Embed Size (px)
Citation preview

Care of Critically Ill Adults
Nursing role in monitoring during cardiopulmonaryresuscitation and in the peri-arrest period: A review
Chrysovalantis Pothitakis, MDa, Konstantinos A. Ekmektzoglou, MDb,Maria Piagkou, PhDb, Theodoros Karatzas, PhDc, Theodoros Xanthos, PhDb,*
aDepartment of Anaesthesiology, 401 General Army Hospital of Athens, GreecebDepartment of Anatomy and MSc Program in Cardiopulmonary Resuscitation, University of Athens, Medical School, Athens, Greece
cDepartment of Experimental Surgery and Surgical Research, University of Athens, Medical School, Athens, Greece
a r t i c l e i n f o
Article history:Received 30 May 2010Revised 23 October 2010Accepted 24 November 2010Online 16 March 2011
Keywords:Adult nursingCritical careCardiac arrestCardiopulmonary resuscitationMonitoring
* Corresponding author: Theodoros Xanthos,E-mail address: theodorosxanthos@yahoo
0147-9563/$ - see front matter � 2011 Elsevidoi:10.1016/j.hrtlng.2010.11.006
a b s t r a c t
Objective: The study objective was to present a comprehensive literaturereview on the monitoring of patients with cardiac arrest (CA) and the nursingcontribution in this crucial situation. Monitoring techniques during cardio-pulmonary resuscitation and in the peri-arrest period (just before or after CA)are included.
Methods: Approaches used to access the research studies included a compre-hensive search in relevant electronic databases (Medline, CINAHL, EMBASE,Cochrane Review, British Nursing Index) using relevant keywords (eg, cardiacarrest, resuscitation, monitoring, nurse, survival, outcome). Books and journalsknown to the authors were also used.
Results: The nurse’s role in patients with CA is extremely significant and ifperformed correctly adds great insight to treatment planning and correctmanagement.
Conclusion: Early recognition of CA and invasive (methods and equipment thatrequire endarterial or intravenous access) and noninvasive monitoring shouldbe prompt and appropriate for early return of spontaneous circulation andimproved neurologic outcome in patients.
Cite this article: Pothitakis, C., Ekmektzoglou, K. A., Piagkou, M., Karatzas, T., & Xanthos, T. (2011,
NOVEMBER/DECEMBER). Nursing role in monitoring during cardiopulmonary resuscitation and in the
peri-arrest period: A review. Heart & Lung, 40(6), 530-544. doi:10.1016/j.hrtlng.2010.11.006.
Cardiac arrest (CA) is the cessation of cardiacmechanical activity confirmed by the absence ofsigns of circulation.1 CA is a leading cause of death inEurope, affecting approximately 700,000 individualsper year, whereas approximately 400,000 to 460,000
PhD, 75 Mikras Asias Str.com (T. Xanthos).
er Inc. All rights reserved
people in the United States experience CA each year.When these figures are viewed as a global incidencein an unselected adult population, the overall inci-dence is 1 to 2 per 1000 (0.1%-0.2%) per year.2,3 Theoutcome of CA and cardiopulmonary resuscitation
eet, 11527 Athens, Greece.
.
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4 531
(CPR) is dependent on critical interventions, particu-larly early defibrillation, effective chest compressions,and assisted ventilation. However, despite consider-able efforts to improve the outcome of CA, survival ispoor.4,5 If patient outcomes are to improve, thencontinuous monitoring of the peri-arrest period isessential, not only to identify and prevent CA but alsoto guide treatment planning and immediate inter-ventions during and after CPR.
To determine whether the rescue attempts aresuccessful and to monitor a patient’s progress, thepresence of adequate invasive or noninvasive equip-ment is required, with electrocardiography (ECG) beingthe most essential monitoring tool.6 Furthermore,pupil observation, temperature monitoring, systolicand diastolic blood pressure (BP), and end-tidal carbondioxide (ETCO2) can offer useful information andguidance. New monitoring methods and severalphysiologic parameters are continuously beingexplored and evaluated, such as the bispectral index(BIS), sonography, and coronary perfusion pressure(CPP). The nurse’s role inmonitoring during this criticalperiod is crucial. This review elucidates commonaspects of monitoring during CPR and the peri-arrestperiod, and underlines the importance of earlynursing intervention in patients with CA.
Materials and Methods
The literature review included a comprehensive searchof published literature in the English language datingfrom 1995 to March 2010. A range of electronic data-bases (Medline, CINAHL, EMBASE, Cochrane Review,British Nursing Index) were used. These databaseswere searched using keywords, including cardiac arrest,resuscitation, monitoring, nurse, survival, and outcome.The search was extended using article reference listsand bibliographies of books and reports. Relevantacademic and practitioners’ journals were handsearched. All articles were evaluated for relevancy andconsistency. Inclusion criteria were human studiesdescribingmonitoring during CA, the current EuropeanResuscitation Council (ERC), the American HeartAssociation (AHA) guidelines for CPR, and the nurses’role during and after resuscitation and in the pre-arrestperiod. The literature used in this review is summa-rized in Table 1.
Expert judgment was preferred to determinewhich studies should be presented. Expert judgmentwas carried out by KE and TX, both ERC CourseDirectors, with experience in managing CA and CPR.The authors took into account the most recentlypublished articles, the current guidelines, the orga-nization of responding emergency teams in hospitalsettings, and the developing nursing role in them. Aproposed monitoring approach in patients with CA issummarized in Figure 1.
Results
Noninvasive Monitoring
Noninvasive monitoring refers to methods and equip-ment that do not require endarterial (eg, radial orfemoral) or intravenous (IV) access. It is the type ofmonitoring that is applied first, when the nurse dealswith an emergency situation. Many, if not all, of thenoninvasive monitoring devices are designed to beportable, so they can function in a variety of situationsand locations.
