Embed Size (px)
Citation preview

REVIEW
Fetal neuroimaging: US and MRI
Elida Vazquez & Nuria Mayolas & Ignacio Delgado &
Teresa Higueras
# Springer-Verlag 2009
Introduction
Although MRI has several advantages over US for imagingthe fetal central nervous system (CNS), it cannot replaceUS as a screening modality for fetal anomalies. Nonethe-less, MRI is useful for the diagnosis of fetal CNS anomaliesand is a complementary technique to US. US is performedwith 2.5–5.0-MHz transducers, with the additional use ofvaginal US with 5–7-MHz transducers when the fetus is incephalic or breech positions or when a neural tube defect orspinal abnormality is suspected. When neurosonography isperformed by a trained experienced physician, MR imagingmight not contribute substantially to the US findings [1–4].It is, therefore, very relevant to establish the true indicationsfor fetal MR imaging, depending on the US findings.
Advantages and limitations of fetal MR imaging
Advantages
Fetal MR imaging has several advantages over prenatal US,such as improved contrast resolution and direct visualiza-tion of both sides of the fetal brain, and overcomes some ofthe difficulties encountered with US (decreased amniotic
fluid volume, fetal positioning, and acoustic shadowingfrom the ossifying calvarium). Several reports have shownthat fetal MR imaging can detect sonographically occultabnormalities in up to 50% of cases examined for a varietyof indications. These reports have shown that fetal MRimaging results affect patient counselling and causechanges in pregnancy management in nearly half of cases[5–7].
Limitations
Even with the modern rapid image acquisition advances incoil design, such as parallel imaging with an increasingnumber of channels, fetal motion and maternal claustro-phobia and discomfort during the scan can still affect thequality of the study, particularly in the case of young-gestational-age fetuses [4]. Owing to the potential risk tothe developing fetus and the current limitations of fetal MRimaging, it is prudent to wait until after the first trimesterbefore performing fetal MR imaging; this will also mini-mize the problems created by the small size and excessivemotion. Sedation and intravenous contrast administrationare not recommended in fetal MR imaging because of thepotential risk to the fetus.
Imaging techniques
MRI examinations are usually performed on a 1.5-Tsuperconducting system using an eight-element, phased-array surface coil, with a radiologist monitoring the studyas it is performed. Patients are in the supine or lateralposition with the feet entering the magnet bore first tominimize feelings of claustrophobia. Ultrafast MR imagingtechniques known as single-shot fast spin-echo (SSFSE) or
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435DOI 10.1007/s00247-009-1221-x
E. Vazquez (*) :N. Mayolas : I. DelgadoDepartment of Paediatric Radiology,Hospital Universitario Vall d’Hebron,Psg. Vall d’Hebron, 112-119,08035 Barcelona, Spaine-mail: [email protected]
T. HiguerasFetal Medicine Unit, Hospital Universitario Vall d’Hebron,Barcelona, Spain
half-Fourier acquired single-shot turbo spin-echo (HASTE)are mainly used. Using these rapid pulse sequences, asingle T2-W image can be acquired in less than 1 s,reducing the likelihood of fetal motion. In certain cases,such as imaging of twins or a fetus with a myelomeningo-cele, the coil may need to be repositioned during theexamination. Each sequence is used as the scout forsubsequent sequences. In this manner, axial, sagittal andcoronal image sets of the fetal brain are obtained.
For T1-W imaging, fast multiplanar gradient-recalled-echo techniques, such as FMPSPGR, are used to detect
haemorrhage or calcification, with images acquired during asingle maternal breath hold. Gradient-echo echo-planarT2*-W images and diffusion-weighted imaging (DWI) arealso routinely obtained. In total, scanning time for anexamination ranges from 15 to 20 min.
