Embed Size (px)
Citation preview

Community-base
d Pr
ojec
ts
Report Series
Family Holistic Health Community Promotion Project
Best Science • Best Practice最好的科學‧最好的實踐
Evidence-based & Evidence generating實証為本‧提証為人
Positive Psychology正向心理學
FAMILY Health, Happiness and Harmony - 3Hs 家庭健康、快樂、和諧 - 家有康和樂
TABLE OF CONTENTS Preface (1)….…. ................................................................................................................... 1
Preface (2).……. ................................................................................................................... 2
Preface (3).....…. ................................................................................................................... 3
FAMILY: A Jockey Club Initiative for a Harmonious Society .................................................. 4
Executive summary ............................................................................................................... 8
CHAPTER 1 Introduction ............................................................................................. 10
1.1 Background ...................................................................................................... 10
1.2 Project objectives ............................................................................................. 11
1.3 Project hypotheses ........................................................................................... 11
1.4 Literature review ............................................................................................... 11
CHAPTER 2 Project design and methods .................................................................. 17
2.1 Project design .................................................................................................. 17
2.2 Cluster randomised controlled trial design ........................................................ 19
2.3 Data analysis.................................................................................................... 28
CHAPTER 3 Public education event ........................................................................... 29
3.1 Objectives ........................................................................................................ 29
3.2 Event summary ................................................................................................ 29
CHAPTER 4 Opening Ceremony ................................................................................. 30
4.1 Objectives ........................................................................................................ 30
4.2 Ceremony summary ......................................................................................... 30
4.3 Statistical analyses and results ........................................................................ 31
4.4 Discussion ........................................................................................................ 37
4.5 Conclusions ..................................................................................................... 37
CHAPTER 5 Train-the-Ambassador Programme ....................................................... 39
5.1 Introduction ...................................................................................................... 39
5.2 Objectives ........................................................................................................ 39
5.3 Recruitment ...................................................................................................... 39
5.4 Design .............................................................................................................. 40
5.5 Training content ............................................................................................... 42
5.6 Evaluation ........................................................................................................ 44
5.7 Quantitative evaluation ..................................................................................... 46
5.8 Qualitative evaluation ....................................................................................... 79
5.9 Discussion and conclusion ............................................................................... 96
CHAPTER 6 Community-based programme .............................................................. 98
6.1 Introduction ...................................................................................................... 98
6.2 Community-based programme study design .................................................... 98
6.3 Recruitment and retention .............................................................................. 104
6.4 Community-based programme process evaluation ......................................... 114
6.5 Quantitative evaluation: statistical analysis and results .................................. 123
6.6 Qualitative evaluation: community-based programme focus groups ............... 148
CHAPTER 7 Sharing Session cum Awards Ceremony ............................................ 170
7.1 Objectives ...................................................................................................... 170
7.2 Ceremony summary ....................................................................................... 170
7.3 Statistical analyses and results ...................................................................... 171
7.4 Discussion ...................................................................................................... 176
7.5 Conclusions ................................................................................................... 177
CHAPTER 8 Results Sharing Session ...................................................................... 178
8.1 Objectives ...................................................................................................... 178
8.2 Session summary ........................................................................................... 178
CHAPTER 9 Project evaluation ................................................................................. 180
9.1 Qualitative evaluation: in-depth interviews ...................................................... 180
CHAPTER 10 Project summary, discussion and conclusion .................................... 245
10.1 Project summary and discussion .................................................................... 245
10.2 Strengths and limitations ................................................................................ 247
10.3 Implications and suggestions for future planning ............................................ 249
Acknowledgements ........................................................................................................... 251
References……. ............................................................................................................... 252
Appendices……. ............................................................................................................... 258

PROJECT TEAM Project Title: Family Holistic Health Community Promotion Project
Funder: The Hong Kong Jockey Club Charities Trust
Organisers: Hong Kong Island Women’s Association in collaboration with School of Public Health of The University of Hong Kong Project Consultants: Professor LAM Tai Hing, Sir Robert Kotewall Professor in Public Health Chair Professor of Community Medicine, School of Public Health, The University of Hong Kong; Principal Investigator, FAMILY Project Ms. CHEUNG Carol, Chair, Hong Kong Island Women’s Association Ms. CHAN Kally, Secretary-General, Hong Kong Island Women’s Association
Project Working Group (Hong Kong Island Women’s Association): Ms. HE Qinqin, Piana, Director-General (Secretariat Office) Ms. SUEN Hoiha, Secretary (Secretariat Office)
Project Working Group (FAMILY Project): Ms. WAN Ngai Teck, Alice, Project Administrator Dr. LAI Yuen Kwan, Agnes, Research Officer Dr. NG Yin Lam, Danice, Post-Doctoral Fellow (till Oct 10, 2015) Ms. LAU Chieh Grace, Team Coordinator Ms. LEE Letitia, Research Assistant Ms. LEUNG Ho Ting, Sally, Research Assistant (till Dec 23, 2016) Ms. SUN Yangbo, Viola, Research Assistant (till Mar 31, 2016) Ms. ZHOU Jingwen, Research Assistant (till Aug 31, 2016)
Participating Units: Carnation Women’s Association Chaiwan Women’s Association Hong Kong Central and Western District Women’s Association Hong Kong Southern District Women’s Association Kellett Bay Women’s Association Kin Ngai Society Shek O Woman’s Association Limited South Horizons Women’s Association Wah Fu Estate Women’s Association Wan Chai Yin Ngai Society Women Gather Association Women’s Department of Causeway Bay Association Limited Women’s Department of Hong Kong Soong Ching Ling Goldkey Training Foundation Limited Women’s Department of Shau Kei Wan & Chai Wan Community
Women’s Department of the Hong Kong Executive Administrative & Clerical Staff Association
Women’s Department of the Hong Kong Wan Chai District Association Limited Women’s Department of Wan Chai District Arts, Cultural, Recreational and Sports
Association Limited
FAMILY Project Team, School of Public Health, The University of Hong Kong: Principal Investigator (Family Holistic Health Community Promotion Project): Professor LAM Tai Hing, Sir Robert Kotewall Professor in Public Health; Chair Professor of Community Medicine, School of Public Health, The University of Hong Kong; Principal Investigator, FAMILY Project
Co-Investigators (Family Holistic Health Community Promotion Project): Dr. LAI Yuen Kwan, Agnes Ms. SUN Yangbo, Viola (till Mar 31, 2016) Project Administrator: Ms. WAN Ngai Teck, Alice Research Officer: Dr. FABRIZIO Cecilia (till Aug 31, 2015)
Post-Doctoral Fellows: Dr. CHU Ting Wai, Joanna (till Jun 30, 2016) Dr. HO Chun Yip, Henry (till Jul 31, 2017) Dr. LEE Ka Yiu, Kyle (till Sep 17, 2015) Dr. NG Yin Lam, Danice (till Oct 10, 2015) Dr. SHEN Chen
Team Coordinators: Ms. LAU Chieh Grace Ms. YUEN Cheuk Yam, Edith (till Mar 4, 2015) Senior Research Assistant: Ms. WANG Xin (till Jul 3, 2015) Research Assistants: Ms. CHAN Yan Tung, Jamie Mr. CHENG Ka Man Ms. CHAN Ka Ying (till Mar 2, 2017) Ms. DENG Yuanjie, Sasha (till Feb 28, 2017) Ms. HO I Tong, Hermia (till Apr 7, 2016) Mr. KING Chie Yung, Jackie Ms. KWOK Cheuk Ting, Joanna (till Aug 3, 2015) Ms. LEE Letitia Ms. LEUNG Ho Ting, Sally (till Dec 23, 2016) Ms. MA Ke Ms. NG Yuen Kiu Ms. SUEN Man Tung, Michelle Mr. YAU Yue Chi (till Aug 13, 2016) Ms. ZHOU Jingwen (till Aug 31, 2016) Ms. ZHOU Yi (till Sep 1, 2017)
1
PREFACE (1) Joining our community partners to build a harmonious society
Demographic shifts, economic upheavals and changing societal norms and values are steadily creating new processes and relationships within families, as is immigration across borders. As a result, family structure in society is becoming more complex and diverse, creating many areas of discord in family life.
To address these evolving challenges, The Hong Kong Jockey Club Charities Trust earmarked funding of HK$250 million in 2007 to launch a citywide project titled “FAMILY: A Jockey Club Initiative for a Harmonious Society” (the FAMILY Project), in collaboration with the School of Public Health of The University of Hong Kong. Approaching the issue from a public health perspective, the project is aimed at devising suitable preventive measures and strengthening the message of FAMILY Health, Happiness and Harmony (“the FAMILY 3Hs”) for better holistic family health.
Over the past ten years, a wide range of community partners have come together to implement more than 20 community-based intervention programmes under the FAMILY Project. At the same time, diversified, interactive capacity training workshops have been organised for social service practitioners to help them promote the FAMILY 3Hs and holistic FAMILY health more effectively. Altogether, the FAMILY Project has directly benefited over 350,000 members of the public.
In addition, we have published a series of practice manuals and project reports to share the valuable data and experiences collected for the FAMILY Project from household surveys and community-based programmes. These serve as useful resources for policy makers and social service providers to help foster a more harmonious community.
The Family Holistic Health Community Promotion was successfully implemented in 2015 in collaboration with the Hong Kong Island Women’s Association (HKIWA). More than 1,200 participants participated in this meaningful project, which was aimed at building participants’ commitment to physical activity and a healthy diet. The project also encouraged mutual support amongst participants and their family members in achieving healthy living habits. Through this report, we hope to demonstrate that simple interventions with the involvement of the primary carer of a family can be effective in improving individual and family well-being.
On behalf of The Hong Kong Jockey Club Charities Trust, I would like to express my deepest gratitude to the FAMILY Project Team of the School of Public Health of The University of Hong Kong, HKIWA, as well as their member organizations and other collaborating parties involved in the project. It is our partners’ incredible support that has made the project such a success, and is helping to spread the FAMILY 3Hs and FAMILY holistic health messages to everyone in the community.
Mr. Leong CHEUNG Executive Director, Charities and Community, The Hong Kong Jockey Club

2
PREFACE (2) As the saying goes “happiness lies, first of all, in health”, which means health is the cornerstone of harmonious society. As one of the charity organizations in Hong Kong, Hong Kong Island Women’s Association (HKIWA) not only cares about women’s affairs, but also the construction of a harmonious society. It thus treats helping citizens to stay healthy as its own responsibility.
With the full support of The Hong Kong Jockey Club Charities Trust, we were very honored to have the opportunity to collaborate with the School of Public Health, The University of Hong Kong to hold the Family Holistic Health Community Promotion Project (one of the projects of “FAMILY: A Jockey Club Initiative for a Harmonious Society”) and promote FAMILY Health, Happiness and Harmony (3Hs) on Hong Kong Island.
During January 2016 to December 2016, we formed eight working groups to track participants’ physical activity behaviours, healthy diet behaviours and fitness through workshops, follow-up meetings, and telephone interviews. The data were given to the School of Public Health, The University of Hong Kong for analysis. The research approach of this project is regarded as the perfect combination of practice and academic research.
The Family Holistic Health Community Promotion Project aims at promoting the ideas of doing more exercise and having low sugar diet, thereby helping citizens to keep fit and stay healthy. During the implementation of this project, we held 38 activities, with an attendance count of more than 12,000 over the course of the project. It was one of the most influential and meaningful projects for us.
On behalf of Hong Kong Island Women’s Association, I would like to express my sincere thanks to The Hong Kong Jockey Club Charities Trust and the School of Public Health, The University of Hong Kong. Although the Family Holistic Health Community Promotion Project has come to an end, we hope our citizens can still keep fit, stay healthy, and bring the positive attitude toward healthy lifestyle to their friends and family.
Ms. Carol CHEUNG, MH Chair, Hong Kong Island Women’s Association
3
PREFACE (3) We are most grateful to The Hong Kong Jockey Club Charities Trust which initiated and donated HK$250 million to fund and launch a citywide project entitled “FAMILY: A Jockey Club Initiative for a Harmonious Society”, in collaboration with the School of Public Health of The University of Hong Kong (HKU-SPH). Since 2008, the FAMILY Project Team has successfully completed many community-based and public education projects to develop brief and cost-effective preventive measures to promote FAMILY Health, Happiness and Harmony (3Hs).
In view of growing health challenges locally and globally to increase physical activity in the population, the current phase of FAMILY Project focused on Family Holistic Health. We have designed a simple approach, namely “Zero-time Exercise” which are simple movements and stretching that can be done anytime, anywhere, and by anybody, that do not require extra time (hence zero time), money or equipment.
The Family Holistic Health Community Promotion Project, led by the Hong Kong Island Women’s Association (HKIWA), in collaboration with the FAMILY Project Team, is one of the major intervention projects under FAMILY Project. This project gathered the power, experiences and networks of community leaders from the HKIWA firstly to support the Train-the-Ambassador (volunteers) Programme. These Health Ambassadors then went on to recruit and engage participants for the project’s community-based programme, which encouraged healthy lifestyles involving physical activity (Zero-time Exercise) and a healthy diet (reduce sugar intake). The Family Holistic Health Community Promotion Project has been completed with great success and its benefits have been extended from service workers to the participants and their families. I wish that this report can be shared with community partners and other stakeholders, and the messages and strategies using Zero-time Exercise and reducing sugary drinks to promote healthy lifestyle can be spread across the territory.
On behalf of the FAMILY Project Team, I express my sincerest gratitude to HKIWA, their member organisations and other collaborating parties for their professionalism, commitment and hard work. We are particularly grateful to the Ambassadors and other volunteers who had gone through the Train-the-Ambassador Programme and contributed a lot to the project.
Professor LAM Tai Hing Principal Investigator, FAMILY: A Jockey Club Initiative for a Harmonious Society Sir Robert Kotewall Professor in Public Health Chair Professor of Community Medicine, School of Public Health, The University of Hong Kong
4
FAMILY: A JOCKEY CLUB INITIATIVE FOR A HARMONIOUS SOCIETY
Background To help build a more harmonious society, The Hong Kong Jockey Club Charities Trust invited the School of Public Health, Li Ka Shing Faculty of Medicine, The University of Hong Kong (HKU) to collaboratively launch a project entitled FAMILY: A Jockey Club Initiative for a Harmonious Society (“FAMILY Project”) with funding of HK$250 million. The project aims to identify the sources of family problems, to devise, implement and evaluate preventive measures, and to promote FAMILY Health, Happiness and Harmony (3Hs) through a territory-wide household survey, intervention projects and public education.
The project The project comprises three components:
1. Social barometer
a) Territory-wide Household Survey
The FAMILY Cohort, a population-based cohort study focusing on the family as a unit, was carried out from 2007 to 2014. It aimed to identify the source of domestic problems and derive preventive responses that are complementary, wide-reaching, pervasive and cost-effective. Survey findings can provide useful information to relevant organisations for the planning of future programmes and initiatives.
5
b) Hong Kong Family and Health Information Trends Survey (HK-FHInTS)
During 2009 to 2017, the FAMILY Project Team has conducted one Hong Kong population cross-sectional telephone survey almost every year to assess changes in family and health information seeking behaviours among the general public and the impact of the Project’s programmes in promoting FAMILY 3Hs. Six surveys were completed in 2009, 2010, 2012, 2013, 2016 and 2017 respectively, with extensive media coverage which have helped raise public awareness of FAMILY 3Hs messages.
2. Intervention and community-based programmes
The FAMILY Project Team has been working closely with government departments and numerous social service and related organisations to develop and implement interventions to strengthen family relationships across generations throughout Hong Kong. These include intervention projects to enhance family and parent-child relationships; school-based projects to spread FAMILY 3Hs to hundreds of schools; and community-based projects with Social Welfare Department, Department of Health and various NGOs to promote 3Hs to entire district and the community. The study methods and results of these projects have been shared with the government, NGOs and community service workers and the general public.
The seven intervention projects were:
H.O.P.E. (Hope Oriented Parents Education for Families in Hong Kong) Project
Harmony @ Home Project
Effective Parenting Programme
Happy Transition to Primary One
Share the Care, Share the Joy
Boosting Positive Energy Programme
Be Healthy, So Easy: FAMILY Education Project
The four school-based intervention programmes were:
FAMILY Goes Green
3Hs Family Drama Project
3Hs Family Drama Project II: Family Interactive Drama with Exercise and Fun
More Appreciation and Less Criticism Project
6
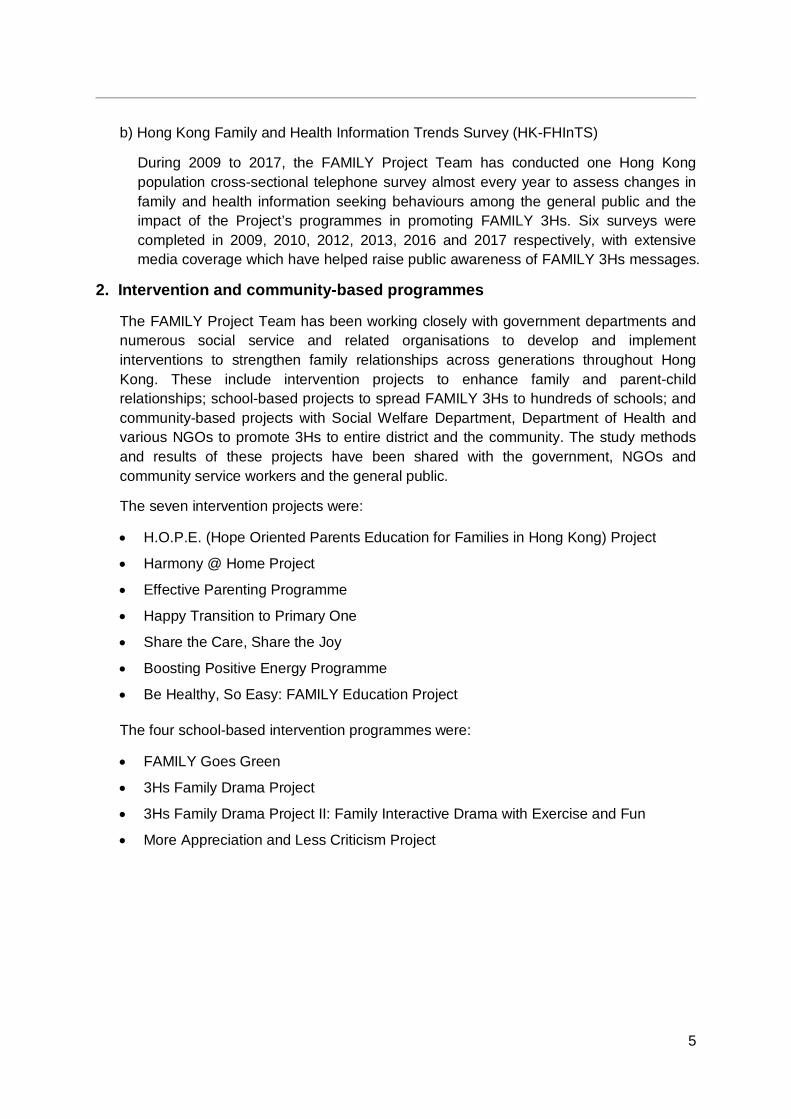
The eight community-based engagement projects were:
Happy Family Kitchen I & II Projects
Learning Families Project
Enhancing Family Well-being Project
Happy Family Kitchen Movement Project
Community Health Campaign: Fitter Families Project
Holistic Health Family Project
Family Holistic Health Community Promotion Project
All of the project interventions were designed using a public health framework, so they were brief, preventive, cost-effective, and targeted a large number of people at the same time. The community-science partnership between academia, government departments and NGOs also ensured that the projects were developed by practitioners who understood the needs of the Hong Kong people, delivered by key community stakeholders, and conducted with scientific rigour to generate evidence for future social health programmes and policies.
3. Health communication and public education
Apart from engaging different community stakeholders in various intervention projects, the key messages of the FAMILY Project were spread far and wide into the community to promote positive family values and harmonious relationships. FAMILY Health, Happiness and Harmony (3Hs) and FAMILY
Holistic Health messages have been disseminated to the general public through various channels to raise public awareness and create a positive environment for family participation. These have been complemented by community-based projects and community-wide events to promote FAMILY 3Hs all around Hong Kong.
7
Train-the-Trainer and Ambassador Programmes
From April 2015 to January 2017, a number of Train-the-Trainer and Ambassador workshops have been organised to train community leaders, teachers, social service workers and volunteers as Health Ambassadors, or health role models so that they can enjoy the benefits, then promote the benefits to others. Trained Health Ambassadors have helped with the implementation of community-based programmes, led simple physical activities to targeted audiences and promoted knowledge of healthy living to participants and the community.
Health promotion events
The FAMILY Project Team has actively co-organised and participated in various community events with social service units and community organisations, with the aim of promoting FAMILY 3Hs messages by means of exhibitions, game booths and talks, etc.
Updated in November 2017
8
EXECUTIVE SUMMARY The Family Holistic Health Community Promotion Project (FHHCPP) was implemented by the Hong Kong Island Women’s Association (HKIWA) in collaboration with the School of Public Health, The University of Hong Kong (HKU-SPH) during January 2016 to December 2016. The project adopted physical activity (多動) and healthy diet (識食) as platforms and main principles to target unhealthy diet (by reducing dietary sugar intake) and physical inactivity (through Zero-time Exercise (ZTEx), and improve the participants’ FAMILY Health, Happiness and Harmony (3Hs).
Participating member associations of the HKIWA formed eight clusters that were randomised using computerised number generation into eight study groups in a cluster randomised controlled trial (cRCT). Each study group utilised a different combination of intervention components, including:
1. Either the Healthy Diet (HD) or the Physical Activity (PA) core and booster intervention programmes;
2. The formation of social chat groups for volunteers (Health Ambassadors) on WhatsApp (an instant messaging platform); and
3. The use of reminders such as bring-home tools like a table mat with healthy diet information or a handgrip, and e-message reminders sent through WhatsApp.
The project harnessed the power and connection of community leaders to recruit and provide training to volunteers (or Health Ambassadors) in the project’s Train-the-Ambassador Programme (TTA) workshops. The Health Ambassadors went on to recruit and engage participants in the project’s community-based programmes, promoting the FAMILY 3Hs and encouraging healthy lifestyles involving physical activity and healthy diets. In the TTA, a core session (2 hours and 15 minutes) and two booster sessions (2 hours each) were held in January to February 2016 for 138 Health Ambassadors. Data were collected from the Health Ambassadors pre-intervention, immediately after the first session, before and immediately after the second session at 1 month, 3 months, 4 months, 6 months, 9 months, and 12 months. The TTA workshops benefited the ambassadors and their families and enhanced the Health Ambassadors’ competence and performance in designing and implementing the community-based intervention programmes.
The family intervention programme began in April 2016. A total of eight core sessions (2 to 2.5 hours each) consisting of interactive talks on either healthy diet or physical activity according to the group as allocated were delivered by interventionists from the FAMILY Project Team, and 1,256 individuals attended. Eight booster sessions (5.5 to 8 hours each) were designed and implemented by the Health Ambassadors, and 1,150 individuals attended. The booster sessions took the form of day trips and the Health Ambassadors were required to include at least 24 to 30 minutes on activities related to healthy diet or physical activity accordingly during the day. Data were collected through self-administered questionnaires pre-intervention, immediately after the core sessions, and before and immediately after the booster sessions at 1 month. The Health Ambassadors then conducted two batches of telephone follow-up interviews on the community-based participants at 3 months and 6 months.
9
In the community-based programmes, both the HD groups and the PA groups showed significant increases in the frequency of performing ZTEx for the hands, legs, and balance. Both the HD groups and the PA groups also showed significant increases in the frequency of having healthy diet- and physical activity-related interactions with their family members over the 6-month study period. Moreover, in comparison with the PA groups, the HD groups showed greater increases in encouraging their family members to choose low-sugar beverage or food options as well as in making low-sugar choices together with their family members at 3 months and 6 months. Both the HD groups and the PA groups showed significant increases in self-reported personal health and happiness, and self-reported FAMILY health, happiness, and harmony. Compared with the PA groups, the HD groups showed a significantly greater increase in self-reported FAMILY health at 1 month after the core sessions. The participants rated the project activities and events highly and indicated that they felt the content was applicable to their daily lives.
The positive outcomes of this project show that people can be motivated to adopt and encourage health-promoting changes for themselves and others. The TTA offers a practical example of a capacity-building training programme, with the Health Ambassadors successfully volunteering their efforts and facilitating the enhancement of the community-based participants’ health awareness and behaviours. Community organisations like the HKIWA and its affiliated member organisations have the commitment and capacity to develop and implement effective large but brief family health intervention projects in collaboration with academics. In the future, other similar non-governmental organisations or community groups can also be empowered to integrate scientific practices into their programmes and policies, and mobilised to promote healthy lifestyles for individuals and their families, building a healthier, happier, and more harmonious society.
10
CHAPTER 1 INTRODUCTION
1.1 Background The 2011 United Nations Political Declaration on the Prevention and Control of Non-communicable Diseases (NCDs) highlighted that NCDs, also known as chronic diseases, are a major cause of global death [1]. NCDs include cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes, amongst other diseases [2]. According to the World Health Organization (WHO) [2], 38 million people die each year as a result of NCDs. The United Nations General Assembly [1] and the WHO [2] recognise four main modifiable risk factors of NCDs: lack of physical activity, unhealthy diet, tobacco use, and harmful use of alcohol. Overweight and obesity, mainly due to physical inactivity and unhealthy diet, also cause NCDs [3, 4]. Globally, the prevalence of obesity has more than doubled since 1980 [4]. Overweight and obesity are linked to more deaths than underweight, and as a result of overweight or obesity, 2.8 million people die each year [3, 4]. In 2014, 39% of adults aged 18 years or over were overweight and 13% were obese [4].
In Hong Kong, 38.8% of Chinese adults aged 18 to 64 are overweight or obese, with a body mass index (BMI) of 23 or above [5]. Over half (55.9%) of the local population is not sufficiently physically active and do not meet the WHO’s recommendations for physical activity [6]. Less than one-quarter (20.5%) have a healthy diet complying with the WHO’s recommendations [7].
One way in which the prevalence of NCDs may be reduced is to reduce the common modifiable risk factors such as insufficient physical activity and unhealthy diet [2]. Thus, Beaglehole et al. [8] suggested four cost-effective population-wide immediate priority interventions in “Priority actions for the non-communicable disease crisis”: the promotion of healthy diets and physical activity, salt reduction, accelerated tobacco control, and the reduction of harmful alcohol consumption.
The current project, the Family Holistic Health Community Promotion Project (FHHCPP) (愛家睦鄰好: 多動 • 識食 • Go!), was part of a larger umbrella project, “FAMILY: A Jockey Club Initiative for a Harmonious Society” (the “FAMILY Project”), which aimed to enhance FAMILY Health, Happiness and Harmony (3Hs) in Hong Kong through a series of interventions. The FHHCPP was launched in collaboration with the Hong Kong Island Women’s Association (HKIWA) and targeted overweight and obesity, physical inactivity, and unhealthy diet through the promotion of healthy diet and physical activity using brief community-based interventions for simple behavioural changes in participants during January 2016 to December 2016. Participants were encouraged to reduce their intake of sugary beverages and food, and to practise “Zero-time Exercise” (ZTEx) (exercises that do not require extra time, money or equipment (3 Zeros), are enjoyable, easy and effective (3Es), and can be performed anywhere, at any time and by anyone (3As)). Using physical activity and healthy diets as platforms and the main principles, the FHHCPP sought to improve the FAMILY 3Hs.

11
1.2 Project objectives The current project had four main objectives:
1. To examine the effectiveness of physical activity and healthy diet interventions for the promotion of FAMILY 3Hs, physical activity behaviours, and healthy diet behaviours;
2. To enhance the participants’ physical activity, healthy diet behaviours, and holistic health;
3. To encourage mutual support among participants and their family members in working towards achieving healthy living habits; and
4. To examine the physical fitness and FAMILY 3Hs of the participants.
1.3 Project hypotheses The intervention programmes were hypothesised to:
1. Encourage and sustain physical activity and healthy diet behaviours; 2. Improve FAMILY 3Hs; and 3. Promote physical fitness and health.
1.4 Literature review Socioeconomic changes have resulted in the rapid increase of risk factors for NCDs, such as physical inactivity and unhealthy diets, contributing to the widespread rise in the prevalence of overweight and obesity [3, 8-10]. In Hong Kong, 38.8% of adults aged 18 to 64 years are overweight or obese, defined by a BMI of 23 or above [5]. Given the high proportion of overweight or obese individuals in Hong Kong, achieving even modest behavioural changes for individuals in the population could potentially lead to significant improvements in public health.
1.4.1 Physical activity Physical activity is defined as “any bodily movement produced by skeletal muscles that requires energy expenditure,” and is not to be mistaken with exercise, a subcategory of physical activity that is “planned, structured, repetitive, and purposeful in the sense that the improvement or maintenance of one or more components of physical fitness is the objective” [11].
The health benefits of physical activity are well-established: in adults, sufficient physical activity can reduce the risk of NCDs, depression, and falls; improve bone and functional health; and is a key factor to energy balancing and weight control [12]. Nevertheless, physical inactivity is common in Hong Kong, with over half the local population being insufficiently physically active [6].
The promotion of physical activity has been recommended as a cost-effective priority intervention [8]. In Hong Kong, the Leisure and Cultural Services Department has jointly launched the “Healthy Exercise for All Campaign” with the Department of Health [13]. Although the campaign encourages public interest in exercise and the incorporation of
12
exercise into daily routine, it does not appear to directly address the major barriers to physical activity, such as lack of time or time constraints due to study or work commitments, finding exercise boring or not finding exercise enjoyable, and lacking confidence in one’s ability to be physically active or having low self-efficacy [14-19].
In a review of past interventions attempting to increase physical activity, Kahn et al. [20] noted that informational interventions are effective; cognitive behavioural strategies are also effective if they provide specific and realistic goals [21]. Moreover, when adopting behavioural change, self-monitoring is important in addition to scheduled follow-up sessions in group-based interventions [21].
1.4.2 Healthy diet The health benefits of a healthy diet have also been well-established; for instance, an adequate consumption of fruit and vegetables can reduce the risks for cardiovascular diseases, and various cancers [3]; whilst a reduction in sugar consumption can lower body weight [22].
Nevertheless, 14 million deaths, or 40% of all deaths, per year may be attributed to the consumption of foods high in saturated or industrially produced sugar, salt, and trans fats [8]. Research shows that compared with children with a low intake of sugar-sweetened beverages, children with the highest intakes of these beverages are more likely to be overweight or obese [22]. Since underlying influences of risk factors of NCDs are overweight and obesity, they are thus also more susceptible to the risks of NCDs [3, 4]. However, despite the WHO recommendations to limit the consumption of sugar-sweetened beverages, sales of such beverages are increasing worldwide [23], and the Centre for Food Safety [24] in Hong Kong has shown that carbonated drinks and fruit juices, beverages that are frequently sugar-sweetened, are popular amongst residents.
The promotion of healthy diets has been recommended as a cost-effective priority intervention [8]. In Hong Kong, an International Advisory Panel on Reduction of Salt and Sugar was established in 2014 to offer advice on the reduction of salt and sugar intake by the local population in Hong Kong, and on the promotion and public education strategy to be taken [25]. The Centre for Food Safety is also making efforts to promote healthy diets by implementing a nutrition labelling scheme. Effective interventions promoting healthy dietary habits or targeting chronic NCDs are often multi-component programmes linked with community stakeholders such as community organisations, and may involve the family and provide individual behaviour change strategies and self-monitoring; such interventions are supported by targeted information delivered by trained professionals [26].
1.4.3 Family-based interventions The maintenance of weight loss through diet or physical activity is difficult unless individuals have support [27-30]. In fact, one major barrier that is cited for not adopting more physically active lifestyles is the lack of encouragement, support, or companionship from family and friends [15, 17, 18]. Gruber and Haldeman [27] suggested that the social context most likely to support making healthy behaviour changes, through the establishment of supportive social and interpersonal context, is the family. Dietary and physical activity behaviours are both well-suited as targets of family-based interventions as meals and recreational physical
13
activities may and often involve the entire family [27]. It is argued that to combat childhood obesity, a family environment promoting healthy behaviours and habits is crucial; this includes parents being informed regarding healthy diets and adopting physically active lifestyles [27, 31-33].
With this in mind, it is unsurprising that family-based interventions are associated with weight loss in overweight or obese children and parents [34]. Epstein et al. [35] reported that weight loss is more successfully achieved and maintained when there is family involvement. Berry et al. [36] reviewed studies on family-based interventions designed to treat childhood obesity using nutrition education and exercise, and found that behavioural modification interventions can be successful in improving weight loss outcomes for both the parents and the children. Magarey et al. [37] have also found that programmes that specifically target parents as the agents of change for the implementation of family lifestyle changes can achieve a relative weight loss of -10% in moderately obese pre-adolescent children that can be maintained for 2 years.
A further advantage of a family-based approach is the unique cost-effective platform it presents for effective obesity interventions [34].
1.4.4 Mobile reminders Information and Communication Technologies (ICTs) refer to a cluster of technologies that are used to share, distribute, gather, and communicate information, and underpin modern digital culture. ICTs encompass hardware that is often Internet-capable such as computers, smartphones, and tablets, as well as the software and applications, such as e-mail, social media sites, and video conferencing, which are used on these devices [38-43].
The Digital Revolution has seen a dramatic rise in the use of ICTs in the last few decades. For instance, according to The World Bank [44], whereas there were only 0.45 Internet users per 100 people in 1994, there were 14.2 Internet users per 100 people in 2004, and by 2014, there were 40.7 Internet users per 100 people. Similarly, the number of fixed broadband subscriptions per 100 people has more than tripled in the last decade [44]. The Internet and other ICT tools that we use in conjunction, such as smartphones, are becoming ubiquitous and pervasive features of this Information Age. Mobile phones in particular have become an increasingly important and well-placed platform for the delivery of health interventions [45].
One of the biggest challenges that face-to-face intervention programmes face is diminished reach and impact due to barriers to accessibility and cost-efficiency [46, 47]. Mobile phones are well-placed to facilitate access to intervention content from a large variety of settings at all times, bringing the intervention to the participants at times convenient to them without active effort on the individual’s part, diminishing the influence of situational constraints [45, 48-50]. Evidence suggests that ICTs such as mobile phones may enable access to high quality information and support across demographics [51, 52]. Moreover, as many software or applications used in conjunction with ICT devices such as mobile phones are freely accessible, intervention materials delivered in this way may be more readily disseminated than through traditional face-to-face interventions [53], offering a cost-effective way to widen access to health interventions and improve support for individuals [54].
14
A common way in which mobile technology is being used for health interventions is to send individuals informational messages or reminders that are relevant to the targeted health behaviours. It has been demonstrated that such frequent or regular reminders may be helpful in improving people’s health behaviours. Ramachandran et al. [55] reported that a mobile phone messaging intervention, wherein participants received frequent mobile phone messages, was an effective method to deliver advice and support aimed at lifestyle changes to prevent type 2 diabetes. Hurling et al. [56] demonstrated that a physical activity programme with mobile phone and email reminders was effective, with their test group reporting a significantly greater increase than the control group for perceived control and intention to exercise, as well as a greater body fat percentage loss than the control group. Parker and Ellis’s [57] findings also support the use of electronic messages to increase physical activity. Haines et al. [58] also demonstrated that a walking program, supplemented by a computer programme and weekly emails had a moderate effect on improving participants’ fitness, mood, health, awareness, and nutrition.
1.4.5 Public health approach Whereas the medical model or clinical approach often focuses on single individuals with an emphasis on disease diagnosis and treatment, the public health approach addresses health issues at the local or national level and is concerned with disease prevention and health promotion for whole communities [59, 60]. Thus, public health interventions are often community- or population-based, seeking to have the maximum benefit for the largest population [59]. Although such a mass approach may only offer a small benefit to each single individual, the mass gain can be unexpectedly large [61]; an intervention with wide penetration can lead to powerful impact even when effect sizes are small [48].
1.4.6 Community-based participatory research Community-based participatory research (CBPR) is an approach that combines research methods and community capacity-building strategies to bridge the gap between knowledge produced through research and translation of this research into interventions and policies [62, 63]. Community-based participatory research is defined as:
“A collaborative approach to research that equitably involves all partners in the research process and recognises the unique strengths that each brings. CBPR begins with a research topic of importance to the community and has the aim of combining knowledge with action and achieving social change…” [64].
Such an approach is attractive to academics and public health professionals as it aims to combine knowledge and action for social changes to improve community health and eliminate disparities.
Nine key principles of CBPR have been identified [63, 65], which are to:
Recognise community as a unit of identity; Build on strengths and resources within the community; Facilitate collaborative, equitable involvement of all partners in all phases of the
research; Integrate knowledge and intervention for the mutual benefit of all partners; Promote a co-learning and empowering process that attends to social inequalities;
15
Involve a cyclical and iterative process; Address health from both positive and ecological perspectives; Disseminate findings and knowledge gained to all partners; and Involve long-term commitment by all partners.
Israel et al. [63] caution that these principles are not intended to be binding on a project; rather, they should be adopted and can vary according to research purposes, context, and participants.
1.4.7 Brief interventions Some of the biggest barriers to delivering and receiving traditional face-to-face intervention programmes, associated with diminished reach and impact, are access to and cost-efficiency (in terms of time, money, or other resources) of the interventions [46, 47, 66, 67]. In family or parenting interventions, for instance, these barriers may manifest as a lack of attendance or adherence to the intervention programme due to the need to juggle scheduling conflicts such as children’s extracurricular classes or parents’ work demands, or the time and monetary costs of attending intervention sessions over a lengthy period of time [46]. Brief interventions (also known as minimal interventions, brief counselling, simple advice, or short-term counselling) provide a promising method of addressing these barriers.
Brief interventions are far from a homogenous entity, varying in setting, length, structure, targets, personnel acting as interventionists, and media of communication used [68], with or without additional written materials such as workbooks or other forms of self-monitoring or self-help [69]. However, as the name of this family of interventions suggests, they are brief in nature, typically consisting of five or fewer sessions that may be as short as several minutes to an hour [69, 70]. In this short time, particularly during the first session, brief interventions primarily aim to help initiate, continue, or accelerate behavioural change in subjects by raising awareness of problems and recommending specific relevant changes or activities; any follow-up sessions provide opportunities to monitor the subject’s progress and enhance the subject’s motivation to make or maintain positive behavioural changes [69]. As such, in contexts where time, monetary, or human resources may be limited, and traditional individual face-to-face interventions are not feasible, brief interventions may be a valuable alternative, cutting down on the resources needed and encouraging better attendance and adherence. It is worth noting that brief interventions can be compatible with and may go toward supporting the public health approach [71].
Past studies of brief interventions and reviews of such studies suggest that brief interventions have merit across settings and targets including, but not limited to, tobacco use, substance abuse, parent-child relationships, physical activity, and dietary adherence [67, 69, 72-82]. However, diet and physical activity are two subjects that are less frequently tackled through brief interventions; Michie et al. [83] reported in a review of healthy eating and physical activity interventions that whilst 16% of treatments were brief or less than one day, and 9% were less than one month in duration, the majority of treatments were longer. Nevertheless, there is a growing body of evidence supporting the efficacy of brief interventions for diet or physical activity.

16
For instance, Berg-Smith et al. [72] reported that a 5 to 30 minute intervention to improve dietary adherence in adolescents showed a significant decrease in the mean proportion of calories from fat consumed, whilst Glasgow, Toobert, and Hampson [77] found that a brief intervention condition produced greater improvements than the usual care condition on a number of dietary measures, such as eating habits and calories from saturated fat. Stevens et al. [81] reported that an experimental condition of two 45-minute sessions plus two brief follow-up telephone contacts showed significantly greater consumption of fruit and vegetables, and significantly less fat consumption, than a control group. Similarly, Kellar and Abraham [79] found that a brief intervention group had eaten more fruit and vegetables than the control group.
In a review of physical activity interventions, Eakin, Glasgow, and Riley [75] concluded that brief physical activity interventions can produce moderate short-term improvements in self-reported physical activity levels. Bolognesi et al. [74] showed that compared with the control group after a 5- to 6-month follow-up, the experimental group receiving brief physical activity counselling had better BMI and abdominal girth. Likewise, Purath et al. [80] found that a brief intervention significantly improved the amount of physical activity performed in a group of sedentary working women.
Considering the growing body of evidence in the West for the efficacy of brief interventions, as well as universal concerns regarding cost-effectiveness in treatment or intervention, and interest in shorter interventions [69], further research on brief interventions in Hong Kong is warranted.

17
CHAPTER 2 PROJECT DESIGN AND METHODS
2.1 Project design
2.1.1 Conceptual framework The FHHCPP utilised the public health approach and the CBPR approach to promote healthy diet, physical activity, and the FAMILY 3Hs through community-based interventions. The project was guided by a conceptual framework (as shown in Figure 2.1) with three stages: Stage 1, spark and start; Stage 2, spread and serve; and Stage 3, share and sustain. A Train-the-Ambassador Programme (TTA) was organised to empower the recruited volunteers (Health Ambassadors) to assist in the project and lead the participants of the community-based programme throughout the project.
Figure 2.1 Conceptual framework of the FHHCPP

18
2.1.1.1 Stage 1: Spark and start A major aim of Stage 1 was to motivate and empower the Health Ambassadors and community-based participants to adopt the healthy diet and physical activity behaviours promoted in the intervention programme. Stage 1 included a public education event and an opening ceremony to publicise the project. The core session of the TTA (2 hours and 15 minutes) and the core sessions of the community-based programme (2 to 2.5 hours each) aimed to raise awareness regarding the health behaviours and empowered the Health Ambassadors and community-based participants to act in order to combat unhealthy diets and insufficient physical activity. Misconceptions and knowledge gaps were highlighted, and Health Ambassadors and community-based programme participants were shown that it can be easy to adopt the simple health behaviours, thus increasing their confidence to help and influence others. Evaluation of the TTA and the community-based programmes began just prior to the core sessions of the respective workshop and programmes, and continued throughout the project until the end of the community-based programme.
2.1.1.2 Stage 2: Spread and serve The key aim of Stage 2 was for Health Ambassadors and community-based programme participants to influence their family or friends to adopt healthy lifestyles involving healthy diet or physical activity. The Health Ambassadors also aimed to influence the participants through the community-based programmes that they designed, planned, and implemented, as well as through the delivery of anti-inertia reminders through WhatsApp, an instant messaging platform. Ongoing evaluation was conducted using questionnaires.
2.1.1.3 Stage 3: Share and sustain In order to evaluate whether the introduced health behaviours were sustained in the community-based programme participants, the Health Ambassadors conducted two batches of telephone follow-up interviews on the participants. Stage 3 also included the Sharing Session cum Awards Ceremony, as well as focus groups and in-depth interviews. At the Sharing Session, the top-performing groups were awarded, and the Health Ambassadors as well as community-based programme participants shared their experiences from the programmes. Focus groups and in-depth interviews were also conducted to collect information about the thoughts and feelings of the Health Ambassadors, community-based programme participants, and community leaders regarding the project overall. The Health Ambassadors and participants were encouraged to use their multiple social roles (for instance, mother, wife, or daughter-in-law) to encourage the adoption of health behaviours both within their own families and beyond. Through them, the HKIWA would have the potential and experience to influence and build the community’s capacity for sustaining health promotion efforts in the future.
19
2.1.2 Project publicity Various strategies were utilised to publicise and promote the project:
Public education and community events, including the Opening Ceremony; Home visits; Street booths; Websites and social media; and Posters and banners.
2.2 Cluster randomised controlled trial design The current project adopted a cluster randomised controlled trial (cRCT) design.
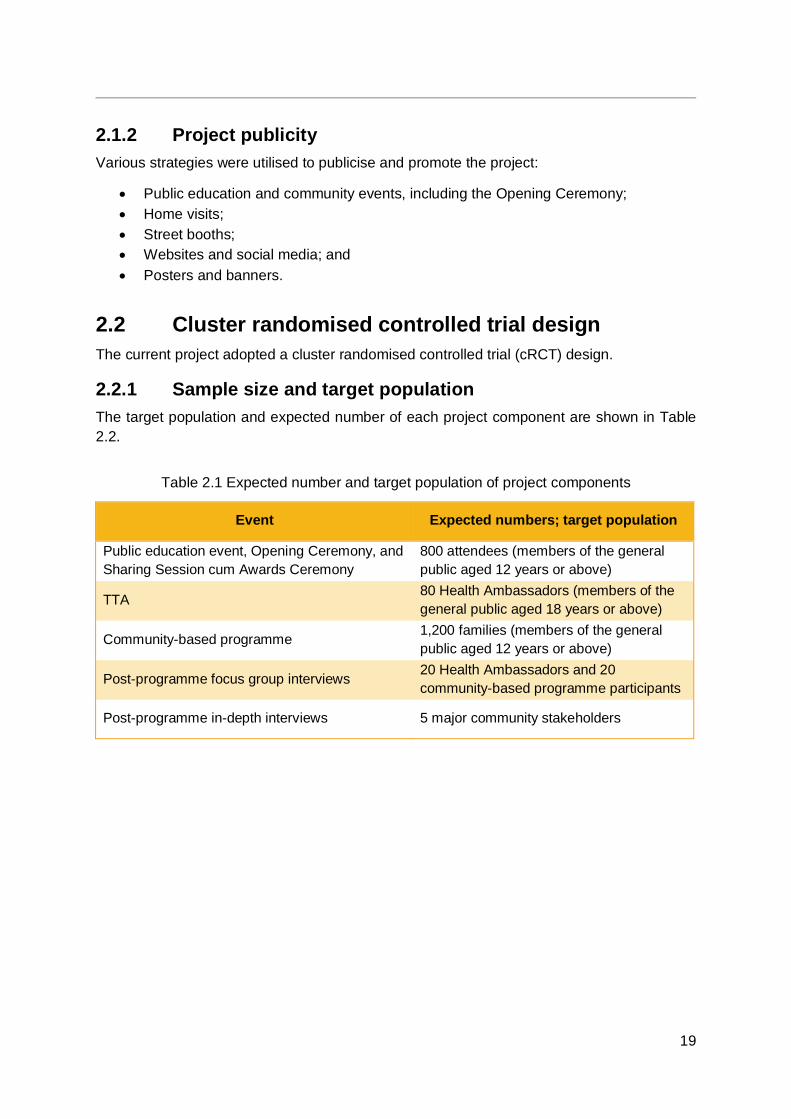
2.2.1 Sample size and target population The target population and expected number of each project component are shown in Table 2.2.
Table 2.1 Expected number and target population of project components
Event Expected numbers; target population
Public education event, Opening Ceremony, and Sharing Session cum Awards Ceremony
800 attendees (members of the general public aged 12 years or above)
TTA 80 Health Ambassadors (members of the general public aged 18 years or above)
Community-based programme 1,200 families (members of the general public aged 12 years or above)
Post-programme focus group interviews 20 Health Ambassadors and 20 community-based programme participants
Post-programme in-depth interviews 5 major community stakeholders
20
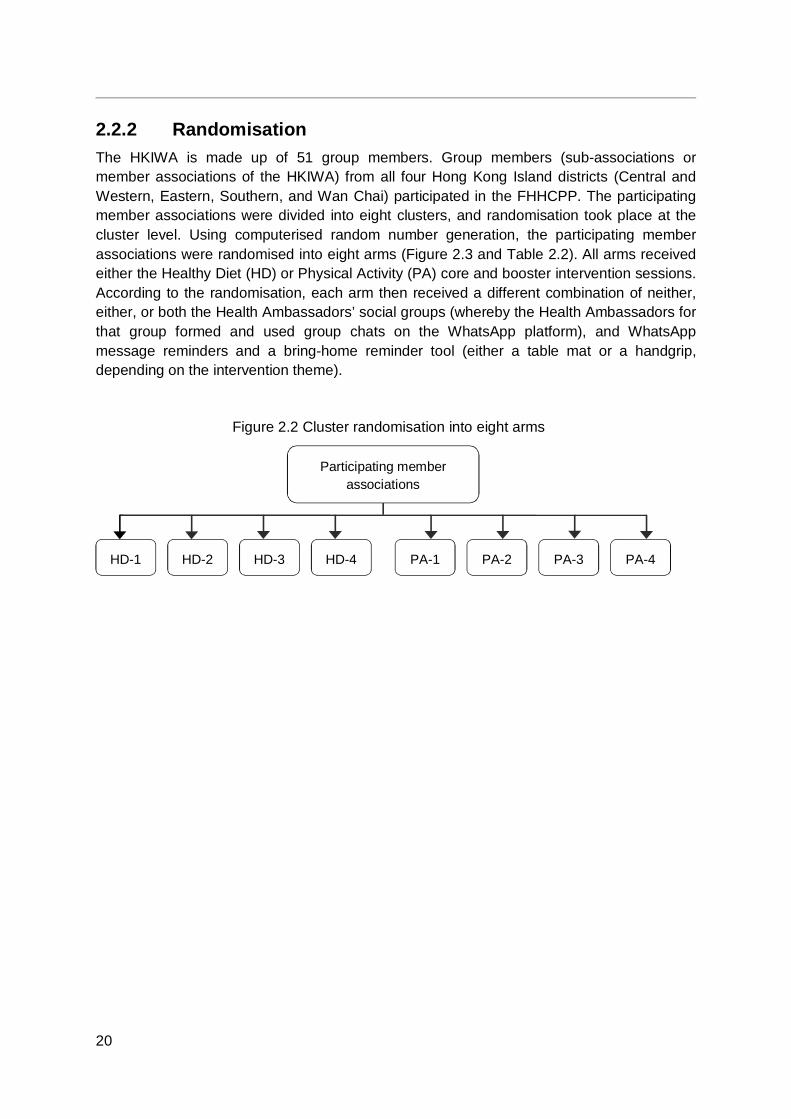
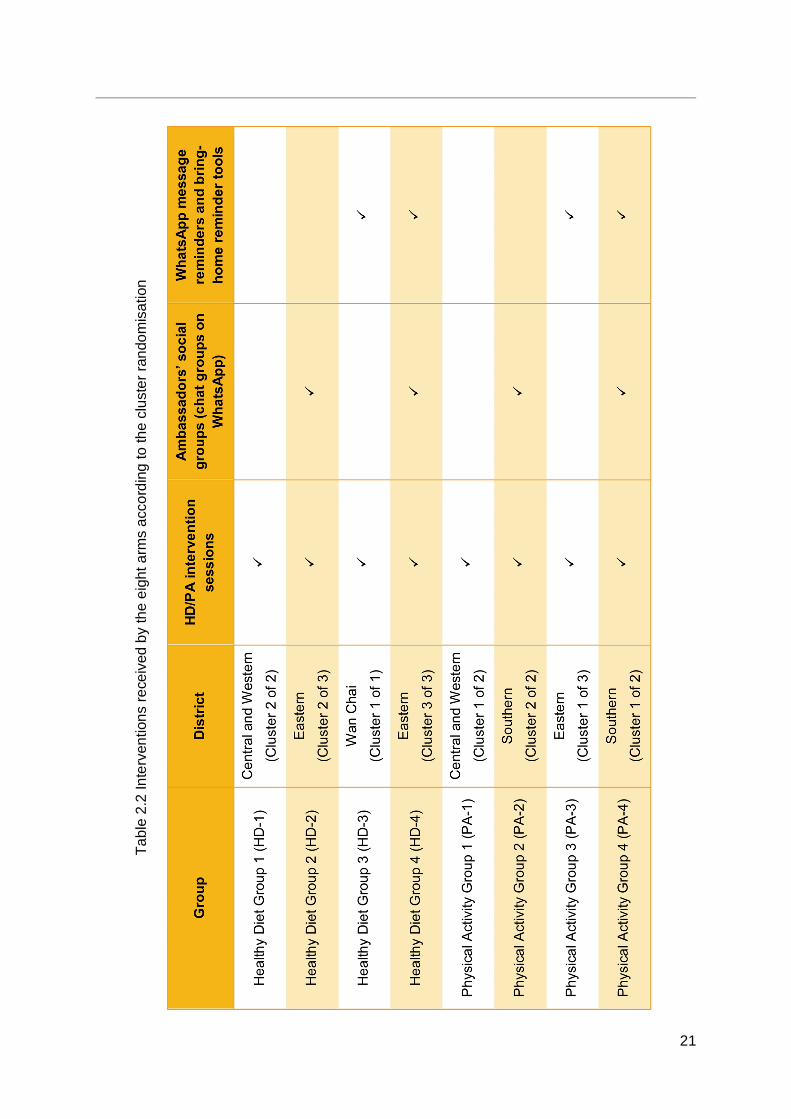
2.2.2 Randomisation The HKIWA is made up of 51 group members. Group members (sub-associations or member associations of the HKIWA) from all four Hong Kong Island districts (Central and Western, Eastern, Southern, and Wan Chai) participated in the FHHCPP. The participating member associations were divided into eight clusters, and randomisation took place at the cluster level. Using computerised random number generation, the participating member associations were randomised into eight arms (Figure 2.3 and Table 2.2). All arms received either the Healthy Diet (HD) or Physical Activity (PA) core and booster intervention sessions. According to the randomisation, each arm then received a different combination of neither, either, or both the Health Ambassadors’ social groups (whereby the Health Ambassadors for that group formed and used group chats on the WhatsApp platform), and WhatsApp message reminders and a bring-home reminder tool (either a table mat or a handgrip, depending on the intervention theme).
Figure 2.2 Cluster randomisation into eight arms
HD-1 HD-2 HD-3 HD-4 PA-1 PA-2 PA-3 PA-4
Participating member associations
21
Tabl
e 2.
2 In
terv
entio
ns re
ceiv
ed b
y th
e ei
ght a
rms
acco
rdin
g to
the
clus
ter r
ando
mis
atio
n

22
2.2.3 Project evaluation Questionnaires were used to evaluate the project outcome measures. A process evaluation was also conducted for the intervention programmes through questionnaires, focus groups, and in-depth interviews.
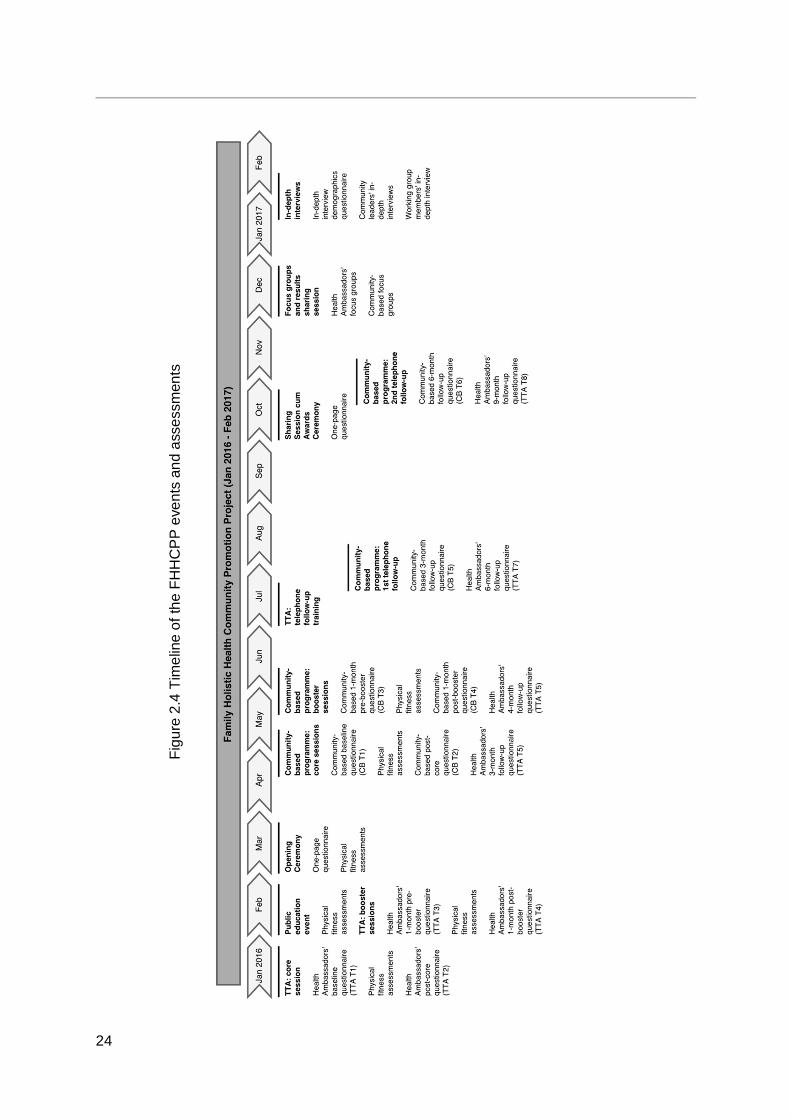
According to the randomisation detailed in Chapter 2.2.2, the intervention programmes and assessments that the Health Ambassadors and community-based participants took part in were planned to run as shown in Figure 2.3. Figure 2.4 shows an overall timeline of project events including project events occurring before and after the intervention programmes. Table 2.3 shows the details of the evaluation framework.

23
Figu
re 2
.3 T
TA a
nd c
omm
unity
-bas
ed p
rogr
amm
e st
udy
desi
gn
N
.B.:
TTA=
Trai
n-th
e-Am
bass
ador
Pro
gram
me;
CB=
com
mun
ity-b
ased
pro
gram
me;
HD
=Hea
lthy
Die
t; PA
=Phy
sica
l Act
ivity
; H
D-1
: H
D in
terv
entio
n on
ly;
HD
-2:
HD
in
terv
entio
n, A
mba
ssad
ors’
soc
ial
grou
p; H
D-3
: H
D i
nter
vent
ion,
HD
Wha
tsAp
p re
min
der
mes
sage
s an
d br
ing-
hom
e re
min
der
tool
; H
D-4
: H
D i
nter
vent
ion,
Am
bass
ador
s’ s
ocia
l gro
up, H
D W
hats
App
rem
inde
r mes
sage
s an
d br
ing-
hom
e re
min
der t
ool;
PA-1
: PA
inte
rven
tion
only
; PA-
2: P
A in
terv
entio
n, A
mba
ssad
ors’
soc
ial
grou
p; P
A-3:
PA
inte
rven
tion,
PA
Wha
tsAp
p re
min
der
mes
sage
s an
d br
ing-
hom
e re
min
der
tool
; PA
-4:
PA i
nter
vent
ion,
Am
bass
ador
s’ s
ocia
l gr
oup,
Wha
tsAp
p re
min
der m
essa
ges
and
brin
g-ho
me
rem
inde
r too
l
24
Figu
re 2
.4 T
imel
ine
of th
e FH
HC
PP
even
ts a
nd a
sses
smen
ts
25
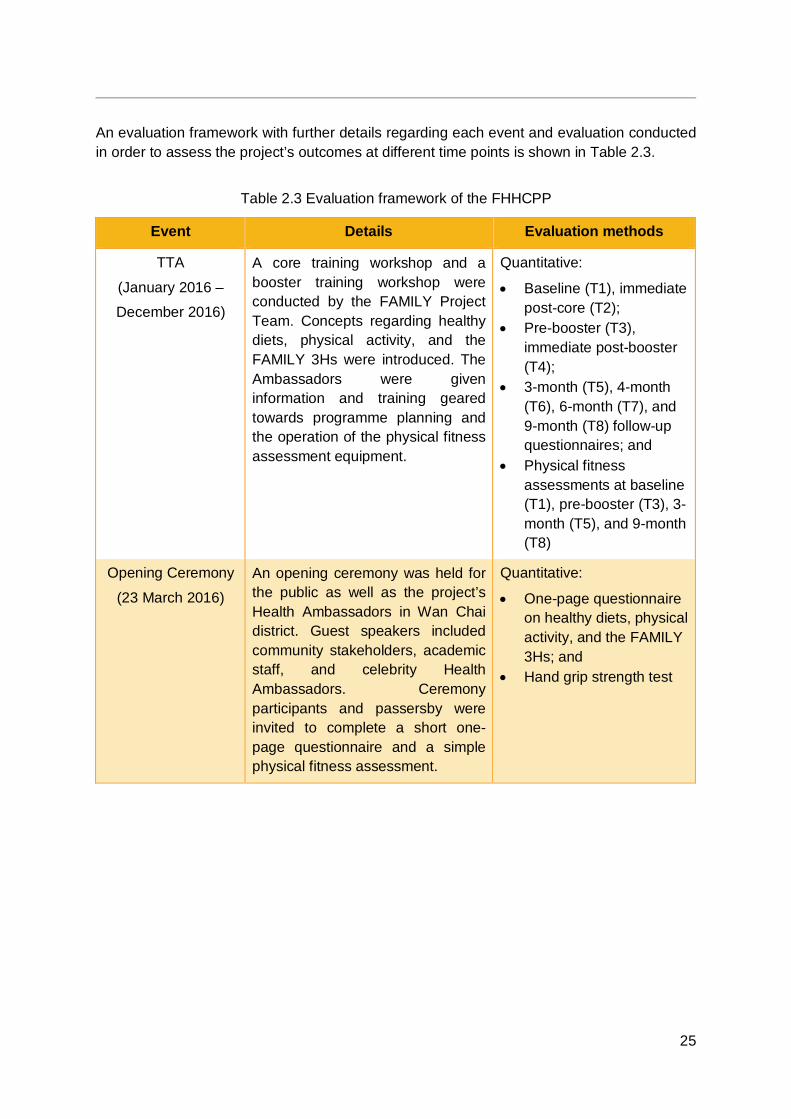
An evaluation framework with further details regarding each event and evaluation conducted in order to assess the project’s outcomes at different time points is shown in Table 2.3.
Table 2.3 Evaluation framework of the FHHCPP
Event Details Evaluation methods
TTA
(January 2016 –
December 2016)
A core training workshop and a booster training workshop were conducted by the FAMILY Project Team. Concepts regarding healthy diets, physical activity, and the FAMILY 3Hs were introduced. The Ambassadors were given information and training geared towards programme planning and the operation of the physical fitness assessment equipment.
Quantitative:
Baseline (T1), immediate post-core (T2);
Pre-booster (T3), immediate post-booster (T4);
3-month (T5), 4-month (T6), 6-month (T7), and 9-month (T8) follow-up questionnaires; and
Physical fitness assessments at baseline (T1), pre-booster (T3), 3-month (T5), and 9-month (T8)
Opening Ceremony
(23 March 2016)
An opening ceremony was held for the public as well as the project’s Health Ambassadors in Wan Chai district. Guest speakers included community stakeholders, academic staff, and celebrity Health Ambassadors. Ceremony participants and passersby were invited to complete a short one-page questionnaire and a simple physical fitness assessment.
Quantitative:
One-page questionnaire on healthy diets, physical activity, and the FAMILY 3Hs; and
Hand grip strength test
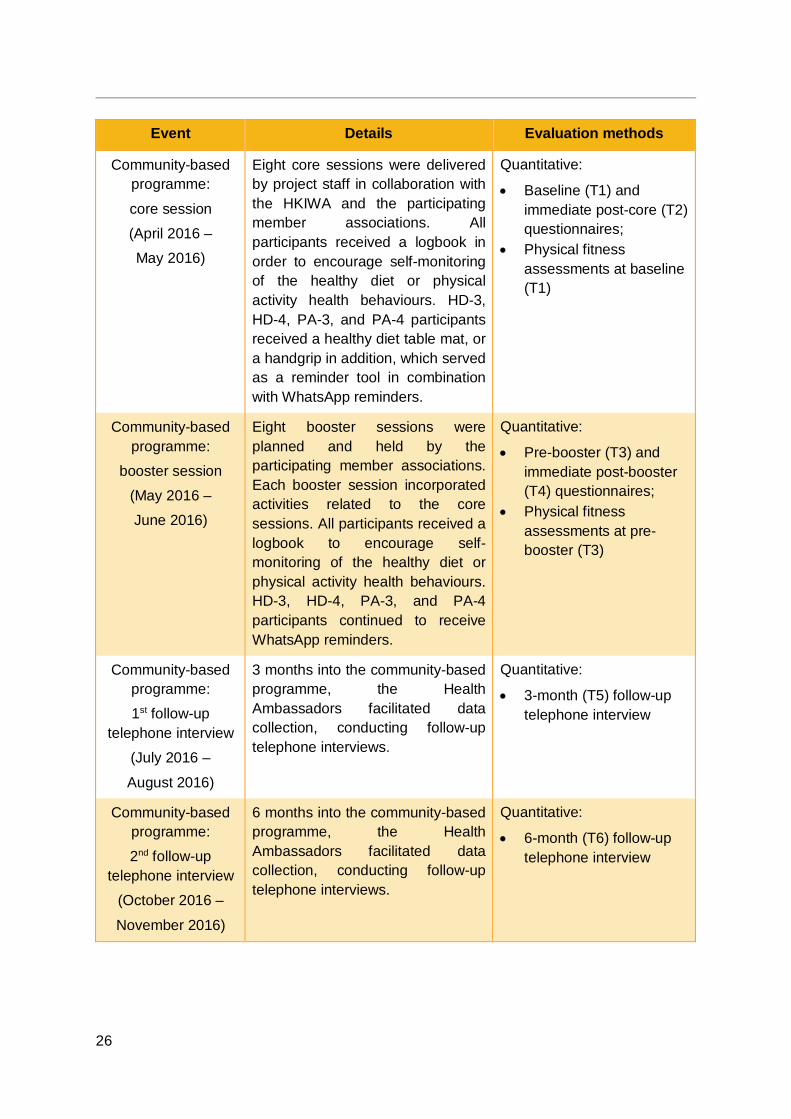
26
Event Details Evaluation methods
Community-based programme:
core session
(April 2016 –
May 2016)
Eight core sessions were delivered by project staff in collaboration with the HKIWA and the participating member associations. All participants received a logbook in order to encourage self-monitoring of the healthy diet or physical activity health behaviours. HD-3, HD-4, PA-3, and PA-4 participants received a healthy diet table mat, or a handgrip in addition, which served as a reminder tool in combination with WhatsApp reminders.
Quantitative:
Baseline (T1) and immediate post-core (T2) questionnaires;
Physical fitness assessments at baseline (T1)
Community-based programme:
booster session
(May 2016 –
June 2016)
Eight booster sessions were planned and held by the participating member associations. Each booster session incorporated activities related to the core sessions. All participants received a logbook to encourage self-monitoring of the healthy diet or physical activity health behaviours. HD-3, HD-4, PA-3, and PA-4 participants continued to receive WhatsApp reminders.
Quantitative:
Pre-booster (T3) and immediate post-booster (T4) questionnaires;
Physical fitness assessments at pre-booster (T3)
Community-based programme:
1st follow-up telephone interview
(July 2016 –
August 2016)
3 months into the community-based programme, the Health Ambassadors facilitated data collection, conducting follow-up telephone interviews.
Quantitative:
3-month (T5) follow-up telephone interview
Community-based programme:
2nd follow-up telephone interview
(October 2016 –
November 2016)
6 months into the community-based programme, the Health Ambassadors facilitated data collection, conducting follow-up telephone interviews.
Quantitative:
6-month (T6) follow-up telephone interview
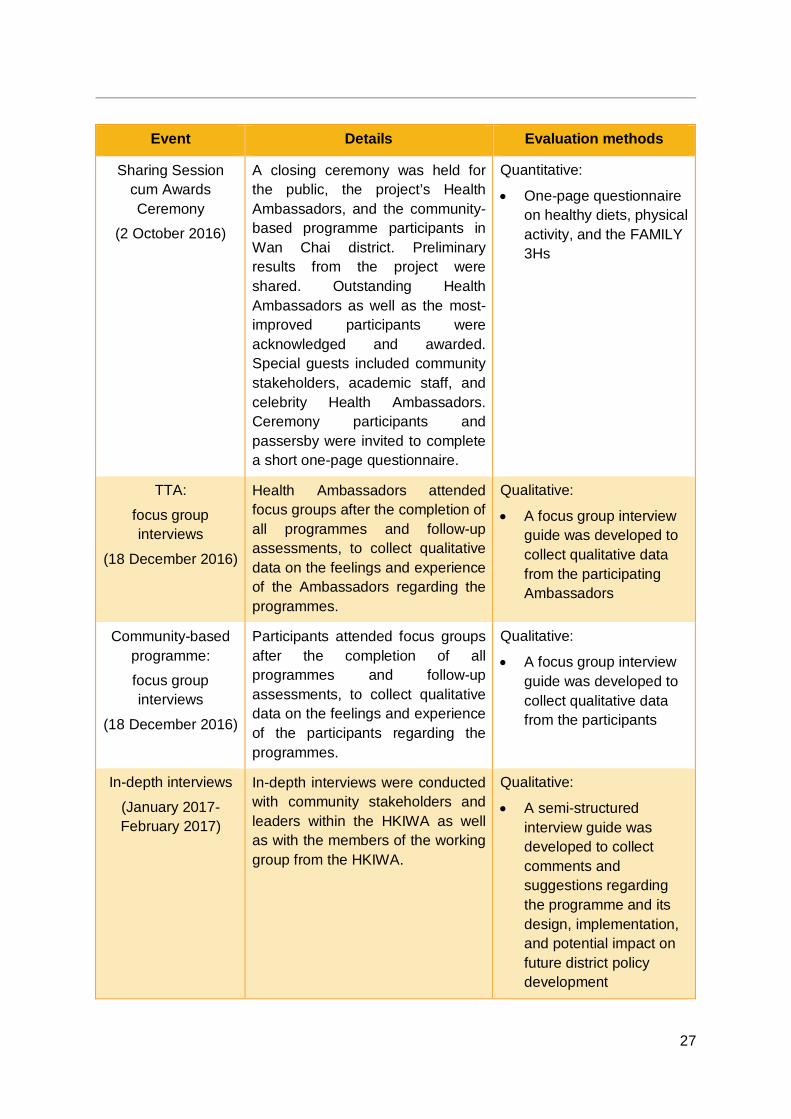
27
Event Details Evaluation methods
Sharing Session cum Awards Ceremony
(2 October 2016)
A closing ceremony was held for the public, the project’s Health Ambassadors, and the community-based programme participants in Wan Chai district. Preliminary results from the project were shared. Outstanding Health Ambassadors as well as the most-improved participants were acknowledged and awarded. Special guests included community stakeholders, academic staff, and celebrity Health Ambassadors. Ceremony participants and passersby were invited to complete a short one-page questionnaire.
Quantitative:
One-page questionnaire on healthy diets, physical activity, and the FAMILY 3Hs
TTA:
focus group interviews
(18 December 2016)
Health Ambassadors attended focus groups after the completion of all programmes and follow-up assessments, to collect qualitative data on the feelings and experience of the Ambassadors regarding the programmes.
Qualitative:
A focus group interview guide was developed to collect qualitative data from the participating Ambassadors
Community-based programme:
focus group interviews
(18 December 2016)
Participants attended focus groups after the completion of all programmes and follow-up assessments, to collect qualitative data on the feelings and experience of the participants regarding the programmes.
Qualitative:
A focus group interview guide was developed to collect qualitative data from the participants
In-depth interviews
(January 2017-February 2017)
In-depth interviews were conducted with community stakeholders and leaders within the HKIWA as well as with the members of the working group from the HKIWA.
Qualitative:
A semi-structured interview guide was developed to collect comments and suggestions regarding the programme and its design, implementation, and potential impact on future district policy development
28
2.3 Data analysis
2.3.1 Quantitative analysis Descriptive statistics were used to give a general overview of the demographic characteristics and outcomes of the participants in both the TTA and the community-based programme. Baseline characteristics were compared between groups using t-tests or Pearson’s chi-square tests, as appropriate. Mixed models were used to analyse differences in outcome changes between groups. All analyses were conducted using the statistical software SPSS 24.0.
2.3.2 Qualitative analysis The focus groups and in-depth interviews were tape-recorded and transcribed verbatim. Transcripts were analysed by thematic content analysis, following the guidelines recommended by Morse and Field [84]. Each transcript was analysed sentence by sentence and coded for the respondents’ meanings. Initial open coding of the data used differing codes, which were subsequently organised into categories. These categories were then integrated into themes within and across groups. Data comparisons within and between groups were also conducted. Field notes were continuously reviewed alongside the transcripts during the process. The software NVivo 11.0 was employed to assist with qualitative data administration, including creating codes, organising and summarising data, searching for interrelationships between codes, and suggesting themes.
2.3.3 Process evaluation analysis Process evaluation data were collected on-site using various forms and checklists. The data were analysed using a combination of quantitative and qualitative methods. Close-ended questions were analysed using descriptive statistics (quantitative method), whilst open-ended questions were analysed by thematic content analysis (qualitative method).
29
CHAPTER 3 PUBLIC EDUCATION EVENT
3.1 Objectives As part of the 2016 Chinese New Year Gathering cum Volunteer Award Ceremony (2016 丙
申年新春團拜暨義工嘉許禮) hosted by the HKIWA, a promotional booth was set up for the FHHCPP.
The promotional booth was set up in order to accomplish two main objectives:
1. To promote and recruit for the Opening Ceremony and community-based programme of the FHHCPP; and
2. To conduct physical fitness assessments and inform attendees of standard reference values for various physical fitness indicators.
3.2 Event summary On 23 February 2016, the HKIWA hosted the 2016 Chinese New Year Gathering cum Volunteer Award Ceremony at Times Square in Causeway Bay. Approximately 60 individuals attended the event. Amongst those in attendance were Mrs. Leung Tong Ching-yee Regina, Spouse of the Chief Executive of Hong Kong; Mr. Chen Wei-feng, Deputy Director General of the Hong Kong Island Sub-Office of the Liaison Office of the Central People’s Government in the Hong Kong Special Administrative Region; Hon. Chung Shu-kun Christopher, Legislative Council Member; and Mrs. Cheung Nga-lai, Chair of the HKIWA.
Mrs. Cheung announced that the HKIWA would be launching the FHHCPP in collaboration with the FAMILY Project Team and The Hong Kong Jockey Club Charities Trust. The programme was described as a family-based programme aiming to promote health for households in Hong Kong through physical activity and a healthy diet, with the help of community Health Ambassadors.
With assistance from several Health Ambassadors and volunteers from the HKIWA, a promotional booth was set up at the venue with equipment, such as blood pressure monitors, electronic body scales, stadiometers, and hand dynamometers. The Health Ambassadors and volunteers were instructed on how to use the equipment by the FAMILY Project Team in advance. The staff, Ambassadors, and volunteers approached and engaged attendees at the event. Physical fitness assessments were conducted for ten attendees, measuring blood pressure, body composition, hand grip strength or hand dynamometry, and flexibility. The attendees approached were also given information on the standard reference values for the physical fitness indicators, as well as information about the FHHCPP and its upcoming Opening Ceremony and community-based programme. The promotional booth ran for approximately 2 hours and 30 minutes.
30
CHAPTER 4 OPENING CEREMONY
4.1 Objectives As part of the FHHCPP, an Opening Ceremony was held and hosted by the HKIWA in March 2016, prior to the commencement of the community-based programme.
There were four main objectives for the Opening Ceremony:
1. To promote and recruit for the community-based programme of the FHHCPP; 2. To assess attendees’ healthy diet and physical activity behaviours and attitudes, as
well as FAMILY 3Hs; 3. To recognise and encourage the recruited Health Ambassadors (who were at the
time, 2 months into the TTA); and 4. To deliver key messages regarding the importance of
a. Physical activity and a healthy diet for health; and b. Loving one’s family.
4.2 Ceremony summary On 19 March 2016, the HKIWA hosted the Opening Ceremony for the FHHCPP in collaboration with the FAMILY Project at the World Trade Centre Club at the World Trade Centre in Causeway Bay. The event was open to the general public and passersby, although some guests were especially invited. Approximately 200 individuals attended the event. Amongst those in attendance by invitation were Professor Lam Tai Hing, Chair Professor of Community Medicine, Sir Robert Kotewall Professor in Public Health, and Principal Investigator of the FAMILY Project, School of Public Health, The University of Hong Kong (HKU-SPH); Professor Sophia Chan, Under Secretary for Food and Health; Ms. Macy Chui, Jockey Club Charities Manager; Mrs. Cheung Nga-lai, Chair of the HKIWA; Mrs. Young Cheung Sun Yuet Nicola, a Hong Kong television and film actress and celebrity Health Ambassador of the project; Mr. Young Chit On Jeremy, Mrs. Young’s husband; and the Health Ambassadors from the project’s TTA, which at the time had been running for 2 months.
Upon arrival, attendees mingled and were invited to complete a one-page questionnaire regarding their healthy diet and physical activity behaviours and attitudes, as well as FAMILY 3Hs. The questionnaires were collected by FAMILY Project Team members, and each attendee received a small FAMILY Project souvenir towel.
At the commencement of the main programme, the guests of honour were invited onto the stage for a series of group photographs; the Health Ambassadors were also recognised and invited onto the stage for group photographs. The guests of honour then took part in an opening ceremony for the official launch of the FHHCPP, and the beginning of healthy behaviours such as physical activity and healthy diets.
Mrs. Young and Mr. Young, along with their two daughters, were invited onto the stage for a brief interview, and were asked how they maintain a healthy diet and keep physically active and fit. Mrs. Young shared that the family tries to maintain a healthy diet low in sugar, and
31
that she skips rope in her spare time, whilst Mr. Young and their daughters demonstrated some home exercises that they do. Attendees were enthusiastic about the family’s tips and demonstrations, and the family received much applause.
Professor Lam and Professor Chan, in their respective speeches, both emphasised the importance of healthy diets and physical activity for health. Professor Lam demonstrated a variety of simple but effective ZTEx, such as vigorously clapping one’s hands, repeatedly contracting one’s abdominal muscles, neck stretches, and raising the legs. Professor Lam also encouraged attendees to recognise that one of the important reasons to promote health, for both oneself and one’s family, is that it can be an expression of love for one’s family; because of love for our families, we should share the benefits of a healthy diet and ZTEx with our family. Professor Lam motivated the attendees to pledge loudly that they would share these key messages with their families.
4.3 Statistical analyses and results A total of 95 questionnaires were collected at the opening ceremony; of these, 76 were valid.
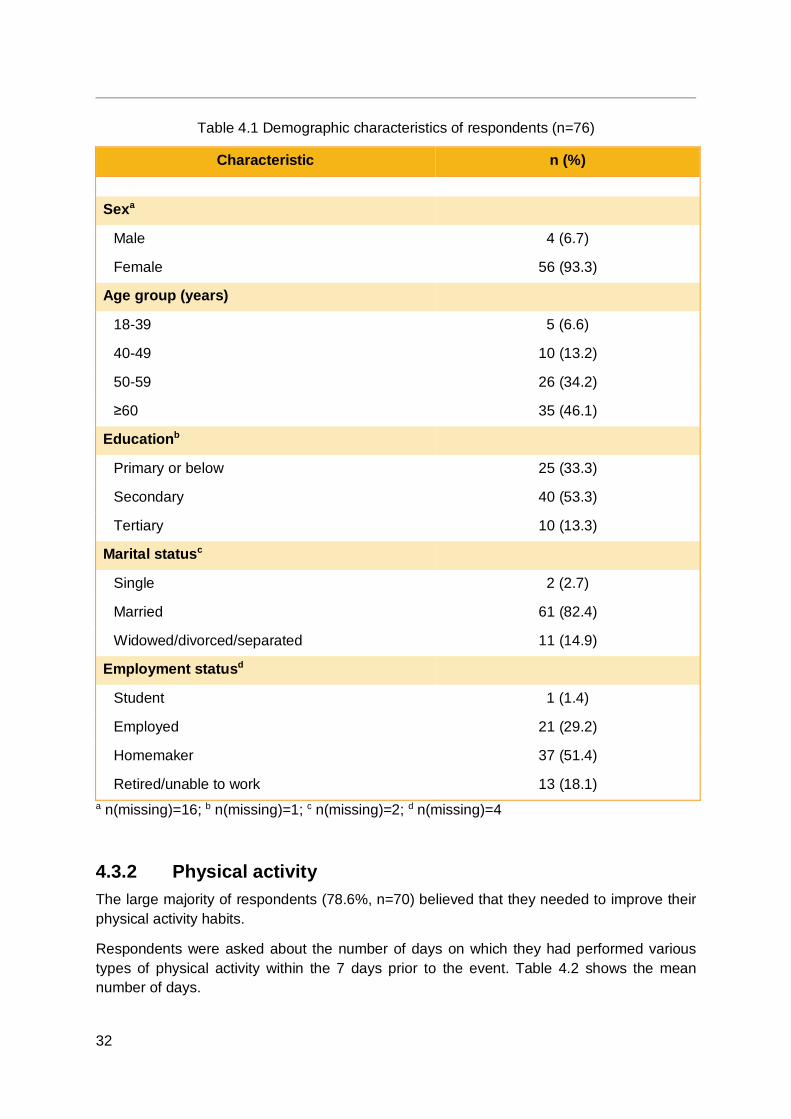
4.3.1 Demographic characteristics The demographic characteristics of the respondents are presented in Table 4.1.
The majority (93.3%) of the respondents were female. About one-third (34.2%) were aged 50-59 years, and nearly half (46.1%) were aged 60 years or above. Over half (53.3%) were educated to secondary level, and a large majority (82.4%) were married. About half (51.4%) were homemakers, and about 30% (29.2%) were employed.
32
Table 4.1 Demographic characteristics of respondents (n=76)
Characteristic n (%) Sexa
Male 4 (6.7)
Female 56 (93.3)
Age group (years)
18-39 5 (6.6) 40-49 10 (13.2) 50-59 26 (34.2) ≥60 35 (46.1)
Educationb
Primary or below 25 (33.3) Secondary 40 (53.3) Tertiary 10 (13.3)
Marital statusc
Single 2 (2.7) Married 61 (82.4) Widowed/divorced/separated 11 (14.9)
Employment statusd
Student 1 (1.4) Employed 21 (29.2) Homemaker 37 (51.4) Retired/unable to work 13 (18.1)
a n(missing)=16; b n(missing)=1; c n(missing)=2; d n(missing)=4
4.3.2 Physical activity The large majority of respondents (78.6%, n=70) believed that they needed to improve their physical activity habits.
Respondents were asked about the number of days on which they had performed various types of physical activity within the 7 days prior to the event. Table 4.2 shows the mean number of days.
33
Table 4.2 Number of days within the 7 days prior to the event on which respondents performed various types of physical activity
Type of physical activity n Mean (SD)
At least ten minutes of moderate physical activities 70 3.95 (2.48)
At least ten minutes of vigorous physical activities 64 2.05 (2.23)
At least ten minutes of any physical activity together with family members 66 2.80 (2.67)
Move the head, neck, shoulders, waist, back, arms, or legs whilst seated 68 3.97 (2.53)
Move the head, neck, shoulders, waist, back, arms, or legs whilst standing 69 4.22 (2.50)
Move the head, neck, shoulders, waist, back, arms, or legs whilst walking 68 4.32 (2.61)
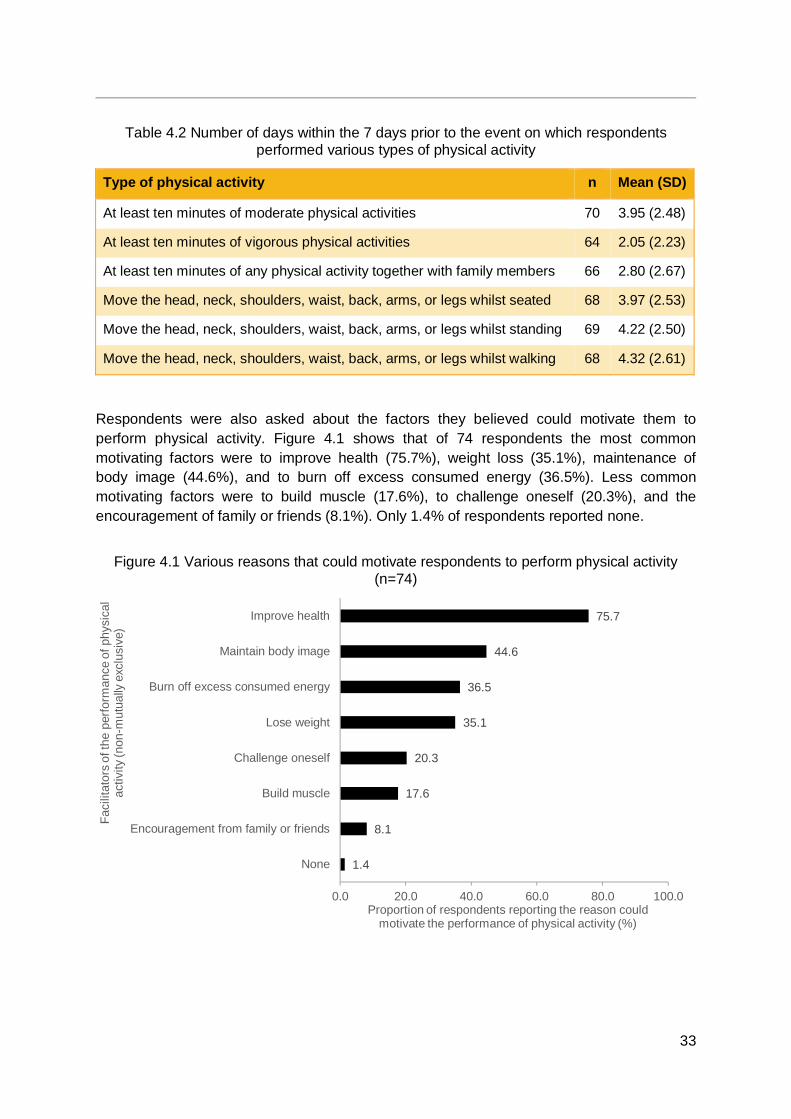
Respondents were also asked about the factors they believed could motivate them to perform physical activity. Figure 4.1 shows that of 74 respondents the most common motivating factors were to improve health (75.7%), weight loss (35.1%), maintenance of body image (44.6%), and to burn off excess consumed energy (36.5%). Less common motivating factors were to build muscle (17.6%), to challenge oneself (20.3%), and the encouragement of family or friends (8.1%). Only 1.4% of respondents reported none.
Figure 4.1 Various reasons that could motivate respondents to perform physical activity (n=74)
1.4
8.1
17.6
20.3
35.1
36.5
44.6
75.7
0.0 20.0 40.0 60.0 80.0 100.0
None
Encouragement from family or friends
Build muscle
Challenge oneself
Lose weight
Burn off excess consumed energy
Maintain body image
Improve health
Proportion of respondents reporting the reason couldmotivate the performance of physical activity (%)
Faci
litat
ors
of th
e pe
rform
ance
of p
hysi
cal
activ
ity (n
on-m
utua
lly e
xclu
sive
)
34
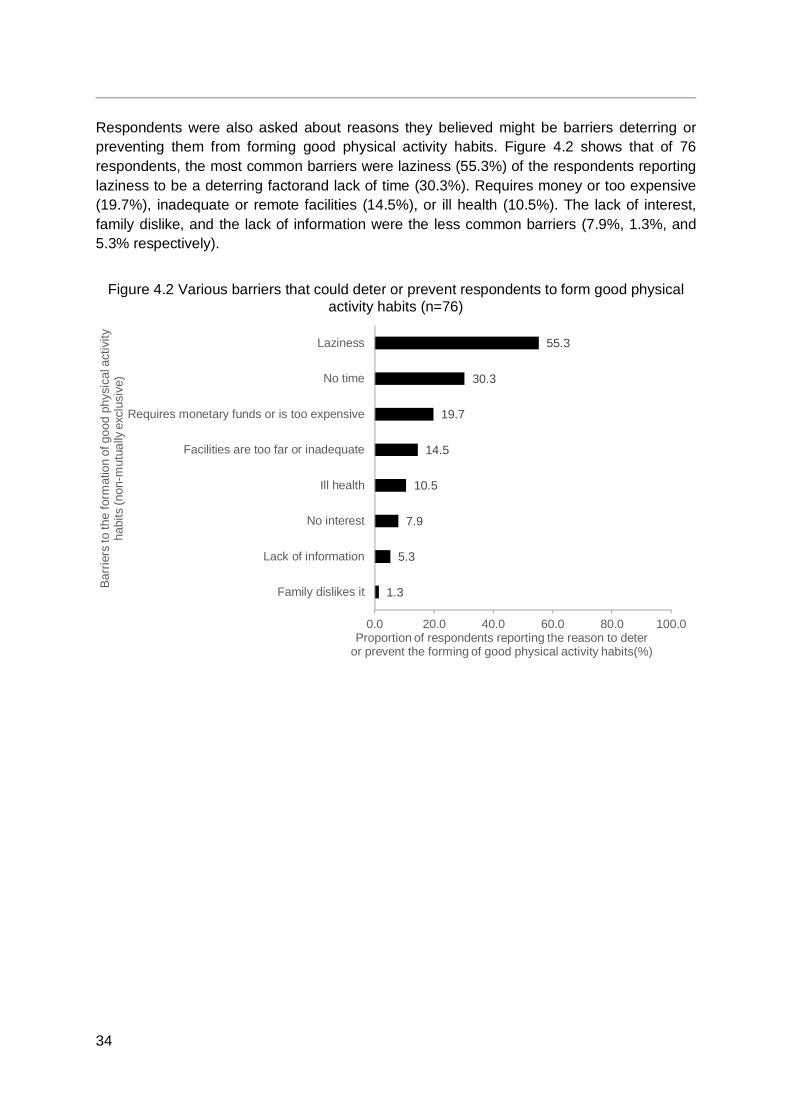
Respondents were also asked about reasons they believed might be barriers deterring or preventing them from forming good physical activity habits. Figure 4.2 shows that of 76 respondents, the most common barriers were laziness (55.3%) of the respondents reporting laziness to be a deterring factorand lack of time (30.3%). Requires money or too expensive (19.7%), inadequate or remote facilities (14.5%), or ill health (10.5%). The lack of interest, family dislike, and the lack of information were the less common barriers (7.9%, 1.3%, and 5.3% respectively).
Figure 4.2 Various barriers that could deter or prevent respondents to form good physical activity habits (n=76)
1.3
5.3
7.9
10.5
14.5
19.7
30.3
55.3
0.0 20.0 40.0 60.0 80.0 100.0
Family dislikes it
Lack of information
No interest
Ill health
Facilities are too far or inadequate
Requires monetary funds or is too expensive
No time
Laziness
Proportion of respondents reporting the reason to deteror prevent the forming of good physical activity habits(%)
Barr
iers
to th
e fo
rmat
ion
of g
ood
phys
ical
act
ivity
ha
bits
(non
-mut
ually
exc
lusi
ve)
35
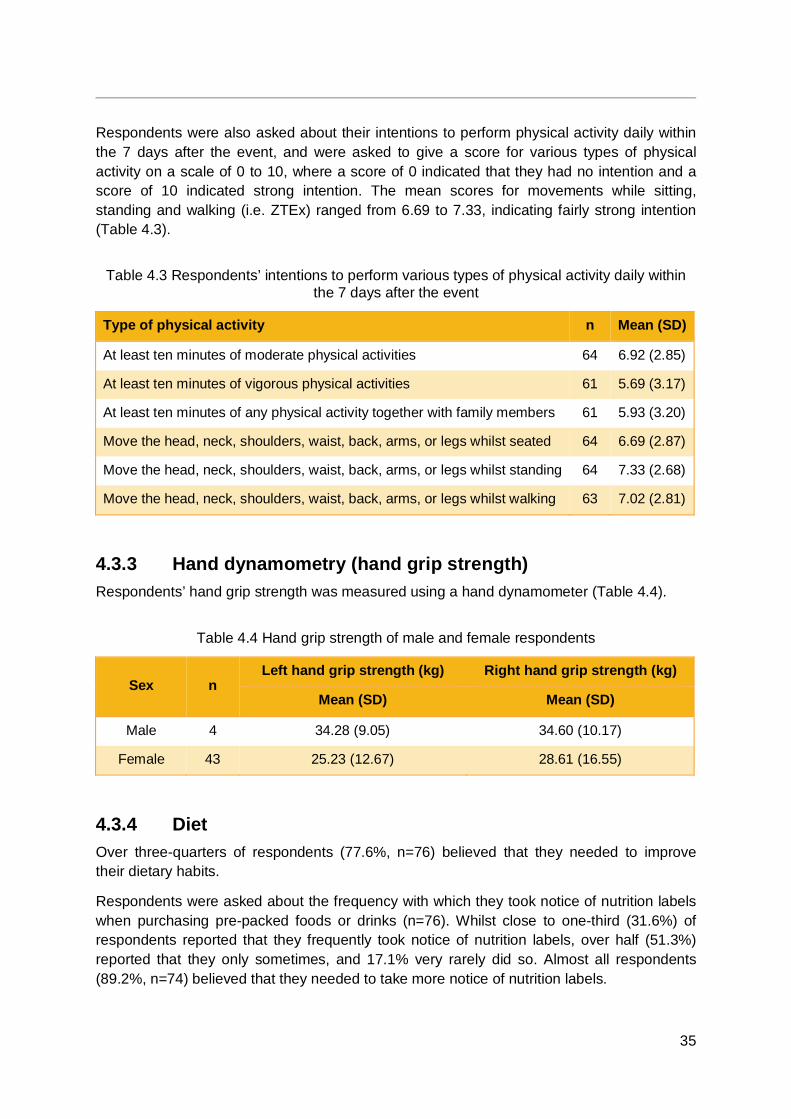
Respondents were also asked about their intentions to perform physical activity daily within the 7 days after the event, and were asked to give a score for various types of physical activity on a scale of 0 to 10, where a score of 0 indicated that they had no intention and a score of 10 indicated strong intention. The mean scores for movements while sitting, standing and walking (i.e. ZTEx) ranged from 6.69 to 7.33, indicating fairly strong intention (Table 4.3).
Table 4.3 Respondents’ intentions to perform various types of physical activity daily within the 7 days after the event
Type of physical activity n Mean (SD)
At least ten minutes of moderate physical activities 64 6.92 (2.85)
At least ten minutes of vigorous physical activities 61 5.69 (3.17)
At least ten minutes of any physical activity together with family members 61 5.93 (3.20)
Move the head, neck, shoulders, waist, back, arms, or legs whilst seated 64 6.69 (2.87)
Move the head, neck, shoulders, waist, back, arms, or legs whilst standing 64 7.33 (2.68)
Move the head, neck, shoulders, waist, back, arms, or legs whilst walking 63 7.02 (2.81)
4.3.3 Hand dynamometry (hand grip strength) Respondents’ hand grip strength was measured using a hand dynamometer (Table 4.4).
Table 4.4 Hand grip strength of male and female respondents
Sex n Left hand grip strength (kg) Right hand grip strength (kg)
Mean (SD) Mean (SD)
Male 4 34.28 (9.05) 34.60 (10.17)
Female 43 25.23 (12.67) 28.61 (16.55)
4.3.4 Diet Over three-quarters of respondents (77.6%, n=76) believed that they needed to improve their dietary habits.
Respondents were asked about the frequency with which they took notice of nutrition labels when purchasing pre-packed foods or drinks (n=76). Whilst close to one-third (31.6%) of respondents reported that they frequently took notice of nutrition labels, over half (51.3%) reported that they only sometimes, and 17.1% very rarely did so. Almost all respondents (89.2%, n=74) believed that they needed to take more notice of nutrition labels.
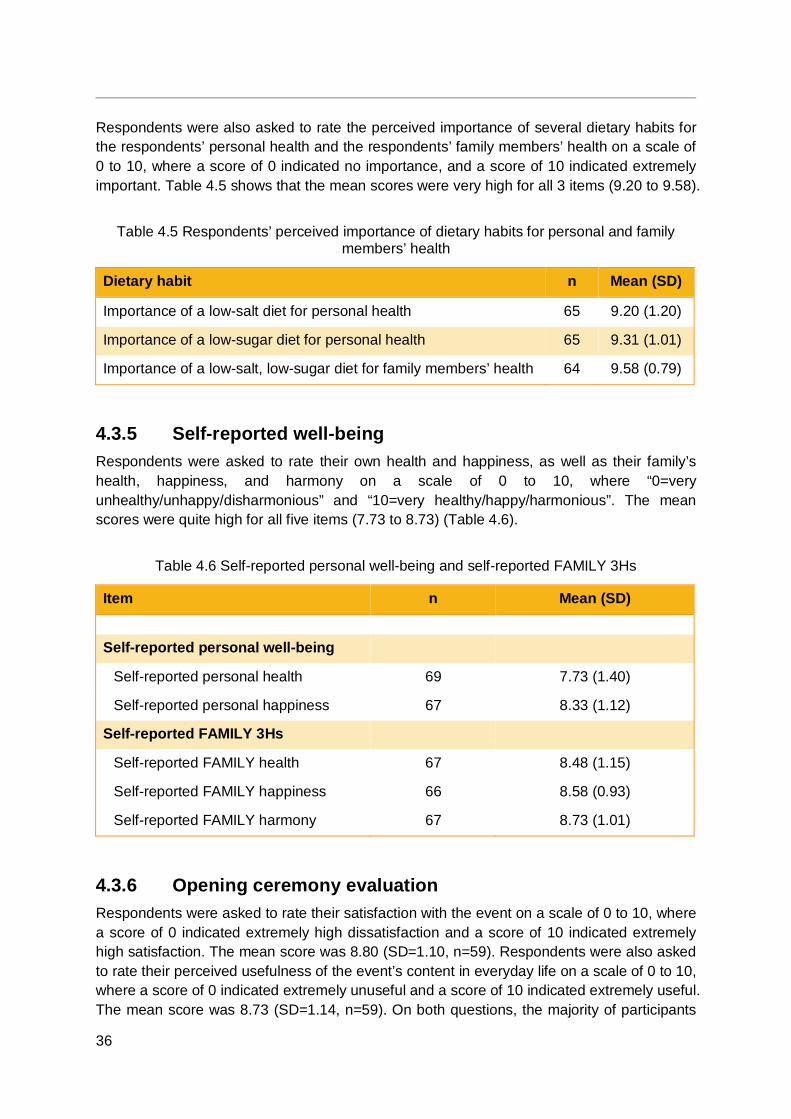
36
Respondents were also asked to rate the perceived importance of several dietary habits for the respondents’ personal health and the respondents’ family members’ health on a scale of 0 to 10, where a score of 0 indicated no importance, and a score of 10 indicated extremely important. Table 4.5 shows that the mean scores were very high for all 3 items (9.20 to 9.58).
Table 4.5 Respondents’ perceived importance of dietary habits for personal and family members’ health
Dietary habit n Mean (SD)
Importance of a low-salt diet for personal health 65 9.20 (1.20)
Importance of a low-sugar diet for personal health 65 9.31 (1.01)
Importance of a low-salt, low-sugar diet for family members’ health 64 9.58 (0.79)
4.3.5 Self-reported well-being Respondents were asked to rate their own health and happiness, as well as their family’s health, happiness, and harmony on a scale of 0 to 10, where “0=very unhealthy/unhappy/disharmonious” and “10=very healthy/happy/harmonious”. The mean scores were quite high for all five items (7.73 to 8.73) (Table 4.6).
Table 4.6 Self-reported personal well-being and self-reported FAMILY 3Hs
Item n Mean (SD) Self-reported personal well-being
Self-reported personal health 69 7.73 (1.40) Self-reported personal happiness 67 8.33 (1.12)
Self-reported FAMILY 3Hs
Self-reported FAMILY health 67 8.48 (1.15) Self-reported FAMILY happiness 66 8.58 (0.93) Self-reported FAMILY harmony 67 8.73 (1.01)
4.3.6 Opening ceremony evaluation Respondents were asked to rate their satisfaction with the event on a scale of 0 to 10, where a score of 0 indicated extremely high dissatisfaction and a score of 10 indicated extremely high satisfaction. The mean score was 8.80 (SD=1.10, n=59). Respondents were also asked to rate their perceived usefulness of the event’s content in everyday life on a scale of 0 to 10, where a score of 0 indicated extremely unuseful and a score of 10 indicated extremely useful. The mean score was 8.73 (SD=1.14, n=59). On both questions, the majority of participants
37
gave a score of 8 or more out of 10 (event satisfaction: 93.2%; perceived usefulness of content: 88.1%). 100.0% (n=69) of respondents answered that they would recommend the event to other people.
4.4 Discussion Although respondents had relatively high scores for self-reported personal health and happiness, as well as self-reported FAMILY health, happiness, and harmony, the majority respondents believed that they needed to make changes to their physical activity habits and dietary habits. However, the high scores implied that further increase by interventions would be difficult (ceiling effect).
About 80% of respondents believed that they needed to make changes to their physical activity habits, and the mean scores for intentions to perform various types of physical activity daily within the week following the opening ceremony suggested that they were ready to make a change. The prospects of improving health and losing weight were major facilitating factors or motivators, but laziness, perceived lack of time, and perceived need for money were major barriers. Such barriers have been previously reported elsewhere (e.g. [14-16, 18, 19]). Hence, interventions for physical activity that address and can overcome these barriers are needed.
About three quarters of respondents believed that they needed to improve their dietary habits. They clearly saw the importance of a low-salt, low-sugar diet for their personal health and their family members’ health with very high mean scores of 9 out of 10 (Table 4.5). However, only about one-third had taken frequent notice of nutrition labels when buying pre-packaged foods or drinks even though 90% believed they needed to do so. Future interventions for healthy diets should include empowering people to read and understand nutrition labels.
Due to the convenience sampling method, volunteer bias cannot be ruled out. The event was advertised as the Opening Ceremony of the FHHCPP, a project focused on the improvement of the health of its participants, and as such had higher self-reported FAMILY 3Hs scores, more ambitious physical activity intentions, and greater willingness and readiness to change their physical activity and dietary habits. Attendees of the ceremony might be more health conscious and proactive about their health than others who did not attend this event. Nevertheless, these participants could be the most appropriate to be trained as voluntary Health Ambassadors or they could become role models in community health programmes to benefit others.
4.5 Conclusions The Opening Ceremony of the FHHCPP successfully recruited a good number of particiaptns and promoted the FHHCPP. Overall, attendees were satisfied with the event and perceived its content to be useful and applicable in daily life.
The one-page questionnaire assessment showed that respondents generally perceived themselves and their family members to be healthy, happy, and harmonious, and felt that they needed to improve or change their physical activity habits or dietary habits and take

38
notice of nutrition labels. Common barriers to forming good physical activity habits included self-perceived laziness, lack of time, and the need of money.
Future interventions need to address and overcome such barriers. Some attendees could be target trainees to become Health Ambassadors.

