Embed Size (px)
Citation preview

Nanobioceramic coatings for biomedicalapplications
T. M. Sridhar*
The development of biomaterials for the repair or replacement of hard tissue is a challenging and
a promising area of research. Engineering cell and tissue behaviour at biomaterial surfaces at the
nanoscale level can be accomplished by chemically modifying surfaces with biologically active
macromolecules or physically modifying the surface topography at the nanoscale. Bioceramics
have been used very successfully within the human body for many years. They are commonly
used in orthopaedic surgery and dentistry but they are potentially suitable for a wide range of
important applications within the medical device industry. The fabrication, microstructure and
properties of this highly active area of research and the significance of a range of nanobioceramic
coatings by electrochemical techniques are discussed. Bio-inspired materials open new
approaches for manufacturing implants for bone replacement. The application of these
nanobioceramic coating techniques to develop biomimetic coatings and scaffolds along with
tissue engineering would set new trends in health care delivery system. The clinical applications
of bioceramic coatings in joint replacement, bone grafts, tissue engineering, drug delivery
systems and dentistry would serve as a useful resource for biomaterials scientists and engineers,
as well as for clinicians and the academic community.
Keywords: Metallic implants, Hydroxyapatite coatings, Electrochemical coatings, Biomimetic, Scaffolds, Tissue engineering
This paper is part of a special issue on biomaterials and bio-medical engineering
Introduction: Metallic implantsThe increasing affluence around the world has a directand tangible impact of increasing the average lifespan of apopulation world wide. Yet, it brings forth a myriad ofnew challenges such as dealing with health issues of anaging population and the modern challenges of disabil-ities due to diseases.1 Metallic materials such as stainlesssteels, Co–Cr alloys, titanium and its alloys, have beenused extensively for centuries in restoration of anatomicalstructures due to their superior mechanical properties.2,3
The most important considerations for their selection inthe human body are their biocompatibility, corrosionresistance, tissue reactions, surface conditions andosseointegration (a bone bed formed through directattachment to bone). Titanium implants have been usedwidely and successfully for various types of boneanchored reconstructions.4,5 It is believed that propertiesof oxide films covering titanium implant surfaces are ofcrucial importance for a successful osseointegration, inparticular at compromised bone sites.
Metallic implants are unique in that they are exposedto living cells, tissues and biological fluids, which are not
only dynamic but also form a hostile environment forthe implant. Clinical experience has shown that metallicimplants are susceptible to localised corrosion in thehuman body, releasing metal ions into the surroundingtissues. As a result, these materials and means tooptimise their biocompatibility have been extensivelystudied over the past decades.6–8 Prosthetic materialshave been implanted for centuries. While prosthesisperformance and biocompatibility are still beingimproved by means of more traditional approachessuch as tribology studies, surface topographic designsand surface electrochemical modifications, newerapproaches are currently being evolved. These includethe design of surface chemistry on a molecular level(allowing chemical reactions with the contacting tissuesand cells), purposeful incorporation of material trig-gered biological responses (e.g. preventing blood coagu-lation in catheters and vascular grafts or providingadhesion molecules for attaching tissues and cells), orthe use of prosthetic biomaterials with living biologicalsubstrates (e.g. meniscus replacement grafts contactingcartilage cells, or implants that contain insulin andproduce living cells).9
Failures of implant devicesMetallic orthopaedic implants are often mounted intothe skeletal system of the human body as consti-tuents of reconstructive devices (e.g. hip or knee joint*Corresponding author, email [email protected]
Department of Biomedical Engineering, SMK FOMRA Institute ofTechnology, Thaiyur Village, Kelambakkam, Chennai 603 103, India
184
� 2010 W. S. Maney & Son Ltd.Received 10 December 2009; accepted 08 February 2010DOI 10.1179/175355510X12723642365449 Materials Technology 2010 VOL 25 NO 3/4

replacement) or fracture fixation products (e.g. plates,screws and nails). The design of these implants isdictated by the anatomy and restricted by the physiologyof the skeletal structure of the human body.10 Themechanical and chemical stabilities and biocompatibilityof the implant materials in the environment of tissuesand body fluids are of fundamental importance for thesuccessful treatment of bone fractures and bonereplacements.11 An orthopaedic implant is consideredto have failed if it has to be prematurely removed fromthe body.
Unfortunately, many failures of stainless steelimplants have been reported and related to corrosion.12
Clinical experience has shown that such implants aresusceptible to crevice and pitting corrosion in the humanbody,13–17 causing release of metallic ions into thesurrounding tissue. This might cause local irritations orsystemic effects and, in some cases, removal of implantsis necessary. Moreover, allergenic reactions sometimesoccur as well. Pure Ti and Ti–6Al–4V alloy are known tobe more susceptible to wear than stainless steels, thusgenerating greater amounts of metallic particles for aloose functional implant. Although Co–Cr alloys aregenerally known to have excellent wear and corrosionresistance in vivo, they do occasionally generate particlesand release ions to their surroundings by mechanisms ofcorrosion and wear. Cobalt can be carcinogenic andmay cause inheritable damage in exposed humans.Hence, it is difficult to demonstrate an advantage oftitanium or Co–Cr alloys over stainless steels for in vivoapplications. These shortcomings limit the use oftitanium and Co–Cr alloys for implant applications.11
Corrosion is the major problem affecting the servicelife of orthopaedic implants.18–21 In industry, commonpractices to control this phenomenon include theaddition of inhibitors, changing the pH of the electrolyteand its composition, reducing temperature, applyingprotective coatings, applying electrical current, etc.Unfortunately, most of these approaches cannot beused for orthopaedic implants since the body environ-ment is fixed and cannot be altered without destructivebiological effects. The application of anodic or cathodicprotections which involve applied currents is impracticalfor surgical implants. The alternate ways to reducecorrosion of orthopaedic implants are materialsselection and surface modification by protectivecoatings.20–26 With respect to materials selection, thelist of potential materials is somehow limited because ofmechanical strength and biocompatibility requirements.One of the great challenges facing materials science andtechnology today is the development of a new genera-tion of biomaterials to function effectively in the bodyenvironment.3
Bioactive ceramicsBioactive resorbable materials offer an alternative to theestablishment of a stable implant/tissue interface. Abioactive material is one that elicits a specific biologicalresponse at the interface, which results in the formationof a bond between the tissues and the material.27 Thisconcept is based on the control of surface chemistry ofthe material. A bioactive implant reacts chemically withthe body fluids in a manner that is compatible with therepair process of the tissues. Formation of the fibrouscapsule is prevented by the adhesion of repairing tissues.
Because the chemical reactions are restricted to thesurface, the material does not degrade in strength. Theimportant point is that failure does not occur at theinterface.
Hydroxyapatite: structure and propertiesThe interest in calcium phosphates stems from the factthat bones and teeth contain a high percentage ofmineralised calcium phosphate. De Jong28 first observedin 1926 the similarity between the powder X-raydiffraction patterns of the in vivo mineral and the basiccalcium phosphate, HAP [Ca10(PO4)6(OH)2]. Basiccalcium phosphates precipitated from aqueous solutionsform a non-stoichiometric series, partly because ofsubstitutions by other ions and surface effects, but alsodue to extremely small crystallite sizes formed by thislow solubility mineral. The chemical and crystallo-graphic similarity of HAP to bone mineral allows it toform very strong biological bonds.29 Hydroxyapatite is abioactive material and has been shown to have asimulating effect on bone formation, also known asosseoinduction. The biological performance of HAPlayers is based on a rapid osteointegration with apronounced increase in the load carrying capacity of theimplant. Hydroxyapatite ceramics obviously showattractive properties such as lack of toxicity, absenceof intervening fibrous tissue, the possibility of forming adirect contact with bone, and the possibility to stimulatebone growth. However, their brittle nature and poormechanical properties curtail their use directly asimplantation materials. This has paved the way for thedevelopment of HAP coatings on commonly used type316L stainless steel, Co–Cr alloys, and Ti and its alloys,mainly for bone replacement.30–33
Development of bioceramic coatingsAt present, for all those clinical applications where loadbearing properties are required, most of the implantsused are metallic, with subsequent and serious problems.An alternative option is to coat the metallic implantswith bioceramics. This technique is being used nowa-days, both for dental implants and hip joint prosthesis.There is still a long way to follow, but several metallicimplants with bioceramic coatings are commerciallyavailable already, and the research in problem solving isunderway.34 The bioceramic coating process on ametallic substrate is quite complicated, and severalmethods are available in this sense. A great deal of theclinical success depends on this coating, since the qualityand durability of the interface attachment greatlydepends on the purity, particle size, chemical composi-tion of the coating, layer thickness and surfacemorphology of the substrate. An additional advantageof bioceramic coating is the reduction of release of ionsfrom the metal alloy. The bioceramic coating representsa truly effective barrier that hinders the metallic ionkinetics of release towards the living body.
Bioceramics/tissue interfacesBone formation around a metallic implant is a complexprocess that involves micro- and nanometric interac-tions. The mechanism of tissue attachment is directlyrelated to the type of tissue response at the implantinterface.35 The relative levels of reaction of the implant
Sridhar Nanobioceramic coatings for biomedical applications
Materials Technology 2010 VOL 25 NO 3/4 185
influence the thickness of the interfacial zone or layerbetween the material and tissues. The concept behindmicroporous bioceramics is the in growth of tissues intothe pores on the surface, as described by Hulbert et al.36
The increased interfacial area between the implant andthe tissues results in increased inertial resistance. It iscapable of withstanding more complex stress states thanimplants that reach only biological fixation. All of thesebioactive materials form an interfacial bond with theadjacent tissue. However, the type of bonding, itsstrength, and the thickness of the bonding zone differfor different materials.
