Embed Size (px)
Citation preview

Journal of Clinical Immunology, Vol. 3, No. 1, 1983
Inherited Deficiency of C8 in a Patient with Recurrent Meningococcal Infections: Further Evidence for a Dysfunctional C8 Molecule and Nonlinkage to the HLA System
P. D E N S E N , ~ E. J. BROWN, 2 G. J. O ' N E I L L , 3 F. TEDESCO, 4 R. A. CLARK, 1 M. M. FRANK, 2 D. WEBB, 5 and J. MYERS 6
Accepted: September 1, 1982
An adult male with recurrent meningococcal infections is reported whose serum lacked functional C8 activity but possessed antigenic C8. The addition of 1500 U of puri- fied C8/ml of serum restored hemolytic activity to nor- mal. Four to five times more C8 was required to restore bactericidal activity than to restore hemolytic activity. Bactericidal activity could also be restored by mixing the patient's serum with a second C8-deficient serum that lacked detectable antigenic or functional C8. The pa- tient's serum contained bactericidal antibody for groups A, B, C, and Y meningococci and specific antibody to group Y capsular polysaccharide. There was two to three times more bactericidal antibody activity in the serum than in a pool of normal sera for the infecting strain. Family studies disclosed a sibling who was HLA identical to the patient but whose serum contained normal amounts of total hemolytic and C8 functional activity. KEY WORDS: C8 deficiency; recurrent meningococcaI infec- tion; HLA linkage.
1Evans Memorial Department of Clinical Research and Depart- ment of Medicine, Boston University Medical Center, Boston, Massachusetts 02118.
2Laboratory of Clinical Investigation, National Institute of Aller- gy and Infectious Diseases, National Institutes of Health, Bethesda, Maryland 20205.
3Memorial Sloan-Kettering Cancer Center, New- York, New York 10021. 4Centro Trasfusionale e di Immunologia dei Trapianti, Ospedale Policlinico, Milano, Italy.
5Department of Medicine, U.S. Public Health Service Hospital, Boston, Massachusetts 02135.
6Department of Medicine, Mountainside Hospital, Montclair, New Jersey 07042.
INTRODUCTION
The complement system is an important element in host defense, the inflammatory response, and the production of tissue injury (1). Investigations of patients with complement deficiency states have been particularly valuable in elucidating the role played by the system as a whole as well as by individual components in each of these important responses (1, 2). Clinical and laboratory investiga- tions have established that patients with early com- plement component deficiencies (through C3) have an increased f requency of autoimmune disorders and, in some instances, of bacterial infection caused by multiple pathogens (2). The latter association is believed to be a direct consequence of impaired antimicrobial defenses, while the former associa- tion may reflect genetic linkage of some of the early complement components to the H L A system. Pa- tients with a deficiency of one of the terminal complement components are selectively susceptible to systemic infections caused by Neisser ia but not other bacteria (3). An association between deficien- cies of terminal complement components and auto- immune disorders is not as striking as with the early component deficiencies (4). Studies of a possible genetic linkage between deficiencies of the late components and the H L A system have yielded contradictory results but, in general, have not sup- ported linkage (5-9). In this paper, we report the results of the immunologic and genetic evaluation of an individual with recurrent Neisser ia meningi t idis infection whose complement deficiency is due to a dysfunctional C8 molecule.
90 0271-9142/83/0100-0090503.00/0 ~ 1983 Plenum Publishing Corporation

C8 DYSFUNCTION AND MENINGOCOCCAL DISEASE 91
Case Report. This previously healthy, Caucasian male experienced his first episode of meningococcal infection at 16 years of age. The details of that illness were published previously to illustrate the management of disseminated intravascular coagula- tion (10). Briefly, following a 3-day prodromal ill- ness, the patient developed shock with meningeal signs and a purpuric rash. Laboratory values showed a mild leukocytosis, pronounced thrombo- cytopenia, markedly prolonged prothrombin and partial thromboplastin times, and elevated fibrin degradation products. The cerebrospinal fluid (CSF) contained 42 leukocytes/mm 3, 66% of which were neutrophils, but the glucose and protein were normal. Cultures of the CSF and blood were nega- tive but a nasopharyngeal culture yielded group C N. meningitidis. Therapy with fluid replacement, antibiotics, steroids, and heparin resulted in gradual improvement and the patient was discharged after 27 days, with eventual complete recovery.
He developed his second episode of meningococ- cal infection 5 years later, at age 21 years, during a stint in the coast guard. Over the course of a day, he developed gastrointestinal symptoms, meningeal signs, and a petechial, purpuric rash. Although alert on admission, he rapidly became comatose and his course was complicated by grand real seizures. The peripheral blood contained 25,300 leukocytes and 86,000 platelets/mm 3, and a mild abnormality of clotting function was evident. The CSF contained 131 leukocytes/mm 3 (32% neutrophils); the glucose and protein were 68 and 52 mg/dl, respectively. Cultures of the blood and CSF grew group Y N. meningitidis. Treatment was initiated with antibiot- ics, dilantin, and mannitol. Repeat lumbar puncture on hospital day 3 demonstrated a CSF formula more typical of bacterial meningitis with a marked leuko- cytosis, moderately elevated protein, and de- pressed glucose. Despite antibiotic therapy, culture of the CSF remained positive. CSF obtained on hospital day 7 was sterile and demonstrated a marked improvement in all laboratory parameters. Skull films and examination for a CSF leak were negative. Serum immunoglobulins were normal. The total hemolytic complement was < 10 hemolyt- ic units (normal, 99-126). The patient was dis- charged after 2 weeks of therapy and 1 week of observation off antibiotic therapy.
