Embed Size (px)
Citation preview






1
N e l o f e r A m i r
E j a z A h m a d K h a n
S a l e e m M . R a n a
Long-lasting insecticide-treated bed nets In Pakistan
THE LAMBERT PUBLISHING

2
If every moment is to be spent in offering the prayers of Almighty Allah, even then we
cannot thank the manifold blessings. Acknowledge with whom man makes rather spending
his life.
All praises for the holy prophet Mohammad (peace be upon him) whose teaching is a
complete code of life and has been sent as Rehmat-UL-Almeen (The Mercy to the Universe).
I am extremely grateful to my family: my husband Mohammad Nazim Saleem and my three
children Kanwal, Kashan and Kinza, for being extremely helpful during my studies, and all
the research work.
I acknowledge scholarly inputs from my co-authors, Dr Ejaz Ahmad Khan and Dr Saleem M
Rana. Their profound intellectual help made this book possible for publication. I thank all
from the malaria Control Programme of Pakistan, both at the federal and provincial levels for
their cooperation and support.
Last but not the least , I am indebt to the participants, the women of rural Pakistan who
despite of their difficult situation due to various cultural and economic reasons, were happy
to be part of our study with the hope that their children and they themselves one day would be
free of this deadly disease.
Dr. Nelofar Amir

3

4

5
Figure 1: Malaria annual parasite incidence in Pakistan (Courtesy to Directorate of Malaria
Pakistan). .................................................................................................................................. 10
figure 2source:http://lsspace.blogspot.com/2008/07/049-discovery-of-key-malaria-
proteins.htmlource: ..................................................................................................................21
figure 3 Source: World Malaria Report, 2008 (who, malaria control and rollback malaria,
current status and trend of malaria) .........................................................................................21
figure 4 source: National Malaria Control Program, Ministry Of Health - Government of
Pakistan. ...................................................................................................................................24
figure 5 source: Ministry of Health - Government of Pakistan malaria.mht.....................24
figure 6 shows both the extrinsic and intrinsic risk factors for malarial transmission . ..........25
figure 7 Source: conceptual framework of the study based on Theory of Reasoned Action
(Martin Fishbone and Icek Ajzen: (1975 1980) Journal of society for Development in new net
environment in B&H) ..............................................................................................................29
figure 8 Source: Nation Master Encyclopedia Mardan. mht ..................................................31

6
INTRODUCTION
Background
History of malaria can be tracked to ancient times, when the Plasmodium remained one of the
most important pathogenic microorganism causing malaria around the world[1].In 400 B.C.,
Airs, Waters, and
During ancient times, long before the term malaria was adopted, the disease used to
be described as:
. He related quartan fevers to the impure air
resulting in deaths under specific conditions in populations. [2].
In 1846, a patient named Adelheid B died at the age of 43 after 24 years in various hospices
for mentally challenged persons. Her autopsy found out brain laden with brown pigment and
spleen coated with brown colour. They concluded that the blood carried some brown pigment
causing death of the patient (Malaria was never among the differential diagnoses) [3].
Discovery of the malarial parasite is an interesting historical event.In 1903, Fritz Schaudinn
observed female Anopheles mosquito injecting sporozoites into the bloodstream. After
which, the sporozoites entered red blood cells. Schaudinn had been struggling for some time
to solve the mystery of the mode of entrance into the body by malaria parasites. From 1901
1904, he worked at the malaria station in Rovigno, a small town in Dalmatia (now Rovinj,
Croatia), which was notorious for its high rate of malarial infection. He performed a set of
five experiments in which he allowed mosquitoes to feed on his maid, who had Plasmodium
vivax crescents in her blood, and subsequently used his own blood for invasion experiments.
In the first four experiments, he failed to find any evidence of direct red cell invasion. In the
last experiment, however, he observed the malarial sporozoite (the endstage form in the
sexual cycle of the parasite) directly entering a red cell. The sporozoites did not develop
further within the red cell (Figure 9) [4]. No appropriate controls were used, and the
7
experiment was not replicated. Unfortunately, Schaudinn died on 22 June, 1906 at the age of
of erythrocytes by infective sporozoites of P. vivax dominated scientific opinion until 1947,
when Henry Shortt and Cyril Garnham showed that a phase of division in the liver preceded
the development of parasites in the blood [5].
Long-lasting insecticidal bed nets (LLINs) are considered a vital component in the worldwide
effort to prevent malaria transmission in malaria-endemic countries [6]. In 2007, the World
Programme recommended immediate scale up of LLIN
distribution from national programmes and partners. As a result, large-scale distribution
efforts have been launched to meet this goal, particularly in sub-Saharan Africa, by a host of
governments, non-governmental organizations and collaborations with local governments and
international charitable organizations. Ethio -up of net distribution
started after the development of a new strategic plan in 2005, and resulted in household
ownership of at least one net (any type) increasing from 4.5% in 2005 to 72.5% by 2007 [7].
In 2006, LLINs were instituted as one of the primary methods of vector control as they
removed the need for regular re-treatment of impregnated nets with insecticide [1]. These
Pesticide Evaluation Scheme (WHOPES), requiring that LLINs retain effective insecticidal
activity for at least 20 laboratory washes and under field conditions for at least three years
[8 ed
on the results of these types of studies; in particular the length of time and the number of
laboratory washes a net can endure before insecticidal activity is lost. However, most
evaluations to date of LLIN performance and durability have been restricted to laboratory
tests, experimental hut studies and limited field trials [9,10].

8
Malaria is a major public health problem. Both the treatment and the control are
compromised by emerging resistance to common antimalarial drugs. In this context, multi-
drug-resistant malaria is highly prevalent [11]. Chloroquine resistance in Plasmodium
falciparum (P.falciparum) contributes to increasing malaria-attributable morbidity and
mortality in Sub-Saharan Africa [12,13] reported SPR 41.8% in district Zhob, Balochistan,
and Pakistan in blood smear slides. Cerebral malaria was reported among 4% and severs
malaria anemia among 17% of all malaria admissions in Afghanistan [14]. Malaria
prevalence was 34% with highest prevalence in children and teenagers in Pakistan [15].
Malaria is accounting for an estimated 300 to 500 million new cases and 1.5 million to 2.7
million deaths annually, majority of these deaths occur in sub-Saharan Africa [16]. There are
four species of Plasmodium causing human malaria P.falciparum, P.vivax, P.ovale and
P.malariae [17]. Falciparum malaria is a complex disease particularly; young children,
pregnant women, and non-immune visitors to malarious areas are at greatest risk of severe or
fatal illness. The world population is increasingly at risk from this disease because of the
difficulties in eradicating the vector mosquito and spread of parasite resistance [18]. World
Health Organization [19] reported that:
Malaria is life threatening disease.
A child dies of malaria in every 30 seconds.
There were 247 million cases in 2006, causing about 880, 000 deaths, mostly among
African children.
Malaria is preventable and curable.
living in lower-income countries.

9
Travelers from malaria free areas are especially vulnerable to the disease.
Malaria takes an economic toll-cutting economic growth rates by as much as 1.3% in
countries with high disease rates.
There are 23 countries in the WHO Eastern Mediterranean Region (EMR), reaching from
Morocco in the west to Pakistan in the east and from Iran in the north to Somalia in the south.
One out of every three deaths in EMR is due to communicable diseases that are 3500 people
every day. Communicable diseases account for 32% of the total burden in Disability Adjusted
Life Years (DALYs) in the region. Vector-borne diseases contribute 7% of the all-
communicable diseases in the region and malaria is on the top [20].
Malaria in Pakistan threatens millions of people, due to poor conditions which are conducive
to spread the disease throughout the country. Malaria in Pakistan is typically unstable.
P.falciparum and P.vivax are widely distributed in Pakistan. Major transmission period is
moon soon i.e. from July to November, but a short spring transmission during April and May
is also evident [21]. Figure 1.1 showed annual parasite incidence.
Dynamics of malaria in Pakistan during the last several years can be seen that in 2004, the
lowest malaria incidence was confined to two provinces Punjab and AJK with combined
population of more than 56% of total population of the country. Out of the total of 105
districts, 91 districts (86.7%) had been affected by malaria. Two provinces, namely
Balochistan and FATA reported highest malaria incidence, while Sindh and NWFP provinces
reported moderate, as compared with the two last, malaria incidence [22].

