Embed Size (px)
Citation preview
http://informahealthcare.com/dreISSN 0963-8288 print/ISSN 1464-5165 online
Disabil Rehabil, Early Online: 1–15! 2014 Informa UK Ltd. DOI: 10.3109/09638288.2014.978508
REVIEW PAPER
How is physical activity monitored in people following stroke?
Natalie A. Fini1,2, Anne E. Holland1,3, Jenny Keating4, Jacinta Simek4, and Julie Bernhardt1,5
1Department of Physiotherapy, La Trobe University, Melbourne, Australia, 2Department of Physiotherapy, Caulfield Hospital, Alfred Health,
Melbourne, Australia, 3Department of Physiotherapy, Alfred Health, Melbourne, Australia, 4Department of Physiotherapy, Monash University,
Melbourne, Australia, and 5Stroke Division, Florey Department, Florey Institute of Neurosciences and Mental Health University of Melbourne,
Melbourne, Australia
Abstract
Purpose: To describe how physical activity is monitored following stroke; to summarise methodsand devices used across the stroke pathway and document their psychometric properties.Methods: Searches of five databases identified studies that included stroke survivors whosephysical activity was quantitatively measured. Two reviewers independently determinedinclusion. A descriptive synthesis was undertaken and reliability data for specific methods ofmonitoring physical activity were pooled where possible. Results: Ninety-one papers (60 usingdevices and 31 using observational methods) met inclusion criteria, with 3479 participants aged21–96 years. Twenty-nine devices (72% accelerometers) were identified. Devices were typicallyused to measure ambulant participants more than 6 months following stroke. Directobservation of physical activity was commonly used for inpatients. No outcome measurementswere common to all methods/devices. Test–retest reliability was not reported for 23 devices; forthe remaining six it ranged from r¼ 0.44 to r¼ 0.99. Inter-rater reliability of observationalmethods ranged from 0.51 to 1.0. Validity was infrequently reported. Conclusions: Physicalactivity outcomes were variable. Devices allow for unobtrusive, sustained monitoring in free-living environments. Observational methods suit inpatient settings but are time and labourintensive. No single approach appears superior but standardisation of outcomes wouldimprove the field.
� Implications for Rehabilitation
� Physical activity measurement is highly variable following stroke and better definition ofphysical activity outcomes would enhance the field.
� Accelerometry and behavioural mapping are most commonly used to measure physicalactivity following stroke, each have advantages and disadvantages depending on the settingand the outcome of interest.
� There is no single device ideal for CLINICAL application for people following stroke.
Keywords
Activity monitoring, acute, community,device, observation
History
Received 8 May 2014Revised 13 October 2014Accepted 15 October 2014Published online 6 November 2014
Introduction
Stroke is a major cause of disability worldwide. A recent reviewof global data concluded that incidence rates of stroke range from41 to 316 cases per 100 000 people per year [1]. The highfinancial and social burden of stroke impacts the community, theindividual, their family and carers [2]. Physical mobility limita-tions are common following a stroke [3] and frequently lead topoor participation in physical activity. Physical activity is definedas ‘‘any bodily movement produced by skeletal muscles thatresults in energy expenditure’’ [4]. Low physical activity is animportant cardiovascular risk factor [5–8]. The American Heart
Association advises that 30 min of exercise per day can reducerisk of heart disease [9] and 10 000 steps per day is considered thepoint at which an individual is classified as active [10]. Strokesurvivors do not meet recommended guidelines for physicalactivity as they demonstrate limited activity [11] and low stepcounts per day (average 1389–6679) [11–17], adding to the risk offurther cardiovascular events.
Increasing physical activity is a relevant treatment target overthe entire stroke recovery pathway [17–21]. Despite this, physicalactivity levels are not routinely monitored after stroke. Thelimitations of subjective monitoring techniques (e.g. question-naires) are well documented and include recall errors and highlevels of over-reporting [13]. Many objective measurementmethods have been reported in healthy populations [22,23],however it is unclear whether these would be valid or feasible foruse following stroke. There is a need to determine which objective
Address for correspondence: Natalie Fini, Department of Physiotherapy,Caulfield Hospital, 260 Kooyong Road, Caulfield, VIC 3162, Australia.Tel: +61 3 9076 6000. E-mail: [email protected]
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.

methods of measuring physical activity in stroke survivors arevalid and clinically applicable.
The primary aim of this review was to describe how physicalactivity is monitored following stroke, including identification ofmethods and devices used across the stroke pathway (from acutecare to community). The secondary aim was to describe thereported psychometric properties (reliability and validity) of thesemeasurements.
Methods
Search strategy
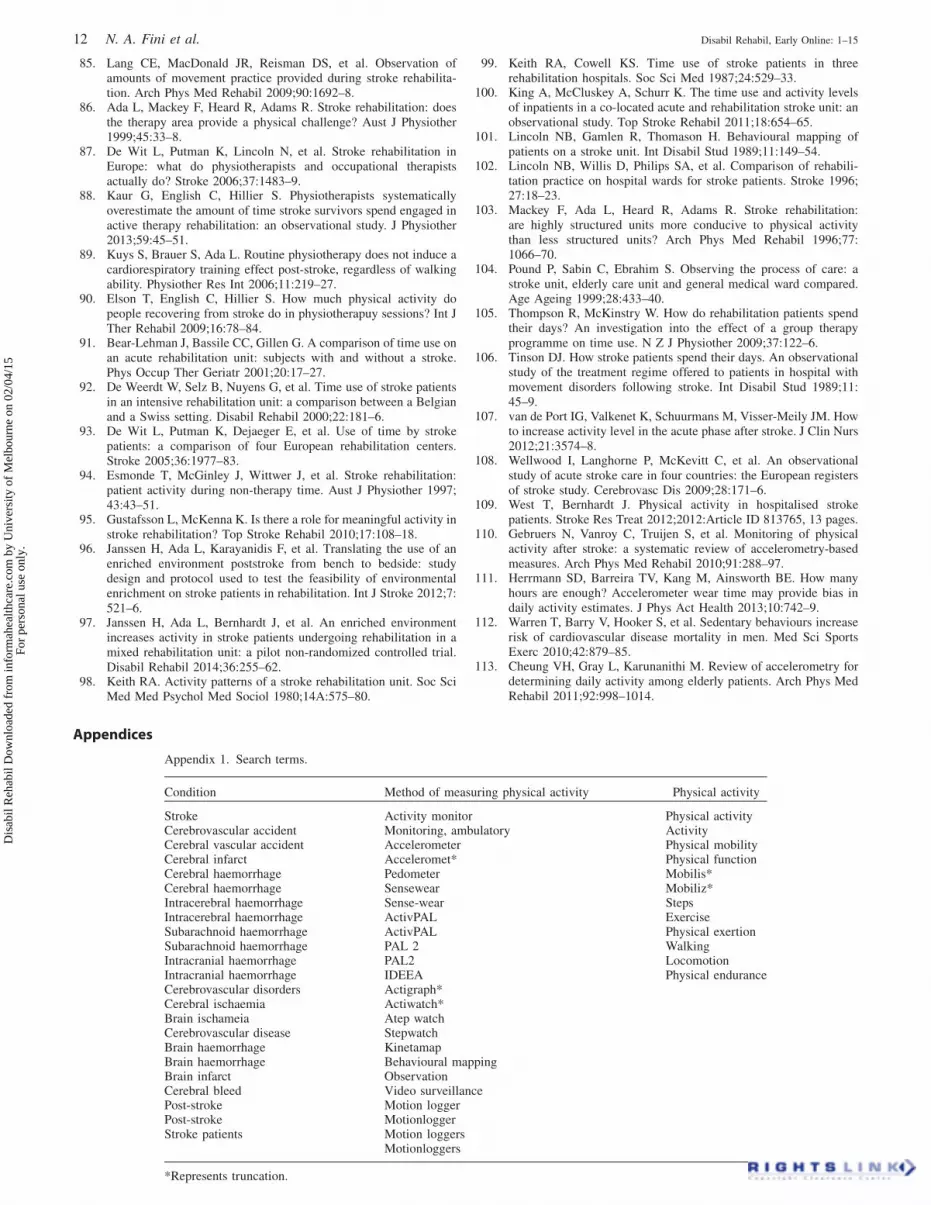
To identify all papers relating to activity monitoring in strokepatients, searches were conducted in MEDLINE (1966 to 26February 2014), CINAHL (1982–26 February 2014), EMBASE(1988–26 February 2014), the Cochrane Library (1970–26February 2014) and PEDro (26 February 2014). The searchterms were grouped into three categories: condition (wordsrelated to stroke), the method of measuring physical activity(e.g. accelerometer, behavioural mapping) and words related tophysical activity (Appendix 1). Reference lists of included studieswere checked for relevant studies. This review is registered onPROSPERO (registration no. CRD42012003448).
Inclusion criteria
Studies of any design published in peer reviewed journals wereeligible, excluding opinion articles and reviews. We aimed tocapture all reports of objective physical activity monitoring ofstroke patients as well as studies that assessed the psychometricproperties of physical activity measurements. Participants wereadults with a clinical diagnosis of stroke. Studies with a mixedpopulation were included if data for stroke participants could beextracted. To be included the method of measuring physicalactivity (device, behavioural mapping techniques or videotaping)had to be specified and an objective measure of physical activity(aim 1) or a level of agreement between independent measure-ments of physical activity (aim 2) reported. Examples of objectivemeasures of physical activity were time engaged in physicalactivity, time spent standing, sedentary time, energy expenditure,number of transitions (e.g. sit to stand) or steps per day.
Exclusion criteria
Studies were excluded if they were not reported in English, if thephysical activity outcome was derived from self-report orquestionnaire responses or if physical activity was predominantlyupper limb or single limb movement.
Study selection
Two reviewers (NF and JB) independently reviewed the title andabstract of retrieved reports. Where it was unclear whether anarticle met the inclusion criteria, the full text was obtained and thetwo reviewers applied the criteria to the full text.