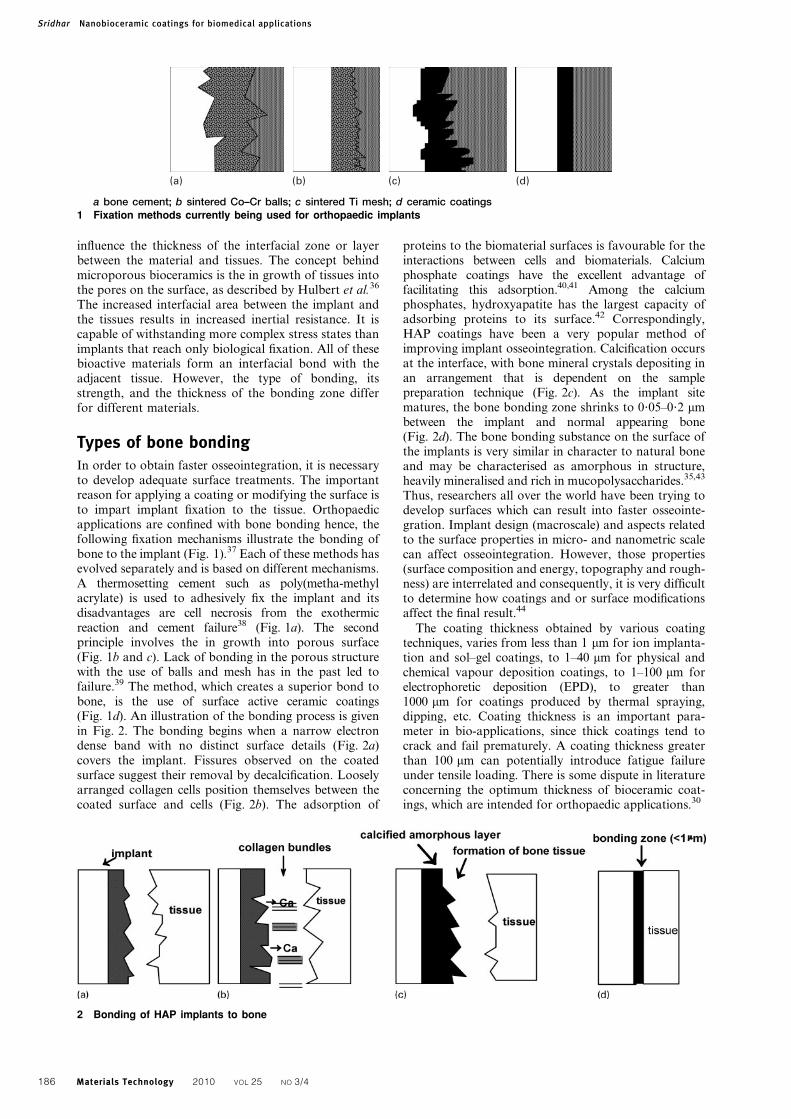
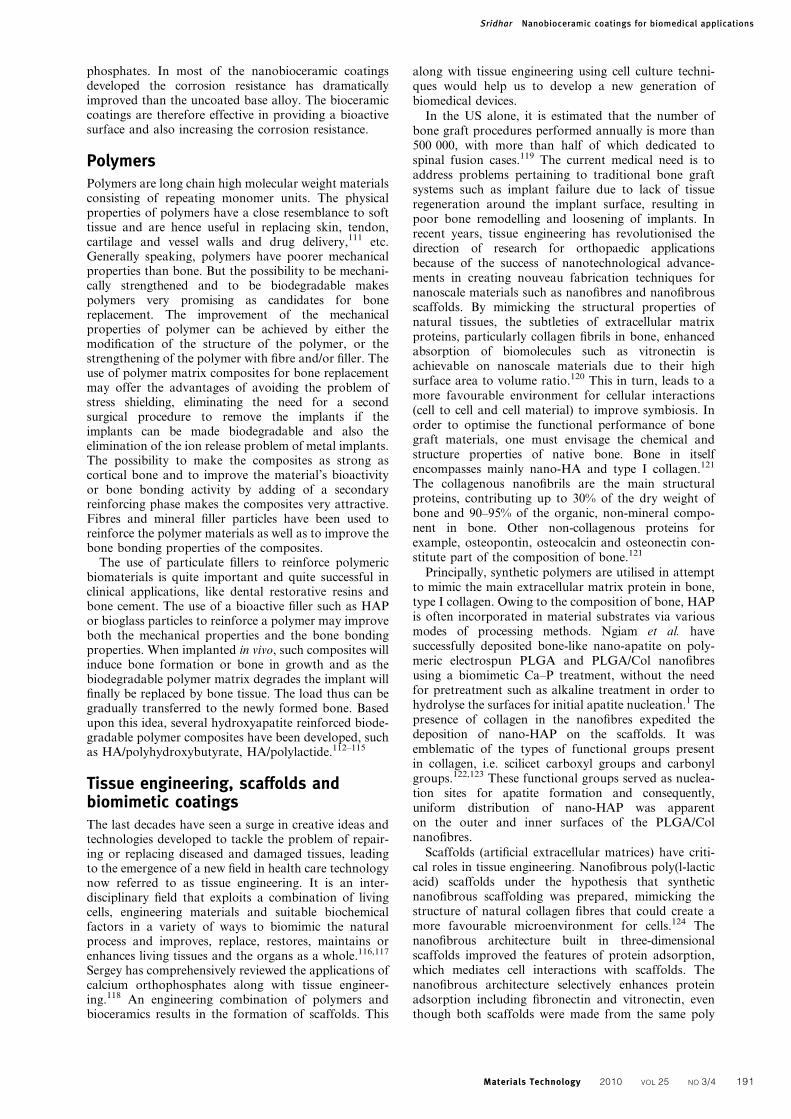
Types of bone bondingIn order to obtain faster osseointegration, it is necessaryto develop adequate surface treatments. The importantreason for applying a coating or modifying the surface isto impart implant fixation to the tissue. Orthopaedicapplications are confined with bone bonding hence, thefollowing fixation mechanisms illustrate the bonding ofbone to the implant (Fig. 1).37 Each of these methods hasevolved separately and is based on different mechanisms.A thermosetting cement such as poly(metha-methylacrylate) is used to adhesively fix the implant and itsdisadvantages are cell necrosis from the exothermicreaction and cement failure38 (Fig. 1a). The secondprinciple involves the in growth into porous surface(Fig. 1b and c). Lack of bonding in the porous structurewith the use of balls and mesh has in the past led tofailure.39 The method, which creates a superior bond tobone, is the use of surface active ceramic coatings(Fig. 1d). An illustration of the bonding process is givenin Fig. 2. The bonding begins when a narrow electrondense band with no distinct surface details (Fig. 2a)covers the implant. Fissures observed on the coatedsurface suggest their removal by decalcification. Looselyarranged collagen cells position themselves between thecoated surface and cells (Fig. 2b). The adsorption of
proteins to the biomaterial surfaces is favourable for theinteractions between cells and biomaterials. Calciumphosphate coatings have the excellent advantage offacilitating this adsorption.40,41 Among the calciumphosphates, hydroxyapatite has the largest capacity ofadsorbing proteins to its surface.42 Correspondingly,HAP coatings have been a very popular method ofimproving implant osseointegration. Calcification occursat the interface, with bone mineral crystals depositing inan arrangement that is dependent on the samplepreparation technique (Fig. 2c). As the implant sitematures, the bone bonding zone shrinks to 0?05–0?2 mmbetween the implant and normal appearing bone(Fig. 2d). The bone bonding substance on the surface ofthe implants is very similar in character to natural boneand may be characterised as amorphous in structure,heavily mineralised and rich in mucopolysaccharides.35,43
Thus, researchers all over the world have been trying todevelop surfaces which can result into faster osseointe-gration. Implant design (macroscale) and aspects relatedto the surface properties in micro- and nanometric scalecan affect osseointegration. However, those properties(surface composition and energy, topography and rough-ness) are interrelated and consequently, it is very difficultto determine how coatings and or surface modificationsaffect the final result.44
The coating thickness obtained by various coatingtechniques, varies from less than 1 mm for ion implanta-tion and sol–gel coatings, to 1–40 mm for physical andchemical vapour deposition coatings, to 1–100 mm forelectrophoretic deposition (EPD), to greater than1000 mm for coatings produced by thermal spraying,dipping, etc. Coating thickness is an important para-meter in bio-applications, since thick coatings tend tocrack and fail prematurely. A coating thickness greaterthan 100 mm can potentially introduce fatigue failureunder tensile loading. There is some dispute in literatureconcerning the optimum thickness of bioceramic coat-ings, which are intended for orthopaedic applications.30
(a) (b) (c) (d)
a bone cement; b sintered Co–Cr balls; c sintered Ti mesh; d ceramic coatings1 Fixation methods currently being used for orthopaedic implants
2 Bonding of HAP implants to bone
Sridhar Nanobioceramic coatings for biomedical applications
186 Materials Technology 2010 VOL 25 NO 3/4

NanobioceramicsBone itself is a composite consisting of HAP nanorodsembedded in the collagen matrix.45 Human teeth arenatural composites which comprise of nano-HAP rods(typically smaller than 100 nm) arranged in lamellae andbound to collagen.46,47 Owing to their nanosize, HAPcrystals have a very large surface area which enableshomogenous resorption by osteoclasts.48,49 NanosizedHAP particles are desirable when biocompatibility isconsidered.50 In recent years, with the rapid develop-ment of nanometric HAP materials, an understanding ofits characteristic has lead to many new ways of using thenanometre HAP.51 The shape of HAP crystal can affectmany characteristics of HAP, such as surface character-istics, bioactivity and so on.52 In addition, nanometricbiomaterials are in favour of cellular adhesion andproliferation, synthesis of alkaline phosphatase and thedeposition of calcium containing minerals on the surfaceof these materials.53 Therefore, nano-HAP exhibitssuperiority in the field of orthopedic implants for itsimproved biological and biomechanical properties.45,54
Moreover, new developments on the production ofnanosized HAP particles have led to many newapplications. For example, nanosized HAP particlescan retard multiplication of cancer cells and be used asan efficient drug delivery agent. It is reported thatnano-HAP particles have suppressive effect on theproliferation of tumour cells.55,56 Apparently differentcharacteristics of HAP particles, such as morphology,size and crystallinity, have shown different biologicalconsequences.57
The drawbacks and salient features of bioceramicsand metallic implants has lead to the development of acombination of both, along with nanotechnologicalmodification of HAP, metallic surfaces or both. Thishas lead to the advancement of a new generation ofmaterials such as surface coatings, scaffolds, tissueengineering, biomimetics and graded structures.
