Embed Size (px)
Citation preview

Send Orders for Reprints to [email protected]
Infectious Disorders – Drug Targets, 2014, 14, 125-132 125
Knowledge, Attitude and Practice (KAP) Survey Concerning Antimicro-bial Use among Australian Hajj Pilgrims
Mohammad Azeem1,2*, Mohamed Tashani1,2, Osamah Barasheed1,2, Leon Heron1, Grant A. Hill-Cawthorne3,4, Elizabeth Haworth5, Dominic E. Dwyer2,6, Harunor Rashid1,2 and Robert Booy1,2,4
1National Centre for Immunisation Research and Surveillance of Vaccine Preventable Diseases, Kids Research Institute, The Children’s Hospital at Westmead, Australia; 2Sydney Medical School, The University of Sydney, Australia; 3Sydney School of Public Health, The University of Sydney, Australia; 4Marie Bashir Institute for Infectious Diseases and Biose-curity, The University of Sydney, Australia; 5Menzies Research Institute Tasmania, Hobart, Tasmania, Australia; 6Centre for Infectious Diseases and Microbiology Laboratory Services, Westmead Hospital, NSW, Australia
Abstract: Resistance to antimicrobial agents has increased for reasons relating to the use and misuse of antimicrobials in human, agriculture and aquaculture. Antimicrobial use is quite high during mass gatherings such as the Hajj pilgrimage. To reduce non-prescription use and inappropriate prescribing of antimicrobials, a more thorough understanding of their use and the motives behind why patients request, even demand, antimicrobials, fail to adhere to the prescription is impor-tant. Therefore, we conducted a knowledge, attitude and practice (KAP) survey among Australian Hajj pilgrims in Mecca during Hajj 2013 using an anonymous, self-administered questionnaire concerning antimicrobial use. Our sample con-sisted of 229 adult Australian subjects. Mean age was 42.4 (SD±12.7) years, 178 (77.9%) were male and 80 (34.9%) used antimicrobials during their stay in Saudi Arabia. Twenty one (26.3%) obtained these in Saudi Arabia without prescription, and about half (38, 47.5%) brought them from Australia. Of the respondents, 55.8% believed that antibiotics are effective against viruses, 53.6% thought that antibiotics are effective against common cold and flu, 78.6 % that humans themselves can become resistant to antibiotics and 75.9% knew that overuse or unnecessary use of antibiotics can cause them to lose effectiveness. This study has revealed that Hajj pilgrims have inappropriate access to antimicrobials in Saudi Arabia as well as in Australia. A large scale education campaign and tighter control on prescribing and dispensing of antimicrobials could improve the appropriate antimicrobial use among Hajj pilgrims.
Keywords: Antimicrobials, Antibiotics, Hajj, Knowledge Attitude and Practice, Survey Mecca.
1. INTRODUCTION
The growing problem of antimicrobial resistance is a major challenge worldwide, placing public health at serious risk. Antibiotic resistance among respiratory pathogens is now a common clinical problem [1-3]. Resistance to antimicrobial agents has increased for many reasons including irrational or over-prescription of antimicrobials by physicians, noncom-pliance with prescribed treatments by patients, self-prescribing or over the counter access, misuse of antimicrobials by un-skilled practitioners and the recent extensive use of antibiot-ics as growth factors in agriculture and aquaculture [4-10]. Prior use of antimicrobials, particularly within four weeks of the current infection is a risk factor for infection or colonisa-tion by antimicrobial resistant organisms [11]. International travel can add to this risk. There are close to 500 million person flights/year internationally and millions of people attend mass gatherings such as the Hajj and Umrah pilgrim-ages, festivals, concerts and sports events. Antibiotics can be used widely, for example to eradicate possible carriage of meningococci in Hajj pilgrims arriving from sub-Saharan *Address correspondence to this author at the National Centre for Immuni-sation Research and Surveillance, Kids Research Institute, The Children’s Hospital at Westmead, Locked Bag 4001, Westmead, NSW 2145, Australia; Tel: +61 421 777 439; Fax: +61 2 9845 1418; E-mail: [email protected]
Africa (i.e. the meningitis belt) [12], or the management of outbreaks and possible international public health implica-tions [13, 14].