10
0.57
0.48
0.38
0.250.21
0.12 0.12 0.130.18
0.04 0.02 0.03 0.06 0.05
0.00
0.10
0.20
0.30
0.40
0.50
0.601
99
6
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
Time (Years)
AP
I
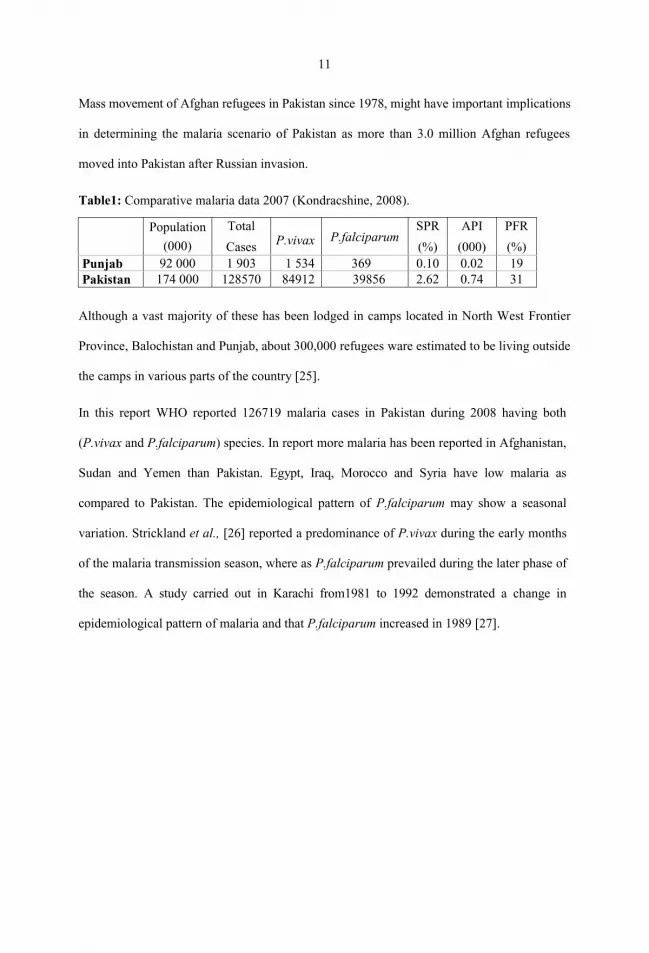
Kondracshine also reported that P.vivax was predominant malaria species, found lowest in
the NWFP. P.falciparum malaria proportion was found highest in Balochistan and Sindh,
although even there it did not exceed 35%. The Annual Blood Examination Rate (ABER)
varied between 1.72% in Punjab to almost 5% in the AJK. Further it is stated by him that
although the population of Punjab province constitutes 53% of the total population of the
country, it constituted only 1.5% of total malaria cases in 2007 (Table 1.1). The Slide
Positivity Rate (SPR) in Punjab Province is 0.10, and Annual Parasite Incidence (API) is
0.02, when ever SPR in Pakistan is 2.62 and API is 0.74.
In 2000 Falciparum Positivity Rate (FPR) in Punjab and Pakistan was 29.6% and 48.7%
respectively [23], which decreased in Punjab up to 19% and increased in Pakistan up to 31%
in 2008 Punjab Malaria Control Programme [24].
11
Mass movement of Afghan refugees in Pakistan since 1978, might have important implications
in determining the malaria scenario of Pakistan as more than 3.0 million Afghan refugees
moved into Pakistan after Russian invasion.
Table1: Comparative malaria data 2007 (Kondracshine, 2008).
Although a vast majority of these has been lodged in camps located in North West Frontier
Province, Balochistan and Punjab, about 300,000 refugees ware estimated to be living outside
the camps in various parts of the country [25].
In this report WHO reported 126719 malaria cases in Pakistan during 2008 having both
(P.vivax and P.falciparum) species. In report more malaria has been reported in Afghanistan,
Sudan and Yemen than Pakistan. Egypt, Iraq, Morocco and Syria have low malaria as
compared to Pakistan. The epidemiological pattern of P.falciparum may show a seasonal
variation. Strickland et al., [26] reported a predominance of P.vivax during the early months
of the malaria transmission season, where as P.falciparum prevailed during the later phase of
the season. A study carried out in Karachi from1981 to 1992 demonstrated a change in
epidemiological pattern of malaria and that P.falciparum increased in 1989 [27].
Population
(000)
Total
Cases P.vivax P.falciparumSPR
(%)
API
(000)
PFR
(%)Punjab 92 000 1 903 1 534 369 0.10 0.02 19Pakistan 174 000 128570 84912 39856 2.62 0.74 31

12
Table 2: Number of laboratory confirmed malaria cases in different endemic countries(World Malaria Report 2008).
Pakistan is a subtropical country with a vast system of irrigation channels and a good rain
fall in most parts of the country, all providing conducive environment for breeding of
mosquitoes. Consequently, malaria remains endemic in most parts of the country. Intensity
of the disease increases during September and October following the rainy season [28]. The
PMCP [15] also noted the same pattern.
Schellenberg et al., [29] described that successful malaria control depends heavily on
efficacious anti-malarial drugs for the treatment of malaria. Artesunate Combination
Treatments (ACT) are increasingly recommended as first line malaria treatment in endemic
countries, but implementation of this recommendation is limited, because of small number of
available and affordable co-formulated anti-malarial drugs. In recent years Intermittent
Preventive Treatment (IPT) has been recommended for malaria control in pregnancy and has
been shown to be potential of public health importance in the prevention of malaria and
anemia in children. Authors suggested concentrating the current understanding of IPT in
Countries Confirmed Cases 2007 Locally transmitted Species
Yemen 223299 P.falciparum, P.vivax
Sudan 2778207 P.falciparum, P.vivax
Afghanistan 433412 P.falciparum
Djibouti 4708 P.falciparum, P.vivaxSomalia 36773 P.falciparum, P.vivaxPakistan 126719 P. vivax, P.falciparum
Saudi Arabia 2864 P.falciparum, P.vivaxSyria 37 P. vivaxMorocco 75 P. vivaxOman 705 P. vivaxEgypt 30 P.falciparumIraq 3 P. vivaxIran 15712 P. vivax, P.falciparum

13
infants and the use of molecular approaches to enhance our understanding of the effects of
interventions on the spread of drug resistance. Yeh and Altman, [30] Over 300 million cases
of malaria each year because significant morbidity and mortality due to limited
implementation of recommendations of Artemether Combination Therapy (ACT).
Malaria remains a major cause of morbidity and mortality in tropical and subtropical regions
of the world, despite decades of malaria control efforts [31]. However Insecticide-Treated-
Nets (ITNs) can reduce malaria transmission by at least 60% and child deaths by 20%. One
of the major breakthroughs of recent decades is the realization that mosquito nets treated with
insecticide, when used properly, give a higher degree of protection against malaria as
compared to untreated nets.[32, 33]. These long lasting-treated bed nets are advanced forms
of ITN, factory impregnated, and are stronger, and remain effective for longer duration[34].
Malaria is caused by a parasite called Plasmodium, i.e. P. falciparum, .P. oval, P. vivax and P
malariae. This is transmitted through bites of infected mosquitoes (vector) to the human body
(definite host). The parasites multiply in liver and then infect red blood cells. Symptoms of
malaria include fever, headache, and vomiting, and usually appear by 10 to 15 days after the
mosquito bite. If not treated, malaria can quickly become life-threatening by disrupting the
blood supply to vital organs. In many parts of the world, the parasites have developed
resistance to a number of anti-malarial drugs. Key interventions to control malaria include:
prompt and effective treatment with Artemisinin-based combination therapies; use of
insecticidal nets by people at risk; and indoor residual spraying with insecticides to control
the vector [35].
Malaria is widely prevalent among tropical and sub-tropical countries with a predominant
effect on the Low and Middle Income Countries (LMICs) making it an issue of great public
health concern. Malaria accounted for estimated deaths of 708 1003 million in 2008, out of
which 89% were in the African region, followed by the Eastern Mediterranean Office

14
(EMRO) (6%) and the South-East Asia (5%). The estimated numbers of deaths are similar to
those reported in the World Malaria Report 2008 [36].
In Pakistan Malaria Disease surveillance program registered 3.5 million slides prepared and
127,825 confirmed cases of malaria in 2006 with Annual Parasite Incidence (API) of 0.8
cases per 1000 populations. API is highest among Baluchistan (5.8/1000 population)
followed by FATA (4.0/1000 population and Sindh (1.08/1000 population) [37].
Malaria has been a major public health issue in the Pakistan due to historic endemicity.
According to conservative estimates approximately half a million Malaria cases occur in the
country annually. These statistics are based on about 21 % of population that uses Govt.
facilities. The sufferers are mostly pregnant women and children under five. This situation
also imposes a negative impact on productivity and the socio economic growth in view of the
main transmission season occurring during harvesting and sowing of the main crops. This
leads to increase in morbidity and mortality and high cost of treatment [38].
In view of the deterioration of global malarial situation, the WHO in partnership with the
World Bank, UNDP and UNICEF, launched global Roll Back Malaria (RBM) initiative in
1998. The six strategic elements are:
1. Early Diagnosis and prompt treatment
2. Multiple prevention
3. Improved detection and response to epidemics.
4. Developing viable partnerships with national and international partners.
5. Focused operational research

15
6. Political commitment
Its objective is to halve the global burden of the disease by 50% in the Malaria endemic
country by the year 2010[27]. Pakistan became a member of the global partnership on the
RBM Programme in 1999 and a project was launched in 2001 to complement the
international efforts in controlling malaria [39].
Long lasting treated bed nets (LLINs) provide physical and chemical barriers and become
extremely effective tool. It is well known that its use leads to large scale killing of the
mosquito [40,41]. LLINs use has become one of the major interventions in National Malaria
Control Program as well as RBM Programme in Pakistan [27]. Bed nets are simple and cost
effective measure and proved to be effective intervention in many countries [42]. A recent
study has shown that the relatively modest coverage of all adults and children can achieve
equitable benefit for the whole community [31]. In 2003 WHO provided 30,000 official
LLINs in the Pakistan. Ideal coverage requirement should be 80% in endemic areas [43].
Directorate of Malaria Control distributed about 400,000 insecticides treated nets till date
[29]. Total distribution of LLINs by Global fund is placed at annexure 5.
During the recent PDHS 2006-2007, the reported coverage is 6%. The availability of nets is
higher in rural (8 percent) than in urban (4 percent) [30]. The efficacy of the LLINs depends
upon the knowledge and attitude of community [44]. The potential contribution of
knowledge, attitude and practices studies to malaria research has not received much attention
in Pakistan. Our study investigated the local community understanding of preventive
measure using LLINs and assessed their practices. .
1. Is community participation achievable?
16
2. How the community participation can be maximally capitalize?
3. What is the best possible method of introducing bed nets to the community?
LITERATURE REVIEW
Global burden
Malaria is one of the communicable diseases which having a high Case Fatality Rate among
tropical and subtropical countries of the world as shown in Fig 1. Most of the deaths are
attributed to malaria occurring in African Region Office (AFRO) of WHO (Fig.2). In 2008,
there were an estimated 243 million cases of malaria. The vast majority of cases (85%) were
in the African Region, followed by the South-East Asia (10%) and Eastern Mediterranean
Regions (4%). The number of cases in the South-East Asia Region is higher, owing to
updated household survey information for Bangladesh and Indonesia on where patients seek
treatment for fever. The estimates also reflect progress in reducing the number of cases in
several countries, but because most reductions have been seen in smaller countries, but their
influence is not much over all regionally and globally [25].
During the last decade, malaria-endemic countries have witnessed a historic increase in the
amount of resources dedicated to fight the disease [45 46 47] Bilateral and multilateral
institutions such as the Global Fund to fight AIDS, Tuberculosis and Malaria, the World
Bank and than doubled funding to
help ease the burden of malaria, especially in sub-Saharan Africa (SSA) [48 49 50 51].
Additionally,
non-profit private sector initiatives, such as the Bill and Melinda Gates Foundation, have
played an important role in changing the debate on financing, design and implementation of
malaria control programmes. Malaria researchers and policy makers have taken advantage