Absence of Respiration: Pulse Palpation
When approaching someone who is in presumed CA,the first task is to determine unresponsiveness,absence of respiration, and circulation. Determiningpulse absence does not require any special equipment,but it is not quick or easy, especially for a non-healthcare professional.7 That is why the ERCsuggests commencing CPR if the patient has no signs oflife (lack of movement, normal breathing, or coughing),until more experienced help arrives or the patientshows signs of life. The AHA, on the other hand,recommends that the healthcare provider should takeno more than 10 seconds to check for a pulse. Nursesexperienced in clinical assessment should palpate thecarotid pulse while simultaneously looking for signs oflife for no more than 10 seconds.8 Carotid pulsationsduring CPR do not indicate the efficacy of coronaryblood flow or myocardial or cerebral perfusion.9
Therefore, checking for carotid pulsations during CPRoffers no data as to the patient’s outcome, and it is notrecommended.9
Other studies have shown that checking forbreathing also can be prone to error. It is notuncommon for agonal gasps to be misdiagnosed asnormal breathing.10 The absence of breathing in anunresponsive person still remains the main sign of CA,according to the 2005 ERC guidelines. Furthermore,identification of agonal gasps is another indication tostart CPR.9
Patients in intensive care units (ICUs) requirefrequent monitoring of vital signs, including heart andrespiratory rate, BP, and saturation of peripheraloxygen (SPO2) to monitor response to medications,nursing procedures, and other therapies. Recognitionof clinical deterioration can be a precursor to CA.11
Pulse Oximetry
Pulse oximetry can be applied quickly and is helpful indetermining oxygenation and adequacy of perfusion tothe site of the probe. However, the pulse oximeter canfail even before the onset of CA because of decreasedlocal blood flow. Pulse oximetry should be used asa real-time “warning system” in patients at risk for
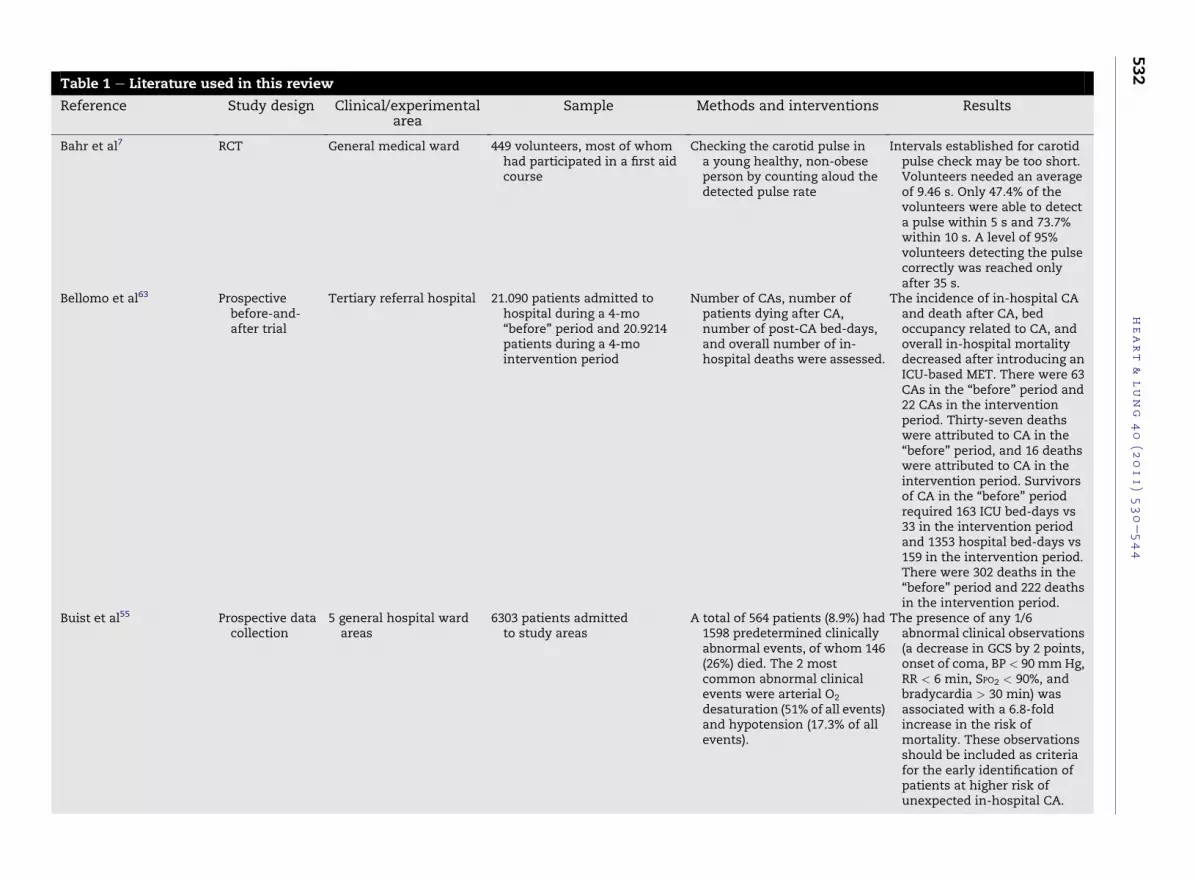
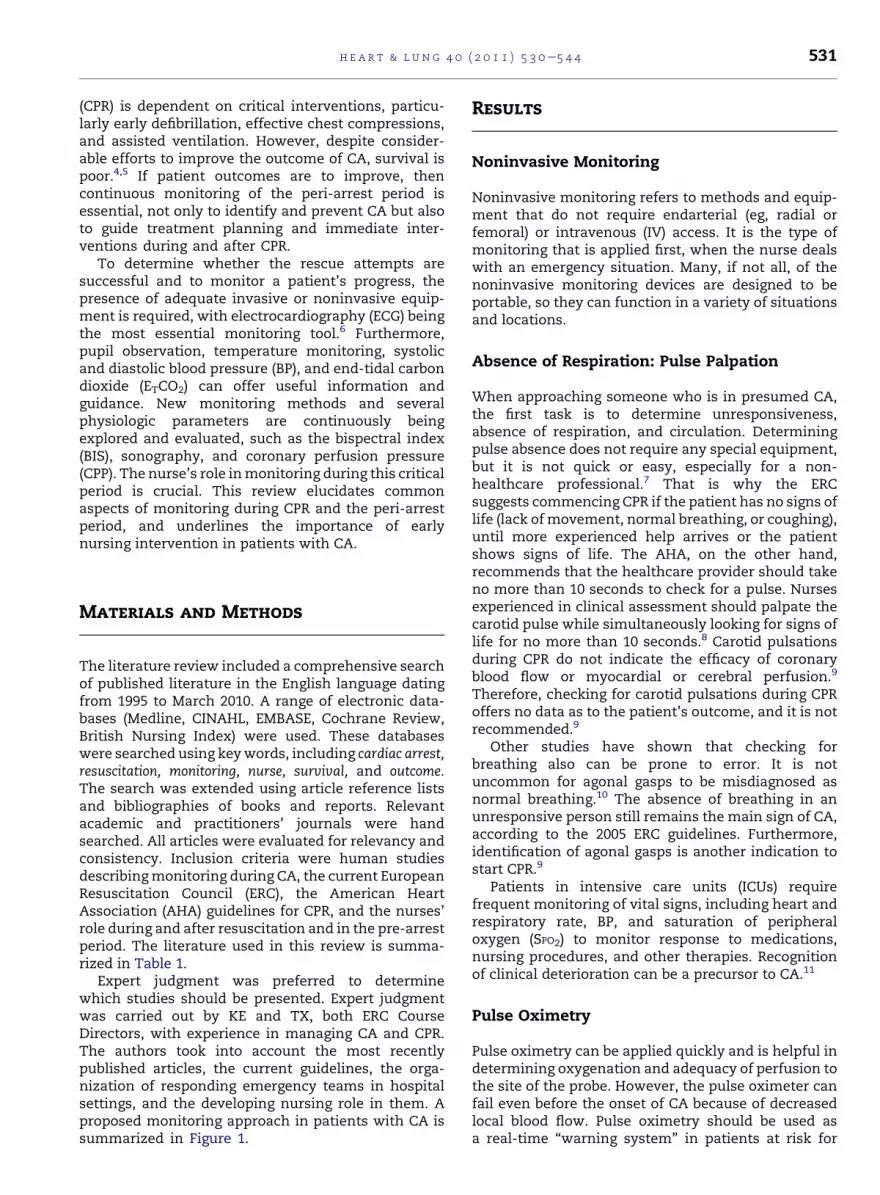
Table 1 e Literature used in this review
Reference Study design Clinical/experimentalarea
Sample Methods and interventions Results
Bahr et al7 RCT General medical ward 449 volunteers, most of whomhad participated in a first aidcourse
Checking the carotid pulse ina young healthy, non-obeseperson by counting aloud thedetected pulse rate
Intervals established for carotidpulse check may be too short.Volunteers needed an averageof 9.46 s. Only 47.4% of thevolunteers were able to detecta pulse within 5 s and 73.7%within 10 s. A level of 95%volunteers detecting the pulsecorrectly was reached onlyafter 35 s.
Bellomo et al63 Prospectivebefore-and-after trial
Tertiary referral hospital 21.090 patients admitted tohospital during a 4-mo“before” period and 20.9214patients during a 4-mointervention period
Number of CAs, number ofpatients dying after CA,number of post-CA bed-days,and overall number of in-hospital deaths were assessed.
The incidence of in-hospital CAand death after CA, bedoccupancy related to CA, andoverall in-hospital mortalitydecreased after introducing anICU-based MET. There were 63CAs in the “before” period and22 CAs in the interventionperiod. Thirty-seven deathswere attributed to CA in the“before” period, and 16 deathswere attributed to CA in theintervention period. Survivorsof CA in the “before” periodrequired 163 ICU bed-days vs33 in the intervention periodand 1353 hospital bed-days vs159 in the intervention period.There were 302 deaths in the“before” period and 222 deathsin the intervention period.
Buist et al55 Prospective datacollection
5 general hospital wardareas
6303 patients admittedto study areas
A total of 564 patients (8.9%) had1598 predetermined clinicallyabnormal events, of whom 146(26%) died. The 2 mostcommon abnormal clinicalevents were arterial O2
desaturation (51% of all events)and hypotension (17.3% of allevents).
The presence of any 1/6abnormal clinical observations(a decrease in GCS by 2 points,onset of coma, BP < 90 mmHg,RR < 6 min, SPO2 < 90%, andbradycardia > 30 min) wasassociated with a 6.8-foldincrease in the risk ofmortality. These observationsshould be included as criteriafor the early identification ofpatients at higher risk ofunexpected in-hospital CA.
heart
&lung
40
(2011)530e544
532

Goldhill et al67 RCT Every adult non-obstetricbed area in a hospital
433 adult non-obstetricinpatients
Recording, on a single ,of RR, HR, systolic BP SPO2,level of consciousnes rineoutput for catheterizpatients, age, and ins ed O2
Simple physiologic observationsidentify high-risk hospitalinpatients. Mortality increasedwith the number ofphysiologic abnormalities: .7%with no abnormalities, 4.4%with 1 abnormality, 9.2% with2 abnormalities, and 21.3%with � 3 abnormalities.
Gwinnutt et al4 RCT 49 hospitals Data on the process andoutcome of CPR afterin-hospital CA: Of 2074 auditforms submitted, 1368 wereincluded in the final analysis.
The initial rhythm mon redwas VF or PVT in 429 tients,of whom 181 (42.2%) redischarged alive, com redwith 6.2% when the i ialrhythm was non-VF/ .Overall, 240 patients .6%)were discharged alive t 6 moafter discharge, 195 ( %) of237 patients were sti live.
Improvement in survival of in-hospital patients with VF/PVTCA. Successful initialresuscitation, defined as ROSC> 20 min was significantlyassociated with VF/PVT as theinitial arrest rhythm, return ofcirculation in < 3 min, age< 70 y, and use of advancedairway. The administration ofany adrenaline wassignificantly associated witha reduced likelihood of ROSC >
20 min or alive discharge.Hauff at al10 Retrospective
data collectionStudy county Reviewed dispatcher audio
recordings and emergencymedical services reports for404 cases of sudden CA
The phase of the record gswas assessed: 1, inst tionsnot offered; 2, instruc nsoffered but declined; 3,instructions offered aaccepted but CPR notimplemented.
