Embed Size (px)
Citation preview
INTERDEPARTMENTAL
CONVERGENCE FOR ADDRESSING
MALNUTRITION
Presented By
Dr. M. Geetha Secretary, WCD
Chhattisgarh

For
Maximum outcome
of government efforts
at field level …. Mantra is......
Convergence..
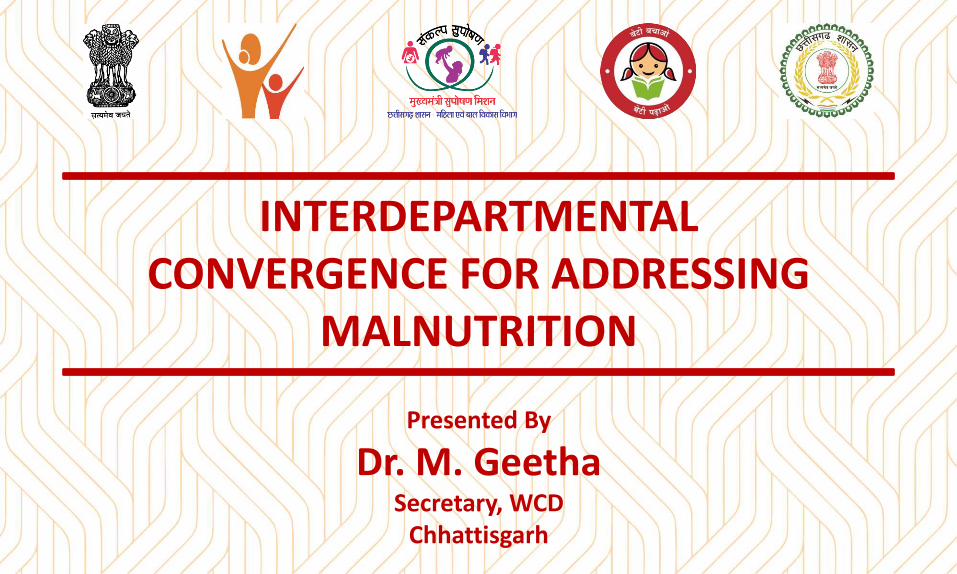
Multi-factorial causes of undernutrition
Points of
Inter Departmental
Convergence at
Root Level
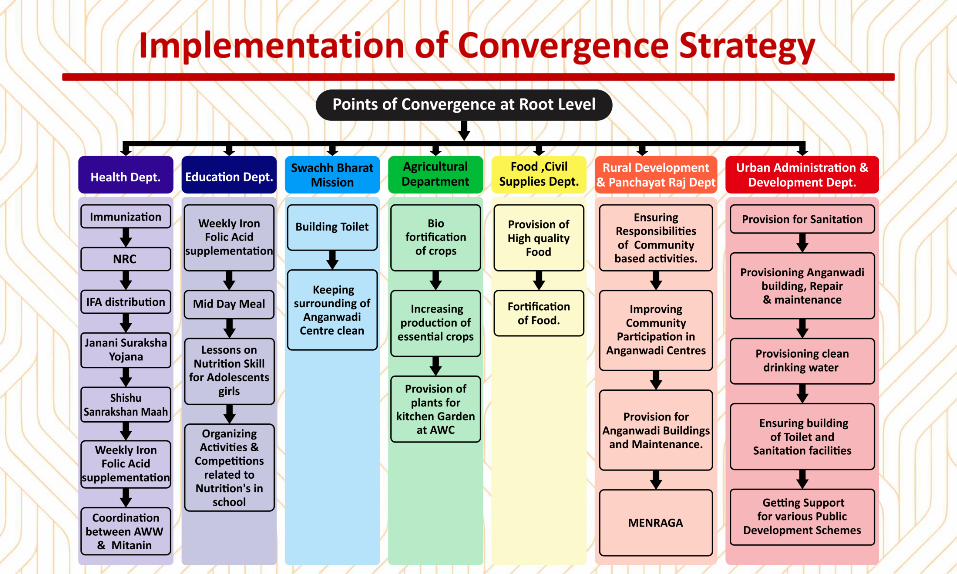
Implementation of Convergence Strategy
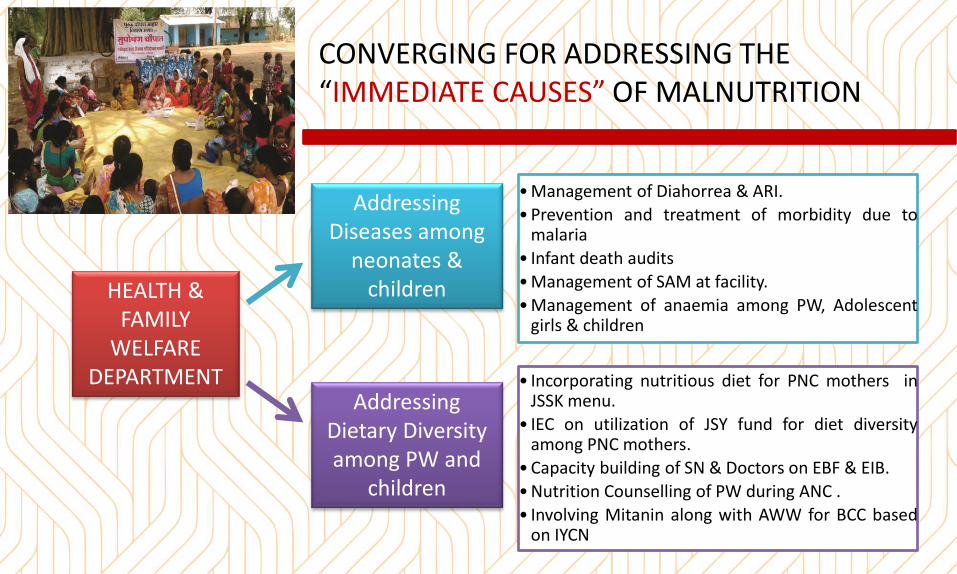
CONVERGING FOR ADDRESSING THE
IMMEDIATE CAUSES OF MALNUTRITION
HEALTH &
FAMILY
WELFARE
DEPARTMENT
Addressing
Diseases among
neonates &
children
Addressing
Dietary Diversity
among PW and
children
• Management of Diahorrea & ARI.
• Prevention and treatment of morbidity due to malaria
• Infant death audits
• Management of SAM at facility.
• Management of anaemia among PW, Adolescent girls & children
• Incorporating nutritious diet for PNC mothers in JSSK menu.
• IEC on utilization of JSY fund for diet diversity among PNC mothers.
• Capacity building of SN & Doctors on EBF & EIB.
• Nutrition Counselling of PW during ANC .
• Involving Mitanin along with AWW for BCC based on IYCN
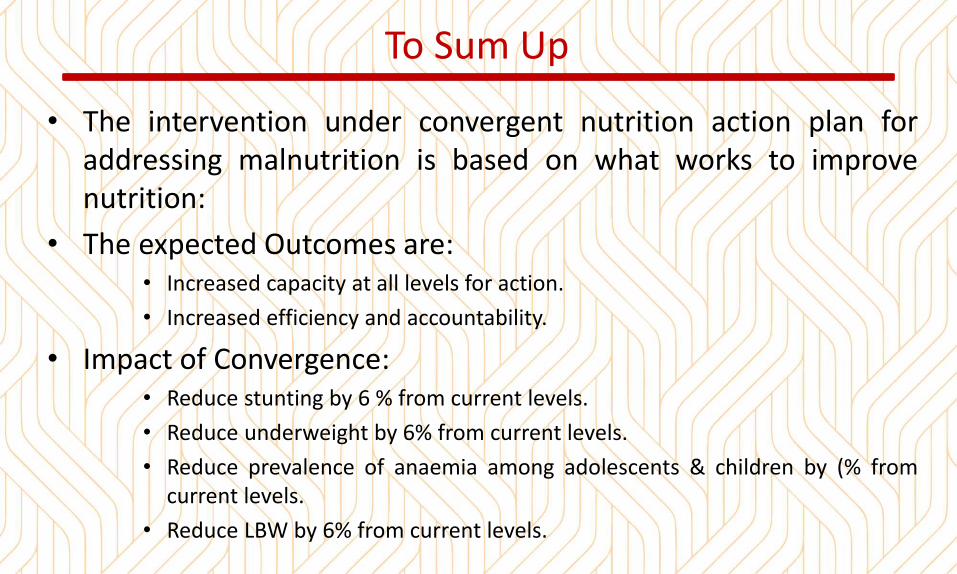
To Sum Up
• The intervention under convergent nutrition action plan for
addressing malnutrition is based on what works to improve
nutrition:
• The expected Outcomes are:
• Increased capacity at all levels for action.
• Increased efficiency and accountability.
• Impact of Convergence:
• Reduce stunting by 6 % from current levels.
• Reduce underweight by 6% from current levels.
• Reduce prevalence of anaemia among adolescents & children by (% from
current levels.
• Reduce LBW by 6% from current levels.

Thank You
Government of U.P.
EXECUTIVE COMMITTEE MEETING,
NATIONAL NUTRITION MISSION,
BALRAMPUR
Nutritional Gaps
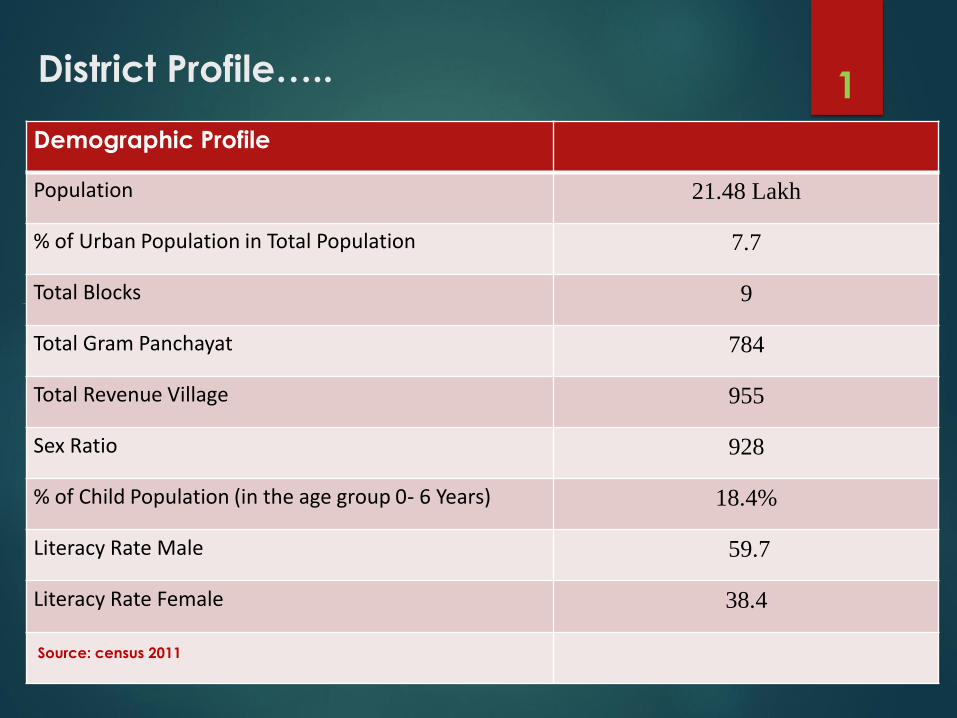
District Profile…..
Demographic Profile
Population 21.48 Lakh
% of Urban Population in Total Population 7.7
Total Blocks 9
Total Gram Panchayat 784
Total Revenue Village 955
Sex Ratio 928
% of Child Population (in the age group 0- 6 Years) 18.4%
Literacy Rate Male 59.7
Literacy Rate Female 38.4
Source: census 2011
1
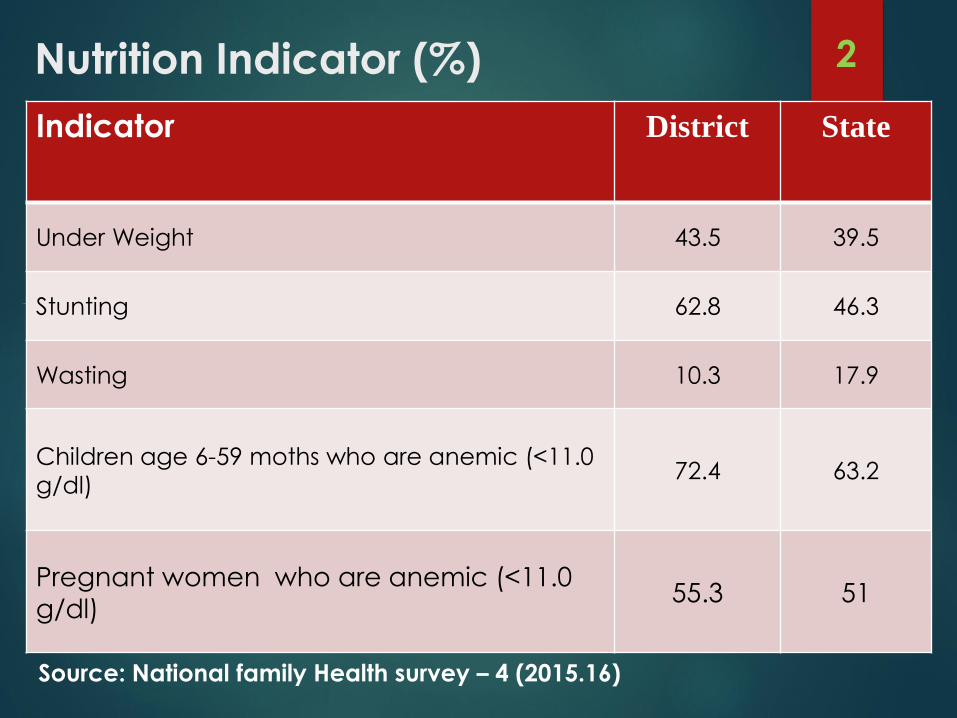
Nutrition Indicator (%)
Indicator District State
Under Weight 43.5 39.5
Stunting 62.8 46.3
Wasting 10.3 17.9
Children age 6-59 moths who are anemic (<11.0
g/dl)72.4 63.2
Pregnant women who are anemic (<11.0
g/dl)55.3 51
Source: National family Health survey – 4 (2015.16)
2
Gaps And ChallengesSystem Level -
o Lack of human resource
o Lack of motivation among staff.
o Lack of logistics & necessary equipment's for Aganwadi Centers.
o Lack of regular capacity building training of AWW and Mukhya Sevika.
o Lack of Sub centers & Anganwadi centers in ratio of population
o Incapability of staff to organize Health and Nutrition Education sessions in the community.
3
Community Level
Lack of awareness related to nutrition.
Improper consumption of THR.
Lack of proper counseling by AWW to beneficiaries.
Cultural practices and superstitions
Poor literacy Status
• Geographical & environmental -• Most of the area is hard to reach so there is a
provision of developing NRC at block CHC/PHC level.• High prevalence of malnourished children• High prevalence of HRP cases • High number of Malnutrition children with worm
infestation.• High prevalence of diarrhea and Pneumonia.
4
Monitoring & Evaluation-
Lack of tool for estimation of Stunted.
Real time monitoring was not available.
5
ACTION PLAN TO
ADDRESS
MALNUTRITION
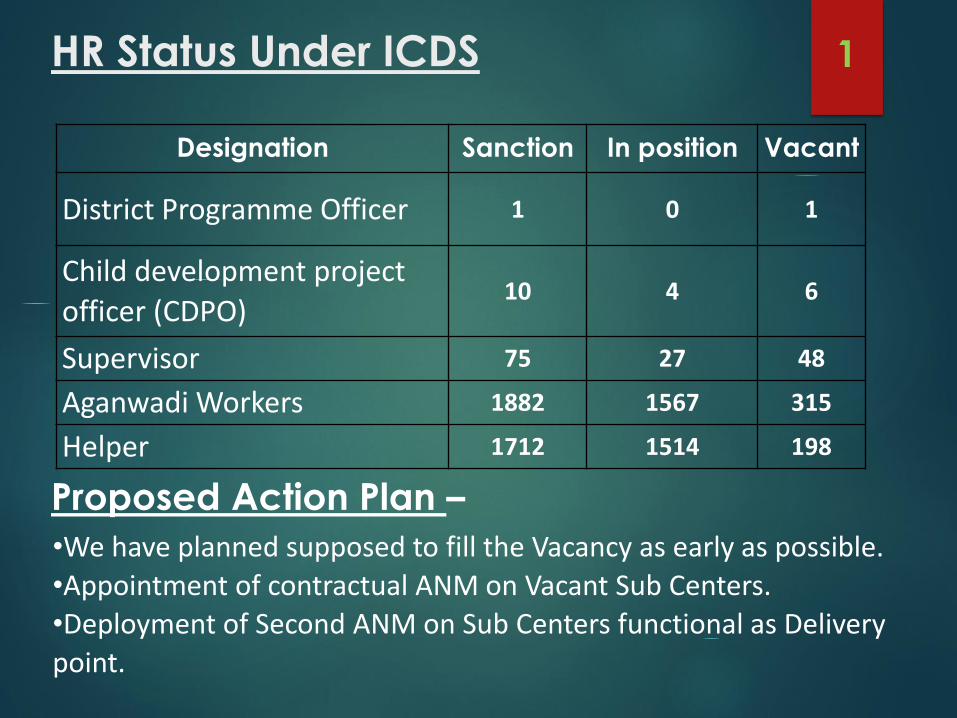
HR Status Under ICDS
Designation Sanction In position Vacant
District Programme Officer 1 0 1
Child development project
officer (CDPO)10 4 6
Supervisor 75 27 48
Aganwadi Workers 1882 1567 315
Helper 1712 1514 198
•We have planned supposed to fill the Vacancy as early as possible.
•Appointment of contractual ANM on Vacant Sub Centers.
•Deployment of Second ANM on Sub Centers functional as Delivery
point.
Proposed Action Plan –
1
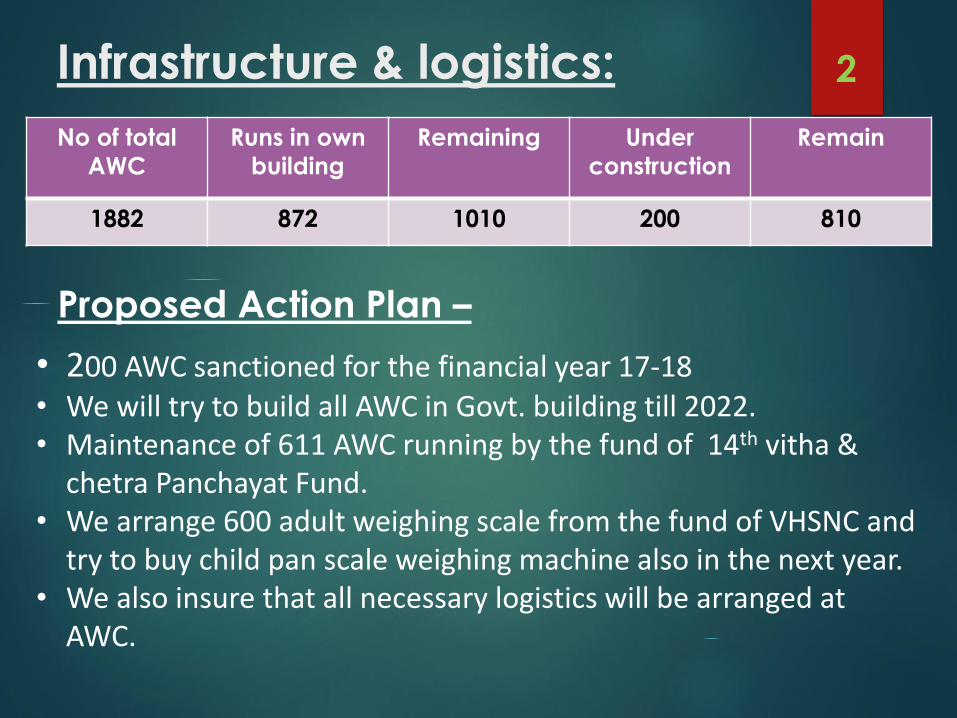
Infrastructure & logistics:
No of total
AWC
Runs in own
building
Remaining Under
construction
Remain
1882 872 1010 200 810
Proposed Action Plan –
• 200 AWC sanctioned for the financial year 17-18• We will try to build all AWC in Govt. building till 2022.• Maintenance of 611 AWC running by the fund of 14th vitha &
chetra Panchayat Fund.• We arrange 600 adult weighing scale from the fund of VHSNC and
try to buy child pan scale weighing machine also in the next year.• We also insure that all necessary logistics will be arranged at
AWC.
2
Proposed Action Plan- Sustaining Health Status ,
Screening of malnourished child & referral
Identification of SAM (Severe Acute Malnutrition) children’s at AWC’s & their referral to NRC will be effectively done by RBSK team.
Regular visits/health checkups by RBSK team will be ensured at every AWC’s twice in a year.
Inter-departmental convergence (Health, PRI, Education, Rural Development & Food supply department & ICDS) to address malnutrition.
Regular tracking of 0 to 3 years (Red & Yellow category Children’s) through SHABRI Sankalp Yojana.
For Kuposhan Mukta Gaon 72 villages were taken by 36 District level officers with the target to free these villages from Malnutrition by March 18.
Sensitization of ASHA, ANM & Anganwadi Workers for timely referral of Severe Acute Malnourished children's in Nutrition Rehabilitation Centre (NRC)
3
Proposed Action Plan
Strengthening VHND through Mega Call Center.
Regular Counseling of mother’s will be ensured by AWW/ASHA & ANM during VHND’s.
Household visits of SUW’s will be ensured by AWW’s.
Identification of HRP’s through effective implementation of
PMSMD(Pradhan Mantri Surakshit Matritwa Diwas). Implementation of PMMVY (Pradhan Mantri Matritwa Vandana Yojna) &
remove challenges of implementation .
Inter-departmental monitoring team for Support & monitor of VHND/IMI sessions
Weekly Iron Folic Acid Supplementation for adolescent girls through WIFS programme.
4
Proposed Action Plan
Strengthening of Routine Immunization Programme
Ensure availability of all equipments & logistics i.e., Weighing machine ,
hub cutter , BP equipments etc.
Regular health checkup & availability of De-worming tablets & iron syrup for
children at Anganwadi centers & Schools through BSPM/NIPI programme.
Capacity building of mother’s on WASH (water sanitation & hygiene) & distribution of ORS & Zinc
Counseling of Pregnant & lactating mother’s and adolescent on health, sanitation & nutrition on Bachpan, Mamta & Ladli Diwas (Held every month on 5,15 & 25).
Community awareness by conducting mothers meeting at AWC & in village.
5
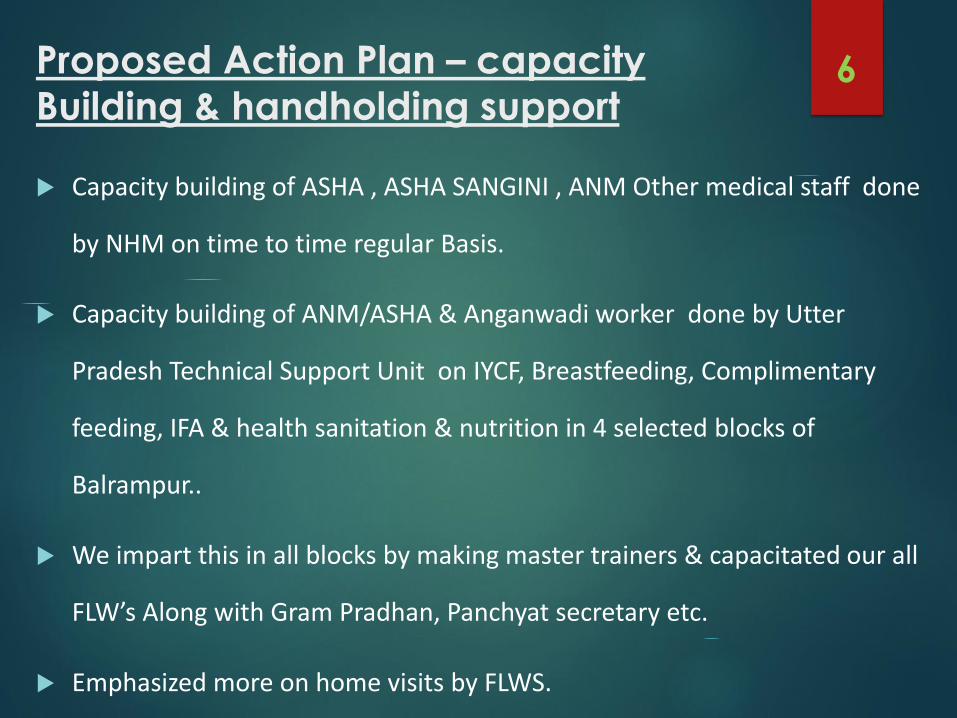
Proposed Action Plan – capacity
Building & handholding support
Capacity building of ASHA , ASHA SANGINI , ANM Other medical staff done
by NHM on time to time regular Basis.
Capacity building of ANM/ASHA & Anganwadi worker done by Utter
Pradesh Technical Support Unit on IYCF, Breastfeeding, Complimentary
feeding, IFA & health sanitation & nutrition in 4 selected blocks of
Balrampur..
We impart this in all blocks by making master trainers & capacitated our all
FLW’s Along with Gram Pradhan, Panchyat secretary etc.
Emphasized more on home visits by FLWS.
6
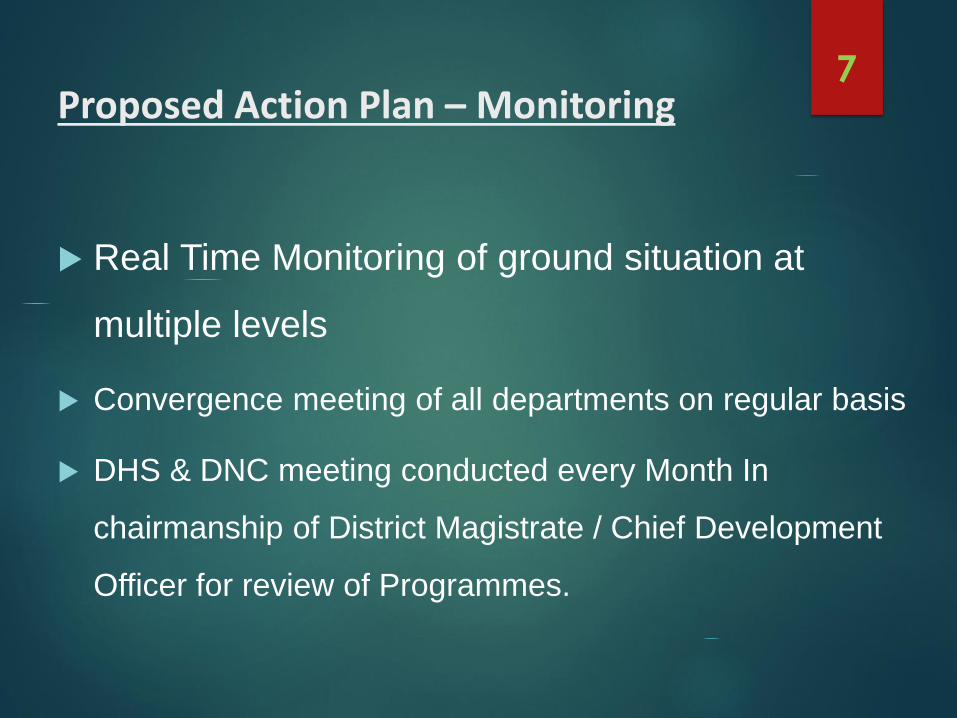
Proposed Action Plan – Monitoring
Real Time Monitoring of ground situation at
multiple levels
Convergence meeting of all departments on regular basis
DHS & DNC meeting conducted every Month In
chairmanship of District Magistrate / Chief Development
Officer for review of Programmes.
7
District Bahraich
Nutrition
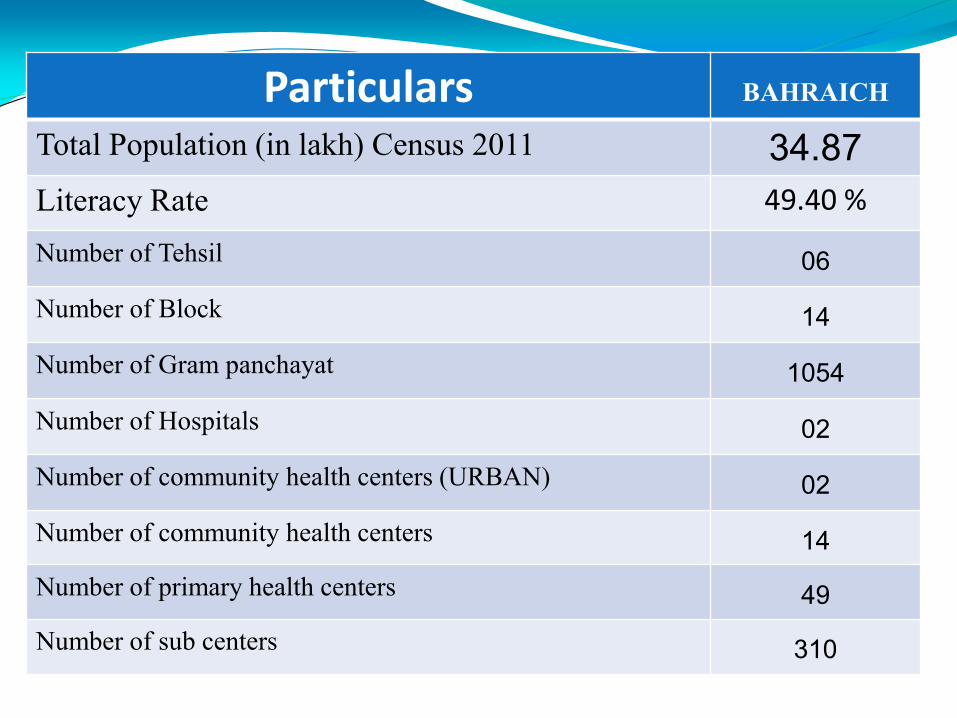
Particulars BAHRAICH
Total Population (in lakh) Census 2011 34.87
Literacy Rate 49.40 %
Number of Tehsil 06
Number of Block 14
Number of Gram panchayat 1054
Number of Hospitals 02
Number of community health centers (URBAN) 02
Number of community health centers 14
Number of primary health centers 49
Number of sub centers 310
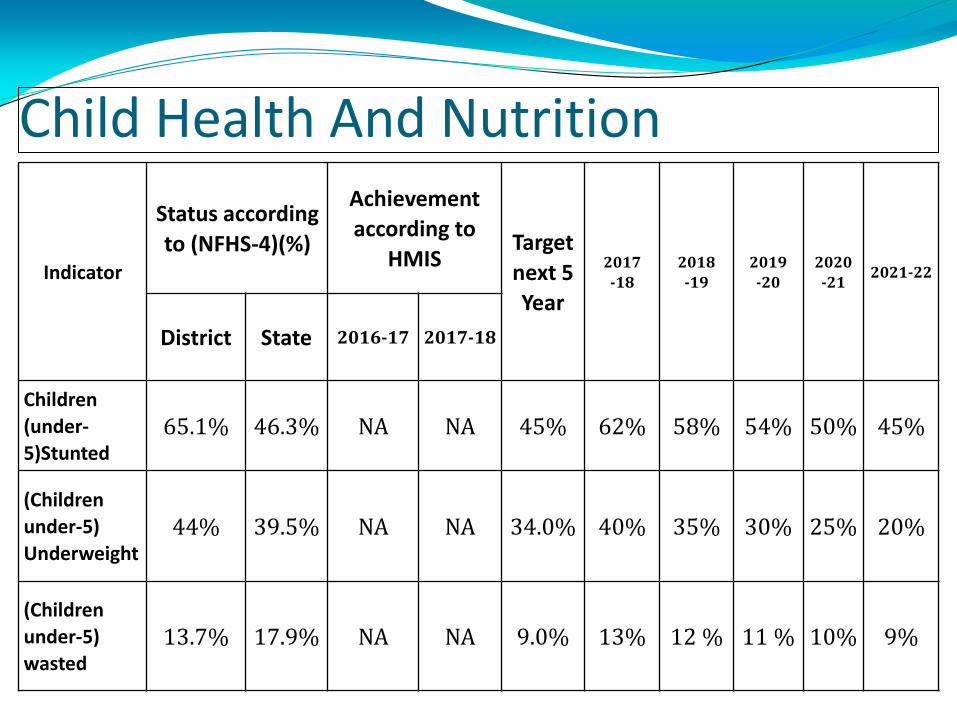
Child Health And Nutrition
Indicator
Status according
to (NFHS-4)(%)
Achievement
according to
HMIS Target
next 5
Year
2017
-18
2018
-19
2019
-20
2020
-21 2021-22
District State 2016-17 2017-18
Children
(under-
5)Stunted 65.1% 46.3% NA NA 45% 62% 58% 54% 50% 45%
(Children
under-5)
Underweight 44% 39.5% NA NA 34.0% 40% 35% 30% 25% 20%
(Children
under-5)
wasted 13.7% 17.9% NA NA 9.0% 13% 12 % 11 % 10% 9%
Gaps And Challenges System Level -
Lack of human resource
Lack of motivation among staff.
Lack of Departmental building & necessary equipment's for Aganwadi Centers.
Lack of regular Training of Anganwadi, ASHA , ANM and other field level Worker.
Lack of regular capacity building training of AWW and MS.
Lack of Infrastructure & logistics
Lack of Sub centers & Anganwadi centers in ratio of population
Un utilization of funds / lack of funds
Incapability of staff to organize Health and Nutrition Education sessions in the community.
Community Level
Lack of awareness related to nutrition.
Improper consumption of THR.
Lack of proper counseling by AWW to beneficiaries.
Cultural practices and superstitions
Poor literacy Status
Monitoring & Evaluation- Lack of tool for estimation of Stunted.
Real time monitoring was not available
AAA / CLUSTER / SECTOR & others meeting not happening on regular basis.
• Geographical & environmental - • Most of the area is hard to reach so there is a provision of developing NRC at
block CHC/PHC level. • High prevalence of malnourished children • High load of deliveries , high prevalence of HRP cases • High number of Malnutrition children with worm infestation. • High prevalence of diarrhea and Pneumonia. • Out of 14 block of Bahraich district 10 blocks are affected with Arsenic & Iron
(un-absorblable) which leads various health issues
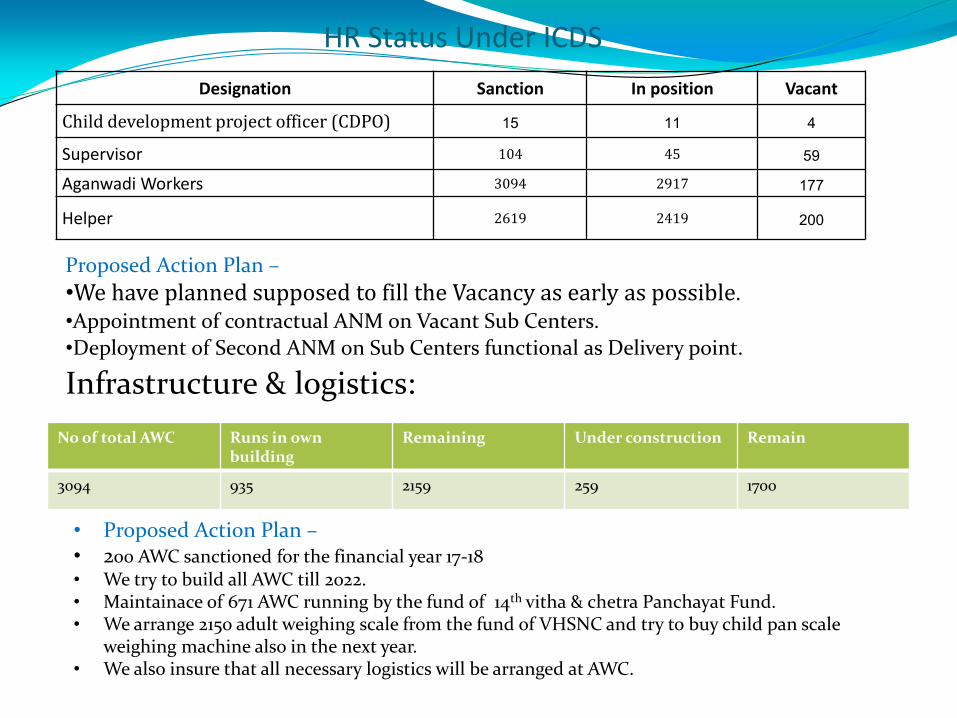
HR Status Under ICDS
Designation Sanction In position Vacant
Child development project officer (CDPO) 15 11 4
Supervisor 104 45 59
Aganwadi Workers 3094 2917 177
Helper 2619 2419 200
Proposed Action Plan –
•We have planned supposed to fill the Vacancy as early as possible.
•Appointment of contractual ANM on Vacant Sub Centers.
•Deployment of Second ANM on Sub Centers functional as Delivery point.
Infrastructure & logistics:
No of total AWC Runs in own building
Remaining Under construction Remain
3094 935 2159 259 1700
• Proposed Action Plan – • 200 AWC sanctioned for the financial year 17-18 • We try to build all AWC till 2022. • Maintainace of 671 AWC running by the fund of 14th vitha & chetra Panchayat Fund. • We arrange 2150 adult weighing scale from the fund of VHSNC and try to buy child pan scale
weighing machine also in the next year. • We also insure that all necessary logistics will be arranged at AWC.
Proposed Action Plan- Sustaining Health Status , Screening of malnourished child & referral
Inter-departmental convergence (Health, PRI, Education, Rural Development & Food supply department & ICDS) to address malnutrition.
Regular tracking of 0 to 3 years (Red & Yellow category Children’s) through SHABRI Sankalp Yojana.
For Kuposhan Mukta Gaon 82 villages were taken by 41 District level officers with the target to free these villages from Malnutrition by March 18.
Sensitization of ASHA, ANM & Anganwadi Workers for timely referral of Severe Acute Malnourished children's in Nutrition Rehabilitation Centre (NRC)
Proposed Action Plan
Strengthening of VHND Routine Immunization Programme Inter-departmental
monitoring team for Support & monitor of VHND/IMI sessions
Ensure availability of all equipments & logistics i.e., Weighing machine , hub cutter , BP
equipments etc.
Regular health checkup & availability of De-worming tablets & iron syrup for children at
Anganwadi centers & Schools.
Capacity building of mother’s on WASH (water sanitation & hygiene) & distribution of ORS & Zinc
Counseling of Pregnant & lactating mother’s and adolescent on health, sanitation & nutrition on Bachpan, Mamta & Ladli Diwas (Held every month on 5,15 & 25).
Community awareness by conducting mothers meeting at AWC & in village.
Inter-departmental monitoring team for Support & monitor of VHND/IMI sessions
Proposed Action Plan – capacity Building & handholding support
Capacity building of ASHA , ASHA SANGINI , ANM Other medical staff done by NHM on time to time regular Basis.
Capacity building of ANM/ASHA & Anganwadi worker done by Utter Pradesh Technical Support Unit on IYCF,
Breastfeeding, Complimentary feeding, IFA & health sanitation & nutrition in 4 selected blocks of Bacharach..
We impart this in all blocks by making master trainers & capacitated our all FLW’s Along with Gram Pradhan,
Panchyat secretary etc.
Emphasized more on home visits by FLWS.
Proposed Action Plan – Monitoring
. Real Time Monitoring of ground situation at multiple levels
Dedicated Focus on Improving Outcomes at District level meeting in every quarter on 10th January 10th April 10th July 10th October
Convergence meeting of all departments on regular basis
DHS & DNC meeting conducted every Month In chairmanship of District Magistrate / Chief
Development Officer for review of Programmes.

