Embed Size (px)
Citation preview

Am J C/in Nutr 1995;62:143-8. Printed in USA. © 1995 American Society for Clinical Nutrition I43
Mortality of infants <6 mo of age supplemented withvitamin A: a randomized, double-masked trial in Nepal�
Keith P West Jr, Joanne Katz, Sharada Ram Shrestha, Steven C LeClerq, Subarna K Khatrv,
Elizabeth K Pradhan, Ramesh Adhikari, Lee Shu-Fune Wu, Ram Prasad Pokhrel, and Alfred Sommer
ABSTRACT The effect of supplementing 1 1 918 infants < 1
mo and 1-5 mo of age with vitamin A (15 000 and 30 000 �tg
retinol equivalents or 50 000 and 100 000 IU, respectively) or a
placebo on subsequent 4-mo mortality was assessed in a random-
ized, double-masked community trial in the rural plains of Nepal.
There were 130 deaths (51.6/1000 child-y) in the control group and
150 deaths (57.1/1000 child-y) in the vitamin A group, yielding a
relative risk of 1.1 1 (95% CI: 0.86, 1.42), which is indicative of no
overall effect on early infant mortality. There was a tendency for
the relative risk of mortality among vitamin A recipients to rise
with improved nutritional status. These results suggest that distri-
bution of a large oral dose of vitamin A to infants < 5-6 mo of age
may not benefit short-term survival. This is in contrast with the
results of trials in which older infants and children in this same
population were supplemented. Am J C’lin Nutr 1995;62: 143-8.
KEY WORDS Vitamin A, supplementation, infant mortal-
ity, verbal autopsy, intolerance
INTRODUCTION
Vitamin A deficiency is widespread in many developing
countries where an estimated I 24 million preschool children
are deficient (1). Between S and 8 million children develop
xerophthalmia each year (2). Beyond its role as the leading
cause of pediatric blindness (3), vitamin A deficiency is an
important underlying cause of early childhood mortality (4);
deficiency apparently comprises the host response to severe
infection (4-6). An estimated 1.3-2.5 million infant and pre-
school child deaths annually can be attributed to vitamin A
deficiency (1).
Over the past decade several studies have examined the
effect of vitamin A on reducing mortality among children aged
� 6 mo at the time of intervention. Six community trials in
Asia (7-1 1 ) and Africa (6) reported mortality reductions of
19-54% after vitamin A supplementation either directly or
through fortification, whereas two trials observed no signifi-
cant effect (12, 13). Meta-analyses based on data from these
trials conclude that vitamin A supplementation can be expected
to reduce mortality of children aged 6-72 mo by 23-34% in
populations where xerophthalmia is at least present
(4, 5, 14, 15).
Five of the above trials observed mortality reductions of
12-62% among infants, most of whom were either stated or
presumed to be aged �‘6-1 1 mo when they were supplemented
with vitamin A (7-11). In two ofthe trials (9, 11), the reduction
was � 50% with 95% CIs that excluded 1.0. These findings
suggest the possibility that vitamin A supplementation earlier
in life, during the first 6 mo, might also reduce mortality from
infection at a time when even a modest proportional effect
could translate into substantial numbers of lives saved. How-
ever, only one of the field trials to date, performed in the
midwestern hills of Nepal (11), has reported any vital data for
infants < 6 mo of age who were supplemented with vitamin A.
Although the number per treatment group was small (ii = 300),
there was no evidence of a survival benefit. In a second, more
recent, hospital-based clinical trial in Indonesia, a significant
reduction in mortality was observed in a cohort of infants after
oral administration of 15 000 jig retinol equivalents (RE)
(SO 000 IU) vitamin A at birth (16).
We report here the findings of a large community trial that
was conducted in the rural floodplains of east central Nepal to
gain a more definitive estimate of the effect that large-dose
vitamin A supplementation in the first 6 mo of life may have on
infant mortality.
I From the Center for Human Nutrition, Department of International
Health and the Dana Center for Preventive Ophthalmology (DCPO), the
Johns Hopkins Schools of Public Health and Medicine, Baltimore; the
Nepal Nutrition Intervention Project-Sarlahi (NNIPS), Kathmandu; the
National Society for the Prevention of Blindness, Kathmandu; and the
Department of Pediatrics and Kanti Children’s Hospital, Tribhuvan Uni-
versity, Kathmandu.
2 This study was carried out under Cooperative Agreement DANO()45-
A-5094 between the Office of Nutrition, US Agency for International
Development (USAID), Washington, DC, and DCPO as a joint undertak-
ing with the National Society for the Prevention of Blindness, Kathmandu,
Nepal, with financial and technical assistance from Task Force Sight and
Life (Roche, Basel, Switzerland), the United Nations Children’s Fund
(UNICEF), Nepal, and NIH grant RRO4O6O. The study supplements(vitamin A and placebo capsules) were a gift of Roche.
3 The Sarlahi Study Group (in addition the authors) included BDChataut, MR Pandey, D Calder, I Gmunder, I Humphrey, I Tielsch,
H Taylor, D Piet, I Canner, NN Achariya, DN Mandal, TR Sakya, BB
Shrestha, and RK Shrestha.
4 Address reprint requests to KP West Jr. Division of Human Nutrition,
Department of International Health, Room 2041, Johns Hopkins School of
Hygiene and Public Health, 615 North Wolfe Street, Baltimore, MD
21205.
