Embed Size (px)
Citation preview
Chinese Herbal Medicine and Acupuncture for Acne Vulgaris: Efficacy, Patient Preferences and Health-Related Quality of Life
A thesis submitted in fulfilment of the requirements for the degree of
Doctor of Philosophy
Suzi Shu Yi Mansu
MAppSc (Chinese Medicine), RMIT University
BAppSc (Chinese Medicine), RMIT University
BHSc (Acupuncture), Victoria University of Technology
School of Health and Biomedical Sciences
College of Science, Engineering and Health
RMIT University
July 2019
Declaration
I certify that, except where due acknowledgement has been made, the work is that of the author
alone; the work has not been submitted previously, in whole or in part, to qualify for any other
academic award; the content of the thesis is the result of work which has been carried out since
the official commencement date of the approved research program; any editorial work, paid or
unpaid, carried out by a third party is acknowledged; and ethics procedures and guidelines have
been followed.
I acknowledge the support I have received for my research through the provision of an
Australian Government Research Training Program Scholarship.
Suzi Mansu ________________________
Date: 26 July 2019

Acknowledgements
I could not have completed a PhD without the support of many people in my life. Firstly, to
my husband, Michael, and daughter, Olivia, for allowing me to forgo household chores and
many weekends that other families we know would have enjoyed, allowing me to focus on the
PhD. I will make it up to you!
I am indebted to my joint senior supervisors, Dr Meaghan Coyle and A/Prof. Tony Zhang, and
consultant supervisor Distinguished Prof. Charlie Xue, for the opportunity to undertake a PhD
at RMIT University. It’s been quite the journey. Thank you, Dr Coyle, for your patience, your
support and making me pay attention to detail to become a better writer. The encouragement
you have given me has been invaluable. You have helped me to think critically and ask, “so
what?” You have been the little voice in my head as I read, write and present, which is
invaluable to me as a lecturer and future researcher. Thank you, A/Prof. Zhang, for your
patience, your guidance especially in the dreaded statistics and for your support throughout this
journey. Thank you, Distinguished Prof. Xue, for planting the seed of undertaking a PhD and
providing ongoing critical input for my project.
I would like to sincerely thank Dr Kevin Kaiyi Wang for his assistance in the Chinese literature
for the systematic reviews and other Chinese references in the thesis; Dr Haiying Liang for the
assistance in the systematic reviews; Dr Iris Wenyu Zhou for reviewing the systematic review
data; and Dr Brian May for his encyclopaedic knowledge of herbs and advice on herbal
medicines in the herbal medicine systematic review. I acknowledge the help and
encouragement of the staff from the China–Australia International Research Centre of Chinese
medicine of RMIT University and Guangdong Provincial Academy of Chinese Medical

iii
Sciences, and all the staff at the Discipline of Chinese Medicine and the School of Health and
Biomedical Sciences.
Finally, to Mary-Jo for your editing services. Professional editor Mary-Jo O’Rourke AE
provided copyediting and proofreading services according to the university-endorsed national
‘Guidelines for editing research theses’.
iv
Table of Contents
Declaration .................................................................................................................................. i
Acknowledgements .................................................................................................................... ii
List of Figures .......................................................................................................................... xii
List of Tables ......................................................................................................................... xiii
Publications .............................................................................................................................. xv
Abbreviations .......................................................................................................................... xvi
Summary .................................................................................................................................... 1
Background ............................................................................................................................ 1
Objectives ............................................................................................................................... 1
Methods .................................................................................................................................. 2
Results .................................................................................................................................... 3
Conclusions ............................................................................................................................ 4
CHAPTER 1 : Introduction ....................................................................................................... 5
1.1 Background ................................................................................................................. 5
1.2 Rationale for the project .............................................................................................. 6
1.3 Objectives and research questions............................................................................... 7
1.3.1 Objectives ............................................................................................................ 7
1.3.2 Research questions ............................................................................................... 7
1.4 Scope of thesis ............................................................................................................. 8
1.5 Organisation of thesis .................................................................................................. 8
CHAPTER 2 : Acne vulgaris ................................................................................................... 11
Overview .............................................................................................................................. 11
2.1 Introduction ............................................................................................................... 11
2.2 Definition of acne vulgaris ........................................................................................ 11
2.3 Prevalence of acne vulgaris ....................................................................................... 12
2.3.1 Global prevalence and regional differences ....................................................... 12
2.3.2 Age differences .................................................................................................. 12

v
2.3.3 Gender differences ............................................................................................. 13
2.3.4 Geographical differences ................................................................................... 14
2.3.5 Severity and prevalence ..................................................................................... 15
2.4 Impact of acne vulgaris ............................................................................................. 16
2.4.1 Economic impact and burden of disease of acne vulgaris ................................. 16
2.4.2 Health-related quality of life .............................................................................. 17
2.5 Pathophysiology of acne vulgaris ............................................................................. 18
2.6 Risk factors and comorbidities .................................................................................. 20
2.6.1 Risk factors ........................................................................................................ 20
2.6.2 Comorbidities ..................................................................................................... 23
2.7 Diagnosis of acne vulgaris ........................................................................................ 23
2.8 Assessment of acne vulgaris ..................................................................................... 24
2.8.1 Severity classification ........................................................................................ 24
2.8.2 Qualify of life assessment .................................................................................. 25
2.9 Treatment and management of acne vulgaris ............................................................ 29
2.9.1 Pharmacological agents ..................................................................................... 30
2.9.2 Non-pharmacological approaches ...................................................................... 35
2.10 Chapter summary ...................................................................................................... 39
CHAPTER 3 : Chinese medicine for acne vulgaris ................................................................. 40
3.1 Introduction to Chinese medicine ............................................................................. 40
3.2 Chinese medicine definition of acne vulgaris ........................................................... 41
3.3 Aetiology and pathophysiology in Chinese medicine ............................................... 41
3.4 Chinese medicine diagnosis and differentiation compared to Western Medicine .... 45
3.5 Chinese medicine syndrome differentiation .............................................................. 46
3.5.1 Heat in the Lungs and wind-heat stagnating in the Lung meridian ................... 47
3.5.2 Heat in the Stomach ........................................................................................... 47
3.5.3 Heat in the Blood and yin deficiency generating internal heat .......................... 48
3.5.4 Stagnation of qi and Blood and heat stagnating in Liver meridian.................... 48
3.5.5 Imbalance of Thoroughfare (Chong) and Conception (Ren) vessels ................. 49
3.5.6 Dampness-heat stagnating in Stomach and Intestines; dampness-heat stagnating in the Spleen and Stomach; accumulation of dampness-heat ........................................... 50
3.5.7 Damp toxin with Blood stasis and toxic heat and Blood stasis ......................... 50
vi
3.5.8 Blood stasis and binding of phlegm ................................................................... 51
3.5.9 Chinese medicine syndromes in clinical trials ........................................................ 53
3.6 Chinese medicine treatment ...................................................................................... 54
3.6.1 Oral Chinese herbal medicine for acne vulgaris ................................................ 55
3.6.2 Topical Chinese herbal medicine for acne vulgaris ........................................... 59
3.7 Acupuncture for acne vulgaris .................................................................................. 62
3.7.1 Acupuncture from textbooks.............................................................................. 62
3.7.2 Acupuncture from treatment guidelines ............................................................. 65
3.8 Other CM treatment factors for acne......................................................................... 65
3.9 Current evidence of Chinese herbal medicine, acupuncture and related manual therapies treatment for acne vulgaris ................................................................................... 66
3.9.1 Chinese herbal medicine systematic reviews .......................................................... 66
3.9.2 Acupuncture systematic reviews ............................................................................. 68
3.9.3 Limitations of Chinese medicine systematic reviews .............................................. 70
3.10 Chapter summary ...................................................................................................... 70
CHAPTER 4 : Health-related quality of life of people with acne vulgaris ............................. 72
4.1 Introduction ............................................................................................................... 72
4.2 Impact of acne on health-related quality of life ........................................................ 73
4.2.1 Psychological impact ......................................................................................... 73
4.2.2 Emotional impact ............................................................................................... 76
4.2.3 Social impact ...................................................................................................... 77
4.2.4 Comparison of health-related quality of life in people with acne and other medical conditions ............................................................................................................ 78
4.3 Factors predictive of impaired health-related quality of life ..................................... 79
4.4 Quality of life scales used in acne vulgaris research studies..................................... 82
4.4.1 General health-related quality of life scales ....................................................... 82
4.4.2 Dermatology-specific health-related quality of life scales ................................ 87
4.4.3 Acne-specific health-related quality of life scales ............................................. 90
4.5 Health-related quality of life in Chinese medicine acne trials .................................. 94
4.6 Discussion ................................................................................................................. 94
4.7 Chapter summary ...................................................................................................... 97
CHAPTER 5 : Acne quality of life and acceptance of Chinese medicine ............................... 98
vii
5.1 Introduction ............................................................................................................... 98
5.1.1 Complementary and alternative medicine for management of acne ....................... 99
5.1.2 Attitudes to treatment ....................................................................................... 100
5.2 Aims and objectives ..................................................................................................... 101
5.2.1 Aims....................................................................................................................... 101
5.2.2 Objectives .............................................................................................................. 101
5.3 Methods ................................................................................................................... 102
5.3.1 Study design ..................................................................................................... 102
5.3.2 Inclusion and exclusion criteria ............................................................................. 102
5.3.3 Survey sampling............................................................................................... 103
5.3.4 Participant recruitment ..................................................................................... 103
5.3.5 Instrument ........................................................................................................ 105
5.3.6 Ethics................................................................................................................ 107
5.3.7 Data collection, storage and security ............................................................... 108
5.3.8 Data analysis .................................................................................................... 108
5.4 Results ..................................................................................................................... 109
5.4.1 Demographic data .................................................................................................. 110
5.4.2 Acne-Specific Quality of Life Questionnaire ........................................................ 115
5.4.3 Complementary and Alternative Medicine (CAM) Questionnaire for Young Adults ........................................................................................................................................ 119
5.4.4 Preferences for CM Treatment .............................................................................. 127
5.5 Discussion ............................................................................................................... 129
5.6 Limitations of survey .............................................................................................. 137
5.7 Conclusions and implications ................................................................................. 140
CHAPTER 6 : Methods for systematic reviews .................................................................... 141
Overview ............................................................................................................................ 141
6.1 Introduction ............................................................................................................. 141
6.2 Study design ............................................................................................................ 142
6.2.1 Participants ....................................................................................................... 142
6.2.2 Intervention ............................................................................................................ 143
6.2.3 Comparators ..................................................................................................... 145
6.2.4 Outcome measures ........................................................................................... 146
6.2.5 Identification of search terms ........................................................................... 148
viii
6.2.6 Process for study selection ............................................................................... 149
6.2.7 Data extraction ................................................................................................. 149
6.2.8 Statistical and meta-analysis ............................................................................ 150
6.2.9 Quality assessment ........................................................................................... 152
6.3 Chapter summary .................................................................................................... 152
CHAPTER 7 : Systematic review of clinical and pre-clinical evidence of Pi Pa Qing Fei Yin for acne vulgaris ..................................................................................................................... 154
Overview ............................................................................................................................ 154
7.1 Introduction ............................................................................................................. 154
7.2 Rationale for selecting Pi Pa Qing Fei Yin ............................................................. 156
7.3 Aims of the systematic review ................................................................................ 157
7.4 Methods ................................................................................................................... 157
7.4.1 Systematic review methods.............................................................................. 157
7.4.2 Experimental evidence methods ...................................................................... 157
7.5 Results ..................................................................................................................... 158
7.5.1 Clinical evidence .............................................................................................. 158
7.5.2 Grading of Recommendations Assessment, Development and Evaluation analysis 178
7.5.3 Experimental evidence ..................................................................................... 179
7.6 Discussion ............................................................................................................... 184
7.7 PPQFY systematic review conclusions ................................................................... 189
7.8 Implications for future clinical research.................................................................. 189
7.9 Implications for clinical practice ............................................................................. 191
7.10 Chapter summary .................................................................................................... 192
CHAPTER 8 : Systematic review of acupuncture for acne vulgaris ..................................... 193
Overview ............................................................................................................................ 193
8.1 Introduction ............................................................................................................. 193
8.2 Rationale for the acupuncture review...................................................................... 195
8.3 Aims ........................................................................................................................ 195
8.4 Results ..................................................................................................................... 196
8.4.1 Search Results .................................................................................................. 196
8.4.2 Characteristics of studies ................................................................................. 196

ix
8.4.3 Risk of bias ...................................................................................................... 210
8.4.4 Primary outcome: therapeutic effective rate .................................................... 212
8.4.5 Secondary outcomes ........................................................................................ 216
8.5 Discussion ............................................................................................................... 218
8.6 Conclusions ............................................................................................................. 220
8.7 Implications for future research .............................................................................. 221
8.8 Implications for clinical practice ............................................................................. 222
8.9 Chapter summary .................................................................................................... 223
CHAPTER 9 : Pi pa qing fei yin for acne vulgaris: A trial protocol ..................................... 224
Overview ............................................................................................................................ 224
9.1 Introduction ............................................................................................................. 225
9.2 Trial justification ..................................................................................................... 227
9.3 Aims ........................................................................................................................ 228
9.4 Research questions .................................................................................................. 228
9.5 Trial design .............................................................................................................. 229
9.5.1 Participant inclusion and exclusion criteria ..................................................... 229
9.5.2 Participants ............................................................................................................ 230
9.5.3 Intervention ...................................................................................................... 233
9.5.4 Comparator ............................................................................................................ 237
9.5.5 Primary outcome measures .............................................................................. 240
9.5.6 Secondary outcome measures .......................................................................... 241
9.6 Trial procedures............................................................................................................ 248
9.6.1 Recruitment ...................................................................................................... 249
9.6.2 Eligibility screening ......................................................................................... 250
9.6.3 Informed consent ............................................................................................. 251
9.6.4 Baseline assessment ......................................................................................... 251
9.6.5 Sequence generation and allocation concealment............................................ 252
9.6.7 Blinding............................................................................................................ 253
9.6.8 Treatment phase ............................................................................................... 253
9.6.9 Follow-up phase ............................................................................................... 255
9.7 Treatment ................................................................................................................ 255
9.7.1 Pi Pa Qing Fei Yin................................................................................................. 255

x
9.7.2 Dispensing and monitoring .............................................................................. 258
9.7.3 Co-medication data collection method ............................................................ 258
9.8 Data collection and storage ..................................................................................... 259
9.9 Sample size calculations.......................................................................................... 260
9.10 Withdrawals and dropouts ....................................................................................... 261
9.11 Trial adherence and preventing drop-outs ............................................................... 262
9.12 Missing data ............................................................................................................ 263
9.13 Data analysis ........................................................................................................... 263
9.14 Early termination of trial ......................................................................................... 264
9.15 Reimbursements ...................................................................................................... 264
9.16 Reporting ................................................................................................................. 264
9.17 Ethical approval....................................................................................................... 264
9.18 Trial registration ...................................................................................................... 265
9.19 Trial compliance ...................................................................................................... 265
9.20 Discussion ............................................................................................................... 265
9.21 Limitations .............................................................................................................. 268
9.22 Conclusions ............................................................................................................. 269
CHAPTER 10 : Discussion and Conclusions ........................................................................ 270
10.1 Introduction ............................................................................................................. 270
10.2 Project summary ...................................................................................................... 271
10.3 Limitations .............................................................................................................. 278
10.4 Implications for research ......................................................................................... 280
10.4.1 Systematic reviews........................................................................................... 280
10.4.2 Trial designs ........................................................................................................ 282
10.4.3 Outcome measures ........................................................................................... 282
10.5 Implications for practice.......................................................................................... 283
10.5.1 Pi Pa Qing Fei Yin ........................................................................................... 283
10.5.2 Acupuncture and related therapies ................................................................... 284
10.5.3 Health-related quality of life ............................................................................ 285
10.6 Conclusions ............................................................................................................. 285
REFERENCES ...................................................................................................................... 286
APPENDICES ....................................................................................................................... 319
xi
Appendix 1 Oral Chinese herbal medicines formulas and herb ingredients .................. 319
Appendix 2 Topical Chinese herbal medicines formulas and herb ingredients ............. 324
Appendix 3 Impact on HRQoL and instruments used .................................................... 326
Appendix 4 Survey questionnaire................................................................................... 329
Appendix 5 Advertising details for survey ..................................................................... 357
Appendix 6 Permissions for the use of the Acne-QoL survey ....................................... 358
Appendix 7 Permissions for the use of the CAM Questionnaire for Young Adults survey ........................................................................................................................................ 362
Appendix 8 CHEAN ethics approval for survey ............................................................ 364
Appendix 9 CHEAN ethics approval for survey amendment 1 ..................................... 367
Appendix 10 CHEAN ethics approval for survey amendment 2 ................................... 370
Appendix 11 CHEAN ethics approval for survey amendment 3 ................................... 373
Appendix 12 CHEAN ethics approval for survey amendment 4 ................................... 376
Appendix 13 Search terms acupuncture and CHM ........................................................ 379
Appendix 14 Published review “Herbal medicine Eriobotrya japonica formula for acne vulgaris: a systematic review” ........................................................................................ 381
Appendix 15 published review “Evidenced-based complementary and alternative medicine” ........................................................................................................................ 394
Appendix 16 Assessment of Reporting of STRICTA items for acupuncture studies .... 407
Appendix 17 Assessment of P. acnes ............................................................................. 410
Appendix 18 SPIRIT statement ...................................................................................... 411
xii
List of Figures
Figure 3.1 Aetiology and pathogenesis of acne in CM ............................................................ 44
Figure 7.1 Flow chart of study selection PPQFY .................................................................. 159
Figure 7.2 Risk of bias PPQFY ............................................................................................. 174
Figure 7.3 PPQFY versus pharmacotherapy: effective rate................................................... 175
Figure 7.4 Subgroup analysis of PPQFY versus comparators: effective rate ........................ 176
Figure 8.1 Study selection flow chart: acupuncture ............................................................... 197
Figure 8.2 Risk of bias summary: acupuncture ..................................................................... 211
Figure 8.3 Forest plot of TER ≥30 per cent change in symptoms acupuncture ..................... 215
Figure 8.4 Forest plot of TER ≥50 per cent change in symptoms acupuncture ..................... 217
Figure 9.1 Example of pragmatic design for acne (adapted from Buch et al. (409)) ............ 238
Figure 9.2 Sample size calculations using the effect estimated from Fehnel et al. (119) ...... 261
xiii
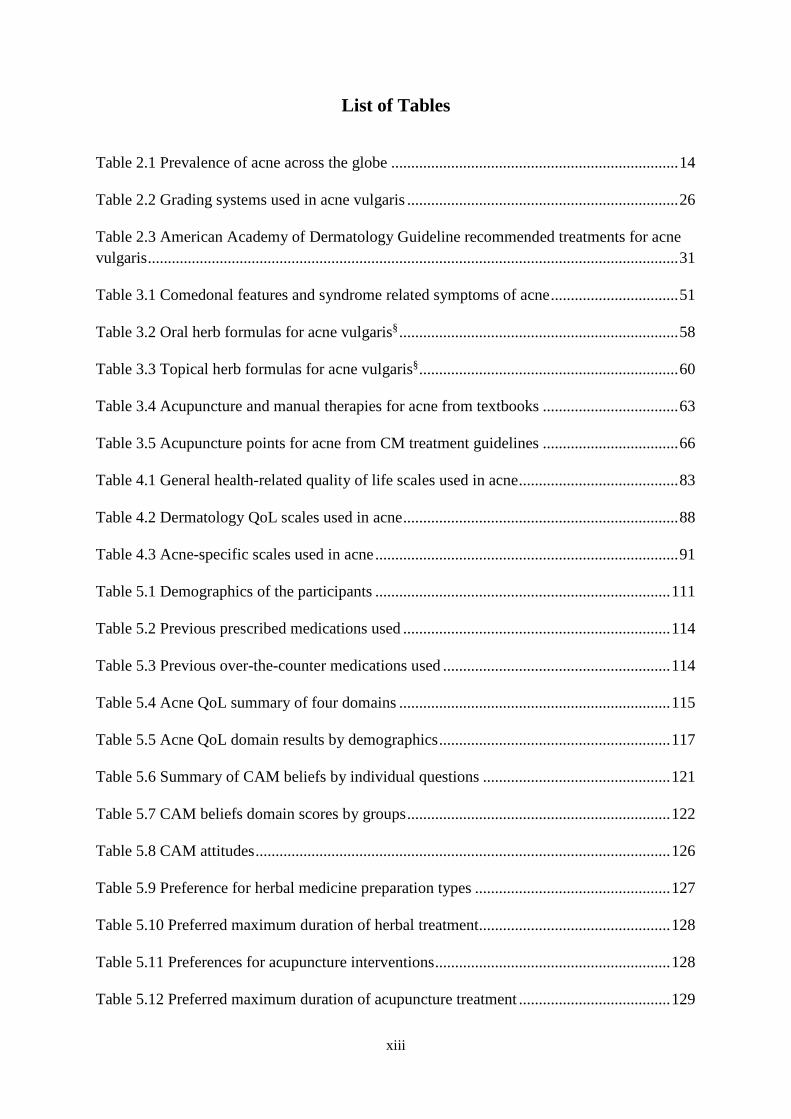
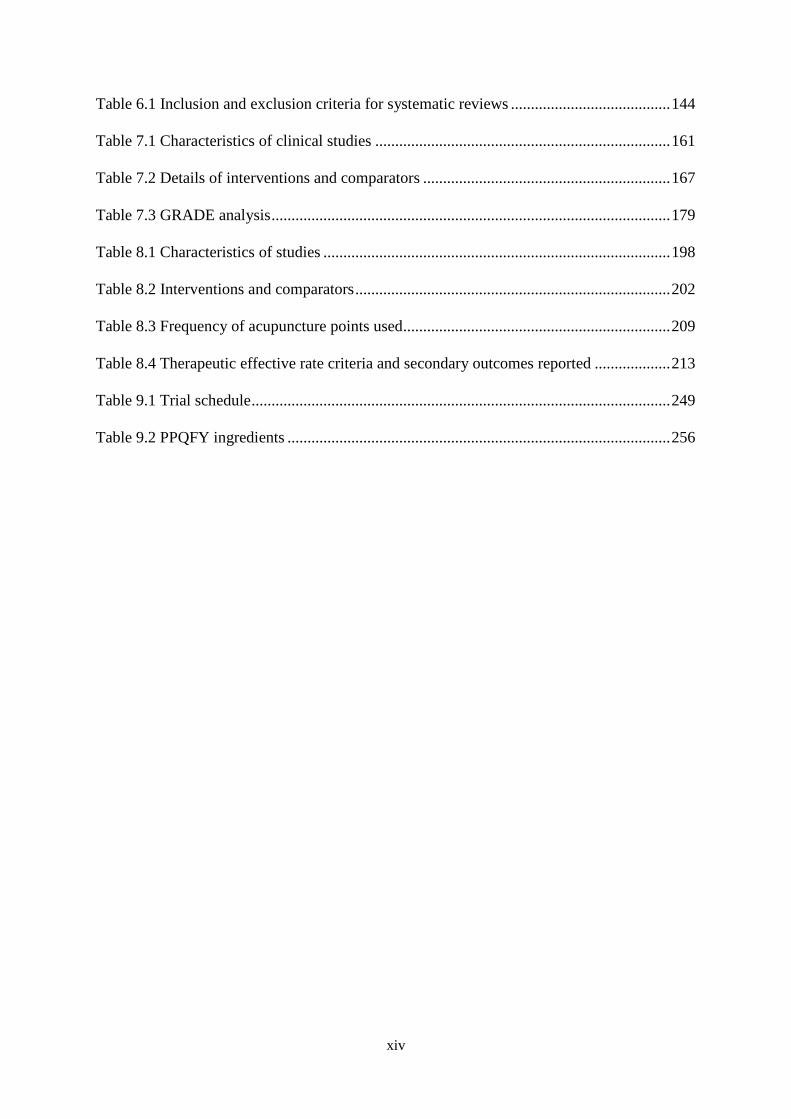
List of Tables
Table 2.1 Prevalence of acne across the globe ........................................................................ 14
Table 2.2 Grading systems used in acne vulgaris .................................................................... 26
Table 2.3 American Academy of Dermatology Guideline recommended treatments for acne vulgaris ..................................................................................................................................... 31
Table 3.1 Comedonal features and syndrome related symptoms of acne ................................ 51
Table 3.2 Oral herb formulas for acne vulgaris§ ...................................................................... 58
Table 3.3 Topical herb formulas for acne vulgaris§ ................................................................. 60
Table 3.4 Acupuncture and manual therapies for acne from textbooks .................................. 63
Table 3.5 Acupuncture points for acne from CM treatment guidelines .................................. 66
Table 4.1 General health-related quality of life scales used in acne ........................................ 83
Table 4.2 Dermatology QoL scales used in acne ..................................................................... 88
Table 4.3 Acne-specific scales used in acne ............................................................................ 91
Table 5.1 Demographics of the participants .......................................................................... 111
Table 5.2 Previous prescribed medications used ................................................................... 114
Table 5.3 Previous over-the-counter medications used ......................................................... 114
Table 5.4 Acne QoL summary of four domains .................................................................... 115
Table 5.5 Acne QoL domain results by demographics .......................................................... 117
Table 5.6 Summary of CAM beliefs by individual questions ............................................... 121
Table 5.7 CAM beliefs domain scores by groups .................................................................. 122
Table 5.8 CAM attitudes ........................................................................................................ 126
Table 5.9 Preference for herbal medicine preparation types ................................................. 127
Table 5.10 Preferred maximum duration of herbal treatment................................................ 128
Table 5.11 Preferences for acupuncture interventions ........................................................... 128
Table 5.12 Preferred maximum duration of acupuncture treatment ...................................... 129
xiv
Table 6.1 Inclusion and exclusion criteria for systematic reviews ........................................ 144
Table 7.1 Characteristics of clinical studies .......................................................................... 161
Table 7.2 Details of interventions and comparators .............................................................. 167
Table 7.3 GRADE analysis .................................................................................................... 179
Table 8.1 Characteristics of studies ....................................................................................... 198
Table 8.2 Interventions and comparators ............................................................................... 202
Table 8.3 Frequency of acupuncture points used ................................................................... 209
Table 8.4 Therapeutic effective rate criteria and secondary outcomes reported ................... 213
Table 9.1 Trial schedule ......................................................................................................... 249
Table 9.2 PPQFY ingredients ................................................................................................ 256

xv
Publications
Thesis-related:
1. Mansu, S. S. Y., Coyle, M., Wang, K., May, B., Zhang, A. L., & Xue, C. C. L. (2018).
Herbal medicine Eriobotrya japonica formula for acne vulgaris: A systematic review.
Journal of Herbal Medicine, 11, 12–23.
2. Mansu, S. S. Y., Liang, H., Parker, S., Coyle, M. E., Wang, K., Zhang, A. L., . . . Xue, C.
C. L. (2018). Acupuncture for acne vulgaris: A systematic review and meta-analysis. Evid
Based Complement Alternat Med, 2018, 4806734. doi:10.1155/2018/4806734.
Conference papers
3. MANSU, Suzi S. Y., COYLE, Meaghan E., WANG, Kaiyi, MAY, Brian, ZHANG,
Anthony L., & XUE, Charlie C. C. L. (2018). Pi Pa Qing Fei Yin for acne vulgaris: A
systematic review. AACMAC, 18–20 May 2018, p. xx (abstract) (RMIT Research Grant).
Additional papers:
4. Wang, K., Coyle, M. E., Mansu, S., Zhang, A. L., & Xue, C. C. (2017). Gentiana scabra
Bunge formula for herpes zoster: Biological actions of key herbs and systematic review of
efficacy and safety. Phytother Res, 31(3), 375–386. doi:10.1002/ptr.5769.

xvi
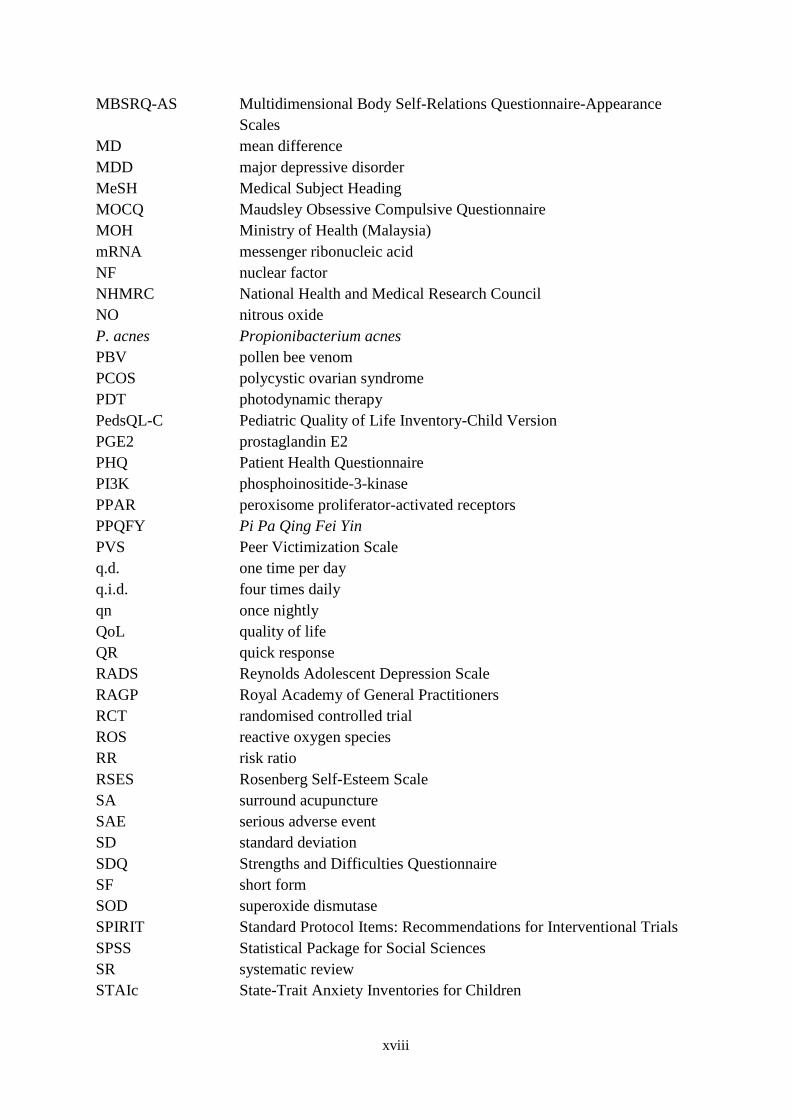
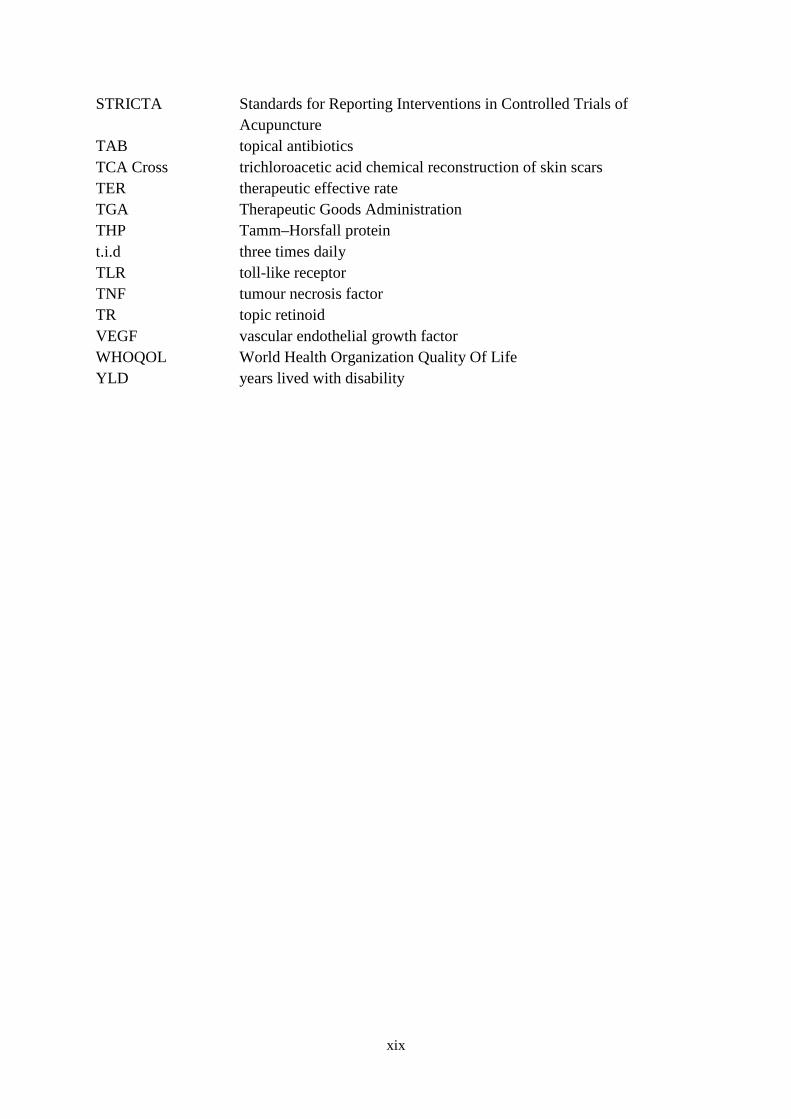
Abbreviations
AA auricular acupressure AAD American Academy of Dermatology Acne-QoL Acne-Specific Quality of Life Questionnaire Acne-QOLI Acne Quality of Life Index ACORN Acne Core Outcome Research Network AD atopic dermatitis ADI Acne Disability Index AE adverse event ANOVA analysis of variance ANZCTR Australian and New Zealand Clinical Trial Register aP adipocyte lipid-binding protein AP auricular pressure APSEA Assessment of the Psychological and Social Effects of Acne AQOL Acne Quality of Life Scale BDI Beck’s Depression Index b.i.d. twice daily BIDQ Body Image Disturbance Questionnaire BMI body mass index BP benzoyl peroxide C control CADI Cardiff Acne Disability Index CAM complementary and alternative medicine CASS Comprehensive Acne Severity Scale CAT catalase CDER Centre for Drug Evaluation and Research CDI Child Depression Inventory CDLQI Children’s Dermatology Life Quality Index CES-D Center for Epidemiologic Studies Depression Scale CHEAN College Human Ethics Advisory Network CHM Chinese herbal medicine CI confidence interval CM Chinese medicine COC combination oral contraceptive pills COMET Core Outcome Measures in Effectiveness Trials CONSORT Consolidated Standard of Reporting Trials COX cyclooxygenase CRF case record form CRP C-reactive protein CSPSCA Capa Social Phobia Scale for Children and Adolescents CSV comma-separated values DHEA dehyroepiandrosterone DHT dihydrotestosterone

xvii
DLQI Dermatology Life Quality Index DNA deoxyribonucleic acid EA electro-acupuncture EADV TF European Academy of Dermatology and Venereology Task Forces ECLA Echelle de Cotation des Lesions d’Acne EGSS Evaluator’s Global Severity Score EQ-5D EuroQoL 5-Dimension Questionnaire ERK extracellular signal-regulated kinase FDA Food and Drug Administration FDLQI Family Dermatology Life Quality Index FNE Fear of Negative Evaluation Scale FoxO1 forkhead box protein O1 GAGS Global Acne Grading System GEA Global Acne Severity Scale GHQ General Health Questionnaire GMP good manufacturing practice GnRH gonadotropin-releasing hormone GPx gutathione peroxidase GRADE Grading of Recommendations, Assessment, Development and
Evaluation HAD Hospital Anxiety and Depression Scale HP haptoglobin HPLC high-performance liquid chromatography HREC Human Research Ethics Committee HRQoL Health Related Quality of Life HSCL Hopkins Symptom Check List HSD hydroxysteroid dehydrogenase I intervention ICD International Classification of Diseases ICH International Conference on Harmonisation of Technical Requirements
for Pharmaceuticals for Human Use IGA Investigator’s Global Assessment IGF insulin growth factor IL interleukin iNOS inducible nitric oxide synthase IP interferon-inducible protein IRF interferon regulatory factor ISGA Investigator’s Static Global Assessment ITT intention-to-treat KC keratinocyte-derived chemokine LPL lipoprotein lipase LPS lipopolysaccharide LSAS Liebowitz Social Anxiety Scale APK mitogen-activated protein kinase
xviii
MBSRQ-AS Multidimensional Body Self-Relations Questionnaire-Appearance Scales
MD mean difference MDD major depressive disorder MeSH Medical Subject Heading MOCQ Maudsley Obsessive Compulsive Questionnaire MOH Ministry of Health (Malaysia) mRNA messenger ribonucleic acid NF nuclear factor NHMRC National Health and Medical Research Council NO nitrous oxide P. acnes Propionibacterium acnes PBV pollen bee venom PCOS polycystic ovarian syndrome PDT photodynamic therapy PedsQL-C Pediatric Quality of Life Inventory-Child Version PGE2 prostaglandin E2 PHQ Patient Health Questionnaire PI3K phosphoinositide-3-kinase PPAR peroxisome proliferator-activated receptors PPQFY Pi Pa Qing Fei Yin PVS Peer Victimization Scale q.d. one time per day q.i.d. four times daily qn once nightly QoL quality of life QR quick response RADS Reynolds Adolescent Depression Scale RAGP Royal Academy of General Practitioners RCT randomised controlled trial ROS reactive oxygen species RR risk ratio RSES Rosenberg Self-Esteem Scale SA surround acupuncture SAE serious adverse event SD standard deviation SDQ Strengths and Difficulties Questionnaire SF short form SOD superoxide dismutase SPIRIT Standard Protocol Items: Recommendations for Interventional Trials SPSS Statistical Package for Social Sciences SR systematic review STAIc State-Trait Anxiety Inventories for Children
xix
STRICTA Standards for Reporting Interventions in Controlled Trials of Acupuncture
TAB topical antibiotics TCA Cross trichloroacetic acid chemical reconstruction of skin scars TER therapeutic effective rate TGA Therapeutic Goods Administration THP Tamm–Horsfall protein t.i.d three times daily TLR toll-like receptor TNF tumour necrosis factor TR topic retinoid VEGF vascular endothelial growth factor WHOQOL World Health Organization Quality Of Life YLD years lived with disability
1
Summary
Background
Acne vulgaris (acne) is a common condition that affects adolescents and adults. Acne
significantly affects people’s health-related quality of life (HRQoL), with reports of low self-
esteem, body image concerns and depression. Acne can be initiated by Propionibacterium
acnes (P. acnes) infection or androgen activity. Conventional medical treatment of acne
includes antibiotics, retinoids, and benzoyl peroxides (BPs). These treatments are not free of
adverse effects.
Chinese medicine (CM) usually attributes mild to moderate acne to heat in the Lung meridian
or damp heat in the Stomach meridian, and severe acne to Blood stasis, toxic heat or binding
of phlegm. CM is used in clinical practice for the treatment of acne; however, there is a lack of
evidence on the clinical benefit and safety of Chinese herbal medicine (CHM) and acupuncture.
While both CM and western medicine (WM) health care paradigms can be used to treat acne,
there are no correlations between CM diagnoses and WM disease states. This PhD describes
mechanisms in both paradigms but does not seek to make correlations between the two.
Objectives
This project aims:
1. To understand the impact of acne on HRQoL and to obtain participant views on CM
treatment options;

2
2. To employ the methods of the Cochrane Handbook for Systematic Reviews of
Interventions to determine the current state of evidence of CHM and acupuncture for
acne; and
3. To develop a randomised controlled trial protocol that evaluates the impact of CHM on
HRQoL in people with acne vulgaris.
Methods
For Objective 1, a review of the current literature on the HRQoL of acne was undertaken with
a focus on the psychological, emotional and social impacts of acne and the predictors of
impairment. There were different general health, dermatology-specific and acne-specific
instruments in the literature to assess the HRQoL of people with acne. The advantages and
disadvantages of each were discussed.
An online survey was conducted to investigate the impact of acne on HRQoL and to obtain
participants’ views on a proposed treatment protocol. Two validated surveys were used.
Questions on patient preferences for CHM and acupuncture treatment duration and frequency
were also included in this survey.
To address Objective 2, two systematic reviews (SRs) were conducted, guided by the methods
of the Cochrane Handbook for Systematic Reviews of Interventions. The first SR evaluated the
CHM formula Pi Pa Qing Fei Yin (PPQFY) and the second evaluated acupuncture and related
modalities. Nine databases were searched for randomised controlled trials (RCTs) for these
two interventions. Following study selection and data extraction, statistical analyses were
conducted using RevMan 5.3. The strength and quality of the evidence were assessed using
Grading of Recommendations Assessment, Development and Evaluation (GRADE).
3
Findings from the HRQoL review and the online survey, and from the two SRs (Objectives 1
and 2) informed the development of the trial protocol, which follows Standard Protocol Items:
Recommendations for Interventional Trials (SPIRIT). A rigorous trial protocol of PPQFY
compared to placebo was designed to address the issues in existing literature and improve the
quality of new data generated from trials.
Results
The review of HRQoL showed that acne had a profound impact on patients’ HRQoL. Anxiety,
depression, and social anxiety were reported to be associated with acne in the literature.
Females, different ethnic groups such as Hispanic, Asian and Maori, and greater severity of
acne tended to correlate with poorer HRQoL. However data on the impact of HRQoL on
Australians was over ten years old. Despite the profound impact of acne on HRQoL reported
in the literature, few CM studies on acne used HRQoL as an outcome measure. Studies that did
use HRQoL had used dermatology-specific rather than acne-specific instruments.
An online survey was conducted using a convenience sampling method, including advertising
in local high schools and through universities in Melbourne. Of the 28 respondents, most were
female, had mild acne and were 15 to 24 years of age. For Acne-QoL, the lowest score was for
the self-perception domain and the highest was for the acne symptoms domain. People with
moderate acne were emotionally affected and worried about their acne. The most commonly
used complementary and alternative medicine (CAM) by participants were alternative medical
systems such as CM, chiropractic and osteopathy. Preferences for CM included topical herbs
and oral pills/tablets and acupuncture; participants preferred four to eight weeks of CHM
treatment and weekly acupuncture treatments.
4
Fifteen trials were included in the SR of PPQFY. PPQFY appeared to have greater benefit
based on change in acne symptoms when compared with pharmacotherapies. None of the
studies used placebo as a control. Twelve trials were included in the SR of acupuncture. There
was no difference between acupuncture and related modalities when compared with
pharmacotherapies. Few studies included in these SRs reported on HRQoL. Both reviews
found methodological design issues such as lack of randomisation and blinding procedures, no
sample size calculations and small sample sizes in the included trials.
The dearth of evidence for the effect of CM on HRQoL and limitations of clinical studies
identified through SRs were addressed with the development of the trial protocol. A
randomised, placebo controlled trial protocol informed by patient preferences was developed
using PPQFY as an example. The proposed participants are 15 years or older with mild to
moderate acne and a CM diagnosis of heat in the Lung. The intervention group will receive
PPQFY capsules while the control group will receive identical placebo capsules. The primary
outcome will be HRQoL using the Acne-QoL. Secondary outcomes include lesion count,
severity grading, and adverse events (AEs).
Conclusions
This project examined the impact of acne on HRQoL, and determined CM treatment
preferences of people with acne. The efficacy and safety of the CHM formula PPQFY and
acupuncture for acne were systematically evaluated. Methodological issues identified in SRs
were addressed in the trial protocol that evaluates the efficacy and safety of PPQFY for patients
with mild to moderate acne. The implementation of the trial protocol may improve treatment
adherence and improve the reliability and quality of future trials.
5
CHAPTER 1 : Introduction
1.1 Background
Acne vulgaris (acne) is a common dermatological condition of the pilosebaceous glands. It
usually begins at adolescence and can affect adults up to 50 years old, while some have adult
onset (1, 2). Acne affects over 9.4 per cent of the world population (3), with adolescents the
most affected (4). Acne affects 79 to 90 per cent of people who live in countries with a high fat
and carbohydrate diet (5). Acne lesions include comedones that range from small pustules and
inflamed papules, to cysts that are located on the face, the upper torso and occasionally the
neck (6). Inflammation can accompany comedones, being more prevalent in adolescents (2).
Genetics, diet, androgen activity and stress have all been implicated in causing acne (7).
Studies have shown that acne can cause psychological, emotional and social issues affecting
health-related quality of life (HRQoL). Low self-esteem, anxiety, depression, body image
concerns and suicidal ideation have been reported in the literature (8-10).
Current conventional treatment therapies such as retinoids are effective for decreasing
inflammation and lesion numbers, but have severe adverse effects (AEs) (11). Retinoids are
teratogenic, and mood changes, depression and suicidal thoughts have been reported (11).
Topical drugs such as topical retinoids and BP can cause skin irritation. The cost of medicines
such as isotretinoin is less than one dollar per day (12). However, due to the severity of the side
effects with these drugs, patients will need to weigh the benefits to their acne condition against
the costs to their general health. Topical and oral antibiotics can become less effective with
long-term use and increase the risk of antibiotic resistance (6). The use of topical antibiotics
(TAB) with BP tends to decrease the risk of resistance, but leaves the skin dry and irritated

6
(13). Combination oral contraceptive pills (COC) are often prescribed to decrease the formation
of androgens in women who also desire contraception, but women taking COC have a higher
risk of thromboembolism (14).
People are increasingly looking for alternatives to conventional medicines when treatments do
not meet their expectations or when AEs from conventional medicines are no longer tolerable
(15-17). Chinese medicine (CM) treatment addresses the root cause of the disease (ben) and
the presenting symptoms (biao), and may be appealing to some people. Chinese herbal
medicine (CHM) and acupuncture have empirically been used for treatment of acne and have
been shown to improve acne in systematic reviews (SR) (18).
1.2 Rationale for the project
The impact of acne on the HRQoL of people in Australia was last evaluated in 1997 (19). More
recent data is needed to improve the understanding of HRQoL of people with acne. An online
survey was conducted to obtain data on the HRQoL of people with acne in Australia. People
with acne are looking to complementary therapies like Chinese medicine as treatments for acne,
yet little is known of their knowledge and beliefs about CAM, and preferences relating to
Chinese medicine treatments. These were assessed as part of the online survey described above.
Knowing patients preferences and values is one part of evidence-based medicine, another part
is knowing the best available evidence. Few SR of CHM and acupuncture for acne have been
published in English. Most of the clinical research on CM treatment of acne has been conducted
in China and very few high-quality methodological trials have been published. There are
limitations to these studies, such as no reporting of the type of acne-grading method and lack
of the use of appropriate controls such as placebo as a control (20), and few studies have
7
examined the burden of acne on HRQoL. The quality of the evidence provided in previous
systematic reviews is limited by the number of databases in their searches and the inclusion
criteria of randomised controlled trials (RCTs) (18, 21). SRs of the two main treatment
techniques of CM practice, CHM and acupuncture, were conducted in this study to inform the
selection of the intervention for the trial protocol. The experimental findings on CHM were
reviewed to gain an understanding of the pathophysiological effect of CHM. Systematic
reviews of CHM and acupuncture highlighted methodological shortcomings. As a case
example of how challenges in Chinese medicine research could be overcome, a trial protocol
for the formula PPQFY was developed. The trial protocol was informed by participants
preferences for CM treatments.
1.3 Objectives and research questions
1.3.1 Objectives
This project aims to evaluate the clinical evidence on CM and acupuncture treatment for acne,
the HRQoL of patients with acne in Australia, and patient preferences in CM treatment for
acne.
Objective 1: To understand the impact of acne on HRQoL and to obtain participant views on
CM treatment options
Objective 2: To use the methods of the Cochrane Handbook for Systematic Reviews of
Interventions to review the efficacy and safety of CHM and acupuncture for acne ; and
Objective 3: To develop a randomised controlled trial protocol that evaluates the impact of
CHM on HRQoL in people with acne vulgaris.
1.3.2 Research questions
1. What impact does acne have on acne patients’ HRQoL?
8
2. What views do people with acne have of CM treatment approaches?
3. What is the current clinical trial evidence of CHM treatment for acne?
4. What is the current clinical trial evidence of acupuncture treatment for acne?
5. Are acupuncture and CHM safe for treating acne?
6. What is the most appropriate trial design for evaluating the effectiveness of CHM to
improve HRQoL of participants?
1.4 Scope of thesis
This project addresses the research questions by evaluating the evidence on CHM treatments
(such as oral and topical CHM) and treatment by acupuncture and related modalities (such as
body acupuncture/acupressure, electro-acupuncture (EA), auricular acupuncture/acupressure,
laser acupuncture and moxibustion). These CM interventions are commonly used in clinical
practice in Australia. Other CM modalities not commonly used in Australia, such as
acupuncture point injection where saline or herbal medicine products are injected into
acupuncture points, were not evaluated.
1.5 Organisation of thesis
Chapter 1 introduces acne and the project. It provides the background and research objectives
and research questions to be answered.
Chapters 2 and 3 provide an overview of acne from both Western and Chinese medicine
perspectives. Chapter 2 describes the definition of acne, prevalence, pathophysiology and
current pharmacological and non-pharmacological management, and summarises the impact of
acne on HRQoL. This chapter highlights the complex pathophysiology and severity assessment
of acne and the complexity of conventional treatment of acne. Chapter 3 summarises the CM
9
understanding of acne. It describes the aetiology, pathogenesis, syndrome differentiation and
CHM and acupuncture treatment of acne. A summary of the clinical evidence is provided and
this highlights the lack of quality evidence on CM for acne.
Chapter 4 provides a comprehensive review of the HRQoL of people with acne. This chapter
reveals the severe psychological, emotional and social impacts that acne can have on people.
It also describes the numerous ways HRQoL can be assessed using general health surveys and
dermatology- and acne-specific HRQoL instruments, and the lack of consensus on the
evaluation of HRQoL of people with acne. It also highlights the lack of HRQoL outcome
measures used in CM trials.
Chapter 5 presents the findings of an online survey that included two validated instruments:
the Acne-Specific Quality of Life Questionnaire (Acne-QoL) and the Complementary and
Alternative Medicine Questionnaire for Young Adults (CAM Questionnaire). The online
survey also determined acne patients’ preferences in CM treatment and these results are
presented in this chapter.
Chapter 6 provides the methods for conducting the SR which are guided by the Cochrane
Handbook for Systematic Reviews of Interventions. The inclusion criteria, database search and
data analysis methods are presented in this chapter.
Chapters 7 and 8 present the findings of two SRs. Chapter 7 systematically reviews the included
RCTs of the CHM formula Pi Pa Qing Fei Yin (PPQFY). Chapter 8 presents the second SR,
on acupuncture and related therapies including body acupuncture, EA, auricular acupuncture,
auricular acupressure (AA) and moxibustion for acne.

10
Chapter 9 uses the clinical evidence from the burden on HRQoL and participant treatment
preferences for CM described in Chapter 5 and findings from the SRs in Chapters 7 and 8, to
design a trial protocol. This chapter proposes a randomised, double-blind, placebo-controlled,
trial using the CHM formula PPQFY as a case example to improve the reliability and quality
of CM trials for the management of acne. It follows the Standard Protocol Items:
Recommendations for Interventional Trials (SPIRIT) guideline.
Chapter 10 summarises the project and discusses the findings of the research. It also provides
a discussion of the study’s limitations and summarises the implications for research and clinical
practice.
Appendices 1 to 18 present the supplementary data discussed in the above chapters.
11
CHAPTER 2 : Acne vulgaris
Overview
This chapter introduces acne vulgaris (acne), its identifying features and the pathogenesis,
diagnosis and treatment. It also describes the prevalence of acne and the impacts on people’s
health-related quality of life (HRQoL).
2.1 Introduction
Acne is a chronic non-life threatening disease that begins around the time of puberty, with the
highest prevalence in people 15 to 17 years of age (22, 23). The condition can continue to affect
adults up to 50 years of age (24), with reports of adult onset acne (acne tarda) increasing (1).
The course of the condition can wax and wane over time (1). It can severely reduce a person’s
quality of life and can lead to anxiety and suicidal thoughts (25, 26). The exact mechanisms of
disease are still being debated (see section 2.5.3 for a description of the pathophysiology of
acne). The main treatment targets include decreasing hyperkeratinisation, inflammation,
androgen activity and infection due to Propionibacterium acnes (P. acnes) (27).
2.2 Definition of acne vulgaris
Acne vulgaris is defined as a chronic inflammatory disease characterised by open and closed
comedones (blackheads and whiteheads, respectively) and inflammatory nodules (cysts),
papules and pustules. Inflammation of sebaceous glands, increased sebum production and
follicular plugging of keratinocytes can cause papules, pustules, nodules or cysts, and non-
inflamed lesions characterised by open or closed comedones (27, 28).

12
Scarring can occur when there is damage to the skin during the healing process of the acne
lesions. Scars are classified into two types. Atrophic scarring is milder and is the result of a
loss of collagen, whereas hypertrophic scarring is more severe as the result of a gain of collagen
which can lead to keloid scars (29).
2.3 Prevalence of acne vulgaris
2.3.1 Global prevalence and regional differences
Acne vulgaris is estimated to affect 9.4 per cent of the world population (3). Large population
studies from different countries have shown variation in acne prevalence. Prevalence
determined by dermatologist examination was 8.1 per cent in China (17,345 people examined)
(30), 3.9 per cent in Germany (of 90,880 people) (31) and 5.4 per cent in Egypt (of 8,008
people) (32). In household surveys, self-reported acne prevalence was found to be lower in
people from northwest Tanzania (0.1 per cent) (33) and Ethiopia (0.35 per cent) (34). There is
no Australia-wide population data on the prevalence of acne. In Victoria, a study of school-
aged children with acne was conducted in 1997 (22). This study found 36.1 per cent of 4- to
18-year-old children in Victorian schools had acne. No acne was reported in indigenous
household surveys of people from Kitavan, Papua New Guinea, and Aché, Paraguay (5). The
authors speculated that diets low in processed Westernised foods and where food was foraged
or grown by the indigenous populations contributed to this finding (5).
2.3.2 Age differences
Studies have shown the prevalence of acne to be higher in adolescents and young adults (2, 4,
30). Up to 85 per cent of 12- to 24-year-olds reported being affected by acne (1), but it may
persist in 64 per cent of adults in their 20s and in 43 per cent in their 30s (4). Prevalence
increases with adolescent age, with 15- to 17-year-olds reporting higher occurrence of acne

13
(22, 23), and relapse of acne is often reported (2). In an online survey of adolescents and young
adults aged 15 to 24 from seven countries in Europe (Belgium, Czech and Slovak Republics,
France, Italy, Poland and Spain), 57.8 per cent self-reported the presence of acne and
prevalence was highest among the 15- to 17-year-olds (35).
2.3.3 Gender differences
Reporting of gender differences in the literature varies considerably. In a study of global
prevalence of skin diseases, 9.8 per cent of males and 9.0 per cent of females reported having
acne (27). Some studies found more females than males reported acne (36, 37), while others
showed no difference between genders (38, 39). Prevalence was higher in females than males
in adolescents between 10 to 12 years old (22). The opposite was seen in older adolescents,
with higher prevalence in males between 16 to 18 years of age (22), although this finding was
not confirmed by Shen et al. (30). Prevalence increased in males as they reached pubertal age
but was higher again in females in the young adult age group aged 19 to 25 years (30). Other
studies reported higher prevalence in males (40-42). Prevalence of acne in adult women has
been reported as 47.3 per cent (43) and 55.0 per cent (2). In a study by Perkins et al. (2), 50.8
per cent of women had had acne since onset in adolescence and 24.8 per cent reported
substantial periods of relapsed acne. One study showed 76 per cent of women presenting with
acne as adults compared to 24 per cent of men (44). About 18 per cent of women had true adult
onset of acne and 37 per cent of women had hyperandrogenicity (44). Most teenage boys will
have acne that disappears by 20 to 25 years of age, but women can have persistent acne up to
40 years of age (45).
14
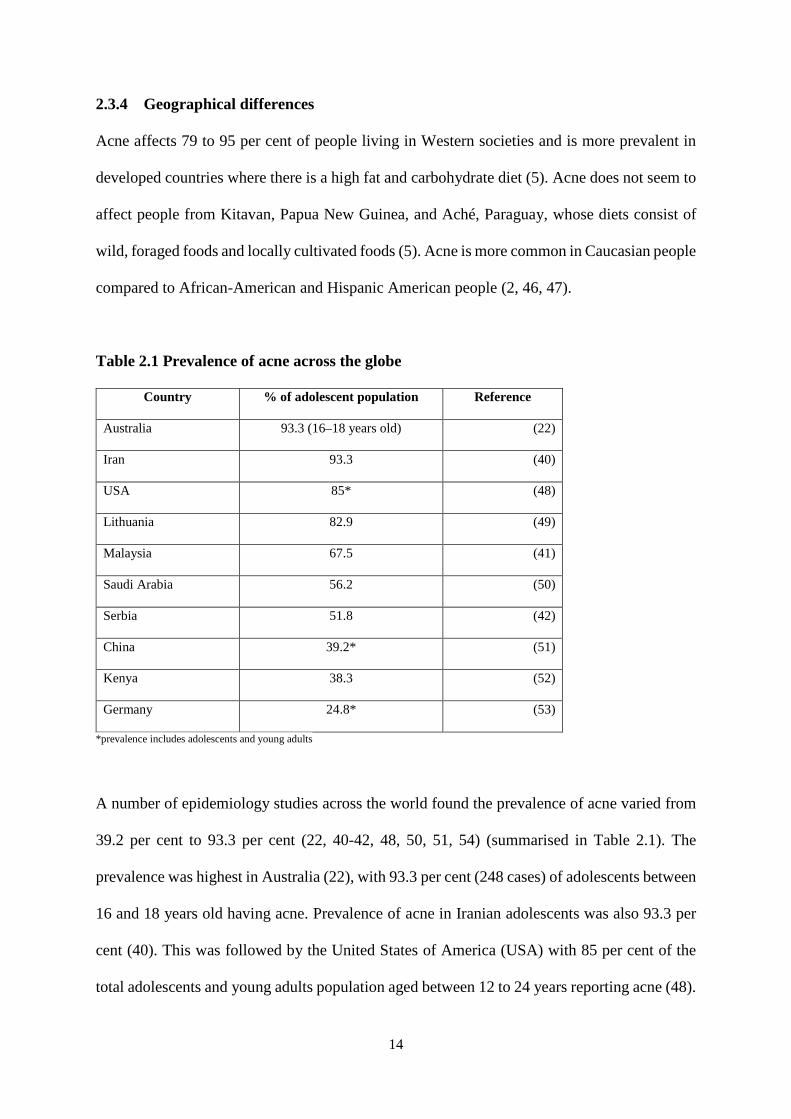
2.3.4 Geographical differences
Acne affects 79 to 95 per cent of people living in Western societies and is more prevalent in
developed countries where there is a high fat and carbohydrate diet (5). Acne does not seem to
affect people from Kitavan, Papua New Guinea, and Aché, Paraguay, whose diets consist of
wild, foraged foods and locally cultivated foods (5). Acne is more common in Caucasian people
compared to African-American and Hispanic American people (2, 46, 47).
Table 2.1 Prevalence of acne across the globe
Country % of adolescent population Reference
Australia 93.3 (16–18 years old) (22)
Iran 93.3 (40)
USA 85* (48)
Lithuania 82.9 (49)
Malaysia 67.5 (41)
Saudi Arabia 56.2 (50)
Serbia 51.8 (42)
China 39.2* (51)
Kenya 38.3 (52)
Germany 24.8* (53)
*prevalence includes adolescents and young adults
A number of epidemiology studies across the world found the prevalence of acne varied from
39.2 per cent to 93.3 per cent (22, 40-42, 48, 50, 51, 54) (summarised in Table 2.1). The
prevalence was highest in Australia (22), with 93.3 per cent (248 cases) of adolescents between
16 and 18 years old having acne. Prevalence of acne in Iranian adolescents was also 93.3 per
cent (40). This was followed by the United States of America (USA) with 85 per cent of the
total adolescents and young adults population aged between 12 to 24 years reporting acne (48).
15
Across Europe, 82.9 per cent of 1,277 Lithuanian schoolchildren had some form of acne (49)
and in a study of 440 Serbian students 51.8 per cent self-reported acne, with prevalence
significantly higher in one city (Uzice, 73.6 per cent) than another (Belgrade, 39.6 per cent)
(42). The authors were unable to determine the reason for this difference. Germany was lower
with 24.8 per cent of adolescents and young adults aged 16 to 20 years from 48,665 employees
of German companies diagnosed with acne (53). In Asia, 67.5 per cent of 409 Malaysian
adolescents between 13 to 18 years old assessed were affected with acne (41) and 56.2 per cent
of 717 Saudi Arabian university students had acne (50). The prevalence in mainland Chinese
adolescents and young adults was lower at 39.2 per cent of 83,008 people from a meta analysis
of 25 epidemiology studies (51).
There is variation in the socioeconomic status of sufferers of acne. In the USA, those with
lower socioeconomic status had higher reports of acne, whereas acne sufferers in Saudi Arabia
reported higher socioeconomic status (55).
2.3.5 Severity and prevalence
Acne is a chronic disease which can last for 10 or more years (56). Severity is commonly
assessed as mild, moderate or severe, although there are several different ways to classify
severity (refer to section 2.7.1 for details). For example, mild and moderate acne is usually
comdeonal acne with fewer lesions and severe acne is higher number of comedones or lesions
are cystic or nodular. A number of cross-sectional and observational studies of primary and
high school students found greater severity of acne in later adolescence (22, 23, 37). Early onset
of acne is a predictor of the severity of acne, as is increasing pubertal age (22, 40, 57). Other
predictors of severity include genetics, where having a mother with acne influenced the severity
of acne (40), and a higher body mass index (BMI) (39, 58).
16
Mild to moderate types of acne with comedonal and inflammatory lesions are seen in
adolescents and is the most common type of acne (2, 22, 30, 38). Older adolescents have been
diagnosed with greater severity of acne (22). In a study of 2,895 female adult acne across three
cities from three countries Los Angeles, United States of America (USA), London, England
and Rome, Italy, there were 57.8 per cent of women with mild acne and 35.6 per cent with
moderate or severe acne had inflammatory acne (2). Clinical acne was seen in women of
African-American and Hispanic origin, rather than Asian or Caucasian origin (59). Patients’
perception of their acne was often worse than assessors’ assessment of their lesions (22, 37,
60).
2.4 Impact of acne vulgaris
2.4.1 Economic impact and burden of disease of acne vulgaris
The global economic impact and burden of disease of acne vulgaris are high. Skin conditions
are ranked fourth overall in years lost due to disability worldwide (3), with 33.7 million years
lived with disability (YLD) collectively for 13 common skin conditions. Acne was only second
to eczema in YLD (61). Acne is the most common condition seen by dermatologists, with 18.1
million visits from 1996 to 2005 and 4.6 million visits to paediatricians for acne in that same
period in the USA alone (62). It is also the most frequent dermatological condition seen in
general practice in the USA (63). In another study on the use of oral and topical retinoids in
mild to moderate acne between 1990 to 1999, 54.2 million medical visits were reported (64).
It is estimated that a total of 12.6 per cent of money spent globally on topical and systemic
treatments for skin conditions was directly related to acne (63). More recent reports suggest 36
per cent of all prescriptions in the USA are related to acne (1) and up to US$3 billion is spent
17
on acne worldwide (4). A United Kingdom (UK) report on the use of antibiotics found 80 per
cent of the 1.2 million topical medicine prescriptions for acne were for topical antibiotics,
dispensed at a cost of £15 million (65). It was also reported that over US$3 billion per year is
lost in the direct and indirect costs of treatment and loss of productivity due to acne (66).
2.4.2 Health-related quality of life
The acne burden of disease is high, with anxiety, depression, body image concerns, poor self-
esteem and suicide ideation and attempts reported in a number of studies (8, 26, 59, 67). More
than 75 per cent of the 215 female respondents of a cross-sectional web-based survey of 15 to
40 years old from the USA “agreed” or “strongly agreed” that acne made them feel less
confident, frustrated, embarrassed and more self-conscious around other people (59). In
another cross-sectional survey in Norway of 3,775 older adolescents aged 18 to 19 years,
suicidal ideation was reported by both girls and boys who suffered substantial acne (self-
reporting of lesions described as “a lot or very much”). The rate of suicidal ideation was twice
as high in girls with substantial acne (25.5 per cent versus 11.9 per cent) and three times as
high in boys (22.6 per cent versus 6.3 per cent) compared to those with less severe acne (9).
These adolescents also reported low attachment to friends, not thriving at school, never having
romantic relationships and never having sexual intercourse (9).
The perception that acne and acne facial scars are negatively viewed by society (68) and
negative attitudes and negative impacts of acne can last for a long time (37). Greater acne
severity does not necessarily translate to worse HRQoL. Some patients with mild acne may
have lower HRQoL compared to those with moderate or severe acne (69, 70).

18
Having acne can prohibit participation in social activities and impair performance at school or
work, or even reduce employment opportunities (25, 59, 71, 72). In a workforce study,
unemployment was higher in those with acne (73). A Turkish study which assessed the HRQoL
of those affected by acne and the impact on their families found that lower HRQoL scores
correlated with higher risk of depression and anxiety (74). Family members were also
negatively affected. Family members who attended their kin’s appointments were asked to fill
out the Family Dermatology Life Quality Index (FDLQI), which assesses social, physical and
psychological wellbeing (75). Acne had a negative impact on family members and the impact
lessened as their kin’s condition improved (74).
2.5 Pathophysiology of acne vulgaris
The mechanisms for the initial development of comedones are not well understood. A number
of factors contribute to acne lesions. These include bacterial infection of P. acnes,
inflammatory mediators on the skin, alteration of the keratinisation of the skin and increased
sebum production with increased androgen activity (27). Mites (Demodex folliculorum) (76,
77) have also been implicated in contributing to this process. Acne was initially reported to be
associated with the bacteria P. acnes (78). However, acne in children younger than 10 years
old is not associated with P. acnes. Increased sebum production and follicular plugging are
seen in this age group (63).
Acne is an inflammatory condition of the pilosebaceous glands of the skin. Comedones and
inflammatory nodules are characteristic lesions in acne vulgaris that result from multifactorial
pathogeneses. Infection from P. acnes and mites (27, 76, 77) stimulates innate and acquired
immune responses and triggers inflammation (79). The initiation of inflammation may be due
to androgens such as testosterone and α-dihydrotestosterone (DHT), with subsequent increase
19
in sebum, enlargement of sebaceous glands and hyperkeratinisation (7, 80). At the onset of
puberty, gonadotropin-releasing hormone (GnRH) release causes dehyroepiandrosterone
(DHEA) to be converted to DHT. Native enzymes in the pilosebaceous gland receptors
forkhead box protein O1 (FoxO1) activate insulin growth factor-1 (IGF-1) to produce
keratinocytes and sebum (60), causing comedone production and oily skin. P. acnes infections
trigger inflammatory responses and lead to tissue damage. This triggers the release of
interleukin-1α (IL-1α), a pro-inflammatory cytokine, from ductal keratinocytes, rupturing the
skin and causing comedones (63, 78, 79). In patients with acne, expression of toll-like receptor
(TLR)-2 by keratinocytes and macrophages and of TLR-4 by keratinocytes is increased,
indicating that innate immunity is active against these microbes (78, 79).
Hyperkeratinisation is caused by altered sebum and lipid content in sebocytes and keratinocytes
(81). Peroxisome proliferator-activated receptors (PPAR) increase human sebum production
(82) and an innate immune response to pathogens such as P. acnes activates adaptive immune
responses from T and B-cells (79). P. acnes stimulates keratinocytes, which produce cytokines,
causing ductal rupture (79). They activate TLR-2 and TLR-4 cytokines. Interleukin-6 (IL-6)
cytokine production caused by lipoxygenase is associated with sebaceous glands and also
increases concomitant PPAR-α and –γ (81). Pro-inflammatory cytokines such as tumour
necrosis factor-α (TNF-α), IL-1, IL-8 and IL-12 are produced with P. acnes infections (79).
Androgens are stimulated at puberty (usually 12 to 14 years of age), increasing sebum
production and the likelihood of acne (83). Sebum production can be stimulated by androgens
and IGF-1. During puberty, the rise of androgens DHT and IGF-1 inhibits FoxO1 regulation (a
receptor that transcribes levels of DHT) and causes excess production of keratinocytes and
sebum. Increase in sebum creates an ideal environment providing nutrients for P. acnes. An
20
increase in bacterial growth and free fatty acids intensifies inflammatory mediators and the
production of extracellular products such as lipases, proteases, hyaluronidases and chemotactic
factors. These inflammatory mediators plug pilosebaceous glands and cause epithelium
overgrowth at the follicular surface to form comedones. The severity of acne is dependent on
the transient IGF-1 levels (60).
Genetics (76), diet (84-86) and neuroendocrine regulatory mechanisms (60) can also contribute
to the occurrence and the severity of acne. Genetics (76) and androgen imbalances can
influence sebaceous gland lipid synthesis (7). Stress may influence acne lesion development.
The level of substance P, which induces neurogenic inflammation in sebaceous glands, was
higher in people with acne compared to healthy controls (87).
2.6 Risk factors and comorbidities
2.6.1 Risk factors
The most common risk factors associated with acne include genetics, diet, cigarette smoking,
alcohol, high BMI and psychological stress. There is an 80 per cent familial risk of persistent
acne in first-degree relatives (88), with reports suggesting 50 to 78 per cent of sufferers of acne
have first-degree relatives who also had acne (22, 37, 38, 40, 89). In an online survey,
participants who reported a history of maternal or paternal acne were associated with increased
probability of having acne (35).
An acne lesion may involve cellular inflammation causing hyperkeratinisation of follicular
ducts (7), with exacerbation due to single or multiple factors such as P. acnes, menstruation,
occupation, sweating, diet and stress. This can lead to cellular inflammation and increase the
number of acne lesions. An online survey of 215 female participants aged 18 to 45 found
21
participants’ acne could be exacerbated around menstrual cycles, or induced by stress,
sweating, cosmetics and humid weather (59).
There are conflicting reports on the implication of diet in acne. A systematic review by Magin
et al. (90) found no effect of diet on the worsening of acne, but a later review suggested the
correlation between diet and acne needed to be revisited (91). Magin et al. (90) looked at diet,
hygiene and sunlight exposure myths associated with acne. They found there were very few
high-quality studies and were unable to provide any recommendations on diet, hygiene or face-
washing. Bowe et al. (91) also reviewed studies on diet, including prospective controlled trials,
retrospective cohort studies, case-control studies and large case series. They found that high
glycaemic load diets may exacerbate acne, while the association between dairy and acne is
weak. They also found a lack of RCTs and suggested further research in this area. Cordain and
colleagues (5) found adolescents and young adult Kitavan Islanders of Papua New Guinea and
Ache hunter gatherers of Paraguay had no incidences of acne, hypothesised to be related to a
diet consisting of wild, foraged and locally cultivated foods. They also suggested high
glycaemic load can lead to hyperinsulinaemia and subsequent endocrine cascade causing high
IGF-1 that can mediate androgen activity as a pathogenesis pathway to acne. One small
randomised controlled study of 43 participants evaluating the effect of low glycaemic index
(GI) food supported this theory. The study compared a low GI diet to a carbohydrate dense diet
in 43 adolescent boys and young adult males 15 to 25 years old. The study found a greater
decrease in total lesion count after 12 weeks in the low GI compared to the carbohydrate dense
group. Insulin sensitivity was improved, and weight loss was also noted in low GI group (86).
Chocolate and other high-sugar foods were associated with acne in studies from Korea and
France (92, 93). Higher milk consumption increased risk of acne in another study in Italy (39).
22
In two studies on milk consumption by 6,094 girls and 4,273 boys (84, 85), total milk intake
was associated with acne in girls (84) and skim milk intake with acne in boys (85). An online
survey of 6,063 young people in Europe found the consumption of chocolate was associated
with an increased probability of having acne (35). In a small Australian RCT, 23 participants
who consumed a low-glycaemic, low-fat diet successfully decreased acne lesions and severity
(86). In Korea, 36.2 per cent of 693 children aged 7 to 12 years had acne, and acne was
associated with obesity (BMI greater than 25 kg/m2) at age 18 (92). Another study from Italy
found a lower BMI reduced the risk of acne (39).
Cigarette smoke contains arachidonic acid and polycyclic aromatic hydrocarbons which induce
phospholipase A2-dependent inflammatory pathways that may lead to acne (63). Cigarette
smoking and alcohol consumption were found to be associated with acne in a study in Korean
students (92). A German study found acne prevalence was significantly higher in active
smokers (54) while two other studies, one in Italy and one in France, found no such association
with smoking (39). Smoking more than 10 cigarettes per day was highly associated with no
acne (93).
Psychological stress is associated with inducing or worsening acne. One study investigating a
correlation between stress and acne surveyed 144 female medical students in their sixth year
and found a high correlation between acne severity and stress (94). Acne severity was graded
and stress levels determined using the Perceived Stress Scale (PSS) questionnaire. They found
higher acne severity in people with higher PSS scores. In a cross-sectional study conducted in
3,778 adolescents aged 18 to 19 years old in Norway, the study found that mental distress
increased when the severity of acne increased (9).
23
2.6.2 Comorbidities
Acne vulgaris can present in isolation or may be associated with conditions such as polycystic
ovaries and polycystic ovarian syndrome (PCOS). PCOS is a common endocrine condition that
presents with oligoanovulation and hyperandrogenism. Hyperandrogenism is a result of
increased insulin levels in the body stimulating ovarian steroidogenesis and increasing the
sensitivity of pituitary gonadotropes and GnRH (95).
Severe acne is associated with sinopulmonary, gastrointestinal and psychological conditions.
Psychological comorbidities included anxiety, depression, migraines, attention deficit
disorder/attention deficit hyperactivity disorder and insomnia (96). In a study by Silverberg
and Silverberg (96), sinus infection, sore throats from causes other than streptococcal infection,
asthma and respiratory allergies such as hayfever were found to be associated with severe acne.
Acne was also found to be associated with reflux/heartburn, abdominal pain, nausea/vomiting
and digestive allergies (excluding diarrhoea and constipation) (96).
2.7 Diagnosis of acne vulgaris
Diagnosis of acne is based on visual observation (13) and it can be classified as acne vulgaris,
conglobata varioliformis, tropical, acne excoriee des jeunes filles (acne that has been
exacerbated by picking, pressing or squeezing) and unspecified acne (97). Other classifications
include infantile acne due to maternal androgens stimulating sebaceous activity, mechanical
acne due to repeated picking or rubbing, tumours such as ovarian tumours that increase
androgen secretion, polycystic ovaries that increase circulating androgens and drug-induced
acne (83). Acneiform drug eruptions can be stimulated by corticosteroids, anabolic steroids,
isoniazid, lithium carbonate and phenytoin, chemical irritants such as oils and cosmetics, and
environmental exposure to dioxins or halogenate phenolic compounds (97). Differentiation of

24
acne vulgaris excludes rosacea and endocrine-related syndromes such as PCOS. Clinical
classifications of acne lesion types are recommended. These include comedonal acne, mild–
moderate papulopustular acne, severe papulopustular acne or moderate nodular acne, and
severe nodular or conglobate acne (28). Diagnosis and differentiation of acne in CM is
discussed in Chapter 3.
2.8 Assessment of acne vulgaris
2.8.1 Severity classification
Acne is graded numerically or by severity, which guides treatment. There is no consensus on
the grading system, with 25 acne-severity grading systems being identified in the literature
(98). Some tools have been developed for research and others for the clinical setting. The tools
developed for research can be complicated and time-consuming, and therefore may not be
appropriate during a short clinical interview (99). There has been a suggestion that lesion count
is superior to grading as it is more objective (100).
The earliest clinical grading system was proposed by Pillsbury in 1956 (101) and estimated the
number and type of lesions and overall involvement (area). Others have used variations of this
system, including a four-point grading system (102), a six-point grading system (103) and a
five-point reference that also includes a comparison with photographs (104, 105). Attempts
have been made to provide a universal scale combining both lesion count and severity grading
that is suitable for research. The Global Acne Grading System (GAGS) (106) is an ordinal scale
used for lesion count and severity for the face, chest and back. The Investigator’s Global
Assessment (IGA), also known as the Investigator’s Static Global Assessment (ISGA) and the
Evaluator’s Global Severity Score (EGSS), is commonly used (98) and is another ordinal
overall grading scale that assesses severity grade based on the dominant lesions and extent of
25
inflammation. The IGA was used in up to 33 per cent of clinical trials published up to 2011
(98) and is the preferred scale used in guidelines for drug development by the Center for Drug
Evaluation and Research (107). Tan et al. (108) modified the IGA to develop the
Comprehensive Acne Severity Scale (CASS), which includes photographic grading.
Two photographic grading scales have also been developed. The Leeds (104) and Leeds
Revised Acne Grading systems (109) are comprised of 15 facial grades, 3 for comedones and
8 for chest and back. It also includes photographic standards. The Echelle de Cotation des
Lesions d’Acne (Acne Lesion Score Scale, ECLA) developed by Dreno and colleagues (110)
for clinical practice takes two minutes to complete. A scale from 0 (absent) to 5 (very severe)
is used. The Global Acne Severity Scale (GEA Scale) was also developed by Dreno and
colleagues for European patients in 2011 (111). A scale from 1 to 5 is used to categorise the
severity of juvenile facial acne. A summary of these grading systems can be found in Table
2.2.
2.8.2 Qualify of life assessment
Various tools are available to assess the QoL of patients with acne. These include general
wellbeing instruments such as the Short Form-36 (SF-36) (112) and Patient Health
Questionnaire-4 (PHQ-4) (113); dermatology QoL instruments such as the Dermatology Life
Quality Index (DLQI) (114), Skindex-16 (115) and Skindex-29 (100, 116, 117); and disease-
specific instruments such as the Acne Quality of Life Index (Acne-QOLI) (118), Acne-Specific
Quality of Life Questionnaire (Acne-QoL) (119-121), Acne Disability Index (ADI) (70),
Cardiff Acne Disability Index (CADI) (122) and Acne Quality of Life Scale (AQOL) (123).
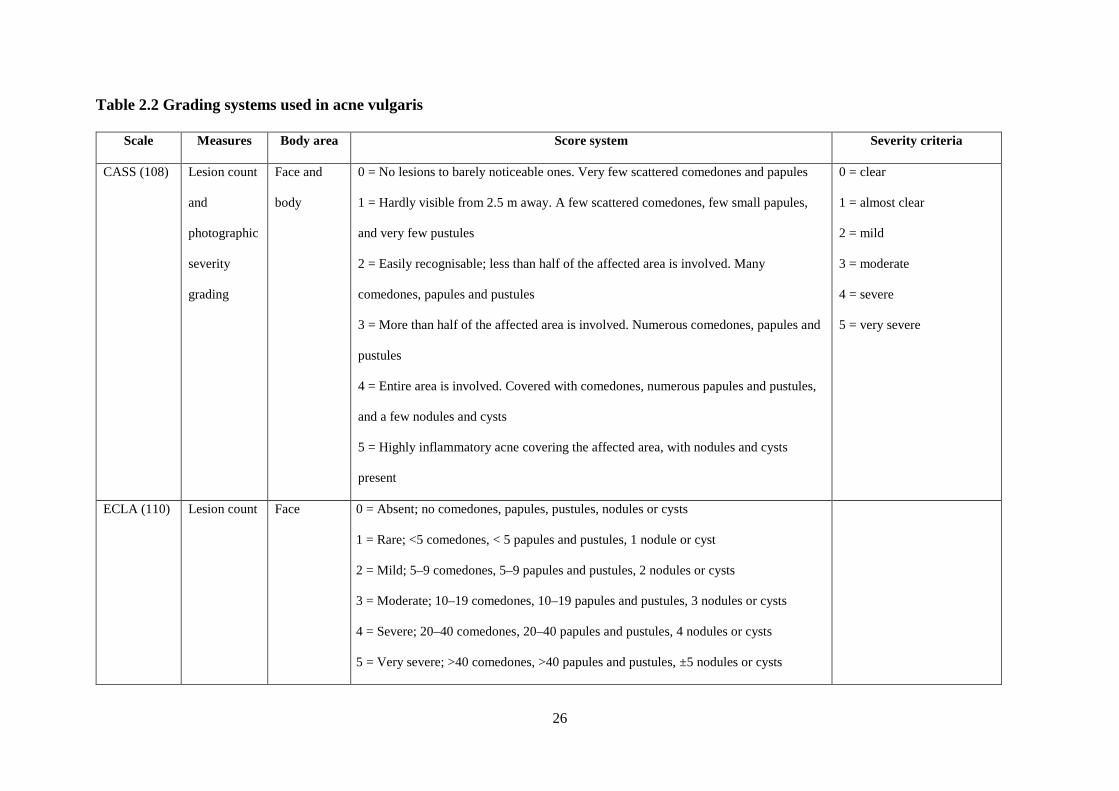
26
Table 2.2 Grading systems used in acne vulgaris
Scale Measures Body area Score system Severity criteria
CASS (108) Lesion count
and
photographic
severity
grading
Face and
body
0 = No lesions to barely noticeable ones. Very few scattered comedones and papules
1 = Hardly visible from 2.5 m away. A few scattered comedones, few small papules,
and very few pustules
2 = Easily recognisable; less than half of the affected area is involved. Many
comedones, papules and pustules
3 = More than half of the affected area is involved. Numerous comedones, papules and
pustules
4 = Entire area is involved. Covered with comedones, numerous papules and pustules,
and a few nodules and cysts
5 = Highly inflammatory acne covering the affected area, with nodules and cysts
present
0 = clear
1 = almost clear
2 = mild
3 = moderate
4 = severe
5 = very severe
ECLA (110) Lesion count Face 0 = Absent; no comedones, papules, pustules, nodules or cysts
1 = Rare; <5 comedones, < 5 papules and pustules, 1 nodule or cyst
2 = Mild; 5–9 comedones, 5–9 papules and pustules, 2 nodules or cysts
3 = Moderate; 10–19 comedones, 10–19 papules and pustules, 3 nodules or cysts
4 = Severe; 20–40 comedones, 20–40 papules and pustules, 4 nodules or cysts
5 = Very severe; >40 comedones, >40 papules and pustules, ±5 nodules or cysts
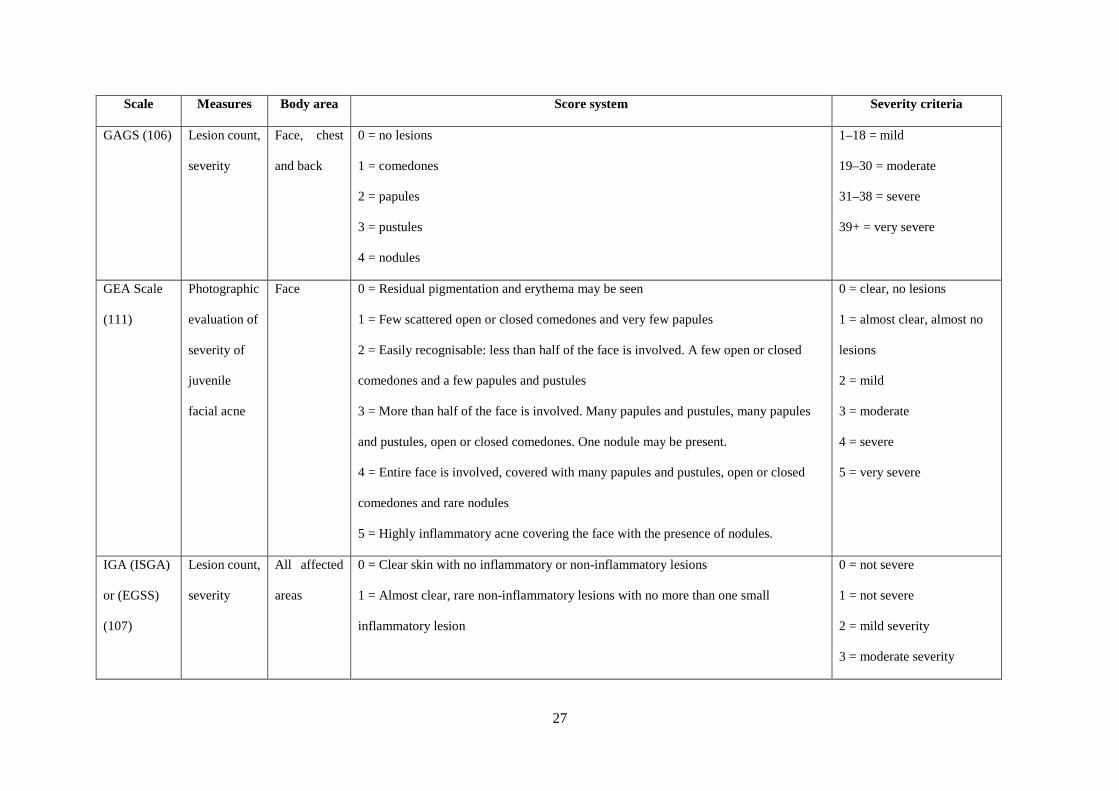
27
Scale Measures Body area Score system Severity criteria
GAGS (106) Lesion count,
severity
Face, chest
and back
0 = no lesions
1 = comedones
2 = papules
3 = pustules
4 = nodules
1–18 = mild
19–30 = moderate
31–38 = severe
39+ = very severe
GEA Scale
(111)
Photographic
evaluation of
severity of
juvenile
facial acne
Face 0 = Residual pigmentation and erythema may be seen
1 = Few scattered open or closed comedones and very few papules
2 = Easily recognisable: less than half of the face is involved. A few open or closed
comedones and a few papules and pustules
3 = More than half of the face is involved. Many papules and pustules, many papules
and pustules, open or closed comedones. One nodule may be present.
4 = Entire face is involved, covered with many papules and pustules, open or closed
comedones and rare nodules
5 = Highly inflammatory acne covering the face with the presence of nodules.
0 = clear, no lesions
1 = almost clear, almost no
lesions
2 = mild
3 = moderate
4 = severe
5 = very severe
IGA (ISGA)
or (EGSS)
(107)
Lesion count,
severity
All affected
areas
0 = Clear skin with no inflammatory or non-inflammatory lesions
1 = Almost clear, rare non-inflammatory lesions with no more than one small
inflammatory lesion
0 = not severe
1 = not severe
2 = mild severity
3 = moderate severity
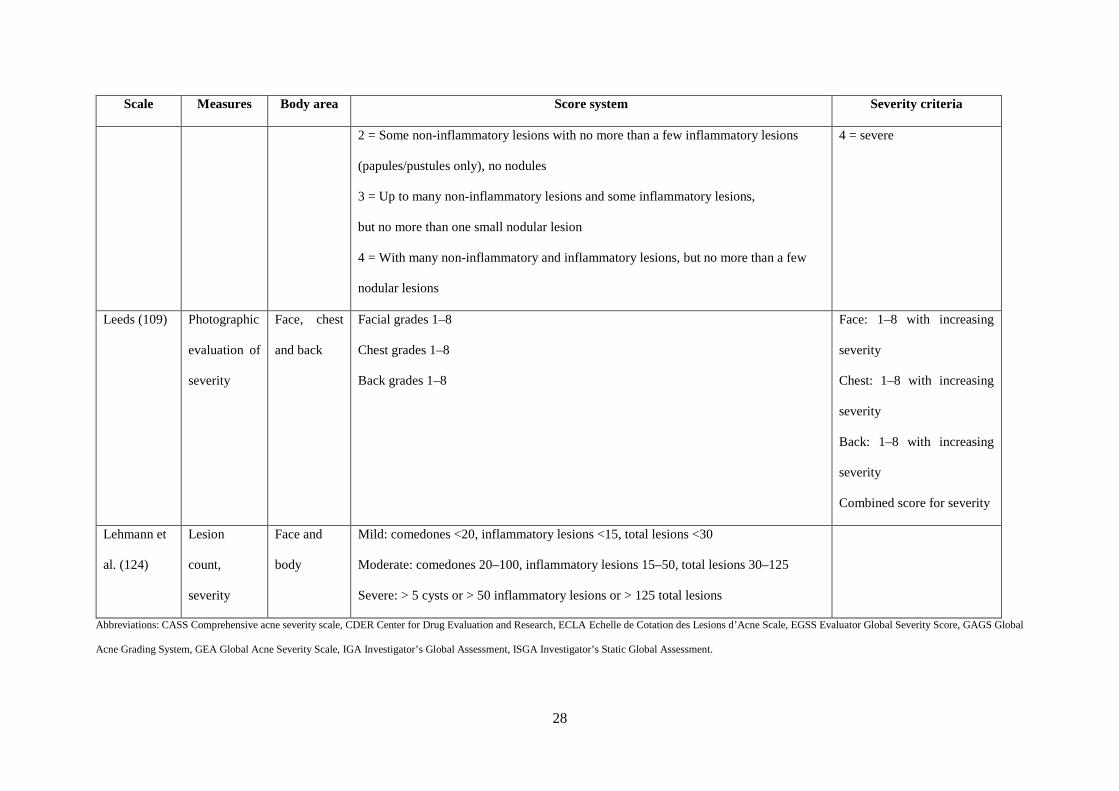
28
Scale Measures Body area Score system Severity criteria
2 = Some non-inflammatory lesions with no more than a few inflammatory lesions
(papules/pustules only), no nodules
3 = Up to many non-inflammatory lesions and some inflammatory lesions,
but no more than one small nodular lesion
4 = With many non-inflammatory and inflammatory lesions, but no more than a few
nodular lesions
4 = severe
Leeds (109) Photographic
evaluation of
severity
Face, chest
and back
Facial grades 1–8
Chest grades 1–8
Back grades 1–8
Face: 1–8 with increasing
severity
Chest: 1–8 with increasing
severity
Back: 1–8 with increasing
severity
Combined score for severity
Lehmann et
al. (124)
Lesion
count,
severity
Face and
body
Mild: comedones <20, inflammatory lesions <15, total lesions <30
Moderate: comedones 20–100, inflammatory lesions 15–50, total lesions 30–125
Severe: > 5 cysts or > 50 inflammatory lesions or > 125 total lesions
Abbreviations: CASS Comprehensive acne severity scale, CDER Center for Drug Evaluation and Research, ECLA Echelle de Cotation des Lesions d’Acne Scale, EGSS Evaluator Global Severity Score, GAGS Global
Acne Grading System, GEA Global Acne Severity Scale, IGA Investigator’s Global Assessment, ISGA Investigator’s Static Global Assessment.

