Embed Size (px)
Citation preview

A MEW
Stacey C. Wilson, RN, PG Dip. Nsg (Mental Health), M.Phil, MNZCMHNSchool of Health and Social Services, Massey University, Palmers ton North
Jenny Carryer, RN, PhD, FCNA(NZ), MNZM, Clinical Chair of Nursing,Massey University/MidCentral District Health Board, Palmerston North
Effective nursing practice requires the ability to recognise emotions and handleresponses in relationships with clients and their families. This emotional competenceincludes nurses managing their own emotional life along with the skill to relateeffectively to the multiple colleagues and agencies that nurses work alongside. Theresearch was designed to explore the views of nurse educators about the challengesthey encounter when seeking to assess a student's development of emotionalcompetence during the three year bachelor of nursing degree. Focus groups wereused to obtain from educators evidence of feeling and opinion as to how theoryand practice environments infiuence student nurses' development of emotionalcompetence. The process of thematic analysis was utilised and three key themesarose as areas of importance to the participants. These were personal and socialcompetence collectively comprises emotional competence in nursing; emotionalcompetence is a key component of fitness to practise; and transforming caring intopractice. The findings of the study indicate a need for definition of what emotionalcompetence is in nursing. It is argued that educators and practicing nurses, whowork alongside students, must uphold the expectation that emotional competenceis a requisite ability and should themselves be able to role model emotionallycompetent communication.
Key Words: Emotional competence, nursing education, emotions, fitness topractise.
Collectively those who choose toundertake education to become aRegistered Nurse are people withwide and varied experiences andcapabilities. In order for nursingstudents to gain confidence, effectivecommunication skills, and the abilityto convey hope and regard for otherswithin their relationships, they must
learn to recognise and understandemotions. Accepting such emotions andvalidating this experience is essentialwhen establishing a relationship.However, managing emotions andworking with the emotions of othersis not a readily teachable skill.
Wilson, S. C, & Carryer, J. (2008). Emotionalcompetence and nursing education: A New Zealandstudy. Nursing Praxis in New Zealand, 24(\), 36-47.
Page 36 Vol. 24 No. 1 2008 Nursing Praxis in New Zealand

It has been argued that there isa connection between a nurse'sability to accept another person'semotional distress and their capacityto accept themselves and their owndistress. Peplau (1988) calls thiscaring neutrality. She suggests thatnurses are required to develop a levelof congruence between what they sayand how they act toward the personswith whom they work. When nurseslearn to process their own emotions,working with another person'semotion is made possible (Horsfall86 Stuhlmiller, 2000). Reflection onone's own unique capabilities andlimitations can assist individuals torecognise these in others. The nurseeducator, working for a recognisedinstitution, is entrusted by the NursingCouncil of New Zealand (the NursingCouncil) to assess the capabilities andcompetence of students in applicationto the professional nursing register,including provision of a statementthat the student is fit to practise(Nursing Council of New Zealand(NCNZ), 2002). The way in whicheducators interpret the competencydomains of practice (NCNZ, 2005), asthey relate to emotional competencehas not been a feature of the nursingliterature. Nor has a collectivedescription of emotional competencebeen established in nursing educationor practice.
The primary aim of this study,undertaken as partial requirement fora Master's degree (Wilson, 2006) wasto explore the challenges encounteredby nurse educators who seek toassess aspects that could be relatedto emotional competence in nursingstudents. Exploration of this research
question was broken down to threeaims:
1. To determine how a group of nurseeducators recognise and describeemotional competence.
2. To facilitate discussion of environ-mental and relational complexitiesthat affect student learning ofemotional competence.
3. To clarify how the competencyassessment framework (NCNZ,2005) can provide a structurefor feedback to students abouttheir development of emotionalcompetence.
