Embed Size (px)
Citation preview
www.pnz.org.nzISSN 1179-7967 (Print)
ISSN 1179-7975 (Online)
THE LATEST NEWS & VIEWS FROM
PHYSIOTHERAPY NEW ZEALAND
MAY 2017
PHYSIOMATTERS
Meeting the Physio Board audit requirements
Also in this issue: •ACC:Astepintherightdirection•Creatingagloballyconnectedphysiocommunity•Casestudy:Achillestendinopathyandrehabisometrics
cOnTEnTS
2 |PHYSIO MATTERS MAY 2017
www.pnz.org.nz
Editorial and Advertising
• SendeditorialitemstotheEditor,[email protected]
• LetterstotheEditorarelimitedto250wordsandmaybeedited.
• SendadvertisementsandcourseinformationtoClaireAnglisspnz@physiotherapy.org.nz
• Advertisingratesandspecificationsareonourwebsite.
• Deadlineforeditorialandadvertisingbookingisno later than 20th of the month, two months before the issue is published.Ifthisdatefallsonaweekendoraholiday,pleasesupplybytheclosestworkingdaybefore.
• MembersmayreadPhysioMattersonourwebsiteandfollowworkablelinks.
The Editor reserves the right to edit material for space and clarity, and to withhold material from publication. Individual views expressed in this publication are not necessarily those of Physiotherapy New Zealand. Inclusion of product or service information or of links to external websites does not imply PNZ endorsement of the product, service or website unless specifically stated. Advertising in Physio Matters does not constitute endorsement of a product and no advertiser may use publication of an advertisement in the magazine to support the marketing of every product. While every endeavour is made to ensure the accuracy of information, no responsibility is accepted for inaccurate information.
Booking deadlines
Issue Booking deadline
February2017 12December2016
March2017 20January
April2017 19February
May2017 18March
June2017 20April
July2017 22May
August2017 20June
September2017 20July
October2017 21August
November2017 20September
December2017 20October
Physiotherapy New Zealand
POBox27386,MarionSquareWellington6141Level6,342LambtonQuay,Wellington6011,NewZealand
Phone:+6448016500|Fax:+6448015571
May 2017
PRESIDENT’S COLUMN 3
NATIONAL OFFICE 4
EDITOR’S NOTE 5
FEATURE: MEETING THE PHYSIO BOARD AUDIT REQUIREMENTS 6
LEARNING AND RESEARCH 10
WCPT: CREATING A GLOBALLY CONNECTED PHYSIOTHERAPY COMMUNITY 12
ACC 15
MEMBER STORY 16
SCHOLARSHIP: SHOULDER BIOMECHANICS AND REHABILITATION 17
PHYSIO BOARD 18
CASE STUDY 20
OF SPECIAL INTEREST 24
SIG: THE CASE FOR ACUPUNCTURE 26
PODCASTS 28
PROFESSIONAL DEVELOPMENT CALENDAR 29
CONTACT DETAILS 31

PRESIdEnT’S cOluMn
PHYSIO MATTERS MAY 2017 | 3
Booking deadlines
Issue Booking deadline
February2017 12December2016
March2017 20January
April2017 19February
May2017 18March
June2017 20April
July2017 22May
August2017 20June
September2017 20July
October2017 21August
November2017 20September
December2017 20October
Physiotherapy New Zealand
POBox27386,MarionSquareWellington6141Level6,342LambtonQuay,Wellington6011,NewZealand
Phone:+6448016500|Fax:+6448015571
Proposal for change update
LIZ BINNS
PRESIDENTPHYSIOTHERAPY NEW ZEALAND
The PNZ proposal for change co-design workshops are now complete and the recommended principles of the future organisational model have been designed. A paper outlining these principles will be distributed to all members, Branches and SIGs, so that everyone has an opportunity to consider the recommendations that your representatives on the co-design group have made.
This recommendation paper will not go deeply into the nitty gritty detail ... the work to do that is immense and will take another 18 months of detailed development with Branch and SIG representatives.
We anticipate being able to have the first vote within the next two months. This will be to give the go ahead for us to progress to the detailed redesign of PNZ based on the principles recommended by the co-design group. This first vote is a ‘general vote’. Essentially what you will be asked to vote on is whether you agree that the proposed recommendations are the right things to do if PNZ is to strengthen its voice and influence for the future. If you agree, then resources will be committed to developing the detailed future operating model and the transition plans. Therefore,
the general vote is the indication that you either do or do not want the work to continue. The work will continue if the vote is a clear majority. So, a very clear “yes” is required but remember, it is only “of those members that vote.” So we need you to have a view and vote.
As above, the process to work up the detailed structure will take 18 or so months. It is important to take the time that is needed to consult widely with you our members, experts in their fields and maybe others who have been through this process. Work will need to be done alongside the chairs, secretaries and treasurers of Branches and SIGs. While it is paramount that this is a considered process, we must not meander
To be what you want us to be and to deliver what you ask, we need you to
participate in deciding the future.
through it. We were urged by Nigel Stirling a constitutional lawyer to be ‘bold’. Sitting on the fence and half measures may feel comfortable now but will cost us in the long-run when any such decisions will need to be revisited – and in his opinion they will have to be if we do not commit to the hard discussions now.
The second vote is a ‘constitutional’ vote.
It is at this point that you will be asked to vote on the fully fleshed out, detailed structure for the future organisation of PNZ (its constitution, governance, operations etc.). A constitutional vote requires a 75% majority as a minimum.
As a parting thought, you will understand the organisation is coming up to a significant crossroad. We cannot move forward alone. To be what you want us to be and to deliver what you ask, we need you to participate in deciding the future. Please take the time to read the recommendation paper when it is sent and please take the time to vote – after all it is your professional body and it is here to serve you.
Liz Binns President
It was fantastic to see another of our members (Margie Olds) attain the Scope of Specialist from the Physiotherapy Board of New Zealand. We now have seven members who are recognised as being at the top of their scope of practice/specialty here in New Zealand. They are our pioneers in achieving this and are navigating uncharted territory. As the number of Specialists grows the opportunities to contribute to the wider health policy agenda, seek out and support opportunities to better position the profession for recognition of Specialists is exciting.

nATIOnAl OFFIcE
4 | PHYSIO MATTERS MAY 2017
Do have a read of our feature article for advice on what to expect if you are selected for audit by
the Board.
Updates from the National Office
jOE ASGHAR
cHIEf ExEcuTIvE OffIcERPHYSIOTHERAPY NEW ZEALAND
You will notice in this edition of Physio Matters that two new columns have popped up – one from Acc and one from the Physio Board. These regular columns aim to provide both organisations an opportunity to keep you informed about their work.In the past few weeks, I have been invited to participate in a number of reviews of Acc including those run by State Services commission and the voice of the customer Group. This provides PNZ a platform to feedback on those issues that members have raised through interactions with Acc. In their column this month on page 15, Acc touch on their reworked pain management service which is part way through its first year of implementation.
We have also been working closely with the Physiotherapy Board to help physiotherapists understand the different but complementary roles that each of us fulfil. Some of the areas we have been working together on have included the review of the Physiotherapy code of Ethics, and how PNZ documents will support the new Board standards. To accompany their
first column on page 18, do have a read of our feature article for advice on what to expect if you are selected for audit by the Board.
Ministry Of Health electronic health record
PNZ has had initial discussions with the team heading the business case development of the national Electronic Health record for the Ministry of health, emphasising the importance and the opportunities that having physiotherapists connected to the record from an early stage would bring. While still at the scoping stage we are looking forward to a continued engagement with the team.
Health Quality and Safety Commission: Incident reporting
As part of the process of reviewing our Adverse Reaction Reporting process, we have met with the
Medical Advisor from the Health
Quality and Safety commission
(HQSc) to help guide and inform
our thinking on how we could best
develop and refresh the existing
reporting system. This is a piece of
work that will unfold with time with
the intent that the process is used to
support practice and to assist you as
members learn from incidents that
occur as part of everyday practice.
joint interests with NZALS
And finally, we have also recently
entered into a Memorandum of
understanding (Mou) with the New
Zealand Artificial Limb Service (NZALS)
and have established the following
joint interests:
•Educatingandsupporting
physiotherapists to improve outcomes
for their clients and patients;
•Collaboratingonprojectsthat
improve outcomes for amputees;
•Communicatingthegreatworkdone
by physiotherapists.
By entering into this Mou, both NZALS
and PNZ have agreed to have at least
one joint collaborative activity each
year. We will keep you up to date as
this develops.
Joe Asghar
Chief Executive
EdITOR’S nOTE
PHYSIO MATTERS MAY 2017 | 5
Important: correction to Ethics Q&A article from March 2017 issue of Physio Matters
It has been brought to our attention that there was an error in our Ethics Q&A column titled ‘Effective communication with patients and other service providers’ published in our March issue.The error occurred in the section under the heading: ‘Are social media sites acceptable in communicating with patients?’
Physio Matters would like clarify that physiotherapists must – rather than should – inform the patient and get consent if the physiotherapist wishes to post identifiable patient information to an online site.
Thank you to our eagle-eyed reader for pointing this out and we apologise for any confusion the original article may have caused.
World Class Education
Professional Instructors
Face to Face Learning
Ongoing Clinical Support
Money Back Guarantee
Treatment techniques combining the IMS and Trigger Point Models maximising clinical outcomes.
REGISTER ONLINE @ www.gemtinfo.com.au
CAA Accredited Courses Osteopathy Australia Endorsed Courses
EARLY
BIRD RATES
APPLY!
For more information, visit our website, call +61 3 9585 8100 or email [email protected]
2017 COURSE LOCATIONS: AUCKLAND, CHRISTCHURCH, MELBOURNE, SYDNEY, KUALA LUMPUR & MORE!
These courses will change the way you view the human body!
TRIGGER POINT DRY NEEDLING COURSES 2017Applications for Pain Management & Sports Injuries
FEATuRE
6 | PHYSIO MATTERS MAY 2017
Meeting the Physio Board audit requirements Every year around 200 Kiwi physiotherapists are audited and big changes are planned for the New Zealand recertification process. Kirstin Mills finds out what these changes are and what you can expect if you are selected for audit.
FEATuRE

PHYSIO MATTERS MAY 2017 | 7
When practising physios apply for their annual practising certificate, they must sign a declaration that they have met continuing professional development (cPD) requirements. Each year 5% of practising physios are randomly selected for audit by the Physiotherapy Board of New Zealand, a requirement under section 41 of the Health Practitioners competence Assurance Act.
The audit is retrospective; focusing on the three years prior to the end of the previous practising year. The board provides a Professional Development Report (PDR) template to complete. Physios must also provide:
•asigneddeclaration;
•anemploymenthistorysummary;
• threereflectivestatementsonanethical, cultural and professional/clinical issue;
•evidenceofprofessionalpeerreview;
• logbookofCPDactivitiesincludingfive pieces of supporting evidence. This is easier to collate with Physiotherapy New Zealand’s free smartphone app for members called Log It, which logs cPD hours, captures evidence using the phone’s camera and creates a secure back up which can be emailed and used for an audit.
Physios choose the five types of evidence they provide, as long as they are across four different learning categories:
•Work-basedCPD
•Professionalactivities
•Formaleducation
•Self-directedCPD
The board’s Recertification Guidelines outline the types of evidence that may be acceptable, and guidance on which category evidence falls into.
When someone is selected for audit, they have two months to get their PDR to the board.
Professional advisor cheryl Hefford says that even though an audit requires physios to send information, there is a reasonable amount of trust involved.
“They send us their log book, but we aren’t able to check up on the whole log book. We ask them to send a few pieces of evidence … but there is still a degree of trust involved in the audit, as well as their declaration.”
The number who fail the audit is tiny. Of the 4500 or so physios who hold an annual practising certificate, 200-220 are audited each year. Typically, less than three fail.
If people do not pass the evaluation of their PDR, they have two to three weeks to remedy their failings and board staff work with them to address the missing information. Senior registration officer Lisa Mansfield says physios can usually provide enough information to meet the requirements. It might be that they have filled in the log book incorrectly or put things in wrong categories.
The main reason people fail is from not providing evidence of enough cPD. Practitioners must do over 100 hours of cPD over three years. Sometimes they record 100 hours in their log book, but include things they cannot claim for (something that is capped or not appropriate for cPD). Because the audit is retrospective they cannot make up hours. They may have other unlogged hours they can claim but, if not, each case is considered individually.
If people are close to meeting requirements or have a good reason for not meeting the hours, they can be asked to be in the audit the following year or, occasionally, the year after.
If they were far off the required hours, then the matter goes to the board. The potential outcome under the HPcA Act might be a competence review. Reviewers assess competence on site: watching the physio treating a patient, looking at patient records and conducting an interview with the physio.
Cheryl Hefford Lisa Mansfield
FEATuRE
8 | PHYSIO MATTERS MAY 2017
cheryl is not aware of anyone having
their registration suspended as the
result of failing an audit, but they may
have a condition for a period of board
supervision imposed on their APc.
The entire recertification programme is
being reviewed, as part of the board’s
strategic plan. The process is likely
to become more of an online one
with people having, for example, an
e-portfolio.
“We’re aware it’s a little bit
cumbersome with the log books and
sending pieces of paper in,” cheryl
says. “The difficulty is getting that
balance between meeting the legal
obligations that practitioners have and
not being too authoritarian. We try
to strike a balance that keeps them
competent, but doesn’t peer over their
shoulder all the time.”
All New Zealand regulatory authorities
have a recertification programme. The
board is looking at these, and others
internationally, for ideas to make
its programme up to date and user
friendly.
