Embed Size (px)
Citation preview
Law and Human Behavior
Criminal Thinking Styles Among People With SeriousMental Illness in JailAmy Blank Wilson, Kathleen Farkas, Karen J. Ishler, Michael Gearhart, Robert Morgan, andMelinda AsheOnline First Publication, April 7, 2014. http://dx.doi.org/10.1037/lhb0000084
CITATIONWilson, A. B., Farkas, K., Ishler, K. J., Gearhart, M., Morgan, R., & Ashe, M. (2014, April 7).Criminal Thinking Styles Among People With Serious Mental Illness in Jail. Law and HumanBehavior. Advance online publication. http://dx.doi.org/10.1037/lhb0000084

Criminal Thinking Styles Among People With SeriousMental Illness in Jail
Amy Blank Wilson, Kathleen Farkas,Karen J. Ishler, and Michael Gearhart
Case Western Reserve University
Robert MorganTexas Tech University
Melinda AsheCase Western Reserve University
The purpose of this study was to extend the investigation of criminal thinking of persons with mentalillness beyond prison and community settings to a jail setting. Participants consisted of 122 individualsincarcerated in a county jail who were diagnosed with a severe mental illness, including schizophreniaspectrum and major mood disorders. Results indicated that people with mental illness in this sample ofjail inmates presented with thinking styles that support a criminal lifestyle, and have criminal thinkingstyles that follow a pattern that is very similar to a sample of prison inmates with serious mental illness.These findings support the need for therapeutic programs for justice-involved persons with seriousmental illness to develop a multipronged treatment approach that integrates interventions for individuals’criminal thinking and antisocial attitudes with treatment for their mental illness and substance abuseissues.
Keywords: jail, mental illness, mentally disordered offender, criminal thinking
Research has consistently demonstrated that people with seriousmental illness (SMIs) are substantially overrepresented in thecriminal justice system (Ditton, 1999; Steadman, Osher, Robbins,Case, & Samuels, 2009; Teplin, Abram, & McClelland, 1996).Estimates of the prevalence of people with mental illness in jailsvary based on study methodology, setting, and definition of mentalillness (Steadman et al., 2009). However, even studies that haveused the most conservative and empirically defensible measures(Steadman et al., 2009; Teplin, 1990; Teplin et al., 1996) havefound that 6.4 to 14.5% of men and 12.2 to 31.0% of women injails have an SMI. These estimates mean that a staggering numberof people with SMI are housed in jails across the United States,given that jails admit over 12 million people each year and releasealmost 9 million (Spaulding et al., 2009).
Recognition among policymakers of the presence of large num-bers of people with mental illness in jails and prisons has led tounprecedented service development for these clients at the federal,
state, and local levels. These services, recently termed “first gen-eration services” (Epperson et al., 2011), were designed to reducecriminal justice involvement by targeting various aspects of con-sumers’ mental illness. They include programs such as pre- andpostjail diversion services (Broner, Lattimore, Cowell, & Sch-lenger, 2004; Compton, Bahora, Watson, & Olivia, 2008), reentryservices (Draine & Herman, 2007; Osher, Steadman, & Barr,2003), specialty community supervision caseloads (probation orparole; Skeem, Peterson, & Silver, 2011), and mental health courts(Boothroyd, Mercado, Poythress, Christy, & Petrila, 2005; Cos-den, Ellens, Schnell, & Yamini-Diouf, 2005). Although there aredifferences in the structure and emphasis of each service model,none have been able to achieve a consistent impact on participants’future involvement in criminal justice settings (Epperson et al.,2011; Morrissey, Meyer, & Cuddeback, 2007; Osher & Steadman,2007; Steadman & Naples, 2005). These findings suggest thatsomething is missing in our current approach to providing treat-ment to this client population (Fisher & Drake, 2007).
Some of the most prominent efforts to explain why mentalhealth treatment programs have struggled to impact public safetyoutcomes focus on identifying what is missing from current treat-ment approaches. One explanation for this lack of impact focuseson the fact that these services do not provide treatment thataddresses risk factors for recidivism (Skeem & Louden, 2006).Another points to the lack of availability of evidence-based mentalhealth treatments for people with mental illness involved in thecriminal justice systems (Osher & Steadman, 2007; Steadman &Naples, 2005). However, a growing body of evidence has foundthat there is no guarantee that access to evidence-based mentalhealth practices will have a significant impact on participants’
Amy Blank Wilson, Kathleen Farkas, Karen J. Ishler, and MichaelGearhart, Jack, Joseph and Morton Mandel School of Applied SocialSciences, Case Western Reserve University; Robert Morgan, PsychologyDepartment, Texas Tech University; Melinda Ashe, School of Arts andSciences, Case Western Reserve University.
This work was funded in part by a Second Chances Grant from the U.S.Department of Justice.
Correspondence concerning this article should be addressed to AmyBlank Wilson, Jack, Joseph and Morton Mandel School of Applied SocialSciences, Case Western Reserve University, 10900 Euclid Ave., Cleve-land, OH 44106. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Law and Human Behavior © 2014 American Psychological Association2014, Vol. 38, No. 1, 000 0147-7307/14/$12.00 DOI: 10.1037/lhb0000084
1

criminal justice outcomes (Morrissey et al., 2007; Osher & Stead-man, 2007; Skeem et al., 2011; Steadman & Naples, 2005).
These discussions have led some to suggest that treatmentprotocols for evidence-based mental health practices for peoplewith mental illness involved in the criminal justice system need tobe modified to include interventions capable of addressing the riskfactors associated with criminal conduct (Morrissey et al., 2007).However, little is known about the nature or extent of criminogenicrisk in this population. The recent attention given to the role thatcriminogenic risk factors may be playing in the criminal involve-ment of people with SMI (e.g., Epperson et al., 2011) has led to thesuggestion that these risk factors, which include antisocial think-ing, behaviors, attitudes, and associates (Andrews, Bonta, &Wormith, 2006), are important co-occurring problems among peo-ple with SMI involved in the justice system. If this hypothesis iscorrect, then finding treatments for these risk factors represents thenext frontier in the development of services for this client popu-lation (Epperson et al., 2011).
Bonta, Law, and Hanson (1998) conducted one of the earlieststudies that looked at the nature of criminogenic risk among peoplewith mental illness. This study used meta-analytic techniques tocompare the predictors of recidivism for people with mental illnesswith those of non-ill offenders. This analysis found that the majorrisk factors for recidivism were the same for people with mentalillness and offenders without mental illness. For example, thestrongest predictors of recidivism among both groups were foundto be criminogenic risk factors associated with the person’s crim-inal history (i.e., the frequency and onset of past criminal behav-ior), whereas clinical variables (any treatment for mental illness)were the weakest. A follow-up meta-analysis produced similarresults: Common criminal risk factors are as relevant for offenderswith mental illness as they are for their nonmentally ill counter-parts, and criminal risk factors remain better predictors of criminaloutcomes than clinical factors (Bonta, Blais, & Wilson, 2013).Although this research offers strong support for the presence ofcriminogenic risk factors among people with mental illness, thestatic nature of the risk factors identified in these studies does littleto inform the development of treatment interventions.
In addition to the Bonta et al. (1998, 2013) meta-analyses, otherresearch has supported the assertion that people with SMI face anumber of criminogenic risk factors. For example, research onadults with schizophrenia has found that they have higher rates ofchildhood conduct disorders than people in the general population(Mueser et al., 2006; Robins, 1993). Epidemiological studies havealso found an association between SMIs, such as schizophrenia,and antisocial personality disorder (Moran & Hodgins, 2004).Information such as this is helpful in developing a clinical profileof people with mental illness involved in the criminal justicesystem. Here again, however, the static nature of identified riskfactors does little to advance the development of interventions;regardless of the focus or intent of an intervention, these factorscannot be changed.
Several recent studies have examined the presence of dynamiccriminogenic risk factors among people with SMI in prisons (Mor-gan, Fisher, Duan, Mandracchia, & Murray, 2010; Wolff, Morgan,& Shi, 2013; Wolff, Morgan, Shi, Fisher, & Huening, 2011). Thesestudies focused on criminal thinking and antisocial attitudes, whichrepresent two critical areas of criminogenic risk. Criminal thinkingis important, in part because it is a dynamic risk factor amenable
to intervention (Friendship, Blud, Erikson, Travers, & Thornton,2003; Walters, Trgovac, Rychlec, Di Fazio, & Olson, 2002). It isalso one of the four criminogenic risk factors that are believed tohave the biggest impact on offending behaviors (Andrews et al.,2006).
