Embed Size (px)
Citation preview

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2083
O B S E RVAT I O N S
Lack of Effect on LDLOxidation andAntioxidant StatusAfter Impro v e m e n tof Metabolic Contro lin Type 2 Diabetes
Type 2 diabetes is associated withi n c reased oxidative stress, whichmay contribute to microvascular and
m a c rovascular complications (1). One ofthe consequences of increased oxidatives t ress may be increased lipid pero x i d a-tion. Improvement of metabolic contro lhas a favorable effect on micro v a s c u l a rand possibly also on macrovascular com-plications (2). Whether reduction of lipidp e roxidation plays a role in this respect isnot known.
We investigated whether impro v e m e n tof metabolic control by insulin therapy hada favorable effect on lipid pero x i d a t i o n .
In this study, 21 patients with type 2diabetes and insufficient metabolic con-t rol despite near-maximal doses of oralblood glucose–lowering agents part i c i-pated (age 58 ± 12 years, diabetes dura-tion 10 years [range 1–38], BMI 29.2 ±7.1 kg/m2, HbA1 c 10.6 ± 1.1%). Four ofthem smoked (10–40 cigarettes/day) andseven of them had clinically evidentm a c rovascular disease. During the study,all patients maintained their diets accord-ing to international nutritional guide-lines. Insulin treatment consisted oftwice-daily injections of a mixture ofs h o rt- and intermediate-acting insulin.The goal of therapy was to achieve fastingand postprandial blood glucose levels ,7and 10 mmol/l, re s p e c t i v e l y, and HbA1 c
,8%. Checkups after 2 weeks andmonthly thereafter consisted of takingm e a s u rements of body weight andH b A1 c. Insulin doses were adjustedweekly on the basis of self-monitoring ofblood glucose levels.
Lipid peroxidation was assessed by 1) thiobarbituric acid reactive substances(TBARS) (3), 2) production of conjugateddienes after copper-induced LDL oxida-tion in vitro (4), and 3) levels of IgG andIgM autoantibodies to oxidized LDL byenzyme-linked immunosorbent assay(5). Vitamin E was determined with high-
p e rf o rmance liquid chro m a t o g r a p h y. Adetailed description of the completemethodology was published pre v i o u s l y(6). Diff e rences between groups wereanalyzed with Student’s t test for paire dsamples. When variables were not nor-mally distributed, Wi l c o x o n ’s signed-rank test was used.
After 3–4 months of insulin therapy,H b A1 c d e c reased to 7.9 ± 0.6% (P ,0.005). The daily insulin dose was 61 U(16–100), and the mean weight gain was5.4 kg. Total cholesterol, LDL cholestero l ,and HDL cholesterol did not change( 6 . 0 ± 1.1, 3.7 ± 0.9, and 1.0 ±0 . 3 mmol/l, respectively), neither dida p o l i p o p rotein B (apoB) and the LDLc h o l e s t e rol/apoB ratio, the latter as arough index of LDL size. Apolipopro t e i nA1 (apoA1) levels increased from 1.45 ±0.28 to 1.63 ± 0.36 g/l, and triglyceridesd e c reased from 2.44 (range 0.95–7.09) to1.74 (0.87–5.67) mmol/l. Fasting insulinlevels increased from 7.6 (2.0–35.5) to12.4 (5.10–58.7) mU/l (P = 0.07). Nod e c rease in TBARS was found (1.83 ±0.79 vs. 1.50 ± 0.39 µmol/l), even whenwe excluded the three patients withtriglycerides .4.5 mmol/l. Lag phase, asan index of the susceptibility of LDL toc o p p e r-induced oxidation, also re m a i n e dunchanged (59 ± 6, resp. 62 ± 10 min),w h e reas the conjugated dienes pro d u c-tion rate decreased from 17.8 ± 2.6 to16.1 ± 3.0 nmol · l– 1 · m i n– 1, P , 0 . 0 0 5 ) .Levels of autoantibodies to oxidized LDLdid not change. Vitamin E levels, cor-rected for LDL cholesterol, re m a i n e du n c h a n g e d .
Some, but not all, studies show evi-dence of increased LDL oxidation in type 2diabetes (6,7). Increased LDL glycationand formation of advanced glycated endp roducts may increase the susceptibilityof LDL to oxidation. Hyperglycemia itselfcan stimulate free-radical production, andsmall dense LDL, more prevalent in type 2diabetes, is prone to oxidation (7). Severalfactors contribute to LDL pero x i d a t i o n ,and this may explain why we, in contrastto our hypothesis, did not find convinc-ing evidence of reduced LDL pero x i d a-tion. The achieved metabolic control maybe of influence: one study found a re d u c-tion in lipid peroxidation only whenH b A1 c d ropped to ,7% (8). In ourpatients who achieved an HbA1 c ,7 . 5 % ,no change was found. Even when HbA1 c
should have been ,7%, the expectede ffect is small and there f o re probably not
clinically relevant. Seven patients hadm a c rovascular disease, but there is noconsensus in the literature on whetherlipid peroxidation in these cases isi n c reased; in a previous study, we did notfind evidence for this (6). Maybe a favor-able effect on LDL peroxidation is coun-teracted by factors that were also changedduring the treatment period and thatstimulate LDL oxidation; for insulin, inv i t ro pro-oxidant pro p e rties have beenshown (9). Obesity is associated withi n c reased LDL peroxidation (10), soweight gain may have influenced theresults, although we think this effect issmall. A change in antioxidant statusseems unlikely; vitamin E levels re m a i n e dunchanged and patients did not changetheir dietary habits during the study. Sul-f o n y l u reas may have an antioxidant eff e c t ,but this has been shown only for gli-clazide in vitro (11). In our study, onlyfour patients used gliclazide. Lipid pero x-idation was tested 2 weeks after the oralagents were stopped, and no change inlipid peroxidation was observed. Thismakes it unlikely that cessation of theseagents should have influenced the re s u l t s .It is uncertain whether the decrease in thep roduction rate of conjugated dienes thatwe found is important. Susceptibility ofLDL to oxidation is explained mainly bythe lag phase. However, the speed atwhich lipid peroxidation products aref o rmed may be also of importance for itsdamaging effect. It is assumed that lipidp e roxidation takes place mainly in thevessel wall, and, there f o re, the questionremains whether serum parameters and inv i t ro parameters are re p re s e n t a t i v e .R e c e n t l y, in agreement with our earlierresults, no association could be foundbetween the prevalence of coro n a ry heartdisease and LDL susceptibility to oxida-tion in type 2 diabetic patients (12).
In conclusion, we found no convinc-ing evidence of reduced LDL oxidationafter improvement of metabolic control intype 2 diabetes. The importance of thereduced conjugated dienes pro d u c t i o nrate remains to be investigated furt h e r.
WILMA A. ORANJE, MD
GABRIELLE J.W.M. RONDAS-COLBERS
GEERTJE N.M. SWENNEN
HANS JANSEN, PHD
BRUCE H.R. WOLFFENBUTTEL, MD, PHD
F rom the Department of Endocrinology and Metabo-lism (W.A.O., G.J.W.M.R.-C., G.N.M.S., B.H.R.W. ) ,
L E T T E R S

2084 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
University Hospital Maastricht and Maastricht Uni-v e r s i t y, Maastricht; and the Department of Intern a lMedicine and Biochemistry (H.J.), University Hospi-tal Dijkzigt, Rotterdam, the Netherlands.
A d d ress correspondence to Dr. W.A. Oranje,D e p a rtment of Endocrinology and Metabolism, Uni-versity Hospital Maastricht, P. Debyelaan 25, P.O. Box5800, 6202 AZ Maastricht, the Netherlands. E-mail:w. o r a n j e @ i n t m e d . u n i m a a s . n l .
R e f e re nc e s1 . Giugliano D, Ceriello A: Oxidative stre s s
and diabetic vascular complications. D i a -betes Care 19:257–267, 1996
2 . U.K. Prospective Diabetes Study Gro u p :Intensive blood-glucose control withs u l p h o n y l u reas or insulin compared withconventional treatment and risk of com-plications in patients with type 2 diabetes(UKPDS 33). Lancet 352:837–853, 1998
3 . Naito C, Kawamura M, Yamamoto Y: Lipidp e roxides as the initiating factor of athero-s c l e rosis. Ann N Y Acad Sci 6 7 6 : 2 7 – 4 5 ,1 9 9 3
4 . Esterbauer H, Striegl G, Puhl H, Rothene-der M: Continuous monitoring of in vitrooxidation of human low density lipopro-tein. F ree Radic Res Commun 6 : 6 7 – 7 5 ,1 9 8 9
5 . Jansen H, Ghanem H, Kuypers JHSAM,Birkenhager JC: Autoantibodies againstm a l o n d i a l d e h y d e - m o d i fied LDL are ele-vated in subjects with an LDL subclassp a t t e rn B. A t h e ro s c l e rosis 1 1 5 : 2 5 5 – 2 6 2 ,1 9 9 5
6 . Oranje WA, Rondas-Colbers GJWM,Swennen GNM, Wo l ffenbuttel BHR: Lipidp e roxidation in type 2 diabetes: re l a t i o n-ship with macrovascular disease? Neth JMed 53:61–68, 1998
7 . Yoshida H, Ishikawa T, Nakamura H: Vi t a-min E/lipid peroxide ratio and susceptibil-ity of LDL to oxidative modification innon-insulin-dependent diabetes mellitus.A rterioscler Thromb Vasc Biol 1 7 : 1 4 3 8 –1446, 1997
8 . Katoh K: Possible relevance of lipid pero x-idation and thromboxane production tothe initiation and/or evolution of micro a n-giopathy in non-hyperlipidemic type 2diabetes mellitus. Diabetes Res Clin Pract18:89–98, 1992
9 . R i fici VA, Schneider SH, KhachadurianAK: Stimulation of low-density lipopro t e i noxidation by insulin and insulin likeg rowth factor I. A t h e ro s c l e rosis 1 0 7 : 9 9 –108, 1994
1 0 . Van Gaal L, Ve rtommen J, de Leeuw I: Thein vitro oxidizability of lipoprotein part i-cles in obese and non-obese subjects. A t h -e ro s c l e rosis 137:S39–S44, 1998
1 1 . O’Brien R, Luo M: The effects of gliclazideand other sulfonylureas on low-densityl i p o p rotein oxidation in vitro. M e t a b o l i s m46:22–25, 1997
1 2 . Leinonen JS, Rantalaiho V, Solakivi T,Koivula T, Wi rta O, Pasternack A, Alho H,Lehtimaki T: Susceptibility of LDL to oxi-dation is not associated with the pre s e n c eof coro n a ry heart disease or renal dysfunc-tion in NIDDM patients. Clin Chim Acta275:163–174, 1998
M e a l - G e n e r a t e dOxidative Stress inD i a b e t e s
The protective effect of red wine
Several epidemiological studies sug-gest that coro n a ry heart diseasem o rtality is lowered by moderate
consumption of red wine (1,2). The car-diovascular benefits of moderate wineconsumption have been thought to stem,at least part l y, from antioxidant activities ofred wine (3).
Recently, a preliminary report sug-gested the possibility that red wine, apolyphenol-rich beverage, increases theantioxidant power of plasma in humans(3). Since then, several authors havepublished results fully confirming thatthe consumption of moderate amountsof red wine elicits a prompt, though tem-p o r a ry, rise of plasma antioxidativedefenses (4,5).
C o n s e q u e n t l y, it has been suggestedthat this pro p e rty may provide a clue tothe role of certain wines in the so-called“ F rench paradox,” according to which theconsumption of moderate amounts of re dwine by the French appears to aff o rd somep rotection against cardiovascular disease,despite their consumption of a diet rich insaturated fat (2). Diabetes is characterizedby a high incidence of cardiovascular dis-ease (6), and oxidative stress has been re c-ognized as a major pathophysiological linkbetween cardiovascular disease and dia-betes (7). In diabetic patients, the con-sumption of meals is accompanied by as i g n i ficant decrease of antioxidantdefenses due to the generation of oxidatives t ress (8). This observation is consistentwith the recent re p o rt by Staprans et al. (9)showing increased postprandial oxidizedlipid levels in poorly controlled diabeticpatients. There f o re, meal consumptionseems to play a crucial role in the genera-tion of oxidative stress in diabetes.
Because red wine ingestion has beendemonstrated to be accompanied by a
s i g n i ficant increase of plasma antioxidantpower (6,7), the aim of this study was toe x p l o re the possibility that red wine con-sumption may reduce oxidative stress pro-duced in diabetic patients during meals.
Informed consent to participate inthe present study was obtained from 10male type 2 diabetic patients (age 55.1 ±1.5 years, mean ± SEM, duration of dia-betes 9.0 ± 1.2 years, BMI 25.6 ±1.1 kg/m2). In each subject, three differ-ent studies were performed in random-ized order on different days: a standardmeal test (8), fasting ingestion of 300 mlof red wine, and a meal plus 300 ml ofred wine. The study protocol wasapproved by the Ethical Committee ofthe University of Udine.
Blood samples, obtained in theabsence of venous stasis, were collectedat baseline and 60, 120, and 180 minafter the meals. In every sample, plasmaglucose, insulin, triglycerides, andplasma total radical-trapping antioxidantparameter (TRAP) were measured. Theassay of TRAP has been recently pro-posed to evaluate plasma antioxidantc a p a c i t y, taking into considerationknown and unknown antioxidants pre s-ent in the plasma as well as their mutualcooperation: A higher TRAP number des-ignates a higher antioxidant capacity(10). The antioxidant power of red wine(Merlot; Azienda Agricola Erm a c o r a ,Ipplis, Udine, Italy) was also tested intriplicate using the method describedabove and compared with the antioxi-dant power of a white wine (10).
By re p e a t e d - m e a s u res analysis ofvariance, plasma glucose (F = 48.0, P =0.001), insulin (F = 42.4, P = 0.001),and triglycerides (F = 26.1, P = 0.001)significantly increased, whereas plasmaTRAP (F = 27.8, P = 0.001) significantlydecreased during the meal test. Fastingconsumption of red wine significantlyincreased TRAP activity, whereas wineingestion with a meal counterbalancedthe decrease of TRAP (F = 8.2, P =0.001). In vitro, red wine showed aTRAP activity of 6.1 ± 0.2 mmol/l,whereas the TRAP of white wine was1.2 ± 0.3 mmol/l.
Our data show that red wine is able top re s e rve plasma from meal-inducedoxidative stress in diabetes, suggesting thatmoderate consumption of red wine duringmeals may have a beneficial effect ind e c reasing the risk of cardiovascular dis-ease in diabetic patients.

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2085
Letters
ANTONIO CERIELLO, MD
NADIA BORTOLOTTI, PHD
ENRICO MOTZ, MD
SEBASTIANO LIZZIO, MD
ASSUNTA RUSSO, MD
VLADIMIR SELMO, MD
BARBARA CATONE, MD
LAURA TONUTTI, MD
CLAUDIO TABOGA, MD
F rom the Department of Clinical and ExperimentalMedicine, the Chair of Internal Medicine (A.C., E.M.,S.L., A.R., V.S., B.C.) and the Chair of Clinical Pathol-ogy (N.B.) and Diabetology Unit (L.T., C.T.), UdineGeneral Hospital, Udine, Italy.
A d d ress correspondence to Dr. Antonio Ceriello,Chair of Internal Medicine, University of Udine, P. l eS. Maria della Misericordia, 33100 Udine, Italy.E-mail: [email protected].
R e f e re n c e s1 . Rimm EB, Giovannucci EL, Willet WC,
Colditz GA, Aschrio A, Rosner B, StampferMJ: Prospective study of alcohol consump-tion and risk of coro n a ry disease in men.L a n c e t 338:464–468, 1991
2 . Renaud S, De Lorgerl M: Wine, alcohol,platelets, and the French paradox for coro-n a ry heart disease. L a n c e t 3 3 9 : 1 5 2 3 –1526, 1993
3 . Maxwell S, Cruickshank A, Thorpe G: Redwine and antioxidant activity in seru m(Letter). L a n c e t 344:193–194, 1994
4 . Whitehead TP, Robinson D, Allaway S,Syms J, Hale A: Effect of red wine on theantioxidant capacity of serum. Clin Chem41:32–35, 1995
5 . Cao G, Russell RM, Lischner N, Prior RL:S e rum antioxidant capacity is increased byconsumption of strawberries, spinach, re dwine or vitamin C in elderly women.J N u t r 128:2383–2390, 1998
6 . Kannel WB, McGee DL: Diabetes and car-diovascular risk factors: the FraminghamS t u d y. C i rc u l a t i o n 59:8–13, 1979
7 . Giugliano D, Ceriello A, Paolisso G: Oxi-dative stress and diabetic vascular com-plications. Diabetes Care 1 9 : 2 5 7 – 2 6 7 ,1 9 9 6
8 . Ceriello A, Bortolotti N, Motz E, Cre s c e n-tini A, Lizzio S, Russo A, Tonutti L, Ta b o g aC: Meal-generated oxidative stress in type 2diabetic patients. Diabetes Care 2 1 : 1 5 2 9 –1533, 1998
9 . Staprans I, Hardman DA, Pan X-M,Feingold KR: Effect of oxidized lipids inthe diet on oxidized lipid levels in post-prandial serum chylomicrons of diabeticpatients. Diabetes Care 2 2 : 3 0 0 – 3 0 6 ,1 9 9 9
1 0 . Ghiselli A, Serafini M, Maiani G, Azzini E,F e rro-Luzzi A: A flu o re s c e n c e - b a s e dmethod for measuring total plasma antiox-idant capability. F ree Radic Biol Med 1 8 : 2 9 –36, 1995
Red Blood CellAutoantibodies With a Shortened E ry t h rocyte LifeSpan as a Cause ofLack of RelationBetween Glycosylated Hemoglobin andMean Blood GlucoseLevels in a Wo m a nWith Type 1 D i a b e t e s
Glycosylated hemoglobin is the testmost widely used to document thed e g ree of glycemic control in patients
with diabetes. The strong statistical re l a-tionship between mean blood glucose lev-els and glycosylated hemoglobin is wellestablished (1); however, clinically signifi-cant diff e rences in average blood glucosef rom individuals with identical glycosy-lated hemoglobin levels have beenre p o rted (2). Diff e rences in ery t h rocyte lifespan among individuals are one of the pro-posed factors that may alter the re l a t i o n-ship between a given glycosylated hemo-globin level and average blood glucose (1).
We re p o rt on a patient in whom lackof relation between glycosylated hemoglo-bin and mean blood glucose levels isexplained by the presence of red blood cella u t o a n t i b o d i e s .
A 30-year-old woman with type 1diabetes of 11 years’ duration was fir s tseen at our clinic for preconception con-t rol. There was no family history ofautoimmune diseases. She had no evi-dence of diabetes complications (norm a ldilated-eye examination and albumine x c retion ,2 0 µg/min) and was on thre einsulin injections per day. She took noother medications re g u l a r l y. Physicalexamination was normal and she wasasymptomatic. She re p o rted habitualgood glycemic control as assessed fro mglycosylated hemoglobin, though sher a rely perf o rmed self-monitoring of bloodglucose levels. Initial glycosylated hemo-globin (high-perf o rmance liquid chro-matography; Bio-Rad, Richmond, CA)was 6.5%. On entering pre c o n c e p t i o nc a re, she started daily capillary blood glu-cose self-monitoring (six to seven mea-
s u rements/day). The glucose meter used( O n e Touch Pro file; LifeScan, Milpitas,CA), with storage capability, allows com-p u t e r-assisted analyses of glucose re a d-ings. After 45 days, her mean blood glu-cose level was 11.3 mmol/l (252 re a d i n g s )and her glycosylated hemoglobin was5.8%. After another period of 45 days, hermean blood glucose level fell to8 . 2 mmol/l (331 readings) and glycosyla-ted hemoglobin to 4.9%. Both glycosyla-ted hemoglobin values are by far lowerthan expected from each average bloodglucose (3). Hemoglobin variants, whichmay lower results of glycosylated hemo-globin (4), were ruled out since the assayused is not affected by these. Ingestion ofv i t a m i n C or E, which has also beenre p o rted to lower glycohemoglobin values(5,6), was also excluded. Red blood celllife span, evaluated with chro m i u m -labeled self-ery t h rocytes, showed areduced half-life: 20 days (normal t1 / 2:28–30 days), with an increased erythro-poietic activity index (2.4) and spleenparticipation in hemolysis. Her levels oflactate dehydrogenase, plasma hemoglo-bin, bilirubin, haptoglobin, and herreticulocyte count were normal. TheCoombs’ antiglobulin test showed thepresence of IgG autoantibodies on thepatient’s red blood cell surface. Furtherevaluation of autoimmune diseaseshowed a positive antinuclear antibodytest, with positive anti-Ro/SSA, anti-La/SSB, and anticardiolipin autoantibod-ies. Anti-DNA, anti-Sm, and anti-RNPautoantibodies were negative.
Immunohemolytic anemia, in itsmildest form with only positive antiery-t h rocyte autoantibodies, seems to beresponsible for the low glycohemoglobinvalues in this patient. Immunohemolyticanemia has been re p o rted as a cause ofd e c reased glycosylated hemoglobin in twopatients with type 1 diabetes (7); however,in both cases, hemolysis, which wasinduced by drugs, was evident. This casesuggests the possibility that the pre s e n c eof red blood cell autoantibodies withs h o rtened ery t h rocyte life span, but noclinical expression, might explain the lackof relation between glycosylated hemoglo-bin and mean blood glucose levels moreoften than has been suspected.
LUCRECIA HERRANZ, MD
CRISTINA GRANDE, SCD
MERCEDES JANEZ, BM
FELIPE PALLARDO, MD
2086 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
F rom the Division of Diabetes, Department ofEndocrinology (L.H., F. P.), the Department of Bio-c h e m i s t ry (C.G.), and the Department of Obstetricsand Gynecology (M.I.), Hospital La Paz, Madrid,S p a i n .
A d d ress correspondence to Lucrecia Herr a n z ,MD, Unidad de Diabetes, Hospital La Paz, Paseo de laCastellana 261, 28046 Madrid, Spain. E-mail:c f a l o n s o @ t e l e l i n e . e s .
R e f e re n c e s1 . Goldstein DE, Little RR, Lorenz RA, Mal-
one JI, Nathan D, Peterson CM: Tests ofglycemia in diabetes. Diabetes Care 1 8 :896–909, 1995
2 . Yudkin JS, Forrest RD, Jackson CA, Ry l eAJ, Davie S, Gould BJ: Unexplained vari-ability of glycated hemoglobin in non-dia-betic subjects not related to glycaemia.Diabetologia 33:208–215, 1990
3 . Nathan DM, Singer DE, Hurxthal K,Goodson JD: The clinical inform a t i o nvalue of the glycosylated hemoglobina s s a y. N EngI J Med 310:341–346, 1984
4 . Allen KR, Hamilton AD, Bodansky AJ,Poon P: Prevalence of haemoglobin vari-ants in a diabetic population and theire ffect on glycated haemoglobin measure-ment. Ann Clin Biochem 29:426–429, 1992
5 . Jain SK, McVie R, Jaramillo JJ, Palmer M,Smith T: Effect of modest vitamin E sup-plementation on blood glycated hemoglo-bin and triglyceride levels and red cellindices in type 1 diabetic patients. J AmColl Nutr 15:458–461, 1996
6 . Davie SJ, Gould BJ, Yudkin JS: Effect of vit-amin C on glycosylation of proteins. D i a -betes 41:167–173, 1992
7 . Tack CJJ, Wetzels JFM: Decreased HbA1 c
levels due to sulfonamide-induced hemol-ysis in two IDDM patients. Diabetes Care19:775–776, 1990
E n t e ro v i rus Antibodies in Relation to Islet CellAntibodies in Tw oPopulations Wi t hHigh and Low Incidence of Type 1 Diabetes
En t e ro v i rus infections are among themost suspect environmental factors inthe pathogenesis of type 1 diabetes
(1–3). The present study was aimed attesting the hypothesis that the markedi n t e rnational variation in the incidence oftype 1 diabetes may re flect diff e rences in
the epidemiology of entero v i rus infectionsin various countries. We measured entero-v i rus antibody levels and islet cell anti-body (ICA) prevalence in healthy school-c h i l d ren in two geographically nearbycountries, Finland and Lithuania, that dif-fer in the incidence of type 1 diabetes. Fin-land has the highest incidence in theworld, whereas in Lithuania, the incidenceis substantially lower (averages of 35 per100,000 and 7 per 100,000, re s p e c t i v e l y,in 0- to 14-year-old children during1983–1992) (4).
S e rum samples were collected during1994 from 1,049 unaffected Lithuanians c h o o l c h i l d ren living within the region ofKaunas and from 3,651 unaff e c t e dFinnish schoolchildren living in nort h e rn
Finland. We analyzed entero v i rus antibod-ies from 200 age- and sex-matched pairsof Finnish and Lithuanian ICA2 c h i l d re n(38% male, mean age 10.8 years). ICA1
s e rum samples were available from 102Finnish children (50% male, mean age11.8 years) and 23 Lithuanian childre n(48% male, mean age 11.6 years).
G ro u p - s p e c i fic IgG class entero v i ru santibodies were analyzed against a syn-thetic peptide and purified Coxsackie Bv i rus (CBV) 4 by enzyme-linked immuno-sorbent assay as previously described (1).S e rotype specific antibodies against CBV4and CBV5 serotypes, which have been con-nected to type 1 diabetes as well asp o l i o v i rus type 1, were analyzed using stan-d a rd plaque neutralization test. Hepatitis A
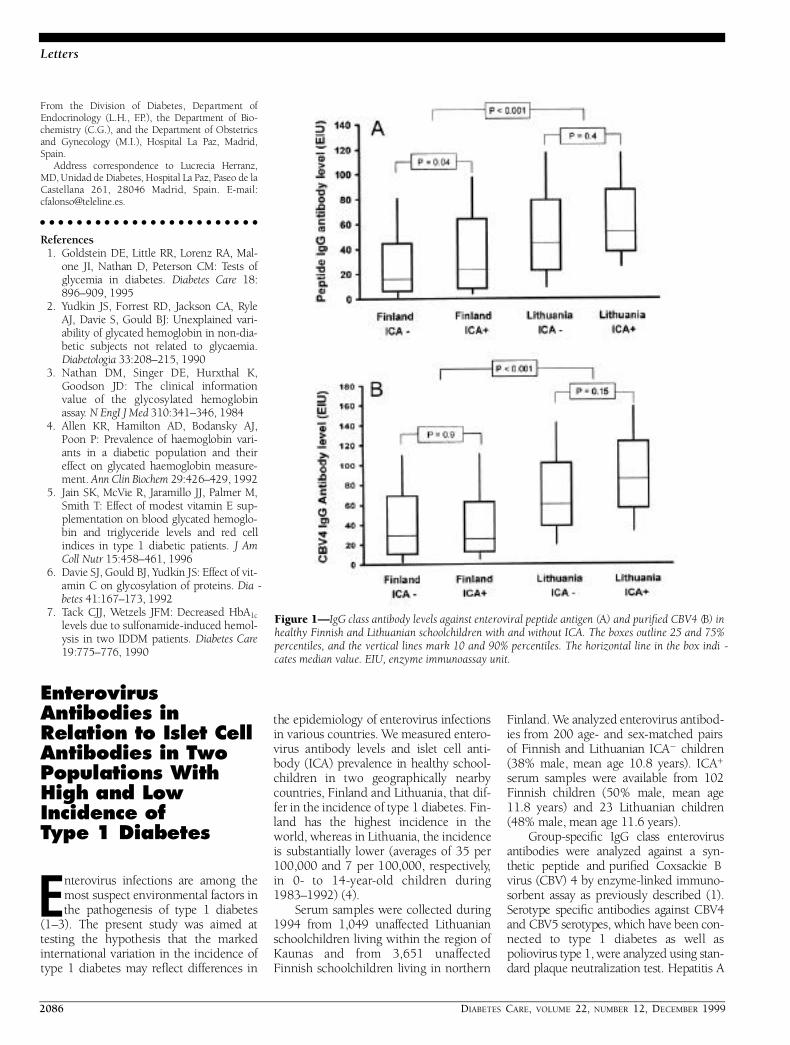
Figure 1—IgG class antibody levels against enteroviral peptide antigen (A) and purified CBV4 (B) inhealthy Finnish and Lithuanian schoolchildren with and without ICA. The boxes outline 25 and 75%percentiles, and the vertical lines mark 10 and 90% percentiles. The horizontal line in the box indi -cates median value. EIU, enzyme immunoassay unit.

