Embed Size (px)
Citation preview

CUTTING EDGE IN AUTOIMMUNITY
Immunoreactivity and avidity of IgG anti-b2-glycoprotein I antibodies from patientswith autoimmune diseases to different peptideclusters of b2-glycoprotein I
A. Artenjak • I. Locatelli • H. Brelih • D. M. Simonic • Z. Ulcova-Gallova •
J. Swadzba • J. Musial • T. Iwaniec • L. Stojanovich • F. Conti • G. Valesini •
T. Avcin • J. W. Cohen Tervaert • Y. Shoenfeld • M. Blank • A. Ambrozic •
S. Sodin-Semrl • B. Bozic • S. Cucnik
� Springer Science+Business Media New York 2014
Abstract The pathogenicity of antibodies against b2-glycoprotein I (anti-b2GPI) depends on multiple factors such as
subclass type, epitope binding and avidity. Due to their large heterogeneity, their impact on antiphospholipid syndrome
(APS) onset is still not fully clarified. We studied the binding characteristics of IgG anti-b2GPI with known avidity from
sera of 201 autoimmune patients (87 with APS, 67 with APS associated with systemic lupus erythematosus (SLE), 47 with
only SLE) to six b2GPI peptides corresponding to amino acid clusters on domains I–II, II, III and III–IV by indirect ELISA
and evaluated their association with clinical features of APS. Peptides A (LKTPRV; domain I–II), B (KDKATF; domain
IV) and C (TLRVYK; domain III) were derived from a hexapeptide phage display library previously shown to react with
pathogenic monoclonal anti-b2GPI. Peptides D (NGPANSK; domain III), E (YNPLWFV; domain II) and F (KMDGNHP;
domain III–IV) represent surface amino acid clusters on b2GPI. The percentage of patients positive for peptides were
observed as follows: 30.3 % for peptide D, 28.90 % for B, 25.9 % for C, 24.9 % for E, 24.4 % for F and 10.0 % for A. The
anti-peptide antibodies in studied serum samples were predominantly of heterogeneous avidity, followed by law avidity
anti-peptide antibodies, whereas only a few were of high avidity. Positive and negative correlations were found between
several anti-peptide antibodies and the rate of thrombosis. Our results indicated diverse reactivity of IgG anti-b2GPI to
different epitopes on b2GPI. Classification of IgG anti-b2GPI into subgroups regarding epitope specificity and avidity
could represent an additional tool in understanding their pathogenicity in APS.
Keywords Antiphospholipid syndrome � Anti-b2GPI antibodies � b2GPI peptides � Anti-b2GPI-related peptides
antibodies � Avidity
A. Artenjak
Lek Pharmaceuticals d.d., Sandoz Biopharmaceuticals Menges,
Kolodvorska 27, 1234 Menges, Slovenia
I. Locatelli � B. Bozic
Faculty of Pharmacy, University of Ljubljana, 1000 Ljubljana,
Slovenia
H. Brelih � D. M. Simonic � A. Ambrozic � S. Sodin-Semrl �B. Bozic � S. Cucnik (&)
Laboratory for Immunology, Department of Rheumatology,
University Medical Centre Ljubljana, Vodnikova 62,
1000 Ljubljana, Slovenia
e-mail: [email protected]
Z. Ulcova-Gallova
Department of Gynaecology and Obstetrics, Genetics and
Medical School of Charles University, 32600 Plzen-Cernice,
Czech Republic
J. Swadzba � J. Musial � T. Iwaniec
Department of Medicine, Jagiellonian University Medical
College, 31-008 Krakow, Poland
L. Stojanovich
Bezhanijska Kosa, University Medical Centre, Belgrade
University, 11080 Belgrade, Serbia
F. Conti � G. Valesini
Dipartimento Medicina Interna e Specialita Mediche,
Rheumatology, Lupus Clinic, La Sapienza, University of Rome,
00161 Rome, Serbia
T. Avcin
Department of Allergology, Rheumatology and Clinical
Immunology, University Medical Centre, University Children’s
Hospital Ljubljana, 1000 Ljubljana, Slovenia
S. Cucnik
123
Immunol Res
DOI 10.1007/s12026-014-8578-0

Introduction
Antiphospholipid syndrome (APS) is an autoimmune dis-
ease defined by vascular (thrombotic) and/or obstetric
complications, in the presence of antiphospholipid anti-
bodies (aPL), i.e., anticardiolipin antibodies, antibodies
against b2-glycoprotein I (anti-b2GPI) and/or lupus anti-
coagulants [1]. The formulation of the original classifica-
tion criteria for APS was performed in Sapporo, Japan
(1998) [2], with a revision in Sydney, Australia, in 2004
[1]. In order for a patient to be diagnosed with APS, one
clinical and one laboratory criterion must be present [1, 3].
APS may be associated with other diseases, mostly sys-
temic lupus erythematosus (SLE) [4]. SLE has been clas-
sified according to the criteria established by the American
Rheumatism Association [5] and revised by the American
College of Rheumatology [6].
aPL are not only a laboratory marker for APS, but can
also be actively involved in disease pathogenesis [7–9].
Furthermore, aPL are considered as a non-traditional risk
factor for atherosclerosis-based cardiovascular diseases,
such as ischemic stroke, coronary artery disease and
peripheral artery disease in patients without overt autoim-
munity [10, 11].
Among the most clinically significant autoantibodies in
APS is anti-b2GPI, directed against b2GPI [8], previously
described as apolipoprotein H. b2GPI is a multifunctional
glycosylated protein present in plasma in concentrations
*180 mg/l (range 20–300 mg/l) [8, 12, 13]. The *50 kDa
protein consists of 326 amino acids, which are folded into
five sushi domains. Domains I–IV are composed of
approximately 60 amino acids, while the 5th domain con-
sists of 82 amino acids. Domain V also has specific char-
acteristics, such as a positively charged, lysine-rich region,
a hydrophobic loop and C-terminal extension, allowing
b2GPI to bind to negatively charged phospholipids [14–
17]. Due to specific interactions between 1st and 5th
domain of b2GPI, the protein exists in two conformations,
i.e., circular plasma and open fishhook conformations [18].
After binding to phospholipids, b2GPI changes the con-
formation from circular to open (‘‘J’’), exposing a cryptic
epitope which is recognized by anti-b2GPI directed against
domain I [19].
Although routine laboratories detect and interpret anti-
b2GPI as one set of autoantibodies, they actually represent
a very heterogeneous group directed against the same
antigen. Due to their polyclonal nature, subpopulations of
anti-b2GPI vary in epitope recognition [8, 20–23], avidity
[24–27] and mechanisms of action [7, 8, 28], which results
in their different pathogenicity and clinical relevance [8,
22, 23, 25, 29, 30]. A subset of IgG anti-b2GPI directed
against domain I on b2GPI seems to have a prominent role
in the pathology of thrombotic complications in patients
with APS [19]. In contrast, a subpopulation of IgA anti-
b2GPI directed against domain IV has been linked to
atherosclerosis in a study using different b2GPI domain-
deleted mutants and native b2GPI [30]. An insight into the
diversity of these autoantibodies was provided by a study
with monoclonal anti-b2GPI. Peptides corresponding to
amino acid sequences on domains I–II, III and IV of b2GPI
were identified using hexamer phage display libraries [28].
These peptides inhibited in vitro/in vivo development of
experimental APS triggered by monoclonal anti-b2GPI,
indicating a possible therapeutic use of synthetic peptides
[28]. Furthermore, a clinical study on 295 patients with
APS and the above-mentioned peptides stressed their
clinical relevance in recognition of different domains of
b2GPI. Antibody positivity for the peptide located on
domain III significantly predicted recurrent spontaneous
abortions, while positivity for the peptide found between
domains I and II was negatively associated with overall
thrombosis [31].