39
CHAPTER 5 TRAIN-THE-AMBASSADOR PROGRAMME
5.1 Introduction Preventive interventions in public health have to be cost-effective, so they must be practical, brief, and easily spread widely across the population. The train-the-trainer educational approach has been used to build capacity in the community [63]. As part of the train-the-trainer approach, experts train professional service workers and lay volunteers to deliver services, reducing demands on time, resources, and manpower on financially strapped and understaffed professional social and health services in the community. Studies have shown that when lay volunteers are provided with training and supervision, their participation in community-based intervention programmes have significant effects on the outcomes [85, 86].
As part of the FHHCPP, a TTA was jointly developed by the FAMILY Project Team and the HKIWA. The TTA was conducted for lay volunteers (Health Ambassadors) to enhance their health-related knowledge and skills and meet the manpower needs of the following large-scale community-based programmes. The training aimed to raise Health Ambassadors’ awareness regarding health behaviours and empower them to combat unhealthy diet and insufficient physical activity. The Health Ambassadors were first empowered to adopt healthy lifestyles involving healthy diet and physical activity, and to share and influence their family and friends, and then influence the participants of their interventions in the FHHCPP.
Two TTA workshops were conducted as part of the programme for the lay volunteers of the HKIWA during January 2016 to March 2016.
5.2 Objectives To increase trainees’ physical activity and improve their dietary habits, family
communication, and personal and family well-being; To invite trainees to share their learning with and influence the health behaviour of
their family members and community participants; To build capacity for the implementation of FHHCPP; and To use mobile messages further enhance healthy diet and physical activity.
5.3 Recruitment Lay volunteers were recruited through the strong networks of the HKIWA and its member associations. With the collaboration with member associations from four districts in Hong Kong (Southern district, Central and Western district, Wan Chai district, and Eastern district), 88 subjects were recruited into the TTA.
40
All trainees fulfilled the following inclusion criteria:
1. Ethnic Chinese, 18 years of age or older; and 2. Able to read Chinese and speak Cantonese.
5.4 Design The effects (or changes) were assessed in all subjects before and after the intervention. We did not use a no-intervention control group. Figure 5.1 shows the design of the cRCT to assess the effectiveness of a two-session intervention and 3 months’ daily electronic health messages. The participating member associations of the HKIWA were randomised into two intervention groups, either the PA group or the HD group. Each group acted as a “placebo” control group for the other.
All trainees in both groups received two 2-hour sessions, including a core session at baseline and a booster session at 1 month. The PA group received the PA booster session whilst the HD group received the HD booster session. The PA group received daily electronic messages related to physical activity and the HD group received daily electronic messages related to healthy diet, all for 3 months.
All trainees were trained as “Health Ambassadors”. They first learned to self-motivate themselves to form healthy living habits. The Health Ambassadors then implemented community-based interventions and health promotion activities for the community-based programme participants. Each Health Ambassador recruited 15-20 participants for the community-based interventions. The Health Ambassadors were also responsible for implementing physical fitness assessments for the community-based programme participants, helping them to complete questionnaires, providing them with reminders and encouragement to adopt health behaviours, and making telephone calls to conduct follow-up assessments.
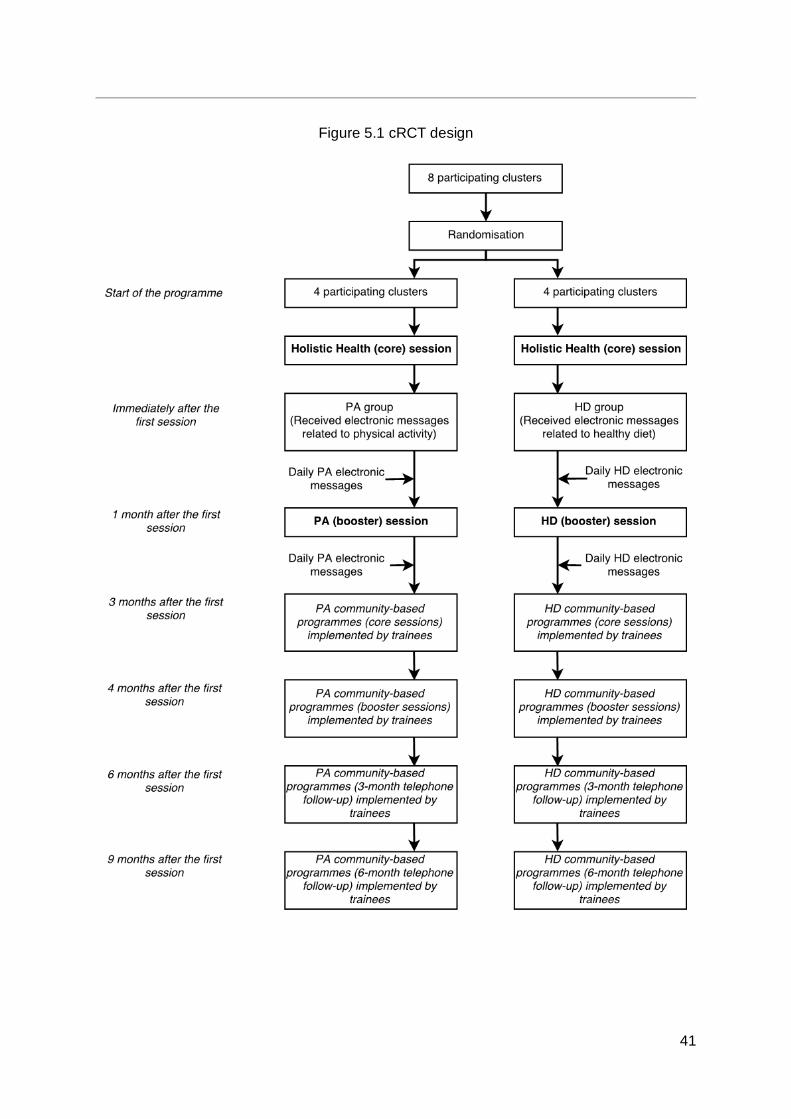
41
Figure 5.1 cRCT design
42
5.5 Training content
5.5.1 Pre-training phase We first conducted a pre-training meeting in January 2016 to obtain the input of the community leaders of the HKIWA to inform the intervention design and planning. The goals were:
1. To identify the needs, resources and feasibility of implementing and evaluating community-based interventions; and
2. To obtain input relevant to enhancing the acceptability and applicability of the TTA and community-based interventions.
5.5.2 Training phase
5.5.2.1 In-class training sessions Two training workshops were conducted, the first at Leighton Hill Community Hall and the second at the training centre at Times Square in Causeway Bay, during January 2016 to March 2016. The workshops were conducted by a multidisciplinary research team from the FAMILY Project Team, with experience in developing health promotion interventions in the community. The team consisted of academic public health professionals (a public health physician and a nurse) and a registered social worker. The TTA aimed not only to promote trainees’ competence (knowledge, self-efficacy and attitude) in implementing the community-based programmes for the general public, but also their personal and family health-related behaviour and well-being.
Both the HD group and the PA group received a 2-hour interactive core session (“Holistic Health session”) at baseline and a 2-hour booster session (PA session for the PA group and HD session for the HD group) at 1 month.
5.5.2.1.1 The core session Session I was a Holistic Health (core) session. The key components of the FHHCPP were introduced, including ZTEx, healthy diet as well as personal and family well-being. The training content of the core session was the same in the PA group and the HD group. The goals were to advocate a healthy lifestyle including regular physical activity and healthy eating habits, and positive family communication and well-being.
To start the session, physical fitness assessments were conducted with the aim of increasing trainees' interest in the intervention that followed. Age- and gender-specific physical fitness reference values and the clinical relevance of these values were presented and discussed with the trainees [87-92], encouraging them to compare their own results with the normative values. We highlighted the harmful effects of physical inactivity and obesity.
The intervention was guided by the Health Action Process Approach [93], and Figure 5.2 shows the essential components and strategies that were used in the model-based intervention.
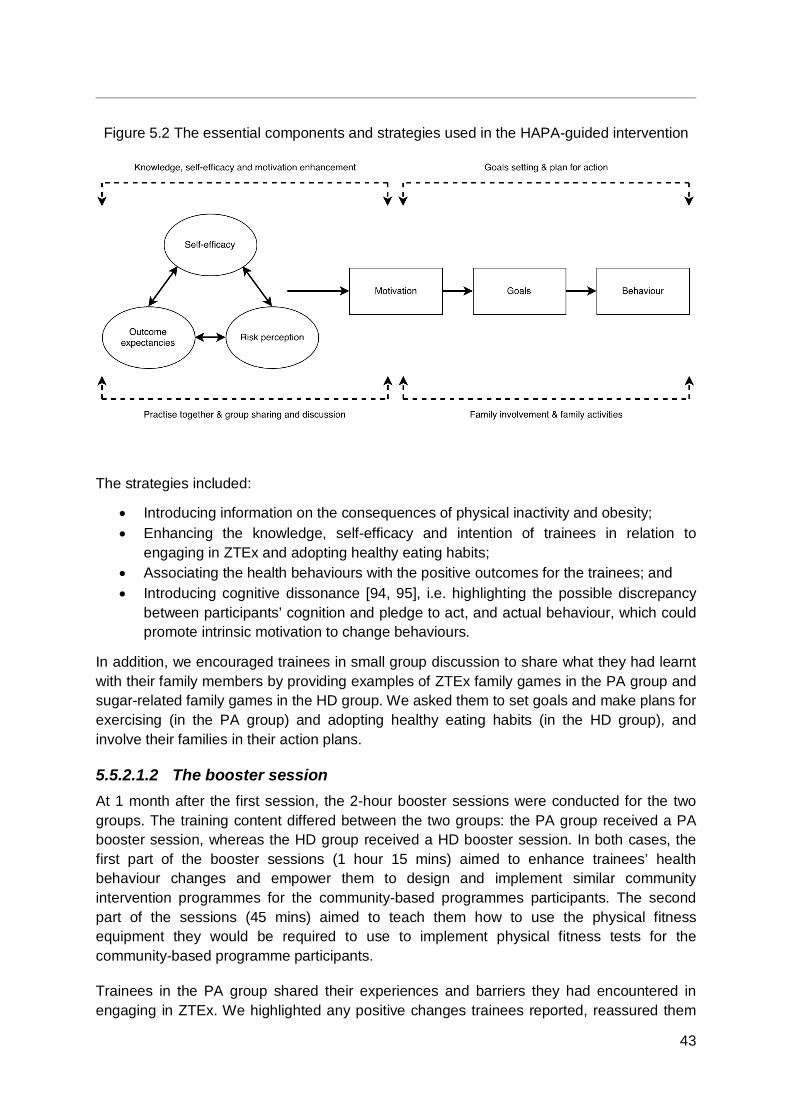
43
Figure 5.2 The essential components and strategies used in the HAPA-guided intervention
The strategies included:
Introducing information on the consequences of physical inactivity and obesity; Enhancing the knowledge, self-efficacy and intention of trainees in relation to
engaging in ZTEx and adopting healthy eating habits; Associating the health behaviours with the positive outcomes for the trainees; and Introducing cognitive dissonance [94, 95], i.e. highlighting the possible discrepancy
between participants’ cognition and pledge to act, and actual behaviour, which could promote intrinsic motivation to change behaviours.
In addition, we encouraged trainees in small group discussion to share what they had learnt with their family members by providing examples of ZTEx family games in the PA group and sugar-related family games in the HD group. We asked them to set goals and make plans for exercising (in the PA group) and adopting healthy eating habits (in the HD group), and involve their families in their action plans.
5.5.2.1.2 The booster session At 1 month after the first session, the 2-hour booster sessions were conducted for the two groups. The training content differed between the two groups: the PA group received a PA booster session, whereas the HD group received a HD booster session. In both cases, the first part of the booster sessions (1 hour 15 mins) aimed to enhance trainees’ health behaviour changes and empower them to design and implement similar community intervention programmes for the community-based programmes participants. The second part of the sessions (45 mins) aimed to teach them how to use the physical fitness equipment they would be required to use to implement physical fitness tests for the community-based programme participants.
Trainees in the PA group shared their experiences and barriers they had encountered in engaging in ZTEx. We highlighted any positive changes trainees reported, reassured them
44
that positive changes were likely to come with doing ZTEx regularly, and reminded them of the negative consequences of physical inactivity and sedentary behaviour.
Trainees in the HD group shared their experiences and barriers they had encountered in adopting low sugar practices. We highlighted any positive changes trainees reported, reassured them that positive changes were likely to come with adopting low sugar dietary practices regularly, and reminded them of the negative consequences of obesity and the related chronic illnesses.
The fidelity of the interventions delivered was assessed by two observers from the FAMILY Project Team separately. They used checklists with items derived from the outline of the training curriculum to ensure the quality of each training session.
5.5.2.2 The electronic messages Immediately after the core session, trainees in both groups received daily mobile messages through the instant messaging platform, WhatsApp. The PA group received well-structured mobile messages related to physical activity, ZTEx, examples of ZTEx, and suggested ZTEx family games (e.g. performing foot pedaling or cycling in the air with family members). The HD group received well-structured mobile messages concerning healthy diet, tips for adopting low sugar practices, and the suggested family games related to low sugar dietary practices (e.g. estimating the sugar content in a drink).
At the completion of training, every trainee was invited to join a graduation ceremony and received a certificate for training completion and an appointment letter for being health promoters.
5.5.3 Post-training phase Post-training support to trainees consisted of ongoing guidance, supervision and consultation. Two post–training support sessions were provided for the trainees, including: (i) an equipment training session that aimed to provide extra guidance on using the fitness measurement equipment; and (ii) a telephone interview training session that aimed to explain the “dos and don’ts” when making telephone calls to the community-based programme participants for the community-based programme 3-month and 6-month follow-up.
5.6 Evaluation
5.6.1 Outcomes
5.6.1.1 Primary outcome Knowledge, self-efficacy and intention in relation to engaging in ZTEx and adopting
low sugar practices
45
5.6.1.2 Secondary outcomes Physical activity; Physical fitness performance; Dietary habits; Family communication in relation to ZTEx and low-sugar dietary practices; Subjective assessment of personal and FAMILY 3Hs (Health, Happiness, Harmony); Confidence in being a Health Ambassador; and Feedback on the training workshops
5.6.2 Measurements Outcomes were assessed by self-reported questionnaires and physical fitness assessments at six time points: baseline, immediately and 1 month after the core session, immediately after the booster session, and 3 months, 4 months, 6 months and 9 months after the core session. Focus group interviews were conducted about 1 year after the core session.
Trainees indicated the extent of their agreement on statements in relation to their perceived knowledge, self-efficacy and intention in relation to engaging in ZTEx and adopting low sugar practice by themselves and with family members (for example, “I am confident that I am able to practise ZTEx regularly”). Each item allowed responses on a scale from “1=strongly disagree” to “6=strongly agree”.
Self-reported physical activity was assessed by questions adopted and modified from the International Physical Activities Questionnaire-Chinese version (IPAQ-C) [96, 97]. We assessed sedentary behaviour by asking two questions (for example, “On a typical weekday in the last 7 days, how many hours per day did you typically spend seated?”). We assessed the frequency (number of days) with which trainees engaged in physical activity in the last seven days by asking two questions (for example, “In the last 7 days, on how many days did you perform at least 10 minutes of moderate physical activity?”). Responses ranged from 0 to 7 days. The practice of positive communication with family members, sharing the information on and engaging in ZTEx and low sugar with family members were assessed by outcome-based questions. Each item allowed responses on a scale from “1=never” to “5=daily”.
Physical fitness assessments with standardised protocols were used to assess trainees’ physical fitness performance, including hand grip strength measured by a dynamometer [98, 99], lower limbs strength assessed by the 30-second chair stand test [100, 101] (the number of sitting-to-standing repetitions the individual was able to complete in 30 seconds), balance assessed by the single leg stance test [102] (the number of seconds that the individual could effectively balance on one leg, up to a maximum of 120 seconds), and flexibility assessed by the chair sit-and-reach test [103] (the distance reached by the hand).
We asked the trainees to indicate their self-reported FAMILY health, happiness and harmony using three questions: “Do you think your family is healthy?”; “Do you think your family is happy?”; and “Do you think your family is harmonious?”. Self-reported personal health and happiness were assessed by asking two questions: “Do you think you are healthy?” and “Do you think you are happy?”. Each item allowed a response on a scale from “0=very unhealthy/unhappy/disharmonious” to “10=very healthy/happy/harmonious”.
46
Fidelity checks were conducted for every training session, which ensured the quality of the training.
The qualitative focus group interviews were audio-taped and transcribed verbatim in Cantonese. Two project team members, one of whom attended the interviews, coded the transcripts. Transcripts were analysed by thematic content analysis, following the guidelines recommended by Morse and Field [84] and the software NVivo 11 was used. Field notes were reviewed with the transcripts to organise and summarise the data. Mixed Method Triangulation design was used to interrelate and interpret the qualitative and quantitative data to validate the results [105].
5.6.3 Statistical analysis Quantitative data were analyzed using SPSS 24.0. The demographic characteristics of the participants were described using frequencies and percentages, and the baseline scores of outcome variables were described using means and standard deviations. To examine whether the cluster randomisation resulted in comparability among the groups, Pearson’s chi-square tests and independent t-tests were conducted to compare the demographic characteristics and baseline scores between the groups. To examine the effectiveness of the training programme, linear mixed model analysis was carried out. This analytical procedure was adopted to assess whether there were differences in the outcome changes between two groups. The principle of intention-to-treat (ITT) analysis was adopted through imputing missing observations from lost to follow-up or decline to complete follow-up questionnaires using the baseline values (i.e., assuming no changes). Sensitivity analysis was performed by using “complete case analysis”, exclusively with trainees with complete evaluations at all assessment time points. An effect size (Cohen’s d) of 0.2 was considered as a small effect, 0.5 as a medium effect, and 0.8 or above as a large effect. All significance tests were two-sided with a 5% level of significance.
5.7 Quantitative evaluation
5.7.1 Recruitment 74 trainees attended the core session and were recruited into the trial. 36 and 38 trainees were randomised into the PA group and the HD group, respectively. Figure 5.3 shows the flow of trainees.
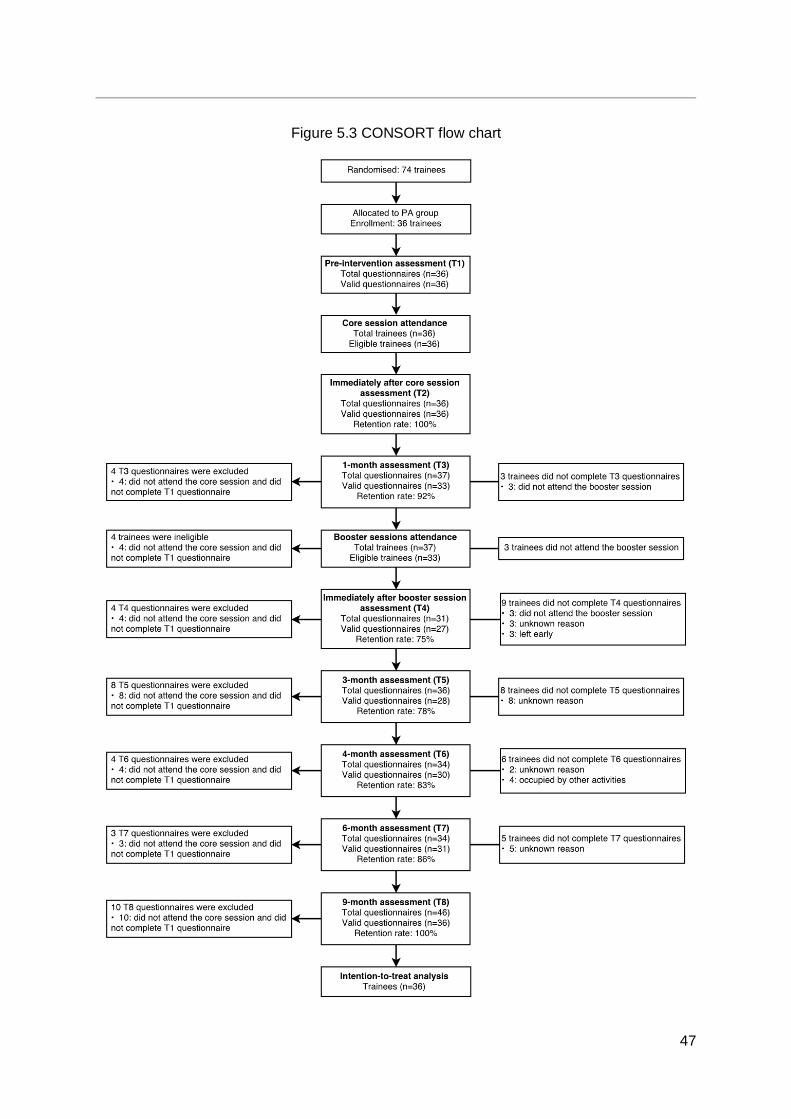
47
Figure 5.3 CONSORT flow chart
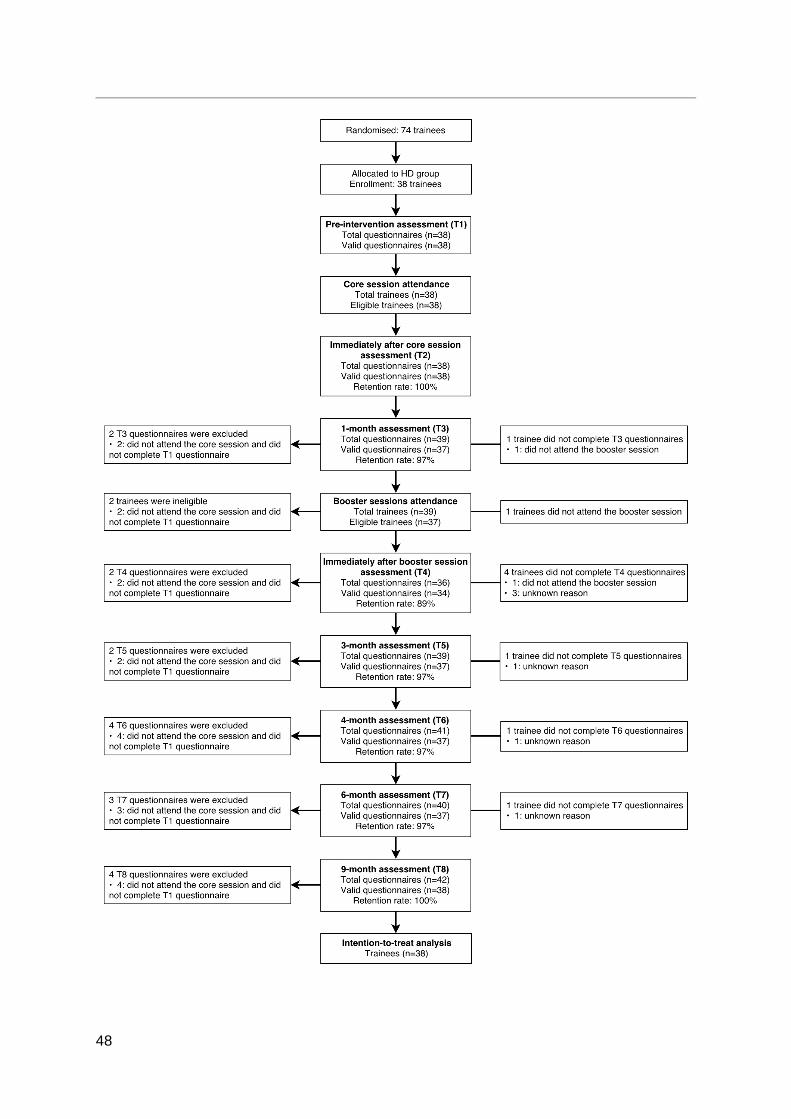
48
49
5.7.2 Characteristics of trainees The trainees were randomised into either the PA group (n=36) or the HD group (n=38). As shown in Table 5.1, most trainees in each group were female (97% in the PA group and 89% in the HD group). Trainees of the HD group were significantly older than those of the PA group (p=0.037). Self-reported personal health was greater in the HD group than in the PA group (p=0.017). Age, sex and baseline values were included as covariates in the subsequent analyses.
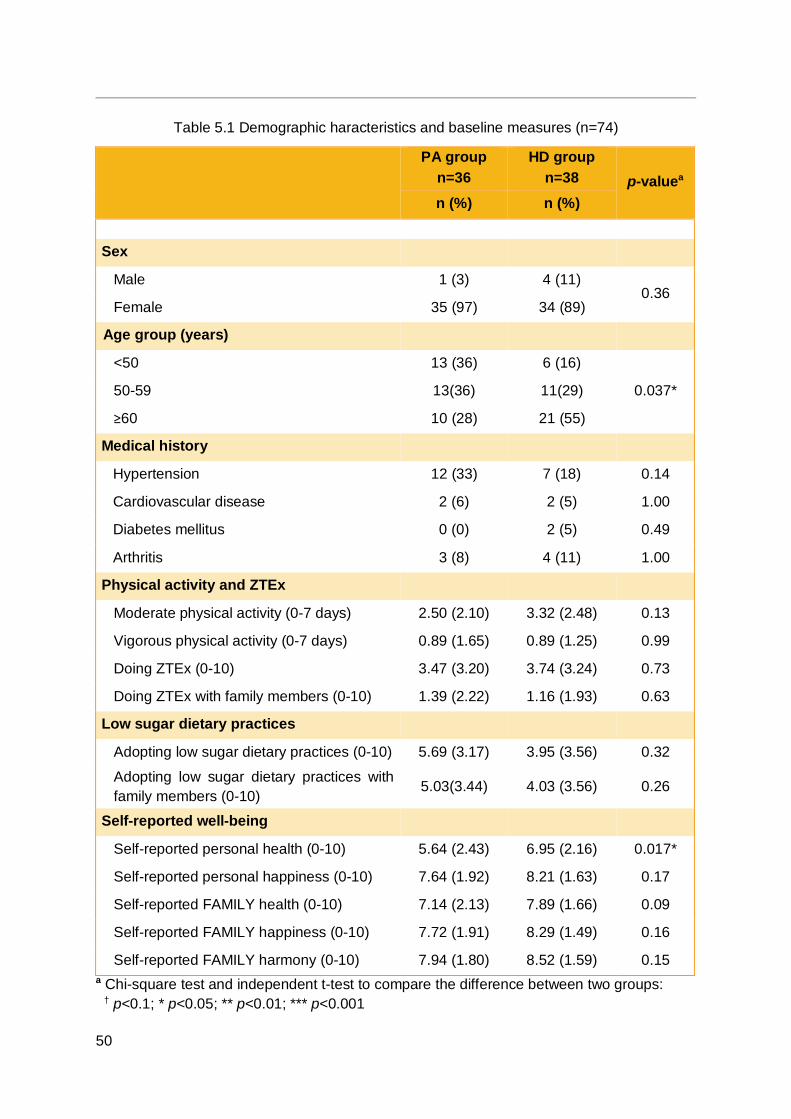
50
Table 5.1 Demographic haracteristics and baseline measures (n=74)
PA group
n=36 HD group
n=38 p-valuea n (%) n (%)
Sex
Male 1 (3) 4 (11) 0.36
Female 35 (97) 34 (89)
Age group (years)
<50 13 (36) 6 (16)
0.037* 50-59 13(36) 11(29)
≥60 10 (28) 21 (55)
Medical history
Hypertension 12 (33) 7 (18) 0.14
Cardiovascular disease 2 (6) 2 (5) 1.00
Diabetes mellitus 0 (0) 2 (5) 0.49
Arthritis 3 (8) 4 (11) 1.00
Physical activity and ZTEx
Moderate physical activity (0-7 days) 2.50 (2.10) 3.32 (2.48) 0.13
Vigorous physical activity (0-7 days) 0.89 (1.65) 0.89 (1.25) 0.99
Doing ZTEx (0-10) 3.47 (3.20) 3.74 (3.24) 0.73
Doing ZTEx with family members (0-10) 1.39 (2.22) 1.16 (1.93) 0.63
Low sugar dietary practices
Adopting low sugar dietary practices (0-10) 5.69 (3.17) 3.95 (3.56) 0.32
Adopting low sugar dietary practices with family members (0-10)
5.03(3.44) 4.03 (3.56) 0.26
Self-reported well-being
Self-reported personal health (0-10) 5.64 (2.43) 6.95 (2.16) 0.017*
Self-reported personal happiness (0-10) 7.64 (1.92) 8.21 (1.63) 0.17
Self-reported FAMILY health (0-10) 7.14 (2.13) 7.89 (1.66) 0.09
Self-reported FAMILY happiness (0-10) 7.72 (1.91) 8.29 (1.49) 0.16
Self-reported FAMILY harmony (0-10) 7.94 (1.80) 8.52 (1.59) 0.15 a Chi-square test and independent t-test to compare the difference between two groups: † p<0.1; * p<0.05; ** p<0.01; *** p<0.001
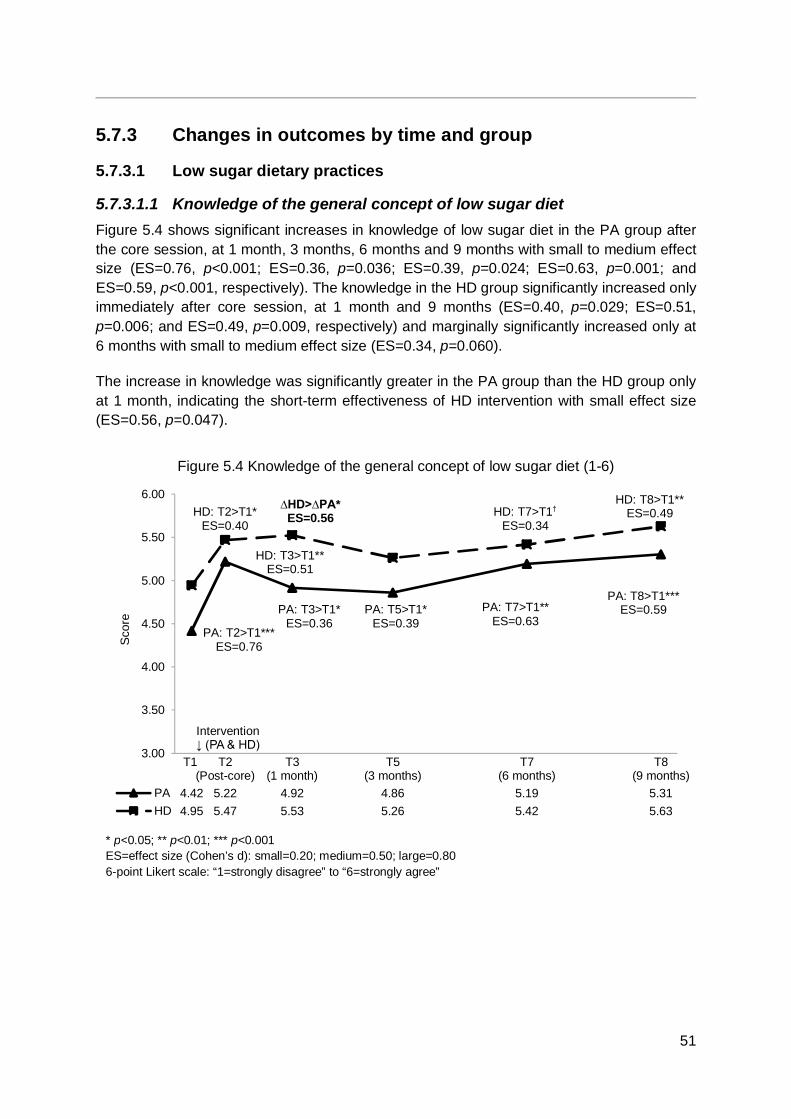
51
5.7.3 Changes in outcomes by time and group
5.7.3.1 Low sugar dietary practices
5.7.3.1.1 Knowledge of the general concept of low sugar diet Figure 5.4 shows significant increases in knowledge of low sugar diet in the PA group after the core session, at 1 month, 3 months, 6 months and 9 months with small to medium effect size (ES=0.76, p<0.001; ES=0.36, p=0.036; ES=0.39, p=0.024; ES=0.63, p=0.001; and ES=0.59, p<0.001, respectively). The knowledge in the HD group significantly increased only immediately after core session, at 1 month and 9 months (ES=0.40, p=0.029; ES=0.51, p=0.006; and ES=0.49, p=0.009, respectively) and marginally significantly increased only at 6 months with small to medium effect size (ES=0.34, p=0.060).
The increase in knowledge was significantly greater in the PA group than the HD group only at 1 month, indicating the short-term effectiveness of HD intervention with small effect size (ES=0.56, p=0.047).
Figure 5.4 Knowledge of the general concept of low sugar diet (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 4.42 5.22 4.92 4.86 5.19 5.31HD 4.95 5.47 5.53 5.26 5.42 5.63
Scor
e
PA: T8>T1***ES=0.59
∆HD>∆PA*ES=0.56
Intervention↓ (PA & HD)
* p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
PA: T7>T1** ES=0.63
HD: T2>T1* ES=0.40
PA: T2>T1*** ES=0.76
HD: T3>T1** ES=0.51
PA: T3>T1* ES=0.36
PA: T5>T1* ES=0.39
HD: T7>T1†
ES=0.34 HD: T8>T1**
ES=0.49

52
5.7.3.1.2 Intention to adopt low sugar dietary practices regularly Figure 5.5 shows a marginally significant increase in intention to adopt low sugar dietary practices in the PA group only immediately after core session (ES=0.39, p=0.057) and significant increases at 6 months and 9 months (ES=0.45, p=0.016 and ES=0.50, p=0.008, respectively) with small to medium effect size. The HD group showed no significant increases.
The increase in intention at 1 month was significantly greater in the HD group than the PA group, indicating the short-term effectiveness of HD intervention with small effect size (ES=0.49, p=0.039).
Figure 5.5 Intention to adopt low sugar dietary practices regularly (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 4.69 5.03 4.89 4.92 5.28 5.42HD 5.37 5.53 5.55 5.24 5.39 5.63
Scor
e
∆HD>∆PA*ES=0.49
Intervention↓ (PA & HD)
† p<0.1; * p<0.05; ** p<0.01 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
PA: T2>T1† ES=0.39
PA: T8>T1** ES=0.50
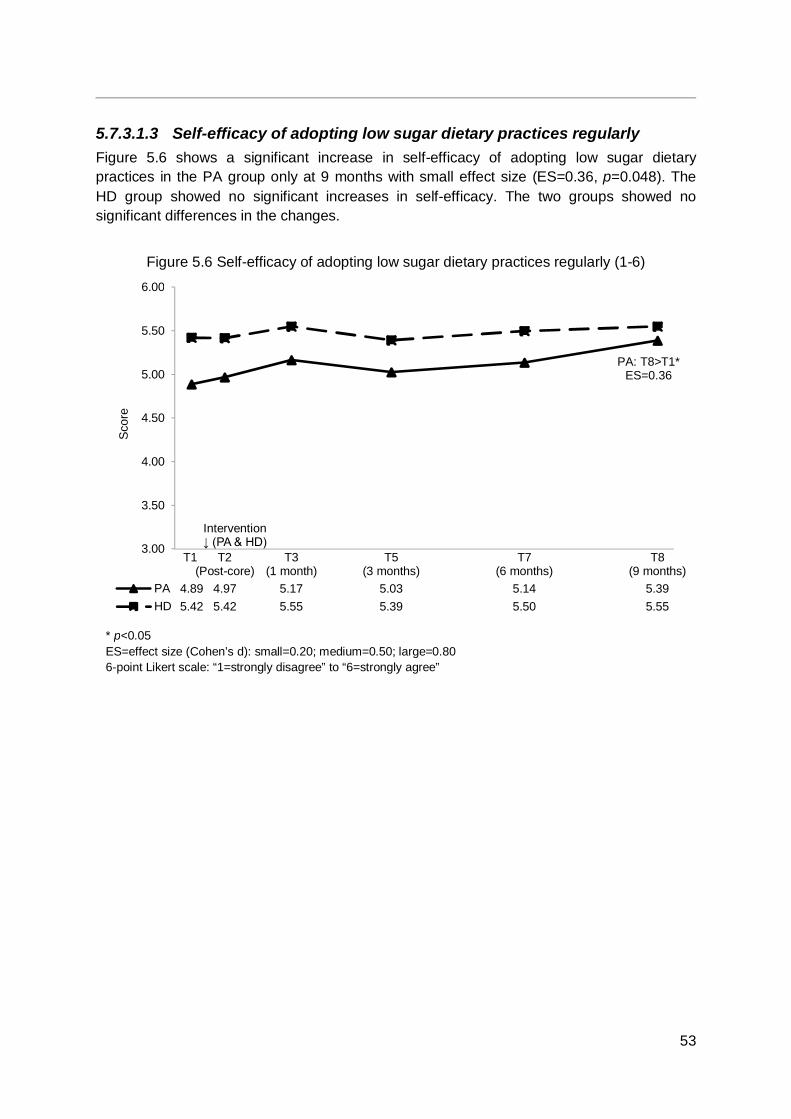
53
5.7.3.1.3 Self-efficacy of adopting low sugar dietary practices regularly Figure 5.6 shows a significant increase in self-efficacy of adopting low sugar dietary practices in the PA group only at 9 months with small effect size (ES=0.36, p=0.048). The HD group showed no significant increases in self-efficacy. The two groups showed no significant differences in the changes.
Figure 5.6 Self-efficacy of adopting low sugar dietary practices regularly (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 4.89 4.97 5.17 5.03 5.14 5.39HD 5.42 5.42 5.55 5.39 5.50 5.55
Scor
e
Intervention↓ (PA & HD)
* p<0.05 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
PA: T8>T1* ES=0.36

54
5.7.3.1.4 Adopting low sugar dietary practices Figure 5.7 shows a significant increase in adopting low sugar dietary practices in the PA group only at 9 months with small effect size (ES=0.42, p=0.019). The low sugar dietary practices in the HD group significantly increased at 1 month, 3 months , 6 months and 9 months with small to large effect size (ES=0.35, p=0.021; ES=0.65, p<0.001; ES=0.90, p<0.001; and ES=1.17, p<0.001, respectively).
The increases were significantly greater in the HD group than the PE group only at 3 months, 6 months and 9 months, indicating the effectiveness of HD intervention with small to medium effect size (ES=0.57, p=0.037; ES=0.59, p=0.014; and ES=0.62, p=0.027, respectively).
Figure 5.7 Adopting low sugar practices (0-10)
2
3
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 5.69 5.54 5.40 5.89 7.17HD 3.95 5.38 6.56 7.22 8.27
Scor
e
∆HD>∆PA*ES=0.57
Intervention↓ (PA & HD)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never” to “10=always”
∆HD>∆PA* ES=0.59
∆HD>∆PA* ES=0.62
HD: T3>T1* ES=0.35
HD: T5>T1*** ES=0.65
HD: T7>T1*** ES=0.90
HD: T8>T1*** ES=1.17
PA: T8>T1* ES=0.42
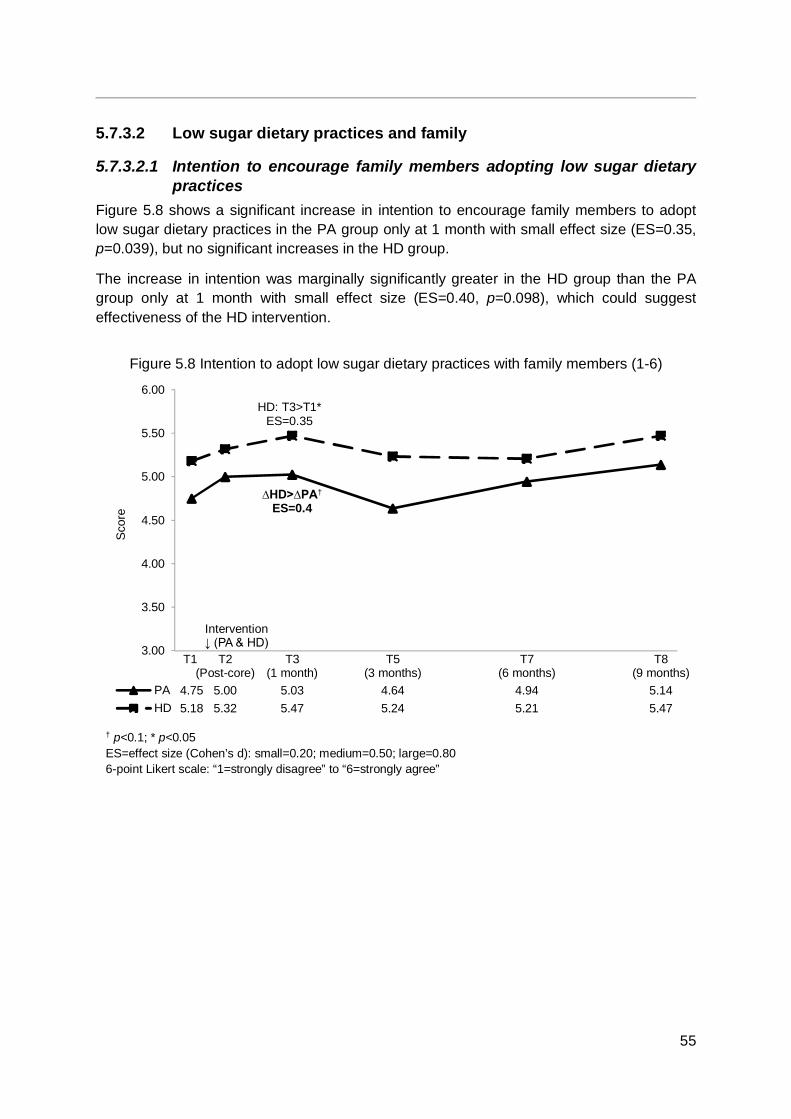
55
5.7.3.2 Low sugar dietary practices and family
5.7.3.2.1 Intention to encourage family members adopting low sugar dietary practices
Figure 5.8 shows a significant increase in intention to encourage family members to adopt low sugar dietary practices in the PA group only at 1 month with small effect size (ES=0.35, p=0.039), but no significant increases in the HD group.
The increase in intention was marginally significantly greater in the HD group than the PA group only at 1 month with small effect size (ES=0.40, p=0.098), which could suggest effectiveness of the HD intervention.
Figure 5.8 Intention to adopt low sugar dietary practices with family members (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 4.75 5.00 5.03 4.64 4.94 5.14HD 5.18 5.32 5.47 5.24 5.21 5.47
Scor
e
∆HD>∆PA†
ES=0.4
Intervention↓ (PA & HD)
† p<0.1; * p<0.05 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
HD: T3>T1* ES=0.35
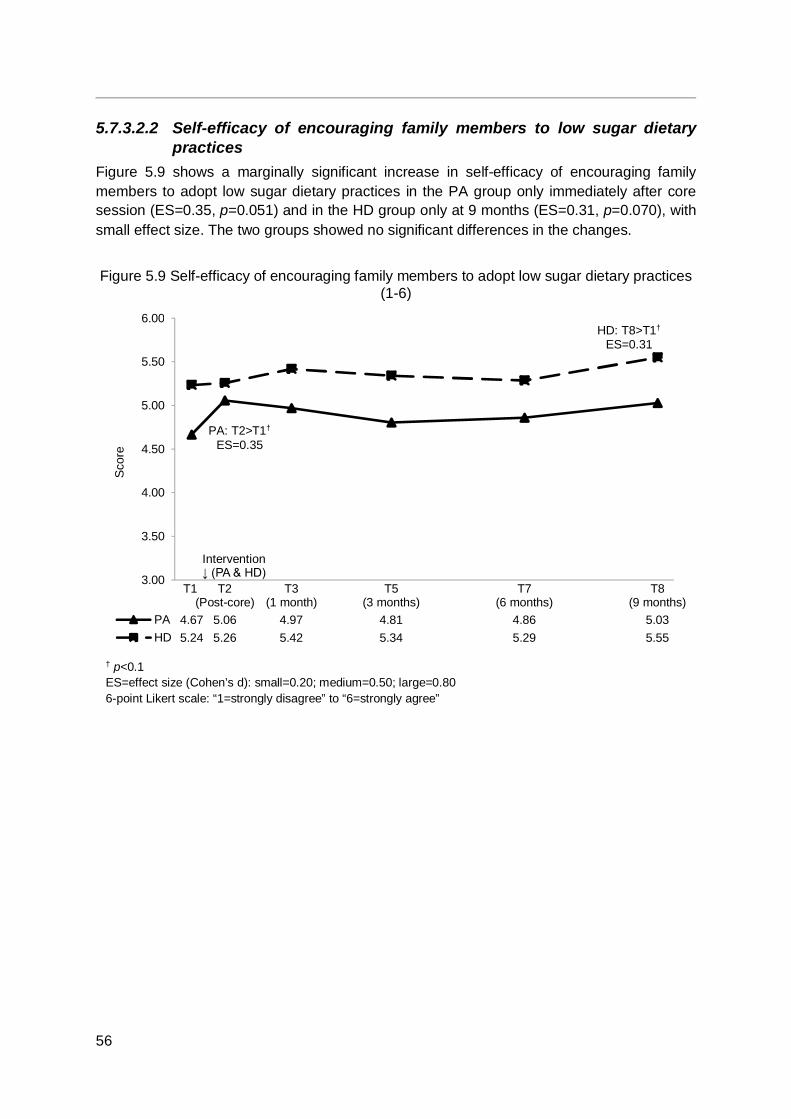
56
5.7.3.2.2 Self-efficacy of encouraging family members to low sugar dietary practices
Figure 5.9 shows a marginally significant increase in self-efficacy of encouraging family members to adopt low sugar dietary practices in the PA group only immediately after core session (ES=0.35, p=0.051) and in the HD group only at 9 months (ES=0.31, p=0.070), with small effect size. The two groups showed no significant differences in the changes.
Figure 5.9 Self-efficacy of encouraging family members to adopt low sugar dietary practices (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 4.67 5.06 4.97 4.81 4.86 5.03HD 5.24 5.26 5.42 5.34 5.29 5.55
Scor
e
Intervention↓ (PA & HD)
† p<0.1 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
PA: T2>T1†
ES=0.35
HD: T8>T1†
ES=0.31
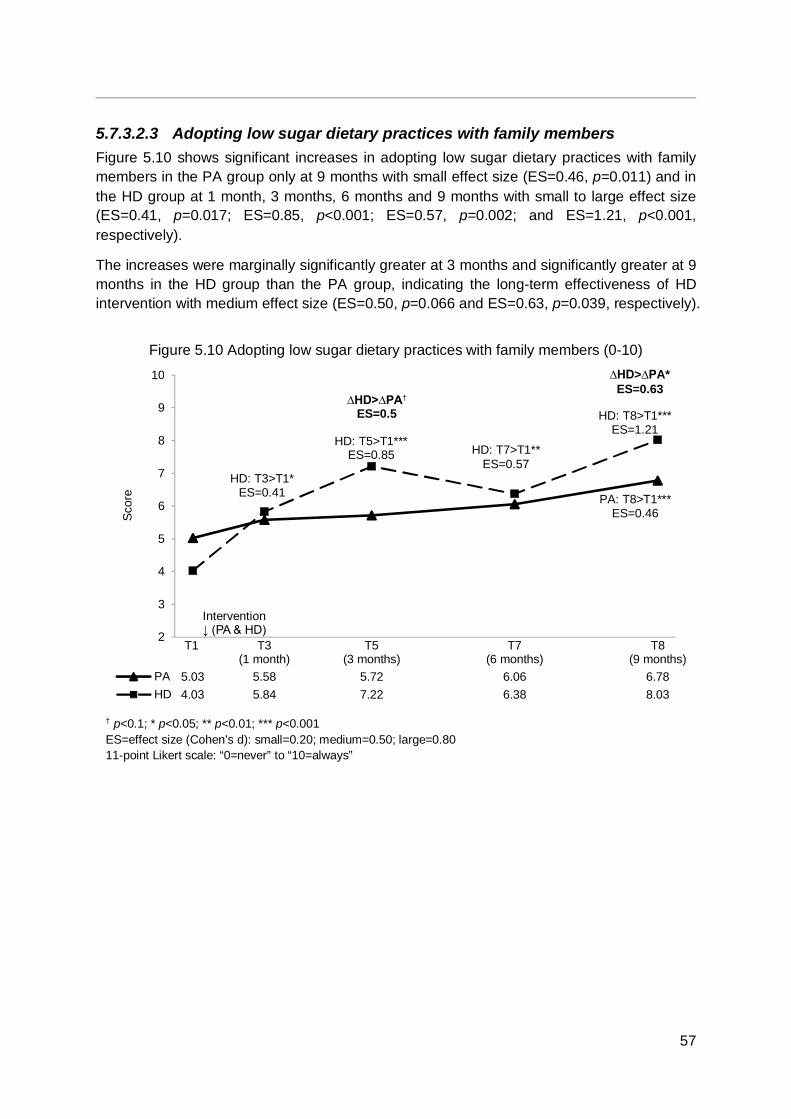
57
5.7.3.2.3 Adopting low sugar dietary practices with family members Figure 5.10 shows significant increases in adopting low sugar dietary practices with family members in the PA group only at 9 months with small effect size (ES=0.46, p=0.011) and in the HD group at 1 month, 3 months, 6 months and 9 months with small to large effect size (ES=0.41, p=0.017; ES=0.85, p<0.001; ES=0.57, p=0.002; and ES=1.21, p<0.001, respectively).
The increases were marginally significantly greater at 3 months and significantly greater at 9 months in the HD group than the PA group, indicating the long-term effectiveness of HD intervention with medium effect size (ES=0.50, p=0.066 and ES=0.63, p=0.039, respectively).
Figure 5.10 Adopting low sugar dietary practices with family members (0-10)
2
3
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 5.03 5.58 5.72 6.06 6.78HD 4.03 5.84 7.22 6.38 8.03
Scor
e
∆HD>∆PA†
ES=0.5
Intervention↓ (PA & HD)
† p<0.1; * p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never” to “10=always”
HD: T8>T1*** ES=1.21
∆HD>∆PA* ES=0.63
PA: T8>T1*** ES=0.46
HD: T7>T1** ES=0.57
HD: T3>T1* ES=0.41
HD: T5>T1*** ES=0.85

58
5.7.3.3 Physical activity and ZTEx
5.7.3.3.1 Knowledge of ZTEx Figure 5.11 shows significant increases in knowledge of ZTEx in the PA group immediately after core session, at 1 month, 3 months, 6 months and 9 months with medium effect size (ES=0.88, p<0.001; ES=0.59, p=0.001; ES=0.65, p=0.001; ES=0.78, p<0.001; and ES=0.74, p<0.001, respectively). The knowledge in the HD group significantly increased only immediately after core session, at 6 months and 9 months with small to medium effect size (ES=0.46, p=0.010; ES=0.41, p=0.018; and ES=0.65, p<0.001, respectively). The two groups did not show significant differences in the changes.
Figure 5.11 Knowledge of ZTEx (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 4.03 5.25 5.03 5.00 5.31 5.31HD 4.92 5.42 5.24 5.16 5.39 5.68
Scor
e
Intervention↓ (PA & HD)
* p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
HD: T2>T1* ES=0.46
PA: T2>T1***
ES=0.88
PA: T3>T1**
ES=0.59 PA: T5>T1** ES=0.65
HD: T7>T1* ES=0.41
PA: T7>T1*** ES=0.78
HD: T8>T1*** ES=0.65
PA: T8>T1*** ES=0.74
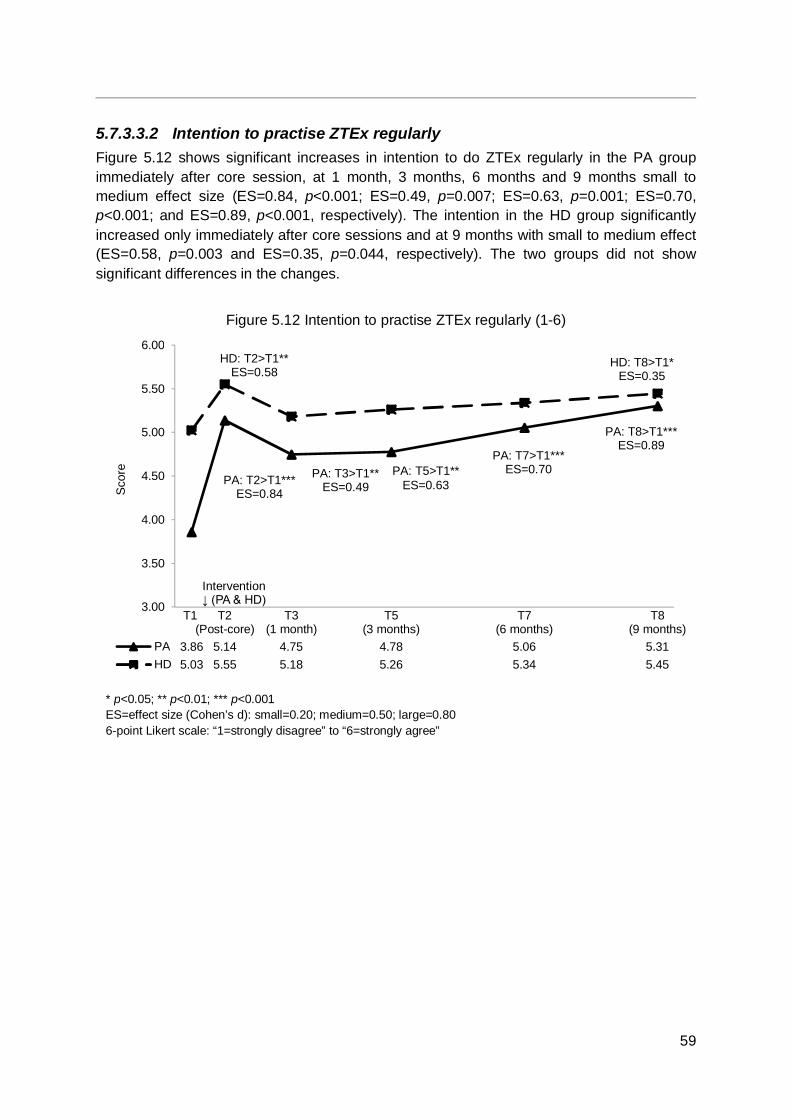
59
5.7.3.3.2 Intention to practise ZTEx regularly Figure 5.12 shows significant increases in intention to do ZTEx regularly in the PA group immediately after core session, at 1 month, 3 months, 6 months and 9 months small to medium effect size (ES=0.84, p<0.001; ES=0.49, p=0.007; ES=0.63, p=0.001; ES=0.70, p<0.001; and ES=0.89, p<0.001, respectively). The intention in the HD group significantly increased only immediately after core sessions and at 9 months with small to medium effect (ES=0.58, p=0.003 and ES=0.35, p=0.044, respectively). The two groups did not show significant differences in the changes.
Figure 5.12 Intention to practise ZTEx regularly (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 3.86 5.14 4.75 4.78 5.06 5.31HD 5.03 5.55 5.18 5.26 5.34 5.45
Scor
e
PA: T2>T1***ES=0.84
PA: T3>T1**ES=0.49
PA: T7>T1***ES=0.70
PA: T8>T1***ES=0.89
HD: T2>T1**ES=0.58
HD: T8>T1*ES=0.35
Intervention↓ (PA & HD)
* p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
PA: T5>T1** ES=0.63

60
5.7.3.3.3 Self-efficacy of practising ZTEx regularly Figure 5.13 shows significant increases in self-efficacy of doing ZTEx regularly in the PA group immediately after core session, at 1 month, 3 months, 6 months and 9 months with medium effect size (ES=0.64, p=0.003; ES=0.66, p=0.001; ES=0.62, p=0.001; ES=0.66, p=0.001; and ES=0.67, p<0.001, respectively). The self-efficacy of doing ZTEx in the HD group significantly increased only immediately after core session (ES=0.69, p<0.001) and marginally significantly increased only at 6 months and 9 months with small effect size (ES=0.27, p=0.091 and ES=0.28, p=0.097, respectively). The two groups did not show significant differences in the changes.
Figure 5.13 Self-efficacy of practising ZTEx regularly (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T6(4 months)
T7(6 months)
T8(9 months)
PA 3.94 4.89 4.86 4.83 4.89 5.06 5.14HD 5.00 5.58 5.26 5.11 5.00 5.32 5.32
Scor
e
PA: T2>T1***ES=0.64
PA:T7>T1**ES=0.66
PA: T8>T1***ES=0.67
HD:T7>T1†
ES=0.27HD: T8>T1†
ES=0.28
Intervention↓ (PA & HD)
† p<0.1; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree” to “6=strongly agree”
PA: T5>T1** ES=0.62
PA: T3>T1** ES=0.66
HD: T2>T1*** ES=0.69

61
5.7.3.3.4 Practising ZTEx Figure 5.14 shows significant increases in doing ZTEx in both the PA and HD groups with medium and large effect size at 1 month, 3 months, 6 months and 9 months (PA group: ES=0.88, p<0.001; ES=0.77, p<0.001; ES=1.19, p<0.001; and ES=1.34, p<0.001, respectively; HD group: ES=0.78, p<0.001; ES=0.66, p<0.001; ES=1.46, p<0.001; and ES=1.18, p<0.001, respectively). The two groups showed no significant differences in the changes.
Figure 5.14 Practising ZTEx (0-10)
2
3
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 3.47 6.31 5.81 6.75 7.92HD 3.74 6.24 5.87 7.39 8.11
Scor
e
PA: T3>T1***ES=0.88
HD: T3>T1***ES=0.78
PA: T5>T1***ES=0.77
HD: T5>T1***ES=0.66
PA: T7>T1***ES=1.19
HD:T7>T1***ES=1.46
PA: T8>T1***ES=1.34
HD: T8>T1***ES=1.18
Intervention↓ (PA & HD)
*** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never” to “10=always”

62
5.7.3.3.5 Moderate physical activity Figure 5.15 shows significant increases in moderate physical activity in the PA group at 1 month, 3 months, 6 months and 9 months with medium and large effect size (ES=0.54, p<0.001; ES=0.69, p<0.001; ES=0.63, p<0.001; and ES=0.80, p<0.001, respectively). Moderate physical activity in the HD group significantly increased only at 9 months with medium effect size (ES=0.51, p<0.001). The two groups did not show significant differences in the changes.
Figure 5.15 Moderate physical activity (0-7 days)
0
1
2
3
4
5
6
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 2.50 3.64 4.00 4.00 4.58HD 3.32 3.34 3.92 3.87 4.84
Day
PA: T5>T1***ES=0.69
PA: T7>T1***ES=0.63
PA: T8>T1***ES=0.83
HD: T8>T1**ES=0.51
PA: T3>T1**ES=0.54
Intervention↓ (PA & HD)
** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
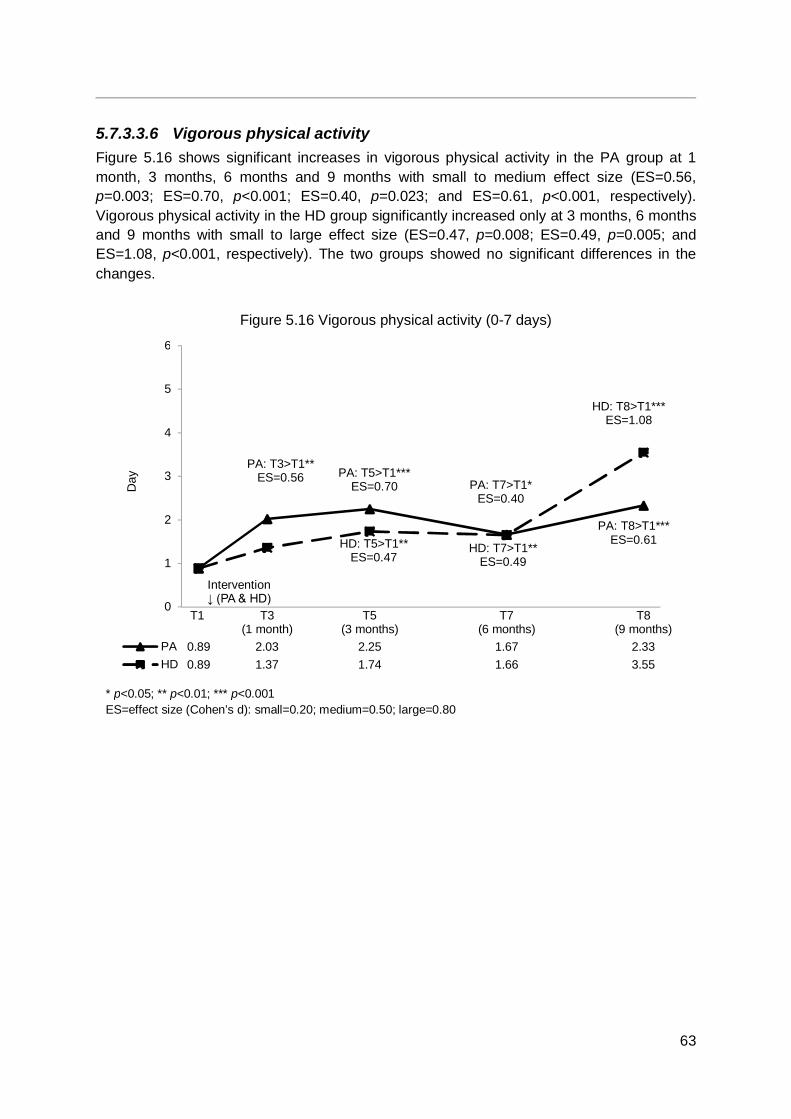
63
5.7.3.3.6 Vigorous physical activity Figure 5.16 shows significant increases in vigorous physical activity in the PA group at 1 month, 3 months, 6 months and 9 months with small to medium effect size (ES=0.56, p=0.003; ES=0.70, p<0.001; ES=0.40, p=0.023; and ES=0.61, p<0.001, respectively). Vigorous physical activity in the HD group significantly increased only at 3 months, 6 months and 9 months with small to large effect size (ES=0.47, p=0.008; ES=0.49, p=0.005; and ES=1.08, p<0.001, respectively). The two groups showed no significant differences in the changes.
Figure 5.16 Vigorous physical activity (0-7 days)
0
1
2
3
4
5
6
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 0.89 2.03 2.25 1.67 2.33HD 0.89 1.37 1.74 1.66 3.55
Day PA: T5>T1***
ES=0.70 PA: T7>T1*ES=0.40
HD: T5>T1**ES=0.47
HD: T7>T1**ES=0.49
HD: T8>T1***ES=1.08
PA: T3>T1**ES=0.56
Intervention↓ (PA & HD)
* p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
PA: T8>T1*** ES=0.61
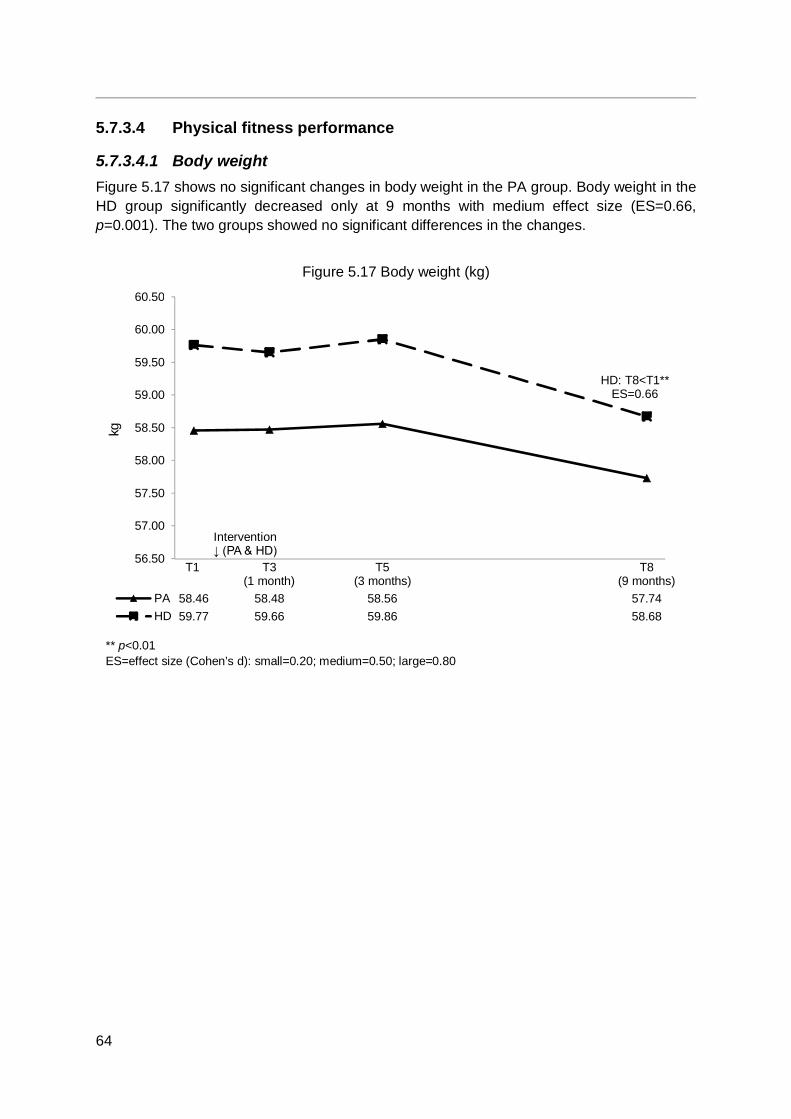
64
5.7.3.4 Physical fitness performance
5.7.3.4.1 Body weight Figure 5.17 shows no significant changes in body weight in the PA group. Body weight in the HD group significantly decreased only at 9 months with medium effect size (ES=0.66, p=0.001). The two groups showed no significant differences in the changes.
Figure 5.17 Body weight (kg)
56.50
57.00
57.50
58.00
58.50
59.00
59.50
60.00
60.50
T1 T3(1 month)
T5(3 months)
T8(9 months)
PA 58.46 58.48 58.56 57.74HD 59.77 59.66 59.86 58.68
kg
Intervention↓ (PA & HD)
** p<0.01 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
HD: T8<T1**
ES=0.66

65
5.7.3.4.2 Right hand grip strength Figure 5.18 shows significant increase in right hand grip strength in the PA group only at 1 month with small effect size (ES=0.46, p=0.022), but no significant increases in the HD group. The increase in right hand grip strength at 1 month was marginally significantly greater in the PA group than the HD group with medium effect size (ES=0.55, p=0.06), which could be suggestive evidence of the short-term effectiveness of PA intervention.
Figure 5.18 Right hand grip strength (kg)
20.00
21.00
22.00
23.00
24.00
25.00
26.00
27.00
28.00
29.00
30.00
T1 T3(1 month)
T5(3 months)
T8(9 months)
PA 24.08 25.87 24.45 23.68HD 25.13 24.85 24.23 24.36
kg
PA: T3>T1*ES=0.46
∆PA>∆HD†
ES=0.55
Intervention↓ (PA & HD)
† p<0.1; * p<0.05 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
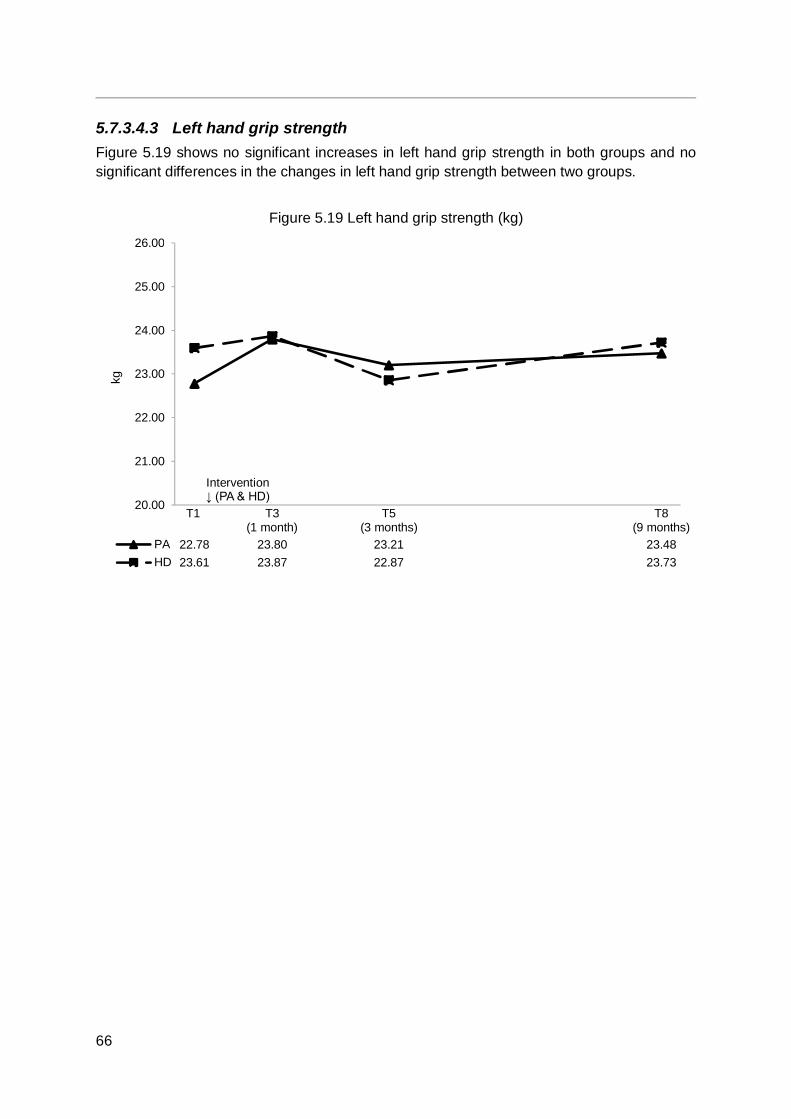
66
5.7.3.4.3 Left hand grip strength Figure 5.19 shows no significant increases in left hand grip strength in both groups and no significant differences in the changes in left hand grip strength between two groups.
Figure 5.19 Left hand grip strength (kg)
20.00
21.00
22.00
23.00
24.00
25.00
26.00
T1 T3(1 month)
T5(3 months)
T8(9 months)
PA 22.78 23.80 23.21 23.48HD 23.61 23.87 22.87 23.73
kg
Intervention↓ (PA & HD)

67
5.7.3.4.4 30-second chair stand test Figure 5.20 shows significant increases in the number of stands completed in the 30-second chair stand test at 1 month, 3 months and 9 months in the PA and HD groups with medium to large effect size (PA group: ES=1.29, p<0.001; ES=0.59, p=0.001; and ES=0.96, p<0.001, respectively; HD group: ES=0.62, p=0.001; ES=0.42, p=0.030; and ES=0.72, p<0.001, respectively). The PA group showed a significantly greater increase at 9 months than the HD group, indicating the long-term effectiveness of PA intervention with medium effect size (ES=0.68, p=0.020)
Figure 5.20 30-second chair stand test (no. of chair stands)
15.00
17.00
19.00
21.00
23.00
25.00
27.00
29.00
31.00
33.00
35.00
T1 T3(1 month)
T5(3 months)
T8(9 months)
PA 22.93 28.89 26.36 28.14HD 22.14 25.14 26.08 24.53
No.
of c
hair
stan
ds
PA: T3>T1***ES=1.29
PA:T5>T1**ES=0.59
HD: T3>T1**ES=0.62
HD: T5>T1*ES=0.42
Intervention↓ (PA & HD)
* p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
PA: T8>T1*** ES=0.96
HD: T8>T1*** ES=0.72
∆PA>∆HD* ES=0.68
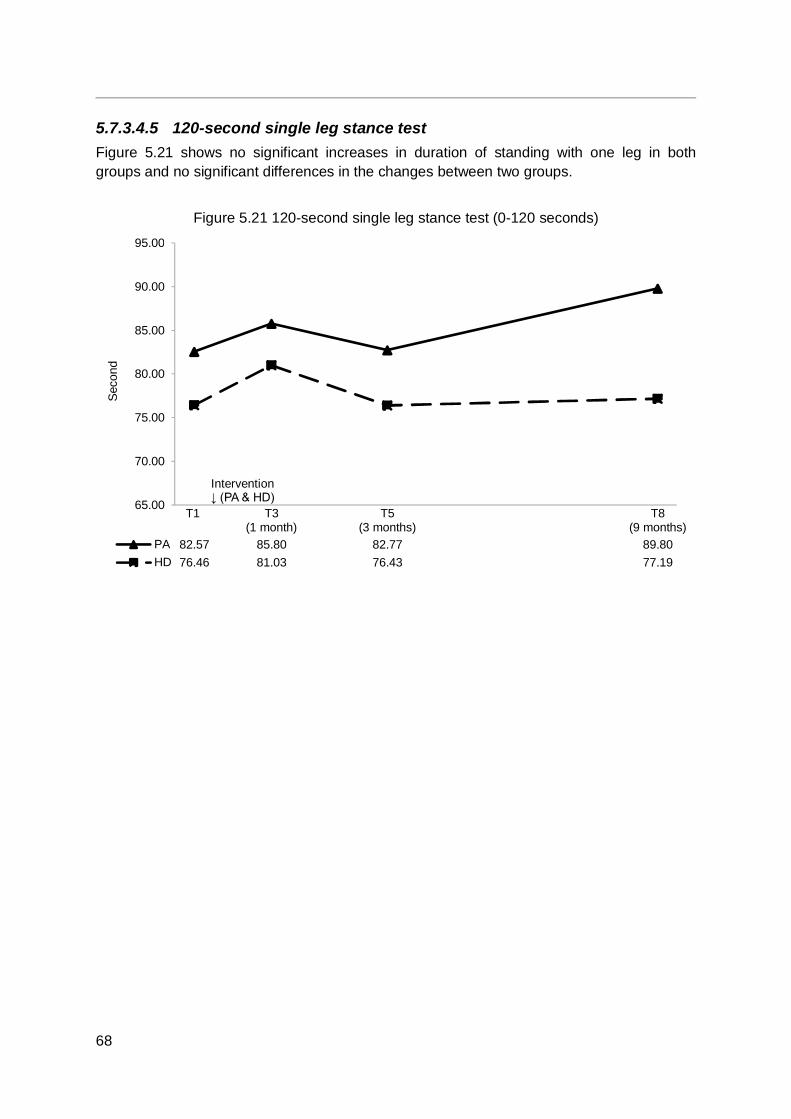
68
5.7.3.4.5 120-second single leg stance test Figure 5.21 shows no significant increases in duration of standing with one leg in both groups and no significant differences in the changes between two groups.
Figure 5.21 120-second single leg stance test (0-120 seconds)
65.00
70.00
75.00
80.00
85.00
90.00
95.00
T1 T3(1 month)
T5(3 months)
T8(9 months)
PA 82.57 85.80 82.77 89.80HD 76.46 81.03 76.43 77.19
Seco
nd
Intervention↓ (PA & HD)
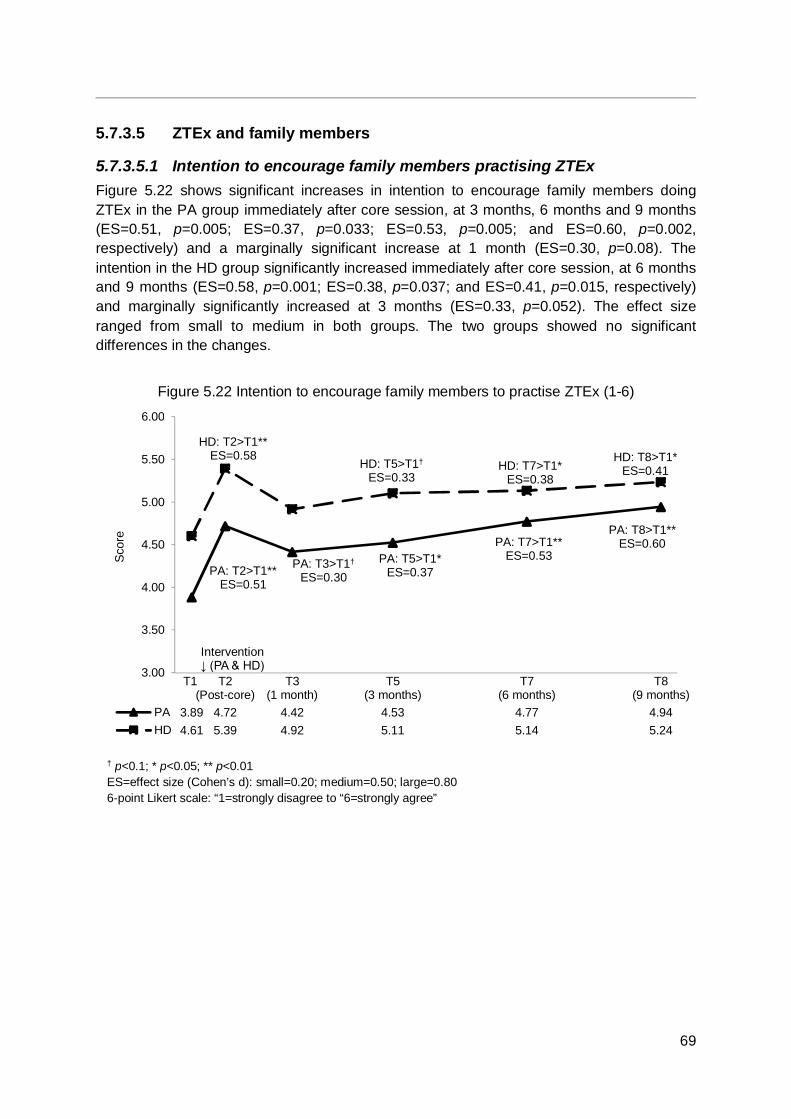
69
5.7.3.5 ZTEx and family members
5.7.3.5.1 Intention to encourage family members practising ZTEx Figure 5.22 shows significant increases in intention to encourage family members doing ZTEx in the PA group immediately after core session, at 3 months, 6 months and 9 months (ES=0.51, p=0.005; ES=0.37, p=0.033; ES=0.53, p=0.005; and ES=0.60, p=0.002, respectively) and a marginally significant increase at 1 month (ES=0.30, p=0.08). The intention in the HD group significantly increased immediately after core session, at 6 months and 9 months (ES=0.58, p=0.001; ES=0.38, p=0.037; and ES=0.41, p=0.015, respectively) and marginally significantly increased at 3 months (ES=0.33, p=0.052). The effect size ranged from small to medium in both groups. The two groups showed no significant differences in the changes.
Figure 5.22 Intention to encourage family members to practise ZTEx (1-6)
3.00
3.50
4.00
4.50
5.00
5.50
6.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 3.89 4.72 4.42 4.53 4.77 4.94HD 4.61 5.39 4.92 5.11 5.14 5.24
Scor
e
PA: T3>T1†
ES=0.30PA: T2>T1**ES=0.51
PA: T5>T1*ES=0.37
PA: T7>T1**ES=0.53
PA: T8>T1**ES=0.60
HD: T2>T1**ES=0.58
HD: T5>T1†
ES=0.33HD: T7>T1*
ES=0.38
HD: T8>T1*ES=0.41
Intervention↓ (PA & HD)
† p<0.1; * p<0.05; ** p<0.01 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree to “6=strongly agree”
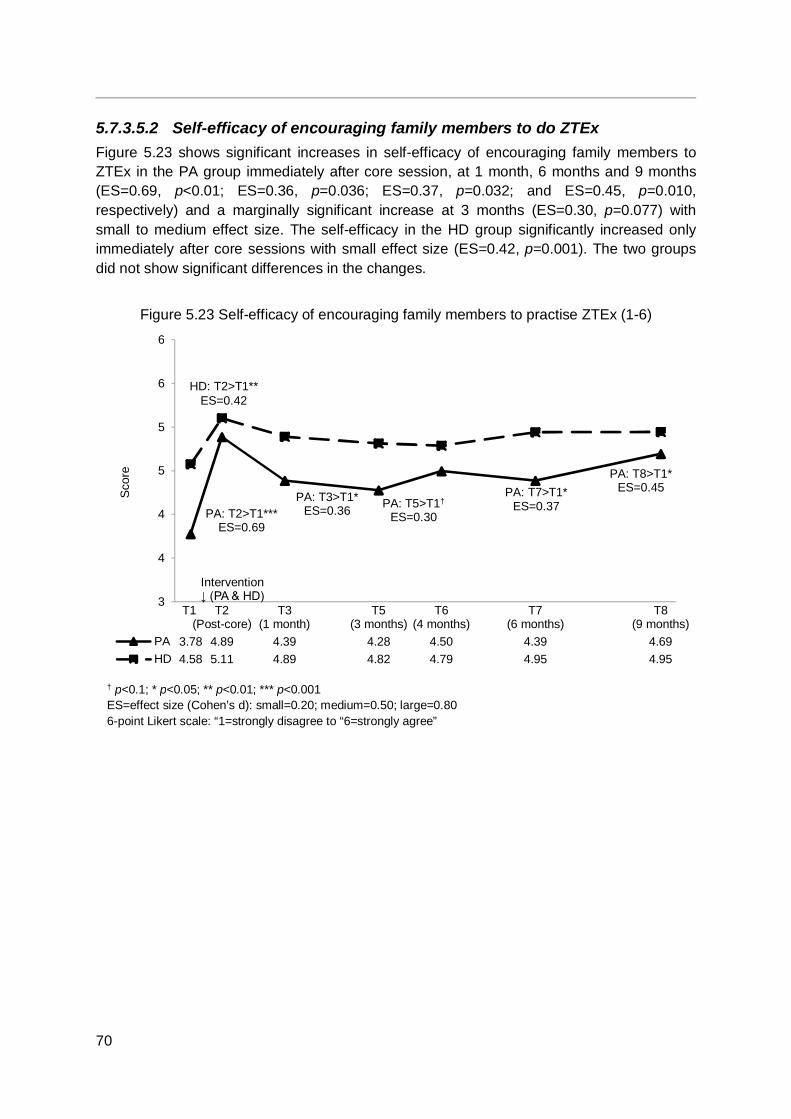
70
5.7.3.5.2 Self-efficacy of encouraging family members to do ZTEx Figure 5.23 shows significant increases in self-efficacy of encouraging family members to ZTEx in the PA group immediately after core session, at 1 month, 6 months and 9 months (ES=0.69, p<0.01; ES=0.36, p=0.036; ES=0.37, p=0.032; and ES=0.45, p=0.010, respectively) and a marginally significant increase at 3 months (ES=0.30, p=0.077) with small to medium effect size. The self-efficacy in the HD group significantly increased only immediately after core sessions with small effect size (ES=0.42, p=0.001). The two groups did not show significant differences in the changes.
Figure 5.23 Self-efficacy of encouraging family members to practise ZTEx (1-6)
3
4
4
5
5
6
6
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T6(4 months)
T7(6 months)
T8(9 months)
PA 3.78 4.89 4.39 4.28 4.50 4.39 4.69HD 4.58 5.11 4.89 4.82 4.79 4.95 4.95
Scor
e
PA: T2>T1***ES=0.69
PA: T3>T1*ES=0.36 PA: T5>T1†
ES=0.30
PA: T8>T1*ES=0.45
Intervention↓ (PA & HD)
† p<0.1; * p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=strongly disagree to “6=strongly agree”
PA: T7>T1* ES=0.37
HD: T2>T1** ES=0.42

71
5.7.3.5.3 Practising ZTEx with family members Figure 5.24 shows significant increases in practising ZTEx with family members in the PA and HD groups at 1 month, 3 months, 6 months and 9 months with medium to large effect size (PA group: ES=0.65, p=0.001; ES=0.78, p<0.001; ES=0.56, p=0.004; and ES=0.65, p<0.001, respectively; HD group: ES=0.86, p<0.001; ES=1.04, p<0.001; ES=0.97, p<0.001; and ES=1.18, p<0.001, respectively).
The increases in doing ZTEx with family members was marginally significantly greater in the HD group than the PA group only at 6 months with medium effect size (ES=0.40, p=0.092), which could be suggestive evidence of the effectiveness of HD intervention.
Figure 5.24 Practising ZTEx with family members (0-10)
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
T1 T2(Post-core)
T3(1 month)
T5(3 months)
T6(4 months)
T7(6 months)
T8(9 months)
PA 1.39 3.61 3.83 4.36 3.45 4.14HD 1.16 3.47 3.84 4.45 3.97 5.58
Scor
e
HD: T3>T1***ES=0.86
HD: T5>T1***ES=1.04
PA: T5>T1***ES=0.78
HD: T7>T1***ES=0.97
PA: T7>T1**ES=0.56
HD: T8>T1***ES=1.18
PA: T8>T1***ES=0.65
Intervention↓ (PA & HD)
† p<0.1; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never” to “10=always”
PA: T3>T1** ES=0.65
∆HD>∆PA† ES=0.40
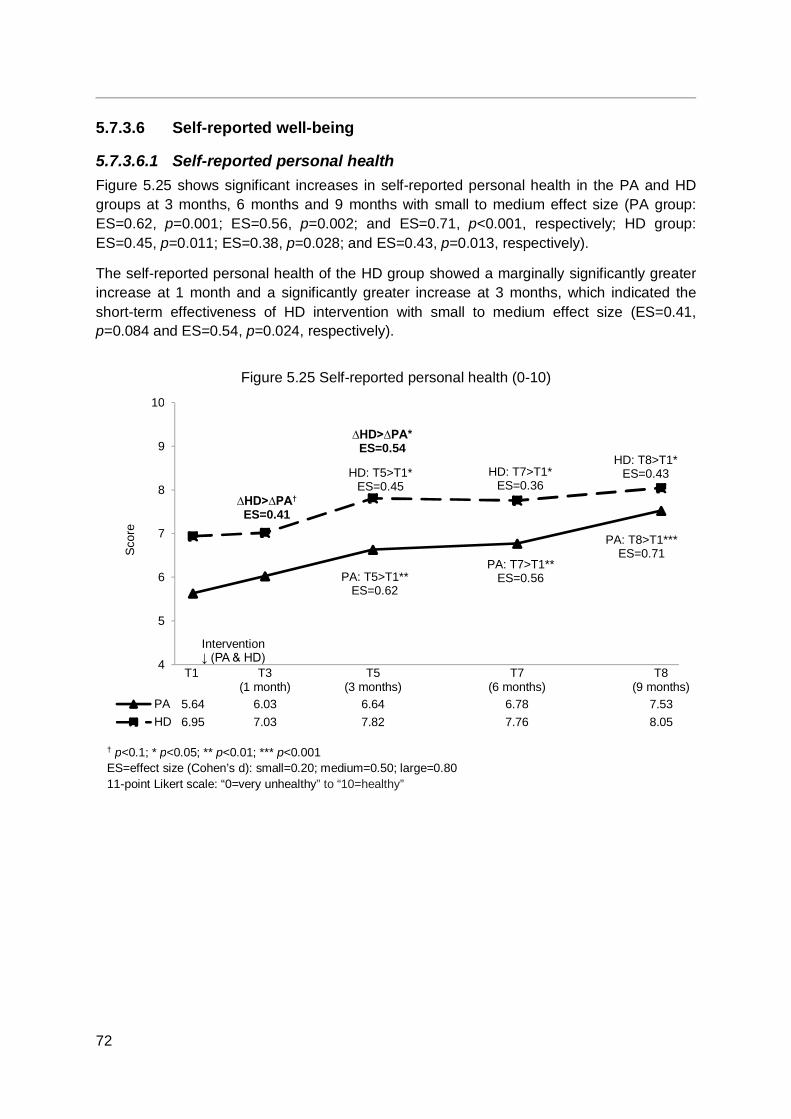
72
5.7.3.6 Self-reported well-being
5.7.3.6.1 Self-reported personal health Figure 5.25 shows significant increases in self-reported personal health in the PA and HD groups at 3 months, 6 months and 9 months with small to medium effect size (PA group: ES=0.62, p=0.001; ES=0.56, p=0.002; and ES=0.71, p<0.001, respectively; HD group: ES=0.45, p=0.011; ES=0.38, p=0.028; and ES=0.43, p=0.013, respectively).
The self-reported personal health of the HD group showed a marginally significantly greater increase at 1 month and a significantly greater increase at 3 months, which indicated the short-term effectiveness of HD intervention with small to medium effect size (ES=0.41, p=0.084 and ES=0.54, p=0.024, respectively).
Figure 5.25 Self-reported personal health (0-10)
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 5.64 6.03 6.64 6.78 7.53HD 6.95 7.03 7.82 7.76 8.05
Scor
e
PA: T5>T1**ES=0.62
HD: T5>T1*ES=0.45
Intervention↓ (PA & HD)
∆HD>∆PA†
ES=0.41
∆HD>∆PA*ES=0.54
PA: T7>T1**ES=0.56
HD: T7>T1*ES=0.36
PA: T8>T1***ES=0.71
HD: T8>T1*ES=0.43
† p<0.1; * p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhealthy” to “10=healthy”
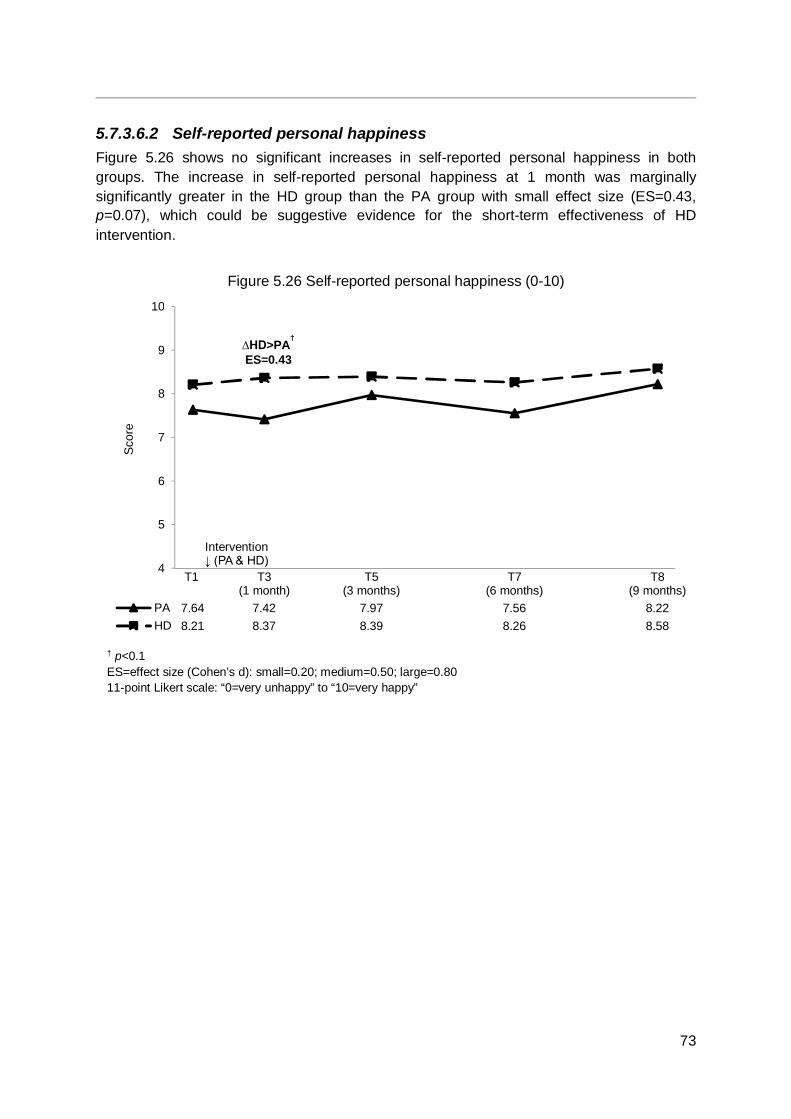
73
5.7.3.6.2 Self-reported personal happiness Figure 5.26 shows no significant increases in self-reported personal happiness in both groups. The increase in self-reported personal happiness at 1 month was marginally significantly greater in the HD group than the PA group with small effect size (ES=0.43, p=0.07), which could be suggestive evidence for the short-term effectiveness of HD intervention.
Figure 5.26 Self-reported personal happiness (0-10)
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 7.64 7.42 7.97 7.56 8.22HD 8.21 8.37 8.39 8.26 8.58
Scor
e
Intervention↓ (PA & HD)
† p<0.1 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhappy” to “10=very happy”
∆HD>PA†
ES=0.43
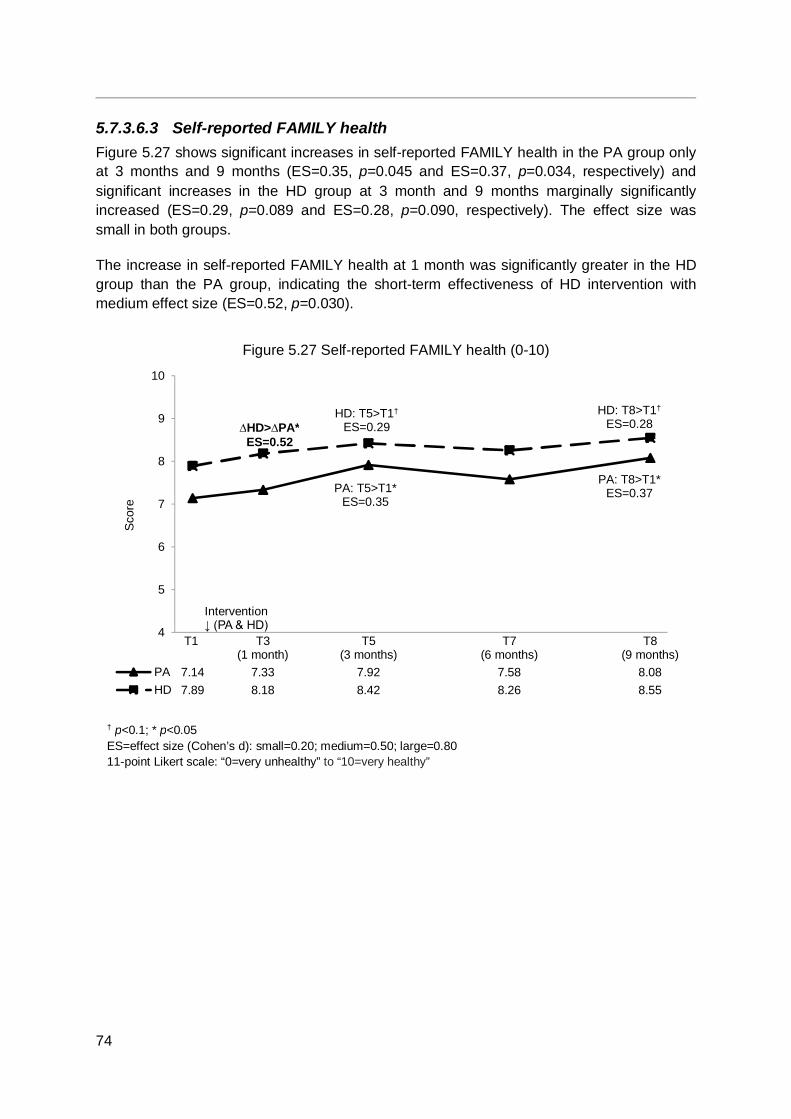
74
5.7.3.6.3 Self-reported FAMILY health Figure 5.27 shows significant increases in self-reported FAMILY health in the PA group only at 3 months and 9 months (ES=0.35, p=0.045 and ES=0.37, p=0.034, respectively) and significant increases in the HD group at 3 month and 9 months marginally significantly increased (ES=0.29, p=0.089 and ES=0.28, p=0.090, respectively). The effect size was small in both groups.
The increase in self-reported FAMILY health at 1 month was significantly greater in the HD group than the PA group, indicating the short-term effectiveness of HD intervention with medium effect size (ES=0.52, p=0.030).
Figure 5.27 Self-reported FAMILY health (0-10)
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 7.14 7.33 7.92 7.58 8.08HD 7.89 8.18 8.42 8.26 8.55
Scor
e
PA: T5>T1*ES=0.35
HD: T5>T1†
ES=0.29
Intervention↓ (PA & HD)
PA: T8>T1*ES=0.37
HD: T8>T1†
ES=0.28
† p<0.1; * p<0.05 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhealthy” to “10=very healthy”
∆HD>∆PA* ES=0.52
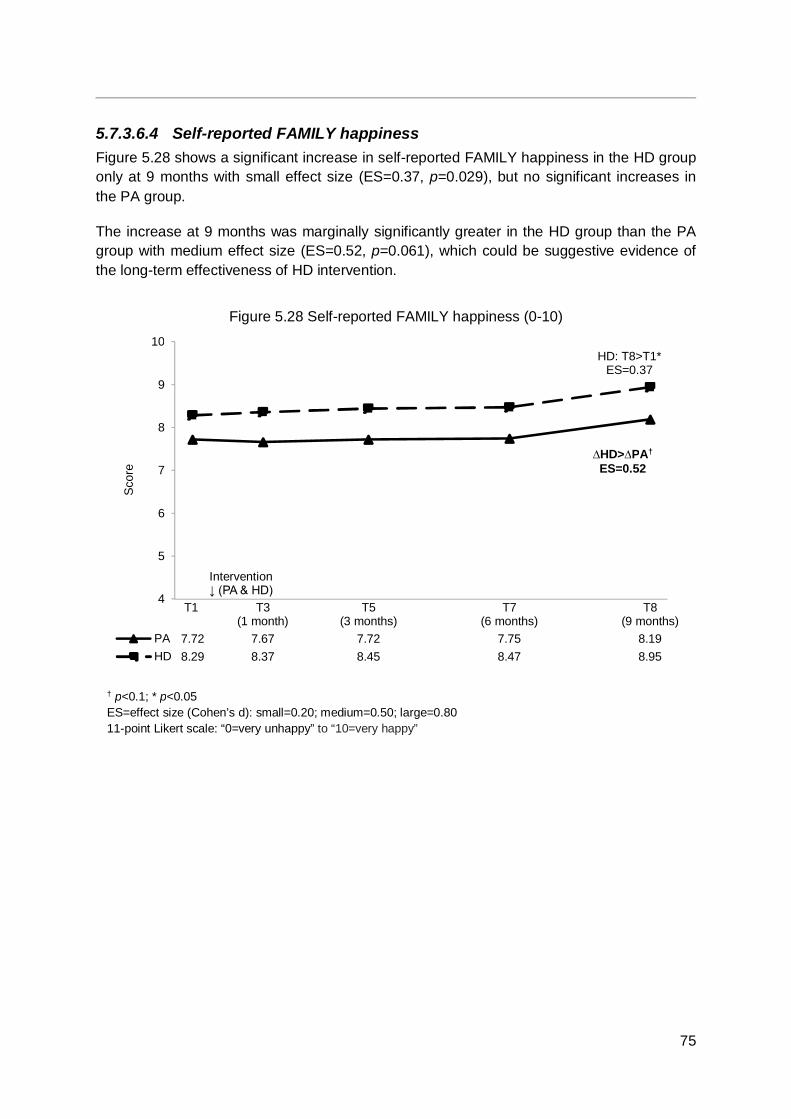
75
5.7.3.6.4 Self-reported FAMILY happiness Figure 5.28 shows a significant increase in self-reported FAMILY happiness in the HD group only at 9 months with small effect size (ES=0.37, p=0.029), but no significant increases in the PA group.
The increase at 9 months was marginally significantly greater in the HD group than the PA group with medium effect size (ES=0.52, p=0.061), which could be suggestive evidence of the long-term effectiveness of HD intervention.
Figure 5.28 Self-reported FAMILY happiness (0-10)
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 7.72 7.67 7.72 7.75 8.19HD 8.29 8.37 8.45 8.47 8.95
Scor
e
Intervention↓ (PA & HD)
HD: T8>T1*ES=0.37
† p<0.1; * p<0.05 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhappy” to “10=very happy”
∆HD>∆PA† ES=0.52