29
Both the Acne-QOLI (118) and the Acne-QoL (119-121) tools have been validated. The Acne-
QoL is a 21-item tool that examines four domains: self-perception, role-emotional, role-social and
acne symptoms. The Acne-QOLI is a 24-item instrument with validated content but the tool itself
is yet to be validated. There is no published consensus guideline on outcome measures for acne,
but there are efforts to gain consensus (99).
2.9 Treatment and management of acne vulgaris
Treatment guidelines published by the American Academy of Dermatology (28), the Royal
Australian College of General Practitioners (125), the Malaysian Ministry of Health with the
Dermatological Society of Malaysia and Academy of Medicine Malaysia (126) and the European
Academy of Dermatology and Venereology (127, 128) all published similar management
strategies for acne across their guidelines. There were four recommended approaches to treatment
including decreasing hyperkeratinisation, microbial colonisation of P. acnes and sebum
production, and inhibiting inflammation (28). Treatment of mild acne includes education about
skin hygiene and debunking myths (13, 125). Topical and oral retinoids are prescribed for
moderate to severe acne and topical BP is combined with TAB to decrease antibiotic resistance
with long-term use (129).
Current conventional treatment therapies are effective but can have adverse effects (AEs).
Retinoids are teratogenic and oral use is associated with mood changes, depression and suicidal
thoughts (11). Topical retinoids and BP can leave the skin dry and cause skin irritation (13). The
effectiveness of topical and oral antibiotics can decrease over time and increase the risk of
antibiotic resistance (129).
30
2.9.1 Pharmacological agents
Topical treatment is generally recommended for eight to twelve weeks (28). Numerous clinical
practice guidelines for acne vulgaris have been published for adults and children. The most recent
publication was by the American Academy of Dermatology (AAD) in 2016, the Guidelines of the
Care of the Management of Acne Vulgaris (28). In Australia, the Acne Best Practice was published
in 2010 by the Royal Australian College of General Practitioners (RACGP) (125). In Europe, the
European Evidence-based (S3) Guidelines for the Treatment of Acne was published in 2012 (127)
with an update in 2016 (130) and in the UK the National Institute for Health and Care Excellence
published clinical knowledge summaries for acne vulgaris in 2014 (131) with an update expected
in 2021. There is one clinical guideline for paediatric acne, Evidence-based Recommendations for
the Diagnosis and Treatment of Pediatric Acne in 2013 by the American Acne and Rosacea
Society (13). The Malaysian Ministry of Health in conjunction with the Dermatological Society of
Malaysia and the Academy of Medicine Malaysia published the Clinical Practice Guidelines
Management of Acne in 2012 (126).
Zaenglein and colleagues (28) gave a simple and clear treatment algorithm for the treatment of
acne (summarised in Table 2.3). This includes first-line treatment for mild, moderate and severe
acne and alternative treatments. For mild acne, topical application of BP or topical retinoid (TR)
alone, or combinations of BP with TAB, BP with TR or BP with TR and TAB are recommended.
For moderate acne, oral antibiotics (OAB) plus topical combination therapy are recommended if
topical treatment alone is ineffective. In severe acne, OAB with topical combination therapy are
recommended. If this is ineffective, oral isotretinoin is recommended.

31
Table 2.3 American Academy of Dermatology Guideline recommended treatments for acne
vulgaris
Mild Moderate Severe
• BP or TR
• BP & TAB
• BP & TR
• BP & TR & TAB
• BP & TAB or TR & BP &
TAB
• OAB plus TR & BP
• OAB plus TR & BP & TAB
• OAB plus topical
combinations
• TR & BP or TR & BP & TAB
• Oral isotretinoin
Abbreviations: BP benzoyl peroxide, TAB topical antibiotics, TR topical retinoid, OAB oral antibiotics (summarised from Zaenglein et al. 2016
(28))
OAB should always be used with topical therapy, with a break-in treatment of two to four weeks
where topical treatment only is used, to reduce the chance of antibiotic resistance. Isotretinoin is
recommended for treatment for up to six months. For moderate acne, a break in treatment can
cause relapse so the full course is recommended.
The AAD Guideline recommended treatments for children and adults are similar, with the
exception that oral tetracycline derivatives (tetracycline, doxycycline and minocycline) are not
recommended for children younger than 8 years old (28). Most of the topical therapies are also not
recommended for children under 10 to 12 years of age and some, such as tetracycline, are not
recommended for children under 8 years of age. Topical and oral retinoids are recommended in
adolescent and younger children if the acne is severe and there is risk of scarring (13). Although
Eichenfield et al. (13) do not indicate an age limit, they suggest careful monitoring of potential
side effects and toxicities, extensive counselling and avoidance during pregnancy.

32
Combination oral contraceptive pills (COC) are recommended for females with no history of
cardiovascular disease. Treatment is long term and treatment response is usually seen after the
third cycle. Second-line treatment of acne vulgaris includes COC for females of any age with
inflammatory lesions (13, 14) to suppress ovarian androgen activity and prevent sebum plugging
in sebaceous glands. COC should not be used in adolescents within two years of first starting
menses and in young girls less than 14 years old. COC are not recommended for males due to
adverse effects such as gynecomastia. Eichenfield et al. (13) recommend COC within one year of
the onset of menstruation. They do not indicate an age limit. Recent studies on prescribing
practices for acne have shown a decrease in prescribing COC for acne (132).
Spironolactone, an aldosterone receptor antagonist that has potent antiandrogen activity, is not
approved by the US Food and Drug Administration (FDA) for the treatment of acne. Nevertheless,
it is still recommended by both the AAD (28) and the American Acne and Rosacea Society (13)
based on expert opinion rather than published data.
Although acne vulgaris is not strictly considered an infection, OAB are prescribed to decrease P.
acnes in sebaceous glands producing inflammation and sebaceous plugging (125, 133-135). P.
acnes can create biofilms which are a physical barrier for antibiotics to penetrate, which may
impact on their effectiveness (Suh and Kwon 2015; Tan and Bhate 2015). Despite the risk of
antibiotic resistance, systemic antibiotic prescriptions for acne by general practitioners have
increased (132, 136).
33
TRs such as adapalene gel normalise desquamation of follicular epithelium, preventing new
comedonal activity. Oral retinoids such as isotreninoin and tretinoin are used long term (up to one
year in eight treatment week intervals with a break of two to four weeks) in severe refractory or
scarring acne, but have AEs including hip growth plate injuries, neutropenia, depression and
suicidal ideation (125, 137) and are teratogenic (137, 138). The number of isotretinoin courses
prescribed for patients with acne by dermatologists and non-dermatologists decreased from 2004
to 2014 (132).
Studies on acne prescribing trends by general practitioners have found increasing prescriptions for
systemic tetracyclines and isotretinoin from 2005 to 2015, with 75 per cent of tetracyclines
prescribed for an average of 2.8 and 3.3 months (136). Prescriptions for spironolactone, COC and
OAB by dermatologists and non-dermatologists all increased between 2004 and 2013 (132).
The European Evidence-Based (S3) Guidelines for the Treatment of Acne 2012 (127) provide
comprehensive guidance on improving management of adult patients with acne, including
diagnosis, reduction of scarring that can occur with cystic or nodular/conglobate acne, promotion
of adherence to treatment and reducing antibiotic resistance. The American Acne and Rosacea
Society (13) has provided consensus treatment recommendations based on a literature review of
current evidence on the various types of acne found in children. The guideline also includes
recommendations on methods of rating severity and clarification of categorisation of paediatric
acne. Treatment algorithms are included to aid practitioners in diagnosis and treatment.

34
The most recent Australian treatment guidelines for acne were published in 2010. The Royal
Australian College of General Practitioners (RACGP) (125) provided treatment recommendations
for mild, moderate, moderate-to-severe and severe acne for both children and adults. There is a
strong emphasis on patient education and countering myths patients might encounter. First- and
second-line treatments described in the Australian guideline are similar to those described in the
guideline of the AAD. A recent review of treatment in Australia suggested that expert consensus
was the basis for treatment guidelines (139). They supported early treatment intervention with
systemic therapy when topical therapy was unsuccessful. The British Association of
Dermatologists and the Royal College of General Practitioners both published guidelines for acne
in 2012 (140). Topical and oral therapies recommended are similar to those of other published
guidelines. No guidelines were provided for severity grading. They do, however, emphasise the
need to refer to specialists if there are diagnostic uncertainties, a failure to respond to recommended
treatments after six months, nodular or moderately severe acne with deeply pigmented skin, or
major psychological disturbances.
The Ministry of Health (MOH) of Malaysia published a clinical practice guideline for the
management of acne in 2012 (141). The main recommendations are similar to those of other
published recommendations for topical and oral treatments, with the exception that it does
recommend single topical therapy such as TRs for mild to moderate acne as well as combined
topical therapy. It also recommends other topical therapies not mentioned in other guidelines, such
as sulfur-based topical combinations and azelaic acid. Salicylic acid used in chemical peels is also
recommended by the MOH. These interventions only provided mild improvements in mild and

35
moderate acne, and the other guidelines do not recommend them as first-line treatments (13, 28,
125).
Four Cochrane reviews evaluated the efficacy and safety of COC, laser therapy, minocycline and
spironolactone for acne (14, 142-144). Arowojolu et al. (14) found, in 31 RCT, that COC reduced
total lesion counts, but no benefit was seen with spironolactone. Jordan et al. (144) found a lack
of controlled studies of laser therapy for acne scars, and evidence was based on 14 case series.
There was some evidence that laser improved scars, but most was visual observation of
improvement without blinded assessments. Garner et al. (143) found that minocycline was
effective for moderate and moderate-to-severe inflammatory acne with the same AE and
antibiotic-resistance profiles as other tetracyclines. Brown et al. (142) evaluated spironolactone
for acne and hirsutism and found no benefit for the management of acne, although spironolactone
did decrease the degree of hirsutism.
2.9.2 Non-pharmacological approaches
2.9.2.1 Cultural and self-management practices
Skin hygiene improves acne by reducing P. acnes and sebum production (145). Gentle face-
washing with cleansers that are not too drying, washing hair that is oily and not picking lesions so
as to prevent scars are advice from the AAD (28). Facial makeup is often used by females and
males to hide lesions and is not thought to worsen lesions (146). It has been shown to improve
QoL for those on treatment for acne (147). Sunlight was previously thought to improve lesions
due to the relationship with P. acnes; however, this is no longer thought to be the case as sunlight
can cause environmental damage to the skin (90).
36
2.9.2.2 Diet
Treatment guidelines currently do not include any dietary changes, although there is limited
evidence that low-glycaemic diets and skim milk may be associated with acne (28). It is suggested
that, due to a significant association between strong IGF-1, high BMI and severe acne, diet may
be a valuable dietary intervention (148). Low glycaemic index diets have been shown to improve
acne in a pilot study, as high glycaemic load foods tend to increase insulin growth factors which
increase sebum production, worsening acne (149, 150).
2.9.2.3 Laser light
Lasers and light devices are yet to be recommended and more studies are needed. The most
promising evidence is for photodynamic therapy (PDT) with a photosensitiser such as
aminolevulinic acid applied for 15 minutes to three hours. Consensus on incubation time and light
sources is yet to be determined (28). The MOH recommends phototherapy and PDT as an
alternative therapy for those who are unable to tolerate standard acne therapies and for those in
whom standard therapies have failed (141).
2.9.2.4 Physical modalities
Surgery is not recommended in any of the treatment guidelines for treatment of acne vulgaris.
Other physical therapies such as chemical peels with agents such as salicylic acid, trichloroacetic
acid chemical reconstruction of skin scars (TCA Cross) technique,
dermabrasion/microdermabrasion and skin needling have been proposed (29), but the strength of
evidence for these treatments is low (28). Comedone removal is only recommended for comedones

37
resistant to other therapies and intralesional corticosteroid injections are recommended for the
treatment of individual acne nodules (28).
2.9.2.5 Complementary and alternative medicine
Many people use complementary and alternative medicine (CAM) for skin conditions (151). Due
to antibacterial resistance, investigations of alternatives to antibacterial treatment have been
conducted (152-154). In a study by Magin et al. (155) of patients recruited from dermatological
practices in Australia, the majority of respondents with acne had used CAM products including
witch hazel (Hamamelis virginiana), tea-tree oil (Leptospermum spp.), citrus washes, aloe vera
(Aloe vera), zinc tablets, herbal remedies, tissue salt tablets, natural oils and evening primrose oil
(Oenothera biennis). In another review of CAM products, basil oil (Ocimum sanctum, Ocimum
basilicum and Ocimum gratissimum) was found to have antimicrobial effects and reduced lesion
counts faster than 10 per cent BP lotion (156). Copaiba oil and green tea are reported to have anti-
inflammatory effects. Green tea and resveratrol also have antimicrobial properties (152). The
traditional Italian herbs Vitis vinifera leaves, Asphodelus microcarpus leaves and Vicia sativa
aerial parts were found to inhibit P. acnes growth and affect the biofilm of the bacteria (153). A
combination of the Ayurvedic herbs Guduchi (Tinospora cordifolia), Manjishtha (Rubia
cordifolia), Sarva (Hemidesmus indicus), Nimba (Azardirachta indica), Khardira (Acacia catechu)
and Kakmachi (Solanum nigrum) extracts had significant anti-inflammatory and antimicrobial
activity (154).
A Cochrane review of CAM included 3,227 participants from 35 trials (157). Trials included in
the review evaluated herbal medicine, acupuncture, wet cupping, diet, purified bee venom (PBV)

38
and tea-tree oil. There was low-quality evidence that low glycaemic load diet, tea-tree oil and PBV
may reduce total skin lesions, but a lack of evidence to support herbal medicine and acupuncture
for acne. Overall, the methodological quality of trials was low and weakened the evidence (157).
A systematic review of botanical and phytochemical treatments for acne vulgaris (20) included 23
clinical trials published in English, 3 of which were trials of Kampo/Chinese herbal formulations.
Meta-analysis was not performed. The herbal preparations showed improvement for mild to
moderate acne, although there were limitations to the studies such as a lack of acne-grading
methods, lack of control or placebo groups, and no assessment of lesion count.
Two systematic reviews of acupuncture, one in English (157) and one in Chinese (18), have been
published. Cao et al. (157) evaluated acupoint-stimulation techniques including acupuncture,
moxibustion, cupping, acupoint injection and acupoint catgut embedding compared with no
treatment, placebo or conventional pharmaceutical medication. They also included combinations
of acupoint-stimulation techniques plus other therapies as interventions, compared to the same or
other therapies alone. The review included 43 trials with 3,453 participants. They described the
methodological quality of the trials as generally poor. They found acupuncture plus herbal
medicine was better than herbal medicine alone and acupuncture plus a herbal facial mask was
better than a herbal facial mask alone. Cupping was significantly better than pharmaceuticals, with
no serious adverse events (SAEs) reported (157). Li et al. (18) evaluated manual acupuncture and
moxibustion compared to routine conventional medicine (isotretinoin and antibiotics) and multiple
Chinese medicine therapies. They included 17 trials with 1,613 participants. They found
acupuncture and moxibustion were better than acupuncture alone and better than routine Western
medicine, although the quality of the evidence again was low (18).

39
Both reviews included studies that compared interventions to other herbal medicines or CM
techniques where the effectiveness of these techniques are not established. Including these studies
into these reviews can dilute the strength of the results. A review that includes studies that
compared controls using placebo or medications with known efficacy will give rigour to the
results. The above reviews included studies of techniques that are not common outside of China
such as catgut embedding and blood cupping as “acupuncture” techniques. The above reviews also
included acupuncture combined with herbal medicines and did not analyse herbal medicines alone.
2.10 Chapter summary
Acne vulgaris is a multifaceted chronic skin condition lasting up to ten years. It can affect patients’
QoL and impact on social and work life. The pathophysiological understanding of acne is evolving,
with current mechanisms including inflammation and hyperkeratinisation. Treatment using topical
and oral antibiotics, and topical and oral retinoids are recommended; these decrease inflammation
and suppress sebum production that causes follicular plugging. Other therapy options include
complementary and alternative medicines and dietary recommendations, although good evidence
for these therapies is lacking.
40
CHAPTER 3 : Chinese medicine for acne vulgaris
3.1 Introduction to Chinese medicine
CM is a health care system that groups symptoms into a pattern of disease (syndrome
differentiation) (158). The aim of CM is to balance yin and yang, which are opposing yet
complementary forces in the body. Environmental, lifestyle, diet and exercise factors can
contribute to an imbalance of yin and yang in the body. Pathogenic factors from external or internal
sources such as wind, heat, summer-heat, dampness and fire can cause dermatological conditions
in CM. Other aetiological factors include insects and parasites (159). These aetiological factors
can affect a person’s zang fu (internal organs) or their meridians where qi (energy) circulates.
During a patient consultation, CM practitioners use their clinical skills to ask a series of questions
about the patient’s main complaint, as well as other questions about their general health. Questions
also relate to emotional, psychological and physical symptoms such as possibility of pain, sleep
disturbances, emotional disturbances, food taste and preferences, chest or abdominal symptoms
and other bodily functions. CM practitioners observe the patient, using their senses of sight, smell
and listening.
Based on the answers given and the observations made, the practitioner uses their clinical
reasoning to formulate a syndrome, taking into consideration the aetiology (cause) and the
pathogenesis (how the disease develops). The practitioner will then differentiate it from other
possible syndromes, arriving at a diagnosis that conforms to CM theory (160). After a diagnosis is
made and a syndrome is differentiated, a treatment principle is formed. Practitioners treat the main
41
complaint, as well as addressing all presenting symptoms together. They also consider the
environmental, dietary, emotional and lifestyle factors of the patient and provide advice according
to CM principles. CM emphasises individualised treatment based on differentiation of the
pathogenic or inherent differences in the patient (161).
3.2 Chinese medicine definition of acne vulgaris
In CM, acne vulgaris (acne) is called cuo chuang and fen ci (162). It is also known as fei feng fen
ci (肺风粉刺) (Lung-wind powder prickles) or fen ci (粉刺) (powder prickles). These terms reflect
the starch-coloured fluid contained within the comedones that is attributed to the Lungs (肺 fei)
(159). Other terms include cuo chuang (痤疮) and an chuang (暗疮) and in lay terms it is called
jiu ci (酒刺) and qing chun ci (青春刺). The name jiu ci (酒刺) is translated as “wine prickles”
related to acne rosacea and qing chun ci (青春刺) translates as “teenage prickles” reflecting the
condition affecting adolescents.
3.3 Aetiology and pathophysiology in Chinese medicine
Acne is a disorder of the sebaceous glands that are distributed on the face, chest and back (6). In
CM, sebaceous glands are associated with the Lungs and Spleen (159). The Lungs protect the
surface of the body (in CM, this is known as wei) to prevent invasion of pathogenic factors. Along
with the Stomach, the Spleen transforms and transports food to produce nutrients (ying in CM)
(158). Figure 3.1 summarises the aetiology and pathogeneses in a flow chart.
In CM there are a few factors that can cause acne. Underlying heat in the Blood is the main
aetiological factor responsible for acne (159). Adolescents are considered more active or warmer
42
in nature and constitutionally tend towards yang (159, 163). The abundant yang, due to
constitutional yang type or Kidney yin deficiency, can lead to heat. Heat in CM describes the nature
of the condition rather than a symptom of inflammation. Heat warms the ying and Blood levels.
The flow of qi and Blood slows in the meridians and collaterals and they become congested,
leading to Blood stagnation. Blood stagnation that stays in the body generates heat in the Blood,
transforming into Blood-heat. Blood and heat push outwards to the surface, causing red eruptions.
Blood-heat can further consume ying and Blood and causes qi and Blood stagnation that can cause
nodular eruptions.
Damp is both an external and internal pathogenic factor that can develop due to environmental
factors or poor diet. Poor diet such as a diet high in greasy, sweet or spicy foods or fish and shellfish
can weaken the transforming and transporting function of the Spleen, leading to damp
accumulation. Dampness manifests in the body with skin symptoms such as acne, vesicles (fluid
filled blisters) and greasy, oily skin (159). Dampness that remains in the body over time can
transform into damp-heat. Damp-heat can accumulate in the Lungs and Stomach. It can transfer to
the Stomach and Large Intestine (Yangming meridians), which reflects on the jaw and around the
nose (159). Damp-heat can also accumulate in the skin and tissues, causing inflammation and
swelling. Damp-heat can transform into fire that steams upwards to the surface of the skin, causing
small red eruptions of papules or comedones (159, 164). Toxins in CM refer to paroxysmal and
extreme pathogenic factors that attack the body or are associated with bacteria, viruses and fungi
(159). An attack of damp toxins can block Blood circulation, resulting in damp toxins with Blood
stasis (165). These previous syndromes are associated with mild-to-moderate comedonal acne.
43
Dampness can block the circulation of body fluids and lead to phlegm accumulation in the body.
This can also lead to blockage of qi and thus Blood circulation over time. When these blockages
manifest on the skin, it can lead to cysts and nodules. Cystic or nodular acne is associated with
toxic heat and/or phlegm and Blood stagnation.
General poor health can allow external pathogenic wind and heat to enter the body, as can washing
in cold water. Both activities can block the pores. Existing heat in the Blood combined with these
factors leads to inflamed comedones. If existing qi and Blood stagnation is aggravated by
emotional disturbances, qi stagnation can further lead to heat in the body which consumes Blood
and body fluids and cause Blood stasis. If there is prolonged heat in the Lungs and Stomach, heat
can transform damp into phlegm, which can cause cystic or nodular acne resulting in toxic heat or
Blood stasis binding with phlegm (159). These last two syndromes are associated with moderate-
to-severe acne.
Constitutional Kidney yin deficiency combined with emotional disturbances resulting in qi
stagnation can cause a disharmony between Chong (冲, Thoroughfare vessel) and Ren (任,
Conception vessel). The “sea of Blood” (Chong and Liver meridians) cannot be nourished and
irregular menstruation and worsening of acne around menstruation can occur (164).
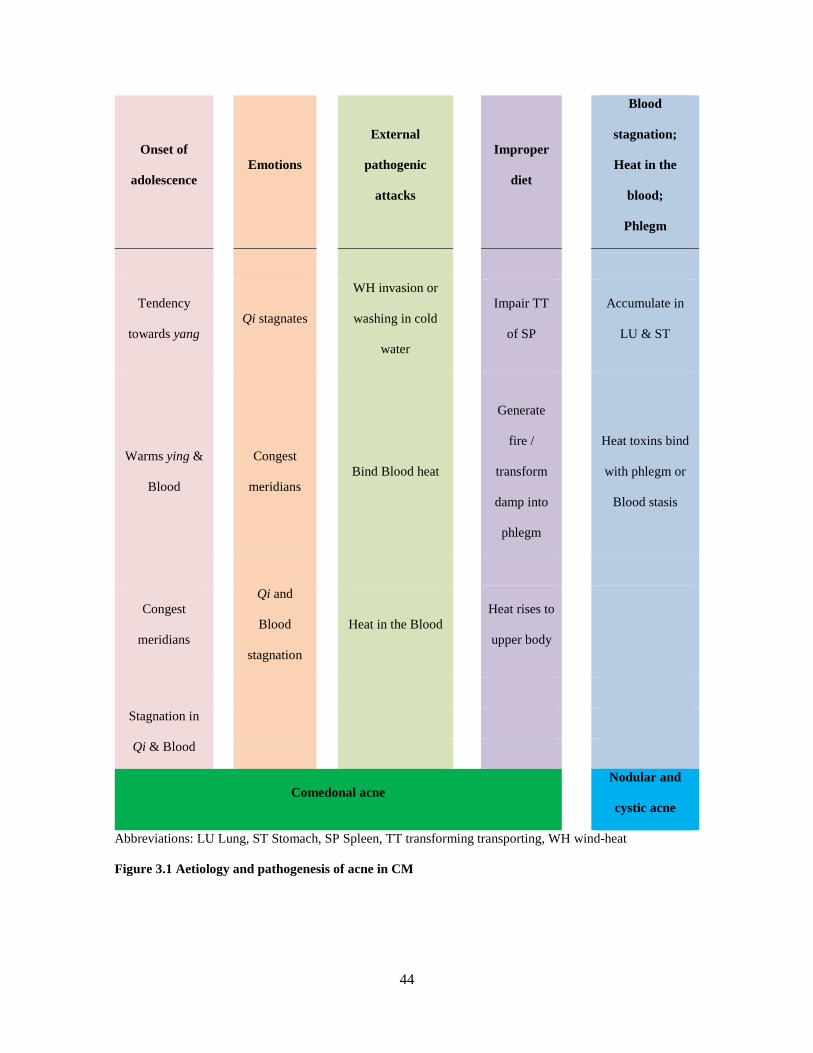
44
Onset of
adolescence Emotions
External
pathogenic
attacks
Improper
diet
Blood
stagnation;
Heat in the
blood;
Phlegm
Tendency
towards yang Qi stagnates
WH invasion or
washing in cold
water
Impair TT
of SP
Accumulate in
LU & ST
Warms ying &
Blood
Congest
meridians Bind Blood heat
Generate
fire /
transform
damp into
phlegm
Heat toxins bind
with phlegm or
Blood stasis
Congest
meridians
Qi and
Blood
stagnation
Heat in the Blood Heat rises to
upper body
Stagnation in
Qi & Blood
Comedonal acne Nodular and
cystic acne
Abbreviations: LU Lung, ST Stomach, SP Spleen, TT transforming transporting, WH wind-heat
Figure 3.1 Aetiology and pathogenesis of acne in CM

45
3.4 Chinese medicine diagnosis and differentiation compared to Western Medicine
CM diagnosis first requires the practitioner to ask a series of questions on the main complaint and
then use “10 traditional questions” to gather information on the patient’s reason for seeking
treatment and their overall health (158). The practitioner will also perform physical examination
using their senses such as observing for skin colour changes or other physical symptoms, olfaction
for different smells that may come from the patient, and auscultation, listening for changes in
voice, lung sounds or cough sounds. This overall narrative of signs and symptoms is then
categorised into a number of syndromes depending on the various CM theories. Examples include
five-element theory, Zang-fu (organ) theory and meridian theory. Similar skills are used during
WM consultations to obtain clinical information from patients. However, a WM practitioner will
not necessarily ask about gastrointestinal function such as appetite or bowel movements when a
patient presents with a headache whereas a CM practitioner will. In clinical practice a consultation
with a CM practitioner is often up to 30 minutes in a new consultation.
Depending on the symptoms and conditions presented, the practitioner would group these
symptoms and diagnose and treat based on this differentiation. For example, a patient with a
common cold may present with a runny nose, clear nasal discharge, headaches and body aches
would be categorised with a “wind-cold” syndrome. Another patient, also presenting with a
common cold, may describe symptoms of a sore throat, cough, thirst and fever; they would be
diagnosed with a “wind-heat” syndrome. CHM and acupuncture treatment will be different based
on the syndrome diagnosis. Diagnosis in WM would be common cold from viral or bacterial
infection. Treatment may or may not differ depending on the patients most bothersome symptoms.
46
3.5 Chinese medicine syndrome differentiation
CM textbooks and treatment guidelines categorises acne lesions into lesion types and syndromes.
Comedonal acne is categorised into three main syndromes (159, 164, 165): heat in the Lung, heat
in the Stomach (sometimes combined as heat in the Lung and Stomach), and heat in the Blood.
Cystic or nodular acne (and severe inflammatory cystic acne, acne conglobata) is categorised into
two syndromes: Blood stasis and Blood stasis with phlegm binding. Cyclic acne is categorised as
qi and Blood stagnation. There are some variations in syndromes, including Kidney yin deficiency
(164) describing the natural yang exuberance of adolescents, and damp toxins with Blood stasis
(165), which has a similar presentation to Blood stasis with phlegm (159). CM treatment guidelines
also have some variations in the syndrome names and have additional syndromes that are not
present in CM textbooks. Syndromes include wind-heat stagnating in the Lung meridian, heat
stagnating in the Liver meridian and imbalance of Chong and Ren vessels, dampness-heat
stagnating in the Stomach and Intestines, dampness-heat stagnating in the Spleen and Stomach,
accumulation of dampness-heat, toxic heat and Blood stasis, and phlegm obstruction and Blood
stasis. A summary of the syndromes and related symptoms seen in comedonal acne are found in
Table 3.1.
The following is a summary of the syndromes described in the textbooks and treatment guidelines.
Three English-language publications describe the syndromes and treatments described below.
These are the books Dermatology in Traditional Chinese Medicine (159), Manual of Dermatology
in Chinese Medicine (165) and Acne and Alopecia (164). Three published treatment CM guidelines
for dermatological conditions were also consulted: Treatment Guidelines for Acne Vulgaris in
China (2014 edition) 中国痤疮治疗指南 (162), Guidelines for Diagnosis and Treatment of
47
Common Diseases of Dermatology in Traditional Chinese Medicine 中医皮肤科常见病诊疗指
南 published by the China Association of Chinese Medicine (166) and the Criteria of Diagnosis
and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine 中医病证诊
断疗效标准 published by the State Administration of Traditional Chinese Medicine of the
People’s Republic of China (167).
3.5.1 Heat in the Lungs and wind-heat stagnating in the Lung meridian
Acne due to heat in the Lungs is the most common clinical presentation. In his book on CM
dermatology, Xu (159) describes comedones due to heat in the Lungs as small (approximately two
millimetres) red or pale red papules. Closed comedones and pustules tend to be located on the
forehead and cheeks and around the nose. The patient may have oily skin and accompanying dry
mouth and nose. The tongue body is red with a thin yellow coating and the pulse will be floating.
CM treatment guidelines consider that wind and heat are both present in acne and describe the
syndrome of wind-heat stagnating in the Lung meridian. Lesions include open and closed
comedones and red papules. Accompanying symptoms and signs include red face, bad breath,
itching, pain, dry mouth and dry stools. The tongue is yellow with a thin coating and there is a
slightly floating or taut or floating and rapid pulse (162, 166).
3.5.2 Heat in the Stomach
Comedones due to heat in the Stomach present in a similar manner to heat in the Lungs; however,
the lesions are distributed around the mouth. Accompanying symptoms include bad breath,
aversion to heat, thirst with a preference for cold drinks, constipation and dark-yellow urine. The

48
tongue body will be red with a thin yellow or greasy coating and the pulse will be slippery and
rapid (159). CM treatment guidelines do not describe heat in the Stomach as a separate syndrome.
However, some of the symptoms in the syndrome wind-heat stagnating in the Lungs such as bad
breath and dry stools may be due to heat in the Stomach.
3.5.3 Heat in the Blood and yin deficiency generating internal heat
Emotional disturbances cause qi to stagnate and transform into heat. This can aggravate existing
heat in the body, causing heat in the Blood. In this syndrome, comedones are concentrated around
the nose and mouth and between the eyebrows. Heat may also cause telangiectasia and a red face.
Comedones can worsen around women’s menstrual cycles. Accompanying symptoms are similar
to those seen with heat in the Stomach and include dry stools and yellow urine. The tip of the
tongue will be red and there will be a yellow coating; the pulse will be thready, slippery and rapid
(159).
Yin deficiency generating internal heat presents with red papules, pustules or nodules on the face.
Additional symptoms include dry mouth, irritability, dream-disturbed sleep, dry and hard stools
and reddish urine. The tongue is red with a thin yellow coating and the pulse is rapid or thready
and rapid (164).
3.5.4 Stagnation of qi and Blood and heat stagnating in Liver meridian
In this syndrome, red or dark papules can be present for several years. Accompanying symptoms
will be associated with a disharmony of the Chong and Ren meridians. In women, it is associated
with irregular menstruation, clots in the menstrual blood and abdominal pain. In men, a darker
49
complexion may result. The stagnation of qi and Blood and heat in the Blood syndromes in women
tend to relate to cyclic acne, but not in all women. Comedones worsen around women’s menstrual
cycles and resolve after their menstrual cycles (159, 164). The tongue body is dark or has dark red
or brown spots and the pulse is deep, thready and choppy.
Heat stagnating in the Liver meridian presents with similar symptoms as the stagnation of qi and
Blood. Inflammatory papules and pustules along with irritability, insomnia, dream-disturbed sleep,
dry mouth, bitter taste and dry stools may be present. In women, breast distension, irregular
menstruation, menorrhagia or hypomenorrhoea may also be present with acne worsening around
the menstrual cycle. The tongue is red with a yellow coating and the pulse is taut and thready or
taut and rapid (166).
3.5.5 Imbalance of Thoroughfare (Chong) and Conception (Ren) vessels
Imbalance of Thoroughfare (Chong) and Conception (Ren) vessels are also described in the CM
treatment guidelines. In this syndrome, lesions also worsen or improve around menstruation.
Lesions are located on the forehead and cheeks or between the eyes. Lesions are aggravated before
menstruation and improve after. Additional symptoms include irregular menstruation,
premenstrual irritability and breast distension. The tongue is pale red with a thin coating and there
is a deep and taut or hesitant pulse (162). These syndromes may be classified as mild-to-moderate
acne.

50
3.5.6 Dampness-heat stagnating in Stomach and Intestines; dampness-heat stagnating in
the Spleen and Stomach; accumulation of dampness-heat
These syndromes described in the CM treatment guidelines include papules and pustules that are
painful, pores that are prominently seen, and skin that is oily and may develop into nodules or
cysts. Additionally, there may be occasional bad breath, lack of thirst, bitter taste, loss of appetite,
loose or sticky stools or constipation, and dark-coloured urine. The tongue is red with a yellow
greasy coating (162, 166, 167). These syndromes may be classified as mild-to-moderate acne.
3.5.7 Damp toxin with Blood stasis and toxic heat and Blood stasis
Damp toxins with Blood stasis result in deep, painful inflamed nodules and pus-filled cysts with
erythema on the face, chest and back. These symptoms are similar to the signs and symptoms
reported in the Blood stasis and binding of phlegm syndrome (below). The affected areas will be
oily and rupture of lesions can result in scarring. Other accompanying symptoms include headache
and feeling hot in the body. The tongue body will be purple with a yellow or white coating. The
pulse will be slow or submerged and choppy (165).
The toxic heat and Blood stasis syndrome presents with similar lesions types and locations as the
damp toxins with Blood stasis. It can also include hyperpigmentation with scarring. It is noted that
this may occur during puberty. Additional signs and symptoms include dry mouth and thirst,
irritability, feverish sensation, bad breath, dry stools and dark urine. The tongue is red with a
yellow coating and the pulse is surging or taut and rapid (166). These types of acne may be
classified as moderate to severe.
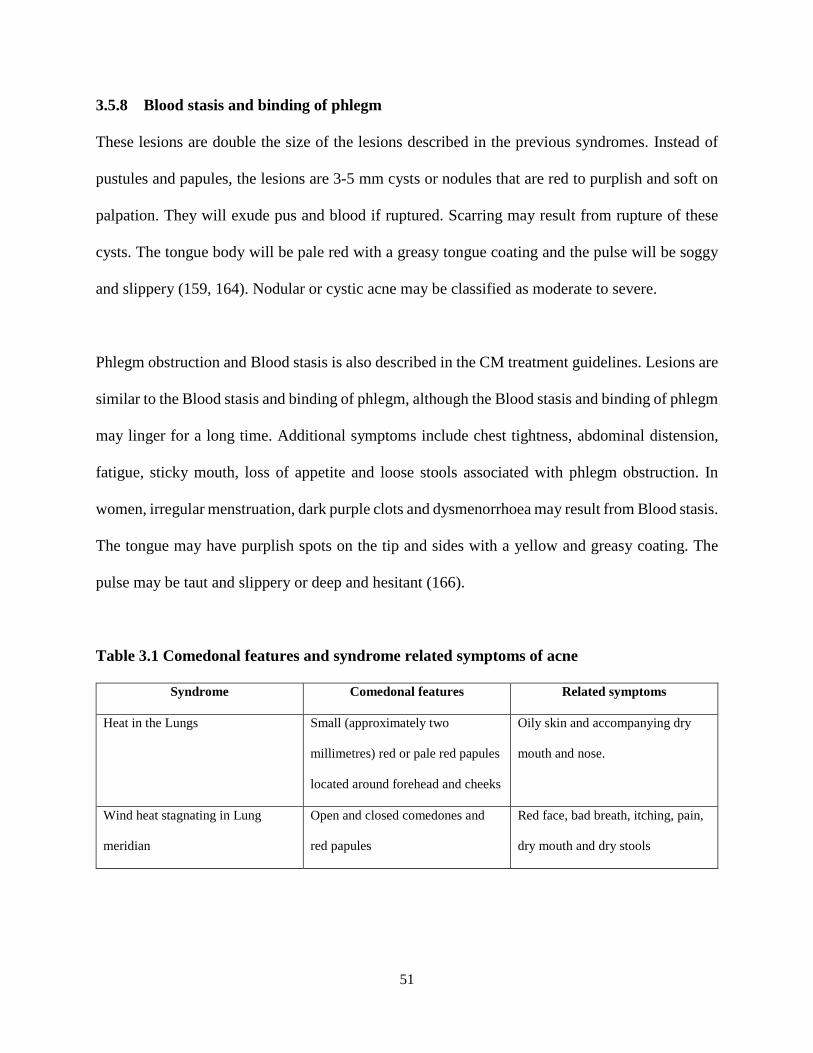
51
3.5.8 Blood stasis and binding of phlegm
These lesions are double the size of the lesions described in the previous syndromes. Instead of
pustules and papules, the lesions are 3-5 mm cysts or nodules that are red to purplish and soft on
palpation. They will exude pus and blood if ruptured. Scarring may result from rupture of these
cysts. The tongue body will be pale red with a greasy tongue coating and the pulse will be soggy
and slippery (159, 164). Nodular or cystic acne may be classified as moderate to severe.
Phlegm obstruction and Blood stasis is also described in the CM treatment guidelines. Lesions are
similar to the Blood stasis and binding of phlegm, although the Blood stasis and binding of phlegm
may linger for a long time. Additional symptoms include chest tightness, abdominal distension,
fatigue, sticky mouth, loss of appetite and loose stools associated with phlegm obstruction. In
women, irregular menstruation, dark purple clots and dysmenorrhoea may result from Blood stasis.
The tongue may have purplish spots on the tip and sides with a yellow and greasy coating. The
pulse may be taut and slippery or deep and hesitant (166).
Table 3.1 Comedonal features and syndrome related symptoms of acne
Syndrome Comedonal features Related symptoms
Heat in the Lungs Small (approximately two
millimetres) red or pale red papules
located around forehead and cheeks
Oily skin and accompanying dry
mouth and nose.
Wind heat stagnating in Lung
meridian
Open and closed comedones and
red papules
Red face, bad breath, itching, pain,
dry mouth and dry stools
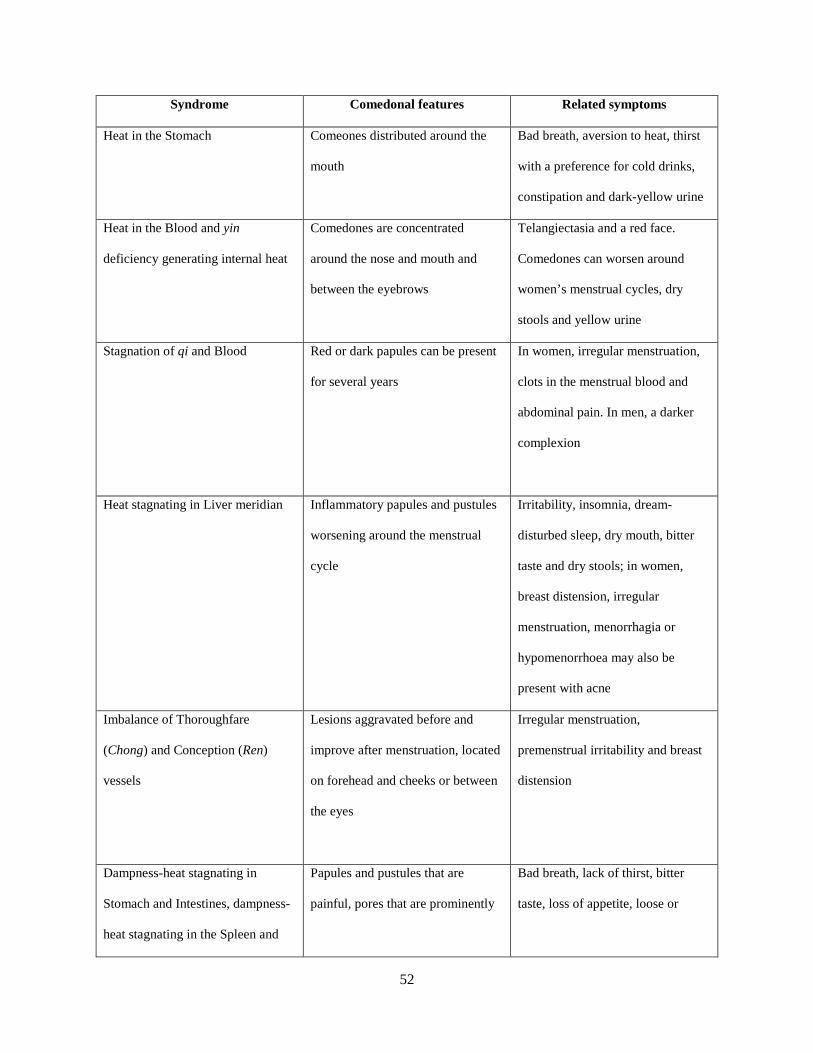
52
Syndrome Comedonal features Related symptoms
Heat in the Stomach Comeones distributed around the
mouth
Bad breath, aversion to heat, thirst
with a preference for cold drinks,
constipation and dark-yellow urine
Heat in the Blood and yin
deficiency generating internal heat
Comedones are concentrated
around the nose and mouth and
between the eyebrows
Telangiectasia and a red face.
Comedones can worsen around
women’s menstrual cycles, dry
stools and yellow urine
Stagnation of qi and Blood Red or dark papules can be present
for several years
In women, irregular menstruation,
clots in the menstrual blood and
abdominal pain. In men, a darker
complexion
Heat stagnating in Liver meridian Inflammatory papules and pustules
worsening around the menstrual
cycle
Irritability, insomnia, dream-
disturbed sleep, dry mouth, bitter
taste and dry stools; in women,
breast distension, irregular
menstruation, menorrhagia or
hypomenorrhoea may also be
present with acne
Imbalance of Thoroughfare
(Chong) and Conception (Ren)
vessels
Lesions aggravated before and
improve after menstruation, located
on forehead and cheeks or between
the eyes
Irregular menstruation,
premenstrual irritability and breast
distension
Dampness-heat stagnating in
Stomach and Intestines, dampness-
heat stagnating in the Spleen and
Papules and pustules that are
painful, pores that are prominently
Bad breath, lack of thirst, bitter
taste, loss of appetite, loose or
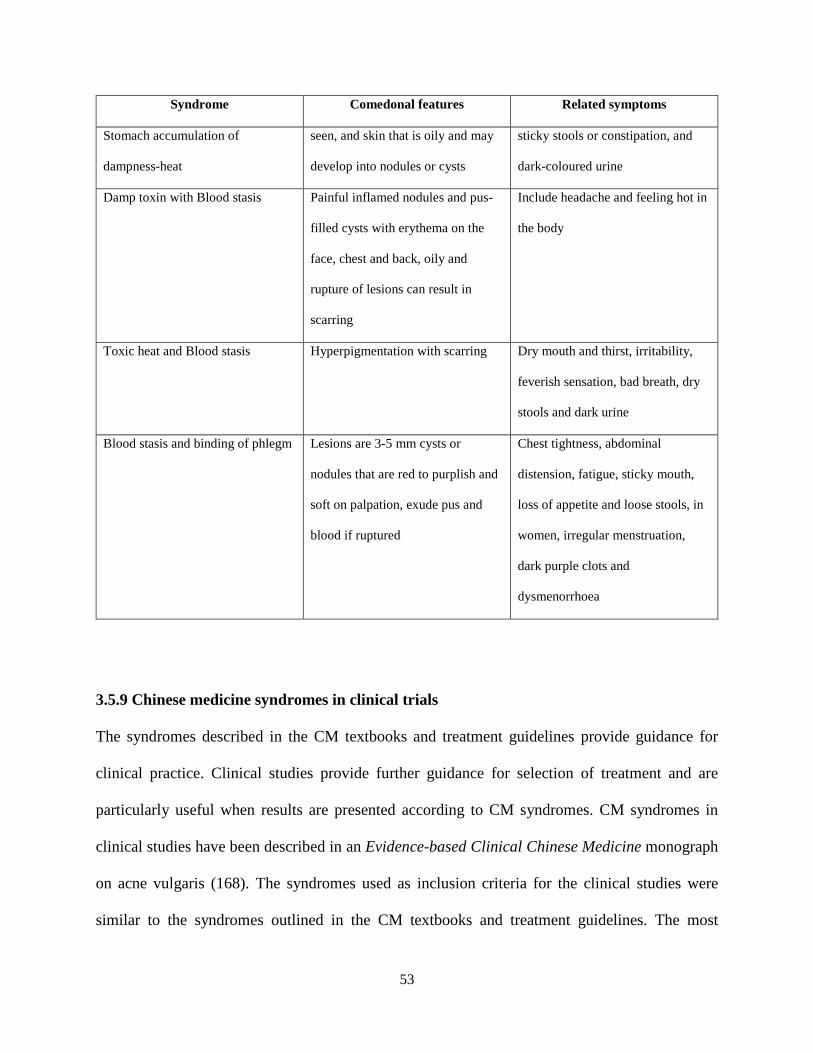
53
Syndrome Comedonal features Related symptoms
Stomach accumulation of
dampness-heat
seen, and skin that is oily and may
develop into nodules or cysts
sticky stools or constipation, and
dark-coloured urine
Damp toxin with Blood stasis Painful inflamed nodules and pus-
filled cysts with erythema on the
face, chest and back, oily and
rupture of lesions can result in
scarring
Include headache and feeling hot in
the body
Toxic heat and Blood stasis Hyperpigmentation with scarring Dry mouth and thirst, irritability,
feverish sensation, bad breath, dry
stools and dark urine
Blood stasis and binding of phlegm Lesions are 3-5 mm cysts or
nodules that are red to purplish and
soft on palpation, exude pus and
blood if ruptured
Chest tightness, abdominal
distension, fatigue, sticky mouth,
loss of appetite and loose stools, in
women, irregular menstruation,
dark purple clots and
dysmenorrhoea
3.5.9 Chinese medicine syndromes in clinical trials
The syndromes described in the CM textbooks and treatment guidelines provide guidance for
clinical practice. Clinical studies provide further guidance for selection of treatment and are
particularly useful when results are presented according to CM syndromes. CM syndromes in
clinical studies have been described in an Evidence-based Clinical Chinese Medicine monograph
on acne vulgaris (168). The syndromes used as inclusion criteria for the clinical studies were
similar to the syndromes outlined in the CM textbooks and treatment guidelines. The most
54
common syndrome encountered was heat in the Lungs or wind-heat stagnating in the Lung
meridian. Damp-heat syndromes such as damp-heat toxins, damp heat in the Stomach and Spleen
or Intestines, and damp-heat and Blood stasis were reported to be used. Phlegm syndromes
included phlegm and dampness, and phlegm and Blood stasis. Heat in the Liver meridian, Liver
qi stagnation, imbalance of Chong and Ren vessels were also used.
3.6 Chinese medicine treatment
There are several different forms of treatment in CM: CHM, acupuncture of body acupuncture
points and acupuncture-related manual therapies. CHM is a common type of treatment used in CM
for acne. For dermatological conditions, it is common for both oral and topical herbs to be
prescribed together. Topical herbs are applied directly to the lesions on the afflicted skin, and oral
herbs are used to address the internal or aetiological factors. Topical herbs have a long history in
CM and are used in various forms from poultices to washes and powders. Oral herbs are
traditionally in the form of decoctions and pills or boluses. In clinical practice, CHM may be
combined with acupuncture treatment for acne.
The common types of acupuncture and acupuncture-related techniques include body acupuncture
(insertion of fine needles into specific loci on the body), auricular acupuncture (insertion of fine
needles into specific loci in the ear), acupressure (applying blunt pressure to specific loci in the
body), moxibustion (heat from burning of artemsia argyi Levl. Et Vant. directed at specific
acupuncture points), warming needles (where a small piece of moxa is placed on top of a needle
and allowed to burn down), cupping (suction of skin and muscles from glasses or other type of
55
cups formed from a vacuum), cutaneous acupuncture (seven-star and plum-blossom needling) and
EA (a mild electrical current applied to acupuncture needles to provide constant stimulation) (169).
Body acupuncture is the most common form of acupuncture technique used in treatment of acne.
Additional acupuncture techniques may also be combined with body acupuncture. The Chinese
term for acupuncture is zhen jiu (针灸), which literally means ‘acupuncture and moxibustion’.
This shows the similarity between the two interventions, which are often combined in clinical
practice. For acne, cupping, cutaneous needling, auricular acupuncture and EA are often combined
with body acupuncture (157, 159, 165). All these acupuncture interventions have been evaluated
in clinical trials of acne. There have been two systematic reviews on acupuncture for acne and one
Cochrane review on complementary medicines for acne (157). A summary is found in Chapter 8:
Systematic review of acupuncture for acne vulgaris.
3.6.1 Oral Chinese herbal medicine for acne vulgaris
The aim of CM treatment is to reduce the number of lesions by addressing the syndrome
differentiation. This may include reducing heat in the Lungs or Stomach, reducing dampness-heat
in the body and preventing dampness-heat from transforming into Blood stasis and phlegm (158),
clearing heat toxins, resolving the phlegm and dissipating Blood stagnation by increasing Blood
circulation (159, 164, 165).
CM treatments are tailored to each syndrome and lesion type. A summary of the acne lesion types,
syndromes and oral and topical formulas is found in Tables 3.2 and 3.3. For the Chinese formula
names and species names of oral herbs, refer to Appendix 1, and for topical herbs, refer to
56
Appendix 2. Ingredients and formulas are sourced from CM dermatology textbooks (159, 164,
165) and CM treatment guidelines (162, 166, 167). There are also recommendations for women to
regulate their menstruation to prevent aggravation of symptoms around menstruation with
acupuncture or CHM (159). For both men and women, it is recommended to regulate
gastrointestinal functions by eating regularly and avoiding aggravating foods such as greasy and
spicy foods. This prevents accumulation of dampness-heat internally which can turn into phlegm
and worsen acne (159).
Individual oral CHM formulas are prescribed for each syndrome. Herbs included in these formulas
act to clear Lung heat, regulate Blood circulation, clear heat toxicity or clear dampness-heat or
phlegm. A summary of the acne lesion types, syndromes and oral formulas is found in Table 3.2.
For comedonal or inflammatory acne, Pi Pa Qing Fei Yin (PPQFY) (枇杷清肺饮) is the key
formula that is commonly prescribed for comedonal acne which acts to clear heat in the Lungs
(159) and wind-heat in Lung meridians (162, 166). It is also recommended for this syndrome by
the China Association of Chinese Medicine in their Guidelines for Diagnosis and Treatment of
Common Disease of Dermatology in Traditional Chinese Medicine (166). The formula consists of
herbs that clear heat in the Lungs and dampness-heat in the upper and middle energisers, tonify
the qi and harmonise the herbs. The ingredients in the formula have been shown to decrease
inflammation (170) and sebum (171).
Liang Xue Qing Fei Yin (凉血清肺饮) (159, 165) is another formula that addresses heat in the
Lung and qi and Blood stagnation. It has similar ingredients to PPQFY. It differs in that it contains
herbs that invigorate Blood circulation and cool the Blood. For heat in the Stomach, Tiao Wei
57
Cheng Qi Tang (调胃承气汤) (159, 165) is used to purge the Stomach heat by purging the
intestines.
For yin deficiency that generates internal heat, Xiao Cuo Tang (消痤汤) (164) contains herbs that
tonify essence (jing 精), clear deficient and pathogenic heat, and invigorate Blood circulation. Tao
Hong Si Wu Tang (桃红四物汤) (159, 164, 165) and Liang Xue Wu Hua Tang (凉血无华汤) (159,
165) are prescribed for heat in the Blood and have ingredients that invigorate Blood circulation,
clear heat from the Blood, tonify Blood and clear pathogenic heat. Tao Hong Si Wu Tang (桃红四
物汤) is combined with modified Wu Wei Xiao Du Yin 五味消毒饮 for toxic heat and stasis
syndrome (167). Finally, for heat toxins Cuo Chuang Jian Ji Tang (Chinese characters not
identified) (165) is prescribed. It contains ingredients that clear pathogenic heat, clear damp-heat
and invigorate Blood circulation, and an ingredient (Jie geng, Platycodon grandiflorum (Jacq.) A.
DC.) that will raise the herbs upwards to the afflicted area and resolve phlegm.
Modified Chai Hu Shu Gan Wan (柴胡疏肝丸加减) (164) can be prescribed for qi and Blood
stagnation and has similar ingredients to Xiao Yao San (逍遥散) and Dan Zhi Xiao Yao San 丹栀
逍遥散加减. Xiao Yao San and Dan Zhi Xiao Yao San are prescribed for heat stagnating in the
Liver meridian (167) and imbalance of Chong and Ren vessels (162), respectively. Herb
ingredients aim to regulate menstruation and clear heat in the Liver. Liang Xue Qing Fei Yin (凉
血清肺饮) (159, 165) is also used in cyclic comedonal acne as it contains herbs that invigorate
Blood circulation and cool the Blood, as well as herbs that clear heat in the Lung. Another
suggested formula is modified Chai Hu Shu Gan Wan (柴胡疏肝丸) combined with ingredients

58
from Xiao Cuo Tang (消痤汤) (164). The formula presented is heavily modified. It contains four
ingredients from the two formulas plus herbs that tonify the Kidney yin, clear heat toxicity and
invigorate Blood circulation.
Formulas that address cystic or conglobate acne have ingredients that clear dampness-heat,
invigorate Blood stasis, clear heat in the Blood and resolve dampness-heat toxins and phlegm. For
damp toxin with Blood stasis, Chu Shi Jie Du Tang (除湿解毒汤) (165) is prescribed. The formula
ingredients clear dampness-heat and resolve toxicity. Hai Zao Yu Hu Tang (海藻玉壶汤) (159) is
prescribed in cases of Blood stasis and binding of phlegm. The ingredients resolve phlegm, clear
damp, regulate the middle energizer qi and clear external pathogens. Ingredients are also added to
resolve hardness (Xia ku cao, Prunella vulgaris L.) and heal wounds (Mu li, Ostrea gigas Thunb.).
Tao Hong Si Wu Tang is combined with modified Hai Zao Yu Hu Tang (海藻玉壶汤) to address
phlegm obstruction and Blood stasis (162, 167).
Table 3.2 Oral herb formulas for acne vulgaris§
Syndrome Oral formula
Comedonal acne
Heat in Lungs Pi Pa Qing Fei Yin (159, 165)
Liang Xue Qing Fei Yin (159, 165)
Wind-heat in Lung meridian Pi Pa Qing Fei Yin (162, 167)
Heat in Stomach Tiao Wei Cheng Qi Tang (159, 165)
Damp-heat stagnating in Stomach and
Intestines; Pattern/syndrome of
Modified Yin Chen Hao Tang (162, 167); modified Qin Lian Ping
Wei San (162)
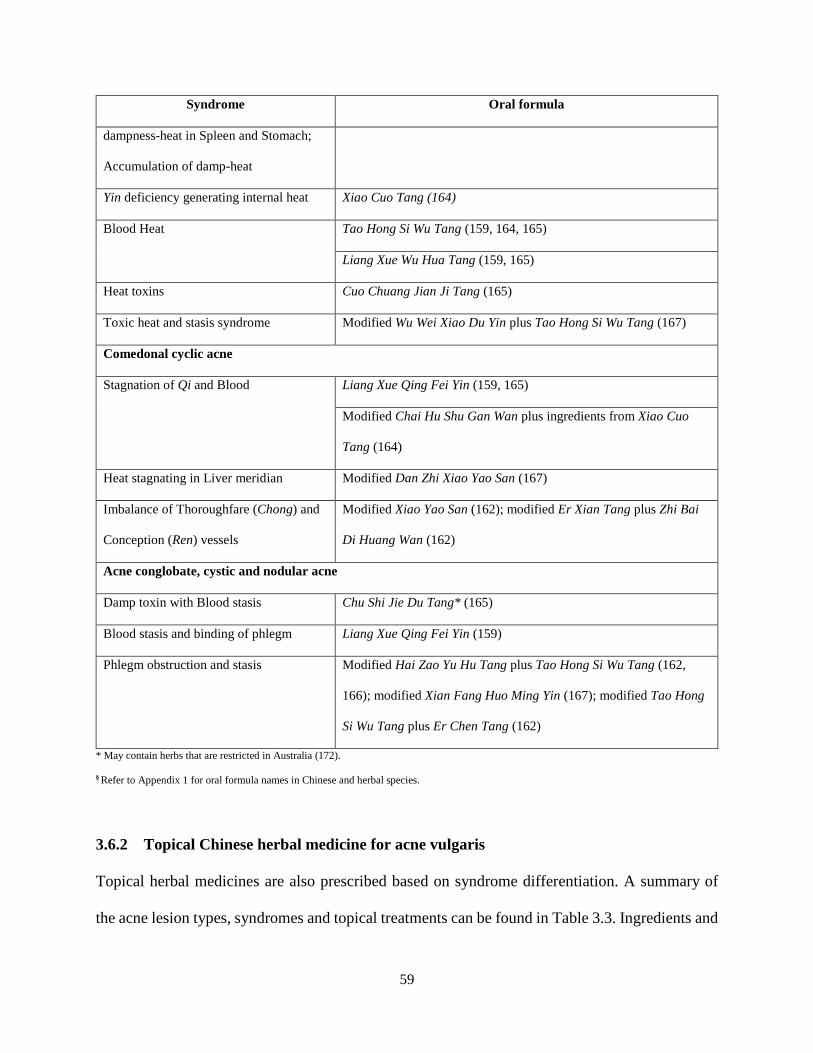
59
Syndrome Oral formula
dampness-heat in Spleen and Stomach;
Accumulation of damp-heat
Yin deficiency generating internal heat Xiao Cuo Tang (164)
Blood Heat Tao Hong Si Wu Tang (159, 164, 165)
Liang Xue Wu Hua Tang (159, 165)
Heat toxins Cuo Chuang Jian Ji Tang (165)
Toxic heat and stasis syndrome Modified Wu Wei Xiao Du Yin plus Tao Hong Si Wu Tang (167)
Comedonal cyclic acne
Stagnation of Qi and Blood Liang Xue Qing Fei Yin (159, 165)
Modified Chai Hu Shu Gan Wan plus ingredients from Xiao Cuo
Tang (164)
Heat stagnating in Liver meridian Modified Dan Zhi Xiao Yao San (167)
Imbalance of Thoroughfare (Chong) and
Conception (Ren) vessels
Modified Xiao Yao San (162); modified Er Xian Tang plus Zhi Bai
Di Huang Wan (162)
Acne conglobate, cystic and nodular acne
Damp toxin with Blood stasis Chu Shi Jie Du Tang* (165)
Blood stasis and binding of phlegm Liang Xue Qing Fei Yin (159)
Phlegm obstruction and stasis Modified Hai Zao Yu Hu Tang plus Tao Hong Si Wu Tang (162,
166); modified Xian Fang Huo Ming Yin (167); modified Tao Hong
Si Wu Tang plus Er Chen Tang (162)
* May contain herbs that are restricted in Australia (172).
§ Refer to Appendix 1 for oral formula names in Chinese and herbal species.
3.6.2 Topical Chinese herbal medicine for acne vulgaris
Topical herbal medicines are also prescribed based on syndrome differentiation. A summary of
the acne lesion types, syndromes and topical treatments can be found in Table 3.3. Ingredients and
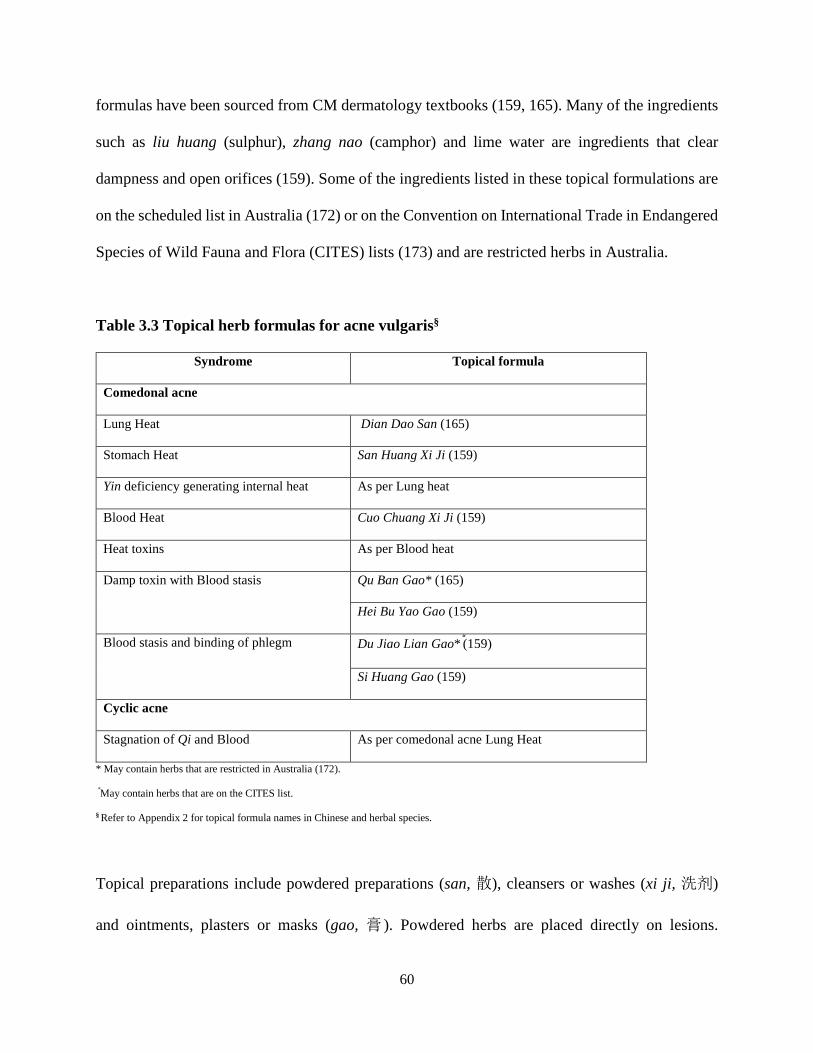
60
formulas have been sourced from CM dermatology textbooks (159, 165). Many of the ingredients
such as liu huang (sulphur), zhang nao (camphor) and lime water are ingredients that clear
dampness and open orifices (159). Some of the ingredients listed in these topical formulations are
on the scheduled list in Australia (172) or on the Convention on International Trade in Endangered
Species of Wild Fauna and Flora (CITES) lists (173) and are restricted herbs in Australia.
Table 3.3 Topical herb formulas for acne vulgaris§
Syndrome Topical formula
Comedonal acne
Lung Heat Dian Dao San (165)
Stomach Heat San Huang Xi Ji (159)
Yin deficiency generating internal heat As per Lung heat
Blood Heat Cuo Chuang Xi Ji (159)
Heat toxins As per Blood heat
Damp toxin with Blood stasis Qu Ban Gao* (165)
Hei Bu Yao Gao (159)
Blood stasis and binding of phlegm Du Jiao Lian Gao* (159)
Si Huang Gao (159)
Cyclic acne
Stagnation of Qi and Blood As per comedonal acne Lung Heat
* May contain herbs that are restricted in Australia (172).
May contain herbs that are on the CITES list.
§ Refer to Appendix 2 for topical formula names in Chinese and herbal species.
Topical preparations include powdered preparations (san, 散), cleansers or washes (xi ji, 洗剂)
and ointments, plasters or masks (gao, 膏 ). Powdered herbs are placed directly on lesions.

61
Cleansers or washes are prepared with raw powdered herbs combined with distilled water and
applied as a wash for two minutes or left on for up to 15 minutes and rinsed off. Ointments, plasters
or masks are usually left on for up to 30 minutes (166) or overnight if necessary. Ointments are
made with beeswax (huang (feng) la – Apis cerana Fabricius), honey (feng mi – Apis cerana
Fabricius) or cold-pressed sesame oil (xiang you – Sesamum indicum L.).
For comedonal inflammatory acne, Dian Dao San (颠倒散) (165) is prescribed for Lung heat. This
formula contains powdered herbs that are purgative and dry dampness. It is also used for cyclic
comedonal acne due to stagnation of qi and Blood as the presentation of comedones is similar. San
Huang Xi Ji (三黄洗剂) (159), prescribed for Stomach heat, contains powdered herbs that clear
dampness-heat. Cuo Chuang Xi Ji (痤疮洗剂) (159) is prescribed for both heat in the Blood and
heat toxins. It contains powdered herbs that clear heat toxicity. For cystic or conglobate acne due
to damp toxins with Blood stasis, Qu Ban Gao (去斑膏) (165) is prescribed. It contains herbs that
resolve toxicity, invigorate Blood circulation and clear heat in the Blood. Hei Bu Yao Gao (黑布
药膏) (159) is also prescribed for this syndrome with herbs that open orifices, extinguish wind and
resolve toxicity. Du Jiao Lian Gao (Giant Typhonium paste – Chinese characters not identified)
(159) is an ointment prescribed for Blood stasis and binding of phlegm. Ingredients in this formula
act to resolve phlegm, clear heat toxicity, resolve abscesses, clear external pathogens and
invigorate Blood circulation. Another ointment used for this syndrome is Si Huang Gao (四黄膏)
(159). It contains herbs that clear dampness-heat, invigorate Blood circulation and purge toxicity.
Many of the formulas and herbs described in the textbooks and clinical guidelines have also been
evaluated in clinical studies. The Evidence-based Clinical Chinese Medicine monograph on acne
62
vulgaris (168) found PPQFY was evaluated in 11 studies. All of the studies used herb ingredients
that differed from the standard formula ingredients of Pi pa ye (Eriobotrya japonica Thunb.
Lindl.), Sang bai pi (Morus alba L.), Huang lian (Coptis chinensis Franch. or Coptis teeta Wall.
or Coptis deltoidea C.Y. Cheng & Hsiao), Huang bai (Phellodendron amurense Rupr. or
Phllodendron chinense Schneid.), Ren shen (Panax ginseng C.A. Mey.) and Gan cao (Glycyrrhiza
glabra L. P. or Glycyrrhiza uralensis Fisch. or Glycyrrhiza inflata BAT.). Run Zao Zhi Yang Jiao
Nang, a commercially available CHM product, was also evaluated in 11 studies.
The review found 171 individual oral herbs and 73 topical herbs included in the studies. The most
frequently evaluated oral CHM was Huang qin (Scutellaria baicalensis Georgi) (80 instances),
followed by Gan cao (Glycyrrhiza glabra L. P. or Glycyrrhiza uralensis Fisch. or Glycyrrhiza
inflata BAT.) (64 instances), Sheng di (Rehmannia glutinosa (Gaertn.) Libosch.) (52 instances)
and Dan shen (Salvia miltiorrhiza Bge.) (52 instances). These herbs are recommended in CM
textbooks; see Appendices 1 and 2.
3.7 Acupuncture for acne vulgaris
3.7.1 Acupuncture from textbooks
Acupuncture treatment can include body acupuncture (insertion of fine needles on different loci
of the body) and auricular acupuncture or acupressure with ear pellets (stimulation of auricular
points from traditional pellets made from Wang bu liu xing (Vaccaria segetalis (Neck.) Garcke)
or stainless-steel ball bearings two millimetres in diameter). Acupuncture treatment can be based
on syndrome differentiation or affected meridians. Treatment frequency varies from once daily to
alternate days or weekly. Treatment duration is usually from seven to ten treatments. A summary
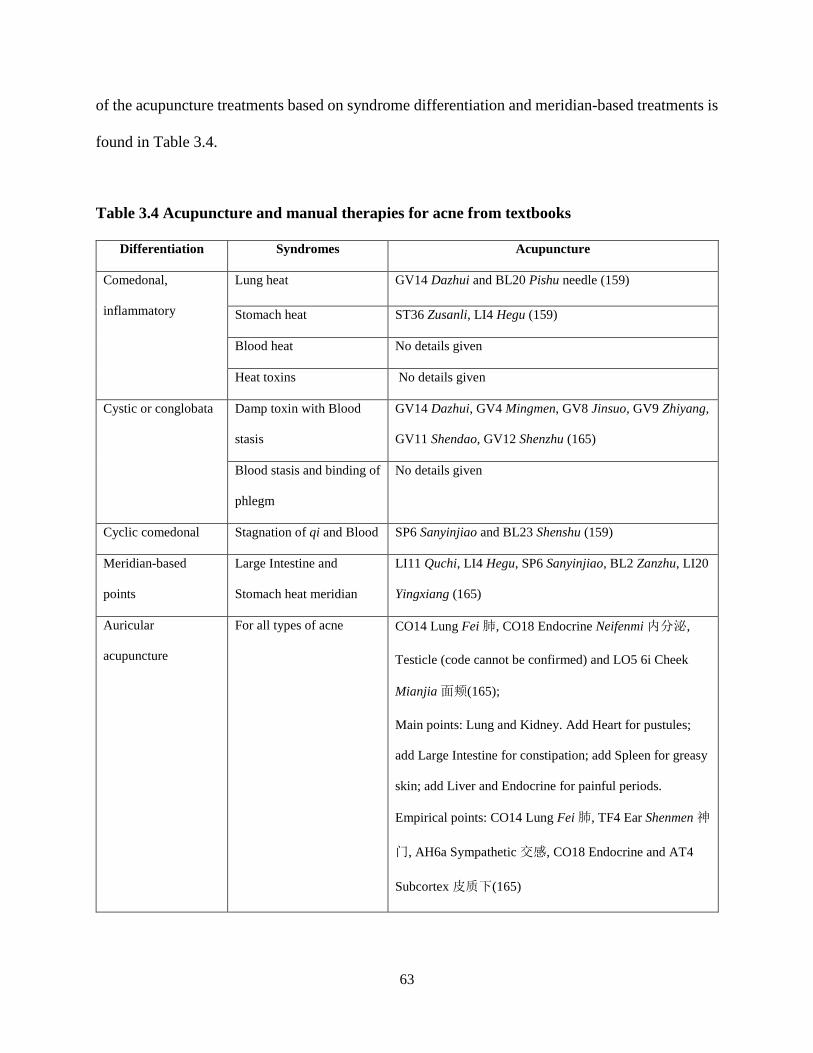
63
of the acupuncture treatments based on syndrome differentiation and meridian-based treatments is
found in Table 3.4.
Table 3.4 Acupuncture and manual therapies for acne from textbooks
Differentiation Syndromes Acupuncture
Comedonal,
inflammatory
Lung heat GV14 Dazhui and BL20 Pishu needle (159)
Stomach heat ST36 Zusanli, LI4 Hegu (159)
Blood heat No details given
Heat toxins No details given
Cystic or conglobata
Damp toxin with Blood
stasis
GV14 Dazhui, GV4 Mingmen, GV8 Jinsuo, GV9 Zhiyang,
GV11 Shendao, GV12 Shenzhu (165)
Blood stasis and binding of
phlegm
No details given
Cyclic comedonal Stagnation of qi and Blood SP6 Sanyinjiao and BL23 Shenshu (159)
Meridian-based
points
Large Intestine and
Stomach heat meridian
LI11 Quchi, LI4 Hegu, SP6 Sanyinjiao, BL2 Zanzhu, LI20
Yingxiang (165)
Auricular
acupuncture
For all types of acne CO14 Lung Fei 肺, CO18 Endocrine Neifenmi 内分泌,
Testicle (code cannot be confirmed) and LO5 6i Cheek
Mianjia 面颊(165);
Main points: Lung and Kidney. Add Heart for pustules;
add Large Intestine for constipation; add Spleen for greasy
skin; add Liver and Endocrine for painful periods.
Empirical points: CO14 Lung Fei 肺, TF4 Ear Shenmen 神
门, AH6a Sympathetic 交感, CO18 Endocrine and AT4
Subcortex 皮质下(165)
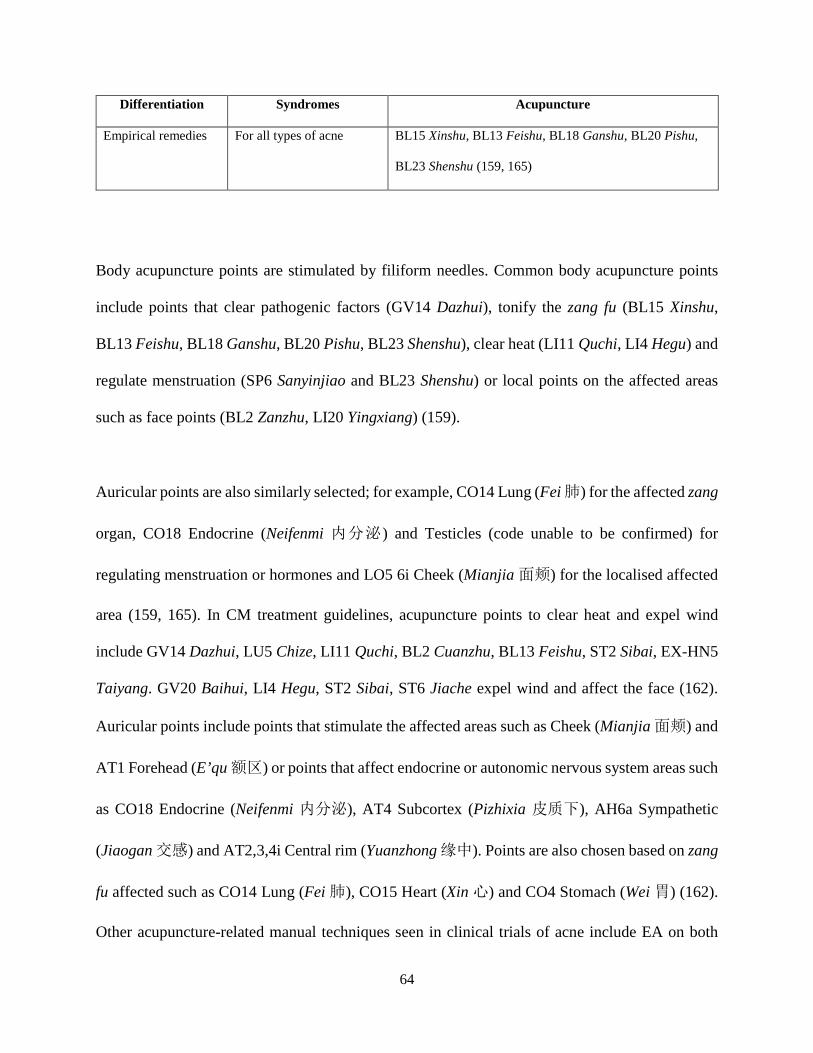
64
Differentiation Syndromes Acupuncture
Empirical remedies For all types of acne BL15 Xinshu, BL13 Feishu, BL18 Ganshu, BL20 Pishu,
BL23 Shenshu (159, 165)
Body acupuncture points are stimulated by filiform needles. Common body acupuncture points
include points that clear pathogenic factors (GV14 Dazhui), tonify the zang fu (BL15 Xinshu,
BL13 Feishu, BL18 Ganshu, BL20 Pishu, BL23 Shenshu), clear heat (LI11 Quchi, LI4 Hegu) and
regulate menstruation (SP6 Sanyinjiao and BL23 Shenshu) or local points on the affected areas
such as face points (BL2 Zanzhu, LI20 Yingxiang) (159).
Auricular points are also similarly selected; for example, CO14 Lung (Fei 肺) for the affected zang
organ, CO18 Endocrine (Neifenmi 内分泌) and Testicles (code unable to be confirmed) for
regulating menstruation or hormones and LO5 6i Cheek (Mianjia 面颊) for the localised affected
area (159, 165). In CM treatment guidelines, acupuncture points to clear heat and expel wind
include GV14 Dazhui, LU5 Chize, LI11 Quchi, BL2 Cuanzhu, BL13 Feishu, ST2 Sibai, EX-HN5
Taiyang. GV20 Baihui, LI4 Hegu, ST2 Sibai, ST6 Jiache expel wind and affect the face (162).
Auricular points include points that stimulate the affected areas such as Cheek (Mianjia 面颊) and
AT1 Forehead (E’qu 额区) or points that affect endocrine or autonomic nervous system areas such
as CO18 Endocrine (Neifenmi 内分泌), AT4 Subcortex (Pizhixia 皮质下), AH6a Sympathetic
(Jiaogan 交感) and AT2,3,4i Central rim (Yuanzhong 缘中). Points are also chosen based on zang
fu affected such as CO14 Lung (Fei 肺), CO15 Heart (Xin 心) and CO4 Stomach (Wei 胃) (162).
Other acupuncture-related manual techniques seen in clinical trials of acne include EA on both
65
auricular and body acupuncture points (174, 175), surround needling around acne lesions (176,
177) and moxibustion (18). A summary of the acupuncture points based on syndrome
differentiation and meridian-based treatments from the CM textbooks is found in Table 3.4.
3.7.2 Acupuncture from treatment guidelines
CM treatment guidelines suggest red and blue light therapy on acne lesions or acupuncture points
for treatment of acne (162) as a related manual therapy. Acupuncture treatment guidelines suggest
the use of local facial acupuncture points and acupuncture points based on syndrome
differentiation. Acupuncture points for acne from treatment guidelines are found in Table 3.5.
3.8 Other CM treatment factors for acne
Dietary advice almost always forms part of CM treatment. Traditionally in CM, a diet of greasy
(for example, high fat, dairy) and fried (oily, which contributes to heat) and spicy foods (for
example, chilli which also contributes to heat) is discouraged as it is may induce or worsen existing
acne though this has not been evaluated in studies. Stress can impair the free flow of Liver Qi. If
Liver Qi is impaired, it may generate heat which can aggravate acne symptoms. Therefore advice
to reduce stress such as traditional exercises, qi gong, tai chi which includes mindfulness
meditation may be encouraged.
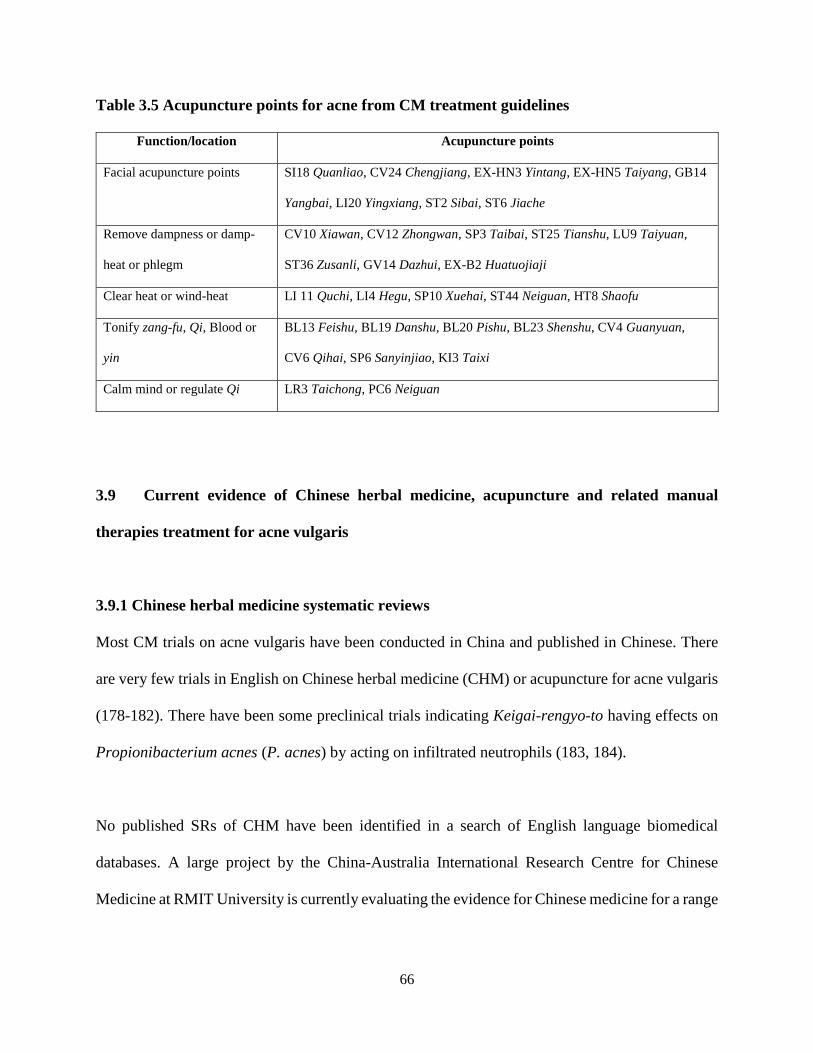
66
Table 3.5 Acupuncture points for acne from CM treatment guidelines
Function/location Acupuncture points
Facial acupuncture points SI18 Quanliao, CV24 Chengjiang, EX-HN3 Yintang, EX-HN5 Taiyang, GB14
Yangbai, LI20 Yingxiang, ST2 Sibai, ST6 Jiache
Remove dampness or damp-
heat or phlegm
CV10 Xiawan, CV12 Zhongwan, SP3 Taibai, ST25 Tianshu, LU9 Taiyuan,
ST36 Zusanli, GV14 Dazhui, EX-B2 Huatuojiaji
Clear heat or wind-heat LI 11 Quchi, LI4 Hegu, SP10 Xuehai, ST44 Neiguan, HT8 Shaofu
Tonify zang-fu, Qi, Blood or
yin
BL13 Feishu, BL19 Danshu, BL20 Pishu, BL23 Shenshu, CV4 Guanyuan,
CV6 Qihai, SP6 Sanyinjiao, KI3 Taixi
Calm mind or regulate Qi LR3 Taichong, PC6 Neiguan
3.9 Current evidence of Chinese herbal medicine, acupuncture and related manual
therapies treatment for acne vulgaris
3.9.1 Chinese herbal medicine systematic reviews
Most CM trials on acne vulgaris have been conducted in China and published in Chinese. There
are very few trials in English on Chinese herbal medicine (CHM) or acupuncture for acne vulgaris
(178-182). There have been some preclinical trials indicating Keigai-rengyo-to having effects on
Propionibacterium acnes (P. acnes) by acting on infiltrated neutrophils (183, 184).
No published SRs of CHM have been identified in a search of English language biomedical
databases. A large project by the China-Australia International Research Centre for Chinese
Medicine at RMIT University is currently evaluating the evidence for Chinese medicine for a range
67
of health conditions. An evidence-based monograph on Chinese medicine for acne vulgaris was
developed during the time of this PhD project, and has subsequently been published (168).
The review of oral CHM included 221 RCTs. More than half the studies combined CHM with
guideline recommended pharmacotherapies and few compared CHM with placebo or no treatment.
Pi Pa Qing Fei Yin (PPQFY) was the most frequently tested traditional formula, evaluated in 11
studies. All of the PPQFY studies made modifications by adding or removing herbs from the
standard formula ingredients. Eighty of the studies used Huang qin (黄芩, Scutellaria baicalensis
Georgi.) as an ingredient in their formulations.
There were 38 studies that used syndrome differentiation in their inclusion criteria, with 21 studies
using one syndrome, seven studies using two syndromes and the remainder using three or more
syndrome. Syndromes included wind-heat in the Lungs, dampness-heat in the either Stomach and
Intestines or in Stomach and Spleen, phlegm obstruction and blood stasis which are common
syndromes reported in textbooks (159, 164, 165).
Only three studies measured health related quality of life (HRQoL), the Dermatology Life Quality
Index (DLQI), the Cardiff Acne Disability Index (CADI) and Skindex-29. The CADI is an acne
specific HRQoL whereas the DLQI and Skindex-29 are general dermatology HRQoL measures.
There were more AEs reported in the control group (1,961 cases) compared to the intervention
group (1,344 cases).
68
There were few meta-analyses conducted in the reported review. Results showed CHM to be
superior to guideline-recommended treatments in reducing acne grading when using both the 1994
guideline (greater than 30% chance of change in symptoms) and 2002 guideline (greater than 50%
chance of change in symptoms). Many comparisons of lesion count and acne grading showed no
difference between CHM and pharmacotherapy at the end of treatment though analysis of change
from baseline to end of treatment did achieve statistically significant improvements from baseline.
Therefore there may be evidence to show CHM may be as effective as guideline recommended
treatments for acne.
3.9.2 Acupuncture systematic reviews
There have been two systematic reviews of randomised controlled trials on acupuncture for acne,
one in Chinese (2009) and one in English (2013) (18, 185). Cao et al (2013) included 43 trials in
their review with 3,453 participants aged between 17 to 43 years old. Interventions reviewed
included acupuncture (electroacupuncture, auricular acupuncture and ear point pressure), cupping,
point injection, catgut embedding, moxibustion and herbal stimulation of acupuncture points or
combined with CHM. The review concluded that the included studies reported “cure rate” as a
major outcome (reduction of lesion count), some gave recurrence rate and one gave quality of life
(QoL) scores. None of the trials reported sample size calculations and have a high risk of bias.
This included selection bias where there was inadequate allocation concealment in all but one trial
and performance bias where blinding was not possible for researchers and patients due to the
comparison of acupoint stimulation to pharmaceutical medications. Six trials reported dropout
rates but did not use intention to treat analysis.
69
The review found that the “cure rate” for acupuncture plus CHM was better than CHM alone but
there was no significant difference when acupuncture was compared to conventional treatment
(pharmaceutical medicines) (185). The authors also reported the efficacy of cupping therapy, point
injection, catgut embedding and moxibustion. Point injection and catgut embedding are not
techniques commonly seen outside of China. Cupping therapy was significantly better than
pharmaceutical medications (tretracycline, ketoconazole) and if combined with CHM was superior
to CHM or acupuncture alone. Point injection on its own or combined with pharmaceutical
medications was significantly better than pharmaceuticals alone but no benefit was seen when it
was combined with CHM. Catgut embedding was better than pharmaceuticals and if combined
with Chinese herbal medicine was better than Chinese herbal medicine on its own. Finally,
moxibustion combined with acupuncture was better than on its own. The authors concluded that
there is some evidence for acupuncture being effective for acne vulgaris however more rigorous
studies are required. A Cochrane review was also conducted by the same authors which provided
similar results to the systematic review (157).
The systematic review on acupuncture for acne published in Chinese (18) also reported overall
poor design in the included 17 trials (involving 1,613 cases) and thus limited the ability to make
conclusions. Nevertheless, all included trials reported cure rate as their main outcome. The authors
conducted a meta-analysis for acupuncture and moxibustion compared to routine western
medicine. The analysis showed the cure rate was higher in the acupuncture and moxibustion group
compared with routine treatment and the combination of acupuncture and moxibustion was better
than acupuncture or moxibustion on its own.
70
3.9.3 Limitations of Chinese medicine systematic reviews
No systematic reviews published in English on CHM for acne have been identified. With the
publication of the Evidence-based Clinical Chinese Medicine monograph on acne vulgaris in 2019
(168), there is evidence to suggest that oral CHM may be at least as effective as conventional
treatments. While this is important, there is still a gap in the evidence for specific CHM formulas
for acne. Publication of these types of SRs will ensure the evidence is accessible to practitioners,
and transferable to clinical practice.
The two systematic reviews and the Cochrane reviews used Chinese medicine as controls as part
of their inclusion criteria. They also included acupuncture techniques not commonly used outside
of China such as wet cupping, cat gut embedding and point injection. Li et al (18) only searched
the Chinese databases and was published in Chinese. The systematic review by Cao et al (185)
published in 2013 was also published later in the Cochrane review by the same authors (157). Both
reviews did state that it was difficult to draw reliable conclusions on the effects of acupuncture for
acne when comparing one unknown intervention with another. To address this issue, there needs
to be a review that looked at more commonly used body or auricular acupuncture compared to
conventional medicine treatments that have established efficacy and are recommended in clinical
practice guidelines.
3.10 Chapter summary
CM treatment is based on syndrome differentiation. For the treatment of acne, oral and topical
CHM and acupuncture techniques are aimed at decreasing lesion numbers, preventing recurrence
and addressing associated hormonal (menstrual) or gastrointestinal (dietary) symptoms (159). The

71
syndromes identified in the CM treatment guidelines and CM textbooks include heat in the Lungs,
heat in the Stomach, heat in the Blood, damp toxins with Blood stasis and Blood stasis with binding
of phlegm. CM syndromes are also related to types of acne lesions such as comedonal and cystic
types. Treatment is based on syndrome differentiation. Oral and topical CHM that clear heat,
resolve phlegm and invigorate stasis are often combined to treat different acne lesions. The
common acupuncture techniques recommended to treat acne include body acupuncture and
auricular acupuncture.
72
CHAPTER 4 : Health-related quality of life of people with acne vulgaris
4.1 Introduction
In the Constitution of the World Health Organization (WHO), the definition of health is “A state
of complete physical, mental and social well-being, not merely the absence of disease” (186).
Many QoL instruments incorporate physical, mental and social dimensions to measure health and
wellbeing. When QoL is measured in the context of a specific disease, this is referred to as health-
related quality of life (HRQoL) (187). This excludes non-health aspects such as economic and
political circumstances (188).
Acne can affect people’s psychological and emotional wellbeing and their social interactions (10,
37, 67). The impact of acne on HRQoL has been well documented in numerous studies and
reviews. Major depression, anxiety, body image concerns and suicidal thoughts and attempts have
been reported (9, 189). Most acne sufferers are adolescents and young adults (4), with adolescents
being most represented. Adolescence is a time of change and desire for social acceptance.
Adolescents with acne have higher social phobia due to their skin condition (190-192). Although
rare, peer victimisation in adolescents can lead to psychological sequelae (193, 194). This chapter
summarises the impact of acne on HRQoL, factors that may predict impaired HRQoL and types
of instruments used to measure HRQoL in people with acne.
73
4.2 Impact of acne on health-related quality of life
4.2.1 Psychological impact
Anxiety, depression, body image concerns, suicidal ideation and suicidal attempts have been
reported in several studies. Depression, anxiety and fear of persistent acne or scarring were present
in adolescents with acne (71). A higher risk of major depressive disorder (MDD) was seen in
people with acne (18.5 per cent) compared to the general population (12.0 per cent) in a
retrospective cohort study in the UK. Risk of MDD was also significantly higher within five years
of acne diagnosis, with the risk decreasing thereafter (189).
In a population-based study in Oslo, Norway, Halvorsen et al. (9) found that adolescents with acne
had social, study and relationship issues. Using the Strengths and Difficulties Questionnaire
(SDQ), they found late adolescents (aged 18 to 19 years) with acne had low attachment to friends,
were not thriving at school and had never had a romantic relationship or sexual intercourse.
Suicidal ideation, mental health problems and social impairment were noted in those with more
severe acne (9). A population-based study in Taiwan found the prevalence of acne was common
in 7- to 12-year-old children and a significant number of females aged 19 to 42 years. They found
an association with major depression that was 1.5 times more common in women who had acne
compared to men who had acne. They also found an increased risk of suicide in women with acne
compared to men (26). A New Zealand survey of students aged 12 to 18 years found that
adolescents who self-reported “problem acne” had a higher frequency of suicidal thoughts and
attempts compared to those without. There was also an increased frequency of depressive
symptoms and anxiety in adolescents with self-reported “problem acne” (25). In a study of the
general population of people born in Dunedin, New Zealand, between April 1972 and March 1973,
people with self-reported “problem acne” were found to have higher rates of anxiety (195).
74
Depression and anxiety were also reported in a US epidemiology survey of adolescents with severe
acne and other comorbidities (96).
Duman et al. (74) assessed the QoL of people 14 to 35 years with acne compared to healthy
volunteers. People with acne filled out the AQOL and the Hospital Anxiety and Depression Scale
(HAD) (196) and age-matched healthy volunteers filled out the HAD only. Both groups filled out
the questionnaires at the time of recruitment and two months later after treatment was administered
to people with acne. In the follow-up evaluation, the researchers did not find an increased risk of
anxiety and depression in people with acne (74). Jankovic et al. (197) translated the Children’s
Dermatology Life Quality Index (CDLQI) and Cardiff Acne Disability Index (CADI) into Serbian
to survey adolescents between 15 to 10 years of age. The CADI and CDLQI scores were low,
indicating a higher HRQoL and only moderate impairment.
Marron et al. (198) also used the HAD to evaluate the HRQoL of people with acne before and after
treatment. They found that anxiety and depression were higher in people with acne compared to
the average population, and that mean scores on HAD decreased after isotretinoin treatment.
Tanghetti et al. (59) used the Patient Health Questionnaire-4 (PHQ-4) and Acne-QoL to assess the
HRQoL of 218 women aged between 25 to 45 years with acne. Results indicated mild-to-moderate
depression and/or anxiety in the past two weeks. All four domains of the Acne-QoL (self-
perception, role-emotional, role-social and acne symptom scores) were lower, indicating a worse
HRQoL in adult women with acne (59).

