Embed Size (px)
Citation preview

Mixed Venous Oxygen Saturation During Cardiopulmonary Bypass Poorly Predicts Regional Venous Saturation Laura B. McDaniel, MD, Joseph B. Zwischenberger, MD, Roger A. Vertrees, CCP, Leta Nutt, BS, Tatsuo Uchida, MS, Thuan Nguyen, MD, and George C. Kramer, PhD
Departments of Anesthesiology and Surgery, and Office of Biostatistics, The University of Texas Medical Branch, Galveston, Texas
Mixed venous oxygen saturation is generally accepted as an indicator of adequacy of systemic oxygen deliv- ery; however, cardiopulmonary bypass (CPB) may al- ter this relationship. Major postoperative complications potentially secondary to inadequate oxygen delivery during CPB indicate that mixed venous oxygen satura- tion may not detect regional venous desaturation dur- ing CPB. We therefore tested the hypothesis that mixed venous oxygen saturation and pH did not predict re- gional venous oxygen saturations and pH during 2 h of bypass in a swine model. Six immature swine (27-34 kg) received standard normothermic CPB. Sagittal si- nus and portal vein oxygen saturations and blood gases were measured at 30, 60, 90, and 120 min of bypass.
Although the venous reservoir oxygen saturation re- mained unchanged during 2 h of bypass, sagittal sinus saturation and pH decreased significantly (66% 2 3.3% to 33% ? 2.2% and 7.38 2 0.04 to 7.23 2 0.05, respec- tively). Likewise in the portal vein, oxygen saturation and pH also decreased (82% + 2.4% to 59.3% ? 3.9% and 7.39 + 0.03 to 7.27 t 0.06, respectively). We conclude that profound regional venous desaturation and progressive regional acidemia may go undetected even when a standard pump flow rate of 100 mL * kg-’ * min-’ is used and mixed venous oxygen saturation is normal.
(Anesth Analg 1995;80:466-72)
M ixed venous oxygen saturation is commonly used to assess the balance of total body oxy- gen delivery to oxygen demand during car-
diopulmonary bypass (CPB). Given an adequate and stable arterial oxygen content and metabolic rate, mixed venous oxygen saturation more than 60% im- plies adequate systemic oxygen delivery (l-3). Despite general acceptance of maintaining mixed venous ox- ygen saturation more than 60% during CPB, major postoperative end-organ complications potentially secondary to undetected regional ischemia during by- pass continue to be reported; for example, acute mes- enteric ischemia (4,5), gastrointestinal bleeding, acute pancreatitis (6), neurocognitive disorders (7,8), isch- emit optic neuropathy (9), choreoathetoid syndromes (lO,ll), cerebral infarction (12), and developmental delay (13,141.
According to the Fick equation, mixed venous oxy- gen saturation reflects total cardiac output, assuming a stable arterial oxygen content and metabolic rate. During CPB, total cardiac output, or pump flow, is a
Accepted for publication October 14, 1994. Address correspondence and reprint requests to Faith McLellan,
Editor, Dept. of Anesthesiology, UTMB #24, Galveston, TX 77555- 0591.
466 An&h Analg 1995;80:466-72
calculated and fixed variable. Likewise, total meta- bolic rate during normothermic bypass should be unchanged from baseline if anesthesia, temperature, hematocrit, and other factors remain fixed. The sensi- tivity of mixed venous oxygen saturation to reflect regional venous oxygen desaturation during bypass is unknown. We therefore hypothesized that, during normothermic CPB, mixed venous oxygen saturation does not predict venous oxygen saturation in the brain and intestinal tract, organs associated with sequelae that drastically increase patient morbidity and mortal- ity @,5,7,8).
Methods
All animal procedures and protocols were performed according to the guidelines approved by The Univer- sity of Texas Medical Branch Animal Care and Use Committee. General anesthesia was induced in six immature Yorkshire female swine (27-34 kg) with in- tramuscular ketamine (10 mg/kg) and atropine (10 pg/kg), followed by a mask inhalational induction with 2% isoflurane (North American Drager Vapor- izer, Telford, PA), oxygen, and air. After endotracheal intubation, the isoflurane was decreased to l.O%- 1.25% and the animals were ventilated with a tidal
01995 by the International Anesthesia Research Society 0003-2999/95/$5.00

ANESTH ANALG CARDIOVASCULAR ANESTHESIA MCDANIEL ET AL. 467 1995;80:466-72 MIXED VENOUS OXYGEN SATURATION DURING BYPASS
volume of 10 mL/kg with a volume-cycled ventilator (Ohio Anesthesia Machine, Madison, WI). Inhaled and expired isoflurane concentrations were analyzed con- tinuously at the endotracheal tube with a Rascal I Gas Analyzer (Ohmeda, Salt Lake City, UT). The respira- tory rate was adjusted to maintain the Pco, between 35 and 40 mm Hg and the inspired oxygen concentra- tion was adjusted to maintain an arterial oxygen ten- sion greater than 100 mm Hg. Anesthesia was main- tained with isoflurane (1.0% to 1.25%). Temporary muscle paralysis was provided by pancuronium, 0.1 mg/kg, which was given immediately before sternot- omy to facilitate opening the chest.
