Embed Size (px)
Citation preview
Evaluation of cadmium and zinc inbiological samples of tobacco andalcohol user male mouth cancerpatients
Tasneem Gul Kazi1, Sham Kumar Wadhwa1, Hassan Imran Afridi1,Naveed Kazi2, Ghulam Abbas Kandhro1, Jameel Ahmed Baig1,Abdul Qadir Shah1, Nida Fatima Kolachi1 and Sumaira Khan1
AbstractThere is compelling evidence in support of positive associations between zinc (Zn) deficiency and highaccumulation of cadmium (Cd) in biological samples of different cancerous patients. The incidence of mouthcancer has been increased among people who possess habit of drinking alcohol, tobacco smoking and chewingwith gradients in Pakistan. In the present study, Cd and Zn contents of blood and scalp hair samples of 92 malemouth cancer patients and 78 referents of same age group (range 35–65 years), socio-economic status, local-ities and dietary habits. Among referent male subjects, 56 consumed tobacco (smoking/chewing), 22 had noneof smoking and chewing tobacco habits, while none of them admitted for alcohol drinking. The scalp hair andwhole blood samples were oxidized by 65% nitric acid and 30% hydrogen peroxide (2:1) ratio in microwaveoven. The Zn in digests was determined by flame atomic absorption while Cd was determined by electrother-mal atomic absorption spectrometry. The average Cd concentration was higher, while level of Zn was lower inthe blood and scalp hair samples of mouth cancer patients as compared to referent subjects (p < .001). Themale referents consuming tobacco (chewing and smoking) have high level of Cd in both their biological samplesas compared to those not smoking or chewing tobacco (p < .012). The Cd/Zn ratio in both biological sampleswas found to be higher in patients than in referent subjects.
Keywordscadmium, zinc, tobacco smoking/chewing, alcohol drinking, mouth cancer, scalp hair and whole blood
Introduction
Cancers of the oral cavity make up 3%–4% of all can-
cers, being in eighth place in men and eleventh in women
when the cancer is caused by smoking and alcohol mis-
use.1 The mouth cancer is the common malignancy
among people who have tobacco smoking and chewing
habits, with a worldwide incidence of over 300,000 new
cases annually.2 The disease is characterized by a high
rate of morbidity and mortality.3 Tobacco use is by far
the most common risk factor for cancers of the mouth
and throat. Both smoking (cigarettes, cigars and pipes)
and ‘smokeless’ tobacco (snuff and chewing tobacco)
have increased the risk of developing oral cancer.4,5
Tobacco smoke can cause cancer anywhere in the
mouth and throat as well as in the lungs, bladder and
many other organs in the body.6 Smokeless tobacco is
linked with cancers of the cheeks, gums and inner sur-
face of the lips.7 Many epidemiologic studies address
the risk of smokeless tobacco for the cancer of oral
cavity and adjacent sites.8,9 Cancers caused by
smokeless tobacco use often begin as leukoplakia or
1 Center of Excellence in Analytical Chemistry, University ofSindh, Jamshoro, Pakistan2 Liaquat University of Medical and Health sciences, Jamshoro,Pakistan
Corresponding author:Tasneem Gul Kazi, Center of Excellence in Analytical Chemistry,University of Sindh, Jamshoro, Pakistan, 76080.E-mail [email protected]
Human and Experimental Toxicology29(3) 221–230
ª The Author(s) 2010Reprints and permission:
sagepub.co.uk/journalsPermissions.navDOI: 10.1177/0960327109360045
het.sagepub.com

erythroplakia, erythroplakia is generally more severe
than leukoplakia and has a higher chance of becoming
cancerous over time.10 The carcinogenic substances
in alcohol and tobacco chewing can cause cancer and
other problems in mouth, because all these materials
remain in contact with gums, inner lining of mouth
and tongue over long periods.11,12
The current estimate is that a nutritional deficiency
of Zn may affect over 2 billion subjects in the
developing world. Growth retardation, immune dys-
function and cognitive impairment are among major
consequences of Zn deficiency.13,14 Zinc deficiency
was associated with increased tumor size and overall
stage of the head and neck cancers.15
Cadmium (Cd) is a toxic metal with sterilizing,
teratogenic and carcinogenic effects.16 Cd exposure
due to industrial pollution or cigarette smoke is an
important risk factor for public health, which may
lead to cancer. It is shown that Cd is an inhibitor of
the enzymes with sulphydryl groups and disrupts the
pathways for the oxidative metabolism.17 In vitro
studies suggest that there is competition for transport
mechanisms between Cd and some essential trace
elements mainly Zn, Se and Cu.18
Determinations of trace metals in human tissues
and fluids (whole blood, serum, plasma and urine)
were used to obtain information on the nutritional sta-
tus for diagnosis of diseases, indication of systemic
intoxication and to obtain information on environ-
mental exposure.19,20 The importance of exploring the
depot-storage capacities of various elements, particu-
larly the toxic ones, remains a vital aspect in elemen-
tal analysis largely met by urine and hair testing.21
The determination of trace metals in biological
samples requires the use of sensitive and selective
techniques such atomic absorption spectrometer.22
This technique has need for solubilization and
enrichment of the analyte and complete or partial
decomposition of the matrix using either convective
systems or microwave ovens and dry ashing.23,24
Chewing tobacco or betel quid is very common in
different parts of Asia, especially Pakistan and India.
It is also popular in some immigrant groups in Europe,
North America and Australia. The term ‘quid’ means
a substance or mixture of substances put in the mouth
and chewed, usually for long periods. It usually con-
tains tobacco, either on its own or mixed with areca
nut (from the Areca catechu tree), slaked lime and
different additives that enhance the toxicity as well
as the psychotropic effect of tobacco.25 This mixture
is wrapped in a leaf (betel leaf), which is where
the name betel quid (also called paan in India and
Pakistan) comes from. The harmful substances in
tobacco and betel quid can cause cancer and other
problems in the mouth, because all these materials
remain in contact with gums, inner lining of the
mouth and tongue for many hours.26
As the rate of mouth cancer has increased in
Pakistan, mainly due to habit of smoking, chewing
unrefined tobacco or tobacco with betel nuts and alco-
hol consumption are considered the important causes
of mouth cancer. The betel nut and paan are not pro-
duced in Pakistan and a huge amount of foreign
exchange is spent on imports of these items. This
hospital-based study is aimed at evaluating the con-
centration of Cd and Zn in whole blood and scalp hair
among male mouth cancer patients (MCPs) and refer-
ents of same age group, from different cities of Sindh,
Pakistan. The biological samples were digested by
microwave prior to analysis of both elements by
flame/electrothermal atomic absorption spectrome-
tery (FAAS/ETAAS).