75
In a study of 18-year-old males in compulsory military service in Brazil, males with lower levels
of education were more dissatisfied with their acne (199). Using the Body Image Disturbance
Questionnaire (BIDQ) and Skindex-16 to investigate body image concerns and QoL, one study
found that, as severity of acne increased, the number of people reporting emotional, social and
occupational impacts increased (8). People with severe acne also modified their behaviour as a
result of their acne (8). Furthermore, almost half of the people with a clinical diagnosis of acne
who had no current acne lesions or mild acne also reported experiencing emotional and
social/occupational impacts. Psychological distress and attentional bias towards acne lesions were
found in a study of people who had acne (200). People with acne tended to be fixated on their acne
lesions and showed a gap in perceived attractiveness compared to controls. In a study looking at
perfectionism, acne and appearance concerns, there was a greater tendency to be concerned with
their acne and their appearance and to have a higher level of socially prescribed perfectionism
(201). Acne patients had higher scores in relation to obsessive compulsive symptoms such as
rumination, checking and slowness compared to controls (202).
Clinical improvement positively affected HRQoL. Whether oral isotretinoin, topical adapalene,
cosmetic interventions or other treatments were used, improvement of the symptoms improved the
HRQoL of people with acne (198, 203-206). Adherence to treatment was also important for
clinical improvement and improvement of HRQoL (207). Reducing emotional symptoms with
cognitive behavioural therapy, patient education and pharmacotherapy was also recommended to
help improve HRQoL (208). One study comparing the use of an acne educational website that had
automated counselling to use of a website without counselling found the website with automated
counselling improved CDLQI scores and general skincare behaviour (209).
76
4.2.2 Emotional impact
Lower self-perception, self-esteem, self-consciousness and self-confidence, and feeling sad, angry
and frustrated are all emotional issues related to acne reported in studies (118, 210). Self-esteem
was lower as acne severity increased (211). One review showed that the presence of acne also
correlated with poor self-attitude in boys and poor self-worth in girls (212). In a qualitative study
of adolescents and adults with acne presenting to general and specialist dermatology practices in
New South Wales, Australia, people with acne were interviewed on the psychological effects of
acne (71). The study found that people with acne immediately had reduced self-esteem and poor
self-image, and were self-conscious and embarrassed when acne appeared. This was exacerbated
by taunting, stigmatisation and perception of being scrutinised (71). Fear of acne not ceasing or
being persistent was also found in a study of children (67) and female adults (59).
Tasoula et al. (213) used the CDLQI to evaluate the HRQoL of adolescents between 11 to 19 years
old. They found that adolescents with moderate-to-severe acne experienced greater psychosocial
and emotional impairment. Decreased self-esteem and embarrassment were seen in 39.8 per cent
adolescents with mild facial acne, 64.6 per cent of adolescents with moderate facial acne and 89.3
per cent of children with severe acne. They also found body image concerns increased
proportionally to acne severity. Feelings of unworthiness and teasing due to acne were seen in 31.4
per cent of adolescents and 21.4 per cent had modified the way they dressed due to their acne
(213). In a study of adolescents aged 12 to 17 years who sought treatment for their acne in a
dermatology clinic, there were no differences found between people with acne and healthy controls
in Rosenberg Self-Esteem Scale (RSES) scores on self-esteem or Capa Social Phobia Scale for
Children and Adolescents (CSPSCA) social anxiety scores (192).
77
4.2.3 Social impact
Social interaction, employment (73), intimate relationships (72) and family relationships (74) are
affected in people with acne. People with acne may be socially phobic and tend to remove
themselves from social activities (71, 211). Social stigma and perception of scrutiny and being
judged due to acne can isolate people in social situations (211). Social anxiety, depression and
anxiety levels in people with acne and vitiligo were significantly higher than healthy controls in a
study using the Liebowitz Social Anxiety Scale (LSAS), HAD and Dermatology Life Quality
Index (DLQI) (191) regardless of clinical acne severity (192). More than half the participants in a
Singaporean study of tertiary students felt embarrassed or self-conscious about their skin
“sometimes” or “all the time”; feelings of embarrassment increased with worsening acne (214).
They also felt their acne interfered with their social or leisure activities, but not their social or
family relationships.
In a study of adolescents aged between 12 to 17 years of age who had had acne for six months or
more, Bahali et al. (193) found no difference between study and control groups (of adolescents
who did not have acne or other appearance-related skin diseases) in the Peer Victimization Scale
(PVS), Child Depression Inventory (CDI), State-Trait Anxiety Inventories for Children (STAIc),
RSES and Pediatric Quality of Life Inventory Child Versions (PedsQL-C) for depression, peer
victimisation, trait anxiety and self-esteem. However, they did find HRQoL was worse with those
who reported peer victimisation (193). Tasoula et al. (213) found that facial acne affected
adolescents’ school work and personal activities in over one-fifth (21.4 per cent) of adolescents in
their study. Nearly one-fifth of adolescents were affected in their hobbies (19.4 per cent) and
78
personal and social lives (19.2 per cent), which also affected their ability to build relationships
with others (213).
Decreased employment was noted in 18- to 30-year-old people with acne compared to controls
(73) and increased stress at work was found in a study of adult females with acne (215). School
and work were affected in women aged 25 to 45 years. One-third of the 218 study participants
reported either missing out on school or poor concentration at work due to their acne (59). One
study that used the Family Dermatology Life Quality Index (FDLQI) on 110 family members of
people with acne showed that the disease progression affected family members. When acne
improved, the FDLQI scores of family members also improved (74). Appendix 3 summarises
studies evaluating the psychological, emotional and social impacts in people with acne and the
instruments used.
4.2.4 Comparison of health-related quality of life in people with acne and other medical
conditions
A number of studies compared acne HRQoL with that of other dermatological or medical
conditions. The impact of acne on HRQoL was comparable to that of psoriasis (116, 216-218),
diabetes and asthma (216, 217). Acne had a greater impact on psychosocial health compared to
psoriasis (218).
In a Danish population study of self-reported skin conditions, people with acne reported a worse
score on the emotions domain of the Skindex-29 compared to those with a rash (psoriasis, atopic
dermatitis and hidradenitis suppurativa) (219). A review comparing atopic dermatitis (AD) and
79
acne showed adolescents with AD had issues with self-identity whereas self-esteem, self-
confidence and self-identity were affected in adolescents with acne (220). Another review by
Nguyen et al. (190) comparing the psychosocial impact of acne with those of vitiligo and psoriasis
found that more adolescents with acne had social phobia compared to those with vitiligo and
psoriasis (190). This was thought to be due to acne occurring around adolescence, which is a time
of identity formation and susceptibility to peer opinions.
4.3 Factors predictive of impaired health-related quality of life
There are conflicting reports of factors that impact on the HRQoL of people with acne. Some
reports supported age of onset, while others did not. Some studies supported acne severity as a
factor in worse HRQoL, but others found more severe acne did not necessarily correlate with
worsening HRQoL. Hispanic, Asian and Pacific Islander/Maori people with acne reported greater
impact on HRQoL compared to Caucasian and African-American people.
The peak acne occurrence is most often reported by adolescents between the ages of 15 to 17 years.
There have also been reports of adult onset acne and an emerging subgroup of female adult onset
of acne. Studies have shown acne has an impact on HRQoL in both adolescents and adults.
Recurrence of acne is common; therefore acne has been redefined as a chronic inflammatory
disease of the pilosebaceous glands (56). Persistent acne and acne breakouts or recurrence can play
a role in HRQoL (59). Most studies have found mild impairment of HRQoL was more commonly
reported (193, 205, 212, 221) but moderate and severe impairment has also been reported in people
with acne (8, 9, 59, 192). Acne severity and gender have also been reported to be associated with
worse HRQoL in people with acne (9, 211).
80
There is a correlation between greater acne severity and worse HRQoL scores (190, 211, 222).
However, some studies have not found this correlation with severity (23, 223). One study of
school-aged children in rural and urban Egypt found that DLQI and CADI scores were influenced
by gender, residence, severity, scarring and previous treatment. Cosmetic concerns were greater
in female students living in urban areas who suffered scarring (37). Another study in Erbil, Iraq,
found HRQoL in females was more affected than in males and severity of acne was linked with
the level of impairment of HRQoL (224). In a study of Victorian adolescents, those with self-
reported moderate acne were more likely to report depression and anxiety, and were in the later
stage of pubertal development (19). CADI was also used in a study investigating HRQoL in
adolescents in Tunisia. Fifty participants (61 per cent) had acne and more than half of these (51
per cent) had altered HRQoL (225). A study in Greece of adolescents aged between 11 to 19 years
using the CDLQI found an impact on HRQoL associated with the severity of symptoms and
treatment (213). Self-reported severity was also correlated with worse DLQI scores in a study
comparing acne and vitiligo to healthy controls (191). Another study of school-aged children found
severe acne was correlated with worse HRQoL on the CDLQI, DLQI and RSES (67). A recent
interview-based study conducted in the UK, Italy and Germany in adolescents and adults who were
having treatment for acne highlighted that moderate-to-severe acne impacted on HRQoL (226).
The type of treatment was also important (226).
Among adults who attended outpatient clinics in Mangalore, India, the location of acne on the
face, the type of lesions and the severity were all influencing factors for worse HRQoL on the
DLQI and CADI (227). Chernyshov et al. (228) found that 75 participants who had sought help
81
from a dermatologist had worse HRQoL on the DLQI and CADI and had more severe acne than
participants who had not sought help from a dermatologist. In a study of Malaysian school-aged
adolescents, males were found to have more severe acne and a higher CADI score, indicating lower
HRQoL (41). However, a study in Hong Kong of late adolescents also found no correlation with
severity and HRQoL (23). Girls had significantly worse HRQoL than boys.
One study compared HRQoL in people with acne with HRQoL in healthy volunteers (74). Using
the AQOL in people with acne and the HAD in healthy volunteers, no relationship was found
between lower HRQoL scores and age, age at disease onset or acne severity (74). Another study
using CADI and the Global Acne Grading Scale (GAGS) to evaluate the HRQoL of senior high
school students in Nigeria found HRQoL was mildly affected in people with mild-to-moderate
acne proportionate to the severity of disease (229). Using the Assessment of the Psychological and
Social Effects of Acne (APSEA) score to evaluate HRQoL, one study found emotional and social
factors influenced HRQoL but not duration of the condition (230).
Lasek and Chren found older people with acne and people whose acne did not improve after three
months of treatment reported greater effects on HRQoL than younger adults (116). Acne severity
alone did not correlate with QoL in one study of university females with acne using the CADI. It
was suggested that other factors such as acne sequelae or social, emotional or other reasons may
contribute to worse HRQoL (223).
There have been studies that evaluated acne in different racial groups. In a population study in the
USA, Gorelick et al. (231) found that the impact of acne was greater among Hispanic and
82
Asian/other participants than among Caucasian and African-American participants. An acne
population study in New Zealand (NZ) found problem acne to be worse in Pacific Islander/Maori
participants compared to NZ European participants (25, 232).
4.4 Quality of life scales used in acne vulgaris research studies
4.4.1 General health-related quality of life scales
Many different general HRQoL scales have been used to evaluate the impact of acne on HRQoL.
A recent position paper by the European Academy of Dermatology and Venereology Task Forces
(EADV TF) on QoL and patient-oriented outcomes for acne, rosacea and hidradenitis suppurativa
(228) identified 24 different instruments used in the evaluation of HRQoL in people with acne. A
summary of the general HRQoL instruments used can be found in Table 4.1.
General wellbeing scales are used to assess the physical, mental and social dimensions to measure
health and wellbeing. These include the Medical Outcome Study 36-item Short Form Health
Survey (SF-36) (112) and its shorter version SF-12, EuroQoL 5-Dimension questionnaire (EQ-
5D) (233), PHQ-4 (113), SDQ (234), General Health Questionnaire (GHQ-28 or GHQ-12) (235,
236) and Hopkins Symptom Checklist (HSCL-90) (237). Some also include economic, political
and/or environmental dimensions, such as the WHO Quality of Life (WHOQOL)-26 (238).
Instruments that directly assess emotional or psychological dimensions have been used in studies.
The Center for Epidemiologic Studies Depression Scale (CES-D) (239), PHQ-4 (113) and
Reynolds Adolescent Depression Scale (RADS) (240) have been used to evaluate the level of
anxiety and/or depression. For social phobia the Fear of Negative Evaluation Scale (FNE) (241)
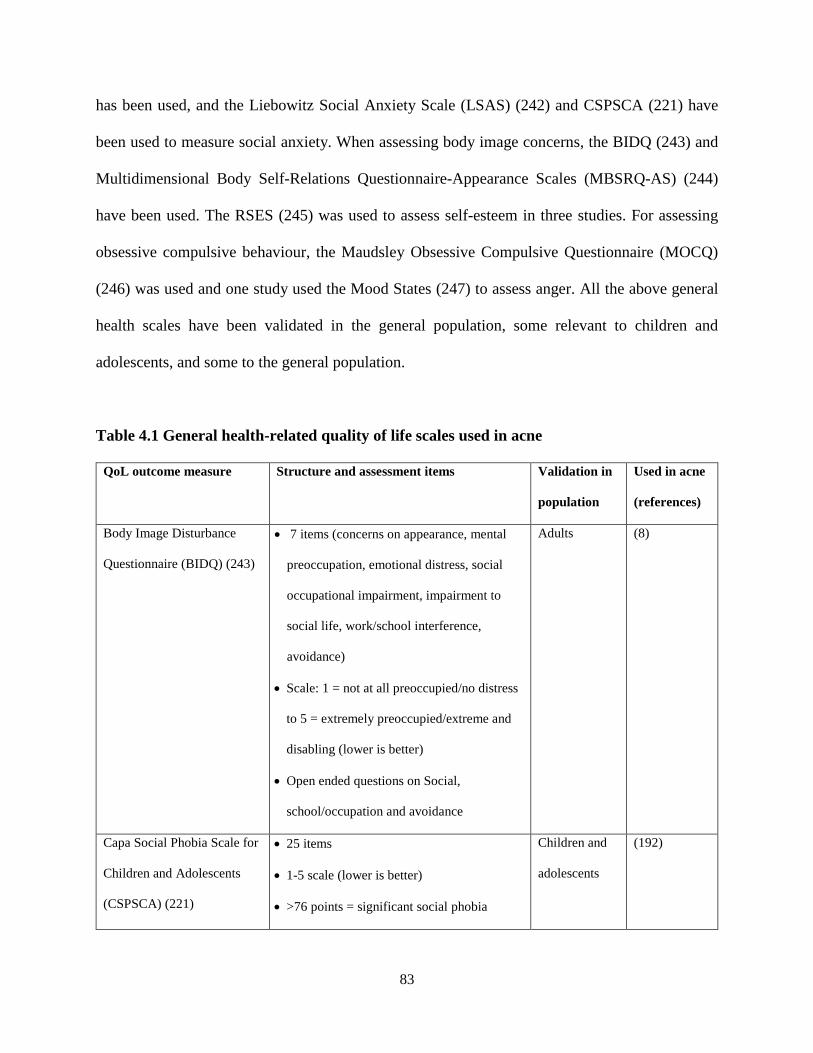
83
has been used, and the Liebowitz Social Anxiety Scale (LSAS) (242) and CSPSCA (221) have
been used to measure social anxiety. When assessing body image concerns, the BIDQ (243) and
Multidimensional Body Self-Relations Questionnaire-Appearance Scales (MBSRQ-AS) (244)
have been used. The RSES (245) was used to assess self-esteem in three studies. For assessing
obsessive compulsive behaviour, the Maudsley Obsessive Compulsive Questionnaire (MOCQ)
(246) was used and one study used the Mood States (247) to assess anger. All the above general
health scales have been validated in the general population, some relevant to children and
adolescents, and some to the general population.
Table 4.1 General health-related quality of life scales used in acne
QoL outcome measure Structure and assessment items Validation in
population
Used in acne
(references)
Body Image Disturbance
Questionnaire (BIDQ) (243)
• 7 items (concerns on appearance, mental
preoccupation, emotional distress, social
occupational impairment, impairment to
social life, work/school interference,
avoidance)
• Scale: 1 = not at all preoccupied/no distress
to 5 = extremely preoccupied/extreme and
disabling (lower is better)
• Open ended questions on Social,
school/occupation and avoidance
Adults (8)
Capa Social Phobia Scale for
Children and Adolescents
(CSPSCA) (221)
• 25 items
• 1-5 scale (lower is better)
• >76 points = significant social phobia
Children and
adolescents
(192)
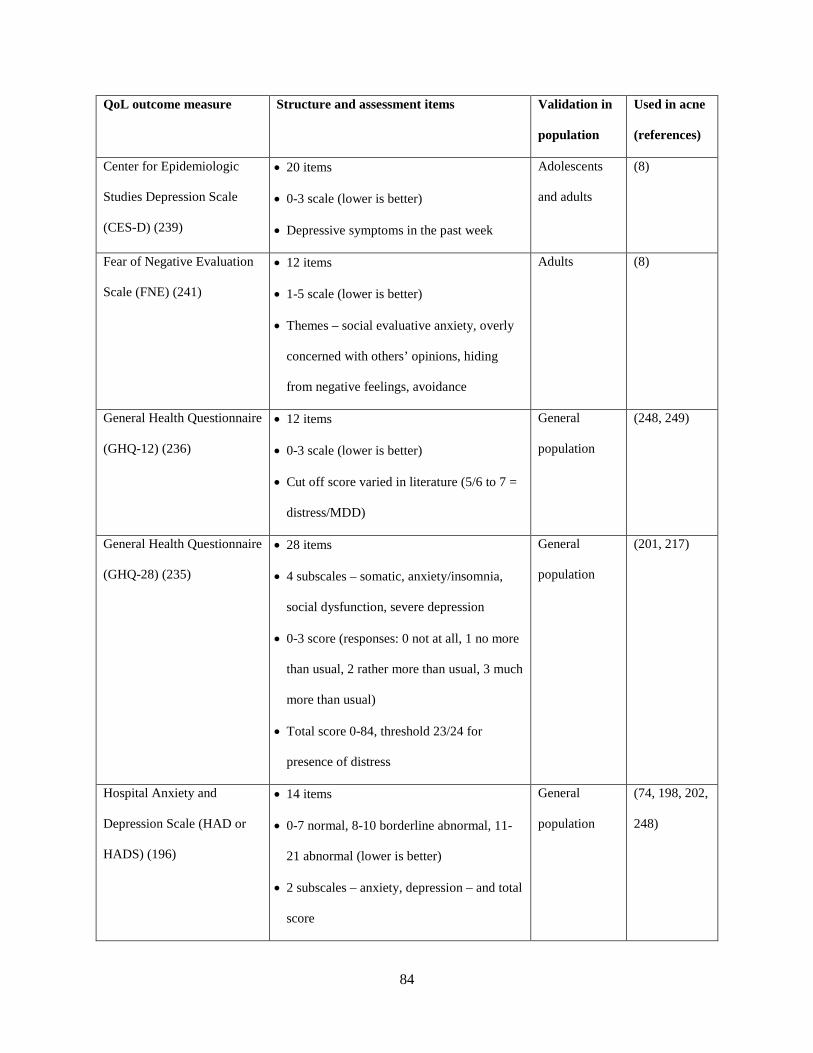
84
QoL outcome measure Structure and assessment items Validation in
population
Used in acne
(references)
Center for Epidemiologic
Studies Depression Scale
(CES-D) (239)
• 20 items
• 0-3 scale (lower is better)
• Depressive symptoms in the past week
Adolescents
and adults
(8)
Fear of Negative Evaluation
Scale (FNE) (241)
• 12 items
• 1-5 scale (lower is better)
• Themes – social evaluative anxiety, overly
concerned with others’ opinions, hiding
from negative feelings, avoidance
Adults (8)
General Health Questionnaire
(GHQ-12) (236)
• 12 items
• 0-3 scale (lower is better)
• Cut off score varied in literature (5/6 to 7 =
distress/MDD)
General
population
(248, 249)
General Health Questionnaire
(GHQ-28) (235)
• 28 items
• 4 subscales – somatic, anxiety/insomnia,
social dysfunction, severe depression
• 0-3 score (responses: 0 not at all, 1 no more
than usual, 2 rather more than usual, 3 much
more than usual)
• Total score 0-84, threshold 23/24 for
presence of distress
General
population
(201, 217)
Hospital Anxiety and
Depression Scale (HAD or
HADS) (196)
• 14 items
• 0-7 normal, 8-10 borderline abnormal, 11-
21 abnormal (lower is better)
• 2 subscales – anxiety, depression – and total
score
General
population
(74, 198, 202,
248)
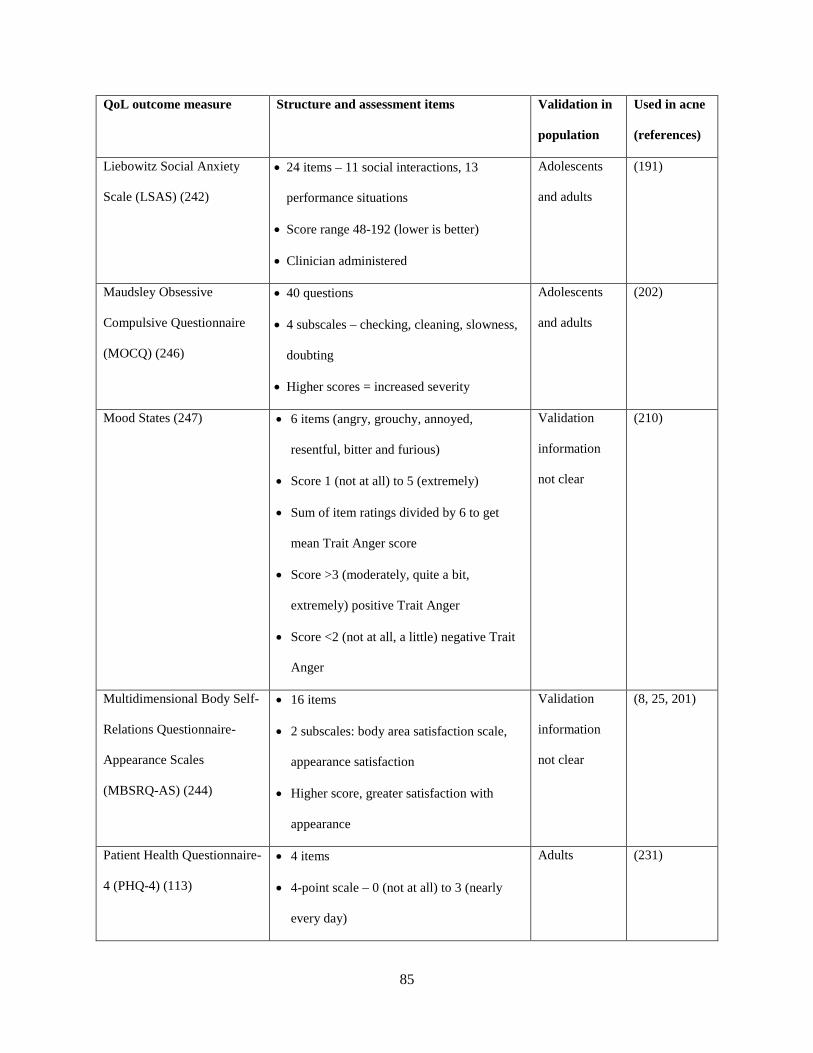
85
QoL outcome measure Structure and assessment items Validation in
population
Used in acne
(references)
Liebowitz Social Anxiety
Scale (LSAS) (242)
• 24 items – 11 social interactions, 13
performance situations
• Score range 48-192 (lower is better)
• Clinician administered
Adolescents
and adults
(191)
Maudsley Obsessive
Compulsive Questionnaire
(MOCQ) (246)
• 40 questions
• 4 subscales – checking, cleaning, slowness,
doubting
• Higher scores = increased severity
Adolescents
and adults
(202)
Mood States (247) • 6 items (angry, grouchy, annoyed,
resentful, bitter and furious)
• Score 1 (not at all) to 5 (extremely)
• Sum of item ratings divided by 6 to get
mean Trait Anger score
• Score >3 (moderately, quite a bit,
extremely) positive Trait Anger
• Score <2 (not at all, a little) negative Trait
Anger
Validation
information
not clear
(210)
Multidimensional Body Self-
Relations Questionnaire-
Appearance Scales
(MBSRQ-AS) (244)
• 16 items
• 2 subscales: body area satisfaction scale,
appearance satisfaction
• Higher score, greater satisfaction with
appearance
Validation
information
not clear
(8, 25, 201)
Patient Health Questionnaire-
4 (PHQ-4) (113)
• 4 items
• 4-point scale – 0 (not at all) to 3 (nearly
every day)
Adults (231)
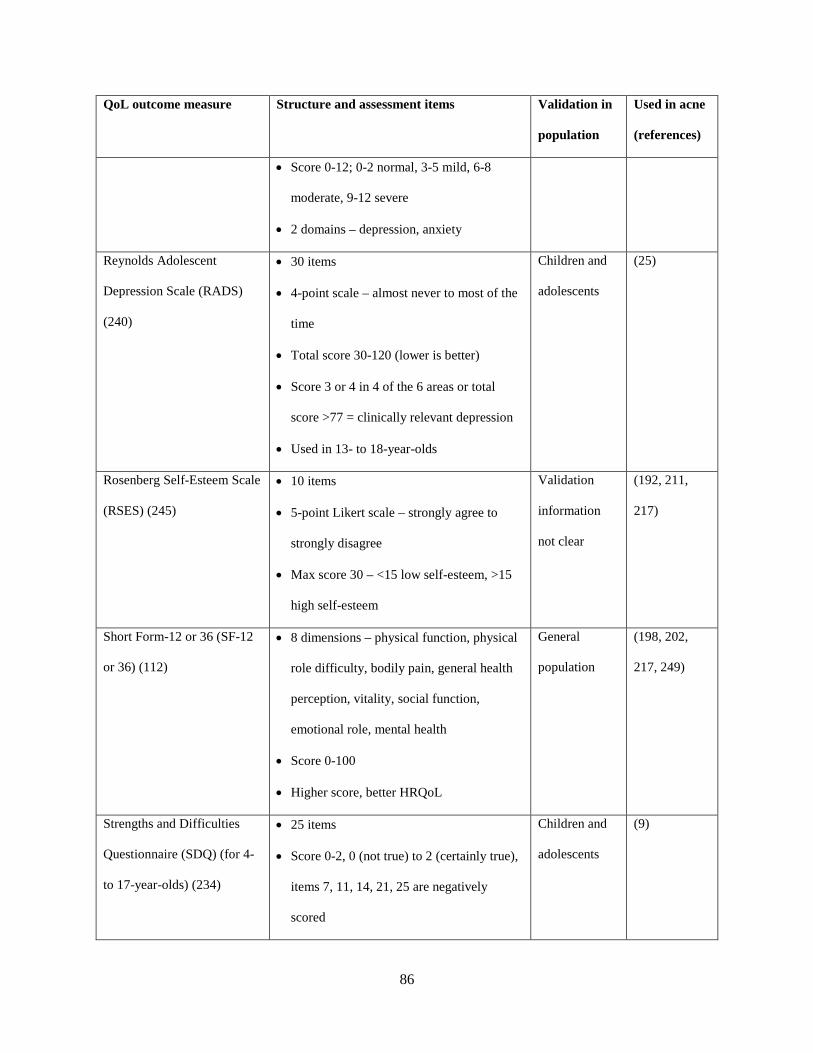
86
QoL outcome measure Structure and assessment items Validation in
population
Used in acne
(references)
• Score 0-12; 0-2 normal, 3-5 mild, 6-8
moderate, 9-12 severe
• 2 domains – depression, anxiety
Reynolds Adolescent
Depression Scale (RADS)
(240)
• 30 items
• 4-point scale – almost never to most of the
time
• Total score 30-120 (lower is better)
• Score 3 or 4 in 4 of the 6 areas or total
score >77 = clinically relevant depression
• Used in 13- to 18-year-olds
Children and
adolescents
(25)
Rosenberg Self-Esteem Scale
(RSES) (245)
• 10 items
• 5-point Likert scale – strongly agree to
strongly disagree
• Max score 30 – <15 low self-esteem, >15
high self-esteem
Validation
information
not clear
(192, 211,
217)
Short Form-12 or 36 (SF-12
or 36) (112)
• 8 dimensions – physical function, physical
role difficulty, bodily pain, general health
perception, vitality, social function,
emotional role, mental health
• Score 0-100
• Higher score, better HRQoL
General
population
(198, 202,
217, 249)
Strengths and Difficulties
Questionnaire (SDQ) (for 4-
to 17-year-olds) (234)
• 25 items
• Score 0-2, 0 (not true) to 2 (certainly true),
items 7, 11, 14, 21, 25 are negatively
scored
Children and
adolescents
(9)
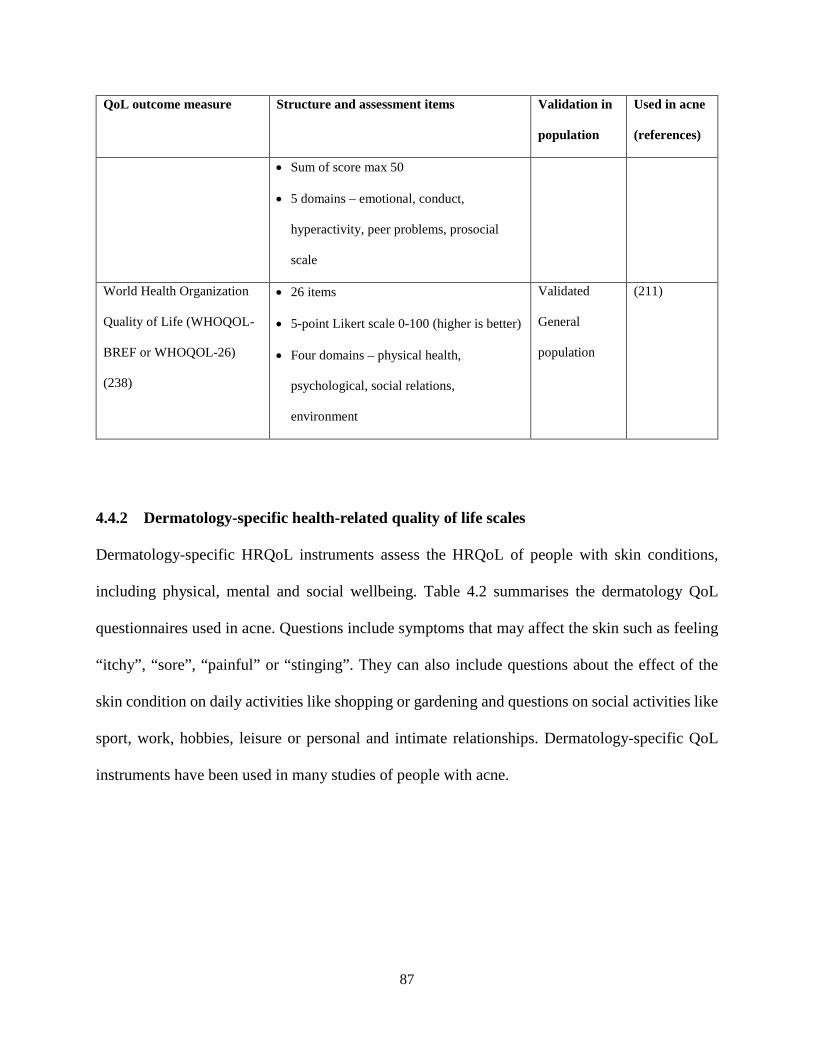
87
QoL outcome measure Structure and assessment items Validation in
population
Used in acne
(references)
• Sum of score max 50
• 5 domains – emotional, conduct,
hyperactivity, peer problems, prosocial
scale
World Health Organization
Quality of Life (WHOQOL-
BREF or WHOQOL-26)
(238)
• 26 items
• 5-point Likert scale 0-100 (higher is better)
• Four domains – physical health,
psychological, social relations,
environment
Validated
General
population
(211)
4.4.2 Dermatology-specific health-related quality of life scales
Dermatology-specific HRQoL instruments assess the HRQoL of people with skin conditions,
including physical, mental and social wellbeing. Table 4.2 summarises the dermatology QoL
questionnaires used in acne. Questions include symptoms that may affect the skin such as feeling
“itchy”, “sore”, “painful” or “stinging”. They can also include questions about the effect of the
skin condition on daily activities like shopping or gardening and questions on social activities like
sport, work, hobbies, leisure or personal and intimate relationships. Dermatology-specific QoL
instruments have been used in many studies of people with acne.

88
Table 4.2 Dermatology QoL scales used in acne
QoL outcome measure Structure and assessment items Validation in
population
Used in acne
(references)
Dermatology Life
Quality Index (DLQI)
(114)
• 10 questions
• Each ranked 0-3 (not at all, a little, a lot,
very much respectively)
• 0-1 no effect, 2-5 small effect, 6-10
moderate effect, 11-20 large effect, 21-30
extreme effect
• Higher score = greater impairment
General
population
(37, 198, 203, 217,
222, 227)
Children’s
Dermatology Life
Quality Index (CDLQI)
(250)
• 10 items
• 4 scores – 0 not at all, 1 only a little, 2
quite a lot, 3 very much
• Max 30 score
• Higher score = greater impairment
Children (197, 213, 251)
Patient-generated
Dermatology Quality of
Life Scales (DQOLS)
• 29 items
• 5-point Likert scale
• 4 psychosocial subscales (embarrassment,
despair, irritableness, distress)
• 4 activity subscales (everyday, summer,
social, sexual)
General
population
Found in skin
studies including
acne
Family Dermatology
Life Quality Index
(FDLQI) (75)
• 10 items
• Each item score 0 to 3
• Domains – emotional impact, burden of
care, physical wellbeing, extra household
expenditure, others’ perceptions
• Higher score = greater impairment
Adults (74)
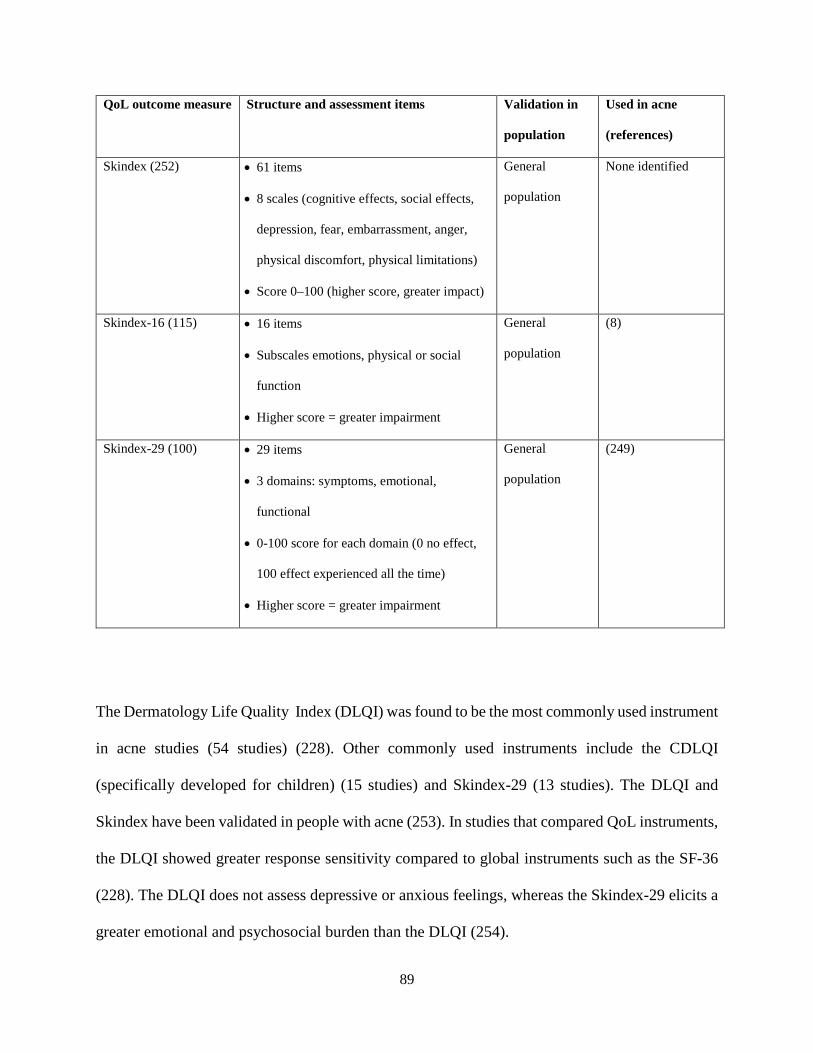
89
QoL outcome measure Structure and assessment items Validation in
population
Used in acne
(references)
Skindex (252) • 61 items
• 8 scales (cognitive effects, social effects,
depression, fear, embarrassment, anger,
physical discomfort, physical limitations)
• Score 0–100 (higher score, greater impact)
General
population
None identified
Skindex-16 (115) • 16 items
• Subscales emotions, physical or social
function
• Higher score = greater impairment
General
population
(8)
Skindex-29 (100) • 29 items
• 3 domains: symptoms, emotional,
functional
• 0-100 score for each domain (0 no effect,
100 effect experienced all the time)
• Higher score = greater impairment
General
population
(249)
The Dermatology Life Quality Index (DLQI) was found to be the most commonly used instrument
in acne studies (54 studies) (228). Other commonly used instruments include the CDLQI
(specifically developed for children) (15 studies) and Skindex-29 (13 studies). The DLQI and
Skindex have been validated in people with acne (253). In studies that compared QoL instruments,
the DLQI showed greater response sensitivity compared to global instruments such as the SF-36
(228). The DLQI does not assess depressive or anxious feelings, whereas the Skindex-29 elicits a
greater emotional and psychosocial burden than the DLQI (254).
90
4.4.3 Acne-specific health-related quality of life scales
Acne-specific HRQoL instruments have been developed to assess the HRQoL effects of acne.
Table 4.3 summarises the acne-specific HRQoL questionnaires. Instruments focus on physical,
mental and social wellbeing specific to acne and exclude questions about generic skin symptoms
such as itching and pain. Often questions have been developed based on focus groups of people
with acne (118, 255). Questions focus on emotions surrounding acne, self-consciousness,
attractiveness or avoidance of social or physical activities. Some have been developed for facial
acne only (for example, the Acne-QoL) and others for acne on the face and other common areas
such as the neck, upper back and upper chest (for example, the CADI). Numerous instruments
have been developed; however, there is no consensus on the most appropriate instruments to use
in clinical or research settings.
The Acne-QoL is the most frequently used acne-specific instrument used in clinical trials of
pharmaceutical interventions (23 studies) (228). It has been recommended for research purposes
by the EADV TF and other reviewers (228, 253). It showed similar results to APSEA and DLQI
instruments (256). The Acne-QoL (119-121) is a 19-item questionnaire separated into four
domains assessing the self-perception, social, emotional and acne symptom impacts on people with
facial acne. It asks questions based on “the past week”. It is a validated instrument for people aged
between 13 to 36 years old, and is scored using a 7-point Likert scale from 0 (extremely or
extensively) to 7 (not at all or none). The maximum score for the domains of self-perception, role-
emotional and symptom scores is 30. The maximum score for the role-social domain is 24. The
higher the score, the better the HRQoL.
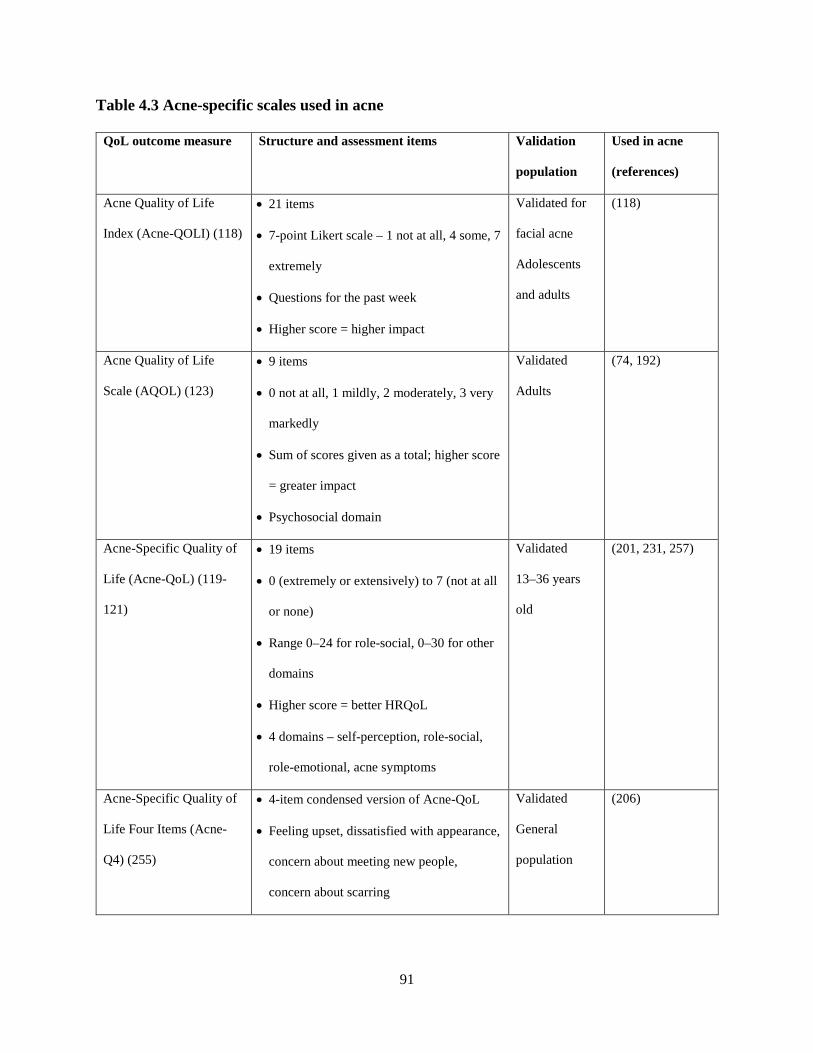
91
Table 4.3 Acne-specific scales used in acne
QoL outcome measure Structure and assessment items Validation
population
Used in acne
(references)
Acne Quality of Life
Index (Acne-QOLI) (118)
• 21 items
• 7-point Likert scale – 1 not at all, 4 some, 7
extremely
• Questions for the past week
• Higher score = higher impact
Validated for
facial acne
Adolescents
and adults
(118)
Acne Quality of Life
Scale (AQOL) (123)
• 9 items
• 0 not at all, 1 mildly, 2 moderately, 3 very
markedly
• Sum of scores given as a total; higher score
= greater impact
• Psychosocial domain
Validated
Adults
(74, 192)
Acne-Specific Quality of
Life (Acne-QoL) (119-
121)
• 19 items
• 0 (extremely or extensively) to 7 (not at all
or none)
• Range 0–24 for role-social, 0–30 for other
domains
• Higher score = better HRQoL
• 4 domains – self-perception, role-social,
role-emotional, acne symptoms
Validated
13–36 years
old
(201, 231, 257)
Acne-Specific Quality of
Life Four Items (Acne-
Q4) (255)
• 4-item condensed version of Acne-QoL
• Feeling upset, dissatisfied with appearance,
concern about meeting new people,
concern about scarring
Validated
General
population
(206)

92
QoL outcome measure Structure and assessment items Validation
population
Used in acne
(references)
Acne-Specific Impact
Scale (ASIS) (256)
• 17 items
• Score (unable to be determined)
• 2 domains (items 1–9 for signs, items 10–
17 on impact)
Validated
Adolescents
and adults
(258)
Assessment of the
Psychological and Social
Effects of acne (APSEA)
(259)
• 15 items
• Score 0–138
• Higher score = worse HRQoL
Validated (230)
Cardiff Acne Disability
Index (122)
• 5 items
• Scores 0–3
• Emotions (2 questions), social, avoidance
and acne symptoms
• Range 0–15; higher score = worse HRQoL
Validated
General
population
(211, 224, 227,
229, 260)
The shortened version of the Acne-QoL, the Acne-Q4 (255), is condensed to four questions about
feeling upset, dissatisfied with appearance, concerns about meeting new people and concerns about
scarring. It has been validated in people with acne and is relevant to all ages. Due to its brevity, it
has been recommended for use in routine clinical practice (254). Testing showed it was a good
predictor of the Acne-QoL total score (255).
The CADI was developed by Motley and Finlay (122). It is the second most frequently used
instrument to measure HRQoL in people with acne in a recent review (41 studies) (228). It has
five questions, two on emotions, one on social activities, one on avoidance of activities and one
on acne symptoms. These are scored 0 (not at all or not a problem) to 3 (very much, severely, all
93
the time). The higher the score, the worse the HRQoL. As it is such a brief instrument, it has been
recommended for use in clinical practice (228, 253, 254).
Other less frequently used acne-specific instruments include the Acne-QOLI (118), AQOL (123),
APSEA (259) and Acne-Specific Impact Scale (ASIS) (256). The Acne-QOLI is similar to the
Acne-QOL, also validated for acne on the face in adolescents and adults. It uses a 7-point Likert
scale of 1 (not at all) to 7 (extremely); in this case, higher scores indicate worse HRQoL. It also
asks questions based on “the past week”, but does not separate questions into domains. It has also
been recommended for clinical practice for a more comprehensive, in-depth view of HRQoL
compared to the CADI or AQOL (254).
The AQOL was developed by Gupta et al. (123) and is a validated instrument for adults over 18
years. It has 9 items on psychosocial domains, and is scored between 0 (not at all) and 3 (very
markedly). A higher score means a greater impact on HRQoL. It is also recommended to be used
in clinical practice due to its brevity (254). The APSEA (259) has 15 items which are summed to
provide a total score between 0 and 138. The first 6 questions of the APSEA relate to rumination
and self-perception. Participants can choose responses ranging from “a great deal of time” to “only
occasionally” for each question. The final 9 questions are on social activities such as shopping and
going out with friends. Participants can indicate their response by placing a line on an unmarked
visual analogue scale (0 to 10, with a blank space in between) or indicating “all the time”. The
APSEA has good correlation with the BDI and is suggested to be used in people with acne with
suspected psychiatric symptoms (254). The ASIS has 17 items divided into two domains. The first
domain relates to signs and symptoms such as oiliness and pimples. The second measures the
94
impacts of acne such as feeling embarrassed, self-conscious or annoyed. The instrument is
validated for facial acne only in adolescents and adults.
4.5 Health-related quality of life in Chinese medicine acne trials
HRQoL outcome is poorly studied in clinical studies of CHM and acupuncture for acne. Few
studies used HRQoL as an outcome measure in CM trials of acne (168). In a Cochrane review of
complementary medicine therapies for acne, only two studies reported on HRQoL (157). None of
the reported trials used an acne-specific HRQoL instrument. The dermatology-specific HRQoL
instruments Skindex-29 and DLQI were used. Recent trials from 2014 onwards have included
Skindex and DLQI. Most trials coming out of China have not reported on HRQoL.
4.6 Discussion
Acne vulgaris can be distressing to people due to the highly visible nature of the skin lesions along
with social stigmatisation (127). Scarring can result from acne and lead to longer term distress
(68). Acne often affects adolescents, at a time when many physiological, social and emotional
changes are occurring (207). Adolescents are trying to navigate through body image expectations,
development of intimate and personal relationships, and other social and sexuality issues. They
could be vulnerable to the psychological effects of skin conditions (261). They have less skills and
experience in coping with the additional stress of a condition that can cause considerable
embarrassment, depression and anxiety (190, 253). Acne HRQoL has also been associated with
gender, severity and late onset or relapses of acne into adulthood. In studies that used physician
assessment of acne severity, HRQoL scores did not correlate with severity; however, studies that
used self-assessment of acne severity had a correlation with worse HRQoL scores (74). Females
95
with acne and having facial acne have also been more associated with worse HRQoL (116, 215).
Other factors can be related to emotions such as anger and satisfaction with treatment (210).
Assessing the impact of acne on a patient’s HRQoL is important for acne management, and
recommendations have been made to include HRQoL assessments as part of routine clinical visits
(228, 253, 254). In the European clinical guidelines for acne, QoL instruments that are easy to use,
readily accessible and have meaningful scores that guide treatment choice have been
recommended. For example, worse HRQoL scores might influence the decision for a more
aggressive therapy (127). The Malaysian MOH Guidelines for Acne Management also state QoL
is an important factor in treatment adherence and subsequent treatment outcomes (126). Education
of the general public and people with acne is lacking and may improve people’s understanding and
lessen the impact on HRQoL (208, 214). Research can improve the understanding of the impact
and burden acne has on people.
The EADV TF (228) recommends brief instruments that are age, culturally and linguistically
appropriate for patients for clinical practice. For research, simultaneous use of general health,
dermatology-specific and acne-specific instruments was suggested, depending on the research
question being answered. The SF-36 is a general health instrument to measure HRQoL in people
with acne, the DLQI, CDLQI and Skindex-29 are dermatology-specific questionnaires, and the
CADI and Acne-QoL are acne-specific measures. Outcome measures for research should also be
language and age appropriate. Some instruments require payment for use; therefore researchers
and clinicians need to consider the financial cost of the instrument, and the limitations or biases
this may introduce in research.
96
Studies have shown that acne duration and severity do not necessarily correlate with acne-related
QoL changes (223); however, there have been more studies that have found a correlation with acne
severity than not (19, 37, 67, 191, 213, 224, 225). The assessment of severity grading is considered
an important factor in helping to understand if there is an impact on HRQoL according to acne
severity, and for clinical assessment and treatment. There is no consensus on the best tool to assess
severity. The AAD has suggested that grading systems need to be reproducible, easy to use and
accepted by dermatologists (145). The MOH has recommended using the Comprehensive Acne
Severity Scale (CASS), which is a modified version of the Investigator Global Assessment (IGA)
of Acne Severity and uses photographs to ensure there is consistency between assessors. It is
simple, reproducible and correlates with the Leeds technique. The Australian guideline – Acne
Best Practice Management (125) – suggests the textual and photographic grading used by Warner
and Plosker (262). The Acne Core Outcome Research Network (ACORN) as part of the Core
Outcome Measures in Effectiveness Trials (COMET) initiative has included HRQoL as one of the
core outcomes for clinical research (263).
Currently there is poor adoption of HRQoL outcomes in trials of CM. There have not been many
reviews on CHM and acupuncture for acne. Few trials used HRQoL as an outcome measure in
previous reviews such as DLQI and Skindex-29 (20, 185). The DLQI asks questions about
itchiness and the effect of acne on social activities such as sport, which may not be as relevant to
someone with acne. It is not sensitive to people with anxiety and depression associated with acne
(253). Similarly, the Skindex-29 also asks questions about itching, burning or stinging which again
are not specific to acne. The Skindex-29 is recommended as a complementary tool as there was no
97
correlation with the direct impact of the cutaneous signs on people with acne (253). Given this, a
study tool needs to be sensitive to emotional, social and symptom changes in relevant cohorts. The
use of an acne-specific HRQoL outcome tool would provide more meaningful data on the impact
of CM on acne.
4.7 Chapter summary
Acne vulgaris has been shown to have a substantial impact on the HRQoL of people with acne
including depression, anxiety, embarrassment and social isolation. There are more than 30
instruments used to evaluate HRQoL in people with acne ranging from general HRQoL scales to
dermatology-specific HRQoL scales and acne-specific HRQoL scales. The use of HRQoL tools
have been suggested in order to assess the impact and possible justification of treatment types for
acne. HRQoL is a poorly assessed outcome measure in CM clinical trials for acne. Previous CM
trials have used general health and generic dermatology instruments as outcome measures.
Previous HRQoL used in CM acne studies have included the Skindex-29 and DLQI. There is a
need to incorporate acne-specific HRQoL in order to assess the effect of CM interventions in
relation to acne on HRQoL.
98
CHAPTER 5 : Acne quality of life and acceptance of Chinese medicine
5.1 Introduction
The previous chapter (Chapter 4) summarised the impact that acne can have on HRQoL. These
included emotional, psychological and social impacts. Acne vulgaris (acne) can adversely affect
people’s HRQoL, with a similar disability impact as psoriasis (216). Clinical severity does not
always correlate with the burden of acne, as mild severity can still have a high impact on QoL
(223). This has been shown in several studies where older adolescents’ perceptions of their acne
were worse than clinicians’ assessments of lesions (22, 37, 60).
Acne has been associated with higher social phobia (190, 191, 195) and higher unemployment
levels (73) than for healthy controls. The perception of acne and acne scars are negatively viewed
(68). One study has shown that people with acne were scored less attractive compared to those
without acne (200). Low self-esteem is also common in people with acne (71, 192, 212). In
interviews conducted with people with acne, interviewees expressed they were worried,
embarrassed and self-conscious about taunting or teasing, and thought they were judged by others
as unclean, unattractive or less worthwhile than other people (71). This affected personal and
family relationships (72).
Facial acne has been shown to negatively affect HRQoL in women (121) and can lead to depression
and anxiety that impact on work and school (59). More than 75 per cent of the 218 female
participants in one study reported that facial acne made them feel less confident, more self-
99
conscious around other people, frustrated and embarrassed (59). Acne can negatively impact on
family members (74) and the negative impact of acne can last for a long time (37).
Australian data from 1997 showed 12 per cent of 2,491 school-aged children between 4 and 18
years old reported a high Acne Disability Index (ADI) score which correlated with clinical severity
(22). The most recent Australian survey on how acne affects the QoL of adolescents was published
in 2010 (248). Adolescents (n = 209) from high school year levels 8, 9 and 11 (aged 14 to 17 years
old) were surveyed three times within a year on the relationship between acne and psychiatric and
psychological comorbidities. The authors found no correlation between acne and psychological
comorbidities in the sample population. Response to the third survey round was low (11 per cent,
n = 25), limiting the reliability of the conclusions. There is no recent data on acne severity and
QoL in Australian adolescents, young people or adults.
5.1.1 Complementary and alternative medicine for management of acne
Most adolescents self-manage their acne. The proportion of people seeking medical management
has been reported to range from 2.4 per cent (264) to 17 per cent (265). In addition to medical
management, the use of complementary and alternative medicine (CAM) for acne is common (151,
155). In a small study of patients’ acne practices in Australia, the common products included witch
hazel (Hamamelis virginiana), tea-tree oil (Leptospermum spp.), citrus washes, aloe vera, zinc
tablets, herbal remedies, tissue salt tablets, natural oils and evening primrose oil (Oenothera
biennis) (155). A review of medicinal plants showed many had inhibitory effects on bacteria,
viruses and fungi in vitro (266).
100
In addition to evidence from experimental studies, there is some evidence for herbal products from
clinical studies. A systematic review of botanical and phytochemical treatments for acne reported
herbal preparations improved mild-to-moderate acne (20). The authors found only a few SAE were
reported, although the studies had methodological issues. AE such as sensitisation of skin from
topical CAM, specifically Chinese herbal medicine (CHM) which is considered a form of CAM,
have been reported but less than for BP (267).
5.1.2 Attitudes to treatment
Patients’ use of CAM including Chinese medicine (CM) is influenced by their perceptions and
beliefs about CAM (268, 269). These include the perception that CAM is a more natural approach
with less potential for adverse effects (267). For CM, beliefs are related to the perceived safety
and efficacy of herbs (269-271), a belief that CM is better for symptomatic relief (269) and herbs
being perceived as being more natural than chemical pharmaceuticals (270). The use of CAM (268)
and CM (270) is also influenced by recommendations from family and friends, and cultural or
educational knowledge of CM (271, 272).
People who have a more positive belief in CAM products are more likely to use such products
(273, 274). Patients’ belief in complementary medicine influences whether they will participate in
a trial (275) and how they participate in a trial (271). In considering trial designs, patient
preferences and stakeholder engagement are suggested to be taken into consideration to improve
participation (276). Tailoring a clinical trial according to stakeholders’ input can improve the
feasibility of a study, recruitment and retention, and adherence with treatment or trial protocol
(277, 278). Other factors for consideration include travel time and cost, and other health issues that
101
may prevent people from attending (277, 279). A recent survey of compliance with CHM in a
community acupuncture clinic highlighted barriers such as cost, efficacy, quality of herbs, side
effect of herbs, taste and product availability (280). A survey on the opinions of adolescents, young
people and adults on their perceptions of and preferences for CM treatments has the potential to
inform clinical trial design to maximise recruitment and adherence. Knowing patient preferences
will help with designing trials that closely reflect patients’ expectations and the reality of clinical
practice. This will provide direct evidence that can be translated into practice.
5.2 Aims and objectives
5.2.1 Aims
This study addresses three aims, to:
1. Determine how facial acne affects the HRQoL of adolescents, young people and adults in
Australia
2. Determine the attitudes towards CAM in adolescents, young people and adults with facial acne
3. Assess the willingness to take CM and preferences for different forms of CM interventions.
5.2.2 Objectives
To meet these aims, the following objectives were developed:
1. Conduct an online survey using Qualtrics including three components:
a. Use of a validated HRQoL for people with facial acne: Acne-Specific Quality of Life
b. Use of a validated questionnaire to assess attitudes about CAM: Complementary and
Alternative Questionnaire for Young Adults
c. Determining preferences for different types of CHM and acupuncture techniques.
102
2. Analyse the results to inform the development of a clinical trial protocol.
5.3 Methods
5.3.1 Study design
The aims of this study were addressed through the use of an online survey. Qualtrics is a secure
tool recommended by the RMIT Human Research Ethics Committee for distributing online
surveys and therefore was chosen to implement the survey. Ethics approval was obtained from the
College Human Ethics Advisory Network (CHEAN; SEHAPP 55-17; Appendices 8-12).
5.3.2 Inclusion and exclusion criteria
The survey was open to adolescents and young people (15 to 24 years old) and adults (≥ 25 years
old) with facial acne. Differences exist between authoritative sources in the definition of
adolescents and young people. The WHO defines the age of adolescents as between 10 and 19
years of age, and of young people as between 10 to 24 years of age (281). The UN defines
adolescents as between 10 and 19 years of age, and youth and young people as between 15 and 24
years of age (282). For the purposes of this study, the definition of youth and young people from
the UN has been adopted.
People with acne usually have lesions on their face, chest, upper back and neck (6). The face is
more visible to the public and more of a concern to patients (121), and is more likely to affect the
QoL. The outcome tool selected for assessment of HRQoL is specific to facial acne; hence one of
the inclusion criteria was people with facial acne.
103
5.3.3 Survey sampling
The survey was aimed at youth and young people (15 to 24 years old) and adults (>25 years old)
living in Australia. A convenience sampling approach was used. Convenience sampling,
particularly online methods, have the potential to reach a larger audience to recruit larger sample
sizes. These methods may reach participants in larger geographical locations and promote higher
engagement with those identifying with a condition or intervention (283). As one of the aims of
the study was to examine the impact of facial acne on QoL generally, it was not necessary to
structure sampling to obtain equal numbers of gender and age groups.
5.3.4 Participant recruitment
Participants were not offered incentives nor were they reimbursed for their participation in the
survey. For the pilot study, fifth year student representatives from the Disciplines of Chinese
Medicine, Chiropractic and Osteopathy in the School of Health and Biomedical Sciences of RMIT
University were contacted and asked to share the study information with their peers in August
2017. The response rate was low with only five pilot participants, so after two months, fourth year
students were also invited to participate and disseminate the pilot survey. Participants were
directed to the online website through a quick response (QR) code or an online link and asked to
answer two additional questions on the time they took to complete the survey and any questions
that were ambiguous to them (Appendix 4, Section 6). These two questions were removed from
the final survey and were not included in the final analysis. No ambiguous questions were
identified during the pilot period and no changes were made to the final survey questions.

104
The full survey was conducted between October 2017 and concluded in August 2018. Recruitment
for the full survey used various strategies. Student representatives from years one to four in the
programs of Chinese Medicine, Chiropractic and Osteopathy in the School of Health and
Biomedical Sciences were contacted to share information about the survey with their classmates.
Posters were placed around Melbourne-based university campuses and e-posters were placed in
the RMIT student and staff online newsletters. A specific Facebook page was developed for the
project. Other established websites were approached to disseminate the survey such as
www.acne.org, an online forum support website for people with acne. Administrators of Facebook
pages for RMIT, RMIT Student Association, RMIT social clubs and RMIT Big Science and Small
Science were also approached to link to the survey Facebook page. Sixty-nine local schools were
approached to advertise in their local school newsletters (see advertising details in Appendix 5).
Recruitment was slower than anticipated and ethics approval was obtained for additional
recruitment strategies including contacting dermatologists and other healthcare professionals such
as acupuncturists and naturopaths to place the advertisements in their practices.
Advertising directed the potential participants to an online website that held the secure Qualtrics
survey. If participants wanted to contact the researchers, telephone and email addresses were added
to the participant information and consent statement at the start of the survey. Participants indicated
consent to participate by selecting “agree to participate” in the survey and continuing on to the
survey. If they selected “I do not agree to participate”, the survey would take them to a thank you
note. Participants were able to close the browser to end participation in the survey at any point in
time.
105
5.3.5 Instrument
The survey was separated into four sections (see Appendix 4):
• Acne-QoL (questions 1 to 19)
• CAM Questionnaire for Young Adults (questions 20 to 37)
• Preferences for CM and trial design (questions 38 to 43)
• Demographics and previous treatment sought for acne (questions 44 to 51).
The Acne-QoL instrument (119, 121, 205) is a validated questionnaire for facial acne. It has 19
questions on participants’ feelings about their acne, medication usage and social interactions.
Questions include how unattractive, embarrassed, self-conscious or upset they feel about their acne.
The questions are grouped into four domains: self-perception, role-social, role-emotional and acne
symptoms. Scores are calculated by summing all items in each domain using an ordinal scale of 0
(“extremely” or “extensive”) to 6 (“not at all” or “none”). Each domain is weighted equally and
the higher the score, the better the HRQoL result. Self-perception, role-emotional and acne
symptoms are scored out of 30; role-social is scored out of 24 (refer to Appendix 4, Section 2).
Permission from the original author was obtained for its use (Appendix 6).
The CAM questionnaire was included into this survey to gain an understanding of the types of
CAM being used by people with acne. Questions in this component was directed at overall prior
use of CAM and not specifically CAM used for their acne. It also used to gauge a negative or
positive attitude to CAM. The CAM Questionnaire for Young Adults has been validated in young
adults (268). Permission has been obtained for its use (Appendix 7). It contains 18 questions in all,
6 on prior use of CAM and 13 on beliefs about CAM. Questions relate to the effectiveness and
106
safety of CAM, social factors influencing choices, and CAM providers. It uses a five-point Likert
scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”) (Appendix 4, Section 3). The
CAM beliefs component (questions 25–37 of the survey) is categorised into three domains –
positive beliefs about CAM (items 25–30, maximum score 30), environmental influences (items
31–34, maximum score 20) and psychological comfort (items 35–37, maximum score 15).
Patterson and Arthur (2009) explained psychological comfort as the reasoning behind people’s
attitudes to CAM. This can include physical, mental and spiritual aspects of health, and people’s
use of CAM due to the fear of discomfort from medical interventions and belief that using CAM
is not harmful. The maximum total score is 65. To determine respondents’ positive or negative
attitude towards CAM and their likelihood of using CAM, the total score is dichotomised at the
median. Participants were asked to answer questions on their beliefs about CAM treatments, their
prior use of CAM and the frequency of their usage of CAM. Some preliminary work has been
published on the validity of the CAM Questionnaire for Young Adults (268).
No existing surveys were identified that explore people’s preferences for CM treatments. The
questions for this section have been developed specifically for this survey. Questions include
preferences relating to the use of CHM and acupuncture therapies, and factors participants would
consider appropriate for the design of a clinical trial (refer to Appendix 4, Section 4). The
additional questions on CM were piloted with 10 people.
Additional questions on the demographics of participants included age, gender, ethnicity, self-
assessment of acne severity, acne duration and previous acne treatments (refer to Appendix 4,
Section 5). These questions were modelled on the Australian Bureau of Statistics Census 2016
107
demographics questions (284). Data was also collected on the length of time to complete the
questionnaire.
As the survey was anonymous and no identifying information was collected, a participant consent
and information form did not form part of the survey. Instead, a statement of participation and
consent was presented to participants prior to beginning the survey (Appendix 4, Section 1). A
question to “agree to participate” or “do not agree to participate” was asked prior to starting the
survey. Agreement for participation was implied through completion of the survey. Participants
could end participation or refuse to continue to participate or withdraw from the survey prior to
completion by closing their browser. Participants were also given the investigators’ contact details
to suggest follow-up if necessary. Should they plan to make a complaint or express concern about
the survey, the RMIT Human Research Ethics Committee details were given.
5.3.6 Ethics
The research was conducted in the College of Science, Engineering and Health, RMIT University.
Ethics was fully granted by the College Human Ethics Advisory Network (CHEAN) in August
2017 (SEHAPP 55-17) (Appendix 8). There were four further applications for amendments
(Appendices 9, 10, 11 and 12) to include additional recruitment methods. The amendments
included recruitment through Facebook and online media (Appendix 9), and two extensions of
time to allow for additional numbers to respond to the survey to (first to 30 May 2018, then to 31
December 2018) (Appendices 10 and 11). The fourth amendment was to gain permission to
approach health practitioners in the Melbourne metropolitan area to place the advertisements in
their health practices (general practitioners, dermatology specialists, CM practitioners and natural
health practitioners) to promote the survey (Appendix 12).
108
5.3.7 Data collection, storage and security
The online survey tool Qualtrics collated anonymous data and no identifying details of participants
were gathered. Data was downloaded into CSV and SPSS formats for further analysis. The data
was stored on a password-protected computer, secured by a password known only to the
investigators. Data will be held on the RMIT secure internet server for a minimum of five years
according to the RMIT research data storage policy.
5.3.8 Data analysis
SPSS (v.24 IBM Corporation) (285) was used to analyse the data. Descriptive statistics were used
for the demographics of the respondents. Inferential statistics were used to analyse the variables
of demographics, Acne-QoL, CAM Questionnaire for Young Adults and CM treatment
preferences. Results with probability (p) values of less than or equal to 0.05 were considered
significant.
Chi-square analysis was used to compare the characteristics of respondents (gender, age, ethnicity,
duration of acne and self-perception of acne severity) in order to examine the differences in their
responses to the Acne-QoL. Age was collapsed into two age groups as defined by the UN for youth
and adults. As respondents were all aged 45 and under, the youth group included 15 to 24 years
and the adult group included 25 to 45 years. Student’s t-test was used to determine the mean
differences between domains in the Acne-QoL survey (self-perception, role-social, role-emotional
and acne symptoms). For data that was not normally distributed, non-parametric tests were used.
Chi-square analysis was also used to examine the differences in CAM use and attitudes to CAM
by the characteristics of respondents. Student’s t-test or one-way analysis of variance (ANOVA)

109
was used to determine the mean difference of the three domains of positive beliefs, environmental
influences and psychological comfort compared between the different groups.
The Acne-QoL authors give instructions for handling missing data. A minimum of three items
must be answered within each domain to calculate domain scores, and a mean value within the
domain was calculated and replaced the missing values. Domain scores were not calculated if the
minimum number of questions was not answered for that domain. There was no missing data in
this section of the survey.
5.4 Results
Local high schools in the metropolitan Melbourne area were contacted in two rounds to place the
posters in their newsletters to advertise the survey. In the first round 29 schools were contacted
and in the second round 40 schools were contacted. Only two schools contacted agreed to place
the advertisement in their online newsletter. There is no data on the number of health practices that
placed the advertisement in their practices.
A few recruitment issues arose during the survey process. The timing of the initial recruitment
phase occurred around the end of the semester, when there were fewer students around to see the
advertisements. Students at the end of the semester were also receiving requests from the
University to complete other learning and teaching surveys, and there is anecdotal evidence that
students can have “survey fatigue” and therefore may be less inclined to complete other surveys.
Online forms of recruitment such as the University Facebook page and RMIT Social Groups’
pages were not successful as these pages limited the type of information they would allow. For

110
example, the RMIT Students’ Facebook page would only allow an advertisement if the project
offered an incentive to students such as vouchers or discounts. Contact with other online sources
such as www.acne.org did not yield a response. Another online recruitment issue was with the
timing of the creation of the Facebook page. During the creation of the page, Facebook was
receiving negative media publicity and the public was protesting by decreasing use of the social
media website (286).
Contacting high schools did not yield many positive responses with only two of the 69 schools
contacted agreeing to advertise in their school newsletters. Most schools responded that they
received many requests to participate in research and would participate if the research aligned with
their school’s mission. Finally, reaching out to health professionals such as dermatologists and
other CAM providers did not yield many responses.
5.4.1 Demographic data
At termination of the survey, 36 responses had been obtained (Table 5.1). Of the 36 respondents,
8 (22.2 per cent) consented only and did not answer any further questions, with 28 continuing on
to the survey questions. Of the 28 remaining respondents, 22 (61.1 per cent) completed all sections
of the survey and 6 (16.7 per cent) partially completed the survey. The number of responses varied
across different sections. Twenty-eight completed the Acne-QoL section (none missing), 27
completed the CAM use component of the CAM questionnaire (one missing), 25 completed the
CAM beliefs component of the CAM questionnaire (3 missing), 22 completed the treatment
preferences (6 missing) and 22 completed the demographics section (6 missing). Data were tested
for normal distribution and no deviations were detected. More respondents were female (17/22)
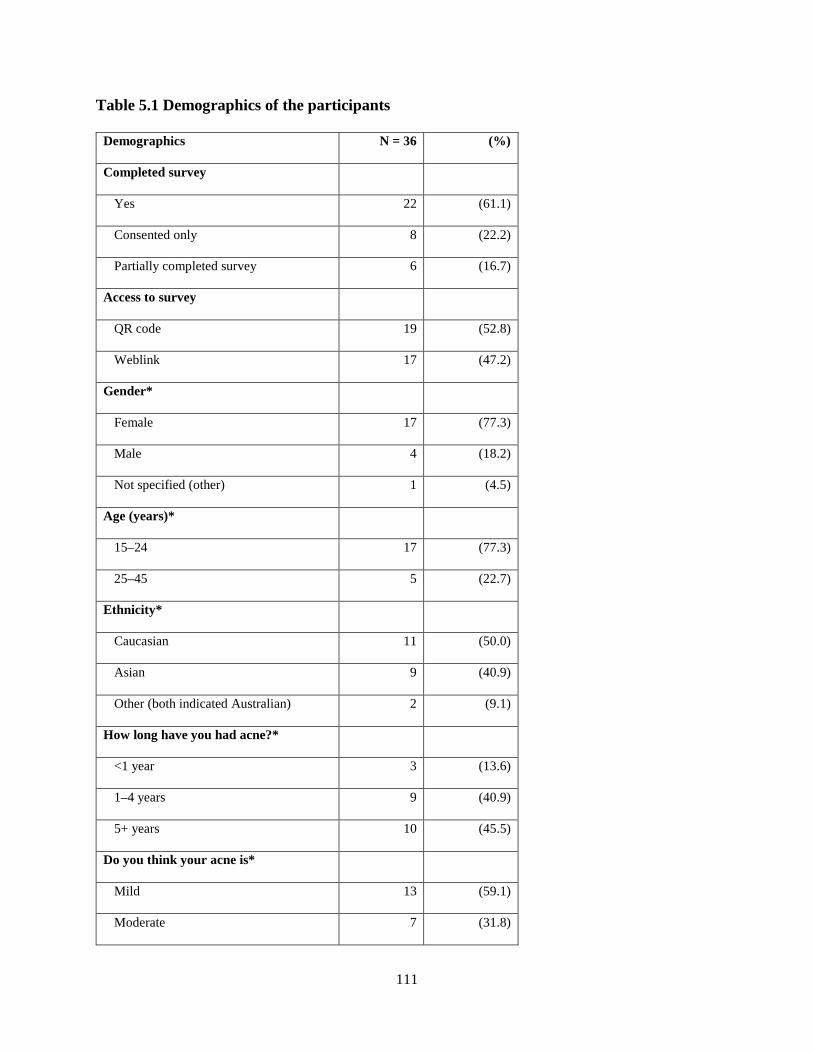
111
Table 5.1 Demographics of the participants
Demographics N = 36 (%)
Completed survey
Yes 22 (61.1)
Consented only 8 (22.2)
Partially completed survey 6 (16.7)
Access to survey
QR code 19 (52.8)
Weblink 17 (47.2)
Gender*
Female 17 (77.3)
Male 4 (18.2)
Not specified (other) 1 (4.5)
Age (years)*
15–24 17 (77.3)
25–45 5 (22.7)
Ethnicity*
Caucasian 11 (50.0)
Asian 9 (40.9)
Other (both indicated Australian) 2 (9.1)
How long have you had acne?*
<1 year 3 (13.6)
1–4 years 9 (40.9)
5+ years 10 (45.5)
Do you think your acne is*
Mild 13 (59.1)
Moderate 7 (31.8)
112
Demographics N = 36 (%)
Severe 2 (9.1)
*Note: demographic information calculated for those “completed survey” (n=22)
than male (4/22). One respondent chose “other” in the question on gender. The youngest
respondents were between 15 and 19 years old, and the oldest was between 36 and 40 years old.
Of the 22 participants who responded to the question of their age, most were between 15 and 24
years old (young people group; 17 respondents, 77.3 per cent) and the remainder were 25 to 45
years old (adult group; 5 respondents, 22.7 per cent). There were no respondents older than 45
years. Respondents mostly identified themselves as Caucasian (11 respondents, 50.0 per cent),
with 40.9 per cent (9 respondents) identifying as Asian. Of the two who responded “other” for
ethnicity, one identified as Australian and the other stated “A”. Compared to the general
population, the age group of the respondents of the survey is within the age range of adolescents
and adults with acne. There are less reports of people with acne over the age of 45 and more at
adolescent and young adults age.
There were slightly more respondents who had had their acne for five or more years (10
respondents, 45.5 per cent) compared to one to four years (9 respondents, 40.9 per cent) and three
respondents who had had their acne for less than a year (13.6 per cent). Most respondents
considered their acne to be mild in severity (13 respondents, 59.1 per cent), with seven who
considered their acne to be moderate (31.8 per cent) and two who considered their acne to be
severe (9.1 per cent). More than half of the respondents who responded to gender reported having
mild acne (11/17 females, 64.7 per cent and 2/4 males, 50 per cent), seven reported moderate acne
(5/17 female, 29.4 per cent, 2/4 males 50 per cent) and one “other” gender reported severe acne

113
(100 per cent) (χ2 = 11.149, df = 4, p = 0.025) with no significant difference in severity across the
different age groups and ethnic groups (χ2 =1.351, df = 2, p=0.509 and χ2 =5.368, df = 4, p=0.252
respectively).
Most had sought medical advice for their acne (14/22 respondents, 63.6 per cent). Just over two-
thirds used prescribed topical medications such as antibiotics, adapalene, retinoids and BP (15/22
respondents, 68.2 per cent). Details of the medications are listed in Table 5.2. Nine respondents
had previously used prescribed oral medications such as antibiotics and isotretinoin. Nine
respondents had used both topical and oral medications, five had used topical medications only
and no respondents had used oral medications only. Two respondents had used oral contraceptive
pills to control their acne. One respondent selected a number of the medications listed and also
selected “none of the above”. Since the respondent also checked many of the drugs, the “none of
the above” response was not applicable and therefore not calculated as a response.
Of the over-the-counter medications, salicylic acid lotions and creams such as Clearasil® were the
most used preparations (16 respondents, 72.7 per cent) (Table 5.3). As with the prescribed
medications section, one respondent chose many over-the-counter medicines and also “none of the
above”; therefore the “none of the above” response was not included in the calculations.

114
Table 5.2 Previous prescribed medications used
Previous prescribed medications used ‡ (N=22) (N=%)
Topical antibiotics and benzoyl peroxide (such as Duac Once Daily
Gel®) 14 (63.6)
Oral antibiotics 9 (40.9)
Topical antibiotics and benzoyl peroxide 6 (27.3)
Topical adapalene (such as Differin Topical Gel® or cream®) 5 (22.7)
Isotretinoin (such as Roaccutane®) 4 (18.2)
Topical retinoids (such as Stieva A Cream®, Re-Trieve Cream®) 4 (18.2)
Topical retinoids and benzoyl peroxide 4 (18.2)
Other (oral contraceptive pill, Chinese medicine, unspecified) 4 (18.2)
Benzoyl peroxide alone (such as Bentonite®) 2 (9.1)
None of the above 6 (27.3)
‡ Participants may have used more than one medication
Table 5.3 Previous over-the-counter medications used
Previous over-the-counter products used ‡ (N=22) (N=%)
Salicylic acid lotions and creams (such as Clearasil® with salicylic
acid) 16 (72.7)
Benzoyl peroxide lotions and creams (such as Proactive® or
Clearasil® with benzoyl peroxide) 15 (68.2)
Azelaic acid preparation (such as Dermatologica® or Ego
Azclear®) 7 (31.8)
Glycolic acid preparations (such as Glycolix®) 4 (18.2)
None of the above 3 (13.6)
Other (unspecified) 1 (4.5)
‡ Participants may have used more than one over-the-counter product
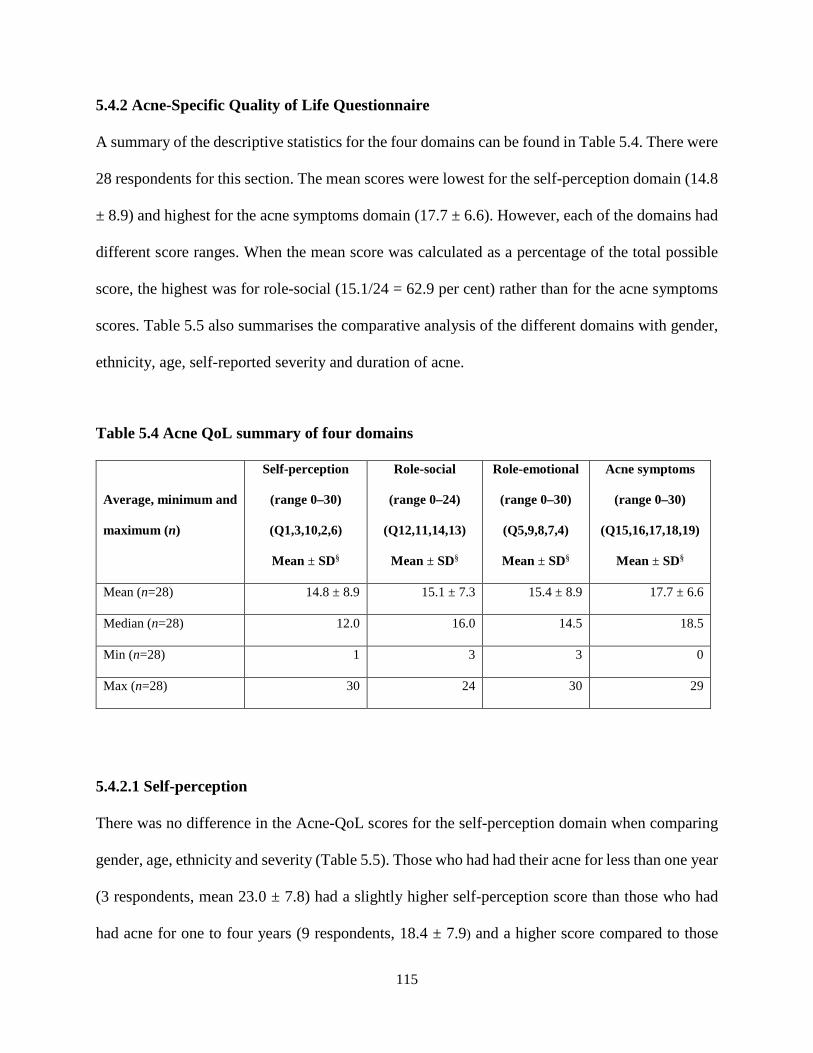
115
5.4.2 Acne-Specific Quality of Life Questionnaire
A summary of the descriptive statistics for the four domains can be found in Table 5.4. There were
28 respondents for this section. The mean scores were lowest for the self-perception domain (14.8
± 8.9) and highest for the acne symptoms domain (17.7 ± 6.6). However, each of the domains had
different score ranges. When the mean score was calculated as a percentage of the total possible
score, the highest was for role-social (15.1/24 = 62.9 per cent) rather than for the acne symptoms
scores. Table 5.5 also summarises the comparative analysis of the different domains with gender,
ethnicity, age, self-reported severity and duration of acne.
Table 5.4 Acne QoL summary of four domains
Average, minimum and
maximum (n)
Self-perception
(range 0–30)
(Q1,3,10,2,6)
Mean ± SD§
Role-social
(range 0–24)
(Q12,11,14,13)
Mean ± SD§
Role-emotional
(range 0–30)
(Q5,9,8,7,4)
Mean ± SD§
Acne symptoms
(range 0–30)
(Q15,16,17,18,19)
Mean ± SD§
Mean (n=28) 14.8 ± 8.9 15.1 ± 7.3 15.4 ± 8.9 17.7 ± 6.6
Median (n=28) 12.0 16.0 14.5 18.5
Min (n=28) 1 3 3 0
Max (n=28) 30 24 30 29
5.4.2.1 Self-perception
There was no difference in the Acne-QoL scores for the self-perception domain when comparing
gender, age, ethnicity and severity (Table 5.5). Those who had had their acne for less than one year
(3 respondents, mean 23.0 ± 7.8) had a slightly higher self-perception score than those who had
had acne for one to four years (9 respondents, 18.4 ± 7.9) and a higher score compared to those
116
who had had acne for more than five years (11.1 ± 7.8). This result was statistically significant (p
= 0.049). In a post-hoc analysis, there was no significant difference between the less than one year
group and the one to four year group (p = 1.000) or the five or more years group (p = 0.099). There
was also no significant difference between the one to four year group and the five or more years
group (p = 0.168).
5.4.2.2 Role-social
There was no difference in the Acne-QoL score for the role-social domain when comparing group
differences in all the characteristics: gender, age, ethnicity, severity of acne and duration of acne.
5.4.2.3 Role-emotional
There was also no difference in the Acne-QoL score in the role-emotional domain when comparing
gender, age, ethnicity and severity. Those with self-reported moderate acne (7 respondents, mean
10.3 ± 4.2) had a lower mean score than those with mild or severe acne, although this result was
not statistically significant (p = 0.064). Those who had had their acne for five or more years (10
respondents, mean 11.0 ± 8.4) were more emotionally affected by their facial acne. In a post-hoc
analysis, there was more emotional impact in people who had had acne for five or more years
compared to the less than one year group (p = 0.031) and in the five or more years group compared
to the one to four years group (p = 0.050). There was no statistical difference between the less than
one year group and the one to four years group (p = 0.979).
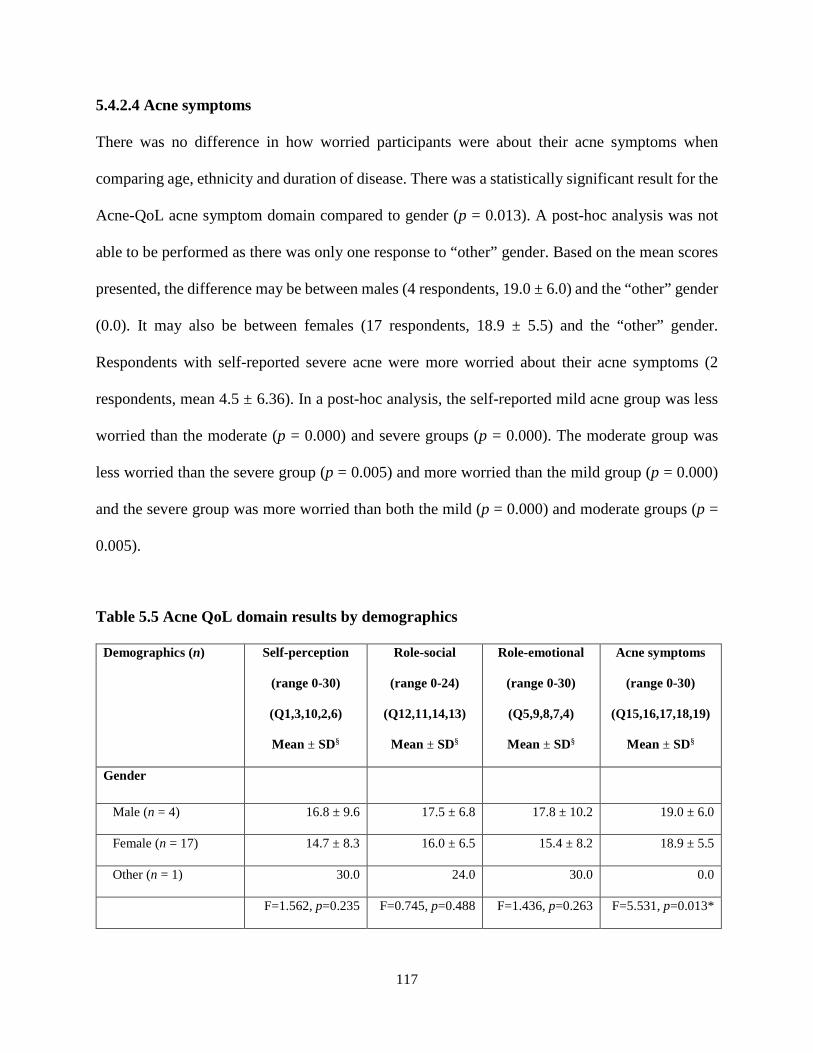
117
5.4.2.4 Acne symptoms
There was no difference in how worried participants were about their acne symptoms when
comparing age, ethnicity and duration of disease. There was a statistically significant result for the
Acne-QoL acne symptom domain compared to gender (p = 0.013). A post-hoc analysis was not
able to be performed as there was only one response to “other” gender. Based on the mean scores
presented, the difference may be between males (4 respondents, 19.0 ± 6.0) and the “other” gender
(0.0). It may also be between females (17 respondents, 18.9 ± 5.5) and the “other” gender.
Respondents with self-reported severe acne were more worried about their acne symptoms (2
respondents, mean 4.5 ± 6.36). In a post-hoc analysis, the self-reported mild acne group was less
worried than the moderate (p = 0.000) and severe groups (p = 0.000). The moderate group was
less worried than the severe group (p = 0.005) and more worried than the mild group (p = 0.000)
and the severe group was more worried than both the mild (p = 0.000) and moderate groups (p =
0.005).
Table 5.5 Acne QoL domain results by demographics
Demographics (n) Self-perception
(range 0-30)
(Q1,3,10,2,6)
Mean ± SD§
Role-social
(range 0-24)
(Q12,11,14,13)
Mean ± SD§
Role-emotional
(range 0-30)
(Q5,9,8,7,4)
Mean ± SD§
Acne symptoms
(range 0-30)
(Q15,16,17,18,19)
Mean ± SD§
Gender
Male (n = 4) 16.8 ± 9.6 17.5 ± 6.8 17.8 ± 10.2 19.0 ± 6.0
Female (n = 17) 14.7 ± 8.3 16.0 ± 6.5 15.4 ± 8.2 18.9 ± 5.5
Other (n = 1) 30.0 24.0 30.0 0.0
F=1.562, p=0.235 F=0.745, p=0.488 F=1.436, p=0.263 F=5.531, p=0.013*

118
Demographics (n) Self-perception
(range 0-30)
(Q1,3,10,2,6)
Mean ± SD§
Role-social
(range 0-24)
(Q12,11,14,13)
Mean ± SD§
Role-emotional
(range 0-30)
(Q5,9,8,7,4)
Mean ± SD§
Acne symptoms
(range 0-30)
(Q15,16,17,18,19)
Mean ± SD§
Age
15–24 (n = 17) 15.6 ± 9.1 16.0 ± 7.0 16.9 ± 8.2 17.0 ± 6.9
25–45 (n = 5) 16.2 ± 8.6 18.8 ± 4.4 14.8 ± 11.4 21.8 ± 4.4
t=-0.134, p=0.895 t=-0.844, p=0.409 t=0.472, p=0.642 t=-1.453, p=0.162
Ethnicity
Caucasian (n = 11) 13.7 ± 8.7 14.7 ± 7.3 13.4 ± 8.4 17.4 ± 5.1
Asian (n = 9) 17.7 ± 7.8 18.8 ± 4.8 18.8 ± 8.4 20.9 ± 5.8
Other (n=2) 18.0 ± 17.0 17.5 ± 9.2 23.0 ± 9.920 9.5 ± 13.424
F=0.550, p=0.586 F=0.986, p=0.391 F=1.664, p=0.216 F=3.004, p=0.073
Severity
Mild (n = 13) 18.6 ± 7.9 18.7 ± 5.5 19.7 ± 8.0 22.5 ± 3.3
Moderate (n = 7) 10.4 ± 4.8 13.4 ± 5.9 10.3 ± 4.2 13.9 ± 1.6
Severe (n = 2) 15.5 ± 20.5 14.5 ± 13.4 17.0 ± 18.4 4.5 ± 6.4
F=2.217, p=0.136 F=1.736, p=0.203 F=3.187, p=0.064 F=37.440, p=0.000*
Duration
Less than 1 year (n = 3) 23.0 ± 7.8 20.7 ± 4.2 24.7 ± 7.5 25.7 ± 4.9
1–4 years (n = 9) 18.4 ± 7.9 17.7 ± 6.2 19.8 ± 5.7 17.0 ± 7.1
5+ years (n = 10) 11.1 ± 7.8 14.5 ± 7.0 11.0 ± 8.4 16.8 ± 5.6
F=3.557, p=0.049* F=1.270, p=0.304 F=5.658, p=0.012* F=2.589, p=0.101
* Statistically significant results
§ Results presented of available responses
119
5.4.3 Complementary and Alternative Medicine (CAM) Questionnaire for Young Adults
There were 27 respondents who started the CAM Questionnaire for Young Adults section of the
survey and 25 who completed this section. For the first question on CAM use: “Have you used
complementary/alternative medicine (CAM)?”, participants were asked to “check all that apply”.
Most respondents had used CAM for treating illness (14 respondents, 51.9 per cent). Twelve
respondents (44.4 per cent) had never used CAM before, 11 (40.7 per cent) had used it to improve
their health and one chose “other” but did not specify the purpose (3.7 per cent). Nine respondents
(33.3 per cent) had used CAM to prevent illness. Nine had used CAM to prevent and treat illness
and to improve their health, three had used it to treat illness only, two had used it to treat illness
and to improve health, and one chose “other” but did not describe why they had used CAM. When
asked to best describe their healthcare practices, six respondents (22.2 per cent) had only used
CAM and not other treatments, and nine (33.3 per cent) had used CAM given by their medical
doctors.
Fifteen participants responded to the questions on which natural health products or therapies they
had used, all having used CAM previously. None of the respondents reported using colour or dance
movement therapy, magnetic therapy, reflexology, shiatsu or therapeutic touch. Respondents were
able to choose more than one CAM. Results presented are categorised according to the National
Center for Complementary and Alternative Medicine (15). All respondents had used at least one
of the alternative medical systems such as traditional CM, Ayurvedic medicine or naturopathy.
Within this group, CM was the most used, with 13 respondents having used “traditional Chinese
medicine”. Twelve had used CAM products, nine had used mind-body therapies, seven had used

