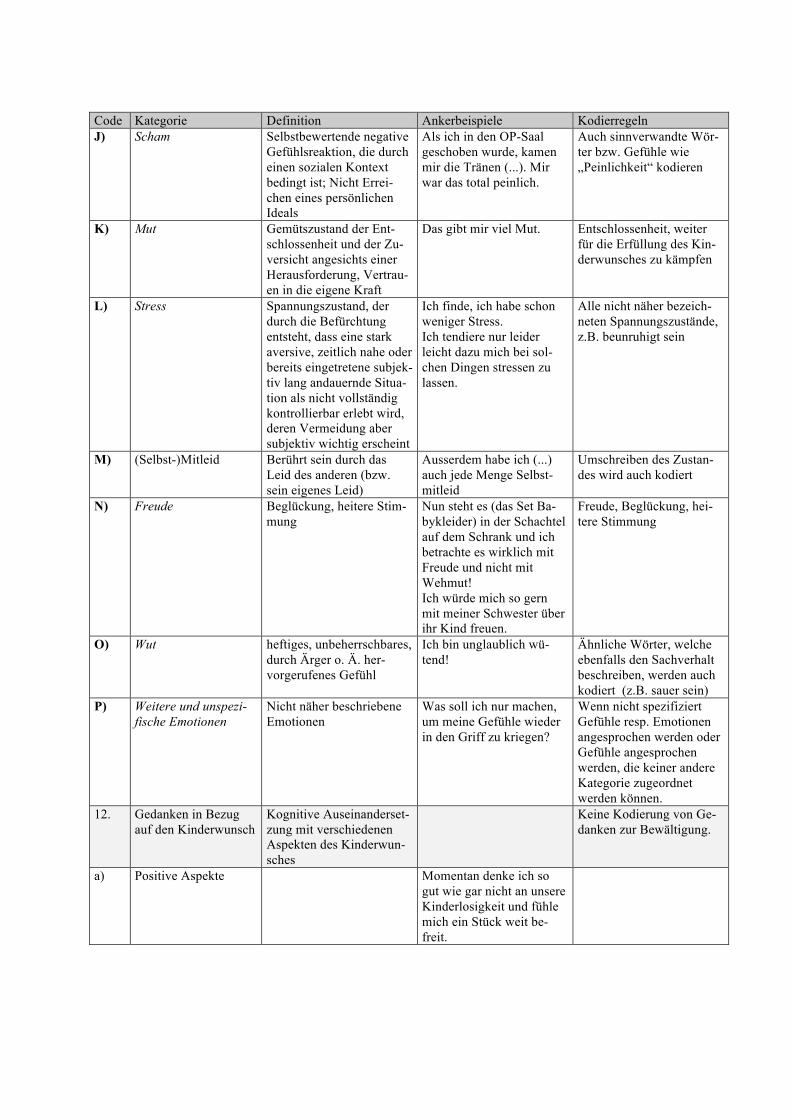
Code Kategorie Definition Ankerbeispiele Kodierregeln J) Scham Selbstbewertende negative
Gefühlsreaktion, die durch einen sozialen Kontext bedingt ist; Nicht Errei-chen eines persönlichen Ideals
Als ich in den OP-Saal geschoben wurde, kamen mir die Tränen (...). Mir war das total peinlich.
Auch sinnverwandte Wör-ter bzw. Gefühle wie „Peinlichkeit“ kodieren
K) Mut Gemütszustand der Ent-schlossenheit und der Zu-versicht angesichts einer Herausforderung, Vertrau-en in die eigene Kraft
Das gibt mir viel Mut. Entschlossenheit, weiter für die Erfüllung des Kin-derwunsches zu kämpfen
L) Stress Spannungszustand, der durch die Befürchtung entsteht, dass eine stark aversive, zeitlich nahe oder bereits eingetretene subjek-tiv lang andauernde Situa-tion als nicht vollständig kontrollierbar erlebt wird, deren Vermeidung aber subjektiv wichtig erscheint
Ich finde, ich habe schon weniger Stress. Ich tendiere nur leider leicht dazu mich bei sol-chen Dingen stressen zu lassen.
Alle nicht näher bezeich-neten Spannungszustände, z.B. beunruhigt sein
M) (Selbst-)Mitleid Berührt sein durch das Leid des anderen (bzw. sein eigenes Leid)
Ausserdem habe ich (...) auch jede Menge Selbst-mitleid
Umschreiben des Zustan-des wird auch kodiert
N) Freude Beglückung, heitere Stim-mung
Nun steht es (das Set Ba-bykleider) in der Schachtel auf dem Schrank und ich betrachte es wirklich mit Freude und nicht mit Wehmut! Ich würde mich so gern mit meiner Schwester über ihr Kind freuen.
Freude, Beglückung, hei-tere Stimmung
O) Wut heftiges, unbeherrschbares, durch Ärger o. Ä. her-vorgerufenes Gefühl
Ich bin unglaublich wü-tend!
Ähnliche Wörter, welche ebenfalls den Sachverhalt beschreiben, werden auch kodiert (z.B. sauer sein)
P) Weitere und unspezi-fische Emotionen
Nicht näher beschriebene Emotionen
Was soll ich nur machen, um meine Gefühle wieder in den Griff zu kriegen?