Morgan et al. (2010) conducted one of the first studies thatassessed the prevalence of criminal thinking among justice-involved people with mental illness. Criminal thinking and anti-social attitudes were assessed in 283 prison inmates (178 men, 105women) with mental illness. This study used the Criminal Senti-ment Scale-Modified (CSS-M; Simourd, 1997) to assess antisocialattitudes. The study found that 85% of men and 72% of women inthe study held antisocial attitudes, values, and beliefs related tocrime. In addition, compared with a sample of offenders withoutmental illness, study participants had higher scores on all CSS-Msubscales, except identification with criminal others (Morgan etal., 2010).
The second measure used by Morgan et al. (2010) to assesscriminal thinking among people with SMI was the PsychologicalInventory of Criminal Thinking Styles (PICTS; Walters, 1995,2006). This measure was designed to assess the extent to whichparticipants engaged cognitive thinking patterns associated withserious criminal behavior. This measure identifies elevated levelsof criminal thinking using gender-specific normative scores. Mor-gan et al.’s analysis found that 66% of their sample endorsed athinking style that indicated the presence of a belief system thatwas supportive of a criminal lifestyle. Furthermore, when Morganet al. examined the average scores on the thinking scales for menand women, only two scales were elevated to a level of clinicalsignificance. Both the Cutoff and Discontinuity scales, whichassessed impulsivity and lack of focus, were elevated to clinicallysignificant levels among men in the sample. Further analysis ofindividual scores found that 71% of individuals had an elevatedscore on at least one criminal thinking scale.
Wolff et al. (2011) also examined antisocial attitudes amongpeople with mental illness incarcerated in prison. In this study,readiness for reentry among 4,204 inmates was assessed using acomputer-assisted, self-administered survey that also used theCSS-M (Simourd, 1997) to assess antisocial attitudes. Wolff et al.(2011) compared the results of the CSS-M by gender across threediagnostic groups: individuals reporting treatment for a SMI(schizophrenia or bipolar disorder), those reporting other mentaldisorders (depression, PTSD, or anxiety), and those reporting nomental disorders. Individuals with SMIs displayed levels of crim-inal thinking comparable with, and at times higher than, those ofoffenders without mental illness. For example, the overall andsubscale scores were generally similar across groups, except thatmen with SMI consistently scored higher than men with no diag-nosis on the overall score and on attitudes toward the law, toler-ance toward law violators, and identification with criminal others(Wolff et al., 2011). In a subsequent study, Wolff et al. (2013)found that male and female inmates with self-reported mentalillness evidenced elevated levels of antisocial attitudes.
Data from Morgan et al. (2010) and Wolff et al. (2011, 2013)offer support for the assertion of others (e.g., Draine, Salzar,Culhane, & Hadley, 2002; Hodgins et al., 2007; Morgan et al.,2010) that treatment programs for justice-involved people withmental illness need to be expanded to address criminogenic needsin addition to mental health and substance use needs. These stud-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
2 WILSON, FARKAS, ISHLER, GEARHART, MORGAN, AND ASHE

ies, however, focused on criminal thinking among people withmental illness incarcerated in prison. Little is known about crim-inal thinking among people with mental illness involved in otherfacets of the criminal justice system. Jails, in particular, couldhouse individuals with mental illness who, as a group, have levelsof criminal thinking that differ from those of prison inmates.Prisons house individuals who have been convicted of serious orrepetitive crimes and, as a result, are serving substantial sentences.Jails, on the other hand, house a more heterogeneous populationthat includes individuals awaiting trial and those serving relativelyshort sentences, which tend to be associated with less severecrimes. Because jails house individuals facing all levels of criminalcharges, jail populations tend to evidence greater variability thanprison populations with respect to the duration of individuals’ priorinvolvement in criminal activities, seriousness of their currentoffenses, and case dispositions. Therefore, it is possible that asubstantial portion of individuals incarcerated in jail could havelower levels of criminal thinking than those incarcerated in prison.
The current study sought to contribute to knowledge in this areaby examining criminal thinking patterns among young adults withSMI incarcerated in a county jail and comparing their levels ofcriminal thinking with those found in a prison population. Thisexamination focused on two questions: (a) To what extent doindividuals with SMI incarcerated in jail engage in thinking pat-terns associated with criminal conduct? and (b) How do the crim-inal thinking patterns of individuals with SMI incarcerated in jailcompare with those of individuals with SMI incarcerated inprison? Based on previous literature examining the prevalence ofcriminal thinking in samples of people with mental illness inprisons (Morgan et al., 2010) and psychiatric settings (Gross &Morgan, 2013), we hypothesized that individuals with mentalillness in this sample of jail inmates would also evidence criminalthinking. Furthermore, due to the differences in the criminal char-acteristics of jail and prison inmates described earlier, we predictedthat the criminal thinking patterns for individuals with SMI incar-cerated in jail would be lower than those found among people withSMI in prison.
Method
Participants
The analysis presented here draws from a study of an enhancedreentry program for young adults with co-occurring SMI andsubstance use disorders incarcerated in a county jail in a midsizeMidwestern city. All individuals with lower-level felony charges,age 18 to 24, who indicated the presence of mental health problemsduring the jail’s booking process, were invited by research staff toparticipate in a screening interview for this study. All researchassociated with this study was approved by the institutional reviewboard at the university at which this research took place.
Screening interviews took place between May 2011 and May2012. One of the goals of the screening interview was to identifyparticipants who had mental health diagnoses that qualified themfor participation in the study of the reentry program. The Mini-International Neuropsychiatric Interview (MINI; Sheehan et al.,1998) was used during screening interviews to assess for thepresence of mental health and substance use disorders.
A total of 171 individuals were approached by research staffregarding participation in this study. Individuals who expressedinterest in participating in this study completed the informedconsent process with research staff prior to the screening inter-view. A total of 138 individuals completed the screening inter-view. Participants included in the analysis presented here weredrawn from the pool of 138 people who completed the screeninginterviews for the reentry study.
Two criteria were used to establish the final sample for thisanalysis. First, results of the MINI (Sheehan et al., 1998) wereused to identify individuals with a diagnosis of an SMI (i.e.,schizophrenia spectrum and/or major affective disorder). Of the138 participants who completed the screening interview, 124 werefound to have a SMI.
Second, participants were included in the present analysis iftheir responses on the PICTS met suggested thresholds for validity.In accordance with the recommendations by Walters (2006), twocases were excluded from analysis. One case was excluded be-cause more than five of the items on the PICTS were missing(Walters, 2006). The second case was excluded because the indi-vidual’s score on one of the validity scales (Confusion-revised)exceeded the recommended limit for use in research (Walters,2006). Thus, the final sample size for the analysis presented herewas 122.
Table 1 provides information related to the sociodemographic,criminal justice, and clinical characteristics of this current sampleof jail inmates. Over 50% of participants had a psychiatric diag-nosis that involved psychotic features (psychotic disorder and/ormood disorder with psychotic features) and over 90% of partici-pants had clinically significant levels of psychiatric symptoms atthe time of the screening interview. As conveyed in the table, thecurrent jail sample was composed of predominantly young, un-married men with substantial levels of prior involvement with thecriminal justice system. According to study follow-up data, only24% of the current jail sample went on to serve a sentence in astate prison.
Measures
The screening interview contained a number of self-report itemsrelated to sociodemographic and criminal justice history variables.This interview also contained formalized measures related to psy-chiatric and substance use diagnoses, criminal thinking, and psy-chiatric symptomatology. Information related to participants’criminal charges and length of time in jail for their instant offensewas collected from criminal justice records.