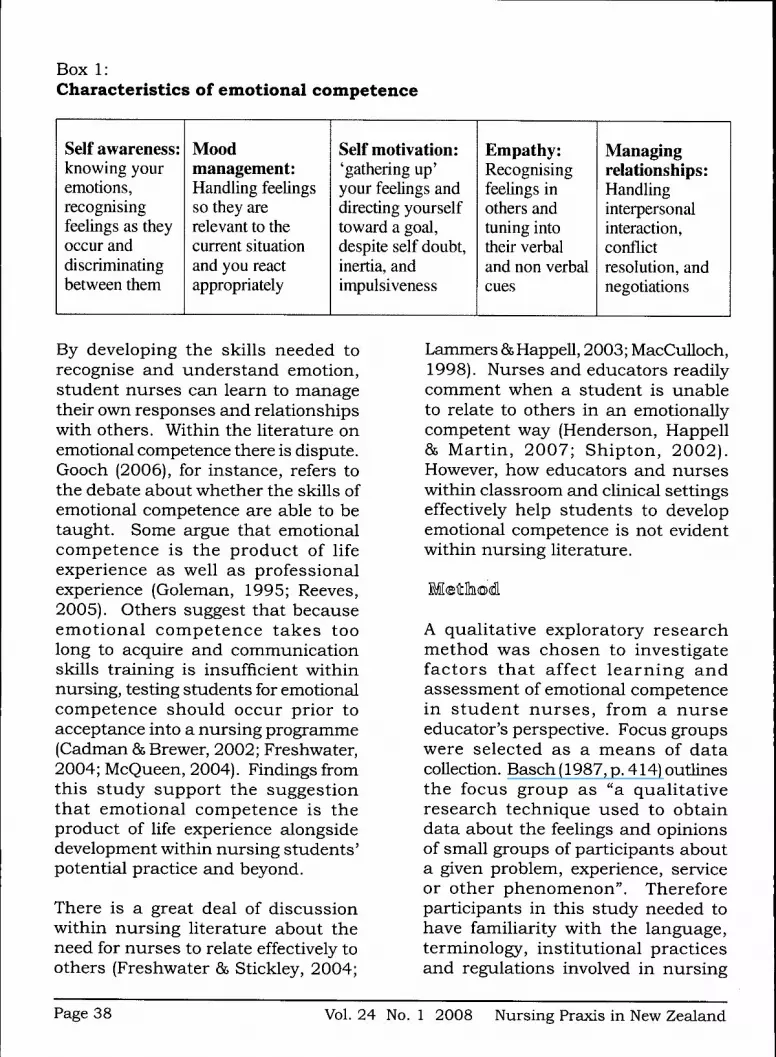
Theories of emotion attempt toexplain the relationship betweensubjective emotional experiencesand an event. However, the sameevent may result in a very differentemotional experience within eachindividual. An understanding ofemotional competence within nursingmay assist educators and nurses toreflect on the individual experiencesstudents have within their learning.Heron (2004) argues that in orderto interact successfully with clientshelping professionals must be able todisplay emotional competence. Withinnursing literature the term 'emotionalcompetence' is used interchangeablywith related terms such as emotionalintelligence (Goleman, 1995; Salovey86 Mayer, 1990), emotional labour(Hocshschild, 1983) and emotionalliteracy (Sharp, 2001). Box 1 shows fivekey characteristics that, collectively,contribute to emotional competence(see Box 1).
Nursing Praxis in New Zealand Vol. 24 No. 1 2008 Page 37
Box 1:Characteristics of emotional competence
Self awareness:knowing youremotions.recognisingfeelings as theyoccur anddiscriminatingbetween them
Moodmanagement:Handling feelingsso they arerelevant to thecurrent situationand you reactappropriately
Self motivation:'gathering up'your feeUngs anddirecting yourselftoward a goal,despite self doubt.inertia, andimpulsiveness
Empathy:Recognisingfeelings inothers andtuning intotheir verbaland non verbalcues
Managingrelationships:Handlinginterpersonalinteraction.conflictresolution, andnegotiations
By developing the skills needed torecognise and understand emotion,student nurses can learn to managetheir own responses and relationshipswith others. Within the literature onemotional competence there is dispute,Gooch (2006), for instance, refers tothe debate about whether the skills ofemotional competence are able to betaught. Some argue that emotionalcompetence is the product of lifeexperience as well as professionalexperience (Goleman, 1995; Reeves,2005), Others suggest that becauseemotional competence takes toolong to acquire and communicationskills training is insufficient withinnursing, testing students for emotionalcompetence should occur prior toacceptance into a nursing programme(Cadman & Brewer, 2002; Freshwater,2004; McQueen, 2004), Findings fromthis study support the suggestionthat emotional competence is theproduct of life experience alongsidedevelopment within nursing students'potential practice and beyond.