Main applications of fetal MR imaging
Fetal MR imaging is used primarily to confirm andcharacterize brain abnormalities detected by routine prena-
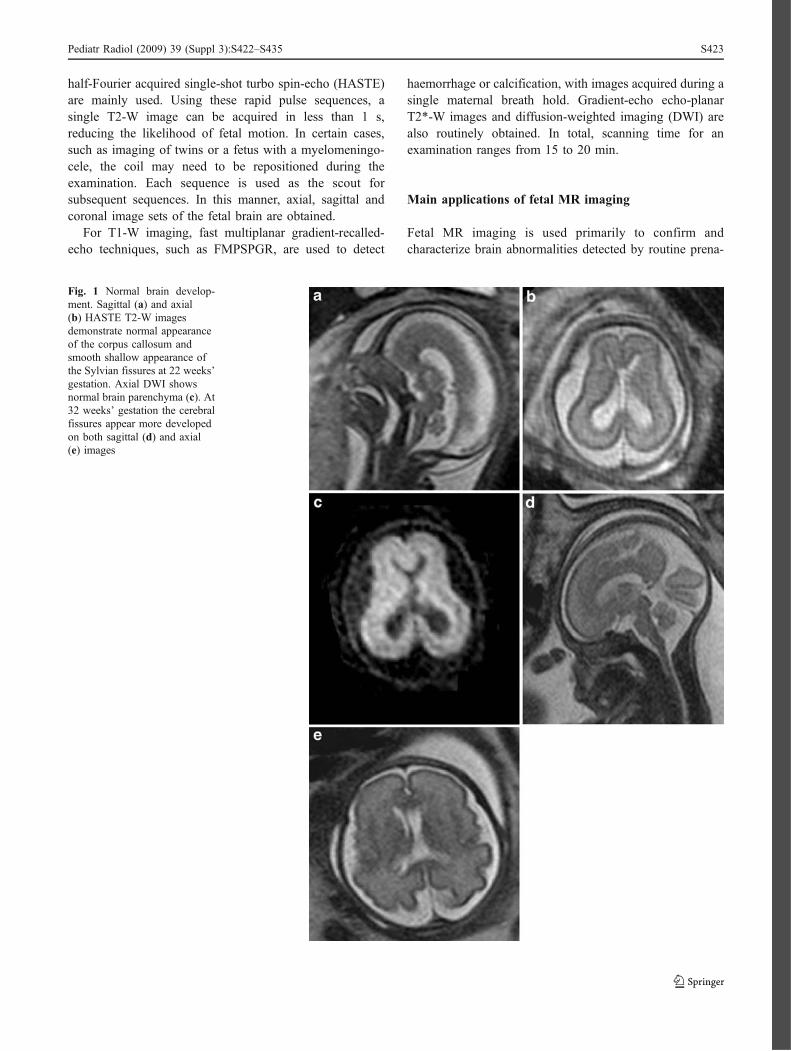
Fig. 1 Normal brain develop-ment. Sagittal (a) and axial(b) HASTE T2-W imagesdemonstrate normal appearanceof the corpus callosum andsmooth shallow appearance ofthe Sylvian fissures at 22 weeks’gestation. Axial DWI showsnormal brain parenchyma (c). At32 weeks’ gestation the cerebralfissures appear more developedon both sagittal (d) and axial(e) images
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435 S423

tal US. Therefore, when a sonographically suspectedabnormality is confirmed, fetal MR is also used to identifyany additional sonographically occult CNS abnormalities[1–4]. Because of the limitations of US, MRI can be used inthese specific situations:
1. When the position of the fetal head is low within thematernal pelvis, in twin pregnancies, and when echo-genicity of the patient is poor, particularly in the latesecond or third trimesters
2. For deep analysis of the fetal posterior fossa (cerebel-lum and tentorial insertion)
3. In pregnancies in which the fetus is at increased risk ofbrain abnormalities, such as in families with a history of aprior child or fetus with CNS anomalies or a geneticdisorder, even in the setting of a normal prenatal US [8]
4. In complications of monochorionic twinning, such astwin-twin transfusion syndrome and co-twin demise
5. To analyze other fetal organs, such as the eyes or inner ears(semicircular canals), which are difficult to assess by US
Fig. 2 Fetal hydrocephalus.Midline sagittal HASTE T2-Wimage (a) demonstrates closureof the Sylvian aqueductin a 36-week-gestation fetus.Severe ventriculomegaly withdestruction of the septumpellucidum is seen on axial(b) and coronal (c) images.Follow-up sagittal (d) and axial(e) T2-W images obtained inthe neonatal period
S424 Pediatr Radiol (2009) 39 (Suppl 3):S422–S435

6. To study the phases of neural development: waves ofmigration and myelination, particularly with DWI
7. For a complete analysis of the whole gyration of thebrain surface
8. Before and after fetal surgical techniques, such asmyelomeningocele repair, ex utero intrapartum treat-ment (EXIT) procedure or diverse laser procedures(selective fetoscopic laser photocoagulation) in twin–twin transfusion syndrome
Specific indications for fetal MR
Normal fetal brain maturation and fetal biometry
The MR imaging morphological changes during pregnancyhave been well documented using conventional T1- andT2-W imaging sequences. Changes in morphology includedeveloping sulcation, decrease of subarachnoid spacevolume and progressive thinning of the periventriculargerminal zone [9, 10]. Changes in signal are related tocontinuous cellular differentiation and organization, myelin
deposition and decrease of water content, predominantlywithin the white matter (Fig. 1).
