Embed Size (px)
Citation preview
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Predicting Premature Termination Within a RandomizedControlled Trial for Binge-Eating Patients
Christoph FlückigerUniversity of Wisconsin-Madison and University of Bern
Andrea MeyerUniversity of Basel
Bruce E. WampoldUniversity of Wisconsin-Madison and Research Institute, Modum Bad Psychiatric Center
Daniel GassmannNadine Messerli-Bürgy
University of Bern
Simone MunschUniversity of Fribourg and University of Lausanne
Understanding the dropout rates of efficacious forms ofpsychotherapy for patients with binge eating disorder (BED)is an unsolved problem within this increasing population.Up until now the role of psychotherapy process character-istics as predictors of premature termination has not beeninvestigated in the BED literature. Within a randomizedcontrolled trial (N=78) we investigated the degree to which
early psychological process characteristics, such as compo-nents of the therapeutic relationship and the experiences ofmastery and motivational clarification, predicted prematuretermination of treatment. We statistically controlled for theinfluences of covariates such as rapid response of treatment,treatment group, body mass index, Axis II disorder, andpatients’ preexisting generalized self-efficacy at baseline.Patients’ postsession reports from Sessions 1 to 5 indicatedthat low self-esteem in-session experiences was a stablepredictor of premature termination. Its predictive valuepersisted after controlling for the above-mentioned covari-ates. Exploratory analyses further revealed low self-esteemexperiences, low global alliance, and low mastery andclarification experiences as predictors in those patients whoexplicitly specified discontentment with therapy as reasonfor premature termination. These results indicate thatpatients’ self-esteem experiences may not be an epiphenom-enon of their specific psychopathology but may representgeneral mechanisms on which remaining or withdrawingfrom psychotherapeutic treatment depends. Early psycho-therapy process characteristics should therefore be considered
www.elsevier.com/locate/bt
Available online at www.sciencedirect.com
Behavior Therapy 42 (2011) 716–725
The authors are grateful to Rick E. Zinbarg for the helpfulcomments of an earlier version of this manuscript. This research wassupported by two grants of the Swiss Science National Foundation:PA00P1_124102 (Christoph Flückiger) and 3200–065588.01/1(Simone Munsch).
Special circumstances: This manuscript is based on a randomizedcontrolled trial presented by Munsch et al. (2007).
Address correspondence to Christoph Flückiger, University ofBern, Department of Clinical Psychology and Psychotherapy,Gesellschaftsstrasse 49, CH-3012 Bern, Switzerland; e-mail:[email protected]/xx/xxx-xxx/$1.00/0© 2011 Association for Behavioral and Cognitive Therapies. Published byElsevier Ltd. All rights reserved.
Author's personal copy
in training and evaluation of psychotherapists carryingthrough BED treatments.
Keywords: premature termination; binge eating disorder; processresearch; rapid response
TO DATE, COGNITIVE BEHAVIORAL THERAPY (CBT),guided self-help CBT, interpersonal therapy (IPT),and behavior weight loss therapy (BWLT) are well-established psychological treatments for patientswith binge eating disorder (BED; Vocks et al.,2009; Wilson, Wilfley, Agras, & Bryson, 2010). Anunresolved although important problem of CBTand BWLT approaches concerns the dropout ratesthat range from 12% (Carter & Fairburn, 1998) to34% (Gorin, Le Grange, & Stone, 2003), therebylimiting treatment efficacy for a substantialgroup of affected individuals (Brownley, Berkman,Sedway, Lohr, & Bulik, 2007). Knowledge aboutpossible predictors of dropout is crucial to under-standing dropout mechanisms, which would inturn lead to ways to keep dropout rates as low aspossible (Kraemer, Wilson, Fairburn, & Agras,2002). Unfortunately, published BED trials withdocumented dropout specifications have notrevealed any systematic treatment baseline pre-dictors of dropouts (Vocks et al., 2009). Up untilnow the role of psychotherapy process variables aspredictors of premature termination, includingexplicit discontentment as reasons of prematuretermination, has not been investigated in the BEDliterature (Dingemans, Spinhoven, & van Furth,2007; Hilbert et al., 2007). Research on mixedeating disorder populations indicates that aspectsof general psychopathology, such as high impul-sivity and high hostility, low self-esteem, highcomorbidity, low cooperativeness, and a lack ofcongruence between patients’ and therapists’ ex-pectations of potential treatment interventions areassociated with premature termination (Coker,Vize, Wade, & Cooper, 1993; Fassino, Pierò,Tomba, & Abbate-Daga, 2009; Wolff & Clark,2001). Meta-analytic overviews of the generaldropout literature indicate that patients’ decisionto terminate treatment prematurely seems to bemoderately related to lower therapeutic alliance,lower expectations of treatment effectiveness,lower patient motivation, lower patient self-efficacy,and higher patient hostility or impulsivity at anearly stage of therapy (Sharf & Primavera, 2009;Wierzbicki & Pekarik, 1993).Further, based on extensive controlled therapy
studies and naturalistic process–outcome studies
(Grawe 1997, 2004; Grawe, Donati, & Bernauer,1994; Orlinsky, Grawe, & Parks, 1994) it can besummarized that the immediate activation ofneed-satisfying experiences (Epstein, 1990) duringtherapy sessions are beneficial preconditions fortherapeutic work on patients’ specific problemsand a lack of need-satisfying experiences can beseen as a risk factor of premature termination.Need-satisfying experiences can be specified aspatients’ evaluation of how the therapeutic inter-action was addressed to experience (i.e., high in-session self-esteem, control, mastery, or motiva-tional clarification; Grawe, 2004).In the present preliminary investigation, we focus
on the early therapeutic process in completerscompared to dropouts in BED treatment. To ourbest knowledge, we are not aware of any BED studyfocusing on this specific question (Brownley et al.,2007). In particular, we investigate the degree towhich early psychological process variables, such ascomponents of the therapeutic relationship and theexperience of mastery and clarification, predictpremature termination of treatment (Grawe, 1997,2004). To test the influence of known disorder-specific factors we account for rapid response ofsymptom reduction as it has been shown to predicttherapy outcome in bulimia nervosa samples (e.g.,Constantino, Arnow, Blasey, & Argas, 2005; Loebet al., 2005; Wilson, Fairburn, Agras, Walsh, &Kraemer, 2002) and in BED samples (Grilo,Masheb,& Wilson, 2006; Hilbert et al., 2007). These prioranalyses, however, were based on restricted samplesof treatment completers and do not include dropouts(Grilo et al., 2006; Hilbert et al., 2007). We furtherincorporated factors such as comorbidity with othermental disorders (Hilbert et al., 2007), BMI (Schlup,Munsch, & Meyer, 2010) and treatment conditionin our analysis. We also explore which variablespredict patient-rated discontentment with therapy asa particular reason for premature termination.