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2087
Letters
v i rus antibodies were measured using theEnzygnost Anti HAV kit (BehringwerkeAG, Marburg, Germany). ICA in theFinnish sera were analyzed as pre v i o u s l ydescribed (5). The detection limit of ICAwas 2.5 Juvenile Diabetes Foundation units( JDF U). ICA in the Lithuanian sera weredetected by indirect immunoflu o re s c e n c emethod on 4-µm cryostat sections of bloodg roup O frozen human pancreas (6). Thel o g2 endpoint titers of test samples werec o n v e rted to JDF U (7). The detection limitof ICA was 5 JDF U.
The Lithuanian ICA2 c h i l d ren hads i g n i ficantly higher entero v i rus antibodylevels than the Finnish children (Fig. 1).This diff e rence was seen in IgG levelsagainst the enteroviral peptide antigen (P , 0.001) and purified CBV4 virions(P , 0.001), as well as in the frequency ofneutralizing antibodies against CBV4( 7 5 vs. 63%, P , 0.01) and CBV5 (65 vs.38%, P , 0.001). Seropositivity in thehepatitis virus A antibody assay was alsom o re common in the Lithuanian than theFinnish children (20 vs. 1%, P , 0 . 0 0 1 ) .H o w e v e r, the Finnish and Lithuanian chil-d ren had similar titers of neutralizing anti-bodies against poliovirus type 1, indicat-ing no diff e rence in the efficacy of poliovaccination pro g r a m s .
ICA prevalence was 2.8% among theFinnish children (8) and 2.2% among theLithuanian children. The Finnish ICA1
c h i l d ren had higher antibody levelsagainst the entero v i rus peptide antigenthan the ICA2 Finnish children (P , 0 . 0 5 ,Fig. 1). The Lithuanian ICA1 c h i l d ren hadhigher antibody levels against CBV4 thanthe Lithuanian ICA2 c h i l d ren, but the dif-f e rence remained statistically nonsignifi-cant (P = 0.15) (Fig. 1). Antibody levelsagainst other entero v i rus antigens, as wellas against hepatitis A virus, were similar inthe ICA2 and ICA1 c h i l d re n .
Higher entero v i rus antibody levels inthe Lithuanian children suggest a higherf requency of entero v i rus infections inLithuania. Higher entero v i rus antibodylevels in the ICA1 c h i l d ren than in theI C A2 c h i l d ren support the role of entero-v i rus infections in b-cell autoimmunity.Thus, the results are discrepant in anintriguing way: entero v i rus infectionsseem to be associated with b-cell autoim-m u n i t y, which is in line with pre v i o u sstudies (1–3), and yet it looks as if theseinfections were more frequent in Lithua-nia, with a lower diabetes incidence, thanin Finland.
In addition to entero v i rus infections,hepatitis A virus infections were alsoshown to be less frequent in Finland thanin Lithuania. The epidemiology of viru s e swith fecal-oral transmission, such ase n t e ro v i ruses and hepatitis A virus, ishighly dependent on climatic and socio-economic factors. Accord i n g l y, climaticd i ff e rences between Finland and Lithuania(mean annual temperatures 2 vs. 6°C inthe regions of serum collection), as well ashigher socioeconomic status in Finland( g ross national products $18,850 vs.$1,350 per capita at the time of the seru mcollection), may explain the lower fre-quency of these infections in Finland.
This is the first study evaluating therelationship between the incidence oft y p e 1 diabetes and the frequency ofe n t e ro v i rus infections in diff e rent popula-tions. The inverse relationship betweenthe two suggests that the high diabetesincidence in Finland is not due to a gener-ally high frequency of entero v i rus infec-tions in the Finnish population. However,it is still possible that diabetogenic entero-v i rus strains are more common in Finlandthan in Lithuania, which could part l yexplain the higher diabetes incidence inFinland. It is also possible that entero v i ru sinfections occurring neonatally or in uterore p resent a greater risk in Finland andother countries with low frequency ofe n t e ro v i rus infections, because in thesecountries, maternal entero v i rus antibodylevels are low and give no protection tothe child. Entero v i rus infections duringthese early ages may be part i c u l a r l yi m p o rtant in the pathogenesis of type 1diabetes, as suggested in recent pro s p e c-tive studies (1,2,9).
Taken together, the results show thatat the population level, a high frequency ofe n t e ro v i rus infections does not necessarilylead to an increased incidence of type 1diabetes. It remains to be determined inf u rther studies whether the inverse re l a-tionship between the frequency of entero-v i rus infections and the incidence of type 1diabetes within a population will beo b s e rved also in other countries.
MARIA LÖNNROT, MD
MIKAEL KNIP, MD, PHD
DALIA MARCIULIONYTE, PHD
JUKKA RAHKO, MD
BRONE URBONAITE, MD, PHD
WILLIAM P.T. MOORE
PEKKA VILJA, PHD
HEIKKI HYÖTY, MD, PHD
F rom the JDFI—Center for Diabetes Prevention inFinland (M.L., M.K., J.R., P. V., H.H.); the Depart-ments of Vi rology (M.L., P. V., H.H.) and Pediatrics(M.K.), University of Ta m p e re Medical School andTa m p e re University Hospital, Ta m p e re; the Depart-ment of Pediatrics ( J.R.), University of Oulu, Oulu;the Department of Vi rology (H.H.), University ofTurku, Turku, Finland; the Institute of Endocrinol-ogy (D.M., B.U.), Kaunas Medical University, Kaunas,Lithuania; and the Department of Diabetes andMetabolism (W. P. T.M.), University of Bristol, Bristol,U . K .
A d d ress correspondence to Maria Lönnrot, MD,University of Ta m p e re, Medical School Depart m e n tof Vi ro l o g y, PO Box 607, FIN-33101 Ta m p e re, Fin-land. E-mail: maria.lonnro t @ u t a . fi.
A c k n o w l e d g m e n t s — This work was sup-p o rted by Juvenile Diabetes Foundation Inter-national Grants 197114 (H.H.) and 197032(M.K.), the European Community INCO-C o p e rnicus Program (contract no. 1615-CT98-0316), the Reino Lahtikari Foundation, theEmil Aaltonen Foundation, the Jalmari andRauha Ahokas Foundation, and the MedicalR e s e a rch Fund of Ta m p e re University Hospital.The Lithuanian part of the study was sup-p o rted by the European Community Con-c e rted Action EURODIAB ACE (contractB M H 1 - C T 9 2 – 0 0 4 3 ) .
We gratefully acknowledge Prof. Edwin A.Gale, Department of Diabetes and Metabolism,University of Bristol, Bristol, U.K., for hisvaluable help in the ICA analyses of theLithuanian children. We are also grateful for thee x p e rt technical assistance of E. Jokela and P.K o r a m o.
R e f e re n c e s1 . Hyöty H, Hiltunen M, Knip M, Laakkonen
M, Vähäsalo P, Karjalainen J, Koskela P,Roivainen M, Leinikki P, Hovi T, ÅkerblomHK, and the Childhood Diabetes in Fin-land (DiMe) Study Group: A pro s p e c t i v estudy of the role of coxsackie B and othere n t e ro v i rus infections in the pathogenesisof IDDM. D i a b e t e s 44:652–657, 1995
2 . Dahlquist GG, Ivarsson S, Lindberg B,F o r s g ren M: Maternal enteroviral infectionduring pregnancy as a risk factor for child-hood IDDM: a population-based case-con-t rol study. D i a b e t e s 44:408–413, 1995
3 . Hiltunen M, Hyöty H, Knip M, Ilonen J,Reijonen H, Vähäsalo P, Roivainen M, Lön-n rot M, Leinikki P, Hovi T, Åkerblom HK,the Childhood Diabetes in Finland (DiMe)Study Group: Islet cell antibody sero c o n-version in children is temporally associ-ated with entero v i rus infections. J Infect Dis175:554–560, 1997
4 . Padaiga Z, Tuomilehto J, Karvonen M,Podar T, Brigis G, Urbonaite B, KohtamakiK, Lounamaa R, Tuomilehto Wolf E,Reunanen A: Incidence trends in child-hood onset IDDM in four countries

2088 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
a round the Baltic sea during 1983–1992.D i a b e t o l o g i a 40:187–192, 1997
5 . Kulmala P, Savola K, Petersen JS, VähäsaloP, Karjalainen J, Löppönen T, Dyrberg T,Åkerblom HK, Knip M: Prediction ofinsulin-dependent diabetes mellitus in sib-lings of children with diabetes: a popula-tion-based study. J Clin Invest 1 0 1 : 3 2 7 –336, 1998
6 . Bottazzo GF, Christensen AF, Doniach D:Islet-cell antibodies in diabetes mellituswith autoimmune polyendocrine defic i e n-cies. L a n c e t ii:1279–1283, 1974
7 . Bonifacio E, Lernmark A, Dawkins RL:S e rum exchange and use of dilutions havei m p roved precision of measurement ofislet cell antibodies. J Immunol Methods106:83–88, 1988
8 . Knip M, Rahko J, Kulmala P, Vähäsalo P,Karjalainen J: Occurrence and persistenceof IDDM-associated autoantibodies inu n a ffected school children (Abstract). D i a -b e t o l o g i a 39 (Suppl. 1):A46, 1996
9 . L ö n n rot M, Korpela K, Knip M, Koskela P,Ilonen J, Simell O, Hyöty H: Entero v i ru sinfection as a risk factor for beta-cellautoimmunity in the prospective birt h -c o h o rt trial DIPP (Abstract). Eur J Endo -c r i n o l 140 (Suppl. 1):34, 1999
Troglitazone Eff i c a c yin a Subject Wi t hG l u c o c o rt i c o i d -Induced Diabetes
Troglitazone is an oral antidiabeticagent that ameliorates insulin re s i s-tance in both peripheral tissues and
liver (1). Troglitazone could be more eff e c-tive in diabetic subjects with gre a t e rinsulin resistance, estimated by homeo-stasis model insulin resistance index(HOMA-R) (2). Glucocorticoid adminis-tration, along with obesity, is one of themost common insulin-resistant conditionsthat we encounter in clinical settings. It isshown that troglitazone improved dis-turbed glucose homeostasis in glucocort i-c o i d - t reated rats (3). A pre l i m i n a ry studyalso reveals that glucocort i c o i d - i n d u c e dinsulin resistance could be reversed byt roglitazone administration in human sub-jects with normal glucose tolerance (4).H o w e v e r, the efficacy of troglitazone hasnot been demonstrated in glucocort i c o i d -induced diabetes in humans.
We have studied a 66-year-old femalein whom diabetes was induced by gluco-c o rticoid. At age 58 years, she had beendiagnosed with polymyositis. Pre d n i s o-
lone 20 mg/day was administered, andthen the dosage was tapered and main-tained at 7.5 mg/day. Before the glucocor-ticoid treatment, her fasting glucose levelwas normal, but she had a family historyof diabetes in her elder bro t h e r. She expe-rienced thirst and polyuria 4 years later (atage 62 years). She was diagnosed with dia-betes, with fasting glucose 11.9 mmol/land HbA1 c 11.6% (normal 4.3–5.8). Adosage of 5 mg glibenclamide/dayd e c reased her HbA1 c levels, but the levelsremained at ,8%. At age 66 years, shewas re f e rred to our division. Her BMI wasas low as 21.3 kg/m2. Her fasting glucosewas 5.50 mmol/l, whereas the maximalpostprandial glucose level in the daily pro-file was as high as 20.8 mmol/l. Seru minsulin concentration was 55.8 pmol/lafter fasting, but it increased to 282 pmol/lp o s t p r a n d i a l l y. Urinary excretion of C-p e p-tide was also as high as 30.8 n m o l / d a y( n o rmal 5.3–39.7). HOMA-R was calcu-lated to be 2.09, not increased to the levelat which drastic effects of tro g l i t a z o n ewould be expected (2). However, in con-sideration of the coexisting postprandialh y p e rglycemia and hyperinsulinemia,which suggests the presence of insulinresistance (5), we initially pre s c r i b e dt roglitazone 200 mg/day in addition toglibenclamide. At 1 month later, she com-plained of hypoglycemic symptoms, andthe dosage of glibenclamide was tapere d .F i n a l l y, 2 years later, 400 mg/day of tro g l i-tazone without sulfonylureas stabilizedher HbA1 c levels at ,6%. Her BMI did notchange throughout the observ a t i o nperiod, but serum leptin concentrationgradually decreased from 13.9 to 4.5 n g / m l .Plasma levels of the soluble fraction oftumor necrosis factor-a receptor 2, whichwas re p o rted to be associated positivelywith body fat and negatively with insulinsensitivity index (6), were 2,320 pg/ml( n o rmal 1,020–2,120) before the additionof troglitazone, and the levels re m a i n e dunchanged during the observation period(data not shown).
G l u c o c o rticoid-induced diabetes isoften characterized by rather normal fast-ing glucose level and abnorm a l l yi n c reased postprandial glucose excursion.In this context, we thought it adequatethat the prediction of insulin re s i s t a n c emay depend on postprandial glucose andinsulin levels rather than HOMA-R andmade a trial of troglitazone administration.C o n s e q u e n t l y, the remarkable and sus-tained efficacy of troglitazone was demon-
strated. In other words, her hyperg l y c e m i amight be attributable mainly to insulinresistance, but not to deficient insulins e c retion. The underlying mechanisms ofg l u c o c o rticoid-induced insulin re s i s t a n c eand its reversal by thiazolidinediones seemto be multifactorial. It seems possible thatboth glucocorticoid and thiazolidine-diones can affect the postreceptor signal-ing cascade of insulin, although few stud-ies have examined the interaction betweenthese agents (7). The thiazolidinedionesbind to peroxisome pro l i f e r a t o r- a c t i v a t e dre c e p t o r-g mainly expressed in adipocytesand ameliorate the “bad” metabolism andsignals that cause insulin resistance (8).The decrease in serum leptin concentra-tions by troglitazone in this subject mayre flect the improvement in such alter-ations of adipocyte metabolism. Furt h e ranalysis is necessary to confirm the benefi-cial effects of thiazolidinediones on gluco-c o rticoid-induced insulin re s i s t a n c e .
KAZUTOSHI FUJIBAYASHI, MD
SHOICHIRO NAGASAKA, MD
NAOKI ITABASHI, MD
AKIO KAWAKAMI, MD
TOMOATSU NAKAMURA, MD
IKUYO KUSAKA, MD
SAN-E ISHIKAWA, MD
TOSHIKAZU SAITO, MD
F rom the Division of Endocrinology and Metabo-lism, Department of Medicine, Jichi Medical School,Minamikawachi, Tochigi, Japan.
A d d ress correspondence to Shoichiro Nagasaka,MD, Division of Endocrinology and Metabolism,D e p a rtment of Medicine, Jichi Medical School,Yakushiji 3311-1, Minamikawachi, Tochigi 329-0498, Japan. E-mail: [email protected].
R e f e re n c e s1 . Saltiel AR, Olefsky JM: Thiazolidinediones
in the treatment of insulin resistance andtype II diabetes. D i a b e t e s 4 5 : 1 6 6 1 – 1 6 6 9 ,1 9 9 6
2 . Nagasaka S, Iwamoto Y, Ishikawa S,Kuzuya T, Saito T: Troglitazone eff i c a c ym e a s u red by insulin resistance index (Let-ter). L a n c e t 350:184, 1997
3 . Okumura S, Takeda N, Takami K, Yo s h i n oK, Hattori J, Nakashima K, Sugimoto M,Ishimori M, Takami R, Yasuda K: Effects oft roglitazone on dexamethasone-inducedinsulin resistance in rats. M e t a b o l i s m 4 7 :351–354, 1998
4 . Willi SM, Kennedy A, Wallace P, GanawayE, Wojciechowski B, Garvey WT: Tro g l i t a-zone prevents glucocort i c o i d - i n d u c e dinsulin resistance in humans (Abstract).D i a b e t e s 48 (Suppl. 1):75A, 1999
5 . Nagasaka S, Ishikawa S, Saito T: Comment

