Embed Size (px)
Citation preview

Journal of Consulting and ClinicalPsychologyD-Cycloserine Augmentation of Cognitive BehavioralGroup Therapy of Social Anxiety Disorder: Prognostic andPrescriptive VariablesJasper A. J. Smits, Stefan G. Hofmann, David Rosenfield, Lindsey B. DeBoer, Paul T. Costa,Naomi M. Simon, Conall O’Cleirigh, Alicia E. Meuret, Luana Marques, Michael W. Otto, andMark H. PollackOnline First Publication, August 12, 2013. doi: 10.1037/a0034120
CITATIONSmits, J. A. J., Hofmann, S. G., Rosenfield, D., DeBoer, L. B., Costa, P. T., Simon, N. M.,O’Cleirigh, C., Meuret, A. E., Marques, L., Otto, M. W., & Pollack, M. H. (2013, August 12).D-Cycloserine Augmentation of Cognitive Behavioral Group Therapy of Social AnxietyDisorder: Prognostic and Prescriptive Variables. Journal of Consulting and ClinicalPsychology. Advance online publication. doi: 10.1037/a0034120

D-Cycloserine Augmentation of Cognitive Behavioral Group Therapy ofSocial Anxiety Disorder: Prognostic and Prescriptive Variables
Jasper A. J. SmitsUniversity of Texas at Austin
Stefan G. HofmannBoston University
David Rosenfield and Lindsey B. DeBoerSouthern Methodist University
Paul T. CostaDuke University School of Medicine
Naomi M. Simon and Conall O’CleirighMassachusetts General Hospital and Harvard Medical School
Alicia E. MeuretSouthern Methodist University
Luana MarquesMassachusetts General Hospital and Harvard Medical School
Michael W. OttoBoston University
Mark H. PollackRush University Medical Center
Objective: The aim of the current study was to identify individual characteristics that (a) predict symptomimprovement with group cognitive behavioral therapy (CBT) for social anxiety disorder (SAD; i.e.,prognostic variables) or (b) moderate the effects of d-cycloserine (DCS) versus placebo augmentation ofCBT for SAD (i.e., prescriptive variables). Method: Adults with SAD (N ! 169) provided LiebowitzSocial Anxiety Scale scores in a trial evaluating DCS augmentation of group CBT. Rate of symptomimprovement during therapy and posttreatment symptom severity were evaluated using multilevelmodeling. As predictors of these 2 parameters, we selected the range of variables assessed at baseline(demographic characteristics, clinical characteristics, personality traits). Using step-wise analyses, wefirst identified prognostic and prescriptive variables within each of these domains and then entered thesesignificant predictors simultaneously in 1 final model. Results: African American ethnicity and cohab-itation status were associated with greater overall rates of improvement during therapy and lowerposttreatment severity. Higher initial severity was associated with a greater improvement during therapybut also higher posttreatment severity (the greater improvement was not enough to overcome the initialhigher severity). DCS augmentation was evident only among individuals low in conscientiousness and
Jasper A. J. Smits, Institute for Mental Health Research and Departmentof Psychology, University of Texas at Austin; Stefan G. Hofmann, De-partment of Psychology, Boston University; David Rosenfield and LindseyB. DeBoer, Department of Psychology, Southern Methodist University;Paul T. Costa, Behavioral Medicine Research Center, Department of Psy-chiatry and Behavioral Science, Duke University School of Medicine;Naomi M. Simon and Conall O’Cleirigh, Department of Psychiatry, Mas-sachusetts General Hospital and Harvard Medical School; Alicia E.Meuret, Department of Psychology, Southern Methodist University; LuanaMarques, Department of Psychiatry, Massachusetts General Hospital andHarvard Medical School; Michael W. Otto, Department of Psychology,Boston University; Mark H. Pollack, Department of Psychiatry, RushUniversity Medical Center.
This report was supported by Grants R01MH075889 and R01MH078308from the National Institute of Mental Health (NIMH). We appreciate thesupport of the NIMH. The content is solely the responsibility of the authorsand does not necessarily represent the official views of the NIMH or theNational Institutes of Health (NIH).
Jasper A. J. Smits receives royalties from various book publishers forwork unrelated to this study. Stefan G. Hofmann has served as a consultantfor Merck and Schering–Plough and receives book royalties from various
book publishers for work unrelated to this study. Paul T. Costa receivesroyalties from the NEO Five-Factor Inventory. Naomi M. Simon reportedunrelated financial affiliations for the past 36 months for providing re-search support from American Foundation for Suicide Prevention, ForestLaboratories, National Institute of Health, and Department of Defense. Shealso receives honoraria for speaking for the Massachusetts General Hos-pital Psychiatry Academy and spousal equity in Elan, Dandreon, G Zero,and Gatekeeper. Michael W. Otto serves as consultant for MicroTranspon-der. and receives royalties from various book publishers for work unrelatedto this study. Mark H. Pollack disclosures over the last 12 months include(a) advisory boards and consultation for Edgemont Pharmaceuticals, EliLilly, Ironwood Pharmaceuticals, Medavante, and Merck; (b) researchgrants: NIH Equity–Doyen, Medavante, Mensante Corp., Mindsite, andTargia Pharmaceutical; (c) royalty/patent: SIGH–A, and SAFER inter-views. David Rosenfield, Lindsey B. DeBoer, Conall O’Cleirigh, Alicia E.Meuret, and Luana Marques report no financial relationships with com-mercial interests.
Correspondence concerning this article should be addressed to JasperA. J. Smits, Institute for Mental Health Research and Department ofPsychology, University of Texas at Austin, 108 E. Dean Keeton StopA8000, Austin, TX 78712–1043. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Journal of Consulting and Clinical Psychology © 2013 American Psychological Association2013, Vol. 81, No. 5, 000 0022-006X/13/$12.00 DOI: 10.1037/a0034120
1

high in agreeableness. Conclusions: African American ethnicity, cohabitation status, and initial severityare prognostic of favorable CBT outcomes in SAD. DCS augmentation appears particularly useful forpatients low in conscientiousness and high in agreeableness. These findings can guide clinicians inmaking decisions about treatment strategies and can help direct research on the mechanisms of thesetreatments.
Keywords: cognitive behavioral therapy, d-cycloserine, social anxiety disorder, social phobia, moderators
Social anxiety disorder (SAD) is among the most commonanxiety disorders (Kessler et al., 2005). Epidemiological surveysfurther show that SAD—particularly the generalized subtype—isassociated with significant personal and societal costs (Schneier etal., 1994; Schneier, Johnson, Hornig, Liebowitz, & Weissman,1992), underscoring the need for effective interventions. Cognitivebehavioral therapy (CBT) has been established as an efficaciousintervention for SAD (Hofmann & Smits, 2008). CBT emphasizesrepeated or prolonged confrontation to feared cues, often in com-bination with cognitive restructuring (Hofmann & Otto, 2008),with the goal of assisting patients in reacquiring a sense of safetyin social interaction and performance situations (Otto, Smits, &Reese, 2004). CBT, delivered in individual or group format, hasbeen shown to outperform both pill and psychological placebotreatment (Davidson et al., 2004; Heimberg et al., 1998) and yieldsmedium to large reductions in symptom severity (Clark et al.,2003). Although efficacious, CBT results in suboptimal outcomesfor many. Indeed, treatment nonresponse rates in large clinicaltrials have been 50% or higher (Davidson et al., 2004), and mostindividuals do not achieve remission (Blanco et al., 2010; David-son et al., 2004).
The observation of suboptimal outcomes of patients receivingCBT for SAD has prompted research on augmentation strategies.One exciting development in this area has been the application ofd-cycloserine (DCS), a partial agonist at the N-methyl-D-aspartate(NMDA) receptor (Anderson & Insel, 2006; Davis, Ressler, Roth-baum, & Richardson, 2006; Hofmann, Smits, Asnaani, Gutner, &Otto, 2011). Following preclinical research demonstrating thatDCS can facilitate extinction learning in rodents by enhancingNMDA receptor function (Davis et al., 2006), initial studies ofDCS for augmenting exposure therapy for the anxiety disordershave yielded promising results (Bontempo, Panza, & Bloch, 2012).With respect to SAD, Hofmann, Meuret, et al. (2006) initiallyshowed that patients receiving DCS 1 hr prior to the last foursessions of a five-session CBT protocol evidenced significantlygreater rates of improvement than patients who received pill pla-cebo. This finding was later replicated by an independent group(Guastella, 2008). Given these positive findings, DCS as an aug-mentation strategy was subsequently applied to a standard 12-session course of group CBT for SAD, examining the degree towhich it extends treatment gains in a full rather than an abbreviatedprotocol (Hofmann et al., 2013).
