Embed Size (px)
Citation preview

NICHD | June 2021
~ , Eunice Kennedy Shriver National Institute IIMlf'./ of Child Health and Human Development
Healthy pregnancies. Healthy children. Healthy and optimal lives.
Promoting Data Harmonization to Accelerate COVID-19 Pediatric Research

I EXECUTIVE SUMMARY Research to understand the impact of the SARS-CoV-2 virus and the COVID-19 pandemic on children is rapidly evolving even though there is a relatively low rate of children hospitalized with severe acute COVID-19 or multisystem inflammatory syndrome in children (MIS-C). Data harmonization is a key strategy to accelerate research on these relatively rare outcomes for which individual studies may be underpowered. Robust data on the physical and mental health of children during and after the pandemic are essential to accelerate our under-standing of the impact of the pandemic and the SARS-CoV-2 virus on children and their immediate and long-term health care needs.
The National Institutes of Health (NIH) convened a Working Group of scientific investigators and representa-tives from partner federal agencies to develop recommendations for common data elements (CDEs) that could be used for studies researching COVID-19 in pediatric participants defined as less than 21 years of age (“chil-dren” will be herein used to describe infants, children, and adolescents). While the NIH defines children as persons under the age of 18, this guidance includes ages 0-21 years because the MIS-C case definition includes ages 0-21.
This report details the approach, efforts, and recommendations of the Working Group. To facilitate the process, the Working Group was divided into two sub-groups: the Biomedical and the Psychosocial/Mental Health/Be-havioral (herein referred to as the “Psychosocial”) Working Groups. These two Pediatric COVID-19 CDE Work-ing Groups operated in parallel through a modified Delphi approach to select and prioritize an inventory of over 600 possible constructs to approximately 100 constructs, and subsequently identified measures or items for each construct.
The recommended CDEs and associated measures are intended for use by any COVID-19 study that includes children. This document should be considered a living document, as more information on the effect of the virus and the pandemic on children becomes available. We strongly recommend researchers include these measures in their studies to maximize the potential for data harmonization while continuing to advance their own study goals. The full set of recommended measures for this effort is available publicly on the NIH Public Health Emergency and Disaster Research Response (DR2) website.
NIH | June 2021 2

~ Common Biomedical Data Common Psychosocial Data Elements and Measures Elements and Measures
Common Biomedical data elements and measures aim to accelerate our understanding of the clinical course of COVID-19 and its effects on children, which will continue to evolve as treatments and vaccines become available. The Biomedical Working Group recommended 49 CDEs across eight domains, which included:
Baseline Child Health Manifestations: Clinical Manifestations: Laboratory
Diagnosis
Manifestations: Cardiopulmonary Diagnostic Assessment Manifestations: Imaging
Treatment Outcomes
+ + +
+
+ + + +
Common Psychosocial1 data elements and measures aim to accelerate our understanding of the psychological, mental health, and social impacts of the virus and the pandemic more broadly on children, which will continue to evolve as society continues to adjust to different phases of the pandemic. The Psychosocial Working Group recommended a total of 50 CDEs across ten domains, which included:
+ Social Determinants of Health + Educational Factors + Community, Family, and Peer Factors + Social Media/Screen Time + Well-being Factors + COVID-19 Stress and Worry + COVID-19 Attitudes, Behaviors and
Experiences + Health-related Behaviors + Mental and Behavioral Health + Health Care
Refer to Key Findings: Biomedical Working Refer to Key Findings: Psychosocial Working Group for additional information. Group for additional information.
Three Domains
Three domains were discussed by both groups:
Demographics (7 elements) Disability/Functional Status (4 elements) Underlying Health Conditions/Health History Prior to Pandemic (1 element)
+ + +
1 For organization of expertise and content, mental health and substance use/abuse are included under the Psychosocial Working Group, although we recognize mental health and substance use/abuse each have biomedical components.
NIH | June 2021 3

I CONTRIBUTORS
FEDERAL PARTNERS* + National Institutes of Health (NIH) + Centers for Disease Control and Prevention (CDC) + Health Resources and Services Administration (HRSA)
COHORTS AND PROGRAMS* + PreVAIL kIds
+ Identifying Biomarker Signatures of Prognostic Value for Multisystem Inflammatory Syndrome in Children (MIS-C)
+ Severity Predictors Integrating Salivary Transcriptomics and Proteomics with Multi Neural Network Intelligence in SARS-CoV-2 Infection in Children (SPITS MISC)
+ COVID-19 Network of Networks Expanding Clinical and Translational Approaches to Predict Severe Illness in Children (CONNECT to Predict Sick Children)
+ Diagnosis of MIS-C in Febrile Children
+ AICORE-kids: Artificial Intelligence COVID-19 Risk AssEssment for kids Identifying Biomarker Signatures of Prognostic Value for Multisystem Inflammatory Syndrome in Children (MIS-C)
+ CARING for Children with COVID
+ Long-Term Outcomes after the Multisystem Inflammatory Syndrome In Children (MUSIC) + Pediatric Research Immune Network on SARS-CoV-2 and MIS-C (PRISM) + Pharmacokinetics, Pharmacodynamics, and Safety Profile of Understudied Drugs
Administered to Children per Standard of Care (POP02)
+ Environmental influences on Child Health Outcomes (ECHO) + Adolescent Brain Cognitive DevelopmentSM Study (ABCD Study®) + National Survey of Children’s Health (NSCH) + National COVID Cohort Collaborative (N3C) + Global Consortium to Study Neurological Dysfunction in COVID-19 (GCS NeuroCOVID) + St. Jude Pediatric COVID-19 U.S. Registry
* The conclusions, findings, and opinions expressed by the contributors do not necessarily reflect the official positions of the NIH, CDC, HRSA, and the Contributing Cohorts and Programs. Rather, the organizations are included simply to highlight their contributions to the process by submitting materials such as case report forms (CRFs) and questionnaires, and providing expertise.
NIH | June 2021 4

Full List of Contributors:
BIOMEDICAL
Aruna Natarajan, NHLBI **
Bob Tamburro, NICHD **
Allison Heath, Children’s Hospital of Philadelphia
Ananth Annapragada, Baylor College of Medicine (PreVAIL kIds)
Andrew Atz, Medical University of South Carolina (ECHO, CARING for Children) †
Angela Campbell, CDC
Audrey Odom John, Children’s Hospital of Philadelphia (PreVAIL kIds)†
Bill Kapogiannis, NICHD (PreVAIL kIds)
Chi Hornick, Duke Pediatric Critical Care Clinical Research (CARING for Children)
Gabriela Maron, St. Jude Children’s Research Hospital (Pediatric COVID-19 U.S. Registry)†
Gina Montealegre, NIAID†
Hannah Calkins, Children’s Hospital of Pennsylvania
Katherine Herbst, Connecticut Children’s Medical Center (PreVAIL kIds)
Liz Amos, NLM
Mary Beth Son, Boston Children’s Hospital†
Matthew Oster, Children’s Healthcare of Atlanta, Emory University School of Medicine, CDC (CARING for Children)†
Michael Cabana, Albert Einstein College of Medicine†
Nina Schor, NINDS
Perdita Taylor-Zapata, NICHD (CARING for Children)
Ravinder Anand, The Emmes Company, LLC (CARING for Children)
Sai Majji , NICHD (PreVAIL kIds)
Steve Webber, Vanderbilt University Medical Center (CARING for Children)
Tellen D. Bennett, University of Colorado School of Medicine (N3C)
Usha Sethuraman, Children’s Hospital of Michigan, Central Michigan University (PreVAIL kIds)
Voula Osganian, NIDDK
PSYCHOSOCIAL Shelli Avenevoli, NIMH **
Bob Tamburro, NICHD **
Brett Miller, NICHD
Christina Park, NIH OD (ECHO)
Courtney K. Blackwell, Northwestern University (ECHO)
Dara Blachman-Demner, NIH OD OBSSR
Elizabeth A. Hoffman, NIDA (ABCD Study®)
Emilia (Emily) Koumans, CDC
Emily D’ Agostino, Duke University
Ericka L. Fink, UPMC Children’s Hospital of Pittsburgh (GCS NeuroCOVID)† Jenae M. Neiderhiser, Penn State University (ECHO)
Jon (Mike) Underwood, CDC
Kaja LeWinn, University of California San Francisco (ECHO)
Lawrence Kleinman, Robert Wood Johnson Medical School (PreVAIL kids) Layla Esposito, NICHD
Michael Kogan, HRSA (NSCH)
Rebecca Hommer, NINDS
Rosalind King, NICHD
Samantha Calabrese, NICHD
Sharon Saydah, CDC
** Indicates co-leads of Pediatric COVID-19 CDE Working Groups. † Indicates participation in the NIH Workshop on Post-acute Sequelae of COVID-19
NIH | June 2021 5

Acknowledgements
Pregnancy CDE + Caroline Signore, NICHD (Project Mentor)
RADxUP + Warren Kibbe, Duke University
RADx Data Coordinating Center (DCC) + Kirk Roberts, UTHealth School of Biomedical Informatics + Peter Rose, UC San Diego
ABCD Study® + Gaya Dowling, NIDA
Pediatric Working Group of the International epidemiology Databases to Evaluate AIDS (IeDEA) Consortium + Rachel Vreeman, Icahn School of Medicine at Mount Sinai
CONNECTS + Josh Fessel, NHLBI
CDE Coordination + Lisa Federer, NLM
Deloitte + Mathini Vaikunthan (Project Coordinator) + Karthika Haridas + Corinne Hausmann
NIH | June 2021 6

I INTRODUCTION Research to understand the impact of COVID-19 and the effect of the pandemic on children is rapidly advanc-ing. As multiple NIH initiatives to study multisystem inflammatory syndrome in children (MIS-C), post-acute sequelae of COVID-19 (PASC), and Return to School were in development, NIH identified several pediatric studies to participate in a data harmonization effort to address the full spectrum of SARS-CoV-2 viral illness in children. Although COVID-19 tends to be a milder disease in most children compared to adults, the spectrum of disease in children is variable ranging from asymptomatic or only mildly affected individuals to those with severe MIS-C. Moreover, the long-term sequelae of SARS-CoV-2 illness in children as well as the effects of the pan-demic itself are only just beginning to be discerned with reports of long-standing debilitating physical and mental health issues. The scope of this initiative is broad: to create a set of common data elements (CDEs) that can be used to assess all aspects of COVID-19 illness in children including acute SARS-CoV-2 infection, MIS-C, and PASC and to encompass the physical, biological, psychological, behavioral, and social factors associated with the virus and the pandemic. Given the relative paucity of specific outcomes in children (e.g., PASC, MIS-C), such harmonization may be pivotal in filling existing knowledge gaps and accelerating progress in addressing the unique health care needs of children during and after the COVID-19 pandemic.
To address this broad task with the necessary scope of expertise, representatives from multiple NIH Institutes and partner federal agencies in conjunction with intramural and extramural investigators convened to develop recommendations for a set of common Biomedical and Psychosocial data elements and measures that, when combined across datasets, may improve our collective understanding of COVID-19 in children. These efforts complement other data harmonization efforts across the NIH. These CDEs and associated measures are recom-mended for use in any COVID-19 study that includes children. Similar to other NIH CDE efforts, a two-tiered approach was used to stratify the recommended CDEs and associated measures for both biomedical and psychosocial-specific studies.
TIER 1 TIER 2
Highly recommended CDEs for all COVID-19 Recommended CDEs for collecting additional studies that include pediatric populations. information for COVID-19 studies that include
pediatric populations. Although Tier 2 measures are highly encouraged, they may pose additional participant or investigator burden that may not be feasible for all studies.
These items and further guidance are described in the Key Findings section below.
NIH | June 2021 7

TIER 1 TIER 2
I APPROACH The two Working Groups (Biomedical and Psychosocial) utilized a modified Delphi approach to: 1) understand the landscape of current and planned COVID-19 research in children; 2) define key scientific questions; 3) prioritize data elements and organize within domains to address key research questions; and 4) define recom-mended common measures using validated measures when possible. The Working Group followed the process outlined in the partner CDE project for Pregnancy (Recommendations for Common Data Elements for COVID-19 Studies Including Pregnant Participants) as delineated here:
Conducted Landscape Analysis: + Collected available Case Report Forms (CRFs), instruments, and protocols from a total
of 42 studies/guidance to better understand the landscape of current and planned COVID-19 research in children. The Group also surveyed existing COVID-19 CDE efforts such as NHLBI CONNECTS, RADxUP, NICHD Pregnancy, and the NIH Clinical Data Coordination Group.
+ Reviewed and catalogued publicly available instruments from sites such as DR2 and PhenX, including validated measures, to understand the broader COVID-19 research landscape both for children and in general.
+ Assessed existing literature regarding the effect of COVID-19 on children to inform later prioritization and research categories.
Defined Key Scientific Questions: + Reviewed existing literature on multidisciplinary research priorities to understand gaps
and create an initial list of scientific questions regarding the effects of SARS-CoV-2 infection and the COVID-19 pandemic on children.
+ Prioritized key scientific questions through a series of discussions based on Working Group member expertise, experience in the field, participation in planning extramural COVID-19 and pediatric studies, published literature, and understanding of the current COVID-19 pediatric research landscape.
Prioritized Data Elements: + Created inventories of data elements (spreadsheets) based on landscape analyses to
identify commonalities and gaps across studies in the field as well as across the Biomedical and Psychosocial inventories.
+ Categorized data elements into domains. + Prioritized domains and CDEs through an iterative, modified Delphi approach to
identify the approximately 50 top data elements per each of the two Working Groups. + Stratified CDEs into two tiers and categorized CDEs within each tier.
NIH | June 2021 8
TIER 1 TIER 2
Defined Data Measures: + Identified potential measures for each Tier 1 and Tier 2 data element based on
existing CRFs, CDEs, tools and questionnaires collected during the landscape analyses, and relevant validated measures from other non-COVID and non-pediatric-specific studies.
+ Prioritized measures through several rounds of review to identify recommended measures for each Tier 1 and Tier 2 data element. A hierarchical approach was used to select measures, with top preference for: 1) known, validated pediatric instruments, followed by 2) measures from COVID-19 studies already in the field, 3) modified versions of existing validated measures, and 4) measures developed by the Working Group(s). Only open-access, publicly available measures were considered.
+ Specified Parent-Self Report, Parent Report About Child, or Child-Self Report for measures obtained via questionnaire. Specified age groups whenever possible.
NIH | June 2021 9

<. <.
KEY FINDINGS The summary below provides details on the number of domains and CDEs prioritized by the Biomedical and Psychosocial Working Groups. Please see the Appendix for the detailed recommendations and guidance.
KEY FINDINGS: BIOMEDICAL WORKING GROUP
The Biomedical Working Group was tasked to create a set of CDEs that would collectively help researchers understand the clinical course of the disease and its effects on children. Building from a baseline set of data elements expected to be collected by all COVID-19 studies (e.g., COVID-19 symptoms, test results, and date(s) of diagnostic test(s)), the Biomedical Working Group prioritized a total of 49 Tier 1 and Tier 2 CDEs to be gathered via medical chart abstraction, downloaded data from electronic health records, research exam, or questionnaire. Recommendations assume that information from patient assessments (e.g., COVID-19 testing, immunizations) can be collected.
It is expected that these measures will be updated as needed to reflect the evolving understanding of the manifestations and concerns of COVID-19 as more data are accumulated on acute COVID, MIS-C, and PASC, and as vaccination and treatment use evolves in pediatric populations.
Summary of Biomedical Recommendations
The Biomedical Working Group prioritized eight total domains (bolded below) to guide recommendations. The summaries below provide the rationale for each domain and the importance of their underlying CDEs to better understand the effects of COVID-19 on children:
Baseline Child Health: This domain, which collects information on current and past health history, provides researchers an opportunity to distinguish between health effects that may result from COVID-19 and those that may result from prior risk factors as well as identifying the impact of COVID-19 on a variety of underlying conditions (e.g., children with cancer or congenital heart disease).
Manifestations
The following four domains relate to the manifestations of SARS-CoV-2 illness identified thus far in children including acute COVID-19, MIS-C, and PASC. The Working Group stressed the importance of collecting all data used to define these SARS-CoV-2 related illnesses, especially as the criteria for diagnoses of acute COVID, MIS-C and PASC may evolve.
Manifestations—Clinical: This domain, which collects information consisting of vital signs, symptoms/physical findings (including infant specific symptoms), duration of symptoms, complications/conditions, is intended to collect data describing the clinical course of SARS-CoV-2 related illness. Note: The Working Group is not prescribing timing of vital signs collection other than an initial set at the time of first encounter; further guidance on data harmonization of vital signs can be found in the Appendix.
NIH | June 2021 10

<. <.
<. <.
<. <. Manifestations—Laboratory: This domain collects the laboratory tests and values associated with
SARS-CoV-2 illness. Note: The Working Group is not prescribing which laboratory tests should be performed in pediatric patients/studies, but rather that the test values should be recorded if performed or “Not Done” should be indicated accordingly. Further guidance on data harmonization of the laboratory values can be found in the Appendix.
Manifestations—Cardiopulmonary Diagnostic Assessments: This domain addresses whether cardiovascular diagnostic assessments (e.g., ECG, Echocardiogram, Cardiac MRI) and pulmonary diagnostic assessments (e.g., pulmonary function tests, co-oximetry) were conducted during the course of infection with SARS-CoV-2 virus, and whether abnormalities were detected. Note: The Working Group is not prescribing which diagnostic assessments should be conducted, but rather, that the abnormalities be recorded if performed or “Not Done” be indicated accordingly. Further guidance on data harmonization of these assessments can be found in the Appendix.
Manifestations—Imaging: This domain collects whether radiographic imaging (e.g., Chest X-ray, CT Scan Brain, Abdominal Ultrasound) was conducted during the course of infection with SARS-CoV-2, and whether abnormalities were detected. Note: Again, the Working Group is not prescribing imaging to be conducted, but rather that the abnormalities be recorded if performed or “Not Done” be indicated accordingly. Further guidance on data harmonization of the imaging results can be found in the Appendix.
Diagnosis: This domain contains the SARS-CoV-2 testing elements that can be used to diagnose infection with SARS-CoV-2.
Treatment: As further understanding of SARS-CoV-2 and COVID-19 is garnered and new treatments become available, it is crucial to track the response of children to various interventions. The logging of treatment and interventions data allows researchers to do so.
Outcomes: This domain aims to capture outcomes specifically related to infection including intensive care unit (ICU) admissions, morbidity, and mortality during COVID hospitalization to inform our understanding of the risks of COVID-19 to children.
NIH | June 2021 11

The Final Biomedical CDE recommendations, organized by domain, are listed below. Items in blue represent Tier 1 CDEs; items in green (with asterisks*) represent Tier 2 CDEs. The Final Biomedical CDE recommendations can be found in the Appendix: COVID-19 Pediatric Biomedical Recommended Measures.
Baseline Child Health 1. Underlying Conditions 2. Premature and Neonatal Conditions* 3. Family History Comorbidities* 4. Health Status (Height/Weight) 5. Breastfeeding* 6. COVID-19 Vaccination History 7. Maternal COVID-19 Vaccination History* 8. Current Vaccination Status* 9. Baseline Medications/Treatment 10. Enrollment Date
Manifestations: Clinical 11. Vital Signs 12. Date and Time of Vital Signs 13. Vital Signs Timepoints 14. Symptoms/Physical Findings 15. Infant-Specific Symptoms/Physical Findings* 16. Duration of Symptoms 17. Complications/Conditions 18. Date of Onset/Diagnosis* 19. Date of Resolution*
Manifestations: Laboratory 20. Labs at Diagnosis 21. Most Abnormal Labs* 22. Date and Time of Lab Sample Collection 23. Other Viral/Bacterial/Fungal Test Positive*
Manifestations: Cardiopulmonary Diagnostic Assessments 24. Cardiovascular Diagnostic Assessment Abnormalities 25. Cardiovascular Diagnostic Assessment Date 26. Pulmonary Diagnostic Assessment Abnormalities 27. Pulmonary Diagnostic Assessment Date
Manifestations: Imaging 28. Radiographic Imaging Abnormalities 29. Date of Radiographic Imaging
Diagnosis 30. SARS-CoV-2 Tested 31. SARS-CoV-2 Test Result 32. Type of Test 33. Date(s) of Test 34. Sample Type Collected*
Treatment 35. Highest Level of Care Required (during COVID-19 episode) 36. Date of Current or Previous Hospital Admission for COVID-19 37. Date of Hospital Discharge 38. Clinical COVID Discharge Diagnosis 39. Date of Current or Any Previous ICU Admission 40. Date of ICU Discharge 41. Medications of Interest 42. Duration of Medications of Interest* 43. Intensive Intervention (Treatment/Device) 44. Do Not Resuscitate/Limitation of Support
Outcomes 45. Patient Survival 46. Death Due to COVID/MIS-C 47. Date of Death 48. Discharged To 49. Severity of COVID-19 Illness
NIH | June 2021 12

Additional Guidance for Biomedical Recommendations
In addition to the above, additional key discussion points identified by the Biomedical Working Group in relation to these measures include the following:
Dates of Service and Patient Zip Code: In order to adhere to the requirements in the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule, this Working Group recognizes that some prioritized elements such as dates and zip code must be limited or de-identified before contributing to a harmonized set of data. More information used by Federal partners such as the National Center for Advancing Translational Sciences (NCATS) N3C on handling data protection can be found on the NCATS website.
Body Mass Index (BMI) and Health Status (Height/Weight): The height (or length in infancy and other situations where standing is not feasible) and weight are listed as Tier 1 elements as elevated BMI (derived from these values) is associated with worse COVID-19 outcomes in adults and children. The Working Group recognizes that in many study protocols, height is not collected, and patient reported height (or parent reported height of a child) is often not reliable. If height is not available in the patient record, it should be marked as “not available.”
NIH | June 2021 13

<.
KEY FINDINGS KEY FINDINGS: PSYCHOSOCIAL WORKING GROUP
The Psychosocial Group aimed to create a set of CDEs that would collectively inform the understanding of the mental health, psychological, social, and behavioral effects of COVID-19 infection and/or the pandemic on the pediatric population.
At the time of this review, research on the psychosocial effects of the COVID-19 pandemic on children was limited and constantly evolving as factors directly impacting children (such as school closure policies) changed over the course of the pandemic. Although the prioritization plan described above was utilized, it was necessary for the Working Group to rely on member expertise, experience in the field, participation in extramural COVID-19 and pediatric studies, and knowledge of the current pediatric COVID-19 research landscape. In contrast to the Biomedical CDE recommendations, the majority of these CDEs require interviews or surveys directly with research participants or their parents.
Summary of Psychosocial Recommendations
The Psychosocial Working Group prioritized 50 elements in ten total domains (bolded below) to guide recom-mendations. The summaries below provide the rationale for each domain and the importance of their underlying CDEs to better understand the effects of COVID-19 and/or the pandemic on children:
Social Determinants of Health (SDOH): This domain captures the factors of Highest education level/degree (household), English proficiency (parent), Employment status (parents), Household income, Housing instability (household), Food insecurity (household), and Racial/ethnic discrimination as Tier 1 elements with additional COVID-19 specific elements in Tier 2. Decades of research have demonstrated that household-level socioeconomic status characteristics are correlated with children’s health through factors such as access to resources, health-related behavior patterns, and household management. Most of these household-level measures are specified as Parent Self-Report for harmonization and data quality.
+ It is important to note that English proficiency is ascertained for the parent, both as an important determinant of health, but also to account for the possible language burden of some of the higher literacy level measures. Investigators should consider anticipated and actual literacy levels of participants when considering implementation of these CDEs, and potential strategies to reduce participant literacy/language proficiency burden. Furthermore, investigators may consider also asking the English proficiency of the child respondent as it relates to literacy levels and burden of the questionnaire, but this was not prioritized as a Tier 1 or Tier 2 SDOH element.
+ For the item Highest education level/degree (household), the guidance from prominent relevant surveys in the field, such as the National Survey of Children’s Health and the National Household Education Survey, recommends asking for information from both parents to attain the highest level in analysis.
NIH | June 2021 14
<. <.
<. <.
<. <.
<. <.
<. Educational Factors: This domain includes Tier 1 elements of Grade level, Current school type, Accommodations for learning difference, Changes to schooling during the pandemic, and Computer access. Tier 2 elements are recommended for garnering additional information on potential exacerbating factors of the pandemic. Researchers who seek a more thorough evaluation of school and educational factors are referred to the National Survey of Children’s Health and the National Household Education Survey for additional items, and may also consider requesting school records and consent to do so. Note: these factors are U.S.-centric, and may need to be adapted for educational factors surveyed internationally.
Community, Family, and Peer Factors: This domain prioritizes Social connection/support as a Tier 1 element due to its importance as a known exacerbating/mitigating factor of the impact of stress on child health. The Tier 2 elements of Emotional support, Peer relationships, Family impact/Household interpersonal conflict, and Community support are recommended to provide additional information on social and emotional support.
Social Media/Screen Time: This short, one item domain is important for understanding children’s use of social media/devices during the pandemic.
Well-being Factors: This domain captures the Tier 1 factor of Well-being (positive affect), and the Tier 2 elements of Coping strategies and Loneliness that may either mitigate or exacerbate COVID-19 pandemic effects and/or represent the outcome of COVID-19 viral manifestations/quarantine and the pandemic.
COVID-19 Stress and Worry: This domain contains elements that were chosen as potential mediators of mental health in the pandemic. These elements include Worry/anxiety about COVID-19 and Stress related to COVID-19 in Tier 2.
COVID-19 Attitudes, Behaviors and Experiences: This domain comprises items including Household COVID-19 exposure, Ability to Isolate, Perception of COVID-19, Adherence to social distancing/face coverings, and Vaccine attitudes.
Health Related Behaviors: This domain includes brief measures of Physical Activity and Sleep Quality/Duration. Nutrition was also considered for this category, and considered important, but a measure that was brief/simple and reliable was not identified.
Mental/Behavioral Health: This domain includes Tier 1 measures on Overall mental/emotional health (both of the parent and child), and Current mental health symptoms (of the child), and Underlying conditions/mental and behavioral health history (also found in the Joint Group Discussion section ). The National Institute of Mental Health (NIMH) recommends the DSM-5 Cross-C utting Symptom measure for assessing current mental health symptoms. Additionally, PROMIS® tools for anxiety, depressive symptoms, and fatigue are also designated Tier 1 due to their particular relevance to COVID-19 and the pandemic. Finally, for younger children (Ages 1-5), the Working Group recommends using the PROMIS Early Childhood parent report measures for Anxiety, Anger/Irritability, Depressive Symptoms, Sleep Health, and Global Health found on HealthMeasures.
Health Care: This domain aims to capture those issues related to health care access and coverage. The elements cover Health insurance status, Changes to health insurance, Changes to health care access during the pandemic, and Receiving mental health or behavioral health treatment/developmental services.
NIH | June 2021 15