Received July 20, 1994.
Accepted for publication January 27, 1995.
by guest on February 22, 2014
ajcn.nutrition.orgD
ownloaded from

144 WEST El AL
SUBJECTS AND METHODS
This trial was part of a large, randomized, double-masked,
placebo-controlled community trial that evaluated the effect of
vitamin A supplementation every 4 mo on preschool child
mortality. Basic methods (10, 17), all-cause mortality findings
for children � 6 mo of age at the time of dosing (10, 18), and
short-term tolerance of infants < 6 mo of age to a large dose of
vitamin A were reported (19). The present study, carried out
between September 1989 and December 1991, addressed the
effects on mortality of supplementing infants < 6 mo of age at
the time of dosing.
Two hundred sixty-one wards in 29 contiguous village de-
velopment areas (VDAs) in the District of Sanlahi were mapped
and ‘�‘33 000 households were numbered. Written consent was
obtained from leaders for the trial to be conducted in their
communities. At the time of household enrollment parental
consent was obtained verbally. Participation was voluntary at
all times.
After a random start, wards were systematically assigned,
blocked on VDAs, for infants to receive an oral dose of vitamin
A [15 000 RE (SO 000 IU) in �3 drops of oil for neonates (< 1
mo of age) and 30 000 RE (100 000 IU) in “�‘6 drops of oil for
infants 1-S mo of age] on placebo [75 RE (250 IU) or 150 RE
(500 IU), respectively] from gelatinous capsules of identical
appearance (Roche, Basel, Switzerland). All supplements also
contained � IU vitamin E pen drop, added as an antioxidant.
A child census was conducted at baseline (visit 1). Infants� S mo of age were enrolled, their dates of birth recorded, a
1-wk morbidity history obtained, left midupper-arm circumfer-
ence (MUAC) measured with an insertion tape (20), and the
age-titened dose of the study supplement was administered. If,
after repeated attempts, a team member failed to dose an infant,
a capsule was left with a responsible adult along with instruc-
tions for dosing. A current history of breast-feeding was ob-
tamed for infants in a 15% random sample of wards. At each
subsequent 4- mo household visit (visits 2-6) these procedures
were repeated and surviving infants born during the last inter-
val were enrolled. Infants 4-S mo of age at any visit remained
in the trial for another 4 mo (ie, until 8-9 mo of age). Infants
who were � 6 mo of age at any visit were excluded from this
analysis.
Births and deaths were reported by the above 4-mo census
and, independently, every 2 mo by a mobile vital surveillance
team. Usually within 3 mo of the reported date of death of an
infant, a “verbal autopsy” interview was conducted in an at-
tempt to reconstruct the occurrence of events in the weeks
preceding the child’s death. Verbal autopsy reports were mdc-
pendently reviewed by two physicians (SKK and RA) who
standardized their reviews for �‘S0 prestudy death reports.
Each assigned up to four associated causes of death. Un-
weighted K scones (with 95% CIs) for deaths nonexclusively
attributed to acute respiratory infection, diarrhea on dysentery,
and wasting malnutrition (three major, associated causes of
death in this study) were 0.92 (0.87, 0.97), 0.82 (0.75, 0.89),
and 0.77 (0.69, 0.84), respectively.
Baseline comparisons were evaluated by the chi-squane test.
All analyses were performed on an intent-to-treat basis, that is,
by randomized treatment group irrespective of individual com-
pliance to the dosing regimen. Mortality rates were calculated
on a person-time (child-y) basis and accumulated oven all 4-mo
intervals of observation. One-third of a child-y follow-up was
assigned for each completed 4-mo interval. Infants who with-
drew on died during an interval were assigned one-sixth of a
child-y of observation for the interval in which the event
occurred. Relative risk (RR) estimates (vitamin A/control mor-
tality rates) were calculated to estimate the overall and strati-
fled effects of vitamin A supplementation on mortality. Ninety-
five percent CIs were computed by the method of Katz et al
(21). All 95% CIs for RR estimates were inflated by 10% (ie,
variances were inflated by 22%) to account for loss in precision
in mortality rate estimation at this age due to the design effect
(22). Data analysis was carried out by using SAS (version 6.1,
SAS Institute, Cany, NC) on a Solbourne microcomputer
(Longmont, CO).
The protocol and procedures for the trial were reviewed and
approved by the Nepal Medical Research Council, Kathmandu,
and the Joint Committee on Clinical Investigation at the Johns
Hopkins University School of Medicine, Baltimore.
RESULTS
A total of 1 1 918 infants (n = 5832 control, ii = 6086
vitamin A) were enrolled during visits 1-6, representing �‘98%
of all surviving infants in the study area at the times of the
household visits. Nearly 90% of enrolled infants were regis-
tered at the visit after their birth. Those not enrolled were
mostly neonates who had been born away from or secluded in
their homes for the first weeks of life; of these, �‘90% were
registered at the next household visit when they were �4 mo of
age.
Infants recruited into the two treatment groups were compa-
nable at entry with respect to sex, age, morbidity in the previous
weeks, nutritional status (MUAC), and proportion being breast-
fed (Table 1). A similar, but atypical, age distribution of
infants in each group was caused by the underenrollment of
newborns and their subsequent enrollment at �4 mo of age and
by the small proportion of infants 4 and S mo of age who were
only eligible to enter the trial at visit 1. Virtually all infants in
the random sample in both groups were currently being breast-
fed, 91% � 10 times per day.
