Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Effect of different modes of therapy on vestibular
and balance dysfunction in Parkinson’s disease
Wafaa Abdel-Hay El-Kholy a, Hesham Mohamed Taha a,*,
Soha Mohamed Hamada b, Mona Abdel-Fattah Sayed b
a Audiology Unit, Otorhinolaryngology Dept., Ain Shams University, Cairo, Egyptb Audiology Department, Hearing & Speech Institute, Giza, Egypt
Received 26 September 2014; accepted 15 February 2015
KEYWORDS
Parkinson’s disease;
Vestibular and balance
dysfunction;
Medical treatment;
Physiotherapy
Abstract Background: Patients with Parkinson’s disease (PD) have difficulties in performing vari-
ous motor tasks such as walking, writing and speaking, together with significant balance dysfunc-
tion. Despite gains made in the field of pharmacotherapy and deep brain stimulation, dopaminergic
medications may produce a limited improvement in postural stability. Sustained improvement in
motor skills can be achieved through physiotherapy.
Aim of the work: To measure the effect of different modes of therapy in controlling vestibular
and/or balance dysfunction in patients with PD.
Methodology: This study was conducted on 20 patients suffering from definite PD, subdivided
into two subgroups according to the mode of therapy they followed. Subgroup I received medical
treatment and physiotherapy, while subgroup II received medical treatment only. The control group
consisted of 10 age- and sex-matched normal subjects. All participants were evaluated using video-
nystagmography (VNG), Computerized Dynamic Posturography (CDP) including sensory impair-
ment, automatic motor and voluntary motor assessment. In addition, patients were evaluated using
functional limitation tests and were asked to fill the Freezing of Gait (FOG) questionnaire.
Results: This research documents vestibular as well as balance dysfunction in patients with PD.
Central vestibular disorders were more common than peripheral ones. The most prevalent balance
abnormality was encountered in the sensory organization subtest, though patients showed signifi-
cant affection in other domains; namely, autonomic motor, voluntary motor and functional
limitation. In general, patients receiving both medication and physiotherapy showed better vestibu-
lar and balance function than those receiving medication only, and approached the normal values in
many test parameters.
Conclusions: Since patients with PD receiving physiotherapy in conjunction with medical treat-
ment showed better control of their vestibular and balance functions, efforts should be directed to
* Corresponding author at: 12 Bagdad Street, Cairo, Egypt. Mobile:
+20 1227431717.
E-mail address: [email protected] (H.M. Taha).
Peer review under responsibility of Egyptian Society of Ear, Nose,
Throat and Allied Sciences.
Egyptian Journal of Ear, Nose, Throat and Allied Sciences (2015) xxx, xxx–xxx
HO ST E D BY
Egyptian Society of Ear, Nose, Throat and Allied Sciences
Egyptian Journal of Ear, Nose, Throat and Allied
Sciences
www.ejentas.com
http://dx.doi.org/10.1016/j.ejenta.2015.02.0052090-0740 ª 2015 Hosting by Elsevier B.V. on behalf of Egyptian Society of Ear, Nose, Throat and Allied Sciences.
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005

start physiotherapy including vestibular rehabilitation as early as possible in order to improve bal-
ance, thus increasing independence in daily life activities.
ª 2015 Hosting by Elsevier B.V. on behalf of Egyptian Society of Ear, Nose, Throat and Allied Sciences.
1. Introduction and rationale
Parkinson’s disease (PD) is a neuro-degenerative disorder
characterized by cardinal features including resting tremors,
rigidity, bradykinesia, and postural difficulties which arise pri-
marily from the loss of dopamine producing neurons and sub-
sequent dysfunction of the basal ganglia–thalamo–cortical
pathway.24 Furthermore, PD leads to abnormalities in two
main components of postural control: orientation (maintain-
ing a normal postural arrangement and alignment) and
stabilization (maintaining equilibrium).44
The pathologic hallmark of PD is degeneration of dopami-
nergic neurons in the substantia nigra pars compacta (SNc),
resulting in the depletion of striatal dopamine.28 This
neurotransmitter regulates excitatory and inhibitory outflow
of the basal ganglia.38 Functional neuro-imaging modalities
such as fMRI, MRS, and DTI have been applied to document
functional deficits in PD. Neuro-imaging is undergoing a shift
from morphological to functional imaging as new technologies
are introduced and technical problems associated with the
local production of radio-isotopes are solved.47
Postural instability (PI) is a disabling disorder, which is
associated with sudden falls, progressive loss of independence
and immobility.16 It usually occurs at the later stages of the
disease and, unlike gait disorders, responds poorly to med-
ication. Marked alteration of gait is common in advanced
PD, although there is evidence suggesting that initial impair-
ment in gait can be detected even early in the course of the dis-
ease.1 Falls occur despite maximal treatment with levodopa,
confirming that axial disability in late stage PD is largely
dopa-resistant (likely due to extranigral and non-dopaminergic
brain lesions). Falls often have dramatic consequences, such as
traumas and fractures. The high risk of fractures was demon-
strated in a large case control study.45
To date, management concepts in PD are still diverse.
Despite gains made in the field of pharmacotherapy and deep
brain stimulation, dopaminergic medications may produce a
limited improvement in PI.4,46 Thus, physiotherapy is the most
commonly used procedure as an adjunct to drug therapy to
treat PD movement disorders.9 Accordingly this study was
designed to measure the effect of different modes of therapy
in controlling vestibular and/or balance dysfunction in patients
with PD.
2. Methodology
2.1. Subjects
The study group consisted of 20 patients with PD diagnosed
by an expert neurologist. Their age ranged from 40 to 60 years
with a mean age of 50.6 years (SD = 4.2 years). They were in
stages I, 2 and 3 according to Hoehm and Yarr staging scale.12
The study group was divided into 2 subgroups according to the
management they received. Patients who were receiving
medical treatment and physiotherapy were assigned to
Subgroup I (n= 8), while Subgroup II patients were receiving
medical treatment only (n = 12). Medical treatment was in the
form of Sinemet (levodopa) twice daily given orally as this is
the mostly utilized drug in this condition, physiotherapy was
twice daily which ranged from 2 to 9 years with a mean of
3.8 years (SD = 3.6 years).
