Embed Size (px)
Citation preview

702 Am J Clin Pathol 2008;130:702-711702 DOI: 10.1309/AJCPNS6K1CYJPDBA
© American Society for Clinical Pathology
Immunopathology / Anti-FLC MonoCLonAL Antibodies
Immunodiagnostic Capabilities of Anti–Free Immunoglobulin Light Chain Monoclonal Antibodies
Sandra Davern, PhD, Lian X. Tang, PhD, Teresa K. Williams, Sallie D. Macy, CMT, Jonathan S. Wall, PhD, Deborah T. Weiss, and Alan Solomon, MD
Key Words: Free light chains; Immunoglobulins; Immunoassay; Multiple myeloma; Amyloidosis
DOI: 10.1309/AJCPNS6K1CYJPDBA
A b s t r a c t
Overproduction of plasma cell–derived monoclonal free κ or λ immunoglobulin light chains (FLCs) is a hallmark of multiple myeloma, AL amyloidosis, and light chain deposition disease. Because these components serve as unique cellular and serologic biomarkers, their detection and quantitation has diagnostic, therapeutic, and prognostic import. In this regard, we have developed monoclonal antibodies (mAbs) that specifically recognize the κ or λ FLC products of all known human variable and constant region light chain genes. We now report the results of our studies that have demonstrated the capability of these reagents to measure, in a modified fluid-phase capture enzyme-linked immunosorbent assay (ELISA), serum κ and λ FLCs at concentrations as low as 5 and 15 ng/mL, respectively. The mAb-based ELISA has greater sensitivity and reproducibility than does the commercially available immunoturbidimetric assay that uses polyclonal anti-FLC antibodies. In addition, the mAbs can immunostain monoclonal FLC-producing plasma cells and pathologic light chain–related amyloid and nonfibrillar tissue deposits. Our anti-FLC mAbs, with their high degree of reactivity and versatility, may provide an invaluable tool in the diagnosis and management of light chain–associated disease.
Monoclonal free κ and λ immunoglobulin light chains (FLCs), ie, LCs that are not covalently bound to heavy chains (as in the case of complete IgG, IgA, IgM, IgD, and IgE molecules), have long been considered unique biomarkers of the human plasma cell–related immunoproliferative dis-orders, which include multiple myeloma, light chain deposi-tion disease, and AL amyloidosis.1 The deposition of these components as renal tubular casts, peritubular deposits, or amyloid fibrils leads to organ dysfunction, resulting in con-siderable morbidity and, eventually, death.2 Thus, the ability to measure accurately serum or urinary FLC concentrations in these patients, as well as identify by immunochemical means the clonal nature of bone marrow–derived plasma cell popula-tions and pathologic tissue deposits, has diagnostic, therapeu-tic, and prognostic import.
Quantification of FLCs in body fluids is necessar-ily dependent on the availability of antibodies that can reli-ably distinguish between such components and those bound to heavy chains. In this regard, efforts have been direct-ed to developing anti-FLC monoclonal antibodies (mAbs) that would prove suitable as diagnostic radioimmunoas-say- or enzyme-linked immunosorbent assay (ELISA)-based reagents.3-6 Unfortunately, in most cases, these were of limit-ed value owing to lack of specificity, eg, their cross-reactivity with immunoglobulin heavy chains or inability to recognize κ and λ FLCs. Furthermore, analyses of normal human serum samples yielded widely disparate results.7 Nevertheless, as part of our long-standing effort to generate mAbs that recog-nize human κ or λ LC variable region (VL) subgroups or gene families (Vκ or Vλ, respectively), as well as epitopes shared among all κ or λ proteins, we identified 2 antibodies, one des-ignated Fκ-C8 and the other Fλ-G9, that reacted exclusively

Am J Clin Pathol 2008;130:702-711 703703 DOI: 10.1309/AJCPNS6K1CYJPDBA 703
© American Society for Clinical Pathology
Immunopathology / originAL ArtiCLe
with κ and λ FLCs, respectively, and that could be used in a fluid-phase ELISA to measure the concentration of such molecules in blood, urine, or cerebrospinal fluid with a high degree of sensitivity and reproducibility.8,9
We now have optimized this assay to include (as the first step) capture of the murine anti-FLC mAbs in wells coated with a goat antimouse IgG (Fc-specific) antibody, in lieu of binding the mAbs directly to the wells. This modification, as we report, has resulted in increased accuracy and reproduc-ibility, with the ability to measure κ and λ FLCs at concentra-tions as low as approximately 5 and 15 ng/mL, respectively. The diagnostic versatility of these reagents also has been evidenced immunocytologically and immunohistochemically, where we showed that they could be used to detect FLC-containing clonal plasma cell populations and establish the light chain nature of pathologic tissue deposits, respectively.
Materials and Methods
Clinical SamplesSerum, urine, and bone marrow specimens were derived
from 71 patients with monoclonal plasma B-cell–related dis-orders (multiple myeloma, light chain deposition disease, AL amyloidosis, Waldenström macroglobulinemia). In addition, sera were obtained from 41 healthy adults. All blood-derived samples were analyzed within 24 hours or frozen at –20°C until use. The study was approved by the University of Tennessee Graduate School of Medicine Institutional Review Board.