Variations of the ADC (apparent diffusion coefficient)values of fetal brain during maturation in utero have beendescribed using DWI [11]. A decrease of the ADC valuesafter a primary rise before the 30th gestational week occursas result of the disappearance of the intermediate zone, incombination with the decrease in water content and thebeginning of higher-order maturation, including myelina-tion. The brainstem and cerebellar hemisphere, as well asthe thalamus, have been shown to undergo much earliermaturation and myelination, with a strong linear negativeage-related correlation of their ADC values. A gestational-age-related decrease in ADCs in the pyramidal tract and thecorpus callosum (with significantly increased fractionalanisotropy) and a trend towards a decrease in the centrumsemiovale have been reported [12].
Although morphometric MR imaging studies havemostly focused on the third trimester, the legal restrictionson abortion timing in many countries has meant that mostfetal MR imaging has to be carried out during the last partof the second trimester, i.e., before the 24th week of
Fig. 3 Isolated mild ventriculomegaly. Normal corpus callosum and posterior fossa can be seen on the sagittal HASTE T2-W image (a) in a 32-week-gestation fetus. There is mild ventriculomegaly (atrial diameter 11 mm) on the axial images (b, c)
Fig. 4 Agenesis of the corpus callosum. Sagittal (a), axial (b) and coronal (c) HASTE T2-W images in a 25-week-gestation fetus demonstrateabsence of the corpus callosum with secondary colpocephaly and abnormally shaped frontal horns
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435 S425

gestation. Since prenatal MR is performed after the 18thweek of gestation, the time available to take crucialdecisions on the basis of clinical and imaging informationis quite limited. Accurate and reliable data on the brainbetween 20 and 24 weeks of gestation has been reported[13]. It is advisable in the day to day practice of fetalimaging to complete the evaluation of the brain taking themeasurements of the main brain structures, includinganteroposterior and superoinferior diameter of the vermis,latero-lateral diameter of the cerebellum, length of thecorpus callosum, fronto-occipital cerebral diameter, cerebral
biparietal and bone biparietal diameters, interhemisphericdistance, and third ventricle and ventricular atria diameters.
Ventriculomegaly
Ventriculomegaly is the most common CNS abnormalityidentified on prenatal sonography. It is defined as atrial width>10 mm on USmeasured at the posterior margin of the glomusof the choroid plexus on an axial plane through the thalami[14]. Counselling women with pregnancies affected by fetalventriculomegaly is difficult because of the wide range of
Fig. 5 Partial agenesis of thecorpus callosum. Sagittal (a),axial (b) and coronal (c) HASTET2-W images in a 28-week-gestation fetus demonstrateabsence of the posterior corpuscallosum. Follow-up sagittalT1-W (d) and axial T2-W(e) images were obtained whenthe baby was 1 month of age
S426 Pediatr Radiol (2009) 39 (Suppl 3):S422–S435
reported outcomes. The severity of ventriculomegaly iscalculated using US measurement of the atrium of the lateralventricles, as follows: mild ventriculomegaly, 10–14 mm;moderate, ≥15 mm with >3 mm of brain parenchyma (corticalmantle) surrounding the ventricles; and severe, ≥15 mm withup to 3 mm of visible cortical mantle (Fig. 2).
Isolated mild ventriculomegaly (10–15 mm) has a goodprognosis, particularly in cases with an atrial diameter<12 mm [15]. US can be limited in its ability to detectadditional abnormalities in the setting of ventriculomegaly,which may occur in 70–80% of cases (Fig. 3). Fetal MRimaging can detect additional sonographically occult CNSabnormalities in up to 40–50% of cases, particularlymalformations of cortical development [4, 16]. MRI isoptional when ventricular size is 10–12 mm, stronglyrecommended >12 mm, and mandatory when there is anincrease in size over time on US follow-up [1].