76
5.7.3.6.5 Self-reported FAMILY harmony Figure 5.29 shows a marginally significant increase in self-reported FAMILY harmony in the HD group at 9 months with small effect size (ES=0.33, p=0.058), but no significant increases in the PA group.
The increases were significantly greater at 6 months and marginally significantly greater at 9 months in the HD group than the PA group with small effect size (ES=0.48, p=0.045 and ES=0.43, p=0.070, respectively), indicating medium-term effectiveness and suggestive evidence of long-term effectiveness of PA intervention.
Figure 5.29 Self-reported FAMILY harmony (0-10)
4
5
6
7
8
9
10
T1 T3(1 month)
T5(3 months)
T7(6 months)
T8(9 months)
PA 7.94 7.92 7.89 7.92 8.42HD 8.53 8.61 8.53 8.76 9.11
Scor
e
Intervention↓ (PA & HD)
HD: T8>T1†
ES=0.33
† p<0.1; * p<0.05 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very disharmonious” to “10=very harmonious”
∆HD>∆PA† ES=0.43
∆HD>∆PA* ES=0.48
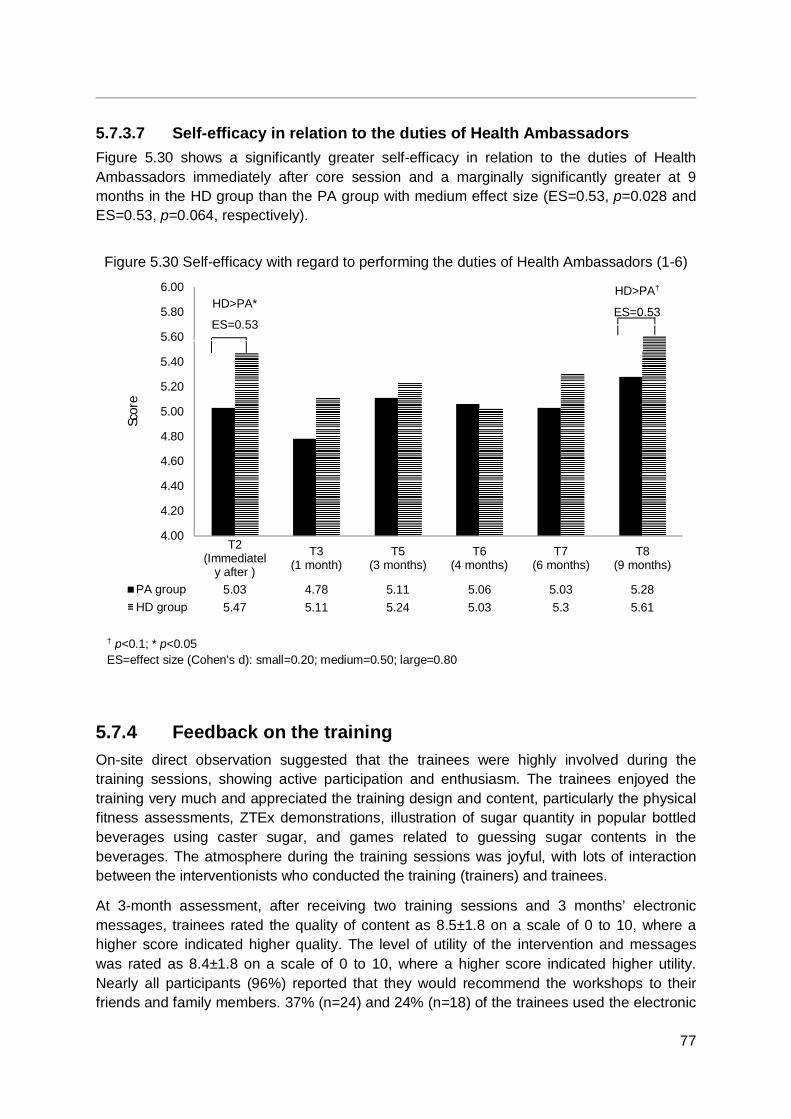
77
5.7.3.7 Self-efficacy in relation to the duties of Health Ambassadors Figure 5.30 shows a significantly greater self-efficacy in relation to the duties of Health Ambassadors immediately after core session and a marginally significantly greater at 9 months in the HD group than the PA group with medium effect size (ES=0.53, p=0.028 and ES=0.53, p=0.064, respectively).
Figure 5.30 Self-efficacy with regard to performing the duties of Health Ambassadors (1-6)
5.7.4 Feedback on the training On-site direct observation suggested that the trainees were highly involved during the training sessions, showing active participation and enthusiasm. The trainees enjoyed the training very much and appreciated the training design and content, particularly the physical fitness assessments, ZTEx demonstrations, illustration of sugar quantity in popular bottled beverages using caster sugar, and games related to guessing sugar contents in the beverages. The atmosphere during the training sessions was joyful, with lots of interaction between the interventionists who conducted the training (trainers) and trainees.
At 3-month assessment, after receiving two training sessions and 3 months’ electronic messages, trainees rated the quality of content as 8.5±1.8 on a scale of 0 to 10, where a higher score indicated higher quality. The level of utility of the intervention and messages was rated as 8.4±1.8 on a scale of 0 to 10, where a higher score indicated higher utility. Nearly all participants (96%) reported that they would recommend the workshops to their friends and family members. 37% (n=24) and 24% (n=18) of the trainees used the electronic
4.00
4.20
4.40
4.60
4.80
5.00
5.20
5.40
5.60
5.80
6.00
T2(Immediatel
y after )
T3(1 month)
T5(3 months)
T6(4 months)
T7(6 months)
T8(9 months)
PA group 5.03 4.78 5.11 5.06 5.03 5.28HD group 5.47 5.11 5.24 5.03 5.3 5.61
Scor
e
† p<0.1; * p<0.05 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
HD>PA*
ES=0.53
HD>PA†
ES=0.53
78
messages to remind themselves to perform ZTEx and adopt low sugar dietary practices respectively.
At 9-month assessment, after the completion of the community-based intervention programmes, the trainees rated the quality of intervention content as 8.4±1.7 and the utility of the intervention was rated as 8.4±1.8. Nearly all participants (97%) reported that they would recommend the intervention programme to their friends and family members. 11% (n=8) and 3% (n=2) of the trainees used the electronic messages to remind themselves to perform ZTEx and adopt low sugar dietary practices respectively.
5.7.5 Summary of quantitative results Overall, the results of the TTA showed that the training was acceptable and effective. The trainees were immersed and actively engaged during the training sessions. Feedback from the trainees indicated that the workshops and souvenirs (including the handgrips, HD table mats and electronic messages) were well-accepted, with the trainees finding the training useful and reporting that they would recommend it to friends and family.
The training workshops and electronic messages were effective in enhancing health-related behaviours, including physical activity, ZTEx, low sugar dietary habits, sharing of learnt knowledge with family members, physical fitness, as well as personal and family well-being in both groups.
The cRCT between-group results comparing the HD group with the PA group showed the positive effects of an additional HD booster session and mobile messages. Trainees in the HD group had significantly greater (i) increases in knowledge, intention and practice of adopting low sugar dietary practice; (ii) reduction in body weight, and (ii) enhancement in personal and family well-being, compared with the PA group. Trainees in the PA group also reported marginally significantly greater increases in moderate physical activity and physical fitness performance, compared with the HD group.
Some outcome measures showed no changes after the intervention, suggesting that the positive responses and improvements were not substantially due to social desirability bias (i.e. the positive responses and improvements were not due to respondents over-reporting socially desirable answers).
The current study shows good evidence for the effectiveness of a TTA that trained lay volunteers to be Health Ambassadors. One unique component of this programme was the emphasis on promoting the concept of being role models. Trainees first engaged themselves in increasing physical activity and low sugar dietary habits before implementing the community-based interventions. The training not only benefited the volunteers themselves but also the community-based programme participants.
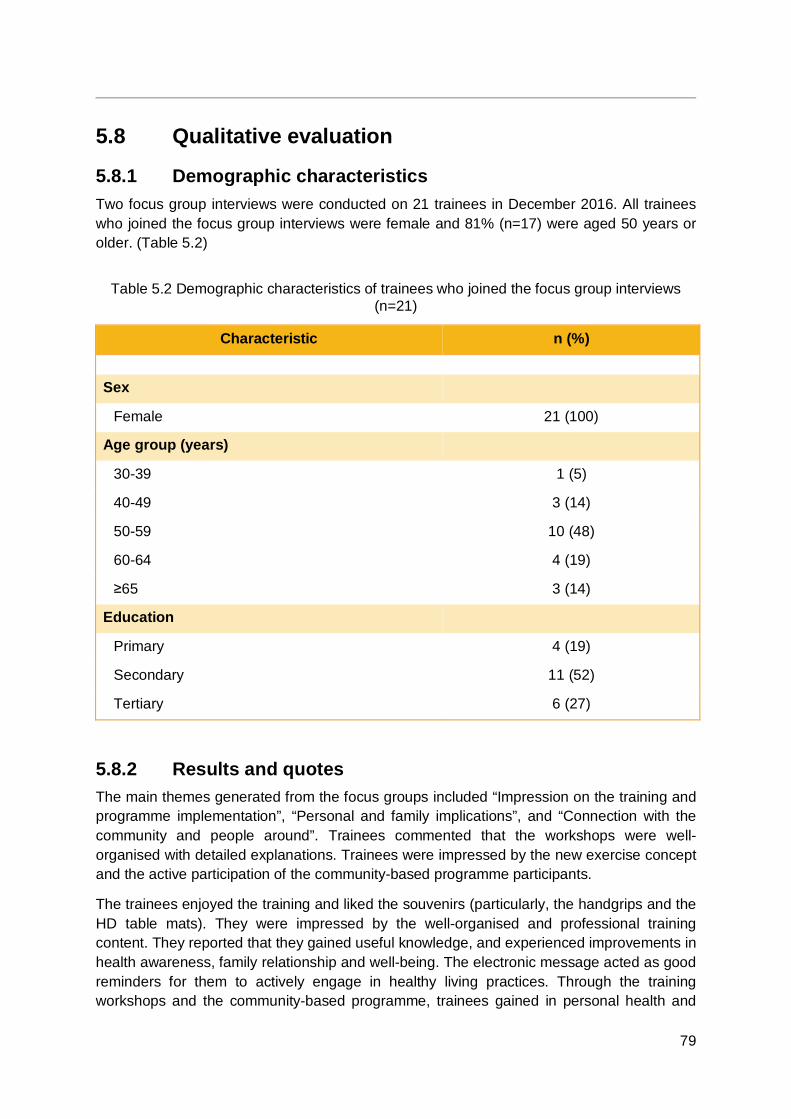
79
5.8 Qualitative evaluation
5.8.1 Demographic characteristics Two focus group interviews were conducted on 21 trainees in December 2016. All trainees who joined the focus group interviews were female and 81% (n=17) were aged 50 years or older. (Table 5.2)
Table 5.2 Demographic characteristics of trainees who joined the focus group interviews (n=21)
Characteristic n (%) Sex
Female 21 (100)
Age group (years)
30-39 1 (5) 40-49 3 (14) 50-59 10 (48) 60-64 4 (19) ≥65 3 (14)
Education
Primary 4 (19) Secondary 11 (52) Tertiary 6 (27)
5.8.2 Results and quotes The main themes generated from the focus groups included “Impression on the training and programme implementation”, “Personal and family implications”, and “Connection with the community and people around”. Trainees commented that the workshops were well-organised with detailed explanations. Trainees were impressed by the new exercise concept and the active participation of the community-based programme participants.
The trainees enjoyed the training and liked the souvenirs (particularly, the handgrips and the HD table mats). They were impressed by the well-organised and professional training content. They reported that they gained useful knowledge, and experienced improvements in health awareness, family relationship and well-being. The electronic message acted as good reminders for them to actively engage in healthy living practices. Through the training workshops and the community-based programme, trainees gained in personal health and
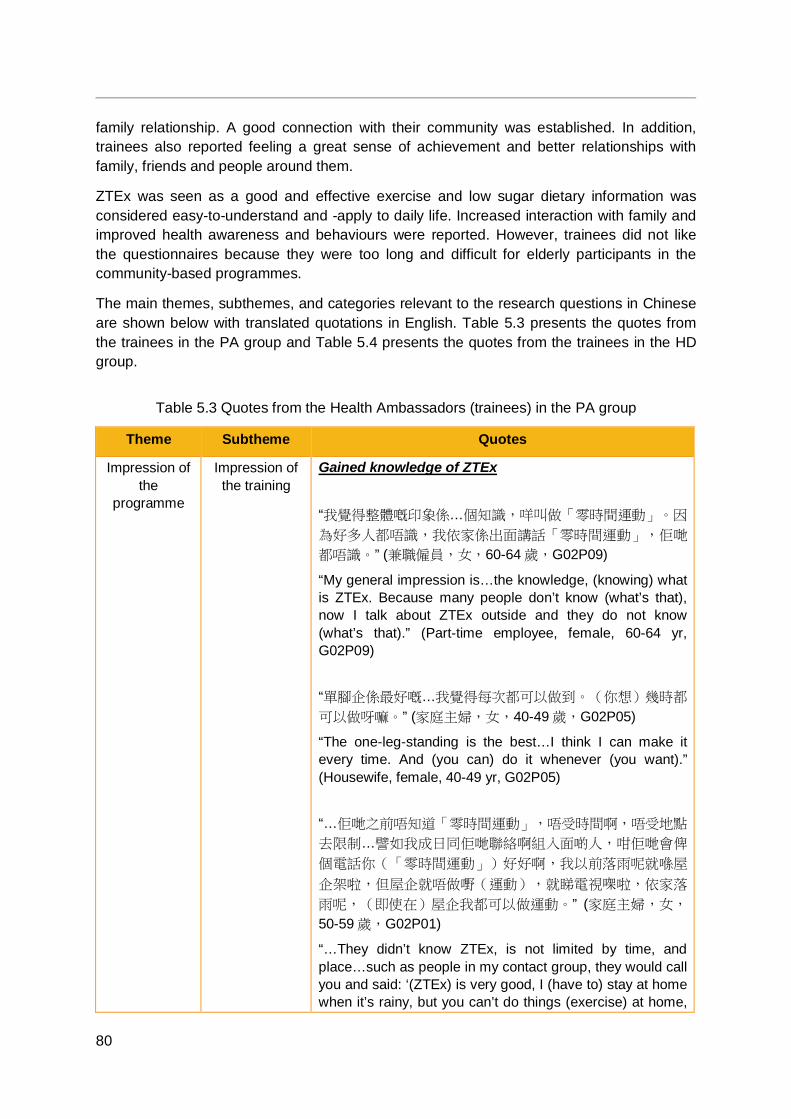
80
family relationship. A good connection with their community was established. In addition, trainees also reported feeling a great sense of achievement and better relationships with family, friends and people around them.
ZTEx was seen as a good and effective exercise and low sugar dietary information was considered easy-to-understand and -apply to daily life. Increased interaction with family and improved health awareness and behaviours were reported. However, trainees did not like the questionnaires because they were too long and difficult for elderly participants in the community-based programmes.
The main themes, subthemes, and categories relevant to the research questions in Chinese are shown below with translated quotations in English. Table 5.3 presents the quotes from the trainees in the PA group and Table 5.4 presents the quotes from the trainees in the HD group.
Table 5.3 Quotes from the Health Ambassadors (trainees) in the PA group
Theme Subtheme Quotes
Impression of the
programme
Impression of the training
Gained knowledge of ZTEx “我覺得整體嘅印象係…個知識,咩叫做「零時間運動」。因
為好多人都唔識,我依家係出面講話「零時間運動」,佢哋
都唔識。” (兼職僱員,女,60-64 歲,G02P09)
“My general impression is…the knowledge, (knowing) what is ZTEx. Because many people don’t know (what’s that), now I talk about ZTEx outside and they do not know (what’s that).” (Part-time employee, female, 60-64 yr, G02P09) “單腳企係最好嘅…我覺得每次都可以做到。(你想)幾時都
可以做呀嘛。” (家庭主婦,女,40-49 歲,G02P05)
“The one-leg-standing is the best…I think I can make it every time. And (you can) do it whenever (you want).” (Housewife, female, 40-49 yr, G02P05) “…佢哋之前唔知道「零時間運動」,唔受時間啊,唔受地點
去限制…譬如我成日同佢哋聯絡啊組入面啲人,咁佢哋會俾
個電話你(「零時間運動」)好好啊,我以前落雨呢就喺屋
企架啦,但屋企就唔做嘢(運動),就睇電視㗎啦,依家落
雨呢,(即使在)屋企我都可以做運動。” (家庭主婦,女,
50-59 歲,G02P01)
“…They didn’t know ZTEx, is not limited by time, and place…such as people in my contact group, they would call you and said: ‘(ZTEx) is very good, I (have to) stay at home when it’s rainy, but you can’t do things (exercise) at home,

81
Theme Subtheme Quotes
just watching television. Now when it’s rainy, (even just) stay at home I could do exercise.’” (Housewife, female, 50-59 yr, G02P01)
Impression of the programme
implement
Massive project “咁我覺得呢我就第一次參加咁大型嘅, 即成幾百人,係咪? 參加做一個運動,我覺得好熱鬧,啊同埋呢就好有氣勢…” (家庭主婦,女,50-59 歲,G02P03)
“I think it’s my first time to participate in such a large scale project, hundreds of people right? To participate in a movement, I think it’s very lifely, and very great…” (Housewife, female, 50-59 yr, G02P03)
Reaction from the community
participants
Good to learn useful health-related information “佢哋嘅投入呢,可以講得係百分之九十呀,唔好講一百啦
下,好多都接受嘅,因為我覺得呢,推廣呢個識食,多動係
對佢哋嘅健康有幫助…依家睇老一代呢好多個啲長者呢…老
咗又要坐輪椅啊,好多病,就算係我哋同輩都有好多都有好
多病,但如果你推廣咗呢一個訊息出去,等佢哋了解咗點樣
叫識食,點樣叫多動,對佢哋嘅健康係好㗎, 唔洗成日叫佢
睇醫生,唔洗成日去食藥。” (兼職僱員,女,60-64 歲,
G02P09) “(How much) they involved themselves into the programme, (I) could say was 90%, not say 100%, many of them accepted it. Because I think, promoting the knowledge of healthy diet, more exercise, is very helpful for their health…Now look at the old generation, there are many elderly, they have to sit on wheelchair when they are old, and have many disease, even our peers have many diseases, but once you promote this message, when they know about how to eat (healthily), how to exercise more, it’s good to their health, and then no need to see doctor or take medication all the time.” (Part-time employee, female, 60-64 yr, G02P09) “…我覺得係整體對一般社會上個啲長者係有幫助。係,最低
限度識食,識郁先…起碼都注重咗…” (兼職僱員,女,60-64 歲,G02P09)
“…I think it (the programme) overall is helpful to the elderly in our society, it is, at the lowest level to know how to eat,
82
Theme Subtheme Quotes
how to exercise…at least (they) pay more attention to it…” (Part-time employee, female, 60-64 yr, G02P09) Enriched participants’ experience “因為有好多人都未,尤其是話喺會展,咁高級嘅地方,好多
人都無去過,尤其是啲老人家…咁去到…個環境咁靚咁咪就
算係去坐下好係好架。 ” (家庭主婦,女,50-59 歲,
G02P02) “Because many people they never…especially the Hong Kong Convention and Exhibition Centre, and then you know such a high class place, many people had never been there before, especially the elderly…and then they went there the environment is so good, even just sit there is good.” (Housewife, female, 50-59 yr, G02P02)
Challenges Hard to do questionnaires among elderly “覺得點算啊,原來要識字架,點解港大個時唔同我哋講…咁
佢唔識字,咁我哋點樣去教佢(做問卷)呀。” (家庭主婦,
女,50-59 歲,G02P04)
“I was thinking what should I do now, they want participants who can read, how come HKU didn’t tell us…they couldn’t read, then how could we teach them (to do the questionnaire).” (Housewife, female, 50-59 yr, G02P04)
“初初我都唔為意㗎,咁呀初初一個兩個,咁多個都要讀嘅。
咁唔係辦法喎…叫晒所有人,一齊,我做讀,你哋做填,你
哋自己揀答案,佢話唔識睇條題目唔識解。” (兼職僱員,
女,50-59 歲,G02P10)
“At first I didn’t notice it, and then at first there was one or two, (later) so many people needed (someone to) read (to them). Then this was not doable…(so I) gathered all of them, (do it) together, I read, you (the participants) choose, and then they said they didn’t know how to choose since they cannot understand.” (Part-time employee, female, 50-59 yr, G02P10)
“就問佢哋,咁就按自己原因就自己個,一個個咁填, 咁樣真
係要俾啲耐性囉,係啊,對啲老人家。” (家庭主婦,女,50-59 歲,G02P03)
“Just ask them, and then they fill it according to their own
83
Theme Subtheme Quotes
reason, one by one to fill, then it really needed some patience, yes, when facing the elderly.” (Housewife, female, 50-59 yr, G02P03)
Implications More exercise engagement
Personal “做運動…我初時係唔知「零時間運動」嘅。咁依家知道呢,
我一起身呢都做下,伸展下,站立下咁樣,係,都做多咗
囉。” (家庭主婦,女,50-59 歲,G02P08)
“Doing exercise…at first I didn’t know ZTEx. Now know it, I do it when I wake up, do some stretching and standing, yes (I think) I have been doing more exercise.” (Housewife, female, 50-59 yr, G02P08)
“我以前番工就真係無嘢做就真係坐喺到,依家就可以企下…
我食飽,我可以企下,先再坐番低咁樣,或者有時,即坐喺
到嘅時間無人嚟,又企得攰嘅, 咁隻腳起落下,咁樣郁下
啦。” (家庭主婦,女,40-49 歲,G02P07)
“Before I went back to work it’s really like if there’s nothing to do, I would sit there (for the whole day), now I can stand. When I’m full I can stand, and then sit down. Or sometimes, when there is no people around, and tired after standing for too long, and then will move legs up and down, and then do some moves.” (Housewife, female, 40-49 yr, G02P07) “我依家呢,嗱煮飯,就蒸魚呢我就喺到單腳企架啦。即個啲
時間就喺到企…嗱搭 lift 呢,又企下,睇電視我又企下咁
咯,唔知邊時得閒我又做下咁囉。” (家庭主婦,女,50-59歲,G02P02)
“Now I. When cooking, I would do single leg stance when I steam the fish. And then I’m standing during at time…when taking the lift, I stand, watching television, I stand, I would do it again whenever I have time.” (Housewife, female, 50-59 yr,G02P02) Family “咁勤力咗做運動囉,同埋屋…即話鼓勵屋企人一齊做咁樣
囉。” (家庭主婦,女,50-59 歲,G02P02)
“I have become more active to do exercise, and the family…will encourage the family to do it together.”
84
Theme Subtheme Quotes
(Housewife, female, 50-59 yr,G02P02) “我呃…參加咗呢個咁嘅活動俾我最多感觸就係可以促進一家
人做運動。” (家庭主婦,女,50-59 歲,G02P03)
“For me…the most touchable thing is (the programme) could facilitate the family to do the exercise.” (Housewife, female, 50-59 yr, G02P03)
Better family relationship
More family communication “我覺得,人多咗話題。同朋友啊,或者同家人啊,都有多啲
嘢傾囉。問下佢哋有無做,關係都好啲啦。” (家庭主婦,
女,40-49 歲,G02P05)
“I think, have more topic to talk with people. With friends, or family, all have more things to talk about. Ask if they have done (the exercise), and then the relationship is better.” (Housewife, female, 40-49 yr, G02P05) Family harmony “起碼…大家主動咗啦,因有時細路有會反轉頭提醒你啊,就
唔係剩係長者去提醒年輕一輩…咁即入面個角色係融和咗
囉。” (家庭主婦,女,50-59 歲,G02P03)
“At least…people get more active, because sometimes the younger kids will remind you (to do exercise), it’s not just the elderly to remind the younger…so the roles (in the family) have blended together into harmony.” (Housewife, female, 50-59 yr, G02P03) “我自己唔認識零時運動,到參加呢個活動認識零時運動,就
同屋企人講,我自己喺屋企做,再鼓勵佢哋,帶動佢哋,呃
…有時進行比賽啊啲,咁我覺得啲入面成個家庭係一有種呃
…好…開心,同埋好熱鬧嘅氣氛囉,變得家庭又融和咗,咁
我就覺得呢個運動係應該值得推廣喺社區啊各方面,係,我
就覺得呢個就我自己最大得益啦哈。” (家庭主婦,女,50-59 歲,G02P03)
“I didn’t know ZTEx, until I have participated in this programme. Then I told my family (about this), and I will do it at home myself, and then will encourage the family to do it too, lead them to do it. Um, sometimes we have competition or what, I feel the whole family has…so happy, and the atmosphere is very lively, and the family is more harmonious, so I think this exercise shuold be promoted to
85
Theme Subtheme Quotes
the community, yes I think this is my biggest gain.” (Housewife, female, 50-59 yr, G02P03)
Better relationship with people
around
With friends “教我哋點樣計 BMI 啊咁樣,咁有時我哋即係同啲朋友傾唉
啊你 BMI 指數高咗喎,咁可以話俾佢聽一齊做運動啦咁樣,
即係由呢個 programme,即我哋健康大使帶動出去我哋自己
去。” (家庭主婦,女,50-59 歲,G02P04)
“(The programme) taught us how to calculate the BMI, so sometimes when we chat with friends would say oh your BMI is a bit high, and then can ask him (the friend) to do exercise together, and then because of this programme, we Health Ambassador could motive us to (convey the health message to friends).” (Housewife, female, 50-59 yr, G02P04) “我有時將我哋健康大使個啲資料放咗喺微信朋友圈呢,啲朋
友反映都好好,係呀,因佢哋都覺得傳遞到呢個健康訊息俾
佢哋…” (家庭主婦,女,50-59 歲,G02P03)
“I sometimes will put the Health Ambassador information post in friend’s circle, and the feedbacks from friends are all good, yes, because they all think it has delivered the healthy message to them…” (Housewife, female, 50-59 yr, G02P03) With colleagues “整體唔錯,最深刻嘅印象就係我哋 5 月 20 號 E 組組織咗 3部車,係百幾人去呃…戶外活動,咁首先喺迪欣湖呢就進行
咗四方舞同埋個個單腳站立,呃…另一部分人呢就去做體能
測試…咁比賽啊咁。咁大家…都好積極,好投入,好團結…
唔錯,整個過程我覺得都…幾好。” (退休,女,60-64 歲,
G02P06) “It’s generally good, the most impressive one was on May 20th, we organised 3 coaches, hundreds of people to…have an outdoor activity. At first we did the square dance and the one-leg-standing at the Inspiration Lake, and the other people went to do the fitness test…and had some competition, and people were very active, and very engaged, very united…it’s not bad, the whole process made me feel very good.” (Retiree, female, 60-64 yr, G02P06)
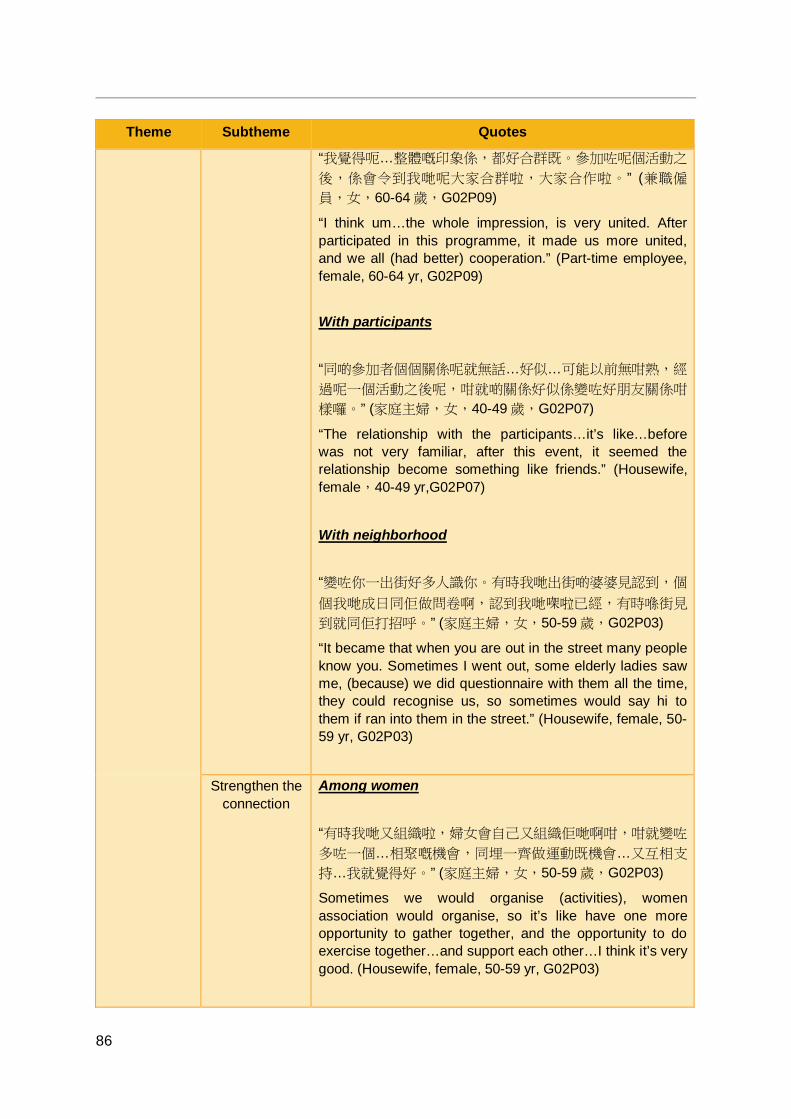
86
Theme Subtheme Quotes
“我覺得呃…整體嘅印象係,都好合群既。參加咗呢個活動之
後,係會令到我哋呢大家合群啦,大家合作啦。” (兼職僱
員,女,60-64 歲,G02P09)
“I think um…the whole impression, is very united. After participated in this programme, it made us more united, and we all (had better) cooperation.” (Part-time employee, female, 60-64 yr, G02P09) With participants “同啲參加者個個關係呢就無話…好似…可能以前無咁熟,經
過呢一個活動之後呢,咁就啲關係好似係變咗好朋友關係咁
樣囉。” (家庭主婦,女,40-49 歲,G02P07)
“The relationship with the participants…it’s like…before was not very familiar, after this event, it seemed the relationship become something like friends.” (Housewife, female,40-49 yr,G02P07)
With neighborhood “變咗你一出街好多人識你。有時我哋出街啲婆婆見認到,個
個我哋成日同佢做問卷啊,認到我哋㗎啦已經,有時喺街見
到就同佢打招呼。” (家庭主婦,女,50-59 歲,G02P03)
“It became that when you are out in the street many people know you. Sometimes I went out, some elderly ladies saw me, (because) we did questionnaire with them all the time, they could recognise us, so sometimes would say hi to them if ran into them in the street.” (Housewife, female, 50-59 yr, G02P03)
Strengthen the connection
Among women “有時我哋又組織啦,婦女會自己又組織佢哋啊咁,咁就變咗
多咗一個…相聚嘅機會,同埋一齊做運動既機會…又互相支
持…我就覺得好。” (家庭主婦,女,50-59 歲,G02P03)
Sometimes we would organise (activities), women association would organise, so it’s like have one more opportunity to gather together, and the opportunity to do exercise together…and support each other…I think it’s very good. (Housewife, female, 50-59 yr, G02P03)
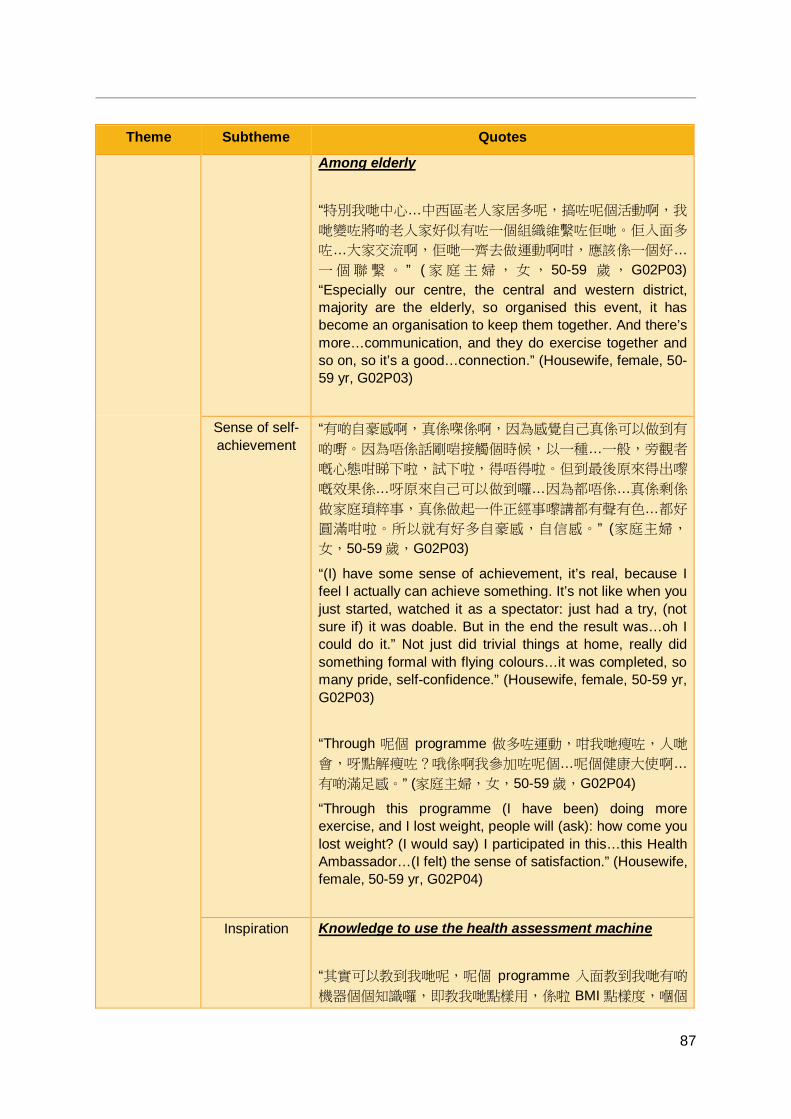
87
Theme Subtheme Quotes
Among elderly “特別我哋中心…中西區老人家居多呢,搞咗呢個活動啊,我
哋變咗將啲老人家好似有咗一個組織維繫咗佢哋。佢入面多
咗…大家交流啊,佢哋一齊去做運動啊咁,應該係一個好…
一 個 聯 繫 。 ” ( 家 庭 主 婦, 女 , 50-59 歲 , G02P03) “Especially our centre, the central and western district, majority are the elderly, so organised this event, it has become an organisation to keep them together. And there’s more…communication, and they do exercise together and so on, so it’s a good…connection.” (Housewife, female, 50-59 yr, G02P03)
Sense of self-achievement
“有啲自豪感啊,真係㗎係啊,因為感覺自己真係可以做到有
啲嘢。因為唔係話剛啱接觸個時候,以一種…一般,旁觀者
嘅心態咁睇下啦,試下啦,得唔得啦。但到最後原來得出嚟
嘅效果係…呀原來自己可以做到囉…因為都唔係…真係剩係
做家庭瑣粹事,真係做起一件正經事嚟講都有聲有色…都好
圓滿咁啦。所以就有好多自豪感,自信感。” (家庭主婦,
女,50-59 歲,G02P03)
“(I) have some sense of achievement, it’s real, because I feel I actually can achieve something. It’s not like when you just started, watched it as a spectator: just had a try, (not sure if) it was doable. But in the end the result was…oh I could do it.” Not just did trivial things at home, really did something formal with flying colours…it was completed, so many pride, self-confidence.” (Housewife, female, 50-59 yr, G02P03) “Through 呢個 programme 做多咗運動,咁我哋瘦咗,人哋
會,呀點解瘦咗?哦係啊我參加咗呢個…呢個健康大使啊…
有啲滿足感。” (家庭主婦,女,50-59 歲,G02P04)
“Through this programme (I have been) doing more exercise, and I lost weight, people will (ask): how come you lost weight? (I would say) I participated in this…this Health Ambassador…(I felt) the sense of satisfaction.” (Housewife, female, 50-59 yr, G02P04)
Inspiration Knowledge to use the health assessment machine “其實可以教到我哋呢,呢個 programme 入面教到我哋有啲
機器個個知識囉,即教我哋點樣用,係啦 BMI 點樣度,嗰個

88
Theme Subtheme Quotes
機器呢,嗰個係好好囉對我哋。有啲咁嘅機,我哋度啲咁嘅
嘢幫到人。” (家庭主婦,女,50-59 歲,G02P04)
“Actually (the programme) could teach us, the programme taught us the knowledge of the machines, taught us how to use them, how to measure BMI, that machine, that is good for us. Having such machines, we can measure such things to help people.” (Housewife, female, 50-59 yr, G02P04) For future event implement “作為大使我哋係學多咗好多。係萌芽知識方面啊…和諧啊,
推廣啊…” (家庭主婦,女,50-59 歲,G02P03)
“As (Health) Ambassador I have learnt a lot. (such as) the bud of knowledge, um harmony, promotion...” (Housewife, female, 50-59 yr, G02P03) “學多咗點同人溝通。因為平時我哋唔係好熟個啲都唔會話打
電話嘛 , 依家就多咗囉。 ” (家庭主婦,女,50-59 歲,
G02P01) “Learnt more how to communicate with others. Because usually we wouldn’t call the ones we are not familiar, now it’s better.” (Housewife, female, 50-59 yr, G02P01) “同埋人與人呢之間個溝通係呢…適應咗好多, 識溝通…” (兼職僱員,女,60-64 歲,G02P09)
“And the communication with other…get used to it a lot, (now) know how to communicate…” (Part-time employee, female, 60-64 yr, G02P09)
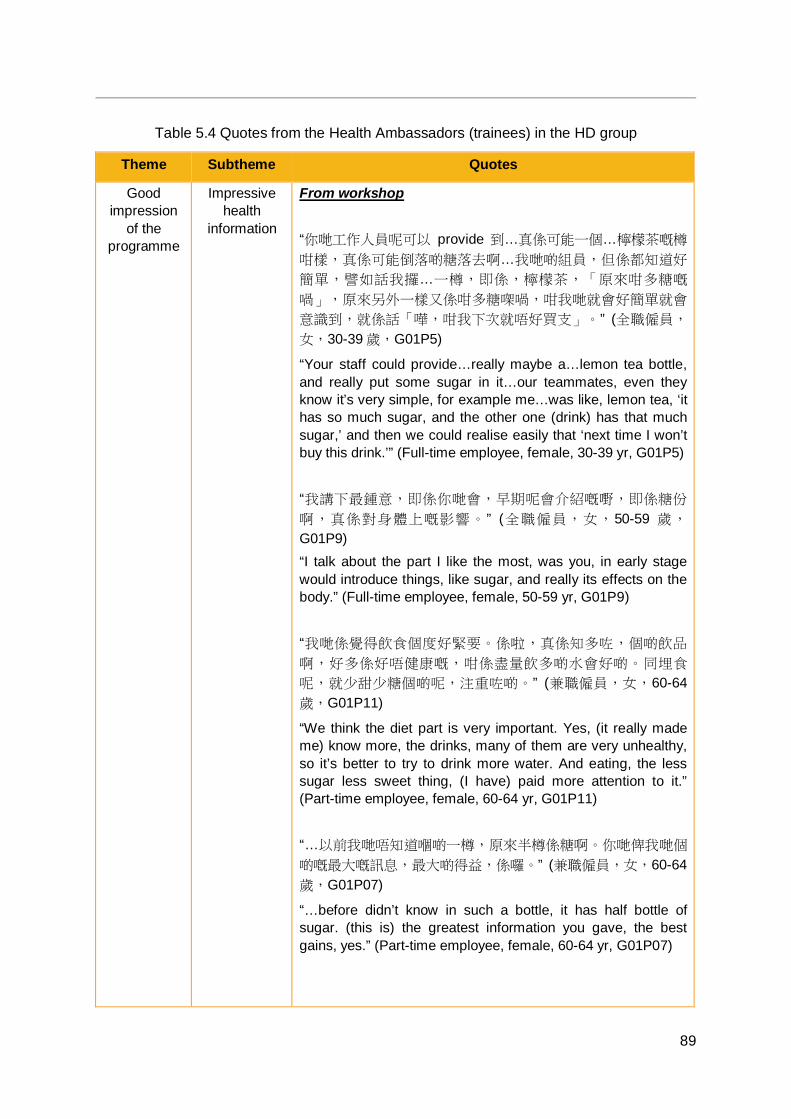
89
Table 5.4 Quotes from the Health Ambassadors (trainees) in the HD group
Theme Subtheme Quotes
Good impression
of the programme
Impressive health
information
From workshop “你哋工作人員呢可以 provide 到…真係可能一個…檸檬茶嘅樽
咁樣,真係可能倒落啲糖落去啊…我哋啲組員,但係都知道好
簡單,譬如話我攞…一樽,即係,檸檬茶,「原來咁多糖嘅
喎」,原來另外一樣又係咁多糖㗎喎,咁我哋就會好簡單就會
意識到,就係話「嘩,咁我下次就唔好買支」。” (全職僱員,
女,30-39 歲,G01P5)
“Your staff could provide…really maybe a…lemon tea bottle, and really put some sugar in it…our teammates, even they know it’s very simple, for example me…was like, lemon tea, ‘it has so much sugar, and the other one (drink) has that much sugar,’ and then we could realise easily that ‘next time I won’t buy this drink.’” (Full-time employee, female, 30-39 yr, G01P5) “我講下最鍾意,即係你哋會,早期呢會介紹嘅嘢,即係糖份
啊,真係對身體上嘅影響。” (全職僱員,女,50-59 歲,
G01P9) “I talk about the part I like the most, was you, in early stage would introduce things, like sugar, and really its effects on the body.” (Full-time employee, female, 50-59 yr, G01P9) “我哋係覺得飲食個度好緊要。係啦,真係知多咗,個啲飲品
啊,好多係好唔健康嘅,咁係盡量飲多啲水會好啲。同埋食
呢,就少甜少糖個啲呢,注重咗啲。” (兼職僱員,女,60-64歲,G01P11)
“We think the diet part is very important. Yes, (it really made me) know more, the drinks, many of them are very unhealthy, so it’s better to try to drink more water. And eating, the less sugar less sweet thing, (I have) paid more attention to it.” (Part-time employee, female, 60-64 yr, G01P11) “…以前我哋唔知道嗰啲一樽,原來半樽係糖啊。你哋俾我哋個
啲嘅最大嘅訊息,最大啲得益,係囉。” (兼職僱員,女,60-64歲,G01P07)
“…before didn’t know in such a bottle, it has half bottle of sugar. (this is) the greatest information you gave, the best gains, yes.” (Part-time employee, female, 60-64 yr, G01P07)
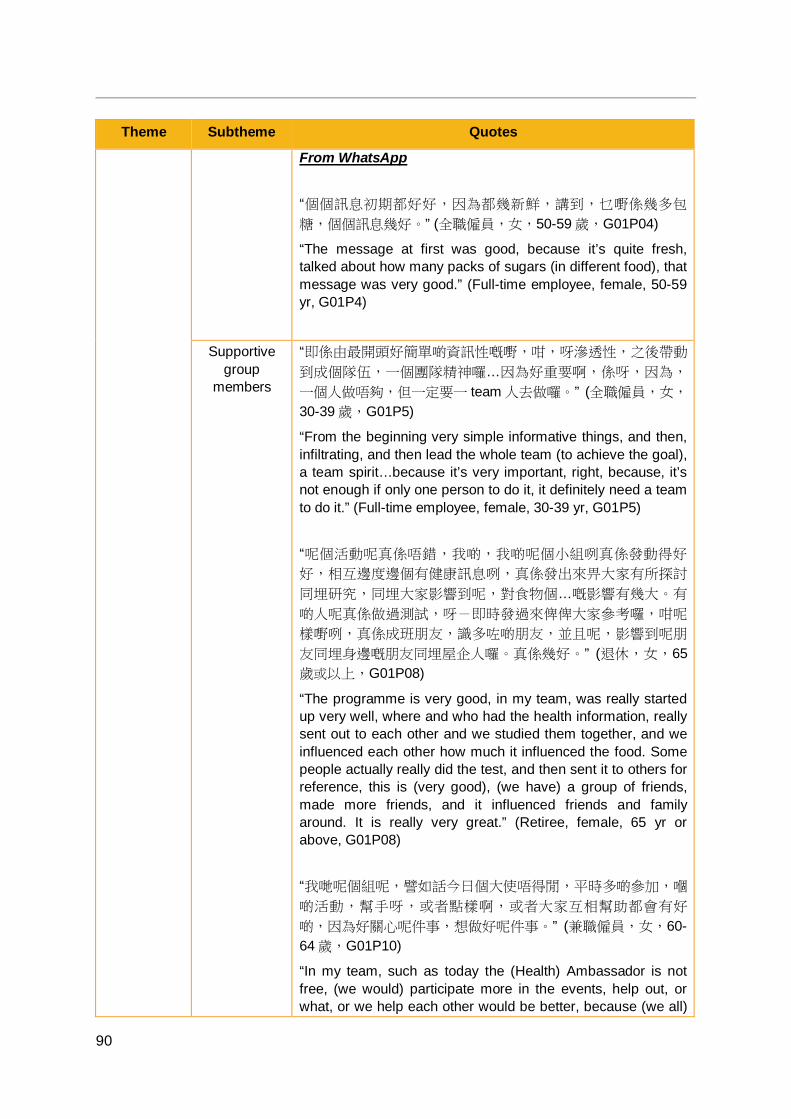
90
Theme Subtheme Quotes
From WhatsApp “個個訊息初期都好好,因為都幾新鮮,講到,乜嘢係幾多包
糖,個個訊息幾好。” (全職僱員,女,50-59 歲,G01P04)
“The message at first was good, because it’s quite fresh, talked about how many packs of sugars (in different food), that message was very good.” (Full-time employee, female, 50-59 yr, G01P4)
Supportive group
members
“即係由最開頭好簡單啲資訊性嘅嘢,咁,呀滲透性,之後帶動
到成個隊伍,一個團隊精神囉…因為好重要啊,係呀,因為,
一個人做唔夠,但一定要一 team 人去做囉。” (全職僱員,女,
30-39 歲,G01P5)
“From the beginning very simple informative things, and then, infiltrating, and then lead the whole team (to achieve the goal), a team spirit…because it’s very important, right, because, it’s not enough if only one person to do it, it definitely need a team to do it.” (Full-time employee, female, 30-39 yr, G01P5) “呢個活動呢真係唔錯,我啲,我啲呢個小組咧真係發動得好
好,相互邊度邊個有健康訊息咧,真係發出來畀大家有所探討
同埋研究,同埋大家影響到呢,對食物個…嘅影響有幾大。有
啲人呢真係做過測試,呀-即時發過來俾俾大家參考囉,咁呢
樣嘢咧,真係成班朋友,識多咗啲朋友,並且呢,影響到呢朋
友同埋身邊嘅朋友同埋屋企人囉。真係幾好。” (退休,女,65歲或以上,G01P08)
“The programme is very good, in my team, was really started up very well, where and who had the health information, really sent out to each other and we studied them together, and we influenced each other how much it influenced the food. Some people actually really did the test, and then sent it to others for reference, this is (very good), (we have) a group of friends, made more friends, and it influenced friends and family around. It is really very great.” (Retiree, female, 65 yr or above, G01P08) “我哋呢個組呢,譬如話今日個大使唔得閒,平時多啲參加,嗰
啲活動,幫手呀,或者點樣啊,或者大家互相幫助都會有好
啲,因為好關心呢件事,想做好呢件事。” (兼職僱員,女,60-64 歲,G01P10)
“In my team, such as today the (Health) Ambassador is not free, (we would) participate more in the events, help out, or what, or we help each other would be better, because (we all)

91
Theme Subtheme Quotes
care a lot about this, and want to do it well.” (Part-time employee, female, 60-64 yr, G01P10) “我就因為係聯絡大使呢,咁就同啲大使熟落咗,因為大家好似
一個,一個 project 要做完,有共同嘅目標,哈,咁就會同佢哋
溝通得多啲啊:你夠人未呀,齊人未呀,咁呀嗰到交流多咗。” (全職僱員,女,50-59 歲,G01P04)
“Because of being the connecting (Health) Ambassador, so I become familiar with other Health Ambassadors, because it’s like we have a, a project to complete, we have the same aim, ha, so then would communicate more with them: do you have enough manpower, has everyone arrived, and then we have more communication.” (Full-time employee, female, 50-59 yr, G01P4)
Practical souvenirs
“最受歡迎係嗰塊布呀, 個條毛巾仔。” (退休,女,60 歲或以
上,G01P08)
“The towel is very popular, the towel.” (Retiree, female, 60 yr or above, G01P08) “黃色個條毛巾仔。一呢又好用,二呢佢攜帶呢方便。總之個個
就,即係毛巾個啲就實用啲。” (兼職僱員,女,60-64 歲,
G01P07) “The yellow towel. Firstly, it’s very good to use, secondly, it’s easy to carry around. All in all, the towel is very practical.” (Part-time employee, female, 60-64 yr, G01P11) “這一條毛巾,我啱啱先跑完 8K,我都圍住嗰條巾。” (全職僱
員,女,50-59 歲,G01P09)
“This towel, I just finished my 8k (run), with the towel round my neck.” (Full-time employee, female, 50-59 yr, G01P9)
Difficulties Verbose questionnaire “之前好多個好細微咁樣(問題),即係有啲重複重複咗,變咗
佢哋(參加者)就話,「又問?」” (全職僱員,女,50-59 歲,
G01P09) “Before there were many detailed (questions), some were duplicated, then turned out they (the participants) would say, ‘ask again?’” (Full-time employee, female, 50-59 yr, G01P9)
92
Theme Subtheme Quotes
“(希望問卷)簡潔啲。” (兼職僱員,女,60-64 歲,G01P11)
“(Hope the questionnaire could be) more concise.” (Part-time employee, female, 60-64 yr, G01P11) Lengthy programme schedule “講困難都有…因為,拖得太長出來…因為有啲參加者呢,唔
expect 咁長嘅,嗰啲活動可能去完一次,一次活動呢,咁就完
啦,跟住我哋仲要不停咁,send 啲短信,有啲甚至係,即係大
使匯報番今日食咗幾多糖啊…應該呢,由一開始呢就應該畀一
個時間表,畀個參加者。” (全職僱員,女,50-59 歲,G01P04)
“There was difficulties…because, (the programme) was too long…because some participants, they didn’t expect this long, they thought maybe only go once, one activity, and then it’s over, and then we also need to continually send the messages, some even, (need to) report to the (Health) Ambassador how much sugar they had that day…should, from the beginning, give a timetable, to the participants.” (Full-time employee, female, 50-59 yr, G01P4)
Implications of the
programme
Increased health
awareness
Personal “都幾好,真係…真係學到嘢都…即係平時我哋,唔係好睇嗰啲
乜嘢標籤呀,細細個咁,即係參加咗呢個活動就, 我哋睇一睇
…” (全職僱員,女,50-59 歲,G01P12)
“It’s very good, really…really learnt something…usually we, don’t really look at the (food) label, so small, (but) after joining this programme, we have a look…” (Full-time employee, female, 50-59 yr, G01P12) Among family “最大嘅分別就係呢,依家我一去買餸,齊齊都話「媽咪,多菜
少肉!」我先生就話,「記得!多啲菜!」呢個好緊要,買嘢
番來個個睇標籤先,邊個買錯呢就話啦:)就呢個最大嘅分
享。” (兼職僱員,女,60-64 歲,G01P07)
“The biggest difference is, now I went to buy food, (the family members) all say: ‘mom, more vegetables and less meat!’ My husband would say: ‘remember get more vegetables!’ This is very important, and will look at the labels after got the food back, (we would) criticise the one who bought the wrong food (laughs), this is the biggest (difference I would like) to share.”

93
Theme Subtheme Quotes
(Part-time employee, female, 60-64 yr, G01P11)
Gained more health
knowledge
“知多啲囉,以前唔知道咁多囉,真係唔知咁多囉。” (兼職僱
員,女,60-64 歲,G01P10)
“Know more (after joining the programme), didn’t know this much before, really didn’t know this much.” (Part-time employee, female, 60-64 yr, G01P10) “我覺得一日糖一日鹽,即係撈埋,會知多啲囉,會記得囉,因
為你一日裡面你都會接觸到糖啊鹽啊咁樣。” (全職僱員,女,
50-59 歲,G01P09)
“I think one day (talking about) sugar, one day (talking about) salt, and put them together, would know more, and would remember, because you will access sugar and salt daily.” (Full-time employee, female, 50-59 yr, G01P09)
Behaviour change
Less sugary diet “(以前)咁我咪檸水兩包糖呢,我真係落,因為好酸嘅嘛。依
家就半包,有時就唔落,咁樣囉。” (兼職僱員,女,60-64 歲,
G01P10) “(Before) I would put two bags of sugar in the lemon water, I really did, because (the lemon water) is too sour. Now I would only put half bag, sometimes don’t put any, that is (what I have changed).” (Part-time employee, female, 60-64 yr, G01P10) “我覺得都有好,大家都有幫助,多少都有啲啟發,譬如你講我
啲識食咧,咁係少糖啊,或者鹽啊。糖啊,平時我飲咖啡,之
前一包多啲啊或者點樣啊,依家我都係半包。” (家庭主婦,
女,40-49 歲,G01P03)
“I think it’s very good, it’s good to all, more or less would have some inspiring, such as you talking about my diet, it’s less sugar, or salt. The sugar, usually when I drink coffee, before (I put) a bag or more, now only half a bag.” (Housewife, female, 40-49 yr, G01P03) More physical activity “咁呢在做運動方面咧,我都覺得有用,譬如零時間活動。搭 lift都可以企個度,單腳企吓等 lift,或者係返工嗰段時中間可以起
身企吓,或者度下腳…之前知道我係要做運動做運動,但係,
94
Theme Subtheme Quotes
其實人都係好被動嘅。你上咗堂,又記得啲…其實好多時間我
哋都可以做吓運動,都可以做到嘅。” (全職僱員,女,50-59歲,G01P09)
“In terms of the exercise part, I think it’s useful, such as ZTEx. You can stand there when you are taking the lift, or do single leg stance when waiting for lift, or stand up during the working hours, or move your legs...before I knew I need to do exercise, but actually I’m quite passive. (Now) you have attended the lectures, and remember some of it… (that made me think) actually there is much time that we can do exercise, we can do it.” (Full-time employee, female, 50-59 yr, G01P09) Read food label “留意多啲標籤上面…糖份啊,真係或者其他啲營養價值啊個
啲。” (全職僱員,女,30-39 歲,G01P5)
“(I have) paid more attention to the label…the sugar amount, or some other nutrition values or so.” (Full-time employee, female, 30-39 yr, G01P5) “參加咗呢個活動啊,真係對我同埋自己身邊人,自己屋企,都
得到一定啲…呀,幫助同埋啟發囉…以前我哋真係唔睇標籤
啊,有時連日期都唔…唔知道留意,而家注重咗…留意標籤,
買嘢首先睇標籤,同埋糖份啊,鹽分啊,有幾多啊,鈣質呀,
同埋營養價值好唔好啊…同埋啲屋企人呢,識食咗之後呢,真
係對身體都有好大幫助。” (退休,女,65 歲或以上,G01P08)
“Joining this activity, was really to me and people around me, my family, are all…got the help and inspiration…Before I really didn’t check the food label, sometimes didn’t even pay attention to…the date, now I pay more attention…to the label, will check the food label before buy it, and (also check) the amount of sugar, salt, how much are there, the calcium, and how’s the other nutritive values…and the family, after knowing how to eat, it’s really very helpful to the body.” (Retiree, female, 65 yr or above, G01P08)
Positively affect people
around to implement
healthier diet
“譬如我哋幾個去飲咖啡,「唉,少啲糖少啲糖」。或者食甜
品,「食少啲食少啲」。其實大家都知,但有時你唔講,成包
糖倒落去,或者食甜品一個食一份,如果一講就係兩個人一份
啦。或者我哋食飯去,「唔好嗌甜品啦,我哋食飽咗了,唔使
再食啦」。咁樣,我覺得,唔會好難。” (家庭主婦,女,40-49歲,G01P03)
“Such as when we go to drink coffee, (I would say): ‘less sugar

95
Theme Subtheme Quotes
less sugar.’ Or when having dessert, (I would say): ‘eat less eat less.’ Actually we call know (about the knowledge of healthy diet), but sometimes if you didn’t mention it, (they would) put the whole bag of sugar in it. Or each one eats a piece of dessert, but if we talk abuot it, we would have two people to share one dessert. Or when we go out to have meals, (I would say): ‘(let’s) don’t order desserts, we are all full, stop eating.’ And then I think it won’t be difficult.” (Housewife, female, 40-49 yr, G01P03) “即係一開始嗰時,咁我哋有好多飯局嘅嘛,我哋就會係呢度,
「喂,少油啊!今晚啊大家唔准食乜嘢!」。” (兼職僱員,
女,60-64 歲,G01P10)
“At the beginning, we have many meals gathering, we would be there (say): ‘hey, less oil! Tonight we should not allow ourselves to eat certain food!’” (Part-time employee, female, 60-64 yr, G01P10)
Better relationship
With friends “我覺得好咗好多,朋友多咗好多。” (家庭主婦,女,65 歲或以
上,G01P06)
“I think I am much better, have many more friends.” (Housewife, female, 65yr or above, G01P06) “就咁睇呢個活動呢,即係真係對我啲,同埋身邊人呢,真係好
大影響,同埋有個凝聚力,同朋友之間呢,即係話多啲話題。
而且呢多啲訊息呢,可以互相…咁家庭有多啲話題囉…做咗呢
個健康大使呢,好多人都,有啲嘢我唔知呢,佢都要來問我,
我知就話俾佢聽囉。” (退休,女,65 歲或以上,G01P08)
“When talking about this event, it’s really have great effects on me and people around me, and (it made us have the) cohesion, with friends we have more topics. And with more information, (we could share) with each other…and the family will have more topics among the family…and as this Health Ambassador, many people, (if) they don’t know about something, they will come and ask me, (if) I know I would tell them.” (Retiree, female, 65 yr or above, G01P08) “全部呢都覺得係好咗了,因為啲朋友呢就覺得,係喎,你有說
服力了,知嘢多咗…” (全職僱員,女,50-59 歲,G01P09)
“I think (the relationship with people around) all are better, because some friends think, right now you are more
96
Theme Subtheme Quotes
convincing, you know more things (after join the programme)…” (Full-time employee, female, 50-59 yr, G01P9) With family “整體都好咗好多,屋企人都好支持我,好好。” (兼職僱員,
女,65 歲或以上,G01P01)
“(The relationship) are overall become better, the family members are all very supportive, it’s really very good.” (Part-time employee, female, 65 yr or above, G01P01)
5.9 Discussion and conclusion Trainees benefitted a lot from the programme. In general, they showed:
High acceptance of the TTA;
Improved competence (knowledge, self-efficacy and attitude) and practice in relation to ZTEx and low sugar dietary habits and paying attention to food nutrient labels;
Enhanced low sugar dietary practices and physical activity (ZTEx) especially;
Improved physical fitness performance and personal and family well-being; and
Enhanced competence in implementing community-based interventions and health promotion activities.
We have (i) designed an innovative brief three-phase evidence-based evidence-generating TTA guided by a theoretical conceptual model to meet the needs of the communities; (ii) implemented our programme with guidelines and provided post-training support; and (iii) systematically evaluated the programme with a model-based approach, using quantitative and qualitative methods.
Experiential teaching and learning methods were used. The training content included the general constructs of positive psychology, health-related (physical activity and healthy diet) information and practices, focusing on ZTEx and sugar reduction, and skills geared toward the implementation of the community-based programmes. Diversified teaching and learning methods, including fitness assessments, experiential learning strategies, role plays, games, group discussions and didactic talks were used. After the training, continuous support including ongoing guidance, supervision and consultation, were provided to the trainees.
Trainees indicated that the training was easy to understand and comprehensive. Trainees felt that the electronic messages were useful and that the souvenirs were practical. Trainees commented that the training not only enhanced their health knowledge, but also improved their health behaviours and benefitted their and their family members’ health and well-being. Trainees derived a great sense of achievement from being Health Ambassadors,

97
successfully designing and implementing community-based interventions for almost 1,300 participants and their family members. The trainees developed better relationships with family members and other people around them. The qualitative feedback corroborated and enriched the quantitative results.
Our evidence-based and evidence-generating TTA offers a practical example of the well-structured development and model-based evaluation of a capacity-building training programme, which should be helpful to others seeking to develop such programmes in diverse communities. Our work has laid a good foundation for deeper collaboration between service organisations and academics, advocating the fusion of “Best Science” with “Best Practice” and empowering service organisations to integrate scientific practices into their existing and future programmes and policy formulation.
98
CHAPTER 6 COMMUNITY-BASED PROGRAMME
6.1 Introduction As the FHHCPP adopted a community-based participatory research approach, the FAMILY Project Team collaborated with the participating community partners to design and implement community-based family intervention programmes in accordance with the theme (HD or PA) assigned during randomisation, working under the same conceptual framework and objectives as described in Chapter 2. The collaborating community partners included the HKIWA, the participating member associations from the Central and Western, Wan Chai, Southern, and Eastern districts, and the Health Ambassadors recruited by the associations for the TTA workshops as described in Chapter 5.
6.2 Community-based programme study design The community-based family intervention programme followed the randomisation and allocation described in Chapter 2. In keeping with the principle of brief interventions, community-based participants received only two intervention sessions throughout the programme: the core session and the booster session. Both sessions were organised by each respective group’s Health Ambassadors. The core sessions were delivered by the FAMILY Project Team, whilst the booster sessions contained content designed by each group’s Health Ambassadors and were delivered by the Health Ambassadors. All groups then completed two rounds of follow-up telephone interviews. Four of the eight groups were sent reminder messages regarding health behaviours taught during the core sessions via WhatsApp (instant messaging platform). Four of the eight groups were supported by Health Ambassadors who had formed social groups (chat groups) on WhatsApp. (Figure 2.3, Chapter 2.2)
Data were collected through questionnaires at six time points:
T1: Baseline, pre-intervention; T2: Immediately post-core session; T3: Pre-booster session (1 month after the core session); T4: Immediately post-booster session (1 month after the core session); T5: 3 months after the core session; and T6: 6 months after the core session.
6.2.1 Core intervention sessions Each intervention group, with topics assigned as described in Chapter 2, held its respective first session (core session) of the community-based intervention programme during April 2016 to May 2016. A total of eight core sessions (lasting 2 to 2.5 hours each) were held, and a total of 1,256 individuals attended these sessions. During the core sessions, each Health Ambassador led and supported groups of approximately 10 to 20 participants as they completed a baseline questionnaire (T1) and a series of physical fitness assessments measuring body composition, muscle strength, and muscle endurance. Body mass, height,

99
hand grip strength, and performance on the single leg stance test1 and 30-second chair stand test2 were measured. FAMILY Project Team then delivered an interactive talk about the FAMILY 3Hs and the group’s corresponding topic (HD or PA) with a duration of about 60 minutes.
In the PA groups, participants were led to recognise the problems of overweight and obesity, and the associated ill-health conditions. Participants were shown World Health Organization standards for physical activity for health and a video clip of Professor Lam explaining ZTEx. The “3 Treasures of PA” were introduced: the single leg stance exercise, hand grip strength, and the chair stand exercise. Participants were given a logbook, or record sheet, in order to facilitate them in self-monitoring their physical activity behaviours. They were encouraged to share the contents of the session with their family members as a way of helping the family achieve the 3Hs, and the FAMILY Project Team and the Health Ambassadors led the participants in making declarations of commitment to practise what they have learnt and increased physical activity. At the end of the session, the participants took part in a creative dance improvised by the participants themselves. In the PA groups with reminders (PA-3 and PA-4), each participant received a handgrip as a souvenir to take home and they were encouraged to use the handgrip as a tool to remind themselves to practise the “3 Treasures”.
In the HD groups, participants were also led to recognise the problems of overweight and obesity, and the associated ill-health conditions. They were shown World Health Organization recommendations for daily sugar intake for health and a video clip showing a family learning about healthy eating and the recommended levels of sugar intake. The “3 Treasures of HD” were introduced: how to read and understand a nutrition label, to consume drinks with low or less sugar, and to consume fewer desserts or desserts with low or less sugar. Participants in the HD groups were given a logbook in order to facilitate them in self-monitoring their healthy diet behaviours. As with the PA groups, the HD groups were encouraged to share the contents of the session with their family members as a way of helping the family achieve the 3Hs, and participants were led to make declarations of commitment to practise what they have learnt and have a healthy diet. Participants in the HD groups with reminders (HD-3 and HD-4) received a healthy diet themed table mat as a souvenir to take home and were encouraged to place the table mat in a prominent position in their home and use it as a tool to remind themselves to adopt the “3 Treasures”.
All groups completed a questionnaire (T2) immediately after the core session.
1 The single leg stance test, or the unipedal stance test, is a balance test. As per the methods used by Springer [106] in a study providing normative values for the test, participants were asked to cross his or her arms over the chest and stand on the foot of their choice (the stance limb) with the other foot raised such that it was near but not touching the stance limb when the timer was started. The test ended when the participant either uncrossed his or her arms, used the raised foot by touching it to the stance limb or the ground, moved the weight-bearing foot, or the maximum time of 120 seconds had elapsed. 2 The 30-second chair stand test is a leg strength and endurance test. Participants were instructed to sit in the middle of their chair with their feet flat on the ground and arms crossed over the chest; when the timer was started, participants rose to a full standing position before sitting back down again, repeating this motion as many times as possible within 30 seconds [107].
100
6.2.2 Booster intervention sessions Each intervention group held its respective second session (booster session) of the community-based intervention programme during May 2016 to June 2015. A total of eight booster sessions were held, and a total of 1,150 individuals attended these sessions.
The booster sessions were organised by the Health Ambassadors and the participating member associations of the HKIWA. All groups chose to hold booster sessions that comprised a day trip as well as intervention-related content regarding healthy diet, physical activity, and family 3Hs knowledge and behaviours. As part of the day trips, each group visited different locations. The locations visited included, but were not limited to: Chi Lin Nunnery, Lingnan Garden, Hong Kong Science Park, Nan Lian Garden, Inspiration Lake, and Sha Tau Kok Farm.
Whilst there was freedom as to the form the session would take and the locations to be visited, the Health Ambassadors were asked to consider and include several requirements when designing the intervention-related content of the sessions:
1. Each group was required to incorporate one activity of at least 8 to 10 minutes in duration for each of the “3 Treasures” that participants learned about during the core sessions, making up a total of at least 24 to 30 minutes of core-related activities; and
2. Each group was required to repeat the declarations of commitment from the core sessions to practicing and adopting the “3 Treasures”.
Each group chose to carry out these requirements differently. In some groups, the activities were led by the Health Ambassadors, whilst in other groups, the activities were led by volunteers or tour guides hired for the day.
At the beginning of the booster sessions, participants completed the pre-booster (T3) questionnaire and physical fitness assessments. Participants were given new logbooks for the upcoming months at the end of the session, and also completed the post-booster (T4) questionnaire.
6.2.3 Telephone follow-up interviews In order to keep tracking the progress of the participants, two batches of telephone follow-up interviews were conducted by the Health Ambassadors as part of the community-based family intervention programme.
In July 2016, a training session was conducted and delivered by the FAMILY Project Team for the Health Ambassadors. About 40 individuals attended the session. The Health Ambassadors in attendance were given a set of guidelines to follow regarding the privacy and confidentiality of participants’ information, the manner in which the interviews were to be conducted, and information that participants should be given should they have any queries regarding the programme or telephone interview. The FAMILY Project Team taught the Health Ambassadors a variety of telephone interviewing techniques, demonstrating the various techniques and highlighting strategies that could be useful, as well as behaviour that should be avoided.
During the period from July 2016 to August 2016, the Health Ambassadors carried out the first batch of telephone follow-up interviews, filling in the 3-month follow-up (T5)
101
questionnaire with participants. The Health Ambassadors carried out the second batch of telephone interviews during the period from October 2016 to November 2016, filling in the 6-month follow-up (T6) questionnaire with participants.
6.2.4 Bring-home anti-inertia reminder tools As part of the community-based programme study, four groups (HD-3, HD-4, PA-3, and PA-4) were randomised to be reminder groups, receiving weekly reminder messages (see Chapter 6.2.5) and bring-home reminder tools at the end of the respective group’s core session. Participants in HD-3 and HD-4 each received a table mat illustrated with information regarding the “3 Treasures of HD” whilst participants in PA-3 and PA-4 each received a handgrip. Participants were instructed to place the reminder tools in a visually prominent place in their home, and were given suggestions: for instance, handgrips could be placed by the television remote control, and table mats could be placed above the kitchen counter. The aim was that the tools would help remind participants of the need to adopt the “3 Treasures” behaviours, and facilitate the implementation of the behaviours; the handgrip could be used when practising hand grip strength, one of the “3 Treasures of PA”, and the table mat could be referred to when preparing meals since it contained information on understanding nutrition labels and daily recommended sugar intake, one of the “3 Treasures of HD”.
6.2.5 WhatsApp anti-inertia reminder messages Mobile phones have become an increasingly important and well-placed platform for the delivery of health interventions [45]. Major advantages of using the mobile phone as a tool for health intervention, as aforementioned in Chapter 1, are cost-effectiveness of interventions and increased accessibility to helpful content and information. As such, two series of mobile messages were designed: one with the theme of healthy diet and one with the theme of physical activity.
6.2.5.1 Operation (delivery of messages) For 27 weeks, HD-3, HD-4, PA-3, and PA-4 received weekly mobile messages via WhatsApp on the topics of healthy diet or physical activity that were designed by the FAMILY Project Team. Each group was sent messages on a weekly basis beginning the week after the respective group’s core intervention session and ending the week of the group’s 6-month follow-up telephone interview.
Each week, the FAMILY Project Team sent the relevant weekly mobile messages to project staff at the HKIWA. The message relevant to each group was then passed through the ranks, from the Health Ambassador Group Leaders of the reminder groups, to the other reminder group Health Ambassadors, to the community-based participants. Thus, HD-3 and HD-4 received weekly healthy diet WhatsApp reminder messages, and PA-3 and PA-4 received weekly physical activity WhatsApp reminder messages. The hierarchy and structure utilised to deliver the weekly messages is depicted in Figure 6.1.
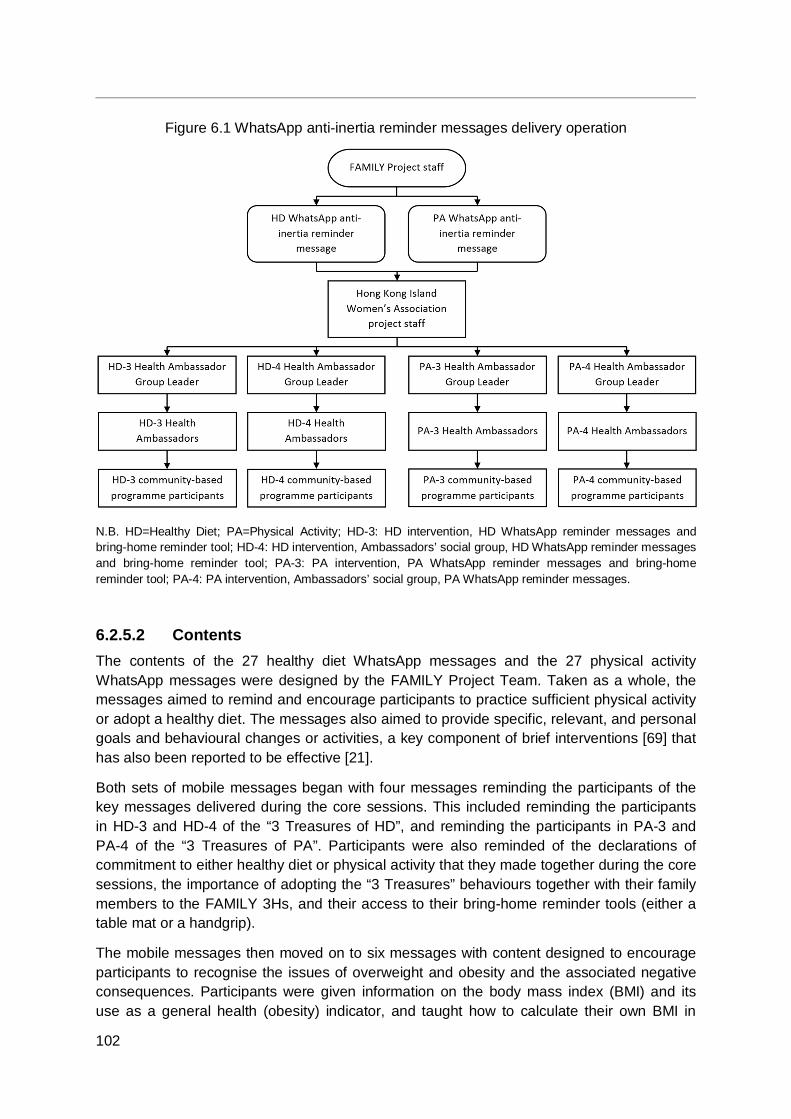
102
Figure 6.1 WhatsApp anti-inertia reminder messages delivery operation
N.B. HD=Healthy Diet; PA=Physical Activity; HD-3: HD intervention, HD WhatsApp reminder messages and bring-home reminder tool; HD-4: HD intervention, Ambassadors’ social group, HD WhatsApp reminder messages and bring-home reminder tool; PA-3: PA intervention, PA WhatsApp reminder messages and bring-home reminder tool; PA-4: PA intervention, Ambassadors’ social group, PA WhatsApp reminder messages.
6.2.5.2 Contents The contents of the 27 healthy diet WhatsApp messages and the 27 physical activity WhatsApp messages were designed by the FAMILY Project Team. Taken as a whole, the messages aimed to remind and encourage participants to practice sufficient physical activity or adopt a healthy diet. The messages also aimed to provide specific, relevant, and personal goals and behavioural changes or activities, a key component of brief interventions [69] that has also been reported to be effective [21].
Both sets of mobile messages began with four messages reminding the participants of the key messages delivered during the core sessions. This included reminding the participants in HD-3 and HD-4 of the “3 Treasures of HD”, and reminding the participants in PA-3 and PA-4 of the “3 Treasures of PA”. Participants were also reminded of the declarations of commitment to either healthy diet or physical activity that they made together during the core sessions, the importance of adopting the “3 Treasures” behaviours together with their family members to the FAMILY 3Hs, and their access to their bring-home reminder tools (either a table mat or a handgrip).
The mobile messages then moved on to six messages with content designed to encourage participants to recognise the issues of overweight and obesity and the associated negative consequences. Participants were given information on the body mass index (BMI) and its use as a general health (obesity) indicator, and taught how to calculate their own BMI in
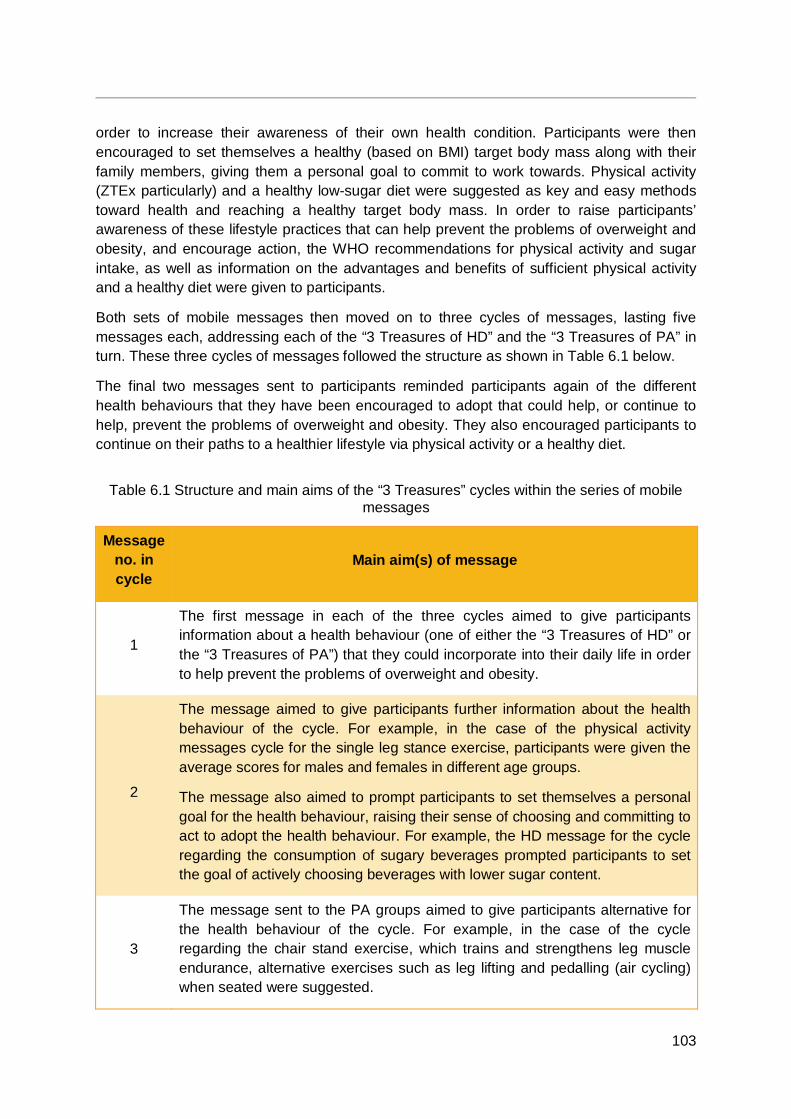
103
order to increase their awareness of their own health condition. Participants were then encouraged to set themselves a healthy (based on BMI) target body mass along with their family members, giving them a personal goal to commit to work towards. Physical activity (ZTEx particularly) and a healthy low-sugar diet were suggested as key and easy methods toward health and reaching a healthy target body mass. In order to raise participants’ awareness of these lifestyle practices that can help prevent the problems of overweight and obesity, and encourage action, the WHO recommendations for physical activity and sugar intake, as well as information on the advantages and benefits of sufficient physical activity and a healthy diet were given to participants.
Both sets of mobile messages then moved on to three cycles of messages, lasting five messages each, addressing each of the “3 Treasures of HD” and the “3 Treasures of PA” in turn. These three cycles of messages followed the structure as shown in Table 6.1 below.
The final two messages sent to participants reminded participants again of the different health behaviours that they have been encouraged to adopt that could help, or continue to help, prevent the problems of overweight and obesity. They also encouraged participants to continue on their paths to a healthier lifestyle via physical activity or a healthy diet.
Table 6.1 Structure and main aims of the “3 Treasures” cycles within the series of mobile messages
Message no. in cycle
Main aim(s) of message
1
The first message in each of the three cycles aimed to give participants information about a health behaviour (one of either the “3 Treasures of HD” or the “3 Treasures of PA”) that they could incorporate into their daily life in order to help prevent the problems of overweight and obesity.
2
The message aimed to give participants further information about the health behaviour of the cycle. For example, in the case of the physical activity messages cycle for the single leg stance exercise, participants were given the average scores for males and females in different age groups.
The message also aimed to prompt participants to set themselves a personal goal for the health behaviour, raising their sense of choosing and committing to act to adopt the health behaviour. For example, the HD message for the cycle regarding the consumption of sugary beverages prompted participants to set the goal of actively choosing beverages with lower sugar content.
3
The message sent to the PA groups aimed to give participants alternative for the health behaviour of the cycle. For example, in the case of the cycle regarding the chair stand exercise, which trains and strengthens leg muscle endurance, alternative exercises such as leg lifting and pedalling (air cycling) when seated were suggested.
104
Message no. in cycle
Main aim(s) of message
The message sent to the HD groups aimed to give participants a specific way in which they could adopt the health behaviour of the cycle. For example, in the cycle regarding the consumption of sugar-sweetened desserts, participants were encouraged to share one dessert with family members rather than consuming one each, lowering the quantity of sugar consumed by each member.
4
The fourth message in each of the three cycles aimed to invite participants to share their knowledge on the HD or PA behaviour with their family members in order to help them make use of their social support network and helping relationships with adopting the health behaviours and healthy lifestyle.
5
The last message in each cycle addressed three aims. Firstly, the message aimed to prompt participants to evaluate their progress with the health behaviour of the cycle. The message also aimed to facilitate participants in forming helping relationships with the Health Ambassador leading them by using words of encouragement. Lastly, the message aimed to remind participants to make use of their bring-home reminder tool in order to help them perform the health behaviours in a consistent context, making the reminder tool a contextual cue for action.
6.3 Recruitment and retention
6.3.1 Inclusion criteria The community-based programme study aimed to recruit at least 1,200 individuals meeting the following inclusion criteria:
Aged 12 years or above; Cantonese-speaking; Have intact verbal and hearing abilities for interpersonal communication; and Have reading and writing abilities suitable for questionnaire completion.
6.3.2 Exclusion criteria Individuals were excluded from the study if he or she:
Failed to meet the aforementioned inclusion criteria; Was unable to sign and give consent; or Had previously attended one or more TTA workshops.
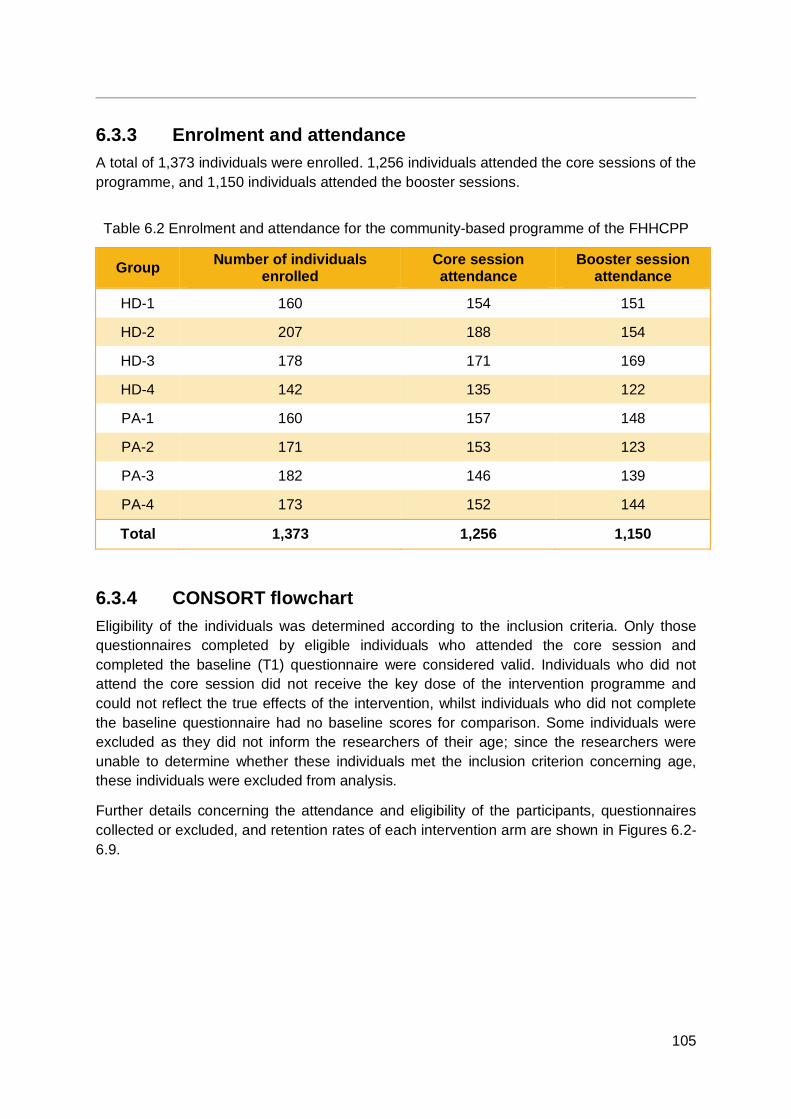
105
6.3.3 Enrolment and attendance A total of 1,373 individuals were enrolled. 1,256 individuals attended the core sessions of the programme, and 1,150 individuals attended the booster sessions.
Table 6.2 Enrolment and attendance for the community-based programme of the FHHCPP
Group Number of individuals enrolled
Core session attendance
Booster session attendance
HD-1 160 154 151
HD-2 207 188 154
HD-3 178 171 169
HD-4 142 135 122
PA-1 160 157 148
PA-2 171 153 123
PA-3 182 146 139
PA-4 173 152 144
Total 1,373 1,256 1,150
6.3.4 CONSORT flowchart Eligibility of the individuals was determined according to the inclusion criteria. Only those questionnaires completed by eligible individuals who attended the core session and completed the baseline (T1) questionnaire were considered valid. Individuals who did not attend the core session did not receive the key dose of the intervention programme and could not reflect the true effects of the intervention, whilst individuals who did not complete the baseline questionnaire had no baseline scores for comparison. Some individuals were excluded as they did not inform the researchers of their age; since the researchers were unable to determine whether these individuals met the inclusion criterion concerning age, these individuals were excluded from analysis.
Further details concerning the attendance and eligibility of the participants, questionnaires collected or excluded, and retention rates of each intervention arm are shown in Figures 6.2-6.9.
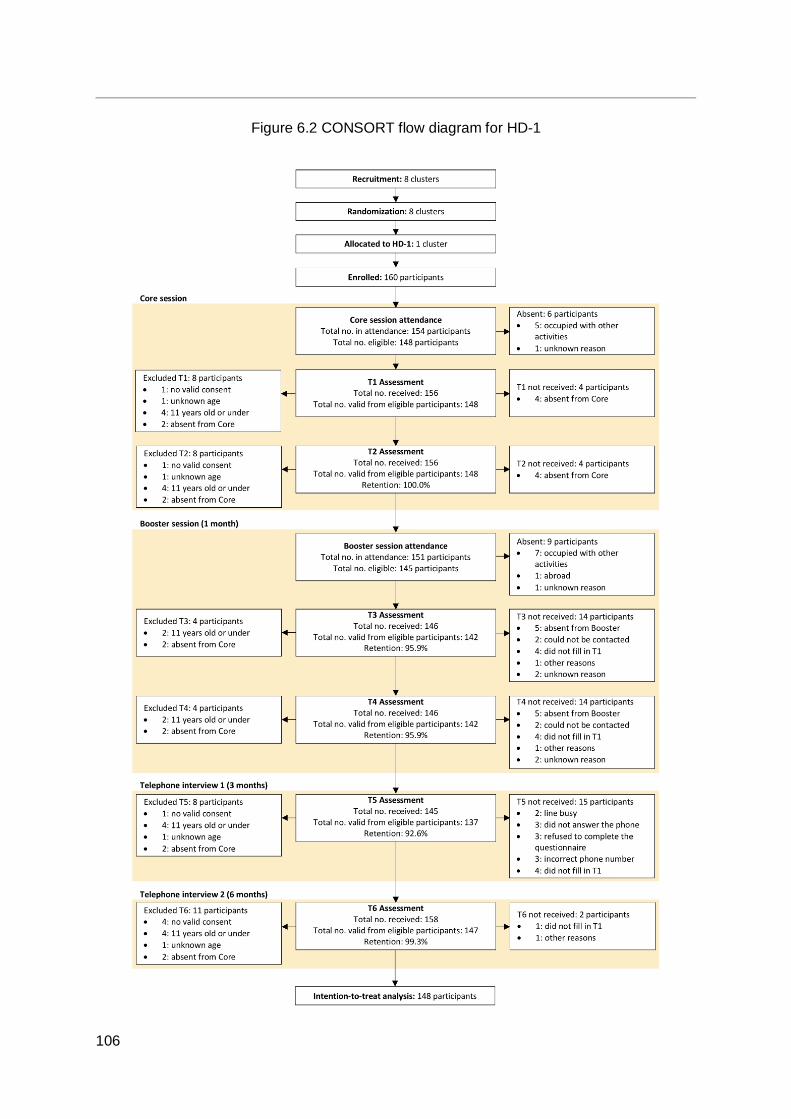
106
Figure 6.2 CONSORT flow diagram for HD-1
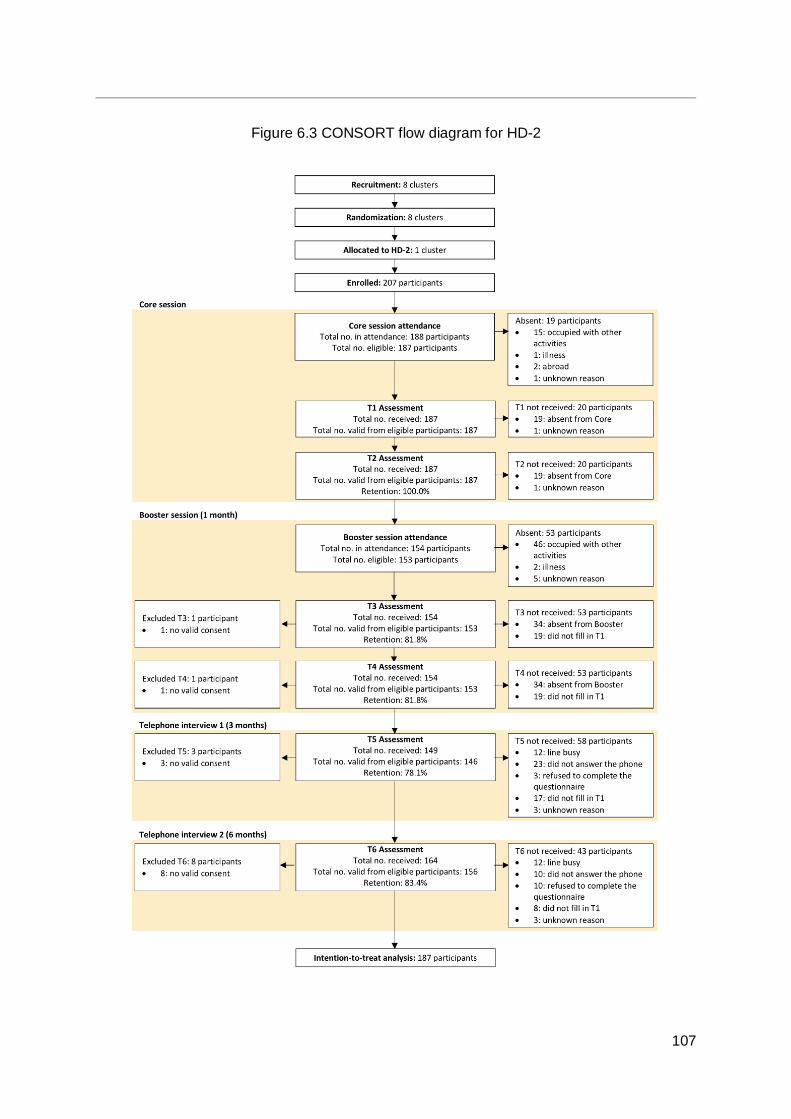
107
Figure 6.3 CONSORT flow diagram for HD-2
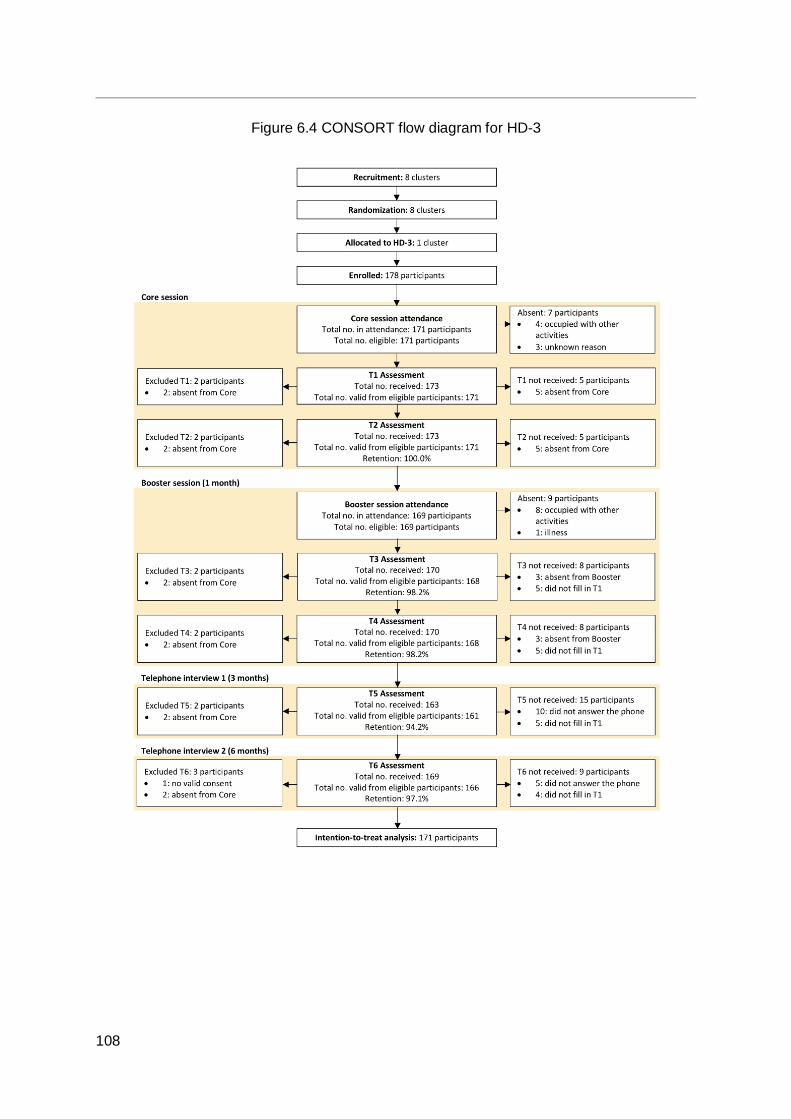
108
Figure 6.4 CONSORT flow diagram for HD-3
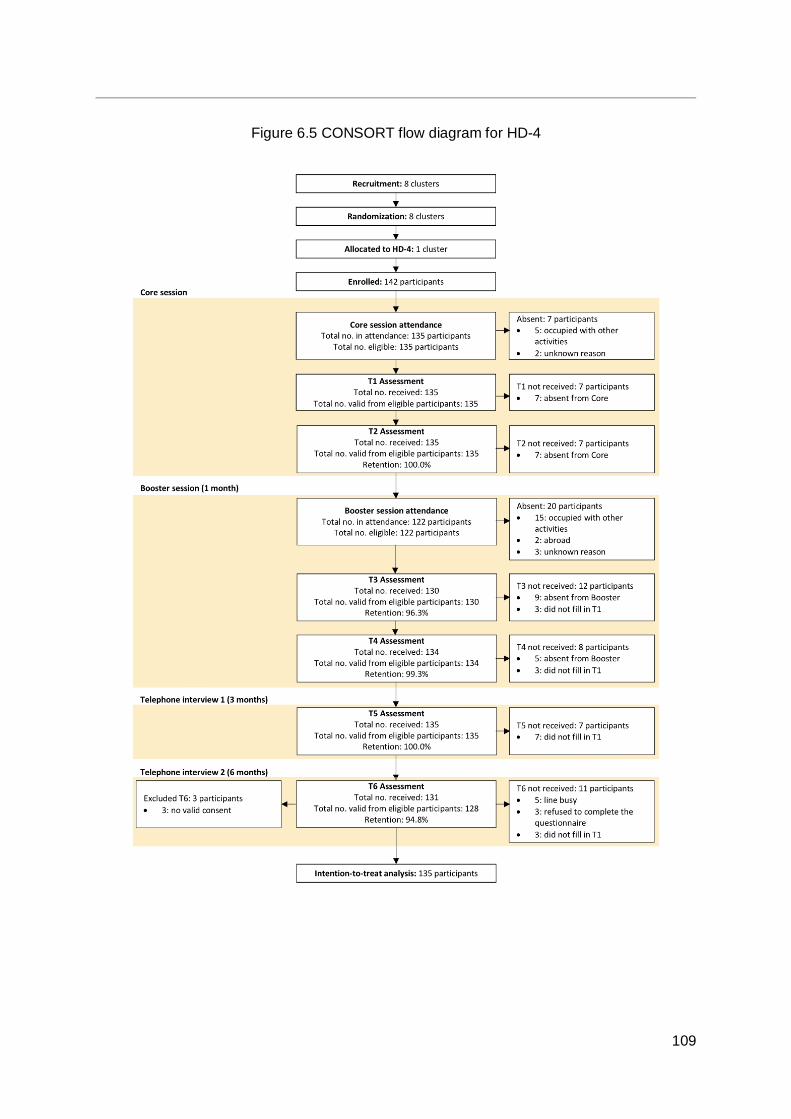
109
Figure 6.5 CONSORT flow diagram for HD-4
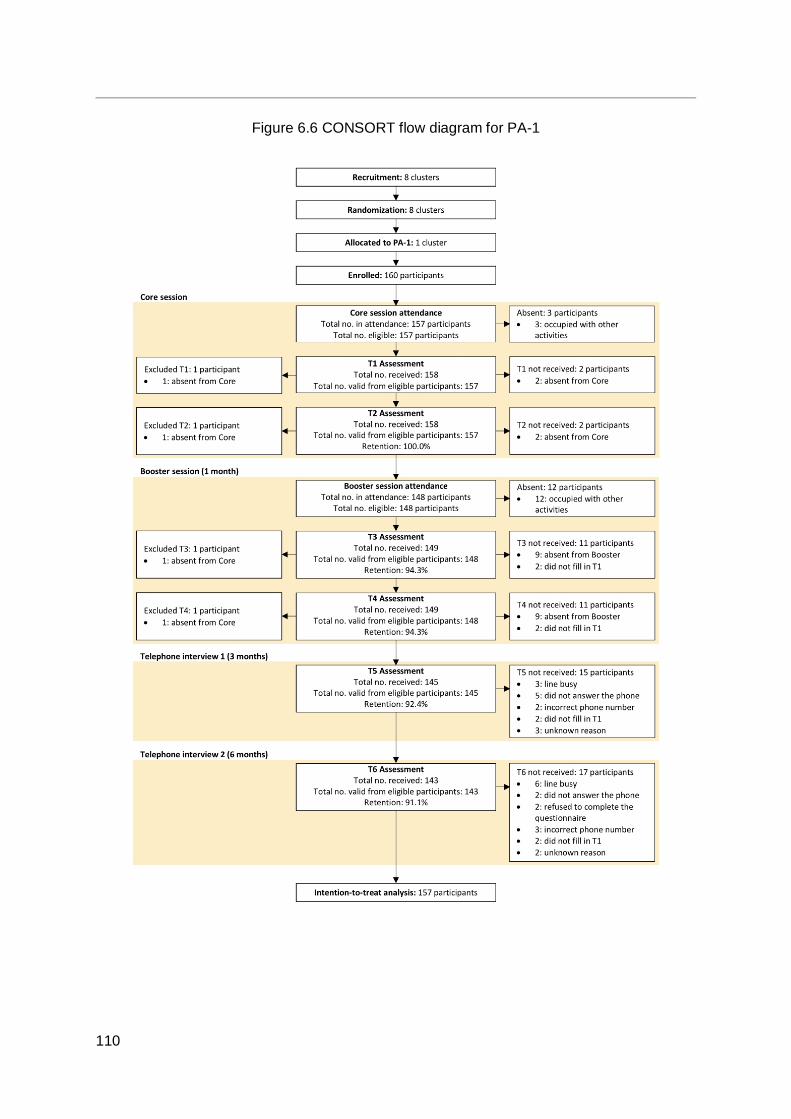
110
Figure 6.6 CONSORT flow diagram for PA-1
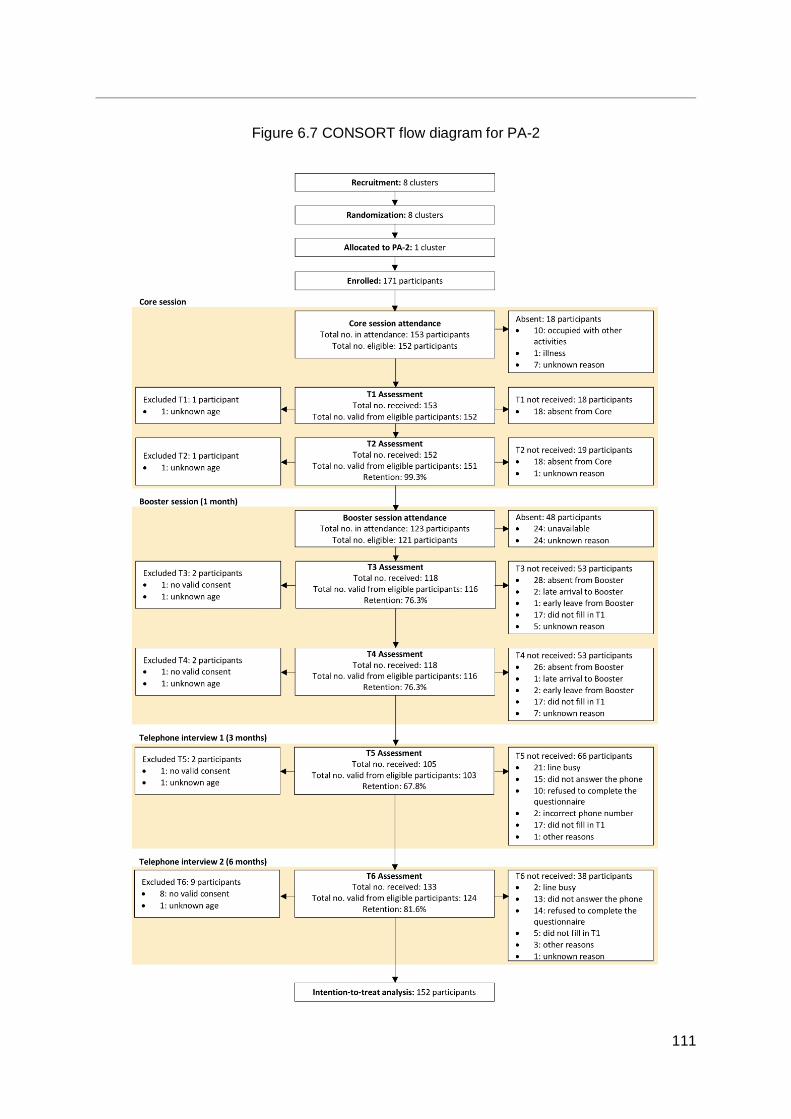
111
Figure 6.7 CONSORT flow diagram for PA-2
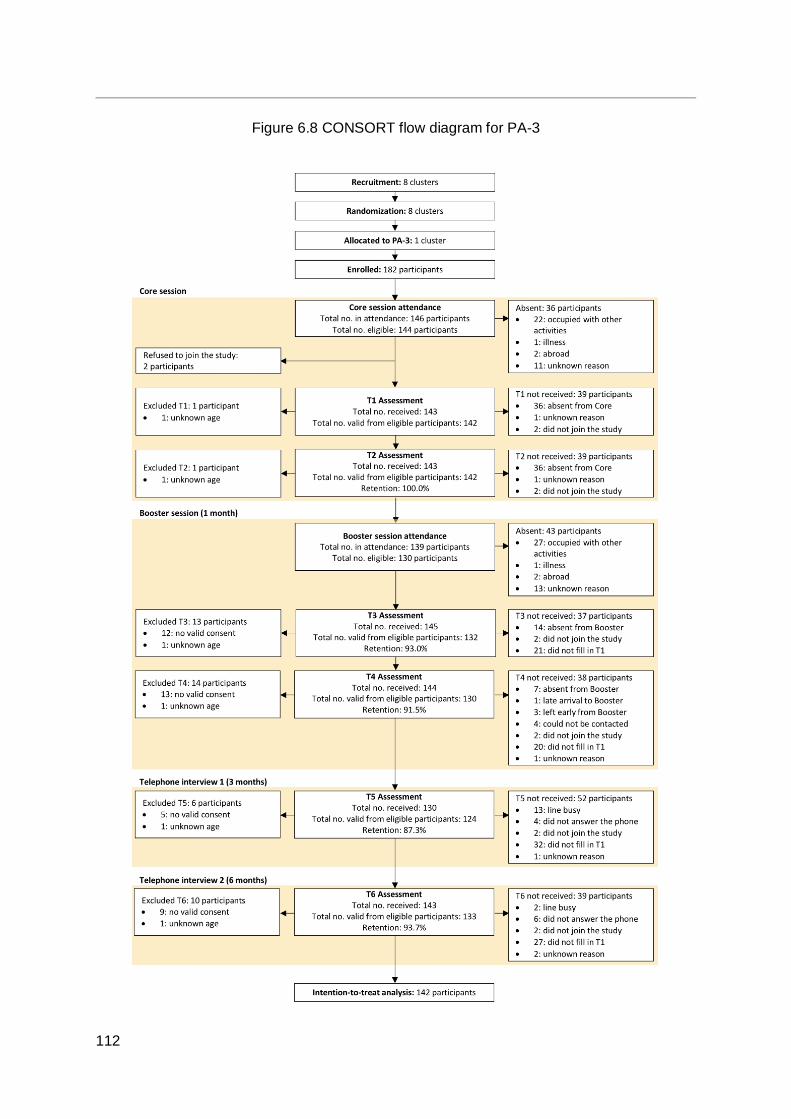
112
Figure 6.8 CONSORT flow diagram for PA-3
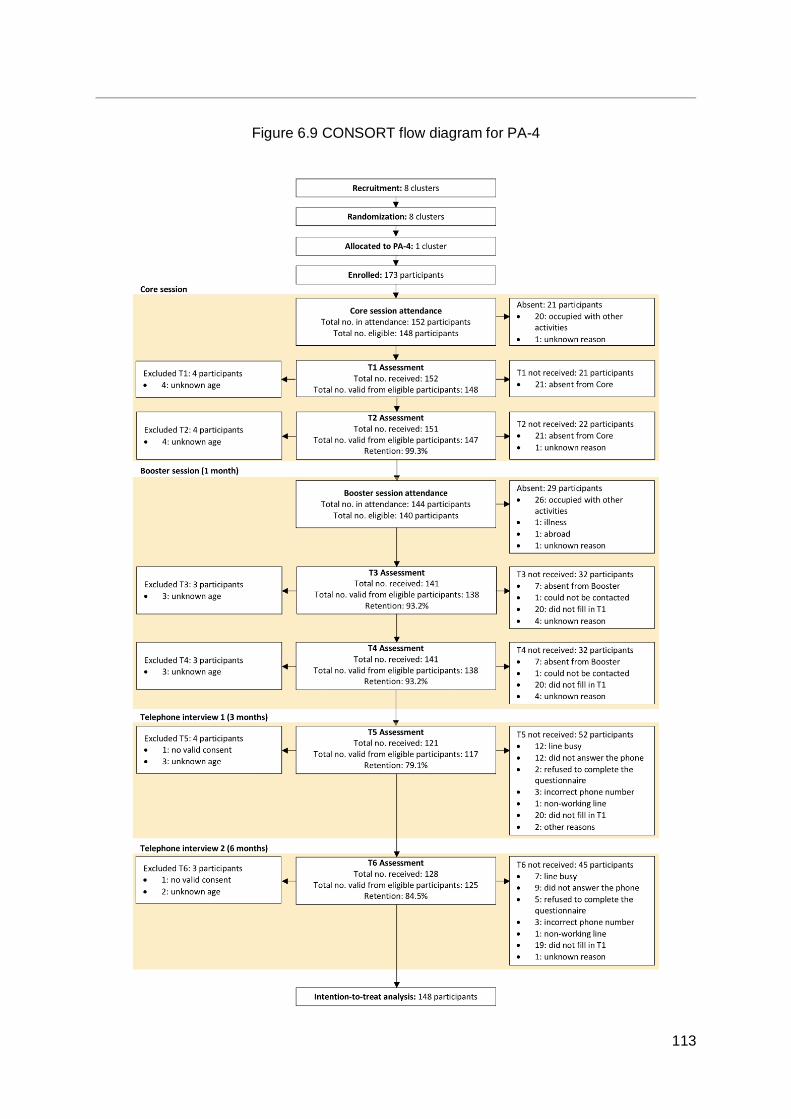
113
Figure 6.9 CONSORT flow diagram for PA-4