17
of heightened global malaria awareness to shift their focus to a rapid expansion of effective
malaria control programmes while downplaying issues related to sustainability of these
programmes. Following the increased awareness, malaria control policies, such as
implementation of large-scale indoor residual spraying with insecticides and universal free
bed net coverage campaigns have seen increased financial support, especially in SSA
[52 53 54 55]. Meanwhile, the last 10 years has seen complete overhaul of policies
addressing malaria case management in endemic settings. Most countries with high malaria
burden have changed their treatment algorithms by adopting more efficacious but expensive
artemisinin-based drug combinations [56 57 58]. Countries have also been urged to improve
malaria diagnostics through adoption of universal testing of all suspected malaria cases by
use of either microscopy or rapid diagnostic tests (RDTs) [14]. Support for preventive
treatments in highly endemic areas through adoption of intermittent preventive treatments in
pregnant women, infants and school-age children have also substantially increased
[59 60 61 62]. The long-term health, economic and social impact of adopting these changes
is not well understood [63 64]. However, given the positive correlation of malaria and
poverty [65], it is important to understand how the current large-scale malaria control policies
are impacting different segments of populations, especially the very poor.
Although initial strategies to scale up insecticide treated nets (ITNs) relied on cost-recovery,
social marketing and targeted distribution strategies (focused on biological and socio-
economically vulnerable groups), increased funding has allowed for universal free bed net
distributions in many SSA countries. While some countries have welcomed the new
financing mechanisms and aligned their policies accordingly, some have shifted largely to
respond to donor mandates alone, and others have defied the call for universal free bed net
distribution

18
as they continue with implementation of targeted bed net distribution [66 67]. Supporters of
universal free bed net distribution have consistently favoured the strategy as the most feasible
way to equitably reach the poor with the life-saving interventions [68 69]. They argue that
cost sharing and targeted interventions dampen demand, enhance inequities and consequently
exacerbate the malaria burden [70]. Despite their arguments, there are potential pitfalls. First,
the claim that free bed net distribution enhances equity is mainly based on limited case
control studies which may be unrepresentative of real-world conditions [71]. As a result, such
studies
are not necessarily generalize able because of infrastructural and large-scale programme
implementation challenges which may threaten the feasibility of reaching out to those most in
need [72 73]. Secondly, given the current global fiscal austerity measures sparked by the
global economic recession and the concomitant overreliance on international development
assistance, the long-term consequences of this strategy in terms of its sustainability remain
uncertain [74 75]. Finally, there has been some skepticism about uniform solutions to a
relatively diverse health problem and whether the disease can ever be eradicated
[76 77 78 79 80 81]. Economists have also
expressed concerns on the need for malaria interventions to do more by incorporating
economic tenets on value for money as well as aspects of programme sustainability [82].
Therefore, any proposed solutions to African economic, socio-political and health, including
those related to malaria, socio-
economic and epidemiologic settings. Despite constituting the largest disease burden
globally, malaria
epidemiology in SSA varies widely [83 84 85]. The variations in malaria policies, strategies
and epidemiology can be attributed to a number of factors, including weather and climate,

19
altitude, physical infrastructure such as water drainage systems, level of economic
development reflected
in population incomes, household structures and investments in public health programmes. It
is important to explore how large-scale malaria control programmes such as targeted free bed
net distribution may impact malaria control efforts, especially among the poorest people. One
study attempted to evaluate the health impact of a large scale malaria control programme in
Zambia [86]. However, the study did not explore how such large-scale interventions
benefited various groups of people with different socio-economic backgrounds. A recent
study from Malawi reported that people living closest to the health facilities were most likely
to have bed nets than those living far away from health clinics [87]. Another study in Zambia
reported households with a woman having attended antenatal clinic or with children under
five years old were twice more likely to have bed nets than those without [29]. In Angola,
people residing more than 15 km outside the capital city of Luanda were almost six times
more likely to test positive for malaria when screened at the health clinic than those living in
the inner-city [88]. Apart from these few studies, little is known about the impact of the large-
scale implementation of malaria programmes, such as universal bed net campaigns, on
household socioeconomic disparities and malaria burden or access and use of effective
malaria control tools. This study aims to understand how implementation of targeted free bed
net distribution has contributed to reduction of childhood malaria infection rates by their
household socioeconomic disparities. The study isunique in the sense that it uses nationally
representative malaria indicator survey data from three sub Saharan Africa countries of
Angola, Tanzania and Uganda. It is the first study to use national data and compare
inequalities in access of bed nets and their consequence in children under-five years of age
malaria infection rates across the three countries with diverse malaria transmission settings
and also their socioeconomic backgrounds. The study uses wealth measured as the proxy for
20
household socio-economic status in exploring these relationships. A list of household assets
including household construction materials, ownership of toilets, use of piped water at home
or community sources of drinking water, furniture, and other assets like bicycles, television
and sofa sets, vehicles etc. were used as detailed in MIS data collection tools [89]. More
specifically, a set of malaria control indicators in children under-five defined as RDT and
microscopy-confirmed positive results on the day of interview, household ownership of bed
across districts/provinces with
and without targeted free bed net distribution programs
Malaria accounted for an estimated 863 000 deaths in 2008, of which 89% were in the
African Region, followed by the Eastern Mediterranean (6%) and the South-East Asia
Regions (5%). The number of deaths in Africa is lower by 34 000, primarily because of a
reduction in the total number of deaths from all causes among children under 5 years of age.
The number of malaria deaths is assumed to follow this trend [25]. In addition to child
mortality, malaria can also cause severe anemia and cerebral complications in young
children. This may have serious consequences for the long-term survival of children, as well
as hinder educational and social development. Economic Burden Estimated decrease in
economic growth due to malaria in highly endemic countries: less than one percentage point
per year. Malaria transmission season generally coincides with the planting and/or harvesting
season. Mostly poor countries are at risk [29].

21
REGIONAL PERSPECTIVE
The WHO Eastern Mediterranean Region Office (EMRO) comprises 22 countries. EMRO
contains Egypt, Libyan Arab Jamahiriya, Morocco, Tunisia (North Africa), Djibouti, Somalia
and Sudan (sub-Saharan Africa), and Afghanistan, Bahrain, Iraq, Islamic Republic of Iran,
Jordan, Kuwait, Lebanon, Oman, Pakistan, Palestine, Qatar, Saudi Arabia, Syrian Arabian
Republic, United Arab Emirates and Yemen (south-west Asia). The total population of
EMRO is 513 million. Communicable diseases account for about 32% in EMRO, where only
8% of total global population lives, burden of vector-borne diseases three million Disability
Adjusted Life Years (DALYs) [90]. In addition, infections such as malaria result in loss of
productivity and school absenteeism. 48% of the regional population (248 million people,
approximately), live in areas at risk of malaria transmission. Reported malaria cases (2.7
million in 2005) with 10.5 million malaria episodes and 49 000 deaths due to malaria occur
every year in the region. Pregnant women and children of young age are at a higher risk in
the south and the central zone of Somalia and Southern Sudan. Malaria among pregnant
women can result in maternal anemia, maternal death, miscarriage, stillbirth, low birth weight
infants and even the neonatal death.

22
In Saudi Arabia, Yemen and the Sub-Saharan countries of the region (Djibouti, Somalia and
Sudan), P. falciparum is in absolute predominance. In the other endemic countries like
Afghanistan, Islamic Republic of Iran and Pakistan, both P. falciparum and P. vivax is
predominant. Due
transmission control strategies are in place. For this reason, they are categorized accordingly
in strategic plan for malaria control and elimination 2006 2010. Nine countries have
eliminated local malaria transmission and they include: Bahrain, Jordan, Kuwait, Lebanon,
Libyan Arab Jamahiriya, Palestine, Qatar, Tunisia and United Arab Emirates. The risk of
malaria reintroduction in these countries still exists. However, among four of the regional
countries ( Oman, Morocco and Syrian Arab Republic), either the malarial transmission has
been interrupted due to interventions or remains as very limited residual foci ( Egypt). Three
of all the regional countries (Islamic Republic of Iran, Iraq and Saudi Arabia) are still malaria
endemic and are in the process of initiating malaria elimination strategy. More than 95% of
the malaria cases are thus concentrated in remaining six countries of Afghanistan, Djibouti,
Pakistan, Somalia, Sudan and Yemen. Sudan alone accounts for almost 50% of the total
regional cases [27].
In Pakistan Malaria is the 2nd most prevalent and devastating disease (figure below) [28].
Malaria is endemic in Pakistan and transmission level is of low to moderate associated with
seasonal transmission and with some epidemic outbreaks in certain geographical entities like
Balochistan, Khyber Pakhtunkhwa and Sindh provinces. The disease is now being recognized
prominent health problem in Federally Administered Tribal Areas (FATA), particularly along
with the international border with Iran and Afghanistan. Malarial epidemics in Pakistan occur
at intervals of 8-10 years. Malaria in Pakistan can be attributed to a number of factors. They
may include seasonal variations, environmental conditions, vector species composition,

23
vector population dynamics, behavior of vector species (zoophiles), and the degree of
immunity among the local population. Yearly trends show that major malaria transmission
season in Pakistan is post monsoon (September-November). . However, along the coastal
areas and the western border areas, the disease prevails throughout the year. A short
transmission season during spring months (March-April) is also documented. However,
during the spring season, most of the cases are delay expression of disease transmitted during
post monsoon season or may be due to the second episode of the disease caused by relapsing
P.vivax malaria [25].
As mentioned above, there are two plasmodia species are present in the country: Plasmodium
vivax and Plasmodium falciparum, of which former is more prevalent (75% cases) than the
later. Nonetheless, later remains most dangerous [25]. These plasmodia are usually
transmitted by two out of 24 commonly found species of Anopheles mosquito. Anopheles
culicifacies and A. stephensi are the documented vectors in malaria transmission in Pakistan.
The roles other suspected species such as, An. Fluviatilis , An. Annularis. A. maculatus
A.superpictus, A. annularus, A. pulcherrimus, A. turkhudi, isstill to be determined [28].

