Embed Size (px)
Citation preview
Community Based Health Insurance Practices in Nepal
Rabindra Ghimire1
Abstract
This paper critically reviews the micro health insurance practices in Nepal practices by governmental and
nongovernmental sectors. The purpose of this paper is to review the existing community based health
insurance practices, assess the opportunities and challenges of micro health scheme and suggest the better
alternatives in Nepalese context. The paper has prepared based on available literature and it is qualitative
in nature. The micro health insurance intervention nominal in Nepal is in infant stage.
Government health post and hospital provides limited health services to public. Most of the Nepalese are far
from the health insurance services. Six community based health insurance schemes have been initiated by
government in 2003. These schemes are running by hospital, health centre, NGOs, Cooperatives, Business
Association and Trade union. Some schemes are self sustained economically whereas most of the schemes
are supported by government and international donor agencies. Micro Health Insurance Schemes are
running in different parts of Nepal which covers almost 50,000 people. From 400 to 18000 clients are
covered by different micro health insurance schemes. are getting health insurance facility. The paper
concludes that the impact of community based social health schemes in Nepal is not significant but it is
essential for poor and marginalized group.
1. INTRODUCTION
1.1 An Overview of Health Insurance in Nepal
Health insurance is new phenomena in Nepalese context even though commercial insurers have been sold health
insurance package since many years. Government have been provided health insurance, medical allowance and free of
health check, consultation and medical treatment through its own organizational structure and resources. Population
having age below 15 and above 75 also get some treatment facilities from state owned hospital. Still large number of
population is outside the schemes of proper health care facilities.
Community health insurance in Nepal had began by international NGO more than 30 years back initiated by the United
Mission to Nepal as “Lalitpur Medical Insurance Scheme" which is regarded as first non-profit health insurance schemes
in Nepal. In 2000, BP Koirala Institute of Health Science (BPKIHS) in Dharan, started health insurance which covered
urban and rural populations, offering the same benefit package at different premium rates. The scheme covered the
organised sector (cooperatives, business groups) and unorganised groups (such as farmers and self-employed groups),
1 Assistant Professor, Pokhara University and currently Research Scholar, Faculty of Commerce, BHU, Varanasi. [email protected]
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 2 of 15
but was unable to expand because of high costs and low premium collection, which created a deficit. Now, more than a
dozen of schemes operated by private sector are in operations by NGOs, Cooperatives and Hospital.
Health insurance providers in Nepal are basically categorized in two broad sectors: Non subsidized (Commercial insurers
and self managed schemes) and subsidized (government managed CBHI schemes, hospital, cooperatives and NGOs
managed schemes). Besides unorganized sector, health insurance is provided by the commercial insurers as per the need
of the customers. Currently, 17 non life insurers are selling health and accidental insurance policies. The rate of health
insurance penetration by commercial insurers is very low due to small volume of risk exposures, lack of awareness and
high claim ratio.
Major health and accidental policies are: Hospital and surgical expenses insurance, medical and health insurance, Group
Medical Insurance, Group Personnel Accident, Medical & Travel Insurance, Medical Aid Insurance, Traveling Medical
Insurance, mediclaim for senior citizen, Overseas Mediclaim, Hospital Cash Plan, Children health policy etc. (Ghimire,
2012). Under the self managed schemes, Health cooperative societies have been providing their members charging
certain premium. The total numbers of such schemes are not well documented either by the Department of Cooperatives
or Insurance Board.
Six pilot schemes were initiated by government and NGOs since 2003 as subsidized insurance schemes. In parallel, some
privately-operated Community Based Health Insurance (CBHI) schemes have been established in financial support of
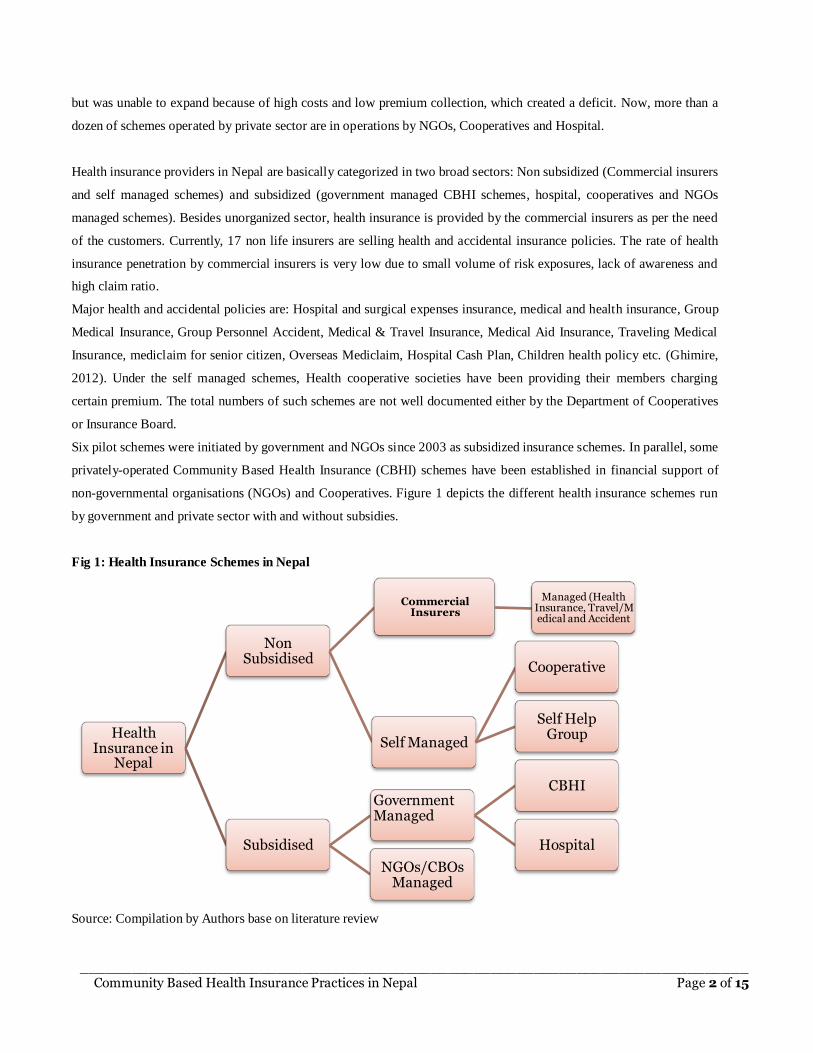
non-governmental organisations (NGOs) and Cooperatives. Figure 1 depicts the different health insurance schemes run
by government and private sector with and without subsidies.
Fig 1: Health Insurance Schemes in Nepal
Source: Compilation by Authors base on literature review
Health Insurance in
Nepal
Non Subsidised
Commercial Insurers
Managed (Health Insurance, Travel/Medical and Accident
Self Managed
Cooperative
Self Help Group
Subsidised
Government Managed
CBHI
Hospital
NGOs/CBOs Managed
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 3 of 15
1.2 Health Financing in Nepal
Major characteristics of public health delivery system of Nepal are poor health facilities rendering by government
hospitals even in cities and capital, unavailability of workable equipments, skilled human resources, effective medicine
in most of the hospital outside the Kathmandu valley and limited services available even in a regional and zonal hospital
committed in policy and programs.