There is a great deal of discussionwithin nursing literature about theneed for nurses to relate effectively toothers (Freshwater 86 Stickley, 2004;
Lammers 85Happell, 2003; MacCulloch,1998), Nurses and educators readilycomment when a student is unableto relate to others in an emotionallycompetent way (Henderson, Happell86 Martin, 2007; Shipton, 2002),However, how educators and nurseswithin classroom and clinical settingseffectively help students to developemotional competence is not evidentwithin nursing literature.
A qualitative exploratory researchmethod was chosen to investigatefactors that affect learning andassessment of emotional competencein student nurses, from a nurseeducator's perspective. Focus groupswere selected as a means of datacollection, Basch (1987, p, 414) outlinesthe focus group as "a qualitativeresearch technique used to obtaindata about the feelings and opinionsof small groups of participants abouta given problem, experience, serviceor other phenomenon". Thereforeparticipants in this study needed tohave familiarity with the language,terminology, institutional practicesand regulations involved in nursing
Page 38 Vol, 24 No, 1 2008 Nursing Praxis in New Zealand

education. Focus groups enabledinteraction among participants andallowed the educators to consider andrespond to the views of others (Kevern&Webb, 2001).
The sample criteria were: to be aRegistered Nurse employed within aNew Zealand pol3^echnic or universitypracticing as a nurse educatorand actively involved in teachingeither classroom or clinical learningexperiences for bachelor of nursingstudents. Permission was soughtfrom the Head of Department at threenursing education schools. A noticewas sent by the researcher to eacheducator working within the schoolsof nursing requesting expressions ofinterest with regard to participationin the study. All volunteers met thecriteria for inclusion and no furthersampling was required once theinitial samples had been recruitedfrom the various institutions. Theresearcher made no attempt to recruitparticipants who held a particular viewof emotional competence, however self
Box 2:Focus group question framework
identiflcation of participants may havecontributed to a bias. This bias may bein favour of the participants believingthe concept of emotional competenceto be relevant in nursing.
Fifteen individual participants tookpart in three separate focus groupsat three different venues. A list ofpotential questions was developedprior to the first focus group to facilitateexplorations around the research aim.The questions (see Box 2) attemptedto strike a balance between generatingdiscussion and the need to limit datacollection according to the purpose ofthe research. The aim was to facilitateand focus discussion rather thancontrol it.
The study was approved by theMassey University Human EthicsCommittee. After the participantsresponded to the advertisement,they were sent an information sheet,question framework, a brief summaryof literature on emotional competenceas shown in Box 1, and a consent form
1. Based on your understanding of what emotional competence is, what do youthink are its key elements?
2. In what ways do you assess your own emotional competence?3. What ways do you communicate or role model emotional competence
personally?4. What ways do you communicate or role model emotional competence as a nurse
educator?5. How do you currently assess emotional competence in nursing students?6. In what ways do the competency framework (NCNZ, 2005) and other
curriculum guidelines inform and guide you when teaching and assessingemotional competence with nursing students?
7. What challenges, tensions, and difficulties do you encounter in relation todemonstrating, teaching or assessing emotional competence?
Nursing Praxis in New Zealand Vol. 24 No. 1 2008 Page 39

to sign. An agreed time and venue wasnegotiated with the separate groups.At the beginning of each focus groupindividual written informed consentwas gained. Participants were invitedto participate in an audio taped focusgroup interview of approximately twohours in length and conducted in theircollective workplace. The researcherhad no educational role in any of theinstitutions involved in this study andfull confidentiality was maintainedthroughout.