Quality assessment
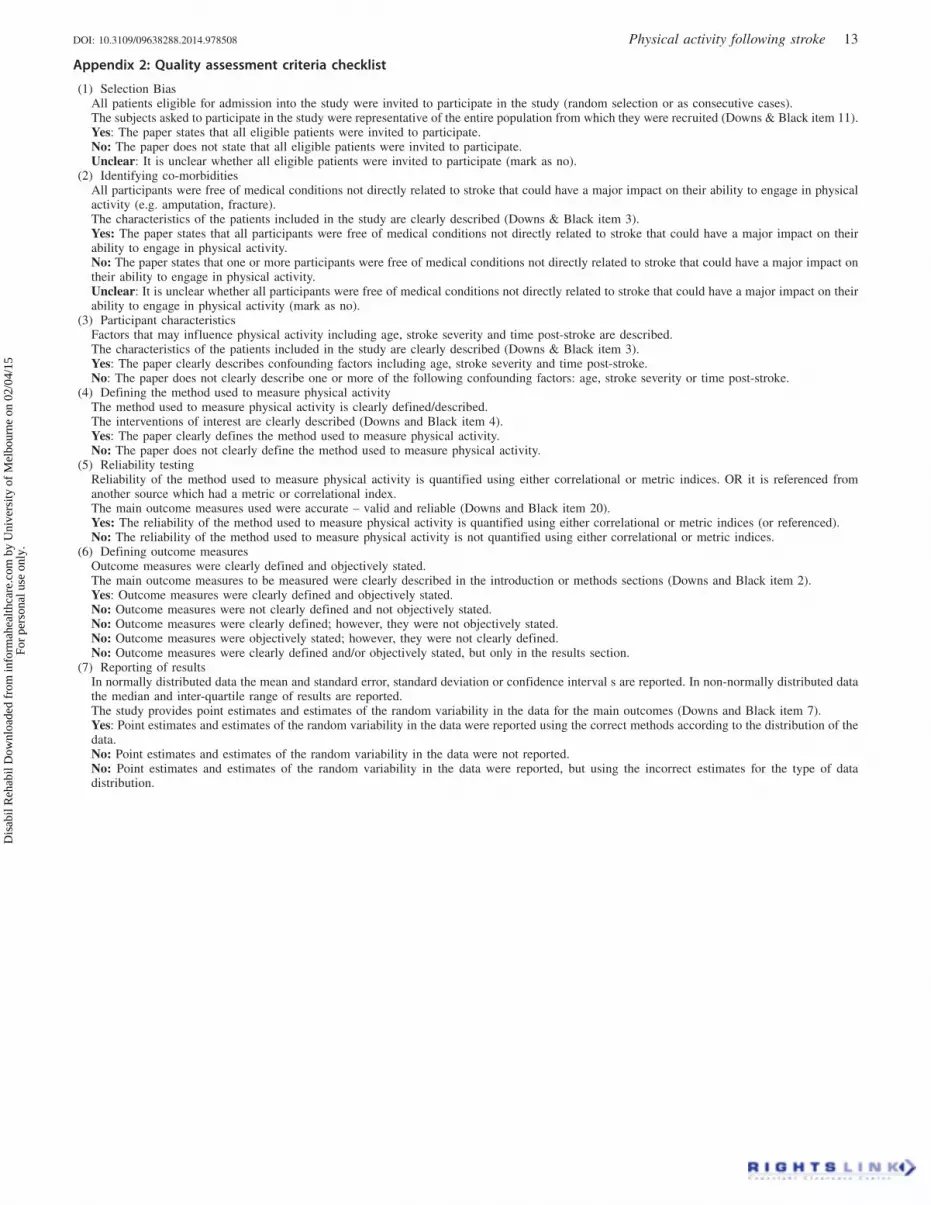
Studies were not excluded on the basis of quality; however theywere screened for quality to assist with interpretation of thereview findings. Six items from the Downs and Black (1998)checklist for measuring study quality [24] were consideredrelevant to this systematic review and were applied by onereviewer (NF). The included quality items and decision rulesassessed selection bias (Item 11), description of participantcharacteristics (Item 3) with particular emphasis on co-morbid-ities that may impact on physical activity participation, descrip-tion of the method of measuring physical activity (Item 4),
reporting of the accuracy of the method of measuring physicalactivity (Item 20), a clear definition of outcome measures (Item 2)and reporting of the estimates of variability and point estimatesfor activity measurements (Item 7). Appendix 2 shows the qualityassessment criteria form.
Data extraction
One reviewer (NF) extracted the following data: full referencedetails, study objective and design, participant and conditiondetails, study method, specifics on activity monitoring, measure-ments of physical activity and reported reliability and validity ofmeasurement methods.
Data analysis
A descriptive synthesis of the methods used to monitor physicalactivity following stroke included the environment in which themethod was used (community, clinical or laboratory), the timepost-stroke at which measurements were taken (acute: 0–14 days,sub-acute: 14 days–6 months or long term: 46 months), partici-pant characteristics of stroke severity and age; and the reliability,validity, simplicity of use, wearability, cost and measurementsassociated with measurement tools.
Where more than one study reported comparable reliabilitystatistics for the same device, the reliability correlation coeffi-cients were pooled using the Hunter–Schmidt method [25].
Results
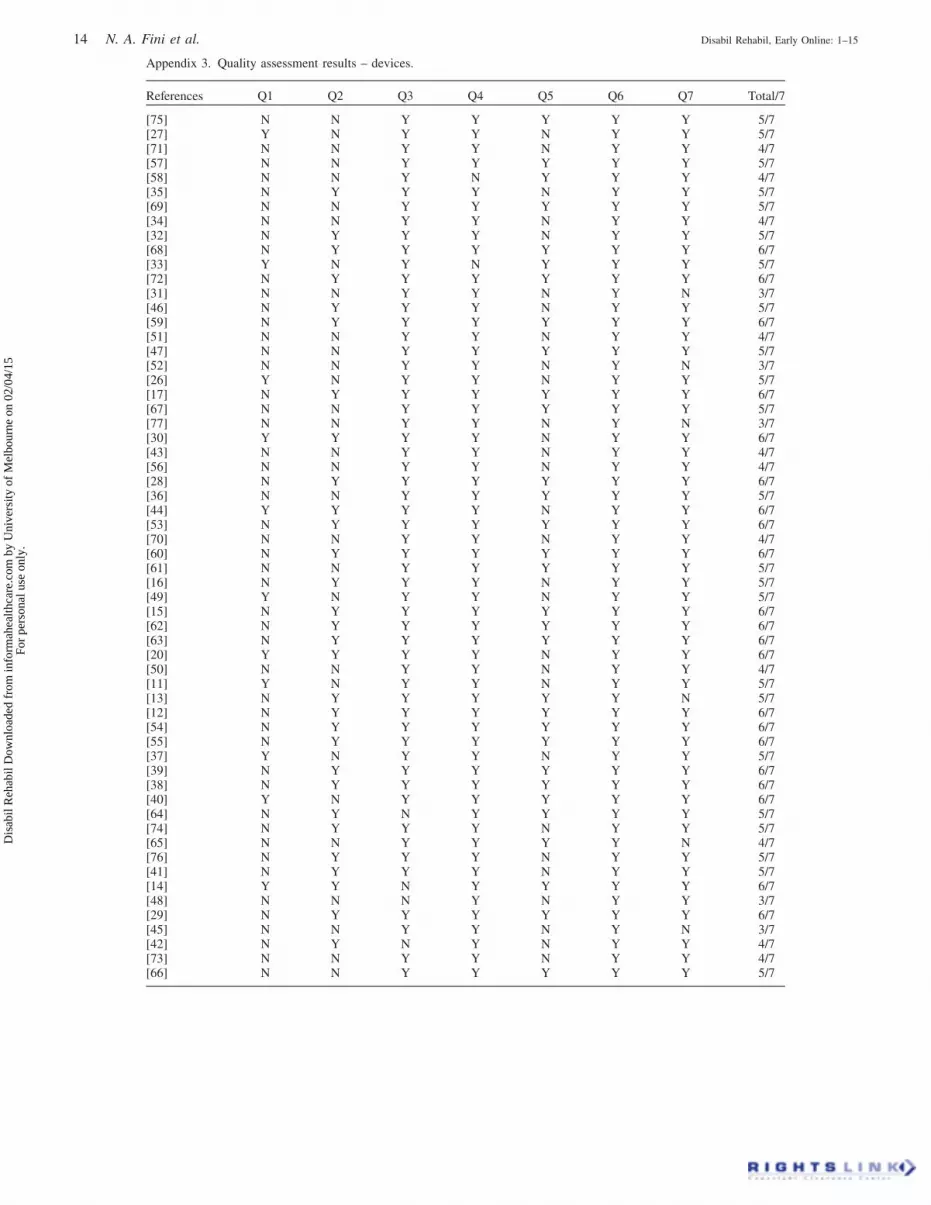
A total of 1547 potential articles were identified through databasesearches. Figure 1 presents the flow of studies into the review.Ninety-one papers were included; 60 used devices and 31 usedobservational methods to measure physical activity. Includedstudies were published between 1980 and 2014; the oldest paperusing a device was from 1998 [26]. There was a dramatic increasein relevant papers published in the past 10 years. Nine studieswere longitudinal and followed participants (all using devices) forlonger than 6 months [11,27–33]. Physical activity was measuredin 3479 stroke survivors (2256 with devices, 1223 with observa-tional methods). Sample sizes of the studies ranged from 1 to 408;the age of participants ranged from 21 to 96. Quality assessmentscores ranged from two to seven out of seven (median¼ 5;Appendices 3 and 4).
Stroke severity
Stroke severity was measured on many different scales, making itdifficult to summarise. Devices were used to assess physicalactivity of ambulant stroke survivors in 95% of studies whilst theremaining five studies [27,30,34–36] included both ambulant andnon-ambulant participants. Studies that used observationalmethods to measure physical activity included participants witha broader range of stroke severity, with approximately half of theincluded participants not independently ambulant.
Study setting and timing
Devices were frequently used to measure physical activity ofpeople living in the community with stroke duration46 months.Observational methods were always used in a clinical setting andmost often in the subacute phase (14 days–6 months). Timing ofdata collection was not specified in one study of a device and sixstudies of observational methods. Figure 2 shows the study settingand timing of physical activity measurement for devices andFigure 3 presents the timing of physical activity measurement forobservational methods.
2 N. A. Fini et al. Disabil Rehabil, Early Online: 1–15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.

Devices
Twenty-nine different devices were used to measure physicalactivity (21 accelerometers, six pedometers and two other,described in Table 1). The device most commonly used was theStep Activity Monitor (SAM; 23 studies) followed by the YamaxDigiwalker SW-200/SW-650/SW-701 (five studies), and theActivPAL (four studies).
There was no common outcome reported across all devices orstudies. Step count was reported in 44 studies (n¼ 1874participants), followed by walking duration in 13 studies(n¼ 623 participants). We classified outcome post-hoc intothree categories: ‘‘Activity Intensity’’ (energy expenditure, peakactivity index and number of steps at specified step rate);‘‘Activity Frequency’’ (step count, activity count and number oftransitions); and ‘‘Activity Duration’’ (time in specified postures,
Figure 1. Study identification and selection.
Records iden�fiedby referencelist checking
n = 41
CINAHLn = 217
EMBASEn = 1052
Cochranen = 184
PEDROn = 109
Medlinen = 458
Duplicate studiesremovedn = 473
Records screened by�tle and abstract
n = 1547
Recordsexcludedn = 1442
Full text ar�clesassessedn = 105
Studiesincluded
n = 91
Full text ar�clesexcluded
n = 55
*Note: some studies test across mul�ple �me points
Community
ClinicalEnvironment
Laboratory
Acute
0 studies
4 studies
n = 192
0 studies
Subacute
24 studies
n = 904
LongerTerm
1 study
n = 17
Time Post Stroke
0 studies 0 studies
0 studies 0 studies
Figure 3. Setting and timing of physical activity measurement usingobservational methods.
*Note: some studies test across mul�ple �me points and se�ngs
Community
ClinicalEnvironment
Laboratory
Acute
1 study
n = 31
4 studies
n = 129
0 studies
Subacute
8 studies
n = 568
8 studies
n = 264
1 study
n = 40
LongerTerm
36 studies
n = 1659
5 studies
n = 115
11 studies
n = 275
Time Post Stroke
Figure 2. Setting and timing of physical activity measurement usingdevices.
