Embed Size (px)
Citation preview

At the Intersection of Health, Health Care and Policy
doi: 10.1377/hlthaff.2010.1102
, 30, no.5 (2011):975-984Health AffairsContinuing Care Retirement Community
Fewer Hospitalizations Result When Primary Care Is Highly Integrated Into AWennberg
Julie P.W. Bynum, Alice Andrews, Sandra Sharp, Dennis McCollough and John E.Cite this article as:
http://content.healthaffairs.org/content/30/5/975.full.html
available at: The online version of this article, along with updated information and services, is
For Reprints, Links & Permissions: http://healthaffairs.org/1340_reprints.php
http://content.healthaffairs.org/subscriptions/etoc.dtlE-mail Alerts : http://content.healthaffairs.org/subscriptions/online.shtmlTo Subscribe:
written permission from the Publisher. All rights reserved.mechanical, including photocopying or by information storage or retrieval systems, without prior
may be reproduced, displayed, or transmitted in any form or by any means, electronic orAffairs HealthFoundation. As provided by United States copyright law (Title 17, U.S. Code), no part of
by Project HOPE - The People-to-People Health2011Bethesda, MD 20814-6133. Copyright © is published monthly by Project HOPE at 7500 Old Georgetown Road, Suite 600,Health Affairs
Not for commercial use or unauthorized distribution
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from
By Julie P.W. Bynum, Alice Andrews, Sandra Sharp, Dennis McCollough, and John E. Wennberg
THE CARE SPAN
Fewer Hospitalizations ResultWhen Primary Care Is HighlyIntegrated Into A Continuing CareRetirement Community
ABSTRACT Meeting the medical and social needs of elderly people is likelyto be costly, disruptive, and at odds with personal preferences if efforts todo so are not well coordinated. We compared two different models ofprimary care in four different continuing care retirement communities.In the first model, used in one community, the physicians and two part-time nurse practitioners delivered clinical care only at that site, coveredall settings within it, and provided all after-hours coverage. In the secondmodel, used in three communities, on-site primary care physician hourswere limited; the same physicians also had independent practices outsidethe retirement community; and after-hours calls were covered by allmembers of the practices, including physicians who did not practice onsite. We found that residents in the first model had two to three timesfewer hospitalizations and emergency department visits. Only 5 percentof those who died did so in a hospital, compared to 15 percent at theother sites and 27 percent nationally. These findings provide insight intowhat is possible when medical care is highly integrated into a residentialretirement setting.
Ninety percent of people age sixty-five or older in the United Stateshave at least one chronic illness.1
As age progresses, chronic condi-tions accumulate, so that more
than 30 percent of people older than age sev-enty-five have four or more of them.2 As if man-aging the complexity of multiple, concurrentconditions were not challenging enough, therisk of loss of independence increases with eachnew condition.3
This trajectory of declining health and abilityto carry out the activities of daily living can resultin repeated care transitions for patients acrossmedical and residential settings. It also can posemajor challenges in care coordination for bothpatients and providers. Ultimately, many pa-
tients on this course experience end-of-life carethat doesnotmeet their expectations orwishes—including spending their final hours in ahospital.4
The medical and social service worlds ap-proach the complex needs of such people fromdifferent perspectives. Clinicians hope that in-creased emphasis on care delivery models thatprovide continuous and coordinated care, suchas patient-centered medical homes, will be theanswer. Social service providers widely endorseprograms for “aging in place” that reduce theneed for changes of residence by providing sup-portive living environments.5 Both approachesare based on the premise that fewer transitionsbetween clinicians and residential settings willlead to better quality of life for elderly adults.
doi: 10.1377/hlthaff.2010.1102HEALTH AFFAIRS 30,NO. 5 (2011): 975–984©2011 Project HOPE—The People-to-People HealthFoundation, Inc.
Julie P.W. Bynum([email protected])is an associate professor ofmedicine and associatedirector of the Center forHealth Policy Research at theDartmouth Institute for HealthPolicy and Clinical Practice,Dartmouth Medical School, inLebanon, New Hampshire.
Alice Andrews is an instructorat the Dartmouth Institute.
Sandra Sharp is a researchassociate at the DartmouthInstitute.
Dennis McCullough is anassociate professor ofcommunity and familymedicine at DartmouthMedical School.
John E. Wennberg is thePeggy Y. Thompson Professor(chair) in the EvaluativeClinical Sciences, DartmouthMedical School, and is thefounder and director emeritusof the Dartmouth Institute.
May 2011 30:5 Health Affairs 975
The Care Span
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from

The continuing care retirement community isa model that merges the medical and social ser-vices approaches in addressing older people’shealth and functional changes, to minimize dis-ruptions and maximize outcomes. Such com-munities traditionally are corporate entities thatprovide theirmemberswith residential care overthe remainder of their lives, allowing them tomove from independent living to assisted livingand to nursing home care within a single com-munity.6
Typically members of continuing care retire-ment communities pay large entry fees followedby monthly fees, although financing modelsvary. Available supportive services also vary; ingeneral, they include such amenities as congre-gate meals, housekeeping, and nurse-assistedmedication management.7 The residential op-tions and additional supports cover the socialand long-term care services typically needed byaging populations.Yet how best to integrate themedical and social services that chronically ill,elderly populations need is unclear, and manyapproaches exist even among continuing carecommunities.In this article we take advantage of a natural
experiment to compare ambulatory and hospitalcare use at four continuing care retirement com-munities. Although all were part of a single non-profit corporation, the manner in which theirresidents were linked to primary care servicesvaried from site to site. At three of the sites, sitesA–C, residents used clinic-based primary carephysicians who also had independent practicesoutside the retirement community. At the fourthsite, site D, residents were served by an on-siteprimary care team whose sole responsibility wasto provide medical visits across all residentialsettings within that community.Examining patterns of care, we found that the
use of Medicare-covered services and deaths inhospitals were much lower when the primarycare practice serving residents was entirely em-bedded in the continuing care retirement com-munity.We discuss why thismodel of health caredelivery may have led to the observed patterns,and which features might be applied to achievesimilar gains in other long-term care settings.