120
manipulative and body-based therapies, two had used creative therapies and two had used others
(aromatherapy and magnet therapy).
Five of these 15 participants (33.3 per cent) took natural health products daily, four (26.7 per cent)
took them weekly and three (20 per cent) took them monthly. Another respondent (2.7 per cent)
took natural health products less often than once a year. Seven (46.7 per cent) saw CAM providers
weekly, two each (13.3 per cent) saw them monthly or less than once per year (13.3 per cent), and
one respondent saw them once per year (6.7 per cent). Participants were not asked about the reason
for their use of CAM.
There were 25 respondents to the CAM beliefs component of the survey. The total score of three
domains ranged from 29 to 61 (maximum score 65) with a mean total score of 48.2 (± 7.4). The
minimum, maximum and mean scores of the three domains are presented in Table 5.6.
For individual question responses, answers for “agree” and “strongly agree” were combined and
answers for “disagree” and “strongly disagree” were combined. Respondents believed young
adults would use CAM if they had more knowledge (question 31, 21 respondents), exposure to
CAM (question 32, 21 respondents) and if their friends were using it (question 33, 21 respondents)
(Table 5.7). Young adults agreed or strongly agreed that CAM providers gave good information
on maintaining a healthy lifestyle (question 25, 19 respondents) and would use CAM if their
coaches or teachers discussed CAM with them (question 34, 18 respondents). Over 60 per cent of
respondents believed that CAM has fewer side effects when taking natural remedies (question 26,
17 respondents), that young adults who believe in physical, mental and spiritual health are more
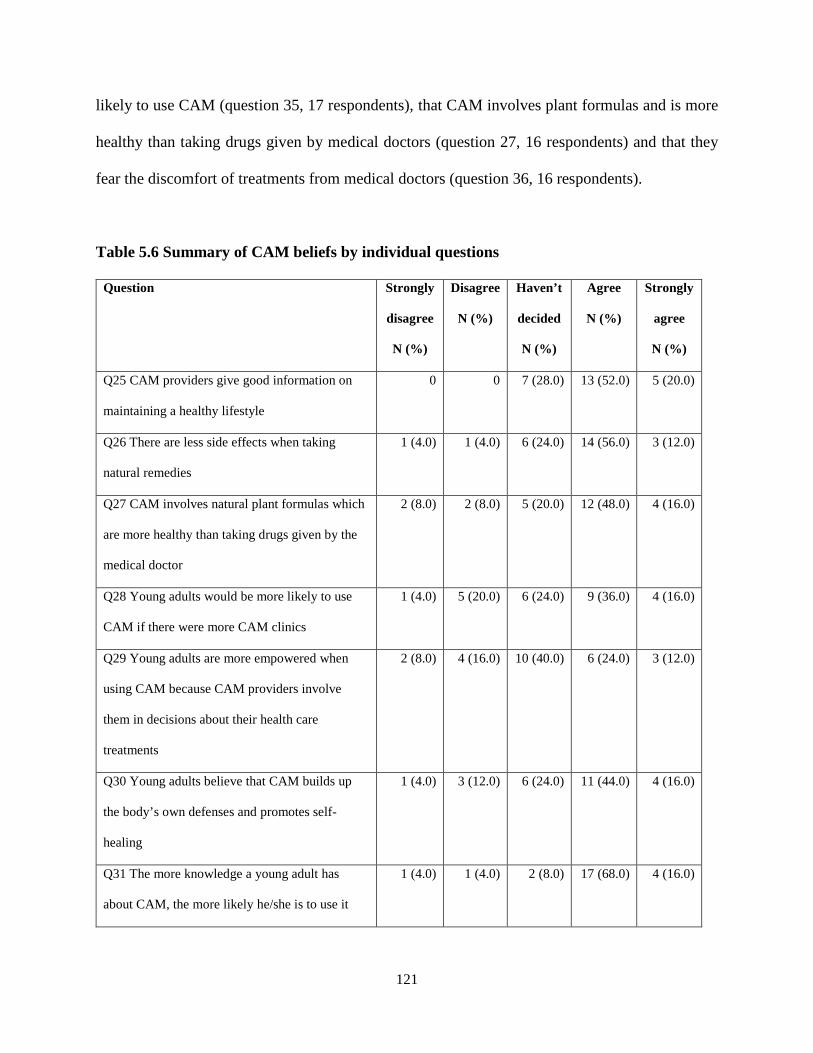
121
likely to use CAM (question 35, 17 respondents), that CAM involves plant formulas and is more
healthy than taking drugs given by medical doctors (question 27, 16 respondents) and that they
fear the discomfort of treatments from medical doctors (question 36, 16 respondents).
Table 5.6 Summary of CAM beliefs by individual questions
Question Strongly
disagree
N (%)
Disagree
N (%)
Haven’t
decided
N (%)
Agree
N (%)
Strongly
agree
N (%)
Q25 CAM providers give good information on
maintaining a healthy lifestyle
0 0 7 (28.0) 13 (52.0) 5 (20.0)
Q26 There are less side effects when taking
natural remedies
1 (4.0) 1 (4.0) 6 (24.0) 14 (56.0) 3 (12.0)
Q27 CAM involves natural plant formulas which
are more healthy than taking drugs given by the
medical doctor
2 (8.0) 2 (8.0) 5 (20.0) 12 (48.0) 4 (16.0)
Q28 Young adults would be more likely to use
CAM if there were more CAM clinics
1 (4.0) 5 (20.0) 6 (24.0) 9 (36.0) 4 (16.0)
Q29 Young adults are more empowered when
using CAM because CAM providers involve
them in decisions about their health care
treatments
2 (8.0) 4 (16.0) 10 (40.0) 6 (24.0) 3 (12.0)
Q30 Young adults believe that CAM builds up
the body’s own defenses and promotes self-
healing
1 (4.0) 3 (12.0) 6 (24.0) 11 (44.0) 4 (16.0)
Q31 The more knowledge a young adult has
about CAM, the more likely he/she is to use it
1 (4.0) 1 (4.0) 2 (8.0) 17 (68.0) 4 (16.0)
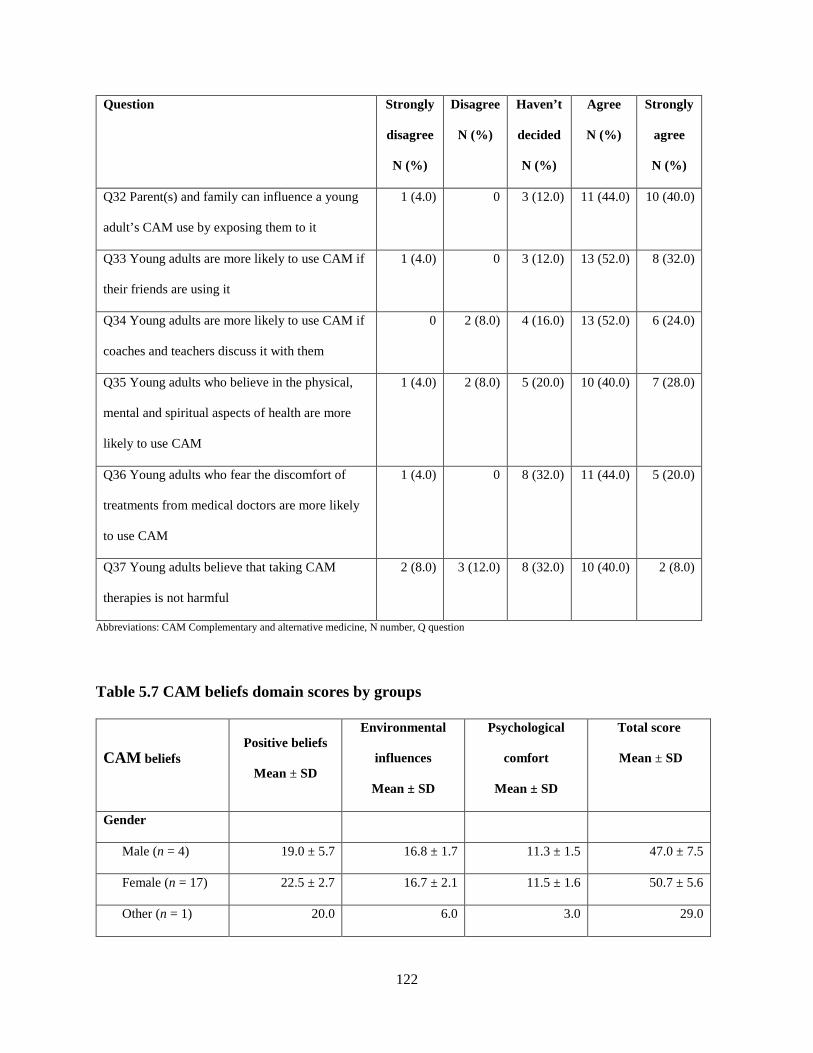
122
Question Strongly
disagree
N (%)
Disagree
N (%)
Haven’t
decided
N (%)
Agree
N (%)
Strongly
agree
N (%)
Q32 Parent(s) and family can influence a young
adult’s CAM use by exposing them to it
1 (4.0) 0 3 (12.0) 11 (44.0) 10 (40.0)
Q33 Young adults are more likely to use CAM if
their friends are using it
1 (4.0) 0 3 (12.0) 13 (52.0) 8 (32.0)
Q34 Young adults are more likely to use CAM if
coaches and teachers discuss it with them
0 2 (8.0) 4 (16.0) 13 (52.0) 6 (24.0)
Q35 Young adults who believe in the physical,
mental and spiritual aspects of health are more
likely to use CAM
1 (4.0) 2 (8.0) 5 (20.0) 10 (40.0) 7 (28.0)
Q36 Young adults who fear the discomfort of
treatments from medical doctors are more likely
to use CAM
1 (4.0) 0 8 (32.0) 11 (44.0) 5 (20.0)
Q37 Young adults believe that taking CAM
therapies is not harmful
2 (8.0) 3 (12.0) 8 (32.0) 10 (40.0) 2 (8.0)
Abbreviations: CAM Complementary and alternative medicine, N number, Q question
Table 5.7 CAM beliefs domain scores by groups
CAM beliefs Positive beliefs
Mean ± SD
Environmental
influences
Mean ± SD
Psychological
comfort
Mean ± SD
Total score
Mean ± SD
Gender
Male (n = 4) 19.0 ± 5.7 16.8 ± 1.7 11.3 ± 1.5 47.0 ± 7.5
Female (n = 17) 22.5 ± 2.7 16.7 ± 2.1 11.5 ± 1.6 50.7 ± 5.6
Other (n = 1) 20.0 6.0 3.0 29.0

123
CAM beliefs Positive beliefs
Mean ± SD
Environmental
influences
Mean ± SD
Psychological
comfort
Mean ± SD
Total score
Mean ± SD
F=1.917, p=0.174 F=13.125, p=0.000* F=13.743, p=0.000* F=6.476, p=0.007*
Ethnicity
Caucasian (n =11) 21.7 ± 2.8 15.9 ± 2.1 11.3 ± 1.7 48.9 ± 5.9
Asian (n = 9) 21.8 ± 4.7 17.7 ± 1.6 11.6 ± 1.4 51.0 ± 6.6
Other (n = 2) 22.0 ± 2.8 11.0 ± 7.1 7.5 ± 6.4 40.5 ± 16.3
F=0.05, p=0.995 F=6.257, p=0.008* F=3.066, p=0.070 F=1.788, p=0.194
Age
15–24 (n = 17) 21.6 ± 3.7 15.8 ± 3.3 10.8 ± 2.4 48.2 ± 7.9
25–45 (n = 5) 22.4 ± 3.0 17.4 ± 1.1 11.8 ± 2.1 51.6 ± 4.7
t=-0.445, p=0.661 t=-1.040, p=0.311 t=-0.814, p=0.425 t=-0.893, p=0.382
Severity
Mild (n = 13) 22.6 ± 3.1 17.0 ± 2.0 11.3 ± 1.6 50.9 ± 6.0
Moderate (n = 7) 20.4 ± 4.5 16.0 ± 2.2 11.9 ± 1.6 48.3 ± 6.6
Severe (n = 2) 21.0 ± 1.4 11.0 ± 7.8 6.5 ± 5.0 39.0 ± 14.1
F=0.926, p=0.413 F=3.727, p=0.043* F=6.530, p=0.007* F=2.691, p=0.094
Duration
< 1 year (n = 3) 22.3 ± 3.2 17.0 ± 2.00 10.0 ± 1.0 49.3 ± 5.9
1–4 years (n = 9) 22.8 ± 3.0 15.7 ± 4.2 11.0 ± 3.1 49.4 ± 9.5
5+ years (n = 10) 20.7 ± 4.1 16.4 ± 1.9 11.4 ± 1.8 48.5 ± 6.2
F=0.859, p=0.440 F=0.254, p=0.778 F=0.392, p=0.681 F=0.039, p=0.962
Abbreviations: CAM complementary and alternative medicine, n number, SD standard deviation
*Statistically significant
124
5.4.3.1 Positive beliefs domain
There was no difference in the CAM questionnaire positive beliefs domain when comparing group
differences in all the characteristics: gender, age, ethnicity, severity of acne and duration of acne.
5.4.3.2 Environmental influences domain
There were no differences when comparing age and duration of acne for the domain of
environmental influences. There was a statistically significant result in gender difference in the
environmental influences domain (p = 0.000). Post-hoc analysis was not able to be performed due
to only one respondent in the “other” gender category. Based on the data presented, the difference
may be between males (4 respondents, 16.8 ± 1.7) and the “other” gender (1 respondent, 6.0). The
difference may also be between females (17 respondents, 16.7 ± 2.1) and the “other” gender. Only
a post-hoc analysis with additional respondents in the “other” gender category can truly show
where the differences lie. Asians had a slightly higher score (9 respondents, mean score 17.7 ±
1.6) than Caucasians (11 respondents 15.9 ± 2.1) and “other” (11.0 ± 7.1) for environmental
influences, indicating that their environment had an influence on their attitudes and possible use
of CAM. In a post-hoc analysis, the differences were seen between the Asian and “other” group (p
= 0.007).
Environmental influences was also scored higher by people who reported their acne as mild (13
respondents, 17.0 ± 2.0) than people with self-reported severe acne (2 respondents, 11.5 ± 7.8). In
a post-hoc analysis, those with self-reported mild acne scored higher on environmental influences
than those with self-reported severe acne (p = 0.041). There was no difference between the
moderate and mild groups (p = 1.000) and no difference between the moderate and severe groups
(p = 0.145).

125
5.4.3.3 Psychological comfort domain
There was no difference in scores in the psychological comfort domain when comparing age and
duration of acne. Similar to the environmental influences domain (p = 0.000), there were
statistically significant gender differences in the psychological comfort domain (p = 0.000). A
post-hoc analysis was not able to be performed due to only one respondent in the “other” gender
category. As with environmental influences, the differences may be between males (4 respondents,
11.3 ± 1.5) and the “other” gender (3.0) and also between females (17 respondents, 11.5 ± 1.6) and
the “other” gender. The self-reported mild severity group (11.3 ± 1.6) scored higher in the
psychological comfort domain compared to the self-reported severe group (6.5 ± 5.0). In a post-
hoc analysis, the mild severity group scored higher in the psychological comfort domain compared
to the severe group (p = 0.010). The moderate group scored higher than the severe group (p =
0.007) and there was no difference between the mild and moderate groups (p = 1.000).
5.4.3.4 Attitudes to CAM
There were 25 valid responses to the questions on CAM attitudes. The median of the total score
was 48 and results were dichotomised at this point. A score of 1 to 48 was defined as a negative
attitude and being less likely to use CAM, whereas a score of 49 to 65 was defined as positive and
being more likely to use CAM. There were 12 respondents with a positive attitude (score 49 and
above) and 13 who had a negative attitude (score 48 and below) (Table 5.8). There were no
differences in the number of people with positive or negative attitudes to CAM when comparing
group differences for all the characteristics: gender, age, ethnicity, severity of acne and acne
duration.

126
Table 5.8 CAM attitudes
CAM attitudes Positive attitude N (%) Negative attitude N (%)
Total (n = 25) 12 (48.0) 13 (52.0)
Gender
Male (n = 4) 1 (25) 3 (75)
Female (n = 17) 11 (64.7) 6 (35.3)
Other (n = 1) 0 (0.0) 1 (100.0)
χ2=3.316, df=2, p=0.191
Ethnicity
Caucasian (n =11) 6 (54.5) 5 (45.5)
Asian (n = 9) 5 (55.6) 4 (44.4)
Other (n = 2) 1 (50.0) 1 (50.0)
χ2= 0.02, df=2, p=0.990
Age
15–24 (n = 17) 8 (47.1) 9 (52.9)
25–45 (n = 5) 4 (80) 1 (20)
χ2= 1.691, df=1, p=0.193
Severity
Mild (n = 14) 8 (61.5) 5 (38.5)
Moderate (n = 7) 3 (42.9) 4 (57.1)
Severe (n = 2) 1 (50) 1 (50)
χ2=0.659, df=2, p=0.719
Duration
< 1 year (n = 3) 2 (66.7) 1 (33.3)
1–4 years (n = 9) 5 (55.6) 4 (44.4)
5+ years (n = 10) 6 (60) 4 (40)
χ2=0.668, df=2, p=0.716

127
5.4.4 Preferences for CM Treatment
Twenty-two respondents provided answers to their preferences on a list of herbal preparations
(Table 5.9). Seventeen (77.3 per cent) chose topical cleansers as their first preference, followed by
four (18.2 per cent) who chose oral pills (round pills) and one (4.5 per cent) who chose oral tablets
(compressed herbs into a flat tablet). For their second preferences, one (4.5 per cent) chose
cleansers, 10 (45.5 per cent) chose pills and five (22.7 per cent) chose tablets. In relation to
treatment duration (Table 5.10), one (4.5 per cent) chose two weeks of treatment, six (27.3 per
cent) chose four weeks of treatment and five (22.7 per cent) chose eight weeks. Five respondents
(22.7 per cent) were willing to take herbs twice or three times daily and 17 (77.3 per cent) were
willing to take herbs less than twice daily.
Table 5.9 Preference for herbal medicine preparation types
Herb type 1st
preference
N (%)
2nd
preference
N (%)
3rd
preference
N (%)
4th
preference
N (%)
5th
preference
N (%)
6th
preference
N (%)
Cleanser (topical) 17 (77.3) 1 (4.5) 2 (9.1) 1 (4.5) 0 (0.0) 1 (4.5)
Pills (oral) 4 (18.2) 10 (45.5) 3 (13.6) 0 (0.0) 2 (9.1) 3 (13.6)
Tablets (oral) 1 (4.5) 5 (22.7) 9 (40.9) 2 (9.1) 3 (13.6) 2 (9.1)
Granules (oral) 0 (0.0) 1 (4.5) 4 (18.2) 12 (54.5) 2 (9.1) 3 (13.6)
Powders (oral) 0 (0.0) 1 (4.5) 2 (9.1) 3 (13.6) 13 (59.1) 3 (13.6)
Liquid (oral) 0 (0.0) 4 (18.2) 2 (9.1) 4 (18.2) 2 (9.1) 10 (45.5)
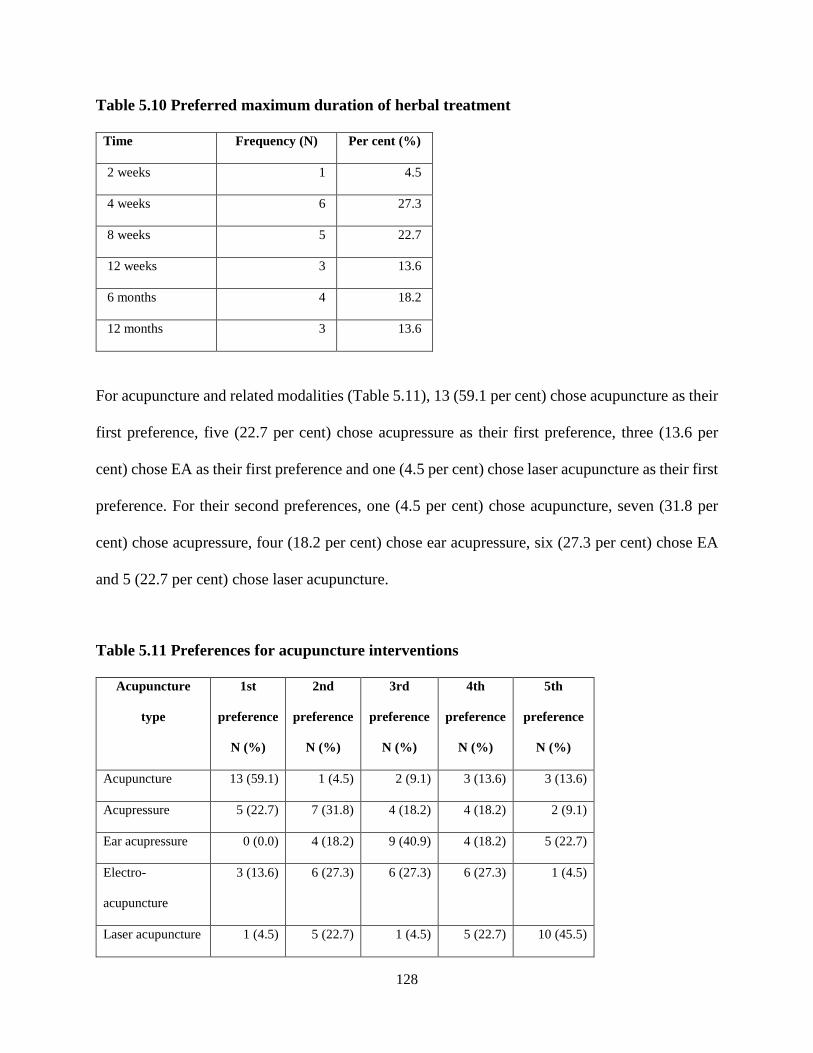
128
Table 5.10 Preferred maximum duration of herbal treatment
Time Frequency (N) Per cent (%)
2 weeks 1 4.5
4 weeks 6 27.3
8 weeks 5 22.7
12 weeks 3 13.6
6 months 4 18.2
12 months 3 13.6
For acupuncture and related modalities (Table 5.11), 13 (59.1 per cent) chose acupuncture as their
first preference, five (22.7 per cent) chose acupressure as their first preference, three (13.6 per
cent) chose EA as their first preference and one (4.5 per cent) chose laser acupuncture as their first
preference. For their second preferences, one (4.5 per cent) chose acupuncture, seven (31.8 per
cent) chose acupressure, four (18.2 per cent) chose ear acupressure, six (27.3 per cent) chose EA
and 5 (22.7 per cent) chose laser acupuncture.
Table 5.11 Preferences for acupuncture interventions
Acupuncture
type
1st
preference
N (%)
2nd
preference
N (%)
3rd
preference
N (%)
4th
preference
N (%)
5th
preference
N (%)
Acupuncture 13 (59.1) 1 (4.5) 2 (9.1) 3 (13.6) 3 (13.6)
Acupressure 5 (22.7) 7 (31.8) 4 (18.2) 4 (18.2) 2 (9.1)
Ear acupressure 0 (0.0) 4 (18.2) 9 (40.9) 4 (18.2) 5 (22.7)
Electro-
acupuncture
3 (13.6) 6 (27.3) 6 (27.3) 6 (27.3) 1 (4.5)
Laser acupuncture 1 (4.5) 5 (22.7) 1 (4.5) 5 (22.7) 10 (45.5)
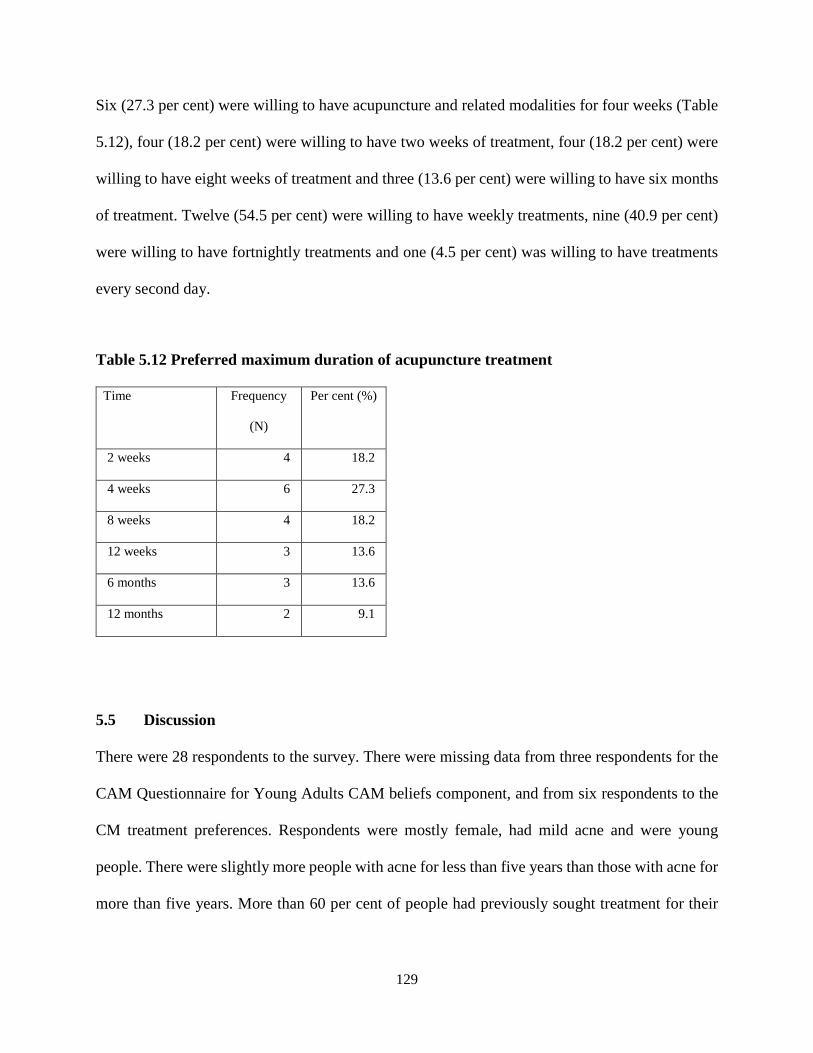
129
Six (27.3 per cent) were willing to have acupuncture and related modalities for four weeks (Table
5.12), four (18.2 per cent) were willing to have two weeks of treatment, four (18.2 per cent) were
willing to have eight weeks of treatment and three (13.6 per cent) were willing to have six months
of treatment. Twelve (54.5 per cent) were willing to have weekly treatments, nine (40.9 per cent)
were willing to have fortnightly treatments and one (4.5 per cent) was willing to have treatments
every second day.
Table 5.12 Preferred maximum duration of acupuncture treatment
Time Frequency
(N)
Per cent (%)
2 weeks 4 18.2
4 weeks 6 27.3
8 weeks 4 18.2
12 weeks 3 13.6
6 months 3 13.6
12 months 2 9.1
5.5 Discussion
There were 28 respondents to the survey. There were missing data from three respondents for the
CAM Questionnaire for Young Adults CAM beliefs component, and from six respondents to the
CM treatment preferences. Respondents were mostly female, had mild acne and were young
people. There were slightly more people with acne for less than five years than those with acne for
more than five years. More than 60 per cent of people had previously sought treatment for their

130
acne and had used medically prescribed TAB and BP to treat their acne. Just under three-quarters
(72.7 per cent) had used over-the-counter medications that contained salicylic acid.
The lowest score on the Acne-QoL was for self-perception and the highest was for acne symptoms.
People were more emotionally affected and worried about their acne if they had moderate acne.
Of note, the self-perception, role-social and role-emotional domains were scored lower in the self-
reported moderate acne group compared to the mild and severe groups, although this was not
statistically significant. The self-reported severe acne group had the lowest score for the acne
symptoms domain. For the CAM questionnaire, just under half of the 27 respondents had not
previously use CAM products. For the overall attitudes to CAM, there were approximately equal
numbers of participants with a positive attitude (n = 12) and a negative attitude (n = 13).
Respondents preferred CHM as a topical cleanser, followed by pills and tablets, and had stronger
preferences for acupuncture and acupressure than for other related interventions. For herbal
medicines, they preferred to take them less than twice daily. Respondents were willing to have
herbal medicines and acupuncture treatment for four to eight weeks. Responses from this survey
informed the clinical trial protocol in Chapter 9.
Respondent fatigue appeared to be a factor in the completion rates for each section of the survey.
The survey was structured with the consent information and consent question given first. This was
followed by the Acne-QoL, then the CAM questionnaire, the CM treatment preferences and finally
the demographics section. Hence as participants completed sections of the survey, the number of
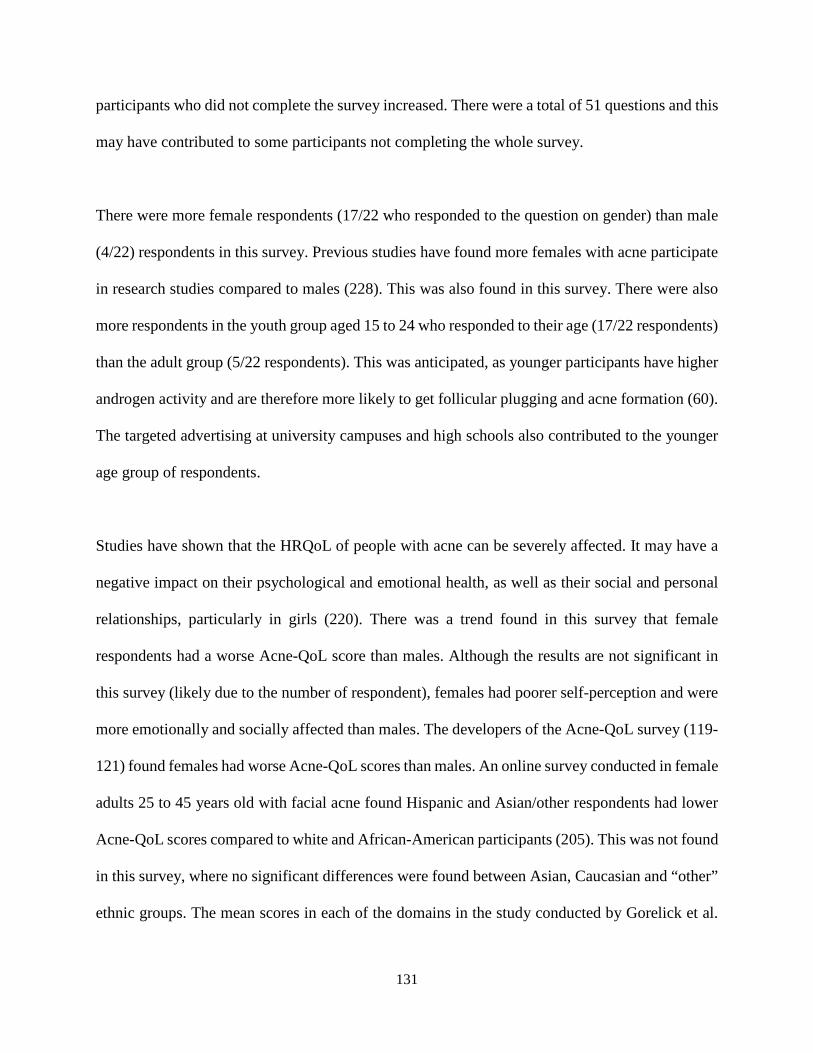
131
participants who did not complete the survey increased. There were a total of 51 questions and this
may have contributed to some participants not completing the whole survey.
There were more female respondents (17/22 who responded to the question on gender) than male
(4/22) respondents in this survey. Previous studies have found more females with acne participate
in research studies compared to males (228). This was also found in this survey. There were also
more respondents in the youth group aged 15 to 24 who responded to their age (17/22 respondents)
than the adult group (5/22 respondents). This was anticipated, as younger participants have higher
androgen activity and are therefore more likely to get follicular plugging and acne formation (60).
The targeted advertising at university campuses and high schools also contributed to the younger
age group of respondents.
Studies have shown that the HRQoL of people with acne can be severely affected. It may have a
negative impact on their psychological and emotional health, as well as their social and personal
relationships, particularly in girls (220). There was a trend found in this survey that female
respondents had a worse Acne-QoL score than males. Although the results are not significant in
this survey (likely due to the number of respondent), females had poorer self-perception and were
more emotionally and socially affected than males. The developers of the Acne-QoL survey (119-
121) found females had worse Acne-QoL scores than males. An online survey conducted in female
adults 25 to 45 years old with facial acne found Hispanic and Asian/other respondents had lower
Acne-QoL scores compared to white and African-American participants (205). This was not found
in this survey, where no significant differences were found between Asian, Caucasian and “other”
ethnic groups. The mean scores in each of the domains in the study conducted by Gorelick et al.
132
(231) were lower in each domain compared to this study. This is likely due to significantly higher
number of respondents to their survey (312 respondents).
There were only two respondents in the severe acne group, which is similar to other cross-sectional
studies, which tended to have lower numbers of people with severe acne compared to those with
mild and moderate acne (8, 37, 203, 222, 227). It has previously been reported that the severity of
acne may not necessarily be associated with a worsening of HRQoL (69). In the study conducted
by Martin et al. (121), higher reported severity was associated with a worse HRQoL score. Many
other studies have also found a correlation between higher severity of acne and worse HRQoL (19,
67, 191, 222, 224). In this survey, one respondent with severe acne had a very high Acne-QoL
score, which means better HRQoL, while the other one with severe acne had a much lower score,
hence the large standard deviation. With only two respondents in the severe acne category, it is
difficult to conclude whether there is a correlation between worse acne and worse HRQoL. Self-
reported acne severity was unable to be verified by a dermatologist in this study as it was an
anonymous online survey. However, with modern technology, future surveys might be able to
consider requesting non-identifiable images of acne areas for verification.
People with prolonged acne duration were found to have lower Acne-QoL scores than those with
shorter duration in a study of 862 respondents from different demographic groups (287). However,
this was not found by Duman et al. (74), who used the AQOL (69). This study also did not find a
correlation between acne duration and worse HRQoL.
133
Twenty-seven respondents answered questions on CAM. Approximately half were previous users
of CAM and just under half had never used CAM. One-third had used CAM to prevent and treat
illness, whereas the developers of the CAM Questionnaire (268) found that three-quarters of their
respondents had used CAM for treating and preventing illness. The most frequently used group
was alternative medical systems and, within this group, CM was the most used system. This may
be related to the recruitment strategies used, including emails to student representatives of Chinese
Medicine, Chiropractic and Osteopathy Disciplines. Although students were not approached
directly, the study investigator is the clinical coordinator and a lecturer in the Chinese Medicine
Discipline and, as a consequence, this may have resulted in more students from CM responding to
the survey. CAM use varied from weekly to once per month and twice per year. CAM users were
more likely to use CAM for treating illness and promote their health which is similar to the findings
from the original survey conducted by Patterson and Arthur (268). In this survey, there were
similar numbers of participants who had a positive attitude to CAM and a negative attitude to
CAM. This is surprising, as one part of the recruitment strategy of this survey was promoted to
students in the CAM areas of CM, chiropractic and osteopathy. A positive attitude to CAM was
interpreted by the original authors as a higher likelihood to use CAM (268). When considering the
previous use of CAM (question 20), about half (n = 15) had previously used CAM and the other
half had not, which may reflect this result. As this was survey was anonymous and no data on
respondent study or employment status, and other recruitment strategies such as posters around
the campus grounds and high schools, there is no certainty that only CAM students responded to
the survey.
134
The original survey did not present results for each domain by demographic characteristics;
therefore no comparisons are able to be made for the different domains. There were gender
differences in the environmental influences and psychological comfort domains; however, due to
only one “other” gender respondent, post-hoc analysis could not be performed. Based on mean
scores, the differences were likely to be between males and the “other” gender and between
females and the “other gender”, rather than between males and females. The environment
influenced Asians and the “other” ethnicity. Environmental influences included prior knowledge
about CAM treatments, whether parents, family or friends used CAM and whether coaches and
teaches discussed CAM with them. Other studies looking at predictors of CAM use by children
and adolescents have reported an association between female gender and parental CAM use (288-
290). There were also differences between the mild and severe acne groups for the environmental
influences and psychological comfort domains. The mild severity group scored higher for both
domains compared to the severe group, indicating the mild group thought that family, friends,
coaches and teachers influenced young people to use CAM and that young people’s reasoning
behind their attitudes to CAM included physical, mental and spiritual aspects of health. Although
there are no other studies on acne severity and CAM use, other studies on CAM use have shown
that it can be influenced by other people, holistic health beliefs (291, 292), belief that it aided
wellbeing (293) and if the user of CAM had a chronic illness (294).
In the individual questions, 21 respondents (84 per cent) agreed or strongly agreed that parents and
family can influence young adults’ CAM use by exposing them to it. CAM use in children and
adolescents is popular (17). In one systematic review on CAM use in children, homeopathy was
the most popular CAM in Germany, the UK and Canada, with herbal product use highest in

135
Germany, Turkey and Brazil (17). The highest predictor for CAM use was higher parental income,
education level and having older children (17). In a survey of adolescents 15 to 19 years old in
Saudia Arabia, the most used CAM product was honey and the least used was acupuncture. This
study also found females tended to use CAM more than males (295). CAM use in the USA also
showed that the most commonly used products were non-vitamin, non-mineral natural products
(15), followed by chiropractic and osteopathy. This survey showed that alternative medical
systems and in particular CM (acupuncture and CHM), followed by mind-body therapies and
manipulative and body-based therapies such as chiropractic and osteopathy, were more commonly
used than other CAM modalities. This is likely related to the recruitment strategies, where students
in the three areas of CAM taught at RMIT University were invited to participate.
There have been no previous studies identified on CM treatment preferences by people with acne.
Respondents were also asked about their preferences for CM treatment methods and length and
frequency of treatment. Although the numbers were low, the data provides insights into people’s
preferences for CM treatment. There was a variation in what respondents were willing to take and
how long participants were willing to have treatment. Topical cleansers was the most preferred of
all the herb preparation types and were the only topical option in the survey. Topical herbs require
no preparation time by the patient and are not orally consumed.
The most preferred preparation type for oral herbs was pills, followed by tablets. The least
preferred was oral liquid (also known as decoctions), despite decoctions being the most common
traditional preparation type. With decoctions, raw herbal medicines are given to patients, who take
them home to boil twice and drink the liquid. They require the most preparation time by the patient,
136
typically between one and a half and two hours. Powders, granules and decoctions are preparations
that are consumed in liquid form. Powders are made by pulverising raw herbs into fine particles
or produced from the liquid extract of boiled herbs. Powder is mixed with water for drinking. A
disadvantage of both decoctions and powders is that the taste of herbal medicines is obvious to the
patient. The taste can be unpalatable for some people (296) and can pose issues for blinding in
clinical trials.
Pills and tablets are common forms of preparation in modern clinical practice. For pills or tablets,
no preparation time is required and patients swallow them whole without needing to prepare herbs
or encounter the taste of the herbs. This feature appeared to be important to respondents in this
survey. Capsules have the same advantages as pills and tablets, but are relatively new to modern
practice. Capsules were not included in the survey, but may be an important preparation type to
achieve blinding in clinical trials.
The most preferred treatment period for herbal medicine was four weeks, followed by eight weeks.
This is a common treatment period encountered in clinical trials (Chapter 7). The treatment
preferences component informed the development of the clinical trial protocol, as it has been
shown that incorporating patient perspectives into interventions can influence participation in trials
(271, 297). In taking into consideration treatment preferences, it is anticipated there would be
greater adherence in trials and clinical practice (276).
137
5.6 Limitations of survey
People with the link to the survey could complete the survey online anonymously without verifying
their identities. This is a common challenge for online surveys. The Acne-QoL survey is limited
to facial acne and does not apply to acne on other parts of the body. It is a self-administered survey
which was initially designed to be implemented in a dermatology office setting where researchers
could be on hand to read questions to participants. If participants could not understand a question,
they were instructed to use their own interpretation and respond about their feelings. The survey
instructions also encouraged participants to complete all questions. As this was an anonymous
online survey, such reminders were unable to be given.
The Acne-QoL survey has been validated for people between 13 to 35 years old and the CAM
Questionnaire for Young adults was validated for adolescents and young adults. The age inclusion
criteria for this survey included people older than 35 years old (one respondent); therefore it is
unknown whether the questions were applicable for the older age group. As most of the
respondents were between 15 and 24 years old (17 respondents), it is possible that the survey
results are representative. Acne severity reported by respondents was unable to be verified by a
dermatologist as it was an online anonymous survey.
Recruitment strategies included advertisements placed on university campuses across Melbourne,
RMIT Facebook student support groups and approaches to high schools to place advertisements
in their newsletters. There were two high schools that agreed to place the advertisement in their
newsletters. Therefore, the age group of 20 to 24 may be overrepresented (10 respondents).

138
Recruitment was also an issue due to the timing of the release of the survey to the public. The
initial pilot study intended for the beginning of the university semester ended up being
implemented at the end of the semester. By the time the full survey was released to the public, it
was semester break and fewer people were on campus to see the advertisements. There were also
limited places where the advertisement could be placed online and on campus. The RMIT
Facebook page and other University online websites limited the type of information that could be
advertised on their websites.
The university student population receives many requests for surveys and, anecdotally, students
can be “over surveyed”. With the promotion of the online survey primarily placed within university
grounds, this limited the reach of the survey. Other marketing approaches such as social media
were similarly unsuccessful. The creation of the survey Facebook page coincided with publicity
of Facebook’s privacy issues and there were reports of a drop in the general use of Facebook during
the time the page was created (286). There were eight hits on the Facebook page. Five responses
were received after dissemination of the survey advertisement to healthcare practitioners later in
the survey period (20 June 2018). As responses for each recruitment strategy were not recorded, it
is unclear which of the advertising methods used were most effective.
The number of respondents to this survey was low. Small survey samples can lead to higher
variability in results and lead to bias (298). There were few statistically significant results in this
set of results and larger standard deviations. Therefore the results should be interpreted with
caution and may not be generalised to the general population of people with acne.

139
There were no incentives given as part of the survey. Incentives may increase participation. In one
survey of plastic surgeons, four different strategies were used (299): an emailed link to an online
survey; regular mail; regular mail with a $1 note; and regular email with a $5 note. Of the 662
surveys sent, 608 were returned. The highest response was from those mailed with a monetary
incentive and the lowest was from emails. Other innovative and timely recruitment strategies may
have increased responses to the survey. These include search engine and banner advertising,
monetary or other types of incentives for participants, collaboration with dermatologists and other
healthcare practitioners, and applying to national or state government departments to enlist high
schools to conduct research.
In the CM preferences section of the survey, no option was provided for a preference for capsules,
as this is not as common traditionally. Pills and tablets may be considered similar products and
some laypersons may not have understood the differences, given that no descriptions or images
were provided. Researchers conducting similar surveys may consider adding capsules as an option,
as this form of herbal medicine is now more popular, with many modern practices being able to
manually create capsules in their private clinics. In addition, providing images or descriptions will
assist participants in understanding the differences between pills, tablets and capsules. This also
applies to granules and powders.
Not all sections of the survey were completed by the respondents. As participants progressed
through each section, the number of respondents declined. The number of questions and the
separation of sections may have contributed to the discontinuation. Future surveys may consider
not separating the sections in surveys or shortening the number of questions.
140
5.7 Conclusions and implications
This survey showed that respondents to the survey were mostly female, young people 15 to 24
years old with mild acne. People with severe acne were more worried about their acne symptoms.
Half of respondents had a positive attitude to CAM. CM treatment preferences included topical
herbs for four to eight weeks and weekly acupuncture treatment. The number of respondents was
low and not many statistically significant results were found. Future surveys will need to use more
creative recruitment strategies and to consider other means such as ethically approved incentives
to recruit more people to complete the survey. The study results therefore cannot be generalised to
the Australian population with acne as a whole. The results from the CM treatment preferences
section of the survey can be used as a guide on treatment preferences to help improve treatment
adherence.
141
CHAPTER 6 : Methods for systematic reviews
Overview
The impact of acne on HRQoL has been described in Chapter 4, and Chapter 5 provided new data
on the emotional, social and psychological impact of acne in young people and adults in Australia.
The next step in this project was to gain an understanding of the effectiveness of CM therapies for
acne vulgaris. Two systematic reviews, one of CHM for acne and one of acupuncture and related
therapies was planned. This chapter describes the methods used to conduct SRs of the efficacy and
safety of two types of CM interventions for acne vulgaris. The results of the first SR on the CHM
formula Pi Pa Qing Fei Yin (Eriobotrya japonica Formula) will be presented in Chapter 7 and the
results of the second SR on acupuncture and related techniques will be presented in Chapter 8.
6.1 Introduction
Systematic reviews provide a summary of the evidence from eligible studies and evaluate the
methodological processes of included studies. They estimate clinical effects and guide clinicians
on clinical decision-making by assessing the confidence in the evidence (300). SRs of RCTs are
considered the highest level of evidence (Level I) according to Australia’s National Health and
Medical Research Council (NHMRC) (301). The methods developed by the Cochrane
Collaboration (302) are considered the best in evaluating RCTs (303).
A monograph currently in press provides a comprehensive evaluation of the evidence for acne,
including CHM (168). A summary of the findings from the monograph relating to CHM and
acupuncture and related techniques can be found in Chapter 3. There are currently no SRs in
142
English on the safety and efficacy of CHM for acne vulgaris. There have been two SRs on RCTs
of acupuncture and related techniques for acne, one in Chinese (18) and one in English (185).
These reviews included CM interventions, placebo and pharmacotherapies as controls, making it
hard to draw reliable conclusions from current reviews. There has also been one English-language
review of botanical and phytochemical therapy for acne vulgaris (20) which included Chinese and
other herbal medicines.
6.2 Study design
The SRs included RCTs involving people with acne vulgaris. Non-controlled studies such as case
series and case-control studies identified in the literature search were excluded.
6.2.1 Participants
Acne vulgaris begins at adolescence but can affect adults (24). It can affect any gender and
ethnicity. As the onset of acne begins at adolescence and the age of puberty can be earlier than 10
years old (304-306) the SRs for the acupuncture-point stimulation and Pi Pa Qing Fei Yin
(PPQFY) did not have an age limit. Acne conglobata was not excluded since some commonly used
acne-grading systems included nodular acne in stage IV or severe acne (106, 107). Although
PPQFY is recommended for comedonal acne, textbooks do not specify that it is used only for mild
or moderate acne. Clinically, most practitioners will use it for mild to moderate acne. Therefore,
there was no limit on acne severity.
143
6.2.2 Intervention
6.2.2.1 Inclusion criteria for PPQFY
A specific search was conducted using the formulation name in Chinese, pin yin and English
variations (Table 6.1). Studies that used the original formula PPQFY or a modified version, alone,
with another formula or as integrative medicine (PPQFY combined with pharmaceuticals), were
included in the review. A modified PPQFY formula was defined as using the original formula with
addition, removal or replacement of one or more herbs.
6.2.2.2 Inclusion criteria for acupuncture
Acupuncture trials that used body acupuncture or acupressure, auricular (ear) acupuncture or
acupressure, EA, electro-stimulation (for example, transcutaneous electrical nerve stimulation),
moxibustion and other forms of direct acupuncture point stimulation such as surround needling or
cutaneous needling were included in the review. Other acupuncture-related techniques such as
laser acupuncture and cupping or integrative medicines (pharmacotherapy) were also eligible for
the review. Techniques not commonly used outside of China were excluded. Studies that included
CM therapies as controls were excluded (Table 6.1).
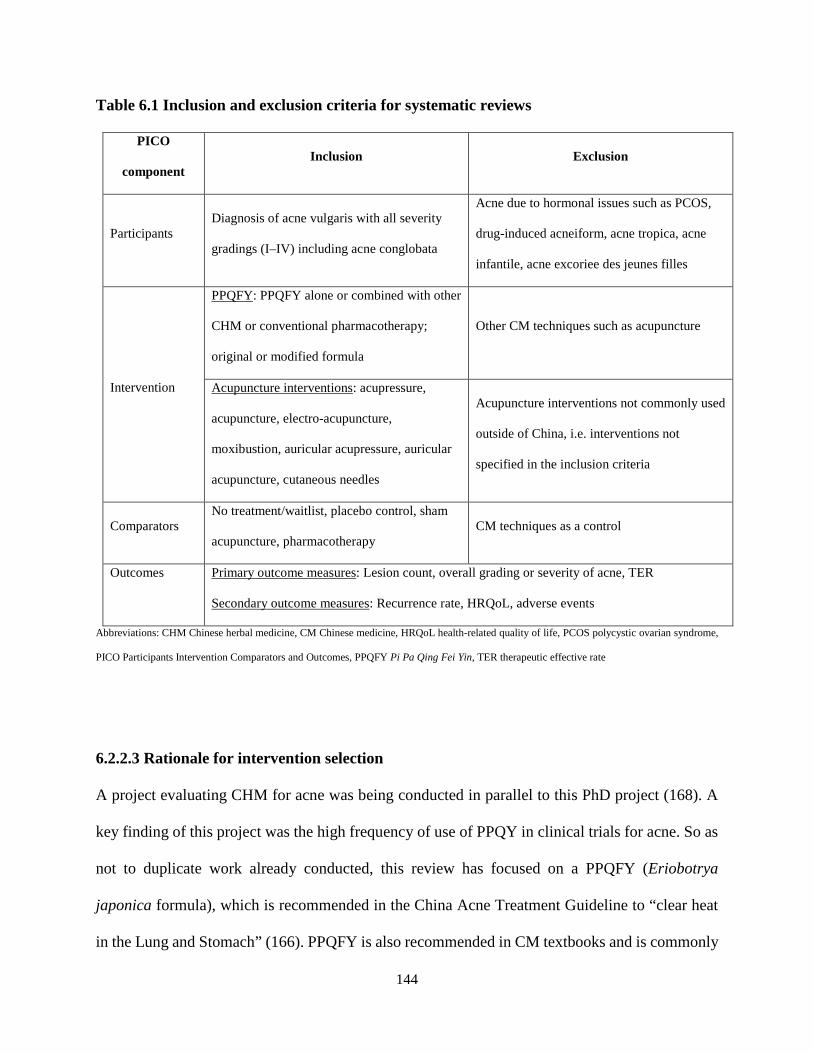
144
Table 6.1 Inclusion and exclusion criteria for systematic reviews
PICO
component Inclusion Exclusion
Participants Diagnosis of acne vulgaris with all severity
gradings (I–IV) including acne conglobata
Acne due to hormonal issues such as PCOS,
drug-induced acneiform, acne tropica, acne
infantile, acne excoriee des jeunes filles
Intervention
PPQFY: PPQFY alone or combined with other
CHM or conventional pharmacotherapy;
original or modified formula
Other CM techniques such as acupuncture
Acupuncture interventions: acupressure,
acupuncture, electro-acupuncture,
moxibustion, auricular acupressure, auricular
acupuncture, cutaneous needles
Acupuncture interventions not commonly used
outside of China, i.e. interventions not
specified in the inclusion criteria
Comparators No treatment/waitlist, placebo control, sham
acupuncture, pharmacotherapy CM techniques as a control
Outcomes Primary outcome measures: Lesion count, overall grading or severity of acne, TER
Secondary outcome measures: Recurrence rate, HRQoL, adverse events
Abbreviations: CHM Chinese herbal medicine, CM Chinese medicine, HRQoL health-related quality of life, PCOS polycystic ovarian syndrome,
PICO Participants Intervention Comparators and Outcomes, PPQFY Pi Pa Qing Fei Yin, TER therapeutic effective rate
6.2.2.3 Rationale for intervention selection
A project evaluating CHM for acne was being conducted in parallel to this PhD project (168). A
key finding of this project was the high frequency of use of PPQY in clinical trials for acne. So as
not to duplicate work already conducted, this review has focused on a PPQFY (Eriobotrya
japonica formula), which is recommended in the China Acne Treatment Guideline to “clear heat
in the Lung and Stomach” (166). PPQFY is also recommended in CM textbooks and is commonly
145
prescribed for comedonal acne (159). There are no standalone reviews of PPQFY in English or in
Chinese. Previous reviews also included acupuncture combined with herbal medicines, did not
analyse herbal medicines alone and did not focus on PPQFY in their reviews (18, 157, 185).
The second review focused on acupuncture and related therapies. Acupuncture is a common
intervention used for the treatment of a range of skin conditions (155). Commonly used
acupuncture techniques that directly stimulate acupuncture points include body acupuncture,
auricular acupuncture and moxibustion. Previous reviews on acupuncture included studies that
combined acupuncture with herbal medicines, or included studies that used CM as a comparator.
Comparing acupuncture with pharmacological treatments that have already been shown to be
effective provides a greater understanding of the effectiveness of acupuncture therapies than
comparing with treatments with unknown efficacy. An acupuncture review specifically on the
aforementioned techniques will clarify whether they are efficacious for acne. Electro-acupuncture
and auricular acupuncture have been shown to decrease inflammatory mediators in various
inflammation pathways (307, 308). Acupuncture has also been shown to decrease sebum
production in combination with BP (309), therefore possibly affecting acne lesions. These
acupuncture-related interventions are also recommended in CM textbooks. Despite the great
potential for using acupuncture for the treatment of acne, there is no good evidence of its safety
and efficacy.
6.2.3 Comparators
Previous systematic reviews included CM as comparators, which diluted the strength of the
evidence when an unknown treatment was compared with another unknown treatment. The
146
comparators for PPQFY review included no treatment or a waitlist, placebo control and
pharmacotherapy. Pharmacotherapy included oral medications such as antibiotics and retinoids
and topical medications such as benzoyl peroxides. In addition to these comparators, the
acupuncture review also included sham acupuncture as a comparator.
6.2.4 Outcome measures
There is no published consensus on outcome measures for research in acne. Lesions may be
assessed using Pillsbury, Leeds, IGA, GAGS or photography (101, 104, 109, 310).
Primary outcomes included an assessment of end-of-treatment differences in:
1. lesion count
2. overall grading (either reported by physician’s assessment or self-reporting and length of
time between recurrence of symptoms); and
3. therapeutic effective rate.
Lesion count is a visual count of the number of inflammatory and non-inflammatory lesions.
Grading is typically assessed using an ordinal grading criterion that indicates levels of severity of
the acne. Therapeutic effective rate (TER) is an outcome frequently used in studies conducted in
China. Criteria for determining clinical effect vary. Two guidelines frequently referenced in
clinical studies are the Clinic Research Guidelines for Chinese Herbal Medicine and New Drugs
(中药新药临床研究指导原则(试行)) (311) and the Criteria of Diagnosis and Therapeutic Effect
of Diseases and Syndromes in Traditional Chinese Medicine (167). The former defines clinical
effect as 50 per cent or greater improvement in lesion count and/or severity grading as effective,
147
while the latter uses a minimum threshold of 30 per cent or greater. Differences exist between the
criteria described in these two guidelines and there is no consensus on which is preferred. A third
guideline published in 2010 (312) also describes a minimum threshold of 30 per cent or greater
change in lesions. The details of the guidelines are below.
The TER of the 2010 guidelines recommends a change of symptoms score by 30 per cent applying
the following parameters:
1. Cure: lesions healed ≥90 per cent, no new lesions
2. Improved: lesions healed ≥30 per cent with a few new lesions
3. No improvement: no changes in lesions
The TER of the 2002 guideline recommended for trials is a change in symptom scores (severity,
location of lesions, symptom score and laboratory tests) applying the following parameters (311):
1. Cure: ≥95 per cent reduction of lesion count
2. Significant improvement: ≥70–95 per cent
3. Improvement: ≥50–70 per cent
4. No improvement: <50 per cent
The TER of the 1994 guideline recommended for trials is a decrease in lesion count applying the
following parameters (167):
1. Cure: lesions and symptoms disappear
2. Improved: ≥30 per cent lesions heal, symptoms improved
3. Not improved: <30 per cent lesions heal, symptoms not improved
148
A similar recommendation for drug trials is made by the Center for Drug Evaluation and Research,
with a 50 per cent improvement considered a success in treatment (107). For the CHM SR, results
for participants who achieved a 50 per cent or greater improvement in signs and symptoms were
analysed. TER is a recommended outcome in Chinese CM research guidelines; however, there are
inconsistencies and no consensus on which is superior. Therefore the acupuncture review included
both criteria and analysed results based on TER of 30 per cent and 50 per cent to ascertain any
differences in effect.
Secondary outcomes included recurrence rate, HRQoL and AE reports. Acne-specific and general
dermatology HRQoL questionnaires were included. General health, dermatology-specific and
acne-specific HRQoL questionnaires have been described in Chapter 4. Acne-specific
questionnaires include the Acne-QoL (119-121), Acne-QOLI (118), ADI (70) and CADI (122).
Dermatology-specific QoL included the DLQI (114), Skindex (252), Skindex-16 (115) and
Skindex-29 (100).
6.2.5 Identification of search terms
A search for the definition and English synonyms for acne vulgaris was conducted in the WHO’s
International Classification of Diseases version 10 (ICD-10) (97) and using medical subject
headings (MeSH) terms in PubMed (313). For the Chinese terms for acne vulgaris, searches in
CM dermatology textbooks (159, 165) and classical texts and medical dictionaries were conducted.
Search results were compiled in an Excel spreadsheet (©Microsoft) (Appendix 13). A comparison
of the terms was conducted and duplicates removed. Details of the search strategy for acupuncture

149
and PPQFY can be found in section 6.2.6, and the methods for identifying experimental studies
are found in section 7.4.2.
6.2.6 Process for study selection
An electronic search of five English (PubMed, Embase, Allied and Complementary Medicine
Database, Cumulative Index to Nursing and Allied Health Literature and Cochrane Library) and
six Chinese-language databases (Chinese National Knowledge Infrastructure, Chongqing VIP
Information Company, Wanfang Data, Chinese Biomedical Literature Database, China’s
Conference Papers Database and China Dissertation database) was conducted from inception to
May 2013 (and updated in February 2015) to identify RCTs of PPQFY and acupuncture. There
were no language restrictions. Search terms were categorised according to intervention (CHM,
traditional Chinese herbs, Chinese drugs and variants; acupuncture, acupressure, acupoint,
auricular acupuncture, auricular acupressure, moxibustion electro-acupuncture, cutaneous needles
and variants), condition (acne vulgaris, acne and variants) and trial design (RCT and variants)
(Appendix 13). The title and abstracts were assessed to identify potential RCTs. Full texts were
retrieved for eligible studies and studies where eligibility could not be determined from the title
and abstract.
6.2.7 Data extraction
Data was extracted into a predefined file including participant characteristics, details of the
intervention and comparator, outcome measures and results. Attempts were made to obtain missing
data by contacting the study authors. Verification of data was conducted by an independent
researcher (Iris Wenyu Zhou).
150
6.2.8 Statistical and meta-analysis
Systematic reviews, with or without meta-analyses are considered the highest level of evidence
(301). Meta-analysis provides a statistical synthesis of the results of multiple studies to estimate a
treatment effect that is not possible from reviewing results of individual studies. Consideration
was given to how to group results of studies in a way that allows meaningful translation into
clinical practice.
For the PPQFY SR, important features were the use of PPQFY alone, combined with other oral
CHM formulas, and combined with topical CHM treatments. Each of these three combinations are
suitable for clinical practice, and having evidence of the effect of each can provide reassurance for
practitioners in prescribing treatments. Conversely, a lack of evidence of effect allows practitioners
to understand where treatments have no evidence of benefit, which prevents unnecessary expense
for patients.
The comparator drug class was an important feature relating to the comparators. Additional
analyses were conducted to identify the benefits of PPQFY compared to OAB, topical BP,
retinoids, and oral antibiotics. The actions of these drugs on pathophysiological pathways have
been established, and included antibacterial effects, reducing hyperkeratinisation and
inflammation. If PPQFY is found to be equally or more effective than acne treatments, this may
provide insight into the potential mechanisms of action for PPQFY as a whole, or for individual
herb ingredients.
151
For the acupuncture SR, analysing contributions of individual acupuncture points is possible, but
is complex, and likely has little bearing on clinical practice. As all studies used a combination of
points, analysing effect of single points was not possible. Diversity in points used prevented
grouping of like studies for meta-analysis. Subgrouping for this review was limited to the
intervention type (acupuncture, auricular acupuncture, auricular acupressure), and comparators (as
described for the PPQFY SR above). Studies reported outcomes with different thresholds for
effectiveness: TER of 30% or greater improvement in lesion count (according to the 1994
guideline), and TER of 50% or greater improvement in lesion count (according to the 2002
guideline). Additional subgroup analyses were conducted for these features.
Meta-analyses was conducted according to the factors outlined above. For dichotomous data, risk
ratios (RR) were calculated with a confidence interval (CI) of 95 per cent. For continuous data, the
mean difference (MD) with a 95 per cent CI was performed. Analysis was conducted using
available data, with a random effects model used. Substantial heterogeneity was defined as I2
greater than 50 per cent. Review Manager version 5.2.4 software (314) was used to analyse data
for the CHM SR. An updated version (version 5.3) became available during the research and the
updated version was used for the acupuncture SR. A sensitivity analysis of primary outcomes was
intended to be performed by excluding studies with low risk of bias in randomisation based on
sequence generation. Publication bias was intended to be explored where at least 10 trials were
included in a meta-analysis by visual inspection of funnel plots for asymmetry. Subgroup analyses
according to intervention and comparators were performed where possible. Details of such
analyses are included in the relevant chapters. For the acupuncture review, subgroup analysis was
also performed based on TER (as described above).
152
6.2.9 Quality assessment
Risk of bias followed the Cochrane Handbook’s Risk of Bias Assessment Tool (302). Two
reviewers independently assessed the risk of bias. Trials included in the review were assessed as
high, low or unclear risk based on the guidance in the handbook. The domains assessed included
random sequence generation, allocation concealment, blinding of participants, personnel and
outcome assessors, incomplete outcome data, selective reporting and other forms of bias such as
conflicts of interest. A third assessor was consulted if disagreement occurred that could not be
resolved through discussion. An assessment of unclear risk was given if there was lack of data
presented in the trials.
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) (315)
was used to assess the quality of the evidence and the strength of recommendations for the CHM
SR. For the acupuncture SR, the Standards for Reporting Interventions in Controlled Trials of
Acupuncture (STRICTA) (316) checklist was applied to assess the transparency of published
reports and the interpretation of results.
6.3 Chapter summary
This chapter summarises the methods used for the SRs of RCTs of the CHM formula PPQFY and
acupuncture and related techniques. The reviews followed the methods of the Cochrane Handbook
for Systematic Reviews of Interventions (302). Studies that used guideline-recommended
comparators such as pharmacotherapies, placebo and no treatment were included in both reviews.
In addition, for the acupuncture review RCTs that used no treatment, sham or placebo needle
treatment were also included in the review. The primary outcome measures of the SRs were

153
changes in lesion count, overall severity grading and therapeutic effective rate. Secondary
outcomes include HRQoL outcomes and AEs.

154
CHAPTER 7 : Systematic review of clinical and pre-clinical evidence of Pi Pa
Qing Fei Yin for acne vulgaris
Overview
Chapter 6 outlined comprehensive methods used in conducting SRs and meta-analyses for CHM
and acupuncture related therapies. This chapter presents the findings from an SR and meta-analysis
of RCTs of the CHM formula Pi Pa Qing Fei Yin (PPQFY) (Eriobotrya Japonica formula) for
acne vulgaris. This review has been published in a modified form in the Journal of Herbal
Medicine in March 2018 (317) (Appendix 14). To better understand the six PPQFY ingredients,
the mechanism of actions from experimental studies are synthesised and presented in this chapter.
7.1 Introduction
Many people use CAM including CHM for skin conditions (151, 318). Despite their common use,
there have been very few reviews of the efficacy and safety of CAM treatments for acne vulgaris.
An SR of botanical and phytochemical treatments for acne included 23 clinical trials (20), three of
which were CHM/Kampo formulations. The CHM preparations showed improvement for mild-to-
moderate acne. Limitations of these clinical trials included the lack of acne-grading methods and
lack of a control or placebo group. No SR have been identified in the English-language databases
that have evaluated the efficacy of CHM generally, or PPQFY specifically, for acne.
An SR on acupoint stimulation (185) included combination therapy of acupuncture with herbal
medicine. The review included 3453 participants from 43 trials. They found the combination of
acupuncture plus herbal medicine showed significant differences in increasing the number of cured
155
patients compared to herbal medicine alone. They also found that acupuncture plus a herbal mask
was better than a herbal mask alone. All trials were assessed as having high risk of bias.
A Cochrane review on CAM for acne that included 35 trials with 3227 participants found
inconsistent effects of acupuncture and herbal medicine for acne (157). Trials comparing CHM
and antibiotics showed no difference between groups for the primary outcome of change in
inflammatory and non-inflammatory lesion counts or total skin lesion counts, or change in acne
severity scores. Trials that compared CHM and retinoic acid did not report on lesion count
reduction and only reported the secondary outcome of “remission”. The results were mixed.
Xiaocuo decoction and adapalene gel were better than oral viaminate capsules, whereas Qingbu
decoction was no better. Two acupuncture trials were evaluated against Western drugs.
Acupuncture was significantly better than oral azithromycin and topical clindamycin phosphate
gel. The other trial showed no difference between acupuncture and oral isotretinoin. The review
also included a low-glycaemic diet, tea-tree oil and pollen bee venom (PBV). The authors found
no clear evidence that a low glycaemic load diet had an effect on non-inflammatory lesion count
between the intervention and control groups. They found that tea-tree oil and PBV reduced skin
lesion count in single trials. AEs in the acupuncture group included itching, redness and pain
following needle insertion. Both herbal medicines and Western drugs caused gastrointestinal upset
and dizziness. Tea-tree oil also caused itchiness, dryness and flaking of the skin. None of the trials
reported any SAEs. This Cochrane review only included trials that had a low risk of bias for
sequence generation. They found that nearly all trials had a high risk for blinding and selective
reporting. Overall, the authors concluded that the strength of evidence was low due to the small
sample sizes and poor methodological designs of the trials.
156
7.2 Rationale for selecting Pi Pa Qing Fei Yin
There are currently no systematic reviews published in English on the safety and efficacy of
PPQFY for acne vulgaris. PPQFY is a common CHM formula recommended by CM textbooks
(159, 165). PPQFY has been used clinically to treat mild-to-moderate inflammatory comedones in
people with acne. It acts to clear heat in the Lungs and cool the Blood. In a recently published
evidence-based CM monograph (168), an analysis was conducted on the efficacy and safety of
CHM as a whole. Overall findings of meta-analyses showed CHM to be more effective than
guideline-recommended treatments in reducing acne severity, and in increasing the number of
participants who achieved a clinical improvement. Given that this work was already underway,
and any addition of recently published trials was unlikely to alter the results found in the 221 RCTs
included in Coyle’s review (168), it was considered unnecessary to conduct a SR of CHM as a
whole. In this monograph, PPQFY was the most common traditional formula tested. This finding,
combined with the inclusion of PPQFY in clinical textbooks, led to the decision to focus on
PPQFY for the SR.
This formula contains six herbs, Pi pa ye (Eriobotrya japonica Thunb. Lindl.), Sang bai pi (Morus
alba L.), Huang lian (Coptis chinensis Franch., Coptis teeta Wall. or Coptis deltoidea C.Y. Cheng
& Hsiao), Huang bai (Phellodendron amurense Rupr. or Phellodendron chinense Schneid.), Ren
shen (Panax ginseng C.A. Mey.) and Gan cao (Glycyrrhiza glabra L. P., Glycyrrhiza uralensis
Fisch. or Glycyrrhiza inflata BAT.). These herbs have anti-inflammatory, anti-lipogenic and
antibacterial effects on P. acnes (319, 320). PPQFY has been evaluated in clinical studies;
however, there are no SR evaluating the efficacy of PPQFY for acne vulgaris to date. This review
evaluates the efficacy and safety of the CHM formula PPQFY alone and in combination with other
157
CHM in the treatment of acne vulgaris. The HRQoL of people with acne can be severely affected
(190). Treatments that improve the acne symptoms also improve HRQoL. This review will also
evaluate the impact of PPQFY on the HRQoL of people with acne.
7.3 Aims of the systematic review
This SR aims to:
1. Evaluate the clinical efficacy and safety of PPQFY for acne; and
2. Synthesise the findings from experimental studies of the six PPQFY ingredients in in terms of
actions on P. acnes, inflammation, hyperkeratinisation, androgen and sebum production.
7.4 Methods
7.4.1 Systematic review methods
The methods of the SR have been described in Chapter 6: Methods for systematic reviews.
7.4.2 Experimental evidence methods
A search of the electronic database PubMed was performed from inception to August 2016. The
six ingredients of PPQFY were used as key words. The pharmaceutical, species, English and pin
yin names for Eriobotrya japonica Thunb. Lindl. leaf (Pi pa ye), Morus alba L. root bark (Sang
bai pi), Coptis chinensis Franch. or Coptis teeta Wall. or Coptis deltoidea C.Y. Cheng & Hsiao
stem, (Huang lian), Phellodendron amurense Rupr. or Phllodendron chinense Schneid. cortex
(Huang bai), Panax ginseng C.A. Mey. root (Ren shen) and Glycyrrhiza glabra L. P. or
Glycyrrhiza uralensis Fisch. or Glycyrrhiza inflata BAT. stem (Gan cao) were used as search
terms. These terms were combined with the terms P. acnes, anti-inflammatory, sebum, androgen
158
and hyperkeratinisation. Articles were limited to those published in English. Data was extracted
into a predefined form that included the herb name, active compound in the experiment, author,
year, whether the experiment was an in vivo and in vitro study, type of animal used, whether
western blot analysis was used and the key findings of the experiment.
7.5 Results
7.5.1 Clinical evidence
7.5.1.1 Characteristics of clinical studies
The original comprehensive search (to May 2013) yielded 27,476 records, with one additional
record identified through other sources. A targeted update search for studies of PPQFY
(Eriobotrya Japonica Formula) to February 2015 identified a further 143 studies (Figure 7.1). In
total, 15 studies, all in Chinese, met the inclusion criteria, with 13 included in the quantitative
analysis. No RCTs were found in English.
Fifteen RCTs included 1782 participants (321-334) (Table 7.1). The mean number of participants
was 119 with a sample size ranging from 60 to 228. Fourteen trials included both males and
females and one trial included only female participants. Participants’ age ranged from 14 to 39
years old (median age 24). All trials were conducted in China between 1997 and 2014. Treatment
duration varied from two to eight weeks. Three trials reported a follow-up period which ranged
from three months (334) to one year (327). The diagnostic tool used in the trials included the
Pillsbury scale (321, 326, 328), Gollnick scale (329) and dermatological textbooks (323, 325, 327,
330-332, 334). The diagnostic tool was not specified in four studies (322, 324, 333, 335).

159
Figure 7.1 Flow chart of study selection PPQFY

160
All trials used the oral herbal formula PPQFY as a base formula for the main intervention (Table
7.2). Three trials combined oral PPQFY with topical herbs (325, 326, 328). Two trials used PPQFY
in combination with other oral herbal formulas (326, 335). Comparators included pharmacotherapy
such as topical and oral antibiotics, topical retinoids and topical BP. Topical agents vitamin E,
vitamin B6 and sulfur creams were added in three trials (323, 327, 335). Three trials used viaminate
as a comparator (321, 333, 334). Viaminate is a non-conventional oral retinoid derivative that is
approved in China for clinical treatment of acne (166). One trial used a combination of viaminate
and an antibiotic (335), which is not a common prescribing practice outside of China. None of the
trials used placebo controls.
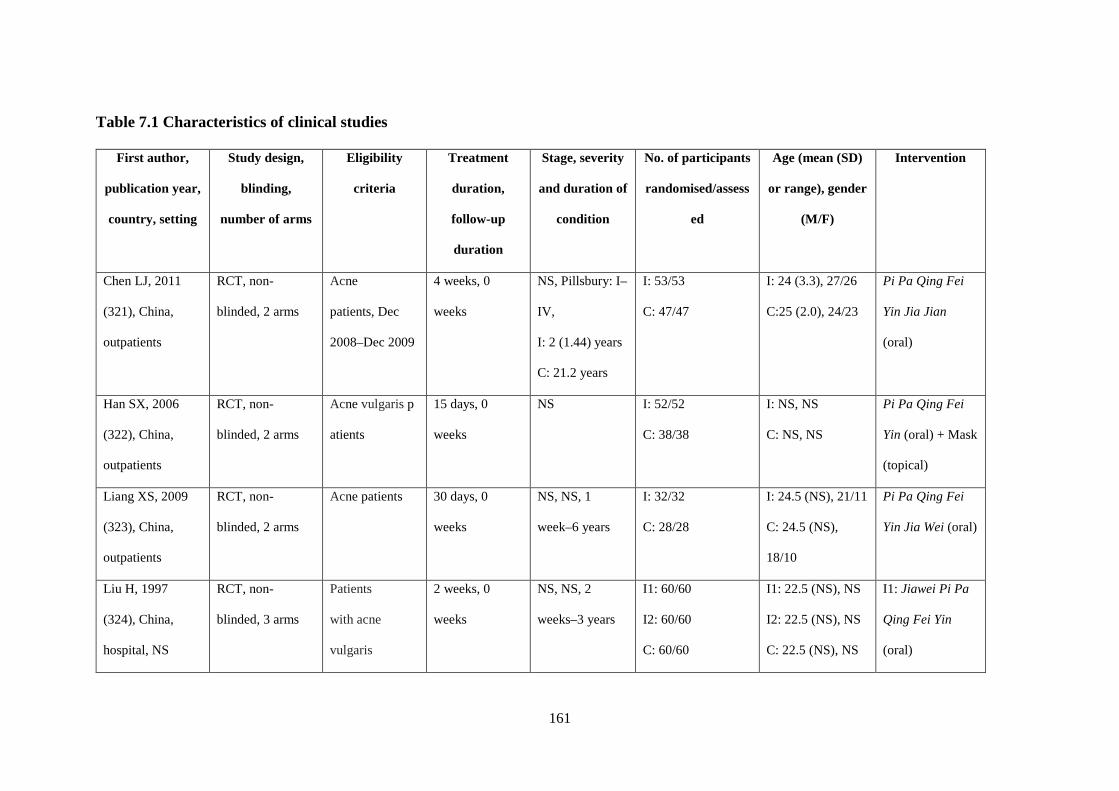
161
Table 7.1 Characteristics of clinical studies
First author,
publication year,
country, setting
Study design,
blinding,
number of arms
Eligibility
criteria
Treatment
duration,
follow-up
duration
Stage, severity
and duration of
condition
No. of participants
randomised/assess
ed
Age (mean (SD)
or range), gender
(M/F)
Intervention
Chen LJ, 2011
(321), China,
outpatients
RCT, non-
blinded, 2 arms
Acne
patients, Dec
2008–Dec 2009
4 weeks, 0
weeks
NS, Pillsbury: I–
IV,
I: 2 (1.44) years
C: 21.2 years
I: 53/53
C: 47/47
I: 24 (3.3), 27/26
C:25 (2.0), 24/23
Pi Pa Qing Fei
Yin Jia Jian
(oral)
Han SX, 2006
(322), China,
outpatients
RCT, non-
blinded, 2 arms
Acne vulgaris p
atients
15 days, 0
weeks
NS I: 52/52
C: 38/38
I: NS, NS
C: NS, NS
Pi Pa Qing Fei
Yin (oral) + Mask
(topical)
Liang XS, 2009
(323), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients 30 days, 0
weeks
NS, NS, 1
week–6 years
I: 32/32
C: 28/28
I: 24.5 (NS), 21/11
C: 24.5 (NS),
18/10
Pi Pa Qing Fei
Yin Jia Wei (oral)
Liu H, 1997
(324), China,
hospital, NS
RCT, non-
blinded, 3 arms
Patients
with acne
vulgaris
2 weeks, 0
weeks
NS, NS, 2
weeks–3 years
I1: 60/60
I2: 60/60
C: 60/60
I1: 22.5 (NS), NS
I2: 22.5 (NS), NS
C: 22.5 (NS), NS
I1: Jiawei Pi Pa
Qing Fei Yin
(oral)
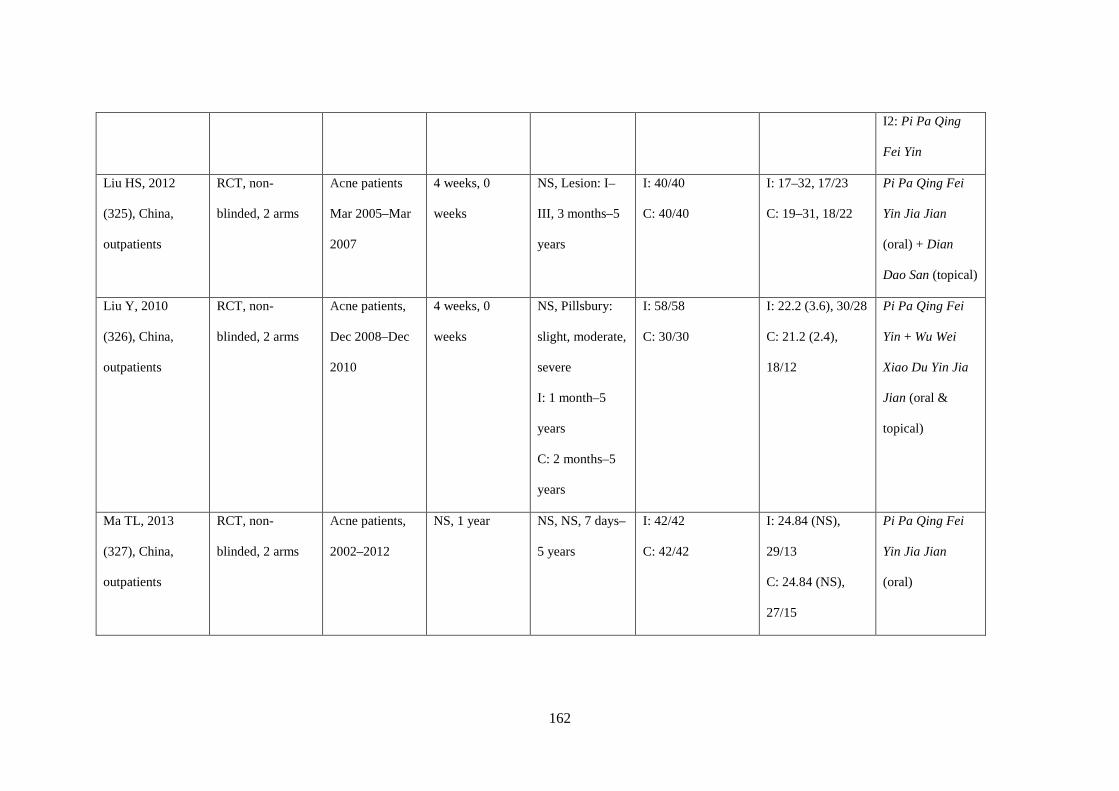
162
I2: Pi Pa Qing
Fei Yin
Liu HS, 2012
(325), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients
Mar 2005–Mar
2007
4 weeks, 0
weeks
NS, Lesion: I–
III, 3 months–5
years
I: 40/40
C: 40/40
I: 17–32, 17/23
C: 19–31, 18/22
Pi Pa Qing Fei
Yin Jia Jian
(oral) + Dian
Dao San (topical)
Liu Y, 2010
(326), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients,
Dec 2008–Dec
2010
4 weeks, 0
weeks
NS, Pillsbury:
slight, moderate,
severe
I: 1 month–5
years
C: 2 months–5
years
I: 58/58
C: 30/30
I: 22.2 (3.6), 30/28
C: 21.2 (2.4),
18/12
Pi Pa Qing Fei
Yin + Wu Wei
Xiao Du Yin Jia
Jian (oral &
topical)
Ma TL, 2013
(327), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients,
2002–2012
NS, 1 year NS, NS, 7 days–
5 years
I: 42/42
C: 42/42
I: 24.84 (NS),
29/13
C: 24.84 (NS),
27/15
Pi Pa Qing Fei
Yin Jia Jian
(oral)
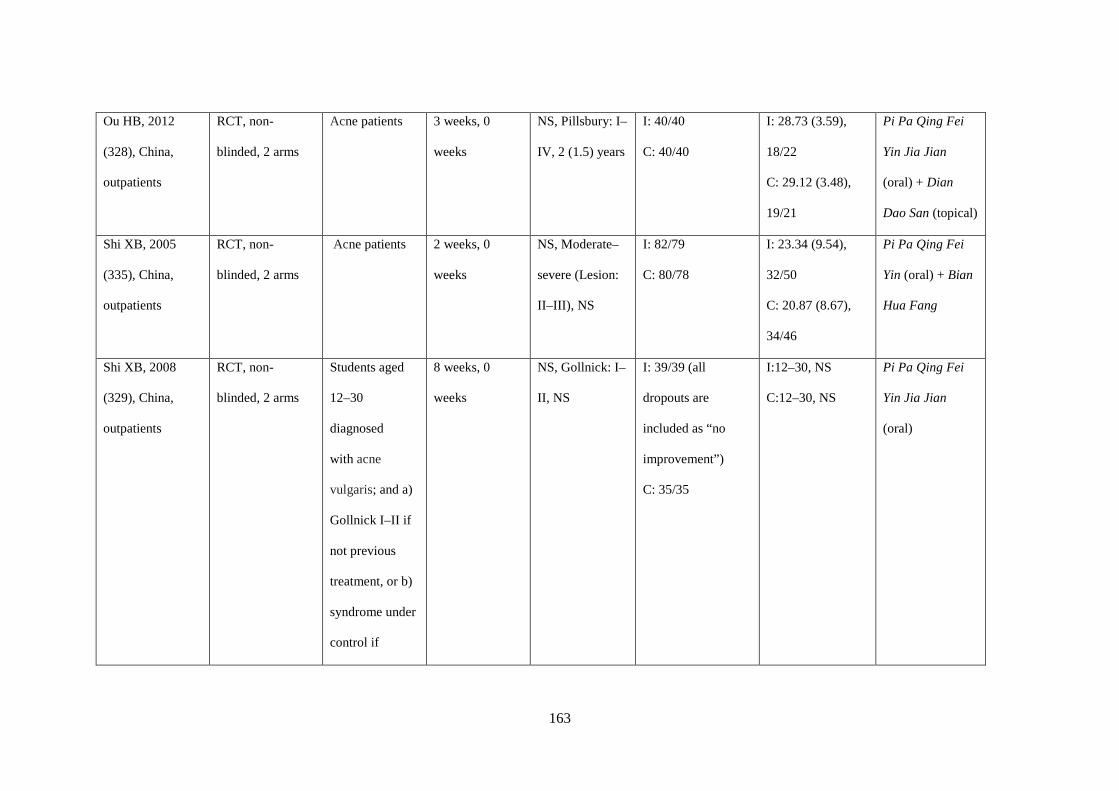
163
Ou HB, 2012
(328), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients 3 weeks, 0
weeks
NS, Pillsbury: I–
IV, 2 (1.5) years
I: 40/40
C: 40/40
I: 28.73 (3.59),
18/22
C: 29.12 (3.48),
19/21
Pi Pa Qing Fei
Yin Jia Jian
(oral) + Dian
Dao San (topical)
Shi XB, 2005
(335), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients 2 weeks, 0
weeks
NS, Moderate–
severe (Lesion:
II–III), NS
I: 82/79
C: 80/78
I: 23.34 (9.54),
32/50
C: 20.87 (8.67),
34/46
Pi Pa Qing Fei
Yin (oral) + Bian
Hua Fang
Shi XB, 2008
(329), China,
outpatients
RCT, non-
blinded, 2 arms
Students aged
12–30
diagnosed
with acne
vulgaris; and a)
Gollnick I–II if
not previous
treatment, or b)
syndrome under
control if
8 weeks, 0
weeks
NS, Gollnick: I–
II, NS
I: 39/39 (all
dropouts are
included as “no
improvement”)
C: 35/35
I:12–30, NS
C:12–30, NS
Pi Pa Qing Fei
Yin Jia Jian
(oral)
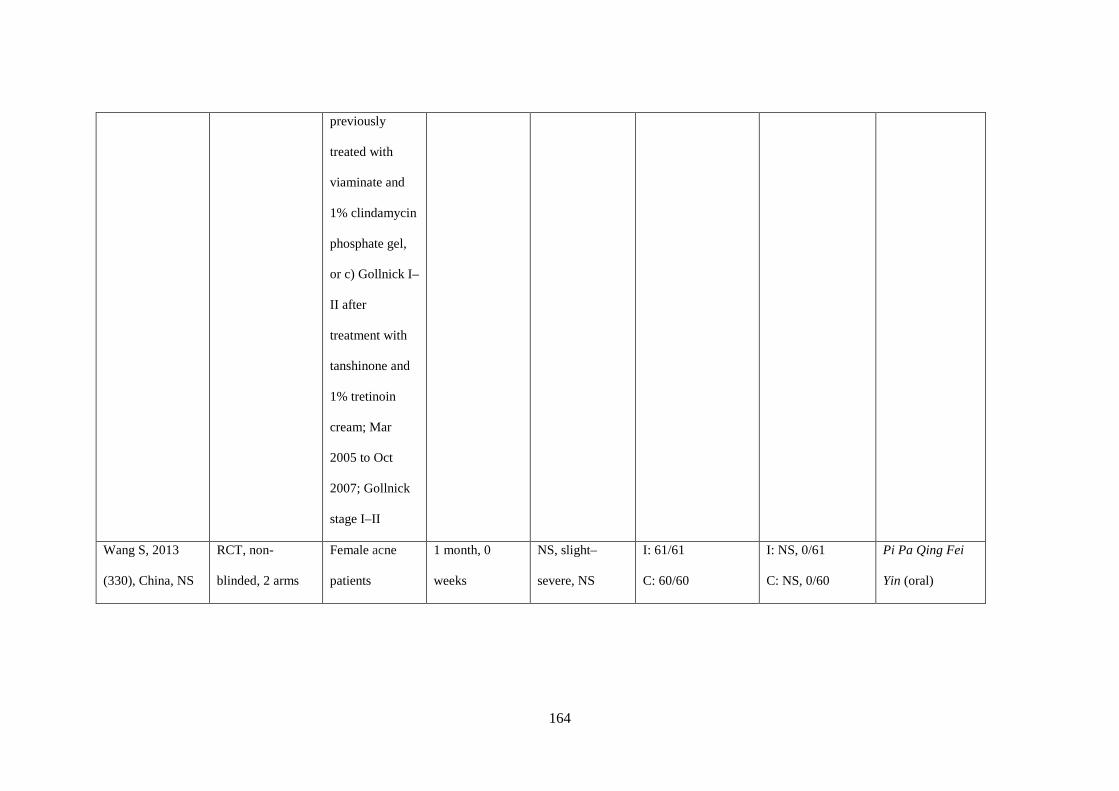
164
previously
treated with
viaminate and
1% clindamycin
phosphate gel,
or c) Gollnick I–
II after
treatment with
tanshinone and
1% tretinoin
cream; Mar
2005 to Oct
2007; Gollnick
stage I–II
Wang S, 2013
(330), China, NS
RCT, non-
blinded, 2 arms
Female acne
patients
1 month, 0
weeks
NS, slight–
severe, NS
I: 61/61
C: 60/60
I: NS, 0/61
C: NS, 0/60
Pi Pa Qing Fei
Yin (oral)

