Embed Size (px)
Citation preview
FUNDAMENTAL AND APPLIED TOXICOLOGY 24, 13-21 (1995)
SYMPOSIUM OVERVIEW
Immunotoxicity—Bridging the Gap between Animal Research andHuman Health Effects1
MARYJANE K. SELGRADE,* KEVIN D. COOPER,! ROBERT B. DEVLIN,* HENK VAN LOVEREN,^:RAYMOND E. BIAGINI,§ AND MICHAEL I. LUSTER||
'Health Effects Research Laboratory, U.S Environmental Protection Agency, Research Triangle Park, North Carolina 27711; ̂ Department ofDermatology, University of Michigan, Ann Arbor, Michigan; \Laboratory of Pathology, National Institute of Public Health and Environmental
Protection, Bilthoven, The Netherlands; ^National Institute of Occupational Health and Safety, Cincinnati, Ohio; and ^Environmental Immunologyand Neurobiology Section, National Institute of Environmental Health Sciences, Research Triangle Park, North Carolina 27709
R e c e i v e d July 5 , 1 9 9 4 ; a c c e p t e d July 11 , 1994
Symposium Overview: Immunotoxicity—Bridging the Gapbetween Animal Research and Human Health Effects. SEL-GRADE, M.-J. K., COOPER, K. D., DEVLIN, R. B., VAN LO-VEREN, H., BIAGINI, R. E., AND LUSTER, M. I. (1995). Fundam.Appl. ToxiCOl. 24, 1 3 - 2 1 . O 1995 Society of Toiicology.
Introduction (M. J. K. Selgrade)
As with other toxicities, uncertainties exist which mayaffect the interpretation of immunotoxicity data in humanhealth risk assessments. The two most problematic issues,extrapolating effects across levels of biologic organizationand extrapolating from animal data to human health ef-fects, are common to most noncancer endpoints. The firstissue involves uncertainties associated with establishing aquantitative relationship between changes in individual im-mune function tests and altered resistance to infectious andneoplastic disease. The second issue involves uncertaintiesassociated with assessing risk to human health based onlaboratory animal studies. The purpose of this symposiumwas to present studies which may help clarify these uncer-tainties.
Toxicant-induced alterations that contribute to the etiol-ogy or functional consequences of a disease may be asso-ciated with any level of biological organization from thepopulation to the molecular level (Table 1). Risk assess-ment attempts to determine the consequences of toxicantexposure at the human population level. Toxicity testing
' The research paper has been reviewed by the HeaJth Effects ResearchLaboratory, U.S. Environmental Protection Agency and approved forpublication. Approval does not signify that the contents necessarily reflectsthe views and policies of the agency, nor does mention of trade names orcommercial products constitute endorsement or recommendation for use.
including immunotoxicity frequently includes cellular ormolecular assays in laboratory rodents. Uncertainties existbecause alterations at each successive biological level mayresult from the interactions of several alterations at a lowerlevel. Furthermore, the fact that these lower-level assays areusually more sensitive raises the concern that statisticallysignificant changes may not be biologically significant. In1991 Luster presented data at an SOT symposium, whichhas subsequently been published (Luster eJ ai, 1992, 1993),that addressed the issue of level of organization. These stud-ies used mathematical analyses to determine which individ-ual immune function tests were most predictive of effectson any of a number of immune function tests, and to estab-lish a relationship between immunosuppression and suscep-tibility to infectious or neoplastic disease using host resis-tance models. As a follow-up, this symposium focused onextrapolation from animal data to human health risk, al-though issues related to extrapolating across levels of organi-zation were also discussed in some presentations.