Nanosurface coatingsThe ability to modify the chemistry and surfacemorphology of the coating by fine control of bathcomposition, pH and temperature makes electroche-mical deposition a versatile process for deposition ofcoatings on implants, with a tailored bodyresponse.30,58,59 A number of novel methods for coatingHAP have been proposed offering the potential forbetter control of film structure such as dip coating, hotisostatic pressing, flame spraying, ion beam deposition,laser ablation and electrochemical deposition along withplasma spraying which has been widely studied over thepast few decades. Plasma spraying is a high temperatureand line of sight process, which has been usedcommercially to produce bioceramic coatings. But,some potential problems include exposure of substratesto intense heat, residual thermal stresses in coatings,poor adherence to the substrate, chemical inhomogene-ity, high porosity and the inability to coat complexshapes with internal cavities.59,60 In plasma sprayingprocess, the high enthalpy of, impurity phases[Ca3(PO4)2, Ca4P2O9, CaO, oxyhydroxyapatite, etc.]and amorphous calcium phosphate are generally identi-fied in the sprayed hydroxyapatite coatings.61 HAP willtransform into metastable phases with a higher solubility
than crystalline HAP, such as tricalcium phosphate(TCP), tetracalcium phosphate, CaO. These impurityand amorphous calcium phosphate have higher dissolu-tion rate than crystalline HAP in aqueous solutions, andit has a problem with decreasing the structural homo-geneity, and the mechanical properties for long termclinical applications of the coatings.50
Although different deposition methods have beenapplied in the last years, sol–gel method offers a goodalternative since the synthesis temperatures are low andit can be applied to a great number of substrates,including those which would oxidise at higher tempera-tures. Sol–gel technology offers a chemically homoge-nous and pure product and has been used for HAPproduction since 1988.62 Several authors have preparedHAP via sol–gel technique using different precursors.Hijon et al. have deposited single phase HAP coatingson Ti–6Al–4V by the sol–gel dipping technique formaqueous solutions containing triethyl phosphite andcalcium nitrate.63 Balamurugan et al. have reported thatthe coating thickness alters the shear strength andcorrosion resistance of sol–gel derived apatite films of316L SS.46,64 Rod-like HAP nanostructures was success-fully prepared by a simple sol–gel precipitation methodby Sanosh et al., which show similar morphology, sizeand crystallinity to HAP crystals of human teeth.46
Further work is focused on a novel way to control thesintering of these HAP nanorods and the possibility ofsimulating a human enamel structure.
Electrophoretic depositionElectrophoretic deposition is evolving as an importantmethod in ceramic processing because it enables theformation of thin ceramic films and nanostructuredlayers. It is also an important tool for preparing thickceramic films and body shaping. The interest in EPD forbiomedical applications stems from a variety of reasons,mainly the possibility of depositing stoichiometric, highpurity material to a degree not easily obtainable by otherprocessing techniques. The deposition of submicrometrepowders offers advantages in fabrication of ceramiccoatings with dense packing, good sinterability andhomogenous microstructure. The development andapplication of EPD for deposition of HAP have beenreviewed.30,65–67 Sridhar et al. have developed new EPDprotocols for the application of thin layers of HAP onthe surface of type 316L SS and studied their electro-chemical properties in vitro.68,69 Both the coating weightand thickness increased with increasing voltage andcoating duration. During deposition, the electric fielddrives the particles towards the electrode and exertspressure. The use of high voltage has the advantage ofshorter deposition times and higher deposition thick-nesses. However, higher voltages resulted in significanthydrogen evolution at the cathode, which in turnincreased the porosity of the deposit. Loss of thickercoatings from the metal surface was observed due todecohesion that occurred between the surface and thecoating. Particle congestion at the cathode resulted inweakly bonded coatings. During the deposition processin this voltage range for 1 to 5 min, no significanthydrogen evolution was observed, and the coatingsobtained were uniformly adhered. The optimum coatingparameters for EPD of HAP on type 316L SS wereidentified at 60 V for 3 min, followed by vacuum(1025 torr) sintering at 800uC for 1 h.70,71
Sridhar Nanobioceramic coatings for biomedical applications
Materials Technology 2010 VOL 25 NO 3/4 187

Recently, it has been reported that nanostructuredcoatings fabricated by EDP have high chemical homo-geneity, reduced flaw size and microstructural uniformity,and require a lower sintering temperature for densifica-tion.72,73 The nanometre sized grains and the high volumefraction of grain boundaries in nanostructured HAP canincrease osteoblasts adhesion, proliferation and miner-alisation.74 Studies on EPD of HAP on different implantalloys have been reported by several investigators.75–78
HAP coated 316L stainless steel fabricated by EPDexhibited higher corrosion resistance than the substrate insimulated body fluids (SBFs), with nobler open circuitpotential and higher pitting and protection poten-tials.69,70 The corrosion behaviour of EPD HAP coatingson the Ti alloys has not been fully studied with respect tothe morphology and size of the starting HAP particles.
Furthermore, HAP coatings reinforced with carbonnanotubes (CNTs) was reported to be a viable route forforming surface composite with higher hardness, elasticmodulus and interlaminar shear strength than that ofthe monolithic HAP layers.79 Addition of CNTs alsohelps to prevent peeling-off of the coating layers byacting as reinforcement network with the deposit. Kwoket al. have utilised cathodic EPD for fabricatingbioactive HAP coatings with and without CNTs onTi–6Al–4V followed by vacuum sintering at 800uC.72
Moreover, CNTs were also used to reinforce the HAPcoating for enhancing its hardness. The designations andaverage particle and crystallite sizes of HAP powdersused are given in Table 1.72 The enhanced propertiescould be attributed to the use of submicrometre sizedHAP particles in the low temperature EDP process.Compared with monolithic HAP coating, the CNTreinforced HAP coating markedly increased the coatinghardness without compromising the corrosion resistanceor adhesion strength.
Electrochemical depositionElectrochemical processes can be an excellent tool toproduce one-dimensional structures due to the provisionof a two-dimensional reaction interface and a precisecontrol of critical reaction parameters.80,81 The occur-rence of lateral self-organised phenomena on thereaction interface can therefore be used to grow three-dimensional nanostructures by electrochemical methods.Especially, the electrochemical formation of self-orga-nised porous nanostructures has attracted much interest,since they possess wide applications in biologicalnanopatterning, high density recording media andtemplates for nanomaterials.
Electrochemical techniques have been used for twopurposes on the surfaces of orthopaedic implants, i.e. for
modifying the oxide layers of the surface and depositionof calcium phosphates. Much interest in electrodeposi-tion has evolved due to:
(i) the low temperatures involved, which enableformation of highly crystalline deposits withlow solubility in body fluids and low residualstresses
(ii) the ability to coat porous, geometrically com-plex, or non-line of sight surfaces
(iii) the ability to control the thickness, compositionand microstructure of the deposit
(iv) the possible improvement of the substrate/coat-ing bond strength
(v) the availability and low cost of equipment.81,82
Electrocrystallisation of hydroxyapatite on titanium wasachieved by cathodic polarisation in solution containingcalcium nitrate and ammonium dihydrogen phosphate.The composition and pH of the bath were found tosignificantly affect the nature and surface morphology ofthe deposit. The formation of well crystallised HAP atpH056?0 occurs at any temperature between 70 and95uC, whereas, at pH054?2, less crystallised, thicker,and more porous coatings that contained traces ofoctacalcium phosphate (OCP) were observed.82 Theinfluence of potassium chloride and sodium nitrite onthe composition and surface morphology of the depositwas also evaluated. A speciation precipitation modelwas applied to better understand the effect of bathconditions. The typical surface morphology of differentcoatings is evident from the SEM images in Fig. 3.82 InFig. 3a, the platelike crystals are typical of monetite. InFig. 3b, typical platelets morphology in this case is muchdifferent from that in Fig. 3a and Ca/P ratio was alsosignificantly higher (1?65). Figure 3c is same as Fig. 3bbut seems to be composed of whiskers and Fig. 3d showsthe typical morphology of a CaP coating. From Fig. 3eit is evident that the surface morphology was changedsignificantly, to needles (likely, hexagons) that protrudeupwards from the substrate. This suggests that syntheticHAP coatings formed by electrocrystallisation are morebiomimetic, at least with respect to their structure andmorphology.58,82
Electrochemical modification of the surface morphol-ogy to increase the biocompatibility of titanium surfacesare typically based on so called spark anodisation, whichtypically leads to formation of rough porous TiO2
layers.83–86 The sparking occurs because of a highapplied voltage, leading to dielectric breakdown of theoxide layer and discharge events. The nanotube layerswere fabricated by electrochemical anodisation oftitanium in fluoride containing electrolytes. Various
Table 1 Designations, average particle and crystallite sizes for various HAP powder coatings on Ti–6Al–4V substrate72
Sample no. Powder Designations Mean crystallite size D, nm Mean particle size, nm1 Spherical HAP powder sHA 16 1752 Flake shaped HAP powder fHA 20 4253 Needle shaped HAP powder nHA 12 5062004 Carbon nanotube powder CNT … 3061000Sample no. Specimens Designations Mean crystallite size D, nm Coating thickness, mm1 As received Ti–6Al–4V Substrate AR–Ti … …2 Heat treated Ti–6Al–4V HT–Ti … …3 Sintered sHAP coating sHA– Ti 17 104 Sintered fHAP coating fHA–Ti 21 105 Sintered nHAP coating nHA–Ti 13 7.56 Sintered sHAP/CNT coating sHA/CNT–Ti 18 10
Sridhar Nanobioceramic coatings for biomedical applications
188 Materials Technology 2010 VOL 25 NO 3/4

nanotube lengths, layers with an individual tubediameter of 100 nm were grown to a thickness ofapproximately 2 mm or 500 nm. The presence ofnanotubes on titanium surface enhances the apatiteformation and that the 2 mm thick nanotube layertriggers deposition faster than the thinner layers. Tubesannealed to anatase, or a mixture of anatase and rutileare clearly more efficient in promoting apatite formationthan the tubes in their ‘as formed’ amorphous state.Electrochemically grown and annealed TiO2 nanotubearrays having anatase structure are expected to be agood precursor system for the formation of HAP.87 Theinitial and later stages of apatite formation from SBF ontitania with different surface morphologies (compact ornanotubular) and different crystal structures (anatase oramorphous) have been reported. In the initial stages ofapatite growth, more nuclei are formed on the nano-tubular surface than on flat compact TiO2. While thecrystallographic structure of the substrate plays a lessimportant role than the morphology in the initialnucleation stages, it is of great importance in the laterstages of apatite crystal growth. The nanotubularmorphology combined with an anatase structure leadsto the formation of apatite layers with a thickness of.6 nm in less than two days.