24
, source: Ministry of Health - Government of Pakistan malaria.mht
Lady Health Workers (LHWs), from all over Pakistan, for the year 2004 reported 12 million
cases of febrile illness. 4.3 million of which were treated for confirmed malaria cases. Health
Management Information System (HMIS) of the country reported 4.5 million clinical cases of
Malaria for that year. Malaria Disease surveillance program registered 3.5 million slides and
127,825 confirmed cases of malaria in 2006 with Annual Parasite Incidence (API) of 0.8
cases per 1000 populations. These results were based on the reports from around 850 malaria
microscopy centers of the country. However, according to another conservative estimate the
actual case load might be 5 times higher than what was officially reported since public sector
diagnosis facilities do not cover more than 20-30% of the attending patients. Approximately,
80% of the patients attend private sector which are not being captured in regular reporting.
The number of serious cases admitted in the hospitals for 2006 was 51000[28].
Pakistan has been actively engaged in malaria control activities since 1950. A malaria control
eradication campaign was launched in 1961 throughout the country. Pakistan then became a
member of the global partnership on the Roll Back Malaria (RBM) Programme in 1999 and
an RBM project was launched in during 2001. The Malaria Control Programme

25
has a Malaria Information Resource Centre that receives monthly morbidity data from each
district of all provinces [29].
shows both the extrinsic and intrinsic risk factors for malarial transmission[91].
Long Lasting Insecticide treated bed Nets (LLINS, ) are the impregnated with slow-release
insecticide, permethrin, a second generation pyrethroid and non-toxic to mammals[92]. Its
use has become one of the major interventions in National Malaria Control Programmes
(MCPs) as well as RBM Programme in Pakistan. The bed nets are effective for 3-5 years and
even after 20 standard washes [27].
Anopheles mosquitoes are nocturnal feeders and using Insecticide Treated Bed Nets (ITNs)
or LLINs can prevent from their bites. Insecticide provides an additional barrier to traditional
physical barrier in preventing mosquito bites. The mosquito, which attempts to bite, is likely
to pick up a lethal dose of the insecticide, which may incapacitate it before biting or at least
kill it after biting, so that it is not able to transmit parasites from the bitten person. Most
pyrethroids also have an excite-repellent effect, which contributes to protective efficacy of
treated nets and this is particularly important where some degree of insecticide resistance
reduces the killing effect. The most effective mechanism of action of ITNs is shortening of

26
life span of mosquitoes to such an extent that they become ineffective to transmit malaria.
When an ITN/LLIN is used correctly, it provides personal protection to individual users and
using them on a community level further decreases the probability of transmission of
infection at community level. This mass effect of prevention advocates use of LLINs in
MCPs. LLINs were developed during late 1990s and are better than the old ITNs, which are
required to be retreated after a 6 months period re
nets that contain an insecticides either incorporated into or coated around fibers, which resist
multiple washes and whose biological activity last as long as the life of net itself i.e. 3 years
for polyester nets and 5 years for polyethylene nets, ese nets normally retain their
biological effectiveness without re-treatment for at least 5 years or up to 20 WHO standard
washes under laboratory conditions and at least 3 years under recommended field conditions.
In the beginning, LLINs were used on trial basis in some selected countries and showed a
significant reduction in disease transmission without repeated treatments. Currently, LLINs
have become one of the best choices of mosquito control for any malaria control program all
over world. During humanitarian crises and resulting population displacements, the use of
LLINs remains the best option of prevention from mosquito bites and disease transmission
[93].
Due to their unique technology, these nets also protect against bedbugs, human lice, fleas,
sand flies (vector of Leishmaniasis), Culex mosquitoes (vectors of Japanese encephalitis,
lymphatic filariasis) spiders and cockroaches. They can also be used to isolate infected and
disease carrier patients in health facilities for disease like yellow fever, Leishmaniasis and
dengue fever besides malaria itself [23].
WHO approved LLINs to be provided free of charge to all children less than five years of age
(one net per child) and to all pregnant women (one net per pregnant woman) in 525 high
transmission union councils in highly endemic districts of Pakistan. LLINs are also to be

27
provided free of charge to all confirmed RTD/Microscopy of P.falciparum cases.8 Free
distribution of bed nets during antenatal clinic visits may be a highly effective way to rapidly
increase the use of bed nets among both pregnant women and their newborn infants in areas
with high levels of Anti Natal Care (ANC) attendance [94].The use of bed nets is widespread
which makes its intensive use viable for malaria control. The high community ownership is
an advantage [95]. A gender and geographical divide in knowledge was observed disfavoring
women and south-eastern area respectively [96]. This study will look into the knowledge,
attitude and practices on use of LLINS among the Pakistani rural population which could

28




32
Basic
Health
Units
Dispensary Hospitals Leprosy
Clinic
MCH
Centers
Rural
Health
Centers
Sub
Health
center
T.B.
Clinic
Total
50 13 4 1 2 6 2 1 79
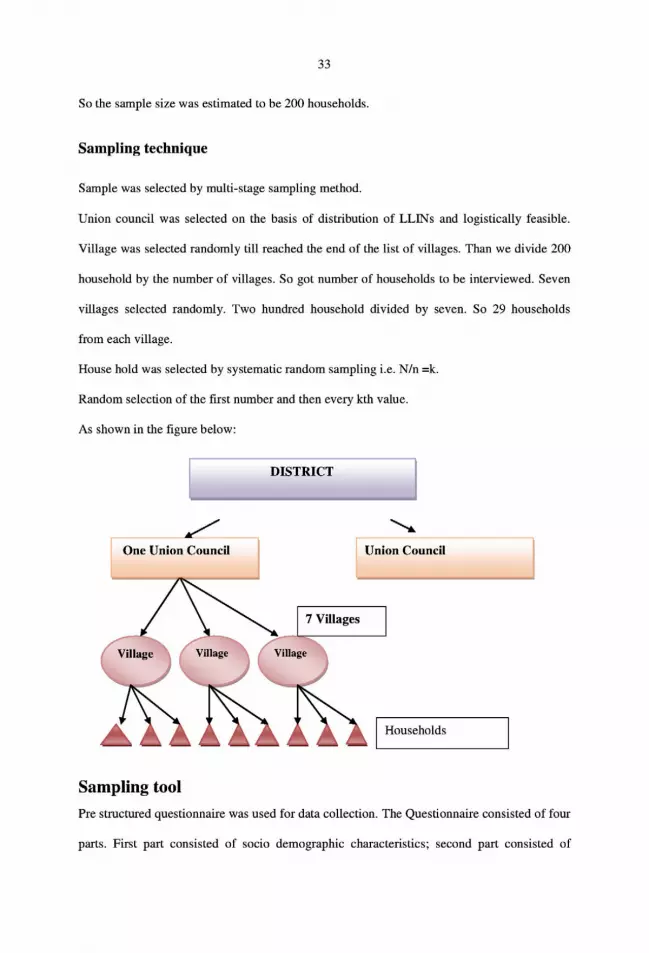
Study design
Cross sectional descriptive study.
Study population
General female population under union council Mohabatabad, District Mardan.
Duration of study
The study period was three months from March till April, 2010.
Sample size estimation
Population size (for finite population correction factor or fpc)(N): 1000000,
Hypothesized % frequency of outcome factor in the population (p): 6%/+/-5.
distribution of LLINs: 6%
Confidence interval: 95%
Design effect: 2
n=[DEFF*Np(1-p]/[d2 /z2 1- -1)+p*(1-p)]
n= 174
= 200 (to overcome non-response or incomplete data gathering)
34
Questions regarding knowledge, third part regarding theory of reasoned actions, and fourth
part regarding practices in using LLINs. Structured questionnaire was administrated to
randomly selected households. One adult person per household was interviewed. The
interviewee should have been the head of the household or in his absence; any adult above
eighteen years (18-years) was to be interviewed.
There were thirty questions in the knowledge part of questionnaire. Scoring for knowledge
was done by yes to No and Do not know . The
knowledge scored to A cut-off point was madeat0-15 fair knowledge , and
from 21-30 to be labeled as good knowledge.
There were twenty questions in the ttitude part of questionnaire. The Likert scace was
used with a s strongly agree
. The score was designated for positive
questions. Reverse scoring was done similarly for the negative questions. All the scores were
then added up to get a range of scores from 20 to100. A cut-off at 50% mark was made for
fair attitude and above 50 score was labeled to be of good attitude.
There were ten questions in the practices part of questionnaire
for a range of 0-10 score, a cutoff point at
5 was made for poor and good practices.
Questionnaire was pre- tested in another union council, , of district Mardan, KPK
province where LLINs intervention was in place.
Inclusion criteriaHouseholds, using LLINs
Adults, above 18 years

