Embed Size (px)
Citation preview
GASTROENTEROLOGY 1996;111:629–637
Nongranulomatous Chronic Idiopathic Enterocolitis:Clinicopathologic Profile and Response to Corticosteroids
EDUARDO A. RUAN,* RICHARD A. KOMOROWSKI,‡ WALTER J. HOGAN,*and KONRAD H. SOERGEL*Departments of *Medicine and ‡Pathology, Medical College of Wisconsin, Milwaukee, Wisconsin
Background & Aims: Nongranulomatous ulcerative en- aged and presented with chronic diarrhea and weight loss.terocolitis has been reported in association with celiac Complicating obstruction, perforation, and hemorrhagesprue, lymphoma, and hypogammaglobulinemia. The were common, and the prognosis was poor. The termsobjective of this study is to present evidence that this ‘‘chronic ulcerative nongranulomatous jejunoileitis’’8 anddisorder exists as a primary entity. Methods: The medi- ‘‘idiopathic chronic ulcerative enteritis’’9 were applied tocal records and histological material of 9 patients these patients. However, many of the patients had celiac(mean age, 45.7 { 5.9 years) who presented with se- sprue (gluten-sensitive enteropathy), and others had intesti-vere chronic diarrhea without specific diagnosis after
nal lymphoma or hypogammaglobulinemia. Consequently,extensive investigations were reviewed. Results: Endo-it has been questioned whether such a syndrome exists asscopically, the duodenum and proximal jejunum werea separate clinical entity.10
inflamed in 6 of 7 patients, with superficial ulcerationsWe present a clinical and histopathologic study of 9in 5 patients. On histology, the lamina propria was infil-
patients with severe chronic diarrhea and nongranulomatoustrated by polymorphonuclear and chronic inflammatorycells, with varying degrees of villous atrophy. There enterocolitis. The majority of the patients had small intesti-were no significant cellular abnormalities of the epithe- nal partial villous atrophy. Although most patients hadlial enterocytes. A similar inflammatory infiltrate was superficial ulcerations, there were no significant cellular ab-present in the colon in 4 of 5 patients. Eight of 9 pa- normalities of the intestinal epithelium. The patients didtients responded to corticosteroids with clinical and not have any recognizable underlying or associated disease.variable histological improvement. Four patients devel- Although the mortality rate was high (3 patients), theoped bleeding from ulcerations in the small or large response to corticosteroids was dramatic, and most patientsintestine. Three patients died: 1 patient who did not
required prolonged maintenance therapy.respond to treatment with corticosteroids and 2 pa-tients with systemic infection. Four of the 6 surviving Materials and Methodspatients required maintenance low-dose corticosteroid
We reviewed the medical records and histological mate-therapy. No underlying disease was discovered duringrial of patients with severe chronic diarrhea hospitalized by ourprolonged follow-up. Conclusions: Idiopathic nongranu-Division of Gastroenterology in whom no specific diagnosis hadlomatous enterocolitis may present as a primary, fre-been obtained after extensive diagnostic testing. Initially, 14 pa-quently fatal disease. Corticosteroid therapy providestients were identified, and 5 patients were excluded: 1 patientimmediate benefit and may be required indefinitely.had intestinal granulomas on histology, 1 patient had hypogam-maglobulinemia, 1 patient had celiac disease antibodies, and his-
T tological material was unavailable in 2 patients. Of the remaininghe differential diagnosis of chronic intestinal in-flammation is extensive (Table 1). It includes 9 patients, none had any of the conditions listed in Table 1. All
patients resided in urban areas in eastern Wisconsin and had noCrohn’s disease, celiac disease, collagen-vascular diseases,history of recent travel or of exposure to farm animals. There waseffects of nonsteroidal anti-inflammatory drugs, and in-no clustering of patients, and no other household members hadfections (including acquired immunodeficiency syn-a diarrheal illness. No patient had used nonsteroidal anti-in-drome), lymphocytic enterocolitis, hypogammaglobuli-flammatory agents. Infectious agents were excluded by repeatednemia, eosinophilic enteritis, immunoproliferative smallstool cultures for bacterial pathogens (including Salmonella, Shi-intestinal disease, autoimmune enteropathy, and intesti-