165
Wang X, 2014
(331), China,
outpatients
RCT, non-
blinded, 3 arms
Acne patients in
outpatients
department; 15–
45 yo; no
topical
treatments in the
past 7 days; no
acne oral
medication in
the past 30 days
1 month, 0
weeks
NS I1: 60/60
I2: 60/60
C: 60/60
15–25; NS Pi Pa Qing Fei
Yin (oral)
Yan LY, 2005
(332), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients 3 weeks, 6
months
NS, light–
severe, 560 days
I: 114/114
C: 114/114
I: 17.6 (NS), 49/65
C: 17.6 (NS),
49/65
Bai Di She Xi Ji
+ Cuo Chuang
Ling + Pi Pa
Qing Fei Yin Jia
Jian (oral)
Zhang LL, 2006
(333), China,
outpatients
RCT, non-
blinded, 2 arms
Acne patients
with CM
diagnosis
4 weeks, 0
weeks
NS, NS,
I: 2 months–7
years
I: 60/60
C: 60/60
I: 22 (2.12), 26/34
C: 24 (2.34), 31/29
Pi Pa Qing Fei
Yin Jia Jian
(oral)
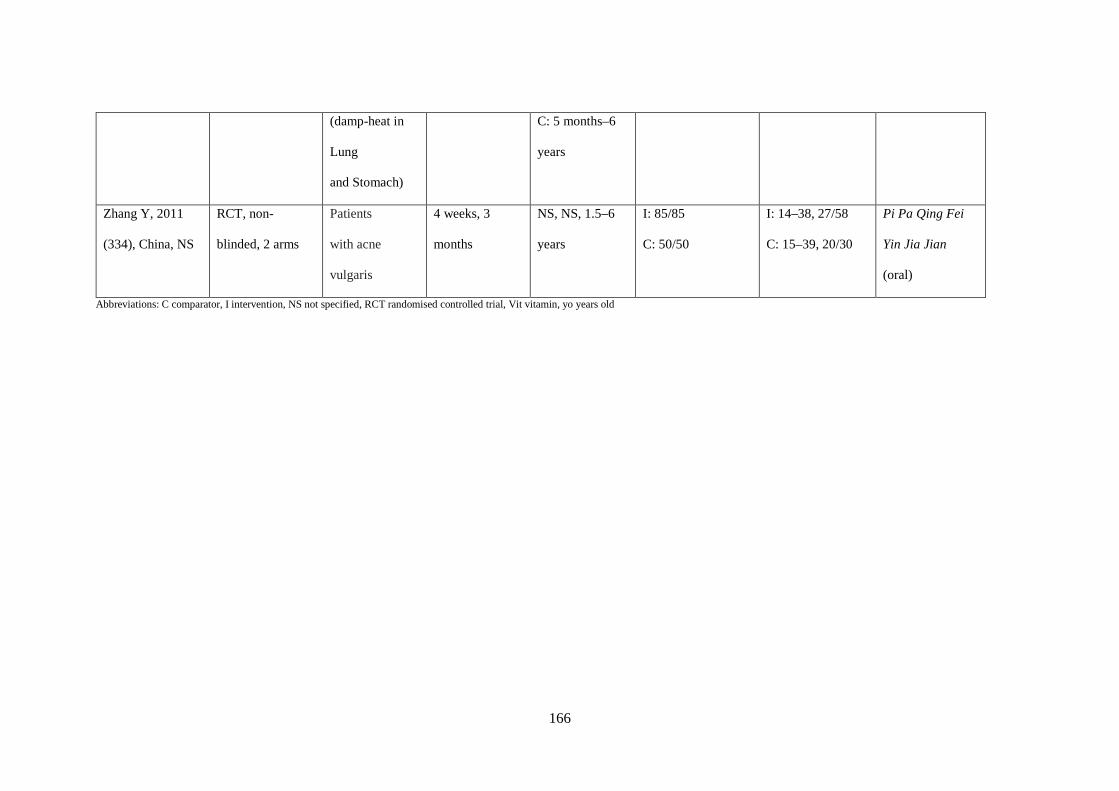
166
Abbreviations: C comparator, I intervention, NS not specified, RCT randomised controlled trial, Vit vitamin, yo years old
(damp-heat in
Lung
and Stomach)
C: 5 months–6
years
Zhang Y, 2011
(334), China, NS
RCT, non-
blinded, 2 arms
Patients
with acne
vulgaris
4 weeks, 3
months
NS, NS, 1.5–6
years
I: 85/85
C: 50/50
I: 14–38, 27/58
C: 15–39, 20/30
Pi Pa Qing Fei
Yin Jia Jian
(oral)
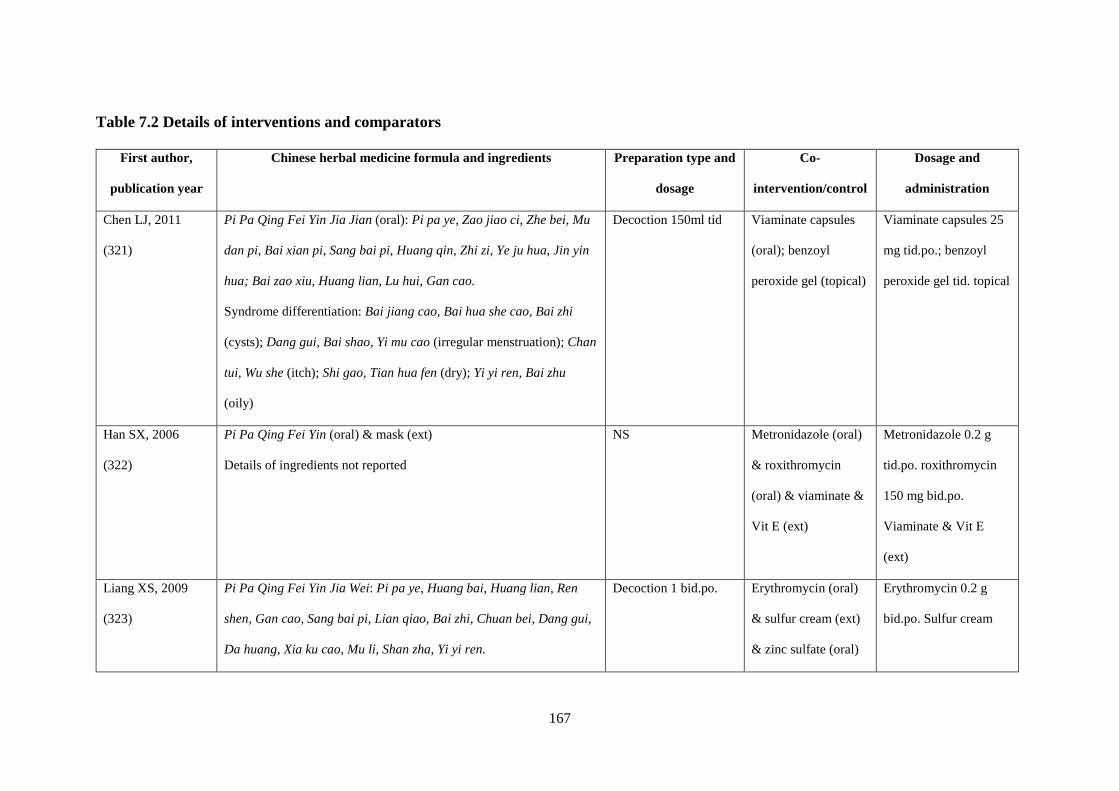
167
Table 7.2 Details of interventions and comparators
First author,
publication year
Chinese herbal medicine formula and ingredients Preparation type and
dosage
Co-
intervention/control
Dosage and
administration
Chen LJ, 2011
(321)
Pi Pa Qing Fei Yin Jia Jian (oral): Pi pa ye, Zao jiao ci, Zhe bei, Mu
dan pi, Bai xian pi, Sang bai pi, Huang qin, Zhi zi, Ye ju hua, Jin yin
hua; Bai zao xiu, Huang lian, Lu hui, Gan cao.
Syndrome differentiation: Bai jiang cao, Bai hua she cao, Bai zhi
(cysts); Dang gui, Bai shao, Yi mu cao (irregular menstruation); Chan
tui, Wu she (itch); Shi gao, Tian hua fen (dry); Yi yi ren, Bai zhu
(oily)
Decoction 150ml tid Viaminate capsules
(oral); benzoyl
peroxide gel (topical)
Viaminate capsules 25
mg tid.po.; benzoyl
peroxide gel tid. topical
Han SX, 2006
(322)
Pi Pa Qing Fei Yin (oral) & mask (ext)
Details of ingredients not reported
NS Metronidazole (oral)
& roxithromycin
(oral) & viaminate &
Vit E (ext)
Metronidazole 0.2 g
tid.po. roxithromycin
150 mg bid.po.
Viaminate & Vit E
(ext)
Liang XS, 2009
(323)
Pi Pa Qing Fei Yin Jia Wei: Pi pa ye, Huang bai, Huang lian, Ren
shen, Gan cao, Sang bai pi, Lian qiao, Bai zhi, Chuan bei, Dang gui,
Da huang, Xia ku cao, Mu li, Shan zha, Yi yi ren.
Decoction 1 bid.po. Erythromycin (oral)
& sulfur cream (ext)
& zinc sulfate (oral)
Erythromycin 0.2 g
bid.po. Sulfur cream
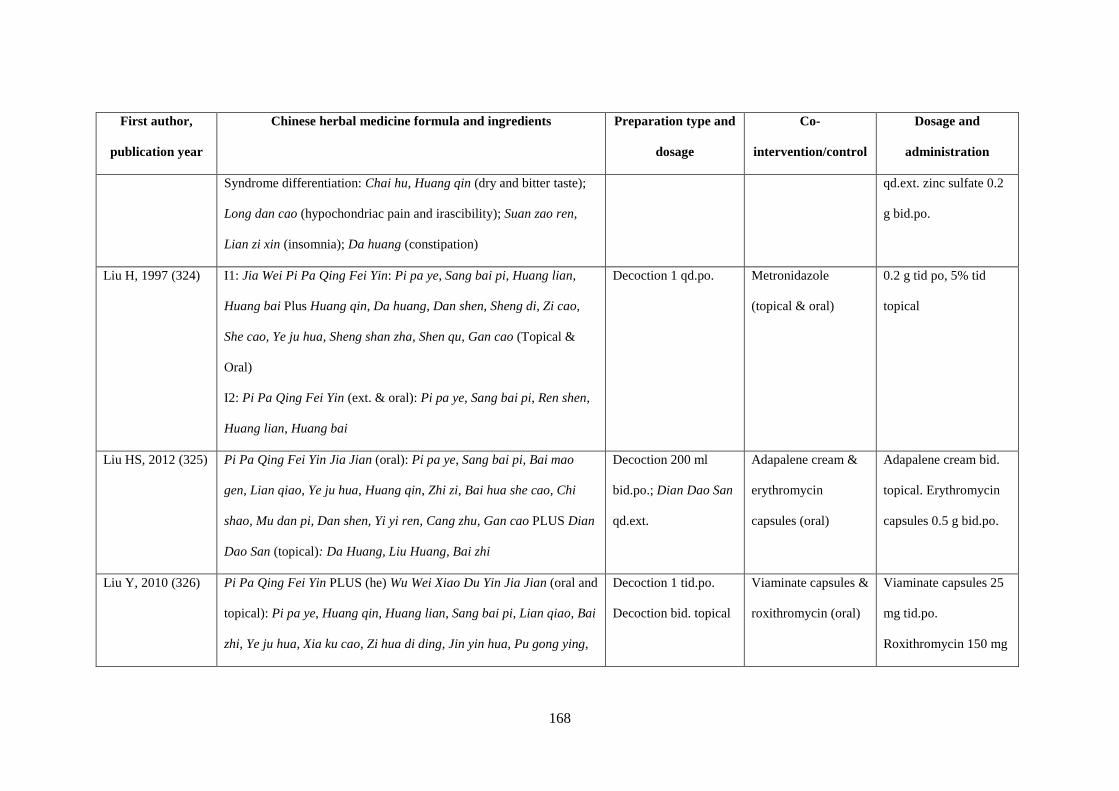
168
First author,
publication year
Chinese herbal medicine formula and ingredients Preparation type and
dosage
Co-
intervention/control
Dosage and
administration
Syndrome differentiation: Chai hu, Huang qin (dry and bitter taste);
Long dan cao (hypochondriac pain and irascibility); Suan zao ren,
Lian zi xin (insomnia); Da huang (constipation)
qd.ext. zinc sulfate 0.2
g bid.po.
Liu H, 1997 (324) I1: Jia Wei Pi Pa Qing Fei Yin: Pi pa ye, Sang bai pi, Huang lian,
Huang bai Plus Huang qin, Da huang, Dan shen, Sheng di, Zi cao,
She cao, Ye ju hua, Sheng shan zha, Shen qu, Gan cao (Topical &
Oral)
I2: Pi Pa Qing Fei Yin (ext. & oral): Pi pa ye, Sang bai pi, Ren shen,
Huang lian, Huang bai
Decoction 1 qd.po. Metronidazole
(topical & oral)
0.2 g tid po, 5% tid
topical
Liu HS, 2012 (325) Pi Pa Qing Fei Yin Jia Jian (oral): Pi pa ye, Sang bai pi, Bai mao
gen, Lian qiao, Ye ju hua, Huang qin, Zhi zi, Bai hua she cao, Chi
shao, Mu dan pi, Dan shen, Yi yi ren, Cang zhu, Gan cao PLUS Dian
Dao San (topical): Da Huang, Liu Huang, Bai zhi
Decoction 200 ml
bid.po.; Dian Dao San
qd.ext.
Adapalene cream &
erythromycin
capsules (oral)
Adapalene cream bid.
topical. Erythromycin
capsules 0.5 g bid.po.
Liu Y, 2010 (326) Pi Pa Qing Fei Yin PLUS (he) Wu Wei Xiao Du Yin Jia Jian (oral and
topical): Pi pa ye, Huang qin, Huang lian, Sang bai pi, Lian qiao, Bai
zhi, Ye ju hua, Xia ku cao, Zi hua di ding, Jin yin hua, Pu gong ying,
Decoction 1 tid.po.
Decoction bid. topical
Viaminate capsules &
roxithromycin (oral)
Viaminate capsules 25
mg tid.po.
Roxithromycin 150 mg
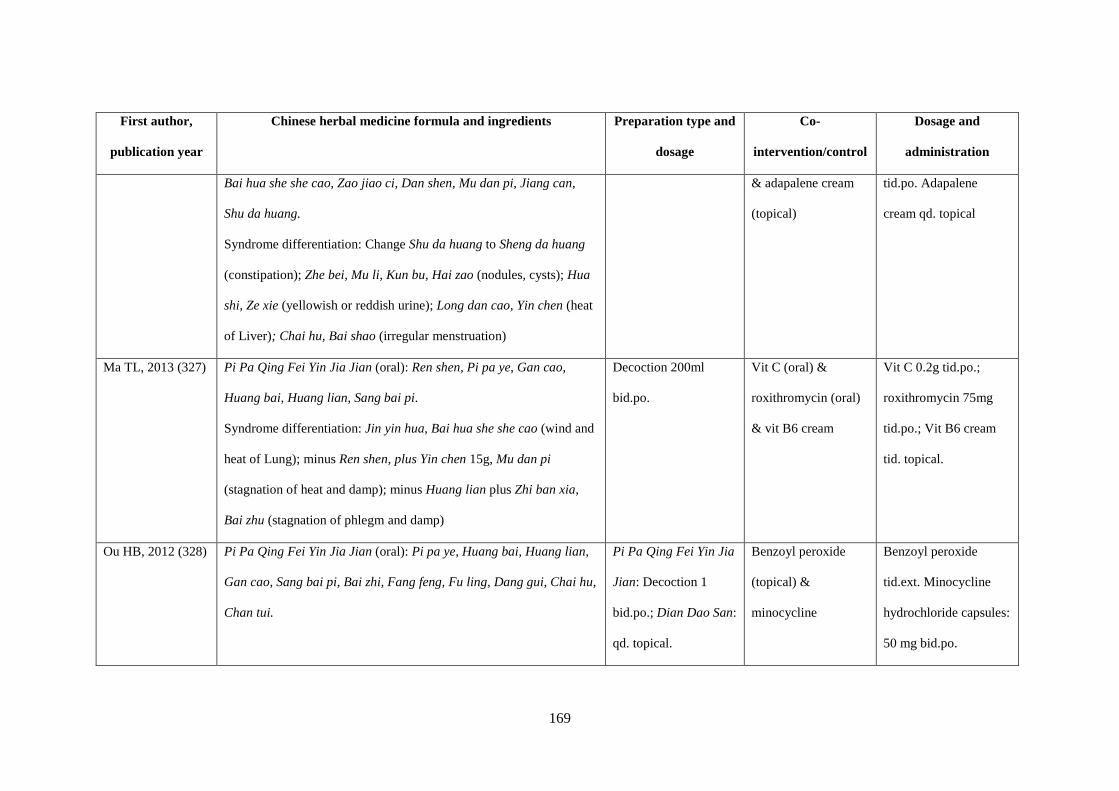
169
First author,
publication year
Chinese herbal medicine formula and ingredients Preparation type and
dosage
Co-
intervention/control
Dosage and
administration
Bai hua she she cao, Zao jiao ci, Dan shen, Mu dan pi, Jiang can,
Shu da huang.
Syndrome differentiation: Change Shu da huang to Sheng da huang
(constipation); Zhe bei, Mu li, Kun bu, Hai zao (nodules, cysts); Hua
shi, Ze xie (yellowish or reddish urine); Long dan cao, Yin chen (heat
of Liver); Chai hu, Bai shao (irregular menstruation)
& adapalene cream
(topical)
tid.po. Adapalene
cream qd. topical
Ma TL, 2013 (327) Pi Pa Qing Fei Yin Jia Jian (oral): Ren shen, Pi pa ye, Gan cao,
Huang bai, Huang lian, Sang bai pi.
Syndrome differentiation: Jin yin hua, Bai hua she she cao (wind and
heat of Lung); minus Ren shen, plus Yin chen 15g, Mu dan pi
(stagnation of heat and damp); minus Huang lian plus Zhi ban xia,
Bai zhu (stagnation of phlegm and damp)
Decoction 200ml
bid.po.
Vit C (oral) &
roxithromycin (oral)
& vit B6 cream
Vit C 0.2g tid.po.;
roxithromycin 75mg
tid.po.; Vit B6 cream
tid. topical.
Ou HB, 2012 (328) Pi Pa Qing Fei Yin Jia Jian (oral): Pi pa ye, Huang bai, Huang lian,
Gan cao, Sang bai pi, Bai zhi, Fang feng, Fu ling, Dang gui, Chai hu,
Chan tui.
Pi Pa Qing Fei Yin Jia
Jian: Decoction 1
bid.po.; Dian Dao San:
qd. topical.
Benzoyl peroxide
(topical) &
minocycline
Benzoyl peroxide
tid.ext. Minocycline
hydrochloride capsules:
50 mg bid.po.

170
First author,
publication year
Chinese herbal medicine formula and ingredients Preparation type and
dosage
Co-
intervention/control
Dosage and
administration
Syndrome differentiation: Lian qiao, Pu gong ying, Zi cao (nodules,
fester); Huang qi (chronic); Mu li, Zhe bei (white head); Tao ren, E
zhu (chromatosis); Da huang (Constipation); Xiang fu (irritability);
Dan shen, Sheng di, Gui zhi, Shi chang pu (pain and itch)
Dian Dao San (ext): Da huang, Liu huang
Hydrochloride
capsules (oral)
Shi XB, 2005 (335) Pi Pa Qing Fei Yin Bian Hua Fang (oral): Pi pa ye, Sang bai pi,
Huang qin, Zhi zi, Pu gong ying, Dan shen, Sheng shan zha, Bai hua
she she cao
Decoction 100ml
bid.po.
Achromycin (oral
antibiotic) &
viaminate & vit E
cream (topical)
Achromycin: 0.5 g, tid.
(first course) po., 0.25
g, tid. (second course);
viaminate & vit E
cream qd. topical.
Shi XB, 2008 (329) Pi Pa Qing Fei Yin Jia Jian (oral): Pi pa ye, Sang bai pi, Huang qin,
Zhi zi, Sheng shan zha, Pu gong ying, Dan shen, Bai hua she she cao
Syndrome differentiation: Gua lou, Zhi shi (Constipation); Pu gong
ying, Zi hua di ding (Heat Toxin); Kun bu, Hai zao (Nodules, cysts);
Yi mu cao (Irregular menstruation)
Decoction 100ml
qd.po.
Tretinoin cream (ext)
and if there is
inflammation will
add clindamycin
(topical)
Tretinoin cream:
qd.ext.;
clindamycin bid.
topical

171
First author,
publication year
Chinese herbal medicine formula and ingredients Preparation type and
dosage
Co-
intervention/control
Dosage and
administration
Pi Pa Qing Fei Yin (Oral): Pi Pa Ye, Sang Bai Pi, Huang Qin, Zhi Zi,
Da Huang, Shan Zha, Dan Shen, Ku Shen, Gan Cao.
Decoction 250 ml
bid.po.
Minocycline
hydrochloride
capsules (oral)
minocycline
hydrochloride capsules
50 mg bid.po.
Wang X, 2014
(331)
Pi Pa Qing Fei Yin (oral): Pi pa ye, Huang lian, Huang qin, Sang bai
pi, Jin yin hua, Mu dan pi, Gan cao
Decoction 50 ml
bid.po.
Doxycycline hyclate
tablets
0.1 g, bid.po.
Yan LY, 2005
(332)
Pi Pa Qing Fei Yin Jia Jian (oral): no details; Bai Di She Xi Ji (ext):
She chuang zi, Bai fan, Di fu zi, Bai ji li; Cuo Chuang Ling (ext.): Xin
yi, Hu po, Bai zhi, Bai ji, Hong hua, Chuan xiong, Huang qin, Shui
zhi, Zhen zhu fen, San qi fen, Bing pian
Bai Di She Xi Ji:
Decoction 1 bid.
topical.
Cuo Chuang Ling:
Cream qd. ext.;
Pi Pa Qing Fei Yin Jia
Jian (Oral): Decoction
1 bid.po.
Benzoyl peroxide
(topical) &
achromycin (oral
antibiotic) & zinc
gluconate (oral)
Benzoyl peroxide
(topical): NS
achromycin (oral
antibiotic): 0.5 g
qid.po.;
zinc gluconate:1 bid.po.
Zhang LL, 2006
(333)
Pi Pa Qing Fei Yin Jia Jian (oral): Pi pa ye 10g, Sang bai pi 15g,
Huang qin 10g, Zhi zi 10g, Huang lian 10g, Da huang 10g, Mu dan pi
Decoction 1 bid.po. Viaminate capsules 25 mg bid.po
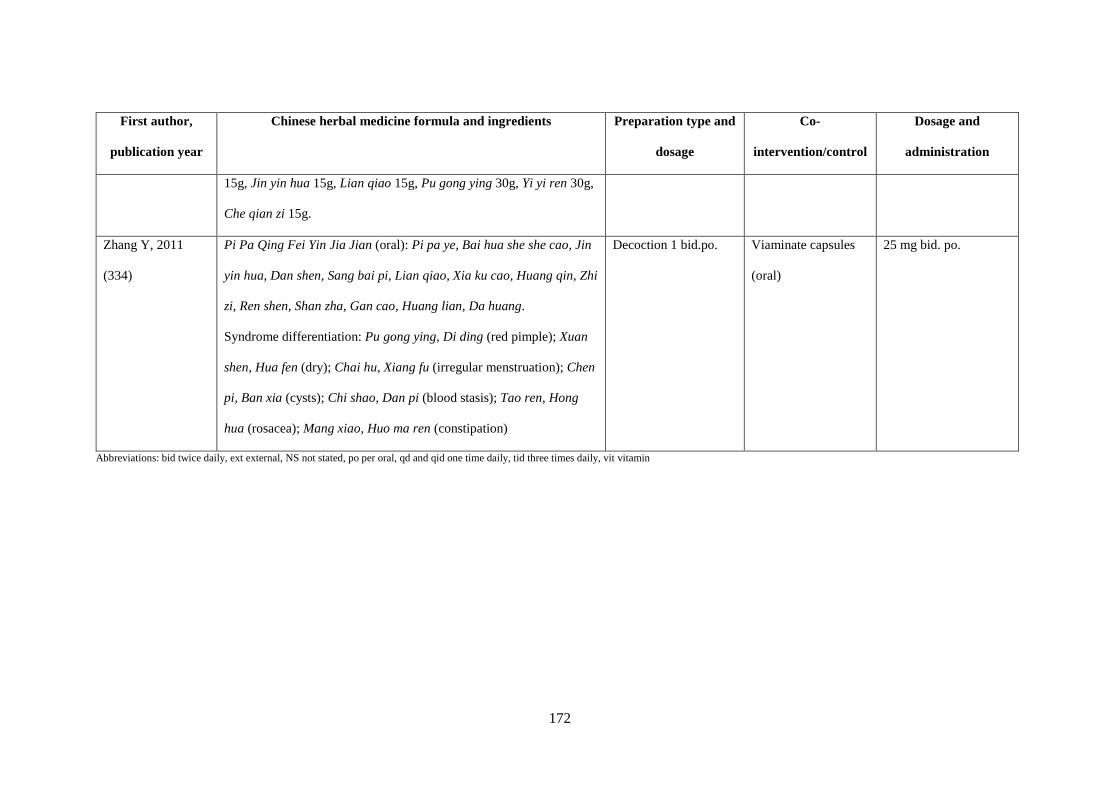
172
First author,
publication year
Chinese herbal medicine formula and ingredients Preparation type and
dosage
Co-
intervention/control
Dosage and
administration
15g, Jin yin hua 15g, Lian qiao 15g, Pu gong ying 30g, Yi yi ren 30g,
Che qian zi 15g.
Zhang Y, 2011
(334)
Pi Pa Qing Fei Yin Jia Jian (oral): Pi pa ye, Bai hua she she cao, Jin
yin hua, Dan shen, Sang bai pi, Lian qiao, Xia ku cao, Huang qin, Zhi
zi, Ren shen, Shan zha, Gan cao, Huang lian, Da huang.
Syndrome differentiation: Pu gong ying, Di ding (red pimple); Xuan
shen, Hua fen (dry); Chai hu, Xiang fu (irregular menstruation); Chen
pi, Ban xia (cysts); Chi shao, Dan pi (blood stasis); Tao ren, Hong
hua (rosacea); Mang xiao, Huo ma ren (constipation)
Decoction 1 bid.po. Viaminate capsules
(oral)
25 mg bid. po.
Abbreviations: bid twice daily, ext external, NS not stated, po per oral, qd and qid one time daily, tid three times daily, vit vitamin
173
Eight trials reported effective rate based on lesion count (324, 325, 329-331, 333-335), six reported
effective rate based on both lesion count and severity (321, 323, 326-328, 332) and one study did
not report details of how the effective rate was calculated (322). Some studies reported using a
specific criterion but modified it. For example, (336) reported using the 2002 guidelines but the
actual threshold was 30 per cent to 70 per cent, which was the 1997 criterion. Four trials (325, 327,
329, 332) reported on recurrence rate. None of the trials reported on the length of time between
recurrences or acne severity, and only one paper (331) reported on the HRQoL measure DLQI.
7.5.1.2 Risk of bias
Overall, the methodological quality of included trials was low to moderate (Figure 7.2). Two trials
(328, 333) were assessed to have a low risk of bias in sequence generation as they used random
number generators. Two trials (321, 331) were assessed as high risk, as Chen and Zhou used
hospital record numbers (321) and Wang et al. used sequence of visit order (331). There was
insufficient information reported on blinding of participants in 14 papers and these were assessed
as unclear. One paper (331) was assessed to have a high risk in the blinding of participants based
on the inclusion of a subjective QoL outcome measure (DLQI). As there was insufficient
information reported on allocation concealment and blinding of personnel and outcome assessors,
all studies were assessed as unclear risk for these domains. All trials were assessed as low risk for
incomplete outcome data and selective reporting. One paper was assessed as high risk for other
biases due to baseline imbalance of participants (334) with no explanation provided. No other
biases such as large differences in sample size between groups or potential conflict of interests
were observed in the other 14 trials (Figure 7.2).
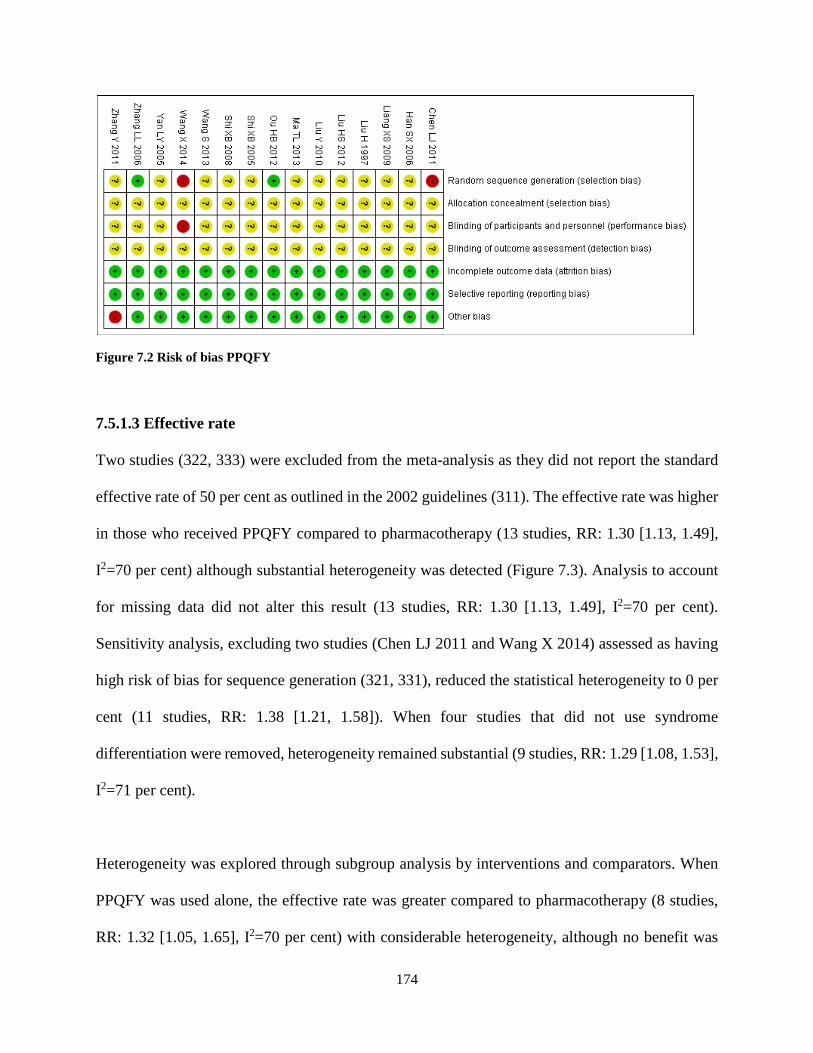
174
Figure 7.2 Risk of bias PPQFY
7.5.1.3 Effective rate
Two studies (322, 333) were excluded from the meta-analysis as they did not report the standard
effective rate of 50 per cent as outlined in the 2002 guidelines (311). The effective rate was higher
in those who received PPQFY compared to pharmacotherapy (13 studies, RR: 1.30 [1.13, 1.49],
I2=70 per cent) although substantial heterogeneity was detected (Figure 7.3). Analysis to account
for missing data did not alter this result (13 studies, RR: 1.30 [1.13, 1.49], I2=70 per cent).
Sensitivity analysis, excluding two studies (Chen LJ 2011 and Wang X 2014) assessed as having
high risk of bias for sequence generation (321, 331), reduced the statistical heterogeneity to 0 per
cent (11 studies, RR: 1.38 [1.21, 1.58]). When four studies that did not use syndrome
differentiation were removed, heterogeneity remained substantial (9 studies, RR: 1.29 [1.08, 1.53],
I2=71 per cent).
Heterogeneity was explored through subgroup analysis by interventions and comparators. When
PPQFY was used alone, the effective rate was greater compared to pharmacotherapy (8 studies,
RR: 1.32 [1.05, 1.65], I2=70 per cent) with considerable heterogeneity, although no benefit was
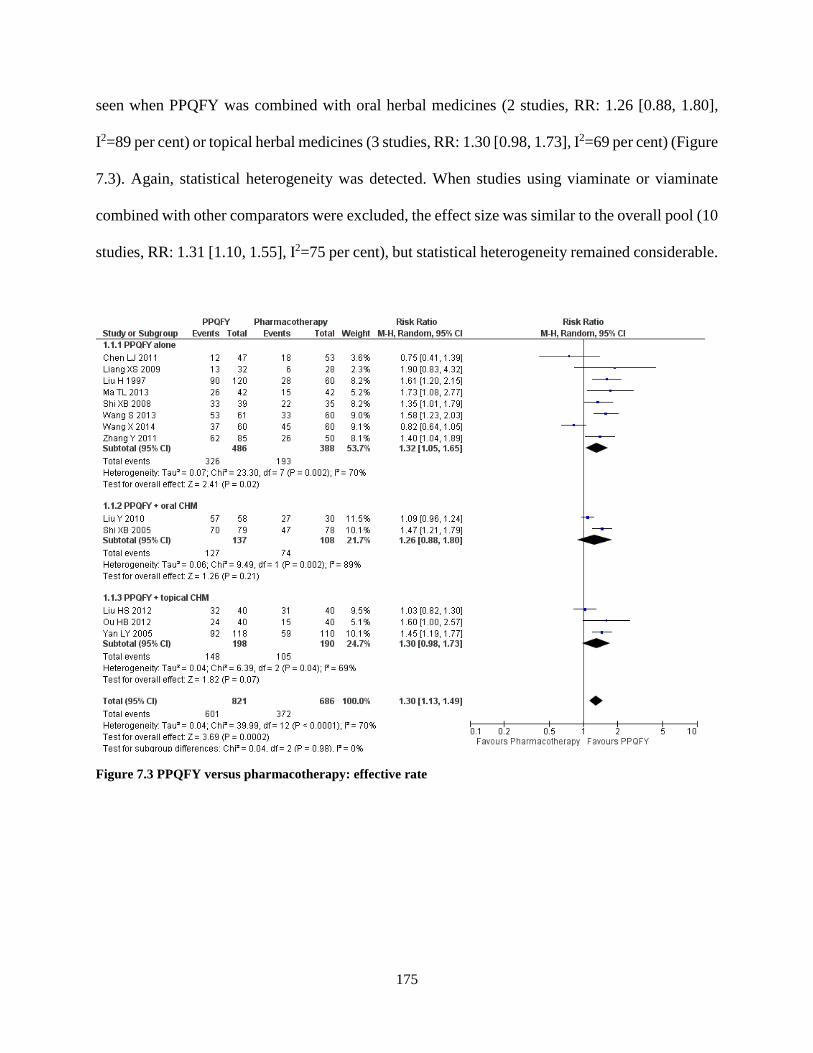
175
seen when PPQFY was combined with oral herbal medicines (2 studies, RR: 1.26 [0.88, 1.80],
I2=89 per cent) or topical herbal medicines (3 studies, RR: 1.30 [0.98, 1.73], I2=69 per cent) (Figure
7.3). Again, statistical heterogeneity was detected. When studies using viaminate or viaminate
combined with other comparators were excluded, the effect size was similar to the overall pool (10
studies, RR: 1.31 [1.10, 1.55], I2=75 per cent), but statistical heterogeneity remained considerable.
Figure 7.3 PPQFY versus pharmacotherapy: effective rate

176
Figure 7.4 Subgroup analysis of PPQFY versus comparators: effective rate
Studies were grouped according to comparator type for further analysis (Figure 7.4). The effective
rate of PPQFY plus topical CHM was greater than those of antibiotics and BP (2 studies, RR: 1.47
177
[1.23, 1.77], I2=0 per cent). PPQFY alone compared to antibiotics with topical supplements
resulted in a greater effective rate (2 studies, RR: 1.77 [1.18, 2.67], I2=0 per cent). No benefit was
seen when PPQFY alone was compared to antibiotics alone (3 studies, RR: 1.27 [0.82, 1.99], I2=89
per cent) and with viaminate alone (2 studies, RR: 1.09 [0.59, 2.01], I2=70 per cent). Results from
single studies showed PPQFY alone produced a higher effective rate than retinoids (RR: 1.35
[1.01, 1.79]) and when combined with oral CHM produced a greater effective rate than antibiotics,
viaminate and supplements (RR: 1.47 [1.21, 1.79]).
7.5.1.4 Recurrence rate
Four studies reported on recurrence rate (325, 327, 329, 332). Two specified the time point at
which the recurrence rate was assessed (327, 332) while two did not (325, 329). Results from two
individual studies showed a lower recurrence rate with PPQFY (RR: 0.29 [0.16, 0.53] (332), RR:
0.17 [0.05, 0.52] (327)) while two showed no statistical significant benefit (RR: 0.25 [0.06, 1.11]
(325), RR: 0.26 [0.06, 1.15] (329)).
7.5.1.5 Health-related quality of life
Only one study reported on HRQoL using the DLQI (331). DLQI scores after one month of
treatment with PPQFY were higher, indicating poorer HRQoL, than with doxycycline (MD: 3.07
[2.42, 3.72]).
7.5.1.6 Adverse events
There were 107 mild AEs reported in 7 of the 15 trials (323-325, 328, 332, 335) with 33 events in
the intervention groups and 74 in the control groups. There were no SAEs reported in the trials. In
the intervention group, AEs included nausea, vomiting or stomach discomfort (29), itching (2),
178
diarrhoea (1) and burning sensation (1). In the control group, AEs included nausea or stomach
discomfort (28), scaling (11), dry mouth (10), itching (9), burning sensation (8), erythema (7),
nausea or vertigo (3) and erythema, itching or scaling (3).
7.5.2 Grading of Recommendations Assessment, Development and Evaluation analysis
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) is an
approach adopted by the Cochrane Collaboration to assess the quality of the evidence and strength
of recommendations for interventions evaluated (337). For the effective rate, 1507 participants
were included from the 13 trials with a treatment range of two to eight weeks. The overall quality
of the evidence was low with a relative effect of 1.30 (RR: 1.30 [1.13-1.19]). The anticipated
absolute effect was 54 per 100 people treated with pharmacotherapies, indicating 54 of those would
have benefit for every 100 people who received pharmacotherapies. For the intervention, there
were 16 more per 100, with an average of 70 people (a range of 7 more to 27 more) benefiting
from PPQFY. With the overall quality of the evidence being low, the effect was limited (Table
7.3).
The data for recurrence was unable to be pooled due to large variations in the data presented in the
studies. The HRQoL assessment for 120 participants (one study) over a one-month treatment
period showed the mean difference for the DLQI was 6.3 points for the pharmacotherapy group
and 3.07 higher for the PPQFY, indicating worse HRQoL for the intervention group. The quality
was moderate. This grading is most likely due to the low numbers included in the analysis from
only one study.
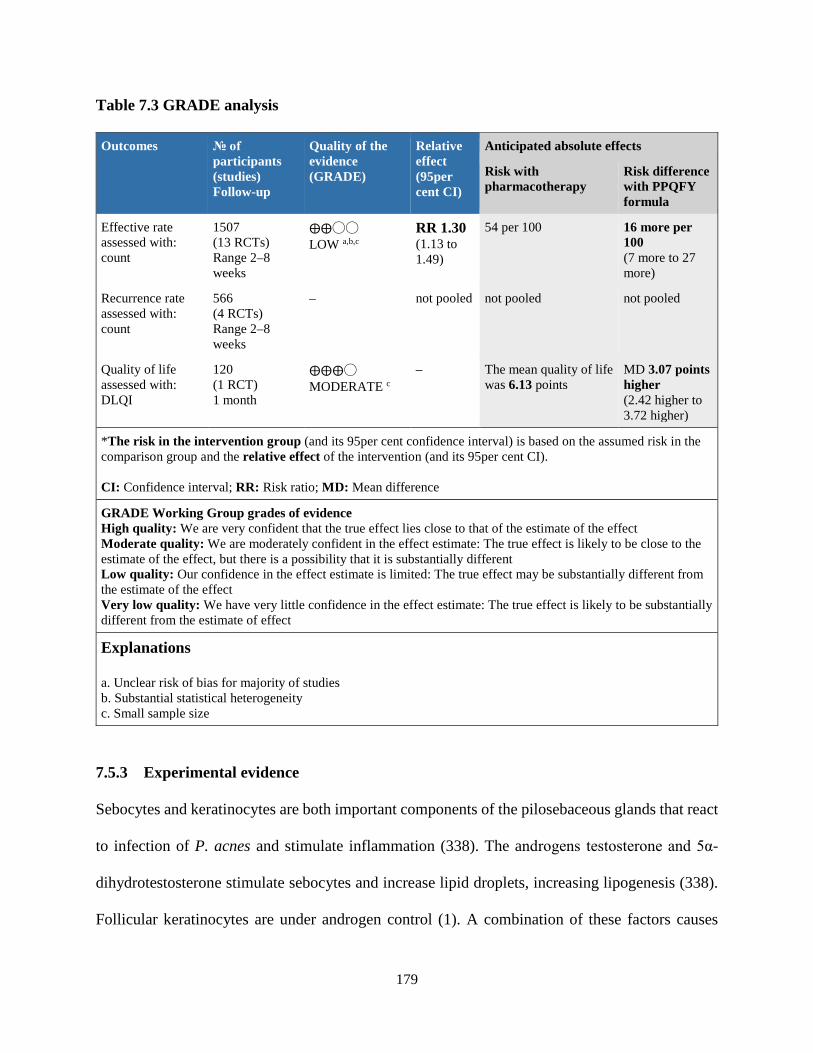
179
Table 7.3 GRADE analysis
Outcomes № of participants (studies) Follow-up
Quality of the evidence (GRADE)
Relative effect (95per cent CI)
Anticipated absolute effects
Risk with pharmacotherapy
Risk difference with PPQFY formula
Effective rate assessed with: count
1507 (13 RCTs) Range 2–8 weeks
⨁⨁◯◯ LOW a,b,c
RR 1.30 (1.13 to 1.49)
54 per 100 16 more per 100 (7 more to 27 more)
Recurrence rate assessed with: count
566 (4 RCTs) Range 2–8 weeks
– not pooled not pooled not pooled
Quality of life assessed with: DLQI
120 (1 RCT) 1 month
⨁⨁⨁◯ MODERATE c
– The mean quality of life was 6.13 points
MD 3.07 points higher (2.42 higher to 3.72 higher)
*The risk in the intervention group (and its 95per cent confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95per cent CI). CI: Confidence interval; RR: Risk ratio; MD: Mean difference
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
Explanations
a. Unclear risk of bias for majority of studies b. Substantial statistical heterogeneity c. Small sample size
7.5.3 Experimental evidence
Sebocytes and keratinocytes are both important components of the pilosebaceous glands that react
to infection of P. acnes and stimulate inflammation (338). The androgens testosterone and 5α-
dihydrotestosterone stimulate sebocytes and increase lipid droplets, increasing lipogenesis (338).
Follicular keratinocytes are under androgen control (1). A combination of these factors causes
180
hyperkeratinisation of cells, contributing to the production of the comedones and pustules seen in
acne. Relevant to the pathogenesis of acne, the six botanicals in PPQFY were found to have anti-
inflammatory, anti-androgenic, anti-adipogenic and anti-lipogenic effects, and were antibacterial
to P. acnes. Key experimental studies of individual herbs identified from the PubMed search were
categorised based on the key pathogenesis described by the AAD 2016 (28) and are presented
below. There were no studies that looked a combination of these herb ingredients.
7.5.3.1 Microbial colonisation with P. acnes
Three of the ingredients had antimicrobial actions. Gan cao (Glycyrrhiza glabra, Glycyrrhiza
uralensis), Huang bai (Phellodendron amurense) and Huang lian (Coptis chinensis) were found
to have antimicrobial actions. The whole-herb extracts of Glycyrrhiza glabra and Glycyrrhiza
uralensis had greater antibacterial potency than erythromycin with no resistance issues (319).
Berberine, a compound common to Phellodendron amurense and Coptis chinensis, inhibited P.
acnes (339). The whole root extract of Panax ginseng prevented P. acnes adhesion to host human
and mouse cell lines (340).
7.5.3.2 Inflammation
All six ingredients of PPQFY had anti-inflammatory effects. The whole-herb extract of Eriobotrya
japonica decreased inducible nitric oxide synthase (iNOS) and the cyclooxygenase-2 (COX-2) in
lipopolysaccharide (LPS) stimulated RAW 264.7 cells (170). The whole-leaf extract of Eriobotrya
japonica inhibited LPS-induced interleukin-8 (IL-8), tumour necrosis factor-α (TNF-α) and IL-1β
in human lung epithelial cells (340), and regulated the production of TNF-α, IL-6 and IL-8 in mast
cells by inhibiting nuclear factor (NF)-κB, p38 mitogen-activated protein kinase (MAPK) and

181
extracellular signal-regulated kinase (ERK) (341). Tormentic acid from Eriobotrya japonica
decreased iNOS and COX-2 in the oedematous paw by increasing the activities of catalase (CAT),
superoxide dismutase (SOD) and glutathione peroxidase (GPx) in the liver of male ICR mice
(342).
Ginsenosides from Panax ginseng inhibited the expression and production of inflammatory
cytokine TNF-α (343). Ginsenoside activated the peroxisome proliferator–activated receptor
gamma (PPAR-γ) nuclear receptor by directly increasing expressions of PPAR-γ2 and its targeting
genes. In addition, ginsenoside sensitised insulin action and promoted the uptake and disposal of
glucose by adipocytes (343, 344). Glabridin from Glycyrrhiza glabra activated PPAR-γ and bound
to it. It also regulated the PPAR-γ gene expression in hepatoma cells (345). Berberine from
Phellodendron amurense inhibited LPS-induced PPAR-γ overexpression and phosphorylation
(346).
Glycyrrhizin from licorice root suppressed the production of cytokines through the inhibition of
lipid raft accumulation and LPS-induced toll-like receptor-3 (TLR)-4 signalling, as well as
suppressing LPS-induced NF-kB and interferon regulatory factor-3 (IRF3) activation (347).
Glycyrrhizic acid and 18β-glycyrrhizic acid had an anti-inflammatory effect. They inhibited the
production of nitrous oxide (NO), prostaglandin E2 (PGE2), TNF-α, IL-6, IL-1β and reactive
oxygen species (ROS). They reduced expression of pro-inflammatory genes (iNOS and COX-2)
and significantly blocked the transcription factors NF-kβ and phosphoinositide-3-kinase (PI3K),
p110δ and p110γ (348).

182
Liquiritigenin from Glycyrrhizae radix blocked the induction of iNOS protein and its messenger
ribonucleic acid (mRNA) at the transcriptional level and significantly inhibited LPS-induced TNF-
α, IL-1β and IL-6 secretions (349). In this study, the inhibition effect was greater on TNF-α, a
secondary cytokine (349). Liquiritigenin inhibited NF-kB activation in macrophages, due to its
inhibition of inhibitory kappa B alpha (I-κBα) phosphorylation (349). A whole-herb extract of
Glycyrrhiza glabra inhibited LPS-induced NO and ROS production, and expression of the
cytokines iNOS, COX-2, TNF-α, IL-1β and IL-6, and protected macrophages from cell death
caused by NO and TNF-α (350).
Berberine chloride, found in Phellodendron amurense and Coptis chinensis, decreased
inflammation by inhibiting IL-6 and IL-8 but not TNF-α (351). However, a whole-herb extract of
Coptis chinensis inhibited TNF-α in human keratinocytes (352). A whole-herb extract of
Phellodendron amurense significantly suppressed the expression of iNOS and COX-2 (353-355)
and decreased nuclear NF-κB and phosphorylated IκBα levels (353). In addition, the whole-herb
extract inhibited IL-6, IL-1β and macrophage chemo-attractant protein-1 (MCP-1) in vitro and in
vivo (353, 354). Berberine may also downregulate the cell-mediated inflammatory response by
directly inhibiting T-cell activation (355). Berberine inhibited LPS-induced PPAR-γ
overexpression and phosphorylation (346). Berberine reduced pro-inflammatory cytokines such as
TNF-α, IL-6, C-reactive protein (CRP) and haptoglobin (HP); and reduction in the expression of
LPL (lipoprotein lipase) was induced by berberine from Phellodendron amurense (171).

183
A whole-herb extract of Morus alba inhibited NO production in LPS-activated RAW 264.7
macrophages and decreased the production of TNF-α (356). It also inhibited NF-κB and
extracellular signal-regulated kinase 1/2 (ERK1/2) activation (357).
7.5.3.3 Follicular hyperkeratinisation
Three ingredients had an effect on adipogenesis, lipogenesis and decreasing serum testosterone
levels. Glycyrrhiza glabra, Glycyrrhiza uralensis and Phellodendron amurense were found to have
anti-adipogenic and lipolytic actions. Glycyrrhizic acid from Glycyrrhiza glabra and Glycyrrhiza
uralensis produced short-term decreases in total serum testosterone and 5α-dihydrotestosterone in
human studies (358). 18β-Glycyrrhetinic acid decreased fat mass by affecting adipogenesis in
maturing preadipocytes and lipolysis in matured adipocyte in 3Te-L1 cells (359). Berberine, an
alkaloid of Phellodendron amurense and Coptis chinensis, reduced secretion of leptin and glycerol
in 3T3-L1 adipocytes and may have reduced the mRNA expression of adipocyte-secreted
inflammatory molecules (171).
7.5.3.4 Sebum production, anti-lipogenic and anti-adipogenic effects
Two of the ingredients had an effect on sebum. Coptis chinensis and Eriobotrya japonica had anti-
lipogenic and anti-adipogenic effects. Coptis chinensis whole-herb extract had a greater effect on
lipogenesis suppression than 0.01per cent retinoic acid in hamster skin (319). Eriobotrya japonica
inhibited lipid accumulation and adipocyte lipid-binding protein (aP2) (360). A whole-leaf extract
of Eriobotrya japonica showed potent inhibition of the glucocorticoid activating enzyme 11β-
hydroxysteroid dehydrogenase 1 (11β-HSD1), an enzyme in adipose tissue (361).
184
7.6 Discussion
PPQFY is a common CHM formula recommended clinically for acne vulgaris in textbooks (159,
165). The clinical evidence from the results of the pooled studies on PPQFY showed that it was
more effective in reducing lesion count, and the effect of the intervention was greatest when
PPQFY was used alone compared to pharmacotherapy, although there was considerable
heterogeneity. The effect of PPQFY varied according to the comparator type, with the highest
effect seen when compared with antibiotics plus topical supplements. There were conflicting
findings when PPQFY was compared with antibiotics alone and in combination with other
medications. The reasons for this are unclear. Some of the studies varied the ingredients for
participants based on syndrome differentiation or modified ingredients of the original formula.
Future research should use original ingredients to evaluate the effect on acne. If modification is
desired, justifications should be provided.
The studies included in this review were of low to moderate methodological quality with
inadequate sequence generation and description of blinding procedures, which may have caused
bias. There were no sample size calculations and sample size in all trials was generally small. The
variability in the interventions and comparators contributed to considerable heterogeneity. The
reporting of effective rate was not consistent among trials. All trials reported on lesion count, but
not all reported on severity of lesions. Although not a validated outcome, reporting of lesion count
and severity are widely used (362). There is a need to establish the criteria for assessing lesion
count.

185
Few studies reported on recurrence rate and follow-up, also lacking description of withdrawals
and drop-outs. None of the studies reported using intention-to-treat analyses to account for missing
data. There was also large variability in comparators and the use of unconventional retinoid
derivatives introduced considerable statistical heterogeneity into this review. Considering the low-
to-moderate methodological quality in study design for most of the trials included in this review,
the results should be interpreted with caution.
The trials used therapeutic effective rate (TER) as a primary outcome measure. TER is based on
the percentage changes of lesion count and severity for improvement. A number of guidelines
(162, 166, 167, 311) exist and variations of 30 per cent and 50 per cent for improvement were
seen. For the PPQFY systematic review, it was decided that a threshold of 50 per cent would be
used for determining clinical effect. This threshold is similar to that described in the CDER (107)
Guidelines for Industry Acne Vulgaris: Developing Drugs for Treatment (107). The CDER
guidelines are the standard with which drug companies in the USA must comply to obtain FDA
approval for a drug (107). The CDER guidelines use the IGA scales to grade lesion severity, with
lesions assessed on a five-point scale from 0 (no lesions) to 4 (severe). An improvement of two
gradings is considered a success, which is similar to 50 per cent improvement in symptoms. This
comparison was used since the IGA is commonly used as a scale for pharmacotherapy trials.
Meta-analysis of herb that only used PPQFY or modified from this formula was statistically
significant, though heterogeneity was considerable. This was in contrast to studies that combined
PPQFY with other oral or topical formulas, where no statistical significance was found. The
combination of PPQFY with other herbal formulas appears to have introduced statistical
186
heterogeneity which may reflect clinical heterogeneity. Some studies included in this review used
only two of the six original ingredients from the formula, while others used four or more
ingredients. Many studies added extensively to the base formula. While this is reflective of clinical
practice, variations in the formula across studies may have produced different clinical effects.
Other factors that could have contributed to statistical heterogeneity include variations in the
severity of disease (mild to severe) across the 15 studies. Statistical heterogeneity was also detected
in several subgroup analyses, but was not able to be explored due to the small numbers of studies.
Therefore, the effect of PPQFY compared with some drugs and drug combinations remains
uncertain.
Acne treatment varies dependent on acne severity and cost. For mild-to-moderate acne in primary
care, the combination of antibiotics with topical medications is first-line therapy (125, 140). OAB
are prescribed for up to six months with 20 per cent improvement within two months and 80 per
cent within six months (140). Second-line therapy includes topical or oral retinoids. This review
included studies using either first- or second-line therapies as the comparator. Several studies
reported acne severity ranging from mild to severe. This may have introduced clinical
heterogeneity and impacted on the potential effect of PPQFY. Pharmacotherapies such as
antibiotics and isotretinoin require four to six months of treatment in order to see clinical benefit
(140).
The Western medicine prescribing practices for acne in the included studies, all of which were
conducted in China, differed to common practices in Europe, Australia and the USA (125, 140,
363). One trial combined OAB with TAB (324). The combination of oral and topical antibiotics is
187
no longer a common prescribing practice due to antibiotic resistance issues (140). Four trials used
an unconventional retinoid derivative (viaminate) (321, 324, 334) that is not recommended in
international guidelines for acne vulgaris (28, 125, 127, 140). Though viaminate is not common
outside of China, it is highly utilised in China. European, US and Australian guidelines are similar
in prescribing practices for retinoids, antibiotics and topical medications. A combination of OAB
with topical BP or topical isotretinoin should be prescribed depending on the severity of the acne.
Photodynamic therapy is recommended in Malaysian and European guidelines, but the US and
Australian guidelines indicates there is less evidence for the efficacy of these interventions.
The number of AEs was lower among those who received PPQFY than those in the control group.
Few studies reported causality assessment of AEs. Monitoring of safe use of herbal products is
important for public safety (364). Many of the comparators used have known side effects, such as
skin irritation and dryness with topical BP (13) and burning, pruritus, scaling and erythema with
topical tretinoin and adapalene (365). Based on the included studies, the formula was well tolerated
by people with acne vulgaris.
There is one published review in English (20) on botanical and phytochemical treatments for acne
reporting on three CHM/Kampo formulations, a herbal face mask, a Kampo formula Kaigei-
rengyo-to and green tea, none of which were PPQFY. Due to the differing scales used in assessing
disease severity, it was not possible to explore the effect of PPQFY on severity subgroups;
therefore we were unable to compare directly with the findings reported in the Fisk et al. review
(20). There is one Cochrane review on CAM that included CHM compared to pharmaceuticals.
None of the included trials used PPQFY. The review found herbal medicines were not better than
188
pharmaceuticals, and there were clinical heterogeneity between trials and incomplete data
reporting. Similar limitations from these reviews such as reporting issues and non-validated
outcome measures were also seen in the trials included in this review.
From the experimental studies, all six ingredients of PPQFY may have an effect in decreasing
inflammation, sebum production and hyperkeratinisation. They may also have an inhibitory effect
on P. acnes, as well as preventing P. acnes from adhering to host cells. Panax ginseng and
glycyrrhizic acid from Glycyrrhiza glabra and Glycyrrhiza uralensis decreased serum testosterone
(358) and encouraged lipolysis in mature adipocytes (Moon et al., 2012). Glycyrrhiza Glabra,
Panax ginseng, Phellodendron amurense and Coptis chinensis all inhibited P. acnes growth (319,
339, 344).
Four of the six ingredients, Glycyrrhiza glabra, Coptis coptidis, Eriobotrya japonica and Panax
ginseng, all inhibit PPAR-γ. Phellodendron amurense, Eriobotrya japonica, Panax ginseng,
liquiritigenin from Glycyrrhiza glabra and a whole-herb extract of Coptis chinensis all inhibit
TNF-α. NF-κB is activated in comedones and strongly expresses IL-1α, which increases
hyperkeratinisation (81, 348, 353, 366). Three of the ingredients, Phellodendron amurense, Morus
alba and Eriobotrya japonica, inhibit NF-κB cytokines and a further three of the ingredients,
Glycyrrhiza glabra, Phellodendron amurense and Eriobotrya japonica, inhibit IL-1β but not IL-
1α (348, 353, 366). Nearly all experimental evidence was from in vivo and in vitro studies. Only
one study was found on the pathophysiological effects of the botanicals in people; caution is
needed when translating effects to people.
189
7.7 PPQFY systematic review conclusions
The six ingredients of PPQFY have anti-inflammatory, antibacterial, anti-lipogenic, anti-
adipogenic and anti-androgenic effects. These actions may contribute to the effects seen in clinical
studies. The number of people achieving a reduction in lesion count was higher with PPQFY
compared with various pharmacotherapies, although statistical heterogeneity was detected in
several meta-analyses. In one study, HRQoL was worse in people who received PPQFY than in
those who received pharmacotherapy. No SAEs were reported in clinical trials, suggesting that
PPQFY was well-tolerated by people with acne. Rigorously designed studies that describe original
formula ingredients, grade the severity of acne and report on clinically relevant outcomes such as
HRQoL are needed.
7.8 Implications for future clinical research
None of the included RCTs were free from bias and methodological shortcomings are highlighted.
Future research should take into consideration:
1. Proper randomisation, allocation concealment and blinding methods (see below)
2. Use of health-related quality of life questionnaires specific to acne as outcome measures
3. Minimised modification of formulations, providing reasoning if modifications are used;
and
4. Comparing interventions with like controls such as placebos and, if using pharmacotherapy
for controls, to use one guideline-recommended treatment at the correct dosage for the
correct age group.
190
Randomisation is used to ensure that there is no selection bias, to control for confounders and to
improve the internal validity of clinical trials (367). Rigorous randomisation procedures prevent
differences between baseline characteristics of participants in different interventions groups. This
is one way to prevent bias in a trial. Trials that do not use randomisation inevitably show that the
intervention assessed has extremely high clinical effects (302).
Concealing group allocation from participants and the research investigators prevents the results
from being influenced by personal biases and beliefs. Knowing which group one is in may lessen
or increase compliance or increase drop-outs. It may make researchers behave differently towards
participants, whether intended or not. Estimates of interventions can be exaggerated in studies with
improper concealment (302). Blinding of participants and researchers would prevent such biases
and control for unobserved cofounders and biases, hence improving the internal validity of the trial
(367).
It is common in CM practice to modify formulas to address the diagnosed syndrome and tailor
treatment to the individual patient as seen in the included trials in this review. This however brings
heterogeneity into the meta-analyses of included clinical trials. The substantial modifications in
the included trials of PPQFY may have contributed to the considerable heterogeneity found in the
meta analysis. Pragmatic trial designs may be one solution to addressing individualised treatments
in trials (PATSOUPOULOS 2011), This type of design requires substantial personnel to
implement the trial and to make timely adjustments to herbs. This type of trial would most closely
reflect real clinical practice however may increase variance in studies and efficacy of the herbs is
difficult to determine.

191
7.9 Implications for clinical practice
From the SR and experimental review, PPQFY has the potential to decrease inflammatory and
non-inflammatory acne lesions, decrease sebum and inhibit P. acnes growth. It may be effective
for mild-to-moderate comedonal acne. All of the studies modified the original formula or added
another formula as an intervention; however, the original formula may not be applicable for all
lesion types or all syndromes. The herbs most commonly added to the formula were Huang qin
(Scutellaria baicalensis Georgi.) followed by (Shan) Zhi zi (Gardenia jasminoides Ellis, fruit), Mu
dan pi (Paeonia suffruticosa Andr., root bark) and Da huang (Rheum palmatum L. or R.
tanguticum Maxim, et Reg. or R. officinale Baill.). All of these herbs are considered ‘cold’ and
have actions that clear heat. Huang qin targets the upper and middle energisers, whereas Huang
bai (Phellodendron amurense Rupr. or P. chinense Schneid.) from the original formula targets the
lower energiser. This is considered a logical modification as the CM syndromes for acne relate to
the upper and middle energisers. Da huang supports draining dampness, clearing heat toxicity and
regulating Blood. Again, these herbs are logical choices due to the CM pathogeneses described in
Chapter 3.
Clinically, the meta-analysis showed that PPQFY produced better outcomes than
pharmacotherapies and with fewer AEs. It may be an alternative to pharmacotherapies for acne.
The studies, however, were not free from biases. Clinicians should use their experience and patient
preferences when prescribing treatment. The main AEs reported with PPQFY included
gastrointestinal AEs such as nausea, abdominal discomfort and intermittent diarrhoea. This may
be explained when considering the actions of the herbs. For example, Da huang is a purgative and
may cause diarrhoea, increased abdominal peristalsis and pain. The other herbs are ‘cold’ in nature
192
and may cause additional gastrointestinal discomfort. The symptoms resolved when the CHM were
discontinued and, although not all trials conducted a follow-up, those trials that did reported no
lingering or residual AEs from the CHM. Therefore the formula is relatively safe with a low risk
of harm. Clinicians should inform patients of the possible risks and strategies to minimise AEs
such as taking herbs after meals.
The trials included in this systematic review did not include integrative medicine, that is, no trials
used a combination of PPQFY with pharmacotherapies compared to pharmacotherapies alone.
Therefore, the safety profile of an integrative medicines was not ascertained in this review.
Practitioners who see patients currently using pharmacotherapies may wish to wait until
pharmacotherapy treatment has ceased before providing CM treatment, given the lack of
information about safety of using CHM and pharmacotherapy concurrently.
7.10 Chapter summary
This chapter has provided the results of the SR and meta-analysis of the targeted CHM formula
PPQFY. The effective rate of PPQFY was better than pharmacotherapies in the treatment of acne
with the exception of HRQoL, although the results should be interpreted with caution due to the
low methodological quality of the trials. There was also only one study that used HRQoL included
in this review which showed pharmacotherapies was better than PPQFY. More studies are needed
that include this outcome measure in order to improve knowledge of the impact of CHM on the
HRQoL of people with acne.
193
CHAPTER 8 : Systematic review of acupuncture for acne vulgaris
Overview
Chapter 6 outlined comprehensive methods used in conducting SRs and meta-analyses for CHM
and acupuncture related therapies. Chapter 7 presented findings on the first SR and meta-analysis
of CHM formula PPQFY for acne. This chapter presents the findings of the second SR of RCTs
of acupuncture and related techniques for acne vulgaris (acne). The SR was published in a modified
form in the journal Evidenced-Based Complementary and Alternative Medicine in March 2018
(368) (Appendix 15).
8.1 Introduction
Acupuncture is an umbrella term for traditional CM techniques that stimulate acupuncture points.
Techniques include body acupuncture (insertion of fine needles at specific loci on the body,
typically for a period of 20 to 30 minutes) and auricular acupuncture (insertion of needles in
specific loci of the auricle). Acupressure is another form of point stimulation that can include using
hands, fingers or other blunt instruments to apply pressure to the acupuncture point with no skin
penetration. Auricular acupressure (AA), similar to body acupuncture point acupressure, is the
placement of blunt instruments such as small metallic ball bearings at specific loci of the auricle.
EA (mild electric stimulation of acupuncture needles) (169) can be used on body acupuncture
points or auricular points. Cutaneous needling (also called plum blossom or seven-star needling)
is a type of device where a cluster of five or seven short needles are spaced out in a circle or star
shape and are taped around a skin lesion or along a meridian (Bertschinger et al., 1993). A form
of indirect point stimulation is moxibustion (burning of Artemisia argii Levl. et Vant or Artemisia
194
vulgaris leaf in a processed form) (369). These techniques for stimulating acupuncture points are
commonly used in the treatment of acne vulgaris.
Several studies have suggested a potential role of acupuncture and related techniques in acne. AA
and surround needling (where two to four needles are inserted superficially around the acne lesion)
have been shown to reduce serum excretion rate (SER) and testosterone (176). When acupuncture
was combined with BP, SER in women was reduced compared to BP alone (309). In animal
studies, auricular acupuncture, auricular EA, body acupuncture and EA have been shown to
decrease inflammation (308, 370-372). Auricular acupuncture may reduce acne inflammation
through peripheral muscarinic receptors (370) and innate and adaptive immune responses (371,
373, 374).
Several reviews have examined the potential benefits of acupuncture techniques in clinical studies.
A Cochrane review on CAM for acne (157) evaluated the efficacy of herbal medicine, acupuncture,
cupping therapy, dietary modifications, purified bee venom (PBV) and tea-tree oil. The review
found there was a lack of evidence to support the use of herbal medicine and acupuncture. Two
SRs of acupuncture for acne have been published, one in English (185) and one in Chinese (18).
Cao et al. (185) included trials which used acupuncture, cupping and other herbal medicines. While
the number of “cured” cases increased when acupuncture was combined with cupping, or oral or
topical herbal medicines, no benefit was found when acupuncture was compared with
pharmacotherapy. The reviewers described the methodological quality of the papers as poor. Li et
al. (18) included trials of manual acupuncture compared to routine conventional medicine
195
(isotretinoin and antibiotics) or multiple CM therapies. The authors were unable to provide
conclusions due to the poor quality of the included trials.
8.2 Rationale for the acupuncture review
The abovementioned reviews included herbal medicines and acupuncture techniques not
commonly used outside of China. Body acupuncture, auricular acupuncture and moxibustion are
commonly used in CM clinical practice for skin conditions. Previous reviews evaluated a
combination of different acupuncture therapies, or combination of herbs with acupuncture or with
pharmacotherapies. They also included studies that used CM as a comparator for which evidence
is lacking. Reviews of the efficacy and safety of body acupuncture, auricular acupuncture and
moxibustion used alone compared with sham or placebo, or conventional acne treatments have not
been identified. This chapter analyses commonly used acupuncture techniques compared to
pharmacotherapies, no treatment, and sham or placebo acupuncture to evaluate their efficacy and
safety for acne vulgaris.
8.3 Aims
This chapter aims to conduct an SR and meta-analysis of the efficacy and safety of acupuncture
and related interventions for acne vulgaris. The methods have been described in Chapter 6:
Methods for systematic reviews.
196
8.4 Results
8.4.1 Search Results
A total of 15,306 records were identified from database searches from inception to May 2013 (and
updated in February 2015) with one additional record sourced through an online search for
acupuncture-related references. After removal of duplicates, screening of titles and abstracts
excluded 7,673 papers, and 2,485 full texts were reviewed (Figure 8.1).
8.4.2 Characteristics of studies
Twelve RCTs involving 1,026 participants met the inclusion criteria (174-177, 336, 375-381). Ten
RCTs with 975 participants were included in the meta-analysis. The data presented from two trials
could not be reanalysed due to data not being available for individual groups; these were excluded
from the quantitative analysis (174, 377). The authors were contacted for additional information;
however, this was unsuccessful. All trials recruited male and female participants except that of
Kim and Kim (377), who recruited only male subjects. Participant age ranged from 13 to 37 with
a median of 23.1 years. Details of trial location, treatment times, follow-up periods and participant
stage and duration of condition are presented in Table 8.1. Most of the studies included in this SR
were conducted in China, however a number of them did not explicitly state their location and
therefore it is not possible to be certain of their exact location. In addition, most trials were not
registered with relevant trial databases.

197
Figure 8.1 Study selection flow chart: acupuncture

198
Table 8.1 Characteristics of studies
First author,
publication year
Trial location Treatment
duration,
follow-up
duration
Stage, severity and duration of condition No. of participants
randomised/assessed;
dropouts or
withdrawals
Age (mean (SD) or
range); gender (M/F)
Han, 2010 (375)
China, hospital
outpatients
8 w, 1 m Stage: NS
Severity: Pillsbury I, II
Duration: I: 2.35±0.86; C: 2.15±0.82
I: 50/46; 4 I: 25.83±5.25; 18/28
C: 50/47; 3 C: 24.68±4.36; 14/33
He, 2009 (376)
China, hospital
outpatients
3 w, NS Stage: NS
Severity: Slight to severe
Duration: I: 20 d to 16 y; C: 1 m to 17 y
I: 24/24; 0 I: 25.2; NS
C: 22/22; 0 C: 23.6; NS
Li, 2002 (176)
NS 6 d, 1 m Stage: NS
Severity: Samuelson 1–9
Duration: I1: 14 d – 15 y, I2: 7 d – 13 y; C:
4 d – 14 y
I1:200/200; 0 I1: 13–37; NS
I2 : 60/60; 0 I2:14–35; NS
C:60/60; 0 C: 14–33; NS
Liu, 2011 (378)
NS 2 w, 6 m Stage: NS
Severity: NS
Duration: I: 1 w – 14 y; C: 1 w – 10 y
I:40/40; 0 I:14–41; 6/34
C:40/40; 0 C:13–30; 7/33
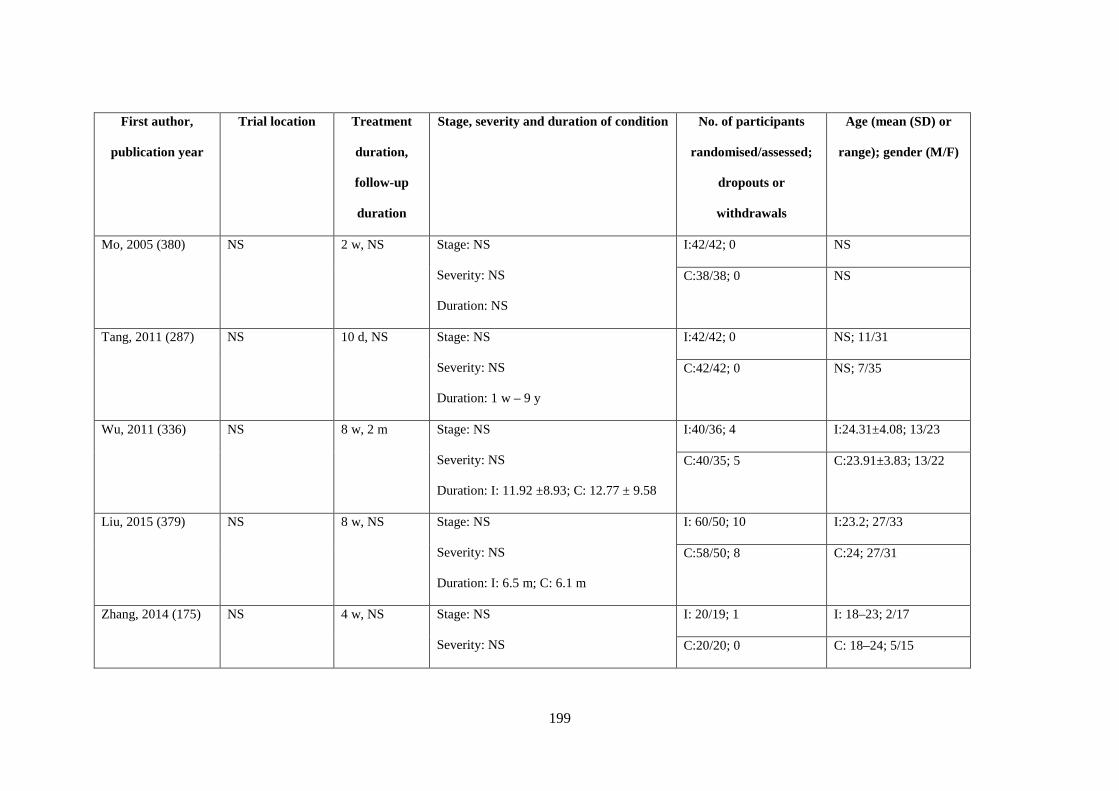
199
First author,
publication year
Trial location Treatment
duration,
follow-up
duration
Stage, severity and duration of condition No. of participants
randomised/assessed;
dropouts or
withdrawals
Age (mean (SD) or
range); gender (M/F)
Mo, 2005 (380)
NS 2 w, NS Stage: NS
Severity: NS
Duration: NS
I:42/42; 0 NS
C:38/38; 0 NS
Tang, 2011 (287)
NS 10 d, NS Stage: NS
Severity: NS
Duration: 1 w – 9 y
I:42/42; 0 NS; 11/31
C:42/42; 0 NS; 7/35
Wu, 2011 (336)
NS 8 w, 2 m Stage: NS
Severity: NS
Duration: I: 11.92 ±8.93; C: 12.77 ± 9.58
I:40/36; 4 I:24.31±4.08; 13/23
C:40/35; 5 C:23.91±3.83; 13/22
Liu, 2015 (379)
NS 8 w, NS Stage: NS
Severity: NS
Duration: I: 6.5 m; C: 6.1 m
I: 60/50; 10 I:23.2; 27/33
C:58/50; 8 C:24; 27/31
Zhang, 2014 (175)
NS 4 w, NS Stage: NS
Severity: NS
I: 20/19; 1 I: 18–23; 2/17
C:20/20; 0 C: 18–24; 5/15
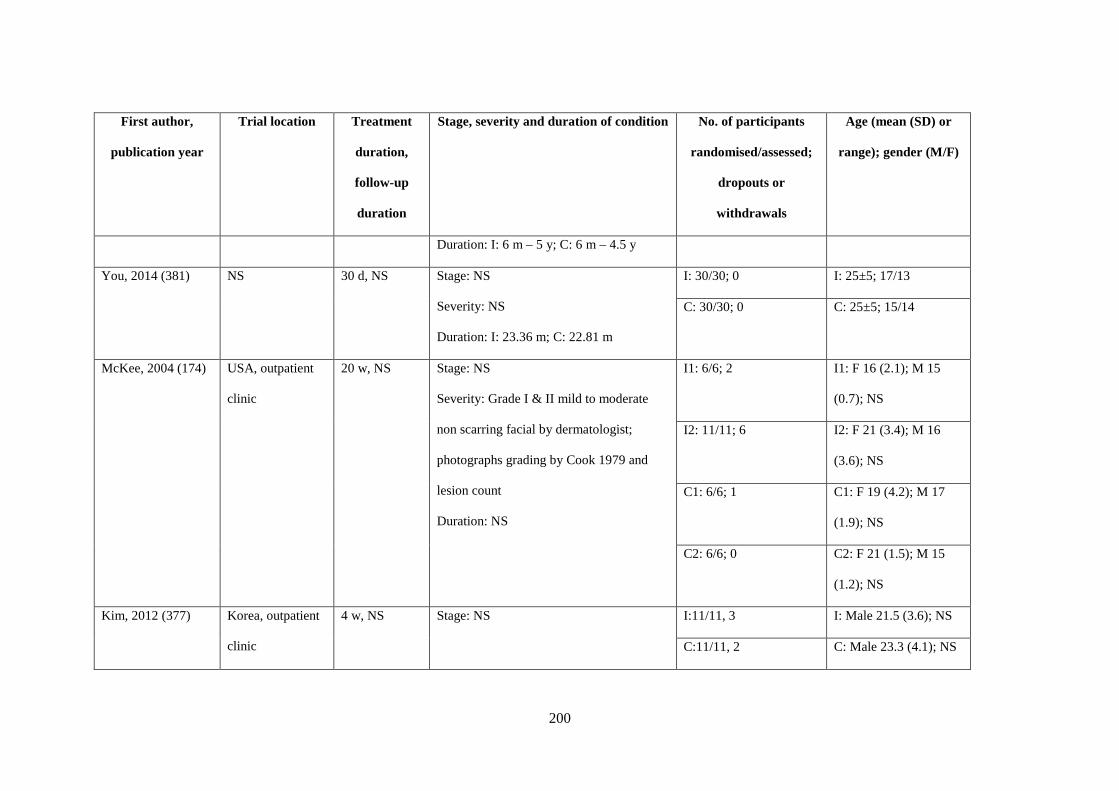
200
First author,
publication year
Trial location Treatment
duration,
follow-up
duration
Stage, severity and duration of condition No. of participants
randomised/assessed;
dropouts or
withdrawals
Age (mean (SD) or
range); gender (M/F)
Duration: I: 6 m – 5 y; C: 6 m – 4.5 y
You, 2014 (381)
NS 30 d, NS Stage: NS
Severity: NS
Duration: I: 23.36 m; C: 22.81 m
I: 30/30; 0 I: 25±5; 17/13
C: 30/30; 0 C: 25±5; 15/14
McKee, 2004 (174)
USA, outpatient
clinic
20 w, NS Stage: NS
Severity: Grade I & II mild to moderate
non scarring facial by dermatologist;
photographs grading by Cook 1979 and
lesion count
Duration: NS
I1: 6/6; 2 I1: F 16 (2.1); M 15
(0.7); NS
I2: 11/11; 6 I2: F 21 (3.4); M 16
(3.6); NS
C1: 6/6; 1 C1: F 19 (4.2); M 17
(1.9); NS
C2: 6/6; 0 C2: F 21 (1.5); M 15
(1.2); NS
Kim, 2012 (377)
Korea, outpatient
clinic
4 w, NS Stage: NS I:11/11, 3 I: Male 21.5 (3.6); NS
C:11/11, 2 C: Male 23.3 (4.1); NS
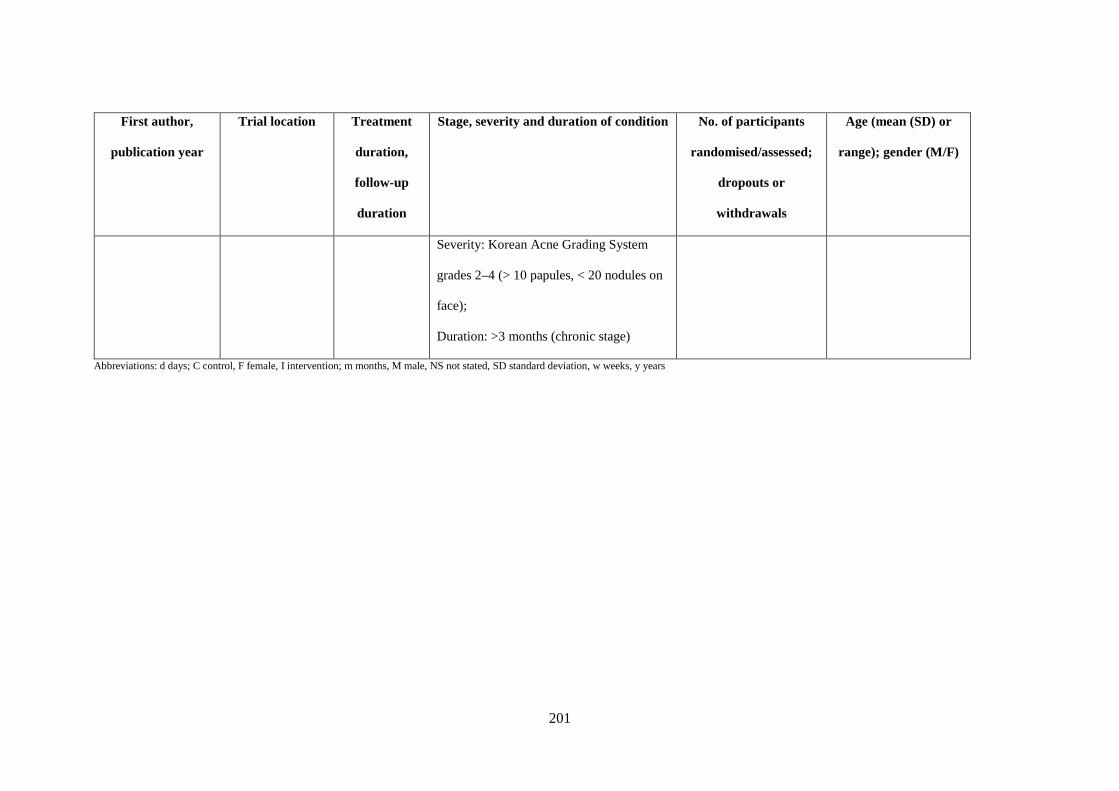
201
First author,
publication year
Trial location Treatment
duration,
follow-up
duration
Stage, severity and duration of condition No. of participants
randomised/assessed;
dropouts or
withdrawals
Age (mean (SD) or
range); gender (M/F)
Severity: Korean Acne Grading System
grades 2–4 (> 10 papules, < 20 nodules on
face);
Duration: >3 months (chronic stage)
Abbreviations: d days; C control, F female, I intervention; m months, M male, NS not stated, SD standard deviation, w weeks, y years

202
Table 8.2 Interventions and comparators
First
author,
publication
year
Intervention type Acupuncture points Intervention treatment
frequency
Control details Control treatment
frequency
Han, 2010
(375)
Acupuncture CV13 Shangwan, CV12 Zhongwan,
CV4 Guanyuan, CV6 Qihai; ST24
Huaroumen, ST26 Wailing; Shangfeng
Shidian (abdominal point 0.5 cun lateral
and superior to ST24); KI13 Qixue, M-
CA-23 Sanjiaojiu (Qipang)
30 mins, 3 times per week Isotretinoin capsules
(oral)
10 mg b.i.d. (first month);
10 mg, q.d. (second
month)
He, 2009
(376)
Acupuncture CV13 Shangwan, CV12 Zhongwan,
CV4 Guanyuan, CV6 Qihai; ST24
Huaroumen, ST26 Wailing; Shangfeng
Shidian (abdominal point 0.5 cun lateral
and superior to ST24); KI13 Qixue, M-
CA-23 Sanjiaojiu (Qipang), M-HN-3
30 mins: body points; 15–20
mins: head points Ashi
Points q.d. (first week), every
2 days (2nd and 3rd weeks)
Metronidazole
(topical)
b.i.d
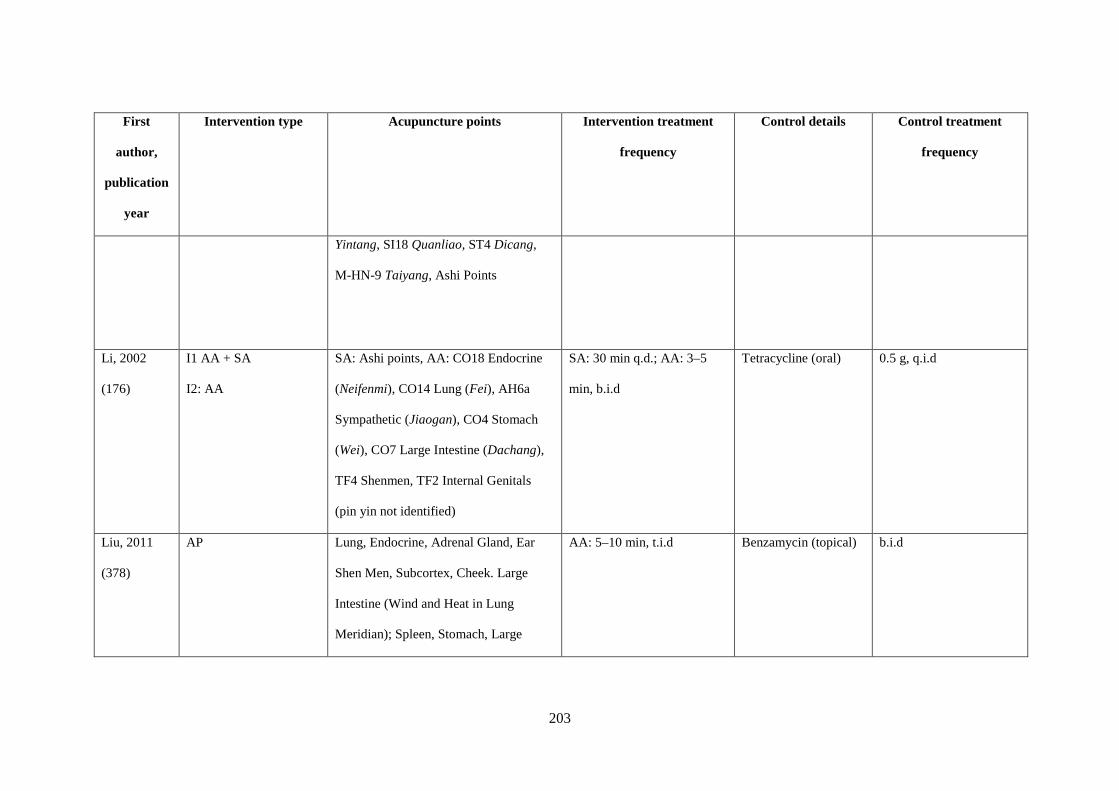
203
First
author,
publication
year
Intervention type Acupuncture points Intervention treatment
frequency
Control details Control treatment
frequency
Yintang, SI18 Quanliao, ST4 Dicang,
M-HN-9 Taiyang, Ashi Points
Li, 2002
(176)
I1 AA + SA
I2: AA
SA: Ashi points, AA: CO18 Endocrine
(Neifenmi), CO14 Lung (Fei), AH6a
Sympathetic (Jiaogan), CO4 Stomach
(Wei), CO7 Large Intestine (Dachang),
TF4 Shenmen, TF2 Internal Genitals
(pin yin not identified)
SA: 30 min q.d.; AA: 3–5
min, b.i.d
Tetracycline (oral) 0.5 g, q.i.d
Liu, 2011
(378)
AP Lung, Endocrine, Adrenal Gland, Ear
Shen Men, Subcortex, Cheek. Large
Intestine (Wind and Heat in Lung
Meridian); Spleen, Stomach, Large
AA: 5–10 min, t.i.d Benzamycin (topical) b.i.d
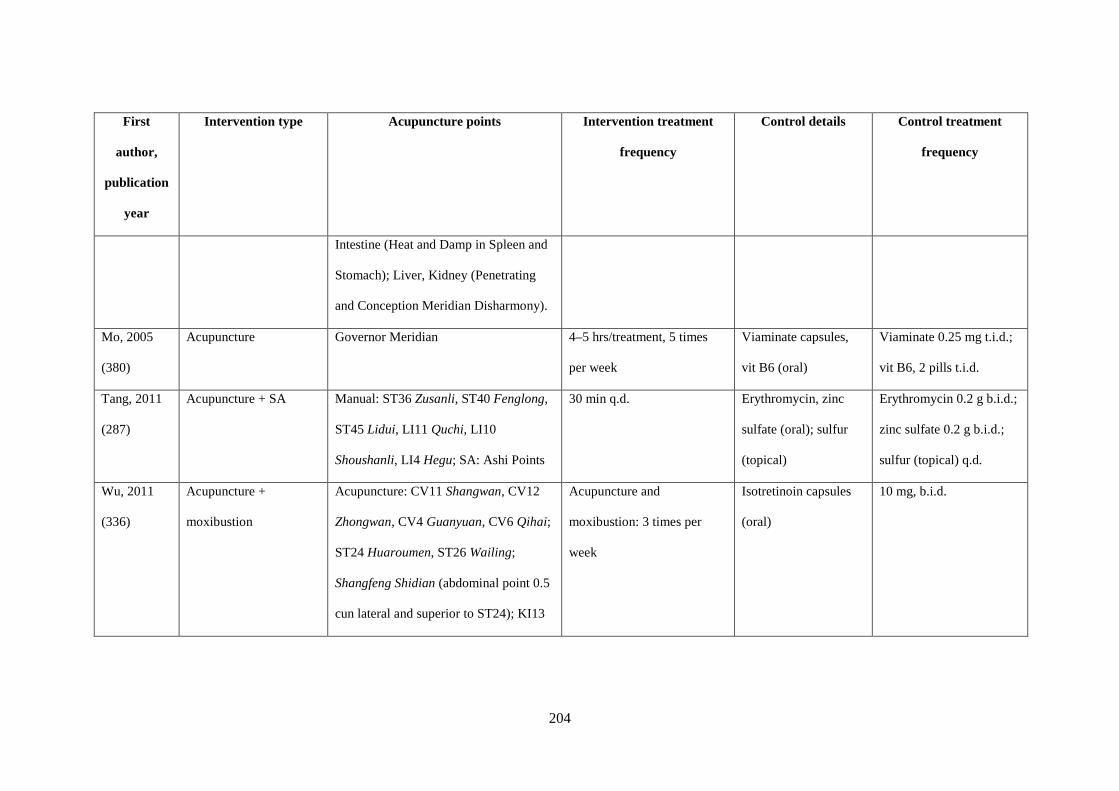
204
First
author,
publication
year
Intervention type Acupuncture points Intervention treatment
frequency
Control details Control treatment
frequency
Intestine (Heat and Damp in Spleen and
Stomach); Liver, Kidney (Penetrating
and Conception Meridian Disharmony).
Mo, 2005
(380)
Acupuncture Governor Meridian 4–5 hrs/treatment, 5 times
per week
Viaminate capsules,
vit B6 (oral)
Viaminate 0.25 mg t.i.d.;
vit B6, 2 pills t.i.d.
Tang, 2011
(287)
Acupuncture + SA Manual: ST36 Zusanli, ST40 Fenglong,
ST45 Lidui, LI11 Quchi, LI10
Shoushanli, LI4 Hegu; SA: Ashi Points
30 min q.d. Erythromycin, zinc
sulfate (oral); sulfur
(topical)
Erythromycin 0.2 g b.i.d.;
zinc sulfate 0.2 g b.i.d.;
sulfur (topical) q.d.
Wu, 2011
(336)
Acupuncture +
moxibustion
Acupuncture: CV11 Shangwan, CV12
Zhongwan, CV4 Guanyuan, CV6 Qihai;
ST24 Huaroumen, ST26 Wailing;
Shangfeng Shidian (abdominal point 0.5
cun lateral and superior to ST24); KI13
Acupuncture and
moxibustion: 3 times per
week
Isotretinoin capsules
(oral)
10 mg, b.i.d.
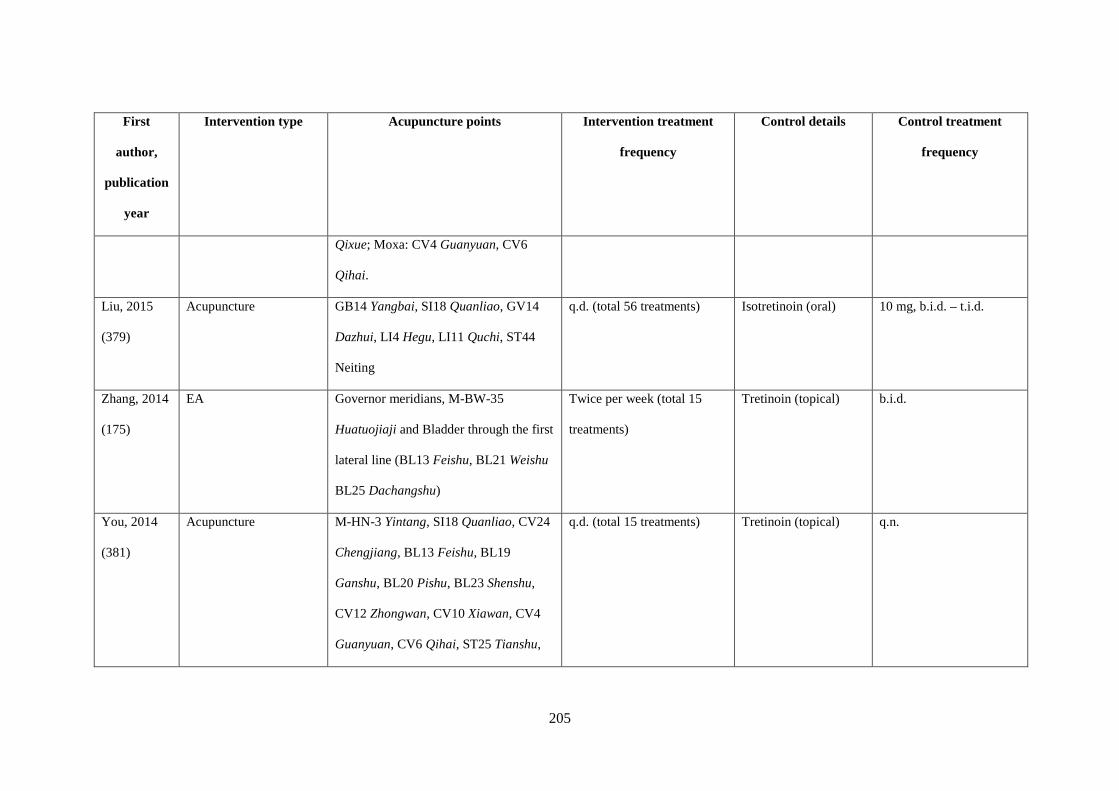
205
First
author,
publication
year
Intervention type Acupuncture points Intervention treatment
frequency
Control details Control treatment
frequency
Qixue; Moxa: CV4 Guanyuan, CV6
Qihai.
Liu, 2015
(379)
Acupuncture GB14 Yangbai, SI18 Quanliao, GV14
Dazhui, LI4 Hegu, LI11 Quchi, ST44
Neiting
q.d. (total 56 treatments) Isotretinoin (oral) 10 mg, b.i.d. – t.i.d.
Zhang, 2014
(175)
EA Governor meridians, M-BW-35
Huatuojiaji and Bladder through the first
lateral line (BL13 Feishu, BL21 Weishu
BL25 Dachangshu)
Twice per week (total 15
treatments)
Tretinoin (topical) b.i.d.
You, 2014
(381)
Acupuncture M-HN-3 Yintang, SI18 Quanliao, CV24
Chengjiang, BL13 Feishu, BL19
Ganshu, BL20 Pishu, BL23 Shenshu,
CV12 Zhongwan, CV10 Xiawan, CV4
Guanyuan, CV6 Qihai, ST25 Tianshu,
q.d. (total 15 treatments) Tretinoin (topical) q.n.
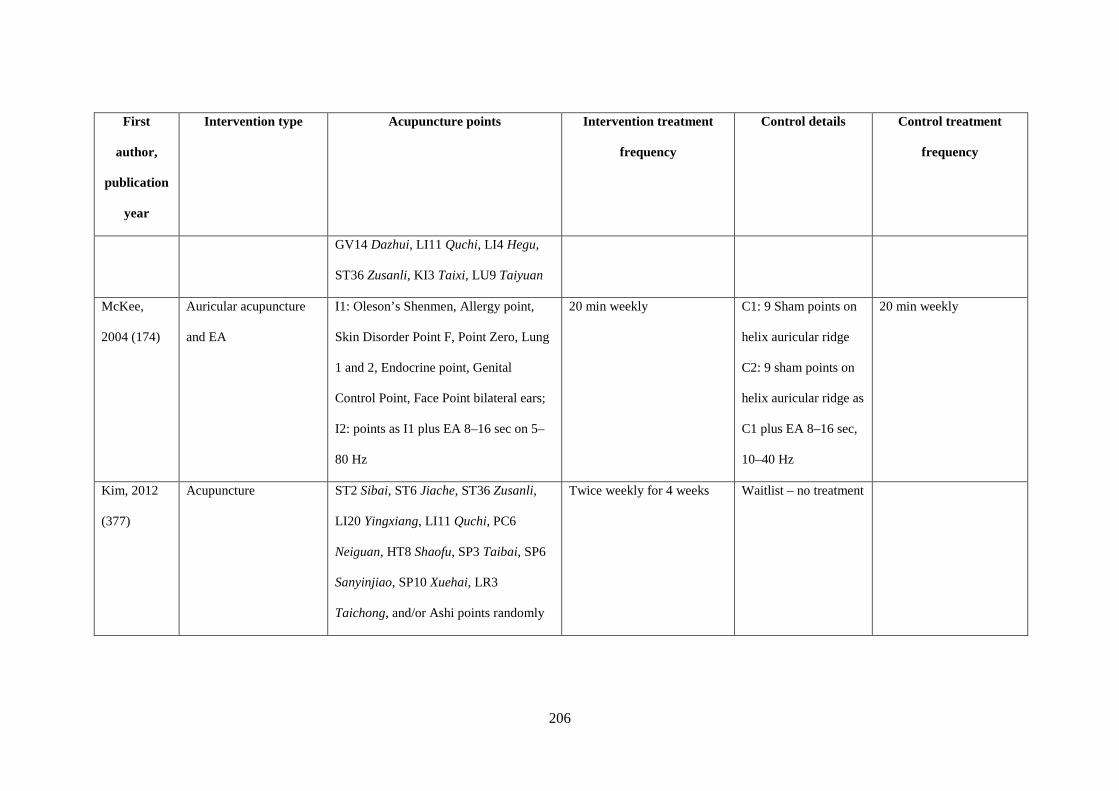
206
First
author,
publication
year
Intervention type Acupuncture points Intervention treatment
frequency
Control details Control treatment
frequency
GV14 Dazhui, LI11 Quchi, LI4 Hegu,
ST36 Zusanli, KI3 Taixi, LU9 Taiyuan
McKee,
2004 (174)
Auricular acupuncture
and EA
I1: Oleson’s Shenmen, Allergy point,
Skin Disorder Point F, Point Zero, Lung
1 and 2, Endocrine point, Genital
Control Point, Face Point bilateral ears;
I2: points as I1 plus EA 8–16 sec on 5–
80 Hz
20 min weekly
C1: 9 Sham points on
helix auricular ridge
C2: 9 sham points on
helix auricular ridge as
C1 plus EA 8–16 sec,
10–40 Hz
20 min weekly
Kim, 2012
(377)
Acupuncture ST2 Sibai, ST6 Jiache, ST36 Zusanli,
LI20 Yingxiang, LI11 Quchi, PC6
Neiguan, HT8 Shaofu, SP3 Taibai, SP6
Sanyinjiao, SP10 Xuehai, LR3
Taichong, and/or Ashi points randomly
Twice weekly for 4 weeks Waitlist – no treatment
207
First
author,
publication
year
Intervention type Acupuncture points Intervention treatment
frequency
Control details Control treatment
frequency
selected at papules and nodules on the
face by acupuncture practitioner
Abbreviations: AA auricular acupressure, b.i.d: twice daily, C control, EA electro-acupuncture, Hz: hertz, I intervention, q.d. one time per day, q.i.d four times daily, qn once nightly, SA surround acupuncture, sec
seconds, t.i.d. three times daily

208
8.4.2.1 Acupuncture interventions used
The intervention most frequently used was acupuncture (six trials) (177, 375, 376, 379-381)
followed by AA (two trials) (176, 378). One trial used EA (and plum blossom needling) (175) and
one trial used acupuncture combined with moxibustion (336). The comparators are described in
Table 8.2. Kim and Kim (377) included three treatment arms, one of acupuncture alone, one of
herbal medicine alone and one where herbal medicine was combined with acupuncture. These
three groups were compared with a waitlist control. Only the data for the acupuncture arm was
included in this analysis. McKee et al. (174) included two treatment arms, auricular acupuncture
and auricular EA, which were compared to placebo control groups, sham auricular acupuncture
and sham auricular EA, respectively.
There was large variation in the acupuncture points used (Table 8.2). Three studies (336, 375, 376)
used CV13 Shangwan, CV12 Zhongwan, CV4 Guanyuan, CV6 Qihai, ST24 Huaroumen, ST26
Wailing, Shang Feng Shi Dian (an abdominal point 0.5 cun lateral to ST 24 Huaroumen) and KI13
Qixue (Table 8.3). Most of the studies used a standardised set of acupuncture points, with one
study using a semi-standardised approach (378). Four studies used Ashi points (176, 177, 336, 376)
for which the location was not specified and two used needles around acne lesions (surround
acupuncture; (176, 177)).
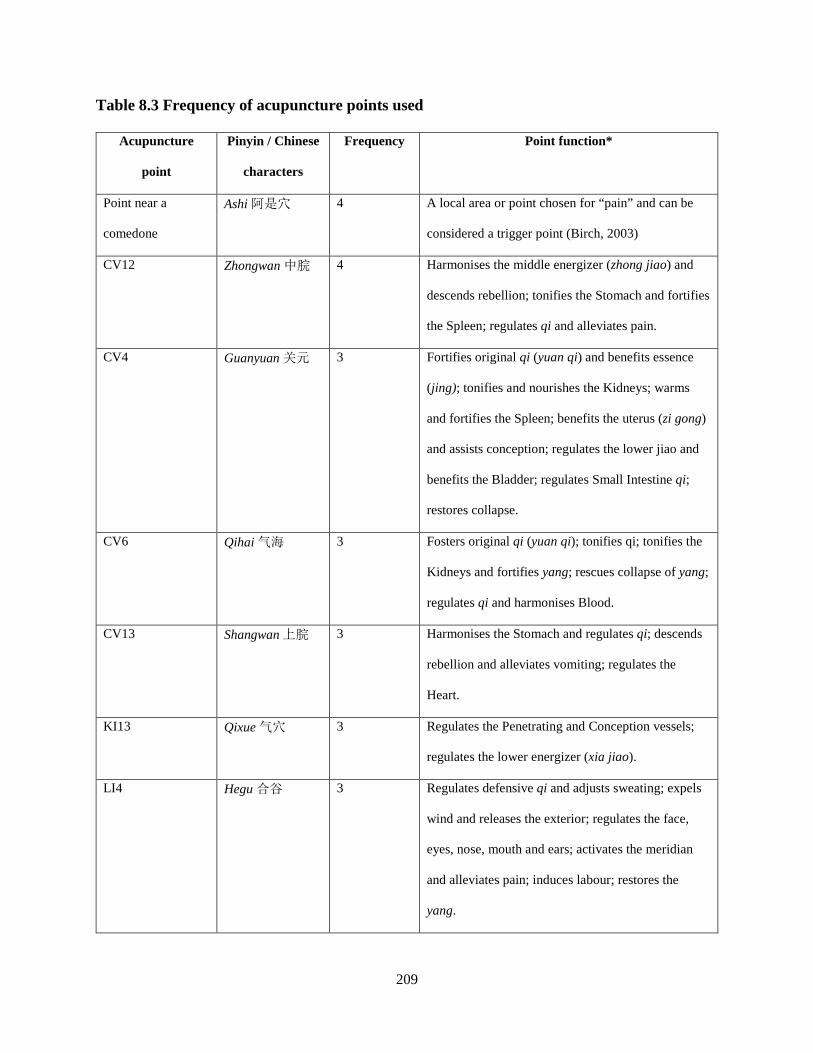
209
Table 8.3 Frequency of acupuncture points used
Acupuncture
point
Pinyin / Chinese
characters
Frequency Point function*
Point near a
comedone
Ashi 阿是穴 4 A local area or point chosen for “pain” and can be
considered a trigger point (Birch, 2003)
CV12 Zhongwan 中脘 4 Harmonises the middle energizer (zhong jiao) and
descends rebellion; tonifies the Stomach and fortifies
the Spleen; regulates qi and alleviates pain.
CV4 Guanyuan 关元 3 Fortifies original qi (yuan qi) and benefits essence
(jing); tonifies and nourishes the Kidneys; warms
and fortifies the Spleen; benefits the uterus (zi gong)
and assists conception; regulates the lower jiao and
benefits the Bladder; regulates Small Intestine qi;
restores collapse.
CV6 Qihai 气海 3 Fosters original qi (yuan qi); tonifies qi; tonifies the
Kidneys and fortifies yang; rescues collapse of yang;
regulates qi and harmonises Blood.
CV13 Shangwan 上脘 3 Harmonises the Stomach and regulates qi; descends
rebellion and alleviates vomiting; regulates the
Heart.
KI13 Qixue 气穴 3 Regulates the Penetrating and Conception vessels;
regulates the lower energizer (xia jiao).
LI4 Hegu 合谷 3 Regulates defensive qi and adjusts sweating; expels
wind and releases the exterior; regulates the face,
eyes, nose, mouth and ears; activates the meridian
and alleviates pain; induces labour; restores the
yang.