According to a study conducted at a hospital in Mecca during Hajj 2003, antibiotics accounted for 43.3% of all medication dispensed during the study period of 15 days [15]. Another study during Hajj 2009 in the Ear, Nose and Throat (ENT) clinic of a Hospital in Mecca found that, de-spite 42.1% (1297 out of 3087) of patients were being diag-nosed with viral upper respiratory tract infections (URTI), more than 95 % of them were treated with antibiotics; the same Saudi study found that, overall, 98.6% (3045/3087) of ENT patients received an antimicrobials [16]. A study con-ducted in Riyadh, Saudi Arabia, found that 77.6% (244/327) of pharmacies recommended and sold antibiotics over the counter [17]. Prudent use of antimicrobials is important to avoid and halt the escalation and transmission of resistant microorgan-isms. Better understanding of current practices and why pa-tient request or demand antibiotics or fail to comply with the prescription is necessary. The use of several intervention tools has been shown to be effective in improving awareness and knowledge as well as changing behaviours of patients and prescribers [18, 19]. Understanding patients’ KAP will aid in the development of
2212-3989/14 $58.00+.00 © 2014 Bentham Science Publishers

126 Infectious Disorders – Drug Targets, 2014, Vol. 14, No. 2 Azeem et al.
strategies and intervention tools to change the practices of patients, clinicians and the public. Therefore, we conducted a survey at Mecca in 2013 to assess Australian Hajj pilgrims’ KAP regarding antimicrobi-als. We also sought to study the prevalence and appropriate-ness of antibiotic use in Australian Hajj pilgrims.
2. METHODS
2.1. Survey Questionnaire
The survey was conducted in Mecca among Australian pilgrims > 18 years of age attending the Hajj pilgrimage dur-ing October 13-19, 2013 using an anonymous self-administered questionnaire. The questionnaire was designed to collect important information and KAP concerning antim-icrobial use, and included questions about self-prescribing and knowledge of antimicrobial effectiveness. It also col-lected participants’ demographics including age, gender, occupation, place of residence (suburb/postcode) and tour operator’s details as well as their underlying medical condi-tions and reasons for antimicrobial use during Hajj. The questionnaire was informed by the appropriate literature and expert opinion and could be completed within 30 minutes.
2.2. Survey
Pilgrims residing in the Australian camps or hotels were approached serially and were invited to participate. The sur-vey was conducted during the last days of Hajj in Mina (an important Hajj location on the outskirts of Mecca) and/or
hotels in Mecca with the collaboration of tour group leaders. The tour group guides arranged for announcements about the study in English and Arabic. All study participants were first briefed about the study and then a verbal consent was ob-tained, after which the survey questionnaire was adminis-tered. Its completion was considered as implied consent for the study. Ten trained volunteer researchers answered the participant queries, provided further explanation as required and, if necessary, recorded dictated responses.
2.3. Ethics Approval
Ethics approval was granted by the Human Research Ethics Committee at Sydney Children’s Hospitals Network, Australia (Ref: 11/SCHN/162).
2.4. Statistical Analysis
All data were first entered into Microsoft Excel 2010 and statistical analysis was performed using the Statistical Pack-age for Social Sciences (SPSS) v.19.0 (SPSS, Inc., Chicago, IL, USA). Categorical variables were compared and analysed by using the chi-squared test. A p value ≤0.05 was consid-ered statistically significant. Logistic regression analysis was used to model the odds of antimicrobial use by knowledge.
3. RESULTS
The study recruited 241 subjects; six were excluded as they were non-Australians (Fig. (1)). The sample therefore consisted of 235 adult subjects, 78% male, 15% female and
Fig. (1). Flow diagram showing recruitment of participant.