Proteins κ- and λ-type Bence Jones proteins were isolated from
the urine of patients with multiple myeloma by zone elec-trophoresis and their purity confirmed by sodium dodecyl sulfate (SDS)/polyacrylamide gel electrophoresis (PAGE), as described previously.10 The LC variable region (VL) subgroup (Vκ1, Vκ2, Vκ3, Vκ4/Vλ1, Vλ2, Vλ3, Vλ6, Vλ8) and constant region (CL) allotype (κm
1,–2, κm1,2, κm
3) or isotype (Cλ1, Cλ2/3, Cλ7) were established serologically and confirmed by amino acid sequence analyses or tandem mass spectrometry.11,12 Polyclonal FLCs were isolated by gel filtration chromatog-raphy of reduced-alkylated IgG (Fr II γ-globulin, Sigma, St Louis, MO), as described.13 Polyclonal IgG, IgA, and IgM preparations were purchased from Sigma. Protein concentra-tions were measured in a bicinchonic acid colorimetric assay (micro BCA assay, Pierce Biotechnology, Rockford, IL).
FLC ImmunoassaysDetails regarding the derivation, purification, and char-
acterization of the IgG1 anti-κ (Fκ-C8) and anti-λ (Fλ-G9) FLC mAbs have been reported previously.8,9 Briefly, Balb/c mice were immunized with thermally denatured κ or λ
Bence Jones proteins and FLC-specific IgG antibodies gen-erated from hybridomas composed of murine immune sple-nocytes fused with SP 2/0 cells, which then were subcloned, propagated, and injected intraperitoneally into pristane-primed mice. The resultant mAbs were purified from ascitic fluid by 40% ammonium sulfate precipitation followed by ion exchange chromatography.
The FLC immunoassay was modified from that origi-nally described9 as follows: Wells in high-titer, polystyrene microtiter plates (Costar, Corning, NY) were coated overnight at 4°C with goat antimouse IgG Fc-specific antibody (Sigma) diluted to a concentration of 4 µg/mL in 0.01 mol/L of sodium bicarbonate buffer, pH 9.6. The wells were washed with 0.05% polysorbate (Tween)-20 in phosphate-buffered saline (PBST) and blocked with 1% bovine serum albumin (BSA) in PBS for 1 hour at room temperature, followed by addition of 50 µL of murine anti-FLC mAb Fκ-C8 or Fλ-G9 that was diluted in working buffer (0.1% BSA/PBS/0.01% thimero-sal) to 4 µg/mL. After incubation (1 hour at 22°C), excess antibody was removed by washing 3 times with PBST. Next, wells were filled with 50-µL volumes of standards composed of equimolar amounts of Bence Jones proteins represent-ing the 4 Vκ or 5 Vλ subgroups diluted in working buffer in the range of 0.001 to 1 µg/mL or individual serum samples (centrifuged at 10,000 rpm for 5 minutes at 4°C to remove any particulates) diluted 1:10, 1:30, 1:100, 1:1,000, 1:3,000, and 1:30,000. After a 1-hour incubation at 22°C and 3 washes with PBST, the wells were filled with 50 µL of horseradish peroxidase (HRP)-conjugated goat F(ab')2 antihuman κ or λ antibodies (Biosource, Camarillo, CA) diluted 1:1,000, the plates were incubated for 1 hour at room temperature, and excess antibody was removed by washing 3 times with PBST. For color development, 50 µL of the 2-component ABTS Peroxidase Substrate System (KPL, Gaithersburg, MD) was added to each well and the enzymatic reaction terminated after 10 minutes by addition of an equal volume of 2% oxalic acid. Absorbance was measured at 405 nm using a microplate reader (BioTek Synergy HT, Winooski, VT). All assays were done in triplicate and considered valid when the R2 values of the standard curves were greater than 0.99.
For the competition ELISA, after capture of the anti-FLC mAbs, wells were filled with 50 µL of a biotinylated κ or λ Bence Jones protein (1 µg/mL) mixed with an equal volume of the same unbiotinylated Bence Jones protein or polyclonal immunoglobulins (0.1-10 µg/mL), and the plates were shaken for 1 hour at 22°C. After washing 3 times with PBST, 50 µL of Immunopure streptavidin-HRP (250 ng/mL; Pierce Biotechnology) was added, and the plates were shaken for 1 hour at room temperature. The wells were washed 3 times with PBST and then filled first with the ABTS substrate and next the oxalic acid solution, after which the absorbance was measured as described in the preceding paragraph.

704 Am J Clin Pathol 2008;130:702-711704 DOI: 10.1309/AJCPNS6K1CYJPDBA
© American Society for Clinical Pathology
Davern et al / Anti-FLC MonoCLonAL Antibodies
For comparative purposes, serum FLC concentrations were measured using the FREELITE Human Kappa and Lambda Free kits purchased from The Binding Site (San Diego, CA) and the Beckman Coulter IMMAGE system (Fullerton, CA), according to the manufacturers’ protocols.