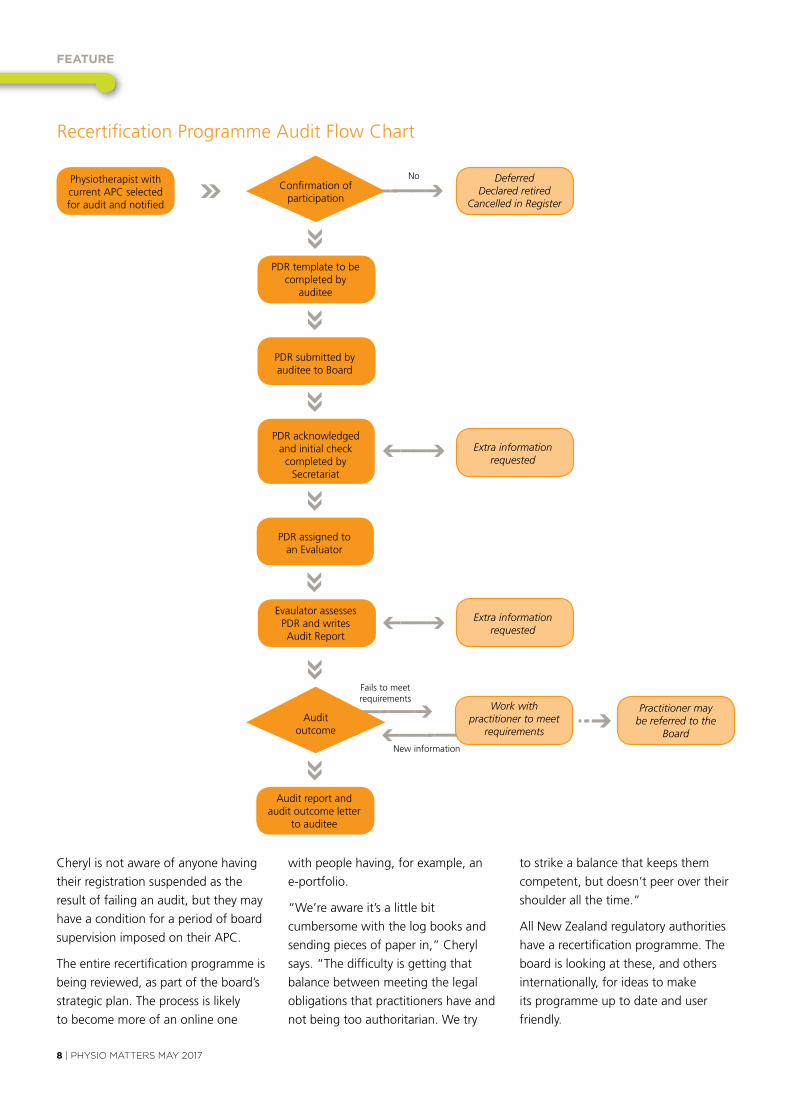
Recertification Programme Audit flow chart
Physiotherapist with current APc selected for audit and notified
PDR template to be completed by
auditee
PDR submitted by auditee to Board
PDR acknowledged and initial check completed by
Secretariat
Evaulator assesses PDR and writes Audit Report
Audit report and audit outcome letter
to auditee
PDR assigned to an Evaluator
Deferred Declared retired
Cancelled in Register
Extra information requested
Extra information requested
Work with practitioner to meet
requirements
Practitioner may be referred to the
Board
confirmation of participation
Audit outcome
No
fails to meet requirements
New information
PHYSIO MATTERS MAY 2017 | 9
and if people are struggling then they’re not going to bring down the reputation of physiotherapists.”
Another positive was that she found the board helpful when she called them for advice over the peer assessment.
Isobel says she would not change any of the cPD she had done following the audit. She received good feedback, particularlyonherreflectivestatements.
Isobel says it was time-consuming to put the information together, but and recommends physios record their cPD regularly.
However, she was uncertain what was required for her reflectivestatements.
“I didn’t know if they wanted me to be really specific about what I did and how I treated people or whether they wanted me to discuss my emotional response to it and how I would manage that.”
Isobel would like to see more technology used, although recognises that not everybody has access to the latest hardware and software. Older physios may not have smartphones or may find technology challenging.
Written by Kirstin Mills
cheryl and the review team are also tapping into the expertise of the International Network of Physiotherapy Regulatory Authorities (INPTRA), a group of international physiotherapy regulators. In a recent INPTRA webinar that cheryl participated in, the British columbia regulatory authority in canada shared its online two-stage system. It includes a quiz and a case scenario.
“That’s quite a different approach to what we have. It’s all online and the practitioner gets immediate feedback and can see how they compare with the rest of the profession in terms of their cPD.”
Another webinar looked at whether authorities are really testing what they think they are testing. cheryl says there is no real consensus on how to test effectively for competence.
“You think you might be doing it the right way, but it is difficult to know for sure. It’s not just our problem, it’s a global problem.”
The revision of the system is a huge project and will require consultation and testing. The aim is to have it running in 2018.
A physio’s view
Wellington physiotherapist Isobel Weeks was audited in 2016. While she understands the importance of audits, she believes the auditing process could be improved.
Isobel, from the united Kingdom, was selected at random for audit in 2015, but because she had only been a New Zealand-registered physio for four months, the audit was deferred for a year.
On the positive side, she says it is good to know she is doing well.
“It was a positive outcome. I understand why they have to do all this and it’s an important process. We want to know that physios working in New Zealand are up to professional standards. I’m quite proud of being a physiotherapist and I would like to know my profession is being taken seriously
Isobel Weeks
Apply now to study in 2017.The University of South Australia’s flexible one-year Professional Certificate in Conservative Management of Pelvic Organ Prolapse provides advanced training to experienced physiotherapists.
Delivered and supported online, you’ll also attend a weekend workshop in Adelaide for practical assessment, and focus on areas including:
• Advanced pelvic floor and prolapse assessment• Biofeedback, electrical stimulation and
transperineal ultrasound• Pessaries in the management of prolapse.
Join Australia’s University of Enterprise. unisa.edu.au/physioprofcert80
9844
0_CR
ICO
S PR
OVID
ER N
O 0
0121
B
ADVANCE YOUR CAREER
IN WOMEN’S HEALTH.
lEARnIng And RESEARcH
10 | PHYSIO MATTERS MAY 2017
Critical Debate: Getting to the ‘point’
Physiotherapists have asserted themselves within healthcare as evidence based practitioners using high quality research to inform, modify, mold and develop practice. This earns physiotherapists the professional respect of other health professionals and ensures the continued support of physiotherapy services by public funding bodies.
Part of the regulatory requirements for a physiotherapist involves continually questioning,reflectingon,andevaluating our practice, in order to change and modify clinical practice as evidence and understanding evolves.
One of the challenges in using research evidence to direct healthcare practice is the enormous pool of literature available and the fact that studies can often be quite confusing and findings contradictory. One minute a study claims a certain technique or approach is the next treatment panacea, and the next minute further findings contradict the original results. There are numerous examples within healthcare; platelet rich plasma for tendons, hyaluronic acid for osteoarthritis, and more recently; arthroscopy for degenerative meniscal tears. This cautions us in becoming wed to any one approach/technique or paradigm.
furthermore, it is common for people exposed to a large body of literature, that individuals or groups of people can have very different interpretations of that literature. An excellent example of this is a literary debate on the existence and constitution of myofascial trigger points (MTPs). This debate has been ongoing over the last twenty years but more recently resurfaced in a series of articles published in The Journal of Rheumatology and The Journal of Body Works and Movement.
The series of articles beautifully demonstrates how individuals can have very different accounts when looking at the same body of literature.
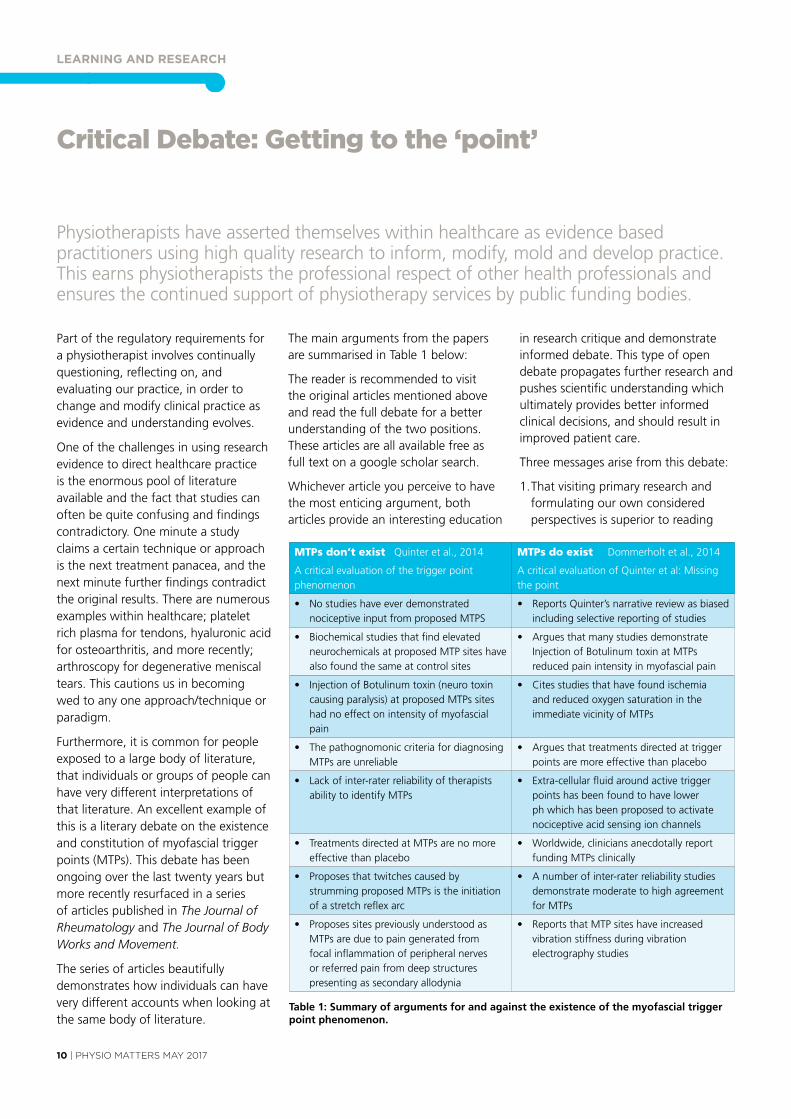
The main arguments from the papers are summarised in Table 1 below:
The reader is recommended to visit the original articles mentioned above and read the full debate for a better understanding of the two positions. These articles are all available free as full text on a google scholar search.
Whichever article you perceive to have the most enticing argument, both articles provide an interesting education
in research critique and demonstrate informed debate. This type of open debate propagates further research and pushes scientific understanding which ultimately provides better informed clinical decisions, and should result in improved patient care.
Three messages arise from this debate:
1. That visiting primary research and formulating our own considered perspectives is superior to reading
MTPs don’t exist Quinter et al., 2014
A critical evaluation of the trigger point phenomenon
MTPs do exist Dommerholt et al., 2014
A critical evaluation of Quinter et al: Missing the point
• Nostudieshaveeverdemonstratednociceptive input from proposed MTPS
• ReportsQuinter’snarrativereviewasbiasedincluding selective reporting of studies
• Biochemicalstudiesthatfindelevatedneurochemicals at proposed MTP sites have also found the same at control sites
• ArguesthatmanystudiesdemonstrateInjection of Botulinum toxin at MTPs reduced pain intensity in myofascial pain
• InjectionofBotulinumtoxin(neurotoxincausing paralysis) at proposed MTPs sites had no effect on intensity of myofascial pain
• Citesstudiesthathavefoundischemiaand reduced oxygen saturation in the immediate vicinity of MTPs
• ThepathognomoniccriteriafordiagnosingMTPs are unreliable
• Arguesthattreatmentsdirectedattriggerpoints are more effective than placebo
• Lackofinter-raterreliabilityoftherapistsability to identify MTPs
• Extra-cellularfluidaroundactivetriggerpoints has been found to have lower ph which has been proposed to activate nociceptive acid sensing ion channels
• TreatmentsdirectedatMTPsarenomoreeffective than placebo
• Worldwide,cliniciansanecdotallyreportfunding MTPs clinically
• Proposesthattwitchescausedbystrumming proposed MTPs is the initiation ofastretchreflexarc
• Anumberofinter-raterreliabilitystudiesdemonstrate moderate to high agreement for MTPs
• ProposessitespreviouslyunderstoodasMTPs are due to pain generated from focalinflammationofperipheralnervesor referred pain from deep structures presenting as secondary allodynia
• ReportsthatMTPsiteshaveincreasedvibration stiffness during vibration electrography studies
Table 1: Summary of arguments for and against the existence of the myofascial trigger point phenomenon.
PHYSIO MATTERS MAY 2017 | 11
pre-digested summaries or secondary evidence.
2. It is valuable to have colleagues constructively challenge our perspectives to stimulate us to progress our individual knowledge (and undertake further research).
3.Akeytoourindividualprofessionalevolutionistoreflecton our own bias and critically challenge our own ideas and practice.
To effectively read primary research, physiotherapists should develop an understanding of how to critically analyse research papers, and do so with the understanding of their own bias and world views. If you are starting out in critical appraisal, a good website to visit is the centre for Evidence Based Medicine which has a wide range of tools and worksheets on critical appraisal; see http://www.cebm.net/critical-appraisal/ or google ‘cEBM’.
Members of Physiotherapy New Zealand have free access to primary research through EBScO; including full text articles
DRY NEEDLINGCOURSES
AdvancedCourseSPECIAL
$329 AUD
Online Theory plus face to face Practical
VISIT www.cpdhealthcourses.com TODAY!
Auckland 2017: Intro & Advanced CoursesComplete all your Dry Needling Intro & Advanced practical training in 1 weekend. Join the Advanced course for only $329 AUD!Save time by completing all your Dry Needling theory ONLINE in your own time.Dr Wayne Mahmoud has over 30 years of clinical & teaching experience and a Masters Degree in Acupuncture.Receive course certificates, free needle starter pack, fully illustrated course manuals and review all techniques on the Video Training Site.
Intro: August 25/26 and Advanced: August 27 (Intro = Fri 5-8pm & Sat 8-5pm. Advanced = Sunday 8-5pm)
"Just wanted to take this opportunity to say BIG THANKS for all your teaching & guidance overthe weekend. Your course was phenomenal. I thoroughly enjoyed it & am sure other studentsdid too. The intermix of online theory followed by practical was great set up. The contentsweren't too challenging and left enough thought provoking questions. I had a fantasticweekend. Very inspirational Wayne." Lockie N (Physiotherapist)
from cINAHL, SPORTDiscus and Rehabilitation Reference centre databases. EBScO provide support resources on how to use the database on the PNZ member website. PNZ will be compiling further resources on critical appraisal of research studies which you will be able to find on the member website by the end of August this year.
Whatever your stance or understanding of the Trigger Point Phenomenon, by reading the debate in these articles you will be impressed by the authors depth of knowledge, considered perspectives, informed critique, and understanding of research methodology.
The key to continuing to develop our professional knowledge isbeingreflectiveofourpracticewithacknowledgmentof our individual bias and challenging our practice. To quote Albert Einstein: “The important thing is not to stop questioning”.
