Embed Size (px)
Citation preview
RESEARCH PAPER
Disturbed eating behaviours and associated psychographiccharacteristics of college studentsV. M. Quick* & C. Byrd-Bredbenner†
*Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, Division of Epidemiology,
Statistics and Prevention Research, Bethesda, MD, USA
†Department of Nutritional Sciences, Rutgers University, New Brunswick, NJ, USA
Keywords
body image, college students, disturbed eating,
psychographic characteristics.
Correspondence
V. M. Quick, Eunice Kennedy Shriver National
Institute of Child Health and Human
Development, National Institutes of Health,
Division of Epidemiology, Statistics and Prevention
Research, 6100 Executive Blvd., Rm 7B13E,
Bethesda, MD, USA.
Tel.: +1 301 435 6936
Fax: +1 301 402 2084
E-mail: [email protected]
How to cite this article
Quick V.M. & Byrd-Bredbenner C. (2013)
Disturbed eating behaviours and associated
psychographic characteristics of college students.
J. Hum. Nutr. Diet.
doi:10.1111/jhn.12060
Abstract
Background: Young adulthood is a stressful transition period that may
increase the risk for disturbed eating, especially for college students. The
present study aimed to explore disturbed eating behaviours and a broad
array of associated psychographic characteristics in a large, diverse sample
of college students.
Methods: College students (n = 2604; 58% white; 63% female) enrolled at
three large, public US universities in 2009 and 2010 were recruited to take
an online survey. The survey included reliable and valid disturbed eating
behaviour and associated psychographic characteristic measures.
Results: Many participants engaged in disturbed eating practices. For exam-
ple, one-quarter of women and one-fifth of men engaged in dietary
restraint. One in seven reported regularly binge eating. One-third used inap-
propriate compensatory behaviours (self-induced vomiting, medicine misuse
and excessive exercise) as a means for controlling weight and/or shape, with
the rate of these behaviours reaching clinically significant levels for 4%, 3%
and 5% of participants, respectively. Examination of psychographic charac-
teristics revealed that one-fifth had moderate levels of depression and anxi-
ety severity and almost half engaged in at least one obsessive–compulsive
disorder type behaviour. Females felt under more pressure to attain the
media physical appearance standard than males.
Conclusions: The findings of the present study suggest that nutrition educa-
tion interventions for college students may be needed to address disturbed
eating behaviours and to provide guidance on how to seek professional
help. The findings also suggest that it may be prudent for healthcare profes-
sionals to routinely screen college students for disturbed eating behaviours
and offer interventions early when treatment is likely to be most effective.
Introduction
Young adults who are college students face many challenges
as they navigate this transitional life stage. This period,
known as ‘emerging adulthood’, is characterised by self-
focus, identity exploration, and major changes in home life
and education/work situations (Arnett, 1997, 1998, 2001).
For most, young adulthood is marked by moving from
their family-of-origin home to independent living, trading
full-time education for full-time work, forming intimate
nonfamily relationships and becoming parents.
These changes are stressful and can impact health-
related behaviours negatively (Bell & Lee, 2006). For
example, emerging adults are at particularly high risk for
weight gain and disturbed eating behaviours (Lewis et al.,
2000; Hoek, 2006). Disturbed eating behaviours are
abnormal practices associated with eating disorders [e.g.
restraint, emotional, disinhibited, binge, and night eating;
ª 2013 The Authors
Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd. 1
Journal of Human Nutrition and Dietetics

weight, shape, and eating concerns; strict dieting; and
controlling body weight and shape through inappropriate
compensatory behaviours (i.e. purging)] that, individu-
ally, do not warrant a psychiatric diagnosis of an eating
disorder, such as anorexia nervosa and bulimia nervosa,
which are clinically defined by DSM-IV (American Psy-
chiatric Association, 2000) criteria. Dietary practices,
sociocultural expectations, body image perceptions and
psychological characteristics may all affect the develop-
ment of disturbed eating behaviours (Striegel-Moore,
1997; Stice, 2002).
Dietary practices of young adults often fall short of rec-
ommendations (Dietary Guidelines for Americans, 2010;
National Cancer Institute, 2010). Intakes of many key
nutrients, including folic acid, calcium, potassium, fibre
and iron (for females), are less than recommended (Ervin
et al., 2004; Barley et al., 2010). By contrast to these defi-
cits, they are consuming excessive amounts of calories,
fat, cholesterol, sugar and sodium (Ervin et al., 2004;
Gunn et al., 2010). Young adults’ unbalanced dietary
intakes increase their risk for chronic disease (Higgins
et al., 1988; Dietz, 1998; Flegal et al., 2010). For women,
insufficient folic acid intake increases their risk of giving
birth to children with neural tube defects (McDowell
et al., 2008).
Sociocultural expectations heavily influence body
image perceptions in Western societies (Thompson et al.,
1999) by promoting a degree of thinness attainable by
few (Hesse-Biber et al., 2006). These expectations are
transmitted via media and exchanges with friends and
family. The pressure to avoid obesity and conform to
cultural or familial ‘standards’ for ‘beauty’ (i.e. thinness)
may prompt disturbed eating behaviours directly and/or
cause distorted body image perceptions (Thompson
et al., 1999; Holsten & Cashwell, 2000; Stice & Hoffman,
2004). Body image distortion is an inaccurate interna-
lised representation of one’s weight, shape and appear-
ance that can lead to body dissatisfaction (Thompson
et al., 1999).
The emotional stress of changes associated with emerg-
ing adulthood also increases the risk of psychological dis-
orders (Misra & McKean, 2000; Sacker & Cable, 2010).
The rates of depression, anxiety, and other mental disor-
ders among young people in the USA have risen steadily
over the last seven decades (Twenge et al., 2010). For
example, five to eight times as many college students
meet the criteria for diagnosis of major depression and/or
anxiety disorder compared to those a century ago, even
when controlling for changes in diagnostic criteria and
measures over the years (Twenge et al., 2010). Poor psy-
chological well-being also is common among individuals
with disturbed eating practices (Crow et al., 1996). For
example, as depression and anxiety severity increase, so
do disturbed eating practices, such as dietary restraint
(i.e. restricting one’s food intake) and disinhibited eating
(i.e. losing control over food intake), which can trigger
binge eating (i.e. eating a large amount of food in a rela-
tively short time and feeling out of control) and purging
(e.g. self-induced vomiting, misuse of laxatives, excessive
exercise) (Bulik, 2002). Similar associations have been
reported for individuals with obsessive–compulsive dis-
order (OCD) severity and eating disorders (Wonderlich,
2002).
Dichotomous thinking is another psychological charac-
teristic associated with disturbed eating behaviours.
Dichotomous thinking is a form of cognitive rigidity
where individuals see reality in polarised categories of
‘either-or’ rather than as a continuum of possibilities
(Byrne et al., 2008). That is, they think of food as being
either ‘good’ or ‘bad’. Individuals who set rigid dietary
‘rules’ are more likely to binge eat after any transgression
from these rules (Fairburn et al., 2003). Dichotomous
thinking is also a key factor in cognitive behavioural
models of eating disorders (Byrne et al., 2008).