Immunohistochemical AnalysisFor immunophenotypic analyses, bone marrow plasma
cells were isolated and immunostained with the anti-κ and anti-λ FLC mAbs and with a mouse antihuman plasma cell mAb (clone VS38c, DAKO, Carpinteria, CA), as described previously.14 Immunohistochemical studies were performed using 4-µm-thick formalin-fixed, paraffin-embedded tissue sections mounted on poly-l-lysine-coated slides that were dried overnight at room temperature and deparaffinized. Sections were immersed in the Glyca, pH 4.0, antigen-retriev-al solution (BioGenex, San Ramon, CA), heated in a micro-wave oven, and immunostained using the ImmPRESS poly-merized reporter enzyme-linked system (Vector Laboratories, Burlingame, CA).
Results
Specificity of Antihuman κ and λ FLC mAbsThe anti-κ (Fκ-C8) and anti- λ (Fλ-G9) FLC mAbs were
shown in a competitive inhibition ELISA to react specifically with monoclonal or polyclonal FLCs, but not with these mol-ecules when they were covalently bound to γ, α, or µ heavy chains (ie, IgG, IgA, or IgM proteins) zTable 1z. As shown in zFigure 1z, κ and λ Bence Jones proteins effectively inhibited
the interaction of mAbs Fκ-C8 and Fλ-G9, respectively, with isotype-matched counterparts coated on ELISA plate wells.
Additional experimental data confirmed that the epitope recognized by the anti-FLC mAbs was confined to the CL domain, as evidenced by the fact that mAbs Fκ-C8 and Fλ-G9 had comparable reactivity with proteins representative of the major human Vκ and Vλ subgroups (Vκ1, Vκ2, Vκ3, and Vκ4 and Vλ1, Vλ2, Vλ3, Vλ6, and Vλ8), respectively. Furthermore, the CL specificity of these reagents was found to be independent of the Cκ allotype (κm
1,–2, κm1,2, κm
3) or Cλ isotype (Cλ1, Cλ2/3, Cλ7) zTable 2z. In addition, the presence of carbohydrate on Bence Jones proteins (as demonstrated in
zTable 1zReactivity of Anti-FLC Monoclonal Antibodies With Monoclonal and Polyclonal Human Immunoglobulins and LCs*
Anti-κ FLC Anti-λ FLC Protein (Fκ-C8) (Fλ-G9)
Monoclonal immunoglobulins IgG 0 0 IgA 0 0 IgD 0 0 IgM 0 0Polyclonal immunoglobulins IgG 0 0 IgA 0 0 IgM 0 0Monoclonal LCs κ + 0 λ 0 +Polyclonal LCs + +
FLC, free LC; LC, light chain.* 0, no difference from background; +, >0.45 optical density.
0.2
0 2
Competitor (� g/mL)
OD
(40
5 n
m)
4 6 8 10
0.4
0.6
0.8
1.0
0
κ IgG IgA IgM
Competitor (� g/mL)
λ
0.2
0 2
OD
(40
5 n
m)
4 6 8 10
0.4
0.6
0.8
1.0
0
IgG IgA IgM
A B
zFigure 1z Anti–free light chain (FLC) specificity of monoclonal antibodies Fκ-C8 and Fλ-G9. Competitive enzyme-linked immunosorbent assay in which 1 µg/mL of a biotinylated κ or λ Bence Jones protein was incubated with 0.1-10 µg/mL of unbiotinylated κ (A) or λ (B) Bence Jones protein and with polyclonal IgG, IgA, or IgM. OD, optical density.
Am J Clin Pathol 2008;130:702-711 705705 DOI: 10.1309/AJCPNS6K1CYJPDBA 705
© American Society for Clinical Pathology
Immunopathology / originAL ArtiCLe
periodic acid–Schiff–stained SDS/PAGE gels) did not affect the assay; similar results were obtained in analyses of mono-mers and dimers isolated from individual samples by gel fil-tration chromatography. In contrast, reduction and alkylation of monoclonal LCs in the presence of 6 mol/L of guanidine HCl or enzymatic cleavage of such molecules into VL and CL fragments15 resulted in loss of reactivity with the anti-FLC mAbs (data not shown).