Patients showing history, symptoms and/or signs of the
following were excluded: Otological disease, neurological
disease (other than PD), systemic disease such as long stand-
ing diabetes and hypertension (more than five years dura-
tion), head trauma and ototoxic drug intake. Patients who
were at stages IV and V of the disease were excluded
because of their severe disability which prevented them from
performing the tests. Also, patients complaining of visual
troubles like cataract or severe errors of refraction were
excluded.
The control group consisted of 10 normal age- and gender-
matched subjects with no symptoms and/or signs of otologic,
vestibular or neurologic disease or any disease affecting
vestibular and balance systems.
2.2. Method
All participants in this study were subjected to the following:
(1) Full history taking, otological and neuro-otological
examination.
(2) Freezing of gait (FOG) questionnaire (for PD patients
only). This detailed gait and falls questionnaire consists
of 6 items that assess gait in daily living, frequency and
severity of FOG, frequency of festinating gait and its
relation to falls, and finally frequency and severity of
falls. Responses to each item are on 5-point scales where
a score of 0 indicates absence of the symptom; while 4
indicates the most severe stage.14 All items were literally
translated to the Arabic language.
(3) Vestibular Assessment (VNG test) using I.C.S Computerized
infrared 4 Channel Video-nystagmography (version 5.1)
and the target being projected by an LCD projector on a
screen about 1.5 meters in front of the subject. VNG
included testing for spontaneous nystagmus, oculomo-
tor, Dix-Hallpike, positional and caloric tests.
(4) Balance Assessment (CDP test results) using Computerized
Dynamic Posturography long forceplate (Neurocom ver-
sion 4 Smart Balance Master). This included the following:
i. Sensory Impairment Assessment – Sensory Organization
Test (SOT): Patients were asked to maintain standing
balance during a combination of three visual and two
support surface conditions. Tasks were performed with
the eyes open and with the eyes closed.32 Participants
were asked to stand quietly and steadily for 3 trials in
each of the 6 conditions.
ii. Automatic Motor Assessment
2 W.A.-H. El-Kholy et al.
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005

– Motor Control Test (MCT): Sequences of small,
medium and large platform translations in forward
and backward directions were used to elicit auto-
matic postural responses. The following parameters
were measured and compared to the default norms
of the equipment: latency, weight symmetry,
strength symmetry and amplitude scaling.36
– Adaptation Test (ADT): Adaptation was assessed
by determining the ability to suppress inappropri-
ate responses to the external disturbance.
Response time was measured to slow toes up
and toes down rotations at 8 degrees/s.21
iii. Voluntary Motor Assessment:
– Limit Of Stability (LOS): The subject was asked
to lean as quickly and accurately as possible
toward a target and to hold steady. The following
measures were recorded: Reaction time, mean
velocity level, directional control level and end-
point excursion percent.33
– Rhythmic Weight Shift (RWS): The subject is
asked to follow an on-screen cue as it moved
between the endpoints, from left to right (lateral)
and from forward to backward (anterior/pos-
terior) between 2 targets at three distinct speeds:
slow, medium, and fast.31
(5) Functional Limitation Tests
i. Tandem walk (TW): Subjects were required to walk
heel to toe along a 10-foot line. They were asked to
walk as quickly as they could without errors. The
performance time of three trials for performance of
each task was averaged for analyses.7
ii. Sit to stand (S-T-S): Subjects were asked to perform
this maneuver 3 times. The following parameters
were measured: weight transfer, rising index and
weight symmetry.26
2.3. Statistical analysis
Data were expressed as mean and standard deviation for
quantitative parametric measures and as median percentiles
for quantitative non-parametric data. Comparison between
two independent groups was done using Student ‘‘t’’ test and
Wilcoxon Rank Sum test for parametric and non-parametric
data respectively. For more than 2 groups, an ANOVA test
was followed by Post-hoc, LSD was used for parametric data
and Kruskall–Wallis test was used for non-parametric data.
Chi-square was used to compare categorical qualitative data.
The probability of error at 0.05 was considered significant.
3. Results
In the study group, the mean age of subjects was 49.1 years
(±4.1) in subgroup I and 51 years (±3.5) in subgroup 2, with
4:1 male-to-female ratio. The mean disease duration was
3.95 years (±2.14) and 4.15 years (±2.65) in subgroups I
and II respectively. Most patients were in stage II of PD dis-
ease (Fig. 1). There were no statistically significant differences
between the 2 study subgroups as regards age (p= 0.179),
gender (p = 0.914), duration of the disease (0.231) and disease
staging (p= 0.912). Moreover, FOG questionnaire scores did
not differ significantly (Table 1). In general, all vestibular and
balance function assessment tests showed better test scores in
subgroup I compared to subgroup II.