Wenn nicht spezifiziert Gefühle resp. Emotionen angesprochen werden oder Gefühle angesprochen werden, die keiner andere Kategorie zugeordnet werden können.
12. Gedanken in Bezug auf den Kinderwunsch
Kognitive Auseinanderset-zung mit verschiedenen Aspekten des Kinderwun-sches
Keine Kodierung von Ge-danken zur Bewältigung.
a) Positive Aspekte Momentan denke ich so gut wie gar nicht an unsere Kinderlosigkeit und fühle mich ein Stück weit be-freit.
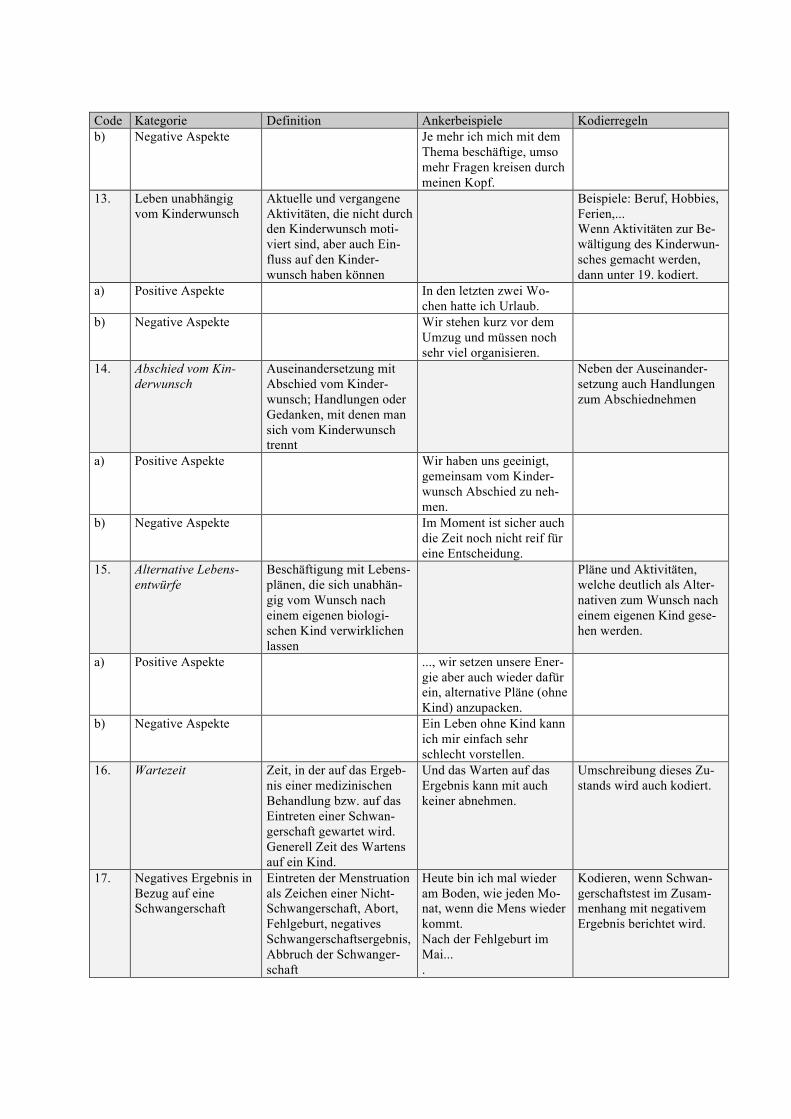
Code Kategorie Definition Ankerbeispiele Kodierregeln b) Negative Aspekte Je mehr ich mich mit dem
Thema beschäftige, umso mehr Fragen kreisen durch meinen Kopf.
13. Leben unabhängig vom Kinderwunsch
Aktuelle und vergangene Aktivitäten, die nicht durch den Kinderwunsch moti-viert sind, aber auch Ein-fluss auf den Kinder-wunsch haben können
Beispiele: Beruf, Hobbies, Ferien,... Wenn Aktivitäten zur Be-wältigung des Kinderwun-sches gemacht werden, dann unter 19. kodiert.
a) Positive Aspekte In den letzten zwei Wo-chen hatte ich Urlaub.
b) Negative Aspekte Wir stehen kurz vor dem Umzug und müssen noch sehr viel organisieren.
14. Abschied vom Kin-derwunsch
Auseinandersetzung mit Abschied vom Kinder-wunsch; Handlungen oder Gedanken, mit denen man sich vom Kinderwunsch trennt
Neben der Auseinander-setzung auch Handlungen zum Abschiednehmen
a) Positive Aspekte Wir haben uns geeinigt, gemeinsam vom Kinder-wunsch Abschied zu neh-men.
b) Negative Aspekte Im Moment ist sicher auch die Zeit noch nicht reif für eine Entscheidung.
15. Alternative Lebens-entwürfe
Beschäftigung mit Lebens-plänen, die sich unabhän-gig vom Wunsch nach einem eigenen biologi-schen Kind verwirklichen lassen
Pläne und Aktivitäten, welche deutlich als Alter-nativen zum Wunsch nach einem eigenen Kind gese-hen werden.
a) Positive Aspekte ..., wir setzen unsere Ener-gie aber auch wieder dafür ein, alternative Pläne (ohne Kind) anzupacken.
b) Negative Aspekte Ein Leben ohne Kind kann ich mir einfach sehr schlecht vorstellen.