After the first focus group took placethe audio tapes were transcribedby the researcher within a week asadvocated by Krueger (2000). Thisassisted with the ongoing analysisand refiection on question structureand relevance for the next group. Theaim of the timeframe was to avoid, asmuch as possible, loss of recall andaccuracy of the observations madeduring the group. Transcription by theresearcher created the opportunity to'listen' differently to the content, toneand interaction that occurred duringthe group - aspects sometimes notapparent while acting as facilitator.At the completion of each group theresearcher negotiated the type offeedback and consultation about thetranscripts and emerging ideas thatbest suited the participants. Theywere offered a choice of an individualcopy of the typed transcripts ora summary. Each of the groupsrequested a four to five page summaryof the transcripts to be posted to themindividually. This took place andthe participants either individuallyor collectively as a group, contactedthe researcher with comments whichwere then incorporated into theanalysis.
There were multiple dimensions toconsider in the analysis of the focusgroup interviews (Kitzinger, 1994;Krueger, 2000; Morgan, 1996). Thefirst steps in the analytic process wereidentifying key questions that relateto the research aim and explorationof the topic, followed by capturingthe data. The next step was tosummarise the key ideas in the data.On completion of the transcribingthe researcher summarised the keypoints according to the researchquestion framework. Answersthroughout the group process wereassigned to a question. Verificationfrom the participants has alreadybeen described above. Participants'written and verbal feedback wasincluded in the data analysis. Thelast step involved debriefing betweenmoderators (Krueger). For thisstudy the principles and process ofthematic analysis (Boyatzis, 1998)were utilised to code and interpretthe data; following this process theidentified themes were discussed withthe participants.
The three major themes arising fromthe thematic analysis of transcriptswere that personal and socialcompetence collectively compriseemotional competence in nursing,emotional competence is a keycomponent of fitness to practise,and the transformation of caring intopractice.
Personal and social competencecollectively comprise emotionalcompetence in nursingThe first aim of this study was todetermine how a group of nurse
Page 40 Vol. 24 No. 1 2008 Nursing Praxis in New Zealand

educators recognise and describewhat emotional competence is innursing. It quickly became apparentduring the focus groups that theeducators had similar ideas as to whatconstituted emotional competence tothem personally, and professionallyhow they sought to recognise atype of emotional competence innursing students when workingwith them. The definition (see Box3) was developed from the variousdescriptions and understandingsoffered by the educators duringthe focus group and focus groupanalysis. It has been summarised bythe researcher based on interpretivequalitative methodology. The definitionis two-fold showing that personaland social competences collectivelyare characteristics of emotionalcompetence in nursing. The educatorsargued that there are few definingcriteria to separate the personalfrom the professional in relation toemotional competence, but that thekey characteristics develop over timewith relational experiences.
A complex challenge for nurseeducators is working with a varied
level of maturity within the studentgroup. Emotional competence ifviewed as a developmental or acquiredcompetence, as suggested by Goleman(1995), means that students needopportunities and support in orderthat they can work on their personalcoping and so become more aware ofhowthey operate with others. Maturityof personal com.petence indicates thatthe student is developing their ownvalue and belief system (Henderson,et al., 2007). The individual natureof gaining emotional competence,increasing consciousness andunderstanding how emotions informand affect behaviour was summed upby an educator in the second focusgroup:
It's an individual experience soit can't be taught, but it can bedeveloped (Gp 2, p. 5).
In doing so, students can then developthe ability to 'tune into' the needs ofthe individuals and communities withwhom they are learning and working(McQueen, 2004). The educatorsargue that this emotional competenceis a key component of developing'fitness to practise' in nursing.
Box 3:Emotional competence a definition for nursing(collectively from the educators)
Personal competence:Is being able to become self-aware andhaving regard for yourself. Beingpersonally competent means youcontinuously work on aspects of yourpersonal coping and emotional reactions,so that you are more aware of how youoperate with others.
Social competence:Is using your self awareness, managing itand moving beyond it. This social abilityenables us to become able to work withanother person's issues or needs.including effective management of conflictin relationships.