Methodparticipants
The study was conducted at the Department ofClinical Psychology and Psychotherapy of theUniversity of Basel, Switzerland, following a ran-domized controlled trial design that contrasted groupCBT and group BWLT (Munsch et al., 2007). Out-patients were recruited through newspaper adver-tisements. It was required that participants meet thefollowing criteria: (a) age between 18 and 70 years;(b) body mass index (BMI; kg/m2) ranging between27 and 40; (c) fulfillment of the criteria for bingeeating disorder according to the German version ofthe Eating Disorder Examination (EDE; Hilbert,Tuschen-Caffier, & Ohms, 2004); (d) absence of
717pred ic t ing premature terminat ion
Author's personal copy
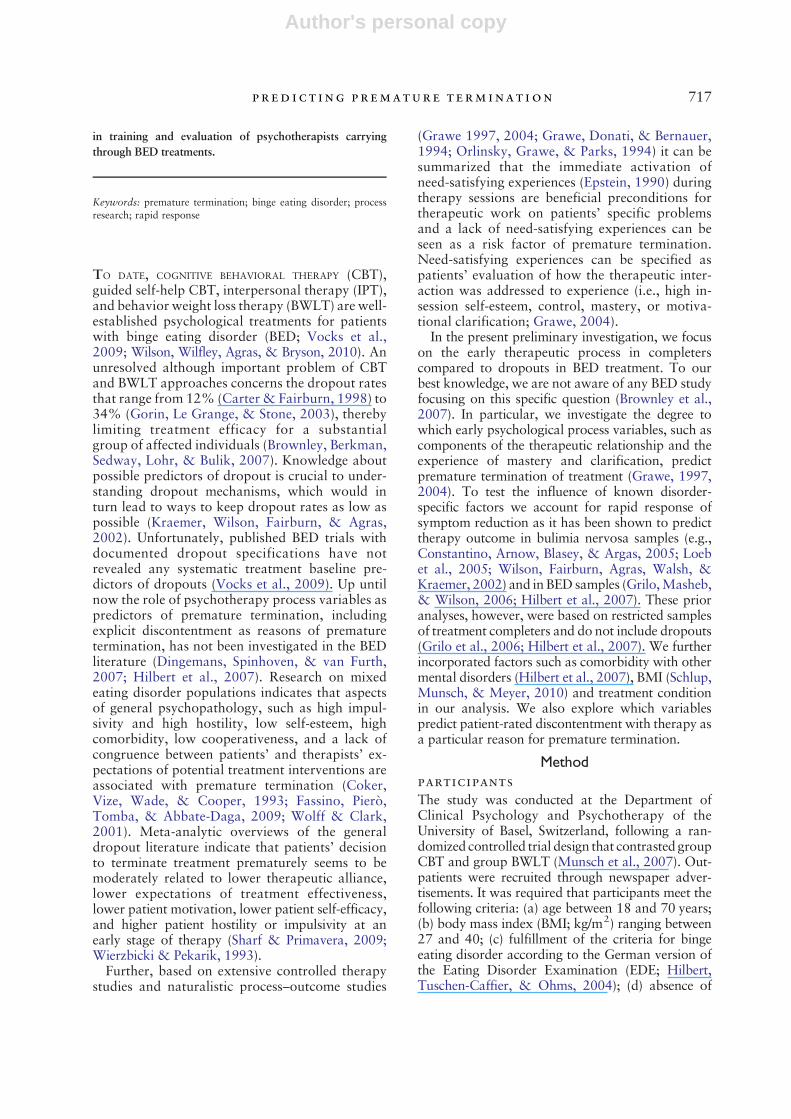
suicidal tendency, psychosis, mania, organic demen-tia, or substance abuse disorder; (e) absence ofpregnancy; (f) absence of participation in a dietprogram or a current psychotherapy or weight lossmedication treatment; and (g) previous surgicaltreatment of obesity. Of the 324 persons whocontacted the department and participated in aphone screening, 80 fulfilled the study criteria andwere randomized to the treatment condition andstarted the therapy (CBT: N=44; BWLT: N=36).Fifty-one patients completed treatment (CBT:N=28;BWLT: N=23), 23 prematurely dropped out beforeend of treatment at Session 16 (CBT:N=13; BWLT:N=10), and 6 dropped out during the six boostersessions (CBT: N=3; BWLT: N=3). For 2 of the 29dropouts no data were available regarding postses-sion reports and they were thus excluded fromsubsequent analyses. The sample characteristics areshown in Table 1. At treatment baseline, completersand dropouts did not differ with respect to sex, age,BMI, frequency of binge eating episodes, depression(Beck Depression Inventory [BDI]), anxiety (BeckAnxiety Inventory [BAI]), and comorbidity withother mental disorders, except for lifetime Axis IIdisorders, which were solely represented in thecompleter sample (see Munsch et al., 2007). Thestudy was approved by the local ethics commission
for medical research and participants gave a writtenconsent before study participation.
treatments
The seven CBT and six BWLT cohorts consisted ofup to sevenmembers with seven therapists (16 week-ly 90-minute group sessions, 6 booster sessions). Theproportion of completers did not differ between thegroup cohorts, χ2(6)=4.8, p=.57. The therapistsconducted both treatment conditions and werepsychotherapists with specialized training in CBTand BWLT. The co-therapists were master's studentsof the department. Therapists and co-therapistswere trained and supervised weekly. The groupCBT followed a manual according to the treatmentapproach of Fairburn, Marcus, and Wilson (1993;Munsch, in press) that focuses on the regulation ofbinge eating behaviors and the modification ofthe body concept. The group BWLT followed themanual from tetrahydrolipstatin-based weight lossthat focuses on balanced nutrition and physicalactivity (Margraf, 2000; Munsch, Biedert, & Keller,2003; for a comparison of the two treatments, seeMunsch et al., 2007, table 2). To minimize alle-giance effects, two treatment manuals were used thatwere developed by the research group (in-housecomparison).