3.1. Vestibular assessment
The most affected group of tests in VNG was oculomotor sub-
tests reflecting central vestibular pattern of dysfunction (58.5%
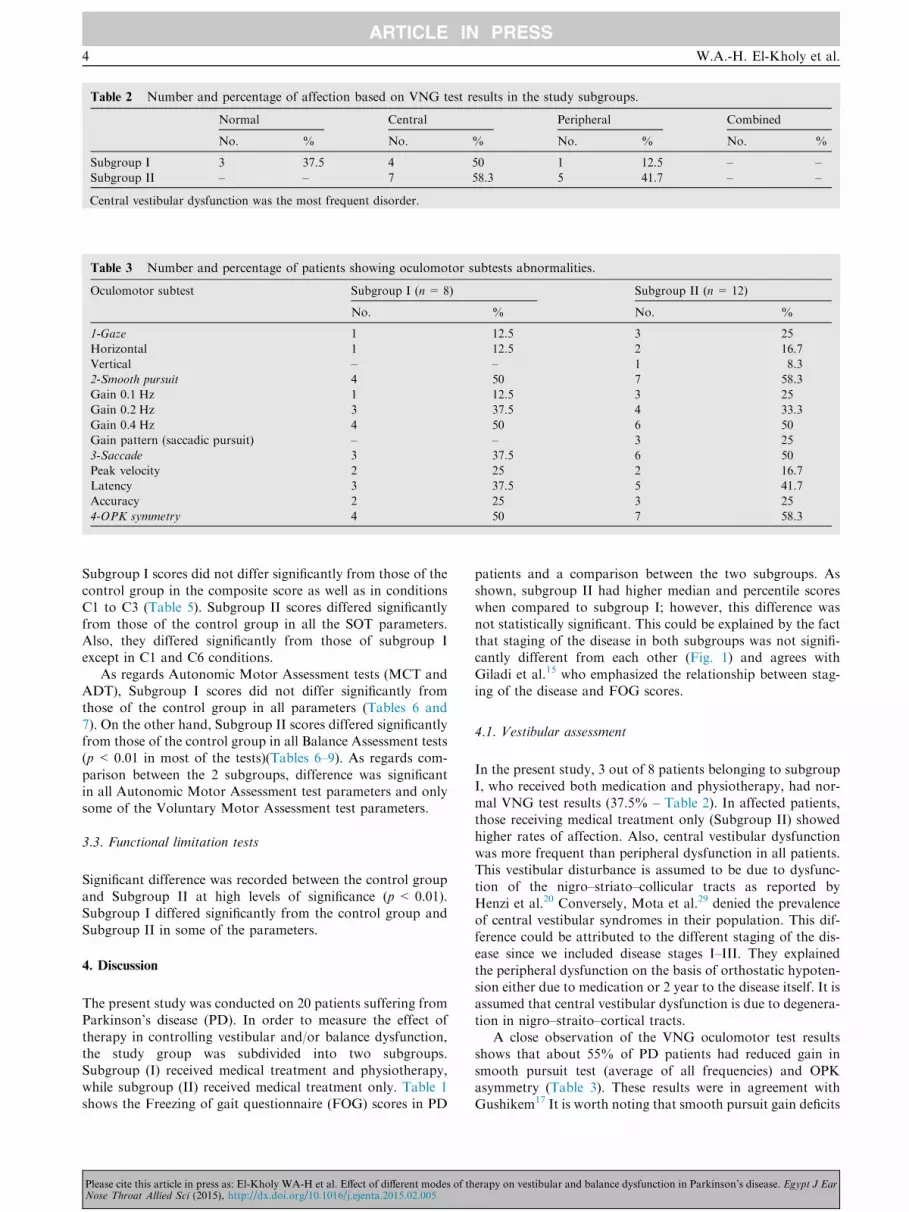
in subgroup I and 50% in subgroup II – Table 2). Table 3
shows the number and percentage of VNG oculomotor test
abnormalities. As shown, the most affected oculomotor
subtests were OPK and smooth pursuit subtests. Subgroup II
consistently showed higher rates of abnormalities. Two
patients in Subgroup I (25%) and 4 patients in subgroup II
(33.3%) showed failure of fixation suppression which is con-
sidered a central vestibular finding. On the other hand, periph-
eral vestibular dysfunction was present in 41.7% in Subgroup
II and 12.5% in subgroup I. Abnormality was in the form of
posterior canal BPPV canalithiasis in 3 patients and unilateral
caloric weakness in another 3 patients. Neither spontaneous
nor positional nystagmus was recorded in any patient.
3.2. Balance assessment
Table 4 shows abnormalities encountered in balance assess-
ment. Similar to vestibular assessment, the percentage of
abnormalities was higher in Subgroup II. The most affected
test was CDP-SOT test (62.5% in Subgroup I and 100% in
Subgroup II), followed by CDP-LOS and TW tests.
0
1
2
3
4
5
6
Subgroup I Subgroup II
stage (1)
stage (2)
stage (3)
Figure 1 Number of patients belonging to the 3 disease stages in
subgroups I and II. Most patients were in stage (2).
Table 1 Comparison between PD subgroups in freezing of
gait (FOG) questionnaire using Kruskall–Wallis Test.
FOG score Subgroup I Subgroup II
Median 7.4 8.5
Percentile 2.00–14.6 2.75–16.00
F value 2.22
P value 0.612
Insignificant statistical difference between 2 subgroups.
Effects of therapy on vestibular and balance dysfunction 3
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005
Subgroup I scores did not differ significantly from those of the
control group in the composite score as well as in conditions
C1 to C3 (Table 5). Subgroup II scores differed significantly
from those of the control group in all the SOT parameters.
Also, they differed significantly from those of subgroup I
except in C1 and C6 conditions.
As regards Autonomic Motor Assessment tests (MCT and
ADT), Subgroup I scores did not differ significantly from
those of the control group in all parameters (Tables 6 and
7). On the other hand, Subgroup II scores differed significantly
from those of the control group in all Balance Assessment tests
(p < 0.01 in most of the tests)(Tables 6–9). As regards com-
parison between the 2 subgroups, difference was significant
in all Autonomic Motor Assessment test parameters and only
some of the Voluntary Motor Assessment test parameters.
3.3. Functional limitation tests
Significant difference was recorded between the control group
and Subgroup II at high levels of significance (p < 0.01).
Subgroup I differed significantly from the control group and
Subgroup II in some of the parameters.
4. Discussion
The present study was conducted on 20 patients suffering from
Parkinson’s disease (PD). In order to measure the effect of
therapy in controlling vestibular and/or balance dysfunction,
the study group was subdivided into two subgroups.
Subgroup (I) received medical treatment and physiotherapy,
while subgroup (II) received medical treatment only. Table 1
shows the Freezing of gait questionnaire (FOG) scores in PD
patients and a comparison between the two subgroups. As
shown, subgroup II had higher median and percentile scores
when compared to subgroup I; however, this difference was
not statistically significant. This could be explained by the fact
that staging of the disease in both subgroups was not signifi-
cantly different from each other (Fig. 1) and agrees with
Giladi et al.15 who emphasized the relationship between stag-
ing of the disease and FOG scores.
