Embed Size (px)
Citation preview
From the Department of Plastic and Reconstruction Surgery, Chang Gung Memorial Hospital, Taipei; Chang Gung University,Taoyuan; Chang Gung Institute of Technology, Taoyuan.Received: May 2, 2005; Accepted: Dec. 20, 2005Correspondence to: Dr. Chien-Tzung Chen, Department of Plastic and Reconstruction Surgery, Chang Gung Memorial Hospital. 5,Fushing Street, Gueishan Shiang, Taoyuan, Taiwan 333, R.O.C. Tel.: 886-3-3281200 ext. 2946; Fax: 886-3-3289582; E-mail:[email protected]
251Review Article
Management of Posttraumatic Enophthalmos
Chien-Tzung Chen, MD; Faye Huang, MD; Yu-Ray Chen, MD
Posttraumatic enophthalmos is one of the common sequelae thatappears after facial injury and remains a challenge to treat for cran-iomaxillofacial surgeons. Several theories have been advocated regard-ing enophthalmos; however, the most well accepted concept is theenlargement of the orbital cavity after displacement due to orbital frac-tures. Generally, a 1 cm3 increase in orbital volume causes 0.8 mm ofenophthalmos. Thorough knowledge of the orbital anatomy is funda-mental and critical for the successful surgical correction of enophthal-mos because most treatment failures are due to inadequate orbital dis-section from fear of injuring the optic nerve and globe. A complete pre-operative plan should be built on a comprehensive clinical examinationof the periorbital soft tissue and bony components, detailed ophthalmicexamination, and high resolution computed tomography scans in theaxial, coronal and reformatted sagittal planes. Based on the anatomicdeformities, there are two major fracture types including orbital blowout fractures and zygomatico-orbital fractures, resulting in posttraumat-ic enophthalmos. Treatment modalities and methods of approach are adapted according tothe severity of the orbital deformities. Minor complications include ectropion, entropion,dystopia, diplopia, and residual enophthalmos. Rare but severe complications such as intra-conal misplacement of the bone graft or retrobulbar hemorrhage with subsequent blindnessmay be encountered. The success of the procedures depend on adequate dissection andmobilization of the displaced soft tissue, correct repositioning of the dislocated or malunitedbony orbit, and proper intra-orbital grafting. (Chang Gung Med J 2006;29:251-61)
Key words: enophthalmos, orbital fracture, endoscope, facial injury.
During the past decade, the treatment principlesof craniomaxillofacial complex bony and soft
tissue injuries have dramatically evolved to an early,aggressive one-stage approach. The standard princi-ples in acute facial trauma including (1) preciseanatomic diagnosis, (2) direct fracture exposure, (3)rigid internal fixation, (4) primary bone grafting, and(5) soft tissue suspension have been well document-ed.(1,2) Lack of recognition of the severity of theseinjuries, failure to understand the principles of recon-
struction, inappropriate application of the techniques,and inadequate exposure have resulted in post-trau-matic secondary facial deformities. These deformi-ties included depressed forehead deformity and tem-poral hollowing in the upper part of the face, malarmalposition, enophthalmos, nasal deformity, andtelecanthus in the middle part of the face, and maloc-clusion related to occlusal problems and temporo-mandibular joint ankylosis in the lower part of theface. The deformities caused functional limitations
Dr. Chien-Tzung Chen
Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
252
and were cosmetically unacceptable, moreover, haveled to emotional and social problems.
Enophthalmos was found to be the most com-mon type among the cases of post-traumatic facialdeformities. It is a sequela of orbital fracture.Although some investigators have suggested thatmost patients are not bothered by enophthalmos,(3,4)
more recent experience has demonstrated that this isnot true. Surgical treatment of post-traumatic enoph-thalmos remains one of the most challenging proce-dures because of the dangers and fear of causinginjury to the optic nerve, globe and its associatedstructures. Moreover, secondary procedures to cor-rect this deformity were frequently unsuccessful.
Anatomic considerationsThorough knowledge of the anatomy of the
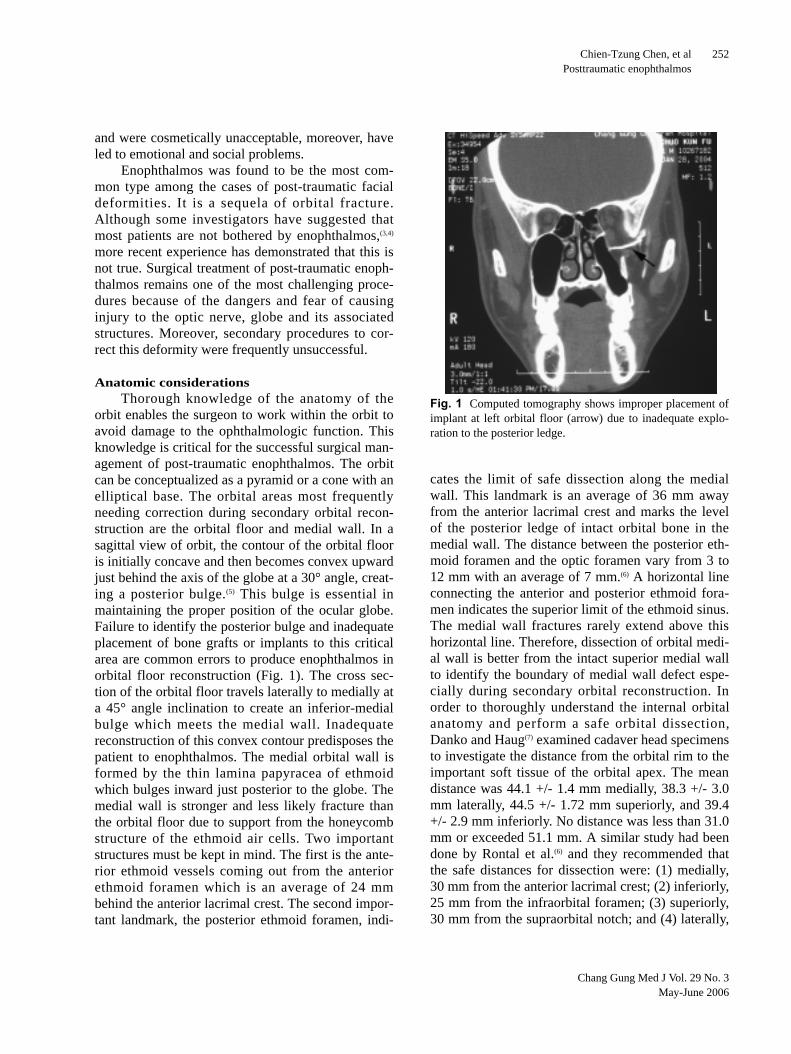
orbit enables the surgeon to work within the orbit toavoid damage to the ophthalmologic function. Thisknowledge is critical for the successful surgical man-agement of post-traumatic enophthalmos. The orbitcan be conceptualized as a pyramid or a cone with anelliptical base. The orbital areas most frequentlyneeding correction during secondary orbital recon-struction are the orbital floor and medial wall. In asagittal view of orbit, the contour of the orbital flooris initially concave and then becomes convex upwardjust behind the axis of the globe at a 30° angle, creat-ing a posterior bulge.(5) This bulge is essential inmaintaining the proper position of the ocular globe.Failure to identify the posterior bulge and inadequateplacement of bone grafts or implants to this criticalarea are common errors to produce enophthalmos inorbital floor reconstruction (Fig. 1). The cross sec-tion of the orbital floor travels laterally to medially ata 45° angle inclination to create an inferior-medialbulge which meets the medial wall. Inadequatereconstruction of this convex contour predisposes thepatient to enophthalmos. The medial orbital wall isformed by the thin lamina papyracea of ethmoidwhich bulges inward just posterior to the globe. Themedial wall is stronger and less likely fracture thanthe orbital floor due to support from the honeycombstructure of the ethmoid air cells. Two importantstructures must be kept in mind. The first is the ante-rior ethmoid vessels coming out from the anteriorethmoid foramen which is an average of 24 mmbehind the anterior lacrimal crest. The second impor-tant landmark, the posterior ethmoid foramen, indi-