Table 1Sample Characteristics at Baseline
Treatment Group Statistic Effect Size c
Completers(n=51)
Dropouts(n=27)
No. of female (%) 46 (90) 24 (89) χ2(1)= .33 1.17Mean age in years (SD) 46 .9 (11.8) 44.1 (11.5) F(1, 77)= .96 0.24Mean BMI (SD) 33.4 (3.8) 33.6 (4.0) F(1, 77)= .02 0.05Generalized self-efficacy (SD) a 27.5 (7.8) 27.1 (4.3) F(1, 77)= .66 0.06No. (%) of Participants WithCurrent comorbidity Axis I 4 (7.8) 3 (11.1) χ2(1)=0.23 0.68Depression 20 (31.4) 8 (29.6) χ2(1)=0.70 1.53Anxiety disorders
Lifetime comorbidity Axis I 23 (45.1) 10 (37.0) χ2(1)= .47 0.68Mood disorders 7 (13.7) 2 (7.4) χ2(1)= .69 1.99Anxiety disorders 9 (17.6) 0 (0) χ2(1)=5.38 b - d
Lifetime comorbidity Axis II 36 (70.6) 17 (62.9) χ2(1)= .47 1.41No. (%) of participants in partnership 10 (19.6) 5 (18.5) χ2(1)= .18 1.07No. (%) of graduate participants 4 (7.8) 4 (14.8) χ2(1)= .93 0.49No. (%) of foreign participants 6 (11.8) 4 (14.8) χ2(1)= .15 0.77No (%) of smokersTreatment group 28 (54.9) 16 (59.3)CBT (%) 23 (45.1) 11 (40.7) χ2(1)= .14BWLT (%) 0.84
Note. BMI = body mass index; CBT = cognitive–behavioral therapy; BWLT = behavior weight loss therapy.a Values ranged between 4 and 40.b pb .024, all other statistics pN .30 (according to Fisher's exact test).c Cohen's d (for metric scales), odds ratio (for proportions).d Could not be computed as one cell frequency was 0.
718 fl u ck iger et al .

Author's personal copy
After completion of all treatment groups, twoindependent raters not being involved in thetreatment trial (students of clinical psychologyholding a bachelor's degree) coded 10 CBT and 10BWLT videotaped sessions using a 29- or 35-itemquestionnaire (number of items depended on treat-ment; unpublished questionnaire is available fromthe authors). For both CBT and BWLT, sessionsfrom different treatment phases were randomlyselected. Raters were blind regarding the sessionand the condition they were rating. The ratingsincluded questions about treatment modality (CBTvs. BWLT), treatment phase (beginning, middle,end of treatment), treatment-specific features (e.g.,for CBT: “Did the therapist train the participant tocope with binge eating?” for BWLT: “Were real-istic weight loss goals targeted?”), and nonspecifictreatment indices (e.g., “Did the therapist struc-ture the session clearly?”). Raters identified 100%of CBT and BWLT sessions correctly. Videotapeswere classified into treatment phase with an accu-racy of 95%, χ2(4) =34.29, pb .001; α= .92,pb .001. Treatment-specific criteria significantly dif-ferentiated among treatment modalities, t(18)=6.17,pb .001 for CBT-specific index, and t(18)=−5.86,pb .001 for BWLT-specific index, whereas nonspe-cific indices did not, t(18)=1.93, p=.07. Interraterreliability was satisfactory with a gamma coefficientof 0.82 for specific indices and 0.62 for unspecificindices.Sixty-seven percent of the completers attended all
sessions. The average number of sessions attendedwas 15.7 (20.2 for completers, 7.7 for prematureterminators). Both treatments led to a fast decline inthe number of weekly binges, which was slightlymore pronounced in the CBT group. At posttreat-ment, CBT was more effective than BWLT at thelevel of the symptoms, but during follow-up, thesedifferences disappeared (Munsch et al., 2007).
assessments
The following assessments were integrated into theanalyses:
Assessment of Mental DisordersAt baseline, BED diagnosis and its core symp-tomatology were identified according to a struc-tured interview for eating disorders (EDE; Hilbertet al., 2004). Mental disorders on Axis I wereassessed using face-to-face diagnostic interviewsfor Axis I (Diagnostisches Interview für PsychischeStörungen für DSM-IV, DIPS; Margraf, Schneider,& Ehlers, 1994) and for Axis II (StrukturiertesKlinisches Interview für DSM-IV, Achse-II,Persönlichkeitsstörungen, SKID-II;Wittchen,Zaudig,& Fydrich, 1997). Both interviews have been shown
to be valid and reliable methods to assess mentaldisorders in clinical and research practice (In-Albon,2008; Suppiger et al., 2009). Standardized adminis-trationwas supervised regularly by twoof the authorsof the main outcome report (Munsch et al., 2007),whereas interrater reliability was not calculated.
Documentation of Premature TerminationAll participants who dropped out before study endwere asked to specify the reasons for prematuretermination by selecting exactly one of 14 offeredcategories and/or writing additional reasons in freetext (Munsch et al., 2007; unpublished question-naire available from the authors). Participantcharacteristics did not differ between completersand dropouts for the following variables: sex, age,BMI, depression (BDI), anxiety (BAI), EDE globalscore, and comorbid mental disorders. None ofthe comparisons between dropouts and completersreached statistical significance (p valuesN .05 for allcomparisons; analyses based on t tests or Fisher'sexact tests/Pearson's χ2 test, respectively). Twodependent variables related to dropout were used:(a) premature termination (27 of all 78 cases), and(b) discontentment with therapy as reason ofpremature termination (8 of the 27 dropouts).
Bern Post-Session Reports for Patients–Short Form2000Patients completed the Bern Post-Session Reportsfor Patients–Short Form 2000 (BPSR-P; Flückiger,Regli, Zwahlen, Hostettler, & Caspar, 2010)measure each week immediately after each therapysession. Therapists had no access to the patients’reports. The seven scales (23 items; see Appendix A)are based on general curative factors proposed byGrawe (1997; for a practical example see Grawe,2004). The scales were constructed using previousversions of these measures (Grawe & Braun, 1994;Grawe, Ohlendorf, Retzmann, & Schröder, 1978)and have shown a satisfactory factor structure usingexplorative and confirmatory factor analysis,SEM: χ2(428)=576; CFI= .94; RMSEA= .057;SRMR=.052. The factor structures of the scaleswere stable over the course of therapy. A comparisonwith the therapist version and observer ratingsdemonstrated satisfactory discriminant and conver-gent validity (Flückiger, Caspar,GrosseHoltforth,&Willutzki, 2009; Flückiger, Regli, et al., 2010). Thepresent analyses are based on the scale means of theavailable reports from Sessions 1 to 5 aggregatedacross each patient.
Rapid ResponseRapid response was defined as a reduction in thenumber of binges by at least 65% during the first4 weeks of treatment (Grilo et al., 2006; Masheb &
719pred ic t ing premature terminat ion
Author's personal copy
Grilo, 2007). Therefore, to compute rapid responsevalues, at least two time points had to be reportedduring the first 4 weeks. For five subjects this wasnot the case and hence no rapid response valuescould be computed. Of the remaining 73 subjects,37 were identified as rapid responders.