Written by Nick Clode
NB: All courses held in Wellington. Both Part A & B courses have an online component requiring successful completion prior to attending the 3 day course. This is approximately 7 hours work. Registration can now be completed online at: www mckenzieinstitute.org/nz
2017 Education Programme
For further info, please contact: Kay Morgon, Branch Manager. Ph: 04 299 6645 or Email: [email protected]
Part D Advanced Cervical and Thoracic Spine & Extremities – Upper Limb (4 days)
27-30 Apr 2017
Part B The Cervical and Thoracic Spine (3 days)
9-11 Jun 2017
Credentialling Examination 29 July 2017
Credentialled Update Day 4 August 2017
Seminar Day 5 August 2017
Part A The Lumbar Spine (3 days) 15-17 Sep 2017
Part C Advanced Lumbar Spine & Extremities – Lower Limb (4 days)
16-19 Nov 2017

WcPT
12 | PHYSIO MATTERS MAY 2017
Creating a globally connected physiotherapy community
As New Zealand’s WcPT representative organisation, we asked the President of WcPT about what’s been going on in the world of physiotherapy.
It’s hard to believe that it has been eight months since my first trip to New Zealand to attend the Physiotherapy New Zealand conference in Auckland in September 2016.
At that time, WcPT had launched its new strategic plan WCPT Move Forward Together, one of the objectives of which is to seek to create a global physiotherapy community where every physiotherapist feels connected.
A globally connected physiotherapy community
creating a connected global physiotherapy community is one aspect of the work of WcPT and we strive to do this in many ways. Probably the most high-profile way we create connections is through our congress – where the world of physiotherapy meets. In July last year, 17 focused Symposia were announced involving 75 global leaders and innovators in the field of physiotherapy. In february, over 1500 physiotherapists were notified
that their abstracts had been accepted for a variety of different presentation formats for congress in cape Town. There will be seminars and networking sessions and a new ‘Indaba’ space for conversation, creation and inspiration. There is great excitement wherever about congress 2017, our first time to host a congress in the WcPT Africa Region.
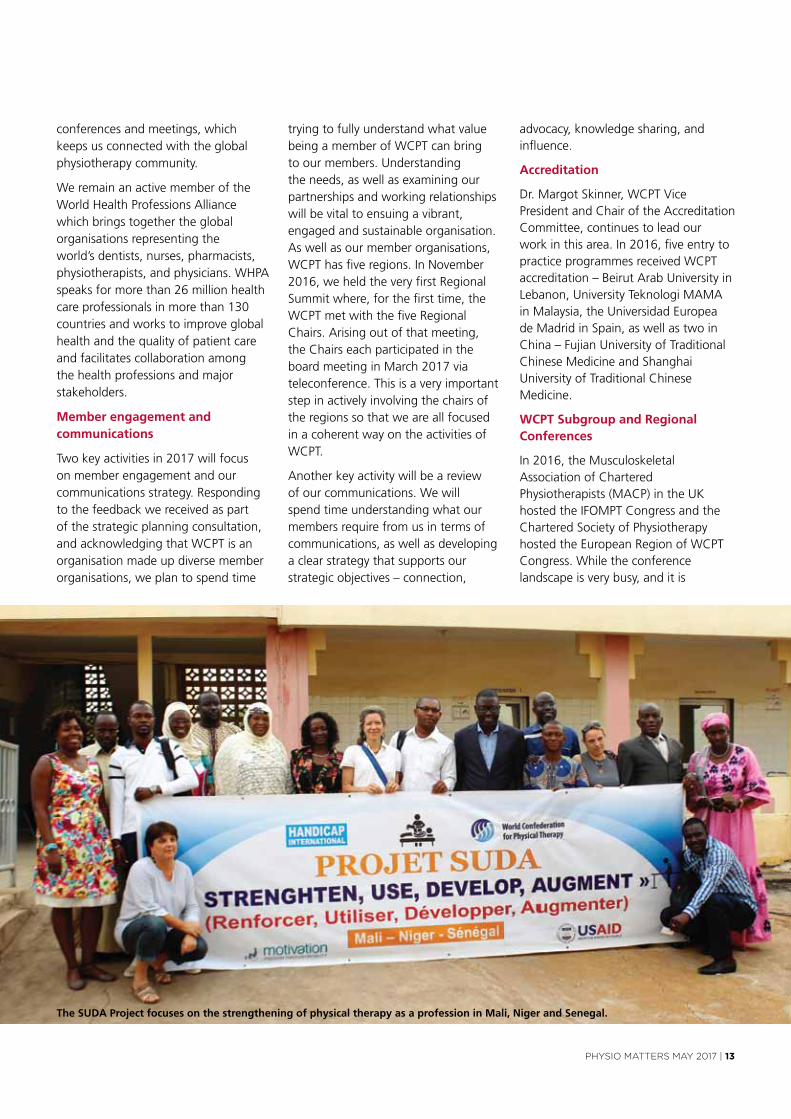
The work of WcPT to implement the activities of the strategic plan is ongoing. Our new chief Executive, Jonathon Kruger, has settled in and we have welcomed four new staff members – Professional Advisers Birgit Mueller-Winkler and Héðinn Jónsson, Head of finance Deborah Williams and Sidi Dieye, our Programme Manager for SuDA (our uSAID funded project).
Growing organisational and educational capacity
SuDA has four main objectives:
1.StrengtheningthreephysiotherapyprofessionalorganisationsinMali,NigerandSenegal;
2.UsingWCPT’sstandardstogrowcapacityinthreeeducationalprogrammesforphysiotherapistsinthosecountries;
3.Developingathoughtleadershippaperonphysiotherapistassistants;
4.Augmentingwheelchairtraininginthephysiotherapysector.
It is the first time WcPT has received development funding to support work key to our strategic objectives and represents an area with great potential
for future exciting projects around the world. We are delighted to be working in collaboration with Handicap International on this project.
International relations and outreach
WcPT is in official relations with the World Health Organisation (WHO) and this relationship is reviewed every three years. In february, we worked with nine international rehabilitation organisations to deliver a statement at the launch of a key call for action for member states and stakeholders in rehabilitation. As part of a response to the call for Action, WcPT committed to facilitate the establishment of a Global Rehabilitation Alliance and the first steps towards considering this will take place when the President and cEO attend the World Health Assembly in Geneva in May 2017.
Recognising the value of global alliances and understanding collaborative advantage was one key topic in a meeting of international sports medicine and physiotherapy organisations held in Monte carlo in advance of the IOc World conference on Prevention of Injury and Illness in Sport. This workshop, hosted by the British Journal of Sports Medicine and involving its member organisations, was a wonderful opportunity to meet the leadership of a number of international sports physiotherapy organisations who are also members of the WcPT subgroup International federation of Sports Physical Therapy.
The WcPT board members continue to travel far and wide meeting with and participating in national
WCPT President Emma Stokes
PHYSIO MATTERS MAY 2017 | 13
conferences and meetings, which keeps us connected with the global physiotherapy community.
We remain an active member of the World Health Professions Alliance which brings together the global organisations representing the world’s dentists, nurses, pharmacists, physiotherapists, and physicians. WHPA speaks for more than 26 million health care professionals in more than 130 countries and works to improve global health and the quality of patient care and facilitates collaboration among the health professions and major stakeholders.
Member engagement and communications
Two key activities in 2017 will focus on member engagement and our communications strategy. Responding to the feedback we received as part of the strategic planning consultation, and acknowledging that WcPT is an organisation made up diverse member organisations, we plan to spend time
trying to fully understand what value being a member of WcPT can bring to our members. understanding the needs, as well as examining our partnerships and working relationships will be vital to ensuing a vibrant, engaged and sustainable organisation. As well as our member organisations, WcPT has five regions. In November 2016, we held the very first Regional Summit where, for the first time, the WcPT met with the five Regional chairs. Arising out of that meeting, the chairs each participated in the board meeting in March 2017 via teleconference. This is a very important step in actively involving the chairs of the regions so that we are all focused in a coherent way on the activities of WcPT.
Another key activity will be a review of our communications. We will spend time understanding what our members require from us in terms of communications, as well as developing a clear strategy that supports our strategic objectives – connection,
advocacy, knowledge sharing, and influence.
Accreditation
Dr. Margot Skinner, WcPT vice President and chair of the Accreditation committee, continues to lead our work in this area. In 2016, five entry to practice programmes received WcPT accreditation – Beirut Arab university in Lebanon, university Teknologi MAMA in Malaysia, the universidad Europea de Madrid in Spain, as well as two in china – fujian university of Traditional chinese Medicine and Shanghai university of Traditional chinese Medicine.
WCPT Subgroup and Regional Conferences
In 2016, the Musculoskeletal Association of chartered Physiotherapists (MAcP) in the uK hosted the IfOMPT congress and the chartered Society of Physiotherapy hosted the European Region of WcPT congress. While the conference landscape is very busy, and it is
The SUDA Project focuses on the strengthening of physical therapy as a profession in Mali, Niger and Senegal.
WcPT
14 | PHYSIO MATTERS MAY 2017
You can register on WCPTs website www.wcpt.org for regular updates and communications, as well as follow WCPT on Facebook and Twitter.
impossible for everyone to get to every congress, increasingly the presentations are made available after the event.
MAcP and IfOMPT have very kindly made the videos of many keynotes available free of charge on their website: https://www.youtube.com/channel/uch4eizx9JRK6_osyxs2uHzA.
The cSP and ER-WcPT have also provided material from the keynotes presented in Liverpool: http://www.liverpool2016.com/programme/presentations.
In June 2017, the Asia Western Pacific Region of WcPT will hold its regional conference in Bangkok, hosted by the Physical Therapy Association of Thailand: http://www.awp2017ptat.com.
What’s next?
The WcPT board is half-way through a four-year term which will be completed at the next General Meeting in Geneva in 2019. The first two years have been a period of great change as we continue to build on the great work of previous decades. A global organisation must continue to be relevant
for its members and its community – and to remain so, must continue to look to the future.
We have been through a period of renewal and there are exciting times ahead for us – do please engage with us through social media by registering on our website, by joining our networks, and by coming to congress.
Emma Stokes WCPT President

Acc
PHYSIO MATTERS MAY 2017 | 15
ACC’s commitment to revolutionising their pain management service: it’s up and running but what happens next?
Every year, Acc supports around 10,000 people with pain management following an accident. Many of these people never fully recover so it’s a lifelong relationship that is focusedontrust,flexibilityandtailoredsupport.
In 2015, Acc began redesigning their pain management service with the objective of providing a more positive client experience and improved outcomes, along with getting back to living their lives as quickly as possible.
following a six month pilot in Auckland, Acc’s new pain management service went live on 1 December 2016. The first year of this new service is important for the service to realise its potential.
A step in the right direction
The introduction of Acc’s new pain management service represents a significant change to the way Acc supports patients with pain. The service aims to improve patient outcomes and experience by reducing the impact of pain following an injury. To do this, the service allows support to be tailored to the needs of each individual with greater autonomy on what’s delivered. Patient education about how to manage pain symptoms, and input from the multidisciplinary team, are central to the service. The service replaced a suite of eight pain management services, including services such as the functional Reactivation Programme and comprehensive Pain Assessment, and its delivered by 22 suppliers across the country.
With any change of this size, it will take time to ensure the service is running smoothly but it’s a step in the right direction and positive client outcomes are expected.
Focused on continuous improvement
Acc used a co-design approach with select representatives from the sector which resulted in the design of the pilot service. This live feedback approach was used to allow refinements to the service delivery model to be made based on feedback from those delivering or receiving the service and changes have already been incorporated into the new service. The focus on continuous improvement has been carried over into the service now it has been implemented nationally, and this commitment will be on going throughout the 3-5 year contract term.
Early results are promising
When delivering new services as complex as pain management, teething problems are always present and there have been some great learnings along the way. A key part of the new service is the introduction of an outcome reporting and benchmarking system called ePPOc (Electronic Persistent Pain Outcome collaboration). Preliminary reporting from ePPOc has shown positive early results. The seven services currently collecting and reporting data to ePPOc have performed well across the areas measured, such as changes in average pain rating and pain catastrophising.
The percentage of patients who have reported clinically significant changes in their average pain rating is 45.7% for New Zealand services, compared to 25.1% for services in Australia. for pain catastrophising the percentage of patients who have reported clinically significant changes in their average pain rating is 75.6% for New Zealand services and 53.1% for Australian services. Data from ePPOc, along with feedback from the sector will support the ongoing development of this service.
Nic Johnson Design Lead, Health System Design, ACC www.acc.co.nz
For more information about the service go to www.acc.co.nz/pain. If you have any questions regarding the new service or would like to provide feedback, please email ACC at [email protected]

MEMBER STORY
16 | PHYSIO MATTERS MAY 2017
MidCentral physio wins emerging leader award
When it comes to providing satisfactory care for patients, there are many areas in which some processes should and can be streamlined in order to make them more efficient. for the past 18 months, Palmerston North physio and PNZ member Emma Lett played a role in developing a new system that does just that – and she won an award for it.
Thanks to Emma’s work, it is now easier for patients to gain access to equipment because physiotherapists and occupational therapists are able to share their resources more freely – without having to ask for approval from the other discipline first.
This means that patients are able to access rehabilitation equipment faster – which in turn reduces wait times and therefore keeps a large number of patients safer.
As the lead allied health practitioner on the project, Emma was responsible for developing the educational material for the 2015 rollout of service accreditation within therapy services while working in the community physio team. She then presented her findings at a number of sessions alongside the professional advisors.
The project took about six months of meetings and presentations before it got off the ground, and the improvements to patient safety since its implementation have been remarkable.
“It has made a significant difference for the patients waiting for separate referrals to be actioned by each team”, explains Allied Health executive director Gabrielle Scott.
Not only have patients been able to access equipment quicker, it has also saved travel, paperwork and consultation time for staff.
“By using service accreditation, simple equipment can be assessed and
organised for delivery at the first point of contact by clinical or assistant staff, [so it’s] better, sooner, [and] more convenient.’
Emma was given her award by Associate Health Minister Peter Dunne during a presentation at Palmerston North hospital in february. During the presentation, Mr. Dunne payed tribute to Emma’s role in the project and the strong focus it put on putting patient safety and wellbeing first.
“Emma did this in a way which was easy to implement, and has resulted in
great benefit for the Midcentral physio
team and patients,” he said.
“This is a great example of quality
improvement”.
Emma is the first of two District Health
Board february award winners of the
inaugural Health Quality and Safety
commission ‘Open for Leadership’
award. The awards recognise, celebrate
and share the work of emerging
healthcare leaders who have made a
difference to patient care.
Written by Erica George
Emma Lett receiving her award from Associate Health Minister Peter Dunne in February.