Factors potentially impedingtelephone CPR can beidentified. Each phase oftelephone CPR processimpeded the implementationof CPR: (1) instructions notoffered in 48%; (2) instructionsoffered but declined in 31%;and (3) instructions offeredand accepted but CPR notimplemented in 21%. Duringthe first phase, telephone CPRwas potentially impeded mostfrequently because the patientwas reported to have signs oflife (64%); during the secondand third phases, telephoneCPR was most often impededbecause of bystander physicallimitation (37%).
(continued on next page)
heart
&lung
40
(2011)530e544
533
day, T,s, uedpir
itopawepanitPVT(17. A82.3ll a
inructioornd

Table 1 e (Continued)
Reference Study design Clinical/experimentalarea
Sample Methods and interventions Results
Herlitz et al5 Prospective datacollection
Hospital setting 557 patients who had an in-hospital CA during a 4-yperiod and in whomresuscitative efforts wereattempted
A total of 292 patients (53%)had CA in wards withmonitoring facilities.
A shortening of the intervalbetween collapse anddefibrillation in patients within-hospital CA might increasesurvival even further. Those ina monitored location morefrequently had a confirmed orpossible AMI judged to be thecause of CA, and the CA waswitnessed more frequently(96% vs 79%). VF/VT wasobserved more often as initialarrhythmia in monitoredwards (56% vs 44%). Themedian interval betweencollapse and first defibrillationwas 1 min in monitored wardsand 5 min in non-monitoredwards. Among patients withCA in monitored wards, 43.2%were discharged alivecompared with 31.1% ofpatients in non-monitoredwards.
Hodgetts at al65 RCT An acute 700-bed districtgeneral hospital
118 consecutive adultpatients with primaryCA in-hospital and 132patients without CA
Risk factors for CA wereassessed: abnormal RR,abnormal breathing indicator(abnormal rate or documentedshortness of breath), abnormalpulse, reduced systolic BP,abnormal T, reduced pulseoximetry, chest pain, andnurse or doctor concern.
Multivariate analysis of CA casesidentified 3 positiveassociations for CA: abnormalbreathing indicator, abnormalpulse, and abnormal systolicBP. Risk factors were weightedand tabulated. Aggregate scoredetermines the grade ofclinical response. Analysisdetermined that a score of 4has 89% sensitivity and 77%specificity for CA; score of 8has 52% sensitivity and 99%specificity. All patients scoring> 10 had CA.
Kause et al64 Prospective,observationalstudy
90 hospitals 638 patients Incidence of antecedents(serious physiologicabnormalities) precedingprimary events (defined asin-hospital deaths, CA, andunanticipated ICU admissions)was studied.
Antecedents are common beforedeath, CA, and unanticipatedICU admission. The mostcommon antecedents werehypotension and a decrease inGCS.
heart
&lung
40
(2011)530e544
534
Laver et al45 Retrospectivestudy
11-bed multidisciplinaryICU in a general hospital
205 patients admitted to ICUafter a CA in the previous24 h
Outcome at hospital di argeand mode of death in on-survivors were record .According to the mod ofdeath, non-survivors ereplaced in 1 of 3 groupmultiple organ failurneurologic, or cardiov culardeath.
Two thirds of the patientsdying after out-of-hospitalCA died of neurologic injury,and this proportion wasapproximately the same forVF/VT and PEA/A.Approximately one quarter ofthe patients dying after in-hospital CA died ofneurologic injury. After CA,22.9% of the in-hospitalpatients and 67.7% of theout-of-hospital patients diedof neurologic injury,irrespective of the primaryCA arrhythmia.
Rivers et al56 RCT ICU of an urban ED 263 patients with severe sepsisor septic shock who received6 h of early goal-directedtherapy or standard therapy(as a control) before admissionto the ICU
A total of 130 patients ( up 1)were randomly assig d toearly goal-directed th apyand 133 patients werrandomly assigned tostandard therapy (gro 2).
Early goal-directed therapyprovides significantbenefits with respect tooutcome in patients withsevere sepsis and septicshock. In-hospital mortalitywas 30.5% in group 1compared with 46.5% ingroup 2. During the intervalfrom 7 to 72 h, group 1 hada significantly higher meancentral venous oxygensaturation, lower lactateconcentration, lower base,and higher pH than group 2.Mean APACHE II scoreswere significantly lower,indicating less severe organdysfunction in group 1 thanin group 2.
(continued on next page)
heart
&lung
40
(2011)530e544
535
schnedews:e,as
groneere
up

Table 1 e (Continued)
Reference Study design Clinical/experimentalarea
Sample Methods and interventions Results
Sandroni et al61 Prospectiveclinical study
A 1400-bed tertiary careteaching hospital
114 patients with CA(37 with VF/VT and 77patients with non-VF/VT)
Factors affecting the outcomeof in-hospital CA wereevaluated; 46% of CAs occurredin monitored areas, 54%occurred in non-monitoredareas; and 32% of patientssurvived to hospital discharge.
Where bystander defibrillationwas not available, the survivalof patients having CA in non-monitored areas stronglydepends on advanced lifesupport provided by the CAT.Patient survival in the wardswas significantly higher whenthe CAT arrival time was < 3min. No patient whose CATarrival time was > 6 minsurvived. CAT arrival time wassignificantly shorter (1.30 �1.70 min) in survivors than innon-survivors (2.51 � 2.37min).
Subbe at al66 Prospectiveclinical study
Hospital setting 1695 patients admitted withacute medical conditions
Effects of introducing MEWscores to identify medicalpatients at risk of catastrophicdeterioration were examined.
MEW score is a suitable scoringtool to identify patients at risk;however, outcomes in medicalemergency admissions areinfluenced by a multitude offactors, and it may be difficultto demonstrate the score’sbenefit. There was no changein mortality of patients withlow, intermediate, or highMEW scores. Rates of CA, ICU,or HDU admission weresimilar. Data analysisconfirmed RR as the bestdiscriminator in identifyinghigh-risk patient groups.
Takasu et al24 Retrospectiveclinical study
ICU 43 resuscitatedpatients with CA
Clinical characteristics ofhyperthermia at an earlystage after resuscitation fromCA were assessed, with thepatients divided into 2 groups:CBD and non-CBD.
Hyperthermia at an early stageafter resuscitation from CAmay be associated with theoutcome of brain death. Meanvalue of peak axillary T within72 h of admission was 39.8�C �.9�C for the CBD group, whichwas significantly greater than38.3�C � .6�C for the non-CBDgroup. In 23 patients witha peak axillary T � 39�C duringthe first 72 h of hospitalization,brain death was diagnosed in20 patients, whereas only 3/20patients with a peak axillary T< 39�C developed brain death.
heart
&lung
40
(2011)530e544
536
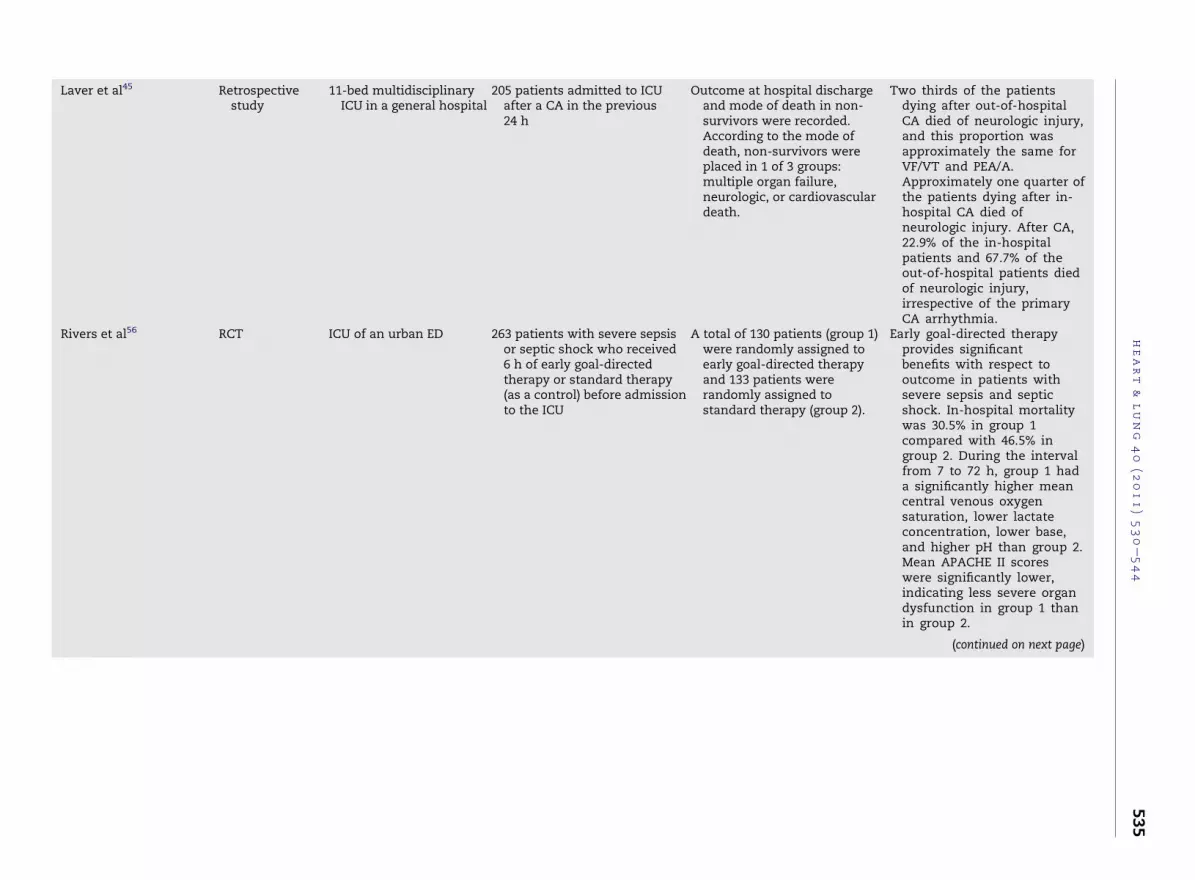
Hypothermia afterCardiac Arrest StudyGroup22
RCT Multicenter setting 273 resuscitated patientswith CA due to VF
Patients were randomlyassigned to undergotherapeutic hypothermia(target T, 32�C-34�C, measuredin the bladder) over a period of24 h or to receive standardtreatmentwith normothermia.