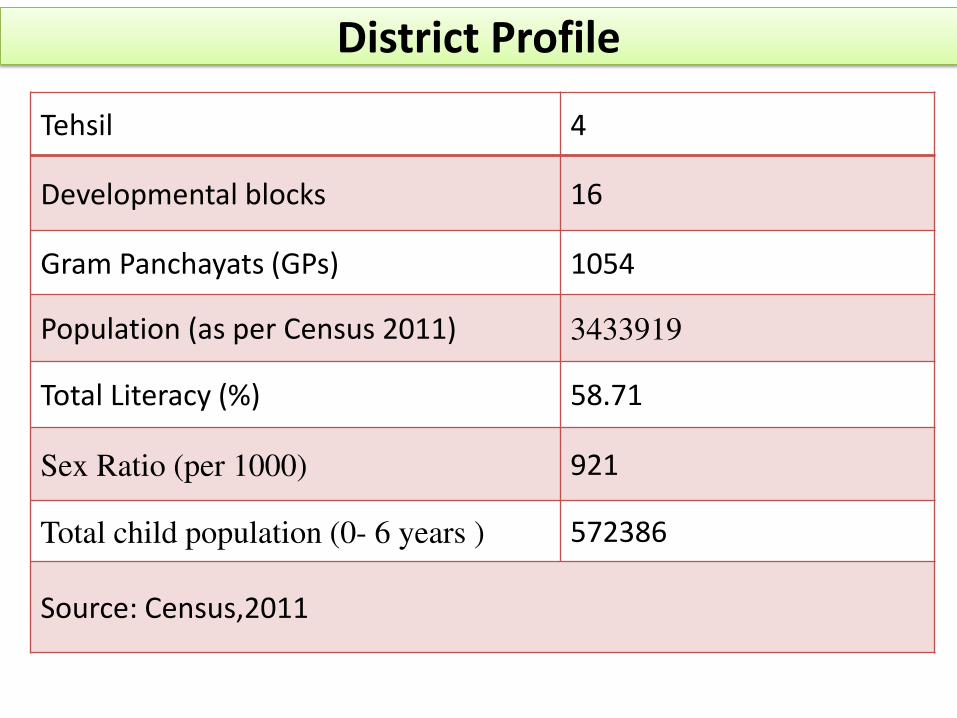
District Profile
Tehsil 4
Developmental blocks 16
Gram Panchayats (GPs) 1054
Population (as per Census 2011) 3433919
Total Literacy (%) 58.71
Sex Ratio (per 1000) 921
Total child population (0- 6 years ) 572386
Source: Census,2011
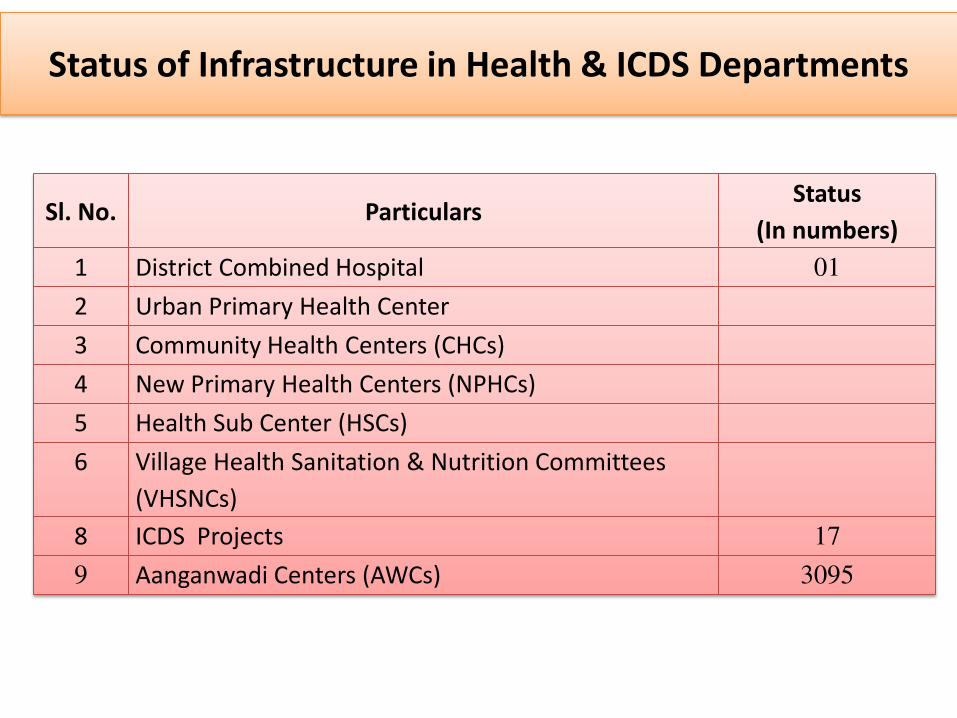
Status of Infrastructure in Health & ICDS Departments
Sl. No. Particulars Status
(In numbers)
1 District Combined Hospital 01
2 Urban Primary Health Center
3 Community Health Centers (CHCs)
4 New Primary Health Centers (NPHCs)
5 Health Sub Center (HSCs)
6 Village Health Sanitation & Nutrition Committees
(VHSNCs)
8 ICDS Projects 17
9 Aanganwadi Centers (AWCs) 3095
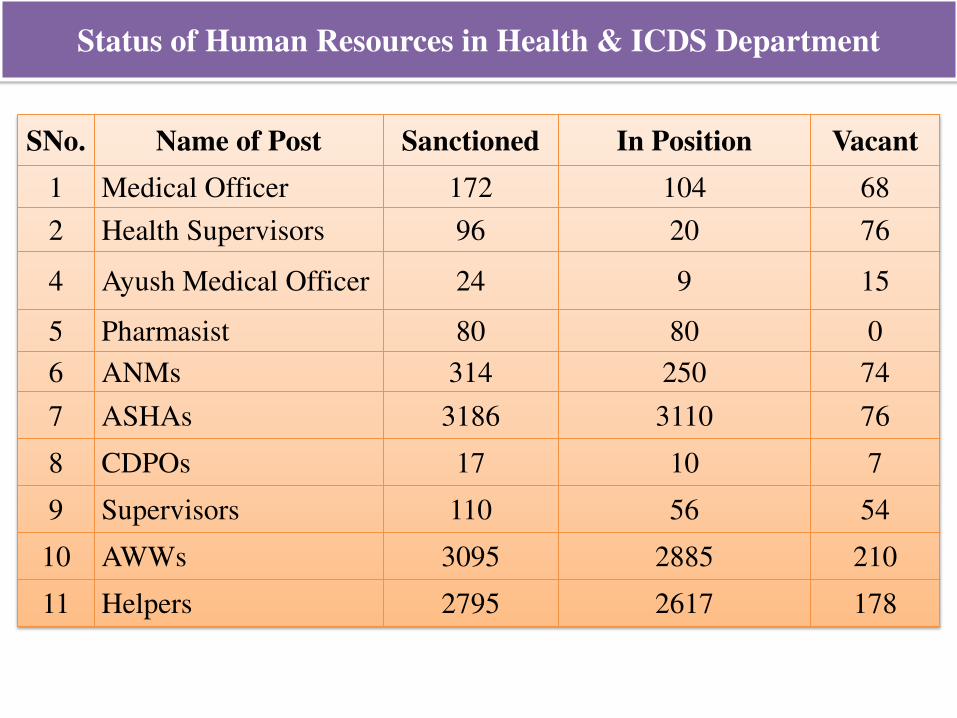
Status of Human Resources in Health & ICDS Department
SNo. Name of Post Sanctioned In Position Vacant
1 Medical Officer 172 104 68
2 Health Supervisors 96 20 76
4 Ayush Medical Officer 24 9 15
5 Pharmasist 80 80 0
6 ANMs 314 250 74
7 ASHAs 3186 3110 76
8 CDPOs 17 10 7
9 Supervisors 110 56 54
10 AWWs 3095 2885 210
11 Helpers 2795 2617 178
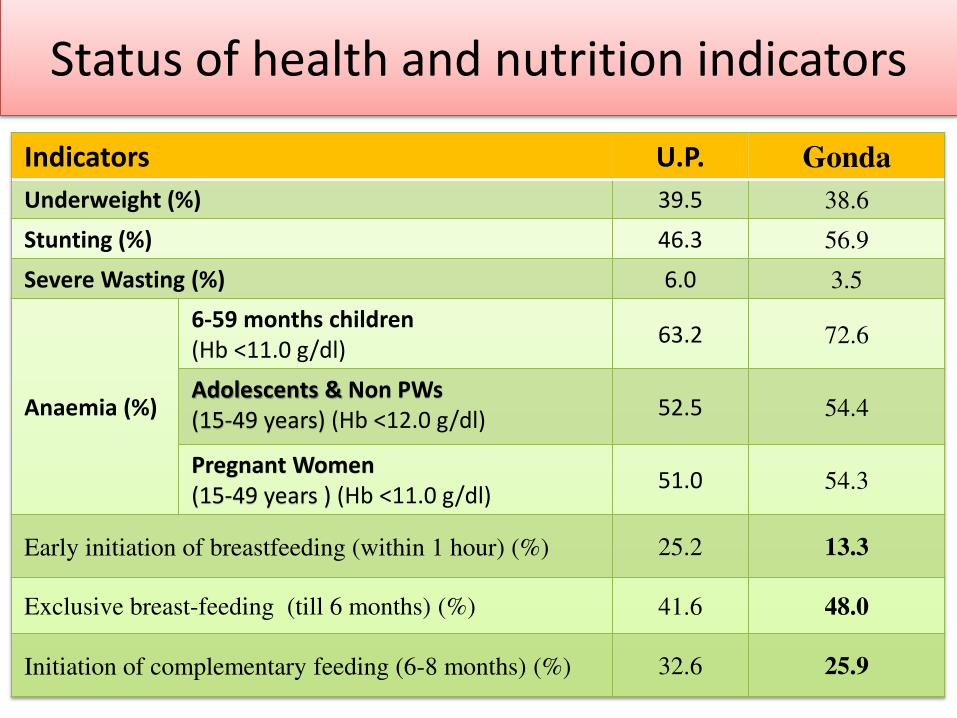
Status of health and nutrition indicators
Indicators U.P. Gonda
Underweight (%) 39.5 38.6
Stunting (%) 46.3 56.9
Severe Wasting (%) 6.0 3.5
Anaemia (%)
6-59 months children
(Hb <11.0 g/dl) 63.2 72.6
Adolescents & Non PWs
(15-49 years) (Hb <12.0 g/dl) 52.5 54.4
Pregnant Women
(15-49 years ) (Hb <11.0 g/dl) 51.0 54.3
Early initiation of breastfeeding (within 1 hour) (%) 25.2 13.3
Exclusive breast-feeding (till 6 months) (%) 41.6 48.0
Initiation of complementary feeding (6-8 months) (%) 32.6 25.9
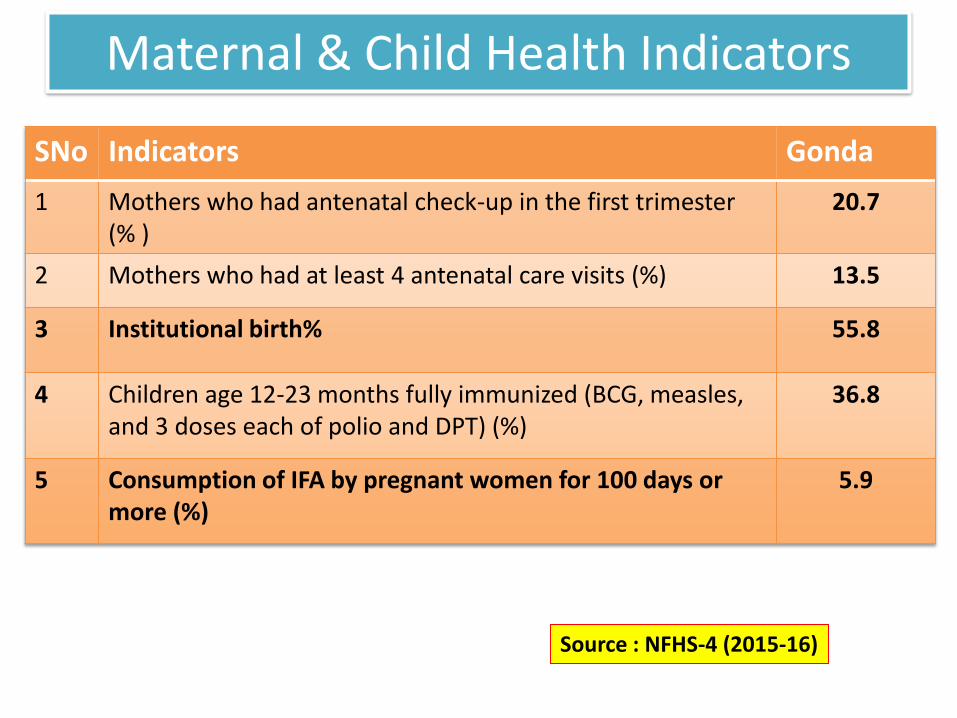
Maternal & Child Health Indicators
SNo Indicators Gonda
1 Mothers who had antenatal check-up in the first trimester
(% )
20.7
2 Mothers who had at least 4 antenatal care visits (%) 13.5
3 Institutional birth% 55.8
4 Children age 12-23 months fully immunized (BCG, measles,
and 3 doses each of polio and DPT) (%)
36.8
5 Consumption of IFA by pregnant women for 100 days or
more (%)
5.9
Source : NFHS-4 (2015-16)
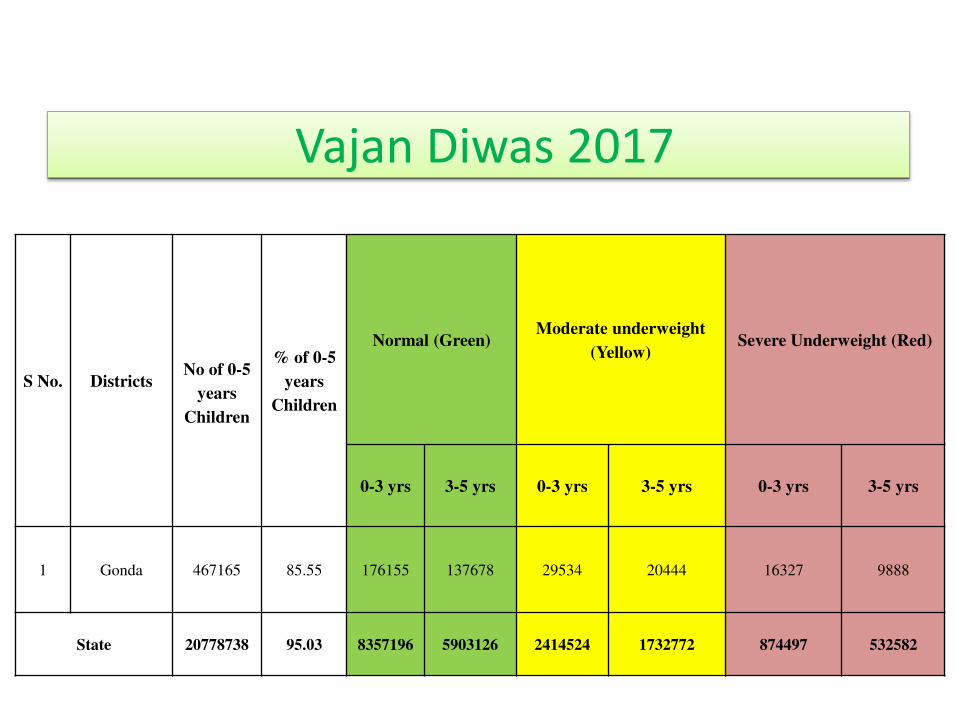
Vajan Diwas 2017
S No. Districts
No of 0-5
years
Children
% of 0-5
years
Children
Normal (Green) Moderate underweight
(Yellow) Severe Underweight (Red)
0-3 yrs 3-5 yrs 0-3 yrs 3-5 yrs 0-3 yrs 3-5 yrs
1 Gonda 467165 85.55 176155 137678 29534 20444 16327 9888
State 20778738 95.03 8357196 5903126 2414524 1732772 874497 532582
• AWWs will identify SUW (red category) children on the basis of weight and age at their AWCs.
• AWWs will ensure distribution of THR to all beneficiaries (7 months to 3 years children, Pregnant women & lactating mothers).
• Regular counseling of mothers will be ensured by AWW, ASHA & ANM during VHND.
• Household visits of SUW children will be ensured by AWWs.
Action Points to Improve Health & Nutrition Indicators
UP Govt has introduced SHABRI (Sustaining Health and nutrition Above Red
Indicator) campaign to improve health and nutrition in 39 Districts of UP in
which Gonda is included.
SHABRI scheme will be implemented with the convergence of 5 departments
viz. ICDS, Health, Panchayti Raj, Rural Development and Food & supply
department.
All SUW (severely underweight or red category) and MUW (moderately
underweight or yellow category) children within the age group of 0-3 years will
be tracked monthly on www.suposhanup.in website.
All convergence departments will ensure to provide their departmental services
to these SUW & MUW children and their families. All the services will be
monitored by e-shabri portal on www.suposhanup.in website.
Kuposhan Mukt Gaon: District level officers will adopt two revenue villages
& make it kuposhan mukt within 6 months with the convergence of 6
departments viz. ICDS, Health, Panchayti Raj, Education, Rural Development
and Food & supply department.
Cont…
• Regular tracking of pregnant women and new born will be ensured by health department to reduce the prevalence of underweight, stunting and wasting in under 5 children.
• Deworming and Iron folic acid consumption by Children, adolescents, pregnant & lactating mothers will be ensured by health department. Which will reduce the prevalence of anaemia in children as well as in mother.
Action Points to Improve Health & Nutrition
Indicators in Children
To ensure the growth of a new born child it is necessary to care for the
mother from the time of first trimester. Severely anemic pregnant women
will be identified and treated before the expected date of delivery. After
birth the child will be visited according the guidelines of HBNC visit and
children who were found to be low in weight will be referred to higher
center.
ASHAs will be motivated for completion of 6 HBNC visits. Moreover
pregnant women will be tracked by ANMs to ensure identification of
severely anemic.
The number of home deliveries must be reduced to ensure clean and aseptic
environment for the new born and mother.
RBSK teams who are responsible for visiting AWW centers and schools
will maintain record of height, weight and mid upper arm circumference of
all children, identify the underweight, stunted and wasted children in the
school and AWW center and refer them to higher health facilities.
Cont..
Cont..
• Screening of 4Ds (Disease, Deficiency, Defects at birth
& developmental delay) and ensure their referral to
DEIC/DH/CHC/NRC will be ensured by RBSK
teams.
• Identification of SAM (Severe acute Malnutrition)
children at AWCs & their referral to NRC will be
effectively done by RBSK teams.
Action Points to Improve Full ANCs & Institutional Delivery
To increase the visits of pregnant women at VHND sites, it is necessary to have a separate due list of pregnant women which will be available with ANM and ASHA so that the eligible pregnant women are mobilized to session site.
All the pregnant women who require medical checkup by a
doctor will be taken to the nearest PHC by free Ambulance services (102). A list of all these pregnant women will be available with ANM at sub center level.
In respect of Women health and nutrition, SHABRI promotes
MCTS registration and ANC check-ups of all PW and THR (Take Home Ration) to all and ensures benefit from PDS.
Cont..
Each pregnant women will be tracked by ASHA and taken to the nearest hospital or delivery system by free ambulance services.
A major reason for pregnant women not getting institutional delivery services is the migration of pregnant women from their house of in laws to parental home (Maika). These PW who are registered with an ASHA from one village move to another village and hence their ANC visits are not completed and they are not tracked for institutional delivery.
To facilitate the tracking of PW who are migrating from one village to other a system for cross notification of such PW will be developed at block level and data of these PW will be shared to the concerned ANM at their parental home.
Action points to Improve Full
immunization in children
• For improving the percentage of fully immunized children in the district, ANMs and their respective ASHAs will be trained at sub center level by MOIC, BCPM and WHO monitor.
• The training will be focused on conducting quality head count survey, updating due list on time, mobilization of children to session site and tracking of left outs or drop outs.
• In respect of children Immunization SHABRI promotes VHND sessions and VHSNC in all villages.
• Repeat monitoring and analysis of these ANMs will be done after two months of their training. The ANMs who have shown improvement in their work will be removed from the list and new ANMs with poor performing sub centers will be added to the list.
• Utilization of central govt. program like intensified Mission Indra Dhanush will be done for improving the coverage.
• A roaster of poor performing ANMs and ASHAs will be prepared at block level and these workers will be a part of annual reorientation training that will be conducted by District Immunization Officer.

Thank
You…
16
NATIONAL NUTRITION MISSION
SHRAVASTI
1
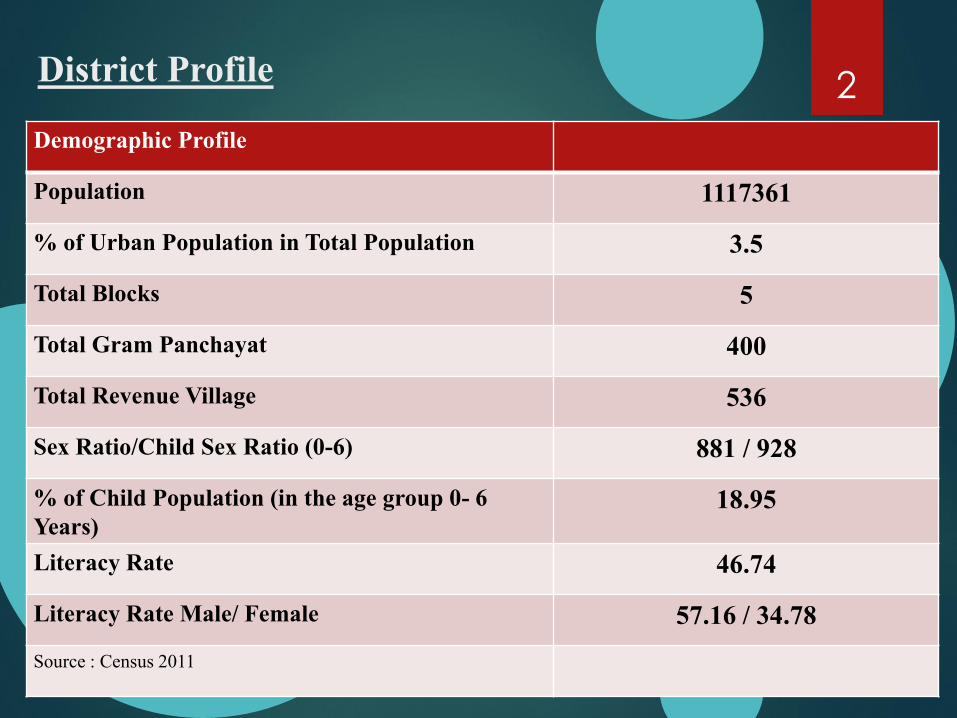
District Profile
Demographic Profile
Population 1117361
% of Urban Population in Total Population 3.5
Total Blocks 5
Total Gram Panchayat 400
Total Revenue Village 536
Sex Ratio/Child Sex Ratio (0-6) 881 / 928
% of Child Population (in the age group 0- 6
Years) 18.95
Literacy Rate 46.74
Literacy Rate Male/ Female 57.16 / 34.78
Source : Census 2011
2
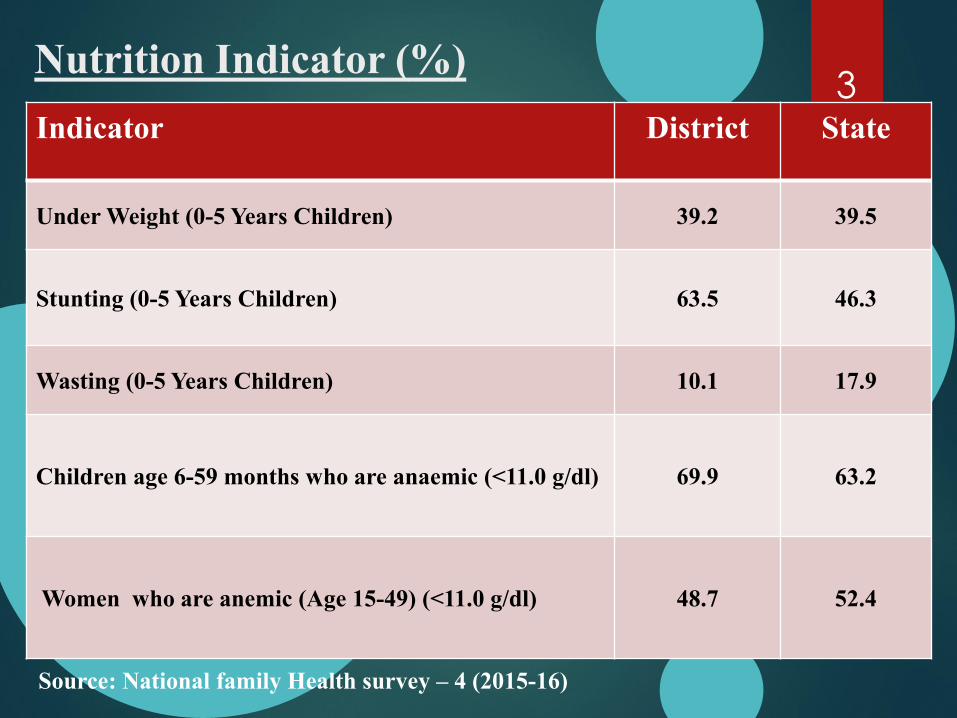
Nutrition Indicator (%)
Indicator District State
Under Weight (0-5 Years Children) 39.2 39.5
Stunting (0-5 Years Children)
63.5 46.3
Wasting (0-5 Years Children) 10.1 17.9
Children age 6-59 months who are anaemic (<11.0 g/dl) 69.9 63.2
Women who are anemic (Age 15-49) (<11.0 g/dl) 48.7 52.4
Source: National family Health survey – 4 (2015-16)
3
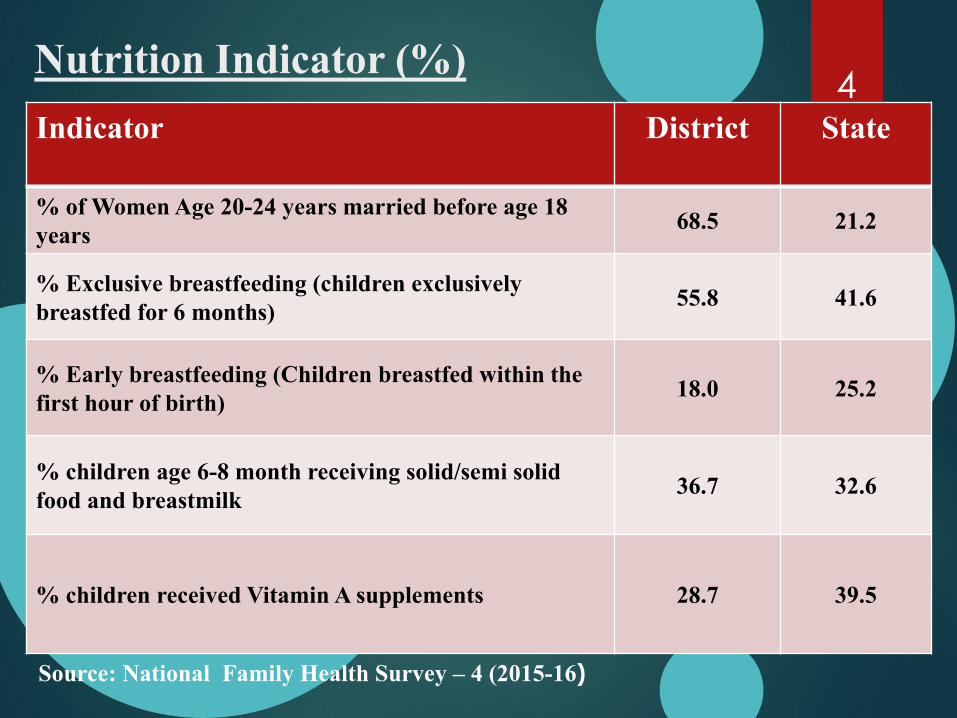
Nutrition Indicator (%)
Indicator District State
% of Women Age 20-24 years married before age 18
years 68.5 21.2
% Exclusive breastfeeding (children exclusively
breastfed for 6 months) 55.8 41.6
% Early breastfeeding (Children breastfed within the
first hour of birth) 18.0
25.2
% children age 6-8 month receiving solid/semi solid
food and breastmilk 36.7 32.6
% children received Vitamin A supplements 28.7 39.5
Source: National Family Health Survey – 4 (2015-16)
4
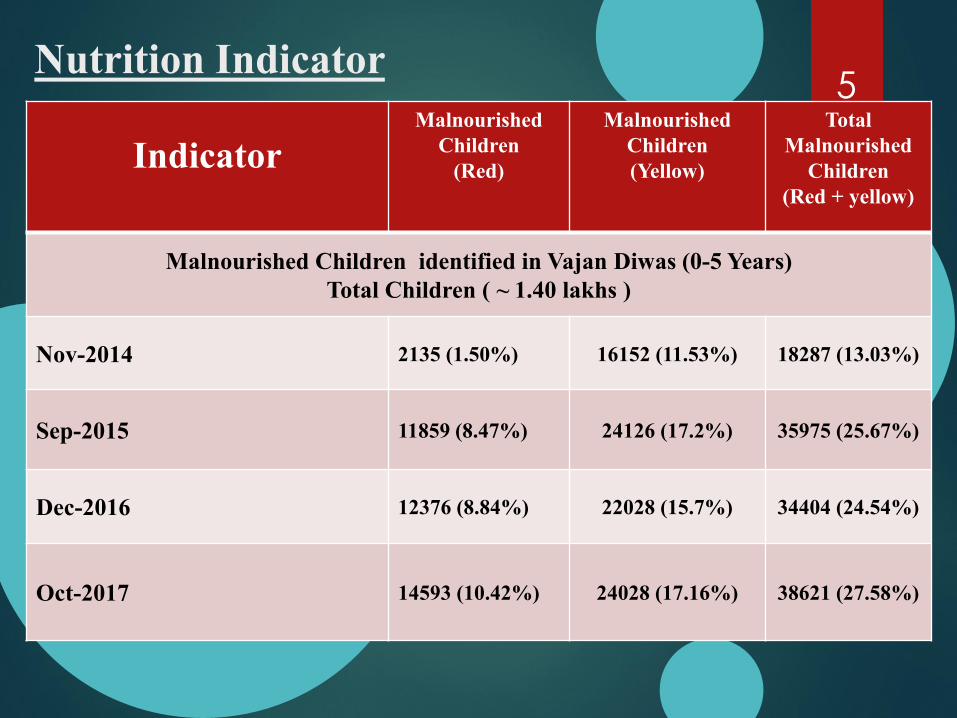
Nutrition Indicator
Indicator Malnourished
Children
(Red)
Malnourished
Children
(Yellow)
Total
Malnourished
Children
(Red + yellow)
Malnourished Children identified in Vajan Diwas (0-5 Years)
Total Children ( ~ 1.40 lakhs )
Nov-2014 2135 (1.50%) 16152 (11.53%) 18287 (13.03%)
Sep-2015 11859 (8.47%) 24126 (17.2%) 35975 (25.67%)
Dec-2016 12376 (8.84%) 22028 (15.7%) 34404 (24.54%)
Oct-2017 14593 (10.42%) 24028 (17.16%) 38621 (27.58%)
5
Constraints o Human Resource ( Supervisors/ AW / AW helper – 20/88/53 )
o Motivation in field staff / Capacity building/ Less honorarium
o Departmental buildings/Equipments ( 529/925)
o Co-ordination issues of AAA
o Lack of AW centers in ratio of population ( 925/1397)
o Frequent strikes
o Improper consumption of THR
o Cultural practices and superstitions
o Awareness Gap
o Terrain ( Indo-Nepal Border )
6
Strategy Proposed
o Filling of vacant posts
o Capacity building
o Convergence for infrastructure/ equipments / services
o Technical support/training
o Real time monitoring ( Shabri Sankalp Yojna )
o Mega Call centre
o NRC/ SNCU utilisation
o Strengthening VHND / Proper utilisation of VHSNC funds
o Tie up with health department ( RI, PMMVY, JSY, JSSK besides others )
o Technological Intervention
7

Initiatives taken in District
o Jeevan Camps were organised in the district to provide better health care to children and pregnant mothers. More than 2 lakh have been covered through these camps
o Operation Kayakalp aims at providing better infrastructure facilities at GP level esp. in schools/Anganwadis.
o Vajan Diwas was conducted at regular intervals to identify the nutrition level of children and tracking them on regular basis
o Transforming Sub health centres to Health and Wellness centres Taken as pilot in one block of district under NHM to provide comprehensive health care
o AAA kits : includes everything they require in field (BP instrument, digital weighing machine, hub cutter, thermometer ,haemoglobin colour check, badges, apron, umbrella, torch, dress, gupshup potli etc
8

THANK YOU

Rajiv Raushan
District Magistrate, Sitamarhi
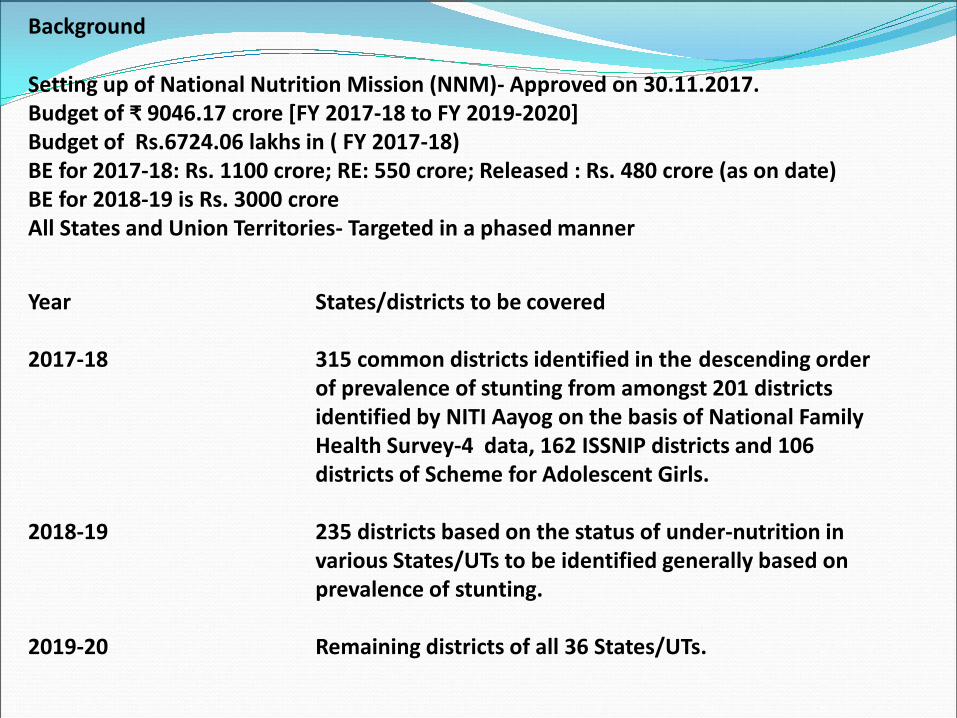
Background
Setting up of National Nutrition Mission (NNM)- Approved on 30.11.2017.
Budget of ₹ 9 4 . crore [FY -18 to FY 2019-2020]
Budget of Rs.6724.06 lakhs in ( FY 2017-18)
BE for 2017-18: Rs. 1100 crore; RE: 550 crore; Released : Rs. 480 crore (as on date)
BE for 2018-19 is Rs. 3000 crore
All States and Union Territories- Targeted in a phased manner
Year States/districts to be covered
2017-18 315 common districts identified in the descending order
of prevalence of stunting from amongst 201 districts
identified by NITI Aayog on the basis of National Family
Health Survey-4 data, 162 ISSNIP districts and 106
districts of Scheme for Adolescent Girls.
2018-19 235 districts based on the status of under-nutrition in
various States/UTs to be identified generally based on
prevalence of stunting.
2019-20 Remaining districts of all 36 States/UTs.
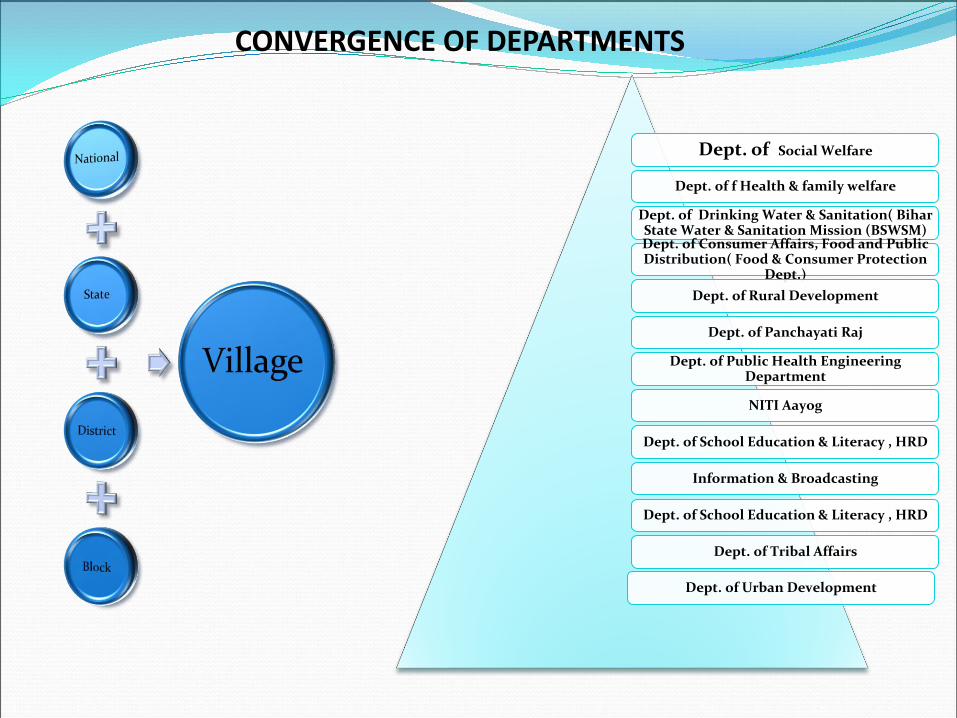
Dept. of Social Welfare
Dept. of f Health & family welfare
Dept. of Drinking Water & Sanitation( Bihar State Water & Sanitation Mission (BSWSM) Dept. of Consumer Affairs, Food and Public Distribution( Food & Consumer Protection
Dept.)
Dept. of Rural Development
Dept. of Panchayati Raj
Dept. of Public Health Engineering Department
NITI Aayog
Dept. of School Education & Literacy , HRD
Information & Broadcasting
Dept. of School Education & Literacy , HRD
Dept. of Tribal Affairs
Dept. of Urban Development
CONVERGENCE OF DEPARTMENTS
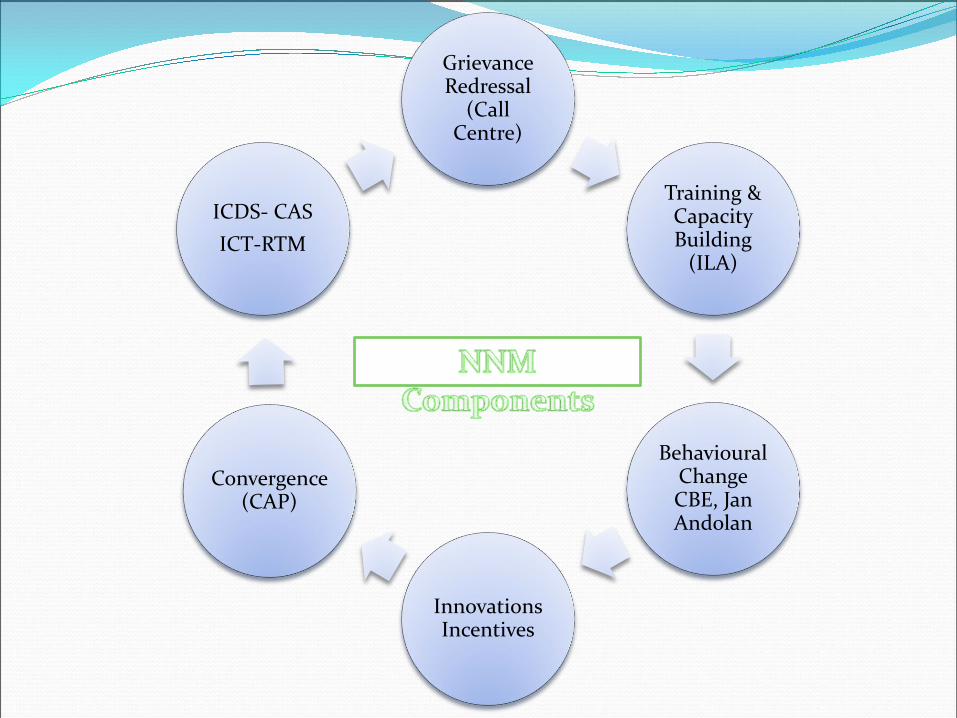
Grievance Redressal
(Call Centre)
Training & Capacity Building
(ILA)
Behavioural Change CBE, Jan Andolan
Innovations Incentives
Convergence (CAP)
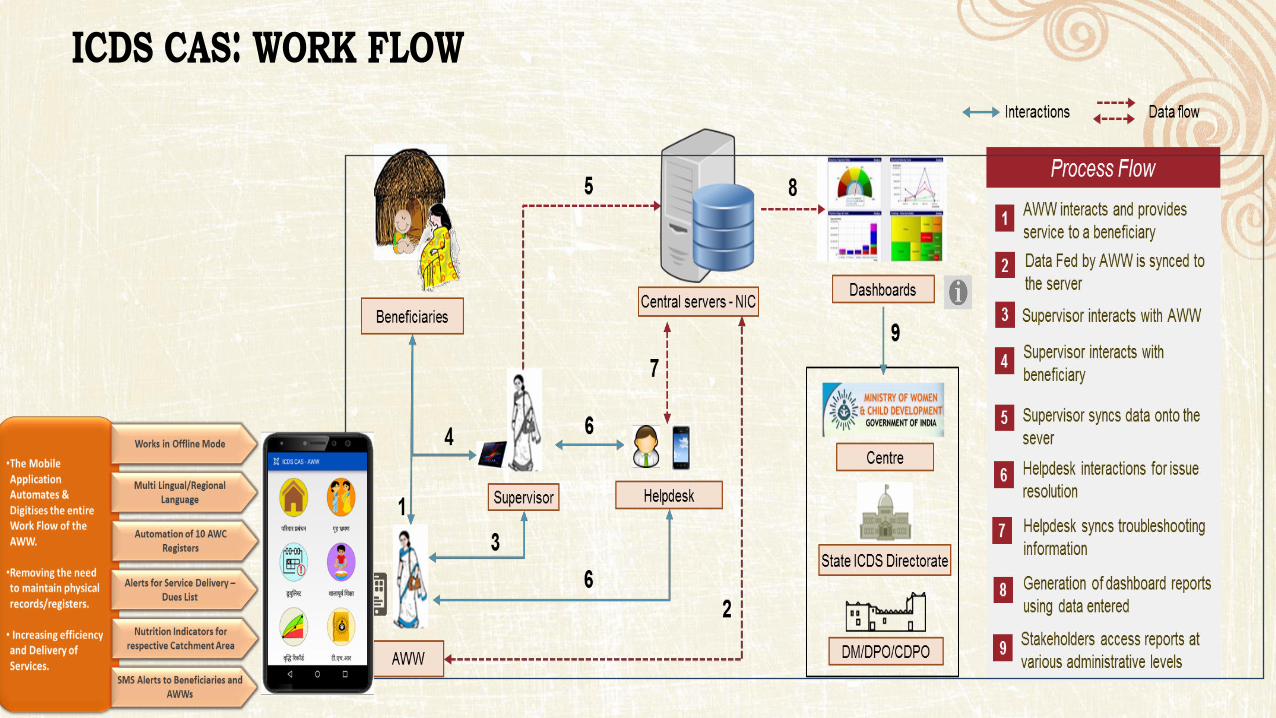
ICDS- CAS
ICT-RTM
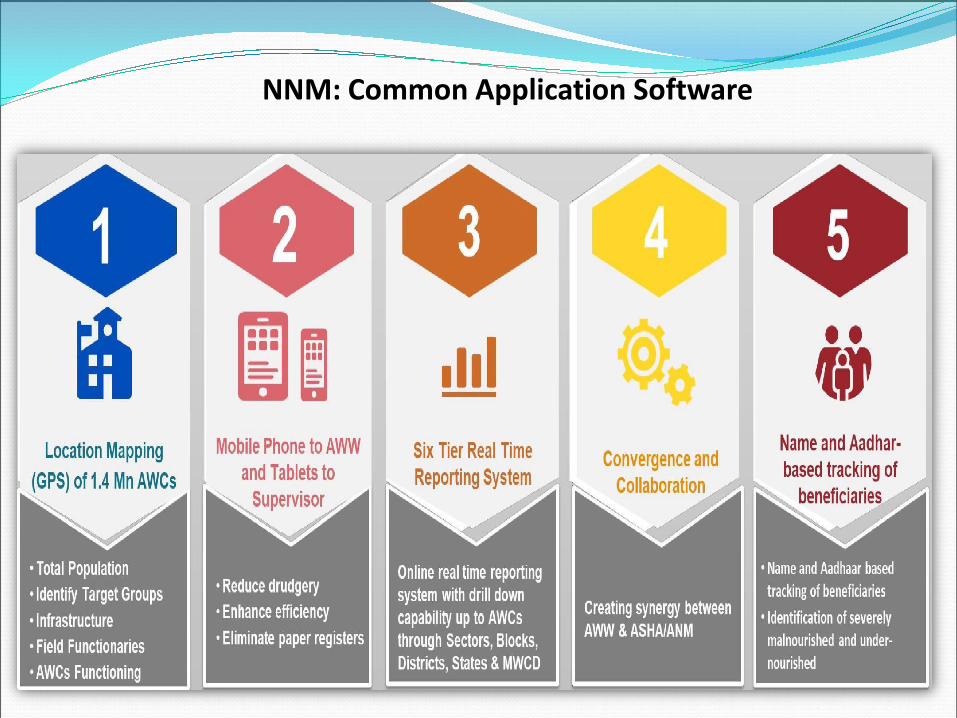
NNM: Common Application Software

