Embed Size (px)
Citation preview
NANOTECHNOLOGY AND INSULIN: A PERFECT MARRIAGE ????
Presented By:Ashwini KumarDoctoral Research ScholarDepartment of BiotechnologyNational Institute of Technology (NIT) RaipurC.G
Awanish Kumar, Ashwini Kumar *
Department of BiotechnologyNIT Raipur
DIABETES….. > 550 million by 2030 (WHO) IDDM and NIDDM Hyperglycemia CVD, Retinopathy, Neuropathy, Nephropathy, Pulmonary Disorders, Infections…..
Oral – Sulfonylureas, Biguanides, TZDs, α-glucosidase inhibitors, Incretin analogs, DPP-4 inhibitors, SGLT2 inhibitors, GSK-3 inhibitors……..
Parenteral – Subcutaneous Insulin
INSULIN….. Peptide hormone (51 a.a) secreted by β-cells of the pancreas.
Regulates the blood glucose level by transporting glucose inside adipocytes and skeletal muscles for further use.
Recombinant Human Insulin (rHI) is currently the final answer to the uncontrolled diabetes (type 1 and type 2).
Formulations – Short acting, Intermediate acting, Long acting, Ultra long acting.
Regulates pre-prandial and post-prandial blood glucose. Parenteral (sub-cutaneous) administration. Injection site morbidity comes as resistance.