Materials and methods
Reagents and glassware
Ultra pure water obtained from a Milli-Q purifier
system Millipore Corp. (Bedford, MA, USA) was used
throughout the work. Concentrated nitric acid (65%),
hydrogen peroxide (30%) and other chemicals were
used as analytical reagent-grade E. Merck (Darmstadt,
Germany) and checked for possible trace metal con-
tamination. Working standard solutions of Cd and Zn
were prepared immediately before their use, by step-
wise dilution of certified standard solution (1000 ppm)
Fluka Kamica (Buchs, Switzerland), with 0.2 mol L–1
HNO3. The stock standard solution of modifier used
for Cd stabilization was 0.05% m/v Pd and 0.03%m/v Mg (NO3)2, which were prepared from, 3.0 g
L�1, Pd 99.999% Aldrich (Milwaukee, WI, USA) and
2.0 g L�1 Mg (NO3)2 solutions (Merck). All solutions
were stored in polyethylene bottles at 4�C. For the
accuracy of methodology, certified reference materials,
human hair BCR 397 (Commission of European com-
munities, Brussels, Belgium) and clincheck control-
lyophilized human whole blood (Recipe, Munich,
Germany) were used. All glassware and plastic materi-
als used were earlier soaked for 24 hours in 2 mol L–1
nitric acid, washed with distilled water and finally
rinsed with ultrapure water, dried and stored in class
100 laminar flow hoods.
222 Human and Experimental Toxicology 29(3)

Apparatus
The analysis of elements was carried out by means of
a double-beam Perkin-Elmer atomic absorption spec-
trometer model A. Analyst 700 (Norwalk, CT, USA),
equipped with a flame burner, graphite furnace
HGA-400 and an autosampler AS-800. The pyro-
coated graphite tubes with an integrated platform
were used. The Cd was measured under optimized
operating conditions by ETAAS. Single element hol-
low cathode lamp for Cd was operated at 4 mA with a
spectral bandwidth of 0.7 nm. The analytical wave-
length was set at 228.8 nm. The graphite furnace heat-
ing program for Cd was set for different steps, drying,
ashing, atomization and cleaning as temperature
range �C/time (sec) (80–120/15, 300–600/15, 1500–
1800/5 and 1800–2000/2), respectively. The acid
digests were transferred to auto sampler cups, and
with a chemical modifier solution introduced 20 mL
of digest and modifier (10 mL þ 10 mL) directly into
the graphite furnace. The Zn was measured under
optimized operating conditions by FAAS with air–
acetylene flame. A wavelength of 213.9 nm was used.
A PEL (PMO23, Osaka, Japan) domestic microwave
oven (maximum heating power at 900 W) was used
to digest the samples. Acid-washed polytetrafluor-
oethylene (PTFE) vessels and flasks were used for
preparing and storing solutions.
Study group
Before the start of this study, all referents and
mouth cancer patients, age range 35–65 years, were
informed through a consent form by the
administration about the aim of study, and all agreed
to participate and signed the form. A questionnaire
was also administered to them in order to collect
details concerning physical data, ethnic origin, health,
dietary habit, age and consent. All participants (refer-
ents and patients) were interviewed personally by the
authors. The standardized interview assessed
socio-demographic characteristics (Table 1). Partici-
pant’s history of cigarette smoking, tobacco chewing
with and without gradient and alcohol consumption,
including initiation age, quantities and years con-
sumed, was also collected. Among study groups,
more than 70% patient’s condition was apparently
worse in terms of chronic illnesses, malnutrition, pov-
erty and ignorance of disease for long time.
Physical examinations were performed in the can-
cer hospitals to measure participant’s weight, height,
blood pressure and biochemical data. The data of
study population (92 mouth cancer patients), admitted
in Nuclear Institute of Medicine and Radiotherapy
(NIMRA) Jamshoro and Larkana institute of nuclear
medicine and radiotherapy (LINAR), situated in dif-
ferent areas of Sindh, Pakistan, in the year 2008, was
obtained by collecting files and extracting important
information. During 1-year study period (2008), the
information department of both the hospitals recorded
>3600 cases of cancers of all types, and mouth cancer
comprised of 2.7%.
The patients were grouped according to their
habits, tobacco smoking (PST), chewing tobacco with
other gradients (PCT) and alcohol consumption with
tobacco smoking (PAST). While control group are
divided into two groups, first group comprises two
sub groups, tobacco smoker (RST) and tobacco
chewing with and without gradients (RCT), while sec-
ond group have none of these habits (RNT) as shown
in Table 1. The anatomical sites used to calculate the
total numbers of cases were gum (23), floor of the
mouth (27) and different part of the mouth (42).
Among MCPs, tobacco chewing with other gradients
(betel quid, calcium and areca nut) included 42.4%,
smokers were 45.6 %, while 12.0% of the total
patients were admitted to alcohol consumption with
tobacco smoking.
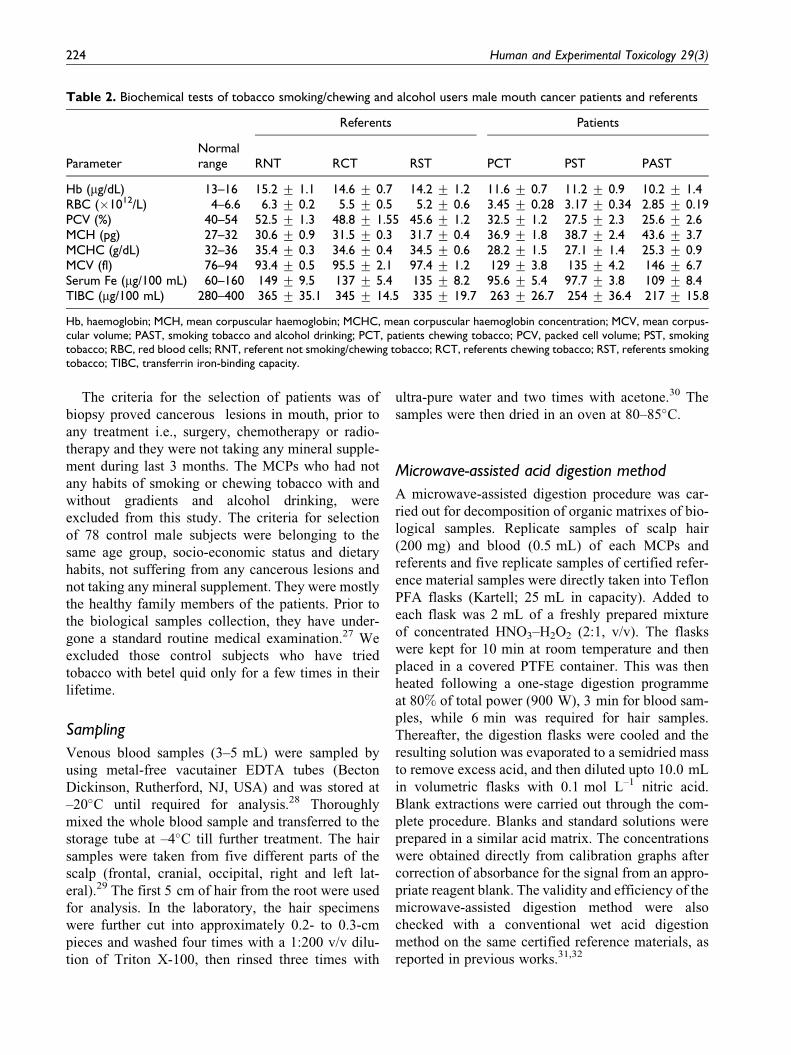
The biochemical tests of patients and referents,
haemoglobin, red blood cells, packed cell volume,
mean corpuscular haemoglobin, mean corpuscular
haemoglobin concentration, mean corpuscular
volume and transferrin iron-binding capacity in the
blood, are shown in Table 2. The histological distribu-
tion is not shown in the present study.