The Final Psychosocial CDE recommendations, organized by domain, are listed below. Items in blue represent Tier 1 CDEs; items in green (with asterisks*) represent Tier 2 CDEs. The Final Psychosocial CDE recommendations can be found in the Appendix: COVID-19 Pediatric Psychosocial Recommended Measures.
Social Determinants of Health 1. Highest Education Level/Degree (Parent) 2. English Proficiency (Parent) 3. Number of household members 4. Employment Status (Parent) 5. Employment Risk for COVID-19 (Family)* 6. COVID 19 Effect on Work* 7. Financial Strain (Family)* 8. Housing Instability (Family) 9. Food Insecurity (Family) 10. Breakfast/Lunch from School* 11. Household Income 12. Racial/Ethnic Discrimination 13. Coronavirus Racial/Ethnic Bias*
Educational Factors 14. Grade Level (School-Age Child) 15. Current School Type 16. Accommodations for Learning Difference 17. Changes to Schooling During Pandemic 18. School Attendance/Absence* 19. Perception of Changes to Schooling* 20. School Risk and Protective Factors* 21. Academic Performance/Achievement 22. Childcare* 23. Computer and Internet Access
Community, Family, and Peer Factors 24. Social Connection/Support 25. Emotional Support/Social Support* 26. Peer Relationships* 27. Family Impact/Household Interpersonal Conflict* 28. Community Support (Cohesion)*
Social Media/Screen Time 29. Time Spent in Front of a Screen*
Well-Being Factors 30. Well-Being 31. Coping Strategies* 32. Loneliness*
COVID-19 Attitudes, Behaviors, and Experiences 33. Household COVID-19 Exposure 34. Ability to Isolate* 35. Belief That COVID Is Serious Disease*
COVID-19 Stress and Worry 36. Adherence to Social Distancing/Face Coverings 37. Vaccine Attitudes* 38. Worry/Anxiety About COVID-19* 39. Stress Related To COVID-19*
Health Related Behaviors 40. Physical Activity* 41. Sleep Quality 42. Sleep Duration* 43. Baseline Child Health
Mental and Behavioral Health 44. Overall Physical and Mental/Emotional Health 45. Current Mental Health Symptoms
Health Care 46. Health Insurance Status 47. COVID-19 Changes to Health Insurance 48. COVID-19 Changes to Health Care Access 49. Receiving Behavioral Health/Mental Health Treatment* 50. Services for Developmental Needs*
NIH | June 2021 16
Additional Guidance for Psychosocial Recommendations
Several key themes were identified by the Working Group relative to the recommended constructs and measures:
COVID-19 relative items: As the goal of this Working Group is to provide CDEs for pediatric COVID-19 projects, many of the prioritized Tier 1 elements are COVID-19 specific and include a reference to the start of the pandemic (herein stated as March 2020). For the most part, COVID-19 specific questions and responses were found in existing COVID-19 questionnaires, protocols, and CRFs. To avoid changing the timelines of validated measures (e.g., PROMIS, NIH Toolbox®) and measures that would be difficult to recall (e.g., sleep, physical activity), the Working Group added supplementary questions to broadly compare the child’s current state versus the child’s state before the pandemic. Investigators may choose to supplement the CDEs with additional questions to evaluate the impact of the pandemic more thoroughly.
Determination of informant for data element and focus of data element: Given that these are pediatric specific data elements, the Working Group deliberated long on two very important considerations relatively unique to research in children: 1) who is the item/measure about (i.e., child, parent, household); and 2) who is the informant of that measure (i.e., child or parent/caregiver/surrogate). With regard to the first, most of the recommended measures gather information about the child study participant, and in only a few cases, measures ask about the parent/caregiver/surrogate or the household. In those few instances, it is believed that the information gathered regarding the parent/caregiver/surrogate or the household (e.g., household income) is most relevant to the assessment of the child.
With regard to the informant, the recommendations of the Working Group vary by construct, in part due to the available measures and in part due to identifying the optimal informant for the construct. As a result, for some constructs, only the parent report about the child is recommended. However, for others, only the child report is solicited, and yet for others, the option of either is provided. Measures were adapted to use “you” or “your child” to account for these distinctions and investigators are encouraged to adapt these accordingly for Parent or Child questionnaires. The nomenclature below is used throughout the recommended measures to clarify these distinctions. + “Parent Self-Report” – refers to parent answering about themselves.
+ “Parent Report About Child” – refers to parent answering about their child.
+ “Child Self-Report” – refers to child answering about themselves.
Age of participant: Age group recommendations (either for Child-Self Report or Parent Report About Child) are provided for existing validated measures and for items drawn from pediatric COVID-19 questionnaires used in the field. In some cases, the age group for Child Self-Report items was modified by leveraging the expertise of the Working Group and referring to the Pediatric patient-reported outcome instruments for research to support medical product labeling: report of the ISPOR PRO good research practices for the assessment of children and adolescents task force. Whether an age group is validated, used, or modified based on best practices will be indicated in the footnotes of each measure. For new or unvalidated COVID-19 specific tools, researchers may consider adjusting age limits to best address their needs.
Child maltreatment or risk of suicide: For the Tier 2 elements Family Impact/Household Interpersonal Conflict and Current Mental Health Symptoms, additional guidance is provided in the Appendix for research related to child maltreatment or suicide due to the federal, state, and institutional regulations and policies that surround these topics.
NIH | June 2021 17

<. <.
<.
KEY FINDINGS KEY FINDINGS: JOINT GROUP DISCUSSIONS
The following domains were discussed by both Working Groups:
Demographics: This domain collects information on demographic information on the participant and has been standardized with PhenX and U.S. Census Bureau. The “Gender Identity” item in PhenX was not recommended by this group for pediatric populations as it has only been validated in adults. In consultation with the NIH Sexual and Gender Minority Research Office (SGMRO), the question set from the ABCD Study® for ages 9+ was instead specified for this element.
Disability/Functional Status: This domain collects information on Disability/Functional Status due to physical and/or mental/emotional conditions. It also includes elements on developmental milestone attainment.
Underlying Conditions: This element contains physical and mental health/behavioral diagnoses prior to, or present at the time of infection with COVID-19 or study enrollment.
+ Physical Conditions: For the categorization of “physical” underlying conditions identified by the Biomedical Working Group, the categorization of the responses may be amplified by using the Pediatric Complex Chronic Conditions (CCC) classification proposed by Feudtner et. al. Indeed, the Tier 2 element for Premature and Neonatal Conditions maps exactly to the Feudtner classifications, whereas the other Tier 1 elements were deliberated by considering the conditions most relevant for COVID-19.
+ National Survey of Children’s Health: For the categorization of mental health / behavioral diagnoses, the Parent-report questions from the National Survey of Children’s Health were used.
NIH | June 2021 18
I OTHER CDE RESOURCES Research projects will collect study variables/questions beyond the minimum CDEs for pediatric participants. In addition to this battery of CDEs, we are encouraging referral to the following NIH recommended repositories for harmonization of additional measures.
+ HealthMeasures: consists of PROMIS, Neuro-QoLTM, ASCQ-Me®, and NIH Toolbox
+ NIH Public Health Emergency and Disaster Research (DR2): provides access to COVID-19 related data collection tools (case report forms (CRFs), data collection forms (DCFs), instruments, surveys, questionnaires) that are currently in use
+ NIH CDE Repository: provides access to structured human and machine-readable definitions of data
+ PhenX Toolkit: catalogs recommended measurement protocols
CONCLUSION AND NEXT STEPS
As the COVID-19 pandemic continues to affect our society, researchers are challenged by the urgency to advance our understanding of the virus on a rapid timeline. As research continues, it is important to plan for data harmonization across studies so that the efforts of each individual study can contribute to a larger, more impact-ful collective body of research. The recommendations in this document can aid in the data harmonization planning process for COVID-19 studies including children. Our recommendations can be especially helpful for researchers who may not be accustomed to designing and performing pediatric-specific research. In this scenario, we hope that Tier 1 recommendations provide important, easily incorporated measures.
In line with the NIH COVID-19 strategy, which promotes collaborative science to address the unprecedented health challenge of the COVID-19 pandemic, these recommendations are publicly available on the NIH Public Health Emergency and Disaster Research Response (DR2) website. We strongly encourage researchers engaged in planning or conducting studies to incorporate these recommendations into their studies wherever possible to help streamline and harmonize data for sharing most effectively. We expect to update these CDEs and measures to reflect the most current research as the understanding of COVID-19 and its treatments progress.
NIH | June 2021 19

APPENDIX

COVID-19 Pediatric Biomedical Recommended Measures The following document includes the Biomedical Pediatric Working Group’s recommended instruments for collecting information on the Group’s Tier 1 and Tier 2 data elements, organized by Domain.
Document Notes: - Navigation: You may use the use the Bookmarks to efficiently navigate the document. To do so,
open the document in Adobe Acrobat and click the Bookmarks icon or hit "F4" on your keyboard - References: References are marked by endnotes; you may click on the endnote to display the
reference, and modifications to the source if applicable.
- Tiers: Tier 1 elements are marked in Blue, Tier 2 elements are marked in Green
Common Data Elements (CDE) User Guidance: - Unless specified, the units for specified age groups are in years.
Baseline Child Health Underlying Conditions1
• Significant underlying medical conditions at the time of COVID-19 testing or diagnosis: • Diabetes type I • Diabetes type II • Obesity • Asthma • Bronchopulmonary dysplasia (BPD) • Cystic fibrosis • Obstructive sleep apnea • Tracheomalacia • Cancer • HIV/AIDS • Hematopoietic cell recipient/bone marrow transplant recipient • Solid organ transplant recipient • Rheumatologic conditions (e.g. rheumatoid arthritis, systemic lupus erythematosus,
vasculitis) • Hypertension • Congenital heart disease • Heart failure • Cardiomyopathy • History of Kawasaki Disease (not a current diagnosis) • History of MIS-C (not a current diagnosis) • Inflammatory bowel disease • Feeding tube dependent • Sickle cell disease • Thrombotic disorders • Chronic liver disease • Chronic kidney disease • Seizure disorder/epilepsy • Eczema
• Physical disability (including cerebral palsy) • Down syndrome • Congenital syndromes/anomalies or genetic conditions including other chromosomal
syndromes • Premature or neonatal conditions • Pregnancy (if of reproductive age) • Other conditions (specify)
• Premature and Neonatal Conditions (Tier 2)2
• Fetal malnutrition • Extreme immaturity • Cerebral hemorrhage at birth • Spinal cord injury at birth • Birth asphyxia • Respiratory diseases • Hypoxic-ischemic encephalopathy • Other
Family History Comorbidities (Tier 2)3
• Have any family members (parent/sibling) been diagnosed with any of the following medical conditions currently or in the past?
• Obesity • Diabetes type I • Diabetes type II • Fibromyalgia (amplified pain syndrome) • Rheumatologic conditions (e.g. rheumatoid arthritis, systemic lupus erythematosus,
vasculitis) • Thrombotic disorders • Other significant comorbidity (specify)
• If the participant is in first year of life, did the participant’s mother test positive for COVID-19 while pregnant or nursing?
• Yes/No/Unknown/Prefer Not to Answer • If participant is in first year of life, did the participant’s father or other caregiver test positive for
COVID-19? • Yes/No/Unknown/Prefer Not to Answer
Health Status (Height/Weight)4
• Height/length • ______ Units • Not available
• Weight • ______ Units • Not available
• Head circumference (only for children less than two years of age) (Tier 2) • _____ Units • Not available
Breastfeeding (Tier 2) • (Ages 0-1 year)

• If the participant is in first year of life, is he or she being breastfed or fed pumped milk? • Yes/No/Unknown/Prefer Not to Answer
COVID-19 Vaccination History5
• Has the participant received a COVID-19 vaccine? • Yes/No/Unknown/Prefer Not to Answer • Date of vaccination
• MM/DD/YYYY • Did the participant receive the second dose of the COVID-19 vaccine?
• Yes/No/ N/A/Unknown/Prefer Not to Answer • Date of vaccination
• MM/DD/YYYY • Which vaccine brand/type did the participant receive?
• Pfizer • Moderna • Johnson and Johnson • AstraZeneca • Unknown • Other (specify)
• Did the participant have any adverse reactions or side effects? • Yes/No/ N/A/Unknown/Prefer Not to Answer • If yes, please specify: _______________
PASC Symptom resolution (Tier 2) • If the participant had long COVID/post-acute sequelae of COVID-19 (PASC) symptoms at the
time of vaccination, did those symptoms change? • Yes, full resolution of symptoms • Yes, some improvement in symptoms • Yes, worsening of symptoms • No, no significant change
Maternal COVID-19 Vaccination History (Tier 2)6
• If participant is in first year of life, did the participant’s mother receive vaccination for COVID-19 while pregnant or nursing?
• Yes/No/Unknown/Prefer Not to Answer Current Vaccination Status (Tier 2)7
• Are the patient's immunizations up to date for their age at the time of COVID-19 diagnosis/assessment?
• Yes/No/Unknown/Prefer Not to Answer • If immunizations are not up to date, what is/are the reason(s) for not being up to date? (Check
all that apply)8
• Parent Report About Child • Clinic was closed because of COVID-19 • Child had symptoms of COVID-19, so you cancelled appointment • You cancelled appointments to avoid being around others/in a healthcare setting • Other reasons related to COVID-19 • Other reasons not related to COVID-19 • Refused to answer
• Has the patient received any MMR vaccinations? • Yes/No/Unknown/Prefer Not to Answer
• Has the patient received the current seasonal influenza vaccine? • Yes/No/Unknown/Prefer Not to Answer
• Has the patient received palivizumab for prevention of respiratory syncytial virus (RSV)? • Yes/No/Unknown/Prefer Not to Answer
• Has the patient received the BCG vaccination? • Yes/No/Unknown/Prefer Not to Answer
• Date of most recent vaccination (excluding vaccination for COVID-19) • MM/DD/YYYY
Baseline Medications/Treatment9
• Current medication name including birth control medications and injections (repeat for each medication)
• Respiratory support prior to onset of COVID-19? • Yes/No
• Specify, check all that apply (Tier 2): • Non-invasive respiratory support (e.g., CPAP, BiPAP) • Invasive respiratory support (e.g. mechanical ventilation via tracheostomy) • Tracheostomy • Supplemental oxygen • Unknown/Uncertain
Enrollment Date • Date participant was enrolled in study (protocol specific)
• MM/DD/YYYY
Manifestations: Clinical Vital signs are routinely collected as part of the baseline visit to determine eligibility to participate in a trial, to serve as a reference point to select vital signs which may be trended during the trial, and to reveal potential indicators of severity and risk that may not otherwise be obvious. Thus, the Working Group recommends transmitting baseline vital signs as a common data point and encourages researchers to supplement this list with other vital signs as dictated by specific criteria in their individual trials.
The Working Group is not currently recommending frequency for documentation of vital signs. Study sites should provide any core vital sign data that are collected for routine monitoring of participants. For example, vital sign data for ICU patients are typically charted every hour, and these data should be available through the electronic health record. For outpatient studies, core vital sign data elements should be taken with any in-person assessment. However, the reference time period for vital signs should be a 24-hour clock from midnight to midnight (00:00-23:59) to allow for consistency across studies.10
Vital Signs11
• Body temperature (degrees Celsius) • Heart rate (beats/min) • Systolic blood pressure (mmHg) • Diastolic blood pressure (mmHg) • Respiratory rate (breaths/min)
• Oxygen saturation (%) o Supplemental oxygen (Yes or No)
• Responses: Values (units), unknown, N/A or not reported Date and Time of Vital Signs
• MM/DD/YYYY • HH:MM
Vital Signs Timepoints12
• Baseline (e.g., at admission, at initial encounter if not admission) • Protocol specific timepoints (e.g., Day 1 AM, Day 1 PM, Day 2 AM, at discharge, etc.) • Unknown
Symptoms/Physical Findings13
Additional Guidance: Note that the two lists below are separated into an acute COVID-19/MIS-C symptom list and a Long COVID/PASC list (which includes the acute COVID-19/MIS-C list).
• Which of the following were experienced during current illness and/or confirmed by physical exam? For each symptom indicate Yes/No/Unknown | Confirmed by Physical Exam
• Acute COVID/MIS-C • Abdominal pain • Bleeding • Chest pain • Cough • Cyanosis (bluish lips/face) • Diarrhea • Fatigue • Fever - documented
Duration in days • Headache • Muscle or body aches • Nasal congestion or runny nose • Nausea/vomiting • Neck pain • New loss of taste or smell • Palpitations • Shortness of breath or difficulty breathing • Skin rash • Sore throat • Subjective fever/chills/rigors/night sweats • Swollen glands
If confirmed by physical exam, cervical lymphadenopathy (at least 1.5 cm in diameter)?
• Conjunctivitis (Red/pink eye(s)) • Oral mucosal change
If confirmed by physical exam were swollen, red, or cracked lips, strawberry tongue, and/or erythema of the oral/pharyngeal mucosa present?
• Changes in hands and feet (Peripheral extremity changes)

• Other symptom(s): • None of the above/asymptomatic
• Long COVID/PASC, including above acute COVID/MIS-C symptoms list plus the following: • Allodynia (pain out of proportion to the stimulus) • Altered level of consciousness/confusion • Anorexia (decrease in appetite) • Anxiety • Cannot move and/or feel one side of body or face • Depressed mood • Dizziness/lightheadedness/blackouts • Exertional fatigue • Forgetfulness • Irritability • Orthostasis (dizziness/lightheadedness/blackouts on sitting up or standing)
If yes, confirmed by changes in heart rate/blood pressure? [Tier 2] • Joint pain • Hallucinations (seeing or hearing things others do not see or hear) [should not be
completed for children <15 years old] • Hypersomnia • Insomnia (difficulty sleeping) • Malaise (including post-exertional malaise) • Muscle weakness • Paresthesia (numbness or tingling somewhere in the body) • Persistent cough
If yes, productive? • Problems with balance • Problems with gait/falls • Toe rashes (red/purple sores or blisters on the feet, including the toes) • Trouble concentrating or difficulty thinking (“brain fog”) • Weight loss • Failure of expected weight gain • Failure of expected linear growth • Other symptom(s):
Infant-Specific Symptoms/Physical Findings (Tier 2) • In addition to the above, which of the following were experienced by the infant during illness?
For each symptom indicate :Yes/No/Unknown | Confirmed by Physical Exam • Dehydration • Full or bulging fontanelle • Fussiness • Increased work of breathing/shallow breathing • Lethargy • Poor feeding
Duration of Symptoms • Date Symptoms Presented (MM/DD/YYYY)

• Date Symptoms Resolved (MM/DD/YYYY) • Ongoing • N/A (No symptoms)
Complications/Conditions14
• Did the patient develop any of the following complications/conditions since the diagnosis of COVID (organized by organ system):
• Fibromyalgia/amplified pain syndrome • Post viral fatigue syndrome • Seizure • Stroke: intracerebral hemorrhage • Stroke: ischemic cerebrovascular
accident • Diabetic ketoacidosis (DKA) • New onset diabetes • Pancreatitis • Acute respiratory distress syndrome
(ARDS) • Bronchiolitis • Deterioration of prior chronic
pulmonary diseases • Lung fibrosis • Pneumonia • Pulmonary embolism • Cardiac arrhythmias • Cardiac failure • Cardiomyopathy • Coronary artery abnormalities
Date of Onset/Diagnosis (Tier 2) • MM/DD/YYYY
Date of Resolution (Tier 2) • MM/DD/YYYY
If there is a venous thrombosis, where is it located? (Tier 2) • Intracranial • Extracranial • Both • Unknown or not reported
Manifestations: Laboratory Labs at Diagnosis (work up of condition)15
• Myocarditis/pericarditis/ pericardial effusion
• Myositis • Shock • Arthritis • Physical disability/muscular
weakness • Acute kidney injury • Acute liver dysfunction • End stage renal disease (ESRD) • Bleeding events • Deep vein thrombosis • Appendicitis • Gastroesophageal reflux
disease (GERD) • Gastrointestinal hemorrhage • Gastrointestinal perforation • Peritonitis • Bacteremia • Pulmonary aspergillosis • Toxic shock syndrome (TSS) • Other (specify)
Additional Guidance: The Tier 1 lab values include, but are not limited to, those parameters necessary for the diagnosis of MIS-C (including markers of inflammation) and other conditions associated with acute and long COVID/PASC. Inclusion in Tier 1 does not suggest that all of these labs are recommended to be performed in all pediatric patients/studies, but rather that the test values or “Not Done” should be reported when performed.
Similar to vital signs, the Working Group is not currently recommending frequency for documentation of specific clinical labs. Study sites are encouraged to provide any lab data that are collected for routine monitoring of participants in addition to the value at diagnosis (i.e., work up of condition), which will vary between outpatient and inpatient settings. However, the reference time period for labs should be a 24-hour clock from midnight to midnight (00:00-23:59) to allow for consistency across studies.
• For each of the below, report test value at diagnosis (i.e., work up of condition) or trial entry with units or “Not Done”
• Any lab tests performed? • Yes • No • Unknown • If yes, lab results have been categorized as Tier 1 or Tier 2 as described below:
Tier 1 Tier 2 • White blood cell count (WBC) • Absolute eosinophil count • Absolute lymphocyte count (ALC) • Absolute monocyte count • Absolute neutrophil count (ANC) • Absolute basophil count • Platelets • Hemoglobin • C-reactive protein (CRP) • Total bilirubin • Erythrocyte sedimentation rate (ESR) • Prothrombin time (PT) • Procalcitonin • International normalized ratio (INR) • Ferritin • Activated partial thromboplastin time • LDH (aPTT) • Albumin • IL-6 • Glucose • Complement • Sodium • Hemoglobin A1C • Creatinine • pH • Blood urea nitrogen (BUN) • pCO2 • Aspartate aminotransferase (AST) • paO2 • Alanine transaminase (ALT) • Calcium • D-dimer • Cerebrospinal fluid (CSF) WBC • Fibrinogen • CSF red blood cell count (RBC) • Troponin (TNI) • CSF Protein • BNP/NT-Pro-BNP • CSF Glucose • Lactate • Other, Specify
Most Abnormal Labs (Tier 2)16
• Any labs repeated during admission that were more abnormal than initial values? • Same list as above
Date and Time of Lab Sample Collection (Repeat as many times as necessary) • MM/DD/YYYY • HH:MM
Other Viral/Bacterial/Fungal Test Positive (Tier 2)17
• Any other viral testing positive?