114
Of the 1,256 individuals attending the core sessions, 1,242 were eligible to join the study according to the inclusion criteria. In total, 1,240 participants were eligible for ITT analyses.
6.3.4.1 Participant retention in HD-1 One cluster was randomly allocated to HD-1, and 160 participants were enrolled.154 individuals attended the core session and 148 were qualified for analyses by ITT.
6.3.4.2 Participant retention in HD-2 One cluster was randomly allocated to HD-2, and 207 participants were enrolled. 188 individuals attended the core session and 187 were qualified for analyses by ITT.
6.3.4.3 Participant retention in HD-3 One cluster was randomly allocated to HD-3, and 178 participants were enrolled. 171 individuals attended the core session and 171 were qualified for analyses by ITT.
6.3.4.4 Participant retention in HD-4 One cluster was randomly allocated to HD-4, and 142 participants were enrolled. 135 individuals attended the core session and135 were qualified for analyses by ITT.
6.3.4.5 Participant retention in PA-1 One cluster was randomly allocated to PA-1, and 160 participants were enrolled. 157 individuals attended the core session and 157 were qualified for analyses by ITT.
6.3.4.6 Participant retention in PA-2 One cluster was randomly allocated to PA-2, and 171 participants were enrolled. 153 individuals attended the core session and 152 were qualified for analyses by ITT.
6.3.4.7 Participant retention in PA-3 One cluster was randomly allocated to PA-3, and 182 participants were enrolled. 146 individuals attended the core session and 142 were qualified for analyses by ITT.
6.3.4.8 Participant retention in PA-4 One cluster was randomly allocated to PA-4, and 173 participants were enrolled. 152 individuals attended the core session and 148 were qualified for analyses by ITT.
6.4 Community-based programme process evaluation
6.4.1 Introduction and methods Process evaluation is widely used to identify components of an intervention that make it practicable, the conditions under which it is feasible, and potential improvements for enhancing programme effectiveness. In order to examine whether the community-based interventions were delivered to the participants with the appropriate dosage (measured by duration) with reasonable quality and fidelity, members of the FAMILY Project Team as well as staff from the HKIWA carried out on-site observation of each intervention programme session (the core session and booster session for each of the eight cluster groups). A
115
process evaluation form was designed to evaluate different aspects of the community-based programmes, and was completed on-site at each of the intervention programmes.
As the core sessions were delivered by the FAMILY Project Team, programme rundowns were prepared by the FAMILY Project Team for the core sessions. However, for the booster sessions, which were designed and implemented by the Health Ambassadors, each group was required to submit a programme rundown to the FAMILY Project Team before the session. Each group was also required to submit a participants’ attendance list after each session.
6.4.2 Results
6.4.2.1 Context The FHHCPP was focused on educating and empowering participants of different socioeconomic backgrounds and their families, targeting physical activity and healthy diet for the promotion of family well-being.
6.4.2.2 Reach The reach of the community-based programme was examined using the programme attendance and participant groups. The affiliated associations of the HKIWA from a total of four districts (Central and Western, Eastern, Wan Chai, and Southern) participated in the programme. Participants were recruited from the affiliated member associations of the HKIWA as well as from the general public. As a result, different kinds of service users were involved in the community-based programmes of the project, differing in age, education level, and income level. In total, 1,256 individuals attended the core sessions. Participants were encouraged to share the health knowledge and experiences they gained from the programmes with their family members, and it is worth noting that the results indicated increases in the frequency with which participants interacted with their family members on either physical activity or healthy diet. Hence, the reach of the programme extended beyond the participants themselves to the participants’ family members.
Table 6.3 Attendance rate at the community-based programme core and booster intervention sessions
Session Attendance rate
n (%)
Overall HD groups PA groups
Core sessions 1,256 (100.00) 648 (100.00) 608 (100.00) Booster sessions 1,150 (91.56) 596 (91.98) 554 (91.12)
6.4.2.3 Recruitment Recruitment refers to the methods used to approach and attract potential participants. The FHHCPP’s community-based programme relied on the HKIWA and its participating affiliated member associations for recruitment. The various associations utilised different means in
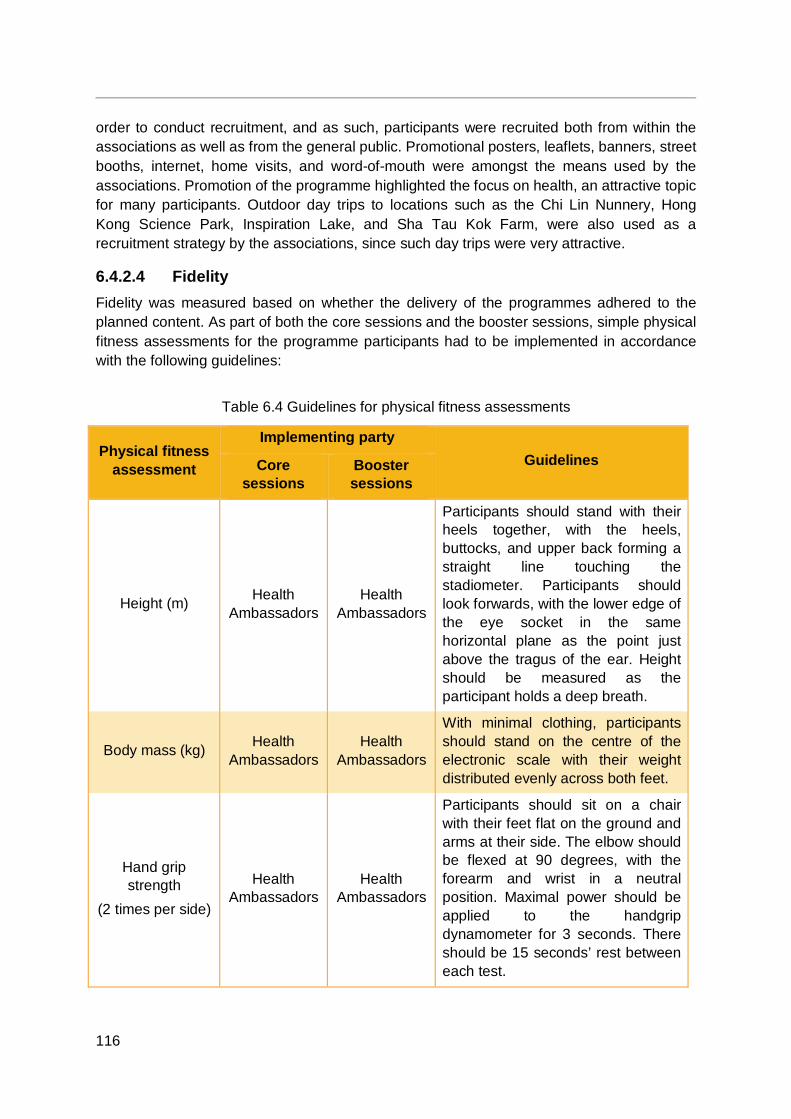
116
order to conduct recruitment, and as such, participants were recruited both from within the associations as well as from the general public. Promotional posters, leaflets, banners, street booths, internet, home visits, and word-of-mouth were amongst the means used by the associations. Promotion of the programme highlighted the focus on health, an attractive topic for many participants. Outdoor day trips to locations such as the Chi Lin Nunnery, Hong Kong Science Park, Inspiration Lake, and Sha Tau Kok Farm, were also used as a recruitment strategy by the associations, since such day trips were very attractive.
6.4.2.4 Fidelity Fidelity was measured based on whether the delivery of the programmes adhered to the planned content. As part of both the core sessions and the booster sessions, simple physical fitness assessments for the programme participants had to be implemented in accordance with the following guidelines:
Table 6.4 Guidelines for physical fitness assessments
Physical fitness assessment
Implementing party Guidelines Core
sessions Booster sessions
Height (m) Health Ambassadors
Health Ambassadors
Participants should stand with their heels together, with the heels, buttocks, and upper back forming a straight line touching the stadiometer. Participants should look forwards, with the lower edge of the eye socket in the same horizontal plane as the point just above the tragus of the ear. Height should be measured as the participant holds a deep breath.
Body mass (kg) Health Ambassadors
Health Ambassadors
With minimal clothing, participants should stand on the centre of the electronic scale with their weight distributed evenly across both feet.
Hand grip strength
(2 times per side)
Health Ambassadors
Health Ambassadors
Participants should sit on a chair with their feet flat on the ground and arms at their side. The elbow should be flexed at 90 degrees, with the forearm and wrist in a neutral position. Maximal power should be applied to the handgrip dynamometer for 3 seconds. There should be 15 seconds’ rest between each test.
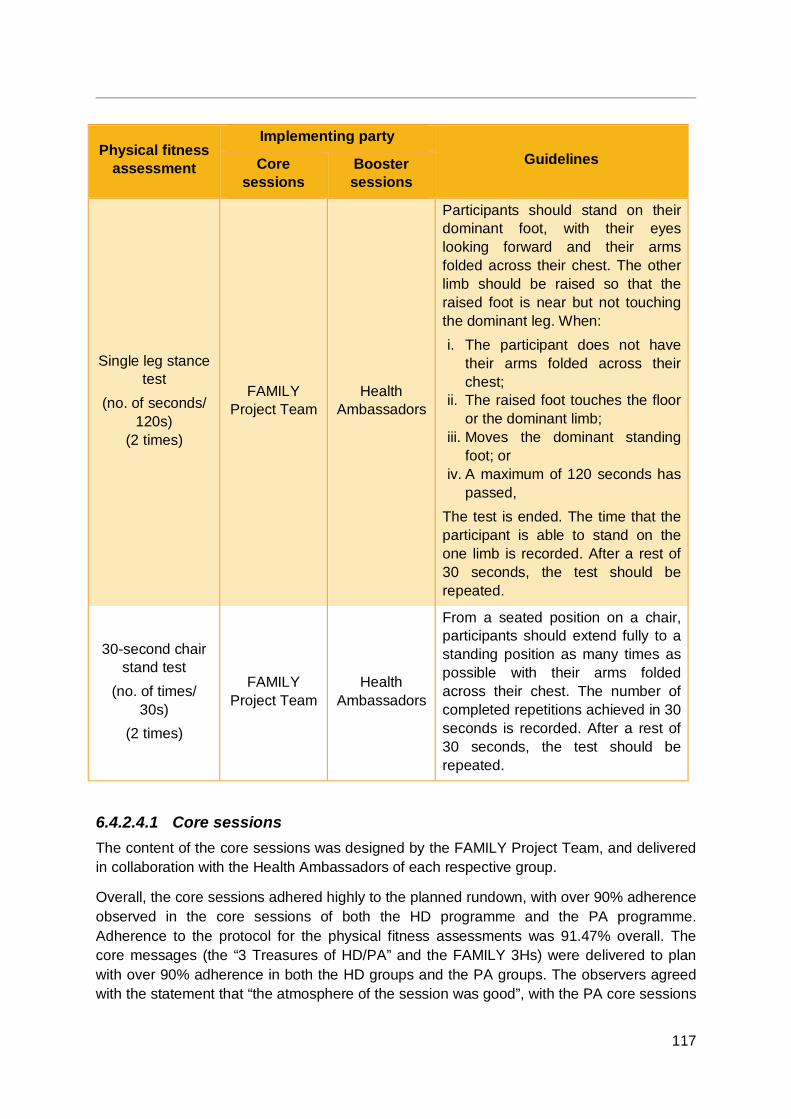
117
Physical fitness assessment
Implementing party Guidelines Core
sessions Booster sessions
Single leg stance test
(no. of seconds/ 120s)
(2 times)
FAMILY Project Team
Health Ambassadors
Participants should stand on their dominant foot, with their eyes looking forward and their arms folded across their chest. The other limb should be raised so that the raised foot is near but not touching the dominant leg. When: i. The participant does not have
their arms folded across their chest;
ii. The raised foot touches the floor or the dominant limb;
iii. Moves the dominant standing foot; or
iv. A maximum of 120 seconds has passed,
The test is ended. The time that the participant is able to stand on the one limb is recorded. After a rest of 30 seconds, the test should be repeated.
30-second chair stand test
(no. of times/ 30s)
(2 times)
FAMILY Project Team
Health Ambassadors
From a seated position on a chair, participants should extend fully to a standing position as many times as possible with their arms folded across their chest. The number of completed repetitions achieved in 30 seconds is recorded. After a rest of 30 seconds, the test should be repeated.
6.4.2.4.1 Core sessions The content of the core sessions was designed by the FAMILY Project Team, and delivered in collaboration with the Health Ambassadors of each respective group.
Overall, the core sessions adhered highly to the planned rundown, with over 90% adherence observed in the core sessions of both the HD programme and the PA programme. Adherence to the protocol for the physical fitness assessments was 91.47% overall. The core messages (the “3 Treasures of HD/PA” and the FAMILY 3Hs) were delivered to plan with over 90% adherence in both the HD groups and the PA groups. The observers agreed with the statement that “the atmosphere of the session was good”, with the PA core sessions

118
getting a mean score of 4.20 out of 5. Overall, the quality of the core sessions was rated with a mean score of 4.10 out of 5.
Table 6.5 Community-based programme core session fidelity
Measure
Feedback by observers Mean (SD)
Overall (n=21)
HD sessions
(n=11)
PA sessions
(n=10) Overall speaking, the degree of adherence of the session to the proposed rundown was approximately ___%. (0-100)
94.38 (7.47)
92.73 (8.17)
96.20 (6.55)
In the delivery of the core messages (“3 Treasures of HD/PA”, FAMILY 3Hs), the degree of adherence to the proposed rundown was approximately ___%. (0-100)
94.48 (7.53)
92.73 (8.17)
96.40 (6.64)
You felt that the degree to which the core messages were conveyed was ___%. (0-100)
96.00 (7.53)
95.00 (8.50)
97.11 (6.62)
The degree to which the physical fitness assessments were executed according to the guidelines was ___%. (0-100)
91.47 (9.81)
92.22 (10.64)
90.63 (9.43)
To what extent do you agree: The atmosphere of the session was good. (1-5a)
3.95 (0.81)
3.73 (0.79)
4.20 (0.79)
Overall speaking, was the quality of session high? (1-5b)
4.10 (0.79)
4.09 (0.94)
4.11 (0.60)
a 5-point Likert scale: “1=strongly disagree” to “5=strongly agree” b 5-point Likert scale: “1=very low” to “5=very high”
119
6.4.2.4.2 Booster sessions In the case of the booster sessions, the content was designed and implemented by the Health Ambassadors of each respective group. For quality control purposes, the following guidelines were given to the Health Ambassadors to follow for the booster sessions:
The session should involve an activity for each of either the “3 Treasures of HD” or the “3 Treasures of PA”, with each activity lasting a minimum of 8 to 10 minutes, making up a minimum of 24 to 30 minutes.
After each activity addressing one of the “3 Treasures,” a sign with the name of the treasure, e.g. “1st Treasure: Single leg stance,” should be held up and the group should read it aloud together.
Once all of the activities for each of the “3 Treasures” have been completed, the group should make declarations of commitment to practising the “3 Treasures:
1. “I will practise the 3 Treasures of PA/the 3 Treasures of HD!” 2. “I will practise the 3 Treasures of PA/the 3 Treasures of HD together with my
family members!”
Proposed rundowns were submitted to the FAMILY Project Team by the Health Ambassadors from the participating affiliated member associations of the HKIWA in advance of the sessions for vetting.
Overall, the sessions adhered highly to the planned rundown, with over 90% adherence observed in the booster sessions of both the HD programme and the PA programme. Adherence to the protocol for the physical fitness assessments was 89.09% overall. The core messages (the “3 Treasures of HD/PA” and the FAMILY 3Hs) were delivered to plan with over 80% adherence in both the HD groups and the PA groups. The observers agreed with the statement that “the atmosphere of the session was good”, with an average rating of 4.19 out of 5. Overall, the quality of the booster sessions was rated with a mean score of 4.31 out of 5.
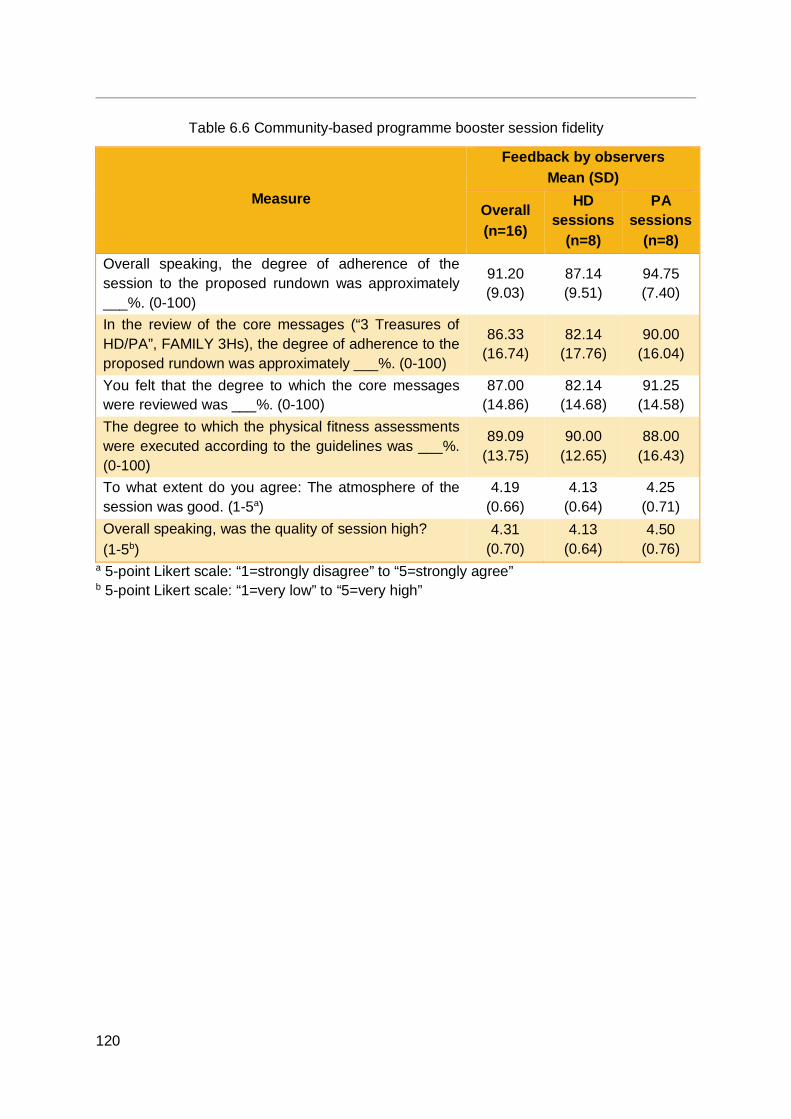
120
Table 6.6 Community-based programme booster session fidelity
Measure
Feedback by observers Mean (SD)
Overall (n=16)
HD sessions
(n=8)
PA sessions
(n=8) Overall speaking, the degree of adherence of the session to the proposed rundown was approximately ___%. (0-100)
91.20 (9.03)
87.14 (9.51)
94.75 (7.40)
In the review of the core messages (“3 Treasures of HD/PA”, FAMILY 3Hs), the degree of adherence to the proposed rundown was approximately ___%. (0-100)
86.33 (16.74)
82.14 (17.76)
90.00 (16.04)
You felt that the degree to which the core messages were reviewed was ___%. (0-100)
87.00 (14.86)
82.14 (14.68)
91.25 (14.58)
The degree to which the physical fitness assessments were executed according to the guidelines was ___%. (0-100)
89.09 (13.75)
90.00 (12.65)
88.00 (16.43)
To what extent do you agree: The atmosphere of the session was good. (1-5a)
4.19 (0.66)
4.13 (0.64)
4.25 (0.71)
Overall speaking, was the quality of session high? (1-5b)
4.31 (0.70)
4.13 (0.64)
4.50 (0.76)
a 5-point Likert scale: “1=strongly disagree” to “5=strongly agree” b 5-point Likert scale: “1=very low” to “5=very high”

121
6.4.2.5 Dose
6.4.2.5.1 Dose delivered On average, observers estimated that the core sessions had addressed the key messages of the intervention (the “3 Treasures of HD/PA” and the FAMILY 3Hs) for approximately 45 minutes. The booster sessions reviewed these messages for over 60 minutes, exceeding the minimum requirement of 24 to 30 minutes set by the guidelines (see Section 6.4.2.4.2).
Table 6.7 Community-based programme dose delivered
Measure
Feedback by observers Mean (SD)
Overall (n=16)
HD sessions (n=8)
PA sessions (n=8)
Core session: The session addressed the core messages for approximately ___ minutes.
45.17 (16.34) 45.20 (19.49) 45.13 (12.65)
Booster session: The session reviewed the core messages for approximately ___ minutes.
64.75 (62.81) 51.50 (60.48) 78.00 (66.28)
6.4.2.5.2 Dose received The effectiveness of intervention programmes can be assessed by evaluating the extent to which participants received programme content.
Participants were asked to evaluate the core session immediately after the session, the booster session immediately after the session, and the FHHCPP overall at 6 months, using the T2, T4, and T6 questionnaire assessments respectively. Participants rated the core sessions, the booster sessions, and the project overall highly. Participants in both the HD groups and PA groups indicated that they were satisfied with the content in the project, and that the content was applicable to their daily lives. Over 90% of participants would recommend the core sessions, the booster sessions, and the project overall to family members or friends.
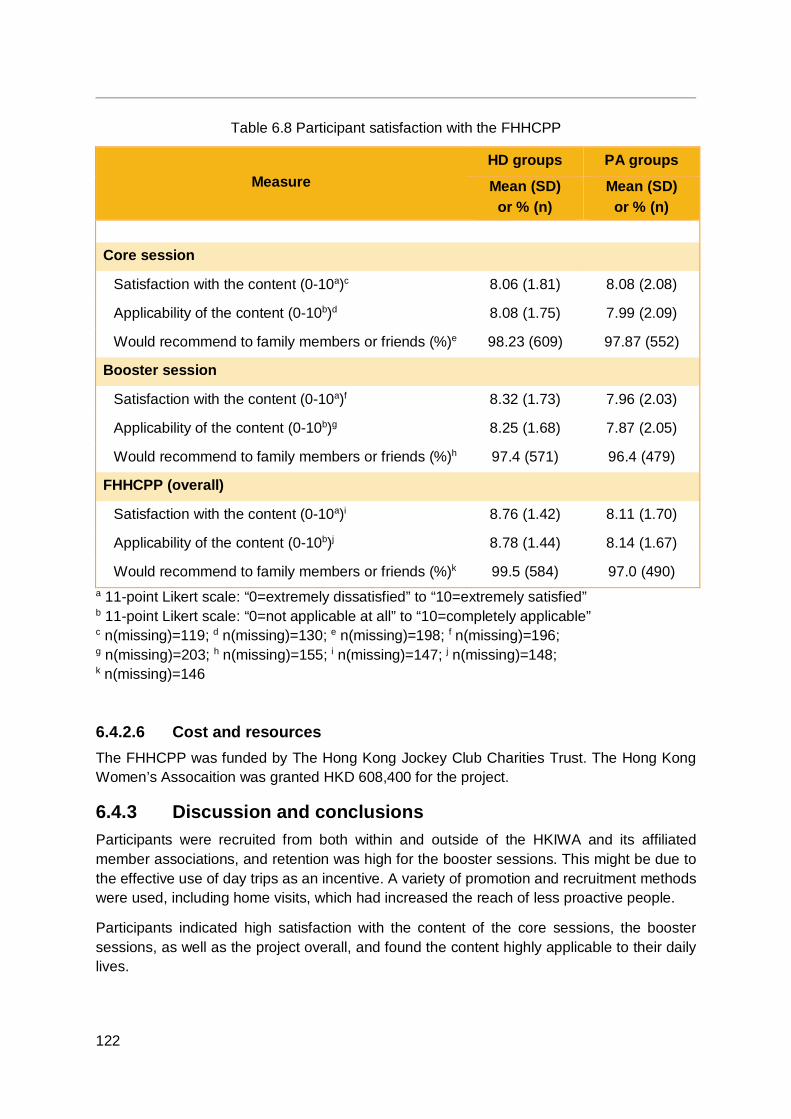
122
Table 6.8 Participant satisfaction with the FHHCPP
Measure HD groups PA groups
Mean (SD) or % (n)
Mean (SD) or % (n)
Core session
Satisfaction with the content (0-10a)c 8.06 (1.81) 8.08 (2.08) Applicability of the content (0-10b)d 8.08 (1.75) 7.99 (2.09) Would recommend to family members or friends (%)e 98.23 (609) 97.87 (552)
Booster session
Satisfaction with the content (0-10a)f 8.32 (1.73) 7.96 (2.03) Applicability of the content (0-10b)g 8.25 (1.68) 7.87 (2.05) Would recommend to family members or friends (%)h 97.4 (571) 96.4 (479)
FHHCPP (overall)
Satisfaction with the content (0-10a)i 8.76 (1.42) 8.11 (1.70) Applicability of the content (0-10b)j 8.78 (1.44) 8.14 (1.67) Would recommend to family members or friends (%)k 99.5 (584) 97.0 (490)
a 11-point Likert scale: “0=extremely dissatisfied” to “10=extremely satisfied” b 11-point Likert scale: “0=not applicable at all” to “10=completely applicable” c n(missing)=119; d n(missing)=130; e n(missing)=198; f n(missing)=196; g n(missing)=203; h n(missing)=155; i n(missing)=147; j n(missing)=148; k n(missing)=146
6.4.2.6 Cost and resources The FHHCPP was funded by The Hong Kong Jockey Club Charities Trust. The Hong Kong Women’s Assocaition was granted HKD 608,400 for the project.
6.4.3 Discussion and conclusions Participants were recruited from both within and outside of the HKIWA and its affiliated member associations, and retention was high for the booster sessions. This might be due to the effective use of day trips as an incentive. A variety of promotion and recruitment methods were used, including home visits, which had increased the reach of less proactive people.
Participants indicated high satisfaction with the content of the core sessions, the booster sessions, as well as the project overall, and found the content highly applicable to their daily lives.
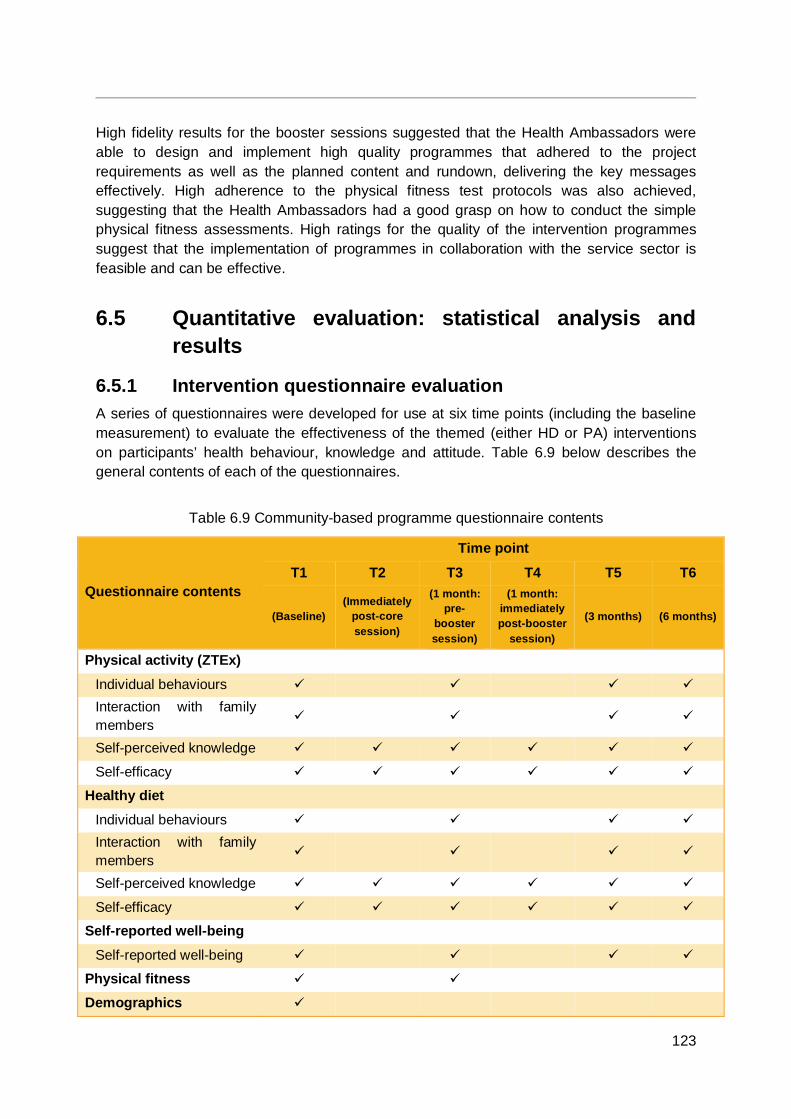
123
High fidelity results for the booster sessions suggested that the Health Ambassadors were able to design and implement high quality programmes that adhered to the project requirements as well as the planned content and rundown, delivering the key messages effectively. High adherence to the physical fitness test protocols was also achieved, suggesting that the Health Ambassadors had a good grasp on how to conduct the simple physical fitness assessments. High ratings for the quality of the intervention programmes suggest that the implementation of programmes in collaboration with the service sector is feasible and can be effective.
6.5 Quantitative evaluation: statistical analysis and results
6.5.1 Intervention questionnaire evaluation A series of questionnaires were developed for use at six time points (including the baseline measurement) to evaluate the effectiveness of the themed (either HD or PA) interventions on participants’ health behaviour, knowledge and attitude. Table 6.9 below describes the general contents of each of the questionnaires.
Table 6.9 Community-based programme questionnaire contents
Questionnaire contents
Time point
T1 T2 T3 T4 T5 T6
(Baseline) (Immediately
post-core session)
(1 month: pre-
booster session)
(1 month: immediately post-booster
session)
(3 months) (6 months)
Physical activity (ZTEx) Individual behaviours Interaction with family members
Self-perceived knowledge
Self-efficacy Healthy diet
Individual behaviours Interaction with family members
Self-perceived knowledge
Self-efficacy Self-reported well-being
Self-reported well-being Physical fitness
Demographics
124
6.5.2 Statistical analysis Of the 1,240 participants eligible for ITT analyses, two were within the age range of 12-17 years. To focus on the adult (18 years or above) participants who made up the majority (99.8%) of the project’s eligible sample with valid baseline assessments, the two younger participants were excluded from the analyses. Thus, 1,238 participants were included in the following analyses.
The baseline characteristics of the participants were described using frequencies and percentages for categorical variables, and means and standard deviations for continuous variables. Baseline comparisons between the groups were performed using the independent t-test for continuous variables and the likelihood ratio chi-square test for categorical variables.
To examine the effectiveness of the HD and PA intervention programmes, outcome changes of the HD groups (HD-1, HD-2, HD-3, and HD-4) were compared with the PA groups (PA-1, PA-2, PA-3, PA-4). Analyses were conducted on an ITT basis, and missing data in assessments following the baseline assessment were imputed from the baseline values (i.e. assuming there were no changes).
For continuous variables, mixed model analysis was used. As the HD groups (four groups in total) were compared with the PA groups (four groups in total), the group of the participant was considered as a random effect to account for cluster randomisation. The baseline measurements, age group, sex, marital status, education, and time point of measurement were considered as fixed effects. The HD groups and PA groups were compared at each time point with reference to the baseline scores. Within-group comparisons were conducted using general linear model analyses. For binary categorical variables, between-group (HD groups versus PA groups) comparisons were conducted using binary logistic regressions. Within-group effects were examined using chi-square and McNemar tests.
All analyses were performed with the statistical software SPSS 24.0. A p-value of less than 0.05 was considered statistically significant. The effect size (Cohen’s d) was computed to measure the size of difference. In accordance with Cohen’s [104] suggestions, an effect size of 0.2 to 0.5 was considered a small effect; an effect size of 0.5 to 0.8 a medium effect; and an effect size of 0.8 or above a large effect.
6.5.3 Baseline demographic characteristics of community-based participants
Table 6.10 shows statistically significant differences amongst the intervention arms across all 6 of the demographic characteristics listed, suggesting that the cluster randomisation process did not result in high comparability of the eight groups.
Despite the differences between the intervention arms, the majority of participants were female or aged 60 years or above, with the second most common age group in each intervention arm being ages 50-59 years. Over half of the participants were married. The majority were educated to either primary or secondary level; in HD-4, PA-1, and PA-2 in particular, over half were educated to primary level only. The majority were not employed, but were either retired or homemakers. The majority of participants had a monthly household income of HKD 29,999 or less.
125
Grouped by intervention theme, the HD groups and the PA groups did not significantly differ in terms of sex or monthly household income (Table 6.11). Over three-quarters of both groups were female, and over three-quarters of both groups had a monthly household income of HKD 29,999 or less.
However, the HD groups and the PA groups differed significantly in terms of age, and other important socioeconomic factors such as education, employment status, and marital status, suggesting that the cluster randomisation process did not result in groups with high comparability.
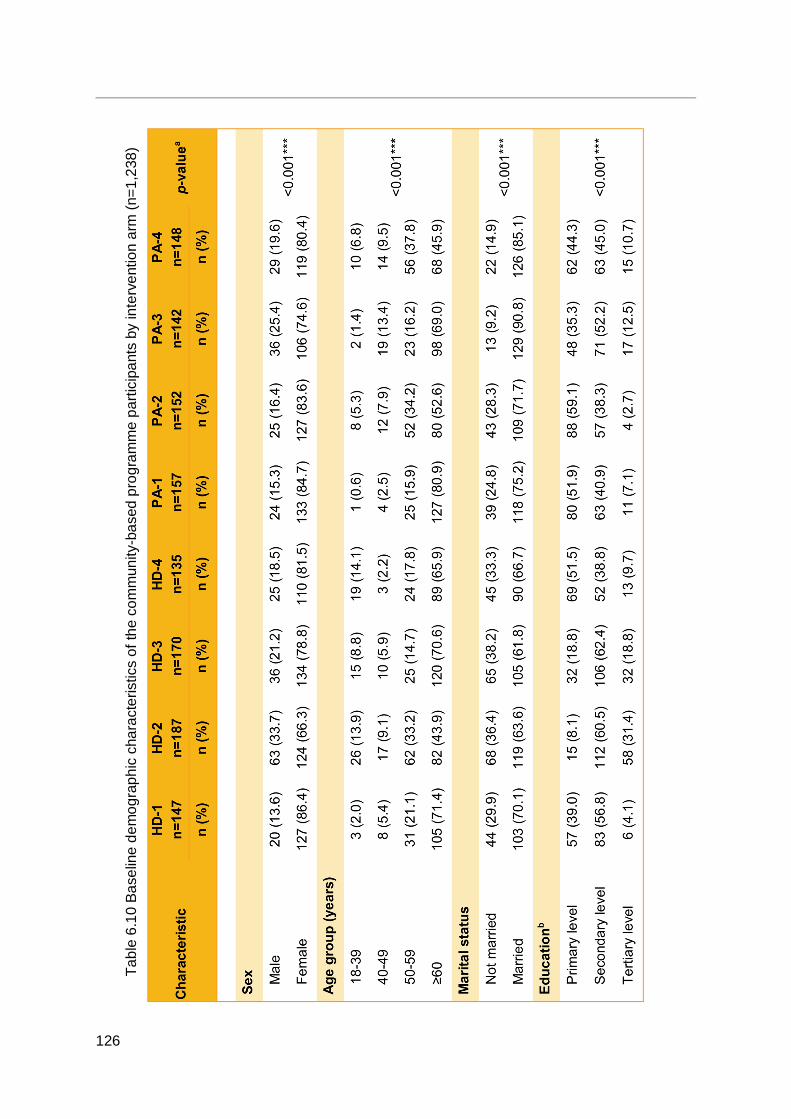
126
Tabl
e 6.
10 B
asel
ine
dem
ogra
phic
cha
ract
eris
tics
of th
e co
mm
unity
-bas
ed p
rogr
amm
e pa
rtici
pant
s by
inte
rven
tion
arm
(n=1
,238
)
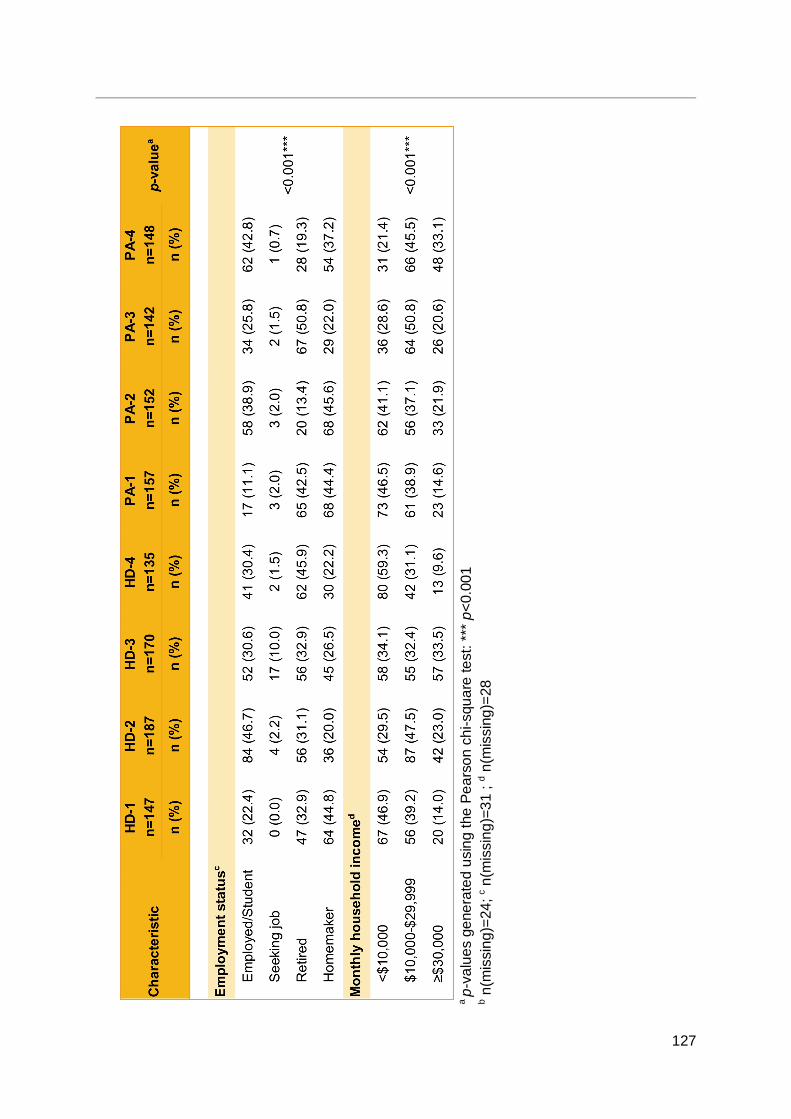
127
a p-
valu
es g
ener
ated
usi
ng th
e Pe
arso
n ch
i-squ
are
test
: ***
p<0
.001
b n(m
issi
ng)=
24; c n
(mis
sing
)=31
; d n
(mis
sing
)=28
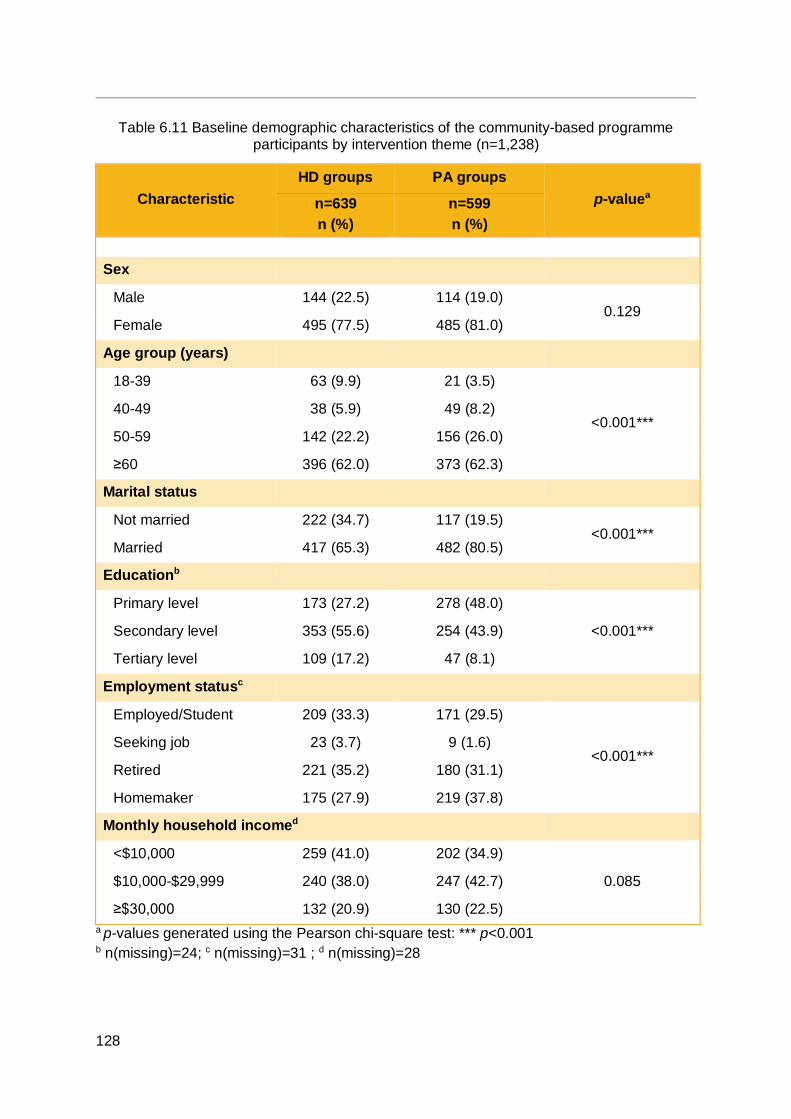
128
Table 6.11 Baseline demographic characteristics of the community-based programme participants by intervention theme (n=1,238)
Characteristic HD groups PA groups
p-valuea n=639 n (%)
n=599 n (%)
Sex
Male 144 (22.5) 114 (19.0) 0.129
Female 495 (77.5) 485 (81.0) Age group (years)
18-39 63 (9.9) 21 (3.5)
<0.001*** 40-49 38 (5.9) 49 (8.2) 50-59 142 (22.2) 156 (26.0) ≥60 396 (62.0) 373 (62.3)
Marital status
Not married 222 (34.7) 117 (19.5) <0.001***
Married 417 (65.3) 482 (80.5) Educationb
Primary level 173 (27.2) 278 (48.0) <0.001*** Secondary level 353 (55.6) 254 (43.9)
Tertiary level 109 (17.2) 47 (8.1) Employment statusc
Employed/Student 209 (33.3) 171 (29.5)
<0.001*** Seeking job 23 (3.7) 9 (1.6) Retired 221 (35.2) 180 (31.1) Homemaker 175 (27.9) 219 (37.8)
Monthly household incomed
<$10,000 259 (41.0) 202 (34.9) 0.085 $10,000-$29,999 240 (38.0) 247 (42.7)
≥$30,000 132 (20.9) 130 (22.5) a p-values generated using the Pearson chi-square test: *** p<0.001 b n(missing)=24; c n(missing)=31 ; d n(missing)=28
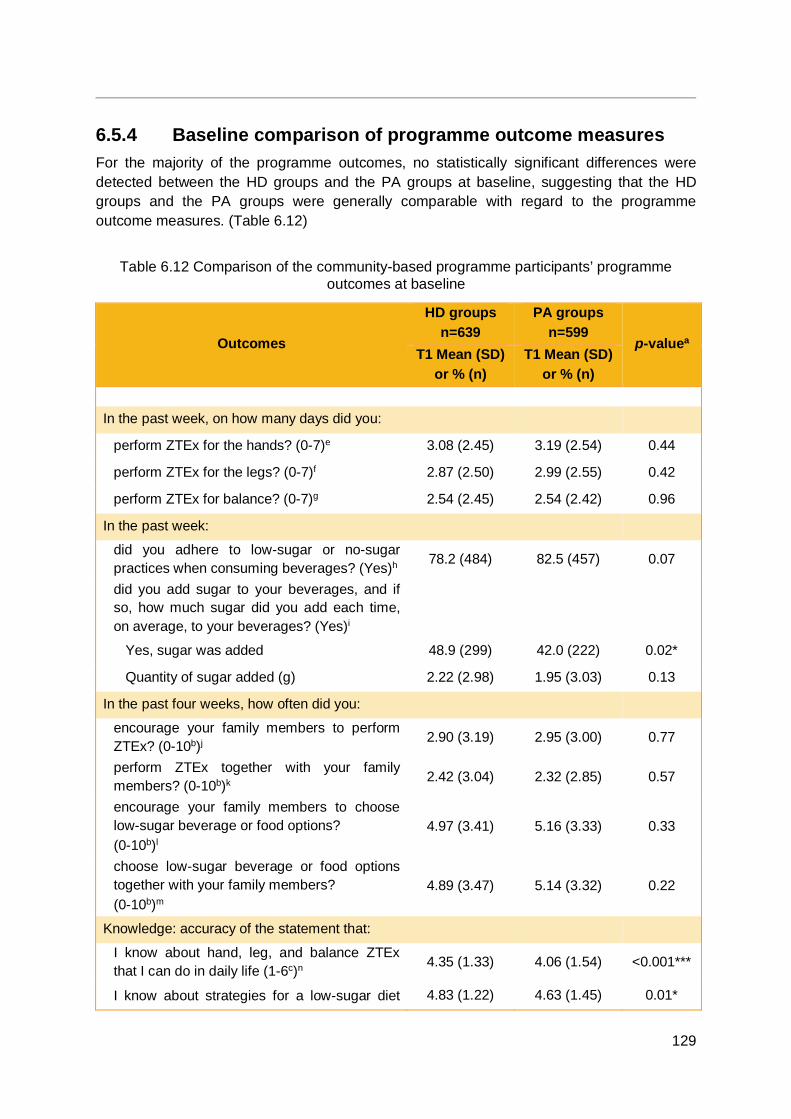
129
6.5.4 Baseline comparison of programme outcome measures For the majority of the programme outcomes, no statistically significant differences were detected between the HD groups and the PA groups at baseline, suggesting that the HD groups and the PA groups were generally comparable with regard to the programme outcome measures. (Table 6.12)
Table 6.12 Comparison of the community-based programme participants’ programme outcomes at baseline
Outcomes
HD groups n=639
PA groups n=599
p-valuea T1 Mean (SD)
or % (n) T1 Mean (SD)
or % (n)
In the past week, on how many days did you:
perform ZTEx for the hands? (0-7)e 3.08 (2.45) 3.19 (2.54) 0.44
perform ZTEx for the legs? (0-7)f 2.87 (2.50) 2.99 (2.55) 0.42
perform ZTEx for balance? (0-7)g 2.54 (2.45) 2.54 (2.42) 0.96
In the past week:
did you adhere to low-sugar or no-sugar practices when consuming beverages? (Yes)h 78.2 (484) 82.5 (457) 0.07
did you add sugar to your beverages, and if so, how much sugar did you add each time, on average, to your beverages? (Yes)i
Yes, sugar was added 48.9 (299) 42.0 (222) 0.02*
Quantity of sugar added (g) 2.22 (2.98) 1.95 (3.03) 0.13
In the past four weeks, how often did you:
encourage your family members to perform ZTEx? (0-10b)j 2.90 (3.19) 2.95 (3.00) 0.77
perform ZTEx together with your family members? (0-10b)k 2.42 (3.04) 2.32 (2.85) 0.57
encourage your family members to choose low-sugar beverage or food options? (0-10b)l
4.97 (3.41) 5.16 (3.33) 0.33
choose low-sugar beverage or food options together with your family members? (0-10b)m
4.89 (3.47) 5.14 (3.32) 0.22
Knowledge: accuracy of the statement that:
I know about hand, leg, and balance ZTEx that I can do in daily life (1-6c)n 4.35 (1.33) 4.06 (1.54) <0.001***
I know about strategies for a low-sugar diet 4.83 (1.22) 4.63 (1.45) 0.01*
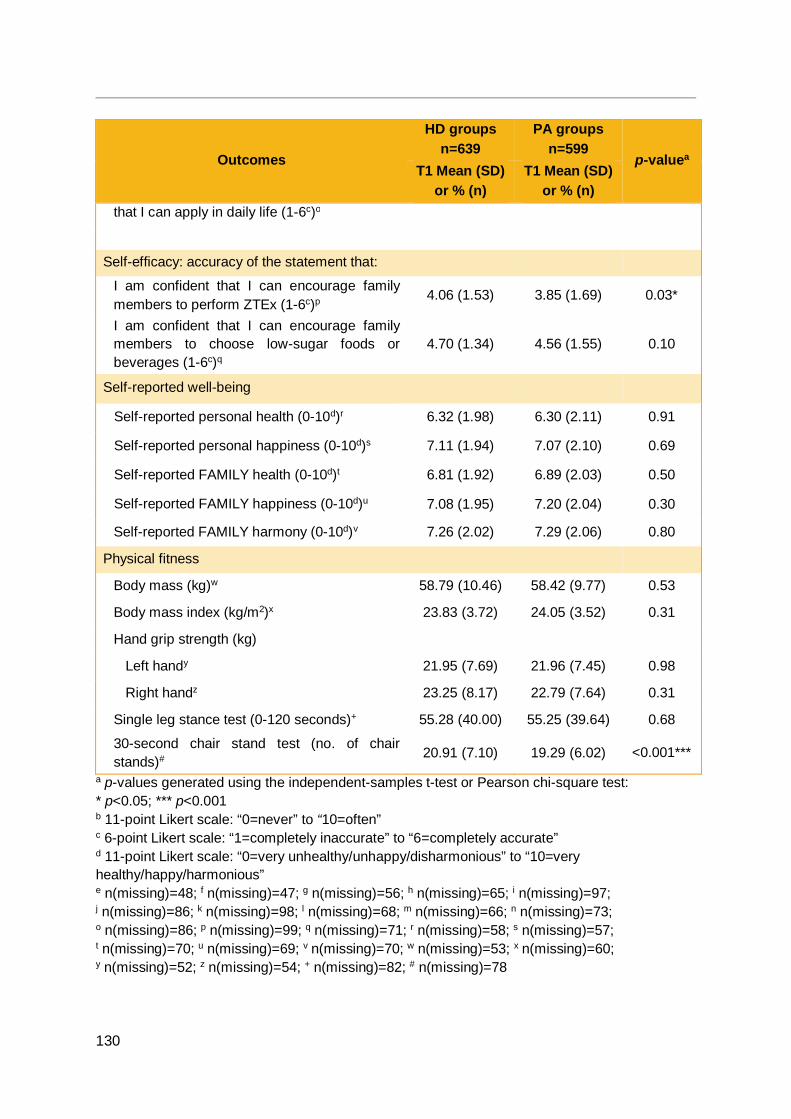
130
Outcomes
HD groups n=639
PA groups n=599
p-valuea T1 Mean (SD)
or % (n) T1 Mean (SD)
or % (n) that I can apply in daily life (1-6c)o
Self-efficacy: accuracy of the statement that:
I am confident that I can encourage family members to perform ZTEx (1-6c)p
4.06 (1.53) 3.85 (1.69) 0.03*
I am confident that I can encourage family members to choose low-sugar foods or beverages (1-6c)q
4.70 (1.34) 4.56 (1.55) 0.10
Self-reported well-being
Self-reported personal health (0-10d)r 6.32 (1.98) 6.30 (2.11) 0.91
Self-reported personal happiness (0-10d)s 7.11 (1.94) 7.07 (2.10) 0.69
Self-reported FAMILY health (0-10d)t 6.81 (1.92) 6.89 (2.03) 0.50
Self-reported FAMILY happiness (0-10d)u 7.08 (1.95) 7.20 (2.04) 0.30
Self-reported FAMILY harmony (0-10d)v 7.26 (2.02) 7.29 (2.06) 0.80
Physical fitness
Body mass (kg)w 58.79 (10.46) 58.42 (9.77) 0.53
Body mass index (kg/m2)x 23.83 (3.72) 24.05 (3.52) 0.31
Hand grip strength (kg)
Left handy 21.95 (7.69) 21.96 (7.45) 0.98
Right handz 23.25 (8.17) 22.79 (7.64) 0.31
Single leg stance test (0-120 seconds)+ 55.28 (40.00) 55.25 (39.64) 0.68
30-second chair stand test (no. of chair stands)# 20.91 (7.10) 19.29 (6.02) <0.001***
a p-values generated using the independent-samples t-test or Pearson chi-square test: * p<0.05; *** p<0.001 b 11-point Likert scale: “0=never” to “10=often” c 6-point Likert scale: “1=completely inaccurate” to “6=completely accurate” d 11-point Likert scale: “0=very unhealthy/unhappy/disharmonious” to “10=very healthy/happy/harmonious” e n(missing)=48; f n(missing)=47; g n(missing)=56; h n(missing)=65; i n(missing)=97; j n(missing)=86; k n(missing)=98; l n(missing)=68; m n(missing)=66; n n(missing)=73; o n(missing)=86; p n(missing)=99; q n(missing)=71; r n(missing)=58; s n(missing)=57; t n(missing)=70; u n(missing)=69; v n(missing)=70; w n(missing)=53; x n(missing)=60; y n(missing)=52; z n(missing)=54; + n(missing)=82; # n(missing)=78

131
6.5.5 Changes in outcomes by time and groups
6.5.5.1 Physical activity
6.5.5.1.1 Physical activity behaviours No significant differences between the HD groups and the PA groups were observed at baseline for the number of days in the previous week on which participants performed ZTEx for the hands, legs, and balance. Both the HD groups and the PA groups showed significant within-group increases in each of the three types of ZTEx at 1 month, 3 months, and 6 months after the core sessions. However, only at 1 month after the core sessions, the PA groups showed significantly greater increases than the HD groups in ZTEx for the legs (p=0.039, d=0.14) and balance (p=0.005, d=0.22), indicating effectiveness of the PA intervention with small effect sze. (Figures 6.10-6.12)
Figure 6.10 Number of days in the previous week on which ZTEx for the hands were performed (0-7 days)
*** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
T1(baseline)
T3(pre-
booster at 1month)
T5(3 months)
T6(6 months)
HD 3.08 3.91 4.68 5.21PA 3.19 4.46 4.61 4.69
0
1
2
3
4
5
6
7
Day
PA: T3>T1 ES =0.45***
HD: T3>T1 ES=0.32***
HD: T5>T1 ES=0.59***
PA: T5>T1 ES=0.55***
HD: T6>T1 ES=0.80***
PA: T6>T1 ES=0.59***
Core session
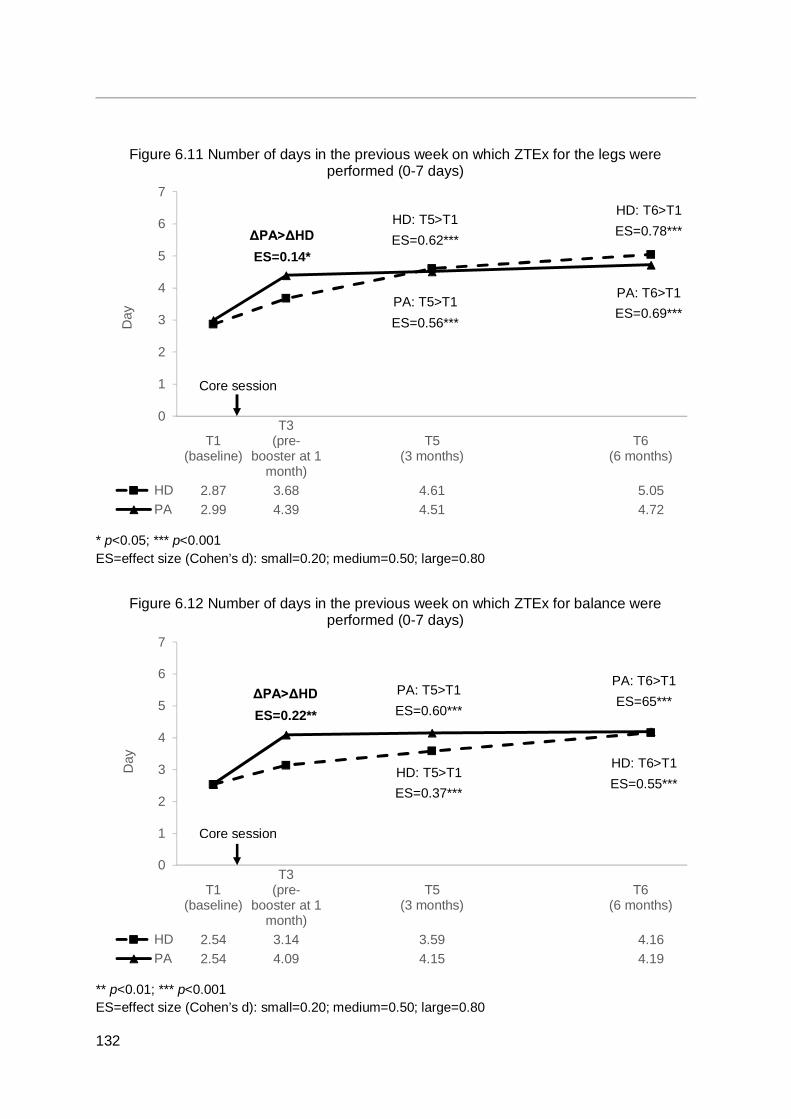
132
Figure 6.11 Number of days in the previous week on which ZTEx for the legs were performed (0-7 days)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
Figure 6.12 Number of days in the previous week on which ZTEx for balance were performed (0-7 days)
** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
T1(baseline)
T3(pre-
booster at 1month)
T5(3 months)
T6(6 months)
HD 2.87 3.68 4.61 5.05PA 2.99 4.39 4.51 4.72
0
1
2
3
4
5
6
7
Day
T1(baseline)
T3(pre-
booster at 1month)
T5(3 months)
T6(6 months)
HD 2.54 3.14 3.59 4.16PA 2.54 4.09 4.15 4.19
0
1
2
3
4
5
6
7
Day
HD: T5>T1 ES=0.62***
PA: T5>T1 ES=0.56***
ΔPA>ΔHD ES=0.14*
HD: T6>T1 ES=0.78***
PA: T6>T1 ES=0.69***
PA: T5>T1 ES=0.60***
HD: T5>T1 ES=0.37***
PA: T6>T1 ES=65***
HD: T6>T1 ES=0.55***
Core session
Core session
ΔPA>ΔHD ES=0.22**
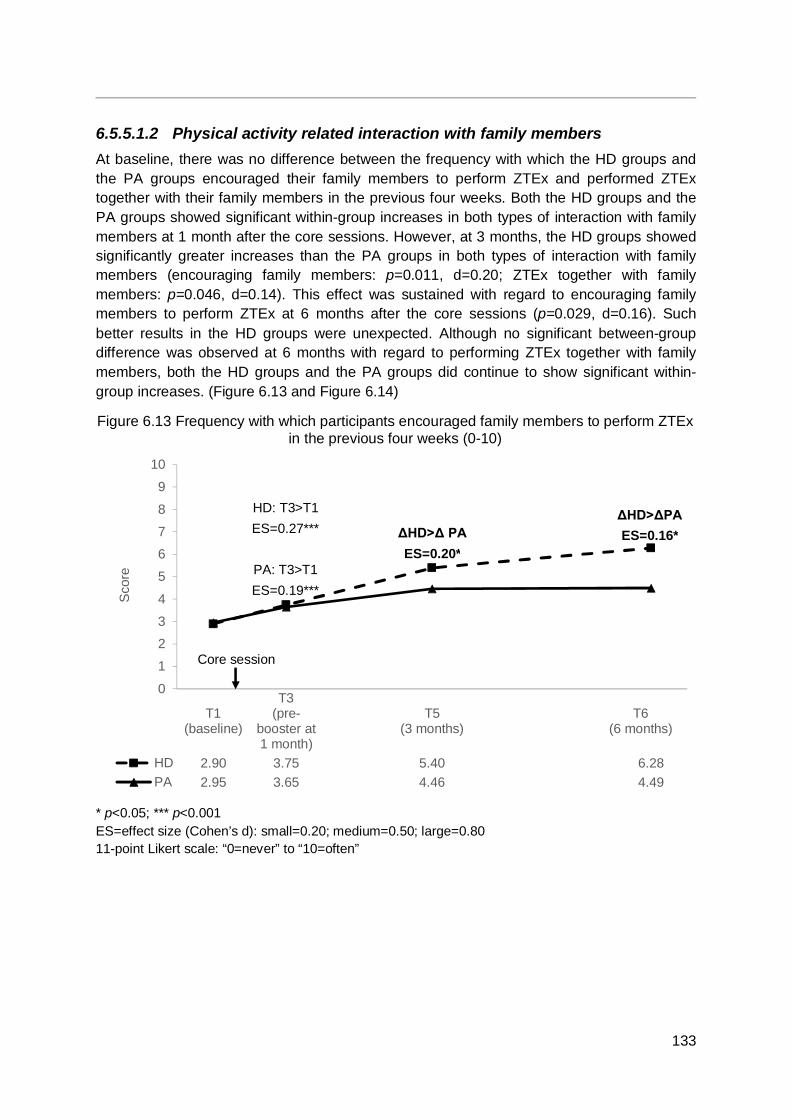
133
6.5.5.1.2 Physical activity related interaction with family members At baseline, there was no difference between the frequency with which the HD groups and the PA groups encouraged their family members to perform ZTEx and performed ZTEx together with their family members in the previous four weeks. Both the HD groups and the PA groups showed significant within-group increases in both types of interaction with family members at 1 month after the core sessions. However, at 3 months, the HD groups showed significantly greater increases than the PA groups in both types of interaction with family members (encouraging family members: p=0.011, d=0.20; ZTEx together with family members: p=0.046, d=0.14). This effect was sustained with regard to encouraging family members to perform ZTEx at 6 months after the core sessions (p=0.029, d=0.16). Such better results in the HD groups were unexpected. Although no significant between-group difference was observed at 6 months with regard to performing ZTEx together with family members, both the HD groups and the PA groups did continue to show significant within-group increases. (Figure 6.13 and Figure 6.14)
Figure 6.13 Frequency with which participants encouraged family members to perform ZTEx in the previous four weeks (0-10)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never” to “10=often”
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 2.90 3.75 5.40 6.28PA 2.95 3.65 4.46 4.49
0
1
2
3
4
5
6
7
8
9
10
Sco
re
HD: T3>T1 ES=0.27***
PA: T3>T1 ES=0.19***
ΔHD>Δ PA ES=0.20*
Core session
ΔHD>ΔPA ES=0.16*

134
Figure 6.14 Frequency with which participants performed ZTEx together with family members in the previous four weeks (0-10)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never” to “10=often”
6.5.5.1.3 Physical activity knowledge and self-efficacy Significant differences between the HD groups and the PA groups were observed at baseline for self-perceived knowledge of ZTEx that could be incorporated in daily life, and for self-efficacy on encouraging family members to perform ZTEx. In both items, the mean score of the HD groups was slightly higher than the PA groups’ mean scores. Both the HD groups and the PA groups showed significant within-group increases for both items immediately after the core session, immediately after the booster session, at 3 months, and at 6 months. Only at 3 months after the core sessions, the HD groups showed a significantly greater increase than the PA groups in the degree to which they felt confident they could encourage their family members to perform ZTEx (p=0.036, d=0.15). Such better results in the HD groups were unexpected. (Figure 6.15 and 6.16)
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 2.9 3.75 5.4 6.28PA 2.95 3.65 4.46 4.49
01
23
4
56
7
89
10
Sco
re
HD: T6>T1 ES=0.88***
PA: T6>T1 ES=0.43***
HD: T3>T1 ES=0.26***
PA: T3>T1 ES=0.21***
ΔHD>ΔPA ES=0.14*
Core session
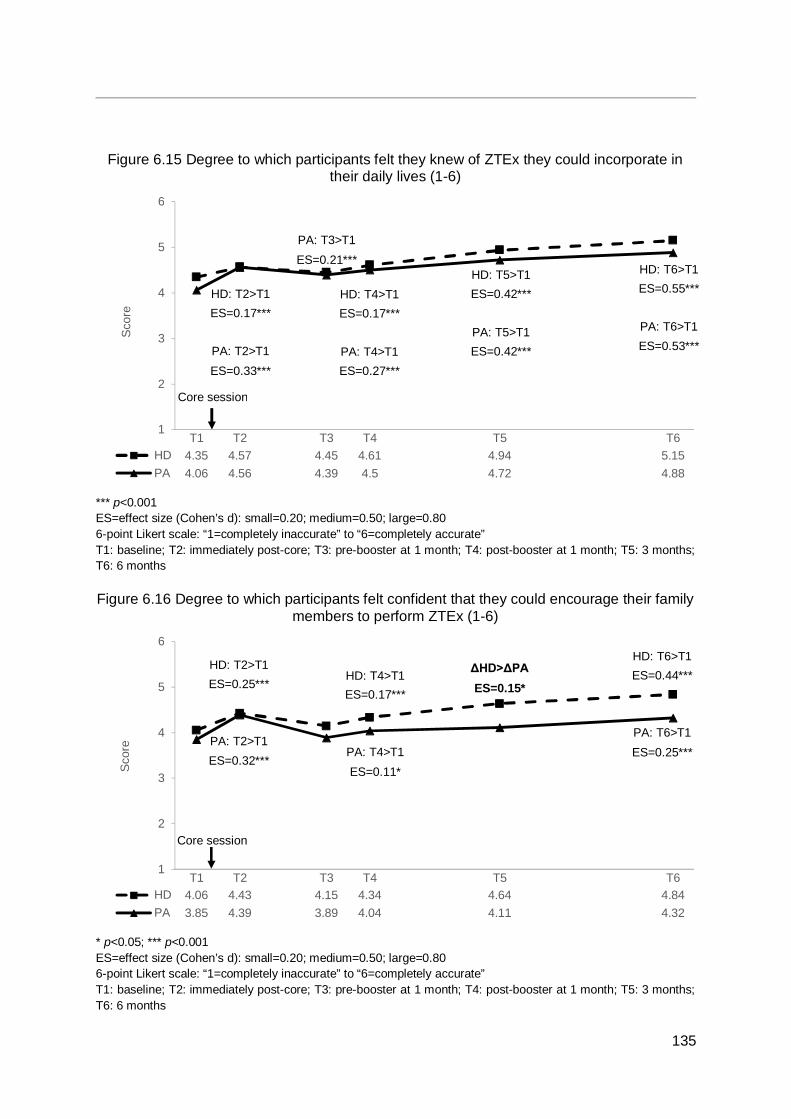
135
Figure 6.15 Degree to which participants felt they knew of ZTEx they could incorporate in their daily lives (1-6)
*** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=completely inaccurate” to “6=completely accurate” T1: baseline; T2: immediately post-core; T3: pre-booster at 1 month; T4: post-booster at 1 month; T5: 3 months; T6: 6 months Figure 6.16 Degree to which participants felt confident that they could encourage their family
members to perform ZTEx (1-6)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=completely inaccurate” to “6=completely accurate” T1: baseline; T2: immediately post-core; T3: pre-booster at 1 month; T4: post-booster at 1 month; T5: 3 months; T6: 6 months
T1 T2 T3 T4 T5 T6HD 4.35 4.57 4.45 4.61 4.94 5.15PA 4.06 4.56 4.39 4.5 4.72 4.88
1
2
3
4
5
6
Scor
e
T1 T2 T3 T4 T5 T6HD 4.06 4.43 4.15 4.34 4.64 4.84PA 3.85 4.39 3.89 4.04 4.11 4.32
1
2
3
4
5
6
Scor
e
HD: T2>T1 ES=0.17***
PA: T2>T1 ES=0.33***
HD: T6>T1 ES=0.55***
PA: T6>T1 ES=0.53***
PA: T3>T1 ES=0.21***
HD: T4>T1 ES=0.17***
PA: T4>T1 ES=0.27***
HD: T5>T1 ES=0.42***
PA: T5>T1 ES=0.42***
HD: T2>T1 ES=0.25***
PA: T2>T1 ES=0.32***
HD: T6>T1 ES=0.44***
PA: T6>T1 ES=0.25***
HD: T4>T1 ES=0.17***
PA: T4>T1 ES=0.11*
ΔHD>ΔPA ES=0.15*
Core session
Core session
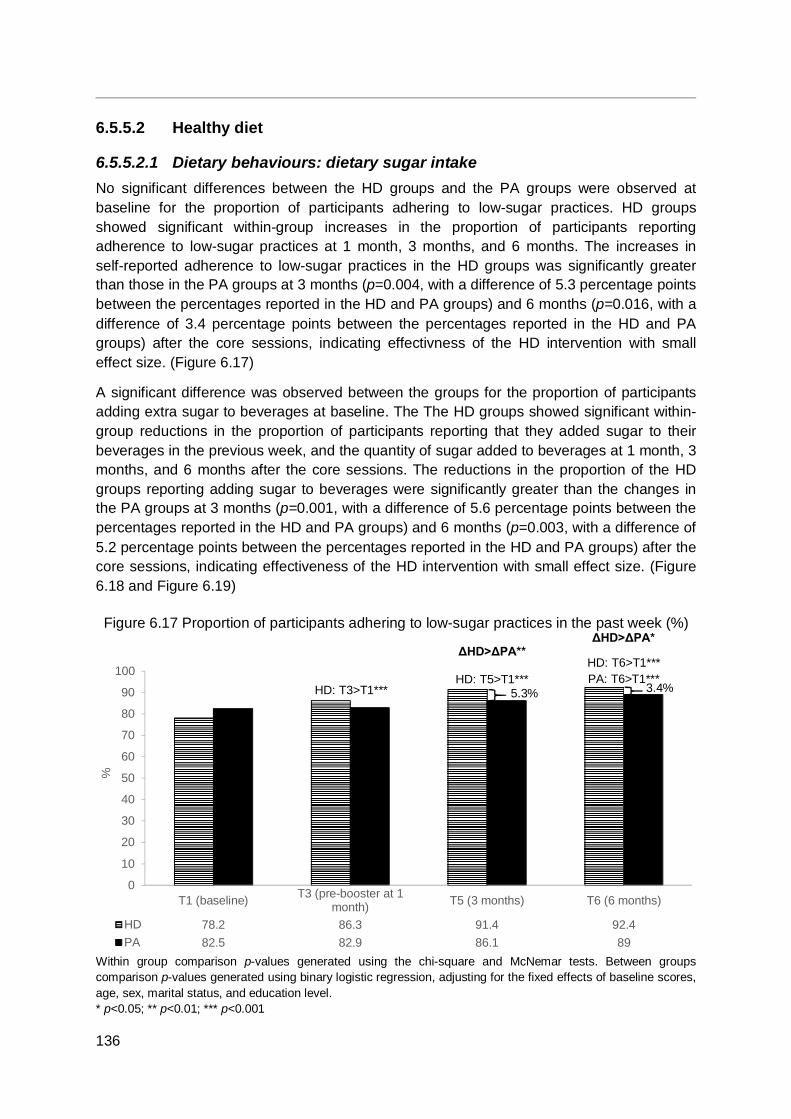
136
6.5.5.2 Healthy diet
6.5.5.2.1 Dietary behaviours: dietary sugar intake No significant differences between the HD groups and the PA groups were observed at baseline for the proportion of participants adhering to low-sugar practices. HD groups showed significant within-group increases in the proportion of participants reporting adherence to low-sugar practices at 1 month, 3 months, and 6 months. The increases in self-reported adherence to low-sugar practices in the HD groups was significantly greater than those in the PA groups at 3 months (p=0.004, with a difference of 5.3 percentage points between the percentages reported in the HD and PA groups) and 6 months (p=0.016, with a difference of 3.4 percentage points between the percentages reported in the HD and PA groups) after the core sessions, indicating effectivness of the HD intervention with small effect size. (Figure 6.17)
A significant difference was observed between the groups for the proportion of participants adding extra sugar to beverages at baseline. The The HD groups showed significant within-group reductions in the proportion of participants reporting that they added sugar to their beverages in the previous week, and the quantity of sugar added to beverages at 1 month, 3 months, and 6 months after the core sessions. The reductions in the proportion of the HD groups reporting adding sugar to beverages were significantly greater than the changes in the PA groups at 3 months (p=0.001, with a difference of 5.6 percentage points between the percentages reported in the HD and PA groups) and 6 months (p=0.003, with a difference of 5.2 percentage points between the percentages reported in the HD and PA groups) after the core sessions, indicating effectiveness of the HD intervention with small effect size. (Figure 6.18 and Figure 6.19)
Figure 6.17 Proportion of participants adhering to low-sugar practices in the past week (%)
Within group comparison p-values generated using the chi-square and McNemar tests. Between groups comparison p-values generated using binary logistic regression, adjusting for the fixed effects of baseline scores, age, sex, marital status, and education level. * p<0.05; ** p<0.01; *** p<0.001
T1 (baseline) T3 (pre-booster at 1month) T5 (3 months) T6 (6 months)
HD 78.2 86.3 91.4 92.4PA 82.5 82.9 86.1 89
0
10
20
30
40
50
60
70
80
90
100
%
ΔHD>ΔPA*
HD: T6>T1*** PA: T6>T1***
ΔHD>ΔPA**
HD: T5>T1*** HD: T3>T1*** 5.3% 3.4%
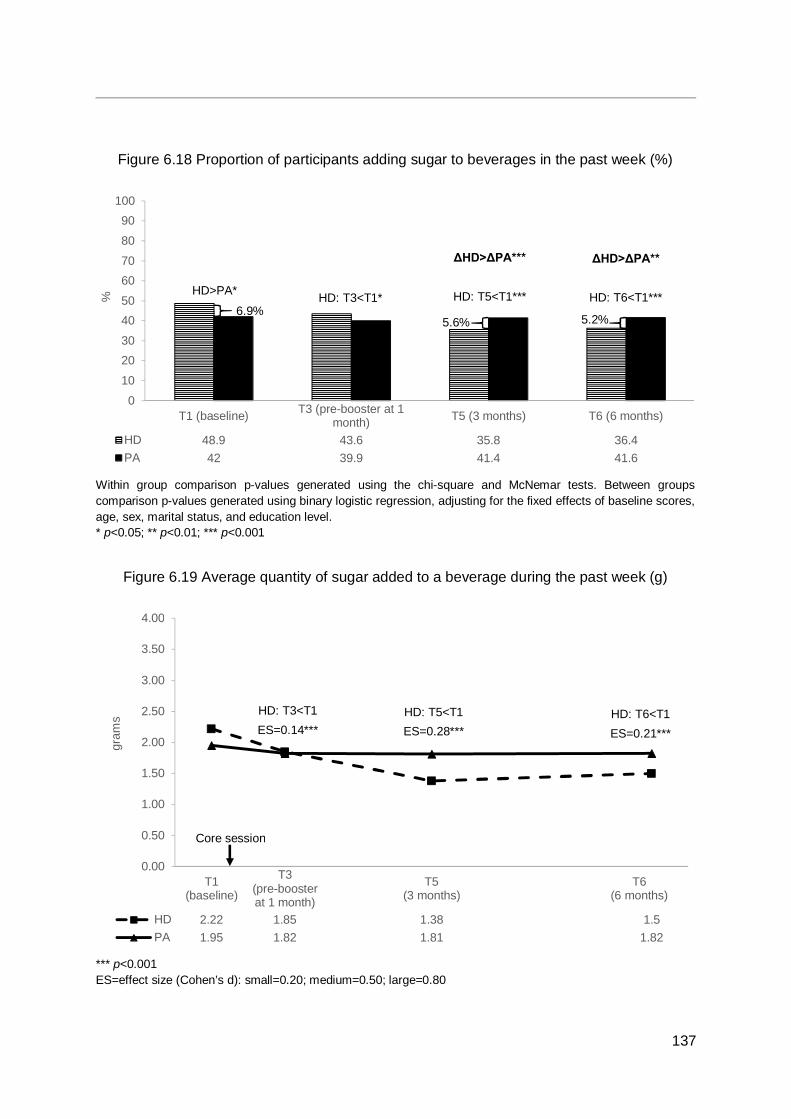
137
Figure 6.18 Proportion of participants adding sugar to beverages in the past week (%)
Within group comparison p-values generated using the chi-square and McNemar tests. Between groups comparison p-values generated using binary logistic regression, adjusting for the fixed effects of baseline scores, age, sex, marital status, and education level. * p<0.05; ** p<0.01; *** p<0.001
Figure 6.19 Average quantity of sugar added to a beverage during the past week (g)
*** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80
T1 (baseline) T3 (pre-booster at 1month) T5 (3 months) T6 (6 months)
HD 48.9 43.6 35.8 36.4PA 42 39.9 41.4 41.6
0102030405060708090
100
%
T1(baseline)
T3(pre-boosterat 1 month)
T5(3 months)
T6(6 months)
HD 2.22 1.85 1.38 1.5PA 1.95 1.82 1.81 1.82
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
gram
s
ΔHD>ΔPA***
HD: T5<T1***
ΔHD>ΔPA**
HD: T6<T1*** HD: T3<T1*
5.6% 5.2%
HD: T3<T1 ES=0.14***
HD: T5<T1 ES=0.28***
HD: T6<T1 ES=0.21***
Core session
6.9%
HD>PA*
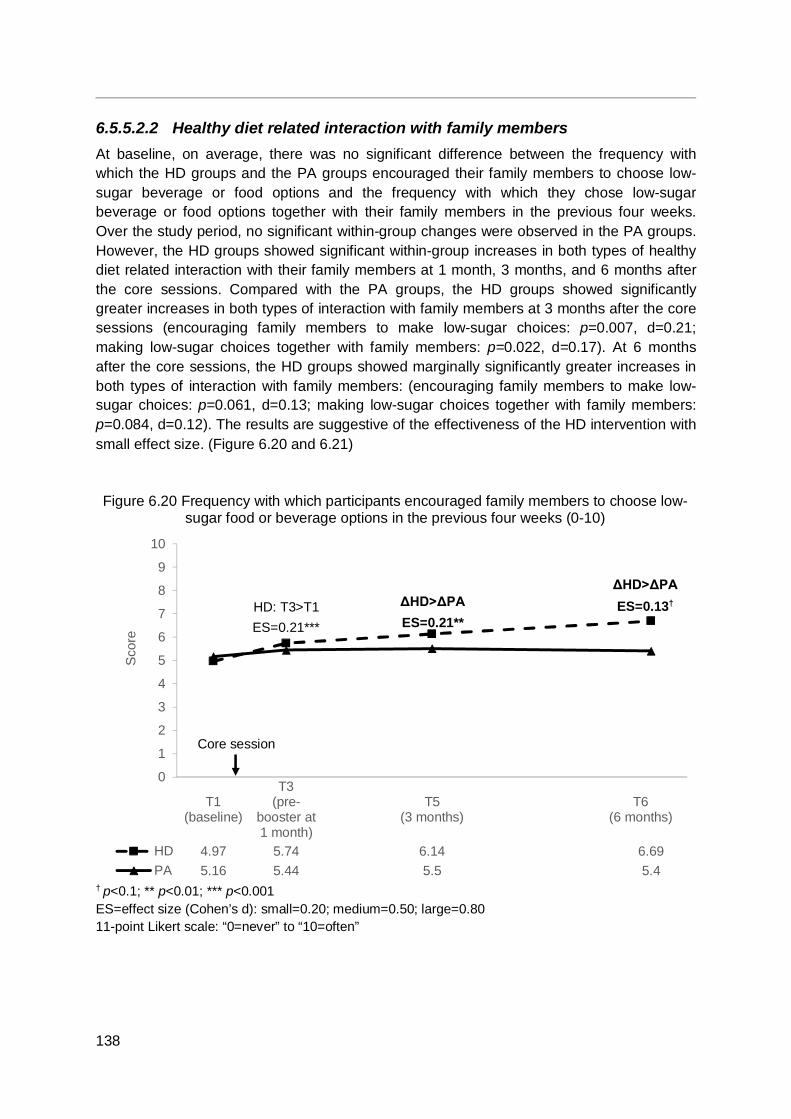
138
6.5.5.2.2 Healthy diet related interaction with family members At baseline, on average, there was no significant difference between the frequency with which the HD groups and the PA groups encouraged their family members to choose low-sugar beverage or food options and the frequency with which they chose low-sugar beverage or food options together with their family members in the previous four weeks. Over the study period, no significant within-group changes were observed in the PA groups. However, the HD groups showed significant within-group increases in both types of healthy diet related interaction with their family members at 1 month, 3 months, and 6 months after the core sessions. Compared with the PA groups, the HD groups showed significantly greater increases in both types of interaction with family members at 3 months after the core sessions (encouraging family members to make low-sugar choices: p=0.007, d=0.21; making low-sugar choices together with family members: p=0.022, d=0.17). At 6 months after the core sessions, the HD groups showed marginally significantly greater increases in both types of interaction with family members: (encouraging family members to make low-sugar choices: p=0.061, d=0.13; making low-sugar choices together with family members: p=0.084, d=0.12). The results are suggestive of the effectiveness of the HD intervention with small effect size. (Figure 6.20 and 6.21)
Figure 6.20 Frequency with which participants encouraged family members to choose low-sugar food or beverage options in the previous four weeks (0-10)
† p<0.1; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never” to “10=often”
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 4.97 5.74 6.14 6.69PA 5.16 5.44 5.5 5.4
0
1
2
3
4
5
6
7
8
9
10
Sco
re
Core session
HD: T3>T1 ES=0.21***
ΔHD>ΔPA ES=0.21**
ΔHD>ΔPA ES=0.13†
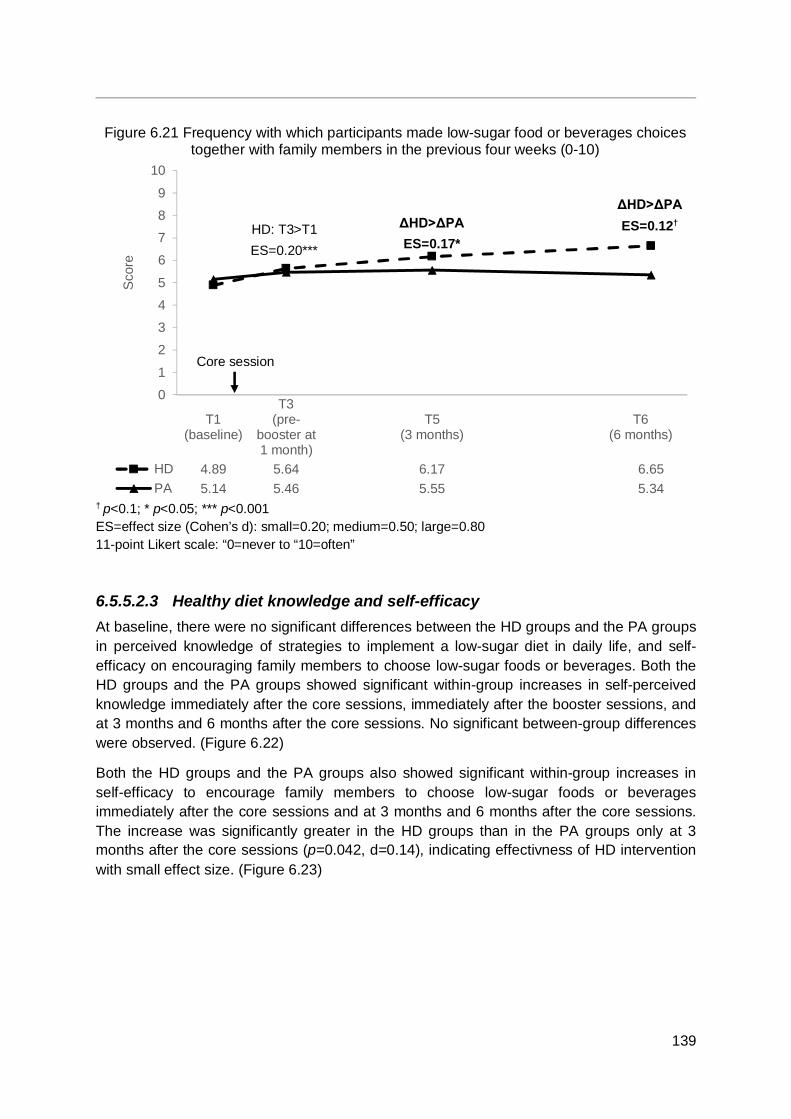
139
Figure 6.21 Frequency with which participants made low-sugar food or beverages choices together with family members in the previous four weeks (0-10)
† p<0.1; * p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=never to “10=often”
6.5.5.2.3 Healthy diet knowledge and self-efficacy At baseline, there were no significant differences between the HD groups and the PA groups in perceived knowledge of strategies to implement a low-sugar diet in daily life, and self-efficacy on encouraging family members to choose low-sugar foods or beverages. Both the HD groups and the PA groups showed significant within-group increases in self-perceived knowledge immediately after the core sessions, immediately after the booster sessions, and at 3 months and 6 months after the core sessions. No significant between-group differences were observed. (Figure 6.22)
Both the HD groups and the PA groups also showed significant within-group increases in self-efficacy to encourage family members to choose low-sugar foods or beverages immediately after the core sessions and at 3 months and 6 months after the core sessions. The increase was significantly greater in the HD groups than in the PA groups only at 3 months after the core sessions (p=0.042, d=0.14), indicating effectivness of HD intervention with small effect size. (Figure 6.23)
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 4.89 5.64 6.17 6.65PA 5.14 5.46 5.55 5.34
0
1
2
3
4
5
6
7
8
9
10
Sco
re
Core session
ΔHD>ΔPA ES=0.17*
HD: T3>T1 ES=0.20***
ΔHD>ΔPA ES=0.12†
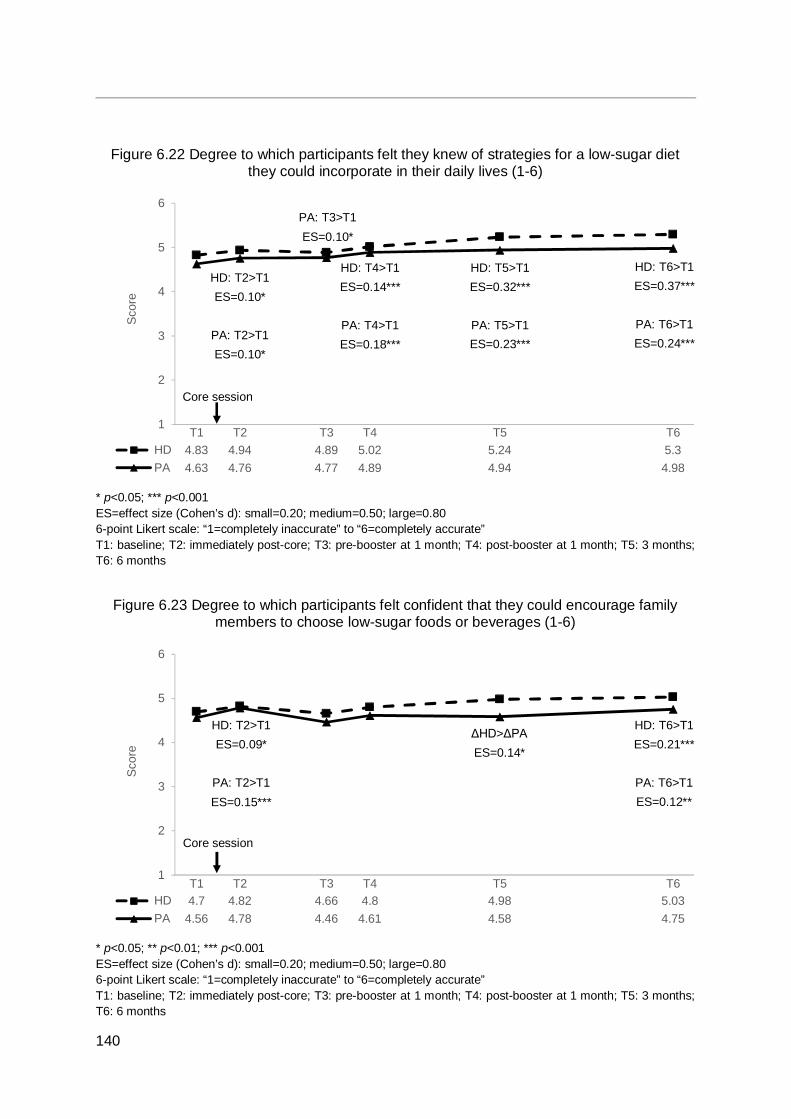
140
Figure 6.22 Degree to which participants felt they knew of strategies for a low-sugar diet they could incorporate in their daily lives (1-6)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=completely inaccurate” to “6=completely accurate” T1: baseline; T2: immediately post-core; T3: pre-booster at 1 month; T4: post-booster at 1 month; T5: 3 months; T6: 6 months
Figure 6.23 Degree to which participants felt confident that they could encourage family members to choose low-sugar foods or beverages (1-6)
* p<0.05; ** p<0.01; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 6-point Likert scale: “1=completely inaccurate” to “6=completely accurate” T1: baseline; T2: immediately post-core; T3: pre-booster at 1 month; T4: post-booster at 1 month; T5: 3 months; T6: 6 months
T1 T2 T3 T4 T5 T6HD 4.83 4.94 4.89 5.02 5.24 5.3PA 4.63 4.76 4.77 4.89 4.94 4.98
1
2
3
4
5
6
Scor
e
T1 T2 T3 T4 T5 T6HD 4.7 4.82 4.66 4.8 4.98 5.03PA 4.56 4.78 4.46 4.61 4.58 4.75
1
2
3
4
5
6
Scor
e
HD: T2>T1 ES=0.09*
PA: T2>T1 ES=0.15***
Core session
Core session
HD: T2>T1 ES=0.10*
PA: T2>T1 ES=0.10*
HD: T6>T1 ES=0.37***
PA: T6>T1 ES=0.24***
PA: T3>T1 ES=0.10*
HD: T6>T1 ES=0.21***
PA: T6>T1 ES=0.12**
HD: T4>T1 ES=0.14***
PA: T4>T1 ES=0.18***
HD: T5>T1 ES=0.32***
PA: T5>T1 ES=0.23***
ΔHD>ΔPA ES=0.14*