cates the limit of safe dissection along the medialwall. This landmark is an average of 36 mm awayfrom the anterior lacrimal crest and marks the levelof the posterior ledge of intact orbital bone in themedial wall. The distance between the posterior eth-moid foramen and the optic foramen vary from 3 to12 mm with an average of 7 mm.(6) A horizontal lineconnecting the anterior and posterior ethmoid fora-men indicates the superior limit of the ethmoid sinus.The medial wall fractures rarely extend above thishorizontal line. Therefore, dissection of orbital medi-al wall is better from the intact superior medial wallto identify the boundary of medial wall defect espe-cially during secondary orbital reconstruction. Inorder to thoroughly understand the internal orbitalanatomy and perform a safe orbital dissection,Danko and Haug(7) examined cadaver head specimensto investigate the distance from the orbital rim to theimportant soft tissue of the orbital apex. The meandistance was 44.1 +/- 1.4 mm medially, 38.3 +/- 3.0mm laterally, 44.5 +/- 1.72 mm superiorly, and 39.4+/- 2.9 mm inferiorly. No distance was less than 31.0mm or exceeded 51.1 mm. A similar study had beendone by Rontal et al.(6) and they recommended thatthe safe distances for dissection were: (1) medially,30 mm from the anterior lacrimal crest; (2) inferiorly,25 mm from the infraorbital foramen; (3) superiorly,30 mm from the supraorbital notch; and (4) laterally,
Fig. 1 Computed tomography shows improper placement ofimplant at left orbital floor (arrow) due to inadequate explo-ration to the posterior ledge.

Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
253
25 mm from the frontozygomatic suture.
PathophysiologyThe exact mechanism of post-traumatic enoph-
thalmos remains incomplete and unclear. Numeroustheories have been proposed to account for enoph-thalmos including: (1) enlargement of the orbital vol-ume by displaced fractures, (2) fat atrophy or necro-sis, (3) scarring of retrobulbar tissues tethering theglobe in a posterior position, (4) loss of ligamentoussupport, and (5) entrapment of the connective-tissueseptal system in a blowout fracture.(8-10) These theo-ries are based on the anatomic concepts of the defor-mities and each emphasized a different viewpoint ofthe orbital anatomy as the cause of enophthalmos.Manson and colleagues(11) studied the orbits of bothcadavers and patients. During the study, they wereable to demonstrate that the principal mechanism ofposttraumatic enophthalmos involved a displacementand change in the shape of orbital soft tissue causedby the loss of bone and ligament support. Fat atrophywas not a prominent feature of posttraumatic enoph-thalmos. Gruss(2) also stressed that posttraumaticenophthalmos was almost entirely due to the dis-placement of the orbital wall with enlargement of thebony orbital cavity. Furthermore, enlarged posteriororbital volumes were common findings on computedtomography (CT) scans of patients with enophthal-mos, suggesting that larger retrobulbar spaces allowthe globes to drop posteriorly in the orbits. However,the cause of residual enophthalmos following orbitalreconstruction may not be the same mechanism as inorbits that did not undergo surgery. The soft tissueatrophy may play some role in the reconstructedorbits.(12)
Since enlargement of the orbital bony volume isthe major cause of enophthalmos, a number ofauthors studied the relationship between the degreeof enophthalmos and the orbital blow out fracturesusing CT scans to identify the patients at risk of lateenophthalmos. Whitehouse et al.(13) found a 1 cm3
increase in orbital volume causing 0.8 mm of enoph-thalmos, providing that measurements were per-formed more than 20 days after the injuries. A recentstudy by Ploder and coworkers(14) demonstrated thatin patients with isolated orbital floor blowout frac-ture, enophthalmos of 2 mm can be expected with3.38 cm2 of the fracture area and 1.62 ml of the dis-placed tissue, and the relationship was valid 10 days
after the injuries. In a study on late post-traumaticenophthalmos, Schuknecht and associates(15) conclud-ed that enophthalmos of 3.5- 5 mm corresponded to amean increase in orbital volume of 7.1 ml, whileenophthalmos of 2.5-3 mm correlated with anincrease in orbital volume of 3.4 ml. In order to pre-cisely correct the late enophthalmos caused by amedial orbital wall defect, Lee(16) used diced cartilagegrafts to fill up the defect and found that 1.37-1.5 mlof the graft material resulted in a 1 mm forwardadvancement of the globe position. Although manyresearchers have conducted studies regarding orbitalvolume measurement, the reports have shown neitherconcurring data nor consistent conclusions. The rea-sons behind the disparity are factors such as differ-ences in measuring tools, software, and radiographictracing points. Timing of intervention and measure-ments may also affect the results. The small volumeof the orbit, only 30-35 cm3 may likewise be a causeof difficulties in these studies.(12) In spite of thisamount of data, the 3-dimensional information of theorbital volume obtained from the CT scans may notbe clinically useful for the surgeons to precisely cor-rect the orbital volume deficiency as most implantsor autogenous graft materials are flat and two-dimen-sional.