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2089
Letters
on glucose-to-insulin ratio as a measure ofinsulin sensitivity in women with PCOS(Letter). J Clin Endocrinol Metab 8 4 : 3 8 3 ,1 9 9 9
6 . F e rnandez-Real J-M, Broch M, Ricart W,Casamitjana R, Gutierrez C, Ve n d rell J,R i c h a rt C: Plasma levels of the solublefraction of tumor necrosis factor receptor 2and insulin resistance. D i a b e t e s 4 7 : 1 7 5 7 –1762, 1998
7 . Weinstein SP, Holand A, O’Boyle E, HaberRS: Effects of thiazolidinediones on gluco-c o rticoid-induced insulin resistance andGLUT4 glucose transporter expression inrat skeletal muscle. M e t a b o l i s m 4 2 : 1 3 6 5 –1369, 1993
8 . Okuno A, Tamemoto H, Tobe K, Ueki K,Mori Y, Iwamoto K, Umesono K, Aka-numa Y, Fujiwara T, Horikoshi H, Ya z a k iY, Kadowaki T: Troglitazone increases thenumber of small adipocytes without thechange of white adipose tissue mass inobese Zucker rats. J Clin Invest 1 0 1 : 1 3 5 4 –1361, 1998
Safety of Human Insulin in P o o r-Sighted ElderlyDiabetic Patients
Pre l i m i n a ry re p o rts and the opinion ofpatients did not completely eliminatethe belief that human insulin may be
d a n g e rous, particularly during the transferf rom animal insulin (1).
It is true that the efficacy of humaninsulin was not fully evaluated on a larg escale or in long-term randomized con-t rolled trials, nor were its adverse eff e c t s .
In one study (2), we assessed theglycemic control and tolerance during thetransfer from animal to human insulin. Wefound that all of our 46 type 1 diabeticpatients were efficiently and safelyswitched from animal to human insulin,without aggravating the incidence ofhypoglycemia, in spite of two major riskfactors, namely advanced age (the oldestpatient was 92 years old) and long-stand-ing diabetes of ,20 years’ duration.
In the present study, we investigatedthe transfer to human insulin adminis-t e red with a pen, as opposed to syringe foranimal insulin, in 30 elderly diabeticpatients (mean age 60.5 ± 15.1 years) whohad a long diabetes duration of 25.7 ±10.9 years and also had deterioratedvision. Diabetic retinopathy was detectedin 69% of patients. Among these, it was
n o n p roliferative in 60%, pre p ro l i f e r a t i v ein 10%, and proliferative in 30%. Of allpatients, 62% had cataracts. Mean visualacuity in the left eye was 5.3/10 ± 3.5,Parinaud scale 3.0 ± 2.6, and in the righteye 5.8/10 ± 3.6, Parinaud scale 3.4 ± 3.3( n o rmal Parinaud value = 2 ) .
The aim of the study in this part i-cular population was evaluation after2 months of glycemic control, hypogly-cemic attacks, treatment satisfaction,and degree of autonomy. The Student’s ttest and the rank-sum test were usedwhen appro p r i a t e .
At the end of study, the median doseof human insulin was 32 U/day (8–74),s i g n i ficantly lower (P = 0.04) than the ini-tial dosage of animal insulin of 36 U/day(14–150). HbA1 c d e c reased from 8.6%(6.4–12.1) to 8.45% (7.0–10.7) (P =0.02). Only one patient experienced a sin-gle severe hypoglycemic episode. Biologi-cal hypoglycemia (,60 mg/dl) was nevero b s e rved in 67% of patients.
At inclusion, patients mildly satisfie dwith the previous treatment were ratherautonomous: 77% were injecting insulinwithout assistance. General health condi-tion was altered, anxiety was a pre d o m i-nant feeling, and 60% were depressed. Atthe end of the study, patients were signifi-cantly (P = 0.009) more satisfied with thenew treatment and the autonomy ratei n c reased: 85% were injecting insulinthemselves. The subjects’ general healthcondition improved significantly (P =0.003). These benefits were remarkable inthe vision-impaired patients: 83% pro-ceeded to auto-injections in comparisonwith 71%, 83% considered the new tre a t-ment more practical, and 50% felt morea u t o n o m o u s .
I m p rovement in the subjects’ qualityof life and autonomy was probably re l a t e dto the use of an insulin pen in poor-sighted elderly patients not frightened bychanging habits. Amelioration of glucosehomeostasis without increase of hypogly-cemia re a s s u res us about the safety ofhuman insulin.
JEAN-JACQUES ALTMAN, MD, PHD
NEGIB ELIAN, MD
MIREILLE BONNEMAIRE, MD
STÉPHANE CALMAR, PHD
SYLVIE FELDMAN, MD
F rom the Service de Diabétologie-Nutrition (J . - J . A . ,N.E., S.F.), Hôpital Laënnec, Paris; and the Labora-t o i re Novo Nordisk (M.B., S.C.), Boulogne-Billan-c o u rt, France.
A d d ress correspondence to Jean-Jacques Altman,MD, PhD, Hôpital Laënnec, 42 rue de Sèvres, 75340Paris Cedex 07, France. E-mail: [email protected] p - h o p - p a r l s . f r.
R e f e re n c e s1 . Hirst J: Adverse effects of human insulin
(Letter). Lancet 352:1710, 19982 . Feldman S, Bonnemaire M, Elian N, Alt-
man JJ, and the investigators of TRANS-F E RT Study: Tr a n s f e rring aged type 1 dia-betic patients from animal to humaninsulin: a randomized study. Diabetes Care21:196–197, 1998
Assessment of In Vivo Stability ofa New InsulinP reparation forImplantable InsulinPumps
A randomized multicenterp rospective trial
Programmable implantable insulinpumps have proven to be safe ande ffective devices for achieving good
metabolic control (1) and decreasing therisk of severe hypoglycemia (2). In 1993,changes in the insulin production pro c e s sresulted in increased insulin pre c i p i t a t i o nin the pumps, worsening the clinical per-f o rmances of the devices. EvaluationDans le Diabète du Traitement parImplants Actifs (EVADIAC) pro p o s e di m p roved pump rinse pro c e d u res and as h o rtening of the interval between re fil l s(3), and the MiniMed catheter wasi m p roved. Hoechst Marion Roussel( F r a n k f u rt, Germany) produced a newinsulin variant (21 PH ETP). EVA D I A Cdesigned a protocol study to examine thein vivo stability of 21 PH ETP using amulticentric, prospective randomizedstudy with intervals of 3 months as com-p a red with 45 days between re fil l s .
A total of 176 patients were random-ized into two groups, G45 (45 days) andG90 (90 days), between re fills. The studycriteria was the accuracy of insulin infu-sion with 21 PH ETP (human semi-synthetic insulin, Genapol stabilized,4 0 0 U/ml; Hoechst).
A total of 196 MiniMed MIP 2001(MiniMed Technologies, Sylmar, CA)pumps were studied: 122 (pumps A)

2090 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
without polyethylene-polypropylene gly-col coating, previously used with otherbatches of insulin and washed with analkaline pro c e d u re before the study, and74 new pumps (pumps B) with polyethyl-e n e - p o l y p ropylene glycol coating on thei n s i d e .
The infusion accuracy (% error) wascalculated as the ratio between theore t i c a land real volume infused diff e rence overthe theoretical volume infused.
The evolution of percent erro r, i.e., t h edelta of % (D%) error at 6, 9, and 12 m o n t h svs. 3 months, was compare d between G4 5
and G9 0 and between pumps A and B,using nonpaire d t tests. An analysis of vari-ance was used to determine whether G4 5,G9 0, pumps A or B, and high percent erro rw e re re l a t e d .
R e s u l t sA total of 88 pumps were randomized intoG4 5 and 108 pumps into G9 0. There wasno diff e rence between G4 5 and G9 0 i nt e rms of D% error at 6, 9, and 12 monthsas compared with 3 months.
H o w e v e r, pumps B showed a gre a t e rD% error at 6 months (P = 0.006 for G4 5
and 0.024 for G9 0). This higher increase inthe percent error tended to attenuate dur-ing the following months. The analysis ofvariance showed that independently fro mg roups G4 5 and G9 0, pumps B presented ahigher percent error than pumps A (P =0 . 0 0 0 3 ) .
On the basis of the results of this studywe may conclude that the stability of 21PH ETP was comparable at 90 days to thatat 45 days in implantable pumps in vivo.As this study was not designed to comparethe two groups of pumps together, the dif-f e rence observed between pumps A andpumps B must be interpreted with cau-tion. This problem is currently underi n v e s t i g a t i o n .
We conclude that using 21 PH ETP,the clinical perf o rmances of implantablepumps are comparable in intervals of 45and 90 days between re fills and that anacceptable 3-month interval betweenre fills may be pro p o s e d .
SOPHIE BOIVIN, MD
PAULINE BELICAR, MD
VINCENT MELKI, MD
EVADIAC GROUP
F rom the Service d’Endocrinologie et MaladiesMétaboliques (S.B.), Hôpitaux Universitaires deS t r a s b o u rg, Strasbourg; Service d’EndocrinologieMaladies Métaboliques et Nutrition (P.B.), CHRU de
Marseille, Hôpital La Timone, Marseille; Serv i c ed’Endocrinologie-Diabétologie (V.M.), CHU Rangueil,Toulouse, France.
A d d ress correspondence to Sophie Boivin, MD,S e rvice d’Endocrinologie et Maladies Métaboliques,Hôpitaux Universitaires de Strasbourg, 1 Place del’Hôpital, 67091 Strasbourg cedex, France.
A c k n o w l e d g m e n t s — We are grateful toSylvie Boullu-Sanchis, MD, for her support instatistical analysis.
R e f e re n c e s1 . Pinget M, Jeandidier N: Long-term safety
and efficacy of intraperitoneal insulin infu-sion by means of implantable pumps.H o rm Met Res 30:475–486, 1998
2 . Jeandidier N, Selam JL, Renard E, Guerc iB, Lassmann-Vague V, Rocher L, Hanaire -B routin H, EVADIAC Study Gro u p :D e c reased severe hypoglycemia fre q u e n c yduring intraperitoneal insulin infusionusing programmable implantable pumps(Letter). Diabetes Care 19:780, 1996
3 . Boivin S, Jeandidier N, Boullu S, Pinget M:Impact of recent changes in the manage-ment of implantable pumps: reduction ofpump/catheter dysfunctioning (Abstract).H o rm Metab Res 29:A2, 1997
In Diabetes Care ,Moving From Compliance toA d h e rence Is NotE n o u g h
Something entirely diff e rent is needed
We had two distinct reactions to theappearance of the recent article byLutfey and Wishner (1) entitled
“Beyond ‘compliance’ is ‘adherence’.” Ourfirst reaction was that it was good to see ana rticle, especially one coauthored by ap rominent endocrinologist, that addre s s e dseveral key issues related to patient-p rovider relationships. We concur withand applaud their discussions of thei m p o rtance of patient-centered care, thes h o rtcomings of traditional compliancea p p roaches, and the need for a more psy-chosocial paradigm.
At the same time, we were disap-pointed that these authors had notre f e rred to a large body of work that hasa d d ressed and gone beyond the adhere n c ea p p roach they recommend. Import a n t
work has been conducted over the past1 5 years that bears directly on the issuesraised. Investigators working in two are a sbegan questioning the terms “compliance”and “adherence,” and the implications ofuse of these terms, about 15 years ago.
Anderson (2) suggested that the use ofthe constructs “compliance” and “adher-ence” were counter- p roductive becausethey both construed the problem to be thep a t i e n t ’s behavior—one of the main pointsin the article by Lutfey and Wi s h n e r. Thiswas one of the earlier articles on theire m p o w e rment approach, which they havere fined and evaluated over the years. Keycontributions of this approach includeexplicitly contrasting the underlyingassumptions and consequences of adopt-ing a traditional compliance-based med-ical model approach with the patient-cen-t e red empowerment approach (3); theexplicit identification of problems with thet e rm “adherence” as an alternative to“compliance” (4); and the developmentand validation of both empowerm e n t -based interventions for patients, ande m p o w e rment training programs for pro-fessionals (4,5).
The second early body of work ques-tioning the usefulness of compliance anda d h e rence terminology was based onempirical, logical, and methodologicalg rounds. Both Johnson and colleagues(6,7) and Glasgow et al. (8) criticized thesea p p roaches based on their lack of utility;sending the wrong message to patientsand to professionals; the multidimensionaln a t u re of adherence behaviors, rather thana d h e rence being a single unitary con-s t ruct; and the dynamic nature of the re g i-men, rather than being a static standardagainst which to compare patient behav-i o r. These authors independently pro-posed the use of terms such as “self-care ”or “self-management” to describe the clus-ter of daily behaviors that patients perf o rmto manage their diabetes. This self-man-agement terminology has been widelyadopted by the American Diabetes Associ-ation and other diabetes org a n i z a t i o n s(9–11) as preferable to the terms “compli-ance” and “adhere n c e . ”
The past 5 years have seen the emer-gence of two additional approaches anda l t e rnative terms that we believe are alsop referable to adherence. The first is psy-chologically based and drawn from thework on self-determination theory by Deciet al. (12). The greatest amount of thisre s e a rch in the diabetes area has been by

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2091
Letters
Williams et al. (13). They prefer the term“autonomy motivation” to refer to the psy-chological process that drives patientbehavior change and the term “autonomys u p p o rt” to refer to actions by health carep rofessionals that enhance patient auton-omy motivation. Like empowerment (4)and self-efficacy (14), there is impre s s i v eand increasing literature supporting theutility of this appro a c h .
F i n a l l y, from a health care delivery andmedical systems perspective, Wagner (16)has promoted the concept “collaborative”or co-management of chronic illnessessuch as diabetes. Like Etzwiler (15) andthe authors cited above, Wagner pro p o s e sthat chronic illness care be based on diff e r-ent principles and concepts than acutec a re. In part i c u l a r, they emphasize thei m p o rtance of collaborative goal settingand on-going self-management support askey elements of successful disease man-agement systems (16,17).
Our second major point is that therecommendations for change proposed byLutfey and Wishner did not go far enough.A p p ropriate diabetes care re q u i res a newand fundamentally diff e rent set of roles forhealth care professionals and patients.M o d i fication of the acute-care model willnot work because its underlying assump-tions are invalid for diabetes care. Diabetesc a re re q u i res a truly collaborativea p p roach, i.e., patients and health carep rofessionals relating as equals, ratherthan the hierarchical approach embeddedin the acute-care model. Unlike the tre a t-ment of acute illnesses, patients with dia-betes are fully responsible for the self-management of their illness (18). Thisresponsibility is non-negotiable andinescapable. Although that statement maysound like a very strong assertion, webelieve it is an accurate description of thereality of diabetes self-management.
The complete responsibility thatpatients have for the self-management ofdiabetes rests on three characteristics of thedisease. First, the most important choicesa ffecting the health and well-being of a per-son with diabetes are made by that person,not by health professionals. Each day,patients make decisions about eating,physical activity, stress management, mon-itoring, etc., that are the major determ i-nants of their diabetes control. Second,patients are in control. No matter what weas health professionals do or say, patientsa re in control of these important daily self-management decisions. When patients
leave the clinic or office, they can and doveto recommendations a health pro f e s-sional makes (19), no matter how impor-tant or relevant the provider believes thoserecommendations to be. Third, the conse-quences of the choices patients make abouttheir diabetes care accrue first and fore-most to patients themselves. We cannots h a re in the risk of developing re t i n o p a t h y,n e u ro p a t h y, or cardiovascular disease norcan we share the cost to the patient’s qual-ity of life of making a commitment to rigor-ous blood glucose control. Diabetes,including its self-management, belongs tothe person with the illness.
When we acknowledge that diabetesis a self-managed disease whose re s p o n s i-bility rests with the patient, we have begunlaying the foundation for a collaborativediabetes care relationship. Collaborationre q u i res us to give up trying to be re s p o n-sible for our patients and instead becomeresponsible to them.
Although we cannot relieve patients oftheir responsibility for the self-manage-ment of diabetes, we can provide expert i s erelated to the self-management of diabetes,help them acquire the knowledge neces-s a ry to make informed decisions aboutself-management, teach self-care tech-niques, provide social and emotional sup-p o rt, offer suggestions for behavior changeand coping strategies, and create opport u-nities for our patients to re flect on thechoices they are making and the goals theyhope to achieve.
Like Lutfey and Wi s h n e r, we believethat the words (and related world views)that we use to describe patient-pro v i d e rrelationships and diabetes self-manage-ment are important. They can either facili-tate or inhibit patient empowerm e n t ,a u t o n o m y, decision-making, sense ofre s p o n s i b i l i t y, and quality of life. This iswhy we prefer terms like “collaborativediabetes management” or simply “self-management.” We believe that such a col-laborative relationship re p resents a tru eparadigm or world view shift, one inwhich the concepts of compliance ora d h e rence have no place.
RUSSELL E. GLASGOW, PHD
ROBERT M. ANDERSON, EDD
F rom the AMC Cancer Research Center, (R.E.G.),D e n v e r, Colorado; and the University of Michigan(R.M.A.), Ann Arbor, Michigan.
A d d ress correspondence to R.E. Glasgow, PhD,AMC Cancer Research Center, 1600 Pierce St., Den-v e r, CO 80214. E-mail: ru s s k p f @ e a rt h l i n k . n e t .
A c k n o w l e d g m e n t s — This article was sup-p o rted in part by National Institutes of Health Grant7 - R O 1 - D K 3 5 5 2 4 - 1 3 .
R e f e re n c e s1 . Lutfey KE, Wishner WJ: Beyond “compli-
ance” is “adherence.” Diabetes Care 2 2 :635–639, 1999
2 . Anderson RM: Is the problem of noncom-pliance all in our heads? Diabetes Educ3:1–34, 1985
3 . Anderson RM: Patient empowerment andthe traditional medical model. D i a b e t e sC a re 18:412–415, 1995
4 . Anderson RM, Funnell MM, Barr PADedrick RF, Davis WK: Learning toempower patients: results of a pro f e s s i o n a leducation program for diabetes educators.Diabetes Care 14:584–590, 1991
5 . Anderson RM, Funnell MM, Butler PM,A rnold MS, Fitzgerald JT, Feste CC:Patient empowerment: results of a ran-domized controlled trial. Diabetes Care18:943–949, 1995
6 . Johnson SB, Silverstein J, Rosenbloom A,C a rter R, Cunningham W: Assessing dailymanagement in childhood diabetes. H e a l t hPsychol 5:545–564, 1986
7 . Johnson SB: Methodological issues in dia-betes re s e a rch: measuring adherence. D i a -betes Care 15 (Suppl. 4):1658–1667, 1992
8 . Glasgow RE, Wilson W, McCaul KD: Regi-men adherence: a problematic construct indiabetes re s e a rch. Diabetes Care 8 : 3 0 0 –301, 1985
9 . Clement S: Diabetes self-managementeducation. Diabetes Care 1 8 : 1 2 0 4 – 1 2 1 4 ,1 9 9 5
1 0 . American Diabetes Association Task Forc eto Revise the National Standards: Nationals t a n d a rds for diabetes self-managementeducation programs. Diabetes Care 1 8 :737–741, 1995
1 1 . American Diabetes Association: Nationals t a n d a rds for diabetes self-managementeducation programs and American Dia-betes Association review criteria. D i a b e t e sC a re 21:S95–S98, 1998
1 2 . Deci EL, Eghrari H, Patrick BC, Loone DR:Facilitating internalization: the self-deter-mination theory perspective. J Pers 6 2 :119–142, 1994
1 3 . Williams GC, Freedman ZR, Deci EL: Sup-p o rting autonomy to motivate patientswith diabetes for glucose control. D i a b e t e sC a re 21:1644–1651, 1998
1 4 . Bandura A: S e l f - E fficacy: The Exercise ofC o n t rol. New York, W.H. Freeman, 1997
1 5 . Etzwiler DD: Chronic care: a need ins e a rch of a system. Diabetes Educ 2 3 : 5 6 9 –573, 1997
1 6 . Wagner EH: Population-based manage-ment of diabetes care. Patient Educ Couns26:225–230, 1995
1 7 . Glasgow RE, Wagner EH, Kaplan RM,
2092 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
Vinicor F, Smith L, Norman J: If diabetes isa public health problem, why not treat it asone? A population-based approach toc h ronic illness. Ann Behav Med 2 1 : 1 – 1 3 ,1 9 9 9
1 8 . Anderson RM, Funnell MM: PuttingHumpty Dumpty back together again.Diabetes Spectrum 12:19–23, 1999
1 9 . Hunt LM, Pugh J, Valenzuela M: Howpatients adapt diabetes self-care re c o m-mendations in everyday life. J Fam Pract46:207–215, 1998
P revalence ofPatients Reachingthe Ta rgets of GoodC o n t rol in Norm a lClinical Practice
A cohort-based study in type 2d i a b e t e s
To prevent chronic complications, thec o n t rol of diabetes must be extendedf rom blood glucose to other card i o-
vascular risk factors (1–3). Euro p e a nguidelines for the target levels of glycatedhemoglobin, blood pre s s u re, lipids, andBMI identified three classes of contro l :good, borderline, and poor (4). Accord i n gto the European Consensus (4), the targ e t sfor good control were as follows:,5 . 2 mmol/l (,200 mg/dl) for total cho-l e s t e rol; ,1.7 mmol/l (,150 mg/dl) fortriglycerides; .1.1 mmol/l (.40 mg/dl)for HDL cholesterol; #25 kg/m2 ( m e n )and #24 kg/m2 (women) for BMI;#140/90 for blood pre s s u re; and within3 SD above the mean value of the re f e r-
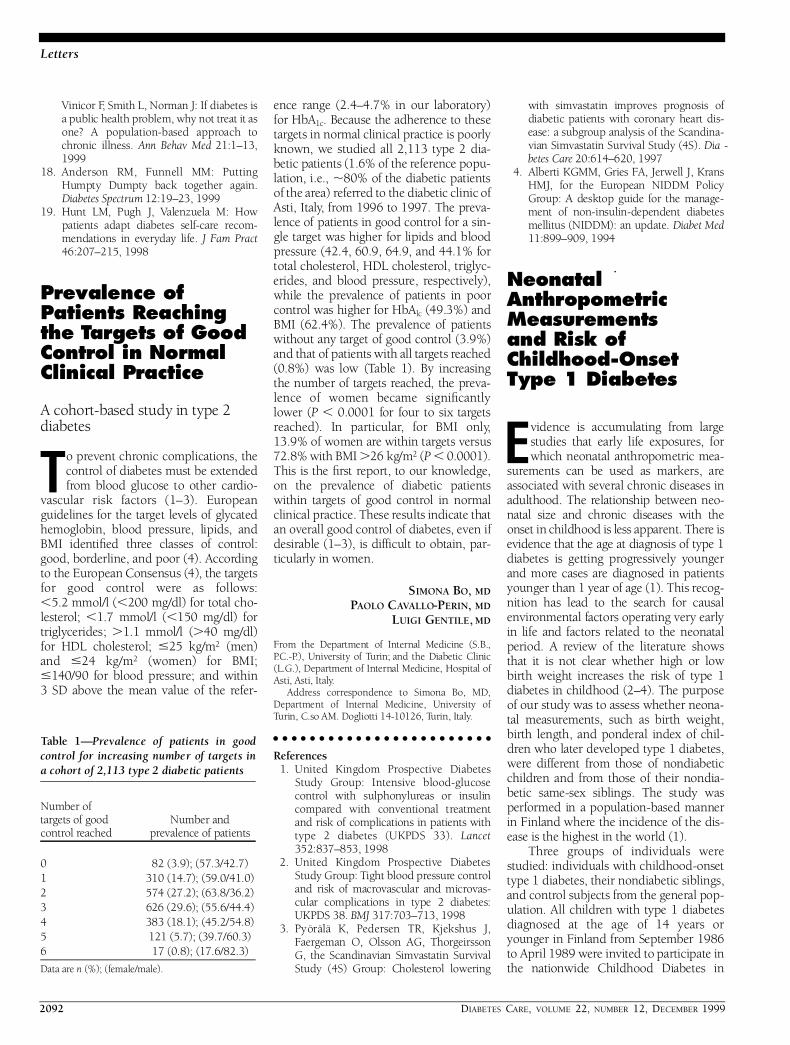
ence range (2.4–4.7% in our laboratory )for HbA1 c. Because the adherence to theset a rgets in normal clinical practice is poorlyknown, we studied all 2,113 type 2 dia-betic patients (1.6% of the re f e rence popu-lation, i.e., ,80% of the diabetic patientsof the area) re f e rred to the diabetic clinic ofAsti, Italy, from 1996 to 1997. The pre v a-lence of patients in good control for a sin-gle target was higher for lipids and bloodp re s s u re (42.4, 60.9, 64.9, and 44.1% fortotal cholesterol, HDL cholesterol, triglyc-erides, and blood pre s s u re, re s p e c t i v e l y ) ,while the prevalence of patients in poorc o n t rol was higher for HbAl c (49.3%) andBMI (62.4%). The prevalence of patientswithout any target of good control (3.9%)and that of patients with all targets re a c h e d(0.8%) was low (Table 1). By incre a s i n gthe number of targets reached, the pre v a-lence of women became signific a n t l ylower (P , 0.0001 for four to six targ e t sreached). In part i c u l a r, for BMI only,13.9% of women are within targets versus72.8% with BMI .26 kg/m2 (P , 0 . 0 0 0 1 ) .This is the first re p o rt, to our knowledge,on the prevalence of diabetic patientswithin targets of good control in norm a lclinical practice. These results indicate thatan overall good control of diabetes, even ifdesirable (1–3), is difficult to obtain, par-ticularly in women.
SIMONA BO, MD
PAOLO CAVALLO-PERIN, MD
LUIGI GENTILE, MD
F rom the Department of Internal Medicine (S.B.,P. C . - P.), University of Tu r i n ; and the Diabetic Clinic(L.G.), Department of Internal Medicine, Hospital ofAsti, Asti, Italy.
A d d ress correspondence to Simona Bo, MD,D e p a rtment of Internal Medicine, University ofTurin, C.so AM. Dogliotti 14-10126, Turin, Italy.
R e f e re n c e s1 . United Kingdom Prospective Diabetes
Study Group: Intensive blood-glucosec o n t rol with sulphonylureas or insulinc o m p a red with conventional tre a t m e n tand risk of complications in patients withtype 2 diabetes (UKPDS 33). L a n c e t352:837–853, 1998
2 . United Kingdom Prospective DiabetesStudy Group: Tight blood pre s s u re contro land risk of macrovascular and micro v a s-cular complications in type 2 diabetes:UKPDS 38. BMJ 317:703–713, 1998
3 . Pyörälä K, Pedersen TR, Kjekshus J,F a e rgeman O, Olsson AG, Thorg e i r s s o nG, the Scandinavian Simvastatin Surv i v a lStudy (4S) Group: Cholesterol lowering
with simvastatin improves prognosis ofdiabetic patients with coro n a ry heart dis-ease: a subgroup analysis of the Scandina-vian Simvastatin Survival Study (4S). D i a -betes Care 20:614–620, 1997
4 . A l b e rti KGMM, Gries FA, Jerwell J, KransHMJ, for the European NIDDM PolicyG roup: A desktop guide for the manage-ment of non-insulin-dependent diabetesmellitus (NIDDM): an update. Diabet Med11:899–909, 1994
Neonatal A n t h ro p o m e t r i cM e a s u rements and Risk of C h i l d h o o d - O n s e tType 1 Diabetes
Evidence is accumulating from larg estudies that early life exposures, forwhich neonatal anthropometric mea-
s u rements can be used as markers, areassociated with several chronic diseases inadulthood. The relationship between neo-natal size and chronic diseases with theonset in childhood is less apparent. There isevidence that the age at diagnosis of type 1diabetes is getting pro g ressively youngerand more cases are diagnosed in patientsyounger than 1 year of age (1). This re c o g-nition has lead to the search for causale n v i ronmental factors operating very earlyin life and factors related to the neonatalperiod. A review of the literature showsthat it is not clear whether high or lowb i rth weight increases the risk of type 1diabetes in childhood (2–4). The purposeof our study was to assess whether neona-tal measurements, such as birth weight,b i rth length, and ponderal index of chil-d ren who later developed type 1 diabetes,w e re diff e rent from those of nondiabeticc h i l d ren and from those of their nondia-betic same-sex siblings. The study wasp e rf o rmed in a population-based mannerin Finland where the incidence of the dis-ease is the highest in the world (1).
T h ree groups of individuals werestudied: individuals with childhood-onsettype 1 diabetes, their nondiabetic siblings,and control subjects from the general pop-ulation. All children with type 1 diabetesdiagnosed at the age of 14 years oryounger in Finland from September 1986to April 1989 were invited to participate inthe nationwide Childhood Diabetes in
Table 1—P revalence of patients in goodc o n t rol for increasing number of targets ina cohort of 2,113 type 2 diabetic patients
Number of t a rgets of good Number and c o n t rol re a c h e d p revalence of patients
0 82 (3.9); (57.3/42.7)1 310 (14.7); (59.0/41.0)2 574 (27.2); (63.8/36.2)3 626 (29.6); (55.6/44.4)4 383 (18.1); (45.2/54.8)5 121 (5.7); (39.7/60.3)6 17 (0.8); (17.6/82.3)
Data are n (%); (female/male).