Suspected abnormalities of the corpus callosum
The corpus callosum develops between gestational weeks 8and 20. Developmental abnormalities of the corpus cal-losum include agenesis (Fig. 4), hypogenesis (or partial
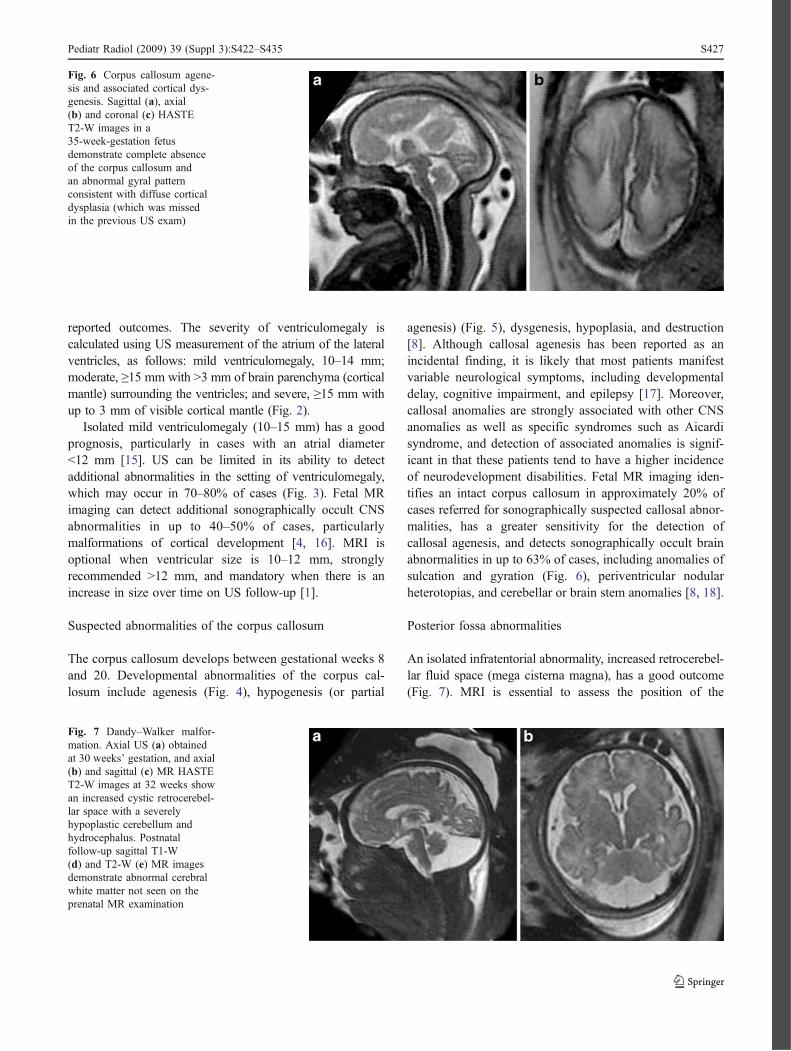
agenesis) (Fig. 5), dysgenesis, hypoplasia, and destruction[8]. Although callosal agenesis has been reported as anincidental finding, it is likely that most patients manifestvariable neurological symptoms, including developmentaldelay, cognitive impairment, and epilepsy [17]. Moreover,callosal anomalies are strongly associated with other CNSanomalies as well as specific syndromes such as Aicardisyndrome, and detection of associated anomalies is signif-icant in that these patients tend to have a higher incidenceof neurodevelopment disabilities. Fetal MR imaging iden-tifies an intact corpus callosum in approximately 20% ofcases referred for sonographically suspected callosal abnor-malities, has a greater sensitivity for the detection ofcallosal agenesis, and detects sonographically occult brainabnormalities in up to 63% of cases, including anomalies ofsulcation and gyration (Fig. 6), periventricular nodularheterotopias, and cerebellar or brain stem anomalies [8, 18].
Posterior fossa abnormalities
An isolated infratentorial abnormality, increased retrocerebel-lar fluid space (mega cisterna magna), has a good outcome(Fig. 7). MRI is essential to assess the position of the
Fig. 7 Dandy–Walker malfor-mation. Axial US (a) obtainedat 30 weeks’ gestation, and axial(b) and sagittal (c) MR HASTET2-W images at 32 weeks showan increased cystic retrocerebel-lar space with a severelyhypoplastic cerebellum andhydrocephalus. Postnatalfollow-up sagittal T1-W(d) and T2-W (e) MR imagesdemonstrate abnormal cerebralwhite matter not seen on theprenatal MR examination
Fig. 6 Corpus callosum agene-sis and associated cortical dys-genesis. Sagittal (a), axial(b) and coronal (c) HASTET2-W images in a35-week-gestation fetusdemonstrate complete absenceof the corpus callosum andan abnormal gyral patternconsistent with diffuse corticaldysplasia (which was missedin the previous US exam)
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435 S427

cerebellar tentorium and cerebellar integrity. However,owing to the low spatial resolution of MRI, inferior vermianagenesis can be overlooked with both techniques [1].