Body Mass IndexTo determine BMI (kg/m2), weight and height weremeasured on an electronic balance scale and by astadiometer at baseline, during treatment, at post-treatment, and during follow-up.
Generalized Self-Efficacy ScaleThe sum of the Generalized Self-Efficacy Scale (GSE;Schwarzer & Jerusalem, 1995) scales represents a
total score on the trait self-efficacy at baseline(α=.86). GSE can be described as an optimisticself-belief in one's ability to cope with future difficultdemands in life.
Treatment GroupsCBT and BWLT were contrasted.
statistical analyses
To assess the relationship among the differentBPSR-P scales, BMI and GSE at baseline, Axis II,treatment group, and rapid response, correlationcoefficients are reported. To test whether thedifferent BPSR-P scales predicted premature termi-nation, we used binary logistic regression models
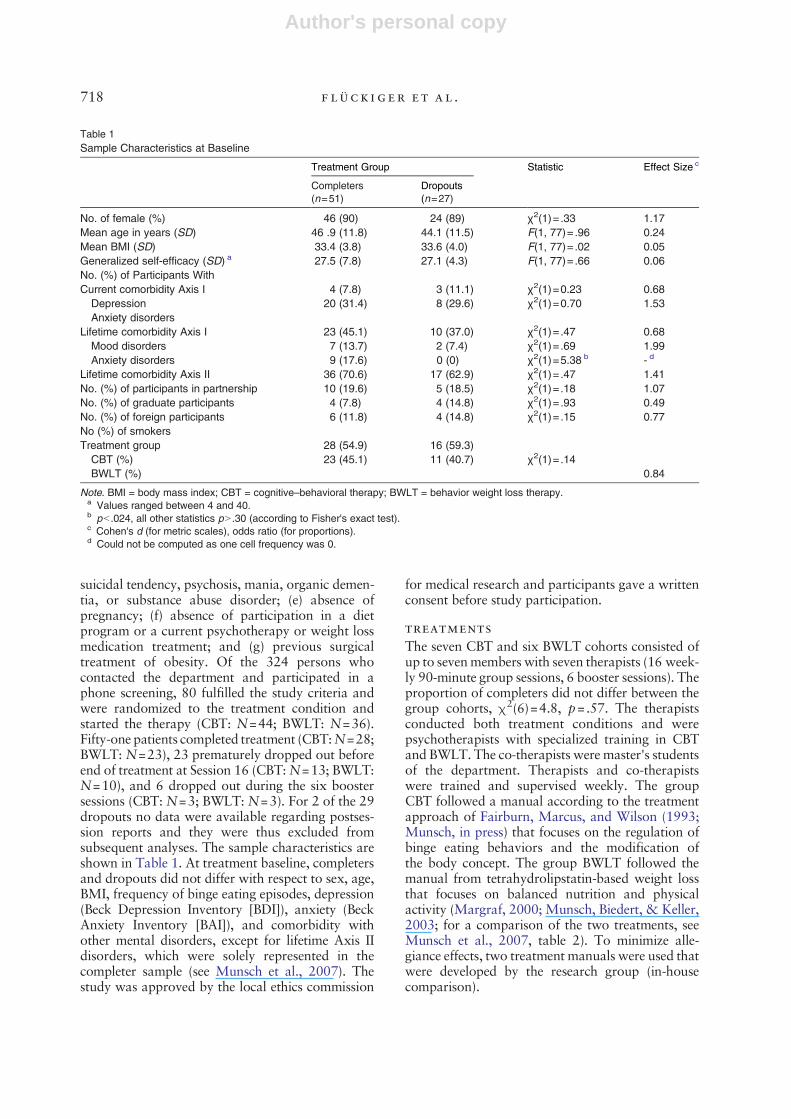
Table 2Correlation Coefficients Between BMI and GSE and Early Therapeutic Process
1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12.
Baseline1. BMI - .12 –.07 .09 .10 .07 .02 .11 .02 .05 .09 –.052. GSE - –.23* –.14 –.08 –.14 –.10 –.13 .10 .11 –.01 –.033. Axis II a .01 .20* .15 .01 .13 .20* .16 .23* .124. CBT(+1)/BWLT (−1) a –.07 –.04 .14 .03 .14 –.02 .03 .13BPSR-P (session 1 to 5)5. Control experiences - .47* .33* .38* .39* .57* .39* –.016. Self-esteem experiences - .72* .84* .42* .64* .73* –.187. Contentment with the bond - .67* .32* .47* .49* –.168. Global alliance - .38* .59* .77* –.159. Problem actuation - .63* .63* .0110. Mastery - .75* .0211. Clarification - –.0512. Rapid response a -
Note. BMI=body mass index; GSE=Generalized Self-Efficacy Scale; CBT=cognitive–behavioral therapy; BWLT=behavior weight losstherapy; BPSR-P=Bern Post-Session Reports for Patients. *pb .05.a Based on Spearman's rank correlation coefficient.
Table 3Self-Reported Reasons for Premature Termination
After Sessions Sessions Sessions Boosters TherapyScreening a 1 to 5 6 to 10 11 to 16 1 to 6 Total
Lack of time (4) 0No interest anymore (3) 1 1 2Conflicting schedule (3) 1 1More appropriate program (3) 0Discontentment with therapy 4 2 2 1 b 9Depression 2 1 3Improvement (4) 1 1 2Pregnancy 1 1 2Accident 1 1No specification (4) 6 b 3 9Total (20) 14 5 4 6 29a Participants who fulfilled all inclusion criteria for treatment admission.b Includes one dropout with no data on the BPSR-P (Bern Post-Session Reports for Patients).
720 fl u ck iger et al .

Author's personal copy
in which each BPSR-P scale was tested separately.As we performed more than one hypothesis testsimultaneously, we adjusted p values accordingto the Holm-Bonferroni method (Holm, 1979). Tocontrol for possible confounders, we also ranmodelsthat included BMI and GSE, treatment group, andrapid response as covariates. Multinominal logisticregression models were applied to predict discon-tentment with therapy as reason for prematuretermination. Categories were (a) treatment comple-tion (reference category), (b) premature terminationdue to discontentment with therapy, and (c) prema-ture termination for other reasons.