Total Number of Respondents = 241
Total Number of Australian Hajj Pilgrims who participated
in Survey = 235
- 6 = Did not answer question on antimicrobial use
Number of Studied participants for Antimicrobial Use = 229
- 11 = Did not answer the questions about KAP survey
Number of Studied participants for KAP Survey = 224
- 6 non Australians
Knowledge, Attitude and Practice (KAP) Survey Concerning Antimicrobial Infectious Disorders – Drug Targets, 2014, Vol. 14, No. 2 127
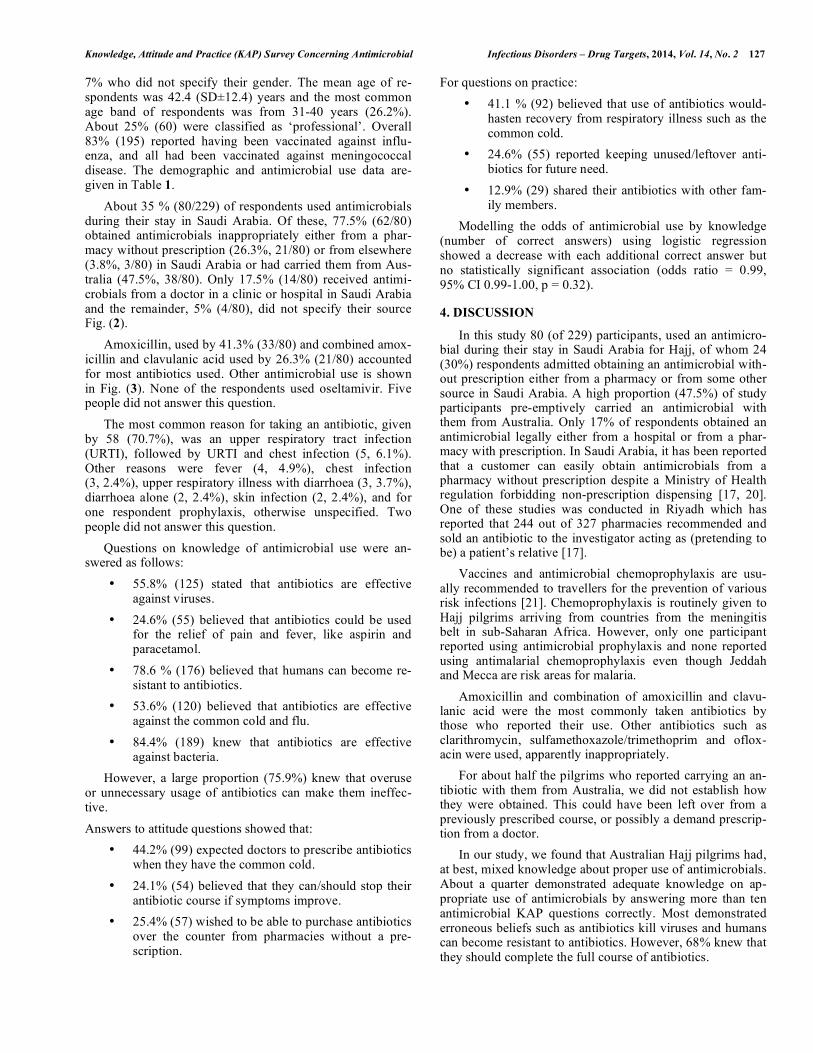
7% who did not specify their gender. The mean age of re-spondents was 42.4 (SD±12.4) years and the most common age band of respondents was from 31-40 years (26.2%). About 25% (60) were classified as ‘professional’. Overall 83% (195) reported having been vaccinated against influ-enza, and all had been vaccinated against meningococcal disease. The demographic and antimicrobial use data are-given in Table 1. About 35 % (80/229) of respondents used antimicrobials during their stay in Saudi Arabia. Of these, 77.5% (62/80) obtained antimicrobials inappropriately either from a phar-macy without prescription (26.3%, 21/80) or from elsewhere (3.8%, 3/80) in Saudi Arabia or had carried them from Aus-tralia (47.5%, 38/80). Only 17.5% (14/80) received antimi-crobials from a doctor in a clinic or hospital in Saudi Arabia and the remainder, 5% (4/80), did not specify their source Fig. (2). Amoxicillin, used by 41.3% (33/80) and combined amox-icillin and clavulanic acid used by 26.3% (21/80) accounted for most antibiotics used. Other antimicrobial use is shown in Fig. (3). None of the respondents used oseltamivir. Five people did not answer this question. The most common reason for taking an antibiotic, given by 58 (70.7%), was an upper respiratory tract infection (URTI), followed by URTI and chest infection (5, 6.1%). Other reasons were fever (4, 4.9%), chest infection (3, 2.4%), upper respiratory illness with diarrhoea (3, 3.7%), diarrhoea alone (2, 2.4%), skin infection (2, 2.4%), and for one respondent prophylaxis, otherwise unspecified. Two people did not answer this question. Questions on knowledge of antimicrobial use were an-swered as follows:
• 55.8% (125) stated that antibiotics are effective against viruses.
• 24.6% (55) believed that antibiotics could be used for the relief of pain and fever, like aspirin and paracetamol.
• 78.6 % (176) believed that humans can become re-sistant to antibiotics.
• 53.6% (120) believed that antibiotics are effective against the common cold and flu.
• 84.4% (189) knew that antibiotics are effective against bacteria.
However, a large proportion (75.9%) knew that overuse or unnecessary usage of antibiotics can make them ineffec-tive. Answers to attitude questions showed that:
• 44.2% (99) expected doctors to prescribe antibiotics when they have the common cold.
• 24.1% (54) believed that they can/should stop their antibiotic course if symptoms improve.