Table 1. Characteristics of study subjects (35–65) agegroups
Referents(n ¼ 78)
Mouth cancerpatients (n ¼ 92)
OccupationLabour 50 (64%) 46 (50.0%)Office worker 28 (36%) 33 (35.9%)Not working —— 13 (14.1%)
HabitsSmoking tobacco 29 (37.2%) 42 (45.6%)Chewing tobacco with
and without gradients(paan, areca nut and slakedlime)
27 (34.6%) 39 (42.4%)
Non-chew tobacco 22 (28.2%) 0 (0%)Smoking þ alcoholdrinkers
0 (0%) 11 (12.0%)
Kazi TG et al. 223
The criteria for the selection of patients was of
biopsy proved cancerous lesions in mouth, prior to
any treatment i.e., surgery, chemotherapy or radio-
therapy and they were not taking any mineral supple-
ment during last 3 months. The MCPs who had not
any habits of smoking or chewing tobacco with and
without gradients and alcohol drinking, were
excluded from this study. The criteria for selection
of 78 control male subjects were belonging to the
same age group, socio-economic status and dietary
habits, not suffering from any cancerous lesions and
not taking any mineral supplement. They were mostly
the healthy family members of the patients. Prior to
the biological samples collection, they have under-
gone a standard routine medical examination.27 We
excluded those control subjects who have tried
tobacco with betel quid only for a few times in their
lifetime.
Sampling
Venous blood samples (3–5 mL) were sampled by
using metal-free vacutainer EDTA tubes (Becton
Dickinson, Rutherford, NJ, USA) and was stored at
–20�C until required for analysis.28 Thoroughly
mixed the whole blood sample and transferred to the
storage tube at –4�C till further treatment. The hair
samples were taken from five different parts of the
scalp (frontal, cranial, occipital, right and left lat-
eral).29 The first 5 cm of hair from the root were used
for analysis. In the laboratory, the hair specimens
were further cut into approximately 0.2- to 0.3-cm
pieces and washed four times with a 1:200 v/v dilu-
tion of Triton X-100, then rinsed three times with
ultra-pure water and two times with acetone.30 The
samples were then dried in an oven at 80–85�C.
Microwave-assisted acid digestion method
A microwave-assisted digestion procedure was car-
ried out for decomposition of organic matrixes of bio-
logical samples. Replicate samples of scalp hair
(200 mg) and blood (0.5 mL) of each MCPs and
referents and five replicate samples of certified refer-
ence material samples were directly taken into Teflon
PFA flasks (Kartell; 25 mL in capacity). Added to
each flask was 2 mL of a freshly prepared mixture
of concentrated HNO3–H2O2 (2:1, v/v). The flasks
were kept for 10 min at room temperature and then
placed in a covered PTFE container. This was then
heated following a one-stage digestion programme
at 80% of total power (900 W), 3 min for blood sam-
ples, while 6 min was required for hair samples.
Thereafter, the digestion flasks were cooled and the
resulting solution was evaporated to a semidried mass
to remove excess acid, and then diluted upto 10.0 mL
in volumetric flasks with 0.1 mol L–1 nitric acid.
Blank extractions were carried out through the com-
plete procedure. Blanks and standard solutions were
prepared in a similar acid matrix. The concentrations
were obtained directly from calibration graphs after
correction of absorbance for the signal from an appro-
priate reagent blank. The validity and efficiency of the
microwave-assisted digestion method were also
checked with a conventional wet acid digestion
method on the same certified reference materials, as
reported in previous works.31,32
Table 2. Biochemical tests of tobacco smoking/chewing and alcohol users male mouth cancer patients and referents
Referents Patients
ParameterNormalrange RNT RCT RST PCT PST PAST
Hb (mg/dL) 13–16 15.2 + 1.1 14.6 + 0.7 14.2 + 1.2 11.6 + 0.7 11.2 + 0.9 10.2 + 1.4RBC (�1012/L) 4–6.6 6.3 + 0.2 5.5 + 0.5 5.2 + 0.6 3.45 + 0.28 3.17 + 0.34 2.85 + 0.19PCV (%) 40–54 52.5 + 1.3 48.8 + 1.55 45.6 + 1.2 32.5 + 1.2 27.5 + 2.3 25.6 + 2.6MCH (pg) 27–32 30.6 + 0.9 31.5 + 0.3 31.7 + 0.4 36.9 + 1.8 38.7 + 2.4 43.6 + 3.7MCHC (g/dL) 32–36 35.4 + 0.3 34.6 + 0.4 34.5 + 0.6 28.2 + 1.5 27.1 + 1.4 25.3 + 0.9MCV (fl) 76–94 93.4 + 0.5 95.5 + 2.1 97.4 + 1.2 129 + 3.8 135 + 4.2 146 + 6.7Serum Fe (mg/100 mL) 60–160 149 + 9.5 137 + 5.4 135 + 8.2 95.6 + 5.4 97.7 + 3.8 109 + 8.4TIBC (mg/100 mL) 280–400 365 + 35.1 345 + 14.5 335 + 19.7 263 + 26.7 254 + 36.4 217 + 15.8
Hb, haemoglobin; MCH, mean corpuscular haemoglobin; MCHC, mean corpuscular haemoglobin concentration; MCV, mean corpus-cular volume; PAST, smoking tobacco and alcohol drinking; PCT, patients chewing tobacco; PCV, packed cell volume; PST, smokingtobacco; RBC, red blood cells; RNT, referent not smoking/chewing tobacco; RCT, referents chewing tobacco; RST, referents smokingtobacco; TIBC, transferrin iron-binding capacity.
224 Human and Experimental Toxicology 29(3)
Statistical analysis
All statistical analyses were performed using com-
puter program Excel X State (Microsoft Corp., Red-
mond, WA, USA) and Minitab 13.2 (Minitab Inc.,
State College, PA, USA). ANOVA was used to assess
the significance of the differences between the vari-
ables investigated in cancerous and non-cancerous
persons. Stepwise multivariate linear regression anal-
ysis was performed using two models, cancerous
patients and referents.