Nursing Praxis in New Zealand Vol. 24 No. 1 2008 Page 41

Emotional competence a keycomponent of fitness to practiseSection 16 of the Health PractitionersCompetence Assurance Act (2003)requires students in application tothe professional nursing registerto demons t ra te the ability tocommunicate effectively. This view ofeffective communication or 'tuning in'is supported by Hocshschild's (1983)claim that nurses engage in emotionallabour. This labour is guided by socialconventions as students relate withothers. As an educator in the firstfocus group asserts:
it means they[the studentjare ableto think about their own personalreactions, acknowledge thosefeelings and challenge themselvesto respond in a way that is goingto be helpful to the person they areworking with (Gp 1, p. 10).
The social rules or expectations ofhow others display emotion, assistsstudents to recognise and regulatetheir own emotional reactions. Saloveyand Mayer (1990) argue that pickingup on people's emotions promotes theability to recognise what others mightbe feeling. The educators discussedcomplex challenges encounteredwhen working with students. Thosechallenges that relate to the emotionalwellbeing and relational ability ofstudents were highlighted as keyfactors determining whether or nota student is seen to be fit to practiseat the completion of the degree.Emotional competence as a keycomponent to being fit to practiseis the second major theme whichresulted from this study.
There was consensus within each ofthe focus groups that students face
multiple life challenges and as a resultstruggle to manage their personalcompetence while learning. As aneducator from the second focus grouppoints out, a student's emotionalproblems can lead to unhelpfulcommunication and impair theirdevelopment of interpersonal ability:
Students come from differentbackgrounds and are at differentlevels and do or not do life well.They come into nursing with theneed to engage patients and staffand it's almost as though they can'tput aside their own stuff [emotionalproblems] in order to work with theneed (Gp 2, p.9).
Quinn (2000) confirms that somestudents may lack confidence in theirclinical and academic ability whichmay lead them to discontinue theirundergraduate education. Therefore,given this understanding that studentsdo struggle, there is a requirementthat educators and nurses considerto what extent they may be failing tosupport distressed and vulnerablestudents in their care.
Transforming caring into practiceThe success of individualised learningoften depends on the student beingan active ra ther than passiveparticipant. Motivation to learn canbe impaired by the student's socialcircumstances. If the circumstancesprevent the student developingpersonal competence then referralor suggestion of personal counsellingmay benefit and enable the studentto focus on learning. Key authors onemotional competence suggest regularpraise, encouragement and positivereinforcement can help studentsto develop emotional competence
Page 42 Vol. 24 No. 1 2008 Nursing Praxis in New Zealand

(Freshwater 86 Stickley, 2004; Humpel86 Caputi, 2001; MacCulloch, 1998),However, the attitude of educatorstoward students with emotional issuesaffecting their learning is a key factoraffecting a student's transformationwith respect to caring capability. Thetransformation of caring into practiceis the third theme resulting from thisstudy.
Freshwater and Stickley (2004) suggestnurse education has been viewed asan essentialist education, this typeof education has an emphasis onproducing individuals who are fitfor practice and "by its very naturemoulds the student" (p, 92), Empathiccommunication from the educator isrequired to understand the studentsthey work alongside. However lack ofemotional competence in educatorsand nurses in practice is an ongoingchallenge that students face in theirlearning. This was summarised by aneducator in the third focus group:
there is this assumption that if youare a nurse you are emotionallycompetent, because you must beif your role is to deal with humanbeings; its communication andprofessionalism but unfortunatelythere is a situation in nursing wherewe [nurses] do not necessarily rolemodel caring communication to ourpeers or our young (Gp 3, p. 45).
Working in partnership with thestudents to develop problem solvingskills and the use of probing (Arnold86 Boggs, 2007) can help them clarifyand focus on their continuum ofdeveloping emotional competence.Learning that takes place in relationto personal and social competencecan promote the development of
professional boundaries, essentialwithin nursing relationships. Oneeducator summed this point up asfollows:
they [the student] need to be ableto step out of their role as mother,partner, friend, and developresponses in a nursing role (Gp 1,p. 8).
The process of educators surfacingissues that affect development ofemotional competence in class and inpractice enables a transformation ofprofessional caring and communicationwithin the student 's developingpractice.
