Embed Size (px)
Citation preview
E973Volume 2
June 8, 2004
Vulnerable Community Development Plan
forNepal Health Sector Programme Implementation Plan
(2004-2009)
submitted to:
The World Bank, Nepal
June 2004
FWE COPY
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
AbbreviationsAAW Assistant Auxiliary WorkerAHW Assistant Health WorkerAIDS Acquired Immuno Deficiency SyndromeAMK Aamaa Milan KendraARH Adolescent Reproductive HealthARI Acute Respiratory InfectionBBC Beyond Beijing ConferenceBCC Behaviour Change CommunicationCBS Centre Bureau of StatisticsCB-IMCI Community Based - Integrated Management of DiseaseCDD Control of Diarrhoeal DiseaseCEDAW Convention on the Elimination of All forms of Discrimination Against WomenCERD International Convention on Elimination of All Forms of Racial DiscriminationCHD Child Health DivisionCRC Convention on the Rights of the ChildCPR Contraceptive Prevalence RateCWIN Child Workers in NepalDACAW Decentralised Action for Children and WomenDALY Disability Adjusted Life YearsDDC District Development CommitteeDWSS Department of Water Supply and SewerageDEIP Dalit Empowerment and Improvement PlanDFID Department for International DevelopmentDoHS Department of Health ServicesEDP External Development PartnersEHCS Essential Health Care ServicesFHD Family Health DivisionEMOC/EOC Emergency Obstetric CareEPI Expanded Programme on ImmunisationFAO Asian Food OrganisationFCHV Female Community Health VolunteerFP Family PlanningFWLD Forum for Women, Law and DevelopmentFWR Far Western RegionFY Fiscal YearGDP Gross Domestic ProductGEFONT General Federation of Nepalese Trade UnionHDI Human Development IndexHEFU Health Economics and Finance UnitHIV Human immunodeficiency VirusHMGN His Majesty's Govenmuent of NepalHRDC Hospital and Rehabilitation for Disabled ChildrenHSPSP Health Sector Program Support ProjectHSRS Health Sector Reform StrategyHSSP/GTZ Health Sector Support Project/GTZHURDIS Human Resource Development Information SystemICIMOD International Centre for Integrated Mountain DevelopmentICPD International Conference on Population and DevelopmentIDA International Development AgencyIEC Information, Education and CommunicationILO International Labour OrganisationIPPF International Planned Parenthood Federation
jj VCDP Health June 2004 10/06/2004
IMR Infant Mortality RateINGO International Non Governmental OrganisationINSEC Informal Sector Support CentreKAP Knowledge, Attitude and PracticeLSGA Local Self Governance ActMCH Maternal and Child HealthMCHW Maternal and Child Health WorkerMDG Millennium Development GoalMGEP Mainstreaming Gender Empowerment ProgrammeML Migrant LabourMLW Migrant Labour WivesMMR Maternal Mortality RateMOES Ministry for Education and SportsMoH Ministry of HealthMTEF Medium Term Expenditure FrameworkMWCSW Ministry of Women, Child and Social WelfareMWR Mid Western RegionNAHD National Adolescent Health and Development StrategyNCASC National Centre for AIDS and STD ControlNDHS Nepal Demographic and Health SurveyNFDIN National Foundation for the Development of Indigenous NationalitiesNFE Non Formal EducationNFHP Nepal Family Health ProjectNHDR Nepal Human Development ReportNHSP-IP Nepal Health Sector Programme - Implementation PlanNPC National Planning CommissionNRHS National Reproductive Health StrategyNSMP Nepal Safer Motherhood ProjectOD Operational DirectivePHCC Primary Health Care CentrePLA Participatory Learning ActionPRSP Poverty Reduction Strategy PaperPWD People With DisabilitiesRH Reproductive HealthSAARC South Asian Association for Regional CooperationSCF UK Save the Children Fund (UK)SLTHP Second Long Term Health PlanSTD Sexually Transmitted DiseaseSTI Sexually Transmitted InfectionSWAP Sector-wide approachTB TuberculosisTBA Traditional Birth AttendantTFR Total Fertility RateTT Tetanus ToxoidU5MIR Under Five Mortality RateUNICEF United Nations Child and Education FundUSAID United States Agency for International DevelopmentVCDP Vulnerable Community Development PlanVDC Village Development CommitteeVDP Village Development PlanVHW Village Health WorkerWFP World Food ProgrammeWHO World Health OrganisationWRLH Women's Right to Life and Health
iii VCDP Health June 2004 10/06/2004
Table of Contents
ABBREVIATIONS 11TABLE OF CONTENTS IVLIST OF ANNEXES V
1. Introduction and Executive Summary of Recommendations 11.1 Executive summary of recommendations 2
1.1.] National level 21.1.2 District level 21.1.3 Community level 2
1.2 Social inclusion 31.3 Consultation, Participation and Disclosure 31.4 Social safeguards 4
2. Legal and Policy Framework 52.1 Background 5
2.1.1 Janajati Communities 52.1.2 Dalit communities 62.1.3 Policies on Women's Development and Gender mainstreaming 62.1.4 People Living with Disabilities 6
2.2 International Policies 62.3 National Policies 7
2.3.1 The Tenth Five Year Plan 72.3.2 Medium Term Expenditure Framework 2002 82.3.3 The Local Self Governance Act (LSGA), 1999 82.3.4 First Long Term Health Plan 82.3.5 National Health Policy 92.3.6 Second Long Term Health Plan 92.3.7 Health Sector Strategy - An Agenda for Reform, 2002 9
3. Parameters of Social Exclusion and health in Nepal: factors impacting exclusionof women, Dalit and Janajatis 113.1 Barriers to Social Inclusion 113.2 Exploring the social barriers to health for vulnerable groups 13
3.2.1 Gender-based exclusion 143.3 Operational linkages between social structure, cultural norms and health service delivery 153.4 Caste and ethnicity based social exclusion 16
3.4.1 Nepal's indigenous peoples 16
4. Programme Components 174.1 Essential Health Care Services (EHCS) 17
4.1.1 Family Planning 174.1.2 Safer Motherhood 194.1.3 Child Health 214.1.4 Communicable disease control 234.1.5 Strengthened Outpatient Services 24
4.2 Decentralisation 244.3 Public Private Partnerships 26
5. Institutionalframework and capacity building 275.1 Institutional capacity of the State 27
5.1.1 Ministry of Health (MoH) 275.1.2 Department of Health Services (DoHS) 275.1.3 National Health Education, Information, Communication (Acting) 30
iv VCDP Health June 2004 10/06/2004
5.1.4 National Centrefor AIDS and STD Control (NCA SC) 305.1.5 National Health Training Centre (NHTC) 315.1.6 Operational Challenges for MOHfor implementation of VCDP 335.1.7 Ministry of Women, Children and Social Welfare (MWCSW) 345.1.8 Ministry of Local Development (MLD) 345.1.9 National Commissions 345.1.10 Local bodies 34
5.2 Civil society 355.2.1 Women 's development organisations 355.2.2 Janajati institutions 355.2.3 Dalit organisations 355.2.4 Children's organisations 355.2.5 Special interest groups 35
5.3 International agencies 365.4 Multilateral and bilateral agencies 36
6. Monitoring and evaluation 366.1 Monitoring and evaluation 366.2 Implementation 37
7. Recommendations 387.1 Core recommendations for actions at the community level 43
7.1.1 Establish block grants to Sub Health Post Management and OperationCommittee (SHPMC) for support from CBOs particularly women 's andadolescent community groups for implementation of NHSP-IP 43
7.1.2 BCC in bilingual languages 457.1.3 HMIS disaggregated data 46
8. Monitoring framework and indicators for VCDP implementation 50
9. Bibliography 54
List of Annexes
Annex-1: Persons met
Annex-2: Hazardous employment and health
Annex-3: Geographic Distribution of Ethnic Groups
Annex-4: Cumulative impact on Social Exclusion from health services in Far Western RegionAnnex-5: Cumulative impact on Social Exclusion from health services in Siraha district
Annex-5a: MDG Goals and Social Inclusion in Health
Annex-6: Budget Formulation and Annual Planning Processes of Local Bodies
Annex-7: Partnership Defined Quality Program: A Partnership Approach to QualityImprovement in Health Services
Annex-8: Social Protection for Vulnerable Communities
Annex-9: Formation of Local Health Management Committee
Annex-i 0: Public Private Partnership
Annex-I 1: Major Health Related Projects Financed by Donors in Nepal
v VCDP Health June 2004 10/06/2004
1. INTRODUCTION AND EXECUTIVE SUMMARY OFRECOMMENDATIONS
This Vulnerable Community Development Plan (VCDP) addresses social exclusion in healthservices in Nepal and the effects and implications for vulnerable people for the Nepal HealthSector Program- Implementation Plan (NHSP-IP). The NHSP-IP is the five year operationalguideline for the Health Sector Reform Strategy - An Agenda for Change'. His Majesty'sGovernment of Nepal (HMGN) is committed to bringing about tangible changes in the health-sector development process. The health sector's vision is:
"A health system in which there is equitable access to coordinated quality healthcare services in rural and urban areas, characterized by: self-reliance, fullcommunity participation, decentralization, gender sensitivity, effective and efficientmanagement, and private and NGO sector participation in the provision andfinancing of health services resulting in improved health status of the population ".2
The key outputs3 , of the NHSP-IP focus on achieving this vision by providing an equitable, highquality health care system for all citizens regardless of their gender, caste, ethnicity, economicstatus and location through:
a. Prioritised Essential Health Care Services,b. Decentralised Management of Health Facilitiesc. Public -Private partnerships
The foundation of the NHSP-IP was set in the objectives of the Second Long Term HealthPlan 1997-2017: "Improve the health status of population particularly those, whose healthneeds often are not met: the most vulnerable groups, women and children, the rural population,the poor, the underprivileged and the marginalised population".
In Nepal's diverse yet hierarchical society, previous experience suggests that citizens' access topublic facilities and resources is highly dependent on social identity (caste, ethnicity andgender), economic status (landowner, sharecropper or business person) and physical location(urban, rural or remote rural). A significant proportion of the total population of Nepal arewomen, Dalits and indigenous people (recent estimates from the 2001 census suggest 16 %Dalits and 36.4 % indigenous population). Due to an absence of reliable data and an institutionalreluctance on the part of earlier governments to implement reforms that fundamentally addressstructural inequality, a number of groups have been excluded from mainstream health policies.The excluded groups are predominantly women and girls, indigenous peoples and occupationalcastes. Because they inhabit all regions and districts of Nepal covered by this broad nationalhealth project, a Vulnerable Communities Development Plan is an essential prerequisite forachieving the stated objective of social inclusion in basic health services as set out in the NHSP-IP Document.
'This Health Sector Strategy is the outcome of considerable work that has been carried out by His Majesty's Govemment of Nepal(HMGN), the NGO and private sectors and External Development Partners (EDPs) over the past three years. This processstarted with a joint review of the sector in autumn 1999 and has continued through a series of workshops and consultationsled by the Health Sector Reform Committee (HSRC) chaired by the Health Minister and a core group. The strategy drawson several key HMGN health sector documents: The 1991 National health policy; the second Long Term Health Plan 1997-2017; the strategic analysis to support that plan (May 2000); the Medium Term Strategic Plan to operationalise that planapproved in 2001; the draft medium term expenditure framework (MTEF) for the first three years of that plan and thepolicy documents for specific programme areas developed by the Department of Health Services, including the 10th planconcept paper or Health Approach paper -a Poverty Reduction Strategy Paper (PRSP) of the Government of Nepal.
2 Second Long Term Health Plan, 1997Final Draft Nepal Health Sector Programme - Implementation Plan (NHSP-IP) 2004 - 09 His Majesty's Government Ministry
of Health, 19 April 2004
1 VCDP Health June 2004 10/06/2004
1.1 Executive summary of recommendations
1.1.1 National level
1. National Advocacy workshop on Conflict and Health with focus on specific constraintsfor girls and women, Dalits and Janajatis in conflict areas
2. Sensitising IEC, Behaviour Change Communication Programmes to include women,Janajati and Dalit health and socio-cultural factors
3. Review health related training given by other line ministries such as Education andLabour.
4. Documentation of forms of abuse women health employees and health seekers face andintroduce a Directive against sexual harassment
5. Building the knowledge base on traditional healers and practices6. Production of instruction manual/social safe guard for NGOs/MOH/DDC/ VDC
employees working in Janajati and Dalit locations.7. Human Resource Development of staff at levels on gender and RH and rights to be
coordinated with the MoH institutional and management capacity developmentprogramme support affirmative action.
8. National Meet of FCHVs from all regions representing different castes and ethnicity toreview the FCHV programme in order to identify constraints ; conduct orientation onRH and gender issues and enhance programme efficiency promote sensitivity to gender,Janajati and Dalits related issues
1.1.2 District level
1. Strengthening Regional Social Inclusion issues related to accessibility, utilization, andimpact of health care provision related to marginalized communities in Far West an MidWestern regions
2. Health Insurance Schemes for Vulnerable Communities3. Instruction/training programme for I/NGOs, VDC and DDC staff working in districts in
Far- and Mid-Western regions to enhance Janajati/Dalit sensitive HSS programmeimplementation.
4. Intersectoral linkages mainstreaming social inclusion issues in health5. Establish networks for emergency travel, supply of medicines, and immediate medical
care to patients with donors and I/NGOs and private sector6. Establish conflict support funds which people without resources can access to for health
care7. Psycho-social support for conflict victims by creating " safe space" for health service
delivery
1.1.3 Community level
1. Development of training programme for community women as assistant health workers inclose relation to the BCC and EHCS tasks of FCHVs.
2. Evaluation role of local bodies as implementer of government policies since 1999towards disadvantaged groups, including IP and Dalits and women
3. Social assessment of the community drug scheme4. Establish block grants scheme for SHPMC to form agreements with selected local
community group5. Establish community based Adolescent Reproductive Health Counseling Center for peer
support.
2 VCDP Health June 2004 10/06/2004
1.2 Social inclusion
is defined in the World Bank Social Analysis Sourcebook as 'the removal of institutionalbarriers and the enhancement of incentives to increase the access of diverse individuals andgroups to development opportunities' (as cited in Bennett 2003. 4). The Ministry of Health has nodefinition of the disadvantaged or socially excluded. The Ministry for Education and Sports(MOES) presents the following definition of the disadvantaged/marginalised: "inclusiveeducation is to 'incorporate learning needs of socially marginalized groups, children withdisabilities, indigenous children and children living in difficult circumstances with specialneeds". MoES further defines 'disadvantaged children' as children with disability, girls, Dalit(23 disadvantaged groups) and other marginalized groups4.
The VCDP assesses NHSP-IP compliance with accepted safeguard policies, primarily TheWorld Bank's Operational Directive (OD) 4.20 on Indigenous Peoples. This directive requiresthat vulnerable people benefit from development projects and that potential adverse effect onthese vulnerable communities resulting from Bank-assisted activities are at best completelyavoided or at least mitigated. It includes the following components, as per recommendations fora thorough Vulnerable Community Development Plan: a presentation of the legal framework forIndigenous People, baseline data, analysis and critique of the proposal under discussion,strategy for local participation, technical identification of development or mitigation activities,institutional capacity, implementation schedule, monitoring and evaluation, cost estimates and afinancing plan. Although the directive on Involuntary Resettlement (8) Operational Directive4.12, is not applicable for the present loan, a separate section details how any sales or donationsof land involved in the programme should be dealt with to ensure that poor or vulnerablehouseholds do not suffer any loss of livelihood due to such sale or donation.Both these WorldBank Directives are in line with Government Policies.
The spectrum of health issues confronting vulnerable people in Nepal is vast and complex.Within a holistic framework of health, this development plan for vulnerable people focuses onpriority health issues that marginalised groups of people such as women, dalits and Janajatis aremost vulnerable to. These include: Child Health and communicable diseases, AdolescentReproductive Health, Safe motherhood and Sexual and Reproductive Health of women,HIV/AIDS and STD infectious diseases, and the impact of conflict.
For the present plan, and for the successful implementation of the NHSP- IP, understanding theeffects and implications of the Maoist insurgency on Nepal's health system is essential.According to a USAID report5 and the experiences of HSSP/GTZ 6 , harassment and threats byboth Maoists and security forces have exacerbated the chronic lack of qualified health staff inremote communities, thus decreasing service delivery in many areas. Health workers haverequested reallocation, but there are no hard figures to indicate whether this is more than usual.The mobility of health workers has decreased, due to reluctance to travel. Outreach clinics aredefunct in affected areas. In some districts the security forces have stringently restricted theprovision of medicines to rural areas, reducing the availability of appropriate treatment. (Source:NSMP. Impact of Conflict on Accessibility of EOC Health Services, By Monique Beun and Basu Dev Neupane, June 20031 76/96/DFD).
1.3 Consultation, Participation and Disclosure
This plan draws on qualitative and quantitative data from primary and secondary sources whichhave been carried out for an intensive social assessment of the health sector. A series ofmeetings and interviews were conducted with a wide range of professionals and scholars
In the Nepalese context this includes women, former "low caste" or Dalits and Indigenous Peoples or Janajati. The latter twogroups especially fir the World bank description in its Operational Directives. i.e. "ethnic minorities. linguistic minorities.children from indigenous groups as per 2002 Act, working children, street children, conflict & calamity affected children,children from remote regions, poor children, children from parents in prisons, those rescued from trafficking and childrenfrom migrant parents." (EFA core document)
5 Martinez, Esperanza C., Hari Koirala, Primary Health Care Services in Nepal, October 20026 Unpublished field visit reports, Health Sector Support Project (HSSP)
3 VCDP Health June 2004 10/06/2004
working in the field of health, language development, gender, conflict, anthropology and socialexclusion issues as part of the consultation. Members of community organisations representingsocially excluded groups, indigenous people and linguistic minorities were interviewed. (ReferAnnex I for list of people met). This document draws extensively on the Vulnerable CommunitiesDevelopment Plan prepared for the Education for Al17 for the Ministry of Education and Sportsin February 2004. On January 8, 2004, separate meetings were held with key nationalstakeholders from the activist communities representing women, Janajatis and Dalits followedby high-level consultation with line ministries and I/NGOs along with representatives. Giventhat the root causes for gender and social exclusion of vulnerable groups in particular, Janajatis,Dalits, and women as a cross- cutting concern for most sectors, these consultations providedvaluable insight for the social assessment for this VCDP.
Specifically for the health sector a Stakeholder Consultation was organised to promote furtherpublic participation, and discuss, inter-alia, the project objectives and activities, focusingparticularly on the findings and draft recommendations of the VCDP. The workshop wassuccessful with the active participation of key stakeholders, about 60 participants, includingHMG/N officials, NGOs, academic institutions and Community Based Associations working inthe health sector. The recommendations of the VCDP were well endorsed. The feedback andrecommendations from the consultation were incorporated into VCDP.
1.4 Social safeguards
Indigenous people social safeguards cover two issues: (i) Indigenous people; (ii) Involuntarysettlement. The current document is devoted to ensuring that the recipients of OD 4.20 on IPsare fully met by the NEFA lending operation.
Safeguard related risks and measures proposed: Based on findings of the Social AssessmentTeam's review, the program will not entail any involuntary resettlement or land acquisition. Theproject does not envisage any land purchase. Land for the construction of public health centresin Nepal is not purchased; rather wealthier members of the community donate it or healthcentres are built on public land that is not owned by any individual. Therefore this program doesnot trigger the OP/BP 4.12 on Involuntary Resettlement.
However, OD 4.20 on Indigenous Peoples does apply. After conducting a separate and detailedstudy, the Government prepared this Vulnerable Communities Development Plan (VCDP).The VCDP lays out a number of steps that the MoH will take to comply with OD 4.20 onIndigenous People by ensuring that the program not only will not have negative impacts on IPand other vulnerable groups, but that it also provides the necessary measures to insure that theyget equal access to project benefits. (See recommendationsfor details).
Rules of taking possession of land: DDC will not resort to any involuntary land acquisition.All donations and purchases will be voluntary. Mechanisms will be developed not only toensure that any land donations are fully voluntary, but also that such donations do not involvephysical displacement or any significant adverse impacts upon incomes of the donor household.All voluntary land transactions will meet the following criteria:
(i) The land in question will be free of squatters, encroachers or other claims ofencumbrances;
(ii) Land will be chosen by the community after ensuring that it will not be disturbing anyother land related resources available in that particular piece of land;
(iii) Verification of the voluntary nature of land donations in each case;(iv) Land transfers will be completed through registration, with land title vested in the SMC;(v) Provision will be made in DDC procedures for redressal of any grievances related to the
land acquisition.
7Vulnerable Community Development Plan by Kiran Bhatia for the World Bank, June 2004
4 VCDP Health June 2004 10/06/2004
Procedure: Lands will not be accepted from such land owners whose holding will be less thanthe minimum economical viable stipulated size. This size of land might vary from one localityto another. In this case, an agreement of minimum stipulation size will be determined by theSAs in the local context.
Land to be used may also not be registered with government (Ailani) and the possibility thatsuch land may have been occupied by landless (Sukumbasi) is high. If Ailani land is occupied, itwill not be accepted for the project.
All land transactions will be subject to registration (as per market transactions) under theownership of SMCs of community health centres that are involved in the project and will bedone only after ensuring that water will indeed be available in that particular piece of land.Essentially, Social Analysis will arrange for field verification of all cases of land purchases insuch a way as to ensure that land has not been taken under any psychological, social, andeconomic domination and that the above obligations and criteria have been fulfilled. Wheresuch land donation involves vulnerable household, the DDC may wish to seek assistance fromlocal organisations for field verification. The DDC Portfolio Chairman should visit the field andconsult with the community for final verification. Information obtained from the community canbe used to verify that the correct procedures for the land acquisition have been carried out by thelocal organisations and the community.
2. LEGAL AND POLICY FRAMEWORK
2.1 Background
There has been considerable commitment by HMGN in investing in the health of its people andextending better health services to the Nepalese populace. Nepal became a party to the 1978global declaration on "Health for All by 2000" and since then significant policy and programmedevelopments have been implemented to meet the challenge of improving the health status ofthe people despite poverty, wide socio-economic disparities and a difficult geographical terrainand health indicators that at present are among the worse in the world. A brief overview of thelegal and policy framework of Nepal's commitment to International obligations and nationalpolicies relating to women, Dalits and ethnic and linguistic minorities is presented below.
2.1.1 Janajati Communities
The Nepalese Constitution and HMG/N's policies indicate the government's increasingemphasis on the development of Nepal's Janajati groups. The 1990 Constitution defines Nepalas a 'multiethnic, multilingual, democratic, independent, sovereign, Hindu and ConstitutionalMonarchical Kingdom', officially recognising Nepal's ethnic diversity. The Constitution alsomakes 'promot[ing] the interests of economically and socially backwards groups' a keydirective principle of the state. Furthermore, a proviso to Article 11, Rights to Equality, statesthat 'special provisions may be made by law for the protection and advancement of the interestsof ... those who belong to a class which is socially, economically or educationally backward.'This proviso accords recognition to positive discrimination for disadvantaged groups8 .Article 6 of Part 1 of the constitution, relating to the 'Language of the Nation', states: (1) TheNepali language in the Devanagari script is the language of the nation. The Nepali languageshall be the official language. (2) All the languages spoken as the mother language in thevarious parts of Nepal are the national languages of Nepal.Article 18 of Part 3 (in the section on Fundamental Rights) states that: (1) Each communityresiding within the Kingdom of Nepal shall have the right to preserve and promote its language,
' NEFEN: Janajati Empowerment Project, Project Document Submitted to Enabling State Programme 3 February 2004
5 VCDP Health June 2004 10/06/2004
script and culture. (2) Each community shall have the right to operate schools up to the primarylevel in its own mother tongue for imparting education to its children.The Government formed the National Committee for Formulating Cultural Policy and Programsin 1992 to conceive and realise concrete plans to help preserve and promote Nepalese culture. Inorder to implement the provision of the 10th Plan, the Nepali Parliament issued an Act in 2002 toestablish the National Foundation for the Development of Indigenous Nationalities (NFDIN) whichhad a broad mandate to ensure the social, economic and cultural development and upliftment ofindigenous peoples, as well as their mainstreaming and equal participation in national development.While these policies do highlight the rights for indigenous people, the real concern is theimplementation modalities and political climate that enables socially excluded people to access theserights.
2.1.2 Dalit communities
Dalit communities have not witnessed much change since the fall of the Rana regime duringwhich they were the most religiously, culturally, socially and economically oppressedpopulation of Nepal. An exception was the introduction of the New Legal Code (Naya MulkiAin) in 1963. According to this Code, nobody could claim inferiority or superiority on the basisof race, caste and creed; everybody was equal before the law. Two recent measures, the LocalSelf-Governance Act, 1999 and the establishment of the National Dalit Commission, aim toincrease Dalit participation in governance with improved protection of rights. Despite this, andthe signing of other national and international acts and conventions (in particular CERD), casteideology has continued to exert a strong influence on Nepalese society and Dalits, particularlyDalit women and girls, continue to have the lowest social, economic and political indicators.Life expectancy of Dalits is 50 years when the national average is 59.
2.1.3 Policies on Women's Development and Gender mainstreaming
Nepal continues to present poor improvement in the HDI for girls and women in most sectors inspite of significant efforts at all levels to confront gender-based inequality and discrimination.This is indicative of the deep-rooted socio-cultural norms and practices of a patriarchal societythat both government and civil society continue to struggle with. Nepal has been signatory tonumerous International Conventions (Beijing Platform for Action, CEDAW and CRC) and isproviding increasing policy reform and resources for women's development and gendermainstreaming. Recent policy reform includes Laws guaranteeing women's right to property,rights against sexual offences, the formation of the National Women's Commission. Lawsrelating to abortion, which was liberalised two years ago to ensure the availability of safe andaccessible abortion, have been passed. The Tenth Plan, building on the efforts of the Ninth Plan,has a specific focus on social inclusion that has created a strong and positive policy environmentfor the empowerment of women and girls.
2.1.4 People Living with Disabilities
Disabled Persons (Protection and Welfare) Act is the only comprehensive legal arrangementmade for the welfare of persons with disabilities. It spells out specific rights of PWDs such as:Right to health - Free medical check ups in all governmental health service institutions; Right toequality in all matters and right to live with dignity; Right to Education; Priority in governmentand semi-government jobs and free legal aid.
2.2 International Policies
Over the past few decades the international development agenda has witnessed rapid progress inpolicy reform on health. There has been a shift from traditional centre driven targeted delivery ofhealth services to an attempt at introducing a more rights based holistic approach to meeting thehealth needs of all. Among the main components of the rights-based approach are: gender equity andequality; sexual and reproductive rights and client-centred health care. The rights-based approach
6 VCDP Health June 2004 10/06/2004
to sexual and reproductive health emerging from the International Conference on Population andDevelopment (ICPD) in 1994 reflects a new global policy consensus on the relationships betweenpopulation policy and sexual and reproductive health and rights: if women are empowered andpeople's needs for sexual and reproductive health are met, population stabilization will be achievedby virtue of choice and opportunity, not coercion and control. The rights-based approach wasreaffirmed and extended at the Fourth World Conference on Women in Beijing in 1995, andagain at the Beijing +5 and ICPD+5 review in 1999. The World Social Forum and the MillenniumDevelopment Goals reaffirm the global commitment to priority for addressing rights of marginalisedmen and women. (Refer Annex 2for details)
2.3 National Policies
Historically Ayurvedic medicines, and different forms of faith healing, were the principal meansof treatment amongst Nepal's traditional communities. Numerous alternative beliefs, knowledgeand practices of health and non-formal medical traditions have been in practice. Despite thesetraditional systems and the subsequent establishment of a government public hospital inKathmandu, access to public health facilities for the common people was extremely restricted.The new Constitution of 1990 established Nepal as a much more inclusive state by explicitlydescribing it as "multi-ethnic, multi-lingual and democratic country". A number of key reformshave been introduced to strengthen the focus on equity and decentralisation, most significantlythe Local Self-Governance Act, 19999.
