Embed Size (px)
Citation preview

Cutaneous CD41 CD561 hematologic malignancies
Cynthia M. Magro, MD,a Pierluigi Porcu, MD,c Jochen Schaefer, MD,a Jack W. Erter, MD,c
Richard R. Furman, MD,b Paul K. Shitabata, MD,d and A. Neil Crowson, MDe
New York, New York; Columbus, Ohio; Torrance, California; and Tulsa, Oklahoma
From
og
si
St
M
O
Fund
Conf
Repr
W
N
Publ
0190
ª 20
doi:1
292
Background: Hematologic malignancies expressing CD4 and CD56 are most commonly associated withthe recently described CD41 CD561 hematodermic neoplasm.
Methods: Thirteen cases of CD41 CD561 hematologic malignancies were prospectively encountered inthe routine and referral practices of the authors.
Results: Patients 1 and 2 were elderly men exhibiting an acute onset of skin, bone-marrow, and peripheralblood involvement, both dying of their disease within less than 12 months. CD31 phenotype and a clonalT-cell receptor b rearrangement indicated categorization as a CD41 natural killer T-cell lymphoma. Patient3 developed a CD561 anaplastic large cell lymphoma and is without disease after excision and radiation.Indolent CD41 CD561 poikilodermatous mycosis fungoides defined case 4. There were 7 patients withCD1231 CD41 CD561 hematodermic neoplasm, 4 dying within 18 months of presentation with peripheralblood/marrow involvement in 6 of the 7 cases. Two patients with granulocytic sarcoma dying within 100days of presentation defined the last two cases.
Limitations: There were relatively small numbers in each of the categories and the follow-up was limitedin those cases where death was not reported.
Conclusion: Cutaneous malignancies composed of CD41 CD561 hematopoietic cells define a variedgroup and oftentimes have an aggressive clinical course although not in every case. ( J Am Acad Dermatol2010;63:292-308.)
Key words: cutaneous; hematologic; malignancy.
Abbreviations used:
AML: acute myelogenous leukemiaEBV: Epstein-Barr virusIL: interleukinMDS: myelodysplastic syndromeMF: mycosis fungoidesMxA: myxovirus proteinNK: natural killer
Natural killer (NK) and NK-like T-celllymphomas are aggressive hematologicmalignancies that frequently have an
extranodal presentation. The main affected organsites include the gastrointestinal tract, skin, and nasalcavities. These neoplasms have been broadly cate-gorized as nasal versus nonnasal in type.1-3 All of
TCL1: T-cell leukemia 1 oncogeneTCR: T-cell receptorUV: ultraviolet
the Department of Pathologya and Division of Hematol-
y and Oncology,b Weill Medical College of Cornell Univer-
ty, New York; Division of Hematology and Oncology, Ohio
ate Universityc; Pathology Inc, Torranced; and Regional
edical Laboratories, St John Medical Center, University of
klahoma.e
ing sources: None.
licts of interest: None declared.
int requests: Cynthia M. Magro, MD, Department of Pathology,
eill Cornell Medical Center, 1300 York Ave, F-309A, New York,
Y 10044. E-mail: [email protected].
ished online June 11, 2010.
-9622/$36.00
09 by the American Academy of Dermatology, Inc.
0.1016/j.jaad.2009.08.044
these neoplasms can present initially in the skinand/or involve the skin as part of a multiorgandisseminated lymphoma, developing concurrentlyand/or after presentation at other sites.
In both NK and NK-like T-cell lymphomas, theneoplastic cells express CD2 and CD56; true NKlymphomas are CD4e and CD8e (ie, null pheno-type). NK-like T-cell lymphomas are characteristi-cally of the null or CD8 phenotype.1-3 The distinctionof NK versus NK-like T-cell lymphoma is based on

J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 293
the T-cell receptor (TCR)b and/or gamma (g) generearrangement and surface CD3 expression; thosethat lack these features are categorized as NK lym-phomas; those that manifest surface CD3 expressionand exhibit a TCR rearrangement are considered NK-like T-cell lymphomas.1-3
In the original classification scheme there was
CAPSULE SUMMARY
d CD41 CDD561 malignancies are mostfrequently observed in the context of theCD41 CD561 hematodermic neoplasm.
d Thirteen cases of cutaneousmalignancies exhibiting this distinctivephenotypic profile were examined.
d CD41 CD561 malignancies are aheterogeneous group including theCD41 CD561 hematodermic neoplasm,granulocytic sarcoma, and conventionalcutaneous T-cell lymphoma.
d Although the course can be aggressive,other common forms of cutaneous T-celllymphoma with this phenotypic profilemay be indolent. A broader array ofimmunohistochemical studies in concertwith molecular studies enables correctcategorization.
a distinctive NK neoplasmphenotypically differentfrom the other reported NKand NK-like T-cell lympho-mas, as it manifested CD4positivity. This tumor fell un-der the designation of blasticNK-like T-cell lymphoma. Inthe revised World HealthOrganization-European Org-anization for Research andTreatment of Cancer classifi-cation, blastic NK-cell lym-phoma was considered aclinically aggressive T-cellneoplasm with a high inci-dence of skin involvementand a significant risk of leu-kemic dissemination.1-3
A blastic cytomorphologyand expression of CD56were held to be evidence ofan NK-precursor cell origin.More recently, however, ithas been established that the
cell of origin is a plasmacytoid dendritic cell.4-6Consequently the term ‘‘blastic NK-like T-cell lym-phoma’’ has been supplanted by the term ‘‘CD41
CD561 hematodermic neoplasm’’ (HD) and mostrecently ‘‘blastic plasmacytoid dendritic cell neo-plasm.’’4-6 In those neoplasms categorized as trueNK lymphomas, there is a frequent association withEpstein-Barr virus (EBV), especially in Asian patientswith nasopharyngeal involvement7,8; EBV has notbeen pathogenetically implicated in CD41 CD561.CD41 CD561 hematodermic neoplasms (HD) areaggressive tumors that typically lead to patientdemise within 12 months of presentation.4-6
Although the dominant literature addressingCD41 CD561 malignancies is in the context ofCD41 CD561 hematodermic neoplasm, there areother hematologic malignancies that may expressthis particular phenotypic profile. We present aspectrum of CD41 CD561 cutaneous malignanciescomprising agranular CD41 CD561 T-cell lym-phoma, classic cutaneous T-cell lymphoma, CD41
CD561 hematodermic neoplasm, and cutaneousgranulocytic sarcoma.
METHODSAll cases were encountered in the consultative
and routine dermatopathology files at the WeillMedical College, New York Presbyterian Hospital.In all cases paraffin-embedded formalin-fixed tissuewas available for routine light microscopy andimmunohistochemistry. On all cases a comprehen-
sive battery of phenotypicmarkers was conducted in-cluding CD2, CD3, CD4,CD8, CD62L, CD7 EBV-en-coding small nonpolyadeny-lated RNA, CD56, granzyme,FoxP3, cutaneous lympho-cyte antigen, CD123 myxovi-rus protein (MxA), CD83,CD123, and T-cell leukemia1 oncogene (TCL1). The pro-cedures for MxA, CD83, andTCL1 will be described ingreater detail. The study re-ceived institutional reviewboard approval in August2007. One of the cases hasbeen previously published.9
ImmunophenotypingSections (5 �m) of forma-
lin-fixed paraffin-embeddedtissues were cut on to plusslides (Fisher Inc, Pittsburgh,PA). Routine deparaffiniza-
tion from xylene to 95% alcohol and rehydrationbefore patented microwave antigen recovery werecarried out. The detection of the antigens wasperformed using a two-step immunohistochemistryprocedure. After a 30-minute incubation with theprimary antibodies, staining was performed usingthe commercially available Vision BioSystems DefineKit (Norwell, MA) adhering to the protocol.Incubation with the primary antibodies was con-ducted using the following dilutions: CD83 1:80(Novocastra, part number NCL CD83,Bannockburn, IL), MxA 1:1600 (Dr Otto Haller,Freiburg, Germany), TCL1 1:50 (Cell Signalling,Danvers, MA).
CD41 CD561 MALIGNANCY ASSOCIATEDWITH T-CELL CLONALITY (NK T-CELLLYMPHOMA, ANAPLASTIC LARGE CELLLYMPHOMA, AND MYCOSIS FUNGOIDES)NK T-cell lymphoma (cases 1 and 2)
The two patients were both men, ages 62 and 76years. One patient presented initially with a suddenonset of ulcerative skin tumors whereas the other

Table I. Natural killerelike CD4 T-cell lymphoma (current series and previously reported cases)
NK-like T-cell lymphoma with a CD41 CD561 phenotypeCase 1 2 312 413 513 615 714
Age, y 62 76 15 32 37 55 79Sex M M F F F M MAffected site Head, chest,
shoulders,axillae, back,spleen, bonemarrow
Bone marrow,trunk, lymphnode
Inner aspectof left thigh
Thighs, glutealregions, trunk,upper limbs
Trunk, head,gingival,extremities,bone marrow
Back, flank,chest,abdomen
Skin, peripheralblood, bonemarrow
Treatment Chemotherapy Chemotherapy Chemotherapyand allogeneicSCT
Chemotherapy Chemotherapy Chemotherapyand allogeneicSCT
Chemotherapy
Outcome Death within6 mo ofpresentation
Death within 12mo ofpresentation
Free of disease1 y afterchemotherapy
Death within 10mo ofpresentation
Multiplerelapsesand died
Still alive attime ofpublication
Death within6 mo ofdiagnosis
ImmunophenotypeCD2 1/� 1 1 1 � 1
CD3 1 1 � 1 � 1
CD4 1 1 1 1 1 1
CD56 1 1 1 1 1 1 1
Granzyme ND 1
TIA ND 1
EBER � 1 � � �TCRb 1 1 ND �TCRg 1 1 1 1 1
EBER, Epstein-Barr virus-encoding small nonpolyadenylated RNA; F, female; M, male; ND, not done; NK, natural killer; SCT, stem cell transplantation; TCR, T-cell receptor; TIA, T-cell intracellular
antigen.
