Embed Size (px)
Citation preview
Int Urogynecol J (1992)3:212-221 �9 1992 The International Urogynecology Journal International
Urogynecology Journal
Review Article
Imaging for Urogynecology, Including New Modalities G. M. Ghoniem 1, M. S. Shoukry 1, A. Yang 2, and J. M o s t w i n 3
1Department of Urology, Tulane University School of Medicine, New Orleans; and 2Departments of Radiology and 3Urology Brady Urological Institute and Johns Hopkins Medical Institutions, Baltimore, USA
Abstract: Radiologic evaluation is the mainstay in urogynecology. Currently videofluorourodynamics is the most precise diagnostic tool for evaluating disturb- ances of micturition. However, evolving application of ultrasonography, when combined with urodynamics, constitutes an attractive alternative for such evalua- tions. Magnetic resonance imaging (MRI) may prove to be a powerful research and clinical tool. Advantages and limitations of each imaging modality are discussed.
Keywords: Imaging; Urogynecology
Introduction
It is common for female patients with an anatomical pelvic abnormality to present to both the gynecologist and the urologist. Such abnormalities are: cystocele, rectocele, enterocele, urethral diverticulum and vesico- or urethrovaginal fistulas. These conditions occur with or without urinary incontinence. Even after repair of such conditions, urinary incontinence can result from either a condition undiagnosed preoperatively, or an iatrogenic one due to weakening of the supporting structures. X-ray evaluation of these conditions, so far, remains the mainstay of the evaluation. However, it is not considered the last word since our tools and approaches are constantly changing. As our imaging capabilities become more sophisticated, a re-evaluation of the general approach is always in order.
In this review we will try to answer the following questions: When and why should each technique be
Correspondence and offprint requests to: Dr Gamal M. Ghoniem, Delta Primate Research Center, Three Rivers Road, Covington, Louisana 70433, USA.
used? What are the strengths and weaknesses of each modality? How can we best maximize our diagnostic accuracy and at the same time minimize the cost, the radiation exposure, the discomfort and the risk? What is best for one physician and one facility may not be best, or even possible, in another.
While stress urinary incontinence may be associated with genital prolapse, these are two separate problems. Correction of genital prolapse is not necessarily follow- ed by cure of stress incontinence or residual urine. On the other hand, correction of cystocele in a continent patient may result in urinary incontinence. The use of chain cystourethrogram pointed out that a cystocele may be, and often is, presenting with an entirely normal urethral vesical relationship [1].
Urinary incontinence in females is created by loss of the equilibrium of compensating forces, and no single factor is responsible for maintaining continence. Classi- cally, stress urinary incontinence can result from one of two mechanisms. In the first, and by far the most common condition, there is urethral and bladder-neck hypermobility with sudden increase of abdominal pressure. The unequal transmission of abdominal pressure to the continence zone provokes incontinence. It is classically stated that due to loss of support of the vesical neck during stress, it descends to a position that is 'outside the abdominal cavity'. That concept led to this condition being thought of as a 'hernia' of the vesical neck. This is supported by the fact that opera- tions designed to 'repair the hernia' are generally successful, with reported cure rates in excess of 90% [2-10]. However, it is not uncommon to find some continent females who have failing abdominal pressure transmission. Also there are females with weak intrin- sic mechanisms but who are still continent due to normal pressure transmission to the urethra. While hypermobility of the urethra and bladder base have

Imaging for Urogynecology 213
been documented by many investigators to be accom- panied by stress urinary incontinence, others [11-13] have questioned the validity of these findings. Hyper- mobility of the urethra is not necessary for inconti- nence, nor is any degree of urethral hypermobility related to the severity of incontinence [14]. Moreover, Fantl et al. [15] studied 145 incontinent patients and found that 78% of them showed sphincter weakness. This suggests that most patients with stress inconti- nence have a certain degree of a sphincter weakness and that the anatomical defect is not the only problem.
In the second condition, the urethra loses its function as a sphincter. Proximal urethral pressure is often low and the closing urethral pressure at that point is usually below 10 cmH20 [14]. Typically, but not invariably, the female patients have had multiple prior pelvic operations resulting in a fibrotic rigid urethra. In addi- tion, this condition occurs in patients with decentraliza- tion (sympathetic injury) of the bladder neck and urethra, as in cases of myelodysplasia, spinal cord infarction, after abdominoperineal resection for carci- noma of the rectum and after Wertheim hysterectomy. Typically, but again not invariably, the urethra is fixed in its position due to fibrosis. However, a few cases will show hypermobility and still weak sphincter mechan- isms. The usual urethropexy operations have a failure rate of at least 15%-50% in these cases [16-20]. On the other hand, surgical repair with a pubovaginal sling has been effective in over 95% of these patients [21,22].
Though medical history and physical examination are of paramount importance, they are usually not suffi- cient to give a precise diagnosis and prognosis of the condition. The accuracy and validity of the Bonney or Marshall test [23] as a prognostic indicator has been greatly emphasized in the literature but its reliability has been questioned because of an inherent concern that compression of the urethra and urethrovesical junction may occur when performing the test [24,14].
The Q-tip test is an inexpensive and easy way to evaluate urethral hypermobility [25,26]; it is proved to be of low specificity and sensitivity as shown by Montz and Stanton [27]. In their study, 32% of patients with positive Q-tip tests had either pure detrusor instability or pure sensory urgency (false-positive) and 24% of patients who had a negative Q-tip test had a diagnosis of pure genuine stress incontinence. The sensitivity and specificity was found to be better for young patients. Bergman in 1984 [28] demonstrated that the vaginal pessary test is a reliable preoperative prognostic test in women with urinary incontinence. However, it does not specify the anatomical defect and its degree, and it may produce a compressive effect over the urethra and the bladder neck which is a potential source of error.
From the above discussion and because of medicole- gal concerns and peer pressure, it can be seen that imaging and urodynamics are being more utilized for diagnosis of the exact etiology and documentation of the condition, as well as for discussing with the patient the prognosis of her condition.
Imaging Techniques
Simple and Chain Cystourethrography
In these techniques, urethral configuration and bladder outline are sharply detailed in the anterior, posterior and lateral positions [29]. The dynamic effects of strain- ing are well demonstrated and the relationship between the urethra and bladder on the one hand and the symphysis pubis on the other is easily noted.
Interpretation of the cystourethrography. Loss of sup- port to the bladder floor, in the anteroposterior view, would be shown by a low position of the bladder floor with more descent below the lower edge of the symphy- sis pubis during abdominal straining. On the lateral view the bladder base shows a backward and downward rotation with a conical shape. Loss of support of the bladder neck and urethra would be shown in the anteroposterior view by a normal or low bladder base in relation to the symphysis pubis. However, the blad-
d e r floor slopes gradually downwards to the internal meatus where it assumes a pointed appearance. On a lateral view there is a conical-shaped bladder base and the internal meatus is located at the most dependent part of the bladder base. There is an increased urethro- vesical angle (more than 100 ~ with an increase of more than 30 ~ in the angle of inclinication of the urethral axis from the vertical line.