Avidity must also be considered when describing the
diversity of anti-b2GPI subpopulations and their clinical
relevance. Several research groups/clinical studies indi-
cated that difference in strength of binding to the same
antigen/same epitope could be an important marker of the
pathogenicity of the specific anti-b2GPI subgroups [25, 29,
32]. An association between high avidity (HAv) IgG anti-
b2GPI and thrombotic or obstetric complications in
patients with APS was reported. This is in contrast to low
avidity (LAv) IgG anti-b2GPI, which were more prevalent
in autoimmune patients without APS [29, 33]. The
involvement of HAv IgG anti-b2GPI in the pathogenesis of
APS was also confirmed in an in vitro study on human
coronary artery endothelial cells [34]. In this study, HAv
IgG anti-b2GPI were shown to increase the expression of
inflammatory and chemotactic cytokines leading to higher
migration of monocytes. These effects were further inten-
sified in the presence of the major acute-phase protein
serum amyloid A [34], denoting that along with
J. W. Cohen Tervaert
Clinical and experimental Immunology, Maastricht University,
Universiteitssingel 40, 6229 ER Maastricht, The Netherlands
Y. Shoenfeld � M. Blank
Sheba Medical Center, The Zabludowicz Center for
Autoimmune Diseases, 52621 Tel-Hashomer, Israel
M. Blank
Department of Human Microbiology, Sackler Faculty of
Medicine, Tel Aviv University, 69978 Ramat Aviv, Israel
S. Sodin-Semrl
Faculty of Mathematics, Natural Sciences and Information
Technologies, University of Primorska, 6000 Koper, Slovenia
Cutting Edge in Autoimmunity
123

lipopolysaccharide [7], serum amyloid A as a marker of
inflammation also represents a trigger or a second hit
uncovering the full pathological potential of anti-b2GPI
[34]. Using heptamer phage display libraries, two binding
epitopes of HAv IgG anti-b2GPI have been characterized:
FNPYWYV and QGOAHSK [27]. These sequences mim-
icked specific amino acid clusters on domains II and III of
b2GPI and are accessible to HAv IgG anti-b2GPI in the
fishhook and circular conformations. In contrast, the
sequence KMDGNHP has been characterized as a surface-
binding epitope for LAv IgG anti-b2GPI and is located
between domains III and IV of b2GPI. It is accessible for
binding of LAv IgG anti-b2GPI only in open fishhook
conformation [27].
The major aim of this study was to identify and define
the binding characteristics of IgG anti-b2GPI from sera of
autoimmune patients with defined diagnoses (APS in the
absence and the presence of SLE and SLE alone) to sep-
arate b2GPI peptides corresponding to amino acid clusters
on domains I–II, II, III and III–IV. The binding and avidity
of IgG anti-b2GPI to the selected six peptide sequences of
b2GPI were addressed and evaluated for their clinical
value and association with clinical/serological features of
APS.
Materials and methods
Selection of patients’ sera
The study which was approved by the National Ethical
Committee (#163/02/09) and is a part of the National
Research Programme #P3-0314 was primarily conducted
on 479 serum samples from patients with different auto-
immune diseases (predominantly APS, APS associated
with SLE, SLE, etc.). The patients enrolled in this study
were collected from seven European centers within the
framework of the European Forum on aPL [29]. Due to the
lack of inter-laboratory standardization for detection of
aPL [35], all samples were retested for positivity of IgG
anti-b2GPI by our in-house indirect enzyme-linked
immunosorbent assay (ELISA) [36, 37]. Positivity for IgG
anti-b2GPI was confirmed in 226 samples, and clinical
relevance of IgG anti-b2GPI avidity was previously tested
and reported by Cucnik et al. [29]. In the current cross-
sectional study, we used 201 of 226 serum samples for
determination of immunoreactivity and avidity of IgG anti-
b2GPI to six b2GPI-related peptides that correspond to
sequence or surface amino acids on different domains of
b2GPI (see section ‘‘Selection of peptides’’). From the
starting 226 samples which were positive for IgG anti-
b2GPI and had determined their avidity, nine were omitted
due to insufficient volume of the sera for all experiments/
studies and 16 due to diagnostic overlaps with other
autoimmune diseases (Sjogren‘s syndrome, systemic scle-
rosis, urticarial vasculitis and autoimmune thrombocyto-
penic purpura). From 201 serum samples appropriate for
the b2GPI-related IgG anti-peptide antibodies (anti-pep-
tide) immunoreactivity and avidity study, 87 patients were
diagnosed with APS, 67 with APS associated with SLE and
47 with only SLE (Fig. 1). The following clinical param-
eters were evaluated in correlation to anti-peptide positivity
and avidity: (a) thrombotic events together or separate as
arterial, venous or microvascular thrombosis and (b) in
female patients also obstetric manifestations.
Selection of peptides
Immunoreactivity and avidity against six b2GPI-related
peptide sequences corresponding to different domains of
b2GPI were studied with a set of in-house indirect IgG anti-
peptide ELISA (Fig. 2). Peptides A (58LKTPRV63; domains
I–II), B (208KDKATF213; domain IV) and C (133TLRVYK138;
domain III) were derived from a hexapeptide phage display
library as epitope targets for pathogenic monoclonal anti-
Fig. 1 Patient enrollment. *Patients positive for IgG anti-b2GPI with
Sjogren‘s syndrome, systemic sclerosis, urticarial vasculitis and
autoimmune thrombocytopenic purpura were excluded due to small
frequencies/group sizes and for sake of clarity of statistical analysis.
Anti-b2GPI antibodies against b2-glycoprotein I, APS antiphospho-
lipid syndrome, SLE systemic lupus erythematosus
Cutting Edge in Autoimmunity
123

b2GPI [28] and were previously shown to have clinical rele-
vance [31]. Peptides D (N143G142P139A141N144S140K138;
domain III), E (Y96N98P116L115W111F81V64; domain II) and F
(K231M161D165G163N164H159P157; domains III–IV) represent
surface amino acid clusters on b2GPI and were found, using a
heptapeptide phage display library by Zager et al. [27], to have
binding epitopes for HAv and LAv IgG anti-b2GPI.
