Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Multicenter Comparison of 18F-FDG and 68Ga-DOTA-PeptidePET/CT for Pulmonary Carcinoid
Filippo Lococo, MD,* Germano Perotti, MD,† Giuseppe Cardillo, MD,‡ Chiara De Waure, MD,§Angelina Filice, MD,|| Paolo Graziano, MD,¶ Giulio Rossi, MD,# Giorgio Sgarbi, MD,*
Antonella Stefanelli, MD,† Alessandro Giordano, PhD,† Pierluigi Granone, PhD,** Guido Rindi, PhD,††Annibale Versari, MD,|| and Vittoria Rufini, MD†
Purpose: The aims of this study were to retrospectively evaluate and comparethe detection rate (DR) of 68Ga-DOTA-peptide and 18F-FDG PET/CT in thepreoperative workup of patients with pulmonary carcinoid (PC) and to assessthe utility of various functional indices obtained with the 2 tracers in predictingthe histological characterization of PC, that is, typical versus atypical.Methods: Thirty-three consecutive patients with confirmed PC referred for18F-FDG and 68Ga-DOTA-peptide PET/CT in 2 centers between January 2009and April 2013 were included. The semiquantitative evaluation included theSUVmax, the SUV of the tumor relative to the maximal liver uptake for18F-FDG (SUVT/L) or the maximal spleen uptake for 68Ga-DOTA-peptides(SUVT/S), the ratio between SUVmax of 68Ga-DOTA-peptides PET/CT,and the SUVmax of
18F-FDG PET/CT (SUVmax ratio). Histology was usedas reference standard.Results: Definitive diagnosis consisted of 23 typical carcinoids (TCs) and10 atypical carcinoids. 18F-FDG PET/CTwas positive in 18 cases and negativein 15 (55% DR). 68Ga-DOTA-peptide PET/CT was positive in 26 cases andnegative in 7 (79% DR). In the subgroup analysis, 68Ga-DOTA-peptide PET/CT was superior in detecting TC (91% DR; P < 0.001), whereas 18F-FDGPET/CTwas superior in detecting atypical carcinoid (100% DR; P = 0.04). TheSUVmax ratio was the most accurate semiquantitative index in identifying TC.Conclusions: Overall diagnostic performance of PET/CT in detecting PC isoptimal when integrating 18F-FDG and 68Ga-DOTA-peptide PET/CT findings.In the subgroup analysis, the SUVmax ratio seems to be the most accurate indexin predicting TC. Both methods should be performed when PC is suspected orwhen the histological subtype is undefined.
Key Words: pulmonary carcinoid, PET/CT, 18F-FDG, 68Ga-DOTA-peptides
(Clin Nucl Med 2015;00: 00–00)
P ulmonary carcinoids (PCs) represent about 1% to 2% of all lungcancers. From the histopathological point of view, they may be
subclassified into typical carcinoids (TCs) and atypical carcinoids(ACs) based on the number of mitoses and the extent of necrosis.1 BothTC and AC are low-grade malignant tumors, being TC usually relatedwith a better prognosis with respect to AC.2 It would be clinically
Received for publication July 7, 2014; revision accepted October 24, 2014.From the *Unit of Thoracic Surgery, IRCCS-Arcispedale Santa Maria Nuova, Reggio
Emilia; †Institute of Nuclear Medicine, Università Cattolica del Sacro Cuore;‡Unit of Thoracic Surgery, Azienda Ospedaliera San Camillo Forlanini; and§Institute of Hygiene, Università Cattolica del Sacro Cuore, Rome; ||Departmentof Nuclear Medicine, IRCCS-Arcispedale Santa Maria Nuova, Reggio Emilia;¶Unit of Pathology, Azienda Ospedaliera San Camillo Forlanini, Rome;#Unit of Pathology, IRCCS-Arcispedale Santa Maria Nuova, Reggio Emilia;**Department of Thoracic Surgery, and ††Institute of Pathology, UniversitàCattolica del Sacro Cuore, Rome, Italy.
Filippo Lococo and Germano Perotti have contributed equally to the article and sharethe first authorship.
Conflicts of interest and sources of funding: Supported in part by Internal UniversityGrants (Line D1/2011-2013 to GR and VR, Università Cattolica del Sacro Cuore)and by the Associazione Italiana Ricerca sul Cancro- AIRC IG 2013 14696 to GR.
Reprints: Vittoria Rufini MD, Istituto di Medicina Nucleare, Policlinico UniversitarioA. Gemelli, Largo A. Gemelli 8, 00168 Roma, Italy. E-mail: [email protected].
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.ISSN: 0363-9762/15/0000–0000
Clinical Nuclear Medicine • Volume 00, Number 00, Month 2015
Copyright © 2015 Wolters Kluwer Health, Inc. Unaut
relevant that the diagnosis of PC and possibly the differentiationbetween TC and AC could be made preoperatively because it may havean impact on surgical management as well as prognostic implications.3
Indeed, the preoperative diagnosis of PC by histopathology is notalways feasible, especially for small peripheral PC; when feasible, itdoes not always ensure an accurate differentiation between TC andAC, which is generally performed on surgical specimens only. Inaddition, CT imaging findings are often similar in both subtypes.4
Functional imaging with 18F-FDG PET/CT, which is routinelyused for metabolic characterization of lung nodules,5 is considered ofpoor utility in PC, mainly the typical ones, because of their indolentgrowth and low glucose metabolism.6,7 After the use of somatostatinreceptor scintigraphy (SRS) with 111In-DTPA-octreotide in neuroendo-crine tumors (NETs), PET/CTwith 68Ga-labeled somatostatin analogsput itself forward as a new tool in the diagnostic assessment ofPCs,8–11 which are tumors characterized by high expression ofsomatostatin receptors.12 Preliminary data on the use of 18F-FDGPET/CT compared with SRS or 68Ga-DOTA-peptide PET/CT basedon small series of PC suggest an added value in terms of sensitivityand specificity by combining the double functional information—the glucose consumption explored by 18F-FDG and the expressionof somatostatin receptors explored by 111In-DTPA-octreotide or68Ga-DOTA-peptides.13–17
The aims of this multicenter study were (a) to retrospectivelyevaluate and compare the detection rate (DR) of 68Ga-DOTA-peptideand 18F-FDG PET/CT in the preoperative workup of a group of patientswith proven PC and (b) to assess the utility of various functional indicesobtainedwith the 2 tracers in predicting the histological characterizationof PC, that is, typical versus atypical.
MATERIALS AND METHODSAll consecutive patients with pathologically confirmed PC
referred for 18F-FDG and 68Ga-DOTA-peptide PET/CT in 2 centersbetween January 2009 and April 2013 were enrolled. Inclusion criteriafor this study were availability of clinical charts; chest CT, 18F-FDGPET/CT, and 68Ga-DOTA-peptide PET/CT performed in a 2-month pe-riod; and the availability of a postsurgical histopathological diagnosis.
Institutional review board approval was obtained for the use ofpersonal data for research purposes. Percutaneous biopsy was obtainedbased on CT morphology when technically feasible.