ResultsTo test whether the process variables were inde-pendent from the characteristics at baseline andinterdependent from each other, correlation co-efficients between the patient's evaluation of theearly therapeutic process (BPSR-P), BMI, GSE atbaseline, treatment condition, Axis II, and rapidresponse are presented in Table 2. None of thecorrelations between the BPSR-P scales and BMI orGSE were significant. BPSR-P scales, however, werehighly intercorrelated, especially self-esteem expe-riences with global alliance, contentment of thebond and clarification, clarification with mastery,and problem actuation (rN .70 for all these relation-ships). Self-reported reasons for premature termi-nation are presented in Table 3.
predicting premature termination
Results of binary logistic regressionmodels (BPSR–P)indicate that individuals with lower self-esteemexperiences, lower alliance, lower mastery, andlower clarification were more likely to terminate.All other process variables did not significantly
predict premature termination (see Table 4).1
When all BPSR-P scales were used together in thesame model, they explained 29.4% of the totaldeviance, based onNagelkerke's pseudoR2;χ2(7)=18.7, p=.009. Only self-esteem experiences re-mained predictive (R2=.182), when simultaneouslycontrolling for BMI and GSE at baseline, treatmentgroup, rapid response, and Axis II (see Table 4).Further, self-esteem experiences did not distinguishbetween early (Sessions 1 to 5) and later drop-outs after Session 5, Wald(1)=1.2, p=.28. BMIχ2(1)= .02, p=.89; GSE χ2(1)=.07, p=.79; treat-ment groups χ2(1)=.14, p=.72; and rapid responsen=73; χ2(1)=1.21, p=.27, did not significantlyaffect premature termination. Axis II predictedpremature termination, χ2(1)=8.25, p=.004, butwhen included with the other covariates, this effectdisappeared χ2(5)=7.6, p=.18.
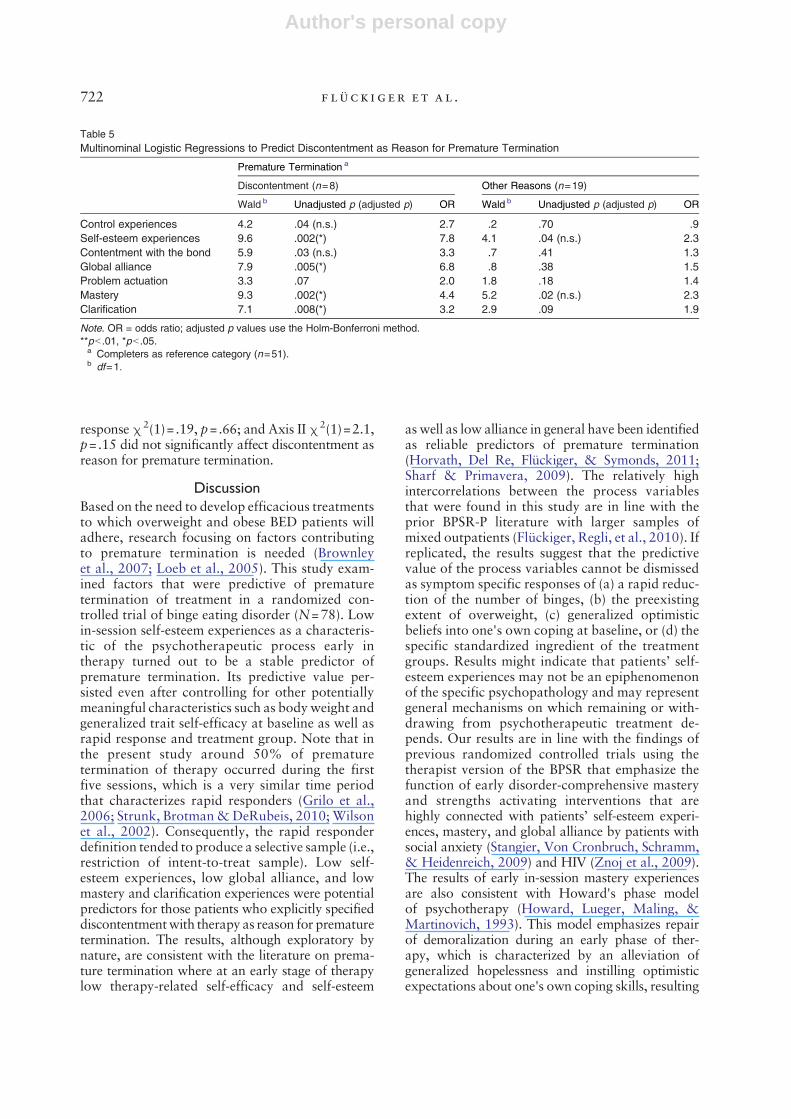
predicting discontentment as reasonfor premature termination
Multinominal logistic regressionmodels (BPSR–P)—low self-esteem experiences, low alliance, low mas-tery, and low clarification—were significant pre-dictors of discontentment as reason for prematuretermination relative to treatment completion (seeTable 5). None of the process variables were sig-nificant predictors of other reasons for prematuretermination, relative to treatment completion (seeTable 5). BMI χ2(1)=.60, p=.44; GSE χ2(1)=1.6,p=.20; treatment groups χ2(1)=1.3, p=.25; rapid
Table 4Binary Logistic Regressions to Predict Premature Termination
Premature Termination a
Without Controlling for Covariates (n=27) Covariates Included (n=22)
χ2 b Unadjusted p (adjusted p) OR χ2 b Unadjusted p (adjusted p) OR
Control experiences .6 .45 1.2 .2 .65 1.4Self-esteem experiences 11.0 .001 (**) 3.1 5.9 .02 (*) 3.0Contentment with the bond 3.2 .07 1.6 2.0 .16 1.6Global alliance 6.2 .01 (*) 2.2 2.6 .13 2.1Problem actuation 3.6 .06 1.6 .4 .55 1.2Mastery 11.5 .001 (**) 2.8 3.8 .05 (ns) 2.1Clarification 7.3 .007 (*) 2.2 1.1 .30 1.5
Note. OR = odds ratio; adjusted p values use the Holm-Bonferroni method.**pb .01, *pb .05.a Completers as reference category (n=51).b df=1.
1We further analyzed intercepts and slopes from Session 1 to 5based on a longitudinal MLM. Aggregated means and MLMintercepts produced comparable results. We did not find anysystematical results on MLM slopes.
721pred ic t ing premature terminat ion
Author's personal copy
response χ2(1)= .19, p=.66; and Axis II χ2(1)=2.1,p=.15 did not significantly affect discontentment asreason for premature termination.