Anti-peptide elisa for immunoreactivity and avidity
detection
Synthetic b2GPI-related peptides (GL Biochem (Shanghai)
Ltd., Shanghai, PR China) were diluted with phosphate-
buffered saline, pH 7.4, 0.15 M (PBS) to final concentra-
tions 10 lg/ml/well for peptides B, D, E, F and 20 lg/ml/
well for A, C and used in the in-house indirect IgG anti-
peptide ELISA. Briefly, 100 ll of diluted peptides were
added into each well of 96-well plates (high binding Costar
EIA-RIA plates, clear, flat bottom, non-sterile, polystyrene;
Corning Incorporated, Corning, NY, USA) and incubated
overnight (*16 h) at 4 �C. The plates were then washed
one time with 250 ll of PBS and blocked with 200 ll of
3 % bovine serum albumin (BSA)-PBS for 1 h at room
temperature (RT). After washing the plates four times with
250 ll PBS, 100 ll of serum samples diluted with 0.5 %
BSA-PBS 1:100 were added onto the plates and incubated
for 2 h at RT. For determination of relative strength of
binding (avidity), serum samples were diluted 1:100 in
0.5 % BSA-PBS with increasing concentrations of NaCl:
0.15, 0.25, 0.5, 1 and 2 M. In the next step, the plates were
washed four times with 250 ll of PBS and incubated with
100 ll of 1:1,000 diluted goat anti-human IgG (Fc) con-
jugate (Accurate Chemical and Scientific corp., Westbury,
NY, USA) for 1 h at RT. In the final step, the plates were
again washed four times with 250 ll of PBS and 100 ll of
the substrate p-nitrophenylphosphate in diethanolamine
solution (pH 9.8) was added onto the plates. The reaction
was stopped when the positive control reached the value of
1000 mili optical density (mOD) at wavelength 405 nm
with reference wavelength being 680 nm. A serum sample
from a patient with APS highly positive for IgG anti-b2GPI
served as a positive control and in our preliminary anti-
peptide ELISA studies was shown to be highly immuno-
reactive to all six peptides. Cutoff values for determination
of positivity to each peptide were set for each peptide
separately as 99th percentile in mOD based on results/
responses of 100 tested sera from health blood donors. The
relative binding strength (avidity) was determined with
chaotropic variant of anti-peptide ELISA and presented as
% of binding at higher ionic strength (500 mM NaCl)
compared with binding at 150 mM NaCl. Avidity was
arbitrarily defined as LAv, heterogeneous (HetAv) and
HAv, if the binding at higher ionic strength (500 mM
NaCl) was under 25 %, between 25 and 65 %, or [65 %,
respectively, as compared to binding at 150 mM NaCl.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Sta-
tistics program version 22 (IBM Corporation, Armong,
NY, USA) for applying logistic regression, multinomial
logistic regression, Mann–Whitney U test and Kruskal–
Wallis test. Logistic regression model was developed for
assessment of influence of anti-peptide positivity on the
occurrence of clinical manifestations (e.g., venous, arterial,
microvascular, overall thrombosis and obstetric manifes-
tations) or underlying disease-type subgroups (APS vs.
APS ? SLE, APS vs. SLE and APS ? SLE vs. SLE). In
this model, the presence of anti-peptide positivity was used
as an independent dichotomous variable. In total, 18 dif-
ferent dichotomous variables were produced (six separate
peptides and some selected combinations of different
peptides), namely positivity of each peptide (A, B, C, D, E
and F), mutual positivity of selected pairs of peptides
(A&E, B&C, B&D, B&F, C&D, C&F and D&F), mutual
positivity of selected triplets of peptides (B&C&D,
B&C&F, B&D&F and C&D&F) and the mutual positivity
of a quadruplet of peptides (B&C&D&F). Selection of
pairs, triplets and quadruplets was based on the peptide
position of domains of b2GPI, as estimated by previous
research (clinical and pathological relevance of anti-
b2GPI) [8, 22, 23, 26, 27, 29, 30]. Consequently, we
selected combinations of peptides A and E that are located
Fig. 2 Schematic presentation of peptide positions on b2GPI
domains. Only the peptide position on the domains is exact
Cutting Edge in Autoimmunity
123

on domains I and II and all combinations of peptides B, C,
D and F that are located on domains III and IV (Fig. 2).
Due to the large number of variables tested in the regres-
sion model, the forward conditional method was used for
choosing the significant variables.
Multinomial logistic regression was used for studying
the relationship between anti-peptide positivity and IgG
anti-b2GPI avidity presented as three arbitrarily defined
categories (HAv, HetAv or LAv). As before the multi-
nomial logistic regression model, anti-peptide positivity
was tested as 18 independent dichotomous variables and
forward conditional method was used for choosing the
significant variables.
For studying the influence of binding strength of anti-
peptide antibodies on the occurrence of clinical manifes-
tations or underlying disease type, Mann–Whitney U test or
Kruskal–Wallis test were used depending on whether there
were two or three groups compared. The results were
considered statistically significant when p \ 0.05 (i.e.,
significance level). In case of multiple pairwise compari-
sons, the Bonferroni correction was applied resulting in
significance level to be set at 0.0167, if three groups were
compared.
Results
From 201 enrolled patients, 43.3 % had APS, 33.3 % had
APS associated with SLE and 23.4 % had SLE. The mean
age of patients was 40.3 years and ranged between 12 and
80 years. The majority of patients were female (77.1 %).
76.6 % experienced thrombotic complications (arterial,
venous or microvascular) and 34.8 % of female patients
experienced obstetric manifestations. All included patients
were positive for IgG anti-b2GPI and had IgG anti-b2GPI
avidity determined. From 67 patients with HAv IgG anti-
b2GPI, 88.1 % were diagnosed with APS (independently
or as associated with SLE) and 11.9 % that had only SLE.
73.1 % of these patients had thrombotic complications
(venous, arterial and/or microvascular) and 53.3 % of
female patients had obstetric manifestations. In compari-
son, from 45 patients with LAv IgG anti-b2GPI, 64.4 %
were diagnosed with APS (independently or associated
with to SLE), whereas 35.6 % had SLE. Patients positive
for LAv IgG anti-b2GPI experienced 57.8 % thrombotic
disorders (venous, arterial and/or microvascular) and
27.0 % of female patients had obstetric episodes.
Observed numbers of positive sera for anti-peptide
antibodies were as follows: 20 for A (LKTPRV; domains
I–II), 58 for B (KDKATF; domain IV), 52 for C
(TLRVYK; domain III), 61 for peptide D (NGPANSK;
domain III), 50 for E (YNPLWFV; domain II) and 49 for F
(KMDGNHP; domains III–IV) (Table 1). Due to
insufficient amount of sera, some samples positive for
peptides were excluded in the coming step (5 positive
samples for peptide A, 1 for B, 2 for C, 9 for D, 7 for E and
4 for F), when binding strength for anti-peptide antibodies
was determined. The median binding strength was 28.7 %
for peptide A, 37.1 % for B, 32.7 % for C, 33.8 % for D,
27.5 % for E and 28.2 % for F. The anti-peptide antibodies
in studied serum samples were predominantly of HetAv (8
for peptide A, 43 for B, 40 for C, 37 for D, 29 for E and 29
for F) followed by LAv anti-peptide antibodies (4 for
peptide A, 11 for B, 10 for C, 13 for D, 13 for E and 14 for
F), whereas only a few were of HAv (3 for peptides A and
B, 2 for D and F and 1 for E) (Table 2). Further, statistical
analyses were conducted on determined anti-peptide avid-
ity presented as binding strength and not categorically as
arbitrarily defined groups (e.g., high, heterogeneous and
low anti-peptide avidity).
In order to evaluate the influence of anti-peptide posi-
tivity on the occurrence of clinical manifestations or
underlying disease-type subgroups or anti-b2GPI avidity, a
logistic regression modeling was applied. Here, mutual
positivity of selected combinations of peptides was also
tested. Among 201 patients, the number of serum samples
with mutual positivity of pairs of peptides A&E, B&C,
B&D, B&F, C&D, C&F and D&F were 17, 38, 47, 36, 39,
41 and 39, respectively. Number of serum samples with
mutual positivity of triplets of peptides B&C&D, B&C&F,
B&D&F and C&D&F were 32, 31, 33 and 34, while 28
serum samples were mutually positive for peptides
B&C&D&F. Using logistic regression, we observed a
statistically significant negative prediction of the positivity
for peptide D on the occurrence of venous thrombosis
(odds ratio (OR) 0.465, 95 % confidence interval (CI)
(95 % CI) 0.247–0.879, p = 0.018). We also observed a
positive prediction of positivity for peptide E on arterial
thrombosis occurrence (OR 3.441, 95 % CI 1.331–8.901,
p = 0.011), while mutual positivity for peptides B and F
had a negative prediction for arterial thrombosis (OR
0.153, 95 % CI 0.045–0.517, p = 0.003). Patients mutually
positive for peptides B, C and F had a *2.5 times smaller
odds to experience overall thrombosis (either venous,
arterial and/or microvascular) as compared to patients
negative for any of these peptides (OR 0.407, 95 % CI
0.185–0.874, p = 0.021). Patients positive for peptide B
had a *4.1 times higher odds for having only APS without
SLE as compared to patients diagnosed with APS associ-
ated with SLE (OR 0.242, 95 % CI 0.087–0.673,
p = 0.007), while on the other hand, positivity for peptides
C and F was a significant predictor for diagnosis of APS
associated with SLE as compared to only the APS diag-
nosis (OR 7.105, 95 % CI 2.292–22.028, p = 0.001). A
significant negative prediction was also observed for pos-
itivity to peptide A and the presence of HAv IgG anti-
Cutting Edge in Autoimmunity
123
b2GPI in comparison with LAv IgG anti-b2GPI (OR
0.167, 95 % CI 0.033–0.845, p = 0.031). A negative pre-
diction was observed for overall thrombosis in the HAv
anti-b2GPI patients subgroup when samples were positive
for peptide C and F (OR 0.170, 95 % CI 0.036–0.805,
p = 0.026) (Table 3).