Study Data And MethodsStudy Design We conducted an observationalcohort study of health care use among residentsof four continuing care retirement communities.All four, located in the Midwest, Mid-Atlantic,and New England regions of the United States,provide a full spectrum of residential servicesand belong to the same parent corporation.We conducted telephone interviews with staff
at each site and the national corporate office toobtain information about the sites, focusing onhow primary care is delivered.We also obtainedinformation fromUS census data about the townwhere each continuing care retirement commu-nity was located.We then used Medicare claimsdata for residents at all four sites to assess use ofambulatory, inpatient, and emergency care andto determine place of death. We also comparedthese patterns among residents to those of peo-ple living in the same towns but not in the con-tinuing care communities.Continuing Care Community Sites Aspart of
the same corporation, the four continuing careretirement community sites studied shared a fi-nancial model and philosophy toward care. Res-idents paid an up-front fee andmonthly fees thatdid not change as level of care increased. Eachcommunity had a medical clinic on site, whoseorganization was determined by a local gov-erning board.Communities And Surrounding Towns
Membership in each site was determined usingpostal codes, because members live on site andeach site has a unique ZIP+4 code. Residents ofthe surrounding towns were also identified byZIP code. To be included in the analysis, resi-dents of the retirement communities and sur-rounding towns had to be enrolled in fee-for-service Medicare and be at least seventy-fiveyears old. Residents at the sites do not partici-pate in managed care, and the average age atmove-in ranged from seventy-four to eightyyears.Asa result,oursample included90–96per-cent of all residents at the sites. We excludedyounger residents, to keep the comparisongroups across the four sites as similar aspossible.Measuring Health Care Use Health care use
was measured using Medicare administrativedata. For a detailed description of methods,see the Technical Appendix.8 In brief, we in-cluded data from the period 1997–2006 for eachperson, andwecalculateduseover thenumberofyears the person lived in the continuing careretirement community, reported as annual ratesper person-years of observation. This methodallowed data from people who moved or diedto contribute to the analysis.We chose utilization measures that character-
ized ambulatory care and examined differencesin the use of hospital-based services. Measuresincluded the number of visits to clinicians (pri-mary care providers, medical specialists, andmid-level providers such as nurse practitionersand physician assistants); rates of emergencydepartment visits; and rates of medical and sur-gical hospitalizations. Measures of continuityincluded the average number of unique (differ-
The Care Span
976 Health Affairs May 2011 30:5
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from

ent) physicians visited and the percentage ofresidents seeing more than ten different physi-cians in a year.Finally, the percentage of deaths that occurred
in a hospital was determined. All measures werecalculated separately for residents of the retire-ment communities and for residents of the sur-rounding towns. Because of data availability, themeasures came from different size samples ofthe Medicare data and years within the studyperiod; see the Technical Appendix for details.8
Analysis Standard statistical methods wereapplied (see the Technical Appendix8). Severalpoints warrant special comment. The resultswere all adjusted for demographic characteris-tics (age, sex, and race), but not for severity ortype of illness. Claims-based illness adjustmentmay create biased estimates because having adiagnosis is dependent on having a visit or pro-cedure, not on the actual presence of disease.9
The likelihood of bias is high when one grouphas many fewer visits or hospitalizations, whichwas the case in this study. One solution mighthave been to use objective measures of func-tional status, but these arenot reported in billingdata. By limiting the analysis to residents ageseventy-five or older, we tried to keep the com-parison groups as similar as possible in terms of
functional status and illness across the four sites.Data were not available to adjust for socio-
economic status. However, residents of the com-munities pay high out-of-pocket fees, which sug-gests that subjects at all four sites are relativelyaffluent. The relative homogeneity of our studysite populations—generally white, affluent, andreceiving care in a setting subsidizedbyhighout-of-pocket expenses—has the advantage of im-proving the validity of the comparisons in spiteof our inability to adjust for socioeconomicstatus.At the same time, that relative homogeneity
may limit the application of our results to morediverse populations. However, the same demo-graphics tend to characterize assisted living res-idents in general. Moreover, with nearly onemillion elders in assisted living communitiesnationwide, understanding the design of caredelivery and its impacts in these settings hasinherent value.7,10
ResultsCharacteristics Of Sites And Their Resi-dents The four continuing care retirement com-munity sites sharedmanycharacteristicsbut alsohad several key differences (Exhibit 1). Each site
Exhibit 1
Comparison Of Residents, Clinical Services, And Surrounding Communities Across Four Continuing Care Retirement Community Sites
Site A Site B Site C Site D
Resident characteristics
Number of residents 358 441 1,110 559Mean age in 2006 (years) 85.4 84.6 85.6 84.4Percent white 100.0% 100.0% 97.4% 99.2%Percent female 71.1% 62.9% 68.2% 65.9%
Health care and residential care services
No. of assisted living beds 24 36 104 50No. of nursing home beds 42 35 109 42No. of independent living units 211 213 504 250On-site nurse practitioner coverage 1 full time 1 full time 1 full time 2 half timeOn-site physician coverage 3 on site, each for
a half-day per weekAny credentialedcommunityphysician may be on site
2 on site, each for2 half-days per week
2 half time practicingsolely at the continuingcare retirementcommunity
Residents receiving primarycare on site
90% 80% 95% 98%
After-hours (on-call) coveragesource
Community-basedpractices
Community-basedpractices
Community-basedpractices
Only clinicians whowork on site
Hospital proximity 2 miles 4 miles 2 miles 2 miles
Surrounding community characteristics
College or university Yes Yes Yes YesPercent white 71.9% 84.1% 92.7% 88.8%Percent families in poverty 6.7% 7.3% 2.7% 1.0%Population size 8,195 18,198 6,451 10,850
SOURCES Authors’ analysis and survey of continuing care retirement community sites, 2000 US census data.