DOI: 10.3109/09638288.2014.978508 Physical activity following stroke 3
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
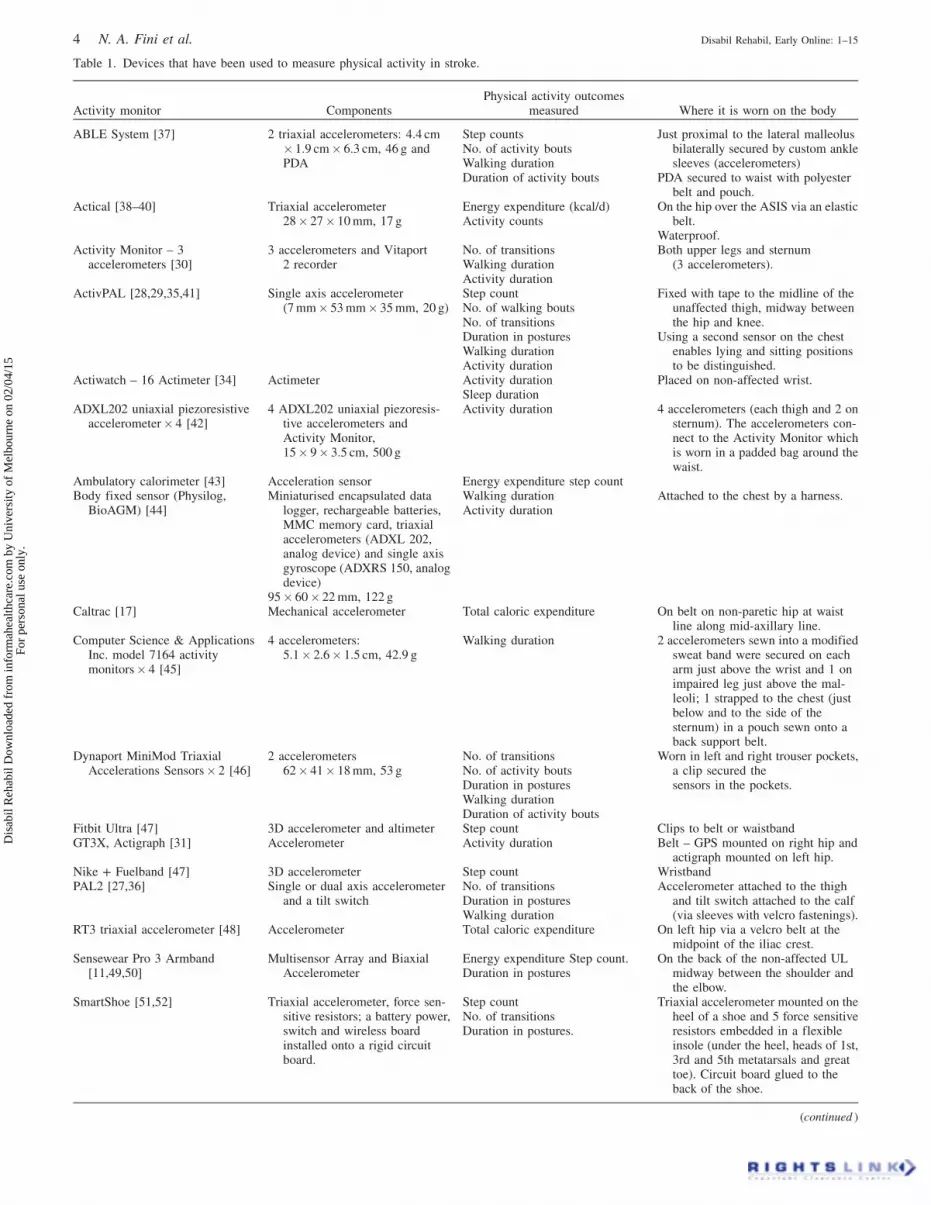
Table 1. Devices that have been used to measure physical activity in stroke.
Activity monitor ComponentsPhysical activity outcomes
measured Where it is worn on the body
ABLE System [37] 2 triaxial accelerometers: 4.4 cm� 1.9 cm� 6.3 cm, 46 g andPDA
Step countsNo. of activity boutsWalking durationDuration of activity bouts
Just proximal to the lateral malleolusbilaterally secured by custom anklesleeves (accelerometers)
PDA secured to waist with polyesterbelt and pouch.
Actical [38–40] Triaxial accelerometer28� 27� 10 mm, 17 g
Energy expenditure (kcal/d)Activity counts
On the hip over the ASIS via an elasticbelt.
Waterproof.Activity Monitor – 3
accelerometers [30]3 accelerometers and Vitaport
2 recorderNo. of transitionsWalking durationActivity duration
Both upper legs and sternum(3 accelerometers).
ActivPAL [28,29,35,41] Single axis accelerometer(7 mm� 53 mm� 35 mm, 20 g)
Step countNo. of walking boutsNo. of transitionsDuration in posturesWalking durationActivity duration
Fixed with tape to the midline of theunaffected thigh, midway betweenthe hip and knee.
Using a second sensor on the chestenables lying and sitting positionsto be distinguished.
Actiwatch – 16 Actimeter [34] Actimeter Activity durationSleep duration
Placed on non-affected wrist.
ADXL202 uniaxial piezoresistiveaccelerometer� 4 [42]
4 ADXL202 uniaxial piezoresis-tive accelerometers andActivity Monitor,15� 9� 3.5 cm, 500 g
Activity duration 4 accelerometers (each thigh and 2 onsternum). The accelerometers con-nect to the Activity Monitor whichis worn in a padded bag around thewaist.
Ambulatory calorimeter [43] Acceleration sensor Energy expenditure step countBody fixed sensor (Physilog,
BioAGM) [44]Miniaturised encapsulated data
logger, rechargeable batteries,MMC memory card, triaxialaccelerometers (ADXL 202,analog device) and single axisgyroscope (ADXRS 150, analogdevice)
95� 60� 22 mm, 122 g
Walking durationActivity duration
Attached to the chest by a harness.
Caltrac [17] Mechanical accelerometer Total caloric expenditure On belt on non-paretic hip at waistline along mid-axillary line.
Computer Science & ApplicationsInc. model 7164 activitymonitors� 4 [45]
4 accelerometers:5.1� 2.6� 1.5 cm, 42.9 g
Walking duration 2 accelerometers sewn into a modifiedsweat band were secured on eacharm just above the wrist and 1 onimpaired leg just above the mal-leoli; 1 strapped to the chest (justbelow and to the side of thesternum) in a pouch sewn onto aback support belt.
Dynaport MiniMod TriaxialAccelerations Sensors� 2 [46]
2 accelerometers62� 41� 18 mm, 53 g
No. of transitionsNo. of activity boutsDuration in posturesWalking durationDuration of activity bouts
Worn in left and right trouser pockets,a clip secured thesensors in the pockets.
Fitbit Ultra [47] 3D accelerometer and altimeter Step count Clips to belt or waistbandGT3X, Actigraph [31] Accelerometer Activity duration Belt – GPS mounted on right hip and
actigraph mounted on left hip.Nike + Fuelband [47] 3D accelerometer Step count WristbandPAL2 [27,36] Single or dual axis accelerometer
and a tilt switchNo. of transitionsDuration in posturesWalking duration
Accelerometer attached to the thighand tilt switch attached to the calf(via sleeves with velcro fastenings).
RT3 triaxial accelerometer [48] Accelerometer Total caloric expenditure On left hip via a velcro belt at themidpoint of the iliac crest.
Sensewear Pro 3 Armband[11,49,50]
Multisensor Array and BiaxialAccelerometer
Energy expenditure Step count.Duration in postures
On the back of the non-affected ULmidway between the shoulder andthe elbow.
SmartShoe [51,52] Triaxial accelerometer, force sen-sitive resistors; a battery power,switch and wireless boardinstalled onto a rigid circuitboard.
Step countNo. of transitionsDuration in postures.
Triaxial accelerometer mounted on theheel of a shoe and 5 force sensitiveresistors embedded in a flexibleinsole (under the heel, heads of 1st,3rd and 5th metatarsals and greattoe). Circuit board glued to theback of the shoe.
(continued )
4 N. A. Fini et al. Disabil Rehabil, Early Online: 1–15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.

time walking, time spent active). Figure 4 shows device capabilityfor measuring outcomes in these categories. Two devices werecapable of measuring across all three domains of activityintensity, frequency and duration: the SAM and the SensewearPro 3.
Physical activity was measured from one hour (duringlaboratory testing) to 12 days. In 19 studies, physical activitywas measured for less than 12 h and in 31 studies physical activitywas measured for more than 3 days. The devices involved wearingbetween one and five sensors on different parts of the body. Nodevice algorithms or normative data were reported. Samplingrates were reported for 41% of devices. The cost of the device wasreported in two papers. Five devices were able to detectimprovements in activity level in the longitudinal studies: theactivPAL, activity monitor – 3 accelerometers, PAL 2, SAM andthe Sensewear Pro3 [11,27–30,33].
Observational methods
The observational methods used to measure physical activity werebehavioural mapping (25 studies), videotape observation(4 studies) and counting repetitions of activities (2 studies).Many different activity classifications were noted, however moststudies had three major items of interest: activity, location andpeople present with the patient. In 58% of studies, specific detailsabout the type of activity observed (e.g. walking, transferring oraffected upper limb use) and the position of the participant (e.g.
sitting, standing or in bed) was provided. In two studies,‘‘therapeutic versus non-therapeutic activity’’ [78,79] wasreported and three studies classified activities into pre-determinedcategories [80–83]. Studies in which physical activity was
Activity monitor ComponentsPhysical activity outcomes
measured Where it is worn on the body
StepWatch Activity Monitor orStep Activity Monitor (SAM)[12–17,20,33,47,53–66]
Micro-processor linked acceler-ometer and electronic filter
75� 50� 20 mm, 38 g.
No. of steps at specified step ratePeak activity indexStep countsNo. of activity boutsDuration of activity bouts
Just above the lateral malleolus of theunaffected leg.
Waterproof.
TriTrac RT3 Accelerometer [67] Triaxial accelerometer, 65 g Activity counts On waist belt in a central back positionas close to the body’s COG aspossible.
Wireless Triaxial Accelerometers[68]
2 accelerometers: 100 g,1� 2� 5 cm with a USB portfor charging and downloading.
Step countsNo. of activity boutsWalking durationDuration of activity bouts
Above each ankle on the bony tibia,3 cm above the medial malleolusattached by velcro to a soft snapband.
Pedometer (Conventional) [53] Step counts On waist belt on non-paretic hip atmidline of the thigh
Pedometer (Digimax) [32] Step countsPedometer (model 650 Yamasa
Tokei Co.) [26]Step counts On the waist belt above the hip joint
on the non-paretic side.OMRON HJ-113-E Piezoelectric
Pedometers [69]Horizontal cantilevered beam with
a weight on the end with apiezoelectric crystal.
Step counts Around the neck, or on the waistbandabove either hip.
Pedometer (Yamax DigiwalkerSW-200/SW-650/SW-701)[47,70–73]
Spring lever arm mechanism Step counts Midway between iliac crest andumbilicus over right leg (clipped tobelt via waistband) OR lateral sideof the non-paretic knee (proximalfibula) with a patella brace.
VKR Fitness Twin Step Pedometer[74]
Step counts At the waistband of the pants or at thetop of the sock.
IDEEA – the Intelligent Device forEnergy Expenditure andActivity [75,76]
1 data collection recorderdevice: 70� 55� 24 mm,58 g and 5 small sensors:20� 15� 2 mm, 2 g.
Step countsActivity countsNo. of transitionsDuration in posturesWalking durationActivity duration
5 sensors (chest, front of both thighsand bottom of both feet). Recorderdevice attached to a belt or waist ofpants.
Pulmonary Gas ExchangeMeasurement System [77]
Energy expenditure
PDA, personal digital assistant; No., number; kcal/d, kilocalories per day; ASIS, anterior superior iliac spine; MMC, MultiMediaCard; GPS, gobalpositioning system; COG, centre of gravity; USB, universal serial bus.
n = number of devices
Intensity
Dura�onFrequency
n=3
n=0n=2
n=5n=9n=8
n=2
Figure 4. Device capability for measuring outcomes following stroke(n¼ number of devices).
DOI: 10.3109/09638288.2014.978508 Physical activity following stroke 5
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
measured during therapy included specific information about theactivity, for example number of steps or transfers [84,85], timespent in exercises targeting activity limitations [86–89] and timespent active or inactive [88–90].
Physical activity was measured from 30 min to 12 h on 1 to 10days. Observations of each participant were most commonly madeevery 10 min and ranged from 8 to 30 min. One study reportedcontinuous observation [83] (as did the counting repetitions andvideotape observation papers) [84,85,87–90].