JA
MA
CA
DD
ER
MA
TO
L
AU
GU
ST
20
10
294
Ma
groet
al

Fig 1. Biopsy specimen shows striking pandermal nodu-lar infiltrate assuming interstitial, perivascular, and peri-adnexal disposition. Infiltrate is associated with dermaleffacement (case 2 of natural killer T-cell lymphomacases).
Fig 2. In addition there is extension of infiltrate into fat.Infiltrate is largely nonepidermotropic (case 2 of naturalkiller T-cell lymphoma cases).
Fig 3. Higher-power magnification reveals that cells areintermediate in size, manifesting markedly atypicalalthough monomorphic appearance. Cells have round tooval nuclei, which are eccentrically disposed and associ-ated with perinuclear hoff (case 2 of natural killer T-celllymphoma cases).
J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 295
patient developed fatigue, weakness, and lymphad-enopathy followed several months later by a duskyerythematous truncal-based rash. Both patientsunderwent bone-marrow and skin biopsies disclos-ing a malignant T-cell infiltrate, the results of whichare detailed below. Neither patient had peripheralblood involvement although patient 2 exhibitedlymphopenia (1.2 3 103/�L) and marked thrombo-cytopenia (15 3 103/�L); both patients had mildanemia at 11.7 g/dL and 10.1 g/dL, respectively.Despite aggressive multiagent chemotherapy bothpatients died within 6 and 12 months, respectively, ofpresentation (Table I).
PathologyBoth patients underwent skin biopsies disclosing
a morphologically and phenotypically similar malig-nant process. There was an effacing diffuse andnodular infiltrate. There was some involvement ofthe adventitia of the hair follicle with focal epithelio-tropism in case 1 (Figs 1 and 2). The infiltrate wasdefined by a monomorphous population of inter-mediate-sized lymphoid forms. The nuclei wereround to reniform with an eccentric dispositionwithin the cell. The chromatin was evenly dispersed;there were single, small discernible centrally locatednucleoli (Fig 3).
The neoplastic cells strongly expressed CD3. Inaddition, they were CD101, CD41, CD561, andCD431 (Fig 4, A to C ). They did not expressgranzyme, CD34, CD68, CD79a, CD20, CD30, orterminal deoxynucleotidyl transferase. The cellswere focally TCL1 positive, however, they did notstain for MxA or CD123. Although there was CD2staining, the majority of the cells were negative incase 1. The cutaneous lymphocyte antigen stainrevealed a distinct perinuclear dotlike staining pat-tern. The FoxP3 stain did not disclose any positive
staining cells. Scattered CD8-expressing lympho-cytes were present. In situ hybridization studies forexpression of kappa and lambda light chain andEBV-encoding small nonpolyadenylated RNA werenegative in case 1 although showed extensive pos-itivity in case 2 (Fig 5, A).
T-cell clonality was identified on the skin biopsyspecimen in case 1 and bone-marrow biopsy spec-imen in case 2 using the technique of multiplexpolymerase chain reaction TCRb fragment size anal-ysis (Figs 4, D, and 5, B). Cytogenetics performed onthe marrow aspirate in case 2 revealed 4 copies ofmost chromosomes; an absence of the Y chromo-some; a deletion in chromosomes 11, 16, and 18; andan isochrome 7q in duplicate (Fig 5, C ).
CD41 561 ANAPLASTIC LARGE CELLLYMPHOMACase 3
The patient was a 79-year-old man who was ingood health until the fall of 2006 when he was stung

Fig 4. Cells are CD561 (A), CD31 (B), and CD41 (C) (case1 of natural killer T-cell lymphoma cases). Dominant T-cellclone compatible with clonal T-cell receptor gene rear-rangement is detected in skin biopsy specimen (D).
Fig 5. A, Cells are focally Epstein-Barr virus-encodingsmall nonpolyadenylated RNA positive (case 2 of naturalkiller T-cell lymphoma cases). B, Dominant T-cell clone isdemonstrated in marrow aspirate indicative of clonalT-cell rearrangement. C, Cytogenetics performed on mar-row aspirate revealed 4 copies of most chromosomes,absence of Y chromosome, and deletion in chromosomes11, 16, and 18 and isochrome 7q in duplicate.
J AM ACAD DERMATOL
AUGUST 2010
296 Magro et al
on the back by a hornet while on his tractor. The areawhere he sustained the sting progressively enlargedover a 4-month period leading to a biopsy that wasperformed in October 2006. After a diagnosis wasmade of anaplastic large cell lymphoma subsequentinvestigations revealed a monoclonal paraprotein ofIgM isotype. Based on subsequent bone-marrowassessment a diagnosis was made of Waldenstrommacroglobulinemia. The skin lymphoma wasexcised in its entirety and was radiated with no
subsequent recurrence and/or development ofadditional nodules as of February 2009. He hasreceived rituximab to treat his Waldenstrom macro-globulinemia with normalization of his immuno-globulin levels although still has symptoms relatedto cold agglutinins. His medical history was remark-able for adenocarcinoma of the colon that wasresected without recurrence in 2000. His only med-ication was ibuprofen (Table II).
PathologyThe biopsy specimen showed a striking pander-
mal infiltrate of very atypical epithelioid-appearing

J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 297
mononuclear cells along with numerous bizarremultinucleated neoplastic giant cells (Fig 6, A).
Phenotypic cells revealed that the cells wereCD301, CD21, CD41, and CD561 and TCR generearrangement studies were positive (Fig 6, B). Therewas a loss of the pan T-cell markers CD3, CD5, andCD7. Immunoreactivity for CD123, MxA, and/orTCL1 was not observed.
CD41 CD561 MYCOSIS FUNGOIDESCase 4
The patient was a 52-year-old man who presentedwith a several-year history of a poikilodermatouseruption involving his trunk. The clinical impressionwas poikilodermatous mycosis fungoides (MF).Apart from pruritus the patient was asymptomatic.He is currently alive and well and being treated withnarrowband ultraviolet (UV) B therapy (Table III).
PathologyA biopsy specimen showed a bandlike lympho-
cytic infiltrate in close apposition to the epidermis.The cells had a distinct cerebriform appearance andwere predominantly small to intermediate in size.Phenotypic studies were conducted and revealedthat the dominant cell in the dermis and epidermiswas a CD41 T cell. The cells were also CD21, CD31,and CD51. A substantial reduction was observed forCD7. The neoplastic cells within the epidermis werehighlighted by a CD56 stain. A few atypical cells inthe dermis were also CD561. There was no immu-noreactivity of the cells for CD123, MxA, TCL1, andCD83.
CD41 CD561 HEMATODERMIC NEOPLASM(BLASTIC PLASMACYTOID DENDRITICCELL NEOPLASM) (CASES 5-11)Clinical summary
The 7 patients were men aged 25, 31, 70, 71, 75,and 76 years and one woman aged 46 years. Thedisease was heralded in all patients by a rash bestcharacterized as a violaceous, plaquelike eruptionmost frequently involving the trunk, proximal arms,and face (Figs 7 and 8). Medical histories wereremarkable for myelodysplasia in one patient andHIV infection in another (see Table IV). This laterpatient had received antiretroviral therapy for 10years before the onset of his cutaneous malignancy.Concurrent bone-marrow involvement was seen in 5of the 7 patients, whereas two patients had spleno-megaly. Although no patients had palpable lym-phadenopathy, two patients had extensive chest,abdominal, and pelvic lymphadenopathy on radiog-raphy. One patient had tumor cells identified in thecerebrospinal fluid, and one patient demonstrated
nasopharyngeal involvement. Four of the 7 patientsdied, 3 less than 12 months from their initial clinicalpresentation; all of these patients received chemo-therapy only. One patient declined treatment anddeveloped progressive disease. Combination che-motherapy was started in one patient in preparationfor an allogeneic stem cell transplantation. The lastpatient exhibited cutaneous confined disease. Hehad a partial response to bexarotene and interferonalfa and will be undergoing an allogenic bone-marrow transplantation. The specific drugs adminis-tered are presented in Table IV.
PathologyAll biopsy specimens appeared similar demon-
strating a massive effacing pandermal infiltrate withfocal angiocentric accentuation. The infiltrate wascomposed of a monomorphic population of mono-cytoid-appearing cells in the 10- to 15-�m range(Fig 9). Red cell extravasation was observed. In all 3cases, phenotypic studies revealed that the cells wereCD41, CD561, CD1231, and cutaneous lymphocyteantigen positive. Other markers that were variablypositive included CD2 (1/6), CD7 (1/6), MxA (3/6),CD83 (1/6), and TCL1 (3/6) (Figs 10 to 12). The cellsdid not express granzyme and T-cell intracellularantigen (TIA). TCR clonality studies revealed agermline configuration and/or a polyclonal T-cellpopulation. Cytogenetic studies in one case showeda monosomy 7 and a deletion of 7q31 via flourescentin situ hybridization analysis.