Major source of health financing in Nepal is private sector (60%) which is followed by government (21%) and rest is
finance by the donor and charity (19%). Most of the private source financing comes from individual's out of pocket
(91%) and rest of the amount is financed by the NGOs and corporations ( MoHP, 2012). This figure shows that health
financing in Nepal entirely depends on private source however, government also contributed one fifth of the total
expenditure in health sector. There is a wider disparity in health care expenditure between better off and poor. A person
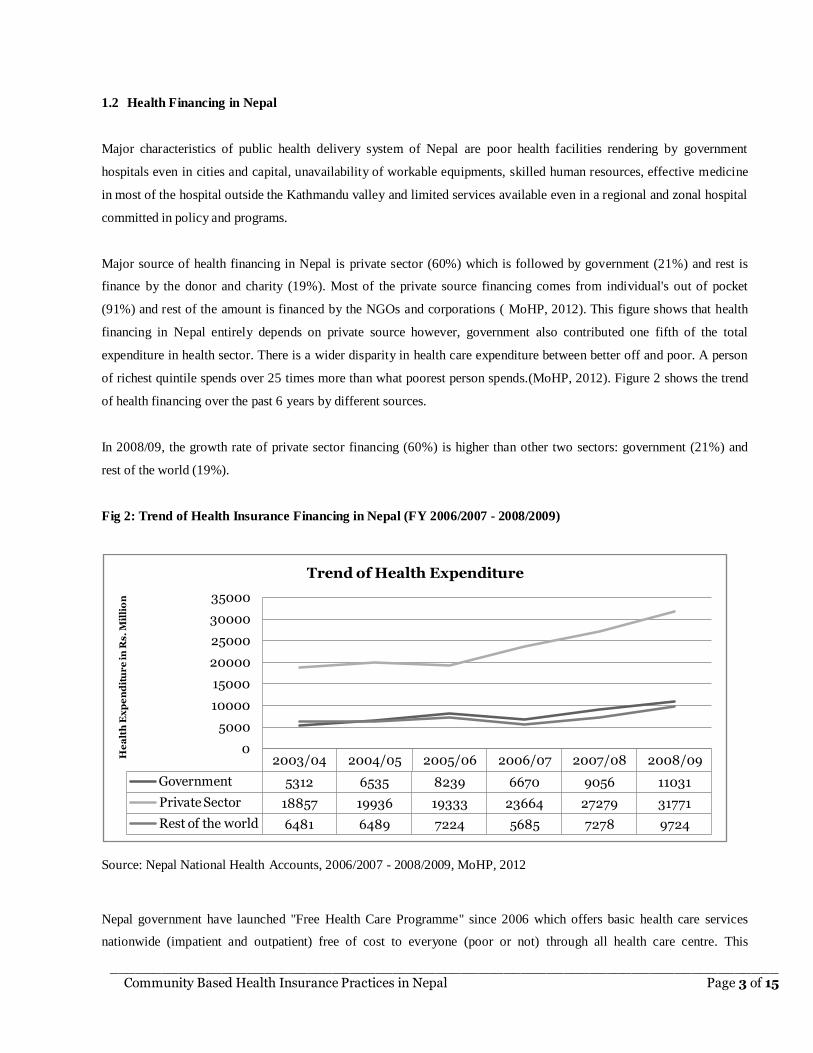
of richest quintile spends over 25 times more than what poorest person spends.(MoHP, 2012). Figure 2 shows the trend
of health financing over the past 6 years by different sources.
In 2008/09, the growth rate of private sector financing (60%) is higher than other two sectors: government (21%) and
rest of the world (19%).
Fig 2: Trend of Health Insurance Financing in Nepal (FY 2006/2007 - 2008/2009)
Source: Nepal National Health Accounts, 2006/2007 - 2008/2009, MoHP, 2012
Nepal government have launched "Free Health Care Programme" since 2006 which offers basic health care services
nationwide (impatient and outpatient) free of cost to everyone (poor or not) through all health care centre. This
2003/04 2004/05 2005/06 2006/07 2007/08 2008/09
Government 5312 6535 8239 6670 9056 11031
Private Sector 18857 19936 19333 23664 27279 31771
Rest of the world 6481 6489 7224 5685 7278 9724
0
5000
10000
15000
20000
25000
30000
35000
He
alt
h E
xp
en
dit
ur
e i
n R
s.
Mil
lio
n
Trend of Health Expenditure
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 4 of 15
programme provides 22 to 40 different medicines free of cost to all. But, additional service (consultations and treatment,
minor surgery, emergency obstetric care (either comprehensive or basic), x-rays and laboratory services) are provided to
target groups only (poor, ultra poor, helpless, disabled, senior citizens above 60 years of age and female community
health volunteers) only.
2. SYNOPSIS OF LITERATURE REVIEW
Most of the poor people in the world are suffering from the health related expenses. Microinsurance is emerging as a
global solution for breaking the cycle of poverty and vulnerability. Locally, it provides an opportunity to plan for ill
health by organizing regular payments, making health expenses predictable and affordable. Micro health insurance is
especially designed to poor and vulnerable people to provide them health and medical facilities since they couldn't afford
the cost of medicine and hospitalization as other normal income people from the ordinary market. The poorest citizens of
the poorest countries are typically exposed to the greatest risks (Murdoch, 1995). They are inherently more vulnerable to
illness due to their living conditions, limited resources and exclusion from social security systems.
In Nepal, families face multiple barriers in accessing healthcare. Delays in the decision to seek care arise from financial
constraints as 72% of people finance health costs “out-of-pocket” (World Bank, 2011). In order to cope with these costs
families may borrow money with interest or sell productive assets, pushing them further into poverty. Access to micro
health insurance has been shown to decrease out-of-pocket expenditure, especially for catastrophic health events, and
improve access to care for insured members (Carrin, Waelkens and Criel 2012). As health insurance coverage is only
5% in Nepal, the opportunity to deliver an innovative solution is substantial (Stoermer et al., 2011).
Illness and crop failure often cause severe economic damage to rural households in Cambodia that more farmer sell their
land due to illness than due to crop failure (Kanjiro, 2005). Crop failure is generally considered to be a common shock,
while illness is considered idiosyncratic. According to recent World Health Organization estimates, every year 25
million households (more than 100 million people) are forced into poverty by illness.
According to WHO (2005) 100 million people every year are driven into poverty due to catastrophic health expenditure.
It is imaginable that most reside in resource poor settings such as Sub Saharan Africa with very weak modern health care
systems and in most cases without any functioning health insurance schemes (WHO, 2003; Carrin et al, 2005).
The highest demand from poor people was for health products and life products, followed by property insurance and
accidental death and disability cover. Roth, Michael and Liber (2007) states that Micro Health Insurance schemes over
the world are found in large numbers but their membership is limited in numbers and growth of membership is slow.
Community Based Health Insurance Schemes (CBHISs) are promising alternatives for a cost sharing health care system
which hopefully also leads to better utilization of health care services, reduce illness related income shocks and
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 5 of 15
eventually lead to a sustainable and fully functioning universal health care system (Shimeles, 2010). But, the experience
of CBHI in different places is different, however, the objective is the same to deliver the health service to poor and
marginalized population in affordable price.
CBHI schemes as observed in different regions of developing world are quite diverse. Nevertheless, certain features
common to most of the schemes can be readily identified, such as, the voluntary participation of the people, not-for-
profit objective in organizing the scheme, scheme management by the community itself, and some degree of risk
pooling. These schemes are reported to have made positive contribution in terms of financial protection, resource
mobilization, social exclusion, and in health care provision (Ahuja, et al. 2003).