141
6.5.5.3 Physical fitness Majority of the physical fitness measures taken showed no significant differences between the HD and PA groups. The exception was the 30-second chair stand test, on which the HD groups scored slightly higher than the PA groups (Table 6.5). At 1 month after the core sessions, the HD groups showed significant within-group reductions in body mass (weight) and body mass index, and significant within-group increases in hand grip strength for both hands, performance on the single leg stance test, and the 30-second chair stand test. The PA groups showed significant within-group increases in hand grip strength for both hands and the 30-second chair stand test. However, the performance of the PA groups on the single leg stance test significantly decreased unexpectedly. No significant differences were observed between the HD groups and the PA groups for the physical fitness assessments.
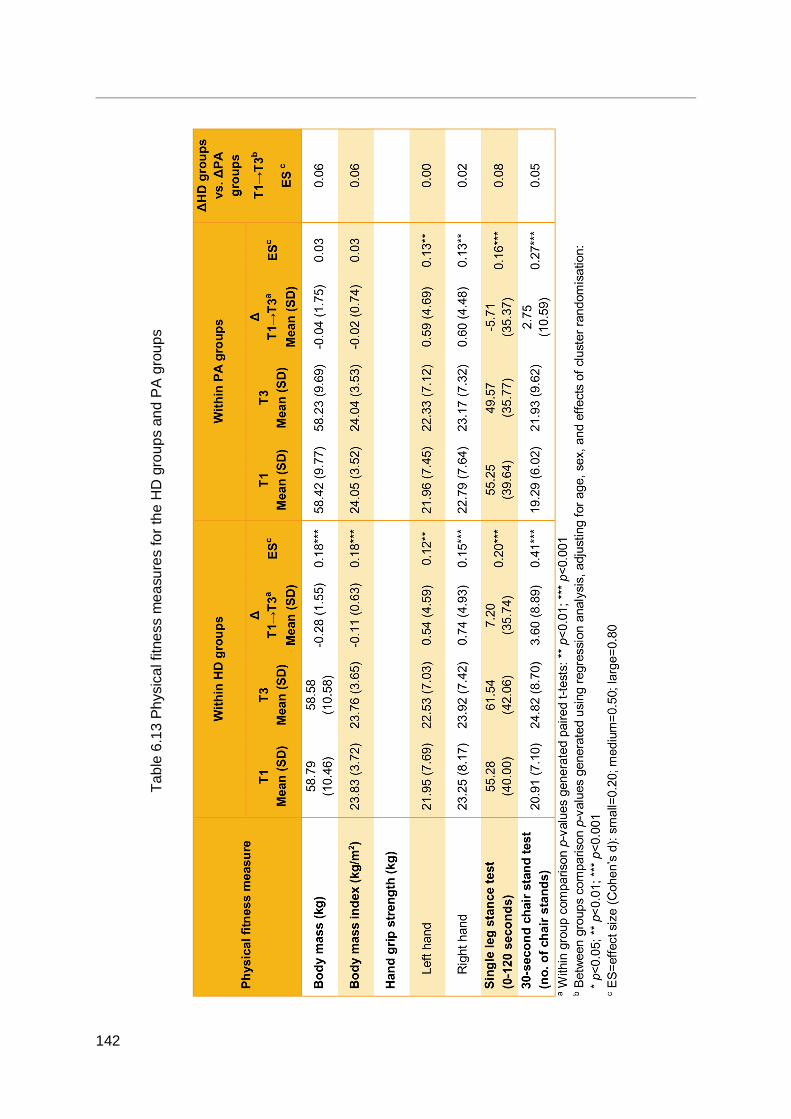
142
Tabl
e 6.
13 P
hysi
cal f
itnes
s m
easu
res
for t
he H
D g
roup
s an
d P
A gr
oups
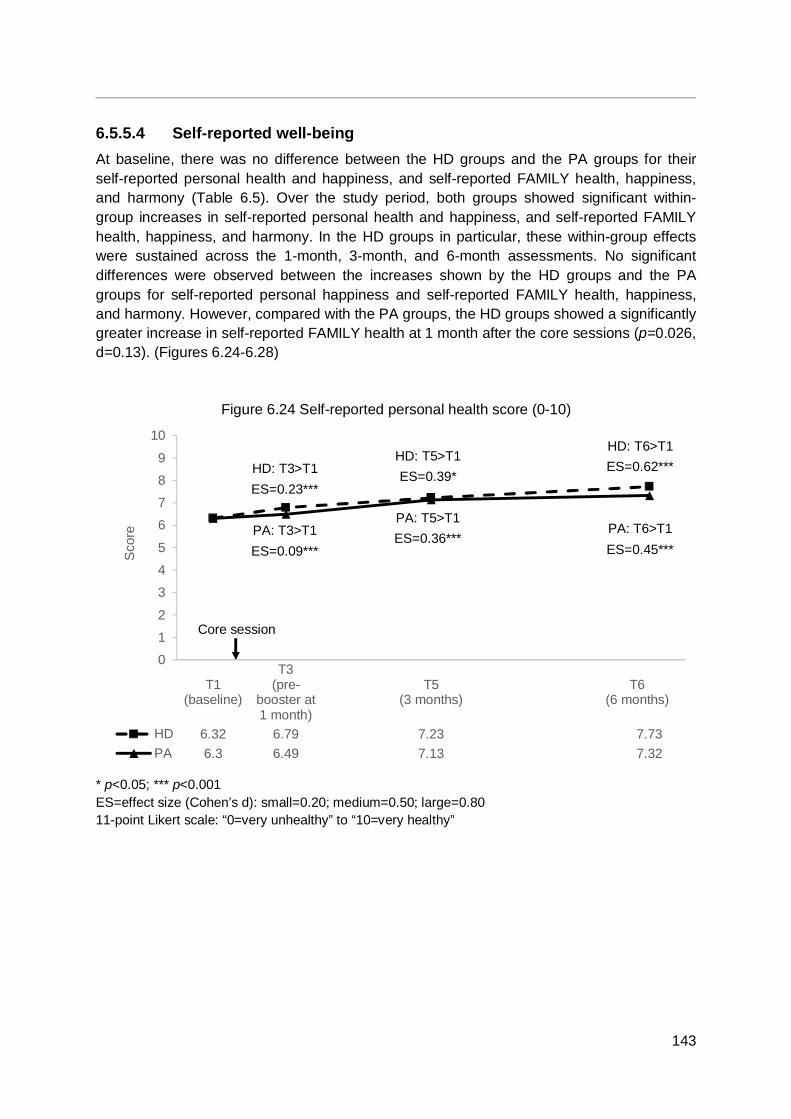
143
6.5.5.4 Self-reported well-being At baseline, there was no difference between the HD groups and the PA groups for their self-reported personal health and happiness, and self-reported FAMILY health, happiness, and harmony (Table 6.5). Over the study period, both groups showed significant within-group increases in self-reported personal health and happiness, and self-reported FAMILY health, happiness, and harmony. In the HD groups in particular, these within-group effects were sustained across the 1-month, 3-month, and 6-month assessments. No significant differences were observed between the increases shown by the HD groups and the PA groups for self-reported personal happiness and self-reported FAMILY health, happiness, and harmony. However, compared with the PA groups, the HD groups showed a significantly greater increase in self-reported FAMILY health at 1 month after the core sessions (p=0.026, d=0.13). (Figures 6.24-6.28)
Figure 6.24 Self-reported personal health score (0-10)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhealthy” to “10=very healthy”
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 6.32 6.79 7.23 7.73PA 6.3 6.49 7.13 7.32
0
1
2
3
4
5
6
7
8
9
10
Sco
re
Core session
HD: T3>T1 ES=0.23***
PA: T3>T1 ES=0.09***
HD: T5>T1 ES=0.39*
PA: T5>T1 ES=0.36***
HD: T6>T1 ES=0.62***
PA: T6>T1 ES=0.45***

144
Figure 6.25 Self-reported personal happiness score (0-10)
*** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhappy” to “10=very happy”
Figure 6.26 Self-reported FAMILY health score (0-10)
* p<0.05; *** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhealthy” to “10=very healthy”
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 7.11 7.41 7.83 8.13PA 7.07 7.21 7.73 7.91
0
1
2
3
4
5
6
7
8
9
10
Sco
re
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 6.81 7.24 7.45 7.88PA 6.89 7.09 7.33 7.6
0123456789
10
Sco
re
Core session
HD: T3>T1 ES=0.15***
HD: T5>T1 ES=0.32***
PA: T5>T1 ES=0.32***
HD: T6>T1 ES=0.45***
PA: T6>T1 ES=0.38***
HD: T5>T1 ES=0.29***
PA: T5>T1 ES=0.20***
HD: T6>T1 ES=0.48***
PA: T6>T1 ES=0.31***
ΔHD>ΔPA ES=0.13*
Core session
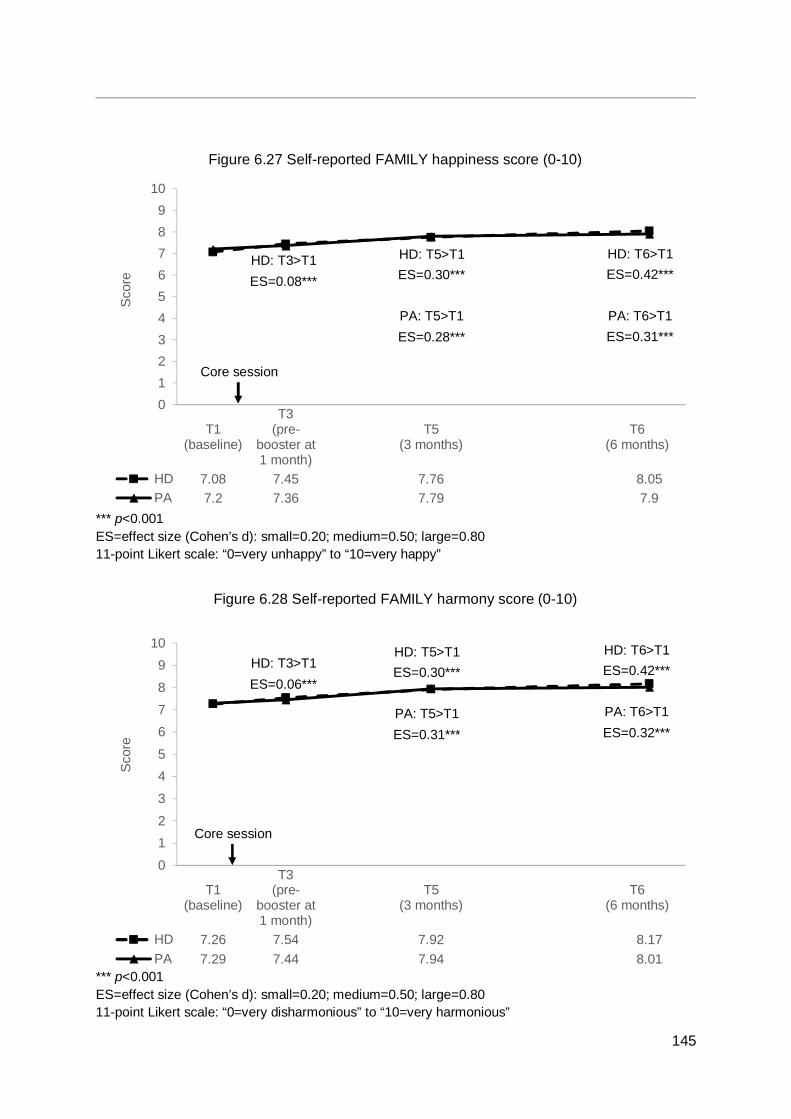
145
Figure 6.27 Self-reported FAMILY happiness score (0-10)
*** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very unhappy” to “10=very happy”
Figure 6.28 Self-reported FAMILY harmony score (0-10)
*** p<0.001 ES=effect size (Cohen’s d): small=0.20; medium=0.50; large=0.80 11-point Likert scale: “0=very disharmonious” to “10=very harmonious”
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 7.08 7.45 7.76 8.05PA 7.2 7.36 7.79 7.9
0123456789
10
Sco
re
T1(baseline)
T3(pre-
booster at1 month)
T5(3 months)
T6(6 months)
HD 7.26 7.54 7.92 8.17PA 7.29 7.44 7.94 8.01
0
12
3
45
67
8
910
Sco
re
Core session
HD: T3>T1 ES=0.08***
HD: T5>T1 ES=0.30***
PA: T5>T1 ES=0.28***
HD: T6>T1 ES=0.42***
PA: T6>T1 ES=0.31***
Core session
HD: T3>T1 ES=0.06***
HD: T5>T1 ES=0.30***
PA: T5>T1 ES=0.31***
HD: T6>T1 ES=0.42***
PA: T6>T1 ES=0.32***
146
6.5.6 Summary and discussion of quantitative results As anticipated, the HD groups showed significant within-group improvements across the study period in their adherence to low-sugar practises and the quantity of sugar added to beverages, whereas the PA groups showed minimal within-group improvements. Compared with the PA groups, the HD groups showed significantly greater increases than the PA groups in the proportion of participants reporting adherence to low-sugar practices at 3 months and 6 months after the core sessions. The reductions in the proportion of the HD groups reporting adding sugar to beverages were also significantly greater than the changes in the PA groups at 3 months and 6 months. The HD groups also showed significant within-group reductions in the quantity of sugar added to beverages at 1 month, 3 months, and 6 months. These results were strong evidence that the HD intervention programme was effective in improving participants’ healthy diet behaviours, particularly in relation to dietary sugar intake, with small effect size.
In terms of physical fitness indicators, the HD groups showed significant within-group reductions in body mass and body mass index, whilst the PA groups did not, indicating that the HD intervention programme (particularly the core session) was more effective than the PA intervention programme in promoting body mass reduction. One reason might be that the reduction of dietary sugar intake in the HD groups might have resulted in a greater reduction in calories intake than the extra energy consumed by the increase of physical activity in the PA groups. Moreover, the reduction of dietary sugar intake might be more easily implemented than the regular performance of physical activity for both the individuals and their families. One-third of participants were homemakers, who typically are heavily involved in cooking and the family’s diet. For this subgroup, the implementation of dietary changes when cooking can be more easily achieved than physical activity changes for the family. Also, as shown by the qualitative results below (see Section 6.6), reducing sugar intake from beverages was easily accomplished by some participants and their family members.
At 1 month after the core sessions, participants in the PA groups showed a significantly greater increase than the participants in the HD groups in the frequency with which they performed physical activity behaviours (ZTEx for the hands, legs, and balance), indicating that the physical activity-based intervention (in particular, the core session) was effective in this respect. However, it should be noted that both the HD groups and the PA groups showed significant within-group improvements, and the between-group differences was not sustained over the study period. Contrary to expectation, the HD groups also showed significantly greater increases than the PA groups in self-efficacy on performing physical activity together with family members and the frequency with which they had physical activity-related interactions with family members at 3 months after the core sessions. On physical fitness indicators addressed specifically by the PA intervention programmes (i.e. hand grip strength, single leg stance test, and 30-second chair stand test), no significant differences were observed between the groups despite the PA groups showing within-group improvements in hand grip strength and the 30-second chair stand test because the HD groups also showed similar within-group improvements.
The improvements shown by the HD groups on physical fitness indicators addressed specifically by the PA intervention programme and on other physical activity-related outcomes could be due to a several reasons. It is worth noting that whilst the PA groups

147
were taught very specific physical activity behaviours and the intervention programme focused on motivating participants to practise these behaviours more frequently, the HD groups were taught more cognitive skills (e.g. reading nutrition labels or calculating the quantity of sugar in a portion of a food product). It is possible that the cognitive nature of the HD intervention programme, in conjunction with an enhanced health awareness and understanding of the problems of overweight and obesity, lent itself to changes in participants’ attitude toward health, prompting participants to seek out health information and make health behaviour changes beyond the domain of healthy diet. Furthermore, participants’ success in reducing body mass in the HD groups may have prompted a virtuous cycle in which participants in the HD groups were further motivated to improve beyond healthy diet to enhance their personal health. Finally, as individuals could influence their family members more easily in reducing sugar intake than increasing physical activity, the family improvements could also reinforce and expand the individuals’ improvements from a healthy diet to more physical activity.
Both the HD groups and the PA groups showed significant within-group improvements in terms of self-reported personal health and happiness, but no significant between-group differences were observed. These results suggest that both the HD and the PA interventions were effective in enhancing self-reported personal health and happiness, although neither intervention was more effective than the others. Additionally, both groups showed significant within-group improvements in self-reported FAMILY health, happiness and harmony. These results suggest that our intervention programmes with emphasis on family health and strategies for sharing and adopting health behaviours together with family members were effective on FAMILY 3Hs. The HD groups did show a significantly greater increase than the PA groups at 1 month after the core sessions in self-reported FAMILY health. It was possible that participants, especially those who were homemakers, found healthy diet changes easier to implement as a family than physical activity changes since healthy diet changes can be made in the kitchen by one person and benefit the whole family whereas physical activity changes would require other family members to change actively.
6.5.7 Conclusions Both the HD groups and the PA groups showed improvements in physical activity and healthy diet behaviours and attitudes, physical fitness, and self-reported well-being. The community-based intervention programmes significantly improved participants’ self-reported personal health and happiness with small to medium effect size, as well as self-reported FAMILY health, happiness, and harmony with small effect size. Notably, there was a significantly greater increase in self-reported FAMILY health in the HD groups than in the PA groups, indicating that the HD intervention was more effective in enhancing self-reported FAMILY health than the PA intervention.
The HD groups also showed significantly greater imrpovements than the PA groups in the proportion of participants reporting adding sugar to beverages, the quantity of sugar added to beverages, and the frequency with which participants engaged in healthy diet-related interactions with family members, with small effect size. Participants in the HD intervention programmes were also successful in reducing their body mass and thus body mass index with small effect size. This suggests that the HD intervention programmes are able to significantly increase the proportion of partipants reporting adherence to low-sugar practices
148
with small effect size, significantly reduce the quantity of sugar added to beverages with small effect size, increase the frequency of healthy diet-related interaction with family members with small effect size, and bring about body mass and body mass index reduction with small effect size.
Overall, these results are encouraging and support the further development of community-based programmes using healthy diet (reducing sugar intake) or physical activity (ZTEx) as platforms to enhance individual and family well-being.
6.6 Qualitative evaluation: community-based programme focus groups
6.6.1 Introduction and objectives A total of four focus groups were conducted in December 2016 at the K. K. Leung Building, HKU. The inclusion criteria were as follows:
To explore the opinions and experiences of community-based participants related to the project, particularly the community-based programme;
To assess the extent to which the community-based intervention programmes had enhanced the participants’ health knowledge, behaviours, and attitudes; and
To examine whether the community-based intervention programmes had helped to improve the participants’ FAMILY 3Hs.
6.6.2 Methods
6.6.2.1 Data collection A total of four focus groups were conducted for community-based programme participants in December 2016 at the K. K. Leung Building, HKU. The inclusion criteria for participants were as follows:
Participated in the core or booster session of the community-based programme; Aged 12 years or above; Able to speak in Cantonese; and Able to understand the content and conversation during the focus group interview.
Participation was voluntary, and written consent was collected from each participant before the focus group discussion began.
The discussions were semi-structured, and questions on the interview guide provided to the moderators and note-takers were open-ended and designed based on the objectives of the project and the community-based programme overall. The discussions were conducted in Cantonese and audio-taped. Each focus group interview lasted for about 30 minutes and was managed by a panel of one moderator and one note-taker from the FAMILY Project.
6.6.2.2 Data analysis All of the recordings of the focus group interviews were transcribed verbatim in Cantonese, and the transcripts were double-checked against the tape recordings. The transcripts were
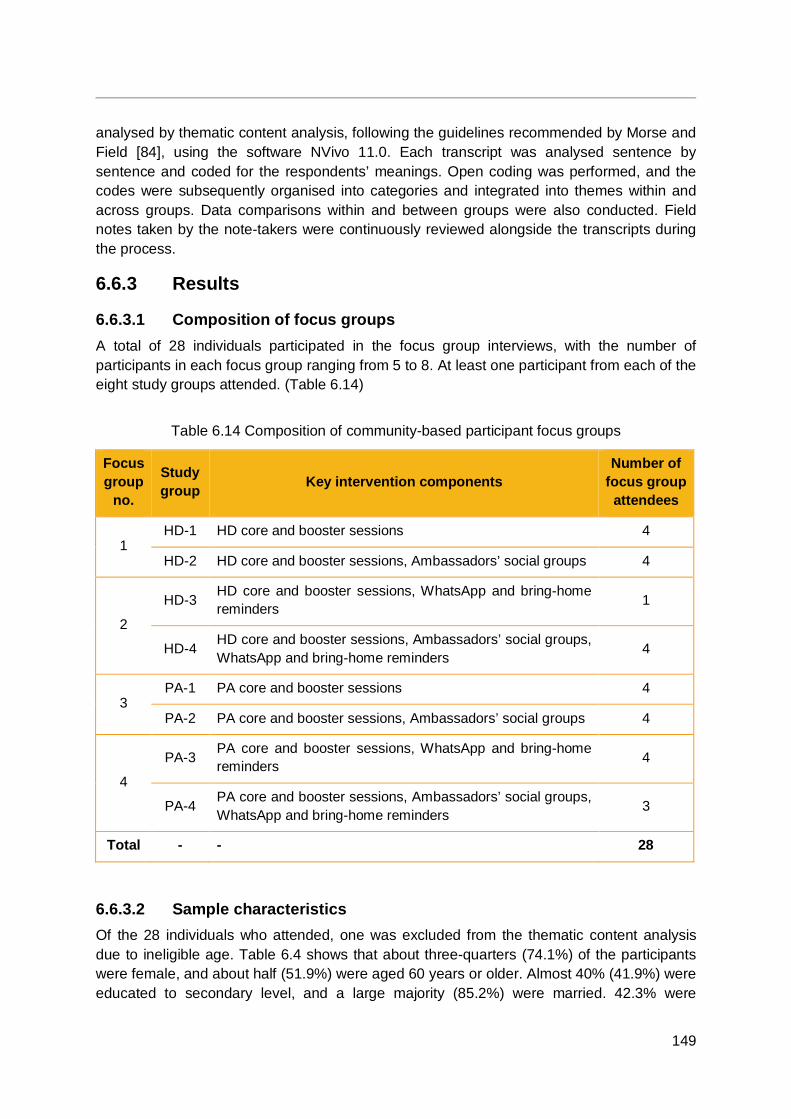
149
analysed by thematic content analysis, following the guidelines recommended by Morse and Field [84], using the software NVivo 11.0. Each transcript was analysed sentence by sentence and coded for the respondents’ meanings. Open coding was performed, and the codes were subsequently organised into categories and integrated into themes within and across groups. Data comparisons within and between groups were also conducted. Field notes taken by the note-takers were continuously reviewed alongside the transcripts during the process.
6.6.3 Results
6.6.3.1 Composition of focus groups A total of 28 individuals participated in the focus group interviews, with the number of participants in each focus group ranging from 5 to 8. At least one participant from each of the eight study groups attended. (Table 6.14)
Table 6.14 Composition of community-based participant focus groups
Focus group
no.
Study group Key intervention components
Number of focus group
attendees
1 HD-1 HD core and booster sessions 4
HD-2 HD core and booster sessions, Ambassadors’ social groups 4
2
HD-3 HD core and booster sessions, WhatsApp and bring-home reminders 1
HD-4 HD core and booster sessions, Ambassadors’ social groups, WhatsApp and bring-home reminders 4
3 PA-1 PA core and booster sessions 4
PA-2 PA core and booster sessions, Ambassadors’ social groups 4
4
PA-3 PA core and booster sessions, WhatsApp and bring-home reminders 4
PA-4 PA core and booster sessions, Ambassadors’ social groups, WhatsApp and bring-home reminders 3
Total - - 28
6.6.3.2 Sample characteristics Of the 28 individuals who attended, one was excluded from the thematic content analysis due to ineligible age. Table 6.4 shows that about three-quarters (74.1%) of the participants were female, and about half (51.9%) were aged 60 years or older. Almost 40% (41.9%) were educated to secondary level, and a large majority (85.2%) were married. 42.3% were
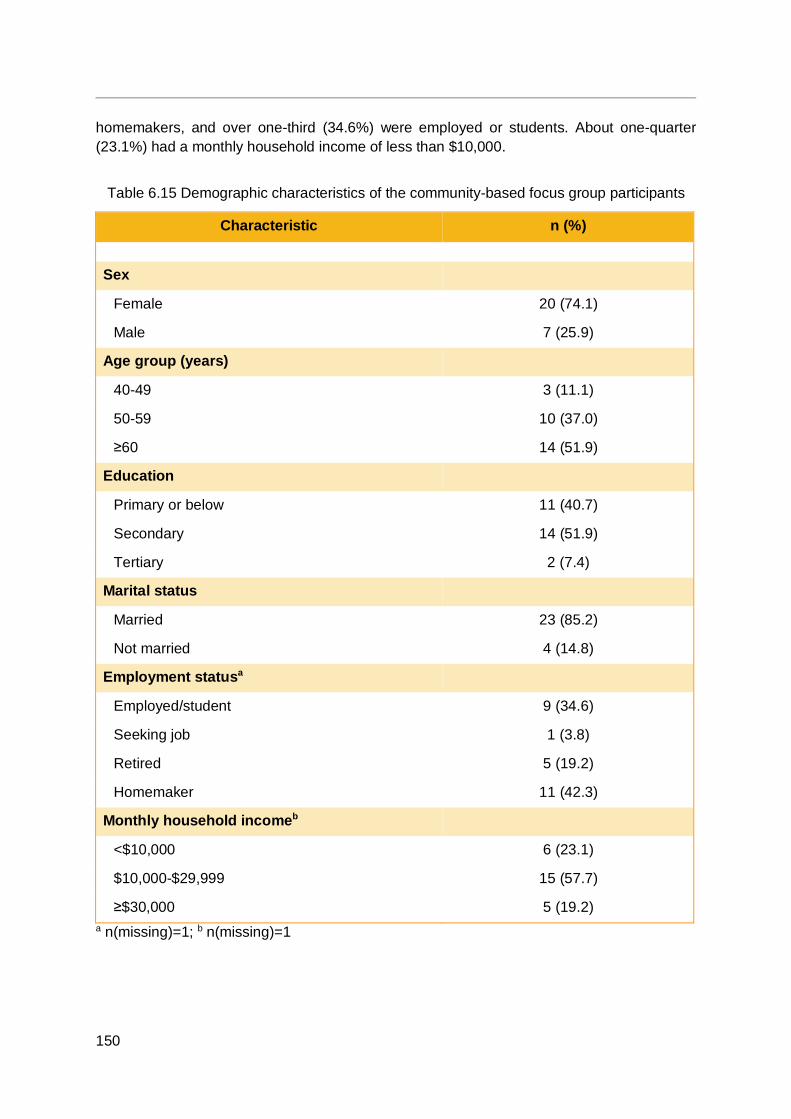
150
homemakers, and over one-third (34.6%) were employed or students. About one-quarter (23.1%) had a monthly household income of less than $10,000.
Table 6.15 Demographic characteristics of the community-based focus group participants
Characteristic n (%) Sex
Female 20 (74.1)
Male 7 (25.9)
Age group (years)
40-49 3 (11.1)
50-59 10 (37.0)
≥60 14 (51.9)
Education
Primary or below 11 (40.7)
Secondary 14 (51.9)
Tertiary 2 (7.4)
Marital status
Married 23 (85.2)
Not married 4 (14.8)
Employment statusa
Employed/student 9 (34.6)
Seeking job 1 (3.8)
Retired 5 (19.2)
Homemaker 11 (42.3)
Monthly household incomeb
<$10,000 6 (23.1)
$10,000-$29,999 15 (57.7)
≥$30,000 5 (19.2) a n(missing)=1; b n(missing)=1
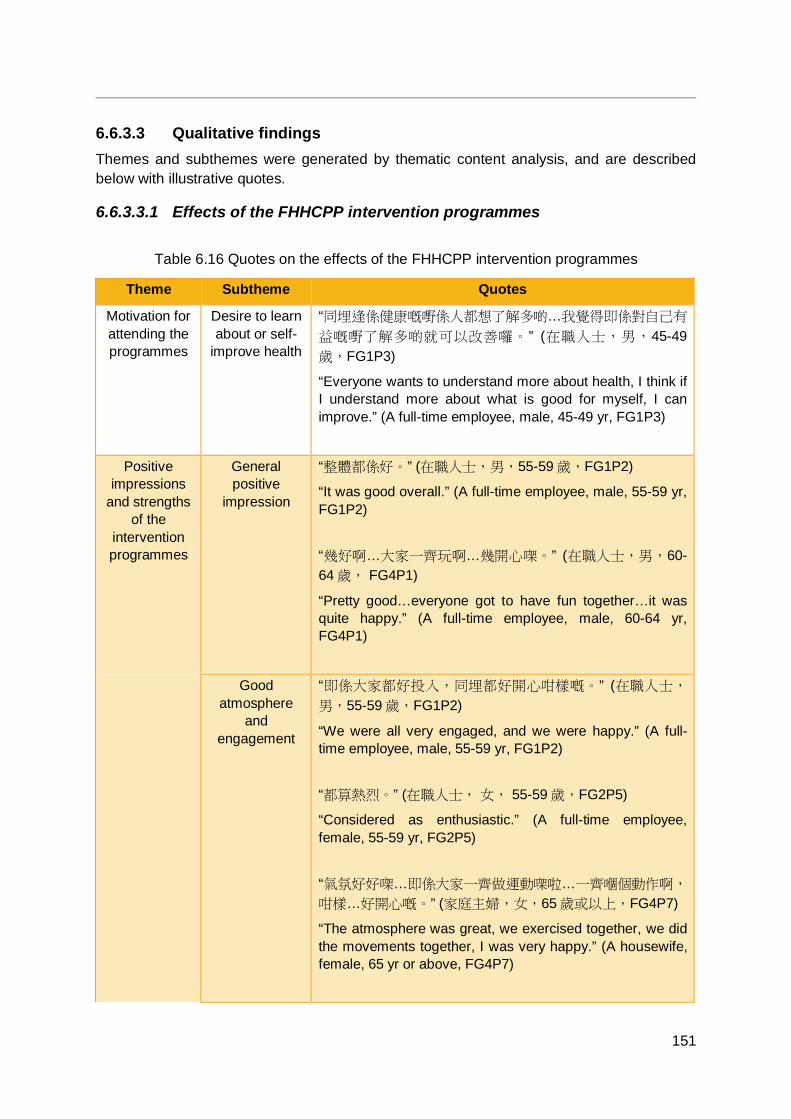
151
6.6.3.3 Qualitative findings Themes and subthemes were generated by thematic content analysis, and are described below with illustrative quotes.
6.6.3.3.1 Effects of the FHHCPP intervention programmes
Table 6.16 Quotes on the effects of the FHHCPP intervention programmes
Theme Subtheme Quotes
Motivation for attending the programmes
Desire to learn about or self-
improve health
“同埋逢係健康嘅嘢係人都想了解多啲…我覺得即係對自己有
益嘅嘢了解多啲就可以改善囉。” (在職人士,男,45-49歲,FG1P3)
“Everyone wants to understand more about health, I think if I understand more about what is good for myself, I can improve.” (A full-time employee, male, 45-49 yr, FG1P3)
Positive impressions
and strengths of the
intervention programmes
General positive
impression
“整體都係好。” (在職人士,男,55-59 歲,FG1P2)
“It was good overall.” (A full-time employee, male, 55-59 yr, FG1P2) “幾好啊…大家一齊玩啊…幾開心㗎。” (在職人士,男,60-64 歲, FG4P1)
“Pretty good…everyone got to have fun together…it was quite happy.” (A full-time employee, male, 60-64 yr, FG4P1)
Good atmosphere
and engagement
“即係大家都好投入,同埋都好開心咁樣嘅。” (在職人士,
男,55-59 歲,FG1P2)
“We were all very engaged, and we were happy.” (A full-time employee, male, 55-59 yr, FG1P2) “都算熱烈。” (在職人士, 女, 55-59 歲,FG2P5)
“Considered as enthusiastic.” (A full-time employee, female, 55-59 yr, FG2P5) “氣氛好好㗎…即係大家一齊做運動㗎啦…一齊嗰個動作啊,
咁樣…好開心嘅。” (家庭主婦,女,65 歲或以上,FG4P7)
“The atmosphere was great, we exercised together, we did the movements together, I was very happy.” (A housewife, female, 65 yr or above, FG4P7)
152
Theme Subtheme Quotes
Core sessions Good quality content Healthy diet content “估唔到一支可樂咁多糖囉…用個沙糖嚟比例會好好多囉,即
係平時你唔會諗住飲…飲支嘢有兩匙糖,原來成支可樂飲晒
係成好多…差唔多半支可樂(樽)嘅糖份咁高…即係完全估
唔到。” (家庭主婦,女,60-64 歲,FG1P1)
“I wouldn’t guess that a bottle of coke contains that much sugar…it is much better to show the proportion of sugar using caster sugar. Normally, you wouldn’t think that drinking a bottled beverage would be 2 spoonfuls of sugar. It turns out that drinking a whole bottle of coke is a lot…the caster sugar takes up almost half the coke bottle…I wouldn’t have guessed that at all.” (A housewife, female, 60-64 yr, FG1P1) “測試嗰方面…即係測試吓你自己嗰個體能去到邊度啊…” (退休人士,男,55-59 歲,FG1P4)
“In terms of the (physical fitness) assessments…they test the level of your physical fitness…” (A retiree, male, 55-59 yr, FG1P4) Physical activity content “有用嘅…譬如你嗰啲平衡啊嗰啲呢我哋平時唔駛話要咩地方
都可以做到,隨時都做…你等車都可以做。” (家庭主婦,
女,65 歲或以上,FG4P7)
“It is useful…for example, for the balance exercises, we do not need a certain place to do them, we can do them at any time…even when you are waiting for a ride.” (A housewife, female, 65 yr or above, FG4P7) “依家有呢個方便簡單嘅做下咁大家一齊玩又好…” (家庭主
婦,女,40-44 歲,FG4P4)
“Now there are some convenient and simple exercises that we can do, it is good that we can have fun together…” (A housewife, female, 40-44 yr, FG4P4)

153
Theme Subtheme Quotes Group activities were enjoyable “戶外又…又開心…齊齊玩呢…又開心因為大家一齊開心。” (家庭主婦,女, 50-54 歲,FG4P5)
“(I) was happy at the outdoor (activity)…(we) had fun together…it was joyful because all were happy together.” (A housewife, female, 50-54 yr, FG4P5) Good instructor “OK 啦, 無問題,個個都幾好。” (在職人士,女,65 歲或以
上,FG2P4; 在職人士,女,55-59 歲,FG2P3)
“(The instructors) were okay, no problems, everyone was quite good.” (A part-time employee, female, 65 yr or above, FG2P4; A full-time employee, female, 55-59 yr, FG2P3) “導師幾好囉,係啊…好親切。” (在職人士,男,60-64 歲, FG4P1) “The instructor was quite good, yes… (the instructor was) very nice.” (A full-time employee, male, 60-64 yr, FG4P1)
Booster sessions (day
trips) were enjoyable
“我覺得有一次係搞…旅行活動…咁我又覺得佢搞得好,同埋
係嗰度呢,就 eh 同我哋講咗一啲又係教我哋呢啲活動嘅嘢
嘅推廣我都覺得…即係好好囉…好有印象。” (在職人士,
女,65 歲或以上,FG2P4)
“I felt a day trip was organised…I thought they (the organisers) organised it well. When we were there, (they) told us and taught us things related to the programme and health promotion. I thought…that was very good…it left a deep impression.” (A part-time employee, female, 65 yr or above, FG2P4) “嗰度(旅行活動場地)又…即空曠啲,開揚啲咁又舒服啲…
戶外會好啲嘅,即係你戶外嗰度無咁侷促。” (在職人士,
男,45-49 歲,FG1P3)
“The venue (of day trip) was...more spacious, more open and more comfortable…outdoor (venues) are better, it is less cramped outdoors.” (A full-time employee, male, 45-49 yr, FG1P3)
154
Theme Subtheme Quotes
Sufficient manpower and
resources
“(資源配套)都不錯…人手方面啊…場地嗰啲…幾好。” (待業人士,男,40-44 歲,FG1P5)
“(Resources support was) not bad…in terms of manpower…the venue... pretty good.” (An unemployed individual, male, 40-44 yr, FG1P5)
Changes in participants
Increased general health knowledge or
awareness
“引發咗我哋會去注意咗呢個身體呀各方面。” (在職人士,
女,65 歲或以上,FG2P4)
“This has led us to pay more attention to various aspects of the body.” (A part-time employee, female, 65 yr or above, FG2P4) “原來要注意咁多嘢。” (在職人士,女,55-59 歲,FG2P5)
“It turns out there is a lot (I) need to pay attention to.” (A full-time employee, female, 55-59 yr, FG2P5)
Healthy diet-related
changes
Enhanced healthy diet awareness, knowledge, or attitude “即係本身食嘢唔係好垃雜,即係做咗之後再…清楚多啲啦,
了解多啲啦。” (退休人士,男,55-59 歲,FG1P4)
“I didn’t eat much junk food anyway, but after joining this programme…I know more, understand more.” (A retiree, male, 55-59 yr, FG1P4) “參加呢個節目呢認識咗好多嘢囉,知道加糖呢要少啲,加少
啲囉,不要加咁多囉。” (家庭主婦,女,60-64 歲,FG1P1)
“I know more after joining this programme, I know less sugar should be added, add less, don’t add that much.” (A housewife, female, 60-64 yr, FG1P1) “或者…飲食嗰方面會可以再好啲呢…” (退休人士,男,55-59 歲,FG1P4)
“Maybe…the diet can be improved…” (A retiree, male, 55-59 yr, FG1P4)
155
Theme Subtheme Quotes Positive behavioural changes More attention paid to nutrition labels “我本來去超級市場買嘢都無去睇標籤,而家一定要去睇。” (在職人士,女,50-54 歲, FG1P6)
“I was not used to read the nutrition labels when I shopped at the supermarket. Now, I always read them.” (A part-time employee, female, 50-54 yr, FG1P6) “會留意下啲標籤,啲糖份會唔會太高呀咁樣囉,即係注重身
體。” (在職人士, 女,65 歲或以上,FG2P4)
“(I) would pay attention to the nutrition labels, “is the sugar content too high?”, pay attention to health.” (A part-time employee, female, 65 yr or above, FG2P4) Increased healthy diet behaviour: decreased dietary sugar intake from food or drinks “飲品嗰啲咁咪以往…啲飲品好多糖啊,依家落少啲糖啊…知
道無益。” (在職人士,男,45-49 歲,FG1P3)
“In the past, I drank beverages with a lot of sugar. Now I add less sugar…I know it is bad for me.” (A full-time employee, male, 45-49 yr, FG1P3) “係啊,糖…食少咗好多。” (家庭主婦,女,60-64 歲,
FG1P1) “Yes, sugar…I eat a lot less.” (A housewife, female, 60-64 yr, FG1P1)
Physical activity-related
changes
Enhanced physical activity awareness, knowledge, or attitude “學到好多啊…能力又好咗啦。” (在職人士,女,50-54 歲,
FG4P6) “(I) learnt a lot…am more capable.” (A part-time employee, female, 50-54 yr, FG4P6) “我覺得,即係你哋嘅團體搞咗呢個運動,係幫到我哋認識多
啲呢方面嘅嘢,即係識食,多做運動,咁我就即係嗰啲最深
156
Theme Subtheme Quotes 刻感受就係呢樣。” (在職人士,女,65 歲或以上,FG2P4)
“I think, this programme that your institution organised has helped us to learn a lot about this topic (health), that is, adopting a healthy diet, exercising more, that is what left the deepest impression on me.” (A part-time employee, female, 65 yr or above, FG2P4) Positive behavioural changes “以前唔會…即係特登抽啲時間去做運動啊,依家就會無時無
刻都做啦,有時喺屋企摘菜啊,即係有時整緊嘢,煮緊…炒
菜啊。” (家庭主婦,女,60-64 歲,FG3P6)
“In the past, I wouldn’t… intentionally squeeze time out to exercise. Now I do it all the time, sometimes when I am at home preparing the vegetables, doing other things, cooking…stir-frying vegetable.” (A housewife, female, 60-64 yr, FG3P6) “係工作嗰陣時做囉…即係單腳企嗰個…同埋坐企高嗰個…” (在職人士,女,60-64 歲,FG4P3)
“I do it (physical activity) whilst working…I do the single leg stance…and the chair stand (exercise)…” (A full-time employee, female, 60-64 yr, FG4P3) Felt physical health or fitness improvements after doing physical activity “單腳企,平衡嗰啲呢…最好就等車等得耐…個人好無聊又好
心急嗰陣時呢就唔知點樣放鬆…隻腳咁樣企下。” (家庭主
婦,女,40-44 歲,FG4P4)
“The single leg stance for balance…is bestwhen you have been waiting for a ride for a long time…when you are really bored and anxious, and you do not know how to relax…you can stand on one leg like that.” (A housewife, female, 40-44 yr, FG4P4) “因為我成日拗柴。即係就,好咗好多囉…係喇…即係你就少
咗拗柴囉…(靠練習)單腳(企)嗰個…得閒就做囉…” (在職人士,女,60-64 歲,FG4P3)
“Because I sprain my ankle a lot. It is much better now…I sprain it less…(since practising) the single leg stance…I do it when I am free…” (A full-time employee, female, 60-64
157
Theme Subtheme Quotes yr, FG4P3)
Enhanced friendships
Made friends through the FHHCPP “我難忘呢,識咗你哋(其他參加者)呢班人呢,我覺得好開
心喇。因為個個都老友記嚟㗎嘛,依家變咗做朋友喇。真係
呢個係好難忘嘅…即係變咗大家有得溝通呀,大家買乜嘢
呀,即係都係街坊街尾㗎依家,「喂買乜嘢你有無睇標籤
呀?」” (在職人士,女,55-59 歲,FG2P3)
“It is unforgettable that I met you (other participants), I feel delighted because we are all elderly, and now we have become friends. This is really unforgettable…we can communicate with each other about what we are buying, we are in the same neighbourhood now, “Have you read the food label when you bought that?” (A full-time employee, female, 55-59 yr, FG2P3) Shared knowledge with or influenced friends “咁就介紹下啲朋友呀,認識多啲呀,叫佢哋注意健康嗰啲
囉。” (在職人士,女,55-59 歲,FG2P5)
“(I) introduced it to my friends, so they know more, asked them to pay attention to health.” (A full-time employee, female, 55-59 yr, FG2P5) “我如果同啲朋友一齊呢,佢叫我去食甜品呢我…我就話少食
喇,我哋可以轉下去食第二樣嘅食物。咁變咗就即係,帶埋
佢哋都會走向即係話,少甜,或者少咸嗰啲咁樣囉。即係食
嘢的時候一齊…一齊即係要叫嘢食呀咁我自己就提點囉。咁
同埋又話俾佢哋聽,我參加咗呢個活動呀,「嗱,咁樣咁樣
係好有益嘅」,咁樣提俾佢哋。” (在職人士,女,65 歲或以
上,FG2P4)
“If I am with my friends and they ask me to go for dessert, I…I say to eat less (dessert), we can eat something else instead. So as a result, I have influenced them to go toward a low sugar or low salt diet. That is, when we eat together…when we have to order food together, I remind them, and I also tell them that I have joined this programme, ‘See, this and that are healthy,’ I remind them like that.” (A part-time employee, female, 65 yr or above, FG2P4)
158
Theme Subtheme Quotes
Changes in participants’
family
Family health Participants adopted health behaviours together with family members “咁變咗我哋食嘢方面都會節制…即係份量細小啲咁樣係喇,
咁糖當然就…就要少啲啦…” (在職人士,男,45-49 歲,
FG1P3) “We control our diet, eat smaller portions, and of course for sugar…we have to eat less…” (A full-time employee, male, 45-49, FG1P3) “同埋自己屋企人添,更加推廣,同埋多啲一齊做運動。” (在職人士,女,65 歲或以上,FG2P4)
“With family, promote more, and we exercise together more.” (A part-time employee, female, 65 or above, FG2P4) Participants practised physical activity together with family members “同埋拉筋嗰啲呢,因為我不嬲都有拉筋咁嘛。我又跟住同佢
兩個一齊呢,有時,禮拜六、日放假嗰陣時一齊玩呢咁樣。” (家庭主婦,女,40-44 歲,FG4P4)
“Also with the stretching, because I always do stretching. Somtimes, Saturday and Sunday, holiday, I play together with my two children.” (A housewife, female, 40-44 yr, FG4P4)
Family harmony
Communication or interaction with family members regarding the FHHCPP (not theme-specific) “食飯嗰陣時咪討論返內容…咁咪大家可以溝通多啲,了解多
啲大家互相了解多啲健康上面嘅嘢,咁對屋企和睦都好啲。” (在職人士,男,45-49 歲,FG1P3)
“We discuss the (programme) content during meal times…so we communicate more, understand more about each other’s health, which is good for family harmony.” (A full-time employee, male, 45-49 yr, FG1P3) “多咗啲話題分享下啊。” (家庭主婦,女,65 歲或以上,
FG3P2) “(We) have more topics to share on.” (A housewife, female,
159
Theme Subtheme Quotes 65 yr and above, FG3P2) Communication or interaction with family members regarding healthy diet “我就覺得,即係你參加咗就會認識多咗,識多咗咁你就…屋
企人有時有啲都唔知,分享咗俾佢聽,啊咁,咁又覺得會好
啲。” (在職人士,男,45-49 歲,FG1P3)
“I think, you know more after participating (in this programme), when you know more, you can share with your family since they might not know, I think that is better.” (A full-time employee, male, 45-49, FG1P3) “(同家人關係)好咗,即係都係為大家健康著想囉。叫佢唔
好整咁咸呀咁濃味呀嗰啲嘢,咁成家人都有幫助㗎嘛。” (在職人士,女,55-59 歲,FG2P5)
“It (the relationship with family members) has got better, it’s for the sake of everyone’s health, asking him (husband) not to cook too salty or strong dishes, it helps the whole family.” (A full-time employee, female, 55-59 yr, FG2P5) Communication or interaction with family members regarding physical activity “即係同埋先生一齊,都講俾佢聽,「你唔使,嗱,特登去行
山啊咩嘢…你喺屋企啊都可以做㗎」…成日都將呢啲訊息講
俾佢聽囉。” (家庭主婦,女,60-64 歲,FG3P6)
“With my husband, I tell him ‘You don’t need to specially go hiking or anything…you can do it (physical activity) at home’…I always tell him these messages.” (A housewife, female, 60-64 yr, FG3P6) Mutual support and encouragement “所以同佢呢,因為佢不嬲都有跳舞,佢自己拉筋嘅。但係同
我一齊…同佢, 我有個伴囉…做得開心啲囉。” (家庭主婦,
女,40-44 歲,FG4P4)
“So, with her (daughter). She always dances, and she does stretching. But when I do it (stretching) with her…I have company…I am happier doing it.” (A housewife, female, 40-44 yr, FG4P4)
160
Theme Subtheme Quotes “我媽會揸下呢個(手握力器)囉…初初合唔埋嘅…咁佢話無
心機 。我話「你練吓練吓啦,耐啲就得㗎啦。」” (在職人
士,女,60-64 歲,FG4P3)
“My mother does squeeze the handgrip…at first, she couldn’t close it…and she said she was dispirited. I told her ‘With more practice, in time you will be able to do it.’” (A full-time employee, female, 60-64 yr, FG4P3)
Personal changes in
family members
Increased healthy diet behaviours “係呀係呀(影響到家人),食得健康。” (退休人士,女,65歲或以上,FG2P2)
“Yes, yes (I was able to influence my family), to eat more healthily.” (A retiree, female, 65 yr or above, FG2P2) “咁就變咗屋企人…好似我哋今朝早出去食早餐嘅,飲咖啡嘅
唔放糖囉,樣樣都少啲囉。” (在職人士,女,55-59 歲,
FG2P3) “With my family, for instance, when we went out for breakfast this morning, we didn’t add sugar to the coffee, we have cut down on everything.” (A full-time employee, female, 55-59 yr, FG2P3) Participants were unsure if family members made physical activity changes “無(行為轉變)啊佢哋…返學…屋企佢哋一返來就係功課…
閂晒門入房做功課㗎啦…唔見到佢哋點樣做運動㗎啦即係。” (家庭主婦,女, 50-54 歲,FG4P5)
“They have not had any behavioural change…they go to school…as soon as they get home, they work on their homework…they go to their room and close the door to do their homework…(I) can’t see how they exercise.” (A housewife, female, 50-54 yr, FG4P5)
Motivation for behavioural
changes
Motivation for healthy diet-
related behavioural
changes
Enhanced health awareness or knowledge “排隊做測試嗰時呢覺得亦都好想了解自己嗰個身體狀況啊…
同埋嗰啲握力測試啊咁樣…亦都覺得啊原來咁樣差咗,或者
咁係正常,覺得有啲…要改善啊。” (在職人士,男,45-49歲,FG1P3)

161
Theme Subtheme Quotes “When I was queueing for the fitness assessments, I also really wanted to understand more about my body condition…and the hand grip strength test…I thought oh, so this is worse, or this is normal, I felt that...(I) needed to improve.” (A full-time employee, male, 45-49 yr, FG1P3) “引發咗我哋會去注意咗呢個身體呀各方面,呢件事啦,咁樣
就令到我哋去希望多啲去跟住去做,即係照呢一個你哋呢個
話咁樣做運動呀, 食方面留意啲注意啲。” (在職人士,女,
65 歲或以上,FG2P4)
“This has led us to pay more attention to various aspects of the body…which has made us hope that we can follow the recommendations more, that is, what you have told us about how to exercise and pay more attention to our diet.” (A part-time employee, female, 65 yr or above, FG2P4) “我覺得,即係你哋嘅團體搞咗呢個運動,係幫到我哋認識多
啲呢方面嘅嘢,即係識食,多做運動。咁我就即係嗰啲最深
刻感受就係呢樣,因為如果唔係呢,唔係你哋推廣呢,可能
我哋…就無咁多呢個叫咩, 知識添呀。同埋就唔會話去實踐
去做呢個行動。” (在職人士,女,65 歲或以上,FG2P4)
“I think, this programme that your institution organised has helped us to learn a lot about this topic (health), that is, adopting a healthy diet, exercising more, that is what left the deepest impression on me, because otherwise, if you had not promoted this, maybe we wouldn’t have so much knowledge, and also we would not practise and take action.” (A part-time employee, female, 65 or above, FG2P4)
Barriers to behavioural
changes
Barriers to practising physical activity
Lack of time or energy “因為我要返工㗎嘛…返到屋企就好…即係好攰啦…” (在職人
士,女,60-64 歲,FG4P3)
“Because I have to go to work…when I get home, I am already very tired…” (A full-time employee, female, 60-64 yr, FG4P3) “佢(女)無咩時間啊… ” (在職人士,女,50-54 歲,
FG4P6) “She (daughter) does not have time…” (A part-time employee, female, 50-54 yr, FG4P6)
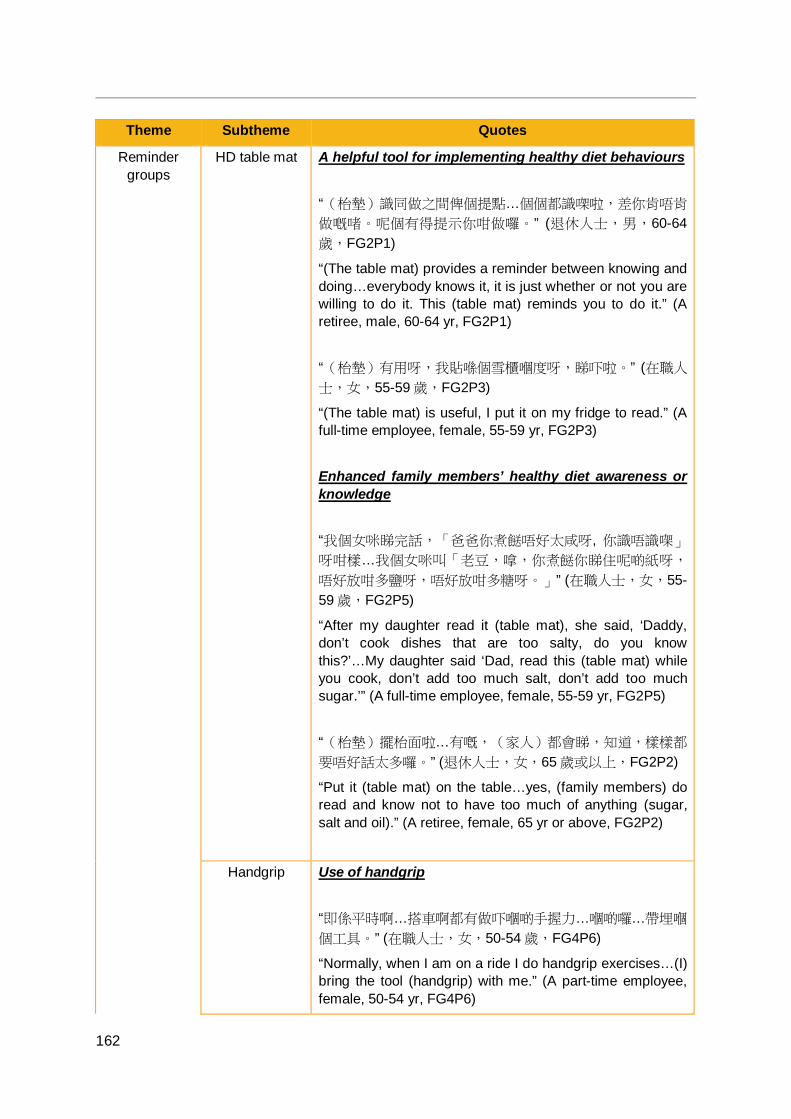
162
Theme Subtheme Quotes
Reminder groups
HD table mat A helpful tool for implementing healthy diet behaviours “(枱墊)識同做之間俾個提點…個個都識㗎啦,差你肯唔肯
做嘅啫。呢個有得提示你咁做囉。” (退休人士,男,60-64歲,FG2P1)
“(The table mat) provides a reminder between knowing and doing…everybody knows it, it is just whether or not you are willing to do it. This (table mat) reminds you to do it.” (A retiree, male, 60-64 yr, FG2P1) “(枱墊)有用呀,我貼喺個雪櫃嗰度呀,睇吓啦。” (在職人
士,女,55-59 歲,FG2P3)
“(The table mat) is useful, I put it on my fridge to read.” (A full-time employee, female, 55-59 yr, FG2P3) Enhanced family members’ healthy diet awareness or knowledge “我個女咪睇完話,「爸爸你煮餸唔好太咸呀, 你識唔識㗎」 呀咁樣…我個女咪叫「老豆,嗱,你煮餸你睇住呢啲紙呀,
唔好放咁多鹽呀,唔好放咁多糖呀。」” (在職人士,女,55-59 歲,FG2P5)
“After my daughter read it (table mat), she said, ‘Daddy, don’t cook dishes that are too salty, do you know this?’…My daughter said ‘Dad, read this (table mat) while you cook, don’t add too much salt, don’t add too much sugar.’” (A full-time employee, female, 55-59 yr, FG2P5) “(枱墊)擺枱面啦…有嘅,(家人)都會睇,知道,樣樣都
要唔好話太多囉。” (退休人士,女,65 歲或以上,FG2P2)
“Put it (table mat) on the table…yes, (family members) do read and know not to have too much of anything (sugar, salt and oil).” (A retiree, female, 65 yr or above, FG2P2)
Handgrip Use of handgrip “即係平時啊…搭車啊都有做吓嗰啲手握力…嗰啲囉…帶埋嗰
個工具。” (在職人士,女,50-54 歲,FG4P6)
“Normally, when I am on a ride I do handgrip exercises…(I) bring the tool (handgrip) with me.” (A part-time employee, female, 50-54 yr, FG4P6)
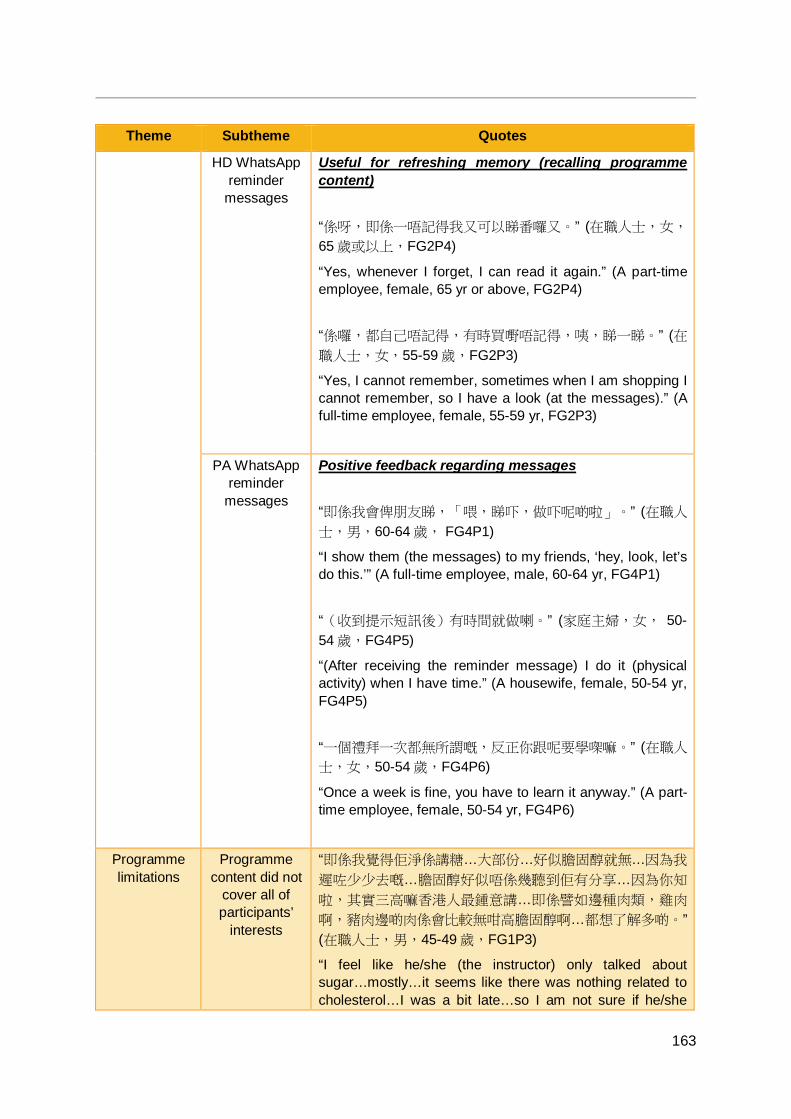
163
Theme Subtheme Quotes
HD WhatsApp reminder
messages
Useful for refreshing memory (recalling programme content) “係呀,即係一唔記得我又可以睇番囉又。” (在職人士,女,
65 歲或以上,FG2P4)
“Yes, whenever I forget, I can read it again.” (A part-time employee, female, 65 yr or above, FG2P4) “係囉,都自己唔記得,有時買嘢唔記得,咦,睇一睇。” (在職人士,女,55-59 歲,FG2P3)
“Yes, I cannot remember, sometimes when I am shopping I cannot remember, so I have a look (at the messages).” (A full-time employee, female, 55-59 yr, FG2P3)
PA WhatsApp reminder
messages
Positive feedback regarding messages “即係我會俾朋友睇,「喂,睇吓,做吓呢啲啦」。” (在職人
士,男,60-64 歲, FG4P1)
“I show them (the messages) to my friends, ‘hey, look, let’s do this.’” (A full-time employee, male, 60-64 yr, FG4P1) “(收到提示短訊後)有時間就做喇。” (家庭主婦,女, 50-54 歲,FG4P5)
“(After receiving the reminder message) I do it (physical activity) when I have time.” (A housewife, female, 50-54 yr, FG4P5) “一個禮拜一次都無所謂嘅,反正你跟呢要學㗎嘛。” (在職人
士,女,50-54 歲,FG4P6)
“Once a week is fine, you have to learn it anyway.” (A part-time employee, female, 50-54 yr, FG4P6)
Programme limitations
Programme content did not
cover all of participants’
interests
“即係我覺得佢淨係講糖…大部份…好似膽固醇就無…因為我
遲咗少少去嘅…膽固醇好似唔係幾聽到佢有分享…因為你知
啦,其實三高嘛香港人最鍾意講…即係譬如邊種肉類,雞肉
啊,豬肉邊啲肉係會比較無咁高膽固醇啊…都想了解多啲。” (在職人士,男,45-49 歲,FG1P3)
“I feel like he/she (the instructor) only talked about sugar…mostly…it seems like there was nothing related to cholesterol…I was a bit late…so I am not sure if he/she

164
Theme Subtheme Quotes shared on cholesterol…You know, the “3 Highs” (blood pressure, blood sugar and blood lipid) is a hot topic in Hong Kong. For instance, which type of meat...chicken, which part of the pork meat contains less cholesterol…I want to know more.” (A full-time employee, male, 45-49 yr, FG1P3) “佢完全無提到睡眠個問題。足夠嘅睡眠好重要。即係佢可能
…覺得個個都知㗎啦,唔駛講咁樣。” (退休人士,男,60-64 歲,FG2P1)
“He/she did not mention the issue of sleep at all. Getting enough sleep is very important. Maybe he/she thought that everyone knew and there was no need to mention it.” (A retiree, male, 60-64 yr, FG2P1)
Suggestions for
improvements
Questionnaires should be simplified
“問卷都可以簡化啲。” (家庭主婦,女,60-64 歲,FG3P3)
“The questionnaire could be simplified.” (A housewife, female, 60-64 yr, FG3P3) “問卷又要簡化啲。” (退休人士,女,60-64 歲,FG3P8)
“The questionnaire should be simplified.” (A retiree, female, 60-64 yr, FG3P8)
Programmes do not have to
be held at large venues
“唔一定大型呢啲㗎嘛。 ” (在職人士,女,55-59 歲,
FG2P3) “It does not have to be so large scale.” (A full-time employee, female, 55-59 yr, FG2P3)
Promotion should be
accomplished through more
means
“多啲途徑宣傳,係喇,多啲途徑咁即係多啲人知道…咁希望
你如果多啲可以好似話,係其他嘅,即係公開式嘅途徑呢,
咁就變咗全香港多啲人都知道, 提醒佢哋多啲做呢個…動
作。” (在職人士,女,65 歲或以上,FG2P4)
“Promote through more channels, yes, using more channels means that more people will get to know about it…use of more channel, more people get to know it…hopefully if you use more channels, like public channels, then more people in Hong Kong will know about it, remind them to exercise more.” (A part-time employee, female, 65 or above, FG2P4) “多啲宣傳下啦。” (在職人士,女,55-59 歲,FG2P3)
“Promote more.” (A full-time employee, female, 55-59 yr,
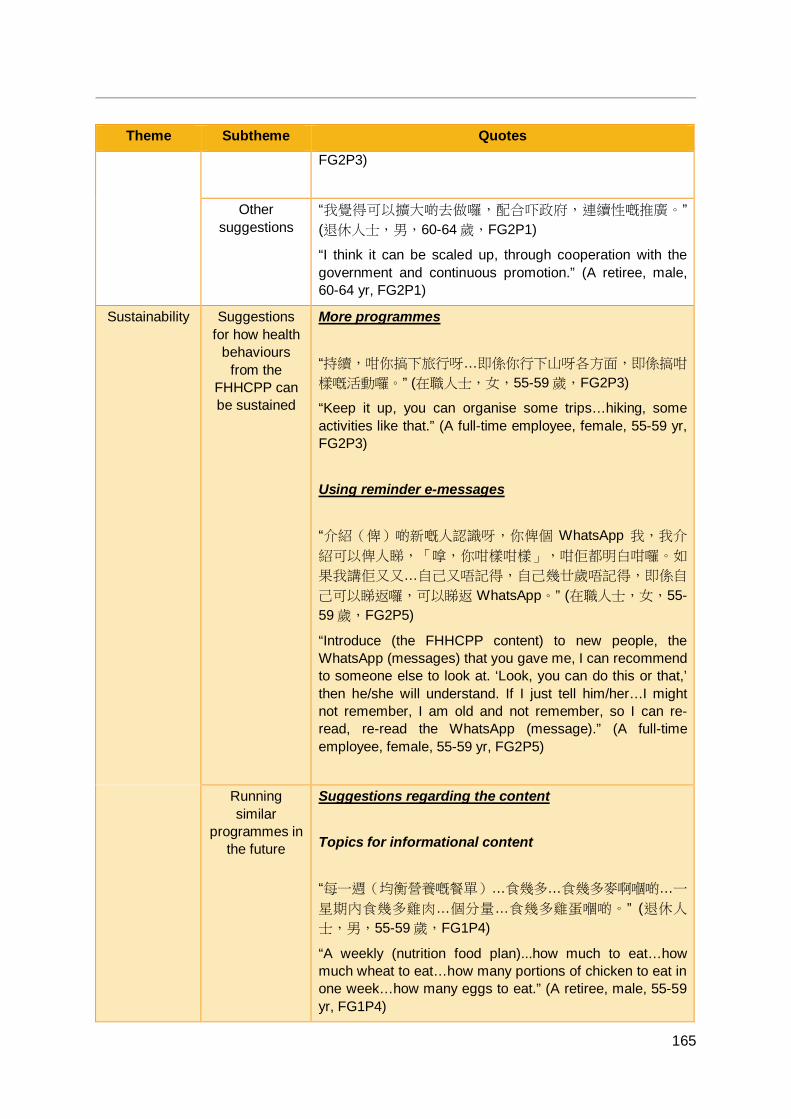
165
Theme Subtheme Quotes FG2P3)
Other suggestions
“我覺得可以擴大啲去做囉,配合吓政府,連續性嘅推廣。” (退休人士,男,60-64 歲,FG2P1)
“I think it can be scaled up, through cooperation with the government and continuous promotion.” (A retiree, male, 60-64 yr, FG2P1)
Sustainability Suggestions for how health
behaviours from the
FHHCPP can be sustained
More programmes “持續,咁你搞下旅行呀…即係你行下山呀各方面,即係搞咁
樣嘅活動囉。” (在職人士,女,55-59 歲,FG2P3)
“Keep it up, you can organise some trips…hiking, some activities like that.” (A full-time employee, female, 55-59 yr, FG2P3) Using reminder e-messages “介紹(俾)啲新嘅人認識呀,你俾個 WhatsApp 我,我介
紹可以俾人睇,「嗱,你咁樣咁樣」,咁佢都明白咁囉。如
果我講佢又又…自己又唔記得,自己幾廿歲唔記得,即係自
己可以睇返囉,可以睇返 WhatsApp。” (在職人士,女,55-59 歲,FG2P5)
“Introduce (the FHHCPP content) to new people, the WhatsApp (messages) that you gave me, I can recommend to someone else to look at. ‘Look, you can do this or that,’ then he/she will understand. If I just tell him/her…I might not remember, I am old and not remember, so I can re-read, re-read the WhatsApp (message).” (A full-time employee, female, 55-59 yr, FG2P5)
Running similar
programmes in the future
Suggestions regarding the content Topics for informational content “每一週(均衡營養嘅餐單)…食幾多…食幾多麥啊嗰啲…一
星期內食幾多雞肉…個分量…食幾多雞蛋嗰啲。” (退休人
士,男,55-59 歲,FG1P4)
“A weekly (nutrition food plan)...how much to eat…how much wheat to eat…how many portions of chicken to eat in one week…how many eggs to eat.” (A retiree, male, 55-59 yr, FG1P4)
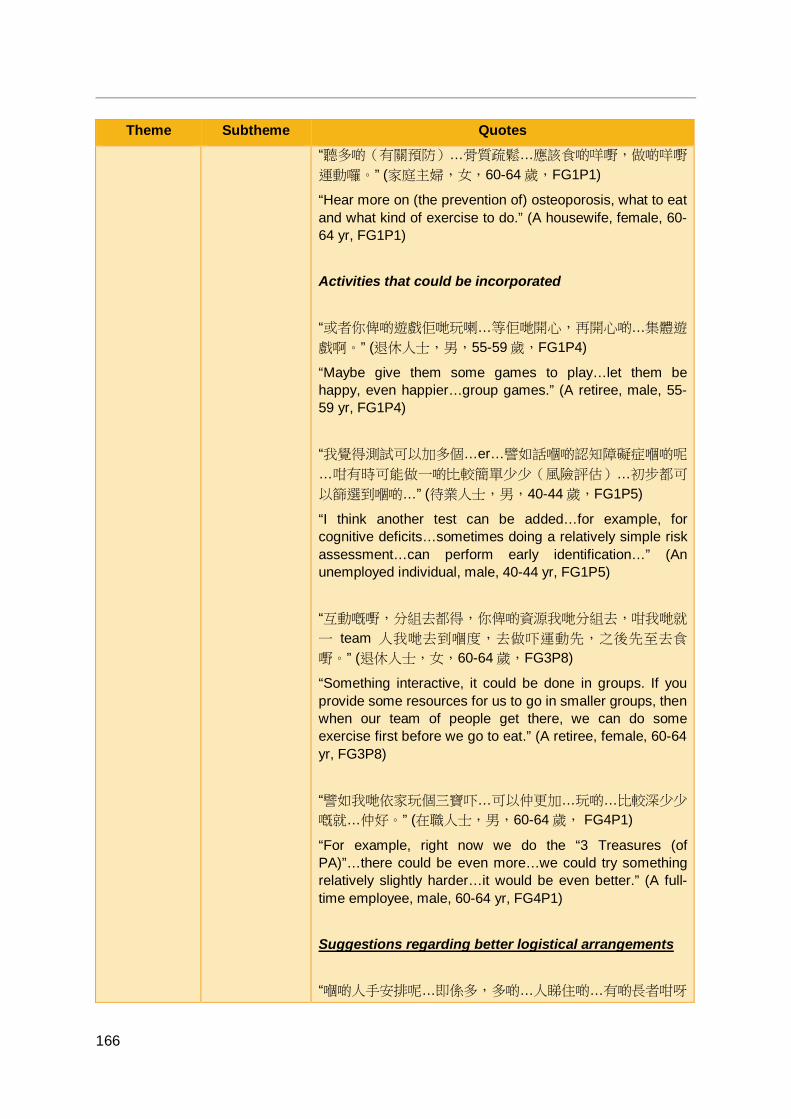
166
Theme Subtheme Quotes “聽多啲(有關預防)…骨質疏鬆…應該食啲咩嘢,做啲咩嘢
運動囉。” (家庭主婦,女,60-64 歲,FG1P1)
“Hear more on (the prevention of) osteoporosis, what to eat and what kind of exercise to do.” (A housewife, female, 60-64 yr, FG1P1) Activities that could be incorporated “或者你俾啲遊戲佢哋玩喇…等佢哋開心,再開心啲…集體遊
戲啊。” (退休人士,男,55-59 歲,FG1P4)
“Maybe give them some games to play…let them be happy, even happier…group games.” (A retiree, male, 55-59 yr, FG1P4) “我覺得測試可以加多個…er…譬如話嗰啲認知障礙症嗰啲呢
…咁有時可能做一啲比較簡單少少(風險評估)…初步都可
以篩選到嗰啲…” (待業人士,男,40-44 歲,FG1P5)
“I think another test can be added…for example, for cognitive deficits…sometimes doing a relatively simple risk assessment…can perform early identification…” (An unemployed individual, male, 40-44 yr, FG1P5) “互動嘅嘢,分組去都得,你俾啲資源我哋分組去,咁我哋就
一 team 人我哋去到嗰度,去做吓運動先,之後先至去食
嘢。” (退休人士,女,60-64 歲,FG3P8)
“Something interactive, it could be done in groups. If you provide some resources for us to go in smaller groups, then when our team of people get there, we can do some exercise first before we go to eat.” (A retiree, female, 60-64 yr, FG3P8) “譬如我哋依家玩個三寶吓…可以仲更加…玩啲…比較深少少
嘅就…仲好。” (在職人士,男,60-64 歲, FG4P1)
“For example, right now we do the “3 Treasures (of PA)”…there could be even more…we could try something relatively slightly harder…it would be even better.” (A full-time employee, male, 60-64 yr, FG4P1) Suggestions regarding better logistical arrangements “嗰啲人手安排呢…即係多,多啲…人睇住啲…有啲長者咁呀
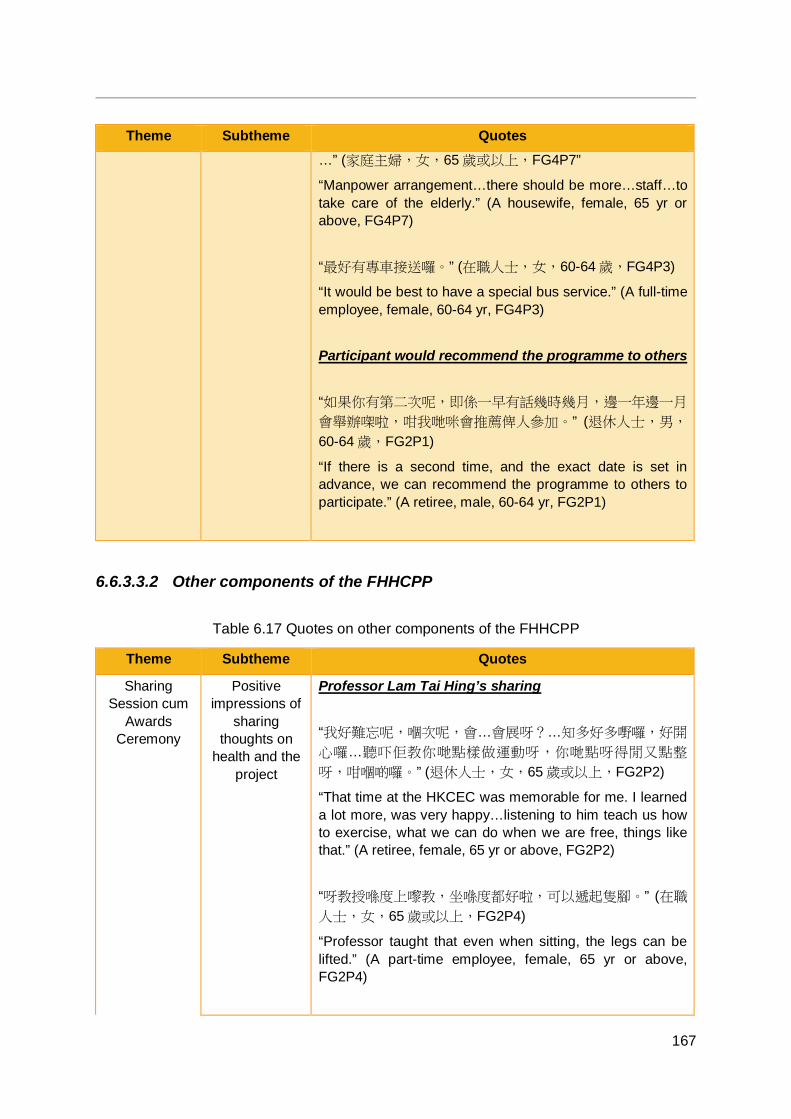
167
Theme Subtheme Quotes …” (家庭主婦,女,65 歲或以上,FG4P7”
“Manpower arrangement…there should be more…staff…to take care of the elderly.” (A housewife, female, 65 yr or above, FG4P7) “最好有專車接送囉。” (在職人士,女,60-64 歲,FG4P3)
“It would be best to have a special bus service.” (A full-time employee, female, 60-64 yr, FG4P3) Participant would recommend the programme to others “如果你有第二次呢,即係一早有話幾時幾月,邊一年邊一月
會舉辦㗎啦,咁我哋咪會推薦俾人參加。” (退休人士,男,
60-64 歲,FG2P1)
“If there is a second time, and the exact date is set in advance, we can recommend the programme to others to participate.” (A retiree, male, 60-64 yr, FG2P1)
6.6.3.3.2 Other components of the FHHCPP
Table 6.17 Quotes on other components of the FHHCPP
Theme Subtheme Quotes
Sharing Session cum
Awards Ceremony
Positive impressions of
sharing thoughts on
health and the project
Professor Lam Tai Hing’s sharing “我好難忘呢,嗰次呢,會…會展呀?…知多好多嘢囉,好開
心囉…聽吓佢教你哋點樣做運動呀,你哋點呀得閒又點整
呀,咁嗰啲囉。” (退休人士,女,65 歲或以上,FG2P2)
“That time at the HKCEC was memorable for me. I learned a lot more, was very happy…listening to him teach us how to exercise, what we can do when we are free, things like that.” (A retiree, female, 65 yr or above, FG2P2) “呀教授喺度上嚟教,坐喺度都好啦,可以遞起隻腳。” (在職
人士,女,65 歲或以上,FG2P4)
“Professor taught that even when sitting, the legs can be lifted.” (A part-time employee, female, 65 yr or above, FG2P4)
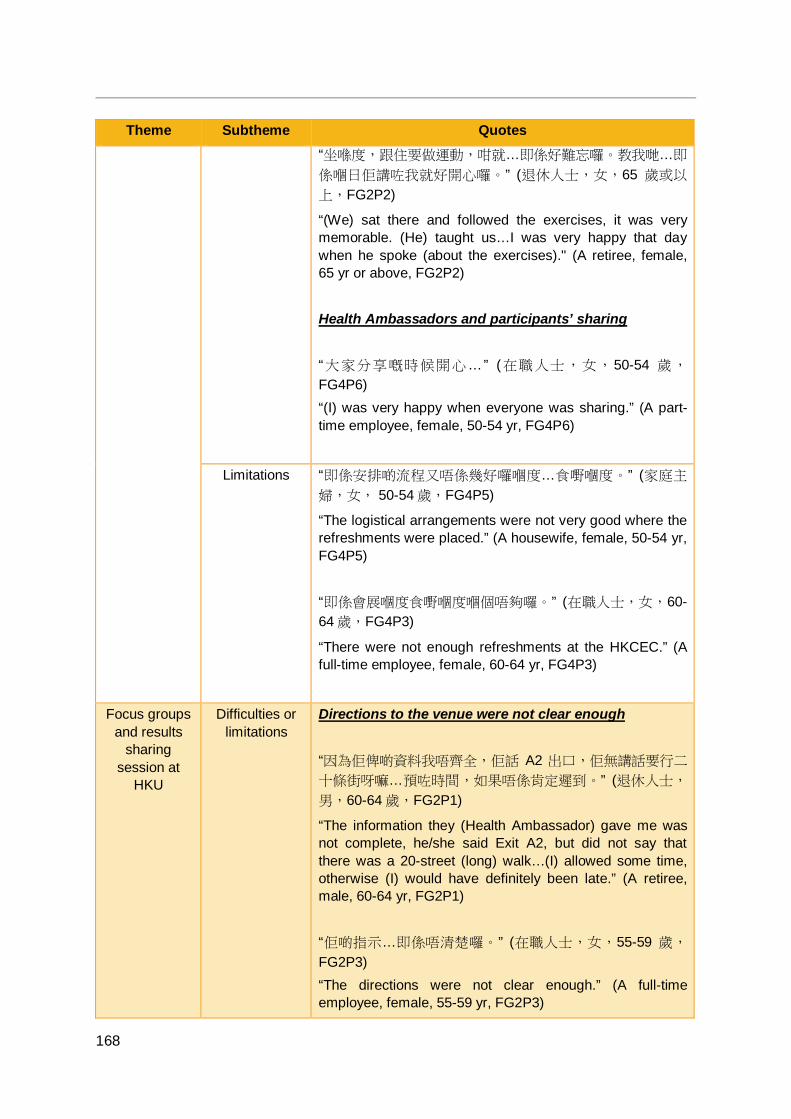
168
Theme Subtheme Quotes “坐喺度,跟住要做運動,咁就…即係好難忘囉。教我哋…即
係嗰日佢講咗我就好開心囉。” (退休人士,女,65 歲或以
上,FG2P2)
“(We) sat there and followed the exercises, it was very memorable. (He) taught us…I was very happy that day when he spoke (about the exercises)." (A retiree, female, 65 yr or above, FG2P2) Health Ambassadors and participants’ sharing “大家分享嘅時候開心… ” (在職人士,女,50-54 歲,
FG4P6) “(I) was very happy when everyone was sharing.” (A part-time employee, female, 50-54 yr, FG4P6)
Limitations “即係安排啲流程又唔係幾好囉嗰度…食嘢嗰度。” (家庭主
婦,女, 50-54 歲,FG4P5)
“The logistical arrangements were not very good where the refreshments were placed.” (A housewife, female, 50-54 yr, FG4P5) “即係會展嗰度食嘢嗰度嗰個唔夠囉。” (在職人士,女,60-64 歲,FG4P3)
“There were not enough refreshments at the HKCEC.” (A full-time employee, female, 60-64 yr, FG4P3)
Focus groups and results
sharing session at
HKU
Difficulties or limitations
Directions to the venue were not clear enough “因為佢俾啲資料我唔齊全,佢話 A2 出口,佢無講話要行二
十條街呀嘛…預咗時間,如果唔係肯定遲到。” (退休人士,
男,60-64 歲,FG2P1)
“The information they (Health Ambassador) gave me was not complete, he/she said Exit A2, but did not say that there was a 20-street (long) walk…(I) allowed some time, otherwise (I) would have definitely been late.” (A retiree, male, 60-64 yr, FG2P1) “佢啲指示…即係唔清楚囉。” (在職人士,女,55-59 歲,
FG2P3) “The directions were not clear enough.” (A full-time employee, female, 55-59 yr, FG2P3)