Preoperative evaluationIn forming a thoughtful preoperative plan, com-
prehensive clinical examination and complete radi-ographic evaluation of the orbit must be carried out.Careful review of the patient’s medical historyincluding the injury mechanism and previous opera-tions on the facial skeleton not only allows for betterunderstanding the extent of periorbital fractures butalso alerts the surgeon to other possible causes ofpost-traumatic enophthalmos. Preoperative pho-tographs including the premorbid photographs arebeneficial not only as baseline records but also asvaluable assets in treatment planning.(17)
Documentation of the patient’s subjective complaintsand wishes are important because it may affect thesurgeon’s decisions. For example, in a certain casethe enophthalmos was caused by inadequate reduc-tion of the zygomatic fracture and reconstruction.However, in some situations, the patients may justwish for enophthalmos correction without mobiliza-tion of the deformed zygoma. The surgeon is thenrequired to judge and balance between patient’s

Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
254
wishes and surgical procedure and outcome.The periorbital examination including the soft
tissue and bony components must be analyzed. Thedisplaced position of the brow, the medial and lateralcanthi as well as the changes of the lengths of thepalpebral fissures reflect the changes in the underly-ing position of the orbital rim structures that need tobe corrected. The presence of infraorbital nervenumbness as well as evidence of lacrimal ductobstruction should be noted. The projection themalar body and the contour of the arch should becompared with the uninjured site. The presence of adeepening supratarsal sulcus and hypoglobus indi-cates loss of support inferiorly and posteriorly. Therelative anterior-posterior position of the globe isassessed most accurately through an inferior view.Hertel exophthalmometry is accurate in defining thedifferences between the globe position of the injuredand uninjured side provided that the lateral orbitalrim is in the correct and symmetrical position. If thelateral orbital rim is malpositioned, examining thepatient from the lateral view using the superiororbital rim as reference points is recommended.
Preoperative ophthalmology consultation is rou-tinely sought. Ocular examination should includeassessment of the visual acuity, visual field, pupillaryfunction, extraocular muscle function, and slit lampexamination to rule out corneal perforation orhyphyema. A dilated fundus examination is carriedout to identify any optic nerve and retinal patholo-gies. A forced duction test advocated by Putterman(18)
must be considered when restriction in ocular move-ment is detected. The presence of diplopia is fre-quently associated with limitations of extraocularmuscle movements. One must differentiate the caus-es of diplopia which may result from (1) orbital tis-sue entrapment, (2) injured cranial nerve inducedmalfunction of eye muscle, and (3) malposition ofglobe.
Image studies may include plain radiographsand CT scans. Recently, the development of the heli-cal CT scan has changed the types of studies neededto diagnose and evaluate orbital trauma. The helicalCT scan allows for continuous acquisition of vol-umes of tissue, which permits multi-planar recon-structions of additional image planes. This techniquepromises to reduce the number of examinations andradiation exposure of the patient while improving thequality of the images.(19) In addition, the radiation
dose delivered to the lens is much less than that ofconventional CT scans. Total scanning time isreduced (18 seconds for a helical scan comparedwith 104 seconds for conventional CT axial andcoronal scans).(20) CT scanning has much improvedour preoperative assessment capability of post-trau-matic enophthalmos and has become a standardexamination tool in our practice. The fine-cut CTscans are taken both in axial and coronal planes, withsoft tissue and bone windows. The reformed sagittalsections that connect the apex of the orbit and themidpoint of the globe are particularly helpful toassess the situation and adequacy of previous recon-struction of the orbital floor fractures. The CT scansshould be used to show the adjacent cavity and struc-tures and detect associated periorbital deformities toaid the surgeon in making a proper therapeutic plan.Three-dimensional CT images serve as a quickoverview of the pathologic condition but they areseldom of value in the internal portion of the orbit.(9)
TreatmentTessier, a pioneer in the field of craniofacial sur-
geon, documented the principles of correction ofpost-traumatic enophthalmos including: (1) completesubperiosteal dissection to free the periorbital tissuefrom displaced orbital fragments, (2) repositioning ofthe orbital framework with osteotomies, and (3)reconstruction of the walls and framework with bonegrafts.(21) In order to obtain adequate exposure andsoft tissue mobilization, the 360-degree circumferen-tial subperiosteal dissection of the orbit down to theorbital cone through coronal and lower lid incisionshas been advocated.(2,22,23) However, this concept hasbeen found to be unnecessary to correct globe posi-tion, even in cases of long-standing enophthalmos. Infact, this may aggravate problems of the globe posi-tion and vision function. The intraorbital dissectionneed only be confined to the area of previous dam-age.(12,24)