There is a need to extrapolate from animal data to hu-man health effects not only because most of the data comefrom animal studies, but also because animal studies relievesome of the uncertainties associated with human epidemio-logic studies (reviewed below by Biagini). Fortunately, theimmune system is highly conserved across species such thatthe organs and cells of the immune system in humans,mice, and rats are similar. Hence, if toxicokinetic propertiesare similar, it is reasonable to test for potentially adverseeffects on the human immune system using laboratory ro-dents. Also, in instances where controlled human studieshave been possible, results of immune function studies inmice have been accurate predictors of effects in humans. Asexamples, human clinical studies with ultraviolet radiationand with ozone were presented by Cooper and Devlin, re-spectively, and are described below. Immunosuppressive
13 0272-0590/95 $6.00Copyright C 1995 by the Society of Toxicology.All rights of reproduction in any form reserved.
14 SELGRADE ET AL.
TABLE 1Levels of Organization
Population Incidence of infectious, neoplastic, allergic, orautoimmune disease
Organism Enhanced susceptibility to infection (e.g., increasednumbers of microbes in target organs ordissemination to other organs; delayed clearance)
Organ/tissue Hematology or histopathology of lymphoid organsCellular Immune function, lymphocyte subpopulationsSubcellular Cytokine mRNA; receptors, etc.
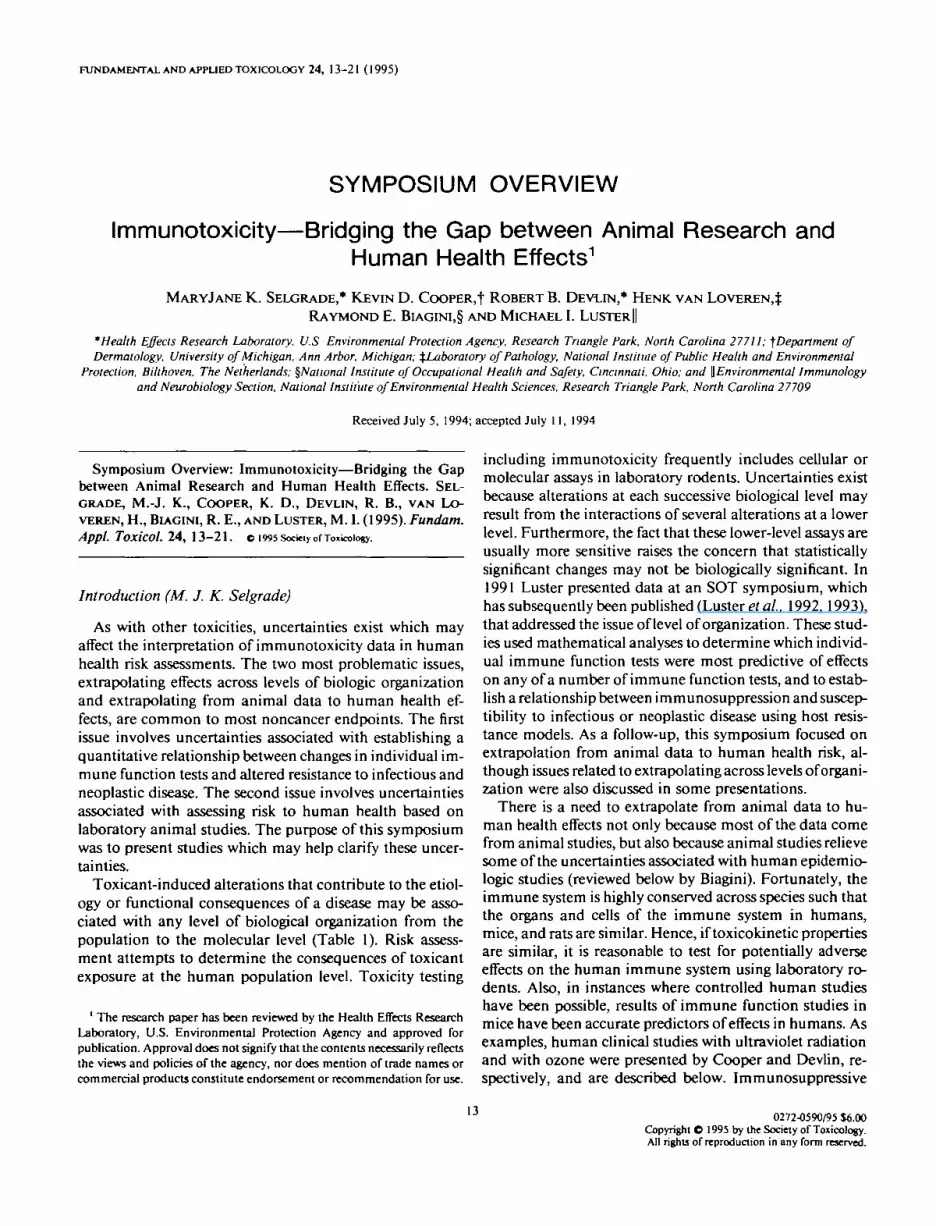
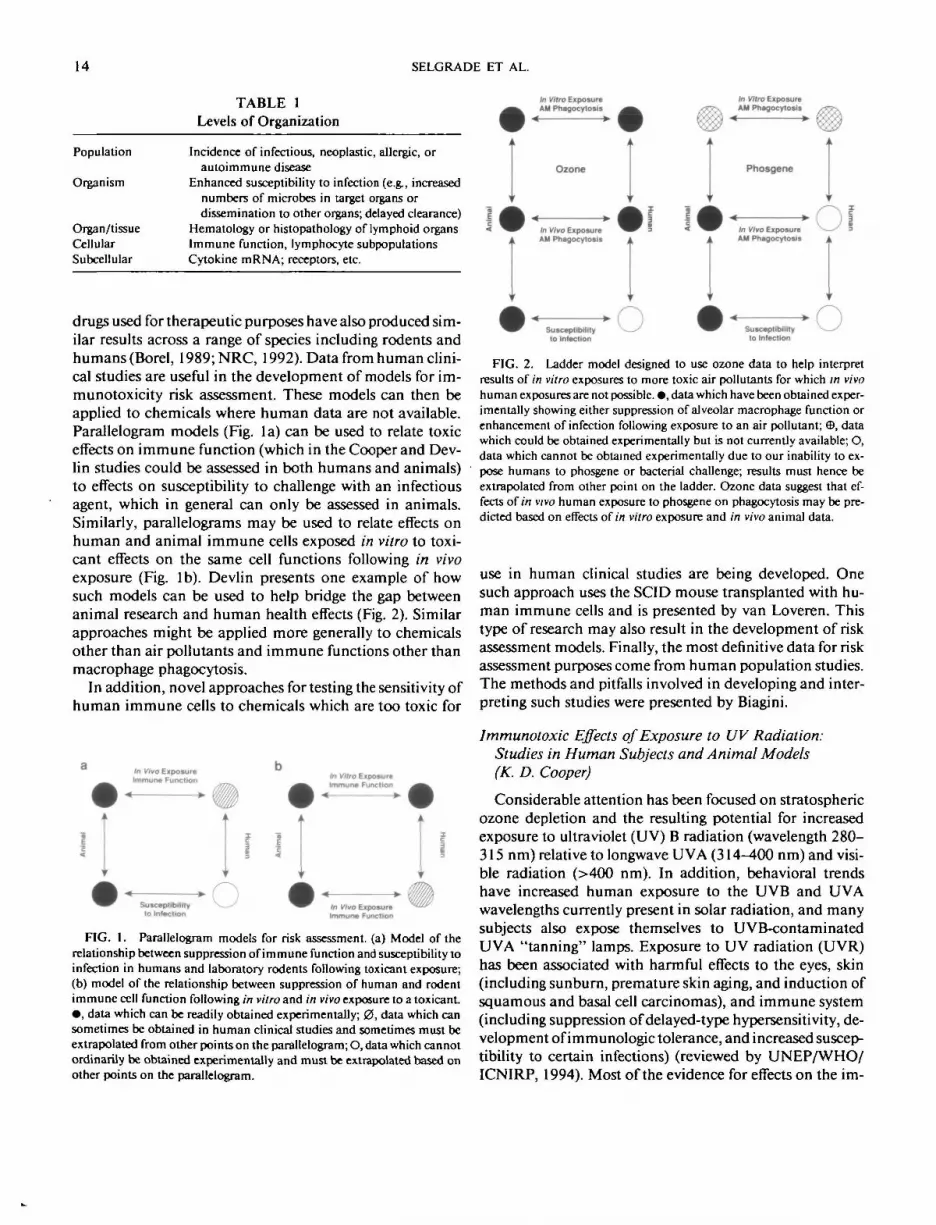
drugs used for therapeutic purposes have also produced sim-ilar results across a range of species including rodents andhumans (Borel, 1989; NRC, 1992). Data from human clini-cal studies are useful in the development of models for im-munotoxicity risk assessment. These models can then beapplied to chemicals where human data are not available.Parallelogram models (Fig. 1 a) can be used to relate toxiceffects on immune function (which in the Cooper and Dev-lin studies could be assessed in both humans and animals)to effects on susceptibility to challenge with an infectiousagent, which in general can only be assessed in animals.Similarly, parallelograms may be used to relate effects onhuman and animal immune cells exposed in vitro to toxi-cant effects on the same cell functions following in vivoexposure (Fig. lb). Devlin presents one example of howsuch models can be used to help bridge the gap betweenanimal research and human health effects (Fig. 2). Similarapproaches might be applied more generally to chemicalsother than air pollutants and immune functions other thanmacrophage phagocytosis.
In addition, novel approaches for testing the sensitivity ofhuman immune cells to chemicals which are too toxic for
In Vivo ExposureImmure Function In Vitro Exposure
Immune Function
Susceptibilityto Infection
In Vivo ExposureImmune Function
FIG. 1. Parallelogram models for risk assessment (a) Model of therelationship between suppression of immune function and susceptibility toinfection in humans and laboratory rodents following toxicant exposure;(b) model of the relationship between suppression of human and rodentimmune cell function following in vitro and in vivo exposure to a toxicant• , data which can be readily obtained experimentally; 0 , data which cansometimes be obtained in human clinical studies and sometimes must beextrapolated from other points on the parallelogram; O, data which cannotordinarily be obtained experimentally and must be extrapolated based onother points on the parallelogram.
