Embed Size (px)
Citation preview

SCHOLARLY PAPER
Cognitive Deficits Following Stroke
M Jane Riddoch Glyn W Humphreys Andrew Bateman
Key Words Stroke, stroke rehabilitation, cognitive deficits, unilateral neglect, exfindion, arousal, dyspraxia, assessment.
Summary The rehabilitation of survivors of stroke places heavy demands on NHS resources. Studies investigating the efficacy of stroke rehabilitation have produced equivocal results. In this paper we focus on the effects of cognitive deficits on motor functioning (in particular, disorders of praxis and attention) and report some results of particular relevance to physiotherapists. For instance, a symmetrical approach to treatment may not only improve motor function but may also help reduce the severity of unilateral neglect (ie encouraging the patient to orient visually to the affected side should improve the ability to attend to and to be aware of the affected side of space. Motor cues are more likely to be effective than visual cues if motor performance is required, and in particular cueing is,most likely to be effective if it is initiated by a patient rather than a therapist. Simultaneous bi-lateral exer- cises should be avoided unless attempts are made to overcome any effect of extinction, where a patient may attend only to the unaffected limb. In addition, cases of dyspraxia show that pa- logical functioning may be transferred between the hemispheres. Sequential bi-lateral exercises are to be preferred; the effect of the intact limb performing a pattern of movement may provide the visual experience of what the movement should be, and there also may be actjvation of homologous motor areas via the corpus callosum which may facilite the normal movement pattern.
Introduction Cognitive impairment in stroke patients is thought to be a poor prognostic indicator of recovery (see Jeffery and Good, 1995, for a review). The incidence of cognitive deficits following stroke has been put at 35.2% (Tatemichi et al, 1994). A number of different cognitive deficits may result from stroke, and any one patient may have a selective cognitive deficit or may have a number of different cognitive deficits. In broad terms these include language production and comprehension deficits (eg the aphasias); reading disorders (the dyslexias); writing disor- ders (the dysgraphias); recognition deficits (which may be specific to a given sensory modality, eg visual agnosia, tactile agnosia, etc, or may be multi-modal as may be seen in some of the demen- tias); memory deficits (there are a number of Werent sorb of memory deficit, two being short- and long-term memory deficits); attentional and praxic deficits (more detail on these two types of deficit will be presented below). Depending on the
severity of these deficits there may be signi6cant effects on ability to function normally. Tradition- ally, diagnosis of a particular deficit (or deficits) has been made by a neuropsychologist following administration of appropriate tests. Over recent years the relatively new discipline of cognitive neuropsychology has developed; this has done much to inform us of the precise nature and level of impairment of Merent cognitive deficits. Using theories and experimental procedures derived from cognitive psychology, detailed study of Merent patients has significantly contributed to the development of theoretical models of cogni- tive processing. These models are important for the understanding not only of complex cognitive fucntions but also for rehabilitation. A basic assumption of cognitive neuropsychology is that when one or more components of a normal processing system is impaired by brain damage, the remaining components will operate normally (although ifa damaged component lies ‘upstream’ in the processing system, the ‘down-stream’ components will not get their normal input and functioning may be affected). The essence of cogni- tive neuropsychology is the single-case approach. The argument is that any processing system is likely to be extremely complex. Damage may affect any component or combinations of compo- nents within this system. A vast number of different processing impairments could result. Identification of the specific impaired components can be achieved only by detailed assessment of an individual case.
Cognitive neuropsychology provides a more detailed diagnosis than traditional neuropsycho- logical assessments and therefore more detailed information about the precise nature of (for instance) language deficits. It can provide valu- able cues to therapists as to where therapy should be targeted (Riddoch and Humphreys, 1994). There are a t least three different ways that treatment may be implemented: restoration, reconstitution or compensation. The restoration approach focuses on the damaged component within the system; thus, ifdorsitlexion of the foot is impaired, specific dorsiflexion exercises are practised. The reconstitution approach avoids the impaired process by getting a patient to do the task in another way, using intact abilities (for instance, full abduction and elevation of the shoulder via the long head of biceps and triceps,
pectoralis major and the spinati when the deltoid is paralysed (Wynn Parry, 1981). The compensa- tion approach aims to get patients to function as well as possible by using whatever abilities remain intact. Each approach has a Werent aim: restoration is intended to enable patients to operate normally by normal means; reconstitution aims for normal performance using unusual methods, while compensation aims a t patients performing abnormally but optimally. In order for functional performance to be as similar as possible to a premorbid level, the treatment of choice must be the restoration approach - however, in some circumstan ces the nature and/or extent of the damage will preclude it. In such circumstances, the reconstitution or compensa- tion approaches should be adopted. Asseasmerit of a patient’s cognitive deficits using a cognitive neuropsychological approach will allow a more precise diagnosis. In the following section we focus on two disorders of cognition (attentional impairments and dyspraxia) which may have particular signifwince in the design of rehabilita- tion programmes by physiotherapists. In the case of dytspraxia we argue that if one component of the system is. damaged (eg the visual component of the action system) a reco&tution approach could be adopted (ie a verbally mediated treatment focusing on the intact verbal component of the action system) - see figure on page 471.
Msordere of Attention Attentional deficits have major implications for physiotherapists. At least five studies have demonstrated that patients with attentional deficits (in particular, uni-lateral neglect) show impaired recovery in activities of daily living relative to patients with no attentional deficits, and the presence of neglect appears more problematic than seventy of lesion, aphasia and intellectual capacity (Denes et al, 1982; Fullerton et al, 1986; Henley et al, 1985; Kinsella and Ford,. 1980; Wade et al, 1983). In the following section, we shall discuss three different attentional deficits: the disorders of unilateral neglect, extinction and arousal.