nal lymphoma.Abbreviation used in this paper: EGD, esophagogastroduodenos-A number of reports of patients with idiopathic nongran-
copy.ulomatous intestinal inflammation and ulceration have ap- q 1996 by the American Gastroenterological Association
0016-5085/96/$3.00peared in the literature. The patients were typically middle
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro

630 RUAN ET AL. GASTROENTEROLOGY Vol. 111, No. 3
copy (EGD), there was duodenal erythema. The small bowelTable 1. Some Causes of Acute and Chronic Enterocolitisradiographs showed thickened jejunal mucosal folds and
Crohn’s diseaseflocculation of contrast material. Duodenal biopsy specimensCeliac sprueshowed severe acute and chronic inflammatory infiltrate inCollagenous spruethe lamina propria and partial villous atrophy. ColonoscopyIntestinal lymphoma
Hypogammaglobulinemia was normal, and colonic biopsy specimens were normal. ADrugs (nonsteroidal anti-inflammatory agents, potassium tablets, 4-week trial of a strict gluten-free diet had no effect. The
antineoplastic agents) patient was hospitalized in December 1992 for fluid replace-Malnutrition
ment. The stool volume was 1225 g/24 h containing 3.7 gAmyloidosisof fat. Celiac disease antibody results were negative. TwentyCollagen-vascular diseases (dermatomyositis polyarteritis nodosa)
Ischemia milligrams prednisone daily was begun, and the diarrheaRadiation resolved promptly. In August 1993, the result of an EGD wasArsenate poisoning normal and duodenal biopsy specimens showed near completeInfections (Salmonella, Campylobacter, tuberculosis, syphilis,
resolution with only minimal inflammation in the laminacytomegalovirus, acquired immunodeficiency syndrome)propria. The patient remains asymptomatic.Eosinophilic enteritis
Patient 3. A 22-year-old woman presented in AugustLymphocytic enterocolitis1
Pericrypt eosinophilic enterocolitis2 1990 with a 4-week history of watery diarrhea and vomitingGranulomatous enterocolitis3
and a 17-lb weight loss. A sigmoidoscopy showed mucosalImmunoproliferative small intestinal disease friability and fibrinous exudate, and the patient was treatedAcute jejunoileitis4
with olsalazine with no effect. An EGD showed severe in-Enteritis necroticans (pig bel)flammation with ulceration in the duodenum. Duodenal biopsyAutoimmune enteropathy5
specimens showed severe acute and chronic inflammation in theCryptogenic multifocal ulcerous stenosing enteritis6
Torkelson syndrome7 lamina propria with crypt abscesses and total villous atrophy. Atrial of a gluten-free diet was ineffective. The patient washospitalized in December 1990 and treated with parenteralnutrition. Forty milligrams prednisone daily was administered
gella, Campylobacter, and Yersinia) and stool examinations for ova, for 4 weeks, and the patient soon experienced the return ofparasites, Cryptosporidium, and Clostridium difficile toxin. No infec- solid stools. In February 1991, she had a relapse of diarrhea,tious agents were recognized on light and electron microscopy of was hospitalized, and was treated with a course of intravenousmucosal biopsy specimens. corticosteroids with improvement. By March 1993, she was
Mucosal biopsy specimens were processed routinely and stained asymptomatic while being treated with 30-mg prednisone onwith H&E. Specimens for electron microscopy were processed in alternating days. The duodenal biopsy specimens showed com-glutaraldehyde. The small intestinal epithelial and villous mor- plete resolution of the histopathologic abnormalities.phology was assessed according to standard criteria.11 A histopath- Patient 8. A 64-year-old man with a history of adult-ologic score was devised for small intestinal biopsy specimens. onset diabetes presented with 6 months of diarrhea, weight loss,The presence of minimal epithelial abnormalities on light micros- and progressive extremity edema. His serum albumin was 3.1 g/copy (loss of the brush border, cellular atypia, or increased mitotic dL. An EGD showed erosive duodenitis, and duodenal biopsy