In patients who have beensuccessfully resuscitated afterCA due to VF, therapeutic mildhypothermia increased therate of a favorable neurologicoutcome and reducedmortality; 55% had a favorableneurologic outcome (cerebral-performance category, 1 [goodrecovery] or 2 [moderatedisability]), compared with39% in the normothermiagroup. Mortality at 6 mo was41% in the hypothermia groupand 55% in the normothermiagroup.
Zeiner et al25 RCT University clinic 151 resuscitated patientswith CA
T was recorded on admissionto the ED and after 2, 4, 6, 12,18, 24, 36, and 48 h. The lowestT within 4 h and the highest Tduring the first 48 h after ROSCwere recorded and correlatedto the best-achieved cerebralperformance categories’ scorewithin 6 mo.
Hyperthermia is a potentialfactor for an unfavorablefunctional neurologic recoveryafter successful CPR. Patientswith a favorable neurologicrecovery showed a higherlowest T within 4 h (35.8�C vs35.2�C and a lower highest Tduring the first 48 h ROSC(37.7�C vs 38.3�C). For each �C>
37�C, the risk of an unfavorableneurologic recovery increases,with an OR of 2.26.
APACHE II, Acute Physiology and Chronic Health Evaluation II; RCT, randomized controlled trial; CA, cardiac arrest; ICU, intensive care unit; GCS, Glasgow Coma Score; RR,respiratory rate; HR, heart rate; BP, blood pressure; A, asystole; T, temperature; SPO2, oxygen saturation; O2, oxygen; CPR, cardiopulmonary resuscitation; VF, ventricularfibrillation; PVT, pulseless ventricular tachycardia; ROSC, return of spontaneous circulation; AMI, acute myocardial infarction; VT, ventricular tachycardia; PEA, pulselesselectrical activity; ECG, electrocardiography; ED, emergency department; CAT, cardiac arrest team;MEW, modified early warning;MET, medical emergency team; CBD, chronicbrain death; HDU, high dependency unit; OR, odds ratio.
heart
&lung
40
(2011)530e544
537
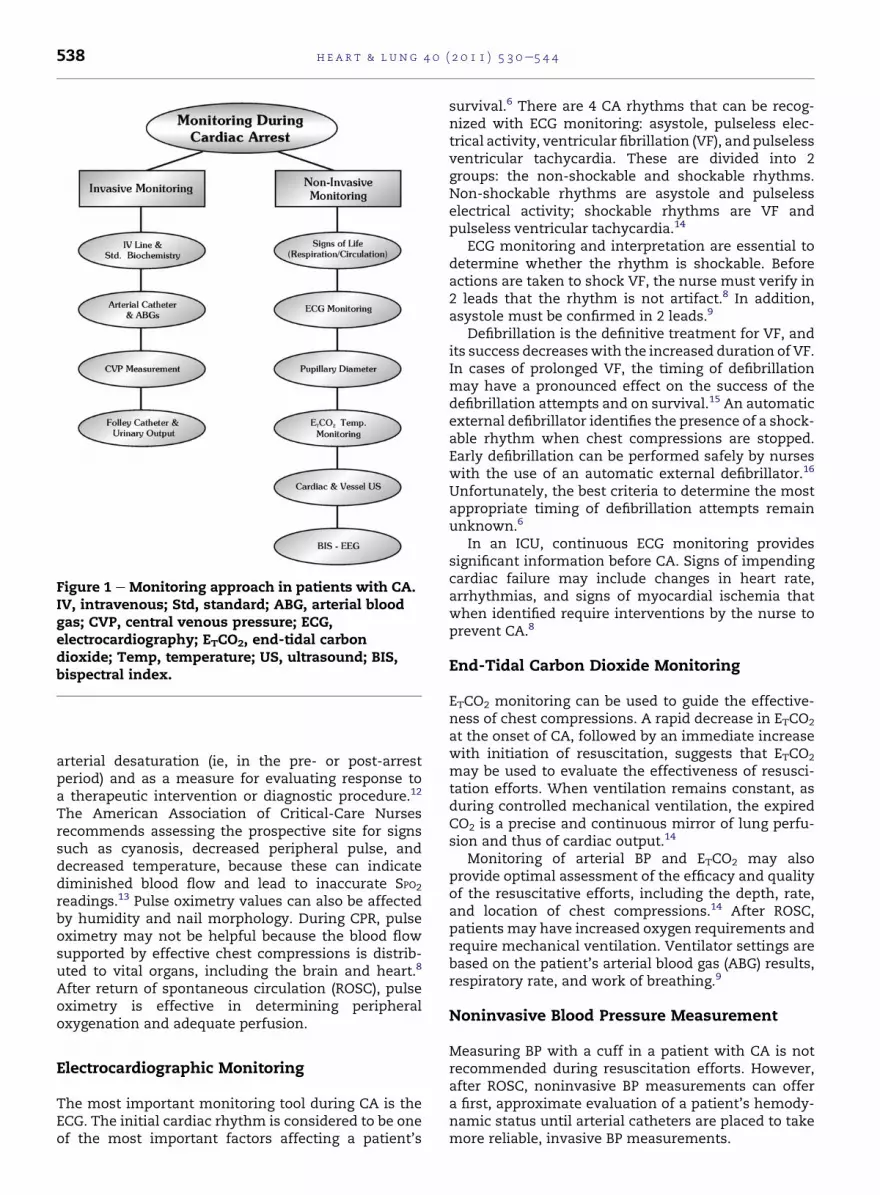
Figure 1 e Monitoring approach in patients with CA.IV, intravenous; Std, standard; ABG, arterial bloodgas; CVP, central venous pressure; ECG,electrocardiography; ETCO2, end-tidal carbondioxide; Temp, temperature; US, ultrasound; BIS,bispectral index.
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4538
arterial desaturation (ie, in the pre- or post-arrestperiod) and as a measure for evaluating response toa therapeutic intervention or diagnostic procedure.12
The American Association of Critical-Care Nursesrecommends assessing the prospective site for signssuch as cyanosis, decreased peripheral pulse, anddecreased temperature, because these can indicatediminished blood flow and lead to inaccurate SPO2
readings.13 Pulse oximetry values can also be affectedby humidity and nail morphology. During CPR, pulseoximetry may not be helpful because the blood flowsupported by effective chest compressions is distrib-uted to vital organs, including the brain and heart.8
After return of spontaneous circulation (ROSC), pulseoximetry is effective in determining peripheraloxygenation and adequate perfusion.