DiscussionBased on the need to develop efficacious treatmentsto which overweight and obese BED patients willadhere, research focusing on factors contributingto premature termination is needed (Brownleyet al., 2007; Loeb et al., 2005). This study exam-ined factors that were predictive of prematuretermination of treatment in a randomized con-trolled trial of binge eating disorder (N=78). Lowin-session self-esteem experiences as a characteris-tic of the psychotherapeutic process early intherapy turned out to be a stable predictor ofpremature termination. Its predictive value per-sisted even after controlling for other potentiallymeaningful characteristics such as body weight andgeneralized trait self-efficacy at baseline as well asrapid response and treatment group. Note that inthe present study around 50% of prematuretermination of therapy occurred during the firstfive sessions, which is a very similar time periodthat characterizes rapid responders (Grilo et al.,2006; Strunk, Brotman&DeRubeis, 2010; Wilsonet al., 2002). Consequently, the rapid responderdefinition tended to produce a selective sample (i.e.,restriction of intent-to-treat sample). Low self-esteem experiences, low global alliance, and lowmastery and clarification experiences were potentialpredictors for those patients who explicitly specifieddiscontentmentwith therapy as reason for prematuretermination. The results, although exploratory bynature, are consistent with the literature on prema-ture termination where at an early stage of therapylow therapy-related self-efficacy and self-esteem
as well as low alliance in general have been identifiedas reliable predictors of premature termination(Horvath, Del Re, Flückiger, & Symonds, 2011;Sharf & Primavera, 2009). The relatively highintercorrelations between the process variablesthat were found in this study are in line with theprior BPSR-P literature with larger samples ofmixed outpatients (Flückiger, Regli, et al., 2010). Ifreplicated, the results suggest that the predictivevalue of the process variables cannot be dismissedas symptom specific responses of (a) a rapid reduc-tion of the number of binges, (b) the preexistingextent of overweight, (c) generalized optimisticbeliefs into one's own coping at baseline, or (d) thespecific standardized ingredient of the treatmentgroups. Results might indicate that patients’ self-esteem experiences may not be an epiphenomenonof the specific psychopathology and may representgeneral mechanisms on which remaining or with-drawing from psychotherapeutic treatment de-pends. Our results are in line with the findings ofprevious randomized controlled trials using thetherapist version of the BPSR that emphasize thefunction of early disorder-comprehensive masteryand strengths activating interventions that arehighly connected with patients’ self-esteem experi-ences, mastery, and global alliance by patients withsocial anxiety (Stangier, Von Cronbruch, Schramm,& Heidenreich, 2009) and HIV (Znoj et al., 2009).The results of early in-session mastery experiencesare also consistent with Howard's phase modelof psychotherapy (Howard, Lueger, Maling, &Martinovich, 1993). This model emphasizes repairof demoralization during an early phase of ther-apy, which is characterized by an alleviation ofgeneralized hopelessness and instilling optimisticexpectations about one's own coping skills, resulting
Table 5Multinominal Logistic Regressions to Predict Discontentment as Reason for Premature Termination
Premature Termination a
Discontentment (n=8) Other Reasons (n=19)
Wald b Unadjusted p (adjusted p) OR Wald b Unadjusted p (adjusted p) OR
Control experiences 4.2 .04 (n.s.) 2.7 .2 .70 .9Self-esteem experiences 9.6 .002(*) 7.8 4.1 .04 (n.s.) 2.3Contentment with the bond 5.9 .03 (n.s.) 3.3 .7 .41 1.3Global alliance 7.9 .005(*) 6.8 .8 .38 1.5Problem actuation 3.3 .07 2.0 1.8 .18 1.4Mastery 9.3 .002(*) 4.4 5.2 .02 (n.s.) 2.3Clarification 7.1 .008(*) 3.2 2.9 .09 1.9
Note. OR = odds ratio; adjusted p values use the Holm-Bonferroni method.**pb .01, *pb .05.a Completers as reference category (n=51).b df=1.
722 fl u ck iger et al .

Author's personal copy
in early-stage enhancement of patients' subjectivewell-being.From a clinical perspective, our findings indicate
that even though disorder-specific treatments suchas CBT and BWLT foster mastery experiences bysymptom reduction, a considerable group ofpatients might need tailored interventions aimedat increasing self-esteem experiences, mastery, andalliance beyond symptom reduction (Bohart &Tallman, 2010; Gilbert & Leahy, 2009; Linehan,1997; Wilson, 1998). Such strategies could includestrengths-fostering microinterventions, whichcould be systematized within disorder-specific treat-ments (Flückiger, Wüsten, Zinbarg, & Wampold,2010; Gassmann & Grawe, 2006; Grawe, 2004,p. 432 ff; Zinbarg, Mashal, Black, & Flückiger,2010).This study has various limitations. First, the small
sample size in this study limits the generalizabilityof the results as well as analyses of potential sub-groups. Second, there is still a lack of informationover the long-term course on samples includingboth dropouts and completers. For example,dropout samples may include proactive patients,who after terminating one treatment actively selectother treatments or therapists more appropriate forthem (e.g., Seligman, 1995). Third, group processessuch as coherence are not integrated into thepresent study (e.g., Burlingame, McClendon, &Alonso, 2011). Fourth, we only analyzed thepatient's perspective of the process variables andfuture studies might consider the therapist's per-spective. Nevertheless, keeping these limitations inmind, the current study adds knowledge to researchfocusing on factors influencing premature termi-nation of generally efficacious treatments. Psycho-therapy process characteristics seem to contributeto a meaningful extent to the adherence or with-drawal from eating disorder treatments andshould be considered in training, individualizedtherapy plans, and supervision and evaluation ofpsychotherapists conducting disorder-specifictreatments.
Appendix A. Scales of the Bern Post-SessionReports for Patients (BPSR-P Short Form 2000)
BPSR-PIn-SessionExperiences
Meaning Example of an Item(Cronbach's α)
1. Controlexperiences
Patient's perceptionof possibilities to takean active part duringtherapy
During therapy, thetherapist lets me gomy own way. (.80)
Appendix A (continued)
BPSR-PIn-SessionExperiences
Meaning Example of an Item(Cronbach's α)
2. Self-esteemexperiences
Patient's attribution ofhow therapistreinforced/fosteredpatient's self-esteem
The therapist letsme feel my ownstrengths. (.81)
3. Contentmentof the bond
Patient's (dis)contentment withtherapist/therapy
Today I feel that thetherapist is thinkingdifferently about methan what he or sheis saying. (−) (.85)
4. Globalalliance
Patient's perceptionof successfulcollaborationbetween patient andtherapist
The therapist andI appreciate eachother. (.83)
5. Problemactuation
Patient's evaluation ofhow intense patientand therapist workedon “hot topics”
What we did todayreally affected me.(r=.73)
6. Masteryexperiences
Patient's evaluationof progress tocope with hisor her own problems
Now I feel betterprepared forsituations I couldnot handle before.(.85)
7. Clarificationexperiences
Patient's evaluationof progress tounderstand his orher ownproblems/situation
I understand myselfand my problemsbetter now. (.80)
ReferencesBohart, A. C., & Tallman, K. (2010). Clients: The neglected
common factor in psychotherapy. In B. L. Duncan, S. D.Miller, B. E. Wampold, & M. A. Hubble (Eds.), The heartand soul of change: Delivering what works in therapy(pp. 83–111). Washington, DC: APA.