35
Exclusion criteria
Critically ill persons
Technical person working in Malaria Control Program
Elderly with disabilities
Ethical consideration
The study complied with the ethical principles being approved by the ethical
committee of Health Services Academy.
Informed consent was obtained from all the participants after explaining them the
nature of study.
Confidentiality of all the information obtained was ensured.
General ethical principles, including respect for persons, were observed.
RESULTS
Descriptive Analysis
Socio-demographic
Two hundred households were surveyed with a refusal of 0.5%. All the eligible adults (18
years and above) were interviewed. All the study participants were females. (Maximum
participants were of the age group 21-30 years (55.3%), one third were of 31-40 years age
group (37.2%).
Regarding their educational levels, majority of the participants were illiterate (73.9%) and
only a few acquired primary (11.6%) and secondary (8%) educations. Mostly, females were
house wives (98%) and only a few (2%) were in the government job. Most of the housing
types were Pakka (brick house) Makkan (60.8%) while others was Kacha (mud house)
Makkan (38.7%)

36
TABLE-1: Socio demographic characteristics of respondents (n=199)
Socio demographic variables Number Percentages
Age1- < 20 2- 21-303- 1-404- 41=
5110
74
10
2.5%55.3%
37.2%
5%
Gender:1- Females 199 100%
Marital status:1- Married 199 100%
Relation to the head of the house hold:1- Spouse2- Daughter3- Head of H.H.
19711
99%0.5%0.5%
Education:1- No education2- Primary3- Middle4- Secondary5- Higher
147
238
165
73%
11.6%4%
8%2.5%
Occupation:House wivesGovt: job
1945
97%2%
Type of house hold:Pakka MakkanKacha Makkan
12177
60.8%38.7%
Knowledge regarding use of LLINs
Majority of the respondents have had heard about Malaria. Most of them knew that malaria
could be prevented. Regarding personal protective measures, majority of the participants
heard about bed nets while some of them did not. Most (92.5%) of them knew about LLINs
(Fig10). They received LLINs from the Lady Health Workers (LHWs). Majority were having
bed nets in selected areas. When knowledge regarding disease and insect
37
prevention was explored, majority (88.9 %) knew about malaria prevention. Mostly had good
knowledge (71.9%) about prevention from mosquito bite, and less than one fourth (23.6%)
had some knowledge about LLINs protection against other insects. Regarding knowledge
about LLINs use, mostly knew how to use it. Most of the information about LLINs was
conveyed by the LHWs. Almost all the respondents knew that the LLINs should be washed.
Less than one third (29%) knew how to wash them and after six months. However, majority
had knowledge to wash them once they were dirty (63%). In most of the cases (97.5 %),
LHWs have had described the procedure. Majority (95.5%) knew how to dry it after washing
whereas some of them (3%) did not know how to do it. Knowledge regarding sleeping under
bed nets showed that respondents knew that all family members should have slept (77.9%)
under bed nets. Very few had this knowledge for the pregnant women (18.6%), and for less
than five years children (3.01%) (Fig: 10). Overall, there was good level of knowledge about
the efficacy of the use of LLINs. Majority also appreciated its proxy use for privacy and they
did not have the knowledge on mechanism of action of the LLINs in preventing disease.
Nonetheless, they were confident that the LLINs were safe for use. Importantly, most of them
(about two-thirds) were found ready to buy LLINs for themselves and rest were not. In
malaria prevention, participants helped themselves (42.7%). LHWs were instrumental in
providing LLINs and in educating the participants about using LLINs. More than half of the
respondents acquired LLINs from the LHWs. there was good knowledge base regarding
using, washing and efficacy of the LLINs among the respondents.

38
Table: 2 Response of the participant regarding knowledge about LLINs
Question yes No Do not know
1-Respondents heardabout malaria
197(99%) 2(1%) 0(0%)
2-respondents think malariacan be prevented.
194(97.5%) 3(1.5%) 2(1%)
3- respondents know aboutpersonal protective measures
124(62.3%) 75(37.3%) 0(0%)
4-respondents heard aboutbed nets.
184(92.5%) 15(7.5%) 0(0%)
5-respondents know aboutimpregnated and non impregnatedbed nets.
160(80.4%) 39(19.6%) 0(0%)
6-respondents know LLINs. 184(92.5%) 15(7.5%) 0(0%)7- Respondents has bed nets. 198(99.5% 1(0.5%) 0(0%)
8- respondents know the use of LLINs 196(98.5%) 2(1%) 1(0.5%)
9-respondents know use of LLINs by any one. 192(96.5%) 5(2.5%) 2(1%)
10- whether he or she describe the procedure 194(97.5%) 5(2.5%) 0(0%)
11-respondents know how to wash it.
12-respondents know how to dry it.
13- bed nets provide privacy.
14-respondents know bed nets are made up of.
15respondents know bed nets are coated withInsecticides.
16-respondents know bed nets are safe forHumans.17-bed nets are affordable.
18-respondents like to buy it
193(97.0%)
190(95.5%)
164(82.4%)
16(8%)
149(74.9%)
193(97%)
158(79.4%)
135(67.8%)
5(2.5%)
6(3%)
12(6%)
174(87.4%)
17(8.5%)
2(1%)
3(1.5%)
62(31.2)
1(0.5%)
3(1.5%)
23(11.6%)
9(4.5%)
33(16.6%)
4(2%)
38(19.1%)
2(1%)

39
Question Numbers Frequencies
Who help in malaria prevention?YourselfGovernmentNGOs
856252
42.7%31.2%26.1%
Came to know about LLINs from?Radio and T.V.MCPDoctorsNGOsLHWs
22228165
1%1%1%14.1%82.9%
Having number of bed nets123
185131
93%6.5%0.5%
Respondents got bed nets fromGovernmentNGOsLHWs
387109
1.5%43.7%54.8%
Disease that could be prevented by bed netsMalariaOthers
17722
88.9%11.1%
Insect could be prevented by bed netsmosquitosand flybugs
143947
71.9%4.5%23.6%
Respondents learn the use of LLIN fromMCPDoctorNGOsLHWs
1128178
5.5%1%4%89.4%
It should be washed afterWeeklyMonthlySix monthlyWhen dirty
11558125
0.5%7.5%29.1%62.8%
Mainly slept under bed netsAllHead of the familyPregnant womanLess than five years
1551376
77.9%0.5%18.6%3%

40
Question Number FrequenciesRespondents think about its effectivenessNot satisfactorySatisfactoryGoodExcellent
2217322
1%1%86.9%11.1%
Change in mosquito numbersnot satisfactorysatisfactoryexcellent
81856
4%93%3%
Majority of the respondents showed good level of attitude regarding the use of LLINs.
Participants were found in an agreement with most of the positive and in disagreement with
most of the negative statements as shown in Table 4.
Table: 4 Attitudes of the Participants Regarding Use of LLINs.
Questions. Stronglydisagree
Disagree
Neither agreenor disagree
Agree Stronglyagree
Mosquito causes fever 0(0%) 1(0.5%) 1(0.5%) 83(41.7%)
114(57.3%)
Bed nets prevent fromfever.
0(0%) 2(1.0%) 2(1.0%) 71(35.7)
124(62.3%)
Bed nets are use full inpreventing Malaria.
0(0%) 0(0%) 2(1.0%) 84(42.2)
113(56.8%)
Mosquito bites preventfrom fever.
2(1%) 183(92%)
6(3%) 8(4%) 0(0%)
In your opinion, you wouldget mosquito bites despiteuse of bed nets.
1(0.5%) 184(92.5%)
6(3%) 4(2%) 4(2%)
Bed nets should be usedonly at night.
1(0.5%) 44(22.1%)
4(2.0%) 109(54.8%)
41(20.6%)
Bed nets good for children. 2(1.0%) 94(47.2%)
3(1.5%) 64(32.2%)
36(18.1%)
Bed nets useless for adults. 1(0.5%) 185(93. 3(1.5%) 10(5.0 0(0%)

41
Questions. Stronglydisagree
Disagree
Neither agreenor disagree
Agree Stronglyagree
0%) %)Bed nets used by femalesmostly.
2(1.0%) 161(80.9%)
21(10.6%) 12(6.0%)
3(1.5%)
Protect from nuisanceinsects or. Animal
0(0%) 39(19.6%)
9(4.5%) 89(44.7%)
62(31.2%)
Feel better privacy while sleeping under bed nets.
0(0%) 0(0%) 2(1.0%) 79(39.7%)
118(59.3%)
Feel hotness under bednets.
0(0%) 27(13.6%)
1(0.5%) 116(58.3%)
55(27.6%)
Neighbor would like to buy bed nets.
O(0%) 7(3.5%) 13(6.5%) 103(51.8%)
76(38.2%)
Prefer to receive it fromhealth authority.
0(0%) 22(11.1%)
43(21.6%) 87(43.7%)
47(23.6%)
Bed nets coated withinsecticides to killmosquitoes.
0(0%) 3(1.5%) 1(.5%) 89(44.7%)
106(53.3%)
Insecticide treated nets aresafe for human.
0(0%) 7(3.5%) 2(1.0%) 66(33.2%)
124(62.3%)
Worry about possible toxiceffects.
1(0.5%) 170(85.4%)
2(1%) 9(4.5%)
17(8.5%)
Washing bed nets reducesits effectiveness.
0(0%) 182(91.5%)
6(3%) 10(5%)
1(0.5%)
Animal also needprotection.
0(0%) 71(35.7%)
98(49.2%) 27(13.6%)
3(1.5%)
Practices regarding use of LLINsPractices were found of good level (Table 4). With regard to personal protective measures,
most of the respondents used bed nets most frequently followed by repellent oils and less
frequently burning cow dung to repel mosquitoes. For the last six months, most of them were
using bed nets and did not find any loss in efficacy in due course of time of the use. . Mostly
they used bed nets by tied with nails, or covered themselves as chadder or use as hanging.
Mostly they were using at bed. It was found that the washing practices were not good as most