Electrocardiographic Monitoring
The most important monitoring tool during CA is theECG. The initial cardiac rhythm is considered to be oneof the most important factors affecting a patient’s
survival.6 There are 4 CA rhythms that can be recog-nized with ECG monitoring: asystole, pulseless elec-trical activity, ventricular fibrillation (VF), and pulselessventricular tachycardia. These are divided into 2groups: the non-shockable and shockable rhythms.Non-shockable rhythms are asystole and pulselesselectrical activity; shockable rhythms are VF andpulseless ventricular tachycardia.14
ECG monitoring and interpretation are essential todetermine whether the rhythm is shockable. Beforeactions are taken to shock VF, the nurse must verify in2 leads that the rhythm is not artifact.8 In addition,asystole must be confirmed in 2 leads.9
Defibrillation is the definitive treatment for VF, andits success decreaseswith the increased duration of VF.In cases of prolonged VF, the timing of defibrillationmay have a pronounced effect on the success of thedefibrillation attempts and on survival.15 An automaticexternal defibrillator identifies the presence of a shock-able rhythm when chest compressions are stopped.Early defibrillation can be performed safely by nurseswith the use of an automatic external defibrillator.16
Unfortunately, the best criteria to determine the mostappropriate timing of defibrillation attempts remainunknown.6
In an ICU, continuous ECG monitoring providessignificant information before CA. Signs of impendingcardiac failure may include changes in heart rate,arrhythmias, and signs of myocardial ischemia thatwhen identified require interventions by the nurse toprevent CA.8
End-Tidal Carbon Dioxide Monitoring
ETCO2 monitoring can be used to guide the effective-ness of chest compressions. A rapid decrease in ETCO2
at the onset of CA, followed by an immediate increasewith initiation of resuscitation, suggests that ETCO2
may be used to evaluate the effectiveness of resusci-tation efforts. When ventilation remains constant, asduring controlled mechanical ventilation, the expiredCO2 is a precise and continuous mirror of lung perfu-sion and thus of cardiac output.14
Monitoring of arterial BP and ETCO2 may alsoprovide optimal assessment of the efficacy and qualityof the resuscitative efforts, including the depth, rate,and location of chest compressions.14 After ROSC,patients may have increased oxygen requirements andrequire mechanical ventilation. Ventilator settings arebased on the patient’s arterial blood gas (ABG) results,respiratory rate, and work of breathing.9
Noninvasive Blood Pressure Measurement
Measuring BP with a cuff in a patient with CA is notrecommended during resuscitation efforts. However,after ROSC, noninvasive BP measurements can offera first, approximate evaluation of a patient’s hemody-namic status until arterial catheters are placed to takemore reliable, invasive BP measurements.
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4 539
There are few randomized trials evaluating the roleof BP on the outcome after CA. In the absence ofdefinitive data, the nurse, who has been shown to bemore vigilant in the measurement of BP than doctors,should target the mean arterial BP to achieve anadequate urine output, taking into consideration thepatient’s normal BP.8,17
Pupillary Diameter
Pupil diameter, pupil equality, and pupil response tolight are evaluated to assess for potential brain pathol-ogies after CA. Although the majority of the populationhave equal pupils, up to 1 of 5 patients can present withanisocoria and no underlining pathology.18 During CPR,dilatedpupilsmaybeattributed toatropine. Theclinicalfinding of bilateral pupillary dilation with loss ofpupillary light reflexes is a late sign of ischemic braininjury.19
There are no neurologic signs that can predictoutcome in the first hours after ROSC. The ERC guide-lines state that the absence of pupil light reflexes onday 3 is predictive of a poor outcome (death or vege-tative state) with high specificity.8 The AHA goes onestep further stating that an absent pupillary response24 hours after resuscitation strongly predicts poorneurologic outcome.9 The absence of pupillary responseis such a strong negative predictor that the AmericanCollege of Surgeons and the National Association ofEmergency Medical Services Physicians suggest with-holding resuscitation in traumatic CA.20 Little attentionhas been given to pupil diameter in response to thera-peutic interventions during CPR.6
Temperature Monitoring
Recent data suggest that hypothermia (core tempera-tures of 33�C-36�C) in patients post-CA is beneficial forneurologic recovery. It is strongly advised to keep thepatient’s temperature under constant surveillancewitha thermometer. The nurse can use traditional means ofcooling (cold fluids, extracorporeal circuits, body cavitylavage, whole-body ice water immersion, continuousveno-venous hemofiltration, and air-conductionhypothermia) or modern devices (commercial surfaceand intravascular cooling); the latter have advantagesin ease of application, patient safety, maintenance oftarget temperature, and control of decooling.21
It is currently recommended that post-arrestpatients should not be rewarmed unless the coretemperature is less than 33�C ; in that case, they shouldbe rewarmed to 34�C . In a controlled trial with 6months of follow-up that included 275 patients, mildhypothermia was more effective than standardnormothermia for improving neurologic outcome afterCA due to VF.22
A period of hyperthermia (hyperpyrexia) is commonin the first 48 hours after CA.23,24 The risk of a poorneurologic outcome increases for each degree of bodytemperature > 37�C .25 Hyperthermia occurring in the
first 72 hours after CAmay be treated with antipyreticsor active cooling. The optimum target temperature,rate of cooling, duration of hypothermia, and rate ofrewarming have yet to be determined. Gastric, perito-neal, pleural, or bladder lavage with cold water lowersthe core temperature. Intravascular cooling techniquesinclude the use of cold IV fluids, IV cooling catheters,and extracorporeal circuits.26 Nursesmust be educatedon the cooling methods that are available in theirinstitutions.
A patient’s temperature during resuscitation effortscan be measured if continuous temperature moni-toring is already in place (Foley or pulmonary arterycatheter); this can provide the healthcare professionalwith significant insight because hypothermia orhyperthermia may occur (eg, after drug overdose). Incase of severe hypothermia, defibrillation attemptsshould be limited to 3, and IV drugs should be withhelduntil the core body temperature exceeds 30�C. Cardio-pulmonary bypass is the optimal method of activeinternal rewarming because it also provides circula-tion, oxygenation, and ventilation while graduallyincreasing core body temperature. However, it is notthe preferred method, because other less invasivetechniques are available (forced-air warming viaheating blankets, airway warming through ventilatoradjustments, and heated irrigation ranging fromgastric and bladder lavage with warm fluids to perito-neal dialysis and thoracic lavage).27 It goes withoutsaying that the method of temperature measurement(esophageal, bladder, rectal, or tympanic) should be thesame throughout resuscitation and rewarming.26
Other Monitoring Techniques: Sonographyand Bispectral Index Monitoring
Sonography is being used to evaluate resuscitationefforts. Transesophageal echocardiography (TEE) isdifficult to perform during resuscitation but can bedone after resuscitation with ROSC.28 Transthoracicechocardiography can be performed during resuscita-tion efforts because it is noninvasive, but it cannot beperformed during CPR.29 TEE can diagnose themajorityof specific cardiovascular abnormalities associatedwith CA. A sudden decrease in aortic blood flow fol-lowed by a decrease in ETCO2 suggests CA, despitecontinuation of the ECG signal. With the initiation ofCPR, the improvement in aortic blood flow and ETCO2
levels indicates the efficiency of the resuscitationeffort.30 In patients with intraoperative CA, TEE can beapplied to measure aortic blood flow, aortic diameter,and blood velocity at the same anatomic level contin-uously. This additional diagnostic information alongwith the identification of cardiac pathology (eg,ischemia) may directly guide specific, potentially life-saving therapy.31
Cardiac sonography is a sensitive tool in monitoringpost-CA contractile dysfunction.32 Sonographic evalu-ation within the first 24 hours after CA is useful toguide ongoing management because it can document
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4540
myocardial dysfunction and low cardiac output.9
Persistent and worsening hemodynamic instability isregarded as a clear indication for sonography. Sonog-raphy can be taught to medical and nursing staff withlittle or no previous experience.33
The addition of nursing personnel to the sono-graphic practice has enhanced the assessment anddiagnosis of cardiovascular disease.34 TEE imaging bycritical care nurses has been shown to be a safemethodfor measuring cardiac index and estimating intravas-cular volume in patients requiring hemodynamicmonitoring in medical and surgical ICUs, becausemeasurements obtained via Doppler imaging corre-lated well with those obtained via pulmonary arterycatheterization.35
BIS has the potential to offer information about theadequacy of cerebral blood flow and oxygenation,although changes in BIS readings often lag behindchanges in arterial pressures.6 BIS is one of severalsystems used in anesthesiology to measure the effectsof specific anesthetic drugs on the brain and to trackchanges in a patient’s level of sedation or hypnosis. BISis measured using a statistically based algorithm thatallows a computer inside an anesthesia monitor toanalyze data from a patient’s electroencephalogramduring surgery.36 When BIS monitoring is used duringCPR, it can be used as a potential predictor of cerebralperfusion, therefore helping the resuscitating team inassessing the cerebral response to the CPR.37,38 A highBIS value reflects cerebral activity and shouldencourage the team to continue CPR.39 However,others support that BIS predicts neither ROSC norsurvival after admission to ICU.40,41
BIS is of limited value during the early phase of post-resuscitative care.42 BIS values of zero help predicta poor neurologic outcome after CA and inducedhypothermia. However, a non-zero BIS is insufficientas a sole predictor of good neurologic survival.43,44
Invasive Monitoring
Invasive monitoring refers to methods and equipmentthat require endarterial or IV access. It is usuallyapplied after some type of noninvasivemonitoring is inplace, because setting up the equipment and securingthe sensors on the patients can be a time-consumingtask. However, when in place, invasive monitoringprovides continuous and precise readings of thepatient’s status, allowing modification of any thera-peutic interventions. Furthermore, after ROSC, themetabolic changes and the tendency of the injuredheart to develop some type of arrhythmia make inva-sive monitoring even more essential.45 Althoughcatheters are usually placed by physicians, it is thenurses who are called to interpret the reading of thatkind of monitoring and take care of the catheter.Invasive monitoring is used to assess the patient’sresponse to therapies during and after CA in the ICU.46