May 2011 30:5 Health Affairs 977
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from
offered similar residential services, including in-dependent living, assisted living, and nursinghome beds that were also certified for skillednursing use.Residents’ out-of-pocket expenses were simi-
lar, but they varied based on the local cost ofliving. A single person in a one-bedroom apart-ment would pay $185,000–$230,000 to join thecommunity and $2,700–$3,300 per month infees to cover housing, services, and health carefor the rest of his or her life.The residents included in this study were sim-
ilarly elderly (average age 84–85 years), pre-dominantly female (63–71 percent), and white(97–100 percent) across the four sites. Selectedresidents of surrounding townshad similar dem-ographics (mean age 83, 64 percent female,94 percent white).On-Site Medical Services All four sites had at
least one on-site nurse practitioner in their clin-ics, plus an on-site registered nurse for after-hours coverage. At site D only, the nurse practi-tioners took after-hours calls alternating withthe physicians.At all sites, physicians offered on-site office
hours. Yet there were distinct differences inhow physician coverage was provided. At sitesA–C, on-site physician hours were limited, andthe same physicians saw nonresidents at practi-ces outside of the continuing care retirementcommunity. After-hours calls were covered bymembers of the physician’s practice, including
physicians who did not practice on site.In contrast, the physicians and two part-time
nurse practitioners at site D delivered clinicalcare only at that site, covered all settings withinit, and provided all after-hours coverage. Be-cause of the dedicated team structure at site D,we characterized that site as having the mostintegrated primary care.Visits And Continuity All of the continuing
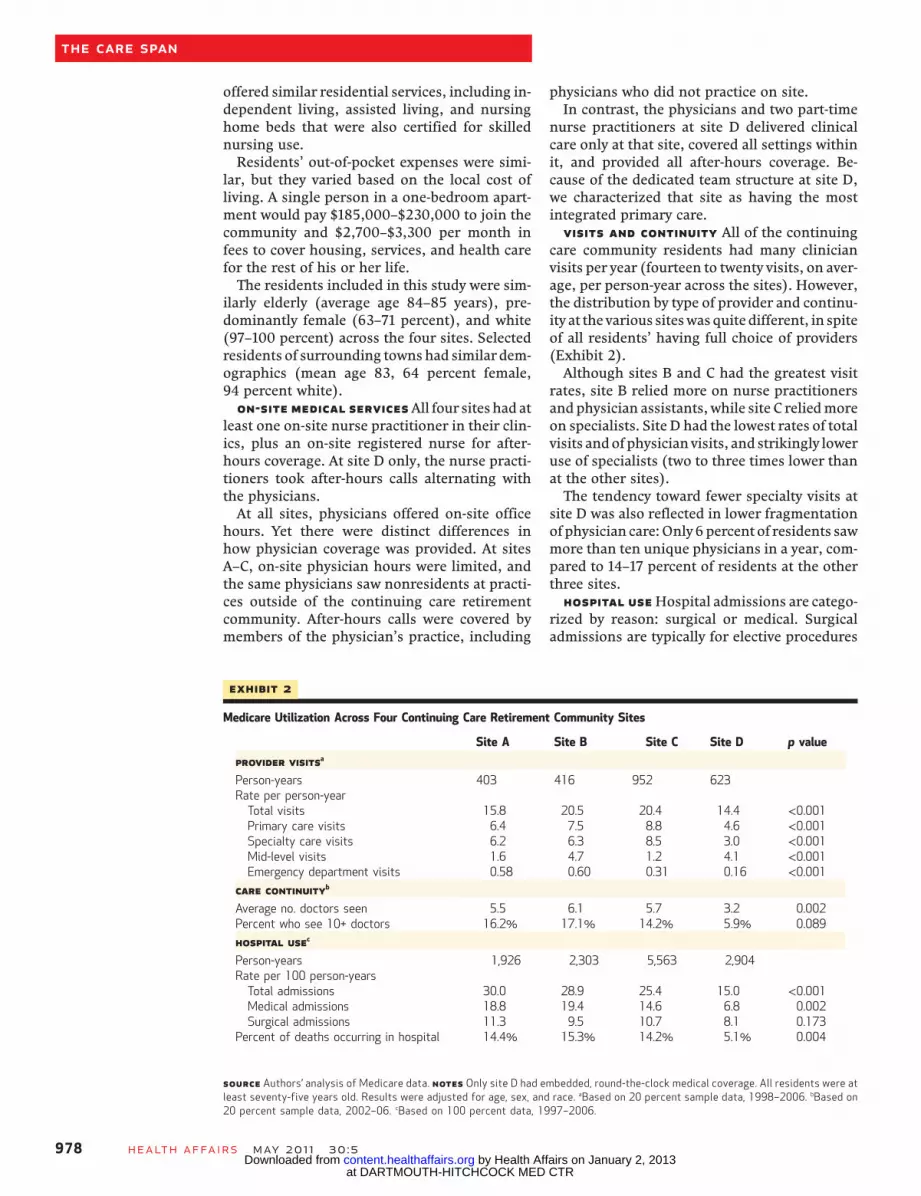
care community residents had many clinicianvisits per year (fourteen to twenty visits, on aver-age, per person-year across the sites). However,the distribution by type of provider and continu-ity at the various siteswasquite different, in spiteof all residents’ having full choice of providers(Exhibit 2).Although sites B and C had the greatest visit
rates, site B relied more on nurse practitionersand physician assistants, while site C reliedmoreon specialists. Site D had the lowest rates of totalvisits andof physicianvisits, and strikingly loweruse of specialists (two to three times lower thanat the other sites).The tendency toward fewer specialty visits at
site D was also reflected in lower fragmentationof physician care:Only6percent of residents sawmore than ten unique physicians in a year, com-pared to 14–17 percent of residents at the otherthree sites.Hospital UseHospital admissions are catego-
rized by reason: surgical or medical. Surgicaladmissions are typically for elective procedures
Exhibit 2