Electrochemically deposited nanograined calcium phos-phate coatings were produced on titanium alloy substratesusing aqueous electrolyte maintained at acidic pH byNarayanan et al.88 Ultrasonated bath produced coatingscontaining dicalcium phosphate dehydrate and the grainsizes were in the range of 50–100 nm. An electrochemicalmethod of producing nanocrystalline hydroxyapatitecoatings on titanium surface is reported by Narayananet al.89,90 The bath contained Ca(NO3)2 and NH4H2PO4
in the molar ratio of 1?67 : 1. The electrolyte wasmaintained at physiological pH and was ultrasonicallyagitated throughout the time of electrolysis. Coatingscontained monohydroxyapatite phase whose crystal sizeswere lower than 30 nm. These sizes are comparable to thesize of the bone hydroxyapatite crystals. Small globules ofhydroxyapatite covered the coating surface completely.Ultrasonic agitation promoted the formation of nano-crystalline structure which will help in better attachmentof bone tissues to the implant surface. They containedvery small crystals of the size of few nanometres, as shownby the bright field transmission electron micrographs andelectron diffraction patterns shown in Fig. 4.89 Figure 4cshows rings corresponding to HAP.
Fluorine, which exists in human bone and enamel,can be incorporated into HAP crystal structure by
a pH54?2, 60uC, 2 h; b pH54?2, 85uC, 4 h; c pH56?0, 80uC, 3 h; d pH56?0, 90uC, 3 h; e pH56?0, 90uC, 3 h, addition of0?01M KCl; f pH56?0, 90uC, 3 h, addition of 1?00M NaNO2 (Ref. 82)
3 Typical surface morphologies (SEM images) of CaP coatings deposited under different conditions
Sridhar Nanobioceramic coatings for biomedical applications
Materials Technology 2010 VOL 25 NO 3/4 189

substituting OH2 groups with F2 ions to formfluoridated hydroxyapatite (FHA).60 Fluoridated hydro-xyapatite possesses lower solubility than pure HAPwhile maintaining the comparable bioactivity andbiocompatibility.91 Recently, many researchers focusedon the application of FHA as bioactive coatings toprovide both early stability and long term perfor-mance.92,93 In comparison with HAP coating, FHAcoatings could provide lower dissolution, better apatite-like layer deposition, better protein adsorption, compar-able or better cell attachment and improved alkalinephosphatase activity in cell culture.94–97 Hydroxyapatiteand FHA coatings were deposited on titanium sub-strates using an electrochemical technique. Typicalapatite structures were obtained for all the coatingsafter electrodeposition and subsequent post-treatment,including alkaline immersion and vacuum calcination.The coatings were uniform and dense, with a thicknessof y5 mm. Compared with pure Ti, FHA and HAPcoatings exhibited higher biological affinity like cellproliferation and alkaline phosphatase activity. Clinicalapplications suggest that a moderate content of F, suchas Ca5(PO4)3(OH)0?375–0?5F0?5–0?625, be most suitable as acompromise among cell attachment, cell proliferation,apatite deposition and dissolution resistance.
Alternative immersion method (AIM)Apatite depositions from SBF have been widely used forthe in vitro assessment of the bioactivity of bone anddental implant materials. Titanium based implantmaterials can be coated with an anodic TiO2 nanotubelayer which can significantly stimulate apatite forma-tion. The tubular nature of such coatings makes themhighly suitable for the application of a treatment called‘alternative immersion method’, which preloads thecoatings with synthetic hydroxyapatite.2 This treatmentis indeed found to additionally promote natural apatiteformation significantly. Layers of nanotubes withvarious diameters and crystal structures (amorphous,anatase/rutile) were produced, AIM treated, and theformation of apatite in SBF10 (10 mmol L21 HCO{
3 )was evaluated. The results show a drastic enhancementof apatite deposition rates for AIM treated TiO2
nanotube layers in comparison with non-treated TiO2
surfaces. The thickness of the nanotube layers can beinfluenced by varying the anodisation time and pH ofthe electrolyte.98 The AIM is schematically outlined inFig. 5.2 On anodised light metals such as Al and Mg thathave surfaces with mesoporous morphology, the AIMtreatment can be used to efficiently deposit synthetic
HAP.99 Key factors that influence the deposition werefound to be the pore size and the ion content in the oxidematerial.100–103
Chen et al. have reported the formation of nanocrys-talline HAP coatings.50 A kind of bilayer HAP coatingson the pure titanium substrates was prepared were thecoatings were first sprayed by coarse powder underspraying power of 35 kW and then fine powder underspraying power of 45 kW. Bilayer HAP coatings wereheat treated followed by immersion in SBF. Nano-HAPis comparatively stable during immersion in SBF. Heattreated nanoparticles are in favour of the adhesion ofcells. With culture time, osteoblasts spread favourablyand form a kind of anchor structure impinging on thesurface of coatings. The results show that nano-HA heattreated coatings are comparatively stable during immer-sion in SBF and favours adhesion of osteoblasts.Therefore, nanoparticles materials are greatly promisingin the development of more valuable orthopaedic anddental implants. However, the mechanism of nano-HAP–osteoblast interaction is expected to investigatethoroughly, which will promote the research of bioma-terials with better biological performance.
Modification of titanium surface by using phosphorusion implantation followed by oxidation accelerates theformation of calcium phosphates and increases thecorrosion resistance of titanium.104 After the implanta-tion, the corrosion resistance of titanium increased.105–108
Examinations of titanium exposed to body fluidsimulating solutions have shown that calcium phosphateforms spontaneously on the titanium surface.109 Thiscalcium phosphates layer is very thin; after 30 days ofexposure, its thickness is of the order of a fewnanometres. In explaining the mechanism of the forma-tion of calcium phosphate, they assume that, in the firststage, phosphate ions are present in the solution areadsorbed onto the surface of the oxide layer.109,110
This is followed by introduction of phosphate ions intothe titanium surface to accelerate the formation of
5 Schematic outline of AIM treatment leading to deposi-
tion of Ca–P enriched layers2
a b c
4 a SEM and TEM of electrochemical coatings, b micrograph showing HA grains and c electron diffraction pattern indi-
cating rings for HAP89
Sridhar Nanobioceramic coatings for biomedical applications
190 Materials Technology 2010 VOL 25 NO 3/4
phosphates. In most of the nanobioceramic coatingsdeveloped the corrosion resistance has dramaticallyimproved than the uncoated base alloy. The bioceramiccoatings are therefore effective in providing a bioactivesurface and also increasing the corrosion resistance.
PolymersPolymers are long chain high molecular weight materialsconsisting of repeating monomer units. The physicalproperties of polymers have a close resemblance to softtissue and are hence useful in replacing skin, tendon,cartilage and vessel walls and drug delivery,111 etc.Generally speaking, polymers have poorer mechanicalproperties than bone. But the possibility to be mechani-cally strengthened and to be biodegradable makespolymers very promising as candidates for bonereplacement. The improvement of the mechanicalproperties of polymer can be achieved by either themodification of the structure of the polymer, or thestrengthening of the polymer with fibre and/or filler. Theuse of polymer matrix composites for bone replacementmay offer the advantages of avoiding the problem ofstress shielding, eliminating the need for a secondsurgical procedure to remove the implants if theimplants can be made biodegradable and also theelimination of the ion release problem of metal implants.The possibility to make the composites as strong ascortical bone and to improve the material’s bioactivityor bone bonding activity by adding of a secondaryreinforcing phase makes the composites very attractive.Fibres and mineral filler particles have been used toreinforce the polymer materials as well as to improve thebone bonding properties of the composites.