16. Wartezeit Zeit, in der auf das Ergeb-nis einer medizinischen Behandlung bzw. auf das Eintreten einer Schwan-gerschaft gewartet wird. Generell Zeit des Wartens auf ein Kind.
Und das Warten auf das Ergebnis kann mit auch keiner abnehmen.
Umschreibung dieses Zu-stands wird auch kodiert.
17. Negatives Ergebnis in Bezug auf eine Schwangerschaft
Eintreten der Menstruation als Zeichen einer Nicht-Schwangerschaft, Abort, Fehlgeburt, negatives Schwangerschaftsergebnis, Abbruch der Schwanger-schaft
Heute bin ich mal wieder am Boden, wie jeden Mo-nat, wenn die Mens wieder kommt. Nach der Fehlgeburt im Mai... .
Kodieren, wenn Schwan-gerschaftstest im Zusam-menhang mit negativem Ergebnis berichtet wird.
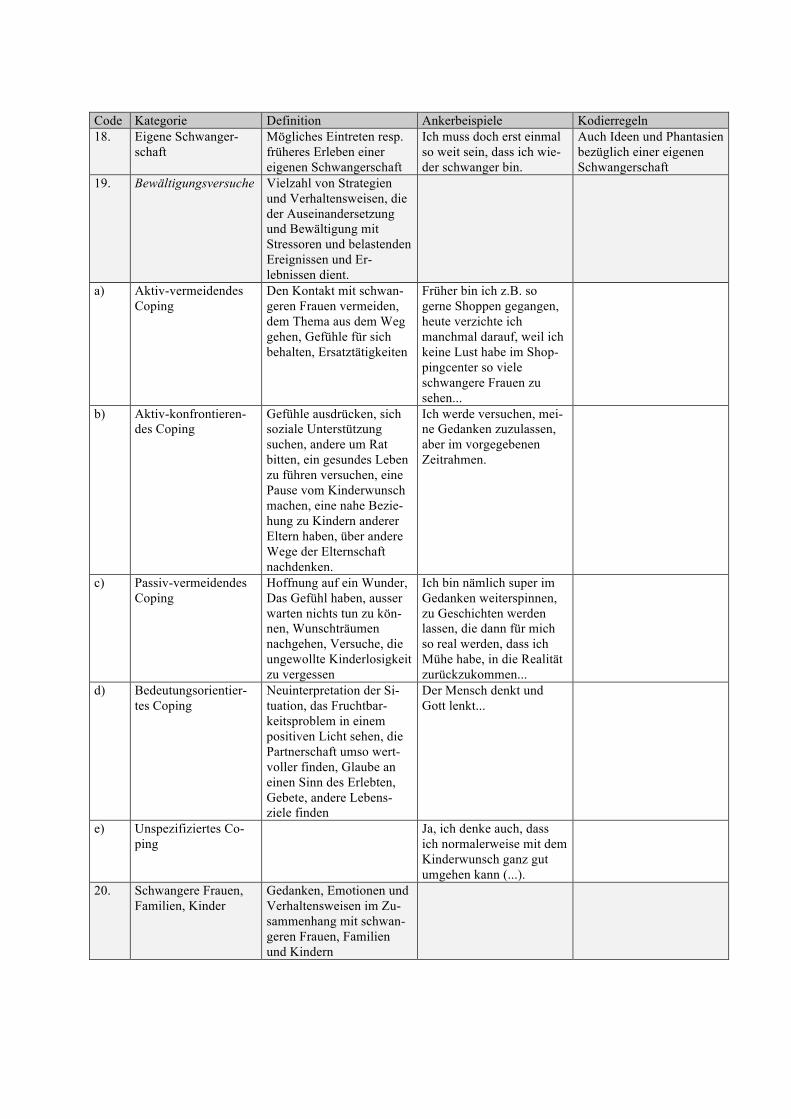
Code Kategorie Definition Ankerbeispiele Kodierregeln 18. Eigene Schwanger-
schaft Mögliches Eintreten resp. früheres Erleben einer eigenen Schwangerschaft
Ich muss doch erst einmal so weit sein, dass ich wie-der schwanger bin.
Auch Ideen und Phantasien bezüglich einer eigenen Schwangerschaft
19. Bewältigungsversuche Vielzahl von Strategien und Verhaltensweisen, die der Auseinandersetzung und Bewältigung mit Stressoren und belastenden Ereignissen und Er-lebnissen dient.
a) Aktiv-vermeidendes Coping
Den Kontakt mit schwan-geren Frauen vermeiden, dem Thema aus dem Weg gehen, Gefühle für sich behalten, Ersatztätigkeiten
Früher bin ich z.B. so gerne Shoppen gegangen, heute verzichte ich manchmal darauf, weil ich keine Lust habe im Shop-pingcenter so viele schwangere Frauen zu sehen...
b) Aktiv-konfrontieren-des Coping
Gefühle ausdrücken, sich soziale Unterstützung suchen, andere um Rat bitten, ein gesundes Leben zu führen versuchen, eine Pause vom Kinderwunsch machen, eine nahe Bezie-hung zu Kindern anderer Eltern haben, über andere Wege der Elternschaft nachdenken.