Medicare Utilization Across Four Continuing Care Retirement Community Sites
Site A Site B Site C Site D p value
Provider visitsa
Person-years 403 416 952 623Rate per person-yearTotal visits 15.8 20.5 20.4 14.4 <0.001Primary care visits 6.4 7.5 8.8 4.6 <0.001Specialty care visits 6.2 6.3 8.5 3.0 <0.001Mid-level visits 1.6 4.7 1.2 4.1 <0.001Emergency department visits 0.58 0.60 0.31 0.16 <0.001
Care continuityb
Average no. doctors seen 5.5 6.1 5.7 3.2 0.002Percent who see 10+ doctors 16.2% 17.1% 14.2% 5.9% 0.089
Hospital usec
Person-years 1,926 2,303 5,563 2,904Rate per 100 person-yearsTotal admissions 30.0 28.9 25.4 15.0 <0.001Medical admissions 18.8 19.4 14.6 6.8 0.002Surgical admissions 11.3 9.5 10.7 8.1 0.173
Percent of deaths occurring in hospital 14.4% 15.3% 14.2% 5.1% 0.004
SOURCE Authors’ analysis of Medicare data. NOTES Only site D had embedded, round-the-clock medical coverage. All residents were atleast seventy-five years old. Results were adjusted for age, sex, and race. aBased on 20 percent sample data, 1998–2006. bBased on20 percent sample data, 2002–06. cBased on 100 percent data, 1997–2006.
The Care Span
978 Health Affairs May 2011 30:5
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from
and therefore tend to be planned events. In con-trast, medical admissions usually are unplannedevents resulting from acute illness or exacerba-tion of chronic conditions that require ur-gent care.We found little difference across the sites in
rates of surgical admissions, but large differenc-es in rates of medical admissions and emergencydepartment visits. Residents at sites A and B hadsimilar rates of medical admissions (nineteenper hundred person-years) and emergency de-partment visits (0.60 per person-year). Site Chad significantly fewer medical admissions (fif-teenperhundredperson-years) andhalf asmanyemergency visits (0.31 per person-year).Site D had many fewer of both types of admis-
sions: only seven medical admissions per hun-dred person-years and 0.16 emergency room vis-its per person-year. Compared to siteD, theothersites had 2.0–3.8 times higher rates of medicaladmissions and emergency room visits; see Ap-pendix Figure A.8,11
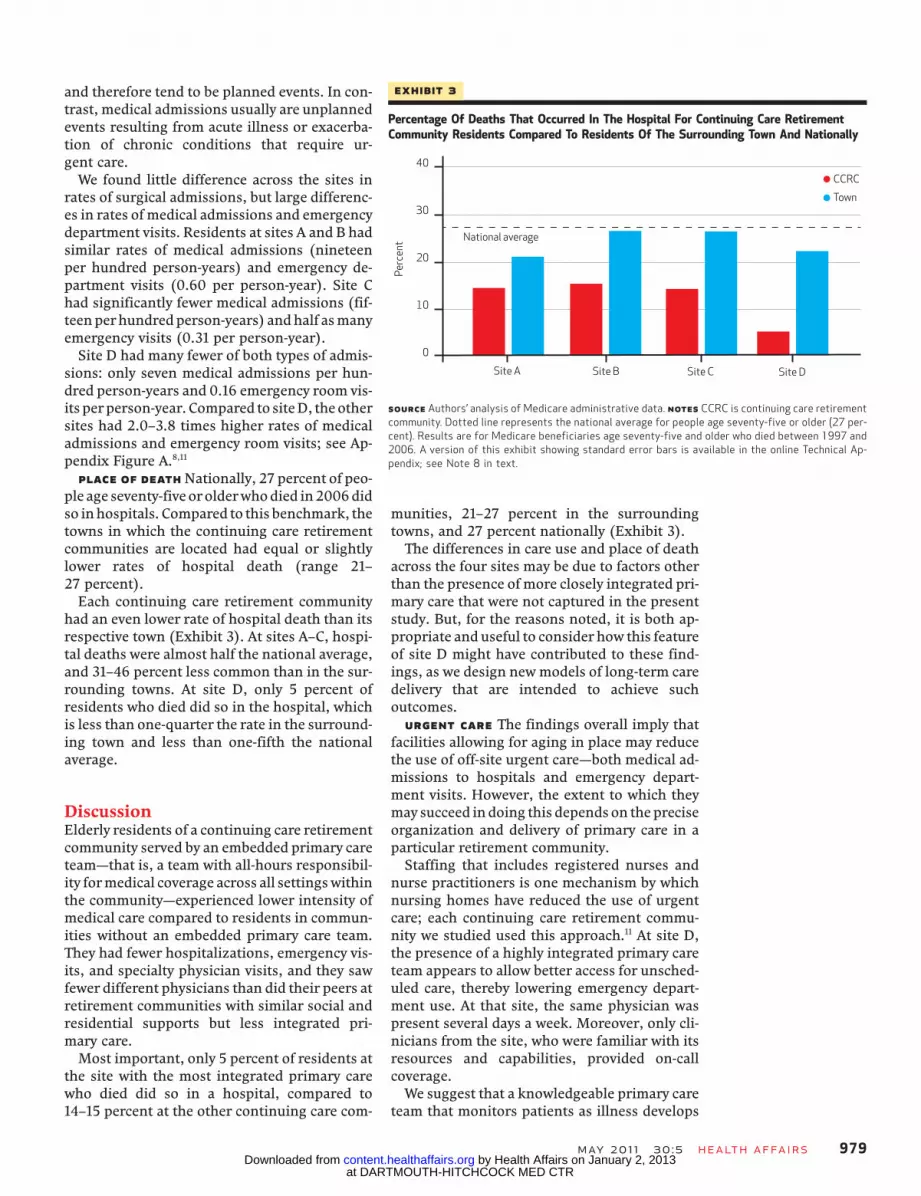
Place Of Death Nationally, 27 percent of peo-ple age seventy-fiveorolderwhodied in2006didso inhospitals. Compared to this benchmark, thetowns in which the continuing care retirementcommunities are located had equal or slightlylower rates of hospital death (range 21–27 percent).Each continuing care retirement community
had an even lower rate of hospital death than itsrespective town (Exhibit 3). At sites A–C, hospi-tal deaths were almost half the national average,and 31–46 percent less common than in the sur-rounding towns. At site D, only 5 percent ofresidents who died did so in the hospital, whichis less than one-quarter the rate in the surround-ing town and less than one-fifth the nationalaverage.