Socioeconomic and demographic characteristics of house-
holds with � 1 infant in the trial were similar by treatment
group. Three percent of study households in both groups cx-
penienced an infant death in the previous 12 mo; �36% of
mothers in both groups had one or more child die previously.
Approximately 85% of newly enrolled infants in each group
were supplemented directly by field staff whereas capsules
were left at home for ‘�13%; �2% in each group did not
receive their first intended dose. Periodic follow-up of parents
during the trial suggested that, in both groups, �6O% of cap-
sules left for administration had been given to infants. Thus, on
average, > 90% of enrolled infants were dosed at each visit.
Oven the six 4-mo intervals 5832 and 6086 infants pantici-
pated in the trial, generating 7666 and 7998 infant visits or
2517 and 2625 child-y of observation in the control and vita-
mm A groups, respectively (Table 2). There were 130 deaths
among control subjects and 150 deaths among vitamin A-sup-
plemented infants yielding mortality rates of 51.6 and 57.1
deaths per 1000 child-y, respectively, and a RR of 1.11 (95%
CI: 0.86, 1.42), indicative of no overall effect on mortality.
by guest on February 22, 2014
ajcn.nutrition.orgD
ownloaded from
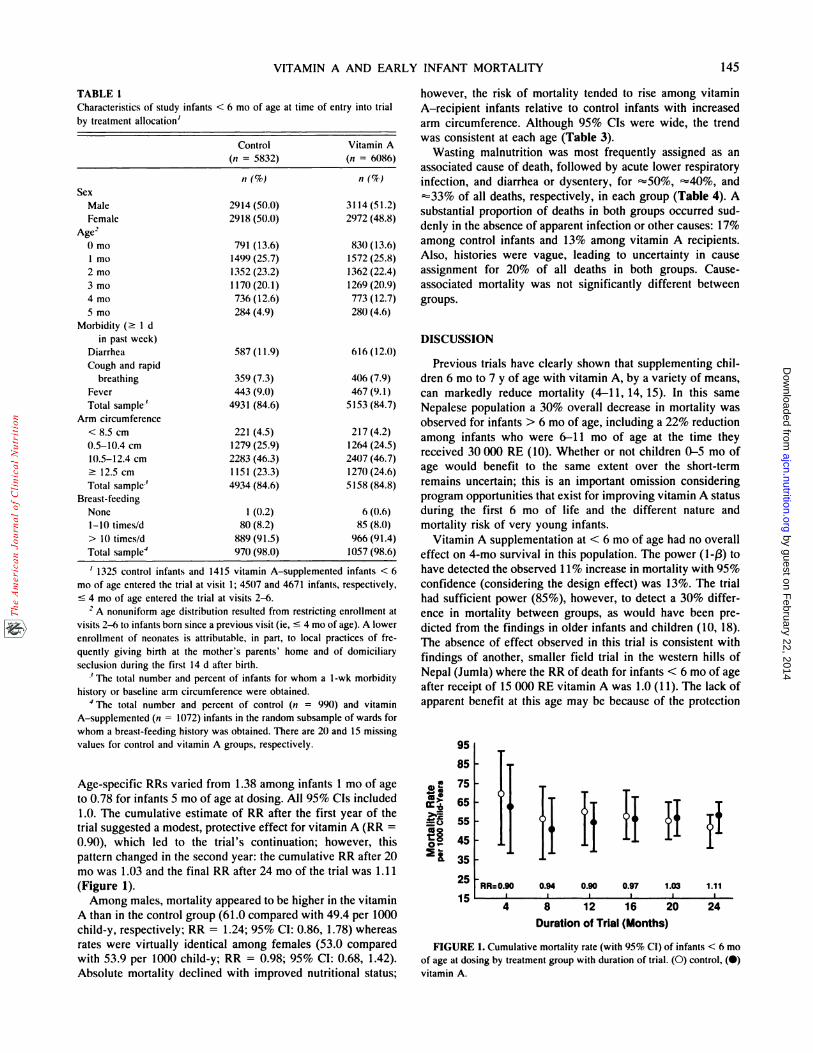
TABLE 1
Characteristics of study infants < 6 mo of age at time of entry into trial
by treatment allocation’
85
� 75
� 65
= 0
�45
�35
25
15
VITAMIN A AND EARLY INFANT MORTALITY 145
Control(n = 5832)
Vitamin A(n 6086)
n(%) n(%)
SexMale 2914 (50.0) 3114 (51.2)
Female 2918 (50.0) 2972 (48.8)
Age20 mo 791 (13.6) 830(13.6)
1 mo 1499(25.7) 1572 (25.8)
2 mo 1352 (23.2) 1362 (22.4)
3 mo 1170(20.1) 1269 (20.9)
4 mo 736 (12.6) 773 (12.7)
S mo 284 (4.9) 280(4.6)
Morbidity (� I d
in past week)
Diarrhea 587 (1 1.9) 616 (12.0)
Cough and rapid
breathing 359 (7.3) 406 (7.9)
Fever 443 (9.0) 467 (9.1)
Total sample3 4931 (84.6) 5153 (84.7)
Arm circumference
< 8.5 cm 221 (4.5) 217 (4.2)
0.5-10.4 cm 1279 (25.9) 1264 (24.5)
10.5-12.4 cm 2283 (46.3) 2407 (46.7)
� 12.5 cm 1 151 (23.3) 1270 (24.6)
Total sample1 4934 (84.6) 5158 (84.8)
Breast-feeding
None 1 (0.2) 6 (0.6)
1-10 times/d 80 (8.2) 85 (8.0)
> 10 times/d 889 (91.5) 966 (91.4)
Total sample4 970 (98.0) 1057 (98.6)
‘ 1325 control infants and 1415 vitamin A-supplemented infants < 6mo of age entered the trial at visit 1; 4507 and 4671 infants, respectively,
� 4 mo of age entered the trial at visits 2-6.