One week following discharge, he again devel- oped fever, vomiting, and meningeal signs. There was no rash but an acutely enlarged, tender anterior cervical lymph node was noted. Studies of clotting
function were normal. The CSF contained 39 leuko- cytes/mm 3, 89% of which were lymphocytes, and the glucose and protein were 58 and 48 mg/dt, respectively. Cultures and gram stain of the CSF were negative for organisms but blood cultures grew N. meningitidis. The isolate was not sero- grouped. The patient defervesced promptly with antibiotic therapy. At the time of discharge, addi- tional therapeutic measures included bivalent-me- ningococcal vaccine, fresh-frozen plasma to restore complement function, and prophylactic minocy- cline and rifampicin, which were continued for 4 weeks.
Two months following the discontinuation of prophylactic antibiotics, he presented to another hospital with fever, myalgias, vomiting, diarrhea, headache, meningismus, and rash and was thought to have aseptic meningitis. On transfer the next day, he was lethargic, febrile, and hypotensive and had a purpuric truncal rash. Petechiae were present on mucosal membranes and he again had tender right cervical and supraclavicular adenopathy. Lab- oratory studies demonstrated a leukocytosis of 40,000/ram 3 with a marked left shift. The platelet count was normal but the prothrombin and partial thromboplastin times were moderately prolonged. The CSF contained 3 cells/ram 3, of which 2 were neutrophils; the glucose and protein were normal. Cultures of the CSF and blood were negative. Dramatic clinical improvement occurred within 24 hr of starting penicillin, which was then continued for 2 weeks. The patient again received meningo- coccal vaccine and was discharged on antibiotic prophylaxis. One year later prophylaxis was dis- continued, and the patient has remained healthy during the ensuing 2 years.
MATERIALS AND METHODS
Sera. Blood was collected from the patient and members of his family, allowed to clot at room temperature for t hr, and centrifuged at 1500g for 15 rain at 4°C. The serum was removed and stored in small aliquots at -70°C. In some studies, a pool of normal human sera (PHS) from I0 men and 10 women who were not taking antibiotics and who denied any history of neisserial infection was used as a control.
Meningococci. The identity of the group Y me- ningococcus isolated from the patient during his second meningococcal infection was reconfirmed by sugar fermentation, positive oxidase test, typical
Journal o f Clinical l?mrnunology, Vol. 3, No. 1, 1983

92 DENSEN, BROWN, O'NEILL, TEDESCO, CLARK, FRANK, WEBB, AND MYERS
appearance on gram stain, and serogrouping using anticapsular antibody specific for group Y meningo- cocci. This strain was used in most studies employ- ing bacteria. Where indicated, other clinical neis- serial isolates were utilized. Neisseria were grown to log phase in proteose peptone broth containing 0.82% glucose and washed twice in 0.01 M potassi- um phosphate buffer, pH 7.0, containing 0.1% bo- vine serum albumin prior to use.
Neutrophils. Human polymorphonuclear neutro- phils (PMN) were purified from venous blood by dextran sedimentation and hypotonic lysis of the contaminating erythrocytes. This method routinely yields leukocyte preparations that are 85-90% neu- trophils.
Assays of Complement Function. Total hemolyt- ic complement activity in serum was measured by the method of Mayer (11) and expressed as the reciprocal of the serum dilution sufficient to lyse 50% of the sensitized sheep erythrocytes (Z = 0.69) used in the assay. In some experiments, deficient serum was reconstituted with partially purified hu- man C8 (Cordis Laboratories, Inc., Miami, FL) prior to the determination of total hemolytic activi- ty. Assays of total hemolytic complement were performed in Veronal-buffered saline (t2).
The titer of functional C8 in serum was measured by a previously described method (12). Briefly, sheep erythrocytes sensitized through C7 (EAClgp4-7hu; Cordis Laboratories, Inc.) are incu- bated with serial twofold dilutions of the serum being tested in the presence of excess C9 (Cordis Laboratories, Inc.). Functional C8 activity is ex- pressed as the reciprocal of the serum dilution sufficient to provide one hemolytic site per celt (Z = 1.0). Hemolytic C8 assays were carried out in low- ionic strength (Ix = 0.065) dextrose-veronal-buff- ered saline (12).
The functional activity of other complement com- ponents in the patient's serum was determined by previously described methods (12). The concentra- tion of factor B in serum was determined by radial immunodiffusion.
HLA Typing and HLA-Linked Marker Studies. Family members were genotyped for HLA-A, -B, and -C locus antigens by the standard two-stage microcytotoxicity typing technique using a large battery of well-characterized antisera. HLA-DR typing was carried out using B- cells prepared by filtering peripheral blood lymphocytes through ny- lon-wool columns (13) in a modified two-stage mi- crocytotoxicity test with VIII International Work-
shop reagents. HLA-D typing was performed in a one-way system using 5 x 10 4 responding and 5 x 10 4 stimulating cells. The stimulating cells were irradiated with 2000 rads as previously described (14). Typing for the HLA-linked complement mark- ers, C2, C4, and BF, and the red-cell enzyme, GLO, was carried out by previously described methods (15-18).