Uni-lateral Negbct (or Inattention) Patients with uni-lateral neglect fail to respond to events occurring on the side of space opposite to their lesion (thus a patient with damage to the right hemisphere will fail to react or to respond to eventa occurring on the lefk). This problem ia most pronounced after right hemisphere lesions, though it can also occur with left hemisphere lesiona (Humphreys and Riddoch, 1993; Riddoch and Humphreys, 1986). Over recent years it has become clear that there is not just one single
disorder that can be called ‘neglect’ but neglect may be considered a global term for a number of (frequently) independent deficits. For instance, patients may show neglect in some but not all sensory modalities (ie they may show neglect for visual objects on the left but not for auditory sounds and vice versa) (Barbieri and De Renzi, 1989). Neglect may be shown for near space and not for far space and vice versa (Bisiach et al, 1986; Halligan and Marshall, 1991) and the patient may show ‘motor’ neglect (failure to use the neglected limb, despite intact power and sensation) and no visual neglect (although the reverse pattern is more common) (Laplane and Degos, 1983).
While not directly identifying the problem of uni- lateral neglect, early proponents of the Bobath method of physiotherapy did in fact address the problem when standard treatment procedures were implemented. For instance, Todd explicitly stated that ’treatment must be directed towards using the affected side rather than ignoring it, so that a whole symmetrical man evolves’ (Todd, 1974). She subsequently stated that T h e bed should be placed so that the locker, food televi- sion, visitors or objects of interest are on the patient’s affected side. Presentation of bedpans and other nursing procedures can be carried out from the same side to reinforce treatment objec- tives’ (Todd, 1974; see also Davies, 1985)’. A primary aim for the symmetrid approach was to improve function, but clearly there were also implications for reducing neglect since attention was cued to the side. A number of studies have shown that such cueing ameliorates neglect (Halligan et al, 1991; Humphreys and Riddoch, 1992; Riddoch and Humphreys, 1983).
Cueing and Neglect: Mcnfulity of cue and task Recent work has also shown that, for maximal effect, the modality of the cue and the modality of the task should be congruent (Riddoch et al, 1995). Their patient (EL) was relatively unusual in that he had a left-sided lesion (neglect can occul aRer left-side lesions but tends not to be so severe or so long-lasting as neglect following right-side lesion - Caramazza and Hillis, 1990; Ogden, 1987; Patterson and Wilson, 1990). Their patient also showed left-side neglect in some circumstances (eg he read SAND as LAND, and also made lefbside errors in naming pictures with
‘The positioning of items in the patient‘s immediate environment on the contralesional side may be advocated by (at least some) physcotherapists; interestingly (at least some) neurologists have argued for the complete opposite. Heilman (1979, 1993) proposed that if patients have negkt then an activity calling for their response should occur in the ipsilesional side of space.
487
left-side identifying featuresI2. However, he showed right-side neglect in cancellation and copying tasks. The side neglected varied according to the task he was asked to perform. Thie same effect has been reported in other patients (Costello and Warrington, 1987; Humphrep and Riddoch, 1992, 1994; Kashiwagi et al, 1990). With EL it appeared that it was the nature of the task material that was important (ie whether EL was processing a single item such as a word or a picture, or multiple items). Riddoch ef al looked at this in more detail using two tasks. reading single four-letter words (in normal readers individual words are processed as a single object) or copying the same words (the task requires each letter to be processed separately). EL’S performance was measured as percentage correct according to letter position in both conditions. In the reading task, EL scored only 53% correct for the first letter while scoring maximally for the remaining letters (ie left-side neglect). When asked to copy the same words, he scored 91% correct for the first letter and thereafter performance deteriorated until he was scoring only 35% for the last letter in the word tie right-side neglect).
Typically, the cues used to help improve the performance of patients with neglect in reading consist of coloured strips placed in the (neglected) margin, or the use of the forefinger to orient atten- tion to the beginning of the line (Riddoch and Humphreys, 1986). Riddoch et a1 (1995) explored the use of visual and motor (positioning of the forefinger) cues more formally with EL. They found that, relative to the no-cue (baseline) condi- tion, EL’S performance was significantly improved with a left-side visual cue when reading words; other cue conditions (right visual cue, left or right motor cue) did not significantly affect perfor- mance relative to the baseline condition. However, when a similar procedure was used in a copying task they found a significant improve- ment in performance in the ‘mtor-cue’ (ie a finger positioned to the right of the word) condition - performance in the visual-cue condition now did not differ significantly from the baseline condi- tion. EL’S data suggest that it would be unwise to use the same sort of cue for all occasions, but rather that therapists should consider the tasks that patients have to perform and attempt to match cue and task modality. The significant effects of a visual cue for visual tasks are consis- tent with the proposals put forward by Davies (1985) and Todd (1974) regarding the organisa- tion of the environment of a patient in the early
‘A fox pictured with the head on the left and tail on the right was described simply as an animal with a tail, while an elephant pictured with the head on the tight was named COneCtty.
days following brain damage (see above). The visual cues provided by pereonnel approaching and interacting wi th a patient on the contralei- sional side wiU encourage viaral orienting to that side. However, most aepeete of physiotherapy are concerped with b c t i d improvement and the mechanisms underlying motor re-education (in particular). The leeson to be learned from EL is that a visual cue ie not likely to be as effective as a motor cue in encouraging the orientation of attention towards the affected side during the performance of motor tasks. The motor cue may result from movement of the affected limb by the therapist, or active movement of that limb by the patient (see below).