CD41 CD561 GRANULOCYTICSARCOMA/ACUTE MYELOGENOUSLEUKEMIA CUTIS WITH MONOCYTICDIFERENTIATION MIMICKING CD41
CD561 HEMATODERMIC NEOPLASM(CASE 12 AND 13)Clinical summary
The patient was a 46-year-old woman who hadbeen treated for a 2-cm invasive breast cancer forwhich she underwent lumpectomy and axillary nodedissection followed by high-dose Adriamycin andradiation therapy. In the summer of 2007 the patientpresented with a papular rash on her extremities thatwas biopsied and diagnostic of acute monocyticleukemia; she was subsequently established to havebone-marrow involvement. She underwent chemo-therapy with daunorubicin and cytarabine alongwith an allogeneic stem cell transplantation. Sheobtained a complete remission on bone-marrowbiopsy. Her course was complicated by severegraft-versus-host disease with prominent gastroin-testinal involvement. She died in November of 2007

Table II. CD561 anaplastic large cell lymphoma (current series and previously reported cases)
CD561 variants of anaplastic large cell lymphoma
Case 1, Current
series
225 326 428 529 633 733 831 932
Age, y 76 57 56 4 14 33 56 58 4
Sex M F M F M F M M F
Medical
history
Previously
healthy
Previously
healthy
Kidney
transplantation;
prednisone,
azathioprine,
and
cyclosporine
Previously
healthy
Previously
healthy
Kidney
transplantation;
azathioprine
for 2 y
Kidney
transplantation;
cyclosporine,
azathioprine,
prednisone 6 y
Previously
healthy
Previously
healthy
Affected
site
Back Forehead
and scalp
Forehead and
right hand
Head, chest,
jaw (right
vertical
ramus)
Back, neck,
front of thigh,
cervical 1
inguinal node,
large periaortic
and retrocrural
mass, CNS
Abdomen, chest,
arms, lung,
myocardium,
pancreas
Lower aspect
of left leg
Elbow, in a
background
of more
generalized
plaquelike
rash
Thigh
Treatment Excision,
radiation,
because of
subsequent
paraprotein
rituximab
Chemotherapy,
stem cell
transplantation
Chemotherapy Chemotherapy Chemotherapy D/C azathioprine
and cyclosporine
and increase
prednisone
Chemotherapy,
radiotherapy,
relapsed
Excision and
2 cycles of
chem
Complete
excision
Outcome No evidence
of recurrent
disease;
reduction in
paraprotein,
persistent
cold
agglutinins
Complete
remission 6 y
Complete
remission
for 6 mo
Complete
remission
for 4 y
Two relapses
with new
course of
chemotherapy
leading to
resolution,
ongoing
treatment
2.75 y after
diagnosis
After discontinuing
immunosuppressiv
therapy nodules
resolved in 4 mo;
recurrence 14 mo
later and then died
of widespread
disease
Relapsed 7 mo
later and
died 15 mo
later of renal
failure,
recurrent
lymphoma
No response
because of
side effects
no further
therapy, no
additional
follow-up
Free of
disease
44
mo
later
Immunophenotype
CD2 1 ND ND \50% 1 ND �CD3 � � 1 1 1/� 1 � � �CD4 1 � 1 \50% � � 1 ND �CD8 � 1 � � 1 � � � �CD7 � 1 � 1 ND ND �CD56 1 1 1 1 1 1 1 1 1
JA
MA
CA
DD
ER
MA
TO
L
AU
GU
ST
20
10
298
Ma
groet
al
e

Gra
nzy
me
11
1?
1�
�1
1
TIA
ND
11
?1
�N
D1
1
TC
Rb
ND
ND
ND
ND
ND
1N
DN
SN
D
TC
Rg
ND
Re
arra
ng
em
en
tR
ear
ran
ge
men
tR
ear
ran
ge
me
nt
Ge
rmlin
eN
D1
�EB
ER�
��
ND
��
=
CN
S,C
en
tral
ne
rvo
us
syst
em
;D
/C,
dis
con
tin
ue
d;
EBER
,Ep
stei
n-B
arr
viru
s-e
nco
din
gsm
all
no
np
oly
ade
nyl
ate
dR
NA
;F,
fem
ale
;M
,m
ale;
ND
,n
ot
do
ne
;TC
R,
T-c
ell
rece
pto
r.
Fig 6. Biopsy specimen shows sheetlike infiltrate of verypleomorphic large hematopoietic cells with binucleationand multinucleation. Cells have abundant cytoplasm.There is background population of neutrophils and eo-sinophils (A). Cells are CD301 (B) (case 1 of anaplasticlarge cell lymphoma group).
J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 299
after developing Klebsiella pneumonia and hemor-rhagic cystitis (Table V).
Case 13The patient was a 64-year-old man; his medical
history was remarkable for prostate and lung cancer.In December 2007 he developed fatigue and wasfound to be cytopenic. Subsequent bone-marrowassessment was compatible with an intermediategrade myelodysplastic syndrome (MDS) favoringrefractory anemia with excess blasts type I; thedetails of the marrow findings are described below.Shortly after the administration of long-acting gran-ulocyte colony-stimulating factor he developed nod-ular lesions on the scalp and axillae. Despitechemotherapy he continued to develop dissemi-nated skin nodules and a retro-orbital mass. Hewas to receive an allogeneic stem cell transplanta-tion, however, within 4 months of presentation hedied; the immediate cause of death was a stroke. Anautopsy was not performed.
PathologyIn both cases the skin biopsy specimens showed a
very striking pandermal mononuclear cell infiltrate.The cells demonstrated round to oval nuclei with a

Table III. CD561 mycosis fungoides (current case and previously reported cases)
CD56 variants of mycosis fungoides
Case 1 (current
series)
2 (Current
series)
340 441 541 641 742 839 939
Age, y 62 47 33 45 6 37 26 NA NA
Sex M M (Asian) M (Asian) F (Asian) M (Somali) F F NA NA
Affected
site
Truncal
poikilodermatous
skin lesions
Truncal
poikilodermatous
skin lesions
Extremities,
trunk
Poikiloderma
elbow left
arm
poikiloderma
hyperpigmented
areas of
thighs, buttocks,
and groin
Abdomen and
then other
areas
to involve
90% of his
skin
hypopigmented
with follicular
accentuation
5-y History of
truncal rash
and then
nodule on
lower aspect
of back,
poikiloderma
Erythroderma
and
poikiloderma,
peripheral
blood
involvement
tumors
No details
available
No details
available
Treatment Light
therapy
Narrowband
UVB
Psoralen light
treatment
Topical steroids
and local
radiotherapy
with limited
response
Psoralen and light Psoralen and
light,
excision
of tumor
Steroids,
then UVB
Light and
psoralen
Light and
psoralen
Outcome In remission,
without
evidence of
disease
In remission,
without
evidence
of disease
Stage IB
responded
with no
evidence of
disease 1 y
later
Limited stage IA
disease 6 y
since
diagnosis
Stage IB residual
areas of
hypopigmentation
no disease
progression
No further
tumors, skin
poikiloderma
in remission
Stage IA,
responded to
light and
psoralen
Stage IA,
responded to
light and
psoralen
Immunophenotype
CD2 1 1 1 1 1 1 1 1
CD3 1 1 1 1 1 1 1 1 1
CD4 1 � � � � 1 � � �CD8 � 1 � 1 � � 1 � �CD56 1 1 1 1 1 1 1 1
TIA 1 1 1 1 1 1
Granzyme 1 � 1 1
TCRb ND ND
TCRg 1 1 1 1 1
EBER � ND � � �
EBER, Epstein-Barr virus-encoding small nonpolyadenylated RNA; F, female; M, male; NA, not available; ND, not done; TCR, T-cell receptor; TIA, T-cell intracellular antigen; UVB, ultraviolet B.
JA
MA
CA
DD
ER
MA
TO
L
AU
GU
ST
20
10
300
Ma
groet
al
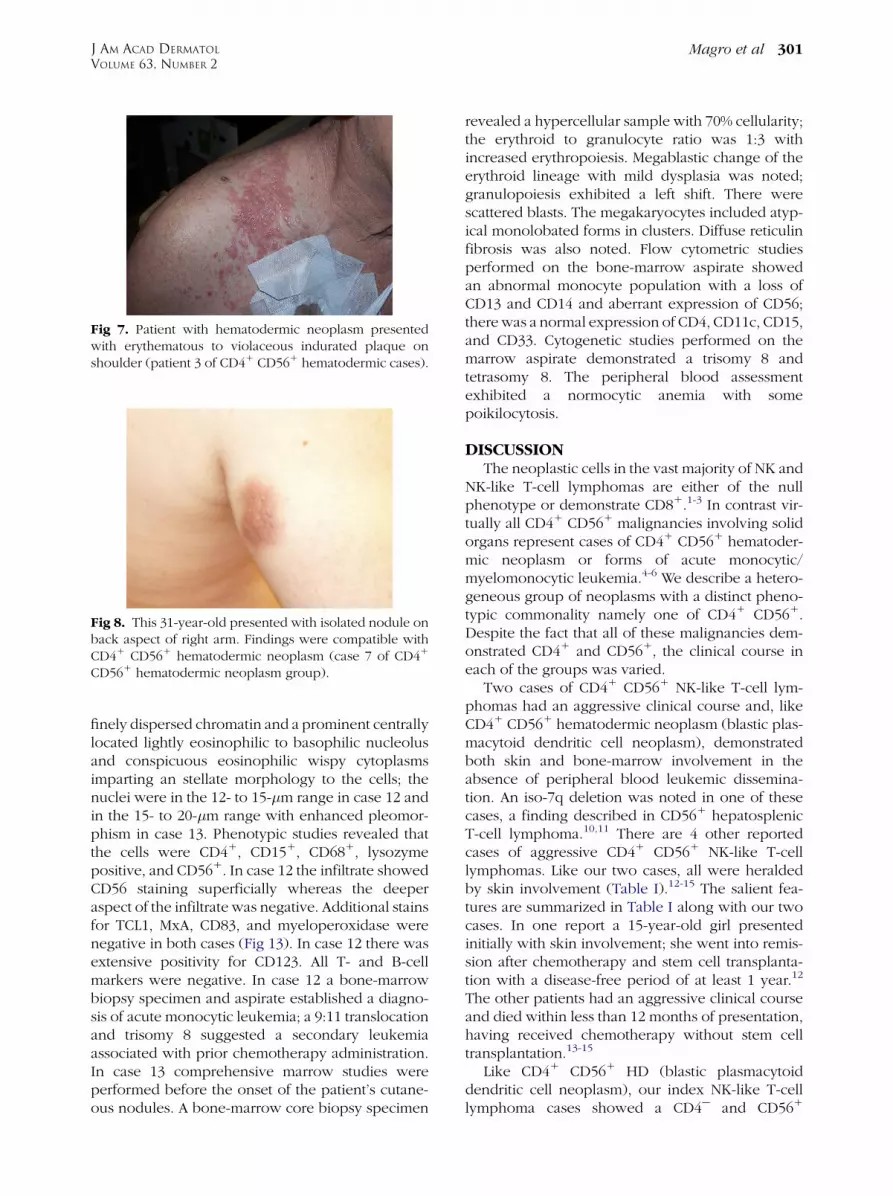
Fig 7. Patient with hematodermic neoplasm presentedwith erythematous to violaceous indurated plaque onshoulder (patient 3 of CD41 CD561 hematodermic cases).