Psychometric properties
Validity
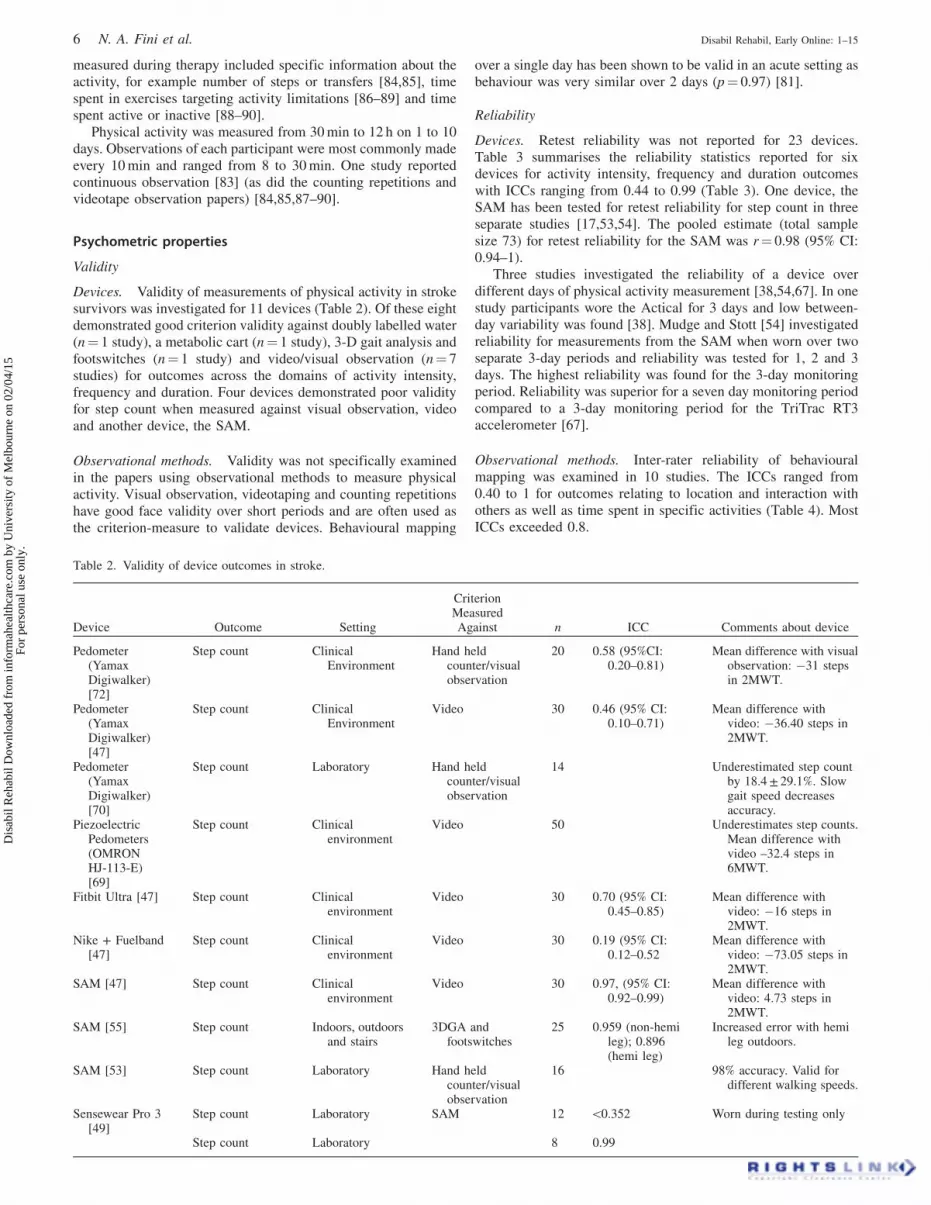
Devices. Validity of measurements of physical activity in strokesurvivors was investigated for 11 devices (Table 2). Of these eightdemonstrated good criterion validity against doubly labelled water(n¼ 1 study), a metabolic cart (n¼ 1 study), 3-D gait analysis andfootswitches (n¼ 1 study) and video/visual observation (n¼ 7studies) for outcomes across the domains of activity intensity,frequency and duration. Four devices demonstrated poor validityfor step count when measured against visual observation, videoand another device, the SAM.
Observational methods. Validity was not specifically examinedin the papers using observational methods to measure physicalactivity. Visual observation, videotaping and counting repetitionshave good face validity over short periods and are often used asthe criterion-measure to validate devices. Behavioural mapping
over a single day has been shown to be valid in an acute setting asbehaviour was very similar over 2 days (p¼ 0.97) [81].
Reliability
Devices. Retest reliability was not reported for 23 devices.Table 3 summarises the reliability statistics reported for sixdevices for activity intensity, frequency and duration outcomeswith ICCs ranging from 0.44 to 0.99 (Table 3). One device, theSAM has been tested for retest reliability for step count in threeseparate studies [17,53,54]. The pooled estimate (total samplesize 73) for retest reliability for the SAM was r¼ 0.98 (95% CI:0.94–1).
Three studies investigated the reliability of a device overdifferent days of physical activity measurement [38,54,67]. In onestudy participants wore the Actical for 3 days and low between-day variability was found [38]. Mudge and Stott [54] investigatedreliability for measurements from the SAM when worn over twoseparate 3-day periods and reliability was tested for 1, 2 and 3days. The highest reliability was found for the 3-day monitoringperiod. Reliability was superior for a seven day monitoring periodcompared to a 3-day monitoring period for the TriTrac RT3accelerometer [67].
Observational methods. Inter-rater reliability of behaviouralmapping was examined in 10 studies. The ICCs ranged from0.40 to 1 for outcomes relating to location and interaction withothers as well as time spent in specific activities (Table 4). MostICCs exceeded 0.8.
Table 2. Validity of device outcomes in stroke.
Device Outcome Setting
CriterionMeasuredAgainst n ICC Comments about device
Pedometer(YamaxDigiwalker)[72]
Step count ClinicalEnvironment
Hand heldcounter/visualobservation
20 0.58 (95%CI:0.20–0.81)
Mean difference with visualobservation: �31 stepsin 2MWT.
Pedometer(YamaxDigiwalker)[47]
Step count ClinicalEnvironment
Video 30 0.46 (95% CI:0.10–0.71)
Mean difference withvideo: �36.40 steps in2MWT.
Pedometer(YamaxDigiwalker)[70]
Step count Laboratory Hand heldcounter/visualobservation
14 Underestimated step countby 18.4 ± 29.1%. Slowgait speed decreasesaccuracy.
PiezoelectricPedometers(OMRONHJ-113-E)[69]
Step count Clinicalenvironment
Video 50 Underestimates step counts.Mean difference withvideo –32.4 steps in6MWT.
Fitbit Ultra [47] Step count Clinicalenvironment
Video 30 0.70 (95% CI:0.45–0.85)
Mean difference withvideo: �16 steps in2MWT.
Nike + Fuelband[47]
Step count Clinicalenvironment
Video 30 0.19 (95% CI:0.12–0.52
Mean difference withvideo: �73.05 steps in2MWT.
SAM [47] Step count Clinicalenvironment
Video 30 0.97, (95% CI:0.92–0.99)
Mean difference withvideo: 4.73 steps in2MWT.
SAM [55] Step count Indoors, outdoorsand stairs
3DGA andfootswitches
25 0.959 (non-hemileg); 0.896(hemi leg)
Increased error with hemileg outdoors.
SAM [53] Step count Laboratory Hand heldcounter/visualobservation
16 98% accuracy. Valid fordifferent walking speeds.
Sensewear Pro 3[49]
Step count Laboratory SAM 12 50.352 Worn during testing only
Step count Laboratory 8 0.99
(continued )
6 N. A. Fini et al. Disabil Rehabil, Early Online: 1–15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.

Device Outcome Setting
CriterionMeasuredAgainst n ICC Comments about device
Wireless TriaxialAcceleromet-ers [68]
Visualobservation
High construct and conver-gent validity with activ-ity logs and bouts ofwalking.
SmartShoe [51] Number oftransitions andstep count
Laboratory Video 12 0.99 Fast and self –selectedspeeds. Accuracy forcorrectly identifyingpostures: 97.2%
IDEEA [75] Activity counts Community Visualobservation
3 94% accuracy
ComputerScience &ApplicationsInc. ActivityMonitors [45]
Walking duration Community andclinicalenvironment
Video 9 0.99
IDEEA [75] Time on feet Community Visualobservation
3 99% accuracy
PAL 2 [36] Time upright Clinicalenvironment
Visualobservation
20 0.72 (95% CI:0.43–0.88)
Measured over 8 h.
PAL 2 [36] Time sitting Clinicalenvironment
Visualobservation
20 0.68 (95% CI:0.36–0.86)
Measured over 8 h.
PAL 2 [36] Time lying Clinicalenvironment
Visualobservation
20 0.74 (95% CI:0.46–0.89)
Measured over 8 h.
Sensewear Pro 3[50]
Energyexpenditure
Community Doubly labelledwater
9 0.850 Mean difference: 3.8%.Measured for 10 days
Sensewear Pro 3[49]
Energyexpenditure
Laboratory Metabolic cart 12 0.702 (non-hemiarm) 0.586(hemi arm)
Worn during testing only
ICC, Intraclass Correlation Coefficient; CI, Confidence Interval; 2MWT, 2-min walk test; 6MWT, 6-min walk test; hemi, hemiplegic.
Table 3. Retest reliability of device outcomes in stroke.
Activity monitorOutcomemeasure n Statistic 95% CI Setting
Days of PAmeasurement
Pedometer(Conventional) [53]
step count 16 r¼ 0.64 Clinical environment 2� 6 min (walk tests),on 2 separate days
SAM [17] Step count 17 r¼ 0.96 Community 2� 2 days, within 3weeks
SAM [53] Step count 16 r¼ 0.975 Clinical environment 2� 6 min (walk tests),on 2 separate days
SAM [54] Step count 40 ICC¼ 0.989 Community 2� 3 days, 1 week apartActical [38] Activity counts 40 ICC¼ 0.95 0.92–0.97 Community 3 consecutive daysIDEEA [75] Activity counts 42 ICC¼ 0.8 Community 2� 1 day, 1 week apartTriTrac RT3Accelerometer [67]
Activity counts 20 ICC¼ 0.68 0.36–0.86 Community 2� 7 days, 8 weeksapart
IDEEA [75] Time on feet 42 ICC¼ 0.69 Community 2� 1 day, 1 week apartSAM [54] No. steps at
medium andhigh rate(430 steps/min)
40 ICC¼ 0.969 Community 2� 3 days, 1 week apart
SAM [54] No. steps at lowrate (530steps/min)
40 ICC¼ 0.953 Community 2� 3 days, 1 week apart
SAM [54] Peak activityindex
40 ICC¼ 0.955 Community 2� 3 days, 1 week apart
Caltrac [17] Activity calories 17 r¼ 0.44 Community 2� 2 days, within 3weeks
Actical [38] Energyexpenditure
40 ICC¼ 0.95 0.92–0.97 Community 3 consecutive days
CI, Confidence Interval; r, Pearson correlation coefficient; ICC, Intraclass correlation coefficient; LOA, Limits of agreement.