Ich werde versuchen, mei-ne Gedanken zuzulassen, aber im vorgegebenen Zeitrahmen.
c) Passiv-vermeidendes Coping
Hoffnung auf ein Wunder, Das Gefühl haben, ausser warten nichts tun zu kön-nen, Wunschträumen nachgehen, Versuche, die ungewollte Kinderlosigkeit zu vergessen
Ich bin nämlich super im Gedanken weiterspinnen, zu Geschichten werden lassen, die dann für mich so real werden, dass ich Mühe habe, in die Realität zurückzukommen...
d) Bedeutungsorientier-tes Coping
Neuinterpretation der Si-tuation, das Fruchtbar-keitsproblem in einem positiven Licht sehen, die Partnerschaft umso wert-voller finden, Glaube an einen Sinn des Erlebten, Gebete, andere Lebens-ziele finden
Der Mensch denkt und Gott lenkt...
e) Unspezifiziertes Co-ping
Ja, ich denke auch, dass ich normalerweise mit dem Kinderwunsch ganz gut umgehen kann (...).
20. Schwangere Frauen, Familien, Kinder
Gedanken, Emotionen und Verhaltensweisen im Zu-sammenhang mit schwan-geren Frauen, Familien und Kindern
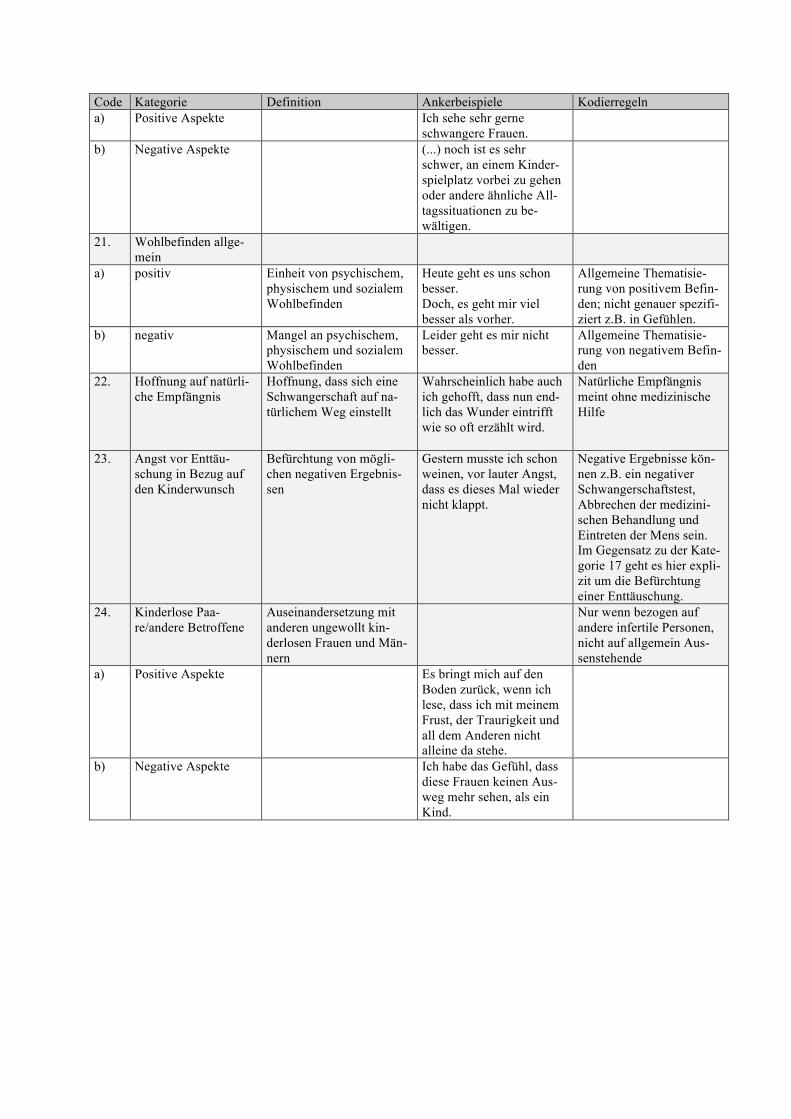
Code Kategorie Definition Ankerbeispiele Kodierregeln a) Positive Aspekte Ich sehe sehr gerne
schwangere Frauen.
b) Negative Aspekte (...) noch ist es sehr schwer, an einem Kinder-spielplatz vorbei zu gehen oder andere ähnliche All-tagssituationen zu be-wältigen.
21. Wohlbefinden allge-mein
a) positiv Einheit von psychischem, physischem und sozialem Wohlbefinden
Heute geht es uns schon besser. Doch, es geht mir viel besser als vorher.
Allgemeine Thematisie-rung von positivem Befin-den; nicht genauer spezifi-ziert z.B. in Gefühlen.
b) negativ Mangel an psychischem, physischem und sozialem Wohlbefinden
Leider geht es mir nicht besser.
Allgemeine Thematisie-rung von negativem Befin-den
22. Hoffnung auf natürli-che Empfängnis
Hoffnung, dass sich eine Schwangerschaft auf na-türlichem Weg einstellt
Wahrscheinlich habe auch ich gehofft, dass nun end-lich das Wunder eintrifft wie so oft erzählt wird.
Natürliche Empfängnis meint ohne medizinische Hilfe
23. Angst vor Enttäu-schung in Bezug auf den Kinderwunsch
Befürchtung von mögli-chen negativen Ergebnis-sen
Gestern musste ich schon weinen, vor lauter Angst, dass es dieses Mal wieder nicht klappt.