In order to evaluate the impact of anti-peptide avidity,
the relationships between binding strength of anti-peptide
positive samples and clinical/serological parameters were
analyzed. A significant difference was observed between
binding strengths to peptides B and F in groups with
present HAv, HetAv and LAv IgG anti-b2GPI. For peptide
B, we observed the highest median binding strength in
HAv IgG anti-b2GPI group, followed by HetAv and LAv
IgG anti-b2GPI groups (44.3 vs. 36.6 vs. 31.7 %,
p = 0.021). Similarly, for peptide F, the highest median
binding strength was noted for HAv IgG anti-b2GPI
positive group, followed by LAv and HetAv anti-b2GPI
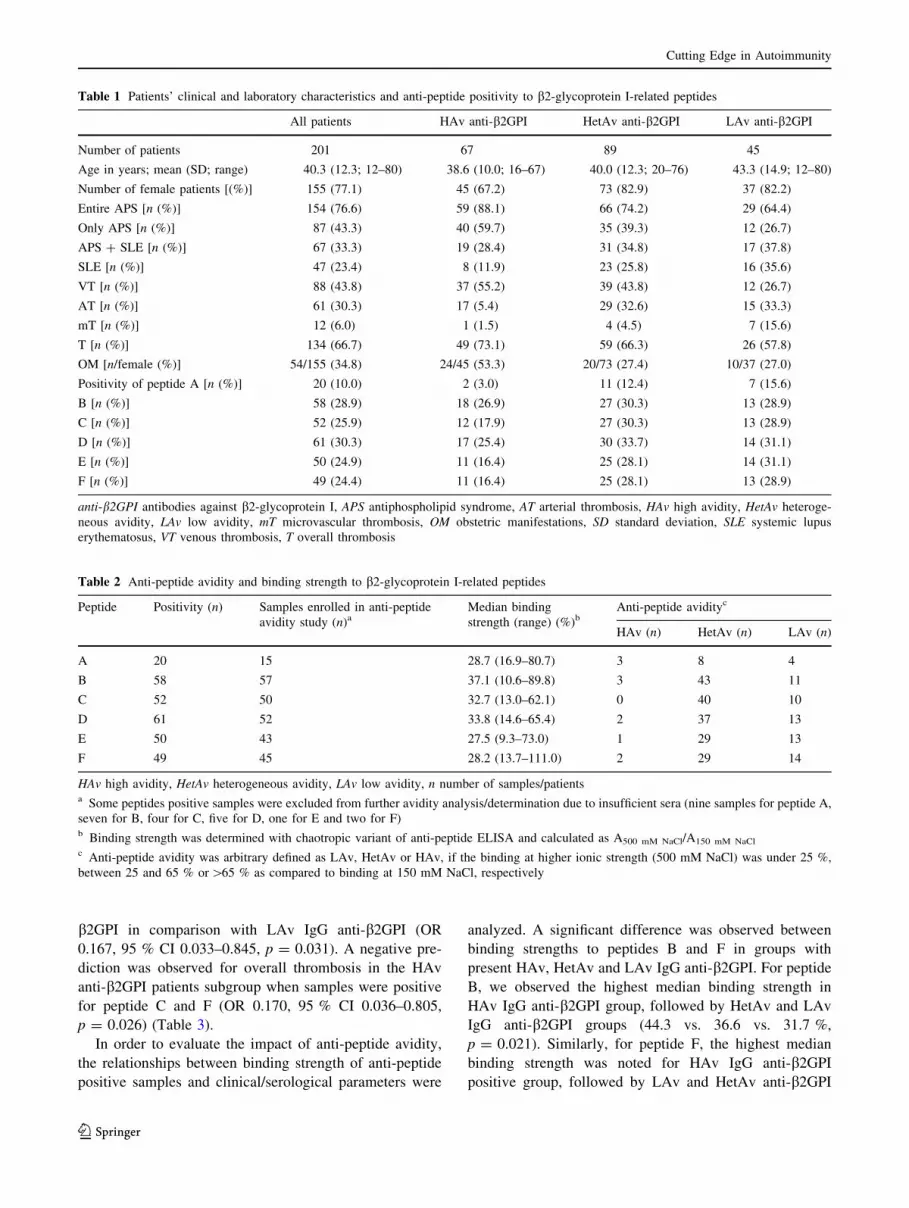
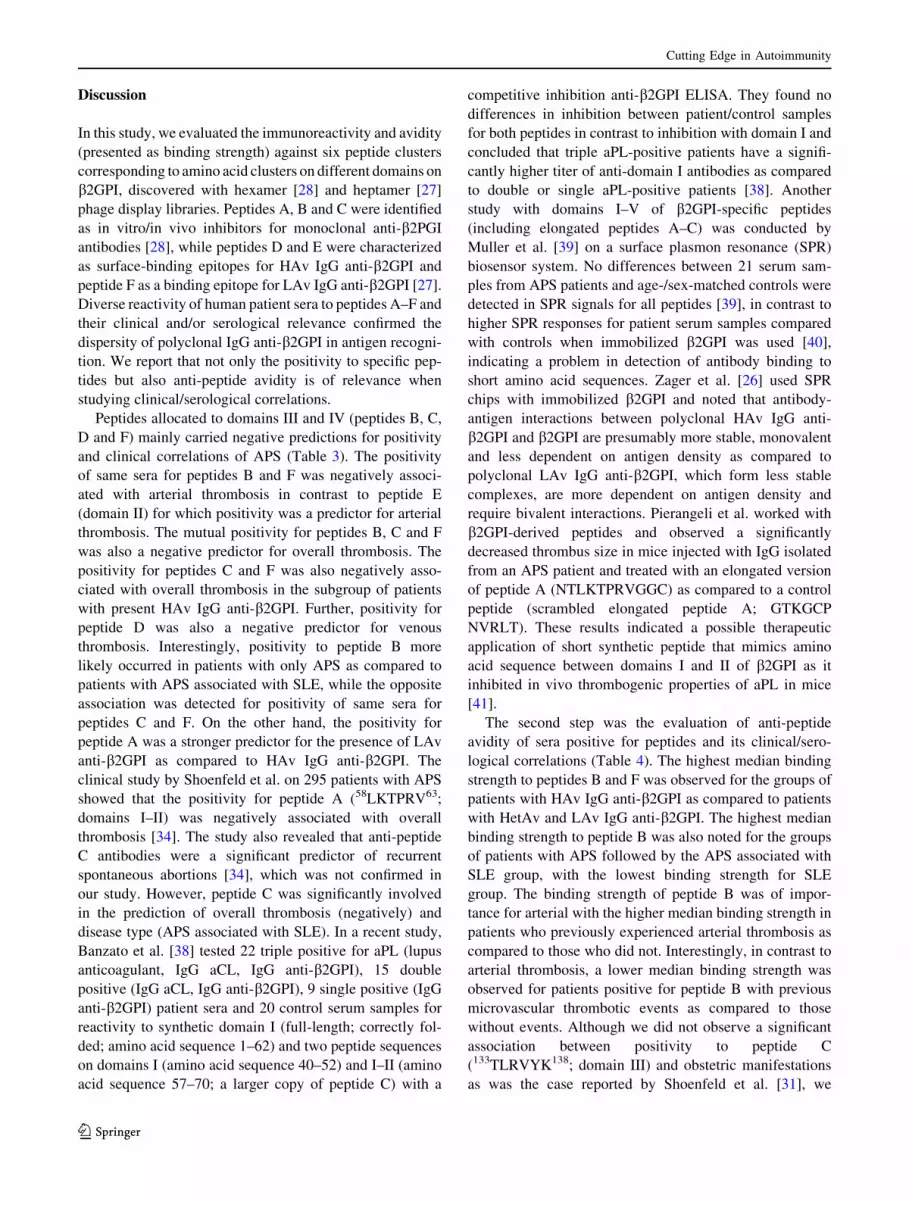
Table 1 Patients’ clinical and laboratory characteristics and anti-peptide positivity to b2-glycoprotein I-related peptides
All patients HAv anti-b2GPI HetAv anti-b2GPI LAv anti-b2GPI
Number of patients 201 67 89 45
Age in years; mean (SD; range) 40.3 (12.3; 12–80) 38.6 (10.0; 16–67) 40.0 (12.3; 20–76) 43.3 (14.9; 12–80)
Number of female patients [(%)] 155 (77.1) 45 (67.2) 73 (82.9) 37 (82.2)
Entire APS [n (%)] 154 (76.6) 59 (88.1) 66 (74.2) 29 (64.4)
Only APS [n (%)] 87 (43.3) 40 (59.7) 35 (39.3) 12 (26.7)
APS ? SLE [n (%)] 67 (33.3) 19 (28.4) 31 (34.8) 17 (37.8)
SLE [n (%)] 47 (23.4) 8 (11.9) 23 (25.8) 16 (35.6)
VT [n (%)] 88 (43.8) 37 (55.2) 39 (43.8) 12 (26.7)
AT [n (%)] 61 (30.3) 17 (5.4) 29 (32.6) 15 (33.3)
mT [n (%)] 12 (6.0) 1 (1.5) 4 (4.5) 7 (15.6)
T [n (%)] 134 (66.7) 49 (73.1) 59 (66.3) 26 (57.8)
OM [n/female (%)] 54/155 (34.8) 24/45 (53.3) 20/73 (27.4) 10/37 (27.0)
Positivity of peptide A [n (%)] 20 (10.0) 2 (3.0) 11 (12.4) 7 (15.6)
B [n (%)] 58 (28.9) 18 (26.9) 27 (30.3) 13 (28.9)
C [n (%)] 52 (25.9) 12 (17.9) 27 (30.3) 13 (28.9)
D [n (%)] 61 (30.3) 17 (25.4) 30 (33.7) 14 (31.1)
E [n (%)] 50 (24.9) 11 (16.4) 25 (28.1) 14 (31.1)
F [n (%)] 49 (24.4) 11 (16.4) 25 (28.1) 13 (28.9)
anti-b2GPI antibodies against b2-glycoprotein I, APS antiphospholipid syndrome, AT arterial thrombosis, HAv high avidity, HetAv heteroge-
neous avidity, LAv low avidity, mT microvascular thrombosis, OM obstetric manifestations, SD standard deviation, SLE systemic lupus