Usually weakness or loss of support of the bladder base occurs together with loss of support of the urethra and bladder neck, but these changes do not necessarily happen together. If a cystocele is present without urinary incontinence, the downward and backward rotation of the bladder causes a relative elevation of the level of the internal meatus away from the area of maximum hydrostatic pressure. It appears possible that the partially weakened sphincteric mechanism could function fairly Well under such circumstances [30].
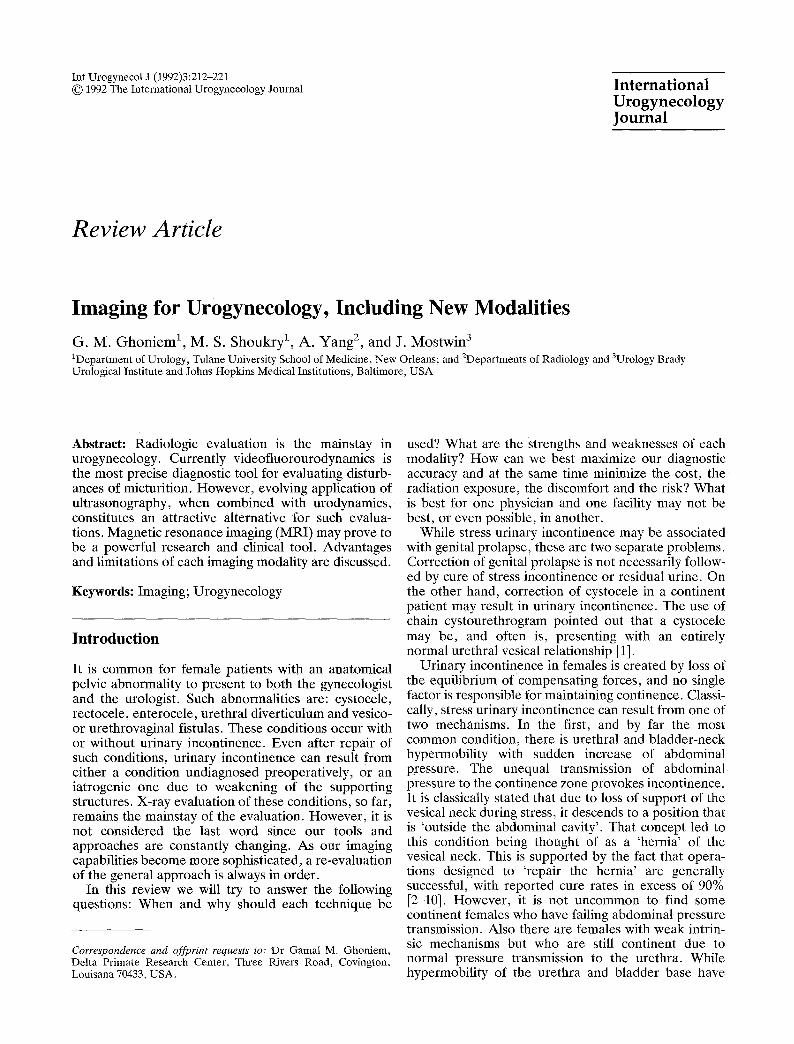
A voiding cystourethrogram or urethogram can de- monstrate a urethral diverticulum. Using a special Foley catheter, urethral diverticulae are easily de- monstrated (Fig. 1). In this technique, one balloon is used to occlude the bladder neck, and the other to occlude the external urinary meatus.
Disadvantages. The major deficiency of these tests used in the investigation of urinary incontinence is the inability to detect detrusor instability, which is a major source of incontinence in females. The cystogram does not determine bladder and urethral function as could be done with urodynamic measurements at the time of the test.
Videofluorocystourethrography
Radiographic visualization of the lower urinary tract is usually combined with urodynamic studies using a multichannel recorder measuring intravesical, in-
214 G.M. Ghoniem et al.
Fig. 1. Intubated urethrogram showing multiple posterior urethral diverticulae in 55-year-old female with recurrent urinary tract infec- tions.
on a television monitor. This can be achieved by a separate television camera sending the video image (from urodynamic tracing and X-ray) to a video splitter which mixes the information and displays it on a single video screen. Alternatively, computer digitization of the X-ray and urodynamic data can be displayed on a television screen and printed on paper. This test is considered the 'gold standard' for the evaluation of voiding abnormalities [31-35]. The whole event can be videotaped for later review and for documentation.
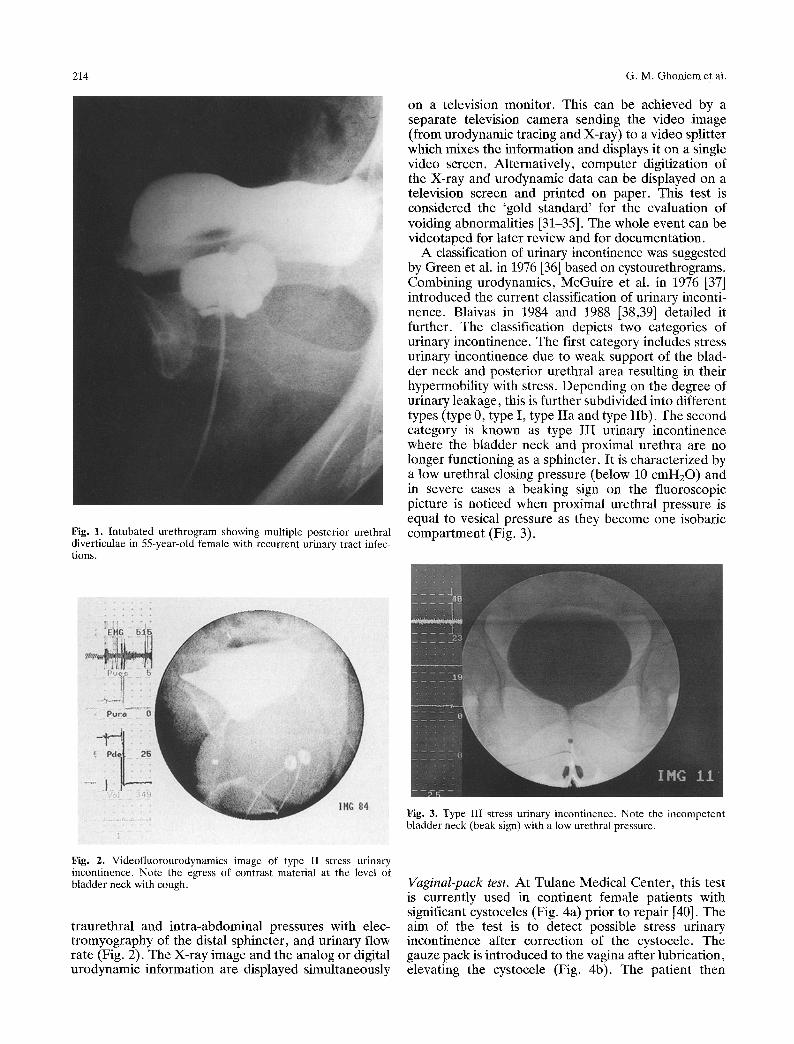
A classification of urinary incontinence was suggested by Green et al. in 1976 [36] based on cystourethrograms. Combining urodynamics, McGuire et al. in 1976 [37] introduced the current classification of urinary inconti- nence. Blaivas in 1984 and 1988 [38,39] detailed it further. The classification depicts two categories of urinary incontinence. The first category includes stress urinary incontinence due to weak support of the blad- der neck and posterior urethral area resulting in their hypermobility with stress. Depending on the degree of urinary leakage, this is further subdivided into different types (type 0, type I, type IIa and type IIb). The second category is known as type IIl urinary incontinence where the bladder neck and proximal urethra are no longer functioning as a sphincter. It is characterized by a low urethral closing pressure (below 10 cmH20) and in severe cases a beaking sign on the fluoroscopic picture is noticed when proximal urethral pressure is equal to vesical pressure as they become one isobaric compartment (Fig. 3).