Serum Bactericidal Assay. Either 2 x 106 or 2 x 10 7 meningococcal colony-forming units were inocu- lated, respectively, into 10 or 30% human serum in either Hanks balanced salt solution (GIBCO Labo- ratories, Grand Island, NY) or 0.01 M potassium phosphate buffer containing 0.1% bovine serum albumin in a final volume of 0.25 ml. The reaction mixtures were tumbled (12-15 rpm) at 37°C and survival of organisms was quantitated after 60 min by plating aliquots on gonococcal agar base (Difco Laboratories, Detroit, MI) containing 1% isovitalex supplement. Survival is expressed as a percentage of the inoculum at time zero.
Opsonophagocytic Assay. Human neutrophils (2 X 106) were added to 10% human serum in 0.01 M phosphate buffer containing 2 x 10 6 meningococcal colony-forming units in a total volume of 0.25 ml and the mixture was tumbled (12-15 rpm) at 37°C for 60 min. Survival, assessed by dilution plating on agar, was expressed as a percentage of the inocu- lure at time zero.
Assays for Meningococcal Antibody. Antibody titers to groups A, B, C, and Y meningococci were kindly determined by Dr. Carl E. Frasch (Bureau of Biologics, FDA, Bethesda, MD) using a previously described microbactericidal assay (19). In separate experiments, the titer of bactericidal antibody activ- ity for group Y meningococci in the patient's serum was compared to that in PHS. In these experiments, serial dilutions of heated serum (56°C, 30 rain) serving as the antibody source were mixed with 5% hypogammaglobulinemic human serum serving as a complement source. The hypogammaglobulinemic serum by itself was devoid of bactericidal activity for the group Y meningococcus at this concentra- tion. These serum mixtures were then employed in the low-inoculum bactericidal assay described pre- viously. These assays detect total bactericidal anti- body activity in serum but not antigen-specific activity. The amount of anticapsular antibody to group Y meningococci present in the patient's se- rum was kindly determined by Dr. J. MacLeod Griffiss (Channing Laboratory, Boston, MA) using a previously described technique (20) which mea-
Journal of Clinical Immunology, Vol. 3, No. 1, 1983

C8 DYSFUNCTION AND MENINGOCOCCAL DISEASE 93
Table I, Immunoglobulin Concentration in Patient Serum and Pooled Fractions of Sera o
Ig concentration (mg/dl)
Ig source IgG IgM IgA
PHS 1450 52 100 IgG pool 450 <5 <4.2 IgM pool <18 64 <4.2
C8D 620 190 50 IgG pool 1750 <5 <4.2 IgM pool <18 96 2.3
-Delipidated sera were fractionated by sequential molecular sieve and ion exchange chromatography. Appropriate fractions were pooled and concentrated and the immunoglobulin concen- tration was determined by radial immunodiffusion. Ig, immuno- globulin; PHS, pooled human serum; C8D, serum deficient in the eighth complement component.
sures the ability of the test serum to precipitate radioactively labeled group Y capsular polysaccha- ride of a known specific activity. The class of antibody responsible for bactericidal activity was assessed by purifying IgG and IgM from PHS and the patient's serum by a combination of molecular- sieve and ion-exchange chromatography as previ- ously described (21). The purity of these prepara- tions is shown in Table I. An amount of immuno- globulin equivalent to 30% of its concentration in PHS was added to 30% hypogammaglobulinemic serum in 0.01 M phosphate buffer containing 0.1% bovine serum albumin. This reconstituted hypo- gammaglobulinemic serum was then utilized in the high-inoculum bactericidal assay described above.
Neutrophil Function Studies. Previously de- scribed techniques were utilized to assess oxygen consumption (22) and chemotaxis (23) in response to a standard stimulus.
R E S U L T S
Studies o f the Patient's Complement System. The patient's serum lacked hemolytic activity in both the total hemolytic assay and the C3-C9 assay, which provides a measure of terminal component activity. Further studies (Table II) demonstrated that the patient lacked functional C8 activity.
Hemolytic activity in the patient's serum could be restored to normal by the addition of 1500 U of partially purified (Cordis) C8/ml of serum. In con- trast, in excess of 2000 U of (Cordis) C8/ml of serum was required to restore complement-dependent bactericidal activity in the patient's serum to a level comparable to that in PHS for his own infecting meningococcal isolate. The precise amount of Cor-
dis C8 required to restore serum bactericidal activi- ty completely could not be ascertained due to inhibition by other constituents contained in the relatively large amounts of the C8 preparation re- quired in the assay. The addition of 6666-8333 U of highly purified C8 (activity adjusted to that in the Cordis preparation by the ability to restore total hemolytic activity in C8-deficient serum to normal) restored bactericidal activity in the deficient serum to normal.
The possibility that the patient's serum might contain a functionally nonreactive but immuno- chemically reactive C8 molecule was examined using rabbit anti-human C8 (Fig. 1). The patient's serum reacted with the antibody to give a line of partial identity with C8 in normal serum. No immu- noreactive C8 was detected in the serum from a previously reported patient with C8 deficiency ex- amined concurrently using the same antiserum as well as three additional antisera with C8 specificity. These results suggested that the biochemical basis for these two deficiencies might be different. Conse- quently, equal volumes of the two C8-deficient sera were combined and the mixture was examined for bactericidal and hemolytic activity. The results of these studies (Table III) demonstrate that, although neither deficient serum alone possesses significant activity, the mixture of the two has potent bacteri- cidal and substantial hemolytic activity.