Fig 8. This 31-year-old presented with isolated nodule onback aspect of right arm. Findings were compatible withCD41 CD561 hematodermic neoplasm (case 7 of CD41
CD561 hematodermic neoplasm group).
J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 301
finely dispersed chromatin and a prominent centrallylocated lightly eosinophilic to basophilic nucleolusand conspicuous eosinophilic wispy cytoplasmsimparting an stellate morphology to the cells; thenuclei were in the 12- to 15-�m range in case 12 andin the 15- to 20-�m range with enhanced pleomor-phism in case 13. Phenotypic studies revealed thatthe cells were CD41, CD151, CD681, lysozymepositive, and CD561. In case 12 the infiltrate showedCD56 staining superficially whereas the deeperaspect of the infiltrate was negative. Additional stainsfor TCL1, MxA, CD83, and myeloperoxidase werenegative in both cases (Fig 13). In case 12 there wasextensive positivity for CD123. All T- and B-cellmarkers were negative. In case 12 a bone-marrowbiopsy specimen and aspirate established a diagno-sis of acute monocytic leukemia; a 9:11 translocationand trisomy 8 suggested a secondary leukemiaassociated with prior chemotherapy administration.In case 13 comprehensive marrow studies wereperformed before the onset of the patient’s cutane-ous nodules. A bone-marrow core biopsy specimen
revealed a hypercellular sample with 70% cellularity;the erythroid to granulocyte ratio was 1:3 withincreased erythropoiesis. Megablastic change of theerythroid lineage with mild dysplasia was noted;granulopoiesis exhibited a left shift. There werescattered blasts. The megakaryocytes included atyp-ical monolobated forms in clusters. Diffuse reticulinfibrosis was also noted. Flow cytometric studiesperformed on the bone-marrow aspirate showedan abnormal monocyte population with a loss ofCD13 and CD14 and aberrant expression of CD56;there was a normal expression of CD4, CD11c, CD15,and CD33. Cytogenetic studies performed on themarrow aspirate demonstrated a trisomy 8 andtetrasomy 8. The peripheral blood assessmentexhibited a normocytic anemia with somepoikilocytosis.
DISCUSSIONThe neoplastic cells in the vast majority of NK and
NK-like T-cell lymphomas are either of the nullphenotype or demonstrate CD81.1-3 In contrast vir-tually all CD41 CD561 malignancies involving solidorgans represent cases of CD41 CD561 hematoder-mic neoplasm or forms of acute monocytic/myelomonocytic leukemia.4-6 We describe a hetero-geneous group of neoplasms with a distinct pheno-typic commonality namely one of CD41 CD561.Despite the fact that all of these malignancies dem-onstrated CD41 and CD561, the clinical course ineach of the groups was varied.
Two cases of CD41 CD561 NK-like T-cell lym-phomas had an aggressive clinical course and, likeCD41 CD561 hematodermic neoplasm (blastic plas-macytoid dendritic cell neoplasm), demonstratedboth skin and bone-marrow involvement in theabsence of peripheral blood leukemic dissemina-tion. An iso-7q deletion was noted in one of thesecases, a finding described in CD561 hepatosplenicT-cell lymphoma.10,11 There are 4 other reportedcases of aggressive CD41 CD561 NK-like T-celllymphomas. Like our two cases, all were heraldedby skin involvement (Table I).12-15 The salient fea-tures are summarized in Table I along with our twocases. In one report a 15-year-old girl presentedinitially with skin involvement; she went into remis-sion after chemotherapy and stem cell transplanta-tion with a disease-free period of at least 1 year.12
The other patients had an aggressive clinical courseand died within less than 12 months of presentation,having received chemotherapy without stem celltransplantation.13-15
Like CD41 CD561 HD (blastic plasmacytoiddendritic cell neoplasm), our index NK-like T-celllymphoma cases showed a CD4e and CD561
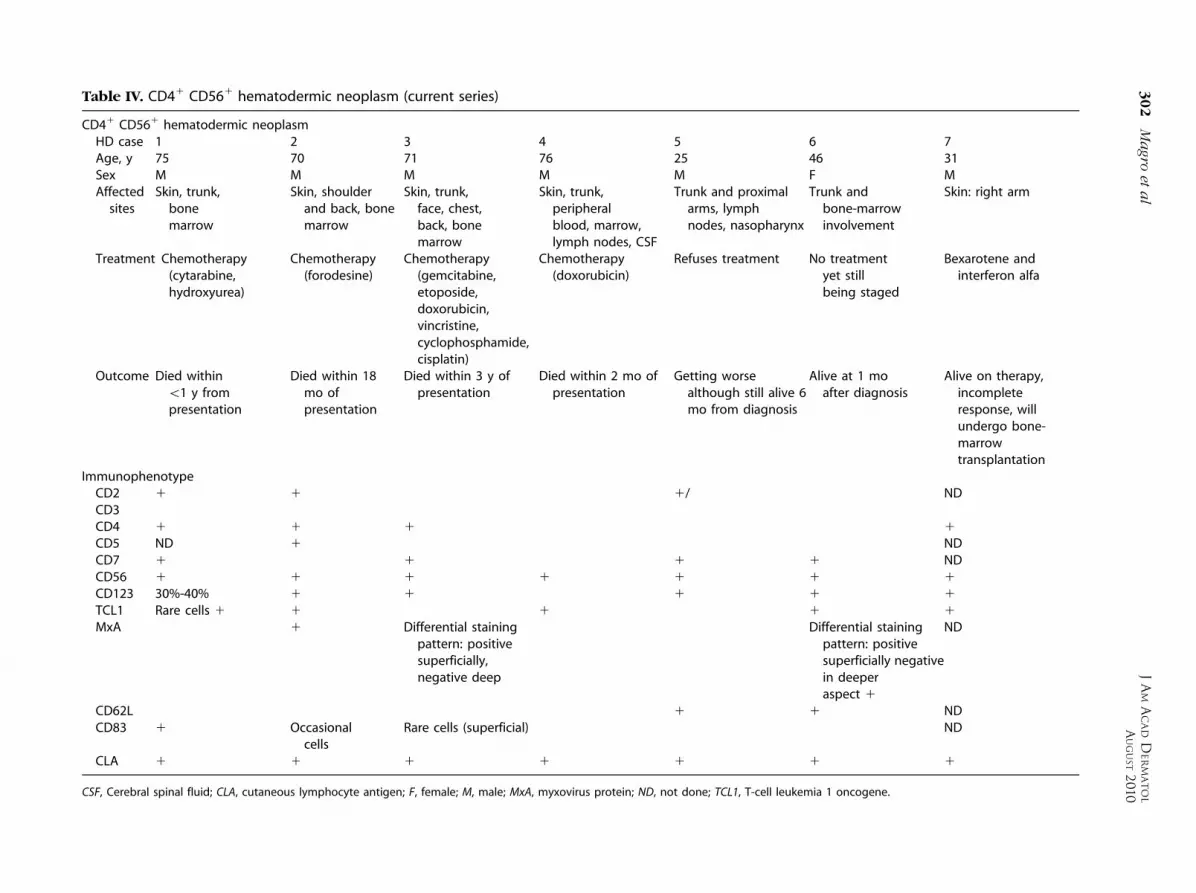
Table IV. CD41 CD561 hematodermic neoplasm (current series)
CD41 CD561 hematodermic neoplasmHD case 1 2 3 4 5 6 7Age, y 75 70 71 76 25 46 31Sex M M M M M F MAffected
sitesSkin, trunk,
bonemarrow
Skin, shoulderand back, bonemarrow
Skin, trunk,face, chest,back, bonemarrow
Skin, trunk,peripheralblood, marrow,lymph nodes, CSF
Trunk and proximalarms, lymphnodes, nasopharynx
Trunk andbone-marrowinvolvement
Skin: right arm
Treatment Chemotherapy(cytarabine,hydroxyurea)
Chemotherapy(forodesine)
Chemotherapy(gemcitabine,etoposide,doxorubicin,vincristine,cyclophosphamide,cisplatin)
Chemotherapy(doxorubicin)
Refuses treatment No treatmentyet stillbeing staged
Bexarotene andinterferon alfa
Outcome Died within\1 y frompresentation
Died within 18mo ofpresentation
Died within 3 y ofpresentation
Died within 2 mo ofpresentation
Getting worsealthough still alive 6mo from diagnosis
Alive at 1 moafter diagnosis
Alive on therapy,incompleteresponse, willundergo bone-marrowtransplantation
ImmunophenotypeCD2 1 1 � 1/� � NDCD3 � � � � �CD4 1 1 1 1
CD5 ND 1 NDCD7 1 � 1 1 1 NDCD56 1 1 1 1 1 1 1
CD123 30%-40% 1 1 1 1 1
TCL1 Rare cells 1 1 � 1 � 1 1
MxA � 1 Differential stainingpattern: positivesuperficially,negative deep
� � Differential stainingpattern: positivesuperficially negativein deeperaspect 1
ND
CD62L 1 1 NDCD83 1 Occasional
cellsRare cells (superficial) � � ND
CLA 1 1 1 1 1 1 1
CSF, Cerebral spinal fluid; CLA, cutaneous lymphocyte antigen; F, female; M, male; MxA, myxovirus protein; ND, not done; TCL1, T-cell leukemia 1 oncogene.