erythematosus, VT venous thrombosis, T overall thrombosis
Table 2 Anti-peptide avidity and binding strength to b2-glycoprotein I-related peptides
Peptide Positivity (n) Samples enrolled in anti-peptide
avidity study (n)aMedian binding
strength (range) (%)bAnti-peptide avidityc
HAv (n) HetAv (n) LAv (n)
A 20 15 28.7 (16.9–80.7) 3 8 4
B 58 57 37.1 (10.6–89.8) 3 43 11
C 52 50 32.7 (13.0–62.1) 0 40 10
D 61 52 33.8 (14.6–65.4) 2 37 13
E 50 43 27.5 (9.3–73.0) 1 29 13
F 49 45 28.2 (13.7–111.0) 2 29 14
HAv high avidity, HetAv heterogeneous avidity, LAv low avidity, n number of samples/patientsa Some peptides positive samples were excluded from further avidity analysis/determination due to insufficient sera (nine samples for peptide A,
seven for B, four for C, five for D, one for E and two for F)b Binding strength was determined with chaotropic variant of anti-peptide ELISA and calculated as A500 mM NaCl/A150 mM NaCl
c Anti-peptide avidity was arbitrary defined as LAv, HetAv or HAv, if the binding at higher ionic strength (500 mM NaCl) was under 25 %,
between 25 and 65 % or [65 % as compared to binding at 150 mM NaCl, respectively
Cutting Edge in Autoimmunity
123

groups (41.8 vs. 28.4 vs. 26.5 %, p = 0.044). The binding
strength for peptide B differed in patients with/without
arterial and microvascular thrombosis with the higher
median binding strength for the presence of arterial
thrombosis compared with those without arterial throm-
bosis (41.9 vs. 34.4 %, p = 0.033). Interestingly, the
median binding strength was higher in patients positive for
peptide B without microvascular thrombosis compared
with patients positive for peptide B with microvascular
thrombosis (38.8 vs. 24.3 %, p = 0.049). Additionally, a
difference between binding strength to peptide B was
observed also among patients diagnosed either with APS,
APS associated with SLE or SLE alone with the highest
median binding strength for APS group followed by APS
associated with SLE and SLE groups (41.2 vs. 34.3 vs.
32.2 %, p = 0.022). A difference in strength of binding for
peptide C was also observed in female patients with pre-
vious obstetric manifestation compared with female
patients without such complications (36.8 vs. 32.0 %,
p = 0.039) (Table 4).