• Yes/No • If yes, list other viral tests that were positive
• Positive blood cultures? • Organism • Date
Manifestations: Cardiopulmonary Diagnostic Assessments Additional Guidance: Similar to vital signs and clinical labs, the Working Group is not currently recommending frequency for documentation of specific cardiopulmonary assessments. Study sites are encouraged to provide any cardiopulmonary assessment data that are collected for monitoring of participants, in addition to the data reporting abnormality.
Cardiovascular Diagnostic Assessment Abnormalities18
• Did the patient have any cardiovascular diagnostic assessment performed (beyond physical exam) • Yes - abnormalities detected
• If abnormalities detected, was there • Abnormal function • Pericardial effusion • Coronary artery abnormalities
• Yes – normal • No – not performed • Unknown • If yes specify:
• ECG (Tier 2): • Yes – abnormalities detected, Yes – normal, No – not performed, Unknown
• ECHO (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
• Cardiac MRI (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
• Other tests (specify test) performed (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
Cardiovascular Diagnostic Assessment Date • MM/DD/YYYY Pulmonary Diagnostic Assessment Abnormalities19
• Did the patient have any pulmonary diagnostic testing (beyond physical exam and radiographic imaging) • Yes – abnormalities detected • Yes – normal • No – not performed • Unknown • If yes specify:
• 6-Minute Walk Test (Tier 2) [only ages 6+]20: • Yes – abnormalities detected, Yes – normal, No – not performed, Unknown
• Pulmonary Function Test (Tier 2) [only ages 6+]: • Yes – abnormalities detected, Yes – normal, No – not performed, Unknown
• Co-oximetry (Tier 2): • Yes – abnormalities detected, Yes – normal, No – not performed, Unknown

• 2-Minute Walk Test (Tier 2) [only ages 6+]21: • Yes – abnormalities detected, Yes – normal, No – not performed, Unknown
• Other tests (specify test) performed (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
Additional Guidance: Please note that while the 6-Minute Walk Test (6-MWT) is currently grouped with the Pulmonary Diagnostic Assessments, it is also used as a Cardiovascular Diagnostic Assessment. Please refer to the footnote for 6-MWT assessment in MIS-C patients.
Pulmonary Diagnostic Assessment Date • MM/DD/YYYY
Manifestations: Imaging Radiographic Imaging Abnormalities22
Additional Guidance: Similar to vital signs and clinical labs, the Working Group is not currently recommending frequency for documentation of specific radiographic imaging. Study sites are encouraged to provide any radiographic imaging data that are collected for monitoring of participants, in addition to the data reporting abnormality. • Did the patient have a chest x-ray performed?
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown • Did the patient have any other radiographic imaging performed?
• Yes - abnormalities detected • Yes – normal • No – not performed • Unknown • If yes specify: • CT Brain (Tier 2):
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown • CT Chest (Tier 2):
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown • CT Abdomen (Tier 2):
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown • Lung Ultrasound (Tier 2):
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown • Vascular Ultrasound (Tier 2):
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown • Abdominal Ultrasound (Tier 2):
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown • Neonatal Ultrasound Brain (Tier 2):
• Yes - abnormalities detected, Yes – normal, No – not performed, Unknown (Only performed on infants with open anterior fontanelle)
• MRI Brain (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
• MRI Spine (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
• MRI Abdomen (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
• Other radiographic imaging (specify test) performed (Tier 2): • Yes - abnormalities detected, Yes – normal, No – not performed, Unknown
Date of Chest-X-ray • MM/DD/YYYY • HH:MM
Date of CT Brain (Tier 2) • MM/DD/YYYY
Date of CT Chest (Tier 2) • MM/DD/YYYY
Date of CT Abdomen (Tier 2) • MM/DD/YYYY
Date of Lung Ultrasound (Tier 2) • MM/DD/YYYY
Date of Vascular Ultrasound (Tier 2) • MM/DD/YYYY
Date of Abdominal Ultrasound (Tier 2) • MM/DD/YYYY
Date of Neonatal Ultrasound (brain) (Tier 2) • MM/DD/YYYY
Date of MRI Brain (Tier 2) • MM/DD/YYYY
Date of MRI Spine (Tier 2) • MM/DD/YYYY
Date of MRI Abdomen (Tier 2) • MM/DD/YYYY
Date of Other Radiographic Imaging (Tier 2) • MM/DD/YYYY
Diagnosis SARS-CoV-2 Tested23
• Has the participant been tested for SARS-CoV-2? • Tested • Not Tested • Unknown
SARS-CoV-2 Test Result24 (Repeat as many times as necessary) • If tested, what was the result?
• Positive • Negative • Unknown
Type of test (Repeat as many times as necessary) 25,26
• What test was performed (Select one)?
• Molecular amplification test (RT PCR) • SARS-CoV-2 RNA level Quantitative • SARS-CoV-2 RNA detection Qualitative
• SARS-CoV-2 Antigen • SARS-CoV-2 Rapid Antigen
• Serology • SARS CoV-2 IgM • SARS CoV-2 IgG or Neutralizing Antibody/Serologic
• If yes, what is the antibody to: • Spike antibody • Nucleocapsid antibody
• Other, specify: • For each item: Detected/Not Detected/Not detected in pooled specimen/Inconclusive/
Not Done/N/A or Not reported/Unknown Date(s) of Test (Repeat as many times as necessary)
• MM/DD/YYYY Sample Type Collected (Tier 2)27
• Nasal • Nasopharyngeal • Saliva • Endotracheal aspirate • Bronchoalveolar lavage (BAL) fluid • Blood • Stool • Cord Blood
Treatment Highest Level of Care Required (during COVID-19 episode)28
• Highest level of care received during the COVID-19 episode? • Admitted to the intensive care unit (ICU) • Admitted to the hospital • Emergency Department assessment • Outpatient (in-person and telemedicine) • Self-care alone/over-the-counter medications • Unknown
Date of Current or Any Previous Hospital Admission for COVID-19 (repeat as many times as necessary) • MM/DD/YYYY
Date of Hospital Discharge (repeat as many times as necessary) • MM/DD/YYYY Clinical COVID Discharge Diagnosis (repeat as many times as necessary)29
• Were any of the following conditions listed as a discharge diagnosis for this COVID-19 related admission (mark all that apply)?
• Acute COVID
• MIS-C • Kawasaki Disease • Long COVID/Post-Acute Sequelae of COVID (PASC) • None of the above
Date of Current or Any Previous ICU Admission (repeat as many times as necessary) • MM/DD/YYYY
Date of ICU Discharge (repeat as many times as necessary) • MM/DD/YYYY
Medications of Interest (Acute COVID/MIS-C/Long COVID (PASC) directed)30
• What medications did the patient take or receive to treat Acute COVID-19/MIS-C/Long COVID(PASC)? For each item: Yes/No/Unknown/Not reported:
• Anti-coagulant • Antiplatelets/Aspirin therapy • Heparin • Enoxaparin • Warfarin • Direct oral anticoagulant (DOAC)
• Systemic antibiotics • Specify antibiotic ______
• Immune modulators/Immunosuppressants • Anakinra • Tocilizumab • Convalescent plasma • SARS-CoV-2 monoclonal antibodies • Intravenous immunoglobulins (IVIG) • Interferon • Tumor necrosis factor (TNF) inhibitors (i.e. infliximab, etanercept, adalimumab) • NSAID-Ibuprofen
• Anti-viral/Anti-COVID • Remdesivir • Ribavirin
• Diabetic Medications • Insulin
• Inhaled Medications • Inhaled steroids • Albuterol • Ipratropium
• Systemic Steroids • Dexamethasone • Methylprednisolone • Prednisone/prednisolone • Hydrocortisone • Fludrocortisone
• Other medications (specify____)
Duration of Medications of Interest (repeat for each medication) (Tier 2)31
• Date Medication started (MM/DD/YYYY) • Date Medication stopped (MM/DD/YYYY) • Ongoing • N/A (No support)
Timing of medications, particularly immune modulators/immunosuppressants, may be important for assessing other relevant data elements, such as lab values. Therefore, as appropriate, the Working Group recommends documenting the time as well as the date when these specific medications are administered. Intensive Intervention (Treatment/Device)32
• Did the patient receive the following for treatment of COVID in the hospital? For each item: Yes/No/Unknown/Not reported
• Invasive mechanical ventilation (e.g., endotracheal intubation, mechanical ventilation via tracheostomy)
• New tracheostomy • Noninvasive mechanical ventilation (e.g., CPAP, BiPAP, NIPPV) • Extracorporeal membrane oxygenation (ECMO) • Vasoactive medications • Arterial catheter placement • Cardiopulmonary resuscitation with/without return of spontaneous circulation • Central venous catheter placement • Low flow oxygen therapy (e.g. nasal cannula, simple mask, face tent) • High flow oxygen therapy • Invasive management of thrombosis (e.g., surgical thrombectomy, endovascular thrombectomy,
catheter-directed thrombolysis) • Renal replacement therapy (RRT) • Pacemaker placement • Left ventricular assist device (LVAD) • Other, specify
Duration of Intensive Intervention (Treatment/Device) Support (Tier 2)33
• Date intensive treatment started (MM/DD/YYYY) • Date intensive treatment stopped (MM/DD/YYYY) • Ongoing • N/A (No support)
Do Not Resuscitate/Limitation of Support34
• Was there a “Do Not Resuscitate” order or any other limitation of support? • Yes • No • Unknown/Not reported
Outcomes Patient Survival35
• Did the patient die? • Yes • No • Unknown
Death due to COVID/MIS-C?36
• If yes, was the death COVID-19 related (including MIS-C)? • Yes • No • Unknown • N/A or not reported
Date of Death • MM/DD/YYYY
Discharged To37
• If hospitalized for suspected or diagnosed COVID-19 and survived, to where was the participant discharged?
• Home • Rehabilitation Facility/Nursing Facility • Other, specify ______ • N/A or not reported
Severity of COVID-19 Illness38
• What is the COVID-19 severity at time of maximum severity of illness? • Asymptomatic/presymptomatic infection • Mild illness • Moderate illness • Severe illness • Critical illness • Unknown • N/A or not reported
NIH Severity Definitions: - Asymptomatic or Presymptomatic Infection: Individuals who test positive for SARS-CoV-2 using a virologic test (i.e., a
nucleic acid amplification test [NAAT] or an antigen test) but who have no symptoms that are consistent with COVID-19.
- Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste and smell) but who do not have shortness of breath, dyspnea, or abnormal chest imaging.
- Moderate Illness: Individuals who show evidence of lower respiratory disease during clinical assessment or imaging and who have an oxygen saturation (SpO2) ≥94% on room air at sea level.
- Severe Illness: Individuals who have SpO2 <94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mm Hg, or lung infiltrates >50%.
- Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction. - In pediatric patients, radiographic abnormalities are common and, for the most part, should not be the only criteria
used to determine the severity of illness. The normal values for respiratory rate also vary with age in children; thus, hypoxia should be the primary criterion used to define severe COVID-19, especially in younger children.

COVID-19 Pediatric| Psychosocial Recommended Measures
The following document includes the Psychosocial Pediatric Working Group’s recommended instruments for collecting information on the Group’s Tier 1 and Tier 2 recommended data elements, organized by Domain. Document Notes: - Navigation: You may use the use the Bookmarks to efficiently navigate the document. To do so, open the document in Adobe Acrobat and click the Bookmarks icon or hit "F4" on your keyboard
- References: References are marked by endnotes; you may click on the endnote to display the reference, and modifications to the source if applicable.
- Tiers: Tier 1 elements are marked in Blue, Tier 2 elements are marked in Green
Common Data Elements (CDE) User Guidance: • Unless specified as “Parent Self-Report”, questions refer to the child study participant. Studies should
choose between you/your child depending on if they are collecting information via child or parent/caregiver report. When information appears in brackets (such as [you/your child]), please choose the option relevant to the questionnaire.
• “Parent Self-Report” – refers to parents answering about themselves. • “Parent Report About Child” – refers to parent answering about their child. Please note, sometimes the
verbiage “this child” or “the child” is used rather than “your child” to maintain consistency with the language in the original measure.
• “Child Self-Report” – refers to children answering about themselves. o Child Self-Report measures are recommended for specific age groups based on the following:
Validated: Recommendation is based on validation data, for example, PROMIS®, NIH Toolbox®, PhenX protocols validated in specified age ranges.
Used in COVID-19 Questionnaires: Recommendation is based on use of the items in pediatric cohort studies, for example, the Adolescent Brain Cognitive Development Study SM (ABCD Study®), Adolescent Behaviors and Experiences Survey (ABES), Environmental influences on Child Health Outcomes (ECHO) COVID-19 Questionnaires.
Modified*: For measures modified from adult questionnaires, this Working Group recommends implementing a 13+ age range. The Working Group has justified this approach using the Report of the ISPOR PRO good research practices for the assessment of children and adolescents task force; comparing the measures to existing measures asked of adolescents; and modifying questions to verify that the subject matter was appropriate for adolescents. These “modified” age groups will have an asterisk next to them to mark that they are NOT yet validated or specifically used in pediatric populations, but the Working Group has found the recommendation reasonable.
• Investigators may choose to consistently add “Prefer not to answer” or “Don’t know” response choices to these questions. The Working Group has kept the question responses from the original source and has not added these answer choices uniformly. Participants have the right to refuse or skip any item.
• The superscript “†” indicates that the element is “COVID-19 specific” (either a change from before the pandemic or language specific to the pandemic).
• Unless specified, the units for specified age groups are in years.

Domain: Social Determinants of Health Highest Education Level/Degree (Parent)39
Parent Self-Report • What is the highest grade or level of school that you have completed?
• 8th grade or less • 9th to 12th grade; no diploma • High school graduate or GED completed • Completed a vocational, trade, or business school program • Some college credit, but no degree • Associate Degree (AA, AS) • Bachelor's Degree (BA, BS, AB) • Master’s Degree (MA, MS, MSW, MBA) • Doctorate (PhD, EdD) or Professional Degree (MD, DDS, DVM, JD) • Prefer not to answer • Don't know
Does this child have another parent or adult caregiver who lives in this household? • Yes • No • If yes, what is the highest grade or level of school this caregiver has completed?
• 8th grade or less • 9th to 12th grade; no diploma • High school graduate or GED completed • Completed a vocational, trade, or business school program • Some college credit, but no degree • Associate Degree (AA, AS) • Bachelor's Degree (BA, BS, AB) • Master’s Degree (MA, MS, MSW, MBA) • Doctorate (PhD, EdD) or Professional Degree (MD, DDS, DVM, JD) • Prefer not to answer • Don't know
English Proficiency (Parent)40
Parent Self-Report • Do you speak a language other than English at home?
• Yes • No • Prefer not to answer • (If yes) Since you speak a language other than English at home, we are interested in your own
opinion of how well you speak English. Would you say you speak English… • Very well • Well • Not well • Not at all
Number of Household Members41
Parent Self-Report or Child Self-Report (Ages 13+)* • How many people live in your household now?

• Please indicate the number of adults living in your household: • Please indicate the number of children (<18 years old) living in your household:
Employment Status (Parent)42
Parent Self-Report • Which of the following best describes your current employment status? Mark all that apply
• Employed full-time • Employed part-time • Working without pay • Not employed, but looking for work • Not employed and not looking for work • Retired • Disabled, permanently or temporarily • Student • Other • Don’t know
• Does this child have another parent or adult caregiver who lives in this household? • Yes • No • If yes, which of the following best describes this caregiver’s current employment status? Mark all
that apply • Employed full-time • Employed part-time • Working without pay • Not employed, but looking for work • Not employed and not looking for work • Retired • Disabled, permanently or temporarily • Student • Other • Don’t know
†Employment Risk for COVID-19 “Frontline Status” (Family) (Tier 2)43
Parent Self-Report • Are you or is anyone in your household employed in healthcare and have direct patient contact?
• Yes • No • Unknown
• Are you or is anyone in your household a frontline or essential worker other than in healthcare (such as employed at a grocery store or factory)?
• Yes • No • Unknown
†COVID 19 Effect on Work (Tier 2) Parent Self-Report44
• Have you, or has anyone in your household, experienced a loss of employment income since the start of the COVID-19 pandemic (since March 2020)?
• Yes
• No †COVID-19 Changes to Work (Tier 2) Parent Self-Report45
• Which of the following changes in employment have occurred due to the COVID-19 pandemic? (Check all that apply)
Self Partner Yes No N/A Yes No N/A
(1) Move to remote work, telework (2) Loss of hours (3) Decreased pay (4) Furloughed (5) Loss of job (6) Decreased job security (7) Disruptions due to childcare challenges (8) Increased hours (9) Another change (specify)
†Financial Strain (Family) (Tier 2)46
Parent Self-Report • How difficult is/was it to meet each of the following needs for you and/or your family during the
COVID-19 pandemic (since March 2020)? Not difficult Somewhat difficult Very difficult
Have enough money for food
Have enough money to pay for electricity, heating, or water Have enough money to pay for housing
Get help from community organizations that I trust Get help from family members and friends See a healthcare provider if you or your family needs it Get routine / essential medications
Get transportation when you need it
Use the internet for things like work, school, medical visits, socializing • Thinking about the future, over the next 3 months how challenging will it be to make ends meet?
• A lot more challenging than usual • A little more challenging than usual • No more challenging than usual • Less challenging than usual • Don’t know

†Housing Instability (Family)47
Parent Self-Report • Have any of the following occurred during the COVID-19 pandemic (since March 2020)?
• Relocation or moving from where you lived before March 2020 due to financial strain (e.g., downsizing, moving in with family, etc.)
• Yes • No
• Faced possible eviction since March 2020 • Yes • No
• Loss of your housing, or becoming homeless since March 2020 • Yes • No
†Food Insecurity (Family)48
Parent Self-Report • The following are several statements that people have made about their food situation. Please tell me
whether the statement was “often”, “sometimes”, or “never” true for you and for other members of your household in the last 12 months, since [date 12 months ago]
• 1. "The food that we bought just didn't last, and we didn't have money to get more." • Often true • Sometimes true • Never true • Don’t know
• 2. "We couldn't afford to eat balanced meals." • Often true • Sometimes true • Never true • Don’t know
• 3. In the last 12 months, since [date 12 months ago], did you or other adults in your household ever cut the size of your meals or skip meals because there wasn't enough money for food?
• Yes • No (Skip to 5) • Don’t know (Skip to 5)
• Optional Screener: If any of the first 3 questions are answered affirmatively (i.e., if either Q1 or Q2 are "often true" or "sometimes true" or Q3 is "yes"), proceed to the next question. Otherwise, skip to question 5.
• If yes, please answer the following question. If no, skip to question 5 below 3a. How often did this happen—almost every month, some months but not every
month, or in only 1 or 2 months? • Almost every month • Some months but not every month • Only 1 or 2 months • Don’t know
• 4. In the last 12 months, did you ever eat less than you felt you should because there wasn't enough money to buy food?
• Yes
• No • Don’t know
• 5. In the last 12 months, were you ever hungry but didn't eat because you couldn't afford enough food? • Yes • No • Don’t know
• Modified by Pregnancy CDE Working Group • 6. In the last 12 months, if you didn’t have enough to eat or what you wanted to eat, why was that?
Choose all that apply.49
• Couldn’t get out to buy food (for example, didn’t have transportation, or had mobility or health problems that prevented you from getting out)
• Didn’t want to go out to buy food • Afraid to go out because of the chance of contracting COVID-19 • Couldn’t get groceries or meals delivered to me • The stores didn’t have the food I wanted • Other (specify) • I always had enough to eat and what I wanted to eat
†Breakfast/Lunch from School (Tier 2)50
Parent Report About Child • Did your child get breakfast and/or lunch from the school in the 2019-2020 school year before the
COVID-19 pandemic? • No • Yes • Don’t Know
• If yes, did the school continue to provide breakfast and/or lunch during the COVID-19 pandemic (since March 2020)?
• No • Yes, less frequently • Yes, same frequency • Yes, more frequently
Household Income51
Parent Self-Report • Thinking about members of your family living in this household, what is your combined annual income,
meaning the total pre-tax income from all sources earned in the past year? • $0 to $9,999 • $10,000 to $14,999 • $15,000 to $19,999 • $20,000 to $34,999 • $35,000 to $49,999 • $50,000 to $74,999 • $75,000 to $99,999 • $100,000 to $199,999 • $200,000 or more • Don’t know/Not sure • Prefer not to answer

†Racial/Ethnic Discrimination Child Self-Report (Ages 13+)
• During your life, how often have you felt that you were treated badly or unfairly because of your race or ethnicity?52
• Never • Rarely • Sometimes • Most of the time • Always
• Since the start of the pandemic (since March 2020), have you felt that you were treated badly or unfairly because of your race or ethnicity53:
• Less • Same amount • More • Not applicable (N/A)
†Coronavirus Racial/Ethnic Bias (Tier 2) Child Self-Report (Ages 15+)54
• Please answer the following questions on your beliefs about how the coronavirus is affecting people of your race/ethnicity
Strongly disagree
Somewhat disagree
Somewhat agree
Strongly agree
I believe the country has become more dangerous for people in my racial/ethnic group because of fear of the coronavirus.
1 2 3 4
People of my race/ethnicity are more likely to lose their job because of the coronavirus.
1 2 3 4
I worry about people thinking I have the coronavirus simply because of my race/ethnicity.
1 2 3 4
Most social and mass media reports about the coronavirus create bias against people of my racial/ethnic group.
1 2 3 4
People of my race/ethnicity are more likely to get the coronavirus.
1 2 3 4
People of my race/ethnicity will not receive coronavirus healthcare as good as the care received by other groups.
1 2 3 4
Due to the coronavirus, I have been cyberbullied because of my race/ethnicity.
1 2 3 4
Since the coronavirus, I have seen a lot more cyberbullying of people of my race/ethnicity.
1 2 3 4
Negative social media posts against people of my race/ethnicity have increased because of the coronavirus.
1 2 3 4
Domain: Educational Factors Grade Level (School-age Child) Parent Report About Child55
• What is this child’s current grade, grade equivalent, or year of school? If this child is not assigned a specific grade or is homeschooled, mark the grade level of the curriculum the child receives. If between school years, mark the last grade level attended.
• Child has not yet started kindergarten • Full-day kindergarten • Partial-day kindergarten • 1st grade • 2nd grade • 3rd grade • 4th grade • 5th grade • 6th grade • 7th grade • 8th grade • 9th grade • 10th grade • 11th grade • 12th grade
Child Self-Report (Ages 12+)56
• Think about the school you [currently/last] [attend/attended]. What grade [are/were] you in? • 4th grade • 5th grade • 6th grade • 7th grade • 8th grade • 9th grade • 10th grade • 11th grade • 12th grade
Current School Type57
Parent Report About Child • Is your child’s current school a... [mark all that apply]
• A public school, including charter school or magnet school • A private school, including private religious schools • Bureau of Indian Affairs (BIA) or tribal school • Early Childhood Center (school/center includes preschool and/or early elementary grades) • Special Education school – primarily serves children with disabilities • College, community college, or university • Homeschool, including co-ops • Full-time cyber school
Child Self-Report (Ages 13+)*

• Is your current school a... [mark all that apply] • A public school, including charter school or magnet school • A private school, including private religious schools • Bureau of Indian Affairs (BIA) or tribal school • Special Education school – primarily serves children with disabilities • College, community college, or university • Homeschool, including co-ops • Full-time cyber school
Note: for the remaining elements in this Domain, the questions are primarily for grades K-12: †Accommodations for Learning Difference58
Parent Report About Child • Does your child have an Individualized Education Plan (IEP) or 504 plan?
• No • Yes • Don’t know • If yes, was your child receiving specialized services or resources on an Individualized Education
Plan (IEP) or 504 plan in the 2019-2020 school year before the pandemic?59
• No • Yes • Don’t know
• During the pandemic (since March 2020) were the child’s services less, the same, or more frequent compared to before the pandemic?60
• Less • Same • More • N/A
†Changes to Schooling During Pandemic61
Additional Guidance: This is a high level element to capture predominant forms of schooling during the different school years spanning the COVID-19 pandemic. For studies that want more detailed assessment of the length of time spent in the different forms of schooling during the COVID-19 pandemic, the Working Group proposes two strategies for investigators to consider: 1) using an event history calendar as a visual guide to obtain more specific month to month information on changes to schooling; from parents, and/or 2) obtaining the school district information on changes to schooling during the pandemic, noting this may only be applicable to students attending public schools (i.e., if the student answers Current School Type with “A public school, including charter school or magnet school”).
Parent Report About Child • From March 2020-June 2020, what was the predominant form of schooling for your child:
o Attend school in person ONLY o Attend school remotely ONLY o Attend school via a hybrid model that included in person schooling and remote distance learning o Not attend school because school was cancelled o Not attend school because child dropped out o Not attend school for other reason (please specify) o Not applicable (N/A)
• From Sept 2020-June 2021, what was the predominant form of schooling for your child: o Attend school in person ONLY o Attend school remotely ONLY o Attend school via a hybrid model that included in person schooling and remote distance learning o Not attend school because school was cancelled o Not attend school because child dropped out o Not attend school for other reason (please specify) o Not applicable (N/A)
• From Sept 2021-present, what was the predominant form of schooling for your child: o Attend school in person ONLY o Attend school remotely ONLY o Attend school via a hybrid model that included in person schooling and remote distance learning o Not attend school because school was cancelled o Not attend school because child dropped out o Not attend school for other reason (please specify) o Not applicable (N/A)
†School Attendance/Absence (Tier 2)62
Parent Report About Child Additional Guidance: Parent-reported absenteeism may be unreliable. Studies may alternatively seek to use school district records to calculate absences during each school year.63
• Since start of the current school year (or past school year if on summer break), about how many days did this child miss school (including missing remote learning)?
• No missed school days [skip next question] • 1-3 days • 4-6 days • 7-10 days • 11-15 days • 15 or more days • This child was not enrolled in school [skip next question] • Don’t know [skip next question]
• If more than 1 day was missed, about how many days did this child miss school (including missing remote learning) because of illness of you or a family member from COVID-19?
• No missed school days • 1-3 days • 4-6 days • 7-10 days • 11-15 days • 15 or more days • This child was not enrolled in school • Don’t know
†Perception of Changes to Schooling (Tier 2)64
Parent Report About Child