The use of particulate fillers to reinforce polymericbiomaterials is quite important and quite successful inclinical applications, like dental restorative resins andbone cement. The use of a bioactive filler such as HAPor bioglass particles to reinforce a polymer may improveboth the mechanical properties and the bone bondingproperties. When implanted in vivo, such composites willinduce bone formation or bone in growth and as thebiodegradable polymer matrix degrades the implant willfinally be replaced by bone tissue. The load thus can begradually transferred to the newly formed bone. Basedupon this idea, several hydroxyapatite reinforced biode-gradable polymer composites have been developed, suchas HA/polyhydroxybutyrate, HA/polylactide.112–115
Tissue engineering, scaffolds andbiomimetic coatingsThe last decades have seen a surge in creative ideas andtechnologies developed to tackle the problem of repair-ing or replacing diseased and damaged tissues, leadingto the emergence of a new field in health care technologynow referred to as tissue engineering. It is an inter-disciplinary field that exploits a combination of livingcells, engineering materials and suitable biochemicalfactors in a variety of ways to biomimic the naturalprocess and improves, replace, restores, maintains orenhances living tissues and the organs as a whole.116,117
Sergey has comprehensively reviewed the applications ofcalcium orthophosphates along with tissue engineer-ing.118 An engineering combination of polymers andbioceramics results in the formation of scaffolds. This
along with tissue engineering using cell culture techni-ques would help us to develop a new generation ofbiomedical devices.
In the US alone, it is estimated that the number ofbone graft procedures performed annually is more than500 000, with more than half of which dedicated tospinal fusion cases.119 The current medical need is toaddress problems pertaining to traditional bone graftsystems such as implant failure due to lack of tissueregeneration around the implant surface, resulting inpoor bone remodelling and loosening of implants. Inrecent years, tissue engineering has revolutionised thedirection of research for orthopaedic applicationsbecause of the success of nanotechnological advance-ments in creating nouveau fabrication techniques fornanoscale materials such as nanofibres and nanofibrousscaffolds. By mimicking the structural properties ofnatural tissues, the subtleties of extracellular matrixproteins, particularly collagen fibrils in bone, enhancedabsorption of biomolecules such as vitronectin isachievable on nanoscale materials due to their highsurface area to volume ratio.120 This in turn, leads to amore favourable environment for cellular interactions(cell to cell and cell material) to improve symbiosis. Inorder to optimise the functional performance of bonegraft materials, one must envisage the chemical andstructure properties of native bone. Bone in itselfencompasses mainly nano-HA and type I collagen.121
The collagenous nanofibrils are the main structuralproteins, contributing up to 30% of the dry weight ofbone and 90–95% of the organic, non-mineral compo-nent in bone. Other non-collagenous proteins forexample, osteopontin, osteocalcin and osteonectin con-stitute part of the composition of bone.121
Principally, synthetic polymers are utilised in attemptto mimic the main extracellular matrix protein in bone,type I collagen. Owing to the composition of bone, HAPis often incorporated in material substrates via variousmodes of processing methods. Ngiam et al. havesuccessfully deposited bone-like nano-apatite on poly-meric electrospun PLGA and PLGA/Col nanofibresusing a biomimetic Ca–P treatment, without the needfor pretreatment such as alkaline treatment in order tohydrolyse the surfaces for initial apatite nucleation.1 Thepresence of collagen in the nanofibres expedited thedeposition of nano-HAP on the scaffolds. It wasemblematic of the types of functional groups presentin collagen, i.e. scilicet carboxyl groups and carbonylgroups.122,123 These functional groups served as nuclea-tion sites for apatite formation and consequently,uniform distribution of nano-HAP was apparenton the outer and inner surfaces of the PLGA/Colnanofibres.
Scaffolds (artificial extracellular matrices) have criti-cal roles in tissue engineering. Nanofibrous poly(l-lacticacid) scaffolds under the hypothesis that syntheticnanofibrous scaffolding was prepared, mimicking thestructure of natural collagen fibres that could create amore favourable microenvironment for cells.124 Thenanofibrous architecture built in three-dimensionalscaffolds improved the features of protein adsorption,which mediates cell interactions with scaffolds. Thenanofibrous architecture selectively enhances proteinadsorption including fibronectin and vitronectin, eventhough both scaffolds were made from the same poly
Sridhar Nanobioceramic coatings for biomedical applications
Materials Technology 2010 VOL 25 NO 3/4 191

(l-lactic acid) material. These results demonstrate thatthe biomimetic nanofibrous architecture serves as super-ior scaffolding for tissue engineering. The material,however, still remains to be developed to overcome theconcern of pathogen transmission, the difficulties inhandling, and less control over the mechanical proper-ties, biodegradability, and batch to batch consistency ofnatural materials from biological sources.125 Cell attach-ment, migration, and growth on the polymer surfacesare believed to be mediated by proteins, either adsorbedfrom serum proteins or secreted by the cells.
Bone marrow stromal cells are a potential source ofosteoblasts and chondrocytes and can be used toregenerate damaged tissues using a tissue engineeringapproach. These strategies require the use of anappropriate scaffold architecture that can support theformation de novo of either bone and cartilage tissue, orboth, as in the case of osteochondral defects. The laterhas been attracting a great deal of attention since it isconsidered a difficult goal to achieve. Joaquim et al.have developed a novel HA/chitosan bilayered scaffoldby combining a sintering and a freeze drying techniqueto show the potential of such type of scaffolds for beingused in tissue engineering of osteochondral defects.126
Therefore, on the basis of the osteochondral approaches,the development of bilayered osteochondral scaffoldscombining both HAP and chitosan layers thus seems agood approach but there is a need for more simple andreliable strategies to manufacture bilayered scaffolds forosteochondral applications.127,128
To achieve improvement of implant osseointegration,the most promising approaches is to bestow a nano-HAP/collagen surface to mimic bone on bone contactingimplants.129 Such a surface would probably make use ofspeciality from each one of nano-HAP and collagen inthe interactions at the implant/bone interface, andthereby, probably produce a good bone tissue reactionand a bone bonding interface. Nano-HAP sol andcollagen gel were mixed and coated on different titaniumsurfaces by the deposition method. By cell culturing,investigations were conducted into cell responses tonano-HAP, nano-HAP/collagen, native, and anodisedtitanium surfaces. The in vitro studies showed thatporous structures produced by anodic oxides ontitanium served as positive anchorage sites for cellfilopodia to connect, and nano-HAP decreased cellattachment of osteoblasts and induced well developedlong filopodia and broad lamellipodia, thereby enhan-cing cellular motility. Collagen involvement enhancedcell adhesion to nano-HA. Cell reactions to nano-HA,nano-HA/collagen, native, and porous titanium surfacesprovide some guidance for an optimal osseointegrationby their application in surface modifications forimplants.
Santos et al. have evaluated the relative role of thecalcium phosphate surface chemistry and surface topo-graphy on human osteoblast behaviour.130 Highly densephosphate ceramics (single phase HAP and b-TCPs)presenting two distinct nanoroughnesses were produced.The phosphate chemistry was responsible for changes inadhesion, proliferation and cell differentiation.131–134 OnTCP, it was shown that the main influent parameter wassurface chemistry, which negatively affected the initialcell adhesion but positively affected the subsequent stageof proliferation and differentiation. On HAP, the main
influent parameter was surface topography, whichincreased cell differentiation but lowered proliferation.
Among the processes producing the thinner andresorbable HAP coatings, biomimetic and electrochemi-cal deposition are two of the most promising newprocesses.40 Moreover, these processes can producenano-HAP on the metallic substrate surface.135–137
Barrere et al. have reported that a biomimetic processcan produce an apatite coating within 72 h.138 Thisprocess has been applied to deposit the CaP coating on aroughened surface, which demonstrated that a 25 mmcoating formed on the roughened surface, and OCP andHAP both appeared in the coating.139 Octacalciumphosphate has been identified as one of the CaP thatparticipates in the early stage of biomineralisation ofcalcified tissues. The biodegradability and osteoconduc-tivity of OCP have been demonstrated in vivo.140
An attractive strategy for fabricating mimics ofdifferent types of composite biomaterials is to electivelygrow apatite on polymers with control of structure,mechanical properties, and function.141 Silk/apatitecomposites were prepared by growing apatite onfunctionalised nanodiameter silk fibroin fibres preparedby electrospinning. The functionalised fibres were spunfrom an aqueous solution of silk/polyethylene oxide(78 : 22 w/w) containing poly(L-aspartate), which wasintroduced as an analogue of non-collageous proteinsnormally found in bone. Apatite mineral growthoccurred preferentially along the longitudinal directionof the fibres, a feature that was not present in theabsence of the combination of components at appro-priate concentrations. The results suggest that thisapproach can be used to form structures with potentialutility for bone related biomaterials based on the abilityto control the interface wherein nucleation and crystalgrowth occur on the silk fibroin. With this level ofinorganic–organic control, coupled with the uniquemechanical properties, slow rates of biodegradation,and polymorphic features of this type of proteins, newopportunities emerge for utility of biomaterials. Manyorganic polymers have been studied as substratesfor hydroxyapatite nucleation and crystal growth,including electrospun silk fibres are used as templatesfor growth of apatite as a route to generate newcomposite biomaterials with a broader range of proper-ties. The electrospinning process offers an alternativeapproach to protein fibre formation that can generatenanometre diameter fibres, a useful feature in somebiomaterial and tissue engineering applications due tothe increased surface area for cell interactions and tissueingrowth.142–145
Many papers have reported on the importance of siliconon the bone formation, the growth and development ofbone, teeth and some invertebrate skeletons.146–148
Recently, Si element was introduced into hydroxyapatiteceramic by different techniques to further improveosseointegration. Increasing evidences have shown thatthe presence of Si contributes to the enhanced bioac-tivity of some bioactive ceramics in vitro. Siliconsubstituted hydroxyapatite (Si-HAP) coatings with0?14 to 1?14 at-%Si on pure titanium were prepared bya biomimetic process.146 The prepared Si-HAP coatingsand HAP coating were only partially crystallised or innanoscaled crystals. The introduction of Si element inHAP significantly reduced P and Ca content, but
Sridhar Nanobioceramic coatings for biomedical applications
192 Materials Technology 2010 VOL 25 NO 3/4

densified the coating. Both the HAP and the Si-HAPcoatings demonstrated a significantly higher cell growthrate than the uncoated pure titanium in all incubationperiods while the Si-HAP coating exhibited a signifi-cantly higher cell growth rate than the HAP coating. Thesynthesis mode of HAP and Si-HAP coatings insimulated body environments contribute significantlyto good cell biocompatibility in the biomimetic process.Silicon substituted hydroxyapatite [Ca10(PO4)6–
x(SiO4)x(OH)2–x] composite coatings on a bioactivetitanium substrate were prepared by EPD techniquewith the addition of triethanolamine to enhance theionisation degree of Si-HAP suspension.149 The deposit-ing thickness and the images of Si-HA coating can bechanged with the variation of deposition time. Thebioactive TiO2 coating formed may improve the bondstrength of the coatings. The interaction of Ti/Si-HAPcoating with bovine serum albumin is much greater thanthat of Ti/HAP coating, suggesting that the incorpora-tion of silicon in HAP is significant to improve thebioactive performance of HAP.