DOI: 10.3109/09638288.2014.978508 Physical activity following stroke 7
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
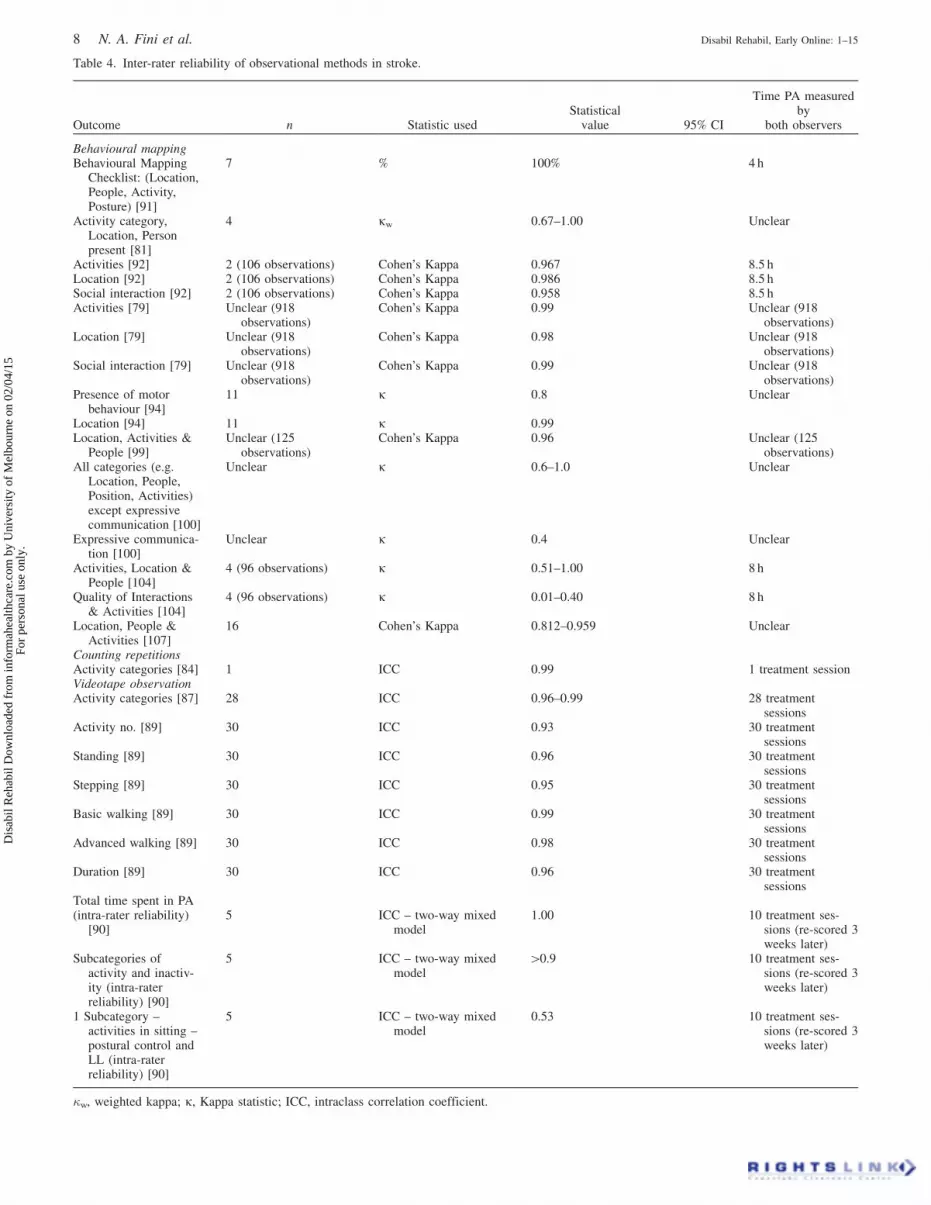
Table 4. Inter-rater reliability of observational methods in stroke.
Outcome n Statistic usedStatistical
value 95% CI
Time PA measuredby
both observers
Behavioural mappingBehavioural Mapping
Checklist: (Location,People, Activity,Posture) [91]
7 % 100% 4 h
Activity category,Location, Personpresent [81]
4 kw 0.67–1.00 Unclear
Activities [92] 2 (106 observations) Cohen’s Kappa 0.967 8.5 hLocation [92] 2 (106 observations) Cohen’s Kappa 0.986 8.5 hSocial interaction [92] 2 (106 observations) Cohen’s Kappa 0.958 8.5 hActivities [79] Unclear (918
observations)Cohen’s Kappa 0.99 Unclear (918
observations)Location [79] Unclear (918
observations)Cohen’s Kappa 0.98 Unclear (918
observations)Social interaction [79] Unclear (918
observations)Cohen’s Kappa 0.99 Unclear (918
observations)Presence of motor
behaviour [94]11 k 0.8 Unclear
Location [94] 11 k 0.99Location, Activities &
People [99]Unclear (125
observations)Cohen’s Kappa 0.96 Unclear (125
observations)All categories (e.g.
Location, People,Position, Activities)except expressivecommunication [100]
Unclear k 0.6–1.0 Unclear
Expressive communica-tion [100]
Unclear k 0.4 Unclear
Activities, Location &People [104]
4 (96 observations) k 0.51–1.00 8 h
Quality of Interactions& Activities [104]
4 (96 observations) k 0.01–0.40 8 h
Location, People &Activities [107]
16 Cohen’s Kappa 0.812–0.959 Unclear
Counting repetitionsActivity categories [84] 1 ICC 0.99 1 treatment sessionVideotape observationActivity categories [87] 28 ICC 0.96–0.99 28 treatment
sessionsActivity no. [89] 30 ICC 0.93 30 treatment
sessionsStanding [89] 30 ICC 0.96 30 treatment
sessionsStepping [89] 30 ICC 0.95 30 treatment
sessionsBasic walking [89] 30 ICC 0.99 30 treatment
sessionsAdvanced walking [89] 30 ICC 0.98 30 treatment
sessionsDuration [89] 30 ICC 0.96 30 treatment
sessionsTotal time spent in PA(intra-rater reliability)
[90]5 ICC – two-way mixed
model1.00 10 treatment ses-
sions (re-scored 3weeks later)
Subcategories ofactivity and inactiv-ity (intra-raterreliability) [90]
5 ICC – two-way mixedmodel
40.9 10 treatment ses-sions (re-scored 3weeks later)
1 Subcategory –activities in sitting –postural control andLL (intra-raterreliability) [90]
5 ICC – two-way mixedmodel
0.53 10 treatment ses-sions (re-scored 3weeks later)
�w, weighted kappa; k, Kappa statistic; ICC, intraclass correlation coefficient.
8 N. A. Fini et al. Disabil Rehabil, Early Online: 1–15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.

In two studies, the inter-rater reliability of videotape observa-tion was reported with ICCs ranging from 0.93 to 0.99 for timespent in specific activities (Table 4). In one study, intra-raterreliability was examined for time spent in subcategories ofactivity with ICCs ranging from 0.53 to 1.00.
Discussion
Accelerometry and behavioural mapping are the most commonmethods used to measure physical activity following stroke andstep count is the outcome most frequently reported.Accelerometry is commonly used in a community setting forambulant stroke survivors in the longer term. Behaviouralmapping is always used in a clinical environment, mostcommonly in the subacute phase. Physical activity measurementis highly variable following stroke and many different outcomeshave been reported. This makes it difficult to compare resultsacross studies to enable a wider understanding of the issue.
There are advantages and disadvantages associated with bothdevices and observational methods to measure physical activityfollowing stroke. Devices allow stroke survivors’ activity to bemonitored in their natural environments for long, uninterruptedperiods. Many devices are quite small and unobtrusive with onlyone sensor. However, devices are generally costly, can be complexto use and the validity and reliability data for monitoring activityfollowing stroke is limited. Observational methods on the otherhand are only suitable for a clinical environment, are obtrusiveand time and labour intensive. Observational methods do notcapture activity intensity and can over or under estimate theamount of activity performed due to the low sampling rate(assumes the activity observed is continued until the nextobservation) [36]. However, inter-rater reliability is overall highfor observational methods and they can detect a low threshold ofactivity (i.e. distinguish between lying, sitting up in bed andsitting out of bed) and provide additional information on patientlocation and who they are with [109]. Many accelerometers havedifficulty distinguishing between lying and sitting postures [51]and only one device identified in this review could do this in astroke population (PAL 2), although there were issues with correctposture identification when lying with the knees bent and sittingwith the knees straight [36]. The method chosen by the user willdepend on their resources and the aims of physical activitymeasurement.
The psychometric properties of devices need to be addressedmore frequently and adequately in the stroke population. Manypapers report validity of device outcomes in other populations;however, this is not likely to be relevant to stroke survivors. Thereare certain issues characteristic of this population such asasymmetry, slow movement speed and use of gait aids that mayinfluence a device’s ability to accurately measure physicalactivity [17,38,53,55,70]. The papers that report on devicevalidity in stroke have very small sample sizes, generally 30 orless and replication would strengthen confidence in validity. Thesampling rate of a device may also affect the validity of deviceoutcomes. Knarr and colleagues [56] showed that changing thesampling rate could dramatically influence the outcomesreported. They demonstrated that a 60-s sampling epoch over-estimated the walking duration by 40% and underestimated thenumber of walking bouts by 83% when compared to a 5-ssampling rate. They discovered that these deviations were worstfor low activity days. The sampling rate chosen needs to beconsidered against an appropriate monitoring duration (thisrelates to the device memory and data storage). In addition tothese issues, content and construct validity of device outcomesneeds to be further explored: is step count alone an adequatemeasure of physical activity? [75] Do measurements of activity
intensity, frequency and duration all need to be considered tounderstand the nature of physical activity?
Further to this, the psychometric property of retest reliabilityneeds to be established for many devices, to ensure theirconsistency of measurement across time and subsequent usefor longitudinal activity monitoring. Retest reliability has onlybeen established for a few devices in stroke and only onedevice, the SAM has been tested on multiple occasions forstep counts and demonstrates very high reliability. Days ofphysical activity measurement is another issue to consider andonly three studies have examined this. Two of the three studiesfound that longer measurement periods are more reliable.Employment and weekly activity patterns and variability arepossible influences on the ideal number of days of measurement[38,67], as are device failure and non-compliance [110]. Ithas been suggested in a population of healthy adults that aminimum of 13 h per day is required for valid measures of dailyphysical activity [111] and this should be explored in the strokepopulation. Future research should comprehensively address thevalidity and retest reliability of devices to be used in the strokepopulation.
Reaching a consensus in reporting of outcomes for bothdevices and observational methods would be useful for futureresearch using physical activity measurement in stroke. Currentlythe available research is fragmented in terms of methods used andoutcomes reported. There is an opportunity to consider usingsimilar outcomes in each area of activity intensity, frequency andduration. For example, someone may do the recommendednumber of steps per day, but at a very low intensity or someonemay work at a high intensity, but for a very short period of timewith prolonged bouts of sedentary behaviour. We do not currentlyknow which category or combination of categories is mostimportant for long term benefits, specifically reduction incardiovascular morbidity and mortality in stroke survivors.However, the cardiovascular risks of sedentary behaviour in anormal population are well known [7,112]. We need to considercollaborative opportunities across different research groups to usesimilar methods of measurement and common outcomes to allowpooling of data for hypothesis generation for future research.Consensus in physical activity measurement would also facilitateevaluation of physical treatment and health programs followingstroke.
For a physical activity, measurement device to be useful inthe clinical environment, to both patients and clinicians, itneeds to be simple to use, inexpensive and able to provide dataor feedback that is meaningful to stroke survivors in a timelyfashion [52]. Immediate feedback could include informationsuch as activity targets and sedentary time. This would enablephysical activity monitoring to be used as a motivation andbehaviour change tool in this population who are known to berelatively inactive and at risk of cardiovascular illnesses[11,15,17]. Ideally devices should be able to provide data in thethree categories of activity: intensity, frequency and duration;only two devices identified in this review (the SAM andSensewear Pro 3) are capable of measuring all three categoriesin stroke. Data provided also needs to be valid and reliable, butparameters for establishing adequate reliability and validity havenot been defined. For ease of use and wear, devices should also beunobtrusive, lightweight, comfortable and acceptable to strokesurvivors. In addition, a long battery life, waterproofing andability to transmit data wirelessly would be advantageous [113].No devices identified in this review meet all of these criteria.However, given the rapid rise in use of devices in stroke researchover the past 10 years, we are optimistic that closer collaborationbetween device manufacturers and users may result in betterdevices for clinical application.
DOI: 10.3109/09638288.2014.978508 Physical activity following stroke 9
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.