JA
MA
CA
DD
ER
MA
TO
L
AU
GU
ST
20
10
302
Ma
groet
al
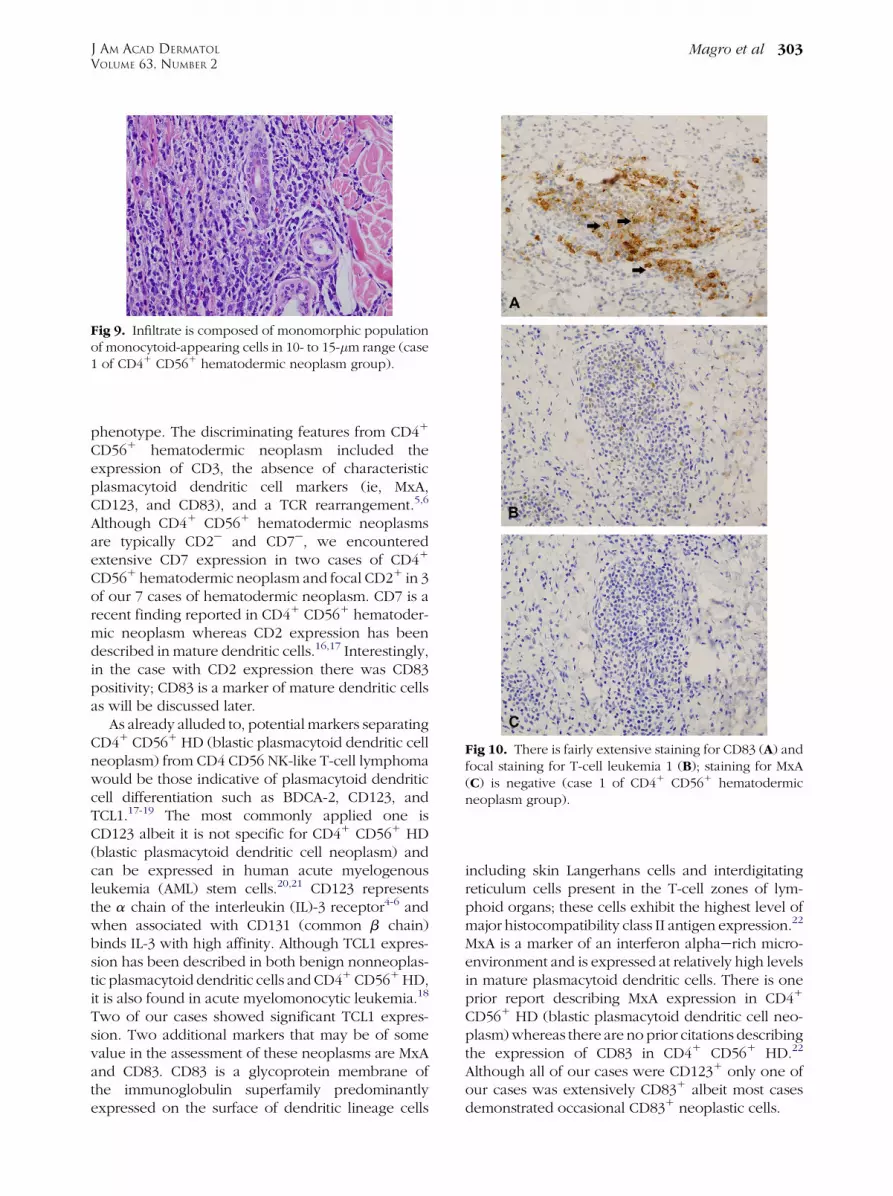
Fig 9. Infiltrate is composed of monomorphic populationof monocytoid-appearing cells in 10- to 15-�m range (case1 of CD41 CD561 hematodermic neoplasm group).
Fig 10. There is fairly extensive staining for CD83 (A) andfocal staining for T-cell leukemia 1 (B); staining for MxA(C) is negative (case 1 of CD41 CD561 hematodermicneoplasm group).
J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 303
phenotype. The discriminating features from CD41
CD561 hematodermic neoplasm included theexpression of CD3, the absence of characteristicplasmacytoid dendritic cell markers (ie, MxA,CD123, and CD83), and a TCR rearrangement.5,6
Although CD41 CD561 hematodermic neoplasmsare typically CD2e and CD7e, we encounteredextensive CD7 expression in two cases of CD41
CD561 hematodermic neoplasm and focal CD21 in 3of our 7 cases of hematodermic neoplasm. CD7 is arecent finding reported in CD41 CD561 hematoder-mic neoplasm whereas CD2 expression has beendescribed in mature dendritic cells.16,17 Interestingly,in the case with CD2 expression there was CD83positivity; CD83 is a marker of mature dendritic cellsas will be discussed later.
As already alluded to, potential markers separatingCD41 CD561 HD (blastic plasmacytoid dendritic cellneoplasm) from CD4 CD56 NK-like T-cell lymphomawould be those indicative of plasmacytoid dendriticcell differentiation such as BDCA-2, CD123, andTCL1.17-19 The most commonly applied one isCD123 albeit it is not specific for CD41 CD561 HD(blastic plasmacytoid dendritic cell neoplasm) andcan be expressed in human acute myelogenousleukemia (AML) stem cells.20,21 CD123 representsthe a chain of the interleukin (IL)-3 receptor4-6 andwhen associated with CD131 (common b chain)binds IL-3 with high affinity. Although TCL1 expres-sion has been described in both benign nonneoplas-tic plasmacytoid dendritic cells and CD41 CD561 HD,it is also found in acute myelomonocytic leukemia.18
Two of our cases showed significant TCL1 expres-sion. Two additional markers that may be of somevalue in the assessment of these neoplasms are MxAand CD83. CD83 is a glycoprotein membrane ofthe immunoglobulin superfamily predominantlyexpressed on the surface of dendritic lineage cells
including skin Langerhans cells and interdigitatingreticulum cells present in the T-cell zones of lym-phoid organs; these cells exhibit the highest level ofmajor histocompatibility class II antigen expression.22
MxA is a marker of an interferon alphaerich micro-environment and is expressed at relatively high levelsin mature plasmacytoid dendritic cells. There is oneprior report describing MxA expression in CD41
CD561 HD (blastic plasmacytoid dendritic cell neo-plasm) whereas there are no prior citations describingthe expression of CD83 in CD41 CD561 HD.22
Although all of our cases were CD1231 only one ofour cases was extensively CD831 albeit most casesdemonstrated occasional CD831 neoplastic cells.
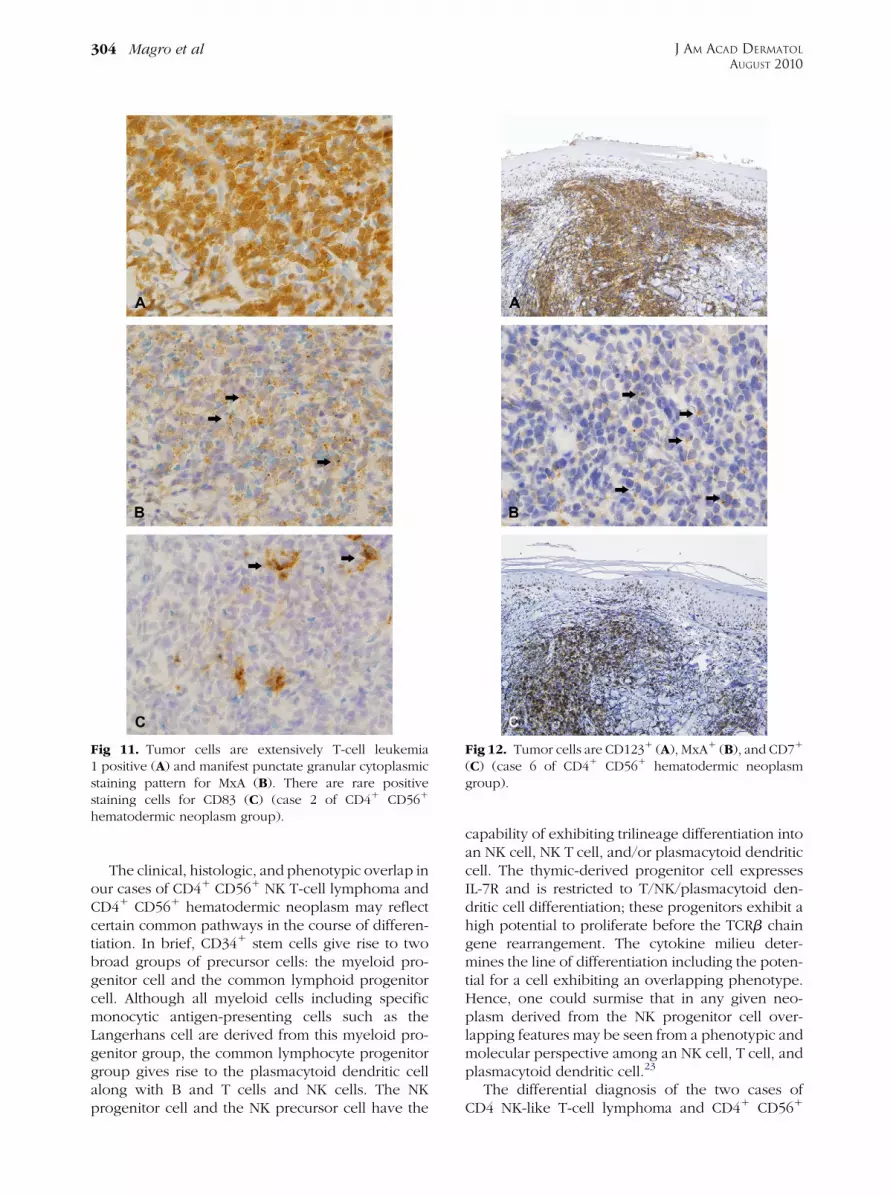
Fig 11. Tumor cells are extensively T-cell leukemia1 positive (A) and manifest punctate granular cytoplasmicstaining pattern for MxA (B). There are rare positivestaining cells for CD83 (C) (case 2 of CD41 CD561
hematodermic neoplasm group).