A femoral artery catheter (l&gauge) was inserted by cut-down for pressure measurements and blood sampling. An Oximetric pulmonary artery catheter (Abbott Critical Care Systems, N. Chicago, IL), which was inserted in the femoral vein, was used for pulmo- nary artery and pulmonary artery occlusion pressure measurements, thermodilution cardiac output deter- minations, mixed venous blood sampling, and contin- uous mixed venous oximetry data. Nasopharyngeal and rectal temperatures were recorded by a thermistor (Yellow Springs Instruments, Yellow Springs, OH) cal- ibrated before each experiment. An additional catheter (lbgauge, B-cm catheter; Cook Critical Care, Bloom- ington, IN) was placed in the external jugular vein and threaded into the thorax for central venous pressure measurements. A celiotomy incision allowed exposure of the portal vein, which was cannulated with a 16- gauge catheter. The temporalis muscle was dissected from the cranium and a 1 X 1 cm midline craniectomy was performed with a Drimmel drill. The dura and sagittal sinus were identified and PE 50 polyethylene tubing was inserted in the sagittal sinus for a distance of 1 cm.
A median sternotomy was performed and the peri- cardium was opened and tented. Heparin sodium, 400 IU/kg, was administered through the central venous cannula before aortic cannulation. The activated clot- ting time was maintained at more than 500 s with additional heparin given as needed. A single 40 X 32 Fr double-stage venous return cannula (Model 14992; Sarns 3M Health Care Division, Ann Arbor, MI) was inserted through the right atria1 appendage. A 20-Fr cannula (DLP Cannula; DLP; Grand Rapids, MI) was inserted into the ascending aorta. The extracorporeal circuit consisted of a membrane oxygenator (Plexus Oxygenator; Sarns, Irvine, CA), and a 40-l.~ arterial filter (Pall SP3840; Pall, Glen Cove, NY), and polyvinyl chloride tubing. Lactated Ringer’s solution (1000 mL) and 500 mL of 6% hydroxyethyl starch were required to prime the circuit. Perfusion was conducted using nonpulsatile flow, hemodilution, and normothermia
with a nonarrested, nonejecting heart. The tempera- ture was maintained at 38°C with a thermostatically controlled water bath (Sarns Dual Cooler-Heater; Sarns, Irvine, CA).
Normal acid-base status was maintained by adjust- ments in gas flow and composition during CPB. The mean arterial pressure during CPB (53.3 + 4.5, range 45-58 mm Hg) was not manipulated pharmacologi- cally. The pump flow rate, 100 mL * kg-’ * min-‘, was maintained throughout 2 h of bypass by adding lac- tated Ringer’s solution to maintain a steady venous reservoir level of 300 mL.
Arterial and mixed venous blood was sampled from the arterial cannula and pulmonary artery catheter for baseline blood gas analysis, oxygen saturation, and hematocrit. During CPB arterial blood was sampled from the pump oxygenator and mixed venous blood from the venous reservoir. Blood from the portal vein and sagittal sinus was sampled for blood gas analysis, hematocrit, and oxygen saturation. Venous oxygen saturation was measured on a CO-Oximeter (Instru- mentation Laboratory, Lexington, MA).
The animals were allowed to stabilize for 30 min after the surgical preparation before CPB. The meas- urements recorded after stabilization were taken as baseline data. After initiation of CPB, measurements were obtained at 30, 60, 90, and 120 min. Then the animals were killed with an intravenous injection of saturated potassium chloride solution (0.35 mL/kg).
Four data sets (% oxygen saturation, pH, Pvco2, and venous bicarbonate) were analyzed separately for each data set as a three-factor factorial experiment. The three factors were location (mixed venous, portal, and sagittal sinus), time (0, 30, 60, 90, 120 min), and animals (random effect). Fisher’s least-significant dif- ference procedure with Bonferroni adjustment was used to assess location differences. Each time point was compared with baseline (0 min) using Dunnett’s test. All effects, interactions, contrasts, and tests were assessed at the 0.05 level of significance. Data are reported as mean + SEM.
Results
Arterial oxygenation variables, including pH,, Pace,, and Pao2, did not vary significantly (Table 1). Arterial bicarbonate levels during bypass were significantly less than baseline at 30 min (P < 0.05), but did not change throughout the remainder of CPB. Bypass he- matocrit was significantly less throughout CPB when compared with baseline hematocrit. Baseline temper- ature did not differ from temperature during CPB.