Conclusions
Physical activity measurement and outcomes following strokevary considerably. Devices allow for unobtrusive, longer moni-toring in free-living environments. Observational methods suitinpatient settings but are time and labour intensive. No singledevice is ideal for clinical application for people following strokebut there are several devices that provided comprehensiveassessment data. Future research should focus on the psychomet-ric properties of devices and investigate common outcomes acrossthe activity intensity, frequency and duration domains to enablepooling of physical activity data across multiple studies in thestroke population.
Acknowledgements
The authors would like to thank Dr Tania Pizzari for herassistance with the protocol design of this review. We thank theVictorian State Government for infrastructure support provided toThe Florey Institute of Neuroscience and Mental Health.
Declaration of interest
The primary author is a recipient of a National Heart Foundationof Australia Postgraduate Scholarship (award no: PP 12 M 6983).This study was supported by a Caulfield Hospital Major ResearchGrant and a Victorian Stroke Clinical Network PostgraduateScholarship in Stroke Care. None of the authors have any conflictsof interest to declare in relation to this manuscript.
References
1. Thrift AG, Cadilhac DA, Thayabaranathan T, et al. Global strokestatistics. Int J Stroke 2014;9:6–18.
2. National Stroke Foundation. National stroke audit – rehabilitationservices report 2012. Melbourne, Australia: National StrokeFoundation; 2012.
3. Senes S. AIHW: how we manage stroke in Australia. AIHW cat. no.CVD 31. Canberra: Australian Institute of Health and Welfare;2006.
4. Casperson CJ, Powell KE, Christenson GM. Physical activity,exercise, and physical fitness: defintiions and distinctions for health-related research. Public Health Reports 1985;100:126–31.
5. Australian Institute of Health and Welfare. Australia’s health 2012.Australia’s health series no.13. Cat. no. AUS 156. Canberra: AIHW;2012.
6. Smith SC, Benjamin EJ, Bonow RO, et al. AHA/ACCF secondaryprevention and risk reduction therapy for patients with coronary andother atherosclerotic vascular disease: 2011 update: a guideline fromthe american heart association and american college of cardiologyfoundation. Circulation 2011;124:2458–73.
7. Owen N, Sparling P, Healy G, et al. Sedentary behaviour: emergingevidence for a new health risk. Mayo Clin Proc 2010;85:1138–41.
8. Lieberman DA, Chamberlin B, Medina Jr E, et al. The power ofplay: innovations in getting active summit 2011: a science panelproceedings report from the American Heart Association.Circulation 2011;123:2507–16.
9. ACSM and AHA. Physical activity and public health in older adults:recommendation from the American College of Sports Medicine &the American Heart Association. Circulation 2007;116:1094–105.
10. Tudor-Locke C, Bassett Jr DR. How many steps/day are enough?Preliminary pedometer indices for public health. Sports Med 2004;34:1–8.
11. Moore SA, Hallsworth K, Plotz T, et al. Physical activity, sedentarybehaviour and metabolic control following stroke: a cross-sectionaland longitudinal study. PLoS One 2013;8:e55263.
12. Mudge S, Barber PA, Stott NS. Circuit-based rehabilitationimproves gait endurance but not usual walking activity in chronicstroke: a randomized controlled trial. Arch Phys Med Rehabil 2009;90:1989–96.
13. Mudge S, Stott NS. Timed walking tests correlate with daily stepactivity in persons with stroke. Arch Phys Med Rehabil 2009;90:296–301.
14. Shaughnessy M, Michael KM, Sorkin JD, Macko RF. Steps afterstroke: capturing ambulatory recovery. Stroke 2005;36:1305–7.
15. Michael K, Macko RF. Ambulatory activity intensity profiles,fitness and fatigue in chronic stroke. Top Stroke Rehabil 2007;2:5–12.
16. Manns PJ, Baldwin E. Ambulatory activity of stroke survivorsmeasurement options for dose, intensity, and variability of activity.Stroke 2009;40:864–7.
17. Haeuber E, Shaughnessy M, Forrester LW, et al. Accelerometermonitoring of home- and community-based ambulatory activityafter stroke. Arch Phys Med Rehabil 2004;85:1997–2001.
18. Bernhardt J, Indredavik B, Langhorne P. When should rehabilitationbegin after stroke? Int J Stroke 2013;8:5–7.
19. Karin D, Michel P, Bogousslavsky J. Early mobilisation after stroke:review of the literature. Cerebrovasc Dis 2006;22:183–90.
20. Moore JL, Roth EJ, Killian C, Hornby TG. Locomotor trainingimproves daily stepping activity and gait efficiency in individualspoststroke who have reached a ‘‘plateau’’ in recovery. Stroke 2010;41:129–35.
21. Stuart M, Chard S, Roettger S. Exercise for chronic stroke survivors:a policy perspective. J Rehabil Res Dev 2008;45:329–36.
22. Warren JM, Ekelund U, Besson H, et al. Assessment of physicalactivity – a review of methodologies with reference to epidemio-logical research: a report of the exercise physiology section of theEuropean Association of Cardiovascular Prevention andRehabilitation. Eur J Cardiovasc Prev Rehabil 2010;17:127–39.
23. Herrmann S, Ragan BG. Outcome assessment part 1: measurementof physical activity. Athletic Ther Today 2008;13:25–8.
24. Downs SH, Black N. The feasibility of creating a checklist for theassessment of the methodological quality both of randomised andnon-randomised studies of health care interventions. J EpidemiolCommun Health 1998;52:377–84.
25. Diener MJ, Hilsenroth MJ, Weinberger J. A primer on meta-analysisof correlation coefficients: the relationship between patient-reportedtherapeutic alliance and adult attachment style as an illustration.Psychother Res 2009;19:519–26.
26. Hachisuka K, Tsutsui Y, Furusawa K, Ogata H. Gender differencesin disability and lifestyle among community-dwelling elderly strokepatients in Kitakyushu, Japan. Arch Phys Med Rehabil 1998;79:998–1002.
27. Askim T, Bernhardt J, Churilov L, et al. Changes in physical activityand related functional and disability levels in the first six monthsafter stroke: a longitudinal follow-up study. J Rehabil Med 2013;45:423–8.
28. Kottink AI, Hermens HJ, Nene AV, et al. A randomized controlledtrial of an implantable 2-channel peroneal nerve stimulator onwalking speed and activity in poststroke hemiplegia. Arch Phys MedRehabil 2007;8:971–8.
29. Touillet A, Guesdon H, Bosser G, et al. Assessment of compliancewith prescribed activity by hemiplegic stroke patients after anexercise programme and physical activity education. Ann PhysRehabil Med 2010;53:250–65.
30. Janssen W, Bussmann J, Selles R, et al. Recovery of the sit-to-standmovement after stroke: a longitudinal cohort study. NeurorehabilNeural Repair 2010;24:763–9.
31. Evans CC, Hanke TA, Zielke D, et al. Monitoring communitymobility with global positioning system technology after a stroke: acase study. J Neurol Phys Ther 2012;36:68–78.
32. Dean CM, Rissel C, Sherrington C, et al. Exercise toenhance mobility and prevent falls after stroke: the communitystroke club randomized trial. Neurorehabil Neural Repair 2012;26:1046–57.
33. Duncan PW, Sullivan KJ, Behrman AL, et al. Body-weight-supported treadmill rehabilitation after stroke. N Engl J Med2011;364:2026–36.
34. Cavalcanti P, Campos T, Araujo J. Actigraphic analysis of the sleep-wake cycle and physical activity level in patients with stroke:implications for clinical practice. Chronobiol Int 2012;29:1267–72.
35. Britton E, Harris N, Turton A. An exploratory randomizedcontrolled trial of assisted practice for improving sit-to-stand instroke patients in the hospital setting. Clin Rehabil 2008;22:458–68.
36. Kramer SF, Cumming T, Churlov L, Bernhardt J. Measuring activitylevels at an acute stroke ward: comparing observations to a device.BioMed Res Int 2013;2013:Article ID 460482, 8 pages.
37. Prajapati SK, Gage WH, Brooks D, et al. A novel approach toambulatory monitoring: investigation into the quantity and control of
10 N. A. Fini et al. Disabil Rehabil, Early Online: 1–15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
everyday walking in patients with subacute stroke. NeurorehabilNeural Repair 2011;25:6–14.
38. Rand D, Eng JJ, Tang PF, et al. How active are people with stroke?:use of accelerometers to assess physical activity. Stroke 2009;40:163–8.
39. Rand D, Eng JJ, Tang PF, et al. Daily physical activity and itscontribution to the health-related quality of life of ambulatory indi-viduals with chronic stroke. Health Qual Life Outcomes 2010;8:80–7.
40. Rand D, Eng JJ. Disparity between functional recovery and daily useof the upper and lower extremities during subacute stroke rehabili-tation. Neurorehabil Neural Repair 2012;26:76–84.
41. Salbach NM, Brooks D, Romano J, et al. Cardiorespiratoryresponses during the 6-minute walk and ramp cycle ergometertests and their relationship to physical activity in stroke.Neurorehabil Neural Repair 2014;28:111–19.
42. Van Den Berg-Emons RJ, Bussmann JB, Stam HJ. Accelerometry-based activity spectrum in persons with chronic physical conditions.Arch Phys Med Rehabil 2010;91:1856–61.
43. Katoh J, Murakami M, Hirayama M, et al. Correlation of pedometricmeasurement of daily physical activity with exercise endurance byoxygen uptake kinetics in ambulatory stroke patients. J Phys TherSci 2002;14:77–80.
44. Lindemann U, Moe-Nilssen R, Nicolai SE, et al. Assessment ofbalance in unsupported standing with elderly inpatients by forceplate and accelerometers. Aging-Clin Exp Res 2012;24:37–41.
45. Uswatte G, Miltner WH, Foo B, et al. Objective measurement offunctional upper-extremity movement using accelerometer record-ings transformed with a threshold filter. Stroke 2000;31:662–7.
46. Frazer SWT, Hellebrand WEH, Keijsers NLW. Variation andachievement of ambulatory activity among patients with chronicstroke. J Rehabil Med 2013;45:848–53.
47. Fulk GD, Combs SA, Danks KA, et al. Accuracy of 2 activitymonitors in detecting steps in people with stroke and traumatic braininjury. Phys Ther 2014;94:222–9.
48. Singh A, Stewart A, Franzsen D, MacKay-Lyons M. Energyexpenditure of dressing in patients with stroke. Int J Ther Rehabil2011;18:683–93.
49. Manns PJ, Haennel RG. SenseWear armband and stroke: validity ofenergy expenditure and step count measurement during walking.Stroke Res Treat 2012;2012:Article ID 247165, 8 pages.
50. Moore SA, Hallsworth K, Bluck LJ, et al. Measuring energyexpenditure after stroke: validation of a portable device. Stroke2012;43:1660–2.
51. Fulk GD, Edgar SR, Bierwirth R, et al. Identifying activity levelsand steps of people with stroke using a novel shoe-based sensor.J Neurol Phys Ther 2012;36:100–7.
52. Fulk GD, Sazonov E. Using sensors to measure activity in peoplewith stroke. Top Stroke Rehabil 2011;18:746–57.
53. Macko RF, Haeuber E, Shaughnessy M, et al. Microprocessor-basedambulatory activity monitoring in stroke patients. Med Sci SportsExerc 2002;34:394–9.
54. Mudge S, Stott NS. Test-retest reliability of the StepWatch ActivityMonitor outputs in individuals with chronic stroke. Clin Rehabil2008;22:871–7.
55. Mudge S, Stott NS, Walt SE. Criterion validity of the stepwatchactivity monitor as a measure of walking activity in patients afterstroke. Arch Phys Med Rehabil 2007;88:1710–15.
56. Knarr B, Roos MA, Reisman DS. Sampling frequency impactsmeasurement of walking activity after stroke. J Rehabil Res Dev2013;50:1107–12.