Fig 12. Tumor cells are CD1231 (A), MxA1 (B), and CD71
(C) (case 6 of CD41 CD561 hematodermic neoplasmgroup).
J AM ACAD DERMATOL
AUGUST 2010
304 Magro et al
The clinical, histologic, and phenotypic overlap inour cases of CD41 CD561 NK T-cell lymphoma andCD41 CD561 hematodermic neoplasm may reflectcertain common pathways in the course of differen-tiation. In brief, CD341 stem cells give rise to twobroad groups of precursor cells: the myeloid pro-genitor cell and the common lymphoid progenitorcell. Although all myeloid cells including specificmonocytic antigen-presenting cells such as theLangerhans cell are derived from this myeloid pro-genitor group, the common lymphocyte progenitorgroup gives rise to the plasmacytoid dendritic cellalong with B and T cells and NK cells. The NKprogenitor cell and the NK precursor cell have the
capability of exhibiting trilineage differentiation intoan NK cell, NK T cell, and/or plasmacytoid dendriticcell. The thymic-derived progenitor cell expressesIL-7R and is restricted to T/NK/plasmacytoid den-dritic cell differentiation; these progenitors exhibit ahigh potential to proliferate before the TCRb chaingene rearrangement. The cytokine milieu deter-mines the line of differentiation including the poten-tial for a cell exhibiting an overlapping phenotype.Hence, one could surmise that in any given neo-plasm derived from the NK progenitor cell over-lapping features may be seen from a phenotypic andmolecular perspective among an NK cell, T cell, andplasmacytoid dendritic cell.23
The differential diagnosis of the two cases ofCD4 NK-like T-cell lymphoma and CD41 CD561
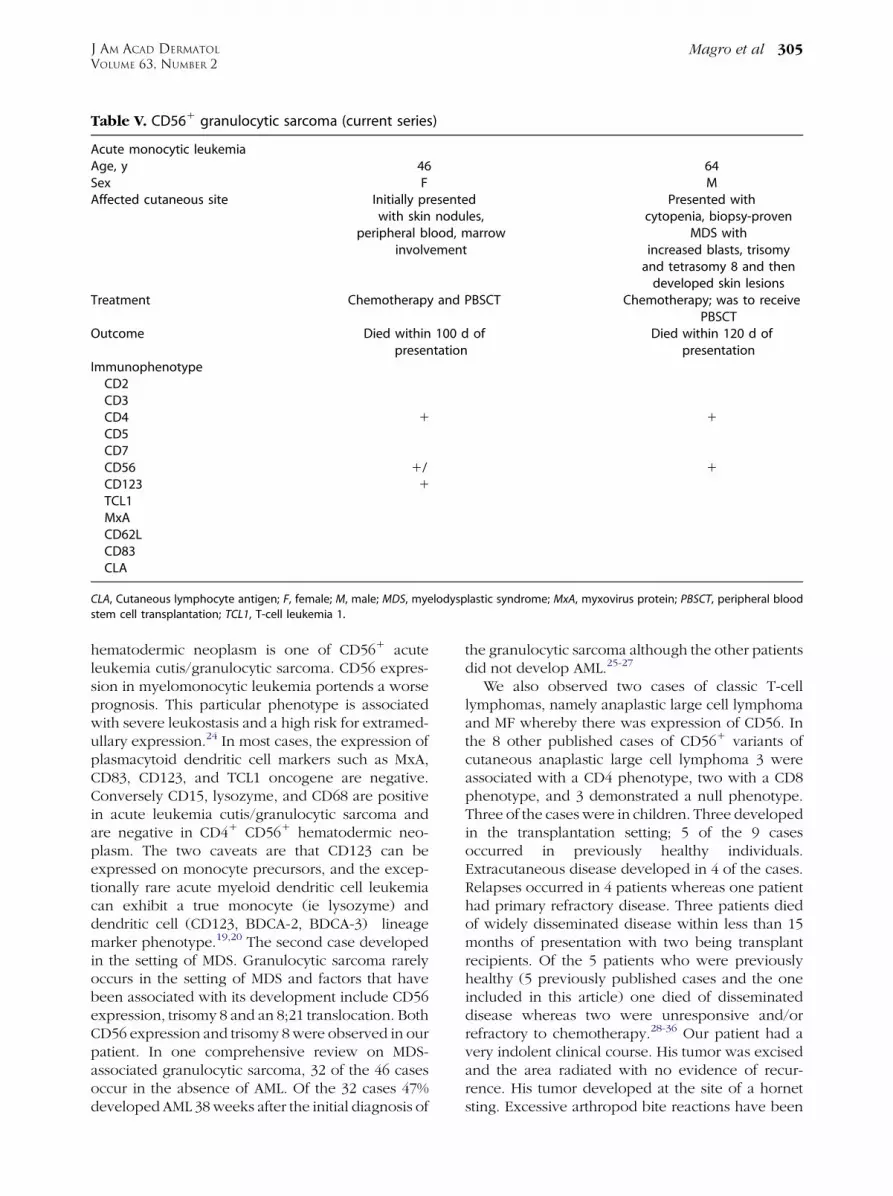
Table V. CD561 granulocytic sarcoma (current series)
Acute monocytic leukemiaAge, y 46 64Sex F MAffected cutaneous site Initially presented
with skin nodules,peripheral blood, marrow
involvement
Presented withcytopenia, biopsy-proven
MDS withincreased blasts, trisomy
and tetrasomy 8 and thendeveloped skin lesions
Treatment Chemotherapy and PBSCT Chemotherapy; was to receivePBSCT
Outcome Died within 100 d ofpresentation
Died within 120 d ofpresentation
ImmunophenotypeCD2 �CD3 � �CD4 1 1
CD5 � �CD7 � �CD56 1/� 1
CD123 1 �TCL1 � �MxA � �CD62L �CD83 �CLA
CLA, Cutaneous lymphocyte antigen; F, female; M, male; MDS, myelodysplastic syndrome; MxA, myxovirus protein; PBSCT, peripheral blood
stem cell transplantation; TCL1, T-cell leukemia 1.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 305
hematodermic neoplasm is one of CD561 acuteleukemia cutis/granulocytic sarcoma. CD56 expres-sion in myelomonocytic leukemia portends a worseprognosis. This particular phenotype is associatedwith severe leukostasis and a high risk for extramed-ullary expression.24 In most cases, the expression ofplasmacytoid dendritic cell markers such as MxA,CD83, CD123, and TCL1 oncogene are negative.Conversely CD15, lysozyme, and CD68 are positivein acute leukemia cutis/granulocytic sarcoma andare negative in CD41 CD561 hematodermic neo-plasm. The two caveats are that CD123 can beexpressed on monocyte precursors, and the excep-tionally rare acute myeloid dendritic cell leukemiacan exhibit a true monocyte (ie lysozyme) anddendritic cell (CD123, BDCA-2, BDCA-3) lineagemarker phenotype.19,20 The second case developedin the setting of MDS. Granulocytic sarcoma rarelyoccurs in the setting of MDS and factors that havebeen associated with its development include CD56expression, trisomy 8 and an 8;21 translocation. BothCD56 expression and trisomy 8 were observed in ourpatient. In one comprehensive review on MDS-associated granulocytic sarcoma, 32 of the 46 casesoccur in the absence of AML. Of the 32 cases 47%developed AML 38 weeks after the initial diagnosis of
the granulocytic sarcoma although the other patientsdid not develop AML.25-27
We also observed two cases of classic T-celllymphomas, namely anaplastic large cell lymphomaand MF whereby there was expression of CD56. Inthe 8 other published cases of CD561 variants ofcutaneous anaplastic large cell lymphoma 3 wereassociated with a CD4 phenotype, two with a CD8phenotype, and 3 demonstrated a null phenotype.Three of the cases were in children. Three developedin the transplantation setting; 5 of the 9 casesoccurred in previously healthy individuals.Extracutaneous disease developed in 4 of the cases.Relapses occurred in 4 patients whereas one patienthad primary refractory disease. Three patients diedof widely disseminated disease within less than 15months of presentation with two being transplantrecipients. Of the 5 patients who were previouslyhealthy (5 previously published cases and the oneincluded in this article) one died of disseminateddisease whereas two were unresponsive and/orrefractory to chemotherapy.28-36 Our patient had avery indolent clinical course. His tumor was excisedand the area radiated with no evidence of recur-rence. His tumor developed at the site of a hornetsting. Excessive arthropod bite reactions have been
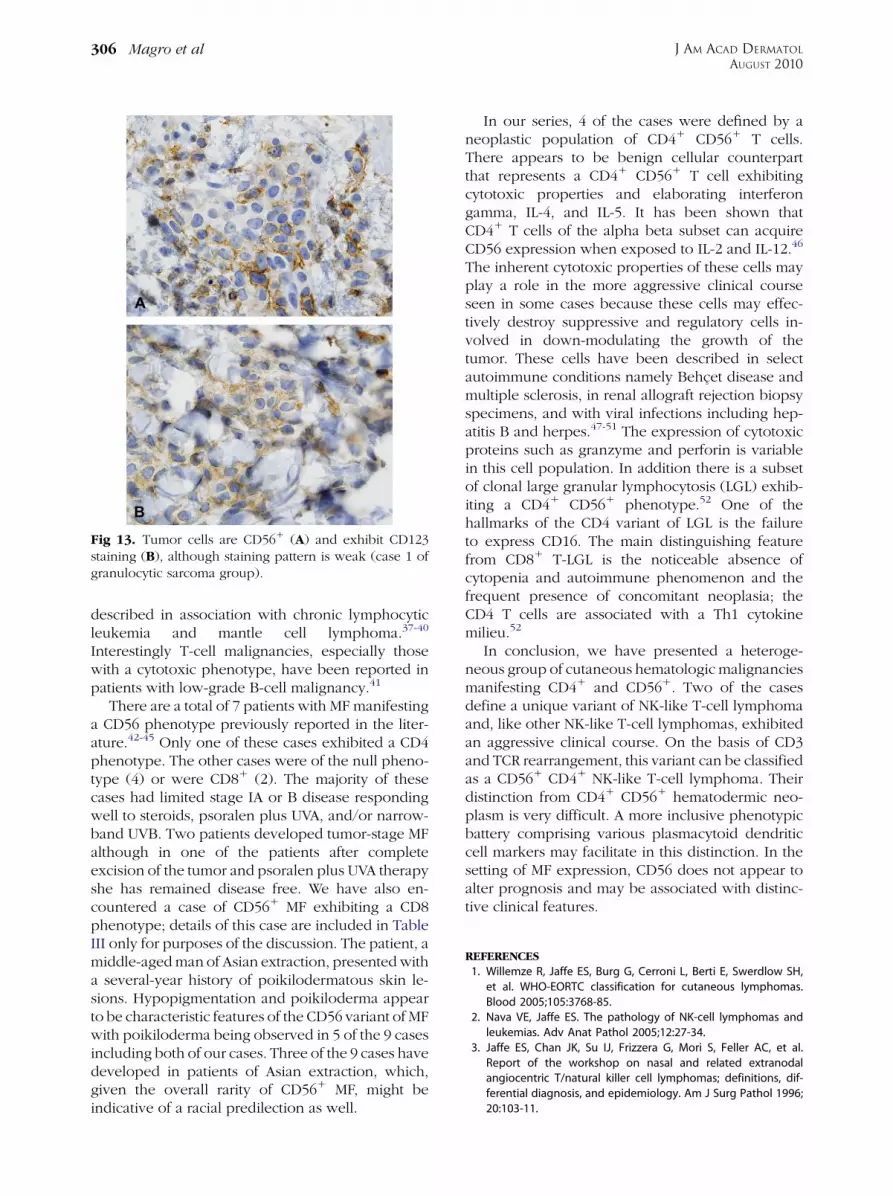
Fig 13. Tumor cells are CD561 (A) and exhibit CD123staining (B), although staining pattern is weak (case 1 ofgranulocytic sarcoma group).