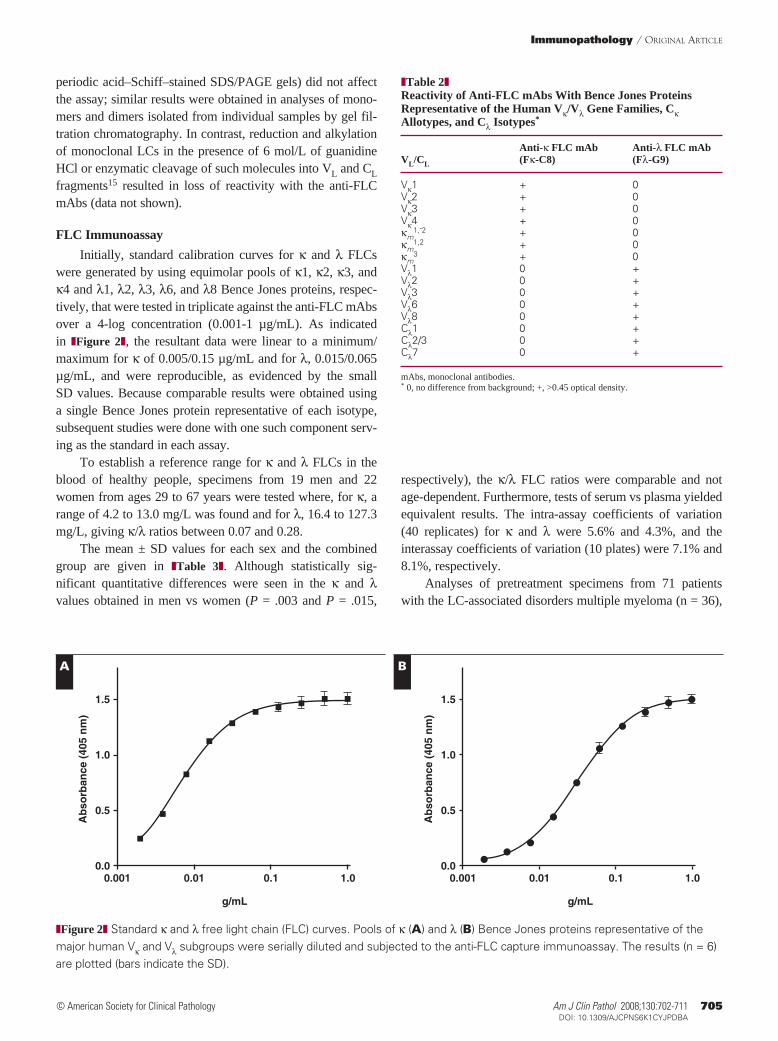
FLC ImmunoassayInitially, standard calibration curves for κ and λ FLCs
were generated by using equimolar pools of κ1, κ2, κ3, and κ4 and λ1, λ2, λ3, λ6, and λ8 Bence Jones proteins, respec-tively, that were tested in triplicate against the anti-FLC mAbs over a 4-log concentration (0.001-1 µg/mL). As indicated in zFigure 2z, the resultant data were linear to a minimum/maximum for κ of 0.005/0.15 µg/mL and for λ, 0.015/0.065 µg/mL, and were reproducible, as evidenced by the small SD values. Because comparable results were obtained using a single Bence Jones protein representative of each isotype, subsequent studies were done with one such component serv-ing as the standard in each assay.
To establish a reference range for κ and λ FLCs in the blood of healthy people, specimens from 19 men and 22 women from ages 29 to 67 years were tested where, for κ, a range of 4.2 to 13.0 mg/L was found and for λ, 16.4 to 127.3 mg/L, giving κ/λ ratios between 0.07 and 0.28.
The mean ± SD values for each sex and the combined group are given in zTable 3z. Although statistically sig-nificant quantitative differences were seen in the κ and λ values obtained in men vs women (P = .003 and P = .015,
respectively), the κ/λ FLC ratios were comparable and not age-dependent. Furthermore, tests of serum vs plasma yielded equivalent results. The intra-assay coefficients of variation (40 replicates) for κ and λ were 5.6% and 4.3%, and the interassay coefficients of variation (10 plates) were 7.1% and 8.1%, respectively.
Analyses of pretreatment specimens from 71 patients with the LC-associated disorders multiple myeloma (n = 36),
zTable 2zReactivity of Anti-FLC mAbs With Bence Jones Proteins Representative of the Human Vκ/Vλ Gene Families, Cκ Allotypes, and Cλ Isotypes*
Anti-κ FLC mAb Anti-λ FLC mAb VL/CL (Fκ-C8) (Fλ-G9)
Vκ1 + 0Vκ2 + 0Vκ3 + 0Vκ4 + 0κm
1,-2 + 0κm
1,2 + 0κm
3 + 0Vλ1 0 +Vλ2 0 +Vλ3 0 +Vλ6 0 +Vλ8 0 +Cλ1 0 +Cλ2/3 0 +Cλ7 0 +
mAbs, monoclonal antibodies.* 0, no difference from background; +, >0.45 optical density.
� g/mL
0.5
0.001 0.01 0.1
Ab
sorb
ance
(40
5 n
m)
1.0
1.0
1.5
0.0
� g/mL
0.5
0.001 0.01 0.1
Ab
sorb
ance
(40
5 n
m)
1.0
1.0
1.5
0.0
A B
zFigure 2z Standard κ and λ free light chain (FLC) curves. Pools of κ (A) and λ (B) Bence Jones proteins representative of the major human Vκ and Vλ subgroups were serially diluted and subjected to the anti-FLC capture immunoassay. The results (n = 6) are plotted (bars indicate the SD).