2.3.1 The Tenth Five Year Plan
The Tenth Five Year Plan (2002-2007), Nepal's Poverty Reduction Strategy, is the first nationalplan to have social inclusion as one of its four pillars. It has recognized gender-based disparitiesin income and human development as important elements of the poverty profile in Nepal. ThePlan also gave priority consideration to major social variables, such as gender, ethnicity, andcaste related differentials, which exacerbate the intensity and depth of poverty for the affectedgroups. The PRSP has identified: (1) the sociological factors that constrain women's access tohousehold income and resources in male-headed families and that the absence of this access is acrucial factor for women to receive health services. (2) the many indigenous ethnic (Janajatis)and caste (Dalits) groups that have been historically disadvantaged. (3) the health sector as acritical area of human development, improving living standards in rural areas for mainstreamingmarginalised groups and communities. (4) that service delivery remains weak due to lack oftrained staff, drugs and medicines and inadequate or misallocation of resources. (4) that womendevelopment has been regarded as cross cutting theme across the four pillars (P-155)PRSP's health sector objective is to extend Essential Health Care Services (EHCS) to all,especially to rural, remote, and poor populations. In order to mainstream the marginalisedgroups and regions, the plan has emphasized access to health facility within one hour's walk toall, and to prioritise special programs in the Mid and Far Western regions as it presents specificchallenges to women and vulnerable communities. The plan sets explicit objectives of reducingexisting gaps between these groups and the rest of the population through monitoringmechanisms of targeted programs to ensure equal attention to the deprived communities throughthe Ministry of Local Development, together with Nepal Dalit Commission and NationalAcademy for the Upliftment of the Indigenous People.
However specific strategies for behaviour change of health personnel towards the poor womenand socially excluded groups for service delivery and representation of the women andmarginalised groups in the management committees of Health posts are not clearly statedincreasing the risk of limited social inclusion.
9 LSGA Governance Act 1999: The LSGA, 1999 stipulates that representatives from 'socially and economically backward tribesand ethnic communities, downtrodden and indigenous groups' shall be nominated to each village, municipality and districtcouncil. This clearly includes the Dalits. Clause 43 (3) of the act requires VDCs to prioritise projects that provide 'directbenefits' to the so-called 'backward classes' (Dalits)
7 VCDP Health June 2004 10/06/2004
2.3.2 Medium Term Expenditure Framework 2002
HMG/N's Medium Term Expenditure Framework 2002 has categorised public health activitieswith Essential Health Care Services as a first priority. HMGN is implementing an annualImmediate Action Plan for priority reform and has initiated an incremental transfer of sub-health posts to local management committees and contracting out of district hospitals. In all thepolicies, decentralisation is presented as a core strategy with health to be managed locally withincreased community participation.
2.3.3 The Local Self Governance Act (LSGA), 1999
The LSGA has emphasized priority areas of local bodies to "enhance the living standards,income and employment of, and render direct benefits to, the village people and contribute topoverty alleviation". This Act has sanctioned authority to village committees to operate andmanage health centres, health posts and sub health posts, primary health care services includingfamily planning and maternity and child care services. It has made the provision ofrepresentation of women, economically backward tribes, ethnic communities and indigenouspeople at village and ward level development committees The Act has directed the bodies toallocate funds earned from their sources in the health sector on a priority basis'°.Social analysis: the LSGA in its provisions does not address issues of inequity and vulnerabilityas a result of gender, caste or ethnicity. Directions to recognize and address specific barriersfaced by such vulnerable groups, are absent. The absence of such specific directives has resultedin very few women being elected to executive positions of local institutions" with onlymarginal representation of women in elected institutions except for the reserved grass rootspositions. There were no women mayors, vice mayors or DDC chairpersons (Bhusal, 1998 andShrestha, 1998). Both VDCs and municipalities do not have gender-disaggregated data of their staff,beneficiaries, user groups, development project and services to women. (Gender Budget Audit; MeenaAcharya)
The Gender Budget Audit carried out recently, has found that the VDCs and DDCs budgetformulation process has negligible involvement of women, Dalits and Janajatis. (Refer Annex-6fordetails on VDCs and DDC budgetformulation process). Among women, 71% (compared to 57 percent of men)have little or no involvement in planning village health programmes and 67 per cent of women(compared to 59% of men) are only marginally involved in implementation. A sharper genderdifferential is found among the Dalits: 75 per cent either do not participate or participate verylittle in the planning of village health services, compared to 58 per cent of the advantagedgroups (largely Brahmin and Chettri men.) This difference parallels that of implementationwhere non-participation is 74 per cent for Dalits compared to 56 per cent for the advantagedgroups. (Neilson)
2.3.4 First Long Term Health Plan
The government prepared The First Long Term Health Plan (1976-92) to address the majorhealth requirements of the population. Though a comprehensive strategic document, this Planwas never operationalised. Primarily a centre driven plan, it was not developed through aparticipatory approach and was not shared and disseminated with the concerned partners andfailed to bring the desired results.
"' A Manual Prepared for Transfer and Operation of Local Health Institutions 2060 (2004) His Majesty's Govemment, Ministry OfHealth, Department of Health Services
Only 289 women were elected as ward chairpersons in a total of 35217 wards, where election was completed. Among nearly eightthousand chairpersons and vice chairpersons only 26 were women. Only one woman had managed to be elected to theposition of vice chairperson of DDC. Altogether, only three women had fought for the DDC chairperson and vicechairperson positions. Among 26 women who had fought for DDC membership, only eight got elected. This was less thannine percent of 924 members in the 75 DDCs to which election had been completed in 1997. (Meena Acharya: GenderBudget Audit ofMinistry ofLocal Development: MWCSW/ MGEP/UNDP. 2003)
8 VCDP Health June 2004 10/06/2004
m~~ ~ ~~~~~~ 1
2.3.5 National Health Policy
The National Health Policy (1991) provided the key guiding instrument for the policyframework for health sector development in Nepal. Its objectives include: (i) extension of basicprimary health care services up to the village level; (ii) provide opportunity to rural people toenable them to obtain the benefit of modem medical facilities; (iii) Priority targets for womenand children (MMR, IMR and TFR). It focuses on local resource mobilization to reach peoplewith special needs. It has directed for the adoption of micro planning process in health planningto target all groups with special efforts to reach the underprivilegedHowever, the policy lacks recognition of the rights of women dalit, and ethnic groups and nomechanisms to ensure representation of these groups in the planning process. It also lacks anycommitment to the need to develop a data base and monitoring systems of disaggregated data bygender, caste and ethnicity.
2.3.6 Second Long Term Health Plan
Building on the National Health Policy and to further guide health sector development theSecond Long Term Health Plan (SLTHP)-1997 - 2017) was developed. The SLTHP hasconsidered health as a human rights issue1 2 and emphasized improvement in the health status ofthe population particularly those, whose health needs often are not met: the most vulnerablegroups, women and children, the rural population, the poor, the underprivileged and themarginalised population. However, strategies and clear mechanisms of service provision for theeconomically and socially deprived populations including people living with disabilities andwomen are again not clearly stated.
2.3.7 Health Sector Strategy - An Agenda for Reform, 2002
The Health Sector Reform Strategy draws on key HMGN health sector documents including the1991 National Health Policy; the Second Long Term Health Plan 1997-2017; the StrategicAnalysis to support that plan (May 2000); the draft Medium Term Expenditure Framework(MTEF), and the policy documents for specific programme areas developed by the Departmentof Health Services as well as the 10th plan concept paper or Health Approach paper - a PovertyReduction Strategy Paper (PRSP) of the Government of Nepal. There is considerablecommitment by HMGN and its EDPs to poverty reduction and achieving the millenniumdevelopment goals (MDGs). The key issues identified for reform are: Ensuring access of thepoor and vulnerable to EHCS; Ensuring that public health services are run in a most efficientmanner; Ensuring services out side the EHCS with the provision of safety nets; Monitoring andtracking sector performance.
Strengths for Social Inclusion: Major equity issues are related to gender, age, caste, ethnicity,income and area of residence. Transportation cost causes significant restriction to the pooraccessing health care in remote areas and the largest equity discrepancies relate to area ofresidence. The document focuses in particular on how the health sector would make itscontribution to poverty reduction and to improving health outcomes for the poor and thoseliving in remote areas. Health expenditure is very low in Nepal in spite of some real increasesover recent years. The strategy has emphasized the importance to ensure that pubic financewould be directed to the EHCS and the poor and vulnerable. This would only be achieved ifalternative financing schemes for these services are developed along side resource allocationpolicies for pubic finance that target the EHCS and the poor and vulnerable.There are serious concerns about access to services by the poor. Access to both public andprivate inpatient facilities varies considerably by income group with the wealthier having higherutilization of both public and private facilities. Need of monitoring data from benefit incidencestudies as to which socio economic groups are accessing health care at all levels is.
12 SLTHP, Health Policy Context, pp-10
9 VCDP Health June 2004 10/06/2004
Challenges for Social Exclusion* The strategy is silent about the ongoing political conflict and its implications on the
health sector - the requirements of children, widows, female headed householdsparticularly from dalit and Janajati households have been excluded due to conflict.
* There had been many policy commitments in the past but were not translated in topractice due to lack of realistic implementation plan. In the present strategy too these gapsare evident and may inhibit full implementation.
* Though the strategy has emphasized for the implementation of decentralisation in thesector, the required process has not been defined.
* During the process of developing the strategy there was no involvement of stakeholders atthe district and level below.
Review of NHSP - IP
The Nepal Health Sector Programme -Implementation Plan's (2003-07) key focus is to"ensure access by the poor and vulnerable to EHCS": increase the coverage and raise the qualityof EHCS, with special emphasis on improved access for poor and vulnerable groups (pp-7).Selected outputs are directly related to social inclusion strategies (pp-16) and one key indicatorstates: "by the end of 5 years (in 2006/7) XX% of the poor and vulnerable groups areutilizing the prioritized EHCS" (pp-23).Systems for priority access to poor and vulnerable groups have been outlined in the projectdocument in major areas: to develop criteria to identify the poor, expansion of EHCS,subsidized drugs and services, safety net, rehabilitation (of the conflict affected), andparticipation (pp-23). For the implementation of NHSP-IP a, "Statement of Intent" to guide thepartnership for health sector development in Nepal, has been signed by major ExternalDevelopment Partner (EDP) representatives in health and the Ministry of Health. Theframework suggests that all support will be consistent with HSRS.Strengths for social inclusion
NHSP -IP has clearly outlined social inclusion strategies. Systems for priority access topoor and vulnerable groups have been detailed.
* It emphasises the need to ensure that the poorest people, receive the greatest share ofpublic subsidies for essential services (i.e. services which produce the greatest reductionin health burden)
* NHSP has outlined five Sector Management Outputs to ensure effective implementation.* The emphasis of the reform strategy is on outputs and health outcomes. The HSRS isreqarded as a move towards strateajic pIanning and a sector-wide approach (SWAP).* NHSP-IP has been developed after wide consultations with key stakeholders at different
levels and is based on various studies including one on social assessment13 .Challenges for social inclusion* Lack of conceptual clarity on social inclusion: A review from the perspective of gender
and social inclusion reveals that conceptual clarity on gender and mainstreaming is stilllacking, and a substantive rights based approach is absent.
* Clear recognition of the specific needs and concerns of Dalits and Janajatis is absent inNHSP-IP. While it states that criteria to identify the poor will be finalised andincorporated in the decentralised reform actions, it has not defined who the vulnerable areand lacks a clear definition of vulnerability with relevance to by gender, caste or age.
* The indicators in the NHSP-IP are not disaggregated by gender, caste and ethnicity andthus specific initiatives necessary for social inclusion of women, Dalits and Janajatis maynot occur.
13 Social Assessment in consideration of gender and marginalised population including in conflict areas (February 2003)
10 VCDP Health June 2004 10/06/2004
* While the NHSP has recognised the health needs for rehabilitation due to the ongoingconflict it has not provided the necessary resources or strategic plan to manage the impactof conflict on non-functioning of health facilities, the rising needs for curative services,psycho-social consequences and infrastructure. The special health concerns of conflictaffected children, widows, female-headed households and resource poor families ofJanajati and Dalits in remote locations have not been recognised.
The NHSP-IP explicitly reflects a poverty focus, coherent with the HSS, both in policystatement and strategy. However, both the HSS and NHSP-IP make no reference to the currentconflict in the country. While arguably this may be justified for a "long term" strategy, it wouldbe highly relevant to include reference to the conflict and the negative consequences onimplementation of services and reforms over the next 3 years. The NHSP-IP generally does notaddress other types of inequity and vulnerability in depth. such as by gender, caste, or age. Thefew explicit references to services for vulnerable groups are found in the Output 1 statement("Clear systems in place to ensure that the poor and vulnerable have priority for access"), in theHIV programme emphasis, and in the Disaster Management activities. However, lacking adetailed Annual Work Plan and Budget, it is difficult to judge how these statements are to bemade real. (Joint Review of the Nepal Health Sector Programme - Implementation Plan, 15-26 March 2004)
Social analysis of other health policies
HMG/N has developed various national policies and strategies for different health components.Those relevant to the prioritised areas of this VCDP are child and adolescent health, nationalreproductive health strategy (NRHS), 1998 and national HIV/AIDS strategy (2002-2006). (ReferAnnex 3for details).
3. PARAMETERS OF SOCIAL EXCLUSION AND HEALTH IN NEPAL:FACTORS IMPACTING EXCLUSION OF WOMEN, DALIT ANDJANAJATIS
This section includes specific primary and secondary data on the types of barriers that differentsocial groups of Nepal face, the socio-cultural framework including structures, which governrural economic life, and the key factors of social exclusion, which impact the health of thepeople of Nepal.
3.1 Barriers to Social Inclusion
Barriers to social inclusion in all facets of life in Nepal include gender-based socialstratification, which in turn must be placed in the prevailing ethnic, and caste based hierarchiesthat structure econornic and social relationships in Nepal. This defines how the lives of girls andboys, men and women will be shaped according to the caste and ethnic groups they are born in,their religion and the location of their community and the rules and norms that these socialstructures define. These social structures govern all spheres of an individual's daily life. Thehealth status of the people in Nepal remains low on account of four main barriers: economic,social, physical/mental, and geographical.
3.1.1 Economic barriers: Nepal is predominantly an agricultural country, drawing about40 percent of its Gross Domestic Product from this sector with approximately 85 percent of itspopulation still earning their living from farming. The annual per capita income of Nepal is nowUSD $240 and around 42 percent of the population are estimated to be living in poverty. Themajority of the population is rural-based, where poverty is at its worst, particularly in the mid-western and far-western regions of the country which are beset by the double problem ofcontinuing food shortages and the ongoing impact of the State-Maoist conflict. Poverty presentsmany disincentives for families to invest in health seeking care, especially for girls and womenwho are historically less valued and hold a lower social status than men and boys in almost allcommunities. The user charge, levied to provide additional income for the hospitals, generallydiscourage children, elderly and the low-income groups from seeking care because of the
11 VCDP Health June 2004 10/06/2004
unavailability of money during sickness. (Public Expenditure Review of the Health Sector in Nepal, HEFU, MoH,2003, page 18). There are certain systematic associations between social identity and economicstatus. Ninety percent of Nepal's Dalits live below poverty line with an average per capitaincome of only $ 39.60.
3.1.2 Geographic barriers: Nepal is one of the poor est and most mountainous countries inthe world with great diversity in terrain that presents a range of challenges for access andinfrastructure. Significant geographical variations mirror the existing income povertydifferentials. The HDI for urban areas (0.616) far outstrips that for rural areas (0.446), becauseof better access to services, resources and opportunities. Similarly, there are significantdifferences among ecological zones. The HDI for mountains (0.378) is well below that for thehills (0.51). The broad scattering of communities in the mountains limits access to services andresources and severely disadvantages people who live there. Human development in the hills ishigher than in the Terai (and the national average). The central and eastern regions of thecountry have the highest proportion of indigenous peoples, but the data overwhelminglyindicate that Janajatis primarily occupy the hilly and mountainous regions of Nepal, and thatthese districts are often remote and accessible only by foot.All available data in Nepal suggest that poverty is deeper and more severe in rural areasespecially in the mid and far Western regions. Hill districts with a high concentration HillDalits are Surkhet, Kailali and Kaski; Terai districts with a high concentration of Dalits areSiraha and Saptari. Gender-based development indicators are low in almost all these samedistricts.
Poverty is more extensive in the hills and the mountains as compared to both urban areas, aswell as the (rural) terai. Over 90% of the poor live in rural areas. Poverty in both the Terai andthe Central Hills is close to the national average, but is much higher (56%) in the Mountainregion. The poverty rate is the highest in the more remote rural areas-the Mid-Western andFar-Western hills and mountain regions where it is as high as 72%. The highest proportion ofpeople with disability without access to education was found in the mountains (77%) as compared tothe hills (58%)14. Relative to people in other parts of the country, residents of rural and remoteareas in Nepal have lower life expectancy and suffer more from chronic and acute illness. As aresult, the impoverished populations of the underserved areas depend heavily on public sectorfacilities, which are most deficient in those very areas. These regional disparities are among theworst in the world. (Report No. 19613 Nepal Operational Issues and Prioritization of Resources in the Health Sector June 8,2000 Health, Nutrition and Population Unit, South Asia Region)
Drinking water containing high amounts of arsenic has adverse affects on human health,including increased risks for cancer, diabetes and heart disease. (http://www.south-asia.com/USA/hub_arsenic.html) In Nepal no medical case of arsenicosis has been reported15 so far. But arseniccontamination has been detected in 11 Terai districts of Nepal.3.1.3 Mental and Physical Barriers for children with special needs: Children withdisabilities are the most visible group of those targeted in the MoES definition of disadvantagedpeople and there is a specific focus on special needs education. WHO estimates that 10 percentof the total population of Nepal suffers from disability with the number being higher in womenand comparatively worse in the case of women above 25 years of age 35% were under 19years of age (UNICEF 2003, Lansdown). More than 50 percent of disabilities are seen in childrenbelow five (A Situation Analysis on Disabilityv in Nepal, 2001).
In rural Nepal, many girls suffer disability due to lack of timely access to vaccine for polio andother related diseases. A study of eight surveyed districts in 1995 indicated that 12.4 percent ofthe population was mentally retarded with many cases being acquired retardation caused byneglect of disease, especially high fever, severe diarrhea, typhoid, pneumonia, measles, polio,encephalitis and paralysis (A Situation Analysis of Disability in Nepal, 2001. Chitrakar, 2004)
14 Source: Disabled Children in Nepal Progress in implementing the Convention on the Rights of ihe Child, Gerison Lansdown, 20035 Reports on the Household survey on the health impact of arsenic contaminated ground water I nNawalparasi, 2001, Drinking
water quality programme NRCS/JRCS/ENPHO
12 VCDP Health June 2004 10/06/2004
Studies done on disabilities so far have traditionally used a gender-blind approach. (Dhungana,2003). Absence of barrier-free development is a fundamental need of disabled people and theyneed access to these services (Hema 1966; Ototake, 2000; Maqbool, 2003).
3.1.4 Barriers caused by Maoist conflict: In the most severely affected areas, Maoists havereduced health service availability since health staff have often left their postings due toharassment. The security forces have restricted delivery of medicines. The conflict has had amajor impact on transport during the night, when curfews are imposed and mobility is severelyrestricted. The number of male household members has been significantly reduced, leaving thedecisions concerning health expenses to the female household members.Since the Maoist conflict started more than 35 thousands pregnant women have died and postpartum haemorrhage is the main cause of maternal death. (The Space Times daily newspaper dated 01 April04). Particularly at night, it has become more difficult to ask advice from relatives, neighbours,and nearby TBA and FCVH who would otherwise be consulted before taking major stepsinvolving financial expense. Uneducated, poorer, low-caste people in particular, are not awarethat they can get permission for night travel (Source: NSMP: Impact of Conflict on Accessibility of EOC HealthServices, By Monique Beun and Basu Dev Neupane, June 2003 176/96/DFD). A new emerging concern is thegrowing number of physically handicapped children who will require special health care. Thoseseparated from parents and families in the midst of conflict are amongst the most vulnerable. Ithas been estimated that 2000 children have lost at least one parent and over 4000 have beendisplaced from their villages in the conflict-affected areas and forced to migrate.Impact of conflict on women, Dalits and Janajatis: The insurgency has had severalconsequences on vulnerable and disadvantaged groups. The safety, livelihood and status ofwomen and girls have been especially negatively impacted, with a sharp rise in male migration.Dalits too have become victims as both the warring parties and the general public treat themwith suspicion. Forces have committed violent acts, including gang rape, torture and murderagainst women who were believed to support Maoists or who were hiding informationconcerning their husbands or sons- there are 24 documented cases of pregnancies caused byrape.
Psycho social impact: Ongoing research16 has revealed that out of 37 respondents (of whom 25were women and 16% Janajatis), 31 (84%) have admitted to behavioural disturbances such assleeplessness, anxiety disorders, and feelings of guilt and sadness. Three quarters of thepopulation was in substantial emotional distress (74%).Given the far-reaching impact of the conflict it is unrealistic to speak of a "National" Healthplan where whole districts are without more than a few functioning health facilities. HisMajesty's Government of Nepal's most immediate task must be to seek a speedy and completeresolution to the present conflict. Without this, NHSP-IP may be implemented in Kathmandubut will remain a distant dream in most of rural Nepal.3.1.5 Social Barriers: Social barriers include gender-based social stratification, which in turnmust be placed in the prevailing ethnic and caste-based hierarchies that structure economic andsocial relationships in Nepal. The lives and opportunities of girls and boys and men and womenare shaped according to the caste and ethnic groups into which they are born, their religion andthe location of their community and the rules and norms that these social structures define.These social structures govern all spheres of an individual's daily life.
3.2 Exploring the social barriers to health for vulnerable groups
The primary focus in this analysis is to understand the various barriers for exclusion of peoplefrom improved health status. Past research has concluded that social exclusion occurs due toinequality in:
1 UNU/swisspeace: Case Study on Gender perspectives in Small Arms and Light Weapons, HURDEC, INSEC, IHRICON, 2004
13 VCDP Health June 2004 10/06/2004
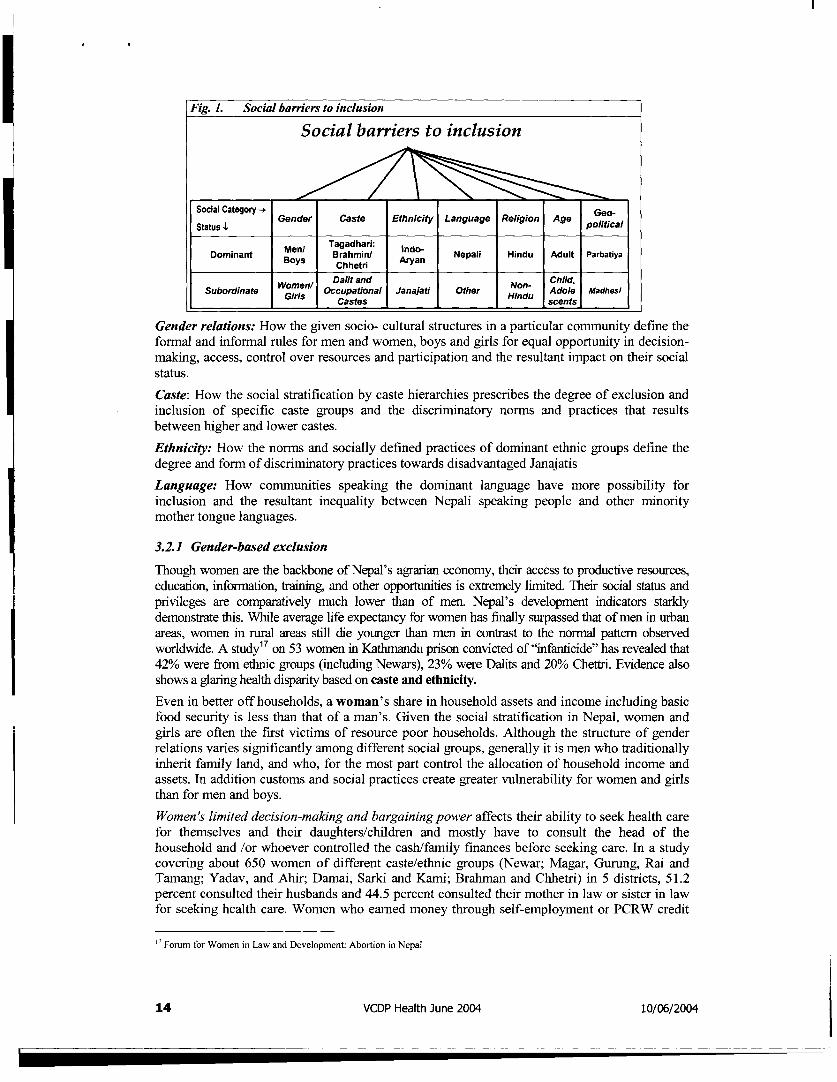
Fig. 1. Social barriers to inclusion
Social barriers to inclusion
Social Category- |
5ttuso C Gender Caste Ethnicity Language Religion Age pola
Moeyns aharin Anrydan Nepali Hindu Adult Parbatiya
Woel Dalit and Non- Child,.Subordinate Occupational Janajati Other du Adole /Madhsi_
Gender relations: How the given socio- cultural structures in a particular community define theformal and informal rules for men and women, boys and girls for equal opportunity in decision-making, access, control over resources and participation and the resultant impact on their socialstatus.
Caste: How the social stratification by caste hierarchies prescribes the degree of exclusion andinclusion of specific caste groups and the discriminatory norms and practices that resultsbetween higher and lower castes.
Ethnicity: How the norms and socially defined practices of dominant ethnic groups define thedegree and form of discriminatory practices towards disadvantaged JanajatisLanguage: How communities speaking the dominant language have more possibility forinclusion and the resultant inequality between Nepali speaking people and other minoritymother tongue languages.
3.2.1 Gender-based exclusion
Though women are the backbone of Nepal's agrarian economy, their access to productive resources,education, informnation, training, and other opportunities is extremely limited. Their social status andprivileges are comparatively much lower than of men. Nepal's development indicators starklydernonstrate this. While average life expectancy for women has finally surpassed that of men in urbanareas, women in rural areas still die younger than men in contrast to the nonnal pattem observedworldwide. A study17 on 53 women in Kathimandu prison convicted of "infanticide" has revealed that42% were from ethnic groups (including Newars), 23% were Dalits and 20% Chettri. Evidence alsoshows a glaring health disparity based on caste and ethnicity.Even in better off households, a woman's share in household assets and income including basicfood security is less than that of a man's. Given the social stratification in Nepal, women andgirls are often the first victims of resource poor households. Although the structure of genderrelations varies significantly among different social groups, generally it is men who traditionallyinherit family land, and who, for the most part control the allocation of household income andassets. In addition customs and social practices create greater vulnerability for women and girlsthan for men and boys.