J AM ACAD DERMATOL
AUGUST 2010
306 Magro et al
described in association with chronic lymphocyticleukemia and mantle cell lymphoma.37-40
Interestingly T-cell malignancies, especially thosewith a cytotoxic phenotype, have been reported inpatients with low-grade B-cell malignancy.41
There are a total of 7 patients with MF manifestinga CD56 phenotype previously reported in the liter-ature.42-45 Only one of these cases exhibited a CD4phenotype. The other cases were of the null pheno-type (4) or were CD81 (2). The majority of thesecases had limited stage IA or B disease respondingwell to steroids, psoralen plus UVA, and/or narrow-band UVB. Two patients developed tumor-stage MFalthough in one of the patients after completeexcision of the tumor and psoralen plus UVA therapyshe has remained disease free. We have also en-countered a case of CD561 MF exhibiting a CD8phenotype; details of this case are included in TableIII only for purposes of the discussion. The patient, amiddle-aged man of Asian extraction, presented witha several-year history of poikilodermatous skin le-sions. Hypopigmentation and poikiloderma appearto be characteristic features of the CD56 variant of MFwith poikiloderma being observed in 5 of the 9 casesincluding both of our cases. Three of the 9 cases havedeveloped in patients of Asian extraction, which,given the overall rarity of CD561 MF, might beindicative of a racial predilection as well.
In our series, 4 of the cases were defined by aneoplastic population of CD41 CD561 T cells.There appears to be benign cellular counterpartthat represents a CD41 CD561 T cell exhibitingcytotoxic properties and elaborating interferongamma, IL-4, and IL-5. It has been shown thatCD41 T cells of the alpha beta subset can acquireCD56 expression when exposed to IL-2 and IL-12.46
The inherent cytotoxic properties of these cells mayplay a role in the more aggressive clinical courseseen in some cases because these cells may effec-tively destroy suppressive and regulatory cells in-volved in down-modulating the growth of thetumor. These cells have been described in selectautoimmune conditions namely Behcet disease andmultiple sclerosis, in renal allograft rejection biopsyspecimens, and with viral infections including hep-atitis B and herpes.47-51 The expression of cytotoxicproteins such as granzyme and perforin is variablein this cell population. In addition there is a subsetof clonal large granular lymphocytosis (LGL) exhib-iting a CD41 CD561 phenotype.52 One of thehallmarks of the CD4 variant of LGL is the failureto express CD16. The main distinguishing featurefrom CD81 T-LGL is the noticeable absence ofcytopenia and autoimmune phenomenon and thefrequent presence of concomitant neoplasia; theCD4 T cells are associated with a Th1 cytokinemilieu.52
In conclusion, we have presented a heteroge-neous group of cutaneous hematologic malignanciesmanifesting CD41 and CD561. Two of the casesdefine a unique variant of NK-like T-cell lymphomaand, like other NK-like T-cell lymphomas, exhibitedan aggressive clinical course. On the basis of CD3and TCR rearrangement, this variant can be classifiedas a CD561 CD41 NK-like T-cell lymphoma. Theirdistinction from CD41 CD561 hematodermic neo-plasm is very difficult. A more inclusive phenotypicbattery comprising various plasmacytoid dendriticcell markers may facilitate in this distinction. In thesetting of MF expression, CD56 does not appear toalter prognosis and may be associated with distinc-tive clinical features.
REFERENCES
1. Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH,
et al. WHO-EORTC classification for cutaneous lymphomas.
Blood 2005;105:3768-85.
2. Nava VE, Jaffe ES. The pathology of NK-cell lymphomas and
leukemias. Adv Anat Pathol 2005;12:27-34.
3. Jaffe ES, Chan JK, Su IJ, Frizzera G, Mori S, Feller AC, et al.
Report of the workshop on nasal and related extranodal
angiocentric T/natural killer cell lymphomas; definitions, dif-
ferential diagnosis, and epidemiology. Am J Surg Pathol 1996;
20:103-11.

J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Magro et al 307
4. Petrella T, Comeau MR, Maynadie M, Couillault G, De Muret A,
Maliszewski CR, et al. Agranular CD41 CD561 hematodermic
neoplasm (blastic NK-cell lymphoma) originates from a pop-
ulation of CD561 precursor cells related to plasmacytoid
monocytes. Am J Surg Pathol 2002;26:852-62.
5. Khoury JD, Medeiros LJ, Manning JT, Sulak LE, Bueso-Ramos C,
Jones D. CD561 TdT1 blastic natural killer cell tumor of the
skin. Cancer 2002;94:2401-8.
6. Shiman M, Marchione R, Ricotti C, Romanelli P, Alonso-
Llamazares J. CD41/CD561 hematodermic neoplasm (plasma-
cytoid dendritic cell tumor). Dermatol Online J 2008;14:5.
7. Kluin PM, Feller A, Gaulard P, Jaffe ES, Meijer CJ, Muller-
Hermelink HK, et al. Peripheral T/NK-cell lymphoma: a report
of the IXth workshop of the European Association for Hema-
topathology. Histopathology 2001;38:250-70.
8. Greer JP, Kinney MC, Loughran TP. T cell and NK cell
lymphoproliferative disorders. Hematology Am Soc Hematol
Educ Program 2001;259-81.
9. Hamadani M, Magro CM, Porcu P. CD41 CD561 hematodermic
tumor (plasmacytoid dendritic cell neoplasm). Br J Haematol
2008;140:122.
10. Alonsozana EL, Stamberg J, Kumar D, Jaffe ES, Medeiros LJ,
Frantz C, et al. Isochromosome 7q: the primary cytogenetic
abnormality in hepatosplenic gamma delta T cell lymphoma.
Leukemia 1997;11:1367-72.
11. Tamaska J, Adam E, Kozma A, Gopcsa L, Andrikovics H, Tordai
A, et al. Hepatosplenic gammadelta T-cell lymphoma with ring
chromosome 7, an isochromosome 7q equivalent clonal
chromosomal aberration. Virchows Arch 2006;449:479-83.
12. Liu XY, Atkins R, Feusner JH, Rowland JM. Blastic NK-cell-like
lymphoma with T-cell receptor gene rearrangement. Am J
Hematol 2004;57:251-3.
13. Hofbauer GF, Kamarachev J, Kempf W, Burg G, Pestalozzi BC,
Dummer R. A CD41CD561 natural killer-like T-cell systemic
lymphoma with hemorrhagic cutaneous manifestations. Br J
Dermatol 2001;144:414-48.
14. Aoyama Y, Yamane T, Hino M, Ohta K, Nakamae H, Yamamura
R, et al. Blastic NK cell lymphoma/leukemia with T-cell recep-
tor-gamma rearrangement. Ann Hematol 2001;80:752-4.
15. Stetsenko GY, McFarlane R, Kalus A, Olerud J, Cherian S,
Fromm J, et al. CD41/CD561 hematodermic neoplasm: report
of a rare variant with a T-cell receptor gene rearrangement. J
Cutan Pathol 2008;35:579-84.
16. Jaye DL, Geigerman CM, Herling M, Eastburn K, Waller EK, Jones
D. Expression of the plasmacytoid dendritic cell marker BDCA-2
supports a spectrum of maturation among CD41 CD561
hematodermic neoplasms. Mod Pathol 2006;19:1555-62.