Table 3 Significant influences of anti-peptide positivity on clinical/serological outcomes
Outcome Anti-peptide positivity Odds ratio
(95 % CI)
p value
Venous thrombosis D 0.465 (0.247–0.879) 0.018
Arterial thrombosis E 3.44 (1.33–8.90) 0.011
B&F 0.153 (0.045–0.517) 0.003
Overall thrombosis B&C&F 0.407 (0.185–0.874) 0.021
APS ? SLE versus APSa B 0.242 (0.087–0.673) 0.007
C&F 7.11 (2.29–22.0) 0.001
HAv versus LAv anti-b2GPIb A 0.167 (0.033–0.845) 0.031
Overall thrombosis (HAv anti-b2GPI subgroup) C&F 0.170 (0.036–0.805) 0.026
anti-b2GPI antibodies against b2-glycoprotein I, APS antiphospholipid syndrome, HAv high avidity, HetAv heterogeneous avidity, LAv low
avidity, SLE systemic lupus erythematosusa Multiple comparisons of dependent variable were performed (APS vs. APS ? SLE, APS vs. SLE and APS ? SLE vs. SLE) and Bonferroni
correction used—significant result when p \ 0.0167b Multinominal logistic regression model was used to asses this correlation (HAv vs. HetAv, HAv vs. LAv and HetAv vs. LAv anti-b2GPI
groups). Significant results are shown for relation between HAv vs. LAv anti-b2GPI groups
Table 4 Significant relationships between anti-peptide binding strength and serological/clinical outcomes
Peptide Testing outcome Median (range) binding strength (%) n p value Statistical test
B AT- 34.4 (10.6–89.8) 44 0.033 M–W (U = 174.0)
AT? 41.9 (32.4–62.8) 13
B mT- 38.8 (10.6–89.8) 53 0.049 M–W (U = 43.0)
mT? 24.3 (15.7–37.1) 4
B APS 41.2 (21.9–89.8) 27 0.022 K–W (v22 = 7.661)
APS ? SLE 34.3 (15.7–49.1) 15
SLE 32.2 (10.6–51.7) 15
B HAv 44.3 (26.5–85.5) 17 0.021 K–W (v22 = 7.769)
HetAv 36.6 (16.0–89.8) 27
LAv 31.7 (10.6–50.1) 13
C OM-a 32.0 (13.0–56.6) 30 0.039 M–W (U = 117.0)
OM?a 36.8 (24.2–62.1) 13
F HAv 41.8 (14.5–50.6) 10 0.044 K–W (v22 = 6.229)
HetAv 26.5 (14.8–111.0) 22
LAv 28.4 (13.7–74.8) 13
Anti-b2GPI antibodies against b2-glycoprotein I, APS antiphospholipid syndrome, AT arterial thrombosis, HAv high avidity, HetAv heteroge-
neous avidity, K–W Kruskal–Wallis test, LAv low avidity, mT microvascular thrombosis, M–W Mann–Whitney U test, n number of patients, OM
obstetric manifestations, SLE systemic lupus erythematosusa Only female patients positive for peptide F were enrolled in this model
Cutting Edge in Autoimmunity
123
Discussion
In this study, we evaluated the immunoreactivity and avidity
(presented as binding strength) against six peptide clusters
corresponding to amino acid clusters on different domains on
b2GPI, discovered with hexamer [28] and heptamer [27]
phage display libraries. Peptides A, B and C were identified
as in vitro/in vivo inhibitors for monoclonal anti-b2PGI
antibodies [28], while peptides D and E were characterized
as surface-binding epitopes for HAv IgG anti-b2GPI and
peptide F as a binding epitope for LAv IgG anti-b2GPI [27].
Diverse reactivity of human patient sera to peptides A–F and
their clinical and/or serological relevance confirmed the
dispersity of polyclonal IgG anti-b2GPI in antigen recogni-
tion. We report that not only the positivity to specific pep-
tides but also anti-peptide avidity is of relevance when
studying clinical/serological correlations.
Peptides allocated to domains III and IV (peptides B, C,
D and F) mainly carried negative predictions for positivity
and clinical correlations of APS (Table 3). The positivity
of same sera for peptides B and F was negatively associ-
ated with arterial thrombosis in contrast to peptide E
(domain II) for which positivity was a predictor for arterial
thrombosis. The mutual positivity for peptides B, C and F
was also a negative predictor for overall thrombosis. The
positivity for peptides C and F was also negatively asso-
ciated with overall thrombosis in the subgroup of patients
with present HAv IgG anti-b2GPI. Further, positivity for
peptide D was also a negative predictor for venous
thrombosis. Interestingly, positivity to peptide B more
likely occurred in patients with only APS as compared to
patients with APS associated with SLE, while the opposite
association was detected for positivity of same sera for
peptides C and F. On the other hand, the positivity for
peptide A was a stronger predictor for the presence of LAv
anti-b2GPI as compared to HAv IgG anti-b2GPI. The
clinical study by Shoenfeld et al. on 295 patients with APS
showed that the positivity for peptide A (58LKTPRV63;
domains I–II) was negatively associated with overall
thrombosis [34]. The study also revealed that anti-peptide
C antibodies were a significant predictor of recurrent
spontaneous abortions [34], which was not confirmed in
our study. However, peptide C was significantly involved
in the prediction of overall thrombosis (negatively) and
disease type (APS associated with SLE). In a recent study,
Banzato et al. [38] tested 22 triple positive for aPL (lupus
anticoagulant, IgG aCL, IgG anti-b2GPI), 15 double
positive (IgG aCL, IgG anti-b2GPI), 9 single positive (IgG
anti-b2GPI) patient sera and 20 control serum samples for
reactivity to synthetic domain I (full-length; correctly fol-
ded; amino acid sequence 1–62) and two peptide sequences
on domains I (amino acid sequence 40–52) and I–II (amino
acid sequence 57–70; a larger copy of peptide C) with a
competitive inhibition anti-b2GPI ELISA. They found no
differences in inhibition between patient/control samples
for both peptides in contrast to inhibition with domain I and
concluded that triple aPL-positive patients have a signifi-
cantly higher titer of anti-domain I antibodies as compared
to double or single aPL-positive patients [38]. Another
study with domains I–V of b2GPI-specific peptides
(including elongated peptides A–C) was conducted by
Muller et al. [39] on a surface plasmon resonance (SPR)
biosensor system. No differences between 21 serum sam-
ples from APS patients and age-/sex-matched controls were
detected in SPR signals for all peptides [39], in contrast to
higher SPR responses for patient serum samples compared
with controls when immobilized b2GPI was used [40],
indicating a problem in detection of antibody binding to
short amino acid sequences. Zager et al. [26] used SPR
chips with immobilized b2GPI and noted that antibody-
antigen interactions between polyclonal HAv IgG anti-
b2GPI and b2GPI are presumably more stable, monovalent
and less dependent on antigen density as compared to
polyclonal LAv IgG anti-b2GPI, which form less stable
complexes, are more dependent on antigen density and
require bivalent interactions. Pierangeli et al. worked with
b2GPI-derived peptides and observed a significantly
decreased thrombus size in mice injected with IgG isolated
from an APS patient and treated with an elongated version
of peptide A (NTLKTPRVGGC) as compared to a control
peptide (scrambled elongated peptide A; GTKGCP
NVRLT). These results indicated a possible therapeutic
application of short synthetic peptide that mimics amino
acid sequence between domains I and II of b2GPI as it
inhibited in vivo thrombogenic properties of aPL in mice
[41].
The second step was the evaluation of anti-peptide
avidity of sera positive for peptides and its clinical/sero-
logical correlations (Table 4). The highest median binding
strength to peptides B and F was observed for the groups of
patients with HAv IgG anti-b2GPI as compared to patients
with HetAv and LAv IgG anti-b2GPI. The highest median
binding strength to peptide B was also noted for the groups
of patients with APS followed by the APS associated with
SLE group, with the lowest binding strength for SLE
group. The binding strength of peptide B was of impor-
tance for arterial with the higher median binding strength in
patients who previously experienced arterial thrombosis as
compared to those who did not. Interestingly, in contrast to
arterial thrombosis, a lower median binding strength was
observed for patients positive for peptide B with previous
microvascular thrombotic events as compared to those
without events. Although we did not observe a significant
association between positivity to peptide C
(133TLRVYK138; domain III) and obstetric manifestations
as was the case reported by Shoenfeld et al. [31], we
Cutting Edge in Autoimmunity
123

observed a significantly higher anti-peptide C avidity
between female patients who experienced obstetric mani-
festations and those who did not. Avidity is an important
aspect in describing the binding characteristics of anti-
bodies; however, it seems that in our tests (indirect anti-
peptide ELISA with BSA blocking) avidity was affected by
shorter amino acid sequences, because the measured anti-
peptide avidity was lower (Table 2) compared with anti-
b2GPI avidity from our previous studies [24, 29, 32, 33].