Mental health and substance use diagnoses were assessed usingthe MINI (Sheehan et al., 1998). The MINI is a short, structureddiagnostic interview that was developed and standardized based onthe Composite International Diagnostic Interview (CIDI) and in-formed by the Diagnostic and Statistical Manual of Mental Dis-orders (4th ed., text rev.; American Psychiatric Association, 2000)and ICD-10 (World Health Organization, 1992). It takes about 15min to complete and has been used in correctional settings (Black,Arndt, Hale, & Rogerson, 2004). Studies have found that theinterrater and test–retest reliabilities for the MINI were acceptableand that the validity of the MINI compared favorably with otherstructured diagnostic interviews (Sheehan et al., 1998). The mea-sure was designed to screen for the presence of a number of mental
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
3CRIMINAL THINKING AMONG PEOPLE WITH SMI IN JAIL
health disorders, including past or current episodes of major de-pression or mania, lifetime or current episodes of psychotic disor-ders, current alcohol dependence or abuse and/or drug dependenceor abuse, and lifetime history of antisocial personality disorder.
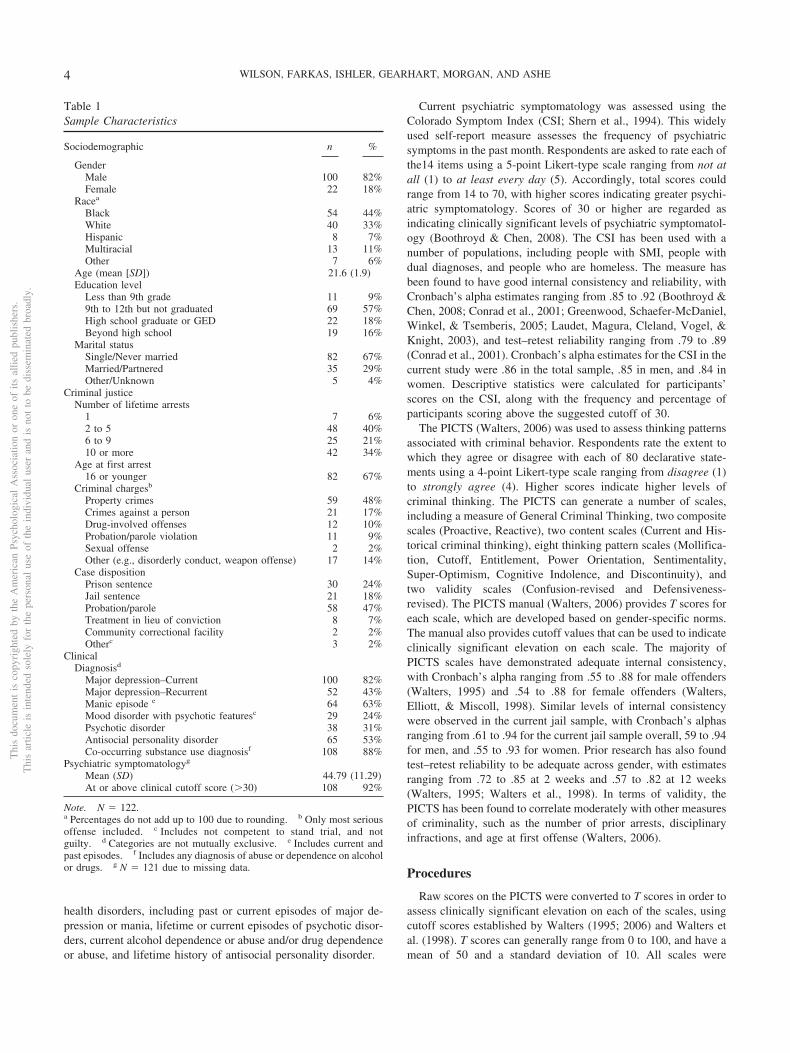
Current psychiatric symptomatology was assessed using theColorado Symptom Index (CSI; Shern et al., 1994). This widelyused self-report measure assesses the frequency of psychiatricsymptoms in the past month. Respondents are asked to rate each ofthe14 items using a 5-point Likert-type scale ranging from not atall (1) to at least every day (5). Accordingly, total scores couldrange from 14 to 70, with higher scores indicating greater psychi-atric symptomatology. Scores of 30 or higher are regarded asindicating clinically significant levels of psychiatric symptomatol-ogy (Boothroyd & Chen, 2008). The CSI has been used with anumber of populations, including people with SMI, people withdual diagnoses, and people who are homeless. The measure hasbeen found to have good internal consistency and reliability, withCronbach’s alpha estimates ranging from .85 to .92 (Boothroyd &Chen, 2008; Conrad et al., 2001; Greenwood, Schaefer-McDaniel,Winkel, & Tsemberis, 2005; Laudet, Magura, Cleland, Vogel, &Knight, 2003), and test–retest reliability ranging from .79 to .89(Conrad et al., 2001). Cronbach’s alpha estimates for the CSI in thecurrent study were .86 in the total sample, .85 in men, and .84 inwomen. Descriptive statistics were calculated for participants’scores on the CSI, along with the frequency and percentage ofparticipants scoring above the suggested cutoff of 30.
The PICTS (Walters, 2006) was used to assess thinking patternsassociated with criminal behavior. Respondents rate the extent towhich they agree or disagree with each of 80 declarative state-ments using a 4-point Likert-type scale ranging from disagree (1)to strongly agree (4). Higher scores indicate higher levels ofcriminal thinking. The PICTS can generate a number of scales,including a measure of General Criminal Thinking, two compositescales (Proactive, Reactive), two content scales (Current and His-torical criminal thinking), eight thinking pattern scales (Mollifica-tion, Cutoff, Entitlement, Power Orientation, Sentimentality,Super-Optimism, Cognitive Indolence, and Discontinuity), andtwo validity scales (Confusion-revised and Defensiveness-revised). The PICTS manual (Walters, 2006) provides T scores foreach scale, which are developed based on gender-specific norms.The manual also provides cutoff values that can be used to indicateclinically significant elevation on each scale. The majority ofPICTS scales have demonstrated adequate internal consistency,with Cronbach’s alpha ranging from .55 to .88 for male offenders(Walters, 1995) and .54 to .88 for female offenders (Walters,Elliott, & Miscoll, 1998). Similar levels of internal consistencywere observed in the current jail sample, with Cronbach’s alphasranging from .61 to .94 for the current jail sample overall, 59 to .94for men, and .55 to .93 for women. Prior research has also foundtest–retest reliability to be adequate across gender, with estimatesranging from .72 to .85 at 2 weeks and .57 to .82 at 12 weeks(Walters, 1995; Walters et al., 1998). In terms of validity, thePICTS has been found to correlate moderately with other measuresof criminality, such as the number of prior arrests, disciplinaryinfractions, and age at first offense (Walters, 2006).
Procedures
Raw scores on the PICTS were converted to T scores in order toassess clinically significant elevation on each of the scales, usingcutoff scores established by Walters (1995; 2006) and Walters etal. (1998). T scores can generally range from 0 to 100, and have amean of 50 and a standard deviation of 10. All scales were
Table 1Sample Characteristics
Sociodemographic n %
GenderMale 100 82%Female 22 18%
Racea
Black 54 44%White 40 33%Hispanic 8 7%Multiracial 13 11%Other 7 6%
Age (mean [SD]) 21.6 (1.9)Education level
Less than 9th grade 11 9%9th to 12th but not graduated 69 57%High school graduate or GED 22 18%Beyond high school 19 16%
Marital statusSingle/Never married 82 67%Married/Partnered 35 29%Other/Unknown 5 4%
Criminal justiceNumber of lifetime arrests
1 7 6%2 to 5 48 40%6 to 9 25 21%10 or more 42 34%
Age at first arrest16 or younger 82 67%
Criminal chargesb
Property crimes 59 48%Crimes against a person 21 17%Drug-involved offenses 12 10%Probation/parole violation 11 9%Sexual offense 2 2%Other (e.g., disorderly conduct, weapon offense) 17 14%
Case dispositionPrison sentence 30 24%Jail sentence 21 18%Probation/parole 58 47%Treatment in lieu of conviction 8 7%Community correctional facility 2 2%Otherc 3 2%
ClinicalDiagnosisd
Major depression–Current 100 82%Major depression–Recurrent 52 43%Manic episode e 64 63%Mood disorder with psychotic featuresc 29 24%Psychotic disorder 38 31%Antisocial personality disorder 65 53%Co-occurring substance use diagnosisf 108 88%
Psychiatric symptomatologyg
Mean (SD) 44.79 (11.29)At or above clinical cutoff score (�30) 108 92%
Note. N � 122.a Percentages do not add up to 100 due to rounding. b Only most seriousoffense included. c Includes not competent to stand trial, and notguilty. d Categories are not mutually exclusive. e Includes current andpast episodes. f Includes any diagnosis of abuse or dependence on alcoholor drugs. g N � 121 due to missing data.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
4 WILSON, FARKAS, ISHLER, GEARHART, MORGAN, AND ASHE
constructed according to the procedures established in the PICTSVersion 4.0 manual (Walters, 2006). Overall T scores and gender-specific T scores are reported in this analysis for two reasons. FirstT scores for the PICTS are developed based on gender-specificnorms published in the manual (Walters, 2006), or obtained di-rectly from Walters (G. Walters, personal communication, March13, 2013), and, as such, are generally reported by gender. Second,although T scores can be computed and are reported here for thetotal sample, gender-specific scores are also included to facilitatecomparison between the T scores for the current jail sample andthose for the sample in Morgan et al. (2010).