PET/CT ProtocolsPET/CT studies were performed in 2 Italian centers, the PET/CT
center of Santa Maria Nuova Hospital in Reggio Emilia (center A) andthe PET/CT center of Policlinico A. Gemelli in Rome (center B).Before data collection and analysis, the adhesion to standard protocolsfor patient preparation, image acquisition and reconstruction, and semi-quantitative analysis in the clinical routine was checked to minimize theinterinstitute variability.18 In center A, PET/CT was performed on ahybrid scanner (Discovery STE; GE Healthcare, Chalfont St Giles,United Kingdom) with a sensitivity according to National ElectricalManufacturers Association 2001 equal to 9.365 cps/kBq. The CT
www.nuclearmed.com 1
horized reproduction of this article is prohibited.

Lococo et al Clinical Nuclear Medicine • Volume 00, Number 00, Month 2015
attenuation correction acquisition parameterswere 120-kV voltage, 80-mAtube current, and 3.75-mm slice thickness. Images were reconstructedusing the 3-dimensional ordered-subsets expectation maximization, witha 256 � 256 matrix and a voxel size of 2.73 � 2.73 � 3.27 mm3.In center B, PET/CTwas performed on a hybrid scanner (Gemini GXL;Philips Medical Systems, Cleveland, Ohio), with a sensitivity accord-ing to National Electrical Manufacturers Association 2001 equal to8.056 cps/kBq. The CT attenuation correction acquisition parameterswere 120-kV voltage, 80-mA tube current, and 5-mm slice thickness.Images were reconstructed using the iterative method of line of response(RAMLA LOR-3D) implemented by Philips, with a 144� 144 matrixand a voxel size of 4 � 4 � 4 mm3.
PET/CT with 18F-FDG and 68Ga-DOTA-peptides in the singlepatient were performed in the same center within a 2-month period.The use of a 68Ga somatostatin analog was approved by the local ethicscommittee of each center. All patients gave written informed consentfor the 2 PET/CT studies and for the use of personal data.
18F-FDG PET/CT ProtocolIn both centers, patients were asked to fast for at least 5 hours
before 18F-FDG injection. Before PET/CTacquisition, the patients werehydrated with 500 mL of water. At the time of tracer injection, allpatients had a blood glucose level under 150 mg/dL. PET imageswere recorded from the skull base to the mid thigh. Acquisition started60 ± 10 minutes after the IV administration of 3.7 MBq/kg body weightof 18F-FDG in both centers. PET images were recorded for 3.5 minutesper bed position in center A and for 3 minutes per bed position in center B.
68Ga-DOTA-Peptides PET/CT ProtocolIn center A, 68Ga was obtained from a commercially available
68Ge/68Ga generator (Ciclotron, Napa, Calif) with a nominal activityof 1.85 GBq. DOTATOC or DOTATATE were labeled with 68Gaaccording to previously described protocols.19,20 The administered doseof 68Ga DOTATOC and 68Ga DOTATATE was 2 MBq/kg, and theuptake time was 60 ± 10 minutes after tracer injection; PET imageswere acquired for 5 minutes per bed position. In center B, 68Ga wasobtained from a 68Ge/68Ga generator (IGG 100; Eckert & ZieglerIsotope Products, Berlin, Germany), with a nominal activity of1.85 GBq. DOTANOCwas labeled with 68Ga according to a previouslydescribed protocol.21 The administered dose of 68Ga DOTANOC was2 MBq/kg, and the uptake time was 60 ± 10 minutes after tracer injec-tion; PET images were acquired for 4 minutes per bed position.
Image AnalysisThe PET/CT findings were independently reviewed by 2 experi-
enced nuclear medicine physicians who reread all studies blinded tothe clinical reports and reached a consensus. Any focal accumulationof each tracer in the lung nodule higher than the surrounding uptakewas considered an abnormal finding. The DR for both tracerswas deter-mined on a per-patient basis from the number of positive studies and thenumber of patients with PC, according to histological diagnosis.SUVmax was calculated as the highest tumor voxel value for the primarylung tumor in each patient; SUV was normalized by body weight inboth centers.
The SUVof the tumor relative to the maximal liver uptake (for18F-FDG) or the maximal spleen uptake (for 68Ga-DOTA-peptides)was calculated by dividing the SUVmax of the tumor by the SUVmax
of the liver (SUVT/L) or spleen (SUVT/S), respectively. To limit theinfluence of the use of 3 different peptides in semiquantitative analysis,possible variations in splenic uptake (SUVS) among the 3 68Ga peptidesused were calculated.
In addition, the ratio between SUVmax of 68Ga-DOTA-peptide PET/CT and SUVmax of
18F-FDG PET/CT (SUVmax ratio)was calculated.
2 www.nuclearmed.com
Copyright © 2015 Wolters Kluwer Health, Inc. Unaut
SurgeryDespite some unavoidable variability in the surgical technique
among the 3 centers involved, the surgical strategies were substantiallysimilar in all centers. In detail, surgical approach was always performedvia lateral thoracotomy. Similarly, the policy adopted when planningthe extension of pulmonary resection was influenced by the sameassumptions as follows: (1) sublobar resection (wedge resection orsegmentectomy) was indicated in selected cases of TC (peripheralnode–negative TC) and AC (peripheral node–negative lesions and/orpoor pulmonary function); (2) lobectomy was indicated in the remain-ing cases, including those without a preoperative diagnosis or whenan histological distinction between AC and TC was not feasible atfrozen section evaluation; and (3) lymph node dissection was indicatedin all patients with PC apart from patients with TC who underwentsublobar resection. In such cases, a mediastinal lymph node samplingwas performed.
HistologyAll pathological specimens were reviewed and classified as TC
or AC according to World Health Organization criteria.1 Completeresection was confirmed when the bronchial stump was free of tumorusing both the intraoperative frozen sections and paraffin-embeddedpermanent sections.
Statistical AnalysisA descriptive analysis was performed by means of absolute and
relative frequencies for qualitative variables and median and interquar-tile range (IQR) and mean (SD) for quantitative variables. Histologywas used as reference standard. The effectiveness of PET/CT with18F-FDG and 68Ga-DOTA-peptides in identifying carcinoid tumorsand distinguishing TC from AC was assessed through DR and 95%confidence intervals (CIs). Mann-Whitney U and Student t tests wereused to determine statistically significant differences (P < 0.05)between patient characteristics in the 2 groups (TC and AC), whenappropriated. Kruskal-Wallis 1-way test was used to determine statisti-cally significant differences (P < 0.05) among the SUVS of the 3 pep-tides. McNemar symmetry test was used to test for differences in theprevalence of categorical variables. Finally, the accuracy of SUVT/L
for 18F-FDG and SUVT/S for 68Ga-DOTA-peptides and that of theSUVmax ratio were assessed by receiver operating characteristic(ROC) and area under the curve (AUC). In particular, anAUC of at least0.70 was considered satisfactory. In this case, a cutoff maximizingsensitivity and specificity was chosen. SPSS software (version 16,released 2007; SPSS Inc, Chicago, Ill) was used to run the analysis.