2 A nonuniform age distribution resulted from restricting enrollment at
visits 2-6 to infants born since a previous visit (ie, � 4 mo of age). A lower
enrollment of neonates is attributable, in part, to local practices of fre-
quently giving birth at the mother’s parents’ home and of domiciliary
seclusion during the first 14 d after birth.
3 The total number and percent of infants for whom a 1-wk morbidity
history or baseline arm circumference were obtained.
4 The total number and percent of control (n = 990) and vitamin
A-supplemented (n 1072) infants in the random subsample of wards for
whom a breast-feeding history was obtained. There are 20 and 15 missing
values for control and vitamin A groups, respectively.
Age-specific RRs varied from 1.38 among infants I mo of age
to 0.78 for infants S mo of age at dosing. All 95% CIs included
1 .0. The cumulative estimate of RR after the first year of the
trial suggested a modest, protective effect for vitamin A (RR =
0.90), which led to the trial’s continuation; however, this
pattern changed in the second year: the cumulative RR after 20
mo was 1.03 and the final RR after 24 mo of the trial was 1.11
(Figure 1).
Among males, mortality appeared to be higher in the vitamin
A than in the control group (61.0 compared with 49.4 per 1000
child-y, respectively; RR = 1.24; 95% CI: 0.86, 1.78) whereas
rates were virtually identical among females (53.0 compared
with 53.9 per 1000 child-y; RR 0.98; 95% CI: 0.68, 1.42).
Absolute mortality declined with improved nutritional status;
however, the risk of mortality tended to rise among vitamin
A-recipient infants relative to control infants with increased
arm circumference. Although 95% CIs were wide, the trend
was consistent at each age (Table 3).
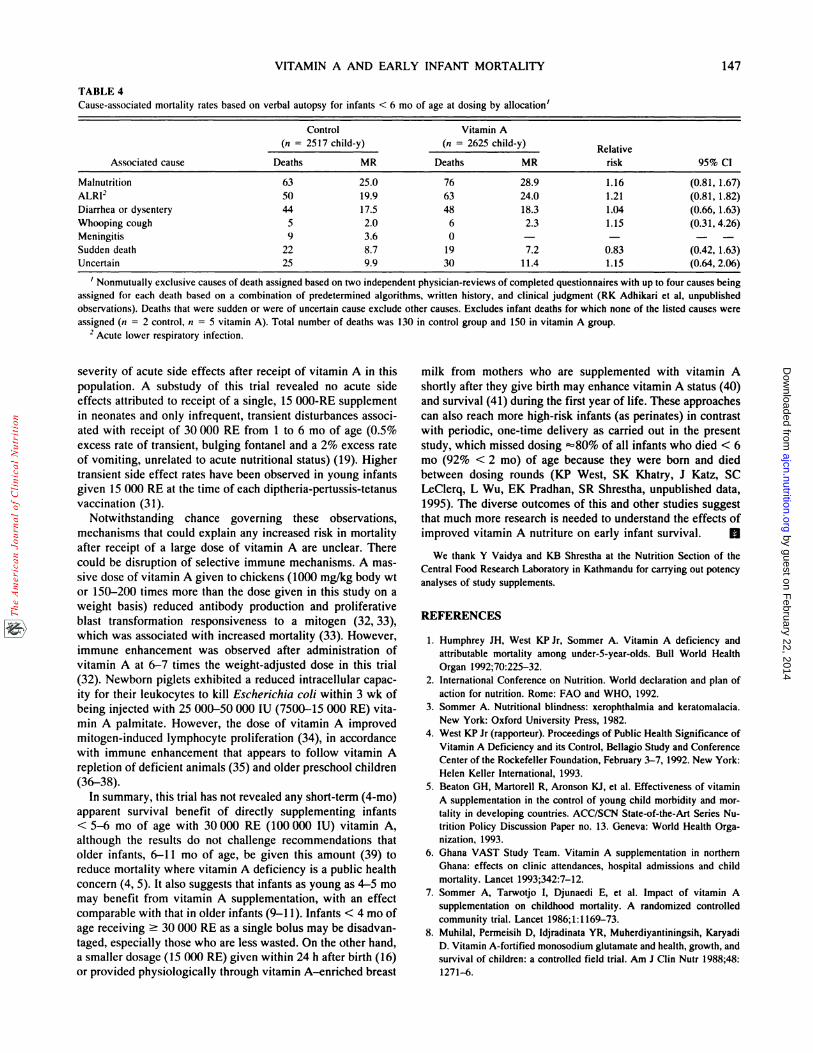
Wasting malnutrition was most frequently assigned as an
associated cause of death, followed by acute lower respiratory
infection, and diarrhea on dysentery, for “SO%, �cc40%, and
=33% of all deaths, respectively, in each group (Table 4). A
substantial proportion of deaths in both groups occurred sud-
denly in the absence of apparent infection or other causes: 17%
among control infants and 13% among vitamin A recipients.