42
of them did not wash their bed nets at the time of the survey. Some were found having them
washed after 6 months and monthly and daily washes to the least extent. Most of them
washed with plain water. Some of them washed with detergents. Mostly dried bed nets under
shades while some of them dried under sun. They showed very good practices of hanging bed
nets when not in use.
Table 5: Respondents Practices Regarding Use of Long Lasting Insecticide Treated Bed
Nets.
Questions number %
Using personal protective measure along with bed nets1- oil as repellent 38 19.1%
2- cow dung fumes 4 2.0%
3- bed nets only 150 75.4%
Respondents had bed nets.
1- Less than one month 21 10.6%2- Less than six months 100 50.3%
3- More than six months 78 39.2%
Respondents using bed nets
1- Less than one month 48 24.1%
2- Less than six months 121 60.8%
3- More than six months 30 15.1%
Noticed reduction in the efficacy of bed nets
1- No 194 97.5%
2-donot know 5 2.5%
How Respondents used bed nets
1- Hanging 17 8.5%
2- tie with robe 5 2.5%
3- tie with nail 127 63.8%
4- use as chadder 50 25.1%

43
Questions number %
Where they used bed nets.
1- Bed 196 98.5%
2- Windows 1 0.5%
They Washed bed nets
1- Daily 1 0.5%
2- monthly 18 9.0%
3- six monthly 72 36.2%
4- not yet 108 54.3%
They Washed bed nets with
1- plain water 150 75.4%
2- detergent 6 3%
3- not yet 43 21.6%
Respondents dry bed nets with
1- under sun 11 5.5%
2- under shades 187 94.0%
Respondents do when bed nets not in use
1- fold 60 30.2%
2-hang 138 69.3%
3- others 1 0.5%
Categorization of knowledge, attitude and practices
Table 8.Cumulative Level of Knowledge, Attitude and Practices
Numbers PercentageKnowledge
Good knowledge
Fair knowledge
188
11
94.5%
5.5%
Attitude

44
Good attitude
Fair attitude
72
127
36.2%
63.8%Practices
good practices 199 100%
When the variables of KAP were transformed and re-coded and analyzed for scoring, it was
revealed that almost all of the participants (94.5%) had good knowledge regarding the use of
LLINs and majority (63.8%) had fair attitude. All of them (100%) had good practices
regarding the use of LLINs.
Association between Socio Demographic variables and KAP categories
Cross tab was done and chi square was applied to see the association between
socio demographic variables and KAP but no statistically significant association
was found.

45
DISCUSSIONRespondents of the study were hundred percent married and mostly spouses of the head of
the household. Mostly respondents were illiterate. So the lower educational status of women
suggests that verbal campaigns rather than written literature may be the best way to spread
messages about personal protective measures. Most of the respondents were living in Pakka
be given to the residents of Kacha
Makkan.
The knowledge about use of LLINs was good (94.5%) among the community. The results
show that most people had information about Malaria. The most important source of
information was LHWs. Which is comparable with the knowledge of community documented
by Khumbulani W Hlongwana et al conducted in Swaziland, Africa where knowledge were
also high (78%) but they got information from health facilities[102].
Bed nets were provided free of cost to the community. Freely distributed bed nets are
acceptable, feasible and result in high usage. It was documented in the study conducted in
Kinshasa, Sub Saharan Africa, by Pettifog A, et al where free distribution of bed nets during
antenatal clinic visits may be a highly effective way ( 80% use by women and their new born)
to rapidly increase the use of bed nets among both pregnant women and their newborn
infants[103].
Personal protection use among the participants was high (62.3%). This aspect has been
reported to be fair enough (43.4%) by Khumbulani W Hlongwana et al in their survey
conducted in Swaziland, Africa [48].
The two most important predictors of use of personal protection were age and education. As
shown in my results participants with forty years and above were more knowledgeable than
the other age groups. So community participation could be benefitted by this age group.
46
There is need to direct general education as well health education towards youth. Need to be
more focused campaigns for other age groups for the improvement of their knowledge,
attitude and practices regarding use of LLINs. Overall more educated people used personal
protection more frequently and also had better knowledge of malaria. A similar trend (75.4%)
was found by a survey conducted in Lao by Uza M et al, Which showed that education was
predictive of knowledge about use of bed nets [46].
Hearing about malaria is not enough but should be seen as foundation through which the
whole range of issue should be understood. Observation regarding preventive measures
showed that most respondents (97.5%) believed that malaria is preventable. Which is
comparable with the survey where (78.1%) believed that Malaria is preventable conducted in
Swaziland, Africa [32].
Despite this positive response some did not know about prevention. This may be due to the
fact that most people are dependent on interventions by the Malaria Control Programmes for
protection against malaria infection. Most of the respondents knew about impregnated and
non impregnated bed nets. Target group (pregnant women and under five children) was
facilitated by the distribution of LLINs. Most of them had one bed net given by global fund.
Some also had more than one, where pregnant women were more than one in one household.
Regarding disease and insect prevention from the bed nets, respondents related Malaria and
Mosquito mostly prevented by bed nets. Community showed good response to buy bed nets
(67.8%). This showed their ownership for LLINs. While the study conducted in Tanzania by
Humphrey D et al, documented (77.3%) and Khumbulani W Hlongwana et al documented
(38.8%) owner ship regarding bed nets [42, 32].
Mostly respondents knew how to use, how to wash and wash it when dirty. They also knew
Respondents thought well about its effectiveness. They were satisfied with the change in

47
mosquito numbers. Generally, there was lack of knowledge about insecticide treated bed nets
among the surveyed population, yet they knew that it was coated with some insecticide, and it
was safe for human beings. Majority (>70%) , stated that bed nets protected from nuisance
insects. There is a common perception that mosquitoes are nuisance, and this might explain
why women were more likely to use bed nets, coils and repellents. Similar results have been
documented by Sarah J Moore et al in China [41].
The awareness of the respondents that malaria was caused and transmitted by the bite of
mosquito was excellent (99%). The results are comparable to the study conducted by Syed
Masud Ahmed et al in the most endemic areas of Bangladesh where more than 90% knew
about it. Almost all (99.7%) made correct association in a study conducted by Khumbulani
W Hlongwana et al in Swaziland [43, 32].
Most of them disagreed that washing reduced its effectiveness. When inquired about animal
protection from economic point of view almost half of the respondents were neither agree nor
disagree because it was strange for them to protect animals. Practices regarding use of LLINs
were good. Most of them used bed nets at bed and tied it with nails. They hung their bed nets
when not in use. Most of them did not wash bed nets yet. Those who washed their bed nets
dried in the shade. This is actually required to maintain the efficacy of insecticide treated bed
nets. Respondents were using LLINs 100% and it was comparable with the survey conducted
by Khumbulani W Hlongwana et al in Swaziland (Africa) where the use was 65.3% [32].
Limitations
The interviewees were not representative of the population as a whole, with hundred percents
females and mostly house-wives. The data collectors were the LHWs and there was a
and training augmented by surprise visits by the principal researcher and data cleaning.


50
REFERENCES
1. Schlitzer, M., 2007. History of antimalarial drug development, currently used therapeutics
and drugs in clinical development. Chem.Med. Chem., 2(7):944-986
2. Hippocrates: On Airs, Waters, and Places. 400 BCE, The Internet Classics Archive 1994;
Book 2, Part 7. English translation: Adams F. The Genuine Works of Hippocrates. London:
Sydenham Society; 1849:179 222.
3. Meckel H: Ueber schwarzes Pigment in der Milz und dem Blute einer Geisteskranken.
Allgemeine Zeitschrift für Psychiatrie und psychisch-gerichtliche Medicin 1847, 4:198 226
4. Schaudinn F: Studien über krankheitserregende Protozoen. Plasmodium vivax (Grassi &
Feletti), der Erreger des Tertianfiebers beim Menschen. Arb Kaiserl Gesundheitsamte 1903,
19:169 250
5. Cox F: History of the discovery of the malaria parasites and their vectors. Parasit Vectors
2010, 3:5.
6. WHO: Global Malaria Programme. Insecticide-treated mosquito nets: a WHO position
statement. Geneva: World Health Organization; 2007.
7. Shargie EB, Ngondi J, Graves PM, Getachew A, Hwang J, Gebre T, Mosher AW, Ceccato
P, Endeshaw T, Jima D, Tadesse Z, Tenaw E, Reithinger R,Emerson PM, Richards FO Jr,
Ghebreyesus TA T: Rapid Increase in ownership and use of long-lasting insecticidal nets and
decrease in prevalence of malaria in three regional states of Ethiopia (2006 2007). J
TropMed 2010, 2010(Article ID 750978):12. doi:10.1155/2010/750978.
8. WHO: Guidelines for laboratory and field testing of long-lasting-insecticida mosquito nets.
Geneva: World Health Organization; 2005. WHO/CDS/ WHOPES/GCDPP/2005.11.
9. Miller JE, Lindsay SW, Armstrong JRM: Experimental hut trials of bednets impregnated
with synthetic pyrethroid or organophosphate insecticide for mosquito control in the Gambia.
Med Vet Entomol 1991, 5:465 476.
10. Irish S, N'Guessan R, Boko P, Metonnou C, Odjo A, Akogbeto M, Rowland M: Loss of
protection with insecticide-treated nets against pyrethroidresistant Culex quinquefaciatus
mosqutoes once nets become holed: an experimental hut study. Parasit Vectors 2008, 1:17.