In Vitro ExposureAM Phagocytosis
< »•
Ozone
In Vivo ExposureAH Phagocytosis
Susceptibility O
in Vitro ExposureAM Phagocytosis
Phosgene
In Vivo ExposureAH Phagocytosis
Susceptibilityto Infection
FIG. 2. Ladder model designed to use ozone data to help interpretresults of in vitro exposures to more toxic air pollutants for which in vivohuman exposures are not possible. • , data which have been obtained exper-imentally showing either suppression of alveolar macrophage function orenhancement of infection following exposure to an air pollutant; ffi, datawhich could be obtained experimentally but is not currently available; O,data which cannot be obtained experimentally due to our inability to ex-pose humans to phosgene or bacterial challenge; results must hence beextrapolated from other point on the ladder. Ozone data suggest that ef-fects of in vivo human exposure to phosgene on phagocytosis may be pre-dicted based on effects of in vitro exposure and in vivo animal data.
use in human clinical studies are being developed. Onesuch approach uses the SCID mouse transplanted with hu-man immune cells and is presented by van Loveren. Thistype of research may also result in the development of riskassessment models. Finally, the most definitive data for riskassessment purposes come from human population studies.The methods and pitfalls involved in developing and inter-preting such studies were presented by Biagini.
Immunoloxic Effects of Exposure to UV Radiation:Studies in Human Subjects and Animal Models(K. D. Cooper)
Considerable attention has been focused on stratosphericozone depletion and the resulting potential for increasedexposure to ultraviolet (UV) B radiation (wavelength 280-315 nm) relative to longwave UVA (314-400 nm) and visi-ble radiation (>400 nm). In addition, behavioral trendshave increased human exposure to the UVB and UVAwavelengths currently present in solar radiation, and manysubjects also expose themselves to UVB-contaminatedUVA "tanning" lamps. Exposure to UV radiation (UVR)has been associated with harmful effects to the eyes, skin(including sunburn, premature skin aging, and induction ofsquamous and basal cell carcinomas), and immune system(including suppression of delayed-type hypersensitivity, de-velopment of immunologic tolerance, and increased suscep-tibility to certain infections) (reviewed by UNEP/WHO/ICNIRP, 1994). Most of the evidence for effects on the im-
IMMUNOTOXICITY RISK ASSESSMENT 15
mune system and all of the evidence for effects on in-fectious disease have come from animal studies. Althoughestimates of incremental changes in cataract incidence andcancer incidence have been formulated, as yet, it has notbeen possible to estimate the impact that increased UVBexposure has on infectious disease and vaccine effective-ness. The first step in this process is to gain a quantitative(dose response) assessment of UVR effects on human im-mune reactivity. Toward this end we performed experi-ments in humans to determine: (a) whether immunosup-pression occurs as it does in mice after UV radiation, (b) ifso, the dose-response relationship, and (c) the role pigmen-tation may have in modulating such effects.
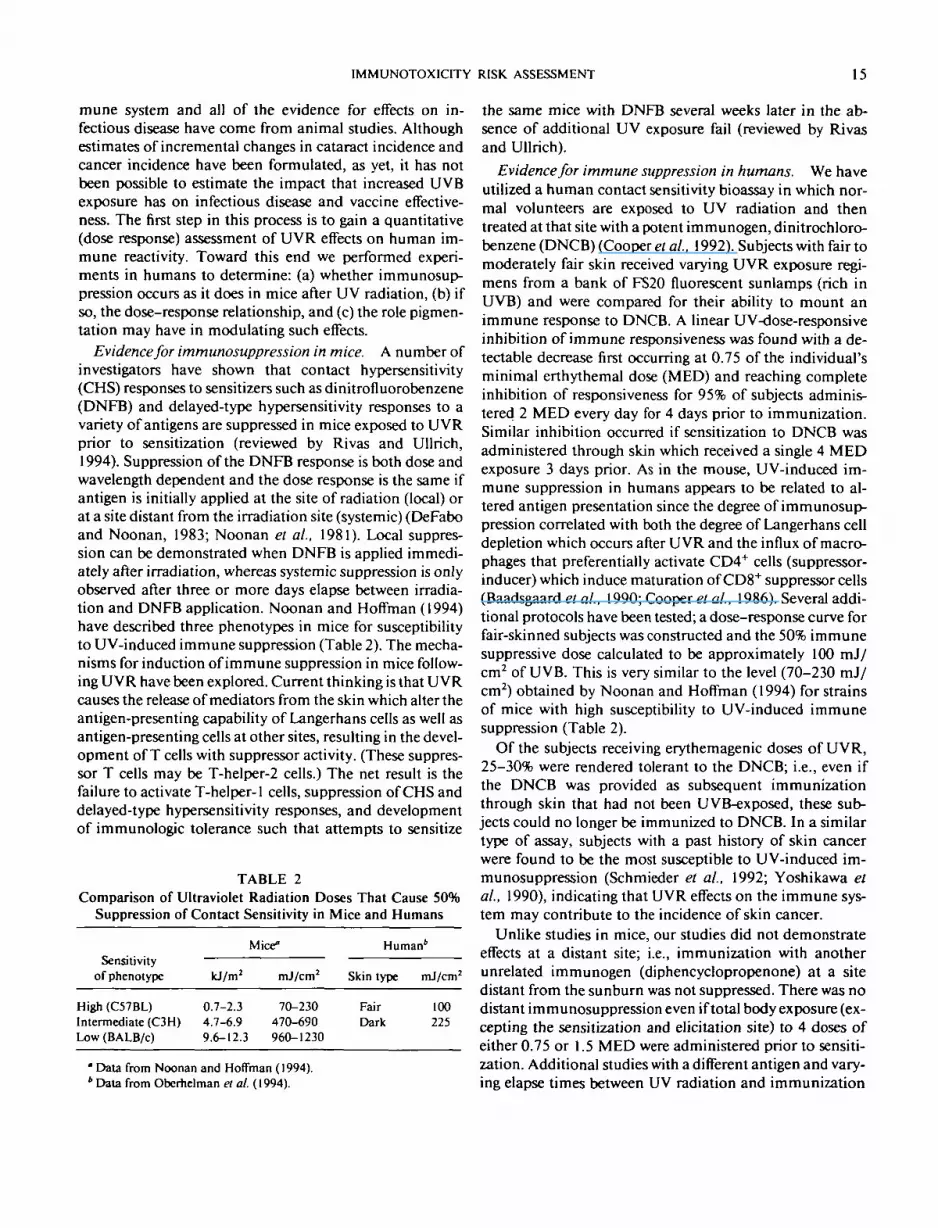
Evidence for immunosuppression in mice. A number ofinvestigators have shown that contact hypersensitivity(CHS) responses to sensitizers such as dinitrofluorobenzene(DNFB) and delayed-type hypersensitivity responses to avariety of antigens are suppressed in mice exposed to UVRprior to sensitization (reviewed by Rivas and Ullrich,1994). Suppression of the DNFB response is both dose andwavelength dependent and the dose response is the same ifantigen is initially applied at the site of radiation (local) orat a site distant from the irradiation site (systemic) (DeFaboand Noonan, 1983; Noonan et ai, 1981). Local suppres-sion can be demonstrated when DNFB is applied immedi-ately after irradiation, whereas systemic suppression is onlyobserved after three or more days elapse between irradia-tion and DNFB application. Noonan and Hoffman (1994)have described three phenotypes in mice for susceptibilityto UV-induced immune suppression (Table 2). The mecha-nisms for induction of immune suppression in mice follow-ing UVR have been explored. Current thinking is that UVRcauses the release of mediators from the skin which alter theantigen-presenting capability of Langerhans cells as well asantigen-presenting cells at other sites, resulting in the devel-opment of T cells with suppressor activity. (These suppres-sor T cells may be T-helper-2 cells.) The net result is thefailure to activate T-helper-1 cells, suppression of CHS anddelayed-type hypersensitivity responses, and developmentof immunologic tolerance such that attempts to sensitize
TABLE 2Comparison of Ultraviolet Radiation Doses That Cause 50%
Suppression of Contact Sensitivity in Mice and Humans
Sensitivityof phenotype
High (C57BL)Intermediate (C3H)Low (BALB/c)
kJ/m2
0.7-2.34.7-6.99.6-12.3
Mice"
mj/cm2
70-230470-690960-1230
Human*
Skin type mJ/cm2
Fair 100Dark 225
' Data from Noonan and Hoffman (1994).* Data from Oberhelman a at. (1994).
the same mice with DNFB several weeks later in the ab-sence of additional UV exposure fail (reviewed by Rivasand Ullrich).