Also, histories were vague, leading to uncertainty in cause
assignment for 20% of all deaths in both groups. Cause-
associated mortality was not significantly different between
groups.
DISCUSSION
Previous trials have clearly shown that supplementing chil-
dren 6 mo to 7 y of age with vitamin A, by a variety of means,
can markedly reduce mortality (4-11, 14, 15). In this same
Nepalese population a 30% overall decrease in mortality was
observed for infants > 6 mo of age, including a 22% reduction
among infants who were 6-i 1 mo of age at the time they
received 30 000 RE (10). Whether or not children 0-S mo of
age would benefit to the same extent oven the short-term
remains uncertain; this is an important omission considering
program opportunities that exist for improving vitamin A status
during the first 6 mo of life and the different nature and
mortality risk of very young infants.
Vitamin A supplementation at < 6 mo of age had no overall
effect on 4-mo survival in this population. The power (1-/3) to
have detected the observed 1 1 % increase in mortality with 95%
confidence (considering the design effect) was 13%. The trial
had sufficient power (85%), however, to detect a 30% differ-
ence in mortality between groups, as would have been pre-
dicted from the findings in olden infants and children (10, 18).
The absence of effect observed in this trial is consistent with
findings of another, smaller field trial in the western hills of
Nepal (Jumla) where the RR of death for infants < 6 mo of age
after receipt of 15 000 RE vitamin A was 1.0 (1 1). The lack of
apparent benefit at this age may be because of the protection
95
�. IfD ff If ifRR=O.90 0.94 0.90 0.97 1.03 1.11
I I I I I I
4 8 12 16 20 24
Duration of Trial (Months)
FIGURE 1. Cumulative mortality rate (with 95% CI) of infants < 6 moof age at dosing by treatment group with duration of trial. (0) control, (#{149})vitamin A.
by guest on February 22, 2014
ajcn.nutrition.orgD
ownloaded from

146 WEST El AL
I Excludes 33 and 34 children with missing MUAC values for control and vitamin A groups, respectively. MR, mortality rate per 1000 child-y.
TABLE 2
Effect of vitamin A on cumulative 4-mo mortality of infants < 6 mo of age at time of dosing’
Treatment variables
and mortality
< 1 Mo
Vitamin
Control A
1 Mo
Vitamin
Control A
2 Mo
Vitamin
Control A
3 Mo
Vitamin
Control A
4 Mo
Vitamin
Control A
5 Mo
Vitamin
Control A
0-5 Mo
Vitamin
Control A
Infantvisits 791 830 1499 1572 1352 1362 1263 1361 1355 1379 1406 1494 7666 7998
Withdrawals 6 11 21 21 16 19 21 12 14 17 21 14 99 94
Deaths 34 38 32 46 20 22 11 15 15 14 18 15 130 150
Child-y 256.9 268.4 490.8 512.8 444.7 447.2 415.7 449.2 446.8 454.5 462.2 493.2 2517.1 2625.3
Mortality rate 132.3 141.6 65.2 89.7 45.0 49.2 26.5 33.4 33.6 30.8 38.9 30.4 51.6 57.1
Relative risk 1.07 1.38 1.09 1.26 0.92 0.78 1.11
95% CI (0.66, 1.72) (0.85, 2.24) (0.56, 2.12) (0.54, 2.95) (0.41, 2.03) (0.37, 1.65) (0.86, 1.42)
1 Infants < 1 mo of age received 15 000 �ig RE; those 1-S mo of age received 30 000 �g RE. Mortality rate expressed as deaths per 1000 child-y.
from vitamin A deficiency already conferred by extensive
breast-feeding early in life. Olden infants may be more suscep-
tible to vitamin A deficiency as vitamin A intake diminishes
with less breast-feeding, which may result in inadequate vita-
mm A to meet metabolic demands, as has been observed
among older children with respect to risk of xerophthalmia in
this (23) and other populations (24-26).
There was a suggestion that mortality risk may be increased
among infants 1-3 mo of age receiving 30 000 RE (100 000
IU) vitamin A. Although not statistically significant (ie, 27%
for 1-3 mo combined, 95% CI: - 1 1%, 89%), the finding
raises concern that this single dose may be excessive for very
young infants, although no untoward effects were observed in
a previous, smaller placebo-controlled trial in Jordan where 90
young infants received three times this dosage (100 000 RE)
(27). In infants aged 4 and S mo the protective effect of 30 000
RE vitamin A began to emerge, reflected by 8% and 22%
reductions in mortality at these ages, respectively, which were
consistent with the 22% reduction observed among infants
given this same amount of vitamin A in the second 6 mo of life
(10). Similar age effects were observed by Clausen (28) in
1932: whereas cod liver oil administered to infants < 6 mo of
age had no apparent effect on severity of illnesses, in older
infants (6-24 mo) there was a 10-fold decrease in the incidence
TABLE 3
of severe infections (eg, pneumonia, septicemia) compared
with control infants. The smaller dose (15 000 RE) given in the
first month of life did not appear problematic.