DiscussionElderly residents of a continuing care retirementcommunity served by an embedded primary careteam—that is, a team with all-hours responsibil-ity formedical coverage across all settingswithinthe community—experienced lower intensity ofmedical care compared to residents in commun-ities without an embedded primary care team.They had fewer hospitalizations, emergency vis-its, and specialty physician visits, and they sawfewer different physicians than did their peers atretirement communities with similar social andresidential supports but less integrated pri-mary care.Most important, only 5 percent of residents at
the site with the most integrated primary carewho died did so in a hospital, compared to14–15 percent at the other continuing care com-
munities, 21–27 percent in the surroundingtowns, and 27 percent nationally (Exhibit 3).The differences in care use and place of death
across the four sites may be due to factors otherthan the presence of more closely integrated pri-mary care that were not captured in the presentstudy. But, for the reasons noted, it is both ap-propriate and useful to consider how this featureof site D might have contributed to these find-ings, as we design newmodels of long-term caredelivery that are intended to achieve suchoutcomes.Urgent Care The findings overall imply that
facilities allowing for aging in place may reducethe use of off-site urgent care—both medical ad-missions to hospitals and emergency depart-ment visits. However, the extent to which theymay succeed indoing this dependson thepreciseorganization and delivery of primary care in aparticular retirement community.Staffing that includes registered nurses and
nurse practitioners is one mechanism by whichnursing homes have reduced the use of urgentcare; each continuing care retirement commu-nity we studied used this approach.11 At site D,the presence of a highly integrated primary careteam appears to allow better access for unsched-uled care, thereby lowering emergency depart-ment use. At that site, the same physician waspresent several days a week. Moreover, only cli-nicians from the site, who were familiar with itsresources and capabilities, provided on-callcoverage.We suggest that a knowledgeable primary care
team that monitors patients as illness develops
Exhibit 3
Percentage Of Deaths That Occurred In The Hospital For Continuing Care RetirementCommunity Residents Compared To Residents Of The Surrounding Town And Nationally
Perc
ent
Site A Site B Site C Site D
National average
CCRC
Town
SOURCE Authors’ analysis of Medicare administrative data. NOTES CCRC is continuing care retirementcommunity. Dotted line represents the national average for people age seventy-five or older (27 per-cent). Results are for Medicare beneficiaries age seventy-five and older who died between 1997 and2006. A version of this exhibit showing standard error bars is available in the online Technical Ap-pendix; see Note 8 in text.
May 2011 30:5 Health Affairs 979
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from

over several days may be able to respond in arangeofways to anacute, unscheduled situation.In other words, the existence of an “embedded”team may allow for responses beyond simply anemergency department visit for an affectedpatient.Using Resources To Maximize Choices For
Site Of Care In ourdiscussionswith theprimarycare team at site D, we learned that a close col-laboration between clinicians and continuingcare retirement community residents led to aconsensus favoring the conservative manage-ment of acute and chronic illnesses, with an ex-pressed preference among most members toavoid hospitalization if at all possible.12 Becausethe primary care team served all settings withinthe continuing care retirement community, itwas able to deploy residential resources in pur-suit of this preference—including direct admis-sion to the community’s Medicare-qualifiedskilled nursing facility as a way of avoiding hos-pital admission.Under ordinary fee-for-service Medicare pay-
ment policy, a skilled nursing facility stay mustbe preceded by a three-day hospital admission toqualify for reimbursement. The philosophy ofcare and ability to cross-subsidize within thecontinuing care community made the use of itsskillednursingbeds a viable option, even thoughnot reimbursed by Medicare.With clinicians on site and providing after-
hours coverage, it was also possible for the pri-mary care team at site D to accept an early hos-pital discharge without a qualifying stay to askilled nursing bed, or to manage borderlinecases in the community’s skilled nursing bedsrather than in the hospital. The skilled nursingbeds were also used to support members whowere at the end of life, either preventing or sub-stituting for hospitalization.The ability to use nursing home beds certified
for skilled nursing use as flexibly as possibledepends not only on the way the beds are fi-nanced, but also on the presence of a medicalteam that can make an immediate assessmentand do a skilled bed admission on the spot, thenfollow up with daily monitoring of more acutelyill patients. All sites were certified to use theirnursing home beds flexibly, but informants’comments revealed that access to clinicianswas not consistent enough at sites A–C to makethe practice as routine as it was at site D.Other programs for high-risk elderly people
that have been shown to reduce hospital use,such as the Program for All-Inclusive Care, alsocapitalize on the ability to deploy services in adifferentmanner and ina timely fashionbyusinga dedicated medical team, albeit through capi-tated financing.13,14
Patient-Provider Continuity Over TimeAnd Setting Another reason why more highlyintegrated primary care in the continuing carecommunity is associated with less-intense medi-cal caremay be that it results in greater provider-patient continuity, both over time and acrosssettings within the community. Greater physi-cian continuity has been associated with lessemergency department and hospital care.15–17
Continuity and visits with the primary care pro-vider, in particular, have been associated withless aggressive end-of-life care.16,18