• Using a scale of 1-5 where 1 is not at all true, and 5 is completely true, how true would you say each of the following statements is for your child’s school/college, regarding how your experiences were/are during the COVID-19 pandemic (since March 2020)
Not at all true (1)
(2) (3) (4) Completely true (5)
Remote learning is as effective as live/traditional classroom lectures for my child. My child can meet his/her educational goals with remote learning. My child has sufficient social interaction with peers during remote learning. It seems my child experiences a lack of interest during remote learning. It seems my child experiences frustration during remote learning.
School Risk and Protective Factors (Tier 2)65
Child Self-Report (Ages 12-18) Strongly Disagree, Disagree, Neither Agree or Disagree, Agree, Strongly Agree:
Teacher Relationships 1. Teachers understand my problems 2. Teachers and staff seem to take a real interest in my future 3. Teachers are available when I need to talk with them 4. It is easy to talk with teachers 5. Students get along well with teachers 6. At my school, there is a teacher or some other adult who notices when I’m not there 7. Teachers at my school help us children with our problems 8. My teachers care about me 9. My teacher makes me feel good about myself School Connectedness 10. My schoolwork is exciting 11. Students can make suggestions on courses that are offered 12. Students are publicly recognized for their outstanding performances in speech, drama, art, music, etc. 13. If this school had an extra period during the day, I would take an additional academic class 14. This school makes students enthusiastic about learning 15. Students are frequently rewarded or praised by faculty and staff for following school rules Academic Support 16. I usually understand my homework assignments

17. Teachers make it clear what work needs to be done to get the grade I want 18. I believe that teachers expect all students to learn 19. I feel that I can do well in this school 20. My teachers believe that I can do well in my school work 21. I try hard to succeed in my classes Order and Discipline 22. Classroom rules are applied equally 23. Problems in this school are solved by students and staff 24. Students get in trouble if they do not follow school rules 25. The rules of the school are fair 26. School rules are enforced consistently and fairly 27. My teachers make it clear to me when I have misbehaved in class 28. Discipline is fair (Only answer if in-person schooling) School Physical Environment 29. The school grounds are kept clean 30. My school is neat and clean 31. My school buildings are generally pleasant and well maintained 32. My school is usually clean and tidy School Social Environment 33. I am happy with kinds of students who go to my school 34. I am happy, in general, with the other students who go to my school Perceived Exclusion/Privilege 35. At my school, the same person always gets to help the teacher 36. At my school, the same kids get chosen every time to take part in after-school or special activities 37. The same kids always get to use things, like a computer, a ball or a piano, when we play Academic Satisfaction 38. I am happy about the number of tests I have 39. I am happy about the amount of homework I have
†Academic Performance/Achievement66
Child Self-Report (Ages 10+)/Parent Report About Child • In the months before the pandemic (2019-February 2020) how would you describe [your/your child’s]
grades in school? • Below Average (D’s or F’s) • Average (C’s) • Good (B’s) • Very Good (A’s and B’s) • Excellent (A’s) • I/my child was not graded • Refused • Don’t know
• During the current school year (or most recent school year if on summer break) how would you describe [your/your child’s] grades in school? • Below Average (D’s or F’s) • Average (C’s)

• Good (B’s) • Very Good (A’s and B’s) • Excellent (A’s) • I/my child was not graded • Refused • Don’t know
†Childcare (Tier 2) Parent Self-Report67
• How has the COVID-19 outbreak affected your regular childcare/supervision of school aged children (K-12)? (Mark all that apply)
• I had difficulty arranging for childcare/supervision • I had to pay more for childcare/supervision • My co-parent or I no longer needed child care • My co-parent or I had to change our work schedule or quit our job to care for our children • My regular childcare/supervision was not affected by the COVID-19 outbreak • I do not have a school-age child who needed regular supervision
†Computer and Internet Access68
Parent Report About Child • How often is a computer/laptop or other digital device (e.g., tablet) available to your child for
educational purposes to support remote distance learning? Select only one answer. • Always available • Usually available • Sometimes available • Rarely available • Never available • N/A
• Is/are the computer(s) or other digital device(s) …? Select all that apply. • Provided by the child’s school or school district to use outside of school • Provided by someone in the household or family, or it is the child’s • Provided by another source • N/A
• How often is the Internet available to your child for educational purposes to support remote distance learning? Select only one answer. • Always available • Usually available • Sometimes available • Rarely available • Never available • N/A
• Are Internet services …? Select all that apply. • Paid for by the children’s school or school district • Paid for by someone in the household or family • Paid for by another source • N/A

Domain: Community, Family, and Peer Factors †Social Connection/Support Child Self-Report (Age 13+)69
• Compared to before the COVID-19 outbreak (before March 2020), do you feel • Much less socially connected • Less socially connected • Slightly less socially connected • Slightly more socially connected • More socially connected • Much more socially connected
Parent Report About Child (Age 8+)70
• Compared to before the COVID-19 outbreak (before March 2020), does your child seem • Much less socially connected • Less socially connected • Slightly less socially connected • Slightly more socially connected • More socially connected • Much more socially connected
†Emotional Support/Social Support (Tier 2)71
NIH Toolbox Emotional Support FF v2.0 Child Self-Report (Ages 8-17) • Respond by marking one box per row • In the past month, please describe how often…
Never Rarely Sometimes Usually Always I have someone who understands my problems I have someone who will listen to me when I need to talk I have someone to talk with when I have a bad day There is someone around to help me if I need it I can get helpful advice from others when dealing with a problem I get useful advice about important things in my life I have someone to talk with about school problems
• Working Group addition: • Compared to before the COVID-19 pandemic (before March 2020)…
Less The same More I have someone who understands my problems I have someone who will listen to me when I need to talk I have someone to talk with when I have a bad day

There is someone around to help me if I need it I can get helpful advice from others when dealing with a problem I get useful advice about important things in my life I have someone to talk with about school problems
†Peer Relationships (Tier 2)72
Parent Report About Child (Ages 1-5): PROMIS Early Childhood Parent Report Item Bank v1.0 – Social Relationships – Peer Relationships – Short Form 4a
• Please respond to each question or statement by marking one box per row • In the past 7 days…
Never Rarely Sometimes Usually Always My child shared with other kids My child played well with other children My child laughed and smiled with other children My child showed interest in other children
• Working Group addition: • Compared to before the COVID-19 pandemic (before March 2020)…
Less The same More My child shares with other kids My child plays well with other children My child laughs and smiles with other children My child shows interest in other children
Parent Report About Child (Ages 5-17): PROMIS Parent Proxy Bank v2.0 – Peer Relationships – Short Form 7a
• Please respond to each question or statement by marking one box per row • In the past 7 days…
Never Rarely Sometimes Usually Always My child felt accepted by other kids his/her age My child was able to count on his/her friends My child was good at making friends My child and his/her friends helped each other out Other kids wanted to be my child's friend
Other kids wanted to be with my child Other kids wanted to talk to my child
• Working Group addition: • Compared to before the COVID-19 pandemic (before March 2020)…
Less The same More My child feels accepted by other kids his/her age My child is able to count on his/her friends My child is good at making friends My child and his/her friends help each other out Other kids want to be my child's friend Other kids want to be with my child Other kids want to talk to my child
Child Self-Report (Ages 8-17): PROMIS Pediatric Item Bank v2.0 – Peer Relationships – Short Form 8a
• Please respond to each question or statement by marking one box per row • In the past 7 days…
Never Rarely Sometimes Usually Always I felt accepted by other kids my age I was able to count on my friends I was able to talk about everything with my friends I was good at making friends
My friends and I helped each other out Other kids wanted to be my friend Other kids wanted to be with me Other kids wanted to talk to me
• Working Group addition: • Compared to before the COVID-19 pandemic (before March 2020)…
Less The same More I feel accepted by other kids my age I am able to count on my friends I am able to talk about everything with my friends I am good at making friends My friends and I help each other out

Other kids want to be my friend Other kids want to be with me Other kids want to talk to me
†Family Impact/Household Interpersonal Conflict (Tier 2)73
Parent Self-Report • How [have/were] you and your child(ren) (been) getting along during the COVID-19 outbreak (since
March 2020)? • Very well – no problems or tension • Well – occasional tension, some tension, but manageable • Okay – some tension and sometimes things get out of hands (a few heated arguments) • Not very well – tense, lots of arguing, unsettled feeling, definite problems • Terribly
• Is this a change from how you were getting along before the outbreak (before March 2020)? • No • Yes
Child Self-report (Ages 13+) • How [have/were] YOU and your parent(s) (been) getting along during the COVID-19 outbreak (since
March 2020)? • Very well – no problems or tension • Well – occasional tension, some tension, but manageable • Okay – some tension and sometimes things get out of hands (a few heated arguments) • Not very well – tense, lots of arguing, unsettled feeling, definite problems • Terribly
• Is this a change from how you were getting along before the outbreak (before March 2020)? • No • Yes
If study approval and privacy ensured; INTERVIEWER: IF CONDUCTING PHONE INTERVIEW, PLEASE SAY THE FOLLOWING: For the next 3 questions, I am going to ask you about some private matters, so please turn your speakerphone off.
• During the COVID-19 outbreak (since March 2020), did things ever get to the point where an adult you were living with got physically violent with a child (for example, shoved, hit, kicked, or shook [her/him/them])?
• No • Yes
• During the COVID-19 outbreak (since March 2020), was an adult in your household ever physically violent with you (for example, shoved, hit, kicked, or shook you)?
• No • Yes
• During the COVID-19 outbreak (since March 2020), did things ever get to the point where an adult you were living with got physically violent with someone else (for example, shoved, hit, kicked, or shook someone else)?
• No • Yes
Additional Guidance: Guidance for conducting child maltreatment research and reporting varies depending on the scope of the project, study participants, setting of the study (school, hospital, etc.) and state mandatory reporting laws. More information on state statutes can be found at the HHS Childwelfare.gov site: https://www.childwelfare.gov/pubPDFs/manda.pdf (2019). Researchers should consult with their IRBs to minimize risks to study participants, appropriately consent and adhere to ethical practices and regulatory requirements for including vulnerable children in research: https://www.hhs.gov/ohrp/regulations-and-policy/guidance/special-protections-for-children/index.html. Additional NICHD resources for forensic or evidence-based interviewing of children include: http://nichdprotocol.com/, https://youth.gov/content/nichd-investigative-interview-protocol.
Community Support (Cohesion) (Tier 2)74
Parent Self-Report • Now I’m going to read some statements about things that people in your neighborhood may or may not do. • For each of these statements, please tell me whether you strongly agree, agree, neither agree nor disagree,
disagree or strongly disagree. • This is a close-knit neighborhood. • People around here are willing to help their neighbors. • People in this neighborhood generally don’t get along with each other. • People in this neighborhood do not share the same values. • People in this neighborhood can be trusted.
• For each of the following, please tell me if it is very likely, likely, neither likely nor unlikely, unlikely, or very unlikely that people in your neighborhood would act in the following manner. • If a group of neighborhood children were skipping school and hanging out on a street corner, how likely
is it that your neighbors would do something about it? • If some children were spray-painting graffiti on a local building, how likely is it that your neighbors
would do something about it? • If a child was showing disrespect to an adult, how likely is it that people in your neighborhood would
scold that child? • If there was a fight in front of your house and someone was being beaten or threatened, how likely is it
that your neighbors would break it up? • Suppose that because of budget cuts the fire station closest to your home was going to be closed down
by the city. How likely is it that neighborhood residents would organize to try to do something to keep the fire station open?
Domain: Social Media/Screen Time †Time Spent in Front of a Screen (Tier 2) Child Self-Report (Ages 13+)*/Parent Report About Child75
• ON MOST WEEKDAYS, about how much time did [you/your child] spend in front of a TV, computer, cellphone or other electronic device watching programs, playing games, accessing the Internet or using social media? Do not include time spent doing schoolwork.
• Less than 1 hour • 1 hour • 2 hours • 3 hours • 4 or more hours
• Compared to before the COVID-19 outbreak (before March 2020), how much are [you/your child] now doing of the following76:
• Spending time watching TV/videos (such as YouTube), playing video/computer games, or using social media for educational purposes, including schoolwork
• Less • Same amount • More
• Spending time watching TV/videos (such as YouTube), playing video/computer games, or using social media for non-educational purposes
• Less • Same amount • More
Domain: Well-being Factors †Well-being77
Child Self-Report (Ages 13+) • Since becoming aware of the COVID-19 outbreak, how often have you felt happy and satisfied with your
life • Not at all • Rarely • Sometimes • Often • Very often
Parent Report About Child (age 1+) • Since becoming aware of the COVID-19 outbreak, how often has your child seemed happy and satisfied
with his/her life? • Not at all • Rarely • Sometimes • Often • Very often
Well-being (Tier 2)78
NIH Toolbox Positive Affect Fixed Form v2.0 Child Self-Report (Ages 8-12)
• In the past 7 days, Not at all A little bit Somewhat Quite a bit Very much
I felt attentive I felt delighted I felt calm I felt at ease I felt enthusiastic I felt interested I felt confident I felt energetic
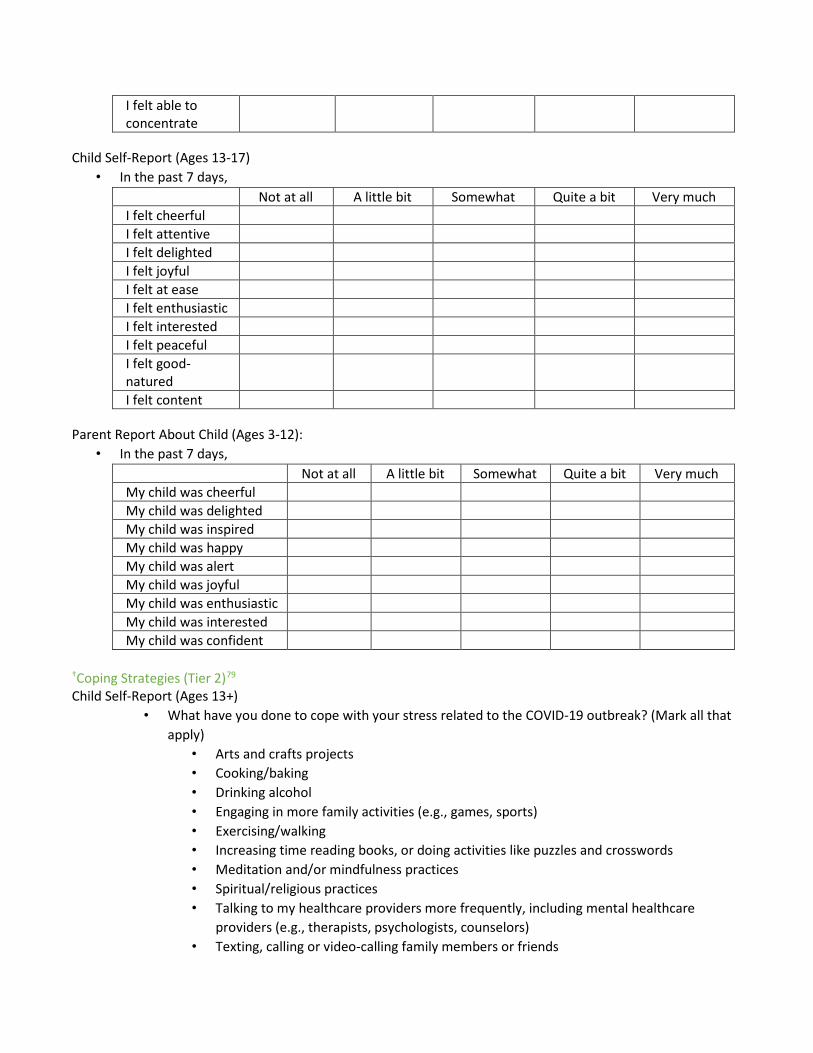
I felt able to concentrate
Child Self-Report (Ages 13-17) • In the past 7 days,
Not at all A little bit Somewhat Quite a bit Very much I felt cheerful I felt attentive I felt delighted I felt joyful I felt at ease I felt enthusiastic I felt interested I felt peaceful I felt good-natured I felt content
Parent Report About Child (Ages 3-12): • In the past 7 days,
Not at all A little bit Somewhat Quite a bit Very much My child was cheerful My child was delighted My child was inspired My child was happy My child was alert My child was joyful My child was enthusiastic My child was interested My child was confident
†Coping Strategies (Tier 2)79
Child Self-Report (Ages 13+) • What have you done to cope with your stress related to the COVID-19 outbreak? (Mark all that
apply) • Arts and crafts projects • Cooking/baking • Drinking alcohol • Engaging in more family activities (e.g., games, sports) • Exercising/walking • Increasing time reading books, or doing activities like puzzles and crosswords • Meditation and/or mindfulness practices • Spiritual/religious practices • Talking to my healthcare providers more frequently, including mental healthcare
providers (e.g., therapists, psychologists, counselors) • Texting, calling or video-calling family members or friends
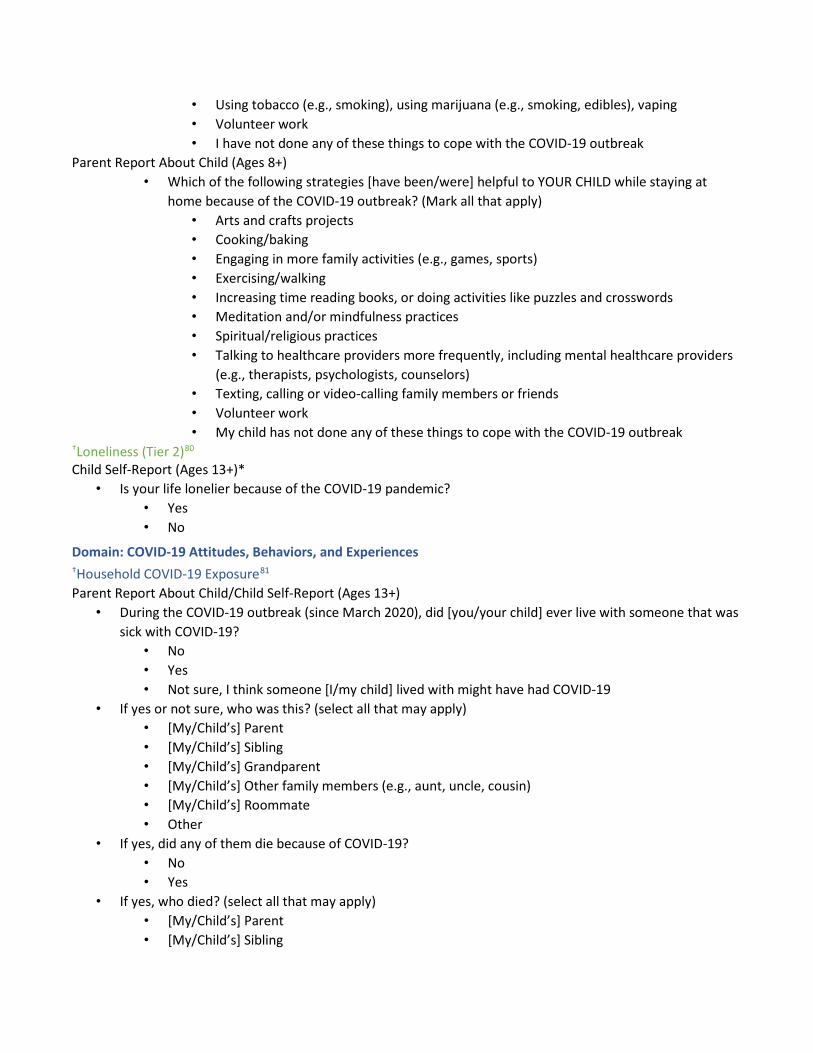
• Using tobacco (e.g., smoking), using marijuana (e.g., smoking, edibles), vaping • Volunteer work • I have not done any of these things to cope with the COVID-19 outbreak
Parent Report About Child (Ages 8+) • Which of the following strategies [have been/were] helpful to YOUR CHILD while staying at
home because of the COVID-19 outbreak? (Mark all that apply) • Arts and crafts projects • Cooking/baking • Engaging in more family activities (e.g., games, sports) • Exercising/walking • Increasing time reading books, or doing activities like puzzles and crosswords • Meditation and/or mindfulness practices • Spiritual/religious practices • Talking to healthcare providers more frequently, including mental healthcare providers
(e.g., therapists, psychologists, counselors) • Texting, calling or video-calling family members or friends • Volunteer work • My child has not done any of these things to cope with the COVID-19 outbreak
†Loneliness (Tier 2)80
Child Self-Report (Ages 13+)* • Is your life lonelier because of the COVID-19 pandemic?
• Yes • No
Domain: COVID-19 Attitudes, Behaviors, and Experiences †Household COVID-19 Exposure81
Parent Report About Child/Child Self-Report (Ages 13+) • During the COVID-19 outbreak (since March 2020), did [you/your child] ever live with someone that was
sick with COVID-19? • No • Yes • Not sure, I think someone [I/my child] lived with might have had COVID-19
• If yes or not sure, who was this? (select all that may apply) • [My/Child’s] Parent • [My/Child’s] Sibling • [My/Child’s] Grandparent • [My/Child’s] Other family members (e.g., aunt, uncle, cousin) • [My/Child’s] Roommate • Other
• If yes, did any of them die because of COVID-19? • No • Yes
• If yes, who died? (select all that may apply) • [My/Child’s] Parent • [My/Child’s] Sibling

• [My/Child’s] Grandparent • [My/Child’s] Other family members (e.g., aunt, uncle, cousin) • [My/Child’s] Roommate • Other
†Ability to Isolate (Tier 2)82
Parent Self-Report • If it were necessary, could a member of your household isolate themselves from the rest of your household
due to suspected COVID-19 infection for as long as needed? To effectively isolate during a COVID-19 infection, the infected family member would need to stay in a specific “sick room” away from other people or animals and, if possible, use a separate bathroom.
• Yes • No • Unknown
†Belief That COVID is Serious Disease (Tier 2)83
Parent Self-Report/Child Self-Report (Ages 13+)* • I believe that COVID-19 is a serious disease.
• Yes • No • Unsure (or don’t know)
†Adherence to Social Distancing/Face Coverings (Tier 1)84
Parent Self-Report/Child Self-Report (Ages 13+)* • To the best of your knowledge, which of the following can protect you and your family from COVID-19?
(Mark all that apply) • Standing 6 feet from another person • Wearing a face mask • Working from home • Distance learning (or taking school classes over the computer or remotely) • Vaccination for COVID-19
†Vaccine Attitudes (Tier 2) Parent Self-Report85
• Which of the following applies to your plans about the COVID vaccine for your child(ren)? • My child(ren) is/are already vaccinated • I plan on getting the COVID vaccine for my child(ren) as soon as it is available • I plan on getting the COVID vaccine for my child(ren) eventually • I do not plan on getting the COVID vaccine for my child(ren) • I am unsure
• If you do not plan on getting the COVID vaccine for your child(ren), why not (mark all that apply)?86
• Not available • Doctor/healthcare provider did not recommend • My friends and family did not recommend • I have read information that suggests it is unsafe • The vaccine was not well tested in ethnically diverse people • The vaccine was not well tested among children • I cannot afford the vaccine