Mean arterial pressure and central venous pressure throughout bypass were significantly less than baseline values. The calculated pump flow of 100
468 CARDIOVASCULAR ANESTHESIA MCDANIEL ET AL. ANESTH ANALG MIXED VENOUS OXYGEN SATURATION DURING BYPASS 1995;80:466-72
Table 1. Oxygenation Variables During Normothermic Bypass
Bypass interval (min)
Variable Baseline 30 60 90 120
PH 7.46 I+I 0.02 7.47 + 0.1 7.45 If: 0.1 7.46 k 0.2 7.46 It 0.1 Pace, 37.3 + 2.4 32.4 2 1.9 34.3 k 1.8 33.8 k 1.8 33.4 2 1.9 Pao, 310 2 20.1 312 + 34.1 244 + 32.7 269 t 42.1 284 -c 42.0 Arterial bicarbonate 27.1 k 1.2 24.4 + 0.8* 23.9 -c 0.8* 23.4 + 0.6* 22.0 + 0.7* Hct 26.3 ? 2.2 14.6 + 1.6* 15.9 t- 1.5* 16.4 t 1.6* 14.4 +- 1.5% Temperature (“C) 37.3 + 0.4 37.4 t 0.3 37.6 + 0.1 37.6 + 0.2 37.6 2 1.4
Hct = hematocrit. a Temperature was measured nasopharyngeally. * P < 0.05 compared with baseline value.
mL * kg-’ * min-’ did not vary during CPB but was significantly less than baseline cardiac output (Table 2).
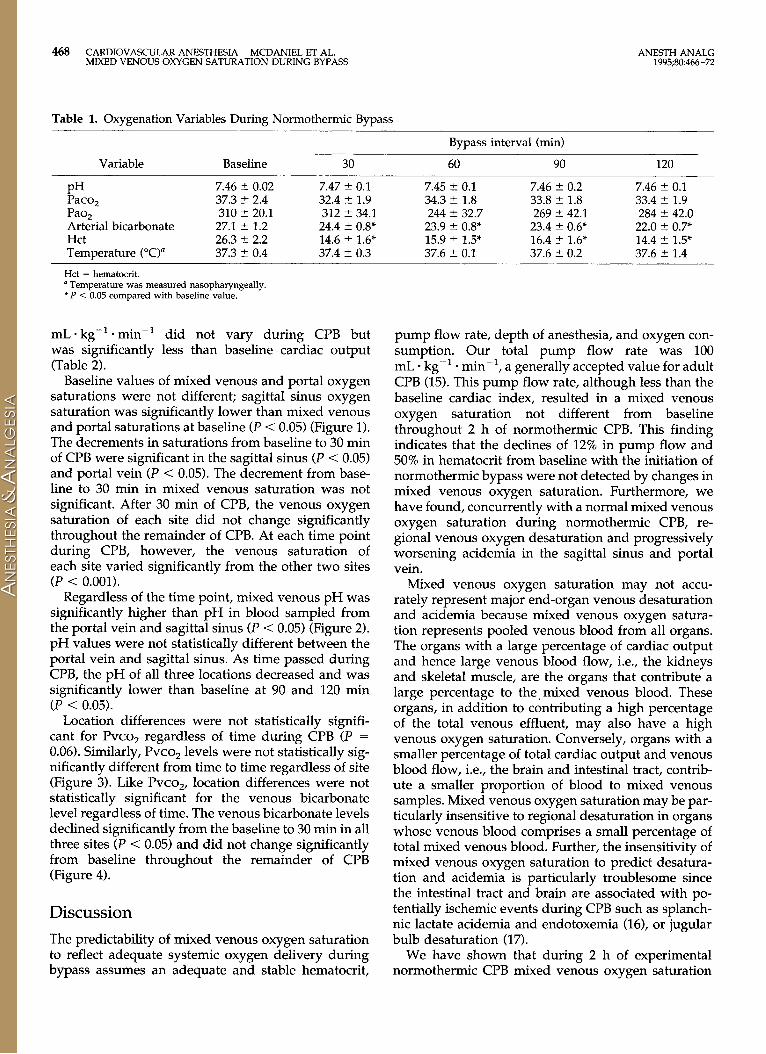
Baseline values of mixed venous and portal oxygen saturations were not different; sagittal sinus oxygen saturation was significantly lower than mixed venous and portal saturations at baseline (P < 0.05) (Figure 1). The decrements in saturations from baseline to 30 min of CPB were significant in the sagittal sinus (P < 0.05) and portal vein (P < 0.05). The decrement from base- line to 30 min in mixed venous saturation was not significant. After 30 min of CPB, the venous oxygen saturation of each site did not change significantly throughout the remainder of CPB. At each time point during CPB, however, the venous saturation of each site varied significantly from the other two sites (P < 0.001).