Tobor (2005) in his study concludes that the main weaknesses of CBHI are the low level of revenues that can be
mobilized from poor communities, the frequent exclusion of the poorest of the poor from participation in such schemes
without some form of subsidy, the small size of the risk pool, the limited management capacity that exists in rural and
low-income contexts, and their isolation from the more comprehensive benefits that are often available through more
formal health financing mechanisms and provider networks.
CBHI schemes are run in different modalities in international practices such as community owned, run by local or central
government or both, run by hospitals or clinics, run by international NGOs or donors, by cooperatives or trade unions.
3. OBJECTIVES AND METHODOLOGY
Objective of this paper is to review the existing community based health insurance practices in Nepal, assess
effectiveness of health insurance program run by government and private sector and provide suggestions regarding the
suitable model for the better delivery of the health insurance to the poor and vulnerable community with the best possible
way. The paper also shed lights the prospects and challenges of community based micro health insurance schemes.
The paper has been prepared based on secondary information available from different literature. Sufficient literature has
been reviewed and required data have been gathered from the various relevant publications published from Department
of Health Services, bilateral and multilateral development organizations, INGOs, NGOs. Relevant literature in the field
of community based health insurance in Nepal and health insurance financing in Nepal has been collected. Government’s
health related rules, strategic plan and policy have been also been consulted. The study is descriptive and qualitative in
nature based on available secondary information from the published and unpublished sources including the web search.
Experts in the field were consulted to validate the information.
We have taken total 22 CBHI schemes for this study. Six CBHI schemes are run by government run and 16 are privately
run. For government run CBHI, medicine, diagnosis, hospitalization and total benefits variables are taken for analysis
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 6 of 15
whereas in private owned CBHI scheme, Number of Beneficiaries and coverage of area, types of beneficiaries and
supporting agency are taken as variables for discussion.
4. COMMUNITY BASED HEALTH INSURANCE PRACTICES
Micro Health Insurance schemes have been run in different name and modality in Nepal but they are still not operated as
per the insurance guidelines and not registered under Insurance Board. Government and private sector run different
schemes are discussed in this section.
4.1 Government Run CBHI
Health insurance has gained momentum among policy makers in Nepal over the last couple of years. The Ministry of
Health and Population is in the process of drafting a health insurance policy and a new health financing strategy. At the
implementation level, the Ministry of Health and Population has been piloting community-based health insurance
schemes since 2003/04 and for the effective implementation of the scheme, Community Health Insurance Operational
Guidelines, 2006 is on operation.
Currently, CBHI are run either in two modalities: low cost high frequency of illness and high cost low frequency of
illness model.
i. Low cost high frequency of illness model: This model covers the primary health care services at
Dumkauli,Tikapur, Lamahi, Chandranigahapur and Katari PHC.
ii. High cost, low frequency of illness model: This model covers primary health care services with referral services
at Mangalbare.
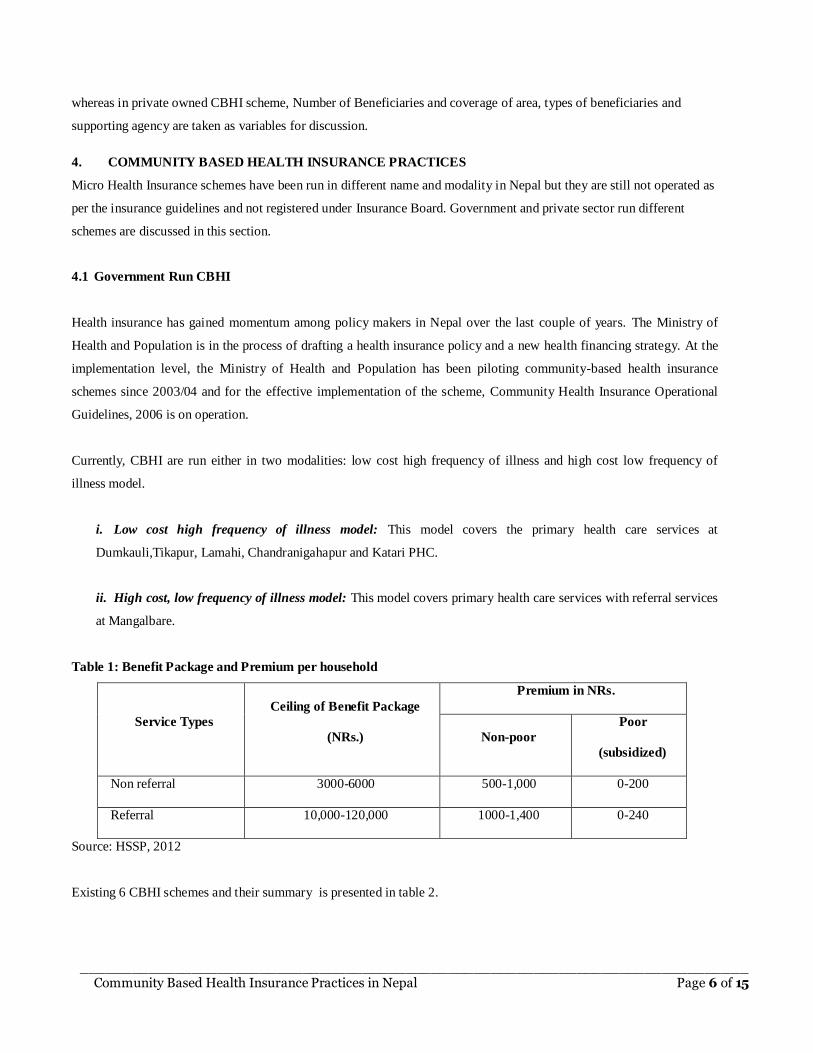
Table 1: Benefit Package and Premium per household
Service Types
Ceiling of Benefit Package
(NRs.)
Premium in NRs.
Non-poor
Poor
(subsidized)
Non referral 3000-6000 500-1,000 0-200
Referral 10,000-120,000 1000-1,400 0-240
Source: HSSP, 2012
Existing 6 CBHI schemes and their summary is presented in table 2.