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2093
Letters
Finland Study (DiMe). Of the 801 familiesinvited, 782 participated. The pre s e n tstudy included 373 boys and 289 girlswith type 1 diabetes. Data were also col-lected for 773 siblings aged 3–19 years. Ofthose, 311 boys and 352 girls had theirb i rth-size data available. The sibling con-t rol subjects were selected on the basis ofbeing the oldest child of the same sex inthe family of the proband. There were 54siblings who had developed diabetes whow e re excluded from analyses. Birth date–and sex-matched nondiabetic control chil-d ren, 363 boys and 313 girls, were ran-domly selected from the Finnish nationalpopulation re g i s t ry. In all three studyg roups, pre m a t u re ($2 weeks beforet e rm) children and children born to dia-betic mothers or mothers with gestationaldiabetes were excluded from the analysis.
Means of birth weight (g), birth length(cm), and ponderal index {weight [kg]:[length (m)]3} between groups were com-p a red with the paired Student’s t t e s t .
The results are given in Table 1. Nei-ther birth weight, birth length, nor pon-deral index was significantly diff e re n tbetween type 1 diabetic case subjects andtheir nondiabetic sibling control subjectsin either sex (P . 0.1 in all instances).Boys with type 1 diabetes had a slightly,but not signific a n t l y, higher birth weightand birth length than their nondiabeticsiblings and a significantly higher birt hweight and birth length compared withthe control boys (P = 0.035 and P = 0.007,respectively). The girls with type 1 dia-betes were taller at birth than the contro lgirls (P = 0.042). The correlation analysisrevealed that neither birth weight, birt h
length, nor ponderal index was related tothe age at diagnosis of type 1 diabetes (r ,0.05 in all instances).
It has been documented that childre nwith type 1 diabetes are taller than theirpeers before or at the time of diagnosis (5).We may speculate that this observation isto some extent true already at birth. Onthe other hand, we were not able to docu-ment any diff e rences in birth length withinfamilies of type 1 diabetic probands. Theoldest siblings of the same sex of thep roband did not differ in neonatal mea-s u rements in any respect from thep roband. This could mean that both birt hlength and weight are genetically deter-mined in families to a greater extent thantype 1 diabetes is. On the other hand, thepower to obtain statistically significant dif-f e rence between the boys with type 1 dia-betes and their siblings was not high. Therea re no previous studies where the anthro-pometric parameters at birth of type 1 d i a-betic children were compared with thoseof their nondiabetic siblings.
B i rth weight was higher in boys withtype 1 diabetes, but not in girls, compare dwith matched control subjects from thegeneral population. In 1989, Rewers et al.(6) in Poland showed that newborn seither .4,000 or ,2,000 g were at ani n c reased risk of type 1 diabetes. In 1992,Metcalfe and Baum (7) found the birt hweight of British children who developedtype 1 diabetes to be higher than that ofthe control subjects. Also, Dahlquist et al.(8) re p o rted in 1996 that lower birt hweight and intrauterine growth re t a rd a-tion were associated with a lower risk oftype 1 diabetes in Sweden.
If there is an association between theb i rth weight and the risk of type 1 diabetes,it may be U-shaped instead of linear. Atvalues in the physiological range and itsv i c i n i t y, the effect of reduced weight andintrauterine growth might be in favor ofreducing the risk of type 1 diabetes. Inc h i l d ren with a severe weight deficit atb i rth, various disturbances of the develop-ing organism might take the pre p o n d e r-ance. The risk of type 1 diabetes due tolower birth weight might thus be modifie dby two diff e rent factors: 1) by decre a s i n gthe demand of insulin at moderate birt hweight deficit (and perhaps increasing it athigher birth weight values); and 2) by pre-disposing to diabetes by a qualitatively dif-f e rent mechanism at more severe birt hweight deficit and pre m a t u r i t y.
In conclusion, birth length influ e n c e dthe risk of developing type 1 diabetes inchildhood more than birth weight: Babieswho developed type 1 diabetes in child-hood were taller at birth than their nondi-abetic peers. Basic neonatal anthro p o m e t-ric parameters of children with type 1 dia-betes do not differ from those of theirnondiabetic siblings of the same sex in theFinnish population.
TOOMAS PODAR, MD
PÄIVI ONKAMO, MSC
TOM FORSEN, MD
MARJATTA KARVONEN, MD
EVA TUOMILEHTO-WOLF, MD
JAAKKO TUOMILEHTO, MD
THE DIME STUDY GROUP
F rom the Hospital of Endocrinology (T. P.), Clinicumof the University of Ta rtu, Ta rtu, Estonia; and theDiabetes and Genetic Epidemiology Unit (P.O., T. F. ,M.K., E.T. - W., J.T.), Department of Epidemiologyand Health Promotion, National Public Health Insti-tute, Helsinki, Finland.
A d d ress correspondence to Jaakko Tu o m i l e h t o ,MD, Diabetes and Genetic Epidemiology Unit,D e p a rtment of Epidemiology and Health Pro m o t i o n ,National Public Health Institute, Mannerh e i m i n t i e166, FIN-00300 Helsinki, Finland. E-mail: jaakko.t u o m i l e h t o @ k t l . fi.
R e f e re n c e s1 . Tuomilehto J, Vi rtala E, Karvonen M,
Lounamaa R, Pitkäniemi J, Reunanen A,Tu o m i l e h t o - Wolf E, Toivanen L: Incre a s ein incidence of insulin-dependent diabetesmellitus among children in Finland. Int JE p i d e m i o l 24:984–992, 1995
2 . Khan N, Couper JJ: Low-birt h - w e i g h tinfants show earlier onset of IDDM. D i a -betes Care 17:653–656, 1994
3 . L a w l e r-Heavner J, Cruickshanks KJ, Hay
Table 1—B i rth weight, birth length, and ponderal index in type 1 diabetic probands, nondiabeticsiblings, and control children by sex
P ro b a n d s Type 1 P ro b a n d sversus d i a b e t i c v e r s u s C o n t ro l
S i b l i n g s s i b l i n g s p ro b a n d s c o n t rol subjects c h i l d re n
B o y sB i rth weight (g) 3,671 ± 482 0 . 7 5 1 * 3,716 ± 461 0 . 0 3 5 3,639 ± 484B i rth length (cm) 50.9 ± 2.2 0 . 2 8 9 51.2 ± 1.9 0 . 0 0 7 50.8 ± 2.0Ponderal index 27.5 ± 2.3 0 . 3 0 1 27.7 ± 2.5 0 . 3 5 4 27.6 ± 2.4
G i r l sB i rth weight (g) 3,569 ± 488 0 . 1 3 2 3,564 ± 480 0 . 4 9 0 3,520 ± 460B i rth length (cm) 50.4 ± 2.0 0 . 9 8 0 50.4 ± 1.9 0 . 0 4 2 50.1 ± 1.8Ponderal index 27.7 ± 2.6 0 . 1 8 1 27.7 ± 2.4 0 . 1 1 0 27.9 ± 2.4
Data are means ± SD or P. There were 129 pairs of boys and 103 pairs of girls for matched pro b a n d - s i b l i n ganalysis and 335 pairs of boys and 282 pairs of girls for matched pro b a n d – c o n t rol subject analysis. *P v a l u erefers to the matched pair analysis.
2094 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
W W, Gay EC, Hamman RF: Birth size andrisk of insulin-dependent diabetes mellitus(IDDM). Diabetes Res Clin Pract 2 4 : 1 5 3 –159, 1994
4 . Bock T, Pedersen CR, Volund A, PallesenCS, Buschard K: Perinatal determ i n a n t samong children who later develop IDDM.Diabetes Care 17:1154–1157, 1994
5 . Blom L, Persson LA, Dahlquist G: A highlinear growth is associated with ani n c reased risk of childhood diabetes melli-tus. D i a b e t o l o g i a 35:528–533, 1992
6 . Rewers MJ, Grudziak A, Orzegowska E,Zygmunt A, Machczynski M, Stone RA,Walczak M, Norris J, Jozwiak M: The riskof development of type 1 (insulin-depen-dent) diabetes in childhood depends onm a t e rnal age and birth weight (Abstract).D i a b e t o l o g i a 32:532A, 1989
7 . Metcalfe MA, Baum JD: Family character-istics and insulin-dependent diabetes. A rc hDis Child 67:731–736, 1992
8 . Dahlquist G, Sandberg S, Källen B: Intra-uterine growth pattern and risk of child-hood onset insulin dependent (type 1 )diabetes: population based case-contro ls t u d y. B M J 313:1174–1177, 1996
All Patients Wi t hWe rn e r ’s Syndro m eA re Insulin Resistant,But Only Those WhoAlso Have Impaire dInsulin Secre t i o nDevelop OvertD i a b e t e s
Ab n o rmalities in insulin secre t i o n ,insulin action, or both contribute tothe development of diabetes, but the
relative contributions of these two factorsa re not fully elucidated. Insulin re s i s t a n c eis usually associated with glucose intoler-ance and diabetes, but insulin re s i s t a n c emay not necessarily result in glucose intol-erance if hypersecretion of insulin cancompensate for the insulin resistance. Ifthis is the case, then only subjects withi m p a i red insulin secre t o ry capacity willdevelop diabetes in the presence of insulinresistance. One way to address this possi-bility is to study the relationship betweenglucose tolerance and insulin secre t o rycapacity in syndromes with extre m einsulin resistance, such as insulin re c e p t o rmutations and We rn e r ’s syndro m e .
We rn e r ’s syndrome is a rare disord e rwith autosomal recessive inheritance, char-
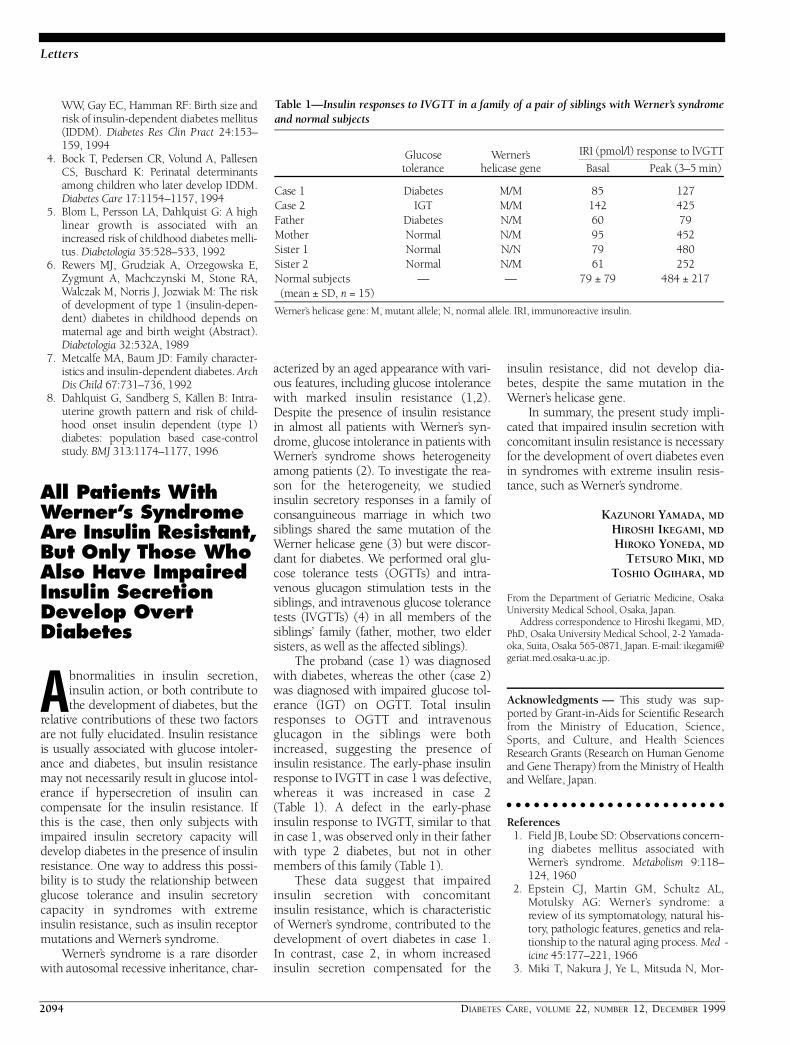
acterized by an aged appearance with vari-ous features, including glucose intolerancewith marked insulin resistance (1,2).Despite the presence of insulin re s i s t a n c ein almost all patients with We rn e r ’s syn-d rome, glucose intolerance in patients withWe rn e r ’s syndrome shows hetero g e n e i t yamong patients (2). To investigate the re a-son for the hetero g e n e i t y, we studiedinsulin secre t o ry responses in a family ofconsanguineous marriage in which twosiblings shared the same mutation of theWe rner helicase gene (3) but were discor-dant for diabetes. We perf o rmed oral glu-cose tolerance tests (OGTTs) and intra-venous glucagon stimulation tests in thesiblings, and intravenous glucose tolerancetests (IVGTTs) (4) in all members of thesiblings’ family (father, mother, two eldersisters, as well as the affected siblings).
The proband (case 1) was diagnosedwith diabetes, whereas the other (case 2)was diagnosed with impaired glucose tol-erance (IGT) on OGTT. Total insulinresponses to OGTT and intravenousglucagon in the siblings were bothi n c reased, suggesting the presence ofinsulin resistance. The early-phase insulinresponse to IVGTT in case 1 was defective,w h e reas it was increased in case 2( Ta b l e 1). A defect in the early-phaseinsulin response to IVGTT, similar to thatin case 1, was observed only in their fatherwith type 2 diabetes, but not in othermembers of this family (Table 1).
These data suggest that impaire dinsulin secretion with concomitantinsulin resistance, which is characteristicof We rn e r ’s syndrome, contributed to thedevelopment of overt diabetes in case 1.In contrast, case 2, in whom incre a s e dinsulin secretion compensated for the
insulin resistance, did not develop dia-betes, despite the same mutation in theWe rn e r ’s helicase gene.
In summary, the present study impli-cated that impaired insulin secretion withconcomitant insulin resistance is necessaryfor the development of overt diabetes evenin syndromes with extreme insulin re s i s-tance, such as We rn e r ’s syndro m e .
KAZUNORI YAMADA, MD
HIROSHI IKEGAMI, MD
HIROKO YONEDA, MD
TETSURO MIKI, MD
TOSHIO OGIHARA, MD
F rom the Department of Geriatric Medicine, OsakaUniversity Medical School, Osaka, Japan.
A d d ress correspondence to Hiroshi Ikegami, MD,PhD, Osaka University Medical School, 2-2 Ya m a d a-oka, Suita, Osaka 565-0871, Japan. E-mail: ikegami@g e r i a t . m e d . o s a k a - u . a c . j p .
A c k n o w l e d g m e n t s — This study was sup-p o rted by Grant-in-Aids for Scientific Researc hf rom the Ministry of Education, Science,S p o rts, and Culture, and Health SciencesR e s e a rch Grants (Research on Human Genomeand Gene Therapy) from the Ministry of Healthand We l f a re, Japan.
R e f e re n c e s1 . Field JB, Loube SD: Observations concern-
ing diabetes mellitus associated withWe rn e r ’s syndrome. M e t a b o l i s m 9 : 1 1 8 –124, 1960
2 . Epstein CJ, Martin GM, Schultz AL,Motulsky AG: We rn e r ’s syndrome: areview of its symptomatology, natural his-t o ry, pathologic features, genetics and re l a-tionship to the natural aging process. M e d -i c i n e 45:177–221, 1966
3 . Miki T, Nakura J, Ye L, Mitsuda N, Mor-
Table 1—Insulin responses to IVGTT in a family of a pair of siblings with We rn e r ’s syndro m eand normal subjects
G l u c o s e We rn e r ’s IRI (pmol/l) response to lVGTT
t o l e r a n c e helicase gene B a s a l Peak (3–5 min)
Case 1 D i a b e t e s M / M 8 5 1 2 7Case 2 I G T M / M 1 4 2 4 2 5F a t h e r D i a b e t e s N / M 6 0 7 9M o t h e r N o rm a l N / M 9 5 4 5 2Sister 1 N o rm a l N / N 7 9 4 8 0Sister 2 N o rm a l N / M 6 1 2 5 2N o rmal subjects — — 79 ± 79 484 ± 217(mean ± SD, n = 15)
We rn e r ’s helicase gene: M, mutant allele; N, normal allele. IRI, immunoreactive insulin.
DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2095
Letters
ishima A, Sato N, Kamino K, Ogihara T:Molecular and epidemiological studies ofWe rner Syndrome in the Japanese popula-tion. Mech Ageing Dev 98:255–265, 1997
4 . Yoneda H, Ikegami H, Yamamoto Y, Ya m-ato E, Cha T, Kawaguchi Y, Tahara Y, Ogi-hara T: Analysis of early-phase insulinresponses in nonobese subjects with mildglucose intolerance. Diabetes Care 1 5 :1517–1521, 1992
Youth-Onset Type 2Diabetes (Y2DM)Associated Wi t hH N F 1 A S 3 1 9in Aboriginal C a n a d i a n s
A f o rm of diabetes, youth-onset type 2diabetes (Y2DM), has emerged as an e w, significant public health con-
c e rn in several ethnic groups (1). Y2DM isactually more common in some Canadianaboriginal communities than type 1 dia-betes is in the general pediatric population(2–6). Aboriginal Canadians with Y2DMa re typically nonketotic obese female ado-lescents or young adults (2–6). This phe-notype resembles typical type 2 diabetesthat is associated with obesity and hyper-insulinemia. It is definitely distinct fro mmaturity-onset diabetes of the young(MODY) (1–6). Most clinicians haveassumed that the striking Y2DM pheno-type has a component of genetic suscepti-bility (2–6). Recently, we identified agenetic marker, HNF1A S319, in adult Oji-C ree with type 2 diabetes (7). The H N F 1 AS319 variant was private to Oji-Cree anda l t e red a conserved glycine residue withinthe DNA binding domain of hepatocytenuclear factor- 1a. HNF1A S319/S319homozygotes and S319/G319 h e t e ro z y-gotes had odds ratios for type 2 diabetes of4.0 and 2.0, re s p e c t i v e l y, compared withG319/G319 homozygotes (7).
To evaluate the relationship betweenHNF1A S319 and Y2DM, we studied 317O j i - C ree subjects aged 10–25 years fro mthe Sandy Lake re s e rve in nort h e rnOntario (7). We identified 16 subjectswith type 2 diabetes (14 of whom werefemales), 15 subjects with impaired glu-cose tolerance (IGT) (12 of whom werefemales), and 286 subjects with norm a lglucose tolerance (162 of whom weref e m a l e s ) .
Table 1 shows the clinical, biochemi-cal, and genetic features of Oji-Cree sub-jects with Y2DM, IGT, and norm o-glycemia. Compared with norm o g l y c e m i csubjects, those with Y2DM had signifi-cantly increased BMI, glucose concentra-tions after fasting and 2 h after 75-g glu-cose challenge, and fasting plasma insulinand C-peptide concentrations (all P ,0.001). The values for all continuous traitsin subjects with IGT were interm e d i a t e ,with values between those for subjectswith Y2DM and those for norm o g l y c e m i cs u b j e c t s .
All observed genotype frequenciesfollowed the expectations of the Hardy-Weinberg law. The frequency of HNF1AS319 was 0.343 and 0.086 in subjectswith Y2DM and normoglycemic sub-jects, respectively (P = 0.00005). The fre-quency of HNF1A S319 was 0.167 insubjects with IGT, which was not statisti-cally different from that of subjects withY2DM or normoglycemia. H N F 1 AS319/S319 homozygotes and S319/G319heterozygotes had odds ratios for Y2DMof 119 (95% CI 6.1–2,320) and 2.9(1.5–5.8), respectively, compared withsubjects with the HNF1A G319/G319genotype. HNF1A S319/G319 heterozy-gotes had an odds ratio for IGT of 1.9(0.91–4.2). The Y2DM subjects whowere homozygous for HNF1A S319/S319were not different from the HNF1A sub-jects for any clinical or biochemical phe-notype (data not shown).
The cellular basis for the developmentof type 2 diabetes in Oji-Cree subjectswith HNF1A S319 is not yet established.
Most mutations in HNF1A have beeno b s e rved with MODY3, which typicallyoccurs in lean younger adults and is asso-ciated with defective insulin secre t i o nf rom pancreatic b-cells (8). In contrast,Y2DM in the Oji-Cree appears to be typi-cal type 2 diabetes, associated with obesityand hyperinsulinemia (1–7). It is possiblethat adolescent obesity and insulin re s i s-tance in the Oji-Cree population mays t ress the capacity of HNF1A S319 c a rr i e r sto mount an adequate insulin re s p o n s e ,but this would re q u i re confirmation withcellular and/or physiological studies. It isof interest that the adolescent subjectswith Y2DM had a significantly highermean fasting plasma insulin concentrationthan the other groups, suggesting that aninsulin response is present, but is insuff i-cient or ineffective in preventing the devel-opment of diabetes.
The emergence of Y2DM in Canadianaboriginal people has been attributed torecent population-wide increases in obe-sity and insulin resistance (2–6). These, int u rn, have resulted from the decline inphysical activity and the increased re l i a n c eon store-bought food (2–6). HNF1A S319appears to be a strong and significant con-tributor to the Y2DM phenotype. It mightp rove to be a useful marker for identifyingyoung subjects at risk for developing dia-betes. These subjects would be candidatesfor interventions, such as exercise and/ord i e t a ry modification. Similar associationswith diff e rent genetic variants may exist inother ethnic minorities (1) for whomY2DM is also an incipient public healthd i l e m m a .
Table 1—Clinical, biochemical, and genetic variables in Oji-Cree subjects aged #25 years
D i a b e t e s I G T N o rm o g l y c e m i a
n ( f e m a l e ) 16 (14) 15 (12) 286 (162)Age (years) 19.6 ± 4.3 17.1 ± 4.7 17.0 ± 4.4BMI (kg/m2) 32.8 ± 5.1 28.1 ± 6.1 23.8 ± 5.5*Blood glucose levels (mmol/l)
F a s t i n g 9.4 ± 4.4 5.8 ± 0.70 5.3 ± 0.46*2-h p.c. 14.9 ± 7.5 8.7 ± 0.67 5.1 ± 1.3*
Fasting insulin (U/l) 409 ± 450 231 ± 171 104 ± 61*C-peptide (U/l) 1.37 ± 1.11 0.73 ± 0.43 0.55 ± 0.35*H N F 1 A g e n o t y p e s
S 3 1 9 / S 3 1 9 2 (2) 0 0S 3 1 9 / G 3 1 9 7 (6) 5 (3) 49 (23)G 3 1 9 / G 3 1 9 7 (6) 10 (9) 237 (139)
Data are n (female) or means ± SD. *Significantly diff e rent from subjects with diabetes and IGT at P , 0 . 0 0 1 .p.c., post challenge with 75-g oral glucose.