4.1. Vestibular assessment
In the present study, 3 out of 8 patients belonging to subgroup
I, who received both medication and physiotherapy, had nor-
mal VNG test results (37.5% – Table 2). In affected patients,
those receiving medical treatment only (Subgroup II) showed
higher rates of affection. Also, central vestibular dysfunction
was more frequent than peripheral dysfunction in all patients.
This vestibular disturbance is assumed to be due to dysfunc-
tion of the nigro–striato–collicular tracts as reported by
Henzi et al.20 Conversely, Mota et al.29 denied the prevalence
of central vestibular syndromes in their population. This dif-
ference could be attributed to the different staging of the dis-
ease since we included disease stages I–III. They explained
the peripheral dysfunction on the basis of orthostatic hypoten-
sion either due to medication or 2 year to the disease itself. It is
assumed that central vestibular dysfunction is due to degenera-
tion in nigro–straito–cortical tracts.
A close observation of the VNG oculomotor test results
shows that about 55% of PD patients had reduced gain in
smooth pursuit test (average of all frequencies) and OPK
asymmetry (Table 3). These results were in agreement with
Gushikem17 It is worth noting that smooth pursuit gain deficits
Table 2 Number and percentage of affection based on VNG test results in the study subgroups.
Normal Central Peripheral Combined
No. % No. % No. % No. %
Subgroup I 3 37.5 4 50 1 12.5 – –
Subgroup II – – 7 58.3 5 41.7 – –
Central vestibular dysfunction was the most frequent disorder.
Table 3 Number and percentage of patients showing oculomotor subtests abnormalities.
Oculomotor subtest Subgroup I (n= 8) Subgroup II (n = 12)
No. % No. %
1-Gaze 1 12.5 3 25
Horizontal 1 12.5 2 16.7
Vertical – – 1 8.3
2-Smooth pursuit 4 50 7 58.3
Gain 0.1 Hz 1 12.5 3 25
Gain 0.2 Hz 3 37.5 4 33.3
Gain 0.4 Hz 4 50 6 50
Gain pattern (saccadic pursuit) – – 3 25
3-Saccade 3 37.5 6 50
Peak velocity 2 25 2 16.7
Latency 3 37.5 5 41.7
Accuracy 2 25 3 25
4-OPK symmetry 4 50 7 58.3
4 W.A.-H. El-Kholy et al.
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005

increased in more challenging tasks; appear to be more
affected in 0.4 Hz compared to 0.1 and 0.2 Hz frequencies in
the 2 study subgroups (Table 3). This is expected and agrees
with that of Hain et al.19 who stated that as the frequency or
acceleration of head movements increases (>1–2 Hz,
>2000 deg/s2), the efficacy of tracking of eye movement
decreases.
In both study subgroups, there is a general agreement in the
percentage of abnormalities in smooth pursuit and OPK tests
(Table 3), which agrees with that of Krauzlis.25 The pursuit
system is chiefly responsible for generating slow phases of
optokinetic nystagmus (OKN), which limit full-field motion
of the visual environment upon the retina during head move-
ment. In addition, much of the neural machinery of the pursuit
Table 5 Comparison between the control group and the study subgroups as regards SOT test scores.
Equilibrium-E (deg/s)
Strategy-S (deg)
Control group (n= 10) Subgroup I (n= 8) Subgroup II (n = 12) ANOVA test
F value P valueX (SD) X (SD) X (SD)
C 1 E 93.0 (2.3)a 90.9 (1.8)a 89.1 (3.9)a 2.4 0.118
S 99.0 (0.4)a 98.7 (1.7)a 94.0 (3.3)a 4.0 0.118
C 2 E 92.0 (1.4)a 90.1 (1.2)a 79.5 (6.0)b 5.4 0.023
S 97.0 (0.7)a 96.0 (0.9)a 83.5 (5.6)b 6.1 0.042
C 3 E 93.0 (2.3)a 87.3 (6.9)a 73.4 (10.2)b 6.3 0.025
S 98.0 (1.7)a 97.0 (1.3)a 85.0 (6.0)b 5.0 0.01
C 4 E 86.1 (5.5)a 80.4 (5.6)a 69.5 (14.3)b 7.2 0.003
S 83.2 (4.8)a 74.3 (3.6)b 66.8 (10.3)c 7.0 0.001
C 5 E 85.2 (9.7)a 75.3 (6.8)b 60.9 (16.1)c 16.3 0.002
S 77.6 (10.6)a 75.0 (4.7)a 57.5 (12.9)b 8.3 0.0
C 6 E 80.0 (10.2)a 70.4 (10.8)b 52.0 (18.5)b 22.4 0.0
S 76.5 (11.4)a 70.7 (11.7)b 56.0 (15.5)b 12.7 0.0
Significant difference between the control group and the study subgroups in condition (C2 and C3), highly significant difference in conditions
(C4–C6) and in the composite scores.
Table 6 Comparison between the control group and the study subgroups as regards MCT test parameters.
MCT Control group Subgroup I Subgroup II ANOVA test
X (SD) X (SD) X (SD) F value P value
Weight symmetry forward 98 (6.8)a 100 (8.8)a 125.7 (30.2)b 4.9 0.015
Weight symmetry backward 95.3 (7.6)a 98.5 (11.6)a 129 (24.7)b 11.04 0.00
Latency forward 140 (13)a 132.7 (22)a 162.5 (22.08)b 4.2 0.002
Latency backward 163 (10.6)a 147.4 (23.8)a 152.5 (17.7)a 2.3 0.117
Strength symmetry forward 115.3 (8.6)a 119 (22.06)a 122 (20.6)a 2.6 0.092
Kruskall–Wallis test
Median Median Median H value P value
Strength symmetry backward 96a 110a 124b 7.5 0.023
Amplitude forward 4.0a 3.7a 4.5a 0.2 0.89
Amplitude backward 4 3 5.15 0.28 0.23
Medians with different letters are significantly different from each other. Highly significant difference between the control group and the study
subgroups in weight symmetry backward and latency forward and significant statistical difference in Weight symmetry forward, and Strength
symmetry backward.