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 7 of 15
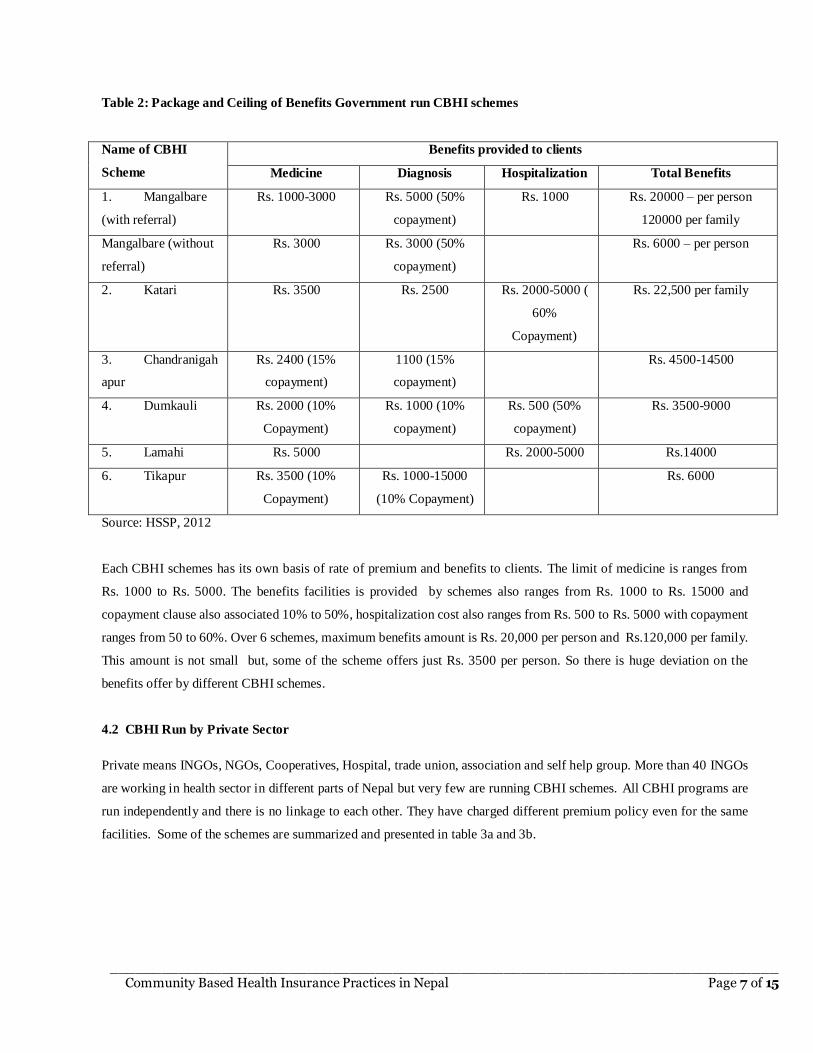
Table 2: Package and Ceiling of Benefits Government run CBHI schemes
Name of CBHI
Scheme
Benefits provided to clients
Medicine Diagnosis Hospitalization Total Benefits
1. Mangalbare
(with referral)
Rs. 1000-3000 Rs. 5000 (50%
copayment)
Rs. 1000 Rs. 20000 – per person
120000 per family
Mangalbare (without
referral)
Rs. 3000 Rs. 3000 (50%
copayment)
Rs. 6000 – per person
2. Katari Rs. 3500 Rs. 2500 Rs. 2000-5000 (
60%
Copayment)
Rs. 22,500 per family
3. Chandranigah
apur
Rs. 2400 (15%
copayment)
1100 (15%
copayment)
Rs. 4500-14500
4. Dumkauli Rs. 2000 (10%
Copayment)
Rs. 1000 (10%
copayment)
Rs. 500 (50%
copayment)
Rs. 3500-9000
5. Lamahi Rs. 5000 Rs. 2000-5000 Rs.14000
6. Tikapur Rs. 3500 (10%
Copayment)
Rs. 1000-15000
(10% Copayment)
Rs. 6000
Source: HSSP, 2012
Each CBHI schemes has its own basis of rate of premium and benefits to clients. The limit of medicine is ranges from
Rs. 1000 to Rs. 5000. The benefits facilities is provided by schemes also ranges from Rs. 1000 to Rs. 15000 and
copayment clause also associated 10% to 50%, hospitalization cost also ranges from Rs. 500 to Rs. 5000 with copayment
ranges from 50 to 60%. Over 6 schemes, maximum benefits amount is Rs. 20,000 per person and Rs.120,000 per family.
This amount is not small but, some of the scheme offers just Rs. 3500 per person. So there is huge deviation on the
benefits offer by different CBHI schemes.
4.2 CBHI Run by Private Sector
Private means INGOs, NGOs, Cooperatives, Hospital, trade union, association and self help group. More than 40 INGOs
are working in health sector in different parts of Nepal but very few are running CBHI schemes. All CBHI programs are
run independently and there is no linkage to each other. They have charged different premium policy even for the same
facilities. Some of the schemes are summarized and presented in table 3a and 3b.
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 8 of 15
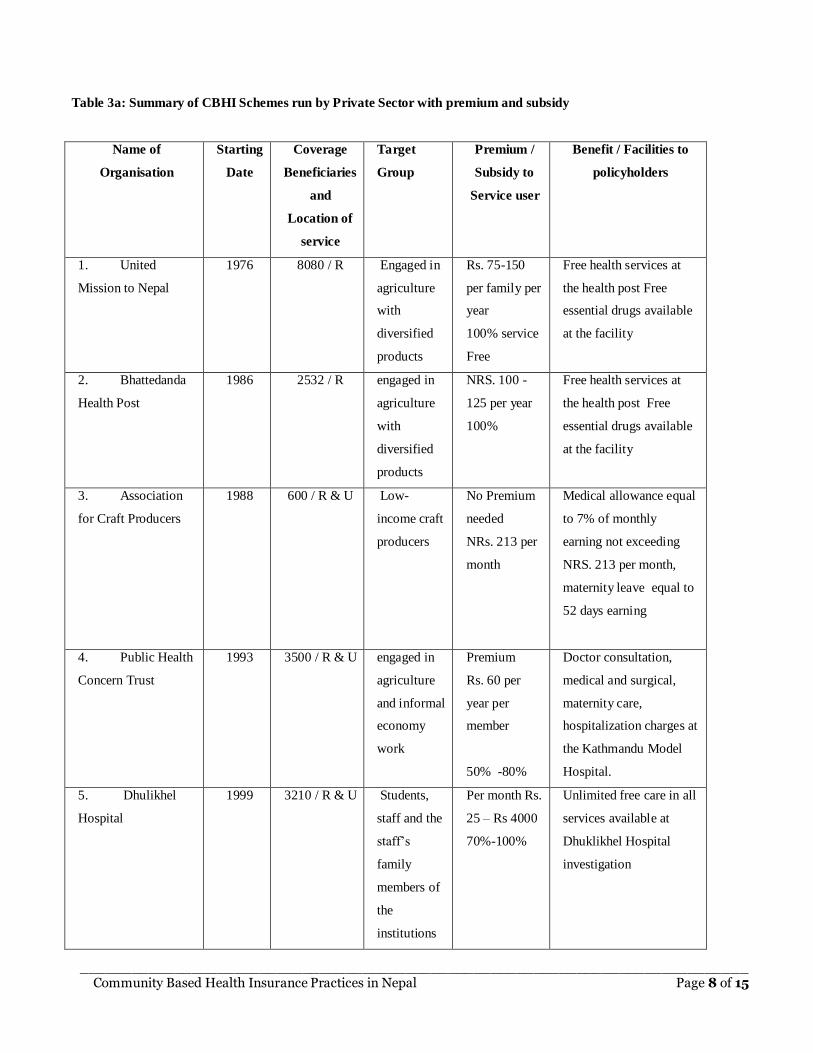
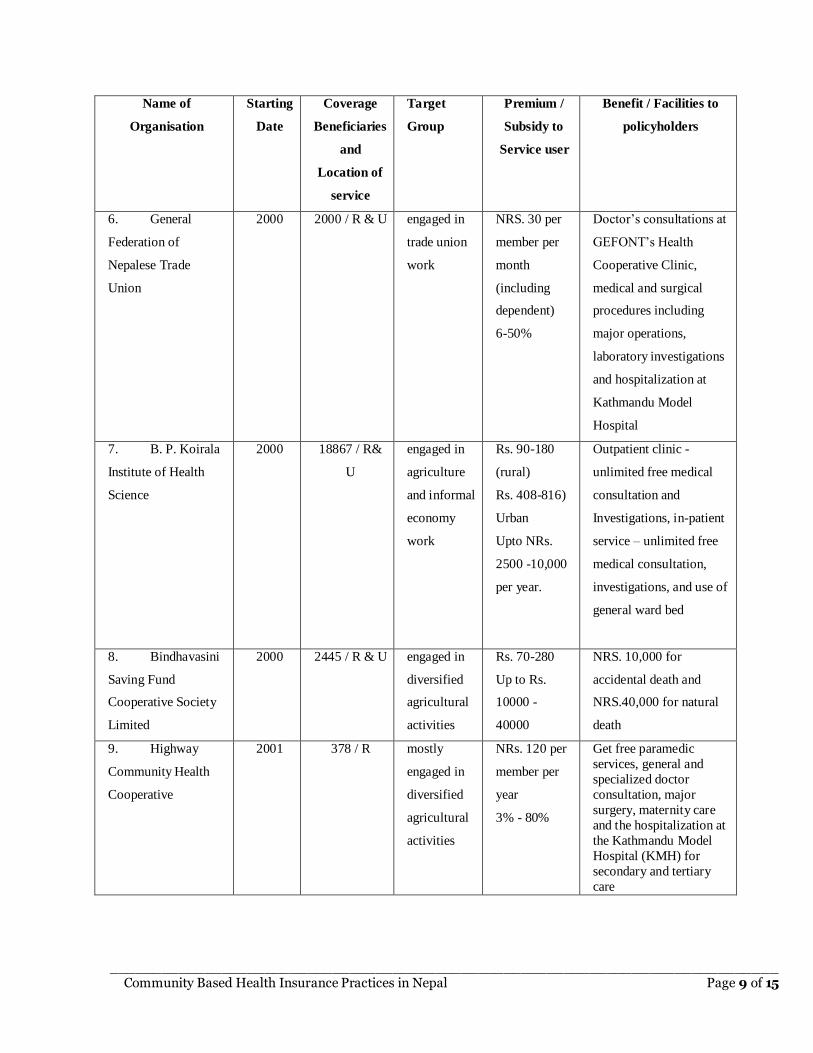
Table 3a: Summary of CBHI Schemes run by Private Sector with premium and subsidy
Name of
Organisation
Starting
Date
Coverage
Beneficiaries
and
Location of
service
Target
Group
Premium /
Subsidy to
Service user
Benefit / Facilities to
policyholders
1. United
Mission to Nepal
1976 8080 / R Engaged in
agriculture
with
diversified
products
Rs. 75-150
per family per
year
100% service
Free
Free health services at
the health post Free
essential drugs available
at the facility
2. Bhattedanda
Health Post
1986 2532 / R engaged in
agriculture
with
diversified
products
NRS. 100 -
125 per year
100%
Free health services at
the health post Free
essential drugs available
at the facility
3. Association
for Craft Producers
1988 600 / R & U Low-
income craft
producers
No Premium
needed
NRs. 213 per
month
Medical allowance equal
to 7% of monthly
earning not exceeding
NRS. 213 per month,
maternity leave equal to
52 days earning
4. Public Health
Concern Trust
1993 3500 / R & U engaged in
agriculture
and informal
economy