Evidence for immune suppression in humans. We haveutilized a human contact sensitivity bioassay in which nor-mal volunteers are exposed to UV radiation and thentreated at that site with a potent immunogen, dinitrochloro-benzene (DNCB) (Cooper et ai, 1992). Subjects with fair tomoderately fair skin received varying UVR exposure regi-mens from a bank of FS20 fluorescent sunlamps (rich inUVB) and were compared for their ability to mount animmune response to DNCB. A linear UV-dose-responsiveinhibition of immune responsiveness was found with a de-tectable decrease first occurring at 0.75 of the individual'sminimal erthythemal dose (MED) and reaching completeinhibition of responsiveness for 95% of subjects adminis-tered 2 MED every day for 4 days prior to immunization.Similar inhibition occurred if sensitization to DNCB wasadministered through skin which received a single 4 MEDexposure 3 days prior. As in the mouse, UV-induced im-mune suppression in humans appears to be related to al-tered antigen presentation since the degree of immunosup-pression correlated with both the degree of Langerhans celldepletion which occurs after UVR and the influx of macro-phages that preferentially activate CD4+ cells (suppressor-inducer) which induce maturation of CD8+ suppressor cells(Baadsgaard et ai, 1990; Coopers ai, 1986). Several addi-tional protocols have been tested; a dose-response curve forfair-skinned subjects was constructed and the 50% immunesuppressive dose calculated to be approximately 100 mJ/cm2 of UVB. This is very similar to the level (70-230 mJ/cm2) obtained by Noonan and Hoffman (1994) for strainsof mice with high susceptibility to UV-induced immunesuppression (Table 2).
Of the subjects receiving erythemagenic doses of UVR,25-30% were rendered tolerant to the DNCB; i.e., even ifthe DNCB was provided as subsequent immunizationthrough skin that had not been UVB-exposed, these sub-jects could no longer be immunized to DNCB. In a similartype of assay, subjects with a past history of skin cancerwere found to be the most susceptible to UV-induced im-munosuppression (Schmieder et ai, 1992; Yoshikawa etai, 1990), indicating that UVR effects on the immune sys-tem may contribute to the incidence of skin cancer.
Unlike studies in mice, our studies did not demonstrateeffects at a distant site; i.e., immunization with anotherunrelated immunogen (diphencyclopropenone) at a sitedistant from the sunburn was not suppressed. There was nodistant immunosuppression even if total body exposure (ex-cepting the sensitization and elicitation site) to 4 doses ofeither 0.75 or 1.5 MED were administered prior to sensiti-zation. Additional studies with a different antigen and vary-ing elapse times between UV radiation and immunization

16 SELGRADE ET AL.
need to be examined before the possibility of systemic ef-fects in humans can be completely dismissed.
In order to assess whether pigmentation has a role inprotecting against UVR-induced immunosuppression,light- and dark-skinned human subjects were prospectivelyrandomized into groups receiving single doses of 1 -4 MEDat an immunization site 3 days prior to sensitization withDNCB. Upon administration of a biologically equalizeddose of 4 MED, the reduced percentage of successful immu-nizations was similar in both light-skinned subjects (MEDof 20-40 mJ/cm2) and dark-skinned subjects (MED of 60-110 mJ/cm2) at 25 and 33%, respectively (Oberhelman etai, 1994). The point dose at which 50% of subjects werehyporesponsive was 100 mJ/cm2 for light-skinned subjectsand 225 mJ/cm2 for dark-skinned subjects. Although thedose-response curves differ, immunosuppressive UVRdoses in dark-skinned subjects were only 2.25-fold overthose of light-skinned subjects. Such doses are easilyachieved during occupational or recreational exposure.However, immunosuppression in dark skin occurred withless observable redness than in light skin, making it moredifficult for the individual to judge their own degree ofUVR exposure.
Summary and conclusions. These studies indicate thatas in mice "local" immune suppression occurs in humansfollowing exposure to highly relevant, commonly encoun-tered, levels of UVR. Also, as in mice, a certain proportionof exposed subjects develop immunologic tolerance. Thelevels of UVR required to produce 50% suppression of CHSin humans and in genetically susceptible strains of mice aresimilar (Table 2); however, unlike mice, systemic immuno-suppression has yet to be demonstrated in humans.
Immunotoxicity of Ozone: A Comparison between AnimalModels and Human Subjects (R. B. Devlin)
More than 120 million people in the United States areexposed to levels of ozone which exceed the current EPANational Ambient Air Quality Standard (0.125 ppm). Thisubiquitous oxidant gas has been shown to cause decrementsin lung function, increases in airway reactivity, and inflam-mation in humans exposed for short periods of time to lowlevels of ozone in controlled clinical studies. Animals ex-posed to ozone have also been shown to have altered lungfunction and increased inflammation, as well as decreasedresistance to bacterial infection. This decreased resistancehas been attributed to suppression of alveolar macrophagephagocytic function (reviewed by Selgrade and Gilmour,1994). Since it is faster and cheaper to expose animals (incontrast to humans) to ozone, and a wider array of end-points is available in animals (e.g., morphological studies oflung tissue, post-ozone challenge with microorganisms), itis important to be able to extrapolate from the very largeanimal toxicology database on ozone to human health risk.
In this report, we describe an approach in which ozone-in-duced decrements in phagocytic capability of alveolar mac-rophages from humans and mice were directly comparedby in vitro exposure of these cells to ozone. The phagocyticcapability of macrophages removed from humans and miceexposed to comparable doses of ozone in vivo is also com-pared. We report that human and mouse alveolar macro-phages have essentially the same response to both in vitroand in vivo ozone exposure, indicating that, in this case, themouse provided a good model for assessing potential hu-man health effects.