706 Am J Clin Pathol 2008;130:702-711706 DOI: 10.1309/AJCPNS6K1CYJPDBA
© American Society for Clinical Pathology
Davern et al / Anti-FLC MonoCLonAL Antibodies
systemic AL amyloidosis (n = 23), and light chain deposition disease (n = 7), as well as Waldenström macroglobulinemia (n = 5), revealed abnormal κ/λ FLC ratios of more than 0.3 in subjects having monoclonal κ-type serum immunoglobu-lins and/or urinary Bence Jones proteins (as evidenced by immunofixation electrophoresis) or, alternatively, less than 0.07 for those with λ-type molecules. In all cases, there was concordance between the κ or λ nature of the serum or urinary monoclonal protein and its predominance in the FLC ratio. In general, a value that was abnormally high or low resulted from an increase in the amount of the monoclonal immunoglobulin; however, the extent of deviation of FLC values from normal was not necessarily related to the concentration of the patho-logic component. This contrasted with the unaffected isotype, which was within normal limits or reduced. In patients who responded to therapy, a reduction in the concentration of the monoclonal serum or urinary immunoglobulin was reflected by normalization of the κ/λ FLC ratio, although even when such molecules could no longer be detected posttherapy by immunofixation electrophoresis, a normal FLC ratio was not necessarily found.
Comparison of mAb- and Polyclonal Antibody–Based FLC Immunoassays
The results of our analyses of sera using our mAb-based ELISA method vs the FREELITE immunoturbidimetric method that uses polyclonal reagents revealed marked quantitative dif-ferences in the κ and λ values; in the case of FREELITE, these were generally lower (especially for λ) than those obtained by ELISA, thus affecting the absolute FLC κ/λ ratios. As shown in zTable 4z, these trends also were apparent when the same 12 serum specimens were analyzed in our laboratory and in that of Jerry A. Katzman, PhD, Mayo Clinic, Rochester, MN, where the most notable discrepancy involved case 3 with an IgGλ gammopathy. Furthermore, in our studies of 71 mono-clonal immunoglobulin-containing serum samples, κ and λ data could be obtained directly in all specimens by the ELISA method, whereas this was possible in only 39 cases using the standard 1:10 dilution specified by the FREELITE protocol. (In the other 32, it was necessary to repeat the study using, as appropriate, undiluted or offline diluted specimens.)
Immunohistochemical ResultsThe specific recognition of κ and λ FLCs by mAbs
Fκ-C8 and Fλ-G9 also was demonstrated immunocytochemi-cally when these reagents were tested against cell suspensions prepared from the bone marrow of patients with multiple myeloma or AL amyloidosis. Among more than 30 cases studied, the monoclonal immunoglobulin immunophenotype of the plasma cells was apparent by a predominance of κ or λ cytoplasmic reactivity zImage 1z, even in patients with AL amyloidosis in whom the percentage of this cell population was relatively low, ie, <5%. There was complete agreement between the type of FLC documented immunocytochemically
zTable 3zEnzyme-Linked Immunosorbent Assay Monoclonal Antibody–Derived FLC Values in Normal Adult Serum Samples*
κ FLC λ FLC κ/λ FLC†
Men (n = 19) 6.6 ± 2.3 49.8 ± 21.5 0.15 ± 0.06Women (n = 22) 8.9 ± 2.8 66.1 ± 27.5 0.14 ± 0.04Combined (n = 41) 7.9 ± 2.8 58.5 ± 26.0 0.15 ± 0.05
FLC, free light chain.* Data are given as mean ± SD in milligrams per liter.† Average of all individual patient values.
zTable 4zComparison of FLC Immunoquantitative Data
Anti-FLC Polyclonal Antibodies† Anti-FLC Monoclonal Antibodies‡
Case No./ Monoclonal Diagnosis Immunoglobulin* κ FLC§ λ FLC§ κ/λ FLC κ FLC§ λ FLC§ κ/λ FLC
1/AL IgGλ 1.1 10.9 0.10 0.6 27.7 0.022/MM IgGκ 4.1 0.6 6.83 6.6 6.2 1.063/AL IgGλ 1.2 1.9 0.63 1.3 50.5 0.034/AL IgGκ 12.1 1.6 7.56 18.1 19.9 0.915/AL BJPκ 101.0 0.2 505.0 141.5 4.1 34.516/AL IgGλ/BJPλ 0.8 40.0 0.02 1.3 43.3 0.037/MM IgGκ 68.1 0.26 261.9 27.2 2.8 97.18/MM/AL BJPκ 39.1 4.20 9.31 282.1 25.6 11.029/MM BJPλ 0.15 74.7 0.002 0.7 71.4 0.0110/AL IgAλ 0.62 8.1 0.08 0.7 217.3 0.00311/AL BJPλ 0.96 48.7 0.02 1.2 27.8 0.0412/MM BJPκ 35.8 1.1 32.5 35.5 6.0 5.92
AL, AL amyloidosis; BJP, Bence Jones protein; FLC, free light chain; MM, multiple myeloma.* Based on immunofixation electrophoresis.† FREELITE anti-κ FLC and anti-λ FLC reagents. Normal values, κ, 3.3-19.4 mg/L; λ, 5.71-26.3 mg/L; κ/λ, 0.26-1.65.‡ Anti-κ FLC (Fκ-C8) and anti-λ FLC (Fλ-G9) monoclonal antibodies. Normal values, κ, 4.2-13.0 mg/L; λ, 16.4-127.3 mg/L; κ/λ, 0.07-0.28.§ In milligrams per liter.