210
Acupuncture
point
Pinyin / Chinese
characters
Frequency Point function*
LI11 Quchi 曲池 3 Clears heat; cools the Blood, eliminates wind, drains
damp and alleviates itching; regulates qi and Blood;
activates the meridians and alleviates pain.
SI18 Quanliao 颧髎 3 Eliminates wind and alleviates pain; clears heat and
reduces swelling.
ST24 Huaroumen 滑肉
門
3 Transforms phlegm and calms the spirit (shen);
harmonises the Stomach and alleviates vomiting.
ST26 Wailing 外陵 3 Regulates qi and alleviates pain.
Upper wind-damp
point (an
abdominal point
0.5 cun lateral to
ST24 Huaroumen)
Shang Feng Shi
Dian
上风湿点
3 Functions not identifiable.
Indications: postoperative complaints in the wrist
joint and palm, pain, swelling, limitation of
movement and numbness of wrist and pain in the
palm (Sun, 2007).
* Point indications sourced from Deadman, 2009 (382) unless otherwise indicated.
8.4.3 Risk of bias
The methodological quality of the trials was generally low (Figure 7.2). Four trials (176, 376, 380,
381) were assessed as having high risk of bias in the domain of sequence generation as they used
sequence of visit for randomisation. Five trials (175, 336, 375, 377, 379) were assessed as low risk
as random number generators were used. Three trials were assessed as unclear as there was
insufficient information (174, 177, 378). All trials were assessed as having unclear risk in blinding
of participants. Two trials were assessed as low risk for blinding of outcome assessors (174, 377)
and ten were at unclear risk due to insufficient information. One trial was assessed as having
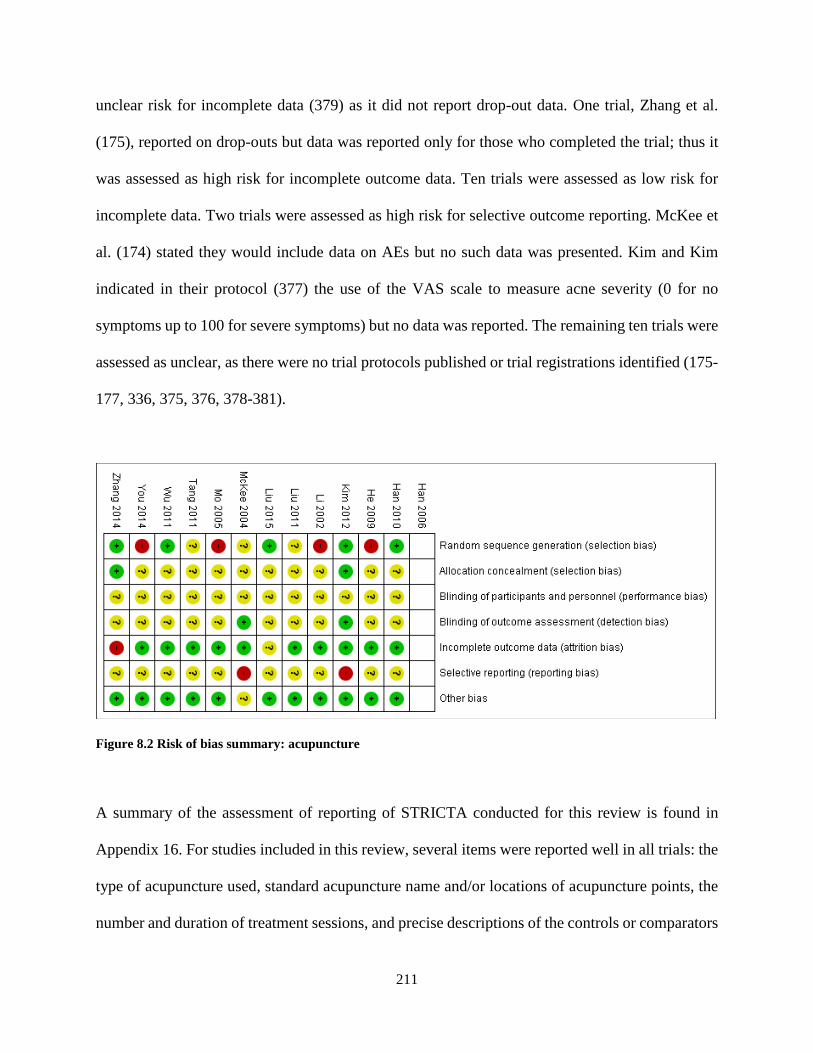
211
unclear risk for incomplete data (379) as it did not report drop-out data. One trial, Zhang et al.
(175), reported on drop-outs but data was reported only for those who completed the trial; thus it
was assessed as high risk for incomplete outcome data. Ten trials were assessed as low risk for
incomplete data. Two trials were assessed as high risk for selective outcome reporting. McKee et
al. (174) stated they would include data on AEs but no such data was presented. Kim and Kim
indicated in their protocol (377) the use of the VAS scale to measure acne severity (0 for no
symptoms up to 100 for severe symptoms) but no data was reported. The remaining ten trials were
assessed as unclear, as there were no trial protocols published or trial registrations identified (175-
177, 336, 375, 376, 378-381).
Figure 8.2 Risk of bias summary: acupuncture
A summary of the assessment of reporting of STRICTA conducted for this review is found in
Appendix 16. For studies included in this review, several items were reported well in all trials: the
type of acupuncture used, standard acupuncture name and/or locations of acupuncture points, the
number and duration of treatment sessions, and precise descriptions of the controls or comparators
212
(Table 8.2). The trials conducted in China did not provide information about the practitioners, the
setting and context of treatment, the instructions to practitioners, or the information and
explanations to the patients.
8.4.4 Primary outcome: therapeutic effective rate
One trial (176) reported on TER based on lesion count and severity, and also reported on serum
testosterone and recurrence rate. Four trials (336, 375, 379, 381) reported on TER according to the
2002 Guideline for New Chinese Herbal Medicine in Clinical Practice and Research (中药新药
临床研究指导原则 (试行)) (311). Three trials (175, 376, 380) used the 1994 CM research
guidelines (167). One trial did not refer to a guideline for judgement of TER but indicated that an
improvement in lesions of 95 per cent was a cure and 60 per cent was a significant improvement;
this data was included in the meta-analysis (378). Another trial (177) also did not specify a
guideline for judgement of TER and indicated no lesions as a cure, 80 per cent as significant
improvement and >30 per cent as improvement; this data was also included in the meta-analysis
(177). The criteria for determining clinical effect are described in Table 8.4. Only one trial reported
measuring QoL, using the Skindex-29 (377).
Figure 8.3 presents the forest plot for the meta-analysis of TER ≥30 per cent change in symptoms.
Meta-analysis showed the chance of achieving a 30 per cent or greater change in lesion count in
the acupuncture group was not different to the combined pharmacotherapy group (retinoids,
antibiotics and other supplements) (four studies, RR: 1.07 [95 per cent CI 0.98, 1.17], I2=8 per
cent) (175, 177, 376, 380) with low heterogeneity. Subgroup analysis of studies where the
comparator was antibiotics plus other supplements showed the chance of a 30 per cent or greater
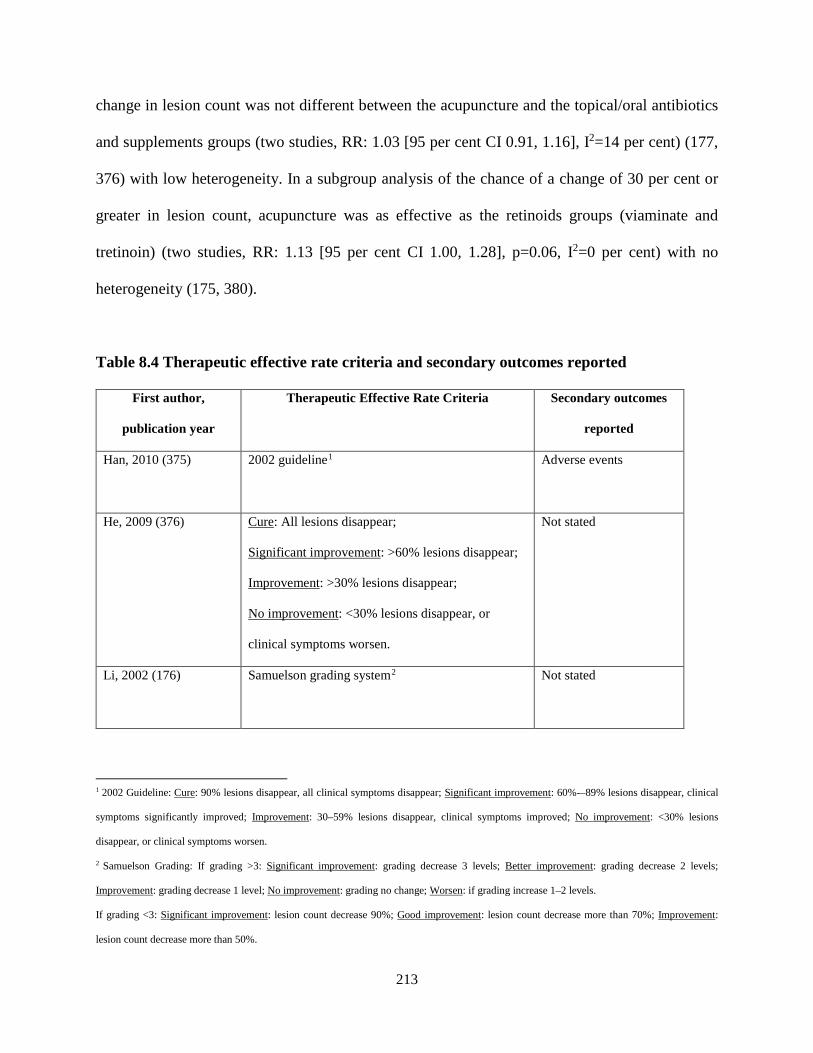
213
change in lesion count was not different between the acupuncture and the topical/oral antibiotics
and supplements groups (two studies, RR: 1.03 [95 per cent CI 0.91, 1.16], I2=14 per cent) (177,
376) with low heterogeneity. In a subgroup analysis of the chance of a change of 30 per cent or
greater in lesion count, acupuncture was as effective as the retinoids groups (viaminate and
tretinoin) (two studies, RR: 1.13 [95 per cent CI 1.00, 1.28], p=0.06, I2=0 per cent) with no
heterogeneity (175, 380).
Table 8.4 Therapeutic effective rate criteria and secondary outcomes reported
First author,
publication year
Therapeutic Effective Rate Criteria Secondary outcomes
reported
Han, 2010 (375) 2002 guideline1
Adverse events
He, 2009 (376) Cure: All lesions disappear;
Significant improvement: >60% lesions disappear;
Improvement: >30% lesions disappear;
No improvement: <30% lesions disappear, or
clinical symptoms worsen.
Not stated
Li, 2002 (176) Samuelson grading system2
Not stated
1 2002 Guideline: Cure: 90% lesions disappear, all clinical symptoms disappear; Significant improvement: 60%-–89% lesions disappear, clinical
symptoms significantly improved; Improvement: 30–59% lesions disappear, clinical symptoms improved; No improvement: <30% lesions
disappear, or clinical symptoms worsen.
2 Samuelson Grading: If grading >3: Significant improvement: grading decrease 3 levels; Better improvement: grading decrease 2 levels;
Improvement: grading decrease 1 level; No improvement: grading no change; Worsen: if grading increase 1–2 levels.
If grading <3: Significant improvement: lesion count decrease 90%; Good improvement: lesion count decrease more than 70%; Improvement:
lesion count decrease more than 50%.
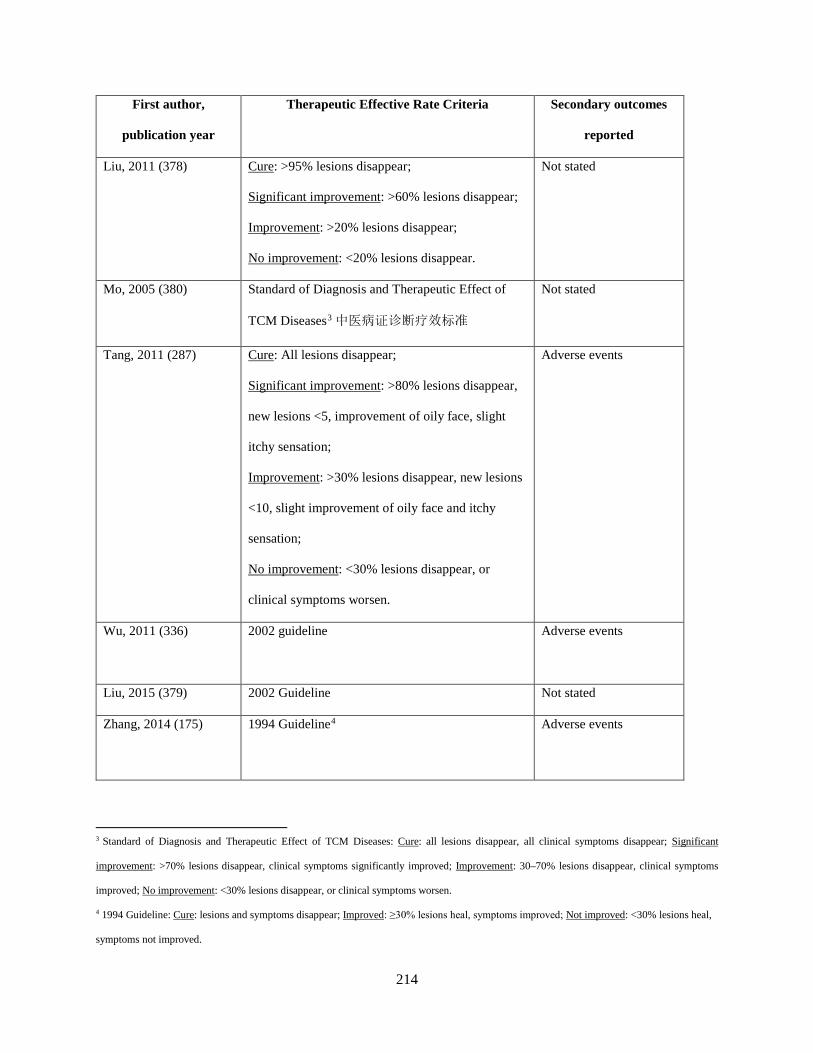
214
First author,
publication year
Therapeutic Effective Rate Criteria Secondary outcomes
reported
Liu, 2011 (378) Cure: >95% lesions disappear;
Significant improvement: >60% lesions disappear;
Improvement: >20% lesions disappear;
No improvement: <20% lesions disappear.
Not stated
Mo, 2005 (380) Standard of Diagnosis and Therapeutic Effect of
TCM Diseases3 中医病证诊断疗效标准
Not stated
Tang, 2011 (287) Cure: All lesions disappear;
Significant improvement: >80% lesions disappear,
new lesions <5, improvement of oily face, slight
itchy sensation;
Improvement: >30% lesions disappear, new lesions
<10, slight improvement of oily face and itchy
sensation;
No improvement: <30% lesions disappear, or
clinical symptoms worsen.
Adverse events
Wu, 2011 (336) 2002 guideline Adverse events
Liu, 2015 (379) 2002 Guideline Not stated
Zhang, 2014 (175) 1994 Guideline4
Adverse events
3 Standard of Diagnosis and Therapeutic Effect of TCM Diseases: Cure: all lesions disappear, all clinical symptoms disappear; Significant
improvement: >70% lesions disappear, clinical symptoms significantly improved; Improvement: 30–70% lesions disappear, clinical symptoms
improved; No improvement: <30% lesions disappear, or clinical symptoms worsen.
4 1994 Guideline: Cure: lesions and symptoms disappear; Improved: ≥30% lesions heal, symptoms improved; Not improved: <30% lesions heal,
symptoms not improved.
215
First author,
publication year
Therapeutic Effective Rate Criteria Secondary outcomes
reported
You, 2014 (381) 2002 Guideline
Severity grading: Global
Acne Grading System
McKee, 2004 (174) Not applicable Photographic grading.
Kim, 2012 (377) Not applicable Skindex-29;
photographic grading;
Korean Acne Severity
Scale.
Figure 8.3 Forest plot of TER ≥30 per cent change in symptoms acupuncture
One study (380) used viaminate (a retinoid vitamin A derivative), which is only recommended in
Chinese treatment guidelines. When this study was excluded from the meta-analysis of TER ≥30
per cent change in symptoms, there were only minor differences in the results, although
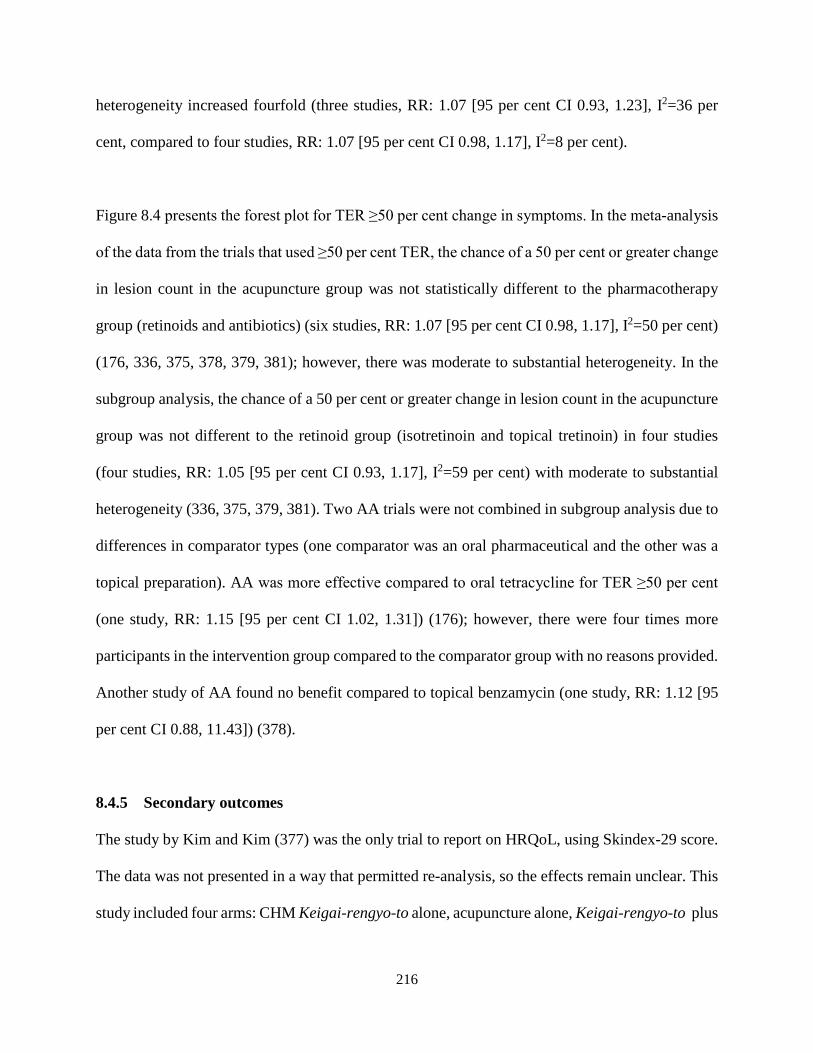
216
heterogeneity increased fourfold (three studies, RR: 1.07 [95 per cent CI 0.93, 1.23], I2=36 per
cent, compared to four studies, RR: 1.07 [95 per cent CI 0.98, 1.17], I2=8 per cent).
Figure 8.4 presents the forest plot for TER ≥50 per cent change in symptoms. In the meta-analysis
of the data from the trials that used ≥50 per cent TER, the chance of a 50 per cent or greater change
in lesion count in the acupuncture group was not statistically different to the pharmacotherapy
group (retinoids and antibiotics) (six studies, RR: 1.07 [95 per cent CI 0.98, 1.17], I2=50 per cent)
(176, 336, 375, 378, 379, 381); however, there was moderate to substantial heterogeneity. In the
subgroup analysis, the chance of a 50 per cent or greater change in lesion count in the acupuncture
group was not different to the retinoid group (isotretinoin and topical tretinoin) in four studies
(four studies, RR: 1.05 [95 per cent CI 0.93, 1.17], I2=59 per cent) with moderate to substantial
heterogeneity (336, 375, 379, 381). Two AA trials were not combined in subgroup analysis due to
differences in comparator types (one comparator was an oral pharmaceutical and the other was a
topical preparation). AA was more effective compared to oral tetracycline for TER ≥50 per cent
(one study, RR: 1.15 [95 per cent CI 1.02, 1.31]) (176); however, there were four times more
participants in the intervention group compared to the comparator group with no reasons provided.
Another study of AA found no benefit compared to topical benzamycin (one study, RR: 1.12 [95
per cent CI 0.88, 11.43]) (378).
8.4.5 Secondary outcomes
The study by Kim and Kim (377) was the only trial to report on HRQoL, using Skindex-29 score.
The data was not presented in a way that permitted re-analysis, so the effects remain unclear. This
study included four arms: CHM Keigai-rengyo-to alone, acupuncture alone, Keigai-rengyo-to plus

217
acupuncture and a wait-list control. The authors combined the results and did not separate the
herbal results and the acupuncture results. The study authors were contacted but no response was
received. The study authors concluded that the use of acupuncture and Chinese herbal medicine
Keigai-rengyo-to could be used for inflammatory acne lesions but that further research was
required.
Figure 8.4 Forest plot of TER ≥50 per cent change in symptoms acupuncture
A total of 127 AEs were reported in three trials (177, 336, 375). The other nine trials did not
mention any AEs. There were more AEs in the control group (98 in the control group, 29 in the
intervention group). AEs in the intervention group included painful sensation (11 cases),
ecchymosis (9 cases), flushing (5 cases) and itchy sensation after needle withdrawal (4 cases),
which are common AEs seen after needle penetration and acupressure (383, 384). In the control

218
group, AEs that included dry mouth (75 cases), dry skin and desquamation (17 cases) and
gastrointestinal discomfort (6 cases) are also common AEs following topical benzoyl peroxide and
retinoid treatment (28, 385). No SAEs were reported in the included trials.
8.5 Discussion
This SR showed that the chance of ≥30 per cent and ≥50 per cent improvement in acne symptoms
with body acupuncture, EA and AA was not statistically different from that of pharmaceuticals for
acne vulgaris. Interestingly, the magnitude of the treatment effect and the 95 per cent CI were the
same for the primary meta-analyses, regardless of which criteria were used to measure clinical
change. There were more AEs in the pharmacotherapy/control group than in the
acupuncture/intervention group. Based on the included studies, acupuncture was well tolerated by
participants with acne vulgaris.
TER is a common measure of effect in CM trials. The TER for acne vulgaris is a subjective
outcome that includes a change in lesion count and/or severity. It is not clear whether this outcome
measure has been validated. The Chinese research guidelines for acne from 2002 (311) suggest a
≥50 per cent change in lesion count or severity, whereas the 1994 guidelines (167) suggested ≥30
per cent change in lesion count and symptoms. In this review, acupuncture was as effective as
antibiotics in trials that used the TER criterion of a ≥30 per cent improvement in symptoms. In the
trials that used a ≥50 per cent improvement in symptoms, AA was as effective as antibiotics, and
acupuncture was as effective as topical and oral retinoids. There is currently no consensus on
outcome measures for acne, although there are efforts underway to standardise them (99). There
was only one trial that reported on an HRQoL measure, the Skindex-29, even though there is

219
mounting evidence that sufferers of acne vulgaris may experience a considerable psychological
and emotional burden (59).
All trials in the quantitative analysis used retinoids or antibiotics as the comparator. Retinoids and
antibiotics have demonstrated efficacy for acne (28); however, long-term antibiotic use can
contribute to antibiotic resistance (386). Retinoids have SAEs such as teratogenicity and should
be used with caution in people of childbearing age (13). Acupuncture and AA were shown in this
analysis not to be statistically different to guideline-recommended treatments but with fewer side
effects, and may be an option for those wanting an alternative treatment to pharmaceuticals.
Treatment times varied considerably across the trials. Such variations in treatment times could
have introduced clinical heterogeneity. The typical treatment duration for body acupuncture is 20
to 30 minutes for each treatment and treatment frequency may vary from one to five times per
week depending on the local clinical practice environment. Fibromyalgia and tension headache
studies have found 20 to 30-minute needle retention, repeated stimulation on acupuncture points
(the de-qi sensation) and daily or twice weekly treatment to have better clinical outcomes
compared to less needle retention time and once-weekly treatment (387, 388).
The findings of this review are similar to those of previous reviews (18, 185); however, previous
reviews included trials that compared CM interventions against each other such as acupuncture
compared to herbal medicines. This review faced the same limitations as the others in terms of the
methodological quality of the included trials. The methodological quality of the included studies
was low, with four of the twelve studies assessed as having high risk of bias and three unclear in
220
the domain of sequence generation. There was also insufficient information on the blinding of
outcome assessors and participants.
Sample sizes were small and none of the included studies reported sample size calculations. Not
all trials reported on the severity of lesions. There were no follow-up assessments in the included
trials. Statistical heterogeneity was also detected in several subgroup analyses, but was not able to
be explored due to the small numbers of studies. Detailed reporting of trial information was
lacking; none of the trials addressed all items from the Consolidated Standard of Reporting Trials
(CONSORT) (389) or STRICTA (316) standard reporting conventions. The STRICTA guidelines
are important in order to improve the transparency of intervention reporting in acupuncture clinical
trials. The lack of standardised reporting in included studies can pose an issue with the
reproducibility of studies and may be a source of bias. Reporting of such details would enhance
accurate analysis and interpretation of data, and improve research reliability in acupuncture
interventions (390). GRADE was not applied to the acupuncture SR due to time constraints at the
time of publication of the manuscript.
8.6 Conclusions
There was no statistical difference in the efficacy of acupuncture compared to pharmacotherapies
for acne vulgaris; however, acupuncture interventions reported fewer AEs. Poor methodological
quality of trial designs and lack of consistent reporting of outcome measures from some trials were
found in this review; therefore results should be interpreted with caution. Future trials should
include rigorous methodological design and reporting should follow standard reporting
221
conventions such as CONSORT and STRICTA. QoL measures and further investigation of the
mechanisms of acupuncture on acne should also be considered in future studies.
8.7 Implications for future research
Many of the limitations of the studies included in this review were also identified in the SR of Pi
Pa Qing Fei Yin (see Chapter 7). The key considerations for studies of both CHM and acupuncture
include:
1. Proper randomisation, allocation concealment and blinding methods (see below)
2. Use of health-related quality of life questionnaires specific to acne as outcome measures
3. Comparing interventions with like controls such as sham acupuncture or placebo needling
and, if using pharmacotherapy for controls, use of guideline-recommended treatments at
the correct dosage for the correct age group as controls.
For further discussion of these issues, see section 7.8 in Chapter 7.
In addition to the above items, future acupuncture studies should provide reasoning for the
selection of acupuncture points, and consider a standardised time for treatment duration and
treatment period. Standard acupuncture needle retention time and treatment frequency in Australia
are normally 20 to 30 minutes every day for ten treatments (391). One study had a 4 to 5-hour
treatment duration five times per week. Having standard treatment times may help to reduce
clinical heterogeneity and facilitate translation of research findings into clinical practice. Having
interventions and controls that appear the same or similar is recommended for rigorous evaluation

222
of treatment efficacy (392-394). Future trials should consider using placebo needles or sham
acupuncture as controls.
8.8 Implications for clinical practice
The meta-analysis of results showed that there was no statistical difference between acupuncture
and related manual techniques and pharmacotherapies. Acupuncture may be an alternative
treatment for those seeking treatment other than pharmacotherapies. Acupuncture had fewer AEs
than pharmacotherapies. AEs with acupuncture were similar to those encountered in acupuncture
practice. Acupuncture AEs included bleeding, bruising and itching at needle sites. Minimising pain
and bleeding while performing acupuncture is a common goal for practitioners. Strategies such as
using the correct needle size for the patient, improving acupuncture skills and using a longer
duration of applying pressure to the acupuncture point upon needle withdrawal, particularly when
using face points, will minimise pain, bleeding and bruising.
Both auricular acupuncture/acupressure trials and body acupuncture trials featured in this review.
Results were similar for both; therefore practitioners should consider using AA for those who have
a fear of needles. Acupuncture points featured in the review include textbook-recommended
acupuncture points such as CV13 Shangwan, CV12 Zhongwan, CV4 Guanyuan, CV6 Qihai. Ashi
points were also used in four studies, which conforms with clinical practice using points on or near
the affected area. Common auricular points included CO18 Endocrine (Neifenmi), CO14 Lung
(Fei), AH6a Sympathetic (Jiaogan), CO4 Stomach (Wei), CO7 Large Intestine (Dachang), TF4
Shenmen and may be an alternative to body acupuncture points.

223
8.9 Chapter summary
This chapter summarises the findings of the SR and meta-analysis conducted of RCTs of common
acupuncture and related techniques for acne vulgaris. Overall, acupuncture was no different to
pharmacotherapies for the treatment of acne, although the methodological quality of the included
studies was low. As with the PPQFY review, only one trial used HRQoL as an outcome measure.
More studies are needed in order to understand the impact of acupuncture and related manual
techniques on the HRQoL of people with acne.
224
CHAPTER 9 : Pi pa qing fei yin for acne vulgaris: A trial protocol
Overview
This project has reviewed the current literature and has summarised the epidemiology, diagnosis,
pathophysiology and treatments for acne vulgaris (Chapter 2). The project also described CM
theory underpinning acne vulgaris and summarised the different types of CM treatments prescribed
for acne (Chapter 3). Chapter 4 showed that many people who have acne vulgaris may be
significantly affected by their acne emotionally, socially or psychologically. There are numerous
instruments used to measure the impact of HRQoL however there is no consensus on which
instrument should be used in clinical practice and for research.
A survey was conducted to provide current data on how acne affects HRQoL of Australian young
people and adults (Chapter 5). It also acquired data on the types of CM treatments people with
acne would find acceptable. The respondents to the survey were under 45 years old, most with
mild to moderate acne. People with self-reported moderate acne were more emotionally affected
and worried about their acne. Chinese medicine treatment preferences suggested that CHM or
acupuncture treatment for four to eight weeks would be acceptable, which reflects clinical practice.
The SRs (Chapters 7 and 8) have shown that CHM formula PPQFY has a greater effective rate
than pharmacotherapies though acupuncture is no better but no worse than pharmacotherapies.
Both reviews found the quality of the included trials were low with many methodological issues
identified in the trials. This chapter focuses on a trial procotol to address the methodological issues
highlighted in the SRs, such as randomisation and allocation of participants, blinding of
participants and researchers, using appropriate controls, and herbal medicine quality control. The
use of syndrome differentiation will assist translation of trial findings into clinical practice, and
225
the primary outcome will be HRQoL. The formula PPQFY will be used as an exemplar for
conducting a CM trial.
9.1 Introduction
People with acne can be emotionally, socially and psychologically affected by their skin condition
(190, 192, 216). There is a negative perception of acne (200) and it can have a significant impact
on HRQoL (74). Improving HRQoL should be a goal of healthcare in clinical treatment (395).
Using patient HRQoL information can lead to optimised care and help with decisions on treatment
(126, 222) and facilitate patient-centred care (395).
There has been a Cochrane review on CAM for acne which included CM modalities (157), two
systematic reviews on CM for acne (18, 185) and two conducted as part of this project. All reviews
found that the randomised trials included in the reviews were mostly of low quality. Many of the
studies compared CHM to CHM or other acupuncture related techniques, comparing unknown
effects against others. There were also poor randomisation and blinding procedures in the included
trials. Therefore, more rigorously designed studies are needed to address these methodological
flaws and to confirm the clinical efficacy of acupuncture and CHM for acne. All reviews also
found few trials used HRQoL as an outcome measure. Therefore, there is a need for a rigorously
designed trial to assess the efficacy of CM treatment in reducing acne severity and improving the
HRQoL of people with acne.
Chapter 5 details the preferences of survey participants in relation to CM treatments. In terms of
acceptability of treatment, there was a slightly higher preference for CHMs (topical) over
226
acupuncture treatment. Participants preferred topical treatments (cleansers) over oral pills or
tablets (72.2 per cent). Respondents also preferred oral pills and tablets over granules and raw
herbs. This is similar to clinical practice. Pills and tablets are more popular than raw herbs. Raw
herbs require more time for preparation and both raw herbs and granules are less palatable to some,
whereas swallowing pill and tablets is quick and the taste of herbs is not as strong. Participants
preferred taking herbs once daily. In clinical practice, oral CHM would be prescribed twice to
three times daily depending on the different forms of herbs. Oral decoction is prescribed twice
daily, and capsules, pills and tablets are usually three times daily. For treatment length, survey
respondents preferred four weeks (26.1 per cent) to eight weeks (21.7 per cent) of CHM treatment,
which is similar to the length of time used in the trials included in the SR (Chapter 7). Treatment
duration in clinical practice is dependent on acne severity. A typical course of herbal treatment for
acne is twice daily herbs over one to three months (159). In acupuncture preferences, 60.9 per cent
preferred body acupuncture and 95.7 per cent would like the treatment to be weekly or fortnightly.
More participants also preferred a treatment period of four to eight weeks for acupuncture. The
frequency and duration of treatment are similar to clinical practice.
The methodological issues outlined in Chapters 7 and 8 included lack of proper randomisation, no
sample size calculations, lack of blinding of participants and personnel, and lack of reporting
against recommended trial guidelines. This trial protocol is developed, using PPQFY as a case
example, to improve the quality of evidence for CM effects on HRQOL in people with acne. There
have also been no SRs published in English and none on Pi Pa Qing Fei Yin (PPQFY) alone
without modification of the original ingredients. The SR described in Chapters 7 and 8 showed
that PPQFY-based treatments achieved a higher reduction in lesion count than various

227
pharmacotherapies, while acupuncture showed no difference. In addition, the subgroup analysis of
PPQFY alone (which included herbs from the original formula and modifications based on
syndrome differentiation) showed greater improvement than pharmacotherapies, whereas, studies
that combined other topical or oral formulations did not. Although the first preference in Chapter
5 was for topical CHM, the evidence from the systematic review for PPQFY was for the oral route
of administration, and not topical. Oral herbal medicine was the second preference from survey
respondents. Therefore, with the evidence from the SRs, the trial protocol will include oral
PPQFY.
This chapter presents an RCT protocol and details the steps used to develop the protocol. The
findings from the survey described in Chapter 5 have informed the design of this trial protocol, as
have the SRs of CHM and acupuncture described in Chapters 7 and 8.
9.2 Trial justification
The SRs in Chapter 7 and Chapter 8 have highlighted methodological shortcomings in previous
research. These include a lack of rigorous study design and a lack of reporting against guidelines
such as STRICTA and CONSORT. This trial protocol will improve on trial design by including
more rigorous randomisation procedures, sample size calculations, allocation concealment and
blinding procedures, which were rarely described in the trials included in the SRs. This trial
protocol will follow the recommendations on reporting according to CONSORT and in particular
the CONSORT Extension for Chinese Herbal Medicine Formulas (396).
228
In addition, there were only two CM RCTs in the SRs that used HRQoL as an outcome measure
(331, 377). The HRQoL instruments used were not acne-specific. There is a need to fill this gap
in acne research in CM. The gaps identified in the SRs relating to trial design are addressed to
improve the quality of CHM research in acne vulgaris. Details of the trial design can be found in
section 9.5.
9.3 Aims
This trial protocol aims to:
1. Develop rigorous trial procedures informed by existing evidence and consumer preferences;
and
2. Ensure the trial protocol meets the reporting standards of the Standard Protocol Items:
Recommendations for Interventional Trials (SPIRIT).
9.4 Research questions
1. Does the Chinese herbal medicine Pi Pa Qing Fei Yin improve the health-related quality
of life of people with acne vulgaris compared to placebo?
2. Does the Chinese herbal medicine Pi Pa Qing Fei Yin decrease lesion count and severity
in people with acne vulgaris?
3. Does Pi Pa Qing Fei Yin decrease the Propionibacterium acnes count on the skin of people
with acne vulgaris?
4. Is Pi Pa Qing Fei Yin safe to use in people with acne vulgaris?
229
9.5 Trial design
This protocol is for a prospective, randomised, double-blind, placebo-controlled trial using PPQFY
as the intervention. A summary of the inclusion criteria for participants, the interventions, controls
and outcome measures and the rationale for selection are described. The implementation of the
trial does not form part of this PhD project. Prior to undertaking this trial, researchers will be
responsible for obtaining funding and complying with all ethical and regulatory requirements for
a clinical trial.
9.5.1 Participant inclusion and exclusion criteria
The target study group is people:
1. Diagnosed with mild-to-moderate facial acne vulgaris (with or without other areas affected) as
defined by the American Academy of Dermatology (AAD): an inflammatory disease of the
pilosebaceous units in the skin of the face, neck, chest and upper back (28)
2. Of any gender
3. Who are adolescents and young people (15 to 24 years old), as defined by the United Nations
(UN) (United Nations, 2008) or adults (25 to 45 years old)
4. Who meet the Chinese medicine diagnosis criteria of heat in the Lung; and
5. Who give written consent to participate in the trial.
Participants will be excluded if they:
1. Are under the age of 15 or over the age of 45
2. Are unable to read or speak English
230
3. Are unable to give informed consent or obtain consent from parents or guardians to participate
in the trial
4. Have endocrine-related acneiform (polycystic ovarian syndrome, PCOS), rosacea, chloracne,
acne varioformis, acne tropica, acne venenata, acne necrotica miliaris or acneiform eruptions
from drugs
5. Have acne severity greater than 4 using the Comprehensive Acne Severity Scale (CASS)
6. Have used any Chinese herbal medicines within the previous three months
7. Have known allergies to the Chinese herbal medicine or placebo ingredients
8. Are females who are pregnant or planning to become pregnant during the trial, or females who
are breastfeeding; or
9. Have severe medical conditions including heart, liver or kidney disease.
9.5.2 Participants
Eligible participants will be people aged 15 to 45 with facial acne diagnosed according to the AAD
guidelines and the CM syndrome of heat in the Lung.
9.5.2.1 Rationale for participant selection
Acne begins at adolescence but can continue into adulthood, with higher occurrence of acne
reported in 15- to 17-year-olds (22, 23). According to Australian legislation, children under 18
years old have limited competence or capacity to make independent decisions about their health
care (397). However, a child between 14 (South Australia) and 16 (New South Wales) can validly
consent to their own treatment in some states in Australia as they may be “capable of understanding
231
the nature, consequences and risks” involved in medical treatment (397, 398). Consent to
participate in a trial from a parent or guardian would still be required.
Acne is reported to be most prevalent in the 12- to 24-year-old age group, but reports of adult onset
acne are increasing (1), with acne reported in 64 per cent of adults in their 20s and 43 per cent in
their 30s (76). It is rare for people over 45 to have acne. They are also more likely to have other
medical conditions and higher risk of comorbidities (399). Therefore, due to the prevalence and
capability of adolescents to understand the medical intervention, adolescents 15 years and older,
young people and adults between 25 and 45 will be the target participant group.
9.5.2.2 Chinese medicine diagnostic criteria
The CHM PPQFY used in this trial is traditionally prescribed to people with the CM diagnosis of
heat in the Lung (see Chapter 3) (159), which corresponds to the comedonal type acne. In this
syndrome, open and closed comedones (including red papules and pustules) are distributed mainly
around the cheeks, forehead and nose, and may also involve the chest and back. Shiny, oily skin
and a dry mouth and nose may also be present. The tongue body is red with a thin yellow coating
and the pulse is floating.
CM practitioners use a synthesis approach to diagnosis compared to WM practitioners who use a
reductive approach (400). In evaluating evidence for CM trials, practitioners may find modern
research methods reductive and at odds with the traditional concepts of CM. Syndrome
differentiation is a key concept (see Chapter 3, section 3.5) and individualised treatment according
to syndrome differentiation is the cornerstone of CM treatment. Including syndrome differentiation

232
as an inclusion criterion in modern trials may be one way to bridge this disconnect from research
to clinical practice (401).
Using syndrome differentiation as part of the inclusion criteria will limit the number of participants
included in the trial, but will ensure that the results are relevant to clinical practice. As this trial
protocol aims to be acceptable to participants and relevant to clinical practice, where syndrome
differentiation is common, syndrome differentiation is a desired component of this protocol. The
intervention proposed for this protocol is PPQFY (9.5.3), which addresses the CM syndrome heat
in the Lung; therefore this syndrome will be an inclusion criterion.
The CM syndromes heat in the Stomach, stagnation of qi and Blood, and imbalance of
Thoroughfare (Chong) and Conception (Ren) vessels describe lesions similar to those described
for heat in the Lungs. However, the ingredients of PPQFY have not traditionally been used for
these three syndromes; other herbs for these three syndromes are described in Chapter 3.
Additional syndromes identified in Chapter 3 included damp toxins with Blood stasis and Blood
stasis with binding of phlegm. Lesions seen with the syndrome damp toxins with Blood stasis
include nodules and cysts that are deep, painful, inflamed and pus-filled. Lesions with the
syndrome Blood stasis with binding of phlegm include nodules and cysts that are 3–5 mm, red to
purple in colour and soft on palpation. The description of these lesions would correspond to the
severe acne severity grading. Therefore people diagnosed with these syndromes will be excluded.
Acne vulgaris is defined as a “chronic inflammatory dermatosis notable for open or closed
comedones (black and whiteheads) and inflammatory lesions, including papules, pustules and

233
nodules (also known as cysts)” (28). Although many of the trials in the SR in Chapter 7 did not
exclude participants with severe acne, the intended Chinese herbal formula PPQFY is traditionally
used for mild-to-moderate comedonal acne. The symptoms listed in the above syndrome
differentiation correspond to mild-to-moderate severity gradings (see Chapter 2) in the IGA tool
(107), the GAGS (106) and the CASS (108). Therefore, to reflect clinical practice, the participant
inclusion criteria will be mild-to-moderate acne. Severity grading will be made by a study
dermatologist using the CASS (108), which is a modified and validated version of the IGA tool
(107). Acne conglobata, acne venenata and acne necrotica miliaris are considered to be greater
than grade 4 severity on the CASS (108).
9.5.3 Intervention
The intervention will be the Chinese herbal formula Pi Pa Qing Fei Yin (PPQFY).
9.5.3.1 Rationale for intervention selection
The intervention was selected based on the SRs described in Chapters 7 and 8, and after
considering participant preferences in Chapter 5. In the literature review of CHM (Chapter 3),
PPQFY was recommended in key CM clinical guidelines and textbooks, and was also the most
frequently used in clinical studies (168). The SR on CHM PPQFY (Eriobotrya Japonica Formula;
see Chapter 7) found the number of people achieving a reduction in lesion count was higher with
PPQFY compared with various pharmacotherapies. The greatest effect was found when the
original formula was modified, rather than combined with other formulations of CHM (for
example, topical or oral). There were no SAEs reported, suggesting that the formula was well
tolerated. Experimental studies also showed that all six ingredients of PPQFY may have an effect
234
in decreasing inflammation, sebum production and hyperkeratinisation. These herbs showed an
inhibitory effect on P. acnes, as well as preventing P. acnes from adhering to host cells in vivo and
in vitro (Chapter 7).
Clinically, patients are frequently prescribed oral CHM and topical CHM at the same time. The
SRs did not find evidence that the combination of topical applications and oral CHM was more
effective than pharmacotherapies. Further, there was only one experimental study identified
relating to the mechanisms of action of topical herbs with topical Ren shen (Panax ginseng C.A.
Mey.) preventing P. acnes from adhering to host cells (340). Therefore, topical CHM will not be
included in this protocol (159, 165).
The second SR was conducted on acupuncture and acupressure for acne. This review found that
there was no statistical difference in the efficacy of acupuncture compared to pharmacotherapies;
however, acupuncture interventions reported fewer AEs. Again, the quality of the evidence was
low. In the subgroup analysis of AA compared to oral tetracyclines, AA was more effective than
tetracycline; however, there were four times the number of people in the AA group compared to
the tetracycline group. Acupuncture has been found to decrease inflammation in animal studies
(371, 372) and auricular acupuncture may reduce acne inflammation through regulating innate and
adaptive immune responses (370). As the SR found more promising evidence for PPQFY than for
acupuncture, acupuncture was not selected as the intervention for this trial protocol. Clinically and
in CM textbooks (159, 165), CHM is considered the main treatment method and acupuncture is
used as an adjunct therapy.

235
PPQFY oral capsules will be used (see 9.7.1 for details of ingredients and dosing). Each capsule
will contain 0.5 g of the granulated herbal ingredients (refer to section 9.7.1). Adult participants
18 to 45 years old will be prescribed four capsules twice daily (total of 4 g daily) over an eight-
week treatment period. An eight-week treatment period was a common period encountered in
previous trials (Chapter 7) and it was also the preferred period by respondents in the survey
conducted in this project (Chapter 5). A recent protocol also considered the effect time of the
intervention (although no details were given on how this was determined) and tolerability and
compliance by participants (402). The CHM Advanced Textbook on Traditional Chinese Medicine
and Pharmacology, Volume II (403) age-to-dose guidelines suggests a dose range of two-thirds to
the total adult dosage for children aged 14 to 18 years. Two capsules is half the adult dosage and,
as it is not possible to give half-capsule dosages, younger participants 15 to 17 years of age will
be given three-quarter dosage, that is, three capsules twice daily (total of 3 g daily). This is still
within the recommended dosing for this age group.
All capsules will be wholly enclosed opaque capsules to prevent tampering and decrease visibility
of the ingredients inside the capsules in order to maximise blinding. Having wholly enclosed
capsules will also decrease the risk of the capsules breaking open and the ingredients being
identified. Although the respondents from the survey preferred pills and tablets, capsules are
another form of preparation which is swallowed whole and are a similar size and shape to tablets.
Capsules are generally softer than tablets and pills, and so easier to swallow. They also mask the
smell of herbs better than tablets or pills. One study looking at the blinding of capsules of ginger
compared to placebo found the participants were not able to determine which type of capsule they
received, but were able to distinguish them from the smell inside of the bottles (404). The study
236
suggested using blister packs to prevent the smell of ginger from breaking the blinding. In a
pharmacokinetic study comparing the bioequivalence of pirfenidone tablets and capsules, the
investigators found the larger 801 mg tablet was similar to three 267 mg capsules (405).
Bioequivalence in this example was dependent on the dosage of tablets and capsules, and not the
type of preparation. In extension, there is no difference in the bioavailability of capsules compared
to tablets. Therefore, for this study, using smaller capsules will improve blinding, making them
easier to swallow in order to improve compliance.
CHM is traditionally prescribed in raw form. With modern processing methods, granulated and
powder concentrated herbs are now commonly prescribed. The convenience of not having to boil
up herbs is more acceptable to patients in clinical practice and compliance is higher. Granulated
and powdered herbs are extracted using water or alcohol extraction methods usually at an average
concentration ratio of 5:1. Based on the calculations of the herb ingredients (section 9.7.1), the
daily dosage of the herbs would be 4 g per day for adults and 3 g per day for children aged 15 to
17.
Capsules come in various sizes and the smallest is 0. As children will be included in the trial, the
smallest size is more appropriate as they would be easier to swallow. Since the smallest size would
hold less herbs, around 0.5 g, adult participants would need to take four capsules twice daily and
participants aged 15 to 17 would need to take three capsules twice daily. Most people would not
be amenable to taking eight capsules at a time. Traditionally, the recommended dosing for CHM
is twice to three times daily (403). In modern practice, twice daily is more common as most patients
would be at either school or work and so would have less opportunity or forget to take a dose in
237
the middle of the day. Thus, practitioners in clinical practice prescribe twice daily, at breakfast and
dinner time. In addition, given that most AEs reported in the CHM review (Chapter 7) were
gastrointestinal symptoms, taking eight capsules at a time can increase the chance of AEs.
Therefore, to minimise the risk of gastrointestinal AEs and to improve compliance, four capsules
twice daily will be prescribed for adults and three capsules twice daily for participants aged 15 to
17.
9.5.4 Comparator
The comparator will be placebo capsules made from a vegetable corn/potato starch that does not
include any active constituents. Placebo capsules will look, taste and smell the same and be the
same colour as the intervention.
9.5.4.1 Rationale for comparator selection
Most studies in the SR of PPQFY used active controls of current guideline-recommended
treatments. Actively controlled studies require more participants for statistical power (406). The
number of participants in individual CHM trials for acne described in the Evidence-based Clinical
Chinese Medicine monograph (168) ranged between 30 and 320 (median 90). For some trials, the
number of participants may not have enough statistical power to determine non-inferiority to
current treatment controls. In pragmatic study designs, multiple interventions or comparators can
be used (see Figure 9.1 for example). Pragmatic study designs are ideal, but require larger numbers
of participants and so are more expensive to conduct (407, 408). Pragmatic study designs also
increase variance in studies and so it is more difficult to determine efficacy (407). It is suggested
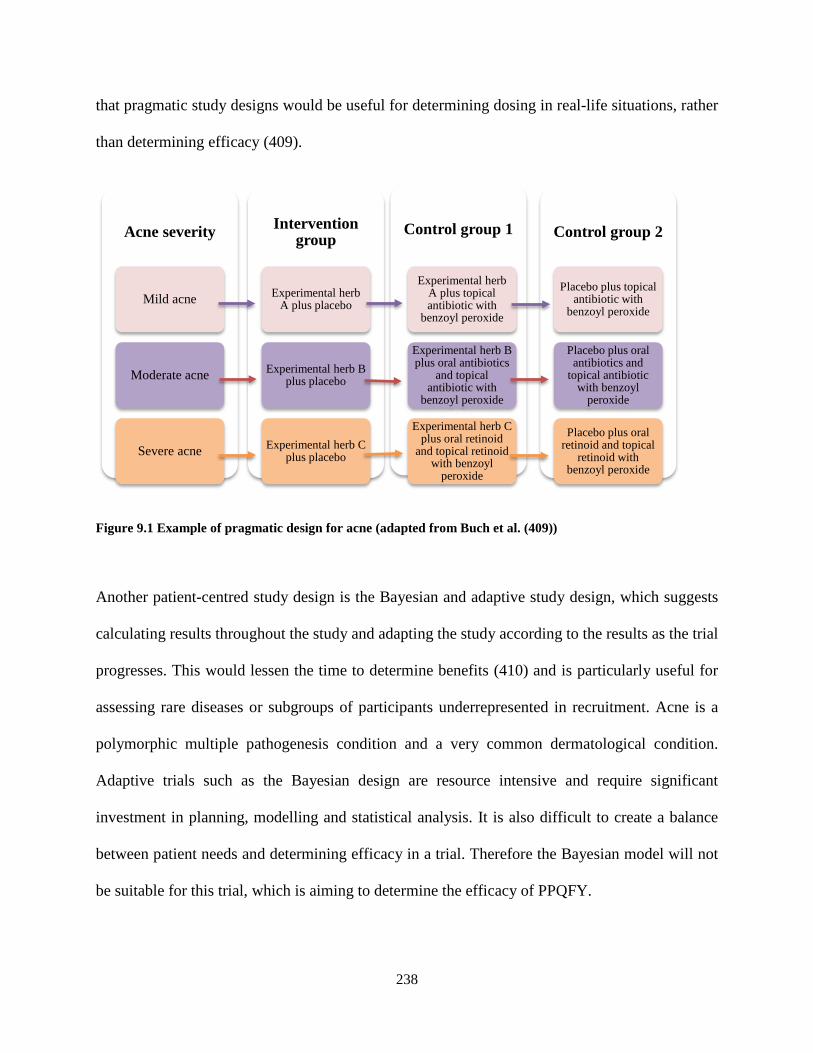
238
that pragmatic study designs would be useful for determining dosing in real-life situations, rather
than determining efficacy (409).
Figure 9.1 Example of pragmatic design for acne (adapted from Buch et al. (409))
Another patient-centred study design is the Bayesian and adaptive study design, which suggests
calculating results throughout the study and adapting the study according to the results as the trial
progresses. This would lessen the time to determine benefits (410) and is particularly useful for
assessing rare diseases or subgroups of participants underrepresented in recruitment. Acne is a
polymorphic multiple pathogenesis condition and a very common dermatological condition.
Adaptive trials such as the Bayesian design are resource intensive and require significant
investment in planning, modelling and statistical analysis. It is also difficult to create a balance
between patient needs and determining efficacy in a trial. Therefore the Bayesian model will not
be suitable for this trial, which is aiming to determine the efficacy of PPQFY.
Acne severity
Mild acne
Moderate acne
Severe acne
Intervention group
Experimental herb A plus placebo
Experimental herb B plus placebo
Experimental herb C plus placebo
Control group 1
Experimental herb A plus topical antibiotic with
benzoyl peroxide
Experimental herb B plus oral antibiotics
and topical antibiotic with
benzoyl peroxide
Experimental herb C plus oral retinoid
and topical retinoid with benzoyl
peroxide
Control group 2
Placebo plus topical antibiotic with
benzoyl peroxide
Placebo plus oral antibiotics and
topical antibiotic with benzoyl
peroxide
Placebo plus oral retinoid and topical
retinoid with benzoyl peroxide
239
Efficacy (explanatory) trial designs have limitations in extrapolating findings to real-life situations
(409). Explanatory trials are considered the gold standard, as they minimise confounders and bias,
are able to provide clear comparison of experimental intervention compared to control, and
determine clinical equivalence (409, 410). Clinical trials using like interventions with like controls
provide a rigorous evaluation of treatment efficacy (392-394). Although CHM has been used in
clinic settings for millennia, this does not necessarily indicate efficacy.
The recommendations for determining efficacy are to compare like interventions with like controls
(393, 394). Only a few studies from both the CHM and acupuncture reviews (Chapters 7 and 8)
used placebo controls. As this trial aims to determine the efficacy of PPQFY, a placebo control
treatment arm will be used. Therefore, this trial design will use PPQFY as the intervention and a
placebo as the control. The comparator will be a placebo capsule with vegetable starch that has no
active ingredients and has a similar appearance, packaging, colour, smell and taste to the
intervention to reduce bias (396, 411).
The NHMRC’s National Statement on Ethical Conduct in Human Research update in 2018 states
that it is unethical to withhold treatment if there is known risk of significant harm in the absence
of treatment (412). Acne is not considered a life-threatening condition, although it does have a
large impact on HRQoL. Not everyone with acne will seek medical treatment and some will use
over-the-counter products only (222). Therefore a lack of treatment with an active control such as
pharmacotherapies is unlikely to pose serious harm and therefore a placebo control is considered
an appropriate comparator.

240
9.5.5 Primary outcome measures
The primary outcome measure will be HRQoL using the Acne-QoL (119, 121, 205). The change
in domain scores from baseline (week 0) to end of treatment (week 8), and from baseline to end of
follow-up (week 12), will be compared between the two groups.
9.5.5.1 Justification of selection of primary outcome
Acne-QoL is the most used HRQoL tool in clinical trials (228). It is a validated tool that assesses
the HRQoL of people with facial acne. It has 19 questions in four domain areas: self-perception,
role-social, role-emotional and acne symptoms, which assesses feelings about acne, medication
usage and social interaction. Questions include how unattractive, embarrassed, self-conscious or
upset people feel about their acne. The questions use a seven-answer code ranging from 0
(‘extremely’ or ‘extensively’) to 7 (‘not at all’ or ‘none’). The domains of self-perception, role-
emotional and acne symptoms are scored from 0 to 30, and the role-social domain has a maximum
score of 24. Higher scores indicate better HRQoL. Acne-QoL is a self-administered tool that takes
approximately 10 minutes to complete. After permission for use has been obtained, administration
of the Acne-QoL will follow the instructions given by the developers. The Acne-QoL is
recommended by the European Academy of Dermatology and Venereology Task Force on Quality
of Life and Patient Oriented Outcomes and Acne, the Rosacea and Hidradenitis Suppurativa (228)
and other reviewers of acne HRQoL instruments (253, 254). Therefore the Acne-QoL is well suited
to assessing the HRQoL outcome of this trial.
There is one other acne-specific validated HRQoL instrument for facial acne, the Acne-QOLI
(118). It is more commonly used for clinical purposes than for research (254). Other acne-specific
241
and dermatological HRQoL tools have been recommended by the above organisations and
publications. The Skindex-29 and DLQI are dermatology-specific tools validated for acne.
However, they are not specific to acne and include questions that may not be relevant to acne, such
as about itching (refer to Chapter 4). The CADI has also been used in acne trials and is
recommended for routine clinical practice and trials (228), but it is not specific to facial acne.
9.5.6 Secondary outcome measures
Secondary outcomes will include photographic lesion counts, severity grading using the CASS,
self-reported current medications, P. acnes levels present on the skin and AEs.
9.5.6.1 Lesion count
Lesion count will be assessed using photographs at baseline (week 0), end of treatment (week 8)
and follow-up (week 12). Changes in lesion count will be compared between the two groups.
Lesion count includes the entire face and the chin, and excludes the neck. The different types of
non-inflammatory lesions (open comedones and closed comedones) and inflammatory lesions
(papules, pustules and nodules) will be recorded.
9.5.6.1.1 Justification for including lesion count as a secondary outcome measure
Lesion count is a common objective outcome assessment used in clinical practice and research
trials. Lesion counts include counting the number of open and closed comedones, papules, pustules
and nodules, and inflammation. A table listing the different types of lesions will be used to record
the count. Lesions are categorised into inflammatory and non-inflammatory, and a total count will
be recorded at each visit. Inflammatory lesions are ruptured papules, pustules and nodules (open
242
comedones) that are often painful. Non-inflammatory lesions include closed comedones (papules,
pustules and nodules) that have no redness or pain.
The process of identifying a lesion and counting can vary from assessor to assessor, as can severity
assessment. Photographs of participants’ skin lesions may differ if the lighting or other factors
change at each visit. This will be minimised by taking photographs at the same location with
appropriate lighting and using the same equipment each time. To minimise the variability in
assessment, standard definitions of lesion types and an image with a description will be used as
standard examples. Research investigators will be given training on identifying and counting lesion
types in order to improve reproducibility (111). An independent researcher will be responsible for
lesion count.
9.5.6.2 Severity grading
The CASS will be used to grade acne severity. Severity will be assessed at baseline (week 0), end
of treatment (week 8) and follow-up (week 12). Changes in severity from baseline to end of
treatment and follow-up will be compared between the two groups.
9.5.6.2.1 Justification for assessing severity using Comprehensive Acne Severity Scale
The AAD has suggested that grading systems need to be reproducible, easy to use and accepted
by dermatologists (145). Severity grading includes lesion size, density, type and the distribution
and intensity of involvement of affected sites (413). The CASS was developed from the IGA by
Tan et al. (108). The CASS can be used for lesions on the face, neck, chest and upper back. It has
an ordinal grading scale that assesses overall severity based on the dominant lesions and extent of

243
inflammation and lesion distribution. Scoring ranges from 0 (no lesions or barely noticeable
lesions) to 5 (very severe acne with highly inflammatory acne covering the affected area with
nodules and cysts present).
The CASS also recommends photographic grading to provide an opportunity for review of lesions
if there are discrepancies and for independent assessment. With modern photographic equipment
and good lighting, photographic inconsistencies can be minimised. This grading scale has a high
correlation with the Leeds photonumeric system and has a positive correlation with the Acne-QoL.
As Acne-QoL will be used as a primary outcome measure for this study, this severity scale will be
a suitable tool for severity grading.
The CASS includes both descriptive and numerical scales that have clear descriptions for assessing
severity. It is flexible and comprehensive. A key advantage is that it does not rely on lesion count
like other severity scales that grade severity. As the protocol already intends to record lesion count
as a secondary outcome, this will not need to be repeated for determination of severity. It has been
recommended for severity grading by the Malaysian MOH’s Management of Acne Clinical
Practice Guidelines (126). To date, the CASS (108) is the only validated acne severity grading
scale. Permission to use the CASS should be sought by researchers.
Various other instruments used for severity grading include photographs, descriptive text and
ordinal scales such as 0 (mild) to 4 (severe) with descriptions, or a combination of these criteria (a
summary can be found in Chapter 2). The Leeds system requires a more complicated photonumeric
scale including 16 facial, 8 chest and 8 back categories which may be time-consuming to

244
administer. The CASS was better able to differentiate between the “clear” and “mild” categories
compared to the Leeds system (108).
The GEA Scale (111) has a similar grading scale as the CASS with an ordinal scale of 0 (residual
pigmentation and erythema may be seen) to 4 (entire face is involved, covered with many papules
and pustules, open or closed comedones and rare nodules). It is a photographic evaluation of
severity for juvenile facial acne. This trial will include participants from 15 to 45 years old;
therefore the CASS is more suitable for this age group. The GAGS (106) separates the area of
assessment into regions. Each region is given a numerical value of 1 to 4 based on the most severe
lesion within that location. That number is then multiplied by the number of lesions in the region
to allocate a global severity score. It does not take into consideration the density or intensity of
lesions and is less suitable for grading in this trial.
9.5.6.3 Propionibacterium acnes identification
P. acnes count will be assessed at baseline (week 0), end of treatment (week 8) and follow-up
(week 12) using the surface scrub technique. The changes in P. acnes will be compared between
the two groups.
9.5.6.3.1 Justification for Propionibacterium acnes collection technique
P. acnes is a commensal gram-negative bacterium that lives on human skin. It is well documented
that P. acnes is present in acne lesions (134, 414, 415) and may initiate inflammation that forms
microcomedones (81). Skin punch biopsy is recommended to investigate the presence of P. acnes
in the epidermis and hair follicles; this is a minor surgical procedure performed by a dermatologist

245
(415). This technique is not feasible for this trial, as it is cumbersome and exposes the skin to
chemicals, which can cause cross-contamination (415).
Gel biopsy is another technique used to collect skin samples. A gel is placed on the skin to form a
polymerised adhesive. Due to variation in skin humidity, pH and environmental factors, this
technique is hard to standardise (415). Sebum can also cause uncertain effects; therefore gel biopsy
is not suitable for this trial. Materials that have direct contact with the skin such as pads or stripping
tape have also been previously used to obtain P. acnes samples. This is non-invasive and able to
obtain 14 layers of stratum corneum. Variation in tapes can lead to differences in the number of
stratum corneum layers being removed, making it difficult to standardise the method (415).
A skin swab is quick and easy to perform, and provides useful information on the skin surface
stratum corneum microbiota if the sample is taken directly from lesions (415); however, it is hard
to standardise.
The surface scrub technique is non-invasive, using a blade to gently scrape the skin surface of a
lesion in the same site in triplicate to minimise the quantification variations and make it easier to
quantify. At each visit, sample sites will be chosen depending on the locations of lesions. Scrapings
will be placed in a sterile, sealed pathology bag and sent for laboratory analysis. This technique
will be used for this trial. The total number of P. acnes from the scrapings will be counted. As
laboratories require patient samples be labelled with the patient’s details, the samples will be sent
to a person not involved in conducting the trial to enter the data in order to ensure the blinding of
assessors. A mean change in P. acnes count from baseline to end of treatment will be calculated
246
(416) and the changes in P. acnes will be compared between groups. Appendix 17 provides an
example of the P. acnes data collection form.
9.5.6.4 Medications used during the trial
Co-medication or concomitant medications will be allowed during the study period with the
exception of prescribed oral isotretinoin. Oral isotretinoin is usually prescribed for people with
severe acne. The inclusion criterion is mild-to-moderate acne and it is anticipated that people who
are on oral isotretinoin will be excluded. Other oral and topical medications commonly prescribed
for mild-to-moderate acne will be allowed. Oral prescription medications include antibiotics and
contraceptive pills. Topical prescription medications such as BP with antibiotics or retinoids
(Stieva A Cream) may also be used. Participants will be allowed to use other over-the-counter
products such as Clearasil® or ProActive®. Participants will be required to record co-medications
and other over-the-counter products used during the trial period.
9.5.6.5 Adverse events and safety monitoring
AEs will be documented on the case record form (CRF) by trial researchers. AEs will be
categorised as expected or unexpected. An expected AE is a reaction known to be associated with
the use of the herbs as reported in CHM pharmacopeia (369). An unexpected AE is defined as a
reaction not identified or consistent with the use of the herb. SAEs are defined by the Australian
Therapeutic Goods Administration (TGA) (417) as follows:
• results in death
• is life-threatening
• results in inpatient hospitalisation or prolonged hospitalisation

247
• results in persistent or significant disability or incapacity
• is associated with a congenital anomaly or birth defect; or
• is a medically important event or reaction.
Based on the SR of PPQFY, oral herbal medicines can cause some gastrointestinal discomfort
including nausea or vomiting, stomach discomfort, diarrhoea and dry mouth. Another reported
symptom is vertigo. Participants will be instructed to report AEs at any time during the trial to
researchers, who will refer them to the trial doctor. The trial doctor will assess whether the AE is
possibly, likely or unlikely to be related to the intervention. Participants will be referred to relevant
medical intervention from their general practitioner, dermatologist or hospital as required. SAEs
will be reported to the product manufacturer, the relevant institution Human Research Ethics
Committees and the TGA as per the Good Practice Guidelines. They will also be recorded in each
participant’s CRF. SAE reports will also be reviewed by the trial doctor, as will other AEs, to
ensure participants are directed to the medical care needed.
For safety, participants will be requested to have a full blood examination incorporating renal and
liver function tests at baseline and at follow-up. If an abnormal blood result is present at baseline,
the investigators will refer the participant to the trial doctor to review their results and to assess
whether it is safe for the participant to proceed in the trial or needs to be excluded from the trial.
The trial doctor will determine whether the patient should also be referred to their relevant medical
practitioner for further follow-up.

248
Liver and kidney functions tests will be conducted again at follow-up. The trial doctor will assess
the clinical implications and determine the appropriate medical steps to take or refer as required.
The participant will be followed up until the AEs have resolved or stabilised to ensure there are no
further issues. Trial insurers should be notified to ensure future care needs are met.
9.5.6.6 Procedures for breaking codes
Emergency 24-hour access to the participant identification and treatment codes will be made
available to authorised study investigators at the site of study. Should the need arise to unmask the
treatment code, an authorised study investigator will have access to the treatment code with
confirmation from one other researcher. Emergency unblinding will be documented.
9.6 Trial procedures
Trial participation will be for 12 weeks (Table 9.1). Participants will be asked to attend a total of
four visits during this time. There will not be a run-in period, as the life cycle of acne lesions varies
from week to week, and hence is unlikely to stabilise. The treatment period will be eight weeks,
which is in line with other current CHM trials for acne (402) and was the preferred duration from
the survey results. The recommended duration of treatment with interventions such as antibiotics
is up to three months, with a change in treatment if there is little or no improvement after three
months (126). The survey identified eight weeks as the preferred treatment duration (refer to
Chapter 5). Many trials included in the SR also provided treatment for eight weeks (Chapter 7);
this duration is considered a reasonable timeframe to see changes in acne.
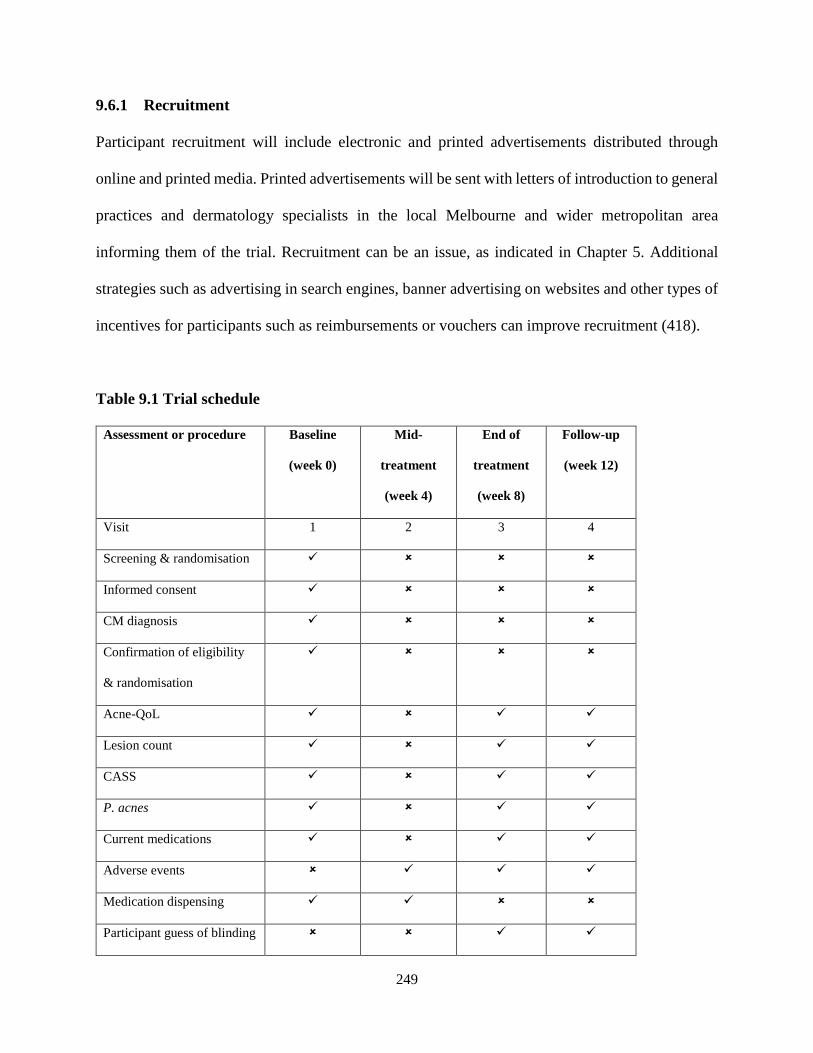
249
9.6.1 Recruitment
Participant recruitment will include electronic and printed advertisements distributed through
online and printed media. Printed advertisements will be sent with letters of introduction to general
practices and dermatology specialists in the local Melbourne and wider metropolitan area
informing them of the trial. Recruitment can be an issue, as indicated in Chapter 5. Additional
strategies such as advertising in search engines, banner advertising on websites and other types of
incentives for participants such as reimbursements or vouchers can improve recruitment (418).
Table 9.1 Trial schedule
Assessment or procedure Baseline
(week 0)
Mid-
treatment
(week 4)
End of
treatment
(week 8)
Follow-up
(week 12)
Visit 1 2 3 4
Screening & randomisation
Informed consent
CM diagnosis
Confirmation of eligibility
& randomisation
Acne-QoL
Lesion count
CASS
P. acnes
Current medications
Adverse events
Medication dispensing
Participant guess of blinding

250
Abbreviations: Acne-QoL Acne-Specific Quality of Life, CASS Comprehensive Acne Severity Scale, CM Chinese medicine, P. acnes
Propionibacterium acnes
Individuals may contact the trial coordinators to obtain further information and the participant
information and consent form (PICF). Interested individuals will attend initial assessment of
eligibility and provide written informed consent.
9.6.2 Eligibility screening
Eligibility of participants will be checked against the inclusion criteria. Randomisation will be
performed after confirming eligibility at the initial assessment. Individuals who meet the inclusion
criteria and agree to participate in the study by signing the consent form will be assigned a
participant number.
CM syndrome differentiation can vary between assessors (419). Procedures will be put in place to
minimise assessor variation by using a participant-completed questionnaire about symptoms and
signs. Study practitioners can then make a diagnosis using the information provided. Inter-rater
reliability of the instrument will be conducted to determine the reliability of the CM diagnosis of
the syndrome heat in the Lung. A number of different types of inter-rater reliability methods have
been reported (420-423). Good inter-rater reliability requires practitioner training before trial
commencement on the use of the questionnaire-based checklist and calibration of results between
assessors using methods such as the Delphi process (424). Study investigators should discuss and
calibrate their diagnoses prior to intake of participants. Based on previous studies, this may need
to be done up to six times before a reduction in variability is seen (422).

251
9.6.3 Informed consent
Participants will be given a written plain-language statement and a verbal explanation of the study
at the initial assessment. Prior to participants signing the consent form, any questions they have
will be answered and signed written consent will be given in front of a witness. Participants who
are under 18 years old will require a parent or guardian in attendance. Both the child and the parent
or guardian will be given the written plain-language statement and the verbal explanation of the
study. The consenting parent or guardian will sign the consent form in front of the witness with
the agreement of the child.
9.6.4 Baseline assessment
Participants will be asked to fill out four questionnaires:
1. General information (demographics, general health status regarding current medical
conditions, medical history, current and previous medications)
2. Screening questionnaire
3. Acne-QoL; and
4. Self-administered Chinese medicine syndrome differential diagnosis checklist.
Participants will also be asked to do a blood test for full blood examination, and liver and kidney
function. As there is limited data on herbal medicine safety in pregnancy, serum human chorionic
gonadotropin will also be measured in females of reproductive age to exclude pregnancy.
Pregnancy is an exclusion criterion for the trial. The study investigators will take photographs of
the face to perform the lesion count, assess acne severity using the CASS and take skin samples
for P. acnes assessment at baseline assessment.
252
9.6.5 Sequence generation and allocation concealment
Participants will be randomly assigned to the intervention group (PPQFY) or control group using
block randomisation, with block sizes of four and six with a ratio of 1:1. The randomisation
schedule will be computer-generated by an independent researcher who will hold the password-
protected list. Randomisation numbers will be placed into sealed, numbered envelopes to ensure
they stay in sequence order and are opened in sequential order. Each envelope will contain a
randomisation and medication number that is concealed to the treatment allocation. A study
investigator will provide the participant with the study medication (PPQFY or placebo) based on
the number allocated. Participants will also be given the medication diaries and AE diaries, and
instructed on how to fill out the forms daily to monitor adherence and AEs. The dispenser, who
will also be blinded to group allocation, will dispense oral capsules sufficient for four weeks of
use.
Due to the length of time between visits, adherence may be an issue. In one review on acne
treatment adherence, the reviewers found a weak physician–patient relationship, fear of adverse
reactions, lack of results, complex regimens and forgetfulness as hurdles to adherence (425). To
improve adherence, participants will be given detailed verbal and written instructions with a
‘frequently asked questions’ brochure on how to take the medications and how to fill out the forms.
Modern technology can also help with engagement (426). A website will be developed with the
same information given to participants and a contact form within the website for participants to
easily ask questions of research investigators. Electronic recording of adherence will reduce the
253
burden on participants to attend the trial site. Every two weeks, participants will be sent
personalised email reminders to take the trial medication. By using secure online forms,
participants will have easier access to forms and there will be less risk of losing hardcopy forms
(426). Participants will be provided with the contact details of investigators should they have any
further questions during the trial period.
9.6.7 Blinding
This is a double-blind trial design. The randomisation sequence and allocation will be unknown to
the participants, the study investigators (who will conduct scheduled visits and outcome
assessment) and the trial medication dispenser. The data will be analysed by a statistician who is
blind to the treatment codes using a two-stage unblinding process. The final unblinding will be
conducted after the completion of the statistical analysis. At week eight and at follow-up, study
participants will be asked whether they thought they were in the real or placebo group, or whether
they were unsure of their group allocation. The Bang blinding index will be used to assess the
degree of blinding, response bias and different behaviour between the two study arms. The
Bang blinding index is scaled to an interval of −1 to 1, 1 being complete lack of blinding, 0 being
consistent with perfect blinding and −1 indicating opposite guessing, which may be related to
unblinding (427). This will support the credibility of the blinding process.
9.6.8 Treatment phase
Visit 1 (week 0)
After completion of baseline assessments (section 9.6.4), participants will be dispensed the first
four weeks of trial medication.