The results on immunoreactivity and avidity in the current
study are in part controversial. For instance, the immuno-
reactivity to peptide D (domain III) was negatively asso-
ciated with venous thrombosis (Table 3); however, in
previous studies, peptide D was found as a possible-bind-
ing epitope for HAv anti-b2GPI, associated with throm-
botic as well as obstetric complications in APS patients
[24, 29, 32, 33]. Positivity for peptide E (domain II) rec-
ognized by HAv anti- b2GPI [27], was a predictor for
arterial thrombosis (Table 3). Expectedly, positivity for
peptide F (domains III–IV) found as a binding epitope for
LAv anti-b2GPI [27] was involved in negative prediction
of arterial and overall thrombosis and as a predictor for
APS ? SLE as compared to diagnosis of only APS
(Table 3). However, interestingly, although peptide F was
found to be a binding epitope for LAv anti-b2GPI [27], we
observed a significant correlation between anti-peptide F
binding strength and anti-b2GPI avidity. The highest
median anti-peptide F avidity was detected for HAv anti-
b2GPI (Table 4), which once again elucidates the diversity
of human polyclonal IgG anti-b2GPI subpopulations.
In conclusion, in the last few years, a theory has been
emerging that points to IgG anti-b2GPI directed against
domain I as having the most clinical relevance [7, 8, 19].
However, current as well as previous clinical and transla-
tional studies [25, 27–29] on anti-b2GPI and peptide pos-
itivity also clearly indicate that other anti-b2GPI
subpopulations have to be taken into account to delineate
APS pathology. Furthermore, anti-b2GPI and anti-peptide
avidity should be considered, especially in context of APS
clinical manifestations, such as thromboses and obstetric
complications. Our results indicate a wide dispersity in
antibody avidity and recognition of peptides corresponding
to amino acid sequences on different domains of b2GPI
and their clinical relevance. Direct comparison between
anti-b2GPI and anti-peptide positivity/avidity cannot be
equally evaluated due to different interactions between
antibody/whole antigen and antibody/peptides. This delin-
eation depends on the secondary structure of b2GPI, which
can strengthen the epitope/paratope recognition and bind-
ing strength, versus the lack of these interactions in pep-
tides. Thus, classification of anti-b2GPI into subgroups
regarding epitope specificity and avidity could represent an
additional tool in understanding the pathogenicity of IgG
anti-b2GPI in APS. In the future, studying IgG anti-b2GPI
subpopulations as evaluated by positivity/avidity of anti-
bodies against all domains and specific domains of b2GPI
should be addressed, especially in the context of their
clinical impact.
Acknowledgments The study is in accordance with the Helsinki
Declaration of 1975, revised in 1983 and was approved by the
National Ethical Committee (No. 163/02/09). This work was funded
by the National Research Program Grant No. P3-0314 from the
Ministry of Higher Education, Science and Technology, Slovenia.
Conflict of interest The authors declare no conflict of interest.
References
1. Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL,
Cervera R, et al. International consensus statement on an update
of the classification criteria for definite antiphospholipid syn-
drome (APS). J Thromb Haemost. 2006;4(2):295–306. doi:10.
1111/j.1538-7836.2006.01753.x.
2. Wilson WA, Gharavi AE, Koike T, Lockshin MD, Branch DW,
Piette JC, et al. International consensus statement on preliminary
classification criteria for definite antiphospholipid syndrome:
report of an international workshop. Arthritis Rheum. 1999;42(7):
1309–11. doi:10.1002/1529-0131(199907)42:7\1309:AID-ANR1[3.
0.CO;2-F.
3. Cervera R, Asherson RA. Antiphospholipid syndrome. In:
Shoenfeld Y, Cervera R, Gershwin ME, editors. Diagnostic criteria
in autoimmune diseases. Totowa: Humana Press; 2008. p. 9–14.
4. Cervera R, Piette JC, Font J, Khamashta MA, Shoenfeld Y,
Camps MT, et al. Antiphospholipid syndrome: clinical and
immunologic manifestations and patterns of disease expression in
a cohort of 1,000 patients. Arthritis Rheum. 2002;46(4):1019–27.
doi:10.1002/art.10187.
5. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield
NF, et al. The 1982 revised criteria for the classification of sys-
temic lupus erythematosus. Arthritis Rheum. 1982;25(11):
1271–7.
6. Hochberg MC. Updating the American College of Rheumatology
revised criteria for the classification of systemic lupus erythe-
matosus. Arthritis Rheum. 1997;40(9):1725.
7. Meroni PL, Borghi MO, Raschi E, Tedesco F. Pathogenesis of
antiphospholipid syndrome: understanding the antibodies. Nat
Rev Rheumatol. 2011;7(6):330–9. doi:10.1038/nrrheum.2011.52.
8. de Laat B, Mertens K, de Groot PG. Mechanisms of disease:
antiphospholipid antibodies-from clinical association to patho-
logic mechanism. Nat Clin Pract Rheumatol. 2008;4(4):192–9.
doi:10.1038/ncprheum0740.
9. Espinosa G, Cervera R. Antiphospholipid syndrome: frequency,
main causes and risk factors of mortality. Nat Rev Rheumatol.
2010;6(5):296–300. doi:10.1038/nrrheum.2010.47.
10. Artenjak A, Lakota K, Frank M, Cucnik S, Rozman B, Bozic B,
et al. Antiphospholipid antibodies as non-traditional risk factors
in atherosclerosis based cardiovascular diseases without overt
autoimmunity. A critical updated review. Autoimmun Rev.
2012;11(12):873–82. doi:10.1016/j.autrev.2012.03.002.
11. Shoenfeld Y, Gerli R, Doria A, Matsuura E, Cerinic MM, Ronda
N, et al. Accelerated atherosclerosis in autoimmune rheumatic
diseases. Circulation. 2005;112(21):3337–47. doi:10.1161/
CIRCULATIONAHA.104.507996.
Cutting Edge in Autoimmunity
123

12. Lin F, Murphy R, White B, Kelly J, Feighery C, Doyle R, et al.
Circulating levels of beta2-glycoprotein I in thrombotic disorders
and in inflammation. Lupus. 2006;15(2):87–93.
13. Horstman LL, Jy W, Bidot CJ, Ahn YS, Kelley RE, Zivadinov R,
et al. Antiphospholipid antibodies: paradigm in transition.
J Neuroinflammation. 2009;6:3. doi:10.1186/1742-2094-6-3.
14. Lozier J, Takahashi N, Putnam FW. Complete amino acid
sequence of human plasma beta 2-glycoprotein I. Proc Natl Acad
Sci USA. 1984;81(12):3640–4.
15. Hunt JE, Simpson RJ, Krilis SA. Identification of a region of beta
2-glycoprotein I critical for lipid binding and anti-cardiolipin antibody
cofactor activity. Proc Natl Acad Sci USA. 1993;90(6):2141–5.
16. Schwarzenbacher R, Zeth K, Diederichs K, Gries A, Kostner GM,
Laggner P, et al. Crystal structure of human beta2-glycoprotein I:
implications for phospholipid binding and the antiphospholipid
syndrome. EMBO J. 1999;18(22):6228–39. doi:10.1093/emboj/
18.22.6228.
17. Sodin-Semrl S, Frank M, Ambrozic A, Pavlic J, Sustar V, Cucnik S,
et al. Interactions of phospholipid binding proteins with negatively
charged membranes: b2-glycoprotein I as a model mechanism. In:
Leitmannova Liu A, editor. Advances in planar lipid bilayers and
liposomes, 1st ed. Amsterdam: Elsevier; 2008. p. 243–73.
18. Agar C, van Os GM, Morgelin M, Sprenger RR, Marquart JA,
Urbanus RT, et al. Beta2-glycoprotein I can exist in 2 confor-
mations: implications for our understanding of the antiphospho-
lipid syndrome. Blood. 2010;116(8):1336–43. doi:10.1182/blood-
2009-12-260976.