Results
The elemental contents in the biological samples,
especially in blood samples, varied widely among
individuals; thus, a significantly large number of sam-
ples were required for statistical interpretation of the
data to achieve a meaningful correlation between phy-
siological disorders and concentrations of trace and
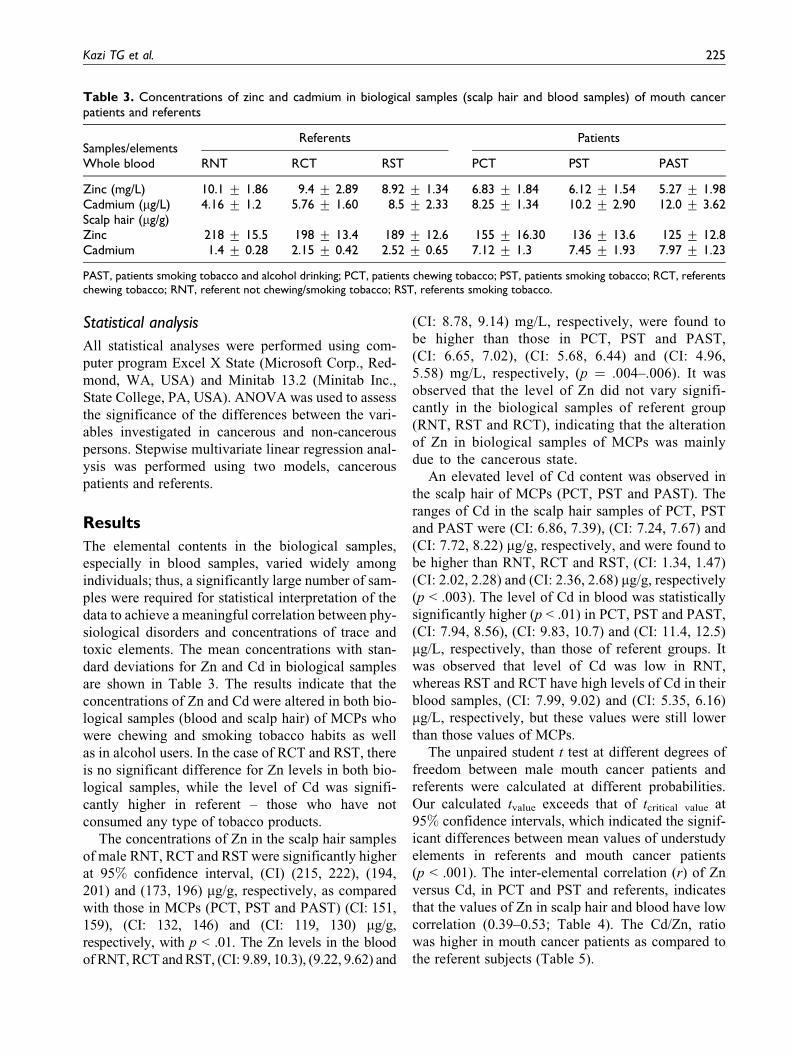
toxic elements. The mean concentrations with stan-
dard deviations for Zn and Cd in biological samples
are shown in Table 3. The results indicate that the
concentrations of Zn and Cd were altered in both bio-
logical samples (blood and scalp hair) of MCPs who
were chewing and smoking tobacco habits as well
as in alcohol users. In the case of RCT and RST, there
is no significant difference for Zn levels in both bio-
logical samples, while the level of Cd was signifi-
cantly higher in referent – those who have not
consumed any type of tobacco products.
The concentrations of Zn in the scalp hair samples
of male RNT, RCT and RST were significantly higher
at 95% confidence interval, (CI) (215, 222), (194,
201) and (173, 196) mg/g, respectively, as compared
with those in MCPs (PCT, PST and PAST) (CI: 151,
159), (CI: 132, 146) and (CI: 119, 130) mg/g,
respectively, with p < .01. The Zn levels in the blood
of RNT, RCT and RST, (CI: 9.89, 10.3), (9.22, 9.62) and
(CI: 8.78, 9.14) mg/L, respectively, were found to
be higher than those in PCT, PST and PAST,
(CI: 6.65, 7.02), (CI: 5.68, 6.44) and (CI: 4.96,
5.58) mg/L, respectively, (p ¼ .004–.006). It was
observed that the level of Zn did not vary signifi-
cantly in the biological samples of referent group
(RNT, RST and RCT), indicating that the alteration
of Zn in biological samples of MCPs was mainly
due to the cancerous state.
An elevated level of Cd content was observed in
the scalp hair of MCPs (PCT, PST and PAST). The
ranges of Cd in the scalp hair samples of PCT, PST
and PAST were (CI: 6.86, 7.39), (CI: 7.24, 7.67) and
(CI: 7.72, 8.22) mg/g, respectively, and were found to
be higher than RNT, RCT and RST, (CI: 1.34, 1.47)
(CI: 2.02, 2.28) and (CI: 2.36, 2.68) mg/g, respectively
(p < .003). The level of Cd in blood was statistically
significantly higher (p < .01) in PCT, PST and PAST,
(CI: 7.94, 8.56), (CI: 9.83, 10.7) and (CI: 11.4, 12.5)
mg/L, respectively, than those of referent groups. It
was observed that level of Cd was low in RNT,
whereas RST and RCT have high levels of Cd in their
blood samples, (CI: 7.99, 9.02) and (CI: 5.35, 6.16)
mg/L, respectively, but these values were still lower
than those values of MCPs.
The unpaired student t test at different degrees of
freedom between male mouth cancer patients and
referents were calculated at different probabilities.