Nutrition education has the potential to help young
adults develop and maintain healthy, rather than dis-
turbed, eating patterns. The most effective educational
interventions are targeted and tailored to specific audi-
ences (Maibach et al., 1996; Institute of Medicine, 2002;
Bernhardt, 2004). Our understanding of disturbed eating
practices and the many factors associated with these prac-
tices in young adults is limited because previous research
has defined disturbed eating behaviours narrowly,
explored a restricted array of characteristics related to dis-
turbed eating, focused on females and/or clinical groups,
and/or used instruments with modest reliabilities (Kashu-
beck-West et al., 2001; Fairburn & Brownell, 2002;
Ogden, 2003; Reas & Grilo, 2004; Mitchell & Peterson,
2005; Olmsted et al., 2007). The limitations of existing
research thereby hinder the development of nutrition
education interventions designed to help this age group
maintain nondisturbed eating patterns. The high rate and
exorbitant costs of treating those with disturbed eating
practices indicate that a more comprehensive understand-
ing of this audience is needed (Ma et al., 2003; McCor-
mick & Stone, 2007). Thus, the present study aimed to
describe a broad array of disturbed eating practices and
psychographic characteristics linked with disturbed eating
behaviours in a large, diverse sample of free-living young
adults who are college students and to compare differ-
ences between sexes.
Materials and methods
This cross-sectional research study was approved by the
Institutional Review Board at Rutgers University.
ª 2013 The Authors
2 Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd.
Disturbed eating among college students V. M. Quick and C. Byrd-Bredbenner

Sample
Young adults, ages 18–26 years, enrolled in college were
recruited via verbal announcements, listservs, web post-
ings and flyers at three large US public universities from
2009 to 2010. In addition, university instructors of large
general education courses (e.g. psychology, health) were
invited to recruit students in their classes. Recruitment
materials indicated that the study involved spending
approximately 30 min completing an online survey and a
chance to win one of 10 cash prizes ($25). Participants
enrolled in courses taught by a participating professor
also were awarded a few bonus points for participation
and/or research participation credits that were required
by the course.
Instrument
The survey instrument had three sections. The first sec-
tion established the participant’s basic demographic char-
acteristics, such as age, sex and race/ethnicity. Self-report
height and weight data were used to calculate body mass
index (BMI; kg m�2).
The second section examined eating behaviours and
the third section investigated psychographic characteris-
tics associated with eating behaviours. The development
of these sections began with an extensive literature search
to identify a comprehensive array of salient eating behav-
iours and associated psychographic characteristics, as well
as existing valid, reliable, brief self-report measures
appropriate for assessing them in young adults. A panel
of experts (n = 9) in nutrition, eating disorder treatment,
psychology and public health reviewed the list of eating
behaviours and psychographic characteristics to ensure
their comprehensiveness and contextual value with regard
to the aims of the study. The panel also assisted with the
selection of existing scales for assessing eating behaviours
and psychographic characteristics. In addition to the
extant scales used in the present study, the experts recom-
mended creating a method for assessing body image
distortion. The final draft was reviewed by the panel of
experts for contextual value of each item in a scale, clar-
ity, fluidity, grammar, relevance to research purpose and
audience, and to establish content validity of the items
assessing each characteristic.
The contents of sections two and three are described
below. All scales in these sections were scored in accor-
dance with standard procedures established by the existing
scale creators (i.e. averaging all items in a scale), unless
otherwise indicated. In addition, higher scores indicate a
greater presence of the eating behaviour or psychographic
characteristics, unless otherwise indicated.
Disturbed eating behaviours
The second section of the survey examined eating behav-
iours using seven scales, four of which were from the
Eating Disorder Examination Questionnaire (EDE-Q), 6th
edition (Fairburn & Beglin, 1994; Mond et al., 2004; Fair-
burn et al., 2008). The EDE-Q Restraint scale measured
attempts to restrict food intake to influence body shape
and weight. The Eating Concerns scale measured preoccu-
pation with and feelings towards eating food. The EDE-Q
Binge Eating Disorder Module assessed frequency of
binge eating (i.e. eating an unusually large amount of
food accompanied by a sense of loss of control) and the
use of inappropriate compensatory behaviours as a means
for controlling shape or weight (Fairburn et al., 2008).
Inappropriate Compensatory Behaviour scale items were
scored from 0 to 6 based on the frequency the participant
engaged in the behaviours. Scoring took clinical signifi-
cance of the frequency of these behaviours into consider-
ation (i.e. self-induced vomiting, medicine misuse and
excessive exercise are considered clinically significant
when performed � 4, � 4, or >20 times in the past
28 days, respectively) (Luce et al., 2008; Lavender et al.,
2010). For self-induced vomiting and medication misuse
items, a score of 0 to 5 indicated zero to five occurrences
of the behaviour and 6 indicated engaging in the behav-
iour six or more times. For excessive exercise, a score of
0 indicated that no excessive exercise occurred; scores
between 1 and 6 equalled excessively exercising for 1–5,6–10, 11–15, 16–20, 21–25 or >25 times in the past
28 days, respectively. This coding was used for inappro-
priate compensatory behaviours because a score of four
indicated clinical significance and is just above the scale
mid-point, which also allowed for assignment of higher
scores reflecting more frequent occurrences (i.e. severity)
of the behaviour.
Emotional Eating and Disinhibited Eating were assessed
with Three Factor Eating Questionnaire-18 scales (Karls-
son et al., 2000). The Emotional Eating scale assessed
how emotions influence the urge to eat and the Disinhib-
ited Eating scale assessed the extent of loss of control over
eating (Karlsson et al., 2000). To lower participant bur-
den, the Disinhibited Eating scale was reduced to the
items with the strongest factor loadings reported
previously (Karlsson et al., 2000).
The Night Eating Questionnaire assessed night eating
syndrome using only items pertaining to individuals who
get up in the middle of the night and have cravings or
urges to eat (Allison et al., 2008). These items represent
the most salient features of night eating syndrome. Partic-
ipants were coded as a night eater if they got up in the
middle of night and ate � 50% of their daily food intake
after suppertime.
ª 2013 The Authors
Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd. 3
V. M. Quick and C. Byrd-Bredbenner Disturbed eating among college students

Psychographic characteristics associated with eating
behaviours
The third section of the survey explored psychographic
characteristics associated with eating behaviours. Psycho-
graphic characteristics were grouped into three areas:
body image attributes, psychological characteristics and
sociocultural environment.
Body image attributes
Five scales were used to assess body image attributes. The
Weight Concerns scale from the EDE-Q (Fairburn & Beg-
lin, 1994; Mond et al., 2004; Fairburn et al., 2008) mea-
sured feelings about body weight. The EDE-Q (Fairburn
& Beglin, 1994; Mond et al., 2004; Fairburn et al., 2008)
Shape Concerns scale assessed feelings about body shape
and size.
The Self-Evaluative Salience and Motivational Salience
scales from the Appearance Schema Inventory-Revised
(Cash & Labarge, 1996) assessed the extent to which indi-
viduals define or measure themselves and their self-worth
by their physical appearance, as well as the extent to
which persons attend to their appearance and engage in
appearance management behaviours, respectively. These
two scales were reduced in length to reduce repetition
and participant burden.