The emphasis for nursing educationis on producing an individual fit forpractice. Each facility or nursingschool must state that the student iseligible to sit the state examinationby providing endorsement to theNursing Council that the studentis a fit person to practise nursingwithout compromise to public safety(NCNZ, 2002), When the school ofnursing endorses a student as fit topractise, they are implying that thestudent has demonstrated ability inrelation to the competency domains ofpractice (NCNZ, 2005) and educationallearning outcomes. However, as Drakeand Stokes (2004) point out, thereis a lack of clarity about how thesecompetencies and learning outcomesare utilised to assess students. Thethird aim of this research was todiscuss how the Nursing Councilcompetency assessment frameworkcan provide structure for feedback tostudents about their development ofemotional competence. The educators
Nursing Praxis in New Zealand Vol, 24 No, 1 2008 Page 43

suggested that emotional competenceis a core component of assessingfitness to practise in nursing students,however currently the nominatedNursing Council (2005) competenciesto practise do not reflect a requirementof personal and social competence orhow it might be assessed.
In preparation for interpersonalengagement, with a variety ofindividuals and groups duringtheir learning, nursing studentsmust develop the ability to managetheir emotions and responses andcommunicate effectively with others.It seems that while nurse educatorsare sensitive to the potential andactual challenges experienced byundergraduate students, at thesame time there appears to bean unwarranted assumption thatstudents are responsible for, andable to resolve these issues. It isassumed all that is needed is for themto recognise and learn to effectivelymanage such issues. Yet, given thefactors that inhibit development ofemotional competence such as a lackof clarity of the concept in nursing,limited understanding of how suchcompetence is linked to learningoutcomes in the curriculum, and thepresence of multiple life stressorsthat inhibit learning, along with anyemotional problems a student mayhave, it is not reasonable to expectstudents to self manage their learningalone. Clearly there is a need tolink emotional competence withinthe current Nursing Council (2005)competency assessment framework.
The competency framework providesa structured series of feedbackopportunities to students while they
are in practice and underpins thecurriculum and learning outcomeswithin the bachelor of nursingdegree (NCNZ, 2002). The statutoryrequirement that learning mustbe measured and documented inaccordance with the Nursing Council(2005) competency domains of practiceleads to an underlying tension withinrelationships between educator andstudent. This challenges educatorsto articulate subjective experiencesand understanding of the students'learning into objective language oroutcomes. Educators argue againstthe requirements of objective checklistswithin an assessment process. Theysuggest this requirement, at times,undermines the learning aims andrelational experiences of students.
As students progress through thedegree, they practise new relationalskills. Assessment opportunities innursing education include written,oral and practical experiences inwhich the student can demonstrateknowledge and skill in relational ability.Within the assessment relationshipwith students, the educators useobjective criteria as well as theirsometimes intuitive knowledge tofacilitate awareness of those relationalcapabilities. Therefore assessment ofemotional competence needs to be anindicator within the Nursing Councilcompetency framework.
Facilitation of learning, from aneducator's perspective, requires beingflexible and adaptive to the variouslearning styles and capabilities ofthe students (Heron, 2004). Theissue of having to write reports onstudents in the form of summativeassessments and match a student's
Page 44 Vol. 24 No. 1 2008 Nursing Praxis in New Zealand

ability to a criterion means thateducators are forced to put to thestudent objectively what is essentially,a subjective appraisal of learning.This is in direct opposition to theeducator's proposal of valuing emotionwithin the teaching relationship, andpromoting assessment as an ongoingopportunity to appraise the student'sability. In this current paradigm ofscientific and outcome based ideologyin nursing the use of subjectiveknowledge and understanding, whichis informed partially by emotionsexperienced within relationships, hasbeen discouraged (Freshwater, 2007;Reeves, 2005; Williams, 2001).