The catheters used during invasive monitoring can beapplied to central veins (eg, jugular vein, subclavian
vein) or peripheral arteries (eg, radial artery, femoralartery). Invasive monitoring may be necessary tomeasure BP accurately and to determine the mostappropriate combination of medications to optimizeblood flow.9
A central venous catheter can be of value inmeasuring central venous pressure, ensuring venousaccess when no peripheral veins are available, andproviding access for administration of drugs thatcannot be given peripherally.8 Central venous pressureis often used tomake estimates of circulatory function,in particular cardiac function and blood volume. Theabsolute value is not as important as serial measure-ments and the change in response to therapy. Anormal value in a spontaneous breathing patient is 5 to10 cmH2O (3.7-7.4 mm Hg).47 The flow-directedballoon-tipped pulmonary artery catheter (alsoknown as the Swan-Ganz or right heart catheter) isanother diagnostic clinical tool used for bedsidemonitoring (measurement of pulmonary artery resis-tance and right ventricular function).48
Hemodynamic optimization can be achieved in thepre- and post-arrest period using central venousoxygen saturation (ScvO2) as a surrogate, via afiberopticpulmonary artery catheter. Continuous measurementof ScvO2 will alert the nurse to major derangements inoxygen balance, which allows for timely implementa-tion of appropriate interventions.49-51 ScvO2 indirectlyreflects how much oxygen was consumed by thetissues. Poor ScvO2 measurements strongly correlatewith poor patient outcome. Minimally invasive,continuous near-infrared spectroscopy measuresintracellular oxygen levels, quantifies intracellularfunction, and identifies other conditions that mightaffect intracellular work.52
CPP, the only reliable prognostic factor for success-ful resuscitation,8,9 measured by a health professional,can guide therapeutic interventions during CA. If directarterial and central venous monitoring is available, thecalculation of CPP can be useful. In addition, invasivemonitoring of systemic BP may help to improve effec-tiveness of chest compression but must not delay theprovision of basic or advanced resuscitation.8
When the need arises, arterial and central venouscatheters can be used when a blood sample is requiredto check a patient’s biochemical status. For patientswith CA, if possible, it is strongly suggested to sendblood samples for ABG and electrolytes. Monitoringboth arterial and mixed venous blood gases and pHlevels during CA can be invaluable in determining thechanges in acid-base equilibrium and can offer thenecessary guidance to modify the acid-base balancetherapy.53 It would be best to repeat ABG, acid-basevalues, and potassium every 10 to 15 minutes. ABGreadings alone cannot give the full picture of thepatient and are not a reliable indicator of the severity oftissue hypoxemia, hypercarbia, or tissue acidosis.9
There are no data to support the targeting ofa specific arterial PCO2 after resuscitation from CA, butit is reasonable to adjust ventilation to achieve
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4 541
normocarbia and to monitor this using PCO2 and ABGvalues.8
Monitoring blood glucose levels is of significantimportance during and after resuscitation efforts.Blood glucose should be checked frequently, andhypoglycemia or hyperglycemia should be correctedcarefully. It is important not to cause hyperglycemiaand thus promote osmotic diuresis.54 Hyperglycemiadramatically augments the effects of hypoxia onischemia, increases the extent of central nervoussystem damage, and reduces survival of patients withCA.8 Additional studies are needed, however, to iden-tify the optimal target range of blood glucose concen-tration and the effect of tight glucose control onoutcomes of patients after CA.9
Catheterization of the urinary bladder is essential tomeasure hourly urinary output, reflecting both cardiacoutput and renal function. Significantly decreasedurinary volumemight be an early sign of compromisedcardiac and renal function and should alert the nurseto act accordingly.
Discussion
A significant body of research demonstrates that manyhospitalized patients exhibit signs of clinical deteriora-tion before experiencing CA (altered level of conscious-ness, oxygenation status, trends in systolic BP).55
In-hospital CA is associated with an increasedmortality rate, and it isassumedthat interventionduringthe pre-arrest period will translate into saved patients’lives.56 Investigators have reported that 60% to 76% ofpatientshadaperiodof instability or deterioration in the1 to 8 hours before CA.57
The majority of patients hospitalized with CA orrequiring emergency transfer to the ICU haveabnormal physiologic values recorded in the hoursbefore the event. Many studies document that physi-ologic measurements are often not made or recordedduring this critical time of clinical deterioration. Suchphysiologic abnormalities can be associated withadverse outcome. Measurements of abnormal physi-ology, including temperature, pulse rate, BP, respira-tory rate, hemoglobin, oxygen saturation by pulseoximetry, and deterioration of mental status, aretherefore important to any system designed for earlydetection of physiologic instability. At a minimum,these measurements must be obtained accurately andrecorded with appropriate frequency. A system thatrecognizes both significantly abnormal values andtriggers an immediate and appropriate treatmentresponse is required.58 Because patients have signifi-cantly greater metabolic requirements (blood and fluidloss, pain, infection, trauma) post-CA, they oftenrequire hourly or more frequent documentation.59
With the introduction of oximetry and mass spec-trometry in the 1980s, continuous assessment of
oxygenation is done by arterial catheterization. Afterresuscitation, nurses should evaluate the patient’sECG, radiographs, and laboratory analyses of serumelectrolytes and cardiac biomarkers.9
The nursing staff play a pivotal role in the effectivemanagement and monitoring of in-hospital CAbecause they are usually the first respondents in the in-hospital setting. They are, therefore, the first to initiateresuscitation, even before arrival of the medicalemergency team (MET).60 The traditional response toCA is a reactive one in which hospital staff attend thepatient after CA has occurred. CA teams seem toimprove survival after CA in circumstances where noteam has previously existed.61 In some hospitals, theCA team has been replaced by a MET that responds notonly to patients in CA but also to those with acutephysiologic deterioration.62,63 The MET is usuallycomposed of medical and nursing staff from intensivecare and general medicine and responds to specificcalling criteria.
Patients’ monitoring within any hospital organiza-tion is primarily a nursing responsibility, because it isthe nurses who most often apply the Early WarningScore (EWS) or call the MET.57 The clinical signs ofacute illness are similar whatever the underlyingprocess, because they reflect failing respiratory,cardiovascular, and neurologic systems. Abnormalphysiology is common in clinical departments, yet themeasurement and recording of important physiologicobservations of sick patients occur less frequently thanis desirable.64 To assist in the early detection of criticalillness, many hospitals now use EWS systems.65-67
EWS systems allocate points to routine vital signsmeasurements. Risk factors for CA have been identi-fied, quantified, and formulated into a table of activa-tion criteria to help predict and avert CA by alertinga clinical response. A graded clinical response takinginto account abnormal breathing, abnormal pulse, andabnormal systolic BP has resulted in a tool that hasboth high sensitivity and specificity for predicting CA.In one of the studies, statistical analysis determinedthat an EWS of 4 had 89% sensitivity and 77% specificityfor CA and that an EWS score of 8 had 52% sensitivityand 99% specificity. All patients with an EWS > 10 hadCA.56 The weighted score of � 1 vital sign observations,or the total EWS, may be used to suggest increasing thefrequency of vital signs monitoring to nurses or to callthe MET.66
A highly professional and skilled nurse is an integralpart of the hospital MET. The role of the nurse is torecognize a patient who is clinically unstable and alertthe appropriate personnel to initiate treatment. Ina unstable patient, traditional monitoring falls short;heart rate may not adequately reflect the patient’sdegree of compromise; BP is a function of cardiacoutput and systemic vascular resistance rather thantissue perfusion itself; urine output is unreliable asa resuscitation guide; body temperature is also unreli-able because temperature regulation is significantlyimpaired by shock; and hemodynamic monitoring via
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4542
pulmonary artery catheters can provide more infor-mative data, but also has limitations.52
Nurse educators need to develop teaching methodsthat promote critical thinking skills and foster quickproblem-solving in the novice nurse. Novice nursingstudents and nurseswho are just starting in the clinicalenvironment struggle withmany challenges (acquiringvital signs, interpreting them to determinewhether thevalues are within an acceptable range, and deter-mining whether any nursing action is needed). BasicPrinciples, Foundations, and Fundamentals of Nursingare often the first nursing courses offered, in whichstudents learn the theoretic background. These arefollowed by skill demonstration in the clinical simu-lation laboratory and by practice in the clinical envi-ronment.68 Educators need to teach nurses how torespond to situations that are not expected. With theadvent of human patient simulators, educators candesign complex events, so that nurses have an oppor-tunity to make decisions similar to those in the realworld, complete with the complexity and time pressurewithout harming a patient.57 Algorithms provide guid-ance in evaluating and determining cause and inter-ventions, promoting critical thinking, and providingnurses with a systematic decision-making tool. The useof algorithms alone does not promise a positiveoutcome but establishes a standard of care to be fol-lowed, appropriate to the needs of the individualpatient. This is why monitoring is of the utmostimportance.68
Protocols about CA and proper management requireconstant updating to implement an internationallyaccepted algorithm for therapeutic interventions anddecision-making. Except for basic research, clinicalstudies need to focus on comparing monitoringschemes and making correlations about treatmentstrategies to fill any gaps in evidence and providea robust clinical algorithm regarding in- and out-of-hospital CA management, therefore improvingsurvival of those with CA.