Body Image Distortion was assessed by comparing actual
self-reported BMI weight category [i.e. underweight
(BMI < 18.5 kg m�2), normal weight (BMI = 18.5–24.9 kg m�2), overweight (BMI > 25 kg m�2), scored 1,
2 and 3, respectively] to perceived current body weight
(i.e. very thin/thin, average, slightly heavy/overweight,
scored 1, 2 and 3, respectively). Perceived current body
weight was assessed by asking participants, ‘How would
you describe your weight?’, with responses ranging from
very thin to overweight. A Body Image Distortion score
was derived by subtracting actual BMI weight category
score from perceived current body weight score. Scores
could range from �2 to 2. Scores close to zero indicate
accurate body image perception. Positive scores indicate
individuals perceive they are heavier than they actually are,
whereas negative values indicate that individuals perceive
they are thinner than they actually are.
Psychological characteristics
Psychological characteristics were assessed with five
scales. The Patient Health Questionnaire-8 measured the
frequency a person experienced each of the DSM-IV cri-
teria for depression (Spitzer et al., 1999; Kroenke et al.,
2001). The Generalized Anxiety Disorder scale assessed
severity of anxiety (e.g. feeling nervous, anxious or on
the edge) (Spitzer et al., 2006). The Florida Obsessive
Compulsive Inventory (Storch et al., 2007) was used to
assesses presence and severity of OCD symptoms. The
OCD score is calculated only for those who had OCD
symptoms.
Self-esteem was measured using items from the Rosen-
berg Self Esteem scale (Rosenberg, 1965) with the highest
factor loadings (Henkel, 1976). In addition, the original
Likert scale was increased from 4 to 5 points to provide a
broader array of answers and to make it more consistent
with other scales used in this study. Higher scores
indicate lower self-esteem.
The Dichotomous Eating subscale from the Dichoto-
mous Thinking in Eating Disorders Scale (Byrne et al.,
2008) assessed the presence of a rigid, ‘black-and-white’
cognitive thinking style. Scores were computed only for
those who reported dieting because this scale is not
applicable to those who do not diet.
Sociocultural environment
Sociocultural environment was evaluated using seven
scales that focused on media and family environments.
Three scales from the Sociocultural Attitudes Towards
Appearance Questionnaire (Thompson et al., 2004) mea-
sured media influences on body image. The Internaliza-
tion-General scale assessed the influence of media (e.g.
television, magazines) on body image. The Pressures-
Media scale measured perceived pressure from the media
on body image. The Information-Media scale evaluated
awareness of societal appearance norms conveyed by the
media. These scales were shortened to reduce repetition
or to better reflect current media used by young adults.
Retained items were those with highest factor loadings
reported by others (Thompson et al., 2004).
Family eating environment was assessed using Child-
hood Family Mealtime Questionnaire scales, which
assessed recollections of family mealtime experiences dur-
ing childhood (Miller et al., 1993). These scales were
reduced in length to improve their relevance to the target
audience. The Mealtime Communication-Based Stress
scale assessed stress felt during mealtimes as a child. The
Mealtime Structure scale assessed family mealtime pres-
sures as a child. The Appearance Weight Control scale
evaluated the importance of weight management as a
child. The Emphasis on Mother’s Weight scale assessed
the attention participants felt was given to their mothers’
weight during childhood.
Statistical analysis
Internal consistency scores (i.e. Cronbach-a) were calcu-
lated for all eating behaviour and psychographic charac-
teristic instruments. Descriptive statistics (e.g. mean, SD,
frequency) were generated for all demographic items,
eating behaviour measures and psychographic characteris-
tic scales by sex. To determine whether males differed
ª 2013 The Authors
4 Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd.
Disturbed eating among college students V. M. Quick and C. Byrd-Bredbenner

significantly from females, independent sample t-tests
were conducted on all measures. P < 0.05 was considered
statistically significant. All analyses were conducted using
PASW STATISTICS, version 19.0 (SPSS Inc., Chicago, IL,
USA).
Results
A total of 2730 individuals completed the survey during
2009 and 2010. Participants who were not in the age
range of 18 to 26 years (n = 99), non-students (n = 21)
or those who omitted key demographic information (i.e.
height, weight or sex; n = 6) were eliminated from the
data analysis. Thus, the total sample size was 2604.
The majority of participants were female (63%) and
first- or second-year college students (64%). Participants
also were primarily white (58%) and Asian (21%). Black/
African Americans and Hispanics each represented
approximately 8% of participants with the remaining 5%
being from other racial/ethnic groups. Participant mean
(SD) age was 19.72 (1.53) years and mean (SD) BMI
was in the healthy range [23.34 (4.04) kg m�2; range
13–55 kg m�2], with few participants being underweight
(6%) or obese/morbidly obese (7%). Most participants
were at a healthy weight (68%) and approximately one-
fifth were overweight. Dieting behaviours were reported
by more than one-third (38%) of participants.
Cronbach-a internal consistency scores were computed
for the scales used to measure eating behaviours and psy-
chographic characteristics. Cronbach-a for all measure-
ments were good to excellent (i.e. range = 0.71 to 0.92)
(Table 1), except for the Inappropriate Compensatory
Behaviour scale (a = 0.51).
Disturbed eating behaviours
As shown in Table 1, mean Eating Concerns and
Restraint scale scores were low, indicating that partici-
pants did not have negative eating concerns and were
infrequently restricting food intake. However, females
scored significantly higher on both these scales than
males.
Specifically, 1.6% of females and 0.2% of males had
clinically significant Eating Concerns scores (i.e. mean
score � 4) that met eating disorder criteria. One-quarter
of women and one-fifth of men reported restricting
their food intake for � 8 h at least once in the past
28 days as a means of controlling their weight or shape.
In addition, almost one-quarter engaged in binge eating
in the past 28 days. Regular occurrences of binge eating
(i.e. � 4 binge eating episodes in the past 28 days) were
reported by approximately one in seven men and
women.
An examination of use of inappropriate compensatory
behaviours as a means for controlling weight and/or
shape indicated that 6% used self-induced vomiting in
the past 28 days, and 4% reporting a frequency that
reached clinically significant levels for meeting eating dis-
order criteria. Similarly, 6% misused medicine and 3%
had a misuse rate sufficiently high to be categorised as
clinically significant for meeting eating disorder criteria.
Excessive exercise was reported by almost one-third of
participants, with 5% reaching a clinically significant level
for meeting eating disorder criteria. Males and females
did not differ in their frequency of self-induced vomiting
or misusing medicine; however, males excessively exer-
cised significantly more than females.
Participants had moderate Emotional and Disinhibited
Eating scale scores. Females scored significantly higher on
the Emotional Eating scale, but there were no sex differ-
ences on the Disinhibited Eating scale.
Almost 2% of participants met the criteria to be classi-
fied as night eaters. Males had significantly higher night
eating scores than females.
Body image attributes
Although Shape Concerns and Weight Concerns scale
scores were low, 15% and 10% of participants had Shape
Concerns and Weight Concerns scores, respectively, that
were � 4 and are considered clinically significant for
meeting eating disorder criteria. Mean Self-Evaluative Sal-
ience and Motivational Salience scale scores were slightly
above the mid-point, indicating that appearance played a
moderate role in participants’ assessment of their self-
worth and that they did invest some resources in their
physical appearance. Compared with males, females had
significantly greater concerns about their shape and
weight, were more likely to base their self-worth on phys-
ical appearance, and placed a greater value on overall
appearance.
A comparison of actual and perceived BMI weight cate-
gory (i.e. Body Image Distortion) indicated that both
males and females perceived their weights somewhat
accurately. However, male participants were significantly
more likely than females to perceive themselves as being
lighter than their actual body weight.