Modification of the chemistry and surface topographyof nanophase ceramics was used to provide biomaterialformulations designed to direct the adhesion andproliferation of human mesenchymal stem cells.150
Human mesenchymal stem cell adhesion was dependentupon both the substrate chemistry and grain size, butnot on surface roughness or crystal phase. The resultsdemonstrated the potential of nanophase ceramicsurfaces to modulate functions of human mesenchymalstem cells, which are pertinent to biomedical applica-tions such as implant materials and devices.
NanocompositesGenerally two critical factors involved in producingnanocomposites with bone-like properties are a goodinterfacial adhesion between organic polymers andinorganic HAP, and the uniform dispersion of HAP atnanolevel in the polymer matrix. The former contributesto the improved mechanical properties of nanocompo-sites and the latter is responsible for the enhancedprotein adsorption and cell adhesion/proliferation dueto the larger specific surface area. Lee et al., attemptedto improve these properties by modifying the surface ofHAP nanocrystals with a diverse class of couplingagents and polymers.151 The effect of surface modifiedHAP nanocrystals on the biocompatibility of a new typenanocomposite consisting of poly(e-caprolactone) andHAP was studied. Poly(e-caprolactone) grafted HAP innanocomposites provided more favourable environ-ments for protein adsorption, positive effects onadhesion and proliferation of fibroblasts compared withunmodified HAP.
Future directions and outlookThe clinical ramifications of increase in metal content inbody fluids and remote organs of patients who have ametal implant need to be elucidated. Surface engineer-ing, bioceramics and functionally graded coatings arethe promising techniques to battle corrosion of bioma-terials. In spite of the immense growth, further researchon nanobioceramics coupled with orthopaedic implantsand tissue engineering would lead to the development ofnew biomedical devices with the better understandingof the structure–property relationship. Modification of
biomaterial surface properties through control of thecharacteristic length scale is one promising approach tomodulate select cell functions. In the case of nanoscaleceramics, the length scale of the material approaches thelength scale of the proteins which mediate cell materialinteractions. This aspect affects the type, amount andconformation of adsorbed proteins and in turn mod-ulates select cell functions. Biomimetic coatings andscaffolds would pave the way for advanced futureresearch in this area of nanobiomaterials.
Although all compounds in the calcium phosphategroup have similar chemical constitutions, their solubi-lity varies. It is generally known that TCP in its twoallotropic forms (a-TCP or b-TCP) is more soluble thanHAP at physiologic pH and consequently more suscep-tible to bioresorption. Thus, when fast bone remodellingis desired, a biphasic ceramics can be applied. Cellularbehaviour largely depends on the physical and chemicalcharacteristics of materials surface. Therefore, thediscussion about the importance of chemistry versussurface topography in influencing cell response is stillopen and this would lead to the development offunctionally graded materials and coatings. Despite thepromises of tissue engineering applications, no investi-gation has to date addressed the effects of nanoscaledimensions on the cell functions of undifferentiatedmesenchymal stem cells and other sensitive tissues. Amore systematic and multinational research approach isneeded to develop and standardise protocols forevaluation of tissue engineered products. In future, itshould be feasible to design a new generation of geneactivating nanobioceramics based implants and scaf-folds tailored for specific patients and disease states.
Acknowledgements
The author expresses his sincere thanks to Professor N.V. Pundarikanthan, Director, and Professor L. MaheshKumar, Principal, SMK Fomra Institute of Technologyfor their keen interest support to publish this review.Thanks are also due to the contributors, who kindlyagreed to permit reprinting the figures.
References1. M. Ngiam, S. Liao, A. J. Patil, Z. Cheng, C. K. Chan and
S. Ramakrishna: Bone, 2009, 45, 4–16.
2. A. Kodama, S. Bauer, A. Komatsu, H. Asoh, S. Ono and
P. Schmuki: Acta Biomater., 2009, 5, 2322–2330.
3. U. Kamachi Mudali, T. M. Sridhar and B. Raj: Sadhana, 2003,
28, 601–637.
4. Y. T. Sula, C. B. Johanssona, S. Petronisc, A. Krozerd, Y. Jeonge,
A. Wennerberga and T. Albrektssona: Biomaterials, 2002, 23,
491–501.
5. X. Zhu, O. Eibl, L. Scheideler and J. G. Gerstorfer: J. Biomed.
Mater. Res. 2006, 79A, 114–127
6. D. F. Williams (ed.): ‘Definitions in biomaterials: proceedings of a
consensus conference of the European Society for Biomaterials,
Chester, England, March 3–5, 1986’, 3; 1987, Amsterdam, New
York, Elsevier.
7. X. Liu, P. K. Chu and C. Ding: Mater. Sci. Eng. R, 2004, R47, 29–
121.
8. B. D. Ratner: in ‘Titanium in medicine’, (ed. D. M. Brunette et al),
2; 2001, Berlin, Springer.
9. D. Muster, B. Demri and M. H. Ali: in ‘Encyclopedic handbook
of biomaterials and bioengineering, part A: materials’, (ed. D. L.
Wise et al), Vol. 1, 785; 1995, New York, Marcel Dekker, Inc.
10. F. Williams: Mater. Sci. Technol., 1987, 3, 797–803.
11. N. Eliaz: in ‘Corrosion science and technology: mechanism,
mitigation and monitoring’, (ed. U. Kamachi Mudali and B. Raj),
356–397; 2008, New Delhi, Narosa Publishing House.
Sridhar Nanobioceramic coatings for biomedical applications
Materials Technology 2010 VOL 25 NO 3/4 193

12. U. Kamachi Mudali, T. M. Sridhar, N. Eliaz and B. Raj: Corros.
Rev., 2003, 21, 231–267.
13. M. Sivakumar, U. Kamachi Mudali and S. Rajeswari: J. Mater.
Sci. Lett., 1995, 14, 148–151.
14. M. Sivakumar, K. S. Kumar Dhanadurai, S. Rajeswari and
V. Thulasiraman: J. Mater. Sci. Lett., 1995, 14, 351–353.
15. M. Sivakumar, S. Rajeswari and V. Thulasiraman: J Mater. Sci.
Lett., 1996, 15, 2192–2194.
16. M. Sivakumar, U. Kamachi Mudali and S. Rajeswari: J. Mater.
Eng. Perform., 1994, 3, 744–753.
17. M. Sivakumar and S. Rajeswari: J. Mater. Sci. Lett., 1992, 11,
1039–1042.
18. N. Eliaz and O. Nissan: J. Biomed. Mater. Res. A, 2007, 83A, 546–
557.
19. L. Thair, U. Kamachi Mudali, S. Rajagopalan, K. G. M. Nair,
R. Asokamani and B. Raj: Corros. Sci., 2003, 45, 1951–1967.
20. S. Kumar, T. S. N. Sankara Narayanan, S. G. S. Raman and S. K.
Seshadri: Corros. Sci., 2010, 52, 711–721.
21. E. M. Sachs, S. M. Allen and R. M. Latanision: Corros. Sci.,
2001, 43, 1781–1791.
22. S. Kumar, T. S. N. Sankara Narayanan, S. G. S. Raman and S. K.
Seshadri: Mater. Chem. Phy., 2010, 119, 337–346.
23. L. Thair, U. Kamachi Mudali, S. Rajagopalan, K. G. M. Nair, R.
Asokamani and B. Raj: Corros. Sci., 2002, 44, 2439–2457.
24. S.-B. Hong, N. Eliaz, G. G. Leisk, E. M. Sachs, R. M. Latanision
and S. M. Allen: J. Dent. Res., 2001, 80, 860–863.
25. S. Kumar and T. S. N. Sankarnarayanan: J. Dent., 2008, 36, 500–
507.
26. S. Kumar, T. S. N. Sankara Narayanan, S. G. S. Raman and S. K.
Seshadri: Mater. Sci. Eng. C, 2009, C29, 1942–1949.
27. J. P. Collier, V. A. Surprenant, R. E. Jensen and M. B. Mayor:
Clin. Orthop., 1991, 271, 305–312.