specimens showed severe acute and chronic inflammation of thefigures) received 1 point, and severe epithelial abnormalities re-lamina propria and subtotal villous atrophy. Small intestinal ra-ceived 2 points. Partial villous atrophy received 1 point, and totaldiographs were normal. The colonic mucosa was grossly normalvillous atrophy received 2 points. Mild inflammation, defined byon colonoscopy. However, on biopsy, there was moderate in-a slight increase in the number of plasma cells or by the presenceflammatory infiltration of the lamina propria. In June 1994, anof small numbers of lymphocytes or neutrophils, received 1 point.in-hospital trial of a gluten-free diet for 2 weeks had no effect.Moderate inflammation, defined as a moderately increased densityCeliac disease antibody results were negative. Twenty milligramsof inflammatory cells, received 2 points. Severe inflammation,prednisone daily by mouth for 2 weeks had no effect. The patient’sdefined by complete filling of the lamina propria by inflammatorystool volume was 10,820 g/24 h with 21 g of fat. Bowel restinfiltrate, received 3 points. The maximum score was 7 points.with parenteral nutrition caused only a moderate reduction ofQuantitative variables were expressed as mean { SE. Thestool output. However, the patient continued to deteriorate anddifference in the histopathologic scores before and after cortico-died in August 1994. On postmortem examination, there wassteroid therapy was tested with the Wilcoxon signed rank test.autolysis of the intestinal mucosa, but there was no inflammatoryA P value of °0.05 was considered significant.involvement of the remaining intestinal wall.
Selected Case Summaries ResultsPatient 2. A 41-year-old woman presented in Octo- Demographic and Clinical Characteristics
ber 1992 with a 1-month history of diarrhea, nausea, andNine patients (5 women and 4 men; mean age,vomiting and a 10-lb weight loss. An empirical trial of metro-
nidazole had been ineffective. On esophagogastroduodenos- 45.7 { 5.9 years; age range, 22–74 years) presented
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro
NONGRANULOMATOUS CHRONIC ENTEROCOLITIS 631September 1996
Table 2. Demographic and Clinical Characteristics at Presentation
Age Duration of Weight loss Stool volume Stool fat Serum albuminPatient (yr) Sex symptoms (% preillness weight) (g/24 h) (g/24 h) (g/dL)
1 35 F 2 mo 28 3718 23.8 1.92 41 F 1 mo 21 1225 13.7 3.63 22 F 1 mo 12 817 80.7 2.54 46 M 1 wk 11 528 2.6 1.95 74 F 6 mo 30 3926 25.6 2.26 23 M 2 mo 18 1853 132.5 3.57 57 F 2 wk 31 1077 13.6 1.18 64 M 6 mo 23 10,820 21 3.19 49 M 1 wk 15 8205 15 1.9
with an acute onset of large-volume (ú500 g/24 h), showing thickening or effacement of folds and floccula-tion or fragmentation of the barium column. Thesenonbloody, watery diarrhea (Table 2). The mean duration
of symptoms before our initial evaluation was 8.4 { 3.1 changes were limited to the duodenum in 2 patients andextended to the jejunum and ileum in 3 patients. Noweeks (range, 1 week to 6 months). Four patients initially
presented with associated nausea and vomiting, and 2 ulcerations were recognized radiologically in any patient.Two patients had normal small bowel radiographs.patients presented with abdominal cramps. Two patients
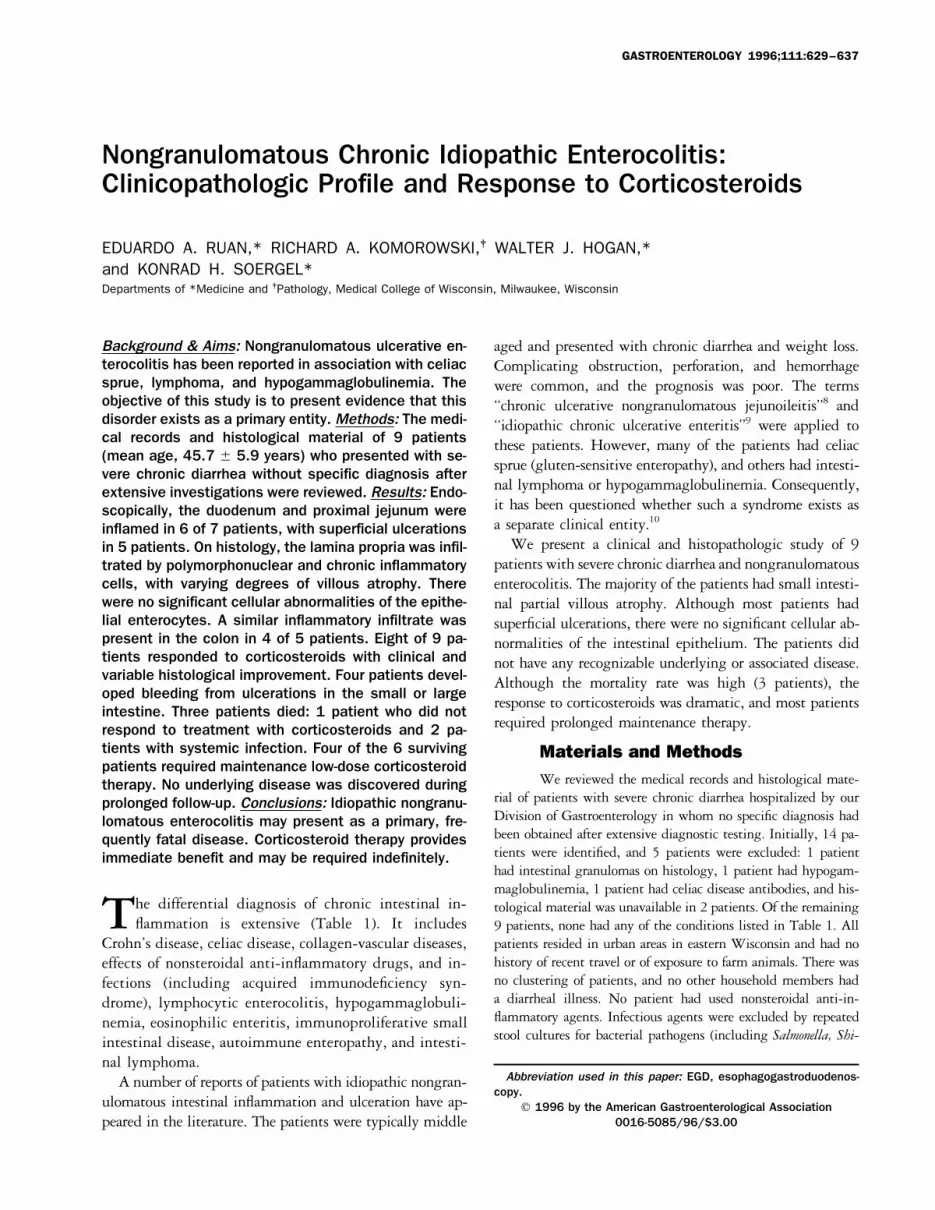
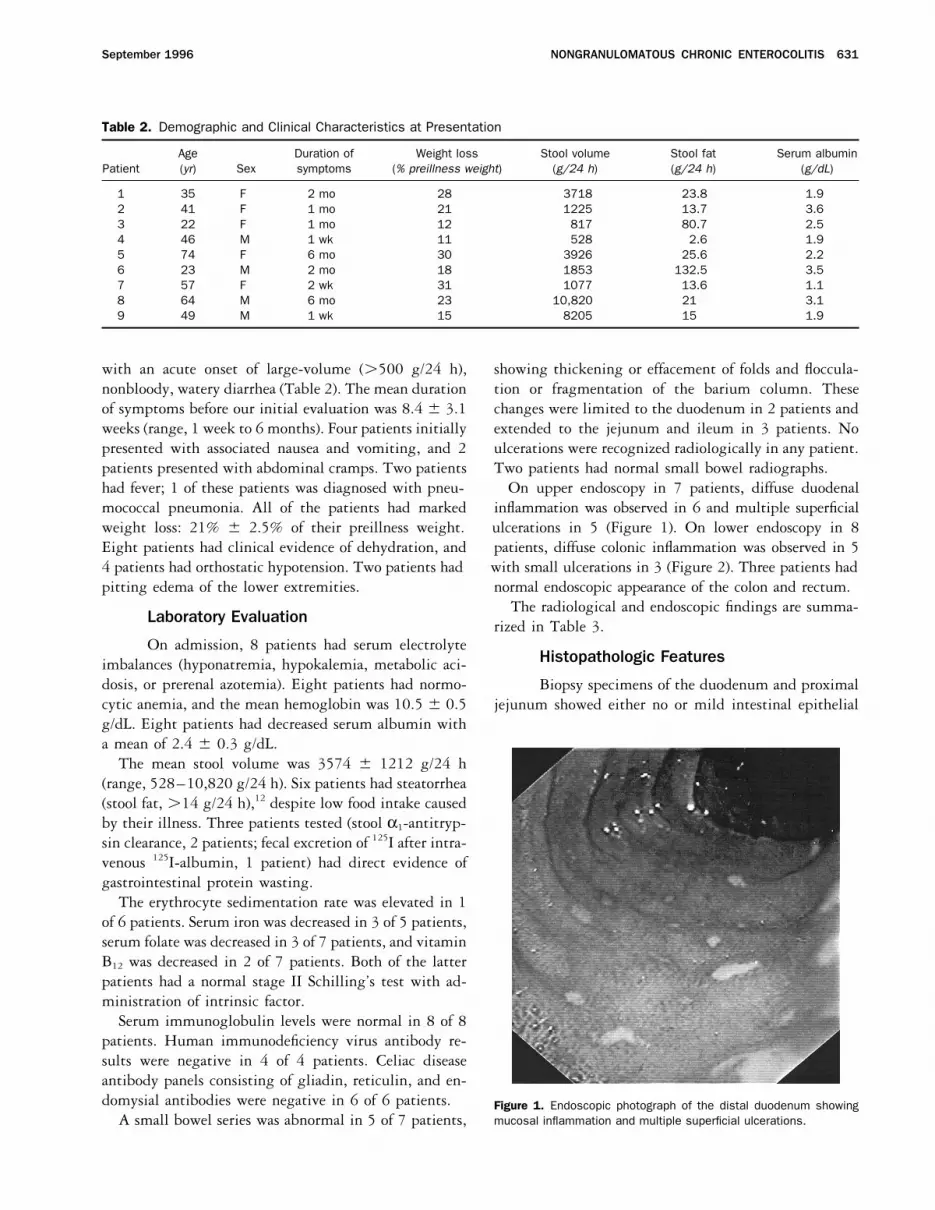
had fever; 1 of these patients was diagnosed with pneu- On upper endoscopy in 7 patients, diffuse duodenalinflammation was observed in 6 and multiple superficialmococcal pneumonia. All of the patients had marked
weight loss: 21% { 2.5% of their preillness weight. ulcerations in 5 (Figure 1). On lower endoscopy in 8patients, diffuse colonic inflammation was observed in 5Eight patients had clinical evidence of dehydration, and
4 patients had orthostatic hypotension. Two patients had with small ulcerations in 3 (Figure 2). Three patients hadnormal endoscopic appearance of the colon and rectum.pitting edema of the lower extremities.
The radiological and endoscopic findings are summa-Laboratory Evaluation rized in Table 3.On admission, 8 patients had serum electrolyte
Histopathologic Featuresimbalances (hyponatremia, hypokalemia, metabolic aci-dosis, or prerenal azotemia). Eight patients had normo- Biopsy specimens of the duodenum and proximalcytic anemia, and the mean hemoglobin was 10.5 { 0.5 jejunum showed either no or mild intestinal epithelialg/dL. Eight patients had decreased serum albumin witha mean of 2.4 { 0.3 g/dL.