ALTERNATIVES…..
INHALED INSULIN FORMULATIONS Lungs are highly vascularized, surface area 50-140 m2 .
Thin alveolar-capillary barrier, rapid absorption.
No peptidases or proteases No pH variation Enhanced absorption with particle size 1-3µm in diameter; larger particles are often swollowed through upper respiratory tract.
Dry powder (Exubera and Technosphere) and Liquid (AERx iDMS).
A. EXUBERA Pfizer/Nektar Pharmaceuticals Dry powder formulation First ever non-parenteral insulin; reached market in 2006; withdrawn in late 2007
Peak insulin concentration more quickly than sub-cutaneous route (45 minutes vs. 105 minutes).
Spray-dried (lyophilized); excipients were mannitol, glycine, sodium citrate.
1 unit (≈3 mg) insulin or 3 units insulin per blister; particle diameter < 5 µm.
DRAWBACKS OF EXUBERA Not suitable for smokers, asthamatic patients COPD patients.
Lung deposition. Decreased the respiratory volumes. A few patients were diagnosed with pulmonary malignancy (IGF-1 activity)
Low market acceptibility
B. AFREZZA Developed by MannKind Corp. CA (USA); Approved by USFDA in June 2014.
Technosphere Insulin (TI); rHI combined with fumaryl diketopiperazine.
Technosphere particles were prepared by pH controlled crystallization of FDKP, polysorbate 80, acetic acid and water.
Median particle size 2-2.5 micron (µm) FDKP and Insulin are absorbed independently; former excreted unchanged in urine.
CONTD….. Insulin release mimics the pancreatic release pattern.
Median Tmax from lungs to blood is 15 minutes. TI was found to ne non-cytotoxic to the bronchial cell lines (no membrane or tight junction damage).
Hypoglycemic and weight gain events lesser than the SC injection.
Better result in COPD and pulmonary patients as compared to Exubera, but still should be used with utmost precaution.
ADVANTAGES…..
Better bioavailibility; no 1st pass metabolism
Ease of access Easy storage and transportaion No chance of microbial contamination
ORAL INSULIN FORMULATIONS….. Insulin is a peptide !!!! PROTEASE INHIBITORS (trypsin, chymotrypsin, elastase, carboxypeptidase, aminopeptidase, insulin degrading enzymes).
pH variation, chemical degradation (1-7.5) Must adhere to the mucus layer…..MUCOADHESIVE
Intestinal cell permeability (hydrophillic & large MW)…..ABSORPTION and PERMEATION ENHANCERS (ZOT & 4-CNAB).
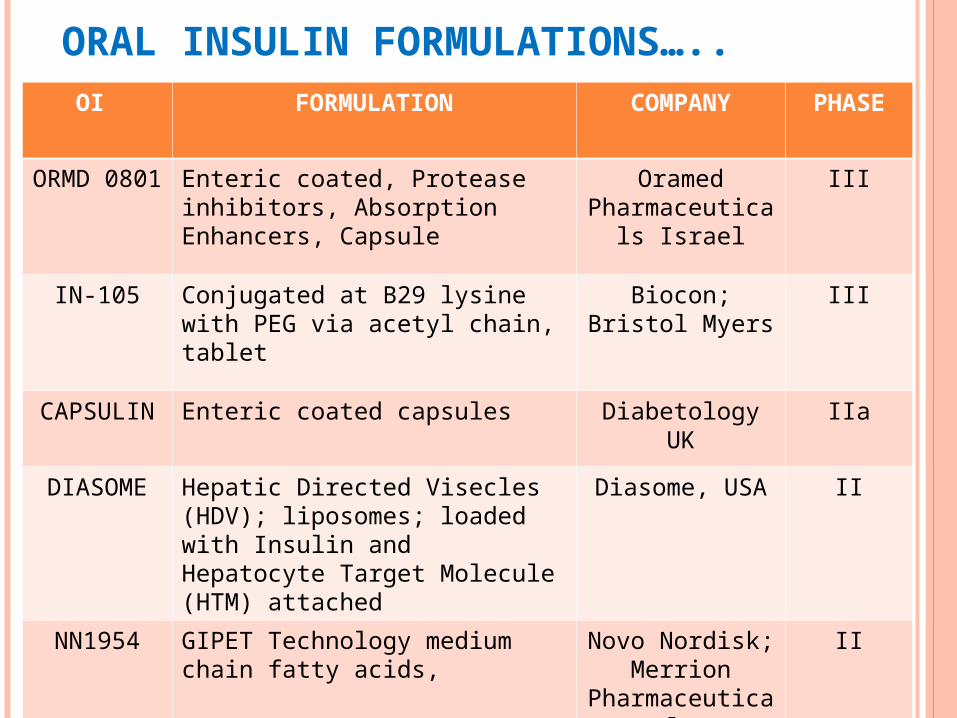
ORAL INSULIN FORMULATIONS…..OI FORMULATION COMPANY PHASE
ORMD 0801 Enteric coated, Protease inhibitors, Absorption Enhancers, Capsule
Oramed Pharmaceutica
ls Israel
III
IN-105 Conjugated at B29 lysine with PEG via acetyl chain, tablet
Biocon; Bristol Myers
III
CAPSULIN Enteric coated capsules Diabetology UK
IIa
DIASOME Hepatic Directed Visecles (HDV); liposomes; loaded with Insulin and Hepatocyte Target Molecule (HTM) attached
Diasome, USA II
NN1954 GIPET Technology medium chain fatty acids,
Novo Nordisk; Merrion
Pharmaceuticals
II
ADVANTAGES…..
Easiest way of delivery. Low immunogenecity Low mitogenecity Low dosage forms and good bioavailibility
NIDDK STUDY
ON-GOING EXPERIMENTS….. Chitosan, Alginate, Chitosan-Alginate, Liposomes, Dextran, Pectin, Cyclodextrin
PLGA (FDA approved), PLA, PCL, Poly Acrylic Acid (PAA)
Thiolated chitosan, better mucoadhesive and extended drug release.
PAA-Cys; Mucoadhesive, permeation enhancer, protease protection.
PolyElectrolyte Complexes (PECs) by mixing oppositely charged ions

C. BUCCAL INSULIN Aerosol spray in the oralpharyngeal cavity.
Presystemic metabolism in GIT and Liver is avoided.
Better accessibility Low pH variation Good surface area Only animal for test is pig
ORAL- LYN Generex Biotechnology, Ontaraio, Canada Aerosol insulin preparation. Average produced micelles is > 10 µm so can’t go to lungs.
Each puff 10 U insulin; stable at RT for approx 6 months
Surfactant, solubilizer, micelles forming agent. Appear in circulation within 5-10 minutes after administration.
Short Tmax and faster time to peak glucose uptake than SC route.
WITHDRAWN !!!! AutoImmune, Biosante, Coremed, Eligen, Nobex in phase II trials.
Aerodose (by Aerogen) Unknown (by Abott) HIIP (Eli Lilly) Alveair (Coremed) BioAir (Biosante) Unknown (Epic Therapeutics) Spiros (Elan Pharmaceuticals)
WHY NANOTECHNOLOGY ???? Better than conventional – drug loading, delivery
Large diabetic population and increasing Large scope Easy for difficult molecules (peptides and proteins)

THANK YOU





