As has been the case for CBT as a single modality treatment,response to DCS-augmented CBT has been variable across indi-viduals with SAD (Hofmann et al., 2013; Hofmann, Pollack, &Otto, 2006). Our aim in the present study was to identify individualcharacteristics that differentiate response to DCS augmentation ina large-scale clinical trial comparing DCS-augmented group CBTwith placebo-augmented group CBT in medication-free adults
with generalized SAD (Hofmann et al., 2013). In the context ofthis study, individual characteristics associated with differences inoutcome between the experimental and the control condition wereconsidered moderators (Kraemer, Wilson, Fairburn, & Agras,2002) or prescriptive variables (Fournier et al., 2009), whereasindividual characteristics associated with outcome regardless ofstudy condition were considered predictor or prognostic variables(Fournier et al., 2009). Accordingly, we hoped that in addition torevealing individual characteristics that differentiate responding toDCS, this analysis could help in identifying individual character-istics that are prognostic of responding to CBT for SAD regardlessof DCS augmentation. We hope that the findings of this study willstimulate research aiming to refine the understanding of the mech-anisms by which CBT (with or without DCS) reduces anxietypathology and thereby aid in achieving the goal of personalizedtherapy (Anderson & Insel, 2006).
Constrained by the limitations of the assessment protocol for theparent trial, we evaluated the patient characteristics available inour database that are also routinely assessed in clinical practice(e.g., demographic characteristics, clinical characteristics, and per-sonality traits). Research relating the efficacy of DCS augmenta-tion to these patient characteristics is limited to some preliminarywork in posttraumatic stress disorder (PTSD). Recently, de Kleine,Hendriks, Kusters, Broekman, and van Minnen (2012) reportedthat differences between DCS-augmented CBT and placebo-augmented CBT with respect to symptom reduction were greateramong patients who presented with more severe symptoms thanpatients who presented with less severe symptoms at baseline.However, because this post hoc moderator analysis did not includeany covariates, it is impossible to rule out possible third-variableexplanations (e.g., comorbid diagnoses, sex, and so forth) for theclinical severity–DCS efficacy relation observed in that study.
Extant research on the relation between patient characteristicsand CBT outcome for SAD has frequently pointed to depressionseverity as an important predictor (i.e., prognostic factor), althoughthe findings have been mixed. Specifically, baseline depressionseverity has been associated with greater symptom severity at theend of CBT for SAD (Collimore & Rector, 2012; Erwin, Heim-berg, Juster, & Mindlin, 2002; Ledley et al., 2005; Turner, Beidel,Wolff, Spaulding, & Jacob, 1996) and with less symptom improve-ment during CBT (Chambless, Tran, & Glass, 1997; Ledley et al.,2005). Several studies have, however, failed to observe the relationbetween depression and rate of change during CBT for SAD(Erwin et al., 2002; Joormann, Kosfelder, & Schulte, 2005; Turneret al., 1996), suggesting that baseline depression severity maysimply be associated with greater symptom severity before andafter treatment, but not necessarily the efficacy of CBT for SAD.Interestingly, McEvoy, Nathan, Rapee, and Campbell (2012) didnot identify comorbid depression as a predictor of CBT for SAD
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
2 SMITS ET AL.

outcome in an analysis that also included a number of otherindividual characteristic variables (e.g., age, gender, social anxietysymptom severity, number of comorbid diagnosis, degree of lifeinterference). Instead, social anxiety symptom severity and num-ber of comorbid diagnosis emerged as prognostic factors in thisanalysis. Together, these findings highlight the importance ofevaluating multiple prospective prognostic or prescriptive vari-ables simultaneously rather than in isolation.
Although it has been proposed that personality traits have im-plications for the outcome of psychotherapy for anxiety disorders(Zinbarg, Uliaszek, & Adler, 2008), we know of no researchevaluating the prognostic (or prescriptive) value of personalitytraits (e.g., agreeableness, conscientiousness, extraversion, neurot-icism, and openness) with respect to the outcome of CBT for SAD(or DCS augmentation). Given findings in the literature linkingconscientiousness to health behaviors and greater treatment adher-ence (Axelsson, Brink, Lundgren, & Lotvall, 2011; Hill & Roberts,2011), it is plausible that those low in conscientiousness are lessable to comply with or utilize treatment. Because the advantagesfor DCS augmentation are much greater in very brief treatments(Guastella et al., 2008; Hofmann, Meuret, et al., 2006) than in thecurrent 12-session protocol (Hofmann et al., 2013), it is possiblethat patients low in conscientiousness, who may not receive thefull dose of CBT, may benefit more from enhancement with DCS.Should it be the case that the DCS augmentation effects are indeedstronger for individuals for whom a standard course of CBT leavesample room for improvement (see de Kleine et al., 2012), highagreeableness may also emerge as a prognostic and prescriptivevariable in our analysis, as it has been associated with suboptimalresponding to exposure-based intervention for panic disorder (Har-court, Kirkby, Daniels, & Montgomery, 1998).
Because extant research on predictors of the efficacy of CBT forSAD and DCS augmentation of CBT, respectively, is limited inscope and has yielded inconsistent findings, we employed anexploratory, hypothesis-generating—rather than hypothesis-driv-en—framework in the present study. Here, we specifically aimedto determine the unique prescriptive or prognostic value of eachpatient characteristic by evaluating its predictive value while con-trolling for the influence of other patient characteristics. Acknowl-edging that multiple tests increase the risk of Type 1 error, weadopted an approach to handling this concern that was developedby Fournier et al. (2009) and later used by Amir, Taylor, andDonohue (2011). Specifically, we selected the patient characteris-tics assessed at the baseline visit and categorized these into mean-ingful domains (e.g., demographic characteristics, clinical charac-teristics, and personality traits). The first step involved a step-wiseprocedure to identify significant prognostic and prescriptive vari-ables within each domain. The second step involved the simulta-neous entry of these prescriptive and prognostic variables identi-fied for each domain in one final model.
Method
Participants
A description of the study design, procedures, and main out-come findings have been reported elsewhere (Hofmann et al.,2013). The sample consisted of 169 adults diagnosed with gener-alized SAD as determined by the Structured Clinical Interview for
DSM–IV Diagnosis (SCID–I; First, Spitzer, Gibbon, & Williams,2001) and a score 60 or higher on the Liebowitz Social AnxietyScale (LSAS; Liebowitz, 1987) at intake. Exclusion criteria were(a) clinically significant medical disorders; (b) lifetime history ofobsessive–compulsive disorder, bipolar disorder, schizophrenia,psychosis, or delusional disorders; (c) diagnosis of PTSD, sub-stance abuse or dependence, or eating disorder within the previous6 months; (d) organic brain syndrome, mental retardation, or othercognitive dysfunction; (e) clinically significant suicidal ideation orbehavior within the previous 6 months; (f) concurrent psychotropicmedication; (g) concurrent psychotherapy; (h) prior nonresponseto exposure therapy; and (i) women who were pregnant or lactatingor who could potentially become pregnant and were not usingmedically accepted forms of contraception. Figure 1 depicts theparticipant flow.
Study Design and Treatments
Eligible participants were enrolled at three study sites: BostonUniversity (BU), Massachusetts General Hospital (MGH), andSouthern Methodist University (SMU). Participants at each siteparticipated in an identical 12-session CBT protocol and wererandomly assigned to treatment condition at Session 3 via acomputer-generated allocation schedule that stratified by baselineSAD severity (i.e., LSAS score ! 70 or " 70; Liebowitz et al.,1992). Patients were randomized in a double-blind fashion andreceived 50 mg of DCS (n ! 87) or an identical-looking placebopill (n ! 82) at Sessions 3–7, 1 hr prior to each of these fivesessions.
Primary outcome variables were assessed throughout the treat-ment phase (at baseline, Sessions 2–8, 10, and 12), at posttreat-ment (Week 13), and during a treatment-free follow-up phase (at1, 3, and 6 months). In the present study, we report only datacollected during the acute phase (i.e., baseline to posttreatment).The institutional review boards of BU, MGH and SMU approvedthe study protocol, and patients at each institution provided writteninformed consent.
CBT. Therapists at each site used a treatment protocolfitting the general timing of Heimberg’s cognitive behavioralgroup therapy (i.e., 12 weekly 2.5-hr sessions; Heimberg &Becker, 2002) but adhering to the exposure targets and strate-gies described by Hofmann and Otto (2008), which were basedon the model described by Hofmann (2007). Treatment groupswere led by two therapists and composed of between four andsix patients. The first two sessions were devoted to educatingpatients about the nature and treatment of SAD and introducedcognitive restructuring. In Sessions 3–7, patients were ledthrough repeated and prolonged confrontation of feared situa-tions with the purpose of achieving fear extinction. Participantscontinued exposure practice in Sessions 8 –12 while utilizingthe cognitive restructuring strategies learned in earlier sessions.All therapists were trained and supervised by Stefan G. Hof-mann and Jasper A. J. Smits.
Medication. Study capsules were prepared containing (a) 50mg DCS or (b) pill placebo and administered orally by therapists.In order to maintain the blind, the appearances of the DCS andplacebo capsules were identical.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
3PREDICTORS OF DCS AUGMENTATION OF CBT FOR SAD

Outcome Measure
The LSAS (Liebowitz, 1987), the gold standard 24-item symp-tom severity measure for SAD, was used as the primary outcomemeasure in the present study. This scale was administered byindependent evaluators blind to treatment condition (Hofmann etal., 2013).