Agenesis or hypoplasia of the cerebellar vermis inassociation with an enlarged posterior fossa, elevated tento-
rium, and cystic dilation of the fourth ventricle is diagnostic ofthe Dandy–Walker malformation (Fig. 8). Milder forms ofvermian hypoplasia with a more normal-appearing posteriorfossa have been referred to as the Dandy–Walker variant(Fig. 9), though the terms Dandy–Walker and Dandy–Walker
Fig. 8 Dandy–Walker variant.Sagittal (a) and axial(b) HASTE T2-W images ina 33-week-gestation fetusdemonstrate vermian hypoplasiaand normal posterior fossa size.The supratentorial structures arenormal (c)
S428 Pediatr Radiol (2009) 39 (Suppl 3):S422–S435

variant have at times been confused [8, 19]. Nevertheless, wehave to be aware that fetal cerebellar development is gradual,steady, and largely comparable to the development of thesupratentorial brain. Archicerebellar (flocculonodular lobe)and paleocerebellar (vermis) structures develop first, whereasthe neocerebellum (cerebellar hemispheres) develops slowly,and largely after birth [20, 21].
Despite the rapid progress in fetal imaging, prenataldiagnosis of posterior fossa dysgenesis remains challengingdue to both false-positive and false-negative diagnoses. In arecent study focused on fetuses with posterior fossaanomalies surviving pregnancy, fetal MRI showed limita-tions in both sensitivity and specificity when comparedwith postnatal MRI, with only 60% of prenatal diagnosesconfirmed postnatally [22]. Early gestational age at the timeof fetal MRI was a significant predictor of discrepancybetween the fetal and postnatal MRI posterior fossafindings (Figs. 10 and 11).
Malformations of cortical development
MRI confirms suspected pathology seen on US and helps todetermine the true extension and importance of the lesions.
One of the most valuable contributions of MRI, however, isits ability to assess normal brain gyration [5, 6]. Theoptimum time to perform the examination is between 30and 32 weeks’ gestation. If an earlier examination isperformed, it should be repeated after this gestational age.Different authors have shown a mean lag of 1.9–2.2 weeksin the appearance of sulci on fetal MR imaging comparedwith neuropathology data. The delay is likely due tolimitations of MR resolution. Sulcation has been observedto be delayed in twin gestations and to have some right-to-left asymmetry [9, 10, 23].
Fetal MR imaging has been reported to be superior toUS in identifying schizencephaly (Fig. 12), lissencephaly(Fig. 13), polymicrogyria, and grey matter heterotopias in astudy of 20 fetuses confirmed on either postnatal imagingor autopsy [23].
Complications of monochorionic twin pregnancies
Monochorionic twins share a common placenta that maycontain abnormal intertwin vascular connections. Theseabnormal vascular connections can result in abnormalities ofblood flow to the fetuses with resulting twin–twin transfusion
Fig. 10 Partial rhombencepha-losynapsis. Axial (a) and sagittal(b) HASTE T2-W images in a22-week-gestation fetus showmild ventriculomegaly and anabnormal cerebellar vermis.Follow-up MR imaging(c–e) performed at 31 weeksmore clearly depicts anabnormal inferior vermis andpersistent mild ventriculomegaly
Fig. 9 Cerebellar vermian hypoplasia. Sagittal (a) and axial (b) HASTE T2-W images in a 20-week-gestation fetus show a small inferior vermis.Note also the hypoplastic corpus callosum. The pregnancy was interrupted and Wolf–Hirschhorn (4p-) syndrome was eventually diagnosed
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435 S429

syndrome (TTTS), with a high morbidity and risk for cerebralischaemia in both twins. Another complication of monochor-ionic twinning is co-twin demise, with increased risk ofneurological impairment in the surviving co-twin (Fig. 14),perhaps because of resultant acute cerebral hypoperfusion orthromboembolic events [8, 24, 25].