Active versus Paessive Motor Cues, bbertaon and North (1992,1993) have performed some intereeting experiments with regard to active or passive motor cueing (all involving patients with left-side neglect following right hemisphere lesions). They used a cancellation task as the objective measure of neglect in their studiess. A measure of neglect may be obtained from the number of items the patient fails to cancel on the contralesional side. Robertson and North (1992) have found that performance on cancellation tash is improved if a patient is instructed periodically by an examiner to move the fingers of the left hand (placed on the table on the left side of the cancellation sheet) relative to no movement of the hand or movement of the hand by the examiner on the left side of space. The improvement was found to occu even when the moving left finger was out of sight of the patient (his hand was placed on bie knee under the table). Robertson and North (1992) argue that their data support the ’recruitment hypothesis’ which state that perception and action are so closely inte- grated that it is reasonable to assume that activation of one system must lead to recruitment of the other (see Rizzolatti and Berti, 1990,1993; Rizzolatti et al, 1987). Robertson and North’s experiment therefore suggests motor activation can facilitate the orienting of visual perception to the neglected side. It is entirely plausible to consider that the reverse relationship might also
Jone example of a cmdktion test is the star cancebtion test - a subtest of the Behavioural Inattention Test. It consists of a number of large and small stars scatterad at random m a stan- &Id A4 sheet of paper ( w i i , 1987). Interspersed between the stafsam leitersandwords. Thepatienrstsskistocrossthrwgh all the small stars on the page. Typically, patients with a right hemilesiOn(andleffneglect)WillstarttheEask~th9li$lt side of the page and will cross wt the smell starsassiduously. After a while, they will indicate that they have tinished even thoughanumberofstarsmaymnah unaussedonthe left side of the page. Even pmmpting them (‘Are YOU sure YOU have crossed out all the stars?‘) often fails to help them detect the ulwxossad stars.
hold true, that is visual orientation to the af€ected side might facilitate motor action. We have argued above that a motor cue is likely to be more effective than a visual cue in a motor task. However, following stroke, the movement in the affected arm may be zero. Nonetheless, it is considered important to maintain a full range of movement and to inhibit spastic patterns (Bobath, 1970; Davies, 1985). The patient should be encouraged to fixate the limb visually during the application of these procedures; by doing so, recruitment of the motor system may be facilitated. This may increase the likelihood of an active motor response when motor cueing might be instigated.
Long-term Effects of Cueing Neglect deficits are likely to coincide with decreased arousal and any treatment of neglect should be coupled with treatment for that condi- tion (see below). While cueing may result in a significant reduction of neglect, its effects may be transitory. Thus, HaUgan and colleagues (1992) have shown that the significant benefits derived from cueing in a line bisection task virtually disappear after ten seconds. It is therefore important to maintain an alert state so that maximal benefit might accrue from cueing.
Extinction While patients with neglect appear to be unaware of stimuli presented to the side opposite their lesion, patients with extinction are able to identify such stimuli correctly. However, if two stimuli are presented simultaneously, one on each side of a patient, he will report only the stimulus on his unimpaired (non-hemiplegic) side. There are important implications of the extinction phenomenon for treatment. These can be illustrated by a further study by Robertson and North (1994). A form of cancellation task was again used as the objective measure; however, on this occasion the patient was required to read all the letters and numbers he could see rather than cancelling them out (there were 40 items in total, randomly scattered across the paper). Robertson and North (1994) demon- strated that the patient was able to report significantly more letters when simultaneously moving the fingers of the left hand on the left knee. No such effect was found ae a result of moving the fingers of the right hand on the left knee or of moving the fingers of left and right hands on left and right knees respectively. Robertson and North (1994) also noted that the patient had more difficulty when required to move hia left hand simultaneously with the right, than when hia left hand was moved alone.
There are important implications here for physio-
therapy. Bi-lateral movements of the arms, whether on both left and right sides of space or on either left or right sides of space, do not reduce neglect to anything like the same degree as a single movement of the left hand in patients with leR neglect. In the therapeutic situation, when the focus of treatment is initiation of movement, greater benefits are to be expected if uni-lateral movements are performed. In daily life, patients with problems of this sort should be encouraged to position the arm appropriately (ie so that i t is within view and may act as a visual cue), but bi- lateral activities should be avoided unless attempts are made to reduce extinction effects by increasing awareness of the hemiplegic side.
Arousal In order to respond appropriately to events occur- ring in the environment, we need to be alert in order to detect those events. Recent evidence from positron emission tomography indicates that the right hemisphere is dominant in the arousal mechanism (Corbetta et al, 1993); and a number of studies have shown that right as compared with left hemisphere lesions cause hypoarousal (Heilman et al, 1978; Posner and Peterson, 1990; Zoccolotti et al, 1982). The negative effect of hypoarousal is clearly described by Seron et a1 (1989) in their account of a 60-year old businessman who developed a tumour at the junction of the temporal and occipital lobes in the right hemisphere. His behaviour following removal of the tumour was described as follows: 'The patient seemed aware of his trouble but indifferent to it. There was some apathy and depression and the patient spent long periods sitting in a chair without doing anything. When questioned about his lack of activity, he replied that he could not see well, so he preferred sitting still' (Seron et al, 1989, pages 329-301). The patient did indeed have a left hemianopia (loss of vision in the left half of his visual fields) and uni-lateral neglect, but these are unlikely to account for the degree of lethargy he exhibited.