Conclusions
Training can improve patient monitoring during CAand the peri-arrest period. Nurses can also take moreresponsibility for managing these patients, taking intoaccount the equipment provided, the availablepersonnel, and the previous experience and ability tofunction as part of a team. Physiologic criteria thatsignal a patient’s status deterioration can guide deci-sions about the initiation of emergency interventionsand the call of the MET team. Intervention protocolsmust be continuously reevaluated through controlledstudies to determine their appropriateness for patientswith CA, regardless of their pathophysiologic back-ground. Research is needed to identify, by thoroughmonitoring, patient populations at risk for CA, to
describe the effects of routine nursing procedures andidentify those that improve or even restore ROSCand tissue oxygenation. However, it is the promptinterventions, based on clinical assessment andmonitoring values, that will eventually improvepatients’ outcomes.
Acknowledgments
The authors thank Elia Delaporta for the linguisticediting of this article.
References
1. Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE,Bossaert L, et al. International Liaison Committee onResuscitation; American Heart Association; EuropeanResuscitation Council; Australian ResuscitationCouncil; New Zealand Resuscitation Council; Heartand Stroke Foundation of Canada; InterAmericanHeart Foundation; Resuscitation Councils of SouthernAfrica; ILCOR Task Force on Cardiac Arrest andCardiopulmonary Resuscitation Outcomes. Cardiacarrest and cardiopulmonary resuscitation outcomereports: update and simplification of the Utsteintemplates for resuscitation registries: a statement forhealthcare professionals from a task force of theInternational Liaison Committee on Resuscitation(American Heart Association, European ResuscitationCouncil, Australian Resuscitation Council, NewZealand Resuscitation Council, Heart and StrokeFoundation of Canada, InterAmerican HeartFoundation, Resuscitation Councils of SouthernAfrica). Circulation 2004;110:3385-97.
2. Sans S, Kesteloot H, Kromhout D. The burden ofcardiovascular diseases mortality in Europe. TaskForce of the European Society of Cardiology onCardiovascular Mortality and Morbidity Statistics inEurope. Eur Heart J 1997;18:1231-48.
3. Myerburg RJ, Wellens H. Epidemiology of cardiacarrest. In: Priori S, Zipes D, editors. Sudden cardiacdeath. Oxford: Blackwell Publishing; 2006. p. 3-20.
4. Gwinnutt CL, Columb M, Harris R. Outcome aftercardiac arrest in adults in UK hospitals: effect of the1997 guidelines. Resuscitation 2000;47:125-35.
5. Herlitz J, Bang A, Aune S, Ekstrom L, Lundstrom G,Holmberg S. Characteristics and outcome amongpatients suffering in-hospital cardiac arrest inmonitored and nonmonitored areas. Resuscitation2001;48:125-35.
6. Hayes MM, Berg RA, Otto CW. Monitoring duringcardiac arrest: are we there yet? Curr Opin Crit Care2003;9:211-7.
7. Bahr J, Klingler H, Panzer W, Rode H, Kettler D. Skillsof lay people in checking the carotid pulse.Resuscitation 1997;35:23-6.
8. Nolan JP, Deakin CD, Soar J, Bottiger BW, Smith G.European Resuscitation Council. EuropeanResuscitation Council guidelines for resuscitation2005. Section 4. Adult advanced life support.Resuscitation 2005;67:S39-86.
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4 543
9. 2005 American Heart Association Guidelines forCardiopulmonary Resuscitation and EmergencyCardiovascular Care. ECC Committee, Subcommitteesand Task Forces of the American Heart Association.Circulation 2005;112:IV1-203.
10. Hauff SR, Rea TD, Culley LL, Kerry F, Becker L,Eisenberg MS. Factors impeding dispatcher-assistedtelephone cardiopulmonary resuscitation. Ann EmergMed 2003;42:731-7.
11. Sapo M, Wu S, Asgari S, McNair N, Buxey F, Martin N,et al. A comparison of vital signs charted by nurseswith automated acquired values using waveformquality indices. J Clin Monit Comput 2009;23:263-71.
12. Valdez-Lowe C, Ghareeb SA, Artinian NT. Pulseoximetry in adults. Am J Nurs 2009;109:52-9, quiz 60.
13. Day MW. Oxygen saturation monitoring by pulseoximetry. In: Lynn-McHale Wiegand DJ, editor. AACNprocedure manual for critical care. Philadelphia:Elsevier/Saunders; 2010. p. 121-8.
14. Deakin CD, Nolan JP. European ResuscitationCouncil. European Resuscitation Council guidelinesfor resuscitation 2005. Section 3. Electricaltherapies: automated external defibrillators,defibrillation, cardioversion and pacing.Resuscitation 2005;67:S25-37.
15. Pellis T, Bisera J, Tang W, Weil MH. Expandingautomatic external defibrillators to includeautomated detection of cardiac, respiratory andcardiorespiratory arrest. Crit Care Med 2002;30:S176-8.
16. Handley AJ, Koster R, Monsieurs K, Perkins GD,Davies S, Bossaert L. European Resuscitation Council.European Resuscitation Council guidelines forresuscitation 2005. Section 2. Adult basic life supportand use of automated external defibrillators.Resuscitation 2005;67(Suppl 1):S7-23.
17. Padfield PL. Measuring blood pressure: who and how?J Hypertens 2009;27:216-8.
18. Littlejohns L. Routine consensual pupil checks inacute monitoring. Crit Care Nurse 2007;27:62-4.
19. Dawes E, Durham L. Monitoring and recordingpatients’ neurological observations. Nurs Stand 2007;22:40-5.
20. Hopson LR, Hirsh E, Delgado J, Domeier RM, Krohmer J,McSwain NE Jr, et al. National Association of EMSPhysicians Standards and Clinical Practice Committee;American College of Surgeons Committee on Trauma.Guidelines for withholding or termination ofresuscitation in prehospital traumaticcardiopulmonary arrest. J AmColl Surg2003;196:475-81.
21. Seder DB, Van der Kloot TE. Methods ofcooling: practical aspects of therapeutictemperature management. Crit Care Med 2009;37:S211-22.
22. The Hypothermia After Cardiac Arrest Study Group.Mild therapeutic hypothermia to improve theneurologic outcome after cardiac arrest. N Engl J Med2002;346:549-56.
23. Hickey RW, Kochanek PM, Ferimer H, Alexander HL,Garman RH, Graham SH. Induced hyperthermiaexacerbates neurologic neuronal histologic damageafter asphyxial cardiac arrest in rats. Crit Care Med2003;3:531-5.
24. Takasu A, Saitoh D, Kaneko N, Sakamoto T, Okada Y.Hyperthermia: is it an ominous sign after cardiacarrest? Resuscitation 2001;49:273-7.
25. Zeiner A, Holzer M, Sterz F, Schorkhuber W,Eisenburger P, Havel C, et al. Hyperthermia after
cardiac arrest is associated with an unfavorableneurologic outcome. Arch Intern Med 2001;161:2007-12.
26. Soar J, Deakin CD, Nolan JP, Abbas G, Alfonzo A,Handley AJ, et al. European Resuscitation Council.European Resuscitation Council guidelines forresuscitation 2005. Section 7. Cardiac arrest in specialcircumstances. Resuscitation 2005;67(Suppl 1):S135-70.
27. Lasater M. Treatment of severe hypothermia withintravascular temperature modulation. Crit CareNurse 2008;28:24-9, quiz 31.
28. van der Wouw PA, Koster RW, Delemarre BJ, de Vos R,Lampe-Schoenmaeckers AJ, Lie KI. Diagnosticaccuracy of transesophageal echocardiographyduring cardiopulmonary resuscitation. J Am CollCardiol 1997;30:780-3.
29. Varriale P, Maldonado JM. Echocardiographicobservations during in hospital cardiopulmonaryresuscitation. Crit Care Med 1997;25:1717-20.
30. Kolar M, Krizmaric M, Klemen P, Grmec S. Partialpressure of end-tidal carbon dioxide successfulpredicts cardiopulmonary resuscitation in the field:a prospective observational study. Crit Care 2008;12:R115.
31. Memtsoudis SG, Rosenberger P, Loffler M,Eltzschig HK, Mizuguchi A, Shernan SK, et al. Theusefulness of transesophageal echocardiographyduring intraoperative cardiac arrest in noncardiacsurgery. Anesth Analg 2006;102:1653-7.