Potential Prognostic or Prescriptive Variables
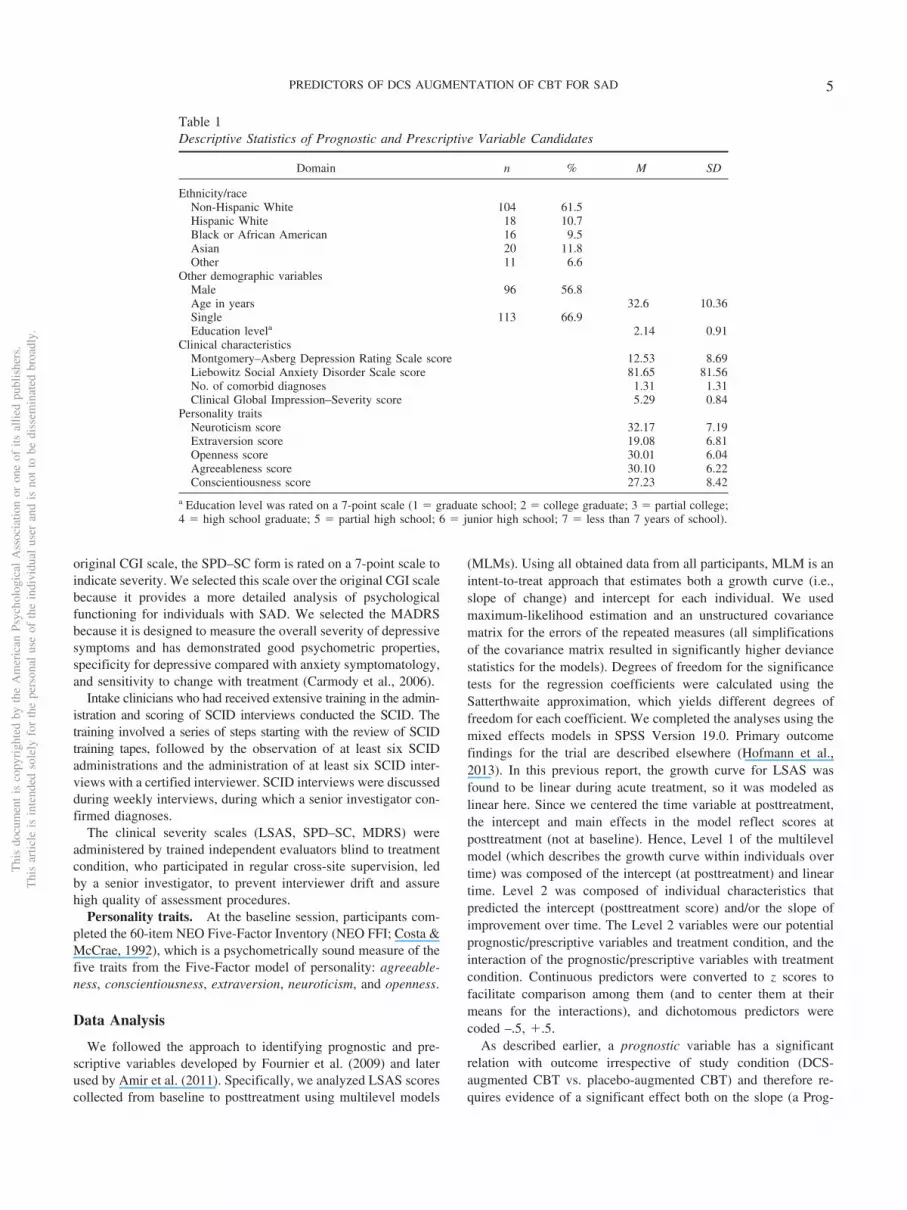
All potential prognostic or prescriptive variables were assessedat baseline, prior to randomization (see Table 1). To facilitate theanalyses (discussed later), we grouped the variables into the fol-lowing categories:
Race/ethnicity. Given there was meaningful representation("10% of the sample; Fournier et al., 2009) of Hispanic, Asian,and African American patients, we compared non-Hispanic Whiteto Hispanic White, African American, Asian, and other (i.e., Amer-ican Indian/Alaska Native, Native Hawaiian or other Pacific Is-
lander). We examined this category separately from other demo-graphic characteristics to reduce the number of terms in the initialmodels.
Other demographic characteristics. This domain comprisedsex, age, highest education level, and cohabitation status (dichot-omized; i.e., single, divorced, widowed, or separated vs. married orliving with partner). Demographic information was collected usinga questionnaire.
Clinical characteristics. Baseline psychiatric functioningwas assessed by clinician-rated measures. This domain comprisedclinical severity (as assessed by the Social Phobic Disorders Se-verity Form, or SPD-SC; Liebowitz et al., 1992), depressive symp-tom severity (as assessed by the Montgomery–Asberg DepressionRating Scale, or MADRS (Montgomery & Asberg, 1979) and AxisI comorbidity (i.e., number of comorbid Axis I disorders as as-sessed by the SCID–I; Hofmann et al., 2013).
The SPD–SC is an expansion and adaptation of the ClinicalGlobal Impression Scale (CGI; Guy, 1976) to SAD. Similar to the
Figure 1. Patient flow. DCS ! d-cycloserine.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
4 SMITS ET AL.
original CGI scale, the SPD–SC form is rated on a 7-point scale toindicate severity. We selected this scale over the original CGI scalebecause it provides a more detailed analysis of psychologicalfunctioning for individuals with SAD. We selected the MADRSbecause it is designed to measure the overall severity of depressivesymptoms and has demonstrated good psychometric properties,specificity for depressive compared with anxiety symptomatology,and sensitivity to change with treatment (Carmody et al., 2006).
Intake clinicians who had received extensive training in the admin-istration and scoring of SCID interviews conducted the SCID. Thetraining involved a series of steps starting with the review of SCIDtraining tapes, followed by the observation of at least six SCIDadministrations and the administration of at least six SCID inter-views with a certified interviewer. SCID interviews were discussedduring weekly interviews, during which a senior investigator con-firmed diagnoses.
The clinical severity scales (LSAS, SPD–SC, MDRS) wereadministered by trained independent evaluators blind to treatmentcondition, who participated in regular cross-site supervision, ledby a senior investigator, to prevent interviewer drift and assurehigh quality of assessment procedures.
Personality traits. At the baseline session, participants com-pleted the 60-item NEO Five-Factor Inventory (NEO FFI; Costa &McCrae, 1992), which is a psychometrically sound measure of thefive traits from the Five-Factor model of personality: agreeable-ness, conscientiousness, extraversion, neuroticism, and openness.
Data Analysis
We followed the approach to identifying prognostic and pre-scriptive variables developed by Fournier et al. (2009) and laterused by Amir et al. (2011). Specifically, we analyzed LSAS scorescollected from baseline to posttreatment using multilevel models
(MLMs). Using all obtained data from all participants, MLM is anintent-to-treat approach that estimates both a growth curve (i.e.,slope of change) and intercept for each individual. We usedmaximum-likelihood estimation and an unstructured covariancematrix for the errors of the repeated measures (all simplificationsof the covariance matrix resulted in significantly higher deviancestatistics for the models). Degrees of freedom for the significancetests for the regression coefficients were calculated using theSatterthwaite approximation, which yields different degrees offreedom for each coefficient. We completed the analyses using themixed effects models in SPSS Version 19.0. Primary outcomefindings for the trial are described elsewhere (Hofmann et al.,2013). In this previous report, the growth curve for LSAS wasfound to be linear during acute treatment, so it was modeled aslinear here. Since we centered the time variable at posttreatment,the intercept and main effects in the model reflect scores atposttreatment (not at baseline). Hence, Level 1 of the multilevelmodel (which describes the growth curve within individuals overtime) was composed of the intercept (at posttreatment) and lineartime. Level 2 was composed of individual characteristics thatpredicted the intercept (posttreatment score) and/or the slope ofimprovement over time. The Level 2 variables were our potentialprognostic/prescriptive variables and treatment condition, and theinteraction of the prognostic/prescriptive variables with treatmentcondition. Continuous predictors were converted to z scores tofacilitate comparison among them (and to center them at theirmeans for the interactions), and dichotomous predictors werecoded –.5, #.5.