• 25.4% (57) wished to be able to purchase antibiotics over the counter from pharmacies without a pre-scription.
For questions on practice: • 41.1 % (92) believed that use of antibiotics would-
hasten recovery from respiratory illness such as the common cold.
• 24.6% (55) reported keeping unused/leftover anti-biotics for future need.
• 12.9% (29) shared their antibiotics with other fam-ily members.
Modelling the odds of antimicrobial use by knowledge (number of correct answers) using logistic regression showed a decrease with each additional correct answer but no statistically significant association (odds ratio = 0.99, 95% CI 0.99-1.00, p = 0.32).
4. DISCUSSION
In this study 80 (of 229) participants, used an antimicro-bial during their stay in Saudi Arabia for Hajj, of whom 24 (30%) respondents admitted obtaining an antimicrobial with-out prescription either from a pharmacy or from some other source in Saudi Arabia. A high proportion (47.5%) of study participants pre-emptively carried an antimicrobial with them from Australia. Only 17% of respondents obtained an antimicrobial legally either from a hospital or from a phar-macy with prescription. In Saudi Arabia, it has been reported that a customer can easily obtain antimicrobials from a pharmacy without prescription despite a Ministry of Health regulation forbidding non-prescription dispensing [17, 20]. One of these studies was conducted in Riyadh which has reported that 244 out of 327 pharmacies recommended and sold an antibiotic to the investigator acting as (pretending to be) a patient’s relative [17]. Vaccines and antimicrobial chemoprophylaxis are usu-ally recommended to travellers for the prevention of various risk infections [21]. Chemoprophylaxis is routinely given to Hajj pilgrims arriving from countries from the meningitis belt in sub-Saharan Africa. However, only one participant reported using antimicrobial prophylaxis and none reported using antimalarial chemoprophylaxis even though Jeddah and Mecca are risk areas for malaria. Amoxicillin and combination of amoxicillin and clavu-lanic acid were the most commonly taken antibiotics by those who reported their use. Other antibiotics such as clarithromycin, sulfamethoxazole/trimethoprim and oflox-acin were used, apparently inappropriately. For about half the pilgrims who reported carrying an an-tibiotic with them from Australia, we did not establish how they were obtained. This could have been left over from a previously prescribed course, or possibly a demand prescrip-tion from a doctor. In our study, we found that Australian Hajj pilgrims had, at best, mixed knowledge about proper use of antimicrobials. About a quarter demonstrated adequate knowledge on ap-propriate use of antimicrobials by answering more than ten antimicrobial KAP questions correctly. Most demonstrated erroneous beliefs such as antibiotics kill viruses and humans can become resistant to antibiotics. However, 68% knew that they should complete the full course of antibiotics.

128 Infectious Disorders – Drug Targets, 2014, Vol. 14, No. 2 Azeem et al.
Table 1. Demographics of the participants and antimicrobial use during Hajj 2013.
Antimicrobial use during Hajj 2013
Characteristics Total Number of Participants
n (% of total) Yes n (%)
No n (%)
No answer n (%)
Gender
Male 183 (77.9) 66 (36.1) 114 (62.3) 3 (1.6)
Female 35 (14.9) 7 (20.0) 26 (74.3) 2 (5.7)
No answer 17 (7.2) 7 (41.2) 9 (52.9) 1 (2.6)
Age Group
21-30 years 46 (19.6) 14 (31.8) 30 (68.2) 2 (4.3)
31-40 years 60 (25.5) 19 (31.7) 41 (68.3) 0 (0.0)
41-50 years 43 (18.3) 12 (27.9) 30 (69.8) 1 (2.3)
51-60 years 46 (19.6) 21 (45.7) 24 (52.2) 1 (2.2)
61-70 years 21 (8.9) 9 (42.9) 10 (47.6) 2 (9.5)
No Answer 19 (8.1) 5 (26.3) 14 (73.7) 0 (0.0)
Occupation
Professional 56 (23.8) 20 (35.7) 36 (64.3) 0 (0.0)
Other White Collar 37 (15.7) 21 (56.8) 16 (43.2) 0 (0.0)
Trade Worker 29 (12.3) 7 (24.1) 21 (72.4) 1 (3.4)
Home Maker 13 (5.5) 3 (23.1) 9 (69.2) 1 (7.7)
Retired 9 (3.8) 4 (44.4) 3 (33.3) 2 (22.2)
Student 9 (3.8) 2 (22.2) 7 (77.8) 0 (0.0)
Self Employed 14 (6.0) 3 (21.4) 11 (78.6) 0 (0.0)
No answer 68 (28.9) 20 (29.4) 46 (67.6) 2 (2.9)
Residence
New South Wales 121 (51.5) 46 (38) 72 (59.5) 3 (2.5)
Victoria 43 (18.3) 8(18.6) 33(76.7) 2 (4.7)
Other States 40 (17.0) 13 (32.5) 27 (67.5) 0 (0.0)
No answer 31 (13.2) 13 (41.9) 17 (54.8) 1 (3.7)
Knowledge
Good 59 (25.1) 20 (33.9) 38 (64.4) 1 (1.7)
Average 97 (41.3) 33 (34.0) 62 (63.9) 2 (2.1)
Below average 67 (28.5) 25 (37.3) 41 (61.2) 1 (1.5)
No answer 12 (5.1) 2 (16.7) 8 (66.7) 2 (16.7)

Knowledge, Attitude and Practice (KAP) Survey Concerning Antimicrobial Infectious Disorders – Drug Targets, 2014, Vol. 14, No. 2 129
Fig. (2). Antimicrobial use by Australian Hajj Pilgrims during Hajj 2013 (n = 229).