As discussed earlier, displacement of the orbitalwall with increased bony orbital cavity was the mainreason of post-traumatic enophthalmos. The aim ofenophthalmos correction is restoration of the bonyvolume of the orbit. The concepts of the 3-stepapproach to correct post-traumatic orbital deformitiesadvocated by Grant et al.(12) consist of mobilization ofthe soft tissues in the area of fracture, repositioningof the anterior and middle sections of the bony

Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
255
orbital rim followed by reconstruction of the innerorbital wall, and reattachment of the soft tissue to thebone at the proper location. They emphasized thatrestoration of the position and shape of the orbitalsoft tissue by mobilization and reconstruction of thebony orbit significantly improved enophthalmos.(11)
Contemporary treatment of post-traumatic enoph-thalmos and surgical approaches are based on theseverity of the orbital deformities and fracture types.In general, two fracture types including orbital blowout fracture and zygomatico-orbital fracture are themain etiologies causing late enophthalmos.(25)
Deformity with orbital blow out fracture
Usually an enlarged orbital wall is caused by anunrepaired orbital medial wall fracture, inadequatefloor reconstruction or combination of both factors.Inadequate primary internal orbital reconstructionfrequently results from fear of injury to the opticnerve and then failure to identify the posterior ledgeof the orbital floor. On the other hand, the medialorbital blowout fractures also play an important roleof late enophthalmos, because there is a high inci-dence of occurrence, a low rate of diagnosis, and ahigh severity of defect. Pearl and Vistnes(26) foundthat 50% of patients with blow out fractures hadassociated medial wall fractures. Late enophthalmoswas found in 76 % of patients with medial wall frac-tures in the study by Burm et al. of 76 patients withpure orbital blowout fracture.(27)
Many methods have been used to explore theorbital medial wall including the remote coronalincision, direct local medial canthal incision(28) andW-shaped incision.(29) The incision may extend to theinfraorbital rim to explore the orbital floor.(30)
Alternatively, a medial transconjunctival incisionusing rigid endoscopic assistance provides adequateexposure to the medial orbital wall with excellentcosmetic and functional results.(31,32) This technique isapplicable to all sizes of defects, and is especiallyuseful for those involving the superior and posteriormedial orbit, which is difficult to dissect through alower lid incision. In general, the endoscopic tech-nique can be applied for primary and secondaryrepairs of medial orbital wall defects and the correc-tion of enophthalmos.(5)
The deformities limited to the orbital floor arebest accessed through either a lower eyelid subciliaryincision or an inferior transconjunctival incision. If
the transconjunctival incision is used, a lateral can-thotomy and cantholysis may be added to providewider exposure and placement of larger graft forreconstruction of the orbital floor. Although thetransconjunctival approach leaves no facial scars andhas lower incidence of ectropion than standard sub-ciliary incision, one should be cautious when usingthis approach on patients who have had previoustranscutaneous incisions because of a high incidenceof post-operative ectropion.(33) In addition, the pres-ence of orbicularis muscle weakness or lower lidshortening must be taken into consideration indesigning a lower eyelid incision. Additional expo-sure of the orbital floor may be obtained by inferiororbitotomy.(34) Using a marginal osteotomy along theinferior orbital rim, the prolapsed orbital tissuebecomes easier to be released from the maxillarysinus without injury to the infraorbital nerve and canbe moved back to the orbital cavity.
After the reduction of all herniated periorbitalcontents, the orbital defects are clearly identified andthe surrounding bony shelves are delineated to facili-tate placement and decision of the shape and dimen-sions of the grafts. The choice of metal, alloplasticmaterial, or autogenous bone graft depends on opera-tor preference, and the need to achieve a stable con-struct. These grafts are placed on the delineated bonyshelves from the posterior orbit to the anterior orbit.Whenever possible, the grafts must be rigidly fixedwith microscrews or microplates to the orbital rim incases with extensive orbital wall defects. Fixationimproves the predictability of reconstruction and pre-vents migration of the material.(35) Figures 2 shows aclinical case.
Orbito-zygomatic deformity
Pearl(36) stated that the most common causes ofenophthalmos were not blow-out fractures but inade-quate reduction of zygomatic fractures. Inadequatereduction of displaced orbitozygomatic fractures pro-duce flattened malar areas, increasing facial widthand external rotation of the lateral orbital walls,which result in markedly increased orbital volumesand subsequent enophthalmos. Therefore, treatmentof enophthalmos relies on the degree of displacementof the lateral orbital wall and rim as well as thepatient’s preference or choice. If a patient is not will-ing to undergo a zygoma repositioning procedurethrough an orbitozygomatic osteotomy or presents
Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
256
with a deformity involving only minor rotation of thezygomatic body, the surgical procedure is similar tothe method for repairing a deformity caused by anorbital blow out fracture. The correction of enoph-thalmos should focus on the reconstruction of theinternal orbital wall, especially adding grafts on thelateral orbital wall. As outlined previously, the basicprinciples of a successful correction rely on adequateexposure, complete release of periorbital tissue in theinjured area and sufficient onlay grafting.