169
6.6.4 Summary of community-based focus group findings Findings from the four focus groups showed that participants generally had very positive impressions of the intervention programmes. Participants highlighted some of the strengths of the programmes, including the good atmosphere and engagement, the high quality content regarding healthy diet and physical activity that was delivered at the core sessions, and the enjoyable day trips that participants took as part of the booster sessions. Professor Lam Tai Hing’s sharing at the Sharing Session cum Awards Ceremony also left a deep impression on the participants.
Participants indicated that as a result of the intervention programmes, they experienced increases in healthy diet or physical activity knowledge or awareness. In turn, this enhanced awareness motivated positive healthy diet-related or physical activity-related behavioural changes. Those in the PA groups also reported feeling physical health or fitness improvements after making physical activity behavioural changes and increasing their practice of physical activity. The intervention programmes also affected the participants’ socially. Participants connected with and made new friends through the project, and also influenced their friends by sharing knowledge that they had gained from the intervention programmes with their friends. Moreover, the intervention programmes provided participants with more topics on which they could interact with their family members, enhancing family communication and harmony. Participants adopted healthy diet behaviours as well as physical activity behaviours together with their family members, and participants and their family members were mutually supportive of each other in making healthy behavioural changes.
The groups within the HD groups and the PA groups that had received WhatsApp reminder messages as well as a bring-home reminder tool (either a HD-themed table mat or a handgrip) found that the WhatsApp reminder messages were useful as a memory aid. The table mat was also a helpful tool for reminding about healthy diet behaviours. It also helped to enhance family members’ awareness and knowledge of healthy diet.
The focus group participants suggested that to encourage sustainability of the effects of the programmes, more programmes on the topics could be held, or e-message reminders similar to the WhatsApp reminders sent out by the programmes could be used. Several limitations of and suggestions were also highlighted. Participants felt felt that the programmes did not cover all of the health topics that they were interested in, and future programmes could cover a broader range of health topics and also incorporate a larger variety of activities. The questionnaires used for evaluation could be simplified, and better logistical arrangements could be made in terms of manpower in order to support more elderly participants. Nevertheless, should similar programmes be run in the future, participants would recommend the programme to others.
Overall, the results of the community-based focus groups showed that the intervention programmes were successful in improving participants’ health behaviours as well as their personal health and family health and harmony, supporting and enriching the findings of the quantitative evaluation.
170
CHAPTER 7 SHARING SESSION CUM AWARDS CEREMONY
7.1 Objectives As part of the FHHCPP, a Sharing Session cum Awards Ceremony was held in October 2016.
The main objectives were:
1. To acknowledge the Health Ambassadors’ involvement in the design and implementation of the community-based programme;
2. To acknowledge the Health Ambassadors and community-based participants’ fitness progress;
3. To assess attendees’ healthy diet and physical activity behaviours and attitudes, as well as FAMILY 3Hs;
4. To provide a platform for community leaders and stakeholders, Health Ambassadors, and community-based participants to share their personal experiences and thoughts regarding the project and its effects on the community, their families, and themselves; and
5. To encourage attendees to keep working toward healthier lifestyles in order to achieve FAMILY 3Hs.
7.2 Ceremony summary The Sharing Session cum Awards Ceremony was held on 2 October 2016 at the Hong Kong Convention and Exhibition Centre in Wan Chai. The event was open to the general public and invited guests. About 800 people attended the event.
Amongst those in attendance as officiating guests of honour were Mrs. Leung Tong Ching-yee Regina, Spouse of the Chief Executive of Hong Kong; Dr. Ko Wing-man, Secretary for Food and Health; Ms. Song Wei, Deputy Head of the Liason Office of the Central People’s Government in the Hong Kong Special Administrative Region; Ms. Chan Imelda, Executive Manager of Charities of the Hong Kong Jockey Club Charities Trust; Ms. Ip Lau Suk-yee Regina, Non-official Member of the Executive Council and Legislative Council Member; Hon. Kwok Wai-keung, Legislative Council Member; Hon. Cheung Kwok-kwan Horace, Legislative Council Member; Mrs. Cheung Nga-lai, Chair of the HKIWA; and Professor Lam Tai Hing, Chair Professor of Community Medicine, Sir Robert Kotewall Professor in Public Health, and Principal Investigator of the FAMILY Project, HKU-SPH.
Upon arrival and registration, attendees were greeted with many display boards showing photos and from and summaries of the results of the core sessions and booster sessions of the community-based family intervention programme. Photo props were placed around the venue and attendees were invited to take photos using the colourful props. A special photograph area with a large frame was set up. Attendees were invited to have physical
171
fitness measurements taken by the FAMILY Project Team for their own reference, and attendees who did so were given small souvenirs.
Inside the hall, speeches were given by Mrs. Cheung, Dr. Ko, and Ms. Chan. All praised the FHHCPP highly, and highlighted the successes of the project as well as the contributions to society. Experiences regarding the benefits of healthy diet and physical activity were also shared. An athlete from the 2016 Paralympic Games, So Wah Wai, was invited for an interview on stage, and he talked about the importance of a healthy diet and sufficient physical activity, not just for physical fitness but for mental well-being. Professor Lam also delivered a short talk on the benefits of ZTEx as a form of simple physical activity.
The Health Ambassadors were recognised, acknowledged and awarded. The top performing groups in terms of body weight loss were also recognised and awarded. The Health Ambassadors as well as community-based family intervention programme participants were given the opportunity to share their experiences of the programme, with many sharing anecdotes about not just the positive effect the programme had on their personal health but also on their family members’ health and the well-being, happiness, health, and harmony of their family as a unit.
Before leaving the Sharing Session cum Awards Ceremony, attendees were invited to complete a one-page questionnaire regarding their healthy diet and physical activity behaviours and attitudes, as well as FAMILY 3Hs. Each attendee also received a memorial tote bag with the project logo, as well as a souvenir towel.
7.3 Statistical analyses and results A total of 169 questionnaires were collected at the Sharing Session cum Awards Ceremony; of these, 155 were valid.
7.3.1 Demographic characteristics The demographic characteristics of the respondents are presented in Table 7.1.
The majority (89.1%) were female, and most were aged 50 years or above, 42.4% were educated to primary level or below, whilst almost half (49.7%) were educated to secondary level. About three-quarters (73.4%) were married, and about half were homemakers (48.3%).
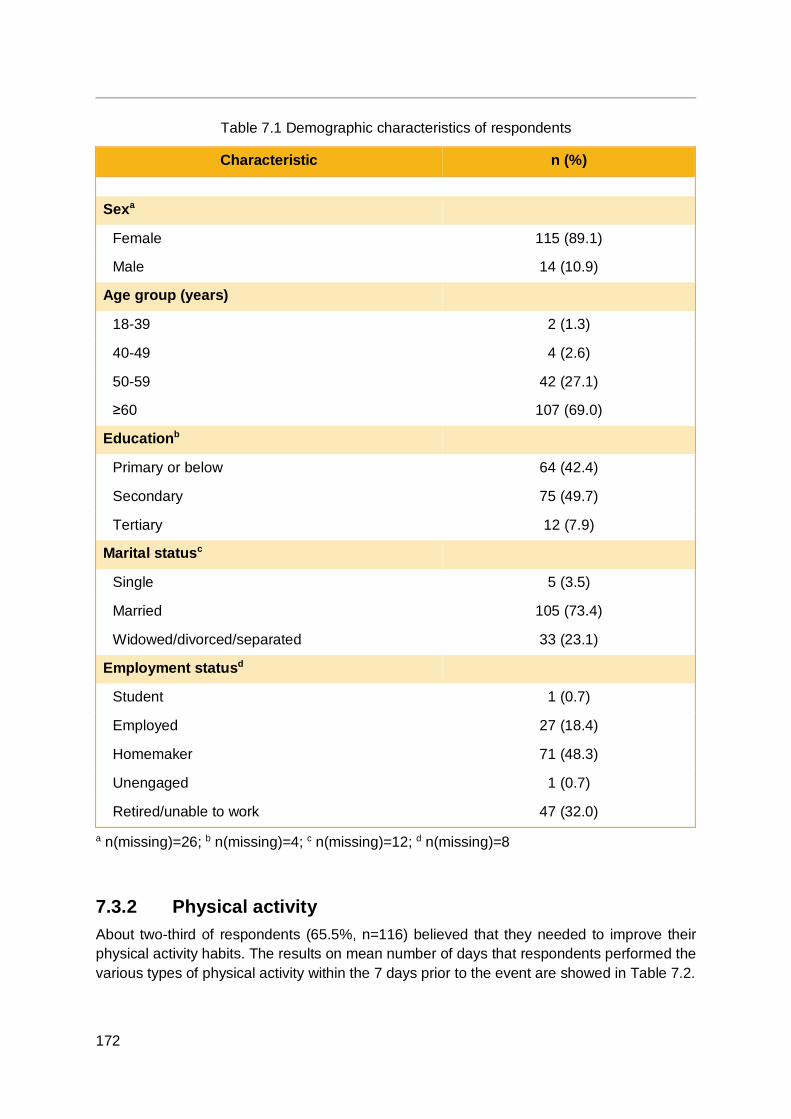
172
Table 7.1 Demographic characteristics of respondents
Characteristic n (%) Sexa
Female 115 (89.1)
Male 14 (10.9)
Age group (years)
18-39 2 (1.3)
40-49 4 (2.6)
50-59 42 (27.1)
≥60 107 (69.0)
Educationb
Primary or below 64 (42.4)
Secondary 75 (49.7)
Tertiary 12 (7.9)
Marital statusc
Single 5 (3.5)
Married 105 (73.4)
Widowed/divorced/separated 33 (23.1)
Employment statusd
Student 1 (0.7)
Employed 27 (18.4)
Homemaker 71 (48.3)
Unengaged 1 (0.7)
Retired/unable to work 47 (32.0)
a n(missing)=26; b n(missing)=4; c n(missing)=12; d n(missing)=8
7.3.2 Physical activity About two-third of respondents (65.5%, n=116) believed that they needed to improve their physical activity habits. The results on mean number of days that respondents performed the various types of physical activity within the 7 days prior to the event are showed in Table 7.2.
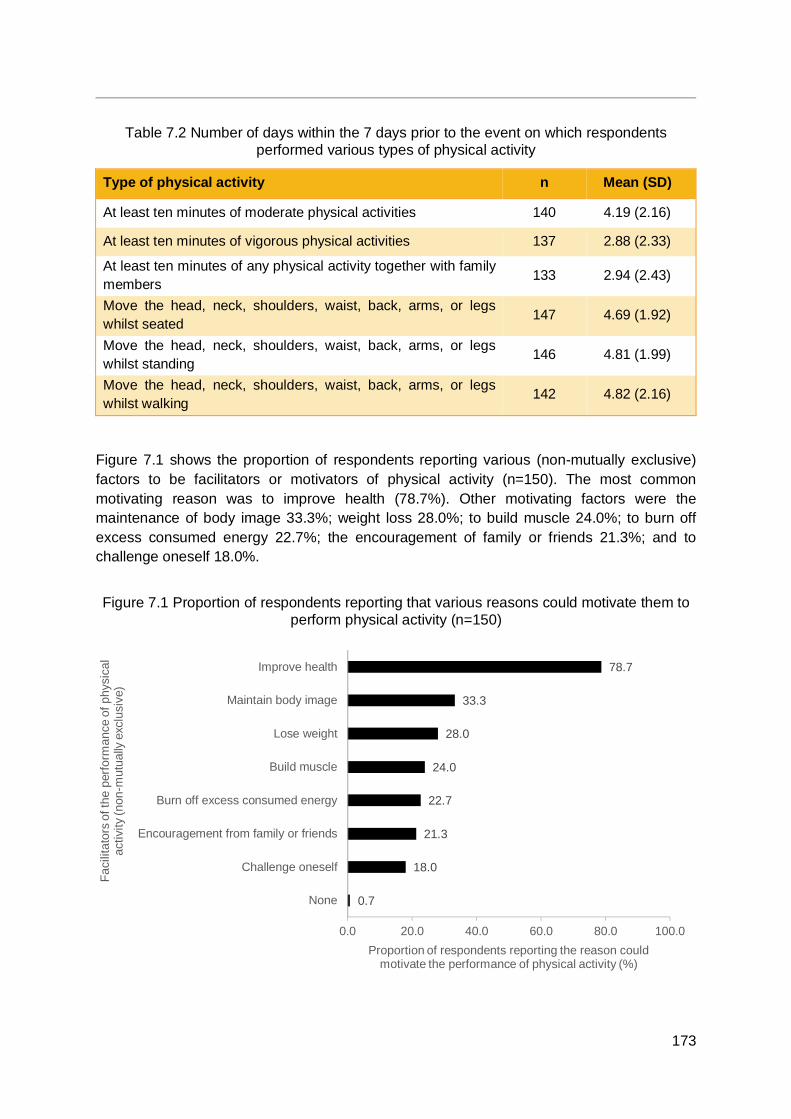
173
Table 7.2 Number of days within the 7 days prior to the event on which respondents performed various types of physical activity
Type of physical activity n Mean (SD)
At least ten minutes of moderate physical activities 140 4.19 (2.16)
At least ten minutes of vigorous physical activities 137 2.88 (2.33)
At least ten minutes of any physical activity together with family members 133 2.94 (2.43)
Move the head, neck, shoulders, waist, back, arms, or legs whilst seated 147 4.69 (1.92)
Move the head, neck, shoulders, waist, back, arms, or legs whilst standing
146 4.81 (1.99)
Move the head, neck, shoulders, waist, back, arms, or legs whilst walking
142 4.82 (2.16)
Figure 7.1 shows the proportion of respondents reporting various (non-mutually exclusive) factors to be facilitators or motivators of physical activity (n=150). The most common motivating reason was to improve health (78.7%). Other motivating factors were the maintenance of body image 33.3%; weight loss 28.0%; to build muscle 24.0%; to burn off excess consumed energy 22.7%; the encouragement of family or friends 21.3%; and to challenge oneself 18.0%.
Figure 7.1 Proportion of respondents reporting that various reasons could motivate them to perform physical activity (n=150)
0.7
18.0
21.3
22.7
24.0
28.0
33.3
78.7
0.0 20.0 40.0 60.0 80.0 100.0
None
Challenge oneself
Encouragement from family or friends
Burn off excess consumed energy
Build muscle
Lose weight
Maintain body image
Improve health
Proportion of respondents reporting the reason couldmotivate the performance of physical activity (%)
Faci
litat
ors
of th
e pe
rform
ance
of p
hysi
cal
activ
ity (n
on-m
utua
lly e
xclu
sive
)
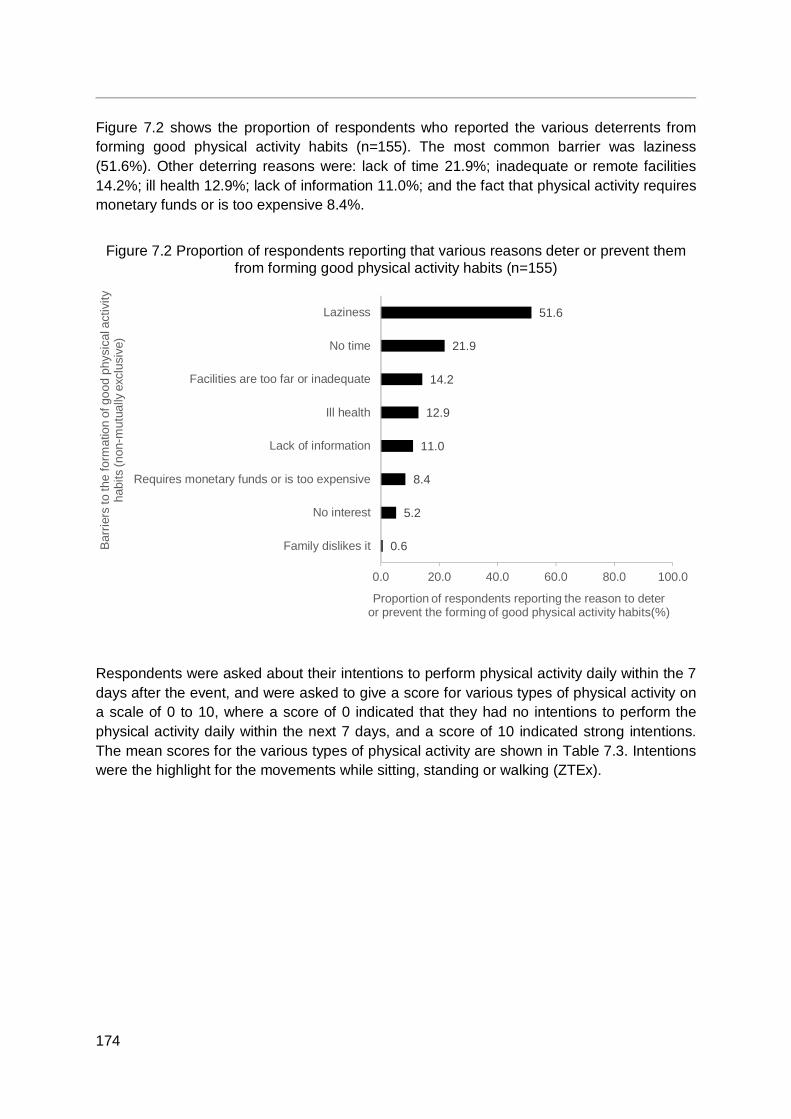
174
Figure 7.2 shows the proportion of respondents who reported the various deterrents from forming good physical activity habits (n=155). The most common barrier was laziness (51.6%). Other deterring reasons were: lack of time 21.9%; inadequate or remote facilities 14.2%; ill health 12.9%; lack of information 11.0%; and the fact that physical activity requires monetary funds or is too expensive 8.4%.
Figure 7.2 Proportion of respondents reporting that various reasons deter or prevent them from forming good physical activity habits (n=155)
Respondents were asked about their intentions to perform physical activity daily within the 7 days after the event, and were asked to give a score for various types of physical activity on a scale of 0 to 10, where a score of 0 indicated that they had no intentions to perform the physical activity daily within the next 7 days, and a score of 10 indicated strong intentions. The mean scores for the various types of physical activity are shown in Table 7.3. Intentions were the highlight for the movements while sitting, standing or walking (ZTEx).
0.6
5.2
8.4
11.0
12.9
14.2
21.9
51.6
0.0 20.0 40.0 60.0 80.0 100.0
Family dislikes it
No interest
Requires monetary funds or is too expensive
Lack of information
Ill health
Facilities are too far or inadequate
No time
Laziness
Proportion of respondents reporting the reason to deteror prevent the forming of good physical activity habits(%)
Barr
iers
to th
e fo
rmat
ion
of g
ood
phys
ical
act
ivity
ha
bits
(non
-mut
ually
exc
lusi
ve)

175
Table 7.3 Respondents’ intentions to perform various types of physical activity daily within the 7 days after the event
Type of physical activity n Mean (SD)
At least ten minutes of moderate physical activities 124 6.87 (2.68)
At least ten minutes of vigorous physical activities 122 5.83 (3.19)
At least ten minutes of any physical activity together with family members 118 5.58 (3.17)
Move the head, neck, shoulders, waist, back, arms, or legs whilst seated 121 7.27 (2.28)
Move the head, neck, shoulders, waist, back, arms, or legs whilst standing
122 7.27 (2.24)
Move the head, neck, shoulders, waist, back, arms, or legs whilst walking
121 7.11 (2.55)
7.3.3 Diet Three-quarters (75.2%, n=153) of respondents believed that they needed to improve their dietary habits.
Respondents were asked about the frequency with which they took notice of nutrition labels when purchasing pre-packed foods or drinks (n=148). About half (49.3%) frequently took notice of nutrition labels; 38.5% sometimes; 9.5% rarely; and only 2.7% never did so. Almost all (91.6%, n=154) reported that they needed to take notice of or take more notice of nutrition labels.
Respondents were also asked to rate the perceived importance of several dietary habits for health for the respondents’ personal health and the respondents’ family members’ health on a scale of 0 to 10, where a score of 0 indicated that they viewed the habit to be of no importance, and a score of 10 indicated extremely important. The mean scores were very high (9.03 to 9.22). (Table 7.4)
Table 7.4 Respondents’ perceived importance of dietary habits for personal and family members’ health
Dietary habit n Mean (SD)
Importance of a low-salt diet for personal health 129 9.03 (1.19)
Importance of a low-sugar diet for personal health 129 9.05 (1.20)
Importance of a low-salt, low-sugar diet for family members’ health 127 9.22 (1.13)
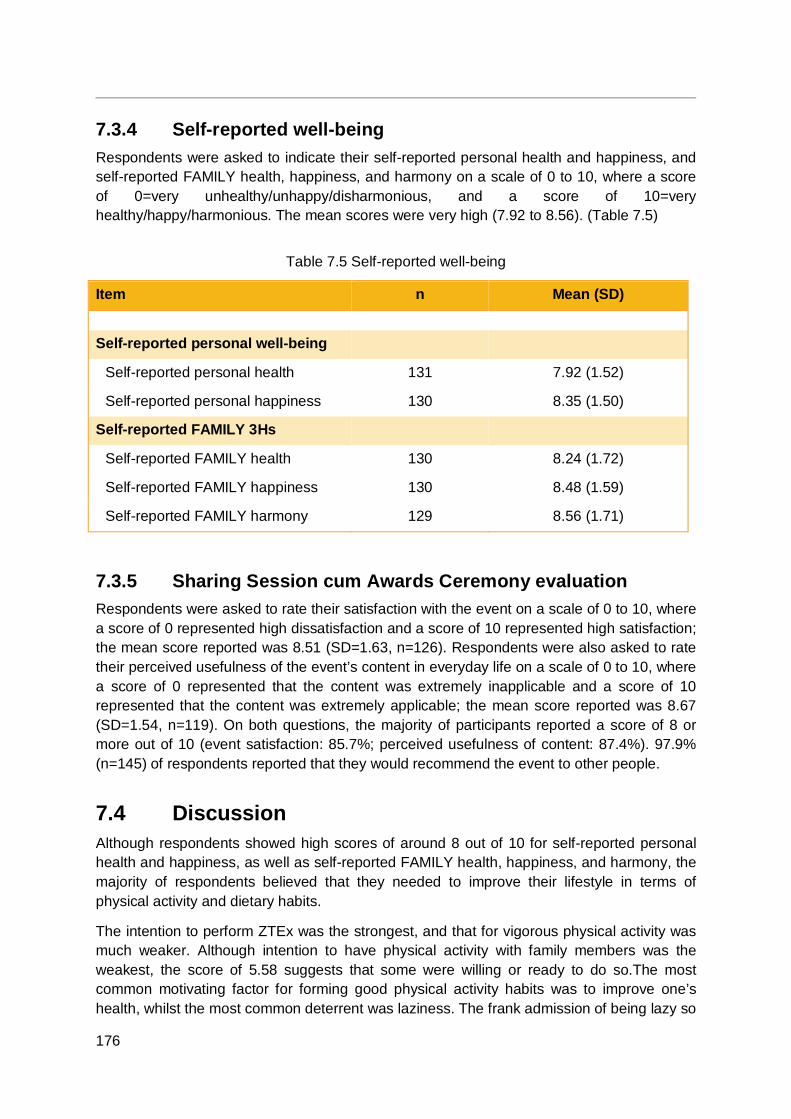
176
7.3.4 Self-reported well-being Respondents were asked to indicate their self-reported personal health and happiness, and self-reported FAMILY health, happiness, and harmony on a scale of 0 to 10, where a score of 0=very unhealthy/unhappy/disharmonious, and a score of 10=very healthy/happy/harmonious. The mean scores were very high (7.92 to 8.56). (Table 7.5)
Table 7.5 Self-reported well-being
Item n Mean (SD) Self-reported personal well-being
Self-reported personal health 131 7.92 (1.52)
Self-reported personal happiness 130 8.35 (1.50)
Self-reported FAMILY 3Hs
Self-reported FAMILY health 130 8.24 (1.72)
Self-reported FAMILY happiness 130 8.48 (1.59)
Self-reported FAMILY harmony 129 8.56 (1.71)
7.3.5 Sharing Session cum Awards Ceremony evaluation Respondents were asked to rate their satisfaction with the event on a scale of 0 to 10, where a score of 0 represented high dissatisfaction and a score of 10 represented high satisfaction; the mean score reported was 8.51 (SD=1.63, n=126). Respondents were also asked to rate their perceived usefulness of the event’s content in everyday life on a scale of 0 to 10, where a score of 0 represented that the content was extremely inapplicable and a score of 10 represented that the content was extremely applicable; the mean score reported was 8.67 (SD=1.54, n=119). On both questions, the majority of participants reported a score of 8 or more out of 10 (event satisfaction: 85.7%; perceived usefulness of content: 87.4%). 97.9% (n=145) of respondents reported that they would recommend the event to other people.
7.4 Discussion Although respondents showed high scores of around 8 out of 10 for self-reported personal health and happiness, as well as self-reported FAMILY health, happiness, and harmony, the majority of respondents believed that they needed to improve their lifestyle in terms of physical activity and dietary habits.
The intention to perform ZTEx was the strongest, and that for vigorous physical activity was much weaker. Although intention to have physical activity with family members was the weakest, the score of 5.58 suggests that some were willing or ready to do so.The most common motivating factor for forming good physical activity habits was to improve one’s health, whilst the most common deterrent was laziness. The frank admission of being lazy so
177
many highlights that future interventions on physical activity need to tackle and overcome participants’ laziness. ZTEx being easy, enjoyable and effective (3Es) could be a new approach and deserve further research and development.
Slightly more respondents believed that they needed to improve their dietary habits than physical activity. Almost all recognised that a low-salt or low-sugar diet as highly important for their personal and family health, and that they needed to note the nutrition labels when purchasing pre-packaged foods and drinks. These results indicate the need and the great potential for further interventions to promote a healthy low-sugar and low-saly diet in Hong Kong.
Due to the convenience sampling method, the possible effect of volunteer bias cannot be ruled out. The attendees of the event might be more health conscious and proactive about their health. Some of the respondents might have been community-based programme participants and Health Ambassadors who had received the project’s interventions and thus already had enhanced awareness about healthy physical activity and dietary habits.
7.5 Conclusions The Sharing Session cum Awards Ceremony of the FHHCPP successfully highlighted and celebrated the contributions of the Health Ambassadors in the design and implementation of the community-based programme, with display boards, videos, and speeches with appreciative and encouraging remarks on the community-based programme activities and the Health Ambassadors’ contributions and their acheivements.
Overall, attendees were very satisfied with the event and perceived its content to be useful and applicable in daily life. The key findings from the one-page questionnaire assessment were very useful for future developments of intervention programmes.

178
CHAPTER 8 RESULTS SHARING SESSION
8.1 Objectives As part of the FHHCPP, a Results Sharing Session was held in December 2016.
The main objectives were:
1. To acknowledge the hard work of the Health Ambassadors in implementing the community-based programme;
2. To share some preliminary findings with key community leaders within the HKIWA and the Health Ambassadors; and
3. To encourage attendees to keep working toward healthier lifestyles to enhance FAMILY 3Hs.
8.2 Session summary The Results Sharing Session was held on 18 December 2016 at HKU. The event was open for Health Ambassadors of the project as well as key community leaders within the HKIWA. About 100 people attended including the Chair, Vice-chairs, and Secretary-general of the HKIWA. Reporters from several daily news outlets, including Headline Daily (頭條日報), Hong Kong Commercial Daily (香港商報), Sing Tao Daily (星島日報), and Wen Wei Po (文匯
報) were also present.
To start, the Chair of the HKIWA, Mrs. Cheung Nga-lai, gave a short speech about the FHHCPP, highlighting that the project was one of the largest and most wide-reaching projects that the HKIWA had organised. Mrs. Cheung emphasised the importance of physical activity and healthy diets in her speech, and noted that one of the goals of the project was to encourage these behaviours amongst its grassroots participants.
Following Mrs. Cheung’s speech, some preliminary findings from the project’s TTA and community-based programme were presented by Professor Lam Tai Hing, Chair Professor of Community Medicine, Sir Robert Kotewall Professor in Public Health, and the Principal Investigator of the FAMILY Project, HKU-SPH. Preliminary and encouraging findings from the 3-month follow-up with community-based programme participants and from the 6-month follow-up with the Health Ambassadors were presented.
Backed by the findings that participants’ physical activity had increased, sugar consumption decreased, and FAMILY 3Hs increased, Professor Lam encouraged the attendees to keep working towards healthy lifestyles and FAMILY 3Hs by using physical activity and healthy diet as platforms to motivate family members and others. Professor Lam also highlighted the efforts of the Health Ambassadors in recruiting large numbers of participants for the community-based programme and in maintaining high retention rates throughout the programme. The high mean scores for satisfaction reported by community-based programme participants for the Core session and the Booster session were presented and were used to highlight and acknowledge the success of the Health Ambassadors in implementing the community-based programme.

179
At the conclusion of the Results Sharing Session, attendees were each given a souvenir tote bag printed with the project’s logo. Each tote bag contained a handgrip and a table mat featuring knowledge regarding healthy diet. Attendees also received a star-shaped foam stress ball that could double as a handgrip, as well as packets of red envelopes (or lai see). The souvenirs were met with enthusiasm, and many attendees asked for another.
Each of the news outlets that were present during the Results Sharing Sessionpublished an article on the FHHCPP on 22 December 2016, which could further publicise the project to the whole of Hong Kong.
180
CHAPTER 9 PROJECT EVALUATION
9.1 Qualitative evaluation: in-depth interviews
9.1.1 Introduction and objectives Upon the completion of all other programmes and events within the FHHCPP (addressed in Chapters 3 through 8), the FAMILY Project Team conducted in-depth interviews with several leaders and stakeholders within the HKIWA, including the Chair, the Vice-chairs (also Chairs of the various member associations of the HKIWA), and the Secretary-general. Member associations from all four districts (Central and Western, Eastern, Southern, and Wan Chai) involved in the project under the HKIWA were included. In-depth interviews were also conducted with members of the project’s working group from the HKIWA. The objectives of the in-depth interviews were as follows:
To explore the opinions of community leaders and working group members regarding the design and implementation of the project;
To capture any community or social impact of the FHHCPP; To collect suggestions regarding the dissemination of the project, its messages, and
its results; To collect comments for future improvements; and, To explore possible resources and support from the interviewees’ organisations for
similar projects in the future.
9.1.2 Methods A total of nine in-depth interviews were conducted. Participation was voluntary, and written consent was collected from the interviewees before the in-depth interviews began.
The interviews were semi-structured, and questions on the interview guide provided to the moderators and note-takers were open-ended and designed based on the overall objectives of the FHHCPP and the interviews. The interviews were conducted in Cantonese and audio-taped. Each interview lasted for about 60 minutes and was managed by a panel of one to two moderators and one note-taker from the FAMILY Project Team.
9.1.2.1 Data analysis All of the recordings of the in-depth interviews were transcribed verbatim in Cantonese, and the transcripts were double-checked against the tape recordings. The transcripts were analysed by thematic content analysis, following the guidelines recommended by Morse and Field [84], using the software NVivo 11.0. Each transcript was analysed sentence by sentence and coded for the respondents’ meanings. Open coding was performed, and the codes were subsequently organised into categories and integrated into themes within and across groups. Data comparisons within and between groups were also conducted. Field notes taken by the note-takers were continuously reviewed alongside the transcripts during the process.

181
9.1.3 Results
9.1.3.1 Sample characteristics A total of 18 community stakeholders or leaders within the HKIWA were interviewed. The interviewees could be grouped into two main categories: community leaders (n=16), and working group members (n=2). The community leaders included the Chairs, Vice-chairs, and Secretary-generals of the participating member associations as well as the HKIWA. The working group members interviewed were HKIWA staff memebers who worked closely with the FAMILY Project Team throughout the project.
The working group members were likely to have a more in-depth understanding overall of the project, including the difficulties experienced during the design and implementation stages, whilst the community leaders were likely to have a broader grasp on the community or societal effects of the project, and its future dissemination within districts and beyond. Community leaders of the HKIWA who were also leaders within their own member associations were also likely to have a more in-depth understanding of the specific difficulties their respective member association encountered during the project.
Table 9.1 shows that all of the interviewees were female and had been involved in the implementation of the FHHCPP. More than one-third were 40-49 years of age. Half were educated to tertiary level. About two-thirds had been members of the organisation or association they represented for more than 10 years.
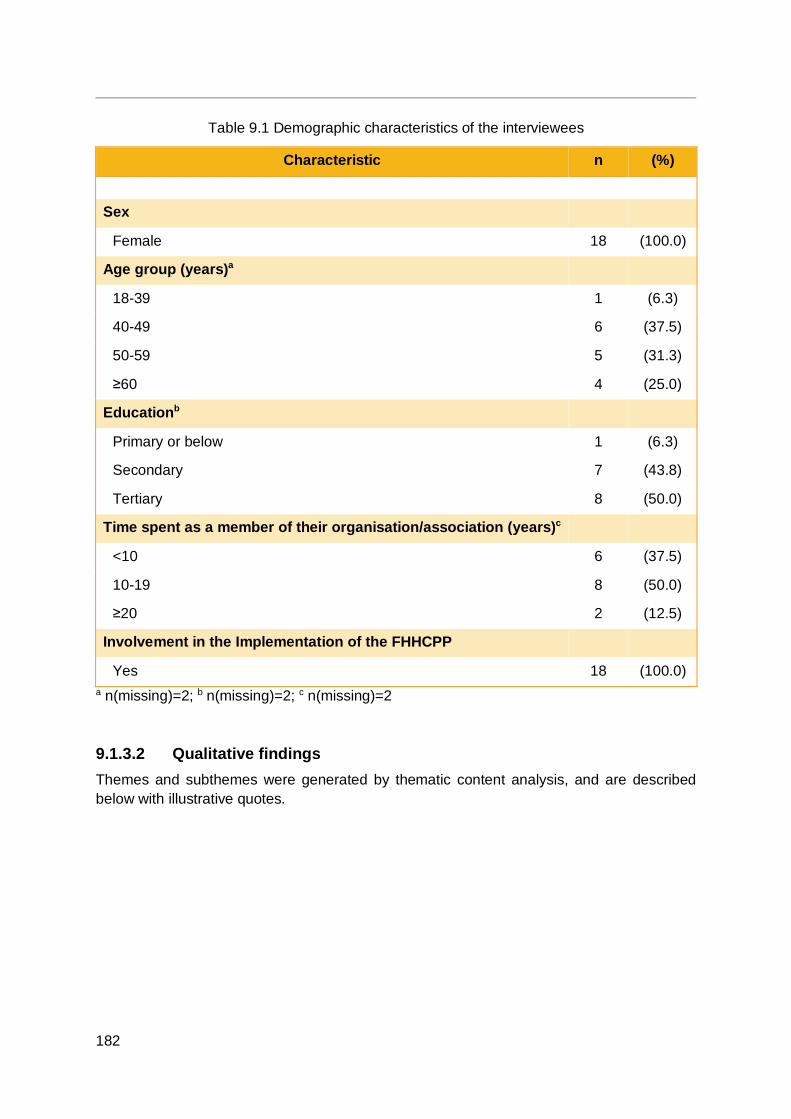
182
Table 9.1 Demographic characteristics of the interviewees
Characteristic n (%)
Sex
Female 18 (100.0)
Age group (years)a
18-39 1 (6.3)
40-49 6 (37.5)
50-59 5 (31.3)
≥60 4 (25.0)
Educationb
Primary or below 1 (6.3)
Secondary 7 (43.8)
Tertiary 8 (50.0)
Time spent as a member of their organisation/association (years)c
<10 6 (37.5)
10-19 8 (50.0)
≥20 2 (12.5)
Involvement in the Implementation of the FHHCPP
Yes 18 (100.0) a n(missing)=2; b n(missing)=2; c n(missing)=2
9.1.3.2 Qualitative findings Themes and subthemes were generated by thematic content analysis, and are described below with illustrative quotes.
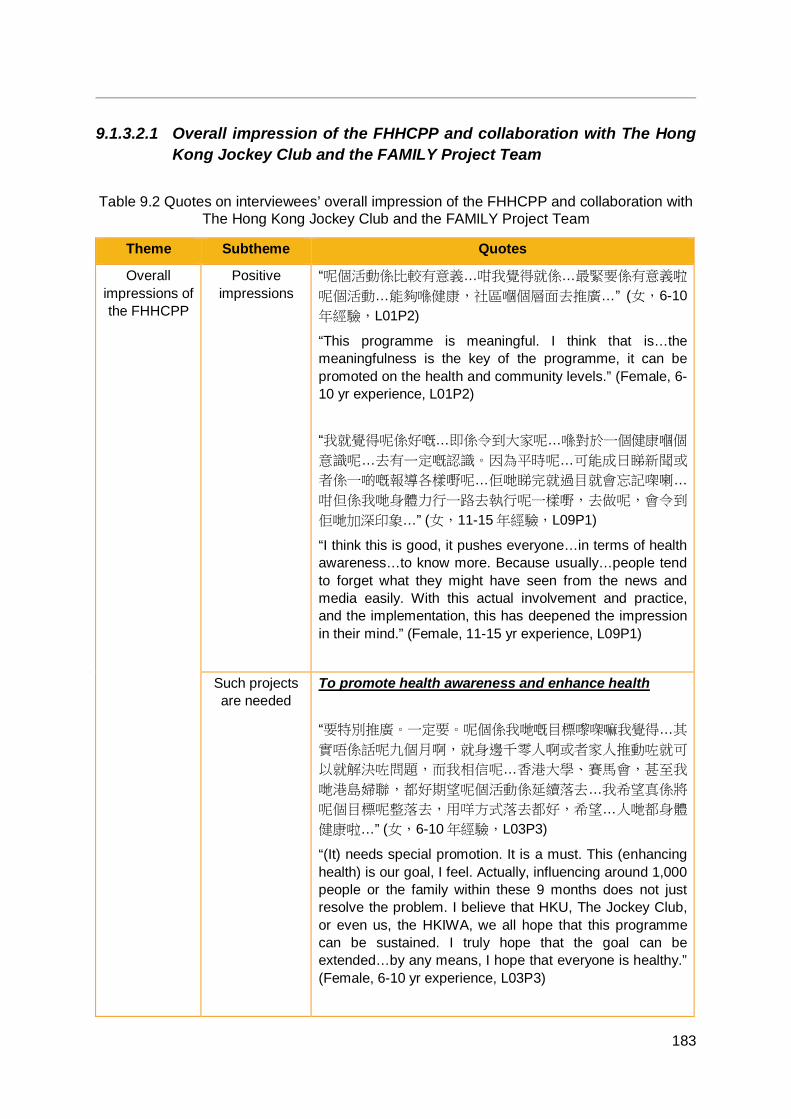
183
9.1.3.2.1 Overall impression of the FHHCPP and collaboration with The Hong Kong Jockey Club and the FAMILY Project Team
Table 9.2 Quotes on interviewees’ overall impression of the FHHCPP and collaboration with The Hong Kong Jockey Club and the FAMILY Project Team
Theme Subtheme Quotes
Overall impressions of the FHHCPP
Positive impressions
“呢個活動係比較有意義…咁我覺得就係…最緊要係有意義啦
呢個活動…能夠喺健康,社區嗰個層面去推廣…” (女,6-10年經驗,L01P2)
“This programme is meaningful. I think that is…the meaningfulness is the key of the programme, it can be promoted on the health and community levels.” (Female, 6-10 yr experience, L01P2) “我就覺得呢係好嘅…即係令到大家呢…喺對於一個健康嗰個
意識呢…去有一定嘅認識。因為平時呢…可能成日睇新聞或
者係一啲嘅報導各樣嘢呢…佢哋睇完就過目就會忘記㗎喇…
咁但係我哋身體力行一路去執行呢一樣嘢,去做呢,會令到
佢哋加深印象…” (女,11-15 年經驗,L09P1)
“I think this is good, it pushes everyone…in terms of health awareness…to know more. Because usually…people tend to forget what they might have seen from the news and media easily. With this actual involvement and practice, and the implementation, this has deepened the impression in their mind.” (Female, 11-15 yr experience, L09P1)
Such projects are needed
To promote health awareness and enhance health “要特別推廣。一定要。呢個係我哋嘅目標嚟㗎嘛我覺得…其
實唔係話呢九個月啊,就身邊千零人啊或者家人推動咗就可
以就解決咗問題,而我相信呢…香港大學、賽馬會,甚至我
哋港島婦聯,都好期望呢個活動係延續落去…我希望真係將
呢個目標呢整落去,用咩方式落去都好,希望…人哋都身體
健康啦…” (女,6-10 年經驗,L03P3)
“(It) needs special promotion. It is a must. This (enhancing health) is our goal, I feel. Actually, influencing around 1,000 people or the family within these 9 months does not just resolve the problem. I believe that HKU, The Jockey Club, or even us, the HKIWA, we all hope that this programme can be sustained. I truly hope that the goal can be extended…by any means, I hope that everyone is healthy.” (Female, 6-10 yr experience, L03P3)
184
Theme Subtheme Quotes To enhance interpersonal relationships and societal harmony “多咗一啲共同嘅話題,咁成個 family 成個家庭就會容易
啲,多啲溝通嘅嘢…咁正面咁樣溝通就大家會接受好多,咁
所以對於全香港嘅和諧穩定,其實呢啲活動我絕對覺得係好
好嘅…好 positive 嘅。” (女,6-10 年經驗,L04P2)
“Have more common topics, so the whole family, (its communication) becomes easier and more frequent…all of us accept positive communication like this. It brings positive impact to the societal harmony in Hong Kong, I absolutely think that such programme is excellent, very positive…” (Female, 6-10 yr experience, L04P2)
Collaboration with The Hong Kong Jockey Club and the
FAMILY Project Team
Positivity toward
collaborating with the FAMILY
Project Team
“呢一個活動我諗最大特色就係我哋都有講緊就係將學術研究
同埋呢地區服務呢兩樣嘢有個結合囉,一個實踐。即係以前
應該未試過嘅。” (女,5 年經驗或以下,L06P1)
“The combination of academic research and community service, the implementation, makes this programme unique. Never been tried before.” (Female, 5 yr or less experience, L06P1)
Gratitude shown by the
HKIWA toward the FAMILY
Project Team
“我都話,港大咁高嘅學府,係香港最高嘅學府,即係話作為
我哋喺地區基層嘅層面,能夠同港大合作搞活動,都係我哋
嘅一個榮譽。” (女,6-10 年經驗,L01P2)
“Like I have said, from us, a community level, having a chance to collaborate with HKU, a top university, the highest university in HK, is our honour.” (Female, 6-10 yr experience, L01P2)
“我哋都開心㗎。即係多謝港大搞一個咁嘅活動啦…” (女,
L01P1)
“We are happy, we appreciate that HKU conducted such a project.” (Female, L01P1)
Advantages Combination of research with community-based activities enhanced the HKIWA “我覺得婦聯搞呢個活動呢其實真係一個,對於我哋自己嚟
(講)係一個提升嘅…咁呢個係一年嘅,所以係,即係我覺
得,即係我哋自己…港大係一個學術研究啦,咁婦聯嘅話,
其實就係一個實踐,實踐方面…所以呢兩個係好好咁
185
Theme Subtheme Quotes combine 埋一齊咯…所以呢個係好特別咯。” (女,5 年經驗
或以下,W01P2)
“I think this programme that HKIWA organised is really a…for us, this is level-raising. In this year, I think, we…HKU is an academic research institution, HKIWA is about practice, the implementation…so this is a great combination, this is very special.” (Female, 5 yr or less experience, W01P2) HKU brand or reputation “因為我哋有個品牌係香港大學啦,香港大學嘅…即係大家都
好明白到香港大學呢個咁專業嘅、咁有權威性嘅機構、學校
嚟架嘛,咁依家我哋基層嘅婦女團體能夠同香港大學,即係
港島婦聯或者再屬下嘅團體能夠同香港大學推行呢一個運動
呢,都肯定好㗎啦…加上我哋係街頭嘅招募嘅時候,都有品
牌效應嘅。唔係我哋南區婦女嘅效應,而係香港大學做過呢
樣嘢嘅係會比較有呢個說服力囉。” (女,11-15 年經驗,
L03P6) “Because we have a brand, HKU, we all understand HKU is a professional institution, school with good authoritative reputation. Now our community-based women’s associations are able to (collaborate) with HKU…I mean HKIWA and its member associations implemented this programme with HKU…must be good…plus, when we were doing recruitment on street, there was a branding effect. Not the effect from our Southern district women association, but HKU who have done this before, it was more convincing.” (Female, 11-15 yr experience, L03P6) The FAMILY Project Team’s work standard “我覺得你哋比較有系統性,即係有成 set 嘢,即係有計
劃。” (女,6-10 年經驗,L02P1)
“I think you (FAMILY Project Team) is more systematic, that is, you have a set of materials, a plan.” (Female, 6-10 yr experience, L02P1)
186
Theme Subtheme Quotes The FAMILY Project Team provided sufficient resources and support Valuable information was provided “好㗎呢件事真係。能夠同你哋合作,將呢啲咁專業嘅訊息攞
到嚟我哋基層,先至係都受用,唔係單純係嗰啲知識分子或
者中產或者啲 好想健康嘅人,但係呢好多基層其實都好想知
嘅。” (女,11-15 年經驗,L03P6)
“It is truly a good thing...being able to cooperate with you, to bring these professional messages to our community, that’s beneficial. Not only the well-educated or middle-class or those who really want to be healthy want to know, but a lot of low-income people also very much want to know as well.” (Female, 11-15 yr experience, L03P6) Manpower support was provided at programmes “都覺得足夠…資源呢,你哋人手應該係 OK 嘅。” (女,16-20 年經驗,L07P1)
“There were enough…resources, the manpower you provided was fine.” (Female, 16-20 yr experience, L07P1) The HKIWA felt supported by the FAMILY Project Team in the working relationship “支援都夠嘅,即係港大嗰邊嘅支援呢,其實都好充足嘅,即
係我哋有啲咩問題呀,基本上你哋都俾到個 support 我哋。” (女,5 年經驗或以下,L06P1)
“The backup, the backup from HKU was sufficient, that is when we had enquiries, basically, you were able to provide support.” (Female, 5 yr or less experience, L06P1) Mutually beneficial collaboration “其實係好創新,咁就變咗有唔同嘅 party 呢…俾佢哋可以了
解到唔同 party 嘅運作囉,即係譬如 for 婦聯本身,我哋就可
以睇到呀原來係即係港大佢哋做嘢係點,係好緊密嘅,要求
好高嘅,咁俾返我哋自己會員睇到一個借鑒囉,亦都係一個
提升。咁可能 for 返你哋,你哋…可能都未話真係好可以係
…即係落區去做呢啲,亦都可以更加深入去對地區人士嗰種
187
Theme Subtheme Quotes 了解囉,所以呢個係一個好處,即係大家都係一個互相增
長,一個增值喺度。” (女,5 年經驗或以下,L06P1)
“This is innovative, several parties got involved, they could understand how different parties work. For instance, HKIWA could learn how HKU works in a programme, how detailed…with high standard. Our members saw it as a model, and an enhancement. From your side, you might not have a deep understanding about working with the community, so it is an advantage...for us to learn from each other, adding value.” (Female, 5 yr or less experience, L06P1) Funding support “資源又係馬會資源喎,馬會又好厲害啊嘛,喺香港嚟講係一
個有錢…” (女,6-10 年經驗,L01P2)
“Resources are provided by The Jockey Club, The Jockey Club is really great, has great resouces in Hong Kong…” (Female, 6-10 yr experience, L01P2)
Difficulties Cultural differences between the FAMILY Project Team and the HKIWA, member associations, or participants “其實即係優點亦都係困難嚟嘅,即係工作起身嘅時候呢,可
能會吃力少少啦,即係話譬如你哋嘅訊息可能落到去我哋地
區參加人士嘅時候我哋要用我哋,我哋要將一啲語言呢係少
少改變返,等地區人士係更加去了解究竟係咩嚟嘅,即係呢
一個,呢一個過程,即係所以港島婦聯嗰個角色喺呢度囉,
即係中間嗰個過程,點樣去可以順利咁樣去將訊息係交到俾
佢哋。” (女,5 年經驗或以下,L06P1)
“This is an advantage as well as a difficulty. During the implementation, it might be a bit hard. For example, when you wanted to send your messages to our participants in the community, we rephrased the messages to let them understand more easily. This is a process, this is the process where HKIWA took up the mediating role, to deliver the messages to the participants smoothly.” (Female, 5 yr or less experience, L06P1) Other difficulties “我覺得…挑戰我自己係我即係有好多不足啦…即係要就係學
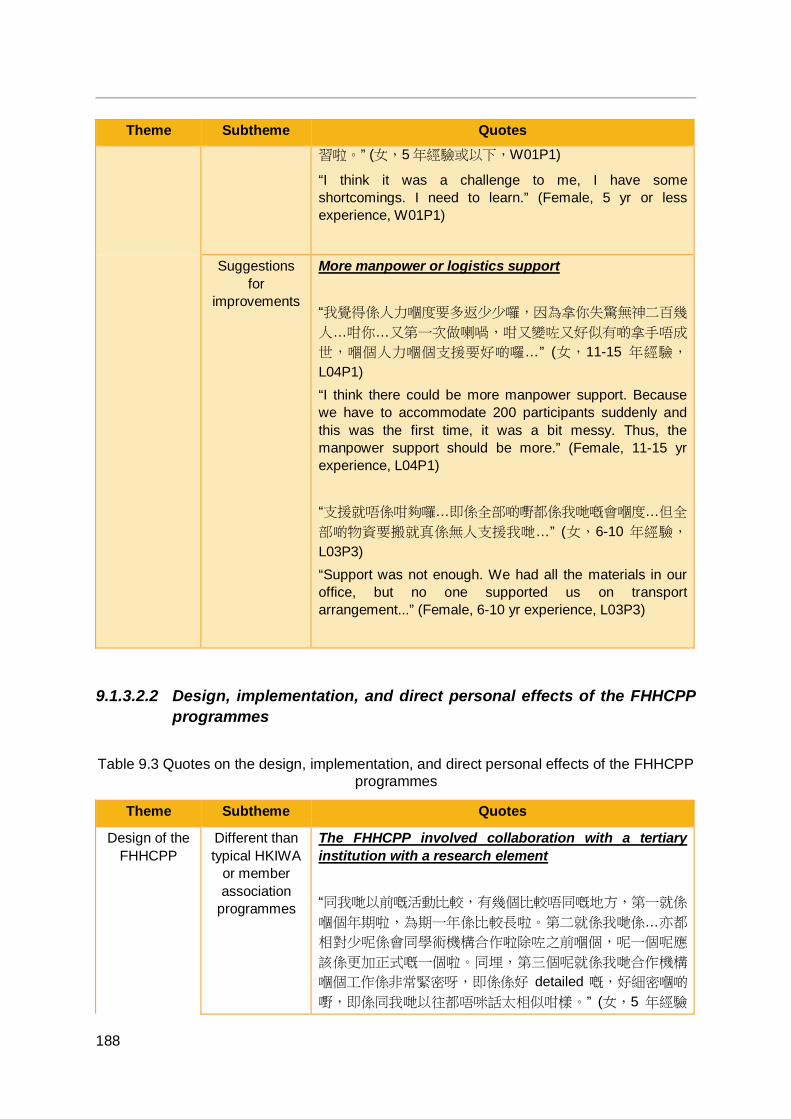
188
Theme Subtheme Quotes 習啦。” (女,5 年經驗或以下,W01P1)
“I think it was a challenge to me, I have some shortcomings. I need to learn.” (Female, 5 yr or less experience, W01P1)
Suggestions for
improvements
More manpower or logistics support “我覺得係人力嗰度要多返少少囉,因為拿你失驚無神二百幾
人…咁你…又第一次做喇喎,咁又變咗又好似有啲拿手唔成
世,嗰個人力嗰個支援要好啲囉…” (女,11-15 年經驗,
L04P1) “I think there could be more manpower support. Because we have to accommodate 200 participants suddenly and this was the first time, it was a bit messy. Thus, the manpower support should be more.” (Female, 11-15 yr experience, L04P1) “支援就唔係咁夠囉…即係全部啲嘢都係我哋嘅會嗰度…但全
部啲物資要搬就真係無人支援我哋…” (女,6-10 年經驗,
L03P3) “Support was not enough. We had all the materials in our office, but no one supported us on transport arrangement...” (Female, 6-10 yr experience, L03P3)
9.1.3.2.2 Design, implementation, and direct personal effects of the FHHCPP programmes
Table 9.3 Quotes on the design, implementation, and direct personal effects of the FHHCPP programmes
Theme Subtheme Quotes
Design of the FHHCPP
Different than typical HKIWA
or member association
programmes
The FHHCPP involved collaboration with a tertiary institution with a research element “同我哋以前嘅活動比較,有幾個比較唔同嘅地方,第一就係
嗰個年期啦,為期一年係比較長啦。第二就係我哋係…亦都
相對少呢係會同學術機構合作啦除咗之前嗰個,呢一個呢應
該係更加正式嘅一個啦。同埋,第三個呢就係我哋合作機構
嗰個工作係非常緊密呀,即係係好 detailed 嘅,好細密嗰啲
嘢,即係同我哋以往都唔咪話太相似咁樣。” (女,5 年經驗
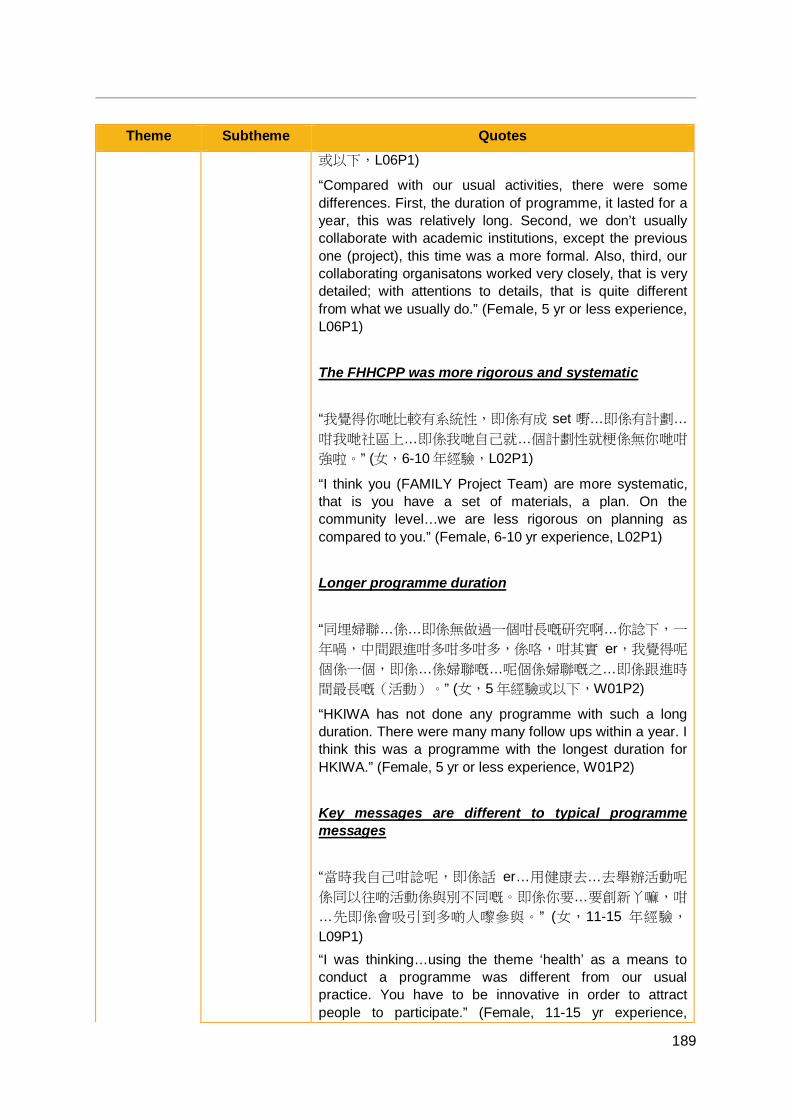
189
Theme Subtheme Quotes 或以下,L06P1)
“Compared with our usual activities, there were some differences. First, the duration of programme, it lasted for a year, this was relatively long. Second, we don’t usually collaborate with academic institutions, except the previous one (project), this time was a more formal. Also, third, our collaborating organisatons worked very closely, that is very detailed; with attentions to details, that is quite different from what we usually do.” (Female, 5 yr or less experience, L06P1) The FHHCPP was more rigorous and systematic “我覺得你哋比較有系統性,即係有成 set 嘢…即係有計劃…
咁我哋社區上…即係我哋自己就…個計劃性就梗係無你哋咁
強啦。” (女,6-10 年經驗,L02P1)
“I think you (FAMILY Project Team) are more systematic, that is you have a set of materials, a plan. On the community level…we are less rigorous on planning as compared to you.” (Female, 6-10 yr experience, L02P1) Longer programme duration “同埋婦聯…係…即係無做過一個咁長嘅研究啊…你諗下,一
年喎,中間跟進咁多咁多咁多,係咯,咁其實 er,我覺得呢
個係一個,即係…係婦聯嘅…呢個係婦聯嘅之…即係跟進時
間最長嘅(活動)。” (女,5 年經驗或以下,W01P2)
“HKIWA has not done any programme with such a long duration. There were many many follow ups within a year. I think this was a programme with the longest duration for HKIWA.” (Female, 5 yr or less experience, W01P2) Key messages are different to typical programme messages “當時我自己咁諗呢,即係話 er…用健康去…去舉辦活動呢
係同以往啲活動係與別不同嘅。即係你要…要創新丫嘛,咁
…先即係會吸引到多啲人嚟參與。” (女,11-15 年經驗,
L09P1) “I was thinking…using the theme ‘health’ as a means to conduct a programme was different from our usual practice. You have to be innovative in order to attract people to participate.” (Female, 11-15 yr experience,
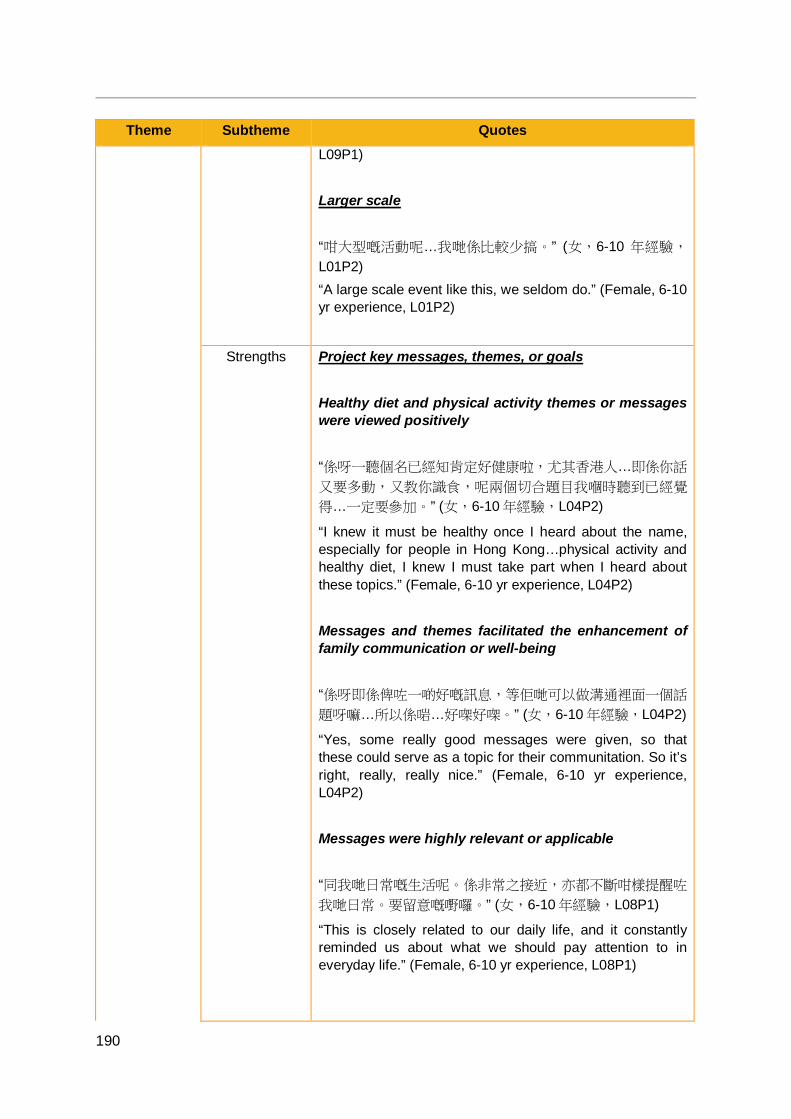
190
Theme Subtheme Quotes L09P1) Larger scale “咁大型嘅活動呢…我哋係比較少搞。” (女,6-10 年經驗,
L01P2) “A large scale event like this, we seldom do.” (Female, 6-10 yr experience, L01P2)
Strengths Project key messages, themes, or goals Healthy diet and physical activity themes or messages were viewed positively “係呀一聽個名已經知肯定好健康啦,尤其香港人…即係你話
又要多動,又教你識食,呢兩個切合題目我嗰時聽到已經覺
得…一定要參加。” (女,6-10 年經驗,L04P2)
“I knew it must be healthy once I heard about the name, especially for people in Hong Kong…physical activity and healthy diet, I knew I must take part when I heard about these topics.” (Female, 6-10 yr experience, L04P2) Messages and themes facilitated the enhancement of family communication or well-being “係呀即係俾咗一啲好嘅訊息,等佢哋可以做溝通裡面一個話
題呀嘛…所以係啱…好㗎好㗎。” (女,6-10 年經驗,L04P2)
“Yes, some really good messages were given, so that these could serve as a topic for their communitation. So it’s right, really, really nice.” (Female, 6-10 yr experience, L04P2) Messages were highly relevant or applicable “同我哋日常嘅生活呢。係非常之接近,亦都不斷咁樣提醒咗
我哋日常。要留意嘅嘢囉。” (女,6-10 年經驗,L08P1)
“This is closely related to our daily life, and it constantly reminded us about what we should pay attention to in everyday life.” (Female, 6-10 yr experience, L08P1)
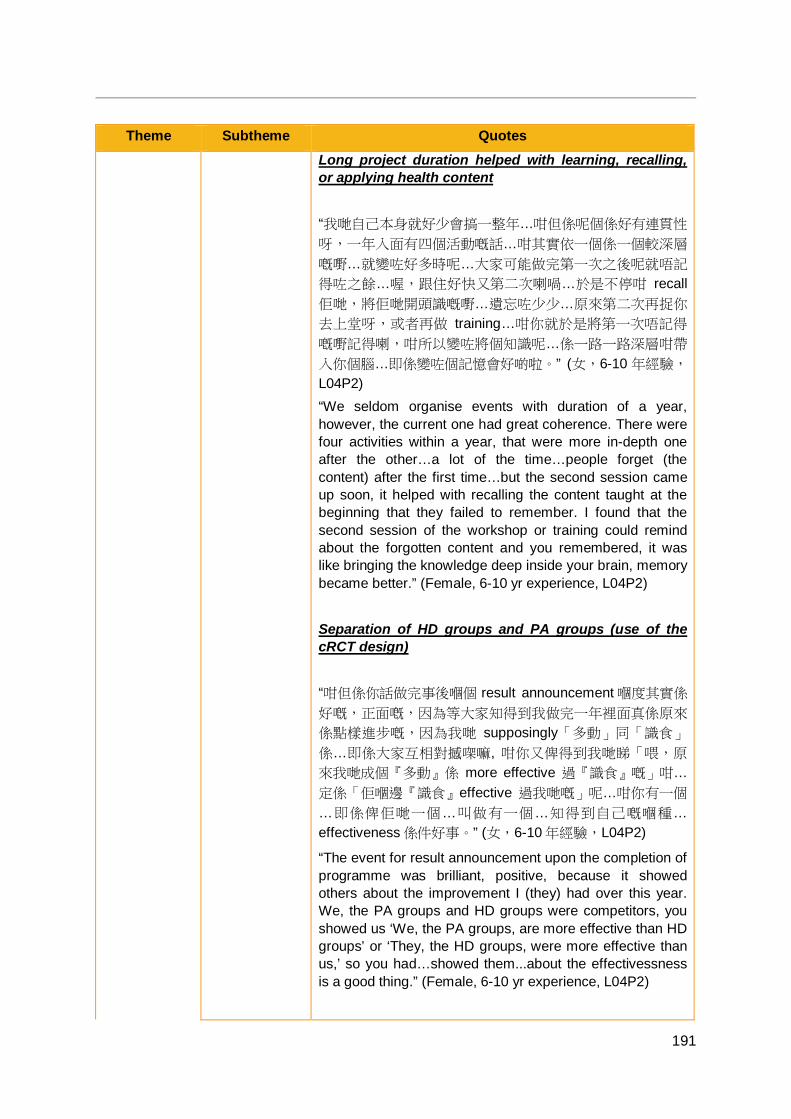
191
Theme Subtheme Quotes Long project duration helped with learning, recalling, or applying health content “我哋自己本身就好少會搞一整年…咁但係呢個係好有連貫性
呀,一年入面有四個活動嘅話…咁其實依一個係一個較深層
嘅嘢…就變咗好多時呢…大家可能做完第一次之後呢就唔記
得咗之餘…喔,跟住好快又第二次喇喎…於是不停咁 recall佢哋,將佢哋開頭識嘅嘢…遺忘咗少少…原來第二次再捉你
去上堂呀,或者再做 training…咁你就於是將第一次唔記得
嘅嘢記得喇,咁所以變咗將個知識呢…係一路一路深層咁帶
入你個腦…即係變咗個記憶會好啲啦。” (女,6-10 年經驗,
L04P2) “We seldom organise events with duration of a year, however, the current one had great coherence. There were four activities within a year, that were more in-depth one after the other…a lot of the time…people forget (the content) after the first time…but the second session came up soon, it helped with recalling the content taught at the beginning that they failed to remember. I found that the second session of the workshop or training could remind about the forgotten content and you remembered, it was like bringing the knowledge deep inside your brain, memory became better.” (Female, 6-10 yr experience, L04P2) Separation of HD groups and PA groups (use of the cRCT design) “咁但係你話做完事後嗰個 result announcement 嗰度其實係
好嘅,正面嘅,因為等大家知得到我做完一年裡面真係原來
係點樣進步嘅,因為我哋 supposingly「多動」同「識食」
係…即係大家互相對撼㗎嘛, 咁你又俾得到我哋睇「喂,原
來我哋成個『多動』係 more effective 過『識食』嘅」咁…
定係「佢嗰邊『識食』effective 過我哋嘅」呢…咁你有一個
…即係俾佢哋一個…叫做有一個…知得到自己嘅嗰種…
effectiveness 係件好事。” (女,6-10 年經驗,L04P2)
“The event for result announcement upon the completion of programme was brilliant, positive, because it showed others about the improvement I (they) had over this year. We, the PA groups and HD groups were competitors, you showed us ‘We, the PA groups, are more effective than HD groups’ or ‘They, the HD groups, were more effective than us,’ so you had…showed them...about the effectivessness is a good thing.” (Female, 6-10 yr experience, L04P2)
192
Theme Subtheme Quotes Systematic approach “因為我哋義工係彈性處理嘅,亦都係持續性嘅,係你做咗我
哋義工,我哋每一個活動都歡迎你嚟參加,歡迎你俾意見,
但係呢就無規定你要出席啊,無規定你咁多,即係無規定你
…你要做啲乜嘢,但今次係有系統嘅。” (女,6-10 年經驗,
L08P1) “We handle our (HKIWA) volunteers with flexibility, and it is a sustained (programme). When you become our volunteer, we welcome your participation on every single occasion, welcome your suggestions, but there is no compulsory attendance. We don’t have many rules, that is not many rules about what you need to do, but this time, it was systematic.” (Female, 6-10 yr experience, L08P1)
Limitations Sample size was too rigid “我覺得可能你哋嘅計算方法…嘅問題,我哋都認同,即係都
係會配合嘅,但係我覺得譬如話我哋主要嘅目的呢…係希望
更多嘅人唔係千六囉,係更多人嘅。” (女,6-10 年經驗,
L08P1) “I think it was maybe a calculation issue. We agreed and accommodated, but if this is the primary goal…to reach more people, not just 1600, but more people.” (Female, 6-10 yr experience, L08P1)
Suggestions for
improvements
More programmes “真係要加多少少嘅活動落去會比較好少少囉…太過長嘅時候
呢,一定要有啲嘢俾佢哋做呢、玩呢,佢先至有嗰個參與能
力…即強啲囉…” (女,20 年經驗或以上,L03P1)
“More programmes should be included and it would be better. Long duration programmes must include more activities for them to participate in, to play, so they have stronger sense of participation.” (Female, 20 yr or more experience, L03P1) “我覺得攪多個 programme 囉。” (女,6-10 年經驗,L08P1)
“Orgainise more programmes.” (Female, 6-10 yr experience, L08P1)
193
Theme Subtheme Quotes Increase reach using a snowballing approach “我反而覺得可以做一樣嘢…一人帶一人嘅運動…「你身邊有
邊個你覺得值得推薦佢…一齊過嚟聽嚟個分享會㗎?」…咁
令到佢都覺得「原來我呢唔單止係我」,佢個潛意識都知
「唔單止我自己受惠喎,其實我應該留意吓我身邊有邊個
人,我係值得帶埋佢嚟嘅,或者可以帶我個孫,我個孫女都
因為呢個活動佢都受惠嘅,咁呢可以帶過嚟」…咁你話一人
帶一人嘅運動,已經好快將你嗰個(受惠人數)已經係
double 咗啦。” (女,6-10 年經驗,L08P1)
“I think there is one thing that can be done…a snowballing approach to the programme…‘who would you recommend to come with you to the Sharing Session?’, this brings them an awareness that ‘I am not alone’, they have in mind that ‘it is not only beneficial to myself, but I should also pay attention to the people around me, who should I bring in, maybe I can bring my grandchild. My granddaughter benefitted from the activity, so I can bring her,’… the snowballing approach can double the number of people benefitted really quickly.” (Female, 6-10 yr experience, L08P1) Different topics Mental health “我哋係想做多啲係同心靈嘅。即係譬如話係…即係香港可能
好多人情緒問題呀嗰類,可能會係從呢一方面去走轉…雖然
你(「多動」、「識食」)都係令人開心啲都會有,但係始
終可能個 focus 可能再去多啲真係 focus 返喺即係
psychological 嗰方面會好啲。” (女,5 年經驗或以下,
L06P1) “We want to have some programmes for the mind. For instance, there may be quite a lot of people in Hong Kong suffering from mood problems, maybe we can start from this perspective...although yours (PA, HD) are also intended to make people happy. But we can turn the focus…to have the main focus on psychological perspective might be better.” (Female, 5 yr or less experience, L06P1)
The HKIWA’s experience
The HKIWA’s goals for the
“大家真係想做好呢件事囉,咁變成好多潛意識入邊已經係揸
到個目標。” (女,6-10 年經驗,L08P1)
194
Theme Subtheme Quotes FHHCPP “We really wanted to do this well, so we unconsciously had
a clear target to hold on to.” (Female, 6-10 yr experience, L08P1) “好㗎呢件事真係。能夠同你哋合作,將呢啲咁專業嘅訊息落
到嚟我哋基層,先至係都受用,唔係單純係嗰啲知識分子或
者中產或者啲…好想健康嘅人,但係呢好多基層其實都好想
知嘅…唔通過熟悉呢個活動,根本你唔知…其實出呢啲慢慢
去潛移默化去推廣先至係我哋嘅目標。” (女,11-15 年經
驗,L03P6)
“It is truly a good thing...being able to cooperate with you, to bring these professional messages to our community, that’s beneficial. Not only the well-educated or middle-class or those who really want to be healthy want to know, but a lot of low-income people also very much want to know as well. Without knowing about this programme, I wouldn’t know…to promote, change and influence gradually and imperceptibly is our goal.” (Female, 11-15 yr experience, L03P6)
The HKIWA’s role within FHHCPP
Facilitating and supporting member associations and Health Ambassadors Coordinating member associations “都一個統籌啦,一個領導啦。” (女,5 年經驗或以下,
L06P1) “(HKIWA) was a co-ordinator, a leader.” (Female, 5 yr or less experience, L06P1) Providing HKIWA’s perspective and resources “其實我哋秘書處呢,對佢哋好大嘅協助嘅…我哋同佢哋…其
實佢哋去按照佢哋提出嘅意見,或者我有啲咩諗法…我哋都
會提供啲唔同嘅意見,一齊去參與囉。” (女,6-10 年經驗,
L08P1) “Actually, our Secretariat, offered them (the member assications) a lot of assistance, with them, we…they gave their opinions, or maybe I had mine…we provided different opinions, and participated together.” (Female, 6-10 yr experience, L08P1)
195
Theme Subtheme Quotes “除咗預算之外,其實仲有好多我哋可以資助佢有啲咩材料
啊,或者我哋有啲咩專業意見可以提供俾佢呀。” (女,6-10年經驗,L08P1)
“Apart from the budget, actually there was a lot that we could subsidise; maybe we could provide some professional advices.” (Female, 6-10 yr experience, L08P1) Encouraging or comforting Health Ambassadors “當佢哋有啲唔同嘅意見嘅時候或者唔同嘅諗法,有陣時都會
有情緒波動嘅時候,我哋就係去幫佢,一個緩和啦。” (女,
6-10 年經驗,L08P1)
“When they had different suggestions or different thoughts, sometimes they got emotional; we helped them to alleviate this.” (Female, 6-10 yr experience, L08P1) Liaising between HKU and Health Ambassadors “呢啲(活動安排)所以就係我哋中間人嘅(挑戰)…即係…
其實都可以話一個餅乾夾…係喇,夾心餅你中間嗰度嘅…係
喇,其實呢個溝通…其實我哋嘅…點解話我哋…即係婦聯嘅
作用喺呢度,其實婦聯一直都係呢個角色嘅…無論係各區咁
樣嘅,因為我哋都係一個中間統籌嘅角色…我哋都要同你哋
溝通咁交返俾下面嘅,下面嘅一個好清晰嘅話俾佢知。” (女,5 年經驗或以下,W01P2)
“The arrangement became the challenge for us, the mediator. It was like a sandwich biscuit, the filling of it…yes…the communication, actually our…the function of HKIWA was there…actually HKIWA have been taking up this role, of all districts, because we were the coordinator, we had to communicate with you and then get clear instructions to pass on to the member associations.” (Female, 5 yr or less experience, W01P2)
Working relationship
with member associations and Health
Ambassadors
Non-hierarchical dynamic between the HKIWA and member associations and Health Ambassadors “其實雖然話屬會咁咯…其實我哋係平級㗎嘛…唔係嗰啲上下
級嘅關係嘅…佢唔玩就走㗎啦,我唔 buy 你,我就唔玩㗎
啦。” (女,5 年經驗或以下,W01P2)
“They are named as member associations, but we are equal, it is not a hierarchical relationship…if they don’t take
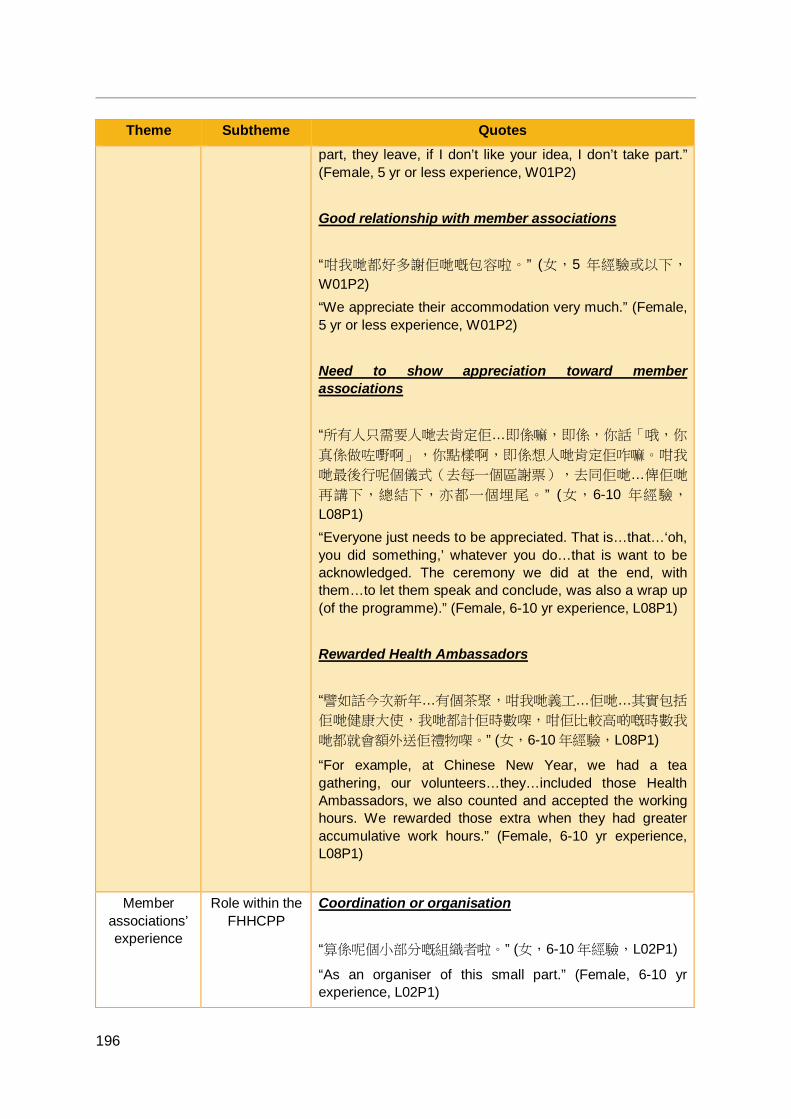
196
Theme Subtheme Quotes part, they leave, if I don’t like your idea, I don’t take part.” (Female, 5 yr or less experience, W01P2) Good relationship with member associations “咁我哋都好多謝佢哋嘅包容啦。” (女,5 年經驗或以下,
W01P2) “We appreciate their accommodation very much.” (Female, 5 yr or less experience, W01P2) Need to show appreciation toward member associations “所有人只需要人哋去肯定佢…即係嘛,即係,你話「哦,你
真係做咗嘢啊」,你點樣啊,即係想人哋肯定佢咋嘛。咁我
哋最後行呢個儀式(去每一個區謝票),去同佢哋…俾佢哋
再講下,總結下,亦都一個埋尾。” (女,6-10 年經驗,
L08P1) “Everyone just needs to be appreciated. That is…that…‘oh, you did something,’ whatever you do…that is want to be acknowledged. The ceremony we did at the end, with them…to let them speak and conclude, was also a wrap up (of the programme).” (Female, 6-10 yr experience, L08P1) Rewarded Health Ambassadors “譬如話今次新年…有個茶聚,咁我哋義工…佢哋…其實包括
佢哋健康大使,我哋都計佢時數㗎,咁佢比較高啲嘅時數我
哋都就會額外送佢禮物㗎。” (女,6-10 年經驗,L08P1)
“For example, at Chinese New Year, we had a tea gathering, our volunteers…they…included those Health Ambassadors, we also counted and accepted the working hours. We rewarded those extra when they had greater accumulative work hours.” (Female, 6-10 yr experience, L08P1)
Member associations’ experience
Role within the FHHCPP
Coordination or organisation “算係呢個小部分嘅組織者啦。” (女,6-10 年經驗,L02P1)
“As an organiser of this small part.” (Female, 6-10 yr experience, L02P1)
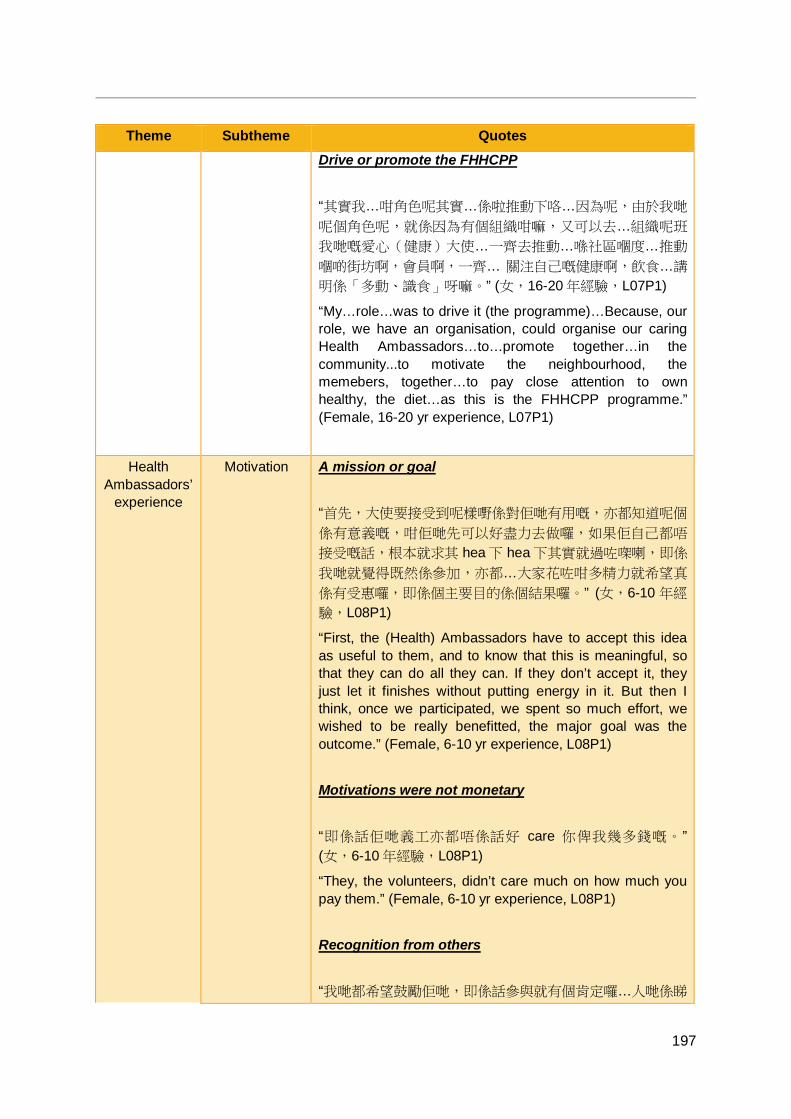
197
Theme Subtheme Quotes Drive or promote the FHHCPP “其實我…咁角色呢其實…係啦推動下咯…因為呢,由於我哋
呢個角色呢,就係因為有個組織咁嘛,又可以去…組織呢班
我哋嘅愛心(健康)大使…一齊去推動…喺社區嗰度…推動
嗰啲街坊啊,會員啊,一齊… 關注自己嘅健康啊,飲食…講
明係「多動、識食」呀嘛。” (女,16-20 年經驗,L07P1)
“My…role…was to drive it (the programme)…Because, our role, we have an organisation, could organise our caring Health Ambassadors…to…promote together…in the community...to motivate the neighbourhood, the memebers, together…to pay close attention to own healthy, the diet…as this is the FHHCPP programme.” (Female, 16-20 yr experience, L07P1)
Health Ambassadors’
experience
Motivation A mission or goal “首先,大使要接受到呢樣嘢係對佢哋有用嘅,亦都知道呢個
係有意義嘅,咁佢哋先可以好盡力去做囉,如果佢自己都唔
接受嘅話,根本就求其 hea 下 hea 下其實就過咗㗎喇,即係
我哋就覺得既然係參加,亦都…大家花咗咁多精力就希望真
係有受惠囉,即係個主要目的係個結果囉。” (女,6-10 年經
驗,L08P1)
“First, the (Health) Ambassadors have to accept this idea as useful to them, and to know that this is meaningful, so that they can do all they can. If they don’t accept it, they just let it finishes without putting energy in it. But then I think, once we participated, we spent so much effort, we wished to be really benefitted, the major goal was the outcome.” (Female, 6-10 yr experience, L08P1) Motivations were not monetary “即係話佢哋義工亦都唔係話好 care 你俾我幾多錢嘅。” (女,6-10 年經驗,L08P1)
“They, the volunteers, didn’t care much on how much you pay them.” (Female, 6-10 yr experience, L08P1) Recognition from others “我哋都希望鼓勵佢哋,即係話參與就有個肯定囉…人哋係睇
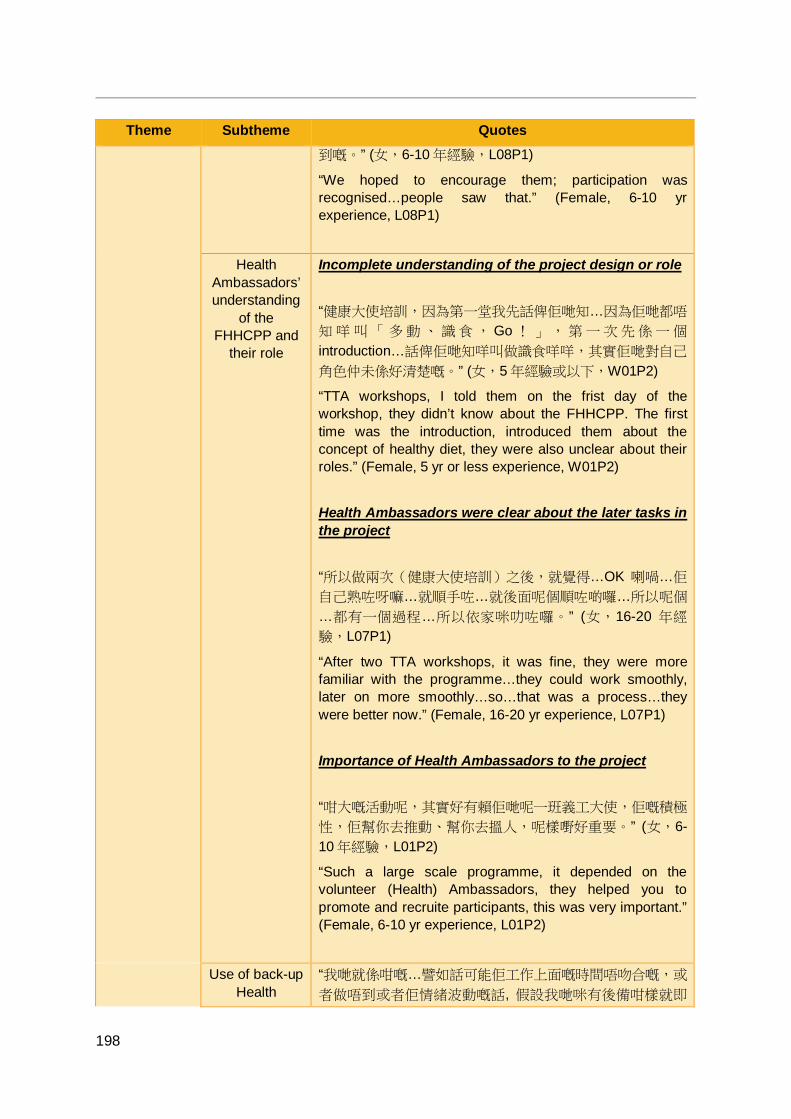
198
Theme Subtheme Quotes 到嘅。” (女,6-10 年經驗,L08P1)
“We hoped to encourage them; participation was recognised…people saw that.” (Female, 6-10 yr experience, L08P1)
Health Ambassadors’ understanding
of the FHHCPP and
their role
Incomplete understanding of the project design or role “健康大使培訓,因為第一堂我先話俾佢哋知…因為佢哋都唔
知 咩 叫 「 多 動 、 識食 , Go ! 」 , 第 一 次先係 一 個
introduction…話俾佢哋知咩叫做識食咩咩,其實佢哋對自己
角色仲未係好清楚嘅。” (女,5 年經驗或以下,W01P2)
“TTA workshops, I told them on the frist day of the workshop, they didn’t know about the FHHCPP. The first time was the introduction, introduced them about the concept of healthy diet, they were also unclear about their roles.” (Female, 5 yr or less experience, W01P2) Health Ambassadors were clear about the later tasks in the project “所以做兩次(健康大使培訓)之後,就覺得…OK 喇喎…佢
自己熟咗呀嘛…就順手咗…就後面呢個順咗啲囉…所以呢個
…都有一個過程…所以依家咪叻咗囉。” (女,16-20 年經
驗,L07P1)
“After two TTA workshops, it was fine, they were more familiar with the programme…they could work smoothly, later on more smoothly…so…that was a process…they were better now.” (Female, 16-20 yr experience, L07P1) Importance of Health Ambassadors to the project “咁大嘅活動呢,其實好有賴佢哋呢一班義工大使,佢嘅積極
性,佢幫你去推動、幫你去搵人,呢樣嘢好重要。” (女,6-10 年經驗,L01P2)
“Such a large scale programme, it depended on the volunteer (Health) Ambassadors, they helped you to promote and recruite participants, this was very important.” (Female, 6-10 yr experience, L01P2)
Use of back-up Health
“我哋就係咁嘅…譬如話可能佢工作上面嘅時間唔吻合嘅,或
者做唔到或者佢情緒波動嘅話, 假設我哋咪有後備咁樣就即
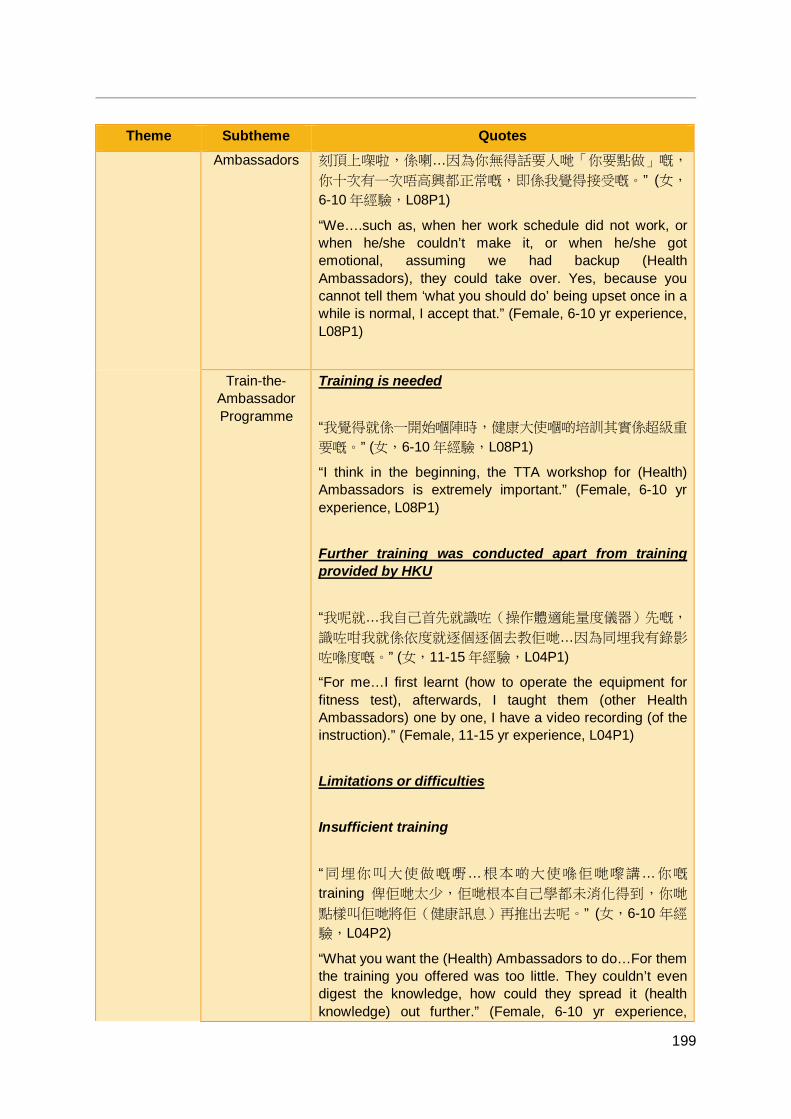
199
Theme Subtheme Quotes Ambassadors 刻頂上㗎啦,係喇…因為你無得話要人哋「你要點做」嘅,
你十次有一次唔高興都正常嘅,即係我覺得接受嘅。” (女,
6-10 年經驗,L08P1)
“We….such as, when her work schedule did not work, or when he/she couldn’t make it, or when he/she got emotional, assuming we had backup (Health Ambassadors), they could take over. Yes, because you cannot tell them ‘what you should do’ being upset once in a while is normal, I accept that.” (Female, 6-10 yr experience, L08P1)
Train-the-Ambassador Programme
Training is needed “我覺得就係一開始嗰陣時,健康大使嗰啲培訓其實係超級重
要嘅。” (女,6-10 年經驗,L08P1)
“I think in the beginning, the TTA workshop for (Health) Ambassadors is extremely important.” (Female, 6-10 yr experience, L08P1) Further training was conducted apart from training provided by HKU “我呢就…我自己首先就識咗(操作體適能量度儀器)先嘅,
識咗咁我就係依度就逐個逐個去教佢哋…因為同埋我有錄影
咗喺度嘅。” (女,11-15 年經驗,L04P1)
“For me…I first learnt (how to operate the equipment for fitness test), afterwards, I taught them (other Health Ambassadors) one by one, I have a video recording (of the instruction).” (Female, 11-15 yr experience, L04P1) Limitations or difficulties Insufficient training “同埋你叫大使做嘅嘢…根本啲大使喺佢哋嚟講…你嘅
training 俾佢哋太少,佢哋根本自己學都未消化得到,你哋
點樣叫佢哋將佢(健康訊息)再推出去呢。” (女,6-10 年經
驗,L04P2)
“What you want the (Health) Ambassadors to do…For them the training you offered was too little. They couldn’t even digest the knowledge, how could they spread it (health knowledge) out further.” (Female, 6-10 yr experience,
200
Theme Subtheme Quotes L04P2) Training was rushed “可能就我哋前期 prepare 其實唔夠嘅…因為真係…時間好逼
啊,我哋雖然…proposal…即係十二月底咁馬會批咗啦,咁
我哋一月份就即刻就上馬咁啦,一月份就要培訓健康大使啦
…咁其實係一個…差唔多一個星期就各個區去發散嗰個健康
大使去搵嗰啲參加者。” (女,5 年經驗或以下,W01P2)
“The preparation at the early stage was not enough, because it was true that the time was really rushed. We…the proposal...was approved by The Jockey Club in late December, we started immediately in January, trained the Health Ambassadors in January...it was like a…almost a week later, the Health Ambassadors were already asked to recruite participants from different districts.” (Female, 5 yr or less experience, W01P2) Suggestions for improvements More flexible time slots “(出席健康大使培訓)都困難㗎…所以呢…可能會彈性少
少,即係譬如話未必一定要一次過係…佢哋(全部健康大
使)出席晒…可能分開幾個 group 咁樣囉,即係每一次我哋
俾啲…可能唔同嘅日期時間俾佢揀,可能每一次有廿個人,
十幾個人,即係小組少少可能會好啲囉。” (女,5 年經驗或
以下,L06P1)
“(Attending the TTA workshops) was difficult, so…should be more flexible. For example, all the Health Ambassadors attending the same session might not be neccessary, maybe we they could be divided into groups. We could give them options on different time slots, maybe 10-20 people in each time slot, training with smaller groups is better.” (Female, 5 yr or less experience, L06P1) More training (either number of sessions or duration) “上多幾堂唔緊要,可能有啲重複…或者有時間嘅…我哋一,
二節去埋唔緊要,聽多啲咁嘛叫做自己加深啲認識,記得好
啲,同人哋講又好啲。” (女,16-20 年經驗,L03P5)
“More sessions is fine, might be a bit repetitive…maybe if
201
Theme Subtheme Quotes time allowed, it is okay for us to attend both, learning more can deepen my knowledge, memorise better, introduce to others better.” (Female, 16-20 yr experience, L03P5) More training on the operation of physical fitness equipment “儀器嗰個說明呀,嗰個培訓可能再著重多啲,即係可能,可
能要拍個 video 俾佢哋,即係 send 出嚟俾佢哋,等佢哋可
以唔記得就睇返,唔記得就睇返,呢樣嘢係比較緊要啲囉。” (女,5 年經驗或以下,L06P1)
“The operation of the equipement can be focused on more in the training. Maybe offer them a video recording of it, send to them. For them to watch when they fail to recall, watch again when fail to recall, this is quite important.” (Female, 5 yr or less experience, L06P1) More training on the design of the FHHCPP “我諗你可以略略帶過(有關計劃模式、內容、科研簡介),
但係大部分未必明白,但係始終都要將呢件事好簡略咁有個
框㗎咁講一講出嚟囉…少量嘅呢啲資料。” (女,5 年經驗或
以下,L06P1)
“I think you can briefly mention (about plan, content, research brief introduction), the majority of them might not understand, but eventually the framework of this programme ought to be mentioned, a little such information.” (Female, 5 yr or less experience, L06P1) More training on recruitment “因為其實呢我上咗兩次堂之後就要出街招人,咁我點樣介紹
呢個產品出嚟呢?就唔夠勁呀…點樣招得好 d 呢咁樣?” (女,20 年經驗或以上,L03P1)
“I started the recruitment on the street after two sessions of training, but how should I introduce this product? Not convincing enough…how could I recruit better?” (Female, 20 or more yr experience, L03P1)
202
Theme Subtheme Quotes Training should use different means “可能用唔同嘅形式呀,唔同嘅聚會,令佢哋呢就係更加能夠
了解佢哋自己嘅角色同埋之後嗰個(知識)點樣去運用呀。” (女,5 年經驗或以下,L06P1)
“Maybe in different forms, various types of gathering, lead them to have a better understanding of their roles and the application of knowledge.” (Female, 5 yr or less experience, L06P1) Trainer to trainee ratio “一個對八十個你係得唔到效果,但係唔係代表即係八十人上
堂係唔好嘅,而係就係話,如果係你上完之後再分小組啦,
譬如一個對十個(咁樣)再分小組咁所以咪得囉…我就會覺
得八十人一齊上堂無問題,至緊要就係話你上完第一個
section 係教完喇…你再有小組俾佢哋上依啲堂呢…等佢哋每
一個人都有機會發問佢哋唔明嘅地方。” (女,11-15 年經
驗,L04P1)
“The ratio of 1 to 80 couldn’t reach the optimal outcome, but it doesn’t mean that having 80 in one session is not good. I am saying it is fine if there are some small group activities with ratio of 1 to 10. The most important thing is after the first session, there are small group activities…a chance for everyone to ask questions.” (Female, 11-15 yr experience, L04P1)
Changes in Health
Ambassadors’ personal or
FAMILY 3Hs
Positive changes in health attitude, knowledge, or behaviour “我覺得係…佢哋嗰個健康大使就覺得係佢哋嘅知識層面呢闊
咗…闊咗好多…即係…佢哋就覺得…其實佢唔只係會煮飯嘅.煮飯係有分健康嘅…佢哋係提升咗好多…即係佢哋會話佢哋
好開心。” (女,5年經驗或以下,W01P2)
“I think…the Health Ambassadors have widened their horizon on knowledge…much wider…that is…they think…they don’t just know how to cook, but cook healthily…they have improved a lot, they said they are very happy.” (Female, 5 yr or less experience, W01P2) “我覺得呢個運動好好。因為我有個委員,都係大使嚟,佢
keep 住做,佢真係減到肥…起碼個肚腩無咁大啦。” (女,6-
203
Theme Subtheme Quotes 10 年經驗,L03P3)
“I think this exercise is great. There is a committee member from the association, she is also a (Health) Ambassador, she kept doing it, and she lost weight…at least her belly became smaller.” (Female, 6-10 yr experience, L03P3) Increased happiness “今次做完之後,個個都好開心。” (女,6-10 年經驗,
L08P1) “After this programme, everyone is very happy.” (Female, 6-10 yr experience, L08P1) Enhanced harmony (communication or networks) “即係每一次嘅活動,佢哋都會 er 返番去同家人分享啦…” (女,5 年經驗或以下,W01P2)
“They shared with the family after each event…” (Female, 5 yr or less experience, W01P2) Family members’ perception of Health Ambassador enhanced “老公讚啦,啊仔就話,「哦,原來係…亞媽都識咁多知識
嘅」…” (女,5 年經驗或以下,W01P2)
“My husband praised, my son said ‘Oh, I didn’t know my mother knows that much knowledge’…” (Female, 5 yr or less experience, W01P2)
Strengths or positive
characteristics
Health Ambassadors were highly committed or responsible despite the challenging work “大家好 committed 呀呢樣嘢…都好落力去做。其實成日佢
哋都會打來,「啊,好辛苦啊,原來咁難,哎呀原來…點解
原來之前都無預計咁咁咁」,但係出到來嘅效果大家都覺得
好,所以開心嘅。” (女,5年經驗或以下,L06P1)
“The Health Ambassadors were committed to it…so into it. They called all the time and said ‘huh, it is tiring, I found it so hard, huh…I didn’t expect that.’ But they were glad with the outcomes, therefore happy.” (Female, 5 yr or less experience, L06P1)
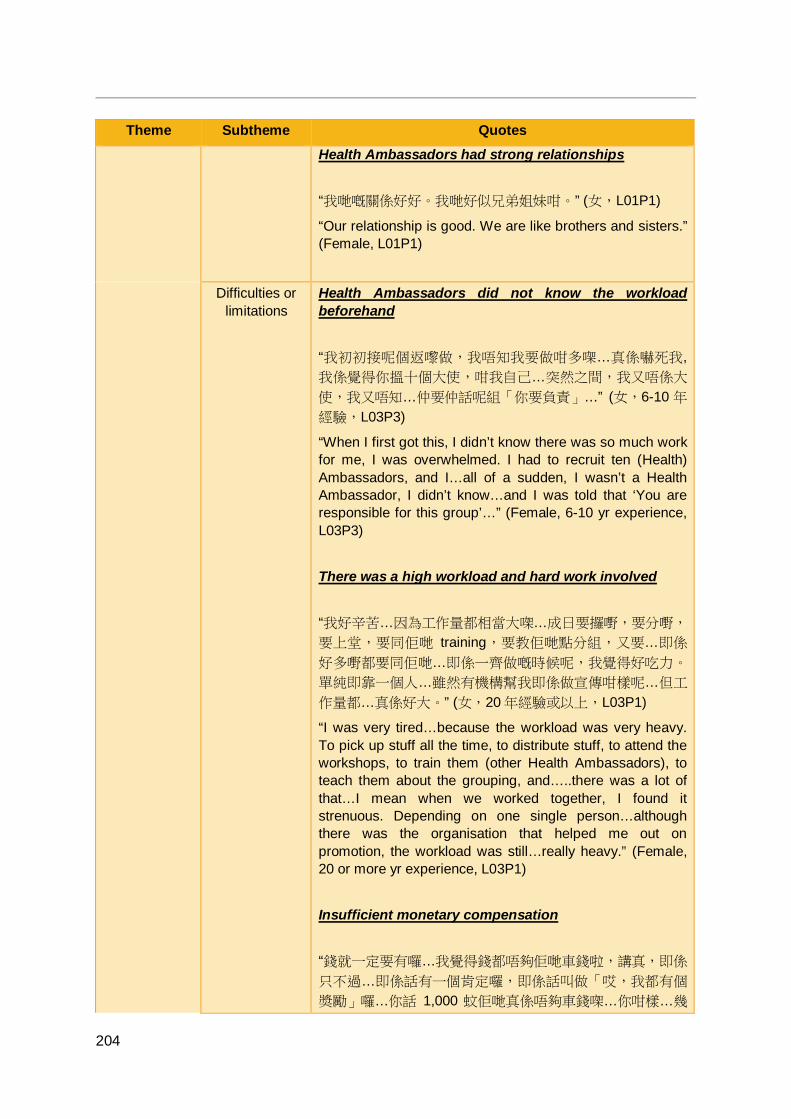
204
Theme Subtheme Quotes Health Ambassadors had strong relationships “我哋嘅關係好好。我哋好似兄弟姐妹咁。” (女,L01P1)
“Our relationship is good. We are like brothers and sisters.” (Female, L01P1)
Difficulties or limitations
Health Ambassadors did not know the workload beforehand “我初初接呢個返嚟做,我唔知我要做咁多㗎…真係嚇死我, 我係覺得你搵十個大使,咁我自己…突然之間,我又唔係大
使,我又唔知…仲要仲話呢組「你要負責」…” (女,6-10 年
經驗,L03P3)
“When I first got this, I didn’t know there was so much work for me, I was overwhelmed. I had to recruit ten (Health) Ambassadors, and I…all of a sudden, I wasn’t a Health Ambassador, I didn’t know…and I was told that ‘You are responsible for this group’…” (Female, 6-10 yr experience, L03P3) There was a high workload and hard work involved “我好辛苦…因為工作量都相當大㗎…成日要攞嘢,要分嘢,
要上堂,要同佢哋 training,要教佢哋點分組,又要…即係
好多嘢都要同佢哋…即係一齊做嘅時候呢,我覺得好吃力。
單純即靠一個人…雖然有機構幫我即係做宣傳咁樣呢…但工
作量都…真係好大。” (女,20 年經驗或以上,L03P1)
“I was very tired…because the workload was very heavy. To pick up stuff all the time, to distribute stuff, to attend the workshops, to train them (other Health Ambassadors), to teach them about the grouping, and…..there was a lot of that…I mean when we worked together, I found it strenuous. Depending on one single person…although there was the organisation that helped me out on promotion, the workload was still…really heavy.” (Female, 20 or more yr experience, L03P1) Insufficient monetary compensation “錢就一定要有囉…我覺得錢都唔夠佢哋車錢啦,講真,即係
只不過…即係話有一個肯定囉,即係話叫做「哎,我都有個
奬勵」囉…你話 1,000 蚊佢哋真係唔夠車錢㗎…你咁樣…幾