Seron and colleagues employed a number of different tasks to try and reduce the neglect shown by their patient. For instance, he was given exercises which encouraged visual scanning from the intact to the defective side of space. These exercises were very effective and the patient was scoring maximally even on the most difiicult tasks after only two weeks (four sessions per week). However, there was no generalisation to everyday life. At the end of the therapy session the patient would fail to notice the therapist's extended hand to shake hands and would frequently bump into the door jamb. His spatial disorientation in the hospital corridors persisted; he could not

tell the time correctly and when eating he neglected the food on the left side of his plate. Seron et a1 (1989) then attempted to extend the scanning exercises into everyday life situations. The therapist would provide a verbal cue to the patient if he failed to scan the neglected side during various activities (eg cooking, painting, playing chess, walking, catching a ball, conversing, etch Therapy took place over a longer time period (eight weeks) and was coincidental with his occupational therapy sessiona. Again, while performance was very good during the therapy 8essions, there appeared to be no gener- alisation to his home environment. A selfcueing strategy was then used, the patient was trained to prompt himself with slogans such as ‘The left space does exist’ and ‘I must move my eyes in that direction’. Again, there was no sign of transfer outside the therapy setting. During the fourth week of the 8elfaeing therapy, a dramatic event occurred. When playing with hie dog in the garden the patient ran headfirst into some barbed wire on his left and seriously injured his face. Seron and colleagues then made a radical change in the rehabilitation programme. The patient was supplied with a buzzer which emitted a high-pitched noise at random intervals of five to twenty seconds. The buzzer fitted into the patient’s left shirt pocket, and was provided with a switch to turn off the noise. This device had a significant effect on behaviour in both the therapy and the home situation and his family reported a significant improvement in his daily activities. Seron et al suggest that the buzzer acted as a reminder to the patient to direct atten- tion to the left side but an alternative explanation may be that it had the effect of increasing general arousal. Therapists should perhaps consider the use of such a buzzer as an adjunct to therapy. In the initial acute stage following a stroke, periods of its use should be limited. Patients are frequently drowsy and need some time to recover from the cerebral insult. The amount of time the buzzer is operational during the day (ie periods of time when random buzzes will occur) should grad- ually be increased as their condition stabilises.
Dimrdera of Praxis Praxic disorders (apraxiddyspraxia) may be defined as disorders of skilled movement which are not caused by weakness, akinesia, de-af€eren- tiation, abnormality of tone or posture, abnormal movements such as tremor or chorea, intellectual deterioration, poor comprehension or unco-opera- tiveness (Heilman, 1979). Praxic dieorders have been argued to be relatively common (occuming in approximately 50% of patients with left brain
damage); but an, generaIIy not mportui beauma they rarely appear in everyday dtuationm when motor behaviour is spontaneow, but rather in artificial situationa such u when the patisat ir
1986). Apraxia may be -tad with aphada, which may makeitdifaeult todetect.
asked to mime parts& move-. (De Rerrts,
Initiation of Movemeat in bbrpon# to vtmrlclrer An inbmting illustration of the dhrder coma from Jantraet d (1992). Their patient, a 61-year- old man, had a five-year history of dimculty in waking following rightride brain damage M a result of a etrdte. On edminrirrn toarehbilitatba unit, he was fbund to have a mild ledt hemipararir with no sensory d-t. He wan aletrt, oriented and showed no evidence of cerebellar dysfunction, tremor ot rigidity. Although his motor recovery was good, he was unable to walk. Initial rehabil- itation included ‘traditional gait training, a general exercise programme, and d e t y educa- tion’ (Jantra et al, 1992, page 96) which did not appear to have any marked effect on functional performance. However, when the patient wan askedtostepavergrey andredcolouredetripeeon the floor, his walking improved, only to regmm when the stripes were removed. Colour cuee appeared to have facilitated performana, but how could the environment be 80 arm& that colour cues were always present? Jantra and c o l l v devised a solution - bright orange projectiom were attachedtothebaseofhis&icka. Thepmjec- tiom were aligned horizontally and about six inches long. The patient’s task wae to step over these projections during the mbg p h a ~ of gait. This strategy proved very succe~ful, the patient progressed quickly from two sticks to one, and was discharged after 23 days. Follow-up at one year showed that the patient had maintained hia independence, ueing no et icb within the h o w , and one when he walked outaide.
The treatment was effective - but why? The authors give no account as to the reason that colour cues facilitated performance. Without having an underlying theoretical rationale for treatment, it becomes difficult to know whether such cues will also be effective in other cases of patients with walking difficulty.
Initiation of Movement in &erponre to verbal cues We have been able to perform a detailed study of a patient (CD) who showed the oppaeiite pattern of performance to the patient d d b e d above: visual cues did not help him to genetate the appmpriate action while a verbal command did (Riddoch et al,
1989)'. CD suffered a left-hemisphere stroke secondary to hypertension. Initially, he had a profound right hemiplegia but this quickly resolved leaving minimal weakness. He was able to walk with one stick, and had minimal weak- ness of his right arm. He was referred to us for testing by the speech therapist who noted that he seemed to find it dif€icult to demonstrate how objects are used in the test situation. Occasionally such difficulties were also noted at home, his wife indicating that he used his shaving brush inap- propriately, or that he would fail to cut through his meat, thus taking a large slice to his mouth. One possible reason for his difficulty with objects could be that he simply did not recognise them (ie visual agnosia); however, detailed testing showed that this was not the case. We performed an extensive study of CDs ability to demonstrate the use of objects using two main conditions. In one (the visual condition), objects were placed on the table in front of him and he was asked to demon- strate their use (he was allowed to pick up the object if he wished). In the other (the verbal condi- tion), no objects were present and he was asked to pantomime the use of named objects (eg 'Show me how you might use a hammer'). In both instances, our patient was asked to perform the action with either his left or his right hand. Our patient performed well in the verbal condition, scoring nearly 100% correct with both left and right hand. The visual condition yielded some interesting results performance was very good with the left hand, but he made many errors with the right. The hemiparesis was not the cause of the problem, since the patient was able to do the equivalent movements well in the verbal condi- tion. He appeared to have a specific difficulty with visual input when he had to use his right hand. Riddoch and colleagues used these data to argue that there must be separate action programmes for each hand (the left and right action programmes being located in the right and left hemispheres respectively). Furthermore, we can activate these programmes either by visual input (the actual object) or by verbal input (the command to pantomime the use of the objecty.