Fig. 3. Type III stress urinary incontinence. Note the incompetent bladder neck (beak sign) with a low urethral pressure.
Fig. 2. Videofluorourodynamics image of type II stress urinary incontinence. Note the egress of contrast material at the level of bladder neck with cough.
traurethral and intra-abdominal pressures with elec- tromyography of the distal sphincter, and urinary flow rate (Fig. 2). The X-ray image and the analog or digital urodynamic information are displayed simultaneously
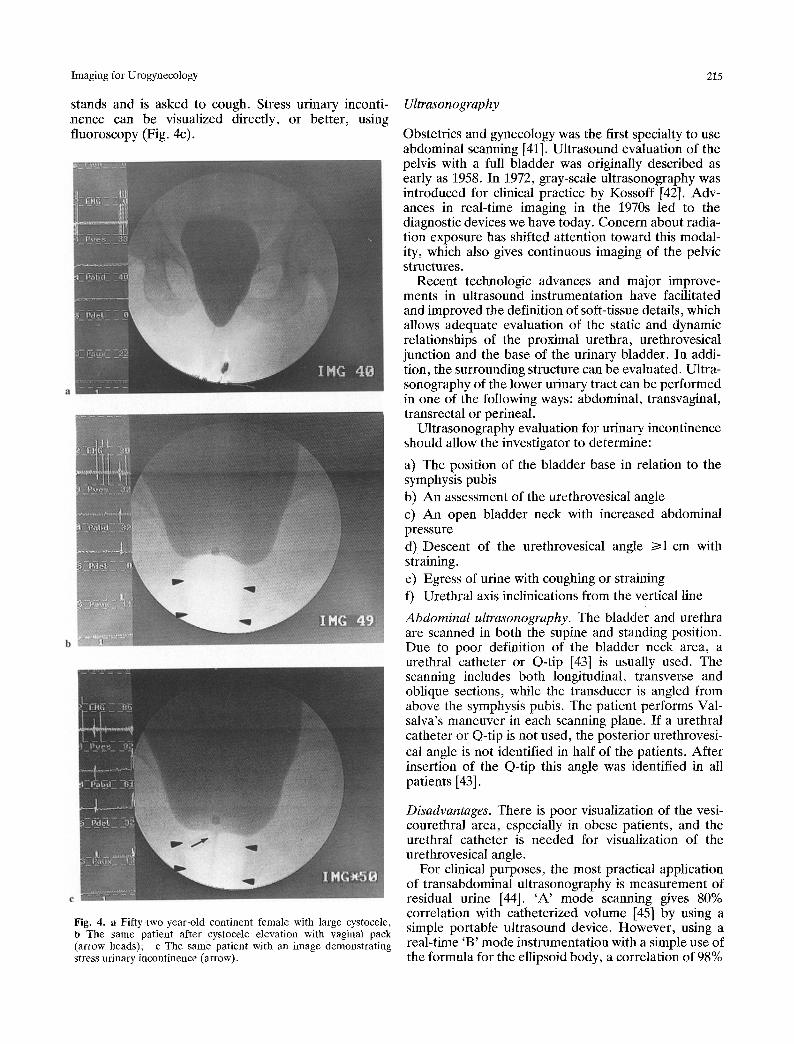
Vaginal-pack test. At Tulane Medical Center, this test is currently used in continent female patients with significant cystoceles (Fig. 4a) prior to repair [40]. The aim of the test is to detect possible stress urinary incontinence after correction of the cystocele. The gauze pack is introduced to the vagina after lubrication, elevating the cystoeele (Fig. 4b). The patient then
Imaging for Urogynecology 215
stands and is asked to cough. Stress urinary inconti- nence can be visualized directly, or better, using fluoroscopy (Fig. 4c).
Ultrasonography
Obstetrics and gynecology was the first specialty to use abdominal scanning [41]. Ultrasound evaluation of the pelvis with a full bladder was originally described as early as 1958. In 1972, gray-scale ultrasonography was introduced for clinical practice by Kossoff [42]. Adv- ances in real-time imaging in the 1970s led to the diagnostic devices we have today. Concern about radia- tion exposure has shifted attention toward this modal- ity, which also gives continuous imaging of the pelvic structures.
Recent technologic advances and major improve- ments in ultrasound instrumentation have facilitated and improved the definition of soft-tissue details, which allows adequate evaluation of the static and dynamic relationships of the proximal urethra, urethrovesical junction and the base of the urinary bladder. In addi- tion, the surrounding structure can be evaluated. Ultra- sonography of the lower urinary tract can be performed in one of the following ways: abdominal, transvaginal, transrectal or perineal.
Ultrasonography evaluation for urinary incontinence should allow the investigator to determine:
a) The position of the bladder base in relation to the symphysis pubis b) An assessment of the urethrovesical angle c) An open bladder neck with increased abdominal pressure d) Descent of the urethrovesical angle I>1 cm with straining. e) Egress of urine with coughing or straining f) Urethral axis inclinications from the vertical line
Abdominal ultrasonography. The bladder and urethra are scanned in both the supine and standing position. Due to poor definition of the bladder neck area, a urethral catheter or Q-tip [43] is usually used. The scanning includes both longitudinal, transverse and oblique sections, while the transducer is angled from above the symphysis pubis. The patient performs Val- salva's maneuver in each scanning plane. If a urethral catheter or Q-tip is not used, the posterior urethrovesi- cal angle is not identified in half of the patients. After insertion of the Q-tip this angle was identified in all patients [43].
Fig. 4. a Fifty-two-year-old continent female with large cystocele, b The same patient after cystocele elevation with vaginal pack (arrow heads); c The same patient with an image demonstrating stress urinary incontinence (arrow).
Disadvantages. There is poor visualization of the vesi- courethral area, especially in obese patients, and the urethral catheter is needed for visualization of the urethrovesical angle.
For clinical purposes, the most practical application of transabdominal ultrasonography is measurement of residual urine [44]. 'A' mode scanning gives 80% correlation with catheterized volume [45] by using a simple portable ultrasound device. However, using a real-time 'B' mode instrumentation with a simple use of the formula for the ellipsoid body, a correlation of 98%
216 G.M. Ghoniem et al.
was found between the estimated and catheterized residual urine [46,47]. For cases in which ultrasound fails to show residual urine it was found to be less than 20 ml. The ellipsoid formula is simplified to
V = . 5 x D l x D 2 x D 3
(V = volume, D1 = breadth, D2 -= height and D3 = length).