The mean stool volume was 3574 { 1212 g/24 h(range, 528–10,820 g/24 h). Six patients had steatorrhea(stool fat, ú14 g/24 h),12 despite low food intake causedby their illness. Three patients tested (stool a1-antitryp-sin clearance, 2 patients; fecal excretion of 125I after intra-venous 125I-albumin, 1 patient) had direct evidence ofgastrointestinal protein wasting.
The erythrocyte sedimentation rate was elevated in 1of 6 patients. Serum iron was decreased in 3 of 5 patients,serum folate was decreased in 3 of 7 patients, and vitaminB12 was decreased in 2 of 7 patients. Both of the latterpatients had a normal stage II Schilling’s test with ad-ministration of intrinsic factor.
Serum immunoglobulin levels were normal in 8 of 8patients. Human immunodeficiency virus antibody re-sults were negative in 4 of 4 patients. Celiac diseaseantibody panels consisting of gliadin, reticulin, and en-domysial antibodies were negative in 6 of 6 patients. Figure 1. Endoscopic photograph of the distal duodenum showing
mucosal inflammation and multiple superficial ulcerations.A small bowel series was abnormal in 5 of 7 patients,
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro

632 RUAN ET AL. GASTROENTEROLOGY Vol. 111, No. 3
Figure 3. Pretreatment distal duodenal biopsy specimen showing to-tal villous atrophy. The lamina propria is filled with a mixture of acuteand chronic inflammatory cells. The arrows indicate a mucosal mi-croabscess (H&E stain; original magnification 251).
Figure 2. Endoscopic photograph of the colon showing mucosal in-flammation and multiple superficial ulcerations.
sive postmortem autolysis of the mucosa; however, therewas no inflammatory involvement of the submucosa, themuscularis propria, or the serosa. No fistulae, fibrosis, orabnormalities on light microscopy. In all specimens, thethickening of the intestinal wall was observed. Mesen-normal cylindrical enterocytic shape was preserved withteric and retroperitoneal lymph nodes were normal onno change in their nuclear polarity, and there was nogross inspection and light microscopy.increase in intraepithelial lymphocytes. On ultrastruc-
tural examination, 2 of 5 patients had loss of the epithe-Treatment and Outcomelial brush border, and it was intact in 3 patients. Five
patients had partial villous atrophy, and 2 patients had All patients were hospitalized at initial presenta-tion for fluid and electrolyte replacement and for diagnos-total villous atrophy (Figure 3). In all patients, a diffuse
inflammatory infiltrate was present in the lamina propria, tic evaluation. Five patients required temporary treat-ment with parenteral nutrition; 4 of these patientsconsisting of a mixture of plasma cells and lymphocytes
with abundant polymorphonuclear cells. Crypt abscesses experienced a decrease of the stool output but not cessa-tion of the diarrhea during temporary fasting. Two pa-of the small intestinal mucosa were observed in 3 pa-
tients. The inflammatory infiltrate was also present in tients were treated empirically with metronidazole, 1patient was treated with doxycycline, 3 patients werethe colon in 4 of 5 patients, with crypt abscesses in 3
patients. The normal crypt architecture was generally treated with sulfasalazine, and 2 patients were treatedwith octreotide injections, all without benefit. Four of 4preserved except in some areas of severe colitis (Figure
4); no granulomas were found. patients had no response to a strict gluten-free diet.All patients eventually were treated with corticoste-In the necropsy material of 3 patients, there was exten-
Table 3. Endoscopic and Radiological Findings
Patient Duodenum Rectum/colon Small bowel radiographs
1 Inflammation and ulcerations Inflammation and ulcerations Mucosal thickening in the duodenum2 Inflammation Normal Mucosal thickening in the jejunum3 Inflammation and ulcerations Inflammation —4 Inflammation and ulcerations Normal Mucosal thickening in the duodenum5 Inflammation and ulcerations Inflammation Normal6 — — Mucosal thickening in the jejunum and ileum7 — Normal Mucosal thickening in the jejunum and ileum8 Inflammation and ulcerations Inflammation and ulcerations Normal9 Normal Inflammation and ulcerations —
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro

NONGRANULOMATOUS CHRONIC ENTEROCOLITIS 633September 1996
Figure 4. Pretreatment colonic biopsy specimen showing chronic ac-tive colitis and crypt distortion. The arrow indicates a crypt abscess(H&E stain; original magnification 301).