'Recent evidence from primates indites that there are at least eight different motor amas controlling the limbs and body in the frontal cortex, in a d d i i to two further areas being specialised for eye movements. Two areas are of particular relevance here: the dorsal and ventral aspects ofthepmmotorcorter. The dorsal af8aisthougMtoclonbkrtetomOt0r~ . by-- neuralprogrammesnecsssruyfwmeMendedecdbnandtoexecw Ibndthebehavbw.Thevenbelar6amaybemorespedallgedfor ~ B x e a w c n l m d e r r r i l s u e l ~ ( K u r a t e , 1994).
5Jantra et el (1992) may have had the reverse diifiiulty, good performance with vieually presented objects and poor perfor- mance on pantomime, however there is no indication whether this was ever fonnaHy assemed.
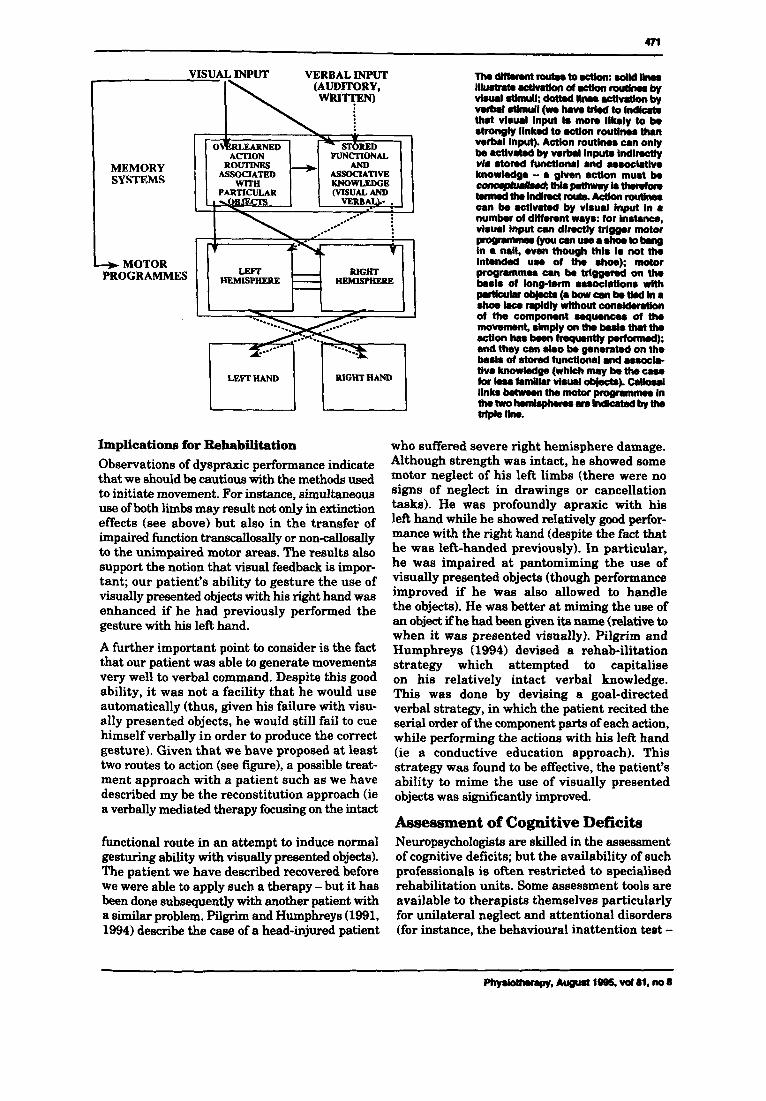
Left and Right Hemisphere Action programmes Frequently when CD failed to demonstrate the use of a visually presented object with his right hand, we would ask him to perform the task with his left hand. He had no difficulty in doing this. If he was then asked again to demonstrate the use with his right hand he was then able to do so. This improvement could have come about either by visual feedback (from observing the left hand performance) or from some interaction between the left and right hemisphere motor programmes via the corpus callosum. We think the latter was more likely on the basis of some other aspects of his performance. For instance, we asked him to perform some sequences of movements with both hands; thus, we placed a teapot, a mug and a jug in front of him and asked him to show how he would pour out a cup of tea. He started by pouring from the teapot (using his left hand) directly inta his cup. We then asked whether he took milk with his tea. He started the sequence again. This time he poured from the teapot into the jug (using his left hand) and then from the jug into the cup (using his right hand), he then pretended to drink from the cup (holding it in his right hand). Remember that gestures using the left hand with single objects were very good. When the activity required the co-ordinated action of both hands, errors then developed in left-hand performance. This suggests that normal co-cordinated func- tioning of the two upper limbs requires 'cross-talk' between the left and right hemisphere motor programming areas (inter-hemispheric transfer time as measured by visual evoked responses indi- cates that there are both callosal and non-callosal linkages between the two motor areas (Jeeves, 1969). As a result of this cross-talk, faulty func- tioning may spread from the impaired to the intact hemisphere. This supposition was given further credence by some further observations with our patient. If he was asked to perform a simple move- ment (eg tapping the hand on the table) for a reasonably long time period (30 seconds) we found he was then unable to inhibit the tapping to perform a different movement (flipping the hand, first palm down then palm up on the table). When we observed this, we attempted to overcome the motor perseveration in the impaired limb by prolonged attempts to initiate the required move- ment (both patient initiated and therapist assisted). Following this, however, we observed motor penseveration of the flipping movement m w in the intact limb. As a result of our observations of CD and other dyspraxic patients (Pilgrim and Humphreys, 1991,1994) we have attempted to identify a t least some of the component abilities which allow interactions with objects. These components are illustrated in the figure opposite.