In most situations, the “malunited” and dis-placed zygoma needs to be repositioned into its cor-rect anatomic position. Accurate re-establishment of
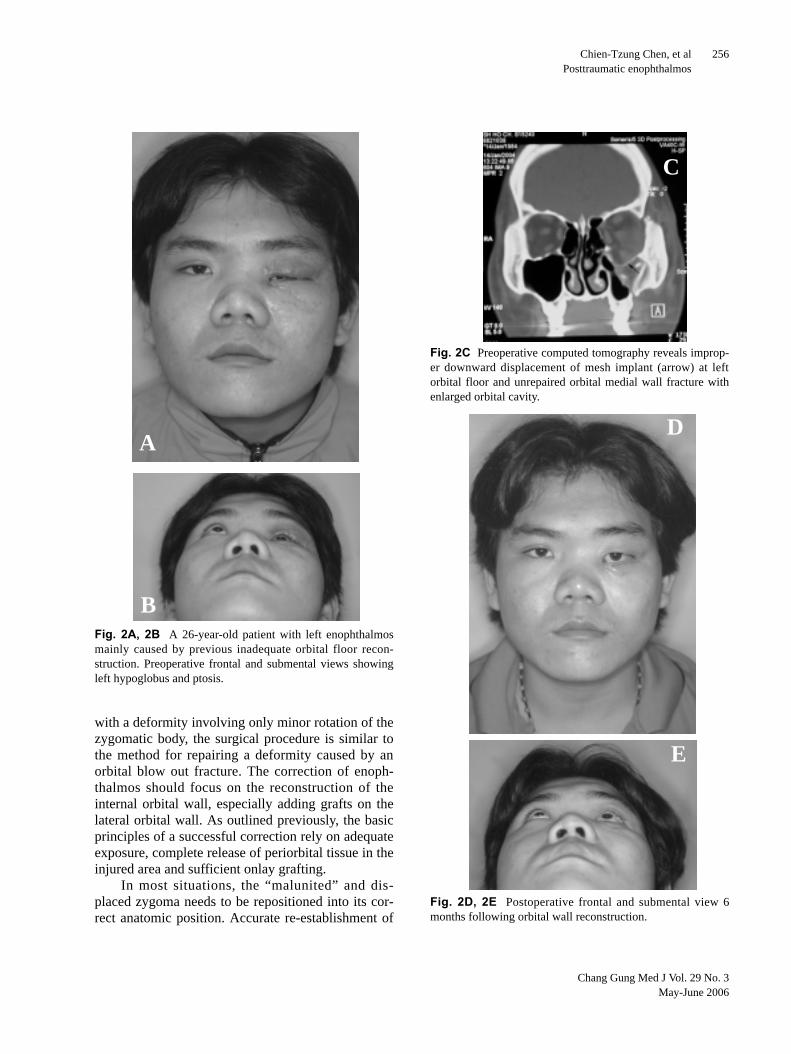
Fig. 2A, 2B A 26-year-old patient with left enophthalmosmainly caused by previous inadequate orbital floor recon-struction. Preoperative frontal and submental views showingleft hypoglobus and ptosis.
A
B
Fig. 2C Preoperative computed tomography reveals improp-er downward displacement of mesh implant (arrow) at leftorbital floor and unrepaired orbital medial wall fracture withenlarged orbital cavity.
Fig. 2D, 2E Postoperative frontal and submental view 6months following orbital wall reconstruction.
D
E
C
Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
257
the correct position of the zygoma body and theorbital rim helps restore the correct orbital volumeand, combined with deep orbital bone grafting, cor-rects enophthalmos.(2) The orbitozygomatic deformityis corrected by recreating the fracture pattern andrepositioning the bone. Following the old fracturelines as a guide for osteotomy has been advocated tocorrect the posttraumatic orbitozygomatic malposi-tion.(37-39) The corrective osteotomies are performed atthe fronto-zygomatic suture, infraorbital rim, zygo-matic arch and lateral maxillary buttress. To accom-plish this, the traditional coronal, cutaneous lowereyelid and intraoral incisions are used to obtain wideexposure of the orbito-zygomatic complex and facili-tate deep orbital exploration.(2,22,25)
Based on considerable their experience,Longaker and Kawamoto(24) used limited exposurevia the lateral upper blepharoplasty, transconjuncti-val without canthotomy and intraoral incisions torecreate the fracture, mobilize and reposition themalunited zygoma instead of the conventional coro-nal approach. The advantages of this approach arereduced morbidity and hospital stay, shorter operat-ing time, and avoidance of blood transfusions. Theauthors agree with the concepts advocated byLongaker and Kawamoto(9) using a limited accesstechnique instead of extensive exposure for mobi-lization of malunited zygoma to correct posttraumat-ic enophthalmos. The limited exposure is performed
only via an extended infraciliary incision with lateralcanthotomy and upper buccal incision. The extendedinfraciliary incision with lateral extension is used toexpose the fronto-zygomatic junction, lateral orbitalwall, infraorbital rim, and zygomatic arch. Thisapproach obviates the eyebrow incision, which isvisible in some patients.(36) All the osteotomies can bedone under direct vision except for the zygomaticarch at which the bony cut is made using an angledoscillating saw with the assistance of a 4 mm, 30°endoscope. Therefore, the deformed zygoma is com-pletely mobilized and repositioned to restore anatom-ic alignment. Following the anatomic reduction ofthe fracture, the remaining orbital defect is repairedwith grafts when necessary. The most difficult part inthis procedure is determination of the precise posi-tion of the mobilized zygoma in a three-dimensionalspace. Hammer and Prein(40) stressed the value of thelateral orbital wall as a reliable landmark during sec-ondary revisions. However, this maneuver is usefulonly when the lateral orbital wall has not been dis-rupted severely by the injury.(25) Recently, advance-ment in computer and navigational technologieshelps ensure the position of the repositioned bonycomplex precisely and improve accuracy of theorbital reconstruction.(41,42) Figures 3 demonstrates aclinical case.
ComplicationThe complication rate of 10 to 15% after orbital
reconstruction has been reported.(43) The commonpostsurgical sequelae are ectropion with sclera show-ing or entropion, both of which are related to surgicalincisions and may be minimized with meticulous
Fig. 2F Coronal view of postoperative CT scan after recon-struction of the orbital floor, medial and lateral wall withMedpor implants which is not visible on CT scan. Please notesymmetric position of medial rectus muscle and inferior rec-tus muscle on both orbital cavities.
F
Fig. 3A Preoperative view of patient with right enophthal-mos and malar depression.