As described earlier, a prognostic variable has a significantrelation with outcome irrespective of study condition (DCS-augmented CBT vs. placebo-augmented CBT) and therefore re-quires evidence of a significant effect both on the slope (a Prog-
Table 1Descriptive Statistics of Prognostic and Prescriptive Variable Candidates
Domain n % M SD
Ethnicity/raceNon-Hispanic White 104 61.5Hispanic White 18 10.7Black or African American 16 9.5Asian 20 11.8Other 11 6.6
Other demographic variablesMale 96 56.8Age in years 32.6 10.36Single 113 66.9Education levela 2.14 0.91
Clinical characteristicsMontgomery–Asberg Depression Rating Scale score 12.53 8.69Liebowitz Social Anxiety Disorder Scale score 81.65 81.56No. of comorbid diagnoses 1.31 1.31Clinical Global Impression–Severity score 5.29 0.84
Personality traitsNeuroticism score 32.17 7.19Extraversion score 19.08 6.81Openness score 30.01 6.04Agreeableness score 30.10 6.22Conscientiousness score 27.23 8.42
a Education level was rated on a 7-point scale (1 ! graduate school; 2 ! college graduate; 3 ! partial college;4 ! high school graduate; 5 ! partial high school; 6 ! junior high school; 7 ! less than 7 years of school).
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
5PREDICTORS OF DCS AUGMENTATION OF CBT FOR SAD

nostic Variable $ Time interaction) and the intercept (Fournier etal., 2009). A prescriptive variable, on the other hand, predictseither the direction or magnitude of the differential rates of im-provement between DCS-augmented and placebo-augmentedCBT. As such, a prescriptive variable requires evidence of asignificant interaction effect both on the slope (a PrescriptiveVariable $ Condition $ Time interaction) and intercept (Fournieret al., 2009). Accordingly, all analyses included the followingpredictors: Condition, Time, and Condition $ Time. For all prog-nostic/prescriptive variables, we added their main effect and theirinteractions with Condition, Time, and Condition $ Time asadditional predictors of outcome. Finally, because initial severity(as indexed by Social Phobic Disorders Severity Form; Liebowitzet al., 1992) has been associated with treatment outcome in thisdata set (Hofmann et al., 2013) and because sex has been associ-ated with treatment condition in this data set (Hofmann et al.,2013), we included Initial Severity, Initial Severity $ Time, andSex as control variables in every analysis.
Following Fournier et al. (2009) and Amir et al. (2011), we firstconducted a step-wise procedure for each domain of predictors(race/ethnicity, other demographic characteristics, clinical charac-teristics, personality traits), separately. In Step 1, we tested amodel including all variables for a given domain (as well as theirinteractions with Condition, Time, and Condition $ Time). Step 2retained the terms from Step 1 that were significant at p % .20.Step 3 retained the terms from Step 2 that were significant at p %.10. Finally, Step 4 retained the terms from Step 3 that weresignificant at p % .05. In all these steps, lower level main effectsand interactions of a higher level interaction were retained if thehigher order interaction was retained, regardless of their signifi-cance (i.e., a main effect was retained if its interaction with anyother variable was retained, regardless of the significance of themain effect). Finally, each term that was significant at p % .05 inStep 4 (within each domain) was included in a final model (acrossdomains), allowing the testing of the effects of each variable whilecontrolling for the effects of other variables.
Results
Step-Wise Analyses Within Each Domain
The results of the step-wise procedure for each domain arepresented in Table 2. In the text, we report only the significantresults of Step 4 for each domain. We discuss the form andinterpretation of each significant finding in the last section of theResults, under the subheading Final Model.1
Race/ethnicity. In Step 4 for the race/ethnicity domain, Afri-can American ethnicity was a significant predictor of faster linearchange in LSAS scores, African American Ethnicity $ Timeinteraction: b ! &1.30 (SE ! 0.52), t(151) ! &2.51, p ! .013.Accordingly, African American patients had lower posttreatmentLSAS scores than patients who were not African American, b !&13.79 (SE ! 5.23), t(150) ! &2.64, p ! .009. No other race/ethnicity prognostic or prescriptive variables were identified.
Other demographic characteristics. In Step 4 of this do-main, cohabitation status was a significant predictor of both fasterlinear change in LSAS, Cohabitation Status $ Time interaction:b ! &0.84 (SE ! 0.32), t(148) ! &2.60, p ! .010, and lowerposttreatment LSAS scores, b ! &9.19 (SE ! 3.25), t(147) !
&2.83, p ! .005. No other demographic prognostic or prescriptivevariables were identified.
Clinical characteristics. Neither depressive symptom sever-ity nor the number of comorbid Axis I comorbid disorders(whether log transformed to reduce skewness or not) were relatedto the slope of improvement in LSAS or posttreatment LSASscores. It should be noted that initial severity on the on theSPD–SC was included in all analyses. Its relation with LSAS isreported in the section under the “Final Model.”
Personality traits. In Step 4 for the personality traits domain,agreeableness was a moderator of the treatment effects on slope ofLSAS over time, Agreeableness $ Condition $ Time interaction:b ! 0.69 (SE ! 0.31), t(154) ! 2.21, p ! .029, but not onposttreatment LSAS scores (see Table 2). In this Step 4, consci-entiousness also interacted with treatment condition to predict theslope of change in LSAS, Conscientiousness $ Condition $ Timeinteraction: b ! –0.85 (SE ! 0.30), t(149) ! &2.83, p ! .005, andwas not significantly associated with the effect of treatment con-dition on posttreatment LSAS scores, Conscientiousness $ Con-dition interaction: b ! &5.98 (SE ! 3.97), t(147) ! &1.95, p !.053. Last, neuroticism was associated with posttreatment LSASscores (but not as a moderator) in Step 4, suggesting that neurot-icism was positively associated with posttreatment LSAS scoresirrespective of condition or time (see Table 2).
Final Model With All Significant Prognostic andPrescriptive Variables
The final model included the simultaneous entry of the prescrip-tive and prognostic variables found to be significant in Step 4 ofthe previous sets of analyses (and again included initial severity,Initial Severity $ Time, and sex). The results are presented inTable 2 and Figures 2 and 3. All prescriptive and prognosticvariables that were significant in the step-wise analyses for eachdomain (see Table 2) retained significance in the final model.Specifically, African American patients evidenced greater rates ofimprovement during CBT, African American Ethnicity $ Timeinteraction: b ! &1.50 (SE ! 0.51), t(152) ! &2.95, p ! .004,and lower posttreatment LSAS scores, b ! &16.44 (SE ! 5.10),t(152) ! &3.23, p ! .002, than patients who were not AfricanAmerican. Compared with patients who are not African American,African American patients showed a 49% faster rate of improve-ment in LSAS scores during treatment (see Figure 2a). Similarly,cohabitation status remained associated with faster linear changein LSAS, Cohabitation $ Time interaction: b ! 0.88 (SE ! 0.31),t(149) ! 2.81, p ! .006, and lower posttreatment LSAS scores,b ! &9.30 (SE ! 3.17), t(149) ! 2.93, p ! .004; see Figure 2b.Those cohabitating showed a 29% faster rate of improvement inLSAS over time compared with those who were not cohabitating.In these analyses, greater initial severity also remained a signifi-cant predictor of faster linear change in LSAS, Initial Severity $Time interaction: b ! &0.82 (SE ! 0.15), t(149) ! &5.63, p %.001, but also of higher posttreatment LSAS scores, b ! 4.54(SE ! 1.48), t(15) ! &3.06, p ! .003; see Figure 2c.
1 Per suggestion of a reviewer, we tested whether the results varied as afunction of site. We did not observe any significant moderator effects ofsite.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
6 SMITS ET AL.

Table 2Step-Wise Analyses
Domain/predictor
Change over time Posttreatment score
b (SE)a p b (SE)b p
Domain: Ethnicity/raceStep 1
Hispanic 0.06 (0.52) &5.21 (5.25)Black or African American &1.38 (0.54) ! &13.31 (5.41) !
Asian 0.06 (0.50) 1.53 (5.04)Other &0.75 (0.69) &3.77 (6.92)Hispanic $ Condition 0.41 (1.04) 4.88 (10.46)Black or African American $ Condition 0.23 (1.07) 9.21 (10.69)Asian $ Condition 1.34 (1.00) †† 10.34 (10.06)Other $ Condition 1.43 (1.37) 23.36 (13.73) †
Step 2 (retain effects at p % .20)c
Black or African American &1.33 (0.52) ! &13.95 (5.28) !!
Asian 0.07 (0.50) 1.53 (5.02)Other 1.40 (3.25)Asian $ Condition 1.22 (0.98) 9.76 (9.96)Other $ Condition 8.12 (6.42)
Step 3 (retain effects at p % .10)c
Black or African American &1.30 (0.52) ! &13.79 (5.23) !!
Step 4 (retain effects at p % .05)c
Black or African American &1.30 (0.52) ! &13.79 (5.23) !!
Domain: Other demographic variablesStep 1
Age 0.13 (0.17) 0.99 (1.73)Education 0.04 (0.16) &0.19 (1.62)Single &0.95 (0.36) !! &9.48 (3.65) !!
Age $ Condition &0.56 (0.34) † &3.73 (3.42)Education $ Condition 0.37 (0.32) 1.10 (3.20)Single $ Condition 0.62 (0.72) 9.11 (7.27)
Step 2 (retain effects at p % .20)c
Age 0.12 (0.16) &0.69 (1.67)Single &0.99 (0.35) !! &10.04 (3.54) !!