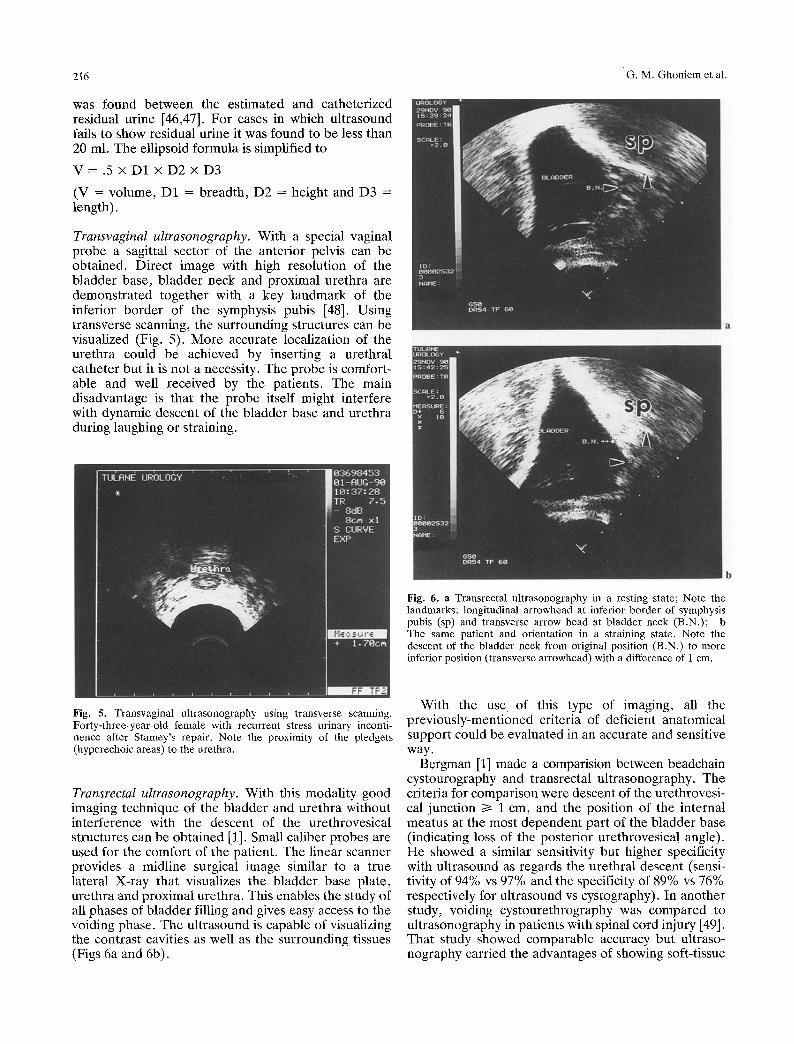
Transvaginal uItrasonography. With a special vaginal probe a sagittal sector of the anterior pelvis can be obtained. Direct image with high resolution of the bladder base, bladder neck and proximal urethra are demonstrated together with a key landmark of the inferior border of the symphysis pubis [48]. Using transverse scanning, the surrounding structures can be visualized (Fig. 5). More accurate localization of the urethra could be achieved by inserting a urethral catheter but it is not a necessity. The probe is comfort- able and well received by the patients. The main disadvantage is that the probe itself might interfere with dynamic descent of the bladder base and urethra during laughing or straining.
Fig. 6. a Transrectal ultrasonography in a resting state; Note the landmarks: longitudinal arrowhead at inferior border of symphysis pubis (sp) and transverse arrow head at bladder neck (B.N.); b The same patient and orientation in a straining state. Note the descent of the bladder neck from original position (B.N.) to more inferior position (transverse arrowhead) with a difference of I cm.
Fig. S. Transvaginal ultrasonography using transverse scanning. Forty-three-year-old female with recurrent stress urinary inconti- nence after Stamey's repair. Note the proximity of the pledgets (hyperechoic areas) to the urethra.
Transrectal ultrasonography. With this modality good imaging technique of the bladder and urethra without interference with the descent of the urethrovesical structures can be obtained [1]. Small caliber probes are used for the comfort of the patient. The linear scanner provides a midline surgical image similar to a true lateral X-ray that visualizes the bladder base plate, urethra and proximal urethra. This enables the study of all phases of bladder filling and gives easy access to the voiding phase. The ultrasound is capable of visualizing the contrast cavities as well as the surrounding tissues (Figs 6a and 6b).
With the use of this type of imaging, all the previously-mentioned criteria of deficient anatomical support could be evaluated in an accurate and sensitive way.
Bergman [1] made a comparision between beadchain cystourography and transrectal ultrasonography. The criteria for comparison were descent of the urethrovesi- cal junction >i 1 cm, and the position of the internal meatus at the most dependent part of the bladder base (indicating loss of the posterior urethrovesical angle). He showed a similar sensitivity but higher specificity with ultrasound as regards the urethral descent (sensi- tivity of 94% vs 97% and the specificity of 89% vs 76% respectively for ultrasound vs cystography). In another study, voiding cystourethrography was compared to ultrasonography in patients with spinal cord injury [49]. That study showed comparable accuracy but ultraso- nography carried the advantages of showing soft-tissue
Imaging for Urogynecology 217
details and muscle contractions which were not seen by voiding cystourethrography.
Combining ultrasound with multichannel urodyna- mic testing has increased the value of the tests and probably makes it comparable to the videofluorourody- namic studies [50-55].
Computed Tomography
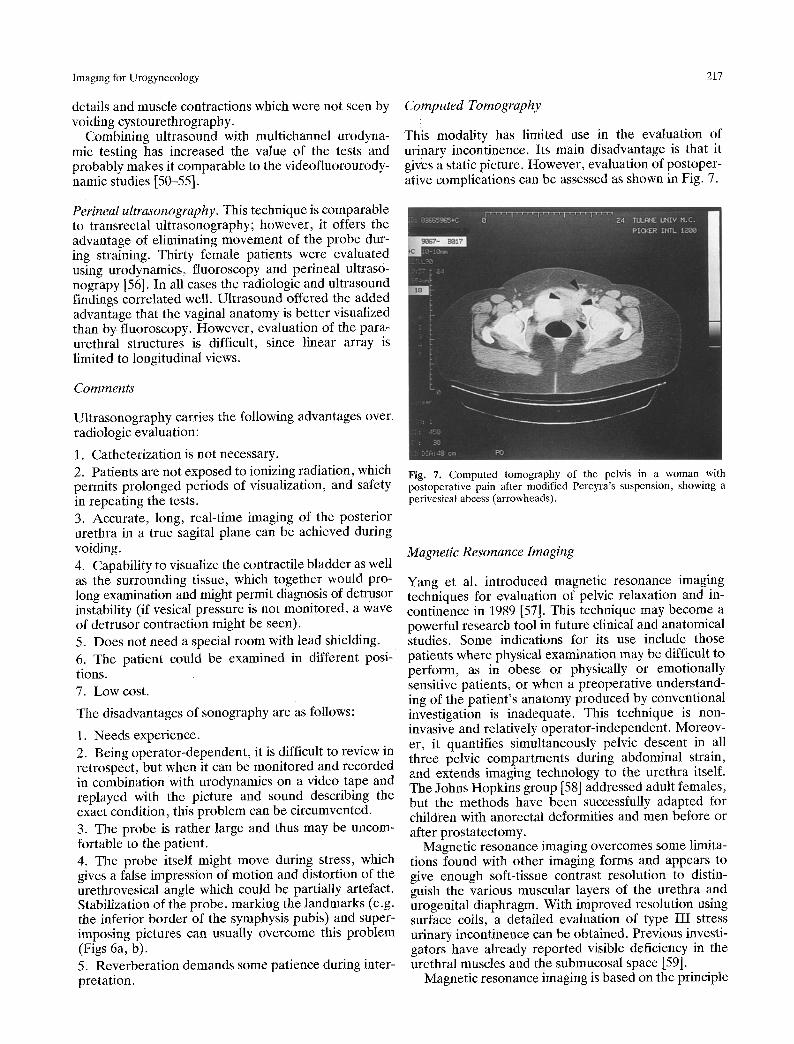
This modality has limited use in the evaluation of urinary incontinence. Its main disadvantage is that it gives a static picture. However, evaluation of postoper- ative complications can be assessed as shown in Fig. 7.