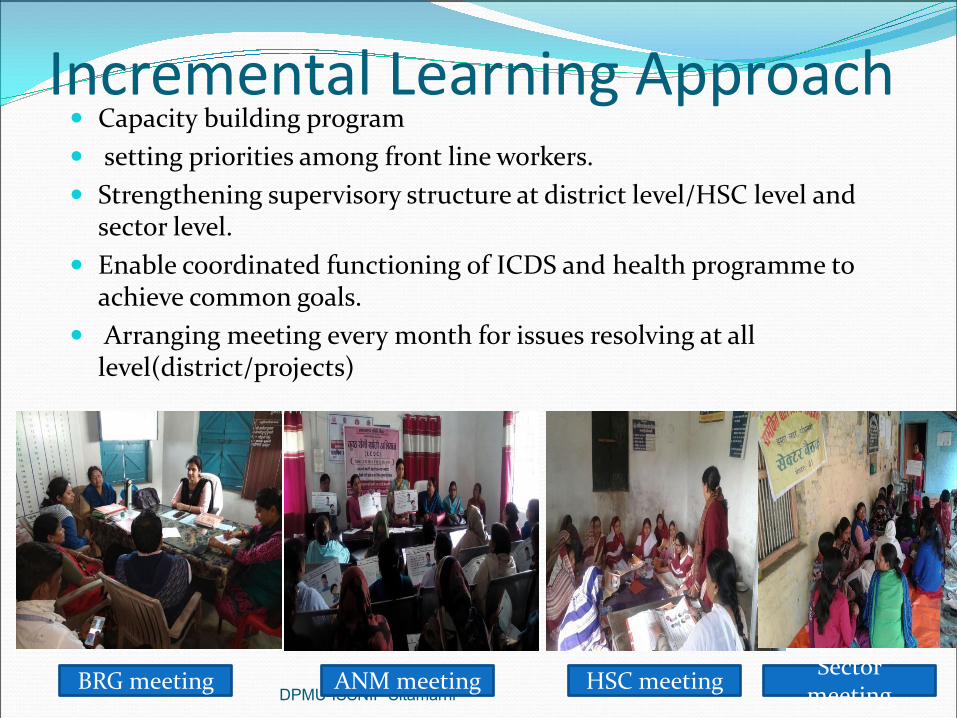
Incremental Learning Approach Capacity building program
setting priorities among front line workers.
Strengthening supervisory structure at district level/HSC level and sector level.
Enable coordinated functioning of ICDS and health programme to achieve common goals.
Arranging meeting every month for issues resolving at all level(district/projects)
DPMU-ISSNIP Sitamarhi BRG meeting ANM meeting HSC meeting
Sector meeting
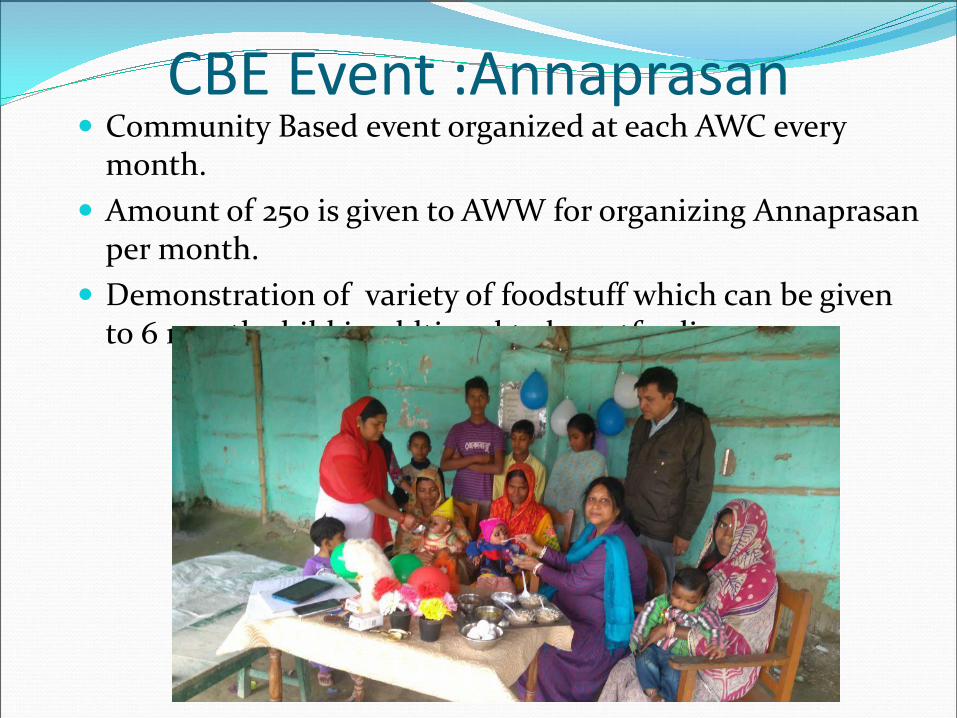
CBE Event :Annaprasan Community Based event organized at each AWC every
month.
Amount of 250 is given to AWW for organizing Annaprasan per month.
Demonstration of variety of foodstuff which can be given to 6 month child inaddtional to breastfeeding.
DPMU-ISSNIP Sitamarhi
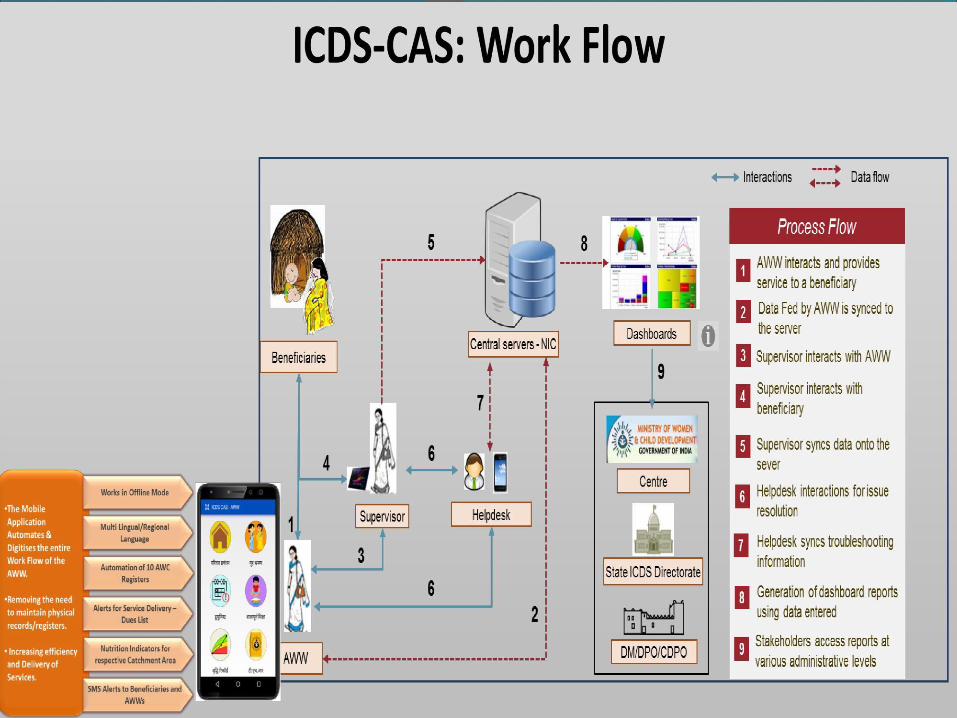
ICT-RTM (Information and
Communication technology-Real
Time Monitoring)
Mobile for AWC and Tablets given to Lady Supervisors
ICDS-CAS(AWW) App for AWW and ICDS-CAS(LS) for LS and ICDS-CAS(issue tracker) for District & Block helpdesk.
Sitamarhi succeeded as pilot project and till feb-18, 81% sevika is working/active on ICDS-CAS.
DPMU-ISSNIP Sitamarhi
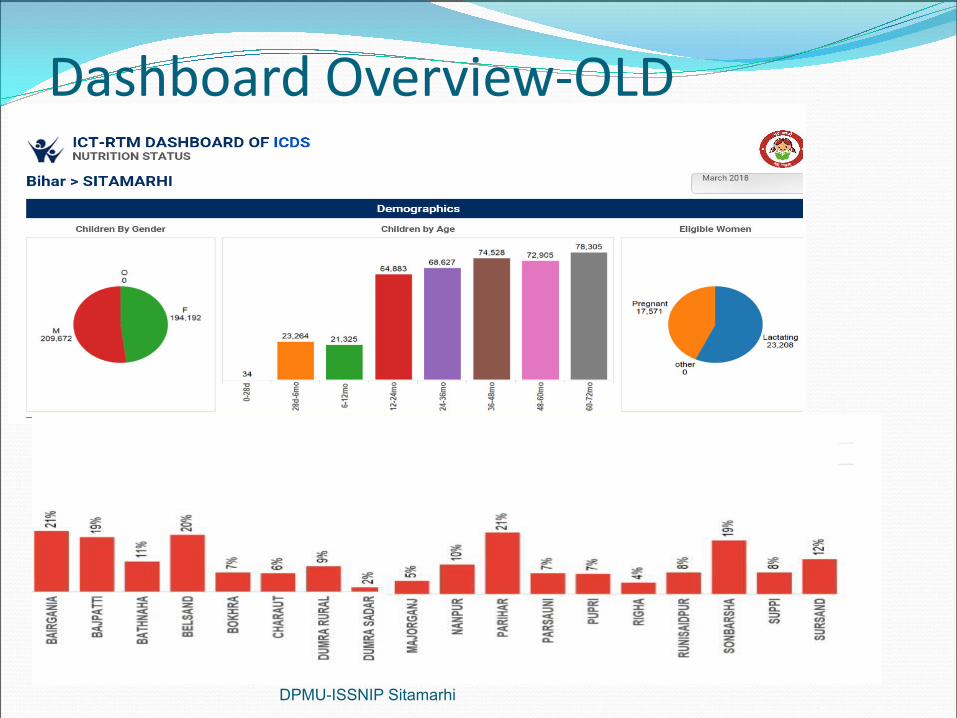
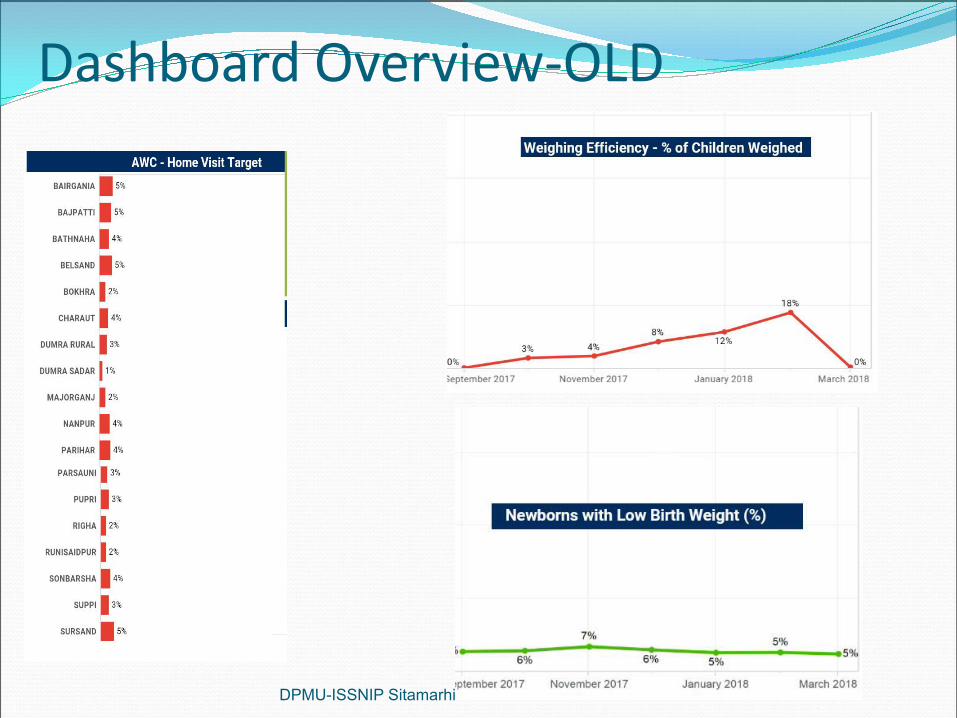
Dashboard Overview-OLD
DPMU-ISSNIP Sitamarhi
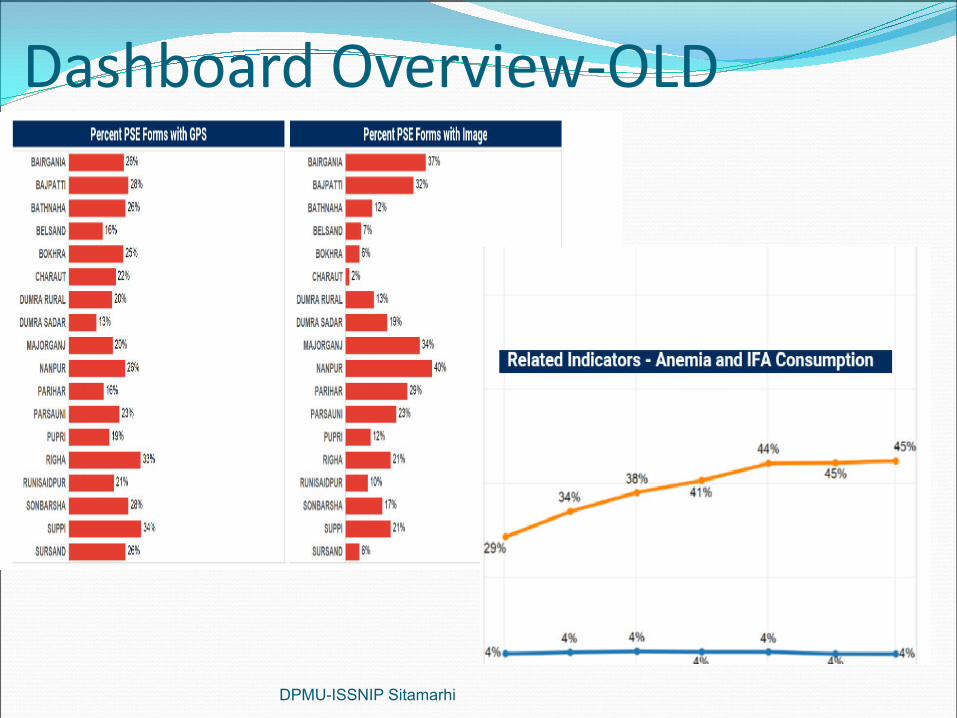
Dashboard Overview-OLD
DPMU-ISSNIP Sitamarhi
Dashboard Overview-OLD
DPMU-ISSNIP Sitamarhi
NNM Respected Prime minister Mr. Narendra Modi will launch NNM on 8th
March 2018 with the help of ICT-RTM, and this programe will be telecasted on WCD site and NIC.
Improve Nutrition services delivery.
Analyzing nutrition data.
Monitor and make stetegies for its improvement based on ICT-RTM.
AIM Mapping nutrition gap
Reduce low birth weight.
Reduce Anemia in Adolescence.
Make Bihar mal-nutrition free .
Reduce slunting.
DPMU-ISSNIP Sitamarhi
NNM Praphat feri In Sitamarhi NNM Prabhat pheri inaugration was
done by DDC sir and DPO(ICDS) sir .
DPMU-ISSNIP Sitamarhi

Convergence meeting with all
Concern department

Executive Committee MeetingExecutive Committee MeetingExecutive Committee MeetingNational Nutrition MissionNational Nutrition MissionNational Nutrition Mission
SiddharthnagarSiddharthnagarSiddharthnagar
Dated-13-03-2018Dated-13-03-2018Dated-13-03-2018
Presented by-Presented by-
KUNAL SILKUKUNAL SILKU
District MagistrateDistrict Magistrate
SiddharthnagarSiddharthnagar
Presented by-
KUNAL SILKU
District Magistrate
Siddharthnagar
Siddharthnagar Demographic Details
Indicators under Ni� Aayog Aspira�onal District
Underweight children under 0‐5 years
Stun�ng among children under 5 years
Percentage of Infants Aged 6‐23 months Receiving an Adequate Diet.
Severe Acute Malnourishment
Percentage of women taking Supplementary Nutri�on
Children age 6‐59 months who are Anemic
Prevalence of anemia in women and girls (15‐49 years)
Strategy
Way forward/Sugges�on
CONTENT
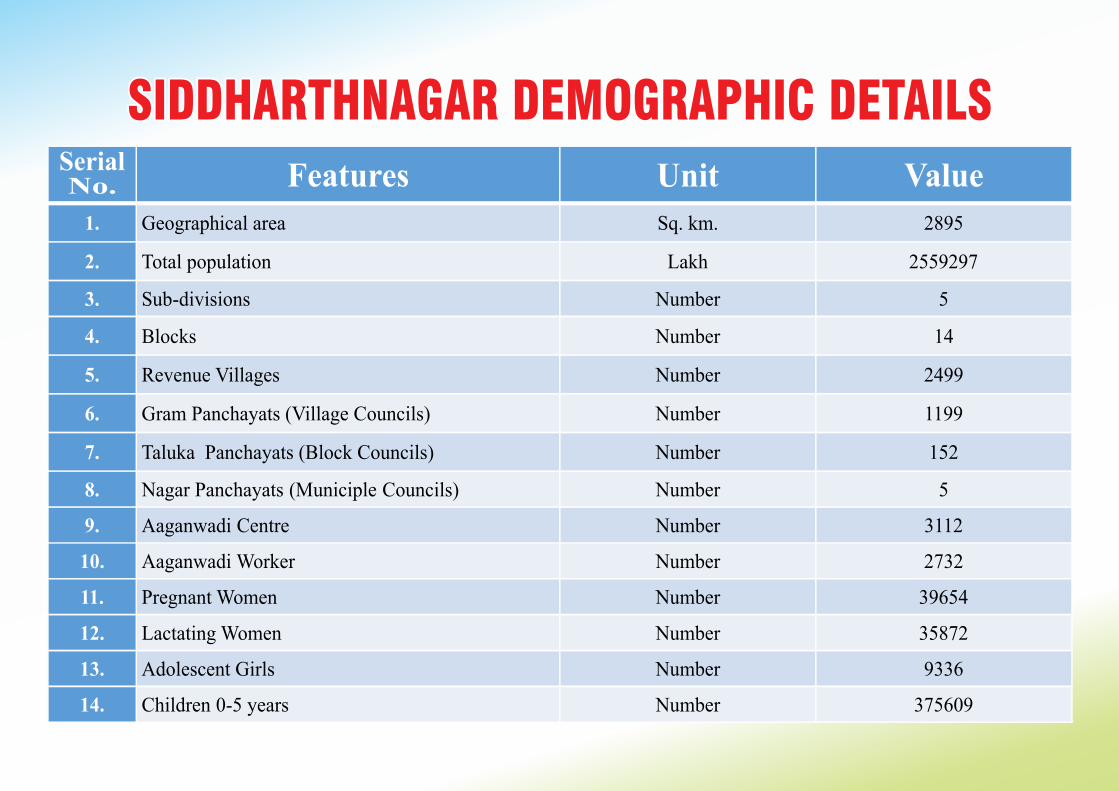
SIDDHARTHNAGAR DEMOGRAPHIC DETAILSSIDDHARTHNAGAR DEMOGRAPHIC DETAILSSIDDHARTHNAGAR DEMOGRAPHIC DETAILSSerial No. Features Unit Value
1. Geographical area Sq. km. 2895
2. Total population Lakh 2559297
3. Sub-divisions Number 5
4. Blocks Number 14
5. Revenue Villages Number 2499
6. Gram Panchayats (Village Councils) Number 1199
7. Taluka Panchayats (Block Councils) Number 152
8.
Nagar Panchayats
(Municiple
Councils)
Number
5
9.
Aaganwadi
Centre
Number
3112
10.
Aaganwadi
Worker
Number
2732
11.
Pregnant Women
Number
39654
12.
Lactating Women
Number
35872
13.
Adolescent Girls
Number
9336
14.
Children
0-5 years
Number
375609
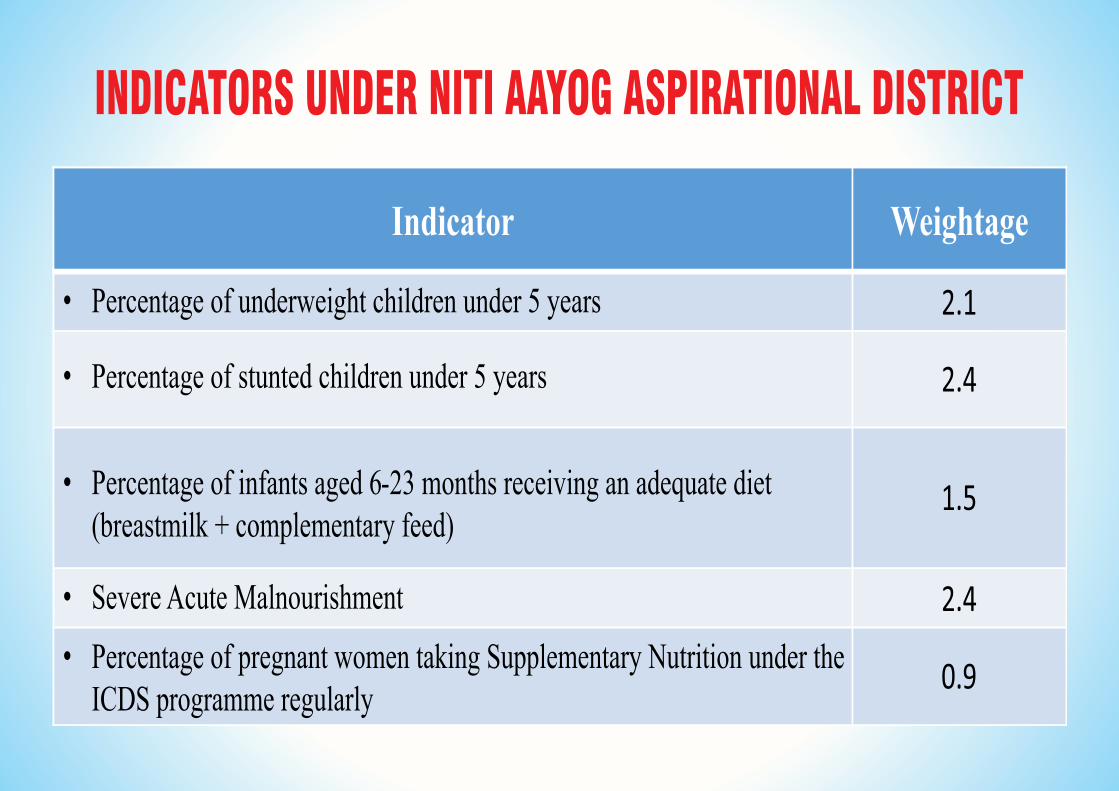
INDICATORS UNDER NITI AAYOG ASPIRATIONAL DISTRICT
Indicator Weightage
• Percentage of underweight children under 5 years
• Percentage of stunted children under 5 years
• Severe Acute Malnourishment
• Percentage of infants aged 6-23 months receiving an adequate diet (breastmilk + complementary feed)
• Percentage of pregnant women taking Supplementary Nutrition under the ICDS programme regularly
2.1
2.4
1.5
2.4
0.9
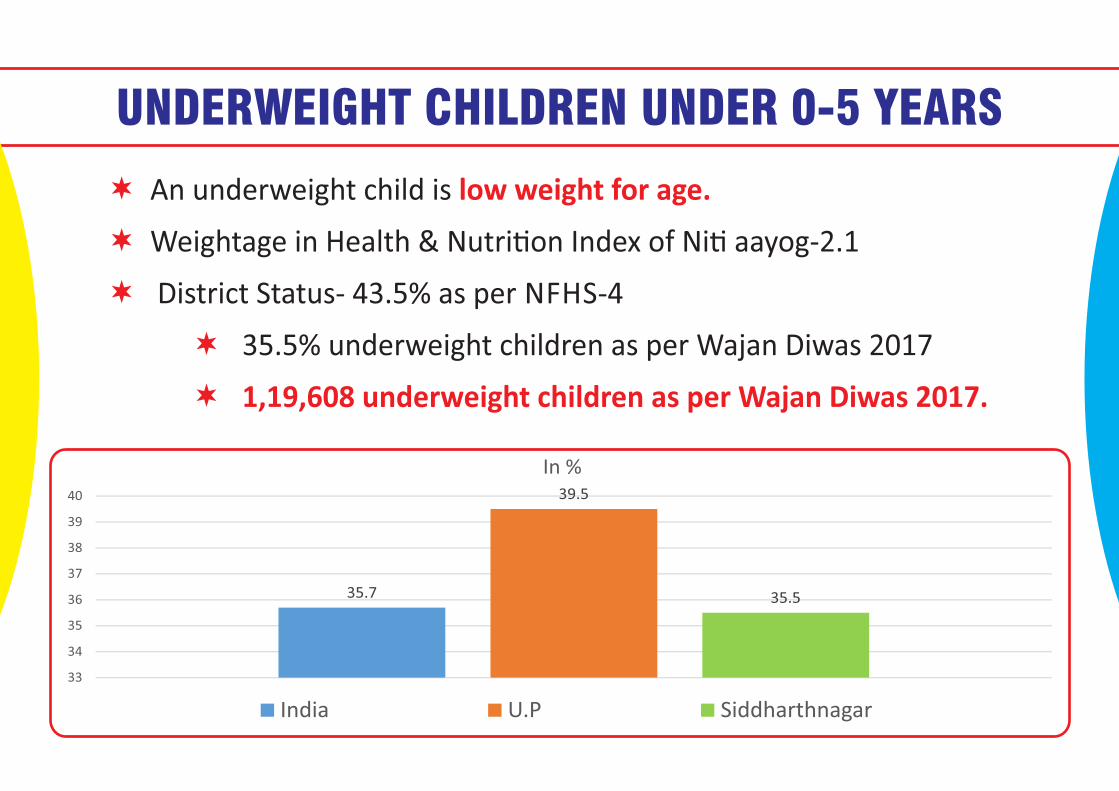
UNDERWEIGHT CHILDREN UNDER 0-5 YEARS
An underweight child is An underweight child is low weight for age.low weight for age.
Weightage in Health & Nutri�on Index of Ni� aayog‐2.1 Weightage in Health & Nutri�on Index of Ni� aayog‐2.1
District Status‐ 43.5% as per NFHS‐4 District Status‐ 43.5% as per NFHS‐4
35.5% underweight children as per Wajan Diwas 2017 35.5% underweight children as per Wajan Diwas 2017
1,19,608 underweight children as per Wajan Diwas 2017.1,19,608 underweight children as per Wajan Diwas 2017.
An underweight child is low weight for age.
Weightage in Health & Nutri�on Index of Ni� aayog‐2.1
District Status‐ 43.5% as per NFHS‐4
35.5% underweight children as per Wajan Diwas 2017
1,19,608 underweight children as per Wajan Diwas 2017.
35.7
39.5
35.5
33
34
35
36
37
38
39
40
In %
India U.P Siddharthnagar
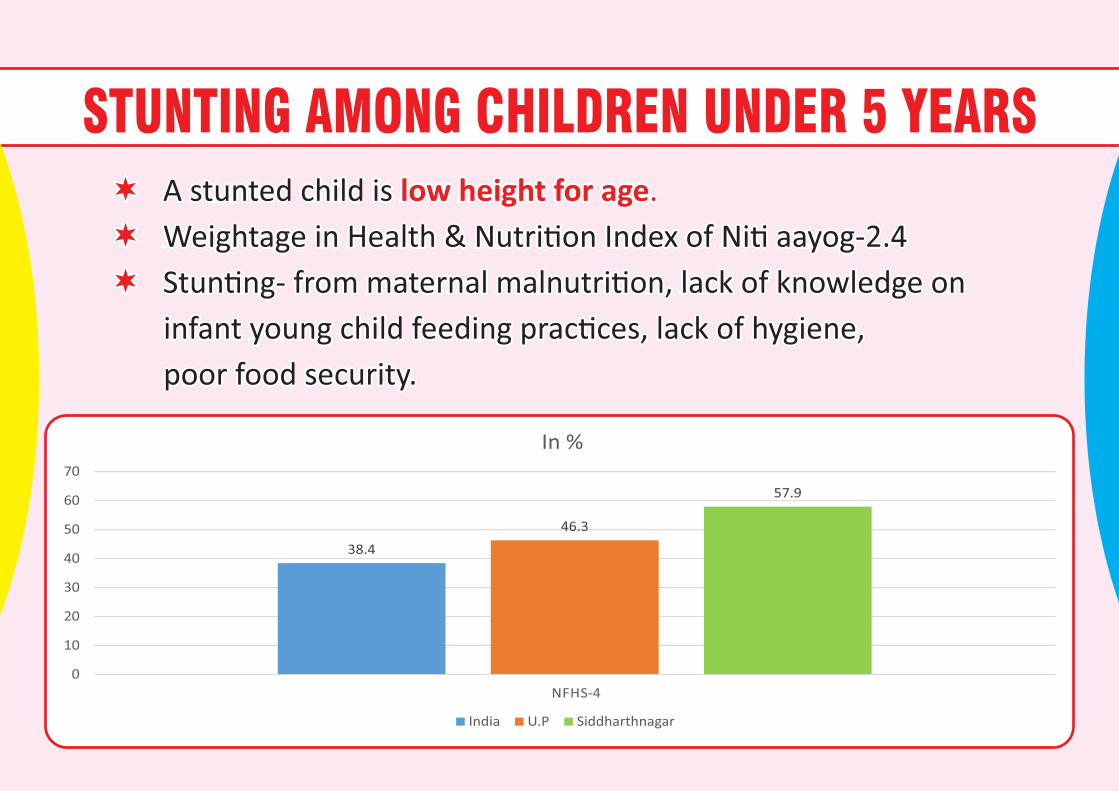
STUNTING AMONG CHILDREN UNDER 5 YEARS low height for age. low height for age. A stunted child is A stunted child is
Weightage in Health & Nutri�on Index of Ni� aayog‐2.4 Weightage in Health & Nutri�on Index of Ni� aayog‐2.4
Stun�ng‐ from maternal malnutri�on, lack of knowledge on Stun�ng‐ from maternal malnutri�on, lack of knowledge on
infant young child feeding prac�ces, lack of hygiene, infant young child feeding prac�ces, lack of hygiene,
poor food security. poor food security.
low height for age. A stunted child is
Weightage in Health & Nutri�on Index of Ni� aayog‐2.4
Stun�ng‐ from maternal malnutri�on, lack of knowledge on
infant young child feeding prac�ces, lack of hygiene,
poor food security.
38.4
46.3
57.9
0
10
20
30
40
50
60
70
NFHS‐4
In %
India U.P Siddharthnagar
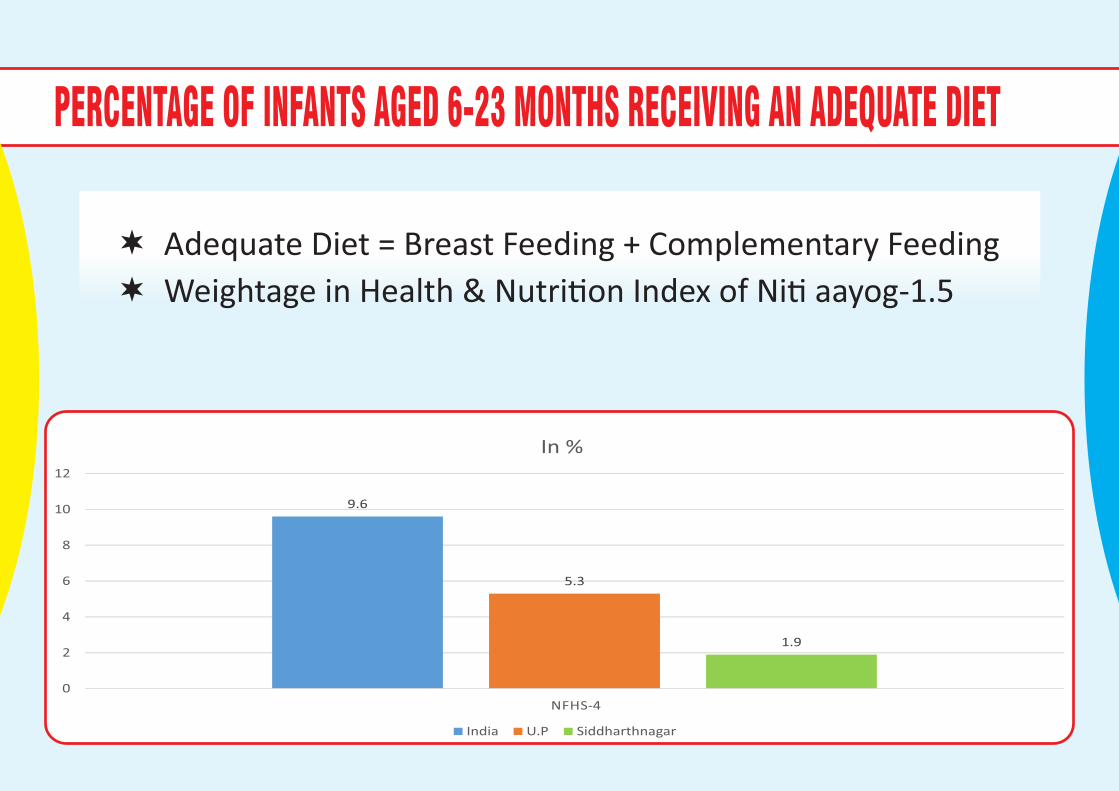
PERCENTAGE OF INFANTS AGED 6-23 MONTHS RECEIVING AN ADEQUATE DIET
Adequate Diet = Breast Feeding + Complementary Feeding
Weightage in Health & Nutri�on Index of Ni� aayog‐1.5
9.6
5.3
1.9
0
2
4
6
8
10
12
NFHS‐4
In %
India U.P Siddharthnagar
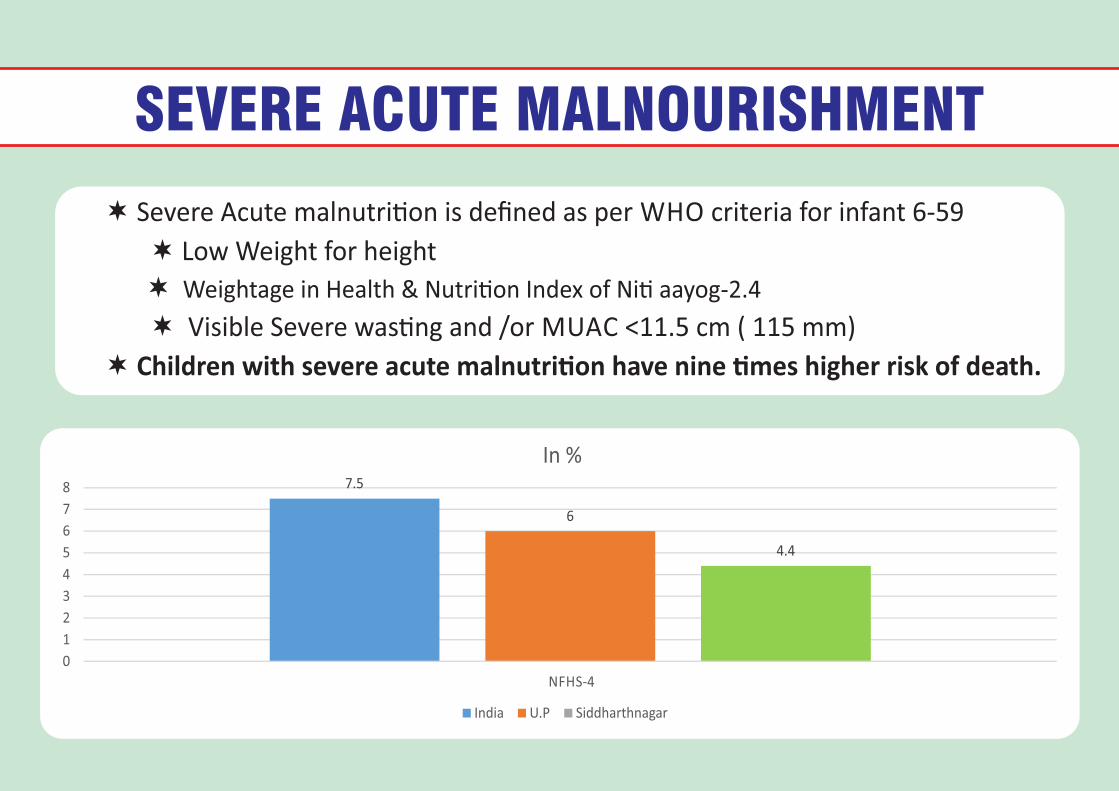
SEVERE ACUTE MALNOURISHMENT
Severe Acute malnutri�on is defined as per WHO criteria for infant 6‐59
Low Weight for height
Weightage in Health & Nutri�on Index of Ni� aayog‐2.4
Visible Severe was�ng and /or MUAC <11.5 cm ( 115 mm)
Children with severe acute malnutri�on have nine �mes higher risk of death.
7.5
6
4.4
0
1
2
3
4
5
6
7
8
NFHS‐4
In %
India U.P Siddharthnagar
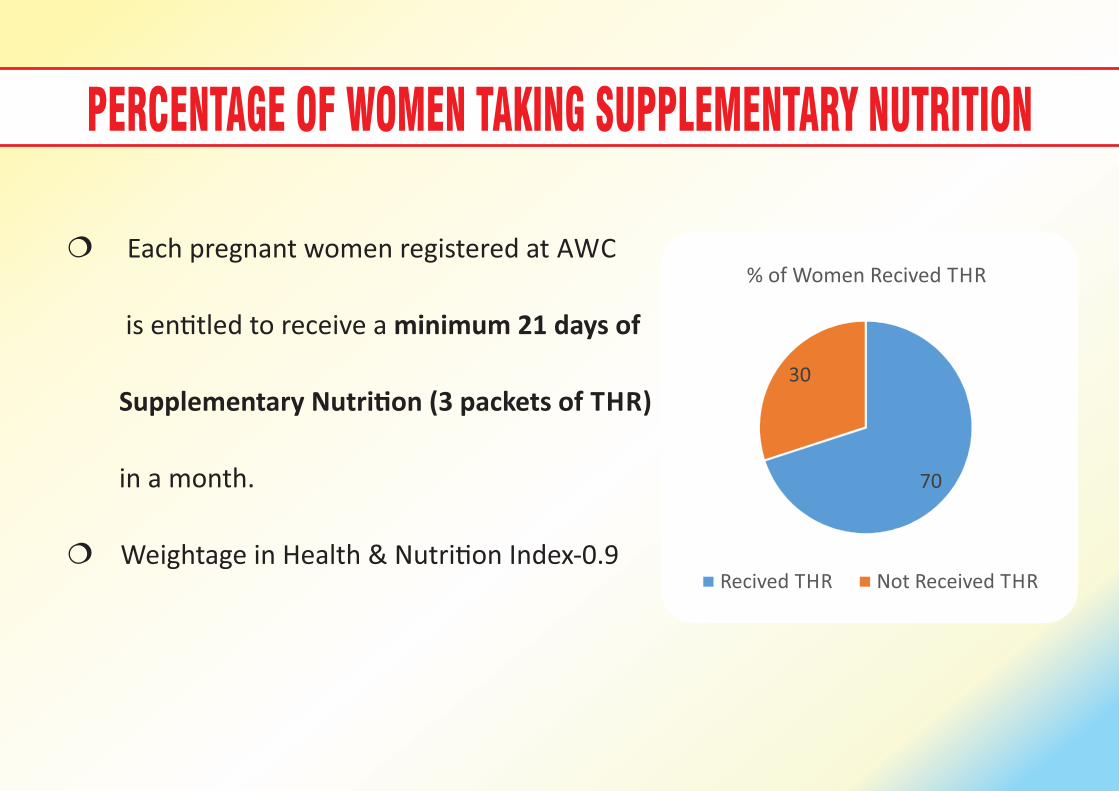
PERCENTAGE OF WOMEN TAKING SUPPLEMENTARY NUTRITION
Each pregnant women registered at AWC
is en�tled to receive a minimum 21 days of
Supplementary Nutri�on (3 packets of THR)
in a month.
Weightage in Health & Nutri�on Index‐0.9
70
30
% of Women Recived THR
Recived THR Not Received THR
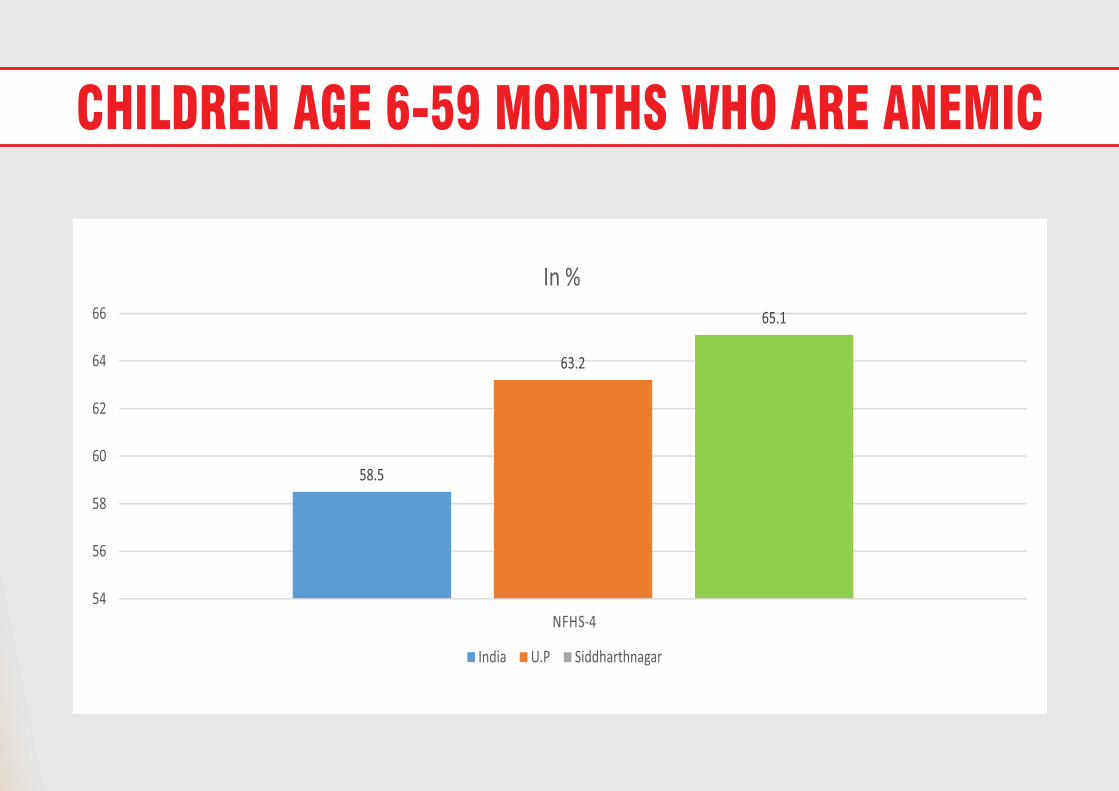
CHILDREN AGE 6-59 MONTHS WHO ARE ANEMIC
58.5
63.2
65.1
54
56
58
60
62
64
66
NFHS‐4
In %
India U.P Siddharthnagar
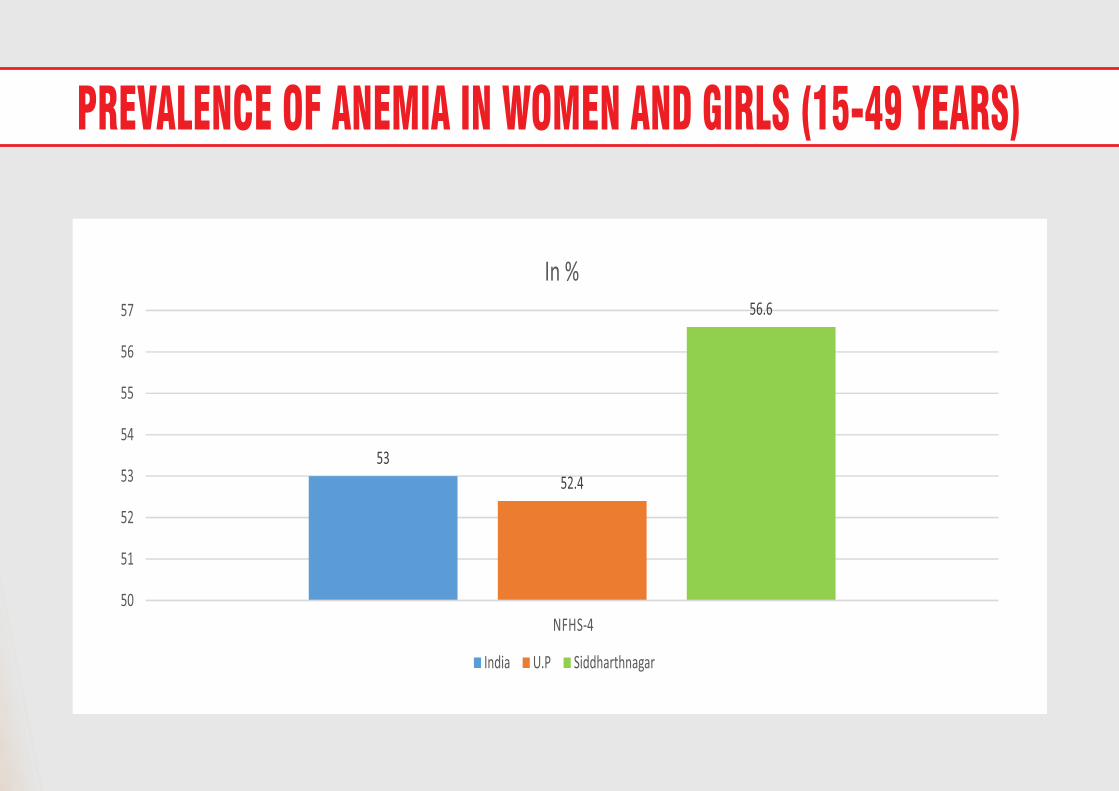
PREVALENCE OF ANEMIA IN WOMEN AND GIRLS (15-49 YEARS)
53
52.4
56.6
50
51
52
53
54
55
56
57
NFHS‐4
In %
India U.P Siddharthnagar
DN ERU N OF UO RE IL SC HY MC EE NF TIL
DN ERU N OF UO RE IL SC HY MC EE NF TIL
DN ERU N OF UO RE IL SC HY MC EE NF TIL
STRATEGY FOR UNDERWEIGHT CHILDREN
Regular tracking/weighing using growth chart.
Focus on 1000 days. Early ini�a�on of breast feeding, exclusive breast
feeding and con�nued breast feeding �ll 2 years of age.
Linking of severely under weight children’s family to Antayodaya
scheme to ensure food security.
Providing job card to parents of SAM children to upgrade their
economic status.
Focus on home visit by front line workers as part of BCC (Behavior
Change Communica�on.
Rou�ne health check up, treatment and regular follow up of health
status of sever underweight children.
STRATEGY FOR MATERNAL HEALTH
100% tracking and registra�on of pregnant women by Health
and ICDS
Ensure 4 Antenatal check ups compulsorily.
Iron folic Acid supplementa�on as per norms.
Ensure 100% tracking and home visit by FLW of high risk
pregnancy cases and referral.
100% supplementary nutri�on from ICDS (THR).
STRATEGY FOR ADOLESCENT GIRLS
Weekly Iron Folic Acid supplementa�on through WIFS
programme.
Organizing Ladli Diwas for awareness genera�on among
adolescent girls related to health and hygiene.
Educa�ng adolescent girls regarding health, hygiene and
sanita�on by Health, ICDS and Educa�on departments.
Preven�ve and correc�ve measures for reducing
malnutri�on in adolescent girls.
COMMON STRATEGY1. 96 villages have been adopted by 49 district level officers to set them free from severe malnutri�on
as per State Nutri�on Mission guidelines.
2. To tackle malnutri�on effec�vely, ac�ve as well as cohesive support and convergence among
a. ICDS,
b. Health,
c. PRI,
d. Rural Development,
e. Educa�on and
f. Civil Supply departments has been ensured and regular monitoring and review is done in District
Nutri�on Commi�ee mee�ng every month.
3. Improving water and sanita�on facility, making district open defeca�on free.
4. Real �me monitoring of THR distribu�on by district and block level officials.
5. Focus on home visit by front line workers as part of BCC (Behavior Change Communica�on).
6. Promo�on of diet diversity for all, using home visit and mid media pla�orms
7. For be�er prac�ces of complementary feeding ECCE (Early Childhood Care and Educa�on) sessions are
being organized at AWC, VHND, Annaprashan and mothers mee�ngs.
WAY FORWARD / SUGGESTION In place of Panjiri as THR, THR in the form of candies, biscuits and other protein rich packaged powder products. (It will
help in preven�ng diversion in form of ca�le feed)
Development of IEC materials related to Maternal Infant and Young Child Nutri�on and Infant Young Child Feeding
prac�ces.(Should be taken up by state and center similar to Swatch Bharat Mission Scheme)
Procurement of new weighing scale where weighing scale are not func�onal. (Can be done using un�ed fund of ANM.)
Recruitment of Aaganwadi and Mukhya Sevika (State should try to get the HC stay vacated.)
Handholding required in iden�fying and preven�ng stun�ng.
a. Currently our program focusses on matnutri�on. Our FLWs are trained for iden�fica�on, measuring as well as
preven�on and cure for malnutri�on.
b. However, no such literature, tools or training has been provided for iden�fica�on, measurement, preven�on or cure
of stun�ng.
c Currently neither ASHA nor AWW are measuring stun�ung.
So as a way forward
a. Requirement of height‐weight‐age chart for tracking of stunted children (Currently only weight‐Age chart has been
provided)
b. To ensure tools and training to FLWs for iden�fica�on of stunted children.
c .Convergence with Health Department for rapid screening of 0‐5 years children and iden�fica�on of stunted children.
Ensuring home visit of severely underweight children by FLW as well as District level officials. (To be done at district level)
Training/sensi�za�on of AWW, Mukhya Sevika and CDPO on Maternal Infant and Young Child Nutri�on and Infant Young
Child Feeding prac�ces. (To be done at district level. However some training partners can be provided to us by state /
center)