PICTS T scores were analyzed for the two composite scales(Reactive and Proactive) to determine what percentage of thecurrent jail sample held belief systems that were supportive of acriminal lifestyle (T score �55). Then T scores for each of theeight thinking patterns and two content scales were analyzed todetermine which ones were elevated to a point of clinical signif-icance in this current jail sample (T score �60).
To compare the levels and styles of criminogenic thinkingamong these jail inmates with SMI to those displayed by individ-uals with SMI in prison, the PICTS T scores for the validity andthinking style scales for the current jail sample were comparedwith the T scores for the same scales reported in the Morgan et al.(2010) published report. Independent sample t tests were used tocompare differences in mean T scores between the samples, overalland by gender.
As part of this comparison, the background characteristics ofthese two samples were examined on all variables when thenecessary data were available in both samples. The samples werecompared by age, gender, race/ethnicity, marital status, and edu-cational level using t tests and chi-square tests based on the type ofvariable being compared. Statistically significant differences wereobserved on each of these characteristics. However, the effect sizes
for all but one comparison were small—for example, phi rangedfrom .14 (for race/ethnicity) to .19 (for gender and level of edu-cation). As might be expected, the age restrictions used in theselection of the current jail sample resulted in a mean difference inage between the two samples of 14.1 years—a large effect size, asindicated by Cohen’s d � 1.92. In addition to being markedlyyounger, the current jail sample also differed from the Morgan etal. (2010) sample in the following ways. The current jail samplewas comprised of a greater proportion of men (82% vs. 63%).Among those who reported no postsecondary education, individ-uals in the current jail sample were less likely to have successfullycompleted 12th grade than those in the prison sample (18% vs.33%). More participants in the current jail sample reported them-selves to be currently married or partnered than did those inMorgan et al.’s (2010) sample (29% vs. 16%). Additionally, thecurrent jail sample had a higher proportion of individuals whoidentified as a person of color (67% vs. 52%). Another differencebetween these two samples that is important to note here is thatonly 24% of the current jail sample went on to serve time in prison;in contrast, all participants in Morgan et al.’s (2010) sample wereserving prison sentences (median sentence length � 10 years).
Results
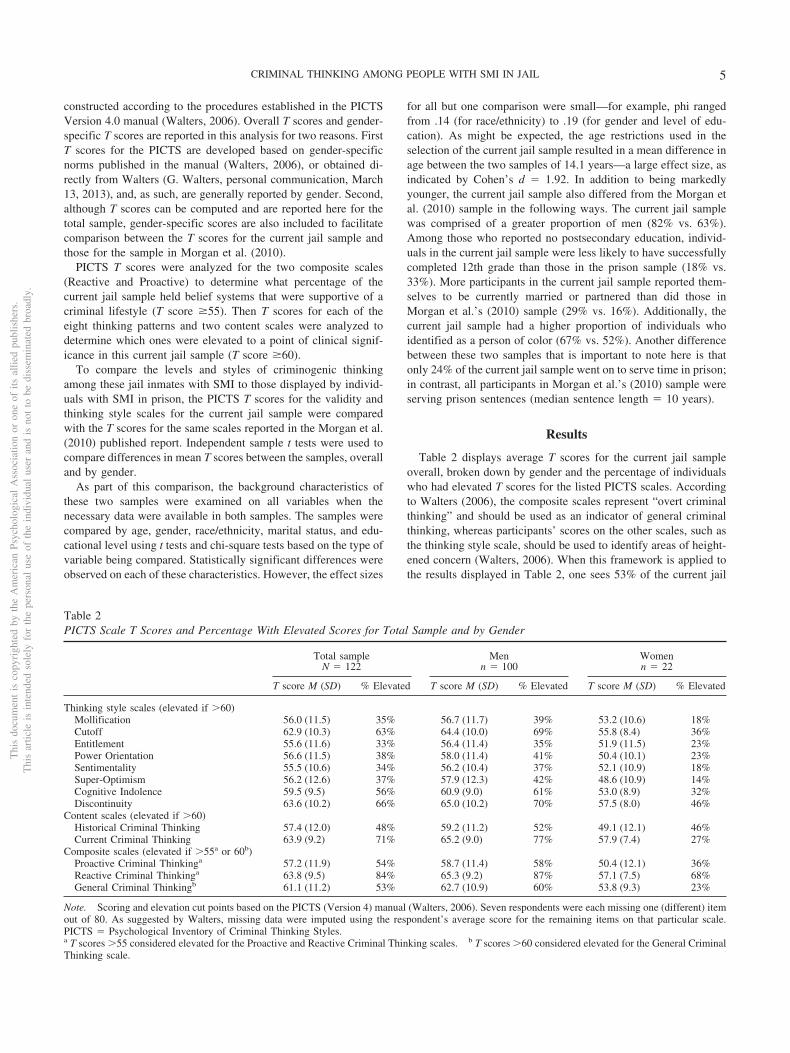
Table 2 displays average T scores for the current jail sampleoverall, broken down by gender and the percentage of individualswho had elevated T scores for the listed PICTS scales. Accordingto Walters (2006), the composite scales represent “overt criminalthinking” and should be used as an indicator of general criminalthinking, whereas participants’ scores on the other scales, such asthe thinking style scale, should be used to identify areas of height-ened concern (Walters, 2006). When this framework is applied tothe results displayed in Table 2, one sees 53% of the current jail
Table 2PICTS Scale T Scores and Percentage With Elevated Scores for Total Sample and by Gender
Total sampleN � 122
Menn � 100
Womenn � 22
T score M (SD) % Elevated T score M (SD) % Elevated T score M (SD) % Elevated
Thinking style scales (elevated if �60)Mollification 56.0 (11.5) 35% 56.7 (11.7) 39% 53.2 (10.6) 18%Cutoff 62.9 (10.3) 63% 64.4 (10.0) 69% 55.8 (8.4) 36%Entitlement 55.6 (11.6) 33% 56.4 (11.4) 35% 51.9 (11.5) 23%Power Orientation 56.6 (11.5) 38% 58.0 (11.4) 41% 50.4 (10.1) 23%Sentimentality 55.5 (10.6) 34% 56.2 (10.4) 37% 52.1 (10.9) 18%Super-Optimism 56.2 (12.6) 37% 57.9 (12.3) 42% 48.6 (10.9) 14%Cognitive Indolence 59.5 (9.5) 56% 60.9 (9.0) 61% 53.0 (8.9) 32%Discontinuity 63.6 (10.2) 66% 65.0 (10.2) 70% 57.5 (8.0) 46%
Content scales (elevated if �60)Historical Criminal Thinking 57.4 (12.0) 48% 59.2 (11.2) 52% 49.1 (12.1) 46%Current Criminal Thinking 63.9 (9.2) 71% 65.2 (9.0) 77% 57.9 (7.4) 27%
Composite scales (elevated if �55a or 60b)Proactive Criminal Thinkinga 57.2 (11.9) 54% 58.7 (11.4) 58% 50.4 (12.1) 36%Reactive Criminal Thinkinga 63.8 (9.5) 84% 65.3 (9.2) 87% 57.1 (7.5) 68%General Criminal Thinkingb 61.1 (11.2) 53% 62.7 (10.9) 60% 53.8 (9.3) 23%
Note. Scoring and elevation cut points based on the PICTS (Version 4) manual (Walters, 2006). Seven respondents were each missing one (different) itemout of 80. As suggested by Walters, missing data were imputed using the respondent’s average score for the remaining items on that particular scale.PICTS � Psychological Inventory of Criminal Thinking Styles.a T scores �55 considered elevated for the Proactive and Reactive Criminal Thinking scales. b T scores �60 considered elevated for the General CriminalThinking scale.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
5CRIMINAL THINKING AMONG PEOPLE WITH SMI IN JAIL
sample held criminal belief systems supportive of a criminallifestyle. As a group, men displayed elevated T scores on theGeneral Criminal Thinking scale, two composite scales (Reactive,Proactive), and one content scale (Current). The elevated meanscores on the Current and the General criminal thinking scalesindicate that the men in the current jail sample displayed thinkingstyles at the time of the interview that were supportive of acriminal lifestyle. The mean scores for women on the compositeand content scales showed very similar patterns of elevation,except that women’s’ overall mean score on the Proactive com-posite scale did not reach the suggested clinical cutoff. Elevatedscores on the Reactive composite scale indicate a “cognitive pro-cess characterized by impulsivity, hostility, and emotionality”(Morgan et al., 2010, p. 330). Elevated scores on the proactivecomposite scale indicate that a substantial portion of the men in thecurrent jail sample demonstrated a criminal thinking style bestcharacterized as “planned, cold blooded, and goal directed” (Wal-ters, 2006, p. 6).