Negative Ergebnisse kön-nen z.B. ein negativer Schwangerschaftstest, Abbrechen der medizini-schen Behandlung und Eintreten der Mens sein. Im Gegensatz zu der Kate-gorie 17 geht es hier expli-zit um die Befürchtung einer Enttäuschung.
24. Kinderlose Paa-re/andere Betroffene
Auseinandersetzung mit anderen ungewollt kin-derlosen Frauen und Män-nern
Nur wenn bezogen auf andere infertile Personen, nicht auf allgemein Aus-senstehende
a) Positive Aspekte Es bringt mich auf den Boden zurück, wenn ich lese, dass ich mit meinem Frust, der Traurigkeit und all dem Anderen nicht alleine da stehe.
b) Negative Aspekte Ich habe das Gefühl, dass diese Frauen keinen Aus-weg mehr sehen, als ein Kind.

Anhang E Review of the manuscript „Internet-Based Support for Infertile Patients: A Randomized Con-
trolled Study“ from the Journal of Behavioral Medicine
Von: "Tracey Revenson" <[email protected]> Datum: 10. Juni 2009 18:20:18 GMT+02:00 An: [email protected] Betreff: Decision on your manuscript #JOBM672 RE: Internet-Based Support for Infertile Patients: A Randomized Controlled Study JOBM672 Dear Dr. Haemmerli: I have now received three expert reviews of your manuscript, and I have also read the paper carefully. The reviewers felt that the paper was interesting and was in an emerging area in behavioral medicine that deserves attention. At the same time, all three reviewers felt that flaws in the design of the study limited its contribution to the field. Based on the reviews and my own reading of the paper, I am inviting a major revision of the paper and resubmission of a manuscript that is shorter and that more accurately reports the findings, given the limitations of the design. All three reviewers give detailed yet different feedback on the manuscript, and I will not re-peat the specific issues here. I urge you to pay close attention to their specific critiques when revising. I will point out some of the central ones here and also add some of my own. All three reviewers felt that the manuscript could be more streamlined, without losing any detail. There was a good deal of redundancy in the writing (in fact, throughout the whole manu-script). Even with the additions requested by the reviewers, I would like the revised manu-script to be no more than 30 pages maximum. I am numbering the overall comments so that you can reply to them more easily in your cover letter. The first four are central to the acceptance of a revised manuscript. 1. The Results are written in a misleading manner and give the impression of more findings than there are. This may be my most serious problem with the manuscript. Given there are no group-x-time interactions, this needs to be said first and said briefly, without presenting all the effects that are non-significant. The group means can be presented in a table, but the message needs to be accurate: there were no group-x-time effects. 2. Reviewer 1 and myself both felt that the subgroup analyses starting on p. 13 - the analyses of change within the intervention group only -- were post-hoc and "gilding the lily", as these were not a prior hypotheses, were underpowered, and basically ignored the basic principles of an RCT. It is also unclear whether the cutoff score for the IDS and CES-D are valid for this particular population. There would need to be much more empirical justification for that. This section should be deleted, but you can raise this possibility (without data) in the discussion section. Similarly the delayed effects of the control group should be deleted as again, there are many threats to validity. 3. I had major concerns about the fact that 40 of the participants in the study were (20) mar-ried couples and thus, their data are not independent. Moreover, this affects analyses of gen-der. You may need to talk with a statistician about how to address these issues in data ana-lyses; it is complicated because only a subset of your participants are married to each other, but it seems that all the men are married to another participant. Please clarify this as well. Similarly, I was surprised that gender differences were not discussed in any way. And was
random assignment done stratifying for gender? How many couples ended up (together) in the intervention condition? This also could skew the effects. 4. There is some confusion about the intention-to-treat paradigm and handling missing data at post-test. They are separate statistical issues. Intention-to-treat involves including people who complete baseline but do not complete the intervention in the experimental group, but does not say that one should replace missing data at post-test. Moreover, there is some controversy over LOCF, and this should be addressed in the discussion section. 5. The first paragraph is inaccurate, given the findings of the RCT and not the post-hoc within-group change over time. The discussion is quite long, given the few RCT results. Once the changes in the results/analyses requested above are done, I think you will have an easy time cutting the discussion section. The section starting on page 20 goes off on a tan-gent; it should be 1-2 sentences, hypothesizing that such interventions may only be effective for those in distress, but again, you do not have valid data to support this, only a weak sugges-tion. You will need to come to a recommendation, based on your data, on whether an internet intervention is appropriate for everyone or just for those in high distress. As currently written, you are going in both directions. Subheadings in the discussion section would also help the reader follow, but use only 2-3. Other important issues raised by the reviewers: * The design issues raised by Reviewer 2 need to be addressed. Many of the additional details about the medical and clinical status of your intervention and control groups can be said quite briefly. * What was the race/ethnicity composition of your sample? This should be noted. * There needs to be more description of the intervention; for example, both Reviewers 2 and 3 ask about interaction with therapists which seems to be a key element of your interven-tion. Did the participants have and phone contact or was it exclusively by internet? All three reviewers' comments ask specific questions about this. * It is also not clear exactly what the controls were doing during their waiting time, and this is critical to making conclusions about the intervention's effects. Did any of the control participants have counseling or therapy? How much did they talk to others? Was this co-varied in your major analyses? * The alpha coefficient for the IDS scale was acceptable for research purposes but just barely. Did you factor it with your sample? From the items given, it sounds like there may be two subscales - one's own distress and relationship distress. * The section on adherence and acceptability of the intervention can be tightened and the additional information requested by Reviewer 3 added in a brief fashion. As internet therapy is fairly new, I am sure that JOBM readers would like to know how participants felt about it. As these reviewers' comments and this letter suggests, there is a fairly large amount of work to do on the paper, but we all feel that there is something very new and important to be said here. When preparing your revised manuscript, carefully consider both the issues raised in