Our calculated tvalue exceeds that of tcritical value at
95% confidence intervals, which indicated the signif-
icant differences between mean values of understudy
elements in referents and mouth cancer patients
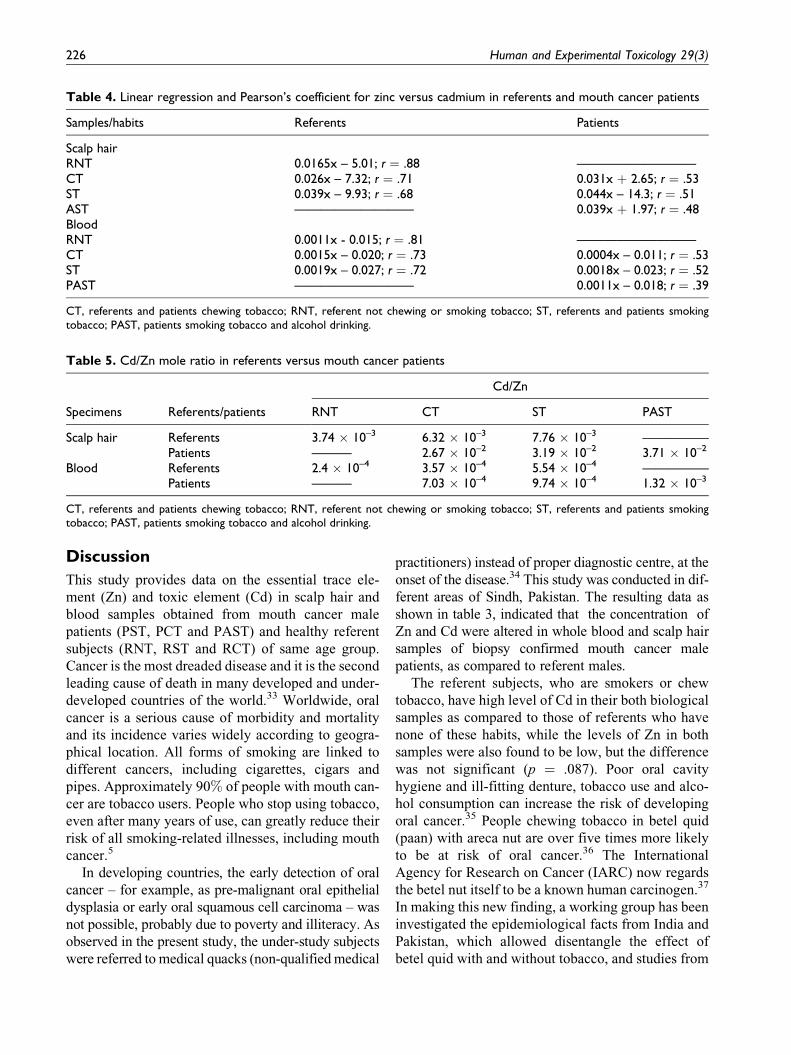
(p < .001). The inter-elemental correlation (r) of Zn
versus Cd, in PCT and PST and referents, indicates
that the values of Zn in scalp hair and blood have low
correlation (0.39–0.53; Table 4). The Cd/Zn, ratio
was higher in mouth cancer patients as compared to
the referent subjects (Table 5).
Table 3. Concentrations of zinc and cadmium in biological samples (scalp hair and blood samples) of mouth cancerpatients and referents
Samples/elementsReferents Patients
Whole blood RNT RCT RST PCT PST PAST
Zinc (mg/L) 10.1 + 1.86 9.4 + 2.89 8.92 + 1.34 6.83 + 1.84 6.12 + 1.54 5.27 + 1.98Cadmium (mg/L) 4.16 + 1.2 5.76 + 1.60 8.5 + 2.33 8.25 + 1.34 10.2 + 2.90 12.0 + 3.62Scalp hair (mg/g)Zinc 218 + 15.5 198 + 13.4 189 + 12.6 155 + 16.30 136 + 13.6 125 + 12.8Cadmium 1.4 + 0.28 2.15 + 0.42 2.52 + 0.65 7.12 + 1.3 7.45 + 1.93 7.97 + 1.23
PAST, patients smoking tobacco and alcohol drinking; PCT, patients chewing tobacco; PST, patients smoking tobacco; RCT, referentschewing tobacco; RNT, referent not chewing/smoking tobacco; RST, referents smoking tobacco.
Kazi TG et al. 225
Discussion
This study provides data on the essential trace ele-
ment (Zn) and toxic element (Cd) in scalp hair and
blood samples obtained from mouth cancer male
patients (PST, PCT and PAST) and healthy referent
subjects (RNT, RST and RCT) of same age group.
Cancer is the most dreaded disease and it is the second
leading cause of death in many developed and under-
developed countries of the world.33 Worldwide, oral
cancer is a serious cause of morbidity and mortality
and its incidence varies widely according to geogra-
phical location. All forms of smoking are linked to
different cancers, including cigarettes, cigars and
pipes. Approximately 90% of people with mouth can-
cer are tobacco users. People who stop using tobacco,
even after many years of use, can greatly reduce their
risk of all smoking-related illnesses, including mouth
cancer.5
In developing countries, the early detection of oral
cancer – for example, as pre-malignant oral epithelial
dysplasia or early oral squamous cell carcinoma – was
not possible, probably due to poverty and illiteracy. As
observed in the present study, the under-study subjects
were referred to medical quacks (non-qualified medical
practitioners) instead of proper diagnostic centre, at the
onset of the disease.34 This study was conducted in dif-
ferent areas of Sindh, Pakistan. The resulting data as
shown in table 3, indicated that the concentration of
Zn and Cd were altered in whole blood and scalp hair
samples of biopsy confirmed mouth cancer male
patients, as compared to referent males.
The referent subjects, who are smokers or chew
tobacco, have high level of Cd in their both biological
samples as compared to those of referents who have
none of these habits, while the levels of Zn in both
samples were also found to be low, but the difference
was not significant (p ¼ .087). Poor oral cavity
hygiene and ill-fitting denture, tobacco use and alco-
hol consumption can increase the risk of developing
oral cancer.35 People chewing tobacco in betel quid
(paan) with areca nut are over five times more likely
to be at risk of oral cancer.36 The International
Agency for Research on Cancer (IARC) now regards
the betel nut itself to be a known human carcinogen.37
In making this new finding, a working group has been
investigated the epidemiological facts from India and
Pakistan, which allowed disentangle the effect of
betel quid with and without tobacco, and studies from
Table 4. Linear regression and Pearson’s coefficient for zinc versus cadmium in referents and mouth cancer patients
Samples/habits Referents Patients
Scalp hairRNT 0.0165x – 5.01; r ¼ .88 —————————CT 0.026x – 7.32; r ¼ .71 0.031x þ 2.65; r ¼ .53ST 0.039x – 9.93; r ¼ .68 0.044x – 14.3; r ¼ .51AST ————————— 0.039x þ 1.97; r ¼ .48BloodRNT 0.0011x - 0.015; r ¼ .81 —————————CT 0.0015x – 0.020; r ¼ .73 0.0004x – 0.011; r ¼ .53ST 0.0019x – 0.027; r ¼ .72 0.0018x – 0.023; r ¼ .52PAST ————————— 0.0011x – 0.018; r ¼ .39
CT, referents and patients chewing tobacco; RNT, referent not chewing or smoking tobacco; ST, referents and patients smokingtobacco; PAST, patients smoking tobacco and alcohol drinking.
Table 5. Cd/Zn mole ratio in referents versus mouth cancer patients
Specimens Referents/patients
Cd/Zn
RNT CT ST PAST
Scalp hair Referents 3.74 � 10–3 6.32 � 10–3 7.76 � 10–3 —————Patients ——— 2.67 � 10–2 3.19 � 10–2 3.71 � 10–2
Blood Referents 2.4 � 10–4 3.57 � 10–4 5.54 � 10–4 —————Patients ——— 7.03 � 10–4 9.74 � 10–4 1.32 � 10–3
CT, referents and patients chewing tobacco; RNT, referent not chewing or smoking tobacco; ST, referents and patients smokingtobacco; PAST, patients smoking tobacco and alcohol drinking.