2096 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
ROBERT A. HEGELE, MD
ANTHONY J.G. HANLEY, MSC
BERNARD ZINMAN, MD
STEWART B. HARRIS, MD
CAROL M. ANDERSON, BSC
F rom the Samuel Lunenfeld Research Institute andthe Department of Medicine (A.J.G.H., B.Z.), Univer-sity of To ronto, To ronto; and the Thames Valley Fam-ily Practice Research Centre (S.B.H.) and the John P.R o b a rts Research Institute and Departments of Medi-cine and Biochemistry (R.A.H., C.M.A.), Universityof We s t e rn Ontario, London, Ontario, Canada.
A d d ress correspondence to Robert A. Hegele,MD, Blackburn Cardiovascular Genetics Laboratory,John P. Robarts Research Institute, 406-100 Pert hD r., London, ON, Canada N6A 5K8. E-mail: ro b e rt .h e g e l e @ rr i . o n . c a .
A c k n o w l e d g m e n t s — This work was sup-p o rted by grants from the National Institutes ofHealth (1-R21-DK44597-01), the OntarioM i n i s t ry of Health (#04307), the CanadianDiabetes Association (in honor of Rheta MaudeG i l b e rt), the Medical Research Council ofCanada (#MA13430), and general supportf rom the Blackburn Group. R.A.H. is a Care e rInvestigator of the Heart and Stroke Founda-tion of Ontario (#CI-2979). S.B.H. is a Care e rInvestigator of the Ontario Ministry of Health.A.J.G.H. was supported by Health Canadat h rough a National Health Research and Devel-opment Program Research Training Aw a rd.
We acknowledge the assistance of the chiefand council of the community of Sandy Lake;the Sandy Lake community surveyors; theSandy Lake nurses; and the staff of the Univer-sity of To ronto Sioux Lookout Pro g r a m.
R e f e re n c e s1 . Young RS, Rosenbloom AL: Type 2 (non-
insulin dependent) diabetes in minorityyouth: conference re p o rt. Clin Pediatr 3 7 :63–66, 1998
2 . Dean HJ, Mundy RL, Moffatt M: Non-insulin-dependent diabetes mellitus inIndian children in Manitoba. C M A J 1 4 7 :52–57, 1992
3 . H a rris SB, Perkins BA, Whalen-Brough E:Non-insulin-dependent diabetes mellitusamong First Nations children: new entityamong First Nations people of nort h w e s t-e rn Ontario. Can Fam Physician 4 2 : 8 6 9 –876, 1996
4 . B l a n c h a rd JF, Dean H, Anderson K, Wa j d aA, Ludwig S, Depew N: Incidence andp revalence of diabetes in children aged0–14 years in Manitoba, Canada, 1985–1993. Diabetes Care 20:512–515, 1997
5 . Dean H: NIDDM-Y in First Nation chil-d ren in Canada. Clin Pediatr 3 7 : 8 9 – 9 6 ,1 9 9 8
6 . Dean HJ, Young TK, Flett B, Wo o d -Steiman P: Screening for type-2 diabetes inaboriginal children in nort h e rn Canada.
Lancet 352:1523–1524, 19987 . Hegele RA, Cao H, Harris SB, Hanley AJG,
Zinman B: The hepatic nuclear factor- 1alpha G319S variant is associated withearly-onset type 2 diabetes in CanadianO j i - C ree. J Clin Endocrinol Metab 8 4 : 1 0 7 7 –1082, 1999
8 . Velho G, Froguel P: Genetic, metabolicand clinical characteristics of maturityonset diabetes of the young. Eur J Endo -c r i n o l 138:233–239, 1998
Two-Hour P o st–Glucose Loading Plasma Glucose Is the Main D e t e rminant for theP ro g ression Fro mI m p a i red GlucoseTolerance to Diabetes in Hong Kong Chinese
The category of impaired glucose toler-ance (IGT) was created in 1979 by theWorld Health Organization and the
National Diabetes Data Group to identify ag roup of subjects who were at higher riskfor cardiovascular disease and subsequentdevelopment of type 2 diabetes (1,2).T h e re have been few re p o rts on the risk ofp ro g ression to diabetes in Chinese peoplewith IGT. We followed up 123 Chinesesubjects with IGT with yearly oral glucosetolerance tests (OGTTs) and aimed toexamine their risk of pro g ression to dia-betes and the risk factors for pro g re s s i o n .
Between 1988 and 1995, 123 Chinesesubjects with IGT were re c ruited for ayearly OGTT until they had pro g ressed todiabetes or up to June 1997, which iswhen all of the data were analyzed. Gly-cated hemoglobin (HbA1 c) and fasting, 1-h, and 2-h plasma glucose (PG) levelsw e re measured during the OGTT. Insulinassays of fasting, 1-h, and 2-h plasma sam-ples were also perf o rmed, but they wereavailable in 66 subjects only. Of these 123subjects, 15 (12.2%) were men and 108(87.8%) were women. The subjects were22–66 years of age. After a mean follow-up period of 1.71 ± 1.35 years (range0.92–7.64, median 1.06), 29 (23.6%) pro-g ressed to diabetes, 34 (27.6%) re m a i n e dwith IGT, and 60 (48.8%) re v e rted to nor-mal OGTT. The 50% “survival time” (95%
CI) from IGT to diabetes was 4.34 y e a r s(3.72–5.41) with the Kaplan-Meier analy-sis. With use of Cox re g ression analysis top redict the pro g ression to diabetes withage, sex, BMI, blood pre s s u re, HbA1 c, andfasting, 1-h, and 2-h PG as predictor vari-ables, 2-h PG was the only signific a n tindependent parameter with b = 0.616,SEM = 0.203, P = 0.002, and relative risk(RR) (95% CI) = 1.85 (1.24–3.76). Forthose with 2-h PG $10.1 mmol/l (mean1 1 SD), the pro g ression from IGT to dia-betes was much higher, with the 50%“ s u rvival time” of 2.03 (1.53–2.53) yearsas compared with 6.16 (2.37–9.95) yearsfor those with 2-h PG , 10.1 mmol/l (log-rank test: P , 0.01) (Fig. 1). Of the 66subjects whose plasma insulin levels hadbeen made available, there was no statisti-cally significant diff e rence in the insulinlevels among subjects with diabetes, IGT,or normal OGTT. Through the use of Coxre g ression analysis with age; sex; BMI;blood pre s s u re; HbA1 c; fasting, 1-h, and 2-h PG and insulin; insulinogenic indexes;and insulin resistance (calculated with ac o m p u t e r-solved homeostasis modelassessment method) as predictor variables,2-h PG was the only significant indepen-dent variable with b = 0.837, SEM =0.326, P = 0.010, and RR (95% CI) = 2.31( 1 . 2 2 – 4 . 3 7 ) .
The rate of pro g ression from IGT todiabetes was re p o rted to be 11.3% peryear in the Da Qing IGT and DiabetesStudy involving Chinese subjects inn o rt h e rn Mainland China (3). In thep resent study, 50% of our patients withIGT pro g ressed to diabetes in 4.34 years.A crude rate of pro g ression was hencecalculated to be 11.5% per year in Chi-nese individuals in Hong Kong. Similarto most other studies (3–5), the mosti m p o rtant risk factor predicting subse-quent pro g ression from IGT to diabetes isthe baseline 2-h PG concentration. Wefound that subjects whose 2-h PG$1 0 . 1 mmol/l, in comparison with thosewhose 2-h PG ,10.1, had a rate of pro-g ression three times higher. In addition,for every 1 mmol/l increase in the 2-h PGlevel, there is a 1.85-fold higher risk forp ro g ression from IGT to diabetes. Someother risk factors for pro g ression fro mIGT to diabetes, such as age and obesity(4–6), have been re p o rted. However,both of these disappeared as independentrisk factors once plasma glucose (and/orinsulin) had been introduced into themultivariate analysis.
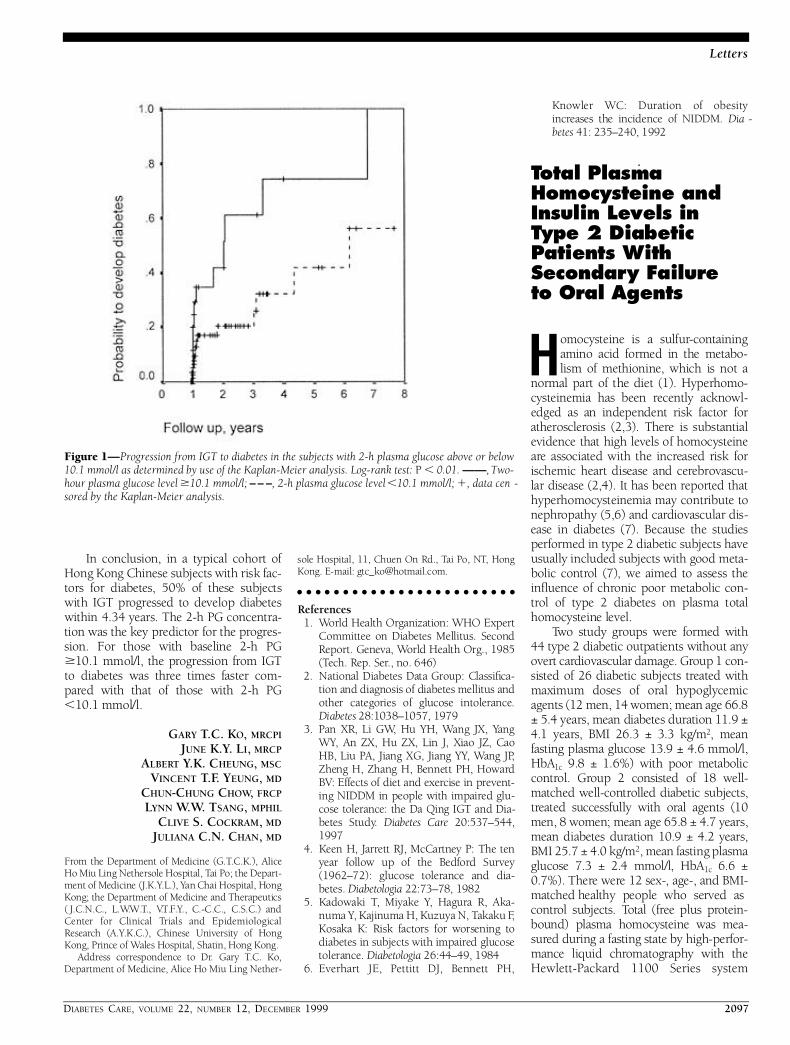
DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2097
Letters
In conclusion, in a typical cohort ofHong Kong Chinese subjects with risk fac-tors for diabetes, 50% of these subjectswith IGT pro g ressed to develop diabeteswithin 4.34 years. The 2-h PG concentra-tion was the key predictor for the pro g re s-sion. For those with baseline 2-h PG$10.1 mmol/l, the pro g ression from IGTto diabetes was three times faster com-p a red with that of those with 2-h PG,10.1 mmol/l.
GARY T.C. KO, MRCPI
JUNE K.Y. LI, MRCP
ALBERT Y.K. CHEUNG, MSC
VINCENT T.F. YEUNG, MD
CHUN-CHUNG CHOW, FRCP
LYNN W.W. TSANG, MPHIL
CLIVE S. COCKRAM, MD
JULIANA C.N. CHAN, MD
F rom the Department of Medicine (G.T.C.K.), AliceHo Miu Ling Nethersole Hospital, Tai Po; the Depart-ment of Medicine (J.K.Y.L.), Yan Chai Hospital, HongKong; the Department of Medicine and Therapeutics( J.C.N.C., L.W. W. T., V. T. F. Y., C.-C.C., C.S.C.) andCenter for Clinical Trials and EpidemiologicalR e s e a rch (A.Y.K.C.), Chinese University of HongKong, Prince of Wales Hospital, Shatin, Hong Kong.
A d d ress correspondence to Dr. Gary T.C. Ko,D e p a rtment of Medicine, Alice Ho Miu Ling Nether-
sole Hospital, 11, Chuen On Rd., Tai Po, NT, HongKong. E-mail: [email protected].
R e f e re n c e s1. World Health Organization: WHO Expert
Committee on Diabetes Mellitus. SecondR e p o rt. Geneva, World Health Org., 1985( Tech. Rep. Ser., no. 646)
2 . National Diabetes Data Group: Classific a-tion and diagnosis of diabetes mellitus andother categories of glucose intolerance.Diabetes 28:1038–1057, 1979
3 . Pan XR, Li GW, Hu YH, Wang JX, Ya n gW Y, An ZX, Hu ZX, Lin J, Xiao JZ, CaoHB, Liu PA, Jiang XG, Jiang YY, Wang JP,Zheng H, Zhang H, Bennett PH, HowardB V: Effects of diet and exercise in pre v e n t-ing NIDDM in people with impaired glu-cose tolerance: the Da Qing IGT and Dia-betes Study. Diabetes Care 2 0 : 5 3 7 – 5 4 4 ,1 9 9 7
4 . Keen H, Jarrett RJ, McCartney P: The tenyear follow up of the Bedford Surv e y(1962–72): glucose tolerance and dia-betes. D i a b e t o l o g i a 22:73–78, 1982
5 . Kadowaki T, Miyake Y, Hagura R, Aka-numa Y, Kajinuma H, Kuzuya N, Takaku F,Kosaka K: Risk factors for worsening todiabetes in subjects with impaired glucosetolerance. D i a b e t o l o g i a 26:44–49, 1984
6 . E v e rh a rt JE, Pettitt DJ, Bennett PH,
Knowler WC: Duration of obesityi n c reases the incidence of NIDDM. D i a -b e t e s 41: 235–240, 1992
Total Plasma Homocysteine andInsulin Levels inType 2 DiabeticPatients With S e c o n d a ry Failure to Oral Agents
Homocysteine is a sulfur- c o n t a i n i n gamino acid formed in the metabo-lism of methionine, which is not a
n o rmal part of the diet (1). Hyperh o m o-cysteinemia has been recently acknowl-edged as an independent risk factor fora t h e ro s c l e rosis (2,3). There is substantialevidence that high levels of homocysteinea re associated with the increased risk forischemic heart disease and cere b ro v a s c u-lar disease (2,4). It has been re p o rted thath y p e rhomocysteinemia may contribute ton e p h ropathy (5,6) and cardiovascular dis-ease in diabetes (7). Because the studiesp e rf o rmed in type 2 diabetic subjects haveusually included subjects with good meta-bolic control (7), we aimed to assess thei n fluence of chronic poor metabolic con-t rol of type 2 diabetes on plasma totalhomocysteine level.
Two study groups were formed with44 type 2 diabetic outpatients without anyo v e rt cardiovascular damage. Group 1 con-sisted of 26 diabetic subjects treated withmaximum doses of oral hypoglycemicagents (12 men, 14 women; mean age 66.8± 5.4 years, mean diabetes duration 11.9 ±4.1 years, BMI 26.3 ± 3.3 k g / m2, meanfasting plasma glucose 13.9 ± 4.6 mmol/l,H b A1 c 9.8 ± 1.6%) with poor metabolicc o n t rol. Group 2 consisted of 18 well-matched well-controlled diabetic subjects,t reated successfully with oral agents (10men, 8 women; mean age 65.8 ± 4.7 years,mean diabetes duration 10.9 ± 4.2 years,BMI 25.7 ± 4.0 kg/m2, mean fasting plasmaglucose 7.3 ± 2.4 mmol/l, HbA1 c 6.6 ±0.7%). There were 12 sex-, age-, and BMI-matched healthy people who served asc o n t rol subjects. Total (free plus pro t e i n -bound) plasma homocysteine was mea-s u red during a fasting state by high-perf o r-mance liquid chromatography with theHewlett-Packard 1100 Series system
Figure 1—Progression from IGT to diabetes in the subjects with 2-h plasma glucose above or below10.1 mmol/l as determined by use of the Kaplan-Meier analysis. Log-rank test: P , 0.01. ——, Two-hour plasma glucose level $10.1 mmol/l; – – –, 2-h plasma glucose level ,10.1 mmol/l; 1, data cen -sored by the Kaplan-Meier analysis.