Subgroup analyses also revealed a perplexing, dose-respon-
sive rise in RRs of mortality among supplemented children
who were least wasted (as measured by arm circumference).
Although not statistically significant for any one comparison,
the trend was consistent at each age, irrespective of the abso-
lute RR observed in the most wasted group, suggesting that the
effect (though underpowered and not easily explained) may
have been real. This effect was not apparent, however, from
verbal autopsy findings in which the estimated RR of mortality
associated with wasting malnutrition was 1.16 (Table 4). These
data are also not easily resolved with findings of a hospital-
based vitamin A dosing trial of newborns in Indonesia where
vitamin A (SO 000 IU) dramatically reduced mortality in the
better-nourished infants (16). One striking observation in the
present study (unrelated to vitamin A supplementation) is the
enormous potential impact that the elimination of wasting
malnutrition, reflected by a low MUAC, could have on reduc-
ing early infant mortality, an observation that has been repeat-
edly made in older children (10, 29, 30).
Adverse effects of vitamin A supplementation in the first 6
mo of life could not be predicted from the occurrence or
Effect of vitamin A on mortality of infants < 6 mo of age by allocation and midupper-arm circumference (MUAC) at time of dosing’
MUAC
Control Vitamin A .
Relative
risk 95% CIDeaths Child-y MR Deaths Child-y MR
< 1 Mo of age
< 8.5 cm8.5-10.4cm
� 10.5 cm
34
1110
1
257
25119
28
132
44488
36
38
108
2
268
26119
31
142
38567
64
1.07
0.870.80
1.76
(0.65, 1.76)
(0.36, 2.10)(0.29,2.21)
(0.13, 24.45)
1-3 Mo of age
<8.5cm
8.5-10.4 cm
10.5-12.4cm
� 12.5 cm
63
16
17
10
2
1351
42
283
619
234
47
376
60
16
9
83
16
26
18
8
1409
39
280
651
264
59
413
93
28
30
1.26
1.10
1.55
1.71
3.52
(0.88,1.80)
(0.54,2.25)
(0.80, 3.02)
(0.73,4.00)
(0.64, 19.42)
4-S Mo of age< 8.5 cm8.5-10.4 cm
10.5-12.4 cm
� 12.5 cm
33S
10
8
7
909S
37
304454
36
962
268
26
15
29
3
6
8
11
948
6
33
320
480
31
546
180
25
23
0.84
0.57
0.67
0.95
1.49
(0.49, 1.45)
(0.14, 2.33)
(0.23, 1.97)
(0.32, 2.79)
(0.52, 4.23)
by guest on February 22, 2014
ajcn.nutrition.orgD
ownloaded from
VITAMIN A AND EARLY INFANT MORTALITY 147
TABLE 4
Cause-associated mortality rates based on verbal autopsy for infants < 6 mo of age at dosing by allocation’
Associated cause
(n
Control2517 child-y)
Vitami(n = 2625
n A
child-y)Relative
risk 95% CIDeaths MR Deaths MR
Malnutrition 63 25.0 76 28.9 1.16 (0.81, 1.67)
ALRI2 SO 19.9 63 24.0 1.21 (0.81, 1.82)Diarrhea or dysentery 44 17.5 48 18.3 1.04 (0.66, 1.63)
Whooping cough S 2.0 6 2.3 1.15 (0.31, 4.26)Meningitis 9 3.6 0 - - - -
Sudden death 22 8.7 19 7.2 0.83 (0.42, 1.63)
Uncertain 25 9.9 30 11.4 1.15 (0.64, 2.06)
, Nonmutually exclusive causes of death assigned based on two independent physician-reviews of completed questionnaires with up to four causes being
assigned for each death based on a combination of predetermined algorithms, written history, and clinical judgment (RK Adhikari et al, unpublished
observations). Deaths that were sudden or were of uncertain cause exclude other causes. Excludes infant deaths for which none of the listed causes wereassigned (n = 2 control, n = S vitamin A). Total number of deaths was 130 in control group and 150 in vitamin A group.
2 Acute lower respiratory infection.
severity of acute side effects after receipt of vitamin A in this
population. A substudy of this trial revealed no acute side
effects attributed to receipt of a single, 15 000-RE supplement
in neonates and only infrequent, transient disturbances associ-
ated with receipt of 30 000 RE from 1 to 6 mo of age (0.5%
excess rate of transient, bulging fontanel and a 2% excess rate
of vomiting, unrelated to acute nutritional status) (19). Higher
transient side effect rates have been observed in young infants
given 15 000 RE at the time of each diptheria-pertussis-tetanus
vaccination (31).