A
Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
258
surgical dissection and soft tissue resuspension.Transient exophthalmos and diplopia are expectedand usually resolve within 2-3 months. However,worsening of double vision and dystopia had beenobserved postoperatively after correction of lateenophthalmos.(44) Residual enophthalmos has beenseen commonly due to the difficulty in accuratelyassessing orbital volume intra-operatively and limita-tions from the increased intraocular pressure. Theendpoint of orbital reconstruction is reached whenthe globe feels tight on palpation and can not be
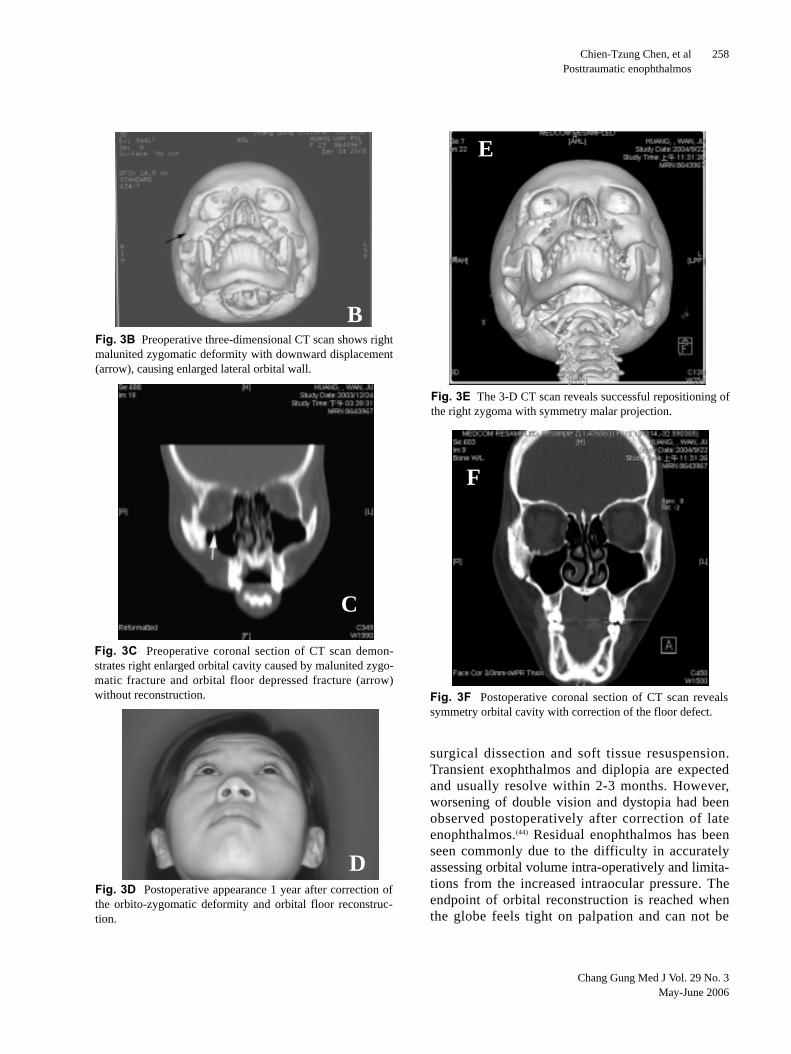
Fig. 3B Preoperative three-dimensional CT scan shows rightmalunited zygomatic deformity with downward displacement(arrow), causing enlarged lateral orbital wall.
B
Fig. 3C Preoperative coronal section of CT scan demon-strates right enlarged orbital cavity caused by malunited zygo-matic fracture and orbital floor depressed fracture (arrow)without reconstruction.
C
Fig. 3D Postoperative appearance 1 year after correction ofthe orbito-zygomatic deformity and orbital floor reconstruc-tion.
D
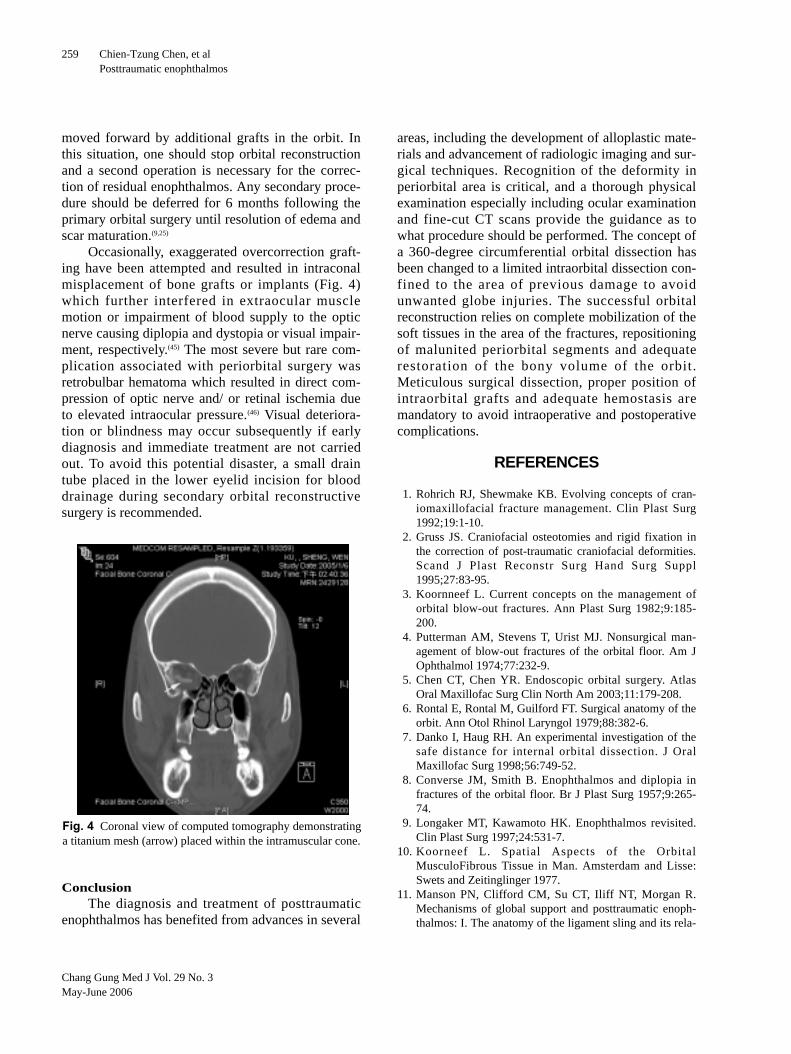
Fig. 3E The 3-D CT scan reveals successful repositioning ofthe right zygoma with symmetry malar projection.