Age $ Condition &0.36 (0.30) &2.01 (3.07)Step 3 (retain effects at p % .10)c
Single &0.84 (0.32) !! &9.19 (3.25) !!
Step 4 (retain effects at p % .05)c
Single &0.84 (0.32) !! &9.19 (3.25) !!
Domain: Clinical characteristicsStep 1d
Baseline Montgomery–Asberg DepressionRating Scale (MADRS) score &0.07 (0.16) 1.58 (1.63)
No. of comorbid diagnoses &0.03 (0.16) 0.63 (1.65)Baseline MADRS $ Condition 0.35 (0.32) 2.34 (3.27)No. of Comorbid Diagnoses $ Condition 0.33 (0.32) 0.55 (3.30)
Domain: Personality traitsStep 1
Neuroticism 0.004 (0.18) 3.12 (1.83) †
Extraversion &0.17 (0.17) &.49 (1.74)Openness 0.21 (0.15) †† .39 (1.57)Agreeableness 0.13 (0.16) 2.21 (1.61) ††
Conscientiousness &0.04 (0.17) &1.37 (1.76)Neuroticism $ Condition 0.48 (0.35) †† .52 (3.63)Extraversion $ Condition &0.10 (0.34) &3.03 (3.47)Openness $ Condition 0.15 (0.31) 1.45 (3.17)Agreeableness $ Condition 0.71 (0.31) ! 4.92 (3.22) ††
Conscientiousness $ Condition &0.66 (0.34) † &4.73 (3.53) ††
Step 2 (retain effects at p % .20)c
Neuroticism 0.05 (0.17) 3.08 (1.78) †
Openness 0.19 (0.15) 0.43 (1.55)Agreeableness 0.12 (0.16) 2.04 (1.60)Conscientiousness &0.07 (0.17) &1.47 (1.72)Neuroticism $ Condition 0.48 (0.34) †† 1.46 (3.49)
(table continues)
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
7PREDICTORS OF DCS AUGMENTATION OF CBT FOR SAD
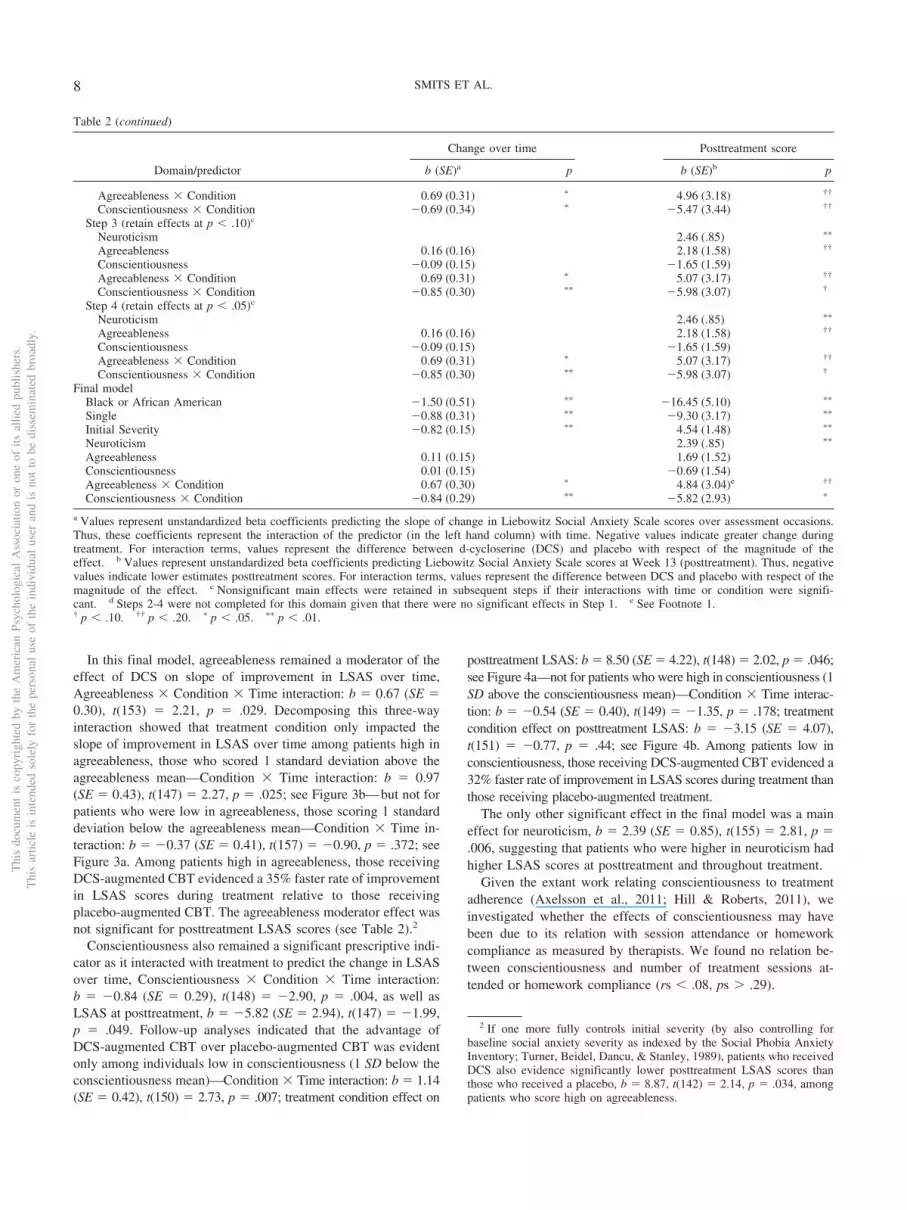
In this final model, agreeableness remained a moderator of theeffect of DCS on slope of improvement in LSAS over time,Agreeableness $ Condition $ Time interaction: b ! 0.67 (SE !0.30), t(153) ! 2.21, p ! .029. Decomposing this three-wayinteraction showed that treatment condition only impacted theslope of improvement in LSAS over time among patients high inagreeableness, those who scored 1 standard deviation above theagreeableness mean—Condition $ Time interaction: b ! 0.97(SE ! 0.43), t(147) ! 2.27, p ! .025; see Figure 3b—but not forpatients who were low in agreeableness, those scoring 1 standarddeviation below the agreeableness mean—Condition $ Time in-teraction: b ! &0.37 (SE ! 0.41), t(157) ! &0.90, p ! .372; seeFigure 3a. Among patients high in agreeableness, those receivingDCS-augmented CBT evidenced a 35% faster rate of improvementin LSAS scores during treatment relative to those receivingplacebo-augmented CBT. The agreeableness moderator effect wasnot significant for posttreatment LSAS scores (see Table 2).2
Conscientiousness also remained a significant prescriptive indi-cator as it interacted with treatment to predict the change in LSASover time, Conscientiousness $ Condition $ Time interaction:b ! &0.84 (SE ! 0.29), t(148) ! &2.90, p ! .004, as well asLSAS at posttreatment, b ! &5.82 (SE ! 2.94), t(147) ! &1.99,p ! .049. Follow-up analyses indicated that the advantage ofDCS-augmented CBT over placebo-augmented CBT was evidentonly among individuals low in conscientiousness (1 SD below theconscientiousness mean)—Condition $ Time interaction: b ! 1.14(SE ! 0.42), t(150) ! 2.73, p ! .007; treatment condition effect on
posttreatment LSAS: b ! 8.50 (SE ! 4.22), t(148) ! 2.02, p ! .046;see Figure 4a—not for patients who were high in conscientiousness (1SD above the conscientiousness mean)—Condition $ Time interac-tion: b ! &0.54 (SE ! 0.40), t(149) ! &1.35, p ! .178; treatmentcondition effect on posttreatment LSAS: b ! &3.15 (SE ! 4.07),t(151) ! &0.77, p ! .44; see Figure 4b. Among patients low inconscientiousness, those receiving DCS-augmented CBT evidenced a32% faster rate of improvement in LSAS scores during treatment thanthose receiving placebo-augmented treatment.
The only other significant effect in the final model was a maineffect for neuroticism, b ! 2.39 (SE ! 0.85), t(155) ! 2.81, p !.006, suggesting that patients who were higher in neuroticism hadhigher LSAS scores at posttreatment and throughout treatment.
Given the extant work relating conscientiousness to treatmentadherence (Axelsson et al., 2011; Hill & Roberts, 2011), weinvestigated whether the effects of conscientiousness may havebeen due to its relation with session attendance or homeworkcompliance as measured by therapists. We found no relation be-tween conscientiousness and number of treatment sessions at-tended or homework compliance (rs % .08, ps " .29).
2 If one more fully controls initial severity (by also controlling forbaseline social anxiety severity as indexed by the Social Phobia AnxietyInventory; Turner, Beidel, Dancu, & Stanley, 1989), patients who receivedDCS also evidence significantly lower posttreatment LSAS scores thanthose who received a placebo, b ! 8.87, t(142) ! 2.14, p ! .034, amongpatients who score high on agreeableness.