Perineal ultrasonography. This technique is comparable to transrectal ultrasonography; however, it offers the advantage of eliminating movement of the probe dur- ing straining. Thirty female patients were evaluated using urodynamics, fluoroscopy and perineal ultraso- nograpy [56]. In all cases the radiologic and ultrasound findings correlated well. Ultrasound offered the added advantage that the vaginal anatomy is better visualized than by fluoroscopy. However, evaluation of the para- urethral structures is difficult, since linear array is limited to longitudinal views.
Comments
Ultrasonography carries the following advantages over radiologic evaluation:
1. Catheterization is not necessary. 2. Patients are not exposed to ionizing radiation, which permits prolonged periods of visualization, and safety in repeating the tests. 3. Accurate, long, real-time imaging of the posterior urethra in a true sagital plane can be achieved during voiding. 4. Capability to visualize the contractile bladder as well as the surrounding tissue, which together would pro- long examination and might permit diagnosis of detrusor instability (if vesical pressure is not monitored, a wave of detrusor contraction might be seen). 5. Does not need a special room with lead shielding. 6. The patient could be examined in different posi- tions. 7. Low cost.
The disadvantages of sonography are as follows:
1. Needs experience. 2. Being operator-dependent, it is difficult to review in retrospect, but when it can be monitored and recorded in combination with urodynamics on a video tape and replayed with the picture and sound describing the exact condition, this problem can be circumvented. 3. The probe is rather large and thus may be uncom- fortable to the patient. 4. The probe itself might move during stress, which gives a false impression of motion and distortion of the urethrovesical angle which could be partially artefact. Stabilization o f the probe, marking the landmarks (e.g. the inferior border of the symphysis pubis) and super- imposing pictures can usually overcome this problem (Figs 6a, b). 5. Reverberation demands some patience during inter- pretation.
Fig. 7. Computed tomography of the pelvis in a woman with postoperative pain after modified Pereyra's suspension, showing a perivesicat abeess (arrowheads).
Magnetic Resonance Imaging
Yang et al. introduced magnetic resonance imaging techniques for evaluation of pelvic relaxation and in- continence in 1989 [57]. This technique may become a powerful research tool in future clinical and anatomical studies. Some indications for its use include those patients where physical examination may be difficult to perform, as in obese or physically or emotionally sensitive patients, or when a preoperative understand- ing of the patient's anatomy produced by conventional investigation is inadequate. This technique is non- invasive and relatively operator-independent. Moreov- er, it quantifies simultaneously pelvic descent in all three pelvic compartments during abdominal strain, and extends imaging technology to the urethra itself. The Johns Hopkins group [58] addressed adult females, but the methods have been successfully adapted for children with anorectal deformities and men before or after prostatectomy.
Magnetic resonance imaging overcomes some limita- tions found with other imaging forms and appears to give enough soft-tissue contrast resolution to distin- guish the various muscular layers of the urethra and urogenital diaphragm. With improved resolution using surface coils, a detailed evaluation of type III stress urinary incontinence can be obtained. Previous investi- gators have already reported visible deficiency in the urethral muscles and the submucosal space [59].
Magnetic resonance imaging is based on the principle
218 G.M. Ghoniem et al.
that protons wobble at a frequency dependent on the strength of the magnetic field in which they are found. By imposing a magnetic field gradient stronger on one side of the patient than the other, protons in different parts of the body can be made to wobble at different frequencies and therefore their localization may be differentiated. Once stimulated by radiofrequency or gradient pulse (like plucking a guitar string) Wotons gradually returned to the baseline state, emitting a radiofrequency signal (the tone from a guitar string). The rate of return to the relaxed state depends on the proton environment. Protons in water, muscle or fat relax at different rates. By tuning into the echo (or tone) at different times after stimulation, different signal mixes will be obtained. This indicates different tissue composition. Protons can be stimulated or ex- cited with different pulse sequences and the echo listened to several times to gain further information about tissue composition (air and calcium do not contain protons, have no signal and therefore appear black on the images). The radiofrequency signal is analyzed and an image resembling a conventional CT image is generated. Unlike CT, it may be generated in any orthogonal or oblique plane, and is ideal for evaluating complex anatomical relationships in any plane of interest. Radio antennae or surface coils placed close to the area of interest increase resolution significantly (up to 3 mm slices and 300 • 300 micron pixels).
Contraindications. Patients with pacemakers, foreign metal objects in the retina, old cerebral aneurysm clips; patients unable to cooperate and those with severe claustrophobia cannot undergo MRI. Less than 5% in Johns Hopkins' series were disqualified or could not tolerate the study.