work
Premium
Rs. 60 per
year per
member
50% -80%
Doctor consultation,
medical and surgical,
maternity care,
hospitalization charges at
the Kathmandu Model
Hospital.
5. Dhulikhel
Hospital
1999 3210 / R & U Students,
staff and the
staff’s
family
members of
the
institutions
Per month Rs.
25 – Rs 4000
70%-100%
Unlimited free care in all
services available at
Dhuklikhel Hospital
investigation
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 9 of 15
Name of
Organisation
Starting
Date
Coverage
Beneficiaries
and
Location of
service
Target
Group
Premium /
Subsidy to
Service user
Benefit / Facilities to
policyholders
6. General
Federation of
Nepalese Trade
Union
2000 2000 / R & U engaged in
trade union
work
NRS. 30 per
member per
month
(including
dependent)
6-50%
Doctor’s consultations at
GEFONT’s Health
Cooperative Clinic,
medical and surgical
procedures including
major operations,
laboratory investigations
and hospitalization at
Kathmandu Model
Hospital
7. B. P. Koirala
Institute of Health
Science
2000 18867 / R&
U
engaged in
agriculture
and informal
economy
work
Rs. 90-180
(rural)
Rs. 408-816)
Urban
Upto NRs.
2500 -10,000
per year.
Outpatient clinic -
unlimited free medical
consultation and
Investigations, in-patient
service – unlimited free
medical consultation,
investigations, and use of
general ward bed
8. Bindhavasini
Saving Fund
Cooperative Society
Limited
2000 2445 / R & U engaged in
diversified
agricultural
activities
Rs. 70-280
Up to Rs.
10000 -
40000
NRS. 10,000 for
accidental death and
NRS.40,000 for natural
death
9. Highway
Community Health
Cooperative
2001 378 / R mostly
engaged in
diversified
agricultural
activities
NRs. 120 per
member per
year
3% - 80%
Get free paramedic
services, general and
specialized doctor
consultation, major
surgery, maternity care
and the hospitalization at
the Kathmandu Model
Hospital (KMH) for
secondary and tertiary
care
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 10 of 15
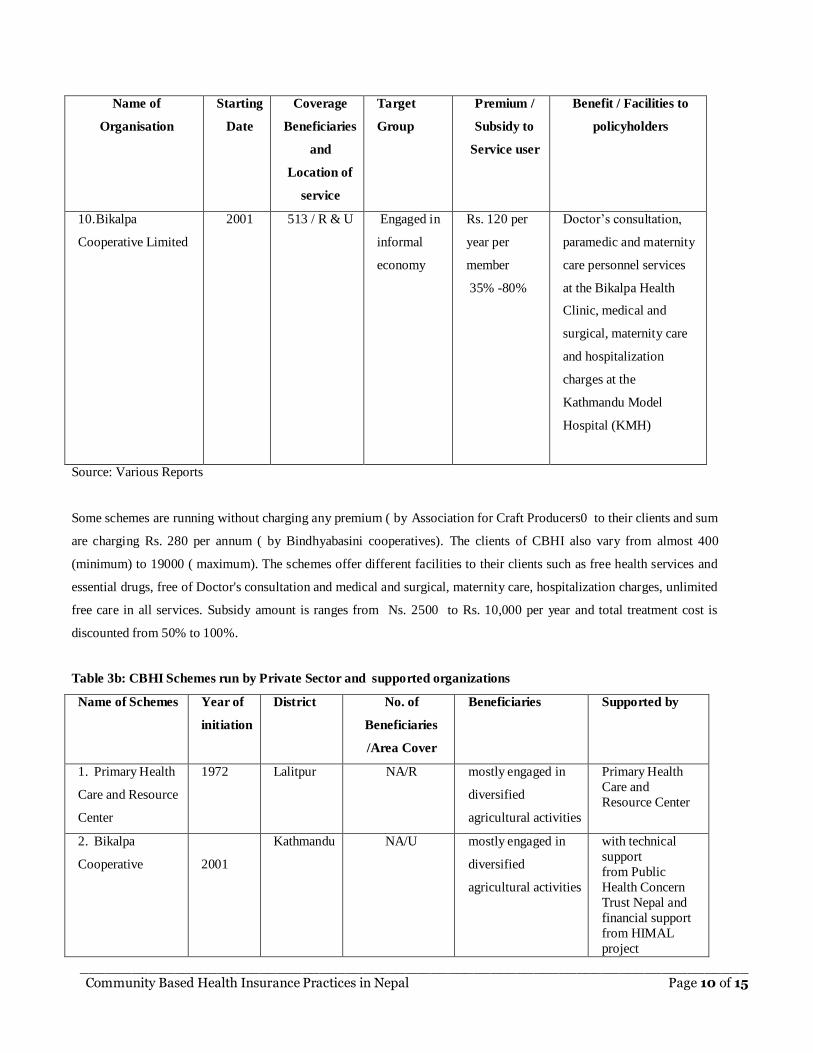
Name of
Organisation
Starting
Date
Coverage
Beneficiaries
and
Location of
service
Target
Group
Premium /
Subsidy to
Service user
Benefit / Facilities to
policyholders
10. Bikalpa
Cooperative Limited
2001 513 / R & U Engaged in
informal
economy
Rs. 120 per
year per
member
35% -80%
Doctor’s consultation,
paramedic and maternity
care personnel services
at the Bikalpa Health
Clinic, medical and
surgical, maternity care
and hospitalization
charges at the
Kathmandu Model
Hospital (KMH)
Source: Various Reports
Some schemes are running without charging any premium ( by Association for Craft Producers0 to their clients and sum
are charging Rs. 280 per annum ( by Bindhyabasini cooperatives). The clients of CBHI also vary from almost 400
(minimum) to 19000 ( maximum). The schemes offer different facilities to their clients such as free health services and
essential drugs, free of Doctor's consultation and medical and surgical, maternity care, hospitalization charges, unlimited
free care in all services. Subsidy amount is ranges from Ns. 2500 to Rs. 10,000 per year and total treatment cost is
discounted from 50% to 100%.