Table 4 Number and percentage of patients showing Computerized Dynamic Posturography and Functional Limitation tests
abnormalities in the study subgroups.
Test Subgroup I (n= 8) Subgroup II (n= 12)
No. % No. %
CDP (Sensory impairment assessment) SOT 5 62.5 12 100
CDP (Automatic motor assessment) MCT 2 25 6 50
ADT 2 25 5 33.3
CDP (Voluntary motor assessment) RWS 3 37.5 6 50
LOS 5 62.5 8 66.7
Functional limitation tests TW 2 25 9 75
S-T-S 2 25 6 50
Effects of therapy on vestibular and balance dysfunction 5
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005

system contributes to the suppression or enhancement of the
VOR by visual inputs. Thus, dysfunction of smooth pursuit,
OKN slow phases, and visual modulation of the VOR nearly
always parallel each other. In our study, six patients showed
failure of fixation suppression in caloric test (30%).
As regards the pattern of abnormality, 3 patients showed
cog-wheel appearance in smooth pursuit test (Table 3). A
similar pattern was reported by Campbell et al.6 They reported
that saccades are commonly used instead of smooth pur-
suits when following an object in PD being a basal ganglia
disease.
About 45% of PD patients showed saccade test abnormal-
ity; delayed latency being the most prevalent abnormality
(Table 3). These results agree with those of Jankovic23 who
reported prolonged saccade latency and hypometric saccades
in patients with PD. On the other hand, some authors reported
normal values.8,41 Others such as13 studied only mildly affected
patients. White et al.48 reported that L-DOPA had no effect on
the peak velocity performance index and suggested that
differences in anti-parkinsonian treatment do not account for
the discrepancies between reports. Differences in the severity
of the disease could provide an explanation.
When comparing the different oculomotor subtest results,
both smooth pursuit and OPK showed higher rates of affec-
tion compared to saccades. This agrees with that of Sparks39
and is based on the different pathways responsible for both
eye movements. The standard descending pathways for sac-
cades likewise contain cortico–ponto–cerebellar connections.
These include direct projections from cortical eye fields to
eye-movement-related structures in the brainstem such as the
superior colliculus (SC) and premotor including nuclei in the
reticular formation (PMN), and also pathways through the
basal ganglia, including the caudate nucleus (CN) and the sub-
stantia nigra pars reticulata (SNr). Thus, these pathways
include some degree of direct cortical control over the motor
output. On the other hand, the standard pathways for pursuit
simply link visual sensory areas to the cerebellum, consistent
with pursuit’s presumed role as a visuomotor reflex.
Table 7 Comparison between the control group and the study subgroups as regards ADT test parameters.
ADT Control group Subgroup I Subgroup II ANOVA test
X (SD) X (SD) X (SD) F value P value
Toes up 48.3 (6.9)a 53.9 (8.3)a 86.9 (21.4)b 7.5 0.000
Kruskall–Wallis test
Toes down Median Median Median H value P value
31.2a 32.7a 49.7b 16.4 0.000
Medians with different letters are significantly different from each other. Highly significant statistical differences between the study subgroups and
the control group in toes up and toes down tests.
Table 8 Comparison between the control group and the study subgroups as regards RWS test parameters.
RWS Control group Subgroup1 Subgroup2 ANOVA test
Median Median Median H value P value
LT–RT velocity (deg/s) 4.9a 3.8ab 2.0b 11.7 0.003
Front–back velocity
(deg/s) 3.3a 2.4ab 1.1b 13.0 0.001
Front–back DCL (%) 81ab 68.5a 53b 16.3 0
Kruskall–Wallis test
LT–RT DCL (%) X (SD) X (SD) X (SD) F value P value
85.2 (1.9)a 83.2 (4.02)a 65.3 (9.6)b 30.0 0.00
Medians with different letters are significantly different from each other. Highly significant statistical differences between 2 groups in all RWS test
parameters.
Table 9 Comparison between the control group and the study subgroups as regards LOS test parameters.
LOS Control group Subgroup I Subgroup II Kruskall–Wallis test
Median Median Median H value P value
Reaction time (sec) 0.66a 0.9b 1.55b 14.6 0.001
Mean velocity level (deg/s) 4.6a 3.0b 1.5b 15.3 0.00
Directional control level (%) 69.5a 72.0a 42.0b 17.65 0.00
(End point excursion – Maximum excursion end) (%) 71.0a 68.7b 48.5c 20.54 0.00
Medians with different letters are significantly different from each other. Highly significant statistical differences between the study subgroups and
the control group in all LOS parameters.
6 W.A.-H. El-Kholy et al.
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005

Six out of 20 patients had peripheral vestibular disorder in
the form of BPPV (3 patients–15%) and unilateral caloric
weakness (3 patients–15%). Bloem3 reported a lower percent-
age for BPPV in their PD group (8%). Caloric weakness was
also reported by Silveira et al.37 who stated that the reduction
in the response to the caloric tests was perceived as one of the
modifications of the vestibular system in relation to the PD
process. Several studies mention the loss of ciliated cells of
the ampullary crests and the maculae, decline in the number
of neurons of the vestibular ganglion, degeneration of the oto-
conia, decrease in the labyrinthine blood flow, progressive
depression of neural stability, reduction in the compensation
capacity of the vestibulo–ocular and vestibulospinal reflexes,
which contribute to a decrease in the speed of pursuit move-
ments and to rotational and caloric hypoactivity of the
vestibular system, at both the peripheral and central levels in
those patients37 However, no studies set explanation for the
unilateral affection encountered in our patients.