The solo practitioner of yore who managedpatients in the clinic, hospital, home, and nurs-ing home embodied the provision of high con-tinuity in all its dimensions: informational(sharing health data), management (developingand executing treatment plans), and relation-ship (maintaining an ongoing therapeutic con-nection).19 To some degree, the integratedmodelat site D emulates this traditional role of clini-cians that crosses multiple settings. The rela-tional continuity that having a very small groupof clinicians fosters may improve the likelihoodof patients’ trust in decisions and providers’knowledge of patients’ preferences.15,19
Role Of Preferences Several alternative ex-planations, other than the design of primarycare, may account for the observed differencesin utilization rates across the four sites. One isthat patients’preferences for amount and type ofhospital service use could vary systematicallyacross the sites.We do not have any informationabout individual residents’ preferences at thesites we studied. Yet there is some informationabout the preferences of residents of continuingcare communities from other studies.Previousworkhasdocumented that40percent
of continuing care retirement community resi-dents reported considering place of death intheir decision to enter such a community, and
Close collaborationbetween clinicians andresidents led to aconsensus favoringthe conservativemanagement ofillnesses.
The Care Span
980 Health Affairs May 2011 30:5
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from
most preferred to die on the community cam-pus.20 Other studies of preferences among con-tinuing care residents have shown that the ma-jority preferred not to die in the hospital.21,22
Additionally, it has been shown that prefer-ences for the intensity of end-of-life care donot vary by region.23 These findings tend to re-duce the likelihood that differences in residents’preferences at the four siteswere large enough toaccount for the observed differences in placeof death.
Community Influence In addition to partici-pating in the design of its primary care deliverysystem, each retirement communityprobablyde-velops social and cultural norms that also influ-ence decisions regarding hospitalization andthe intensity of end-of-life care. There may beopportunities for learning, development of self-management skills, support groups, and sharedcommunity resources that lead todifferential useof the hospital.Clinicians at site D described participating in
community discussions that led to the develop-ment of an approach that placed a high priorityon individual patients’ preferences. But this de-velopment of a community norm might emergeindependent of the integrated primary careteam.
Exceptions To The Regional Practice Pat-ternMany studies have shown that one’s regionof residence can be related to as much as a two-fold difference in physician and hospital use andspending.24,25 In fact, some studies have shownregion to be the strongest predictor of end-of-lifecare intensity and place of death.4,20,26 Therefore,location of the continuing care communities inregions with higher or lower hospital utilizationrates might be expected to influence those rates.Yet the continuing care retirement commun-
ities we studied appear to deliver care that devi-ates from the local norm. At site D, in particular,the difference is very large. Although the per-centage dying in the hospital was lower at all
sites compared to theMedicarenational average,hospital deaths were even lower at continuingcare community sites than in their surroundingtowns. And at the site with integrated primarycare, the percentage dying in the hospital wasless than one-quarter that of the surroundingtown and one-fifth the national average (see Ap-pendix Figure B for additional utilization com-parisons).8
We cannot know definitively, from these data,whether philosophy of care, role of patients’preferences, insulation from Medicare fee-for-service forces, design of primary care delivery,or other as yet unidentified features led to thesetreatment patterns that are strikingly differentfrom local norms.With further investigation, wecould learn more from these collaborative mod-els about the drivers of variation in health caredelivery.Policy Implications The example of dramati-
cally lower hospital use at the end of life and theuse of fewer physician, emergency, and hospitalvisits in a care delivery system that serves theelderly is an important demonstration of “whatis possible.” We could not find any other pub-lished reports with such low proportions ofdeaths occurring in the hospital. But what fea-tures of a continuing care retirement communitywith embedded primary care can be adoptedmore broadly?The features that are not reproducible are the
affluence of the residents and subsidization byhigh out-of-pocket expenses. Yet other key fea-tures are transferrable.The spectrum of on-site clinic services can be
expanded to cover urgent care if the physicianscan provide more in-person access or consulta-tion and support for the nurse practitioner dur-ing regular working hours. Physicians and nursepractitioners can provide continuous care acrossall relevant settings: clinic, nursing home, andskilled nursing care.On-call coverage canbeprovidedbyphysicians
and nurse practitioners who are knowledgeableabout, and comfortable with, the urgent careservices that can be delivered on site. Nursinghome beds can be used more flexibly, for urgentor end-of-life care, if there are alternative fund-ing streams and accessible clinicians.The adoption of these features on a broader
scale might not seem feasible under the fee-for-service paymentmodel, andwhen financing fallsonpublic payers or onpeoplewith less affluence.But new policies included in the Affordable CareAct of 2010 may lower barriers to this type ofpatient-centered, coordinated care. Several pol-icy changes affect long-term care (such as theCommunity Living Assistance Services and Sup-ports Act and Medicaid incentives to increase
New policies includedin the AffordableCare Act of 2010may lower barriers topatient-centered,coordinated care.