RESULTSPatient data are reported in Table 1. Among 85 patients with
PC admitted to both centers between January 2009 and April 2013,33 patients with the mean (SD) age of 59.7 (14) years (range, 23–76years) fulfilled the inclusion criteria. In particular, 28 patients who firstunderwent 18F-FDG PET/CT had been also submitted to 68Ga-DOTA-peptide PET/CT due to low or no 18F-FDG uptake and cytological orradiological suspicion of PC; 5 patients who first underwent 68Ga-DOTA-peptide PET/CT for cytological or radiological suspicion ofPC had been also submitted to 18F-FDG PET/CT due to low or no68Ga-DOTA-peptide uptake. A preoperative cytological/histologicaldiagnosis of PC was available in 8 cases (7 central, 1 peripheral).Complete resection was pathologically confirmed in all cases exceptfor 1 patient with central AC and N2 disease in whom a macroscopicdisease was left. Definitive diagnosis consisted of 23 TC and 10 AC.All pulmonary lesions measured more than 10 mm. Lymph nodeinvolvement was detected in 4 cases—3 AC (2 N1 diseases and 1 N2disease) and 1 TC with N1 extension. In the 3 cases with N1 disease,the lymph node involvement was microscopic only. Atypical carcinoid
© 2015 Wolters Kluwer Health, Inc. All rights reserved.
horized reproduction of this article is prohibited.
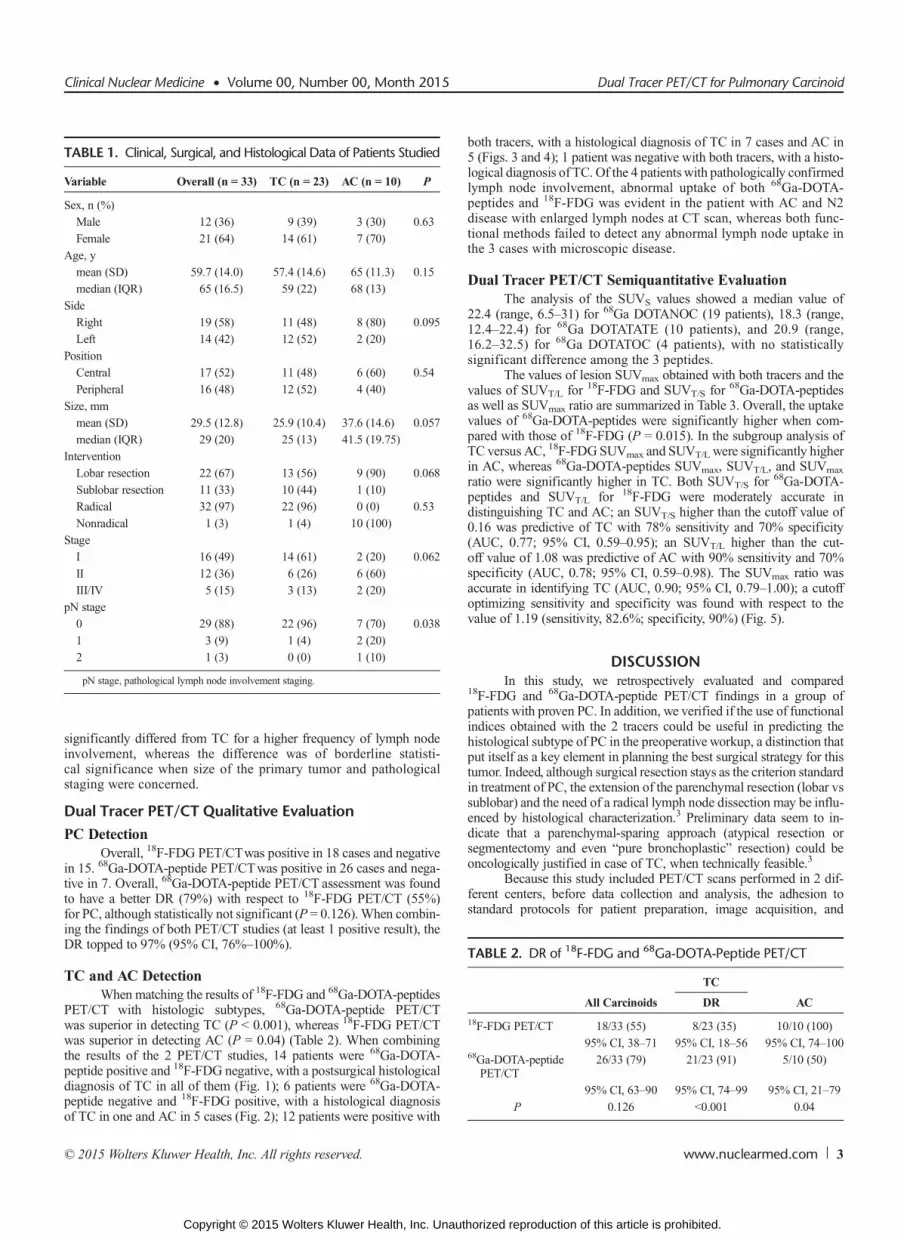
TABLE 1. Clinical, Surgical, and Histological Data of Patients Studied
Variable Overall (n = 33) TC (n = 23) AC (n = 10) P
Sex, n (%)
Male 12 (36) 9 (39) 3 (30) 0.63
Female 21 (64) 14 (61) 7 (70)
Age, y
mean (SD) 59.7 (14.0) 57.4 (14.6) 65 (11.3) 0.15
median (IQR) 65 (16.5) 59 (22) 68 (13)
Side
Right 19 (58) 11 (48) 8 (80) 0.095
Left 14 (42) 12 (52) 2 (20)
Position
Central 17 (52) 11 (48) 6 (60) 0.54
Peripheral 16 (48) 12 (52) 4 (40)
Size, mm
mean (SD) 29.5 (12.8) 25.9 (10.4) 37.6 (14.6) 0.057
median (IQR) 29 (20) 25 (13) 41.5 (19.75)
Intervention
Lobar resection 22 (67) 13 (56) 9 (90) 0.068
Sublobar resection 11 (33) 10 (44) 1 (10)
Radical 32 (97) 22 (96) 0 (0) 0.53
Nonradical 1 (3) 1 (4) 10 (100)
Stage
I 16 (49) 14 (61) 2 (20) 0.062
II 12 (36) 6 (26) 6 (60)
III/IV 5 (15) 3 (13) 2 (20)
pN stage
0 29 (88) 22 (96) 7 (70) 0.038
1 3 (9) 1 (4) 2 (20)
2 1 (3) 0 (0) 1 (10)
pN stage, pathological lymph node involvement staging.
TABLE 2. DR of 18F-FDG and 68Ga-DOTA-Peptide PET/CT
TC
All Carcinoids DR AC
18F-FDG PET/CT 18/33 (55) 8/23 (35) 10/10 (100)
95% CI, 38–71 95% CI, 18–56 95% CI, 74–10068Ga-DOTA-peptide
PET/CT26/33 (79) 21/23 (91) 5/10 (50)
95% CI, 63–90 95% CI, 74–99 95% CI, 21–79
P 0.126 <0.001 0.04
Clinical Nuclear Medicine • Volume 00, Number 00, Month 2015 Dual Tracer PET/CT for Pulmonary Carcinoid
significantly differed from TC for a higher frequency of lymph nodeinvolvement, whereas the difference was of borderline statisti-cal significance when size of the primary tumor and pathologicalstaging were concerned.
Dual Tracer PET/CT Qualitative Evaluation
PC DetectionOverall, 18F-FDG PET/CTwas positive in 18 cases and negative
in 15. 68Ga-DOTA-peptide PET/CTwas positive in 26 cases and nega-tive in 7. Overall, 68Ga-DOTA-peptide PET/CT assessment was foundto have a better DR (79%) with respect to 18F-FDG PET/CT (55%)for PC, although statistically not significant (P = 0.126). When combin-ing the findings of both PET/CT studies (at least 1 positive result), theDR topped to 97% (95% CI, 76%–100%).