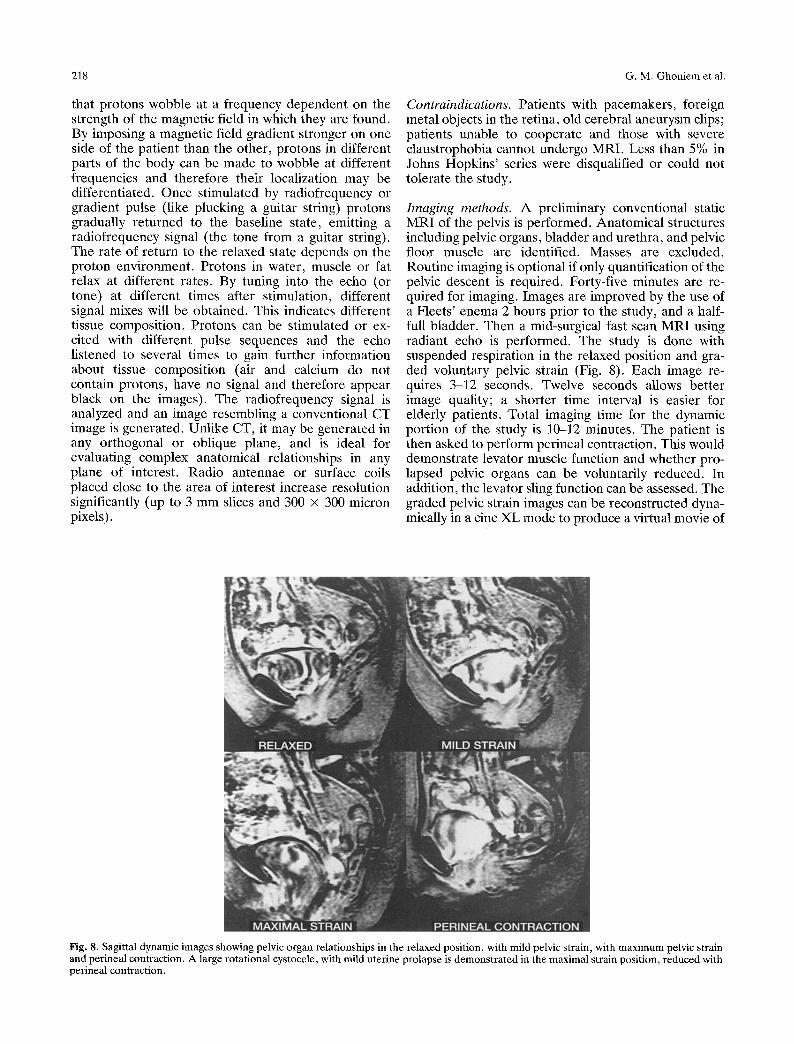
Imaging methods. A preliminary conventional static MRI of the pelvis is performed. Anatomical structures including pelvic organs, bladder and urethra, and pelvic floor muscle are identified. Masses are excluded. Routine imaging is optional if only quantification of the pelvic descent is required. Forty-five minutes are re- quired for imaging. Images are improved by the use of a Fleets' enema 2 hours prior to the study, and a half- full bladder. Then a mid-surgical fast scan MRI using radiant echo is performed. The study is done with suspended respiration in the relaxed position and gra- ded voluntary pelvic strain (Fig. 8). Each image re- quires 3-12 seconds. Twelve seconds allows better image quality; a shorter time interval is easier for elderly patients. Total imaging time for the dynamic portion of the study is 10-12 minutes. The patient is then asked to perform perineal contraction. This would demonstrate levator muscle function and whether pro- lapsed pelvic organs can be voluntarily reduced. In addition, the levator sling function can be assessed. The graded pelvic strain images can be reconstructed dyna- mically in a cine XL mode to produce a virtual movie of
Fig. 8. Sagittal dynamic images showing pelvic organ relationships in the relaxed position, with mild pelvic strain, with maximum pelvic strain and perineal contraction. A large rotational cystocele, with mild uterine prolapse is demonstrated in the maximal strain position, reduced with perineal contraction.
Imaging for Urogynecology 219
the relationship between prolapsing organs. For static evaluation of the urethra, the Johns Hop-
kins group recently began using an intravaginal surface coil (Medrad Corp., Pittsburg, PA) adapted from its initial design for intrarectal imaging. The location pro- vided the necessary proximity for high resolution neces- sary to image periurethral structures.
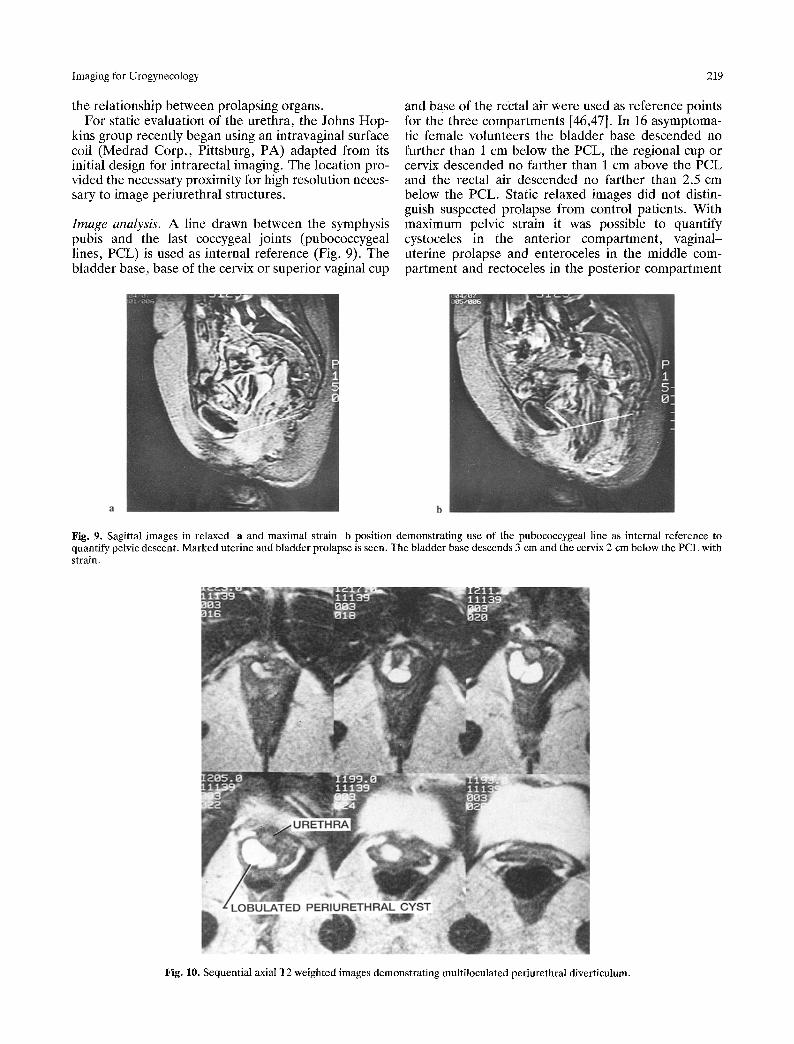
Image analysis. A line drawn between the symphysis pubis and the last coccygeal joints (pubococcygeal lines, PCL) is used as internal reference (Fig. 9). The bladder base, base of the cervix or superior vaginal cup
and base of the rectal air were used as reference points for the three compartments [46,47]. In 16 asymptoma- tic female volunteers the bladder base descended no further than 1 cm below the PCL, the regional cup or cervix descended no farther than 1 cm above the PCL and the rectal air descended no farther than 2.5 cm below the PCL. Static relaxed images did not distin- guish suspected prolapse from control patients. With maximum pelvic strain it was possible to quantify cystoceles in the anterior compartment, vaginal- uterine prolapse and enteroceles in the middle com- partment and rectoceles in the posterior compartment
Fig. 9. Sagittal images in relaxed a and maximal strain b position demonstrating use of the pubococcygeal line as internal reference to quantify pelvic descent. Marked uterine and bladder prolapse is seen. The bladder base descends 3 cm and the cervix 2 cm below the PCL with strain.
Fig. 10. Sequential axial T2 weighted images demonstrating multiloculated periurethral diverticulum.
220 G .M. Ghoniem et al.
Muscular layer Urethral mucosa
Areolar tissue smooth m. / ~ i t u r a t o r knt . . . . . .