Fig. (3). Reported antibiotic use.
Did nnot use : 149 Used: 80
Brouhome (38
ught from , 47.5%)
Purchasepharmac
prescriptioArabia (2
ed from a cy without on in Saudi 21, 26.3%)
No Ans
Prescribedby a docto
/ hospitaArabia (1
Obtaineprescrip
elsewher
swer, (4, 5%)
d / provided or in a clinic al in Saudi 14, 17.5%)
ed without ption from re, (3 ,3.8%)
)
Amoxicillin, 41%
Amoxicillin / Clavulanic acid, 26%
Clarithromycin, 4%
Cephalexin, 3%
Cefaclor, 3%
Metronidazole, 3%
Sulfamethoxazole / Trimethoprim, 2%
Azithormycin, 1%Ofloxacin, 1%
Other/Multiple, 10%
No answer, 6%

130 Infectious Disorders – Drug Targets, 2014, Vol. 14, No. 2 Azeem et al.
Fig. (4). Responses of Australian Hajj Pilgrims to KAP survey questions concerning antimicrobials (n = 224, shown as percentage). The response to the question about practice indicated that about 40 % in our survey would use an antibiotic for respira-tory illness such as the common cold and influenza. This was lower than or similar to recent Malaysian studies (82%), lower than a European study (53%) and higher than in Tai-wan (17%) [22-25]. In our study, 23.7% respondents reported keeping left over antibiotics at home for future need, higher than for KAP surveys conducted in the US and UK but lower than in Jor-dan [26-28]. Also about 12% in our study indicated that they share their antibiotics with other family members which was lower than Chen et al found in Taiwan [24]. A number of studies recommend educational interven-tions aimed at patients and clinicians to improve their awareness and knowledge and change behaviours [19, 29, 30]. Some studies have shown reduction in antimicrobial prescribing by doctors trained to use methods such as inter-active booklets, enhanced communication skills and delayed prescribing for the management of respiratory infections [10, 31-34]. Our study has shown a continuing and urgent need for education on the appropriate use of antimicrobials for pil-grims before and during Hajj and on the mechanisms and dangers of antimicrobial resistance. This could be done via Hajj tour groups, Islamic Associations, local mosques, Is-lamic youth centres and Islamic media such as religious websites and radio channels. To the best of our knowledge, this is the first KAP survey examining antimicrobial use among Australian Hajj pil-
grims. While it has clearly inappropriate use of antimicrobi-als by Australian Hajj pilgrims, the study has several limita-tions. Firstly, ours was a minority sample of Australian Hajj 2013. Secondly, because it used a self-reported question-naire, we infer rather than objectively measure behaviours. Thirdly, the excess of male participants may have skewed our findings.
5. CONCLUSION
This study has found that Australian Hajj 2013 pilgrims had many misconceptions regarding antimicrobial use and had easy access to non-prescribed antimicrobials. We rec-ommend a large scale education campaign to improve ap-propriate antimicrobial use among Hajj pilgrims. Relevant health authorities should improve the enforcement of pre-scription only dispensing of antimicrobials in community pharmacies and assure quality antimicrobial use with evi-dence-based guidelines including appropriate chemoprophy-laxis for travellers. A validated study is needed to further explore attitudes and practices to achieve better antimicrobial control.