m
VISUAL INPUT VERBAL INPUT Th.dmamntrorR#to.ctkn:.oMd~ lllurtna.ahntknol.c(knroutkwrby visual dimull; d0tt.d llnos .cthntkn by v e h l dimull (wa h v o trl.d to I n d i c r ( . that Vl8Ud input Is mom llkely to k BtrOngly Ilnkul to action routha than v.rb.1 Input). AcHon routlnes can only be .ctlvated by wrbd Input. tndlmtly wla rtond functional and as.otlrtlw knowledge - a glven action muat be ~ L i a p m t h m y b t I m W o m t.nndth.lndimcl roum Aakn routkwr can be .ctlvated by visual Input In a numbw of dlffemnt ways: for Instance, vlsual Input can dlnctly trlgger motor P w m - - ( m - - a - @ ~ in a nail, even t h w h thl8 I 8 not the intendad use of the shoe); motor programme8 mn k trlggamd on tho
r#rticuhr-(a bow a n ktlrd in I shoe bWdlywithoutcon.ld.lrtlon of the component saqumcos of the movemsnt, slmply on the buk tha the actlonhIl8k.ntnq~tlyp.rtomlul); and they can also be gpnemled on the
tlve knowledge (whkh may k the c a u tor ku familiar v l u d objects). c.Houl links betmm th. motor m m m In t h O t W O ~ ~ M s l n d ~ b y U l O tripk Ilrw.
+ MOTOR b.818 Of hg-tWltl a8SOCblh8 wlth HEMISPHERE
bad8 of 8 t O d fUnctiOMl Ind ~ U O c i O -
RSGHT HAND
Implications for Rehabilitation Observations of dyspraxic performance indicate that we should be cautious with the methods used to initiate movement. For instance, simultaneous use of both limbs may result not only in extinction effects (see above) but also in the transfer of impaired fundion tranacallosally or nondosally to the unimpaired motor areas. The results also support the notion that visual feedback is impor- tant; our patient’s ability to gesture the use of visually presented objeets with his right hand was enhanced if he had previously performed the gesture with his left hand.
A further important point to consider is the fact that our patient was able to generate movements very well to verbal command. Despite this good ability, it was not a facility that he would use automatically (thus, given his failure with visu- ally presented objects, he would still fail to cue himself verbally in order to produce the correct gesture). Given that we have proposed at least two routes to action (see figure), a possible treat- ment approach with a patient such as we have described my be the reconstitution approach (ie a verbally mediated therapy focusing on the intact
functional route in an attempt to induce normal gesturing ability with visually presented objects). The patient we have described recovered before we were able to apply such a therapy - but it has been done subsequently with another patient with a similar problem. pilgrim and Humphrep (1991, 1994) describe the case of a head-injured patient
who suffered severe right hemisphere damage. Although strength was intact, he showed some motor neglect of his left limbs (there were no signs of neglect in drawings or cancellation tasks). He was profoundly apraxic with his left hand while he showed relatively good perfor- mance with the right hand (despite the fact that he was left-handed previously). In particular, he was impaired at pantomiming the use of visually presented objects (though performance improved if he was also allowed to handle the objects). He was better at miming the use of an object if he had been given ita name (relative to when it was presented visually). Pilgrim and Humphreys (1994) devised a rehab-ilitation strategy which attempted to capitalise on his relatively intact verbal knowledge. This was done by devising a goal-directed verbal strategy, in which the patient recited the serial order of the component parts of each action, while performing the actions with his left hand (ie a conductive education approach). This strategy was found to be effective, the patient’s ability to mime the use of visually presented objecta was significantly improved.
Assessment of Cognitive Deficits Neuropsychologists are skilled in the assessment of cognitive deficits; but the availability of such professionals is often restricted to specialised rehabilitation units. Some assessment tools are available to therapists themselves particularly for unilateral neglect and attentional disorders (for instance, the behavioural inattention test -

472
Wilson et al , 1987 - and the test of everyday attention - Robertson et al, 1994). However, if departmental budgets are limited, and it is not possible to buy such tests, therapists can easily devise assessment tools of their own. These may include simple cancellation tests for neglect. This could consist of a sheet of paper with a large number of letters printed a t random. All the letters of the alphabet or a subset of letters can be used. The patient is asked to cross out all exam- ples of one particular letter. The greater the number of letters on the page, the harder the task will be, particularly if a la& number of different letters is used (Riddoch and Humphreys, 1987). If target letters are missed out on one side of the page more than the other, the patient is likely to have visual neglect (left-side omissions indicate left-side neglect which is usually found following a right cerebral lesion although not always, as was the case with EL (see above), while the converse is true if right-side omissions are shown). Assessment of extinction can also be very simple; for example, a therapist touches a patient on either the left, right or both arms. The patient is asked to report ‘left’, ‘right’ or ‘both‘. Once it is clear that the patient understands what is required, the test is repeated with the patient’s eyes shut. If the patient is able to report a single touch to either right or left arms but fails to report correctly when both arms are touched, then that patient is exhibiting extinction. In order to assess for dyspraxia, the therapist should collect a number of everyday objects and assess the patient’s ability to gesture the use of such objects with each hand independently, if the patient is able to use both hands (otherwise the patient should be asked to demonstrate the use of the object with the unimpaired hand). The patient’s ability to pantomime the same objects (in the absence of those objects) should also be assessed. If the patient shows impaired performance in either of these conditions (to the visually presented object, or to the name of the object) or if normal performance is dependent on the hand use, a diagnosis of dyspraxia may be made.