/ k///N/ vagina J / " ~ ~ ~ Pertvaginal
Median raphe
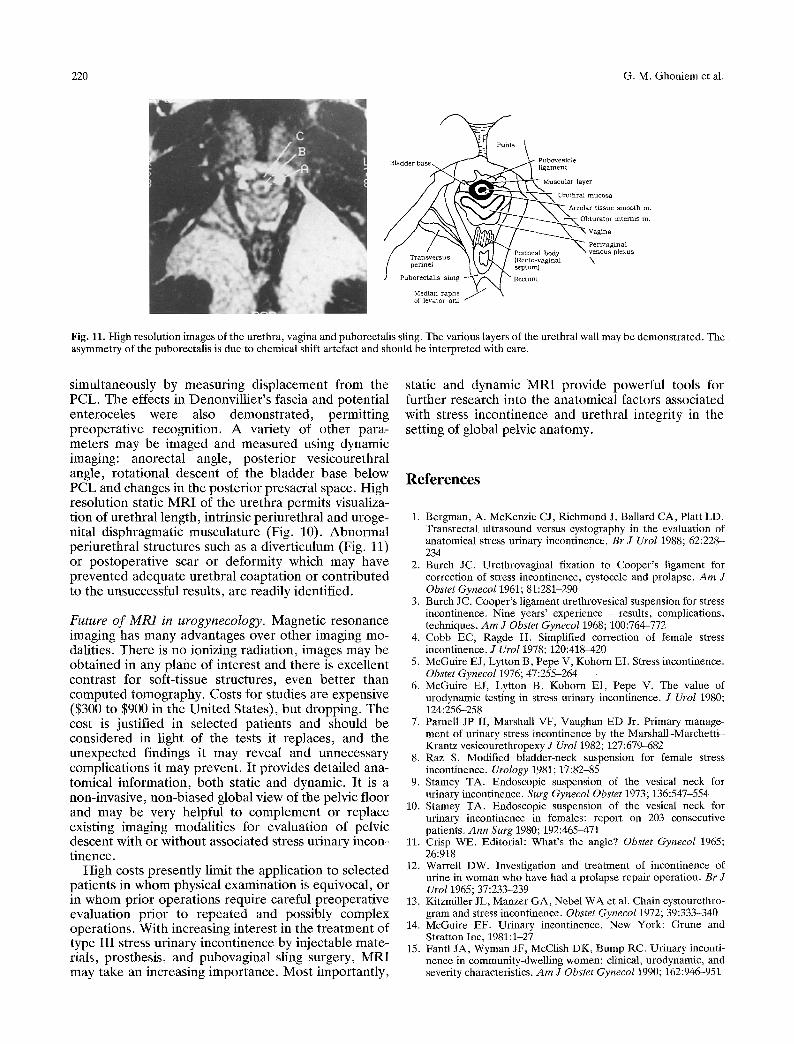
Fig. 11. High resolution images of the urethra, vagina and puborectalis sling. The various layers of the urethral wall may be demonstrated. The asymmetry of the puborectalis is due to chemical shift artefact and should be interpreted with care.
simultaneously by measuring displacement from the PCL. The effects in Denonvillier's fascia and potential enteroceles were also demonstrated, permitting preoperative recognition. A variety of other para- meters may be imaged and measured using dynamic imaging: anorectal angle, posterior vesicourethral angle, rotational descent of the bladder base below PCL and changes in the posterior presacral space. High resolution static MRI of the urethra permits visualiza- tion of urethral length, intrinsic periurethral and uroge- nital disphragmatic musculature (Fig. 10). Abnormal periurethral structures such as a diverticulum (Fig. 11) or postoperative scar or deformity which may have prevented adequate urethral coaptation or contributed to the unsuccessful results, are readily identified.
Future of MRI in urogynecology. Magnetic resonance imaging has many advantages over other imaging mo- dalities. There is no ionizing radiation, images may be obtained in any plane of interest and there is excellent contrast for soft-tissue structures, even better than computed tomography. Costs for studies are expensive ($300 to $900 in the United States), but dropping. The cost is justified in selected patients and should be considered in light of the tests it replaces, and the unexpected findings it may reveal and unnecessary complications it may prevent. It provides detailed ana- tomical information, both static and dynamic. It is a non-invasive, non-biased global view of the pelvic floor and may be very helpful to complement or replace existing imaging modalities for evaluation of pelvic descent with or without associated stress urinary incon- tinence.
High costs presently limit the application to selected patients in whom physical examination is equivocal, or in whom prior operations require careful preoperative evaluation prior to repeated and possibly complex operations. With increasing interest in the treatment of type III stress urinary incontinence by injectable mate- rials, prosthesis, and pubovaginal sling surgery, MRI may take an increasing importance. Most importantly,
static and dynamic MRI provide powerful tools for further research into the anatomical factors associated with stress incontinence and urethral integrity in the setting of global pelvic anatomy.
References
1. Bergman, A. McKenzie CJ, Richmond J, Ballard CA, Platt LD. Transrectal ultrasound versus cystography in the evaluation of anatomical stress urinary incontinence. Br J Urol 1988; 62:228- 234
2. Burch JC. Urethrovaginal fixation to Cooper's ligament for correction of stress incontinence, cystocele and prolapse. A m J Obstet Gynecol 1961; 81:281-290
3. Burch JC. Cooper's ligament urethrovesical suspension for stress incontinence. Nine years' experience - results, complications, techniques. A m J Obstet Gynecol 1968; 100:764-772
4. Cobb EC, Ragde H. Simplified correction of female stress incontinence. J UroI 1978; 120:418-420
5. McGuire EJ, Lytton B, Pepe V, Kohorn EI. Stress incontinence. Obstet Gynecol 1976; 47:255-264
6. McGuire EJ, Lytton B, Kohorn EI, Pepe V. The value of urodynamic testing in stress urinary incontinence. J Urol 1980; 124:256--258
7. Parnell JP II, Marshall VF, Vaughan ED Jr. Primary manage- ment of urinary stress incontinence by the Marshall-Marchetti- Krantz vesicourethropexy J Urol 1982; 127:679-682
8. Raz S. Modified bladder-neck suspension for female stress incontinence. Urology 1981; 17:82-85
9. Stamey TA. Endoscopic suspension of the vesical neck for urinary incontinence. Surg Gynecol Obstet 1973; 136:547-554
10. Stamey TA. Endoscopic suspension of the vesical neck for urinary incontinence in females: report on 203 consecutive patients. Ann Surg 1980; 192:465-471
11. Crisp WE. Editorial: What's the angle? Obstet Gynecol 1965; 26:918
12. Warrell DW. Investigation and treatment of incontinence of urine in woman who have had a prolapse repair operation. Br J Urol 1965; 37:233-239
13. Kitzmiller JL, Manzer GA, Nebel WA et al. Chain cystourethro- gram and stress incontinence. Obstet Gynecol 1972; 39:333-340
14. McGuire EF. Urinary incontinence. New York: Grune and Stratton Inc, 1981:1-27
15. Fantl JA, Wyman JF, McClish DK, Bump RC. Urinary inconti- nence in community-dwelling women: clinical, urodynamic, and severity characteristics. A m J Obstet Gyneco11990; 162:946--951
Imaging for Urogynecology 221
16. Marshall VF, Segaul RM. Experience with suprapubic vesi- courethral suspension after previous failure to correct stress incontinence in women. J UroI 1968; 100:647-648
17. Parnell JP III, Marshall VF, Vaughan ED Jr. Management of recurrent urinary stress incontinence by the Marshall-Marchetti- Krantz vesicourethropexy. J Urol 1984; 132:912-914
18. Blaivas JG, Salinas J. Type III stress urinary incontinence: importance of proper diagnosis and treatment. Surg Forum 1984; 35:473-475
19. Sand PK, Bowen LW, Pangamiban R, Ostergard DR. The low pressure urethra as a factor in failed retropubic urethropexy. Obstet Gynecol 1987; 69:339-402