• I do not have time to take my child to be vaccinated • My child is at low risk and does not need it • It is riskier to go and get it than to stay at home • Worried about side effects • The vaccine’s technology hasn’t been tested enough • The vaccine was approved too fast • No long-term safety data available • Concerned about vaccine storage • My child already had COVID-19 • Other (please specify):
Domain: COVID-19 Stress and Worry †Worry/Anxiety About COVID-19 (Tier 2)87
Child Self-Report (Ages 9+) • During the COVID-19 pandemic (since March 2020)
Not at all Slightly Moderately Very Extremely How worried have you been about coronavirus (COVID-19)? How worried have others around you been about coronavirus (COVID-19)? How worried have you been about changes to schooling in the 2020-2021 school year (e.g., missing school in-person)? How much do you think your life has changed due to coronavirus (COVID-19)? How hopeful have you been that the coronavirus/COVID-19 crisis in your area will end soon?
• In the past week: Not at all Slightly Moderately Very Extremely
How worried have you been about coronavirus (COVID-19)? How worried have others around you been about coronavirus (COVID-19)? How worried have you been about changes to schooling in the 2020-2021 school year (e.g., missing school in-person)? How much do you think your life has changed due to coronavirus (COVID-19)?
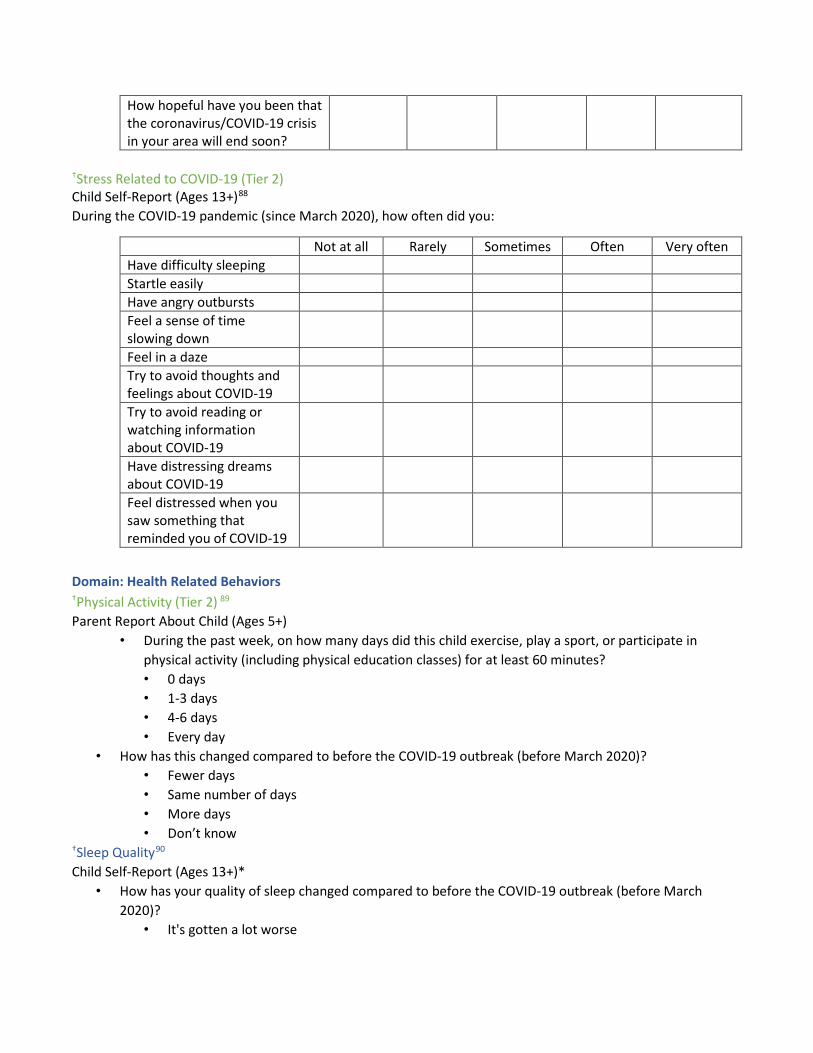
How hopeful have you been that the coronavirus/COVID-19 crisis in your area will end soon?
†Stress Related to COVID-19 (Tier 2) Child Self-Report (Ages 13+)88
During the COVID-19 pandemic (since March 2020), how often did you:
Not at all Rarely Sometimes Often Very often Have difficulty sleeping Startle easily Have angry outbursts Feel a sense of time slowing down Feel in a daze Try to avoid thoughts and feelings about COVID-19 Try to avoid reading or watching information about COVID-19 Have distressing dreams about COVID-19 Feel distressed when you saw something that reminded you of COVID-19
Domain: Health Related Behaviors †Physical Activity (Tier 2) 89
Parent Report About Child (Ages 5+) • During the past week, on how many days did this child exercise, play a sport, or participate in
physical activity (including physical education classes) for at least 60 minutes? • 0 days • 1-3 days • 4-6 days • Every day
• How has this changed compared to before the COVID-19 outbreak (before March 2020)? • Fewer days • Same number of days • More days • Don’t know
†Sleep Quality90
Child Self-Report (Ages 13+)* • How has your quality of sleep changed compared to before the COVID-19 outbreak (before March
2020)? • It's gotten a lot worse
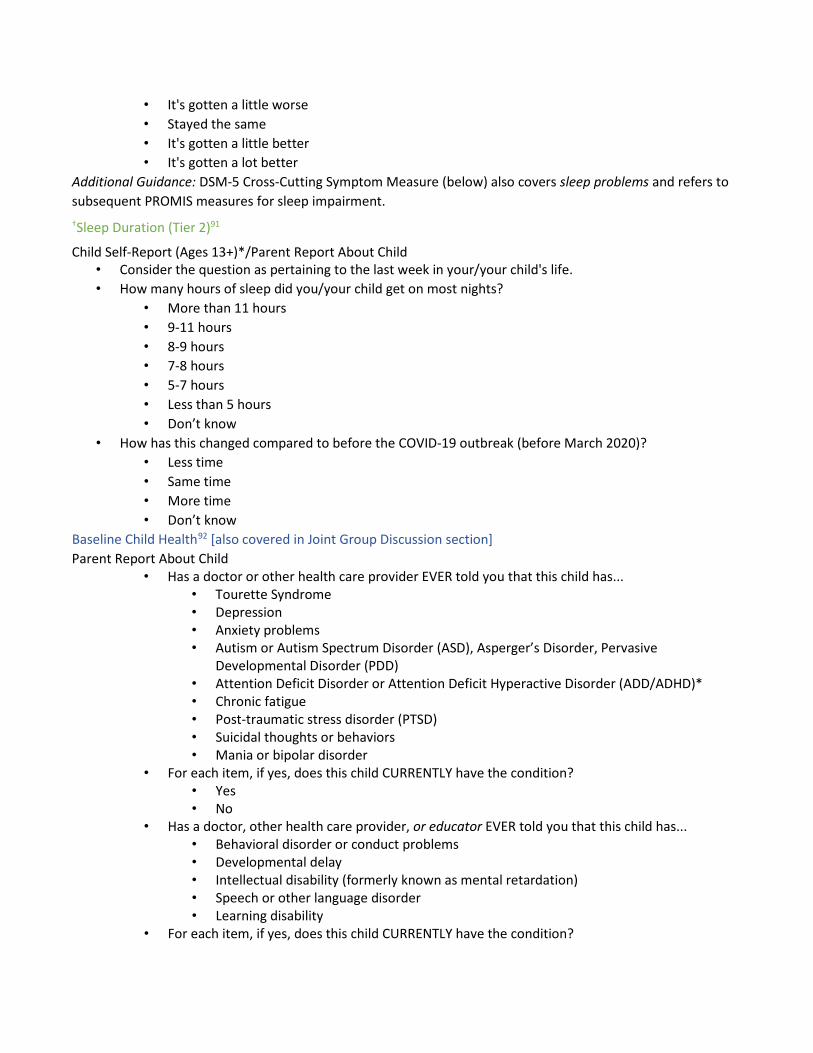
• It's gotten a little worse • Stayed the same • It's gotten a little better • It's gotten a lot better
Additional Guidance: DSM-5 Cross-Cutting Symptom Measure (below) also covers sleep problems and refers to subsequent PROMIS measures for sleep impairment. †Sleep Duration (Tier 2)91
Child Self-Report (Ages 13+)*/Parent Report About Child • Consider the question as pertaining to the last week in your/your child's life. • How many hours of sleep did you/your child get on most nights?
• More than 11 hours • 9-11 hours • 8-9 hours • 7-8 hours • 5-7 hours • Less than 5 hours • Don’t know
• How has this changed compared to before the COVID-19 outbreak (before March 2020)? • Less time • Same time • More time • Don’t know
Baseline Child Health92 [also covered in Joint Group Discussion section] Parent Report About Child
• Has a doctor or other health care provider EVER told you that this child has... • Tourette Syndrome • Depression • Anxiety problems • Autism or Autism Spectrum Disorder (ASD), Asperger’s Disorder, Pervasive
Developmental Disorder (PDD) • Attention Deficit Disorder or Attention Deficit Hyperactive Disorder (ADD/ADHD)* • Chronic fatigue • Post-traumatic stress disorder (PTSD) • Suicidal thoughts or behaviors • Mania or bipolar disorder
• For each item, if yes, does this child CURRENTLY have the condition? • Yes • No
• Has a doctor, other health care provider, or educator EVER told you that this child has... • Behavioral disorder or conduct problems • Developmental delay • Intellectual disability (formerly known as mental retardation) • Speech or other language disorder • Learning disability
• For each item, if yes, does this child CURRENTLY have the condition?

• Yes • No
Domain: Mental and Behavioral Health Overall Physical and Mental/Emotional Health Note: Collect BOTH Parent-Self Report and either Child-Self Report or Parent Report About Child Parent Self-Report93
• In general, how is your physical health? • Excellent • Very good • Good • Fair • Poor
• In general, how is your mental or emotional health? • Excellent • Very good • Good • Fair • Poor
Parent Report About Child94
• In general, how is your child’s physical health? • Excellent • Very good • Good • Fair • Poor
• In general, how is your child’s mental or emotional health? • Excellent • Very good • Good • Fair • Poor
Child Self-Report (Ages 8+)95
• In general, how would you rate your physical health? • Excellent • Very good • Good • Fair • Poor
• In general, how would you rate your mental health, including your mood and your ability to think? • Excellent • Very good • Good • Fair • Poor
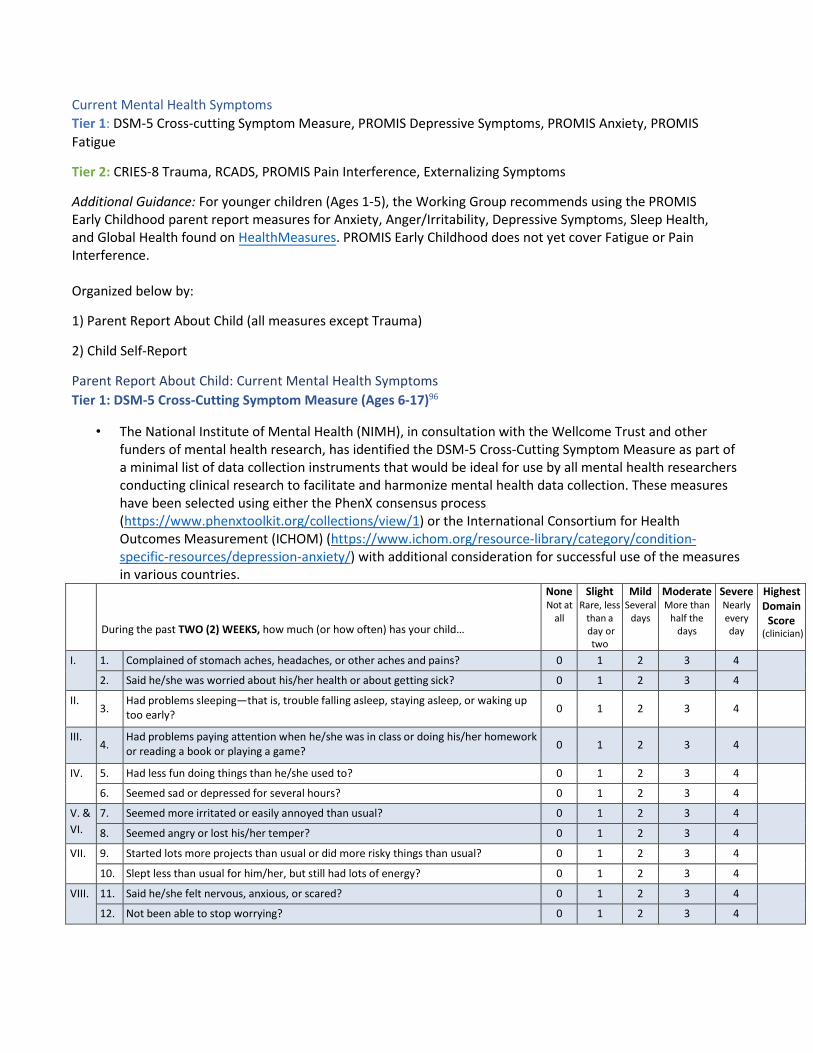
Current Mental Health Symptoms Tier 1: DSM-5 Cross-cutting Symptom Measure, PROMIS Depressive Symptoms, PROMIS Anxiety, PROMIS Fatigue
Tier 2: CRIES-8 Trauma, RCADS, PROMIS Pain Interference, Externalizing Symptoms
Additional Guidance: For younger children (Ages 1-5), the Working Group recommends using the PROMIS Early Childhood parent report measures for Anxiety, Anger/Irritability, Depressive Symptoms, Sleep Health, and Global Health found on HealthMeasures. PROMIS Early Childhood does not yet cover Fatigue or Pain Interference.
Organized below by:
1) Parent Report About Child (all measures except Trauma)
2) Child Self-Report
Parent Report About Child: Current Mental Health Symptoms Tier 1: DSM-5 Cross-Cutting Symptom Measure (Ages 6-17)96
• The National Institute of Mental Health (NIMH), in consultation with the Wellcome Trust and other funders of mental health research, has identified the DSM-5 Cross-Cutting Symptom Measure as part of a minimal list of data collection instruments that would be ideal for use by all mental health researchers conducting clinical research to facilitate and harmonize mental health data collection. These measures have been selected using either the PhenX consensus process (https://www.phenxtoolkit.org/collections/view/1) or the International Consortium for Health Outcomes Measurement (ICHOM) (https://www.ichom.org/resource-library/category/condition-specific-resources/depression-anxiety/) with additional consideration for successful use of the measures in various countries.
During the past TWO (2) WEEKS, how much (or how often) has your child…
None Not at
all
Slight Rare, less
than a day or two
Mild Several
days
Moderate More than
half the days
Severe Nearly every day
Highest Domain
Score (clinician)
I. 1. Complained of stomach aches, headaches, or other aches and pains? 0 1 2 3 4
2. Said he/she was worried about his/her health or about getting sick? 0 1 2 3 4
II. 3.
Had problems sleeping—that is, trouble falling asleep, staying asleep, or waking up too early? 0 1 2 3 4
III. 4.
Had problems paying attention when he/she was in class or doing his/her homework or reading a book or playing a game? 0 1 2 3 4
IV. 5. Had less fun doing things than he/she used to? 0 1 2 3 4
6. Seemed sad or depressed for several hours? 0 1 2 3 4
V. & VI.
7. Seemed more irritated or easily annoyed than usual? 0 1 2 3 4
8. Seemed angry or lost his/her temper? 0 1 2 3 4
VII. 9. Started lots more projects than usual or did more risky things than usual? 0 1 2 3 4
10. Slept less than usual for him/her, but still had lots of energy? 0 1 2 3 4
VIII. 11. Said he/she felt nervous, anxious, or scared? 0 1 2 3 4
12. Not been able to stop worrying? 0 1 2 3 4

13. Said he/she couldn’t do things he/she wanted to or should have done, because they made him/her feel nervous?
0 1 2 3 4
IX. 14. Said that he/she heard voices—when there was no one there—speaking about him/her or telling him/her what to do or saying bad things to him/her?
0 1 2 3 4
15. Said that he/she had a vision when he/she was completely awake—that is, saw something or someone that no one else could see?
0 1 2 3 4
X. 16.
Said that he/she had thoughts that kept coming into his/her mind that he/she 0 1 2 3 4would do something bad or that something bad would happen to him/her or to
someone else?
17. Said he/she felt the need to check on certain things over and over again, like whether 0 1 2 3 4a door was locked or whether the stove was turned off?
18. Seemed to worry a lot about things he/she touched being dirty or having germs or being poisoned?
0 1 2 3 4
19. Said that he/she had to do things in a certain way, like counting or saying special 0 1 2 3 4things out loud, in order to keep something bad from happening?
In the past TWO (2) WEEKS, has your child …
XI. 20. Had an alcoholic beverage (beer, wine, liquor, etc.)? Yes No Don’t Know
21. Smoked a cigarette, a cigar, or pipe, or used snuff or chewing tobacco? Yes No Don’t Know
22. Used drugs like marijuana, cocaine or crack, club drugs (like ecstasy), hallucinogens (like LSD), heroin, inhalants or solvents (like glue), or methamphetamine (like speed)?
Yes No Don’t Know
23. Used any medicine without a doctor’s prescription (e.g., painkillers [like Vicodin], stimulants [like Ritalin or Adderall], sedatives or tranquilizers [like sleeping pills or Valium], or steroids)?
Yes No Don’t Know
XII. 24. In the past TWO (2) WEEKS, has he/she talked about wanting to kill himself/herself or about wanting to commit suicide?
Yes No Don’t Know
25. Has he/she EVER tried to kill himself/herself? Yes No Don’t Know
Tier 2 (After Meeting Thresholds)
Domain Domain Name Threshold to guide further inquiry
DSM-5 Level 2 Cross-Cutting Symptom Measure available online
I. Somatic Symptoms Mild or greater LEVEL 2—Somatic Symptom—Parent/Guardian of Child Age 6–17 (Patient Health Questionnaire 15 Somatic Symptom Severity (PHQ-15)
II. Sleep Problems Mild or greater LEVEL 2—Sleep Disturbance—Parent/ Guardian of Child Age 6–17 (PROMIS— Sleep Disturbance—Short Form)1
III. Inattention Slight or greater LEVEL 2—Inattention—Parent/Guardian of Child Age 6–17 (SNAP-IV) IV. Depression Mild or greater LEVEL 2—Depression—Parent/Guardian of Child Age 6–17 (PROMIS Emotional
Distress—Depression—Parent Item Bank) V. Anger Mild or greater LEVEL 2—Anger—Parent/Guardian of Child Age 6–17 (PROMIS Emotional
Distress—Calibrated Anger Measure—Parent) VI. Irritability Mild or greater LEVEL 2—Irritability—Parent/Guardian of Child Age 6–17 (Affective Reactivity
Index) VII. Mania Mild or greater LEVEL 2—Mania—Parent/Guardian of Child Age 6–17 (adapted from the Altman
Self-Rating Mania Scale) VIII. Anxiety Mild or greater LEVEL 2—Anxiety—Parent/Guardian of Child Age 6–17 (adapted from PROMIS
Emotional Distress—Anxiety—Parent Item Bank) IX. Psychosis Slight or greater None
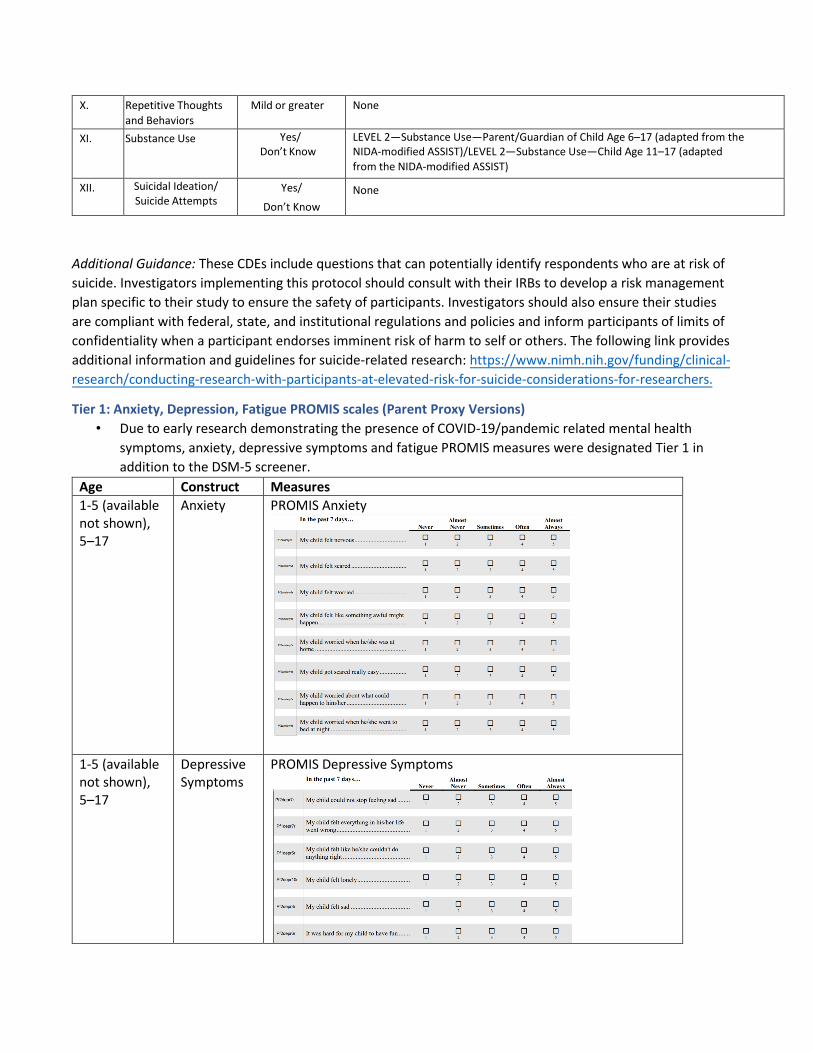
In Che pasc 7 days .. Almost AlmOit Ntn-r Nt\·tr Sometimn Ofte n Ahu .n
My child felt nervous ... D D D D D
' ) )
My chi ld felt scared ... D D D D D ' ) .
My child felt worried ... D D D D D ' ' ) . )
My child felt like something awful might D D D D D happen ... ' ) )
My child worried when he/she was at D D D D D home ... ) )
My chi ld got scared really easy ... D D D D D
My child worried about what could D D D D D happen to him/her .... ' ' ) . )
My child worried when he/she went to D D D D D bed at night .. ' .
In the pasc 7 days .. . Almos! Almost Newr Ne,'t r SomNimes or1en Alwa,•s
Pl2depr7r My child could not stop feeling sad ... D D D D D ' ' ) ' )
Plldepr7r My child felt everything in his/her life went wrong ...
D D D D D
~'"""' My child felt like he/she couldn't do D D D D D anything right .. '
Pf2depr10r My child felt lonely ... D D D D D
~,...,.,, My child felt sad .. D D D D D
~,- It was hard for my chi ld to have fun ... D D D D D 2 ) )
X. Repetitive Thoughts and Behaviors
Mild or greater None
XI. Substance Use Yes/ Don’t Know
LEVEL 2—Substance Use—Parent/Guardian of Child Age 6–17 (adapted from the NIDA-modified ASSIST)/LEVEL 2—Substance Use—Child Age 11–17 (adapted from the NIDA-modified ASSIST)
XII. Suicidal Ideation/ Suicide Attempts
Yes/
Don’t Know None
Additional Guidance: These CDEs include questions that can potentially identify respondents who are at risk of suicide. Investigators implementing this protocol should consult with their IRBs to develop a risk management plan specific to their study to ensure the safety of participants. Investigators should also ensure their studies are compliant with federal, state, and institutional regulations and policies and inform participants of limits of confidentiality when a participant endorses imminent risk of harm to self or others. The following link provides additional information and guidelines for suicide-related research: https://www.nimh.nih.gov/funding/clinical-research/conducting-research-with-participants-at-elevated-risk-for-suicide-considerations-for-researchers.
Tier 1: Anxiety, Depression, Fatigue PROMIS scales (Parent Proxy Versions) • Due to early research demonstrating the presence of COVID-19/pandemic related mental health
symptoms, anxiety, depressive symptoms and fatigue PROMIS measures were designated Tier 1 in addition to the DSM-5 screener.
Age Construct Measures 1-5 (available not shown), 5–17
Anxiety PROMIS Anxiety
1-5 (available not shown), 5–17
Depressive Symptoms
PROMIS Depressive Symptoms
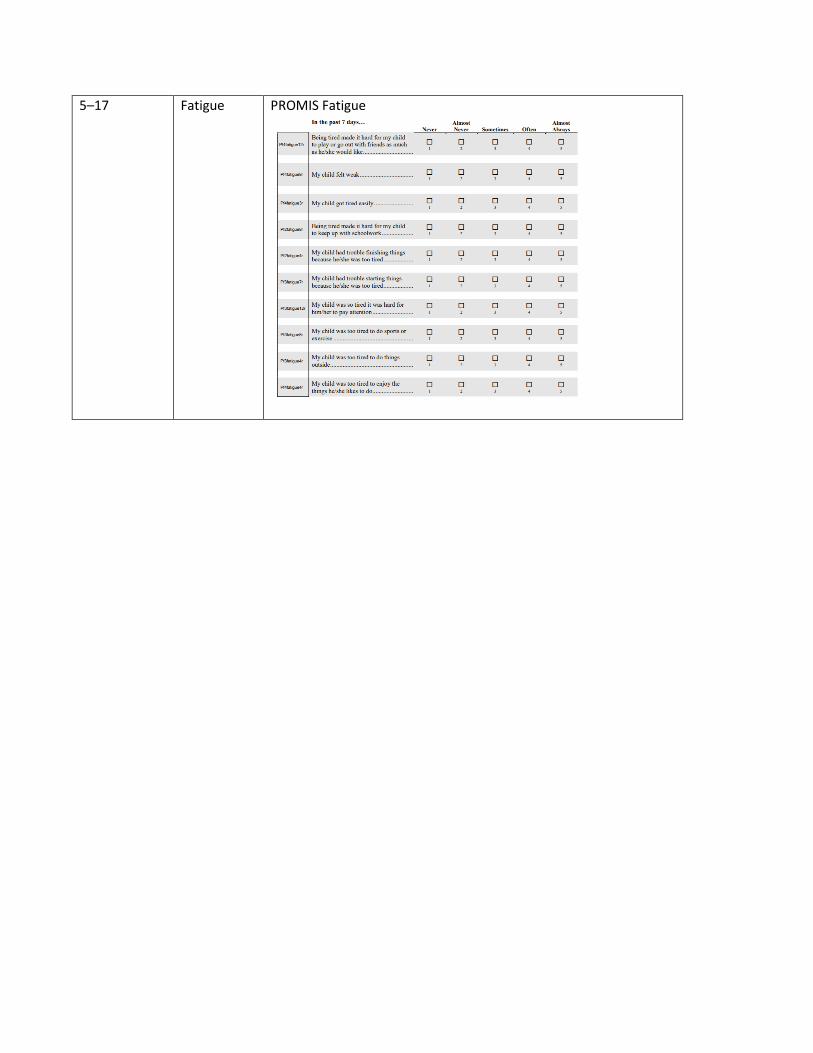
n the past 7 d a)' ...
Being tired made it hard for my child PMfaligue12r to play or go out with friends as much
as he/she would like ....
Pf:itar.v<-121'
My child felt weak ...
My child got tired easily ...
Being tired made it hard for my child to keep up with schoolwork ...
My child had trouble finishing things because he/she was too tired ...
My child had trouble starting things because he/she was too tired ...
My child was so tired it was hard for him/her to pay attent ion ...
My child was too tired lo do sports or exercise.
My child was too tired 10 do things outside ...
'
Almost Ne,·er Somelimn Often
' ' '
' ' '
' ' ' ' ' ' ' ' ' '
' ' ' ' '
' ' '
5–17 Fatigue PROMIS Fatigue
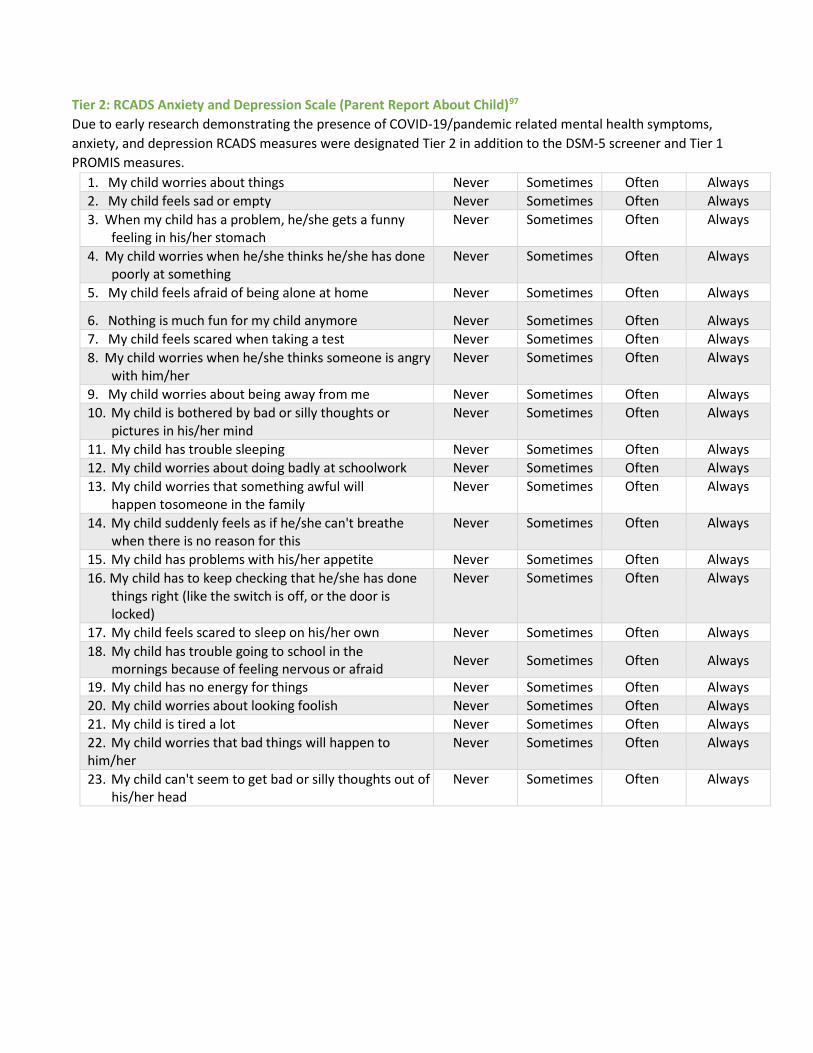
Tier 2: RCADS Anxiety and Depression Scale (Parent Report About Child)97
Due to early research demonstrating the presence of COVID-19/pandemic related mental health symptoms, anxiety, and depression RCADS measures were designated Tier 2 in addition to the DSM-5 screener and Tier 1 PROMIS measures.
1. My child worries about things Never Sometimes Often Always 2. My child feels sad or empty Never Sometimes Often Always 3. When my child has a problem, he/she gets a funny
feeling in his/her stomach Never Sometimes Often Always
4. My child worries when he/she thinks he/she has done poorly at something
Never Sometimes Often Always
5. My child feels afraid of being alone at home Never Sometimes Often Always
6. Nothing is much fun for my child anymore Never Sometimes Often Always 7. My child feels scared when taking a test Never Sometimes Often Always 8. My child worries when he/she thinks someone is angry
with him/her Never Sometimes Often Always
9. My child worries about being away from me Never Sometimes Often Always 10. My child is bothered by bad or silly thoughts or
pictures in his/her mind Never Sometimes Often Always
11. My child has trouble sleeping Never Sometimes Often Always 12. My child worries about doing badly at schoolwork Never Sometimes Often Always 13. My child worries that something awful will
happen tosomeone in the family Never Sometimes Often Always
14. My child suddenly feels as if he/she can't breathe when there is no reason for this
Never Sometimes Often Always
15. My child has problems with his/her appetite Never Sometimes Often Always 16. My child has to keep checking that he/she has done
things right (like the switch is off, or the door is locked)
Never Sometimes Often Always
17. My child feels scared to sleep on his/her own Never Sometimes Often Always 18. My child has trouble going to school in the
mornings because of feeling nervous or afraid Never Sometimes Often Always
19. My child has no energy for things Never Sometimes Often Always 20. My child worries about looking foolish Never Sometimes Often Always 21. My child is tired a lot Never Sometimes Often Always 22. My child worries that bad things will happen to him/her
Never Sometimes Often Always
23. My child can't seem to get bad or silly thoughts out of his/her head
Never Sometimes Often Always