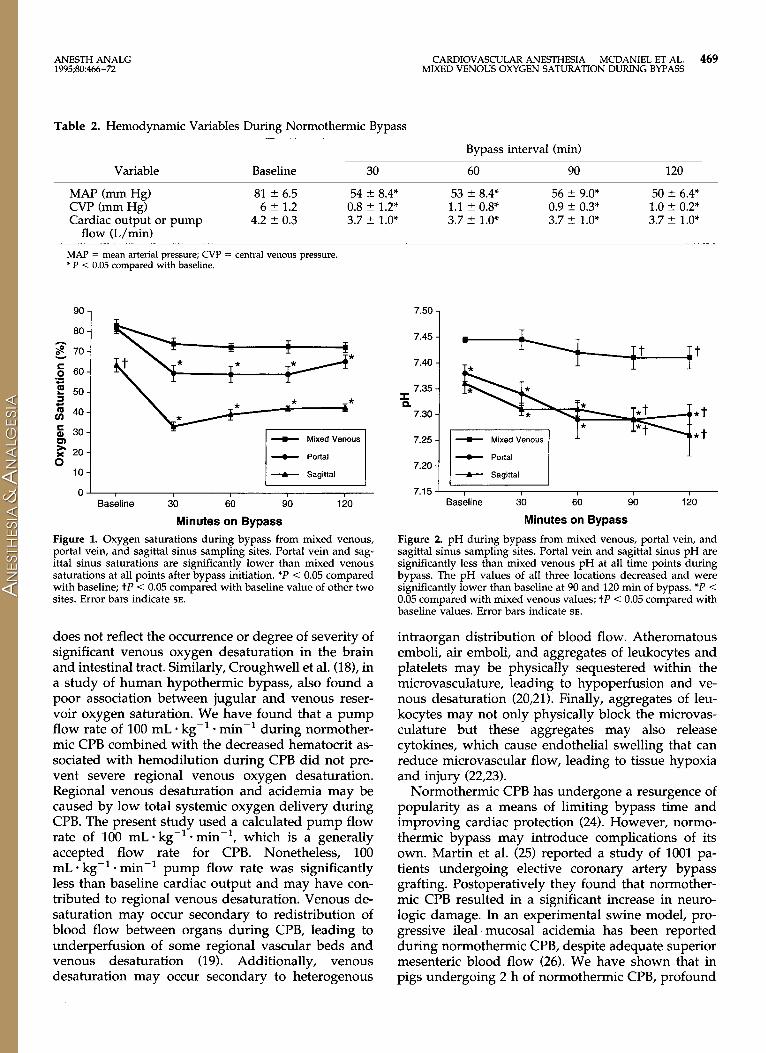
Regardless of the time point, mixed venous pH was significantly higher than pH in blood sampled from the portal vein and sagittal sinus (P < 0.05) (Figure 2). pH values were not statistically different between the portal vein and sagittal sinus. As time passed during CPB, the pH of all three locations decreased and was significantly lower than baseline at 90 and 120 min (P < 0.05).
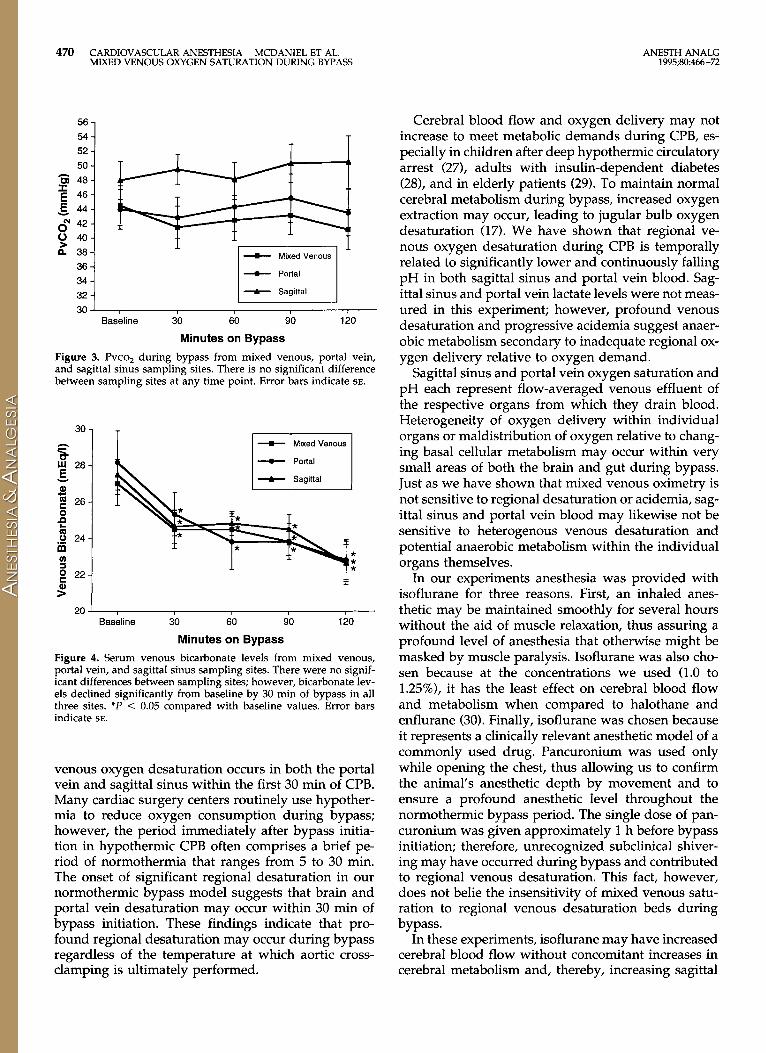
Location differences were not statistically signifi- cant for Pvco, regardless of time during CPB (P = 0.06). Similarly, Pvco, levels were not statistically sig- nificantly different from time to time regardless of site (Figure 3). Like PVCO~, location differences were not statistically significant for the venous bicarbonate level regardless of time. The venous bicarbonate levels declined significantly from the baseline to 30 min in all three sites (P < 0.05) and did not change significantly from baseline throughout the remainder of CPB (Figure 4).