When the scores on the thinking style scales are examined, wesee the mean score for men in the current jail sample exceeded aclinically significant elevation point (T score �60) for three of theeight thinking style scales. As a group, men in the current jailsample scored relatively high on the Cutoff scale, which indicatesissues with emotional control and impulsivity. Individuals withclinically elevated scores on this thinking style have been de-scribed as “having a hot tempter with a propensity to maintain ascrew it approach to dealing with problems” (Morgan et al., 2010,p. 331). Men also scored high on the Cognitive Indolence scale, forwhich clinically elevated scores indicates “short cut thinking,”which involves a lack of critical reasoning skills as they relate topersonal ideas and plans, combined with a tendency to look for theeasy way around everyday problems (Walters, 1995, 2006). Theaverage Discontinuity scale score was also elevated among men.This scale measures consistency in an individual’s thought andactions. Elevated scores on this scale indicate a tendency forindividuals to be easily distracted by events going on around themand a tendency to lose sight of one’s goals (Morgan et al., 2010;Walters, 2006). As shown in Table 2, none of the mean scores forwomen on the eight thinking style scales reached a clinicallysignificant elevation point (T score �60).
Although mean T scores are informative, it is useful to considerthe proportion of each sample or subsample who scored above theclinical cutoff for each scale. These data are presented as percent-ages in Table 2 (see Columns 3, 5, and 7). For the most part, thesefigures mirror the average T-score results, in that those scales forwhich the mean score of the sample exceeded the suggestedclinical cutoff were those for which a majority of individuals in thesample scored in the elevated range. For example, the highestaverage thinking style score for men was Discontinuity; accord-ingly, 70 of men scored above the clinical cutoff on this scale. Inaddition to providing support for the use of mean scores in thecurrent jail sample, these percentages provide valuable ancillaryinformation. For instance, even though the average Discontinuityscore for women in the current jail sample did not exceed therecommended clinical cutoff (T �60), nearly half of women (46%)did have a score above this value. Similar to the findings for men,the other thinking style scales with the highest percentages ofelevated scores among the women were Cutoff and CognitiveIndolence.
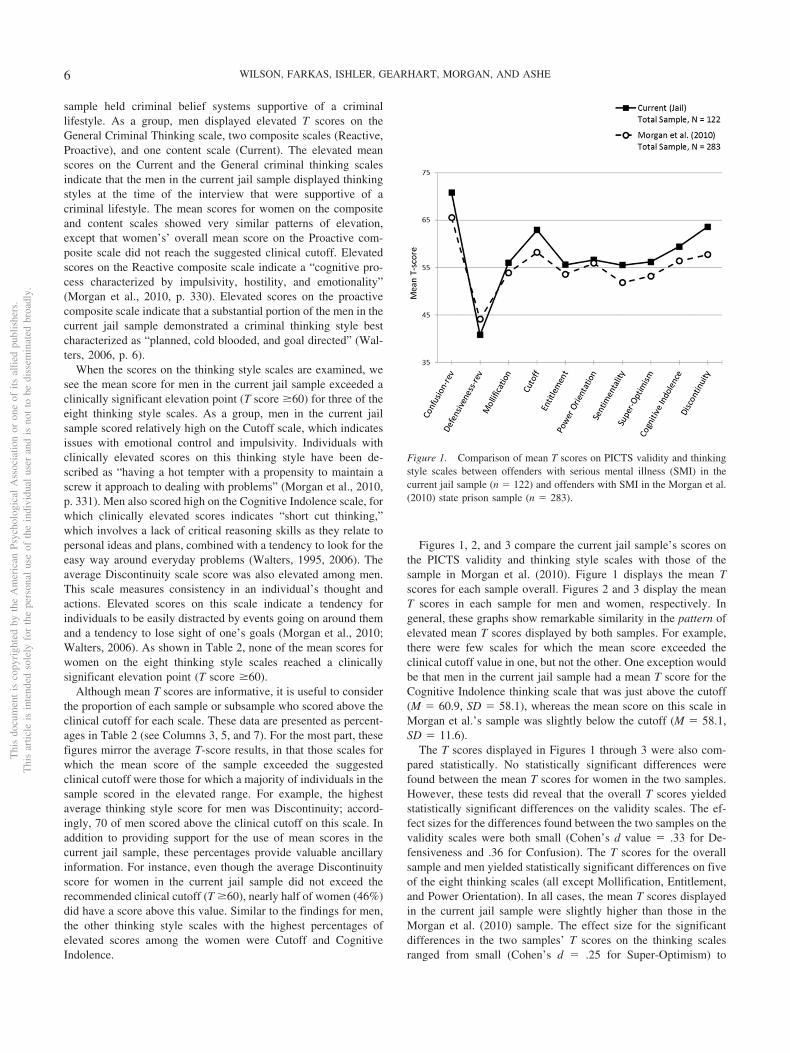
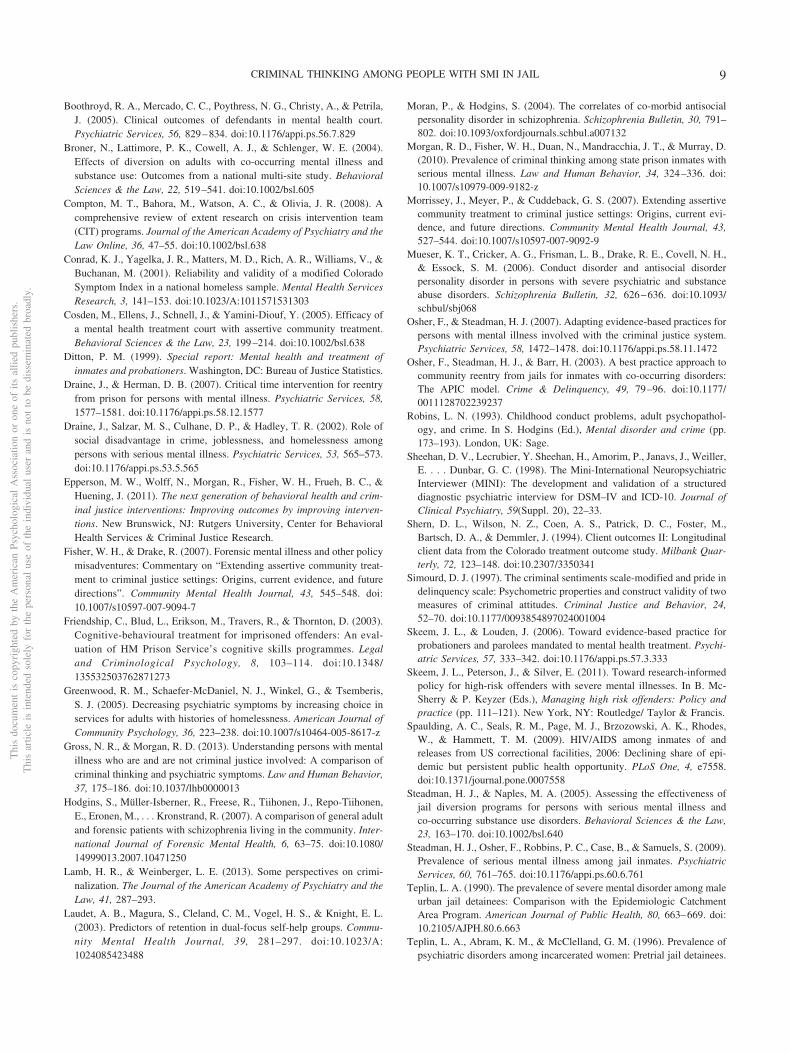
Figures 1, 2, and 3 compare the current jail sample’s scores onthe PICTS validity and thinking style scales with those of thesample in Morgan et al. (2010). Figure 1 displays the mean Tscores for each sample overall. Figures 2 and 3 display the meanT scores in each sample for men and women, respectively. Ingeneral, these graphs show remarkable similarity in the pattern ofelevated mean T scores displayed by both samples. For example,there were few scales for which the mean score exceeded theclinical cutoff value in one, but not the other. One exception wouldbe that men in the current jail sample had a mean T score for theCognitive Indolence thinking scale that was just above the cutoff(M � 60.9, SD � 58.1), whereas the mean score on this scale inMorgan et al.’s sample was slightly below the cutoff (M � 58.1,SD � 11.6).