ScHOlARSHIP
PHYSIO MATTERS MAY 2017 | 17
Shoulder biomechanics and rehabilitation
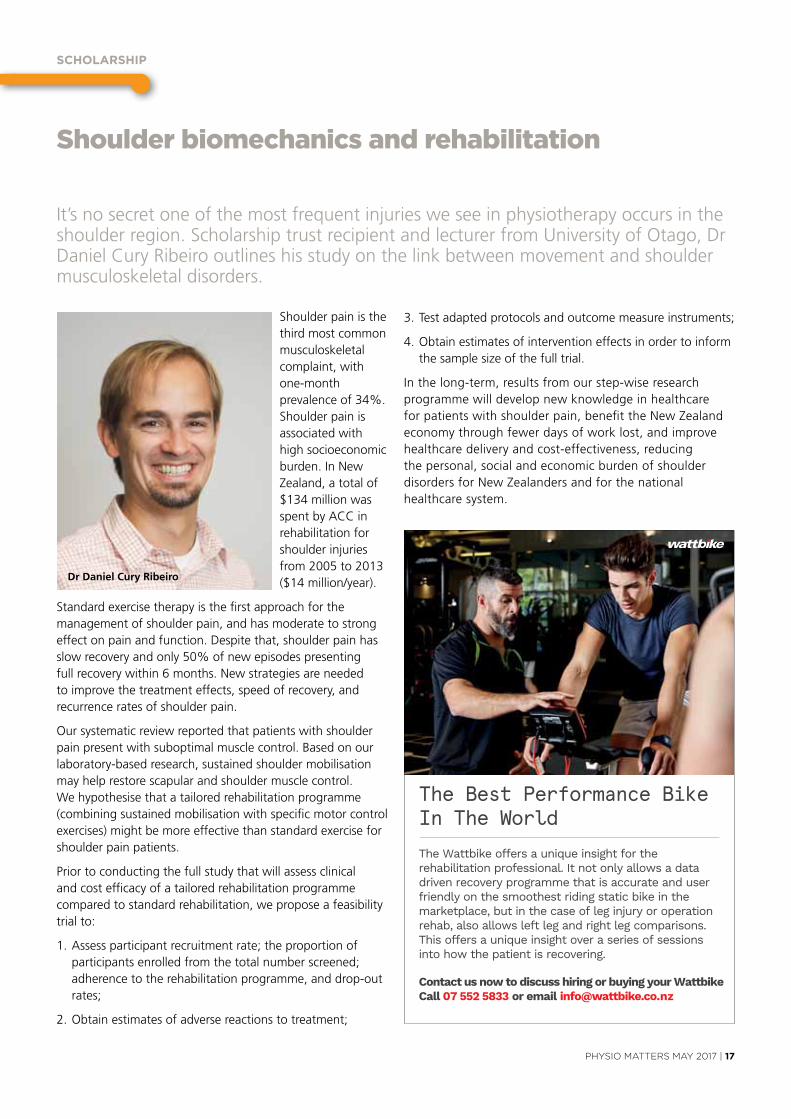
It’s no secret one of the most frequent injuries we see in physiotherapy occurs in the shoulder region. Scholarship trust recipient and lecturer from university of Otago, Dr Daniel cury Ribeiro outlines his study on the link between movement and shoulder musculoskeletal disorders.
Shoulder pain is the third most common musculoskeletal complaint, with one-month prevalence of 34%. Shoulder pain is associated with high socioeconomic burden. In New Zealand, a total of $134 million was spent by Acc in rehabilitation for shoulder injuries from 2005 to 2013 ($14 million/year).
Standard exercise therapy is the first approach for the management of shoulder pain, and has moderate to strong effect on pain and function. Despite that, shoulder pain has slow recovery and only 50% of new episodes presenting full recovery within 6 months. New strategies are needed to improve the treatment effects, speed of recovery, and recurrence rates of shoulder pain.
Our systematic review reported that patients with shoulder pain present with suboptimal muscle control. Based on our laboratory-based research, sustained shoulder mobilisation may help restore scapular and shoulder muscle control. We hypothesise that a tailored rehabilitation programme (combining sustained mobilisation with specific motor control exercises) might be more effective than standard exercise for shoulder pain patients.
Prior to conducting the full study that will assess clinical and cost efficacy of a tailored rehabilitation programme compared to standard rehabilitation, we propose a feasibility trial to:
1. Assess participant recruitment rate; the proportion of participants enrolled from the total number screened; adherence to the rehabilitation programme, and drop-out rates;
2. Obtain estimates of adverse reactions to treatment;
3. Test adapted protocols and outcome measure instruments;
4. Obtain estimates of intervention effects in order to inform the sample size of the full trial.
In the long-term, results from our step-wise research programme will develop new knowledge in healthcare for patients with shoulder pain, benefit the New Zealand economy through fewer days of work lost, and improve healthcare delivery and cost-effectiveness, reducing the personal, social and economic burden of shoulder disorders for New Zealanders and for the national healthcare system.
Dr Daniel Cury Ribeiro
The Best Performance BikeIn The World
The Wattbike offers a unique insight for the rehabilitation professional. It not only allows a data driven recovery programme that is accurate and user friendly on the smoothest riding static bike in the marketplace, but in the case of leg injury or operation rehab, also allows left leg and right leg comparisons. This offers a unique insight over a series of sessions into how the patient is recovering.
Contact us now to discuss hiring or buying your Wa bike Call 07 552 5833 or email info@wa bike.co.nz

PHYSIOTHERAPY BOARd OF nEW ZEAlAnd
18 | PHYSIO MATTERS MAY 2017
Making physiotherapy better, togetherThis month marks the start of the Physiotherapy Board’s consultation on our professional and practice standards and the Aotearoa New Zealand code of Ethics and Professional conduct (code of Ethics) which we’re reviewing jointly with Physiotherapy New Zealand (PNZ).
Together with the Physiotherapy Practice Thresholds of Australia and Aotearoa New Zealand, which we now share with our colleagues across the ditch, these documents provide the framework for the future of New Zealand physiotherapy practice and our vision to foster excellence and actively make a difference.
On Wednesday, May 10th we will hold a symposium with invited members of the profession and stakeholders to launch the consultation on the standards, and the final round of consultation on the code of Ethics. We are looking for feedback on these. After that, we’ll be taking the draft standards out to all physiotherapists, educators, and relevant health professionals to make sure we get all your feedback.
As a profession, it’s important we all move forward together. Part of the Board’s responsibility is to make sure that happens through consultation. We see ourselves as one of the guardians of physiotherapy in Aotearoa New Zealand, not just as a regulator.
But how do these pieces fit together? That’s something we’re keen on all physios understanding as part of this consultation.
We like to think of it in terms of lifelong learning – for you, for us, and for our profession. That’s about making sure physiotherapists in New Zealand are always progressing, always informed by evidence-based practice, and applying the adage ‘trust but verify’. The core of our vision for practitioners and the profession as a whole is to foster excellence and to
make a difference. And the best way we can do this is together.
Our Educational Standard for Physiotherapy Practitioner Programmes in Aotearoa New Zealand (Accreditation) is the first step. This sets out the minimum requirements to be met by teaching institutions to deliver entry-level physiotherapy programmes that provide students with the knowledge, clinical skills and professional attributes to practice physiotherapy in New Zealand. We’ve just finished consultation on these and will be rolling them out once the feedback has been considered and the standards finalised.
We’ve got the physiotherapy practice thresholds, which describe the threshold competence (standards)
requirements for initial and continuing registration. finally, and most importantly, we have the code of Ethics, which are reviewing jointly with PNZ, and the Board’s draft Standards. It’svitalthesedocumentsreflectyourprofession and your views, which is why your feedback is so important.
Everyone in physiotherapy has a serious stake in both the code of Ethics and the Standards. That’s why it’s so important that we hear from you as we develop them, and why we’re looking forward to talking with you about them soon.
Jon Warren MSC Physiotherapy Board Professional Advisor
www.physioboard.org.nz
The Annual Hawkes Bay Symposium
Dynamic Wellness Embracing the Four Pillars of Healthfor Allied Health Professionals
Join us for a jam-packed day in The Bay listening to a diverse range of speakers who will share their expertise in creating dynamic wellness for clients by embracing the Four Pillars of Health.
HAWKES BAY PHYSIOTHERAPY BRANCH presents
DATE: Saturday September 16th
VENUE: The Education Centre at Hastings Memorial Hospital, Canning Road, Hastings.
TIME: 8.30am – 5.30pm (9 CPD hours)
Key Note Speaker: Warren Bernard - “Psychology and the Body”
Warren works as a clinical psychologist in the cancer, renal and chronic pain service at the HBDHB.
More information about Warren is available on his website: www.wiseandshine.co.nz
Our topics throughout the day will include issues such as:
• Mental Health• Community Services• Chronic Pain• Pain Management.
Book now for the Early Bird Price (Book before August 20th)
$150Regular price
$175Closing date: Friday September 8thRegistrations available online through PNZ website.For further information contact [email protected]
The Annual Hawkes Bay Symposium
Dynamic Wellness Embracing the Four Pillars of Healthfor Allied Health Professionals
Join us for a jam-packed day in The Bay listening to a diverse range of speakers who will share their expertise in creating dynamic wellness for clients by embracing the Four Pillars of Health.
HAWKES BAY PHYSIOTHERAPY BRANCH presents
DATE: Saturday September 16th
VENUE: The Education Centre at Hastings Memorial Hospital, Canning Road, Hastings.
TIME: 8.30am – 5.30pm (9 CPD hours)
Key Note Speaker: Warren Bernard - “Psychology and the Body”
Warren works as a clinical psychologist in the cancer, renal and chronic pain service at the HBDHB.
More information about Warren is available on his website: www.wiseandshine.co.nz
Our topics throughout the day will include issues such as:
• Mental Health• Community Services• Chronic Pain• Pain Management.
Book now for the Early Bird Price (Book before August 20th)
$150Regular price
$175Closing date: Friday September 8thRegistrations available online through PNZ website.For further information contact [email protected]

cASE STudY
20 | PHYSIO MATTERS MAY 2017
Case Study: Achilles tendinopathy and rehab isometrics
As part of the Australian college of Physiotherapists specialisation process, candidates must undertake a case study. Here, vassilia (Lia) Giovanovits, Australian Physiotherapy Association (APA) Sports Physiotherapist, explores the use of isometrics in the rehabilitation of a runner with chronic insertional Achilles tendinopathy.
Achilles tendinopathy, especially those involving the insertion of the tendon, are a common and poorly understood pathology without a clear and preferred treatment pathway. Evidence is now emerging that isometric exercises (IE) may be effective in the management of tendinopathies but further research is needed.
Tendinopathy is described as tendon pain (Rio et al 2015) which commonly presents with deficits in strength, endurance and plyometric ability (Silbernagel & crossley 2015) limiting participation in activities of daily living and sport (carcia et al 2010). The cumulative incidence of Achilles tendinopathy (AT) in runners is high, with 42 per cent of runners diagnosed with Achilles pathology or rupture during their lifetime (Kujala et al 2005). The pathogenesis of tendinopathy appears to be related to an unaccustomed increase in tensile and or compressive load (cook & Purdam 2012) but the exact mechanism is unknown. changes in cellularity and collagen disruption are observed in pathological tendons but improvements in symptoms do not appear to be related to changes in tendon structure (Drew et al 2014), nevertheless understanding tendon pathology may provide indirect support for management approaches.
Pathophysiology
Proximal to the insertion, the Achilles tendon transitions into fibrocartilage from the deep to the superficial aspect, creating two layers of fibrocartilage.
Duringdorsiflexiontheselayersoffibrocartilage, tendon and bursa are compressed against each other and the underlying bone (Benjamin et al 2006). compression of the tendon or transitional zone may cause a reduction in bound water, triggering the synthesis of large water binding proteoglycans (cook & Purdam et al 2012). If the compressive load continues or time for recovery is inadequate, disruption of the collagen matrix can occur (cook & Purdam et al 2009).
The exact mechanism behind tendon pain is unknown but changes in local tendon signalling, altered central modulation of pain and non-nociceptive mechanisms have all been proposed as potential mechanisms (Rio et al 2014).
Management
The conservative management of mid-substance tendinopathies has received a significant amount of attention in the literature but research for insertional Achilles tendinopathy (IAT) is less extensive (Wiegerinck et al 2013). Lower success rates reported for IAT (Alfredson & cook 2007) compared to the mid portion, may be related to increased compressive loads at the insertion (Benjamin et al 2006).
current trends in management focus on improving load tolerance of the tendon by load modification and then graded exposure (Malliaras et al 2015).
History
A 35-year-old recreational runner (KA) presented with a four-month history
of bilateral Achilles pain and stiffness which started two to three days after competing in a 30km trail run.
After developing pain, KA had three weeks off running then gradually reintroduced his training.
Symptoms in the left Achilles had reduced but overall pain levels in the right Achilles were gradually increasing, KA now experienced onset of symptoms with walking and increased morning pain and stiffness (5–6/10 visual analogue scale (vAS)). If KAremainedontheflatandlimitedhisruns to 45–60 minutes, he could run with minimal symptoms, however, KA regularly completed trail runs causing an increase in symptoms after cessation of activity.
Preceding the development of Achilles pain, KA had been running four to five times per week and approximately 70 km per week predominantly on trails. The only modification since the development of pain was a reduction in the long run. KA had been attending the gym two times per week, focusing on core exercises, hamstring, quadriceps and gluteal strengthening.
KA had been gradually changing his technique from a heel strike towards a forefoot pattern in an attempt to improve performance, and had been running in that style for the past 12 months.
The main goal for KA was to be able to participate in the 19km Triple Top Mountain run in Tasmania, in four months.
PHYSIO MATTERS MAY 2017 | 21
Examination
KA presented with localised pain in the region of the right Achilles insertion during a single leg calf raise and immediate pain when standing on an incline. Both Achilles were thickened and tender on palpation at the insertion.