57. Bowden MG, Balasubramanian CK, Behrman AL, Kautz SA.Validation of a speed-based classification system using quantitativemeasures of walking performance poststroke. Neurorehabil NeuralRepair 2008;22:672–5.
58. Bowden MG, Behrman AL, Neptune RR, et al. Locomotorrehabilitation of individuals with chronic stroke: difference betweenresponders and nonresponders. Arch Phys Med Rehabil 2013;94:856–62.
59. Fulk GD, Reynolds C, Mondal S, Deutsch JE. Predicting home andcommunity walking activity in people with stroke. Arch Phys MedRehabil 2010;91:1582–6.
60. Manns PJ, Tomczak CR, Jelani A, et al. Use of the continuous scalephysical functional performance test in stroke survivors. Arch PhysMed Rehabil 2009;90:488–93.
61. Manns PJ, Tomczak CR, Jelani A, Haennel RG. Oxygen uptakekinetics: associations with ambulatory activity and physical
functional performance in stroke survivors. J Rehabil Med 2010;42:259–64.
62. Michael KM, Allen JK, Macko RF. Reduced ambulatory activityafter stroke: the role of balance, gait, and cardiovascular fitness.Arch Phys Med Rehabil 2005;86:1552–6.
63. Michael K, Goldberg AP, Treuth MS, et al. Progressive adaptivephysical activity in stroke improves balance, gait, and fitness:preliminary results. Top Stroke Rehabil 2009;16:133–9.
64. Resnick B, Michael K, Shaughnessy M, et al. Inflated perceptions ofphysical activity after stroke: pairing self-report with physiologicmeasures. J Phys Act Health 2008;5:308–18.
65. Roos MA, Rudolph KS, Reisman DS. The structure of walkingactivity in people after stroke compared with older adults withoutdisability: a cross-sectional study. Phys Ther 2012;92:1141–7.
66. Zalewski KR, Dvorak L. Barriers to physical activity between adultswith stroke and their care partners. Top Stroke Rehabil 2011;18:666–75.
67. Hale LA, Pal J, Becker I. Measuring free-living physical activity inadults with and without neurologic dysfunction with a triaxialaccelerometer. Arch Phys Med Rehabil 2008;89:1765–71.
68. Dobkin BH, Xu X, Batalin M, et al. Reliability and validity ofbilateral ankle accelerometer algorithms for activity recognition andwalking speed after stroke. Stroke 2011;42:2246–50.
69. Carroll SL, Greig CA, Lewis SJ, et al. The use of pedometers instroke survivors: are they feasible and how well do they detect steps?Arch Phys Med Rehabil 2012;93:466–70.
70. Manns PJ, Orchard JL, Warren S. Accuracy of pedometry forambulatory adults with neurological disabilities. Physiother Can2007;59:208–17.
71. Baert I, Feys H, Daly D, et al. Are patients 1 year post-stroke activeenough to improve their physical health? Disabil Rehabil 2012;34:574–80.
72. Elsworth C, Dawes H, Winward C, et al. Pedometer step counts inindividuals with neurological conditions. Clin Rehabil 2009;23:171–5.
73. van Swigchem R, Vloothuis J, den Boer J, et al. Is transcutaneousperoneal stimulation beneficial to patients with chronic stroke usingan ankle-foot orthosis? A within-subjects study of patients’satisfaction, walking speed and physical activity level. J RehabilMed 2010;42:117–21.
74. Robinson CA, Shumway-Cook A, Ciol MA, Kartin D. Participationin community walking following stroke: subjective versus objectivemeasures and the impact of personal factors. Phys Ther 2011;91:1865–76.
75. Alzahrani MA, Ada L, Dean CM. Duration of physical activity isnormal but frequency is reduced after stroke: an observational study.J Physiother 2011;57:47–51.
76. Sakamoto K, Nakamura T, Sajima Y, et al. Physical activities andsteps in daily living after stroke. J Wakayama Med Soc 2008;59:67–72.
77. Houdijk H, ter Hoeve N, Nooijen C, et al. Energy expenditure ofstroke patients during postural control tasks. Gait Posture 2010;32:321–6.
78. Huijben-Schoenmakers M, Gamel C, Hafsteinsdottir TB. Filling upthe hours: how do stroke patients on a rehabilitation nursing homespend the day? Clin Rehabil 2009;23:1145–50.
79. De Weerdt W, Nuyens G, Feys H, et al. Group physiotherapyimproves time use by patients with stroke in rehabilitation. Aust JPhysiother 2001;47:53–61.
80. Skarin M, Sjoholm A, Nilsson AL, et al. A mapping study onphysical activity in stroke rehabilitation: establishing the baseline.J Rehabil Med 2013;45:997–1003.
81. Bernhardt J, Dewey H, Thrift A, Donnan G. Inactive and alone:physical activity within the first 14 days of acute stroke unit care.Stroke 2004;35:1005–9.
82. Bernhardt J, Chitravas N, Meslo IL, et al. Not all stroke units arethe same: a comparison of physical activity patterns in Melbourne,Australia, and Trondheim, Norway. Stroke 2008;39:2059–65.
83. Gage WH, Zabjek KF, Sibley KM, et al. Ambulatory monitoring ofactivity levels of individuals in the sub-acute stage followingstroke: a case series. J Neuroeng Rehabil 2007;4:Article no. 41,10 pages.
84. Lang CE, MacDonald JR, Gnip C. Counting repetitions: anobservational study of outpatient therapy for people with hemipar-esis post-stroke. J Neurol Phys Ther 2007;31:3–10.
DOI: 10.3109/09638288.2014.978508 Physical activity following stroke 11
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
85. Lang CE, MacDonald JR, Reisman DS, et al. Observation ofamounts of movement practice provided during stroke rehabilita-tion. Arch Phys Med Rehabil 2009;90:1692–8.
86. Ada L, Mackey F, Heard R, Adams R. Stroke rehabilitation: doesthe therapy area provide a physical challenge? Aust J Physiother1999;45:33–8.
87. De Wit L, Putman K, Lincoln N, et al. Stroke rehabilitation inEurope: what do physiotherapists and occupational therapistsactually do? Stroke 2006;37:1483–9.
88. Kaur G, English C, Hillier S. Physiotherapists systematicallyoverestimate the amount of time stroke survivors spend engaged inactive therapy rehabilitation: an observational study. J Physiother2013;59:45–51.
89. Kuys S, Brauer S, Ada L. Routine physiotherapy does not induce acardiorespiratory training effect post-stroke, regardless of walkingability. Physiother Res Int 2006;11:219–27.
90. Elson T, English C, Hillier S. How much physical activity dopeople recovering from stroke do in physiotherapuy sessions? Int JTher Rehabil 2009;16:78–84.
91. Bear-Lehman J, Bassile CC, Gillen G. A comparison of time use onan acute rehabilitation unit: subjects with and without a stroke.Phys Occup Ther Geriatr 2001;20:17–27.
92. De Weerdt W, Selz B, Nuyens G, et al. Time use of stroke patientsin an intensive rehabilitation unit: a comparison between a Belgianand a Swiss setting. Disabil Rehabil 2000;22:181–6.
93. De Wit L, Putman K, Dejaeger E, et al. Use of time by strokepatients: a comparison of four European rehabilitation centers.Stroke 2005;36:1977–83.
94. Esmonde T, McGinley J, Wittwer J, et al. Stroke rehabilitation:patient activity during non-therapy time. Aust J Physiother 1997;43:43–51.
95. Gustafsson L, McKenna K. Is there a role for meaningful activity instroke rehabilitation? Top Stroke Rehabil 2010;17:108–18.
96. Janssen H, Ada L, Karayanidis F, et al. Translating the use of anenriched environment poststroke from bench to bedside: studydesign and protocol used to test the feasibility of environmentalenrichment on stroke patients in rehabilitation. Int J Stroke 2012;7:521–6.
97. Janssen H, Ada L, Bernhardt J, et al. An enriched environmentincreases activity in stroke patients undergoing rehabilitation in amixed rehabilitation unit: a pilot non-randomized controlled trial.Disabil Rehabil 2014;36:255–62.
98. Keith RA. Activity patterns of a stroke rehabilitation unit. Soc SciMed Med Psychol Med Sociol 1980;14A:575–80.
99. Keith RA, Cowell KS. Time use of stroke patients in threerehabilitation hospitals. Soc Sci Med 1987;24:529–33.
100. King A, McCluskey A, Schurr K. The time use and activity levelsof inpatients in a co-located acute and rehabilitation stroke unit: anobservational study. Top Stroke Rehabil 2011;18:654–65.
101. Lincoln NB, Gamlen R, Thomason H. Behavioural mapping ofpatients on a stroke unit. Int Disabil Stud 1989;11:149–54.
102. Lincoln NB, Willis D, Philips SA, et al. Comparison of rehabili-tation practice on hospital wards for stroke patients. Stroke 1996;27:18–23.
103. Mackey F, Ada L, Heard R, Adams R. Stroke rehabilitation:are highly structured units more conducive to physical activitythan less structured units? Arch Phys Med Rehabil 1996;77:1066–70.
104. Pound P, Sabin C, Ebrahim S. Observing the process of care: astroke unit, elderly care unit and general medical ward compared.Age Ageing 1999;28:433–40.
105. Thompson R, McKinstry W. How do rehabilitation patients spendtheir days? An investigation into the effect of a group therapyprogramme on time use. N Z J Physiother 2009;37:122–6.
106. Tinson DJ. How stroke patients spend their days. An observationalstudy of the treatment regime offered to patients in hospital withmovement disorders following stroke. Int Disabil Stud 1989;11:45–9.
107. van de Port IG, Valkenet K, Schuurmans M, Visser-Meily JM. Howto increase activity level in the acute phase after stroke. J Clin Nurs2012;21:3574–8.
108. Wellwood I, Langhorne P, McKevitt C, et al. An observationalstudy of acute stroke care in four countries: the European registersof stroke study. Cerebrovasc Dis 2009;28:171–6.
109. West T, Bernhardt J. Physical activity in hospitalised strokepatients. Stroke Res Treat 2012;2012:Article ID 813765, 13 pages.
110. Gebruers N, Vanroy C, Truijen S, et al. Monitoring of physicalactivity after stroke: a systematic review of accelerometry-basedmeasures. Arch Phys Med Rehabil 2010;91:288–97.
111. Herrmann SD, Barreira TV, Kang M, Ainsworth BE. How manyhours are enough? Accelerometer wear time may provide bias indaily activity estimates. J Phys Act Health 2013;10:742–9.
112. Warren T, Barry V, Hooker S, et al. Sedentary behaviours increaserisk of cardiovascular disease mortality in men. Med Sci SportsExerc 2010;42:879–85.
113. Cheung VH, Gray L, Karunanithi M. Review of accelerometry fordetermining daily activity among elderly patients. Arch Phys MedRehabil 2011;92:998–1014.
Appendices
Appendix 1. Search terms.
Condition Method of measuring physical activity Physical activity
Stroke Activity monitor Physical activityCerebrovascular accident Monitoring, ambulatory ActivityCerebral vascular accident Accelerometer Physical mobilityCerebral infarct Acceleromet* Physical functionCerebral haemorrhage Pedometer Mobilis*Cerebral haemorrhage Sensewear Mobiliz*Intracerebral haemorrhage Sense-wear StepsIntracerebral haemorrhage ActivPAL ExerciseSubarachnoid haemorrhage ActivPAL Physical exertionSubarachnoid haemorrhage PAL 2 WalkingIntracranial haemorrhage PAL2 LocomotionIntracranial haemorrhage IDEEA Physical enduranceCerebrovascular disorders Actigraph*Cerebral ischaemia Actiwatch*Brain ischameia Atep watchCerebrovascular disease StepwatchBrain haemorrhage KinetamapBrain haemorrhage Behavioural mappingBrain infarct ObservationCerebral bleed Video surveillancePost-stroke Motion loggerPost-stroke MotionloggerStroke patients Motion loggers
Motionloggers
*Represents truncation.