The T scores displayed in Figures 1 through 3 were also com-pared statistically. No statistically significant differences werefound between the mean T scores for women in the two samples.However, these tests did reveal that the overall T scores yieldedstatistically significant differences on the validity scales. The ef-fect sizes for the differences found between the two samples on thevalidity scales were both small (Cohen’s d value � .33 for De-fensiveness and .36 for Confusion). The T scores for the overallsample and men yielded statistically significant differences on fiveof the eight thinking scales (all except Mollification, Entitlement,and Power Orientation). In all cases, the mean T scores displayedin the current jail sample were slightly higher than those in theMorgan et al. (2010) sample. The effect size for the significantdifferences in the two samples’ T scores on the thinking scalesranged from small (Cohen’s d � .25 for Super-Optimism) to
Figure 1. Comparison of mean T scores on PICTS validity and thinkingstyle scales between offenders with serious mental illness (SMI) in thecurrent jail sample (n � 122) and offenders with SMI in the Morgan et al.(2010) state prison sample (n � 283).
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
6 WILSON, FARKAS, ISHLER, GEARHART, MORGAN, AND ASHE
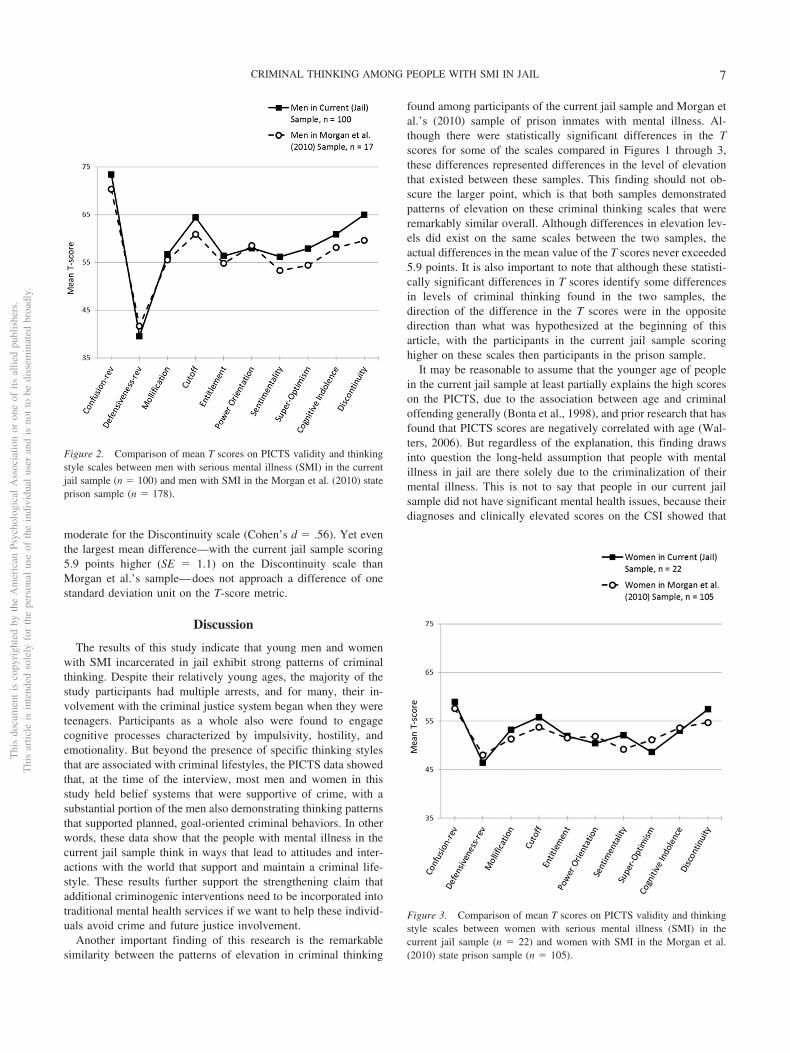
moderate for the Discontinuity scale (Cohen’s d � .56). Yet eventhe largest mean difference—with the current jail sample scoring5.9 points higher (SE � 1.1) on the Discontinuity scale thanMorgan et al.’s sample—does not approach a difference of onestandard deviation unit on the T-score metric.
Discussion
The results of this study indicate that young men and womenwith SMI incarcerated in jail exhibit strong patterns of criminalthinking. Despite their relatively young ages, the majority of thestudy participants had multiple arrests, and for many, their in-volvement with the criminal justice system began when they wereteenagers. Participants as a whole also were found to engagecognitive processes characterized by impulsivity, hostility, andemotionality. But beyond the presence of specific thinking stylesthat are associated with criminal lifestyles, the PICTS data showedthat, at the time of the interview, most men and women in thisstudy held belief systems that were supportive of crime, with asubstantial portion of the men also demonstrating thinking patternsthat supported planned, goal-oriented criminal behaviors. In otherwords, these data show that the people with mental illness in thecurrent jail sample think in ways that lead to attitudes and inter-actions with the world that support and maintain a criminal life-style. These results further support the strengthening claim thatadditional criminogenic interventions need to be incorporated intotraditional mental health services if we want to help these individ-uals avoid crime and future justice involvement.
Another important finding of this research is the remarkablesimilarity between the patterns of elevation in criminal thinking
found among participants of the current jail sample and Morgan etal.’s (2010) sample of prison inmates with mental illness. Al-though there were statistically significant differences in the Tscores for some of the scales compared in Figures 1 through 3,these differences represented differences in the level of elevationthat existed between these samples. This finding should not ob-scure the larger point, which is that both samples demonstratedpatterns of elevation on these criminal thinking scales that wereremarkably similar overall. Although differences in elevation lev-els did exist on the same scales between the two samples, theactual differences in the mean value of the T scores never exceeded5.9 points. It is also important to note that although these statisti-cally significant differences in T scores identify some differencesin levels of criminal thinking found in the two samples, thedirection of the difference in the T scores were in the oppositedirection than what was hypothesized at the beginning of thisarticle, with the participants in the current jail sample scoringhigher on these scales then participants in the prison sample.
It may be reasonable to assume that the younger age of peoplein the current jail sample at least partially explains the high scoreson the PICTS, due to the association between age and criminaloffending generally (Bonta et al., 1998), and prior research that hasfound that PICTS scores are negatively correlated with age (Wal-ters, 2006). But regardless of the explanation, this finding drawsinto question the long-held assumption that people with mentalillness in jail are there solely due to the criminalization of theirmental illness. This is not to say that people in our current jailsample did not have significant mental health issues, because theirdiagnoses and clinically elevated scores on the CSI showed that
Figure 2. Comparison of mean T scores on PICTS validity and thinkingstyle scales between men with serious mental illness (SMI) in the currentjail sample (n � 100) and men with SMI in the Morgan et al. (2010) stateprison sample (n � 178).
Figure 3. Comparison of mean T scores on PICTS validity and thinkingstyle scales between women with serious mental illness (SMI) in thecurrent jail sample (n � 22) and women with SMI in the Morgan et al.(2010) state prison sample (n � 105).