Women's limited decision-making and bargaining power affects their ability to seek health carefor themselves and their daughters/children and mostly have to consult the head of thehousehold and /or whoever controlled the cash/family finances before seeking care. In a studycovering about 650 women of different caste/ethnic groups (Newar; Magar, Gurung, Rai andTamang; Yadav, and Ahir; Damai, Sarki and Kami; Bralman and Chhetri) in 5 districts, 51.2percent consulted their husbands and 44.5 percent consulted their mother in law or sister in lawfor seeking health care. Women who earned money through self-employment or PCRW credit
" Forum for Women in Law and Development: Abortion in Nepal
14 VCDP Health June 2004 10/06/2004
sometimes used their earnings to pay for health care, but most women would only seek care ontheir own accord if services were free. (World Bank: Understanding Access, Demand and Uitlisation of HealthServices in Nepal and their Constraints, June 2001)
Neglect: The same study states that in all districts women were recognized to be ill by familymembers only when they were bedridden or unable to perform their daily tasks. Familymembers and women themselves place a very low value on women's lives, thus women's healthis often ignored. Fear of domestic violence contributed to women's reluctance to voice theirneed for healthcare services.
Janajati women: Women's position relative to men varies by caste and ethnic group. Ironicallywomen from the dominant "high caste" groups are among the most severely restricted in termsof access to assets, opportunity and voice. The status of women and girls among the ethnicgroups speaking Tibeto-Burman languages and among the lower caste Hindus is much higherthan among the dominant high-caste Indo-Aryan groups (Bennett 2003). Janajati women arerelatively better off in terms of gender equality within their own communities as compared toupper caste Hindu women. Janajati women are in the paradoxical role of being at onceoppressed by state and national forces yet relatively better off in terns of gender equality withintheir own communities as compared to caste Hindu women. However, education and literacyare particularly low among Janajati women, while literacy in Nepali - a language which is amother-tongue for very few - is lower still.Dalit women: Dalit women constitute 50.6 percent of the total population of Nepal, as per the1991 census. It is estimated that more than 98 percent of the Dalit women live in the rural areas.Dalit women's literacy is much lower to that of Dalit men. The literacy rate is more than 3 timeshigher among Hill Dalit women (14.7%) than among Terai Dalit women (4.0%). Dalit womenface triple discrimination in their daily lives -as a woman, as a Dalit, and as a Dalit woman.Dalit women have to face more discrimination than men in places like water taps, markets,training centres, wage payment and food distribution for agricultural work. The majority oftrafficked girls and women are from the Dalit and Janajati community.Women with special needs: Women and girls with disabilities in Nepalese society experienceadditional discrimination because of their disabilities as they are exposed to greater risk ofphysical and sexual abuse, denial of reproductive rights and reduced opportunity to entermarriage and family life. Apart from birth affected disabilities, women and girls in Nepal alsobecome disabled due to discriminatory social and economic practices and issues of gender basedviolence. Service delivery programs largely ignore these social dimensions of disability.
3.3 Operational linkages between social structure, cultural norms and health service deliveryGender, caste and ethnicity -along with geographic location and distance from the seat of powerin Kathmandu - remain highly correlated with poverty and vulnerability in Nepal'8 . Availabledata demonstrates how the presence of several barriers (e.g. poverty, residence in a remote area(especially in the Mid and Far Westem Hills), being a girl, being from a Dalit or Janajati groupand being disabled) can lead to multiple exclusions and compounded disadvantage. Yetmembership in some sorts of excluded groups can actually help to reduce other forms ofexclusion. For example, Janajati children face a linguistic barrier and often suffer from lowenrolment and high drop out rates because of their unfamiliarity with Nepali as the medium ofinstruction. Yet districts with a high Janajati population are found to have a lower gender gap inliteracy. Conversely, although children from districts with a high proportion of Hindu Castepopulations (both high and low) who grow up speaking Nepali do not suffer linguisticdisadvantage, girls from these districts face the highest gender-based barriers. Those districtswhere the Hindu caste population is dominant (clustered in the mid and Far Western regions)also have the highest gap between male and female. (Refer to Annexes 11, 12 and 13 for geographicdistributions of ethnic groups and representations of barrier linkages in the Far West Region and Siraha district)
18 World Bank, 2004, Concept Note on Nepal Gender and Social Exclusion Assessment
15 VCDP Health June 2004 10/06/2004
3.4 Caste and ethnicity based social exclusionThe Dalits, as historically disadvantaged groups, lag behind in their income and asset levels, intheir education and other human development indicators - and in the extent to which they arerepresented in the power structure. There are 205 types of caste-based discrimination currentlypracticed against the Dalits that have been documented in a recent national survey. The nationalaverage Dalit literacy rate for 6 years and above is only 23 percent (12 percent for Dalit womenand 33 percent Dalit men) and only 30 percent of Dalit children go to school.'9The Dalit children outnumber other groups in the worst form of child labour prevalent in Nepalisociety. U5MR (Under 5 Children Mortality Rate) was 171.2 compared to 79 of the nationalaverage (per 1000 live births) in 1996 (NEsAc, 1998). IMR (Infant mortality rate) was 116.5(compared to 52.5 for Brahmin) per 1000 live births in 1996 (NESAC, 1998). Immunisationcoverage on Dalit children is 43 per cent, which is less by 20 per cent than the national average.Regarding the young age mortality, the child mortality was reported 15 out of 33 from the Dalits(TEAM Consult. 1999: Table A4.2a: 256).
3.4.1 Nepal's indigenous peoples
Various definitions2 0 on indigenous people exist (Cohen 1999. Gurung 2001). On basis of the NationalAcademy for the Upliftment of Indigenous People/ Nationalities Act, 2058 (2001) the law hasidentified 59 indigenous peoples, which may be changed after periodic review.Of the estimated 300 million indigenous peoples of the world, 8.27 million live in Nepal.Currently, there are 59 cultural groups identified as indigenous nationalities or Adibasi Janajatisby the government. The indigenous peoples possess distinct identities, cultures, languages,religions, histories, institutional structures (Human Rights Yearbook, 2004), health care practices,medication practices, utilization of specific shaman healers, worshiping, health seekingbehaviours with spiritual relationship to their land and with their unique customary laws,knowledge system, values and world views, the indigenous peoples from different societiesapart from those with rigid hierarchy of the Hindu caste system in Nepal.The discrimination and exclusion, which is often structural and systematic, based on theirethnicity, language or religion, has barred the indigenous peoples from exercising theirindividual and collective rights for non-discrimination, and to effective participation andcultural identity. The failure to observe civil and political as well as economic, social andcultural rights is a major concern for promoting an equitable, inclusive and peaceful society inNepal (Human Rights Yearbook, 2004). Of the estimated 300 million indigenous peoples of the world,8.27 million live in Nepal. Currently, there are 59 cultural groups identified as indigenousnationalities or Adibasi Janajatis by the govermnent. Discrimination and marginalization ofindigenous peoples represent a major threat to the rich diversity and democracy in contemporaryNepal. Janajatis are disadvantaged due to. Nepali, the 'language of the nation' is the only'official language', which is reportedly spoken as a mother tongue by 48.61 percent of the totalpopulation (CBS 2001) There are also large populations in the Terai who are not Janajati but whospeak Maithili, Hindi or other distinct languages as their mother tongue. If health serviceproviders are not conversant with the languages, access for Janajati people becomes constrained.Family poverty - especially among disadvantaged Janajati groups -leads children to seek workand exposes them to health risks.
Representatives of indigenous population groups consider language as one the most severeaccess barriers experienced by indigenous people in accessing basic health care, - even biggerthan barriers connected to economic and resource limitations. The language barrier is thereforeperceived as leading to significant under-utilization of public health services.
'9 Situational Analysis of Dalits in Nepal, 2002
20 Definition on indigenous peoples relies on the three variables: I) language, 2) self-perception, and 3) geographical concentration.These variables are used in different combinations and are given different priorities depending on the country under investigation.The definition has been applied in World Bank investigation on poverty among indigenous peoples of Latin America. (Cohen 1999)
16 VCDP Health June 2004 10/06/2004
Chepang: Chepangs, also known as 'Prajas' have depended on forests and forestproducts for food for generations. With decreasing natural resources, they arecaught in a vicious cycle of insufficient food, increasing poverty, chronic starvationleading to various types of illnesses.* Distance: Living high up on mountains, slopes, Chepangs are far from healthservice centres and other facilities. In Chit wan, they have to walk for sevenhours before they can reach a sub-health post or a school. The strainsometimes results in their contracting other illnesses, leading to morecomplications of arranging emergency funds. Disillusioned with the availableservices (no medicines, no health workers) most Chepangs today are unwillingto make the effort.* Language issues: Most health workers are not Chepangs making language ahuge barrier. In Chit wan, out of 20 teachers, only two (kept locally by theChepangs themselves) were Chepangs.* Discrimination: The humiliating language and the discriminatory behaviour ofthe health workers are additional barriers, forcing them to prefer their traditionalmethods. Women find it more difficult to access health centres because ofgender specific constraints.This state of starvation and ill health bears direct impact on children's education.Only when children are able to cope with staying hungry and walking long distance,which usually only be adolescents, can manage do they start aKtending schools.(Source: SNV: Can Orange Trees Blossom On A Barren Land, 1997; Interviews with SNV staff)
4. PROGRAMME COMPONENTSSelected initiatives of the Government and other agencies supporting the programmecomponents of NHSP-IP are reviewed from a social inclusion and gender perspective in thissection. The progranime components are linked to those included in the PAD and categorisedaccordingly.
4.1 Essential Health Care Services (EHCS)21
4.1.1 Family Planning
HMG/N's long term goal in famnily planning is to reduce fertility and under -five mortality.Programme strategies are (i) increasing demand for services through Behaviour ChangeCommunication (BCC); (ii) increasing access to integrated family planning and reproductivehealth services; (iii) improving care quality with counselling, infection prevention andmanagement of side effects and complications; and (iv) increasing access to condoms throughmultiple channels. DOHS's Family Health Division (FHD) implements the program.Challenges for social inclusion
Contraceptive Prevalence Rate2 2: Nepal continues to experience high levels of populationgrowth (2.27 per annum). Numbers of women of reproductive age is projected to increase upto71 percent (Nepal Health Profile on Women, Health and Development 2001, Planning andForeign Aid Division, DoHS/MoH) indicate the need for massive FP services in the future.
2 The Program will support the expansion and/or strengthening of eleven priority cost-effective services by: (i) developing andimplementing technical standards to improve service quality;(ii) providing in-service training to upgrade the technical skills ofabout field workers; (iii) ensuring drug availabilitv in health facilities by improved drug procurement and distribution; (iv)using behaviour change communication (BCC) to inform the public about services; to promote healthy behaviours; and topromote a client focused, gender-sensitive attitude among providers; (v) improving outreach activities especially in the Midand Far-Westem Regions; (vii) contracting NGOs for service deliverv in eight municipalities; and (viii) conducting ServiceDeliverv Surveys (SDS) to obtain client and provider experience of and perceptions about the quality and adequacy of healthservices(PAD, World Bank April 2004)22 CPR expresses the percentage of married women of reproductive age (MWRA) using any contraceptive device at any time
17 VCDP Health June 2004 10/06/2004
More men than women are well-informed about family planning methods due to men's accessto information and mobility being higher than women's across geographic, age, caste andethnicity diversity. However, contraceptive prevalence rate (CPR), which is a direct indicator ofpeople's conscious efforts to control fertility, is 38%23 in Nepal with forty-nine districts havingCPRs below the national average 24.Women have poor access to sexual and reproductive rights National studies indicate that despite92% men agreeing that contraception is not a woman's responsibility alone; almost 70% menbelieve that male sterilization is the same as being castrated (NDHS 2001). The most widely usedform of sterilization is female sterilization, which is 15% among currently married women whilemale sterilization is only 6%. Data reveals that only about 24% of men are among new FPacceptors. In fact Voluntary surgical contraception of men has increased in the MWR andFWDR, but has actually decreased nationally over the past three years as per the latest DoHSannual report. New acceptors of different spacing methods have decreased except for condomuse. Wide differences exist between districts in the range and quality of FP services provided(e.g. IUCDs and Norplant are available in 60 and 55 districts only).
Womens unmet need: There is a high unmet need25 with two in every three Nepalese womendemanding FP services but only three/fifths are receiving it. Approximately 35% of teenagers26have an unmet need for FP services , and the wanted fertility rate amongst adolescents is 2.5.These factors lead to unwanted pregnancies, sometimes leading to abortions, which untilrecently was illegal.Social exclusion impact on Total Fertility Rate:(1) A strong linkage between education and fertility has been clearly established. Whilewomen had a TFR of 4.8, women with some secondary education had a TFR of 2.3 (NDHS 2001).The total fertility rate27 estimated at 4.1 per woman is quite high. There are vast geographicaldisparities with urban TFR (at 2.1/woman) and rural (at 4.4/woman) and the TFR is the highestin the mountain- 4.8 births/woman.(2) The under-5-year mortality rates for children of uneducated mothers in Nepal is 121 per1000 births, 64 per cent higher than for children of mothers who have some primary educationand nearly double that of children of mothers who have some secondary education (DIIS 2002).Compared with children of mothers with SLC and above children of uneducated mothers have 8times higher risk of dying. Reducing one key social risk exposure - such as lack of education -might decrease the vulnerability of women to the effects of other health risks (WHO 1998, Ostlin et al2001). (Refer Annex 5, Figure 3for correlation between mother 's education and U5MR.)
Research has indicated that contrary to other population groups in Nepal, Dalit women have notexperienced any progress in indicators such as use of family planning devices, girls attendingschools and increases in life expectancy in recent years (Koirala 2002).Social norms: In Nepalese society women are often viewed as a biological means of humanreproduction. Various socio-cultural, socio-economic, religious cultural and political factorshave been influencing the women's health and relevant attitudes, traditions and behaviours(Rajbhandari et al., 1998). These factors are deeply rooted in our social structure, where women havesubordinate status resulting in low self-esteem. There is lack of knowledge among widepopulation groups, particularly rural women, about women's health concerns. Indigenousknowledge, technology, experience and plant resource of medicinal values have been graduallydisappearing and at the same time resorting to health facilities is very low in rural areas. Muslimwomen for example, face religious constraints in the use of FP services. Mobility constraints
23 NDHS 2001: The respondents in the NDHS survey were: Brahman/Chhettri/Newar: 31 %; Janajati: 24%; Occupational castes:21%, Muslim: 4.6; Rajbhanshi/Yadav/Ahir:10%; Others: 10%24 Differences between districts: Maximum: Kathmandu: 77.42%, Kalikot: 7.87%25 Unmet Need: Women who want to wait before another child but are not using any contraceptive are considered to have an unmetneed.26 Adolescent and Youth Reproductive Health in Nepal: Status, Issues, Policies, and Programs, Policy Project, 200327 TFR expresses the number of children a woman will bear by the end of her reproductive life under prevailing fertility conditions.(Annual Report 2002-03)
18 VCDP Health June 2004 10/06/2004
also hamper their access.2 8 Social realities in Nepal would constrain access to FP services for
unmarried women, especially girls.
Discussion within couples about contraceptive use is still uncommon due to women's poor
bargaining power. One in two married women has stated that their husbands alone have the final
say in the wife's health care (NDHS 2001). 16% of women, who have no say in household
decisions, are using a modern method of contraception compared to 42% women who actively
participate in household decisions. Use also varies with attitudes towards wife beating. 36
percent of women who believe that a man is not justified in wife beating are using modern FP
methods compared to 26 percent of women who believe otherwise. Thus women's status is
strongly linked to access to family planning services (NDHS 2001). Research by Engender health2 9
has indicated that while men take majority of the decisions, they are not informed decisions
because men are unaware of FP/RH issues. Due to unavailability of disaggregated data, the
specific issues of Dalits and Janajatis could not be identified. [Responses of government and other agencies
(Please refer to annex ... for examples)]
Gender, Caste and Ethnic issues: Various I/NGOs and projects are supporting the Family
Planning programme of HMG/N. But apart from SCF US, specific strategies or guidelines to
reach the socially excluded have not been adopted. While gender concerns have been addressed
to a certain extent, needs and interests of Dalits and Janajatis have not been consciously
recognized.
Female Community Health Volunteers (FCHVs) have become key delivery agents and many
activities are focused on increasing their skills. Most FCHVs are from families, which have a
more secure economic background than others in their community. Due to the work without
pay, some examples of FCHVs facing domestic violence from husbands and mothers-in-law
were found where the women were beaten for attending meetings 30 .
The overall caste ethnicity disaggregation of the 47000 FCHVs is unavailable but it is generally
recognized that most FCHVs are of Brahman/Chettri caste and very few are Dalits or
Janajatis31. Lower caste representation can be found only in areas with a high concentration of
lower caste people. Poor people were found to have more trust in FCHVs, and those who were
further from health facilities consulted them more often. People with education did not consult
FCHVs as they had better access to health services
4.1.2 Safer Motherhood
The FHD's National Safe Motherhood Plan (2002-2017) plans, over 15 years, the establishment
of basic and comprehensive emergency obstetric care (B/CEOC) in all 75 districts, skilled
attendance at all births and increased access to emergency fund and transport services. NHSP-IP
will establish CEOC in 10 hospitals, place midwives at the village level and improve basic
obstetric care with competency based training to outreach female providers.
Prioritised Health Service Achievers and Social Exclusion
Gender based inequality results in several additional constraints for women and girls that cause
maternal death and several illnesses. Women 15-44 years old experience a 26 percent higher
loss of DALYs than men in the same age group. Much of this excess loss is related to problems
related to pregnancy.
* Heavy workload: No rest during pregnancy and after childbirth.
* Deprivation: Inadequate food during pregnancy and after delivery; deprived of love and
care during pregnancy and during the adolescent period; deprive of education, health
28 Interviews with key informants29 Interview with project staff3 Matemal and Neonatal Health and HMG/N: A Study of the Concept of Volunteerism: Focus on Community Based Health
Volunteers in Selected Areas of Nepal, February 2003.
3' Interviews with key stakeholders
19 VCDP Health June 2004 10/06/2004
care, expression of feelings; lack of financial security; deprived of information due to
language.* Cultural Practices: food restrictions during pregnancy, lactation or post partum (certain
food restrictions during menstruation 48%, lactation 23% and post partum 43% is an
example)3 2 ; Chhaupadi (field observation)3 3 ; hazardous practices such as - practice of
making the women vomit forcefully in retention of placenta.
* Dropping out from school, child labour, gender discrimination, violence and abuses
including girl trafficking and prostitution.
Significant effects on women's reproductive health amongst women workers were identified,
including over bleeding, miscarriage, loss of reproductive capacity, high infant mortality, under
weight child, and disabled baby. The agriculture sector showed the highest effect followed by
the tea sector, mainly from over bleeding and miscarriage. 27.2 women workers have suffered
from over bleeding, 13.3 from loss of reproductive capacity, 20.3 from miscarriage, 13.4 from
under weight children, 13.3. from high infant mortality and 10.8 from disabled children.(Gefont/KAD Study Report on Women Worker issues, Searchfor Alternatives, 2003)
Heath seeking behavior is deeply influenced by caste and ethnicity with some traditional
practices providing treatment based on natural remedies and indigenous knowledge (see chart
below). The findings of a study in Baglung revealed that the Mangol and Dalit population as a
proportion of the total population in Baglung (29% and 25% respectively) are relatively higher
in comparison to the national proportion. However, their representation of the population using
caesarean section is disproportionately small (only 10% & 13% respectively). Conversely the
percentage of caesarean sections by the Brahmin, Chhetri and Newar is disproportionately high.(NSMP/DFID: Assessing the quality of Comprehensive Essential Obstetric care using an audit of the 100 Caesarean sections in
Baglung District - Pandit Upendra*; Clapham Susan). Refer to Annex 4 for table Women's Major Health
Problems in Rural Nepal and Effective Health Remedies
Challenges for social inclusion
Nepal has one of the highest maternal mortality rate in the world (539 per 100,000 women) and
neonatal mortality rate of 39/1000 live births. Around 50% infant mortality is due to deaths
during neonatal and perinatal periods. Delivery conducted by trained health personnel is 13%
only. Antenatal and post natal care is very limited (NHsp-Jp).
Nepalese women of reproductive age comprise 23% of the population. Women 15-44 years old
experience a 26 percent higher loss of DALYs3 4 than men in the same age group. Much of this
excess loss is directly related to pregnancy complications. 70% women are anaemic. 90%
deliveries take place at home, most deaths occurring at the community (79%) and 21% at the
health institution levels. Only 28% women receive care from doctor, nurse or midwife or ANM;
11% from health assistant, AHW; 3% from MCHV; 6% from VHW (NDHS 2001).
Abortion complication is a major problem and 20-27% of maternal deaths in the hospital are
due to complication of abortion (Maternity' Hospital, 1993). The Maternal Mortality and Morbidity
study in 1998 showed that in the community 5% of the deaths are due to abortion. 46% maternal
deaths are due to bleeding (NFHP).
Disparities based on geographic access and education have been documented e.g. 23 percent of
rural adolescents have begun childbearing as compared to 13 percent in urban areas for the same
age group (Nepal Demographic and Health Survey 20001). The number of pregnancies among women who
had attended school compared with those who had never attended school was 2.1 vs. 4.4 in
Achham district and 2.5 vs. 3.7 for Doti. (GTZ/UNFPA: Reproductive Morbidity - A Neglected Issue?)
32 Reproductive Morbidity a neglected issue? report of a clinic-based study in Far Westem Nepal, GTZ/IlNFPA, 2002, pp-2 3
33 Chhaupadi is the system in Far Westem region that menstruating women have to stay in a separate small room outside the house
or at the cowshed.3 DALY is a summary measure of population health, developed as a means of combining morbidity and mortality in a single index.
World Bank, World Development Report 1993
20 VCDP Health June 2004 10/06/2004
Social norms and practices have a profound effect women's health. Young mothers are forced to
follow food restrictions during critical periods, such as pregnancy, menstruation and lactation.
Practices like Chhaupadi goth (cowsheds where women are kept in isolation during childbirth and
menstruation) in the Mid and Far Westem Regions expose women to high risks of infection, mental
trauma and even increase sexual vulnerability (there have been many cases of rape reported)35 .
While largely undocumented, discriminatory behavior within communities and by health service
providers has been stated by women and men from different vulnerable groups and increase the
constraints faced by Dalits and Janajatis.
Significant gender specific effects on women's reproductive health were identified in a study on
women's work and occupational hazards. Women workers suffered from over-bleeding,
miscarriage, loss of reproductive capacity, high infant mortality, under weight and giving birth
to children with disability. The agriculture sector showed the highest effect followed by the tea
sector, mainly from over bleeding and miscarriage. Carpet and hotel show the highest % of
infant mortality; agriculture, tea and construction show the highest % of disabled children. In
the garbage sector, 66.7% women suffered from over -bleeding.
A review of Tharu and Magar obstetric practices3 6 revealed that there was only fragmented
documentation about birthing practices, decision-making, and sources of information, health
care-seeking beliefs and behaviour, and other related aspects of social organisation in many
ethnic groups in the different parts of Nepal. But considerable ethnic differences exist3 7, enough
to highlight the importance of understanding localised knowledge to the increasing access
component of the project. [Responsefrom Government and other agencies (Please refer to Annex 8for examples)]
4.1.3 Child Health
The DOHS's Child Health Division (CHD) implements child survival programs with priority
focus on ARI, Immunisation and Nutrition. The programme faces an enormous challenge of
reaching preventive and curative services to women and children.
CDD, ARI, Immunization, Nutrition are being integrated with the community based integrated
management of child illnesses (CB-IMCI). The ARI Control Programme covers 75 districts,
with 10 having the community-based IMCI.
Prioritised Health Service Achievers and Social Exclusion
Gender inequality affects girls throughout the life cycle. Female children are more likely to be
stunted (52% for girls, 49% for boys) or severely stunted than male children (24 for girls, 19 for
boys) due to neglect and less access to food, care and timely treatment. (NDHS, 2001). Children in
rural areas are more likely to be stunted i.e. 52% than those in urban areas: 37%, children in
mountain areas are more likely to be stunted (61%) (NDHS, 2001) 43.7 percent of adolescent girls
are currently married of which 23 percent of female adolescents in rural Nepal have begun
childbearing as compared to 13 percent in urban areas for the same age group and percentage of
adolescent mothers and pregnant mothers is highest in Terai as compared to hill and mountains.(Adolescent and Youth Reproductive Health in Nepal: Status, Issues. Policies, and Programs, Policy Prqject, 2003)Refer Annex 4
for tablefor Situation of Adolescents in Nepal.)
I Interviews with key informants and NGO field staff
36 NSMP: Obstetric Health Perspectives Of Magar And Tharu Communities: A Social Research Report To Inform The Nepal Safer
Motherhood Project's IEC Strategy, Mary Manadhar, 1999
A Needs Assessment conducted by Nepal Safe Motherhood Project
37 The role of the traditional healer (lamajhankri among Magars, and guruwas among Tharu) is central. Apart from the traditional
healers, the most common additional sources of help and information are the private medical shop, and the untrained
traditional birth attendant, rather than trained govemmental health service providers. Decision-making is characterized by
many different types of delay at all stages of the process, from the woman's first recognition of something abnormal to a
decision to her take to the hospital. Men generally showed little awareness of women's obstetric and menstrual problems,
but some, especially the younger men, did express an interest in leaming about it. For their part, women were largely
skeptical of any benefit of increasing knowledge of these issues among men. Some traditional systems that can operate to
organise and provide help in emergencies were found. (NSMP: Obstetric Health Perspectives Of Magar And Tharu
Communities: A Social Research Report To Inform The Nepal Safer Motherhood Project s IEC Strategy, Mary Manadhar,
1999)
21 VCDP Health June 2004 10/06/2004
Challenges for social inclusion
The highest risk groups are children under five, particularly girls, who account for 52.5 percent
of all female deaths. One in every 11 children born dies before reaching age five (NDHS 2001).
Although children under 5 years old represent only 16 percent of the population, they account
for over 50 percent of the total DALYs lost from all causes and 80 percent of the under-five
deaths are due to causes in Group I.
The statistics regarding children's health bear evidence to the double impact of poverty and
exclusion. One in two Nepalese children under five years is stunted; 10% wasted; 48%
underweight and 27% women fall below cut-off for body mass index. One-third children with
diarrhoea are not given any treatment at all and one in four children is taken to health facilities
for treatment of ARI symptoms (NDHS 2001). Evidence suggests that only 60% of children aged
12-23 months are fully vaccinated (2002)38. Cases of respiratory infection and diarrhoeal
diseases are found to confront people from all age groups. Only in four children is taken to the
health facility for treatment of ARI symptoms (NDHS 2001).
More than 50% of children suffer chronic malnutrition and stunting, forever crippling their
potential for growth, development and productivity.3 9 . The proportion of malnourished children
is 14% in Nepal, with the highest in the FWR at 16.4%. Prevalence of anaemia among the
preschool children was higher (78%) and the highest was among the infant age 6-11 months
(90%) (DHS Annual Report 2001-2002). One in four Nepali women suffers from malnutrition.
Girl children under five face violent assaults more than twice as many than boy children. A very
significant proportion of the children who run away from home are actually escaping violence
and brutality at home (Gerison, 2003). Of 200,000 women trafficked: 20% girls below 18 years;
Age group most vulnerable for trafficking4 0 is 11-18 for girls and 6-12 for boys. A higher
number of girl children, mostly ex-Kamaiya Tharu girls, work as domestic servants. 43 percent
of women convicted for infanticide 41 were adolescents.
The limited data that is available about Dalit children reveals that U5MR was 171.2 compared
to 79 of the national average (per 1000 live births) in 1996 (NESAC, 1998) and IMR was 116.5
(compared to 52.5 for Brahmin) per 1000 live births in 1996 (NESAC, 1998). The immunization
coverage on Dalit children is a mere 43 per cent, which is less by approximately 20 per cent
than the national average.
In a study on Dalits in Siraha, 20 cases of disabilities were found out of the sample population
of Dalits in Siraha whom 16 were male and 4 were female. The 'Chamars' seemed to have the
highest instances of disability followed by Danuwars and Teli/Sudi and Musahars.