Psychological characteristics
Mean scores indicated depression and anxiety were mild
for almost half of the participants, with females scoring sig-
nificantly higher on both these scales than males. Almost
half of participants (n = 1224) reported OCD-related
symptoms. Of these participants, OCD severity was low,
with no sex differences. Self-esteem mean scores were
ª 2013 The Authors
Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd. 5
V. M. Quick and C. Byrd-Bredbenner Disturbed eating among college students
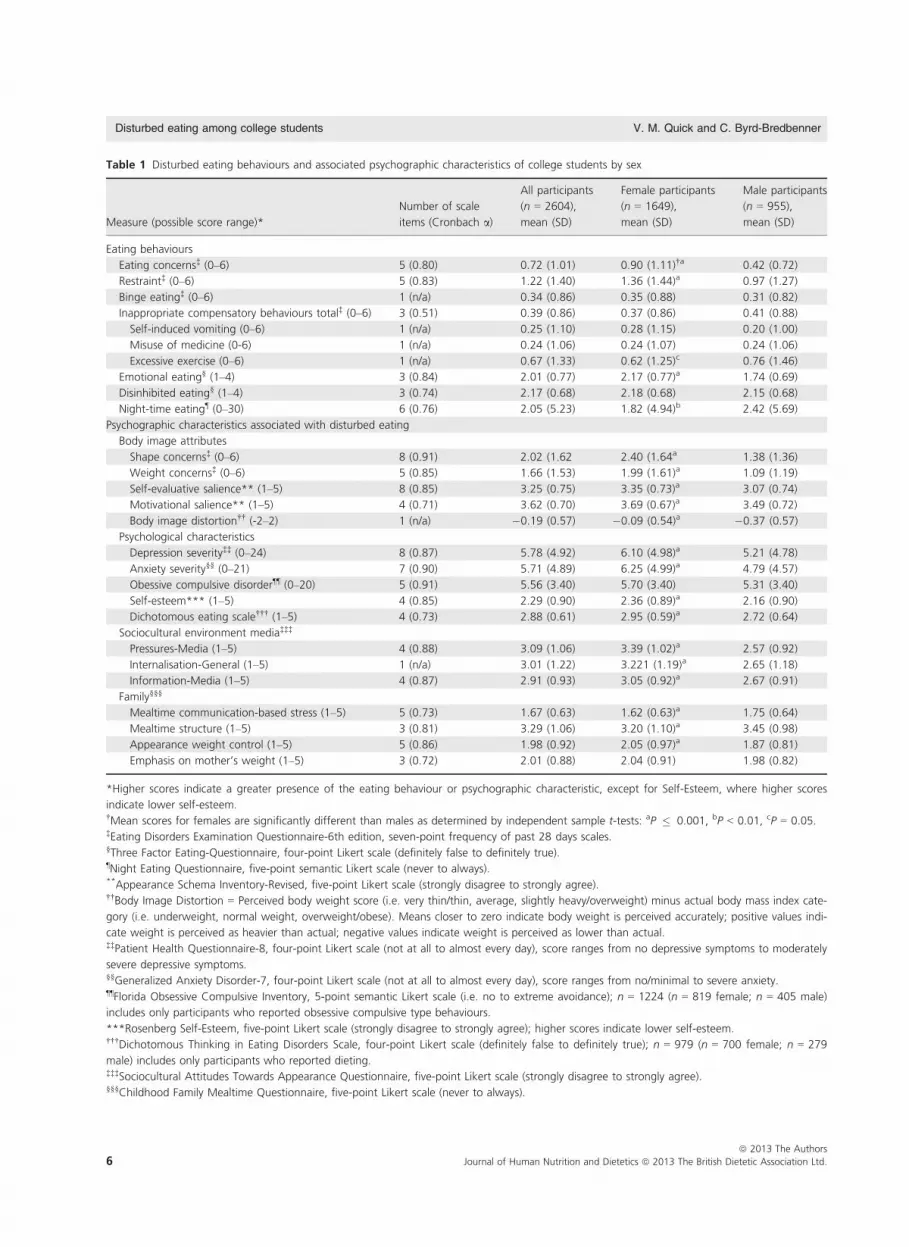
Table 1 Disturbed eating behaviours and associated psychographic characteristics of college students by sex
Measure (possible score range)*
Number of scale
items (Cronbach a)
All participants
(n = 2604),
mean (SD)
Female participants
(n = 1649),
mean (SD)
Male participants
(n = 955),
mean (SD)
Eating behaviours
Eating concerns‡ (0–6) 5 (0.80) 0.72 (1.01) 0.90 (1.11)†a 0.42 (0.72)
Restraint‡ (0–6) 5 (0.83) 1.22 (1.40) 1.36 (1.44)a 0.97 (1.27)
Binge eating‡ (0–6) 1 (n/a) 0.34 (0.86) 0.35 (0.88) 0.31 (0.82)
Inappropriate compensatory behaviours total‡ (0–6) 3 (0.51) 0.39 (0.86) 0.37 (0.86) 0.41 (0.88)
Self-induced vomiting (0–6) 1 (n/a) 0.25 (1.10) 0.28 (1.15) 0.20 (1.00)
Misuse of medicine (0-6) 1 (n/a) 0.24 (1.06) 0.24 (1.07) 0.24 (1.06)
Excessive exercise (0–6) 1 (n/a) 0.67 (1.33) 0.62 (1.25)c 0.76 (1.46)
Emotional eating§ (1–4) 3 (0.84) 2.01 (0.77) 2.17 (0.77)a 1.74 (0.69)
Disinhibited eating§ (1–4) 3 (0.74) 2.17 (0.68) 2.18 (0.68) 2.15 (0.68)
Night-time eating¶ (0–30) 6 (0.76) 2.05 (5.23) 1.82 (4.94)b 2.42 (5.69)
Psychographic characteristics associated with disturbed eating
Body image attributes
Shape concerns‡ (0–6) 8 (0.91) 2.02 (1.62 2.40 (1.64a 1.38 (1.36)
Weight concerns‡ (0–6) 5 (0.85) 1.66 (1.53) 1.99 (1.61)a 1.09 (1.19)
Self-evaluative salience** (1–5) 8 (0.85) 3.25 (0.75) 3.35 (0.73)a 3.07 (0.74)
Motivational salience** (1–5) 4 (0.71) 3.62 (0.70) 3.69 (0.67)a 3.49 (0.72)
Body image distortion†† (-2–2) 1 (n/a) �0.19 (0.57) �0.09 (0.54)a �0.37 (0.57)
Psychological characteristics
Depression severity‡‡ (0–24) 8 (0.87) 5.78 (4.92) 6.10 (4.98)a 5.21 (4.78)
Anxiety severity§§ (0–21) 7 (0.90) 5.71 (4.89) 6.25 (4.99)a 4.79 (4.57)
Obessive compulsive disorder¶¶ (0–20) 5 (0.91) 5.56 (3.40) 5.70 (3.40) 5.31 (3.40)
Self-esteem*** (1–5) 4 (0.85) 2.29 (0.90) 2.36 (0.89)a 2.16 (0.90)
Dichotomous eating scale††† (1–5) 4 (0.73) 2.88 (0.61) 2.95 (0.59)a 2.72 (0.64)
Sociocultural environment media‡‡‡
Pressures-Media (1–5) 4 (0.88) 3.09 (1.06) 3.39 (1.02)a 2.57 (0.92)
Internalisation-General (1–5) 1 (n/a) 3.01 (1.22) 3.221 (1.19)a 2.65 (1.18)
Information-Media (1–5) 4 (0.87) 2.91 (0.93) 3.05 (0.92)a 2.67 (0.91)
Family§§§
Mealtime communication-based stress (1–5) 5 (0.73) 1.67 (0.63) 1.62 (0.63)a 1.75 (0.64)
Mealtime structure (1–5) 3 (0.81) 3.29 (1.06) 3.20 (1.10)a 3.45 (0.98)
Appearance weight control (1–5) 5 (0.86) 1.98 (0.92) 2.05 (0.97)a 1.87 (0.81)
Emphasis on mother’s weight (1–5) 3 (0.72) 2.01 (0.88) 2.04 (0.91) 1.98 (0.82)
*Higher scores indicate a greater presence of the eating behaviour or psychographic characteristic, except for Self-Esteem, where higher scores
indicate lower self-esteem.†Mean scores for females are significantly different than males as determined by independent sample t-tests: aP � 0.001, bP < 0.01, cP = 0.05.‡Eating Disorders Examination Questionnaire-6th edition, seven-point frequency of past 28 days scales.§Three Factor Eating-Questionnaire, four-point Likert scale (definitely false to definitely true).¶Night Eating Questionnaire, five-point semantic Likert scale (never to always).**Appearance Schema Inventory-Revised, five-point Likert scale (strongly disagree to strongly agree).††Body Image Distortion = Perceived body weight score (i.e. very thin/thin, average, slightly heavy/overweight) minus actual body mass index cate-
gory (i.e. underweight, normal weight, overweight/obese). Means closer to zero indicate body weight is perceived accurately; positive values indi-
cate weight is perceived as heavier than actual; negative values indicate weight is perceived as lower than actual.‡‡Patient Health Questionnaire-8, four-point Likert scale (not at all to almost every day), score ranges from no depressive symptoms to moderately
severe depressive symptoms.§§Generalized Anxiety Disorder-7, four-point Likert scale (not at all to almost every day), score ranges from no/minimal to severe anxiety.¶¶Florida Obsessive Compulsive Inventory, 5-point semantic Likert scale (i.e. no to extreme avoidance); n = 1224 (n = 819 female; n = 405 male)
includes only participants who reported obsessive compulsive type behaviours.
***Rosenberg Self-Esteem, five-point Likert scale (strongly disagree to strongly agree); higher scores indicate lower self-esteem.†††Dichotomous Thinking in Eating Disorders Scale, four-point Likert scale (definitely false to definitely true); n = 979 (n = 700 female; n = 279
male) includes only participants who reported dieting.‡‡‡Sociocultural Attitudes Towards Appearance Questionnaire, five-point Likert scale (strongly disagree to strongly agree).§§§Childhood Family Mealtime Questionnaire, five-point Likert scale (never to always).
ª 2013 The Authors
6 Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd.