Studies of the Complement System and Genetic Markers in the Patient's Family. The results of investigations of the complement system, HLA genotype, and genetic markers for the sixth chro- mosome in the patient and his family are presented in Tables IV and V. In spite of the fact that the mother and father are obligate heterozygotes for C8
Table II. Complement Levels in C8-Deficient Serum-
U/ml
Component assay Patient Normal
Total hemolytic complement (CHso) 0 58-103 C3-C9 0 20-40 C3 69,000 50,000-100,000 C5 137,000 100,000-300,000 C6 18,000 20,000-70,000 C7 450,000 200,000-500,000 C8 0 1.9,000-71,000 C9 24,570 10,000-20,000
Factor B 17.4 mg/dl 13-22 mg/dt
~Functional complement assays were performed as described under Materials and Methods. Factor B was quantitated by radial immunodiffusion.
Journal of Clinical Immunology, Vol. 3, No. 1, 1983

94 DENSEN~ BROWN, O'NEILL, TEDESCO, CLARK, FRANK~ WEBB~ AND MYERS
Fig. 1. Examination of sera deficient in the eighth component of complement (CSD) for immunoreactive C8 by double diffusion in agarose. The central well contains rabbit antihuman C8. Peripheral wells 1 and 2 contain pooled normal human serum; wells 3 and 6, C8D~ (subject of the present report); and wells 4 and 5, C8Dz [subject of a previous report (33)].
deficiency, there is no clear correlation among the heterozygous state, functional C8 activity, and total hemolytic activity. The data in these two tables also indicate that the patient has an HLA-identical brother. Despite identity at the HLA loci and other loci on the sixth chromosome, the patient and his brother clearly differ with respect to C8 activity. These studies provide strong evidence for the lack of linkage of the C8 locus with HLA loci.
Table III. Reconstitution of Complement-Dependent Serum Bactericidal and Hemolytic Activity in Two C8-Deficient Sera.
CHso Condition % survival ~ (U/ml) c
30% PHS <0.04 68.5 15% PHS 5.2 - - 15% C8D1 >161 0 15% C8D2 84.5 0 15% C8D1 +
15% C8D~ 2.0 75
aResults represent the means of two separate experiments per- formed in duplicate. PHS, pooled human serum; C8D, serum deficient in the eighth component of complement; C8D~, subject of the present report; CSD~, subject of a previous report (33).
bLog-phase group Y meningococci (2 × 107 colony-forming units) isolated from patient C8D~ were incubated for 1 hr under the stated conditions. Survival is expressed as a percentage of the initial inoculum.
"Total hemolytic complement.
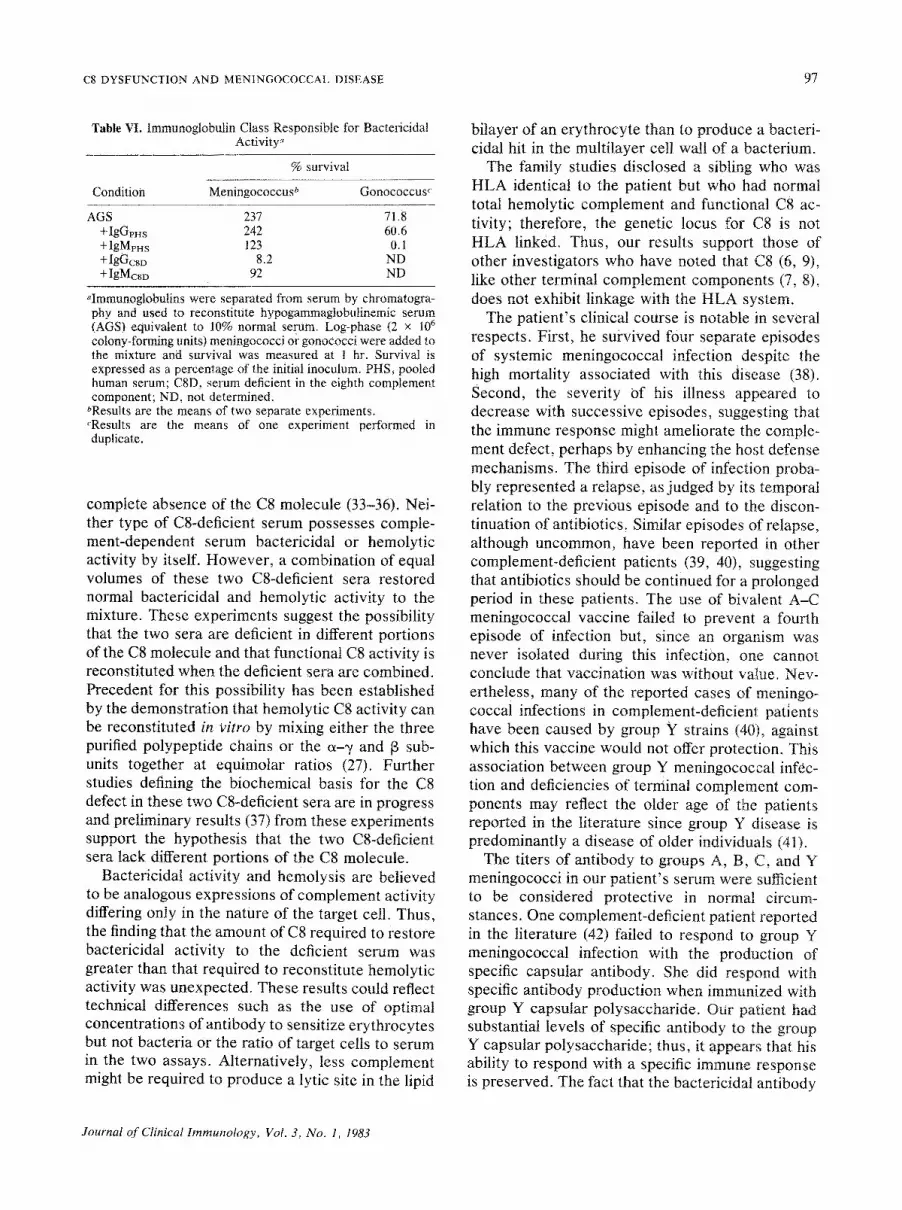
Studies of Antimeningococcal Antibody. There was no serum available from the patient at an early stage of his illness, so all studies of antimeningococ- cal antibody were performed using serum obtained from the patient after his recovery. This convales- cent serum had serogroup-specific antibody at titers of >--1/512 for group A, 1/128 for group B, 1/256 for group C, and 1/64 ~br group Y meningococci. The serum had a capacity to bind 58 ng of group Y capsular polysaccharide/25 txl. Bactericidal anti- body specific for the infecting meningococcal iso- late was measured in PHS and in the patient's serum (Fig. 2). There was 2-2.5 times as much bactericidal antibody in the patient's serum as in PHS. The immunoglobulin class responsible for bactericidal activity was examined by reconstitut- ing hypogammaglobulinemic serum with IgG or IgM purified from the two sera (Table VI). The results of these studies clearly demonstrate that IgG is primarily responsible for the killing of the group Y meningococcus in C8-deficient serum, but they fail to identify the class of immunoglobulin respon- sible for bactericidal activity in normal serum. From these data, we cannot exclude the presence of some activity in the IgM pools since bacterial growth in IgM-supplemented hypogammaglobuline- mic serum was inhibited relative to that in hypo-