Figure 5. Repeat duodenal biopsy specimen (same patient as in Fig-ure 3) after steroid therapy showing regeneration of villi and markeddecrease in the inflammatory infiltrate (H&E stain; original magnifica-tion 401).roids (20–50 mg/day prednisone or the equivalent) in
an effort to control their unrelenting symptoms. Theresults of this therapy are summarized in Table 4. Eightpatients had a prompt and dramatic clinical response was discontinued after 8 months of treatment. One year
later, the patient remained asymptomatic; however, in-within several days. Solid stools returned in 4 patients,and 4 patients experienced a marked decrease in the testinal biopsy specimens showed only partial resolution
of the histopathologic abnormalities.daily stool volume (mean reduction in daily stool volume,74.8% { 9%). Marked improvement in the histopatho- Six patients required prolonged therapy with low-dose
corticosteroids (5–15 mg/day prednisone) and could notlogic abnormalities was observed in 5 of the 9 patientson follow-up small intestinal biopsy specimens, obtained be weaned from the treatment without recurrence of the
diarrhea. These patients were followed up for a mean of1–28 months (mean, 14.6{ 5.8 months) after initiationof therapy (Figure 5). The histopathologic features on 63.4 { 22 months (range, 6 months to 16 years). Two
of the patients died. Patient 1 developed fulminantpresentation and after corticosteroid therapy are summa-rized in Table 5. There was a significant reduction in staphylococcal sepsis 1 year after initial presentation. No
focus of the infection could be identified. The patient’sthe histopathologic score (4.6 { 0.4 and 2.7 { 0.7; Põ 0.05) (Table 5). One patient (patient 8) did not re- diarrhea had been controlled with 12.5 mg/day predni-
sone, but intestinal biopsy specimens had shown no im-spond to corticosteroid therapy clinically or histologicallyand died after 6 months. One patient (patient 2) experi- provement after 1 year of treatment. Patient 7 had been
on corticosteroid maintenance for 12 years with control ofenced symptomatic remission, and corticosteroid therapy
Table 4. Response to Corticosteroid Treatment and Outcome
Initial clinical Histological Daily maintenance of Duration ofPatient response response Outcome Cause of death oral prednisone (mg) follow-up
1 Improved No response Death Staphylococcal sepsis — 1 yr2 Asymptomatic Improved Survival — None for 24 mo 3 yr3 Asymptomatic Resolution Survival — 15 4 yr4 Improved Improved Survival — 15 5 yr5 Improved Improved Survival — 5 4 yr6 Improved No response Survival — 10 13 yr7 Asymptomatica No response Death Invasive aspergillosis — 16 yr8 No response No response Death Disease progression — 6 mo9 Asymptomatic Improved Survival — None for 7 mo 13 mo
aThis patient was a 57-year-old woman who had been asymptomatic on low-dose corticosteroid maintenance therapy for 12 years, althoughher intestinal biopsy specimens had shown no improvement. She presented with bleeding ileal ulcerations positive for cytomegalovirus thatwere resected. Corticosteroid therapy was discontinued, and postoperative recurrence of the diarrhea occurred. Brief trials of prednisonetherapy had no effect. The patient gradually deteriorated and eventually died with invasive aspergillosis.
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro

634 RUAN ET AL. GASTROENTEROLOGY Vol. 111, No. 3
Table 5. Histopathologic Features of Small Intestinal Biopsy Specimens Before and After Corticosteroid Therapy
Before treatment After treatment
Villous Crypt Villous CryptPatient Inflammation atrophy abscesses Scorea Inflammation atrophy abscesses Scorea
1 Severe Total Yes 6 Severe Total Yes 62 Severe Partial No 5 Mild None No 13 Severe Total Yes 6 None None No 04 Mild None No 2 Mild None No 15 Severe Partial No 5 Mild None No 16 Moderate Partial No 4 Moderate Partial No 47 Moderate None No 3 Moderate None No 38 Severe Partial No 5 Severe Partial No 59 Moderate Partial Yes 5 Mild Partial No 3
aThe score is based on 0–7 points histopathologic severity score defined as follows: epithelial abnormalities (loss of microvilli, cellular atypia,or increased mitotic figures): minimal, 1 point; severe, 2 points; partial villous atrophy, 1 point; total villous atrophy, 2 points; mild inflammation,1 point; moderate, 2 points; severe, 3 points.
symptoms with 5 mg/day prednisone, although intestinal served in the duodenum (5 of 7 patients) and colon (3of 5 patients). Small intestinal radiographs showed non-biopsy specimens had shown no improvement after the
first year of therapy. The patient presented with bleeding specific changes of the mucosal fold pattern affecting theproximal or the entire small bowel in 5 of 7 patients.ileal cytomegalovirus ulcerations that required resection.
The prednisone was discontinued, and the patient experi- Intestinal biopsy specimens showed a unique diffuse in-flammatory infiltrate of the lamina propria with plasmaenced diarrhea recurrence. Brief trials of prednisone ther-
apy resulted in no improvement. She subsequently devel- cells, lymphocytes, and abundant polymorphonuclearcells frequently associated with crypt abscesses. Of note,oped invasive aspergillosis and died.