Discussion
The predictability of mixed venous oxygen saturation to reflect adequate systemic oxygen delivery during bypass assumes an adequate and stable hematocrit,
pump flow rate, depth of anesthesia, and oxygen con- sumption. Our total pump flow rate was 100 mL - kg-’ - min-l , a generally accepted value for adult CPB (15). This pump flow rate, although less than the baseline cardiac index, resulted in a mixed venous oxygen saturation not different from baseline throughout 2 h of normothermic CPB. This finding indicates that the declines of 12% in pump flow and 50% in hematocrit from baseline with the initiation of normothermic bypass were not detected by changes in mixed venous oxygen saturation. Furthermore, we have found, concurrently with a normal mixed venous oxygen saturation during normothermic CPB, re- gional venous oxygen desaturation and progressively worsening acidemia in the sagittal sinus and portal vein.
Mixed venous oxygen saturation may not accu- rately represent major end-organ venous desaturation and acidemia because mixed venous oxygen satura- tion represents pooled venous blood from all organs. The organs with a large percentage of cardiac output and hence large venous blood flow, i.e., the kidneys and skeletal muscle, are the organs that contribute a large percentage to the, mixed venous blood. These organs, in addition to contributing a high percentage of the total venous effluent, may also have a high venous oxygen saturation. Conversely, organs with a smaller percentage of total cardiac output and venous blood flow, i.e., the brain and intestinal tract, contrib- ute a smaller proportion of blood to mixed venous samples. Mixed venous oxygen saturation may be par- ticularly insensitive to regional desaturation in organs whose venous blood comprises a small percentage of total mixed venous blood. Further, the insensitivity of mixed venous oxygen saturation to predict desatura- tion and acidemia is particularly troublesome since the intestinal tract and brain are associated with po- tentially ischemic events during CPB such as splanch- nit lactate acidemia and endotoxemia (16), or jugular bulb desaturation (17).
We have shown that during 2 h of experimental normothermic CPB mixed venous oxygen saturation
ANESTHANALG CARDIOVASCULAR ANESTHESIA MCDANIEL ET AL. 469 1995;80:466-72 MIXED VENOUS OXYGEN SATURATION DURING BYPASS
Table 2. Hemodynamic Variables During Normothermic Bypass
Variable Baseline 30
Bypass interval (min)
60 90 120
MAP (mm Hg) 81 ? 6.5 54 t 8.4* 53 ? 8.4* 56 5 9.0* 50 2 6.4* CVP (mm Hg) 6 + 1.2 0.8 + 1.2* 1.1 ? 0.8* 0.9 ? 0.3* 1.0 k 0.2* Cardiac output or pump 4.2 2 0.3 3.7 -c 1.0* 3.7 2 1.0% 3.7 +- 1.0* 3.7 + 1.0*
flow (L/min)
MAP = mean arterial pressure; CVP = central venom pressure. l P < 0.05 compared with baseline.
90
00
q e 70
-5 60 ii 5 50
G m 40
5 30
E x 20 0
10
0
-C Mixed Venous
- Portal
--C Sagittal i
Baseline i0 $0 40
Minutes on Bypass
1;o
Figure 1. Oxygen saturations during bypass from mixed venous, portal vein, and sagittal sinus sampling sites. Portal vein and sag- ittal sinus saturations are significantly lower than mixed venous saturations at all points after bypass initiation. *P < 0.05 compared with baseline; tP < 0.05 compared with baseline value of other two sites. Error bars indicate SE.