Notwithstanding chance governing these observations,
mechanisms that could explain any increased risk in mortality
after receipt of a large dose of vitamin A are unclear. There
could be disruption of selective immune mechanisms. A mas-
sive dose of vitamin A given to chickens (1000 mg/kg body wt
on 150-200 times more than the dose given in this study on a
weight basis) reduced antibody production and proliferative
blast transformation responsiveness to a mitogen (32, 33),
which was associated with increased mortality (33). However,
immune enhancement was observed after administration of
vitamin A at 6-7 times the weight-adjusted dose in this trial
(32). Newborn piglets exhibited a reduced intracellular capac-
ity for their leukocytes to kill Escherichia coli within 3 wk of
being injected with 25 000-SO 000 IU (7500-15 000 RE) vita-
mm A palmitate. However, the dose of vitamin A improved
mitogen-induced lymphocyte proliferation (34), in accordance
with immune enhancement that appears to follow vitamin A
repletion of deficient animals (35) and older preschool children
(36-38).
In summary, this trial has not revealed any short-term (4-mo)
apparent survival benefit of directly supplementing infants
< 5-6 mo of age with 30 000 RE (100 000 IU) vitamin A,
although the results do not challenge recommendations that
older infants, 6-11 mo of age, be given this amount (39) to
reduce mortality where vitamin A deficiency is a public health
concern (4, 5). It also suggests that infants as young as 4-S mo
may benefit from vitamin A supplementation, with an effect
comparable with that in older infants (9-1 1). Infants < 4 mo of
age receiving � 30 000 RE as a single bolus may be disadvan-
taged, especially those who are less wasted. On the other hand,
a smaller dosage (15 000 RE) given within 24 h after birth (16)
on provided physiologically through vitamin A-enriched breast
milk from mothers who are supplemented with vitamin A
shortly after they give birth may enhance vitamin A status (40)
and survival (41) during the first year of life. These approaches
can also reach more high-risk infants (as peninates) in contrast
with periodic, one-time delivery as carried out in the present
study, which missed dosing =80% of all infants who died < 6
mo (92% < 2 mo) of age because they were born and died
between dosing rounds (KP West, 5K Khatry, J Katz, SC
LeClenq, L Wu, EK Pradhan, SR Shrestha, unpublished data,
1995). The diverse outcomes of this and other studies suggest
that much more research is needed to understand the effects of
improved vitamin A nutniture on early infant survival. A
We thank Y Vaidya and KB Shrestha at the Nutrition Section of the
Central Food Research Laboratory in Kathmandu for carrying out potency
analyses of study supplements.
REFERENCES
1. Humphrey JH, West KP Jr. Sommer A. Vitamin A deficiency andattributable mortality among under-S-year-olds. Bull World Health
Organ 1992;70:225-32.
2. International Conference on Nutrition. World declaration and plan of
action for nutrition. Rome: FAO and WHO, 1992.
3. Sommer A. Nutritional blindness: xerophthalmia and keratomalacia.
New York: Oxford University Press, 1982.4. West KP Jr (rapporteur). Proceedings of Public Health Significance of
Vitamin A Deficiency and its Control, Bellagio Study and Conference
Center of the Rockefeller Foundation, February 3-7, 1992. New York:Helen Keller International, 1993.
S. Beaton GH, Martorell R, Aronson KI, et al. Effectiveness of vitamin
A supplementation in the control of young child morbidity and mor-
tality in developing countries. ACC/SCN State-of-the-Art Series Nu-
trition Policy Discussion Paper no. 13. Geneva: World Health Orga-
nization, 1993.
6. Ghana VAST Study Team. Vitamin A supplementation in northernGhana: effects on clinic attendances, hospital admissions and childmortality. Lancet 1993;342:7-12.
7. Sommer A, Tarwotjo I, Djunaedi E, et al. Impact of vitamin A
supplementation on childhood mortality. A randomized controlled
community trial. Lancet 1986;1:1 169-73.8. Muhilal, Permeisih D, Idjradinata YR. Muherdiyantiningsih, Karyadi
D. Vitamin A-fortified monosodium glutamate and health, growth, andsurvival of children: a controlled field trial. Am I Clin Nutr 1988;48:
1271-6.
by guest on February 22, 2014
ajcn.nutrition.orgD
ownloaded from

148 WEST El AL
9. Rahmathullah L, Underwood BA, Thulasiraj RD. et al. Reduced mor-
tality among children in Southern India receiving a small weekly dose
of vitamin A. N Engl I Med 1990;323:929-3S.10. West KP Ir, Pokhrel RP, Katz I, et al. Efficacy of vitamin A in
reducing preschool child mortality in Nepal. Lancet 1991;338:67-71.1 1. Daulaire NMP, Starbuck ES, Houston RM, Church MS. Stukel TA,
Pandey MR. Childhood mortality after a high dose of vitamin A in ahigh risk population. Br Med I 1992;304:207-10.
12. Vijayaraghavan K, Radhalah G, Surya Prakasam BS, Rameshwar
Sarma Ky, Reddy V. Effect of massive dose vitamin A on morbidityand mortality in Indian children. Lancet 1990;2:1342-5.
13. Herrera MG, Nestel P. El Amin A, Fawzi WW, Mohamed Kit, Weld
L. Vitamin A supplementation and child survival. Lancet 1992;340:267-71.
14. Fawzie WW, Chalmers TC, Herrera MG, Mosteller F. Vitamin Asupplementation and child mortality: a meta-analysis. JAMA 1993;
269:898-903.
15. Glasziou PP, Mackerras DEM. Vitamin A supplementation in infec-
tious diseases: a meta-analysis. Br Med I 1993;306:366-70.