Brownley, K. A., Berkman, N. D., Sedway, J. A., Lohr, K. N.,& Bulik, C. M. (2007). Binge eating disorder treatment:A systematic review of randomized controlled trials.International Journal of Eating Disorders, 40, 337–348.doi:10.1002/eat.20370
Burlingame, G. M., McClendon, D. T., & Alonso, J. (2011).Cohesion in group therapy. Psychotherapy, 48, 34–42. doi:10.1037/a0022063
Carter, J. C., & Fairburn, C. G. (1998). Cognitive–behavioralself-help for binge eating disorder: A controlled effectivenessstudy. Journal of Consulting and Clinical Psychology, 66,616–623. doi:10.1037/0022-006X.66.4.616
Coker, S., Vize, C., Wade, T., & Cooper, P. J. (1993). Patientswith bulimia nervosa who fail to engage in cognitive behaviortherapy. International Journal of Eating Disorders, 13,35–40. doi:10.1002/1098-108X(199301)13:1b35::AID-EAT2260130105N3.0.CO;2-N
Constantino, M. J., Arnow, B. A., Blasey, C., & Agras, W. S.(2005). The association between patient characteristics andthe therapeutic alliance in cognitive–behavioral and inter-personal therapy for bulimia nervosa. Journal of Consulting
723pred ic t ing premature terminat ion
Author's personal copy
and Clinical Psychology, 73, 203–211. doi:10.1037/0022-006X.73.2.203
Dingemans, A. E., Spinhoven, P., & van Furth, E. F. (2007).Predictors and mediators of treatment outcome in patientswith binge eating disorder. Behaviour Research and Therapy,45, 2551–2562. doi:10.1016/j.brat.2007.06.003
Epstein, S. (1990). Cognitive-experiental self-theory. In L. A.Pervin (Ed.),Handbook of personality: Theory and research(pp. 165–192). New York: Guilford Press.
Fairburn, C. G., Marcus, M. D., & Wilson, G. T. (1993).Cognitive–behavioral therapy for binge eating and bulimianervosa: A comprehensive treatment manual. In C. G.Fairburn & G. T. Wilson (Eds.), Binge eating—Nature,assessment and treatment New York: Guilford Press.
Fassino, S., Pierò, A., Tomba, E., & Abbate-Daga, G. (2009).Factors associated with dropout from treatment foreating disorders: A comprehensive literature review. BMCPsychiatry, 9, 67.
Flückiger, C., Caspar, F., Grosse Holtforth, M., &Willutzki, U.(2009). Working with the patient's strengths—A micropro-cess approach. Psychotherapy Research, 19, 213–223. doi:10.1080/10503300902755300.
Flückiger, C., Regli, D., Zwahlen, D., Hostettler, S., & Caspar, F.(2010). Der Berner Patienten- und Therapeutenstundenbogen2000 [The Bern Post-Session Reports for Patients andTherapists 2000]. Zeitschrift für Klinische Psychologie undPsychotherapie. doi:10.1026/1616-3443/a000015
Flückiger, C., Wüsten, G., Zinbarg, R. E., & Wampold, B. E.(2010). Resource activation—Using client's own strengths inpsychotherapy and counseling. Cambridge, MA: Hogrefe.
Gassmann, D., & Grawe, K. (2006). General change mechanisms:The relation between problem activation and resource activa-tion in successful and unsuccessful therapeutic interactions.Journal of Clinical Psychology and Psychotherapy, 13, 1–11.
Gilbert, P., & Leahy, R. L. (2009). The therapeutic relationshipin the cognitive behavioral psychotherapies. London:Routledge.
Gorin, A. A., Le Grange, D., & Stone, A. A. (2003).Effectiveness of spouse involvement in cognitive behavioraltherapy for binge eating disorder. International Journal ofEating Disorders, 33, 412–433. doi:10.1002/eat.10152
Grawe, K. (1997). Research-informed psychotherapy. Psycho-therapy Research, 7, 1–19.
Grawe, K. (2004). Psychological therapy. Cambridge, MA:Hogrefe.
Grawe, K., & Braun, U. (1994). Qualitätskontrolle in derPsychotherapie [Quality management in psychotherapy].Zeitschrift für Klinische Psychologie und Psychotherapie,23, 242–267.
Grawe, K., Donati, R., & Bernauer, F. (1994). Psychotherapie imWandel. Von der Konfession zur Profession [Psychotherapy intransition. Fromconfession toprofession].Göttingen,Germany:Hogrefe.
Grawe,K.,Ohlendorf,H., Retzmann, A.,&Schröder,M. (1978).Der Gruppenbeurteilungsbogen [The group postsessionreport]. In R. Ullrich & R. Ullrich de Muynck (Eds.), SozialeKompetenz (pp. 36–71). München, Germany: Pfeiffer.
Grilo, C. M., Masheb, R. M., & Wilson, G. T. (2006). Rapidresponse to treatment for binge eating disorder. Journal ofConsulting and Clinical Psychology, 74, 602–613. doi:10.1037/0022-006X.74.3.602
Hilbert, A., Saelens, B. E., Stein,R. I.,Mockus,D. S.,Welch,R.R.,Matt, G. E., & Wilfley, D. E. (2007). Pretreatment andprocess predictors of outcome in interpersonal and cognitivebehavioral psychotherapy for binge eating disorder. Journal ofConsulting and Clinical Psychology, 75, 645–651. doi:10.1037/0022-006X.75.4.645
Hilbert, A., Tuschen-Caffier, B., & Ohms, M. (2004). Eatingdisorders examination: A German version of the structuredeating disorder interviews. Diagnostica, 50, 98–106.
Holm, S. (1979). A simple sequentially rejective multiple testprocedure. Scandinavian Journal of Statistics, 6, 65–70.
Horvath, A., Del Re, A. C., Flückiger, C., & Symonds, D.(2011). The alliance in adult psychotherapy. In J. E.Norcross (Ed.), Relationships that works (pp. 25–69).New York, NY: Oxford University Press.
Howard, K. I., Lueger, R. J., Maling, M. S., & Martinovich, Z.(1993). A phase model of psychotherapy outcome: Causalmeditation of change. Journal of Consulting and ClinicalPsychology, 61, 678–685.
In-Albon, T. (2008). Validity of the “Diagnostisches Interview beipsychischen Störungen (DIPS für DSM-IV-TR).Zeitschrift fürklinische Psychologie und Psychotherapie, 37, 33–42.