Am J Clin Pathol 2008;130:702-711 707707 DOI: 10.1309/AJCPNS6K1CYJPDBA 707
© American Society for Clinical Pathology
Immunopathology / originAL ArtiCLe
and that of the serum or urinary monoclonal protein. Notably, κ or λ FLCs could be detected in plasma cells from the patients who had monoclonal serum immunoglobulins, but no evident Bence Jones protein, even when urine specimens were tested at a concentration of 100 mg/mL or more.
The anti-FLC mAbs also immunostained AL amyloid tissue deposits zImage 2z, as well as other types of pathologic LC precipitates, including those found in the form of κ- or λ-containing casts in renal tubules or as peritubular punctate lesions, as found in multiple myeloma or light chain deposi-tion disease, respectively zImage 3z.
Discussion
We have developed a robust fluid-phase capture ELISA that uses specific murine antihuman FLC mAbs to measure, with a high degree of sensitivity and reproducibility, con-centrations of κ and λ FLCs in serum and other body fluids. Furthermore, these mAbs have proven to be useful as immu-nodiagnostic reagents to establish the monoclonality of bone marrow–derived plasma cells, especially in the case of AL amyloidosis, in which, in contrast with multiple myeloma, the percentage is typically low, ie, 5% to 10%.16 In addition, in
A A A
DDD
C C C
B B B
zImage 1z Immunocytochemical detection of κ or λ free light chains (FLCs) in bone marrow–derived plasma cells. Cytocentrifuged suspension of preparations obtained from patients with multiple myeloma (A and B) or AL amyloidosis (C and D) and immunostained, using as primary reagents an anti–plasma cell antibody (left) or the anti-κ (center) and anti-λ (right) FLC monoclonal antibodies (A-D, ×400).

708 Am J Clin Pathol 2008;130:702-711708 DOI: 10.1309/AJCPNS6K1CYJPDBA
© American Society for Clinical Pathology
Davern et al / Anti-FLC MonoCLonAL Antibodies
was not detected on pepsin-derived or naturally occurring CL fragments. In this respect, we previously reported that sero-logic identification of κ and λ epitopes, as well as κm allotypes (located in the Cκ region), also was dependent on the native polypeptide.15,28-30 In studies involving a nonsecreted aber-rant κ LC product, which due to a missense mutation had a completely anomalous sequence after position 187 (including the absence of the Cys 194 residue required for an intrachain disulfide bond with Cys 146), we found that this component was nonreactive with the anti-κ FLC mAb and posited that the epitope recognized by this antibody was located between
immunohistochemical studies, the κ or λ nature of amyloid and nonfibrillar pathologic deposits found in tissue biopsy specimens was readily evidenced. As shown by others,17-26 measurement of FLCs in serial blood or urine specimens obtained from patients before and after chemotherapy can be used to document response to treatment and/or relapse. The clinical import of such information is the subject of a recent review article.27
Although it is presumed that the FLC epitope recognized by mAbs Fκ-C8 and Fλ-G9 is located in the CL domain, its expression requires the intact LC molecule, inasmuch as it
A A A
DDD
C C C
B B B
zImage 2z Immunohistochemical detection of κ- or λ-containing AL amyloid deposits. Formalin-fixed, deparaffinized sections of kidney (A and B) and heart (C and D) were stained with Congo red and examined by polarizing microscopy (left), as well as immunostained with the anti-κ (center) or anti-λ (right) free light chain monoclonal antibodies (A-D, ×400).

Am J Clin Pathol 2008;130:702-711 709709 DOI: 10.1309/AJCPNS6K1CYJPDBA 709
© American Society for Clinical Pathology
Immunopathology / originAL ArtiCLe
A A
B B
C C
zImage 3z Immunohistochemical detection of κ- or λ-containing pathologic deposits. Formalin–fixed, deparaffinized sections of kidney obtained from patients with multiple myeloma (A and B) and light chain deposition disease (C) immunostained with the anti-κ (left) or anti-λ (right) free light chain monoclonal antibodies (A-C, ×400).

710 Am J Clin Pathol 2008;130:702-711710 DOI: 10.1309/AJCPNS6K1CYJPDBA
© American Society for Clinical Pathology
Davern et al / Anti-FLC MonoCLonAL Antibodies
as recommended,6,7 international reference standards and vali-date the FLC immunoassays designed for clinical use.
From the Human Immunology and Cancer Program, Department of Medicine, University of Tennessee Graduate School of Medicine, Knoxville.
Supported in part by USPHS research grant CA10056 from the National Cancer Institute, Bethesda, MD. Dr Tang was an American Cancer Society Harry and Elsa Jiler International Visiting Scientist, and Dr Solomon is an American Cancer Society Clinical Research Professor.
Address reprint requests to Dr Solomon: Human Immunology and Cancer Program, University of Tennessee Graduate School of Medicine, 1924 Alcoa Hwy, Knoxville, TN 37920.
Acknowledgments: We thank Craig Wooliver and James Foster for technical assistance and Keira Clark for manuscript preparation.