CONFLICT OF INTEREST
Leon Heron and Robert Booy have received funding from Baxter, CSL, GSK, Merck, Novartis, Pfizer, Roche, and Sanofi Pasteur for the conduct of sponsored research, travel to present at conferences or consultancy work; all funding received is directed to research accounts at The
12.9
24.1
24.6
25.4
44.2
41.1
24.6
53.6
55.8
84.4
75.9
78.6
84.8
83
71.4
71.4
71.4
50.9
54.5
72.3
42
42.4
11.2
17
17
9.4
4
4.5
4
3.1
4.9
4.5
3.1
4
1.8
4.5
7.1
4.5
5.8
0 10 20 30 40 50 60 70 80 90 100
If my family member is sick, I usually give my antibiotics to them
You can stop taking a full course of antibiotic if your symptoms areimproving
It is good to keep leftover antibiotics at home in case of future need
It would be good to be able to purchase antibiotics in pharmacies withoutprescription
I expect antibiotics to be prescribed by my doctor if I suffer from commoncold symptoms
When I get a respiratory illness like common cold and Flu, I takeantibiotics to help me get better more quickly
Antibiotics are the same as medications used to relieve pain and fever suchas aspirin and paracetamol
Antibiotics are effective against cold and flu
Antibiotics are effective against viruses
Antibiotics are effective against bacteria
Overuse/Unnecessary use of antibiotics can cause antibiotics to loseeffectiveness
Humans can become resistant to antibiotics
Bacteria can become resistant to antibiotics
Yes No No Answer

Knowledge, Attitude and Practice (KAP) Survey Concerning Antimicrobial Infectious Disorders – Drug Targets, 2014, Vol. 14, No. 2 131
Children’s Hospital at Westmead. The other authors have declared no conflict of interest in relation to this work.
ACKNOWLEDGEMENTS
We would like to thank following volunteers for their support in data collection: M Alfelali, H Bokhary, M Als, Y Alghamdi, D Alansari, A Al-‐Hetairshi, M Chow, D Sakabumi, S Melebari, N Dibi, A Al-‐Beladi, D Tashkandi, W Al-‐Otaiby, R Abu Zahirah, S Alhadramy, Z Siyam, M Bakhaidar, A Basalamah, S Jiman, A Alotaibi, M Hijan, S Abuzidbarabwan, M Al-‐Sudais, S Alghamdi, S Alghamdi, M Sheikh, T Almalki, A Alaklubi, M Alzahrani, A Alharthi, A Alrashed, O Jamal, A Qasim, I Alhomoud, A Alqahtani, H Akil, H Alzahrani, S Alsaedi, M Alsubeiy, M Alhazmi, A Alfawzan, Y Alharbi, R Alharbi, Y Alobeisy, A Aljohani, I Malawi, E Matar, A Tawakoul, A ALnami, A Alshareif, I Kalantan, A Arbaeen, E Alalawi, A AlGhamdi, A Koshak, A Alkhaldi, I Al-Nami, A Howsawi, B Fairaq, B Maghrabi, T Murad, H Alzahrani, K Almehma-di, D Milibari, R Hafiz, R Kalantan, S Al-Ansari, A Rajab, A Alfahmy, G Ali, F Abu naji, L Hassan, L Althumali, L Far-hat, N Baddour, H Alandanusi, W Alqurashi, S Fallata, A Alharbi, J Bahakeem, A Alshareef, B Rawa, D Alnemari, A Alghamdi, A Muqadimi, A Bimah, O Alamri, J Qutub, A Al-Ghamdi, A Mirza, A Alandijani, O Qoqandi, F Mandourah, M Alghamdi, M Mahboob, M Alsulami, M Hinnawi, N Hawsawi, N Dhabab, A Balamash, M Bawazir, J Samkari, R Nassir, M AlAsmari, F Alzahrani, A Alomari and A Ma-keen.
REFERENCES [1] World Health Organisation. Antimicrobial Resistance : Global
Report on. Surveillance 2014. http://www.who.int/drugresistance/ documents/surveillancereport/en/ (Accessed May 15, 2014).
[2] Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A. D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. B. M. J., 2010, 340, 2096.
[3] Centers for Disease Control and Prevention : Antibiotic / Antimicrobial Resistance. http://www.cdc.gov/drugresistance/ about.html (AccessedApril 22, 2014).
[4] Antimicrobial resistance: measures need to tackle global use. Vet. Rec., 2013, 172(11), 277-278.
[5] Alvarez-Fernandez, E.; Alonso-Calleja, C.; Garcia-Fernandez, C.; Capita, R. Prevalence and antimicrobial resistance of Salmonella serotypes isolated from poultry in Spain: comparison between 1993 and 2006. Int. J. Food Microbiol., 2012, 153(3), 281-287.