Disturbed eating among college students V. M. Quick and C. Byrd-Bredbenner

below the score range mid-point, indicating high levels of
self-esteem. Females had significantly lower self-esteem
than males. Dichotomous Thinking mean scores were
significantly higher in female dieters than male dieters.
Sociocultural environment
Pressures-Media, Internalization-General, and Informa-
tion-Media mean scale scores were slightly above the
mid-point, indicating that participants neither agreed,
nor disagreed that they felt pressure to attain the media
‘thin ideal’. However, females scored significantly higher
on all of these scales than males, indicating that they felt
more pressure to attain the media physical appearance
standard, were more aware of societal appearance norms
set by the media, and more frequently compared their
bodies with those in the media.
Participants recalled little mealtime communication-
based stress, importance placed on weight management,
and did not recall much emphasis being placed on their
mothers’ weight. However, most participants reported
sometimes feeling pressure during meals as a child. Males
reported significantly greater mealtime communication-
based stress and mealtime pressure than females. Con-
versely, females had significantly higher Appearance
Weight Control mean scores than males, indicating that
they recalled a greater importance placed on weight
management.
Discussion
The present study indicates that college students engage
in a variety of disturbed eating behaviours, similar to pre-
vious studies (Luce et al., 2008; Lavender et al., 2010).
Restraint, Eating Concerns, and Binge Eating findings are
comparable to normative data for this audience (Luce
et al., 2008; Lavender et al., 2010); however, regular
occurrences of binge eating (i.e. � 4 times in the past
28 days) in women were double the rate previously
reported (Luce et al., 2008). This finding may indicate
that binge eating prevalence is increasing or was
previously under-reported.
The finding that one-third of participants engaged in
inappropriate compensatory behaviours as a means for
controlling weight and/or shape is troubling. Although
the rate of regular occurrences of self-induced vomiting
in males was comparable to normative data for male col-
lege students, medicine misuse by males was three times
higher than previously reported (Lavender et al., 2010).
This higher rate of medicine misuse could reflect the
more inclusive nature of medicines considered in the
present study (i.e. laxatives, diuretics, insulin), an increase
in medicine misuse for weight control purposes, and/or a
greater willingness to report this behaviour in a confiden-
tial online survey.
By contrast to the higher rate of self-induced vomiting
and medicine misuse by young adult college females
versus males reported by others (Neumark-Sztainer et al.,
2002; Luce et al., 2008), these sex differences did not
emerge in the present study. The similarity between the
sexes may be because the sample in the present study
was much more racially/ethnically diverse than previous
studies, and certain racial groups (e.g. Asian women)
have a lower incidence of unhealthy weight control
behaviours (Mintz & Kashubeck, 1999; Regan & Cach-
elin, 2006). In addition, this similarity could indicate that
males are increasing their use of inappropriate compen-
satory behaviours and/or were more willing to reveal this
information.
The significantly higher rates of excessive exercise
reported by men may illustrate the dual nature of the
male body ideal: low body fat and high muscularity (Lav-
ender et al., 2010). Thus, for males, excessive exercise
may be a muscle-gaining behaviour rather than an inap-
propriate compensatory behaviour (McElhone et al.,
1999). Future research should clarify why excessive exer-
cise is used by males to a greater extent than females.
Body image attributes are important to consider
because they can affect eating behaviours (Heinberg,
1996; Hesse-Biber et al., 2006). The present study lends
support to others (Luce et al., 2008; Lavender et al.,
2010) in that females, compared to males, put greater
emphasis on defining their self-worth and value by their
physical appearance (Cash & Labarge, 1996; Thompson
et al., 2004; Karazsia & Crowther, 2008) and had greater
shape and weight concerns (Luce et al., 2008; Lavender
et al., 2010). The more intense feelings of cultural pres-
sures to be thin typically reported by females (Brown &
Dittmar, 2005) may explain their greater weight and
shape concerns.
Anxiety, depression, and OCD findings confirm that
substantial numbers of young adults suffer from these
psychological problems (Horwath & Weissman, 2000;
Robins et al., 2001; Eisenberg et al., 2007; Mulfinger,
2007; Byrne et al., 2008). Fortunately, these problems are
mild for most, although one in five had moderate levels
of depression and anxiety severity and almost half
engaged in at least one OCD behaviour. The finding that
males had higher self-esteem than females reveals that
sex-specific self-esteem differences reported for children
and teens extend into young adulthood (Raevuori et al.,
2007). Women’s self-esteem continues to lag behind men
after transitioning from adolescence to young adulthood
(Block & Robins, 1993).