TC and AC DetectionWhen matching the results of 18F-FDG and 68Ga-DOTA-peptides
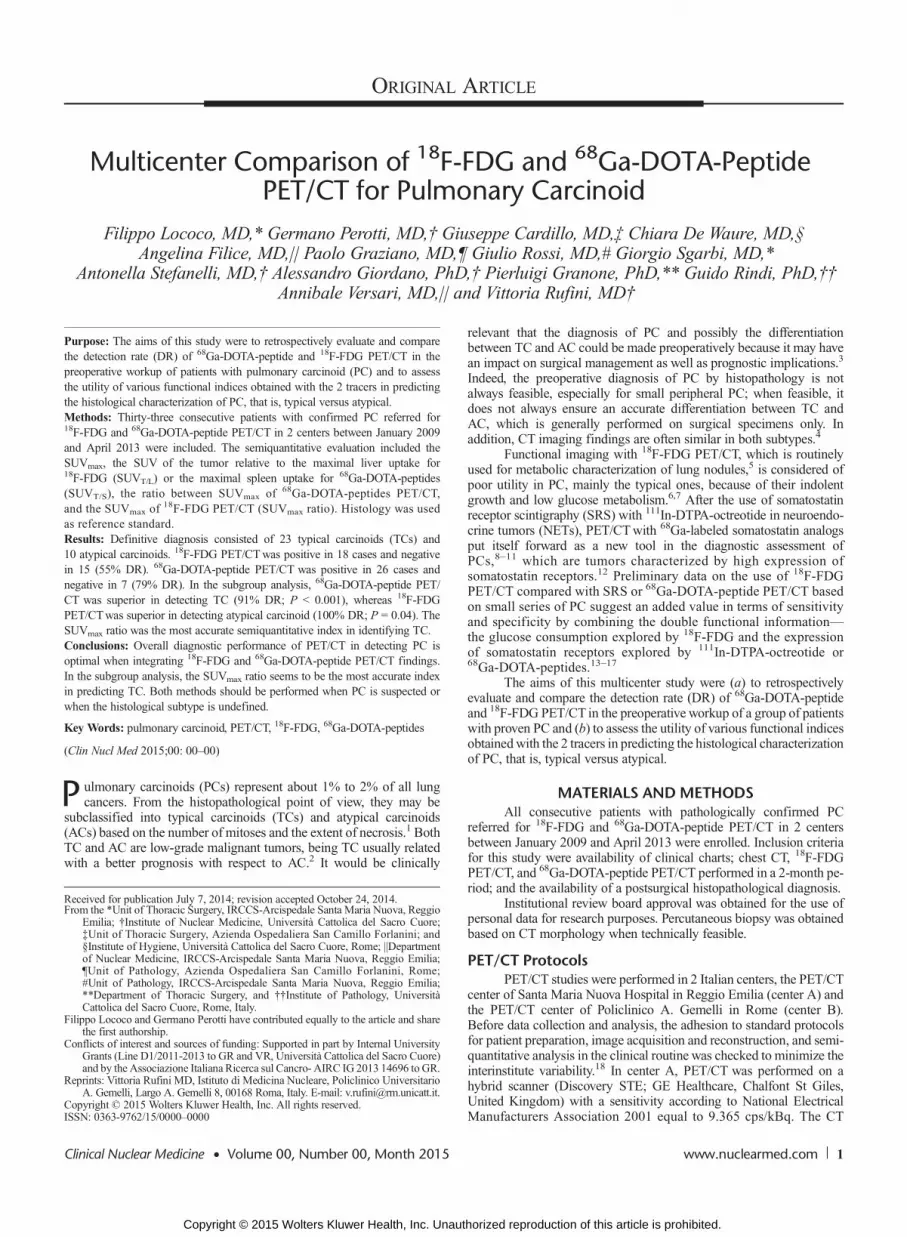
PET/CT with histologic subtypes, 68Ga-DOTA-peptide PET/CTwas superior in detecting TC (P < 0.001), whereas 18F-FDG PET/CTwas superior in detecting AC (P = 0.04) (Table 2). When combiningthe results of the 2 PET/CT studies, 14 patients were 68Ga-DOTA-peptide positive and 18F-FDG negative, with a postsurgical histologicaldiagnosis of TC in all of them (Fig. 1); 6 patients were 68Ga-DOTA-peptide negative and 18F-FDG positive, with a histological diagnosisof TC in one and AC in 5 cases (Fig. 2); 12 patients were positive with
© 2015 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2015 Wolters Kluwer Health, Inc. Unaut
both tracers, with a histological diagnosis of TC in 7 cases and AC in5 (Figs. 3 and 4); 1 patient was negative with both tracers, with a histo-logical diagnosis of TC. Of the 4 patientswith pathologically confirmedlymph node involvement, abnormal uptake of both 68Ga-DOTA-peptides and 18F-FDG was evident in the patient with AC and N2disease with enlarged lymph nodes at CT scan, whereas both func-tional methods failed to detect any abnormal lymph node uptake inthe 3 cases with microscopic disease.
Dual Tracer PET/CT Semiquantitative EvaluationThe analysis of the SUVS values showed a median value of
22.4 (range, 6.5–31) for 68Ga DOTANOC (19 patients), 18.3 (range,12.4–22.4) for 68Ga DOTATATE (10 patients), and 20.9 (range,16.2–32.5) for 68Ga DOTATOC (4 patients), with no statisticallysignificant difference among the 3 peptides.
The values of lesion SUVmax obtained with both tracers and thevalues of SUVT/L for 18F-FDG and SUVT/S for 68Ga-DOTA-peptidesas well as SUVmax ratio are summarized in Table 3. Overall, the uptakevalues of 68Ga-DOTA-peptides were significantly higher when com-pared with those of 18F-FDG (P = 0.015). In the subgroup analysis ofTC versus AC, 18F-FDGSUVmax and SUVT/L were significantly higherin AC, whereas 68Ga-DOTA-peptides SUVmax, SUVT/L, and SUVmax
ratio were significantly higher in TC. Both SUVT/S for 68Ga-DOTA-peptides and SUVT/L for 18F-FDG were moderately accurate indistinguishing TC and AC; an SUVT/S higher than the cutoff value of0.16 was predictive of TC with 78% sensitivity and 70% specificity(AUC, 0.77; 95% CI, 0.59–0.95); an SUVT/L higher than the cut-off value of 1.08 was predictive of AC with 90% sensitivity and 70%specificity (AUC, 0.78; 95% CI, 0.59–0.98). The SUVmax ratio wasaccurate in identifying TC (AUC, 0.90; 95% CI, 0.79–1.00); a cutoffoptimizing sensitivity and specificity was found with respect to thevalue of 1.19 (sensitivity, 82.6%; specificity, 90%) (Fig. 5).