does not reflect the occurrence or degree of severity of significant venous oxygen desaturation in the brain and intestinal tract. Similarly, Croughwell et al. (18), in a study of human hypothermic bypass, also found a poor association between jugular and venous reser- voir oxygen saturation. We have found that a pump flow rate of 100 mL * kg-’ * min-’ during normother- mic CPB combined with the decreased hematocrit as- sociated with hemodilution during CPB did not pre- vent severe regional venous oxygen desaturation. Regional venous desaturation and acidemia may be caused by low total systemic oxygen delivery during CPB. The present study used a calculated pump flow rate of 100 mL * kg-’ * min-‘, which is a generally accepted flow rate for CPB. Nonetheless, 100 mL * kg-’ * min-’ pump flow rate was significantly less than baseline cardiac output and may have con- tributed to regional venous desaturation. Venous de- saturation may occur secondary to redistribution of blood flow between organs during CPB, leading to underperfusion of some regional vascular beds and venous desaturation (19). Additionally, venous desaturation may occur secondary to heterogenous
7.50
7.45
7.40
7.35 I 0.
7.30
7.25
7.20 -0- Portal
I
.L
* Sagittal
7.15 LL Baseline 30 60 90 120
Minutes on Bypass
Figure 2. pH during bypass from mixed venous, portal vein, and sagittal sinus sampling sites. Portal vein and sagittal sinus pH are significantly less than mixed venous pH at all time points during bypass. The pH values of all three locations decreased and were significantly lower than baseline at 90 and 120 min of bypass. *P < 0.05 compared with mixed venous values; tP < 0.05 compared with baseline values. Error bars indicate SE.
intraorgan distribution of blood flow. Atheromatous emboli, air emboli, and aggregates of leukocytes and platelets may be physically sequestered within the microvasculature, leading to hypoperfusion and ve- nous desaturation (20,21). Finally, aggregates of leu- kocytes may not only physically block the microvas- culature but these aggregates may also release cytokines, which cause endothelial swelling that can reduce microvascular flow, leading to tissue hypoxia and injury (22,23).
Normothermic CPB has undergone a resurgence of popularity as a means of limiting bypass time and improving cardiac protection (24). However, normo- thermic bypass may introduce complications of its own. Martin et al. (25) reported a study of 1001 pa- tients undergoing elective coronary artery bypass grafting. Postoperatively they found that normother- mic CPB resulted in a significant increase in neuro- logic damage. In an experimental swine model, pro- gressive ileal mucosal acidemia has been reported during normothermic CPB, despite adequate superior mesenteric blood flow (26). We have shown that in pigs undergoing 2 h of normothermic CPB, profound
470 CARDIOVASCULAR ANESTHESIA MCDANIEL ET AL. MIXED VENOUS OXYGEN SATURATION DURING BYPASS
56 -
54 -
52 -
50 -
2 48-
E 46-
E. 44- o” 42 -
0 40-
p’ 3a-
36 -
34 -
32 -
+ Portal
__ Basksline i0 $0 sb ii0
Minutes on Bypass
Figure 3. Pvco, during bypass from mixed venous, portal vein, and sagittal sinus sampling sites. There is no significant difference between sampling sites at any time point. Error bars indicate SE.
30 -
s W 28-
-5 al
5 26-
8 t
.o 24- m Y g 22-
>”
- Portal
20 J I I Baseline 30 60 90 120
Minutes on Bypass
Figure 4. Serum venous bicarbonate levels from mixed venous, portal vein, and sagittal sinus sampling sites. There were no signif- icant differences between sampling sites; however, bicarbonate lev- els declined significantly from baseline by 30 min of bypass in all three sites. *P < 0.05 compared with baseline values. Error bars indicate SE.
venous oxygen desaturation occurs in both the portal vein and sagittal sinus within the first 30 min of CPB. Many cardiac surgery centers routinely use hypother- mia to reduce oxygen consumption during bypass; however, the period immediately after bypass initia- tion in hypothermic CPB often comprises a brief pe- riod of normothermia that ranges from 5 to 30 min. The onset of significant regional desaturation in our normothermic bypass model suggests that brain and portal vein desaturation may occur within 30 min of bypass initiation. These findings indicate that pro- found regional desaturation may occur during bypass regardless of the temperature at which aortic cross- clamping is ultimately performed.
ANESTH ANALG 1995;80:466-72
Cerebral blood flow and oxygen delivery may not increase to meet metabolic demands during CPB, es- pecially in children after deep hypothermic circulatory arrest (271, adults with insulin-dependent diabetes (28), and in elderly patients (29). To maintain normal cerebral metabolism during bypass, increased oxygen extraction may occur, leading to jugular bulb oxygen desaturation (17). We have shown that regional ve- nous oxygen desaturation during CPB is temporally related to significantly lower and continuously falling pH in both sagittal sinus and portal vein blood. Sag- ittal sinus and portal vein lactate levels were not meas- ured in this experiment; however, profound venous desaturation and progressive acidemia suggest anaer- obic metabolism secondary to inadequate regional ox- ygen delivery relative to oxygen demand.
Sagittal sinus and portal vein oxygen saturation and pH each represent flow-averaged venous effluent of the respective organs from which they drain blood. Heterogeneity of oxygen delivery within individual organs or maldistribution of oxygen relative to chang- ing basal cellular metabolism may occur within very small areas of both the brain and gut during bypass. Just as we have shown that mixed venous oximetry is not sensitive to regional desaturation or acidemia, sag- ittal sinus and portal vein blood may likewise not be sensitive to heterogenous venous desaturation and potential anaerobic metabolism within the individual organs themselves.