In the past 7 days .. . Almost Almost Never Neve.- Sometimes Often Alwavs -
Pf2paWl5r My child had trouble sleeping when D D D D D he/she had pain .. I ' ] • '
Pf3pain7r My child felt angry when he/she had D D D D D pain ..... I ' ] • '
Pf2pain2r My child had trouble doing schoolwork D D D D D when he/she had pain .. I ' ] • '
pf3pain2r It was hard for my child to pay anention D D D D D when he/she had pain .. I ' ] • '
Pf2pain4r It was hard for my child to run when D D D D D he/she had pain .. I ' ] • '
Pflpain4r It was hard for my child to walk one D D D D D block when h she had pain .. I ' ] • '
Pf3pain4r It was hard for my chi ld to have fun D D D D D when he/she had pain .. I ' ] • '
Pf4pain6r It was hard for my chi ld to stay standing D D D D D when he/she had pain ......... I 2 ] • ' ~
Cognitive Function - Short Form 7a
Please respond 10 each ques tion or statement by marking one box per row.
In the past 4 weeks ... None of AIHrleof Some of Mos1of AU oflhe the time 1hetime the time the rime time
Your child has to use written lists D D D D D pedSPCF5_FA more often than other people his/her
' 4 ] ' I age so he/she will not forget things .....
NOCOG44_2 It is hard for your child to pay
D D D D D A, attention to one thing for more than
' 4 ] ' I 5. IO minutes ..... ............................... . ..
NOCOG65_2 Your child has trouble keeping track
D D D D D A, of what he/she is doing if he/she gets
' 4 ] ' I interrupted ..
p810_FA Your child has to read things severa l D D D D D times to understand them .. .. .. ... .. .. ... . ... ' 4 ] 2 I
p88_FA Your child forgets things easily ....... ... . D D D D D
' 4 ] ' I
Your child has to work really hard to D D D D D pedsPCF8_FA pay attention or he/she makes
' 4 ] 2 I mistakes ...............................................
Your child has trouble remembering D D D D D pedsPCF6_FA to do things like school projects or
chores ................................................... ' . ] ' I
Tier 2: Pain, Cognitive Function Age Construct Measures 8-17 Pain Pain Interference Parent Proxy
8-17 Cognitive Function
Cognitive Function Parent Proxy
Tier 2: Externalizing Symptoms • While prioritized as a Tier 2 measure, this Working Group does not recommend specific measures since
the most commonly used measures (Child Behavior Checklist and Strengths and Difficulties Questionnaire) require licensing. The Multidimensional Assessment Profile of Disruptive Behavior (MAP-DB), is available for use as well and does not require a license.
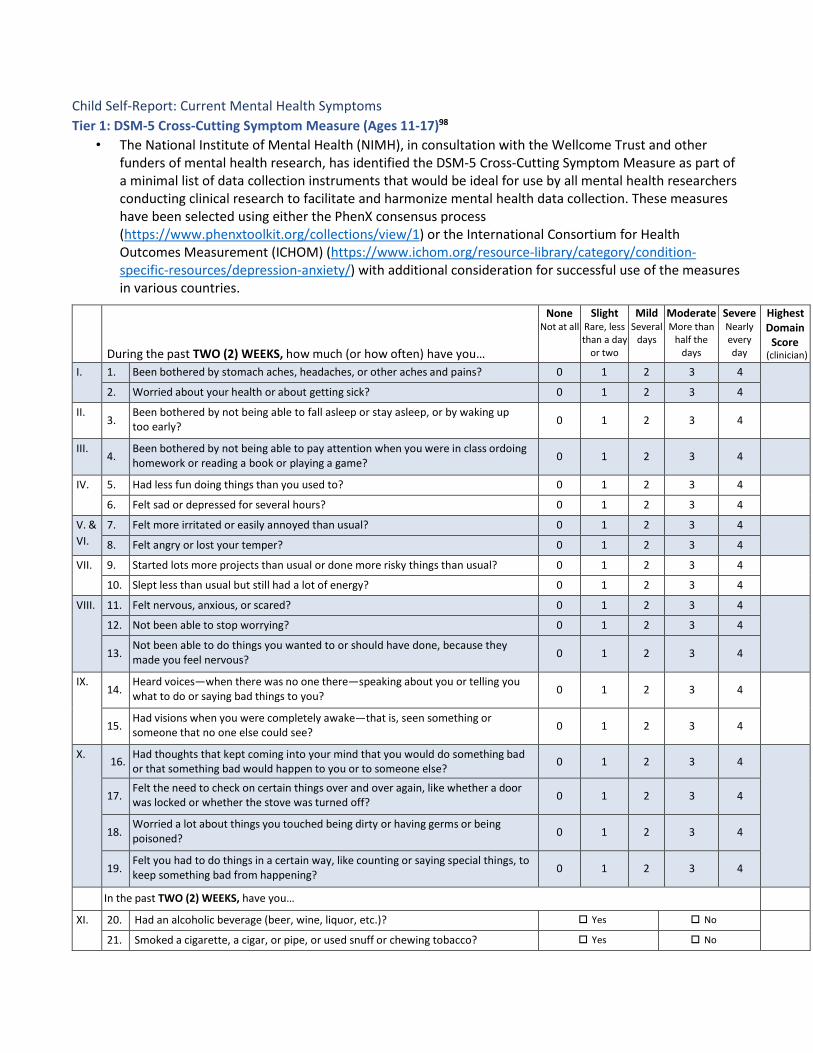
Child Self-Report: Current Mental Health Symptoms Tier 1: DSM-5 Cross-Cutting Symptom Measure (Ages 11-17)98
• The National Institute of Mental Health (NIMH), in consultation with the Wellcome Trust and other funders of mental health research, has identified the DSM-5 Cross-Cutting Symptom Measure as part of a minimal list of data collection instruments that would be ideal for use by all mental health researchers conducting clinical research to facilitate and harmonize mental health data collection. These measures have been selected using either the PhenX consensus process (https://www.phenxtoolkit.org/collections/view/1) or the International Consortium for Health Outcomes Measurement (ICHOM) (https://www.ichom.org/resource-library/category/condition-specific-resources/depression-anxiety/) with additional consideration for successful use of the measures in various countries.
During the past TWO (2) WEEKS, how much (or how often) have you…
None Not at all
Slight Rare, less than a day
or two
Mild Several
days
Moderate More than
half the days
Severe Nearly every day
Highest Domain
Score (clinician)
I. 1. Been bothered by stomach aches, headaches, or other aches and pains? 0 1 2 3 4
2. Worried about your health or about getting sick? 0 1 2 3 4
II. 3.
Been bothered by not being able to fall asleep or stay asleep, or by waking up too early? 0 1 2 3 4
III. 4.
Been bothered by not being able to pay attention when you were in class ordoing 0 1 2 3 4homework or reading a book or playing a game?
IV. 5. Had less fun doing things than you used to? 0 1 2 3 4
6. Felt sad or depressed for several hours? 0 1 2 3 4
V. & VI.
7. Felt more irritated or easily annoyed than usual? 0 1 2 3 4
8. Felt angry or lost your temper? 0 1 2 3 4
VII. 9. Started lots more projects than usual or done more risky things than usual? 0 1 2 3 4
10. Slept less than usual but still had a lot of energy? 0 1 2 3 4
VIII. 11. Felt nervous, anxious, or scared? 0 1 2 3 4
12. Not been able to stop worrying? 0 1 2 3 4
13. Not been able to do things you wanted to or should have done, because they made you feel nervous? 0 1 2 3 4
IX. 14.
Heard voices—when there was no one there—speaking about you or telling you what to do or saying bad things to you? 0 1 2 3 4
15. Had visions when you were completely awake—that is, seen something or someone that no one else could see? 0 1 2 3 4
X. 16. Had thoughts that kept coming into your mind that you would do something bad 0 1 2 3 4or that something bad would happen to you or to someone else?
17. Felt the need to check on certain things over and over again, like whether a door
0 1 2 3 4was locked or whether the stove was turned off?
18. Worried a lot about things you touched being dirty or having germs or being poisoned? 0 1 2 3 4
19. Felt you had to do things in a certain way, like counting or saying special things, to keep something bad from happening? 0 1 2 3 4
In the past TWO (2) WEEKS, have you…
XI. 20. Had an alcoholic beverage (beer, wine, liquor, etc.)? Yes No
21. Smoked a cigarette, a cigar, or pipe, or used snuff or chewing tobacco? Yes No