205
Theme Subtheme Quotes 廿百次活動…咁你話 1,000 蚊 1 年其實就真係…有啲少囉。” (女,6-10 年經驗,L08P1)
“Sufficient funding is a must…I think the monetary compensation didn’t even cover their transportation fee, to be honest, it served as a recognition. It was like ‘oh, I have a reward.’ 1,000 dollars was not enough for transportation fee, you had so many activites, 1,000 dollars for a year was really…too little.” (Female, 6-10 yr experience, L08P1) Health Ambassadors showing low commitment were a concern for the HKIWA “反而我哋最驚嗰啲完全係乜都話好好,好完就無咗影嗰啲,
我哋反而最擔心呢啲。” (女,6-10 年經驗,L08P1)
“We worried most about those Health Ambassadors who said everything was very good, but then they went missing afterwards, we were most worried about this.” (Female, 6-10 yr experience, L08P1) Health Ambassadors often have no time as they are employed “因為我哋依家嗰個健康大使呢…有好多返緊工,好多時唔得
閒。咁呢…變咗係搵佢哋出席係難。” (女,L01P1)
“Our Health Ambassadors…most of them had to go to work and they were often busy. So…it was difficult to get them to attend (the workshops and programme).” (Female, L01P1)
Suggestions for
improvements
Shared workload between Health Ambassadors pairs “如果可以嘅話呢,可以自己搵一個 partner,你兩個自己協
調,俾佢哋一個主動性…一係就你出(出席活動)一係就我
出,你有乜嘢一係你打(電話)一係我打…咁我覺得亦都加
強咗佢哋兩個嘅關係,咁亦都令到大家呢(可以輕鬆些),
因為始終…我覺得始終都係義工,佢哋真係唔係全職。” (女,6-10 年經驗,L08P1)
“If it is possible allow each to find a partner, you two coordinate yourselves, give them autonomy, either you attend (the event) or I do, whatever happens either you make the phoe call or I do. This strengthens their relationship, and is more relaxed, because…I think they were volunteers afterall, they weren’t full-time employees
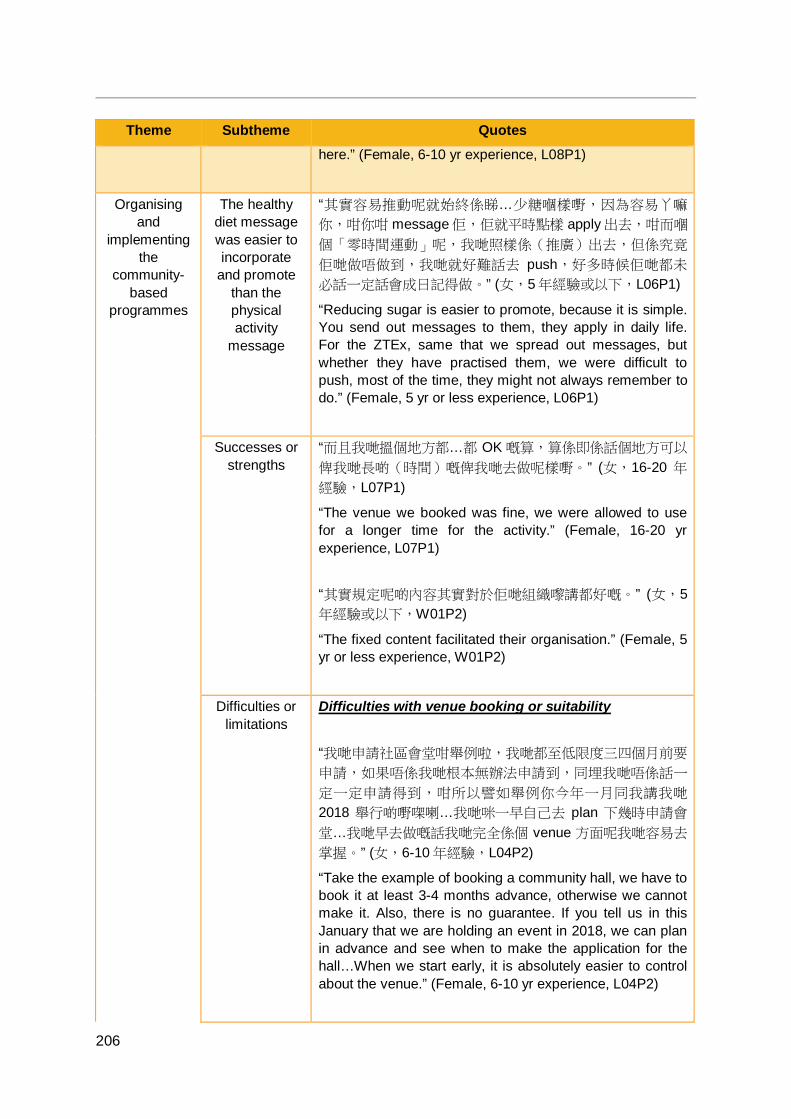
206
Theme Subtheme Quotes here.” (Female, 6-10 yr experience, L08P1)
Organising and
implementing the
community-based
programmes
The healthy diet message was easier to incorporate
and promote than the physical activity
message
“其實容易推動呢就始終係睇…少糖嗰樣嘢,因為容易丫嘛
你,咁你咁 message佢,佢就平時點樣 apply 出去,咁而嗰
個「零時間運動」呢,我哋照樣係(推廣)出去,但係究竟
佢哋做唔做到,我哋就好難話去 push,好多時候佢哋都未
必話一定話會成日記得做。” (女,5年經驗或以下,L06P1)
“Reducing sugar is easier to promote, because it is simple. You send out messages to them, they apply in daily life. For the ZTEx, same that we spread out messages, but whether they have practised them, we were difficult to push, most of the time, they might not always remember to do.” (Female, 5 yr or less experience, L06P1)
Successes or strengths
“而且我哋搵個地方都…都 OK 嘅算,算係即係話個地方可以
俾我哋長啲(時間)嘅俾我哋去做呢樣嘢。” (女,16-20 年
經驗,L07P1)
“The venue we booked was fine, we were allowed to use for a longer time for the activity.” (Female, 16-20 yr experience, L07P1) “其實規定呢啲內容其實對於佢哋組織嚟講都好嘅。” (女,5年經驗或以下,W01P2)
“The fixed content facilitated their organisation.” (Female, 5 yr or less experience, W01P2)
Difficulties or limitations
Difficulties with venue booking or suitability “我哋申請社區會堂咁舉例啦,我哋都至低限度三四個月前要
申請,如果唔係我哋根本無辦法申請到,同埋我哋唔係話一
定一定申請得到,咁所以譬如舉例你今年一月同我講我哋
2018 舉行啲嘢㗎喇…我哋咪一早自己去 plan 下幾時申請會
堂…我哋早去做嘅話我哋完全係個 venue 方面呢我哋容易去
掌握。” (女,6-10 年經驗,L04P2)
“Take the example of booking a community hall, we have to book it at least 3-4 months advance, otherwise we cannot make it. Also, there is no guarantee. If you tell us in this January that we are holding an event in 2018, we can plan in advance and see when to make the application for the hall…When we start early, it is absolutely easier to control about the venue.” (Female, 6-10 yr experience, L04P2)

207
Theme Subtheme Quotes Difficulties organising participants for day trips and accommodating their requests “安排啲人好大問題…俾人覺得有啲唔係咁公平…即係之前無
講到明…無講到明…呀要參加(「多動、識食,Go!」)嗰
啲(先)有免費去旅行…係啦,就變咗有啲人有得去有啲人
無。流程上有啲困難囉…” (女,6-10 年經驗,L03P3)
“Organising participants was a big problem…some of them think it was unfair…because no pre-condition was mentioned, not clear that only those who take part in FHHCPP are entitled with a free trip…yes…so it turned out that some were offered and some weren’t. There was a bit problematic logistically…” (Female, 6-10 yr experience, L03P3) The core session was rushed “時間太急…我哋借個場呢…佢就限制,所以第一晚呢…我哋
就好急好急要交場俾人。” (女,16-20 年經驗,L03P4)
“Too rushed, the venue we booked came with rules, so the first night, we had to return the venue in a hurry.” (Female, 16-20 yr experience, L03P4)
Suggestions for
improvements
More time and better planning “一路培訓一路攪(program)會好啲…或者你一培訓完即刻
就攪會好啲,即係譬如話我頭先講可能做 4 次培訓,咁可能
你去到第 3 次就已經叫佢哋 prepare 開始攪活動喇,咁可能
要第 4 次培訓嗰陣呢做多啲一齊 review 呀嗰啲,嗰啲工作囉
會好啲,都係需要一個比較貼身嘅帶領…地區嘅工作人員。” (女,5 年經驗或以下,L06P1)
“Attending the workshop and organising the programme at the same time would be better…maybe immediately after the training would be better. Like I said, maybe if there are four training sessions, you tell them to start preparing for the programme on the third training, so we could have a review on the fourth session together...review on the tasks, need a close guidance for the community staff.” (Female, 5 yr or less experience, L06P1) “即係時間上唔好黐咁埋囉,同埋加上即係…喺 5 月啦,可能
5 月都有啲假期呢,變咗就唔係咁好。” (女,6-10 年經驗,
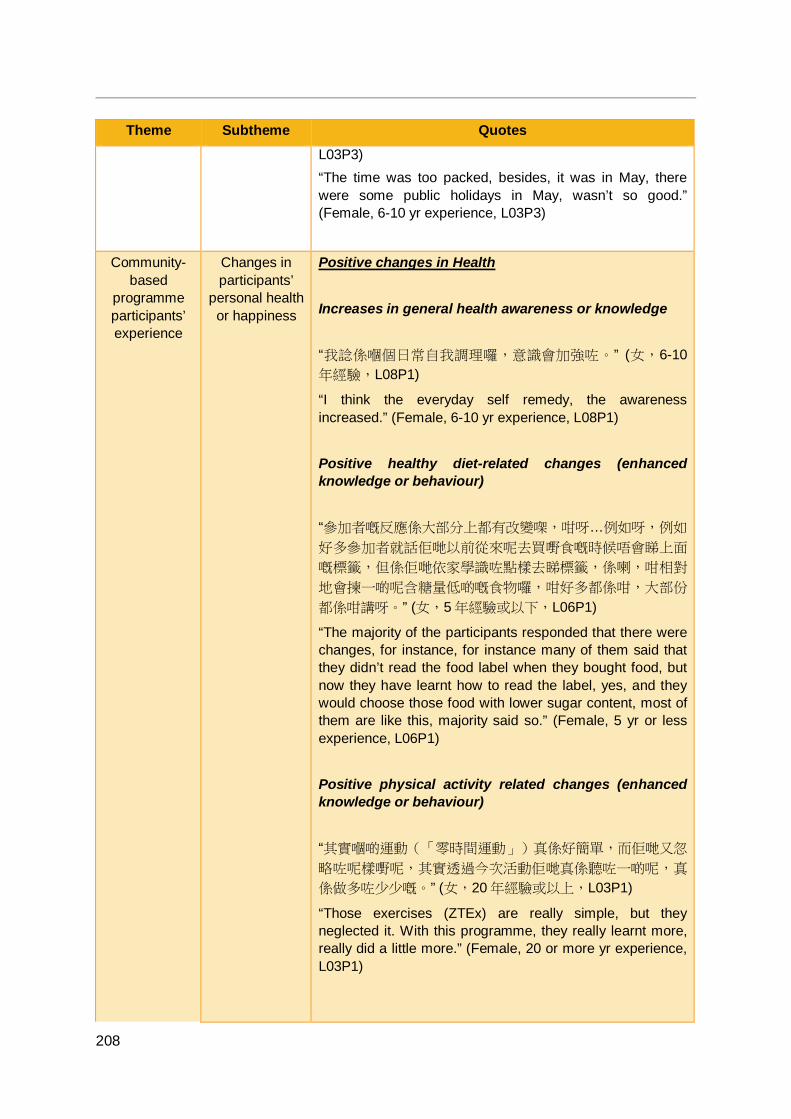
208
Theme Subtheme Quotes L03P3) “The time was too packed, besides, it was in May, there were some public holidays in May, wasn’t so good.” (Female, 6-10 yr experience, L03P3)
Community-based
programme participants’ experience
Changes in participants’
personal health or happiness
Positive changes in Health Increases in general health awareness or knowledge “我諗係嗰個日常自我調理囉,意識會加強咗。” (女,6-10年經驗,L08P1)
“I think the everyday self remedy, the awareness increased.” (Female, 6-10 yr experience, L08P1) Positive healthy diet-related changes (enhanced knowledge or behaviour) “參加者嘅反應係大部分上都有改變㗎,咁呀…例如呀,例如
好多參加者就話佢哋以前從來呢去買嘢食嘅時候唔會睇上面
嘅標籤,但係佢哋依家學識咗點樣去睇標籤,係喇,咁相對
地會揀一啲呢含糖量低啲嘅食物囉,咁好多都係咁,大部份
都係咁講呀。” (女,5 年經驗或以下,L06P1)
“The majority of the participants responded that there were changes, for instance, for instance many of them said that they didn’t read the food label when they bought food, but now they have learnt how to read the label, yes, and they would choose those food with lower sugar content, most of them are like this, majority said so.” (Female, 5 yr or less experience, L06P1) Positive physical activity related changes (enhanced knowledge or behaviour) “其實嗰啲運動(「零時間運動」)真係好簡單,而佢哋又忽
略咗呢樣嘢呢,其實透過今次活動佢哋真係聽咗一啲呢,真
係做多咗少少嘅。” (女,20 年經驗或以上,L03P1)
“Those exercises (ZTEx) are really simple, but they neglected it. With this programme, they really learnt more, really did a little more.” (Female, 20 or more yr experience, L03P1)

209
Theme Subtheme Quotes Increases in self-knowledge about one’s own physical fitness or health condition “咁個脂肪磅係最好嘅…咁 check 咗變咗佢哋係知道個身體
上好多嘢「唉,原來我重咗幾多呀」…同埋啲手握力…咁呢
依家佢哋知啦,原來可以訓練下多啲力嘅「我係個手唔係咁
夠力」嘅…即係會接觸到呢啲嘢。” (女,6-10 年經驗,
L03P3) “The body fat machine is the best one, after the measurement, they know more about their body, ‘Oh, I gained this much weight,’ and the grip strength. Now, they know, grip strength can be trained, ‘My hand is not strong enough,’ to know about this kind of thing.” (Female, 6-10 yr experience, L03P3) Increases in Happiness “我覺得分享真係…令佢哋開心咗好多嘅。” (女,5 年經驗或
以下,W01P1)
“I think the sharing…made them much happier.” (Female, 5 yr or less experience, W01P1)
Changes in participants’
FAMILY 3Hs or family
interaction
Increases in Harmony with family members Enhanced family harmony (general) “我相信佢哋係融洽咗囉,就係呢個融洽咗囉。” (女,6-10年經驗,L08P1)
“I believe they became more harmonious.” (Female, 6-10 yr experience, L08P1) Enhanced family harmony, communication or interaction via healthy diet as a platform “佢哋仲有覺得係有咗一個分享嘅行動…因為呢之前即係話…
可能就係一個甜品呢就係…即係自己食…但係學咗呢個「識
食」活動…之後…就呢可能會覺得原來分享呢係最開心嘅…” (女,5 年經驗或以下,W01P1)
“They think that it is about the act of sharing too…Maybe if there was a dessert, I ate it myself…but after I learnt about healthy diet, maybe sharing is the happiest thing.” (Female,
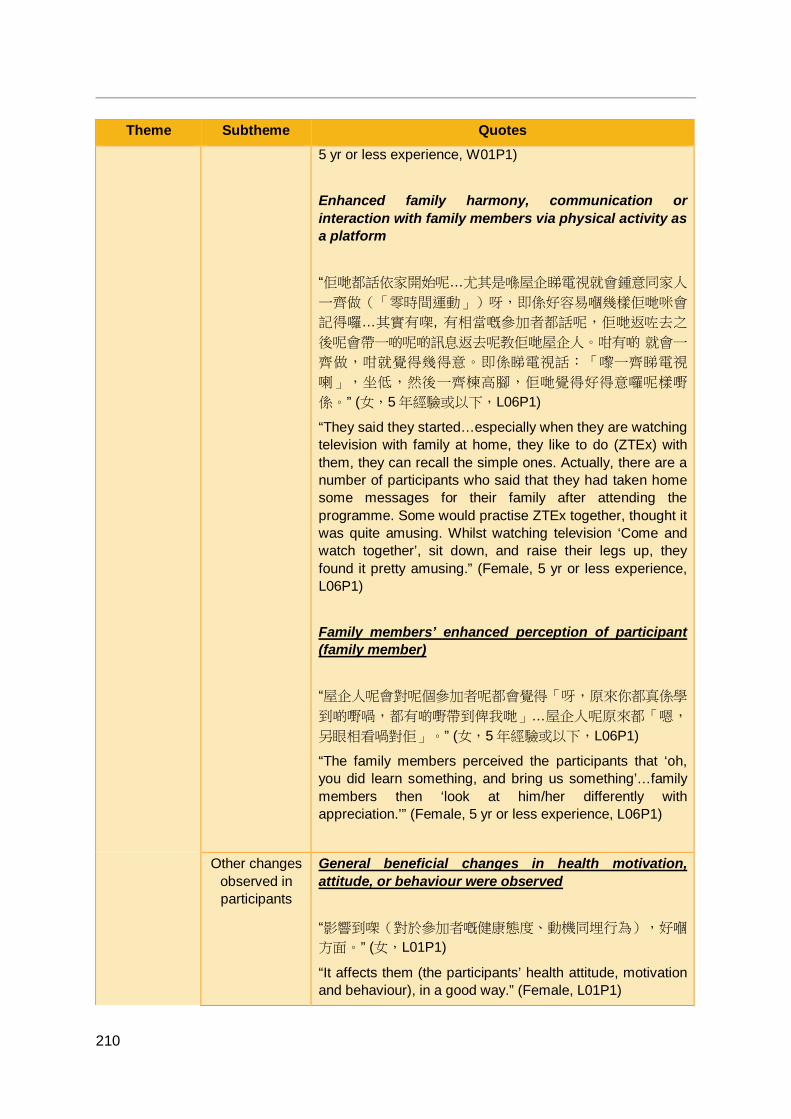
210
Theme Subtheme Quotes 5 yr or less experience, W01P1) Enhanced family harmony, communication or interaction with family members via physical activity as a platform “佢哋都話依家開始呢…尤其是喺屋企睇電視就會鍾意同家人
一齊做(「零時間運動」)呀,即係好容易嗰幾樣佢哋咪會
記得囉…其實有㗎, 有相當嘅參加者都話呢,佢哋返咗去之
後呢會帶一啲呢啲訊息返去呢教佢哋屋企人。咁有啲 就會一
齊做,咁就覺得幾得意。即係睇電視話:「嚟一齊睇電視
喇」,坐低,然後一齊楝高腳,佢哋覺得好得意囉呢樣嘢
係。” (女,5 年經驗或以下,L06P1)
“They said they started…especially when they are watching television with family at home, they like to do (ZTEx) with them, they can recall the simple ones. Actually, there are a number of participants who said that they had taken home some messages for their family after attending the programme. Some would practise ZTEx together, thought it was quite amusing. Whilst watching television ‘Come and watch together’, sit down, and raise their legs up, they found it pretty amusing.” (Female, 5 yr or less experience, L06P1) Family members’ enhanced perception of participant (family member) “屋企人呢會對呢個參加者呢都會覺得「呀,原來你都真係學
到啲嘢喎,都有啲嘢帶到俾我哋」…屋企人呢原來都「嗯,
另眼相看喎對佢」。” (女,5 年經驗或以下,L06P1)
“The family members perceived the participants that ‘oh, you did learn something, and bring us something’…family members then ‘look at him/her differently with appreciation.’” (Female, 5 yr or less experience, L06P1)
Other changes observed in participants
General beneficial changes in health motivation, attitude, or behaviour were observed “影響到㗎(對於參加者嘅健康態度、動機同埋行為),好嗰
方面。” (女,L01P1)
“It affects them (the participants’ health attitude, motivation and behaviour), in a good way.” (Female, L01P1)
211
Theme Subtheme Quotes “我覺得佢哋已經用咗係自己生活中啦,因為畢竟係一年
啊。” (女,5 年經驗或以下,W01P1)
“I think they have got it applied in their daily lives, it has been a year after all.” (Female, 5 yr or less experience, W01P1) Positive changes in self-efficacy or sense of responsibility “我哋嗰啲家庭主婦,佢會覺得自己嗰個 er,價值,係啦,
提高咗,地位都提高咗。” (女,5 年經驗或以下,L06P1)
“Our…housewives, they think about their values, yes, have raised, and the status was also raised.” (Female, 5 yr or less experience, L06P1)
Participants motivated to
make behavioural
changes due to others’
influence
“大家會見到 「你真係做咗一排(「零時間運動」),你真
係瘦咗喎」,「你識食咗一排,你真係瘦咗」,即係佢哋會
覺得羨慕你瘦咗之餘,佢哋會扚起心肝 「我都要咁樣㗎喇」
…即係會有個互相鞭策互相鼓勵嘅作用走出嚟,同埋真係開
開 心 心 去 participate , 而 裡 面 有好 多 活 動 係我 哋 去
encourage 啲屋企人一齊去參與㗎嘛…活動嘅成功與否其實
屋企人嘅支持同參與係好重要嘅。” (女,6-10 年經驗,
L04P2) “We noticed ‘Oh, after some times of practice (of ZTEx), you really got thinner,’ ‘After adopting the heathy diet for a while, you really got thinner’. That is they envied that you got thinner, they were more determined, ‘I have to do this as well’…it is a mutually spurring, a mutual encouragement, so they participated very happily. There were a lot of acitivies for us to encourage our family to take part together…the support and participation of the family are essential to the success of the activity.” (Female, 6-10 yr experience, L04P2) “咁而嗰個「零時間運動」呢,我哋照樣係(推廣)出去,但
係究竟佢哋做唔做到,我哋就好難話去 push,好多時候,
佢哋都未必話一定話會成日記得做,咁但係呢…都我哋問好
多,佢哋都話依家開始呢…尤其是喺屋企睇電視就會鍾意同
家人一齊做呀,即係好容易嗰幾樣佢哋咪會記得囉。” (女,
5 年經驗或以下,L06P1)
“For the ZTEx, that we spread out the same messages, but whether they have practised them, we were difficult to push, most of the time, they might not often remember. But
212
Theme Subtheme Quotes we had a lot of follow-up questions, they said they have started…especially when they are watching television with family members at home, they like to do (ZTEx) with them, they can recall the simple ones.” (Female, 5 yr or less experience, L06P1)
Participants would welcome more face-to-face sessions
“好多人話「攪完係咪真係就完咗呢?」” (女,5 年經驗或以
下,W01P2)
“Many of them quesitoned ‘Has it really ended after completing (the tasks of the programme)?’” (Female, 5 yr or less experience, W01P2) “嗰啲參加者就會…(對於活動之數)多就唔會話太多。譬如
你成班人走出去做一個活動,或者咩,就唔會多。” (女,
L01P1) “Those participants would not consider it (the number of sessions) as excessive. If a group was organising an event or what, not too many.” (Female, L01P1)
Relationship between Health
Ambassadors and
community-based
programme participants
Health Ambassadors
helped community-
based participants
Explained the study to participants “你又有你哋嘅解釋囉,我哋都有咁講,你上次唔知你有無進
步啊嗎,或者退步呢唔聽話呢咁,佢哋又唔會話你講得唔啱
囉咁。” (女,6-10 年經驗,L02P1)
“You also have your own explanation. We have said so. You did not know whether you improved last time. Or got worse or did not follow the advice…They would not say you said wrongly. (Female, 6-10 yr experience, L02P1) Reminded participants of health behaviours “咁我覺得係…即係(提醒)佢哋(健康大使)係好嘅…即係
間中你提醒下…「 唉呀你又提醒我」…我哋有時都唔記得
㗎。” (女,11-15 年經驗,L04P1)
“I think…reminding them is beneficial…you remind them occasionally…‘Oh, you remind me again’…sometimes we also forget.” (Female, 11-15 yr experience, L04P1)
Relationship enhanced
through the
“即係以前可能舉例可能你 call 嗰啲長者,根本無人 call 過佢
嘅,根本無人理過佢,但因為呢個活動裡面呀 X 成日都 call佢哋,咁令到佢哋又會開心囉,係咪先…有人關懷囉…即係
213
Theme Subtheme Quotes FHHCPP 每一樣嘢就俾到…即係傳達嘅訊息就係話多咗關懷你,call
呀…WhatsApp 呀都係一種關懷嚟㗎。” (女,6-10 年經驗,
L04P2) “That is, in the past, for example, you might call the elderly, actually no one had called them, no one had actually paid attention to them, but because of this programme, X always calls them, and this makes them happy, right…someone cares…that is, every single thing gives…that is, conveys the message that (we) care more about you (now). Calls…WhatsApp (messages) are both ways of caring.” (Female, 6-10 yr experience, L04P2) “我覺得大使呢,同佢哋啲參加者接觸得比較多啲嘅。” (女,
6-10 年經驗,L08P1)
“I think the (Health) Ambassadors, they have more contact with the participants.” (Female, 6-10 yr experience, L08P1)
Participant satisfaction
Participants were happy
with the programmes
“有時我喺街度撞到佢哋…「X 姑娘幾時又再搞啊,快啲通知
我啊」咁。” (女,L01P1)
“Sometime, when I bumped into them on the street…they would say, ‘Ms. X, when you gonna hold the programme again, inform me quickly.’” (Female, L01P1) “整體上呢我哋嗰班老友記都好開心…都好開心。” (女,16-20 年經驗,L03P4)
“In general, our old friends are very happy, very happy.” (Female, 16-20 yr experience, L03P4)
Use of WhatsApp reminder
messages
Community-based
programme
Positive reaction to use of weekly e-messages “即係你哋…即係港大每一星期都發套片啦,即係提醒佢哋
啦,其實呢個係非常之好嘅活動…每個健康大使都覺得,
哦,原來係即係有一個責任咁嘅…所以佢哋都係好開心嘅。” (女,5 年經驗或以下,W01P2)
“You, HKU, send out video weekly, to remind them, this is a really good act. Every (Health) Ambassador reckoned that they have a responisibility, so they were happy.” (Female, 5 yr or less experience, W01P2)
214
Theme Subtheme Quotes Implementation Timing and motivation are important for effectiveness “接收訊息嘅人呢,第一個佢有無興趣睇,第二個佢有無時間
去推動…其實呢個好重要。” (女,6-10 年經驗,L01P2)
“Message recipients...first, if he/she is interested, second, if he/she has time to promote…these are very important.” (Female, 6-10 yr experience, L01P2) Health Ambassadors successfully sent out the messages to participants “做俾訊息出去嗰個無問題。” (女,6-10 年經驗,L01P2)
“To be the one to send out messages is fine.” (Female, 6-10 yr experience, L01P2) Difficulties or limitations Too much material or messages too frequent “有唔少人呢反映呢 WhatsApp,短訊,一星期一次呢就太頻
密喇。” (女,5 年經驗或以下,L06P1)
“Some participants fed back that the WhatsApp, the text, once a week was too frequent.” (Female, 5 yr or less experience, L06P1) Not all Health Ambassadors or participants have or know how to use WhatsApp “對於有啲係無 WhatsApp 嘅係真係…所以話 「啊我點呢?
我係咪打個電話去同佢講呢?」” (女,5 年經驗或以下,
W01P2) “For those who have no WhatsApp…I was uncertain ‘What should I do? Should I call and talk to him/her?’” (Female, 5 yr or less experience, W01P2)
215
Theme Subtheme Quotes Health Ambassadors were unclear about the duration of the e-messages “大家 send send send,所以後邊就問 「仲要 send 到幾時
啊?」…係啊,所以我哋要問返你…咁你哋再俾個時間話,
啊,到咗…” (女,5 年經驗或以下,W01P2)
“They kept sending out messages, and later on, they asked ‘When is it gonna end?’…yes, so I had to ask you and you told me about the time, oh, it’s there.” (Female, 5 yr or less experience, W01P2) Participants do not pay attention to the messages “即係我哋 send 個訊息出去呢…係無用㗎…睇完過眼雲煙。” (女,L01P1)
“We send out messages…useless…forget quickly after reading it.” (Female, L01P1)
Train-the-Ambassador Programme
Positive reaction to use of e-messages “一開始,特別係…我覺得一開始特別係健康大使嗰度呢,
嗯,你哋係要佢哋每一日交功課嘅…嗰個其實幾…嗯…一開
始係幾 work 嘅。” (女,5 年經驗或以下,W01P2)
“At the beginning, especially…I think at the beginning with the Health Ambassdaors, you assigned them with daily homework...that is actually…um…quite some work at the start.” (Female, 5 yr or less experience, W01P2)
Suggestions for
improvements
More engaging content “其實單 send 一張圖片,其實係少啲…如果有個 video 咁樣
俾佢哋,動畫嘅形式…佢哋可能會更加…生動啲,佢真係會
點開去睇。” (女,5 年經驗或以下,W01P1)
“Simply sending an image…that was too little…If there is a video for them, in the form of animation…they might be…more lively, he/she is likely to click in and watch.” (Female, 5 yr or less experience, W01P1)
216
Theme Subtheme Quotes
Scientific evaluation
Positivity toward
methods and understanding of importance of evaluation
Positivity toward the use of different evaluation methods Using a mixed methods approach “其實我覺得研究係真係要咁樣嘅…要全面嘅,要多好多嘅角
度,唔係話你係真係話你填咗問卷返嚟就 OK 嘅,即係你譬
如依家嘅 focus group 啦…個人嘅 face-to-face 嘅 interview啦呢啲…其實都係非常非常之好嘅…因為研究真係需要咁
嘅,所以我哋理解嘅…係啦,所以其實都好歡迎。” (女,5年經驗或以下,W01P1)
“I think research should really be like this…all-rounded, with many perspectives; it is not onlt about filling in and returning a questionnaire. Like now, the focus group, the individual face-to-face interview, these are very very good…Because research need these, we understand…yes, so we very much welcomed.” (Female, 5 yr or less experience, W01P1) Using quantitative methods “Questionnaires 問佢哋嘅話…佢哋先可以 self-assess 到…
即係你係從問題裡面佢先會知得到「原來咁至係喎」,「點
解我無醒起呢?嗰個又無醒起呢?」即係 recall 返佢哋應該
要醒起嘅嘢,咁佢哋就透過你個 questionnaire 去做。 ” (女,6-10 年經驗,L04P2)
“It is only by surveying them with questionnaires that they can self-assess…that is, they can only realise through the questions, ‘So that is what it should be’, ‘Why didn’t I remember? I didn’t remember that either?’ That is, they recalled things that they should have remembered, and they did this through your questionnaire.” (Female, 6-10 yr experience, L04P2) Using qualitative methods “我個人覺得好喎…譬如嗰啲(聚焦)小組,你又咁做,呀可
以咁做好啲喎,咁我又可以好啲…我覺得好好。即係唔駛成
日自己做,人哋分享下,OK 嘅…我覺得…分享嗰度幾好幾
happy 呀可?” (女,6-10 年經驗,L03P3)
“I personally think that it is good…for instance, to use (focus) groups. ‘You did that, oh, doing it like that would be

217
Theme Subtheme Quotes better, I can improve’…I think that’s very good. It means that you aren’t just doing it by yourself all the time, it’s okay when people share…I think the sharing (at the focus groups) was quite good, quite happy, right?” (Female, 6-10 yr experience, L03P3) Understanding of the importance of evaluation to generate evidence for effectiveness “我覺得係需要㗎,因為你咁做…即係 go through 成個…我
哋叫好專業性嘅呢一個成個研究嘅過程,咁先至…你出嚟結
果先有公信力㗎嘛,呢個係需要,即係,當然係複雜,即係
做起身係複雜,同我哋…同參加者解釋嘅時候都吃力,都複
雜,但係係需要㗎囉呢樣嘢。” (女,5 年經驗或以下,
L06P1) “I think this is necessary, because you…I mean going through the whole…we called it a professional research process, with this…the result would be credible, this is essential. Of course it is complicated, it is complicated in practice, and when we…explained to the participants it was exhaustive, and complex, but such things were really needed.” (Female, 5 yr or less experience, L06P1)
Physical fitness
measurements
Difficulties with the physical fitness measurement equipment Health Ambassadors had difficulties operating the equipment “磅脂肪嗰個…嗰個就比較有啲難度…” (女,16-20 年經驗,
L07P1) “The one for measuring body fat…that was more difficult...” (Female, 16-20 yr experience, L07P1) Insufficient equipment “其實我哋嗰時要 book 儀器我哋係五套,其實我依家諗返起
呢,其實係唔夠嘅…咁其實實則我哋應該係擺八套嘅…” (女,5 年經驗或以下,W01P2)
“That time when we needed to book the equipment, we needed 5 sets, but when I looked back, acutally there weren’t enough, we needed to have 8 sets.” (Female, 5 yr
218
Theme Subtheme Quotes or less experience, W01P2)
Difficulties with questionnaires
Telephone follow-up interviews were difficult to implement “如果係會員自己識嘅話仲 OK 啦,同佢傾下計,咁有啲唔識
嘅話,佢可能就 cut 咗你嘅電話嘅喇,所以呢啲就比較難。” (女,5 年經驗或以下,W01P2)
“It is still okay if he/she is a member and you know them yourself, chatting with them; then there are those who if you don’t know them, he/she might cut off your call, so those are relatively hard.” (Female, 5 yr or less experience, W01P2) Participants needed Health Ambassadors to help with reading or explaining the questionnaires “有時要幫佢哋做,要讀要講俾佢哋聽點樣做。” (女,6-10年經驗,L01P2)
“Sometimes had to help them, to read and to explain to them.” (Female, 6-10 yr experience, L01P2) Participants gave unreliable responses “因為呢個社區好多都係獨居啦,同埋嗰啲兩夫婦…嗰啲仔女
…即係唔係同埋一齊住。所以我哋問返佢「有無同屋企人做
運動啊?」,「哎呀, 我一個人住,點同屋企人做運動,我
打電話佢都唔聽我支笛啦,佢來都唔來探下我啊」…即係話
…譬如我打電話俾個女叫佢做,佢有無做你唔知㗎嘛。” (女,L01P1)
“Because there are many people living alone in this community, and the couples…are not living together with their children. So, when we ask them ‘Did you exercise with your family members?’, ‘Ah, I live by myself, how can I exercise with my family members, they don’t listen to me even when I call them, they don’t even come to visit me’…That is…if I call my daughter and tell her to exercise, and she doesn’t do it, you wouldn’t know.” (Female, L01P1)
219
Theme Subtheme Quotes Content of questionnaires was repetitive “但係有好多係重複又重複。” (女,11-15 年經驗,L04P1)
“A lot were repeated and repeated.” (Female, 11-15 yr experience, L04P1) Content was too complex “個 questionnaire 入面係太過 details,太過 sophisticated,同埋太多私隱嘢喺嗰度,即係如果以一個 questionnaire 嚟
講,係有時都唔需要做得咁 sophisticated 嘅。” (女,6-10年經驗,L04P2)
“The content of the questionnaire was too detailed, too sophisticated, and too many private information. For a questionnaire, sometimes it is not essential to be this sophisticated.” (Female, 6-10 yr experience, L04P2) Questionnaire had too many questions or was implemented too frequently “即係問卷太多…佢哋就…有少少難接受,特別…你話如果有
長者嗰啲就更加之啦咁樣,咁戴住放大鏡佢都仲…仲要…咩
(填問卷)囉…始終…即係…都係繁複啊覺得…問卷多啦,
頁數多啦。” (女,11-15 年經驗,L09P1)
“Too many questionnaires. They felt a bit unacceptable, especially for the elderly. They (filled in the questionnaire) by wearing magnifying glasses. Anyway, the questionnaires were complicated and too many…too many pages.” (Female, 11-15 yr experience, L09P1)
Understanding of academic
needs
“即係你哋係俾咗一個好標準嘅 standard…譬如係話一啲問
卷呢,你哋就會好…即係好長或者點樣啦…咁其實我哋係理
解嘅。” (女,5 年經驗或以下,W01P2)
“You provided a standard, for example, the questionnaires, you would be really too long or what…actually we understood.” (Female, 5 yr or less experience, W01P2) “其實我哋都明白你哋諗咩嘅其實,事實譬如話…就好似份問
卷咁樣…但係呢就係一定有作用嘅。” (女,6-10 年經驗,
L03P3) “We understand your thought, like, the
220
Theme Subtheme Quotes questionnaires…there must be some use.” (Female, 6-10 yr experience, L03P3)
Suggestions for
improvements
Questionnaire content should be simplified “即係譬如你話做問卷,咪就係話嗰啲字句點樣令佢哋容易理
解, 容易消化呢咁樣。始終係街坊嘅嘛,即係..唔係話個個都
係好高學識啊,即係個理解能力(唔)係太…太好啊嗰啲囉。
最好啲問卷就係簡單易明, 易做嘅咁樣。” (女,11-15 年經
驗,L09P1)
“For example, with the questionnaires, how can the phrases be made to be easy for them to understand, easy, simple? In the end, they are community members (basic education), that is…not all of them are highly educated, which means that their (reading) comprehension capabilities are (not) too…too good. It would be best if the questionnaires are simple, easy to understand, easy to complete.” (Female, 11-15 yr experience, L09P1) Implementation of questionnaires Face-to-face methods should be used instead of telephone interviews 「多動、識食,Go!」嘅電話問卷嘅話可以…其實可以取消
…可以搞一個活動咯…團聚…因為佢哋更加鍾意嗰個 face-to-face 啊即係面對面嘅…大家有個小小啊飲茶啦…茶會啦…
你就 call 埋你嗰個健康大使一齊飲個早茶做下呢個問卷…對
於社區來講…好過你打個電話咁,其實打電話都要嘅…我哋
仲係要俾啊…有時買下卡啦,或者係你做打電話,電話費啊
呢啲其實都好重(成本)嘅。” (女,5 年經驗或以下,
W01P2) “With the FHHCPP’s phone interviews…actually, they could be cancelled…an event could be organised…a reunion…because they (the participants) prefer face-to-face (activities)…everyone could have a bit of tea…you could call your Health Ambassadors together to have morning tea and to complete the questionnaires…for community(-based programmes)…that would be better than calling. Actually, to make calls…we also sometimes need to buy (SIM) cards. If you are making calls, the phone bill is actually quite costly.” (Female, 5 yr or less experience, W01P2)
221
Theme Subtheme Quotes Use of ICT or visual aids “其實係咪可以改善(問卷)係電腦上面呢,或者依家…科技
咁先進,點解仲要整咁多問卷呢?其實你根本就係電腦上
面,俾人哋自己禁晒落去,你哋又唔使再入,你又好我哋又
好…話俾佢聽,「喂,你上呢個電腦邊一版,剔剔剔」,剔
完之後就 send 過來俾你哋(HKU)啦…咁其實你整體嘅資
源、環保啊,其實所有嘅嘢同埋減少你嘅時間性嗰個去操作
呢,其實…大家都好。” (女,6-10 年經驗,L08P1)
“Actually, could it (the questionnaire) be improved by putting it on the computer? Nowadays…with such advanced technology, why do we still need so many hardcopies of the questionnaires? You could actually just let people fill it in themselves on the computer; you wouldn’t need to re-enter (the data) either; it would be good for you and good for us…Tell them, ‘Hey, go onto this webpage and tick, tick, tick (the responses),’ after completing, it will be sent to you (HKU)…actually, your resources in general will be environmental. Actually, it would (save on) everything and also reduce your operation time. Actually…it would be good for everyone.” (Female, 6-10 yr experience, L08P1) “(用個 powerpoint)一齊去答呢個無問題喎。因為佢唔
識,可以即刻問到你啊嘛。” (女,L01P3)
“(Using a PowerPoint) to answer it (the questionnaire) together is not a problem, because if they don’t understand, they can ask you immediately.” (Female, L01P3)
Interviewees’ experience
Changes in the interviewees
Enhanced healthy diet attitude, knowledge, or behaviour “我哋就會打(完)波嘅時候聚會呀 咁我哋往時就食完飯就
食甜品嗰啲呢,往時就一人一盅個隻呢咁呀正常呢依家就分
㗎喇,通常都係減一半呀,「我同你 share 啦」咁,即係好
好多㗎。” (女,11-15 年經驗,L04P1)
“We gather after exercise (ballsport). We used to have dessert after the meal, we used to have one portion per person; now, we normally share. We usually have half less, ‘I’ll share with you,’ it’s much better.” (Female, 11-15 yr experience, L04P1) “至少食個 cake 嘅時候都諗緊,我會囉,以前我會食咗先講
222
Theme Subtheme Quotes 囉,依家你會諗下,「哇你知唔知幾多(糖)啊,唔好食
啦。」” (女,6-10 年經驗,L08P1)
“At least when eating cake, I am also thinking (about the sugar content), I do. Before, I would just eat it first. Now, you would think, ‘Wow, do you know how much (sugar) that is, better not eat it.’” (Female, 6-10 yr experience, L08P1) Enhanced physical activity attitude, knowledge, or behaviour “喺張床度…我就開始,踢下腳啊,搓下手啊,總之係,將自
己嗰個身體郁下佢,咁呀熱身下,先至起身。” (女,16-20年經驗,L07P1)
“On the bed…I start to kick my legs, rub my arms…in short, I move my body and warm up before I get up.” (Female, 16-20 yr experience, L07P1) “同埋我自己企地鐵啊,我自己都會郁動下啊咁樣。” (女,6-10 年經驗,L08P1)
“When I am standing on the train, I move around too.” (Female, 6-10 yr experience, L08P1)
Eager to get feedback for
self-improvement
“我又倒返轉頭了解返呢,即係我哋喺嗰個協青社,嗰日搞嗰
個四月廿四呢,我哋搞呢場活動,你都有參與啦…即係你對
我哋搞嗰次嘅活動呢,你睇到我哋喺邊方面做得同你哋嘅要
求呢有啲差距啊?有無啲咩嘅意見話俾我哋聽呢?” (女,6-10 年經驗,L01P2)
“I am thinking back and want to understand (more about) the programme that we organised at the Youth Centre on April 24th, which you also took part in…your view of the programme we organised that time, what did you observe that we did that was different than what you required? Do you have any comments for us?” (Female, 6-10 yr experience, L01P2) “我都想聽聽你哋嘅意見,即係話譬如話呢個過程途中,我哋
有啲咩…其實我都想睇下自己,都會改善㗎嘛。” (女,6-10年經驗,L08P1)
“I want to know your suggestions, for instance, during the process, did we have…I actually want to know about myself, would improve.” (Female, 6-10 yr experience, L08P1)
223
Theme Subtheme Quotes
Planning and preparation
The FHHCPP provided
experience for the future
“因為始終第一次去做,就未去考慮好多嘢,我哋就以為可以
咁做咁做咁做,但真係 execute 嗰陣就發覺呀原來咁係唔得
嘅,即係嗰個規限比較多嘅,咁就我哋之前無預料到嘅,但
係經過今次之後我哋大概知道嗰個要求係點樣樣…呢個俾咗
好多,好多建議㗎。” (女,5 年經驗或以下,L06P1)
“Since it was our first time doing this, there was a lot that we hadn’t considered yet. We thought that such and such could be done, but when it came to actually executing it, we found that it turned out that it couldn’t be done. There were quite a lot of limitations, which we hadn’t expected before. However, through this time, we know roughly what the requirements are…this has provided a lot, a lot of suggestions.” (Female, 5 yr or less experience, L06P1) “咁我哋呢一次會俾一個經驗俾「多動、識食,Go!二」
啦。” (女,5 年經驗或以下,W01P2)
“This time (the FHHCPP) will serve as experience for the FHHCPP II.” (Female, 5 yr or less experience, W01P2)
Difficulties or limitations
Insufficient time for planning or preparation “前期方面時間唔夠啦…時間緊咯,做 prepare 嘅話呢其實真
係唔係好夠咯。” (女,5 年經驗或以下,W01P2)
“There was not enough time in the early stages…time was tight, (we) really didn’t have enough preparation (time).” (Female, 5 yr or less experience, W01P2) Timing for programmes was a difficulty “即係當時好似話係,每個區都會有一啲嘅物資係配套落去俾
佢哋做呀呢一個練習啊咁樣㗎嘛。但咁啱佢哋個 booking呢,booking 又 book 到差唔多係嗰啲時間…所以呢就走來走
去喇,咁啲物資…好急咁樣…即係要將時間調轉尺來配合呢
個物資嘅運送咁樣囉。呢度就爭啲啦咁樣。” (女,11-15 年
經驗,L09P1)
“At the time, supposedly, every district would have some materials coordinated so that they could practise. But it happened to be that the bookings were made for around the same time…so (the materials) had to go back and forth, the materials…it seemed rushed…like we had to change the timings to accommodate the delivery of the materials. This was a bit of a limitation.” (Female, 11-15 yr
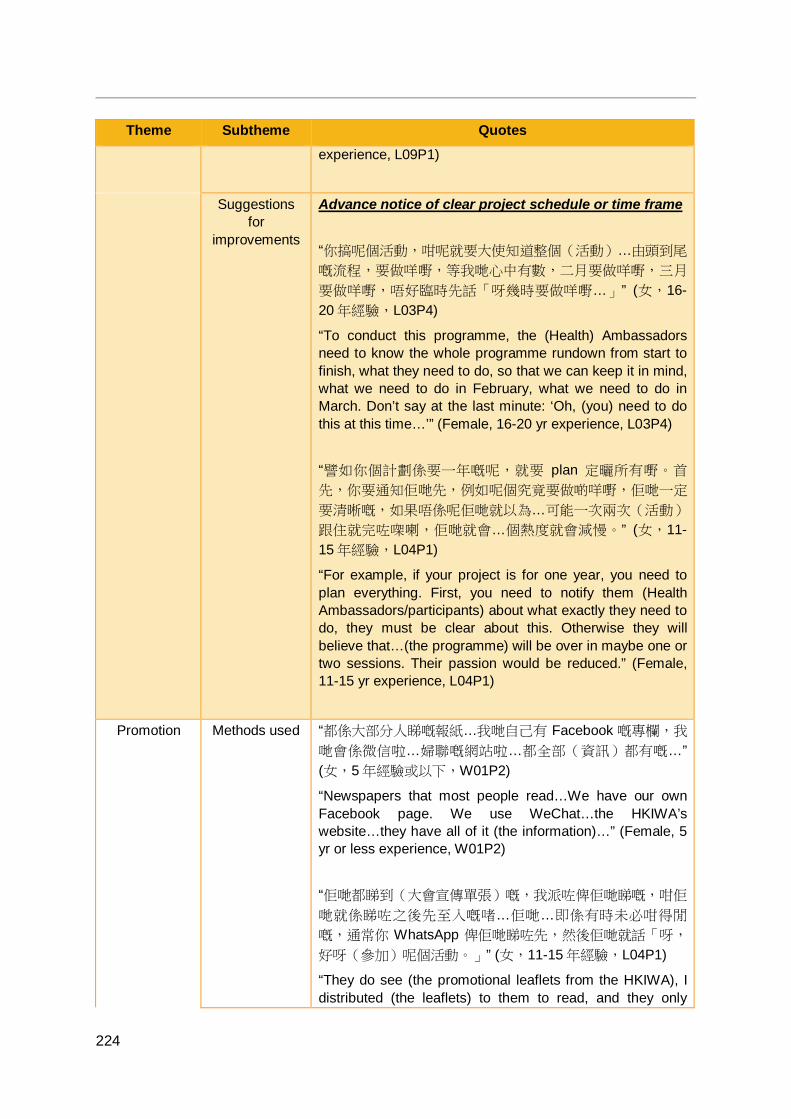
224
Theme Subtheme Quotes experience, L09P1)
Suggestions for
improvements
Advance notice of clear project schedule or time frame “你搞呢個活動,咁呢就要大使知道整個(活動)…由頭到尾
嘅流程,要做咩嘢,等我哋心中有數,二月要做咩嘢,三月
要做咩嘢,唔好臨時先話「呀幾時要做咩嘢…」” (女,16-20 年經驗,L03P4)
“To conduct this programme, the (Health) Ambassadors need to know the whole programme rundown from start to finish, what they need to do, so that we can keep it in mind, what we need to do in February, what we need to do in March. Don’t say at the last minute: ‘Oh, (you) need to do this at this time…’” (Female, 16-20 yr experience, L03P4) “譬如你個計劃係要一年嘅呢,就要 plan 定曬所有嘢。首
先,你要通知佢哋先,例如呢個究竟要做啲咩嘢,佢哋一定
要清晰嘅,如果唔係呢佢哋就以為…可能一次兩次(活動)
跟住就完咗㗎喇,佢哋就會…個熱度就會減慢。” (女,11-15 年經驗,L04P1)
“For example, if your project is for one year, you need to plan everything. First, you need to notify them (Health Ambassadors/participants) about what exactly they need to do, they must be clear about this. Otherwise they will believe that…(the programme) will be over in maybe one or two sessions. Their passion would be reduced.” (Female, 11-15 yr experience, L04P1)
Promotion Methods used “都係大部分人睇嘅報紙…我哋自己有 Facebook 嘅專欄,我
哋會係微信啦…婦聯嘅網站啦…都全部(資訊)都有嘅…” (女,5 年經驗或以下,W01P2)
“Newspapers that most people read…We have our own Facebook page. We use WeChat…the HKIWA’s website…they have all of it (the information)…” (Female, 5 yr or less experience, W01P2) “佢哋都睇到(大會宣傳單張)嘅,我派咗俾佢哋睇嘅,咁佢
哋就係睇咗之後先至入嘅啫…佢哋…即係有時未必咁得閒
嘅,通常你 WhatsApp 俾佢哋睇咗先,然後佢哋就話「呀,
好呀(參加)呢個活動。」” (女,11-15 年經驗,L04P1)
“They do see (the promotional leaflets from the HKIWA), I distributed (the leaflets) to them to read, and they only

225
Theme Subtheme Quotes joined (the programme) after reading…they…might not necessarily be free. Usually, if you WhatsApp it (the leaflet) to them to read first, then they will say, ‘Ah, this programme would be good (to join).’” (Female, 11-15 yr experience, L04P1)
Limitations “我覺得我哋喺電視啦,或者一啲其他嘅嗰個圖像,就係少咗
啲嘅。” (女,5 年經驗或以下,W01P2)
“I feel that for television, or pictoral (visual) ones (promotion), we have been a bit lacking.” (Female, <5 yr or less experience, W01P2)
Suggestions for
improvements
“即係唔係淨係我哋婦女團體個社區嗰度,我覺得…譬如話一
啲學校呀…即係你哋港大都要推廣下囉。” (女,11-15 年經
驗,L04P1)
“So it is not only within our women’s associations community, I feel that…for example, some academic institutions…that is, you, HKU, needs to do some promotion too.” (Female, 11-15 yr experience, L04P1) “大家都用得比較多嘅嗰個,睇電視啦…搭地鐵嘅時候會有少
少嗰個…燈箱(廣告)嗰個啦。” (女,5 年經驗或以下,
W01P2) “Everyone uses (does) that quite a lot, watching television…when you take the MTR, there could be some…adverts.” (Female, 5 yr or less experience, W01P2)
Recruitment Methods used by the member
associations
“你啲人成日都喺街度派街招,佢攞完都無件事…我話唔係
啦,我哋有啲會員…我哋有咁多會員,上樓招…我哋上樓招
…拍門囉!” (女,6-10 年經驗,L03P3)
“People always distribute leaflets on the street to recruit. People take the leaflets and forget about them…I said, no, we have some members…we have so many members, we should recruit door-to-door…make home visits!” (Female, 6-10 yr experience, L03P3) “咁我哋就喺街度開個 booth 啦…一路呢就盡量(派單張)出
去…講明係做乜嘢…係咁專業呢,起碼佢哋會明呀…明白我
做緊乜嘢…即係你知…擺個帳篷咁靚,都有人望㗎…” (女,
11-15 年經驗,L03P6)
“We set up a booth on the street and distributed (the leaflets) as much as possible…say exactly what (the
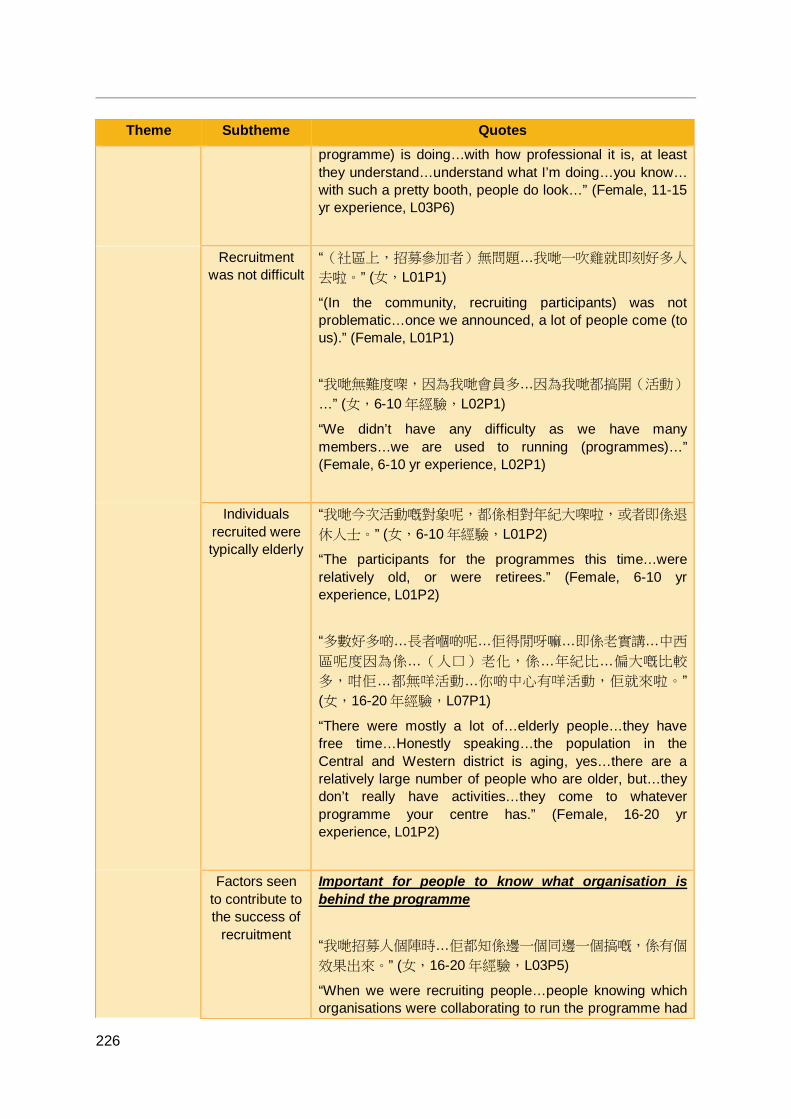
226
Theme Subtheme Quotes programme) is doing…with how professional it is, at least they understand…understand what I’m doing…you know… with such a pretty booth, people do look…” (Female, 11-15 yr experience, L03P6)
Recruitment was not difficult
“(社區上,招募參加者)無問題…我哋一吹雞就即刻好多人
去啦。” (女,L01P1)
“(In the community, recruiting participants) was not problematic…once we announced, a lot of people come (to us).” (Female, L01P1) “我哋無難度㗎,因為我哋會員多…因為我哋都搞開(活動)
…” (女,6-10 年經驗,L02P1)
“We didn’t have any difficulty as we have many members…we are used to running (programmes)…” (Female, 6-10 yr experience, L02P1)
Individuals recruited were typically elderly
“我哋今次活動嘅對象呢,都係相對年紀大㗎啦,或者即係退
休人士。” (女,6-10 年經驗,L01P2)
“The participants for the programmes this time…were relatively old, or were retirees.” (Female, 6-10 yr experience, L01P2) “多數好多啲…長者嗰啲呢…佢得閒呀嘛…即係老實講…中西
區呢度因為係…(人口)老化,係…年紀比…偏大嘅比較
多,咁佢…都無咩活動…你啲中心有咩活動,佢就來啦。” (女,16-20 年經驗,L07P1)
“There were mostly a lot of…elderly people…they have free time…Honestly speaking…the population in the Central and Western district is aging, yes…there are a relatively large number of people who are older, but…they don’t really have activities…they come to whatever programme your centre has.” (Female, 16-20 yr experience, L01P2)
Factors seen to contribute to the success of
recruitment
Important for people to know what organisation is behind the programme “我哋招募人個陣時…佢都知係邊一個同邊一個搞嘅,係有個
效果出來。” (女,16-20 年經驗,L03P5)
“When we were recruiting people…people knowing which organisations were collaborating to run the programme had
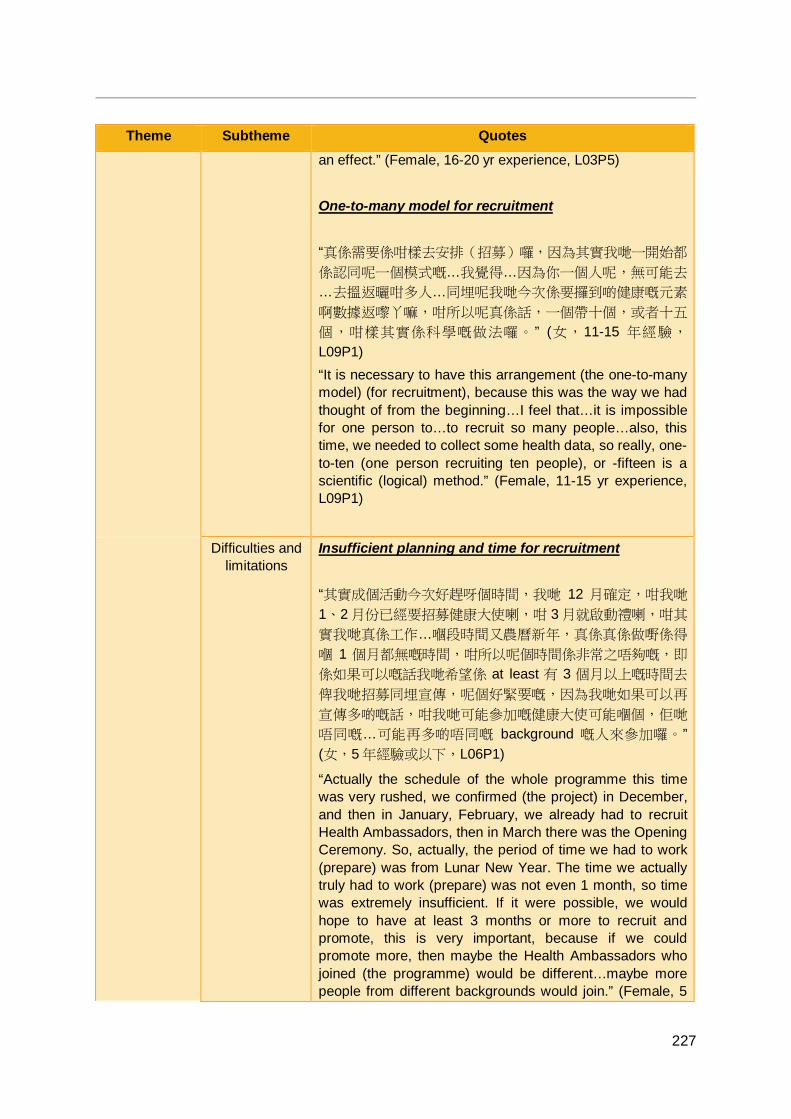
227
Theme Subtheme Quotes an effect.” (Female, 16-20 yr experience, L03P5) One-to-many model for recruitment “真係需要係咁樣去安排(招募)囉,因為其實我哋一開始都
係認同呢一個模式嘅…我覺得…因為你一個人呢,無可能去
…去搵返曬咁多人…同埋呢我哋今次係要攞到啲健康嘅元素
啊數據返嚟丫嘛,咁所以呢真係話,一個帶十個,或者十五
個,咁樣其實係科學嘅做法囉。 ” (女,11-15 年經驗,
L09P1) “It is necessary to have this arrangement (the one-to-many model) (for recruitment), because this was the way we had thought of from the beginning…I feel that…it is impossible for one person to…to recruit so many people…also, this time, we needed to collect some health data, so really, one-to-ten (one person recruiting ten people), or -fifteen is a scientific (logical) method.” (Female, 11-15 yr experience, L09P1)
Difficulties and limitations
Insufficient planning and time for recruitment “其實成個活動今次好趕呀個時間,我哋 12 月確定,咁我哋
1、2 月份已經要招募健康大使喇,咁 3 月就啟動禮喇,咁其
實我哋真係工作…嗰段時間又農曆新年,真係真係做嘢係得
嗰 1 個月都無嘅時間,咁所以呢個時間係非常之唔夠嘅,即
係如果可以嘅話我哋希望係 at least 有 3 個月以上嘅時間去
俾我哋招募同埋宣傳,呢個好緊要嘅,因為我哋如果可以再
宣傳多啲嘅話,咁我哋可能參加嘅健康大使可能嗰個,佢哋
唔同嘅…可能再多啲唔同嘅 background 嘅人來參加囉。” (女,5 年經驗或以下,L06P1)
“Actually the schedule of the whole programme this time was very rushed, we confirmed (the project) in December, and then in January, February, we already had to recruit Health Ambassadors, then in March there was the Opening Ceremony. So, actually, the period of time we had to work (prepare) was from Lunar New Year. The time we actually truly had to work (prepare) was not even 1 month, so time was extremely insufficient. If it were possible, we would hope to have at least 3 months or more to recruit and promote, this is very important, because if we could promote more, then maybe the Health Ambassadors who joined (the programme) would be different…maybe more people from different backgrounds would join.” (Female, 5
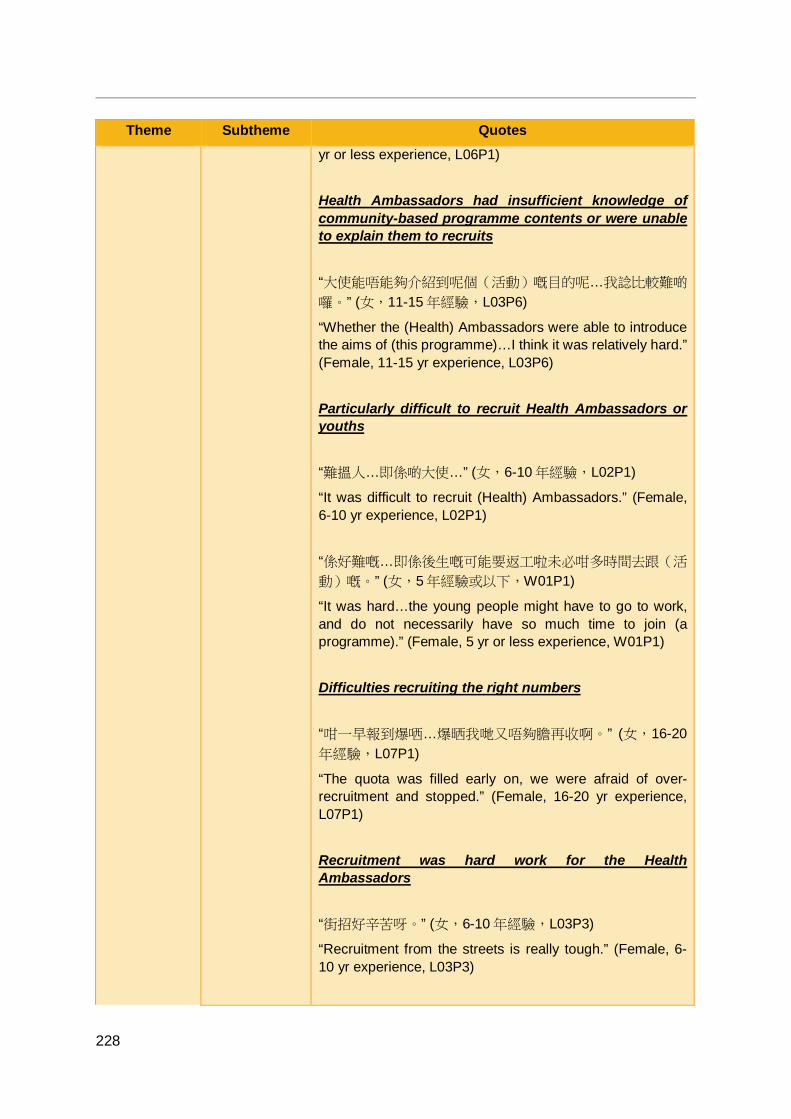
228
Theme Subtheme Quotes yr or less experience, L06P1) Health Ambassadors had insufficient knowledge of community-based programme contents or were unable to explain them to recruits “大使能唔能夠介紹到呢個(活動)嘅目的呢…我諗比較難啲
囉。” (女,11-15 年經驗,L03P6)
“Whether the (Health) Ambassadors were able to introduce the aims of (this programme)…I think it was relatively hard.” (Female, 11-15 yr experience, L03P6) Particularly difficult to recruit Health Ambassadors or youths “難搵人…即係啲大使…” (女,6-10 年經驗,L02P1)
“It was difficult to recruit (Health) Ambassadors.” (Female, 6-10 yr experience, L02P1) “係好難嘅…即係後生嘅可能要返工啦未必咁多時間去跟(活
動)嘅。” (女,5年經驗或以下,W01P1)
“It was hard…the young people might have to go to work, and do not necessarily have so much time to join (a programme).” (Female, 5 yr or less experience, W01P1) Difficulties recruiting the right numbers “咁一早報到爆哂…爆晒我哋又唔夠膽再收啊。” (女,16-20年經驗,L07P1)
“The quota was filled early on, we were afraid of over-recruitment and stopped.” (Female, 16-20 yr experience, L07P1) Recruitment was hard work for the Health Ambassadors “街招好辛苦呀。” (女,6-10 年經驗,L03P3)
“Recruitment from the streets is really tough.” (Female, 6-10 yr experience, L03P3)
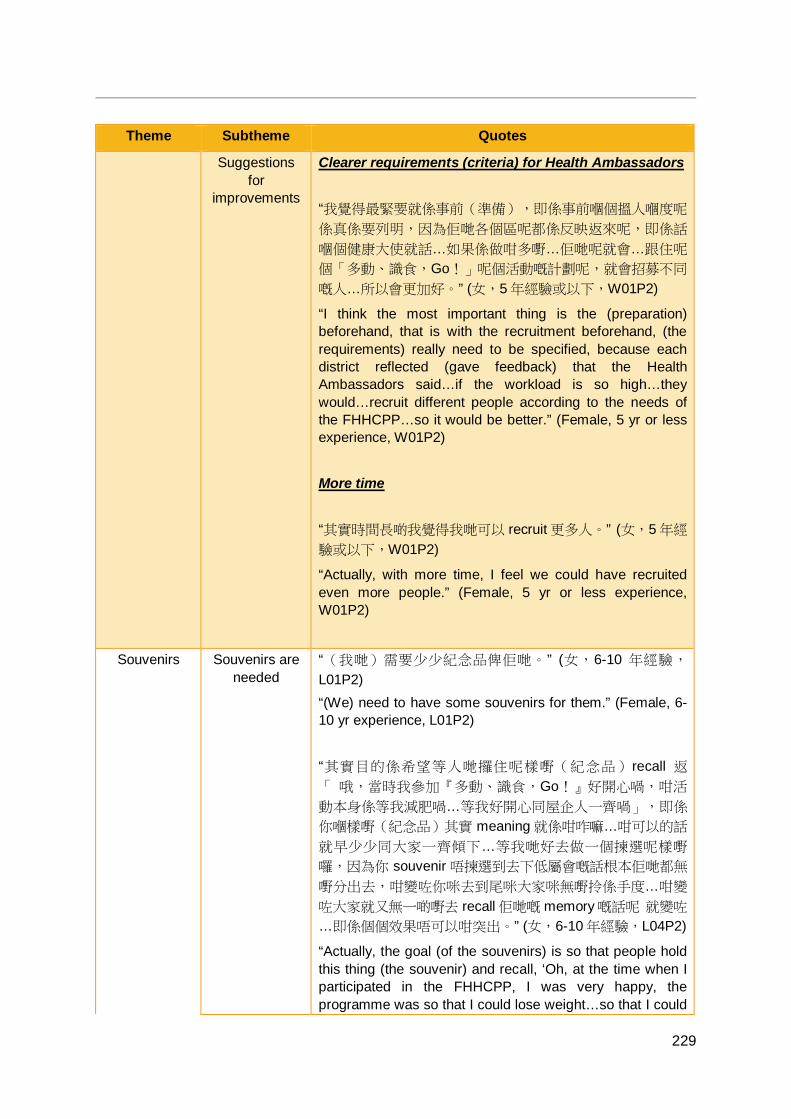
229
Theme Subtheme Quotes
Suggestions for
improvements
Clearer requirements (criteria) for Health Ambassadors “我覺得最緊要就係事前(準備),即係事前嗰個搵人嗰度呢
係真係要列明,因為佢哋各個區呢都係反映返來呢,即係話
嗰個健康大使就話…如果係做咁多嘢…佢哋呢就會…跟住呢
個「多動、識食,Go!」呢個活動嘅計劃呢,就會招募不同
嘅人…所以會更加好。” (女,5 年經驗或以下,W01P2)
“I think the most important thing is the (preparation) beforehand, that is with the recruitment beforehand, (the requirements) really need to be specified, because each district reflected (gave feedback) that the Health Ambassadors said…if the workload is so high…they would…recruit different people according to the needs of the FHHCPP…so it would be better.” (Female, 5 yr or less experience, W01P2) More time “其實時間長啲我覺得我哋可以 recruit 更多人。” (女,5 年經
驗或以下,W01P2)
“Actually, with more time, I feel we could have recruited even more people.” (Female, 5 yr or less experience, W01P2)
Souvenirs Souvenirs are needed
“(我哋)需要少少紀念品俾佢哋。” (女,6-10 年經驗,
L01P2) “(We) need to have some souvenirs for them.” (Female, 6-10 yr experience, L01P2) “其實目的係希望等人哋攞住呢樣嘢(紀念品)recall 返
「 哦,當時我參加『多動、識食,Go!』好開心喎,咁活
動本身係等我減肥喎…等我好開心同屋企人一齊喎」,即係
你嗰樣嘢(紀念品)其實 meaning 就係咁咋嘛…咁可以的話
就早少少同大家一齊傾下…等我哋好去做一個揀選呢樣嘢
囉,因為你 souvenir 唔揀選到去下低屬會嘅話根本佢哋都無
嘢分出去,咁變咗你咪去到尾咪大家咪無嘢拎係手度…咁變
咗大家就又無一啲嘢去 recall 佢哋嘅 memory 嘅話呢 就變咗
…即係個個效果唔可以咁突出。” (女,6-10 年經驗,L04P2)
“Actually, the goal (of the souvenirs) is so that people hold this thing (the souvenir) and recall, ‘Oh, at the time when I participated in the FHHCPP, I was very happy, the programme was so that I could lose weight…so that I could
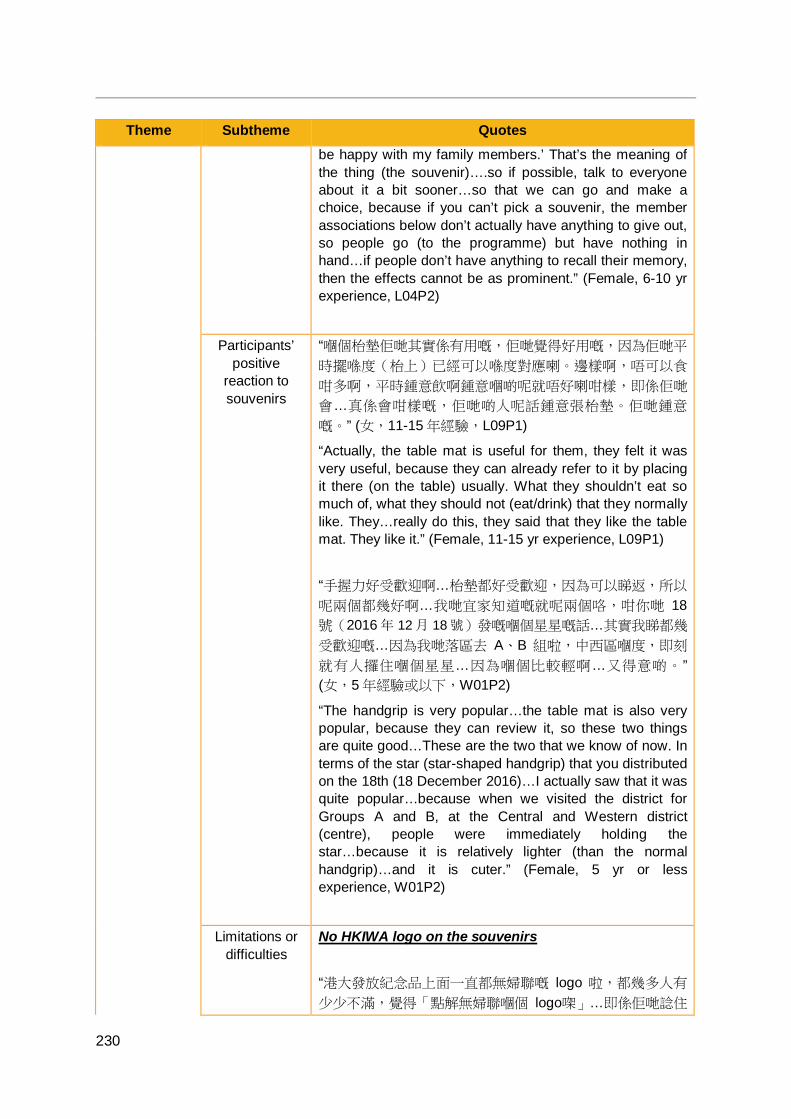
230
Theme Subtheme Quotes be happy with my family members.’ That’s the meaning of the thing (the souvenir)….so if possible, talk to everyone about it a bit sooner…so that we can go and make a choice, because if you can’t pick a souvenir, the member associations below don’t actually have anything to give out, so people go (to the programme) but have nothing in hand…if people don’t have anything to recall their memory, then the effects cannot be as prominent.” (Female, 6-10 yr experience, L04P2)
Participants’ positive
reaction to souvenirs
“嗰個枱墊佢哋其實係有用嘅,佢哋覺得好用嘅,因為佢哋平
時擺喺度(枱上)已經可以喺度對應喇。邊樣啊,唔可以食
咁多啊,平時鍾意飲啊鍾意嗰啲呢就唔好喇咁樣,即係佢哋
會…真係會咁樣嘅,佢哋啲人呢話鍾意張枱墊。佢哋鍾意
嘅。” (女,11-15 年經驗,L09P1)
“Actually, the table mat is useful for them, they felt it was very useful, because they can already refer to it by placing it there (on the table) usually. What they shouldn’t eat so much of, what they should not (eat/drink) that they normally like. They…really do this, they said that they like the table mat. They like it.” (Female, 11-15 yr experience, L09P1) “手握力好受歡迎啊…枱墊都好受歡迎,因為可以睇返,所以
呢兩個都幾好啊…我哋宜家知道嘅就呢兩個咯,咁你哋 18號(2016 年 12 月 18 號)發嘅嗰個星星嘅話…其實我睇都幾
受歡迎嘅…因為我哋落區去 A、B 組啦,中西區嗰度,即刻
就有人攞住嗰個星星…因為嗰個比較輕啊…又得意啲。” (女,5 年經驗或以下,W01P2)
“The handgrip is very popular…the table mat is also very popular, because they can review it, so these two things are quite good…These are the two that we know of now. In terms of the star (star-shaped handgrip) that you distributed on the 18th (18 December 2016)…I actually saw that it was quite popular…because when we visited the district for Groups A and B, at the Central and Western district (centre), people were immediately holding the star…because it is relatively lighter (than the normal handgrip)…and it is cuter.” (Female, 5 yr or less experience, W01P2)
Limitations or difficulties
No HKIWA logo on the souvenirs “港大發放紀念品上面一直都無婦聯嘅 logo 啦,都幾多人有
少少不滿,覺得「點解無婦聯嗰個 logo㗎」…即係佢哋諗住
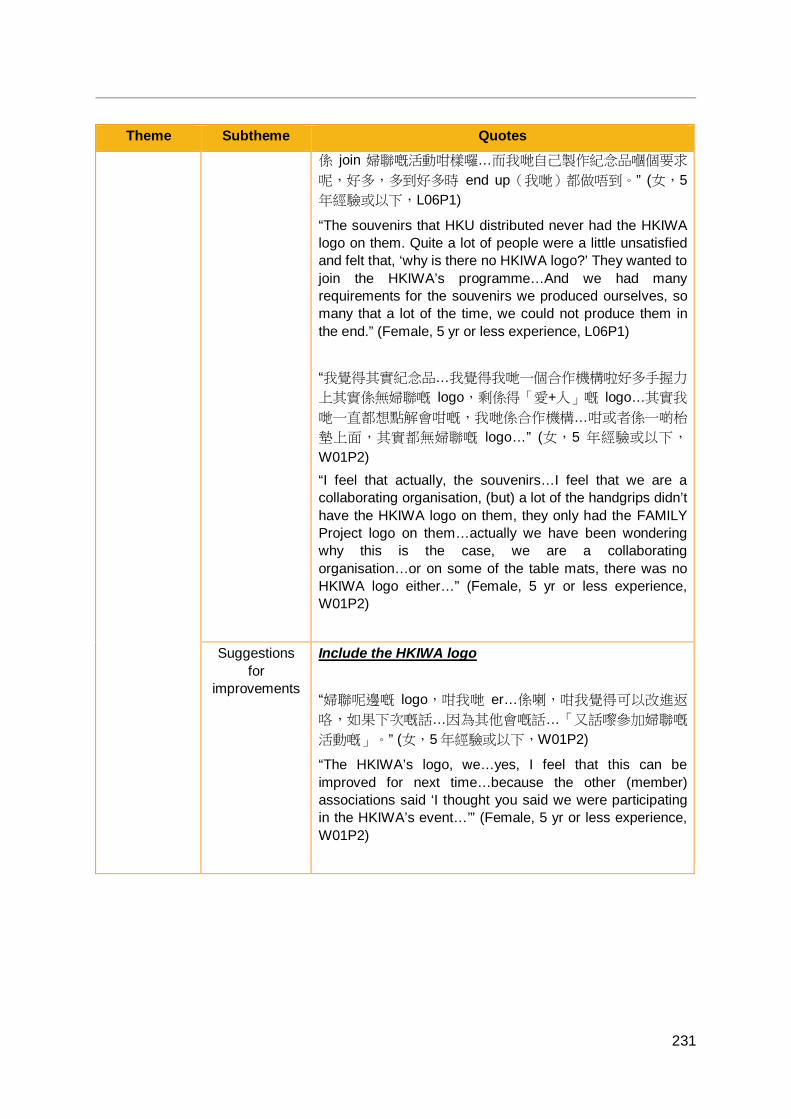
231
Theme Subtheme Quotes 係 join 婦聯嘅活動咁樣囉…而我哋自己製作紀念品嗰個要求
呢,好多,多到好多時 end up(我哋)都做唔到。” (女,5年經驗或以下,L06P1)
“The souvenirs that HKU distributed never had the HKIWA logo on them. Quite a lot of people were a little unsatisfied and felt that, ‘why is there no HKIWA logo?’ They wanted to join the HKIWA’s programme…And we had many requirements for the souvenirs we produced ourselves, so many that a lot of the time, we could not produce them in the end.” (Female, 5 yr or less experience, L06P1) “我覺得其實紀念品…我覺得我哋一個合作機構啦好多手握力
上其實係無婦聯嘅 logo,剩係得「愛+人」嘅 logo…其實我
哋一直都想點解會咁嘅,我哋係合作機構…咁或者係一啲枱
墊上面,其實都無婦聯嘅 logo…” (女,5 年經驗或以下,
W01P2) “I feel that actually, the souvenirs…I feel that we are a collaborating organisation, (but) a lot of the handgrips didn’t have the HKIWA logo on them, they only had the FAMILY Project logo on them…actually we have been wondering why this is the case, we are a collaborating organisation…or on some of the table mats, there was no HKIWA logo either…” (Female, 5 yr or less experience, W01P2)
Suggestions for
improvements
Include the HKIWA logo “婦聯呢邊嘅 logo,咁我哋 er…係喇,咁我覺得可以改進返
咯,如果下次嘅話…因為其他會嘅話…「又話嚟參加婦聯嘅
活動嘅」。” (女,5 年經驗或以下,W01P2)
“The HKIWA’s logo, we…yes, I feel that this can be improved for next time…because the other (member) associations said ‘I thought you said we were participating in the HKIWA’s event…’” (Female, 5 yr or less experience, W01P2)
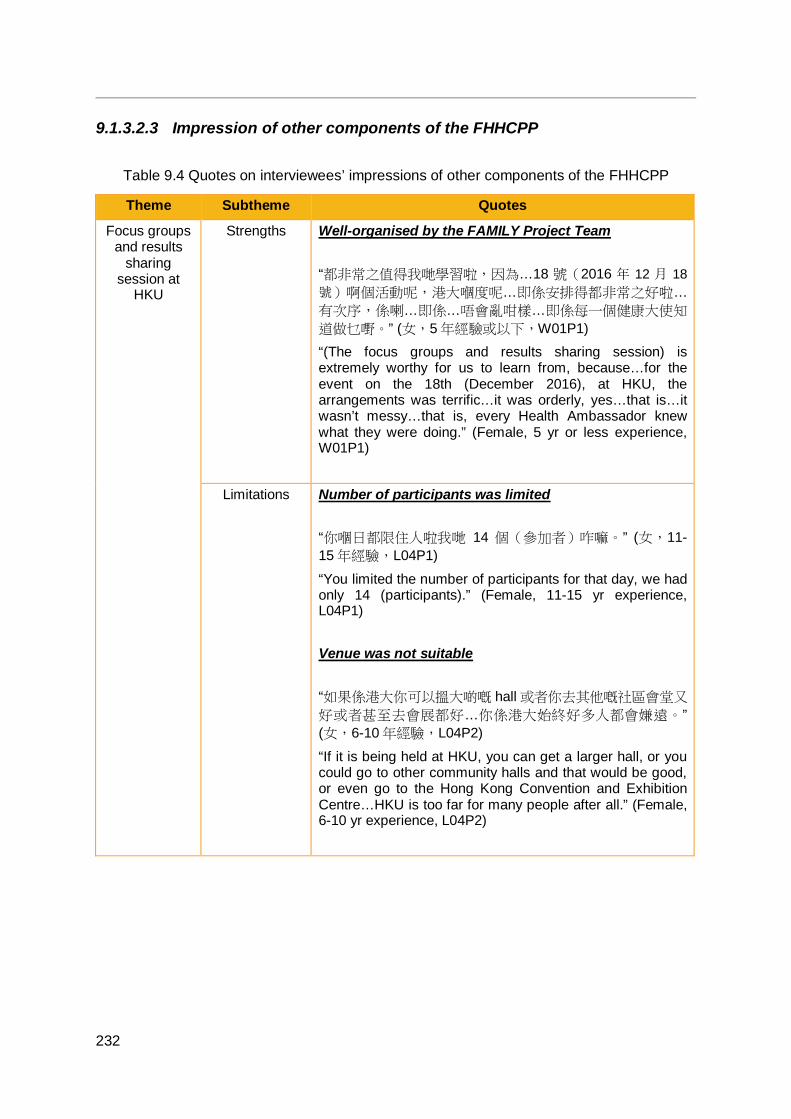
232
9.1.3.2.3 Impression of other components of the FHHCPP
Table 9.4 Quotes on interviewees’ impressions of other components of the FHHCPP
Theme Subtheme Quotes
Focus groups and results
sharing session at
HKU
Strengths Well-organised by the FAMILY Project Team “都非常之值得我哋學習啦,因為…18 號(2016 年 12 月 18號)啊個活動呢,港大嗰度呢…即係安排得都非常之好啦…
有次序,係喇…即係…唔會亂咁樣…即係每一個健康大使知
道做乜嘢。” (女,5 年經驗或以下,W01P1) “(The focus groups and results sharing session) is extremely worthy for us to learn from, because…for the event on the 18th (December 2016), at HKU, the arrangements was terrific…it was orderly, yes…that is…it wasn’t messy…that is, every Health Ambassador knew what they were doing.” (Female, 5 yr or less experience, W01P1)
Limitations Number of participants was limited “你嗰日都限住人啦我哋 14 個(參加者)咋嘛。” (女,11-15 年經驗,L04P1)
“You limited the number of participants for that day, we had only 14 (participants).” (Female, 11-15 yr experience, L04P1) Venue was not suitable “如果係港大你可以搵大啲嘅 hall 或者你去其他嘅社區會堂又
好或者甚至去會展都好…你係港大始終好多人都會嫌遠。” (女,6-10 年經驗,L04P2)
“If it is being held at HKU, you can get a larger hall, or you could go to other community halls and that would be good, or even go to the Hong Kong Convention and Exhibition Centre…HKU is too far for many people after all.” (Female, 6-10 yr experience, L04P2)
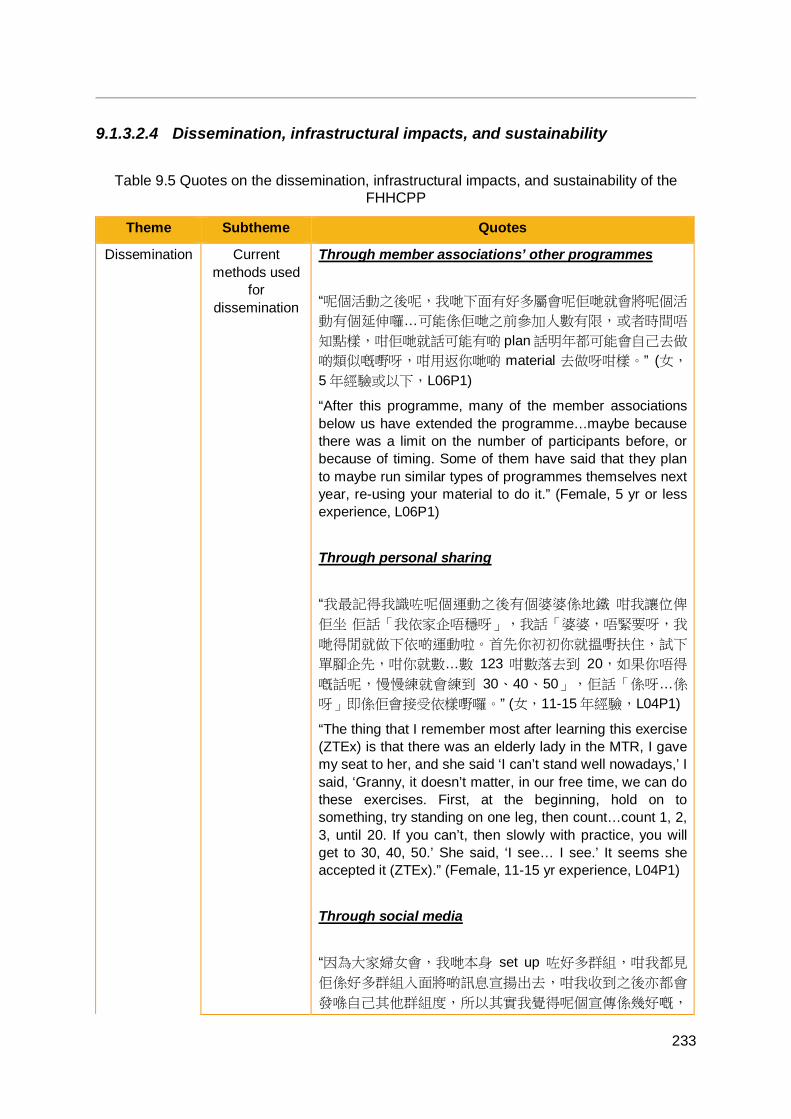
233
9.1.3.2.4 Dissemination, infrastructural impacts, and sustainability
Table 9.5 Quotes on the dissemination, infrastructural impacts, and sustainability of the FHHCPP
Theme Subtheme Quotes
Dissemination Current methods used
for dissemination
Through member associations’ other programmes “呢個活動之後呢,我哋下面有好多屬會呢佢哋就會將呢個活
動有個延伸囉…可能係佢哋之前參加人數有限,或者時間唔
知點樣,咁佢哋就話可能有啲 plan 話明年都可能會自己去做
啲類似嘅嘢呀,咁用返你哋啲 material 去做呀咁樣。” (女,
5 年經驗或以下,L06P1)
“After this programme, many of the member associations below us have extended the programme…maybe because there was a limit on the number of participants before, or because of timing. Some of them have said that they plan to maybe run similar types of programmes themselves next year, re-using your material to do it.” (Female, 5 yr or less experience, L06P1) Through personal sharing “我最記得我識咗呢個運動之後有個婆婆係地鐵 咁我讓位俾
佢坐 佢話「我依家企唔穩呀」,我話「婆婆,唔緊要呀,我
哋得閒就做下依啲運動啦。首先你初初你就搵嘢扶住,試下
單腳企先,咁你就數…數 123 咁數落去到 20,如果你唔得
嘅話呢,慢慢練就會練到 30、40、50」,佢話「係呀…係
呀」即係佢會接受依樣嘢囉。” (女,11-15 年經驗,L04P1)
“The thing that I remember most after learning this exercise (ZTEx) is that there was an elderly lady in the MTR, I gave my seat to her, and she said ‘I can’t stand well nowadays,’ I said, ‘Granny, it doesn’t matter, in our free time, we can do these exercises. First, at the beginning, hold on to something, try standing on one leg, then count…count 1, 2, 3, until 20. If you can’t, then slowly with practice, you will get to 30, 40, 50.’ She said, ‘I see… I see.’ It seems she accepted it (ZTEx).” (Female, 11-15 yr experience, L04P1) Through social media “因為大家婦女會,我哋本身 set up 咗好多群組,咁我都見
佢係好多群組入面將啲訊息宣揚出去,咁我收到之後亦都會
發喺自己其他群組度,所以其實我覺得呢個宣傳係幾好嘅,
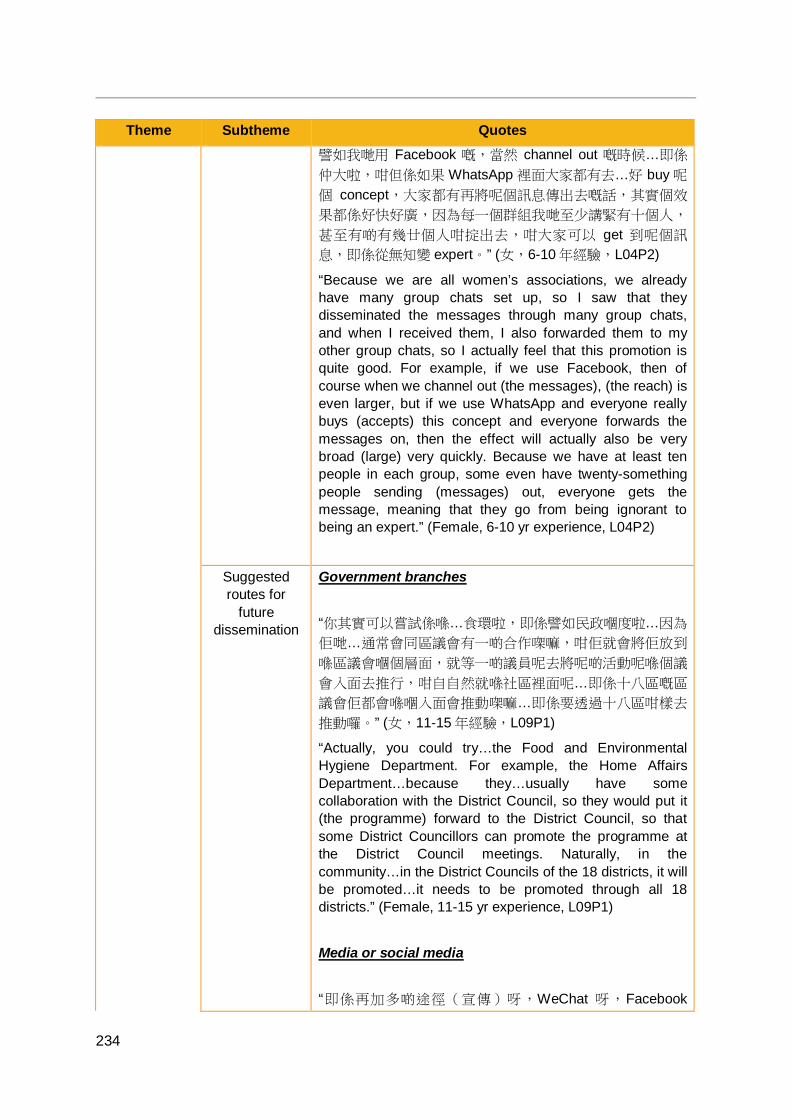
234
Theme Subtheme Quotes 譬如我哋用 Facebook 嘅,當然 channel out 嘅時候…即係
仲大啦,咁但係如果 WhatsApp 裡面大家都有去…好 buy 呢
個 concept,大家都有再將呢個訊息傳出去嘅話,其實個效
果都係好快好廣,因為每一個群組我哋至少講緊有十個人,
甚至有啲有幾廿個人咁掟出去,咁大家可以 get 到呢個訊
息,即係從無知變 expert。” (女,6-10 年經驗,L04P2)
“Because we are all women’s associations, we already have many group chats set up, so I saw that they disseminated the messages through many group chats, and when I received them, I also forwarded them to my other group chats, so I actually feel that this promotion is quite good. For example, if we use Facebook, then of course when we channel out (the messages), (the reach) is even larger, but if we use WhatsApp and everyone really buys (accepts) this concept and everyone forwards the messages on, then the effect will actually also be very broad (large) very quickly. Because we have at least ten people in each group, some even have twenty-something people sending (messages) out, everyone gets the message, meaning that they go from being ignorant to being an expert.” (Female, 6-10 yr experience, L04P2)
Suggested routes for
future dissemination
Government branches “你其實可以嘗試係喺…食環啦,即係譬如民政嗰度啦…因為
佢哋…通常會同區議會有一啲合作㗎嘛,咁佢就會將佢放到
喺區議會嗰個層面,就等一啲議員呢去將呢啲活動呢喺個議
會入面去推行,咁自自然就喺社區裡面呢…即係十八區嘅區
議會佢都會喺嗰入面會推動㗎嘛…即係要透過十八區咁樣去
推動囉。” (女,11-15 年經驗,L09P1)
“Actually, you could try…the Food and Environmental Hygiene Department. For example, the Home Affairs Department…because they…usually have some collaboration with the District Council, so they would put it (the programme) forward to the District Council, so that some District Councillors can promote the programme at the District Council meetings. Naturally, in the community…in the District Councils of the 18 districts, it will be promoted…it needs to be promoted through all 18 districts.” (Female, 11-15 yr experience, L09P1) Media or social media “即係再加多啲途徑(宣傳)呀,WeChat 呀,Facebook
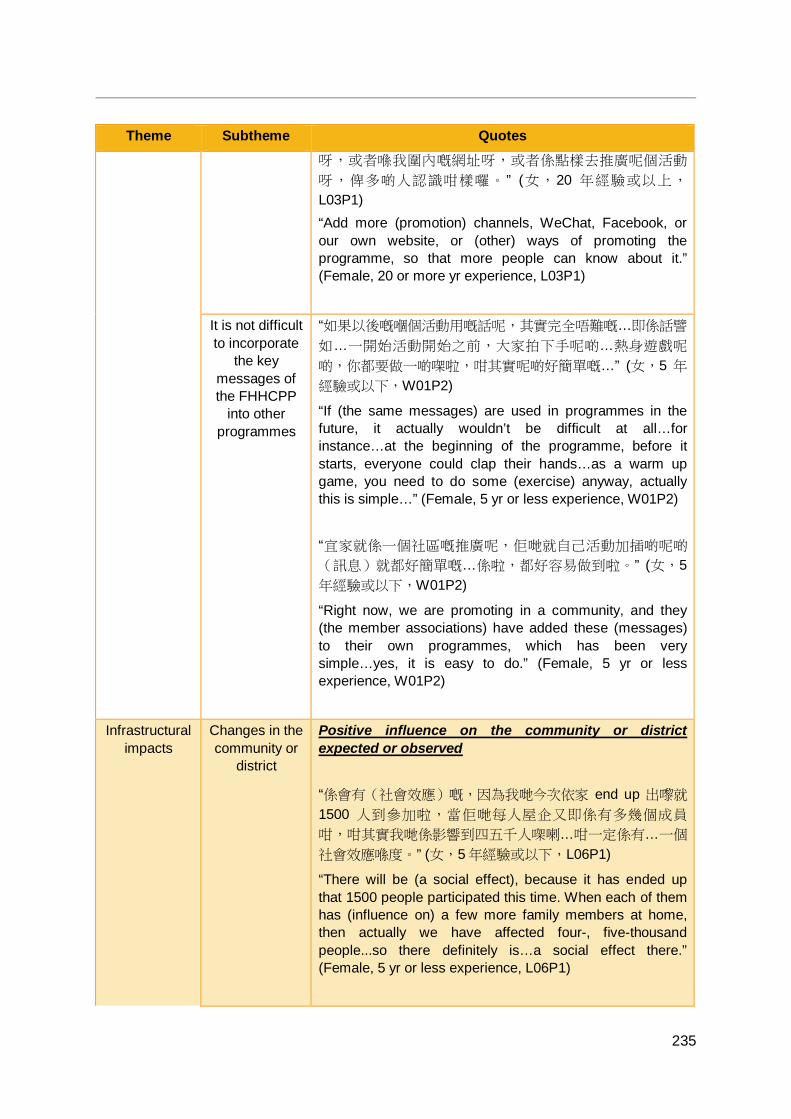
235
Theme Subtheme Quotes 呀,或者喺我圍內嘅網址呀,或者係點樣去推廣呢個活動
呀,俾多啲人認識咁樣囉。 ” (女,20 年經驗或以上,
L03P1) “Add more (promotion) channels, WeChat, Facebook, or our own website, or (other) ways of promoting the programme, so that more people can know about it.” (Female, 20 or more yr experience, L03P1)
It is not difficult to incorporate
the key messages of the FHHCPP
into other programmes
“如果以後嘅嗰個活動用嘅話呢,其實完全唔難嘅…即係話譬
如…一開始活動開始之前,大家拍下手呢啲…熱身遊戲呢
啲,你都要做一啲㗎啦,咁其實呢啲好簡單嘅…” (女,5 年
經驗或以下,W01P2)
“If (the same messages) are used in programmes in the future, it actually wouldn’t be difficult at all…for instance…at the beginning of the programme, before it starts, everyone could clap their hands…as a warm up game, you need to do some (exercise) anyway, actually this is simple…” (Female, 5 yr or less experience, W01P2) “宜家就係一個社區嘅推廣呢,佢哋就自己活動加插啲呢啲
(訊息)就都好簡單嘅…係啦,都好容易做到啦。” (女,5年經驗或以下,W01P2)
“Right now, we are promoting in a community, and they (the member associations) have added these (messages) to their own programmes, which has been very simple…yes, it is easy to do.” (Female, 5 yr or less experience, W01P2)
Infrastructural impacts
Changes in the community or
district
Positive influence on the community or district expected or observed “係會有(社會效應)嘅,因為我哋今次依家 end up 出嚟就
1500 人到參加啦,當佢哋每人屋企又即係有多幾個成員
咁,咁其實我哋係影響到四五千人㗎喇…咁一定係有…一個
社會效應喺度。” (女,5 年經驗或以下,L06P1)
“There will be (a social effect), because it has ended up that 1500 people participated this time. When each of them has (influence on) a few more family members at home, then actually we have affected four-, five-thousand people...so there definitely is…a social effect there.” (Female, 5 yr or less experience, L06P1)
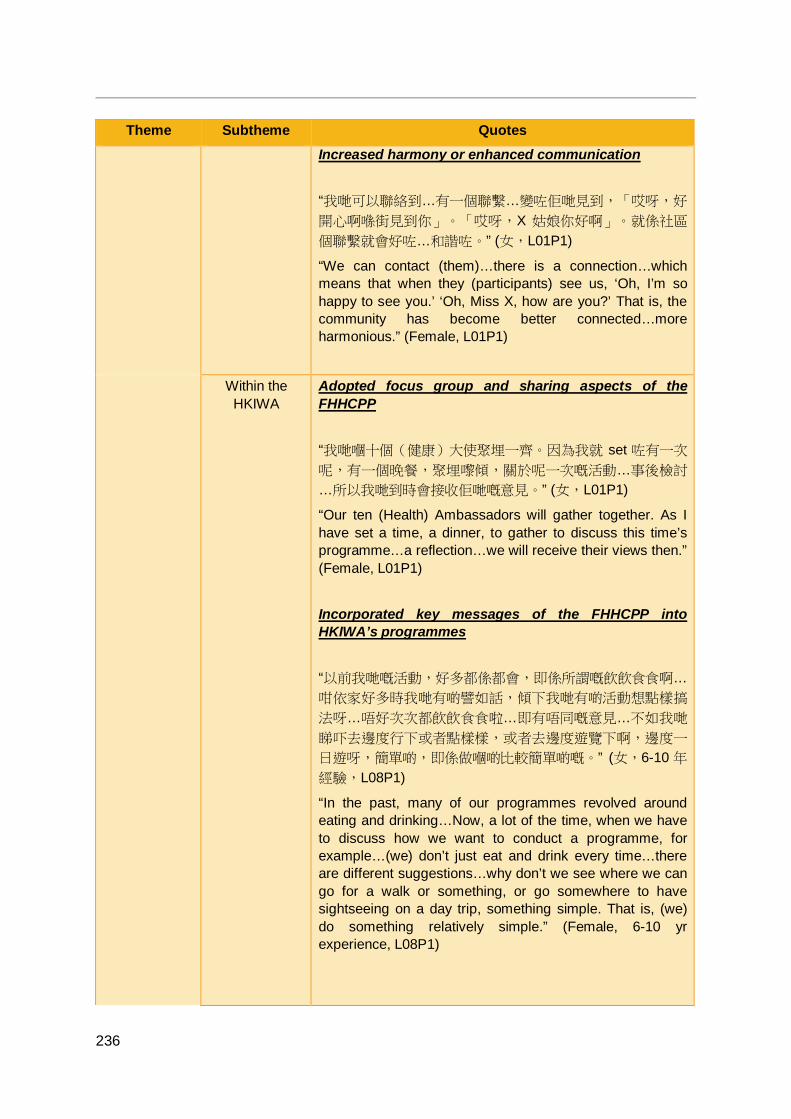
236
Theme Subtheme Quotes Increased harmony or enhanced communication “我哋可以聯絡到…有一個聯繫…變咗佢哋見到,「哎呀,好
開心啊喺街見到你」。「哎呀,X 姑娘你好啊」。就係社區
個聯繫就會好咗…和諧咗。” (女,L01P1)
“We can contact (them)…there is a connection…which means that when they (participants) see us, ‘Oh, I’m so happy to see you.’ ‘Oh, Miss X, how are you?’ That is, the community has become better connected…more harmonious.” (Female, L01P1)
Within the HKIWA
Adopted focus group and sharing aspects of the FHHCPP “我哋嗰十個(健康)大使聚埋一齊。因為我就 set 咗有一次
呢,有一個晚餐,聚埋嚟傾,關於呢一次嘅活動…事後檢討
…所以我哋到時會接收佢哋嘅意見。” (女,L01P1)
“Our ten (Health) Ambassadors will gather together. As I have set a time, a dinner, to gather to discuss this time’s programme…a reflection…we will receive their views then.” (Female, L01P1) Incorporated key messages of the FHHCPP into HKIWA’s programmes “以前我哋嘅活動,好多都係都會,即係所謂嘅飲飲食食啊…
咁依家好多時我哋有啲譬如話,傾下我哋有啲活動想點樣搞
法呀…唔好次次都飲飲食食啦…即有唔同嘅意見…不如我哋
睇吓去邊度行下或者點樣樣,或者去邊度遊覽下啊,邊度一
日遊呀,簡單啲,即係做嗰啲比較簡單啲嘅。” (女,6-10 年
經驗,L08P1)
“In the past, many of our programmes revolved around eating and drinking…Now, a lot of the time, when we have to discuss how we want to conduct a programme, for example…(we) don’t just eat and drink every time…there are different suggestions…why don’t we see where we can go for a walk or something, or go somewhere to have sightseeing on a day trip, something simple. That is, (we) do something relatively simple.” (Female, 6-10 yr experience, L08P1)