51
11. Touré, A.O., Koné, L.P., Jambou, R., Konan, T.D., Demba, S., Beugre, G.E. and Koné,
M., 2008. In vitro susceptibility of Plasmodium falciparum isolates from Abidjan (Côte
d'Ivoire) to quinine, artesunate and chloroquine. Sante, 18(1):43-47.
12. Ogungbamigbe, T.O., Ojurongbe, O., Ogunro, P.S., Okanlawon, B.M. and Kolawole,
S.O., 2008. Chloroquine resistant Plasmodium falciparum malaria in Nigeria: efficacy of
amodiaquine + sulfadoxinepyrimethamine and chloroquine + chlorpheniramine for treatment.
Mem. Inst. Oswaldo. Cruz., 103(1):79-84.
13. Asinzai, M.I. and Kakar Suleman khel, J.K., 2008. Incidence of human malaria infection
in northern hilly region of Balochistan, adjoining with NWFP, Pakistan: district Zhob. Pak
J Biol Sci., 11(12):1620-1624.
14. Okiro, E.A., Al-Taiar, A., Reyburn, H., Idro, R., Berkley, J.A. and Snow, R.W., 2009.
Age patterns of severe paediatric malaria and their relationship to Plasmodium falciparum
transmission intensity. Malar J., 8:4-6.
15. Syafruddin, D., Krisin, K., Asih, P., Sekartuti, S., Dewi, R.M., Coutrier, F., Rozy, I.E.,
Susanti, A.I., Elyazar, I.R., Sutamihardja, A., Kinzer, M. and Rogers, W.O., 2009. Seasonal
prevalence of malaria in West Sumba district, Indonesia. Malar J., 8(1): 8-10.
16. Stoppacher, R. and Adams, S.P., 2003. Malaria deaths in the United States: Case report
and review of deaths, 1979-1998. J. Forensic. Sci., 48(2): 404-408.
17. Lee, B.J, and Durand, R., 2003. The mechanisms of resistance to antimalarial drugs in
Plasmodium falciparum. Fundam. Clin.Pharmacol., 17: 147-153.
18. Bloland, P.B., 2001. Drug resistance in malaria. WHO/CDC/CSR/DRS., 4:1-5.
19. World Health Organization, 2009. World Malaria Report (2009).
20. World Health Organization, 2003. Roll Back Malaria, Regional Strategic Plan, 2003-
2006., 2-10.

52
21. Punjab Strategic Plan., 2005. National Malaria Control Programme, Ministry of Health,
Government of Pakistan. Strat. Plan,15-21.
22. Kondracshine, A., (2008). Situation Analysis of malaria situation in the province of
Punjab. Draft Report, WHO., 2-3.
23. National HMIS Report., 2000. Situation of clinical malaria (fever) in Pakistan. National
HMIS Cell Ministry of Health Government of Pakistan, Islamabad, 1-13.
24. Punjab Malaria Control Programme., 2008. Annual report of Punjab Malaria Control
Programme, 8-10.
25. Suleman, M., 1988. Malaria in Afghan refugees in Pakistan. Trans. R. Soc. Trop. Med.
Hyg., 82: 44-47.
26. Strickland, G.T., Zafar, L., Fox, E., Khaliq, A.A. and Choudhry, M.A., 1987. Endemic
malaria in four villages of the Pakistani province Punjab. Trans. R. Soc. Trop. Med. Hyg.,
81: 36-41.
27. Rafi, S., Memon, M.A., Rao, M.H. and Billo, A.G., 1994. A change of Plasmodium
species infecting children in Karachi over the last decade. J. Pakistan. Med. Assoc., 44(7):
162-164.
28. Hafiz, R.A., 1994. The role of cytochrome P 450 and glycoprotein in the development of
resistance by Plasmodium falciparum to chloroquine. Ph.D Thesis, University of Aberdeen.
UK., 45-49.
29. Schellenberg, D., Abdulla, S. and Roper, C., 2006. Current issues for anti-malarial drugs
to control Plasmodium falciparum malaria. Curr. Mol. Med., 6(2): 253-260
30. Yeh, I. and Altman, R.B., 2006. Drug Targets for Plasmodium falciparum: a post-
genomic review/survey. Mini. Rev. Med. Chem., 6(2): 177-202
53
31. Snow RW, Guerra CA, Abdisalan M, Myint HY, Hay SI. The global distribution of
clinical episodes of plasmodium falciparum malaria. Nature. 2005;343:214-217.doi:
1038/nature03343. [pub med]
32. Akande TM, Musa IO. Epidemiology of Malaria in Africa; Afri J Clin Experiment 2005;
9: 107-11.
33. Federal Ministry of Health (FMOH). The Abuja declaration on Roll Back Malaria in
Africa; Extract from African summit on Roll Back Malaria. World Health Organization
(WHO) Fact sheet 2000; p2-12.
34. Insecticide treated mosquito nets: a WHO Position Statement, Global Malaria
Programme, World Health Organization
35. Malaria, World Health Organization [On line] available at www.who.int/topics/malaria/en/.
Accessed at 12/3/2010
36. WHO: World Malaria report, 2009, page 27 [On line]. Available at
http://whqlibdoc.who.int/publications/2009/9789241563901_eng.pdf. accessed at 7/ 7/
2010
37. Strategic planning for Malaria control and elimination EMRO region by WHO 2006-
2010; page 8-9 [On line]. Available from. http://www.emro.who.int/dsaf/dsa741.pdf.
Accessed at 11/3/2010
38. Directorate of Malaria Pakistan [On line]. available from:
http://202.83.164.26/wps/portal/Moh/!ut/p/c0/04_SB8K8xLLM9MSSzPy8xBz9CP0os3h_Nx
9_SzcPIwP_MAsDA6MQL3NXtxBvIwNzA_2CbEdFAOW90ZM!/?WCM_GLOBAL_CON
TEXT=/wps/wcm/connect/MohCL/ministry/home/sahomegeneral/sageneralright/national+m
alaria+control+programme:Accessed at 10/4/2010
39. Malaria Participants Manual. Behavioral change communication services project; funded
by GFATM Round II, Malaria component. Implemented by Adgroup-HRDI Consortium
Islamabad;p. 7, 2006

54
40. Sultan M, Ali S. Malaria: Pakistan demographic Health survey. 2006-2007. Pages 147-
151.
41. Binka FN, Income F, Smith T. Impact of spatial distribution of permethrin-impergnated
bed nets on child mortality in rural northern Ghana. American journal of Topical Medicine
and Hygiene, 1998, 59(1):8085.
42. Hawley, WA et al. Community-wide effect of permethrin-treated bed nets on child
mortality and malaria morbidity in Western Kenya. American Journal of Tropical Medicine
and Hygiene, 2003, 68(4):121127.
43. Khumbulani W, Hlongwana LH, Musawenkosi LH, Simon K, Govender K, Maharaja R,
et al. Community knowledge, attitudes and practices (KAP) on malaria in Swaziland: A
country earmarked for malaria elimination. Malaria J. 2009 Feb. 19; 8: 29. 1.
44. Personal communication with Dr. Qutab uddin Kakar, technical advisor WHO, National
Malaria Control Programme.
45 Snow RW, Marsh K: Malaria in Africa: progress and prospects in the decade since the
Abuja Declaration. Lancet 2010, 376:137 139.
46 Snow RW, Okiro EA, Gething PW, Atun R, Hay SI: Equity and adequacy of international
donor assistance for global malaria control: an analysis of populations at risk and external
funding commitments. Lancet 2010, 376:1409 1416.
47 Sarbib J-L, Nankani G, Patel P: The booster program for malaria control: putting
knowledge and money to work. Lancet 2006, 368:253 257.
48 History of the Global Fund. http://www.theglobalfund.org/en/about/history/.

55
49
http://www.fightingmalaria.gov/about/index.html.
50 Grabowsky M: The billion-dollar malaria moment. Nature 2008, 451:1051 1052.
51 Pigott D, Atun R, Moyes C, Hay S, Gething P: Funding for malaria control 2006 2010: a
comprehensive global assessment. Malar J 2012, 11:246.
52 Kilian A, Boulay M, Koenker H, Lynch M: How many mosquito nets are needed to
achieve universal coverage? Recommendations for the quantification and allocation of long-
lasting insecticidal nets for mass campaigns. Malar J 2010, 9:330.
53 Kiszewski A, Johns B, Schapira A, Delacollette C, Crowell V, Tan-Torres T,
Ameneshewa B, Teklehaimanot A, Nafo-Traoré F: Estimated global resources needed to
attain international malaria control goals. Bull World Health Organ 2007, 85:623 630.
54 World Health Organization: Global Malaria Programme: Insecticide-Treated Mosquito
Nets: A WHO Position Statement, Global Malaria Programme. 2nd edition. Geneva: WHO;
2010.
55 Guerin PJ, Olliaro P, Nosten F, Druilhe P, Laxminarayan R, Binka F, Kilama WL, Ford N,
White NJ: Malaria: current status of control, diagnosis, treatment, and a proposed agenda for
research and development. Lancet Infect Dis 2002, 2:564 573.
56 Bosman A, Mendis KN: A major transition in malaria treatment: the adoption and
deployment of artemisinin-based combination therapies. Am J Trop Med Hyg 2007, 77:193
197.