Thank You.
Government of U.P.
ANALYSIS ON GAPS IN NUTRITION
SECTOR
DISTRICT- SITAPUR
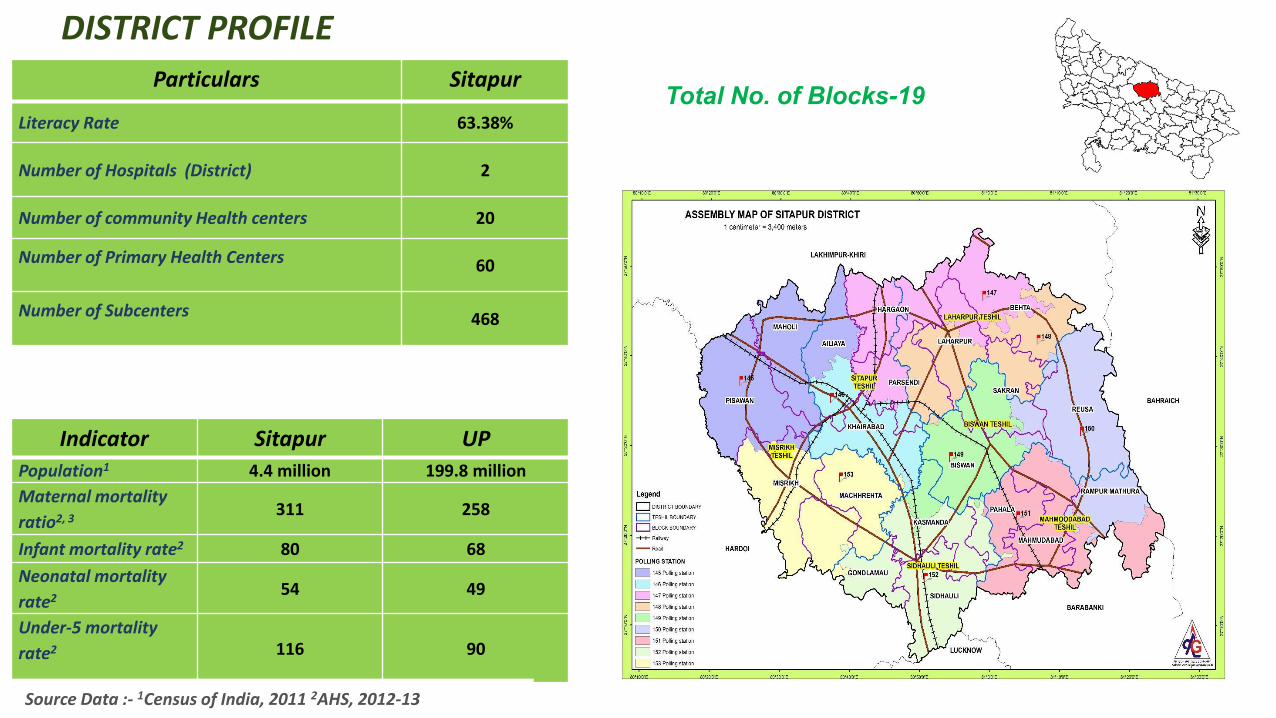
Total No. of Blocks-19
Indicator Sitapur UP
Population1 4.4 million 199.8 million
Maternal mortality
ratio2, 3 311 258
Infant mortality rate2 80 68
Neonatal mortality
rate2 54 49
Under-5 mortality
rate2
116 90
Source Data :- 1Census of India, 2011 2AHS, 2012-13
DISTRICT PROFILE
Particulars Sitapur
Literacy Rate 63.38%
Number of Hospitals (District) 2
Number of community Health centers 20
Number of Primary Health Centers 60
Number of Subcenters 468
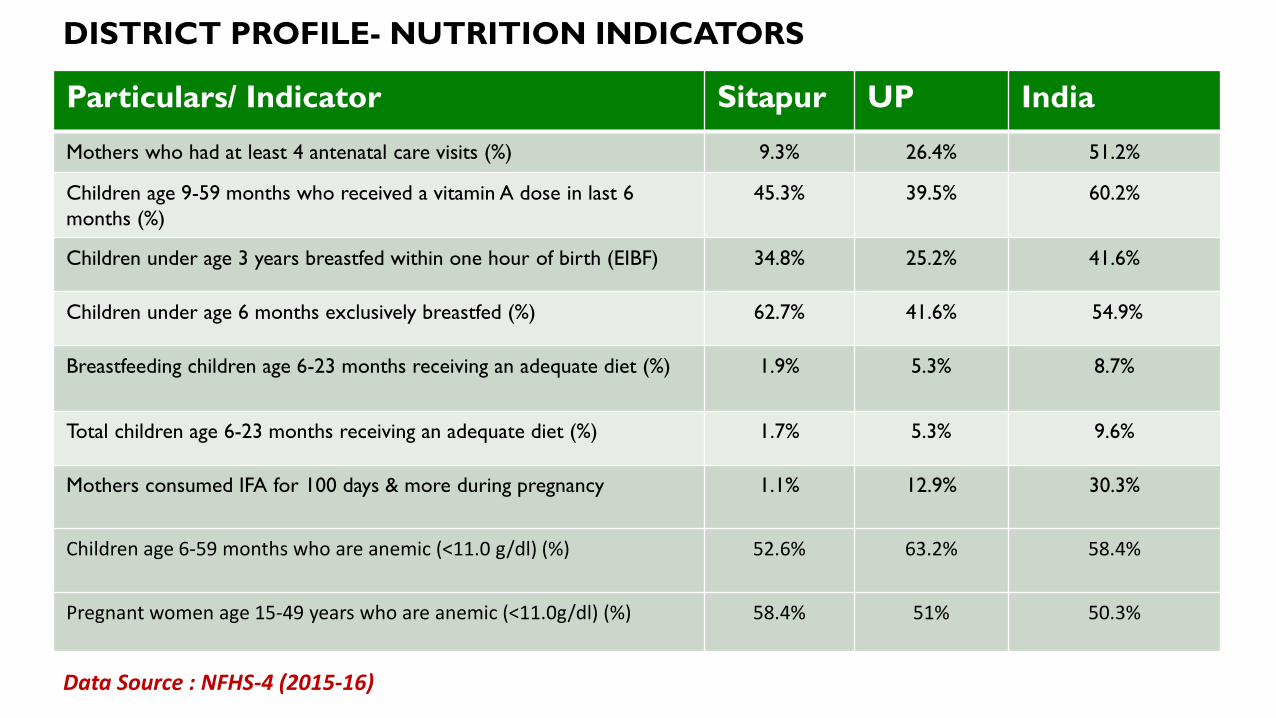
DISTRICT PROFILE- NUTRITION INDICATORS
Particulars/ Indicator Sitapur UP India
Mothers who had at least 4 antenatal care visits (%) 9.3% 26.4% 51.2%
Children age 9-59 months who received a vitamin A dose in last 6 months (%)
45.3% 39.5% 60.2%
Children under age 3 years breastfed within one hour of birth (EIBF) 34.8% 25.2% 41.6%
Children under age 6 months exclusively breastfed (%) 62.7% 41.6% 54.9%
Breastfeeding children age 6-23 months receiving an adequate diet (%) 1.9% 5.3% 8.7%
Total children age 6-23 months receiving an adequate diet (%) 1.7% 5.3% 9.6%
Mothers consumed IFA for 100 days & more during pregnancy 1.1% 12.9% 30.3%
Children age 6-59 months who are anemic (<11.0 g/dl) (%) 52.6% 63.2%
58.4%
Pregnant women age 15-49 years who are anemic (<11.0g/dl) (%) 58.4% 51% 50.3%
Data Source : NFHS-4 (2015-16)
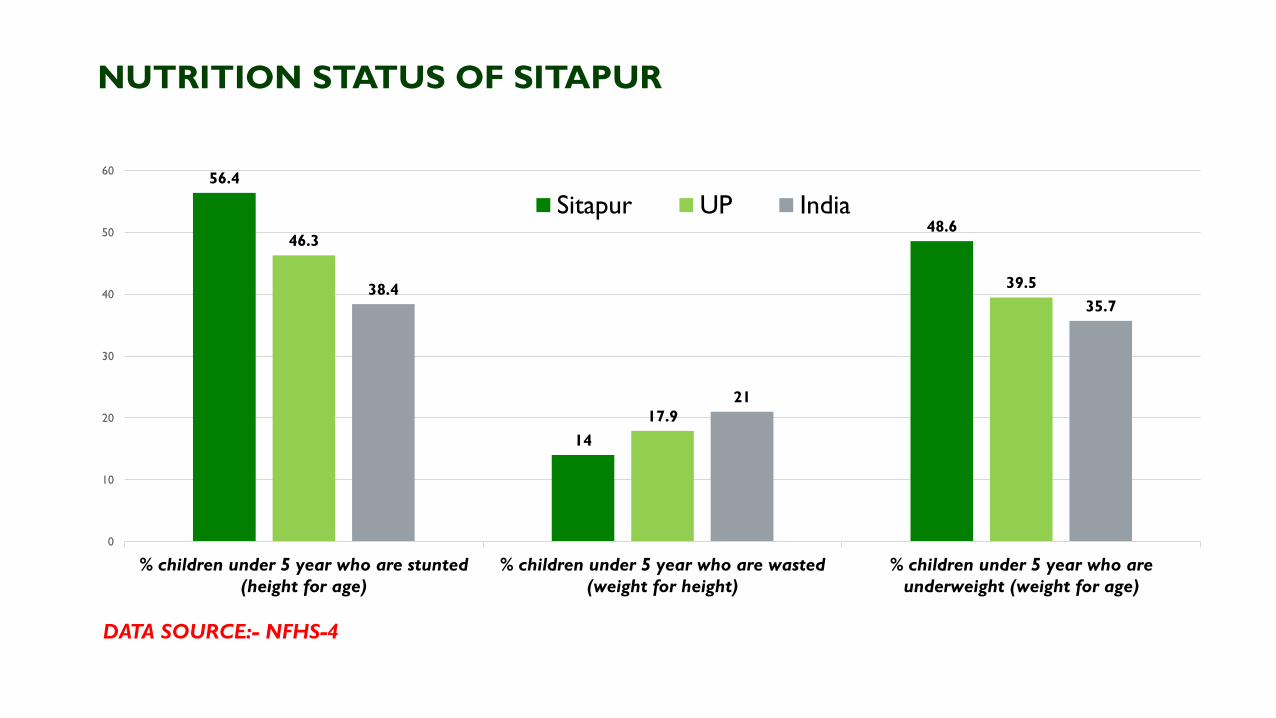
NUTRITION STATUS OF SITAPUR
56.4
14
48.6 46.3
17.9
39.5 38.4
21
35.7
0
10
20
30
40
50
60
% children under 5 year who are stunted(height for age)
% children under 5 year who are wasted(weight for height)
% children under 5 year who areunderweight (weight for age)
Sitapur UP India
DATA SOURCE:- NFHS-4
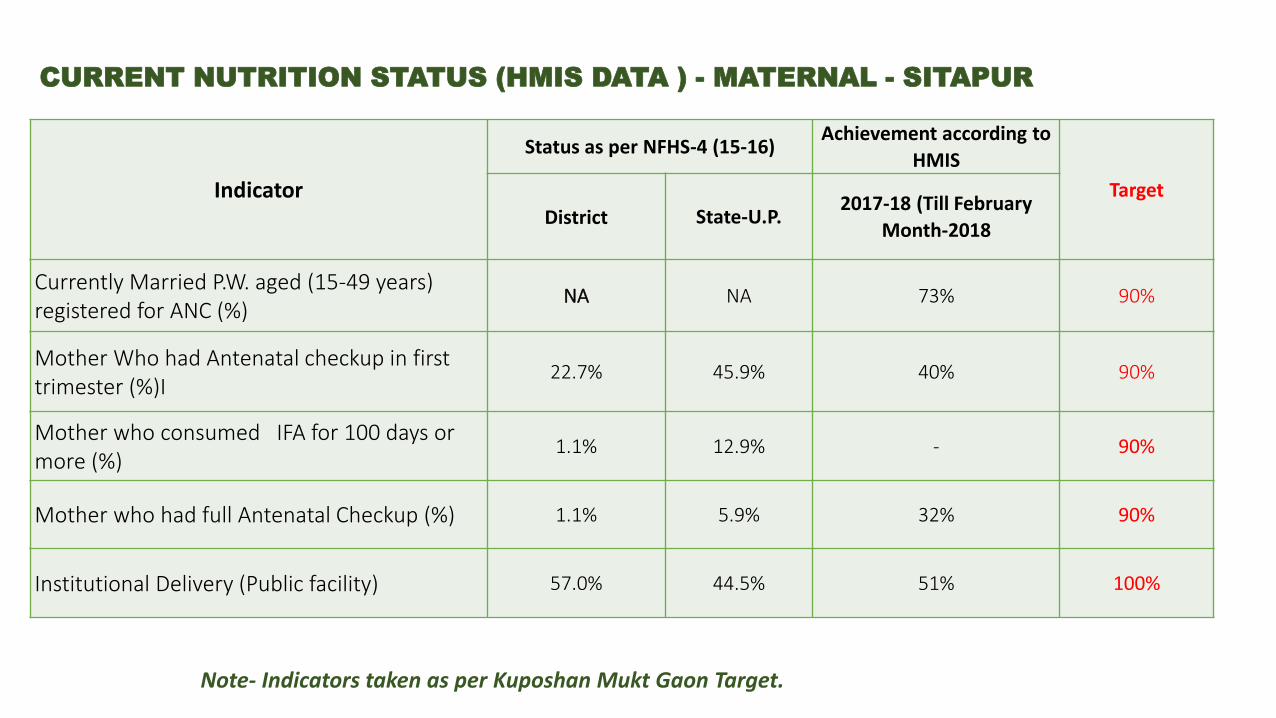
CURRENT NUTRITION STATUS (HMIS DATA ) - MATERNAL - SITAPUR
Indicator
Status as per NFHS-4 (15-16) Achievement according to
HMIS
Target
District State-U.P. 2017-18 (Till February
Month-2018
Currently Married P.W. aged (15-49 years)
registered for ANC (%) NA NA 73% 90%
Mother Who had Antenatal checkup in first
trimester (%)I 22.7%
45.9%
40% 90%
Mother who consumed IFA for 100 days or
more (%) 1.1% 12.9% - 90%
Mother who had full Antenatal Checkup (%) 1.1% 5.9% 32% 90%
Institutional Delivery (Public facility) 57.0% 44.5% 51% 100%
Note- Indicators taken as per Kuposhan Mukt Gaon Target.
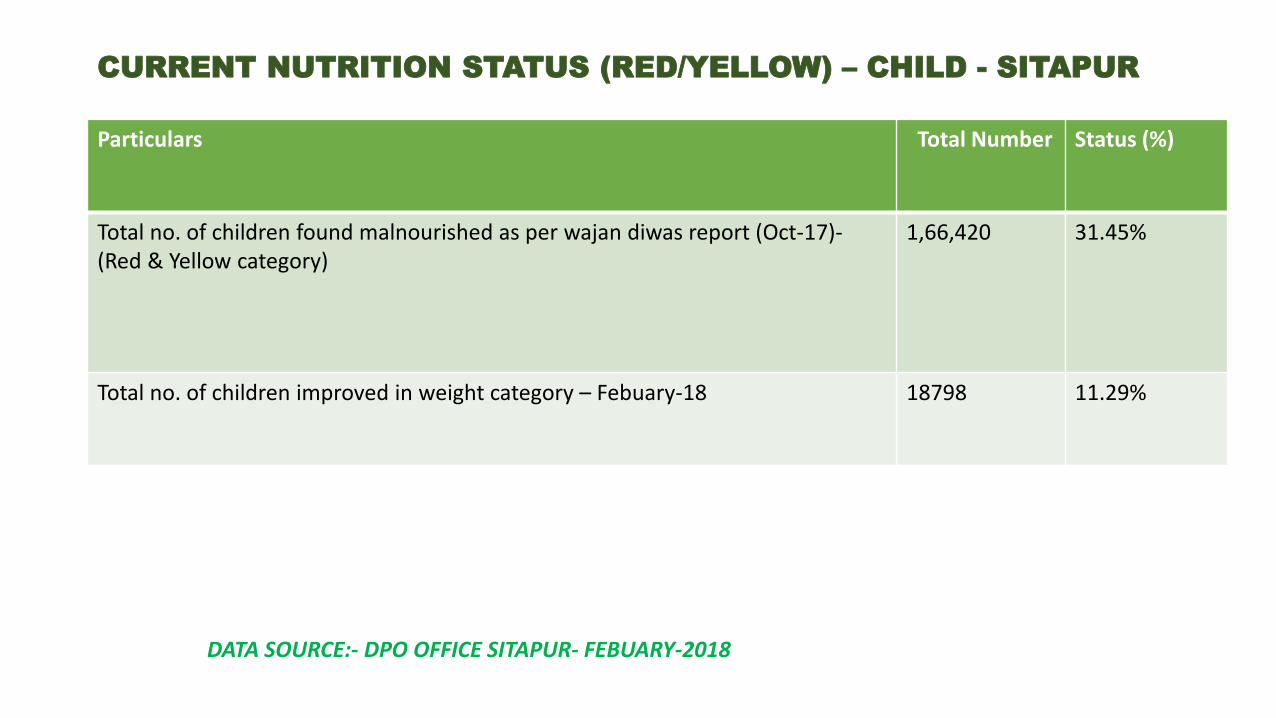
CURRENT NUTRITION STATUS (RED/YELLOW) – CHILD - SITAPUR
Particulars Total Number Status (%)
Total no. of children found malnourished as per wajan diwas report (Oct-17)-
(Red & Yellow category)
1,66,420 31.45%
Total no. of children improved in weight category – Febuary-18 18798 11.29%
DATA SOURCE:- DPO OFFICE SITAPUR- FEBUARY-2018
PERSISTANCE OF GAPS & CHALLENGES IN ACHIVEING LOW NUTRITION AMONG MATERNAL & CHILD NUTRITION.
Poor coordination in convergence in-between different departments at district and block level.
Poor quality in delivering a health services, shortage of essential drugs at block level (like - Iron-sucrose).
Not having regular & effective monitoring systems to check over program.
Poor Infrastructure & necessary equipment's (Weighing machine) of Aganwadi centers.
Lack of human resource to cater a health services (ICDS + Health Dept.)
Lack of motivation among staff.
Un utilization of funds / Lack of funds.
Health service providers (AWW ,ASHA & ANM) are in-capable to organize Health & Nutrition Education sessions at community level.
Due to long distance & geographical constraint community face problem to reach NRC for treatment of SAM children.
High load of deliveries and high prevalence of HRP cases among pregnant women.
Lack of knowledge on Health , nutrition & sanitation at community level.
Lack of participation at community level.
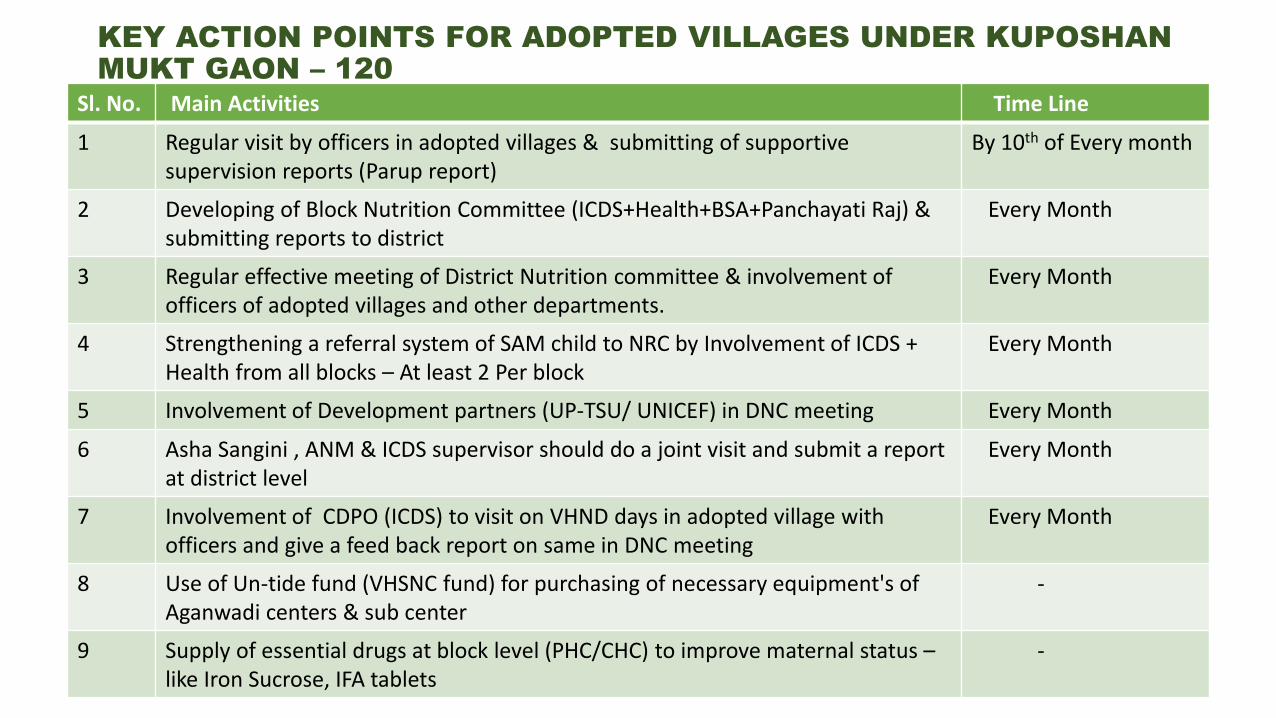
KEY ACTION POINTS FOR ADOPTED VILLAGES UNDER KUPOSHAN MUKT GAON – 120
Sl. No. Main Activities Time Line
1 Regular visit by officers in adopted villages & submitting of supportive
supervision reports (Parup report)
By 10th of Every month
2 Developing of Block Nutrition Committee (ICDS+Health+BSA+Panchayati Raj) &
submitting reports to district
Every Month
3 Regular effective meeting of District Nutrition committee & involvement of
officers of adopted villages and other departments.
Every Month
4 Strengthening a referral system of SAM child to NRC by Involvement of ICDS +
Health from all blocks – At least 2 Per block
Every Month
5 Involvement of Development partners (UP-TSU/ UNICEF) in DNC meeting Every Month
6 Asha Sangini , ANM & ICDS supervisor should do a joint visit and submit a report
at district level
Every Month
7 Involvement of CDPO (ICDS) to visit on VHND days in adopted village with
officers and give a feed back report on same in DNC meeting
Every Month
8 Use of Un-tide fund (VHSNC fund) for purchasing of necessary equipment's of
Aganwadi centers & sub center
-
9 Supply of essential drugs at block level (PHC/CHC) to improve maternal status –
like Iron Sucrose, IFA tablets
-
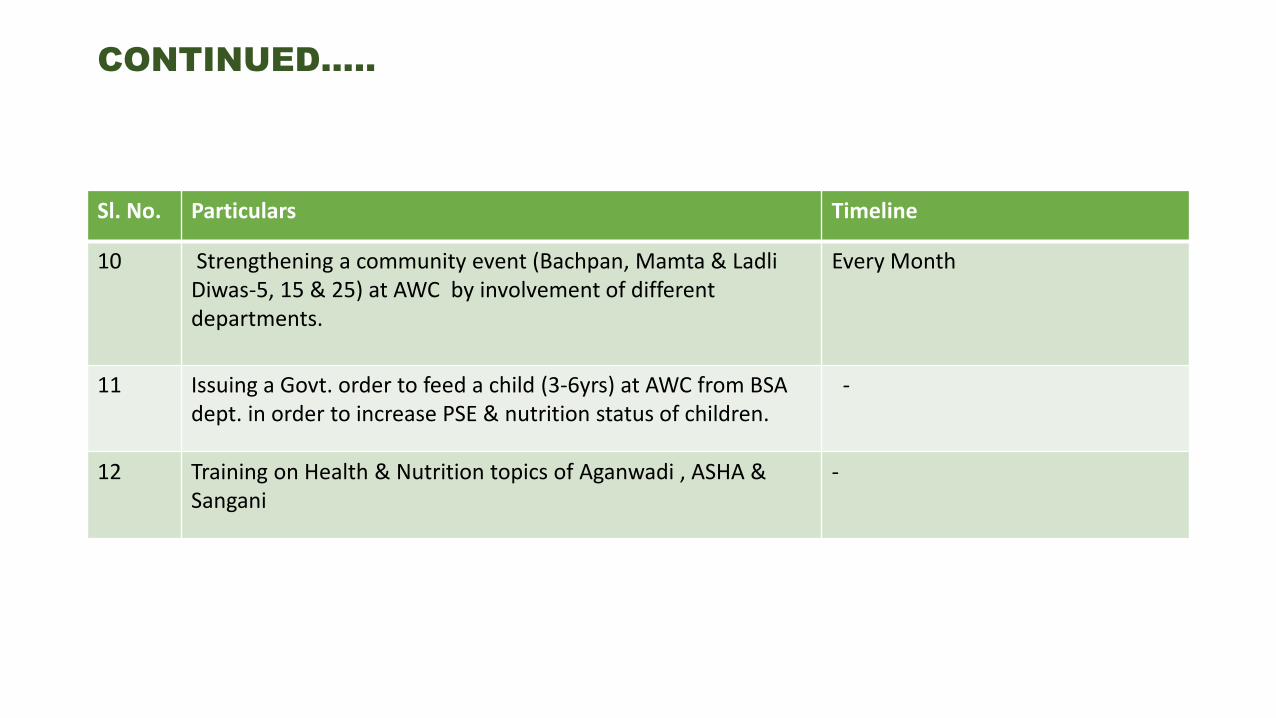
CONTINUED…..
Sl. No. Particulars Timeline
10 Strengthening a community event (Bachpan, Mamta & Ladli
Diwas-5, 15 & 25) at AWC by involvement of different
departments.
Every Month
11 Issuing a Govt. order to feed a child (3-6yrs) at AWC from BSA
dept. in order to increase PSE & nutrition status of children.
-
12 Training on Health & Nutrition topics of Aganwadi , ASHA &
Sangani
-

GOOD PRACTICES ON IMPROVING NUTRITION STATUS AT COMMUNITY LEVEL WITH DEVELOPMENT PARTNERS – UP-TSU.
Community Events
Joint visit of Development Partners (TSU- DN)
with Health & ICDS Dept. DNC Meeting BSPM Inaugration
THANK YOU….
By – Dr. Sharikha Mohan (D.M. Sitapur)
Dept. of Women & Child Development,
Govt. of Karnataka

Setting up of National Nutrition Mission (NNM)- Approved on 30.11.2017.
Budget of ₹ 9 . rore [FY -18 to FY 2019-2020]
BE for 2017-18: Rs. 1100 crore; RE: 550 crore; Released : Rs. 480 crore (as on date)
BE for 2018-19 is Rs. 3000 crore
All States and Union Territories- Targeted in a phased manner
Year States/districts to be covered
2017-18
315 common districts identified in the descending order of prevalence of
stunting from amongst 201 districts identified by NITI Aayog on the basis
of National Family Health Survey-4 data, 162 ISSNIP districts and 106 districts
of Scheme for Adolescent Girls.
2018-19
235 districts based on the status of under-nutrition in various States/UTs to be
identified generally based on prevalence of stunting.
2019-20 Remaining districts of all 36 States/UTs.
FEATURES OF NNM 1. The NNM, as an apex body, will monitor, supervise, fix targets and guide the
nutrition related interventions across the Ministries
2. The proposal consists of
• Mapping of various Schemes contributing towards addressing malnutrition
• Introducing a very robust convergence mechanism
• ICT based Real Time Monitoring system
• Incentivizing States/UTs for meeting the targets
• Incentivizing Anganwadi Workers (AWWs) for using IT based tools
• Eliminating registers used by AWWs · introducing measurement of height of
children at the Anganwadi Centres (AWCs)
• Social Audits
• Setting-up Nutrition Resource Centres, involving masses through Jan
Andolan for their participation on nutrition through various activities, among
others.
The programme through the targets will strive to
Reduction in the level of stunting
under-nutrition,
anemia and
low birth weight babies
Major impact:

one great step toward
Improving Nutrition
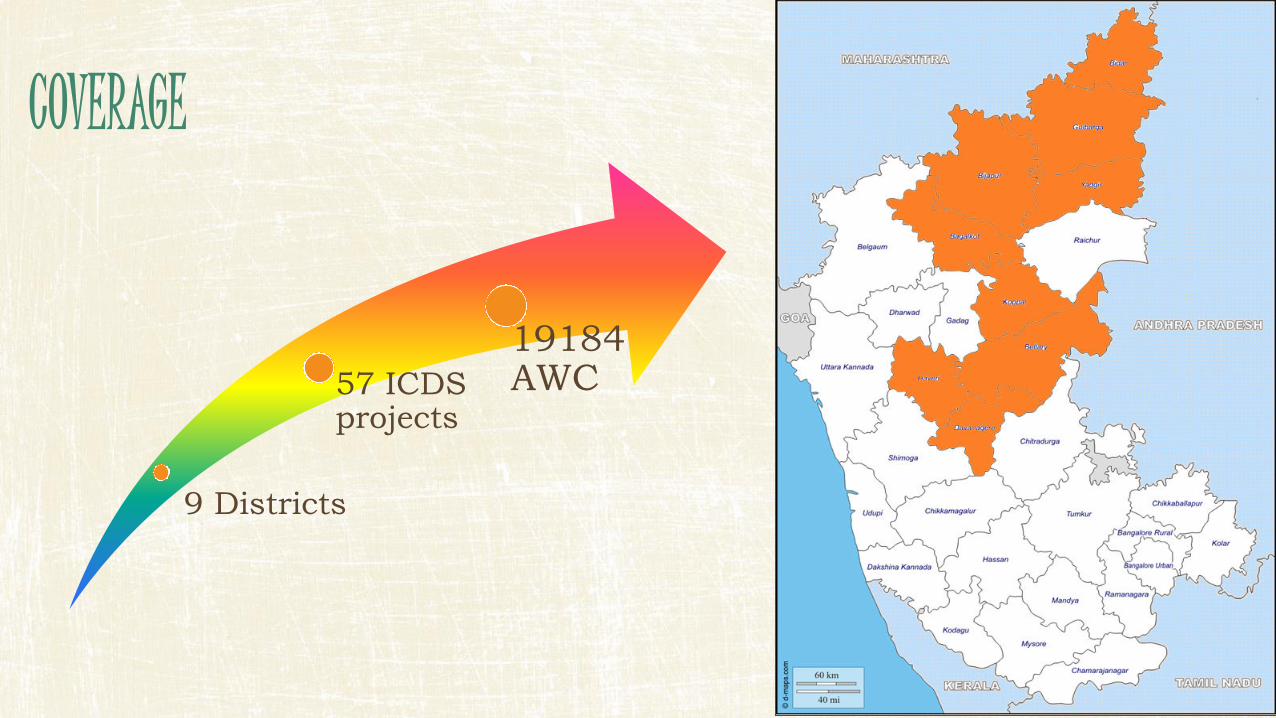
9 Districts
57 ICDS projects
19184 AWC
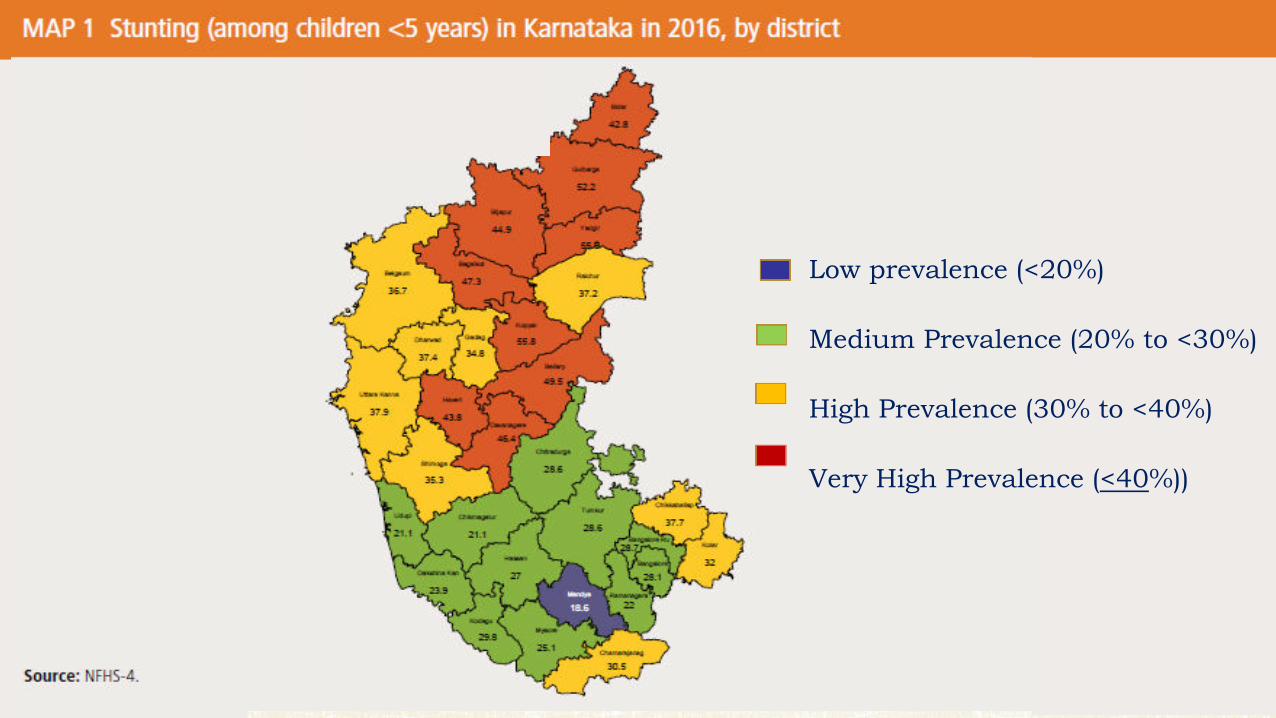
Low prevalence (<20%)
Medium Prevalence (20% to <30%)
High Prevalence (30% to <40%)
Very High Prevalence (<40%))
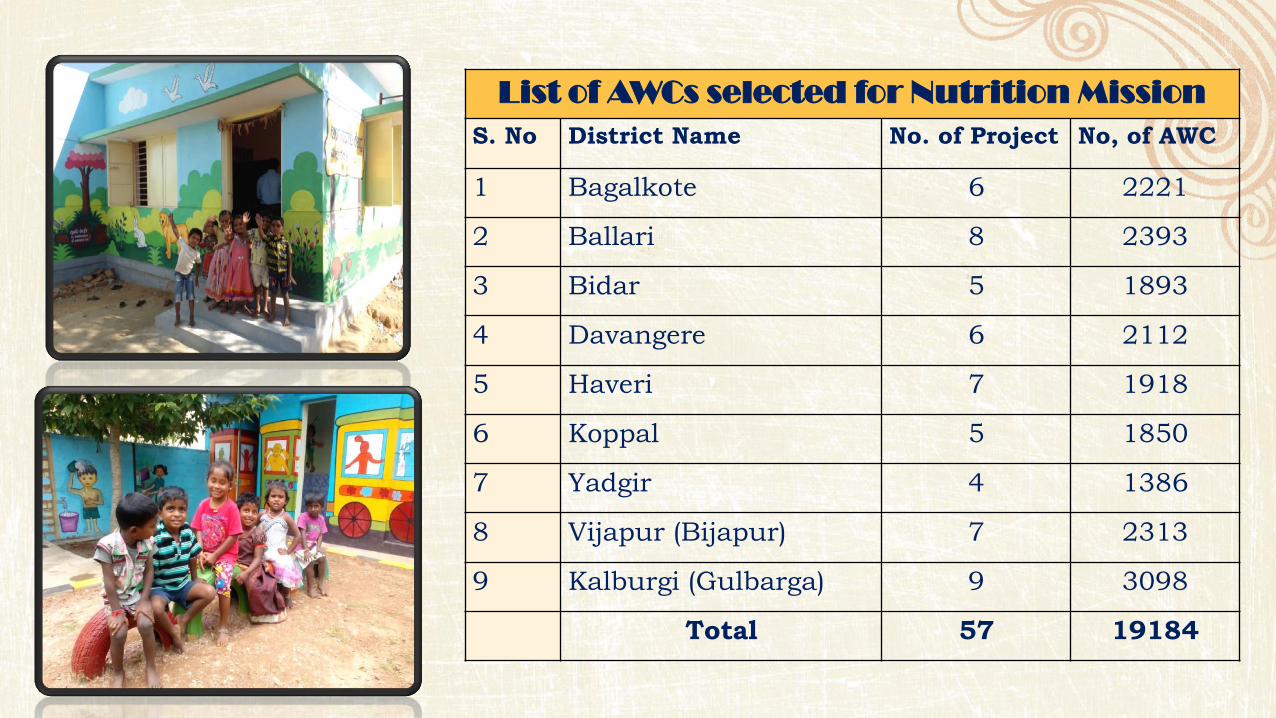
List of AWCs selected for Nutrition Mission
S. No District Name No. of Project No, of AWC
1 Bagalkote 6 2221
2 Ballari 8 2393
3 Bidar 5 1893
4 Davangere 6 2112
5 Haveri 7 1918
6 Koppal 5 1850
7 Yadgir 4 1386
8 Vijapur (Bijapur) 7 2313
9 Kalburgi (Gulbarga) 9 3098
Total 57 19184
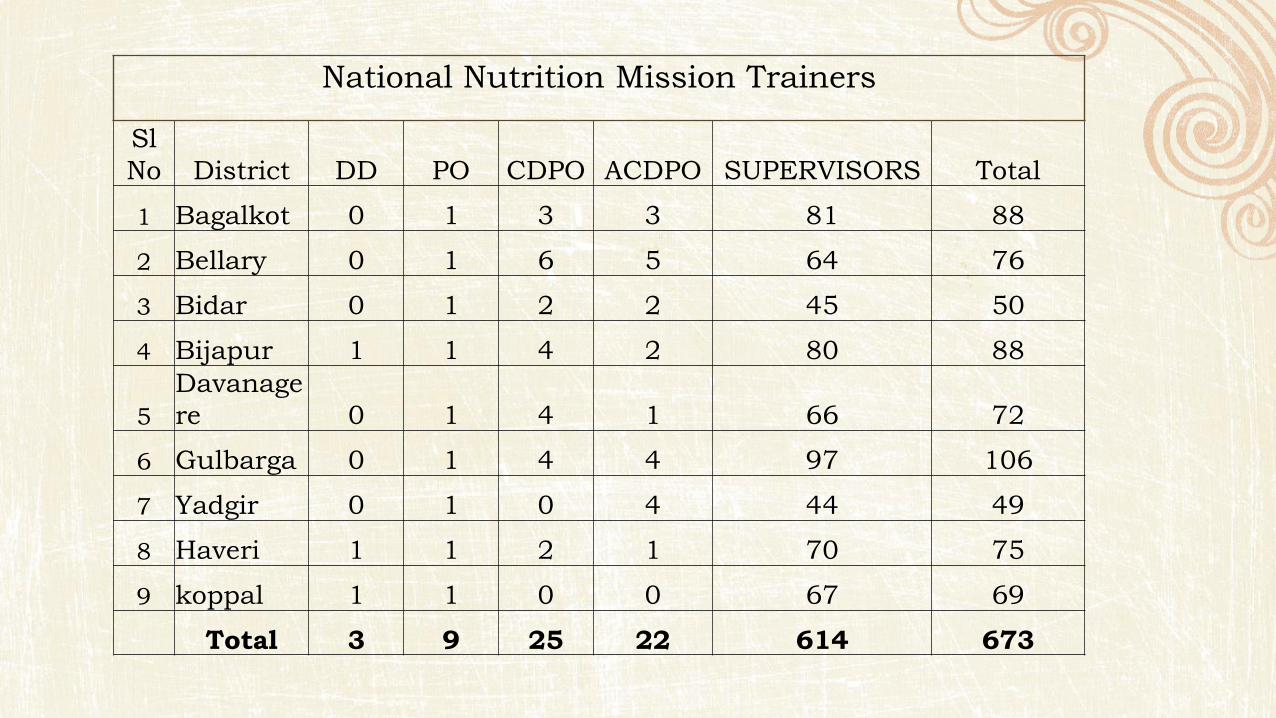
National Nutrition Mission Trainers
Sl
No District DD PO CDPO ACDPO SUPERVISORS Total
1 Bagalkot 0 1 3 3 81 88
2 Bellary 0 1 6 5 64 76
3 Bidar 0 1 2 2 45 50
4 Bijapur 1 1 4 2 80 88
5
Davanage
re 0 1 4 1 66 72
6 Gulbarga 0 1 4 4 97 106
7 Yadgir 0 1 0 4 44 49
8 Haveri 1 1 2 1 70 75
9 koppal 1 1 0 0 67 69
Total 3 9 25 22 614 673
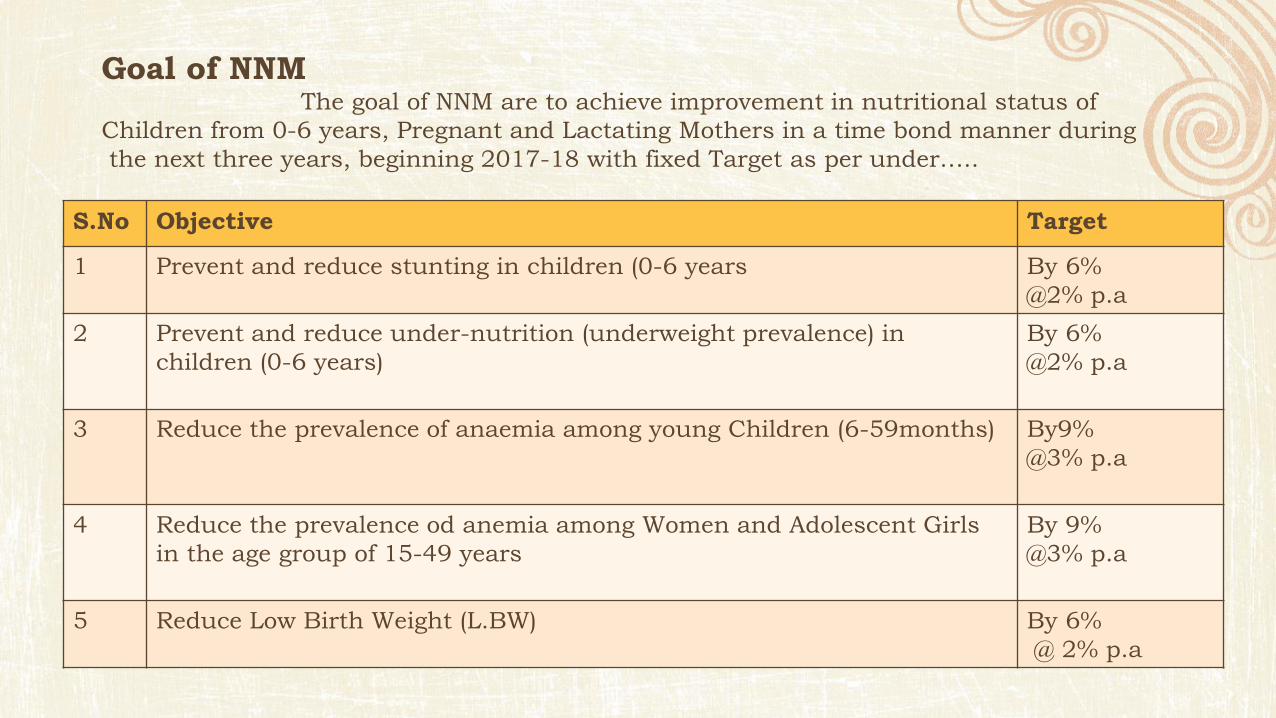
Goal of NNM The goal of NNM are to achieve improvement in nutritional status of
Children from 0-6 years, Pregnant and Lactating Mothers in a time bond manner during
the next three years, beginning 2017-18 with fixed Target as per under…..
S.No Objective Target
1 Prevent and reduce stunting in children (0-6 years By 6%
@2% p.a
2 Prevent and reduce under-nutrition (underweight prevalence) in
children (0-6 years)
By 6%
@2% p.a
3 Reduce the prevalence of anaemia among young Children (6-59months) By9%
@3% p.a
4 Reduce the prevalence od anemia among Women and Adolescent Girls
in the age group of 15-49 years
By 9%
@3% p.a
5 Reduce Low Birth Weight (L.BW) By 6%
@ 2% p.a

Targets- for the next three years, beginning 2017-18 as per under…..
Prevent and
reduce stunting in
children (0-6
years)
Prevent and reduce
under-nutrition
(underweight prevalence)
in children (0-6 years)
Reduce the
prevalence of
anemia among
young Children (6-
59months)
Reduce the prevalence
of anemia among
Women and
Adolescent Girls 15-49
years
Reduce Low
Birth Weight
(L.BW)
NNM By 6%
@2% p.a
By 6%
@2% p.a
By9%
@% p.a
By 9%
@3% p.a
By 6%
@ 2% p.a
Koppal
(59.8%)
By 53.8%
(49.9%)
By 43.9%
(68.5)
By 59.5%
(68.1%)
By 59.1%
Yadgir (55.5%)
By 49.5%
(50.3%)
By 44.3%
(74.00%)
By 65.00%
(74.00%)
By 65.00%
Kalburgi (52.2%)
By 46.2%
(56.7%)
By 50.7%
(72.4%)
By 63.4%
(72.4%)
By 63.4%
Bellari (47.3%)
By 41.2%
(39.4%)
By 33.4%
(72.3%)
By (63.3%)
(69.1%)
By 60.1%

Targets- for the next three years, beginning 2017-18 as per under…..
Prevent and
reduce stunting in
children (0-6 years
Prevent and reduce
under-nutrition
(underweight prevalence)
in children (0-6 years)
Reduce the
prevalence of
anemia among
young Children (6-
59months)
Reduce the prevalence
of anemia among
Women and
Adolescent Girls 15-49
years
Reduce Low
Birth Weight
(L.BW)
Bagalkote (47.3)
By 41.3%
(44.6%)
By 38.6%
(62.9%)
By 53.9%
(66.6%)
By 57.6%
Davangere
(46.4%)
By 40.4%
(41.9%)
By 35.9%
(65.9%)
By 56.9%
(65.9%)
By 56.9%
Vijaypur (44.9 %)
By 38.9%
(38.9%)
By 32.9%
(68.00%)
By 59.00%
(68.00%)
By 59.00%
Haveri
(43.4%)
By 37.4%
(36.5%)
By 30.5%
(63.9%)
By 54.9%
(63.9%)
By 54.9%
Bidar (42.8%)
By 36.8%
(39.4%)
By 33.4%
(69.1%)
By 60.1%
(69.1%)
By 60.1%
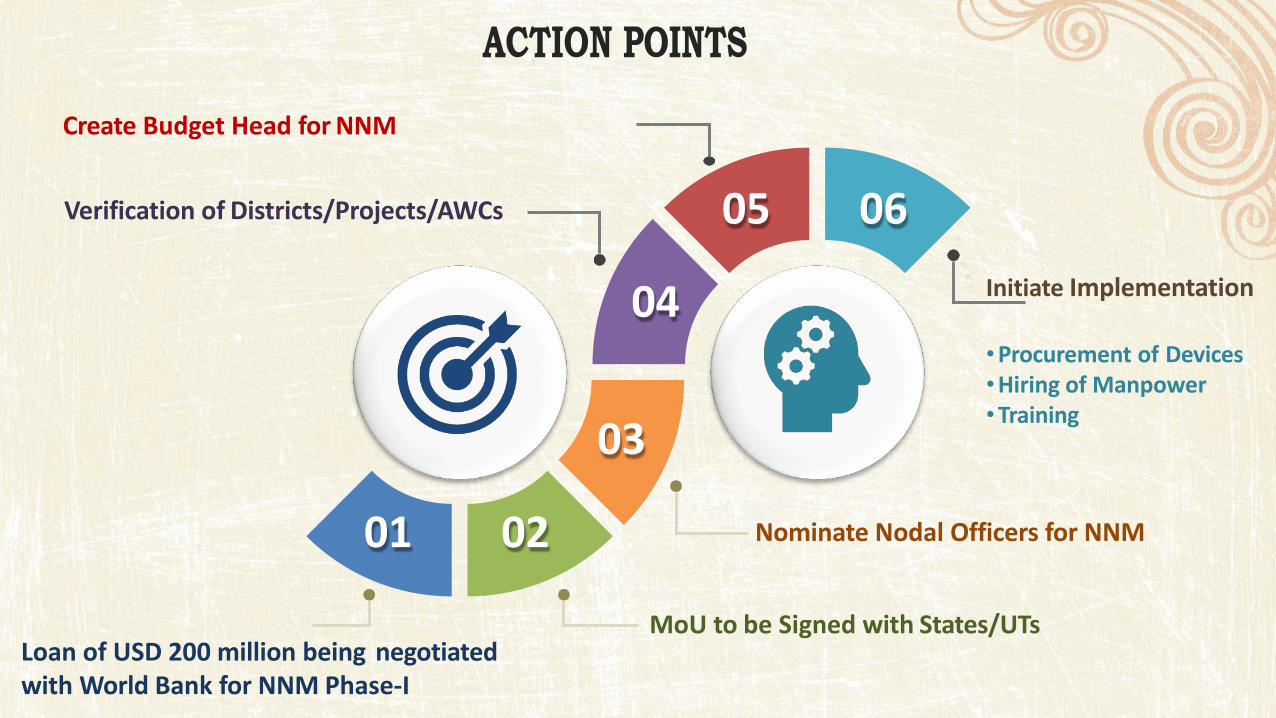
03
06
04
05
01 02
Loan of USD 200 million being negotiated
with World Bank for NNM Phase-I
MoU to be Signed with States/UTs
Nominate Nodal Officers for NNM
Verification of Districts/Projects/AWCs
Create Budget Head for NNM
Initiate Implementation
•Procurement of Devices
•Hiring of Manpower
•Training
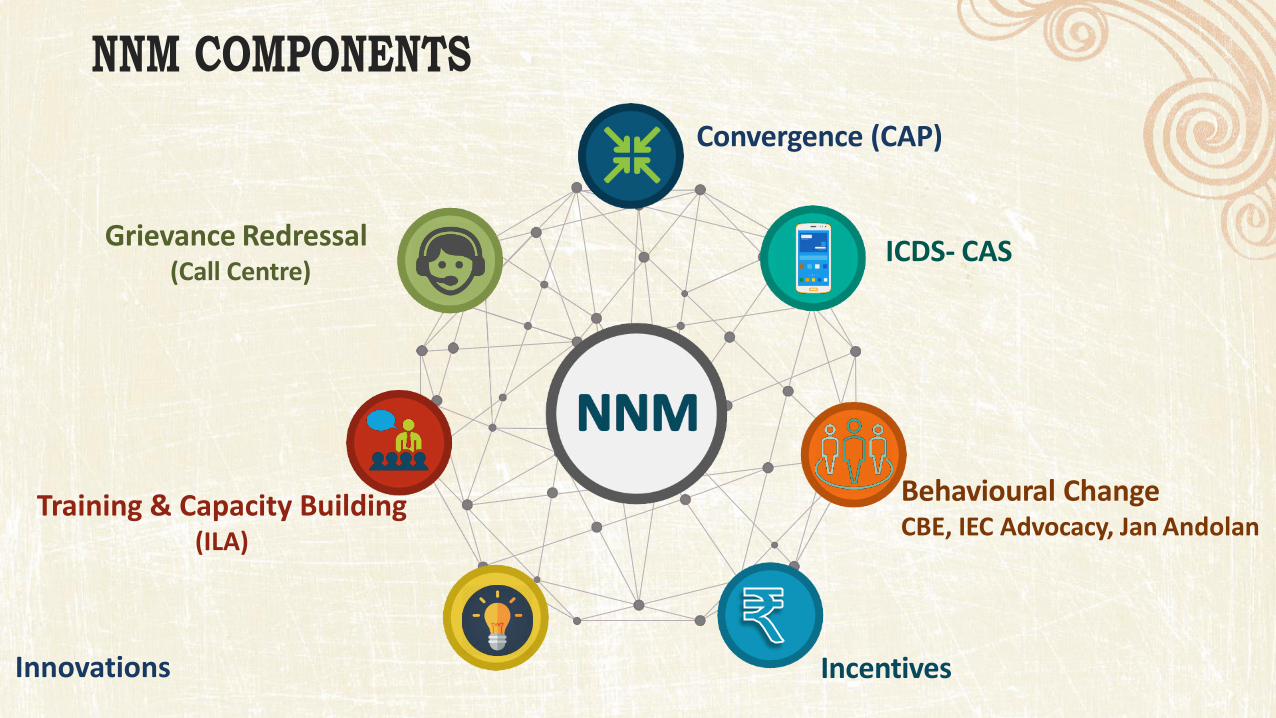
Convergence (CAP)
ICDS- CAS Grievance Redressal
(Call Centre)
Behavioural Change CBE, IEC Advocacy, Jan Andolan
Training & Capacity Building (ILA)
Innovations Incentives
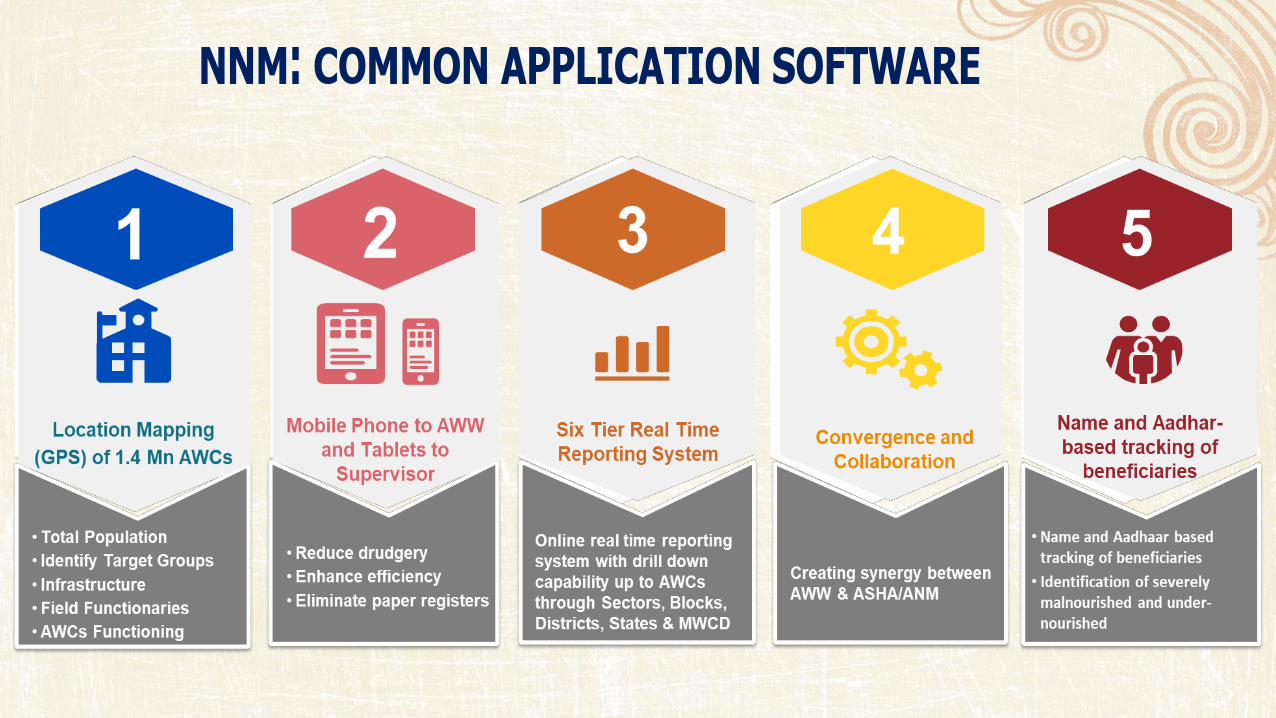
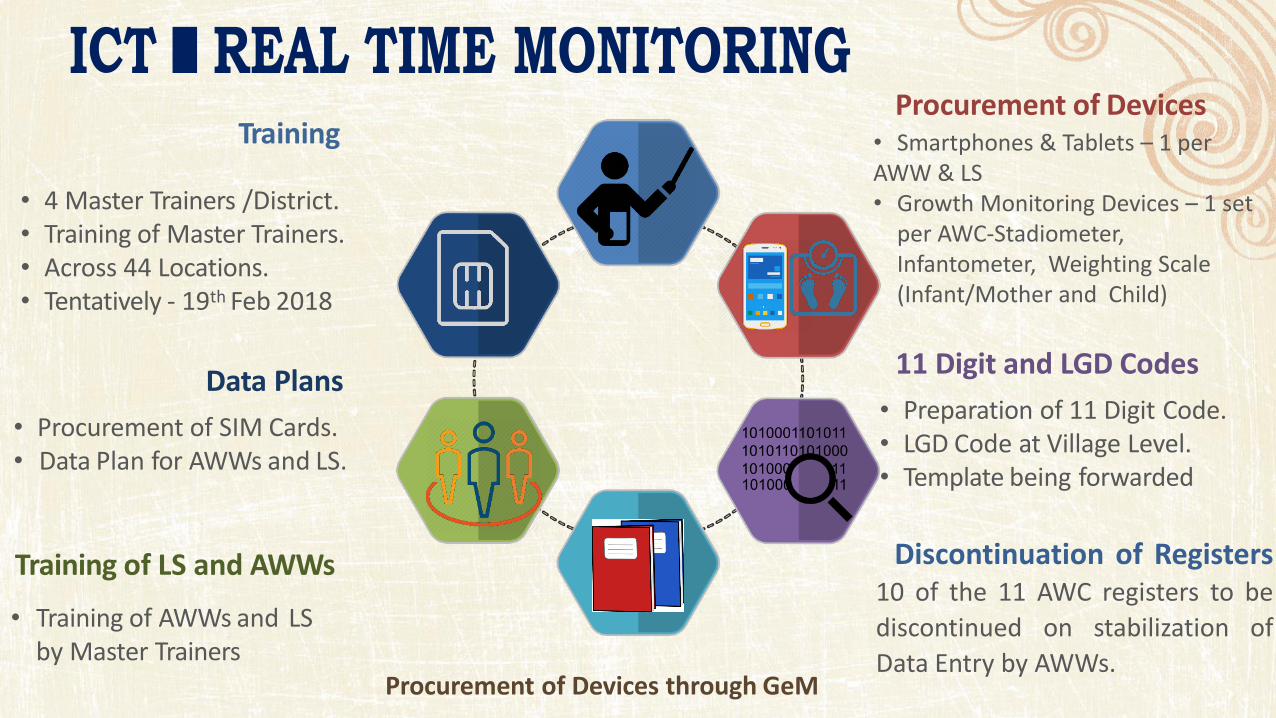
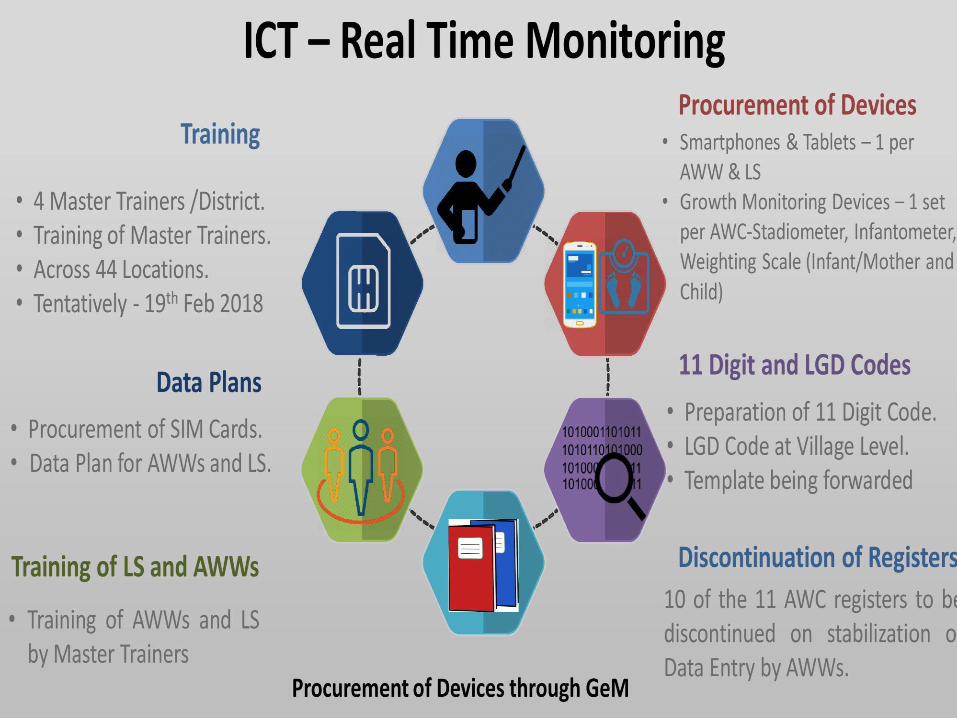
11 Digit and LGD Codes
• Preparation of 11 Digit Code.
• LGD Code at Village Level.
• Template being forwarded
Discontinuation of Registers
10 of the 11 AWC registers to be
discontinued on stabilization of
Data Entry by AWWs.
Data Plans
• Procurement of SIM Cards.
• Data Plan for AWWs and LS.
Training of LS and AWWs
• Training of AWWs and LS
by Master Trainers
Procurement of Devices
• Smartphones & Tablets – 1 per
AWW & LS
• Growth Monitoring Devices – 1 set
per AWC-Stadiometer,
Infantometer, Weighting Scale
(Infant/Mother and Child)
Training
• 4 Master Trainers /District.
• Training of Master Trainers.
• Across 44 Locations.
• Tentatively - 19th Feb 2018
Procurement of Devices through GeM
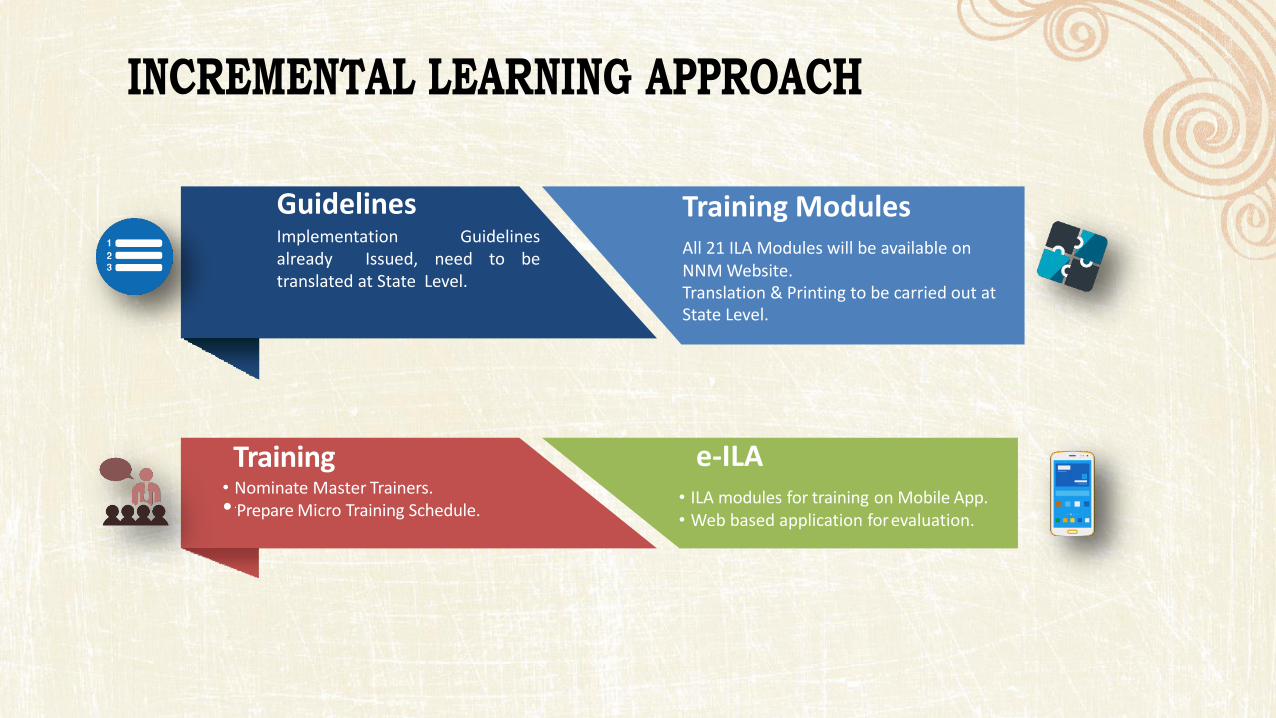
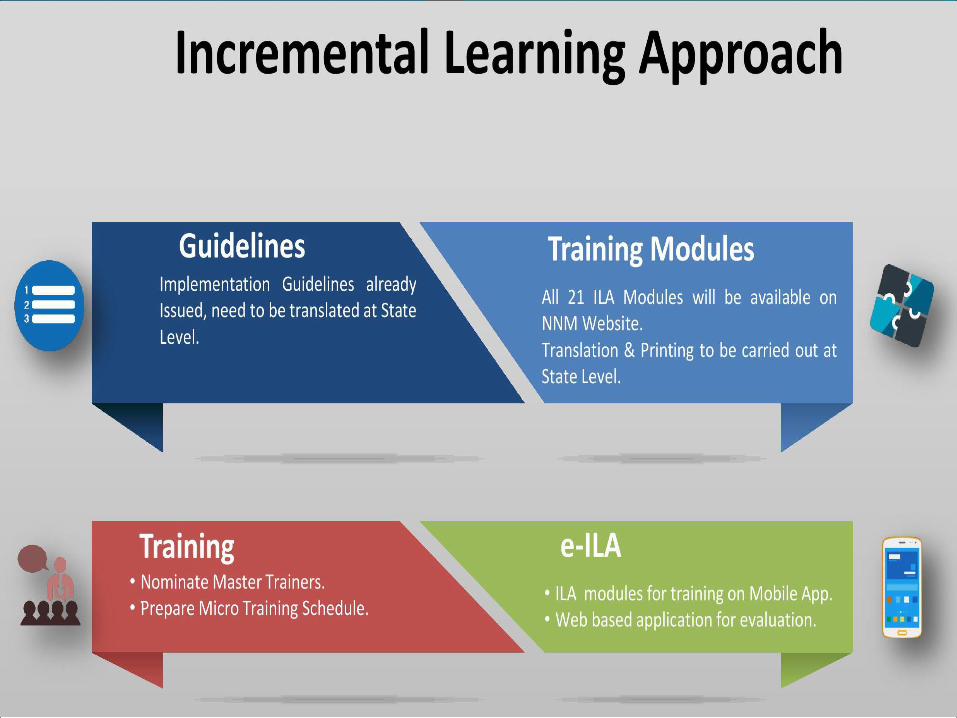
e-ILA
• ILA modules for training on Mobile App.
• Web based application for evaluation.
Training Modules
All 21 ILA Modules will be available on
NNM Website.
Translation & Printing to be carried out at
State Level.
Guidelines Implementation Guidelines
already Issued, need to be
translated at State Level.
Training • Nominate Master Trainers.
• .Prepare Micro Training Schedule.
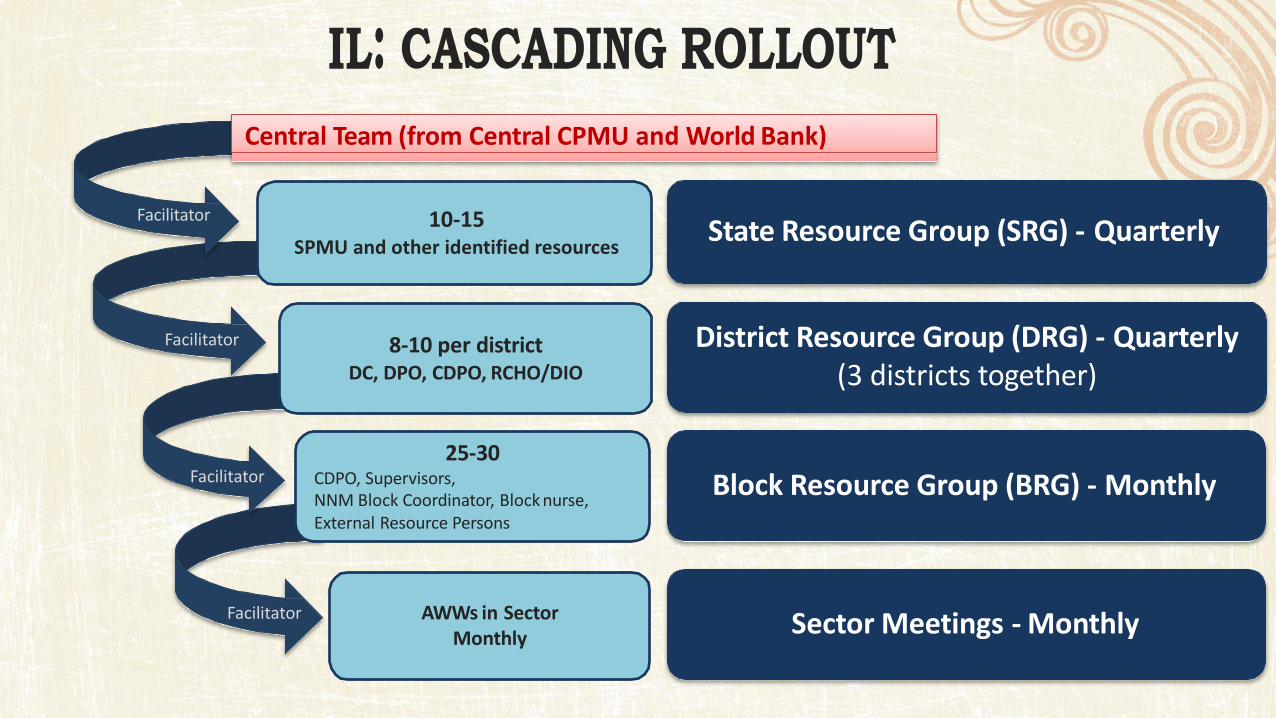
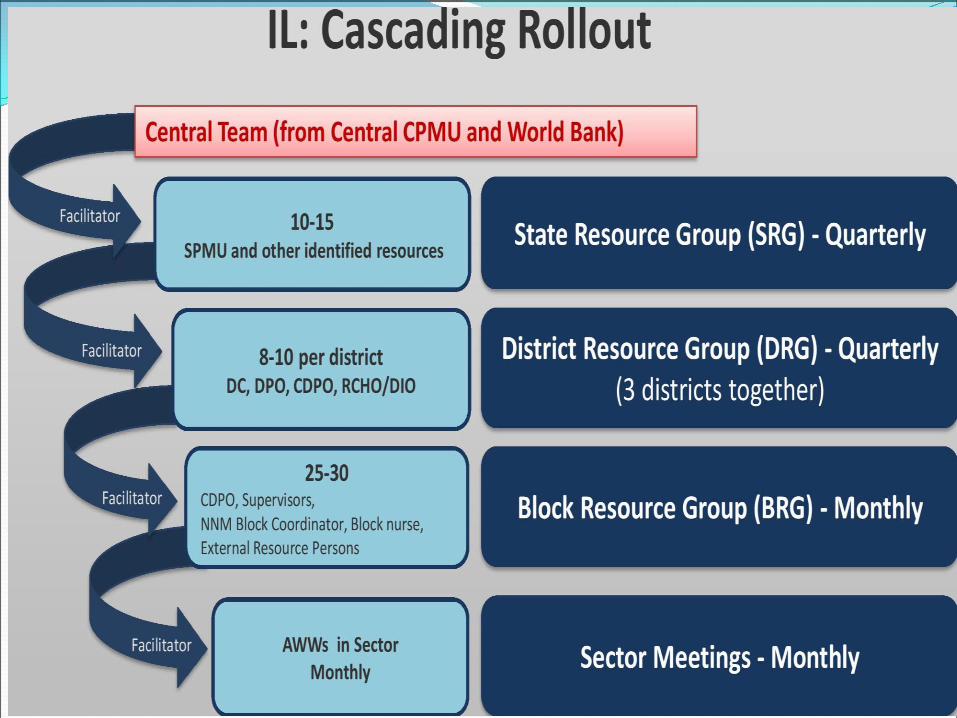
State Resource Group (SRG) - Quarterly
District Resource Group (DRG) - Quarterly
(3 districts together)
Block Resource Group (BRG) - Monthly
Sector Meetings - Monthly
8-10 per district DC, DPO, CDPO, RCHO/DIO
25-30 CDPO, Supervisors,
NNM Block Coordinator, Block nurse,
External Resource Persons
AWWs in Sector
Monthly
10-15
SPMU and other identified resources
Central Team (from Central CPMU and World Bank)
Facilitator
Facilitator
Facilitator
Facilitator
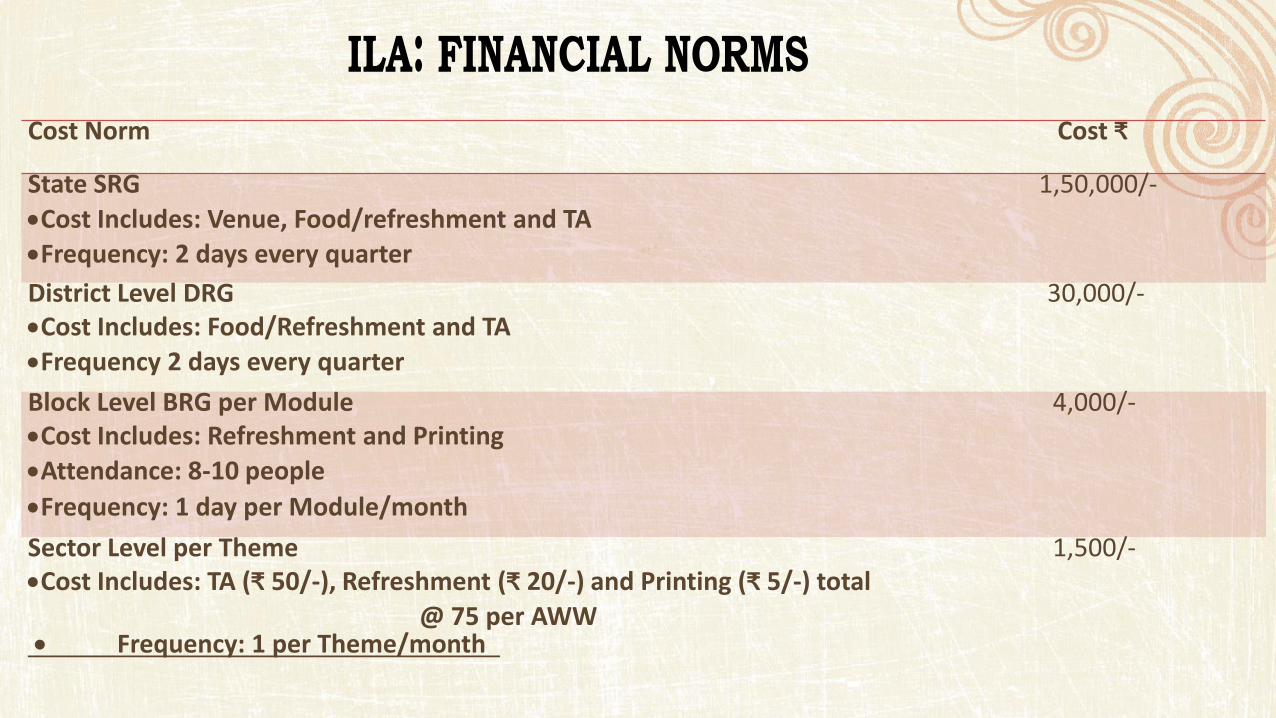
Cost Norm Cost ₹
State SRG
Cost Includes: Venue, Food/refreshment and TA
Frequency: 2 days every quarter
1,50,000/-
District Level DRG
Cost Includes: Food/Refreshment and TA
Frequency 2 days every quarter
30,000/-
Block Level BRG per Module
Cost Includes: Refreshment and Printing
Attendance: 8-10 people
Frequency: 1 day per Module/month
4,000/-
Sector Level per Theme
Cost I ludes: TA ₹ /- , Refresh e t ₹ /- a d Pri ti g ₹ /-) total
@ 75 per AWW Frequency: 1 per Theme/month
1,500/-
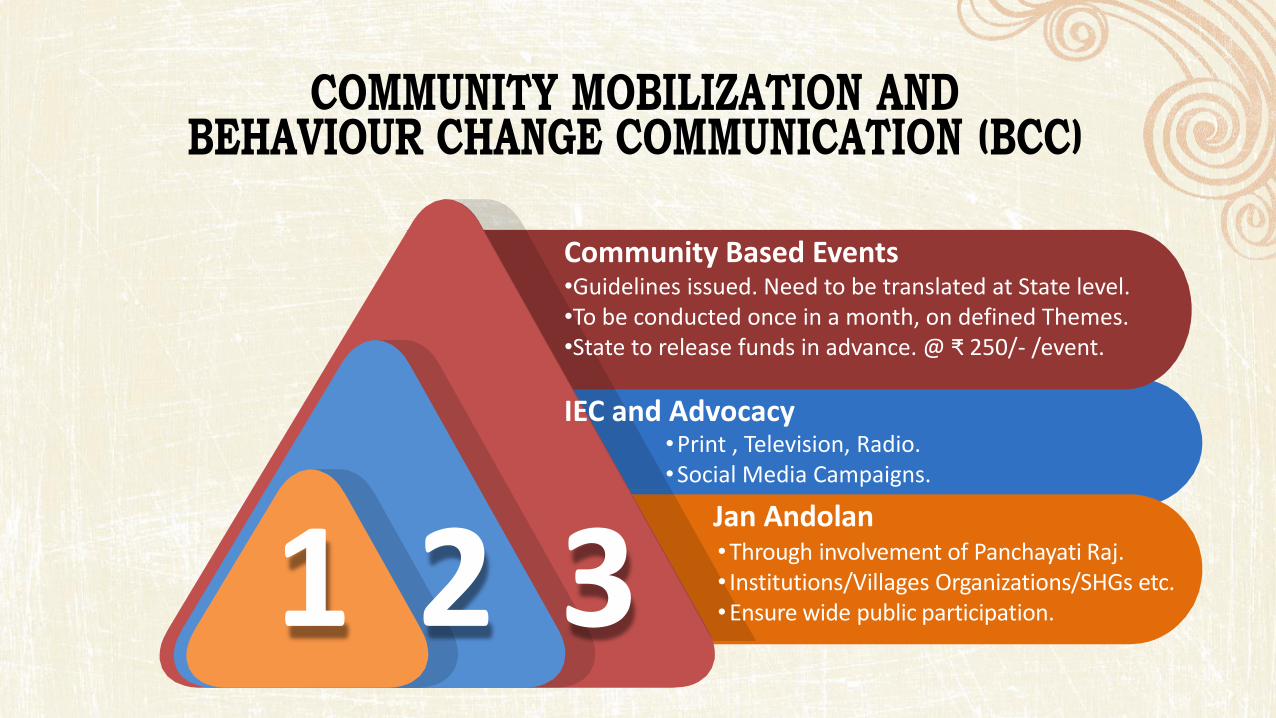
1 2 3
Community Based Events •Guidelines issued. Need to be translated at State level.
•To be conducted once in a month, on defined Themes.
•State to release funds in advance. @ ₹ 5 /- /event.
IEC and Advocacy •Print , Television, Radio.
•Social Media Campaigns.
Jan Andolan •Through involvement of Panchayati Raj.
• Institutions/Villages Organizations/SHGs etc.
•Ensure wide public participation.
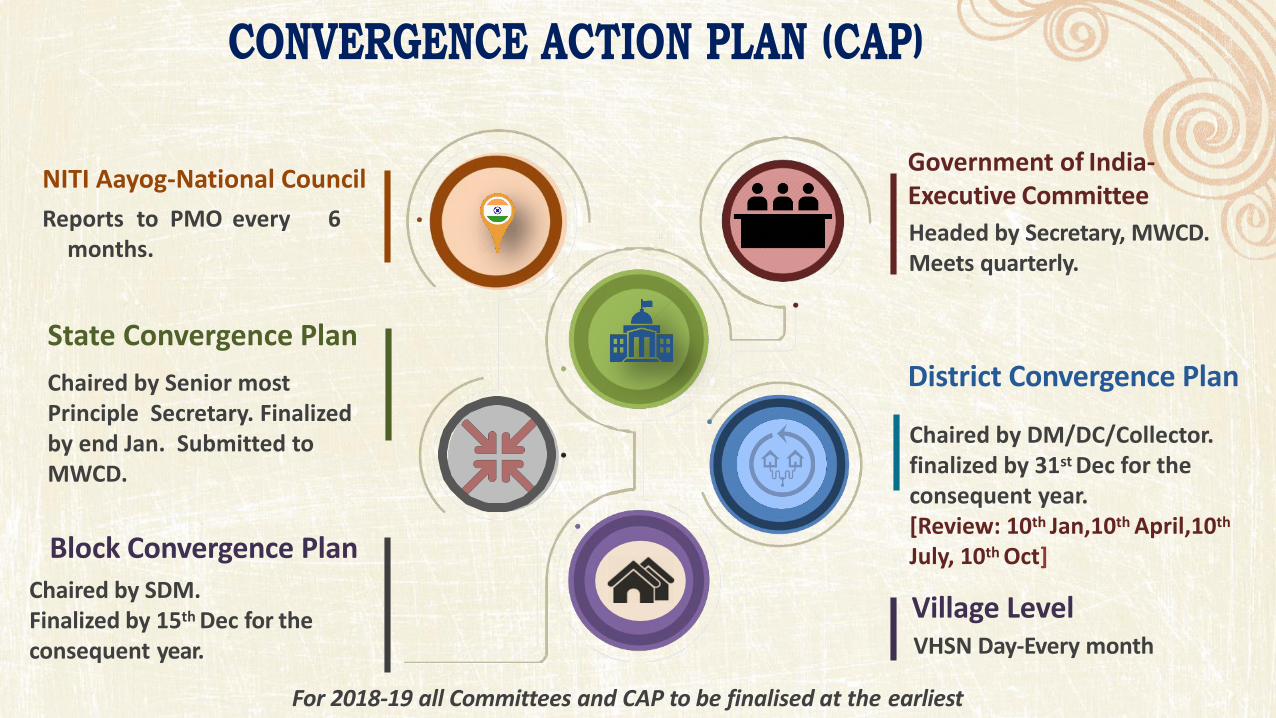
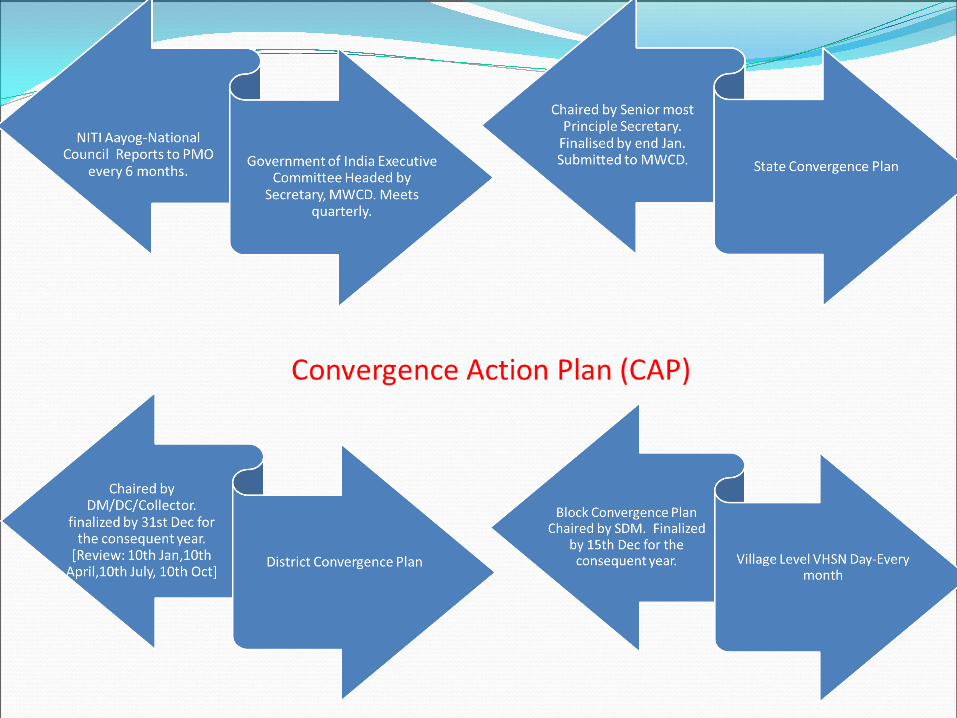
District Convergence Plan
Chaired by DM/DC/Collector.
finalized by 31st Dec for the
consequent year.
[Review: 10th Jan,10th April,10th
July, 10th Oct]
Village Level VHSN Day-Every month
State Convergence Plan
Chaired by Senior most
Principle Secretary. Finalized
by end Jan. Submitted to
MWCD.
Block Convergence Plan
Chaired by SDM.
Finalized by 15th Dec for the
consequent year.
Government of India-
Executive Committee
Headed by Secretary, MWCD.
Meets quarterly.
NITI Aayog-National Council
Reports to PMO every 6
months.
For 2018-19 all Committees and CAP to be finalised at the earliest