20. McGuire EJ. Urodynamic findings in patients after failure of stress incontinence operation. Prog Clin Biol Res 1981; 78:351- 36O
21. McGuire EJ, Lytton B. Pubovaginal sling procedure for stress incontinence. J Urol 1978; 119:82-84
22. Blaivas JG, Salinas J. Type III stress urinary incontinence: importance of proper diagnosis and treatment. Surg Forum 1984; 35:473-475
23. Bonney V. On diurnal incontinence of urine of women. J Obstet Gynaecol Br Emp 1923; 30:358
24. Migliorini GD, Glenning PP. Bonney's test - fact or fiction? BrJ Obstet Gynaecol 1987; 94:157-159
25. Crystale CD, Charme LS, Copeland WE. Q-tip test in stress urinary incontinence. Obstet Gynecol 1971; 38:313-315
26. Bergman A, Koonings PP, Ballard CA. Negative Q-tip test as a risk factor for failed incontinence surgery in women. J Reprod Med 1989; 34:193-197
27. Montaz FJ, Stanton SL. Q-tip test in female urinary inconti- nence. Obstet Gynecol 1986; 67:258-260
28. Bergman A, Bhatia NN. Pessary test: simple prognostic test in women with stress urinary incontinence. Urology 1984; 24:109- 110
29. Hodgkinson CP, Dank HP, Kelly WT. Urethrocystogram: metallic bead chain technique. CIin Obstet Gynecol 1958; 1:668- 677
30. Hodgkinson CP. Stress urinary incontinence. Am J Obstet Gyne- col 1970; 108:1141-1168
31. Enhorning G, Miller ER, Hinman F Jr. Urethral closure studies with cineroentgenography and simultaneous bladder and urethral pressure recording. Surg Gynecol Obstet 1964; 118:507
32. Bates CP, Corney LE. Synchronous cine-pressure-flow cystog- raphy: a method for routine urodynamic investigation. Br J Radiol 1971; 44:44--50
33. McGuire EJ. Combined radiographic and manometric assess- ment of urethral sphincter function. J Uro11977; 118:632-635
34. Yalla SV, Rossier AB, Faro Ba. Synchronous cystosphinctero- metry in patients with spinal cord injury. Urology 1975; 6:777- 788
35. Blalvas JG, Fischer DM. Combined radiographic and urodyna- mic monitoring: advances in technique. J Urol 1981; 125:693-694
36. Green TH Jr. Development of a plan for the diagnosis and treatment of urinary stress incontinence. Am J Obstet Gynecol 1962; 83:632-648
37. McGuire EJ, Lytton B, Pepe V, Kohorn EI. Stress urinary incontinence. Obstet Gynecol 1976; 47:255-264
38. Blaivas JG. Classification of stress urinary incontinence. Neurol Urodynam 1984; 2:103-116
39. Blaivas JG. Stress incontinence: classification and surgical approach. J Urol 1988; 139:727-731
40. Ghoniem GM. Vaginal pack test in women with significant cystoceles. Unpublished data.
41. Donald I, Brown TG. Investigation of abdominal masses by pulsed ultrasound. Lancet 1958; 1:1188-1194
42. Kossoff G, Improved techniques in ultrasound cross sectional ecography. Ultrasonics 1972; 10:221-227
43. Bhatia NN, Ostergard DR. Urodynamics in women with stress urinary incontinence. Obstet Gynecol 1982; 60:552-559
44. McLean GK, Edell SL. Determination of bladder volumes by gray-scale uttrasonography. Radiology 1978; 128:181-182
45. Cardenas DD, Kelly E, Krieger JN et al. Residual urine volumes in patients with spinal cord injury: measurement with a portable ultrasound instrument. Arch Phys Med Rehab 1988; 69:514-516
46. Roehrbern CG, Peters PC. Can transabdominal ultrasound estimation of postvoiding residual (PVR) replace catheterization? Urology 1988; 31:445-449
47. Roehrbern CG, McConnell JD. Ultrasound of the bladder. Contemporary Urology March 1990:58-76
48. Quinn MJ, Beynon J, Mortensen NJ, Smith PJ. Transvaginal endosonography: a new method to study the anatomy of the lower urinary tract in urinary stress incontinence. Br J Uro11988; 62:414-418
49. Fellows GJ, Cannefl LB, Ravichandran G. Transrectal ultraso- nography compared with voiding cystourethrography after spinal cord injury. Br J Urol 1987; 59:218-221
50. Nishizawa O, Moriya I, Satoh S, Harada T, Tsuchida S. A new video urodynamics: combined ultrasonotomographic and urody- namic monitoring. Neurol Urodynam 1982; 1:295-301
51. Shapeero LG, Friedland GW, Perkash I. Transrectal reno- graphic voiding cystourethrography studies in neuromuscular bladder dysfunction. Am J Roentgeno11983; 141:83-90
52. Shabsigh R, Fishman IF, Krebs M. The use of transrectal longitudinal real-time ultrasonography in urodynamics. J Urol 1987; 138:1416-1419
53. Shabsigh R, Fishman I J, Krebs M. Combined transrectal ultraso- nography and urodynamics in the evaluation of detrusor- sphincter dyssynergia. Br J grol 1988; 62:326-330
54. Brown MC, Sutherst JR, Murray A, Richmond DH. Potential use of ultrasound in place of X-ray fluoroscopy in urodynamics. Br J Urol 1985;57:8890
55. Perkash I, Friedland GW. Transrectal ultrasonography of the lower urinary tract: evaluation of bladder-neck problems. Neurol Urodynam 1986; 5:299-306
56. Kohorn El, Scioscia AL, Jearty P, Hobbins JC. Ultrasound eystourethrography by perineal scanning for the assessment of female stress urinary incontinence. Obstet Gynecol I986; 68:269- 272
57. Yang A, Mostwin JL, Radebaugh LC, Rosenshein N, Zerhouni EA. Dynamic evaluation of pelvic prolapse using fastscan mag- netic resonance imaging (MRI) and cinematic display. Compari- son with cystometrogram. J Urol 1989; 141(Pt 2):200A
58. Yang A, Mostwin JL, Rosenshein NB, Zerhouni EA. Dynamic evaluation of pelvic prolapse with fastscan MRI and cinematic display. Radiology (in press)
59. Klutke CG, Little NA, Raz S. The anatomy of stress inconti- nence. AUA Update Series 1990; 9, Lesson 39:306-311





