Congenital infections
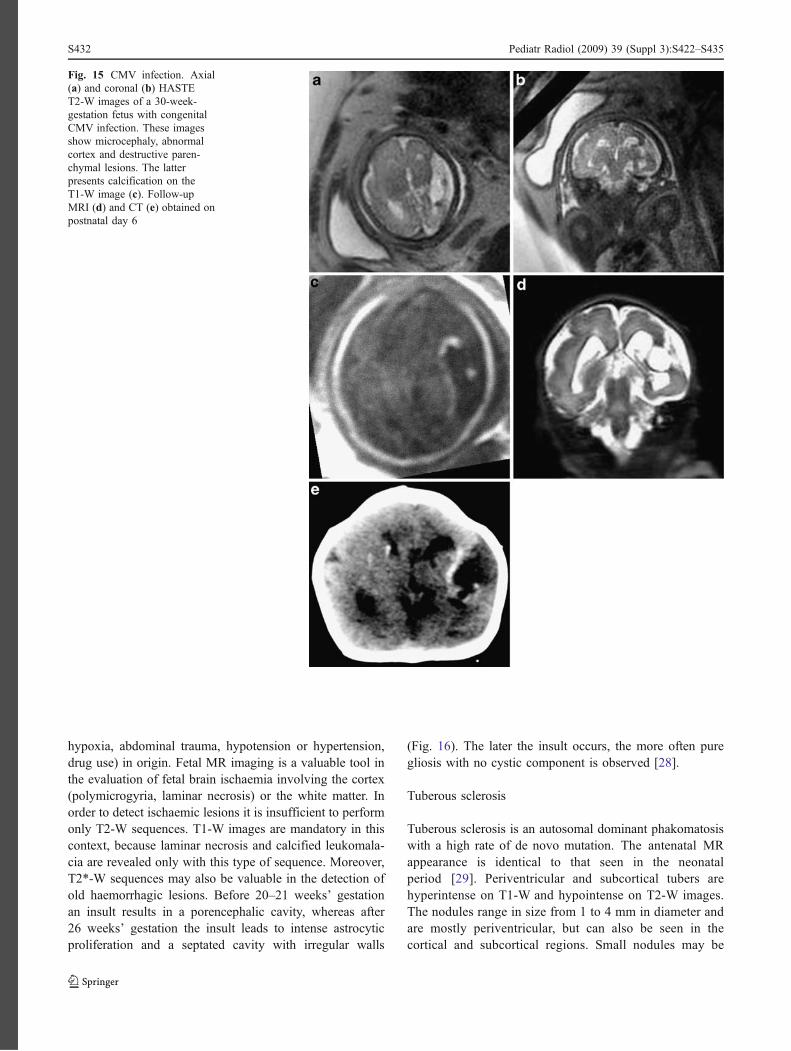
The most common cause of congenital viral infection iscytomegalovirus (CMV; Fig. 15). Other viruses that canalso affect the fetal brain include varicella zoster virus,parvovirus B19, rubella, and lymphocytic choriomeningitis
virus. The parasite Toxoplasma gondii can also result infetal brain abnormalities. Areas of chronic parenchymalinjury typically appear bright on T2-W images and can befocal or diffuse. Chronic injury can also manifest as volumeloss and ventricular enlargement [8, 26]. The mostfrequently reported cerebral lesions induced by CMVinclude ventricular dilatation, subependymal cysts, micro-cephaly and periventricular calcifications [27].
Ischaemic lesions
The causes of fetal ischemia can be placental, fetal(infection, anasarca), or maternal (hypovolaemic shock,
Fig. 11 Mega cisterna magna.Sagittal (a) and axial(b) HASTE T2-W images in a34-week-gestation fetus demon-strate a large cisterna magna.The vermis is identified and isnormal in size
S430 Pediatr Radiol (2009) 39 (Suppl 3):S422–S435

Fig. 13 Classic lissencephaly.Sagittal (a) and axial(b) HASTE T2-W images in a28-week-gestation fetus showminimal formation of theSylvian fissures consistent withclassic lissencephaly
Fig. 14 Monochorionic twin-ning with co-twin demise. Thesurviving fetus is also abnormalwith a left germinal matrix hae-morrhage seen on the coronal(a) and axial (b) HASTE T2-Wimages
Fig. 12 Schizencephaly. Sagittal (a), axial (b) and coronal HASTE T2-W images in a 31-week-gestation fetus demonstrate bilateral open-lipschizencephalic defects. The septum pellucidum is absent
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435 S431
hypoxia, abdominal trauma, hypotension or hypertension,drug use) in origin. Fetal MR imaging is a valuable tool inthe evaluation of fetal brain ischaemia involving the cortex(polymicrogyria, laminar necrosis) or the white matter. Inorder to detect ischaemic lesions it is insufficient to performonly T2-W sequences. T1-W images are mandatory in thiscontext, because laminar necrosis and calcified leukomala-cia are revealed only with this type of sequence. Moreover,T2*-W sequences may also be valuable in the detection ofold haemorrhagic lesions. Before 20–21 weeks’ gestationan insult results in a porencephalic cavity, whereas after26 weeks’ gestation the insult leads to intense astrocyticproliferation and a septated cavity with irregular walls
(Fig. 16). The later the insult occurs, the more often puregliosis with no cystic component is observed [28].