In vitro ozone exposure of human and murine macro-phages. Human alveolar macrophages were obtainedfrom volunteers who underwent bronchoalveolar lavage(BAL) as described elsewhere (Koren el ai, 1989). Mousealveolar macrophages were also obtained by bronchoalveo-lar lavage (methods described by Gilmour et ai, 1993).Cells from both species were adhered to plastic chamberslides in culture medium for 1 hr. Medium was replacedwith PBS and cells were then placed in a rocking CO2 incu-bator and exposed to 0.8 ppm ozone for 3 hr. Macrophageswere washed with PBS to remove nonadherant cells and thenumber of fluorescent particles ingested per 100 adheredmacrophages was assessed (phagocytic index) as previouslydescribed (Devlin et ai, 1991). Both human and murinemacrophage phagocytic capability was suppressed follow-ing ozone exposure (Table 3). These data demonstrate that
TABLE 3Effect of Ozone Exposure on Alveolar
Macrophage Phagocytosis
Treatment
In vitro air
In vitro ozone(0.8 ppm; 3 hr)
% Suppression
In vivo air
In vivo ozone'
% Suppression% Suppression corrected''
for dosimetric difference
Mice
369.2 (26.4),"n = 6
291.7(17.4),*n = 621%
330.6(10.4),n = 4
194.0(19.7),** = 442%
28%
Humans
386.7 (50.5),n = 6
275.0(45.1),*n-629%
714.9(46.1),n " 10
539.2 (22.3),*n ° 10
25%
25%
' Mean (standard error) of the phagocytic index (number of fluorescentparticles ingested per 100 macrophages).
* Significantly different from air control (p < 0.05; Student's t test).c Mice were exposed to 0.8 ppm for 3 hr, humans were exposed to 0.08
ppm for 6.6 hr while undergoing intermittent exercise.d Based on studies using "O, alveolar macrophages of mice exposed to
0.8 ppm ozone for 3 hr receive roughly 1.5 times more ozone than those ofhumans exposed to 0.08 ppm ozone for 6.6 hr while exercising moderately(see text for more details).

IMMUNOTOXICITY RISK ASSESSMENT 17
human and murine alveolar macrophages respond simi-larly to ozone, with human cells showing a 29% decrease inphagocytic index (PI) compared to 21% in murine cells.
In vivo exposure of humans and mice to ozone. Healthyhuman volunteers 18-35 years old were exposed twice for6.6 hr while undergoing intermittent moderate exercise:once to 0.08 ppm ozone and once to filtered air (Devlin etai, 1991). A randomized double-blind protocol was usedand exposures were separated by at least 3 weeks. Subjectsunderwent BAL 18 hr after each exposure, and macro-phages were obtained as described above. Six-week-oldCD1 mice were exposed to 0.8 ppm ozone or filtered air for3 hr, and macrophages were obtained by BAL. Cells fromboth species were then assessed for phagocytic capability asdescribed above. In vivo exposure resulted in a significantdrop in the phagocytic index of both murine and humanmacrophages (Table 3). Mice exposed to 0.8 ppm ozone for3 hr had a 42% drop in PI, while humans exposed to 0.08ppm ozone for 6.6 hr while exercising had a 25% drop in PI.
The response of an individual to ozone is a function ofozone concentration, duration of exposure, and ventilationrate (CxTxV). Thus, it is not straightforward to comparethe dose of ozone delivered to the lungs of resting mice withthat of exercising humans. One way to compare the dose ofozone delivered to the alveolar macrophages of mice andhumans is to use ozone labeled with a stable oxygen isotope(18O). When ozone, a highly reactive gas, reacts with func-tional groups on the surface of alveolar macrophages, itforms reaction products with a half-life of about 6 hr whichcan be measured by mass spectrometry (Hatch et ai, 1994).This approach has been used to demonstrate that humansexposed to 0.4 ppm ozone for 2 hr while undergoing heavyintermittent exercise receive levels of ozone comparable tothose received by resting rats (Hatch et ai, 1994) or mice(Slade, R., Watkinson, W. P., and Hatch, G. E., personalcommunication) exposed to 2.0 ppm ozone for 2 hr. Simi-lar calculations suggest that mice exposed to 0.8 ppm ozonefor 3 hr receive roughly 1.5 times more ozone than humansexposed to 0.08 ppm ozone for 6.6 hr while exercising mod-erately. Assuming that changes in PI following in vivo expo- .sure are reflective of the dose of ozone delivered to macro-phages and that CxTxV products increase as a linear func-tion, then mice exposed to a comparable dose of ozone asthe humans would have a 28% drop in PI; very close to the25% decrease in PI observed in humans.
Summary and conclusions. Data comparing humanand murine alveolar macrophages exposed to similar dosesof ozone in vitro suggest that cells from both species re-spond almost identically as measured by macrophagephagocytic capability. Also, using 18O-labeled ozone to nor-malize for differences in dose of ozone delivered to restingmice compared with exercising humans, macrophagesfrom both species also appear to have very similar responses
following in vivo exposure. Thus, these data suggest that (1)the effects of ozone exposure on murine alveolar macro-phage function are predictive of effects on human alveolarmacrophage function, and (2) effects of in vitro exposure ofmacrophages to ozone are predictive of effects which resultfrom in vivo exposure. A similar approach has shown thathumans and rats exposed to comparable doses of ozone alsohave comparable increases in two indicators of inflamma-tion: PMN influx into the lung and increased BAL protein(Hatch et ai, 1994). This information could be used to de-velop risk assessment models which might help us to inter-pret data obtained from studies with more toxic air pollu-tants, such as phosgene, for which human in vivo exposureare not possible (Fig. 2).
The Human-SCID Mouse Model in Immunotoxicology(H. van Loveren)
Immunotoxicity can express itself in many differentforms including morphologic changes such as those thatoccur in the thymus following TCDD exposure. Histologi-cal changes in peripheral lymphoid tissues in the respira-tory tract or the skin can also be indicative of immunotoxi-city. Often associated with such morphological changes arefunctional alterations which range from suppression of an-tigen-specific antibody responses to decreased resistance toinfectious or neoplastic diseases. Immunotoxic agents areusually detected by in vivo studies using experimental ani-mals such as mice or rats. Subsequently, it is difficult toaccurately predict on the sole basis of experimental animalstudies the risk of exposure to immunotoxicants in hu-mans. When human exposure occurs, the actual dose isoften difficult to establish, and there is a restriction in po-tential endpoints that may be studied.
Current research activities are, in part, devoted to im-proving extrapolation of animal experiments to humans.One such effort focuses on in vitro systems (such as thatdescribed by Dr. Devlin above), in which relevant cell typesof animal and human origins are exposed to immunotoxi-cants, and "read-outs" are applied to investigate possibledifferences or similarities in sensitivity and mechanism ofaction. Another model that is currently under investiga-tion, and directed to serving the same goal, is the use ofsevere combined immune deficient (SCID) mice that arereconstituted with human immune cells in an attempt toallow for the development of an immune system that moreclosely approximates that of humans.
The SCID mouse has an aberrant gene on chromosome16 that results in malfunctioning of a DNA recombinaseenzyme. This enzyme sustains the genomic rearrangementin lymphocytes during maturation that is required for gener-ation of the specific T cell receptors and antibody repertoireon T and on B lymphocytes, respectively. Because of thisdefect, SCID mice lack functionally active T and B lympho-

18 SELGRADE ET AL.
cytes and are, therefore, excellent hosts for receiving xeno-grafts, including grafts comprising lymphoid tissue.