None of the 3 patients who died showed histological significant cellular abnormalities of the epithelial layer,as are typically present in untreated celiac sprue, wereimprovement with corticosteroid therapy, despite an ini-
tial clinical response in 2 patients (patients 1 and 7). In absent. In several patients, the same type of inflammatoryinfiltrate was also found in the colon. Partial villous atro-contrast, 5 of the 6 surviving patients showed some de-
gree of histological improvement while treated with cor- phy was present in 5 patients, and complete villous atro-phy was present in 2 patients. Corticosteroid therapyticosteroid therapy. One patient (patient 6) had absent
histological improvement, despite adequate symptomatic resulted in a rapid and dramatic response in all except1 patient who continued to deteriorate and died. Mainte-control on maintenance corticosteroid therapy for 13
years. nance therapy was required in 6 patients, including 4 ofthe 6 surviving patients. Two patients have remained
Other Complications asymptomatic for 7 and 24 months, respectively, aftercorticosteroid therapy was discontinued. One patient,Two patients (patients 1 and 7) developed bleed-who was not included in the series because histologicaling ulcerations in the postbulbar duodenum that werematerial was unavailable for review, developed a relapsetreated endoscopically. One of the patients (patient 1)10 years after discontinuing corticosteroid therapy andwas receiving prednisone. This patient also had bleedingresponded to a second course of prednisone. Complica-ulcerative proctitis during prednisone therapy and wastions were as follows: bleeding postbulbar duodenal ul-treated with a course of cyclosporine with improvement.cerations in 2 patients, bleeding cytomegalovirus ileal
Discussion ulcerations in 1 patient, and bleeding rectal ulcerationsin 1 patient. Three patients died. One patient died fromNine previously healthy, middle-aged patientsprogression of the disease, 1 patient died from staphylo-presented with a relatively abrupt onset of severe chroniccoccal sepsis, and 1 patient died from invasive aspergillo-diarrhea and required hospitalization. No infectioussis.agents were identified, and there was no evidence for
In this series, the clinical and radiological featuresa primary underlying disease after extensive diagnosticwere not typical of Crohn’s disease. No patient developedinvestigations. On endoscopy, inflammation and, in
many cases, multiple superficial ulcerations were ob- intestinal stenosis, perforation, or fistulization. In addi-
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro

NONGRANULOMATOUS CHRONIC ENTEROCOLITIS 635September 1996
tion, the histopathologic features were not consistent trate of the lamina propria and the crypt abscesses notedin 3 patients are not typical of celiac sprue. In contrastwith this disorder. Specifically, there were no granulo-
mas, focal or transmural inflammation, deep ulcers, fi- to our patients, many patients with celiac sprue andcomplicating ulceration have deep ulcers that frequentlybrosis, or thickening of the intestinal wall.perforate. In summary, we believe that our patients didSince the original report, credited to Nyman13 innot have celiac sprue; they did not have hypogammaglob-1949, there have been a number of case reports of patientsulinemia, and they were not found to have lymphomawith intestinal inflammation and ulcerations. The termsduring prolonged follow-up or at autopsy (3 patients).chronic ulcerative nongranulomatous jejunoileitis8 and
idiopathic chronic ulcerative enteritis9 were applied. On An interesting feature of our patients was their dra-matic response to corticosteroid therapy. Only half of thereview of the literature,14–50 70 patients have been re-
ported. Thirty-six patients (51%) had underlying dis- patients that were administered such treatment in ourliterature review had a similar response. In the revieweases. Of these, 23 patients (64%) had celiac sprue, 10
patients (29%) had intestinal lymphoma, and 5 patients by Baer et al.,10 only 2 of 13 patients who were treatedwith corticosteroids experienced a lasting benefit. In con-(14%) had hypogammaglobulinemia. When the patients
with and without underlying diseases were compared, trast, 7 of our 9 patients derived a long-term benefitfrom corticosteroid therapy. In addition, there was a rela-deep ulcerations, often associated with stenosis, were
more common in the patients with underlying diseases tionship between clinical and histological improvement(Table 2), except for 1 patient (patient 6) whose symp-(64% vs. 32%), as well as intestinal perforation (33%
vs. 17%) and obstruction (31% vs. 15%). Hemorrhage toms were controlled on maintenance prednisone therapyfor 13 years, despite absence of histological improvement.was more common in the patients without underlying
diseases (6% vs. 29%). The mortality rate was high in In all, there were 4 patients without change in theirhistopathologic score, and 3 of these patients eventuallyboth groups (50% and 51%). The diagnosis of lymphoma
was frequently delayed because intestinal lymphoma is died, despite an initial clinical response in 2 patients(patients 1 and 7). Thus, a negative histological responseknown to cause malabsorption with inflammation and
ulcerations remote from the site of malignant involve- to treatment in these patients can be a predictor of anadverse outcome.ment.51
In a separate series of 47 patients with malabsorption In conclusion, we believe our patients had a distinctclinical syndrome that could not be classified into anyand intestinal ulceration from The Johns Hopkins Hospi-
tal reviewed by Baer et al.,10 22 patients had celiac sprue, previously recognized diagnostic category. The histo-pathologic features were unique in that there was anand 14 patients had miscellaneous underlying disorders
including lymphoma and hypogammaglobulinemia. abundance of polymorphonuclear cells mixed withchronic inflammatory cells in the lamina propria, oftenHowever, 11 patients did not respond to a gluten-free
diet and were designated as ‘‘unclassified sprue.’’ Intesti- with crypt abscesses, involving the small intestine andcolon. Of note, the intestinal epithelial layer had nonal ulceration is a recognized complication of celiac sprue
that is uncommon but frequently fatal.30 Thus, it was significant cellular abnormalities as observed in patientswith celiac sprue. The patients responded dramaticallypostulated that the patients with unclassified sprue actu-
ally had celiac sprue that was not gluten responsive be- to corticosteroid therapy and often required prolongedtreatment. However, complications of gastrointestinalcause of the presence of ulcerations and because of their
older age (56.2 { 11.8 years vs. 48.2 { 10.8 years). hemorrhage and infection were common, and the mortal-ity rate was high (3 of 9 patients). Patients with thisHowever, our patients were younger (45.7 { 5.9 years).