this letter and the reviewer comments (which are attached) and submit a list of responses to the comments. Your responses should be uploaded as a file in addition to your revised manu-script. In addition, please highlight any changes in your revised text (e.g., using red font or your word processor's highlighting feature, but DO NOT retain tracking changes, only high-light) to allow for easy recognition of modifications. In order to submit your revised manuscript electronically, please access the following web site: http://jobm.edmgr.com/ Click login Your login is: Your username is: moonliner Your password is: Your password is: haemmerli28836 Click "Author Login" Click submissions waiting author's revision and proceed through the user friendly submission process. Please note that resubmitting a revised manuscript does not guarantee eventual acceptance for publication. It is likely that I will send the revised manuscript back to at least one of the origi-nal reviewers. Finally, if you do decide to revise and resubmit your paper, you must do so within 90 days or else it will be assumed to be withdrawn from further consideration by our automated computer system. I look forward to receiving your revised manuscript. Sincerely, Tracey A. Revenson, Ph.D. Associate Editor Journal of Behavioral Medicine COMMENTS FOR THE AUTHOR: Reviewer #1: Review - jobm672 Overall, this was an interesting study with design flaws. This is a timely study because we are of a generations that heavily uses web-based information and support. The aim of the study was to evaluate the efficacy of internet-based treatment for infertility. The goals were amiable, but the methods were flawed and conclusions felt to be a reach based on the results. Since a power analysis was done and the indicated number of participants were enrolled, the results need to be honored. The information obtained from the study was considerable and would add to the literature if the results were more concise and the discussion is made more succinct and aimed at what was found and how to avoid the pitfalls of this particular study. 1. Lines 46-50, This sentence was awkward to read because it seems that two important pieces of information are being introducing that do not flow together. I would recommend creating two separate sentences 2. Lines 76-77, There is such an emphasis on this being the only or first Germen language online treatment of its kind; I would suggest leading with or emphasizing the other variables that differentiate it from its Cousineau et al., 2008 predecessor. 3. Line 102, It would be helpful to understand how you ensured that the men or women were suffering from primary or secondary infertility for at least one year and what criteria you
used to identify infertility. 4. Line 112, Please add 'correspondence via postal service' as indicated on line 107. 5. Line 126, grammar, delete the word "with" from, "and four participants did not provide with any reason." 6. Lines 133-134, please start sentence with Eighty percent rather than 80%. Also, please indicate if this means that participants completed all three assessments and weather partici-pants were emailed or mailed questionnaires? 7. Lines 136-137, It is not clear why the five control participants that got pregnant in the course of the online coaching did not complete the questionnaires? 8. Lines 140-144, Please double check your numbers, they appear to be off by one, it adds up to 53 not 52. "Half" or 26 completed the entire guide 15 completed 50% 11 completed less than 50% 1 completed one session 9. Line 146, To be consistent I would recommend presenting the control group data in a consistent fashion, 18(44%) rather than just 44%. 10. Line 165, indicates that there are 13 sessions, but on line 142 there is an indication that the guide consists of 14 sessions, please clarify. 11. Line 201, Please be consistent with numbers, two and 13, (2 and 13 or second and last). 12. Lines 201-208, the content of this paragraph is somewhat confusing to me. It is not clear how someone anonymously publishing their personal experience is taking advantage of "collaborative elements" of the internet or "realizing therapeutic factors associated with group therapy in an individual setting." Please clarify. 13. Line 214, Would recommend changing "messages" to "queries" in order to be consistent with your previous language. 14. Lines 218-223, would suggest simplifying the paragraph by - starting with "There were three female therapists involved.." - deleting "on the one hand" and "on the other hand" - follow the identification of the "psychologist bearing a master's degree in clinical psy-chology" with her experience and supervisory role of the postgraduate students 15. Line 233, delete "used" 16. Line 235, would consider deleting the word "resultant." 17. Lines 246, 252, 302,306, 307, 312, 331, 335, 347, 354, 356, there are more in the rest of the manuscript and in the tables, I believe it should be IDS instead of IBS. 18. Lines 290-291, would suggest adding an "a" to as whole" or getting rid of "as whole" all together. 19. Line 308, I am not sure what Post-Post refers to. 20. Line 320, Paragraph - it appears that you are presenting results as if you intended to run them, but I believe they are post-hoc exploratory analysis and if so should be labeled as such. 21. Line 362, It is unclear how many control women became pregnant during the waiting period because you indicated that 4 on line 362, but 6 on line 127, please clarify. 22. Lines 401-402, suggest taking stats out of discussion. Reviewer #2: Overall, I think that you did a nice job trying to add to the existing intervention literature for this population. The literature suggests other factors regarding psychological adjustment to infertility are at play. See review by Dunkel-Schetter & Lobel (1991) regarding levels of distress in infertility patients.