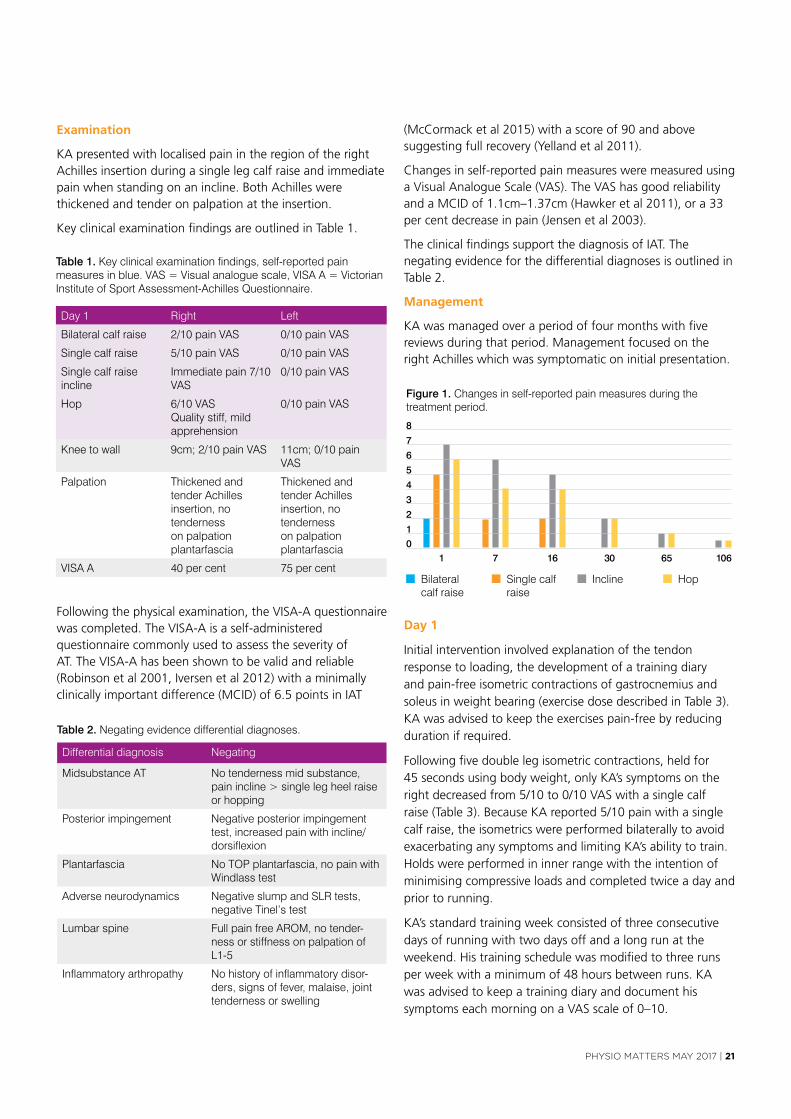
Key clinical examination findings are outlined in Table 1.
(Mccormack et al 2015) with a score of 90 and above suggesting full recovery (Yelland et al 2011).
changes in self-reported pain measures were measured using a visual Analogue Scale (vAS). The vAS has good reliability and a McID of 1.1cm–1.37cm (Hawker et al 2011), or a 33 per cent decrease in pain (Jensen et al 2003).
The clinical findings support the diagnosis of IAT. The negating evidence for the differential diagnoses is outlined in Table 2.
Management
KA was managed over a period of four months with five reviews during that period. Management focused on the right Achilles which was symptomatic on initial presentation.
following the physical examination, the vISA-A questionnaire was completed. The vISA-A is a self-administered questionnaire commonly used to assess the severity of AT. The vISA-A has been shown to be valid and reliable (Robinson et al 2001, Iversen et al 2012) with a minimally clinically important difference (McID) of 6.5 points in IAT
Day 1
Initial intervention involved explanation of the tendon response to loading, the development of a training diary and pain-free isometric contractions of gastrocnemius and soleus in weight bearing (exercise dose described in Table 3). KA was advised to keep the exercises pain-free by reducing duration if required.
following five double leg isometric contractions, held for 45 seconds using body weight, only KA’s symptoms on the right decreased from 5/10 to 0/10 vAS with a single calf raise (Table 3). Because KA reported 5/10 pain with a single calf raise, the isometrics were performed bilaterally to avoid exacerbating any symptoms and limiting KA’s ability to train. Holds were performed in inner range with the intention of minimising compressive loads and completed twice a day and prior to running.
KA’s standard training week consisted of three consecutive days of running with two days off and a long run at the weekend. His training schedule was modified to three runs per week with a minimum of 48 hours between runs. KA was advised to keep a training diary and document his symptoms each morning on a vAS scale of 0–10.
CASE STUDY
80 physiotherapy.asn.au
development of pain was a reduction in the long run. KA had been
attending the gym two times per week, focusing on core exercises,
hamstring, quadriceps and gluteal strengthening.
KA had been gradually changing his technique from a heel strike
towards a forefoot pattern in an attempt to improve performance,
and had been running in that style for the past 12 months.
The main goal for KA was to be able to participate in the 19km
Triple Top Mountain run in Tasmania, in four months.
Examination
KA presented with localised pain in the region of the right Achilles
insertion during a single leg calf raise and immediate pain when
standing on an incline. Both Achilles were thickened and tender on
palpation at the insertion.
Key clinical examination findings are outlined in Table 1.
Following the physical examination, the VISA-A questionnaire
was completed. The VISA-A is a self-administered questionnaire
commonly used to assess the severity of AT. The VISA-A has been
shown to be valid and reliable (Robinson et al 2001, Iversen et al
2012) with a minimally clinically important difference (MCID) of 6.5
points in IAT (McCormack et al 2015) with a score of 90 and above
suggesting full recovery (Yelland et al 2011).
Changes in self-reported pain measures were measured using
a Visual Analogue Scale (VAS). The VAS has good reliability and
a MCID of 1.1cm–1.37cm (Hawker et al 2011), or a 33 per cent
decrease in pain (Jensen et al 2003).
The clinical findings support the diagnosis of IAT. The negating
evidence for the differential diagnoses is outlined in Table 2.
Table 1. Key clinical examination findings, self-reported pain measures in blue. VAS = Visual analogue scale, VISA A = Victorian Institute of Sport Assessment-Achilles Questionnaire.
Day 1 Right Left
Bilateral calf raise 2/10 pain VAS 0/10 pain VAS
Single calf raise 5/10 pain VAS 0/10 pain VAS
Single calf raise incline
Immediate pain 7/10 VAS
0/10 pain VAS
Hop 6/10 VAS Quality stiff, mild apprehension
0/10 pain VAS
Knee to wall 9cm; 2/10 pain VAS 11cm; 0/10 pain VAS
Palpation Thickened and tender Achilles insertion, no tenderness on palpation plantarfascia
Thickened and tender Achilles insertion, no tenderness on palpation plantarfascia
VISA A 40 per cent 75 per cent
Management
KA was managed over a period of four months with five reviews
during that period. Management focused on the right Achilles which
was symptomatic on initial presentation.
Day 1
Initial intervention involved explanation of the tendon response to
loading, the development of a training diary and pain-free isometric
contractions of gastrocnemius and soleus in weight bearing
(exercise dose described in Table 3). KA was advised to keep the
exercises pain-free by reducing duration if required.
Following five double leg isometric contractions, held for 45
seconds using body weight, only KA’s symptoms on the right
decreased from 5/10 to 0/10 VAS with a single calf raise (Table
3). Because KA reported 5/10 pain with a single calf raise, the
isometrics were performed bilaterally to avoid exacerbating any
symptoms and limiting KA’s ability to train. Holds were performed in
inner range with the intention of minimising compressive loads and
completed twice a day and prior to running.
Differential diagnosis Negating
Midsubstance AT No tenderness mid substance, pain incline > single leg heel raise or hopping
Posterior impingement Negative posterior impingement test, increased pain with incline/dorsiflexion
Plantarfascia No TOP plantarfascia, no pain with Windlass test
Adverse neurodynamics Negative slump and SLR tests, negative Tinel’s test
Lumbar spine Full pain free AROM, no tender-ness or stiffness on palpation of L1-5
Inflammatory arthropathy No history of inflammatory disor-ders, signs of fever, malaise, joint tenderness or swelling
Table 2. Negating evidence differential diagnoses.
CASE STUDY
80 physiotherapy.asn.au
development of pain was a reduction in the long run. KA had been
attending the gym two times per week, focusing on core exercises,
hamstring, quadriceps and gluteal strengthening.
KA had been gradually changing his technique from a heel strike
towards a forefoot pattern in an attempt to improve performance,
and had been running in that style for the past 12 months.
The main goal for KA was to be able to participate in the 19km
Triple Top Mountain run in Tasmania, in four months.
Examination
KA presented with localised pain in the region of the right Achilles
insertion during a single leg calf raise and immediate pain when
standing on an incline. Both Achilles were thickened and tender on
palpation at the insertion.
Key clinical examination findings are outlined in Table 1.
Following the physical examination, the VISA-A questionnaire
was completed. The VISA-A is a self-administered questionnaire
commonly used to assess the severity of AT. The VISA-A has been
shown to be valid and reliable (Robinson et al 2001, Iversen et al
2012) with a minimally clinically important difference (MCID) of 6.5
points in IAT (McCormack et al 2015) with a score of 90 and above
suggesting full recovery (Yelland et al 2011).
Changes in self-reported pain measures were measured using
a Visual Analogue Scale (VAS). The VAS has good reliability and
a MCID of 1.1cm–1.37cm (Hawker et al 2011), or a 33 per cent
decrease in pain (Jensen et al 2003).
The clinical findings support the diagnosis of IAT. The negating
evidence for the differential diagnoses is outlined in Table 2.
Table 1. Key clinical examination findings, self-reported pain measures in blue. VAS = Visual analogue scale, VISA A = Victorian Institute of Sport Assessment-Achilles Questionnaire.
Day 1 Right Left
Bilateral calf raise 2/10 pain VAS 0/10 pain VAS
Single calf raise 5/10 pain VAS 0/10 pain VAS
Single calf raise incline
Immediate pain 7/10 VAS
0/10 pain VAS
Hop 6/10 VAS Quality stiff, mild apprehension
0/10 pain VAS
Knee to wall 9cm; 2/10 pain VAS 11cm; 0/10 pain VAS
Palpation Thickened and tender Achilles insertion, no tenderness on palpation plantarfascia
Thickened and tender Achilles insertion, no tenderness on palpation plantarfascia
VISA A 40 per cent 75 per cent
Management
KA was managed over a period of four months with five reviews
during that period. Management focused on the right Achilles which
was symptomatic on initial presentation.
Day 1
Initial intervention involved explanation of the tendon response to
loading, the development of a training diary and pain-free isometric
contractions of gastrocnemius and soleus in weight bearing
(exercise dose described in Table 3). KA was advised to keep the
exercises pain-free by reducing duration if required.
Following five double leg isometric contractions, held for 45
seconds using body weight, only KA’s symptoms on the right
decreased from 5/10 to 0/10 VAS with a single calf raise (Table
3). Because KA reported 5/10 pain with a single calf raise, the
isometrics were performed bilaterally to avoid exacerbating any
symptoms and limiting KA’s ability to train. Holds were performed in
inner range with the intention of minimising compressive loads and
completed twice a day and prior to running.
Differential diagnosis Negating
Midsubstance AT No tenderness mid substance, pain incline > single leg heel raise or hopping
Posterior impingement Negative posterior impingement test, increased pain with incline/dorsiflexion
Plantarfascia No TOP plantarfascia, no pain with Windlass test
Adverse neurodynamics Negative slump and SLR tests, negative Tinel’s test
Lumbar spine Full pain free AROM, no tender-ness or stiffness on palpation of L1-5
Inflammatory arthropathy No history of inflammatory disor-ders, signs of fever, malaise, joint tenderness or swelling
Table 2. Negating evidence differential diagnoses.
CASE STUDY
September 2016 81
KA’s standard training week consisted of three consecutive days of
running with two days off and a long run at the weekend. His training
schedule was modified to three runs per week with a minimum of
48 hours between runs. KA was advised to keep a training diary and
document his symptoms each morning on a VAS scale of 0–10.
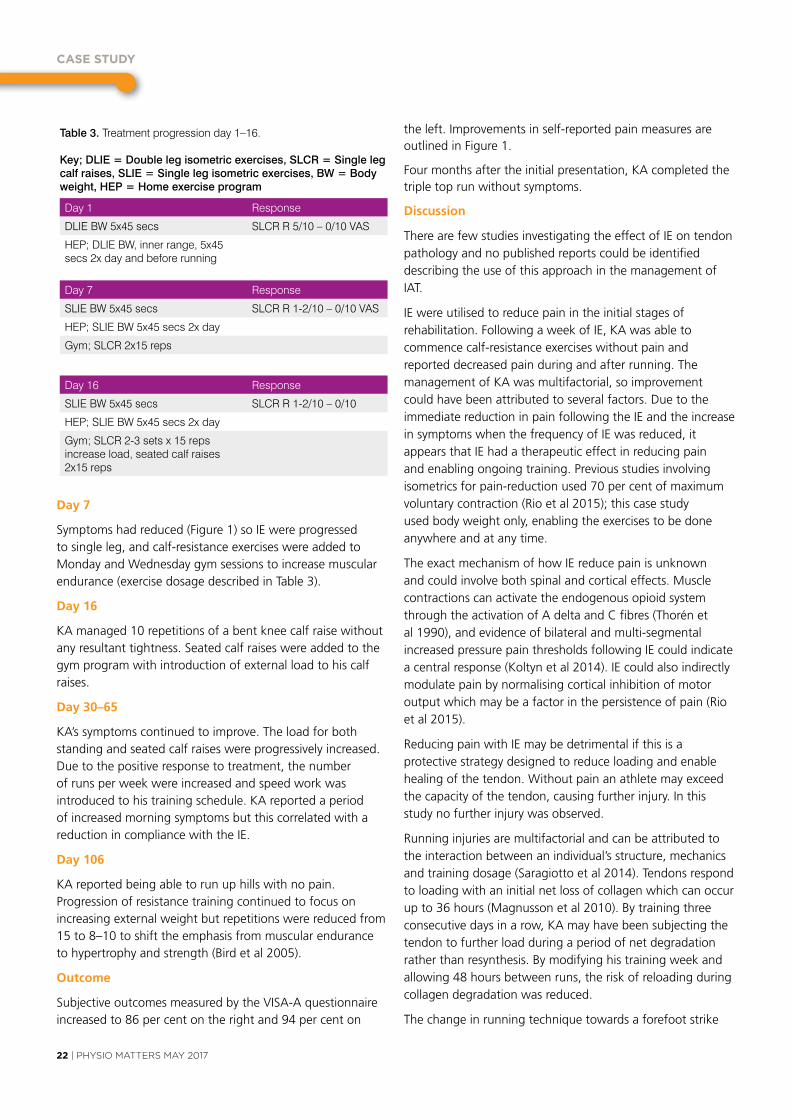
Day 7
Symptoms had reduced (Figure 1) so IE were progressed to
single leg, and calf-resistance exercises were added to Monday
and Wednesday gym sessions to increase muscular endurance
(exercise dosage described in Table 3).
Day 1 Response
DLIE BW 5x45 secs SLCR R 5/10 – 0/10 VAS
HEP; DLIE BW, inner range, 5x45 secs 2x day and before running
Day 7 Response
SLIE BW 5x45 secs SLCR R 1-2/10 – 0/10 VAS
HEP; SLIE BW 5x45 secs 2x day
Gym; SLCR 2x15 reps
Day 16 Response
SLIE BW 5x45 secs SLCR R 1-2/10 – 0/10
HEP; SLIE BW 5x45 secs 2x day
Gym; SLCR 2-3 sets x 15 reps increase load, seated calf raises 2x15 reps
Table 3. Treatment progression day 1–16.