Over the period of five years, there were 52 deaths cases of whom 15 were reported to be
children. The highest number of cases of children's death was found to be among Musahar caste
groups. The Muslims, Musahars and Chamars comprised the largest proportion of those who did
not take vaccines due to lack of immunisation. the instances if not taking TT among the
untouchable castes group. Dalit children outnumber all other groups in the worst form of child
labour prevalent in Nepal (Situational Analysis of Dalits). The caste/ethnicity of child labourers in thecarpet sector is highest of Tamangs with 34 percent boys and 24 percent girls. Though these
children (of 14-16 age groups) work for an average of 15 hours a day, their earnings are
controlled by relatives. And this is more so for girls (36.1 %) than for boys (22.2%) (Child Labourers
ILO)
According to field information, there are several components of the EPI programme that are
currently dysfunctional throughout the country. Some of the difficulties can be attributed to the
conflict in a direct or indirect way, but some others are due to dire and chronic lack of
3 The reported coverage of different antigens at the national level was 94% for BCG, 80.3% for oral polio vaccine (OPV3), 80.3%
for diphtheria, pertussis and tetanus (DPT3) and 75.6% for measles during the last year (Annual Report)
39 Nepal Micronutrient Survey, 1998.4' (UNNIFEM/IIDS: Status and dimensions of trafficking within Nepalese context, 2004)
41 Forum for Women, Law and Development (FWLD); Laws of Nepal have classified many abortion cases as "infanticide" and this
"crime" carries heavy criminal penalties
22 VCDP Health June 2004 10/06/2004
maintenance of equipment or to local decisions based on personal interest. Dissolution of thelocally elected bodies resulted in reduced funds and inadequate coordination as VDC funds,leaders and members were the key for the coordination of volunteers as well as for the provisionof information to the community and of food and shelter for the EPI teams in hilly and
mountainous districts. (Martinez and Koirala) [Responsefrom Government and other agencies (Please refer ta annex ... for
examples)]
4.1.4 Communicable disease control
Tuberculosis and Leprosy has impacted poor households, more and within these, girls and
women are worse off.
Prevention and Control of HIV/AIDS/STI: Strategies include: (i) preventing STIs and HIV
among the high-risk groups; (ii) ensuring safe blood supply; (iii) preventing infections amongthe young; (iv) ensuring care and support for persons infected and affected by HIV/AIDS; (v)
improved monitoring and evaluation; and (v) establishing an effective management system.
Challenges for social inclusion
There are 60,000 people suffering from HIV/AIDS in Nepal of whom 26% are women. 2400
AIDS related deaths have been recorded. Amongst the high-risk group, 40% are migrantlabour4 2 , and 18% are clients of sex-workers. Knowledge of preventive measures was found
lowest amongst Dalits and Tharu migrants and their wives. Ethnicity, education and marital
status were found to be significantly associated with sexual behaviour 4 3 and vulnerability to
HIV AIDS.
Girl child workers suffer sexual harassment which puts them at an increased risk of HIV
infection (CWJN 2000). Women and girls vulnerability is four times greater than that of men and
boys. 64 men, 143 women were HIV affected in the age group 14-19 years, in 2000 (NCASC).
17.3% prevalence of HIV among female sex workers in the Kathmandu Valley 62% of femalesex workers range between 20-29 years in age.4 4; Males make the decision to use condoms
HIV/AlDS prevalence consistently exceeds 5% in one or more sub-groups (Source: NHSP - IP, 2003).
Nepal's epidemic is beginning to show signs that it may be on the verge of becoming
generalized in some communities, especially among those in the Far-Western 45 and Western
regions of Nepal where heavy migration to India occurs. Stigmatization and discrimination of
those infected with HIV have become commonplace - and acceptable. PLWHA have limited
access to care and support services, treatment, and opportunities to create sustainable livelihoodand to participate in decision-making regarding the HIV response.
STI and Gender dimensions: Women are still stigmatised with regard to STI treatment and
care. Almost all health workers, FCHVs and peer educators stated that many of the men, mostly
those from elite and educated groups, are unwilling to support their wives in the treatment of
STIs. It was observed that partner treatment for the ML group was particularly difficult, sincethe men live in India for more than six months in a year (SC, STI Prevalence Study: 2001) and
are thus also hard-to-reach for project interventions.. The vulnerability of MLWs has been
fuelled by economic and social subordination and limited access to information and education.
In a study covering 141 migrant labour, 37.6% were found to be Dalits. Enhanced Supportfor HIV Prevention in Nepal
Programme Phase II (Oct 1999 -Sept. 2002) Final Survey Report, Submitted to: Save the Children US By Deve opment
Resource Centre (DRC) October 2002. Thefield work was in Kailali. Bardiva, Kanchanpur, Banke, Dang
43 With higher levels of education there was an increase in high-risk sexual behaviour such as MSM, oral and anal sex. Respondents
who were educated to grades 1-5 were the most risk indulgent group followed by respondents who had education of more
than grade 10. Unmarried respondents were more likely to indulge in high-risk sexual behaviour. In particular MSM and
oral sex is significantly higher among unmarried respondents. The men having sex with men (MSM) behaviour was higher
among the Newars, Tharus, Gurung and Magars and least among Dalits. Enhanced Support for HIV Prevention in Nepal
Programme Phase 11 (Oct 1999 - Sept. 2002) Final Survey Report; Submitted to: Save the Children US By Deve opment
Resource Centre (DRC) October 200244 Enhanced Support for HIV Prevention in Nepal Programme Phase II (Oct 1999 -Sept. 2002) Final Survey Report, Submitted to:
Save the Children US By Deve opment Resource Centre (DRC) October 2002
45 Among migrants in the Far-West, a recent JICA study in Doti district found 10% of men who had migrated to Mumbai were HIV
positive.
23 VCDP Health June 2004 10/06/2004
It is harder for them to afford the cost of STI treatment, which is, on average, Rs5OO to Rs800,
and some have had to borrow money for the purpose. In addition women are looked down upon
if they are known to suffer from such diseases as STI. Because of the social stigma and fear of
the apprehension of their husbands, MLWs do not like to keep a stock of condoms in theirhouse. A few of the MLWs noted that it creates mistrust between husband and wife, and
breaches the relationship, if the husband finds his wife is keeping condoms when he returns
home. It is the males who make the decision to use condom during sexual intercourse. The
males thought that talking about condom and sexual health is not necessary because they were
having sex with their wives. [Responsefrom Government and other agencies: (Please refer to annex ... for examples)]
4.1.5 Strengthened Outpatient Services
Strategies are (i) expanding the Community Drug Programme (CDP); allowing public facilities
to charge for drugs to have these in stock; (iii) switching to a "pull" system of drug ordering and
local purchasing under central price negotiation; and (iv) improving staff motivation by
decentralizing some personnel functions. MOH will promote rational drug use; implement
standard treatment schedules and essential drug lists through training, monitoring and
supervision; and ensure essential infrastructure, repair and maintenance.
The existing situation: Hospital use data indicates that women access hospital services far less
than men. Even for women above 70 the use of public hospitals is far less than that of a man
(Male: 8; Women: 5).
4.2 Decentralisation46
His Majesty's Government has introduced one of the world's most progressive legislation for
decentralization in the world devolving primary responsibility for local development to elected
local authorities. The Local Self-Governance Act (LSGA) has given authority to the local
bodies (VDC, Municipality and DDC) to operate and manage health centres, health posts and
sub health posts, primary health care services, perform public health related works including
toilet construction, protection of water sources, family planning and maternity and child care
services. The LSGA has emphasized priority areas of the local bodies to "enhance the living
standards, income and employment of, and render direct benefits to, the village people andcontribute to poverty alleviation ". It has directed the bodies to allocate funds earned from their
sources in the health sector on a priority basis. (A Manual Preparedfor Transfer and Operation of Local Health
Institutions 2060 (2004) His Majesty's Government, Ministry Of Health, Department of Health Services).
Government policy with regard to health is consistent with the decentralised and participatory process
of decision making and inplementation, and hence in keeping with the LSGA. However, in
implementation, there is lack of clarity as to the functions and responsibilities of government health
agencies and local bodies. The problem is compounded by gaps in the provisions of the LSGA and the
way health services are currently administered by the public sector agencies. 47
While the LSGA mandates local government bodies to manage and supervise S/HP and their
functioning, local committees and VDC and bodies like HMC should control resources and
management of S/HP. Another discrepancy is the allocation of responsibilities without any
provision for the required resources. These differences in rules and regulations between LSGA,
46 Greater local authority and responsibility over service provision (IDA, GTZ, DflD, SDC): The Program will support capacity
building for the decentralized management of health services. By the conclusion of the five year Program, responsibility
and authority over health posts and sub-health posts throughout the country will be handed over to Local Bodies (i.e., local
government structures). The program will articulate roles and functions of the Local Bodies in the health sector and provide
training in leadership, setting local priorities in health, personnel management, performance appraisal, planning, budgeting,
financial accounting and controls. MOH officials at all levels will receive orientation and guidance regarding their roles in
supporting Local Bodies (Project Appraisal Document, World Bank,April 2004)
4 The World Bank Study on Local Organisations: Roles and Relationships, Review of the Health Sector, National Labour
Academy, Nepal
24 VCDP Health June 2004 10/06/2004
10th Plan and MoH guidelines and the role of local bodies (VDCs and DDCs) are a majorconcern for enhanced community ownership of S/HPs.
The 'Health Sector Reform Strategy: An Agenda for Change' authorizes local bodies to be"responsible and capable of managing health facilities in a participative, accountable andtransparent way with effective support from the MoH and its sector partners" (MoH 2002). TheHSRS recognizes that management of health facilities requires transfer not only of budgets butalso of responsibilities for planning and implementation of health service development withinthe districts and has implications for a new relationship between the Ministry, DDCs and VDCs.Indicators of progress have also been identified.
Current progress in implementation of decentralization has been the following: (Joint Review of the
Nepal Health Sector Programme - Implementation Plan, 15-26 March 2004)
Hospital Autonomy: Hospital Development Boards have been formed for all governmenthospitals above the district level. This has recently been extended to 12 district hospitals. Inaddition to grants from MOH, Hospital Development Boards have to generate there ownresources to recover some portion of the recurrent cost through user charges. According toPublic Expenditure Review of the Health Sector (2003) financial cost recovery rate variesconsiderably, but on average the zonal hospitals recover around a third of the total costs. Inaddition to resource general function, Hospital Development Boards have the responsibility to:
. oversee the day-to-day running of the hospital,* undertake assessment and subsidy for those unable to pay,* ensure smooth functioning of the hospital, and* hire staff.
Sub-health post handover: Since 2002 the MOH has handed over responsibility for themanagement of 922 sub health posts to communities. According to the Guidelines developed by theMinistry of Health for orientation of Health Committees, handover has two broad objectives, i.e.:
* To ensure quick, timely and effective health services in the local level by ensuringtransparency and good governance, and
* To mobilize the available local resources to its possible extent.
Currently Village Development Committees receive central government grant of which 25% areearmarked for social services including health. In addition, VDCs can generate additionalresources to cover the services. No extra central government funds accompany the newarrangements under SHP handover. While the committees have the responsibilities to overseeand monitor the functioning of health staff, they have no responsibility for their hiring andfiring, which remains under the MOH.
The chair of the SHP health committee is the VDC chairman when in post. In the currentclimate the chairman is the VDC secretary. The guidelines state that the committee must havefour women as members and two candidates have to represent the dalit/Janajati community(with one being a woman). The SHP Management Guidelines outline the functions of theSHPMC but no role or responsibility to address gender and social inclusion concerns arestated. The functions are stated in a neutral manner, based on the assumption that services willreach all the members of the community. Experience has indicated that unless directives areestablished, access of Dalits and Janajatis remains limited (Refer Annex 9 for a detailed review of the Local
Institution Health Operation and Management Committee).
A report of Sub-Health Post Decentralisation Process Review pointed out that the MOH'sresponsibilities should not end with the mere handover of local health facilities to localcommunities and giving orientation to its committee members, but continue to provide support,guidelines, build their capacity and monitor their performance. But feedback from informantshas been that the handing over is as yet not effective as the required financial and humanresources have not been transferred.
Decentralisation and EDPs: Decentralisation presents a major challenge to the process of aidcoordination, hannonisation, and sector wide programming, partly because of the absence of
25 VCDP Health June 2004 10/06/2004
detail , but also because many EDPs have a strong presence at district level. However neither
the draft harmonisation paper, nor the NHSP-IP addresses how EDPs are to engage with
government at the different levels. On the one hand there is the need to for EDPs to engage at
central level to promote decentralisation plus all the other reforms, and to engage in sector
dialogue. On the other hand there is the reality of a strong EDP presence at district level
engaged with capacity building for planning and other interventions which necessitates
discussions between local authorities and EDPs about their current and future support. It is not
clear at this stage how this issue can be addressed, but considerable thought needs to be given to
it to ensure that EDPs do not just relocate their highly project focussed debate from the centre to
the districts. This will then need to be reflected in a revised Code of Conduct or Memorandum
of Understanding between MoH and EDPs.
The social issues which affect decentralization include:. High level of poverty and its impact on health needs;. low per capita funding for health care;. relatively limited role of the private health care sector;. problematic allocation of resources in the health sector in the existing
epidemiological and demographic profile;. poor technical efficiency of the government health sector; inequality of the
system particularly in the urban/rural and rich/poor relationship;. ethnic composition of the country and the regional and federal aspirations of
some political groupings;. domination by local elites. existence of an important network of self-help groups
4.3 Public Private Partnerships48
Private sector contributes to about 76% of the total health expenditure (NHSP-IP). This sector
and NGOs already make an important contribution to health provision in Nepal. Various
agreements and operating modalities exist between MoH and NGOs and private providers, and
in many cases these are vital for supporting EHCS programmes and directly providing curative
care that cannot be covered by public expenditure. HMG/N has rightly identified the potential
for developing this contribution further. The HSS states that the 'public sector will develop a
major new role in working with the private / NGO sector', and identifies four areas where this
will operate:
1) sustainable financing2) providing an integrated approach to delivery EHCS;
3) quality assurance by government; and4) pharmaceuticals, other consumables and new technology.
The joint review of the NHSP -IP has carried out an in- depth review of the Public Private
Partnership. Detailed recommendations for addressing the future challenges to improve Public
Private Partnership are presented in Annex-10.
Social Protection Measures for Health
Nepal's middle-income group and the mainly urban, formal economy workforce have been the
beneficiaries of existing social security provisions (e.g. provident fund, maternity leave, medical
care). At present, the formal social security systems (provident fund and citizen's investment
fund) cover mainly civil servants, army, police, and teachers. In total, about 400,000government officials are covered. The Government is the single largest employer in the country.
48 The MOH will appoint a focal point for PPP. The Program will support the development of guidelines, contract standards and
regulatory frameworks, and provide training. New service provider agreements/contracts will be defined with NGOs and
the private sector. Large district/zonal hospitals will be made autonomous, and NGOs/private sector will be contracted to
manage others (Project Appraisal Document, World Bank, April 2004)
26 VCDP Health June 2004 10/06/2004
Any private enterprise with more than 10 employees can join the provident fund on a voluntary
basis. All enterprises can join the retirement plan under the citizen's investment fund. However,
there is no mandatory social insurance provision for the private sector.
The Labor Act and regulations provide some special rights for women workers, who are legally
entitled to equal pay for similar jobs, maternity leave, breast feeding time and creche facilities.But women have to be on a permanent pay roll, which is often not the case. There is norecognition that the poor, caste and ethnic disadvantaged require specific provisions.
Government, employers' organizations, trade unions, community groups and women'scooperatives as well as families, caste based and occupation based groups and communities are
implementing different social protection schemes. Apart from the formal sector social securityprovisions, there are various informal, partly traditional, community-based insurance
arrangements (micro-insurance). (For details on impact on vulnerable communities, see Annex 8 on social protection).
5. INSTITUTIONAL FRAMEWORK AND CAPACITY BUILDING
One of the tasks of a successful Vulnerable Community Development Plan is to identify the
institution or institutions who should and can take responsibility for implementing the
suggestions contained in this report. In many developing countries, government institutionsassigned the responsibility of supporting disadvantaged groups are weak and thus unable toprovide the level of engagement, which vulnerable people deserve. Assessing the track record
and capabilities of these institutions is fundamental to assessing what they can deliver both in
terms of the availability of funds for investments and field operations, the adequacy of
experienced and trained professional staff, the ability of vulnerable peoples' own organisations,local administration authorities and NGOs interacting with government institutions and
stakeholders groups, and the ability of the executing agency or agencies to mobilise other units
to successfully implement the NHSP-IP vision and the recommendations contained within this
Vulnerable Community Development Plan.
5.1 Institutional capacity of the State
The following institutions should be involved in the successful implementation of the NHSP-IP vision
and the recommendations contained within this Vulnerable Community Development Plan. Theirspecific tasks will involve the development of a working system and skilled and motivated staff to
support social inclusion in primary health centres throughout the nation. More than rles, a shift in
attitudes and behaviour are called for to bring social transfornation in health centres.
5.1.1 Ministry of Health (MoH)
With the lead responsibility from the government to manage and oversee the national health
service program, the Ministry of Health (MoH) is best positioned to take the leading role in the
successful implementation of NHSP-IP and the recommendations of this VCDP. With
numerous departments and sections, a large human resource and skilled employees as well as
ongoing donor support, the Ministry has the potential to galvanise interest and support across a
wide range of institutions in government. In order to effectively implement the Vulnerable
Community Development Plan, it will be necessary to establish:
(1) policy directives for increased social diversity in staff;(2) capacity building for improved attitude behaviour and skills towards woman, Janajati and dalits;
(3) more effective partnerships with NGOs for improved responsiveness to vulnerable
communities and their social exclusion from health services
5.1.2 Department of Health Services (DoHS)
The department has the primary responsibility for delivery of all the national health service
programs. It comprises of five divisions, three centres and two sections and has full
27 VCDP Health June 2004 10/06/2004
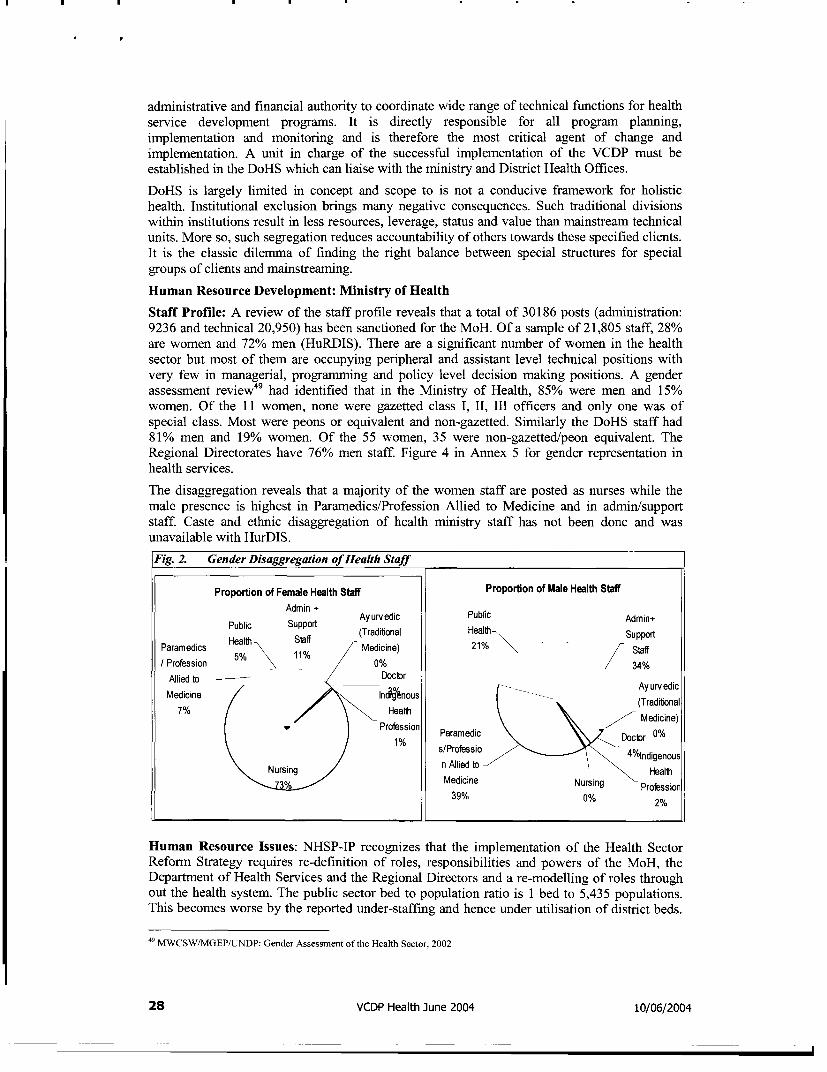
administrative and financial authority to coordinate wide range of technical functions for healthservice development programs. It is directly responsible for all program planning,implementation and monitoring and is therefore the most critical agent of change andimplementation. A unit in charge of the successful implementation of the VCDP must beestablished in the DoHS which can liaise with the ministry and District Health Offices.
DoHS is largely limited in concept and scope to is not a conducive framework for holistichealth. Institutional exclusion brings many negative consequences. Such traditional divisionswithin institutions result in less resources, leverage, status and value than mainstream technicalunits. More so, such segregation reduces accountability of others towards these specified clients.
It is the classic dilemma of finding the right balance between special structures for special
groups of clients and mainstreaming.
Human Resource Development: Ministry of Health
Staff Profile: A review of the staff profile reveals that a total of 30186 posts (administration:9236 and technical 20,950) has been sanctioned for the MoH. Of a sample of 21,805 staff, 28%are women and 72% men (HuRDIS). There are a significant number of women in the healthsector but most of them are occupying peripheral and assistant level technical positions withvery few in managerial, programming and policy level decision making positions. A genderassessment review4 9 had identified that in the Ministry of Health, 85% were men and 15%women. Of the 11 women, none were gazetted class I, II, III officers and only one was ofspecial class. Most were peons or equivalent and non-gazetted. Similarly the DoHS staff had81% men and 19% women. Of the 55 women, 35 were non-gazetted/peon equivalent. TheRegional Directorates have 76% men staff. Figure 4 in Annex 5 for gender representation inhealth services.
The disaggregation reveals that a majority of the women staff are posted as nurses while the
male presence is highest in Paramedics/Profession Allied to Medicine and in admin/supportstaff. Caste and ethnic disaggregation of health ministry staff has not been done and wasunavailable with HurDIS.
Fig. 2. Gender Disaggregation of Health Staff
Proportion of Female Health Staff Proportion of Male Health Staff
Admin + Ayurvedic Public Admin+Public Support (Tradibonal Health Support
Paramedics Health S1 Medicine) 21% Staff
/ Profession 5% 11% 0% 34%
Allied to g Doctor
Medicine IndVgnous (Traditonal
7% Health Medicine)
Profession Paramedic Doctor 0%
s/Professio 4%lndigenous
Nursing n Allied to Health
Medicine Nursing Profession.39% NuOr°s/ln90% 2%
Human Resource Issues: NHSP-IP recognizes that the implementation of the Health SectorReform Strategy requires re-definition of roles, responsibilities and powers of the MoH, theDepartment of Health Services and the Regional Directors and a re-modelling of roles throughout the health system. The public sector bed to population ratio is I bed to 5,435 populations.This becomes worse by the reported under-staffing and hence under utilisation of district beds.
49 MWCSW/MGEP/UNDP: Gender Assessment of the Health Sector, 2002
28 VCDP Health June 2004 10/06/2004
Staff vacancies and absenteeism are widespread - only 60% of sanctioned posts are filled. Thetotal number of staff in proportion to the population is extremely low.
A Strategic Plan for Human Resources for Health has been prepared by MoH covering theperiod 2003-2017. This introduces new policies and operational mechanisms to improve theability of the Ministry to manage systematically the deployment, utilisation, development andcareers of its staff50. The overall distribution of staff in terms of the mix of skills shows adeficiency in the middle technical grades. There is currently a large number of unskilled staffsupport (35% of the total work force). These unskilled staff along with other low level staffmakes up 70% of the workforce. (Strategic Plan for Human Resources for Health)
The MoH has started recently upgrading MCH workers by providing ANM scholarship in 500VDCs and plans to place ANMs in all VDCs. The fact that MCHWs are being upgraded toANMs leading to a decrease in support staff from 70% to 45% and an increase in the mid-levelfrom 18% to 38% is a positive shift. The issue here is of representation of Dalits and Janajatis asit can be assumed that MCHWs5 ' are mainly from the dominant castes. The shift from 12% to
17% in the high-level staff also raises the issues of gender and social inclusion as representationof women is minimal at the higher levels.
The strategic plan identifies the need to produce more graduate nurses. While a caste/ethnicityprofile of the nurse students was unavailable 52 , a micro-survey of four Medical Colleges inKathmandu reveals that out of a total of 758 students for MBBS, only five were Dalits (see Annex 4
table 7for details).
The Institute of Medicine has started its own undergraduate programme to prepare medicalgraduates who will have the skill, knowledge and attitude to work in Nepal's varyingenvironments. Stronger emphasis has been placed on community medicine.
It is estimated that 47,949 medical staff will be recruited between 2003 and 201753. Of these the
highest number is that of ANMs, followed by certificate/staff nurses. This can be used as anopportunity for recruiting representatives from the dalit and Janajati groups, increasing the
diversity of the staff profile.
The staffing proposals for health posts and sub-health posts reveal that a nurse and an ANM willbe added to HP. In sub-health posts, one MCHW will be upgraded to ANM, an additionalMCHW will be added along-with one support staff, taking the total number of service providersat the sub-health post to 6. This again can provide the space for inclusion of Dalits and Janajatisso that issues of caste and language are addressed.
This Strategic Plan for Human Resources has not identified any policy or strategies for increaseof women in decision making positions, when data indicates that there are very few in thegazetted class in higher positions. There appears to be no recognition of the need to adopt
alternative strategies to recruit and retain staff from dalit and Janajati caste/ethnic groups. Theprojected staff requirements do not include measures for caste and ethnic disadvantaged group'sinclusion or address gender issues.
Retention of core health staff - especially women - at the level of health facilities due to lack ofmotivation is a major concern. Most of the time, health workers are absent in the health postsand sub-health posts, limiting the availability of critical safe motherhood and reproductivehealth related services. Only peons and clerks are available to provide services, which furtherconstrains of women as they are reluctant to consult male health workers especially when a
gynecological examination is required. (World Bank: Understanding Access, Demand and Utilisation of Health
Services in Nepal and their Constraints, June 2001)
50 Policy Paper on Health Sector Development of His Majesty's Government of Nepal, Nepal Development Forum- 2004, Pre
Consultation Meeting, Presented by Ministry of Health, HMG/Nepal, February 2004.
SI Since disaggregated data is unavailable, this is based on informant opinions.52 The Lalitpur Nursing Campus was unable to provide the details of the students profile due to intemal regulations.
'3 MoH: Strategic Plan for Human Resources for Health 2003-2017
29 VCDP Health June 2004 10/06/2004
5.1.2.1 District Health Office (DHO): DHO is responsible for planning the delivery andmanagement of all national programs on education at the district level. Potential goals include:the handing over of public health service centres to the community and the coordination andcooperation with traditional health centres. All DHOs are overstretched and are constantlychallenged with far too may targets to complete. Social accountability will be close toimpossible for DHOs without technical support from civil society groups. DoHS needs to dotwo actions to enable this. First, provide directives on the 'how to' for setting up agreementswith NGOs/local groups. Second, facilitate workshops with NGO/local partners to discussmodalities and create a culture for effective partnership.