32. Panchal A, Blumberg A, Schneider J, Torres CA,Aune S, Angelos MG. Cardiac ultrasound to monitorpost-cardiac arrest myocardial dysfunction. AcadEmerg Med 2005;12:69.
33. Price S, Uddin S, Quinn T. Echocardiography incardiac arrest. Curr Opin Crit Care 2010;16:211-5.
34. Gilman G, Nelson JM, Murphy AT, Kidd GM, Stussy VL,Klarich KW. The role of the nurse in clinicalechocardiography. J Am Soc Echocardiogr 2005;18:773-7.
35. Iregui MG, Prentice D, Sherman G, Schallom L, Sona C,Kollef MH. Physicians’ estimates of cardiac index andintravascular volume based on clinical assessmentversus transesophageal Doppler measurementsobtained by critical care nurses. Am J Crit Care 2003;12:336-42.
36. Johansen JW. Update on bispectral index monitoring.Best Pract Res Clin Anaesthesiol 2006;20:81-99.
37. Azim N, Wang CY. The use of bispectral index duringa cardiopulmonary arrest: a potential predictor ofcerebral perfusion. Anaesthesia 2004;59:610-2.
38. Chakravarthy M, Patil T, Jayaprakash K,Shivananda N, Jawali V. Bispectral index is anindicator of adequate cerebral perfusion duringcardiopulmonary resuscitation. J Cardiothorac VascAnesth 2003;17:506-8.
39. Szekely B, Saint-Marc T, Degremont AC,Castelain MH, Fischler M. Value of bispectral indexmonitoring during cardiopulmonary resuscitation. BrJ Anaesth 2002;88:443-4.
40. Chollet-Xemard C, Combes X, Soupizet F, Jabre P,Penet C, Bertrand C, et al. Bispectral index monitoringis useless during cardiac arrest patients’resuscitation. Resuscitation 2009;80:213-6.
41. Fatovich DM, Jacobs IG, Celenza A, Paech MJ. Anobservational study of bispectral index monitoring forout of hospital cardiac arrest. Resuscitation 2006;69:207-12.
h e a r t & l ung 4 0 ( 2 0 1 1 ) 5 3 0e5 4 4544
42. Shibata S, Imota T, Shigeomi S, SatoW Ezan K. Use ofthe bispectral index during the early postresuscitativephase after out-of-hospital cardiac arrest. J Anesth2005;19:243-6.
43. Stammet P, Werer C, Mertens L, Lorang C, Hemmer M.Bispectral index (BIS) helps predicting badneurological outcome in comatose survivors aftercardiac arrest and induced therapeutic hypothermia.Resuscitation 2009;80:437-42.
44. Leary M, Fried DA, Gaieski DF, Merchant RM,Fuchs BD, Kolansky DM, et al. Neurologicprognostication and bispectral index monitoring afterresuscitation from cardiac arrest. Resuscitation 2010;81:1133-7.
45. Laver S, Farrow C, Terner D, Nolan J. Mode of deathafter admission to an intensive care unit followingcardiac arrest. Intensive Care Med 2004;30:2126-8.
46. Wiener B, Chacko S, Cron SG, Cohen MZ. Guidelinedevelopment and education to insure accurate andconsistent pulmonary artery wedge pressuremeasurement by nurses in intensive care units.Dimens Crit Care Nurs 2007;26:263-8.
47. Davidson CJ, Bonow RO. Cardiac catheterization. In:Libby P, Bonow RO, Mann DL, Zipes DP, editors.Braunwald’s heart disease: a textbook ofcardiovascular medicine. Philadelphia: ElsevierScience; 2004. p. 395-422.
48. Maragiannis D, Lazaros G, Aloizos S, Vavouranakis E,Stefanadis C. Pulmonary artery catheter (PAC) underattack? Hellenic J Cardiol 2010;51:49-54.
49. Rivers EP, Ander DS, Powell D. Central venous oxygensaturation monitoring in the critically ill patient. CurrOpin Crit Care 2001;7:204-11.
50. Goodrich C. Continuous central venous oximetrymonitoring. Crit Care Nurs Clin North Am 2006;18:203-9, x.
51. Jesurum J. Tissue oxygenation and routine nursingprocedures in critically ill patients. J Cardiovasc Nurs1997;11:12-30.
52. Schulman C. Is your patient fully resuscitated? NursManage 2003;34:44-7.
53. Soar J, Deakin CD, Nolan JP, Abbas G, Alfonzo A,Handley AJ, et al. European Resuscitation Council.European Resuscitation Council guidelines forresuscitation 2005. Section 7. Cardiac arrest in specialcircumstances. Resuscitation 2005;67(Suppl 1):S135-70.
54. Langhelle A, Tyvold SS, Lexow K, Hapnes SA, Sunde K,Steen PA. In-hospital factors associated withimproved outcome after out-of-hospital cardiacarrest. A comparison between four regions in Norway.Resuscitation 2003;56:247-63.
55. Buist M, Bernard S, Nguyen TV, Moore G, Anderson J.Association between clinically abnormal observationsand subsequent in-hospital mortality: a prospectivestudy. Resuscitation 2004;62:137-41.
56. Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A,Knoblich B, et al. Early goal-directed therapy in thetreatment of severe sepsis and septic shock. N Engl JMed 2001;345:1368-77.
57. Gazarian PK, Henneman EA, Chandler GE. Nursedecision making in the prearrest period. Clin Nurs Res2010;19:21-37.
58. PeberdyMA,CretikosM,AbellaBS,DeVitaM,Goldhill D,KloeckW, et al. International Liaison Committee onResuscitation; American Heart Association; AustralianResuscitation Council; European Resuscitation Council;Heart and Stroke Foundation of Canada; InterAmerican
Heart Foundation; Resuscitation Council of SouthernAfrica; New Zealand Resuscitation Council; AmericanHeart Association Emergency Cardiovascular CareCommittee; American Heart Association Council onCardiopulmonary, Perioperative, and Critical Care;InterdisciplinaryWorking Group onQuality of Care andOutcomes Research. Recommended guidelines formonitoring, reporting, and conducting research onmedical emergency team, outreach, and rapid responsesystems: an Utstein-style scientific statement:a scientific statement from the International LiaisonCommittee on Resuscitation (American HeartAssociation, Australian Resuscitation Council,European Resuscitation Council, Heart and StrokeFoundation of Canada, InterAmerican HeartFoundation, Resuscitation Council of Southern Africa,and the New Zealand Resuscitation Council); theAmericanHeartAssociation EmergencyCardiovascularCare Committee; the Council on Cardiopulmonary,Perioperative, and Critical Care; and theInterdisciplinaryWorking Group onQuality of Care andOutcomes Research. Circulation 2007;116:2481-500.
59. Sapo M, Wu S, Asgari S, McNair N, Buxey F, Martin N,et al. A comparison of vital signs charted by nurseswith automated acquired values using waveformquality indices. J Clin Monit Comput 2009;23:263-71.
60. Gombotz H, Weh B, Mitterndorfer W, Rehak P. In-hospital cardiac resuscitation outside the ICU bynursing staff equipped with automated externaldefibrillatorsdthe first 500 cases. Resuscitation 2006;70:416-22.
61. Sandroni C, Ferro G, Santangelo S, Tortora F,Mistura L, Kavallaro F, et al. In-hospital cardiacarrest: survival depends mainly on the effectivenessof the emergency response. Resuscitation 2004;62:291-7.
62. Hillman K, Chen J, Cretikos M, Bellomo R, Brown D,Doig G, et al; MERIT study investigators. Introductionof the medical emergency team (MET) system:a cluster-randomised controlled trial. Lancet 2005;365:2091-7.
63. Bellomo R, Goldsmith D, Uchino S, Buckmaster J,Hart GK, Opdam H, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust2003;179:283-7.
64. Kause J, Smith G, Prytherch D, Parr M, Flabouris A,Hillman K. A comparison of antecedents to cardiacarrests, deaths and emergency intensive careadmissions in Australia and New Zealand, and theUnited Kingdom-the ACADEMIA study. Resuscitation2004;62:275-82.
65. Hodgetts TJ, Kenward G, Vlachonikolis IG, Payne S,Castle N. The identification of risk factors for cardiacarrest and formulation of activation criteria to alerta medical emergency team. Resuscitation 2002;54:125-31.
66. Subbe CP, Davies RG, Williams E, Rutherford P,Gemmell L. Effect of introducing the Modified EarlyWarning score on clinical outcomes, cardio-pulmonary arrests and intensive care utilization inacute medical admissions. Anaesthesia 2003;58:797-802.
67. Goldhill DR, McNarry AF. Physiological abnormalitiesin early warning scores are related to mortality inadult inpatients. Br J Anaesth 2004;92:882-4.
68. Rathbun MC, Ruth-Sahd LA. Algorithmic toolsfor interpreting vital signs. J Nurs Educ 2009;48:395-400.





