May 2011 30:5 Health Affairs 981
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from
home and community-based services).Most relevant to this discussion are policies
that address chronic care coordination. The stra-tegic lead will come from two new offices: onecharged with improving coordination of Medi-care and Medicaid programs; and a second, theCenter for Medicare and Medicare Innovation,for which development of “patient centeredmedical homes models for high need individ-uals” is a high priority.27(p7)
Some features of the collaboration betweencontinuing care retirement communities andprimary care providers observed at site D couldinform the design ofMedicare pilot projects anddemonstrations that areunderdevelopment. Forexample, pilot programs of bundled paymentsfor hospitalization and care transition demon-stration projects could consider ways to makeflexible skilled nursing home beds more acces-sible, in collaboration with the physicians whowork in those settings.In addition, accountable care organization
payment models offer incentives for a group ofproviders to deploy resources and personnel col-laboratively for high-risk patients. Under theshared savings model or under partial capita-tion, provider groups could design a compensa-tion model that allows providers more manage-ment choices for high-risk elderly people in needof urgent care, beyond sending them to an emer-gency department.The opportunities for alternative models will
be even greater for Medicare beneficiaries whoare also eligible for Medicaid (known as duallyeligible), who also have access to Medicaidwaiver-based home and community-based careservices or arenursinghome residents. For thesevulnerable groups, social and medical care aremanaged exclusively or primarily throughpublicpayers, which creates opportunities for the Cen-ters for Medicare andMedicaid Services to alignpayment policies across the social and medicalcare delivery systems.
ConclusionThe collaboration between continuing care re-tirement communities and primary care provid-ers shows what is possible when the two groupswho provide social and medical care work to-gether to meet the needs of people in their lastdecades of life. A continuing care retirementcommunity offers its members a contract to pro-vide housing and nursing support across a per-son’s remaining life span, regardless of the levelof need.Medical providers could make a similar com-
mitment to redesign their medical practicesaround the need for care across the life span thatgoes beyond the office-based medical home toone that is truly patient centered and encom-passes all residential settings. Learning how suc-cessful models incorporate residential settingsinto the design of medical homes can providevaluable insights on how to improve care forpatients at high risk for functional decline, hos-pitalization, and death. ▪
The authors acknowledge the staff atthe Kendal Corporation who gave theirtime in providing information abouttheir work environment. Julie Bynum’s
work was funded by a Paul B. BeesonCareer Development Award in Agingfrom the National Institute on Aging,NIA AG-07-001. John Wennberg serves
as a paid consultant to the Foundationfor Informed Medical Decision Makingand Health Dialog, and he receivesroyalties from Health Dialog.
Providers could makea commitment toredesign their medicalpractices around theneed for care acrossthe life span.
The Care Span
982 Health Affairs May 2011 30:5
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from
NOTES
1 Anderson G. Chronic care: makingthe case for ongoing care. Princeton(NJ): Robert Wood Johnson Foun-dation; 2010.
2 Wolff JL, Starfield B, Anderson G.Prevalence, expenditures, and com-plications of multiple chronic con-ditions in the elderly. Arch InternMed. 2002;162(20):2269–76.
3 Wolff JL, Boult C, Boyd C, AndersonG. Newly reported chronic condi-tions and onset of functionaldependency. J Am Geriatr Soc.2005;53(5):851–5.
4 Pritchard RS, Fisher ES, Teno JM,Sharp SM, Reding DJ, Knaus WA,et al. Influence of patient prefer-ences and local health system char-acteristics on the place of death. JAm Geriatr Soc. 1998;46(10):1242–50.
5 Wardrip K. Strategies to meet thehousing needs of older adults.Washington (DC): AARP PublicPolicy Institute; 2010 Mar.
6 Centers for Medicaid and MedicareServices. Types of long-term care:continuing care retirement com-munities [Internet]. Baltimore(MD): CMS; 2007 [cited 2010 Jun 1].Available from: http://www.medicare.gov/LongTermCare/Static/CCRC.asp
7 Hawes C, Phillips CD, RoseM, HolanS, Sherman M. A national survey ofassisted living facilities. Gerontolo-gist. 2003;43(6):875–82.
8 To access the Technical Appendix,click on the Technical Appendix linkin the box to the right of the articleonline.
9 Song Y, Skinner J, Bynum J,Sutherland J, Wennberg JE, FisherES. Regional variations in diagnosticpractices. N Engl J Med. 2010;363(4):45–53.
10 Stevenson DG, Grabowski DC.
Sizing up the market for assistedliving. Health Aff (Millwood).2010;29(1):35–43.
11 Bourbonniere M, Evans LK. Ad-vanced practice nursing in the careof frail older adults. J Am GeriatrSoc. 2002;50(12):2062–76.
12 Wennberg JE. Tracking medicine: aresearcher’s quest to understandhealth care. New York (NY): OxfordUniversity Press; 2010.
13 Hirth V, Baskins J, Dever-Bumba M.Program of All-Inclusive Care(PACE): past, present, and future.J Am Med Dir Assoc. 2009;10(3):155–60.
14 Master RJ, Eng C. Integrating acuteand long-term care for high-costpopulations. Health Aff (Millwood).2001;20(6):161–72.
15 Haggerty JL, Reid RJ, Freeman GK,Starfield BH, Adair CE, McKendry R.Continuity of care: a multidiscipli-nary review. BMJ. 2003;327:1219–21.
16 Sharma G, Fletcher KE, Zhang D,Kuo Y-F, Freeman JL, Goodwin JS.Continuity of outpatient and inpa-tient care by primary care physiciansfor hospitalized older adults. JAMA.2009;301(16):1671–80.
17 Wasson JH, Sauvigne AE,Mogielnicki RP, Frey WG, Sox CH,Gaudette C, et al. Continuity of out-patient care in elderly men: a ran-domized trial. JAMA. 1984;252:2413–7.