Fig. 3F Postoperative coronal section of CT scan revealssymmetry orbital cavity with correction of the floor defect.
E
F
Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
259
moved forward by additional grafts in the orbit. Inthis situation, one should stop orbital reconstructionand a second operation is necessary for the correc-tion of residual enophthalmos. Any secondary proce-dure should be deferred for 6 months following theprimary orbital surgery until resolution of edema andscar maturation.(9,25)
Occasionally, exaggerated overcorrection graft-ing have been attempted and resulted in intraconalmisplacement of bone grafts or implants (Fig. 4)which further interfered in extraocular musclemotion or impairment of blood supply to the opticnerve causing diplopia and dystopia or visual impair-ment, respectively.(45) The most severe but rare com-plication associated with periorbital surgery wasretrobulbar hematoma which resulted in direct com-pression of optic nerve and/ or retinal ischemia dueto elevated intraocular pressure.(46) Visual deteriora-tion or blindness may occur subsequently if earlydiagnosis and immediate treatment are not carriedout. To avoid this potential disaster, a small draintube placed in the lower eyelid incision for blooddrainage during secondary orbital reconstructivesurgery is recommended.
ConclusionThe diagnosis and treatment of posttraumatic
enophthalmos has benefited from advances in several
areas, including the development of alloplastic mate-rials and advancement of radiologic imaging and sur-gical techniques. Recognition of the deformity inperiorbital area is critical, and a thorough physicalexamination especially including ocular examinationand fine-cut CT scans provide the guidance as towhat procedure should be performed. The concept ofa 360-degree circumferential orbital dissection hasbeen changed to a limited intraorbital dissection con-fined to the area of previous damage to avoidunwanted globe injuries. The successful orbitalreconstruction relies on complete mobilization of thesoft tissues in the area of the fractures, repositioningof malunited periorbital segments and adequaterestoration of the bony volume of the orbit.Meticulous surgical dissection, proper position ofintraorbital grafts and adequate hemostasis aremandatory to avoid intraoperative and postoperativecomplications.
REFERENCES
1. Rohrich RJ, Shewmake KB. Evolving concepts of cran-iomaxillofacial fracture management. Clin Plast Surg1992;19:1-10.
2. Gruss JS. Craniofacial osteotomies and rigid fixation inthe correction of post-traumatic craniofacial deformities.Scand J Plast Reconstr Surg Hand Surg Suppl1995;27:83-95.
3. Koornneef L. Current concepts on the management oforbital blow-out fractures. Ann Plast Surg 1982;9:185-200.
4. Putterman AM, Stevens T, Urist MJ. Nonsurgical man-agement of blow-out fractures of the orbital floor. Am JOphthalmol 1974;77:232-9.
5. Chen CT, Chen YR. Endoscopic orbital surgery. AtlasOral Maxillofac Surg Clin North Am 2003;11:179-208.
6. Rontal E, Rontal M, Guilford FT. Surgical anatomy of theorbit. Ann Otol Rhinol Laryngol 1979;88:382-6.
7. Danko I, Haug RH. An experimental investigation of thesafe distance for internal orbital dissection. J OralMaxillofac Surg 1998;56:749-52.
8. Converse JM, Smith B. Enophthalmos and diplopia infractures of the orbital floor. Br J Plast Surg 1957;9:265-74.
9. Longaker MT, Kawamoto HK. Enophthalmos revisited.Clin Plast Surg 1997;24:531-7.
10. Koorneef L. Spatial Aspects of the OrbitalMusculoFibrous Tissue in Man. Amsterdam and Lisse:Swets and Zeitinglinger 1977.
11. Manson PN, Clifford CM, Su CT, Iliff NT, Morgan R.Mechanisms of global support and posttraumatic enoph-thalmos: I. The anatomy of the ligament sling and its rela-
Fig. 4 Coronal view of computed tomography demonstratinga titanium mesh (arrow) placed within the intramuscular cone.
Chang Gung Med J Vol. 29 No. 3May-June 2006
Chien-Tzung Chen, et alPosttraumatic enophthalmos
260
tion to intramuscular cone orbital fat. Plast Reconstr Surg1986;77:193-202.
12. Grant MP, Iliff NT, Manson PN. Strategies for the treat-ment of enophthalmos. Clin Plast Surg 1997;24:539-50.
13. Whitehouse RW, Batterbury M, Jackson A, Noble JL.Prediction of enophthalmos by computed tomographyafter ‘blow out’ orbital fracture. Br J Ophthalmol1994;78:618-20.
14. Ploder O, Klug C, Voracek M, Burggasser G, Czerny C.Evaluation of computer-based area and volume measure-ment from coronal computed tomography scans in isolat-ed blowout fractures of the orbital floor. J Oral MaxillofacSurg 2002;60:1267-72.
15. Schuknecht B, Carls F, Valavanis A, Sailer HF. CT assess-ment of orbital volume in late post-traumatic enophthal-mos. Neuroradiology 1996;38:470-5.
16. Lee J. Preplanned correction of enophthalmos using dicedcartilage grafts. Br J Plast Surg 2000;53:17-23.
17. Hardesty RA, Coffey JA, Jr. Secondary craniomaxillofa-cial deformities. Current principles of management. ClinPlast Surg 1992;19:275-300.