Although dichotomous thinking is a key factor in cog-
nitive behavioural models of eating disorders (Byrne
ª 2013 The Authors
Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd. 7
V. M. Quick and C. Byrd-Bredbenner Disturbed eating among college students
et al., 2008), studies of this characteristic have been lim-
ited to female adults diagnosed with an eating disorder
and non-eating disordered overweight/obese women
(Byrne et al., 2008). As expected, this form of cognitive
rigidity was lower in both male and female participants
than that reported for females with an eating disorder
(Byrne et al., 2008), although it was similar to over-
weight/obese women. Given males’ lower eating concerns,
it was not unexpected that they were less likely to think
of food as being either ‘good’ or ‘bad’ than females.
The sociocultural environment can be a powerful influ-
encer of eating behaviours and body image (Heinberg,
1996; Worobey, 2002). Consistent with the literature
(Ogden & Mundray, 1996; Holmstrom, 2004), men felt
less pressure from the media environment to live up to
an unrealistic, media-defined body type. This may be
because media targets women and bombards them with
messages to be thin. For example, magazines targeted to
men have one-tenth as many advertisements focusing on
body weight and dieting as women’s magazines (Malkin
et al., 1999; Andersen, 2002). Although published
research with males could not be located, family eating
environment findings are similar to those reported for
undergraduate females (Worobey, 2002). The findings of
the present study suggest that both males and females
recollect childhood mealtime experiences as being not
especially stressful.
The congruence of many findings with previous research
is important given that participants were much more
racially/ethnically diverse (i.e. reflective of the proportion
of white versus non-white young adult population in the
USA) (Erkolahti et al., 2003) than the vast majority of
studies exploring similar constructs. Accordingly, the find-
ings suggest that the eating behaviours and related psycho-
graphic characteristics studied may not be bound by race/
ethnicity but perhaps reflect this newly-recognised devel-
opmental stage of emerging adulthood (Arnett, 2001).
The value of a study must be balanced by its strengths
and weaknesses. To date, the present study comprises the
most comprehensive assessment of disturbed eating
behaviours and associated psychographic characteristics in
young adults. In addition, the findings obtained in the
present study help to overcome many of the limitations
of previous studies that investigated disturbed eating
practices and associated psychographic characteristics in
this age group (Kashubeck-West et al., 2001; Fairburn &
Brownell, 2002; Ogden, 2003; Reas & Grilo, 2004; Mitch-
ell & Peterson, 2005; Olmsted et al., 2007). First, the
present study defined disturbed eating behaviours broadly
and explored a wide array of salient associated psycho-
graphic characteristics. Second, the sample was large and
included racially/ethnically diverse, free-living male and
female young adults. Third, instrument selection was
guided by a panel of experts and resulted in a survey
comprised of valid, reliable, audience-appropriate scales.
The care taken to reduce the length of many of the scales
used resulted in scales having good reliability, comparable
to their original full length scales. These shortened scales
can help future researchers reliably measure study attri-
butes with lower participant burden. In addition, the
present study demonstrated the utility of some of these
scales with new audiences (e.g. no previously published
studies could be located that used the Dichotomous
Thinking or Childhood Family Mealtime Questionnaire
with men). Online administration of the survey instru-
ment also can be considered a study strength. This
administration method made it easy, convenient and con-
fidential for young adults to participate and yielded valu-
able data and, perhaps, more accurate responses to
sensitive questions.
Despite the many strengths of the present study, it is
important to take into account its limitations. The
cross-sectional nature of the present study limits the
assignment of temporality to the findings; however, these
findings are very useful for hypothesis generating research
and provide the basis for more prospective designs.
Another limitation was the use of a convenience sample
recruited from only three universities; therefore, results
may not be generalisable to the young adult population
as a whole and to all racial/ethnic groups.
Future studies should aim to examine disturbed eating
behaviour risk and associated psychographic characteris-
tics in a large sample of youth who are followed over
time (prospectively) to determine how disturbed eating
behaviours are initiated in the years leading up to young
adulthood. A better understanding of the factors that
promote and impede disturbed eating behaviours can
inform the development of much needed interventions
that help this age group develop health-protective eating
behaviours that will benefit them throughout adulthood.
Conclusions
The present study reveals that many college students
engage in disturbed eating practices, and the rates for
binge eating in females and inappropriate compensatory
behaviours in males may be higher than previously
assumed. Thus, these findings suggest that nutrition edu-
cation interventions for college student audiences should
address disturbed eating behaviours and provide guidance
on how to seek professional help for them. The findings
of the present study also suggest that it may be prudent
for healthcare professionals to routinely screen college
students for disturbed eating behaviours and intervene
early when treatment is likely to be most effective
(DeSocio et al., 2007). In the long term, screenings and
ª 2013 The Authors
8 Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd.
Disturbed eating among college students V. M. Quick and C. Byrd-Bredbenner

interventions could decrease the rate and/or severity of
disturbed eating behaviours and reduce associated medi-
cal complications, ultimately increasing the quality of life
for college students.
Acknowledgments
Virginia Quick conducted this study when at Rutgers
University.
Conflicts of interest, sources of funding andauthorship
The authors declare that there are no conflicts of interest.
This study was supported by a Kappa Omicron Nu
Research Fellowship.
VQ implemented the study, analysed the data and wrote
the manuscript. CB-B helped with the interpretation of
the data, as well as the writing and reviewing of the
manuscript. All authors critically reviewed the manu-
script and approved the final version submitted for
publication.
References
Allison, K., Lundgren, J., O’Rearden, J. Martino, N., Sarwer,
D., Ubdden, T., Crosby, R. & Engel, S. (2008) The Night
Eating Questionnaire (NES): psychometric properties of a
measure of severity of the Night Eating Syndrome. Eat.
Behav. 9, 62–72.
American Psychiatric Association. (2000) Diagnostic and
Statistical Manual of Psychiatric Disorders, 4th edn.
Washington, DC: American Psychiatric Association.
Andersen, A. (2002) Eating disorders in males. In Eating
Disorders and Obesity: A Comprehensive Handbook, 2nd edn.
eds C. Fairburn & K. Brownell, pp. 188–192. New York, NY:
Guilford Press.
Arnett, J. (1997) Young people’s conception of the transition
to adulthood. Youth Soc. 29, 3–21.
Arnett, J. (1998) Learning to stand alone: the contemporary
American transition to adulthood in cultural and historical
context. Hum. Dev. 41, 295–315.
Arnett, J. (2001) Conceptions of the transition to adulthood:
perspectives from adolescence through midlife. J. Adult Dev.
8, 133–143.
Barley, R., Dodd, K., Gahche, J., Dwyer, J., McDowell, M.,
Yetley, E., Sempos, C., Burt, V., Radimer, K. & Picciano, M.
(2010) Total folate and folic acid intake from foods and
dietary supplements in the United States: 2003-2006. Am. J.
Clin. Nutr. 91, 231–237.
Bell, S. & Lee, C. (2006) Does timing and sequencing of
transitions to adulthood make a difference? Stress, smoking,
and physical activity among young Australian women Int. J.