4.2. Balance assessment
Using the CDP equipment, PD patients were assessed in 4
main domains: Sensory impairment, automatic motor, volun-
tary motor and functional limitation. Though a considerable
number of patients from both subgroups showed abnormal
results in many of these tests, a consistently higher prevalence
of abnormalities was encountered in Subgroup II compared to
Subgroup I.
The highest percentage of affection was in the sensory
impairment SOT test (62.5% in subgroup I and 100% in sub-
group II – Table 4). As previously reported by many authors,
organization protocols are useful for the assessment of pos-
tural control under various sensory conditions and generally
accepted as a reliable paradigm of measuring the capacity of
the central nervous system to prioritize and reintegrate sensory
information.32,43 Tagliabue et al.40 reported that these patients
showed a breakdown in the temporal coordination between
postural adjustments and arm reaching during whole body
reaching to a target when closing their eyes. Abnormal pos-
tural coordination when vision was obscured is consistent with
impaired proprioceptive mapping compensated by the use of
vision. PD patients in our study showed a significant shift from
normative values in all conditions except C1 as well as the
composite score (Table 5). This is consistent with a combined
vestibular insult and propioceptive defect. It also points to the
fact that PD patients showed more difficulty in controlling
their balance in more complex sensory conflict situations com-
pared to the control group.
As regards automatic motor assessment MCT test, a signifi-
cant difference between the groups was recorded in forward
latency, weight strength and backward strength symmetry
(Table 6). Inkster and Eng22 reported that strength is a key
component to overall health and has been documented as defi-
cient in individuals with PD.30 This vital aspect of health is
important for integrity of both tendons and muscles, which
may be related to prolonged latency scores, falls and other
associated risk of injuries.31
Strength symmetry test showed significant difference
between the control group and subgroup II, but there was
no significant difference between the control group and sub-
group I (Table 6). In other words, patients who received
additional physiotherapy approximated performance of nor-
mal subjects in their age. Many studies reported that a
decrease in postural stability is commonly observed in levo-
dopa medicated PD patients in contrast to physiotherapy
due to decreased proprioceptive sensitivity.34,2 Thus, strategies
for enhancing balance among older adults with PD are needed,
because in the absence of regular physical activity, balance and
muscle strength deteriorate.
Similar to MCT, Adaptation (ADT) test scores, toes up and
toes down, differed significantly in subgroup II compared to
the control group (Table 7). Performance on the ADT requires
adequate ankle range of motion and muscle strength as well as
effective motor adaptation which is absent in PD. Results
agree with those of Fisher10 who reported that during the first
(unexpected) trials, the initial disruptive responses are cor-
rected by secondary responses in the opposing muscles. With
each subsequent trial, initial reactions are attenuated and sec-
ondary responses strengthened to reduce overall sway.
As regards voluntary motor assessment, both Rhythmic
Weight Shift (RWS) and Limits of Stability (LOS) were
affected, with variability among the parameters measured
(Tables 8 and 9). Rhythmic weight shift test is used to evaluate
the participants’ voluntary ability to move the COG in an
intended direction at different velocities. This agrees with that
of Mazzoni et al.27 who reported that PD patients had strik-
ingly worse directional control compared to the other healthy
elder and more so in the anterior-posterior than in the medio-
lateral direction.
As stated by Franchignomi et al.,11 the slower and smaller
LOS of patients with PD may be related to the perceived diffi-
culty of moving their COG toward the targets. In the present
study, patients belonging to subgroup I showed better LOS
test results than those in subgroup II. This result is in agree-
ment with that of Qutubuddin et al.35 who reported that
patients who had received physiotherapy showed significant
changes in reaction time, movement velocity and endpoint
excursion than other PD groups who received levodopa as a
life time therapy.
Finally, an analysis was done to evaluate the performance
of PD patients on functional limitation tests. Only one forth
of patients in subgroup I showed abnormal scores in this group
of tests, whereas three-quarters and one half of the patients in
subgroup II scored abnormally on Tandem Walk (TW) and
Sit-to-Stand (S-T-S) tests respectively (Tables 10 and 11).
Stated differently, three-quarters of patients who received
additional physiotherapy could successfully perform these
functional tests and, therefore, may be more immune to the
risk of falls. Patients with PD scores significantly lower when
compared to the control group in most of the functional lim-
itation assessment parameters (Tables 10 and 11). Our results
agree with those of Haas et al.18 who reported that tandem
walk is one of the greatest difficulties experienced in individu-
als with PD in overall mobility and gait. This is especially
apparent as the disease progresses increasing the risk of falling
and decreasing overall mobility.
Similarly, rising from a chair is a physically demanding
function that is a common problem in aging, particularly in
individual with PD. Brod et al.5 found that 81% of individuals
with PD self-reported having difficulty standing from a seated
position. Individuals must have adequate lower body strength
and exhibit the ability to control their center of gravity as it
shifts from an initial position over the seat to a location
Effects of therapy on vestibular and balance dysfunction 7
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005

centered over the base of support (feet). This explains the sig-
nificant difference between patients with PD and controls in
measures of weight symmetry and weight transfer (Table 11).
4.3. Effect of additional physiotherapy
In almost all tests of vestibular and balance assessment con-
ducted in this study, patients who received physiotherapy out-
stood their counterparts who did not receive such intervention.
It should be emphasized that, in some tests, their performance
approximated that of normal subjects in their age. They also
had much lower prevalence of functional limitations which
advantageously decrease the risk of falls and improve their
general ambulation and balance.