In our experiments anesthesia was provided with isoflurane for three reasons. First, an inhaled anes- thetic may be maintained smoothly for several hours without the aid of muscle relaxation, thus assuring a profound level of anesthesia that otherwise might be masked by muscle paralysis. Isoflurane was also cho- sen because at the concentrations we used (1.0 to 1.25%), it has the least effect on cerebral blood flow and metabolism when compared to halothane and enflurane (30). Finally, isoflurane was chosen because it represents a clinically relevant anesthetic model of a commonly used drug. Pancuronium was used only while opening the chest, thus allowing us to confirm the animal’s anesthetic depth by movement and to ensure a profound anesthetic level throughout the normothermic bypass period. The single dose of pan- curonium was given approximately 1 h before bypass initiation; therefore, unrecognized subclinical shiver- ing may have occurred during bypass and contributed to regional venous desaturation. This fact, however, does not belie the insensitivity of mixed venous satu- ration to regional venous desaturation beds during bypass.
In these experiments, isoflurane may have increased cerebral blood flow without concomitant increases in cerebral metabolism and, thereby, increasing sagittal

ANESTH ANALG CARDIOVASCULAR ANESTHESIA MCDANIEL ET AL. 471 1995;80:466-72 MIXED VENOUS OXYGEN SATURATION DURING BYPASS
sinus oxygen saturation. However, the isoflurane con- centration during bypass was not different from base- line and sagittal sinus desaturation occurred during bypass, indicating that sagittal sinus desaturation dur- ing bypass was due to factors other than isoflurane. Furthermore, whatever the cause of sagittal sinus and portal vein desaturation during bypass, mixed venous oxygen saturation did not predict the occurrence or degree of desaturation at any point during bypass.
The hematocrit during bypass in these experiments was, indeed, lower than usual clinical standards. Nev- ertheless, the same hematocrit circulated in all three venous beds at the time of each sampling interval and the mixed venous sample did not predict the regional desaturation, even if a low hematocrit contributed to the regional desaturation. An interesting question for future study is whether an improved hematocrit would prevent regional desaturation or whether fac- tors other than regional oxygen delivery participate in regional venous desaturation during bypass.
Paco2, which was reduced by 3-4 mm Hg during bypass (10% reduction when compared to baseline), may, by reducing regional blood flow proportionally, have contributed to the degree of regional desatura- tion seen during bypass. However, the effects of a 10% reduction in Pco, could not explain a nearly 50% reduction in sagittal sinus saturation during bypass; nor do the effects of reduced Pco, alter our basic premise that mixed venous saturation poorly predicts regional oxygen desaturation during bypass.
In conclusion, we have demonstrated that profound venous oxygen desaturation in the sagittal sinus and portal vein occurred during the first 30 min of exper- imental normothermic CPB. The occurrence or sever- ity of regional venous oxygen desaturation in the sag- ittal sinus and portal vein was not predicted by concomitant changes in mixed venous oxygen satura- tions, indicating that better strategies for evaluating regional oxygen delivery during bypass are needed. Further, we found that standard, clinically relevant pump flow rates did not prevent profound regional desaturation even when mixed venous oxygen satu- ration was normal. Strategies to prevent and treat end-organ complications of CPB may be addressed by using regional venous saturation values to indicate matching of oxygen delivery and demand. Further- more, current guidelines for calculating pump flow during normothermic bypass may be reconciled to better match prebypass systemic oxygen delivery with oxygen delivery during CPB.