Tuberous sclerosis
Tuberous sclerosis is an autosomal dominant phakomatosiswith a high rate of de novo mutation. The antenatal MRappearance is identical to that seen in the neonatalperiod [29]. Periventricular and subcortical tubers arehyperintense on T1-W and hypointense on T2-W images.The nodules range in size from 1 to 4 mm in diameter andare mostly periventricular, but can also be seen in thecortical and subcortical regions. Small nodules may be
Fig. 15 CMV infection. Axial(a) and coronal (b) HASTET2-W images of a 30-week-gestation fetus with congenitalCMV infection. These imagesshow microcephaly, abnormalcortex and destructive paren-chymal lesions. The latterpresents calcification on theT1-W image (c). Follow-upMRI (d) and CT (e) obtained onpostnatal day 6
S432 Pediatr Radiol (2009) 39 (Suppl 3):S422–S435

Fig. 16 Ischaemic lesion. Sagittal (a) and axial (b) HASTE T2-Wimages of a 33-week-gestation fetus referred for further investigationof an US finding of ventriculomegaly. An irregular cavity was also
seen in the right periventricular area. c Axial GRE T2* image inanother 20-week-gestation fetus depicts periventricular haemorrhagewith intraventricular (choroid plexus) extension
Fig. 17 Tuberous sclerosis.Sagittal HASTE T2-W image(a) confirms a cardiac mass,consistent with rhabdomyoma,seen on a previous US in a35-week-gestation fetus. AxialHASTE T2-W image(b) also displays hypointensesubependymal nodules.Follow-up neonatal MRI,performed at 5 days of age,more clearly demonstrates manysubependymal and corticaltubers on T1-W (c) and T2-W(d) images
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435 S433

overlooked, even on MRI. US does not depict the tubers;fetuses are usually referred after cardiac rhabdomyoma isdiscovered. The incidence of tuberous sclerosis in fetusespresenting with cardiac tumour is very high (78–87.5%)and MRI is a valuable tool in demonstrating braininvolvement (Fig. 17).
Spinal anomalies
One of the more common fetal spinal anomalies detected byprenatal US is the myelomeningocoele, identified by theabsence of posterior elements of the vertebral bodies ataffected levels and extension of the subarachnoid spaceposteriorly through the bony spina bifida. Myelomeningo-coeles are almost always seen in combination with a ChiariII malformation [8]. Fetal MR imaging is also helpful whena bony spinal abnormality is detected on prenatal sonogra-phy, to rule out an underlying spinal cord anomaly such asdiastematomyelia (Fig. 18) [30].
Conclusion
In conclusion, US and MR imaging are complementarynon-invasive imaging methods in the evaluation of high-risk pregnancies. When a CNS anomaly is detected by US,MR imaging may demonstrate additional findings that mayalter patient counselling and case management. From theperspective of the critical decisions that often need to bemade, the important limitations of the techniques and theirinterpretation persist and need to be considered carefully.Correlation between fetal cerebral imaging (US and MRI)and fetal pathological data and postnatal imaging findingswill improve our knowledge and understanding of brainpathologies and will enable a more confident approach tomanagement of pregnancy and prenatal counselling.
Acknowledgments We thank Gemma Corsellas for her excellentfetal MRI technical assistance and Celine Cavallo for helping withEnglish manuscript preparation.
Fig. 18 Diastematomyelia.Sagittal HASTE T2-W image(a) of a 22-week-gestation fetusdemonstrates abnormalwidening with a septum divid-ing the spinal canal resulting intwo hemicords. Axial (b, c) MRimages better display thedivided spinal cord.Corresponding fetal autopsycoronal view depicts the cordmalformation (d)
S434 Pediatr Radiol (2009) 39 (Suppl 3):S422–S435

Conflicts of interest The authors have declared that there are noconflicts of interest.