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
7CRIMINAL THINKING AMONG PEOPLE WITH SMI IN JAIL

they have SMIs that require treatment. Rather, this finding offerssupport for the contention that criminogenic risk and mental illnessare two separate, but interrelated, challenges facing people withmental illness involved in the criminal justice system, and thatmore must be done to understand the relationship between the twoand how to effectively intervene on both factors.
While the findings presented here make important contributionsto the literature there are several limitations that must be consid-ered. For example, systematic sampling techniques were used toidentify as many potential study participants as possible whoentered the jail during the study time frame. However, no matterhow careful and comprehensive the sampling techniques, theywere not random; thus, the representativeness of these findingsneeds to be confirmed in future research. In addition, although thisanalysis included a comparison with state inmates (Morgan et al.,2010) with mental illness, little is known about the base rate ofcriminal thinking among people with mental illness generally.Studying the levels of criminal thinking among people with mentalillness generally could be an important direction for research inthis area.
The discussion of the differences between the two samples ofpeople with mental illness examined in this article showed thatthese samples were different in some potentially important ways.For example, the current jail sample was much younger than theprison sample, which could contribute to the higher levels ofcriminal thinking found in the current jail sample. Yet despite thisimportant difference, these samples had remarkably similar pat-terns of elevation on the criminal thinking scales associated withimpulsivity and emotionality. Thus, although age may be contrib-uting to the magnitude of criminal thinking in the current jailsample, the comparison of the current jail sample’s scores with theprison sample’s scores shows a pattern of criminal thinking thatsuggests something else besides age is contributing to the types ofcriminal thinking found in these two samples. This possibility isalso supported by the fact that the elevated levels of impulsivityand emotionality found in the criminal thinking patterns of indi-viduals with mental illness in the current jail sample and Morganet al.’s (2010) prison sample were also higher than those reportedin the research on criminal thinking among general populationoffenders housed in federal prison that T scores used in both ofthese studies were based upon (Walters, 1995).
The stability in the pattern of elevation across these two differ-ent samples of people with mental illness raises questions abouthow the presence of mental illness may interact with preexistingcriminal thinking styles to further elevate these thinking styles inways that require further study. The fact that the criminal thinkingscores were highest in the sample of people with mental illnesswith the youngest age also suggests that further research needs tobe done to examine the rates of criminal thinking among peoplewith mental illness generally, so that the potential interactionbetween age and mental illness can be further explored.
It is also important to note that the samples of people withmental illness analyzed in this article had scores on the Confusionvalidity scale that were higher than those reported by Walters(1995). Although the PICTS provides guidelines for acceptablescores on this scale that were followed in both studies, theseelevated scores lend further support to the suggestion that themanifestation and identification of criminal thinking among peoplewith mental illness requires further study. This leads to the last
point for consideration, which relates to using the norms estab-lished in Walters’s work with federal prison inmates to create Tscores and assess elevation among people at other levels of cus-tody and those with mental illness. On the one hand, using thesescores helps to illustrate the extent to which criminogenic thinkingin our samples matches that displayed non-ill offenders. On theother hand, if this measure continues to be used as the benchmarkof criminal thinking across different justice-involved populations,it may be necessary to develop norms specific to other settings(e.g., state prisons) and/or populations (e.g., those with mentalillness).
Conclusions
This study contributes to the growing literature demonstratingthat justice-involved people with SMI exhibit thinking styles thatcontribute to and support a criminal lifestyle. Specifically, thisstudy of jail inmates completes the review of criminal thinkingthroughout the justice system that was previously limited to prisoninmates (Morgan et al., 2010; Wolff et al., 2011, 2013), andjustice-involved people with SMI in psychiatric treatment facilities(Gross & Morgan, 2013). The results of this study are important,given the number of admissions to jails in the United States, aspreviously noted, and the amount of resources and services that arebeing devoted to limiting this population’s future involvementwith the justice system. When the findings of these studies arelooked at collectively, it becomes clear that therapeutic programsfor justice-involved persons with SMI must develop a multiprongtreatment approach that integrates interventions for individuals’criminal thinking and antisocial attitudes specifically, and likelycriminogenic risk (e.g., associates), with treatment for their mentalillness and substance abuse issues (Epperson et al., 2011; Lamb &Weinberger, 2013). Therefore, future research needs examine theeffectiveness of correctional treatment programs designed tochange criminal thinking and antisocial attitudes with offenderswith mental illness, and develop models that are tailored to thespecific learning and treatment needs of this client population.
References
American Psychiatric Association. (2000). Diagnostic and statistical man-ual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Andrews, D. A., Bonta, J., & Wormith, J. S. (2006). The recent past andnear future of risk and/or need assessment. Crime & Delinquency, 52,7–27. doi:10.1177/0011128705281756
Black, D. W., Arndt, S., Hale, N., & Rogerson, R. (2004). Use of the MiniInternational Neuropsychiatric Interview (MINI) as a screening tool inprisons: Results of a preliminary study. Journal of the American Acad-emy of Psychiatry and the Law, 32, 158–162.
Bonta, J., Blais, J., & Wilson, H. A. (2013). The prediction of risk formentally disordered offenders: A quantitative synthesis. Manuscriptsubmitted for publication.
Bonta, J., Law, M., & Hanson, K. (1998). The prediction of criminal andviolent recidivism among mentally disordered offenders: A meta-analysis. Psychological Bulletin, 123, 123–142. doi:10.1037/0033-2909.123.2.123
Boothroyd, R. A., & Chen, H. J. (2008). The psychometric properties of theColorado Symptom Index. Administration and Policy in Mental Healthand Mental Health Services Research, 35, 370 –378. doi:10.1007/s10488-008-0179-6
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
8 WILSON, FARKAS, ISHLER, GEARHART, MORGAN, AND ASHE
Boothroyd, R. A., Mercado, C. C., Poythress, N. G., Christy, A., & Petrila,J. (2005). Clinical outcomes of defendants in mental health court.Psychiatric Services, 56, 829–834. doi:10.1176/appi.ps.56.7.829
Broner, N., Lattimore, P. K., Cowell, A. J., & Schlenger, W. E. (2004).Effects of diversion on adults with co-occurring mental illness andsubstance use: Outcomes from a national multi-site study. BehavioralSciences & the Law, 22, 519–541. doi:10.1002/bsl.605
Compton, M. T., Bahora, M., Watson, A. C., & Olivia, J. R. (2008). Acomprehensive review of extent research on crisis intervention team(CIT) programs. Journal of the American Academy of Psychiatry and theLaw Online, 36, 47–55. doi:10.1002/bsl.638
Conrad, K. J., Yagelka, J. R., Matters, M. D., Rich, A. R., Williams, V., &Buchanan, M. (2001). Reliability and validity of a modified ColoradoSymptom Index in a national homeless sample. Mental Health ServicesResearch, 3, 141–153. doi:10.1023/A:1011571531303
Cosden, M., Ellens, J., Schnell, J., & Yamini-Diouf, Y. (2005). Efficacy ofa mental health treatment court with assertive community treatment.Behavioral Sciences & the Law, 23, 199–214. doi:10.1002/bsl.638
Ditton, P. M. (1999). Special report: Mental health and treatment ofinmates and probationers. Washington, DC: Bureau of Justice Statistics.
Draine, J., & Herman, D. B. (2007). Critical time intervention for reentryfrom prison for persons with mental illness. Psychiatric Services, 58,1577–1581. doi:10.1176/appi.ps.58.12.1577
Draine, J., Salzar, M. S., Culhane, D. P., & Hadley, T. R. (2002). Role ofsocial disadvantage in crime, joblessness, and homelessness amongpersons with serious mental illness. Psychiatric Services, 53, 565–573.doi:10.1176/appi.ps.53.5.565
Epperson, M. W., Wolff, N., Morgan, R., Fisher, W. H., Frueh, B. C., &Huening, J. (2011). The next generation of behavioral health and crim-inal justice interventions: Improving outcomes by improving interven-tions. New Brunswick, NJ: Rutgers University, Center for BehavioralHealth Services & Criminal Justice Research.