226 Human and Experimental Toxicology 29(3)

Taiwan (China), where tobacco is not added to the
betel quid.37,38 It was reported in literature that betel
quid with areca nut produce carcinogenicity in experi-
mental animals.34 Chewing betel quid (with mixture
of tobacco leaves, areca nut and spices) is a signifi-
cant risk factor for oral cancer is also confirmed by
another study.36
Malnutrition is one of the major problems in cancer
patients. Although not prevalent in all types of can-
cers, but mouth cancer, undernourishment is a com-
mon and serious problem.34 Cancer patients usually
have inadequate energy and protein intakes, increased
metabolic rate and abnormalities in carbohydrate,
lipid and protein metabolism.39 Cancer treatment with
chemotherapy and radiation therapy is also potentially
damaging the nutritional status.40 A poor diet may
increase the risk of certain types of mouth cancer,
because of a lack of Zn, vitamins and other essential
minerals. Epidemiological studies also suggest a role
for diet in this context.41 In western countries, the
main risk factors are tobacco and alcohol consump-
tion, which have been shown to account for 75%–
90% of oral cancer, with evidence of a synergistic
effect of these two exposures.42 In industrial regions
of the world, increased consumption of tobacco has
been held responsible for the pronounced increase in
oral cancer.43 It is demonstrating that reactive oxygen
species, such as hydroxyl radical, are formed in the
human oral cavity during areca quid chewing, and that
the activity might cause oxidative DNA damage to the
surrounding tissues.44 It has been suggested that free
radicals, reactive oxygen species and reactive nitro-
gen species in the inhaled tobacco smoke and eating
raw tobacco induce lesions of the mucosa, which are
then transformed into oral cancer.45
Alcohol acts as a solvent that enhances the penetration
of carcinogenic compounds into the mucosa. Ethanol
may facilitate the uptake of environmental carcinogens,
especially from tobacco smoke, through cell membranes
that are damaged and changed in their molecular compo-
sition by the direct effect of alcohol. Furthermore,
chronic alcoholism leads to atrophy and lipomatous
metamorphosis of the parenchyma of the parotid and sub-
maxillary gland and this alteration results in a functional
impairment of saliva flow and its increased viscosity.
Thus, the mucosal surface will be insufficiently rinsed
and is, therefore, exposed to higher concentrations of
locally acting carcinogens in addition to a prolongation
of the contact time of the substances with the mucosa.46
Tobacco leaves naturally accumulate and concen-
trate relatively high levels of Cd, and therefore
smoking of tobacco is an important source of Cd
exposure for smokers.47 The total amount of carcino-
gens in cigarette smoke ranges from one to 3 mg per
cigarette.35 The country of origin and type of the
product play major roles in determining the chemical
composition of cigarette tobacco.48 It was investi-
gated that one pack of cigarettes deposits 2–4 mg Cd
into the lungs of a smoker, whereas some of the
smoke passes into the air to be inhaled by smokers and
nonsmokers alike.49 It was also consistent with
another study that smokers generally exhibit signifi-
cantly higher Cd body burdens than non-smokers,
while smoking with alcohol consumption enhance the
Cd absorption and accumulation in all the tissues.47
The results suggested that although Cd poses a hazard
to essential trace metal homeostasis of various organs,
co-exposure can pose a major threat, while consump-
tion of ethanol may absorb much more Cd than their
unexposed counterparts.50
The results of present study are consistent with the
hypothesis that exposure to Cd oxide fumes by
tobacco smoking or chewing increases the risk of
mortality from oral cancer, due to deficiency of essen-
tial elements like Zn.51 In the past few years, increas-
ing consideration has been given to interactions
occurring in the organism between toxic metals and
bioelements essential for life. These interactions are
complex and involve biometals such as zinc, copper,
iron, selenium, calcium and toxic elements, including
cadmium.52 The basis of Cd toxicity is its negative
influence on enzymatic systems of cells, resulting
from substitution of other essential metal ions (mainly
Zn, Cu and Ca) in metalloenzymes and its very strong
affinity to biological structures containing –SH
groups, such as proteins, enzymes and nucleic acids.53
The relevance of Cd–Zn interactions should be con-
sidered in the light of the general population exposure
to Cd54 and common deficiency of Zn in the world,
mainly due to nutritional factors.55
Zn was considered one of the necessary composi-
tions of many enzymes in human body, involved in
the synthesis of DNA and RNA polymeric enzymes,
took part in the nucleic acid metabolism and immuno
surveillance protection, affecting the process of can-
cer development directly or indirectly. Epidemiologi-
cal studies also indicated that content of Zn in serum
of tumor patients was lower than in healthy persons.56
Zinc is well known to induce production of metal-
lothionein, which is very rich in cysteine, and this is
an excellent scavenger of hydroxyl radical. Thus, it
is clear that Zn has multiple roles as antioxidant and
Kazi TG et al. 227

is, therefore, an excellent candidate for clinical che-
moprevention trials in humans.57
It was reported that the mechanism by which Cd
antagonizes Zn may be from its ability to substitute
for Zn in the Zn finger DNA binding domain, and this
may be the way Cd causes toxicity and cancer.
Cadmium depletes glutathione and protein-bound
sulfhydryl groups, resulting in enhanced production
of reactive oxygen species such as superoxide ion,
hydroxyl radicals and hydrogen peroxide.58 A far
more comprehensive study of the basic mechanism
for alteration of Zn level in blood, and other biologi-
cal samples, and its significance in all malignancies is
needed. Many epidemiologic studies suggest that Zn
deficiency may be associated with increased risk of
cancer.57 Zn supplementation is associated with
decreased oxidative stress and improved immune
function and might aid in the prevention and treat-
ment of cancer. The effect of Zn on the immune sys-
tem strengthens the body’s defense against abnormal
cell growth associated with cancer development.59
The profound Zn deficiency is quite rare in
humans, but mild-to-moderate Zn deficiency may be
relatively common throughout the world in both
less developed and industrial countries,60 and
Zn-deficient persons have increased susceptibility to
a variety of pathogens; although the cause in some
cases may be inadequate dietary intake, Zn absorption
is possibly the most common causative factor.55 The
effects of Zn on the initiation and progression of can-
cer are not well established; although the negative
effects of Zn deficiency on the immune system are
clear.61 Changes in blood Zn have been found in lym-
phoproliferative disorders as well as in breast, lung
and gastrointestinal tumors.62 It was investigated that
the decrease in plasma Zn concentration was observed
after stress, trauma and in several malignancies.63
A balanced diet that includes enough calcium, iron,
protein and Zn will also help to reduce the amount
of Cd that may be absorbed into the body from food
or drink.64
It was also observed in present study that the socio-
economic factors also play a role in higher mortality
rates in patients, such as poor nutrition, irregular
screening, late diagnosis and unequal access to health
care due to poverty. On other side, the cost of treat-
ment for mouth cancer and other types of cancer is
very high, which is commonly not affordable. The
local hygiene center facilities are poor in our country
and there are no routine monitoring and screening
carried out for those people living in small towns.