Behav. Med. 13, 256–274.
Bernhardt, J.M. (2004) Communication at the core of
effective public health. Am. J. Public Health. 94,
2051–2053.
Block, J. & Robins, R. (1993) A longitudinal study of
consistency and change in self-esteem from early
adolescence to early adulthood. Child Dev. 64, 902–923.
Brown, A. & Dittmar, H. (2005) Think ‘thin’ and feel bad:
the role of appearance schema activation, attention
level, and thin-ideal internalization for young women’s
responses to ultra-thin media ideals. J. Soc. Psychol. 24,
1088–1113.
Bulik, C. (2002) Anxiety, depression and eating disorders. In
Eating Disorders and Obesity: A Comprehensive Handbook,
2nd edn. eds C. Fairburn & K. Brownell, pp. 193–198. New
York, NY: Guilford Press.
Byrne, S., Allen, K., Dove, E., Watt, F. & Nathan, P. (2008)
The reliability and validity of the dichotomous thinking in
eating disorders scale. Eat. Behav. 9, 154–162.
Cash, T & Labarge, A. (1996) Development of the appearance
schemas inventory: a new cognitive body-image assessment.
Cog. Ther. Res. 20, 37–50.
Crow, S., Zander, K., Crosby, R., & Mitchell, J. (1996)
Discriminant function analysis of depressive symptoms in
binge eating disorder, bulimia nervosa, and major
depression. Int. J. Eat. Disord. 19, 399–404.
DeSocio, J., O’Toole, J., Nemirow, S. & Lukach, M. (2007)
Screening for childhood eating disorders in primary care.
Prim. Care Comp. J. Clin. Psychiatry. 9, 16–20.
Dietz, W. (1998) Health consequences of obesity in youth:
childhood predictors of adult disease. Pediatrics. 101, 518–525.
Eisenberg, D., Gollust, S., Golberstein, D. & Hefner, J. (2007)
Prevalence and correlates of depression and anxiety, and
suicidality among university students. Am. J. Orthopsychiatry
77, 534–542.
Erkolahti, R., Ilonen, T. & Saarijarvi, S. (2003) Self-Image of
adolescents with diabetes mellitus type 1 and rheumatoid
arthritis. Nordic J. Psychiatr. 57, 309–312.
Ervin, R., Wang, C., Wright, J. & Kennedy-Stephenson, M.
(2004) Dietary Intake of Selected Minerals for the United
States Population: 1999–2008. Hyattsville, MD: National
Center for Health Statistics.
Fairburn, C. & Beglin, S. (1994) Assessment of eating
disorders: interview or self-report questionnaire? Int. J. Eat.
Disord. 16, 363–370.
Fairburn, C. & Brownell, K. (2002) Eating Disorders and
Obesity. New York, NY: Guilford Press.
Fairburn, C., Cooper, Z. & Shafran, R. (2003) Cognitive
behavior therapy for eating disorders: a ‘transdiagnostic’
theory and treatment. Behav. Res. Ther. 41, 509–528.
Fairburn, C., Cooper, Z. & O’Connor, M. (2008) Cognitive
Behavior Therapy and Eating Disorders. New York, NY:
Guilford Press.
Flegal, K., Carroll, M., Ogden, C. & Curtin, L. (2010)
Prevalence and Trends in Obesity Among US Adults 1999-
2008. J. Am. Med. Assoc. 303, 235–241.
ª 2013 The Authors
Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd. 9
V. M. Quick and C. Byrd-Bredbenner Disturbed eating among college students
Gunn, J., Kuklina, E., Keenan, N. & Laborthe, D. (2010)
Sodium intake among adults – United States, 2005–2006.
Morb. Mortal. Wkly. Rep. 59, 764–769.
Heinberg, L. (1996) Theories of body image disturbance:
perceptual, developmental and sociocultural factors. In
Body Image, Eating Disorders, and Obesity: An Integrative
Guide for Assessment and Treatment. ed. J. Thompson,
pp. 27–47. Washington, DC: American Psychological
Association.
Henkel, R. (1976) Tests of Significance. Sage University Paper
Series on Quantitative Applications in the Social Sciences,
07-004. Newbury Park, CA: Sage.
Hesse-Biber, S., Leavy, P., Quinn, C. & Zoino, J. (2006) The
mass marketing of disordered eating and eating disorders:
the social psychology of women, thinness and culture.
Women’s Stud. Int. Forum. 29, 208–224.
Higgins, M., Kannel, W., Garrison, R., Pinsky, J. & Stokes, J.
(1988) Hazards of obesity-the Framingham experience. Acta.
Medica. Scand. 723, 23–36.
Hoek, H. (2006) Incidence, prevalence and mortality of
anorexia and other eating disorders. Curr. Opin. Pyschiatr.
19, 389–394.
Holmstrom, A. (2004) The effects of the media on body
image: a meta-analysis. J. Broadcast and Electr. Media. 48,
196–217.
Holsten, J. & Cashwell, C. (2000) Family functions and eating
disorders among college women. J. Coll. Counsel. 3, 5–16.
Horwath, E. & Weissman, M. (2000) The epidemiology and
cross-national presentation of obsessive–compulsive
disorder. Psychiatric Clini. North Amer. 23, 493–507.
Institute of Medicine. (2002) Speaking of Health: Assessing
Health Communication Strategies for Diverse Populations.
Washington, DC: National Academy Press.
Karazsia, B. & Crowther, J. (2008) Psychological and
behavioral correlates of the SATAQ-3 with males. Body
Image 5, 109–115.
Karlsson, J., Persson, L.O., Sjostrom, L. & Sullivan, M. (2000)
Psychometric properties and factor structure of the Three-
Factor Eating Questionnaire (TFEQ) in obese men and
women: results from the Swedish Obese Subjects (SOS)
study. Int. J. Obes. 24, 1715–1725.
Kashubeck-West, S., Mintz, L. & Saunders, K. (2001)
Assessment of Eating Disorders in Women. Counsel. Psychol.
29, 662–664.
Kroenke, K., Spitzer, R. & Williams, J. (2001) The PHQ-9:
validity of a brief depression severity measure. J. Intern.
Med. 16, 606–613.
Lavender, J., De Young, K. & Anderson, D. (2010) Eating
Disorder Examination Questionnaire (EDE-Q): norms for
undergraduate men. Eat. Behav. 11, 119–121.
Lewis, C., Jacobs, D.R.J., McCreath, H., Kiefe, C., Schreiner,
P., Smith, D. & Williams, O. (2000) Weight gain continues
in the 1990s: 10-year trends in weight and overweight from
the CARDIA study Coronary Artery Risk Development in
Young Adults. Am. J. Epidiemiol. 151, 1172–1181.
Luce, K., Crowther, J. & Pole, M. (2008) Eating Disorder
Examination Questionnaire (EDE-Q): norms for
Undergraduate Women. Int. J. Eat. Disord. 41, 273–276.
Ma, Y., Bertone, E.R., Stanek, E.J., Reed, G., Hebert, J., Cohen,
N., Merriam, P. & Ockene, I. (2003) Association between
eating patterns and obesity in a free-living US adult
population. Am. J. Epidemiol. 158, 85–92.
Maibach, E., Maxfield, A., Ladin, K. & Slater, M. (1996)
Translating health psychology into effective health
communication. J. Health Psychol. 1, 261–277.