28. W. F. de Jong: Rec. Trav. Chim. Pays-Bas, 1926, 45, 445.
29. J. L. Gilbert and J. J. Jacobs: in ‘Modularity of orthopedic
implants’, STP 1301, ASTM, West Conshohoken, PA, 1997, 45–
59.
30. T. M. Sridhar, N. Eliaz, U. Kamachi Mudali and B. Raj: Corros.
Rev., 2002, 20, 255–293.
31. N. Eliaz, W. Kopelovitch, L. Burstein, E. Kobayashi and
T. Hanawa: J. Biomed. Mater. Res. A, 2009, 89A, 270–280.
32. V. Raman, S. Tamilselvi and N. Rajendran: Electrochim. Acta,
2007, 52, 7418–7424.
33. M. Karthega, S. Tamilselvi and N. Rajendran: Trends Biomater.
Artif. Organs, 2006, 20, 31–34.
34. T. M. Sridhar and S. Rajeswari: Corr. Rev., 2009, 287–332.
35. L. A. de Senaa, N. C. C. Rochab, M. C. Andradec and G. A.
Soaresa: Surf. Coat. Technol., 2003, 166, 254–258.
36. S. F. Hulbert, J. C. Bokros, L. L. Hench, J. Wilson and
G. Heimke: in ‘High Tech ceramics’, (ed. P. Vincenzini), 189;
1987, Amsterdam, Elsevier.
37. C. C. Berndt, G. N. Haddad, A. J. D. Farmer and K. A. Gross:
Mater. Forum, 1990, 14, 161–169.
38. B. J. Anderson, M. A. R. Freeman and S. A. Swanson: J. Bone
Joint Surg. B, 1972, 54B, 590–596.
39. H. W. Wevers and T. D. V. Cooke: Clin. Mater., 1987, 2, 67–72.
40. G. L. Yang, F. M. He, J. A. Hu, X. X. Wang and S. F. Zhao: Oral
Surg. Oral Med. Oral Pathol. Oral Radiol. Endod., 2009, 107, 782–
789.
41. H. Zeng, K. K. Chittur and W. R. Lacefield: Biomater., 1999, 20,
377–384.
42. Y. Yang, K. H. Kim and J. L. Ong: Biomaterials.., 2005, 26, 327–
337.
43. T. Kokubo. H. M. Kim and M. Kawashita: in ‘Bone engineering’,
(ed. J. E. Davies), 190–194; 2000, Toronto, EM Squared.
44. C. von Wilmowsky, S. Bauer, R. Lutz, M. Meisel, F. W. Neukam,
T. Toyoshima, P. Schmuki, E. Nkenke and K. A. Schlegel:
J. Biomed. Mater. Res. B, 2009, 89B, 165–171.
45. K. Prabakaran and S. Rajeswari: Spec. Chim. Acta A, 2009, 74A,
1127–1134
46. K. P. Sanosh, M. C. Chu, A. Balakrishnan, Y. J. Lee, T. N. Kim
and S. J. Cho: Curr. Appl. Phy., 2009, 9, 1459–1462.
47. P. Fratzl, H. S. Gupta, E. P. Paschalis and P. Roschger: J. Mater.
Chem., 2004, 14, 2115–2123.
48. H. M. Kim: J. Curr. Opin. Solid State Mater. Sci., 2003, 7, 289–
299.
49. L. L. Hench: J. Am. Ceram. Soc., 1998, 81, 1705–1728.
50. Y. M. Chen, T. F. Xi, Y. P. Lv and Y. D. Zheng: Appl. Surf. Sci.,
2008, 255, 375–378.
51. C. Qiu, X. Xiao and R. Liu: Ceram. Int., 2008, 34, 1747–1751
52. T. J. Webster, R. W. Siegel and R. Bizios: Biomaterials., 1999, 20,
1221–1227.
53. J. S. Bow, S. C. Liou and S. Y. Chen: Biomaterials., 2004, 25,
3155–3161
54. J. L. Xu, K. A. Khor, Z. L. Dong, Y. W. Gu, R. Kumar and
P. Cheang: Mater. Sci. Eng. A, 2004, A374, 101–108.
55. Q. Fu, N. Zhou, W. H. Huang, D. P. Wang, L. Y. Zhang and H.
F. Li: J. Biomed. Mater. Res. A, 2005, 74A, 156–163.
56. M. Z. Yin, Y. C. Han, H. L. Dai and S. P. Li: J. Wuhan Univ.
Technol., 2006, 21, 102–104.
57. P. Laquerriere, A. G. Laquerrier, E. Jallot, G. Balossier,
P. Frayssinet and M. Guenounou: Biomaterials, 2003, 24, 2739–
2747.
58. N. Eliaz and M. Eliyahu: J. Biomed. Mater. Res. A, 2007, 80A,
621–634.
59. H. Wang, N. Eliaz, Z. Xiang, H.-P. Hsu, M. Spector and L. W.
Hobbs: Biomaterials, 2006, 27, 4192–4203.
60. J. Wang, Y. Chao, Q. Wan, Z. Zhu and H. Yu: Acta Biomater.,
2009, 5, 1798–1807.
61. C. W. Yang and T. S. Lui: J. Eur. Ceram. Soc., 2008, 28, 2151–
2159.
62. Y. Masuda, K. Matubara and S. Sakka: J. Ceram. Soc. Jpn, 1990,
98, 84–95.
63. N. Hijon, M. V. Cabanas, I. Izquierdo-Barba and M. Vallet-Regi:
Key Eng. Mater., 2004, 254–256, 363.
64. A. Balamurugan, G. Balossier, S. Kannan and S. Rajeswari:
Mater. Lett., 2006, 60, 2288–2293.
65. I. Zhitomirsky: Adv. Colloid Interf. Sci., 2002, 97, 279–317.
66. P. Sarkar and P. S. Nicholson: J. Am. Ceram. Soc., 1996, 79, (8),
1987.
67. M. Wei, A. Ruys, B. K. Milthorpe and C. C. Sorrell: J. Biomed.
Mater. Res., 1999, 45, 11–19.
68. T. M. Sridhar, T. K. Arumugam, S. Rajeswari and M. Subbaiyan:
J. Mater. Sci. Lett., 1997, 16, 1964–1969.
69. T. M. Sridhar, U. Kamachi Mudali and M. Subbaiyan: Corros.
Sci, 2003, 45, 237–252.
70. T. M. Sridhar, U. Kamachi Mudali and M. Subbaiyan: Corros.
Sci., 2003, 45, 2337–2359.
71. T. M. Sridhar and U. Kamachi Mudali: Trans. Ind. Inst. Met.,
2003, 56, 221–230.
72. C. T. Kwok, P. K. Wonga, F. T. Cheng and H. C. Manc: Appl.
Surf. Sci., 2009, 255, 6736–6744.
73. P. M. Cortez and G. V. Gutieerrez: Adv. Eng. Mater., 2003, 5,
812–815.
74. S. A. Catledge, M. Fries and Y. K. Vohrain: ‘Encyclopedia of
nanoscience and nanotechnology’, Vol. X, 14; 2003, American
Scientific Publishers, Los Angeles.
75. X. Meng, T. Y. Kwon, Y. Yang, J. L. Ong and K. H. Him:
J. Biomed. Mater. Res. B, 2006, 78B, 373–377.
76. I. Zhitomirsky and L. Gal-Or: J. Mater. Sci. Mater. Med., 1997,
8, 213–219.
77. L. Guo and H. Li: Surf. Coat. Technol., 2004, 185, 268–274.
78. P. Mondragon-Cortez and G. Vargas-Gutierrez: Mater. Lett.,
2004, 58, 1336–1339.
79. C. Kaya: Ceram. Int., 2008, 34, 1843–1847.
80. K. Yasuda and P. Schmuki: Electrochim. Acta, 2007, 52, 4053–
4061.
81. N. Eliaz, T. M. Sridhar, U. Kamachi Mudali and B. Raj: Surf.
Eng., 2005, 21, 238–242.
82. N. Eliaz and T. M. Sridhar: Cryst. Growth Des., 2008, 8, 3965–3977.
83. H. Tsuchiya, J. M. Macak, L. Muller, J. Kunze, F. Muller,
P. Greil, S. Virtanen and P. Schmuki: J. Biomed. Mater. Res. A,
2006, 77A, 534–541.
84. B. Yang, M. Uchida, H. M. Kim, X. Zhang and T. Kokubo:
Biomaterials, 2004, 25, 1003–1010.
85. Y. T. Sul, C. B. Johansson, S. Petronis, A. Krozer, Y. Jeong,
A. Wennerberg and T. Albrektsson: Biomaterials, 2002, 23, 491–
501.
86. W. H. Song, Y. K. Jun, Y. Han and S. H. Hong: Biomaterials,
2004, 25, 3341–3349.
87. J. Kunze, L. Muller, J. M. Macaka, P. Greil, P. Schmuk and F. A.
Muller: Electrochim. Acta, 2008, 53, 6995–7003.
88. R. Narayanan, S. Seshadri, T. Kwon and K. Kim: Scr. Mater.,
2007, 56, 229–232.
89. R. Narayanan, T.-Y. Kwon and K.-H. Kim: Mater. Sci. Eng. C,
2008, C28, 1265–1270.
90. R. Narayanan and S. K. Seshadri: Mater. Chem. Phy., 2007, 106,
406–411.
91. S. M Barinov, S. V. Tumanov, I. V. Fadeeva and V. Y. Bibikov:
Inorg. Mater., 2003, 39, 877–880.
Sridhar Nanobioceramic coatings for biomedical applications
194 Materials Technology 2010 VOL 25 NO 3/4

92. E. J. Lee, S. H. Lee, H. W. Kim, Y. M. Kong and H. E. Kim:
Biomaterials, 2005, 26, 3843–3851.