[6] Alvarez-Fernandez, E.; Dominguez-Rodriguez, J.; Capita, R.; Alonso-Calleja, C. Influence of housing systems on microbial load and antimicrobial resistance patterns of Escherichia coli isolates from eggs produced for human consumption. J. Food Prot., 2012,75(5), 847-853.
[7] Carlet, J.; Jarlier, V.; Harbarth, S.; Voss, A.; Goossens, H.; Pittet, D. Ready for a world without antibiotics? The Pensieres Antibiotic Resistance Call to Action. Antimicrob. Resist. Infect. Control, 2012, 1(1), 11.
[8] Weir, M.; Rajic, A.; Dutil, L.; Cernicchiaro, N.; Uhland, F. C.; Mercier, B.; Tusevljak, N. Zoonotic bacteria, antimicrobial use and antimicrobial resistance in ornamental fish: a systematic review of the existing research and survey of aquaculture-allied professionals. Epidemiol. Infect., 2012, 140(2), 192-206.
[9] Okumura, J.; Wakai, S.; Umenai, T. Drug utilisation and self-medication in rural communities in Vietnam. Soc. Sci. Med., 2002, 54(12), 1875-1886.
[10] Aarestrup, F. M.; Wegener, H. C.; Collignon, P. Resistance in bacteria of the food chain: epidemiology and control strategies. Expert Rev. Anti Infect. Ther., 2008, 6(5), 733-750.
[11] Nuorti, J. P.; Butler, J. C.; Crutcher, J. M.; Guevara, R.; Welch, D.; Holder, P.; Elliott, J. A. An outbreak of multidrug-resistant pneumococcal pneumonia and bacteremia among unvaccinated nursing home residents. N. Engl. J. Med., 1998, 338(26), 1861-1868.
[12] Memish, Z. A. The Hajj: communicable and non-communicable health hazards and current guidance for pilgrims. Euro. Surveill., 2010, 15(39), 19671.
[13] Abubakar, I.; Gautret, P.; Brunette, G. W.; Blumberg, L.; Johnson, D.; Poumerol, G.; Memish, Z. A.; Barbeschi, M.; Khan, A. S. Global perspectives for prevention of infectious diseases associated with mass gatherings. Lancet Infect. Dis., 2012, 12(1), 66-74.
[14] World Health Organisation. Communicable disease alert and response for mass gatherings : key considerations. http://www.who.int/csr/ Mass_gatherings2.pdf (Accessed April 10, 2014).
[15] Shakir, H. A.; Gazzaz, Z. J.; Dhaffar, K. O.; Shahbaz, J. Outpatient Services during (1423h) Hajj Season. Sultan Qaboos Univ. Med. J., 2006, 6(1), 47-50.
[16] Alherabi, A. Z. Impact of pH1N1 influenza A infections on the Otolaryngology, Head and Neck Clinic during Hajj, 2009. Saudi Med. J., 2011, 32(9), 933-938.
[17] Bin Abdulhak, A. A.; Altannir, M. A.; Almansor, M. A.; Almohaya, M. S.; Onazi, A. S.; Marei, M. A.; Aldossary, O. F.; Obeidat, S. A.; Obeidat, M. A.; Riaz, M. S.; Tleyjeh, I. M. Non prescribed sale of antibiotics in Riyadh, Saudi Arabia: a cross sectional study. B. M. C. Public Health, 2011, 11, 538.
[18] Meeker, D.; Knight, T. K.; Friedberg, M. W.; Linder, J. A.; Goldstein, N. J.; Fox, C. R.; Rothfeld, A.; Diaz, G.; Doctor, J. N. Nudging guideline-concordant antibiotic prescribing: a randomized clinical trial. J. A. M. A. Intern. Med., 2014, 174(3), 425-431.
[19] Monette, J.; Miller, M. A.; Monette, M.; Laurier, C.; Boivin, J. F.; Sourial, N.; Le Cruguel, J. P.; Vandal, A.; Cotton-Montpetit, M. Effect of an educational intervention on optimizing antibiotic prescribing in long-term care facilities. J. Am. Geriatr. Soc., 2007, 55(8), 1231-1235.
[20] Al-Ghamdi, M. S. Empirical treatment of uncomplicated urinary tract infection by community pharmacist in the Eastern province of Saudi Arabia. Saudi Med. J., 2001, 22(12), 1105-1108.