Table 3b: CBHI Schemes run by Private Sector and supported organizations
Name of Schemes Year of
initiation
District No. of
Beneficiaries
/Area Cover
Beneficiaries Supported by
1. Primary Health
Care and Resource
Center
1972 Lalitpur NA/R mostly engaged in
diversified
agricultural activities
Primary Health
Care and
Resource Center
2. Bikalpa
Cooperative
2001
Kathmandu NA/U mostly engaged in
diversified
agricultural activities
with technical
support
from Public
Health Concern
Trust Nepal and
financial support
from HIMAL
project
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 11 of 15
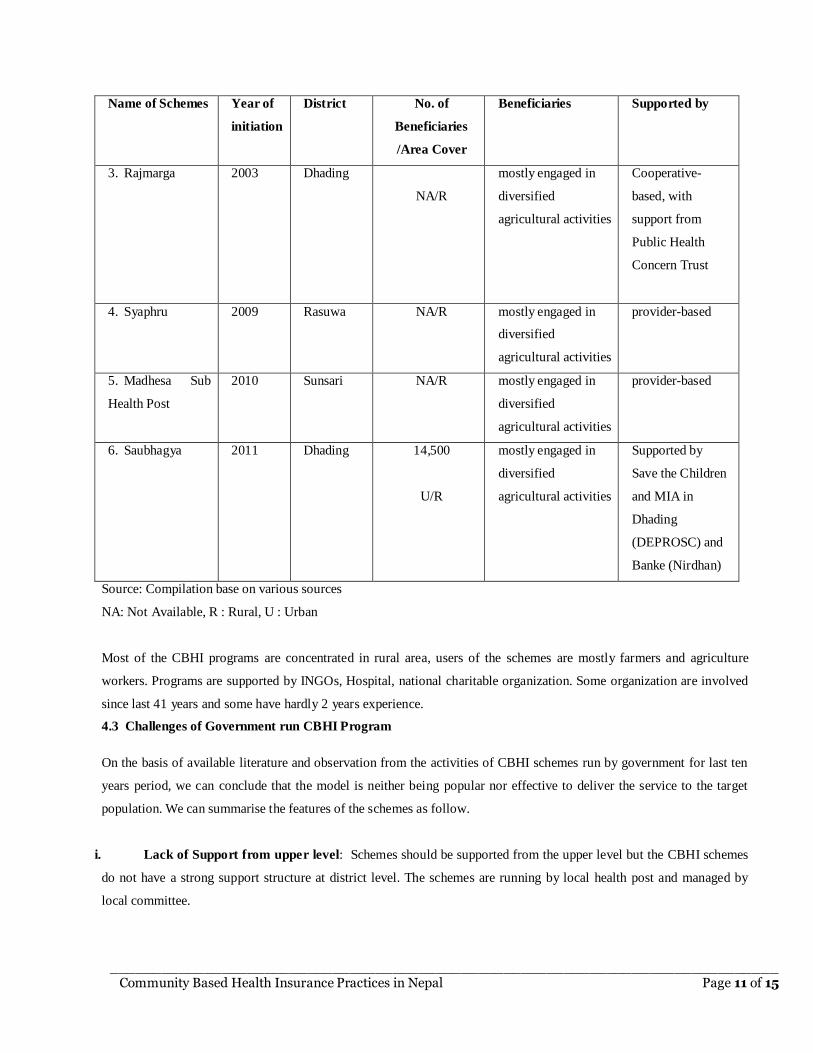
Name of Schemes Year of
initiation
District No. of
Beneficiaries
/Area Cover
Beneficiaries Supported by
3. Rajmarga 2003 Dhading
NA/R
mostly engaged in
diversified
agricultural activities
Cooperative-
based, with
support from
Public Health
Concern Trust
4. Syaphru
2009
Rasuwa NA/R mostly engaged in
diversified
agricultural activities
provider-based
5. Madhesa Sub
Health Post
2010 Sunsari NA/R mostly engaged in
diversified
agricultural activities
provider-based
6. Saubhagya 2011 Dhading 14,500
U/R
mostly engaged in
diversified
agricultural activities
Supported by
Save the Children
and MIA in
Dhading
(DEPROSC) and
Banke (Nirdhan)
Source: Compilation base on various sources
NA: Not Available, R : Rural, U : Urban
Most of the CBHI programs are concentrated in rural area, users of the schemes are mostly farmers and agriculture
workers. Programs are supported by INGOs, Hospital, national charitable organization. Some organization are involved
since last 41 years and some have hardly 2 years experience.
4.3 Challenges of Government run CBHI Program
On the basis of available literature and observation from the activities of CBHI schemes run by government for last ten
years period, we can conclude that the model is neither being popular nor effective to deliver the service to the target
population. We can summarise the features of the schemes as follow.
i. Lack of Support from upper level: Schemes should be supported from the upper level but the CBHI schemes
do not have a strong support structure at district level. The schemes are running by local health post and managed by
local committee.