Nursing is a social practice andnurses are part of a community inwhich they work with individuals,families, and groups in multiplerelationships. De Carvalho (2004)argues that teaching and assessing thepractice of care pragmatics, whetherin or outside of a hospital setting iscomplex. Clear understanding anddisclosure of the teaching activitiesamong the educator group promotestransparency. For the students,transparency permits processes tobe clear and generates a commonunders tanding of expectations(Webber, 2002). This encouragesstudents to become self-directed, goalorientated and take control of theirleaning outcomes. Transparencyof the teaching activities, and aconsistent approach to assessment,can contribute positively to students'overall development of emotionalcompetence. Having a sharedunderstanding of how the NursingCouncil competencies can be usedto recognise and provide feedbackto students with respect to their
development of emotional competenceis vital in this process.
Nursing education has the role ofpreparing competent nurses to meetthe current and future healthcareneeds of the communities in which theywork. Vernon (2000) suggests nurseeducators need to review outcomesof traditional teaching strategiesand seek to explore alternatives thatpromote a satisfactory teaching andlearning environment for educatorsand s tudents alike. There wasagreement within the educator groupsthat consistency in the process ofassessment and learning outcomesis required. However, using tickbox systems and criteria for scoringresults in educators having to stateto those students who do not fit thebox, that they have failed. There isno opportunity to identify with thestudent their current ability andwhere learning may need to take place.Moreover, many of the Nursing Councilcompetencies relate to learning andprogress of an individual's knowledgeand skill development rather thantasks and described actions.
The above distinction is an importantaspect to consider in terms of subjectiveknowing within the student-educatorrelationship. The educators whotook part in the focus groups wereall qualified at post graduate leveland had many years of practice andteaching behind them, so all could beargued to be mature nurses. However,it is important to note that the focusgroup discussion was not implyingthat students become emotionallycompetent in comparison to how theeducators saw their own capability,or that emotional competence was
Nursing Praxis in New Zealand Vol. 24 No. 1 2008 Page 45

assessed by default. Rather thanassuming students were competentunless they didn't "do" something in anemotionally competent way, educatorsconsistently suggested that personaland social competency to manageemotion and enhance relationalability is required within maturingnursing practice. The educators areadvocating the value of emotion, andmoreover that the nature of emotionand the subjective context in whichemotion is experienced, should beacknowledged and valued within theprocess of teaching and assessment.
Emotional competence, in theperception of the nurse educatorparticipants, has emerged as afoundational concept for nursingeducation. The inclusion of emotionalcompetence within the curriculumand learning relationships needs to
be considered within the context ofa community. It is a community inwhich students, educators and clientsbelong. Nursing students need todevelop skills of critical reflectionwithin their practice. There is a needfor educators and students alike tohave a clearer understanding of whatconstitutes emotional competencein nursing and how this knowledgecan be realistically incorporatedinto learning and assessmentopportunities. Adequate preparationand meaningful reflection withininterpersonal situations are vital tothis process. When students aretaught that emotional competenceis a required competence withinprofessional nursing practice, thenursing professionals they workalongside must uphold this expectationand provide opportunities to fosteremotional growth in the students andsupport their learning and practice ofthe competence.
ReferencesArnold, E., & Boggs, K. (2007). Interpersonal relationships: Professional communication skills for
nurses. Philadelphia: Saunders.
Basch, C. E. (1987). Focus group interview: An underutilized research technique for improving theoryand practice in health education. Health Education Quarterly, 14(4), 411-448.
Boyatzis, R. E. (1998). Transforming qualitative information: Thematic analysis and code development.Thousand Oaks: Sage.
Cadman, C , & Brewer, J. (2002). Emotional intelligence: A vital prerequisite for recruitment innursing. Journal of Nursing Management, 9(6), 321-324.
de Carvalho, V. (2004). Caring, researching and teaching: Meaning and implications of nursing practice[electronic version]. Revista Latino-Americana de Enfermagem, 12(5), 806-815.
Drake, M., & Stokes, G. (2004). Managing pre-registration student risk: A professional and legislativeminefield. Nursing Praxis in New Zealand, 20(1), 15-27.
Freshwater, D. (2004). Emotional intelligence: Developing emotionally literate training in mentalhealth. Mental Health Practice, 8(4), 12-15.
Freshwater, D. (2007). Dialogue, conversation and discussion: Reflection upon languagingrelationships. Journal of Psychiatric and Mental Health Nursing, 14, 431-432.