Table 2 (continued)
Domain/predictor
Change over time Posttreatment score
b (SE)a p b (SE)b p
Agreeableness $ Condition 0.69 (0.31) ! 4.96 (3.18) ††
Conscientiousness $ Condition &0.69 (0.34) ! &5.47 (3.44) ††
Step 3 (retain effects at p % .10)c
Neuroticism 2.46 (.85) !!
Agreeableness 0.16 (0.16) 2.18 (1.58) ††
Conscientiousness &0.09 (0.15) &1.65 (1.59)Agreeableness $ Condition 0.69 (0.31) ! 5.07 (3.17) ††
Conscientiousness $ Condition &0.85 (0.30) !! &5.98 (3.07) †
Step 4 (retain effects at p % .05)c
Neuroticism 2.46 (.85) !!
Agreeableness 0.16 (0.16) 2.18 (1.58) ††
Conscientiousness &0.09 (0.15) &1.65 (1.59)Agreeableness $ Condition 0.69 (0.31) ! 5.07 (3.17) ††
Conscientiousness $ Condition &0.85 (0.30) !! &5.98 (3.07) †
Final modelBlack or African American &1.50 (0.51) !! &16.45 (5.10) !!
Single &0.88 (0.31) !! &9.30 (3.17) !!
Initial Severity &0.82 (0.15) !! 4.54 (1.48) !!
Neuroticism 2.39 (.85) !!
Agreeableness 0.11 (0.15) 1.69 (1.52)Conscientiousness 0.01 (0.15) &0.69 (1.54)Agreeableness $ Condition 0.67 (0.30) ! 4.84 (3.04)e ††
Conscientiousness $ Condition &0.84 (0.29) !! &5.82 (2.93) !
a Values represent unstandardized beta coefficients predicting the slope of change in Liebowitz Social Anxiety Scale scores over assessment occasions.Thus, these coefficients represent the interaction of the predictor (in the left hand column) with time. Negative values indicate greater change duringtreatment. For interaction terms, values represent the difference between d-cycloserine (DCS) and placebo with respect of the magnitude of theeffect. b Values represent unstandardized beta coefficients predicting Liebowitz Social Anxiety Scale scores at Week 13 (posttreatment). Thus, negativevalues indicate lower estimates posttreatment scores. For interaction terms, values represent the difference between DCS and placebo with respect of themagnitude of the effect. c Nonsignificant main effects were retained in subsequent steps if their interactions with time or condition were signifi-cant. d Steps 2-4 were not completed for this domain given that there were no significant effects in Step 1. e See Footnote 1.† p % .10. †† p % .20. ! p % .05. !! p % .01.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
8 SMITS ET AL.

Discussion
In the present study, we aimed to identify baseline characteris-tics associated with differential response to DCS augmentation ofCBT and response to CBT for SAD overall. Using a multivariateapproach, we found that African American ethnicity and cohabi-tation status were positive prognostic variables of CBT outcome.In addition, initial severity was associated with a faster rate ofsymptom improvement but remained related to higher symptomseverity at posttreatment. Last, both agreeableness and conscien-tiousness emerged as prescriptive variables, such that the positiveaugmentation effects of DCS (over placebo) were evident onlyamong persons high in agreeableness or low in conscientiousness,respectively.
The findings of the present study extend previous research in anumber of meaningful ways. First, our results suggest that patientspresenting with severe generalized SAD, as defined by the pres-ence of high symptom severity, do not respond more poorly to
Figure 3. Prescriptive variable: Agreeableness. There was no differencein treatment response between d-cycloserine (DCS)- and placebo (PBO)-augmented cognitive behavioral therapy among patients who scored low inagreeableness (Panel A). However, there was a significant differencebetween these groups among patients who scored high on agreeableness(Panel B). High agreeableness was operationalized as 1 standard deviationabove the mean and low agreeableness as 1 standard deviation below themean. LSAS ! Liebowitz Social Anxiety Scale.
Figure 2. Prognostic variables. African American patients showed agreater response to cognitive behavioral therapy (CBT) than patients whowere not African American (Panel A), individuals who were cohabitatingshowed greater response to CBT than those who were not cohabitating(Panel B), and patients presenting with greater initial symptom severityshowed greater response to CBT than those who had less initial severity(Panel C). High severity was operationalized as 1 standard deviation abovethe mean and low severity as 1 standard deviation below the mean.LSAS ! Liebowitz Social Anxiety Scale.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
9PREDICTORS OF DCS AUGMENTATION OF CBT FOR SAD

CBT emphasizing exposure to feared cues coupled with cognitiverestructuring (Hofmann, 2007; Hofmann & Otto, 2008) relative topatients with less severe SAD. Instead, our findings suggest thatpatients who present with high symptom severity actually improvefaster and may simply need longer treatment to achieve equiva-lence with those presenting with low(er) initial severity (Smits,Minhajuddin, Thase, & Jarett, 2012). It is important to note herethat our analyses indicate SAD symptom severity as a prognosticvariable over Axis I comorbidity and depressive symptom severity.Also, our results do not indicate a role for DCS in speeding the rateof improvement for patients high in initial severity as has beenhypothesized (Otto et al., 2010) and observed in a recent smaller-scale trial involving patients with PTSD (de Kleine et al., 2012).
Second, the results of the present study provide much neededinformation on how ethnic minorities fare with CBT relative totheir non-Hispanic White counterparts (Horrell, 2008). Indeed,
research in this area is sparse, particularly as it relates to SAD, andinitial results of studies of CBT for other disorders have providedmixed results (Horrell, 2008). For example, Markowitz, Spielman,Sullivan, and Fishman (2000) found African American ethnicitypredicted poorer response to CBT for depression in HIV-positivemen, while Miranda et al. (2003) noted no differences amongAfrican American, Latina, and White women regarding the effectsof CBT on depressive symptoms. In contrast, our findings indicatethat African Americans respond better to CBT for SAD thanpatients who are not African American. In fact, it was notable thataverage posttreatment score for African Americans was in theremission range. Accordingly, our findings may lessen concernsabout whether empirically supported treatments, such as CBT forSAD, are effective for diverse populations (Hall, 2001). Given thenovelty of this result in relation to existing findings, it seemspremature to speculate on the underlying causes of this finding.However, if our results are replicated, understanding why AfricanAmericans may respond better to CBT for SAD than their non-African American counterparts should be a focus of future work.
Third, controlling for other demographic, clinical severity, andpersonality variables, we found that cohabitation status was asignificant predictor of CBT outcome in our analysis, with cohabi-tating participants evidencing greater symptom improvement andlower posttreatment severity. It has been suggested that personswho cohabitate may do particularly well with CBT because, com-pared with those who do not cohabitate, they tend to have a greatersocial network and because they have more opportunities to prac-tice with their partners or friends the tools they have learned(Fournier et al., 2009). This may be particularly relevant to CBTfor SAD, which stresses repeated exposure to social interactionand performance situation outside the session (Heimberg &Becker, 2002; Hofmann & Otto, 2008). Alternatively, relative toindividuals who are single, those who cohabitate may receivegreater social support, which may confer additional therapeuticeffects.
Fourth, our analyses identified agreeableness and conscientious-ness as (independent) moderators of the efficacy of DCS foraugmenting CBT of SAD. Only individuals low in conscientious-ness or high in agreeableness, respectively, achieved greater ben-efit from DCS compared with placebo augmentation. To ourknowledge, this is the first indication of a potential matchingstrategy (i.e., personality traits) for DCS augmentation of CBT,since no moderators emerged in a recent meta-analysis of small-scale efficacy trials of DCS (Bontempo et al., 2012). In contrast toour hypothesis, follow-up analyses provided no evidence suggest-ing that individuals low in conscientiousness received less treat-ment or utilized treatment less well on the measures available (e.g.,session attendance, homework compliance). Nonetheless, there isevidence, albeit mixed, of potential different central nervous sys-tem characteristics between those low and high in conscientious-ness, which may suggest there may be a specifically biologicalexplanation for the observed effects. Specifically, Hiio et al.(2011) reported that low conscientiousness is a characteristic ofcarriers of the brain-derived neurotrophic factor (BDNF)Val66Met genotype Met-allele, and several studies have shownthat the BDNFMet allele has been associated with an impairment inextinction learning in both mice (Soliman et al., 2010; Yu et al.,2009) and humans (Soliman et al., 2010), likely because of re-duced ventromedial prefrontal activity and increased amygdala
Figure 4. Prescriptive variable: Conscientiousness. There was a signifi-cant difference in treatment response between d-cycloserine (DCS)- andplacebo (PBO)-augmented cognitive behavioral therapy among patientswho scored low in conscientiousness (Panel A). However, there was nosignificant difference between these groups among patients who scoredhigh on conscientiousness (Panel B). High conscientiousness was opera-tionalized as 1 standard deviation above the mean and low conscientious-ness as 1 standard deviation below the mean. LSAS ! Liebowitz SocialAnxiety Scale.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
10 SMITS ET AL.

activity during extinction. Yu and colleagues documented that thisextinction learning deficit exhibited by BDNFMet mice can bereversed by the administration of DCS (Yu et al., 2009).