Key; DLIE = Double leg isometric exercises, SLCR = Single leg calf raises, SLIE = Single leg isometric exercises, BW = Body weight, HEP = Home exercise program
1 7 16 30 65 10601
2
3
4
5
6
7
8
Figure 1. Changes in self-reported pain measures during the treatment period.
Bilateral calf raise
Single calf raise
Incline Hop
Day 16
KA managed 10 repetitions of a bent knee calf raise without any
resultant tightness. Seated calf raises were added to the gym
program with introduction of external load to his calf raises.
Day 30–65
KA’s symptoms continued to improve. The load for both standing
and seated calf raises were progressively increased. Due to the
positive response to treatment, the number of runs per week were
increased and speed work was introduced to his training schedule.
KA reported a period of increased morning symptoms but this
correlated with a reduction in compliance with the IE.
Day 106
KA reported being able to run up hills with no pain. Progression of
resistance training continued to focus on increasing external weight but
repetitions were reduced from 15 to 8–10 to shift the emphasis from
muscular endurance to hypertrophy and strength (Bird et al 2005).
Outcome
Subjective outcomes measured by the VISA-A questionnaire
increased to 86 per cent on the right and 94 per cent on the left.
Improvements in self-reported pain measures are outlined in Figure 1.
Four months after the initial presentation, KA completed the triple
top run without symptoms.
Discussion
There are few studies investigating the effect of IE on tendon
pathology and no published reports could be identified describing
the use of this approach in the management of IAT.
IE were utilised to reduce pain in the initial stages of rehabilitation.
Following a week of IE, KA was able to commence calf-resistance
exercises without pain and reported decreased pain during and
after running. The management of KA was multifactorial, so
improvement could have been attributed to several factors. Due to
the immediate reduction in pain following the IE and the increase in
symptoms when the frequency of IE was reduced, it appears that
IE had a therapeutic effect in reducing pain and enabling ongoing
training. Previous studies involving isometrics for pain-reduction
used 70 per cent of maximum voluntary contraction (Rio et al 2015);
this case study used body weight only, enabling the exercises to be
done anywhere and at any time.
The exact mechanism of how IE reduce pain is unknown and could
involve both spinal and cortical effects. Muscle contractions can
cASE STudY
22 | PHYSIO MATTERS MAY 2017
Day 7
Symptoms had reduced (figure 1) so IE were progressed to single leg, and calf-resistance exercises were added to Monday and Wednesday gym sessions to increase muscular endurance (exercise dosage described in Table 3).
Day 16
KA managed 10 repetitions of a bent knee calf raise without any resultant tightness. Seated calf raises were added to the gym program with introduction of external load to his calf raises.
Day 30–65
KA’s symptoms continued to improve. The load for both standing and seated calf raises were progressively increased. Due to the positive response to treatment, the number of runs per week were increased and speed work was introduced to his training schedule. KA reported a period of increased morning symptoms but this correlated with a reduction in compliance with the IE.
Day 106
KA reported being able to run up hills with no pain. Progression of resistance training continued to focus on increasing external weight but repetitions were reduced from 15 to 8–10 to shift the emphasis from muscular endurance to hypertrophy and strength (Bird et al 2005).
Outcome
Subjective outcomes measured by the vISA-A questionnaire increased to 86 per cent on the right and 94 per cent on
the left. Improvements in self-reported pain measures are outlined in figure 1.
four months after the initial presentation, KA completed the triple top run without symptoms.
Discussion
There are few studies investigating the effect of IE on tendon pathology and no published reports could be identified describing the use of this approach in the management of IAT.
IE were utilised to reduce pain in the initial stages of rehabilitation. following a week of IE, KA was able to commence calf-resistance exercises without pain and reported decreased pain during and after running. The management of KA was multifactorial, so improvement could have been attributed to several factors. Due to the immediate reduction in pain following the IE and the increase in symptoms when the frequency of IE was reduced, it appears that IE had a therapeutic effect in reducing pain and enabling ongoing training. Previous studies involving isometrics for pain-reduction used 70 per cent of maximum voluntary contraction (Rio et al 2015); this case study used body weight only, enabling the exercises to be done anywhere and at any time.
The exact mechanism of how IE reduce pain is unknown and could involve both spinal and cortical effects. Muscle contractions can activate the endogenous opioid system through the activation of A delta and c fibres (Thorén et al 1990), and evidence of bilateral and multi-segmental increased pressure pain thresholds following IE could indicate a central response (Koltyn et al 2014). IE could also indirectly modulate pain by normalising cortical inhibition of motor output which may be a factor in the persistence of pain (Rio et al 2015).
Reducing pain with IE may be detrimental if this is a protective strategy designed to reduce loading and enable healing of the tendon. Without pain an athlete may exceed the capacity of the tendon, causing further injury. In this study no further injury was observed.
Running injuries are multifactorial and can be attributed to the interaction between an individual’s structure, mechanics and training dosage (Saragiotto et al 2014). Tendons respond to loading with an initial net loss of collagen which can occur up to 36 hours (Magnusson et al 2010). By training three consecutive days in a row, KA may have been subjecting the tendon to further load during a period of net degradation rather than resynthesis. By modifying his training week and allowing 48 hours between runs, the risk of reloading during collagen degradation was reduced.
The change in running technique towards a forefoot strike
CASE STUDY
September 2016 81
KA’s standard training week consisted of three consecutive days of
running with two days off and a long run at the weekend. His training
schedule was modified to three runs per week with a minimum of
48 hours between runs. KA was advised to keep a training diary and
document his symptoms each morning on a VAS scale of 0–10.
Day 7
Symptoms had reduced (Figure 1) so IE were progressed to
single leg, and calf-resistance exercises were added to Monday
and Wednesday gym sessions to increase muscular endurance
(exercise dosage described in Table 3).
Day 1 Response
DLIE BW 5x45 secs SLCR R 5/10 – 0/10 VAS
HEP; DLIE BW, inner range, 5x45 secs 2x day and before running
Day 7 Response
SLIE BW 5x45 secs SLCR R 1-2/10 – 0/10 VAS
HEP; SLIE BW 5x45 secs 2x day
Gym; SLCR 2x15 reps
Day 16 Response
SLIE BW 5x45 secs SLCR R 1-2/10 – 0/10
HEP; SLIE BW 5x45 secs 2x day
Gym; SLCR 2-3 sets x 15 reps increase load, seated calf raises 2x15 reps
Table 3. Treatment progression day 1–16.
Key; DLIE = Double leg isometric exercises, SLCR = Single leg calf raises, SLIE = Single leg isometric exercises, BW = Body weight, HEP = Home exercise program
1 7 16 30 65 10601
2
3
4
5
6
7
8
Figure 1. Changes in self-reported pain measures during the treatment period.
Bilateral calf raise
Single calf raise
Incline Hop
Day 16
KA managed 10 repetitions of a bent knee calf raise without any
resultant tightness. Seated calf raises were added to the gym
program with introduction of external load to his calf raises.
Day 30–65
KA’s symptoms continued to improve. The load for both standing
and seated calf raises were progressively increased. Due to the
positive response to treatment, the number of runs per week were
increased and speed work was introduced to his training schedule.
KA reported a period of increased morning symptoms but this
correlated with a reduction in compliance with the IE.
Day 106
KA reported being able to run up hills with no pain. Progression of
resistance training continued to focus on increasing external weight but
repetitions were reduced from 15 to 8–10 to shift the emphasis from
muscular endurance to hypertrophy and strength (Bird et al 2005).
Outcome
Subjective outcomes measured by the VISA-A questionnaire
increased to 86 per cent on the right and 94 per cent on the left.
Improvements in self-reported pain measures are outlined in Figure 1.
Four months after the initial presentation, KA completed the triple
top run without symptoms.
Discussion
There are few studies investigating the effect of IE on tendon
pathology and no published reports could be identified describing
the use of this approach in the management of IAT.
IE were utilised to reduce pain in the initial stages of rehabilitation.
Following a week of IE, KA was able to commence calf-resistance
exercises without pain and reported decreased pain during and
after running. The management of KA was multifactorial, so
improvement could have been attributed to several factors. Due to
the immediate reduction in pain following the IE and the increase in
symptoms when the frequency of IE was reduced, it appears that
IE had a therapeutic effect in reducing pain and enabling ongoing
training. Previous studies involving isometrics for pain-reduction
used 70 per cent of maximum voluntary contraction (Rio et al 2015);
this case study used body weight only, enabling the exercises to be
done anywhere and at any time.
The exact mechanism of how IE reduce pain is unknown and could
involve both spinal and cortical effects. Muscle contractions can
PHYSIO MATTERS MAY 2017 | 23
pattern may have contributed to the development of symptoms by increasing calf activity and possibly Achilles load (Kulmala et al 2013). KA had been running with this gait pattern for eight months before the development of symptoms, so modification of training load and strengthening were addressed first before considering changes in technique. Due to the reduction in symptoms following load modification and strengthening, gait mechanics were not addressed in this study.
various strengthening programs have been reported in the literature but there is no consensus on the optimum loading protocol for tendons. Due to time constraints and practicality for KA, the resistance component of the rehabilitation program consisted of gym sessions two to three times a week, similar to the Heavy Slow Resistance program. Plyometrics were not included as KA was already running, and progression of tendon loading and capacity to tolerate the stretch shortening cycle had been achieved through the addition of hills and interval training.
While further research is needed to compare a combined program of IE and resistance exercises with resistance
only in the management of IAT and other tendons, this case demonstrates that when IE are combined with other resistance exercises and load management, pain-reduction and good functional outcomes can be achieved.
Lia is an APA Sports Physiotherapist and is undertaking the Australian college of Physiotherapists specialisation program. Lia currently works in private practice and is part of the medical network for the Tasmanian Institute of Sport. She has worked for the Australian rowing team, the canadian women’s rowing team, the Australian para-cycling team and volunteered at the London Olympics.
Making Education Easy
Sports MedicineResearch Review
www.researchreview.co.nz
1
a publication
In this issue: Aetiology of sudden death in
sports in the UK
Secondary injury risk in young athletes after ACL reconstruction
Workloads for predicting injury in elite rugby league players
Higher BMI associated with plantar fasciopathy
Injection therapies for tennis elbow
Factors predicting poor patellofemoral pain outcomes
Physical therapy for subacromial pain
Climbing improves low back pain
FAI syndrome: Warwick Agreement
Validity of consumer physical activity monitors
Welcome to the twentieth issue of Sports Medicine Research Review.This issue begins with an interesting read on causes and precipitating factors of sudden cardiac death among athletes, highlighting the need for preventive strategies. There are several meta-analyses included in this issue, covering risk factors for reinjury post-ACL reconstruction, the association between BMI and plantar fasciopathy, injection treatments for lateral epicondylalgia (‘tennis elbow’) and physical therapies for subacromial pain syndrome. This issue concludes with an evaluation of consumer-based physical activity monitors (e.g. ‘Fitbits’, etc) suggesting cautious use for estimating energy expenditure, despite accurate measurements of steps during structured ambulatory activities.
Your feedback and suggestions help us in our selection of studies that we hope you will find helpful and informative, so please keep them coming.
Kind regards
Dr James McGarvey Dr Stuart Armstrong [email protected] [email protected]
Etiology of sudden death in sports: insights from a United Kingdom regional registryAuthors: Finocchiaro G et al.Summary: Between 1994 and 2014, 357 consecutive cases of athletes who died suddenly and unexpectedly in the UK underwent post mortem including evaluation by an expert cardiac pathologist. Clinical information was obtained from referring coroners. The mean age was 29 years, and 92% were males. Sixty-one percent died during intense exertion. A wide range of team and individual sports were represented, the most common being running (25%) and football (25%). Eighty-one percent were asymptomatic leading into the event. Eight percent had palpitations, 6% chest pain, 5% syncope and 1% decreased exercise tolerance. Eight percent had a history of premature sudden death in a first-degree relative. At post mortem, 42% had a normal examination of the heart, indicating sudden arrhythmic death syndrome. Myocardial disease was seen in 35% of cases including most commonly LV hypertrophy or fibrosis (16%), arrhythmogenic RV cardiomyopathy (13%) and hypertrophic cardiomyopathy (6%). Coronary artery anomalies were found in 5%. There were notable trends when evaluated by age. Fifty-six percent of those under the age of 18 years had a structurally normal heart compared with only 26% of those aged over 35 years. Diseases of the myocardium such as LV hypertrophy or arrhythmogenic RV cardiomyopathy were much more common over the age of 35 years and rare under the age of 18 years. However, coronary artery anomalies caused 11% of deaths under age 18 years compared with only 2% of those aged over 35 years. Patients who died at rest were more likely to have sudden arrhythmic death syndrome, e.g. a structurally normal heart. Those who died during exertion were more likely to have arrhythmogenic RV cardiomyopathy, LV fibrosis or coronary artery abnormalities.
Comment (JM): This is an interesting insight into the rare event of sudden cardiac death in young sports people. This study has implications for the high-profile issue of cardiac screening for athletes. The age-related breakdown showed that those aged under 18 years are more likely to have a structurally normal heart but run into trouble due to a primary arrhythmia syndrome. Screening for this age group in particular needs to therefore include an ECG. This is true for all ages given that >80% of athletes died suddenly without warning symptoms. Older individuals more often have structural changes, and echocardiography will statistically become increasingly useful. The authors note, however, that when screening the families of victims of sudden cardiac death with autopsy findings consistent with idiopathic LV hypertrophy, primary arrhythmia syndromes were found in 6 of 13 (46%) and probable hypertrophic cardiomyopathy in only one family. Therefore a finding of hypertrophic cardiomyopathy may be a red herring and should not exclude the possibility that an underlying arrhythmia syndrome is the actual issue. In general, hypertrophic cardiomyopathy was seen to be less of an issue in this series than in others previously published. Athletes with arrhythmogenic RV cardiomyopathy were 6 times more likely to die on exertion compared with those with other cardiac pathologies, reinforcing the current advice for exercise restriction in these patients. In many cases immediate availability of an AED (automated external defibrillator) could be potentially life-saving, so these need to continue to be made more available.