DISCUSSIONIn this study, we retrospectively evaluated and compared
18F-FDG and 68Ga-DOTA-peptide PET/CT findings in a group ofpatients with proven PC. In addition, we verified if the use of functionalindices obtained with the 2 tracers could be useful in predicting thehistological subtype of PC in the preoperative workup, a distinction thatput itself as a key element in planning the best surgical strategy for thistumor. Indeed, although surgical resection stays as the criterion standardin treatment of PC, the extension of the parenchymal resection (lobar vssublobar) and the need of a radical lymph node dissection may be influ-enced by histological characterization.3 Preliminary data seem to in-dicate that a parenchymal-sparing approach (atypical resection orsegmentectomy and even “pure bronchoplastic” resection) could beoncologically justified in case of TC, when technically feasible.3
Because this study included PET/CT scans performed in 2 dif-ferent centers, before data collection and analysis, the adhesion tostandard protocols for patient preparation, image acquisition, and
www.nuclearmed.com 3
horized reproduction of this article is prohibited.
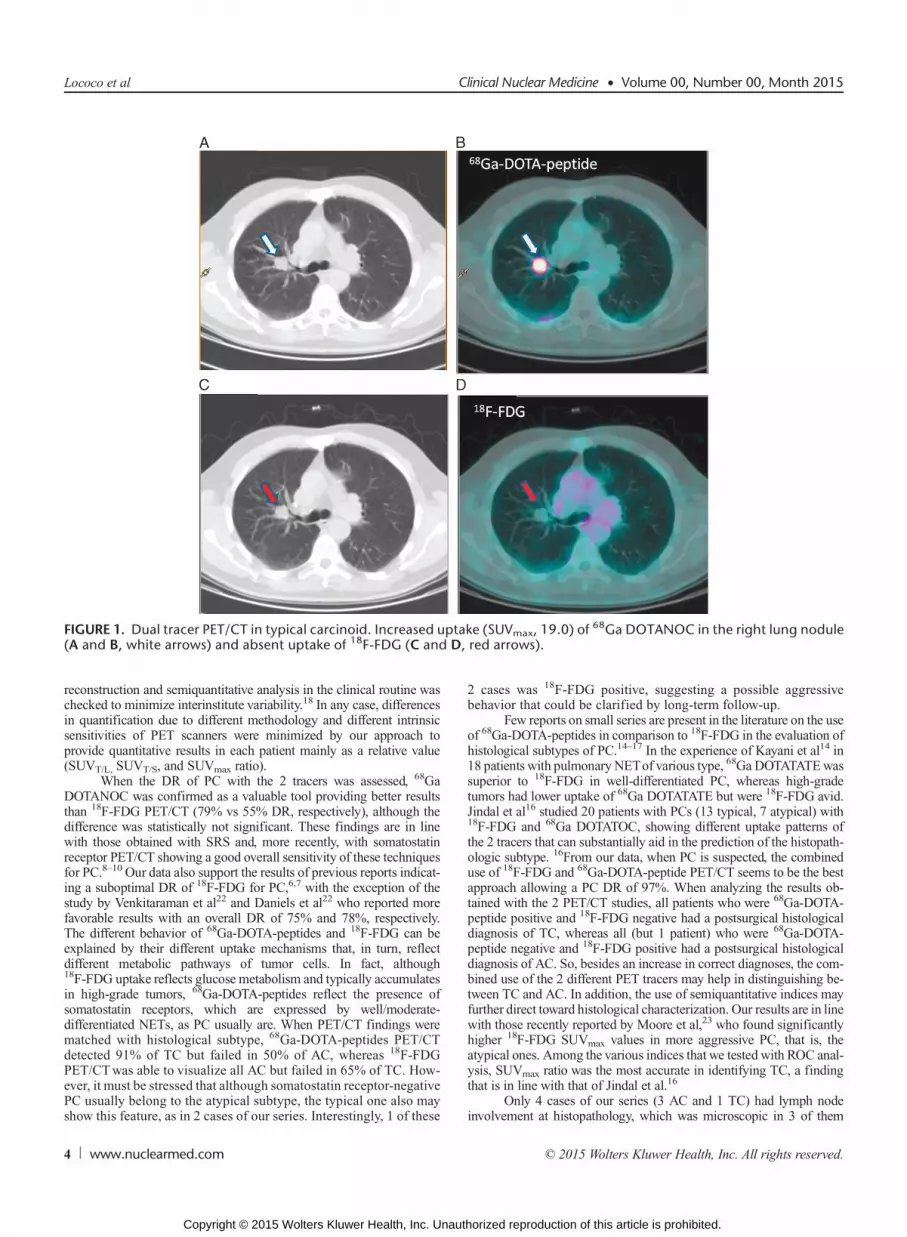
FIGURE 1. Dual tracer PET/CT in typical carcinoid. Increased uptake (SUVmax, 19.0) of68Ga DOTANOC in the right lung nodule
(A and B, white arrows) and absent uptake of 18F-FDG (C and D, red arrows).
Lococo et al Clinical Nuclear Medicine • Volume 00, Number 00, Month 2015
reconstruction and semiquantitative analysis in the clinical routine waschecked to minimize interinstitute variability.18 In any case, differencesin quantification due to different methodology and different intrinsicsensitivities of PET scanners were minimized by our approach toprovide quantitative results in each patient mainly as a relative value(SUVT/L, SUVT/S, and SUVmax ratio).
When the DR of PC with the 2 tracers was assessed, 68GaDOTANOC was confirmed as a valuable tool providing better resultsthan 18F-FDG PET/CT (79% vs 55% DR, respectively), although thedifference was statistically not significant. These findings are in linewith those obtained with SRS and, more recently, with somatostatinreceptor PET/CT showing a good overall sensitivity of these techniquesfor PC.8–10 Our data also support the results of previous reports indicat-ing a suboptimal DR of 18F-FDG for PC,6,7 with the exception of thestudy by Venkitaraman et al22 and Daniels et al22 who reported morefavorable results with an overall DR of 75% and 78%, respectively.The different behavior of 68Ga-DOTA-peptides and 18F-FDG can beexplained by their different uptake mechanisms that, in turn, reflectdifferent metabolic pathways of tumor cells. In fact, although18F-FDG uptake reflects glucose metabolism and typically accumulatesin high-grade tumors, 68Ga-DOTA-peptides reflect the presence ofsomatostatin receptors, which are expressed by well/moderate-differentiated NETs, as PC usually are. When PET/CT findings werematched with histological subtype, 68Ga-DOTA-peptides PET/CTdetected 91% of TC but failed in 50% of AC, whereas 18F-FDGPET/CTwas able to visualize all AC but failed in 65% of TC. How-ever, it must be stressed that although somatostatin receptor-negativePC usually belong to the atypical subtype, the typical one also mayshow this feature, as in 2 cases of our series. Interestingly, 1 of these
4 www.nuclearmed.com
Copyright © 2015 Wolters Kluwer Health, Inc. Unaut
2 cases was 18F-FDG positive, suggesting a possible aggressivebehavior that could be clarified by long-term follow-up.