2098 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
( Wa l d b ronn, Germany). Insulin was mea-sured under the same conditions byradioimmunologic assay (Bio-Rad, Swierk,Poland). HbA1 c was measured by commer-cially available chromatographic assay.Because normality of distribution was con-firmed in each group of data, the Student’st test for unpaired data was used to analyzethe diff e rences between groups. To assessc o rrelation between given parameters, theP e a r s o n ’s correlation analysis was per-f o rmed. Values for P , 0.05 were consid-e red signific a n t .
Mean ± SD fasting plasma total homo-cysteine concentrations were signific a n t l yhigher in group 1 patients (17.1 ± 4.5nmol/l, P ,0.001) than in group 2 patients(8.2 ± 3.9 nmol/l) and healthy control sub-jects (6.5 ± 4.9 nmol/l). HbA1 c v a l u e sshowed positive correlation with homo-cysteine concentration in group 1 (r = 0.41; P , 0.05). Inversely, insulin lev-els were significantly lower in group 1 (8.3 ± 5.2 µU/ml) than in group 2 (14.6 ±5.2 µU/ml, P , 0.001), with no statisticallys i g n i ficant diff e rence between insulin levelsin group 1 (8.3 ± 5.2 µU/ml) and healthyc o n t rol subjects (9.3 ± 6.1 µU/ml). Therewas a negative correlation between homo-cysteine and insulin concentrations in theg roup 1 patients (r = 20.32; P , 0 . 0 5 ) .
T h e re are few studies analyzing therelation between plasma homocysteine andtype 2 diabetes, especially in re g a rd tometabolic control. Lanfredini et al. (6) andHoogeveen et al. (7) recently confirmed thev a s c u l a r-damaging impact of homocysteinein type 2 diabetic individuals. However, inthe study by Hoogeveen et al., unlike inours, the degree of metabolic control didnot show any correlation with plasmahomocysteine concentration. This discre p-ancy may be partly explained by the diff e r-ence in the studies’ designs. Mean HbA1 c
level in the study by Hoogeveen et al. (7)was ,6.0%, whereas our group 1 patientsshowed considerably worse metabolic con-t rol as being in the long-term period of oral-agent failure. Our findings are in agre e m e n twith the observations of Munshi et al. (8),who described greater frequency of hyper-homocysteinemia in type 2 diabetes, andP a s s a ro et al. (9), who also found corre l a-tion between high homocysteine levels andH b A1 c in type 2 diabetic people as well asduration of the disease. The latter was notc o n firmed in our study.
To our knowledge, there have been nore p o rts so far on the relationship betweenplasma homocysteine and endogenous
insulin level in patients with type 2 dia-betes. We have demonstrated an appare n tnegative correlation between these twoparameters in poorly controlled type 2diabetic subjects. This observation seemsto be in accordance with the re p o rts abouttype 1 diabetes. Cronin et al. (10) andRobillon et al. (11) noted lower homocys-teine levels in insulin-treated well-con-t rolled type 1 diabetic subjects than inhealthy control subjects. As shown byH u l t b e rg et al. (12), deterioration of meta-bolic control in type 1 diabetes, typicallycaused by direct or indirect insulin defi-c i e n c y, is accompanied by homocysteineplasma increase. We have found that highplasma homocysteine concentrations areassociated with decreased insulin levels intype 2 diabetes. Fonseca et al. (13) notedthat hyperinsulinemia decreases homocys-teine levels in normal subjects, but not ini n s u l i n - resistant type 2 diabetic subjects.Animal studies published recently byJacobs et al. (14) confirm that insulin isd i rectly involved in the regulation ofhomocysteine metabolism. There f o re, itmay be suggested that the compro m i s e dinsulin action caused by the relative orabsolute insulin deficiency is associatedwith plasma homocysteine level elevation.Insulin thus seems to play a signific a n t ,but yet unclear, role in the altered homo-cysteine metabolism found in diabetes.
In conclusion, we found that chro n i cpoor metabolic control of type 2 diabeteswas characterized by elevation of plasmahomocysteine concentration and that thelatter inversely correlated with endoge-nous insulin levels. Our results may add tothe understanding of the increased fre-quency and mechanisms of vascular dam-age in diabetes.
JÓZEF DRZEWOSKI, MD, PHD
LESZEK CZUPRYNIAK, MD
GRAZYNA CHWATKO, MSC
EDWARD BALD, PHD
F rom the Metabolic Diseases and Gastro e n t e ro l o g yD e p a rtment ( J.D., L.C.), Medical University of Lodz;and the Environmental Chemistry Depart m e n t(G.C., E.B.), University of Lodz, Lodz, Poland.
A d d ress correspondence to Leszek Czupry n i a k ,MD, Metabolic Diseases and Gastro e n t e ro l o g yD e p a rtment, Barlickiego University Hospital No. 1,Ul. Kopcinskiego 22, 90-153 Lodz, Poland. E-mail:c z u p ry n i a k @ y a h o o . c o . u k .
A c k n o w l e d g m e n t s — The study was sup-p o rted by the Mayor of Lodz City Grant num-ber G-4/98 (AM 2 4 0 - 9 9 ) .
R e f e re n c e s1 . Ueland PM, Refsum H, Stabler SP, Mali-
now MR, Andersson A, Allen RH: To t a lhomocysteine in plasma or serum: meth-ods and clinical applications. Clin Chem39:1764–1779, 1993
2 . The European Concerted Action Pro j e c t :Plasma homocysteine as a risk factor forvascular disease. J A M A 2 7 7 : 1 7 7 5 – 1 7 8 1 ,1 9 9 7
3 . Nehler MR, Taylor LM Jr, Porter JM:Homocysteinemia as a risk factor for ath-e ro s c l e rosis: a re v i e w. C a rdiovasc Surg 5 :559–567, 1997
4 . Stehouwer CDA, We i j e n b e rg MP, van derB e rg M, Jakobs C, Feskens EJM,K romhout D: Serum homocysteine andrisk of coro n a ry heart disease and cere-b rovascular disease in elderly men: a1 0-year follow-up. A rterioscler Thro m bVasc Biol 18:1895–1901, 1998
5 . Hofmann MA, Kohl B, Zumbach MS,B o rcea V, Bierhaus A, Henkels M, Amiral J,Schmidt AM, Fiehn W, Ziegler R, Wahl P,N a w roth PP: Hyperh o m o c y s t ( e ) i n e m i aand endothelial dysfunction in IDDM.Diabetes Care 21:841–848, 1998
6 . L a n f redini M, Fiorina P, Peca MG,Ve ronelli A, Mello A, Astorri E, Dall’AglioP, Craveri A: Fasting and post-methionineload homocyst(e)ine values are corre l a t e dwith microalbuminuria and could con-tribute to worsening vascular damage innon-insulin-dependent diabetes mellitussubjects. M e t a b o l i s m 47:915–921, 1998
7 . Hoogeveen EK, Kostense PJ, Beks PJ,Mackaay AJ, Jakobs C, Bouter LM, HeineRJ, Stehouwer CDA: Hyperh o m o c y s t e i n e-mia is associated with an increased risk ofc a rdiovascular disease, especially in non-insulin-dependent diabetes mellitus: apopulation-based study. A rterioscler Thro m bVasc Biol 18:133–138, 1998
8 . Munshi MN, Stone A, Fink L, Fonseca V:H y p e rhomocysteinemia following a methio-nine load in patients with non-insulin-dependent diabetes mellitus and macro-vascular disease. M e t a b o l i s m 45: 133–135,1 9 9 6
9 . P a s s a ro A, Solini A, D’Elia K, Pareschi PL,Carantoni M, Fellin R: Factors influ e n c i n gplasma homocysteine as determinant ofc a rdiovascular risk in type 2 diabetes mel-litus. D i a b e t o l o g i a 41 (Suppl. 1):A337, 1998
1 0 . C ronin CC, McPartlin JM, Barry DG, Fer-riss JB, Scott JM, Weir DG: Plasma homo-cysteine concentrations in patients withtype 1 diabetes. Diabetes Care 2 1 : 1 8 4 3 –1847, 1998
1 1 . Robillon JF, Canivet B, Candito M, SadoulJL, Jullien D, Morand P, Chambon P, Fre y-chet P: Type 1 diabetes mellitus and homo-cyst(e)ine. Diabetes Metab 2 0 : 4 9 4 – 4 9 6 ,1 9 9 4
1 2 . H u l t b e rg B, Agardh CD, Agardh E, Loves-

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2099
Letters
tam-Adrian M: Poor metabolic contro l ,early age at onset, and marginal folate defi-ciency are associated with increasing levelsof plasma homocysteine in insulin-depen-dent diabetes mellitus: a five-year follow-up study. Scand J Clin Lab Invest 5 7 : 5 9 5 –600, 1997
1 3 . Fonseca VA, Mudaliar S, Schmidt B, FinkLM, Kern PA, Henry RR: Plasma homocys-teine concentrations are regulated by acutehyperinsulinemia in nondiabetic but nottype 2 diabetic subjects. M e t a b o l i s m 4 7 :686–689, 1998
1 4 . Jacobs RL, House JD, Brosnan ME, Bro s-nan JT: Effects of stre p t o z o t o c i n - i n d u c e ddiabetes and of insulin treatment onhomocysteine metabolism in the rat. D i a -b e t e s 47:1967–1970, 1998
B e n z o d i a z e p i n eI n t e rru p t i o n
Does it cause hypoglycemia?
We re p o rt on a patient who pre-sented with a reduction in insulinre q u i rements after discontinuing
clonazepam. A 43-year-old diabetic manwas admitted to the endocrinology wardfor glycemic control after incomplete trans-craneal adenomectomy of a pituitaryg rowth horm o n e – s e c reting macro a d e n o m a .After treatment with lanreotide was begun,his daily insulin dose decreased fro m.300 to 142 U and he was discharged on104 insulin U/day, lanreotide 30 mg for 10days, and replacement therapy withh y d ro c o rtisone and levothyroxine. Onemonth after discharge, he was started onclonazepam 6 mg/day because of excru c i-ating headaches that did not respond toother drugs. Three months later, clon-azepam was discontinued. The followingday (which was 3 days after a lanre o t i d einjection), the patient was admitted to ourd a y - c a re center because of hypoglycemiccoma that was induced without changes infood intake, insulin dose, or physicala c t i v i t y. The dosage of insulin was pro g re s-sively decreased to 30 U/day during thefollowing week because of re c u rr i n gepisodes of hypoglycemia, and it stabilizedat 58 U/day 6 months later. Because ofschedule difficulties, the patient declinedan acute test with clonazepam to assess hisg rowth hormone/glucose re s p o n s e .
In rats, clonazepam has beenre p o rted to increase blood glucose (1)and growth hormone (2) levels in vivo,
but not in a pituitary growth horm o n e –s e c reting cell line in vitro (3). In humans,diazepam had been proposed as a stimu-lation test for growth hormone secre t i o n(4), but was later abandoned because ofits inconsistency (5).
Our patient had stable secondary dia-betes, but he presented with an abru p treduction in insulin re q u i rements. Hadthe recent administration of lanre o t i d ebeen the cause, similar episodes wouldhave occurred with previous doses; suchepisodes had not happened. It seems thatonly certain growth horm o n e – p ro d u c i n gcell lines are sensitive to benzodiazepines,which would account for the irre g u l a rresponse observed with diazepam in acro-megalics (5,6). Although definite proof islacking, we propose that our patient’stumor was responsive to clonazepam, andthe interruption of benzodiazepine tre a t-ment caused a decrease in growth hor-mone secretion and insulin re q u i re m e n t s .
ANA M. WÄGNER, MD
SUSAN M. WEBB, MD, PHD
ROSA CORCOY, MD, PHD
F rom the Endocrinology and Nutrition Depart m e n t ,Hospital Sant Pau, Autonomous University ofB a rcelona, Barcelona, Spain.
A d d ress correspondence to Rosa Corc o y, MD,PhD, Endocrinology and Nutrition Depart m e n t ,Hospital Sant Pau, S. Antonio M. Claret 167, 08025B a rcelona, Spain. E-mail: rc o rc o y @ s a n t p a u . e s .
R e f e re n c e s1 . Najim RA, Al-Essa LY, Al-Jawad FH:
E ffects of some drugs acting at the central-type benzodiazepine receptors on bloodglucose in mice. Clin Exp Pharmacol Physiol16:7–12, 1989
2 . Männistö PT, Laakso ML, Järvinen A, RägoL: Effects of central and peripheral typebenzodiazepine ligands on growth hor-mone and gonadotropin secretion in malerats. P h a rmacol To x i c o l 71:75–80, 1992
3 . Black KL, Shiraishi T, Ikezak K, Tabuchi K,Becker D: Peripheral benzodiazepine stim-ulates secretion of growth hormone andmitochondrial proliferation in pituitarytumour GH3 cells. N e u rol Res 1 6 : 7 4 – 8 0 ,1 9 9 4
4 . Kannan V: Diazepam test of growth hor-mone secre t i o n. Horm Metab Res 1 3 : 3 9 0 –393, 1981
5 . Zaccaria M, Giordano G, Ragazzi E, SicoloN, Foresta C, Scandellari C: Lack of eff e c tof im diazepam administration on hGHand hPRL in normal and acromegalic sub-j e c t s . J Endocrinol Invest 8:167–170, 1985
6 . Fanghanel G, Larraza O, Villalobos M,Fanghanel L, Velasco M, Velasco F: Diff e r-
ential response to aminergic stimuli andbiological behavior of growth horm o n es e c reting pituitary adenomas. Can J Neuro lS c i 17:78–82, 1990
A m e r i c a nO rthopaedic Footand Ankle SocietyDiabetic Shoe S u rv e y
It is well accepted that the developmentof a foot ulcer in the diabetic individualis often the precursor of lower- e x t re m i t y
amputation. Once the ulcer develops, thep a t i e n t ’s quality of life decreases appre c i a-bly (1). This increased morbidity utilizes asubstantial proportion of health carere s o u rces (2–4). It is also well accepted thata comprehensive program of patient edu-cation, skin and nail care, protective shoes,and ongoing monitoring decreases thatrisk, thus decreasing patient morbidity andre s o u rce consumption (5–8; J.O. Krause,J . W. Bro d s k y, unpublished observ a t i o n s ) .This information led to the passage of theM e d i c a re Therapeutic Shoe Bill, whichp rovides these benefits to individuals withdiabetes. In spite of this information, moste x p e rts feel that very few patients are pro-vided with comprehensive pro p h y l a c t i cfoot care or protective shoe gear.
Members of the Diabetes Committeeof the American Orthopaedic Foot andAnkle Society randomly surveyed 402 dia-betic individuals during visits to theirendocrinologists. This venue was selectedbecause it was felt to re p resent a “bestpractice” group of patients, i.e., thosepatients receiving the most compre h e n s i v ec a re for their diabetes. The demographicsrevealed that the patients were re p re s e n t a-tive of a typical longstanding diabetic pop-ulation, averaging 61.5 years of age andwith a duration of diabetes of 27.3 years.To re i n f o rce the premise of a “best prac-tice” group, 93.5% had health-care bene-fits through Medicare and/or a privateinsurance carr i e r.
Only 73.4% had any form of patienteducation, which was usually provided bya nurse or podiatrist. The frequency ofexamination of their feet was variable,with only 59.9% having twice-yearlyexaminations and 8.5% never having anexamination. Only 12.2% wore specialshoes, and just 15.4% used any type of

2100 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
custom foot orthosis. Only 7.7% of theshoes or foot orthoses were provided bythe patients’ health care providers (9).
This study highlights a substantialo p p o rtunity for improvement in the careof individuals with diabetes. The mostcommon reason for hospitalization of thediabetic individual is foot infection. It isreasonable to assume that diabetic patientshave their blood sugar levels tested peri-odically and that they meet with their die-titians and diabetes educators. In thislight, it is reasonable to target 100% of dia-betic patients to be educated about thec a re of their feet and methods to pre v e n tinfection or the development of an ulcer. Itis also reasonable to target that 100% ofdiabetic individuals have their feet exam-ined periodically. From available data, areasonable target rate for pro p h y l a c t i cshoe gear is 25%.
P rophylactic foot care programs areless expensive and consume fewerre s o u rces than our current method of tre a t-ment. If we achieve these targets, we cani m p rove the quality of health care for dia-betic individuals, improve their quality oflife, and actually decrease the overall costof care. In the current cost-conscious envi-ronment, these reasonable goals can beattained without “up-front” high-tech capi-tal expenditure. This study will be pub-lished in full in the November issue of F o o tand Ankle Intern a t i o n a l. This issue will bededicated to the care of the diabetic foot.
MICHAEL S. PINZUR, MD
F rom the Loyola University Medical Center, May-wood, Illinois.
A d d ress correspondence to Michael S. Pinzur,MD, Professor of Orthopaedic Surg e ry and Rehabili-tation, Loyola University Medical Center, 2160 S.First Ave., Maywood, IL 60153. E-mail: mpinzu1@l u c . e d u .
R e f e re n c e s1 . Holden JM, Fernie GR: Extent of art i fic i a l
limb use following rehabilitation. J Ort h o pR e s 5:562–568, 1987
2 . Eckman MH, Gre e n field S, Mackey WC,Wong JB, Kaplan S, Sullivan L, Dukes K,Pauker SG: Foot infections in diabeticpatients: decision and cost-eff e c t i v e n e s sanalysis. J A M A 273:712–720, 1995
3 . Gilmer TP, Manning WG, O’Connor PJ,Rush WA: The cost to health plans of poorglycemic control. Diabetes Care 2 0 : 1 8 4 7 –1853, 1997
4 . Selby JV, Zhang D, Ray GT, Colby CJ:Excess costs for medical care for patientswith diabetes in a managed care popula-
tion. Diabetes Care 20:1396–1401, 19975 . G re e n b e rg L: Analysis of Footcare Data fro m
the 1990 National Health Interview Study.Rockville, MD, Health Resources and Ser-vices Administration, Bureau of HealthP rofessions, Division of Medicine, 1992
6 . McGill M, Molyneaux LM, Yue DK, Tu rt l eJR: A single visit diabetes complicationassessment service: a complement to dia-betes management at the primary carelevel. Diabet Med 10:366–370, 1993
7 . Reiber GE, Smith DG, Boone DA, delAguila M, Borchers RE, Mathews D,Joseph AW, Burgess EM: Design and pilottesting of the DVA/Seattle footwear systemfor diabetic patients with foot insensitivity.J Rehabil Res Dev 34:1–8, 1997
8 . Rönnemaa T, Toikka T, Hämäläinen H,Liukkonen I: Evaluation of the impact ofpodiatrist care in the primary pre v e n t i o nof foot problems in diabetic subjects. D i a -betes Care 23:1833–1837, 1997
9 . Pinzur MS, Shields NN, Goelitz B,Slovenkai M, Kaye R, Ross SDK, Suri M:American Orthopaedic Foot and AnkleSociety Diabetic Shoe Surv e y. Foot AnkleI n t. In pre s s
C O M M E N T S A N DR E S P O N S E S
Insulin-Sensitive andI n s u l i n - R e s i s t a n tVariants inNonobese JapaneseType 2 DiabeticP a t i e n t s
The role of triglycerides in insulinre s i s t a n c e
It is well known that two subtypes existin Japanese nonobese type 2 diabeticpatients: one with normal peripheral
insulin sensitivity and the other with pri-m a ry peripheral insulin resistance (1,2). Inthe present study, 70 untreated nonobesetype 2 diabetic patients who visited ourclinic participated. Type 2 diabetes wasdiagnosed based on the criteria of theWorld Health Organization (3). All sub-jects ingested at least 150 g of carbohy-drate for the 3 days preceding the study.None of the subjects had significant re n a l ,hepatic, or cardiovascular disease, nor didthey take any medications known to aff e c t
lipid metabolism. The blood was drawnduring the morning after a 12-h fast.Plasma glucose was measured with theglucose oxidase method and plasmainsulin was measured with a radioim-munoassay kit. The total cholesterol, LDLc h o l e s t e rol, HDL cholesterol, triglycerides,and uric acid were also measured. Theestimate of insulin resistance by home-ostasis model assessment (HOMA-IR) wascalculated with the following form u l a :fasting serum insulin (µU/ml) 3 f a s t i n gplasma glucose (mmol/l)/22.5, as describedby Matthews et al. (4). The HOMA-IRvalue of control subjects was 1.6 ± 0.9(mean ± SD) and we defined any value.2.5 (mean ± SD of normal control sub-jects) as an insulin-resistant state and anyvalue ,2.5 as an insulin-sensitive state.The threshold value for insulin re s i s t a n c ein our study (i.e., 2.5) was similar to that(i.e., 2.77) re p o rted in subjects with nometabolic disorders that was re p o rted byB o rona et al. (5). The clinical characteris-tics and clinical pro files of insulin-sensi-tive (n = 30) and insulin-resistant (n = 40)subtypes were compared. No signific a n td i ff e rence was observed in age, sex, fastingplasma glucose, HbA1 c, and uric acid lev-els between the two groups. The patientswith insulin resistance had higher BMIand higher total cholesterol and LDL cho-l e s t e rol levels than those with norm a linsulin sensitivity, but the diff e rence wasnot statistically significant. In contrast, thepatients with insulin resistance had signifi-cantly higher levels of serum triglyceridesthan those with normal insulin sensitivity.(199.7 ± 20.0 vs. 94.2 ± 5.0 mg/dl, P ,0.001). HDL cholesterol levels weres i g n i ficantly lower in type 2 diabetic sub-jects with insulin resistance (47 ± 2 mg/dl)c o m p a red with those with normal insulinsensitivity (60 ± 3 mg/dl, P , 0 . 0 0 1 ) .T h e re was a positive correlation betweenHOMA-IR values and the levels of seru mtriglycerides in the patients studied (r =0.857, P , 0.0001). It is there f o re sug-gested that hypertriglyceridemia, but notBMI, is associated with insulin re s i s t a n c ein our nonobese type 2 diabetic patients.This finding suggests that pharm a c o l o g i c a lagents that lower serum triglyceride levelsmight improve glucose tolerance innonobese type 2 diabetic patients byreducing insulin resistance. In this re g a rd ,the study by Jones et al. (6) showing thatt reatment of patients with type 2 diabeteswith bezafibrate improves not only glu-cose tolerance but also serum triglyceride