93. H. W. Kim, Y. M. Kong, C. J. Bae, Y. J. Noh and H. E. Kim:
Biomaterials, 2004, 25, 2919–2926.
94. K. Cheng, S. Zhang, W. Weng and X. Zhang: Surf. Coat.
Technol., 2005, 198, 242–246.
95. H. Qu and M. Wei: Acta Biomater., 2006, 2, 113–119.
96. H. W. Kim, H. E. Kim and J. C. Knowles: Biomaterials, 2004, 25,
3351–3358.
97. S. Kannan, J. M. Ventura, and J. M. F. Ferreira: Chem. Mater.,
2005, 17, 3065–3068.
98. J. M. Macak, H. Tsuchiya and P. Schmuki: Angew. Chem. Int.
Ed., 2005, 44, 2100–2102.
99. S. Ono, A. Kiyotake and H. Asoh: ECS Trans., 2008, 11, 1–8.
100. H. Asoh, T. Kawame, W. Shibata and S. Ono: J. Soc. Inorg.
Mater. Jpn, in press.
101. S. Ono, A. Kodama and H. Asoh: J. Jpn Inst. Light Met., 2008,
58, 593–598.
102. S. Ono. M. Saito and H. Asoh: Electrochem. Solid State Lett.,
2004, 7, B21–B24.
103. H. Asoh, S. Ono, T. Hirose, M. Nakao and H. Masuda:
Electrochim. Acta, 2003, 48, 3171–3174.
104. D. Krupa, J. Baszkiewicz, J. W. Sobczak, A. Bilinski, A. Barcz
and B. Rajchel: Vacuum, 2003, 70, 109–113.
105. T. Sundararajan, U. Kamachi Mudali, K. G. M. Nair,
S. Rajeswari and M. Subbaiyan: Mater. Corros., 1999, 50, 344–
349.
106. T. Sundararajan, U. Kamachi Mudali, K. G. M. Nair,
S. Rajeswari and M. Subbaiyan: J. Mater. Eng. Perf., 1999, 8,
252–260.
107. T. Sundararajan, U. Kamachi Mudali, K. G. M. Nair, S.
Rajeswari and M. Subbaiyan: Mater. Trans. JIM, 1998, 39,
759–764.
108. K. M. Veerabadran, U. Kamachi Mudali, K. G. M. Nair and
M. Subbaiyan: Mater. Sci. Forum., 1999, 318–320, 561–568.
109. T. Hanawa and M. Ota: Appl. Surf. Sci., 1992, 55, 269–276.
110. D. Krupa, J. Baszkiewicz, J. A. Kozubowski, A. Barcz, J. W.
Sobczak. A. Bilinski, M. L. Szumie and B. Rajchel: Biomaterials,
2002, 23, 3329–40.
111. B. Sun, B. Ranganthan and S.-S. Feng: Biomaterials, 2008, 29,
475–486.
112. C. Doyle, K. E. and Tanner and W. Bonfield: Biomaterials, 1991,
12, 841–847.
113. J. C. Knowles, G. W. Hastings, H. Ohta, S. Niwa and N. Boeree:
Biomaterials, 1992, 13, 491–496.
114. Q. Liu, J. R. de Wijn, D. Bakker and C. A. van Blitterswijk:
J. Mater. Sci., 1996, 7, 551–557.
115. C. A. van Blitterswijk, D. Bakker, H. Leenders, J. V. D. Brink,
S. C. Hesseling, Y. P. Bovell, A. M. Radder, R. J. Sakker, M. L.
Gallard, P. H. Heinze and G. J. Beumer: in ‘Bone-bonding
biomaterials’, (ed. P. Ducheyne et al), 153–171; 1992, Leidendorp,
Reed Healthcare Comunications.
116. in ‘Nanotechnology and tissue engineering – the scafold’, (ed. C.T.
Laurencin and L. S. Nair), 163; 2008, Boca Raton, FL, CRC Press
117. L. G. Griffith and G. Naughton: Science, 2002, 295, 1009–1014.
118. Sergey V. Dorozhkin: Biomaterials, 2010, 31, 1465–1485.
119. A. S. Greenwald, S. D. Boden, V. M. Goldberg, Y. Khan, C. T.
Laurencin and R. N. Rosier: J. Bone Joint Surg. Am., 2001, 83,
S98–S103.
120. K. M. Woo, V. J. Chen and P. X. Ma: J. Biomed. Mater. Res. A,
2003, 67A, 531–537.
121. M. Vallet-Regi: J. Chem. Soc. Dalton Trans., 2001, 100, 97–108.
122. W. Zhang, K. L. Huang, S. S. Liao and F. Z. Cui: J. Am. Ceram.
Soc., 2003, 86, 1052–1054.
123. W. Zhang, S. S. Liao and F. Z. Cui: Chem. Mater. 2003, 15, 3221–
3226.
124. K. Mi Woo, V. J. Chen and P. X. Ma: J. Biomed. Mater. Res. A,
203, 67A, 531–537.
125. P. X. Ma and R. Zhang: J. Biomed. Mater. Res., 1999, 46, 60–72.
126. J. M. Oliveira, M. T. Rodrigues, S. S. Silvaa, P. B. Malafaya, M.
E. Gomes, C. A. Viegasc, I. R. Diasc, J. T. Azevedod, J. F. Mano
and R. L. Reis: Biomaterials, 2006, 27, 6123–6137.
127. K. Uematsu, K. Hattori, Y. Ishimoto, J. Yamauchi, T. Habata,
Y. Takakura, H. Ohgushi, T. Fukuchi and M. Sato: Biomaterials,
2005, 26, 4273–9.
128. L. Solchaga, J. Temenoff, J. Gao, A. Mikos and V. M. G. Caplan:
Osteoarthr. Cartil., 2005, 13, 297.
129. W. H. Songa,Y. K. Juna, Y. Hana and S. H. Honga: Biomaterials,
2004, 25, 3341–3349.
130. E. A. dos Santos, M. Farina, G. A. Soares and K. Anselme:
J. Biomed. Mater. Res. A, 2009, 89A, 510–520.
131. D. Rokusek, C. Davitt, A. Bandyopadhyay, S. Bose and H. L.
Hosick: J. Biomed. Mater. Res. A, 2005, 75, 588–594.
132. S. V. Dorozhkin and M. Epple: Angew. Chem. Int. Ed., 2002, 41,
3130–3146.
133. M. Bohner: Injury, 2000, 31, S-D37–47.
134. A. Ehara, K. Ogata, S. Imazato, S. Ebisu, T. Nakano and
Y. Umakoshi: Biomaterials, 2003, 24, 831–836.
135. I. O. Smith, L. R. McCabe and M. J. Baumann: Int. J. Nanomed.,
2006, 1, 189–194.
136. M. Sato, A. Aslani, M. A. Sambito, N. M. Kalkhoran, E. B.
Slamovich and T. J. Webster: J. Biomed. Mater. Res. A, 2008,
84A, 265–72.
137. F. Chen, W. M. Lam, C. J. Lin, G. X. Qiu, Z. H. Wu, K. D. Luk
and W. W Lu: J. Biomed. Mater. Res. B, 2007, 82B, 183–91.
138. F. Barrere, P. Layrolle, C. A. van Blitterswijk and K. de Groot:
J. Mater. Sci. Mater. Med., 2001, 12, 529–534.
139. H. Fuming, Y. Guoli, W. Xiaoxiang and Z. Shifang: J. Oral
Rehabil., 2008, 35, 754–765.
140. O. Suzuki, M. Nakamura, Y. Miyasaka, M. Kagayama and
M. Sakurai: Tohoku J. Exp. Med., 1991, 164, 37–50.
141. C. Li, H. J. Jin, G. D. Botsaris and D. L. Kaplana: J. Mater. Res.,
2005, 20, 3374–3384.
142. H. Yoshimoto, Y. M. Shin, H. Terai and J. P. Vacanti:
Biomaterials, 2003, 24, 2077–2082.
143. J. A. Matthews, G. E. Wnek, D. G. Simpson and G. L. Bowlin:
Biomacromolecules, 2002, 3, 232–238.
144. H.-J. Jin, J. Chen, V. Karageorgiou, G. H. Altman and D. L.
Kaplan: Biomaterials, 2004, 25, 1039–1047.
145. J. D. Stitzel, K. Pawlowski, G. E. Wnek, D. G. Simpson and G. L.
Bowlin: J. Biomater. Appl., 2001, 16, 22–33.
146. E. Zhang, C. Zou, G. Yu: Mater. Sci. Eng. C, 2009, C29, 298–305.
147. S. Hayakawa, K. Tsuru, C. Ohtsuki and A. Osaka: J. Am. Ceram.
Soc. 1999, 8, 2155–2160.
148. T. Tian, D. Jiang, J. Zhang and Q. Lin: Mater. Sci. Eng. C, 2008,
C28, 57–63.
149. X. F. Juan, Z. Ying and Y. Jiang: Trans. Non–Ferr. Met. Soc.
Chn, 2009, 19, 125–130.
150. A. J. D. Tulloch, R. Bizios and R. W. Siegel: J. Biomed. Mater.
Res. A, 2009, 90A, 586–594.
151. H. J. Lee, S. E. Kim, H. W. Choi, C. W. Kim, K. J. Kim and S. C.
Lee: Eur. Poly. J., 2007, 43, 1602–1608.
Sridhar Nanobioceramic coatings for biomedical applications
Materials Technology 2010 VOL 25 NO 3/4 195





