5.1.2.2 Sub Health Post Management Committees (SHPMCs): With the meaningfulinvolvement of parents of women, Dalits and Janajatis of vulnerable groups, Sub Health PostManagement Committees (SHPMCs) and local conmmunities should be given responsibility inactual practice of managing the health centres and the health service it provides at the locallevel. The Rules and Regulations for SHPMCs do not provide sufficient practical guidelines forenhancing SHPMCs to address social inclusion. Without capacity building on these socialfactors, SHPMCs will face difficulty in making the strategic shift as the lead body for
addressing social inclusion in primary health centres.
FCHVs and TBAs: The 47,873 Female Health Volunteers 54 (FCHVs) and 12,682 TraditionalBirth Attendants5 5 (TBAs), being unpaid volunteers are not part of the Health Ministry staff. Atthe bottom of the service provider hierarchy and closest to the community, it is on them that
many health programs rely for service delivery. FCHVs are increasingly the entry point formany lINGO supported initiatives and have been acknowledged as the prime contributors forthe success of programmes such as Vitamin A distribution. There is an ongoing debate about theuse of women as volunteers since it reinforces the belief that women are secondary earners andhave the "time" to volunteer. While one recent study56 indicates that FCHVs claim they arehappy doing "dharma", their need to eam and the lack of remuneration has often been cited as a
major de-motivating factor (see box belowfor details).
There is an ongoing discussion about the voluntary status of the FCHVs with one argumentstating that it is better to be an unpaid volunteer than to be the poorly paid lowest member of thestaff 67 . The Ministry made the policy decision early in the programme not to make them part ofthe staff due to lack of funds for sustained remuneration of such large numbers.
5.1.3 National Health Education, Information, Communication (Acting)
The NHEICC plans, implements and reviews the Health Education Programme, the FamilyHealth Programme, the Control of Diarrhoeal Diseases/ Acute Respiratory Infection
Programme, and the Health Literature and Library Information System. The main activitiescarried out by this centre are: (a) Production and distribution of printed materials; (b)Presentation of regular weekly and periodic audio-visual programmes; (c) Dissemination ofhealth messages through mass media, mobile video shows and cinema slide shows; (d)Facilitation of seminars/workshops. The centre coordinates with other GOs and I/NGOs tosupport district and central level IEC programmnes. It would have a lead role in developingmaterials in all languages of the nation for Janajati population to be less excluded.
5.1.4 National Centrefor AIDS and STD Control (NCASC)
This centre could critical role in coordinating the establishment of community based adolescentand youth centres for reproductive health and sexual rights and peer support. This centre couldalso coordinate with development of life skill based package for training of peer educators.
5 Refer above and the annex for more details5 The TBA programme has been phased out from this year.5 Maternal and Neonatal Health and HMG/N: A Study of the Concept of Volunteerism: Focus on Community Based Health
Volunteers in Selected Areas of Nepal, February 20035 Interviews with key informants
30 VCDP Health June 2004 10/06/2004
5.1.5 National Health Training Centre (NHTC)
HRD has been a core part of health services delivery programme and the revision of MoHservices structure in 1993 brought the institutional leadership in HR training. NHTC manages atraining network of regional and district training centres and in addition works closely withI/NGO , private sector and donors to provide technical training to health officials at differentlevels. Numerous types of trainings are organised by NHTC in 2002/03 a total of 7,741 healthstaff were trained achieving 94% of the target at the central level. At the district level as wellover 80,000 FCHVs received training. The cumulative target over the 9h Five year Plan,average target of 75,000 health workers was achieved. A quick review of the central leveltraining programme in 2002/03 indicates a very strong focus on bio medical information andpractically no inclusion on the social dimensions of health. To address social exclusion it wouldbe essential for service providers at all levels to have conceptual clarity on gender and socialinclusion and the socio-cultural dimensions of health. The NHTC and the district traininginstitutions would need first capacity building themselves before they can facilitate effectivepartnerships with NGOs for introducing training for field service providers on gender -socialinclusion and health.
Budget Review of Health Sector Finances: The planned allocations for MoH over the nexttwo years of the Medium Term Expenditure Framework (MTEF), through 2005/06, areexpected to increase to 5.5 percent by 2005/06. This suggests a strong governmentalcommitment to health, as there has been a sharp increase in security and defence budgets,leaving the govemment with little funds. (Refer to Annex 6 for details on Health ExpenditureBudget)
The previous trend has been of the regular budget of HMG being fully spent, but thegovernment and donor development budget remaining heavily under utilized, with theutilization rate of donor fund decreasing from 61% to 27% over the period from 1999 to 2002(HEFU, pg 8). This is mainly due to the low absorptive capacity of the government and thedifferent budget release rules of the EDPs. The proportion of government recurrent funding hasincreased. Much of the increase (77%) has been used to finance wages which have increasedfrom 48 to 55%. Trends suggest a decreasing share of funding going to rural areas. Theybenefit from only 50% of the spending.
MOH expenditure on secondary and tertiary care facilities increased from 14.6 percent of thehealth budget in 1991/92 to 37.5 percent in 1997/98 while the share of spending on primary caredecreased from 76.8 percent to 57.25 percent over the same period. In addition, the portion orresources spent on hospital construction over the last five years has increased three timesfrom 3% to 11% (Maskay et al 2002, NHEA 2002). These tendencies indicate an urban vis-ai-vis ruralresource allocation bias58. Since the most disadvantaged populations live in the rural areas thisurban/rural allocation bias indicates a de facto policy which contradicts the stated politicalcommitment to primary care since initiation of the National Health Policy of 1991. (SocialAssessment of the Nepal Health Sector Reform Submitted to World Bank, Nepal Office (draft
130503) Nielsen et al)
Despite the fact that Nepal spends 5 percent of its GDP on health, most of Nepal's expenditurescome from private out-of-pocket contributions, which in 2000 accounted for approximately 70percent of total health expenditures. This, as the NHSP-IP recognizes, constrains the poor anddisadvantaged from accessing health services as they are less capable of private out-of-pocketcontributions.
58 This needs to be evaluated more in detail since there has been an increase in expenditures to district and below health services (as
a proxy for Essential Health Care Program) which can be seen as a compensation for the indicated recent tendency of urban
bias. But dominance in power structure on the basis caste hierarchy is one potential explanation for the discrepancybetween enunciated policy and actual performance. All but 8.8% of the individuals occupying the top political, bureaucratic
and executive positions in Nepal in 1999 are recruited from high caste Hindu groups (92.2%) (Gurung 2002). People withIP and Dalit identity held respectively 8.4% and 0.3% of total top positions with potential influence on policy enunciation.
Political marginalisation of IPs and Dalits is based on social discrimination and is therefore considered a main reason why
these groups are deprived of economic, educational and overall social well-being (Gurung 2002)
31 VCDP Health June 2004 10/06/2004
Approximately 14 percent of total health expenditures in Nepal are channelled through theMinistry of Health and an additional three percent is spent by other ministries (e.g., MoF, MLD,
and MoE), autonomous bodies (e.g., universities) and local bodies (DDC, VDC andmunicipalities). Direct expenditures by external development partners (EDP) account foranother 13 percent of health expenditures. (NHSP-IP)
Donor contributions are roughly the same size as HMG contributions to public healthexpenditures. Direct EDP assistance is 90% as technical and financial assistance goes directly toMoH and funds are self-executed by donors (for details see Annex-li). This indicates less money
available in the government treasury.
A gender assessment of government programs and budgetary allocation in healthsector revealed the following:* Budgetary allocations (for the health sector) that are was allocated to programs
exclusively targeted to girls and women - such as allocations made to MaternityHospital, Mid-wife (Sudeni) Program, Women Health Volunteer Programme andMother and Child Programme in Ramechap and Dolkha Districts was, duringthe period 1998/99-2000/2001, only about 1.5 to 1.7 percent of the total budgetof the Ministry of Health
* Programmes that did not exclusively target women but contained suchcomponents that benefit women more than other programs60, had about 16 to18 percent of the total budget of the Ministry of Health in 1998/99-1999/2000.However, this share decreased to only 8 percent in the budget for 2000/2001due to a large gap between the allocation and actual expenditure underPopulation and Family Health programs.
* The rest of the allocations in the health sector amount to roughly about 80 to 90percent of the total health budget allocated (on average during 1998/99-2000/2001) to programs that did not target either male or female in particular.(New Era 2001:39). UNIFEM/UNDP: Gender Budget Audit, Meena Acharya, Gender Issues inHealth Sector Budgeting
This assessment study also reports that budget inadequacy is not a major issue at the centrallevel but that management deficiency is the problem. The health budget was found to be highlyinsufficient at the village and the district levels.
Another review of the health budget from a gender perspective covering the period from1995/96 to 2001-0261 found that exclusively women programmes had 1.5 percent of the budgetof 2001-02. Primarily women programmes had 2.0% and programmes benefiting both women
and men had 96.4% (Source; MGEP, Gender Assessment of Health Sector, pg 41).
Women's share of the total health budget is estimated at 50 percent but maternal healthproblems form a very large proportion (11 %) of the total disease burden which indicates asevere gender bias in potential needs. Gender difference in susceptibility, exposure and socialconsequences of ill health argues for an increased share in the health budget to be allocated forwomen health (Neilson et al)
Dalit and Janajati concems are not reflected in the budget. Interviews indicated that next years'sbudget will reflect such concerns especially for trafficking and nutrition6 2
NHSP -IP has presented Resource Envelope estimates for the health sector as well as for EHCSunder different scenarios. This is an estimate of the overall resource envelope that will beavailable to the health sector over the Tenth Plan period. The projections have been made fewerthan three alternative scenarios based on the assumptions regarding the GDP and revenuegrowth rate, proportion of foreign assistance and internal borrowing in GDP, government
5 Meena Acharya,: Gender Budget Audit, Gender Issues in Health Sector Budgeting UINIFEM/UNDP
6 such as allocations made to Family Planning and Matemal Child Welfare Programs, Population and Family Health, Nutrition
Acquired Immuno Deficiency Syndrome (AIDS) and Sexually Transmitted Diseases (STDs) control programs
61 MWCSW/MGEP/UNDP: Gender Assessment in the Health Sector, January 200262 Mr. Tanka Mani Sharma, Hefu/MOH
32 VCDP Health June 2004 10/06/2004
expenditure allocation to health and to basic health care packages. Three alternative scenarioswere set out - a base case (felt to be the most realistic one), a high case (the most optimisticscenario) and a low case (a more pessimistic worst) scenario. The key assumptions involved inmaking the projections are provided. The base case assumptions are the prevailing situation(2000/01) as indicated by major macro economic indicators. For the base case, it is assumed thatthe present situation will continue in future as well. (The three alternative scenarios presented are given in Table
3 in Annex 6.)
According to the budget estimate for 2001/2002, an amount of Rs. 224 (US $3) roughly will bespent on average on a person in the public sector. This is an extremely low amount ofexpenditure. According to an estimate, a developing country should spend around US $ 10-12for ensuring the primary health care package alone (New Era, 2001:3 7).
In Nepal health expenditures external to government is not reported (as much as 85%) andtherefore significant donor contributions are not reflected in the government's budget system(Maskay 2002). Nevertheless, HMGN is gradually incorporating more and more direct funding inthe health budget. This lack of transparency constitutes a major barrier when planning andanalyzing impact.
A major gap in the allocations and the discussions about the budget is the complete absence ofresources necessary for addressing the issues of gender and social inclusion. As has beenrepeatedly identified, there is a persistent inequity in the use of services by girls and women and
for non-maternity care. Boys benefit significantly more from public hospital care than girls; ifmaternal care is excluded, the overall balance service provision favours men and boys withinalmost every age group (Public Expenditure of the Health Sector in Nepal 2003, HEFU/MoH). Issues concerningDalits and Janajajtis have not been recognized at all. To increase access of these groups tohealth services, various innovative strategies will be necessary. Funding for such issues needs to
be planned for.
Another gap has been the complete ignorance of the effects of conflict on health services andthe emerging need to address issues like psycho-social issues, curative services: and
orthopaedics.
5.1.6 Operational Challengesfor MOHfor implementation of VCDP
Although the health policy of the government emphasises three key aspects, namely,decentralisation of planning at the lowest level, decentralisation of health service management,and integration of vertical programs for effective service delivery, the existing system has notbeen able to make progress on all three counts.
Nepal's institutional capacity for strategic planning, policy development, resource mobilization,and coordination of external donors and national stakeholders is extremely limited. Skills inplanning, management, health economics, and financial analysis are lacking. Responsibilitieswithin MoH and DoHS are poorly delineated. The Ministry of Finance lacks an effectivemechanism for monitoring and coordinating domestic and external resources that flow into thehealth sector. Programs are inadequately integrated, resulting in duplication of effort andinefficient implementation. Planning, budgeting, operations and monitoring functions remainoverly centralized. Both quality and quantity of outreach services are diminished by lack ofdrugs, supplies, and qualified health care providers and the problem of staff absenteeism,especially in remote areas. (Nepal Operation Issues and Prioritization of Resources in the Health Sector, World Bank,
June 2000). Whilst health policy, health provision and health finance are all Kathmandu centeredthere are still weaknesses in terms of communication and engagement. Leadership of the healthsector programme by HMGN is a critical requirement; that leaderships needs to be confidant,robust and open to the involvement of all stakeholders. Health workers have been confined todistrict headquarters. Confidence in the service and its accessibility needs to be maintained.Political dissonance of whatever kind undennines the institutional integrity of services whoeverhappens to be the provider.
33 VCDP Health June 2004 10/06/2004
Financial constraints: The main constraint seen in the institutional options available to HMGNin the health sector is finance. Maximizing efficiency, accessing new resources, focusing publicfunds on a limited range of cost-effective interventions and acknowledge the continuedrequirement for personal expenditure on health will all be part of the financial strategy;tempered with pragmatism. Based on relatively optimistic assumptions regarding the growth of
both Government and EDP resources, the 10t Plan envisages per capita public expenditure onhealth increasing from $2.58 to reach just $3.50 by 2006-7.
The main institutional constraints on staff performance are low pay scale, very seldomrecognition of good work, weak supervision and management and lack of sharing of reformvision at all levels. (Institutional Assessment of Nepal Health Sector, World Bank, Verulam Associates for Core Group of
Health Sector Reform Committee, 2002- Page 5)
MOH and related government institutions who are assigned responsibility for the health ofvulnerable sub-population groups, like indigenous people, are found to have weak capabilitiesfor dealing with these matters. In order to enhance the institutional capacity for appropriatelyaddressing issues related to indigenous people, support of the following activities are relevant:(i) Assessing the track record, capabilities, and needs of those institutions is a fundamentalrequirement. Other institutional issues that need to be addressed through Bank assistance are the(ii) availability of funds for investments and field operations; (iii) adequacy of experiencedprofessional staff; (iv) ability of indigenous peoples' own organizations, local administrationauthorities, and local NGOs to interact with specialized government institutions; (v) ability ofMOH to mobilize other agencies involved in the plan's implementation; and (vi) adequacy offield presence. (World Bank social safeguards and the Social Assessment of HSS)
5.1.7 Ministry of Women, Children and Social Welfare (MWCSW9
MWCSW is an important national voice for most of the socially excluded groups and canprovide valuable policy reform for inclusion in the national agenda. It has been appointed thegender focal point for all government programs but the Ministry has poor resources and
visibility in spite of extensive technical support from several donor agencies. Coordination withMinistry is critical for MOH for implementation of the VCDP as gender is a crosscuttingconcern for all socially excluded groups.
5.1.8 Ministry of Local Development (MLD)
The MLD has lead accountability for the management of local bodies and decentralization. Thelinkages with the education sector are essential given the recently approved 7h Amendment of
the Education Act. The MLD has in the past been pivotal in supporting primary health centresthrough District funds and its role needs to be strengthened for this. Harmonisation of thecurrent discrepancies in legal frameworks is an urgent immediate task.
5.1.9 National Commissions
Commissions such as the National Women's Commission, National Dalit Commission, NationalCommittee for the Development of Nationalities and the National Federation of the Disabledhave been working intensively, becoming a strong national voice for their constituencies.Councils and other bodies representing the interests of women, Dalits, and Janajatis andchildren have also been established. All these would be key partnership for addressing severalof the VDCP recommendations. However they are largely young organisations and wouldrequire capacity building, resources and improved accountability measures for improvedfunctioning.
5.1.10 Local bodies
VDCs, DDCs and associations like Association of District Development Committees, Nepal(ADDC/N) advocate the cause of decentralization. Directives for social inclusion and communitymonitoring need to be developed and coordination mechanisms need to be established.
34 VCDP Health June 2004 10/06/2004
Common to all such government agencies would be sustained dialogue and reflection on issuesof social inclusion, affecting women, Dalits, Janajatis and other disadvantaged groups to enablean attitudinal shift towards inclusion.
5.2 Civil society
The past two decades have witnessed steady progress in civil society responsiveness to thedevelopment of the socially excluded. National bodies, district networks, community groupshave mushroomed to respond with commitment and perseverance to getting their daughters intoschools and their women literate. With easy access to donor aid and huge demand for advocacy,training, research and technical support, a growing number of NGO's have taken up communityhealth issues as their priority development program.
5.2.1 Women's development organisations: Nepal at present has a vast network ofcommunity-based groups that have demonstrated a rich range and wide coverage of work bywomen groups in several critical development sectors. At national, district and communitylevel, there are several thousand women's groups and many federations who could be valuablepartners in advocating social inclusion of girls and disadvantaged children and women. Many ofthese groups have demonstrated how to work successfully with communities on issues of genderand caste discrimination, equal representation in local bodies, more equitable resourceallocation and children's and women's well being.
5.2.2 Janajati institutions: The Nepal Federation of Nationalities (NEFEN) is as an umbrellaorganisation and advocacy forum for Nepal's vulnerable peoples, legally recognized as therepresentative organisation of vulnerable communities. In order to implement the provision ofthe 10th Plan, the Nepali Parliament issued an Act in 2002 to establish the National Foundationfor the Development of Vulnerable Nationalities (NFDIN) which had a broad mandate to ensurethe social, economic and cultural development and upliftment of vulnerable peoples, as well astheir mainstreaming and equal participation in national development.
5.2.3 Dalit organisations: The movement of Nepali Dalits against discrimination and socialinjustice began more than five decades ago. There are today over 60 agencies in Nepal workingon Dalit issues. All political parties have sister Dalit organizations though these are moregoverned by political interests. At the national level, the Nepal Dalit Sangh is lobbying thepassing of a Bill in favour of Dalits. The National Dalit Council and Dalit Commission play alead role in advocacy for policy and legislative reform to address Dalit rights. Others like theDalit Welfare Council and many grassroot NGOs target specific Dalit communities for supportthrough scholarships, incentives, literacy and skills development programs.
5.2.4 Children's organisations: There are hundreds of examples of children's clubs andorganisations across Nepal, where children have been actively engaged and taken leadership inimproving community efforts on critical social inclusion issues such as increasing enrolment of girlsand Dalit children, confronting child labour and trafficking, challenging child marriage andparticipating in health centres management. Child clubs, Child Rights Forums and Child RightsAwareness Groups have been formed in many schools and through these forums, children are beinginvolved in the decision making process of health related activities. Similarly, child clubs havestarted playing a dynamic role in VDC meetings. Over the years, children have been activelyparticipating in the electronic media particularly on Frequency Modulation (FM) Radio and TV, aswell as print media.
5.2.5 Special interest groups: A large number of welfare organisations provide service forvaried disabilities. Support is mostly institution based and in a welfare mode with very limitedexamples of social inclusion.
The weakness of Nepali NGOs and the dominance of international NGOs and EDPs in servicedelivery are in part functions of organizational culture and the relationships within and betweenNGOs and NGOs and HMGN. The private sector is also institutionally young. Networks are not
35 VCDP Health June 2004 10/06/2004
strong and there is heavy reliance on external connections particularly with India. (Institutional Assessment
of Nepal Health Sector, World Bank Verulam Associates for Core Group ofHealth Sector Reform Committee, 2002- Page 4)
5.3 International agencies
Numerous I/NGOs in Nepal support district and community program for girls and Dalitseducation. Furthermore agencies such as PLAN, Action Aid have made significant contributionto social inclusion. The results all confirm that communities have the capacity to mobilisethemselves, if the process is right.
5.4 Multilateral and bilateral agencies
Development aid for health today is rising both in quantity and diversity. Amongst the UN agencies,UNIFPA is a lead player with women's and girls' reproductive and sexual health and rights as thenumber one global priority for the agency. Similarly, strategic shifts of UNICEF towardsdecentralization has enabled effective convergence with the local governance structures and theDACAW program today is well established in 15 districts demonstrating a positive example ofmainstreaming the interests of the poor and marginalized particularly children and women.
The World Bank has been a major donor for health care service, providing loans to HMG for nationalhealth programs. A exceptional contribution has been the policy advocacy for social inclusion in theTenth Plan and the support for further analysis to provide the frame work for ensuring that the needs ofsocially excluded groups are addressed appropriately in all planning and sector interventions. DFI) isalso a lead agency and along with the Bank, has supported HMG for social assessment and has beensupporting other programs for social inclusion. This project follows a SWAp where donors have ????resources in an effort to achieve a more cohesive pragmatic synergy and greater impact. UTNDP hasbeen the lead player in Nepal for decentralization and has established programs in 60 districts buildingcapacities of local bodies and setting up local development funds. Gender mainstreaming and socialdevelopment is the second major area of support.
6. MONITORING AND EVALUATION
6.1 Monitoring and evaluation
Since this plan focuses on social issues, it is essential that monitoring and evaluation assessprocess and progress as well as output and outcome indicators. Indicators can come in twoforms: (1) technical and (2) self-reflective indicators using a community-owned and operatedmonitoring system. The main recommendation regarding monitoring and evaluation is thatprogress on the VCDP and various other interventions be evaluated during the first year ofimplementation as a basic requirement for scaling the project up. The monitoring frameworkand indicators presented in section 9 would provide baseline fro monitoring and evaluation.Therefore in the first year a baseline survey should be carried out as per the informationcollected by Community Health Information Management System carried out by the NGOs.Health Management Information System (HMIS) must collect data disaggregated by gender,age, disability, caste (Dalit/non-Dalit) and ethnicity (Janajati/non-Janajati). (Refer to section8.2.3 for further details). Strong monitoring and evaluation is critical for the government anddonors to assess the progress of VCDP, to learn from past experience and to actively improvethe output performance.
VCDP: The MoH and its various offices are responsible for monitoring the VCDPrecommendation and the indicators. While disaggregated data for caste and ethnicity is notavailable as yet, in order to correctly monitor outcomes of the Health Monitoring InformationSystem (HMIS) must produce such disaggregated data for all levels in Nepal. (Please refer to
Monitoring Framework for VCDP implementation, Section 9.)
36 VCDP Health June 2004 10/06/2004
To monitor social development, inclusion and unintended negative effects, annual externalevaluations must be conducted. The evaluation team should include social development experts,health experts, anthropologists and gender specialists. The annual extemal evaluations should besupplemented by independent evaluation by a group of indigenous and dalit representatives.Such evaluation must also include the 'process' aspect of the program's implementation andperformance. For the overall monitoring of health centres management, SMCs and localcommunities must be given responsibility. District and local level NGOs and dalit andindigenous people's organisations may be included in monitoring inputs and outputs and canassist local communities and inexperienced MCs in the formulation of rigorous and culturally-appropriate monitoring techniques.
Mechanisms to monitor the implementation of the agreed plan: Health ManagementInformation System (HMIS) data and appropriate M&E systems will be developed/strengthenedand implemented to ensure accountability of all stakeholders. HMIS will collect datadisaggregated by gender, disability, caste (Dalit/non-Dalit) and ethnicity (Janajati/non-Janajati)and use social inclusion indicators (e.g. issues such as shifts in decision making patterns, genderrelations, inter-caste behaviour). At the health centres level, there may be need for more detailedclassification of gender, caste and ethnic categories. These can be aggregated into user -friendlykey categories for the central level reports.
Community Managed Information System (CMIS) data will support HMIS under MOU withlocal groups for collection of disaggregated data. Mechanisms such as social audits and socialmapping will track health centres participation and drop out rates by gender, caste and ethnicityof children and women from socially marginalised communities, monitor discriminatorybehaviour/practices, support local women recruitment and feed such information to the CMISsystem.
6.2 Implementation
Vulnerable Community Development Plan should include an implementation schedule withbenchmarks by which progress can be measured at appropriate intervals. Pilot programs may beneeded to provide planning information for phasing the project component for Dalit andindigenous peoples with the main investment. The aim must be the long-term sustainability ofproject activities subsequent to completion of disbursement. It is anticipated that almost all theactivities will be initiated within Year 1. National policies, regulations, guidelines and directiveswill be reviewed, revised, and implemented within the first year of the project.
(A) Funding at the Community Level: (i) NRs. 100,000 as a one-time incentive will beprovided to all community-managed health centres. (ii) All government-managed health centreswill get an initial basic grant for the first year. In order to receive the basic grant during year 2,the Management Committee (MC) will need to follow the health centres grants plan. Inaddition, health centres will be eligible for higher levels of funding if they are able to go beyondthe basic level of accountability (audited account statements) and fulfil the higher accountabilityrequirements for level I or level II. Which should be developed in consultation with keystakeholders.
(B) Funding at the Central Level. Central funds will be used (probably on an outsourcingbasis) for: (i) providing technical expertise on integrating positive images of diverse socio-cultural and religious groups into the ongoing BCC, IEC and capacity building and curriculumdevelopment process; (ii) It is recommended that development of the program should beinitiated in Year 1 developing a framework for sanctions against discrimination which will becarried out within six months by the Monitoring and Inspection Section of the MoE.
37 VCDP Health June 2004 10/06/2004
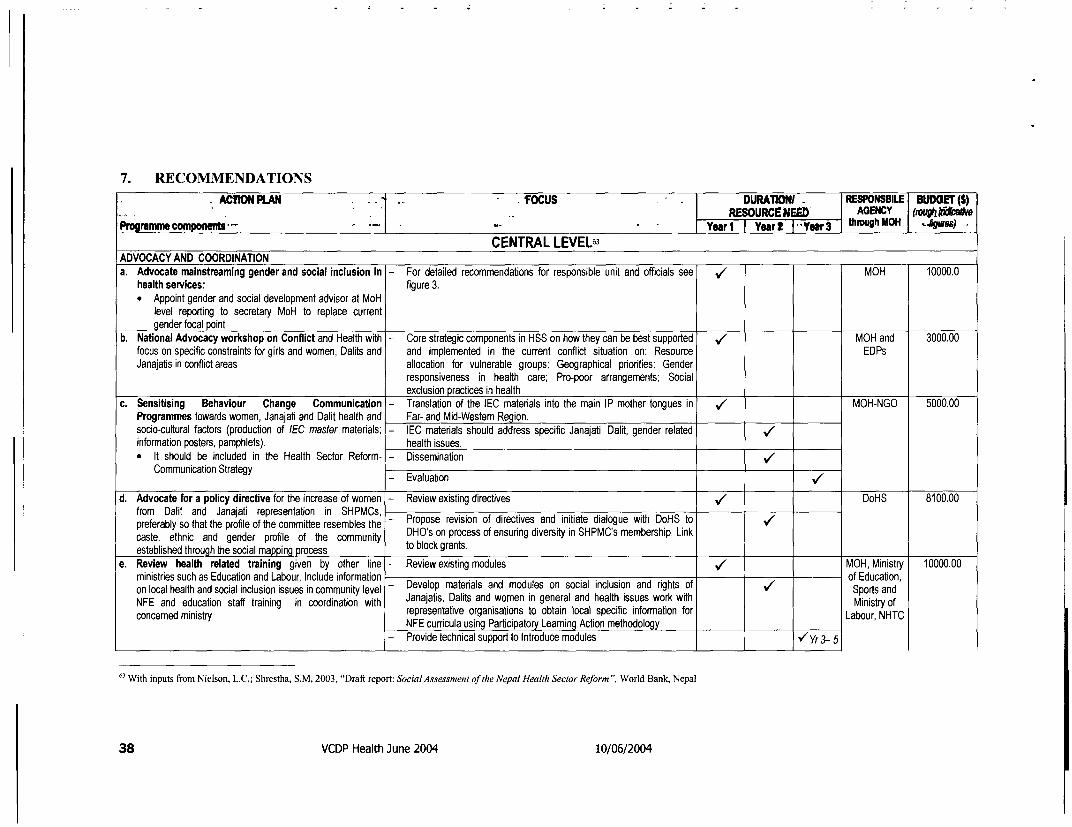
7. RECOMMENDATIONS
ACTION PLAN . . . ^ * - fOCUS . - DURATIONI W RESPONSBILE BUDOET (S).- * . - .- 1 .. .RESOURCtNEED AGENCY (rwugkAtAwProgramme componewb Yearl Y .. aa1 Ye a|h IS t 3 thl . .gacs)CENTRAL LEVEL63
ADVOCACY AND COORDINATIONa. Advocate mainstreaming gender and social inclusion in - For detailed recommendations for responsible unit and officials see MOH 10000.0health services: figure 3.