16. Humphrey I, Agoestina T, Taylor G, Usman A, West KP Jr. Sommer
A. Acute and long term risks and benefits to neonates of 50,000 lU oralvitamin A. Report of the 16th IVACG Meeting, Chiang Rai, Thailand,
October 24-28, 1994. Washington, DC: The Nutrition Foundation,1995.
17. Pradhan EK, Katz I, LeClerq SC, West KP Jr. Data management for
large community trials in Nepal. Control Clin Trials 1994;15:220-34.18. Pokhrel RP, Khatry 5K, West KP Ir, et al. Sustained reduction in child
mortality due to vitamin A in Nepal. Lancet 1994;343:1368-9.
19. West KP Jr. Khatry 5K, LeClerq SC, et al. Tolerance of young infantsto a single, large dose of vitamin A: a randomized community trial in
Nepal. Bull World Health Organ 1992;70:733-9.
20. Zerfas AJ. The insertion tape: a new circumference tape for use in
nutritional assessment. Am I Clin Nutr 197S;28:782-7.
21. Katz D, Baptista I, Azen SP, Pike MC. Obtaining confidence intervals
for the risk ratio in cohort studies. Biometrics 1978;34:469-74.
22. Katz I, Zeger SL. Estimation of design effects in cluster surveys. Ann
Epidemiol l994;4:295-301.
23. Khatry 5K, West KP Jr. Katz I, et al. Epidemiology of xerophthalmiain Nepal: a pattern of household poverty, childhood illness and mor-
tality. Arch Ophthalmol 199S;113:425-9.24. Tarwotjo I, Sommer A, Soegiharto T. Dietary practices and xeroph-
thalmia among Indonesian children. Am I Clin Nutr 1982;3S:S74-81.25. West KP, Chirambo M, Katz I, Sommer A. Breast-feeding, weaning
patterns, and the risk of xerophthalmia. A case-control study in South-ern Malawi. Am I Clin Nutr 1986;44:690-7.
26. Mahalanabis D. Breast feeding and vitamin A deficiency among
children attending a diarrhoea treatment centre in Bangladesh: a case-
control study. Br Med I 1991;303:493-6.
27. Pathwardan VN, Kamel WW, Pharaon H. Studies on vitamin A
deficiency in infants and young children in Jordan. Part II. A pilot trial
of vitamin A prophylaxis in Jordanian infants (February, 1965-
August, 1966). Geneva: Public Health Service Research/World Health
Organization, 1966.
28. Clausen SW. The effects of moderate deficiency of vitamins. Bull N Y
Acad Med 1934;10:471-82.
29. Sommer A, Loewenstein M. Nutritional status and mortality. A pro-
spective validation of the QUAC stick. Am I Clin Nutr 1975;28:287-
92.
30. Pelletier DL. The relationship between child anthropometry and mor-
tality in developing countries: implications for policy, programs and
future research. I Nutr 1994;124:2047S-81S.
31. de Francisco A, Chakraborty I, Chowdhury HR, et al. Acute toxicity
of vitamin A given with vaccines in infancy. Lancet 1993;342:S26-7.
32. Friedman A, Sklan D. Antigen-specific immune response impairment
in the chick as influenced by dietary vitamin A. I Nutr 1989;119:
790-S.
33. Friedman A, Meidovsky A, Leitner G, Sklan D. Decreased resistance
and immune response to Eschermchia co/i infection in chicks with low
or high intakes of vitamin A. I Nutr 1991;121:39S-400.
34. Hoskinson CD, Chew BP, Wong TS. Effects of injectable /3-carotene
and vitamin A on lymphocyte proliferation and polymorphonuclear
neutrophil function in piglets. Biol Neonate 1992;62:32S-36.
35. Ross AC. Vitamin A status: relationship to immunity and the antibody
response. Proc Soc Exp Biol Med 1992;200:303-20.
36. Semba RD. Muhilal, Scott AL, et al. Depressed immune response to
tetanus in children with vitamin A deficiency. I Nutr 1992;122:101-7.
37. Semba RD, Muhilal, Ward BI, et al. Abnormal T-cell subset propor-
tions in vitamin-A-deficient children. Lancet 1993;341:S-8.
38. Coutsoudis A, Kiepiela P, Coovadia HM, Broughton M. Vitamin A
supplementation enhances specific IgG antibody levels and total lym-
phocyte numbers while improving morbidity in measles. Pediatr Infect
Dis I 1992;11:203-9.
39. WHOIUNICEF/IVACG Task Force. Vitamin A supplements. A
guide to their use in the treatment and prevention of vitamin A
deficiency and xerophthalmia. Geneva: World Health Organization,
1988.
40. Stoltzfus RI, Hakimi M, Miller KW, et al. High dose vitamin A
supplementation of breast feeding Indonesian mothers: effects on the
vitamin A status of mother and infant. I Nutr 1993;123:666-7S.
41. de Francisco A, Yasin Y, Chakraborty I. Vitamin A supplementation
given to mothers after delivery reduces infant mortality and increased
symptoms of morbidity. Report of the 16th IVACG Meeting, Chiang
Rai, Thailand, October 24-28, 1994. Washington, DC: The Nutrition
Foundation, 1995.
by guest on February 22, 2014
ajcn.nutrition.orgD
ownloaded from





