56
57 Hoshen M: Artesunate combinations for malaria. Lancet 2004, 363:737.
58 WHO: Guidelines for Malaria Treatment. Geneva: World Health Organization; 2006.
59 World Health Organization: A Strategic Framework for Malaria Prevention and Control
during Pregnancy in Africa Region. Congo Brazzaville: WHO Regional Office for Africa;
2004.
60 Clarke SE, Jukes MCH, Njagi JK, Khasakhala L, Cundill B, Otido J, Crudder C,
Estambale BBA, Brooker S: Effect of intermittent preventive treatment of malaria on health
and education in schoolchildren: a cluster-randomised, double-blind, placebo-controlled trial.
Lancet 2008, 372:127 138.
61 Carneiro I, Smith L, Ross A, Roca-Feltrer A, Greenwood B, Schellenberge JA, Smith T,
Schellenberg D: Intermittent preventive treatment for malaria in infants: a decision-support
tool for sub-Saharan Africa. Bull World Health Organ 2010, 88:807 814.
62 Chandramohan D, Owusu-Agyei S, Carneiro I, Awine T, Amponsa-Achiano K, Mensah
N, Jaffar S, Baiden R, Hodgson A, Binka F, Greenwood B: Cluster randomised trial of
intermittent preventive treatment for malaria in infants in area of high, seasonal transmission
in Ghana. BMJ 2005, 331:727 733.
63 Goodman C, Kara H, Anne M, Virginia W, Worrall E: The Economics of Malaria and Its
Control. In Scientific Working Group on Malaria (WHO/TDR ed). Geneva: WHO; 2003
64 Breman JG, Alilio MS, Mills A: Conquering the intolerable burden of
2004, 71:1 15.
65 Worrall E, Basu S, Hanson K: Is malaria a disease of poverty? A review of the literature.
Trop Med Int Health 2005, 10:1047 1059.

57
66 Sexton A: Best practices for an insecticide-treated bed net distribution programme in sub-
Saharan eastern Africa. Malar J 2011, 10:157.
67 Teklehaimanot A, Sachs JD, Curtis C: Malaria control needs mass distribution of
insecticidal bed nets. Lancet 2007, 369:2142 2146.
68 Kilama WL: The 10/90 gap in sub-Saharan Africa: resolving inequities in health research.
Acta Trop 2009, Supplement 1:S8 S15.
69 Kilian A, Wijayanandana N, Ssekitoleeko J: Review of delivery strategies for insecticide
treated mosquito nets: are we ready for the next phase of malaria control efforts? TropIKAnet
2010, 1. ISSN 2078-8606.
70 Cohen J, Dupas P: Free distribution or cost-sharing? Evidence from a randomized malaria
prevention experiment. Quart J Econ 2010, 125:1 45
71 Grabowsky M: Distributing insecticide-treated bednets during measles vaccination: a low-
cost means of achieving high and equitable coverage. Bull World Health Organ 2005,
83:195 201.
72 . Steketee RW, Eisele TP: Is the scale up of malaria intervention coverage also achieving
equity? PLoS One 2009, 4:e8409.
73 Larsen DA, Keating J, Miller J, Bennett A, Changufu C, Katebe C, Eisele TP: Barriers to
Insecticide-treated mosquito net possession 2 years after a mass free distribution campaign in
Luangwa District, Zambia. PLoS One 2010, 5:e13129.
74 Garrett L: Global health hits crisis point. Nature 2012, 482:7.

58
75 Ordinioha B: The use and misuse of mass distributed free insecticide treated bed nets in a
semi-urban community in Rivers State, Nigeria. Ann Afr Med 2012, 11:163 168.
76 Fryatt R, Mills A, Nordstrom A: Financing of health systems to achieve the health
Millennium Development Goals in low-income countries. Lancet 2010, 375:419 426.
77 Alonso PL, Brown G, Arevalo-Herrera M, Binka F, Chitnis C, Collins F, Doumbo OK,
Greenwood B, Hall BF, Levine MM, Mendis K, Newman RD, Plowe CV, Rodríguez MH,
Sinden R, Slutsker L, Tanner M: A research agenda to underpin malaria eradication. PLoS
Med 2011, 8:e1000406.
78 Alonso PL, Brown G, Arevalo-Herrera M, Binka F, Chitnis C, Collins F, Doumbo OK,
Greenwood B, Hall BF, Levine MM, Mendis K, Newman RD, Plowe CV, Rodríguez MH,
Sinden R, Slutsker L, Tanner M: A research agenda to underpin malaria eradication. PLoS
Med 2011, 8:e1000406.
79 Foster AD: Poverty and illness in low-income rural areas. Amer Econ Rev 1994, 84:216
220.
80 Baird JK: Resurgent malaria at the millennium: control strategies in crisis. Drugs 2000,
59:719 743.
81 Editor L: Is malaria eradication possible? Lancet 2007, 370:1459 1459.
82 . Wilson P, Aizenman Y: Value for money in malaria programming issues and
opportunities, Working Paper 291. Washington D.C: Center for Global Development; 2012.
83 Hay SI, Guerra CA, Tatem AJ, Noor AM, Snow RW: The global distribution and
population at risk of malaria: past, present, and future. Lancet Infect Dis 2004, 4:327 336.

59
84 Hay SI, Guerra CA, Gething PW, Patil AP, Tatem AJ, Noor AM, Kabaria CW, Manh BH,
Elyazar IRF, Brooker S, Smith DL, Moyeed RA, Snow RW: A world malaria Map:
plasmodium falciparum endemicity in 2007. PLoS Med 2009, 6:e1000048.
85 Hay SI, Smith DL, Snow RW: Measuring malaria endemicity from intense to interrupted
transmission. Lancet Infect Dis 2008, 8:369 378.
86 . Ashraf N, Fink G, Weil DN: Evaluating the effects of large scale health interventions in
developing countries: The Zambian Malaria Initiative, SSRN eLibrary. Cambridge,
Massachusetts: NBR Working Paper 16069; 2010
87 Larson P, Mathanga D, Campbell C, Wilson M: Distance to health services influences
insecticide-treated net possession and use among six to 59 month-old children in Malawi.
Malar J 2012, 11:18
88 Thwing JI, Mihigo J, Fernandes AP, Saute F, Ferreira C, Fortes F, de Oliveira AM,
Newman RD: How much malaria occurs in urban Luanda, Angola? A health facility-based
assessment. Am J Trop Med Hyg 2009, 80:487 491.
89 44. MEASURE DHS: Demographic and Health Surveys Data Collection.
http://www.measuredhs.com/data/data-collection.cfm#CP_JUMP_5188
90. World Malaria report 2005.Geneva.RBM/WHO/UNICEF.
91. World Health Organization, World Malaria Report, 2006-7
92. Health Information Management System, 2006.
93. Determinants of Malaria [ On line]. Available at;
http://images.google.com/imgres?imgurl=http://www.ncbi.nlm.nih.gov/bookshelf/picrend
er.fcgi%3Fbook%3Ddcp2%26part%3DA2811%26blobname%3Dch21f1.jpg&imgrefurl=
http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi%3Fbook%3Ddcp2%26part%3DA2870&u
sg=__hSOHmfQEQUu_PDdTx344acglM1g=&h=298&w=297&sz=48&hl=en&start=1&i
tbs=1&tbnid=UoDBJ0sArrV3EM:&tbnh=116&tbnw=116&prev=/images%3Fq%3Ddeter

60
minants%2Bof%2Bmalaria%26hl%3Den%26tbs%3Disch:1. Accessed at 10/3/10
94. Olyster nets, technical information, Sumitomo chemical, page 3-4 [ On line ]. Available
at; www.olyset.net. Accessed at 19/3/10
95. Pettifor A, Taylor E, Nku D, Duvall S, Tabala M, Mwandagalirwa K, et al. Free
distribution of insecticide treated bed nets to pregnant women in Kinshasa: an effective way
to achieve 80% use by women and their newborns. Trop Med Int Health. 2009 Jan;14(1):20-
8.
96. Uza M, Phommpida S, Toma T, Takakura M, Manivong K, Bounyadeth Set al.
Knowledge and behaviour relating to malaria in malaria endemic villages of Khammouane
Province, Lao PDR. Southeast Asian J Trop Med Public Health 2002;33:246 254.
97. Sarah J , Xia M, Nigel H, Caroline J, Zhang Z, Mary M. Border malaria in China
knowledge and use of personal protection by minority populations and implications for
malaria control: a questionnaire-based survey. BMC Public Health 2008; 8: 344.
98. Humphrey D, Emmanuel O, Wilhe l, Paulina M, Maria Zi, Eliningaya J et al. Knowledge,
Attitudes, and Practices about Malaria and Its Control in Rural Northwest Tanzania. Malaria
Research and Treatment 2010; Article ID 794261, 9 pages.
99. Ahmed M, H Rashidul, H Ubydul and H Awlad. Knowledge on the transmission,
prevention and treatment of malaria among two endemic populations of Bangladesh and their
health-seeking behavior, Malar J. 2009; 8: 173. Published online 2009 July 29. doi:
10.1186/1475-2875-8-173.
100. Allen. R. Oxford dictionary. Eight editions. United State: Oxford university press Inc;
1990. Knowledge; p. 656
101. Allen. R. Oxford dictionary. Eight editions. United State: Oxford university press Inc;
1990. Attitude; p. 70.
102. Allen. R. Oxford dictionary. Eight editions. United State: Oxford university press Inc;
1990. Behavior; p. 99.

61
103. Malarial facts, Center for Disease Control and Prevention (CDC) [ On line]. Available
from; http://www.cdc.gov/malaria/index.html. Accessed at 12/4/2010

Buy your books fast and straightforward online - at one of world’s
fastest growing online book stores! Environmentally sound due to
Print-on-Demand technologies.
Buy your books online at
www.get-morebooks.com
Kaufen Sie Ihre Bücher schnell und unkompliziert online – auf einer
der am schnellsten wachsenden Buchhandelsplattformen weltweit!
Dank Print-On-Demand umwelt- und ressourcenschonend produzi-
ert.
Bücher schneller online kaufen
www.morebooks.deVDM Verlagsservicegesellschaft mbH
Heinrich-Böcking-Str. 6-8 Telefon: +49 681 3720 174 [email protected] - 66121 Saarbrücken Telefax: +49 681 3720 1749 www.vdm-vsg.de






