Women &
Child
Developmen
t
Health &
Family
Welfare
Drinking
Water &
Sanitatio
n
Consumer
Affair, Food
& Public
Distribution
Rural
Development
Urban
Development
Tribal Affairs
Panchayat
i Raj
Dept. of
School
Education
& Literacy ,
HRD
Information
&
Broadcastin
g
Converge at
National
State
District
Block
Village
NITI Aayog
AWW/Supervisors
ASHA/ANM
Volunteers/SHGs
AWC as the vibrant platform for convergence of all nutrition programs/Schemes
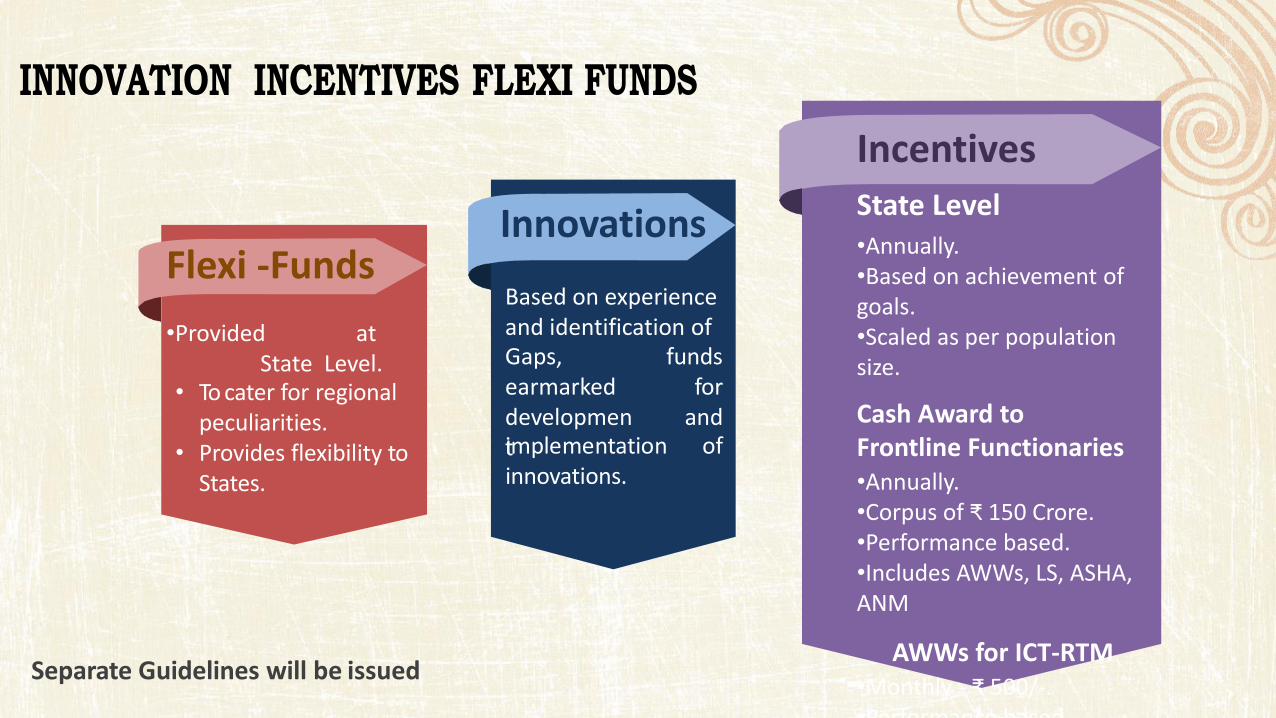
Innovations
Based on experience
and identification of
Gaps,
earmarked
developmen
t
funds
for
and
implementation of
innovations.
Flexi -Funds
•Provided at
State Level.
• To cater for regional
peculiarities.
• Provides flexibility to
States.
Incentives
State Level
•Annually.
•Based on achievement of
goals.
•Scaled as per population
size.
Cash Award to
Frontline Functionaries
•Annually.
•Corpus of ₹ 5 Crore. •Performance based.
•Includes AWWs, LS, ASHA,
ANM
AWWs for ICT-RTM
•Monthly - ₹ 5 /-.
•Performance based.
Separate Guidelines will be issued
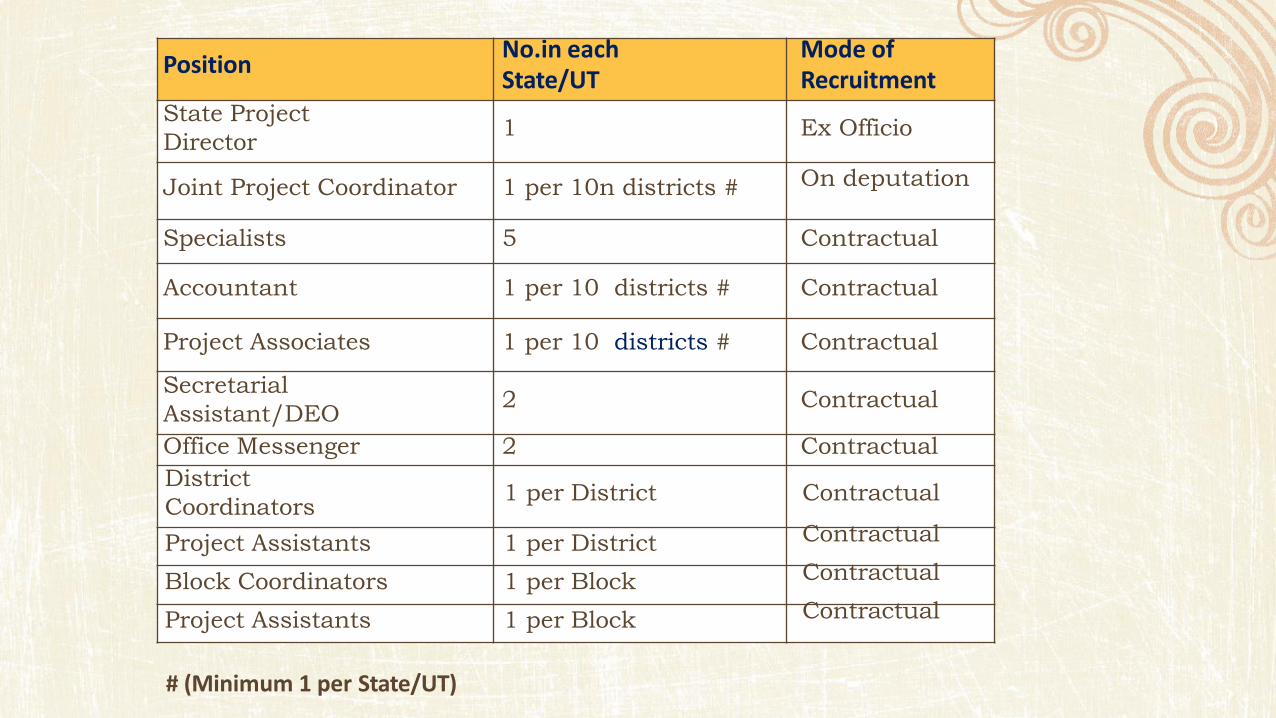
Position No.in each
State/UT
Mode of
Recruitment
State Project
Director 1 Ex Officio
Joint Project Coordinator
1 per 10n districts #
On deputation
Specialists 5 Contractual
Accountant 1 per 10 districts # Contractual
Project Associates 1 per 10 districts # Contractual
Secretarial
Assistant/DEO 2 Contractual
Office Messenger 2 Contractual
District
Coordinators 1 per District Contractual
Project Assistants 1 per District Contractual
Block Coordinators 1 per Block Contractual
Project Assistants 1 per Block Contractual
# (Minimum 1 per State/UT)
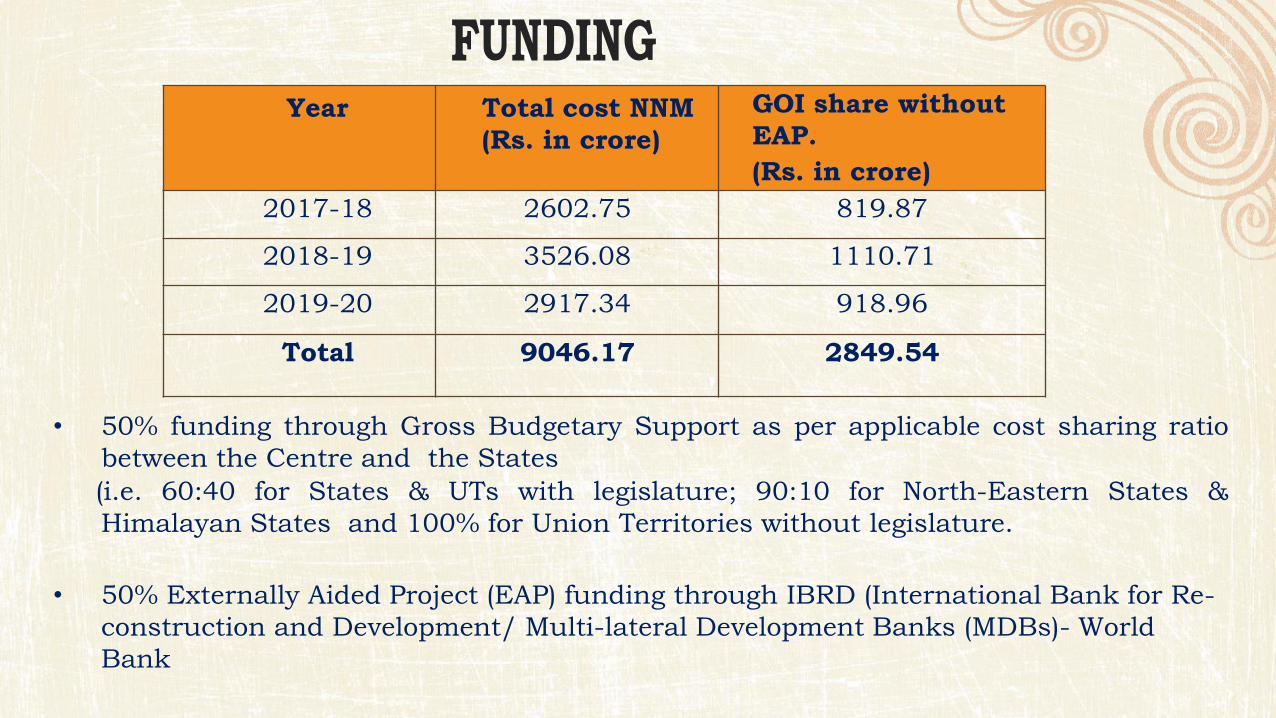
• 50% funding through Gross Budgetary Support as per applicable cost sharing ratio
between the Centre and the States
(i.e. 60:40 for States & UTs with legislature; 90:10 for North-Eastern States &
Himalayan States and 100% for Union Territories without legislature.
• 50% Externally Aided Project (EAP) funding through IBRD (International Bank for Re-
construction and Development/ Multi-lateral Development Banks (MDBs)- World
Bank
Year Total cost NNM
(Rs. in crore)
GOI share without
EAP.
(Rs. in crore)
2017-18 2602.75 819.87
2018-19 3526.08 1110.71
2019-20 2917.34 918.96
Total 9046.17 2849.54
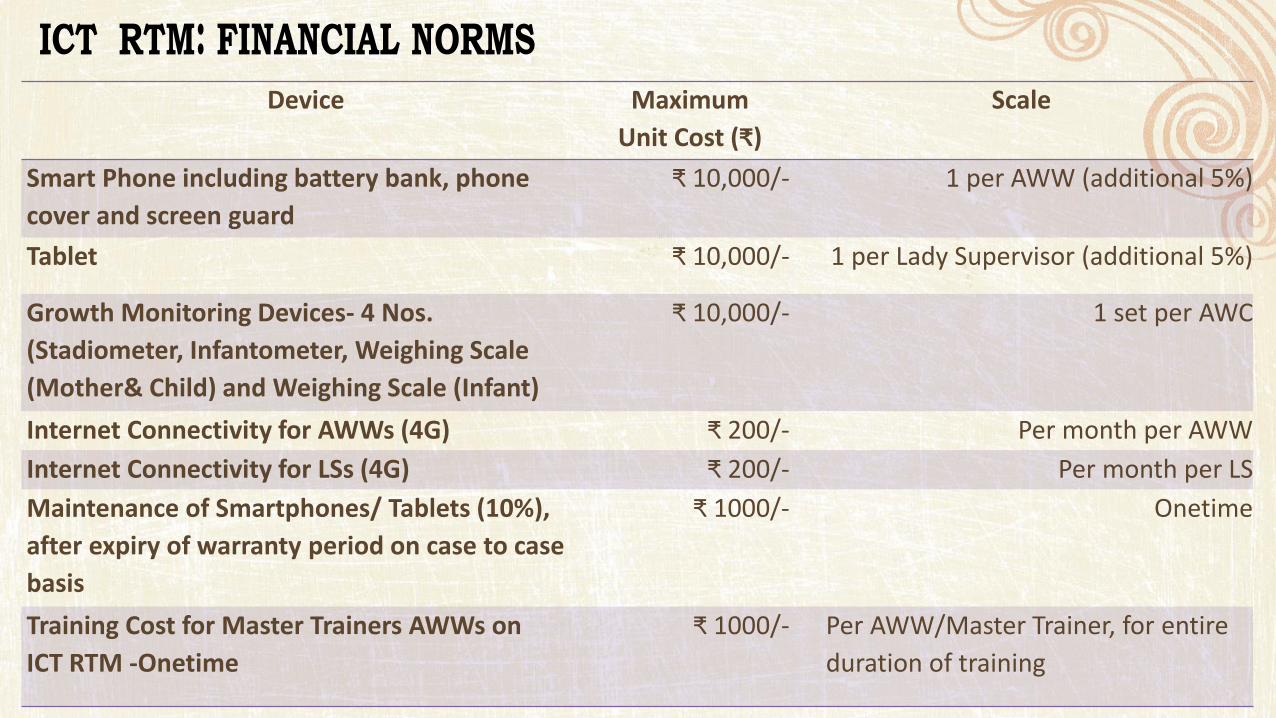
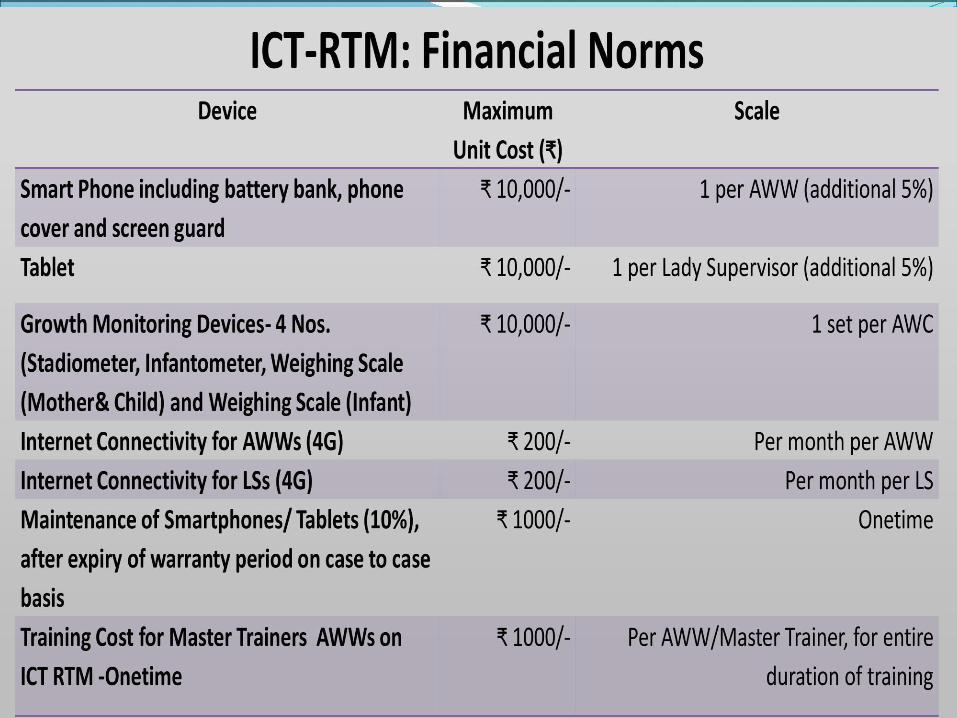
Device Maximum
U it Cost ₹
Scale
Smart Phone including battery bank, phone
cover and screen guard
₹ , /- 1 per AWW (additional 5%)
Tablet ₹ , /- 1 per Lady Supervisor (additional 5%)
Growth Monitoring Devices- 4 Nos.
(Stadiometer, Infantometer, Weighing Scale
(Mother& Child) and Weighing Scale (Infant)
₹ , /- 1 set per AWC
Internet Connectivity for AWWs (4G) ₹ /- Per month per AWW
Internet Connectivity for LSs (4G) ₹ /- Per month per LS
Maintenance of Smartphones/ Tablets (10%),
after expiry of warranty period on case to case
basis
₹ /- Onetime
Training Cost for Master Trainers AWWs on
ICT RTM -Onetime
₹ /- Per AWW/Master Trainer, for entire
duration of training
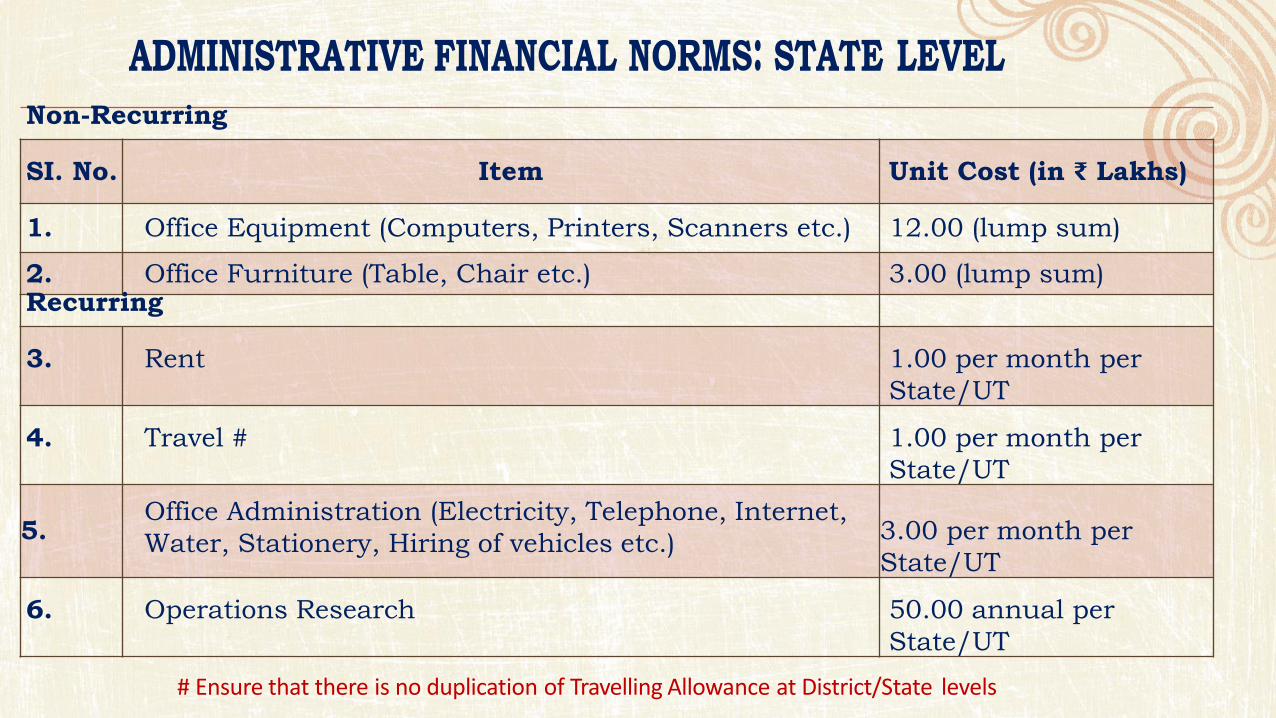
Non-Recurring
SI. No. Item Unit Cost (in ₹ Lakhs)
1. Office Equipment (Computers, Printers, Scanners etc.) 12.00 (lump sum)
2. Office Furniture (Table, Chair etc.) 3.00 (lump sum) Recurring
3. Rent 1.00 per month per
State/UT
4. Travel # 1.00 per month per
State/UT
5. Office Administration (Electricity, Telephone, Internet,
Water, Stationery, Hiring of vehicles etc.)
3.00 per month per
State/UT
6. Operations Research 50.00 annual per
State/UT
# Ensure that there is no duplication of Travelling Allowance at District/State levels
Preparatory Stage
Pre-Launch Stage
Launch
Post Launch Stage
Short Term Activities
Long Term Activities 15 Days
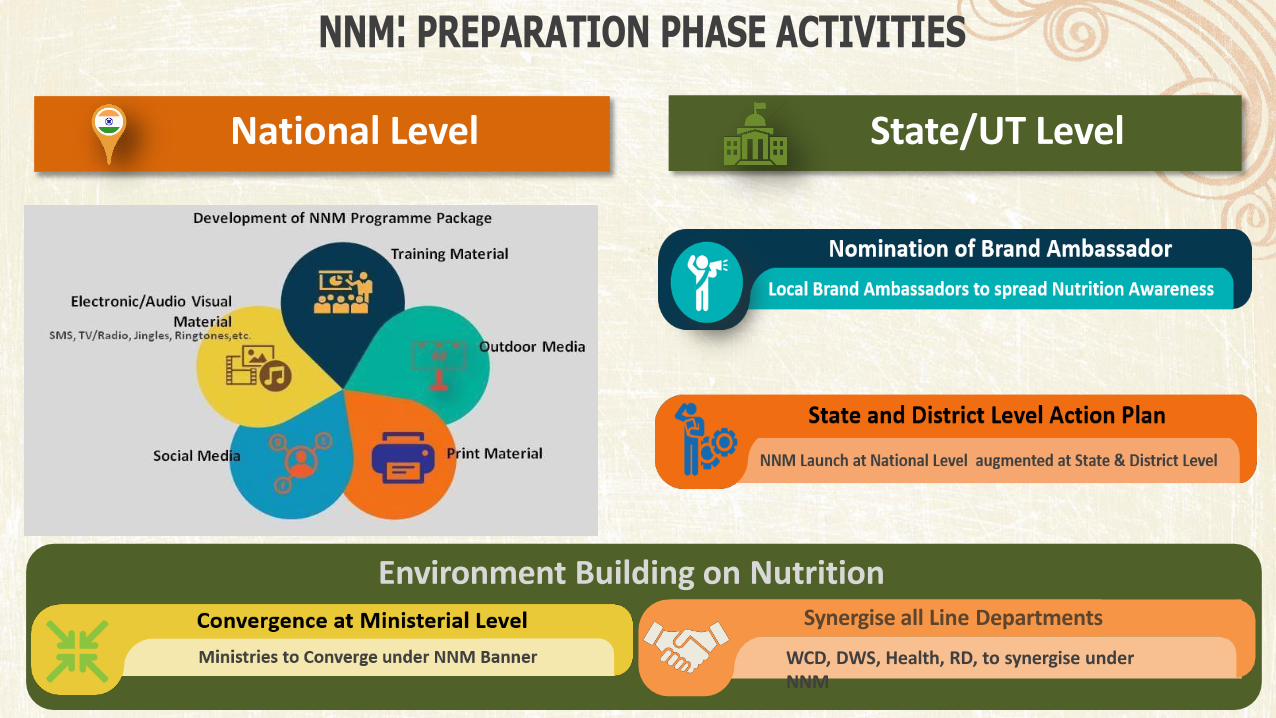
Environment Building on Nutrition
Synergise all Line Departments
National Level State/UT Level
WCD, DWS, Health, RD, to synergise under
NNM

National Level State/UT Level
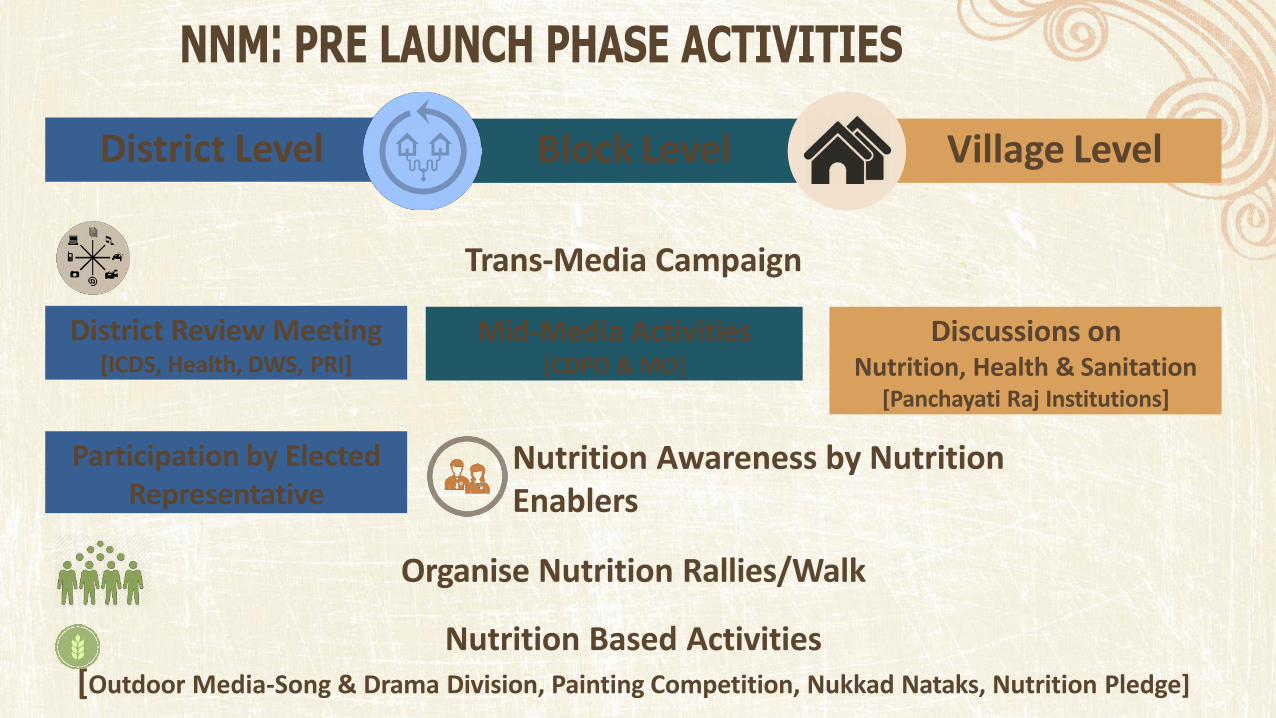
District Level Block Level Village Level
Trans-Media Campaign
District Review Meeting [ICDS, Health, DWS, PRI]
Mid-Media Activities [CDPO & MO]
Discussions on Nutrition, Health & Sanitation
[Panchayati Raj Institutions]
Participation by Elected
Representative Nutrition Awareness by Nutrition
Enablers
Organise Nutrition Rallies/Walk
Nutrition Based Activities
[Outdoor Media-Song & Drama Division, Painting Competition, Nukkad Nataks, Nutrition Pledge]
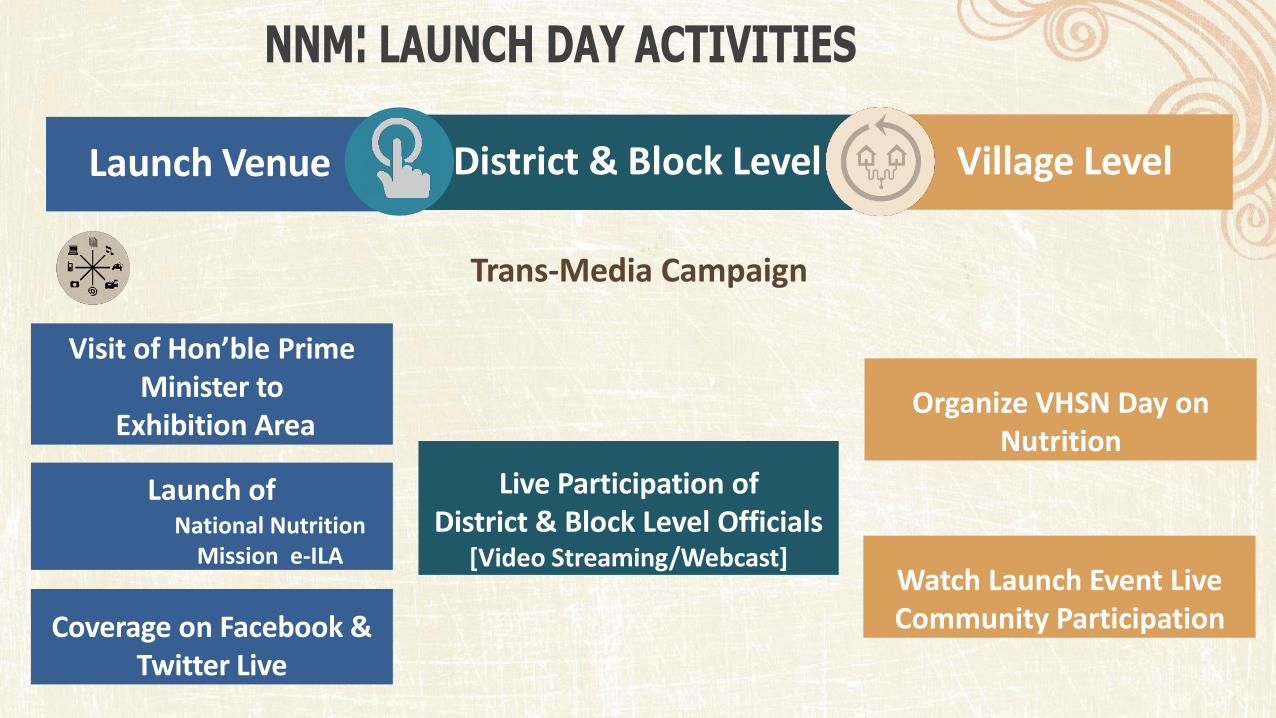
Launch Venue District & Block Level Village Level
Trans-Media Campaign
Coverage on Facebook &
Twitter Live
Live Participation of
District & Block Level Officials [Video Streaming/Webcast]
Organize VHSN Day on
Nutrition
Visit of Ho ’ le Prime
Minister to
Exhibition Area
Launch of National Nutrition
Mission e-ILA Watch Launch Event Live
Community Participation
Launch Minus 15 Days to Minus 10 Days
• District Officers (ICDS, Health, DWs, PRI) to undertake combined reiew meeting focusing on outcome monitoring and nutrtion indicators.
• Ensure Coverage in Local Media
• Post images of activities on social Media page/ handle.
• Participate in Social Media Campaign
Launch Minus 10 Days to Minus 5 Days
• Participation of elected representative in events
• Nutrition Rally/Walk to be organised at District Level.
• Insure Coverage in Local Media
• Post images of activities on social Media Page/handle
• Partcipate in Social Media Campaign
• Outdoor media activation through Song and Drama Division avilable at State Level.
Launch Minus 5 Days to Launch
• Participation of elected representative in events
• District Officers (ICDS, Health, DWs, PRI) to visit
• Insure Coverage in Local Media
• Post images of activities on social Media Page/handle
• Outdoor media activation through Song and Drama Division avilable at State Level.
• Partcipate in Social Media Campaign
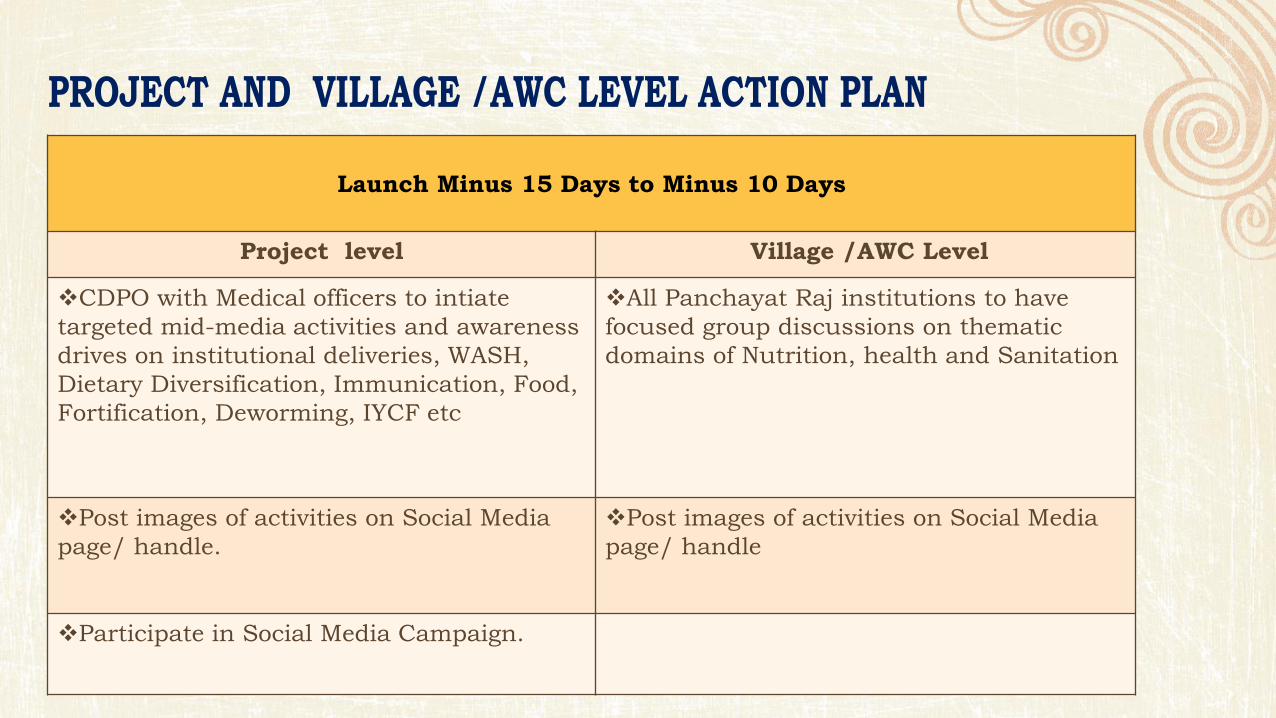
Launch Minus 15 Days to Minus 10 Days
Project level Village /AWC Level
CDPO with Medical officers to intiate
targeted mid-media activities and awareness
drives on institutional deliveries, WASH,
Dietary Diversification, Immunication, Food,
Fortification, Deworming, IYCF etc
All Panchayat Raj institutions to have
focused group discussions on thematic
domains of Nutrition, health and Sanitation
Post images of activities on Social Media
page/ handle.
Post images of activities on Social Media
page/ handle
Participate in Social Media Campaign.
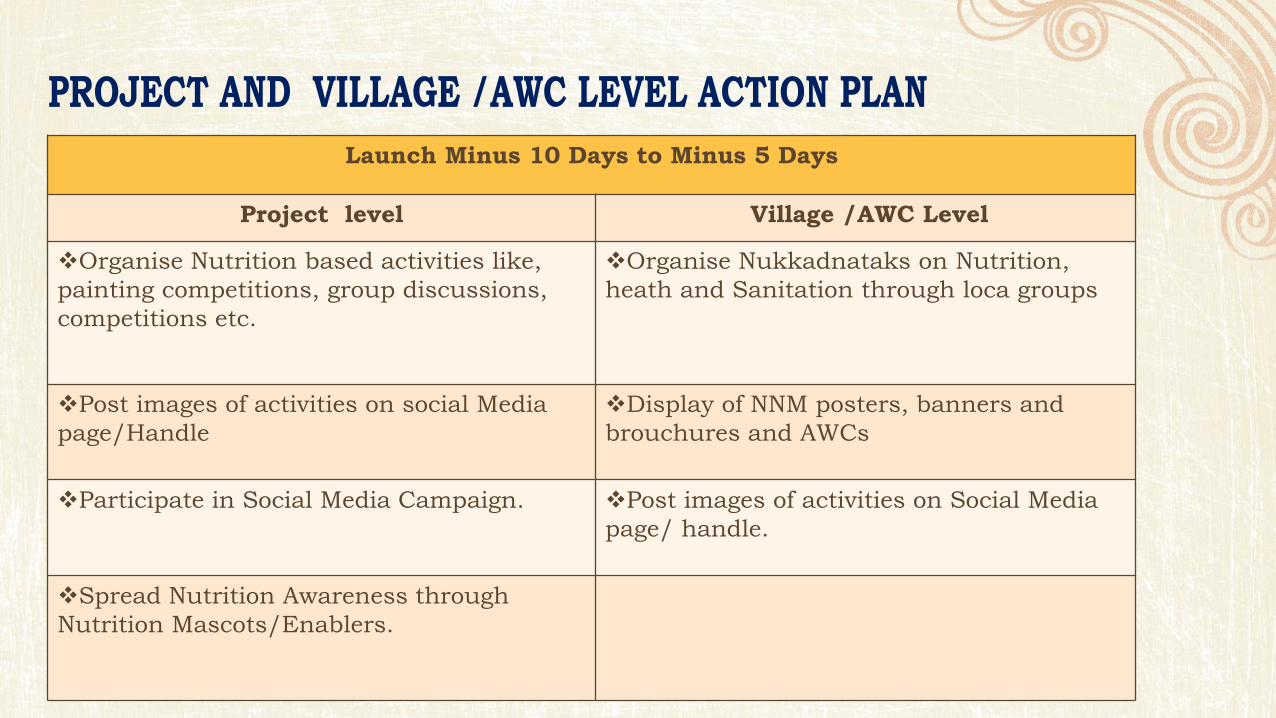
Launch Minus 10 Days to Minus 5 Days
Project level Village /AWC Level
Organise Nutrition based activities like,
painting competitions, group discussions,
competitions etc.
Organise Nukkadnataks on Nutrition,
heath and Sanitation through loca groups
Post images of activities on social Media
page/Handle
Display of NNM posters, banners and
brouchures and AWCs
Participate in Social Media Campaign.
Post images of activities on Social Media
page/ handle.
Spread Nutrition Awareness through
Nutrition Mascots/Enablers.
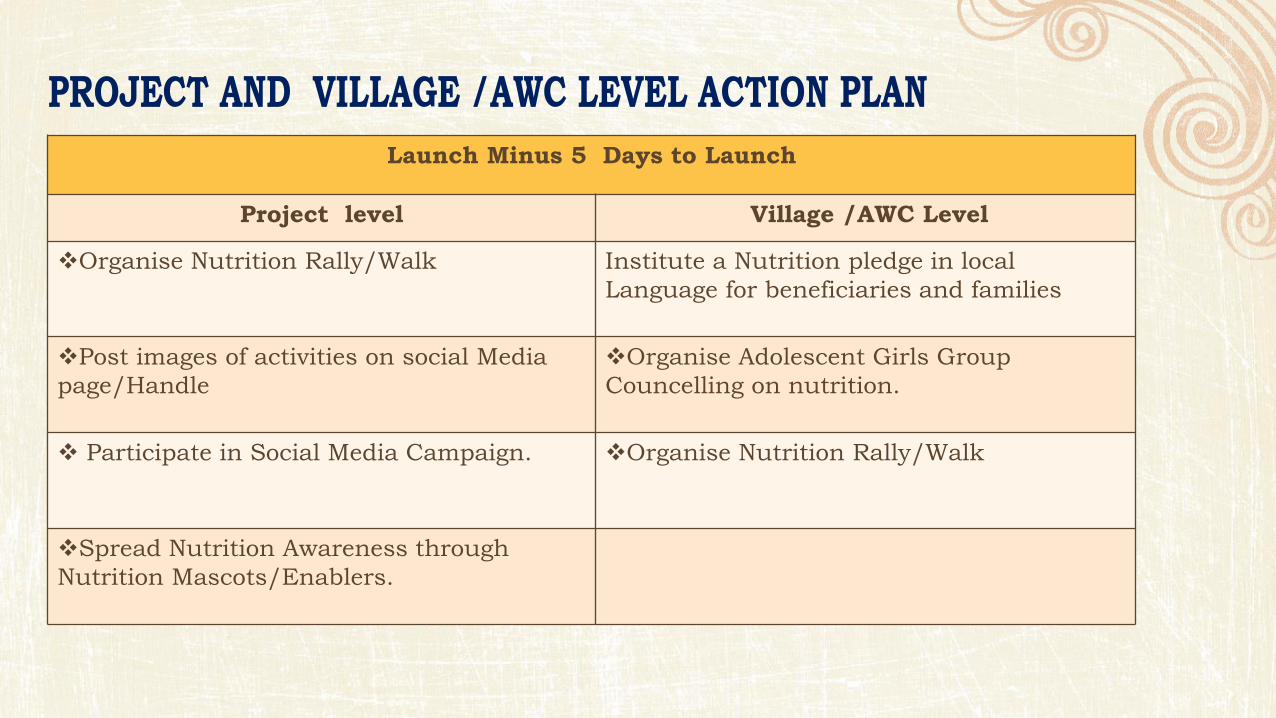
Launch Minus 5 Days to Launch
Project level Village /AWC Level
Organise Nutrition Rally/Walk
Institute a Nutrition pledge in local
Language for beneficiaries and families
Post images of activities on social Media
page/Handle
Organise Adolescent Girls Group
Councelling on nutrition.
Participate in Social Media Campaign.
Organise Nutrition Rally/Walk
Spread Nutrition Awareness through
Nutrition Mascots/Enablers.
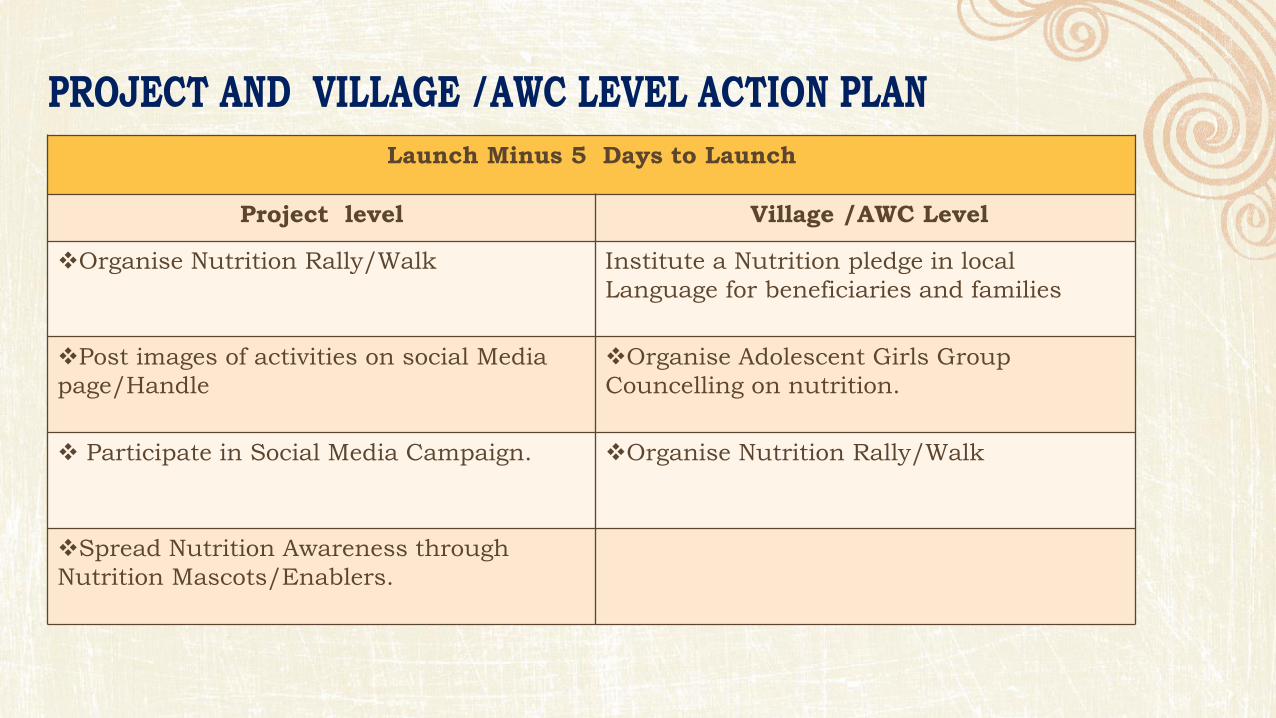
Launch Minus 5 Days to Launch
Project level Village /AWC Level
Organise Nutrition Rally/Walk
Institute a Nutrition pledge in local
Language for beneficiaries and families
Post images of activities on social Media
page/Handle
Organise Adolescent Girls Group
Councelling on nutrition.
Participate in Social Media Campaign.
Organise Nutrition Rally/Walk
Spread Nutrition Awareness through
Nutrition Mascots/Enablers.