Few reports on small series are present in the literature on the useof 68Ga-DOTA-peptides in comparison to 18F-FDG in the evaluation ofhistological subtypes of PC.14–17 In the experience of Kayani et al14 in18 patients with pulmonary NETof various type, 68Ga DOTATATEwassuperior to 18F-FDG in well-differentiated PC, whereas high-gradetumors had lower uptake of 68Ga DOTATATE but were 18F-FDG avid.Jindal et al16 studied 20 patients with PCs (13 typical, 7 atypical) with18F-FDG and 68Ga DOTATOC, showing different uptake patterns ofthe 2 tracers that can substantially aid in the prediction of the histopath-ologic subtype. 16From our data, when PC is suspected, the combineduse of 18F-FDG and 68Ga-DOTA-peptide PET/CT seems to be the bestapproach allowing a PC DR of 97%. When analyzing the results ob-tained with the 2 PET/CT studies, all patients who were 68Ga-DOTA-peptide positive and 18F-FDG negative had a postsurgical histologicaldiagnosis of TC, whereas all (but 1 patient) who were 68Ga-DOTA-peptide negative and 18F-FDG positive had a postsurgical histologicaldiagnosis of AC. So, besides an increase in correct diagnoses, the com-bined use of the 2 different PET tracers may help in distinguishing be-tween TC and AC. In addition, the use of semiquantitative indices mayfurther direct toward histological characterization. Our results are in linewith those recently reported by Moore et al,23 who found significantlyhigher 18F-FDG SUVmax values in more aggressive PC, that is, theatypical ones. Among the various indices that we tested with ROC anal-ysis, SUVmax ratio was the most accurate in identifying TC, a findingthat is in line with that of Jindal et al.16
Only 4 cases of our series (3 AC and 1 TC) had lymph nodeinvolvement at histopathology, which was microscopic in 3 of them
© 2015 Wolters Kluwer Health, Inc. All rights reserved.
horized reproduction of this article is prohibited.
FIGURE 2. Dual tracer PET/CT in atypical carcinoid. Absent uptake of 68Ga DOTANOC in the right lung nodule (A and B, white arrows)and increased uptake of 18F-FDG (SUVmax, 10.6) (C and D, red arrows).
FIGURE 3. Dual tracer PET/CT in typical carcinoid. Highly increased uptake (SUVmax, 27) of68Ga DOTATOC in the left lung nodule
(A and B, white arrows) and lower uptake (SUVmax, 5.3) of18F-FDG (C and D, red arrows); (SUVmax ratio, 5.1).
Clinical Nuclear Medicine • Volume 00, Number 00, Month 2015 Dual Tracer PET/CT for Pulmonary Carcinoid
© 2015 Wolters Kluwer Health, Inc. All rights reserved. www.nuclearmed.com 5
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
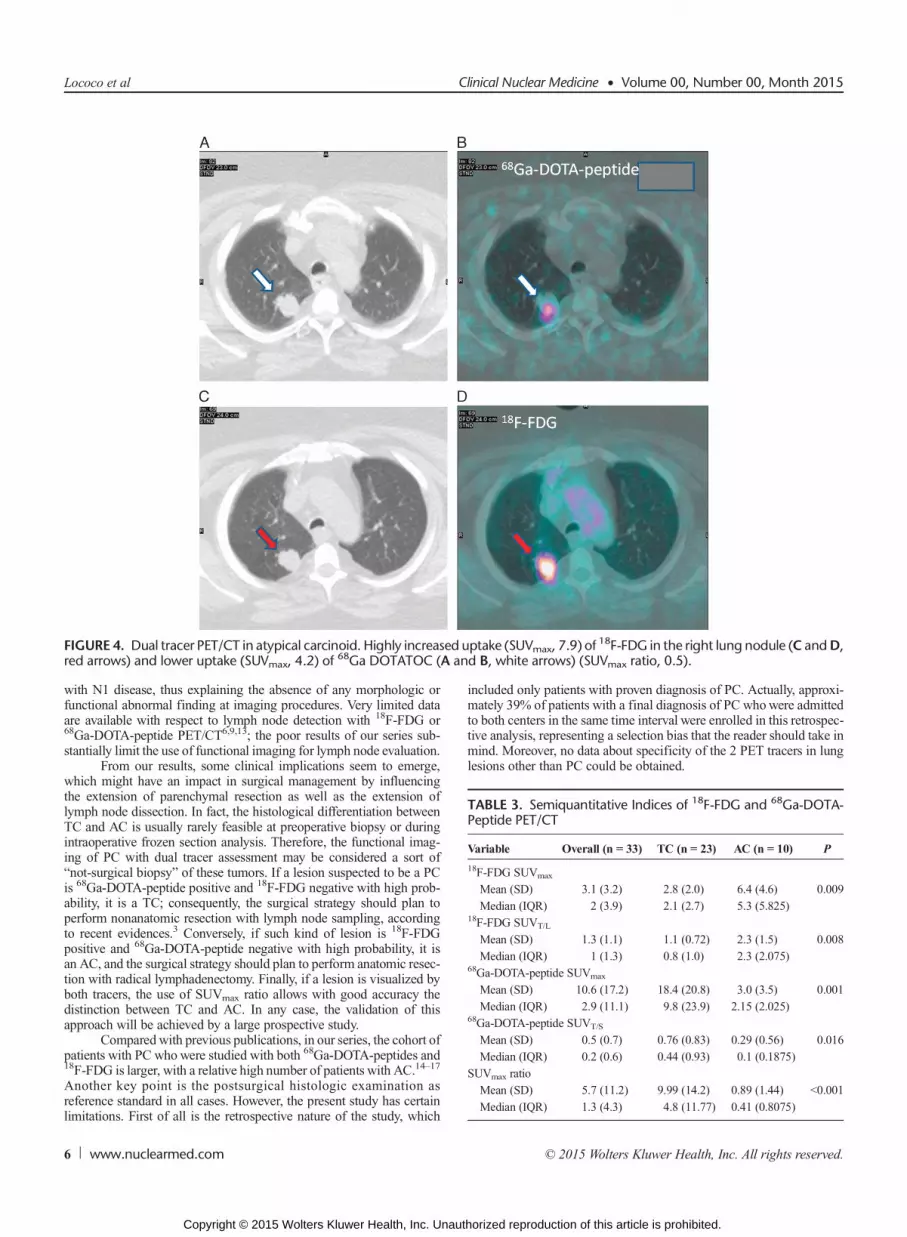
FIGURE 4. Dual tracer PET/CT in atypical carcinoid. Highly increased uptake (SUVmax, 7.9) of18F-FDG in the right lung nodule (C andD,
red arrows) and lower uptake (SUVmax, 4.2) of68Ga DOTATOC (A and B, white arrows) (SUVmax ratio, 0.5).
TABLE 3. Semiquantitative Indices of 18F-FDG and 68Ga-DOTA-Peptide PET/CT
Variable Overall (n = 33) TC (n = 23) AC (n = 10) P
18F-FDG SUVmax
Mean (SD) 3.1 (3.2) 2.8 (2.0) 6.4 (4.6) 0.009
Median (IQR) 2 (3.9) 2.1 (2.7) 5.3 (5.825)18F-FDG SUVT/L
Mean (SD) 1.3 (1.1) 1.1 (0.72) 2.3 (1.5) 0.008
Median (IQR) 1 (1.3) 0.8 (1.0) 2.3 (2.075)68Ga-DOTA-peptide SUVmax
Mean (SD) 10.6 (17.2) 18.4 (20.8) 3.0 (3.5) 0.001
Median (IQR) 2.9 (11.1) 9.8 (23.9) 2.15 (2.025)68Ga-DOTA-peptide SUVT/S
Mean (SD) 0.5 (0.7) 0.76 (0.83) 0.29 (0.56) 0.016
Median (IQR) 0.2 (0.6) 0.44 (0.93) 0.1 (0.1875)
SUVmax ratio
Mean (SD) 5.7 (11.2) 9.99 (14.2) 0.89 (1.44) <0.001
Median (IQR) 1.3 (4.3) 4.8 (11.77) 0.41 (0.8075)
Lococo et al Clinical Nuclear Medicine • Volume 00, Number 00, Month 2015
with N1 disease, thus explaining the absence of any morphologic orfunctional abnormal finding at imaging procedures. Very limited dataare available with respect to lymph node detection with 18F-FDG or68Ga-DOTA-peptide PET/CT6,9,13; the poor results of our series sub-stantially limit the use of functional imaging for lymph node evaluation.