A large number of SCID-human models, and variations,have been described. Two of these models in which SCIDmice are reconstituted with human lymphoid tissue havebeen used in immunotoxicology. One model has been stud-ied in which human peripheral blood lymphocytes (PBLs)are injected intraperitoneally into SCID mice (hu-PBL-SCID). In the other model, liver and thymus tissue fromhuman fetuses or rats are grafted under the kidney capsuleof SCID mice. The effects of chemical exposure on thesehuman grafts have been compared to those by isogeneicgrafts, as well as across species; i.e., the relative toxicantsensitivities of mouse and human immune cells have beencompared in this in vivo situation.
Model 1: hu-PBL-SCID. The model in which PBLs areinjected to simulate certain aspects of the human immunesystem was studied by Pollock et al. (1994). Engraftment ofhu-PBLs into SCID mice provides at least a limited, hu-moral immune repertoire, which may be improved by en-graftment with human fetal tissues such as thymus or liver.In these studies, SCID mice were reconstituted by intraperi-toneal or intravenous injection with either tetanus-immu-nized syngeneic mouse splenocytes (mo-SPL) as a controlor tetanus-immunized human PBLs (hu-PBL) undervarious test conditions. SCID mice from the C.B-17 strainproduced more successful human engraftments than micefrom the C3H-SCID strains. Using optimal conditions, mo-SPL-SCID and hu-PBL-SCID mice were engrafted and ad-ministered either 2, 3, 7, 8-tetrachlorodibenzo-/wlioxin orcyclosporin A and periodically bled to measure tetanus-spe-cific antibody and class-specific immunoglobulin concen-trations. Comparison of the chemical-related changes in im-munoglobulin and tetanus antibody concentrations re-vealed some similarities between control mice andmo-SPL-SCID or hu-PBL-SCID mice, particularly withcyclosporin A groups. However, under the various condi-tions examined, hu-PBL-SCID mice demonstrated consid-erable variability in their ability to provide consistent re-constitution, thus, limiting the ability to determine whetherhuman cells are more or less susceptible than mouse cells tothe test agents. Provided that this system can be refined toprovide consistent reconstitution, hu-PBL-SCID mice maybe a promising in vivo model for assessment of potentialimmunotoxic agents.
Model 2: Fetal thymus/liver-SCID. In the secondmodel, fetal thymus tissue, in conjunction with fetal livertissue from the same donor, was transplanted under thekidney capsule of SCID mice. The liver tissue serves as asource for precursor thymocytes, since fetal liver is a hemo-poietic organ. The material was derived from human fetusof 15-20 gestational weeks; in younger fetuses it is not possi-ble to find thymus tissue while tissue from older fetuses fail
to grow resulting in abnormal thymic architecture. Histo-pathologically, transplantation of fetal thymus and liver re-sults in thymus transplants with an architecture that is simi-lar to a normal thymus. This is underlined by a virtuallyidentical composition of thymocyte phenotypes, i.e., dou-ble-negative cells, CD4/CD8 double-positive cells, andCD4 and CD8 single-positive cells. Heer et al. (1993) de-scribed the control model for this construct, i.e., SCID micegrafted with thymus and liver tissue from Gestational Day17 rat fetuses (SCID-ra). These studies employed normalrats treated with a single dose of TCDD, and also TCDD-treated SCID-ra and SCID mice grafted with human fetalthymus and liver tissue (SCID-hu). Using morphometricalanalysis, preliminary data indicated that the decreased cor-tex to medulla ratio which resulted from TCDD treatmentin control rats also occurred in the human transplants. Thisindicates that human thymus tissue is sensitive to TCDDexposure at doses similar to those which effect rat thymictissue.
As is true for the hu-PBL-SCID model in which lym-phoid cells are injected, the model in which tissue trans-plants are conducted also has limitations. For example, incontrast to the hu-PBL-SCID mice, the lymphocytes in theSCID-ra model gain access to lymphoid organs of the host,possibly as a consequence of their evolutionary closeness.This may in turn affect the thymus, since it is likely that iffeedback mechanisms are operational in this system, theSCID-ra model may provide a more pronounced drain ofcells from the thymus graft compared to the SCID-hu.Moreover, in some SCID-ra mice, in contrast to SCID-humice, evidence of graft versus host in the skin has beenobserved. While indicating the functionality of the donorcells within the host, it also indicates a further differencebetween the SCID-ra and the SCID-hu model. Such differ-ences will need to be taken into account when comparingeffects of exposure to immunotoxicants.
Summary and conclusion. While a considerableamount of refinement prior to their use in conventionalscreening is required, these studies demonstrate the poten-tial utility of SCID models for immunotoxicology studies.The major limitation of the hu-PBL-SCID model is thevariability and lack of grafted lymphocyte functionalitydue, in part, to their inability to respond to murine cyto-kines. The model using fetal thymus and liver transplantsappears to have less of this problem, since the grafts have arelatively normal appearance, but may be restricted to ana-lyzing the thymus, and hence investigation of chemicalsthat have the thymus as their primary target. It should alsobe noted that, for this model, obtaining human material isoften very difficult. However, given our present ability todevelop animal models through cellular and genetic manip-ulation, refinement of such an animal model is highly con-ceivable in the near future.

IMMUNOTOXICITY RISK ASSESSMENT 19
Difficulties Associated with Assessing Immunotoxic Effectsin Human Populations Studies (R. E. Biagini)
Field studies in humans designed to detect immunomod-ulation from exposure to xenobiotics present challengingproblems to epidemiologists and immunotoxicologists. In-vestigators must choose populations with adequate expo-sure levels to detect potential effects, quantitate exposureon an individual basis if possible, and rule out concurrentexposure to other immunomodulatory factors. A controlgroup must be identified which is similar to the exposedgroup in all characteristics except for exposure to the xeno-biotic under study. Many extraneous circumstances can af-fect immune function in an individual, including sunlight,stress, medication, and illness; these factors may produceimmune alterations as great or greater than those predictedfrom occupational or environmental exposure to xenobio-tics (NRC, 1992; PlotnikoffV/ al, 1991; Clement-Lacroixand Dubertret, 1992; Hersey et al., 1993, Baadsgaard et al.,1990). Such confounders can best be evaluated by adminis-tering questionnaires, which must necessarily include sensi-tive topics such as recreational drug use and HIV infection.Sample acquisition (usually of peripheral blood and/or sa-liva) is performed at sites distant from the controlled labora-tory environment, yielding an assortment of problems thatwould not occur in a clinical situation. Some immune as-says require immediate processing of blood samples and aredifficult to conduct when samples must be transported tothe laboratory from remote locales. Some immunologicaland clinical tests which might yield important data (e.g.,vaccination of subjects to measure primary antibody re-sponse) are rarely, if ever, used in field studies because ofconcerns about the risk/benefit ratio to subjects. Subjectsinvolved in immunotoxicity field studies must be briefedabout the nature and purpose of the study, provide in-formed consent, and be notified of their individual testresults and their possible clinical significance in a timelyfashion.