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2101
Letters
levels is very interesting. In summary, ourp resent study demonstrated that non-obese Japanese type 2 diabetic patientsa re divided into two populations: onewith normal insulin sensitivity and theother with insulin resistance. In addition,t h e re is a possibility that hypert r i g l y c-eridemia per se is associated with insulinresistance in nonobese Japanese type 2diabetic populations.
ATARU TANIGUCHI, MD
MITSUO FUKUSHIMA, MD
MASAHIKO SAKAI, MD
KIYOSHI KATAOKA, MD
KUNIHISA MIWA, MD
ITARU NAGATA, MD
KENTARO DOI, MD
KUMPEI TOKUYAMA, PHD
YOSHIKATSU NAKAI, MD
F rom the First (A.T., M.S., I.N.) and Second (K.M.)D e p a rtments of Internal Medicine, Kansai-Denry o k uHospital; the Department of Internal Medicine (M.F. ) ,Hoshida-Minami Hospital, Osaka; the First Depart-ment of Physiology (K.K.), Ehime University, Ehime;the Second Department of Internal Medicine (K.D.)and the Division of the Science of Nursing (Y.N.), Col-lege of Medical Te c h n o l o g y, Kyoto University, Kyoto;and the Laboratory of Biochemistry of Exercise andNutrition (K.T.), Institute of Health and Sports Sci-ence, University of Tsukuba, Tsukuba, Japan.
A d d ress correspondence to Ataru Taniguchi, MD,First Department of Internal Medicine, Kansai-Den-ryoku Hospital, 2-1-7, Fukushima-ku, Fukushima,Osaka City, Osaka 553-0003, Japan. E-mail: k - 5 8 4 0 3 @ k e p c o . c o . j p .
R e f e re n c e s1 . Taniguchi A, Nakai Y, Fukushima M,
Kawamura H, Imura H, Nagata I, To k u-yama K: Pathogenic factors responsible forglucose intolerance in patients withNIDDM. D i a b e t e s 41:1540–1546, 1992
2 . Nagasaka S, Tokuyama K, Kusaka I,Hayashi H, Rokkaku K, Nakamura T,Kawakami A, Higashiyama M, Ishikawa S,Saito T: Endogenous glucose pro d u c t i o nand glucose effectiveness in type 2 diabeticsubjects derived from stable-labeled mini-mal model approach. D i a b e t e s 4 8 : 1 0 5 4 –1060, 1999
3 . World Health Organization: Diabetes Melli -tus: Report of a WHO Study Gro u p. Geneva,World Health Org., 1985 (Tech. Rep. Ser. ,no. 727)
4 . Matthews DR, Hosker JP, Rudenski AS,Naylor BA, Treacher DF, Tu rner RC:Homeostasis model assessment: insulinresistance and beta-cell function from fast-ing plasma glucose and insulin concentra-tions in man. D i a b e t o l o g i a 2 8 : 4 1 2 – 4 1 9 ,1 9 8 5
5 . B o rona E, Kiechl S, Willeit J, Oberh o l l e n-zer F, Egger G, Ta rgher G, Alberiche M,
Bonadonna RC, Muggeo M: Prevalence ofinsulin resistance in metabolic disord e r s :the Bruneck study. Diabetes 4 7 : 1 6 4 3 –1649, 1998
6 . Jones IR, Swai A, Taylor R, Miller M, LakerM F, Alberti KGMM: Lowering of plasmaglucose concentrations with bezafibrate inpatients with moderately contro l l e dNIDDM. Diabetes Care 13:855–863, 1990
Insulin Lispro, P re g n a n c y, andR e t i n o p a t h y
We read with interest the letter titled“Insulin Lispro and the Develop-ment of Proliferative Diabetic
Retinopathy During Pre g n a n c y,” by Kitz-miller et al. (1). We would like to shareour experience in treating pregnant dia-betic patients with insulin lispro .
P reston Acute Hospital NHS Trust issituated in the nort h w e s t e rn area of theU.K. and serves a population of 350,000.We have a combined diabetes and pre g-nancy clinic run by a consultant diabetolo-gist and obstetrician with their re s p e c t i v eregistrars. Every attempt is made to seet h e patients before pregnancy to ensureg o o d glycemic control before conception.Patients are thereafter seen at least every2 weeks until the thirtieth week and thene v e ry week until they deliver. Our targets ofblood glucose control are a fasting levelbetween 4 and 5 mmol/l and a 2-h post-prandial level between 4 and 7 mmol/l.Patients are admitted, if necessary, to ensuresmooth glycemic control. Our ro u t i n ediabetes care also includes annual re t i n a lp h o t o g r a p h y. We have analyzed our data onthe possible effect of diff e rent types ofinsulin on the pro g ression of re t i n o p a t h y.
We analyzed the data of 30 patientswith diabetes (3 with type 2 and the re s twith type 1) going through 40 pre g n a n-cies. They were 24–36 years of age withduration of diabetes of 2–25 years (mean15). There were 24 patients seen in thep re p regnancy clinic, who went thro u g h30 pregnancies; 16 pregnancies that weremanaged with insulin lispro; 21 that weremanaged with regular insulin; and 3 thatw e re managed with pork Velosulin (theyp re f e rred to stay on animal insulin) astheir short-acting insulin. When they wereseen in the pre p regnancy clinic, theirH b A1 c was ,7% (range 6.2–6.8). In allt h ree patients with type 2 diabetes, insulin
l i s p ro was used (lispro was started beforeconception in two of these patients, andafter confirmation in the other one, sinceshe did not attend the pre p re g n a n c yclinic). The main indication for insulinl i s p ro is patient convenience, since there isno gap re q u i red between injection andmeal. On the whole, six patients withretinopathy went through nine pre g n a n-cies (five with background re t i n o p a t h yand four with previously laser- t re a t e dretinopathy) and none worsened. None ofthe patients re q u i red ophthalmologici n t e rvention during pregnancy or duringthe period immediately postpartum. In therest of the patients, there was no re t i n o p a-thy before, during, or after part u r i t i o n .The prevalence of retinopathy was thesame in the lispro and regular gro u p s .
Worsening of retinopathy duringp regnancy is well known, although themechanisms are not completely clear. Thefactors implicated are preconception con-t rol, fluctuation of glycemic state, hyper-tension, diff e rent growth factors, and oth-ers (2–4). Kitzmiller et al. (1) found thatt h ree of their type 1 diabetic patients withno retinopathy who were managed withinsulin lispro developed florid re t i n o p a t h y,which re q u i red urgent treatment duringp re g n a n c y. It is important to note that inthe second and third patient, the initialH b A1 c was 3.7 and 3.4% above the upperlevel of normal laboratory value (whichwas not mentioned), which was suggestiveof poor glycemic control. More o v e r, themid-trimester decline of HbA1 c in all of thet h ree patients was considerable (2.2–3.6%). In the Diabetes in Early Pre g n a n c yS t u d y, the two main important factors fordeterioration or development of re t i n o p a-thy were higher HbA1 c at entry and dura-tion of diabetes .6 years (5). It has beenclearly documented before that deteriora-tion of retinopathy correlates with theplasma glucose at entry and the rate ofi m p rovement of glycemic control in thefirst 6–14 weeks after entry (6). These twofactors might have been responsible forthe deterioration or development ofretinopathy in the above-cited cases ratherthan the type of insulin used.
It is well known that insulin enhancesthe action of IGF-I (7), but that is unlikelyto be diff e rent with diff e rent types ofinsulin. Other than a slightly higher aff i n i t yfor the placental membranes, no other dif-f e rence in other cell lines using humaninsulin and insulin lispro was noticed (8).Anderson et al. (9) re p o rted their experi-

2102 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
ence in using insulin lispro in nonpre g n a n tadults in whom no increase in incidence ofretinopathy was observed. In summary,our experience with using insulin lispro inp regnant diabetic patients does not suggestany deterioration of re t i n o p a t h y, in spite oftheir long duration (mean 15 years) of dia-betes. We would, however, re c o m m e n dc a reful pooling of data on the managementof diabetes in pregnancy to obtain a larg eenough database for evaluation of the eff e c tof diff e rent types of insulin on re t i n o p a t h yduring pre g n a n c y.
AR PA N D E V BH AT TA C H A RY YA, M D, M R C P (U.K. )PATRICIA A. VICE, BSC, FRCP
F rom the Department of Medicine, Division of Dia-betes and Endocrinology, Preston Acute HospitalNHS Trust, Fulwood, Preston, U.K.
A d d ress correspondence to P.A. Vice, ConsultantPhysician, Preston Acute Hospital NHS Trust, Ful-wood, Preston, Lancashire, PR2 9HT, U.K.
R e f e re n c e s1 . Kitzmiller JL, Main E, Wa rd B, Theiss T,
Peterson DL: Insulin lispro and the devel-opment of proliferative diabetic re t i n o p a-thy during pre g n a n c y. Diabetes Care 2 2 :874–876, 1999
2 . Klein BEK, Moss SE, Klein R: Effect ofp regnancy on pro g ression of diabeticre t i n o p a t h y. Diabetes Care 13:34–40, 1990
3 . A x e r-Siegel R, Hod M, Fink-Cohen S,Kramer M, We i n b e rger D, Schindel B, Ya s-sur Y: Diabetic retinopathy during pre g-n a n c y. O p h t h a l m o l o g y 1 0 3 : 1 8 1 5 – 1 8 1 9 ,1 9 9 6
4 . Hill DJ, Flyvbjerg A, Arany E, Lauszus FE,Klebe JG: Increased levels of serum fib ro-blast growth factor-2 in diabetic pre g n a n twomen with re t i n o p a t h y. J Clin EndocrinolM e t a b 82:1452–1457, 1997
5 . Chew EY, Mills JL, Metzger BE, RemaleyLA, Jovanovic-Peterson L, Knoop RH,Conley M, Rand L, Simpson JL, HolmesLB, Aarons JH, for the National Institute ofChild Health and Human DevelopmentDiabetes in Early Pregnancy Study: Meta-bolic control and pro g ression of re t i n o p a-thy: Diabetes in Early Pregnancy Study.Diabetes Care 18:631–637, 1995
6 . Phelps RL, Sakol L, Metzger BE, JampolLM, Frenkel N: Changes in diabetic re t i n o-pathy during pregnancy: correlations withregulation of hyperglycaemia. A rch Oph -t h a l 104:1806–1810, 1986
7 . Merimee T: The interface between diabeticre t i n o p a t h y, diabetes management, andinsulin-like growth factors. J Clin Endo -crinol Metab 82:2806–2808, 1997
8 . D i M a rchi RD, Chance RE, Long HB,Shields JE, Slieker LJ: Preparation of aninsulin with improved pharm a c o k i n e t i c s
relative to human insulin through consid-eration of structural homology withinsulin-like growth factor 1. H o rm Res 4 1(Suppl. 2):93–96, 1994
9 . Anderson JH, Brunelle RL, Koivisto VA :Reduction of postprandial hyperg l y c e m i aand frequency of hypoglycemia in IDDMpatients on insulin-analog treatment. D i a -b e t e s 46:265–270, 1997
Response to B h a t t a c h a ryya and Vi c e
The interest of Bhattacharyya and Vi c e(1) in our observation of three caseswith the development of pro l i f e r a t i v e
diabetic retinopathy (PDR) during pre g-nancy in a group of 10 diabetic womenwith a baseline negative ophthalmologicexamination (2) is appreciated. Since thiso b s e rvation is quite rare (2,3), we werec o n c e rned to note that the 10 pre g n a n ttype 1 or 2 diabetic women were tre a t e dwith insulin lispro. Bhattacharyya andVice (1) are correct to emphasize care f u lp reparation for pregnancy in diabeticwomen (4), which unfortunately was notdone in our three cases of rapidly develop-ing PDR. They re p o rted on 16 pre g n a n c i e sin 15 women with type 1 or 2 diabetest reated with insulin lispro during pre g-n a n c y. Ten of these women with well-con-t rolled diabetes had negative ophthalmo-logic examinations before, during, andafter pre g n a n c y, and three with back-g round diabetic retinopathy and two withp revious laser- t reated retinopathy alsoshowed no pro g ression. To my knowl-edge, there has been only one pre v i o u s l yre p o rted case of the development of flo r i dPDR during pregnancy from a baselinenegative ophthalmologic examination (3).Although the title of that case re p o rtdescribes a gestational diabetes patient,the patient described was probably awoman with undiagnosed type 2 diabetes,since her initial HbA1 c was 16.2% (6%).
To date, there have been at least 314diabetic women re p o rted in the literature(1–3) with negative initial ophthalmologicexaminations who were treated with stan-d a rd insulin, and 1 case developed PDRduring pre g n a n c y. Now, 20 women withnegative initial examinations who weret reated with insulin lispro have beenre p o rted, and 3 developed PDR. To avoidthe trap of anecdotal cases and uncon-
t rolled observations seeming to infer ac a u s e - e ffect relationship, as noted byJovanovic (5) in her invited response toour observation, further studies are neces-s a ry to see if the association of our thre ecases of PDR with use of insulin lisproo c c u red on the basis of chance. With useof the pro p o rtions noted above, a powercalculation indicates that 110 diabeticwomen with initial negative ophthalmo-logic examinations would be re q u i red ineach group to have an 80% power of fin d-ing a significant diff e rence based oninsulin therapy at the 0.05 level, one-tailed. I agree with Bhattacharyya and Vi c e(1) and Jovanovic (5) that the subgroup ofdiabetic women with poor glycemic con-t rol at the onset of pregnancy is at thehighest risk of developing PDR, perh a p sbecause they may already have undetectedperipheral retinal ischemia. The feasibilityof perf o rming a randomized trial of con-tinuing standard insulin therapy duringp regnancy versus switching to insulinl i s p ro or insulin aspart is good even in thiss u b g roup with evidence of chronic hyper-glycemia, since most diabetic women inN o rth America still enter pregnancy with-out effective preconception care (4). Theya re then exposed to rapid intensification ofglycemic control to prevent fetal damage,usually with days to weeks of wide glucoseexcursions (6).
In separate editorials, Merimee (7)and Chantelau and Kohner (8) discussedfactors that might explain the temporaryworsening of diabetic retinopathy in casesof chronic hyperglycemia exposed toi n t e n s i fied glycemic control. They dis-cussed possible roles of IGF-1 and itsbinding proteins (IGFBPs), includingi n c reased circulating IGF-1 with intensifi-cation of insulin treatment (8). Attia et al.(9) observed acute re c i p rocal changes inf ree IGF-1 and IGFBP-1 levels with acuteinsulin withdrawal of up to 8 h (IGFBP-1up, IGF-1 down), followed by insulinreplacement for 2 h (IGFBP-1 down,I G F-1 up) in type 1 diabetic subjects. Mer-imee (7) stated that “increased intracellu-lar transport of glucose initiated by levelsof IGF-1 in local tissue beds can result incellular hypert rophy and hyperplasia.”Demonstrated effects of IGF-1 in the eyeinclude promotion of chemotaxis of re t i-nal endothelial cells, induction of vasodi-lation, micro a n e u rysm formation, neovas-cularization (10), enhanced formation ofcollagenase, which can dissolve capillarybasement membranes and the collagen