References
1. Guibaud L (2009) Contribution of fetal cerebral MRI for diagnosisof structural anomalies. Prenat Diagn doi:10.1002/pd.2171
2. Raybaud C, Levrier O, Brunel H et al (2003) MR imaging of fetalbrain malformations. Childs Nerv Syst 19:455–470
3. Coakley FV, Glenn O, Qayyum A et al (2004) Fetal MRI:a developing technique for the developing patient. AJR 182:243–252
4. Glenn OA, Barkovich AJ (2006) Magnetic resonance imaging ofthe fetal brain and spine: an increasingly important tool in prenataldiagnosis. Part 1. AJNR 27:1604–1611
5. Levine D, Barnes PD, Madsen JR et al (1997) Fetal centralnervous system anomalies: MR imaging augments sonographicdiagnosis. Radiology 204:635–642
6. Simon EM, Goldstein RB, Coakley FV et al (2000) Fast MRimaging of fetal CNS anomalies in utero. AJNR 21:1688–1698
7. Coakley FV, Hricak H, Filly RA et al (1999) Complex fetaldisorders: effect of MR imaging on management—preliminaryclinical experience. Radiology 213:691–696
8. Glenn OA, Barkovich AJ (2006) Magnetic resonance imaging ofthe fetal brain and spine: an increasingly important tool in prenataldiagnosis. Part 2. AJNR 27:1807–1814
9. Garel C (2004) MRI of the fetal brain: normal development andcerebral pathologies. Springer, Berlin
10. Levine D, Barnes PD (1999) Cortical maturation in normal andabnormal fetuses as assessed with prenatal MR imaging. Radiol-ogy 210:751–758
11. Schneider JF, Confort-Gouny S, Le Fur et al (2007) Diffusion-weighted imaging in normal fetal brain maturation. Eur Radiol17:2422–2429
12. Garel C (2006) New advances in fetal MR neuroimaging. PediatrRadiol 36:621–625
13. Parazzini C, Righini A, Rustico M et al (2008) Prenatal magneticresonance imaging: brain normal linear biometric values below 24gestational weeks. Neuroradiology 50:877–883
14. Cardoza JD, Goldstein RB, Filly RA (1988) Exclusion of fetalventriculomegaly with a single measurement: the width of thelateral ventricular atrium. Radiology 169:711–714
15. Kazan-Tannus JF, Dialani V, Kataoka ML et al (2007) MRvolumetry of brain and CSF in fetuses referred for ventriculome-galy. AJR 189:145–151
16. Wagenvoort AM, Bekker MN, Go AT et al (2000) Ultrafast scanmagnetic resonance in prenatal diagnosis. Fetal Diagn Ther15:364–372
17. Goodyear PW, Bannister CM, Russell S et al (2000) Outcome inprenatally diagnosed fetal agenesis of the corpus callosum. FetalDiagn Ther 16:139–145
18. Glenn O, Goldstein R, Li K et al (2005) Fetal MRI in the evaluationof fetuses referred for sonographically suspected abnormalities ofthe corpus callosum. J Ultrasound Med 24:791–804
19. Klein O, Pierre-Kahn A, Boddaert N et al (2003) Dandy–Walkermalformation: prenatal diagnosis and prognosis. Childs Nerv Syst19:484–489
20. Adamsbaum C, Moutard ML, Andre C et al (2005) MRI of thefetal posterior fossa. Pediatr Neurol 35:124–140
21. Triulzi F, Parazzini C, Righini A (2006) Magnetic resonanceimaging of fetal cerebellar development. Cerebellum 5:199–205
22. Limperopoulos C, Robertson RL Jr, Khwaja OS et al (2008) Howaccurately does current fetal imaging identify posterior fossaanomalies? AJR 190:1637–1643
23. Sonigo PC, Rypens FF, Carteret M et al (1998) MR imaging offetal cerebral anomalies. Pediatr Radiol 28:212–222
24. Feldstein VA (2002) Understanding twin-twin transfusion syn-drome: role of Doppler ultrasound. Ultrasound Q 18:247–254
25. Haverkamp F, Lex C, Hanisch C et al (2001) Neurodevelopmentalrisks in twin–twin transfusion syndrome: preliminary findings.Eur J Paediatr Neurol 5:21–27
26. Barkovich AJ, Girard N (2003) Fetal brain infections. Childs NervSyst 19:501–507
27. Benoist G, Salomon LJ, Mohlo M et al (2008) Cytomegalovirus-related fetal brain lesions: comparison between targeted ultra-sound examination and magnetic resonance imaging. UltrasoundObstet Gynecol 32:900–905
28. Garel C, Delezoide AL, Elmaleh-Berges M et al (2004)Contribution of fetal MR imaging in the evaluation of cerebralischemic lesions. AJNR 25:1563–1568
29. Sonigo P, Elmaleh A, Fermont L et al (1996) Prenatal MRIdiagnosis of fetal cerebral tuberous sclerosis. Pediatr Radiol 26:1–4
30. von Koch CS, Glenn OA, Goldstein RB et al (2005) Fetalmagnetic resonance imaging enhances detection of spinal cordanomalies in patients with sonographically detected bony anoma-lies of the spine. J Ultrasound Med 24:781–789
Pediatr Radiol (2009) 39 (Suppl 3):S422–S435 S435





