254
Visit 2 (week 4)
Week four is the middle of the treatment phase. Participants will be asked to return any unused
oral capsules. The study researchers will record the amount of remaining oral capsules in the CRF.
Participants will be dispensed the final four weeks of the oral capsules. The mid-treatment visit
will be used to encourage participants’ adherence in taking the oral capsules. It will also be used
to check for AEs and to take any appropriate action as required. AEs and SAEs will be recorded
on the CRF. SAEs will be notified to the manufacturer, the relevant institution ethics committees
and the TGA using the relevant forms.
Visit 3 (week 8)
Week eight ends the treatment phase. Participants will be asked to return any unused herb capsules.
They will be asked to complete the Acne-QoL, have their photographs taken for lesion count and
severity grading, and have skin scrapings taken of the affected areas. The study researchers will
record the amount of remaining oral capsules, the results of the lesion count and severity
assessment, and the photographs in the CRF. Blood tests for liver and kidney function and full
blood examinations will also be conducted. A check for AEs will be conducted and any appropriate
action taken as required. AEs and SAEs will be recorded on the CRF. SAEs will be notified to the
manufacturer, relevant institution ethics committees and TGA using the relevant forms. No new
oral capsules will be dispensed. Participants will be reminded of the follow-up period in four
weeks.
255
9.6.9 Follow-up phase
Visit 4 (week 12)
Participants will be asked to visit the trial site again for follow-up assessment, including the Acne-
QoL, photographs for lesion count and severity grading, and skin scrapings of affected areas. The
study researchers will record the results of the lesion count and severity assessment, and the
photographs taken at the time of the visit on the CRF. AEs will be checked for the final time. AEs
and SAEs will be recorded on the CRF. SAEs will be notified to the manufacturer, relevant
institution ethics committees and TGA using the relevant forms.
9.7 Treatment
9.7.1 Pi Pa Qing Fei Yin
The intervention will be PPQFY in capsule form (Table 9.2). This formula contains six herbs, Pi
pa ye (Eriobotrya japonica Thunb. Lindl.), Sang bai pi (Morus alba L.), Huang lian (Coptis
chinensis Franch., Coptis teeta Wall. or Coptis deltoidea C.Y. Cheng & Hsiao), Huang bai
(Phellodendron amurense Rupr. or Phellodendron chinense Schneid.), Ren shen (Panax ginseng
C.A. Mey.) and Gan cao (Glycyrrhiza glabra L. P., Glycyrrhiza uralensis Fisch. or Glycyrrhiza
inflata BAT.). All ingredients act on at least one of the four pathophysiologies described for acne
(Chapter 7).
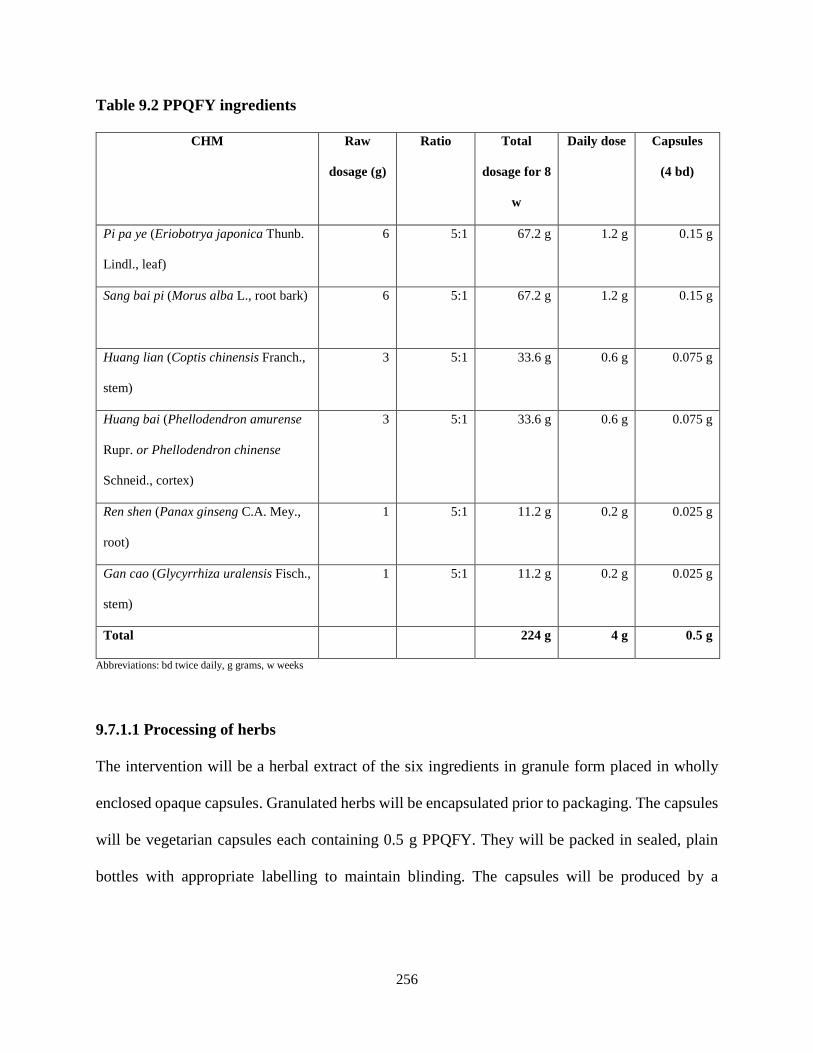
256
Table 9.2 PPQFY ingredients
CHM Raw
dosage (g)
Ratio Total
dosage for 8
w
Daily dose Capsules
(4 bd)
Pi pa ye (Eriobotrya japonica Thunb.
Lindl., leaf)
6 5:1 67.2 g
1.2 g 0.15 g
Sang bai pi (Morus alba L., root bark) 6 5:1 67.2 g
1.2 g 0.15 g
Huang lian (Coptis chinensis Franch.,
stem)
3 5:1 33.6 g 0.6 g 0.075 g
Huang bai (Phellodendron amurense
Rupr. or Phellodendron chinense
Schneid., cortex)
3 5:1 33.6 g 0.6 g 0.075 g
Ren shen (Panax ginseng C.A. Mey.,
root)
1 5:1 11.2 g 0.2 g 0.025 g
Gan cao (Glycyrrhiza uralensis Fisch.,
stem)
1 5:1 11.2 g 0.2 g 0.025 g
Total 224 g 4 g 0.5 g
Abbreviations: bd twice daily, g grams, w weeks
9.7.1.1 Processing of herbs
The intervention will be a herbal extract of the six ingredients in granule form placed in wholly
enclosed opaque capsules. Granulated herbs will be encapsulated prior to packaging. The capsules
will be vegetarian capsules each containing 0.5 g PPQFY. They will be packed in sealed, plain
bottles with appropriate labelling to maintain blinding. The capsules will be produced by a
257
manufacturer that holds a TGA-approved good manufacturing practice (GMP) certificate. Each
capsule of PPQFY will contain granulated herbs as detailed in Table 9.2.
9.7.1.2 Authentication, quality control and safety testing of herbs
As advised by the CONSORT Extension for Chinese Herbal Medicine Formulas, CHM formulas
should ensure quality control of each ingredient in the formula (396). Herbs will be analysed to
confirm authenticity of each ingredient using DNA fingerprint analysis to identify constituents.
Herbs will be tested for contaminants such as pesticides, heavy metals and microbiota. High-
performance liquid chromatography (HPLC) or other techniques such as ultra-performance liquid
chromatography will identify the chemical constituents of herbs and whether the active ingredients
of the herbs are present (428).
Processing of herbs will follow good manufacturing processes for granulated herbs and methods
will provide maximum yield of active constituents. The manufacturer should have the ability to
identify active ingredients, and have risk management and quality process controls in place (428).
9.7.1.3 Placebo
The comparator will be a placebo made from a vegetable corn/potato starch that does not include
any active constituents. Artificial pigments will be added to the starch to mimic the colour of the
PPQFY ingredients. The manufacturer should have a GMP certificate approved by the TGA.
258
9.7.1.4 Dosage and frequency
The dosage of the capsules will be four capsules twice daily for adult participants aged 18 to 45
years, and three capsules twice daily for participants aged 15 to 17 years. Participants will be asked
to take the capsules with warm water twice daily after food (preferably after breakfast and dinner).
Capsules should not be taken with tea or coffee, as there is no data about the interaction or
clearance from the body of CHM when taken with diuretics. Participants will be asked to record
the consumption of the herbs in their medication diary. There must be a minimum of four hours
between dosages; however, the exact time of consumption is not required. Participants may prefer
to take capsules after lunch and dinner, or after lunch and before bed.
9.7.2 Dispensing and monitoring
A medication dispenser who will be blinded to group allocation will instruct participants on the
consumption of the trial medication. Participants will also receive an information leaflet detailing
instructions and frequently asked questions. Online support materials will also be made available
to participants.
9.7.3 Co-medication data collection method
Co-medication or concomitant medications are allowed during the trial, with one exception (refer
to 9.5.6.4). Study participants will be asked to provide a list of daily use of current medications in
their daily diary of medications. These can include guideline-recommended treatments and over-
the-counter oral or topical products. Face-washing is a usual routine for people with or without
acne. Data collected will include the name of the medication, the dosage and frequency, and the
face-washing products used and frequency. This will help monitor if using PPQFY can reduce the
259
need for other medications or other products used for acne. Participants will be requested to
continue using their current medications during the trial and any changes are to be recorded in the
participant medication usage form. Participants who do not take or use any products will be asked
not to begin them during the twelve-week trial period.
9.8 Data collection and storage
Data and results collected will be entered into Microsoft® Excel spreadsheets for cleaning and
transferred into the statistical analysis software package Statistical Package for the Social Sciences
(SPSS) software (IBM SPSS®) or other similar software for further analysis. Only de-identified
aggregated data will be published.
All electronic and hardcopy data will be stored according to the research data storage policy of the
investigators’ institutions. The International Conference on Harmonisation of Technical
Requirements for Pharmaceuticals for Human Use (ICH) Harmonised Guideline with the TGA
Good Practice Guidelines addendums (429) suggests that data be kept for two years after study
completion; however, some institutions, including RMIT University, require data to be kept for 15
years. For children, the records will be kept until they are 25 years old. States and territories of
Australia may require longer periods (or indefinite periods for trials that include children) (430).
Electronic data will be password-protected and stored on a secure internet server. Hardcopy data
will be stored in locked cabinets at the trial site during the trial. At the end of the trial, hardcopy
data will be transferred to institution archives. After 15 years, data will be destroyed following the
relevant institution procedures.
260
9.9 Sample size calculations
Sample size calculation will be based on the primary outcome, the Acne-QoL (119-121). The effect
size will be taken as the change from baseline to end of treatment. With 80 per cent power, the
required number of participants for each group, with allowances for drop-outs, will be calculated
using the software G*Power (431). Fehnel et al. (119) reported the responsiveness of the Acne-
QoL to treatment with Estrostep® (norethindrone acetate/ethinyl estradiol) for moderate acne
vulgaris in placebo-controlled clinical trials. The mean changes in Acne-QoL subscale scores (acne
symptoms) were 7.21+/−5.81 and 4.25+/−6.00 for the intervention and placebo groups,
respectively, giving a Cohen’s D’s effect size of 0.49. Using G*Power 3.1.2 with 80 per cent
power, this suggests a sample size of 134 with 67 in each group (Figure 9.2). For missing data
(refer to 9.12), an intention-to-treat (ITT) analysis will be applied; therefore the sample size does
not include loss to follow-up.
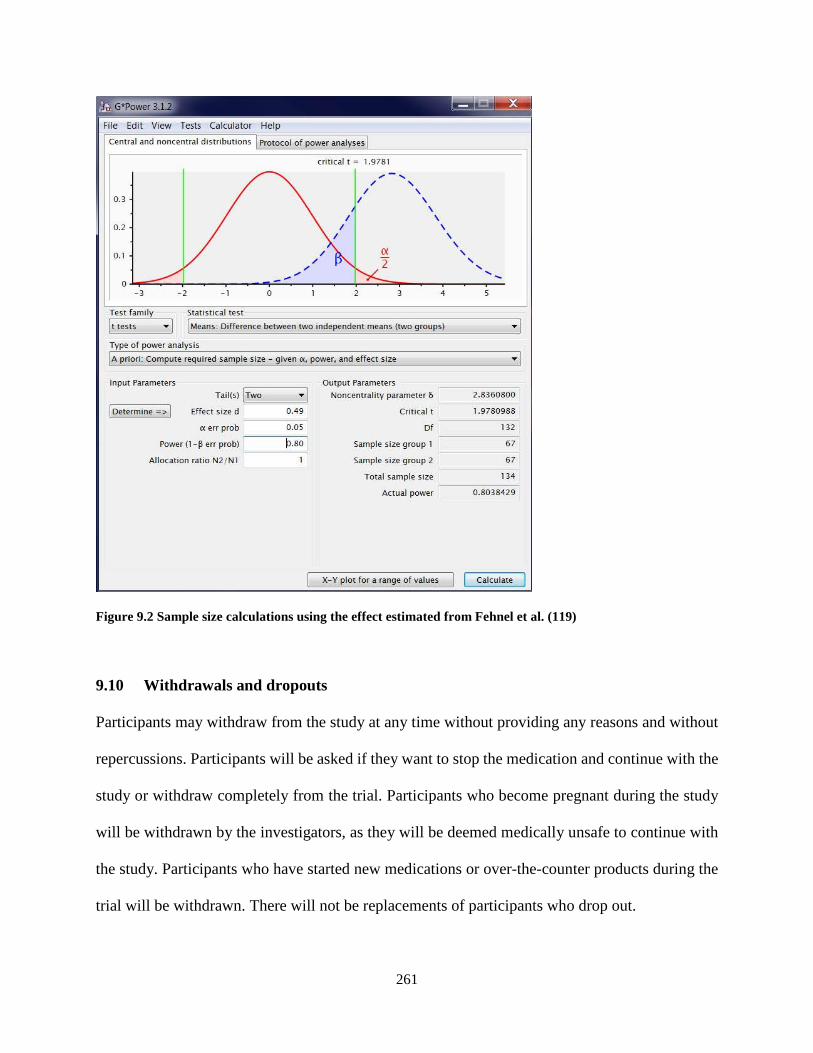
261
Figure 9.2 Sample size calculations using the effect estimated from Fehnel et al. (119)
9.10 Withdrawals and dropouts
Participants may withdraw from the study at any time without providing any reasons and without
repercussions. Participants will be asked if they want to stop the medication and continue with the
study or withdraw completely from the trial. Participants who become pregnant during the study
will be withdrawn by the investigators, as they will be deemed medically unsafe to continue with
the study. Participants who have started new medications or over-the-counter products during the
trial will be withdrawn. There will not be replacements of participants who drop out.
262
9.11 Trial adherence and preventing drop-outs
The researchers should try to minimise drop-outs. In one review of acne treatment adherence,
factors such as lack of knowledge, confusion about the usage or application, and fear of adverse
reactions were reported. Other factors included complex regimens, busy lifestyles and
forgetfulness (425). Adherence to treatment was shown to improve in one trial if the adolescent
was educated about the condition and had a good understanding of acne. In addition, experiencing
fewer side effects and being satisfied with the treatment provide motivation for adherence (432).
Clear instructions on dosing and consumption, and regular reminders can also improve adherence
(425).
Involving participants in trial design is considered good practice, as it prevents exploitation and
maximises partnerships (433). By using survey data from the target participant group on
preferences for treatment types, treatment duration and medication frequency, it is anticipated that
trial participation and adherence will improve (426). Creating a caring and supportive
environment, ensuring patients are accountable for their compliance and maintaining continuous
communication can improve adherence (434). Building trusting relationships between study
researchers and study partners can also improve recruitment and adherence (435).
This study includes verbal and written instructions with a ‘frequently asked questions’ fact sheet
to improve understanding. Modern technology such as secure online forms for ease of access and
personalised email reminders will be implemented to try to improve engagement and adherence
(426, 432).

263
9.12 Missing data
An ITT analysis will be applied to minimise bias in the results. For the primary outcome, the Acne-
QoL, missing data will be imputed as per the developers’ instructions. A minimum of three items
must be answered for each domain in order for domain scores to be calculated. The mean value
within the domain of the answered items should be calculated and the mean value replaces the
missing values. If the minimum number of items is not obtained, the domain score should not be
calculated. For the secondary outcomes, missing responses will be imputed using the method of
the last observation carried forward.
9.13 Data analysis
Data analysis will be conducted by an independent statistician blinded to group allocation.
Baseline demographic comparisons of the two groups will be analysed by using Chi-square or
Student’s t-test and non-parametric tests as appropriate. A test for normality will be performed.
Outcome measures will be presented as means and standard deviations, and the differences
between the two groups will be analysed using repeated-measure ANOVA at baseline, at end of
treatment and at follow-up.
For the primary outcome, the Acne-QoL, a change score for each of the four domains from the
baseline to the end of treatment and from baseline to the end of follow-up will be compared
between groups. Scores for each domain will be calculated by summing scores for all item
responses in each domain. Missing values should be replaced as per the user manual. Routine
scoring checks by checking the range, correlation analysis and manual calculation of domain
scores are also suggested by the developers. For secondary outcome measures, the change score
264
from baseline to the end of treatment and baseline to the end of follow-up will be compared
between groups. Significance is calculated at a probability value of less than 0.05.
9.14 Early termination of trial
An independent data and safety committee will be formed and will meet in the implementation
phase at three months or six months depending on recruitment, and then as necessary. In the event
of an SAE reported during the trial, the independent data and safety monitoring committee will
review data and SAEs. If the SAE is related to the intervention, the independent data and safety
monitoring committee will make a determination on the continuation of the trial.
9.15 Reimbursements
Covering the minimum cost for attending the trial site during the trial period (for example, AU$100
per participant) is a reasonable expectation and highly recommended. Reimbursements may be an
incentive for trial adherence.
9.16 Reporting
Reporting of the trial results will follow the CONSORT statement and extension for herbal
interventions (396). Results should be disseminated through peer-reviewed journals and
conferences.
9.17 Ethical approval
Ethics approval should be sought from the RMIT Human Research Ethics Committee (HREC) or
another HREC, and is the responsibility of the investigators who conduct the research.

265
9.18 Trial registration
The trial should be registered with the relevant trial registration authorities, such as the Australian
and New Zealand Clinical Trial Register (ANZCTR) (www.anzctr.org.au).
9.19 Trial compliance
This trial should comply with the following:
• ICH, Harmonised Guideline Integrated Addendum to ICH E6(R1): Guideline for Good
Clinical Practice – Annotated with Therapeutic Goods Administration (TGA) comments
E6(R2) (429)
• ICH, General Considerations for Clinical Trial (CPMP/ICH/291/95) (436)
• ICH, Statistical Principles for Clinical Trial (CPMP/ICH/363/96) (437)
• NHMRC, National Statement on Ethical Conduct in Research Involving Humans (430);
and
• NHMRC, Guidelines Under Section 95 of the Privacy Act 1988, 2014 (NHMRC, 2014).
9.20 Discussion
This trial protocol illustrates how methodological issues found in the reviews and the lack
inclusion of HRQoL in clinical trials for acne can be addressed, using PPQFY as an example.
Evidence from the literature review of CM and the SRs of RCTs of PPQFY and acupuncture has
informed the development of this trial protocol. The study design improves on the methodological
shortcomings found in the SRs relating to randomisation and blinding procedures. It also takes
into consideration patient treatment preferences in order to improve participant adherence. Having

266
a rigorous study design will minimise bias in results and so practitioners can have confidence in
the study results. Taking into consideration the CM treatment preferences of people with acne in
the trial design makes the trial relevant to them, and using syndrome differentiation and targeting
participants with mild-to-moderate acne ensure the research findings can be translated into
practice. The study design has also taken into consideration participant preferences for CM
treatment types and acceptable treatment frequency and duration from the survey conducted in this
project.
The primary outcome is HRQoL using the Acne-QoL. There were only two previous trials that
reported on QoL as an outcome measure in the SRs. Both trials used general dermatology HRQoL
instruments: Skindex-29 (377) and the DLQI (331). Kim and Kim (377) found no statistically
significant reduction within groups or between groups using the Skindex-29. Wang et al. (331)
found higher DLQI scores (indicating poorer QoL) after one month of treatment with PPQFY than
with doxycycline. Neither the Skindex-29 or DLQI include descriptions of lesions specific to acne;
generic descriptions of skin lesions are included that could be applicable to any skin disease (253).
This trial will provide data on the impact of a common CHM formula, PPQFY, on QoL for people
with acne using a validated, acne-specific HRQoL instrument.
The secondary outcome measures include lesion count, severity grading, P. acnes and AEs. Lesion
count is a common visual outcome measure to rate improvement. It is also used as part of grading
of the severity of acne. The CASS is used for severity grading which includes overall assessment
of lesions and photographic evidence. Lesion count and the CASS can be done concurrently. Both
lesion count and grading will be used as inclusion criteria and as outcome measures. Photographic

267
evidence can be used to standardise study investigators’ perceptions of lesion types and severity,
and allow for independent assessment or review at a later stage. Having severity grading as an
inclusion criterion and as an outcome measure will also provide information on whether the
intervention, PPQFY, is efficacious for mild and/or moderate acne as specified in dermatology
textbooks.
P. acnes is one of the identified pathogeneses of acne. Experimental studies have shown the herbal
ingredients for PPQFY decrease inflammation specifically caused by P. acnes (438), suppress P.
acnes growth (319, 339) and prevent it from adhering to the host (340). Using P. acnes as an
outcome measure will provide information on the potential mechanisms of action of PPQFY.
As this trial aims to determine the efficacy of PPQFY, an efficacy trial design has been chosen
over a pragmatic design. Efficacy trials require a smaller number of participants compared to
pragmatic designs and are less expensive. A placebo control has been chosen over an active control
in the trial protocol as it is the most rigorous test for efficacy (392). Most of the trials encountered
in the SRs used guideline-recommended treatments as active controls and very few placebo-
controlled trials have evaluated the efficacy of PPQFY. Active controlled trials are used to
determine equivalence or superiority, rather than efficacy (392).
Syndrome differentiation has been chosen as an inclusion criterion in the trial design to align with
the traditional use of PPQFY for heat in the Lung. This also coincides with mild-to-moderate acne
in CM (159). Including syndrome differentiation alongside selection of patients with mild and
moderate acne will enable easier translation from research into clinical practice. This may limit

268
the numbers of patients included in the trial. Based on the prevalence of acne severity types
presented in the literature review (Chapter 2) and predictive factors for HRQoL in people with
acne (Chapter 4), most people with acne have mild-to-moderate acne, rather than severe acne.
Therefore, the implications of this limitation are not anticipated to affect trial recruitment. Trial
adherence strategies outlined in this trial protocol and consideration of recruitment strategies
during the planning process will help to minimise drop-outs (439).
9.21 Limitations
This is a trial protocol using the most current information acquired during the project. The narrow
inclusion criteria included in this protocol will not be generalisable to all people with acne, in
particular those with severe acne, cyclical acne or acne scars. It will be generalisable to those with
mild-to-moderate acne. There are a number of pathophysiological processes involved in acne.
These include P. acnes infection, increased levels of sebum causing follicular plugging of the
pilosebaceous gland and hyperkeratinisation, increased androgen activity and inflammation. This
trial does not include serum hormone testing and will not be generalisable to those with hormone-
influenced acne such as PCOS, acne in rosacea or cyclical acne. This trial will determine if PPQFY
alters P. acnes count on the skin. P. acnes can initiate inflammation and alter keratinisation of the
skin (79). There will be visual inspection for inflammation as part of the lesion count, but there
will not be laboratory tests to determine the mechanisms of action of the herbs in humans. Instead,
the protocol will focus on clinical efficacy and safety.
The SR on PPQFY found there was considerable heterogeneity in the results. This was detected in
the groups that used PPQFY as the main formula but with modifications, whether they were small

269
modifications or substantial. Modifications includes removing one or more of the original
ingredients and adding other ingredients or using the original formula and adding more herbs. This
modification reflects clinical practice but may produce different results. Having evidence for the
original six ingredient version of PPQFY can shed light on the effect of making specific
modifications to formulas, as has been done in existing clinical trials.
The survey included 22 participants who indicated their preferences for CHM route of
administration, trial frequency and duration. This small number may limit generalisability to the
whole of the population of people with acne. However, the preferred herbal treatment type and the
treatment frequency and duration of participants align closely with clinical practice; therefore the
results may be generalisable to those with mild and moderate acne.
9.22 Conclusions
This CHM trial protocol takes into consideration stakeholder preference on treatment type and
length of time. The trial design uses rigorous methods such as adequate randomisation techniques,
sample size calculations and blinding of participants and outcome assessors. It follows the
recommendations of the CONSORT Extension for Chinese Herbal Medicine Formulas on trial
design (396) and meets the reporting standards of SPIRIT (Appendix 18). Finally, it addresses the
current lack of evidence for CHM on acne-specific HRQoL.
270
CHAPTER 10 : Discussion and Conclusions
10.1 Introduction
Acne is not a trivial adolescent disease. It is a chronic disease that affects adolescents and adults
up to 50 years old (24), and increasingly affects older women (43). Acne produces visible lesions
on the face that can significantly impact on patients’ HRQoL, with reports of poor self-esteem and
depression (189). Pharmacotherapies used for acne can provide relief of symptoms; however, some
are associated with unwanted AEs that may reduce tolerability (139).
CAM are increasingly popular in the community; however, there is a lack of evidence on the
efficacy and safety of CAM products for acne (151). CM, including body and auricular
acupuncture and CHM, have been commonly used in CM clinical practice to treat acne.
A small number of SRs have evaluated the efficacy and safety of CHM or acupuncture for acne.
Limitations were identified in published SRs. This includes limited numbers of databases searched
and methodological weaknesses in trial designs, such as comparing two CM interventions,
applying outcome measures that have not been validated and inconsistent reporting of acne
severity and AEs. There were also statistical analysis issues, such as lack of ITT analysis to account
for missing data. This project has addressed these gaps through rigorous SR procedures. SRs
involved a comprehensive search of five English and four Chinese databases. Identified citations
were screened against strict inclusion criteria. Reviews were guided by the Cochrane Handbook
for Systematic Reviews of Interventions (302) and assessed the strength and quality of evidence
using the Grading of Recommendations Assessment, Development and Evaluation (GRADE)

271
(315). The reviews also assessed the trial design and reporting standards of the included trials
against CONSORT and STRICTA.
This project has also conducted an online survey to determine the impact of facial acne on QoL in
an Australian population. It also explored stakeholders’ CM treatment preferences. A rigorous trial
protocol has been developed. The findings of the SRs informed the decision on the intervention,
and the findings from the survey guided decisions about treatment frequency and duration.
Incorporating patient preferences into trial design will promote adherence to the trial protocol. The
aim of the trial protocol is to evaluate the efficacy and safety of Pi Pa Qing Fei Yin (PPQFY),
thereby providing new clinical evidence for the treatment of acne.
10.2 Project summary
This thesis includes six components:
1. A general introduction to acne;
2. A review of acne from a CM perspective;
3. A review of the HRQoL of people with acne;
4. An online survey of people of impact of acne on HRQoL, attitudes to CAM and CM
treatment preferences;
5. One SR of the Chinese herbal formula Pi Pa Qing Fei Yin and one SR of acupuncture; and
6. Development of a trial protocol to address the issues highlighted in this research project.
A general literature review was conducted (Chapter 2: Acne vulgaris). Acne affects younger
adolescents, with severity increasing in older adolescents (19, 23) and is more likely to be seen in
272
Caucasians (46) from a Western background (5). The global burden of disease is high, with acne
second only to eczema in years lost due to disability in dermatological conditions (61). The
pathophysiology of acne is complex, with infections from P. acnes, inflammation, androgen
activity, hyperkeratinisation and follicular plugging due to sebum production (28). Both
pharmacological agents and non-pharmacological therapies such as CAM (157), photodynamic
therapy (28) and diet (86) have been described for the treatment of acne. The review highlighted
the multiple number of severity grading instruments encountered in clinical trials for acne. There
is no consensus on one acne grading tool and no consensus on the outcome measures used to
evaluate acne in clinical trials, though there are efforts underway (263). A uniform set of agreed
outcome measures will reduce the uncertainty when evaluating effectiveness of interventions for
acne.
A summary of the CM literature for acne was also conducted (Chapter 3: Chinese medicine). CM
therapies include topical and oral CHM, and body and auricular acupuncture. CM treatment is
based on syndrome differentiation. CHM formulas include PPQFY for the syndrome wind-heat
stagnating in the Lung meridian, Xiao Cuo Tang for yin deficiency generating internal heat and
Tao Hong Si Wu Tang for clearing heat from the Blood, tonifying Blood and clearing pathogenic
heat (159, 165). The main syndromes described and evaluated in trials in the literature include
wind-heat stagnating in the Lung meridian and PPQFY was used to addresses this syndrome (168).
Body acupuncture and auricular acupuncture are commonly used to address similar syndromes.
The HRQoL of people with acne can be affected psychologically, emotionally and socially
(Chapter 4: Quality of life). People with acne have reported depression, suicidal ideation and
273
attempts, poor self-esteem and avoidance of social activities (190, 192). Acne on the face and
severe acne have a correlation with worse HRQoL scores (74). There are many HRQoL
instruments used in the evaluation of people with acne. There were 16 general HRQoL
questionnaires, 7 dermatology-specific questionnaires and 7 acne-specific questionnaires
identified in the literature. General health instruments such as the Medical Outcome Study 36-item
SF-36, dermatology-specific instruments such as the DLQI and the acne-specific CADI are
commonly used to evaluate HRQoL in people with acne. Again, there needs to be agreed upon
instruments used to evaluate HRQoL of people with acne. The use of acne-specific instruments
would provide more accurate meaningful data to people with acne than general health instruments.
Instruments that are age specific may also be beneficial as issues for children, adolescents with
acne have been shown to be different for adults with acne. Despite the importance of HRQoL for
acne patients, this review found few CM trials used HRQoL as an outcome measure. This is an
important outcome measure that should be included in future CM studies.
The online survey (Chapter 5) included three components: the Acne-QoL, CAM Questionnaire
and CM preferences for CM trial design. Recruitment for the study was suboptimal and the
response rate was lower than anticipated. There were 28 respondents; 22 completed the whole
survey and a further 6 partially completed the survey. For data that was available, there was a
greater number of female respondents than males (17 female, 4 male) and most were between 15
to 24 years old. Results for the Acne-QoL showed the lowest score was for the self-perception
domain, compared to the highest score for the acne symptoms domain. For the CAM use
component, the mean domain score was highest for positive beliefs and lowest for psychological
comfort. Most respondents preferred topical cleansers as their first treatment preference, followed
274
by pills and tablets. Weekly acupuncture treatment for between four and eight weeks was the
acupuncture treatment frequency and duration preferred by most respondents. The survey
participants were low. This may have brought some bias and larger variation into the results, and
may not represent all people with acne. There were recruitment issues associated with the survey
and future surveys may need to consider alternative strategies or incentives to improve recruitment.
There were also a large number of questions in the survey. Future surveys may consider separating
each of the components into three separate surveys.
The survey finding that females had worse scores on the Acne-QoL than males was also found by
the survey developers (119-121). Few other studies that assessed HRQoL with the Acne-QoL have
done so in populations similar to those who completed this survey. Given the small sample size
highlighted above, it is difficult to say whether results for this population are the same or different
to other populations.
The number of survey respondents with favourable attitudes to CAM in was similar to the number
with unfavourable attitudes. Findings by Magin et al (155) found positive attitudes in 26 people
who had used CAM for their acne. Use of CAM was perceived as more efficacious in their study,
and was associated with greater self-efficacy. The difference between the results of this study and
those of Magin et al may be due to several reasons. Firstly, this study examined attitudes to CAM
through a survey, while Magin et al conducted interviews. Secondly, approximately half of the
survey respondents in this study had not previously used CAM, which may affect their attitude
toward CAM. Thirdly, the survey used was an existing survey that did not specifically ask about

275
use of CAM for acne. Finally, it was not possible to examine attitudes to CAM for people in this
study who had previously used CAM due to the low response rate (268).
Two SRs were conducted for this project. The first review examined the efficacy and safety of the
CHM formula PPQFY for acne (Chapter 7: Systematic review of Chinese herbal medicine for acne
vulgaris). This contains ingredients that clear Lung heat, clear Stomach heat, resolve phlegm and
tonify qi. Experimental studies have shown inhibition of growth of P. acnes (319), anti-
inflammatory effects (353) and anti-adipogenic effects (440), which may address different acne
pathophysiology pathways. Results of the meta-analysis of the included trials in the SR found there
is some evidence that PPQFY may be effective for acne, with fewer AEs reported compared to
pharmacotherapies. The DLQI (114) was included as an HRQoL outcome measure in one PPQFY
trial (331). There were methodological flaws found in the included trials, including in relation to
randomisation procedures, allocation concealment, blinding procedures and sample size
calculations.
Results in CHM PPQFY meta-analysis showed PPQFY to have a greater effect than
pharmacotherapy though there was considerable heterogeneity. The variation and modification of
ingredients used in trials as well as the inclusion of people with mild to severe acne may have
contributed to this. Only the main ingredients of CHM PPQFY were evaluated in the experimental
studies, and actions included anti-inflammatory (353, 356) and antimicrobial actions (319, 339,
340), and reducing follicular hyperkeratinisation (358, 359) and sebum production (360, 361).
Other herbal medicines may have other physiological effects such as hormonal, endocrinological
or other effects that future reviews may need to investigate.
276
The monograph on acne by Coyle et al evaluated the efficacy of CHM (168). There was some
evidence to show CHM was effective for acne though many comparisons of lesion count and acne
grading show no difference between CHM and pharmacotherapy. Using effective rate in CM trials
is common but may cause some statistical analysis variations as shown in the monograph. This
may be resolved by using standard agreed upon outcome measures in acne trials to resolve this
issue.
Results from the monograph showed CHM may be as effective as guideline recommended
treatments for acne. In comparison, oral PPQFY had a greater effective rate than
pharmacotherapies, in particular for when compared to BP and antibiotics and compared to
retinoids alone. Both the monograph and this review of PPQFY found fewer AEs with CHM than
with pharmacotherapy. The lack of evaluation of HRQoL was also common to both the monograph
and the PPQFY SR. There needs to be more CM studies evaluating this important outcome in acne.
The second SR evaluated acupuncture for acne (Chapter 8: Systematic review of acupuncture for
acne vulgaris). The acupuncture SR found there was no difference between people receiving
acupuncture compared with pharmacotherapies, with low statistical heterogeneity. There were also
fewer AEs in the acupuncture group compared to the pharmacotherapy group. Skindex-29 (100)
was an HRQoL outcome measure used in one acupuncture trial (377). The same shortcomings
found in the PPQFY included trials were also found in the acupuncture included trials. The
acupuncture review in this project included studies that evaluated common acupuncture techniques
such as body acupuncture, auricular acupuncture, electroacupuncture and moxibustion. The
reviews conducted by Li et al (18), Cao et al (185) and the Cochrane systematic review (157)
277
included other techniques that stimulated acupuncture points. They also included studies that
combined acupuncture with CHM interventions and compared interventions with controls that
included CM therapies. This review only included comparators that were of known efficacy such
as pharmacotherapies and or studies that used no treatment/waitlist or placebo. All studies reported
the quality of the included studies were low and methodological issues with the trials. Again, only
one trial measured HRQoL. HRQoL should be given more consideration in future trials to improve
the understanding of the impact CM has on this important outcome for people with acne.
The final component of the project was the trial protocol (Chapter 9). The trial protocol addresses
the methodological issues found in previous trials for PPQFY by using SPIRIT and the CONSORT
Extension for Herbal Interventions as a guide (396). Issues included lack of randomisation in trials,
blinding of personnel and participants, and substantial modification of herbal formulas. As the
evidence from Chapter 7 shows, PPQFY was effective in reducing acne lesion count, and so this
formula was selected as the intervention for the trial protocol. Participants included in the trial will
have mild-to-moderate acne using the proposed validated severity tool CASS (108). Taking into
consideration the survey results of participant preferences, the treatment phase of the trial will run
for eight treatment weeks with follow-up assessment at twelve weeks.
The trial will use an acne-specific HRQoL instrument (the Acne-QoL) as the primary outcome
measure, to address the lack of trials evaluating HRQoL and to provide meaningful data relevant
to patients and clinical practice. It also outlines the trial procedures for recruitment, eligibility
screening and obtaining of informed consent. Randomisation and blinding procedures were
lacking in previous trials and this protocol addresses these gaps. There were also no sample size
278
calculations in many of the included trials and no details on the CHM quality control procedures.
The protocol will also address these issues. Herbs will undergo authentication and safety testing
using a manufacturer that adheres to good manufacturing practices (417). To maintain blinding,
placebo capsules that look and smell the same as the intervention will be used. Blinding will be
assessed using the Bang blinding index (427). There are different trial designs that may be suitable
for evaluating the efficacy of herbal medicine. These include Bayesian, pragmatic and randomised
controlled trials. Bayesian and pragmatic trial designs do not address efficacy as well as
randomised controlled trials. Pragmatic and Bayesian trial designs require substantial personnel.
Bayesian designs are adaptive and require a smaller sample size, but are more beneficial for
diseases that are rare. They are resource intensive and require substantial modelling, design and
statistical analysis. Pragmatic trials reflect real clinical setting scenarios however efficacy has yet
been established for PPQFY and pragmatic designs will introduce variances that make it difficult
to determine efficacy. Given the limitations of pragmatic and Bayesian trial designs, a two-arm
placebo controlled, randomised controlled trial was considered the most appropriate study design
to address the issues found in the SRs. A randomised controlled trial with adequate blinding and
randomisation procedures was presented, using the traditional formula PPQFY as the intervention.
Such a design will improve the reliability of the data and confidence of the efficacy of PPQFY for
people with mild to moderate acne.
10.3 Limitations
The search for both SRs was restricted to Chinese and English databases. Articles were restricted
to these two languages due to the availability of project members who could read and write in these
languages. During the project, English abstracts of articles in other languages such as Korean,
279
Japanese and European languages were encountered. Other databases may contain clinical
evidence that has not been included in this project. Future studies should consider broadening
database searches in other languages to gain a more comprehensive picture of the clinical evidence
for acne.
This project evaluated the efficacy and safety of one CHM formula, PPQFY, which is frequently
used in clinical practice. Future research focusing on other CHM formulas will provide further
evidence of the efficacy of specific CHM formulas for acne. The findings of the SRs are limited
by the low methodological quality of the included trials. Biases were identified in included trials
due to few studies providing information on sequence generation, allocation concealment or
blinding procedures for both participants and assessors. This reduces the reliability of the clinical
outcomes reported. The variation in acne severity in included participants and the variation in the
interventions and comparators included in the trials contributed to considerable heterogeneity,
further reducing the reliability of reported clinical outcomes.
In theory, the advantages of an online survey include ease of use, accessibility, low cost and
reduction of researchers’ time and effort (418). Survey recruitment was challenging. Only two of
the secondary schools approached allowed the survey to be advertised in their newsletters, with
the majority declining due to the limited number of research studies each institution could support.
The online strategies used and the direct mailout to practitioners did not appear to increase
recruitment. Other recruitment strategies may also be a consideration for future research. These
could include banner advertisements, search engine promotions and applying to national or state-

280
based high schools’ education governance departments in order to collaborate with groups of
schools, rather than approaching individual schools.
The low number of participants limits the survey results and they are not able to be generalised to
the Australian population. There is still a need to obtain more data on the HRQoL of people with
acne in Australia in order to gain more contemporary information and to improve the
understanding of the HRQoL of people with acne in Australia.
10.4 Implications for research
10.4.1 Systematic reviews
There were methodological flaws found in the trials included in the SRs. There was a lack of detail
on randomisation or randomisation that was based on hospital record numbers or sequence of
hospital visits. Allocation concealment detail was not reported. There was also a lack of detail on
blinding procedures for both participants and assessors. Some trials in the PPQFY SR used
comparators not recommended by treatment guidelines, such as TAB combined with OAB, and
there was considerable modification of the original ingredients of the formula without justification.
Few studies reported follow-up, with a lack of description of withdrawals and drop-outs. None of
the studies reported using ITT analyses to account for missing data. Further, many trials did not
report AEs. Transparent AE reporting would help to properly assess the safety profile of herbal
medicines (396, 401).
The trials also used the therapeutic effective rate (TER) as a primary outcome measure. The TER
is based on the percentage of change in symptoms such as lesion count and severity, and does not

281
appear to have been validated for acne. Thresholds for improvement were based on two CM
research guidelines: Guideline for New Chinese Herbal Medicine in Clinical Practice and
Research (Vol. 1) (2002) (311) and Criteria of Diagnosis and Therapeutic Effect of Diseases and
Syndromes in Traditional Chinese Medicine (1994) (167). The 2002 guideline suggests a 50 per
cent change in symptoms as an improvement threshold and the 1994 guideline suggests a 30 per
cent improvement threshold. This lack of consensus on the threshold for improvement could bring
confusion to the review results and so the findings of the SRs need to be interpreted with caution.
There was also subjectivity in how the trial authors interpreted descriptions for the different levels
of improvement from the encountered guidelines that trials reported using. In addition, not all trials
followed these guidelines. Although Wu et al. (336) reported using the 2002 guidelines (which
describe improvement of 50 per cent or greater), the actual threshold used to assess improvement
in trial participants was 30 to 70 per cent, which corresponds to the 1994 guidelines (167).
The acupuncture trials included in the SR had the same issues as the PPQFY review. The
acupuncture SR included subgroup analysis of trials that used a 30 per cent threshold for
improvement and those that used a 50 per cent threshold for improvement. Surprisingly, the results
for both subgroups were the same. There is no clear explanation for this occurrence. This may
mean the descriptions are sufficiently subjective that the tool is not able to discriminate between
the two levels. This may also indicate that there is no difference in the two thresholds, whether at
30 per cent or at 50 per cent. In the 2010 research guidelines, the threshold for improvement is 30
per cent (312).

282
10.4.2 Trial designs
Many of the trials encountered in the SRs were assessed as having high risk of bias for sequence
generation. Nearly all were assessed as unclear in relation to allocation concealment. Future trials
should be designed with rigorous randomisation and allocation-concealment procedures. One trial
had three times the number of participants in the first intervention group (n = 200) compared to
the second intervention group (n = 60) and the control group (n = 60) with no explanation (176).
Imbalance in the number of participants in the intervention and control groups can bring bias to
results. Trials need to have sample size calculations.
Few of the trials reported on acne severity. Severity can be based on the number of lesions or the
type of lesions, such as inflamed or non-inflamed comedones, or nodules and cysts. Eight validated
acne-severity grading scales were found in the literature, but none of the included trials in the SRs
used any of the validated scales. Severity grading in the included trials used scales developed by
trial investigators or did not give details. Given that severity also can affect HRQoL, using a
validated severity scale may help to standardise reporting of results.
Many of the trials were assessed as unclear in relation to blinding of assessors and participants.
Trials should follow standard reporting conventions such as STRICTA (316). A more rigorous
trial design to address these issues is presented in this project (Chapter 9).
10.4.3 Outcome measures
Despite increasing reports of people’s HRQoL being affected by acne, HRQoL did not feature
prominently in the CM trials evaluated in the two SRs conducted for this project. None of the trials

283
used acne-specific HRQoL outcome measures. Using an acne-specific HRQoL outcome measure
may give a more accurate picture of the impact of the intervention evaluated for the acne. Although
the DLQI and Skindex-29 have been validated in people with acne and are recommended by the
EADV TF on QoL (228), the DLQI has questions that may not be relevant to someone with acne,
such as about itchiness, and the Skindex-29 also asks questions on itching, burning and stinging.
An acne-specific HRQoL tool would provide meaningful data about people with acne and make it
easier for data to be compared across trials (441).
Attempts have been made to gain consensus for this outcome measure in research, but no
consensus has been achieved (99). There are efforts underway to standardise the outcome measures
used in acne research. CM researchers should consider standardised outcome measures as well as
the TER rate for future trials in order to improve data collection and reduce clinical heterogeneity
when comparing trials. The Acne Core Outcome Research Network (ACORN) is attempting to
standardise the outcome measures used in clinical trials (263) as part of the Core Outcome
Measures in Effectiveness Trials (COMET) initiative. Preliminary identification of measures is
underway; these may include physician and patient assessment of signs and symptoms, global acne
severity and HRQoL measures. The next steps for the group are to identify or develop the outcome
measures set for acne vulgaris.
10.5 Implications for practice
10.5.1 Pi Pa Qing Fei Yin
The ingredients of PPQFY have potential to address the five main pathophysiological pathways of
acne, including inhibiting P. acnes, reducing inflammation and sebum and thus reducing

284
hyperkeratinisation, and affecting androgen activity. The meta-analysis showed that PPQFY was
superior to pharmacotherapies in reducing lesion count though there were many modifications and
additions to the formula. Although there were limitations in the methodological designs, PPQFY
had fewer AEs than pharmacotherapies and appeared to be better tolerated by people with acne.
There is some evidence that PPQFY may be effective for acne, with relatively lower numbers of
AEs than pharmacotherapies. The review found that PPQFY in the included trials was modified
frequently, which reflects clinical practice. Huang qin was commonly substituted for Huang bai,
which changes the focus from the lower energiser (Huang bai) to the upper energiser (Huang qin)
to address the syndrome for wind-heat stagnating in the Lung meridian. The original ingredients
fo the formula addresses mild-to-moderate acne and is the intervention for the trial protocol.
10.5.2 Acupuncture and related therapies
The meta-analysis of the included acupuncture trials found there was no difference between
acupuncture and other common manual therapies such as moxibustion and auricular acupuncture
compared to pharmacotherapies. Although it was not more effective than pharmacotherapies, the
effect size was comparable regardless of the threshold used for TER assessment for those receiving
acupuncture compared to pharmacotherapies. Again, the same methodological design issues were
found in the acupuncture review as in the PPQFY review. Acupuncture and related techniques had
fewer AEs than pharmacotherapies and the reported AEs, such as bruising and pain at the needle
insertion site, are known AEs from acupuncture. Acupuncture may be an alternative for people
who cannot tolerate the AEs from pharmacotherapies such as dryness and burning of the skin and
gastrointestinal disturbances.
285
10.5.3 Health-related quality of life
Findings from the survey show acne has a significant impact on HRQoL. For clinical practice, the
inclusion of HRQoL tools can help to inform decision-making for treatment. For example, if
patients are severely affected although their acne is assessed as mild to moderate, they may benefit
from a multidisciplinary approach to treatment rather than just one modality. Practitioners should
be mindful of the impact acne can have on HRQoL and this line of questioning may be appropriate
as part of the therapeutic consultation. Addressing patients’ HRQoL early will improve patients’
health. A short, easy-to-use tool such as the CADI is recommended in clinical practice by the
EADV TF (228) and other reviewers of HRQoL tools for acne (253, 254).
10.6 Conclusions
This thesis summarises the literature on CM therapies for acne and identifies HRQoL as an
important factor in acne research. The clinical evidence of CM therapies shows PPQFY was more
effective than pharmacotherapies for acne and there was no difference between acupuncture and
pharmacotherapies for acne. PPQFY and acupuncture may be alternatives for those who want
alternatives to conventional medicines. This clinical evidence should be interpreted with caution
due to the methodological flaws of the included studies. This project has attempted to obtain recent
data on how acne impacts the Australian population’s HRQoL and their CM treatment preferences.
A rigorous trial protocol has been designed incorporating stakeholders’ preferences for CM
treatment and addressing the methodological flaws in previous trials to inform future research.
286
REFERENCES
1. Gollnick HP. From new findings in acne pathogenesis to new approaches in treatment. J Eur Acad Dermatol Venereol. 2015;29 Suppl 5:1-7.
2. Perkins AC, Maglione J, Hillebrand GG, Miyamoto K, Kimball AB. Acne vulgaris in women: Prevalence across the life span. J Womens Health. 2012;21(2):223-30.
3. Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavalle RP, Margolis DJ, et al. The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions. J Invest Dermatol. 2014;134(6):1527-34.
4. Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol. 2013;168(3):474-85.
5. Cordain L, Lindeberg S, Hurtado M, Hill K, Eaton SB, Brand-Miller J. Acne vulgaris: A disease of Western civilization. Arch Dermatol. 2002;138(12):1584-90.
6. Williams HC, Dellavalle RP, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361-72.
7. Eichenfield LF, Del Rosso JQ, Mancini AJ, Cook-Bolden F, Stein Gold L, Desai S, et al. Evolving perspectives on the etiology and pathogenesis of acne vulgaris. J Drugs Dermatol. 2015;14(3):263-72.
8. Bowe WP, Doyle AK, Crerand CE, Margolis DJ, Shalita AR. Body image disturbance in patients with acne vulgaris. J Clin Aesthet Dermatol. 2011;4(7):35-41.
9. Halvorsen JA, Stern RS, Dalgard F, Thoresen M, Bjertness E, Lien L. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: A population-based study. J Invest Dermatol. 2011;131(2):363-70.
10. Saitta P, Keehan P, Yousif J, Way BV, Grekin S, Brancaccio R. An update on the presence of psychiatric comorbidities in acne patients, Part 2: Depression, anxiety, and suicide. Cutis. 2011;88(2):92-7.
11. Costa CS, Bagatin E, Martimbianco ALC, da Silva EMK, Lúcio MM, Magin P, et al. Oral isotretinoin for acne. Cochrane Database Syst Rev. 2018(11).
12. Australian Government Department of Health. The Pharmaceutical Benefits Scheme http://www.pbs.gov.au/pbs/home;jsessionid=1eli53p8050x3zyqbj6harg1d accessed 21 Jan 2018. 2018.
13. Eichenfield LF, Krakowski AC, Piggott C, Del Rosso J, Baldwin H, Friedlander SF, et al. Evidence-based recommendations for the diagnosis and treatment of pediatric acne. Pediatrics. 2013;131 Suppl 3:S163-86.
14. Arowojolu AO, Gallo MF, Lopez LM, Grimes DA. Combined oral contraceptive pills for treatment of acne. Cochrane Database Syst Rev. 2012(7).

287
15. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008(12):1-23.
16. Baron SE, Goodwin RG, Nicolau N, Blackford S, Goulden V. Use of complementary medicine among outpatients with dermatologic conditions within Yorkshire and South Wales, United Kingdom. J Am Acad Dermatol. 2005;52(4):589-94.
17. Italia S, Wolfenstetter SB, Teuner CM. Patterns of complementary and alternative medicine (CAM) use in children: A systematic review. Eur J Pediatr. 2014;173(11):1413-28.
18. Li B, Chai H, Du YH, Xiao L, Xiong J. [Evaluation of therapeutic effect and safety for clinical randomized and controlled trials of treatment of acne with acupuncture and moxibustion]. Zhongguo Zhen Jiu. 2009;29(3):247-51. [In Chinese: 黎波, 柴华, 杜元灏, 肖丽, 熊俊. 针灸治
疗痤疮临床随机对照试验疗效及安全性评价. 中国针灸]
19. Kilkenny M, Stathakis V, Hibbert ME, Patton G, Caust J, Bowes G. Acne in Victorian adolescents: Associations with age, gender, puberty and psychiatric symptoms. J Paediatr Child Health. 1997;33(5):430-3.
20. Fisk WA, Lev-Tov HA, Sivamani RK. Botanical and phytochemical therapy of acne: A systematic review. Phytother Res. 2014;28(8):1137-52.
21. Cao H, Yang G, Wang Y, Liu JP. Acupoint Stimulation for Acne: A Systematic Review of Randomized Controlled Trials. Medical Acupuncture. 2012;25(3):173-94.
22. Kilkenny M, Merlin K, Plunkett A, Marks R. The prevalence of common skin conditions in Australian school students: 3. acne vulgaris. Br J Dermatol. 1998;139(5):840-5.
23. Law MP, Chuh AA, Lee A, Molinari N. Acne prevalence and beyond: Acne disability and its predictive factors among Chinese late adolescents in Hong Kong. Clin Exp Dermatol. 2010;35(1):16-21.
24. Collier CN, Harper JC, Cafardi JA, Cantrell WC, Wang W, Foster KW, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58(1):56-9.
25. Purvis D, Robinson E, Merry S, Watson P. Acne, anxiety, depression and suicide in teenagers: A cross-sectional survey of New Zealand secondary school students. J Paediatr Child Health. 2006;42(12):793-6.
26. Yang YC, Tu HP, Hong CH, Chang WC, Fu HC, Ho JC, et al. Female gender and acne disease are jointly and independently associated with the risk of major depression and suicide: A national population-based study. Biomed Res Int. 2014;2014:504279.
27. Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163-96.
288
28. Zaenglein AL, Pathy AL, Schlosser BJ, Alikhan A, Baldwin HE, Berson DS, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-73.e33.
29. Fabbrocini G, Annunziata MC, D'Arco V, De Vita V, Lodi G, Mauriello MC, et al. Acne scars: Pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893080.
30. Shen Y, Wang T, Zhou C, Wang X, Ding X, Tian S, et al. Prevalence of acne vulgaris in Chinese adolescents and adults: A community-based study of 17,345 subjects in six cities. Acta Derm Venereol. 2012;92(1):40-4.
31. Augustin M, Herberger K, Hintzen S, Heigel H, Franzke N, Schafer I. Prevalence of skin lesions and need for treatment in a cohort of 90 880 workers. Br J Dermatol. 2011;165(4):865-73.
32. Abdel-Hafez K, Abdel-Aty MA, Hofny ER. Prevalence of skin diseases in rural areas of Assiut Governorate, Upper Egypt. Int J Dermatol. 2003;42(11):887-92.
33. Gibbs S. Skin disease and socioeconomic conditions in rural Africa: Tanzania. Int J Dermatol. 1996;35(9):633-9.
34. Figueroa JI, Fuller LC, Abraha A, Hay RJ. Dermatology in southwestern Ethiopia: Rationale for a community approach. Int J Dermatol. 1998;37(10):752-8.
35. Wolkenstein P, Machovcová A, Szepietowski JC, Tennstedt D, Veraldi S, Delarue A. Acne prevalence and associations with lifestyle: A cross‐sectional online survey of adolescents/young adults in 7 European countries. J Eur Acad Dermatol Venereol. 2018;32(2):298-306.
36. Darwish MA, Al-Rubaya AA. Knowledge, Beliefs, and Psychosocial Effect of Acne Vulgaris among Saudi Acne Patients. ISRN Dermatol. 2013;2013:929340.
37. El-Khateeb EA, Khafagy NH, Abd Elaziz KM, Shedid AM. Acne vulgaris: Prevalence, beliefs, patients' attitudes, severity and impact on quality of life in Egypt. Public Health. 2014;128(6):576-8.
38. Bagatin E. Adult female acne. Azelaic acid in the treatment of acne in adult females. Introduction. Skin Pharmacol Physiol. 2014;27 Suppl 1:1-2.
39. Di Landro A, Cazzaniga S, Parazzini F, Ingordo V, Cusano F, Atzori L, et al. Family history, body mass index, selected dietary factors, menstrual history, and risk of moderate to severe acne in adolescents and young adults. J Am Acad Dermatol. 2012;67(6):1129-35.
40. Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity, and severity risk factors of acne in high school pupils: A community-based study. J Invest Dermatol. 2009;129(9):2136-41.
41. Hanisah A, Omar K, Shah SA. Prevalence of acne and its impact on the quality of life in school-aged adolescents in Malaysia. J Prim Health Care. 2009;1(1):20-5.

289
42. Peric J, Maksimovic N, Jankovic J, Mijovic B, Reljic V, Jankovic S. Prevalence and quality of life in high school pupils with acne in Serbia. Vojnosanit Pregl. 2013;70(10):935-9.
43. Dreno B. Treatment of adult female acne: A new challenge. J Eur Acad Dermatol Venereol. 2015;29 Suppl 5:14-9.
44. Goulden V, Clark SM, Cunliffe WJ. Post-adolescent acne: A review of clinical features. Br J Dermatol. 1997;136(1):66-70.
45. Holzmann R, Shakery K. Postadolescent acne in females. Skin Pharmacol Physiol. 2014;27 Suppl 1:3-8.
46. Cheng CE, Irwin B, Mauriello D, Liang L, Pappert A, Kimball AB. Self-reported acne severity, treatment, and belief patterns across multiple racial and ethnic groups in adolescent students. Pediatr Dermatol. 2010;27(5):446-52.
47. Freyre EA, Rebaza RM, Sami DA, Lozada CP. The prevalence of facial acne in Peruvian adolescents and its relation to their ethnicity. J Adolesc Health. 1998;22(6):480-4.
48. White GM. Recent findings in the epidemiologic evidence, classification, and subtypes of acne vulgaris. J Am Acad Dermatol. 1998;39(2 Pt 3):S34-7.
49. Karciauskiene J, Valiukeviciene S, Gollnick H, Stang A. The prevalence and risk factors of adolescent acne among schoolchildren in Lithuania: A cross-sectional study. J Eur Acad Dermatol Venereol. 2014;28(6):733-40.
50. Al Robaee AA. Prevalence, knowledge, beliefs and psychosocial impact of acne in University students in Central Saudi Arabia. Saudi Med J. 2005;26(12):1958-61.
51. Li D, Chen Q, Liu Y, Liu T, Tang W, Li S. The prevalence of acne in mainland China: A systematic review and meta-analysis. BMJ Open. 2017;7(4):e015354.
52. Kiprono SK, Wamburu G. Acne vulgaris in general population of rural western Kenya: Cross-sectional community survey. Int J Dermatol. 2016;55(4):e212-4.
53. Schaefer I, Rustenbach SJ, Zimmer L, Augustin M. Prevalence of skin diseases in a cohort of 48,665 employees in Germany. Dermatology. 2008;217(2):169-72.
54. Schafer T, Nienhaus A, Vieluf D, Berger J, Ring J. Epidemiology of acne in the general population: The risk of smoking. Br J Dermatol. 2001;145(1):100-4.
55. Al-Saeed WY, Al-Dawood KM, Bukhari IA, Bahnassy AA. Risk factors and co-morbidity of skin disorders among female schoolchildren in Eastern Saudi Arabia. Invest Clin. 2007;48(2):199-212.
56. Zouboulis CC. Acne as a chronic systemic disease. Clin Dermatol. 2014;32(3):389-96.
57. Lucky AW. A review of infantile and pediatric acne. Dermatology. 1998;196(1):95-7.
290
58. Alan S, Cenesizoglu E. Effects of hyperandrogenism and high body mass index on acne severity in women. Saudi Med J. 2014;35(8):886-9.
59. Tanghetti EA, Kawata AK, Daniels SR, Yeomans K, Burk CT, Callender VD. Understanding the burden of adult female acne. J Clin Aesthet Dermatol. 2014;7(2):22-30.
60. Lynn DD, Umari T, Dunnick CA, Dellavalle RP. The epidemiology of acne vulgaris in late adolescence. Adolesc Health Med Ther. 2016;7:13-25.
61. Karimkhani C, Dellavalle RP, Coffeng LE, Flohr C, Hay RJ, Langan SM, et al. Global skin disease morbidity and mortality: An update from the Global Burden of Disease Study 2013. JAMA Dermatol. 2017;153(5):406-12.
62. Yentzer BA, Irby CE, Fleischer AB, Jr., Feldman SR. Differences in acne treatment prescribing patterns of pediatricians and dermatologists: An analysis of nationally representative data. Pediatr Dermatol. 2008;25(6):635-9.
63. Zouboulis CC, Eady A, Philpott M, Goldsmith LA, Orfanos C, Cunliffe WC, et al. What is the pathogenesis of acne? Exp Dermatol. 2005;14(2):143-52.
64. Balkrishnan R, Fleischer AB, Jr., Paruthi S, Feldman SR. Physicians underutilize topical retinoids in the management of acne vulgaris: Analysis of U.S. National Practice Data. J Dermatolog Treat. 2003;14(3):172-6.
65. What role for topical antibacterials in acne? Drug Ther Bull. 2010;48(12):141-4.
66. Bickers DR, Lim HW, Margolis D, Weinstock MA, Goodman C, Faulkner E, et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J Am Acad Dermatol. 2006;55(3):490-500.
67. Vilar GN, Santos LA, Sobral Filho JF. Quality of life, self-esteem and psychosocial factors in adolescents with acne vulgaris. An Bras Dermatol. 2015;90(5):622-9.
68. Dreno B, Tan J, Kang S, Rueda MJ, Torres Lozada V, Bettoli V, et al. How people with facial acne scars are perceived in society: An online survey. Dermatol Ther. 2016;6(2):207-18.
69. Gupta MA, Gupta AK. Depression and suicidal ideation in dermatology patients with acne, alopecia areata, atopic dermatitis and psoriasis. Br J Dermatol. 1998;139(5):846-50.
70. Motley RJ, Finlay AY. How much disability is caused by acne? Clin Exp Dermatol. 1989;14(3):194-8.
71. Magin P, Adams J, Heading G, Pond D, Smith W. Psychological sequelae of acne vulgaris: Results of a qualitative study. Can Fam Physician. 2006;52:978-9.
291
72. Misery L, Wolkenstein P, Amici JM, Maghia R, Brenaut E, Cazeau C, et al. Consequences of acne on stress, fatigue, sleep disorders and sexual activity: A population-based study. Acta Derm Venereol. 2015;95(4):485-8.
73. Cunliffe WJ. Acne and unemployment. Br J Dermatol. 1986;115(3):386.
74. Duman HT, I. O.; Kocaturk, E.; Duman, M. A. . Evaluation of anxiety, depression, and quality of life in patients with acne vulgaris, and quality of life in their families. DSI. 2016;34(1):6-9.
75. Basra MK, Sue-Ho R, Finlay AY. The Family Dermatology Life Quality Index: Measuring the secondary impact of skin disease. Br J Dermatol. 2007;156(3):528-38.
76. Bhate K, Williams HC. What's new in acne? An analysis of systematic reviews published in 2011-2012. Clin Exp Dermatol. 2014;39(3):273-7; quiz 7-8.
77. Ren X, Zhou S, Zhou J. [Demodex infection in university and middle school students]. Hunan Yi Ke Da Xue Xue Bao. 1997;22(3):281. [In Chinese: 任象琼, 赵双星, 周金春. 大中学
生的蠕形螨调查. 湖南医科大学学报].
78. Beylot C, Auffret N, Poli F, Claudel JP, Leccia MT, Del Giudice P, et al. Propionibacterium acnes: An update on its role in the pathogenesis of acne. J Eur Acad Dermatol Venereol. 2014;28(3):271-8.
79. Dreno B, Gollnick HP, Kang S, Thiboutot D, Bettoli V, Torres V, et al. Understanding innate immunity and inflammation in acne: Implications for management. J Eur Acad Dermatol Venereol. 2015;29 Suppl 4:3-11.
80. Bialecka A, Mak M, Biedron R, Bobek M, Kasprowicz A, Marcinkiewicz J. Different pro-inflammatory and immunogenic potentials of Propionibacterium acnes and Staphylococcus epidermidis: Implications for chronic inflammatory acne. Arch Immunol Ther Exp. 2005;53(1):79-85.
81. Zouboulis CC, Jourdan E, Picardo M. Acne is an inflammatory disease and alterations of sebum composition initiate acne lesions. J Eur Acad Dermatol Venereol. 2014;28(5):527-32.
82. Trivedi NR, Cong Z, Nelson AM, Albert AJ, Rosamilia LL, Sivarajah S, et al. Peroxisome proliferator-activated receptors increase human sebum production. J Invest Dermatol. 2006;126(9):2002-9.
83. Weller R, Hunter J, Savin J, Dahl M. Clinical Dermatology. 2009. Wiley. 4th. [162-76].
84. Adebamowo CA, Spiegelman D, Berkey CS, Danby FW, Rockett HH, Colditz GA, et al. Milk consumption and acne in adolescent girls. Dermatol Online J. 2006;12(4):1.
85. Adebamowo CA, Spiegelman D, Berkey CS, Danby FW, Rockett HH, Colditz GA, et al. Milk consumption and acne in teenaged boys. J Am Acad Dermatol. 2008;58(5):787-93.
292
86. Smith RN, Mann NJ, Braue A, Makelainen H, Varigos GA. A low-glycemic-load diet improves symptoms in acne vulgaris patients: A randomized controlled trial. Am J Clin Nutr. 2007;86(1):107-15.
87. Toyoda M, Nakamura M, Makino T, Kagoura M, Morohashi M. Sebaceous glands in acne patients express high levels of neutral endopeptidase. Exp Dermatol. 2002;11(3):241-7.
88. Goulden V, McGeown CH, Cunliffe WJ. The familial risk of adult acne: A comparison between first-degree relatives of affected and unaffected individuals. Br J Dermatol. 1999;141(2):297-300.
89. Wei B, Pang Y, Zhu H, Qu L, Xiao T, Wei HC, et al. The epidemiology of adolescent acne in North East China. J Eur Acad Dermatol Venereol. 2010;24(8):953-7.
90. Magin P, Pond D, Smith W, Watson A. A systematic review of the evidence for 'myths and misconceptions' in acne management: Diet, face-washing and sunlight. Fam Pract. 2005;22(1):62-70.
91. Bowe WP, Joshi SS, Shalita AR. Diet and acne. J Am Acad Dermatol. 2010;63(1):124-41.
92. Park SY, Kwon HH, Min S, Yoon JY, Suh DH. Epidemiology and risk factors of childhood acne in Korea: A cross-sectional community based study. Clin Exp Dermatol. 2015;40(8):844-50.
93. Wolkenstein P, Misery L, Amici JM, Maghia R, Branchoux S, Cazeau C, et al. Smoking and dietary factors associated with moderate-to-severe acne in French adolescents and young adults: Results of a survey using a representative sample. Dermatology. 2015;230(1):34-9.
94. Zari S, Alrahmani D. The association between stress and acne among female medical students in Jeddah, Saudi Arabia. Clin Cosmet Investig Dermatol. 2017;10:503-6.
95. Gambineri A, Pelusi C, Vicennati V, Pagotto U, Pasquali R. Obesity and the polycystic ovary syndrome. Int J Obes Relat Metab Disord. 2002;26(7):883-96.
96. Silverberg JI, Silverberg NB. Epidemiology and extracutaneous comorbidities of severe acne in adolescence: A U.S. population-based study. Br J Dermatol. 2014;170(5):1136-42.
97. World Health Organisation. International Classification of Diseases-10. Malta: World Health Organisation; 2010 04 Apr 2014.
98. Zarchi K, Jemec GBE. Severity assessment and outcome measures in acne vulgaris. Curr Derm Rep. 2012;1(3):131-6.
99. Tan J, Wolfe B, Weiss J, Stein-Gold L, Bikowski J, Del Rosso J, et al. Acne severity grading: Determining essential clinical components and features using a Delphi consensus. J Am Acad Dermatol. 2012;67(2):187-93.
100. Chren MM. The Skindex instruments to measure the effects of skin disease on quality of life. Dermatol Clin. 2012;30(2):231-6, xiii.

293
101. Pillsbury DM. Dermatology. Philadelphia: Saunders; 1956.
102. James KW, Tisserand JB, Jr. Treatment of acne vulgaris. GP. 1958;18(3):130-9.
103. Christiansen J, Holm P, Reymann F. The retinoic acid derivative Ro 11-1430 in acne vulgaris. A controlled multicenter trial against retinoic acid. Dermatologica. 1977;154(4):219-27.
104. Burke BM, Cunliffe WJ. The assessment of acne vulgaris--the Leeds technique. Br J Dermatol. 1984;111(1):83-92.
105. Cook CH, Centner RL, Michaels SE. An acne grading method using photographic standards. Arch Dermatol. 1979;115(5):571-5.
106. Doshi A, Zaheer A, Stiller MJ. A comparison of current acne grading systems and proposal of a novel system. Int J Dermatol. 1997;36(6):416-8.
107. Center for Drug Evaluation and Research. Guidelines of Care for Acne Vulgaris Management Technical Report. U.S. Department of Health and Human Services; 2005.
108. Tan JK, Tang J, Fung K, Gupta AK, Thomas DR, Sapra S, et al. Development and validation of a comprehensive acne severity scale. J Cutan Med Surg. 2007;11(6):211-6.
109. O'Brien S, Lewis J, Cunliffe W. The Leeds revised acne grading system. J Dermatolog Treat. 1998;9(4):215-20.
110. Dreno B, Bodokh I, Chivot M, Daniel F, Humbert P, Poli F, et al. [ECLA grading: A system of acne classification for every day dermatological practice]. Ann Dermatol Venereol. 1999;126(2):136-41.
111. Dreno B, Poli F, Pawin H, Beylot C, Faure M, Chivot M, et al. Development and evaluation of a Global Acne Severity Scale (GEA Scale) suitable for France and Europe. J Eur Acad Dermatol Venereol. 2011;25(1):43-8.
112. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-83.
113. Kroenke K, Spitzer RL, Williams JB, Lowe B. An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics. 2009;50(6):613-21.
114. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210-6.
115. Chren MM, Lasek RJ, Sahay AP, Sands LP. Measurement properties of Skindex-16: A brief quality-of-life measure for patients with skin diseases. J Cutan Med Surg. 2001;5(2):105-10.
116. Lasek RJ, Chren MM. Acne vulgaris and the quality of life of adult dermatology patients. Arch Dermatol. 1998;134(4):454-8.
294
117. Nijsten T, Sampogna F, Abeni D. Categorization of Skindex-29 scores using mixture analysis. Dermatology. 2009;218(2):151-4.
118. Rapp SR, Feldman SR, Graham G, Fleischer AB, Brenes G, Dailey M. The Acne Quality of Life Index (Acne-QOLI): Development and validation of a brief instrument. Am J Clin Dermatol. 2006;7(3):185-92.
119. Fehnel SE, McLeod LD, Brandman J, Arbit DI, McLaughlin-Miley CJ, Coombs JH, et al. Responsiveness of the Acne-Specific Quality of Life Questionnaire (Acne-QoL) to treatment for acne vulgaris in placebo-controlled clinical trials. Qual Life Res. 2002;11(8):809-16.
120. Girman CJ, Hartmaier S, Thiboutot D, Johnson J, Barber B, DeMuro-Mercon C, et al. Evaluating health-related quality of life in patients with facial acne: Development of a self-administered questionnaire for clinical trials. Qual Life Res. 1996;5(5):481-90.
121. Martin AR, Lookingbill DP, Botek A, Light J, Thiboutot D, Girman CJ. Health-related quality of life among patients with facial acne -- assessment of a new acne-specific questionnaire. Clin Exp Dermatol. 2001;26(5):380-5.
122. Motley RJ, Finlay AY. Practical use of a disability index in the routine management of acne. Clin Exp Dermatol. 1992;17(1):1-3.
123. Gupta MA, Johnson AM, Gupta AK. The development of an Acne Quality of Life scale: Reliability, validity, and relation to subjective acne severity in mild to moderate acne vulgaris. Acta Derm Venereol. 1998;78(6):451-6.
124. Lehmann HP, Andrews JS, Robinson KA, Holloway VL, Goodman SN. Management of acne. Evid Rep Technol Assess (Summ). 2001(17):1-3.
125. Cook D, Krassas G, Huang T. Acne - best practice management. Aust Fam Physician. 2010;39(9):656-60.
126. Ministry of Health Malaysia. Management of Acne: Clinical Practice Guidelines. In: Malaysia MoH, editor. Putrajaya, Malaysia: Ministry of Health Malaysia; 2012.
127. Nast A, Dreno B, Bettoli V, Degitz K, Erdmann R, Finlay AY, et al. European evidence-based (S3) guidelines for the treatment of acne. J Eur Acad Dermatol Venereol. 2012;26 Suppl 1:1-29.
128. Nast A, Rosumeck S, Erdmann R, Alsharif U, Dressler C, Werner RN. Methods report on the development of the European evidence‐based (S3) guideline for the treatment of acne – update 2016. Journal of the European Academy of Dermatology and Venereology. 2016;30(8):e1-e28.
129. Barbieri JS, Spaccarelli N, Margolis DJ, James WD. Approaches to limit systemic antibiotic use in acne: Systemic alternatives, emerging topical therapies, dietary modification, and laser and light-based treatments. J Am Acad Dermatol. 2019;80(2):538-49.
295
130. Nast A, Dreno B, Bettoli V, Bukvic Mokos Z, Degitz K, Dressler C, et al. European evidence-based (S3) guideline for the treatment of acne - update 2016 - short version. J Eur Acad Dermatol Venereol. 2016;30(8):1261-8.
131. National Institute for Health and Care Excellence. Acne vulgaris - NICE CKS. National Institute for Health and Care Excellence (NICE); 2014.
132. Barbieri JS, James WD, Margolis DJ. Trends in prescribing behavior of systemic agents used in the treatment of acne among dermatologists and nondermatologists: A retrospective analysis, 2004-2013. J Am Acad Dermatol. 2017;77(3):456-63.e4.
133. Goulden V. Guidelines for the management of acne vulgaris in adolescents. Paediatr Drugs. 2003;5(5):301-13.
134. Suh DH, Kwon HH. What's new in the physiopathology of acne? Br J Dermatol. 2015;172 Suppl 1:13-9.
135. Tan JK, Bhate K. A global perspective on the epidemiology of acne. Br J Dermatol. 2015;172 Suppl 1:3-12.
136. Odsbu I, Selmer R, Stalsby Lundborg C, Blix HS. Increased prescribing of systemic tetracyclines and isotretinoin for treatment of acne. J Antimicrob Chemother. 2017;72(5):1510-5.
137. Saitta P, Keehan P, Yousif J, Way BV, Grekin S, Brancaccio R. An update on the presence of psychiatric comorbidities in acne patients, part 1: overview of prevalence. Cutis. 2011;88(1):33-40.
138. Tzellos T, Toulis KA, Dessinioti C, Zampeli V, Abdel-Naser MB, Katsambas A, et al. Topical retinoids for the treatment of acne vulgaris. Cochrane Database Syst Rev. 2013(8).
139. Cooper AJ, Harris VR. Modern management of acne. Med J Aust. 2017;206(1):41-5.
140. Archer CB, Cohen SN, Baron SE. Guidance on the diagnosis and clinical management of acne. Clin Exp Dermatol. 2012;37 Suppl 1:1-6.
141. Malaysian Ministry of Health. Clinical Practice Guidelines Management of Acne. In: Health Mo, editor. Putrajaya, Malaysia: Malaysian Government; 2012.
142. Brown J, Farquhar C, Lee O, Toomath R, Jepson RG. Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database Syst Rev. 2009(2):CD000194.
143. Garner SE, Eady A, Bennett C, Newton John N, Thomas K, Popescu CM. Minocycline for acne vulgaris: Efficacy and safety. Cochrane Database Syst Rev. 2012(8).
144. Jordan RE, Cummins CL, Burls AJ, Seukeran DC. Laser resurfacing for facial acne scars. Cochrane Database Syst Rev. 2001(1):CD001866.
296
145. American Academy of Dermatology. Acne: American Academy of Dermatology; 2015 [Acne advice to the public and clinicians].
146. Matsuoka Y, Yoneda K, Sadahira C, Katsuura J, Moriue T, Kubota Y. Effects of skin care and makeup under instructions from dermatologists on the quality of life of female patients with acne vulgaris. J Dermatol. 2006;33(11):745-52.
147. Hayashi N, Imori M, Yanagisawa M, Seto Y, Nagata O, Kawashima M. Make-up improves the quality of life of acne patients without aggravating acne eruptions during treatments. Eur J Dermatol. 2005;15(4):284-7.
148. Seleit I, Bakry OA, Abdou AG, Hashim A. Body mass index, selected dietary factors, and acne severity: Are they related to in situ expression of insulin-like growth factor-1? Anal Quant Cytopathol Histpathol. 2014;36(5):267-78.
149. Smith R, Mann N, Makelainen H, Roper J, Braue A, Varigos G. A pilot study to determine the short-term effects of a low glycemic load diet on hormonal markers of acne: A nonrandomized, parallel, controlled feeding trial. Mol Nutr Food Res. 2008;52(6):718-26.
150. Smith RN, Braue A, Varigos GA, Mann NJ. The effect of a low glycemic load diet on acne vulgaris and the fatty acid composition of skin surface triglycerides. J Dermatol Sci. 2008(1):41-52.
151. Fuhrmann T, Smith N, Tausk F. Use of complementary and alternative medicine among adults with skin disease: Updated results from a national survey. J Am Acad Dermatol. 2010;63(6):1000-5.
152. Fox L, Csongradi C, Aucamp M, du Plessis J, Gerber M. Treatment Modalities for Acne. Molecules. 2016;21(8):1-20.
153. Nelson K, Lyles JT, Li T, Saitta A, Addie-Noye E, Tyler P, et al. Anti-acne activity of Italian medicinal plants used for skin infection. Front Pharmacol. 2016;7:425.
154. Nipanikar S, Chitlange S, Nagore D. Evaluation of anti-inflammatory and antimicrobial activity of AHPL/AYCAP/0413 capsule. Pharmacognosy Res. 2017;9(3):273-6.
155. Magin PJ, Adams J, Heading GS, Pond DC, Smith W. Complementary and alternative medicine therapies in acne, psoriasis, and atopic eczema: Results of a qualitative study of patients' experiences and perceptions. J Altern Complement Med. 2006;12(5):451-7.
156. Orafidiya LO, Agbani EO, Oyedele AO, Babalola OO, Onayemi O. Preliminary clinical tests on topical preparations of Ocimum gratissimum Linn leaf essential oil for the treatment of acne vulgaris. Clin Drug Investig. 2002;22(5):313-9.
157. Cao H, Yang G, Wang Y, Liu JP, Smith CA, Luo H, et al. Complementary therapies for acne vulgaris. Cochrane Database Syst Rev. 2015;1:Cd009436.
297
158. Maciocia Ga. The Foundations of Chinese Medicine: A Comprehensive Text. Third edition. ed. Edinburgh: Elsevier; 2015.
159. Xu YH. Dermatology in Traditional Chinese Medicine. St. Albans: Donica Publishing; 2004.
160. Wang H, Liu X, Lv B, Yang F, Hong Y. Reliable multi-label learning via conformal predictor and random forest for syndrome differentiation of chronic fatigue in traditional Chinese medicine. PLoS One. 2014;9(6):e99565.
161. Koo J, Desai R. Traditional Chinese medicine in dermatology. Dermatol Ther. 2003;16(2):98-105.
162. Xiang L. [Treatment Guidelines for Acne Vulgaris in China (2014 edition)]. J Clin Dermatol. 2015;44(1):52-7. [In Chinese: 项蕾红. 中国痤疮治疗指南. 临床皮肤科杂志].
163. Scott J. Acupuncture in the Treatment of Children. 3rd Edition ed. Seattle: Eastland Press; 1999.
164. Fan R, Xuan G, Hul T. Acne & Alopecia. Beijing: People's Medical Publishing House; 2008.
165. Shen D, Wu X, Wang N. Manual of Dermatology in Chinese Medicine. Seattle: Eastland Press; 1995.
166. China Association of Chinese Medicine. [Guidelines for Diagnosis and Treatment of Common Diseases of Dermatology in Traditional Chinese Medicine]. Beijing: China Press of Traditional Chinese Medicine [In Chinese: 中华中医药学会. 中医皮肤科常见病诊疗指南. 中国中医药出版社]; 2012.
167. State Administration of Traditional Chinese Medicine of People’s Republic of China. [Criteria of Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine]. Nanjing: Nanjing University Publishing House [In Chinese: 国家中医药管理局. 中医
病证诊断疗效标准. 南京大学出版社]; 1994.
168. Coyle M, Liang HY, Wang KY, Zhang AL, Xue CL, Li HY. Evidence-based Clinical Chinese Medicine Volume 11: Acne Vulgaris. In: Xue CL, J. LC, editors.: World Scientific Publishing Co. Pte. Ltd.; 2019.
169. Bertschinger R, Qiu M, Li LY, Zang SC. Chinese Acupuncture and Moxibustion. Bertschinger Re, Qiu Me, Li L-yt, Zang S-ce, editors. Edinburgh: Churchill Livingstone; 1993.
170. Uto T, Suangkaew N, Morinaga O, Kariyazono H, Oiso S, Shoyama Y. Eriobotryae folium extract suppresses LPS-induced iNOS and COX-2 expression by inhibition of NF-kappaB and MAPK activation in murine macrophages. Am J Chin Med. 2010;38(5):985-94.
298
171. Choi BH, Ahn IS, Kim YH, Park JW, Lee SY, Hyun CK, et al. Berberine reduces the expression of adipogenic enzymes and inflammatory molecules of 3T3-L1 adipocyte. Exp Mol Med. 2006;38(6):599-605.
172. The Poisons Standard June 2018 consists of the Standard for the Uniform Scheduling of Medicines and Poisons (2018).
173. Convention on International Trade in Endangered Species of Wild Fauna and Flora. 2018 [https://www.cites.org/] accessed 10 Aug 2018.
174. McKee D, Oring K, Aban I, Lu M, Peele K, Scott B. Treating facial acne in adolescents and young adults with auriculoacupuncture and auriculotherapy: A pilot study Med Acupunct. 2004;16(1):Article 6.
175. Zhang L, Wu F, Xue L, Zhao H. [A controlled study of treating acne vulgaris with electro plum blossom acupuncture treatment]. Lishizhen Medicine and Materia Medica Research. 2014;25(11):2817-8. [In Chinese: 张琳, 吴凡, 薛岚显, 赵宏. 电梅花针叩刺疗法治疗寻常型痤
疮的对照研究. 时珍国医国药].
176. Li F, Wu H, Wang X, Bao Y, Zou R. [Effect of surround needling combined with auricular point sticking on main pathogenetic factors of acne vulgaris]. Chinese Acupuncture and Moxibustion. 2002;22(3):161-3. [In Chinese: 李芳莉, 吴昊, 王晓翠, 包艳东, 邹如政. 围刺结合
耳穴贴压疗法对寻常痤疮主要发病因素的影响.中国针灸].
177. Tang P, Quan Y. [The clinical effect of treating acne vulgaris with manual acupuncture on Yangming meridian and surrounding acupuncture]. Shanghai Journal of Acupuncture and Moxibustion. 2011;30(2):127. [In Chinese: 唐平平, 全英顺. 阳明经针刺配合局部围刺治疗寻
常性痤疮疗效观察. 上海针灸杂志].
178. Kim KS, Kim Y-B. Anti-Inflammatory Effect of Keigai-rengyo-to Extract and Acupuncture in Male Patients with Acne Vulgaris: A Randomized Controlled Pilot Trial. Journal of Alternative & Complementary Medicine. 2012;18(5):501-8.
179. McKee D, Oring K, Aban I. Treating facial acne in adolescents and young adults with auriculoacupuncture and auriculotherapy: a pilot study. Med Acup [Internet]. 2004; 16(1):[30 p.]. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/984/CN-00672984/frame.html.
180. Son B, Yun Y, Choi I. Efficacy of ah shi point acupuncture on acne vulgaris. BMC Complementary and Alternative Medicine. 2012;12.
181. Sun L. He-Ne laser auricular irradiation plus body acupuncture for treatment of acne vulgaris in 36 cases. Journal of Traditional Chinese Medicine. 2006;26(3):193-4.
182. Liu W, Shen D, Song P, Xu X. Clinical observation in 86 cases of acne vulgaris treated with Compound Oldenlandis Mixture. Journal of traditional Chinese medicine = Chung i tsa chih
299
ying wen pan / sponsored by All-China Association of Traditional Chinese Medicine, Academy of Traditional Chinese Medicine. 2003;23(4):255-6.
183. Akamatsu H, Asada Y, Horio T. Effect of keigai-rengyo-to, a Japanese kampo medicine, on neutrophil functions: A possible mechanism of action of keigai-rengyo-to in acne. J Int Med Res. 1997;25(5):255-65.
184. Higaki S, Nakamura M, Morohashi M, Yamagishi T. Propionibacterium acnes biotypes and susceptibility to minocycline and Keigai-rengyo-to. Int J Dermatol. 2004;43(2):103-7.
185. Cao HJ, Yang GY, Wang YY, Liu JP. Acupoint stimulation for acne: A systematic review of randomized controlled trials. Med Acupunct. 2013;25(3):173-94.
186. World Health Organisation. The constitution of the World Health Organisation 46th ed. WHO Chron. 2006;1:29.
187. Post MW. Definitions of quality of life: What has happened and how to move on. Top Spinal Cord Inj Rehabil. 2014;20(3):167-80.
188. Karimi M, Brazier J. Health, health-related quality of life, and quality of life: What is the difference? Pharmacoeconomics. 2016;34(7):645-9.
189. Vallerand IA, Lewinson RT, Parsons LM, Lowerison MW, Frolkis AD, Kaplan GG, et al. Risk of depression among patients with acne in the U.K.: A population‐based cohort study. Br J Dermatol. 2018;178(3):e194-e5.
190. Nguyen CM, Beroukhim K, Danesh MJ, Babikian A, Koo J, Leon A. The psychosocial impact of acne, vitiligo, and psoriasis: A review. Clin Cosmet Investig Dermatol. 2016;9:383-92.
191. Salman A, Kurt E, Topcuoglu V, Demircay Z. Social anxiety and quality of life in vitiligo and acne patients with facial involvement: A cross-sectional controlled study. Am J Clin Dermatol. 2016;17(3):305-11.
192. Unal D, Emiroglu N, Cengiz FP. Evaluation of social anxiety, self-esteem, life quality in adolescents with acne vulgaris. Int J Adolesc Med Health. 2016;30(2):pii.
193. Bahali AG, Bahali K, Biyik Ozkaya D, Bilgic A, Su O, Onsun N. The associations between peer victimization, psychological symptoms and quality of life in adolescents with acne vulgaris. J Eur Acad Dermatol Venereol. 2016;30(12):e184-e6.
194. Magin P, Adams J, Heading G, Pond D, Smith W. Experiences of appearance-related teasing and bullying in skin diseases and their psychological sequelae: Results of a qualitative study. Scand J Caring Sci. 2008;22(3):430-6.
195. Ramrakha S, Fergusson DM, Horwood LJ, Dalgard F, Ambler A, Kokaua J, et al. Cumulative mental health consequences of acne: 23-year follow-up in a general population birth cohort study. Br J Dermatol. 2016;175(5):1079-81.

300
196. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361-70.
197. Jankovic S, Vukicevic J, Djordjevic S, Jankovic J, Marinkovic J. Quality of life among school children with acne: Results of a cross-sectional study. Indian J Dermatol Venereol Leprol. 2012;78(4):454-8.
198. Marron SE, Tomas-Aragones L, Boira S. Anxiety, depression, quality of life and patient satisfaction in acne patients treated with oral isotretinoin. Acta Derm Venereol. 2013;93(6):701-6.
199. Isaacsson VC, Almeida HL, Jr., Duquia RP, Breunig Jde A, Souza PR. Dissatisfaction and acne vulgaris in male adolescents and associated factors. An Bras Dermatol. 2014;89(4):576-9.
200. Lee IS, Lee AR, Lee H, Park HJ, Chung SY, Wallraven C, et al. Psychological distress and attentional bias toward acne lesions in patients with acne. Psychol Health Med. 2014;19(6):680-6.
201. Hanstock TL, Amp, Apos, Mahony JF. Perfectionism, acne and appearance concerns. Pers Individ Dif. 2002;32(8):1317-25.
202. Bez Y, Yesilova Y, Ari M, Kaya MC, Alpak G, Bulut M. Predictive value of obsessive compulsive symptoms involving the skin on quality of life in patients with acne vulgaris. Acta Derm Venereol. 2013;93(6):679-83.
203. Akyazi H, Baltaci D, Alpay K, Hocaoglu Ç. Quality of life in adult patients with acne vulgaris before and after treatment/Eriskin akne vulgaris hastalarinda tedavi öncesi ve sonrasi hayat kalitesi. Dicle Tip Dergisi. 2011;38(3):282-8.
204. Brodell RT, Wertheimer A, Toth D, Bucher D, Rafal E, Kerrouche N, et al. Treatment with adapalene-benzoyl peroxide improve quality of life in patients with severe acne vulgaris. J Am Acad Dermatol. 2013;68(4):AB19.
205. Gieler U, Gieler T, Kupfer JP. Acne and quality of life - impact and management. J Eur Acad Dermatol Venereol. 2015;29 Suppl 4:12-4.
206. Saitta P, Grekin SK. A four-question approach to determining the impact of acne treatment on quality of life. J Clin Aesthet Dermatol. 2012;5(3):51-7.
207. Revol O, Milliez N, Gerard D. Psychological impact of acne on 21st-century adolescents: Decoding for better care. Br J Dermatol. 2015;172 Suppl 1:52-8.
208. Shenefelt PD. Management of psychodermatologic disorders (Advanced Practice) (Report). Dermatol Nurs. 2010;22(4):9.
209. Tuong W, Wang AS, Armstrong AW. Effect of automated online counseling on clinical outcomes and quality of life among adolescents with acne vulgaris: A randomized clinical trial. JAMA Dermatol. 2015;151(9):970-5.

301
210. Rapp DA, Brenes GA, Feldman SR, Fleischer AB, Jr., Graham GF, Dailey M, et al. Anger and acne: Implications for quality of life, patient satisfaction and clinical care. Br J Dermatol. 2004;151(1):183-9.
211. Hosthota A, Bondade S, Basavaraja V. Impact of acne vulgaris on quality of life and self-esteem. Cutis. 2016;98(2):121-4.
212. Dunn LK, O'Neill JL, Feldman SR. Acne in adolescents: Quality of life, self-esteem, mood, and psychological disorders. Dermatol Online J. 2011;17(1):1.
213. Tasoula E, Gregoriou S, Chalikias J, Lazarou D, Danopoulou I, Katsambas A, et al. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An Bras Dermatol. 2012;87(6):862-9.
214. Su P, Chen Wee Aw D, Lee SH, Han Sim Toh MP. Beliefs, perceptions and psychosocial impact of acne amongst Singaporean students in tertiary institutions. J Dtsch Dermatol Ges. 2015;13(3):227-33.
215. Dreno B, Thiboutot D, Layton AM, Berson D, Perez M, Kang S. Large-scale international study enhances understanding of an emerging acne population: Adult females. J Eur Acad Dermatol Venereol. 2015;29(6):1096-106.
216. Cresce ND, Davis SA, Huang WW, Feldman SR. The quality of life impact of acne and rosacea compared to other major medical conditions. J Drugs Dermatol. 2014;13(6):692-7.
217. Mallon E, Newton JN, Klassen A, Stewart-Brown SL, Ryan TJ, Finlay AY. The quality of life in acne: A comparison with general medical conditions using generic questionnaires. Br J Dermatol. 1999;140(4):672-6.
218. Morgan M, McCreedy R, Simpson J, Hay RJ. Dermatology quality of life scales--a measure of the impact of skin diseases. Br J Dermatol. 1997;136(2):202-6.
219. Vinding GR, Knudsen KM, Ellervik C, Olesen AB, Jemec GB. Self-reported skin morbidities and health-related quality of life: A population-based nested case-control study. Dermatology. 2014;228(3):261-8.
220. Nguyen CM, Koo J, Cordoro KM. Psychodermatologic effects of atopic dermatitis and acne: A review on self-esteem and identity. Pediatr Dermatol. 2016;33(2):129-35.
221. Demir T, Karacetin G, Eralp Demir D, Uysal O. Prevalence and some psychosocial characteristics of social anxiety disorder in an urban population of Turkish children and adolescents. Eur Psychiatry. 2013;28(1):64-9.
222. Chernyshov PV, Petrenko A, Kopylova V. What health-related quality of life factors influence the decision of patients with acne to visit a dermatologist? J Clin Aesthet Dermatol. 2018;11(7):21.

302
223. Kokandi A. Evaluation of acne quality of life and clinical severity in acne female adults. Dermatol Res Pract. 2010;2010:pii: 410809.
224. Ismail KH, Mohammed-Ali KB. Quality of life in patients with acne in Erbil city. Health Qual Life Outcomes. 2012;10:60.
225. Zaraa I, Belghith I, Ben Alaya N, Trojjet S, Mokni M, Ben Osman A. Severity of acne and its impact on quality of life. Skinmed. 2013;11(3):148-53.
226. Fabbrocini G, Cacciapuoti S, Monfrecola G. A qualitative investigation of the impact of acne on health-related quality of life (HRQL): Development of a conceptual model. Dermatol Ther. 2018;8(1):85-99.
227. Durai PC, Nair DG. Acne vulgaris and quality of life among young adults in South India. Indian J Dermatol. 2015;60(1):33-40.
228. Chernyshov PV, Zouboulis CC, Tomas‐Aragones L, Jemec GB, Manolache L, Tzellos T, et al. Quality of life measurement in acne. Position Paper of the European Academy of Dermatology and Venereology Task Forces on Quality of Life and Patient Oriented Outcomes and Acne, Rosacea and Hidradenitis Suppurativa. J Eur Acad Dermatol Venereol. 2018;32(2):194-208.
229. Ogedegbe EE, Henshaw EB. Severity and impact of acne vulgaris on the quality of life of adolescents in Nigeria. Clin Cosmet Investig Dermatol. 2014;7:329-34.
230. Zauli S, Caracciolo S, Borghi A, Ricci M, Giari S, Virgili A, et al. Which factors influence quality of life in acne patients? J Eur Acad Dermatol Venereol. 2014;28(1):46-50.
231. Gorelick J, Daniels SR, Kawata AK, Degboe A, Wilcox TK, Burk CT, et al. Acne-related quality of life among female adults of different races/ethnicities. J Dermatol Nurses Assoc. 2015;7(3):154-62.
232. Purvis D, Robinson E, Watson P. Acne prevalence in secondary school students and their perceived difficulty in accessing acne treatment. N Z Med J. 2004;117(1200):U1018.
233. EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208.
234. Goodman R. The Strengths and Difficulties Questionnaire: A research note. J Child Psychol Psychiatry. 1997;38(5):581-6.
235. Goldberg DP, Blackwell B. A user's guide to the General Health Questionnaire. Windsor: NFER-Nelson; 1988.
236. Goldberg DP. Manual of the General Health Questionnaire. Windsor: NFER-Nelson; 1978.
303
237. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins Symptom Checklist (HSCL). A measure of primary symptom dimensions. Mod Probl Pharmacopsychiatry. 1974;7(0):79-110.
238. World Health Organisation. World Health Organization Quality of Life (WHOQOL). 2013 Accessed 13 Sep 2018 http://www.who.int/mental_health/publications/whoqol/en/.
239. Radloff L. The CES-D Scale: A self-reported depression scale for research in the general population. Appl Psychol Meas. 1977;1:385-401.
240. Reynolds WM. Adolescent Depression Scale-High School Version. Odessa Florida: Psychological Assessment Resources; 1987.
241. Leary M. A brief version of the fear of negative evaluation scale. Pers Soc Psychol Rev. 1983;9:371-6.
242. Liebowitz MR. Social phobia. Mod Probl Pharmacopsychiatry. 1987;22:141-73.
243. Cash TF, Phillips KA, Santos MT, Hrabosky JI. Measuring "negative body image": Validation of the Body Image Disturbance Questionnaire in a nonclinical population. Body Image. 2004;1(4):363-72.
244. March J. MSAC Multidimensional Anxiety Scale for Children. New York: Multi-Health Systems Inc.; 1997.
245. Rosenberg M. Society and the Adolescent Self Image. Princeton: Princeton University Press; 1965.
246. Hodgson RJ, Rachman S. Obsessional-compulsive complaints. Behav Res Ther. 1977;15(5):389-95.
247. McNair DM, Lorr M, Droppleman LF. Profile of Mood States Manual. San Diego, CA.: Educational and Industrial Testing Service; 1992.
248. Magin PJ, Pond CD, Smith WT, Goode SM. Acne's relationship with psychiatric and psychological morbidity: Results of a school-based cohort study of adolescents. J Eur Acad Dermatol Venereol. 2010;24(1):58-64.
249. Pagliarello C, Di Pietro C, Tabolli S. A comprehensive health impact assessment and determinants of quality of life, health and psychological status in acne patients. G Ital Dermatol Venereol. 2015;150(3):303-8.
250. Lewis-Jones MS, Finlay AY. The Children's Dermatology Life Quality Index (CDLQI): Initial validation and practical use. Br J Dermatol. 1995;132(6):942-9.
251. Reljic V, Maksimovic N, Jankovic J, Mijovic B, Peric J, Jankovic S. Evaluation of the quality of life in adolescents with acne. Vojnosanit Pregl. 2014;71(7):634-8.
304
252. Chren MM, Lasek RJ, Quinn LM, Mostow EN, Zyzanski SJ. Skindex, a quality-of-life measure for patients with skin disease: Reliability, validity, and responsiveness. J Invest Dermatol. 1996;107(5):707-13.
253. Dreno B. Assessing quality of life in patients with acne vulgaris: Implications for treatment. Am J Clin Dermatol. 2006;7(2):99-106.
254. Barnes LE, Levender MM, Fleischer AB, Jr., Feldman SR. Quality of life measures for acne patients. Dermatol Clin. 2012;30(2):293-300, ix.
255. Tan J, Fung KY, Khan S. Condensation and validation of a 4-item index of the Acne-QoL. Qual Life Res. 2006;15(7):1203-10.
256. Hudgens S, Harper JC, Daniels SR, Banderas B, Varon S, Alexis AF. Validation of a new patient-reported outcome measure for facial acne: The Acne Symptom and Impact Scale (ASIS). J Drugs Dermatol. 2015;14(6):552-9.
257. McLeod LD, Fehnel SE, Brandman J, Symonds T. Evaluating minimal clinically important differences for the acne-specific quality of life questionnaire. Pharmacoeconomics. 2003;21(15):1069-79.
258. Alexis AF, Burgess C, Callender VD, Herzog JL, Roberts WE, Schweiger ES, et al. The efficacy and safety of topical dapsone gel, 5% for the treatment of acne vulgaris in adult females with skin of color. J Drugs Dermatol. 2016;15(2):197-204.
259. Layton AM. Acne scarring-reviewing the need for early treatment of acne. J Dermatolog Treat. 2000;11(1):3-6.
260. Gupta A, Sharma YK, Dash KN, Chaudhari ND, Jethani S. Quality of life in acne vulgaris: Relationship to clinical severity and demographic data. Indian J Dermatol Venereol Leprol. 2016;82(3):292-7.
261. Fried RG, Wechsler A. Psychological problems in the acne patient. Dermatol Ther. 2006;19(4):237-40.
262. Warner GT, Plosker GL. Clindamycin/benzoyl peroxide gel: A review of its use in the management of acne. Am J Clin Dermatol. 2002;3(5):349-60.
263. Layton AM, Eady EA, Thiboutot DM, Tan J. Identifying what to measure in acne clinical trials: First steps towards development of a core outcome set. J Invest Dermatol. 2017;137(8):1784-6.
264. Yeung CK, Teo LH, Xiang LH, Chan HH. A community-based epidemiological study of acne vulgaris in Hong Kong adolescents. Acta Derm Venereol. 2002;82(2):104-7.
265. Corey KC, Cheng CE, Irwin B, Kimball AB. Self-reported help-seeking behaviors and treatment choices of adolescents regarding acne. Pediatr Dermatol. 2013;30(1):36-41.