Freshwater, D., & Stickley, T. (2004). The heart of the art. Nursing Inquiry, 11(2), 91-98.Goleman, D. (1995). Emotional intelligence. New York: Bantam.Gooch, S. (2006). Emotionally smart. Nursing Standard, 20(51), 20-22.
Health Practitioners Competence Assurance Act. (2003). Retrieved March 12, 2005, from ThomsonBrookers Database.
Page 46 Vol. 24 No. 1 2008 Nursing Praxis in New Zealand

Henderson, S., Happell, B., & Martin, T. (2007). Impact of theory and clinical placement onundergraduate students' mental health nursing knowledge, skills and attitudes. InternationalJournal of Mental Health Nursing, 16, 116-125.
Heron, J. (2004). The complete facilitator's handbook. London: Kogan Page. (Original work published1999).
Hocshschild, A. R. (1983). The managed heart: Commercialisation of human feeling. Berkley: Universityof California Press.
Horsfall, J., 86 Stuhlmiller, C. (2000). Interpersonal nursing for mental health. Sydney: MacLennan8s Petty.
Humpel, N., 8s Caputi, P. (2001). Exploring the relationship between work stress, years of experienceand emotional competency using a sample of Australian mental health nurses. Journal ofPsychiatric and Mental Health Nursing, 8(5), 399-403.
Kevern, J., 8s Webb, C. (2001). Focus groups as a tool for critical social research in nurse education.Nurse Education Today, 21(4), 323-333.
Kitzinger, J. (1994). The methodology of focus groups: The importance of interaction between researchparticipants. Sociology of Health and Rlness, 16(1), 103-121.
Krueger, R. A. (2000). Focus Groups: A practical guide for applied research (4* ed.). Thousand Oaks:Sage.
Lammers, J., 86 Happell, B. (2003). Consumer participation in mental health services: Looking froma consumer's perspective. Journal of Psychiatric and Mental Health Nursing, 10, 385-392.
MacCulloch, T. (1998). Emotional competence in professional communication. Journal of Psychiatricand Mental Health Nursing, 6(2), 153-159.
McQueen, A. (2004). Emotional intelligence in nursing work. Journal of Advanced Nursing, 47(1),101-108.
Morgan, D. L. (1996). Focus groups as qualitative research. Csdifornia: Sage.
Nursing Council of New Zealand. (2002). Nursing school/departments handbook for pre-registrationnursing programmes. Wellington: Author.
Nursing Council of New Zealand. (2005). Competency domains of practice for entry into the register ofcomprehensive nurses. Wellington: Author.
Peplau, H. (1988). The art and science of nursing: Similarities, differences and relations. NursingScience Quarterly, 9(1), 8-15.
Quinn, F. (2000). Principles and practice of nurse education (4"'ed.). London: Nelson Thornes.Reeves, A. (2005). Emotional intelligence: Recognising and regulating emotions. AAOHN Journal,
53(4), 172-176.Salovey, P., 8s Mayer, J. (1990). Emotional intelligence. Imagination, Cognition and Personality, 9,
185-211.
Sharp, P. (2001). Nurturing emotional literacy: A practical guide for teachers, parents and those workingin the caring professions. London: David Fulton.
Shipton, S. (2002). The process of seeking stress-care: Coping as experienced by senior baccalaureatenursing students in response to appraised clinical stress. Journal of Nursing Education, 41(6),243-256.
Vernon, R. (2000). New initiatives for nursing education. Vision, 6(11), 33-35.Webber, P. B. (2002). A curriculum framework for nursing. Journal of Nursing Education, 41(1), 15-
24.
Williams, A. (2001). A literature review on the concept of intimacy in nursing. Journal of AdvancedNursing, 33(5), 660-667.
Wilson, S. (2006). A qualitative exploration of emotional competence and its relevance to nursingrelationships. Unpublished thesis presented in partial fulfilment of the requirments for a Masterof Philosophy, Massey University, Palmerston North, New Zealand.
Nursing Praxis in New Zealand Vol. 24 No. 1 2008 Page 47






