22. Used drugs like marijuana, cocaine or crack, club drugs (like Ecstasy), hallucinogens (like LSD), heroin, inhalants or solvents (like glue), or methamphetamine (like speed)?
Yes No
23. Used any medicine without a doctor’s prescription to get high or change the way you feel (e.g., painkillers [like Vicodin], stimulants [like Ritalin or Adderall], sedatives or tranquilizers [like sleeping pills or Valium], or steroids)?
Yes No
XII. 24. In the last 2 weeks, have you thought about killing yourself or committing suicide? Yes No
25. Have you EVER tried to kill yourself? Yes No
Tier 2 (After meeting Thresholds)
Domain Domain Name Threshold to guide further inquiry
DSM-5 Level 2 Cross-Cutting Symptom Measure available online
I. Somatic Symptoms Mild or greater LEVEL 2—Somatic Symptom—Child Age 11–17 (Patient Health Questionnaire Somatic Symptom Severity [PHQ-15])
II. Sleep Problems Mild or greater LEVEL 2—Sleep Disturbance—Child Age 11-17 (PROMIS—Sleep Disturbance— Short Form)1
III. Inattention Slight or greater None IV. Depression Mild or greater LEVEL 2—Depression—Child Age 11–17 (PROMIS Emotional Distress—
Depression—Pediatric Item Bank) V. Anger Mild or greater LEVEL 2—Anger—Child Age 11–17 (PROMIS Emotional Distress—Calibrated
Anger Measure—Pediatric) VI. Irritability Mild or greater LEVEL 2—Irritability—Child Age 11–17 (Affective Reactivity Index [ARI]) VII. Mania Mild or greater LEVEL 2—Mania—Child Age 11–17 (Altman Self-Rating Mania Scale [ASRM]) VIII. Anxiety Mild or greater LEVEL 2—Anxiety—Child Age 11–17 (PROMIS Emotional Distress—Anxiety—
Pediatric Item Bank) IX. Psychosis Slight or greater None X. Repetitive Thoughts
& Behaviors Mild or greater LEVEL 2—Repetitive Thoughts and Behaviors—Child 11–17 (adapted from the
Children’s Florida Obsessive-Compulsive Inventory [C-FOCI] Severity Scale) XI. Substance Use Yes/
Don’t Know LEVEL 2—Substance Use—Child Age 11–17 (adapted from the NIDA-modified ASSIST)
XII. Suicidal Ideation/ Suicide Attempts
Yes/
Don’t Know None
Additional Guidance: These CDEs include questions that can potentially identify respondents who are at risk of suicide. Investigators implementing this protocol should consult with their IRBs to develop a risk management plan specific to their study to ensure the safety of participants. Investigators should also ensure their studies are compliant with federal, state, and institutional regulations and policies and inform participants of limits of confidentiality when a participant endorses imminent risk of harm to self or others. The following link provides additional information and guidelines for suicide-related research: https://www.nimh.nih.gov/funding/clinical-research/conducting-research-with-participants-at-elevated-risk-for-suicide-considerations-for-researchers.
Tier 1: Anxiety, Depression, Fatigue PROMIS scales Pediatric measures Due to early research demonstrating the presence of COVID-19/pandemic related mental health symptoms, anxiety, depressive symptoms, and fatigue PROMIS measures were designated Tier 1 in addition to the DSM-5 screener.
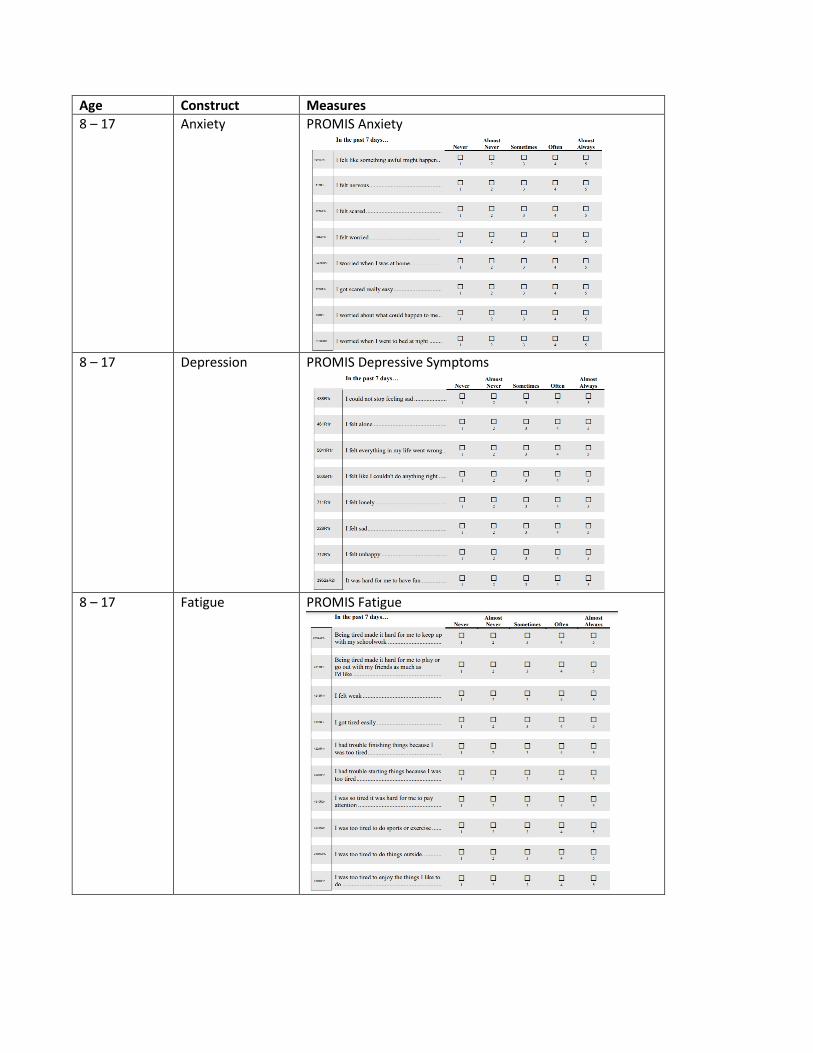
ln l.he pu l 7 day~ ...
I felt like something awful might happen ..
I felt nervous ...
I felt scared ...
I felt worried ...
_,. I worried when I was at home ...
!got scared really easy ...
I worried about what could happen to me ..
•- I worried when I went to bed at night ..
l nlhe pH l 7 d.ays . ..
-I could no1 stop feeling sad ...
I felt alone ..
I felt everything in my life went wrong ..
I felt like I couldn't do anything right ..
I fel t lonely .. .
I felt sad ...
I fel t unhappy ...
It was hard for me to have fun .....
In the pas t 7 days ..
Being tired made it hard for me 10 keep up with my schoolwork: ..
Being tired made it hard for me to play or go out with my friends as much as l'dlik.e ..
!felt weak. ..
I got tired easily ...
I had trouble finishing things because I was too tired ...
I had trouble starting things because I was too tired ...
I was so ti red it was hard for me to pay attention ..
I was too tired to do sports or exercise ...
I was too tired to do things outside . ..
I was too tired to enjoy the things I like 10
do ...
D '
D '
D
D
D '
D '
D
D
D '
D
D '
D
D
D
D
' D
'
Nl"·tt
D
D
D '
D
D
D '
D
D
D '
D
Almost N,n·r Som,limes Oft, n
D D D l l 4
D D D l J 4
D D D
D D D
D D D 2 3 4
D D D 2 l 4
D D D
' ' D D D
' '
Almost Nt,·t r Sometimes Ofttn
D
' D
D
D
D
D
' D
' D
'
Almost Nr,·r r
D
D
' D '
D
D
D
' D
' D
D
' D
D D
' . D D
D D ' D D
D D
D D
' D D
' D D
'
Somrtimes Ofirn
D D
D D
' D D
' D D
D D
D D
' . D D
D D
D D
' D D
Almost Alwan
D ' D ' D
D
D
' D
' D
' D
'
Almost Alwan
D
' D
D ' D
D
D
' D
' D
'
Almost Al"'·a,·s
D
D
' D '
D
D
D
' D
D
D
' D
Age Construct Measures 8 – 17 Anxiety PROMIS Anxiety
8 – 17 Depression PROMIS Depressive Symptoms
8 – 17 Fatigue PROMIS Fatigue
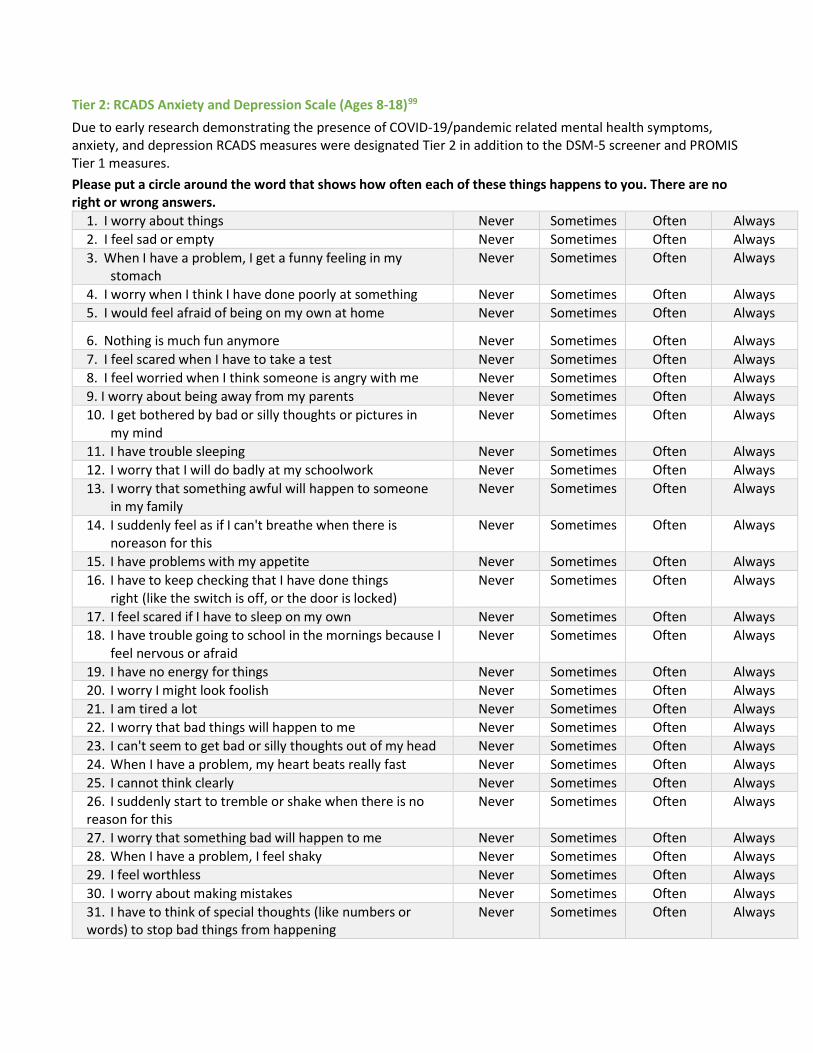
Tier 2: RCADS Anxiety and Depression Scale (Ages 8-18)99
Due to early research demonstrating the presence of COVID-19/pandemic related mental health symptoms, anxiety, and depression RCADS measures were designated Tier 2 in addition to the DSM-5 screener and PROMIS Tier 1 measures. Please put a circle around the word that shows how often each of these things happens to you. There are no right or wrong answers.
1. I worry about things Never Sometimes Often Always 2. I feel sad or empty Never Sometimes Often Always 3. When I have a problem, I get a funny feeling in my
stomach Never Sometimes Often Always
4. I worry when I think I have done poorly at something Never Sometimes Often Always 5. I would feel afraid of being on my own at home Never Sometimes Often Always
6. Nothing is much fun anymore Never Sometimes Often Always 7. I feel scared when I have to take a test Never Sometimes Often Always 8. I feel worried when I think someone is angry with me Never Sometimes Often Always 9. I worry about being away from my parents Never Sometimes Often Always 10. I get bothered by bad or silly thoughts or pictures in
my mind Never Sometimes Often Always
11. I have trouble sleeping Never Sometimes Often Always 12. I worry that I will do badly at my schoolwork Never Sometimes Often Always 13. I worry that something awful will happen to someone
in my family Never Sometimes Often Always
14. I suddenly feel as if I can't breathe when there is noreason for this
Never Sometimes Often Always
15. I have problems with my appetite Never Sometimes Often Always 16. I have to keep checking that I have done things
right (like the switch is off, or the door is locked) Never Sometimes Often Always
17. I feel scared if I have to sleep on my own Never Sometimes Often Always 18. I have trouble going to school in the mornings because I
feel nervous or afraid Never Sometimes Often Always
19. I have no energy for things Never Sometimes Often Always 20. I worry I might look foolish Never Sometimes Often Always 21. I am tired a lot Never Sometimes Often Always 22. I worry that bad things will happen to me Never Sometimes Often Always 23. I can't seem to get bad or silly thoughts out of my head Never Sometimes Often Always 24. When I have a problem, my heart beats really fast Never Sometimes Often Always 25. I cannot think clearly Never Sometimes Often Always 26. I suddenly start to tremble or shake when there is no reason for this
Never Sometimes Often Always
27. I worry that something bad will happen to me Never Sometimes Often Always 28. When I have a problem, I feel shaky Never Sometimes Often Always 29. I feel worthless Never Sometimes Often Always 30. I worry about making mistakes Never Sometimes Often Always 31. I have to think of special thoughts (like numbers or words) to stop bad things from happening
Never Sometimes Often Always
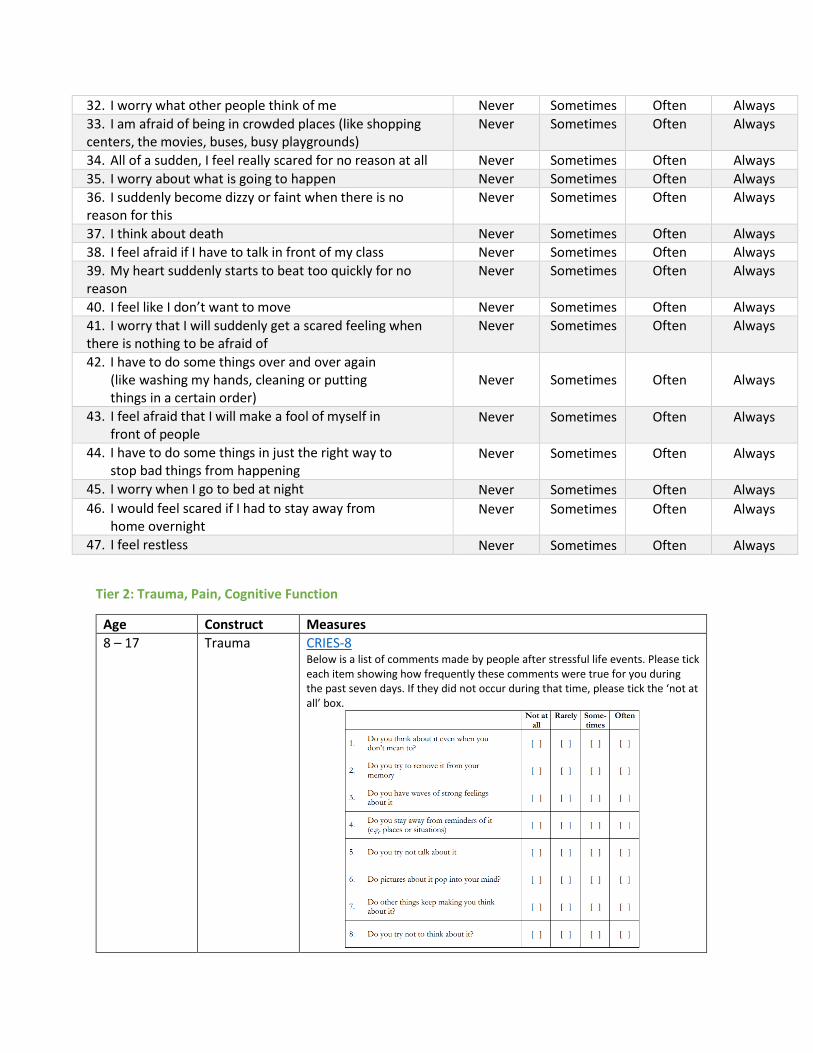
ot at Rarely Some- Often all times
I. Do you think about it even when you
I I I I I I I I don't mean co?
2. Do you try co remove ic from your
I j I j I j I j memory
3. Do you have waves o f strong feelings I I I j I j I j
about it
4. Do you stay away from reminders of it
I I I I I I I I (e.g. places or situations)
5. Do you try no t talk about it I j I j I j I j
6. Do picrurcs about it pop into your mind? I j I j I j I j
7. Do other things keep making you chink I I I I I I I I about it?
8 Do you try not to think about ic? I j I j I j I j
32. I worry what other people think of me Never Sometimes Often Always 33. I am afraid of being in crowded places (like shopping centers, the movies, buses, busy playgrounds)
Never Sometimes Often Always
34. All of a sudden, I feel really scared for no reason at all Never Sometimes Often Always 35. I worry about what is going to happen Never Sometimes Often Always 36. I suddenly become dizzy or faint when there is no reason for this
Never Sometimes Often Always
37. I think about death Never Sometimes Often Always 38. I feel afraid if I have to talk in front of my class Never Sometimes Often Always 39. My heart suddenly starts to beat too quickly for no reason
Never Sometimes Often Always
40. I feel like I don’t want to move Never Sometimes Often Always 41. I worry that I will suddenly get a scared feeling when there is nothing to be afraid of
Never Sometimes Often Always
42. I have to do some things over and over again (like washing my hands, cleaning or putting things in a certain order)
Never Sometimes Often Always
43. I feel afraid that I will make a fool of myself in front of people
Never Sometimes Often Always
44. I have to do some things in just the right way to stop bad things from happening
Never Sometimes Often Always
45. I worry when I go to bed at night Never Sometimes Often Always 46. I would feel scared if I had to stay away from
home overnight Never Sometimes Often Always
47. I feel restless Never Sometimes Often Always
Tier 2: Trauma, Pain, Cognitive Function
Age Construct Measures 8 – 17 Trauma CRIES-8
Below is a list of comments made by people after stressful life events. Please tick each item showing how frequently these comments were true for you during the past seven days. If they did not occur during that time, please tick the ‘not at all’ box.
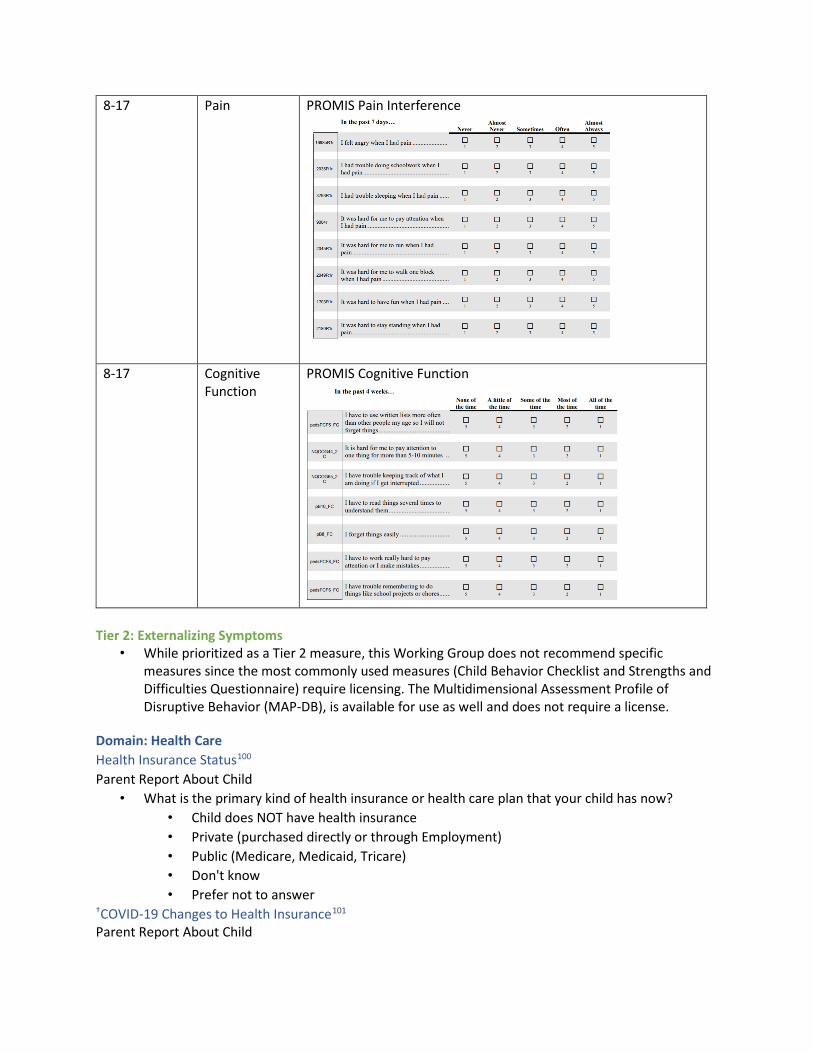
In the past 7days ... Never
1698bR1, I felt angry when I had pain ... '
I had trouble doing schoolwork when I D had pain ...
3793Fllr I had trouble sleeping when I had pain .. '
It was hard for me to pay attention when D I had pain ...
It was hard for me to run when I had pain ...
It was hard for me to walk one block when I had pain ...
It was hard to have fun when I had pain ..
It was hard to stay standing when I had pain ...
In the pas t 4 weeks •..
I have to use wriuen lists more often
pedsPCFS_FC than other people my age so I wi ll not forget things ...
NOCOG<'-2 It is hard for me to pay attention to
C one thing for more than 5• IO minutes .
NOCOG65_2 I have trouble keeping track of what I C am doing if I get interrupted ...
p810_FC I have 10 read things several times to understand them ...
p88_FC I forget things easi ly ...
ped:sPCF8_FC I have to work really hard to pay attention or I make mistakes ...
ped:sPCF8_FC I have trouble remembering to do things like school projects or chores ...
~
'
'
'
None or the time
' D
D
' D
' D
D ' D
Almost Almost Ne,·er Sometimes or,en Alw.1ys
' ' . ' ' ' ' ' ' . ' ' ' ' ' ' . ' ' ' . ' ' ' ' ' . '
Alin leor Some or the Most or All o(the thetime time the time time
' '
D D D D
D D D D
' ' D D D D
' ' D D D D
D D D D . ' ' ' D D D D
8-17 Pain PROMIS Pain Interference
8-17 Cognitive Function
PROMIS Cognitive Function
Tier 2: Externalizing Symptoms • While prioritized as a Tier 2 measure, this Working Group does not recommend specific
measures since the most commonly used measures (Child Behavior Checklist and Strengths and Difficulties Questionnaire) require licensing. The Multidimensional Assessment Profile of Disruptive Behavior (MAP-DB), is available for use as well and does not require a license.
Domain: Health Care Health Insurance Status100
Parent Report About Child • What is the primary kind of health insurance or health care plan that your child has now?
• Child does NOT have health insurance • Private (purchased directly or through Employment) • Public (Medicare, Medicaid, Tricare) • Don't know • Prefer not to answer
†COVID-19 Changes to Health Insurance101
Parent Report About Child

• During this pandemic (since March 2020) has this child had a change in their health insurance coverage?
• Yes • No
• If yes, what change occurred? • Loss of this child’s health insurance • Fewer benefits / less coverage from the insurance • Gaining of insurance, for example as part of emergency coverage of Medicaid expansion
†COVID-19 Changes to Health Care Access Parent Report About Child
• During the COVID-19 pandemic (since March 2020), was there any time when this child needed health care, but it was not received? By health care, we mean medical care as well as other kinds of care like dental care, vision care, and mental health services.102
• Yes • No • If yes, which types of care were not received? Select all that may apply:
• Medical Care • Dental Care • Vision Care • Hearing Care • Mental Health Services • Other (Specify)
• Please rate how much the coronavirus pandemic has changed your family's life in each of the following ways.103
• Medical health care access: • No change • Appointments moved to telehealth • Delays or cancellations in appointments and/or delays in getting prescriptions or
regular vaccinations (e.g., MMR); changes have minimal impact on health • Unable to access needed care resulting in severe risk and/or significant impact
• Mental health treatment access: • No change • Appointments moved to telehealth • Delays or cancellations in appointments and/or delays in getting prescriptions;
changes have minimal impact on health • Unable to access needed care resulting in severe risk and/or significant impact
†Receiving Behavioral Health/Mental Health Treatment (Tier 2)104
Parent Report About Child • During the COVID-19 pandemic (since March 2020), has this child received any treatment or
counseling from a mental health professional? Mental health professionals include psychiatrists, psychologists, psychiatric nurses, and clinical social workers.
• Yes • No, but this child needed to see a mental health professional • No, this child did not need to see a mental health professional

• During the COVID-19 pandemic (since March 2020), has this child taken any medication because of difficulties with their emotions, concentration, or behavior?
• Yes • No
†Services for Developmental Needs (Tier 2)105
• Has this child EVER received special services to meet their developmental needs such as speech, occupational, or behavioral therapy?
• Yes • No
• Is/was this child receiving these special services during the pandemic (since March 2020)? • Yes • No
• Was this child receiving these special services before the pandemic (before March 2020)? • Yes • No

COVID-19 Pediatric Joint Group Discussion Recommended Measures
Domain: Demographics Sex106
• What was the participant’s sex assigned at birth? • Female • Male • Intersex • None of these describe the participant (optional free text) • Prefer not to answer
Age (collected or calculated from MM/DD/YYYY)107
• What is the participant’s current age, including age units (if <2 years, report age in months)? • Calculated from Birth Date (MM/DD/YYYY) and Enrollment Date (MM/DD/YYYY) or
Collected Gestational age at birth (Tier 2)108
(Ages 0-2 years) • If <2 years of age, what was the participant’s gestational age at birth (in weeks)?
• ______ weeks • Unknown • Prefer not to answer
Ethnicity109
• Is the participant of Hispanic, Latino, or Spanish origin? • No, not of Hispanic, Latino, or Spanish origin • Yes, of Hispanic, Latino, or Spanish origin • Prefer not to say
Race110
• What is the participant’s race? Mark one or more boxes • American Indian or Alaska Native • Asian • Black or African American • Native Hawaiian or Other Pacific Islander • White • Some other race • Prefer not to answer
Zip Code111
• What is the participant’s 5-digit zip code? Additional Guidance: Participant’s zip code and birth date are protected health information, please refer to the guidance document for more information.
Gender Identity (Tier 2)112
Additional guidance: The Working Group consulted the NIH Sexual & Gender Minority Research Office (SGMRO) to ascertain whether there is an established measure of Gender Identity validated in children as the PhenX P11801 Measure is for participants 18+ years. As of now, there is not a preferred pediatric-specific validated measure, and this remains an important gap in the SGM data collection repertoire. There are many ongoing efforts to address this gap, including the work of the Measuring Sexual
Orientation and Gender Identity (SOGI) Research Group’s Youth Subgroup, and an in-progress NIH-commissioned consensus report from the National Academies of Sciences, Engineering, and Medicine on collecting sex, gender identity, and sexual orientation data. One measure used in ages 9-10 in the ABCD Study® is presented below, and this data element will be amended if future guidance on the topic is updated:
Child Self-Report (Ages 9+) • Are you transgender?
o Yes o Maybe o No o Did not understand
Parent Report About Child (Ages 9+) • Is your child transgender?
o Yes o Maybe/don’t know o No o Decline to answer
Domain: Disability/Functional Status Disability Status (Tier 2)113
• Child Self-Report (Ages 15+) • 1. Are you deaf, or do you have serious difficulty hearing? • 2. Are you blind, or do you have serious difficulty seeing, even when wearing glasses? • 3. Because of a physical, mental, or emotional condition, do you have serious difficulty
concentrating, remembering, or making decisions? (5 years old or older) • 4. Do you have serious difficulty walking or climbing stairs? (5 years old or older) • 5. Do you have difficulty dressing or bathing? (5 years old or older) • 6. Because of a physical, mental, or emotional condition, do you have difficulty doing
errands alone such as visiting a doctor’s office or shopping? (15 years old or older) • Parent Report About Child (As used in National Survey of Children’s Health)
Ages Questions asked Responses 0-5 • Does this child have any of the following?
• Deafness or problems with hearing? • Blindness or problems with seeing even when wearing
glasses?
Yes No
6-11 • Does this child have any of the following? • Serious difficulty concentrating, remembering, or making
decisions because of a physical, mental, or emotional condition?
• Serious difficulty walking or climbing stairs? • Difficulty dressing or bathing? • Deafness or problems with hearing? • Blindness or problems with seeing even when wearing
glasses?
Yes No
12+ • Does this child have any of the following? Yes No
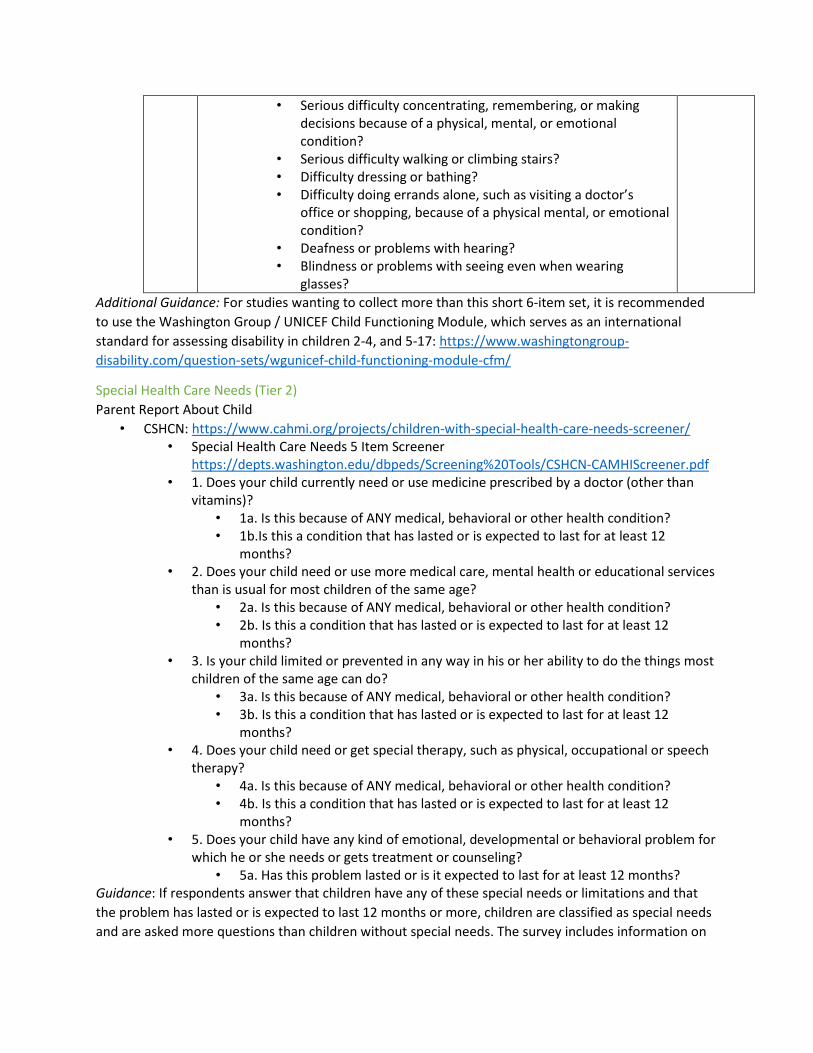
• Serious difficulty concentrating, remembering, or making decisions because of a physical, mental, or emotional condition?
• Serious difficulty walking or climbing stairs? • Difficulty dressing or bathing? • Difficulty doing errands alone, such as visiting a doctor’s
office or shopping, because of a physical mental, or emotional condition?
• Deafness or problems with hearing? • Blindness or problems with seeing even when wearing
glasses? Additional Guidance: For studies wanting to collect more than this short 6-item set, it is recommended to use the Washington Group / UNICEF Child Functioning Module, which serves as an international standard for assessing disability in children 2-4, and 5-17: https://www.washingtongroup-disability.com/question-sets/wgunicef-child-functioning-module-cfm/
Special Health Care Needs (Tier 2) Parent Report About Child
• CSHCN: https://www.cahmi.org/projects/children-with-special-health-care-needs-screener/ • Special Health Care Needs 5 Item Screener
https://depts.washington.edu/dbpeds/Screening%20Tools/CSHCN-CAMHIScreener.pdf • 1. Does your child currently need or use medicine prescribed by a doctor (other than
vitamins)? • 1a. Is this because of ANY medical, behavioral or other health condition? • 1b.Is this a condition that has lasted or is expected to last for at least 12
months? • 2. Does your child need or use more medical care, mental health or educational services
than is usual for most children of the same age? • 2a. Is this because of ANY medical, behavioral or other health condition? • 2b. Is this a condition that has lasted or is expected to last for at least 12
months? • 3. Is your child limited or prevented in any way in his or her ability to do the things most
children of the same age can do? • 3a. Is this because of ANY medical, behavioral or other health condition? • 3b. Is this a condition that has lasted or is expected to last for at least 12
months? • 4. Does your child need or get special therapy, such as physical, occupational or speech
therapy? • 4a. Is this because of ANY medical, behavioral or other health condition? • 4b. Is this a condition that has lasted or is expected to last for at least 12
months? • 5. Does your child have any kind of emotional, developmental or behavioral problem for
which he or she needs or gets treatment or counseling? • 5a. Has this problem lasted or is it expected to last for at least 12 months?
Guidance: If respondents answer that children have any of these special needs or limitations and that the problem has lasted or is expected to last 12 months or more, children are classified as special needs and are asked more questions than children without special needs. The survey includes information on