Reference: J Am Coll Cardiol 2016;67(18):2108–15Abstract
Issue 20 – 2016
Abbreviations used in this issueACL = anterior cruciate ligamentBMI = body mass indexFAI = femoroacetabular impingementL/RV = left/right ventricularOA = osteoarthritisVAS = visual analogue scale
Rehabilitation Counsellors are tertiary qualified allied health professionals who work with individuals with disability, injury or social disadvantage, along with their families, organisations and other health professionals, to deliver work, life and career solutions. The core skills and expertise of Rehabilitation Counsellors include: vocational assessment, job placement support, and career development; rehabilitation and return-to-work services; workplace disability prevention and management.
Kindly supported by
RESEARCH REVIEW
YEARS
MAKING EDUCATION EASYSINCE 2006
RACP MyCPD Program participants can claim one credit per hour (maximum of 50 credits per year) for reading and evaluating Research Reviews.
CLICK HEREFOR MORE INFORMATION
We offer over 50 different Reviews in various clinical areas. Subscription costs nothing – go to www.researchreview.co.nz
SUBSCRIBE
FREEto Rehabilitation Research Review
and Sports Medicine Research Review
Keeping up to date with rehabilitation and sports medicine research couldn’t be easier.
Regular emails to your inbox 4 pages, 10 studies and what they mean for NZ practice according to NZ experts.
Send an email to [email protected] and we will do the rest
Reprinted with permission from the Australian Physiotherapy Association. This case study appeared in the September 2016 issue of InMotion. All references available on request.
Do you have any case studies you’d like to share with Physio Matters? Please send them to the Editor at [email protected].

OF SPEcIAl InTEREST
24 |PHYSIO MATTERS MAY 2017
NZ Football: Fit4Football aims to reduce player injuries
The “old school” casual pre-game jog has been given the red card by New Zealand football and Acc who have teamed up to launch a revolutionary new warm-up programme aimed at tackling the growing frequency and cost of injuries to players.
New Zealand football’s fit4football initiative has been developed as a complete guide to match preparation, performance enhancement and injury prevention for players of all ages and level of competition.
In 2016, New Zealand football created an Injury Prevention Specialists team who work on the guiding principle of enhancing performance through prevention.
fit4football is the overall enhancing performance and injury prevention programme of which the 11+ warm ups are one component of this programme.
NZf National Injury Prevention Manager Megan crockett says the primary goal of fit4football is to address the increasing rate of football-related injuries.
“The number of injuries and the subsequent costs are increasing year-on-year,” said crockett. “The latest Acc figures show there are now more than 48,000 football-related injuries each year, costing the country $36 million annually.”
According to crockett, there are also significant social costs – which include time away from work, time away from sporting groups and social activity, playing with your children, and there is also evidence to show that the academic performance of students side-lined from sport through injury can also suffer when they are isolated.
“The highest injury rate is now in the 15-19 age group,” shesays.“Thatreflectsgrowingplayernumbersbutalsohighlights that we’re not preparing young players as well as we need to. After all, these youngsters are the ones that we want playing, performing and aiming to be our future All Whites and football ferns.”
fit4football’s 11+ warm-up component incorporates fIfA’s 11+ programme, a 20-minute training and match-preparation routine used by many of the top clubs and national teams that has reduced acute injuries by up to 50 percent, and non-acute injuries by up to 30 percent.

PHYSIO MATTERS MAY 2017 | 25
It involves slow to increasing speed running, active dynamic stretching and controlled partner contacts, with exercises developed to improve core and leg strength and balance.
“It’s a fundamental shift in the way we develop our youth to be good functional movers able to withstand the physical demands of football,” adds
crockett. “Old warm-up and cool-down techniques like the jog and static stretch have long been known to be ineffective, but they’re still part of most players’ pre- and post-game routines.
“fit4football changes that mind-set and can benefit players of all ages and ability social to competitive, but our focus is on younger players especially,
to help them develop new and far more effective routines and habits.”
NZ football and Acc have partnered to build a national injury prevention and performance enhancing team, located around New Zealand in the seven federations.
croker says she encourages anyone involved in football, be they players, coaches, referees or team managers, to get along to a roadshow near them to learn about how fit4football can significantly reduce the risk of injury.
“We want more people loving and playing football to the best of their ability, injury-free, for life. It’s about performing on the park, not sitting on the side-lines injured.”
for more information on the fit4football programme visit: www.fit4football.co.nz
• Become a certified APPI Pilates Instructor in 2017• Therapeutic Yoga Training for Health Professionals • Full Matwork Certification Series Available• Online CPD Courses
2017 COURSE DATES Clinical Pilates Training
Book Online / unitehealth.com.au / [email protected] / +61 3 9525 0080
AUCKLANDAPPI Matwork CertificationAPPI Matwork Level 2 9-10 SepAPPI Matwork Level 3 18-19 Nov
APPI Equipment APPI Equipment Level 1 17-18 Jun
CPD Pilates CoursesAPPI Pilates for Runners 21 Oct APPI Pilates for Cyclists 22 Oct
Therapeutic YogaTherapeutic Yoga Training Level 1 15-16 Jul

SIg
26 | PHYSIO MATTERS APRIL 2017
The Case for Acupuncture: Putting sham acupuncture to rest
As a physiotherapist and acupuncturist I’m fascinated by the ever increasing research into the effects of acupuncture. Physiologist Thomas Lundeberg illustrates brilliantly on the YouTube video ‘Physiology 2013 Session 1’ how acupuncture effects various anatomical levels.
Lundeberg describes adenosine being released peripherally resulting in the first stage of pain inhibition and vasodilation. Ergoreceptors in muscle tissue release cGRP triggering further vasodilation and potent trophic effects enhancing healing and repair. Acupuncture stimulation effects the spinal cord, limbic system and Pre frontal cortex (Pfc) (stimulation of Pfc can affect traits such as fear avoidance) resulting in further pain inhibition and either an increase or decrease in sympathetic activity depending on the strength and length of needling. fMRI and other research supports these findings.
However, every now and again an article is written slamming acupuncture as useless because sham acupuncture was shown to be as effective.
Two main styles of sham acupuncture are used in research to act as placebo. Both styles are based on modern chinese acupuncture needling methods, i.e. the needles are inserted into specific acupuncture points and stimulated (usually manually) until deqi (an achy deep sensation) is felt.
Sham acupuncture changes either the location of the needling or the depth of needling by inserting shallowly without causing deqi to be experienced. Often the Streitberger needle is used, which causes the patient to feel a prick. The needle then retracts into the shaft.
Stephen Birch (International Japanese acupuncture teacher and author of numerous books on Japanese acupuncture) claims sham acupuncture is based on an incorrect understanding of acupuncture.
Japanese acupuncture routinely uses shallow needling and does not consider deqi a necessary sensation to be felt for the treatment to be effective.
Because chinese needling is deeper, superficial acupuncture has been considered placebo. Stephen Birch believes that superficial acupuncture is not inert, and further claims that there are no sham acupuncture treatments that act as placebo.
Lundeberg supports sham acupuncture as an invalid form of placebo, claiming that pricking the skin produces afferent nerve activity which will affect the limbic touch response in the brain. In patients with chronic pain especially central sensitisation (cS), light pricking of the skin in the painful area or needling proximally or distally from the painful site can have effects equivalent to needling within the painful area. This results because cS is associated with enlarged receptive neuronal areas causing a greater area of distribution that pain is felt in.
Patients with chronic pain often show abnormalities in descending efferent pathways as well as plasticity changes
in the nervous system. This can cause widespreadinfluencesfromlightpricking of the skin or needling away from the painful area.
In patients with more nociceptive type pain, strong needling (when sham acupuncture elicits deqi) within the affected myotome or nearby myotomes can result in stimulation of the descending pathways to the target painful area.
Because of these reasons Lundeberg states that studies using sham acupuncture are scientifically unacceptable.
Dr Andrew vickers, PhD, conducted a systematic review to identify randomized controlled trials (RcTs) of acupuncture for chronic pain. A total of 29 eligible RcTs with a total of 17,922 patients were analysed for four chronic pain conditions: back and neck pain, osteoarthritis, chronic headache, and shoulder pain.
Dr vickers’s findings were that acupuncture has effects over and above those of sham acupuncture and superior to no acupuncture control for the treatment of chronic pain.
They further claim that because their patient data is of nearly 18,000 randomized patients in high quality RcTs, the case for using acupuncture referral with chronic pain is robust.
Written by Anne Macann
Be part of the APA national conference MOMENTUM 2017, happening in October.
Physiotherapists have always been innovators in health, pushing forward to deliver excellent patient outcomes. As the healthcare landscape becomes more competitive, it is important to keep moving with the changes on a national and global level.
Unite with the rest of the profession to hear from leaders in physiotherapy about the latest clinical research. Meet the people you need to know to help you grow in your profession and discover the newest innovations. Submit your abstract before 17 April.
I C C S Y D N E Y O C T O B E R 1 9 - 2 1
PHYSIOTHERAPY CONFERENCE2 0 1 7
M O M E N T U M
MOM17.24
Early bird registrations open 27 March. apamomentum2017.asn.au
Be part of the APA national conference MOMENTUM 2017, happening in October.
Physiotherapists have always been innovators in health, pushing forward to deliver excellent patient outcomes. As the healthcare landscape becomes more competitive, it is important to keep moving with the changes on a national and global level.
Unite with the rest of the profession to hear from leaders in physiotherapy about the latest clinical research. Meet the people you need to know to help you grow in your profession and discover the newest innovations. Submit your abstract before 17 April.
I C C S Y D N E Y O C T O B E R 1 9 - 2 1
PHYSIOTHERAPY CONFERENCE2 0 1 7
M O M E N T U M
MOM17.24
Early bird registrations open 27 March. apamomentum2017.asn.au
POdcASTS
28 | PHYSIO MATTERS MAY 2017
Podcasting and knowledge translation for physios
Nelson-based physiotherapist Mindy Silva tells Physio Matters how she discovered the world of podcasts and what prompted her to record her own.
I’m a paediatric physiotherapist in Nelson who recently learnt to podcast!
Instead of listening to music when I go for a run or do housework, I stick on headphones and listen to podcasts! constraint Induced Movement Therapy with Dr Taub on Brain Science, or Mindfulness with Dr Harris on the Radio New Zealand (RNZ) App – you can’t beat hearing it from the primary source. I have picked up amazing insights, all for free and without having to try and find extra time to fit it in.
It all started when I was trying to figure out if it was worth self-funding to attend a workshop in Auckland with Beverley cusick. I knew Beverly
was a leader in the management of equinis and inventor of TheraTogs, but I wanted a bit more of an inside scoop. To help me decide, I tried searching the internet for an interview or podcast she had done.
I couldn’t find anything from Beverley though, and I realised that although paediatric therapists are rock stars in my eyes, there’s not a lot of people standing in line to interview them. That’s when I decided to make my own podcast and interview Beverly for our Paediatric Special Interest Group.
It was an amazing opportunity to poke around inside the head of someone with incredible knowledge and
You can listen to Mindy’s podcast at www.wiredondevelopment.com
experience. from organizing the first Bobath course in America to how to run an international business whilst staying focused on being current with the latest research in biomechanics and kinesiology. She had so many nuggets of knowledge to capture and share, and a podcast was the perfect medium for that.
I highly recommend podcasts – and if you can’t find one on a subject you’re interested in, make your own. It’s the most fun you’ll have with knowledge translation.
If you haven’t subscribed or listened to podcasts yet, you should get on to it. Listening to podcasts is one of the easiest ways to learn and hear opinions and tips on how to assess and treat patients across a range of different areas. And the best thing is, you can listen in anytime, anywhere, on any device with a Wi-Fi connection.
Here’s five you might like to check out to get you started:
• StrengthPhysiotherapyPodcast–hostedbyChrisLendrum(iTunes)
A physiotherapist, strength coach and rehab specialist, Lendrum touches on everything from applied movement neurology through to running private practices.
• LiberatedBodyPodcast–hostedbyBrookeThomas(iTunes)
created for both patients and clinicians, this podcast contains interviews with a wide range of practitioners and focuses on “creating healthier, movement rich environments” for children – including a session discussing the importance of standing desks in classrooms.
• PainScienceandSensibility–hostedbySandyHiltonandCoryBlickenstaff(iTunes)
Based in the united States, physical therapists Sandy and cory focus on current research and topics of pain science. They focus on “making information meaningful to practice in the clinic”.
• Cash-BasedPodcast–hostedbyDrJarodCarter(drjarodcarter.com)
Drawing on his own experience in the field, Dr carter shares strategies to help physiotherapists start and run their own practices. Although coming from an American perspective, he does cover interesting topics including marketing, scaling and developing a niche.
• APAPodcastChannel–varioushosts(soundcloud)
for something a bit closer to home, you can check out the Australian Physiotherapy Association’s podcast channel and listen to pre-eminent physio research from Australia and around the world.