12 N. A. Fini et al. Disabil Rehabil, Early Online: 1–15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
Appendix 2: Quality assessment criteria checklist
(1) Selection BiasAll patients eligible for admission into the study were invited to participate in the study (random selection or as consecutive cases).The subjects asked to participate in the study were representative of the entire population from which they were recruited (Downs & Black item 11).Yes: The paper states that all eligible patients were invited to participate.No: The paper does not state that all eligible patients were invited to participate.Unclear: It is unclear whether all eligible patients were invited to participate (mark as no).
(2) Identifying co-morbiditiesAll participants were free of medical conditions not directly related to stroke that could have a major impact on their ability to engage in physicalactivity (e.g. amputation, fracture).The characteristics of the patients included in the study are clearly described (Downs & Black item 3).Yes: The paper states that all participants were free of medical conditions not directly related to stroke that could have a major impact on theirability to engage in physical activity.No: The paper states that one or more participants were free of medical conditions not directly related to stroke that could have a major impact ontheir ability to engage in physical activity.Unclear: It is unclear whether all participants were free of medical conditions not directly related to stroke that could have a major impact on theirability to engage in physical activity (mark as no).
(3) Participant characteristicsFactors that may influence physical activity including age, stroke severity and time post-stroke are described.The characteristics of the patients included in the study are clearly described (Downs & Black item 3).Yes: The paper clearly describes confounding factors including age, stroke severity and time post-stroke.No: The paper does not clearly describe one or more of the following confounding factors: age, stroke severity or time post-stroke.
(4) Defining the method used to measure physical activityThe method used to measure physical activity is clearly defined/described.The interventions of interest are clearly described (Downs and Black item 4).Yes: The paper clearly defines the method used to measure physical activity.No: The paper does not clearly define the method used to measure physical activity.
(5) Reliability testingReliability of the method used to measure physical activity is quantified using either correlational or metric indices. OR it is referenced fromanother source which had a metric or correlational index.The main outcome measures used were accurate – valid and reliable (Downs and Black item 20).Yes: The reliability of the method used to measure physical activity is quantified using either correlational or metric indices (or referenced).No: The reliability of the method used to measure physical activity is not quantified using either correlational or metric indices.
(6) Defining outcome measuresOutcome measures were clearly defined and objectively stated.The main outcome measures to be measured were clearly described in the introduction or methods sections (Downs and Black item 2).Yes: Outcome measures were clearly defined and objectively stated.No: Outcome measures were not clearly defined and not objectively stated.No: Outcome measures were clearly defined; however, they were not objectively stated.No: Outcome measures were objectively stated; however, they were not clearly defined.No: Outcome measures were clearly defined and/or objectively stated, but only in the results section.
(7) Reporting of resultsIn normally distributed data the mean and standard error, standard deviation or confidence interval s are reported. In non-normally distributed datathe median and inter-quartile range of results are reported.The study provides point estimates and estimates of the random variability in the data for the main outcomes (Downs and Black item 7).Yes: Point estimates and estimates of the random variability in the data were reported using the correct methods according to the distribution of thedata.No: Point estimates and estimates of the random variability in the data were not reported.No: Point estimates and estimates of the random variability in the data were reported, but using the incorrect estimates for the type of datadistribution.
DOI: 10.3109/09638288.2014.978508 Physical activity following stroke 13
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
Appendix 3. Quality assessment results – devices.
References Q1 Q2 Q3 Q4 Q5 Q6 Q7 Total/7
[75] N N Y Y Y Y Y 5/7[27] Y N Y Y N Y Y 5/7[71] N N Y Y N Y Y 4/7[57] N N Y Y Y Y Y 5/7[58] N N Y N Y Y Y 4/7[35] N Y Y Y N Y Y 5/7[69] N N Y Y Y Y Y 5/7[34] N N Y Y N Y Y 4/7[32] N Y Y Y N Y Y 5/7[68] N Y Y Y Y Y Y 6/7[33] Y N Y N Y Y Y 5/7[72] N Y Y Y Y Y Y 6/7[31] N N Y Y N Y N 3/7[46] N Y Y Y N Y Y 5/7[59] N Y Y Y Y Y Y 6/7[51] N N Y Y N Y Y 4/7[47] N N Y Y Y Y Y 5/7[52] N N Y Y N Y N 3/7[26] Y N Y Y N Y Y 5/7[17] N Y Y Y Y Y Y 6/7[67] N N Y Y Y Y Y 5/7[77] N N Y Y N Y N 3/7[30] Y Y Y Y N Y Y 6/7[43] N N Y Y N Y Y 4/7[56] N N Y Y N Y Y 4/7[28] N Y Y Y Y Y Y 6/7[36] N N Y Y Y Y Y 5/7[44] Y Y Y Y N Y Y 6/7[53] N Y Y Y Y Y Y 6/7[70] N N Y Y N Y Y 4/7[60] N Y Y Y Y Y Y 6/7[61] N N Y Y Y Y Y 5/7[16] N Y Y Y N Y Y 5/7[49] Y N Y Y N Y Y 5/7[15] N Y Y Y Y Y Y 6/7[62] N Y Y Y Y Y Y 6/7[63] N Y Y Y Y Y Y 6/7[20] Y Y Y Y N Y Y 6/7[50] N N Y Y N Y Y 4/7[11] Y N Y Y N Y Y 5/7[13] N Y Y Y Y Y N 5/7[12] N Y Y Y Y Y Y 6/7[54] N Y Y Y Y Y Y 6/7[55] N Y Y Y Y Y Y 6/7[37] Y N Y Y N Y Y 5/7[39] N Y Y Y Y Y Y 6/7[38] N Y Y Y Y Y Y 6/7[40] Y N Y Y Y Y Y 6/7[64] N Y N Y Y Y Y 5/7[74] N Y Y Y N Y Y 5/7[65] N N Y Y Y Y N 4/7[76] N Y Y Y N Y Y 5/7[41] N Y Y Y N Y Y 5/7[14] Y Y N Y Y Y Y 6/7[48] N N N Y N Y Y 3/7[29] N Y Y Y Y Y Y 6/7[45] N N Y Y N Y N 3/7[42] N Y N Y N Y Y 4/7[73] N N Y Y N Y Y 4/7[66] N N Y Y Y Y Y 5/7
14 N. A. Fini et al. Disabil Rehabil, Early Online: 1–15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.
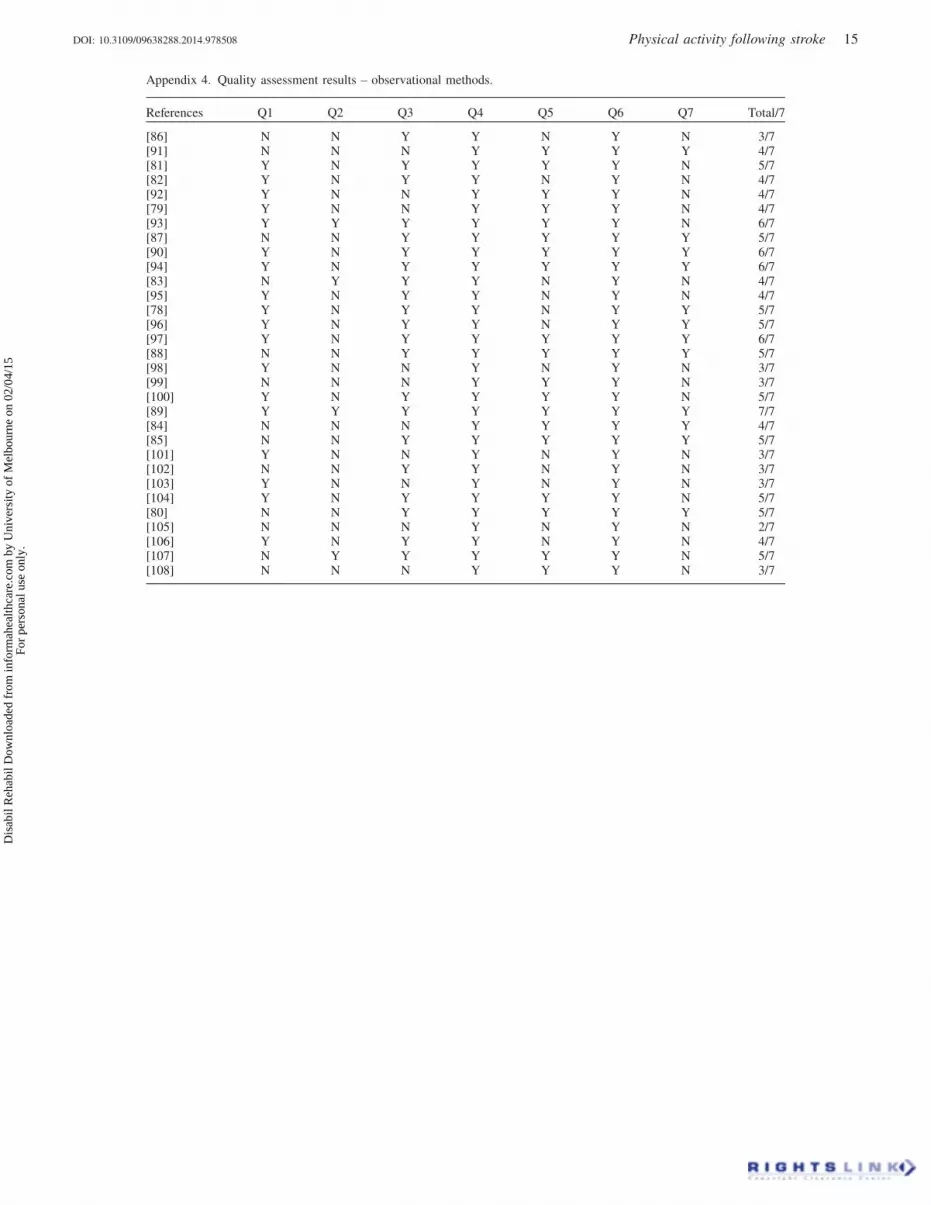
Appendix 4. Quality assessment results – observational methods.
References Q1 Q2 Q3 Q4 Q5 Q6 Q7 Total/7
[86] N N Y Y N Y N 3/7[91] N N N Y Y Y Y 4/7[81] Y N Y Y Y Y N 5/7[82] Y N Y Y N Y N 4/7[92] Y N N Y Y Y N 4/7[79] Y N N Y Y Y N 4/7[93] Y Y Y Y Y Y N 6/7[87] N N Y Y Y Y Y 5/7[90] Y N Y Y Y Y Y 6/7[94] Y N Y Y Y Y Y 6/7[83] N Y Y Y N Y N 4/7[95] Y N Y Y N Y N 4/7[78] Y N Y Y N Y Y 5/7[96] Y N Y Y N Y Y 5/7[97] Y N Y Y Y Y Y 6/7[88] N N Y Y Y Y Y 5/7[98] Y N N Y N Y N 3/7[99] N N N Y Y Y N 3/7[100] Y N Y Y Y Y N 5/7[89] Y Y Y Y Y Y Y 7/7[84] N N N Y Y Y Y 4/7[85] N N Y Y Y Y Y 5/7[101] Y N N Y N Y N 3/7[102] N N Y Y N Y N 3/7[103] Y N N Y N Y N 3/7[104] Y N Y Y Y Y N 5/7[80] N N Y Y Y Y Y 5/7[105] N N N Y N Y N 2/7[106] Y N Y Y N Y N 4/7[107] N Y Y Y Y Y N 5/7[108] N N N Y Y Y N 3/7
DOI: 10.3109/09638288.2014.978508 Physical activity following stroke 15
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
02/0
4/15
For
pers
onal
use
onl
y.





