References 1. Solomon A. Monoclonal immunoglobulins as biomarkers
of cancer. In: Sell S, ed. Cancer Markers: Developmental and Diagnostic Significance. Clifton, NJ: Humana Press; 1980:57-87.
2. Solomon A, Weiss DT, Herrera GA. Renal diseases associated with multiple myeloma and related plasma cell dyscrasias. In: Berenson JR, ed. Biology and Management of Multiple Myeloma. Totowa, NJ: Humana Press; 2004:281-302.
3. Ling NR, Lowe J, Hardie D, et al. Detection of free κ chains in human serum and urine using pairs of monoclonal antibodies reacting with Cκ epitopes not available on whole immunoglobulins. Clin Exp Immunol. 1983;52:234-240.
4. Axiak SM, Krishnamoorthy L, Guinan J, et al. Quantitation of free kappa light chains in serum and urine using a monoclonal antibody based inhibition enzyme-linked immunoassay. J Immunol Methods. 1987;99:141-147.
5. Nelson M, Brown RD, Gibson J, et al. Measurement of free kappa and lambda chains in serum and the significance of their ratio in patients with multiple myeloma. Br J Haematol. 1992;81:223-230.
6. Nakano T, Nagata A. ELISAs for free light chains of human immunoglobulins using monoclonal antibodies: comparison of their specificity with available polyclonal antibodies. J Immunol Methods. 2003;275:9-17.
7. Nakano T, Miyazaki S, Takahashi H, et al. Immunochemical quantification of free immunoglobulin light chains from an analytical perspective. Clin Chem Lab Med. 2006;44:522-532.
8. Abe M, Goto T, Kennel SJ, et al. Production and immunodiagnostic applications of antihuman light chain monoclonal antibodies. Am J Clin Pathol. 1993;100:67-74.
9. Abe M, Goto T, Kosaka M, et al. Differences in kappa to lambda (κ:λ) ratios of serum and urinary free light chains. Clin Exp Immunol. 1998;111:457-462.
10. Solomon A. Light chains of human immunoglobulins. Methods Enzymol. 1985;116:101-121.
11. Murphy CL, Eulitz M, Hrncic R, et al. Chemical typing of amyloid protein contained in formalin-fixed paraffin-embedded biopsy specimens. Am J Clin Pathol. 2001;116:135-142.
12. Murphy CL, Wang S, Williams T, et al. Characterization of systemic amyloid deposits by mass spectrometry. Methods Enzymol. 2006;412:48-62.
residues 187 and 214 but depended on the structural integrity of the entire LC molecule.31
Currently, the only commercially available FLC assay for clinical use is The Binding Site FREELITE system. This immunoassay is based on the interaction of affinity-purified sheep antihuman κ or λ FLC polyclonal antibody–coated latex particles with FLCs contained in serum or urine; the resultant turbidity is compared with reference standards and measured by nephelometry.32,33 The FREELITE protocol specifies that serum specimens first be diluted 1:10; however, owing to its limited measuring range (particularly for λ FLCs), the manu-facturer suggests that out-of-range samples be reanalyzed using a series of offline dilutions. This is seldom a problem with our ELISA-based mAb method because 6 different serum dilutions (1:10 to 1:30,000) are included on each plate and, generally, the results of at least 2 fall within the linear portion of the standard curve; furthermore, in contrast with the immunoturbidimetric assay, it is far more sensitive (ie, 5 and 15 ng/mL vs 3,600 and 5,600 ng/mL32 for κ and λ FLCs, respectively) and encompasses a wider measuring range by a factor of approximately 1,000. Notably, it is not adversely affected by lipemic or hemolyzed serum samples. Although it has been stated that the turbidimetric assay may be more suitable for routine immunochemistry laboratories,32 newer instruments now are available that are capable of ELISA (as well as nephelometric) analyses.
We also have shown that our anti–free κ and λ mAbs react with all LCs, irrespective of their VL or CL composi-tion. Comparison of FLC quantitative data obtained using the FREELITE polyclonal antibody–based immunoturbidimetric method vs our mAb ELISA-based immunoassay revealed that, with the exception of case 3, there was agreement between the κ or λ nature of the monoclonal immunoglobulin and the abnormal κ/λ FLC ratio. However, there were notable differ-ences in the 2 systems in regard to the concentrations of κ and λ FLCs (and the κ/λ ratio) in normal and patient serum samples. The most striking discrepancy involved the lower FREELITE λ values that, in turn, affected the κ/λ ratio. This may be due to the inability of the sheep anti-λ FLC antibodies to recognize all Vλ subgroups or Cλ isotypes, the confounding effect of high-molecular-weight λ-chain polymers,34 interfer-ence by intact Igλ molecules, instrumentation, or unknown technical factors. Other investigators have reported aberrations in measurement of FLCs by this nephelometric-based assay that result from analytic imprecision or discrepancies resulting from dilution.35,36 An additional problem can be the lot-to-lot variation, and, in this regard, the use of monoclonal rather than polyclonal anti-FLC antibodies is obviously advantageous. Nevertheless, given the importance of FLC detection and mea-surement in the diagnosis of clonal plasma cell–related disor-ders, as well as for objective documentation of response to therapy and/or disease progression, it is necessary to develop,

Am J Clin Pathol 2008;130:702-711 711711 DOI: 10.1309/AJCPNS6K1CYJPDBA 711
© American Society for Clinical Pathology
Immunopathology / originAL ArtiCLe
26. Dispenzieri A, Kyle RA, Katzmann JA, et al. Immunoglobulin free light chain ratio is an independent risk factor for progression of smoldering (asymptomatic) multiple myeloma. Blood. 2008;111:785-789.