237
Theme Subtheme Quotes Stronger relationships amongst the HKIWA and/or its member associations “我哋經過今次嘅活動呢,令到我哋同屬會之間個溝通呢…係
絕對加強咗好多嘅。” (女,6-10 年經驗,L08P1)
“After the programme, the communication among member assications became a lot stronger.” (Female, 6-10 yr experience, L08P1) “屬會之間佢哋嘅關係係 close 咗嘅。” (女,5 年經驗或以
下,W01P1)
“The member associations became closer.” (Female, 5 yr or less experience, W01P1) The FHHCPP provided useful learning experience for the future “同埋呢個亦都係一個好好嘅 reference 囉今次…對於下一次
再推廣嗰個時候,咁所以應該都係另外一個影響喺度。” (女,5 年經驗或以下,L06P1)
“Also this time (the FHHCPP) is also a very good reference…for when we promote it next time. So, this is another effect (of the FHHCPP).” (Female, 5 yr or less experience, L06P1)
Potential impact of the
FHHCPP
Hope that the key messages will influence wider society “因為我哋叫做第一(個)咁嘅團體…地區團體去做啦,希望
我哋都可能幫忙推到去其他囉,即係推到去全港咁樣囉。” (女,5 年經驗或以下,L06P1)
“As we count as the first organisation…community-based organisation to do this (implement a project such as the FHHCPP), we hope that we can help to spread it to other (organisations), to the whole of Hong Kong.” (Female, 5 yr or less experience, L06P1) Reducing the health costs and burden on society “(「多動,識食,GO!」)可以推廣到好大,同埋即係好
好嘅一個咯,因為香港依家嘅一啲政府嘅醫療開支係好大嘅
238
Theme Subtheme Quotes …我覺得呢啲,你譬如少糖啊,同埋「零時間運動」啊,你
隨時係可以做到…咁你就會減輕咗,其實你少少嘅一個咁推
廣,就可能減咗好多政府嘅預算咁樣,開支咁,我覺得呢個
係好…即係好值得囉。” (女,5 年經驗或以下,W01P2)
“It (the FHHCPP) can be promoted and scaled up a lot, and be a very good one (project), because the Hong Kong Government’s current medical expenditure is very large…I feel that these things, such as low sugar and ZTEx, can be done at any time…so you will ease (the burden of medical expenditure). Actually, if you promote just a little bit, you might reduce the government’s budget or expenditure by a lot. I feel that this is good…it is very worthwhile.” (Female, 5 yr or less experience, W01P2) Influence at a higher policy or governmental level “其實如果政策上嘅影響嘅話,我哋反而係希望有呢個政策上
嘅影響例如就話…去到醫管局呀或者香港政府依一方面能夠
真係 encourage 依一個活動。首先第一就係話我哋招募(健
康)大使,如果佢係電視度一宣傳嘅話 話依一個活動想大家
一齊去參與,就已經好多人去參與。咁你跟住裡面傳達嘅訊息
就係話等大家可以即係健康啲呀…減到糖呀又多啲運動做
到,咁跟住譬如舉例某一日係俾曬所有會堂係依啲
participants,即係依啲咁多群組都用到佢個會堂嘅,呢個係
非常好嘅你同一日咁多人都做到個個活動喎哇真係…可以入
健力士(世界紀錄)啦老實講句係咪先,咁所以話如果能夠
政府層面上,你哋 influence 到佢哋個 policy 係可以幫手推
廣呢個嘅話 win win 呀 all parties win 嘅 situation 來嘅。” (女,11-15 年經驗,L09P1)
“Actually, if (we are) talking about influence on policy, we actually hope to have influence on policy. For instance…the Hospital Authority or the Hong Kong Government could really encourage (promote) this programme. First of all, the first thing is that with the recruitment of the (Health) Ambassadors, if we promoted on television and said that we want everyone to go and participate in this event, then many people would join in. Then, inside (during the programme), you can deliver the message that everyone can be healthier…by reducing dietary sugar intake, doing more exercise. Then, for instance, to give an example, on a certain day, arrange to have all the community halls, so that every group can use their community hall, it would be excellent if you could have them on the same day since many people would be able to take part, it could go into the Guinness (World Records),
239
Theme Subtheme Quotes honestly speaking. That’s why (I) say that if you are able to influence their policy to help promote this (project) on a governmental level, it is a situation in which all parties win, a win-win.” (Female, 11-15 yr experience, L09P1)
Sustainability Keep holding programmes to
ensure sustainability
“(效能)可以(喺社區延續落去)。但係唔係話今次推完之
後就唔理佢,即係你可能,即係一、兩年之後再有一個繼
續,一個活動落去,即係可能少少改變咁樣樣。即係你係不
斷地係每隔一段時間去做囉,唔係話推完之後就停咗…你停
咗之後可能啲人就無乜記…咁上下之後就唔係好記得㗎喇…
即係我諗你推完出嚟之後頭嗰一、 兩年啲人仲會記得,但係
慢慢一、兩年之後你都再要…再去重新做過。” (女,5 年經
驗或以下,L06P1)
“It (the effects of the FHHCPP) can (continue within the community), but that isn’t to say that we can neglect it after promoting it this time. That is, maybe you (arrange) a follow-up programme 1, 2 years later as a continuation, perhaps with some small changes. In other words, you are continuously doing it (organising programmes) every once in a while, instead of stopping after (this time’s) promotion...(initially) after you stop, this might not (have an effect) on people…but after a while, people don’t really remember…that is, I think for the first 1, 2 years after your promotion, people will still remember, but slowly, after one, two years, you still have to…re-do (re-promote) it again.” (Female, 5 yr or less experience, L06P1) “或者你會 keep 住搞一兩場活動…唔係啲人好易唔記得啊。” (女,6-10 年經驗,L02P1)
“Maybe you will keep organising an event or two (from time to time)…otherwise, people will forget (the programme) easily.” (Female, 6-10 yr experience, L02P1)
Running similar
programmes in the future
Worth organising
Importance of health “健康嘅活動係大家鍾意嘅嘛。咁平時舉辦嘅活動呢就除咗文
娛嘅活動呢,就無其他太多嘅特別嘅認識去…因為健康係同
…越來越同人…即係嗰個息息相關啊,即係佢哋會越來越注
重個健康。依家好多大明星話,「哎,幾努力去搵錢,搵到
錢番來,咁難聽嘅講句就係有無命使呢?」,咁依家佢哋反
而鍾意一個健康…” (女,11-15 年經驗,L09P1)
“Everyone likes health(-related) activities. Usually, apart from recreational activities, there aren’t very many
240
Theme Subtheme Quotes (activities) for especially understanding (health)…because health is becoming more and more closely related to people, that is, they are more and more aware about health. Nowadays, a lot of major celebrities say, ‘Oh, no matter how hard you work to earn money, or how much you earn, to put it crudely, do you have any life left to spend it with?’ Nowadays, they prefer health…” (Female, 11-15 yr experience, L09P1) In order to sustain and disseminate the FHHCPP messages “係一定有(價值去舉行同類活動)嘅…咁一來呢,呢個活動
本身真係好有意義,即係香港你話人口老化,跟住醫療開支
又大,咁其實呢啲咁簡單嘅,一個好簡單嘅訊息出到去之後
呢其實一定對每一個人呢,佢個知識増強咗之後呢都,好多
時佢哋都會慢慢有個改變㗎, 即係健康好啲之後,咁其實係
一個對成個社會係一個,bring 咗一個好 positive 嘅 impact 啦。” (女,5 年經驗或以下,L06P1)
“There definitely is (value in organising similar programmes)…on the one hand, this programme is very meaningful in itself, that is to say, the population in Hong Kong is ageing, and the medical expenditure is large. Actually, something so simple like this, such a simple message, after it is spread out, every person’s knowledge will definitely be strengthened, and a lot of the time they will slowly change. After their health has improved, it (organising similar programmes) will actually be something that is good for the whole society, something that brings a very positive impact.” (Female, 5 yr or less experience, L06P1)
Role of the HKIWA
Coordinate and lead “我希望我哋都係繼續統籌同協調啦。” (女,5 年經驗或以
下,L06P1)
“I hope we can keep taking the management and coordination role.” (Female, 5 yr or less experience, L06P1)
Role of member
associations
Similar role to within the FHHCPP “再繼續舉辦咪頭先咪講咗香港島婦聯咪做一個牽頭嘅 咁我
哋其他全部就埋堆㗎喇嘛我哋。” (女,6-10 年經驗,L04P2)

241
Theme Subtheme Quotes “If there is a second chance, like I said, the HKIWA takes the lead and we follow.” (Female, 6-10 yr experience, L04P2)
More promotion
“我覺得我哋做咗咁多,我覺得宣傳仲爭少少嘅…我哋直接可
以用返 er…甚至可以喺電視啦…做一個好短嘅片啦宣傳「多
動、識食,Go!」,我諗呢個嘅效果…可以推到全港咯,就
唔係香港島。” (女,5 年經驗或以下,W01P2)
“I feel like we have done so much, (but) I feel that there wasn’t enough promotion…we could actually just…(we could) even (promote) on television…produce a very short clip “FHHCPP”, I think the effect of this…could be spread territory-wide, not just within Hong Kong Island.” (Female, 5 yr or less experience, W01P2)
Recruitment Recruiting whole families would be harder “如果你話一次次都係一個 family unit 呢,我諗唔係有咁多人
recruit 到。” (女,5 年經驗或以下,L06P1)
“If they had to come each time as a family unit, I think we wouldn’t be able to recruit so many people.” (Female, 5 yr or less experience, L06P1)
Resources More time for planning or preparation “時間長啲咯,prepare 時間…係啦,咁比較 detail 啲… er,prepare 培訓時間長啲啦,宣傳時間長啲啦,讓嗰個「多
動、識食,Go!」嘅嗰啲大使嘅話可以知道…自己嘅角色,
再更加清晰啲啦咁。” (女,5 年經驗或以下,W01P2)
“A longer time for preparation…yes, it would be more detailed…the time for preparing for the Health Ambassadors’ training could be longer, promotion time could be longer, so that the (Health) Ambassadors know…about their role, even more clearly.” (Female, 5 yr or less experience, W01P2) Need to have sufficient souvenirs “一定要有資源配套嘅…即係譬如…好似你哋之前呢唔咪有一
份…標籤嘅,即係話嗰啲飲品嘅糖分係幾多啊咁樣嘅,嗰個
枱墊佢哋其實係有用嘅…咁呢啲就係一個資源啦。” (女,11-
242
Theme Subtheme Quotes 15 年經驗,L09P1)
“There must be sufficient resources provided…for example…you had a set of (food nutrition) labels before, that is, the label on the drinks with that tells (you) the sugar content. Actually, they (the participants) found the table mat useful…these are resources.” (Female, 11-15 yr experience, L09P1)
Potential problems
“困難主要一個就係我哋喺,如果我哋要擔當一個統籌角色
呢,我哋人力嗰方面呢,即係話統籌嘅人力呢…呢方面係比
較缺乏嘅。” (女,6-10 年經驗,L01P2)
“The major difficulty for us…if we need to take up a coordination role, then in terms of manpower, that is, manpower for coordination…in this aspect we are relatively lacking.” (Female, 6-10 yr experience, L01P2) “即係話如果人(活動嘅對象)係可以相對係年青啲少少嘅,
平均年齡喺五十幾,呢個咁嘅範疇去做呢,就會更加好啲囉
…但係執行上、推行嗰方面呢又未必做到。因為佢哋始終要
返工嘅人多啦,無咁多時間去 keep 住做咁多嘢。你話如果
真係好似教會嗰啲,每個禮拜日去做禮拜,呢啲人如果能夠
咁堅持就真係…呢啲就更加成功囉。” (女,6-10 年經驗,
L01P2) “That is to say that if the people (target participants) could be relatively a little younger, with a mean age of about 50 years, in this context, it would be even better…but in execution and implementation this might not be feasible. Because they (younger people) have to go to work, they don’t have time to keep doing so much. If it were like going to church every Sunday, if the participants could sustain that…this would be even more successful.” (Female, 6-10 yr experience, L01P2)
9.1.4 Summary of the in-depth interview findings Eighteen community stakeholders or leaders of the HKIWA were interviewed. The themes and findings reflected the structures of the HKIWA and the FHHCPP as the interviewees often spoke from the different levels of involvement in the project. Generally, the interviewees had very positive impressions of the project and saw the need for such projects to promote health awareness, enhance health, and improve interpersonal relationships and societal harmony.
243
The FHHCPP differed from the HKIWA or its member associations’ typical programmes in several respects. The project involved collaboration with a tertiary institution and a research element, which meant that the programmes were run in a much more rigorous and systematic manner. It was felt that the combination of research with community-based activities enhanced the HKIWA and built capability. The current project included larger scale programmes of longer duration that promoted different key messages than the associations’ typical programmes. These different key messages, namely healthy diet, physical activity, and 3Hs messages, were seen as the special strengths of the project, highly relevant and applicable to daily life and enhanced family communication and well-being as well as personal well-being. The interviewees observed and gave examples of improvements in personal and family well-being not only in themselves, but in Health Ambassadors and community-based participants as well.
The HKIWA played a key role within the project, facilitating and supporting its member associations and the Health Ambassadors by coordinating, providing resources, and encouraging member associations and the Health Ambassadors. The HKIWA had a good working relationship with the member associations and the Health Ambassadors. The HKIWA also liaised closely between the FAMILY Project Team and the member associations and Health Ambassadors. The in-depth interviews showed that HKU provided sufficient resources and support to the programmes, and that the collaboration with HKU was mutually beneficial. The interviewees felt that collaboration with HKU added the weight of the institution’s brand and reputation behind the project, facilitating recruitment. The information provided by the FAMILY Project Team for the interventions was felt to be of high quality and utility.
The member associations also played a coordinating role within the FHHCPP, with member association organising its own Health Ambassadors. In addition, the member associations were responsible for driving and promoting the project. They used various methods to promote the project and recruit Health Ambassadors and community-based programme participants. The one-to-many model used for recruitment whereby one Health Ambassador was responsible for recruiting ten (or more) community-based programme participants was effective. The difficulties experienced with recruitment were due to insufficient planning and time for recruitment, and an insufficient knowledge of what the programmes would entail and thus a limited ability to explain and persuade potential participants. In future, more time to prepare and familiarise with the project and its contents would help to improve the recruitment process.
The in-depth interviews revealed that the Health Ambassadors’ understanding of the project design and their role was not always complete and they were unclear about the workload beforehand. The Health Ambassadors helped to explain the study to participants and reminded participants to adopt health behaviours. Increased interaction enhanced the relationship between Health Ambassadors and community-based programme participants. Training for the Health Ambassadors was seen as a necessary component of the project given that the Health Ambassadors then have to implement the community-based programme. However, it was felt that the training that was provided was insufficient and rushed. In future, more training on the operation of physical fitness equipment, the design of the project, and recruitment should be conducted with flexible time slots in order to prepare

244
the Health Ambassadors and ensure that they are able to attend. Despite these limitations, the majority of Health Ambassadors were highly committed and responsible in the face of challenging work, and developed strong relationships.
The community leaders and stakeholders interviewed were positive toward the use of the mixed methods used for evaluation as part of the project. However, they observed some difficulties during implementation. For instance, Health Ambassadors had difficulties operating the physical fitness apparatus, telephone interviews were challenging to implement, participants sometimes required help reading the questionnaires, and the questionnaires were complex and repetitive. However, the interviewees understood the importance of rigorous evaluation to generate evidence for effectiveness of the interventions and the need for the same questions to be asked across time points from the academic perspective. In fact, the HKIWA as well as its member associations have adopted some of the evaluation methods used by the project. In particular, the use of focus groups has been adopted in order to gain feedback from volutneers and Health Ambassadors. Nevertheless, simplifying the questionnaires should be considered, and face-to-face methods should be used in addition to telephone interviews.
Apart from the adoption of focus groups, the FHHCPP also had strong impact on the relationships between the HKIWA and its member associations, as well as amongst the member associations themselves. It was felt that these relationships were strengthened through the project. The HKIWA and its member associations have also disseminated the key messages from the project regarding healthy diet, physical activity, and the FAMILY 3Hs through their own programmes. This is in line with the suggestion to organise more programmes to enhance the sustainability of the project’s effects and its messages. It is felt that potentially, the FHHCPP could bring impact to the wider society, beyond the HKIWA, even influencing governmental policy on resource distribution, for example. The project’s preventive health messages could also help toward reducing the burden of healthcare costs on society if the preventive health measures are disseminated and adopted more widely.
To improve the project, or make more beneficial changes if similar projects are run in the future, several suggestions should be considered: running more programmes or sessions, increasing the reach of programmes using a snowball approach to recruit participants, addressing different topics such as mental health, and allowing more time for promotion and recruitment.
245
CHAPTER 10 PROJECT SUMMARY, DISCUSSION AND CONCLUSION
10.1 Project summary and discussion The FHHCPP targeted physical inactivity and unhealthy diets through the promotion of healthy diet (reducing sugar consumption) and physical activity (ZTEx) using brief interventions as a family approach. Using physical activity and healthy diet as platforms, the project ultimately sought to improve FAMILY 3Hs across different sociodemographic groups in Hong Kong using a CBPR approach. As part of the CBPR approach, the FAMILY Project Team worked closely with the HKIWA, a Hong Kong charity focused on empowering women from diverse backgrounds by providing platforms for them to further their learning, exchange, and connect. Two key parts of the project were the TTA and the community-based programme, which the HKIWA and the FAMILY Project Team designed and implemented in collaboration as cRCTs to generate strong evidence on the effectiveness of the interventions. The results of the project demonstrate that the CBPR approach was successful in engaging all the relevant parties, and the vigorious evaluation showed that the participants and their families were benefitted.
The public education event and opening ceremony had served as platforms to promote the project to potential participants as well as to educate on the importance of healthy diet, physical activity, and FAMILY 3Hs. The Opening Ceremony in particular, which was held soon after the intervention sessions for the TTA, provided an opportunity for the community leaders within the HKIWA to exchange with the recruited Health Ambassadors, and for the Health Ambassadors to connect with potential participants for the community-based programme. The public education event and the Opening Ceremony were well received, as were the positive health messages, with respondents at the Opening Ceremony rating the contents of the event and their satisfaction with the event highly.
The TTA provided to volunteer Health Ambassadors recruited by the HKIWA and the participating affiliated member associations successfully utilised a variety of teaching and learning methods, and provided the Health Ambassadors with ongoing guidance as they implemented the community-based intervention programmes. Trainees indicated that the training was easy to understand and comprehensive, enhancing their health knowledge as well as their health behaviour. The qualitative findings from the focus groups discussions with the Health Ambassadors supported the quantitative results that demonstrated the effectiveness of the TTA in enhancing the Health Ambassadors’ physical activity and healthy diet knowledge and behaviours. The programme also enabled the Health Ambassadors to strengthen their relationships with their own family members as well as with the community-based programme participants. A unique value of the TTA was that the training not only benefitted the trainees but also their families and the community-based programme participants.
Eight community-based intervention programmes (comprising a core session and a booster session each) were implemented. Four focused on the theme of healthy diet and four focused on the theme of physical activity. Through collaboration with the HKIWA, its affiliated
246
member associations, and the recruited Health Ambassadors, the community-based programmes reached a wide audience, with participants being recruited from both within and outside the associations. Retention was high for the booster sessions of the community-based programmes. This might be due to the use of day trips as an incentive for the booster session. Participants might have also been motivated to attend the booster sessions as they found the core sessions useful and engaging. The results of the process evaluation showed that participants were highly satisfied with both the HD intervention programmes and the PA intervention programmes. High fidelity check results showed that the Health Ambassadors were able to deliver high quality programmes that were adherent with the requirements of the project and with the planned content, incorporating key health messages. These encouraging results support the continued development and implementation of community-based programmes using a CBPR approach, and TTA involving partnership from the university and community organisations.
The participants completed questionnaires at six time points, showing that the HD intervention programmes were successful in improving participants’ healthy diet behaviours in relation to dietary sugar intake over the study period. The HD groups also showed significant within-group reductions in body mass and body mass index (moving toward the normal range). Both the PA groups and the HD groups showed improvements in knowledge on physical activity and the frequency with which they performed physical activity and had physical activity-related interactions with family members. The improvements in the HD groups on outcomes addressed specifically in the PA intervention programmes could be due to an enhanced health awareness leading to more proactive changes in health behaviours in health domains beyond healthy diet. Both the PA groups and the HD groups showed improvements in self-reported personal health and happiness as well as self-reported FAMILY health, happiness, and harmony, suggesting that the intervention programmes were effective in spreading the FAMILY 3Hs message. The HD groups showed a significantly greater increase than the PA groups in family health at 1 month after the core session, and one possible explanation is that the healthy diet behavioural changes were more easily implemented by participants than the physical activity behavioural changes. Overall, the quantitative results from the community-based programme generated strong evidence supporting the continued development of brief interventions on health topics, including healthy diet and physical activity to promote family well-being and personal health.
Qualitative results from the focus groups with community-based programme participants supported the findings of the quantitative assessments. Participants indicated that they experienced increases in healthy diet or physical activity knowledge, with positive healthy diet or physical activity behavioural changes. The intervention programmes provided participants with more topics on which they could interact with their family members, and they practised healthy diet and physical activity behaviours together with family members, enhancing family communication and harmony.
The Sharing Session cum Awards Ceremony provided a platform for community leaders and stakeholders, the Health Ambassadors, and community-based programme participants to share personal experiences and thoughts regarding the project and its effects on the community, their families, and themselves. Qualitative results from the focus groups indicated that attendees enjoyed hearing other people’s anecdotes and thoughts on the project. However, the logistical arrangements, such as manpower to provide more support to
247
elderly participants, could be improved. Nevertheless, attendees indicated high satisfaction with the event and its contents on the one-page questionnaire.
In-depth interviews with community leaders within the HKIWA showed the need for more projects such as the current one. The FHHCPP made an extremely positive impression. The interviewees reported that the project did not only enhance community-based participants’ and Health Ambassadors’ health awareness, knowledge, and behaviour, but also enhanced the capacity of and relationships among their associations. The CBPR approach was a mutually beneficial arrangement from which the HKIWA and its member associations through the deep collaboration with HKU gained useful experiences for the future. The HKIWA as well as its member associations adopted the use of focus groups or similar gatherings to gain feedback from their volunteers and Health Ambassadors. The associations are also carrying out further dissemination of the key messages from the project regarding healthy diet, physical activity, and the FAMILY 3Hs. A key area in need of improvement was that more time should be allowed for recruitment, Health Ambassadors’ training, and the community-based programmes’ core sessions. The time frame and timeline for events needed to be clearer. Moreover, time and manpower spent by the Health Ambassadors on helping participants with questionnaire completion could be cut down if shorter questionnaires with language more suited for laymen or lower literacy were used. Nevertheless, the project overall had strongly positive impacts on the community-based participants, the Health Ambassadors, the interviewees, and the family members of those involved, and the project has potential to influence district or government policies. In order to sustain the effects of the current project and carry on dissemination work, it is suggested that more similar programmes should be run in the future.
In summary, the FHHCPP, using a CBPR approach with rigorous evaluation by mixed methods, incorporating both quantitative and qualitative evaluation, provided strong evidence for the feasibility and effectiveness of projects implemented by a community organisation in deep collaboration with an academic institution. The continued development and implementation of such projects focusing on the enhancement of FAMILY 3Hs via health-related platforms especially on reducing sugar consumptions and increasing physical activity through ZTEx is warranted.
10.2 Strengths and limitations
10.2.1 Strengths The FHHCPP displayed several strengths that should be noted. Firstly, the project adopted a CBPR approach and was designed and implemented in collaboration between the HKIWA and FAMILY Project Team. The HKIWA’s input maximised the suitability and acceptability of the programmes (especially the community-based programmes) for the participants and ensured the quality of the programmes designed and implemented by the Health Ambassadors for the booster sessions of the community-based programmes. The HKIWA acted as an important coordinator between the FAMILY Project Team and the participating member associations and their Health Ambassadors, helping each party to understand the needs and perspectives of the others. Through this role and capacity, the HKIWA became

248
closer with its affiliated member associations. The CBPR approach used in this project was mutually beneficial for all parties and people involved.
Second, the project was both evidence-based and evidence-generating. The design of the intervention programmes was evidence-based and informed by our literature review on the key concepts and evidence. The project also utilised a cRCT deisgn in order to test the effectiveness of the interventions, and through comprehensive mixed methods evaluation, generated strong evidence for the effectiveness of such intervention programmes.
Third, both the TTA and the community-based programmes were brief interventions. Each programme consisted only of two face-to-face sessions, which were kept short. The use of brief interventions addressed some of the biggest barriers to delivering and receiving interventions: access to and cost-efficiency (in terms of time, money, or other resources) of interventions. The use of brief interventions rather than interventions spread over a longer period of time or sessions of longer duration might have contributed to the high attendance and retention rates as it eased participants’ time costs. In the literature, diet and physical activity have been two lifestyle factors that are less frequently tackled through brief interventions. The findings from this project on the use of such brief interventions to address healthy diet (reducing sugar consumption) and physical activity (ZTEx) can contribute to the growing body of evidence supporting the efficacy of brief interventions.
10.2.2 Limitations Several limitations of this project should be noted. Firstly, because several different member associations of the HKIWA were involved in the project, and each member association had different capabilities, there was some variation in the community-based programme core and booster sessions. For instance, not all of the core or booster sessions were of the same length as different member associations held the sessions at different venues which had varying constraints on time. As the booster sessions were designed and planned by the Health Ambassadors and the member associations, the locations visited and activities involved as part of the day trips also varied. These inconsistencies migh have led to differences in the dose received by and the engagement of participants in the community-based programmes. Further work is needed to standardise the face-to-face sessions of the intervention programmes.
Second, difficulties were experienced when implementing the 3-month and 6-month follow-ups because the Health Ambassadors were required to carry out the follow-up using a telephone interview approach. Health Ambassadors found that using telephone interviews were time consuming as participants did not always answer the phone, and unfamiliar participants would sometimes hang up on the Health Ambassadors. Furthermore, Health Ambassadors found it difficult to get across the meaning of the question sometimes and felt that participants’ responses were rushed or unreliable. This might have led to the lower retention rates for the 3-month follow-up when Health Ambassadors did not have experience for the task. It is suggested that in the future, face-to-face methods could also be used for data collection to facilitate communication and more reliable responses. Simplifying the questionnaires, making use of less complex language, shortening the questionnaires, and increasing incentives are also strategies that should be considered.
249
Third, preparation time in the initial stages of the project was limited. Recruitment for Health Ambassadors was rushed, and as such, not all of the recruited Health Ambassadors were clear on the tasks that they would be required to carry out or the commitment that would be required. Such problems were inevitable as the programme needed to be completed within a short time frame (1 year). In future programmes, more time should be given at the preparation stage in order to allow for the recruitment of suitable Health Ambassadors who can better understand and prepare for the level of commitment needed. More information should also be provided and a clearer time frame or timeline should also be provided to facilitate this process. In turn, Health Ambassadors should also be given more time for the recruitment of suitable participants for the community-based programme.
Additionally, the effect size of different outcomes varied from small to large. For brief interventions, small effect size was expected. As the project was launched in collaboration with a service organisation, it was expected that each participant should receive intervention contents. We could not use a control group with no intervention at all, and hence, intervention contamination could not be avoided. The HD and PA interventions could not be totally separated. For example, the title of the project included both healthy diet and physical activity. Also, large events (such as the Opening Ceremony) could have included attendees who would have received messages on both the healthy diet and physical activity themes and were later allocated to different groups.
Furthermore, some participants were already quite healthy in different aspects and the room for further enhancement was limited (ceiling effect). The repeated questioning whilst completing the questionnaires could have reminded some to take action, or to give socially desirable answers. Finally, the questions or scales could be too crude and insensitive to changes. Nevertheless, some outcomes showed no changes, which suggested social desirability bias would not be substantial.
10.3 Implications and suggestions for future planning The findings from the FHHCPP support the use of the CBPR approach in health promotion with community partners. Community service organisation, such as the HKIWA and its member associations, could collaborate effectively with academia to ensure that high quality and evidence-based content was delivered in a manner acceptable to and suitable for their service targets. Furthermore, volunteers (Health Ambassadors) from the community were involved in the design and implementation of the community-based programmes that also showed evidence of effectiveness through vigorious mixed method evaluation. The successes of the TTA and the community-based programme demonstrate that it is feasible to improve family holistic health in the community using a CBPR approach. Future programmes should also consider adopting such an approach to utilise the expertise of the various parties involved, and the dedicated abd trained volunteers.
Working in a community-based setting, it is often not feasible to adopt the gold standard of randomisation at an individual level, as this presents large challenges in terms of recruitment, follow-up and intervention contamination. Hence, the project utilised a cRCT design, integrating the best science from academia with the best practice from the HKIWA and its member associations. Future community-based programmes may also consider adopting
250
such an approach to generate good evidence. Nevertheless, individual randomisation is preferred if it is feasible.
The project has demonstrated that brief interventions on the topics of healthy diet and physical activity are effective in enhancing personal and family health knowledge, attitude, and behaviour, as well as happiness and harmony. Brief interventions are low cost. Lower time and monetary costs could encourage higher attendance, retention, and engagement. Future public health programmes with similar goals should consider using brief interventions to benefit large numbers of people at comparatively lower costs, although the effect size may not be great.
The impact of the project does not end with the individual participants that were involved or their family members. The project has already inspired the HKIWA and its affiliated member associations to continue disseminating the key health messages and 3Hs messages of the project, with the resources used during the project, such as PowerPoints, notes, or informational content. These are reused and disseminated at the associations’ own programmes beyond the FHHCPP. The associations have also built capacity, are equipped with a large number of well-trained Health Ambassadors, and have gained useful experiences from the current project. The associations have adopted data acquisition methods used during the project such as focus groups, and have developed their knowledge of the research process, enhancing the associations’ capabilities to hold future programmes of a similar nature. Moreover, because the project provided an opportunity for the HKIWA and different member associations to work together toward a common goal, relationships amongst individuals and associations within the HKIWA network have become stronger and closer. This puts the HKIWA and its member associations at an advantage for future programmes and collaboration.
Furthermore, given the wide dissemination of the project and its findings, and the suitable actions to ensure sustainability of its effects, community leaders within the HKIWA hold the view that the project could potentially have an impact on or influence at a district, government, or territory-wide level. Continued and sustained dissemination of the key messages of the project, through programmes and reports, for example, could lead to more focus on preventive programmes, to lower the burden of disease and health costs not just for the individuals and their families but for society as a whole. Ensuring that the effects of enhanced FAMILY 3Hs are sustained, and that the message is spread beyond the HKIWA at a territory-wide level through collaboration with other service organisations could also ultimately enhance societal harmony.
The findings from this project could have important implications not only for future projects at the community level that may adopt the CBPR, brief intervention, and cRCT approaches, but also at the government or policy levels when considering programme planning for the enhancement of family well-being across generations in Hong Kong. Our future publications of scientific papers on the experiences and evidence of this project in international journals would expand the impacts beyond Hong Kong.

251
ACKNOWLEDGEMENTS The FAMILY Project Team would like to thank The Hong Kong Jockey Club Charities Trust for funding this project. We express our sincerest gratitude to the Hong Kong Island Women’s Association and its participating affiliated member associations, including: Carnation Women’s Association, Chaiwan Women’s Association, Hong Kong Central and Western District Women’s Association, Hong Kong Southern District Women’s Association, Kellett Bay Women’s Association, Kin Ngai Society, Shek O Woman’s Association Limited, South Horizons Women’s Association, Wah Fu Estate Women’s Association, Wan Chai Yin Ngai Society, Women Gather Association, Women’s Department of Causeway Bay Association Limited, Women’s Department of Hong Kong Soong Ching Ling Goldkey Training Foundation Limited, Women’s Department of Shau Kei Wan & Chai Wan Community, Women’s Department of the Hong Kong Executive Administrative & Clerical Staff Association, Women’s Department of the Hong Kong Wan Chai District Association Limited, and Women’s Department of Wan Chai District Arts, Cultural, Recreational and Sports Association Limited. We are grateful to the Hong Kong Island Women’s Association, its member associations, and volunteers, for organising this project, their enthusiastic participation, and their strong support in implementation and evaluation. We are also grateful for the hard work put in by many student helpers. Last but not least, we would like to thank all the participants, without whom the project would not have been possible.
252
REFERENCES 1. United Nations General Assembly: Political Declaration of the High-level Meeting of the
General Assembly on the Prevention and Control of Non-communicable Diseases. In: A/RES/66/2. 2012.
2. Noncommunicable diseases [http://www.who.int/mediacentre/factsheets/fs355/en/] 3. Global status report on noncommunicable diseases
[http://www.who.int/nmh/publications/ncd_report_full_en.pdf] 4. Obesity and overweight [http://www.who.int/mediacentre/factsheets/fs311/en/] 5. Body Mass Index (BMI) Distribution [http://www.chp.gov.hk/en/data/1/10/280/6621.html] 6. Level of physical activity by WHO recommendations
[http://www.chp.gov.hk/en/data/1/10/280/6626.html] 7. Consumption of five servings of fruit and vegetables per day
[http://www.chp.gov.hk/en/data/1/10/280/6629.html] 8. Beaglehole R, Bonita R, Horton R, Adams C, Alleyne G, Asaria P, Baugh V, Bekedam H,
Billo N, Casswell S et al: Priority actions for the non-communicable disease crisis. Lancet (London, England) 2011, 377(9775):1438-1447.
9. Geneau R, Stuckler D, Stachenko S, McKee M, Ebrahim S, Basu S, Chockalingham A, Mwatsama M, Jamal R, Alwan A: Raising the priority of preventing chronic diseases: a political process. The Lancet 2010, 376(9753):1689-1698.
10. Rayner G, Hawkes C, Lang T, Bello W: Trade liberalization and the diet transition: a public health response. Health Promotion International 2006, 21(suppl_1):67-74.
11. Health topics: Physical activity [http://www.who.int/topics/physical_activity/en/] 12. Global Strategy on Diet, Physical Activity and Health
[http://www.who.int/dietphysicalactivity/pa/en/] 13. Healthy Exercise for All Campaign [http://www.lcsd.gov.hk/en/healthy/] 14. Allison KR, Dwyer JJM, Makin S: Perceived Barriers to Physical Activity among High
School Students. Preventive Medicine 1999, 28(6):608-615. 15. Overcoming barriers to physical activity
[http://www.cdc.gov/physicalactivity/basics/adding-pa/barriers.html] 16. Chinn DJ, White M, Harland J, Drinkwater C, Raybould S: Barriers to physical activity
and socioeconomic position: implications for health promotion. Journal of Epidemiology and Community Health 1999, 53(3):191.
17. Sallis JF, Hovell MF: Determinants of exercise behavior. Exercise and sport sciences reviews 1990, 18(1):307-330.
18. Sallis JF, Hovell MF, Hofstetter CR: Predictors of adoption and maintenance of vigorous physical activity in men and women. Preventive medicine 1992, 21(2):237-251.
19. Zunft H-JF, Friebe D, Seppelt B, Widhalm K, de Winter A-MR, de Almeida MDV, Kearney JM, Gibney M: Perceived benefits and barriers to physical activity in a nationally representative sample in the European Union. Public health nutrition 1999, 2(1a):153-160.
20. Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, Stone EJ, Rajab MW, Corso P: The effectiveness of interventions to increase physical activity. A systematic review. Am J Prev Med 2002, 22(4 Suppl):73-107.
21. Artinian NT, Fletcher GF, Mozaffarian D, Kris-Etherton P, Van Horn L, Lichtenstein AH, Kumanyika S, Kraus WE, Fleg JL, Redeker NS et al: Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults: a scientific statement from the American Heart Association. Circulation 2010, 122(4):406-441.
253
22. World Health Organization: WHO calls on countries to reduce sugars intake among adults and children. In.; 2015.
23. Reducing consumption of sugar-sweetened beverages to reduce the risk of unhealthy weight gain in adults [http://www.who.int/elena/bbc/ssbs_adult_weight/en/]
24. Reduce Dietary Sugar in Hong Kong [http://www.cfs.gov.hk/english/programme/programme_rdss/FAQ_Sugars_Trade.html]
25. Reduction of Dietary Sodium and Sugar [http://www.cfs.gov.hk/english/programme/programme_rdss/programme_rdss.html]
26. Interventions on diet and physical activity: What works: Summary report [http://www.who.int/dietphysicalactivity/summary-report-09.pdf?ua=1]
27. Gruber KJ, Haldeman LA: Using the Family to Combat Childhood and Adult Obesity. Preventing chronic disease 2009, 6(3):A106.
28. Kelsey K, Earp JAL, Kirkley BG: Is social support beneficial for dietary change? A review of the literature. Family & Community Health 1997, 20(3):70-82.
29. Okun MA, Ruehlman L, Karoly P, Lutz R, Fairholme C, Schaub R: Social support and social norms: Do both contribute to predicting leisure-time exercise? American journal of health behavior 2003, 27(5):493-507.
30. Wing RR, Jeffery RW: Benefits of recruiting participants with friends and increasing social support for weight loss and maintenance. Journal of consulting and clinical psychology 1999, 67(1):132-138.
31. Golan M, Fainaru M, Weizman A: Role of behaviour modification in the treatment of childhood obesity with the parents as the exclusive agents of change. International Journal of Obesity & Related Metabolic Disorders 1998, 22(12):1217-1224.
32. Golan M, Weizman A: Familial approach to the treatment of childhood obesity: conceptual model. Journal of nutrition education 2001, 33(2):102-107.
33. Golan M, Weizman A, Apter A, Fainaru M: Parents as the exclusive agents of change in the treatment of childhood obesity. The American journal of clinical nutrition 1998, 67(6):1130-1135.
34. Epstein LH, Paluch RA, Wrotniak BH, Daniel TO, Kilanowski C, Wilfley D, Finkelstein E: Cost-effectiveness of family-based group treatment for child and parental obesity. Childhood Obesity 2014, 10(2):114-121.
35. Epstein LH, Wing RR, Koeske R, Valoski A: Long-term effects of family-based treatment of childhood obesity. Journal of consulting and clinical psychology 1987, 55(1):91.
36. Berry D, Sheehan R, Heschel R, Knafl K, Melkus G, Grey M: Family-Based Interventions for Childhood Obesity: A Review. Journal of Family Nursing 2004, 10(4):429-449.
37. Magarey AM, Perry RA, Baur LA, Steinbeck KS, Sawyer M, Hills AP, Wilson G, Lee A, Daniels LA: A Parent-Led Family-Focused Treatment Program for Overweight Children Aged 5 to 9 Years: The PEACH RCT. Pediatrics 2011, 127(2):214-222.
38. Carvalho J, Fonseca G, Francisco R, Bacigalupe G, Relvas AP: Information and Communication Technologies and Family: Patterns of Use, Life Cycle and Family Dynamics. In: Journal of Psychology & Psychotherapy: 2016: OMICS International; 2016: 1-3.
39. Gender, Justice and ICTs [http://www.un.org/womenwatch/daw/csw/marcelle.htm] 40. Sharaievska I, Stodolska M: Family satisfaction and social networking leisure. Leisure
Studies 2017, 36(2):231-243. 41. Information and Communication Technology Development Indices
[http://unctad.org/en/Docs/iteipc20031_en.pdf] 42. Are ICT Policies Addressing Gender Equality?
[http://siteresources.worldbank.org/INTICTTOOLKIT/Resources/Ramilo.pdf]
254
43. Walker SK, Rudi JH: Parenting Across the Social Ecology Facilitated by Information and Communication Technology: Implications for Research and Educational Design. Journal of Human Sciences and Extension 2014, 2(2):15-32.
44. Internet users (per 100 people) [http://data.worldbank.org/indicator/IT.NET.USER.P2?end=2014&start=1990]
45. Klasnja P, Pratt W: Healthcare in the pocket: mapping the space of mobile-phone health interventions. Journal of biomedical informatics 2012, 45(1):184-198.
46. Breitenstein SM, Gross D, Christophersen R: Digital delivery methods of parenting training interventions: a systematic review. Worldviews on Evidence‐Based Nursing 2014, 11(3):168-176.
47. Gross D, Johnson T, Ridge A, Garvey C, Julion W, Treysman AB, Breitenstein S, Fogg L: Cost-effectiveness of childcare discounts on parent participation in preventive parent training in low-income communities. The journal of primary prevention 2011, 32(5-6):283-298.
48. Baggett KM, Davis B, Feil EG, Sheeber LL, Landry SH, Carta JJ, Leve C: Technologies for expanding the reach of evidence-based interventions: Preliminary results for promoting social-emotional development in early childhood. Topics in Early Childhood Special Education 2010, 29(4):226-238.
49. Bert SC, Farris JR, Borkowski JG: Parent training: Implementation strategies for adventures in parenting. The journal of primary prevention 2008, 29(3):243-261.
50. Kingston D, Janes-Kelley S, Tyrrell J, Clark L, Hamza D, Holmes P, Parkes C, Moyo N, McDonald S, Austin M-P: An integrated web-based mental health intervention of assessment-referral-care to reduce stress, anxiety, and depression in hospitalized pregnant women with medically high-risk pregnancies: a feasibility study protocol of hospital-based implementation. JMIR research protocols 2015, 4(1):e9.
51. Denney-Wilson E, Laws R, Russell CG, Ong K-l, Taki S, Elliot R, Azadi L, Lymer S, Taylor R, Lynch J: Preventing obesity in infants: the Growing healthy feasibility trial protocol. BMJ open 2015, 5(11):e009258.
52. Fjeldsoe BS, Marshall AL, Miller YD: Behavior change interventions delivered by mobile telephone short-message service. American journal of preventive medicine 2009, 36(2):165-173.
53. Gruver RS, Bishop-Gilyard CT, Lieberman A, Gerdes M, Virudachalam S, Suh AW, Kalra GK, Magge SN, Shults J, Schreiner MS: A Social Media Peer Group Intervention for Mothers to Prevent Obesity and Promote Healthy Growth from Infancy: Development and Pilot Trial. JMIR research protocols 2016, 5(3):e159.
54. Williams G, Hamm MP, Shulhan J, Vandermeer B, Hartling L: Social media interventions for diet and exercise behaviours: a systematic review and meta-analysis of randomised controlled trials. BMJ open 2014, 4(2):e003926.
55. Ramachandran A, Snehalatha C, Ram J, Selvam S, Simon M, Nanditha A, Shetty AS, Godsland IF, Chaturvedi N, Majeed A: Effectiveness of mobile phone messaging in prevention of type 2 diabetes by lifestyle modification in men in India: a prospective, parallel-group, randomised controlled trial. The Lancet Diabetes & Endocrinology 2013, 1(3):191-198.
56. Hurling R, Catt M, De Boni M, Fairley BW, Hurst T, Murray P, Richardson A, Sodhi JS: Using internet and mobile phone technology to deliver an automated physical activity program: randomized controlled trial. Journal of medical Internet research 2007, 9(2):e7.
57. Parker CA, Ellis R: Effect of Electronic Messaging on Physical Activity Participation among Older Adults. In: Journal of aging research. vol. 2016; 2016.
58. Haines DJ, Davis L, Rancour P, Robinson M, Neel-Wilson T, Wagner S: A pilot intervention to promote walking and wellness and to improve the health of college faculty and staff. Journal of American College Health 2007, 55(4):219-225.
255
59. Section I: The Public Health Approach [http://www.cdc.gov/arthritis/temp/pilots-201208/pilot1/online/ph-approach/sectionI.htm]
60. Public Health and Medicine [https://www.hsph.harvard.edu/about/public-health-medicine/] 61. Rose G: Strategy of prevention: lessons from cardiovascular disease. British Medical
Journal (Clinical research ed) 1981, 282(6279):1847-1851. 62. Aguirre-Molina M, Gorman DM: Community-based approaches for the prevention of
alcohol, tobacco, and other drug use. Annual review of public health 1996, 17(1):337-358. 63. Israel BA, Schulz AJ, Parker EA, Becker AB: Review of community-based research:
assessing partnership approaches to improve public health. Annual review of public health 1998, 19(1):173-202.
64. Community-based participatory research [http://www.cbprcurriculum.info/] 65. Israel BA, Schulz AJ, Parker EA, Becker AB, Allen AJ, Guzman JR: Critical issues in
developing and following community based participatory research principles. Community-based participatory research for health 2003, 1:53-76.
66. Agabio R: Non-specialist health workers to treat excessive alcohol consumption and depression. The Lancet 2017, 389(10065):133-135.
67. Dunn C, Deroo L, Rivara FP: The use of brief interventions adapted from motivational interviewing across behavioral domains: a systematic review. Addiction 2001, 96(12):1725-1742.
68. Heather N: Interpreting the evidence on brief interventions for excessive drinkers: the need for caution. Alcohol and alcoholism 1995, 30(3):287-296.
69. Brief Interventions and Brief Therapies For Substance Abuse [https://www.ncbi.nlm.nih.gov/books/NBK64947/pdf/Bookshelf_NBK64947.pdf]
70. Descriptions of Brief Intervention and Brief Therapy [http://www.integration.samhsa.gov/clinical-practice/sbirt/SBIRT_Brief_Therapy_Brief_Intervention_descriptions.pdf]
71. DeMattia L, Lemont L, Meurer L: Do interventions to limit sedentary behaviours change behaviour and reduce childhood obesity? A critical review of the literature. obesity reviews 2007, 8(1):69-81.
72. Berg-Smith S, Stevens V, Brown K, Van Horn L, Gernhofer N, Peters E, Greenberg R, Snetselaar L, Ahrens L, Smith K: A brief motivational intervention to improve dietary adherence in adolescents. Health Education Research 1999, 14(3):399-410.
73. Bien TH, Miller WR, Tonigan JS: Brief interventions for alcohol problems: a review. Addiction 1993, 88(3):315-336.
74. Bolognesi M, Nigg CR, Massarini M, Lippke S: Reducing obesity indicators through brief physical activity counseling (PACE) in Italian primary care settings. Annals of behavioral medicine 2006, 31(2):179-185.
75. Eakin EG, Glasgow RE, Riley KM: Review of primary care-based physical activity intervention studies: effectiveness and implications for practice and future research. The Journal of family practice 2000, 49(2):158-168.
76. Fabrizio CS, Lam TH, Hirschmann MR, Stewart SM: A brief parenting intervention to enhance the parent–child relationship in Hong Kong: Harmony@ Home. Journal of child and family studies 2013, 22(5):603-613.
77. Glasgow RE, Toobert DJ, Hampson S: Effects of a brief office-based intervention to facilitate diabetes dietary self-management. Diabetes Care 1996, 19(8):835-842.
78. Kahan M, Wilson L, Becker L: Effectiveness of physician-based interventions with problem drinkers: a review. CMAJ: Canadian Medical Association Journal 1995, 152(6):851-859.
256
79. Kellar I, Abraham C: Randomized controlled trial of a brief research‐based intervention promoting fruit and vegetable consumption. British journal of health psychology 2005, 10(4):543-558.
80. Purath J, Michaels Miller A, McCabe G, Wilbur J: A Brief Intervention to Increase Physical Activity in Sedentary Working Women Une intervention ponctuelle en vue d'accroître l'activité physique chez les travailleuses sédentaires. CJNR (Canadian Journal of Nursing Research) 2004, 36(1):76-91.
81. Stevens VJ, Glasgow RE, Toobert DJ, Karanja N, Smith KS: One-year results from a brief, computer-assisted intervention to decrease consumption of fat and increase consumption of fruits and vegetables. Preventive medicine 2003, 36(5):594-600.
82. Wilk AI, Jensen NM, Havighurst TC: Meta‐analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers. Journal of general internal medicine 1997, 12(5):274-283.
83. Michie S, Abraham C, Whittington C, McAteer J, Gupta S: Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health psychology : official journal of the Division of Health Psychology, American Psychological Association 2009, 28(6):690-701.
84. Morse J, Field P: Qualitative research methods for health professionals, 2nd edn. California: Sage Publications; 1995.
85. Ayala GX, Vaz L, Earp JA, Elder JP, Cherrington A: Outcome effectiveness of the lay health advisor model among Latinos in the United States: an examination by role. Health education research 2010, 25(5):815-840.
86. Quandt SA, Grzywacz JG, Talton JW, Trejo G, Tapia J, D’Agostino Jr RB, Mirabelli MC, Arcury TA: Evaluating the effectiveness of a lay health promoter-led, community-based participatory pesticide safety intervention with farmworker families. Health promotion practice 2013, 14(3):425-432.
87. Drusini A, Eleazer G, Caiazzo M, Veronese E, Carrara N, Ranzato C, Businaro F, Boland R, Wieland D: One-leg standing balance and functional status in an elderly community-dwelling population in northeast Italy. Aging clinical and experimental research 2002, 14(1):42-46.
88. Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum A, Orlandini A, Seron P, Ahmed SH, Rosengren A, Kelishadi R: Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. The Lancet 2015, 386(9990):266-273.
89. Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E: The association between obesity and low back pain: a meta-analysis. American journal of epidemiology 2009, 171(2):135-154.
90. Vellas BJ, Wayne SJ, Romero L, Baumgartner RN, Rubenstein LZ, Garry PJ: One‐leg balance is an important predictor of injurious falls in older persons. Journal of the American Geriatrics Society 1997, 45(6):735-738.
91. Obesity and overweight [http://www.who.int/mediacentre/factsheets/fs311/en] 92. Zhang F, Ferrucci L, Culham E, Metter EJ, Guralnik J, Deshpande N: Performance on
five times sit-to-stand task as a predictor of subsequent falls and disability in older persons. Journal of aging and health 2013, 25(3):478-492.
93. Schwarzer R: Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Applied Psychology 2008, 57(1):1-29.
94. Draycott S, Dabbs A: Cognitive dissonance 1: An overview of the literature and its integration into theory and practice in clinical psychology. British Journal of Clinical Psychology 1998, 37(3):341-353.
257
95. Draycott S, Dabbs A: Cognitive dissonance 2: A theoretical grounding of motivational interviewing. British Journal of Clinical Psychology 1998, 37(3):355-364.
96. Lee PH, Macfarlane DJ, Lam T, Stewart SM: Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. International Journal of Behavioral Nutrition and Physical Activity 2011, 8(1):115.
97. Macfarlane DJ, Lee CC, Ho EY, Chan K, Chan DT: Reliability and validity of the Chinese version of IPAQ (short, last 7 days). Journal of Science and Medicine in Sport 2007, 10(1):45-51.
98. Roberts HC, Denison HJ, Martin HJ, Patel HP, Syddall H, Cooper C, Sayer AA: A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age and ageing 2011, 40(4):423-429.
99. Trampisch US, Franke J, Jedamzik N, Hinrichs T, Platen P: Optimal Jamar dynamometer handle position to assess maximal isometric hand grip strength in epidemiological studies. The Journal of hand surgery 2012, 37(11):2368-2373.
100. Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, Scherr PA, Wallace RB: A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. Journal of gerontology 1994, 49(2):M85-M94.
101. Jones CJ, Rikli RE, Beam WC: A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Research quarterly for exercise and sport 1999, 70(2):113-119.
102. Newton R: Review of tests of standing balance abilities. Brain injury 1989, 3(4):335-343. 103. Jones CJ, Rikli RE, Max J, Noffal G: The reliability and validity of a chair sit-and-reach
test as a measure of hamstring flexibility in older adults. Research quarterly for exercise and sport 1998, 69(4):338-343.
104. Cohen J: Statistical Power Analysis for the Behavioural Sciences, 2nd edn. Hillsdale, Newark: Lawrence Erlbaum Associates; 1988.
105. Creswell JW, Clark VLP: Designing and conducting mixed methods research. 2007. 106. Springer BA, Marin R, Cyhan T, Roberts H, Gill NW: Normative values for the unipedal
stance test with eyes open and closed. Journal of geriatric physical therapy 2007, 30(1):8-15.
107. The 30-Second Chair Stand Test [https://www.cdc.gov/steadi/pdf/30_second_chair_stand_test-a.pdf]
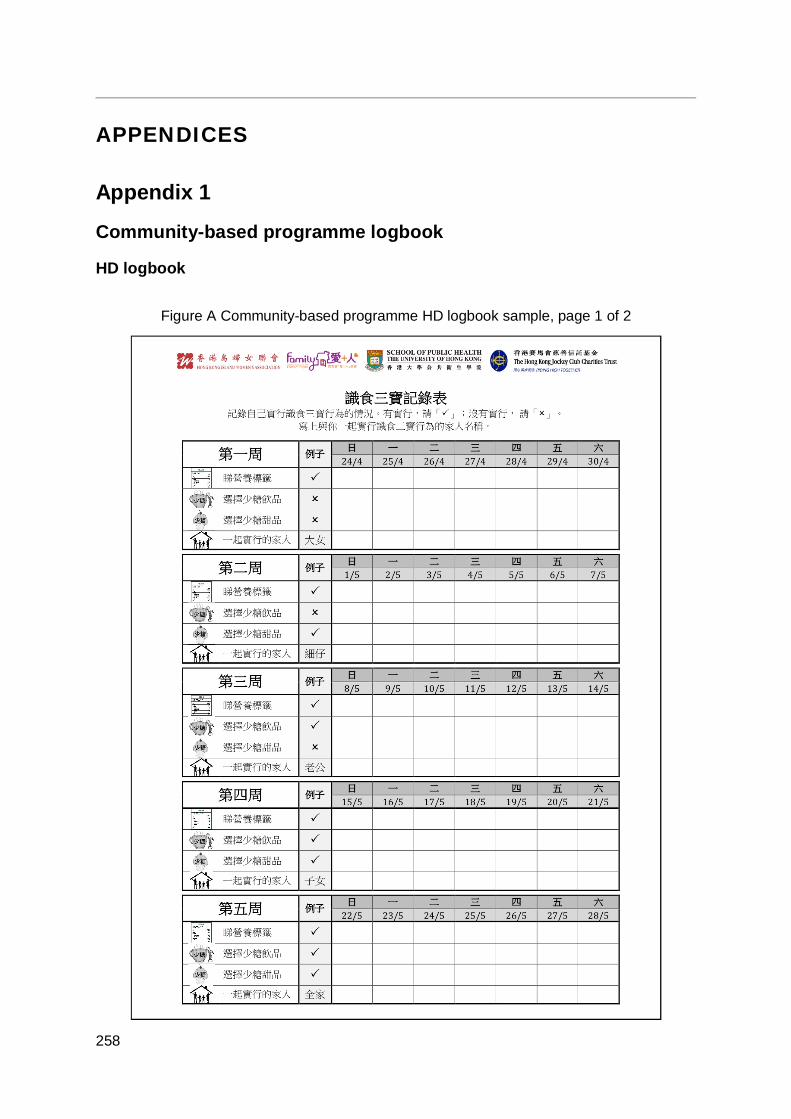
258
APPENDICES
Appendix 1
Community-based programme logbook
HD logbook
Figure A Community-based programme HD logbook sample, page 1 of 2
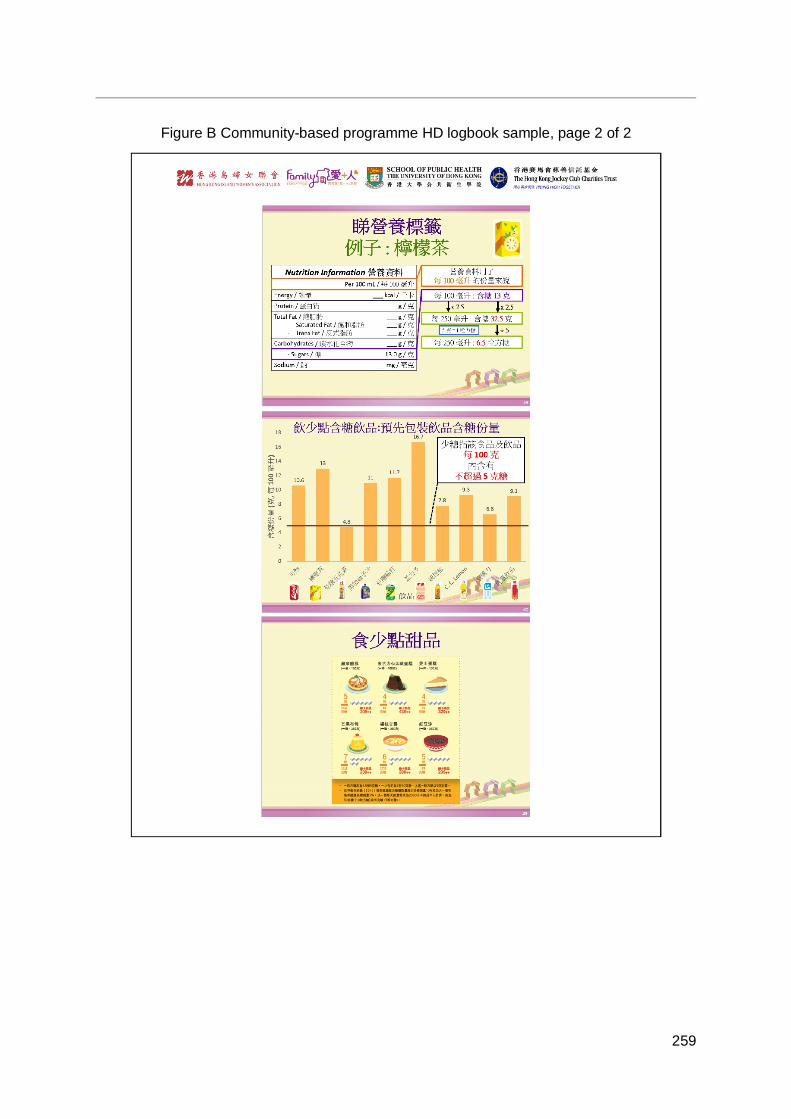
259
Figure B Community-based programme HD logbook sample, page 2 of 2
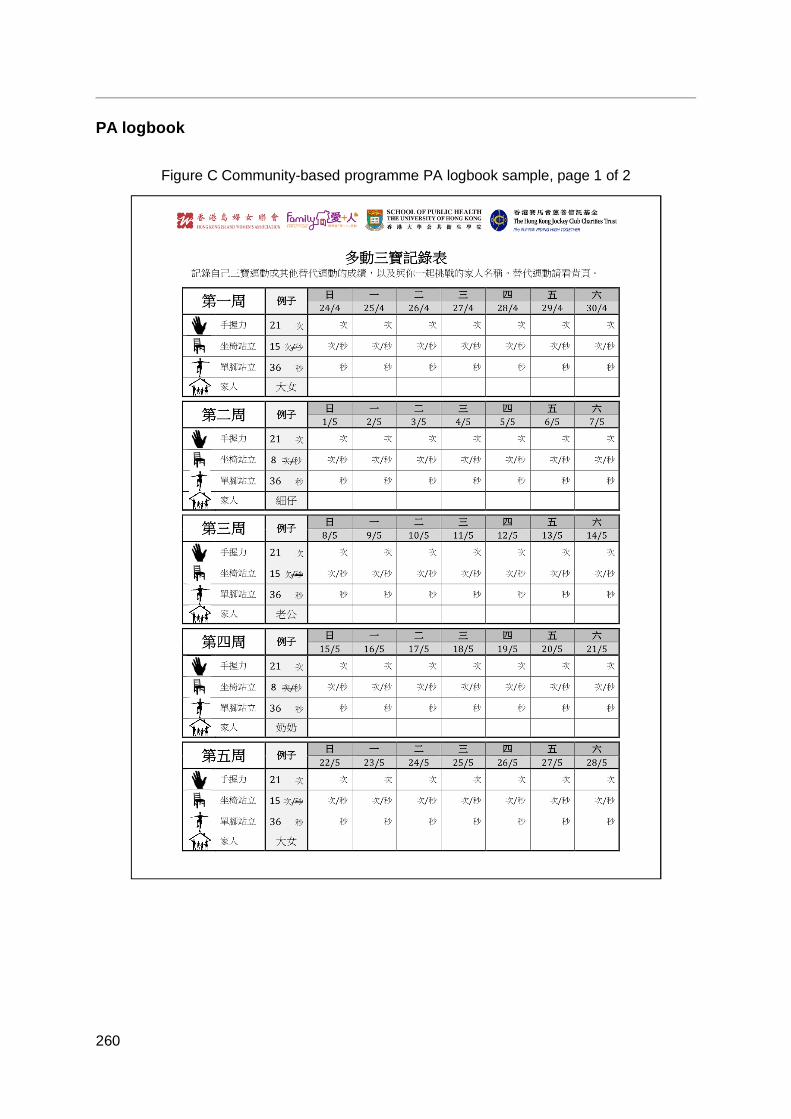
260
PA logbook
Figure C Community-based programme PA logbook sample, page 1 of 2
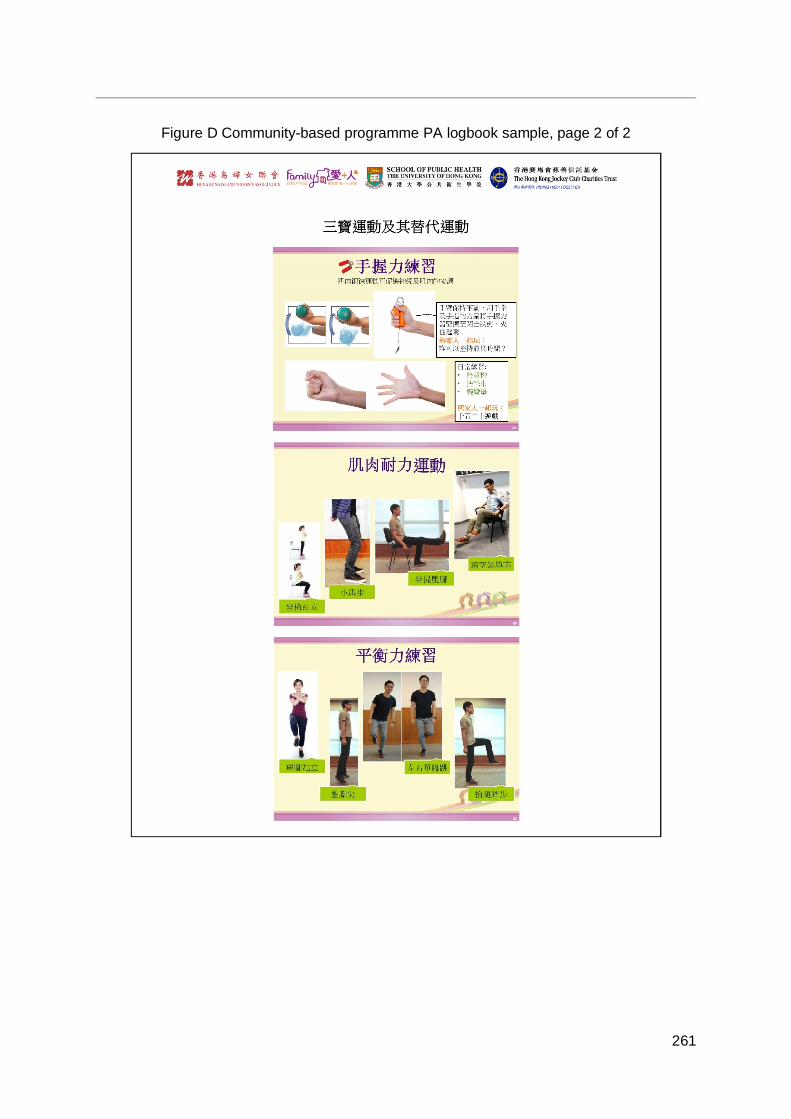
261
Figure D Community-based programme PA logbook sample, page 2 of 2
262
Appendix 2
Publications Chan SS, Viswanath K, Au DW, Ma C, Lam W, Fielding R, Leung G, Lam T-H: Hong Kong
Chinese community leaders’ perspectives on family health, happiness and harmony: a qualitative study. Health education research 2011, 26(4):664-674.
Chen J, Wang M-P, Wang X, Viswanath K, Lam T-H, Chan SS: Secondhand smoke exposure (SHS) and health-related quality of life (HRQoL) in Chinese never smokers in Hong Kong. BMJ open 2015, 5(9):e007694.
Fabrizio CS, Hirschmann MR, Lam TH, Cheung T, Pang I, Chan S, Stewart SM: Bringing scientific rigor to community-developed programs in Hong Kong. BMC public health 2012, 12(1):1129.
Fabrizio CS, Lam TH, Hirschmann MR, Pang I, Yu NX, Wang X, Stewart SM: Parental emotional management benefits family relationships: a randomized controlled trial in Hong Kong, China. Behaviour research and therapy 2015, 71:115-124.
Fabrizio CS, Lam TH, Hirschmann MR, Stewart SM: A brief parenting intervention to enhance the parent-child relationship in Hong Kong: Harmony@Home. Journal of child and family studies 2013, 22(5):603-613.
Fabrizio CS, Stewart SM, Ip AK, Lam TH: Enhancing the parent–child relationship: A Hong Kong community-based randomized controlled trial. Journal of Family Psychology 2014, 28(1):42.
Ho HC, Mui M, Wan A, Ng Y-L, Stewart SM, Yew C, Lam TH, Chan SS: Happy Family Kitchen II: a cluster randomized controlled trial of a community-based family intervention for enhancing family communication and well-being in Hong Kong. Frontiers in psychology 2016, 7:638.
Ho HC, Mui M, Wan A, Ng Y-l, Stewart SM, Yew C, Lam TH, Chan SS: Happy Family Kitchen: A community-based research for enhancing family communication and well-being in Hong Kong. Journal of Family Psychology 2016, 30(6):752.
Ho HC, Mui M, Wan A, Ng Y-l, Stewart SM, Yew C, Lam TH, Chan SS: Happy Family Kitchen II: a cluster randomized controlled trial of a community-based positive psychology family intervention for subjective happiness and health-related quality of life in Hong Kong. Trials 2016, 17(1):367.
Ho HC, Mui M, Wan A, Stewart SM, Yew C, Lam TH, Chan SS: Happy Family Kitchen: behavioral outcomes of a brief community-based family intervention in Hong Kong. Journal of Child and Family Studies 2017, 26: 852–864.
Kavikondala S, Stewart SM, Ni MY, Chan BH, Lee PH, Li KK, McDowell I, Johnston JM, Chan SS, Lam TH, Lam WW: Structure and validity of Family Harmony Scale: an instrument for measuring harmony. Psychological assessment 2016, 28(3):307.
263
Lai AY, Mui MW, Wan A, Stewart SM, Yew C, Lam T-h, Chan SS: Development and two-year follow-up evaluation of a training workshop for the large preventive positive psychology happy family kitchen project in Hong Kong. PLoS one 2016, 11(1):e0147712.
Lai AY, Stewart SM, Mui MW, Wan A, Yew C, Lam TH, Chan SS: An evaluation of a Train-the-Trainer Workshop for social service workers to develop community-based family interventions. Frontiers in public health 2017, 5:141.
Lai AY, Stewart SM, Wan A, Fok H, Lai HY, Lam T-h, Chan SS: Development and evaluation of a training workshop for lay health promoters to implement a community-based intervention program in a public low rent housing estate: The Learning Families Project in Hong Kong. PLoS one 2017, 12(8):e0183636.
Lam T, Stewart S, Hirschmann M, Fabrizio C, Yu N: Can randomized controlled trials be conducted in community social service settings? Public health 2015, 129(5):601-603.
Lam W, Fielding R, McDowell I, Johnston J, Chan S, Leung G, Lam T: Perspectives on family health, happiness and harmony (3H) among Hong Kong Chinese people: a qualitative study. Health education research 2012, 27(5):767-779.
Lee PH, Macfarlane DJ, Lam TH. Factors associated with participant compliance in studies using accelerometers. Gait & posture 2013, 38(4):912-917.
Lee PH, McGrath CP, Kong AY, Lam TH. Self‐report poor oral health and chronic diseases: the Hong Kong FAMILY project. Community dentistry and oral epidemiology 2013, 41(5):451-458.
Lee PH, McGrath CP, Kong AY, Lam TH. Self-reported oral health and quality of life: a latent growth curve analysis. International journal of behavioral medicine 2014, 21(2):358-363.
Lee PH, Nan H, Yu YY, McDowell I, Leung GM, Lam TH. For non-exercising people, the number of steps walked is more strongly associated with health than time spent walking. Journal of science and medicine in sport 2013, 16(3):227-230.
Lee PH, Stewart SM, Lun V, Bond MH, Yu X, Lam TH. Validating the concord index as a measure of family relationships in China. Journal of Family Psychology 2012, 26(6):906-915.
Lee PH, Yu YY, McDowell I, Leung GM, Lam TH. A cluster analysis of patterns of objectively measured physical activity in Hong Kong. Public health nutrition 2013, 16(8):1436-1444.
Leung GM, Ni MY, Wong PTK, Lee PH, Chan BHY, Stewart SM, Schooling MC, Johnston JM, Lam WWT, Chan SSC, McDowell I, Pang H, Fielding R, Lam TH. Cohort profile: FAMILY cohort. International journal of epidemiology 2015, 46(2):1-13.
Leung SS, Lam T: Group antenatal intervention to reduce perinatal stress and depressive symptoms related to intergenerational conflicts: a randomized controlled trial. International journal of nursing studies 2012, 49(11):1391-1402.
264
Li HCW, Chan SS, Mak YW, Lam TH: Effectiveness of a parental training programme in enhancing the parent–child relationship and reducing harsh parenting practices and parental stress in preparing children for their transition to primary school: a randomised controlled trial. BMC public health 2013, 13(1):1079.
Li WH, Mak YW, Chan SS, Chu AK, Lee EY, Lam T: Effectiveness of a play-integrated primary one preparatory programme to enhance a smooth transition for children. Journal of health psychology 2013, 18(1):10-25.
Nan H, Lee PH, McDowell I, Ni MY, Stewart SM, Lam TH. Depressive symptoms in people with chronic physical conditions: prevalence and risk factors in a Hong Kong community sample. BMC psychiatry 2012, 12(1):198.
Nan H, Lee PH, Ni MY, Chan BH, Lam TH. Effects of depressive symptoms and family satisfaction on health related quality of life: the Hong Kong FAMILY study. PLoS one 2013, 8(3):e58436.
Nan H, Ni MY, Lee PH, Tam WW, Lam TH, Leung GM, McDowell, I. Psychometric evaluation of the Chinese version of the Subjective Happiness Scale: evidence from the Hong Kong FAMILY Cohort. International journal of behavioral medicine 2014, 21(4):646-652.
Ni MY, Li TK, Yu NX, Pang H, Chan BH, Leung GM, Stewart SM. Normative data and psychometric properties of the Connor–Davidson Resilience Scale (CD-RISC) and the abbreviated version (CD-RISC2) among the general population in Hong Kong. Quality of Life Research 2016, 25(1):111-116.
Shen C, Wan A, Kwok LT, Pang S, Wang X, Stewart SM, Lam TH, Chan SS: A community based intervention program to enhance neighborhood cohesion: The Learning Families Project in Hong Kong. PLoS one 2017, 12(8):e0182722.
Shen C, Wang MP, Chu JT, Wan A, Viswanath K, Chan SSC, Lam TH: health app possession among smartphone or tablet owners in Hong Kong: population-based survey. JMIR mHealth and uHealth 2017, 5(6):e77.
Soong CS, Wang MP, Mui M, Viswanath K, Lam TH, Chan SS: A “community fit” community-based participatory research program for family health, happiness, and harmony: Design and implementation. JMIR research protocols 2015, 4(4): e126.
Stewart SM, Fabrizio CS, Hirschmann MR, Lam TH: Developing community-based preventive interventions in Hong Kong: a description of the first phase of the family project. BMC Public Health 2012, 12(1):106.
Wang MP, Chu JT, Viswanath K, Wan A, Lam TH, Chan SS: Using information and communication technologies for family communication and its association with family well-being in Hong Kong: FAMILY Project. Journal of medical Internet research 2015, 17(8): e207.
Wang MP, Viswanath K, Lam TH, Wang X, Chan SS: Social determinants of health information seeking among Chinese adults in Hong Kong. PLoS one 2013, 8(8):e73049.

265
Wang MP, Wang X, Lam TH, Viswanath K, Chan SS: Ex‐smokers are happier than current smokers among Chinese adults in Hong Kong. Addiction 2014, 109(7):1165-1171.
Wang MP, Wang X, Lam TH, Viswanath K, Chan SS: Health information seeking partially mediated the association between socioeconomic status and self-rated health among Hong Kong Chinese. PLoS one 2013, 8(12):e82720.
Wang MP, Wang X, Lam TH, Viswanath K, Chan SS: The tobacco endgame in Hong Kong: public support for a total ban on tobacco sales. Tobacco Control 2015, 24(2):162.
Wang MP, Wang X, Viswanath K, Wan A, Lam TH, Chan SS: Digital inequalities of family life information seeking and family well-being among Chinese adults in Hong Kong: a population survey. Journal of medical Internet research 2014, 16(10):e227.
Wang X, Wang MP, Viswanath K, Wan A, Lam TH, Chan SS: smoking and secondhand smoke exposure at home were associated with poor perceived family well-being: findings of FAMILY Project. PLoS one 2016, 11(8):e0161761.
Xie YJ, Stewart SM, Lam TH, Viswanath K, Chan SS: Television viewing time in Hong Kong adult population: associations with body mass index and obesity. PLoS one 2014, 9(1):e85440.
Yu X, Stewart SM, Chui JP, Ho JL, Li AC, Lam TH: A pilot randomized controlled trial to decrease adaptation difficulties in chinese new immigrants to Hong Kong. Behavior therapy 2014, 45(1):137-152.
Yu X, Stewart SM, Liu IK, Lam TH: Resilience and depressive symptoms in mainland Chinese immigrants to Hong Kong. Social psychiatry and psychiatric epidemiology 2014, 49(2):241-249.
Yu X, Tam WW, Wong PT, Lam TH, Stewart SM. The Patient Health Questionnaire-9 for measuring depressive symptoms among the general population in Hong Kong. Comprehensive psychiatry 2012, 53(1):95-102.
Yu XN, Stewart SM, Wong PTK, & Lam TH. Screening for depression with the Patient Health Questionnaire-2 (PHQ-2) among the general population in Hong Kong. Journal of affective disorders 2011, 134(1):444-447.
Yu NX, Lam T, Liu IK, Stewart SM: Mediation of short and longer term effects of an intervention program to enhance resilience in immigrants from mainland China to Hong Kong. Frontiers in psychology 2015, 6:1769.
Zhou Q, Chan SS-c, Stewart SM, Leung CS-c, Wan A, Lam TH: The effectiveness of positive psychology interventions in enhancing positive behaviors and family relationships in Hong Kong: a community-based participatory research project. The Journal of Positive Psychology 2016, 11(1):70-84.
Zhou Q, Stewart SM, Wan A, Leung CS-c, Lai AY, Lam TH, Chan SS-c: Development and evaluation of a train-the-trainer workshop for Hong Kong community social service agency staff. Frontiers in public health 2017, 5:15.

266
Appendix 3
Recognition in the Avant Garde Positive Psychology Clinical Intervention Challenge
267
Appendix 4
Dr. Lai Yuen Kwan Agnes’ Doctor of Philosophy thesis
268
Appendix 5
Conference presentations Lam TH, Leung C, Wan ANT, Soong CSS, Wang C, Chan SSC. Strengthening family
relationship to increase family health, happiness and harmony: findings from a Community-based Participatory Research (CBPR) project under FAMILY: A Jockey Club Initiative for a Harmonious Society Project in Hong Kong. 6th Global Conference of the Alliance for Healthy Cities, Hong Kong, October 29 – November 1, 2014.
Lam TH, Mui M, Wan ANT, Soong CSS, Wang C, Chan SSC. Happy Family Kitchen II, a Community-based Participatory Research (CBPR) to enhance family health, happiness and harmony in Hong Kong: A cluster randomized controlled trial under FAMILY: A Jockey Club Initiative for a Harmonious Society Project. 6th Global Conference of the Alliance for Healthy Cities, Hong Kong, October 29 – November 1, 2014.
Wang X, Wang MP, Lam TH, Viswanath K, Chan SSC. Physically active adults reported higher levels of family health, happiness and harmony: findings from the Hong Kong Family and Health Information and Trends Survey (FHInTs) under FAMILY: A Jockey Club Initiative for a Harmonious Society Project. 6th Global Conference of the Alliance for Healthy Cities, Hong Kong, October 29 – November 1, 2014.
Lam TH, Chen J, Wang MP, Wang X, Soong CSS, Wan ANT, Chan SSC. Secondhand smoke exposure and health-related quality of life in never smokers: The Hong Kong Jockey Club FAMILY Project. 16th World Conference on Tobacco or health - Tobacco and Non-communicable disease, Abu Dhabi, United Arab Emirates, March 17-21, 2015.
Chan BHY, Pang H, Yuan BY, Li TK, Leung GM, Ni MY. A randomised factorial design to examine the effect of requesting Hong Kong identity card (HKID) numbers and participation incentive on participant’s consent to health record linkage: evidence from the FAMILY Cohort. Annual Scientific Meeting, Hong Kong College of Community Medicine, Hong Kong, September 19, 2015.
Ni MY, Li T, Yu NX, Pang H, Chan BHY, Leung GM, Stewart SM. Normative data and psychometric properties of the Connor-Davidson Resilience Scale (CD-RISC) and the abbreviated version (CD-RISC2) among the general population in Hong Kong. Annual Scientific Meeting, Hong Kong College of Community Medicine, Hong Kong, September 19, 2015.
Yao XI, Ni MY, Chan BHY, McDowell I, Leung GM, Pang HH. Systematic evaluation of factors associated with health-related quality of life: a high-dimensional multivariate multilevel analysis in the FAMILY Cohort. Annual Scientific Meeting, Hong Kong College of Community Medicine, Hong Kong, September 19, 2015.
Lai AY, Mui MWK, Wan A, Stewart SM, Yew C, Lam TH, Chan SSC. Development and model-based evaluation of a train-the-trainer workshop for the large preventive positive psychology Happy Family Kitchen Project in Hong Kong, 6th International Nursing Conference, Hong Kong, December 10-11, 2015.
269
Lam TH, Chan BHY, Yuan B, Ni MY. Smoking and family harmony in Hong Kong Chinese: evidence from the FAMILY Cohort, Society for Research on Nicotine and Tobacco Annual Meeting 2016, United States, March 2-5, 2016.
Lai AY, Mui MW, Wan A, Stewart SM, Yew C, Lam TH, Chan SS. Training workshop for applying logic model framework in designing, implementation and evaluation of community-based family intervention in Happy Family Kitchen Project in Hong Kong, 37th Annual Meeting & Scientific Sessions, Society of Behavioral Medicine, Washington DC, United States, March 30-April 2, 2016.
Lam TH. Zero-time Exercise (ZTEx): enjoyable, easy and effective — an innovative concept to promote exercise for anybody, anytime and anywhere: A new initiative from the Hong Kong Jockey Club FAMILY Project, The XIII International Congress on Obesity, United Kingdom, May 1-4, 2016.
Lam TH, Chan BHY, Li TK, Ni MY. Change in body mass index (BMI) among Chinese in a general population: the FAMILY Cohort, The XIII International Congress on Obesity (ICO), Vancouver, Canada, May 1-4, 2016.
Lam TH, Chen S, Wan ANT. Zero-time Exercise, a new approach to promote physical activity — Hong Kong FAMILY Project: A Jockey Club Initiative for a Harmonious Society, The XIII International Congress on Obesity, United Kingdom, May 1-4, 2016.
Lam TH, Lai AY, Wan A, Chu JTW. Zero-time Exercise (ZTEx), a new approach to promote physical activity and mental health: A pilot study under Hong Kong Jockey Club FAMILY Project, The XIII International Congress on Obesity, United Kingdom, May 1-4, 2016.
Ni MY, Chan BHY, Li TK, Lam TH. Child neglect and body mass index (BMI) in adulthood: a sibling study nested in the FAMILY Cohort, The XIII International Congress on Obesity (ICO), Vancouver, Canada, May 1-4, 2016.
Lam TH, Lai AYK, Wan ANT, Chu JTW. Zero-time Exercises (ZTEx), a new approach to promote physical activity and mental health: a pilot study under Hong Kong Jockey Club FAMILY project, FPH Annual Conference and Public Health Exhibition 2016, Brighton, United Kingdom, June 14-15, 2016.
Ho HCY, Wan A, Mui M, Chan SS, Lam TH. The mediating effect of physical exercise on family health, harmony and communication in a community-based family intervention: Happy Family Kitchen Movement under Hong Kong Jockey Club FAMILY Project, Annual Conference on Disaster Preparedness and Response, Hong Kong, October 8, 2016.
Shen C, Wan A, Kwok LT, Lam TH. A community based Intervention of Hong Kong Jockey Club FAMILY Project to enhance Zero-time Exercise and grip strength: Fitter Families, Project Annual Conference on Disaster Preparedness and Response, Hong Kong Academy of Medicine, October 8, 2016.
270
Ho HCY, Wan A, Ki BHS, Chan SS, Lam TH. The mediating effect of positive psychology behaviors on family health, happiness and harmony in a community-based family intervention: Happy Family Kitchen Movement under Hong Kong Jockey Club FAMILY Project, 5th CIFA Regional Symposium, Seoul, Korea, November 3-5, 2016.
Lam TH, Wan A, Mui M, Ho HCY, Chan SS. An innovative and public health approach to promote family holistic health - The FAMILY: A Jockey Club Initiative for a Harmonious Society in Hong Kong, 5th CIFA Regional Symposium, Seoul, Korea, November 3-5, 2016.
Shen C, Wan A, Kwok LT, Pang S, Wang X, Stewart SM, Lam TH, Chan SS. A community based intervention program to enhance family communication and family well-being: The Learning Families Project in Hong Kong, 5th CIFA Regional Symposium, Korea, November 3-5, 2016.
Lai AYK, Wan ANT, Lee DPK, Lam TH. Zero-time Exercise: A cluster randomized control trial to promote physical activity, health, happiness and family harmony under Hong Kong Jockey Club Family Project, The Institute of Cardiovascular Science and Medicine, Twentieth Anniversary Scientific Meeting 2016, Hong Kong, November 19, 2016.
Lam TH, Wan A, Ho HCY, Lau G, Lai A. Zero-time Exercise and Anti-inertia Reminder (AIR) Model: The Hong Kong Jockey Club FAMILY Project, 20th Anniversary Scientific Meeting of the ICSM, Hong Kong, November 19, 2016.
Lam TH, Lai A., Wan A, Lau G, King J. Zero-time Exercises for families: The Hong Kong Jockey Club FAMILY Project, 18th Beijing Hong Kong Medical Exchange, Hong Kong, November 20, 2016.
Lai A, Wan A, Lam TH. FAMILY Project: Training workshops for lay health promoters to implement a community-based intervention program, 215t Research Postgraduate Symposium, Hong Kong, December 1-2, 2016.
Lam TH, Wang MP, Shen C, Wan A, Chan SS. Pattern of health app use and associated sociodemographic factors in Hong Kong smokers - findings from FAMILY Project, Annual Meeting on The Society for Research on Nicotine & Tobacco, Florence, Italy, March 8-11, 2017.
Ho HCY, Wan A, Mui M, Chan SS, Lam TH. The effectiveness of a community-based positive psychology family intervention on physical exercise and fitness of older adults: Happy Family Kitchen Movement under Hong Kong Jockey Club FAMILY Project, 12th International Symposium on Healthy Aging, Hong Kong, March 11-12, 2017.
Lai A, Wan A, Lam TH. Hong Kong Jockey Club FAMILY Project: A 15-min Zero Time Exercise intervention to enhance well-being in older people, 12th International Symposium on Healthy Aging “Wellness and Longevity: From Science to Service”, Hong Kong, March 11-12, 2017.
271
Shen C, Wang MP, Wan A, Chan SS, Lam TH. Zero-time Exercise and subjective happiness in older people: findings from Hong Kong Jockey Club FAMILY Project, 12th International Symposium on Healthy Aging “Wellness and Longevity: From Science to Service”, Hong Kong, March 11-12, 2017.
Lam TH, Ho HCY, Lau G, Wan A, Chan N. Promotion of Zero Time Exercise (ZTEx) through Anti-inertia Reminders (AIR): New initiative from The Hong Kong Jockey Club FAMILY Project, Primary Care Research Symposium, Hong Kong, March 25, 2017.
Lam TH, Lai A, Wan A. Normative data for absolute and relative hand grip strength in Hong Kong: FAMILY Project, a Hong Kong Jockey Club Initiative for a Harmonious Society, International Symposium 2017 Physical Activity & Fitness of Young Generation in Asia-Pacific, Hong Kong, May 20, 2017.
Lai A, Wan A, Lam TH. The effectiveness of a clustered randomized control on Zero-time Exercise to reduce sedentary behaviour, enhance physical activity and improve personal well-being in Hong Kong, ISBNPA 2017Annual Meeting, Victoria, Canada, June 7-10, 2017.
Lam TH, Shen C, Wang MP, Wan A, Chan SS. Factors associated with use of physical activity apps in smartphone and tablet owners in Chinese: findings from Hong Kong Jockey Club FAMILY Project, Annual Meeting on The International Society of Behavioral Nutrition and Physical Activity, Victoria, Canada, June 7-10, 2017.
Shen C, Wang MP, Wan A, Chan SS, Lam TH. Patterns of health apps use in smartphone and tablet owners in Chinese: findings from Hong Kong Jockey Club FAMILY Project, Annual Meeting on The International Society of Behavioral Nutrition and Physical Activity, Victoria, Canada, June 7-10, 2017.
Wan A, Lai A, Lam TH. Train-the-ambassador workshop for a community-based family health promotion project to reduce excess dietary sugar intake: A cluster randomised controlled trial, ISBNPA 2017 Annual Meeting, Victoria, Canada, June 7-10, 2017.
Ho HCY, Wan A, Mui M, Chan SS, Lam TH. Mediating effect of positive psychology behaviors on subjective happiness and life satisfaction in a family intervention: Happy Family Kitchen Movement under Hong Kong FAMILY Project, Fifth World Congress on Positive Psychology, Montreal, Canada, July 13-16, 2017.
272
Copyright © School of Public Health, The University of Hong Kong All rights reserved. Author: School of Public Health, The University of Hong Kong Publisher: The Hong Kong Jockey Club Publication date: November 2017 Disclaimer: The information in this report is for reference only. While endeavors have been made to ensure the accuracy of the information in this report, no express or implied warranty or representation is given to the accuracy or completeness of the information or its appropriateness for use in any particular circumstances. Copyright: The contents available in this report, including but not limited to all text, graphics, drawings, diagrams, and compilation of data or other materials are protected by copyright. Any reproduction, adaptation, distribution, dissemination or making available of such copyright work to the public is strictly prohibited unless prior written authorization is obtained from the School of Public Health, The University of Hong Kong. Please contact the School of Public Health, The University of Hong Kong if you wish to seek permission for use of any material on this report or make inquiries about this report. Acknowledgement is required if this report is used.

Contact Information
Address: G/F, Patrick Manson Building (North Wing), 7 Sassoon Road, Pok Fu Lam, Hong KongTel: (852) 3917 6824 / 3917 6702Fax: (852) 2855 9528E-mail: [email protected]: http://www.family.org.hk
Printed on Recycled Paper





