Conclusions Stroke is one of the most common neurological disorders and treatment of stroke is costly in terms of NHS resources. Attempts to evaluate the efficacy of treatment regimes have proved to be equivocal. The disappointing results of efficacy studies may be due to ahumber of different factors; in particular the heterogeneity of the stroke population. One factor contributing to the heterogeneity is the presence of cognitive impair- ment following stroke. Particular cognitive deficits will vary significantly between patients and will depend on the locus of cerebral damage
and the effect of such damage on other (undam- aged) cortical areas. If the group study approach is to be used in efficacy studies, experimental and control groups should be matched for cognitive deficits (in addition to other factors).
So far as rehabilitation itself is concerned, some cognitive impairments may adversely affect motor functioning. Therapists need to be aware of such deficits and of the need to modify treat- ment appropriately. Assessment should not be restricted to physical problems, but should be extended to include cognitive problems. Treat- ment outcomes will be optimised (provided that some recognition is also taken of social and psychological problems) which must surely have implications not only for NHS resources but also for consumer satisfaction.
Acknowledgments This work was supported by a Stroke Association grant to all three authors and by a Medical Research Council grant to the first two authors. Part of this paper was presented by M J Riddoch at the International Conference on Improving the Q w l i of Phys- ical Therapy ’s Hertogenbosch, The Netherlands, June 1994; ‘N = 1 methodology with particular reference to stroke rehabilitation‘ (keynote address).
Authors and Addmss for Compondence M Jane Riddoch PhD CPsychol MCSP (to whom correspondence should be sent) is a senior lecturer in psychology, Glyn W Humphreys PhD CPsychd FBPS is a professor of psychology, and Andrew Bateman Bscis a research associate in psychology, at the School of Psychology, University of Birmingham, Birm- mgham 615 2lT. Thii article was received on August 14,1994. and acoepted on May 30,1995.
References Barbieri. C and De Renzi, E (1989). ‘Patterns of neglect dissoci- ation’, Behavioural Neuro/ogy, 2,13-24. Bisiach. E, Perani, D, Vallar. G and Berti, A (1986). ‘Uni-lateral neglect: Personal and extrapersonal’, Neuropsychologia. 24,75!3-767.
Bobath, B (1970). Adult Herniplegla: Evaluation and treatment. Heinemann, London. Caramazza, A and Hillis. A E (1990). ‘Levels of representation. co-ordinate frames, and uni-lateral neglect’, Cognitive Neuro- psycho log^ 7,391445. Corbetta. M. Miezin, F M, Shulman, G L and Petersen, S E (1993). ‘A PET study of visuospatial attention’, Journal of Neuro- science, 13.3,1202-26. Costello, A and Warrington. E K (1987). ‘The dissociation of dsu- ospatial neglect and neglect dyslexia’, Journal of Neurohgy, Neurosurgery and Psychiatty, SO, 1 1 10-1 6. Davies, P M (1 985). Steps to Follow, Springer-Verlag, Berlin. De Renzi. E (1985). ‘Methods of limb apraxia examination and their bearing on the interpretation of the disorder‘ in Roy, E A (ed), Neuropsychological Studies of Apraxia and Related Disorders, Elsevier, Amsterdam. Denes, G, Semenza, C, Stoppa, E and Lis. A (1982). ’Uni-lateral spatial neglect and recovery from hemiplegia: A follow-up study‘, Brain, 105, 543-552. Fullerton, K J. McSherry. D and Stout, R W (1986). ‘Albert’s test: A neglected test of visual neglect‘, The Lancet, 430-432.
Phyrlothrcrpy, August l9B5, vol81, no 8
473
Halligan, P W, Donegan. c A and Marshall, J C (1992). ‘When is a cue not a cue? On the intractability of visuospatial neglect’, Neuropsychological Rehabilitation. 4.2, 283-293. Halligan, P W, Manning, Land Marshall. J C (1991). ‘Hemispheric activation vs spatio-motor cueing in visual neglect: A case study’, Neuropsychologia, 29, 165-1 76. HalliQan, P W and Marshall, J C (1991). ‘Left neglect for near but not for far space in man’, Nature, 350,498-500. Heilman. K M (1979). ‘Apraxia’ in: Heilman. K M and Valenstein. E (eds) Clinical Neuropsychology, Oxford University Press, New York.
Heilman, K M, Schwartz. H D and Watson, R T (1978). ’Hypoarousal in patients with the neglect syndrome and emotional indifference’, Neurology, 28.229-232. Heilman, K M, Bowers, D, Valenstein, E and Watson, R T (1993). ‘Disorders of visual attention’ in Kennard, C (ed), Ballidre’s Clin- ical Neurology, Balliere Tindall, London.
Henley, S. Pettit, P. Todd-Pokropek, L and Tupper, J (1985). ’Who goes home? Predictive factors in stroke recovery’, Journal of Neurology, Neurosurgery and Psychiatry, 48.1-6. Humphreys, G W and Rickloch, M J (1992). ‘Interactions between object and space systems revealed through neuropsychology’ in: Meyer, D E and KomMum, S (ed) Attention and Perfonanoe XlV: Synergies in experimental psychology, aflificial intelligence and cognitive science, Massachusetts Institute of Technology Pre& Cambridge, Mass.