Kraemer, H. C., Wilson, G. T., Fairburn, C. G., & Agras, W. S.(2002). Mediators and moderators of treatment effects inrandomized clinical trials. Archive of General Psychiatry,59, 877–883. Retrieved from http://archpsyc.ama-assn.org/cgi/reprint/59/10/877
Linehan, M.M. (1997). Validation and psychotherapy. In A. C.Bohart & L. S. Greenberg (Eds.), Empathy reconsidered:New directions (pp. 353–392). Washington, DC: AmericanPsychological Association.
Loeb, K. L., Wilson, G. T., Labouvie, E., Pratt, E. M., Hayaki,J., Walsh, B. T., Agras, W. S., et al. (2005). Therapeuticalliance and treatment adherence in two interventions forbulimia nervosa: A study of process and outcome. Journal ofConsulting and Clinical Psychology, 73, 1097–1107. doi:10.1037/0022-006X.73.6.1097
Margraf, J. (2000). Aus dick wir nicht dünn. Falsche Erwartung-shaltungen. In E. Roche (Ed.), Hülle und Fülle. Dem Fett aufden Leib gerückt Basel, Switzerland: Hoffmann-La Roche.
Margraf, J., Schneider, S., & Ehlers, A. (1994). DIPS—Diagnostisches Interview bei psychischen Störungen [Diag-nostic interview formental disorders]. Bern, Germany:Huber.
Masheb, R. M., & Grilo, C. M. (2007). Rapid response predictstreatment outcomes in binge eating disorder: Implications forstepped care. Journal of Consulting and Clinical Psychology,75, 639–644. doi:10.1037/0022-006X.75.4.639
Munsch, S. (in press). Kognitive Verhaltenstherapie bei BingeEating Disorder (2nd ed.). Auflage. Weinheim, Germany:Beltz PVU.
Munsch, S., Biedert, E., & Keller, U. (2003). Evaluation of alifestyle change program for the treatment of obesity ingeneral practice. Swiss Medical Weekly, 133, 148–154.
Munsch, S., Biedert, E., Meyer, A., Michael, T., Schlup, B., & Tuc,A. (2007). A randomized comparison of cognitive behavioraltherapy and behavioral weight loss treatment for overweightindividuals with binge eating disorder. International Journal ofEating Disorders, 40, 102–113. doi:10.1002/eat.20350.
Orlinsky,D., Grawe,K.,&Parks, B. (1994). Process and outcomein psychotherapy:Noch einmal. InA. E. Bergin&S.L.Garfield(Eds.), Handbook of psychotherapy and behavior change(pp. 270–376). (4th ed.). New York: Wiley.
Schlup, B., Munsch, S., &Meyer, A. (2010). A non-randomizeddirect comparison of cognitive–behavioral short- and long-term treatment for binge eating disorder. Obesity Facts,3(4), 261–266.
Schwarzer, R., & Jerusalem,M. (1995). Generalized Self-EfficacyScale. In J. Weinman, S. Wight, & M. Johnston (Eds.),Measures in health psychology: A user‘s portfolio. Causal andcontrol beliefs (pp. 35–37). Windsor, UK: NFER-Nelson.
Seligman, M. E. P. (1995). The effectiveness of psychotherapy:The Consumer Reports study. American Psychologist, 50,965–974.
724 fl u ck iger et al .
Author's personal copy
Sharf, J., & Primavera, L. H. (2009). Meta-analysis of psycho-therapy dropout. Manuscript submitted for publication.
Stangier, U., Von Cronbruch, K., Schramm, E., &Heidenreich,T. (2009). Common factors of cognitive therapy andinterpersonal psychotherapy in the treatment of socialphobia. Anxiety, Stress, and Coping. doi:10.1080/10615800903180239
Strunk, D. R., Brotman, M. A., & DeRubeis, R. J. (2010). Theprocess of change in cognitive therapy for depression:Predictors of early inter-session symptom gains. BehaviourResearch and Therapy, 48, 599–606. doi:10.1016/j.brat.2010.03.011
Suppiger, A., In-Albon, T., Hendriksen, S., Hermann, E.,Margraf, J., & Schneider, S. (2009). Acceptance of structureddiagnostic interviews for mental disorders in clinical practiceand research settings. Behavior Therapy, 40, 272–279.
Vocks, S., Tuschen-Caffier, B., Pietrowsky, R., Rustenbach, S. J.,Kersting, A., & Herpertz, S. (2009). Meta-analysis of theeffectiveness of psychological and pharmacological treatmentsfor binge eating disorder. International Journal of EatingDisorders. doi:10.1002/eat.20696
Wierzbicki, M., & Pekarik, G. (1993). A meta-analysis ofpsychotherapy dropout. Professional Psychology: Researchand Practice, 24, 190–195. doi:10.1037/0735-7028.24.2.190
Wilson, G. T. (1998). Manual-based treatment and clinicalpractice. Clinical Psychology, Science and Practice, 5,363–375.
Wilson, G. T., Fairburn, C. C., Agras, W. S., Walsh, B. T., &Kraemer,H. (2002). Cognitive-behavioral therapy for bulimianervosa: Time course and mechanisms of change. Journal of
Consulting and Clinical Psychology, 70, 267–274. doi:10.1037/0022-006X.70.2.267
Wilson, G. T., Wilfley, D. E., Agras, W. S., & Bryson, S. W.(2010). Psychological treatments of binge eating disorder.Archives of General Psychiatry, 67, 94–101. doi:10.1001/archgenpsychiatry.2009.170.
Wittchen, H., Zaudig, M., & Fydrich, T. (1997). StrukturiertesKlinisches Interview für DSM-IV [Structured Clinical Inter-view for DSM-IV]. Bern, Germany: Hogrefe Testzentrale.
Wolff, G. E., & Clark, M. M. (2001). Changes in eating self-efficacy and body image following cognitive–behavioralgroup therapy for binge eating disorder: A clinical study.Eating Behavior, 2, 97–104. doi:10.1016/S1471-0153(01)00021-6
Zinbarg, R. E., Mashal, N. M., Black, D. A., & Flückiger, C.(2010). The future andpromise of cognitive behavior therapy:Acommentary. Psychiatric Clinics of North America, 33,711–727.
Znoj,H. J.,Messerli-Burgy,N., Tschopp, S.,Weber, R., Christen,L., Christen, S., & Grawe, K. (2009). Psychotherapeuticprocess of cognitive–behavioral intervention in HIV-infectedpersons: Results from a controlled, randomized prospectiveclinical trial. Psychotherapy Research. doi:10.1080/10503300903246663
RECEIVED: October 26, 2010ACCEPTED: March 30, 2011Available online 27 May 2011
725pred ic t ing premature terminat ion





