It can be argued that the difference in performance is
mainly due to the applied management protocols rather than
other factors such as age and gender distribution, duration
and staging of the disease since all were not significantly differ-
ent between the two study subgroups (Fig. 1). Many studies
found that balance impairment in older adults with longer
duration PD usually did not respond to levodopa alone;
38% of persons with PD experienced falls; and persons with
PD were 5 times more likely than healthy older adults to suffer
fall-related injuries, such as hip fractures.42
In conclusion, this research documents vestibular as well as
balance dysfunction in patients with PD. Central vestibular
disorders were more common than peripheral ones. The most
prevalent balance abnormality was encountered in the sensory
organization subtest, though patients showed significant affec-
tion in other domains; namely, autonomic motor, voluntary
motor and functional limitation. Physiotherapy, as an adjunct
to medical treatment, showed significant effect in improv-
ing both vestibular and balance dysfunction in patients
with PD; thus improving their functional ability and overall
ambulation in everyday challenging situations. It is, therefore,
recommended to incorporate vestibular rehabilitation in
physiotherapy programs specifically in those who suffer con-
siderable balance and gait disorders.
References
1. Baltadjieva R, Giladi N, Gruendlinger L, Peretz C, Hausdorff J.
Marked alterations in the gait timing and rhythmicity of patients
with de novo Parkinson’s disease. Eur J Neurosci..
2006;24(6):1815–1820.
2. Beuter A, Hernandez R, Rigal R, Modolo J, Blanchet P. Postural
sway and effect of levodopa in early Parkinson’s disease. Can J
Neurol Sci.. 2008;35:65–68.
3. Bloem B. Benign paroxysmal positional vertigo in Parkinson’s
disease: underestimated and undertreated. Mov Disord..
2012;27(Suppl 1):940 [abstract].
4. Bloem B, Beckley D, Van Dijk J, et al. Medium latency stretch
reflexes in young-onset Parkinson’s disease and MPTP-induced
Parkinsonism. J Neurol Sci.., 1878-5883 1994;123(1–2):52–58.
5. Brod M, Mendelsohn G, Roberts B. Patients’ experiences of
Parkinson’s disease. J Gerontol B Psychol Sci Soc Sci..
1998;53B(4):P213.
6. Campbell W, DeJong R, Haerer A. DeJong’s the Neurologic
Examination: Incorporating the Fundamentals of Neuroanatomy and
Neurophysiology. Philadelphia: Lippincott Williams & Wilkins;
2005.
7. Chong R. Factor analysis of the functional limitations test in
healthy individuals. Gait Posture. 2008;28(1):144–149.
8. De Jong J, Jones M, Akinesia G. Hypokinesia, and bradykinesia in
the oculomotor system of patients with Parkinson’s disease. Exp
Neurol.. 1971;32:58–68.
9. Deane K., Jones D., Playford E., Ben-Shlomo Y., Clarke C.
Physiotherapy versus placebo or no intervention in Parkinson’s
disease. In: The Cochrane Library; 2001: No. 4. Available from:
Update Software, Oxford, and ISSN 1469–493 X.
10. Fisher I. Reliability and validity of the modified functional reach
test at the sub-acute stage post-stroke. Disabil Rehabil..
2009;31(3):243–248.
11. Franchignomi F, Martignoni E, Ferriero G, Pasetti C. Balance
and fear of falling in Parkinson’s disease. Parkinsonism Relat
Disord.. 2005;11:427–433.
Table 11 Comparison between the control group and the study subgroups as regards S-T-S test parameters.
S-T-S Control group Subgroup1 Subgroup2 Kruskall–Wallis test
Median Median Median H value P value
Weight transfer (sec) 0.41a 0.8b 2.5b 9.6 0.008
Rising index (%) 28.5a 9.75b 6.0b 13.26 0.001
Sway velocity (deg/s) 4.2a 3.05a 4.5a 4.9 0.083
Weight symmetry (%) 5.5a 5.5a 15.5b 10.8 0.004
Medians with different letters are significantly different from each other. Highly significant statistical difference between the control group and the
study subgroups in Sit to stand test Weight transfer test (WT), rising index test and Weight symmetry.
Table 10 Comparison between the control group and the study subgroups as regards TW test parameters.
TW Control group Subgroup I Subgroup II ANOVA test
Median Median Median H value P value
Speed test(cm/s) 28.7a 14.2b 8.0c 19.3 0.000
Step width (cm) 6.0a 8.5a 10.0a 4.6 0.099
End sway (deg/s) 3.7a 3.6a 7.0b 9.6 0.006
Means with different letters are significantly different from each other. Highly significant statistical differences between the control group and the
2 study subgroups in tandem walk speed test& end sway test.
8 W.A.-H. El-Kholy et al.
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005

12. Geotz CG, Poewe W, Rasaco O, Sampio C, Stibbis GT,
Council C, Giladi N, Holloway RG, Moore GC, Wennig GK,
Yaar MD, Seidi L. Movement Society Task force on rating
scales for Parkinsos disease. Movement society task force on
Hoem and Yarr staging scale: status and recommendation.
Movement Disord. 2004;19(9):1020–1028.
13. Gibson J, Pimlott K, Kennard C. Ocular motor and manual
tracking in Parkinson’s disease and the effect of treatment. J
Neurol Neurosurg Psychiatry. 1987;50:853–860.
14. Giladi N, Shabtai H, et al. Construction of freezing of gait
questionnaire for patients with Parkinsonism. Parkinsonism Relat
Disord.. 2000;6(3):165–170.
15. Giladi N, Tal J, et al. Validation of the freezing of gait
questionnaire in patients with Parkinson’s disease. Mov Disord..
2009;24(5):655–661.
16. Grimbergen Y, Munneke M, Bloem B. Falls in Parkinson’s
disease. Curr Opin Neurol.. 2004;17(4):405–415.
17. Gushikem P. Otoneurologic assessment in elderly patients with
dizziness. 2001. 84f. Thesis. (MSc in Human Communication
Disorders) – Federal University of Sao Paulo-Paulista School of
Medicine, Sao Paulo. Acta A Who; 2001: 21:1–25.
18. Haas C, Turbanski S, Kessler K, Schmidtbleicher D. The effects of
random whole-body-vibration on motor symptoms in Parkinson’s
disease. NeuroRehabilitation., 1878-6448 2006;21(1).
19. Hain T., Ramaswamy T., Hillman M. Anatomy and physiology of
the normal vestibular system. In: HERDMAN, SJ Vestibular
Rehabil. 2nd ed., London: Manole; 1987: 3–24.