Journal of Clinical Immunology, Vol. 3, No. 1, 1983

C8 DYSFUNCTION AND MENINGOCOCCAL DISEASE 95
Table IV. Totat Hemolytic Complement, Functional C8, HLA Typing, and Genetic Markers
CHso C8 (19,000- (58-103) ~ 7t ,000) ~ HLA genotype Bf Glo C4 C2 Chido Rodger
Patient b 0 0 A2; Bt5, (w6); Cw4; D R - SS 1-1 FS C + +
Aw33: B14, (w6); tA4+7
Father 58 41,500 A2; B15 (w6); Cw4; D R - SS 2-I FS C + +
A28; Bw35, (w6); Cw4; DRw4
Mother 56 21,250 A2; Bw39(16), (w6); DRw4 SS 2-1 FS C + +
Aw33; B14, (w6); IA4+7
Brother 47 24,000 A2; BI5, (w6); Cw4: D R - SS 2-1 FS C + +
A2; Bw39(16), (w6); DRw4
Brother b 54 71,000 A2; BI5, (w6); Cw4; D R - SS 1-1 FS C + +
AW33; B14, (w6); IA4+7
Brother 47 43,500 A28; Bw35, (w6); Cw4; DRw4 SS 2-2 FS C + +
A2; Bw39(16), (w6); DRw4
aNormal range in parentheses. bHLA identical.
gammaglobulinemic serum alone. A possible expla- nation for this result is that the bactericidal locus on group Y meningococcal lipopolysaccharide, to which antibody in normal serum is commonly di- rected, is antigenicaily cross-reactive with the agar- ose beads used for the chromatographic separation of immunoglobulins from serum (24). In this cir- cumstance, the chromatographic gel functions as an affinity column to remove cross-reactive (bacteri- cidal) antibody. That the antibody is not functional- ly altered during the separation procedure is dem- onstrated by the finding that purified IgM can kill a serum-sensitive gonococcus as previously reported (25) and that IgG purified from C8-deficient serum can kill the infecting meningococcal strain.
Opsonophagocytic Studies. As a consequence of the functional absence of C8 in the patient's serum,
opsonophagocytic bactericidal activity can be dis- tinguished from complement-dependent serum bac- tericidal activity. The patient's serum readily sup- ported opsonization and killing of the infecting strain of meningococcus by neutrophils (1.7 -+ 0.5% survival in C8-deficient serum plus neutrophils vs 154 -+ 42% survival in C8-deficient serum alone). Analogous studies employing PHS as the source of meningococcal opsonins proved impossible due to an inability to distinguish phagocytic killing from serum bactericidal activity even when tested over a range of serum concentrations.
Neutrophil Function Studies. Neutrophils isolat- ed from the C8-deficient patient demonstrated nor- mal oxygen consumption upon stimulation by phor- bol myristate acetate (17.0 -+ 3.0 ~I O2/106 PMN/hr vs the normal 17.3 -+ 2.2 txl O2/106 PMN/hr). The
Table V. Mixed Lymphocyte Culture (Thymidine Incorporation; cpm)
Stimulating cells
Responder Normal Pool Pool cells Patient Father Mother Brother Brother control I a 2"
Patient b 584 10,858 11,022 470 8,796 15,248 19,696 36,018 Father 17,489 764 27,988 9,224 17,948 30,340 31,472 37,600 Mother 21,546 29,862 3,866 17,002 28,496 35,088 41,902 38,030 Brother b 490 12,530 I6,550 640 8,764 22,104 20,552 27,676 Brother 21,024 19,482 22,822 15,188 1,676 27,528 30,864 35,262 Normal
control 36,856 32,264 43,262 27,902 28,106 524 43,928 42,850
"Pool 1 and Pool 2 are pools of lymphocytes from a large number of normal donors. bHLA identical.