17. Di Pucchio T, Lapenta C, Santini SM, Logozzi M, Parlato S,
Belardelli F. CD21/CD141 monocytes rapidly differentiate into
CD831 dendritic cells. Eur J Immunol 2003;33:358-67.
18. Herling M, Teitell MA, Shen RR, Medeiros LJ, Jones D. TCL1
expression in plasmocytoid dendritic cells (DC2s) and the
related CD41 CD561 blastic tumors of skin. Blood 2003;101:
5007-9.
19. Ferran M, Gallardo F, Ferrer AM, Salar A, Perez-Vila E, Juanpere
N, et al. Acute myeloid dendritic cell leukaemia with specific
cutaneous involvement: a diagnostic challenge. Br J Dermatol
2008;158(5).
20. Munoz L, Nomdedeu JF, Lopez O. Interleukin-3 receptor alpha
chain (CD123) is widely expressed in hematologic malignan-
cies. Haematologica 2001;86:1261-9.
21. Jordan CT, Upchurch D, Szilvassy SJ, Guzman ML, Howard DS,
Pettigrew AL, et al. The interleukin-3 receptor alpha chain is a
unique marker for human acute myelogenous leukemia stem
cells. Leukemia 2000;14:1777-84.
22. Zhou LJ, Tedder TF. CD141 blood monocytes can differentiate
into functionally mature CD831 dendritic cells. Proc Natl Acad
Sci U S A 1996;93:2588-92.
23. Welner RS, Pelayo R, Garrett KP, Chen X, Perry SS, Sun XH, et al.
Interferon-producing killer dendritic cells (IKDCs) arise via a
unique differentiation pathway from primitive c-kitHiCD62L1
lymphoid progenitors. Blood 2007;109:4825-931.
24. Novotny JR, Nucke H, Duhrsen U. Correlation between ex-
pression of CD56/NCAM and severe leukostasis in hyper-
leukocytic acutae myelomonocytic leukemia. Eur J Haematol
2006;76:299-308.
25. Murakami Y, Nagae S, Matsuishi E, Irie K, Furue M. A case of
CD561 cutaneous aleukemic granulocytic sarcoma with mye-
lodysplastic syndrome. Br J Dermatol 2000;143:587-90.
26. Lacronique-Gazaille C, Chaury MP, Le Guyader A, Faucher JL,
Bordessoule D, Feuillard J. A simple method for detection of
major phenotypic abnormalities in myelodysplastic syn-
dromes: expression of CD56 in CMML. Haematologica 2007;
92:859-60.
27. Byrd JC, Edenfield WJ, Dow NS, Aylesworth C, Dawson N.
Extramedullary myeloid cell tumors in myelodysplastic-syn-
dromes: not a true indication of impending acute myeloid
leukemia. Leuk Lymphoma 1996;21:153-9.
28. Boudova L, Kazakov DV, Jindra P, Sima R, Vanecek T, Kuntscher
V, et al. Primary cutaneous histiocyte and neutrophil-rich
CD301 and CD561 anaplastic large-cell lymphoma with
prominent angioinvasion and nerve involvement in the fore-
head and scalp of an immunocompetent woman. J Cutan
Pathol 2006;33:584-9.
29. Kim HK, Jin SY, Lee NS, Won JH, Park HS, Yang WI. Posttrans-
plant primary cutaneous Ki-1 (CD30)1/CD561 anaplastic large
cell lymphoma. Arch Pathol Lab Med 2004;128:96-9.
30. Suzuki R, Kagami Y, Takeuchi K, Kami M, Okamoto M,
Ichinohasama R, et al. Prognostic significance of CD56 expres-
sion for ALK-positive and ALK-negative anaplastic large-cell
lymphoma of T/null cell phenotype. Blood 2000;96:2993-3000.
31. Paulli M, Boveri E, Rosso R, Arico M, Kindl S, Viglio A, et al.
CD56/neural cell adhesion molecule expression in primary
extranodal Ki-1/CD301 lymphoma: report of a pediatric case
with simultaneous cutaneous and bone localizations. Am J
Dermatopathol 1997;19:834-90.
32. Dunphy CH, DeMello DE, Gale GB. Pediatric CD561 anaplastic
large cell lymphoma: a review of the literature. Arch Pathol
Lab Med 2006;130:1859-64.
33. Krenacs L, Wellmann A, Sorbara L, Himmelmann AW, Bagdi E,
Jaffe ES, et al. Cytotoxic cell antigen expression in anaplastic
large cell lymphomas of T- and null-cell type and Hodgkin’s
disease: evidence for distinct cellular origin. Blood 1997;89:
980-9.
34. Chang SE, Park IJ, Huh J, Choi JH, Sung KJ, Moon KC, et al.
CD56 expression in a case of primary cutaneous
CD301 anaplastic large cell lymphoma. Br J Dermatol 2000;
142:766-70.
35. Gould JW, Eppes RB, Gilliam AC, Goldstein JA, Mikkola DL,
Zaim MT, et al. Solitary primary cutaneous CD301 large cell
lymphoma of natural killer cell phenotype bearing the
t(2;5)(p23;q35) translocation and presenting in a child. Am J
Dermatopathol 2000;22:422-8.
36. Coyne JD, Banerjee SS, Bromley M, Mills S, Diss TC, Harris M.
Post transplant T cell lymphoproliferative disorder/T cell
lymphoma: a report of three cases of T anaplastic large cell
lymphoma with cutaneous presentation and a review of the
literature. Histopathology 2004;44:387-93.
37. Walker P, Long D, James C, Marshman G. Exaggerated insect
bite reaction exacerbated by a pyogenic infection in a patient

J AM ACAD DERMATOL
AUGUST 2010
308 Magro et al
with chronic lymphocytic leukemia. Australas J Dermatol 2007;
48:165-9.
38. Kunitomi A, Konaka Y, Yagita M. Hypersensitivity to mosquito
bites as a potential sign of mantle cell lymphoma. Intern Med
2005;44:1097-9.
39. Vassallo C, Passamonti F, Cananzi R, Brazzelli V, Ardigo M,
Lazzarino M, et al. Exaggerated insect bite-like reaction in
patients affected by oncohematological diseases. Acta Derm
Venereol 2005;85:76-7.
40. Barzilai A, Shapiro D, Goldberg I, Yacob-Hirsch Y, Diaz-Cascajo
C, Meytes D, et al. Insect bite-like reaction in patients with
hematologic malignant neoplasms. Arch Dermatol 1999;135:
1503-7.
41. Martinez A, Pittaluga S, Villamor N, Colomer D, Rozman M,
Raffeld M, et al. Clonal T-cell populations and increased risk for
cytotoxic T-cell lymphomas in B-CLL patients: clinicopatho-
logic observations and molecular analysis. Am J Surg Pathol
2004;28:849-58.
42. Santucci M, Pimpinelli N, Massi D, Kadin ME, Meijer CJ, Muller-
Hermelink HK, et al. Cytotoxic natural killer cell cutaneous
lymphomas: report of the EORTC cutaneous lymphoma task
force workshop. Cancer 2003;97:610-27.
43. Klekotka PA, Faulkner-Jones B, Heffernan MP. A case of CD561
mycosis fungoides. Arch Dermatol 2006;142:1370-2.
44. Wain EM, Orchard GE, Mayou S, Atherton DJ, Misch KJ, Russell-
Jones R. Mycosis fungoides with a CD561 immunophenotype.
J Am Acad Dermatol 2005;53:158-63.
45. Ohshima A, Tokura YM, Misawa JM, Yagi HM, Takigawa M.
Erythrodermic cutaneous T cell lymphoma with CD81CD561
leukemic T cells in a young woman. Br J Dermatol 2003;149:891-3.
46. Satoh M, Seki S, Hashimoto W, Ogasawara K, Kobayashi T,
Kumagai K, et al. Cytotoxic gammadelta or alpha beta T cells
with a natural killer cell marker, CD56, induced from human
peripheral blood lymphocytes by a combination of IL-12 and
IL-2. J Immunol 1996;157:3886-92.
47. Taddesse-Heath L, Feldman JI, Fahle GA, Fischer SH, Sorbara L,
Raffeld M, et al. Florid CD41, CD561 T-cell infiltrate associated
with herpes simplex infection simulating nasal NK-/T-cell
lymphoma. Mod Pathol 2003;16:166-72.
48. Eksioglu-Demiralp E, Direskeneli H, Ergun T, Fresko I, Akoglu T.
Increased CD41CD161 and CD41CD561 T cell subsets in
Behcet’s disease. Rheumatol Int 1999;19:23-6.
49. Vergelli M, Le H, van Noort JM, Dhib-Jalbut S, McFarland H,
Martin R. A novel population of CD41CD561 myelin-reactive T
cells lyses target cells expressing CD56/neural cell adhesion
molecule. J Immunol 1996;157:679-88.
50. Bachetoni A, Lionetti P, Cinti P, Alo P, Molajoni ER, Di Tondo U,
et al. Homing of CD41CD561 T lymphocytes into kidney
allografts during tubular necrosis or rejection. Clin Transplant
1995;9:433-7.
51. Barnaba V, Franco A, Paroli M, Benvenuto R, De Petrillo G,
Burgio VL, et al. Selective expansion of cytotoxic T lympho-
cytes with a CD41CD561 surface phenotype and a T helper
type 1 profile of cytokine secretion in the liver of patients
chronically infected with hepatitis B virus. J Immunol 1994;
152:3074-87.
52. Lima M, Almeida J, Dos Anjos Teixeira M, Alguero Md Mdel C,
Santos AH, Balanzategui A, et al. TCRaß1/CD41 large granular
lymphocytosisea new clonal T-cell lymphoproliferative disor-
der. Am J Pathol 2003;163:763-71.





