20. Henzi S, Stanga Z, Ludin H. Vestibular disorders in Parkinson
patients. Schweiz Med Wochenschr. 1990;120:1297–1303.
21. Horak F, Woollacott M. Parkinson’s disease impairs the ability to
change set quickly. J Neurol Sci.. 2000;175(1):57–70.
22. Inkster L, Eng J. Postural control during a sit-to-stand task in
individuals with mild Parkinson’s disease. Exp Brain Res..
2003;154(1):33–38.
23. Jankovic J. Parkinsonism: clinical features and differential
diagnosis. Program for a Comprehensive Review of Movement
Disorders for the Clinical Practitioner. Aspen, CO; 2003: 337–380.
24. Konczak J, Corcos D, Horak F, et al. Proprioception and motor
control in Parkinson’s disease. J Motor Behav..
2009;41(6):543–552.
25. Krauzlis R. Recasting the smooth pursuit eye movement system. J
Neurophysiol.. 2004;91:591–603.
26. Lord S, Murray S, Chapman K, et al. Sit-to-stand performance
depends on sensation, speed, balance, and psychological status in
addition to strength in older people. J Am Geriatr Soc..
2002;57:M539–M543.
27. Mazzoni P, Hristova A, Krakauer J. Why don’t we move faster?
Parkinson’s disease, movement vigor, and implicit motivation. J
Neurosci.. 2007;27(27):7105–7116.
28. McNaught K, Jenner P. Proteasoma impaired in substantia nigra
in Parkinson’s disease. Neurosci Lett.. 2001;297(3):191–194.
29. Mota P, Franco E, Pinto Monteiro A. Study of balance in the
elderly by electronystagmo-graphy. Acta A Who. 2005;21:1–12.
30. Nallegowda M, Singh U, Handa G, et al. Role of sensory input
and muscle strength in maintenance of balance, gait, and posture
in Parkinson’s disease: a pilot study. Am J Phys Med Rehabil..
2004;83:898–908.
31. Nallegowda M, Singh U, Bhan S, Wadwa S, Handa G, Dwivedi
SN. Balance and gait in total hip replacement: a pilot study. Am J
Sports Med Rehabil.. 2003;82:669–677.
32. Nashner LM. Computerized dynamic posturography. In:
Jacobson G, Newman C, Kartush J, editors. Handbook of balance
function and testing. Mosby Year Book; 1993:280–307.
33. Neurocom international Inc, 2012: Rhythmic weight shift test.
www.neurocom.com.
34. O’Suilleabhain P, Bullard J, Dewey R. Proprioception in
Parkinson’s disease is acutely depressed by dopaminergic med-
ications. J Neurol Neurosurg Psychiatry. 2001;71:607–610.
35. Qutubuddin A, Cifu D, Armistead-Jehle P, Carne W, Mcguirk T,
Baron M. A comparison of computerized dynamic posturography
therapy to standard balance physical therapy in individuals with
Parkinson’s disease: a pilot study. NeuroRehabilitation.
2007;22:261–265.
36. Shepard N.T. Clinical Utility of the Motor Control Test (MCT)
and Postural Evoked Responses (PER). NeuroCom Publication;
2000.
37. Silveira S., Taguchi C., Gananca F. Comparative analysis of two
lines of treatment for patients with peripheral vestibular syndrome
over the age of sixty. Acta A WHO. Sao Paulo; 2002: vol. 21, no.
1, p. 1–13, Jan seas.
38. Simuni T. Diagnosis and management of Parkinson’s disease.
Medscape Neurol.. 2007.
39. Sparks D. The brainstem control of saccadic eye movements. Nat
Rev Neurosci.. 2002;3:952–964.
40. Tagliabue M, Ferrigno G, Horak F. Effects of Parkinson’s disease
on proprioceptive control of posture and reaching while standing.
Neuroscience. 2009;158:1206–1214.
41. Teravainen H, Calne D. Studies of Parkinsonian movement: I.
Programming and execution of eye movements. Acta Neurol
Scand.. 1980;62:137–148.
42. Toole T, Hirsch M, Forkink A, Lehman D, Maitland C. The
effects of a balance and strength training program on
Parkinsonism: a preliminary study. J Neurol Rehabil..
2000;14:165–174.
43. Tsang W, Wong V, Fu S, Hui-Chan C. Tai chi improves standing
balance control under reduced or conflicting sensory conditions.
Arch Phys Med Rehabil.. 2004;85:129–137.
44. Vaugoyeau M, Azulay J. Role of sensory information in the
control of postural orientation in Parkinson’s disease. J Neurol
Sci.. 2010;289(1–2):66–68.
45. Vestergaard P, Rejnmark L, Mosekilde L. Fracture risk associated
with Parkinsonism and anti-Parkinson drugs. Calcified Tissue
Int.., 1432-0827 2007;81(3):153–161.
46. Visser J, Allum J, Carpenter M, et al. Effect of subthalamic
nucleus deep brain stimulation on axial motor control and
protective arm responses in Parkinson’s disease. Neuroscience.,
1873-7544 2008;157(4):798–812.
47. Walker R, Purnell G, Jones-Jackson L, Thomas K, Brito J, Ferris
E. Introduction to PET imaging with emphasis on biomedical
research. Neurotoxicology. 2004;25(4):533–542.
48. White O, Saint-Cyr J, Tomlinson R, Sharpe J. Ocular motor
deficits in Parkinson’s disease II. Control of the saccadic and
smooth pursuit systems. Brain. 1983;106:571–587.
Effects of therapy on vestibular and balance dysfunction 9
Please cite this article in press as: El-Kholy WA-H et al. Effect of different modes of therapy on vestibular and balance dysfunction in Parkinson’s disease. Egypt J EarNose Throat Allied Sci (2015), http://dx.doi.org/10.1016/j.ejenta.2015.02.005





