Journal o f Clinical Immunology, Vol. 3, No. 1, 1983

96 DENSEN, BROWN, O'NEILL, TEDESCO, CLARK, FRANK, WEBB, AND MYERS
,2c y 100 t /
/
PHS 0 C8D
I 0 I 1 i I I ~ [ I i ~ I i ~ I l I I 2 40 100 200 400 1000
SERUM CONCENTRATION (reciprocal dilution)
Fig. 2. Bactericidal antibody for group Y meningococci in C8-deficient serum (CSD) and pooled normal human serum (PHS). Log-phase meningococci (2 × 106 colony-forming units) were incubated in a mixture of 5% hypogammaglobulinemic serum and serial dilutions of the test serum. Survival is expressed as a percentage of the initial inoculum. Results are the means -+ SE for three separate experiments performed in duplicate.
80 %
SURVIVAL 60
chemotactic response of the patient's neutrophils to zymosan-activated normal serum (1926 -+ 105 cpm) was normal or increased compared with that of neutrophils from a normal donor. There was no evidence of a chemotactic inhibitor in the C8- deficient serum.
DISCUSSION
The association between recurrent systemic in- fection caused by Neisseria gonorrhoeae or Neis- seria meningitidis and an inherited deficiency of one of the terminal complement components C5-C8 has recently received emphasis in the literature (3). This patient's clinical history prompted us to evalu- ate the possibility of, and ultimately to document, a deficiency of C8 as an explanation for his recurrent episodes of meningococcal infection. Of particular interest was the observation that despite the com- plete absence of functional C8 activity, his serum contained immunoreactive C8. This material pro-
duced a line of partial identity with normal C8 in an Ouchterlony gel and presumably reflects the pres- ence of a dysfunctional C8 molecule. The C8 mole- cule is unusual among complement proteins in that it is composed of three polypeptide chains (26, 27), two of which (a and ~/) are convalently linked and noncovalently associated with the third ([3) chain (27). The t3 chain mediates binding of the C8 mole- cute to the C5-C7 complex (28, 29). Deficiency of C8 due to a dysfunctional molecule has been report- ed (30-32), and the nature of this defect has been delineated recently by Tschopp and associates, who established that three such individuals lacked the C8 13 subunit (32).
Our data, in conjunction with the reported litera- ture (30-36), suggest that there are at least two different types of C8 deficiency, one in which there is a dysfunctional C8 molecule detected antigenical- ly and one in which no immunoreactive material can be detected by conventional means. The latter type of C8 deficiency has been reported to represent the
Journal of Clinical Immunology, Vol. 3, No. 1, 1983
C8 DYSFUNCTION AND MENINGOCOCCAL DISEASE 97
Table VI. Immunoglobulin Class Responsible for Bactericidal Activity -
%survival
Condition Meningococcus ~ Gonococcus ~
AGS 237 71.8 +IgGpHs 242 60.6 + IgMFHs 123 0.1 +IgGcso 8.2 ND + IgMcsD 92 ND
~qmmunogtobulins were separated from serum by chromatogra- phy and used to reconstitute hypogammagtobulinemic serum (AGS) equivalent to 10% normal serum. Log-phase (2 x 10 6 colony-forming units) meningococci or gonococci were added to the mixture and survival was measured at t hr. Survival is expressed as a percentage of the initial inoculum. PHS, pooled human serum; C8D, serum deficient in the eighth complement component; ND, not determined.
~Results are the means of two separate experiments. cResults are the means of one experiment performed in duplicate.
complete absence of the C8 molecule (33-36). Nei- ther type of C8-deficient serum possesses comple- ment-dependent serum bactericidal or hemolytic activity by itself. However, a combination of equal volumes of these two C8-deficient sera restored normal bactericidal and hemolytic activity to the mixture. These experiments suggest the possibility that the two sera are deficient in different portions of the C8 molecule and that functional C8 activity is reconstituted when the deficient sera are combined. Precedent for this possibility has been established by the demonstration that hemolytic C8 activity can be reconstituted in vitro by mixing either the three purified polypeptide chains or the ~-~ and [3 sub- units together at equimolar ratios (27). Further studies defining the biochemical basis for the C8 defect in these two C8-deficient sera are in progress and preliminary results (37) from these experiments support the hypothesis that the two C8-deficient sera lack different portions of the C8 molecule.
Bactericidal activity and hemolysis are believed to be analogous expressions of complement activity differing only in the nature of the target cell. Thus, the finding that the amount of C8 required to restore bactericidal activity to the deficient serum was greater than that required to reconstitute hemolytic activity was unexpected. These results could reflect technical differences Such as the use of optimal concentrations of antibody to sensitize erythrocytes but not bacteria or the ratio of target cells to serum in the two assays. Alternatively, less complement might be required to produce a lytic site in the lipid
bilayer of an erythrocyte than to produce a bacteri- cidal hit in the multilayer cell wail of a bacterium.
The family studies disclosed a sibling who was HLA identical to the patient but who had normal total hemolytic complement and functional C8 ac- tivity; therefore, the genetic locus for C8 is not HLA linked. Thus, our results support those of other investigators who have noted that C8 (6, 9), like other terminal complement components (7, 8), does not exhibit linkage with the HLA system.