In general, the authors did not examine or explore other explanations as to why these indi-viduals are not distressed by infertility (such as social desirability bias in reporting negative affect and optimism). Also, they fail to take examine other types of reproductive loss or fail-ure such as miscarriage or pregnancy or birth complications or seeking fertility treatment. Design: I am concerned about the self-selection of your population. I am not familiar with medical care in Switzerland and Germany. What is the ethnic, occupational, and financial diversity of those seeking fertility treatments? Were individuals or couples compensated for their participation? Were they given feedback as to which distress group they were in? Any differences between primary and secondary infertility? Intervention: The intervention seems novel but appears more psychoeducational than inter-ventional in nature. Please provide more detail and explanation of clarification-oriented therapy techniques. Also, please provide greater detail for use of systems therapy in relation to fertility treatment. In terms of the sessions, session 1 asks for any unrealistic expectations they may have about treatment. Was there any modification of those expectations or cogni-tive themes? We know from the literature that unrealistic expectations can also have a nega-tive impact on treatment. Were there any sessions geared toward communication between partners and communication with medical providers? What was the context of the communi-cation between therapist and participant? It would have been helpful to see examples of the webpages in the appendix. Results: The majority of your sample was female. What challenges did you face in recruiting men into the study? What was the demographical information on the types of treatments re-ceived by the sample (Non-ART vs. ART)? Your sample was relatively young in terms of infertility treatment (experiencing it for about 3 years). Is it possible that they have not ex-perienced as many failures as "longer in treatment" individuals and have less distress and per-haps more optimism? When you stated that your sample as a whole had high levels of mental distress, are you comparing them to the general population or another medical population? Was there any difference between the highly distressed group on any other variables? Were there any gender differences? Interestingly, 31% of your intervention group became pregnant prior to follow-up. What were the statistics for the control group for that same time period? The results indicate that your intervention may be clinically significant but not statistically significant. Do you think that if you had more variance in your sample that you may have a different result? Did you collect data on if individuals were in the middle of treatment or tak-ing a break? The status in treatment can affect distress in this population. Reviewer #3: Child Wish Online Coaching Manuscript Reviewer Comments for JoBM Given Jacky Boivin's findings that only a small proportion of fertility patients actually pursue face-to-face psychological support, developing online interventions is an important next step. Online interventions like this one allow patients to seek support privately, on their own terms, and are quite cost-effective. The authors' description of the efficacy of other psychological interventions (both face-to-face and Internet-based) in the Discussion section provided a rel-evant context for these results. Their use of effect sizes to communicate the clinical import-
ance of these results was also valuable. The intervention was able to produce clinically sig-nificant effects with no face-to-face therapist contact. Improvements were maintained over the 5 month FU period. The authors provide a good rationale for their failure to find multiple statistically significant differences (i.e., small sample size) and their failure to detect a preg-nancy benefit (i.e., short follow-up duration). The authors' choice to use a waiting list control group is a *significant* limitation. They should provide a clear explanation for their choice not to use an educational/attention-control group. General Comments: * It would have been interesting to include some measures of positive psychology (well-being, QOL, stress-related growth, positive states of mind). A future study, perhaps! * Given that group interventions are so helpful in reducing a sense of isolation, an ex-panded discussion of how participants used the online forums would be interesting. (What proportion and which type of patients posted responses to forums? How much discussion or chatting was then generated? How would therapists have moderated these discussions or intervened if content became inappropriate?) Include qualitative examples of comments posted. * What type of communication did participants have with therapists? Requests for help, expression of feelings etc? Can you give an example of the therapists' "brief, motivational messages"? What proportion of the participants wrote/did not write to therapists? * Authors should highlight that only 9 of 64 participants randomized to wait list control dropped out. I feared it would be higher. Line-by-Line Edits/Comments/Questions: * Line 49: Does the author mean that pregnancy rates among infertile pts have NOT been reported? If reported, what are the results? * Line 54: Add one sentence about the psychological benefits of psychological support. * Line 72: In what way are fertility clinic websites inadequate? Provide an example. * Line 79: The sentence beginning with "To Date, only a handful." seems out of place here. Since gender differences are relevant to the results you report later, add a short para-graph about gender differences in mental health outcomes and treatment responses earlier in the Introduction. * Line 126: delete the word "with" * Line 129: replace "According to" with "Following" * Line 140: Move this entire paragraph on proportion of the intervention completed to the very beginning of the Results Section. Combine with "Adherence and sessions completed" paragraph beginning on Line 369. * Line 198: replace "repetition" with "skills consolidation" * Line 199: replace "involves repeating" with "asks participants to repeat several of" * Line 247: replace "Here are some" with "Representative items include" * Line 323: rephrase to indicate that pts with high distress might benefit maximally from the intervention (it is not true that only high distress pts could benefit) * Line 366: Was the 31% pregnancy rate of intervention group participants higher or