Malkin, A., Wornian, K. & Chrisler, J. (1999) Women and
weight: gendered messages on magazine covers. Sex Roles 40,
647–655.
McCormick, B. & Stone, I. (2007) Economic costs of obesity
and the case for government intervention. Obes. Rev. 8
(Suppl. 1), 161–164.
McDowell, M., Lachor, D., Pfeiffer, C., Mulinare, J., Picciano,
M., Rader, J., Yetley, E., Kennedy-Stephenson, M. &
Johnson, C. (2008) Blood Folate Levels: The Latest NHANES
Results. Hyattsville, MD: National Center for Health
Statistics.
McElhone, S., Kearney, J., Giachetti, I., Zurift, H. & Martinez,
J. (1999) Body image perception in relation to recent weight
changes and strategies for weight loss in nationally
represented sample in the European Union. Public Health
Nutr. 2, 143–151.
Miller, D., McCluskey-Fawcett, K. & Irving, L. (1993)
Correlates of bulimia nervosa: early family mealtime
experiences. Adolescence 28, 621–635.
Mintz, L. & Kashubeck, S. (1999) Body image and disordered
eating among Asian American and Caucasion college
students: an examination of race and gender differences.
Psychol. Women Q. 23, 781–796.
Misra, R. & McKean, M. (2000) College students’ academic
stress and its’ relation to their anxiety, time managements
and leisure satisfaction. Am. J. Health Stud. 16, 41–51.
Mitchell, J. & Peterson, C. (2005) Assessment of Eating
Disorders. New York, NY: The Guilford Press.
Mond, J., Hay, P., Rodgers, B., Owen, C. & Beumont, P.
(2004) Temporal stability of the eating disorder examination
questionnaire. Int. J. Eat. Disord. 36, 195–203.
Mulfinger, A. (2007) Comorbidity of Obsessive–Compulsive and
Anorexic Behaviors in Undergraduate Females. Dissertation,
Auburn, AL: Auburn University.
National Cancer Institute. (2010) Usual Dietary Intakes: Food
Intakes, United States Population, 2001-2004. National
Cancer Institute. Available at http://riskfactor.cancer.gov/
diet/usualintakes/pop/ (accessed on 27 August 2011).
Neumark-Sztainer, D., Falkner, N., Story, M., Perry, C.,
Hannan, P. & Mulert, S. (2002) Weight-teasing among
adolescents: correlations with weight status and disordered
eating behaviors. Int. J. Obes. Rel. Metab. Disord. 26, 123–
131.
Ogden, J. (2003) The Psychology of Eating from Healthy to
Disordered Behavior. Berlin: Blackwell Publishing Company.
ª 2013 The Authors
10 Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd.
Disturbed eating among college students V. M. Quick and C. Byrd-Bredbenner

Ogden, J. & Mundray, K. (1996) The effect of the media on
body satisfaction: the role of gender and size. Eur. Eat.
Disord. Rev. 4, 171–182.
Olmsted, M., McFarlane, T., Carter, J. & Trottier, K. (2007)
Assessment of eating disorders. In Annual Review of Eating
Disorders – Part 1. eds S. Wonderlich, J. Mitchell, M. de
Zwaan & H. Steiger, pp. 81–100. New York, NY: Radcliffe
Publishing.
Raevuori, A., Dick, D., Keski-Rahkonen, A., Pulkkinen, L., Rose,
R., Rissanen, A. & Kaprio, J. (2007) Genetic and environment
factors affecting self-esteem from age 14 to 17: a longitudinal
study of Finnish Twins. Psychol. Med. 37, 1625–1633.
Reas, D. & Grilo, C. (2004) Cognitive-behavioral assessment of
body image disturbances. J. Psychiatr. Prac. 10, 314–322.
Regan, P. & Cachelin, F. (2006) Binge eating and purging in a
multi-ethnic community sample. Int. J. Eat. Disord. 39, 523–
526.
Robins, R., Hendin, H. & Trzesniewski, K. (2001) Measuring
global self-esteem: construct validation of a single-item
measure and the Rosenberg Self-Esteem scale. Person Soc.
Psychol. Bull. 27, 151–161.
Rosenberg, M.(1965) Society and the Adolescent Self-Image.
Princeton, NJ: Princeton University Press.
Sacker, A. & Cable, N. (2010) Transitions to adulthood and
psychological distress in young adults born 12 years apart:
constraints on and resources for development. Psychol. Med.
40, 301–313.
Spitzer, R., Kroenke, K. & Williams, J. (1999) Validation and
utility of a self-report version of PRIME-MD: the PHQ
Primary Care Study. J. Am.Med. Assoc. 282, 1737–1744.
Spitzer, R., Kroenke, K., Williams, J. & Lowe, B. (2006) A brief
measure for assessing generalized anxiety disorder. Arch.
Intern. Med. 166, 1092–1097.
Stice, E. (2002) Sociocultural influences on body image
and eating disturbance. In Eating Disorders and Obesity:
A Comprehensive Handbook, 2nd edn. eds C. Fairburn &
K. Brownell, pp. 103–107. New York, NY: Guilford
Press.
Stice, E. & Hoffman, E. (2004) Prevention of eating disorders
In A Handbook of Eating Disorders and Obestiy. ed.
J. Thompson, pp. 33–57. New York, NY: Wiley.
Storch, E., Bagner, D., Merlo, L., Shapira, N., Geffken, G.,
Murphy, T. & Goodman, W. (2007) Florida obsessive–
compulsive inventory: development, reliability and validity.
J. Clin. Psychol. 63, 851–859.
Striegel-Moore, R. (1997) Risk factors for eating disorders.
Ann. N. Y. Acad. Sci. 817, 98–109.
Thompson, J., Heinberg, L. & Altabe, M. & Tantleff-Dunn, S.
(1999) Exacting Beauty: Theory, Assessment and Treatment of
Body Image Disturbance. Washington, DC: American
Psychological Association.
Thompson, J., van den Berg, P., Roehrig, M., Guarda, A. &
Heinberg, L. (2004) The Sociocultural Attitudes Towards
Appearance Questionnaire-3 (SATAQ-3): development and
validation. Int. J. Eat. Disord. 35, 295–304.
Twenge, J., Gentile, B., DeWall, C., Ma, D., Lacefiled, K. &
Schurtz, D. (2010) Birth cohort increases in
psychopathology among young Americans, 1938–2007: a
cross-temporal meta-analysis of the MMPI. Clin. Psychol.
Rev. 30, 145–154.
U.S. Department of Agriculture and US, Department of
Health and Human Services. (2010) Dietary Guidelines for
Americans, 7th edn. Washington, DC: Government
Printing Office.
Wonderlich, S. (2002) Personality and eating disorders. In
Eating Disorders and Obesity, 2nd edn. eds C. Fairburn & K.
Brownell, pp. 204–209. New York, NY: Guilford Press.
Worobey, J. (2002) Early family mealtime experiences and
eating attitudes in normal weight, underweight and
overweight females. Eat Weight Disord. 7, 39–44.
ª 2013 The Authors
Journal of Human Nutrition and Dietetics ª 2013 The British Dietetic Association Ltd. 11
V. M. Quick and C. Byrd-Bredbenner Disturbed eating among college students





