Humphreys, G W and Riddoch, M J (1 993). ‘Interactive attentional systems and uni-lateral visual neglect’ in: Robertson, I and Marshall, J C (eds) Unilateral Neglect, Lawrence Erlbaum Asso- ciates, Hove, pages 139-167. Humphreys, G Wand Riddoch, M J (1994). ‘Attention to within- object and between-object spatial representations’. Cognitive Neuropsychology, 11,207-241. Jantra, P, Trilok, N, Monga, M D, Press, J M, Bradley, J and Gervais, 6 S (1992). ‘Management of apraxic gait in a stroke patient’, Archives of Physical Medicine and Rehabilitation, 73,9&97. Jeeves. M A (1969). ‘A comparison of interhemispheric trans- mission time in acallosals and normals’, Psychonomic Studies, 16,245-246. Jeffery. D R and Good. D C (1995). ‘Rehabilitation of the stroke patient’, Current Opinion in Neurobgy, 8,624. Kashiwagi, A, Kashwagi. T, Nishikawa. T, Tanabe, H and Okuda. J (1990). ‘Hemispatial neglect in a patient with callosal infarction’, Brain, 113, 1005-23. Kinsella. G and Ford, B (1 980). ‘Acute recovery patterns in stroke patients’, Medical Journal of Australia, 2, 663-666. Kurata, K (1994). ‘Information processing for motor control in the primate premotor cortex’, Behavioural Brain Research, 61, 135-1 42. Laplane, D and Degos, J D (1983). ’Motor neglect’, Journalof Neurology, Neurosurgery and Psychiatry, 46.152-1 58. Ogden, J A (1987). ‘The “neglected” left hemisphere’ in: Jean- nerod, M (ed) Neurophysiological and Neuropsychological Aspects of Spatial Neglect, Elsevier. North Holland.
Patterson, K E and Wilson, B (1990). ‘A ROSE is a ROSE or a NOSE: A deficit in initial letter identification’, Cognitive Neuropsy- chology, ’I, 447477. Pilgrim. E and Hurnphreys. G W (1991). ‘Impairment of action to visual objects in a case of ideomotor apraxia’. Cognitive Neumpsycholcgy, 8,459-473. Pilgrim. E and Humphreys, G W (1994). ‘Rehabilitation of a case of ideomotor apraxia’, in: Riddoch, M J and Humphreys. G W
0
(eds) Cognitive Neuropsychology and Cognitive Reha&iltt.gtbn, Lawrence Erlbaum Associates, Hove. Posner, M I and Peterson. S E (1990). ’The attenth the human brain’, Annual Review of
Riddoch, M J and Humphreys, (3 W (lse3). The ol a h g on uni-lateral neglect’, Neuropsychologb, 21, W. Riddoch, M J and Humphreys. G W (1966). ‘unl-bterel negkd, Physiotherapy, 72,425-428. Riddoch. M J and Humphreys. 0 W (1987). ‘Perceptual and action systems in uni-lateral visual neglecy in: Jeanned. M (ed) Neurophysiological and Neurqsyrhobgical Aspects of Spnbial Neglect, Elsevier. North Holland. Riddoch. M J and Humphreys, G W (eds) (1994). Cognitive Neuropsychology and Cognitive Rehabilitation, Lawrence Erlbaum Associates, Hwe. Riddoch, M J. Humphreys, G W, Burroughs. E. Luckhurst, L, Bateman, A and Hill, S (1995). ‘Cueing in a case ot neglect: Modality and automaticity effects’. cognitive ktcpsychdugy, in press. Riddoch, M J, Humphreys, G Wand Price, C J (1989). ‘Routes to action: Evidence from apraxia’, Cognitive Neuropsychology, 6,4374. Aiudatti, G and Berti. A (1990). *Neglect as a neural repmen- tation deficir, Revue N e u w , 146.626-634. Riuolatti, G and Berti, A (1993). ‘Neural mechanisms of spatial neglect’ in: Robertson, I H and Marshall, J C (eds) Unilaleral Neglect: Clinical and experimental studies. Lawrence Erlbaum Associates. Hove. Riuolatti, G, Riggio, L. D a d a , I and UmiP, C (1987). ‘Reori- enting of attention across horizontal and vertical meridians’, Neuropsycholoia, 25.31-40.
lateral left neglect: The role of hemispace. hand and motor actiiation’, Neuropsycbkgia, 30,6.553-563. Robertson, I H and North, N (1993). ‘Active and passive &a- tion of left limbs: Influence on visual and sensory neglect’. Neuropsychohqia, 31,293-300. Robertson, I H and North, N T (1994). ‘One hand is better than two: Motor extinction of left hand advantegein unHatdne#ect‘,
Robertson, I H, Ward, T. Ridgeway, V and Nimmo-Smith. I (1994). The Test of Everyday Attention, Thames Valley Test Company, Bury St Edmunds. Seron. X. Deloche, G and Coyette, F (1989). ‘A retrospectiVe analysis of a single case neglect therapy: A point ot theory‘ in: Seron. X and Deloche, G (eds) Cognitive Approaches in Neuropsychological Rehabilitation, Lawrence Erlbaum Associ- ates, Hillsdale, New Jersey. Tatemichi, T K, Desmond. D W, Stem. Y. Paik. M. Sam, M and Bagiella. E (1994). Cognitive impairment after stroke: Pattern and relationship to functional abilities’, Journal of Neurology, Neurosurgery and Psychiatry, 57.202-207. Todd, J M (1974). ‘Physiotherapy in the early stages of hemi- plegia’, Physiotherapy, 60.336442. Wade, D. Skilbeck, C and Langton Hewer, R (1983). ‘Predicting Barthel ADL score at six months after acute stroke, Archives of Physical Medicine and Rehabilitation, 64.24-28. Wilson. B A. Cockbum, J and Halligan. P (1987). Behavioural lnattention Test, Thames Valley Test Co. Tiichfield. Wynn Party, C B (1981). Rehabilitation of the Hand, 4th edn. Butternorth. London. Zoccolotti, P. Scabini, D and Violani, C (1982). ‘Electrodermal responses in patients with unilateral brain damage’, h u m / of Clinical Neuqsyrhobgia, 4,143-1 50.
13.25-42.
Robertson, I H and North, N (1992). ‘Spatiolllotol cueing in uni-
N W K ~ S Y ~ , =,I-1 1.





