From our results, some clinical implications seem to emerge,which might have an impact in surgical management by influencingthe extension of parenchymal resection as well as the extension oflymph node dissection. In fact, the histological differentiation betweenTC and AC is usually rarely feasible at preoperative biopsy or duringintraoperative frozen section analysis. Therefore, the functional imag-ing of PC with dual tracer assessment may be considered a sort of“not-surgical biopsy” of these tumors. If a lesion suspected to be a PCis 68Ga-DOTA-peptide positive and 18F-FDG negative with high prob-ability, it is a TC; consequently, the surgical strategy should plan toperform nonanatomic resection with lymph node sampling, accordingto recent evidences.3 Conversely, if such kind of lesion is 18F-FDGpositive and 68Ga-DOTA-peptide negative with high probability, it isan AC, and the surgical strategy should plan to perform anatomic resec-tion with radical lymphadenectomy. Finally, if a lesion is visualized byboth tracers, the use of SUVmax ratio allows with good accuracy thedistinction between TC and AC. In any case, the validation of thisapproach will be achieved by a large prospective study.
Compared with previous publications, in our series, the cohort ofpatients with PC whowere studied with both 68Ga-DOTA-peptides and18F-FDG is larger, with a relative high number of patients with AC.14–17
Another key point is the postsurgical histologic examination asreference standard in all cases. However, the present study has certainlimitations. First of all is the retrospective nature of the study, which
6 www.nuclearmed.com
Copyright © 2015 Wolters Kluwer Health, Inc. Unaut
included only patients with proven diagnosis of PC. Actually, approxi-mately 39% of patients with a final diagnosis of PC whowere admittedto both centers in the same time interval were enrolled in this retrospec-tive analysis, representing a selection bias that the reader should take inmind. Moreover, no data about specificity of the 2 PET tracers in lunglesions other than PC could be obtained.
© 2015 Wolters Kluwer Health, Inc. All rights reserved.
horized reproduction of this article is prohibited.
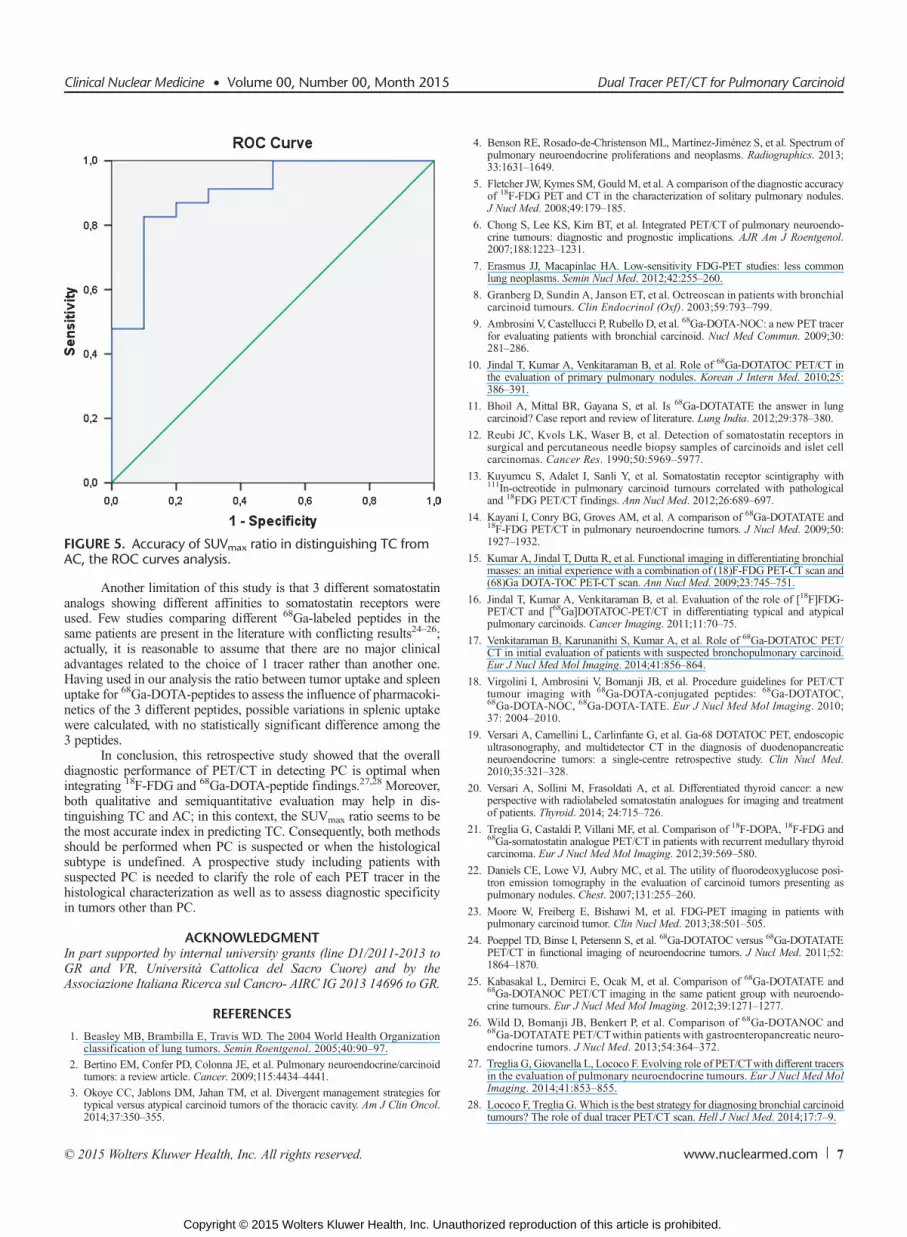
FIGURE 5. Accuracy of SUVmax ratio in distinguishing TC fromAC, the ROC curves analysis.
Clinical Nuclear Medicine • Volume 00, Number 00, Month 2015 Dual Tracer PET/CT for Pulmonary Carcinoid
Another limitation of this study is that 3 different somatostatinanalogs showing different affinities to somatostatin receptors wereused. Few studies comparing different 68Ga-labeled peptides in thesame patients are present in the literature with conflicting results24–26;actually, it is reasonable to assume that there are no major clinicaladvantages related to the choice of 1 tracer rather than another one.Having used in our analysis the ratio between tumor uptake and spleenuptake for 68Ga-DOTA-peptides to assess the influence of pharmacoki-netics of the 3 different peptides, possible variations in splenic uptakewere calculated, with no statistically significant difference among the3 peptides.