Conclusion
The results of this study revealed that mouth cancer
male patients have a different pattern of essential
trace (Zn) and toxic (Cd) elements in their biological
samples as compared to the healthy referents, with the
prevalence being more in smoking and chewing
tobacco patients. However, higher levels of Cd, as
well as a lower level of Zn, correlated well with the
consequences of mouth cancer. The deficiency of the
Zn, which is replaced by Cd, may result in abnormal
physiology disorders, and, in addition to other factors,
which play role in developing mouth cancer. This
study provides some support for the hypothesis that
dietary intake of essential elements and inhalation
of Cd, most probably through drinking alcohol, smok-
ing and chewing tobacco, may increase the risk of
mouth cancer and related disorders, which indicates
that the causal link may be stronger among tobacco
smokers/chewers and alcohol users. We propose that
essential and toxic elemental measurements may be
performed on patients reaching in the emergency
department, to test whether the concentration of it
may serve not only as markers of oral or mouth cancer
and its remedies but also as predictors of adverse
outcomes.
References
1. Lippman SM, Hong WK. Molecular markers of the risk
of oral cancer. N Engl J Med 2001; 344: 1323–1326.
2. Oji C, Chukwuneke FN. Oral cancer in Enugu, Nigeria,
1998–2003. Br J Oral Maxillofacial Surg 2007; 45:
298–301.
3. Macfarlane GI, Boyle P, Evstifeeva TV, Robertson C,
Scully C. Rising trends of oral cancer mortality among
males worldwide: the return of an old public health
problem. Cancer Causes Control 1994; 5: 259–265.
4. Ko YC, Huang YL, Lee CH. Betel quid chewing, cigar-
ette smoking and alcohol consumption related to oral
cancer in Taiwan. J Oral Pathol Med 1995; 24: 450–453.
5. Rodu B, Jansson C. Smokeless tobacco and oral cancer:
a review of the risks and determinants. Crit Rev Oral
Biol Med 2004; 15: 252–263.
6. Avti PK, Kumar S, Pathak CM, Vaiphei K, Lal K. Smo-
keless tobacco impairs the antioxidant defense in liver,
lung, and kidney of rats. Toxicol Sci 2006; 89: 547–553.
7. Lee PN. Circulatory disease and smokeless tobacco in
Western populations: a review of the evidence. Int J
Epidemiol 2007; 36: 789–804.
8. Schildt EB, Eriksson M, Hardell L, Magnuson A. Oral
snuff, smoking habits and alcohol consumption in
228 Human and Experimental Toxicology 29(3)
relation to oral cancer in a Swedish case-control study.
Int J Cancer 1998; 77: 341–346.
9. Muscat JE, Richie JP, Thompson S, Wynder EL.
Gender differences in smoking and risk for oral cancer.
Cancer Res 1996; 56: 5192–5197.
10. Bouquot JE. Reviewing oral leukoplakia. Clinical
concepts for the 1990s. J Am Dent Assoc 1991; 122:
80–82.
11. Stephens WE, Calder A. Source and health implications
of high toxic metal concentrations in illicit tobacco
products. Environ Sci Technol 2005; 39: 479–488.
12. Van Wyk CW, Stander I, Padayachee A, Grobler-
Rabie AF. The areca nut chewing habit and oral
squamous cell carcinoma in South African Indians.
A retrospective study. S Afr Med J 1993; 83: 425–429.
13. Soylak M, Saraymen R, Narin _I, DoGan M. Serum zinc
levels of a poor economic and social region near an
industrial zone. Trace Elements and Electrolytes
1998; 15: 142–144.
14. Prasad AS. Zinc in human health: an update. J Trace
Elem Exp Med 1998; 11: 63–87.
15. Prasad AS, Beck FWJ, Doerr TD, et al. Nutritional and
zinc status of head and neck cancer patients: an inter-
pretive review. J Am Coll Nutr 1998; 17: 409–418.
16. Elinder CG. Cadmium as an environmental hazard.
IARC Sci Publ 1992; 118: 123–132.
17. Goyer RA. Toxic and essential metal interactions.
Annu Rev Nutr 1997; 17: 37–50.
18. Drasch G, Schopfer J, Schrauzer GN. Selenium/
cadmium ratios in human prostates Indicators of
prostate cancer risk of smokers and nonsmokers, and
relevance to the cancer protective effects of selenium.
Biol Trace Element Res 2005; 103: 103–107.
19. Tuzen M. Determination of some trace elements in
whole blood and serum by GFAAS. Trace Elements
and Electrolytes 2002; 19(4):202–204.
20. Soylak M, SaracoGlu S, Divrikli U, Elci L. Copper and
Zinc Concentrations of Serum Samples of Healthy
People Living in Tokat. Turkey. Trace Elements and
Electrolytes 2001;18: 47–50.
21. Soylak M, Saraymen R, Dogan M. Investigation of
Lead, Chromium, Cobalt and Molybdenum Concentra-
tions in Hair Samples Collected from Diabetic Patients.
Fresenius Environmental Bulletin 1995; 4: 485–490.
22. Ghaedi M, Shokrollahi A, Kianfar AH, Mirsadeghi
AS, Pourfarokhi A, Soylak M. The determination of
some heavy metals in food samples by flame atomic
absorption spectrometry after their separation-
preconcentration on bis salicyl aldehyde, 1,3 propan
diimine (BSPDI) loaded on activated carbon. J Hazard
Mater 2008; 154: 128–134.
23. Ghaedi M, Niknam K, Shokrollahi A, Niknam E,
Ghaedi H, Soylak M. A solid phase extraction proce-
dure for Fe3þ, Cu2þ and Zn2þ Ions on 2-phenyl-1H-
benzo[d] imidazole loaded on Triton-X100 coated poly
vinyl chloride. J Hazard Mater 2008; 158: 131–136.
24. Melek E, Tuzen M, Soylak M. Flame atomic
absorption spectrometric determination of cadmiu-
m(II) and lead(II) after their solid phase extraction as
dibenzyldithiocarbamate chelates on Dowex Optipore
V-493.Anal Chim Acta 2006; 578: 213–219.
25. Thomas SJ, MacLennan R. Slaked lime and betel nut
cancer in Papua, New Guinea. Lancet 1992; 340:
577–578.
26. Trivedi AH, Balart DB, Shah PM, et al. Carcinogenic
and genotoxic effects of the tobacco substitute pan
masala: present status and likely future impact on the
Indian population. Canc Treat Rev 1996; 22: 345–354.
27. Zowczak M, Iskra M, Paszkowski J, Manczak M,
Torlinski L. Oxidase activity of ceruloplasmin and
concentrations of copper and zinc in serum of cancer
patients. J Trace Elem Med Biol 2001; 15: 193–196.
28. Cornelis R, Heinzow B, Herber RFM. Sample collec-
tion guidelines for trace elements in blood and urine.
Pure Appl Chem 1995; 67: 1575–608.
29. Kubova J, Hanakova V, Medved J, Stresko V. Determi-
nation of lead and cadmium in human hair by atomic-
absorption spectrometric procedures after solid-phase
extraction. Anal Chim Acta 1997; 337: 329–334.