1
Functional Disability Inventory Child and Adolescent Form
When people are sick or not feeling well it is sometimes difficu lt for them to do their regular activities. In the past two weeks, would you have had any physical trouble or difficulty doing these activities?
No A Little Some A Lot of Trouble Trouble Trouble Trouble Impassible
1. Walking to the bathroom. 0 2 3 4
2. Walking up stairs. 0 2 3 4
3. Doing something with a friend. 0 2 3 4 (For example, playing a game.)
4. Doing chores at home. 0 2 3 4
5. Eating regular meals. 0 2 3 4
6. Being up all day without a nap or rest. 0 2 3 4
7. Riding the school bus or traveling in the car. 0 2 3 4
Remember, you are being asked about difficulty due to physical health.
8. Being at school all day. 0 2 3 4
9. Doing the activities in gym class 0 2 3 4 (or playing sports).
10. Reading or doing homework 0 2 3 4
11. Watching TV. 0 2 3 4
12. Walking the length of a football field. 0 2 3 4
13. Running the length of a football field. 0 2 3 4
14. Going shopping. 0 2 3 4
15. Getting to sleep at night and staying asleep. 0 2 3 4
how often during the past 12 months medical, behavioral, or other health conditions affected the ability of the children identified as having special needs to do things other children of the same age do; how much these conditions affect the children’s ability; and how often children’s health care needs change.
Normative Physical Functional Status [Outcome] (Tier 2)114
• Child-Self Report (Ages 8-17)
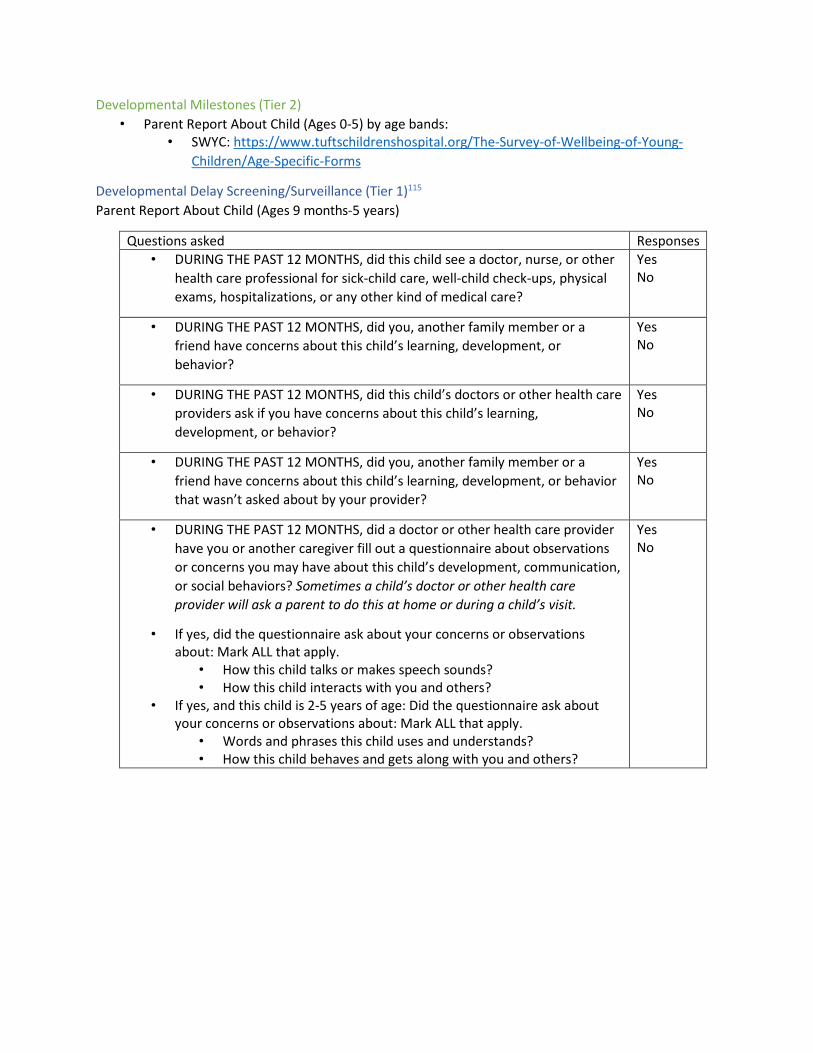
Developmental Milestones (Tier 2) • Parent Report About Child (Ages 0-5) by age bands:
• SWYC: https://www.tuftschildrenshospital.org/The-Survey-of-Wellbeing-of-Young-Children/Age-Specific-Forms
Developmental Delay Screening/Surveillance (Tier 1)115
Parent Report About Child (Ages 9 months-5 years)
Questions asked Responses • DURING THE PAST 12 MONTHS, did this child see a doctor, nurse, or other
health care professional for sick-child care, well-child check-ups, physical exams, hospitalizations, or any other kind of medical care?
Yes No
• DURING THE PAST 12 MONTHS, did you, another family member or a friend have concerns about this child’s learning, development, or behavior?
Yes No
• DURING THE PAST 12 MONTHS, did this child’s doctors or other health care providers ask if you have concerns about this child’s learning, development, or behavior?
Yes No
• DURING THE PAST 12 MONTHS, did you, another family member or a friend have concerns about this child’s learning, development, or behavior that wasn’t asked about by your provider?
Yes No
• DURING THE PAST 12 MONTHS, did a doctor or other health care provider have you or another caregiver fill out a questionnaire about observations or concerns you may have about this child’s development, communication, or social behaviors? Sometimes a child’s doctor or other health care provider will ask a parent to do this at home or during a child’s visit.
• If yes, did the questionnaire ask about your concerns or observations about: Mark ALL that apply.
• How this child talks or makes speech sounds? • How this child interacts with you and others?
• If yes, and this child is 2-5 years of age: Did the questionnaire ask about your concerns or observations about: Mark ALL that apply.
• Words and phrases this child uses and understands? • How this child behaves and gets along with you and others?
Yes No

Domain: Baseline Child Health Underlying Conditions (from Biomedical WG)116
• Significant underlying medical conditions at the time of COVID-19 testing or diagnosis: • Diabetes type I • Diabetes type II • Obesity • Asthma • Bronchopulmonary dysplasia
(BPD) • Cystic fibrosis • Obstructive sleep apnea • Tracheomalacia • Cancer • HIV/AIDS • Hematopoietic cell
recipient/bone marrow transplant recipient
• Solid organ transplant recipient • Rheumatologic conditions (e.g.
rheumatoid arthritis, systemic lupus erythematosus, vasculitis)
• Hypertension • Congenital heart disease • Heart failure • Cardiomyopathy • History of Kawasaki Disease
(not a current diagnosis) • Premature and Neonatal Conditions (Tier 2)117
• Fetal malnutrition • Extreme immaturity • Cerebral hemorrhage at birth • Spinal cord injury at birth • Birth asphyxia • Respiratory diseases • Hypoxic-ischemic encephalopathy • Other
Underlying Conditions (from Psychosocial WG) 118
• History of MIS-C (not a current diagnosis)
• Inflammatory bowel disease • Feeding tube dependent • Sickle cell disease • Thrombotic disorders • Chronic liver disease • Chronic kidney disease • Seizure disorder/epilepsy • Eczema • Physical disability (including
cerebral palsy) • Down syndrome • Congenital syndromes
/anomalies or genetic conditions including other chromosomal syndromes
• Premature or neonatal conditions
• Pregnancy (if of reproductive age)
• Other conditions (specify)
• Significant underlying conditions at the time of COVID-19 testing or diagnosis: • Tourette Syndrome • Depression • Anxiety problems • Autism, Asperger’s Disorder, pervasive developmental disorder or other autism
spectrum disorder • Attention Deficit Disorder or Attention Deficit Hyperactivity Disorder (ADD/ADHD) • Chronic fatigue

• Post-traumatic stress disorder (PTSD) • Suicidal thoughts or behaviors • Mania or bipolar disorder • Behavioral disorder or conduct problems • Developmental delay • Intellectual disability (formerly known as mental retardation) • Speech or other language disorder • Learning disability

Endnotes: links to materials used are provided where available.
1 WHO Post COVID Case Report Form| Biomedical Pediatric Working Group (WG) modifications| https://cdn.who.int/media/docs/default-source/3rd-edl-submissions/who_crf_postcovid_feb9_2021.pdf?sfvrsn=76afd14_1&download=true 2 Feudtner C, Feinstein JA, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014 Aug 8;14:199. doi: 10.1186/1471-2431-14-199. PMID: 25102958; PMCID: PMC4134331.| https://pubmed.ncbi.nlm.nih.gov/25102958/ 3 MUSIC Case Report Form| Biomedical Pediatric WG prioritized response list 4 Clinical Data Coordination Group (Project 5) CDE, Tier 1 |RADxCDE https://www.radxrad.org/resource/guidance-for-use-of-common-data-elements-cdes/ 5 CONNECTS NHLBI Common Data Elements| https://nhlbi-connects.org/common_data_elements 6 Biomedical Pediatric WG 7 St. Jude Pediatric COVID-19 U.S. Registry Case Report Form 8 JHU COVID-19 Community Response Survey Q3a | Modified to use only the COVID-19 related answer choices https://www.phenxtoolkit.org/toolkit_content/PDF/JHU_C4WARD_Health.pdf 9 Clinical Data Coordination Group (Project 5) CDE, Tier 2 10 CONNECTS NHLBI Common Data Elements| https://nhlbi-connects.org/common_data_elements 11 Clinical Data Coordination Group (Project 5) CDE, Tier 1 12 Clinical Data Coordination Group (Project 5) CDE, Tier 1 13 WHO Post COVID Case Report Form | Biomedical Pediatric WG pediatric modifications| https://cdn.who.int/media/docs/default-source/3rd-edl-submissions/who_crf_postcovid_feb9_2021.pdf?sfvrsn=76afd14_1&download=true | RADx CDEs|https://www.radxrad.org/resource/guidance-for-use-of-common-data-elements-cdes/ 14 WHO Post COVID Case Report Form| Biomedical Pediatric WG modifications| https://cdn.who.int/media/docs/default-source/3rd-edl-submissions/who_crf_postcovid_feb9_2021.pdf?sfvrsn=76afd14_1&download=true 15 Clinical Data Coordination Group (Project 5) CDE, Tier 1 | Biomedical Pediatric WG modifications 16 Children’s Hospital of Philadelphia Diagnosis of MIS-C in Febrile Children Case Report Form 17 Children’s Hospital of Philadelphia Diagnosis of MIS-C in Febrile Children Case Report Form 18 WHO Post COVID Case Report Form | Biomedical Pediatric WG modifications| https://cdn.who.int/media/docs/default-source/3rd-edl-submissions/who_crf_postcovid_feb9_2021.pdf?sfvrsn=76afd14_1&download=true 19 WHO Post COVID Case Report Form| Biomedical Pediatric WG modifications| https://cdn.who.int/media/docs/default-source/3rd-edl-submissions/who_crf_postcovid_feb9_2021.pdf?sfvrsn=76afd14_1&download=true| https://pubmed.ncbi.nlm.nih.gov/28637155/ 20 Penner J, Abdel-Mannan O, Grant K, Maillard S, Kucera F, Hassell J, Eyre M, Berger Z, Hacohen Y, Moshal K; GOSH PIMS-TS MDT Group. 6-month multidisciplinary follow-up and outcomes of patients with paediatric inflammatory multisystem syndrome (PIMS-TS) at a UK tertiary paediatric hospital: a retrospective cohort study. Lancet Child Adolesc Health. 2021 Jul;5(7):473-482. doi: 10.1016/S2352-4642(21)00138-3. PMID: 34043958.|https://www.thelancet.com/journals/lanchi/article/PIIS2352-4642(21)00138-3/fulltext 21 Bohannon RW, Wang YC, Bubela D, Gershon RC. Normative Two-Minute Walk Test Distances for Boys and Girls 3 to 17 Years of Age. Phys Occup Ther Pediatr. 2018 Feb;38(1):39-45. doi:
10.1080/01942638.2016.1261981. Epub 2017 Jan 27. PMID: 28129009.| https://pubmed.ncbi.nlm.nih.gov/28129009/ 22 WHO Post COVID Case Report Form| Biomedical Pediatric WG modifications| https://cdn.who.int/media/docs/default-source/3rd-edl-submissions/who_crf_postcovid_feb9_2021.pdf?sfvrsn=76afd14_1&download=true 23 Clinical Data Coordination Group (Project 5) CDE, Tier 1 24 Clinical Data Coordination Group (Project 5) CDE, Tier 1 25 Recommendations for CDEs for COVID-19 Studies Including Pregnant Participants| https://tools.niehs.nih.gov/dr2/index.cfm/resource/24206 26 Clinical Data Coordination Group (Project 5) CDE, Tier 1 27 Acute BRAVE Kids Case Report Form 28 WHO Post COVID Case Report Form | https://cdn.who.int/media/docs/default-source/3rd-edl-submissions/who_crf_postcovid_feb9_2021.pdf?sfvrsn=76afd14_1&download=true 29 Biomedical Pediatric WG 30 CONNECTS NHLBI Common Data Elements| WG modifications| https://nhlbi-connects.org/common_data_elements 31 POP02 Case Report Form 32 Clinical Data Coordination Group (Project 5) CDE, Tier 1 33 POP02 Case Report Form 34 Biomedical Pediatric WG 35 St. Jude U.S. Registry COVID Case Report Form 36 St. Jude U.S. Registry COVID Case Report Form 37 PRISM Case Report Form| Clinical Data Coordination Group (Project 5) CDE, Tier 1 Modified to add “Rehabilitation Facility / Nursing Facility” 38 NIH Clinical Spectrum of SARS-CoV-2 Infection| https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ 39 National Survey of Children’s Health, 2020 Questionnaire|https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents 40 P270201 California Health Interview Survey |https://www.phenxtoolkit.org/protocols/view/270201?origin=search| http://healthpolicy.ucla.edu/chis/design/Documents/2021%20Questionnaires%20and%20Topics%20List /English/CHIS%202021%20CAWI%20%20v1.27%2015APRIL2021%20Adult%20Questionnaire.pdf 41 Rutgers LINK Impact of Social Determinants of Health on Contracting COVID| *Age Group: Modified from Parent Using Best Practices Guidance 42 National Survey of Children’s Health, 2020 Questionnaire| Modified to be “mark all that apply,” added from P11301 “retired”, “disabled, permanently, or temporarily” and “student”|https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents | https://www.phenxtoolkit.org/protocols/view/11301?origin=search 43 Clinical Data Coordination Group (Project 5) CDE, Tier 1 | https://loinc.org/sars-cov-2- and-covid-19/ 44 RADxUP CDE | https://cde.nlm.nih.gov/deView?tinyId=ZwgnESEjK 45 Recommendations for CDEs for COVID-19 Studies Including Pregnant Participants| Modified to add “furloughed” and add “less challenging than usual” to final question| https://tools.niehs.nih.gov/dr2/index.cfm/resource/24206 46 Recommendations for CDEs for COVID-19 Studies Including Pregnant Participants| Modified to specify “financial strain” in first question| https://tools.niehs.nih.gov/dr2/index.cfm/resource/24206

47 Recommendations for CDEs for COVID-19 Studies Including Pregnant Participants| MACS-WIHS Baseline COVID-19 Abbreviated Questionnaire| https://tools.niehs.nih.gov/dr2/index.cfm/resource/24206 48 P270301| PhenX: 6 item standard measure from USDA Economic Research Service| https://www.phenxtoolkit.org/protocols/view/270301#tabsource 49 Recommendations for CDEs for COVID-19 Studies Including Pregnant Participants| https://tools.niehs.nih.gov/dr2/index.cfm/resource/24206 50 ABCD COVID-19 Impact Parent Report| Modified second question responses from Y/N to Y (frequency)/N| https://www.nlm.nih.gov/dr2/ABCD_COVID-19_Impact_Measure-Parent.pdf 51 Recommendations for CDEs for COVID-19 Studies Including Pregnant Participants| Columbia COVID-19 Questionnaire| https://tools.niehs.nih.gov/dr2/index.cfm/resource/24206 52 ABES Modified to remove “in school”| Age group: Used in COVID-19 Questionnaire 53 Added by Working Group 54 Tao, X. (2021). Social Media Use, Online Racial Discrimination, and Mental Health Risks Among Adolescents of Color. Fordham University | Age group: Used in COVID-19 Questionnaire |https://www.phenxtoolkit.org/protocols/view/970201?origin=search 55 National Household Education Survey, 2019| https://nces.ed.gov/nhes/pdf/pfi/2019_pfi.pdf 56 CTC 2010 Youth Survey General School Environment| Age group: Validated| https://www.phenxtoolkit.org/toolkit_content/PDF/PX540501.pdf 57 National Household Education Survey, 2019 | https://nces.ed.gov/nhes/pdf/pfi/2019_pfi.pdf |Modified to remove reference to “in a physical building” and add “Bureau of Indian Affairs or tribal school”, “Early Childhood Center” and “Special Education school”| *Age group: Modified from Parent Report Using Best Practices Guidance 58 ABCD COVID-19 Impact Parent Report| https://www.nlm.nih.gov/dr2/ABCD_COVID-19_Impact_Measure-Parent.pdf 59 GCS Neuro COVID Case Report Form 60 Psychosocial Pediatric WG 61 Psychosocial Pediatric WG 62 National Survey of Children’s Health, 2020 Questionnaire | Modified to specify for illness due to COVID-19, added “Don’t know,” added 15 or more days as it is used sometimes as a cutoff for chronic absenteeism| https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents 63 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6880919/ 64 Rutgers LINK Impact of Social Determinants of Health on Contracting COVID 65 P211001|Age Group: Validated | https://www.phenxtoolkit.org/protocols/view/211001?origin=domain 66 Healthy Pathways| Age group: Validated| Modified to add “I/my child was not graded” | https://link.springer.com/article/10.1007/s11136-010-9687-4 67 ECHO COVID-19 Adult Questionnaire| Modified to add “supervision of school aged children” and added response of “no longer needed child care”|https://www.nlm.nih.gov/dr2/C19-aPV_COVID-19_Questionnaire-Adult_Primary_Version_20200409_v01.30.pdf 68 2020 COVID-19 CENSUS HOUSEHOLD PULSE |Modified to specify for remote learning and changed “children” to “your child” | https://www.phenxtoolkit.org/toolkit_content/PDF/Census_HPS.pdf 69 ECHO Child Self-Report| Age group: Used in COVID-19 Questionnaire| https://www.nlm.nih.gov/dr2/C19-cPV_COVID-19_Questionnaire-Child_Self-Report_Primary_Version_20200608_v01.31.pdf

70 ECHO Child Parent-Report| https://www.phenxtoolkit.org/toolkit_content/PDF/ECHO_Child_Parent_Report_Impacts.pdf 71 NIH Toolbox Emotional Support| Age group: Validated | https://www.healthmeasures.net/explore-measurement-systems/nih-toolbox/intro-to-nih-toolbox/emotion/184-nih-toolbox-emotion 72 PROMIS Peer Relationships| Age group: Validated| https://www.healthmeasures.net/search-view-measures?task=Search.search 73 COVID-19 Experiences (COVEX) |Age group: Used in COVID-19 Questionnaire| https://www.phenxtoolkit.org/toolkit_content/PDF/Fisher_COVEX_Living_Situation.pdf 74 PX210801|https://www.phenxtoolkit.org/toolkit_content/PDF/PX210801.pdf 75 National Survey of Children’s Health, 2020 Questionnaire| *Age group: Modified from Parent Report Using Best Practices Guidance| https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents 76 ECHO Child Self-Report| *Age group: Modified from Parent Report Using Best Practices Guidance | https://www.nlm.nih.gov/dr2/C19-cPV_COVID-19_Questionnaire-Child_Self-Report_Primary_Version_20200608_v01.31.pdf 77 ECHO Child Self-Report| Age group: used in COVID-19 Questionnaire| https://www.nlm.nih.gov/dr2/C19-cPV_COVID-19_Questionnaire-Child_Self-Report_Primary_Version_20200608_v01.31.pdf 78 NIH Toolbox Positive Affect| ABCD COVID-19 Impact Self Report| Age group: Validated| https://www.healthmeasures.net/search-view-measures?task=Search.search 79 ECHO Child Self-Report| Age group: used in COVID-19 Questionnaire| Modified to add COVEX responses and WG responses| https://www.nlm.nih.gov/dr2/C19-cPV_COVID-19_Questionnaire-Child_Self-Report_Primary_Version_20200608_v01.31.pdf 80 JHU COVID-19 Community Response| *Age Group: Modified from Adult Using Best Practices Guidance| https://www.phenxtoolkit.org/toolkit_content/PDF/JHU_C4WARD_Social_Distancing.pdf 81 COVEX| *Age group: Modified Using Best Practices Guidance| https://www.nlm.nih.gov/dr2/COVEX_05_13_20_FINAL_V1.pdf 82 Clinical Data Coordination Group (Project 5) CDE |Modified to add “due to suspected COVID-19” 83 CDC COVID-19 Community survey question bank| *Age group: Modified Using Best Practices Guidance| https://cde.nlm.nih.gov/cde/search?q=serious%20disease 84 CDC COVID-19 Community Survey Question Bank| *Age group: Modified Using Best Practices Guidance| Modified to prioritize social distancing, mask wearing, vaccination| https://cde.nlm.nih.gov/deView?tinyId=rdyjqFW12 85 Novel Coronavirus (COVID) Illness – Patient Report (NCI-PR) | https://disasterinfo.nlm.nih.gov/content/files/COVID_Illness_Patient_Report_NCI-PR.pdf 86 Recommendations for Common Data Elements for COVID-19 Studies Including Pregnant Participants| Vaccine/PASC Addendum 87 ABCD Child Self-Report | Age group: Used in COVID-19 Questionnaire| Modified to add “During the COVID-19 pandemic”| https://www.nlm.nih.gov/dr2/ABCD_COVID-19_Impact_Measure-Youth.pdf 88 ECHO Child Self-Report | Age group: Used in COVID-19 Questionnaire | Modified to be “During the COVID-19 pandemic”| https://www.nlm.nih.gov/dr2/C19-cPV_COVID-19_Questionnaire-Child_Self-Report_Primary_Version_20200608_v01.31.pdf 89 National Survey of Children’s Health, 2020 Questionnaire |Modified to add a “during the pandemic” question and added (including PE) |https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents
90 P960301| *Age Group: Modified Using Best Practices Guidance| https://www.phenxtoolkit.org/protocols/view/960301 91 ABCD COVID-19 Impact Parent Report| *Age Group: Modified Using Best Practices Guidance| https://www.nlm.nih.gov/dr2/ABCD_COVID-19_Impact_Measure-Parent.pdf 92 National Survey of Children’s Health, 2020 Questionnaire| Modified to add “Chronic fatigue”, “PTSD”, “Suicidal thoughts or behaviors” and “mania or bipolar disorder” 93 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4177165/ | National Survey of Children’s Health 94 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4177165/ | National Survey of Children’s Health 95 PROMIS Global Health Pediatric Scale v1.0 | Age Group: Validated 96 DSM-5 |https://www.psychiatry.org/psychiatrists/practice/dsm/educational-resources/assessment-measures | Age Group: Validated 97 RCADS| https://www.childfirst.ucla.edu/resources/ | Age Group: Validated 98 DSM-5 |https://www.psychiatry.org/psychiatrists/practice/dsm/educational-resources/assessment-measures | Age Group: Validated 99 RCADS| https://www.childfirst.ucla.edu/resources/ | Age Group: Validated 100 RADxUP| https://radx-up.org/wp-content/uploads/2021/01/RADx-UP-_-REDCap20201230_codebook-.pdf |Modified to ask about child 101 Pregnancy CDE|MACS-WIHS Baseline COVID-19 Abbreviated Questionnaire| https://dr2.nlm.nih.gov/search/?q=24206 102 National Survey of Children’s Health, 2020 Questionnaire|https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents 103 ABCD COVID-19 Impact Parent Report| Modified to add vaccinations to question stem| Modified to remove “Mild”, “Moderate”, “Severe”| https://www.nlm.nih.gov/dr2/ABCD_COVID-19_Impact_Measure-Parent.pdf 104 National Survey of Children’s Health, 2020 Questionnaire |https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents 105 National Survey of Children’s Health, 2020 Questionnaire| Modified to ask before pandemic |https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents 106 RADxUP CDE https://radx-up.org/wp-content/uploads/2021/01/RADx-UP-_-REDCap20201230_codebook-.pdf | PX011601 https://www.phenxtoolkit.org/protocols/view/%2011601 |Modified to remove “biological” consistent with RADxUP, modified to ask “participant” instead of “you” 107 Clinical Data Coordination Group (Project 5) CDE, Tier 1 |RADx CDE https://www.radxrad.org/resource/guidance-for-use-of-common-data-elements-cdes/ | modified to ask “participant” 108 Biomedical Pediatric WG, https://www.cdc.gov/nchs/nvss/facility-worksheets-guide/30.htm?Sort=URL%3A%3Aasc&Categories=Newborn%20Information 109 Census https://www.phenxtoolkit.org/protocols/view/11901 | modified to ask “participant” 110 RADx, RADxUP | https://www.radxrad.org/wp-content/uploads/2021/03/RADx_rad_CDE_guideline_1.2.pdf 111 Clinical Data Coordination Group (Project 5) CDE, Tier 1 | modified to ask “participant” 112 ABCD| https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6584307/ 113 ACS-6| https://www.cdc.gov/ncbddd/disabilityandhealth/datasets.html 114 Functional Disability Inventory | https://pubmed.ncbi.nlm.nih.gov/16480823/

115 National Survey of Children’s Health| Modified to ask whether the parent had a concern about developmental milestones that was not asked by provider| Note: can add skip logic https://jamanetwork.com/journals/jamapediatrics/fullarticle/2686728 116 WHO Post COVID Case Report Form| WG pediatric modifications https://www.who.int/publications/i/item/global-covid-19-clinical-platform-case-report-form-(crf)-for-post-covid-conditions-(post-covid-19-crf-)#:~:text=WHO's%20Post%20COVID%20case%20report,be%20available%20in%20multiple%20languages 117 Feudtner C, Feinstein JA, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014 Aug 8;14:199. doi: 10.1186/1471-2431-14-199. PMID: 25102958; PMCID: PMC4134331.| https://pubmed.ncbi.nlm.nih.gov/25102958/ 118 National Survey of Children’s Health, 2020 Questionnaire| Modified to add “Chronic fatigue”, “PTSD”, “Suicidal thoughts or behaviors” and “mania or bipolar disorder”|https://mchb.hrsa.gov/data/national-surveys/questionnaires-datasets-supporting-documents





