[21] Hill, D. R.; Ericsson, C. D.; Pearson, R. D.; Keystone, J. S.; Freedman, D. O.; Kozarsky, P. E.; DuPont, H. L.; Bia, F. J.; Fischer, P. R.; Ryan, E. T.; Infectious Diseases Society of America. The practice of travel medicine: guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis., 2006, 43(12), 1499-1539.
[22] Lim, K. K.; Teh, C. C. A Cross Sectional Study of Public Knowledge and Attitude towards Antibiotics in Putrajaya, Malaysia. South. Med. Rev., 2012, 5(2), 26-33.
[23] Grigoryan, L.; Burgerhof, J. G.; Degener, J. E.; Deschepper, R.; Lundborg, C. S.; Monnet, D. L.; Scicluna, E. A.; Birkin, J.; Haaijer-Ruskamp, F. M.; consortium, S. A. R. Attitudes, beliefs and knowledge concerning antibiotic use and self-medication: a comparative European study. Pharmacoepidemiol. Drug Saf., 2007, 16(11), 1234-1243.
[24] Chen, C.; Chen, Y. M.; Hwang, K. L.; Lin, S. J.; Yang, C. C.; Tsay, R. W.; Liu, C. E.; Young, T. G. Behavior, attitudes and knowledge about antibiotic usage among residents of Changhua, Taiwan. J. Microbiol. Immunol. Infect., 2005, 38(1), 53-59.
[25] Ling Oh, A.; Hassali, M. A.; Al-Haddad, M. S.; Syed Sulaiman, S. A.; Shafie, A. A.; Awaisu, A. Public knowledge and attitudes towards antibiotic usage: a cross-sectional study among the general public in the state of Penang, Malaysia. J. Infect. Dev. Ctries., 2011, 5(5), 338-347.
[26] McNulty, C. A.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. The public's attitudes to and compliance with antibiotics. J. Antimicrob. Chemother, 2007, 60(Suppl 1), 63-68.
[27] Shehadeh, M.; Suaifan, G.; Darwish, R. M.; Wazaify, M.; Zaru, L.; Alja'fari, S. Knowledge, attitudes and behavior regarding antibiotics use and misuse among adults in the community of Jordan. A pilot study. Saudi Pharm. J., 2012, 20(2), 125-133.
[28] Schwartz, D. N.; Abiad, H.; DeMarais, P. L.; Armeanu, E.; Trick, W. E.; Wang, Y.; Weinstein, R. A. An educational intervention to improve antimicrobial use in a hospital-based long-term care facility. J. Am. Geriatr. Soc., 2007, 55(8), 1236-1242.
[29] Gjelstad, S.; Hoye, S.; Straand, J.; Brekke, M.; Dalen, I.; Lindbaek, M. Improving antibiotic prescribing in acute respiratory tract infections: cluster randomised trial from Norwegian general

132 Infectious Disorders – Drug Targets, 2014, Vol. 14, No. 2 Azeem et al.
practice (prescription peer academic detailing (Rx-PAD) study). B. M. J., 2013, 347, 4403.
[30] Wilder-Smith, A.; Paton, N. I.; Barkham, T. M.; Earnest, A. Meningococcal carriage in Umra pilgrims returning from Saudi Arabia. J. Travel Med., 2003, 10(3), 147-149.
[31] Husain, E. H.; Dashti, A. A.; Electricwala, Q. Y.; Abdulsamad, A. M.; Al-Sayegh, S. Absence of Neisseria meningitidis from throat swabs of Kuwaiti pilgrims after returning from the Hajj. Med. Princ. Pract., 2010, 19(4), 321-323.
[32] McNulty, C. A.; Nichols, T.; Boyle, P. J.; Woodhead, M.; Davey, P. The English antibiotic awareness campaigns: did they change the
public's knowledge of and attitudes to antibiotic use? J. Antimicrob. Chemother., 2010, 65(7), 1526-1533.
[33] Davey, P.; Garner, S.; Professional Education Subgroup of, S. Professional education on antimicrobial prescribing: a report from the Specialist Advisory Committee on Antimicrobial Resistance (SACAR) Professional Education Subgroup. J. Antimicrob. Chemother., 2007, 60(Suppl 1), 27-32.
[34] Davey, P.; Pagliari, C.; Hayes, A. The patient's role in the spread and control of bacterial resistance to antibiotics. Clin. Microbiol. Infect., 2002, 8(Suppl 2), 43-68.
Received: March 14, 2014 Revised: June 06, 2014 Accepted: June 09, 2014



