27. Pratt G. The evolving use of serum free light chain assays in haematology. Br J Haematol. 2008;141:413-422.
28. McLaughlin CL, Solomon A. A hidden antigenic site localized to the constant region of light chains of immunoglobulins. Science. 1973;179:580-582.
29. Solomon A. Bence Jones proteins and light chains of immunoglobulins, XIV: conformational dependency and molecular localization of the kappa (κ) and lambda (λ) antigenic determinants. Scand J Immunol. 1976;5:685-695.
30. Solomon A, McLaughlin CL, Steinberg AG. Bence Jones proteins and light chains of immunoglobulins, III: inv antigenicity: a genetic expression with serologic dependency on the intact kappa light chain molecule. Immunochemistry. 1970;7:709-713.
31. Coriu D, Weaver K, Schell M, et al. A molecular basis for nonsecretory myeloma. Blood. 2004;104:829-831.
32. Bradwell AR, Carr-Smith HD, Mead GP, et al. Highly sensitive automated immunoassay for immunoglobulin free light chains in serum and urine. Clin Chem. 2001;47:673-680.
33. Katzman JA, Clark RJ, Abraham RS, et al. Serum reference intervals and diagnostic ranges for free and free immunoglobulin light chains: relative sensitivity for detection of monoclonal light chains. Clin Chem. 2002;48:1437-1444.
34. Tate JR, Gill D, Cobcroft R, et al. Practical considerations for the measurement of free light chains in serum. Clin Chem. 2003;49:1957-1958.
35. Daval S, Tridon A, Mazeron N, et al. Risk of antigen excess in serum free light chain measurements [letter]. Clin Chem. 2007;53:1985-1986.
36. Tate JR, Mollee M, Dimeski G, et al. Analytical performance of serum free light-chain assay during monitoring of patients with monoclonal light-chain diseases. Clin Chim Acta. 2007;376:30-36.
13. Fleischman JB, Pain RH, Porter RR. Reduction of gamma-globulins. Arch Biochem Biophys. 1962;(suppl 1):174-180.
14. Solomon A, Weiss DT, Macy SD, et al. Immunocytochemical detection of kappa and lambda light chain V region subgroups in human B-cell malignancies. Am J Pathol. 1990;137:855-862.
15. Solomon A, McLaughlin CL. Bence-Jones proteins and light chains of immunoglobulins, I: formations and characterization of amino-terminal (variant) and carboxyl-terminal (constant) halves. J Biol Chem. 1969;244:3393-3404.
16. Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol. 1995;8:32-59.
17. Drayson M, Tang LX, Drew R, et al. Serum free light-chain measurements for identifying and monitoring patients with nonsecretory multiple myeloma. Blood. 2001;97:2900-2902.
18. Lachman HJ, Gallimore R, Gillmore JD, et al. Outcome in systemic AL amyloidosis in relation to changes in concentration of circulating free immunoglobulin light chains following chemotherapy. Br J Haematol. 2003;122:78-84.
19. Abraham RS, Katzmann JA, Clark RJ, et al. Quantitative analyses of serum free light chains: a new marker for the diagnostic evaluation of primary systemic amyloidosis. Am J Clin Pathol. 2003;119:274-278.
20. Rajkumar SV, Kyle RA, Therneau TM, et al. Presence of monoclonal free light chains in the serum predicts risk of progression in monoclonal gammopathy of undetermined significance. Br J Haematol. 2004;127:308-310.
21. Mead GP, Carr-Smith HD, Drayson MT, et al. Serum free light chains for monitoring multiple myeloma. Br J Haematol. 2004;126:348-354.
22. Tate J, Mollee P, Gill D. Serum free light chains for monitoring multiple myeloma [letter]. Br J Haematol. 2005;128:405-406.
23. Palladini G, Lavatelli F, Russo P, et al. Circulating amyloidogenic free light chains and serum N-terminal natriuretic peptide type B decrease simultaneously in association with improvement of survival in AL. Blood. 2006;107:3854-3858.
24. van Rhee F, Bolejack V, Hollmig K, et al. High serum-free light chain levels and their rapid reduction in response to therapy define an aggressive multiple myeloma subtype with poor prognosis. Blood. 2007;110:827-832.
25. Morris KL, Tate JR, Gill D, et al. Diagnostic and prognostic utility of the serum free light chain assay in patients with AL amyloidosis. Intern Med. 2007;37:456-463.





