District project Village /AWC level
All officials to watch the
Launch of NNM at a central
location and live
participation through Video
Streaming.
Insure Coverage in local
Media.
Post images/ photographs
of activities on Social
Media.
Partcipate in Social Media
Campaign
All officials to watch the
Launch of NNM at a central
location and live
participation through Video
Streaming.
Post images of activities
on social Media
page/Handle.
Partcipate in Social Media
Campaign
Organise VHSN Day on
Nutrition
Watch the Launch on TV
at AWC or Community
Centre etc.
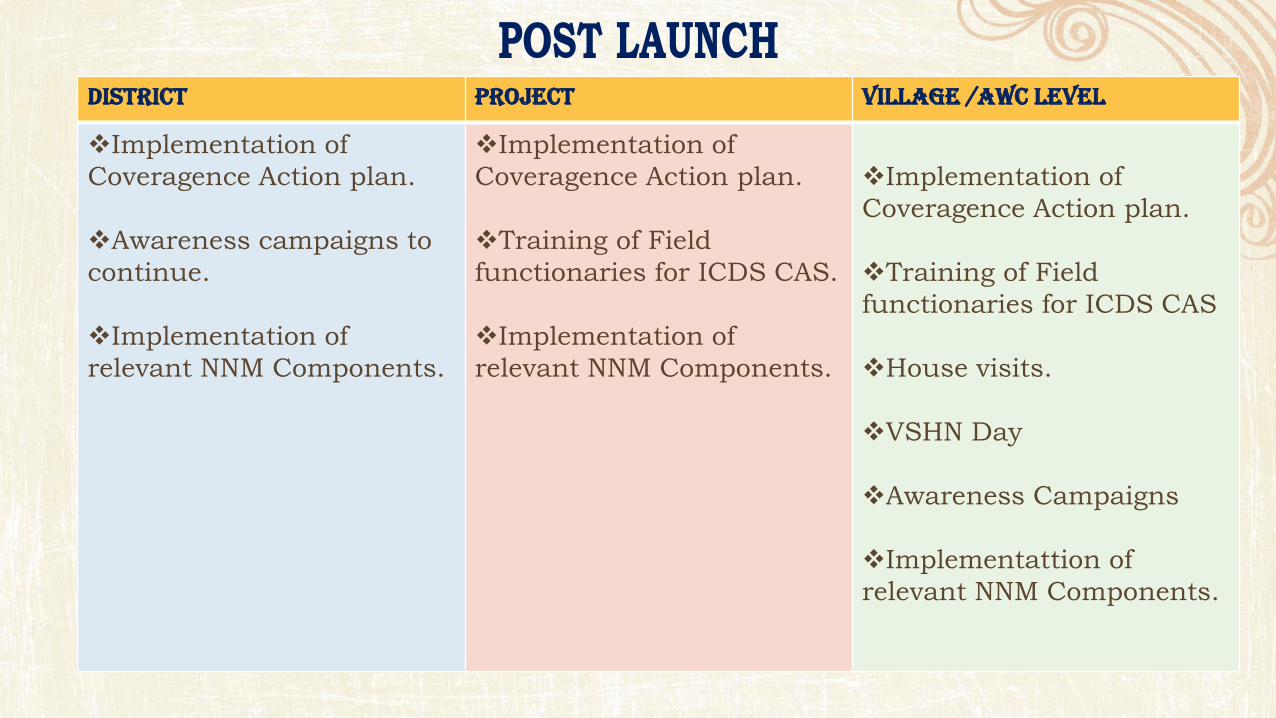
District project Village /AWC level
Implementation of
Coveragence Action plan.
Awareness campaigns to
continue.
Implementation of
relevant NNM Components.
Implementation of
Coveragence Action plan.
Training of Field
functionaries for ICDS CAS.
Implementation of
relevant NNM Components.
Implementation of
Coveragence Action plan.
Training of Field
functionaries for ICDS CAS
House visits.
VSHN Day
Awareness Campaigns
Implementattion of
relevant NNM Components.
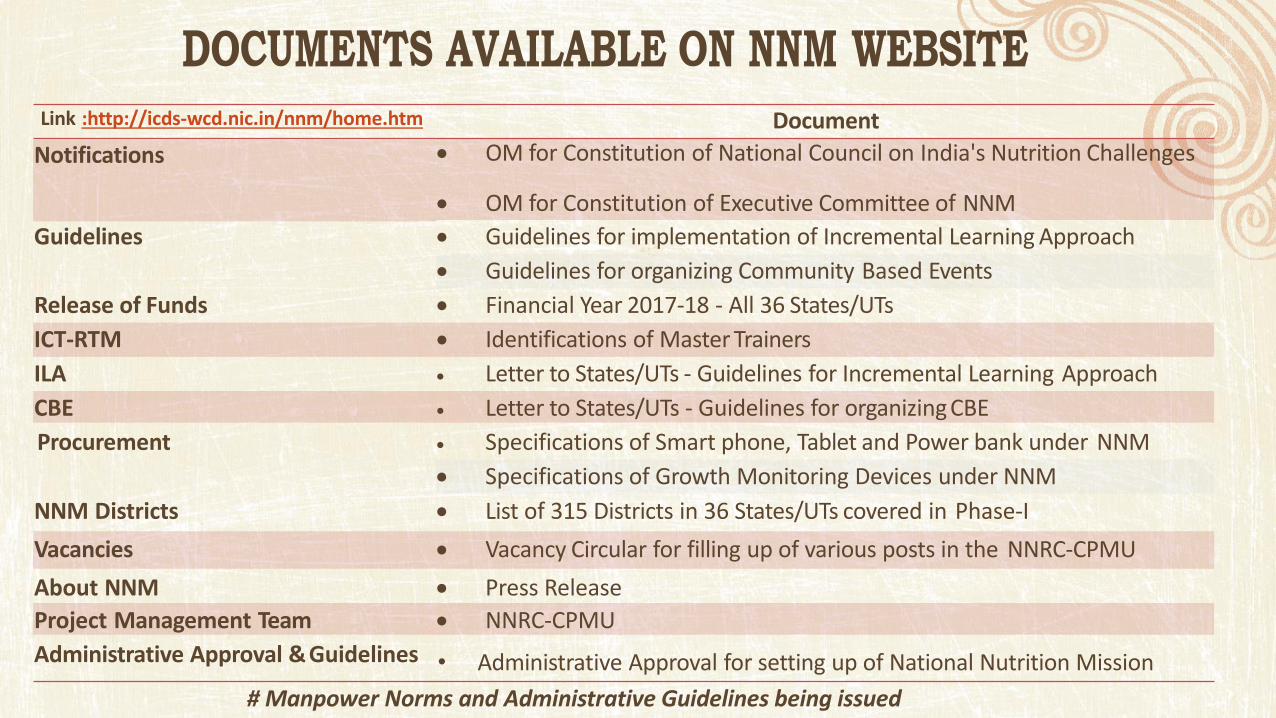
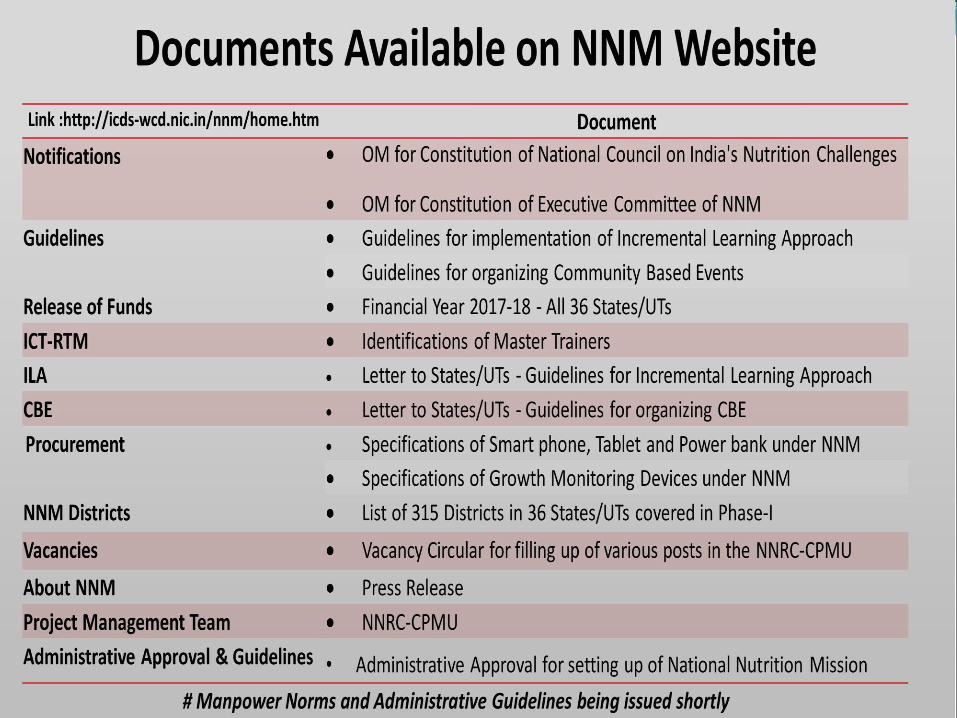
Link :http://icds-wcd.nic.in/nnm/home.htm Document
Notifications OM for Constitution of National Council on India's Nutrition Challenges
OM for Constitution of Executive Committee of NNM
Guidelines Guidelines for implementation of Incremental Learning Approach
Guidelines for organizing Community Based Events
Release of Funds Financial Year 2017-18 - All 36 States/UTs
ICT-RTM Identifications of Master Trainers
ILA Letter to States/UTs - Guidelines for Incremental Learning Approach
CBE Letter to States/UTs - Guidelines for organizing CBE
Procurement Specifications of Smart phone, Tablet and Power bank under NNM
Specifications of Growth Monitoring Devices under NNM
NNM Districts List of 315 Districts in 36 States/UTs covered in Phase-I
Vacancies Vacancy Circular for filling up of various posts in the NNRC-CPMU
About NNM Press Release
Project Management Team NNRC-CPMU
Administrative Approval & Guidelines • Administrative Approval for setting up of National Nutrition Mission
# Manpower Norms and Administrative Guidelines being issued
shortly
Status of Nutrition in
Children Arava Rajkamal
DC West Singhbhum (Jharkhand)
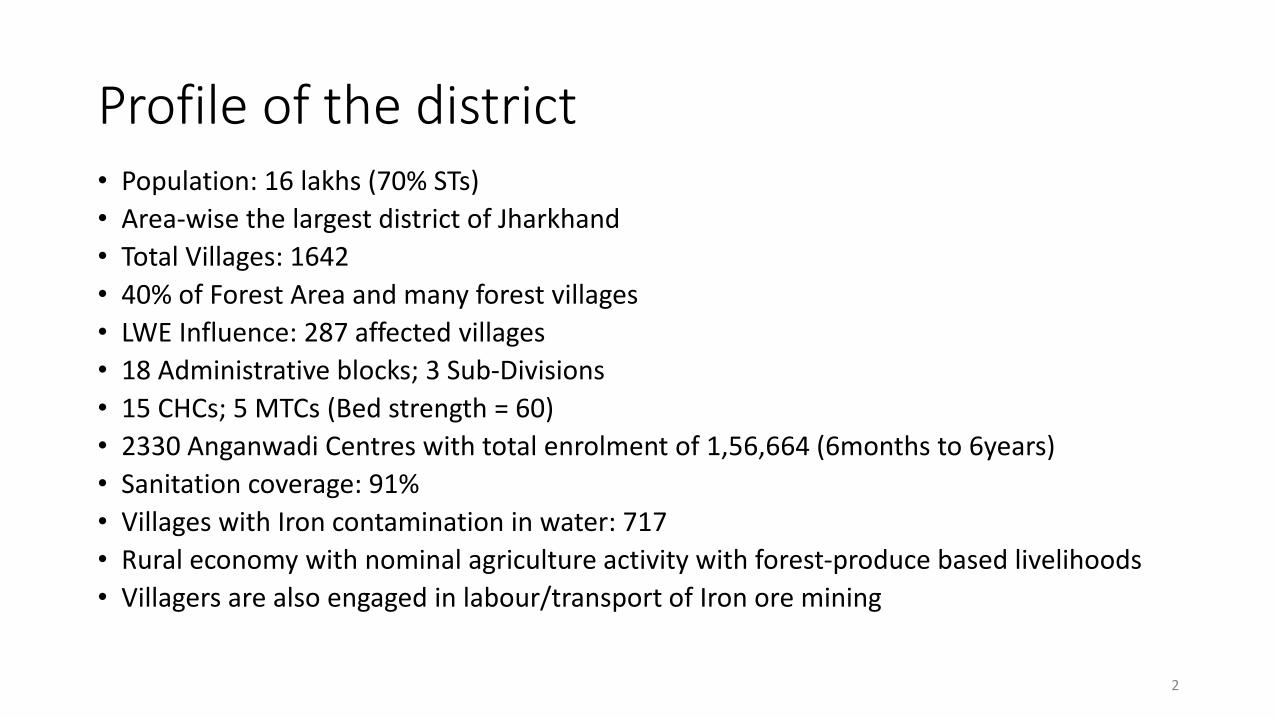
Profile of the district
• Population: 16 lakhs (70% STs)
• Area-wise the largest district of Jharkhand
• Total Villages: 1642
• 40% of Forest Area and many forest villages
• LWE Influence: 287 affected villages
• 18 Administrative blocks; 3 Sub-Divisions
• 15 CHCs; 5 MTCs (Bed strength = 60)
• 2330 Anganwadi Centres with total enrolment of 1,56,664 (6months to 6years)
• Sanitation coverage: 91%
• Villages with Iron contamination in water: 717
• Rural economy with nominal agriculture activity with forest-produce based livelihoods
• Villagers are also engaged in labour/transport of Iron ore mining
2
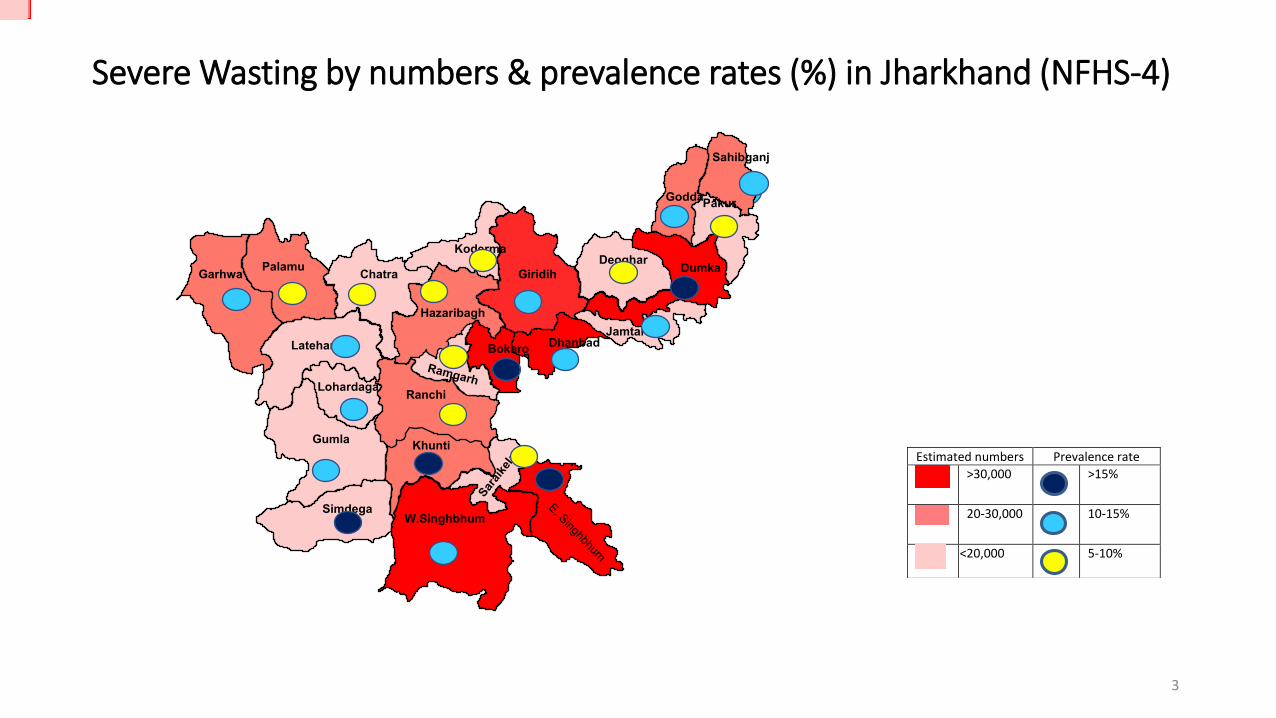
Severe Wasting by numbers & prevalence rates (%) in Jharkhand (NFHS-4)
3
Koderma
Ranchi
Garhwa
Palamu
Chatra
Latehar
Hazaribagh
Giridih
Lohardaga
Gumla
Simdega
W.Singhbhum
Khunti
Bokaro
Dhanbad
Deoghar
Jamtara
Dumka
Godda Pakur
Sahibganj
Estimated numbers Prevalence rate
>30,000
>15%
20-30,000
10-15%
<20,000
5-10%

District: West Singhbhum (Jharkhand) Nutritional status of below 5 years Children
District
Total number of Children
under 5 years who are
stunted (height-for-age)
Total number of
Children under 5 years
who are wasted
(weight-for-height)
Total number of Children
under 5 years who are
severely wasted (weight-
for-height)
Total number of
Children under 5 years
who are underweight
(weight-for-age)
West Singhbhum
142983 *
90267*
31533*
161036*
49.8 45.3
59.4
45.1 39.3
32 29
37.5
23.3
40.6
11.8 11.4 13.1 8.9
19.9
56.5
47.8
66.9
52.6 49.8
0
50
100
NFHS-3
2005-06
(Jharkhand)
NFHS-4
2015-16
(Jharkhand)
NFHS-4
2015-16
(West Singhbhum)
NFHS-4
2015-16
(Saraikela-Kharsawan)
NFHS-4
Y 2015-16
(East Singhbhum)
Children under 5 years who are stunted (height-for-age)(%) Children under 5 years who are wasted (weight-for-height) (%)
Children under 5 years who are severely wasted (weight-for-height)(%) Children under 5 years who are underweight (weight-for-age)(%)
4
Malnutrition’s strong correlation with..
• Poverty / Food insufficiency (leakages and absenteeism in ICDS/NFS/Health services in remote areas)
• Poor complimentary feeding practice (6-23 month children)
• Early marriage and teenage pregnancy
• Lack of access to safe drinking water
• Poor sanitation conditions & lack of hygiene
• Micronutrient deficiencies & Anaemia in adolescent girls
5
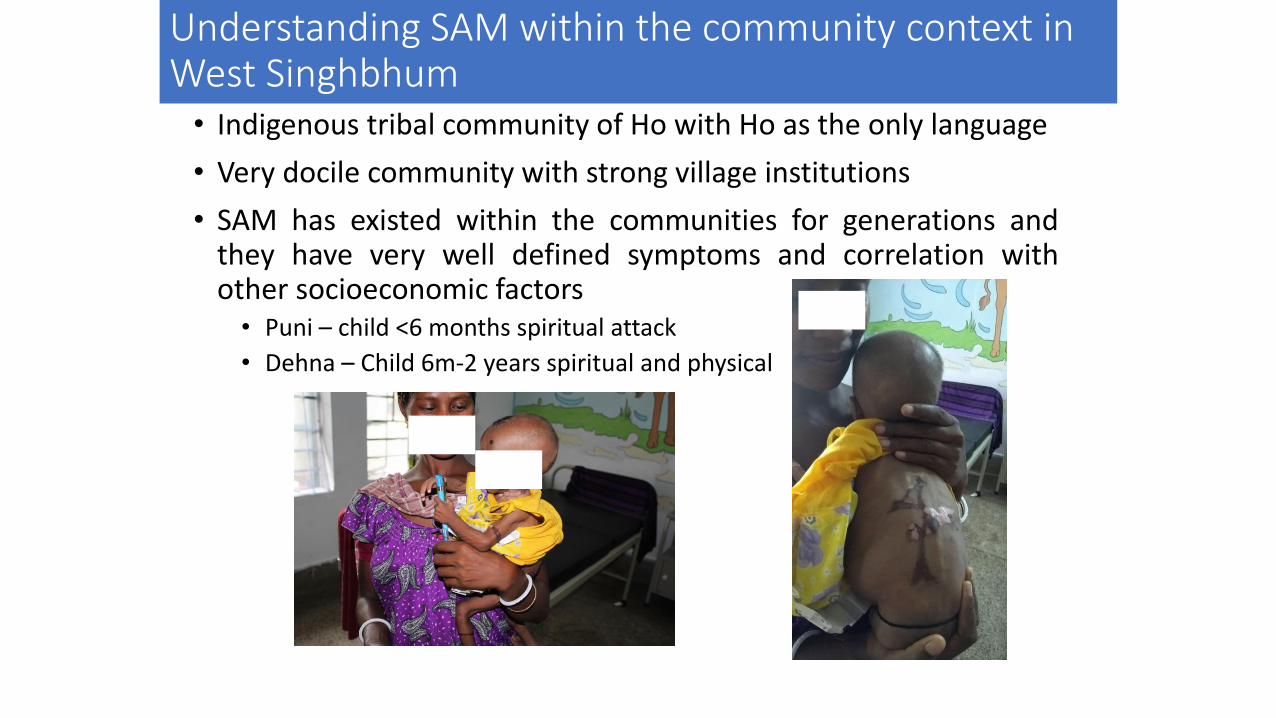
Understanding SAM within the community context in West Singhbhum
• Indigenous tribal community of Ho with Ho as the only language
• Very docile community with strong village institutions
• SAM has existed within the communities for generations and they have very well defined symptoms and correlation with other socioeconomic factors
• Puni – child <6 months spiritual attack
• Dehna – Child 6m-2 years spiritual and physical
Nutritional Intervention Strategy
• Intervention for short-term results: To save the malnourished children with CMAM model pilots in Khuntpani (UNICEF) and Chakradharpur (MSF) blocks. Next 3 months roll-out is planned in 6 other blocks using DMFT support
• Intervention for medium-term results: Expansion of CMAM models to entire district and strengthen the MTC infrastructure & ICDS delivery system (especially in LWE-affected/Forest villages)
• Intervention for long-term results: Address the issue of malnutrition with community-based behavioural change interventions
• Interventions supported by State Nutrition Mission (both blocks), State Health Mission (Chakradharpur) and partners – UNICEF/TATA CSR for Khuntpani and MSF (Doctors without Borders) for Chakradharpur
7
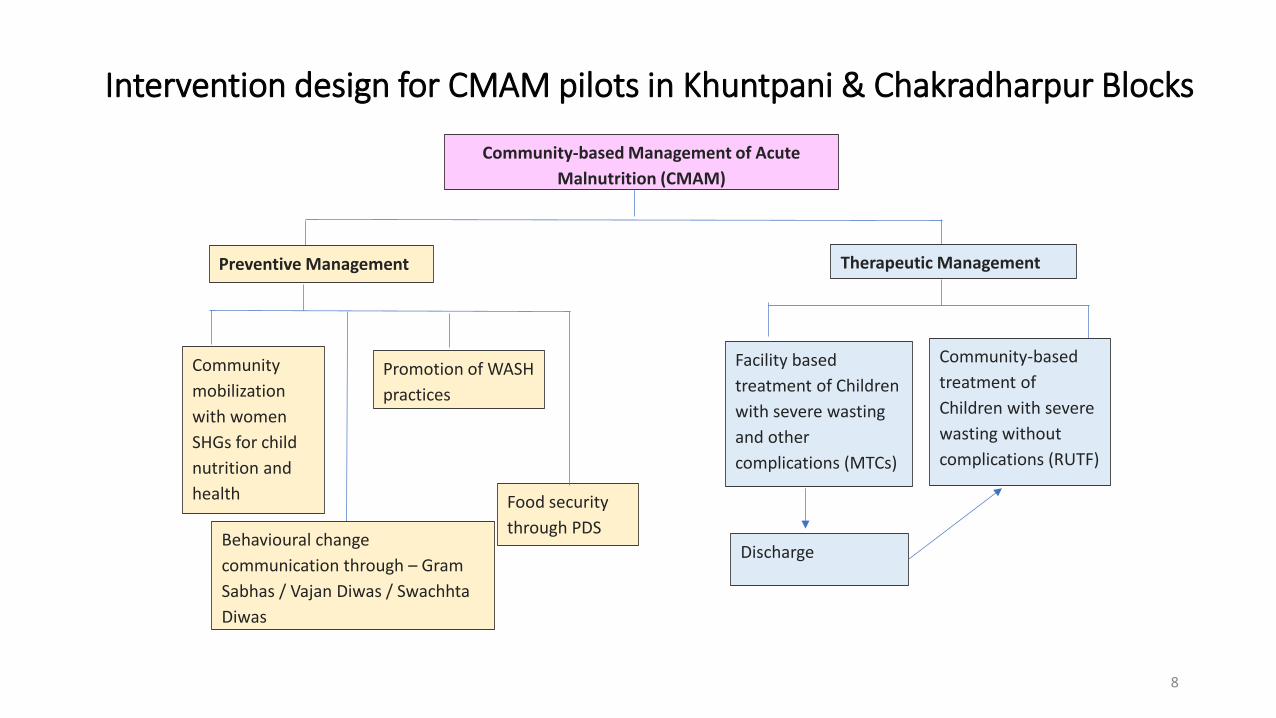
Intervention design for CMAM pilots in Khuntpani & Chakradharpur Blocks
8
Community-based Management of Acute
Malnutrition (CMAM)
Preventive Management Therapeutic Management
Community-based
treatment of
Children with severe
wasting without
complications (RUTF)
Facility based
treatment of Children
with severe wasting
and other
complications (MTCs)
Discharge
Community
mobilization
with women
SHGs for child
nutrition and
health
Promotion of WASH
practices
Behavioural change
communication through – Gram
Sabhas / Vajan Diwas / Swachhta
Diwas
Food security
through PDS
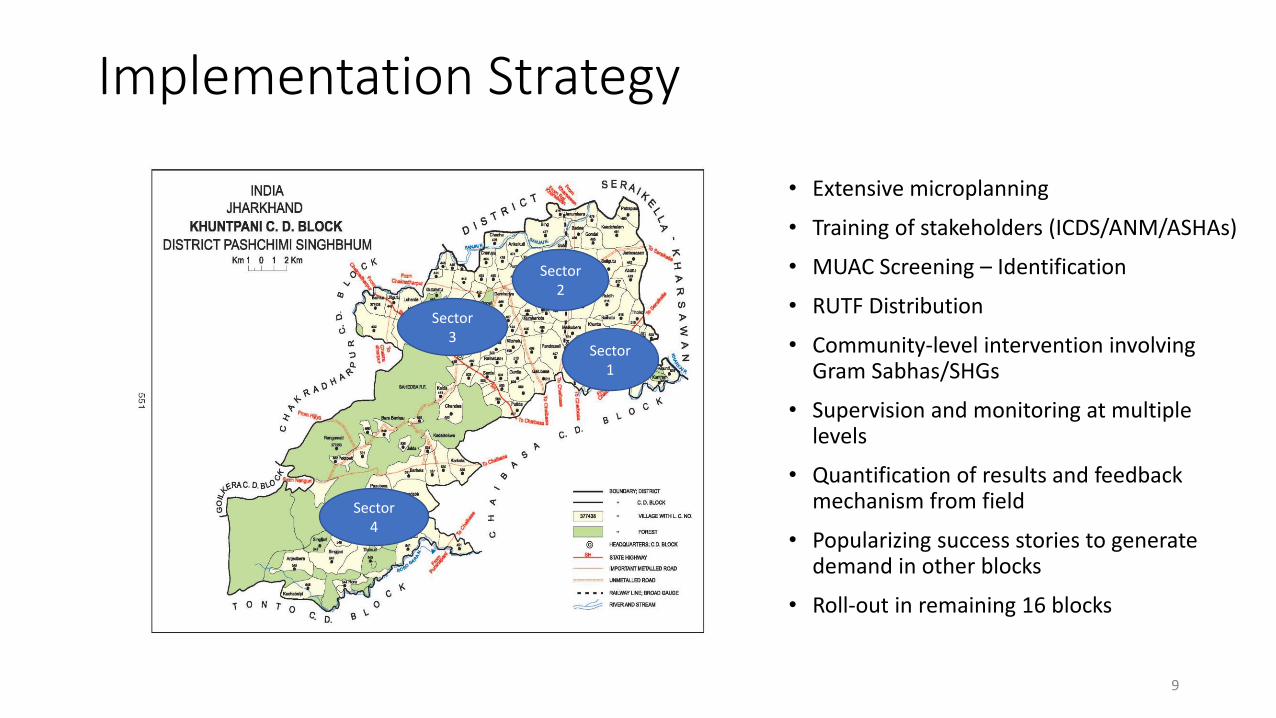
Implementation Strategy
• Extensive microplanning
• Training of stakeholders (ICDS/ANM/ASHAs)
• MUAC Screening – Identification
• RUTF Distribution
• Community-level intervention involving Gram Sabhas/SHGs
• Supervision and monitoring at multiple levels
• Quantification of results and feedback mechanism from field
• Popularizing success stories to generate demand in other blocks
• Roll-out in remaining 16 blocks
9
Sector
4
Sector
3
Sector
2
Sector
1
Massive screening activity of Mid-Upper Arm Circumference
(MUAC)
10

Community Awareness activities involving SHGs
11
RUTF (Nogod Lupu) Distribution
12
Behavioral Change & Sensitization in small groups
13