30. Afridi HI, Kazi TG, Jamali MK, Kazi GH, Arain MB,
Jalbani N, Shar GQ. Analysis of heavy metals in scalp
hair samples of hypertensive patients by conventional
and microwave digestion methods. Spectrosc Lett
2006; 39: 203–214.
31. Kazi TG, Afridi HI, Kazi GH, Jamali MK, Arain MB,
Jalbani N. Evaluation of essential and toxic metals by
ultrasound-assisted acid leaching from scalp hair sam-
ples of children with macular degeneration patients.
Clin Chim Acta 2006; 369: 52–60.
32. Kazi TG, Afridi HI, Kazi N, et al. Distribution of zinc,
copper and iron in biological samples of Pakistani myo-
cardial infarction (1st, 2nd and 3rd heart attack) patients
and controls. Clin Chim Acta 2008; 389: 114–119.
33. Asha G, Vijayalakshmi D, Kumar V. Effect of inter-
vention on the nutritional status of selected cancer
patients. J Hum Ecol 2004; 16: 189–192.
34. Yadav JS, Chadha P. Genotoxic studies in pan masala
chewers: a high cancer risk group. Int J Hum Genet
2002; 2(2): 107–112.
35. Newcomb PA, Carbone PP. The health consequences
of smoking. Cancer Med Clin N Am 1992; 76:
305–331.
Kazi TG et al. 229
36. Ahluwalia KP. Assessing the oral cancer risk of South-
Asian immigrants in New York City. Cancer 2005;
104: 2959–2961.
37. Tomatis L. The IARC monographs program: changing
attitudes towards public health. Int J Occup Environ
Health 2002; 8: 144–152.
38. Warnakulasuriya S, Trivedy C, Peters TJ. Areca nut
use: an independent risk factor for oral cancer. BMJ
2002; 324: 799–800.
39. Rivadeneira DE, Evoy D, Fahey TJ, Lieberman MD,
Daly JM. Nutritional support of the cancer patient.
CA Cancer J Clin 1998; 48: 69–80.
40. Oneschuk D, Younus J. Natural health products and
cancer chemotherapy and radiation therapy. Oncol Rev
2008; 1: 233–242.
41. Spitz MR, Santella RM, Boffetta P, Buffler P. Sub-
group report: head and neck cancer. IARC Sci Publ
2004; 157: p.41–47.
42. Franceschi S, Levi F, Vecchia CL, et al. Comparison of
the effect of smoking and alcohol drinking between oral
and pharyngeal cancer. Int J Cancer 1999; 83: 1–4.
43. Grasso P, Mann AH. Smokeless tobacco and oral can-
cer: an assessment of evidence derived from laboratory
animals. Food Chem Toxicol 1998; 36: 1015–1029.
44. Chen CL, Chi CW, Liu TY. Hydroxyl radical forma-
tion and oxidative DNA damage induced by areca quid
in vivo. J Toxicol Environ Health 2002; 65: 327–336.
45. Yoshida T, Tuder RM. Pathobiology of cigarette
smoke-induced chronic obstructive pulmonary disease.
Physiol Rev 2007; 87: 1047–1082.
46. Maier H, Born IA, Veith S, Adler D, Seitz HK. The
effect of chronic ethanol consumption on salivary
gland morphology and function in the rat. Alcoholism.
Clin Exper Res 1986; 10: 425–427.
47. Csalari J, Szantai K. Transfer rate of cadmium, lead,
zinc and iron from the tobacco-cut of the most popular
Hungarian cigarette brands to the combustion prod-
ucts. Acta Aliment 2002; 31: 279–288.
48. Hecht SS. Tobacco carcinogens, their biomarkers and
tobacco-induced cancer. Nat Rev Cancer 2003; 3:
733–744.
49. Kazi TG, Jalbani N, Arain MB, et al. Toxic metals dis-
tribution in different components of Pakistani and
imported cigarettes by electrothermal atomic absorption
spectrometer. J Hazard Mater 2009; 163: 302–307.
50. Sharma G, Sandhir R, Nath R, Gill K. Effect of ethanol
on cadmium uptake and metabolism of zinc and copper
in rats exposed to cadmium. J Nutr 1991; 121: 87–91.
51. Franceschi S, Barra S, Vecchia CL, Bidoli E, Negri E.
Risk factors for cancer of the tongue and the mouth. A
case-control study from northern Italy. Cancer 1992;
70: 2227–2233.
52. Brzoska MM, Moniuszko-Jakoniuk J, Jurczuk M,
Chraniuk M. The influence of cadmium on bone tissue
in rats. Pol J Environ Stud 1997; 6: 29–32.
53. Stohs SJ, Bagchi D. Oxidative mechanisms in the
toxicity of metal ions. Free Radic Biol Med 1995;
18: 321–336.
54. Waalkes MP, Coogan TP, Barter RA. Toxicological
principles of metal carcinogenesis with special
emphasis on cadmium. Crit Rev Toxicol 1992; 22:
175–201.
55. Lonnerdal B. Dietary factors influencing zinc
absorption. J Nutr 1993; 130: 1378–1383.
56. Dong LH, Qiang WZ, Rong PY, Shu ZT, Zhu XX,
Wang KT. Comparison of serum Zn, Cu and Se con-
tents between healthy people and patients in high, mid-
dle and low incidence areas of gastric cancer of Fijians
Province. World J Gastroenterol 1999; 5: 84–86.
57. Somer E. Health media of America essential guide to
vitamins and minerals. New York: Harper Perennial,
1995, 32, p.139–14.
58. Stohs SJ, Bagchi D, Hassoun E, Bagchi M. Oxidative
mechanisms in the toxicity of chromium and cadmium
ions. J Environ Pathol Toxicol Oncol 2001; 20: 77–88.
59. Timar J, Raso E, Paku S, Kopper L. Oral administra-
tion of trace element preparation and zinc inhibit liver
metastasis of 3LL-HH murine tumor cells. Int J Mol
Med 1998; 2: 105–108.
60. Ganapathy S, Volpe SL. Zinc, exercise and thyroid
hormone function. Crit Rev Food Sci Nutr 1999; 39:
369–390.
61. Linder MC. Nutritional biochemistry and metabolism.
2nd ed. New York: Elsevier Science Publishing Co.
Inc. 1991, p.499–512.
62. Newbern PM, Schrager TF, Broitman S. Esophageal
carcinogenesis in the rat: zinc deficiency and alcohol
effects on tumor induction. Path biology 1997; 65:
39–45.
63. Gupta SK, Shukla V, Vaidya MP. Serum trace ele-
ments and Cu/Zn Ratio in breast cancer patients. J Surg
Oncol 1991; 46: 178–181.
64. Leccia MT, Richard MJ, Favier A, Beani JC. Zinc
protects against ultraviolet A1-induced DNA damage
and apoptosis in cultured human fibroblasts. Biol
Trace Elem Res 1999; 69: 177–190.
230 Human and Experimental Toxicology 29(3)





