19. de Laat B, Derksen RH, van Lummel M, Pennings MT, de Groot PG.
Pathogenic anti-beta2-glycoprotein I antibodies recognize domain I
of beta2-glycoprotein I only after a conformational change. Blood.
2006;107(5):1916–24. doi:10.1182/blood-2005-05-1943.
20. Wang MX, Kandiah DA, Ichikawa K, Khamashta M, Hughes G,
Koike T, et al. Epitope specificity of monoclonal anti-beta
2-glycoprotein I antibodies derived from patients with the anti-
phospholipid syndrome. J Immunol. 1995;155(3):1629–36.
21. Kasahara H, Matsuura E, Kaihara K, Yamamoto D, Kobayashi K,
Inagaki J, et al. Antigenic structures recognized by anti-beta2-gly-
coprotein I auto-antibodies. Int Immunol. 2005;17(12):1533–42.
doi:10.1093/intimm/dxh330.
22. Mahler M, Norman GL, Meroni PL, Khamashta M. Autoanti-
bodies to domain 1 of beta 2 glycoprotein 1: a promising can-
didate biomarker for risk management in antiphospholipid
syndrome. Autoimmun Rev. 2012;12(2):313–7. doi:10.1016/j.
autrev.2012.05.006.
23. Ambrozic A, Avicin T, Ichikawa K, Kveder T, Matsuura E,
Hojnik M, et al. Anti-beta(2)-glycoprotein I antibodies in children
with atopic dermatitis. Int Immunol. 2002;14(7):823–30.
24. Cucnik S, Kveder T, Krizaj I, Rozman B, Bozic B. High avidity
anti-beta 2-glycoprotein I antibodies in patients with anti-
phospholipid syndrome. Ann Rheum Dis. 2004;63(11):1478–82.
doi:10.1136/ard.2003.017939.
25. de Laat B, Derksen RH, de Groot PG. High-avidity anti-beta2
glycoprotein I antibodies highly correlate with thrombosis in
contrast to low-avidity anti-beta2 glycoprotein I antibodies.
J Thromb Haemost. 2006;4(7):1619–21. doi:10.1111/j.1538-
7836.2006.02002.x.
26. Zager U, Irman S, Lunder M, Skarabot M, Musevic I, Hodnik V,
et al. Immunochemical properties and pathological relevance of
anti-beta2-glycoprotein I antibodies of different avidity. Int
Immunol. 2011;23(8):511–8. doi:10.1093/intimm/dxr043.
27. Zager U, Lunder M, Cucnik S, Kveder T, Rozman B, Bozic B.
Immunodominant epitopes of beta2-glycoprotein I for high
avidity antibodies. In: 8th International congress on autoimmu-
nity. Granada, Spain: Geneva: Kenes International; 2012.
28. Blank M, Shoenfeld Y, Cabilly S, Heldman Y, Fridkin M, Kat-
chalski-Katzir E. Prevention of experimental antiphospholipid
syndrome and endothelial cell activation by synthetic peptides.
Proc Natl Acad Sci USA. 1999;96(9):5164–8.
29. Cucnik S, Kveder T, Artenjak A, Ulcova Gallova Z, Swadzba J,
Musial J, et al. Avidity of anti-beta2-glycoprotein I antibodies inpatients with antiphospholipid syndrome. Lupus. 2012;21(7):764–5.
doi:10.1177/0961203312440057.
30. Iverson GM, von Muhlen CA, Staub HL, Lassen AJ, Binder W,
Norman GL. Patients with atherosclerotic syndrome, negative in
anti-cardiolipin assays, make IgA autoantibodies that preferentially
target domain 4 of beta2-GPI. J Autoimmun. 2006;27(4):266–71.
doi:10.1016/j.jaut.2006.09.007.
31. Shoenfeld Y, Krause I, Kvapil F, Sulkes J, Lev S, von Landen-
berg P, et al. Prevalence and clinical correlations of antibodies
against six beta2-glycoprotein-I-related peptides in the anti-
phospholipid syndrome. J Clin Immunol. 2003;23(5):377–83.
32. Cucnik S, Bozic B, Kveder T, Tomsic M, Rozman B. Avidity of
anti-beta2-glycoprotein I and thrombosis or pregnancy loss in
patients with antiphospholipid syndrome. Ann N Y Acad Sci.
2005;1051:141–7. doi:10.1196/annals.1361.055.
33. Cucnik S, Kveder T, Ulcova-Gallova Z, Swadzba J, Musial J,
Valesini G, et al. The avidity of anti-beta2-glycoprotein I anti-
bodies in patients with or without antiphospholipid syndrome: a
collaborative study in the frame of the European forum on anti-
phospholipid antibodies. Lupus. 2011;20(11):1166–71. doi:10.
1177/0961203311406308.
34. Artenjak A, Kozelj M, Lakota K, Cucnik S, Bozic B, Sodin-Semrl S.
High avidity anti-b2-glycoprotein I antibodies activate human cor-
onary artery endothelial cells and trigger peripheral blood mono-
nuclear cell migration. Eur J Inflamm. 2013;11(2):385–96.
35. Favaloro EJ, Wong RC. Laboratory testing for the antiphospho-
lipid syndrome: making sense of antiphospholipid antibody
assays. Clin Chem Lab Med. 2011;49(3):447–61. doi:10.1515/
CCLM.2011.064.
36. Cucnik S, Ambrozic A, Bozic B, Skitek M, Kveder T. Anti-
beta2-glycoprotein I ELISA: methodology, determination of cut-
off values in 434 healthy Caucasians and evaluation of mono-
clonal antibodies as possible international standards. Clin Chem
Lab Med. 2000;38(8):777–83. doi:10.1515/CCLM.2000.111.
37. Avcin T, Ambrozic A, Bozic B, Accetto M, Kveder T, Rozman
B. Estimation of anticardiolipin antibodies, anti-beta2 glycopro-
tein I antibodies and lupus anticoagulant in a prospective longi-
tudinal study of children with juvenile idiopathic arthritis. Clin
Exp Rheumatol. 2002;20(1):101–8.
38. Banzato A, Pozzi N, Frasson R, De Filippis V, Ruffatti A, Bison
E, et al. Antibodies to domain I of beta(2)glycoprotein I are in
close relation to patients risk categories in antiphospholipid
syndrome (APS). Thromb Res. 2011;128(6):583–6. doi:10.1016/
j.thromres.2011.04.021.
39. Muller C, Thaler M, Schlichtiger A, Schreiegg A, Balling G,
Steigerwald U, et al. beta2-glycoprotein I-derived peptides as
antigenic structures for the detection of antiphospholipid anti-
bodies. J Thromb Haemost. 2010;8(9):2073–5. doi:10.1111/j.
1538-7836.2010.03987.x.
40. Metzger J, von Landenberg P, Kehrel M, Buhl A, Lackner KJ,
Luppa PB. Biosensor analysis of beta2-glycoprotein I-reactive
autoantibodies: evidence for isotype-specific binding and differ-
entiation of pathogenic from infection-induced antibodies. Clin
Chem. 2007;53(6):1137–43. doi:10.1373/clinchem.2006.079632.
41. Pierangeli SS, Blank M, Liu X, Espinola R, Fridkin M, Ostertag
MV, et al. A peptide that shares similarity with bacterial antigens
reverses thrombogenic properties of antiphospholipid antibodies
in vivo. J Autoimmun. 2004;22(3):217–25. doi:10.1016/j.jaut.
2004.01.002.
Cutting Edge in Autoimmunity
123





