We are not aware of any research that may provide a possiblebiological explanation for the moderator effects of agreeableness.However, previous research has associated high agreeablenesswith suboptimal responding to exposure-based interventions (Har-court et al., 1998), thus potentially pointing to high agreeablenessas a marker for extinction-learning deficits. Therefore, our findingsmay be consistent with the hypothesis that DCS augmentation isonly indicated for patients who are in some way compromised withrespect to learning with extinction-based therapy. Together, theseobservations call for studies examining the relation among fear-extinction-relevant biological processes or factors (e.g., singlenucleotide polymorphisms); behavioral factors; conscientiousness;agreeableness (or personality traits more broadly); and the efficacyof DCS augmentation of CBT.
Although this research has produced a number of potentiallyuseful findings and has done so while a wide range of possiblethird variables were controlled, a number of limitations deservemention. First, following Fournier et al. (2009) and Amir et al.(2011), we adopted an exploratory approach to identifying prog-nostic and prescriptive variables. Here, we were limited by exam-ining only individual characteristics that had been assessed atbaseline in a study involving adults with generalized SAD whowere randomly assigned to receive 12 sessions of group CBTeither with 50 mg of DCS or placebo during Sessions 3–7. Ac-cordingly, our findings may not generalize to CBT protocols of adifferent duration or individual modality, DCS augmentation of adifferent dose or frequency, or a nongeneralized SAD sample.Moreover, given we had data available on only a limited set ofindividual characteristics, there are plausible third-variable expla-nations (e.g., genetic factors) that may be relevant. Second, as istypical in efficacy trials, we employed a number of exclusioncriteria and therefore may have inadvertently restricted the gener-alizability of the findings to a medication-free SAD sample with-out severe psychiatric or physical health comorbidity. Thus, it ispossible that the predictive value of clinical characteristics wouldhave been different in this study had we included patients whowere taking psychotropic medications or who presented with moresevere comorbid psychopathology. Third, because the comparatorcondition was placebo-augmented CBT, we cannot determinewhether the prognostic factors observed in the present study arespecific to CBT for SAD that is combined with placebo or whetherthese also generalize to CBT without placebo augmentation.Fourth, because we already conducted a large number of tests, wedid not examine interactions among predictor variables. Therefore,we cannot rule out the possibility that the prognostic or prescrip-tive effects observed in the present study vary as a function ofother predictor variables. Examining more such nuanced relationsis an important direction for future research (Fournier et al., 2009).Last, because we limited the analyses to symptom changes duringthe course of treatment, the identified prognostic and prescriptivevariables may be specific to short-term effects and may not gen-eralize to long-term effects.
Despite these limitations, this study is the first to provide infor-mation on patient characteristics that are associated with responseto DCS-augmented CBT for SAD. Clinically, these data, if repli-cated, can offer guidance as practitioners make decisions about
treatment strategies with this patient population. With respect totheory and future research, the observed relations in the presentstudy may be useful for enhancing the understanding of the mech-anisms of CBT for anxiety disorders and thereby ultimately aid inthe development of more potent, personalized interventions forthese disabling conditions.
References
Amir, N., Taylor, C. T., & Donohue, M. C. (2011). Predictors of responseto an attention modification program in generalized social phobia. Jour-nal of Consulting and Clinical Psychology, 79, 533–541. doi:10.1037/a0023808
Anderson, K. C., & Insel, T. R. (2006). The promise of extinction researchfor the prevention and treatment of anxiety disorders. Biological Psy-chiatry, 60, 319–321. doi:10.1016/j.biopsych.2006.06.022
Axelsson, M., Brink, E., Lundgren, J., & Lotvall, J. (2011). The influenceof personality traits on reported adherence to medication in individualswith chronic disease: An epidemiological study in West Sweden. PLoSOne, 6, e18241. doi:10.1371/journal.pone.0018241
Blanco, C., Heimberg, R. G., Schneier, F. R., Fresco, D. M., Chen, H.,Turk, C. L., . . . Liebowitz, M. R. (2010). A placebo-controlled trial ofphenelzine, cognitive behavioral group therapy, and their combinationfor social anxiety disorder. Archives of General Psychiatry, 67, 286–295. doi:10.1001/archgenpsychiatry.2010.11
Bontempo, A., Panza, K., & Bloch, M. H. (2012). D-Cycloserine augmen-tation of behavioral therapy for the treatment of anxiety disorders: Ameta-analysis. Journal of Clinical Psychiatry, 73, 533–537. doi:10.4088/JCP.11r07356
Carmody, T. J., Rush, A. J., Bernstein, I., Warden, D., Brannan, S.,Burnham, D., . . . Trivedi, M. H. (2006). The Montgomery Asberg andthe Hamilton ratings of depression: A comparison of measures. Euro-pean Neuropsychopharmacology, 16, 601–611. doi:10.1016/j.euroneuro.2006.04.008
Chambless, D. L., Tran, G. Q., & Glass, C. R. (1997). Predictors ofresponse to cognitive behavioral group therapy for social phobia. Jour-nal of Anxiety Disorders, 11, 221–240. doi:10.1016/S0887-6185(97)00008-X
Clark, D. M., Ehlers, A., McManus, F., Hackmann, A., Fennell, M.,Campbell, H., . . . Louis, B. (2003). Cognitive therapy versus fluoxetinein generalized social phobia: A randomized placebo-controlled trial.Journal of Consulting and Clinical Psychology, 71, 1058–1067. doi:10.1037/0022-006X.71.6.1058
Collimore, K. C., & Rector, N. A. (2012). Symptom and cognitive predic-tors of treatment response in CBT for social anxiety disorder. Interna-tional Journal of Cognitive Therapy, 5, 157–169. doi:10.1521/ijct.2012.5.2.157
Costa, P. T., & McCrae, R. R. (1992). Revised NEO Personality Inventory(NEO–PI–R) and NEO Five-Factor Inventory (NEO–FFI) manual.Odessa, FL: Psychological Assessment Resources.
Davidson, J. R., Foa, E. B., Huppert, J. D., Keefe, F. J., Franklin, M. E.,Compton, J. S., . . . Gadde, K. M. (2004). Fluoxetine, comprehensivecognitive behavioral therapy, and placebo in generalized social phobia.Archives of General Psychiatry, 61, 1005–1013. doi:10.1001/archpsyc.61.10.1005
Davis, M., Ressler, K., Rothbaum, B. O., & Richardson, R. (2006). Effectsof D-cycloserine on extinction: Translation from preclinical to clinicalwork. Biological Psychiatry, 60, 369–375. doi:10.1016/j.biopsych.2006.03.084
de Kleine, R. A., Hendriks, G. J., Kusters, W. J., Broekman, T. G., & vanMinnen, A. (2012). A randomized placebo-controlled trial ofD-cycloserine to enhance exposure therapy for posttraumatic stressdisorder. Biological Psychiatry, 71, 962–968. doi:10.1016/j.biopsych.2012.02.033
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
11PREDICTORS OF DCS AUGMENTATION OF CBT FOR SAD

Erwin, B. A., Heimberg, R. G., Juster, H., & Mindlin, M. (2002). Comor-bid anxiety and mood disorders among persons with social anxietydisorder. Behaviour Research and Therapy, 40, 19–35. doi:10.1016/S0005-7967(00)00114-5
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (2001).Structured Clinical Interview for DSM–IV Axis-I Disorders–ClinicianVersion. Washington, DC: American Psychiatric Association.
Fournier, J. C., DeRubeis, R. J., Shelton, R. C., Hollon, S. D., Amsterdam,J. D., & Gallop, R. (2009). Prediction of response to medication andcognitive therapy in the treatment of moderate to severe depression.Journal of Consulting and Clinical Psychology, 77, 775–787. doi:10.1037/a0015401
Guastella, A. J., Richardson, R., Lovibond, P. F., Rapee, R. M., Gaston,J. E., Mitchell, P., & Dadds, M. R. (2008). A randomized controlled trialof the effect of D-cycloserine on enhancement of exposure therapy forsocial anxiety disorder. Biological Psychiatry, 63, 544 –549. doi:10.1016/j.biopsych.2007.11.011
Guy, W. (1976). Assessment manual for psychopharmacology. Washing-ton, DC: Government Printing Office.
Hall, G. C. N. (2001). Psychotherapy research with ethnic minorities:Empirical, ethical, and conceptual issues. Journal of Consulting andClinical Psychology, 69, 502–510. doi:10.1037/0022-006X.69.3.502
Harcourt, L., Kirkby, K., Daniels, B., & Montgomery, I. (1998). Thedifferential effect of personality on computer-based treatment of agora-phobia. Comprehensive Psychiatry, 39, 303–307. doi:10.1016/S0010-440X(98)90039-6
Heimberg, R. G., & Becker, R. E. (2002). Cognitive behavioral grouptherapy for social phobia: Basic mechanisms and clinical strategies.New York, NY: Guilford Press.