18. Putterman AM. Management of blow out fractures of theorbital floor. III. The conservative approach. SurvOphthalmol 1991;35:292-8.
19. Maus M. Update on orbital trauma. Curr OpinOphthalmol 2001;12:329-34.
20. Lakits A, Prokesch R, Scholda C, Nowotny R, Kaider A,Bankier A. Helical and conventional CT in the imaging ofmetallic foreign bodies in the orbit. Acta OphthalmolScand 2000;78:79-83.
21. Tessier P, Rougier J, Hervouet F. Sequelae of OrbitalTrauma. Plastic Surgery of the Orbit and Eyelids. NewYork: Matson Publishing; 1981.
22. Kawamoto HK, Jr. Late posttraumatic enophthalmos: acorrectable deformity? Plast Reconstr Surg 1982;69:423-32.
23. Whitaker LA, Yaremchuk MJ. Secondary reconstructionof posttraumatic orbital deformities. Ann Plast Surg1990;25:440-9.
24. Longaker MT, Kawamoto HK, Jr. Evolving thoughts oncorrecting posttraumatic enophthalmos. Plast ReconstrSurg 1998;101:899-906.
25. Kellman RM, Bersani T. Delayed and secondary repair ofposttraumatic enophthalmos and orbital deformities.Facial Plast Surg Clin North Am 2002;10:311-23.
26. Pearl RM, Vistnes LM. Orbital blowout fractures: anapproach to management. Ann Plast Surg 1978;1:267-70.
27. Burm JS, Chung CH, Oh SJ. Pure orbital blowout frac-ture: new concepts and importance of medial orbitalblowout fracture. Plast Reconstr Surg 1999;103:1839-49.
28. Leone CR, Jr., Lloyd WC, III, Rylander G. Surgical repairof medial wall fractures. Am J Ophthalmol 1984;97:349-56.
29. Burm JS, Oh SJ. Direct local approach through a W-shaped incision in moderate or severe blowout fracturesof the medial orbital wall. Plast Reconstr Surg
2001;107:920-8.30. Rauch SD. Medial orbital blow-out fracture with entrap-
ment. Arch Otolaryngol 1985;111:53-5.31. Barone CM, Gigantelli JW. Endoscopic repair of posttrau-
matic enophthalmos using medial transconjunctivalapproach: a case report. J Craniomaxillofac Trauma1998;4:22-6.
32. Chen CT, Chen YR, Tung TC, Lai JP, Rohrich RJ.Endoscopically assisted reconstruction of orbital medialwall fractures. Plast Reconstr Surg 1999;103:714-20.
33. Lorenz HP, Longaker MT, Kawamoto HK, Jr. Primaryand secondary orbit surgery: the transconjunctivalapproach. Plast Reconstr Surg 1999;103:1124-8.
34. Tessier P. Inferior orbitotomy. A new approach to theorbital floor. Clin Plast Surg 1982;9:569-75.
35. Antonyshyn O, Gruss JS, Galbraith DJ, Hurwitz JJ.Complex orbital fractures: a critical analysis of immediatebone graft reconstruction. Ann Plast Surg 1989;22:220-33.
36. Pearl RM. Treatment of enophthalmos. Clin Plast Surg1992;19:99-111.
37. Freihofer HP, van Damme PA. Secondary post-traumaticperiorbital surgery. Incidence and results. JCraniomaxillofac Surg 1987;15:183-7.
38. Perino KE, Zide MF, Kinnebrew MC. Late treatment ofmalunited malar fractures. J Oral Maxillofac Surg1984;42:20-34.
39. Roncevic R. Refracture of untreated fractures of the zygo-matic bone. J Maxillofac Surg 1983;11:252-6.
40. Hammer B, Prein J. Correction of post-traumatic orbitaldeformities: operative techniques and review of 26patients. J Craniomaxillofac Surg 1995;23:81-90.
41. Schmelzeisen R, Gellrich NC, Schoen R, Gutwald R,Zizelmann C, Schramm A. Navigation-aided reconstruc-tion of medial orbital wall and floor contour in cranio-maxillofacial reconstruction. Injury 2004;35:955-62.
42. Gellrich NC, Schramm A, Hammer B, Rojas S, Cufi D,Lagreze W, Schmelzeisen R. Computer-assisted sec-ondary reconstruction of unilateral posttraumatic orbitaldeformity. Plast Reconstr Surg 2002;110:1417-29.
43. Manson PN, Georgiade GS, Georgiade NG, Riefkohl R,Barwick WJ. Management of Midfacial Fractures.Textbook of Plastic, Maxillofacial, and ReconstructiveSurgery, 2nd Ed. Baltimore: Williams & Wilkins; 1992. p409-32.
44. Iliff NT. The ophthalmic implications of the correction oflate enophthalmos following severe midfacial trauma.Trans Am Ophthalmol Soc 1991;89:477-548.
45. Marin PC, Love T, Carpenter R, Iliff NT, Manson PN.Complications of orbital reconstruction: misplacement ofbone grafts within the intramuscular cone. Plast ReconstrSurg 1998;101:1323-7.
46. Chieng HH, Tsai YC, Lin HC, Tseng FY, Yang SJ.Retrobulbar Hemorrhage as a Rare Complication inSurgical Reduction of Blowout Fracture- A Case Report. JPlast Reconstr Surg Assoc R O C 1999;8:316-21.
261
1
(1) (2)
( 2006;29:251-61)
94 5 2 94 12 20333 Tel.: (03)3281200 2946; Fax:
(03)3289582; E-mail: [email protected]


![[Secondary prevention of posttraumatic stress disorder: challenging psychological debriefings]](https://img.dokumen.tips/doc/110x75/635215200e796dacc000516e/secondary-prevention-of-posttraumatic-stress-disorder-challenging-psychological.jpg)


