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2103
Letters
matrix of the retina (6,10), and stimula-tion of mitogenesis of human re t i n a lendothelial cells (11). The latter effect wasenhanced by basic fib roblast growth fac-t o r, which, in pregnant diabetic women,has been ascribed to placental pro d u c t i o nand associated with the development ofPDR (12). Most authors emphasize localretinal production of IGF-1 and the IGF-BPs, but Pfeiffer et al. (13) propose that ab reakdown of the blood retina barrier withi n flux of serum proteins secondary tom i c rovascular disturbances and hypoxia isresponsible for the vitreous alterations ofIGF-1 and IGFBPs found in PDR.
Insulin lispro was developed as aninsulin with improved pharm a c o k i n e t i c srelative to human insulin through con-sideration of structural homology withIGF-1 (14).
B h a t t a c h a ryya and Vice state that “It iswell known that insulin enhances theaction of IGF-1, but that is unlikely to bed i ff e rent with diff e rent types of insulin”(1). One wonders about possible diff e re n-tial effects on the stimulation of IGFBP-3synthesis by insulin in mixed liver cell cul-t u res (15) and the increased IGFBP pro-tease activity of pregnancy (16), since, insome situations, IGFBP-3 may enhancethe cell growth promoting activity ofI G F-1 (17). One wonders about possibled i ff e rential insulin effects on inhibition ofIGFBP-1 production by the liver whilei n c reasing IGF-1 production (18) and onstimulation of IGFBP-1 transport acro s sthe endothelial wall (19), and the fact thatin pregnancy nonphosphorylated forms ofIGFBP-1 have lower affinity for IGF-1 andm o re growth stimulatory activity (17).M o re re s e a rch is needed on the possiblee ffects of insulin analogs on the complexIGF/IGFBP systems, with and withoutp re g n a n c y. Jovanovic (5) stated that“insulin lispro has the same affinity for theIGF-1 receptor as human insulin.” Actu-a l l y, the affinity of insulin lispro for theIGF-1 receptor was increased less thantwofold relative to human insulin in stud-ies at the Lilly Research Laboratories (14).M o re re c e n t l y, Trüb et al. (20) found thatthe IGF-1 receptor affinity (HepG2 cells)of insulin lispro was 141.5% relative tohuman insulin and that the IGF-1 re c e p t o ra ffinity of insulin aspart (B28Asp) was68.8% relative to human insulin. Never-theless, the affinity of any type of insulinfor the IGF-1 receptor is ,1,000-fold lessthan that of IGF-1, ,1% of IGF-1 in cir-culating blood is in the free form (9), and
f ree IGF-1 circulates in nanomolar con-centrations, whereas free insulin circ u l a t e sat picomolar concentrations (21).
Jovanovic (5) cites the work of Ander-son et al. (22) as evidence that contro l l e dtrials of insulin lispro in nonpregnant dia-betic subjects did not show significant dif-f e rences in the frequency of re t i n o p a t h y.H o w e v e r, in my reading of this art i c l ere p o rting the results of a 6-month ran-domized multinational clinical trial per-f o rmed with an open-label cro s s o v e rdesign comparing insulin lispro with re g u-lar human insulin conducted by the LillyR e s e a rch Laboratories in 1,008 type 1 dia-betic subjects, I noticed that re t i n o p a t h ywas not mentioned as an outcome variableor an adverse event (22). It may be likelythat the type of insulin used for intensifie dglycemic control has nothing to do withthe rapid development of PDR in pre g n a n twomen with chronic hyperglycemia andthe beginnings of peripheral re t i n a lischemia, but we will never know withoutp roperly designed controlled trials.
JOHN L. KITZMILLER, MD
F rom the Division of Maternal-Fetal Medicine, GoodSamaritan Hospital, San Jose, Californ i a .
A d d ress correspondence to John L. Kitzmiller,MD, Good Samaritan Hospital, 2425 Samaritan Dr. ,San Jose, CA 95124. E-mail: [email protected].
J.L.K. has received honoraria for speaking engage-ments from Eli Lilly.
R e f e re n c e s1 . B h a t t a c h a ryya A, Vice PA: Insulin lispro ,
p re g n a n c y, and re t i n o p a t h y. Diabetes Care22:2101–2102, 1999
2 . Kitzmiller JL, Main E, Wa rd B, Theiss T,Peterson DL: Insulin lispro and the devel-opment of proliferative diabetic re t i n o p a-thy during pre g n a n c y. Diabetes Care 2 2 :874–876, 1999
3 . Hagay ZJ, Schachter M, Pollack A, Levy R:Development of proliferative re t i n o p a t h yin a gestational diabetes patient followingrapid metabolic control. Eur J ObstetGynecol Reprod Biol 57:211–213, 1994
4 . Kitzmiller JL, Buchanan TA, Kjos S,Combs CA, Ratner RE: Technical Review:P re-conception care of diabetes, congenitalm a l f o rmations, and spontaneous abor-tions. Diabetes Care 19:514–541, 1996
5 . Jovanovic L: Retinopathy risk: what isresponsible? Hormones, hyperg l y c e m i a ,or Humalog? (Commentary) Diabetes Care22:846–848, 1999
6 . Kitzmiller JL, Gavin LA, Gin GD,Jovanovic-Peterson L, Main EK, ZigrangWD: Preconception care of diabetes:glycemic control prevents excess congenital
m a l f o rmations. J A M A 265:731–736, 19917 . Merimee T: Editorial: The interf a c e
between diabetic re t i n o p a t h y, diabetesmanagement, and insulin-like growth fac-tors. J Clin Endocrinol Metab 8 2 : 2 8 0 6 –2808, 1997
8 . Chantelau E, Kohner EM: Why some casesof retinopathy worsen when diabetic con-t rol improves. B M J 315:1105–1106, 1997
9 . Attia N, Caprio S, Jones TW, Heptulla R,Holcombe J, Silver D, Sherwin RS, Ta m-borlane WV: Changes in free insulin-likeg rowth factor-1 and leptin concentrationsduring acute metabolic decompensation ininsulin withdrawn patients with type 1diabetes. J Clin Endocrinol Metab 8 4 : 2 3 2 4 –2328, 1999
1 0 . Grant MB, Mames RN, Fitzgerald C, EllisEA, Aboufrieka M, Guy J: Insulin-likeg rowth factor-1 acts as an angiogenic agentin rabbit cornea and retina: comparativestudies with basic fib roblast growth factor.D i a b e t o l o g i a 36:282–291, 1993
1 1 . Giannini S, Cresci B, Ciucci A, Pala L,Manuelli C, Franchini A, Rotella CM:IGFBP-4/IGFBP-5 ratio regulates theI G F-1 effects on human retinal endothelialcells (HREC) (Abstract). D i a b e t o l o g i a 4 1(Suppl. 1):A18, 1998
1 2 . Hill DJ, Flyvbjerg A, Arany E, Lauszus FF,Klebe JG: Increased serum levels of seru mfib roblast growth factor-2 in diabetic pre g-nant women with re t i n o p a t h y. J ClinEndocrinol Metab 82:1452–1457, 1997
1 3 . P f e i ffer A, Spranger J, Meyer- S c h w i c k e r a t hR, Schatz H: Growth factor alterations inadvanced diabetic retinopathy: a possiblerole of blood retina barrier bre a k d o w n .D i a b e t e s 46 (Suppl. 2):S26–S30, 1997
1 4 . D i M a rchi RD, Chance RE, Long HB,Shields JE, Slieker LJ: Preparation of aninsulin with improved pharm a c o k i n e t i c srelative to human insulin through consid-eration of structural homology withinsulin-like growth factor-1. H o rm Res 4 1(Suppl. 2):93–96, 1994
1 5 . S c h a rf JG, Ramadori G, Braulke T, Hart-mann H: Cellular localization and hor-monal regulation of biosynthesis ofinsulin-like binding proteins and of theacid-labile subunit within rat liver. P ro gG rowth Factor Res 6:175–180, 1995
1 6 . Guidice LC, Farrell EM, Pham H, LamsonG, Rosenfeld RG: Insulin-like growth fac-tor proteins in maternal serum thro u g h o u tgestation and in the puerperium: effects ofa pregnancy-associated serum pro t e a s ea c t i v i t y. J Clin Endocrinol Metab 7 1 : 8 0 6 –816, 1990
1 7 . C o l l e t t - S o l b e rg PF, Cohen P: The role ofthe insulin-like growth factor binding pro-teins and the IGFBP proteases in modulat-ing IGF action. Endocrinol Metab Clin Nort hA m 25:591–614, 1996
1 8 . Brismar K, Fernqvist-Forbes E, Wa h ren J,Hall K: Effect of insulin on the hepatic pro-

2104 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
duction of insulin-like growth factor- b i n d-ing protein-1 (IGFBP-1), IGFBP-3, andIGF-1 in insulin-dependent diabetes. J ClinEndocrinol Metab 79:872–878, 1994
1 9 . Bar RS, Boes M, Clemmons DR, BusbyWH, Sandra A, Dake BL, Booth BA:Insulin diff e rentially alters transcapillarymovement of intravascular IGFBP-1,IGFBP-2 and endothelial cell IGF-bindingp roteins in rat heart. E n d o c r i n o l o g y 1 2 7 :497–499, 1990
2 0 . Trüb T, Hey A, Sorensen AR, Schaffer L,D rejer K, Kurtzhals P: Growth pro m o t i n gactivity of insulin aspart and other insulinanalogues (Abstract). D i a b e t o l o g i a 4 2(Suppl. 1):A179, 1999
2 1 . Le Roith D: Insulin-like growth factors.N Engl J Med 336:633–640, 1997
2 2 . Anderson JH Jr, Brunelle RL, Koivisto VA ,Pfutzner A, Trautmann ME, Vignati L,D i M a rchi R, and the Multicenter InsulinL i s p ro Study Group: Reduction of post-prandial hyperglycemia and frequency ofhypoglycemia in IDDM patients oninsulin-analog treatment. D i a b e t e s 4 6 : 2 6 5 –270, 1997
I m p a i red FastingGlucose Is Not aRisk Factor for C a rdiovascular M o rt a l i t y
In the June 1999 issue of Diabetes Care,Tominaga et al. (1) concluded thati m p a i red glucose tolerance, but not
i m p a i red fasting glucose (IFG), is a risk fac-tor for cardiovascular disease. This conclu-sion was based on the mortality of a cohortof Japanese people over a follow-up periodof 4–6 years, with use of both the Wo r l dHealth Organization and the American Dia-betes Association criteria for the diagnosisof glucose tolerance classes. The IFG gro u pexperienced three deaths per 832 person-years of observation. The odds ratio of thisg roup compared with that of the norm a lglucose tolerance group was 1.32 with ane x t remely wide 95% CI (0.012–140.91),suggesting that the power to detect as i g n i ficant association between IFG andm o rtality was very low (type II erro r ) .
The role of fasting glucose on card i o-vascular mortality has been re c e n t l yre p o rted. Bjørnholt et al. (2) described theexcess risk of cardiovascular deaths innondiabetic men in the upper norm a lrange of fasting blood glucose, and Balkauet al. (3) found a linear re l a t i o n s h i p
between death from coro n a ry heart dis-ease and fasting blood glucose levels. Ifthese observations were valid, namely, thatthe risk of cardiovascular death incre a s e swith increasing fasting blood glucose, onewould expect that people in the IFG cate-g o ry would be at a higher risk than thosein the normal fasting glucose category.
It is possible that the lack of associa-tion found by Tominaga et al. in the Funa-gata Diabetes Study is due to a re l a t i v e l ys h o rt follow-up period of the IFG gro u p ,combined with the low incidence of car-diac deaths, which is a well-known fact inthe Japanese population.
Without challenging the value of the2-h blood glucose levels as a predictor ofc a rdiovascular mort a l i t y, it is pre m a t u re todeny the role of IFG based on the pre-sented data.
SIMON WEITZMAN, MD, MPH
F rom the Department of Epidemiology and the“Fraida” Foundation for Diabetes Research, Ben-Gurion University of the Negev, Beer-Sheva, Israel.
A d d ress correspondence to Simon We i t z m a n ,MD, MPH, Soroka Medical Center, P.O. Box 653,B e e r-Sheva 84105, Israel. E-mail: weitzman@b g u m a i l . b g u . a c . i l .
R e f e re n c e s1 . Tominaga M, Eguchi H, Manaka H,
Igarashi K, Kato T, Sekikawa A: Impaire dglucose tolerance is a risk factor for card i o-vascular disease, but not impaired fastingglucose. Diabetes Care 22:920–924, 1999
2 . B j ø rnholt JV, Erikssen G, Aaser E, SandvikL, Nitter-Hauge S, Jervell J, Erikssen J,Thaulow E: Fasting blood glucose: anu n d e restimated risk factor for card i o v a s-cular death. results from a 22-year follow-up of healthy diabetic men. Diabetes Care22:45–49, 1999
3 . Balkau B, Bertrais S, Ducimetiere P,Eschwege E: Is there a glycemic thre s h o l dfor mortality risk? Diabetes Care 2 2 : 6 9 6 –699, 1999
A Drug InteractionBetween Troglitazone andS i m v a s t a t i n
Since its approval in 1997, tro g l i t a z o n ehas been considered one of the morerecent advances in the treatment of
type 2 diabetes. Troglitazone is a memberof the thiazolidinediones, a class separated
f rom the other oral antidiabetic agents suchas sulfonylureas, a-glucosidase inhibitors,and biguanides by its distinct pharm a c o l-o g y. Troglitazone decreases insulin re s i s-tance, which is thought to be the underly-ing pathophysiology of type 2 diabetes, byi m p roving insulin sensitivity in peripheraltissues (1). It also inhibits hepatic gluco-neogenesis, thus decreasing hepatic glu-cose production (2). In addition to itsinsulin-sensitizing ability, troglitazoneappears to have lipid-lowering effects byinhibiting the synthesis and enhancing theclearance of triglycerides (3).
Limited studies are available to pro v i d edata on the drug interaction pro file oft roglitazone. Human in vivo drug interac-tion trials have indicated that tro g l i t a z o n e ,at clinically relevant doses, behaves as aninducer of the CYP3A4 enzyme (4). Thisconclusion is further supported by the doc-umented interaction of troglitazone withboth oral contraceptives and terf e n a d i n e .Co-administration of troglitazone with oralcontraceptives and terfenadine can decre a s ethe plasma concentration of oral contracep-tives and terfenadine by ,30 and 50–70%,respectively (4,5). To date, there are nopublished studies evaluating the signifi-cance of interaction between tro g l i t a z o n eand other drugs that are also metabolizedby CYP3A4. The majority of HMG-CoAreductase inhibitors, including simvastatin,a re metabolized by CYP3A4, where a spravastatin is believed to be metabolized byisoenzymes other than CYP3A4 (6).
A re t rospective analysis was con-ducted to evaluate a possible drug interac-tion between troglitazone and simvastatin.This was a subgroup analysis of thePravastatin to Simvastatin Conversion-Lipid Optimization Program (PSCOP) thatwas in pro g ress 2 years earlier (7). Thep rogram was designed with the goal ofi n c reasing the percentage of patients meet-ing their LDL cholesterol goal based onNational Cholesterol Education Panelguidelines. Instead of initiating the simvas-tatin dosage according to the dose equiva-lency of two drugs, it was determined bythe lipid pro file and coro n a ry art e ry dis-ease risk factors of the individual patient.
The re t rospective analysis identifie d344 diabetic patients from 1,115 patientsin the original PSCOP. These diabeticpatients were further divided into twog roups: the troglitazone group, whichincluded 21 patients who were tre a t e dwith troglitazone before and after the con-version; and the nontroglitazone gro u p ,

DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999 2105
Letters
which included 323 patients who werenot treated with troglitazone. Additionally,a two-to-one (two nontroglitazone patientsto one troglitazone patient) matchingp rocess was perf o rmed in an eff o rt to con-t rol for the effect of age and weight, whichi d e n t i fied 42 patients. The matching crite-ria for age and weight were ± 3 years and± 4.5 kg, re s p e c t i v e l y.
Pravastatin and simvastatin doses werenot significantly diff e rent between thet roglitazone and the nontro g l i t a z o n epatient groups; the mean doses of pravas-tatin and simvastatin were 24–27 and21–22 mg, re s p e c t i v e l y. There were signifi-cant percentage reductions in total and LDLc h o l e s t e rol levels after antihyperlipidemicmedications were changed from pravastatinto simvastatin in the nonmatched (26 . 4and 210.2%, respectively; P , 0.001) andmatched nontroglitazone (26.6 and211.8%, respectively; P , 0.05) gro u p s .H o w e v e r, no significant reductions in total(22.7%; P = 0.32) and LDL (21.3%; P =0.65) cholesterol were observed in thepatients receiving troglitazone. The per-centage of patients meeting their LDL cho-l e s t e rol goal increased in both nonmatched(48–65%; P , 0.001) and matched non-t roglitazone (52–69%; P = 0.13) patientg roups after converting to simvastatin;h o w e v e r, the increase was significant onlyin the nonmatched group. Nine (42%) ofthe patients treated with troglitazone mettheir LDL cholesterol goal while on pravas-tatin and only eight (38%) after the conver-sion to simvastatin (P = 1.0).
Our re t rospective analysis compare dlipid pro files before and after conversionf rom pravastatin to simvastatin in diabeticpatients who were treated with and with-out troglitazone. Because the mean dosesof pravastatin and simvastatin were simi-l a r, one would expect an additional per-centage reduction (11%) in LDL choles-t e rol after changing pravastatin to simvas-tatin (8,9). However, this was evident onlyin the patients who were not treated witht roglitazone. More o v e r, after these patientsw e re matched according to age and weightwith the troglitazone patients, the re d u c-tions in total and LDL cholesterol were stills i g n i ficant. In addition, the percentage ofpatients meeting their LDL cholestero lgoal after converting to simvastatini n c reased in both nontroglitazone gro u p s .One potential explanation for the re d u c e dlipid-lowering effect of simvastatin in thepatients also taking troglitazone isenhanced enzyme-induced metabolism of
simvastatin. This induction in metabolismby troglitazone is likely to be more pro-nounced with simvastatin than withpravastatin since CYP3A4 is the mainmetabolism isoenzyme for simvastatin,and troglitazone is known to induceCYP3A4 (4,6). Pravastatin has beenshown to exhibit some affinity for CYP3A4(10), even though CYP3A4 may not be thep r i m a ry isoenzyme involved in its metab-olism. Although re t rospectively observ e d ,this interaction between troglitazone andsimvastatin is likely to be clinically re l e-vant and has not been previously re p o rt e d .
On the basis of the results from thisre t rospective analysis, we re c o m m e n dadditional monitoring of lipid pro fil e swhen troglitazone and simvastatin areused concomitantly. Higher simvastatindosage may be re q u i red owing to the pos-sibility that troglitazone may induce themetabolism of simvastatin, thus diminish-ing some lipid-lowering effects of simvas-tatin. To confirm this drug interaction andp rovide more definite information, ap rospective trial is perhaps necessary.
JENNIFER C. LIN, PHARMD
MATTHEW K. ITO, PHARMD, BCPS, FCCP
F rom the School of Pharmacy and Health Sciences,University of the Pacific, Stockton; and the Card i o v a s-cular Pharmacodynamics Laboratory, Veterans Aff a i r sSan Diego Healthcare System, San Diego, Californ i a .
A d d ress correspondence to Matthew K. Ito,P h a rmD, BCPS, FCCP, Veterans Affairs San DiegoH e a l t h c a re System, 3350 La Jolla Village Dr., SanDiego, CA 92161. E-mail: [email protected].
M.K.I. has received honoraria for speakingengagements from Parke-Davis, Merck, and Bristol-Myers Squibb as well as funding for re s e a rch fro mM e rck and Bristol-Myers Squibb.
R e f e re n c e s1 . K e l l e rer M, Kroder G, Tippmer S, Berti L,
Kiehn R, Mostahaf L, Haring HU: Tro g l i t a-zone prevents glucose-induced insulinresistance of insulin receptor in rat-1 fib ro-blasts. D i a b e t e s 43:447–453, 1994
2 . Saltiel AR, Olefsky JM: Thiazolidinedionesin the treatment of insulin resistance andtype II diabetes. D i a b e t e s 4 5 : 1 6 6 1 – 1 6 6 9 ,1 9 9 6
3 . Whitcomb RW, Saltiel AR: Thiazolidine-diones. Exp Opin Invest Dru g s 4 : 1 2 9 9 –1309, 1995
4 . Parke-Davis: Resulin (troglitazone) pack-age insert. Morris Plains, NJ, 1997
5 . Lori CM, Knowlton P, Stern R, Koup JR,Vassos AB, Sedman AJ: Effect of tro g l i t a-zone on terfenadine pharm a c o k i n e t i c swhen dosed 4 hours apart (Abstract). C l i nP h a rmacol Ther 63:228, 1998
6 . Bays HE, Dujovne CA: Drug interactions
of lipid-altering drugs. D rug Saf 1 9 : 3 5 5 –371, 1998
7 . Ito MK, Stolley SN, Morreale AP, Lin JC,M a rcus DB: Rationale, study design, andbaseline results of the Pravastatin to Sim-vastatin Conversion-Lipid OptimizationP rogram (PSCOP). Am J Health Syst Pharm56:1107–1113, 1999
8 . The Simvastatin Pravastatin Study Gro u p :Comparison of the eff i c a c y, safety and tol-erability of simvastatin and pravastatin forh y p e rc h o l e s t e rolemia. Am J Card i o l 7 1 :1408–1414, 1993
9 . Ito MK, Stolley SN, Morreale AP, Lin JC,M a rcus DB: Narrowing the cholestero lt reatment gap: results of the Pravastatin toSimvastatin Conversion-Lipid Optimiza-tion Program (PSCOP) (Abstract). P h a r -m a c o t h e r a p y 19:510, 1999
1 0 . Transon C, Leemann T, Dayer P: In vitrocomparative inhibition pro files of majorhuman drug metabolising cytochro m eP450 isozymes (CY2C9, CYP2D6 andCYP3A4) by HMG-CoA reductase inhibi-tors. Eur J Clin Pharm a c o l 5 0 : 2 0 9 – 2 1 5 ,1 9 9 6
Response to Lin and Ito
E ffect of troglitazone on a t o rvastatin pharm a c o k i n e t i c sand pharm a c o d y n a m i c s
The letter by Lin and Ito (1) raises thepossibility of an interaction betweent roglitazone and simvastatin. We
would like to add further information re l e-vant to the discussion of interactionsbetween HMG-CoA reductase inhibitorsand troglitazone. In vitro studies haveshown that various CYP isozymes, includ-ing CYP3A4, are involved in the metabo-lism of HMG-CoA reductase inhibitors(2–4). Currently available data indicate thatt roglitazone likely induces CYP3A4 activity( 5 , 6 ) . A prospective crossover study wasconducted to evaluate the effect of tro g l i t a-zone on the pharmacokinetics and pharm a-codynamics of atorvastatin, which is a sub-strate of CYP3A4 (7). Although tro g l i t a z o n emoderately reduced the plasma area underthe curve of atorvastatin by 33%, changesin lipids (triglyceride and total, LDL, andHDL cholesterol levels) were similar afteradministration of atorvastatin alone andafter administration of atorvastatin witht roglitazone (8). There f o re, we concur withLin and Ito that a prospective clinical studymight be helpful in clarifying the signifi-

2106 DIABETES CARE, VOLUME 22, NUMBER 12, DECEMBER 1999
Letters
cance of a possible tro g l i t a z o n e - s i m v a s t a t i nd ru g - d rug interaction.
CHO-MING LOI, PHARMD
ALLEN J. SEDMAN, MD, PHD
F rom the Parke-Davis Pharmaceutical Research Divi-sion, Ann Arbor, Michigan.
A d d ress correspondence to Cho-Ming Loi,P h a rmD, Department of Pharmacokinetics, Dynam-ics, and Metabolism, Parke-Davis Pharm a c e u t i c a lR e s e a rch Division, 2800 Plymouth Rd., Ann Arbor,MI 48105. E-mail: [email protected].
C.-M.L. and A.J.S. hold stock in Wa rn e r- L a m b e rt ..
R e f e re n c e s1 . Lin JC, Ito MK: A drug interaction
between troglitazone and simvastatin. D i a -betes Care 22:2104–2105, 1999
2 . Wang RW, Kari PH, Lu AYH, Thomas PE,Guengerich FP, Vyas KP: Biotransform a-tion of lovastatin. IV. Identification ofc y t o c h rome P450 3A proteins as the majorenzymes responsible for the oxidativemetabolism of lovastatin in rat and humanliver microsomes. A rch Biochem Biophys290:355–361, 1991
3 . Transon C, Leemann T, Dayer P: In vitrocomparative inhibition pro files of majorhuman drug metabolising cytochro m eP450 isozymes (CYP2C9, CYP2D6, andCYP3A4) by HMG-CoA reductase inhibi-tors. Eur J Clin Pharm a c o l 5 0 : 2 0 9 – 2 1 5 ,1 9 9 6
4 . P rueksaritanont T, Gorham LM, Ma B, LiuL, Yu X, Zhao JJ, Slaughter DE, Arison BH,Vyas KP: In vitro metabolism of simvas-tatin in humans [SBT]identification of
metabolizing enzymes and effect of thed rug on hepatic P450s. D rug Metab Dispos25:1191–1199, 1997
5 . Koup JR, Anderson GD, Loi CM: Effect oft roglitazone on urinary excretion of6b-h y d ro x y c o rtisol. J Clin Pharm a c o l 3 8 :815–818, 1998
6 . Kaplan B, Friedman G, Jacobs M, Vi s c u s oR, Lyman N, DeFranco P, Bonomini L,Mulgaonkar SP: Potential interaction oft roglitazone and cyclosporine. Tr a n s p l a n t a -t i o n 65:1399–1400, 1998
7 . Parke-Davis: Lipitor (atorvastatin) packagei n s e rt. Morris Plains, NJ, 1999
8 . Loi CM, Stern R, Abel R, Koup JR, Va s s o sAB, Sedman AJ: Effect of troglitazone onp h a rmacokinetics and pharm a c o d y n a m i c sof atorvastatin (Abstract). Clin Pharm a c o lT h e r 65:186, 1999





