In conclusion, this retrospective study showed that the overalldiagnostic performance of PET/CT in detecting PC is optimal whenintegrating 18F-FDG and 68Ga-DOTA-peptide findings.27,28 Moreover,both qualitative and semiquantitative evaluation may help in dis-tinguishing TC and AC; in this context, the SUVmax ratio seems to bethe most accurate index in predicting TC. Consequently, both methodsshould be performed when PC is suspected or when the histologicalsubtype is undefined. A prospective study including patients withsuspected PC is needed to clarify the role of each PET tracer in thehistological characterization as well as to assess diagnostic specificityin tumors other than PC.
ACKNOWLEDGMENTIn part supported by internal university grants (line D1/2011-2013 toGR and VR, Università Cattolica del Sacro Cuore) and by theAssociazione Italiana Ricerca sul Cancro- AIRC IG 2013 14696 to GR.
REFERENCES
1. Beasley MB, Brambilla E, Travis WD. The 2004 World Health Organizationclassification of lung tumors. Semin Roentgenol. 2005;40:90–97.
2. Bertino EM, Confer PD, Colonna JE, et al. Pulmonary neuroendocrine/carcinoidtumors: a review article. Cancer. 2009;115:4434–4441.
3. Okoye CC, Jablons DM, Jahan TM, et al. Divergent management strategies fortypical versus atypical carcinoid tumors of the thoracic cavity. Am J Clin Oncol.2014;37:350–355.
© 2015 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2015 Wolters Kluwer Health, Inc. Unaut
4. Benson RE, Rosado-de-Christenson ML, Martínez-Jiménez S, et al. Spectrum ofpulmonary neuroendocrine proliferations and neoplasms. Radiographics. 2013;33:1631–1649.
5. Fletcher JW, Kymes SM, GouldM, et al. A comparison of the diagnostic accuracyof 18F-FDG PET and CT in the characterization of solitary pulmonary nodules.J Nucl Med. 2008;49:179–185.
6. Chong S, Lee KS, Kim BT, et al. Integrated PET/CT of pulmonary neuroendo-crine tumours: diagnostic and prognostic implications. AJR Am J Roentgenol.2007;188:1223–1231.
7. Erasmus JJ, Macapinlac HA. Low-sensitivity FDG-PET studies: less commonlung neoplasms. Semin Nucl Med. 2012;42:255–260.
8. Granberg D, Sundin A, Janson ET, et al. Octreoscan in patients with bronchialcarcinoid tumours. Clin Endocrinol (Oxf). 2003;59:793–799.
9. Ambrosini V, Castellucci P, Rubello D, et al. 68Ga-DOTA-NOC: a new PET tracerfor evaluating patients with bronchial carcinoid. Nucl Med Commun. 2009;30:281–286.
10. Jindal T, Kumar A, Venkitaraman B, et al. Role of 68Ga-DOTATOC PET/CT inthe evaluation of primary pulmonary nodules. Korean J Intern Med. 2010;25:386–391.
11. Bhoil A, Mittal BR, Gayana S, et al. Is 68Ga-DOTATATE the answer in lungcarcinoid? Case report and review of literature. Lung India. 2012;29:378–380.
12. Reubi JC, Kvols LK, Waser B, et al. Detection of somatostatin receptors insurgical and percutaneous needle biopsy samples of carcinoids and islet cellcarcinomas. Cancer Res. 1990;50:5969–5977.
13. Kuyumcu S, Adalet I, Sanli Y, et al. Somatostatin receptor scintigraphy with111In-octreotide in pulmonary carcinoid tumours correlated with pathologicaland 18FDG PET/CT findings. Ann Nucl Med. 2012;26:689–697.
14. Kayani I, Conry BG, Groves AM, et al. A comparison of 68Ga-DOTATATE and18F-FDG PET/CT in pulmonary neuroendocrine tumors. J Nucl Med. 2009;50:1927–1932.
15. Kumar A, Jindal T, Dutta R, et al. Functional imaging in differentiating bronchialmasses: an initial experience with a combination of (18)F-FDG PET-CT scan and(68)Ga DOTA-TOC PET-CT scan. Ann Nucl Med. 2009;23:745–751.
16. Jindal T, Kumar A, Venkitaraman B, et al. Evaluation of the role of [18F]FDG-PET/CT and [68Ga]DOTATOC-PET/CT in differentiating typical and atypicalpulmonary carcinoids. Cancer Imaging. 2011;11:70–75.
17. Venkitaraman B, Karunanithi S, Kumar A, et al. Role of 68Ga-DOTATOC PET/CT in initial evaluation of patients with suspected bronchopulmonary carcinoid.Eur J Nucl Med Mol Imaging. 2014;41:856–864.
18. Virgolini I, Ambrosini V, Bomanji JB, et al. Procedure guidelines for PET/CTtumour imaging with 68Ga-DOTA-conjugated peptides: 68Ga-DOTATOC,68Ga-DOTA-NOC, 68Ga-DOTA-TATE. Eur J Nucl Med Mol Imaging. 2010;37: 2004–2010.
19. Versari A, Camellini L, Carlinfante G, et al. Ga-68 DOTATOC PET, endoscopicultrasonography, and multidetector CT in the diagnosis of duodenopancreaticneuroendocrine tumors: a single-centre retrospective study. Clin Nucl Med.2010;35:321–328.
20. Versari A, Sollini M, Frasoldati A, et al. Differentiated thyroid cancer: a newperspective with radiolabeled somatostatin analogues for imaging and treatmentof patients. Thyroid. 2014; 24:715–726.
21. Treglia G, Castaldi P, Villani MF, et al. Comparison of 18F-DOPA, 18F-FDG and68Ga-somatostatin analogue PET/CT in patients with recurrent medullary thyroidcarcinoma. Eur J Nucl Med Mol Imaging. 2012;39:569–580.
22. Daniels CE, Lowe VJ, Aubry MC, et al. The utility of fluorodeoxyglucose posi-tron emission tomography in the evaluation of carcinoid tumors presenting aspulmonary nodules. Chest. 2007;131:255–260.
23. Moore W, Freiberg E, Bishawi M, et al. FDG-PET imaging in patients withpulmonary carcinoid tumor. Clin Nucl Med. 2013;38:501–505.
24. Poeppel TD, Binse I, Petersenn S, et al. 68Ga-DOTATOC versus 68Ga-DOTATATEPET/CT in functional imaging of neuroendocrine tumors. J Nucl Med. 2011;52:1864–1870.
25. Kabasakal L, Demirci E, Ocak M, et al. Comparison of 68Ga-DOTATATE and68Ga-DOTANOC PET/CT imaging in the same patient group with neuroendo-crine tumours. Eur J Nucl Med Mol Imaging. 2012;39:1271–1277.
26. Wild D, Bomanji JB, Benkert P, et al. Comparison of 68Ga-DOTANOC and68Ga-DOTATATE PET/CTwithin patients with gastroenteropancreatic neuro-endocrine tumors. J Nucl Med. 2013;54:364–372.
27. Treglia G, Giovanella L, Lococo F. Evolving role of PET/CTwith different tracersin the evaluation of pulmonary neuroendocrine tumours. Eur J Nucl Med MolImaging. 2014;41:853–855.
28. Lococo F, Treglia G.Which is the best strategy for diagnosing bronchial carcinoidtumours? The role of dual tracer PET/CT scan. Hell J Nucl Med. 2014;17:7–9.
www.nuclearmed.com 7
horized reproduction of this article is prohibited.





