References 1. Jamieson WRE, Turnbull KW, Larrieu AJ, et al. Continuous
monitoring of mixed venous oxygen saturation in cardiac sur- gery. Can J Surg 1982;25:538-43.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
McArthur KT, Clark LC, Jr., Lyons C, Edwards S. Continuous recording of blood oxygen saturation in open-heart operations. Surgery 1962;51:121-6. Stanley TH, Isern-Amaral J. Periodic analysis of mixed venous oxygen tension to monitor the adequacy of perfusion during and after cardiopulmonary bypass. Can Anaesth Sot J 1974;21: 454-60. Allen KB, Salam AA, Lumsden AB. Acute mesenteric ischemia after cardiopulmonary bypass. J Vast Surg 1992;16:391-6. Gennaro M, Aster E, Matano R, et al. Acute mesenteric ischemia after cardiopulmonary bypass. Am J Surg 1993;166:231-6. Huddy SPJ, Joyce WI’, Pepper JR. Gastrointestinal complica- tions in 4473 patients who underwent cardiopulmonary bypass surgery. Br J Surg 1991;78:293-6. Newman M, Frasco I’, Kern F, et al. Central nervous system dysfunction after cardiac surgery. Adv Cardiovasc Surg 1992;3: 243- 84. Smith PLC, Newman SP, El1 PJ, et al. Cerebral consequences of cardiopulmonary bypass. Lancet 1986;1:823-5. Larkin DFP, Wood AE, Neligan M, Eustace I’. Ischaemic optic neuropathy complicating cardiopulmonary bypass. Br J Oph- thalmol 1987;71:344-7. DeLeon S, Ilbawi M, Arcilla R, et al. Choreoathetosis after deep hypothermia without circulatory arrest. Ann Thorac Surg 1990; 50:714-9. Robinson RO, Samuels M, Pohl KRE. Choreic syndrome after cardiac surgery. Arch Dis Child 1988;63:1466-9. McDonnell JR, Fleming WH, Chu W-K, et al. Magnetic reso- nance imaging of the brain in infants and children before and after cardiac surgery. Am J Dis Child 1990;144:374-8. Bellinger DC, Wernovsky G, Rappaport LA, et al. Cognitive development of children following early repair of transposition of the great arteries using deep hypothermic circulatory arrest. Pediatrics 1991;87:701-7. Brunberg JA, Reilly EL, Doty DB. Central nervous system con- sequences in infants of cardiac surgery using deep hypothermia and circulatory arrest. Circulation 1974;50:11-60-8. Bregman D, Kesselbrenner M, Sack JB. Pulsatile flow during cardiopulmonary bypass. In: Kay PH, ed. Techniques in extra- corporeal circulation. Oxford: Butterworth-Heinemann Ltd, 1992:211-29. Andersen LW, Landow L, Baek L, et al. Association between gastric intramucosal pH and splanchnic endotoxin, antibody to endotoxin, and tumor necrosis factor-o concentrations in pa- tients undergoing cardiopulmonary bypass. Crit Care Med 1993;21:210-7. Croughwell ND, Frasco I-‘, Blumenthal JA, et al. Warming dur- ing c&diopulmonary bypass is associated with jugula; bulb desaturation. Ann Thorac Sure 1992:53:827-32. Croughwell N, Newman M, White B; et al. Correlation of pump venous and jugular venous saturation during CPB. Anesthesi- ology 1993;7:A143. Lazenby WD, Ko W, Zelano JA, et al. Effects of temperature and flow rate on regional blood flow and metabolism during car- diopulmonary bypass. Ann Thorac Surg 1992;53:957-64. Braude S, Nolop K, Fleming J, et al. Increased pulmonary trans- vascular protein flux after canine cardiopulmonary bypass: as- sociation with lung neutrophil sequestration and tissue peroxi- dation. Am Rev Respir Dis 1986;123:867-71. Rinder CS, Gaal D, Student LA, Smith BR. Platelet-leukocyte activation and modulation of adhesion receptors in pediatric patients with congenital heart disease undergoing cardiopulmo- nary bypass. J Thorac Cardiovasc Surg 1994;107:280-8. Menashe P, Haydar S, Peynet J, et al. A potential mechanism of vasodilation after warm heart surgery: the temperature-depen- dent release of cytokines. J Thorac Cardiovasc Surg 1994;107: 293-9. Schleef RR, Bevilacqua Ml’, Sawdey M, et al. Cytokine activa- tion of vascular endothelium: effects on tissue-type plasmino- gen activator and type 1 plasminogen activator inhibitor. J Biol Chem 1988;263:5797-5803.
472 CARDIOVASCULAR ANESTHESIA MCDANIEL ET AL. ANESTH ANALG MIXED VENOUS OXYGEN SATURATION DURING BYPASS 1995;80:466-72
24. Yau TM, Ikonomidis JS, Weisel RD, et al. Ventricular function after normothermic versus hypothermic cardioplegia. J Thorac Cardiovasc Surg 1993;105:833-44.
_-
25. Martin TD, Craver JM, Gott JP, et al. Prospective, randomized trial of retrograde warm blood cardioplegia: myocardial benefit and neurologic threat. Ann Thorac Surg 1994;57:298-304.
26. Cox CS. Zwischenbereer TB. Fleming RYD. et al. Ileal mucosal hypoperfusion durini c&liopulm&ary ‘bypass. Curr Surg 1992;10:507-10.
27. Greeley WJ, Bracey VA, Ungerleider RM, et al. Recovery of cerebral metabolism and mitochondrial oxidation state is de- layed after hypothermic circulatory arrest. Circulation 1991;84: 111400-6.
28. Croughwell N, Lyth M, Quill TJ, et al. Diabetic patients have abnormal cerebral autoregulation during cardiopulmonary by- pass. Circulation 1990;82:IV407-12.
29. Brusino FG, Reves JG, Smith LR, et al. The effect of age on cerebral blood flow during hypothermic cardiopulmonary by- pass. J Thorac Cardiovasc Surg 1989;97:541-7.
30. Todd MM, Drummond JC, Shapiro HM. Comparative cerebro- vascular and metabolic effects of halothane, enflurane, and isoflurane. Anesthesiology 1982;57:A332.





