Methodologic considerations. The most common de-sign used in immunotoxicity research is the cross-sectionalstudy. In such a study, exposure status and immune func-tion are measured at one point in time or over a short pe-riod of time. The immune function of "exposed" subjects iscompared to the immune function of a comparable groupof "nonexposed" individuals. The first challenge in con-ducting an immune assessment study is to identify the ex-posed group. The study should include populations at theupper end of exposure unless previous studies have alreadyestablished an immunotoxic effect in that range. Where pos-sible, the study should incorporate individual estimates ormeasurement of dose (ideally by biomonitoring of internaldose). Once the exposed group has been identified, a cleardefinition is needed of who is eligible to participate in thestudy. For example, in an occupational study, all exposed
individuals who have worked in a particular departmentmight be considered eligible, while in an environmentalstudy, eligible persons might include all residents of a com-munity or a smaller sample of households. Selection biasoccurs when an individual's willingness to participate varieswith characteristics related to exposure or health status andshould be avoided. A high degree of participation makes itless likely to occur.
Potential immune effects of other chemicals present inthe industrial or residential environment need to be consid-ered such as those used in hobbies or second jobs. In a studyof community residents exposed as a result of a nearby fac-tory, an assessment should be made of other contaminantsin the local environment, as well as potential occupationalchemical exposures.
Known risk factors which might influence the outcomeof immune function tests (e.g., age, gender, cigarette smok-ing, sunlight exposure, stress, use of certain medicationsand recreational drugs) should be matched as much as possi-ble in control and exposed groups or controlled in the analy-sis. However, there are limited quantitative data on the in-fluence of these factors on immune function in the generalpopulation, and it is impossible for an epidemiologic studyto match or analyze all potential factors. For example, dif-ferences in ethnicity, work patterns, socioeconomic status,dietary habits, exercise levels, or community-specific expo-sures to particular viruses might influence comparisons be-tween an exposed and nonexposed population. The studyshould also account for medical factors that might have amajor impact on immune function such as chemotherapyor steroid treatment. Other medications and medical expo-sures (immunizations, radiation) in the recent time periodshould be ascertained and evaluated in the statistical analy-ses. Because many immune function tests have potentialvariability between laboratories or within a laboratory overtime, it is desirable to have each test run by the same labora-tory for all exposed and unexposed subjects in a particularstudy. The laboratory should validate each test procedureto assess measurement and subject variability before theanalysis of study samples begins. Selection of the most ap-propriate tests to perform is frequently dictated by logistics.However, available animal and human literature on theeffects of exposure to a particular xenobiotic as well as thepredictability of immunological endpoints measured in an-imal models to detect immunotoxicity (Luster et al., 1992)must be considered.
Issues important in the interpretation of positive stud-ies. In studies which show significant differences betweenthe exposed and unexposed populations, it is important torecognize that large cross-sectional studies (i.e., studies with100-200 exposed and control subjects) will have adequatestatistical power to detect relatively small differences (onthe order of 10%) in immunological endpoints such as pro-

20 SELGRADE ET AL.
portion of CD4+ and CD8+ cells. Although such studiesmight be interpreted as positive, particularly if there is evi-dence of a dose-response relationship, there will be consid-erable overlap between the values of unexposed and ex-posed individuals, and it is possible that none of the individ-ual values will fall outside the clinically normal range.Interpretation of such findings is difficult because there arelittle quantitative data on the degree to which such parame-ters need to be modified at this end of the response curvebefore there is increased risk of disease. In addition, becausestatistically significant differences measured between thetwo populations may be small in magnitude and of un-known clinical significance, the possibility that they reflectmethodologic problems, such as those described above,rather than a true biological effect is of concern.
Evidence of a dose-response relationship is usually animportant, but not necessary, criterion in the assessment ofa toxic exposure. However, both biological and methodolog-ical factors may complicate the assessment of dose-re-sponse in human immunotoxicity studies. For example, ex-perimental models suggest that high doses may be inhibi-tory, while low doses might be stimulatory (Biagini et al.,1983).
The healthy worker effect (apparent decreased mortalityand morbidity in workers when compared to the generalpopulation) is also a potential confounder in the interpreta-tion of the immunotoxic outcomes from xenobiotic expo-sure, especially when exposed workers are compared to"normal reference values" (Choi, 1992).
Issues important in evaluating negative studies. For anegative study, an important issue is whether the study sizewas adequate to detect a difference of a specified size in theimmune function parameters of interests. The statisticalpower of a study to detect a difference between two popula-tions in the mean of a continuous variable (such as serumIgG level, proportion of CD4+ lymphocytes) depends onthe size of the study groups, the mean and variance of theoutcome in the study groups, the specified type I difference,and the size of the difference to be detected (Colton, 1974).Power calculations are usually performed in planning anepidemiological study. In comparing the results of contra-dictory studies, one issue that should be considered is theprecision of the differences in point estimate (i.e., the confi-dence interval for the estimated difference between groups).
Other study designs. Aside from the cross-sectionalstudy design, two alternative designs may be used in im-munotoxicity studies. In longitudinal studies, groups of peo-ple that are initially free of disease and that differ accordingto extent of exposure to a potential cause of the disease arecompared with respect to incidence of the disease overtime. A variant of this design that might be utilized in im-munotoxicity studies would compare immune function testresults within individuals before and after a defined expo-
sure. Another variant would define exposed and unexposedgroups cross-sectionally, administer immune functiontests, and follow the subjects prospectively to assess rela-tionships between immune function test results and devel-opment of clinical disease.
In case-control studies, persons with a given disease andpersons without the disease are selected: the proportions ofcases and controls who have certain background character-istics or have been exposed to possible risk factors are thendetermined and compared. A case definition may includeindividuals with a continuum of immunologic changes dueto exposure ranging from homeostatic immunologic re-sponses to frank disease. Case-control studies of the etiol-ogy of immunologicalry mediated diseases might identifyincreased risk of previous exposure to particular chemicalsamong the cases; such a finding would be particularly rele-vant if supported by animal studies or evidence of immunefunction changes among humans exposed to the chemical.
Summary and conclusions. The potential problems as-sociated with designing and performing studies to detectimmunomodulation from exposure to xenobiotics in hu-mans include problems common to human epidemiologicstudies in general, as well as problems unique to immunesystem studies. Control and exposed individuals must bewell characterized. Potential confounding factors in boththe exposed and control populations must be factored, tothe extent feasible, into the study design and interpretation.The selection of which immunological endpoints to studymust be directed by both a rigorous review of the literatureconcerning the immunotoxic potential of the exposure inquestion and the potential predictability of measurableendpoints to detect immunomodulation. Minimization oflogistical problems which could effect results is paramountin the design of the study to minimize systematic effects.Validation of the methodology used with respect to repro-ducibility and accuracy and general quality assurance of allacquired data is also desirable. While clinical epidemiologicstudies designed to detect immunomodulation are inher-ently difficult to perform and the acquired results some-times confusing due to wide variabilities in "normalranges," they can be successfully performed with attentionto prestudy planning and constant vigilance for potentialsystematic (or non-exposure related) effects.
ACKNOWLEDGMENTS
Dr. Cooper's work was supported by cooperative agreements CR816177and CR82051O from the Health Effects Research Laboratory, U.S. Envi-ronmental Protection Agency.
REFERENCES
Baadsgaard, O., Salvo, B., Mannie, A., Dass, B., Fox, D. A., and Cooper,K. D. (1990). In vivo ultraviolet-exposed human epidermal cells activate

IMMUNOTOXICITY RISK ASSESSMENT 21
T suppressor cell pathways that involve CD4+CD45RA+ suppressor-in-ducer T cells. J. Immunol. 145, 2854-2861.