Fisher, W. H., & Drake, R. (2007). Forensic mental illness and other policymisadventures: Commentary on “Extending assertive community treat-ment to criminal justice settings: Origins, current evidence, and futuredirections”. Community Mental Health Journal, 43, 545–548. doi:10.1007/s10597-007-9094-7
Friendship, C., Blud, L., Erikson, M., Travers, R., & Thornton, D. (2003).Cognitive-behavioural treatment for imprisoned offenders: An eval-uation of HM Prison Service’s cognitive skills programmes. Legaland Criminological Psychology, 8, 103–114. doi:10.1348/135532503762871273
Greenwood, R. M., Schaefer-McDaniel, N. J., Winkel, G., & Tsemberis,S. J. (2005). Decreasing psychiatric symptoms by increasing choice inservices for adults with histories of homelessness. American Journal ofCommunity Psychology, 36, 223–238. doi:10.1007/s10464-005-8617-z
Gross, N. R., & Morgan, R. D. (2013). Understanding persons with mentalillness who are and are not criminal justice involved: A comparison ofcriminal thinking and psychiatric symptoms. Law and Human Behavior,37, 175–186. doi:10.1037/lhb0000013
Hodgins, S., Müller-Isberner, R., Freese, R., Tiihonen, J., Repo-Tiihonen,E., Eronen, M., . . . Kronstrand, R. (2007). A comparison of general adultand forensic patients with schizophrenia living in the community. Inter-national Journal of Forensic Mental Health, 6, 63–75. doi:10.1080/14999013.2007.10471250
Lamb, H. R., & Weinberger, L. E. (2013). Some perspectives on crimi-nalization. The Journal of the American Academy of Psychiatry and theLaw, 41, 287–293.
Laudet, A. B., Magura, S., Cleland, C. M., Vogel, H. S., & Knight, E. L.(2003). Predictors of retention in dual-focus self-help groups. Commu-nity Mental Health Journal, 39, 281–297. doi:10.1023/A:1024085423488
Moran, P., & Hodgins, S. (2004). The correlates of co-morbid antisocialpersonality disorder in schizophrenia. Schizophrenia Bulletin, 30, 791–802. doi:10.1093/oxfordjournals.schbul.a007132
Morgan, R. D., Fisher, W. H., Duan, N., Mandracchia, J. T., & Murray, D.(2010). Prevalence of criminal thinking among state prison inmates withserious mental illness. Law and Human Behavior, 34, 324–336. doi:10.1007/s10979-009-9182-z
Morrissey, J., Meyer, P., & Cuddeback, G. S. (2007). Extending assertivecommunity treatment to criminal justice settings: Origins, current evi-dence, and future directions. Community Mental Health Journal, 43,527–544. doi:10.1007/s10597-007-9092-9
Mueser, K. T., Cricker, A. G., Frisman, L. B., Drake, R. E., Covell, N. H.,& Essock, S. M. (2006). Conduct disorder and antisocial disorderpersonality disorder in persons with severe psychiatric and substanceabuse disorders. Schizophrenia Bulletin, 32, 626–636. doi:10.1093/schbul/sbj068
Osher, F., & Steadman, H. J. (2007). Adapting evidence-based practices forpersons with mental illness involved with the criminal justice system.Psychiatric Services, 58, 1472–1478. doi:10.1176/appi.ps.58.11.1472
Osher, F., Steadman, H. J., & Barr, H. (2003). A best practice approach tocommunity reentry from jails for inmates with co-occurring disorders:The APIC model. Crime & Delinquency, 49, 79–96. doi:10.1177/0011128702239237
Robins, L. N. (1993). Childhood conduct problems, adult psychopathol-ogy, and crime. In S. Hodgins (Ed.), Mental disorder and crime (pp.173–193). London, UK: Sage.
Sheehan, D. V., Lecrubier, Y. Sheehan, H., Amorim, P., Janavs, J., Weiller,E. . . . Dunbar, G. C. (1998). The Mini-International NeuropsychiatricInterviewer (MINI): The development and validation of a structureddiagnostic psychiatric interview for DSM–IV and ICD-10. Journal ofClinical Psychiatry, 59(Suppl. 20), 22–33.
Shern, D. L., Wilson, N. Z., Coen, A. S., Patrick, D. C., Foster, M.,Bartsch, D. A., & Demmler, J. (1994). Client outcomes II: Longitudinalclient data from the Colorado treatment outcome study. Milbank Quar-terly, 72, 123–148. doi:10.2307/3350341
Simourd, D. J. (1997). The criminal sentiments scale-modified and pride indelinquency scale: Psychometric properties and construct validity of twomeasures of criminal attitudes. Criminal Justice and Behavior, 24,52–70. doi:10.1177/0093854897024001004
Skeem, J. L., & Louden, J. (2006). Toward evidence-based practice forprobationers and parolees mandated to mental health treatment. Psychi-atric Services, 57, 333–342. doi:10.1176/appi.ps.57.3.333
Skeem, J. L., Peterson, J., & Silver, E. (2011). Toward research-informedpolicy for high-risk offenders with severe mental illnesses. In B. Mc-Sherry & P. Keyzer (Eds.), Managing high risk offenders: Policy andpractice (pp. 111–121). New York, NY: Routledge/ Taylor & Francis.
Spaulding, A. C., Seals, R. M., Page, M. J., Brzozowski, A. K., Rhodes,W., & Hammett, T. M. (2009). HIV/AIDS among inmates of andreleases from US correctional facilities, 2006: Declining share of epi-demic but persistent public health opportunity. PLoS One, 4, e7558.doi:10.1371/journal.pone.0007558
Steadman, H. J., & Naples, M. A. (2005). Assessing the effectiveness ofjail diversion programs for persons with serious mental illness andco-occurring substance use disorders. Behavioral Sciences & the Law,23, 163–170. doi:10.1002/bsl.640
Steadman, H. J., Osher, F., Robbins, P. C., Case, B., & Samuels, S. (2009).Prevalence of serious mental illness among jail inmates. PsychiatricServices, 60, 761–765. doi:10.1176/appi.ps.60.6.761
Teplin, L. A. (1990). The prevalence of severe mental disorder among maleurban jail detainees: Comparison with the Epidemiologic CatchmentArea Program. American Journal of Public Health, 80, 663–669. doi:10.2105/AJPH.80.6.663
Teplin, L. A., Abram, K. M., & McClelland, G. M. (1996). Prevalence ofpsychiatric disorders among incarcerated women: Pretrial jail detainees.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
9CRIMINAL THINKING AMONG PEOPLE WITH SMI IN JAIL

Archives of General Psychiatry, 53, 505–512. doi:10.1001/archpsyc.1996.01830060047007
Walters, G. D. (1995). The psychological inventory of criminal thinkingstyles: Part I: Reliability and preliminary validity. Criminal Justice andBehavior, 22, 307–325. doi:10.1177/0093854895022003008
Walters, G. D. (2006). The Psychological Inventory of Criminal ThinkingStyles (PICTS) professional manual (Version 4.0). Allentown, PA: Cen-ter for Lifestyle Studies.
Walters, G. D., Elliott, W. N., & Miscoll, D. (1998). Use of the Psycho-logical Inventory of Criminal Thinking Styles in a group of femaleoffenders. Criminal Justice and Behavior, 25, 125–134. doi:10.1177/0093854898025001008
Walters, G. D., Trgovac, M., Rychlec, M., Di Fazio, R., & Olson, J. (2002).Assessing change with the Psychological Inventory of Criminal Think-ing Styles. Criminal Justice and Behavior, 29, 308–331. doi:10.1177/0093854802029003004
Wolff, N., Morgan, R. D., & Shi, J. (2013). Comparative analysis ofattitudes and emotions among inmates: Does mental illness matter?Criminal Justice and Behavior, 40, 1092–1108. doi:10.1177/0093854813488760
Wolff, N., Morgan, R. D., Shi, J., Fisher, W., & Huening, J. (2011).Comparative analysis of thinking styles and emotional states of male andfemale inmates with and without mental disorders. Psychiatric Services,62, 1485–1493. doi:10.1176/appi.ps.000432011
World Health Organization. (1992). International statistical classificationof diseases and related health problems, 10th Rev. (ICD-10). Geneva,Switzerland: World Health Organization.
Received September 20, 2013Revision received January 9, 2014
Accepted January 9, 2014 �
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
10 WILSON, FARKAS, ISHLER, GEARHART, MORGAN, AND ASHE





