* Appoint gender and social development advisor at MoHlevel reporting to secretary MoH to replace currentgender focal point
b. National Advocacy workshop on Conflict and Health with - Core strategic components in HSS on how they can be best supported / MOH and 3000.00focus on specific constraints for girls and women, Dalits and and implemented in the current conflict situation on: Resource EDPsJanajatis in conflict areas allocation for vulnerable groups; Geographical priorities; Genderresponsiveness in health care; Pro-poor arrangements; Socialexclusion practices in health
c. Sensitising Behaviour Change Communication - Translation of the IEC materials into the main IP mother tongues in ,/ MOH-NGO 5000.00Programmes towards women, Janajati and Dalit health and Far- and Mid-Western Region.socio-cultural factors (production of IEC master matedals; - IEC materials should address specific Janajati, Dalit, gender relatedinformation posters, pamphlets). health issues.* It should be included in the Health Sector Reform- - Dissemination '/Communication Strategy Evaluation
1/
d. Advocate for a policy directive for the increase of women - Review existing directives / DoHS 8100.00from Dalit and Janajati representation in SHPMCs,preferably so that the profile of the committee resembles the - Propose revision of directives and initiate dialogue with DoHS to /caste, ethnic and gender profile of the community DHO's on process of ensuring diversity in SHPMC's membership. Linkestablished through the social mapping process to block grants.
e. Review health related training given by other line - Review existing modules MOH, Ministry 10000.00ministries such as Education and Labour. Include information of Education,on local health and social inclusion issues in community level - Develop materals and modules on social inclusion and rights of / Sports andNFE and education staff training in coordination with Janajats, Dalits and women In general and health Issues work with Ministry ofconcerned ministry representative organisations to obtain local specific information for Labour, NHTCNFE curricula using Participatory Learning Action methodology- Provide technical support to Introduce modules v/'Yr3- 5
63 With inputs from Nielson, L.C.; Shrestha, S.M, 2003, "Draft report: Social Assessment of the Nepal Health Sector Reform ", World Bank, Nepal
38 VCDP Health June 2004 10/06/2004
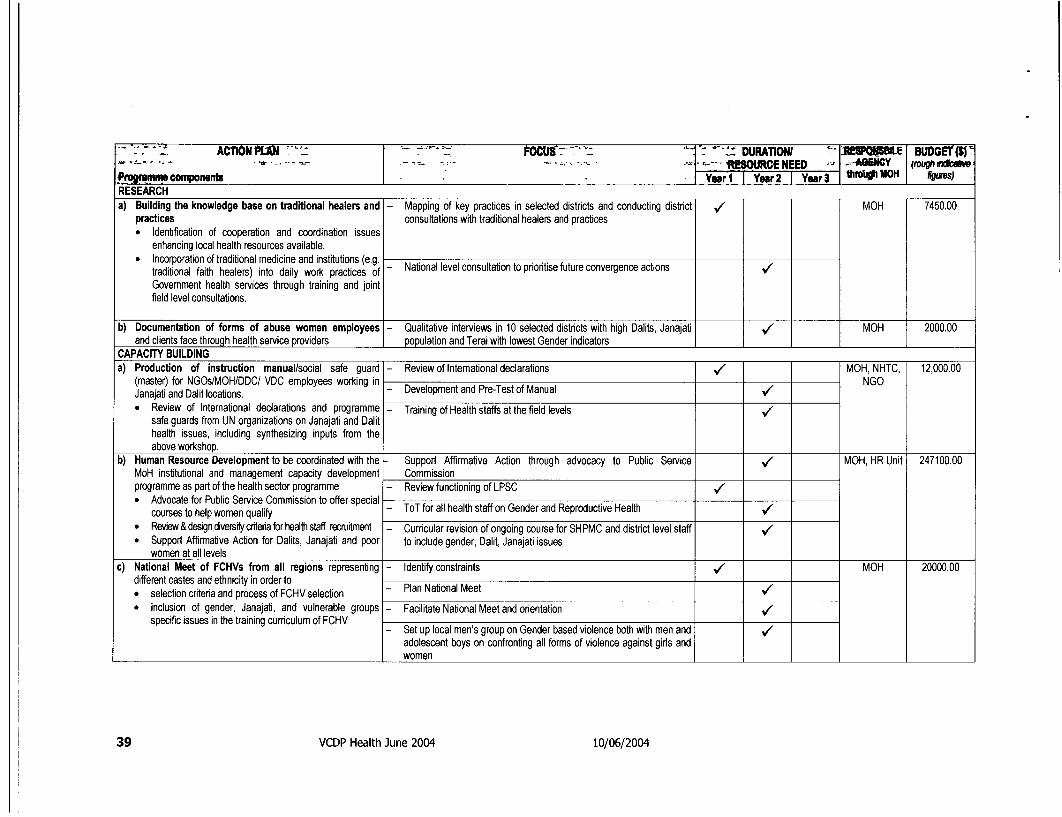
½"- .~~; ACTIONPLAII f-o1 - --' - - - i - ' ' DURATIONI '= tLE T UDCEtIL 'k , _- _ := - r_ ~~ ~ R!Si URCE NEED - -4AHNCY (rough rdcw
PmtWmmm components [ Year I Year 2 Year 3 thfo1IyIUOH figures)RESEARCHa) Building the knowledge base on traditional healers and - Mapping of key practices in selected districts and conducting district V/ MOH 7450.00
practices consultations with traditional healers and practices* Identification of cooperation and coordination issues
enhancing local health resources available.* Incorporation of traditional medicine and institutions (e.g.
traditional faith healers) into daily work practices of - National level consultation to prioritise future convergence actions VGovernment health services through training and jointfield level consultations.
b) Documentation of forms of abuse women employees - Qualitative interviews in 10 selected distncts with high Dalits, Janajati MOH 2000.00and clients face through health service providers population and Terai with lowest Gender indicators
CAPACITY BUILDINGa) Production of instruction manual/social safe guard - Review of Intemational declarations V MOH, NHTC, 12,000.00
(master) for NGOslMOHlDDC/ VDC employees working in NGOJanajati and Dalit locations. - Development and Pre-Test of Manual /* Review of International declarations and programme - Training of Health staffs at the field levels V
safe guards from UN organizations on Janajati and Dalithealth issues, including synthesizing inputs from theabove workshop.
b) Human Resource Development to be coordinated with the - Support Affirmative Action through advocacy to Public Service / MOH, HR Unit 247100.00MoH institutional and management capacity development Commissionprogramme as part of the health sector programme - Review functioning of LPSC /* Advocate for Public Service Commission to offer special - ToT for all health staff on Gender and Reproductive Health
courses to help women qualify* Review & design diversitycrtera for health staff recruitment - Curricular revision of ongoing course for SHPMC and district level staff $* Support Affirmative Action for Dalits, Janajati and poor to include gender, Dalit, Janajati issues
women at all levelsc) National Meet of FCHVs from all regions representing - Identify constraints V MOH 20000.00
different castes and ethnicity in order to* selection criteria and process of FCHV selection - Plan National Meet /* inclusion of gender, Janajati, and vulnerable groups - Facilitate National Meet and orientation
specific issues in the training curriculum of FCHV- Set up local men's group on Gender based violence both with men and /
adolescent boys on confronting all forms of violence against girls andwomen
39 VCDP Health June 2004 10/06/2004
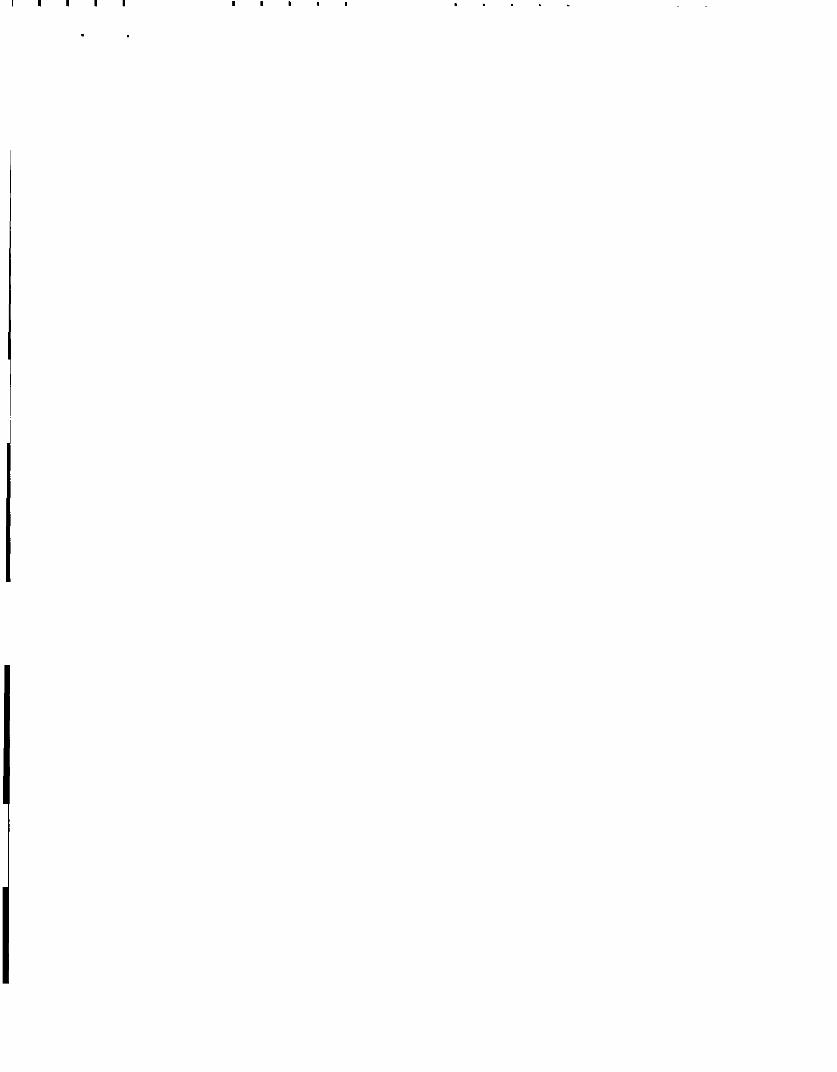
I~||
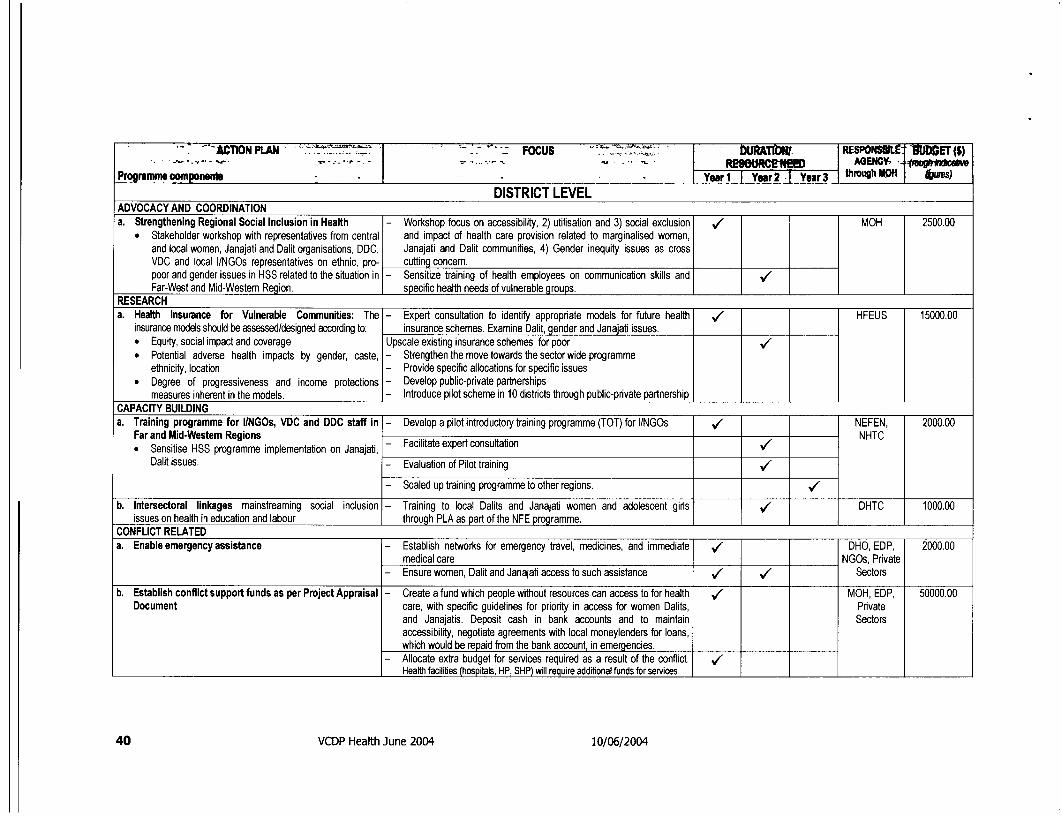
'-ATIONl-M FOCUS A. | tRE SPON4- 'BfI(ET (5)- w E:5:1 -- FtUS I tRiM AGENGC- fv**
Programn componeia - * . Year1 Y90 Year2 ar3 thmiughM WH 6BS)
DISTRICT LEVELADVOCACY AND COORDINATIONa. Strengthening Regional Social Inclusion in Health - Workshop focus on accessibility, 2) utilisation and 3) social exclusion / MOH 2500.00
Stakeholder workshop with representatives from central and impact of health care provision related to marginalised women,and local women, Janajati and Dalit organisations, DDC, Janajati and Dalit communities, 4) Gender inequity issues as crossVDC and local l/NGOs representatives on ethnic, pro- cutting concern.poor and gender issues in HSS related to the situation in - Sensitize training of health employees on communication skills and $Far-West and Mid-Western Region. specific health needs of vulnerable groups.
RESEARCHa. Health Insurance for Vulnerable Communities: The - Expert consultation to identify appropriate models for future health ,/ HFEUS 15000.00
insurance models should be assessed/designed according to: insurance schemes. Examine Dalit, gender and Janajati issues.* Equity, social impact and coverage Upscale existing insurance schemes for poor $* Potential adverse health impacts by gender, caste, - Strengthen the move towards the sector wide programme
ethnicity, location - Provide specific allocations for specific issues* Degree of progressiveness and income protections - Develop public-private partnerships
measures inherent in the models. - Introduce pilot scheme in 10 districts through public-pnvate partnershipCAPACITY BUILDINGa. Training programme for I/NGOs, VDC and DDC staff in - Develop a pilot introductory training programme (TOT) for l/NGOs NEFEN, 2000.00
Far and Mid-Westem Regions . NHTC* Sensitise HSS programme implementation on Janajati, - Facilitateexpertconsultation /
Dalit issues. - Evaluation of Pilot training V/
- Scaled up training programme to other regions. /
b. Intersectoral linkages mainstreaming social inclusion - Training to local Dalits and Janajati women and adolescent girls / DHTC 1000.00issues on health in education and labour through PLA as part of the NFE programme.
CONFLICT RELATEDa. Enable emergency assistance - Establish networks for emergency travel, medicines, and immediate DHO, EDP, 2000.00
medical care NGOs, Private- Ensure women, Dalit and Janajati access to such assistance / / Sectors
b. Establish conflict support funds as per Project Appraisal - Create a fund which people without resources can access to for health / MOH, EDP, 50000.00Document care, with specific guidelines for priority in access for women Dalits, Pnvate
and Janajatis. Deposit cash in bank accounts and to maintain Sectorsaccessibility, negotiate agreements with local moneylenders for loans,which would be repaid from the bank account, in emergencies.
- Allocate extra budget for services required as a result of the conflict. /Health facilibies (hospitals, HP, SHP) will require addibional funds for services.
40 VCDP Health June 2004 10/06/2004
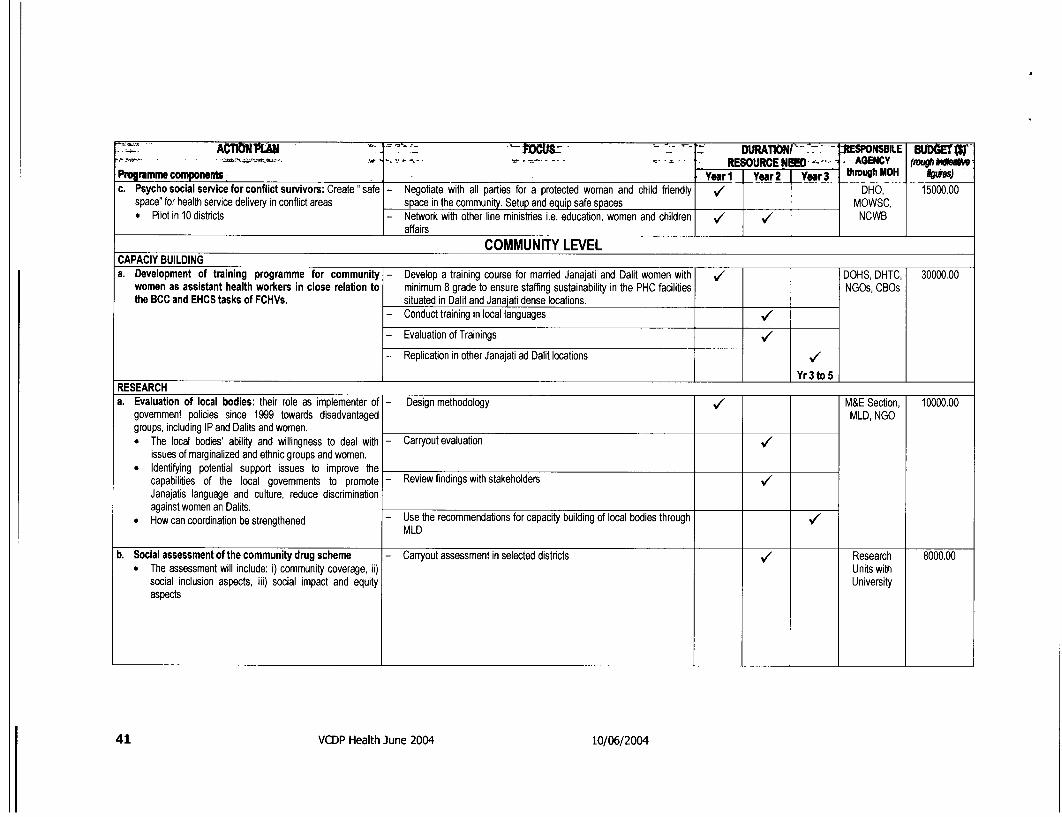
.'''ACMONp U ' ' G_ .7. -DpTIN -' ItNSBILE BUE- - .RESOURCE NEKO--. AGENY (uh e
P?ogramme components - - .. Year I Year 2 JYear 3 through IOH | Wm5)c. Psychosocialserviceforconflictsurvivors:Create"safe - Negotiate with all parties for a protected woman and child friendly V7 DHO, 15000.00
space" for health service delivery in conflict areas space in the community. Setup and equip safe spaces MOWSC,* Pilot in 10 districts - Network with other line ministries i.e. education, women and children ./ / NCWB
affairsCOMMUNITY LEVEL
CAPACIY BUILDINGa. Development of training programme for community - Develop a training course for married Janajati and Dalit women with DOHS, DHTC, 30000.00
women as assistant health workers in close relation to minimum 8 grade to ensure staffing sustainability in the PHC facilities NGOs, CBOsthe BCC and EHCS tasks of FCHVs. situated in Dalit and Janajati dense locations.
- Conduct training in local languages /
- Evaluation of Trainings .7- Replication in other Janajati ad Dalit locations .7
I_Yr3to5 1RESEARCHa. Evaluation of local bodies: their role as implementer of - Design methodology .7 M&E Section, 10000.00
govemment policies since 1999 towards disadvantaged MLD, NGOgroups, including IP and Dalits and women.* The local bodies' ability and willingness to deal with - Carryout evaluation ./
issues of marginalized and ethnic groups and women.* Identifying potential support issues to improve the
capabilities of the local govemments to promote - Review findings with stakeholders ./Janajatis language and culture, reduce discriminationagainst women an Dalits.
* How can coordination be strengthened - Use the recommendations for capacity building of local bodies through MMLD
b. Social assessment of the community drug scheme - Carryout assessment in selected districts . Research 8000.00* The assessment will include: i) community coverage, ii) Units with
social inclusion aspects, iii) social impact and equity Universityaspects
41 VCDP Health June 2004 10/06/2004
ACTION PM. ' FOCI 1 cDURATlONI OW F iii BUDGET (S)mf .$-¢. s .-, - I - - 4- -lESOURCE NEED N3e i; (rou VIiRNdcafb
Programme components - . Yrl Year2 Yur3 a j 11gues)PROGRAMMEa. Establish block grants scheme for SHPMC to form - Develop criteria for grants to SHPMC for making formal agreements / DHO, Local 50000.00
agreements with selected local community groups (CBOs (MoUs) with community level women's and adolescents' groups or Bodies,particularly women and adolescent groups). others NGOs,
Priority to community women's groups such as Mothers - Develop criteria for selection of community groups for MOUs /Club, Women Health Groups, Saving and Credit Groups Establish block grant mechanism in selected Pilot distncts with high /etc. DaliVJanajati population .
b. Establish community based Adolescent Reproductive - Establish adolescent girls and boys groups as peer educators on / Family Health 50000.00Health Counselling Centre for peer support. See table gender and RH rights Department,Community Based Reproductive Health Services for Young - Life skills based training to local youth volunteers NGOs andPeople - Pilot in five distCcts with high indicators of early marriage, violence on RCOs
imTrain motivators suppoe vulnerable communities for women and children, HIV/AIDS, trafficking and low NER of girls. 5 rtimproving health-seeking behaviour cete in eac disric Yr Wh5centres _ each_district
42 VCDP Health June 2004 10/06/2004
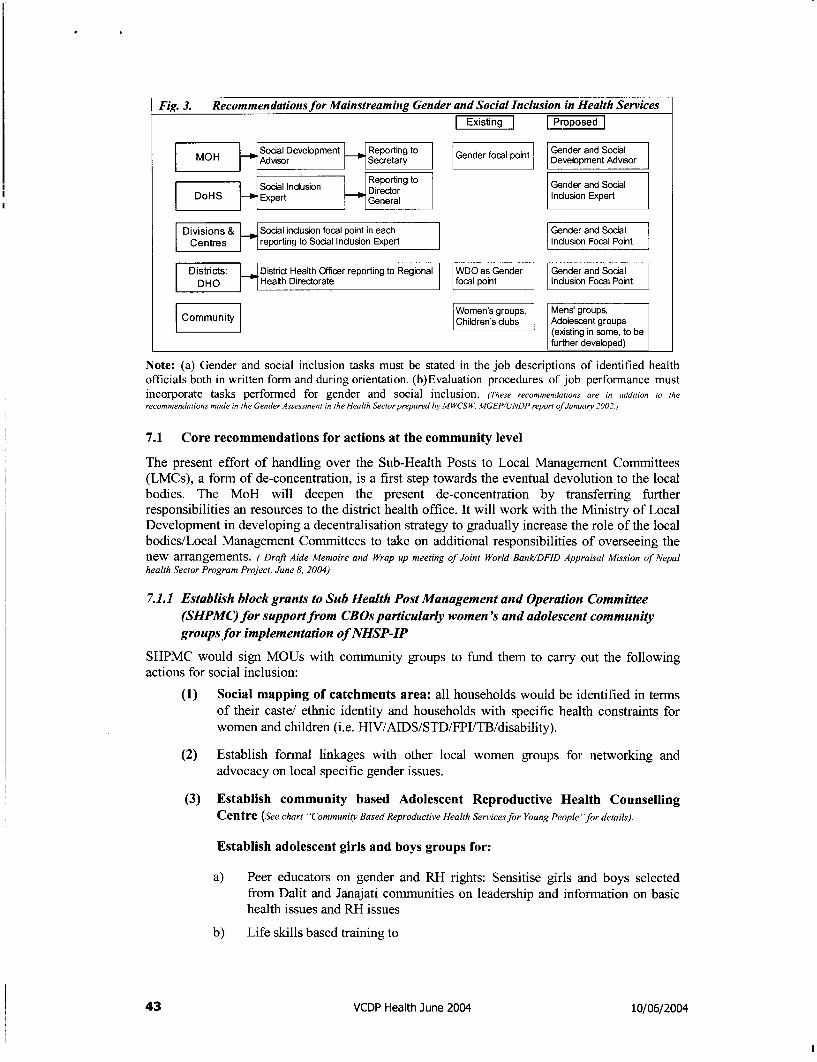
Fig. 3. Recommendationsfor Mainstreaming Gender and Social Inclusion in Health Services
ISocal Devebpment Reportingt° Genderfocal toint Gender and SocialL O i = -vi _ _ SePrtaryDevelopment Advisor
Social Indusion | Reporting to Gender and SocialDoHS Expert Deneral Inndusion Expert
Divisions & I Social indusion focal point in each Gender and SodalCentres |7 reporting to Social Indusion Expert Indusion Focal Point
Districts: | District Health Officer reporting to Regional WDO as Gender Gender and SocialDHO Health Directorate focal point Indusion Focal Point
Women's groups, Mens' groups,Children's dubs Adolescent groups
(existing in some, to befurther developed)
Note: (a) Gender and social inclusion tasks must be stated in the job descriptions of identified healthofficials both in written form and during orientation. (b)Evaluation procedures of job performance mustincorporate tasks performed for gender and social inclusion. (These recommendatons are in addition to therecommendations made in the Gender Assessment in the Health Sector prepared by MWCS W, MGEP/UNDP report of January 2002.)
7.1 Core recommendations for actions at the community level
The present effort of handling over the Sub-Health Posts to Local Management Committees(LMCs), a form of de-concentration, is a first step towards the eventual devolution to the localbodies. The MoH will deepen the present de-concentration by transferring furtherresponsibilities an resources to the district health office. It will work with the Ministry of LocalDevelopment in developing a decentralisation strategy to gradually increase the role of the localbodies/Local Management Committees to take on additional responsibilities of overseeing thenew arrangements. ( Draft Aide Memoire and Wrap up meeting of Joint World BanklDFID Appraisal Mission of Nepalhealth Sector Program Project, June 8, 2004)
7.1.1 Establish block grants to Sub Health Post Management and Operation Committee(SHPMC) for support from CROs particularly women's and adolescent community
groups for implementation of NHSP-IP
SHPMC would sign MOUs with community groups to fund them to carry out the followingactions for social inclusion:
(1) Social mapping of catchments area: all households would be identified in termsof their caste/ ethnic identity and households with specific health constraints forwomen and children (i.e. HIV/AIDS/STD/FPI/TB/disability).