The patient's clinical course is notable in several respects. First, he survived four separate episodes of systemic meningococcal infection despite the high mortality associated with this disease (38). Second, the severity of his illness appeared to decrease with successive episodes, suggesting that the immune response might ameliorate the comple- ment defect, perhaps by enhancing the host defense mechanisms. The third episode of infection proba- bly represented a relapse, as judged by its temporal relation to the previous episode and to the discon- tinuation of antibiotics. Similar episodes of relapse, although uncommon, have been reported in other complement-deficient patients (39, 40), suggesting that antibiotics should be continued for a prolonged period in these patients. The use of bivalent A-C meningococcal vaccine failed to prevent a fourth episode of infection but, since an organism was never isolated during this infection, one cannot conclude that vaccination was without value. Nev- ertheless, many of the reported cases of meningo- coccal infections in complement-deficient patients have been caused by group Y strains (40), against which this vaccine would not offer protection. This association between group Y meningococcal infec- tion and deficiencies of terminal complement com- ponents may reflect the older age of the patients reported in the literature since group Y disease is predominantly a disease of older individuals (41).
The titers of antibody to groups A, B, C, and Y meningococci in our patient's serum were sufficient to be considered protective in normal circum- stances. One complement-deficient patient reported in the literature (42) failed to respond to group Y meningococcal infection with the production of specific capsular antibody. She did respond with specific antibody production when immunized with group Y capsular polysaccharide. Our patient had substantial levels of specific antibody to the group Y capsular polysaccharide; thus, it appears that his ability to respond with a specific immune response is preserved. The fact that the bactericidal antibody
Journal o f Clinical Immunology, Vol. 3, No. 1, 1983

98 DENSEN, BROWN, O'NEILL, TEDESCO, CLARK~ FRANK, WEBB, AND MYERS
present in his serum was of the IgG class, whereas the bactericidal antibody in the pool of normal serum was probably IgM, likely reflects the low prevalence of specific antibody to group Y menin- gococci in the population.
ACKNOWLEDGMENTS
We are i ndeb t ed to Dr. G. F. Brooks , San F r a n -
cisco, for his g e n e r o u s gift o f the s econd C8-
deficient serum. This work was suppor t ed in par t by
Gran t AI16476 f rom the Na t iona l Ins t i tu tes of
Heal th .
REFERENCES
1. Ruddy S, Gigli I, Austen KF: The complement system of man (4 parts). N Engl J Med 287:489-495,545-549,592-596, 642-646, 1972
2. Agnello V: Complement deficiency states. Medicine 57:1- 23, 1978
3. Petersen BH, Lee TJ, Snyderman R, Brooks GF: Neisseria meningitidis and Neisseria gonorrhoeae bacteremia associ- ated with C6, C7 or C8 deficiency. Ann Intern Med 90:917- 920, 1979
4. Zeitz HJ, Miller GW, Lint TF, Ali MA, Gewurz H: Deficien- cy of C7 with systemic lupus erythematosus. Solubilization of immune complexes in complement-deficient sera. Arth Rheum 24:87-93, t981
5. Merritt AD, Petersen BH, Biegel AA, Myers DA, Brooks GF, Hodes ME: Chromosome 6: Linkage Of the eighth component of complement (C8) to the histocompatibility region (HLA). Cytogenet Cell Genet 16:331-334, 1976
6. Giraldo G, Degos L, Beth E, Sasportes M, Marcelli A, Gharbi R, Day NK: C8 deficiency in a family with xero- derma pigrrientosum. Lack of linkage to the HLA region. Clin Immunol Immunopathol 8:377-384, 1977
7. Nemerow GR, Gewurz H, Osofsky SG, Lint TF: Inherited deficiency of the seventh component of complement associ- ated with nephritis. Propensity to formation of C56 and related C7-consuming activity. J Clin Invest 61:1602-1610, 1978
8. Kagan E, Maier GMG, Nurse GT, Miller K, Rabson AR: Further evidence for independent segregation of the HLA system and a structural gene for the sixth component of complement (C6). Tissue Antigens 14:15-21, 1979
9. Raum D, Spence MA, Balavitch D, Tideman S, Merritt AD, Taggart RT, Petersen BH, Day NK, Alper CA: Genetic control of the eighth component of complement..J Ctin Invest 64:858-865, 1979
10. Myers JW, Hasbrouck WH, Corteza B: Disseminated intra- vascular coagulation: Priorities in therapy. J Med Soc NJ 73:325-326, 1976
11. Mayer MM: Complement and complement fixation. In Ex- perimental Immunochemistry, 2nd ed, EA Kabat, MM
Mayer (eds). Springfield, IL, Charles C Thomas, 1961, p 133 12. Gaither TA, Frank MMi Complement. In Clinical Diagnosis
and Management by Laboratory Methods, JB Henry (edL Philadelphia, 16th ed, 1979, pp 1245-1261
13. Lowry R, Goguen J, Carpenter CB, Strom TB, Garovoz MR: Improved B cell typing for HLA-DR using nylon wool column enriched B lymphocyte preparation. Tissue Antigens 14:325-330, 1979
14. Dupont B, Hansen JA, Yunis EJ: Human mixed lymphocyte reaction: Genetics, specificity and biological implications. Adv Immunol 23:107-202, 1976