Biagini, R. E., Moorman, W. J., Smith, R. J., Lewis, T. R., and Bernstein,1. L., (1983). Pulmonary hyperreactivity in cynomologus monkeys (Ma-caca fasiadaris) from nose-only inhalation exposure to disodium hex-achJoroplatinate, Na2Fta6. Toxicol. Appl. Pharmacol. 69, 377-384.
Borel,J.(1989). Pharmacology ofcyclosporine(Sandimmune). V. Pharma-cological properties in vivo. Pharmacol Rev. 41, 259-371.
Choi, B. C. (1992). Definition, sources, magnitude, effect, modifiers andstrategies of reduction of the healthy worker effect. J Occup. Med. 34,979-988.
Clement-Lacroix, P., and Dubertret, L. (1992). Ultraviolet rays and theskin. Modulation of immune functions. Pathol. Biol. (Paris) 40, 178-183.
Colton, T. (1974). Statistics in Medicine. Little, Brown, Boston.Cooper, K. D., Neises, G. R., and Katz, S. I. (1986). Antigen-presenting
OK.M5+ melanophages appear in human epidermis after ultraviolet ra-diation. J. Invest. Dermatol. 86, 363-370.
Cooper, K. D., Oberhelman, B. S., Hamilton, M. S., Baadsgaard, O., Ter-hune, M., LeVee, C , Anderson, T., and Koren, H. (1992). UV exposurereduces immunization rates and promotes tolerance to epicutaneousantigens in humans; relationship to dose, CD 1 a"DR+ epidermal macro-phage induction and Langerhans cell depletion. Proc. Natl. Acad. Sci.USA 89, 8497-8501.
DeFabo, E. C, and Noonan, F. P. (1983). Mechanism of immune suppres-sion by ultraviolet irradiation in vivo. J. Exp. Med. 157, 84-98.
Devlin, R. B., McDonnell, W. F., Mann, R., Becker, S., House, D. E., andKoren, H. S. (1991). Exposure of humans to ambient levels of ozone for6.6 ozone hours causes cellular and biochemical changes in the lung.Am. J. Respir Cell Mol. Biol. 4, 72-81.
Gilmour, M. I., Park, P., and Selgrade, M. J. K. (1993). Ozone-enhancedpulmonary infection with Streptococcus zooeptdemicus in mice: Therole of alveolar macrophage function and capsular virulence factors. AmRev. Respir. Dis. 147, 753-760.
Hatch, G. E., Slade, R., Harris, L. P., McDonald, W. F., Devlin, R. B.,Koren, H. S., Costa, D. L., and McKee, J. (1994). Ozone dose and effectin humans and rats: A comparison using oxygen-18 labeling and bron-choalveolar lavage. Am. Rev. Respir. Cell Mol. Biol. 150, 676-683.
Heer, C. de, Verlaan, A. P. J., Penninks, A. H., Schuurman, H. J., VanLoveren, H. (1993). The SCID-RA mouse: Rat T cell differentiation inthe severe combined immunodeficient mouse. Ada Pathol. Microbiol.Immunol Scand. 101, 467-479.
Hersey, P., Magrath, H., and Wilkinson, F. (1993). Development of an invitro system for the analysis of ultraviolet radiation-induced suppressionof natural killer cell activity. Photochem. Photobiol 57, 279-845.
Koren, H. S., Devlin, R. B., Graham, D. E., Mann, R., McGee, M. P.,Horstman, D. H., Kozumbo, W. J., Becker, S., House, D. E., McDon-
nell, W. F., and Bromberg, P. A. (1989). Ozone induced inflammationin the lower airways of human subjects. Am. Rev. Respir. Dis. 139,404-415.
Luster, M. I., Portier, C, Pait, D. G., White, K. L., Jr., Gennings, C,Munson, A. E., and Rosenthal, G. J. (1992). Risk assessment in immuno-toxicology. I. Sensitivity and predictability of immune tests. Fundam.Appl. Toxicol. 18, 200-210.
Luster, M. I., Portier, C, Pait, D. G., Rosenthal, G. J., Germolec, D. R.,Corsini, E., Blaylock, B. L., Pollock, P., Kouchi, Y., Craig, W., White,D. L., Munson, A. E., and Comment, C. E. (1993). Risk assessment inimmunotoxicology. II. Relationships between immune and host resis-tance tests, Fundam. Appl. Toxicol. 21, 71-82.
Noonan, F. P., DeFabo, E. C, and Kripke, M. L. (1981). Suppression ofcontact hypersensitivity by UV radiation and its relationship to UV-in-duced suppression of tumor immunity. Photochem Pholobiol. 34,683-689.
Noonan, F. P., and Hoffman, H. A. (1994). Susceptibility to immunsup-presion by ultraviolet B radiation in the mouse. Immunogenetics 39,29-39.
NRC (1992). Biologic Markers in Immunotoxicology, pp. 63-82, 206. Na-tional Academy Press, Washington, DC.
Oberhelman, L. J., Koren, H., LeVee, G., and Cooper, K. D. (1994). Doseresponse relationships of immunosuppression by UV radiation in dark-versus light-skinned human subjects. Clin. Res [Abstract]
Plotnikoff, N. P., Faith, R. E., Murgo, A. J., and Wybran, J. (1991). Stressand Immunity, CRC Press, Boca Raton, FL.
Pollock, P. L., Germolec, D. R., Comment, C. E., Rosenthal, G. J., andLuster, M. I. (1994). Development of human lymphocyte-engraftedSCID mice as a model for immunotoxicity assessment. Fundam. Appl.Toxicol. 22, 130-138.
Rivas, J. M., and Ullrich, S. E. (1994). Ultraviolet B radiation and skinimmunology. In Immunotoxicology and Immunopharmacology (J. H.Dean, M. I. Luster, A. E. Munson, and I. Kimber, Eds.), 2nd ed. pp.435-453. Raven Press, New York.
Schmieder, G. J., Yoshikawa, T., Mata, S. M., Streilein, J. W., and Taylor,J. R. (1992). Cumulative sunlight exposure and the risk of developingskin cancer in Florida. J. Dermatol. Surg. Oncol. 18, 517-522.
Selgrade, M. J. K.,andM. I. Gilmour (1994). Effects of gaseous air pollu-tants on immune responses and susceptibility to infectious and allergicdisease. In Immunotoxicology and Immunopharmacology (J. H. Dean,M. I. Luster, A. E. Munson, and I. Kimber, Eds.), 2nd ed. pp. 395-411.Raven Press, New York.
UNEP/WHO/ICNIRP(1994). Environmental Health Criteria UltravioletRadiation. In press, World Health Organization, Geneva.
Yoshikawa, T., Rae, V., Bruins-Slot, W., Van den Berg, J-W., Taylor,J. R., and Streilein, J. W. (1990). Susceptibility to effects of UVB radia-tion on induction of contact hypersensitivity as a risk factor for skincancer in humans. J. Invest Dermatol. 95, 530-536.





