(2) Establish formal linkages with other local women groups for networking andadvocacy on local specific gender issues.
(3) Establish community based Adolescent Reproductive Health CounsellingCentre (See chart "Communitv Based Reproductive Health Servicesfor Young People "for details).
Establish adolescent girls and boys groups for:
a) Peer educators on gender and RH rights: Sensitise girls and boys selectedfrom Dalit and Janajati communities on leadership and information on basichealth issues and RH issues
b) Life skills based training to
43 VCDP Health June 2004 10/06/2004
c) Motivators in vulnerable communities for improving health-seekingbehaviour
d) Providing information to vulnerable communities
(4) Orientation of SHPMC on gender, reproductive health and sexual rights ofwomen and girls.
To reduce gender inequality, men and women positions of authority requireorientation on the gender dimensions of health. Health professional in particularneed to be sensitised on the social and non-biological aspects of health. Orientationshould include:
a) Understanding how different gender and socio-cultural factors impact womenand girls health.
b) The consequences of women and girls gender roles and socio-cultural beliefand practices on access, participation and decision-making regarding theirhealth.
c) Conceptual clarity and tools to address reproductive and sexual rights of girlsand women and the violations of these rights (violence and abuse, forced sexand pregnancies, denial of access to information and services)
(5) Training to local Dalits and Janajati women and adolescent girls through PLAas part of the NFE programme. Given the strong linkage between womeneducation, increased family planning and child survival, women and girls fromvulnerable communities should be enrolled in NFE classes through a special grant.Curricular would focus on reproductive health issues and gender linkages witheducation are essential for cross-sectoral linkages.
(6) Social audit64 of funds and activities to enable community members to be moreinformed on:* Access of vulnerable households specially women and children from
Janajati, Dalit families to services and special benefits* Discriminatory behaviour and practices by service providers, community
members to girls and women and members of Dalit families* use of grant funds from VDC and other special entitlements for Dalits,
Janajatis and women* review of decision-making process within SHPMC to ensure inclusion of
representatives from vulnerable households and their specific concerns.
(7) Documentation of local traditional healing practices for curriculum of healthworkers: collect and document local information on the history and culture ofDalits, Janajatis and linguistic minorities, specially their health related practices,myths and belief patterns related to women and child health
(8) Identification of local women volunteers from Dalit/Janajati groups: AssistingSHPMCs to identify and recruit local women for access to information and servicesby Dalit, Janajati households.
64 Social audit is a framework which allows an organisation to build on existing documentation and reporting and develop a processwhereby it can account for its social performance, report on that performance and draw up an action plan to improve on thatperformance, and through which it can understand its impact on the community and be accountable to its key stakeholders. Theessence of social auditing is therefore: accountingfor what we do and listening to what others have to say so thatfutureperformance can be more effectively targeted at achieving the chosen objectives. http://www.cbs-network.org.uk/socacaud.html
44 VCDP Health June 2004 10/06/2004
(9) Community based Health Management Information System (CMIS): trackinglocal specific health issues by gender, caste and ethnicity of children, adolescentsand women from socially marginalised communities. Child and Adolescent Clubswould be particularly appropriate for carrying out baseline surveys.
(11) Advocacy against discriminatory practices: raising awareness and sensitisinghealth care providers, local bodies, school authorities, teachers and youth on socialinclusion issues and on national policies and directives for sanctions againstdiscriminatory behaviour and practices against girls and women and Dalits/Janajatis seeking health services. Social audit by community-level groups wouldidentify gender based violence, discriminatory behaviour and practiced againstgirls and women, Dalits and Janajatis by health service authorities, teachers andcommunity members.
These will be reported to the relevant grievance cell for action and then bemonitored for implementation by enforcing sanctions against discriminatorypractices and behaviour.
(12) Honouring good practices in social inclusion: acknowledge and honour localbodies, health posts, teachers, students and others who have demonstrated initiativeand good practices in social inclusion in health services:* developing criteria for good practices and informing SHPMCs on selection
process* arranging for wide media coverage on honoured persons
(13) Set up local support group on gender based violence both with men andadolescent boys on confronting all forms of violence against girls and women.
Initiate community based meetings at regular intervals to dialogue on:
* Gender roles and socially prescribed practices and rules that support unequalrelationship between men and women, girls and boys
* Orientation on gender and health- basic information on Pre and anti natalcare, child birth and fathers' role/support
* Develop and introduce BCC on gender specific health consequences forwomen and girls particularly:
* All forms of violence* RH and sexuality* Labour* Access to health information* Decision making on health issues* Include men and boys in social mapping and audit, per educators for school
awareness programmes* Design male leadership campaign for promoting girls education and female
literacy through NFE using successful models of PLA
7.1.2 BCC in bilingual languages
The Local Self-Governance Act (LSGA) of 1999 and the Poverty Reduction Strategy Papers(PRSP) both empower local administration together with civil society, NGOs and relevantethnic and linguistic foundations, committees or commissions to support language and culturalpreservation activities. This VCDP takes the view that the responsibility for ensuring access of
45 VCDP Health June 2004 10/06/2004
non-Nepali speaking community members to the health services recognizes and celebratesdiversity should be shared between the state (central and local governments) and society.
In communities where a large minority/or majority speak another language:
(1) Ensure that at least one sub health post staff is fluent in local language andavailable to assist in communicating patients' health problems to health providerand in communicating instructions from health providers to patients. If thelanguage has a script ensure that signs and key health communication materials areavailable in that script.
(2) develop the necessary training modules in the use of local languages to supportBCC through bilingual medium of instruction to increase sensitivity to culture,language health practices and specific issues related to health of indigenous people,
(3) identify and accredit national and local NGOS to deliver these modules and
(4) bring multilingual, multi ethnic and multi cultural representation in all BCCmaterials
(5) Ensure reaching these campaigns to all socially excluded Janajatis and Dalitsparticularly women
(6) Provide funding these organisations to go to districts to train local health workerswhere communities have demand for bilingual instruction.
Civil society, non-governmental organisations and local government would have theresponsibility to work together to develop modules based on local languages and cultures for thecommunity to use. While the State is therefore involved in the formation of an inclusive andequitable national health policy, society must configure this in a locally meaningful way andtake charge of the culturally sensitive fine-tuning and the successful implementation at acommunity level.
(1) Collecting and documenting information on their own history and culture foruse in the National training curriculum and text books of health staff at alllevels. It is suggested that the National Dalit Commission or the NationalFederation of Nationalities (Nepal Janajati Mahasangh) be provided with somefunds to enable them to make modest grants to communities wishing to do this.
7.1.3 HMIS disaggregated data
(1) Health Management Information System (HMIS) must collect data disaggregatedby gender, age, disability, caste (Dalit/non-Dalit) and ethnicity (Janajati/non-Janajati). At the sub-health post level, there may be a need for a more detailedclassification of categories. These can be aggregated into user-friendly keycategories for the reporting mechanisms.
(2) Use HMIS data collected by local groups under Moue with SHPMCs for baselineinformation in the collection of disaggregated data.
(3) Public private partnership: Partner with philanthropic association and businesshouses to support sub health post/PHCC for drugs and facility
46 VCDP Health June 2004 10/06/2004
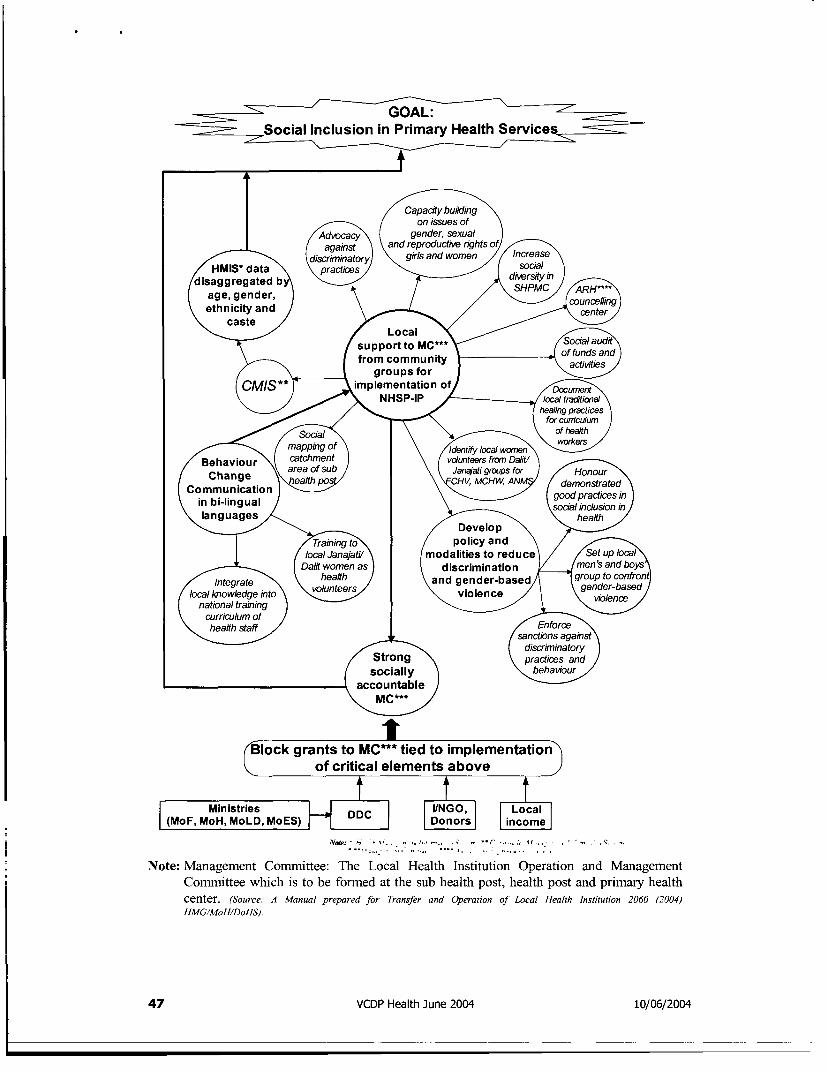
occCal Inclusion in Primary Health Se
on issues ofgAdvocacya gender, sexual
_ against an~~~~d reproductive rights o// discriminatory \ ~girls and women Ices
/ HMISw data pracices \/ soaa/ndiaggregated bieriage, gender,ethnicity and\ caste / /
s ocal bao
T ~ ~~~~~~~ spport to MC*** 03a
cgroups forCMIS** _Aimplementation of/
NHSPNote:/MaagementommitteeTheLoclHealt Institun Operationgracn
_ \ ~~~~~~~~~~~for cunTicumCommittee which is to be formedfat the sub health post, health post and primary health
c mappingo workersyoclwme\ e Beaviou r\ catchmen f dnero nm DaliV 0Change area ofsu Janajattig-ps fO- Hnu
Communica~trio\V MCHW, A ,/deostratedin bi-lingual r goodelprradn ca ein
x ~~~~~~socdal inclusion In4 languages 2/0health
/ evelo'p \ zErainig to\ / policy and \ /
lclJanajt d moai'tie to reduce / SeuplCalJ Dald women as } d iscriminat!o n / mnsandby
/ Integrate \ ~healt /adgne-ased group toconfo
( natioal tramng ) volu\nte gender-based
Srong\paieansocially <bhvor
4 ccountablee
(Bokgrants to MC` tied to implementaton)V of ~critical elements aboveJ
| (MoF,MoH,MoLD,MoES) 3i ;
Note: Management Conurittee: The Local Health Institution Operation and ManagementConmmittee which is to be formed at the sub health post, health post and primary healthcenter. (Source: A Manual prepared for Transfer and Operation of Local Health Institution 2060 (2004)HMG/MoH/DoHS).
47 VCDP Health June 2004 10n/06/2004
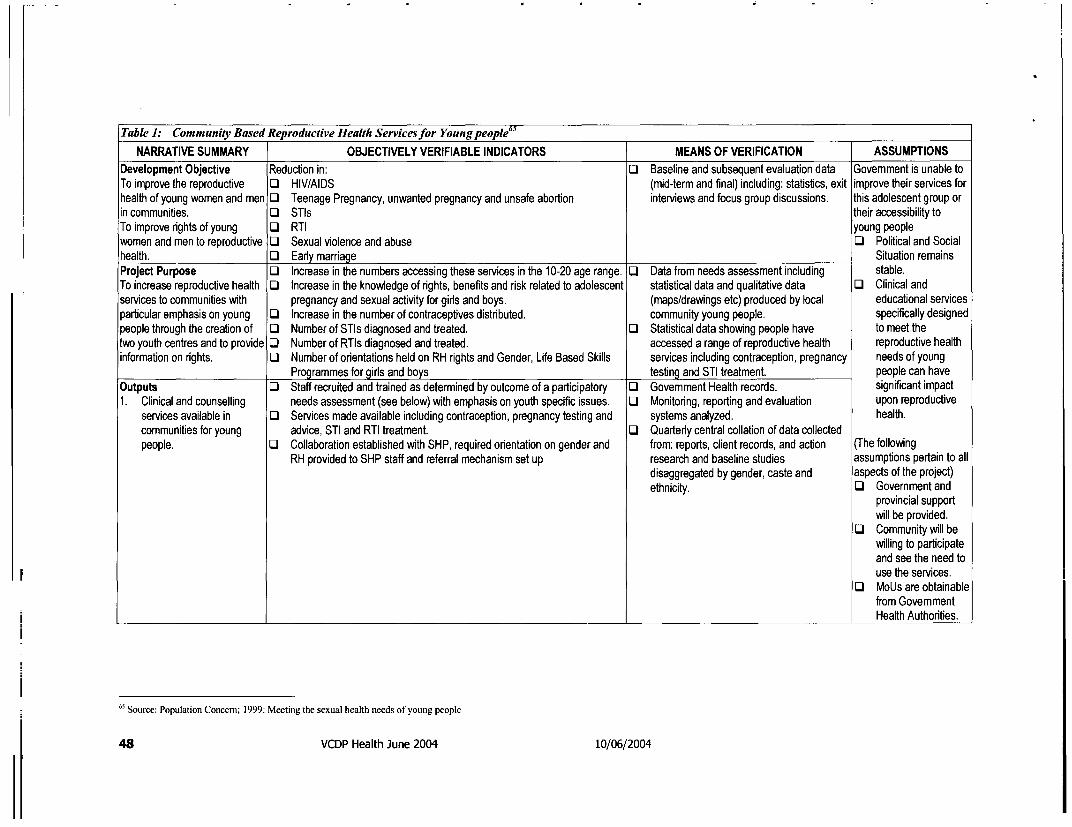
Table 1: Community Based Reproductive Health Servicesfor Young people 65
NARRATIVE SUMMARY OBJECTIVELY VERIFIABLE INDICATORS MEANS OF VERIFICATION ASSUMPTIONSDevelopment Objective Reduction in: O Baseline and subsequent evaluation data Government is unable toTo improve the reproductive O HIV/AIDS (mid-term and final) including: statistics, exit improve their services forhealth of young women and men LI Teenage Pregnancy, unwanted pregnancy and unsafe abortion interviews and focus group discussions. this adolescent group orin communities. Oi STIs their accessibility toTo improve rights of young O RTI young peoplewomen and men to reproductive O Sexual violence and abuse O3 Political and Socialhealth. 0 Early marriage Situation remainsProject Purpose O Increase in the numbers accessing these services in the 10-20 age range. O Data from needs assessment including stable.To increase reproductive health O Increase in the knowledge of rights, benefits and risk related to adolescent statistical data and qualitative data O Clinical andservices to communities with pregnancy and sexual activity for girls and boys. (maps/drawings etc) produced by local educatonal servicesparticular emphasis on young O Increase in the number of contraceptives distributed. community young people. specifically designedpeople through the creation of O Number of STIs diagnosed and treated. O Statistical data showing people have to meet thetwo youth centres and to provide O Number of RTIs diagnosed and treated. accessed a range of reproductive health reproductive healthinformation on rights. U Number of orientations held on RH rights and Gender, Life Based Skills services including contraception, pregnancy needs of young
Programmes for girls and boys testing and STI treatment. people can haveOutputs O Staff recruited and trained as determined by outcome of a participatory O Govemment Health records. significant impact1. Clinical and counselling needs assessment (see below) with emphasis on youth specific issues. LO Monitoring, reporting and evaluation upon reproductive
services available in O Services made available including contraception, pregnancy testing and systems analyzed. health.communities for young advice, STI and RTI treatment. O Quarterly central collation of data collectedpeople. LO Collaboration established with SHP, required orientation on gender and from: reports, client records, and action (The following
RH provided to SHP staff and referral mechanism set up research and baseline studies assumptions pertain to alldisaggregated by gender, caste and aspects of the project)ethnicity. O Government and
provincial supportwill be provided.
LO Community will bewilling to participateand see the need touse the services.
LI MoUs are obtainablefrom GovemmentHealth Authorities.
65 Source: Population Concern; 1999: Meeting the sexual health needs of young people
48 VCDP Health June 2004 10/06/2004
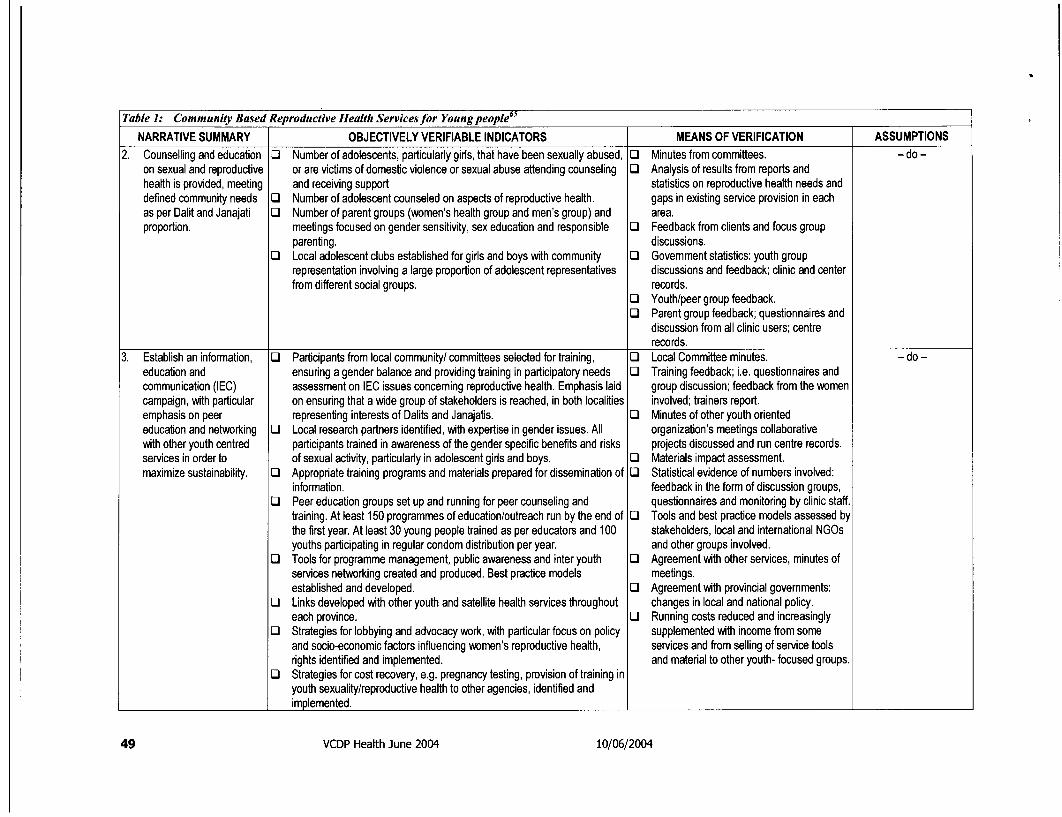
Table 1: Community Based Reproductive Health Servicesfor Young people 65
NARRATIVE SUMMARY OBJECTIVELY VERIFIABLE INDICATORS MEANS OF VERIFICATION ASSUMPTIONS2. Counselling and education U Number of adolescents, particularly girls, that have been sexually abused, O Minutes from committees. - do -
on sexual and reproductive or are victims of domestic violence or sexual abuse attending counseling O Analysis of results from reports andhealth is provided, meeting and receiving support statistics on reproductive health needs anddefined community needs O Number of adolescent counseled on aspects of reproductive health. gaps in existing service provision in eachas per Dalit and Janajati U Number of parent groups (women's health group and men's group) and area.proportion. meetings focused on gender sensitivity, sex education and responsible U Feedback from clients and focus group
parenting. discussions.U Local adolescent clubs established for girls and boys with community U Govemment statistics: youth group
representation involving a large proportion of adolescent representatives discussions and feedback; clinic and centerfrom different social groups. records.
U Youth/peer group feedback.U Parent group feedback; questionnaires and
discussion from all clinic users; centrerecords.
3. Establish an information, U Participants from local community/ committees selected for training, U Local Committee minutes. - do -education and ensuring a gender balance and providing training in participatory needs U Training feedback; i.e. questionnaires andcommunication (IEC) assessment on IEC issues concerning reproductive health. Emphasis laid group discussion; feedback from the womencampaign, with particular on ensuring that a wide group of stakeholders is reached, in both localities involved; trainers report.emphasis on peer representing interests of Dalits and Janajatis. U Minutes of other youth orientededucation and networking U Local research partners identified, with expertise in gender issues. All organization's meetings collaborativewith other youth centred participants trained in awareness of the gender specific benefits and risks projects discussed and run centre records.services in order to of sexual activity, particularly in adolescent girls and boys. U Materials impact assessment.maximize sustainability. U Appropriate training programs and materials prepared for dissemination of U Statistical evidence of numbers involved:
information. feedback in the form of discussion groups,U Peer education groups set up and running for peer counseling and questionnaires and monitoring by clinic staff.
training. At least 150 programmes of education/outreach run by the end of U Tools and best practice models assessed bythe first year. At least 30 young people trained as per educators and 100 stakeholders, local and international NGOsyouths participating in regular condom distribution per year. and other groups involved.
U Tools for programme management, public awareness and inter youth U Agreement with other services, minutes ofservices networking created and produced. Best practice models meetings.established and developed. U Agreement with provincial governments:
U Links developed with other youth and satellite health services throughout changes in local and national policy.each province. O Running costs reduced and increasingly
U Strategies for lobbying and advocacy work, with particular focus on policy supplemented with income from someand socio-economic factors influencing women's reproductive health, services and from selling of service toolsrights identified and implemented. and material to other youth- focused groups.
U Strategies for cost recovery, e.g. pregnancy testing, provision of training inyouth sexuality/reproductive health to other agencies, identified andimplemented.