15. Alper CA: Inherited structural polymorphism in human C2: Evidence for genetic linkage between C2 and Bf. J Exp Med 144:1111-1115, 1976
16. O'Neill GJ, Yang SY, Dupont B: Two HLA-linked loci controlling the fourth component of human complement. Proc Natl Acad Sci USA 75:5165-5169, 1978
17. Alper CA, Boenisch T, Watson L: Genetic polymorphism in human glycine-rich beta-glycoprotein. J Exp Med 135:68- 80, 1972
18. K6mpf J, Bisskort S, Ritter H: Red cell glyoxalase 1 (EC 4.4.1.5): Formal genetics and linkage relations. Humangene- tik 28:249-251, 1975
19. Frasch CE, Chapman SS: Classification of Neisseria menin- gitidis group B into distinct serotypes. I. Serological typing by a microbactericidal method. Infect Immun 5:98-102, 1972
20. Brandt BL, Artenstein MS, Smith CD: Antibody responses to meningococcal polysaccharide vaccines. Infect Immun 8:590-596, 1973
21. Rice PA, Kasper DL: Characterization of gonococcal anti- gens responsible for induction of bactericidal antibody in disseminated infection. J Ctin Invest 60:1149-1158, 1977
22. Densen P, Mandell GL: Gonococcal interactions with poly- morphonuclear neutrophils. Importance of the phagosome for bactericidal activity. J Clin Invest 62:1161-1171, t978
23. Gallin JI, Clark RA, Kimball HR: Granulocyte chemotaxis: An improved in vitro assay employing 51Cr-labeled granulo- cytes. J Immunol 110:233-240, 1973
24. Griffiss JM, Goroff DK: Immunological cross-reaction be- tween a naturally occurring galactan, agarose, and an LPS locus for immune lysis of Neisseria meningitidis by human sera. Clin Exp Immunol 43:20-27, 1981
25. Schoolnik GK, Ochs HD, Buchanan TM: Immunoglobulin class responsible for gonococcal bactericidal activity of normal human sera, J Immunol 122:1771-1779, 1979
26. Kolb WP, Miiller-Eberhard H J: The membrane attack mech- anism of complement: The three polypeptide chain structure of the eighth component (C8). J Exp Med 143:1131-1139, 1976
27. Steckel EW, York RG, Monahan JB, Sodetz JM: The eighth component of human complement. Purification and physico- chemical characterization of its unusual subunit structure. J Biol Chem 255:11,997-12,005, 1980
28. Monahan JB, Sodetz JM: Binding of the eighth comporient of human complement to the soluble cytolytic complex is mediated by its t3 subunit, J Biol Chem 255:10,579-10,582, 1980
29. Monahan JB, Sodetz JM: Role of the 13 subunit in interaction of the eighth component of human complement with the membrane-bound cytolytic complex. J Biol Chem 256:3258- 3262, 1981
30. Matthews N, Stark JM, Harper PS, Doran J, Jones DM:
Journal of Clinical Immunology, Vol. 3, No. I, 1983

c8 DYSFUNCTION AND MENINGOCOCCAL DISEASE 99
Recurrent meningococcal infections associated with a func- tional deficiency of the C8 component of human comple- ment. Clin Exp Immunol 39:53-59, 1980
3l. Tedesco F, Bardare M, Giovanetti AM, Sirchia G: A familial dysfunction of the eighth component of complement (C8). Clin Immunol Immunopathol 16:180-191, 1980
32. Tschopp J, Esser AF, Spira TJ, Mfiller-Eberhard HJ: Occur- rence of an incomplete C8 molecule in homozygous C8 deficiency in man. J Exp Med 154:1599-1607, 1981
33. Petersen BH, Graham JA, Brooks GF: Human deficiency of the eighth component of complement. The requirement of C8 for serum Neisseria gonorrhoeae bactericidal activity. J Clin Invest 57:283-290, 1976
34. Jasin HE: Absence of the eighth component of complement in association with systemic lupus erythematosus-like dis- ease. J Clin Invest 60:709-715, 1978
35. Giraldo G, Degos L, Beth E, Sasportes M, Marcelli A, Gharbi R, Day NK: C8 deficiency in a family with Xero- derma pigmentosum. Clin Immunol Immunopathol 8:377- 384, 1977
36. Agnello V, Pariser KM, Babott D: Association of C8 defi- ciency with sickle-thalassemia hemoglobinopathy. J Immu-
nol 120:1761 (abstr), 1978 37. Tedesco F, Densen P, Sirchia G: Reconstitution of C8
hemolytic activity from the mixture of sera from two groups of C8 deficient subjects. Program and Abstracts, IXth Inter- national Complement Workshop, Miami, Florida, 1981
38. Bacterial meningitis and meningococcemia--United States, 1978. Morbid Mortal Week Rep 28:277-279, 1979
39. Lira D, Gewurz A, Lint TF, Ghaze M, Sepheri B, Gewurz H: Absence of the sixth component of complement in a patient with repeated episodes of meningococcal meningitis. J Pediatr 89:42-47, 1976
40. Peter G, Weigert MB, Bissel AR, Gold R, Kreutzer D, McLean RH: Meningococcal meningitis in familial deficien- cy of the fifth component of complement. Pediatrics 67:882- 886, 1981
41. The Meningococcal Disease Surveillance Groups: Analysis of endemic meningococcal disease by serogroup and evalua- tion of chemoprophylaxis. J Infect Dis 134:201-204, 1976
42. Vogler LB, Newman SL, Stroud RM, Johnston RB Jr: Recurrent meningococcat meningitis with absence of the sixth component of complement: An evaluation of underly- ing immunologic mechanisms. Pediatrics 64:465-467, 1979
Journal of Clinical Immunology, Vol. 3, No. 1, 1983





