18 Kronman A, Ash A, Freund K,Hanchate A, Emanuel E. Can pri-mary care visits reduce hospital uti-lization among Medicare benefici-aries at the end of life? J Gen InternMed. 2008;23(9):1330–5.
19 Guthrie B, Saultz JW, Freeman GK,Haggerty JL. Continuity of carematters. BMJ. 2008;337:548–9.
20 Hays JC, Galanos AN, Palmer TA,
McQuoid DR, Flint EP. Preferencefor place of death in a continuingcare retirement community. Geron-tologist. 2001;41(1):123–8.
21 Resnick B, Andrews C. End-of-lifetreatment preferences among olderadults: a nurse practitioner initiatedintervention. J Am Acad Nurse Pract.2002;14(11):517–22.
22 Nahm ES, Resnick B. End-of-lifetreatment preferences among olderadults. Nurs Ethics. 2001;8(6):533–43.
23 Barnato AE, Herndon MB, AnthonyDL, Gallagher PM, Skinner JS,Bynum JP, et al. Are regional varia-tions in end-of-life care intensityexplained by patient preferences? Astudy of the US Medicare popula-tion. Med Care. 2007;45(5):386–93.
24 Wennberg JE, Fisher ES, Stukel TA,Skinner JS, Sharp SM, Bronner KK.Use of hospitals, physician visits,and hospice care during last sixmonths of life among cohorts loyalto highly respected hospitals in theUnited States. BMJ. 2004;328(7440):607–11.
25 Fisher ES, Wennberg DE, Stukel TA,Gottlieb DJ, Lucas FL, Pinder EL. Theimplications of regional variation inMedicare spending, part 1: the con-tent, quality, and accessibility ofcare. Ann Intern Med. 2003;138(4):273–87.
26 Gruneir A, Mor V,Weitzen S, TruchilR, Teno J, Roy J.Where people die: amultilevel approach to understand-ing influences on site of death inAmerica. Med Care Res Rev. 2007;64(4):351–78.
27 Justice D. Long term services andchronic care coordination: policyadvances enacted by the PatientProtection and Affordable Care Act.Portland (ME): National Academyfor State Health Policy; 2010 Apr.
May 2011 30:5 Health Affairs 983
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from

ABOUT THE AUTHORS: JULIE P.W. BYNUM, ALICE ANDREWS,SANDRA SHARP, DENNIS MCCULLOUGH & JOHN E. WENNBERG
Julie P.W. Bynum isan associateprofessor at theDartmouth Institutefor Health Policyand ClinicalPractice.
Julie Bynum and her colleagues atDartmouth Medical School reporton a study of four continuing careretirement communities withcommon ownership. They foundthat the one with its own on-siteprimary care team that served onlythe retirement community’sresidents experienced the lowestuse of Medicare services, includingthe lowest rate of hospital use anddeaths in hospitals. This is exactlywhat one would hope to see,Bynum observes, when a primarycare practice appears primarilyfocused on residents’ care andgoals.
Bynum is an associate professorof medicine and associate directorof the Center for Health PolicyResearch at the DartmouthInstitute for Health Policy andClinical Practice, DartmouthMedical School. A practicinggeriatrician, Bynum received hermedical degree from the JohnsHopkins Medical School and holdsa master of public health degreefrom the Johns Hopkins BloombergSchool of Public Health.
Alice Andrews is aninstructor at theDartmouthInstitute.
Alice Andrews is an instructor atthe Dartmouth Institute, where sheworks with the Center for Medicineand the Media. She is also seniorcurriculum specialist withDartmouth’s master of health caredelivery science degree program.Andrews holds a master’s degree inhealth policy and clinical practicefrom the Dartmouth Institute and adoctorate in organizationalbehavior from Cornell University.
Sandra Sharp is aresearch associateat the DartmouthInstitute.
Sandra Sharp is a researchassociate at the DartmouthInstitute, where she participates instudies of Medicare utilization andis a lead analyst on the DartmouthAtlas Project. Sharp received hermaster’s degree in populationsciences from the Harvard Schoolof Public Health.
Dennis McCulloughis an associateprofessor atDartmouth MedicalSchool.
Dennis McCullough is anassociate professor in DartmouthMedical School’s Department ofCommunity and Family Medicine.He recently wrote My Mother, YourMother, a guide to the “slowmedicine” approach for elders in
their final years. A practicingfamily physician and geriatricianfor thirty years, McCullough is agraduate of Harvard MedicalSchool.
John E. Wennbergis a professor atthe DartmouthInstitute andDartmouth MedicalSchool.
John Wennberg is the Peggy Y.Thompson Professor (chair) in theEvaluative Clinical Sciences at theDartmouth Medical School, and isfounder and director emeritus ofthe Dartmouth Institute. He hasbeen a professor in the Departmentof Community and Family Medicinesince 1980 and in the Departmentof Medicine since 1989.Wennberg is the founding editor
of the Dartmouth Atlas of HealthCare, which examines patterns ofmedical resource intensity andutilization in the United States. Hecompleted his medical degree atMcGill University, then earned amaster of public health degreefrom the Johns Hopkins School ofHygiene and Public Health (nowthe Bloomberg School of PublicHealth).
The Care Span
984 Health Affairs May 2011 30:5
at DARTMOUTH-HITCHCOCK MED CTR on January 2, 2013Health Affairs by content.healthaffairs.orgDownloaded from









![[Acute and post-acute hospitalizations for stroke in France: recent improvements (2007-2009)]](https://img.dokumen.tips/doc/110x75/63547b6c8db8416a940e2cc8/acute-and-post-acute-hospitalizations-for-stroke-in-france-recent-improvements.jpg)


