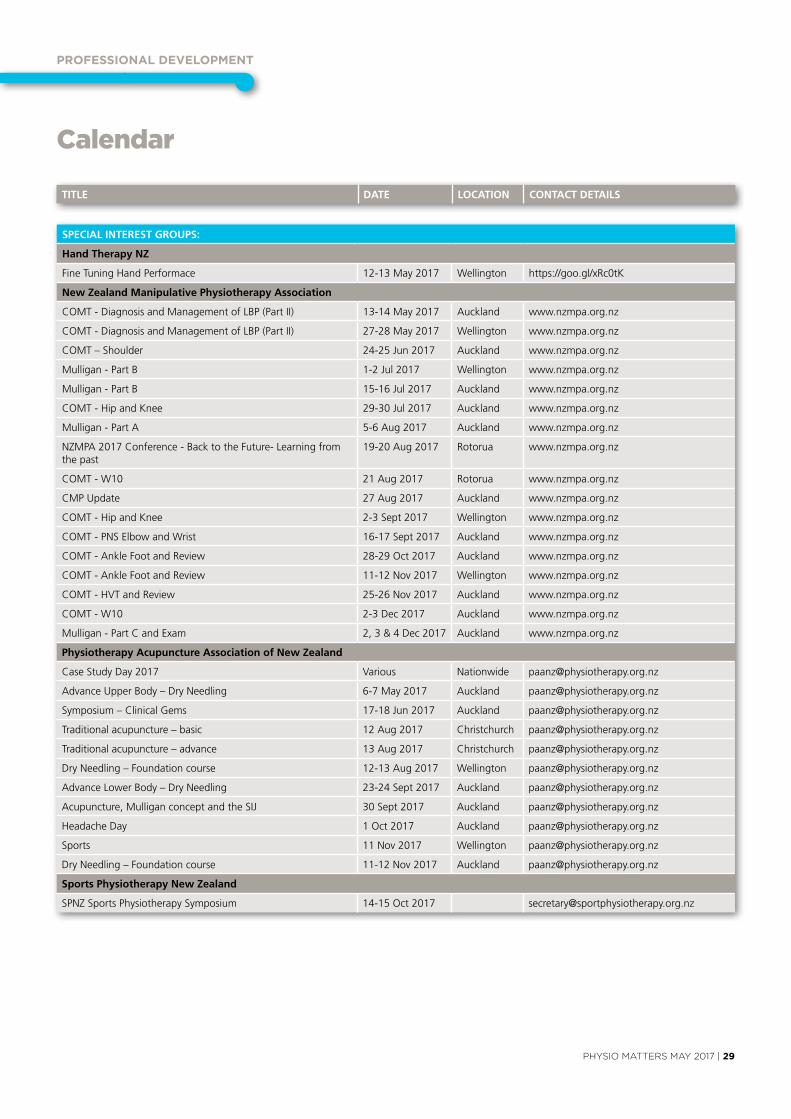
PROFESSIOnAl dEvElOPMEnT
PHYSIO MATTERS MAY 2017 | 29
Calendar
SPECIAL INTEREST GROUPS:
Hand Therapy NZ
fine Tuning Hand Performace 12-13 May 2017 Wellington https://goo.gl/xRc0tK
New Zealand Manipulative Physiotherapy Association
cOMT - Diagnosis and Management of LBP (Part II) 13-14 May 2017 Auckland www.nzmpa.org.nz
cOMT - Diagnosis and Management of LBP (Part II) 27-28 May 2017 Wellington www.nzmpa.org.nz
cOMT – Shoulder 24-25 Jun 2017 Auckland www.nzmpa.org.nz
Mulligan - Part B 1-2 Jul 2017 Wellington www.nzmpa.org.nz
Mulligan - Part B 15-16 Jul 2017 Auckland www.nzmpa.org.nz
cOMT - Hip and Knee 29-30 Jul 2017 Auckland www.nzmpa.org.nz
Mulligan - Part A 5-6 Aug 2017 Auckland www.nzmpa.org.nz
NZMPA 2017 conference - Back to the future- Learning from the past
19-20 Aug 2017 Rotorua www.nzmpa.org.nz
cOMT - W10 21 Aug 2017 Rotorua www.nzmpa.org.nz
cMP update 27 Aug 2017 Auckland www.nzmpa.org.nz
cOMT - Hip and Knee 2-3 Sept 2017 Wellington www.nzmpa.org.nz
cOMT - PNS Elbow and Wrist 16-17 Sept 2017 Auckland www.nzmpa.org.nz
cOMT - Ankle foot and Review 28-29 Oct 2017 Auckland www.nzmpa.org.nz
cOMT - Ankle foot and Review 11-12 Nov 2017 Wellington www.nzmpa.org.nz
cOMT - HvT and Review 25-26 Nov 2017 Auckland www.nzmpa.org.nz
cOMT - W10 2-3 Dec 2017 Auckland www.nzmpa.org.nz
Mulligan - Part c and Exam 2, 3 & 4 Dec 2017 Auckland www.nzmpa.org.nz
Physiotherapy Acupuncture Association of New Zealand
case Study Day 2017 various Nationwide [email protected]
Advance upper Body – Dry Needling 6-7 May 2017 Auckland [email protected]
Symposium – clinical Gems 17-18 Jun 2017 Auckland [email protected]
Traditional acupuncture – basic 12 Aug 2017 christchurch [email protected]
Traditional acupuncture – advance 13 Aug 2017 christchurch [email protected]
Dry Needling – foundation course 12-13 Aug 2017 Wellington [email protected]
Advance Lower Body – Dry Needling 23-24 Sept 2017 Auckland [email protected]
Acupuncture, Mulligan concept and the SIJ 30 Sept 2017 Auckland [email protected]
Headache Day 1 Oct 2017 Auckland [email protected]
Sports 11 Nov 2017 Wellington [email protected]
Dry Needling – foundation course 11-12 Nov 2017 Auckland [email protected]
Sports Physiotherapy New Zealand
SPNZ Sports Physiotherapy Symposium 14-15 Oct 2017 [email protected]
TITLE DATE LOCATION CONTACT DETAILS
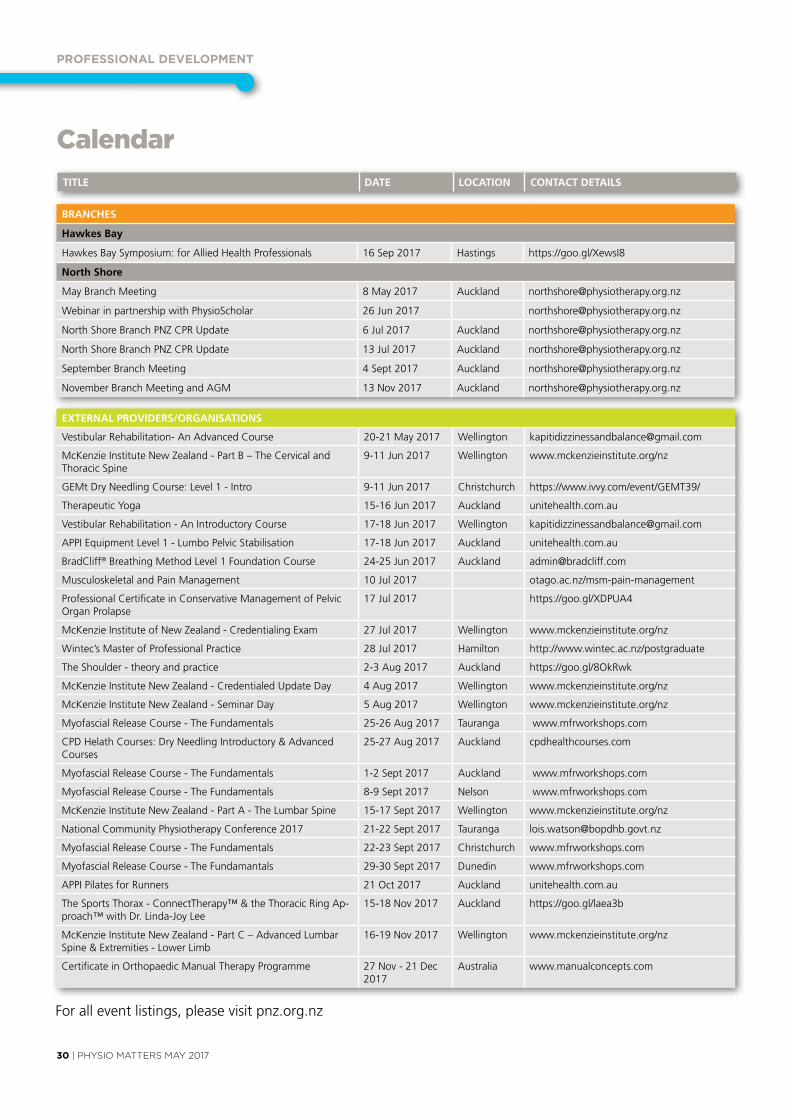
PROFESSIOnAl dEvElOPMEnT
30 | PHYSIO MATTERS MAY 2017
TITLE DATE LOCATION CONTACT DETAILS
ExTERNAL PROVIDERS/ORGANISATIONS
vestibular Rehabilitation- An Advanced course 20-21 May 2017 Wellington [email protected]
McKenzie Institute New Zealand - Part B – The cervical and Thoracic Spine
9-11 Jun 2017 Wellington www.mckenzieinstitute.org/nz
GEMt Dry Needling course: Level 1 - Intro 9-11 Jun 2017 christchurch https://www.ivvy.com/event/GEMT39/
Therapeutic Yoga 15-16 Jun 2017 Auckland unitehealth.com.au
vestibular Rehabilitation - An Introductory course 17-18 Jun 2017 Wellington [email protected]
APPI Equipment Level 1 - Lumbo Pelvic Stabilisation 17-18 Jun 2017 Auckland unitehealth.com.au
Bradcliff® Breathing Method Level 1 foundation course 24-25 Jun 2017 Auckland [email protected]
Musculoskeletal and Pain Management 10 Jul 2017 otago.ac.nz/msm-pain-management
Professional certificate in conservative Management of Pelvic Organ Prolapse
17 Jul 2017 https://goo.gl/xDPuA4
McKenzie Institute of New Zealand - credentialing Exam 27 Jul 2017 Wellington www.mckenzieinstitute.org/nz
Wintec’s Master of Professional Practice 28 Jul 2017 Hamilton http://www.wintec.ac.nz/postgraduate
The Shoulder - theory and practice 2-3 Aug 2017 Auckland https://goo.gl/8OkRwk
McKenzie Institute New Zealand - credentialed update Day 4 Aug 2017 Wellington www.mckenzieinstitute.org/nz
McKenzie Institute New Zealand - Seminar Day 5 Aug 2017 Wellington www.mckenzieinstitute.org/nz
Myofascial Release course - The fundamentals 25-26 Aug 2017 Tauranga www.mfrworkshops.com
cPD Helath courses: Dry Needling Introductory & Advanced courses
25-27 Aug 2017 Auckland cpdhealthcourses.com
Myofascial Release course - The fundamentals 1-2 Sept 2017 Auckland www.mfrworkshops.com
Myofascial Release course - The fundamentals 8-9 Sept 2017 Nelson www.mfrworkshops.com
McKenzie Institute New Zealand - Part A - The Lumbar Spine 15-17 Sept 2017 Wellington www.mckenzieinstitute.org/nz
National community Physiotherapy conference 2017 21-22 Sept 2017 Tauranga [email protected]
Myofascial Release course - The fundamentals 22-23 Sept 2017 christchurch www.mfrworkshops.com
Myofascial Release course - The fundamantals 29-30 Sept 2017 Dunedin www.mfrworkshops.com
APPI Pilates for Runners 21 Oct 2017 Auckland unitehealth.com.au
The Sports Thorax - connectTherapy™ & the Thoracic Ring Ap-proach™ with Dr. Linda-Joy Lee
15-18 Nov 2017 Auckland https://goo.gl/laea3b
McKenzie Institute New Zealand - Part c – Advanced Lumbar Spine & Extremities - Lower Limb
16-19 Nov 2017 Wellington www.mckenzieinstitute.org/nz
certificate in Orthopaedic Manual Therapy Programme 27 Nov - 21 Dec 2017
Australia www.manualconcepts.com
for all event listings, please visit pnz.org.nz
Calendar
BRANCHES
Hawkes Bay
Hawkes Bay Symposium: for Allied Health Professionals 16 Sep 2017 Hastings https://goo.gl/xewsI8
North Shore
May Branch Meeting 8 May 2017 Auckland [email protected]
Webinar in partnership with PhysioScholar 26 Jun 2017 [email protected]
North Shore Branch PNZ cPR update 6 Jul 2017 Auckland [email protected]
North Shore Branch PNZ cPR update 13 Jul 2017 Auckland [email protected]
September Branch Meeting 4 Sept 2017 Auckland [email protected]
November Branch Meeting and AGM 13 Nov 2017 Auckland [email protected]

cOnTAcT dETAIlS
PHYSIO MATTERS MAY 2017 | 31
www.pnz.org.nz
Branch Contacts
Northland
Kimberley Pow [email protected]
North Shore
Lilian van den Bergh [email protected]
Auckland
Tony Westwood [email protected]
Waikato / Bay of Plenty
Rob Neish [email protected]
Hawke’s Bay
Raewyn Newcomb [email protected]
Middle Districts
Bridie Green [email protected]
Wellington
Darragh Kenny [email protected]
Nelson / Marlborough
Sheryl Wilson nelsonmarlborough@physiotherapy. org.nz
Canterbury
Jessie Snowdon [email protected]
Otago
Becky Wilson [email protected]
Southland
fiona Morse [email protected]
Special Interest Groups
Cardiothoracic
Brigitte Eastwood [email protected]
Pelvic, Women’s and Men’s Health
Shelley Solomon [email protected]
District Health Board Leaders
Barbara Saipe [email protected]
Hand Therapists
Marlene Pouri-Lane Ph: 07 854 8949 [email protected]
Neurology
Bridget Dickson [email protected]
NZ Manipulative Physiotherapists Association (NZMPA)
Ingrid du Toit Ph: 09 476 5353 0800 646 000 [email protected] www.nzmpa.org.nz
Occupational Health
Angela Trotter (Administrator) PO Box 27386 Wellington 6141 Ph: 04 894 1685 [email protected]
Paediatrics
Merryn Robertson [email protected]
The Physiotherapy Acupuncture Association (PAANZ)
Angela Trotter (Administrator) PO Box 27386 Wellington 6141 Ph: 04 894 1685 [email protected]
Physiotherapy in Mental Health
Joke van Stavern [email protected]
Physiotherapy for the Older Adult
chrissie Russell [email protected]
Sports Physiotherapy New Zealand
Michael Borich Ph: 021 717 303 [email protected] www.sportsphysiotherapy.org.nz
Chairpersons Standing Committees
contact National Office
Tae Ora Tinana
Sandra Kettle
Professional Standards and Ethics Committee
Ben Hinchcliff fy Dunford
Finance Committee
Sheila Mann
Professional Development Committee
Gill Stotter
National Executive Committee
President
Liz Binns PO Box 27386 Wellington 6141 Ph: 04 801 6500 (National Office) [email protected]
Executive Members
Ricky Bell Melissa Davidson Jess Radovanovich Kurt Thomas
National Office
Office Hours 8.30am - 5.00pm
L6, 342 Lambton Quay PO Box 27 386, Wellington Ph: 04 801 6500 [email protected]
CEO
MN (Joe) Asghar [email protected]
Operations and Business Services Manager
Peter christie [email protected] DD: 04 894 1683
Marketing Manager
Nick Taylor [email protected] DD: 04 894 1686
Professional Advisor
Sue Doesburg [email protected] DD: 04 894 1684
Learning And Research Advisor
Nick clode [email protected] DD: 04 894 1689
Communications and Events Advisor
Erica George [email protected] DD: 04 894 1687
Professional Development Project Officer
Anna Williams [email protected] DD: 04 894 1680
Membership Administrator
claire Angliss [email protected] Ph: 04 801 6500
Accountant
Emma Gillard [email protected] DD: 04 894 1682
Physiotherapy Business Support
Check us out on Facebook, YouTube and Twitter
www.facebook.com/PhysiotherapyNZ www.youtube.com/nzsp1 www.twitter.com/physionz
With over 12,500 online exercise videos and more than 100 added every month, it’s no wonder we are the Number 1 ally of physiotherapists around the world.
We are Physiotec and we help over 3 million patients lead a healthier, more normal life.
12,706THERE ARE
WAYS TO BENEFIT FROM PHYSIOTEC
physiotec.net.au(+64) 0800 445 951





