Supportive Supervision by ICDS
14

Monitoring by PRIs & Officials of District Malnutrition Task Force
15
ATFC Patient Flow
(Chakradharpur)
17
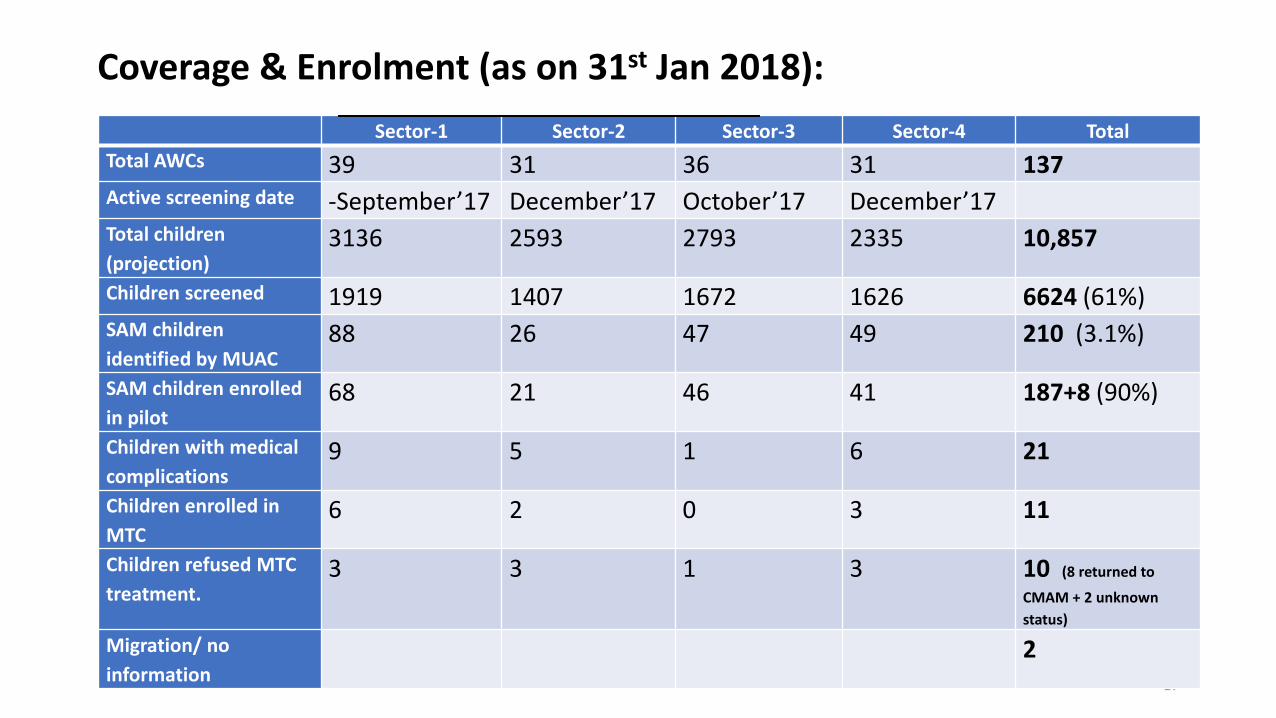
Sector-1 Sector-2 Sector-3 Sector-4 Total
Total AWCs 39 31 36 31 137
Active screening date -Septem er’17 De em er’17 O to er’17 De em er’17
Total children
(projection) 3136 2593 2793 2335 10,857
Children screened 1919 1407 1672 1626 6624 (61%)
SAM children
identified by MUAC 88 26 47 49 210 (3.1%)
SAM children enrolled
in pilot 68 21 46 41 187+8 (90%)
Children with medical
complications 9 5 1 6 21
Children enrolled in
MTC 6 2 0 3 11
Children refused MTC
treatment. 3 3 1 3 10 (8 returned to
CMAM + 2 unknown
status)
Migration/ no
information 2
Coverage & Enrolment (as on 31st Jan 2018):
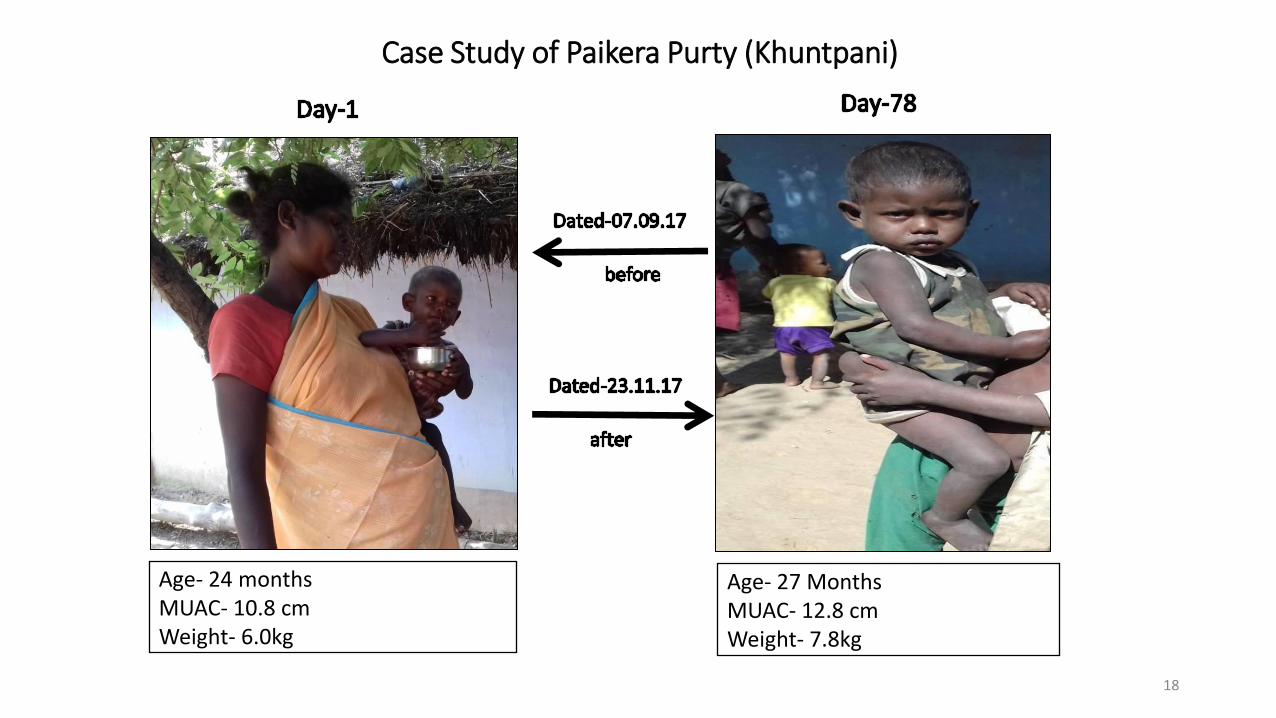
Case Study of Paikera Purty (Khuntpani)
18
Age- 24 months
MUAC- 10.8 cm
Weight- 6.0kg
Age- 27 Months
MUAC- 12.8 cm
Weight- 7.8kg
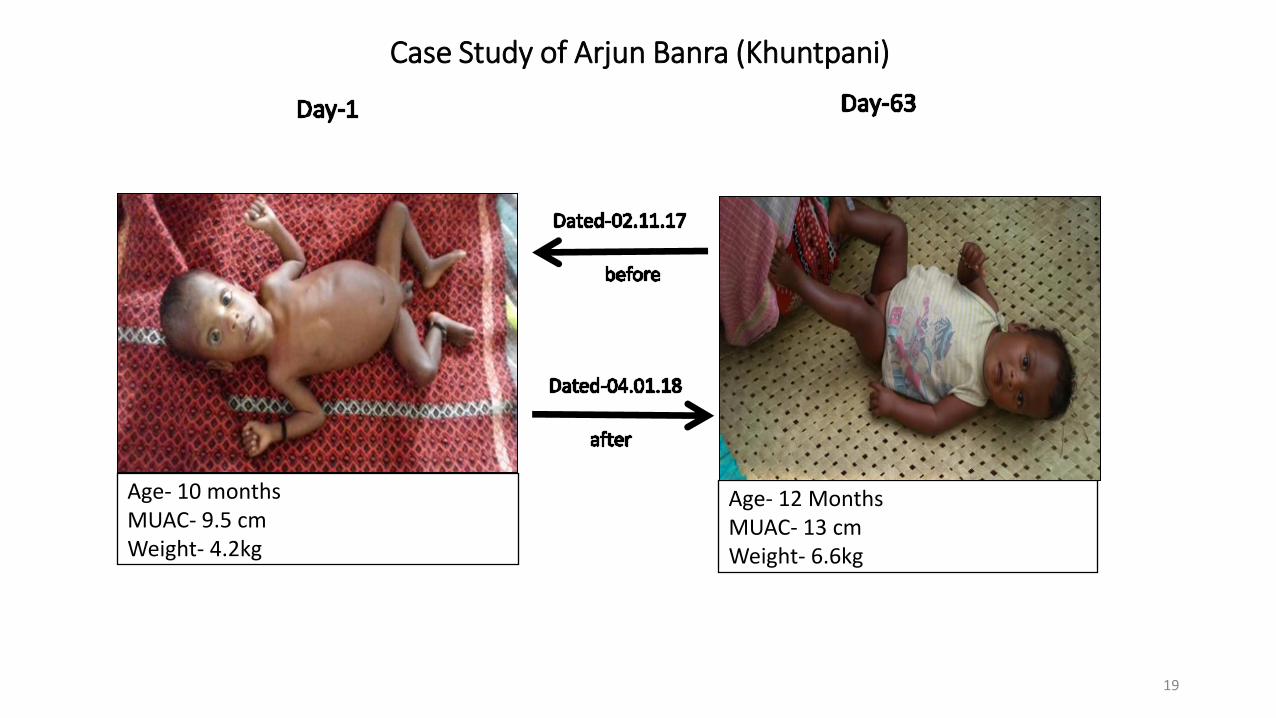
Case Study of Arjun Banra (Khuntpani)
19
Age- 10 months
MUAC- 9.5 cm
Weight- 4.2kg
Age- 12 Months
MUAC- 13 cm
Weight- 6.6kg
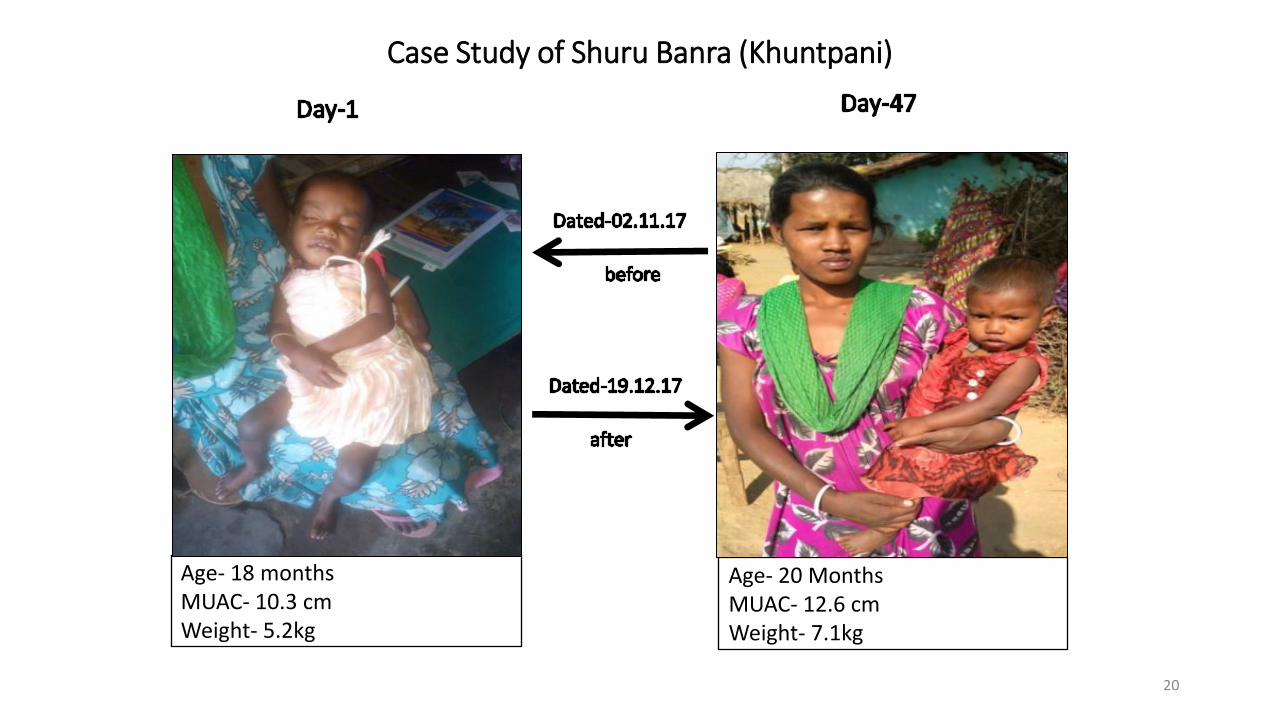
Case Study of Shuru Banra (Khuntpani)
20
Age- 18 months
MUAC- 10.3 cm
Weight- 5.2kg
Age- 20 Months
MUAC- 12.6 cm
Weight- 7.1kg
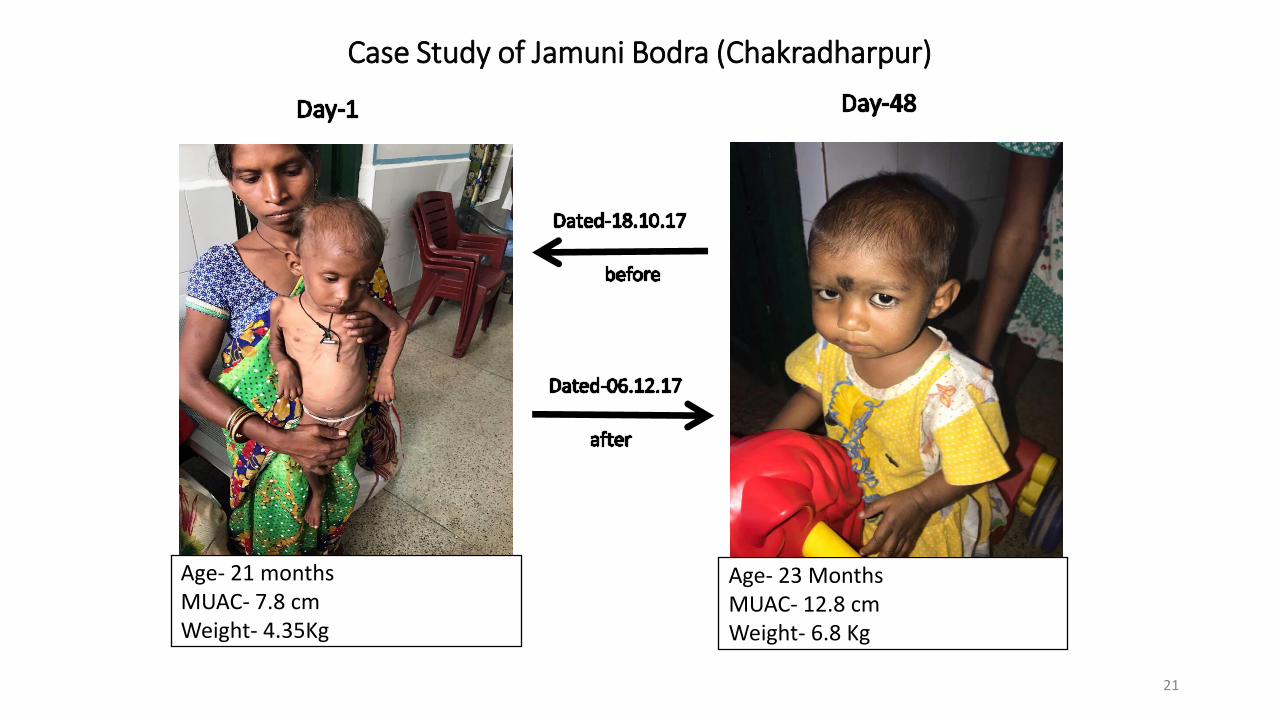
Case Study of Jamuni Bodra (Chakradharpur)
21
Age- 21 months
MUAC- 7.8 cm
Weight- 4.35Kg
Age- 23 Months
MUAC- 12.8 cm
Weight- 6.8 Kg
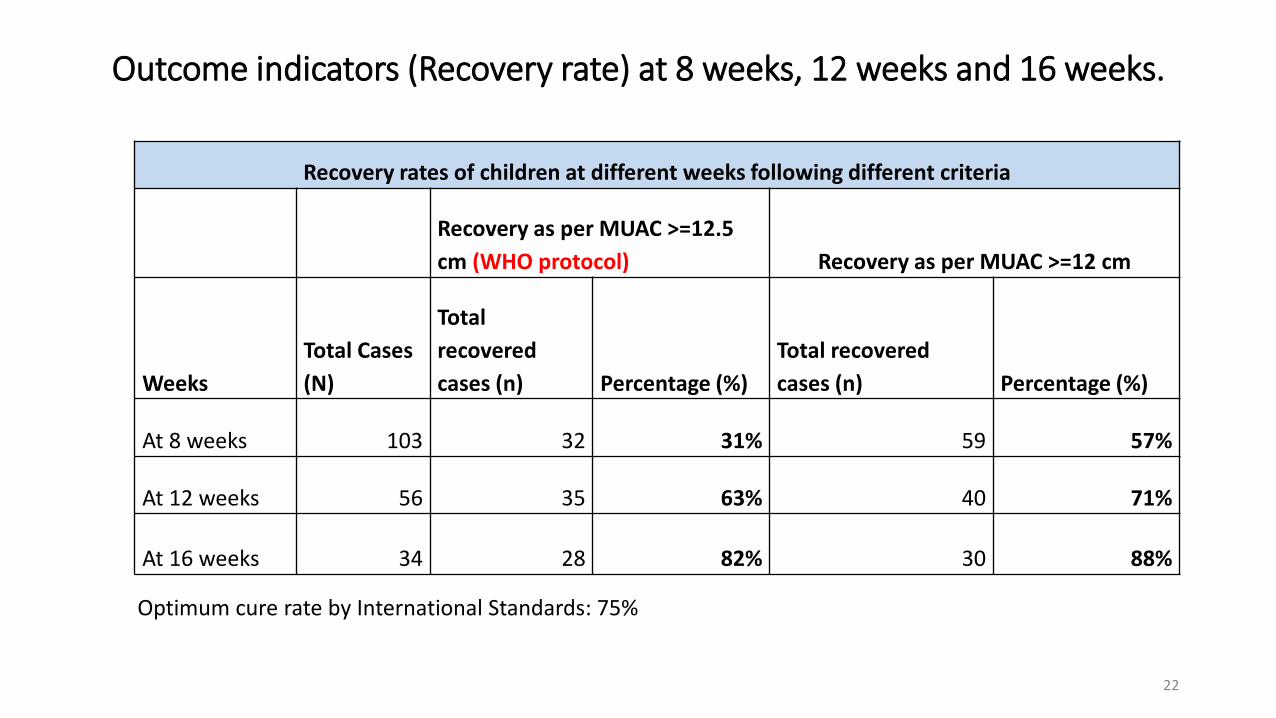
Outcome indicators (Recovery rate) at 8 weeks, 12 weeks and 16 weeks.
22
Recovery rates of children at different weeks following different criteria
Recovery as per MUAC >=12.5
cm (WHO protocol) Recovery as per MUAC >=12 cm
Weeks
Total Cases
(N)
Total
recovered
cases (n) Percentage (%)
Total recovered
cases (n) Percentage (%)
At 8 weeks 103 32 31% 59 57%
At 12 weeks 56 35 63% 40 71%
At 16 weeks 34 28 82% 30 88%
Optimum cure rate by International Standards: 75%
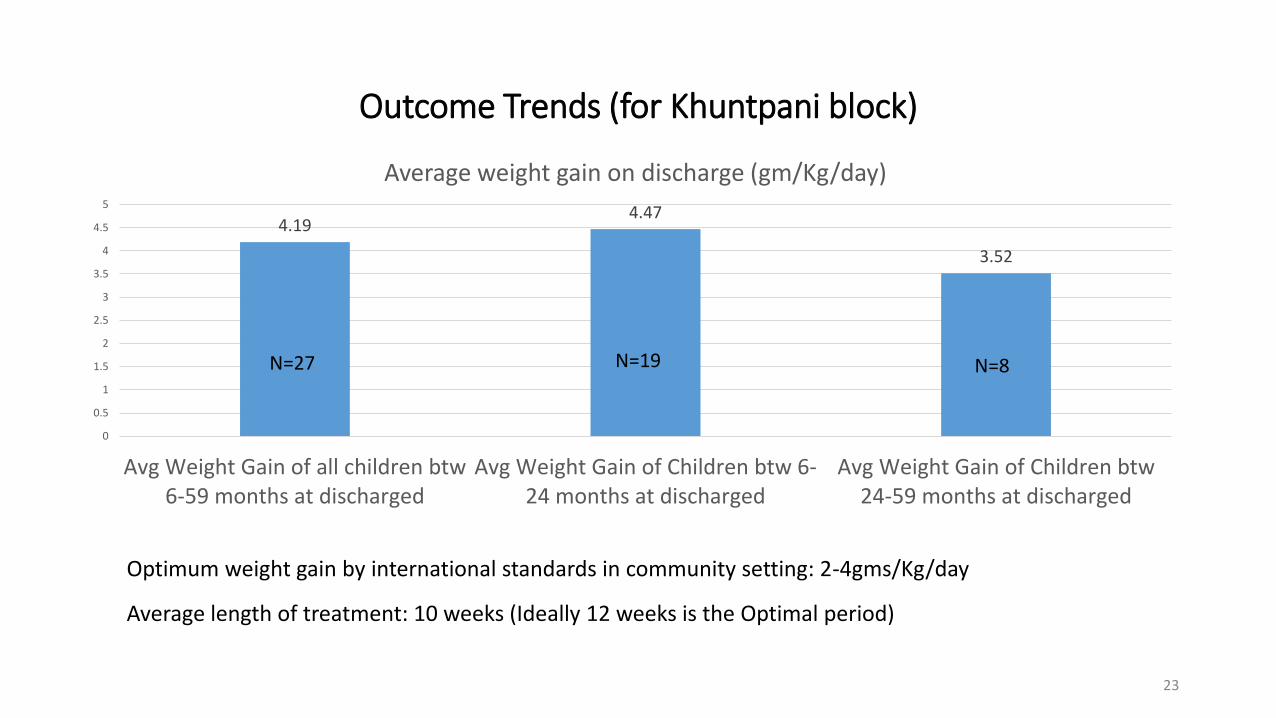
Outcome Trends (for Khuntpani block)
23
4.19 4.47
3.52
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Avg Weight Gain of all children btw
6-59 months at discharged
Avg Weight Gain of Children btw 6-
24 months at discharged
Avg Weight Gain of Children btw
24-59 months at discharged
Average weight gain on discharge (gm/Kg/day)
N=27 N=19 N=8
Average length of treatment: 10 weeks (Ideally 12 weeks is the Optimal period)
Optimum weight gain by international standards in community setting: 2-4gms/Kg/day
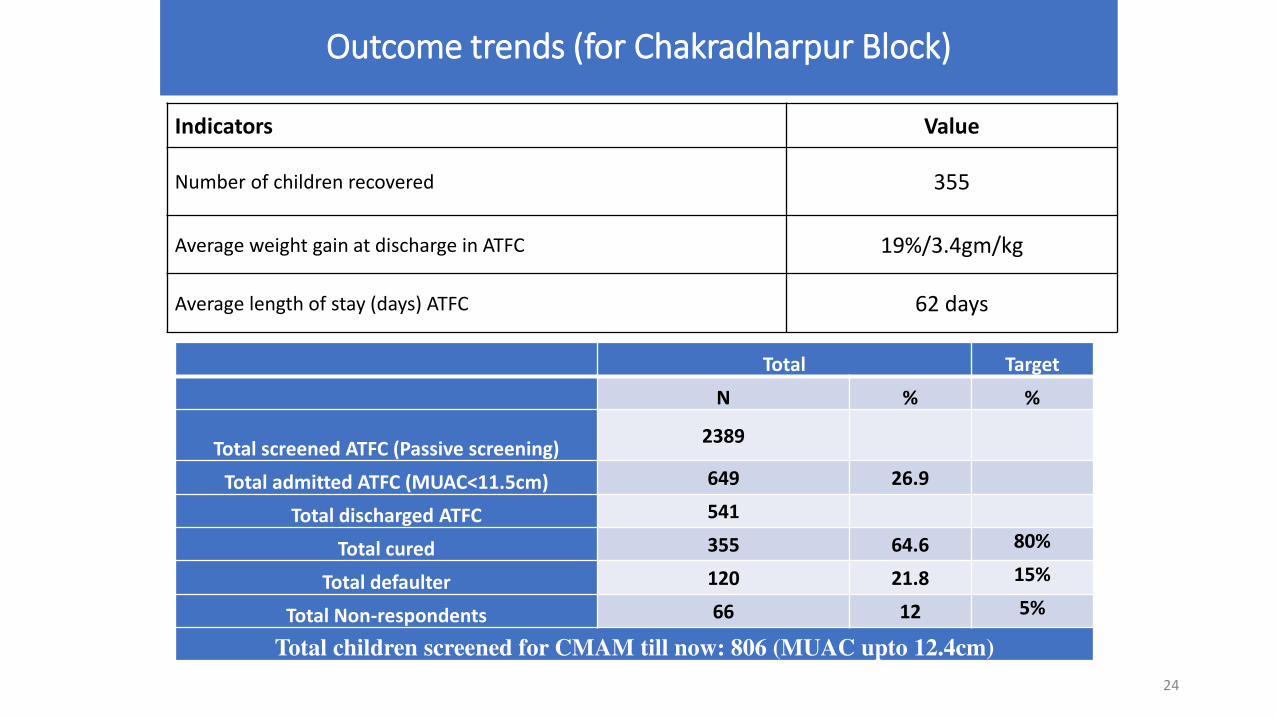
Outcome trends (for Chakradharpur Block)
Indicators Value
Number of children recovered 355
Average weight gain at discharge in ATFC 19%/3.4gm/kg
Average length of stay (days) ATFC 62 days
Total Target
N % %
Total screened ATFC (Passive screening) 2389
Total admitted ATFC (MUAC<11.5cm) 649 26.9
Total discharged ATFC 541
Total cured 355 64.6 80%
Total defaulter 120 21.8 15%
Total Non-respondents 66 12 5%
Total children screened for CMAM till now: 806 (MUAC upto 12.4cm)
24
Learnings & Way forward
• NNM – the gamechanger: HR/Financial/Monitoring support & opportunities through the newly launched National Nutrition Mission
• Instead of Anganwadi Sevika OR ANM/ASHA model – a more holistic model is expected in universal protocol of CMAM (with clearly defined roles to AWW/ASHA/ANM)
• Roll-out in 4 blocks in Phase II (April 2018); 2 more in Phase III (June 2018) and 10 more in Phase IV (September 2018)
• Distribution cum child-friendly MTC Check-up vans (Puni-Dehna Gaadi)
• Focus on using local language-based radio feed/Nukkad nataks/Swachchta Diwas/Vajan Diwas/SHG mobilization to make the fight against malnutrition a Jan Andolan
• Creating examples of cured children as brand ambassadors - Mascots
• Technology-based monitoring of ICDS delivery and mobile app for malnutrition monitoring (underdevelopment for tracking all SAM children)
• Providing safe drinking water & sanitation facilities at all Anganwadi centres from DMFT fund (Total to be covered by 2021)
• Attempt to create a Malnutrition Research & Training Centre at the District (with DMFT support)
25
Thank You
26
one great step toward
Improving Nutrition
4 ICDS projects
1386 AWC

STATUS OF ANGANWADI BUILDINGS
SL.No Name of the
block/project
No.of AWC S Arrangements of centers functioning in
Rent
BUILDI
NGS
Total Sanctioned functioning
Own
BUILDINGS
Panchayat
BUILDINGS
Community
BUILDINGS
Youth
Assitaion
BUILDING
S
Mahila
Asson
BUILDING
S
Temples
School
BUILDING
S
Make
shift
Arrangme
nt AWC Mini
AWC AWC Mini AWC
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
1 Shahapur 386 9 386 9 279 6 9 0 0 0 16 0 85 395
2 Shorapur 451 23 451 23 315 0 20 0 0 0 27 0 112 474
3 yadgir 239 4 239 4 159 4 3 0 0 0 8 0 69 243
4 Guramtakal 260 14 260 14 191 5 5 0 0 0 16 0 57 274
Dist.Total 1336 50 1336 50 944 15 37 0 0 0 67 0 323 1386
1. Gap in Infrastructure – Anganwadi Buildings

Anganwadi Basic Infrastructure Information
Sl.No ICDS Project No of
AWC
No. of
Own
Buildings
Kitchen Room
Availability Garden
Toilets
Availability
Drinking
Water Facility Electricity
Compound
Wall Play Ground
LPG Gas
Connection
Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
1 Shahapur 395 275 210 185 0 395 254 141 147 248 170 225 13 382 13 382 395 0
2 Surpur 474 315 117 357 1 473 49 425 66 408 259 215 61 413 52 422 474 0
3 Yadgir 243 157 84 159 1 242 154 89 83 160 179 64 48 195 54 189 243 0
4 Gurumatkal 274 195 186 88 5 269 171 103 81 193 171 103 37 237 54 220 274 0
Total 1386 942 597 789 7 1379 628 758 377 1009 779 607 159 1227 173 1213 1386 0
2. Gap in Infrastructure – Anganwadi Buildings –other facilities
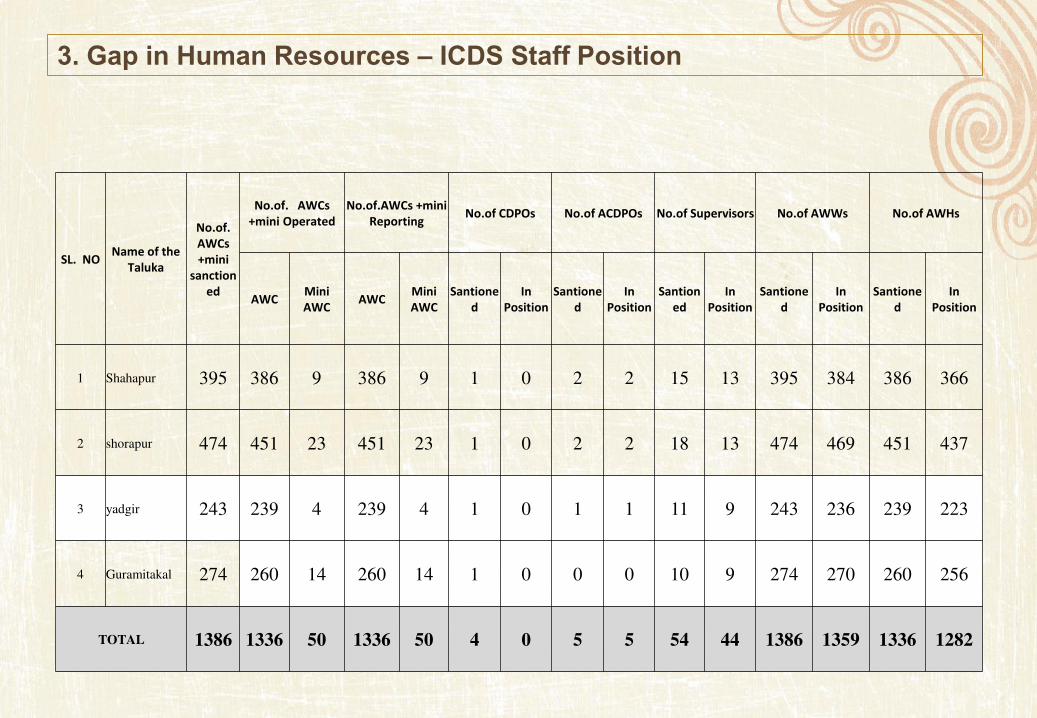
SL. NO Name of the
Taluka
No.of.
AWCs
+mini
sanction
ed
No.of. AWCs
+mini Operated
No.of.AWCs +mini
Reporting No.of CDPOs No.of ACDPOs No.of Supervisors No.of AWWs No.of AWHs
AWC Mini
AWC AWC
Mini
AWC
Santione
d
In
Position
Santione
d
In
Position
Santion
ed
In
Position
Santione
d
In
Position
Santione
d
In
Position
1 Shahapur 395 386 9 386 9 1 0 2 2 15 13 395 384 386 366
2 shorapur 474 451 23 451 23 1 0 2 2 18 13 474 469 451 437
3 yadgir 243 239 4 239 4 1 0 1 1 11 9 243 236 239 223
4 Guramitakal 274 260 14 260 14 1 0 0 0 10 9 274 270 260 256
TOTAL 1386 1336 50 1336 50 4 0 5 5 54 44 1386 1359 1336 1282
3. Gap in Human Resources – ICDS Staff Position
• Poor Attendance in Anganwadi for Pre-School Education Activities
• Parents prefer to send their children to convent school instead of Anganwadis (Urban areas)
• Community Participation is very poor in overall Development of Anganwadi Centers
• Parents are not ready to stay in NRC for complete duration of 15 Days, in every Taluka separate NRC required
• 50% Beneficiary of ICDS do not have toilets in their houses
• All Anganwadis workers and Supervisors need periodic training
• Balavikas Committees need to be strengthened and should be trained regarding ICDS Activities
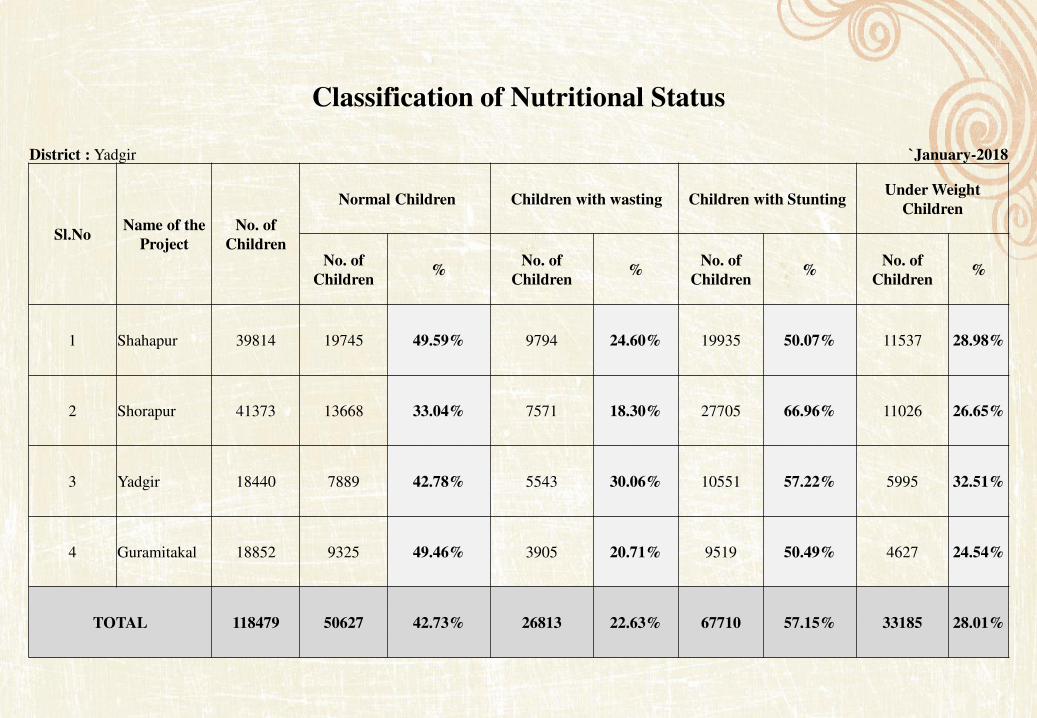
Classification of Nutritional Status
District : Yadgir `January-2018
Sl.No Name of the
Project
No. of
Children
Normal Children Children with wasting Children with Stunting Under Weight
Children
No. of
Children %
No. of
Children %
No. of
Children %
No. of
Children %
1 Shahapur 39814 19745 49.59% 9794 24.60% 19935 50.07% 11537 28.98%
2 Shorapur 41373 13668 33.04% 7571 18.30% 27705 66.96% 11026 26.65%
3 Yadgir 18440 7889 42.78% 5543 30.06% 10551 57.22% 5995 32.51%
4 Guramitakal 18852 9325 49.46% 3905 20.71% 9519 50.49% 4627 24.54%
TOTAL 118479 50627 42.73% 26813 22.63% 67710 57.15% 33185 28.01%
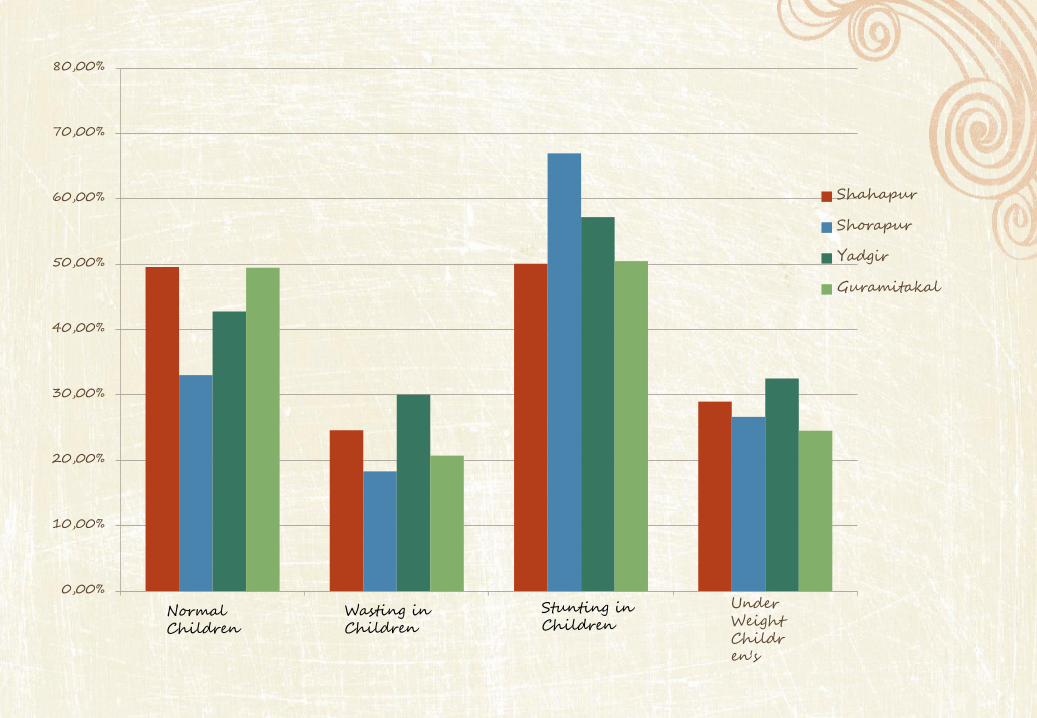
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
70,00%
80,00%
Shahapur
Shorapur
Yadgir
Guramitakal
Normal Children
Wasting in Children
Stunting in Children
Under Weight Children's

Classification of Nutritional Status District : Yadgir (Month Wise)
Sl.No Month & Year
No. of
Weighed
Children
Normal Moderately Severely
No. of
Children %
No. of
Children %
No. of
Children %
1 2 3 4 5 6 7 8 9
1 Apr-17 115020 76976 66.92% 37256 32.39% 788 0.69%
2 May-17 115288 77799 67.48% 36710 31.84% 779 0.68%
3 Jun-17 119255 76953 64.53% 41532 34.83% 770 0.65%
4 Jul-17 113444 76453 67.39% 36179 31.89% 812 0.72%
5 Aug-17 115700 77268 66.78% 37613 32.51% 819 0.71%
6 Sep-17 115729 74454 64.33% 40443 34.95% 832 0.72%
7 Oct-17 112601 75698 67.23% 35985 31.96% 918 0.82%
8 Nov-17 112533 74739 66.42% 36919 32.81% 875 0.78%
9 Dec-17 115611 79022 68.35% 35766 30.94% 823 0.71%
10 Jan-18 116212 83027 71.44% 32399 27.88% 786 0.68%
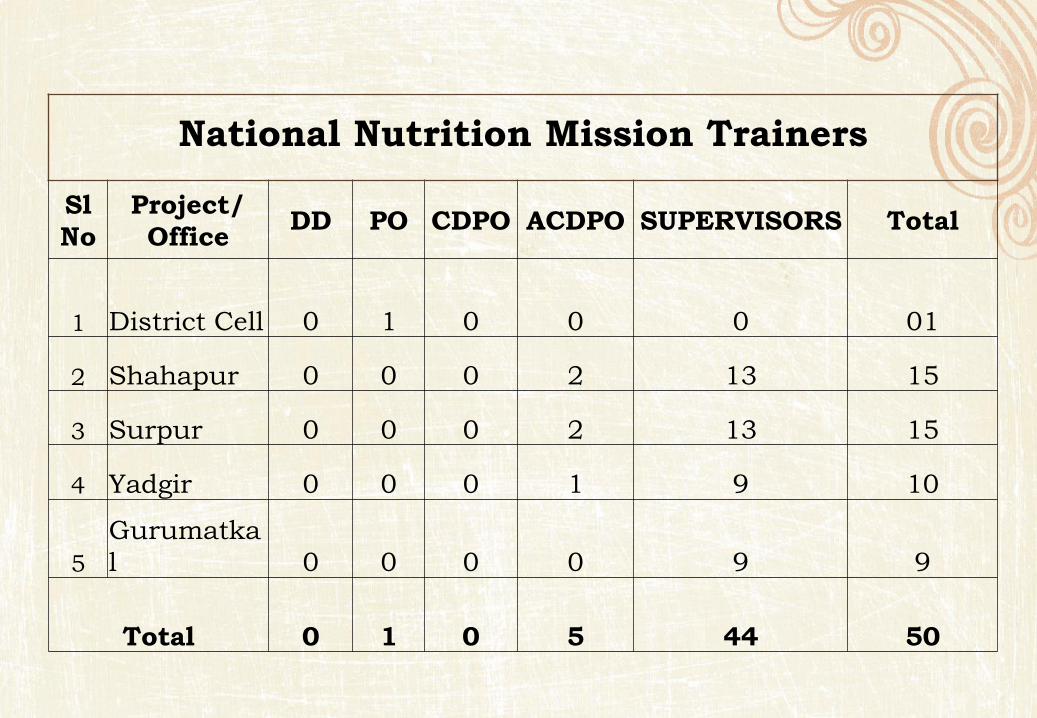
National Nutrition Mission Trainers
Sl
No
Project/
Office DD PO CDPO ACDPO SUPERVISORS Total
1 District Cell 0 1 0 0 0 01
2 Shahapur 0 0 0 2 13 15
3 Surpur 0 0 0 2 13 15
4 Yadgir 0 0 0 1 9 10
5
Gurumatka
l 0 0 0 0 9 9
Total 0 1 0 5 44 50
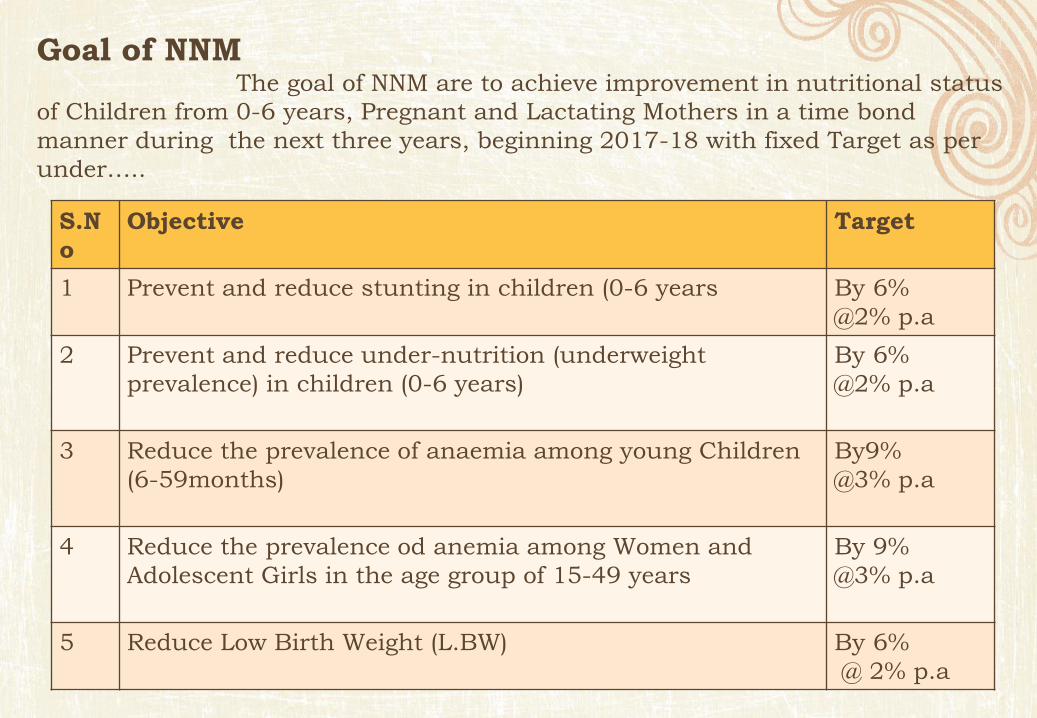
Goal of NNM The goal of NNM are to achieve improvement in nutritional status
of Children from 0-6 years, Pregnant and Lactating Mothers in a time bond
manner during the next three years, beginning 2017-18 with fixed Target as per
under…..
S.N
o
Objective Target
1 Prevent and reduce stunting in children (0-6 years By 6%
@2% p.a
2 Prevent and reduce under-nutrition (underweight
prevalence) in children (0-6 years)
By 6%
@2% p.a
3 Reduce the prevalence of anaemia among young Children
(6-59months)
By9%
@3% p.a
4 Reduce the prevalence od anemia among Women and
Adolescent Girls in the age group of 15-49 years
By 9%
@3% p.a
5 Reduce Low Birth Weight (L.BW) By 6%
@ 2% p.a

Targets- for the next three years, beginning 2017-18 as per under…..
Prevent and
reduce
stunting in
children (0-6
years)
Prevent and reduce
under-nutrition
(underweight
prevalence) in
children (0-6 years)
Reduce the
prevalence of
anemia among
young Children
(6-59months)
Reduce the
prevalence of
anemia among
Women and
Adolescent Girls
15-49 years
Reduce
Low Birth
Weight
(L.BW)
Yadgir (55.5%)
By 49.5%
(50.3%)
By 44.3%
(74.00%)
By 65.00%
(74.00%)
By 65.00%
• District Officers (ICDS, Health, DWs, PRI) to undertake combined reiew meeting focusing on outcome monitoring and nutrtion indicators.
• Ensure Coverage in Local Media
• Post images of activities on social Media page/ handle.
• Participation of elected representative in events
• Nutrition Rally/Walk to be organised at District Level.
• Outdoor media activation through Song and Drama Division avilable at State Level.
• CDPO with Medical officers to intiate targeted mid-media activities and awareness drives on institutional deliveries, WASH, Dietary Diversification, Immunication, Food, Fortification, Deworming, IYCF etc
• All Panchayat Raj institutions to have focused group discussions on thematic domains of Nutrition, health and Sanitation
• Organise Nutrition based activities like, painting competitions, group discussions, competitions etc.
• Spread Nutrition Awareness through Nutrition Mascots/Enablers.
• Organise Adolescent Girls Group Councelling on nutrition.
• Organise Nukkadnataks on Nutrition, heath and Sanitation through loca groups
District project Village /AWC level
Implementation of
Coveragence Action
plan.
Awareness
campaigns to
continue.
Implementation of
relevant NNM
Components.
Implementation of
Coveragence Action
plan.
Training of Field
functionaries for ICDS
CAS.
Implementation of
relevant NNM
Components.
Implementation of
Coveragence Action
plan.
Training of Field
functionaries for ICDS
CAS
House visits.
VSHN Day
Awareness
Campaigns
Implementattion of
relevant NNM
Components.