In addition to their lack of response to gluten withdrawal syndrome may have previously been designated as unclas-sified sprue, chronic ulcerative nongranulomatous jejuno-(4 of 4 patients), celiac disease antibody results (including
endomysial immunoglobulin A antibody, which is ileitis, or idiopathic chronic ulcerative enteritis. The useof the latter two terms should be restricted to thoseknown to have a high sensitivity for celiac sprue52) were
negative (6 of 6 patients). On microscopy, we did not patients in whom celiac sprue, lymphoma, or hypogam-maglobulinemia, as well as other conditions that formobserve the typical features of celiac sprue.11 Although
5 patients had partial villous atrophy and 2 patients part of the differential diagnosis (Table 1) have beenexcluded. The etiology of this syndrome is unclear. Al-had complete villous atrophy, the typical changes of the
villous epithelium were absent, and on electron micros- though known pathogens were excluded by stool testingand light and electron microscopy of the intestine, thecopy, 3 of 5 patients had an intact epithelial brush border.
The intense acute and chronic diffuse inflammatory infil- possibility that an elusive unidentified agent is responsi-
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro
636 RUAN ET AL. GASTROENTEROLOGY Vol. 111, No. 3
23. Smitskamp H, Kuipers FC. Steatorrhea and ulcerative jejunoile-ble cannot be excluded completely. The benefit of corti-itis. Acta Med Scand 1965;177:37–42.costeroids may be related to an effect on intestinal in- 24. Neale G. Royal Postgraduate Medical School: clinicopathological
flammation and/or to effects on intestinal transport. conference: a case of adult onset celiac disease resistant totreatment. BMJ 1968;2:678–684.
References 25. Castleman H, McNeely BU. Case records of the MassachusettsGeneral Hospital. Case 16–1969. N Engl J Med 1969;280:885–
1. DuBois RN, Lazenby AJ, Yardley JH, Hendrix TR, Bayless TM,894.
Giardiello FM. Lymphocytic enterocolitis in patients with ‘refrac-26. Armstrong JK, Ammon RK, Finlay-Jones LR, Joske RA, Vivian AB.tory sprue.’ JAMA 1989;262:935–937.
A further case of chronic ulcerative enteritis. Gut 1973;14:649–2. Clouse RE, Alpers DH, Hockenbery DM, DeSchryver-Kecskemeti652.K. Pericrypt eosinophilic enterocolitis and chronic diarrhea. Gas-
27. Dowling RH. Royal Postgraduate Medical School: clinicopatholog-troenterology 1992;103:168–176.ical conference: non-responsive celiac disease. BMJ 1972;3:3. Zuckerman MJ, Al-Samman M, Boman DA. Granulomatous gas-624–631.troenteritis. Case report with comparison to idiopathic isolated
28. Scully RE, Gadabini JJ, McNeely BU. Case records of the Massa-granulomatous gastritis. Dig Dis Sci 1994;39:1649–1654.chusetts General Hospital. Case 39-1975. N Engl J Med 1975;4. Levine J, Schmidt MH, Burrell MI, Hopkins MS. Acute jejunoileitis,293:712–717.a distinct entity? J Clin Gastroenterol 1992;14:47–51.
29. Klaeveman HL, Gebhard RL, Sessoms C, Strober W. In vitro stud-5. Hill SM, Milla PJ, Botazzo GF, Mirakian R. Autoimmune enteropa-ies of ulcerative ileojejunitis. Gastroenterology 1975;68:572–thy and colitis: is there a generalized autoimmune gut disorder?582.Gut 1991;32:36–42.
30. Bayless TM, Kapelowitz RF, Shelley WM, Ballinger WF, Hendrix6. Perlemuter G, Chaussade S, Kahan A, Delchier JC, Bigard MA,TR. Intestinal ulceration—a complication of celiac disease. NDegoy J, Pariente A, Chagnon JP, Lescut J, Goldfain D, SontagEngl J Med 1967;276:996–1002.D, Coutarel P, Couturier D. Cryptogenic multifocal ulcerous ste-
31. Jones PE, Gleeson MH. Mucosal ulceration and mesentericnosing enteritis: an independent vasculitis or an atypical kind oflymphadenopathy in celiac disease. BMJ 1973;3:212–213.polyarteritis nodosa (abstr)? Gastroenterology 1995;108:A892.
32. Gouffier E, Phan A, Paraf A, Baddaert A, Chevrel JP. Jejuno-ileite7. Smith LJ, Szymanski W, Foulston C, Jewell L, Pabst H. Torkelsonulcereuse d’evolution recurrente. Etude operatoire et endosco-syndrome: life-threatening secretory diarrhea, distinctive smallpique d’un nouveau cas. Gastroenterol Clin Biol 1977;1:545–bowel morphology and variable immunodeficiency (abstr). Gastro-552.enterology 1992;102:698A.
33. Gouerou H, Redelsperger PY, Galian A, Derrichian M, Pappo E,8. Jeffries GH, Steinberg H, Sleisenger MH. Chronic ulcerative (non-Cattan D. Jejuno-ileite ulcereuse chronique avec malabsorption.granulomatous) jejunitis. Am J Med 1968;44:47–59.Gastroenterol Clin Biol 1977;1:561–570.9. Mills PR, Brown IL, Watkinson G. Idiopathic chronic ulcerative
34. Caserta SJ. Non-tropical sprue with several major complications.enteritis: report of 5 cases and review of the literature. Q J MedAm J Gastroenterol 1987;82:689–691.1980;49:133–149.