lower than would be expected to occur clinically? Address this in the Discussion section. * Line 403: replace "results" with "between-group differences" * Line 404: reword sentence beginning "Another reason has to do with.". Suggestion: "The within-group improvements that were observed in the control group across all measures while on the waiting list attenuated between-group differences and therefore also helps to explain the nonsignificant group differences." * Line 407: add an S to "highlight" * Line 421: change "in all groups" to "in all treatment groups" * Line 434: Infertility is not a somatic problem (or cannot be reduced to just a somatic problem). This statement has the potential to offend. Further, Child Wish did not target in-fertility, but rather psychological issues. Omit this sentence altogether. * Line 440: delete "patients with" * Line 443: change to "revealed AT POST TREATMENT" * Line 444: Rephrase to: "In addition, WHEN COMPARING ALL PSYCHOLOGICAL MEASURES AT PRE-TREATMENT TO POST-TREATMENT, within-group effect sizes for this subsample of highly distressed and depressed participants were medium to large" (de-lete last 4 words) * Line 448: Delete this sentence. Rephrase to: "Restricting our overall sample to this highly distressed subsample reduced the statistical power in this analysis and may explain the failure to find significant differences." * Line 485: The first half of this paragraph seems unnecessary (the reader is likely to accept that fertility pts feel stress). Begin paragraph with "Assisted reproductive tx." on line 496. * Line 516: change "by" to "in" * Line 528: change "displayed lower" to "reported shorter" * Line 532: I'm unclear about the statement that the authors did not differentiate medical tx types. Does this mean that they did not differentiate between pts pursuing ART vs. those in earlier diagnostic phases? (Or between patients with ovulatory dysfunction vs. uterine/tubal factor vs. Unexplained infertility etc?) * Line 542: Rephrase sentence: "The main reason GIVEN BY PARTICIPANTS FOR not completing the whole program DELETE was that." * Line 549: change "information" to "psychological support"
Anhang F Curriculum vitae
Curriculum vitae
Hämmerli, Katja
Personal data
Date of birth: September 5, 1982
Nationality: Swiss
Education
1989-1995 Primary school
1995-2001 Secondary school
2001-2006 Licentiate (Psychology), University of Bern
2007-2009 PhD (Psychology), University of Bern
2007- Postgraduate training in psychotherapy, University of Bern
Research and Professional Experience
2007-2009 Scientific assistant, Department of Psychology (Prof. Dr. H. Znoj), Univer-
sity of Bern
Experiences in the Project of the Swiss National Science Foundation (grant
no. 325100 -11375411): Responsible for the executing the study, leading the
group psychotherapy, doing the data analyses and dissemination of results
(publications and presentations at conferences). Development of a manual
of psychological internet-based support for infertile patients. Planning and
executing the study about the internet-based treatment.
Clinical Employment
2007-2009 Group psychotherapy for infertile patients at the University Hospital of Bern
and Basel
2008- Outpatient psychotherapy, Department of Psychology, University of Bern
2009- Psychiatric internship, Private Psychiatric Hospital Wyss, Münchenbuchsee
University Teaching – Seminars
Winter ’07/08 Psychological therapy III (University of Bern)
Winter ‘08/09 Psychological therapy III (University of Bern)
Membership in Professional and Scientific Organisations
Since 2008 Society of Psychotherapy Research (SPR)
Since 2008 Federation of Swiss Psychologists (FSP)
Publications
Haemmerli, K., Znoj, H., Burri, S., Graf, P., Wunder, D., & Perrig-Chiello, P. (2008). Psy-
chological interventions for infertile patients: A review of existing research and a new com-
prehensive approach. Counselling and Psychotherapy Research, 8, 246-252.
Haemmerli, K., Znoj, H., & Barth, J. (2009). The Efficacy of Psychological Interventions for
Infertile Patients: A Meta-analysis Examining Mental Health and Pregnancy Rate. Human
Reproduction Update, 15, 279-295.
Haemmerli, K., Znoj, H., & Berger, T. (2009). Kinderwunsch Online Coaching ein webba-
siertes Selbsthilfeprogramm. Journal für Reproduktionsmedizin und Endokrinologie, 6, 111-
115.
Haemmerli, K, Znoj, H., Stoklas, C, Wunder, D., & Perrig-Chiello, P. (2009). How is Distress
from Infertility Associated with Depression? Geburtshilfe und Frauenheilkunde, 69, 533-536.
In press/submitted:
Haemmerli, K., Znoj, H., & Berger, T. (revised). Internet-based support for infertile patients:
a randomised controlled trial.
Haemmerli, K., Znoj, H., & Berger, T. (submitted). What are the issues infertile women are
dealing with?: A qualitative approach.
Haemmerli, K., Znoj, H., & Barth, J. (submitted). Psychological interventions for infertile
couples: Does gender matter?
Congress Papers and Posters:
Haemmerli, K., Znoj, H., & Barth, J. (2008). Die Wirksamkeit psychologischer Interventio-
nen bei infertilen Patienten auf das psychische Befinden und die Schwangerschaftsrate. Paper
presented at the congress of DGMP and DGMS, Jena, Germany.
Haemmerli, K., Znoj, H., & Berger, T. (2009). Child Wish Online Coaching: Efficacy of the
first German-language Internet-based treatment for infertile patients. Poster presented at the 6.
workshop congress for Clinical Psychology and Psychotherapy of the German society for
psychology, Zuerich, Switzerland.
Haemmerli, K., Znoj, H., & Berger, T. (2009). Internet-based support for infertile patients: a
randomised controlled trial. Paper presented at the congress of 40th SPR International Meet-
ing, Santiago, Chile, America.





