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 12 of 15
ii. Financial efficiency: Most CBHI schemes do not have any data to monitor their financial viability. They are not
aware of their operating expenses as expenses are born by government. So, the incurred expense ratio (incurred
expenses/earned premium) is very high.
iii. Pro Poor Challenges: Another major question is that micro health program does serve the real poor and vulnerable
class? It is said that program are community-based, but they are governed by government not community. The
premium of these schemes is not determined on the actuarial base and risk is not reinsured. The premium is
subsidized in the same rate to rich and poor which is not justifiable.
iv. Sustainability: These schemes need to regulate by Insurance Board otherwise, there is the question of solvency and
sustainability for long run. Schemes are not reinsured and the adverse selection cases are more than normal cases.
v. Limited Coverage: The population of Nepal is 26.6 million, more than 25 percent are below the poverty line and
almost 83 percent are living in rural area. The schemes are running in very small scale and scaling up is also not
done. The impact of micro health insurance over the country is meaningless.(Economic Survey, 2012; CBS, 2011)
vi. Poor Health Care: The reasons behind such poor health care services can be listed as: limited fund available for the
health care services, lack of commitment of professional to work outside the capital city and corruption,
mismanagement and bureaucratic hurdles. The difficult landscape has also contributed to the poor level of access to
healthcare, with rural areas having little or no form of medical treatment available. The healthcare facilities available
in remote areas, the medical professionals are normally poorly trained (Oxfam, 2008)
5. MICRO HEALTH INSURANCE MODEL
Government capacity to deliver free health care to its citizen largely depends on willingness to offer and capacity to
offer. It is also called the fiscal space of government which means “room in a government’s budget that allows it to
provide resources for a desired purpose without jeopardizing the sustainability of its financial position or the stability of
the economy” (Heller P, 2006).
Sustainable sources of government revenue are tax but the tax base is very narrow. The tax to GDP ratio in 2009/10 was
14.3% (average of OECD was 35%). Government has no priority to Health sector since Health Budget to National
Budget ratio never increased than 7.16%. In this context, existing ongoing universal free health care program, maternity
program and other free targeted health care programs might be affected and difficult to maintain and sustain in coming
years.
Worldwide health insurance models are either out of pocket based or government revenue based or mix of the both. Most
of the developing countries, people cannot afford health insurance. In Nepal, more than 80 percent people living in
village and livelihood of 75 percent people is subsistence agriculture so that they cannot purchase life insurance.
Government has not sufficient fund to finance the 100 percent health expenditure to 100 percent population.
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 13 of 15
We have already four different models of health insurance in practices: 1) Private Health Insurance is offering by
commercial insurers for middle and high income class, 2) Micro health insurance is available to low income group by
private sector but the outreach is very poor; 3) Community Based Health Insurance (CBHI) is recently introduced by
government in limited cluster and 4) Social Health Insurance is available to government and corporate employees. None
of the model is perfect and can give the solution of diverse demographic structure having a different income level, health
status, culture and needs. Mix of the above models may give the best result and serve the need of the target population.
According to the objective of this paper, we discuss on the model of micro health insurance. Government should abide
by some fundamental principles while implementing the health insurance program to the poor and vulnerable group.
Need to focus on vulnerable groups, such as women, poor and elderly people, and people suffering to chronic
diseases who are most likely to be excluded by insurance mechanisms.
Need to increase national budgets as well as portion of health budget by increasing the tax base and proper
utilisation of international development budget.
Gradually increase the government support and subsidy to poor and at the same time decrease the amount of
premium. This could be a more promising and more equitable route to universal access.
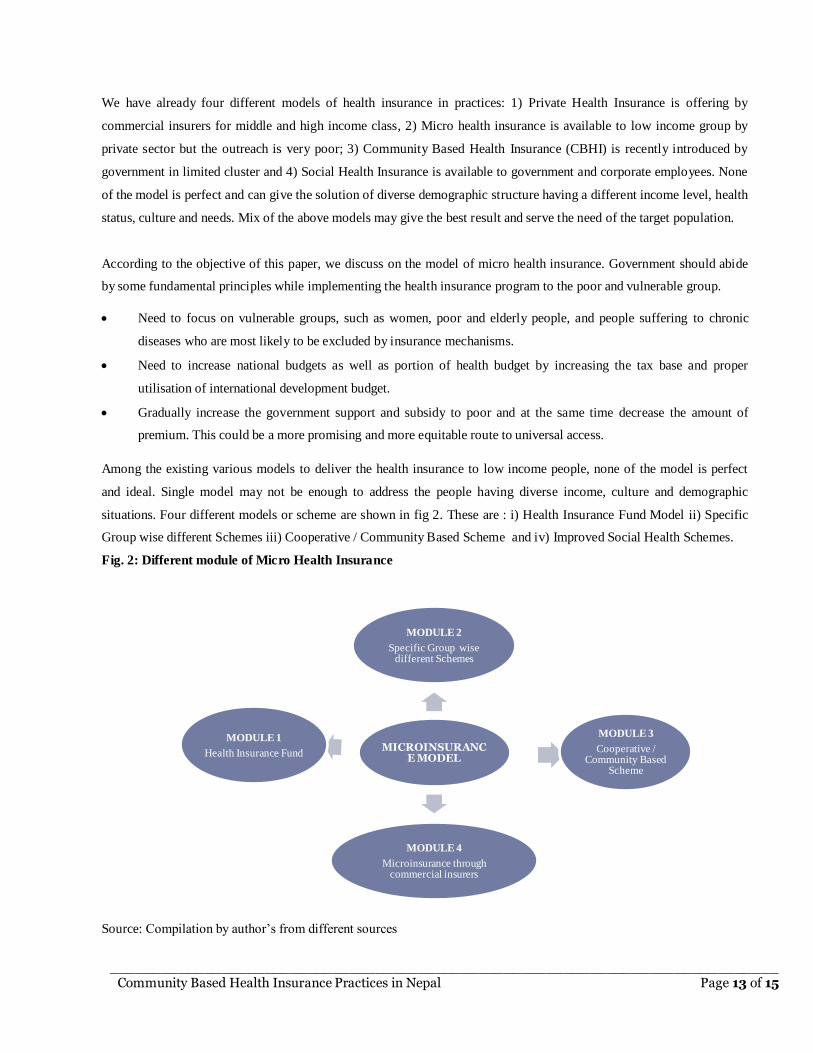
Among the existing various models to deliver the health insurance to low income people, none of the model is perfect
and ideal. Single model may not be enough to address the people having diverse income, culture and demographic
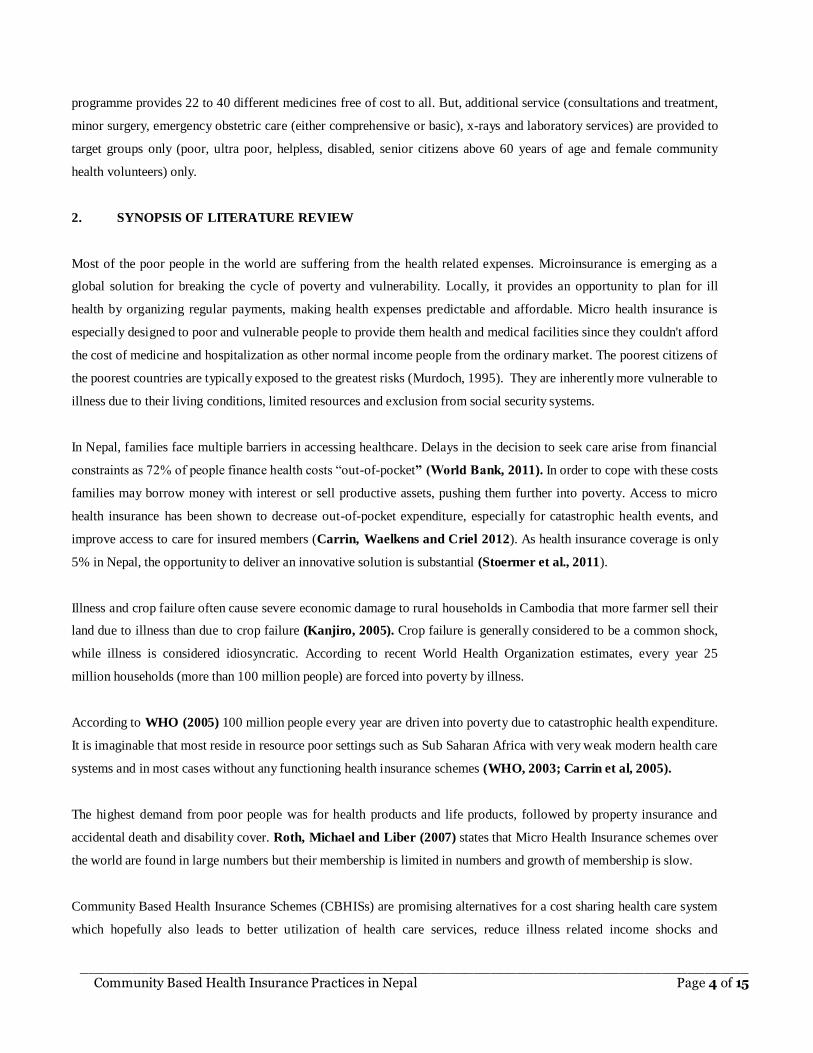
situations. Four different models or scheme are shown in fig 2. These are : i) Health Insurance Fund Model ii) Specific
Group wise different Schemes iii) Cooperative / Community Based Scheme and iv) Improved Social Health Schemes.