35. Aubrey DA. Stenosing jejunitis. Br J Surg 1971;58:633–635.10. Baer AN, Bayless TM, Yardley JH. Intestinal ulceration and malab-36. Kane SP, Parkins RA. Chronic ulcerative jejunitis without symp-sorption syndromes. Gastroenterology 1980;79:754–765.
toms. Postgrad Med J 1979;55:215–217.11. Perera DR, Weinstein WM, Rubin CE. Small intestinal biopsy.37. Neale SP. Royal Postgraduate Medical School: clinicopathologi-Hum Pathol 1975;6:157–217.
cal conference: a case of malabsorption, intestinal mucosal atro-12. Fine KD, Fordtran JS. The effect of diarrhea on fecal fat excretion.phy and ulceration, cirrhosis and emphysema. BMJ 1970;3:Gastroenterology 1992;102:1936–1939.207–212.13. Nyman E. Ulcerous jejuno-ileitis with symptomatic sprue. Acta
38. Himes HW, Gabriel JB, Adlesberg D. Previously undescribed clini-Med Scand 1949;134:275–283.cal and postmortem observations in non-tropical sprue: possible14. Modigliani R, Poitras P, Galian A, Messing B, Guyet-Rousset P,role of prolonged corticosteroid therapy. Gastroenterology 1957;Liebeskind M, Piel-Desruisseaux SL, Rambaud JC. Chronic non-32:60–71.specific ulcerative duodeno-jejuno-ileitis: report of 4 cases. Gut
39. Costello RW, Lyons DJ, Fielding JF. Ulcerative jejunitis: are we1979;20:318–328.missing cases. Ir J Med Sci 1991;160:342–343.15. Lamont CM, Adams FG, Mills PR. Radiology in idiopathic chronic
40. Stuber JL, Wiegman H, Crosby I, Gonzalez G. Ulcers of the colonulcerative enteritis. Clin Radiol 1982;33:283–287.and jejunum in celiac disease. Radiology 1971;99:339–340.16. Robertson DAF, Dixon MF, Scott BB, Simpson FG, Losowsky MS.
41. Brunton FJ, Guyer PB. Malignant histiocytosis and ulcerative jeju-Small intestinal ulceration: diagnostic difficulties in relation tonitis of the small intestine. Clin Radiol 1983;34:251–259.celiac disease. Gut 1983;24:565–574.
42. Zapolsky JH, Janower ML. Idiopathic chronic ulcerative enteritis:17. Goulston KJ, Skyring AP, McGovern VJ. Ulcerative jejunitis associ-a report of two cases. Radiology 1985;155:39–40.ated with malabsorption. Aust Ann Med 1965;14:57–64.
43. London DR, Bamforth J, Creamer B. Steatorrhea presenting with18. Moritz M, Moran JM, Patterson JF. Chronic ulcerative jejunitis:gastrointestinal protein loss. Lancet 1961;2:18–19.report of a case and discussion of classification. Gastroenterol-
44. Freeman M, Shao-Ru C. Non-granulomatous ulcerative jejunoile-ogy 1971;60:96–102.itis. Am J Gastroenterol 1984;79:446–449.19. Jeffries GH, Holman MR, Sleisenger MH. Plasma proteins and
45. Shoesmith JH, Tate GT, Wright CJE. Multiple strictures of thethe gastrointestinal tract. N Engl J Med 1962;266:652–660.jejunum. Gut 1964;5:132–135.20. Lotsberg J, Teisberg P, Myren J, Serek-Hanssen A. Chronic ulcera-
46. Karz S, Guth P, Polonsky L. Chronic ulcerative jejunoileitis. Amtive non-granulomatous jejunitis (abstr). Scand J GastroenterolJ Gastroenterol 1971;56:61–67.1976;11(Suppl):38, 24A.
47. Davidson AR. Recurrent benign ileal ulcer occurring with the ce-21. Corlin RF, Pops MA. Non-granulomatous ulcerative jejunoileitisliac syndrome. BMJ 1969;3:341.with hypogammaglobulinemia: clinical remission after treatment
with g-globulin. Gastroenterology 1972;62:473–478. 48. Green JA, Barkin JS, Gregg PA, Kohen K. Ulcerative jejunitis inrefractory celiac disease: enteroscopic visualization. Gastroin-22. Barry RE, Morris JS, Read AEA. A case of small intestinal atrophy.
Gut 1970;11:743–747. test Endosc 1993;39;4:584–585.
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro

NONGRANULOMATOUS CHRONIC ENTEROCOLITIS 637September 1996
49. Strauch M, Lohr JM, Ottenjann R. Cronische ulzerative jejunitis T. Endomysial antibodies in the diagnosis of celiac disease andthe effect of gluten on antibody titers. Immunol Invest 1989;18:mit malabsorptionssyndrom. Med Klin 1973;68:1113–1116.553.50. Mann NS, Wolfer CF, Mann SK, Kadian RS. Colonic involvement
in chronic ulcerative non-granulomatous jejunoileitis. Am J Proc-tol, Gastroenterology, Colon Rectal Surg 1980;31:17–19. Received January 23, 1996. Accepted May 15, 1996.
51. Isaacson P, Wright DH. Malignant histiocytosis of the intestine. Address requests for reprints to: Konrad H. Soergel, M.D., DivisionHum Pathol 1978;9:661–677. of Gastroenterology, Medical College of Wisconsin, 9200 West Wis-
consin Avenue, Milwaukee, Wisconsin 53226. Fax: (414) 259-1533.52. Kumar V, Lerner A, Valeski JE, Beutner EH, Chorzelski TP, Rossi
/ 5e11$$0017 08-14-96 09:40:48 gasas WBS-Gastro





