49 VCDP Health June 2004 10/06/2004
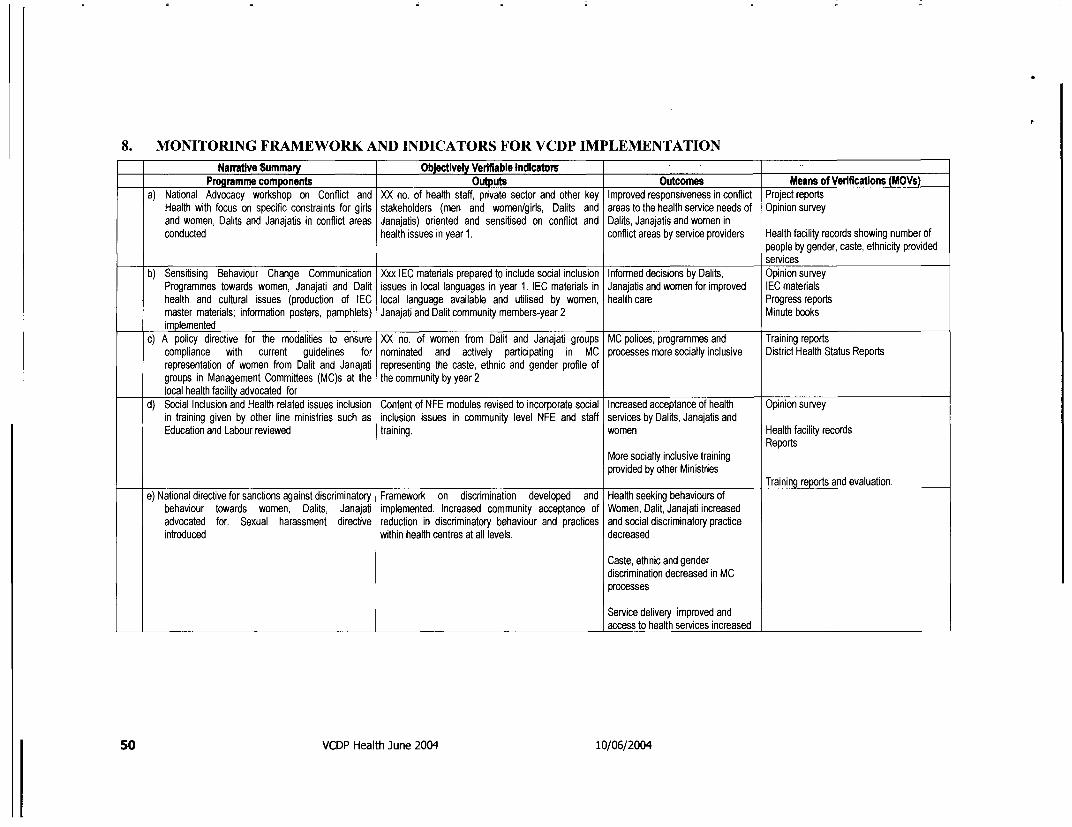
8. MONITORING FRAMEWORK AND INDICATORS FOR VCDP IMPLEMENTATION=___ Narative Summary Objectively Verifiable Indicatoms
Programme components Outputs Outcomes Means of Verifications (MOVs)a) National Advocacy workshop on Conflict and XX no. of health staff, pdvate sector and other key Improved responsiveness in conflict Project reports
Health with focus on specific constraints for girls stakeholders (men and women/gids, Dalits and areas to the health service needs of Opinion surveyand women, Dalits and Janajatis in conflict areas Janajatis) oriented and sensitised on conflict and Dalits, Janajatis and women inconducted health issues in year 1. conflict areas by service providers Health facility records showing number of
people by gender, caste, ethnicity providedservices
b) Sensitising Behaviour Change Communication Xxx IEC materials prepared to include social inclusion Informed decisions by Dalits, Opinion surveyProgrammes towards women, Janajati and Dalit issues in local languages in year 1. IEC materials in Janajatis and women for improved IEC materialshealth and cultural issues (production of IEC local language available and utilised by women, health care Progress reportsmaster materials; information posters, pamphlets) Janajati and Dalit community members-year 2 Minute booksimplemented
c) A policy directive for the modalities to ensure XX no. of women from Dalit and Janajati groups MC polices, programmes and Training reportscompliance with current guidelines for nominated and actively participating in MC processes more socially inclusive District Health Status Reportsrepresentation of women from Dalit and Janajati representing the caste, ethnic and gender profile ofgroups in Management Committees (MC)s at the the community by year 2local health facility advocated for
d) Social Inclusion and Health related issues inclusion Content of NFE modules revised to incorporate social Increased acceptance of health Opinion surveyin training given by other line ministries such as inclusion issues in community level NFE and staff services by Dalits, Janajatis andEducation and Labour reviewed training. women Health facility records
ReportsMore socially inclusive trainingprovided by other Ministries
Training reports and evaluation.e) National directive for sanctions against discriminatory Framework on discrimination developed and Health seeking behaviours of
behaviour towards women, Dalits, Janajati implemented. Increased community acceptance of Women, Dalit, Janajati increasedadvocated for. Sexual harassment directive reduction in discriminatory behaviour and practices and social discriminatory practiceintroduced within health centres at all levels. decreased
Caste, ethnic and genderdiscrimination decreased in MCprocesses
Service delivery improved andaccess to health services increased
50 VCDP Health June 2004 10/06/2004
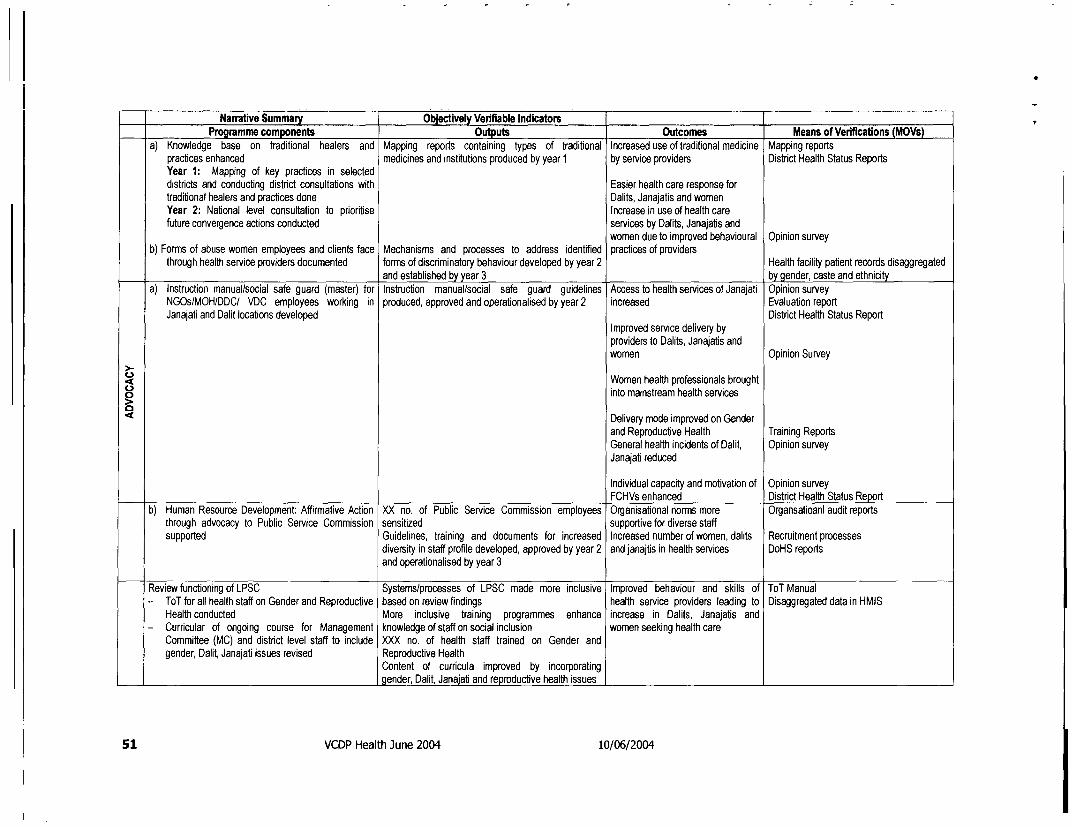
Narrative Summary Obectivey Veiflable lndicatomProgramme components Outputs Outcomes Means of Verifications (MOVs)a) Knowledge base on traditional healers and Mapping reports containing types of traditional Increased use of traditional medicine Mapping reports
practices enhanced medicines and institutions produced by year 1 by service providers District Health Status ReportsYear 1: Mapping of key practices in selecteddistricts and conducting district consultations with Easier health care response fortraditional healers and practices done Dalits, Janajatis and womenYear 2: National level consultation to prioritise Increase in use of health carefuture convergence actions conducted services by Dalits, Janajatis and
women due to improved behavioural Opinion surveyb) Forms of abuse women employees and clients face Mechanisms and processes to address identified practices of providersthrough health service providers documented forms of discriminatory behaviour developed by year 2 Health facility patient records disaggregated
and established by year 3 by gender, caste and ethnicitya) Instruction manual/social safe guard (master) for Instruction manual/social safe guard guidelines Access to health services of Janajati Opinion surveyNGOs/MOH/DDC/ VDC employees working in produced, approved and operationalised by year 2 increased Evaluation reportJanajati and Dalit locations developed District Health Status Report
Improved service delivery byproviders to Dalits, Janajatis andwomen Opinion Survey
Women health professionals brought8 into mainstream health servicesn
Delivery mode improved on Genderand Reproductive Health Training ReportsGeneral health incidents of Dalit, Opinion surveyJanajati reduced
Individual capacity and motivation of Opinion surveyFCHVs enhanced District Health Status Reportb) Human Resource Development: Affirmative Action XX no. of Public Service Commission employees Organisational norms more Organsatioanl audit reportsthrough advocacy to Public Service Commission sensitized supportive for diverse staff
supported Guidelines, training and documents for increased Increased number of women, dalits Recruitment processesdiversity in staff profile developed, approved by year 2 and janajtis in health services DoHS reportsand operationalised by year 3
Review functioning of LPSC Systems/processes of LPSC made more inclusive Improved behaviour and skills of ToT Manual- ToT for all health staff on Gender and Reproductive based on review findings health service providers leading to Disaggregated data in HMISHealth conducted More inclusive training programmes enhance increase in Dalits, Janajatis and- Curricular of ongoing course for Management knowledge of staff on social inclusion women seeking health care
Committee (MC) and distrct level staff to include XXX no. of health staff trained on Gender andgender, Dalit, Janajati issues revised Reproductive Health
Content of curricula improved by incorporatinggender, Dalit, Janajati and reproductive health issues
51 VCDP Health June 2004 10/06/2004
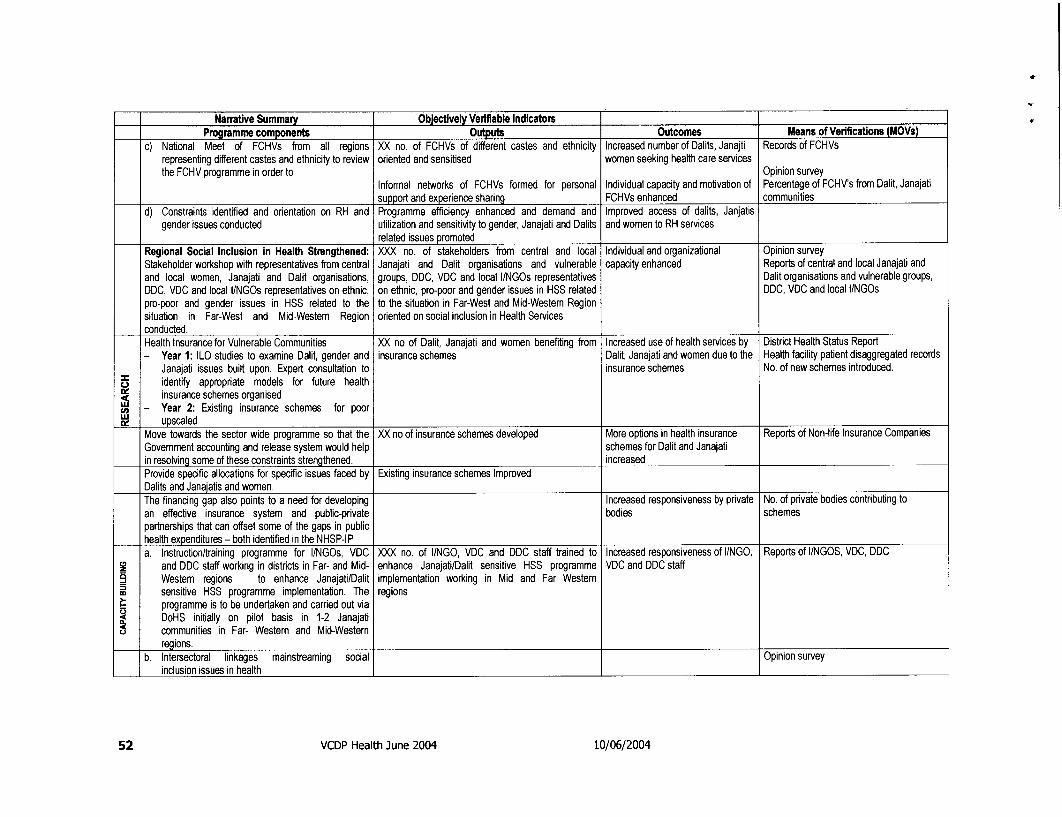
NarTaflve Summary Objectively Verifiable IndicatorsProgramme components Outputs Outcomes Means of Verifications (MOVs)
c) National Meet of FCHVs from all regions XX no. of FCHVs of different castes and ethnicity Increased number of Dalits, Janajti Records of FCHVsrepresenting different castes and ethnicity to review oriented and sensitised women seeking health care servicesthe FCHV programme in order to Opinion survey
Informal networks of FCHVs formed for personal Individual capacity and motivation of Percentage of FCHV's from Dalit, Janajatisupport and experience sharing FCHVs enhanced communities
d) Constraints identified and orientation on RH and Programme efficiency enhanced and demand and Improved access of dalits, Janjatisgender issues conducted utilization and sensitivity to gender, Janajati and Dalits and women to RH services
related issues promotedRegional Social Inclusion in Health Strengthened: XXX no. of stakeholders from central and local Individual and organizational Opinion surveyStakeholder workshop with representatives from central Janajati and Dalit organisations and vulnerable capacity enhanced Reports of central and local Janajati andand local women, Janajati and Dalit organisations, groups, DDC, VDC and local I/NGOs representatives Dalit organisations and vulnerable groups,DDC, VDC and local l/NGOs representatives on ethnic, on ethnic, pro-poor and gender issues in HSS related DDC, VDC and local l/NGOspro-poor and gender issues in HSS related to the to the situation in Far-West and Mid-Westem Regionsituation in Far-West and Mid-Western Region oriented on social inclusion in Health Servicesconducted.Health Insurance for Vulnerable Communities XX no of Dalit, Janajati and women benefiting from Increased use of health services by District Health Status Report- Year 1: ILO studies to examine Dalit, gender and insurance schemes Dalit, Janajati and women due to the Health facility patient disaggregated records
Janajati issues built upon. Expert consultation to insurance schemes No. of new schemes introduced.o identify appropriate models for future health;25 insurance schemes organised
- Year 2: Existing insurance schemes for poor= upscaled
Move towards the sector wide programme so that the XX no of insurance schemes developed More options in health insurance Reports of Non-life Insurance CompaniesGovernment accounting and release system would help schemes for Dalit and Janajatiin resolving some of these constraints strengthened. increasedProvide specific allocations for specific issues faced by Existing insurance schemes ImprovedDalits and Janajatis and women.The financing gap also points to a need for developing Increased responsiveness by private No. of pdvate bodies contributing toan effective insurance system and public-private bodies schemespartnerships that can offset some of the gaps in publichealth expenditures - both identified in the NHSP-IPa. Instruction/training programme for Il/NGOs, VDC XXX no. of I/NGO, VDC and DDC staff trained to Increased responsiveness of I/NGO, Reports of I/NGOS, VDC, DDC
and DDC staff working in distrcts in Far- and Mid- enhance Janajati/Dalit sensitive HSS programme VDC and DDC staffWestern regions to enhance Janajati/Dalit implementation working in Mid and Far Westernsensitive HSS programme implementation. The regionsprogramme is to be undertaken and carried out viaDoHS initially on pilot basis in 1-2 Janajaticommunities in Far- Western and Mid-Westernregions.
b. Intersectoral linkages mainstreaming social Opinion surveyinclusion issues in health
52 VCDP Health June 2004 10/06/2004
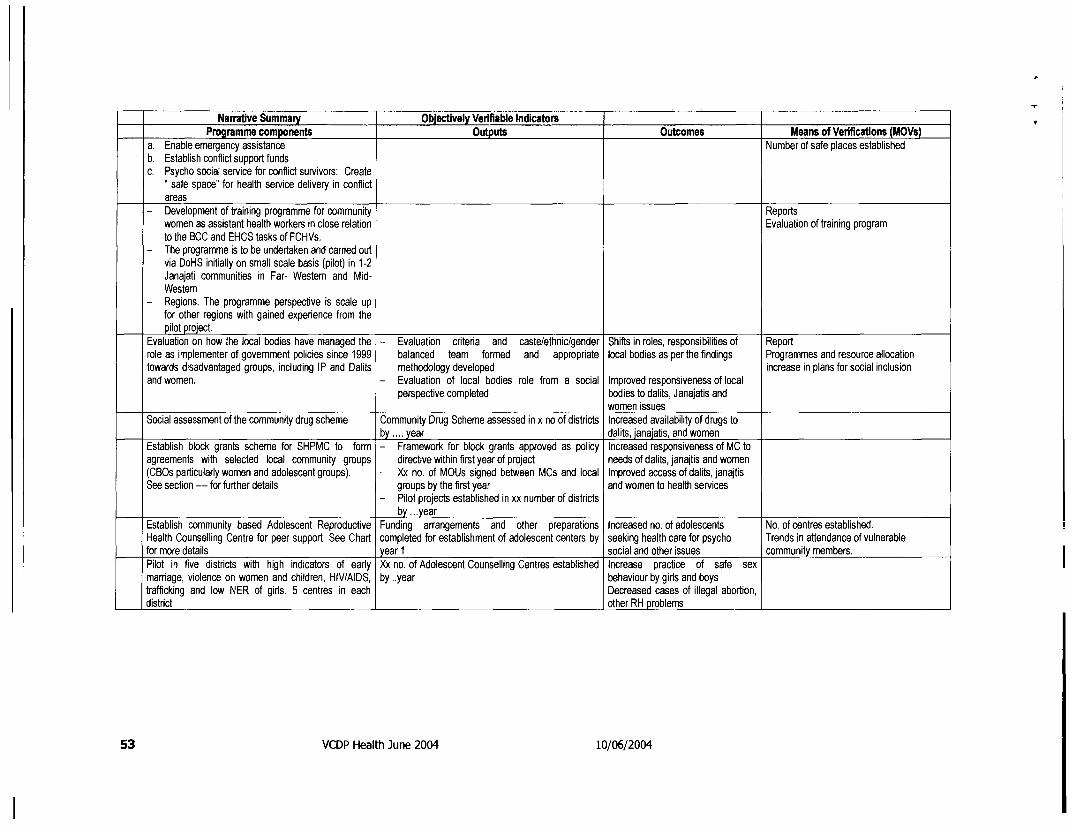
Narratve Summary Objectively Verifiable IndicatorsProgramme components Outputs Outcomes Means of Verifications (MOVs)
a. Enable emergency assistance Number of safe places establishedb. Establish conflict support fundsc. Psycho social service for conflict survivors: Create
" safe space" for health service delivery in conflictareas
- Development of training programme for community Reportswomen as assistant health workers in close relation Evaluation of training programto the BCC and EHCS tasks of FCHVs.
- The programme is to be undertaken and carded outvia DoHS initially on small scale basis (pilot) in 1-2Janajati communities in Far- Westem and Mid-Western
- Regions. The programme perspective is scale upfor other regions with gained experience from the
I pilot proiect.Evaluation on how the local bodies have managed the - Evaluation cdteria and caste/ethnic/gender Shifts in roles, responsibilities of Reportrole as implementer of government policies since 1999 balanced team formed and appropriate local bodies as per the findings Programmes and resource allocationtowards disadvantaged groups, including IP and Dalits methodology developed increase in plans for social inclusionand women. - Evaluation of local bodies role from a social Improved responsiveness of local
perspective completed bodies to dalits, Janajatis andwomen issues
Social assessment of the community drug scheme Community Drug Scheme assessed in x no of districts Increased availability of drugs toby .... year dalits, janajatis, and women
Establish block grants scheme for SHPMC to form - Framework for block grants approved as policy Increased responsiveness of MC toagreements with selected local community groups directive within first year of project needs of dalits, janajtis and women(CBOs particularly women and adolescent groups). - Xx no. of MOUs signed between MCs and local Improved access of dalits, janajtisSee section --- for further details groups by the first year and women to health services
- Pilot projects established in xx number of districtsby ...year
Establish community based Adolescent Reproductive Funding arrangements and other preparations Increased no. of adolescents No. of centres established.Health Counselling Centre for peer support. See Chart completed for establishment of adolescent centers by seeking health care for psycho Trends in attendance of vulnerablefor more details year 1 social and other issues community members.Pilot in five districts with high indicators of early Xx no. of Adolescent Counselling Centres established Increase practice of safe sexmarriage, violence on women and children, HIV/AIDS, by..year behaviour by girls and boystrafficking and low NER of girls. 5 centres in each Decreased cases of illegal abortion,district other RH problems
53 VCDP Health June 2004 10/06/2004
9. BIBLIOGRAPHYACNielson (ORG-MARG) Nepal .2003. "A draft report: Community Based Action Research on
Girls' Education in Nepal" preparedfor UNICEF, October 2003, Kathmandu, NepalAction Aid, 2001, Situation Analysis of DalitsADB (Asian Development Bank).1999. A Country Briefing Paper: Women in Nepal,
Programme Department, Philippines.Bennett, L, 2004, "Concept Note: Nepal Gender and Social Exclusion Assessment", January
2004Bhatia K, 2004, Vulnerable Community Development Plan, World BankCBS. 2002. Population Census of Nepal, National Report, KathmanduCentral Bureau of Statistics. 2003. Population Monograph of Nepal. Kathmandu: His Majesty's
Government National Planning Commission Secretariat.Cohen, Alex et al, 2002, World Mental Health Casebook: Social and Mental Health Programs
in Low-Income CountriesConsequences of torture, CVICTDepartment of Education.2001. School Level Educational Statistics of Nepal, Sanothimi,
Bhaktapur.DHO/GTZ, 2003, Report on First Aid Refresher Training to Freed Kamaiya Leaders: Bardiya,
July 2003DHSP, 2003, Developing Health Sector Decentralisation in Nepal: Collaborative Policy
DevelopmentDHSP/RHDP/HSSP, March 2003, Conflict and Health in Nepal: Action for Peace buildingDhungana, 2003, The Lives of Disabled Women in Nepal; Vulnerability without SupportDoHS/MoH, 2004, A Manual Prepared for Transfer and Operation of Local Health Institutions
2060 (2004)EC/UJNFPA, 2002, Reproductive Health Initiative (RHI) in Nepal: Achievements and
Reflections, August 2002ESP/DFID, 2004, Janajati Empowerment Project, 3 February 2004ESP/DFID ...... Dalit Empowerment Integration Project,FHD/DHS, 1998, Maternal Mortality and Morbidity Study, NepalField Office, CEDPA/Nepal, website.Focus Group Study on Reproductive Health in Nepal from Social -Cultural Perspective, Draft
Report, SAMANTA submitted to UNFPA, 1999FPAN, 2002, "Final Report on Studying FPAN's Policies and Programmes in gender
perspective"GEFONT/KAD, 2003, Study Report on Women Worker issues: Search for AlternativesGTZ/UNFPA, 2002, Reproductive Morbidity a neglected issue? Report of a clinic-based study
in Far Western NepalGurung, Harka. 2001. Nepal Social Demography and Expressions. Kathmandu: New Era.Health Sector Strategy: An Agenda for Change (Reform), Kathmandu, August 2002HMG/ NPC. 1998. The Ninth Plan (1997-2002). Kathmandu, NepalHMG/ NPC. 2003. The Tenth Plan (2003-2007). Kathmandu, NepalHMG/EC/UNFPA, 2002, Reproductive Health Atlas, EC/UNFPA Reproductive Health
Initiative Nepal: A Presentation of Selected Reproductive Health Indicators: 1998-2002HMG/New Era/Orc Macro, 2002, Nepal Demographic and Health Survey 2001, April 2002HMG/UNICEF, 1996, National Maternity Care Guidelines, Nepal,HSSP, 2004, Richshaw Ambulance in Jantanagar, April 2004ICIMOD/CBS/SNV, 2003, Districts of Nepal:, Indicators of Development, update 2003.ICIMOD/CBS/SNV, 2003, Mapping Nepal Census Indicators 2001 and Trends, update 2003.ILO . An Inventory of Micro-Insurance Schemes in NepalILO, 2001, Situation of Child Ragpickers: A Rapid AssessmentILO, 2002, Child Labour in the Nepalese Carpet Sector: A Rapid AssessmentILO, 2004, Sexual harassment at the workplace in NepalILO/STEP, 2003, A Case Study on the Insurance Scheme of the Public Health Concern Trust
(phect) Nepal
54 VCDP Health June 2004 10/06/2004
ILO/STEP, 2003, Alternate Health Care Financing: Synthesis of Existing Experience in Nepal,February 2003
Informal Sector Research and Development Centre .2002. District Demographic Profile ofNepal, Kathmandu, Nepal
Informal Sector Research and Development Centre. 2001. District Development Profile ofNepal, Kathmandu, Nepal
Joint Review of NHSSP-IP, DFIDLansdown Gerison, 2003, Disabled Children in Nepal: Progress in implementing the
Convention on the Rights of the Child.Maternal Mortality and Morbidity Study, FHD/DHS, 1998Ministry of Finance, Office of the Financial Comptroller General. 2003. Report of Expenditure
Tracking Survey of Primary, Lower Secondary and Secondary Schools. Ananmagar,Kathmandu, Nepal, 4 June 2003.
MLD/WFP/GTZ, 2004, Women and Food Security: Reflections and Experiences from theGender Activities of the Rural Community Infrastructure Works Programme, February2004
MOH, 1998, National Reproductive Health Strategy, FHD/ DHS, NepalMoH, 1998, Nepal Safe Motherhood Policy, FHD/DHS/MoH, July 1998MOH, 200, Nepal Country Profile, Women Health and DevelopmentMOH, 2000, National Adolescent Health and Development Strategy,MoH, 2002, Institutional Assessment: Nepal Health Sector, Verulam Associates Ltd/MoH, 2002MOH, 2002, National Safe Motherhood Plan (2002-2017)MoH, 2003, Annual Report- 2001/2002, DHS/MOH, KathmanduMoH, 2003, Public Expenditure of the Health Sector in Nepal, HEFU/MoHMOH, 2055 B.S., Reproductive Health Program, Operational Management Guidelines, (for
District level),MOH, Nepal Family Planning Services Policy 2054 BS (Nepali version)MOH/GTZ, Brochure on Health Sector Support Programme- Nepal, Reproductive Health
ProjectMoH/HMG, 2003, "Final draft Nepal Health Sector Programme -Implementation Plan" 18
August 2003MWCSW/ MGEP/UNDP, 2002, Gender Assessment of Health SectorNational Adolescent Health and Development Strategy, Family Health Division, DHSP,
MOH/HMG, 2000National Adolescent Health and Development Strategy, HMG, MOH, 2000National HIV/AIDS Strategy (2002-2006) Nepal.National RH Health Strategy, 1998 pp- 26-27NCASC, 2000, "Final Draft: Situation Analysis of HIV/AIDS in Nepal, December 2000NDF 2002, "Medium term Expenditure Framework (2002/3 - 2004/5)"NDF/HMG, 2004, "Policy Paper on Health Sector Development of His Majesty's Government
of Nepal"Nepal Family Planning Services Policy 2054 BSNepal Health Profile on Women, Health and Development 2001, Planning and Foreign Aid
Division, DoHS/MoHNepal Safe Motherhood Policy, FHD, DHS, MOH, July 1998NFHP, 2003, Nepal Family Health Programme Behaviour Change Communication Formative
Research and Evaluation Study: Findings on FCHV Survey, July 2003Nielson, L.C.; Shrestha, S.M, 2003, "Draft report: Social Assessment of the Nepal Health Sector
Reform ", World Bank, NepalNRCS/JRCS/ENPHO, 2001, Household survey on the Health Impact of Arsenic Contaminated
Ground water in NawalparasiNSMP, 2004, Draft: Coping with the burden of the costs of maternal health, 17" Feb 2004NSMP: Impact of Conflict on Accessibility of EOC Health Services, By Monique Beun and
Basu Dev Neupane, June 2003 176/96/DFDPandit Upendra; Clapham Susan, 2.... Assessing the quality of Comprehensive Essential
Obstetric care using an audit of the 100 Caesarean sections in Baglung DistrictPolicy Project, 2003, Adolescent and Youth Reproductive Health in Nepal: Status, Issues,
Policies, and Programs
55 VCDP Health June 2004 10/06/2004
r
Project Appraisal Document On A Proposed Credit In The Amount Of Sdr {Amt} Million(US$50 Million Equivalent) To His Majesty's Government of Nepal for A Health SectorProgramme Project, April 20, 2004
Rai, Uma, 2003, Paper in Annual Programme Review Meeting, MalaysiaReproductive Health Initiative in Nepal, Achievements and Reflections EC/UNFPA, August
2002SCF (US), 2003, Maternal and Neonatal Health and HMG/N: A Study of the Concept of
Volunteerism: Focus on Community Based Health Volunteers in Selected Areas of Nepal,February 2003
SCF (US), A report on final survey of Adolescents Sexual and Reproductive Health Project:Kathmandu, 1999-2002
SCF UK, 200 ... ??, A study on governmental plans, programmes and budgets affecting childrenin Nepal,
SCF, 2004, Everyone counts: Dalit children and the right to education in NepalSCF/NNDSWO, 2002, " A Brief Introduction: Nepal Children's Scholarship Endowment
Program", April 2002, KathmanduSDC, 2002, Annual Report of Rural Health Development Project (RHDP) Staff Profile
Information sent by HURDIS/DoHSSpace Times, 01 April 04 - Each year 5 Thousands women Die,STEP/ILO, 2002, Extending Maternity Protection to Women in the Informal Economy, the Case
of NepalUma Rai, UNICEF staff in AMDD Network Conference on 21-23 Oct 2003, Kuala Lumpur
MalaysiaUNAIDS / NCASC, 2003, The HIV/AIDS/STD Situation and The National Response in Nepal:
Country Profile, Jan 2003.UNAIDS/ NCASC, 2003, "The HIV/AIDS/STD Situation and The National Response in Nepal,
Country Profile"UNICEF ROSA, 2001, Emergency Obstetric Care Quality Assessment: Sagarmatha Zonal
Hospital, Rajbiraj, Saptari District, Nepal, Baseline Study, July 2001UNICEF ROSA/NEW ERA, 2001, Emergency Obstetric Care Quality Assessment, Sagarmatha
Zonal Hospital, Rajbiraj, Saptari District, Nepal, Baseline Study, July 2001.UNICEF/National Planning Commission, 2000, A Situation Analysis of Disability in Nepal.UNIFEM/UND, 2..., Gender Budget AuditWomen 'Worst hit' by ongoing conflict, The Kathmandu Post, 01 Apr 04Women and Food Security: Reflections and Experiences from the Gender Activities of the
Rural Community Infrastructure Works Programme, MLD/WFP/GTZ, Feb 2004World Bank, 2000, Nepal Operational Issues and Prioritization of Resources in the Health
Sector, June 8, 2000World Bank, 2001, Understanding Access, Demand and Utilization of Health Services in Nepal
and their Constraints, June 2001World Bank, 2003, "Debriefing note: Study of Best Practices to Include Indigenous People in
Sector Programme Support ", Mission to Nepal, September 2003.World Bank, 2003, Economic Assessment of the Health Sector Strategy, Nepal and Agenda for
Reform, January 2003World Bank, 2004, Concept Note on Nepal Gender and Social Exclusion Assessment.
56 VCDP Health June 2004 10/06/2004





