Fig. 2: Different module of Micro Health Insurance
Source: Compilation by author’s from different sources
MICROINSURANCE MODEL
MODULE 2
Specific Group wise different Schemes
MODULE 3
Cooperative / Community Based
Scheme
MODULE 4
Microinsurance through commercial insurers
MODULE 1
Health Insurance Fund

______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 14 of 15
The best solution can be Mix Model. In mix model, there is government contribution (tax revenue) and personal
contribution (insurance) for health care financing. This can be implemented through different schemes such as through
separate health insurance fund, through association formed by the people of same profession, forming the cooperatives or
CBHI and microinsurance through commercial insurers where subsidies on premium is provided by the government.
Due to the constraints of the length of the paper, detail of each scheme is not possible to discuss in the same paper. These
four schemes can be lunched parallel way as per the situation.
6. CONCLUDING REMARKS
Community Based Health Insurance Nepal was initiated 30 years back but still it is in infant stage. Government of Nepal
has started some CBHI schemes as a pilot study. Moreover, private sector also has offered health insurance in different
modality but the coverage of insurance to public is very limited. There is urgent need of expansion of such services from
Himalayan to Terai and East to West focusing the poor and marginalized community. Since 2006, government has been
providing the different medicines and treatments to public and special groups of people became the milestone in the
history of health care management in Nepal.
It is obvious that CBHI schemes have positive impact on community through various ways for example, it has increased
consciousness on their health, increases utilization rate, increase service coverage, it has provided health security to the
poor, people are getting timely treatment and they are using drug, quality of care improved, community participation and
ownership increased, built referral system. The schemes bear some weakness also which also better to mention for
further improvement of the schemes. These are: inadequate community mobilization for creating awareness on the
benefit of health insurance, low population coverage, high adverse selection Inadequate and weak Monitoring and
Supervision of DOHS and MOHP, increase the trend of moral hazards, higher administration cost, no linkage with other
income generating activities, inadequate ownership taken by community, additional workload for health staffs,
inefficient fund management and there is no legal backing found.
In conclusion, the analysis of community-based health insurance schemes in Nepal shows that their scope and impact is
very limited. In the view of the evaluation team, community-based health insurance, the way it is currently being
implemented, does not look promising in terms of building a comprehensive, equitable, empowering and sustainable
social health insurance system in Nepal, particularly as CBHI schemes do not have a strong support structure at a higher
level. Even though, players and providers in micro insurance sector are big in numbers, their coverage and impact in
Nepal is not significant. Hardly less than 1 per cent get the micro health insurance facilities over the country. Unless and
until all schemes are run under the umbrella of single organized and systematic institution, the result will not be fruitful
and successful.
______________________________________________________________________________ Community Based Health Insurance Practices in Nepal Page 15 of 15
REFFERENCES:
Ahuja, R. And Jutting J. (2003). Design of incentives in community based health insurance schemes. Indian Council For
Research On International Economic Relations. New Delhi.
Carrin ,G.,Waelkens,M. and Criel B. (2005).Community –based health insurance in developing countries: a study of its
contribution to the performance of health financing systems. Tropical Medicine and International Health, Vol
10,No.8, pp 799-811
CBS (2011). Nepal Population Report- 2012. Central Bureau of Statisitcs. Kathmandu
Ghimire, R. (2012). Principles of Insurance and Risk Management. Asmita Books:Kathmandu.
Heller, P. S. (2005). Understanding Fiscal Space. International Monetary Fund.
HSSP(2012).Review of Community-based Health Insurance Initiatives in Nepal. Health Sector Support Programme
Kenjiro, Y. ( )Why Illness Causes More Serious Economic Damage than Crop Failure in Rural Cambodia
MoF (2012). Economic Survey, 2011/12. Government of Nepal. Kathmandu.
MoHP (2011). Nepal Demographic and Health Survey, 2011
MoHP (2012) Nepal national health accounts, 2006/07–2008/09. Kathmandu: Health Economics and Financing Unit,
Ministry of Health and Population, Government of Nepal
MoHP (2012). Nepal National Health Accounts, 2006/2007 - 2008/2009. Ministry of Health and Population
Murdoch, J. (1995), Income Smoothing and Consumption Smoothing, in: Journal of Economic Perspectives, 9, 103–114.
OECD (2011).Health at a Glance, 2011: OECD Indicators.
Oxfam (2008). Government of Nepal scraps user fees for basic health care [Online]. 2008 [cited 2009 Feb 2]; Available
from: URL:http://www.oxfam.org.uk/applications/blogs/policy/2008/01
Roth, J., Michael J. and Liber D. (2007). The landscape of Microinsurance in the world's 100 poorest countries. The
Microinsurance Centre.
Shimeles, A. (2010). Community Based Health Insurance Schemes in Africa: the Case of Rwanda. AFRICAN
DEVELOPMENT BANK GROUP
Stoermer, M; Sharma, SS; Napierala, C; Silwal, PR (2009) Essential drug procurement and supply management system
in Nepal. Options for improvement. Kathmandu: GIZ/GFA Consulting Group GmbH, Health Sector Support
Programme
Tabor, S. R. (2005). Community-Based Health Insurance and Social Protection Policy. World Bank Institute.
WHO (2003).Drug and Money: Price, Affordability and Cost Containment. Amsterdam: IOS Press,
2003.http://archives.who.int/tbs/global/s4912e.pdf
World Bank (2011) Assessing Fiscal Space for Health in Nepal. Health Nutrition and Population, South Asia Region,
The World Bank.
World Health Organization, Geneva , (2003), “ Community based health insurance schemes in developing countries:
facts problems and perspectives”, Discussion Paper.





