Heimberg, R. G., Liebowitz, M. R., Hope, D. A., Schneier, F. R., Holt,C. S., Welkowitz, L. A., . . . Klein, D. F. (1998). Cognitive behavioralgroup therapy vs phenelzine therapy for social phobia: 12-week out-come. JAMA General Psychiatry, 55, 1133–1141. doi:10.1001/archpsyc.55.12.1133
Hiio, K., Merenakk, L., Nordquist, N., Parik, J., Oreland, L., Veidebaum,T., & Harro, J. (2011). Effects of serotonin transporter promoter andBDNF Val66Met genotype on personality traits in a population repre-sentative sample of adolescents. Psychiatric Genetics, 21, 261–264.doi:10.1097/YPG.0b013e32834371e8
Hill, P. L., & Roberts, B. W. (2011). The role of adherence in therelationship between conscientiousness and perceived health. HealthPsychology, 30, 797–804. doi:10.1037/a0023860
Hofmann, S. G. (2007). Cognitive factors that maintain social anxietydisorder: A comprehensive model and its treatment implications. Cog-nitive Behaviour Therapy, 36, 193–209. doi:10.1080/16506070701421313
Hofmann, S. G., Meuret, A. E., Smits, J. A., Simon, N. M., Pollack, M. H.,Eisenmenger, K., . . . Otto, M. W. (2006). Augmentation of exposuretherapy with D-cycloserine for social anxiety disorder. Archives ofGeneral Psychiatry, 63, 298–304. doi:10.1001/archpsyc.63.3.298
Hofmann, S. G., & Otto, M. W. (2008). Cognitive behavioral therapy forsocial anxiety disorder: Evidence-based and disorder-specific treatmenttechniques. London, England: Routledge.
Hofmann, S. G., Pollack, M. H., & Otto, M. W. (2006). Augmentationtreatment of psychotherapy for anxiety disorders with D-cycloserine.CNS Drug Reviews, 12, 208 –217. doi:10.1111/j.1527-3458.2006.00208.x
Hofmann, S. G., & Smits, J. A. (2008). Cognitive behavioral therapy foradult anxiety disorders: A meta-analysis of randomized placebo-controlled trials. Journal of Clinical Psychiatry, 69, 621–632. doi:10.4088/JCP.v69n0415
Hofmann, S. G., Smits, J. A., Asnaani, A., Gutner, C. A., & Otto, M. W.(2011). Cognitive enhancers for anxiety disorders. Pharmacology Bio-chemistry and Behavior, 99, 275–284. doi:10.1016/j.pbb.2010.11.020
Hofmann, S. G., Smits, J. A. J., Rosenfield, D., Simon, N. M., Otto, M. W.,Meuret, A. E., . . . Pollack, M. H. (2013). D-cycloserine as an augmen-tation strategy of cognitive behavioral therapy for social anxiety disor-der. American Journal of Psychiatry, 170, 751–758. doi:10.1176/appi.ajp.2013.12070974
Horrell, S. C. V. (2008). Effectiveness of cognitive behavioral therapy withadult ethnic minority clients: A review. Professional Psychology: Re-search and Practice, 39, 160–168. doi:10.1037/0735-7028.39.2.160
Joormann, J., Kosfelder, J., & Schulte, D. (2005). The impact of comor-bidity of depression on the course of anxiety treatments. CognitiveTherapy and Research, 29, 569–591. doi:10.1007/s10608-005-3340-5
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., &Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributionsof DSM–IV disorders in the National Comorbidity Survey Replication.Archives of General Psychiatry, 62, 593–602. doi:10.1001/archpsyc.62.6.593
Kraemer, H. C., Wilson, G. T., Fairburn, C. G., & Agras, W. S. (2002).Mediators and moderators of treatment effects in randomized clinicaltrials. Archives of General Psychiatry, 59, 877– 883. doi:10.1001/archpsyc.59.10.877
Ledley, D. R., Huppert, J. D., Foa, E. B., Davidson, J. R., Keefe, F. J., &Potts, N. L. (2005). Impact of depressive symptoms on the treatment ofgeneralized social anxiety disorder. Depression and Anxiety, 22, 161–167. doi:10.1002/da.20121
Liebowitz, M. R. (1987). Social phobia. In D. Klein, J. Gorman, A. Fyer,& M. Liebowitz (Eds.), Modern problems of pharmacopsychiatry (pp.141–173). Basel, Switzerland: Karger.
Liebowitz, M. R., Schneier, F., Campeas, R., Hollander, E., Hatterer, J.,Fyer, A., . . . Klein, D. F. (1992). Phenelzine vs. atenolol in socialphobia. A placebo-controlled comparison. Archives of General Psychi-atry, 49, 290–300.
Markowitz, J. C., Spielman, L. A., Sullivan, M., & Fishman, B. (2000). Anexploratory study of ethnicity and psychotherapy outcome among HIV-positive patients with depressive symptoms. Journal of PsychotherapyPractice & Research, 9, 226–231.
McEvoy, P. M., Nathan, P., Rapee, R. M., & Campbell, B. N. (2012).Cognitive behavioural group therapy for social phobia: Evidence oftransportability to community clinics. Behaviour Research and Therapy,50, 258–265. doi:10.1016/j.brat.2012.01.009
Miranda, J., Chung, J. Y., Green, B. L., Krupnick, J., Siddique, J., Revicki,D. A., & Belin, T. (2003). Treating depression in predominantly low-income young minority women: A randomized controlled trial. JAMA:Journal of the American Medical Association, 290, 57–65. doi:10.1001/jama.290.1.57
Montgomery, S. A., & Asberg, M. (1979). A new depression scale de-signed to be sensitive to change. The British Journal of Psychiatry, 134,382–389. doi:10.1192/bjp.134.4.382
Otto, M. W., Smits, J. A., & Reese, H. E. (2004). Cognitive behavioraltherapy for the treatment of anxiety disorders. Journal of ClinicalPsychiatry, 65(Suppl 5), 34–41.
Otto, M. W., Tolin, D. F., Simon, N. M., Pearlson, G. D., Basden, S.,Meunier, S. A., . . . Pollack, M. H. (2010). Efficacy of d-cycloserine forenhancing response to cognitive behavior therapy for panic disorder.Biological Psychiatry, 67, 365–370. doi:10.1016/j.biopsych.2009.07.036
Schneier, F. R., Heckelman, L. R., Garfinkel, R., Campeas, R., Fallon,B. A., Gitow, A., . . . Liebowitz, M. R. (1994). Functional impairmentin social phobia. Journal of Clinical Psychiatry, 55, 322–331.
Schneier, F. R., Johnson, J., Hornig, C. D., Liebowitz, M. R., & Weissman,M. M. (1992). Social phobia. Comorbidity and morbidity in an epide-miologic sample. Archives of General Psychiatry, 49, 282–288. doi:10.1001/archpsyc.1992.01820040034004
Smits, J. A. J., Minhajuddin, A., Thase, M. E., & Jarrett, R. J. (2012).Outcomes of acute phase cognitive therapy in outpatients with anxious
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
12 SMITS ET AL.

versus nonanxious depression. Psychotherapy & Psychosomatics, 81,153–160. doi:10.1159/000334909
Soliman, F., Glatt, C. E., Bath, K. G., Levita, L., Jones, R. M., Pattwell,S. S., . . . Casey, B. J. (2010, February 12). A genetic variant BDNFpolymorphism alters extinction learning in both mouse and human.Science, 327, 863–866. doi:10.1126/science.1181886
Turner, S. M., Beidel, D. C., Dancu, C. V., & Stanley, M. A. (1989). Anempirically derived inventory to measure social fears and anxiety: TheSocial Phobia and Anxiety Inventory. Psychological Assessment, 1,35–40.
Turner, S. M., Beidel, D. C., Wolff, P. L., Spaulding, S., & Jacob, R. G.(1996). Clinical features affecting treatment outcome in social phobia.Behaviour Research and Therapy, 34, 795–804. doi:10.1016/0005-7967(96)00028-9
Yu, H., Wang, Y., Pattwell, S., Jing, D., Liu, T., Zhang, Y., . . . Chen, Z. Y.(2009). Variant BDNF Val66Met polymorphism affects extinction ofconditioned aversive memory. The Journal of Neuroscience, 29, 4056–4064. doi:10.1523/JNEUROSCI.5539-08.2009
Zinbarg, R. E., Uliaszek, A. A., & Adler, J. M. (2008). The role ofpersonality in psychotherapy for anxiety and depression. Journal ofPersonality, 76, 1649–1688. doi:10.1111/j.1467-6494.2008.00534.x
Received August 3, 2012Revision received June 4, 2013
Accepted July 8, 2013 !
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
13PREDICTORS OF DCS AUGMENTATION OF CBT FOR SAD





