305
266. Nasri H, Bahmani M, Shahinfard N, Moradi Nafchi A, Saberianpour S, Rafieian Kopaei M. Medicinal plants for the treatment of acne vulgaris: A review of recent evidences. Jundishapur J Microbiol. 2015;8(11):e25580.
267. Magin PJ, Adams J, Pond CD, Smith W. Topical and oral CAM in acne: A review of the empirical evidence and a consideration of its context. Complement Ther Med. 2006;14(1):62-76.
268. Patterson C, Arthur H. A complementary alternative medicine questionnaire for young adults. Integr Med Insights. 2009;4:1-11.
269. Xue C, Clifton L, Karagiannis J, Li C, Yang A, Zhang L, et al. Public attitudes towards Chinse medicine in Melbourne, Australia. J Complement Integr Med. 2005;2(18):1-11.
270. Kumar S, Rajiah K, Veettil SK, Wei NS. A cross-sectional study on knowledge and attitude toward Traditional Chinese Medicine (TCM) among adults in selected regions of Malaysia. J Complement Integr Med. 2015;12(4):317-23.
271. Mu W, Shang H. Understanding patient values and the manifestations in clinical research with traditional chinese medicine-with practical suggestions for trial design and implementation. Evid Based Complement Alternat Med. 2013;2013:847273.
272. Thorburn J, Cheng M, Bell L, Bell C. Patients’ attitudes towards traditional Chinese medicine and Western medicine in Mainland China and Hong Kong: A mixed methods study. Eur J Integr Med. 2013;5(6):578.
273. Bauml JM, Chokshi S, Schapira MM, Im EO, Li SQ, Langer CJ, et al. Do attitudes and beliefs regarding complementary and alternative medicine impact its use among patients with cancer? A cross-sectional survey. Cancer. 2015;121(14):2431-8.
274. Islahudin F, Shahdan IA, Mohamad-Samuri S. Association between belief and attitude toward preference of complementary alternative medicine use. Patient Prefer Adherence. 2017;11:913-8.
275. Pariera KL, Murphy ST, Meng J, McLaughlin ML. Exploring willingness to participate in clinical trials by ethnicity. J Racial Ethn Health Disparities. 2017;4(4):763-9.
276. Rucker G. A two-stage trial design for testing treatment, self-selection and treatment preference effects. Stat Med. 1989;8(4):477-85.
277. Morton KL, Atkin AJ, Corder K, Suhrcke M, Turner D, van Sluijs EM. Engaging stakeholders and target groups in prioritising a public health intervention: The Creating Active School Environments (CASE) online Delphi study. BMJ Open. 2017;7(1):e013340.
278. Treiman K, McCormack L, Olmsted M, Roach N, Reeve BB, Martens CE, et al. Engaging patient advocates and other stakeholders to design measures of patient-centered communication in cancer care. Patient. 2017;10(1):93-103.

306
279. Loh SY, Lee SY, Quek KF, Murray L. Barriers to participation in a randomized controlled trial of Qigong exercises amongst cancer survivors: Lessons learnt. Asian Pac J Cancer Prev. 2012;13(12):6337-42.
280. Griffin B, Citkovitz C. Survey: Preferences and limitations of herbal medicine use among patients at a community acupuncture clinic. Med Acupunct. 2017;29(1):25-9.
281. Sixty-Fourth World Health Assembly Resolutions and Decisions Annexes, (2011).
282. Definition of Youth, General Assembly Resolutions, A/RES/62/126, 2008 (2008).
283. Owen JE, Bantum EO, Criswell K, Bazzo J, Gorlick A, Stanton AL. Representativeness of two sampling procedures for an internet intervention targeting cancer-related distress: A comparison of convenience and registry samples. J Behav Med. 2014;37(4):630-41.
284. Australian Bureau of Statistics. Census 2016. In: Statistics ABo, editor. Australia: Australian Bureau of Statistics; 2016.
285. IBM Corporation. SPSS 23 ed. 2018.
286. Solon O. Teens are abandoning Facebook in dramatic numbers, study finds. The Guardian. 2018.
287. Tan JKL, Li Y, Fung K, Gupta AK, Thomas DR, Sapra S, et al. Divergence of demographic factors associated with clinical severity compared with quality of life impact in acne. J Cutan Med Surg. 2008;12(5):235-42.
288. Crawford NW, Cincotta DR, Lim A, Powell CV. A cross-sectional survey of complementary and alternative medicine use by children and adolescents attending the University Hospital of Wales. BMC Complement Altern Med. 2006;6:16.
289. Fong DP, Fong LK. Usage of complementary medicine among children. Aust Fam Physician. 2002;31(4):388-91.
290. Yussman SM, Ryan SA, Auinger P, Weitzman M. Visits to complementary and alternative medicine providers by children and adolescents in the United States. Ambul Pediatr. 2004;4(5):429-35.
291. Kristoffersen AE, Stub T, Musial F, Fonnebo V, Lillenes O, Norheim AJ. Prevalence and reasons for intentional use of complementary and alternative medicine as an adjunct to future visits to a medical doctor for chronic disease. BMC Complement Altern Med. 2018;18(1):109.
292. Sirois FM, Salamonsen A, Kristoffersen AE. Reasons for continuing use of complementary and alternative medicine (CAM) in students: A consumer commitment model. BMC Complement Altern Med. 2016;16:75.

307
293. von Conrady DM, Bonney A. Patterns of complementary and alternative medicine use and health literacy in general practice patients in urban and regional Australia. Aust Fam Physician. 2017;46(5):316-20.
294. Italia S, Bruske I, Heinrich J, Berdel D, von Berg A, Lehmann I, et al. Complementary and alternative medicine use among chronically ill adolescents from 2 German birth cohorts. Forsch Komplementmed. 2016;23(4):246-52.
295. Musaiger AO, Abahussain NA. Attitudes and practices of complementary and alternative medicine among adolescents in Saudi Arabia. Glob J Health Sci. 2014;7(1):173-9.
296. Mennella JA, Spector AC, Reed DR, Coldwell SE. The bad taste of medicines: Overview of basic research on bitter taste. Clin Ther. 2013;35(8):1225-46.
297. Cukor D, Cohen LM, Cope EL, Ghahramani N, Hedayati SS, Hynes DM, et al. Patient and other stakeholder engagement in Patient-Centered Outcomes Research Institute funded studies of patients with kidney diseases. Clin J Am Soc Nephrol. 2016;11(9):1703-12.
298. Hackshaw A. Small studies: strengths and limitations. Eur Respir J. 2008;32(5):1141-3.
299. Reinisch JF, Yu DC, Li WY. Getting a valid survey response from 662 plastic surgeons in the 21st century. Ann Plast Surg. 2016;76(1):3-5.
300. Murad MH, Montori VM, Ioannidis JP, Jaeschke R, Devereaux PJ, Prasad K, et al. How to read a systematic review and meta-analysis and apply the results to patient care: Users' guides to the medical literature. JAMA. 2014;312(2):171-9.
301. National Health and Medical Research Council. NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. Canberra: Australian Government.; 2009.
302. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]: The Cochrane Collaboration; 2011.
303. Zeng X, Zhang Y, Kwong JS, Zhang C, Li S, Sun F, et al. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J Evid Based Med. 2015;8(1):2-10.
304. Addo OY, Miller BS, Lee PA, Hediger ML, Himes JH. Age at hormonal onset of puberty based on luteinizing hormone, inhibin B, and body composition in preadolescent U.S. girls. Pediatr Res. 2014;76(6):564-70.
305. Russo G, Brambilla P, Della Beffa F, Ferrario M, Pitea M, Mastropietro T, et al. Early onset of puberty in young girls: An Italian cross-sectional study. J Endocrinol Invest. 2012;35(9):804-8.
306. Tomova A, Robeva R, Kumanov P. Influence of the body weight on the onset and progression of puberty in boys. J Pediatr Endocrinol Metab. 2015;28(7-8):859-65.

308
307. McDonald JL, Cripps AW, Smith PK. Mediators, receptors, and signalling pathways in the anti-inflammatory and antihyperalgesic effects of acupuncture. Evid Based Complement Alternat Med. 2015;2015:975632.
308. Song Q, Hu S, Wang H, Lv Y, Shi X, Sheng Z, et al. Electroacupuncturing at Zusanli point (ST36) attenuates pro-inflammatory cytokine release and organ dysfunction by activating cholinergic anti-inflammatory pathway in rat with endotoxin challenge. Afr J Tradit Complement Altern Med. 2014;11(2):469-74.
309. Xie Y, Gu K, Deng B, Dai Y. [Effects of acupuncture combined with benzoyl peroxide on sebum secretion rate]. J Hainan Med College. 2010;11:1470-2. [In Chinese: 谢芸, 辜孔进, 邓斌, 戴永江. 针刺联合过氧苯甲酰凝胶对皮脂分泌率的影响. 海南医学院学报].
310. Tan JK, Zhang X, Jones E, Bulger L. Correlation of photographic images from the Leeds revised acne grading system with a six-category global acne severity scale. J Eur Acad Dermatol Venereol. 2013;27(3):e414-9.
311. Zheng XY. [Guideline for New Chinese Herbal Medicine in Clinical Practice and Research]: Chinese Medical Science and Technology Publishing House. [In Chinese: 郑筱萸. 中药新药临床研究指导原则. 中国医药科技出版社]; 2002.
312. Wang W. 2010 CM Research Guidelines. Beijing: Scientific and Technical Documentation Press [In Chinese: 王蔚文. 临床疾病诊断与疗效判断标准. 科学技术文献出版社]; 2010.
313. PubMed [Internet]. US National Library of Medicine. 2013.
314. Cochrane Collaboration. Review Manager (RevMan) Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration; 2012.
315. Cochrane Training. Grading of Recommendations, Assessment, Development and Evaluation (GRADE). Cochrane Collaboration. 2018;58.
316. MacPherson H, Altman DG, Hammerschlag R, Youping L, Taixiang W, White A, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. J Altern Complement Med. 2010;16(10):ST1-ST14.
317. Mansu SSY, Coyle M, Wang K, May B, Zhang AL, Xue CCL. Herbal medicine Eriobotrya japonica formula for acne vulgaris: A systematic review. J Herb Med. 2018;11:12-23.
318. Neamsuvan O, Kama A, Salaemae A, Leesen S, Waedueramae N. A survey of herbal formulas for skin diseases from Thailand’s three southern border provinces. J Herb Med. 2015;5(4):190-8.
319. Nam C, Kim S, Sim Y, Chang I. Anti-acne effects of oriental herb extracts: A novel screening method to select anti-acne agents. Skin Pharmacol Appl Skin Physiol. 2003;16(2):84-90.
309
320. Yang Y, Yang X, Xu B, Zeng G, Tan J, He X, et al. Chemical constituents of Morus alba L. and their inhibitory effect on 3T3-L1 preadipocyte proliferation and differentiation. Fitoterapia. 2014;98:222-7.
321. Chen LJ, Zhou JG. [Clinical observation of Chinese Medicine Fomula Pi Pa Jing Fei Yin for Acne Vulgaris Patients]. Asia-Pacific Traditional Medicine. 2011;7(4):48-9. [In Chinese: 陈良金, 周继刚. 枇杷清肺饮加减治疗寻常性痤疮 53 例疗效观察. 亚太传统中医学].
322. Han SX. [Pi Pa Qing Fei Yin Combines with Chinese Medicine Mask to Treat Acne Vulgaris in 90 Patients]. 2006:266. [In Chinese: 韩守信. 摘 枇杷清肺饮配合中药面膜治疗寻常
痤疮 90 例. 河北省崇礼县妇幼保健院].
323. Liang XS, Wang WP. [Modified Pi Pa Qing Fei Yin for 32 Acne Vulgaris Patients]. Journal of New Chinese Medicine. 2009;41(11):87. [In Chinese: 梁希森,王文平. 枇杷清肺饮加味治
疗寻常痤疮 32 例. 新中医].
324. Liu H. [Clinical Observation of Modified Pi Pa Qing Fei Yin for Acne Vulgaris Patients]. Journal of Modern Medicial Doctors. 1997;2(5):55. [In Chinese: 刘红. 加味枇杷清肺饮治疗荨
常型痤疮的临床观察.当代层师杂志].
325. Liu HS, Zhang WJ, Zhuang M, Wu R, Gen J. [Clinical Observation on treatment of Acne with Modified Pipa Qingfei Yin and Supplemented Diandan San]. Anhui Medical and Pharmaceurtical Journal. 2012;16(1):108-9. [In Chinese: 刘汉顺,张文家,庄明,吴蓉,耿娟
. 枇杷清肺饮加减联合加味颠倒散治疗痤疮的临床观察. 安徽医药].
326. Liu Y. [Modified Pi Pa Qing Fei Yin Combines with Wu Wei Xiao Du Yin for 58 Acne Vulgaris Patients]. Journal of Practical Traditional Chinese Medicine. 2010;26(5):305-6. [In Chinese: 刘娅. 枇杷清肺饮合五味消毒饮加减治疗痤疮 58 例观察. 实用中医药杂志].
327. Ma TL. [Modified Pi Pa Qing Fei Yin for 32 Acne Vulgaris Patients]. Menggu Chinese Medicine Journal. 2013;2013(8):12-3. [In Chinese: 马天龙. 枇杷清肺饮加减治疗粉刺 84 例疗
效显著. 内蒙古中医药].
328. Ou HB, Tao XY. [Modified Pi Pa Qing Fei Yin Conbined with Topical treatment of Dian Dao San for 80 Acne Vulgaris Patients]. Journal of Liaoning Chinese Medicine. 2012;39(7):1313-14. [In Chinese: 区鸿斌,陶衔玥. 枇杷清肺饮加减合颠倒散外用治疗寻常型痤疮 80 例. 辽宁
中医杂志].
329. Shi XB, Zhou RE, Zhao YD. [Effects of Loquat Qingfei Decoction Treatment and Prevention Relapse of Acne Vulgaris]. Chin J Dem Venereal. 2008;22(6):375-6. [In Chinese: 石学波, 周仁恩, 赵一栋. 枇杷清肺饮(变化)对寻常痤疮复发的治疗和预防. 中国皮肤性病学杂
志].
330. Wang S, Wu BL, Zhu JT. [The Influence of Pi Pa Qing Fei Yin on Androgen Level in Female Acne Vulgaris Patients]. Journal of Shandong Universityof Chinese Medicine.

310
2013;37(3):230-1. [In Chinese: 王帅,吴蓓玲,朱金土. 枇杷清肺饮对女性寻常性痤疮患者血
清雄激素水平的影响. 山东中医药大学学报.].
331. Wang X, Chen JH, Yao JH, Lin QF. [Influence of Modified Pipa Qingfei Decoction Combined with Bloodletting in Ear on Curative effect and Quality of Life of Patients with Acne]. China Modern Medicine. 2014;21(19):93-4. [In Chinese: 王欣 , 陈建宏, 姚建华, 林青梅. 枇杷清
肺饮加减联合耳尖放血对痤疮患者疗效及生活质量的影响. 中国当代医药].
332. Yan LY, Li JZ. [Clinical Observation on Bai Di She Lotion Combined with Chuo Zhuang Ling for Acne Vulgaris]. Journal of Chinese Medicne for External Treatments. 2005;14(1):17. [In Chinese: 闫凌云,李敬哲. 白地蛇洗剂合痤疮灵治疗痤疮的临床观察. 中医外治杂志].
333. Zhang LL. [Clinical Observation on Modified Pi Pa Qing Fei Yin for Acne Vulgaris Patients with Chinese Medicine Syndrome of Damp-heat in Lung and Stomach]. Journal of Practical Integrated Traditional and Western Medicine. 2006;6(3):31. [In Chinese: 张玲玲. 枇杷
清肺饮加减治疗肺胃湿热型痤疮的药物疗效观察. 实用中西医结合临床].
334. Zhang Y, Huang Y. [Effect Observation of Lonquat Qingfeiyin with Modification for Treating 135 Cases of Acne Vulgaris]. Modern Medicine. 2011;27(3):334-5. [In Chinese: 张 源, 黄 艳. 枇杷清肺饮加减治疗寻常型痤疮 135 例疗效观察. 现代医药卫生].
335. Shi XB, Zhou RE, Zhao YD. [Clinical Observation of Modified Pi Pa Qing Fei Yin for Moderate and Servere Acne Vulgaris]. Jilin Chinese Medicine Journal. 2005;25(8):24-5. [In Chinese: 石学波, 周仁恩, 赵一栋. 枇杷清肺饮(变化)对中、重度寻常性痤疮的临床观察. 吉林中医药].
336. Wu Y. [The clinical research on treating acne of Spleen deficiency combined with Phlegm and Damp with abdominal acupuncture]. The 12th Academic Conference of Acupuncture Association of Guangdong Province; 213-217. [In Chinese: 吴燕珊. 腹针配合灸法治疗脾虚痰
湿型座疮的临床研究. 广东省针灸学会第十二次学术研讨会论文汇编]2011.
337. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-6.
338. Kurokawa I, Danby FW, Ju Q, Wang X, Xiang LF, Xia L, et al. New developments in our understanding of acne pathogenesis and treatment. Exp Dermatol. 2009;18(10):821-32.
339. Higaki S, Nakamura M, Morohashi M, Hasegawa Y, Yamagishi T. Activity of eleven Kampo formulations and eight Kampo crude drugs against Propionibacterium acnes isolated from acne patients: Retrospective evaluation in 1990 and 1995. J Dermatol. 1996;23(12):871-5.
340. Lee JH, Shim JS, Chung MS, Lim ST, Kim KH. Inhibition of pathogen adhesion to host cells by polysaccharides from Panax ginseng. Biosci Biotechnol Biochem. 2009;73(1):209-12.

311
341. Kim EH, Shim B, Kang S, Jeong G, Lee JS, Yu YB, et al. Anti-inflammatory effects of Scutellaria baicalensis extract via suppression of immune modulators and MAP kinase signaling molecules. J Ethnopharmacol. 2009;126(2):320-31.
342. Chang CT, Huang SS, Lin SS, Amagaya S, Ho HY, Hou WC, et al. Anti-inflammatory activities of tormentic acid from suspension cells of Eriobotrya Japonica ex vivo and in vivo. Food Chem. 2011;127(3):1131-7.
343. Gao Y, Yang MF, Su YP, Jiang HM, You XJ, Yang YJ, et al. Ginsenoside Re reduces insulin resistance through activation of PPAR-gamma pathway and inhibition of TNF-alpha production. J Ethnopharmacol. 2013;147(2):509-16.
344. Wang L, Yang X, Yu X, Yao Y, Ren G. Evaluation of antibacterial and anti-inflammatory activities of less polar ginsenosides produced from polar ginsenosides by heat-transformation. J Agric Food Chem. 2013;61(50):12274-82.
345. Rebhun JF, Glynn KM, Missler SR. Identification of glabridin as a bioactive compound in licorice (Glycyrrhiza glabra L.) extract that activates human peroxisome proliferator-activated receptor gamma (PPARgamma). Fitoterapia. 2015;106:55-61.
346. Feng AW, Gao W, Zhou GR, Yu R, Li N, Huang XL, et al. Berberine ameliorates COX-2 expression in rat small intestinal mucosa partially through PPARgamma pathway during acute endotoxemia. Int Immunopharmacol. 2012;12(1):182-8.
347. Fu Y, Zhou E, Wei Z, Song X, Liu Z, Wang T, et al. Glycyrrhizin inhibits lipopolysaccharide-induced inflammatory response by reducing TLR4 recruitment into lipid rafts in RAW264.7 cells. Biochim Biophys Acta. 2014;1840(6):1755-64.
348. Wang CY, Kao TC, Lo WH, Yen GC. Glycyrrhizic acid and 18beta-glycyrrhetinic acid modulate lipopolysaccharide-induced inflammatory response by suppression of NF-kappaB through PI3K p110delta and p110gamma inhibitions. J Agric Food Chem. 2011;59(14):7726-33.
349. Kim JY, Park SJ, Yun KJ, Cho YW, Park HJ, Lee KT. Isoliquiritigenin isolated from the roots of Glycyrrhiza uralensis inhibits LPS-induced iNOS and COX-2 expression via the attenuation of NF-kappaB in RAW 264.7 macrophages. Eur J Pharmacol. 2008;584(1):175-84.
350. Li C, Eom T, Jeong Y. Glycyrrhiza glabra L. Extract Inhibits LPS-Induced Inflammation in RAW Macrophages. J Nutr Sci Vitaminol. 2015;61(5):375-81.
351. Allijn IE, Vaessen SF, Quarles van Ufford LC, Beukelman KJ, de Winther MP, Storm G, et al. Head-to-head comparison of anti-inflammatory performance of known natural products in vitro. PLoS One. 2016;11(5):e0155325.
352. Enk R, Ehehalt R, Graham JE, Bierhaus A, Remppis A, Greten HJ. Differential effect of Rhizoma coptidis and its main alkaloid compound berberine on TNF-alpha induced NFkappaB translocation in human keratinocytes. J Ethnopharmacol. 2007;109(1):170-5.
312
353. Choi YY, Kim MH, Han JM, Hong J, Lee TH, Kim SH, et al. The anti-inflammatory potential of Cortex Phellodendron in vivo and in vitro: Down-regulation of NO and iNOS through suppression of NF-kappaB and MAPK activation. Int Immunopharmacol. 2014;19(2):214-20.
354. Jeong HW, Hsu KC, Lee JW, Ham M, Huh JY, Shin HJ, et al. Berberine suppresses proinflammatory responses through AMPK activation in macrophages. Am J Physiol Endocrinol Metab. 2009;296(4):E955-64.
355. Park EK, Rhee HI, Jung HS, Ju SM, Lee YA, Lee SH, et al. Antiinflammatory effects of a combined herbal preparation (RAH13) of Phellodendron amurense and Coptis chinensis in animal models of inflammation. Phytother Res. 2007;21(8):746-50.
356. Choi EM, Hwang JK. Effects of Morus alba leaf extract on the production of nitric oxide, prostaglandin E2 and cytokines in RAW264.7 macrophages. Fitoterapia. 2005;76(7-8):608-13.
357. Eo HJ, Park JH, Park GH, Lee MH, Lee JR, Koo JS, et al. Anti-inflammatory and anti-cancer activity of mulberry (Morus alba L.) root bark. BMC Complement Altern Med. 2014;14:200.
358. Armanini D, Mattarello MJ, Fiore C, Bonanni G, Scaroni C, Sartorato P, et al. Licorice reduces serum testosterone in healthy women. Steroids. 2004;69(11-12):763-6.
359. Moon MH, Jeong JK, Lee YJ, Seol JW, Ahn DC, Kim IS, et al. 18beta-Glycyrrhetinic acid inhibits adipogenic differentiation and stimulates lipolysis. Biochem Biophys Res Commun. 2012;420(4):805-10.
360. Sharma BR, Oh J, Kim HA, Kim YJ, Jeong KS, Rhyu DY. Anti-obesity effects of the mixture of Eriobotrya japonica and Nelumbo nucifera in adipocytes and high-fat diet-induced obese mice. Am J Chin Med. 2015;43(4):681-94.
361. Gumy C, Thurnbichler C, Aubry EM, Balazs Z, Pfisterer P, Baumgartner L, et al. Inhibition of 11beta-hydroxysteroid dehydrogenase type 1 by plant extracts used as traditional antidiabetic medicines. Fitoterapia. 2009;80(3):200-5.
362. Barratt H, Hamilton F, Car J, Lyons C, Layton A, Majeed A. Outcome measures in acne vulgaris: Systematic review. Br J Dermatol. 2009;160(1):132-6.
363. Dermatological Society Acne Treatment Guidelines Working Group CMDA. [Treatment Guidelines for Acne Vulgaris in China (Draft)]. J Clin Dermatol. 2008;37(5):339-42. [In Chinese: 中国医师协会皮肤科医师分会《中国痤疮治疗指南》专家组. 中国痤疮治疗指南( 讨论稿). 临床皮肤科杂志].
364. Kalaiselvan V, Saurabh A, Kumar R, Singh GN. Adverse reactions to herbal products: An analysis of spontaneous reports in the database of the Pharmacovigilance Programme of India. J Herb Med. 2015;5(1):48-54.

313
365. Ellis CN, Millikan LE, Smith EB, Chalker DM, Swinyer LJ, Katz IH, et al. Comparison of adapalene 0.1% solution and tretinoin 0.025% gel in the topical treatment of acne vulgaris. Br J Dermatol. 1998;139 Suppl 52:41-7.
366. Lee CH, Wu SL, Chen JC, Li CC, Lo HY, Cheng WY, et al. Eriobotrya japonica leaf and its triterpenes inhibited lipopolysaccharide-induced cytokines and inducible enzyme production via the nuclear factor-kappaB signaling pathway in lung epithelial cells. Am J Chin Med. 2008;36(6):1185-98.
367. Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c869.
368. Mansu SSY, Liang H, Parker S, Coyle ME, Wang K, Zhang AL, et al. Acupuncture for acne vulgaris: A systematic review and meta-analysis. Evid Based Complement Alternat Med. 2018;2018:4806734.
369. Bensky D, Clavey S, Stöger E. Chinese Herbal Medicine: Materia medica. 3rd ed. Clavey Sct, Stöger Ect, editors. Seattle, WA, USA: Eastland Press; 2015.
370. Chung WY, Zhang HQ, Zhang SP. Peripheral muscarinic receptors mediate the anti-inflammatory effects of auricular acupuncture. Chin Med. 2011;6(1):3.
371. Fang JQ, Fang JF, Liang Y, Du JY. Electroacupuncture mediates extracellular signal-regulated kinase 1/2 pathways in the spinal cord of rats with inflammatory pain. BMC Complement Altern Med. 2014;14:285.
372. Liu F, Fang J, Shao X, Liang Y, Wu Y, Jin Y. Electroacupuncture exerts an anti-inflammatory effect in a rat tissue chamber model of inflammation via suppression of NF-kappaB activation. Acupunct Med. 2014;32(4):340-5.
373. Du JY, Fang JQ, Liang Y, Fang JF. Electroacupuncture attenuates mechanical allodynia by suppressing the spinal JNK1/2 pathway in a rat model of inflammatory pain. Brain Res Bull. 2014;108:27-36.
374. Wang Z, Chen T, Long M, Chen L, Wang L, Yin N, et al. Electro-acupuncture at acupoint ST36 ameliorates inflammation and regulates Th1/Th2 balance in delayed-type hypersensitivity. Inflammation. 2016.
375. Han B. [A clinical study on abdominal acupuncture for acne by conditioning Liver and Kidney]. [In Chinese: 韩奔 腹钟调理肝肾法治疗瘟疮的 , 广州中医药大学]: Guangzhou University of Chinese Medicine 广州中医药大学; 2010.
376. He X. [24 cases of treating facial acne with abdominal and facial acupuncture]. Inner Mongol Journal of Traditional Chinese Medicine. 2009;28(15):33. [In Chinese: 贺旭艳, 腹针针
刺结合面部浅刺治疗颜面座疮 24 例临床观察, 内蒙古中医药杂志].
314
377. Kim KS, Kim YB. Anti-inflammatory effect of Keigai-rengyo-to extract and acupuncture in male patients with acne vulgaris: A randomized controlled pilot trial. J Altern Complement Med. 2012;18(5):501-8.
378. Liu L. [Clinical observation on treatment of acne vulgaris with auricular point taping and pressing]. Chinese Acupuncture and Moxibustion. 2011;21(10):601. [In Chinese: 刘炼. 耳穴贴压
治疗寻常性痤疮的临床观察. 中国 针灸].
379. Liu S, Shi B. [Effect of acupuncture therapy on immune function in patients with acne]. Chinese Journal of Acupuncture and Moxibustion. 2015;4(2):1-3. [In Chinese: 刘淑梅, 师彬. 针刺治疗痤疮疗效及对免疫功能的影响. 中华针灸电子杂志].
380. Mo X, Jin J. [42 cases of treating acne vulgaris with Cu zhen shen zhu tou ling tai method]. Journal of Traditional Chinese Medical Sciences. 2005;13(5):14. [In Chinese: 莫晓枫, 金君梅. 粗针身柱透灵台治疗寻常性痤疮 42 例临床观察. 中国中医药科技].
381. You M, Liu G. [Therapeutic Observation of Bu Xu Tong Luo Needling Method for Facial Acne]. Shanghai J Acu Mox. 2014;33(9):836-7. [In Chinese: 游妙玲, 刘刚. 补虚通络针刺法治
疗面部痤疮疗效观察. 上海针灸杂志].
382. Deadman P. A Manual of Acupuncture. v.1.2. ed. Deadman P, editor. East Sussex: Journal of Chinese Medicine; 2009.
383. Birch S, Alraek T, Norheim AJ. Acupuncture adverse events in China: A glimpse of historical and contextual aspects. J Altern Complement Med. 2013;19(10):845-50.
384. He W, Zhao X, Li Y, Xi Q, Guo Y. Adverse events following acupuncture: A systematic review of the Chinese literature for the years 1956-2010. J Altern Complement Med. 2012;18(10):892-901.
385. Blasiak RC, Stamey CR, Burkhart CN, Lugo-Somolinos A, Morrell DS. High-dose isotretinoin treatment and the rate of retrial, relapse, and adverse effects in patients with acne vulgaris. JAMA Dermatol. 2013;149(12):1392-8.
386. Lomholt HB, Kilian M. Clonality and anatomic distribution on the skin of antibiotic resistant and sensitive Propionibacterium acnes. Acta Derm Venereol. 2014;94(5):534-8.
387. Hao XA, Xue CC, Dong L, Zheng Z. Factors associated with conflicting findings on acupuncture for tension-type headache: Qualitative and quantitative analyses. J Altern Complement Med. 2013;19(4):285-97.
388. Harris RE, Tian X, Williams DA, Tian TX, Cupps TR, Petzke F, et al. Treatment of fibromyalgia with formula acupuncture: Investigation of needle placement, needle stimulation, and treatment frequency. J Altern Complement Med. 2005;11(4):663-71.
389. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332.

315
390. Liu L, Skinner M, McDonough SM, Kannan P, Baxter GD. STRICTA: Is it time to do more? BMC Complement Altern Med. 2015;15:190.
391. Loyeung BY, Cobbin DM. Investigating the effects of three needling parameters (manipulation, retention time, and insertion site) on needling sensation and pain profiles: A study of eight deep needling interventions. Evid Based Complement Alternat Med. 2013;2013:136763.
392. Castro M. Placebo versus best-available-therapy control group in clinical trials for pharmacologic therapies: Which is better? Proc Am Thorac Soc. 2007;4(7):570-3.
393. Meissner K, Fassler M, Rucker G, Kleijnen J, Hrobjartsson A, Schneider A, et al. Differential effectiveness of placebo treatments: A systematic review of migraine prophylaxis. JAMA Intern Med. 2013;173(21):1941-51.
394. Redberg RF. All placebos are not created equally. JAMA Intern Med. 2013;173(21):1951.
395. Aawar N, Moore R, Riley S, Salek S. Interpretation of Renal Quality of Life Profile scores in routine clinical practice: An aid to treatment decision-making. Qual Life Res. 2016;25(7):1697.
396. Cheng CW, Wu TX, Shang HC, Li YP, Altman DG, Moher D, et al. CONSORT extension for Chinese herbal medicine formulas 2017: Recommendations, explanation, and elaboration. Ann Intern Med. 2017;167(2):112-21.
397. Skene L. Citizen child: Australian law and children's rights Australia: Australian Government; 1996 [cited 2018. Description of children's right and age of consent for medical treatment].
398. Hunter D, Pierscionek BK. Children, Gillick competency and consent for involvement in research. J Med Ethics. 2007;33(11):659-62.
399. Vos T, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-59.
400. Huang CD, Liao KC, Chung FT, Tseng HM, Fang JT, Lii SC, et al. Different perceptions of narrative medicine between Western and Chinese medicine students. BMC Med Educ. 2017;17(1):85.
401. Fung FY, Linn YC. Developing traditional chinese medicine in the era of evidence-based medicine: current evidences and challenges. Evid Based Complement Alternat Med. 2015;2015:425037.
402. Kim K, Kim KI, Lee J. Inhibitory effects of Cheongsangbangpoong-tang on both inflammatory acne lesions and facial heat in patients with acne vulgaris: A randomized controlled trial protocol. BMC Complement Altern Med. 2016;16:21.

316
403. Huang Y. Advanced Textbook on Traditional Chinese Medicine and Pharmacology. Beijing: New World Press. State Administration of Traditional Chinese Medicine; 1995.
404. Zick SM, Blume A, Normolle D, Ruffin M. Challenges in herbal research: A randomized clinical trial to assess blinding with ginger. Complement Ther Med. 2005;13(2):101-6.
405. Pan L, Belloni P, Ding HT, Wang J, Rubino CM, Putnam WS. A pharmacokinetic bioequivalence study comparing pirfenidone tablet and capsule dosage forms in healthy adult volunteers. Adv Ther. 2017;34(9):2071-82.
406. Millum J, Grady C. The ethics of placebo-controlled trials: Methodological justifications. Contemp Clin Trials. 2013;36(2):510-4.
407. Moller HJ. Effectiveness studies: Advantages and disadvantages. Dialogues Clin Neurosci. 2011;13(2):199-207.
408. Patsopoulos NA. A pragmatic view on pragmatic trials. Dialogues Clin Neurosci. 2011;13(2):217-24.
409. Buch MH, Pavitt S, Parmar M, Emery P. Creative trial design in RA: Optimizing patient outcomes. Nat Rev Rheumatol. 2013;9(3):183-94.
410. Mullins CD, Vandigo J, Zheng Z, Wicks P. Patient-centeredness in the design of clinical trials. Value Health. 2014;17(4):471-5.
411. Qi GD, We DA, Chung LP, Fai CK. Placebos used in clinical trials for Chinese herbal medicine. Recent Pat Inflamm Allergy Drug Discov. 2008;2(2):123-7.
412. National Health and Medical Research Council. National Statement on Ethical Conduct in Human Research 2007 (Updated 2018) found in www.nhmrc.gov.au/guidelines/publications/e72. In: Australian Research Council and Universities Australia CoA, editor. Canberra: National Health and Medical Research Council; 2018.
413. Pochi PE, Shalita AR, Strauss JS, Webster SB, Cunliffe WJ, Katz HI, et al. Report of the Consensus Conference on Acne Classification. Washington, D.C., March 24 and 25, 1990. J Am Acad Dermatol. 1991;24(3):495-500.
414. Contassot E, French LE. New insights into acne pathogenesis: Propionibacterium acnes activates the inflammasome. J Invest Dermatol. 2014;134(2):310-3.
415. Omer H, McDowell A, Alexeyev OA. Understanding the role of Propionibacterium acnes in acne vulgaris: The critical importance of skin sampling methodologies. Clin Dermatol. 2017;35(2):118-29.
416. Cunliffe WJ, Holland KT, Bojar R, Levy SF. A randomized, double-blind comparison of a clindamycin phosphate/benzoyl peroxide gel formulation and a matching clindamycin gel with respect to microbiologic activity and clinical efficacy in the topical treatment of acne vulgaris. Clin Ther. 2002;24(7):1117-33.
317
417. Therapeutic Goods Administration. Pharmacovigilance responsibilities of medicine sponsors. In: Department of Health, editor. Australia: Australian Government; 2018.
418. Wright KB. Researching internet-based populations: Advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. J Comput Mediat Commun. 2005;10(3):JCMC1034-JCMC.
419. Popplewell M, Reizes J, Zaslawski C. Consensus in traditional Chinese medical diagnosis in open populations. J Altern Complement Med. 2018.
420. Birkeflet O, Laake P, Vollestad N. Low inter-rater reliability in traditional Chinese medicine for female infertility. Acupunct Med. 2011;29(1):51-7.
421. Grant SJ, Schnyer RN, Chang DH, Fahey P, Bensoussan A. Interrater reliability of chinese medicine diagnosis in people with prediabetes. Evid Based Complement Alternat Med. 2013;2013:710892.
422. Mist S, Ritenbaugh C, Aickin M. Effects of questionnaire-based diagnosis and training on inter-rater reliability among practitioners of traditional Chinese medicine. J Altern Complement Med. 2009;15(7):703-9.
423. O'Brien KA, Abbas E, Zhang J, Guo ZX, Luo R, Bensoussan A, et al. An investigation into the reliability of Chinese medicine diagnosis according to eight guiding principles and zang-fu theory in Australians with hypercholesterolemia. J Altern Complement Med. 2009;15(3):259-66.
424. Chung VCH, Ho RST, Wu X, Wu JCY. Incorporating traditional Chinese medicine syndrome differentiation in randomized trials: Methodological issues. Eur J Integr Med. 2016;8(6):898-904.
425. Moradi Tuchayi S, Alexander TM, Nadkarni A, Feldman SR. Interventions to increase adherence to acne treatment. Patient Prefer Adherence. 2016;10:2091-6.
426. Blodt S, Schutzler L, Huang W, Pach D, Brinkhaus B, Hummelsberger J, et al. Effectiveness of additional self-care acupressure for women with menstrual pain compared to usual care alone: Using stakeholder engagement to design a pragmatic randomized trial and study protocol. Trials. 2013;14:99.
427. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials. 2004;25(2):143-56.
428. Liu C, Guo DA, Liu L. Quality transitivity and traceability system of herbal medicine products based on quality markers. Phytomedicine. 2018;44:247-57.
429. International Conference on Harmonisation. ICH Harmonised Guideline Integrated Addendum to ICH E6(R1): Guideline for Good Clinical Practice E6(R2). In: TGA, editor. Australia: Australian Government; 2016.

318
430. Therapeutic Goods Administration. Australian Clinical Trial Handbook: Guidance on Conducting Clinical Trials in Australia Using 'Unapproved' Therapeutic Goods. In: TGA, editor. 2.2 ed. Australia: Australian Government; 2018.
431. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-91.
432. Miyachi Y, Hayashi N, Furukawa F, Akamatsu H, Matsunaga K, Watanabe S, et al. Acne management in Japan: Study of patient adherence. Dermatology. 2011;223(2):174-81.
433. Gooberman-Hill R, Burston A, Clark E, Johnson E, Nolan S, Wells V, et al. Involving patients in research: Considering good practice. Musculoskeletal Care. 2013;11(4):187-90.
434. Feldman S, Vrijens B, Gieler U, Piaserico S, Puig L, van de Kerkhof P. Treatment Adherence Intervention Studies in Dermatology and Guidance on How to Support Adherence. Am J Clin Dermatol. 2017;18(2):253-71.
435. Lloyd J, McHugh C, Minton J, Eke H, Wyatt K. The impact of active stakeholder involvement on recruitment, retention and engagement of schools, children and their families in the cluster randomised controlled trial of the Healthy Lifestyles Programme (HeLP): A school-based intervention to prevent obesity. Trials. 2017;18(1):378.
436. International Conference on Harmonisation. ICH Topic E 8 General Considerations for Clinical Trial (CPMP/ICH/291/95). 1997.
437. International Conference on Harmonisation. E 9 ICH, Statistical Principles for Clinical Trial (CPMP/ICH/363/96); . 1998.
438. Tsai PJ, Huang WC, Hsieh MC, Sung PJ, Kuo YH, Wu WH. Flavones isolated from Scutellariae radix suppress Propionibacterium acnes-induced cytokine production in vitro and in vivo. Molecules. 2015;21(1):E15.
439. Huang GD, Bull J, Johnston McKee K, Mahon E, Harper B, Roberts JN. Clinical trials recruitment planning: A proposed framework from the Clinical Trials Transformation Initiative. Contemp Clin Trials. 2018;66:74-9.
440. Bae S, Yoon Y. Anti-adipogenic activity of berberine is not mediated by the WNT/beta-catenin pathway. Phytother Res. 2013;27(6):937-43.
441. Core Outcome Measures in Effectiveness Trials (COMET). 2018 [Available from: http://www.comet-initiative.org/, accessed 28 Nov 2018.

319
APPENDICES
Appendix 1 Oral Chinese herbal medicines formulas and herb ingredients
Oral formulas Ingredients (Pinyin, Chinese characters and species name)
Chai Hu Shu Gan Wan modified (柴胡疏肝丸) plus ingredients from Xiao Cuo Tang (Fan et al., 2008)
Chai hu 柴胡 (Bupleurum chinense DC.) Yu jin 郁金 (Curcuma wenyujin Y.H.Chen et C.Ling) Bai shao 白芍 (Paeoniae lactiflora Pall.) Nu zhen zi 女真子 (Ligustrum lucidum Ait.) Han lian cao 旱莲草 (Eclipta prostrata L.) Yu xing cao 鱼腥草 (Houttuynia cordata Thunb.) Pu gong ying 蒲公英 (Taraxacum mongolicum Hand Dan shen 丹参 (Salvia miltiorrhiza Bge.) Shan zha 山楂 (Crataegus pinnatifida Bge. var. major N.E. Br.) Gan cao 甘草 (Glycyrrhiza uranlensis Fischer)
Chu Shi Jie Du Tang (升阳解毒
汤) (Shen et al., 1995)
Bai xian pi 白鲜皮 (Dictamnus dasycarpus Turcz.) Dou juan 豆卷 (Glycines mas (L.) Merr) Yi yi ren 薏苡仁 (Coix lachryma jobi L.) Tu fu ling 土茯苓 (Smilax glabra Roxb.) Shan zhi zi 山栀子(Gardenia jaminoides Ellis) Mu dan pi 牡丹皮 (Paeonia suffruticosa Andr.) Jin yin hua 金银花 (Lonicera japonica Thunb.) Lian qiao 连翘 (Forsythia suspense (Thunb.) Vahl) Zi hua di ding 紫花地丁 (Viola yedoensis Mak.) Mu tong 木通 (Akebia trifoliata (Thunb) Koidz. Var. australis (Diels) Rehd.)* Hua shi 滑石 (Hydrated magnesium silicate) Gan cao 甘草 (Glycyrrhiza uralensis Fischer)
Cuo Chuang Jian Ji Tang (Chinese characters not identified) (Shen et al., 1995)
Jin yin hua 金银花 (Lonicera japonica Thunb.) Lian qiao 连翘 (Forsythia suspense (Thunb.) Vahl) Huang qin 黄芩 (Scutellaria baicalensis Georgi) Chuan xiong 川芎 (Ligusticum chuanxiong Hort.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Jie geng 桔梗 (Platycodon grandiflorum (Jacq.) A. DC.) Niu xi 牛膝 (Achyranthes bidentata Bl.) Ye ju hua 野菊花 (Chrysanthemum indicum L.)
Modified Dan Zhi Xiao Yao San (丹栀逍遥散加减) (State Administration of TCM, 1994)
Mu dan pi 牡丹皮 (Paeonia suffruticosa Andr.) Zhi zi 栀子 (Gardenia jasminoides Ellis) Chai hu 柴胡 (Bupleurum chinense DC.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Bai shao 白芍 (Paeoniae lactiflora Pall.) Bai zhu 白术 (Atractylodes macrocephala Koidz.) Fu ling 茯苓 (Poria cocos (Schw.) Wolf) Zhi gan cao 炙甘草 (honey fried Glycyrrhiza uralensis Fischer)
Modified Er Xian Tang (二仙汤) plus Zhi Bai Di Huang Wan (知柏地黄丸)
(Xiang, 2015)
Er Xian Tang: Xian mao 仙茅 (Curculigo orchioides Gaertn.) Yin yang huo 淫羊藿 (Epimedium grandiflorum Morr., E. sagittatum (Sieb. et Zucc.) Maxim or E. brevicornum Maxim) Ba ji tian 巴戟天 (Morinda officinalis How)

320
Oral formulas Ingredients (Pinyin, Chinese characters and species name)
Huang bai 黄柏 (Phellodendron amurense Rupr.) Zhi mu 知母 (Anemarrhena asphodeloides Bge.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Zhi Bai Di Huang Wan: Zhi mu 知母 (Anemarrhena asphodeloides Bge.) Sheng di huang 生地黃 (Rehmannia glutinosa (Gaertn.) Libosch.) Shan zhu yu 山茱萸 (Cornus officinalis Sieb. et Zucc.) Shan yao 山药 (Dioscorea opposite Thunb.) Fu ling 茯苓 (Poria cocos (Schw.) Wolf) Mu dan pi 牡丹皮 (Paeonia suffruticosa Andr.) Ze xie 泽泻 (Alisma orientalis (Sam) Juzep.)
Hai Zao Yu Hu Tang (海藻玉壶
汤) (Xu, 2004) Hai zao 海藻 (Sargassum pallidum (Turn.) C. Ag.) Kun bu 昆布 (Laminaria japonica Aresch.) Zhe bei mu 浙贝母 (Fritillaria thunbergia Miq.) Zhi ban xia 制半夏 (Pinellia ternate (Thunb.) Breit.) Chen pi 陈皮 (Citrus reticulata Blanco, C. tangerine Hort. Et Tanaka or C. erythrosa Tanaka) Lian qiao 连翘 (Forsythia suspense (Thunb.) Vahl) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Chuan xiong 川芎 (Ligusticum chuanxiong Hort.) Du huo 独活 (Angelica pubescens Maxim) Gan cao 甘草 (Glycyrrhiza uralensis Fischer) Xia ku cao 夏枯草 (Prunella vulgaris L.) Long gu 龙骨 (Fossilised bone - various species) Mu li 牡蛎 (Ostrea gigas Thunb.) Qing pi 青皮 (Citrus reticulata Blanco) Ju he 聚合 (Citrus reticulata Blanco)
Modified Hai Zao Yu Hu Tang (海藻玉壶汤) plus Tao Hong Si Wu Tang (桃红四物汤) (China Association of CM 2012; Xiang, 2015)
Hai Zao Yu Hu Tang: Hai zao 海藻 (Sargassum pallidum (Turn.) C. Ag.) Kun bu 昆布 (Laminaria japonica Aresch.) Hai dai 海带 (Laminaria japonica J.E. Areschoug) Zhe bei mu 浙贝母 (Fritillaria thunbergia Miq.) Zhi ban xia 制半夏 (Pinellia ternate (Thunb.) Breit.) Du huo 独活 (Angelica pubescens Maxim) Chuan xiong 川芎 (Ligusticum chuanxiong Hort.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Qing pi 青皮(Citrus reticulata Blanco, C. tangerine Hort. Et Tanaka or C. erythrosa Tanaka) Chen pi 陈皮(Citrus reticulata Blanco, C. tangerine Hort. Et Tanaka or C. erythrosa Tanaka) Lian qiao 连翘 (Forsythia suspense (Thunb.) Vahl) Gan cao 甘草 (Glycyrrhiza uralensis Fischer) Tao Hong Si Wu Tang: Tao ren 桃仁 (Prunus persica (L.) Batsch.) Hong hua 红花 (Carthamus tinctorius L.) Shu di huang 熟地黄 (Rehmannia glutinosa (Gaertn.) Libosch.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Bai shao 白芍 (Paeoniae lactiflora Pall.)
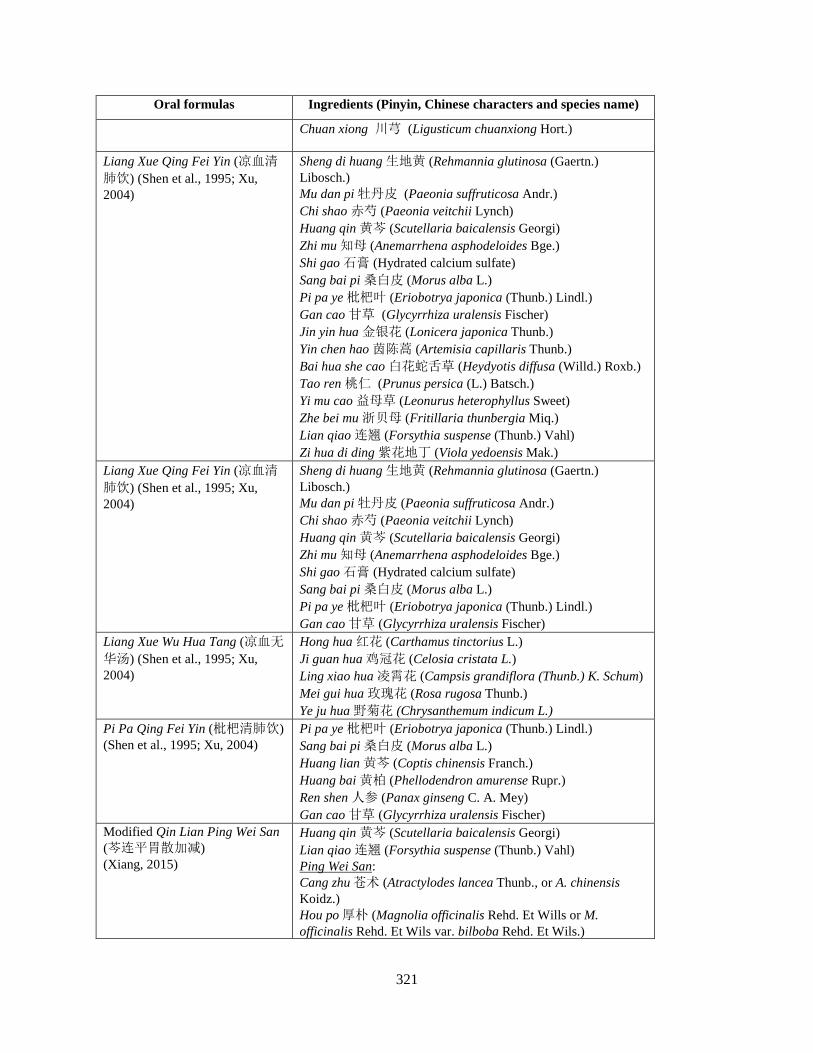
321
Oral formulas Ingredients (Pinyin, Chinese characters and species name)
Chuan xiong 川芎 (Ligusticum chuanxiong Hort.)
Liang Xue Qing Fei Yin (凉血清
肺饮) (Shen et al., 1995; Xu, 2004)
Sheng di huang 生地黄 (Rehmannia glutinosa (Gaertn.) Libosch.) Mu dan pi 牡丹皮 (Paeonia suffruticosa Andr.) Chi shao 赤芍 (Paeonia veitchii Lynch) Huang qin 黄芩 (Scutellaria baicalensis Georgi) Zhi mu 知母 (Anemarrhena asphodeloides Bge.) Shi gao 石膏 (Hydrated calcium sulfate) Sang bai pi 桑白皮 (Morus alba L.) Pi pa ye 枇杷叶 (Eriobotrya japonica (Thunb.) Lindl.) Gan cao 甘草 (Glycyrrhiza uralensis Fischer) Jin yin hua 金银花 (Lonicera japonica Thunb.) Yin chen hao 茵陈蒿 (Artemisia capillaris Thunb.) Bai hua she cao 白花蛇舌草 (Heydyotis diffusa (Willd.) Roxb.) Tao ren 桃仁 (Prunus persica (L.) Batsch.) Yi mu cao 益母草 (Leonurus heterophyllus Sweet) Zhe bei mu 浙贝母 (Fritillaria thunbergia Miq.) Lian qiao 连翘 (Forsythia suspense (Thunb.) Vahl) Zi hua di ding 紫花地丁 (Viola yedoensis Mak.)
Liang Xue Qing Fei Yin (凉血清
肺饮) (Shen et al., 1995; Xu, 2004)
Sheng di huang 生地黄 (Rehmannia glutinosa (Gaertn.) Libosch.) Mu dan pi 牡丹皮 (Paeonia suffruticosa Andr.) Chi shao 赤芍 (Paeonia veitchii Lynch) Huang qin 黄芩 (Scutellaria baicalensis Georgi) Zhi mu 知母 (Anemarrhena asphodeloides Bge.) Shi gao 石膏 (Hydrated calcium sulfate) Sang bai pi 桑白皮 (Morus alba L.) Pi pa ye 枇杷叶 (Eriobotrya japonica (Thunb.) Lindl.) Gan cao 甘草 (Glycyrrhiza uralensis Fischer)
Liang Xue Wu Hua Tang (凉血无
华汤) (Shen et al., 1995; Xu, 2004)
Hong hua 红花 (Carthamus tinctorius L.) Ji guan hua 鸡冠花 (Celosia cristata L.) Ling xiao hua 凌霄花 (Campsis grandiflora (Thunb.) K. Schum) Mei gui hua 玫瑰花 (Rosa rugosa Thunb.) Ye ju hua 野菊花 (Chrysanthemum indicum L.)
Pi Pa Qing Fei Yin (枇杷清肺饮) (Shen et al., 1995; Xu, 2004)
Pi pa ye 枇杷叶 (Eriobotrya japonica (Thunb.) Lindl.) Sang bai pi 桑白皮 (Morus alba L.) Huang lian 黄芩 (Coptis chinensis Franch.) Huang bai 黄柏 (Phellodendron amurense Rupr.) Ren shen 人参 (Panax ginseng C. A. Mey) Gan cao 甘草 (Glycyrrhiza uralensis Fischer)
Modified Qin Lian Ping Wei San (芩连平胃散加减)
(Xiang, 2015)
Huang qin 黄芩 (Scutellaria baicalensis Georgi) Lian qiao 连翘 (Forsythia suspense (Thunb.) Vahl) Ping Wei San: Cang zhu 苍术 (Atractylodes lancea Thunb., or A. chinensis Koidz.) Hou po 厚朴 (Magnolia officinalis Rehd. Et Wills or M. officinalis Rehd. Et Wils var. bilboba Rehd. Et Wils.)

322
Oral formulas Ingredients (Pinyin, Chinese characters and species name)
Chen pi 陈皮 (Citrus reticulata Blanco, C. tangerine Hort. Et Tanaka or C. erythrosa Tanaka) Zhi gan cao 炙甘草 (honey fried Glycyrrhiza uralensis Fischer)
Tao Hong Si Wu Tang (桃红四物
汤) (Fan et al., 2008; Shen et al., 1995; Xu, 2004)
Tao ren 桃仁 (Prunus persica (L.) Batsch.) Hong hua 红花 (Carthamus tinctorius L.) Shu di huang 熟地黄 (Rehmannia glutinosa (Gaertn.) Libosch.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Bai shao 白芍 (Paeoniae lactiflora Pall.) Chuan xiong 川芎 (Ligusticum chuanxiong Hort.)
Modified Tao Hong Si Wu Tang (桃红四物汤) plus Er Chen Tang (二陈汤) (Xiang, 2015)
Tao Hong Si Wu Tang: Tao ren 桃仁 (Prunus persica (L.) Batsch.) Hong hua 红花 (Carthamus tinctorius L.) Shu di huang 熟地黄 (Rehmannia glutinosa (Gaertn.) Libosch.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Bai shao 白芍 (Paeoniae lactiflora Pall.) Chuan xiong 川芎 (Ligusticum chuanxiong Hort.) Er Chen Tang: Zhi ban xia 制半夏 (Pinellia ternate (Thunb.) Breit.) Chen pi 陈皮(Citrus reticulata Blanco, C. tangerine Hort. Et Tanaka or C. erythrosa Tanaka) Fu ling 茯苓 (Poria cocos (Schw.) Wolf) Zhi gan cao 炙甘草 (honey fried Glycyrrhiza uralensis Fischer)
Tiao Wei Cheng Qi Tang (调胃承
气汤) (Shen et al., 1995; Xu, 2004)
Da huang 大黄 (Rheum palmatum L.) Gan cao 甘草 (Glycyrrhiza uralensis Fischer) Mang xiao (Hydrated sodium sulfate)
Modified Wu Wei Xiao Du Yin (五味消毒饮) plus Tao Hong Si Wu Tang (桃红四物汤) (State Administration of TCM,1994)
Wu Wei Xiao Du Yin: Jin yin hua 金银花 (Lonicera japonica Thunb.) Pu gong ying 蒲公英 (Taraxacum mongolicum Hand. -Mazz.) Zi hua di ding 紫花地丁 (Viola yedoensis Mak.) Ye ju hua 野菊花 (Chrysanthemum indicum L.) Zi bei tian kui 紫背天葵 (Begonia fimbristipulata Hance or Semiaquilegia adoxoides (DC.) Mak.) Tao Hong Si Wu Tang: Tao ren 桃仁 (Prunus persica (L.) Batsch.) Hong hua 红花 (Carthamus tinctorius L.) Shu di huang 熟地黄 (Rehmannia glutinosa (Gaertn.) Libosch.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Bai shao 白芍 (Paeoniae lactiflora Pall.) Chuan xiong 川芎 (Ligusticum chuanxiong Hort.)
Modified Xian Fang Huo Ming Yin (仙方活命饮)
(State Administration of TCM, 1994)
Jin yin hua 金银花 (Lonicera japonica Thunb.) Gan cao 甘草 (Glycyrrhiza uralensis Fischer) Zhe bei mu 浙贝母 (Fritillaria thunbergia Miq.) Tian hua fen 天花粉 (Trichosanthes kirilowii Maxim.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Chi shao 赤芍 (Paeonia veitchii Lynch) Ru xiang乳香 (Boswellia carterii Birdw.) Mo yao 没药 (Commiphora myrrha Engl.) Fang feng 防风 (Ledebouriella divaricata (Turcz.), L. seselides (Hoffm.) or Saposhnikovia divaricata (Turcz.) Schischk
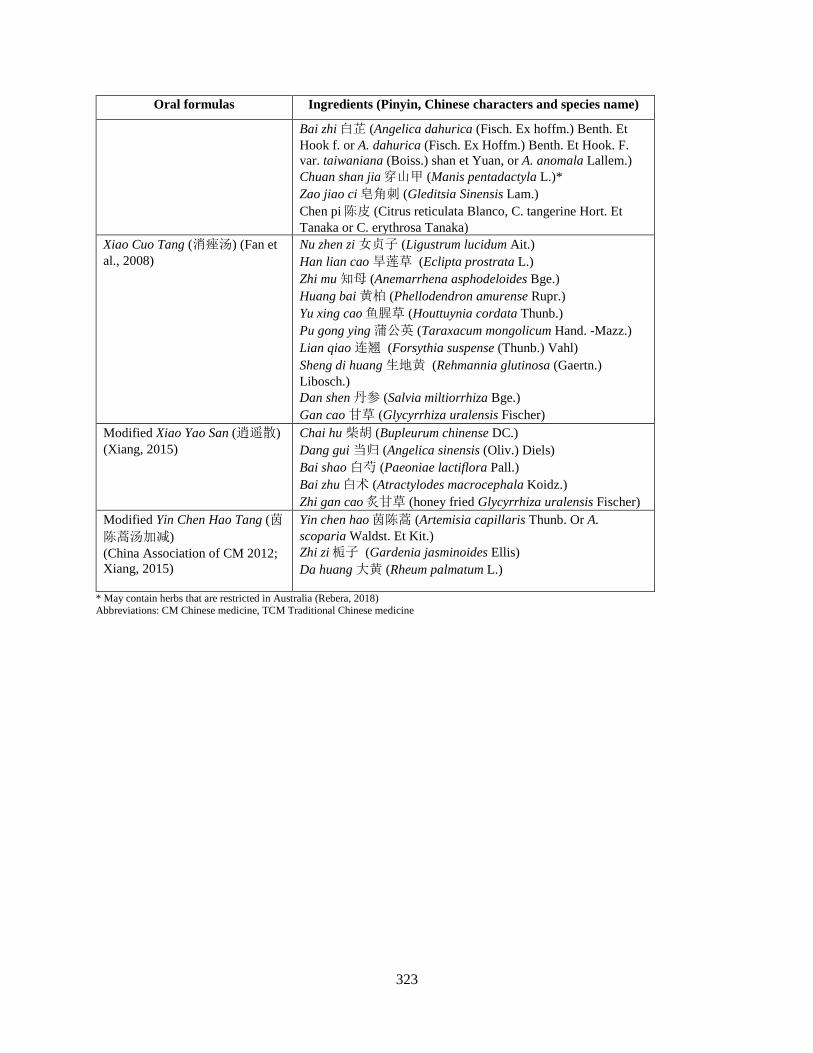
323
Oral formulas Ingredients (Pinyin, Chinese characters and species name)
Bai zhi 白芷 (Angelica dahurica (Fisch. Ex hoffm.) Benth. Et Hook f. or A. dahurica (Fisch. Ex Hoffm.) Benth. Et Hook. F. var. taiwaniana (Boiss.) shan et Yuan, or A. anomala Lallem.) Chuan shan jia 穿山甲 (Manis pentadactyla L.)* Zao jiao ci 皂角刺 (Gleditsia Sinensis Lam.) Chen pi 陈皮 (Citrus reticulata Blanco, C. tangerine Hort. Et Tanaka or C. erythrosa Tanaka)
Xiao Cuo Tang (消痤汤) (Fan et al., 2008)
Nu zhen zi 女贞子 (Ligustrum lucidum Ait.) Han lian cao 旱莲草 (Eclipta prostrata L.) Zhi mu 知母 (Anemarrhena asphodeloides Bge.) Huang bai 黄柏 (Phellodendron amurense Rupr.) Yu xing cao 鱼腥草 (Houttuynia cordata Thunb.) Pu gong ying 蒲公英 (Taraxacum mongolicum Hand. -Mazz.) Lian qiao 连翘 (Forsythia suspense (Thunb.) Vahl) Sheng di huang 生地黄 (Rehmannia glutinosa (Gaertn.) Libosch.) Dan shen 丹参 (Salvia miltiorrhiza Bge.) Gan cao 甘草 (Glycyrrhiza uralensis Fischer)
Modified Xiao Yao San (逍遥散)
(Xiang, 2015)
Chai hu 柴胡 (Bupleurum chinense DC.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Bai shao 白芍 (Paeoniae lactiflora Pall.) Bai zhu 白术 (Atractylodes macrocephala Koidz.) Zhi gan cao 炙甘草 (honey fried Glycyrrhiza uralensis Fischer)
Modified Yin Chen Hao Tang (茵陈蒿汤加减)
(China Association of CM 2012; Xiang, 2015)
Yin chen hao 茵陈蒿 (Artemisia capillaris Thunb. Or A. scoparia Waldst. Et Kit.) Zhi zi 栀子 (Gardenia jasminoides Ellis) Da huang 大黄 (Rheum palmatum L.)
* May contain herbs that are restricted in Australia (Rebera, 2018) Abbreviations: CM Chinese medicine, TCM Traditional Chinese medicine

324
Appendix 2 Topical Chinese herbal medicines formulas and herb ingredients
Topical formulas Ingredients (Pinyin, Chinese characters and species name)
Cuo Chuang Xi Ji (痤疮洗剂) (Xu, 2004)
Liu huang 硫黄 (Sulfur)* Zhang nao 樟脑 (Cinnamomum camphora (L.) Presl)* Xi huang qi jiao 西黄芪胶 (Bummi Tragacanthi) Lime water 柠檬水
Dian Dao San (颠倒散) (Shen et al., 1995)
Da huang 大黄 (Rheum palmatum L.) Liu huang 硫黄 (Sulphur)
Du Jiao Lian Gao (Chinese characters not identified) (Xu, 2004)
Bai fu zi 白附子 (Typhonium giganteum Engl.) Bai zhi 白芷 (Angelica dahurica (Fisch. ex Hoffm.) Benth. Et Hook f.) Zao jiao ci 皂角刺 (Gleditsia sinensis Lam.) Fang ji 防己 (Aristolochia fangchi Wu. or Stephania tetrandra S. Moore.)* Lian qiao 连翘 (Forsythia suspensa (Thunb.) Vahl) Chuan shan jia 穿山甲 (Manis pentadactyla L.)§ Jin yin hua 金银花 (Lonicera japonica Thunb.) Dang gui 当归 (Angelica sinensis (Oliv.) Diels) Hai tong pi 海桐皮 (Erythrina variegate L. var. orientalis (L.) Merr.) Sheng nan xing 生南星 (Arisaema consanguineum Schott) Su mu 苏木 (Caesalpinia sappan L.) Ci wei pi 刺猬皮 (Pellis Erinacei) Hai dai (Kun bu) 昆布 (Laminaria japonica Aresch.) Huo ma ren 火麻仁 (Cannabis sativa L.)* Xue yu tan 血余炭 (Homo sapiens L.) (charred human hair) Xi xian cao 豨莶草 (Siegesbeckia pubescens Makino) Gan chan 干蟾 (Bufo siccus) Ru xiang 乳香 (Boswellia carterii Birdw.) Mo yao 没药 (Commiphora myrrha Engl.) Xiang you 香油 (Sesamum indicum DC.)
Hei Bu Yao Gao (黑布药膏) (Xu, 2004)
Lao hei cu 老黑醋 (Acetum atrum vetum) Wu bei zi 五倍子 (Rhus chinensis Mill.) Wu gong 蜈蚣 (Scolopendra subspinipes mutilans L. Koch.)* Bing pian 冰片 (Dryobalanops aromatica Gaertn.) Feng mi 蜂蜜 (Mel)
Qu Ban Gao (去斑膏) (Shen et al., 1995)
Da feng zi 大风子 (Hydnocarpus anthelmintica Pierre ex Laness) Xing ren 杏仁 (Prunus armeniaca L. var. ansu Maxim.)* Tao ren 桃仁 (Prunus persica (L.) Batsch.) Hong fen 红粉 (Mecuric oxide) Zhang nao 樟脑 (Cinnamomum camphora (L.) Presl)*
San Huang Xi Ji (三黄洗剂) (Xu, 2004)
Ku shen 苦参 (Sophora flavescens Ait.) Da huang 大黄 (Rheum palmatum L.), Huang qin 黄芩 (Scutellaria baicalensis Georgi) Huang bai 黄柏 (Phellodendron amurense Rupr.)
Si Huang Gao (四黄膏) (Xu, 2004)
Huang qin 黄芩 (Scutellaria baicalensis Georgi) Huang lian 黄连 (Coptis chinensis Franch.) Huang bai 黄柏 (Phellodendron amurense Rupr.)
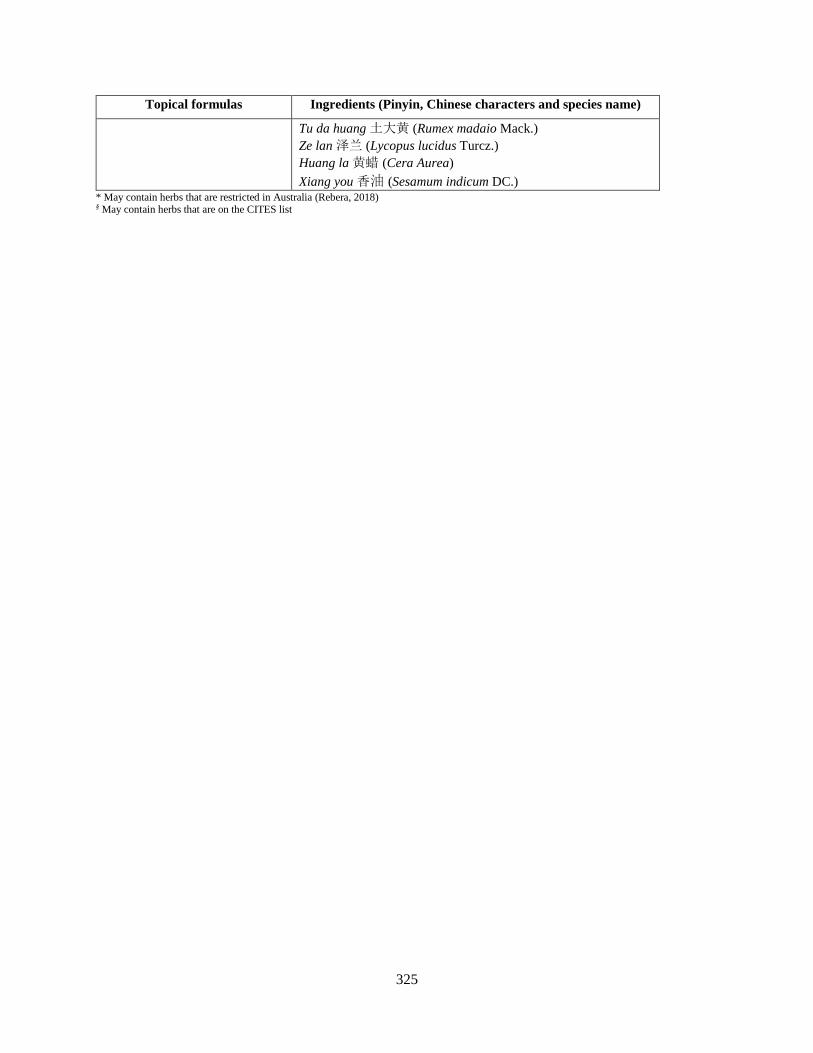
325
Topical formulas Ingredients (Pinyin, Chinese characters and species name)
Tu da huang 土大黄 (Rumex madaio Mack.) Ze lan 泽兰 (Lycopus lucidus Turcz.) Huang la 黄蜡 (Cera Aurea) Xiang you 香油 (Sesamum indicum DC.)
* May contain herbs that are restricted in Australia (Rebera, 2018) § May contain herbs that are on the CITES list

326
Appendix 3 Impact on HRQoL and instruments used
Author, year Sample size (n) Instrument used Findings Akyazi et al., 2011 61 DLQI DLQI was worse in people with acne compared to health
controls. Also worse in severe acne group compared to mild acne group
Bahali et al., 2016 103 PVS, CDI, STAIc, RSES, PedsQL-C
No differences found between study and control groups for peer victimisation, depression, state and trait anxiety, self-esteem or QoL
Bez et al., 2013 146 MOCQ, SF-36, HADS Study group OCD symptoms checking, slowness, rumination greater than control. Study group physical function, physical role, general health perception, vitality, emotional role worse than control
Bowe et al., 2011 52 BIDQ, Skindex-16, MBSRQ-AS, CES-D, FNE
A higher percentage of participants with severe acne were more affected emotionally and experienced greater social/occupational impact than those with mild acne; more than half had body image concerns
Chernyshov et al., 2018 150 DLQI, CADI
People with acne who sought treatment for their condition reported moderate HRQoL impairment compared to people with acne who didn’t consult with a dermatologist
Duman et al., 2016 125 AQOL, FDLQI, HADS Turkish versions
There was no difference between acne group and healthy controls for anxiety and depression (HADS). When HRQoL decreased, risk of anxiety and depression increased. Family members HRQoL was negatively affected
Durai & Nair 2015 140 DLQI, CADI
Age, occupation, marital status, family and treatment history was a factor for HRQoL. Greater acne severity correlated with greater impact on HRQoL
El-Khateeb et al., 2014 2,068 Self-designed questionnaire plus DLQI & CADI
Worse acne severity and scarring resulted in worse HRQoL
Gorelick et al., 2015 312 Acne-QoL, PHQ Acne affected self-perception and social and emotional functioning. There were ethnic differences with Hispanic and Asians more impacted than Caucasian and darker skinned participants
Gupta et al., 2016 100 CADI Hindi version
Males HRQoL was more severely affected than females, particularly males who drank alcohol more than twice per week and who smoked
Halvorsen et al., 2011 3,775 SDQ, HSCL-90 modified Suicidal ideation increased with increasing severity; substantial acne more likely to report mental health problems
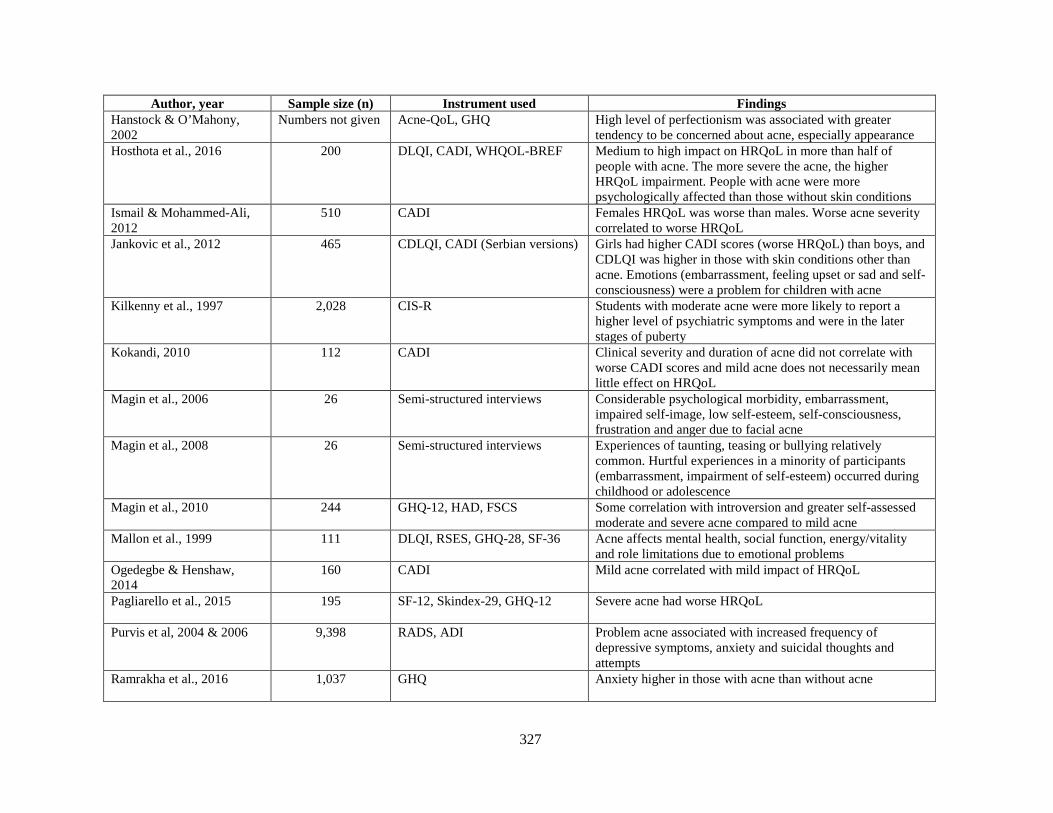
327
Author, year Sample size (n) Instrument used Findings Hanstock & O’Mahony, 2002
Numbers not given
Acne-QoL, GHQ
High level of perfectionism was associated with greater tendency to be concerned about acne, especially appearance
Hosthota et al., 2016 200 DLQI, CADI, WHQOL-BREF Medium to high impact on HRQoL in more than half of people with acne. The more severe the acne, the higher HRQoL impairment. People with acne were more psychologically affected than those without skin conditions
Ismail & Mohammed-Ali, 2012
510 CADI
Females HRQoL was worse than males. Worse acne severity correlated to worse HRQoL
Jankovic et al., 2012 465 CDLQI, CADI (Serbian versions) Girls had higher CADI scores (worse HRQoL) than boys, and CDLQI was higher in those with skin conditions other than acne. Emotions (embarrassment, feeling upset or sad and self-consciousness) were a problem for children with acne
Kilkenny et al., 1997 2,028 CIS-R
Students with moderate acne were more likely to report a higher level of psychiatric symptoms and were in the later stages of puberty
Kokandi, 2010 112 CADI Clinical severity and duration of acne did not correlate with worse CADI scores and mild acne does not necessarily mean little effect on HRQoL
Magin et al., 2006 26 Semi-structured interviews
Considerable psychological morbidity, embarrassment, impaired self-image, low self-esteem, self-consciousness, frustration and anger due to facial acne
Magin et al., 2008 26 Semi-structured interviews
Experiences of taunting, teasing or bullying relatively common. Hurtful experiences in a minority of participants (embarrassment, impairment of self-esteem) occurred during childhood or adolescence
Magin et al., 2010 244 GHQ-12, HAD, FSCS
Some correlation with introversion and greater self-assessed moderate and severe acne compared to mild acne
Mallon et al., 1999 111 DLQI, RSES, GHQ-28, SF-36
Acne affects mental health, social function, energy/vitality and role limitations due to emotional problems
Ogedegbe & Henshaw, 2014
160 CADI
Mild acne correlated with mild impact of HRQoL
Pagliarello et al., 2015 195 SF-12, Skindex-29, GHQ-12
Severe acne had worse HRQoL
Purvis et al, 2004 & 2006 9,398 RADS, ADI Problem acne associated with increased frequency of depressive symptoms, anxiety and suicidal thoughts and attempts
Ramrakha et al., 2016 1,037 GHQ
Anxiety higher in those with acne than without acne

328
Author, year Sample size (n) Instrument used Findings Rapp et al., 2004 479 Mood States
People with acne had anger associated with poorer HRQoL and dissatisfaction with treatment
Reljic et al., 2014 199
CDLQI Impact on HRQOL was mild in the majority of adolescents however there were some severely affected
Salman et al., 2016 148
LSAS, HAD, DLQI
Social anxiety, anxiety and depression were worse in people with acne and vitiligo than healthy controls
Tanghetti et al., 2014 208 Acne-QoL, PHQ-4 Facial acne negatively impacted HRQoL in people with mild and moderate acne with symptoms of anxiety/depression affecting school and work
Tasoula et al., 2012 1,531 CDLQI
People with moderate/severe acne had greater psychosocial and emotional impairment than people with mild acne
Unal et al., 2016 102 CSPSCA, AQOL, RSES Turkish versions
No differences were seen in social anxiety levels and self-esteem between adolescents with acne compared to healthy controls
Vilar et al., 2015 317
CDLQI, DLQI, RSES More severe acne correlated with worse HRQoL. There was no difference with self-esteem (RSES) between those with and without acne
Zaraa et al., 2013 82
CADI French version
Half of participants had a high impact on HRQoL particularly if onset was early and there were presence of pustules
Zauli et al., 2014 100 APSEA
Acne severity was a factor in worse HRQoL before intervention however post intervention, acne reduction of APSEA score did not correlate to reduction of acne severity indicating factors other than acne severity contributed to impact of HRQoL
Abbreviations: Acne-QoL Acne Specific Quality of Life, ADI Acne Disability Index, APSEA, AQOL Acne Quality of Life Scale, BIDQ Body Image Disturbance Questionnaire, CADI Cardiff Acne Disability Index, CDI Child Depression Inventory, CDLQI Children’s Dermatology Life Quality Index, CES-D Centre for Epidemiologic Studies Depression Scale, CIS-R Clinical Interview Schedule, CSPSCA Capa Social Phobia Scale for Children and Adolescents, DLQI Dermatology Life Quality Index, FDLQI Family Dermatology Life Quality Index, FNE Fear of Negative Evaluation Scale, FSCS Fenigstein Self-Consciousness Scale, GHQ General Health Questionnaire, HAD Hospital Anxiety Depression Scale, HSCL Hopkins Symptom Checklist, LSAS Liebowitz Social Anxiety Scale, MBSRQ-AS Multidimensional Body Self-Relations Questionnaire-Appearance Scales, MOCQ Maudsley Obsessive Compulsive Questionnaire, N number, OCD Obsessive compulsive disorder, PedsQL-C Pediatric Quality of Life Inventory Child Versions, PHQ-4 Patient Health Questionnaire, PVS Peer Victimization Scale, QoL quality of life, RADS, RSES Rosenberg Self-Esteem Scale, SF Short Form, SDQ Strengths and Difficulties Questionnaire, STAIc State-Trait Anxiety Inventories for Children, WHOQOL-BREF World Health Organization Quality of Life–BREF

329
Appendix 4 Survey questionnaire
Acne Quality of Life
Survey Flow
Section 1: Participation information (2 Questions) Section 2: Acne Quality of Life (20 Questions) Section 3: CAM Use (9 Questions) Section 3: CAM Beliefs (14 Questions) Section 4: CM Treatment Preferences (6 Questions) Section 5: Demographics (11 Questions) Standard: Pilot Questions (2 Questions)
Start of Block: Participation information
Preamble Statement on Participation You are invited to participate in a research project surveying adolescents, young people and adults on how people feel about their acne, which medications they have used and the impact acne has on their daily life. It will also ask questions on your treatment preferences for Chinese medicine. It should take you 15–20 minutes to complete. Please read this statement carefully and be confident that you understand its contents before deciding whether to participate.
This research is being conducted by Suzi Mansu PhD Candidate and supervised by Associate Professor Anthony Zhang, Dr Meaghan Coyle and Professor Charlie Xue from RMIT University, School of Health and Biomedical Sciences. This project has been approved by RMIT’s Science, Engineering and Health College Human Ethics Advisory Network (CHEAN); The project is jointly supported by the China-Australia International Research Centre for Chinese Medicine (CAIRCCM) – a joint initiative of RMIT University, Australia and the Guangdong Provincial Academy of Chinese Medical Sciences.
Results are intended for publication in a journal article and then dissemination through a conference. It will also be in a chapter as part of the PhD thesis. We don’t anticipate any risks or benefits associated with participating in this study. Some of the questions included in the survey may be embarrassing or make you feel uncomfortable. You have the right to decline to answer particular questions, or to withdraw from the study prior to the completion of the survey by closing down your browser. Once you have completed the survey you will not be able to withdraw, as your responses will not be able to be identified. The information you provide will be confidential, and will only be available to members of the research team.
If there are any questions that make you uncomfortable or raises concerns for you, please contact one of the Investigators, Dr Meaghan Coyle, of this study on 03 9925 7678 or email [email protected]. Dr Coyle will discuss your concerns with you confidentially, and may suggest further follow up if necessary. You may also contact the RMIT Ethics Committee to discuss your concerns if you prefer to have them handled by someone outside the research team. Human Research Ethics Coordinator, Research
330
Integrity, Governance and Systems, RMIT University, GPO Box 2476V VIC 3001. Tel: (03) 9925 2251 or email [email protected].
Consent To be eligible to do the survey, you must be 15 years and older and live in Australia. If you are under 15 years old, or do not live in Australia you are not eligible to participate in this survey. Please close your screen to withdraw from the survey. Thank you for your interest. Because of the nature of data collection, we are not obtaining written informed consent from you. Instead, we ask you to read this statement and click the “agree to participate” or “not agree to participate” check box. We also assume that you have given consent by your completion of the online questionnaire.
o I AGREE to participate (1)
o I DO NOT agree to participate (2)
Skip To: End of Survey If To be eligible to do the survey, you must be 15 years and older and live in Australia. If you are... = I DO NOT agree to participate
Skip To: End of Block If To be eligible to do the survey, you must be 15 years and older and live in Australia. If you are... = I AGREE to participate
End of Block: Participation information
Start of Block: Acne Quality of Life
(C) notice Questions 1-19 are from the Acne-specific Quality of Life Questionnaire (Acne-QoL) Copyright© MERCK & CO., INC., Whitehouse Station, NJ, USA. All Rights Reserved.

331
Q1 In the past WEEK, how unattractive did you feel because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q2 In the past WEEK, how embarrassed did you feel because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q3 In the past WEEK, how self-conscious (uneasy about oneself) did you feel about your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
332
Q4 In the past WEEK, how upset were you about having facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q5 In the past WEEK, how annoyed did you feel at having to spend time every day cleaning and treating your face because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q6 In the past WEEK, how dissatisfied with your self-appearance did you feel because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
333
Q7 In the past WEEK, how concerned or worried were you about not looking your best because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q8 In the past WEEK, how concerned or worried were you that your acne medication/products were working fast enough in clearing up the acne on your face?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q9 In the past WEEK, how bothered did you feel about the need to always have medication or cover-up available for the acne on your face?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o

334
Q10 In the past WEEK, how much was your self-confidence (sure of yourself) negatively affected because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q11 In the past WEEK, how concerned or worried were you about meeting new people because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q12 In the past WEEK, how concerned or worried were you about going out in public because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
335
Q13 In the past WEEK, how much was socializing with people a problem for you because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q14 In the past WEEK, how much was interacting with the opposite sex (or same sex if gay or lesbian) a problem for you because of your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
Q15 In the past WEEK, how many bumps did you have on your face?
extensive (1)
a whole lot (2) a lot (3) a moderate
amount (4) some (5) very few (6) none (7)
Please choose one
(1) o o o o o o o
336
Q16 In the past WEEK, how many bumps full of pus did you have on your face?
extensive (1)
a whole lot (2) a lot (3) a moderate
amount (4) some (5) very few (6) none (7)
Please choose one
(1) o o o o o o o
Q17 In the past WEEK, how much scabbing from your facial acne did you have?
extensive (1)
a whole lot (2) a lot (3) a moderate
amount (4) some (5) very few (6) none (7)
Please choose one
(1) o o o o o o o
Q18 In the past WEEK, how concerned or worried were you about scarring from your facial acne?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o

337
Q19 In the past WEEK, how oily was your facial skin?
extremely (1)
very much (2)
quite a bit (3)
a good bit (4)
somewhat (5)
a little bit (6)
not at all (7)
Please choose one
(1) o o o o o o o
End of Block: Acne Quality of Life
Start of Block: CAM Use
Q20 Have you used complementary/alternative medicine (CAM) for: (check all that apply)
▢ preventing illness (1)
▢ treating illness (2)
▢ promoting health (3)
▢ I have never used CAM (4)
▢ Other (5)
Skip To: End of Block If = I have never used CAM
Skip To: Q20 Other If = Other
Q20 Other If you have chosen “other” please specify:
________________________________________________________________

338
339
Q21 Identify the statement that best describes your healthcare practices:
o I use CAM only (1)
o I use CAM with treatments given to me by my medical doctor (2)
Q22 Which natural health products and therapies do you use or have you used in the past? (check all that apply)
▢ Acupuncture (1)
▢ Acupressure (2)
▢ Aromatherapy (3)
▢ Art therapy (4)
▢ Ayurveda (5)
▢ Bach flower remedies (6)
▢ Chiropractic (7)
▢ Colour therapy (8)
▢ Dance movement therapy (9)
▢ Spiritual healing (10)

340
▢ Herbal medicine (11)
▢ Homeopathy (12)
▢ Hypnosis (13)
▢ Magnetic therapy (14)
▢ Massage (15)
▢ Meditation (16)
▢ Transcendental meditation (17)
▢ Music therapy (18)
▢ Naturopathy (19)
▢ Osteopathy (20)
▢ Reiki (21)
▢ Reflexology (22)
▢ Relaxation/breathing technique (23)
341
▢ Shiatsu (24)
▢ Traditional Chinese medicine (25)
▢ Therapeutic touch (26)
▢ Visualisation (27)
▢ Vitamins and minerals (28)
▢ Yoga (29)
▢ Other (30)
Skip To: Q22 other If Which natural health products and therapies do you use or have you used in the past? (Check all t... = Other
Q22 Other If you have chosen “other” please specify:
________________________________________________________________
342
Q23 Identify the statement that best describes your intake of natural health products. A natural health product includes vitamins and minerals. (check only one box)
o I do not take natural health products (1)
o I take natural health products on a daily basis (2)
o I take natural health products on a weekly basis (3)
o I take natural health products on a monthly basis (4)
o I take natural health products once a year (5)
o I take natural health products less often than once a year (6)
o Other (7)
Skip To: Q23 Other If Identify the statement that best describes your intake of natural health products. A natural heal... = Other
Q23 Other If you have chosen “other” please specify:
________________________________________________________________
343
Q24 Identify the statement that best describes your level of involvement with a CAM provider. (check only one box)
o I do not see CAM providers (1)
o I see CAM providers on a daily basis (2)
o I see CAM providers on a weekly basis (3)
o I see CAM providers on a monthly basis (4)
o I see CAM providers once a year (5)
o I see CAM providers less than once a year (6)
o Other (7)
Skip To: Q24 other If Identify the statement that best describes your level of involvement with a CAM provider. (Check... = Other
Q24 Other If you have chosen “other” please specify:
________________________________________________________________
End of Block: CAM Use
Start of Block: CAM Beliefs
Statement In this section, a young adult is an individual between the ages of 15 and 24 years. Listed below are a number of statements concerning your beliefs about CAM use? For each statement you should circle the number that corresponds most closely to your belief. Choose only one number. Please do not miss any statements.
344
Q25 CAM providers give good information on maintaining a healthy lifestyle
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q26 There are less side effects when taking natural remedies
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q27 CAM involves natural plant formulas which are more healthy than taking drugs given by the medical doctor
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
345
Q28 Young adults would be more likely to use CAM if there were more CAM clinics
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q29 Young adults are more empowered when using CAM because CAM providers involve them in decisions about their healthcare treatments
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q30 Young adults believe that CAM builds up the body’s own defenses and promotes self-healing
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
346
Q31 The more knowledge a young adult has about CAM, the more likely he/she is to use it
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q32 Parent(s) and family can influence a young adult’s CAM use by exposing them to it
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q33 Young adults are more likely to use CAM if their friends are using it
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
347
Q34 Young adults are more likely to use CAM if coaches and teachers discuss it with them
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q35 Young adults who believe in the physical, mental and spiritual aspects of health are more likely to use CAM
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
Q36 Young adults who fear the discomfort of treatments from medical doctors are more likely to use CAM
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o

348
Q37 Young adults believe that taking CAM therapies is not harmful
Strongly disagree (1) Disagree (2) Haven’t decided
(3) Agree (4) Strongly agree (5)
Please choose one (1) o o o o o
End of Block: CAM Beliefs
Start of Block: CM Treatment Preferences
Q38 What type of herbs would you be willing to use for your acne? (rank in order your preference from 1 - 6)
______ Cleanser (topical) (1) ______ Pills (oral) (2) ______ Tablets (oral) (3) ______ Granules (oral) (4) ______ Powders (oral) (5) ______ Liquid (oral) (6)

349
Q39 What is the maximum time would you be willing to try these techniques (please choose one only)?
o 2 weeks (1)
o 4 weeks (2)
o 8 weeks (3)
o 12 weeks (4)
o 6 months (5)
o 12 months (6)
Q40 Herbs can be used at home. How often would you be prepared to use herbs (please choose one only)?
▢ Weekly (1)
▢ Twice weekly (2)
▢ Every second day (3)
▢ Daily (4)
▢ Twice daily (5)
▢ Three times daily (6)
350
Q41 What type of acupuncture and related manual therapies would you be willing to use for your acne? (rank in order your preference from 1–5)
______ Acupuncture (1) ______ Acupressure (like massage) (2) ______ Ear acupressure (3) ______ Electro-acupuncture (mild current through electrodes on acupuncture points) (4) ______ Laser acupuncture (5)
Q42 What is the maximum time would you be willing to try these techniques (please choose one only)?
o 2 weeks (1)
o 4 weeks (2)
o 8 weeks (3)
o 12 weeks (4)
o 6 months (5)
o 12 months (6)
351
Q43 Acupuncture-like treatments require visits to an acupuncturist. How often would you be prepared to use these types of acupuncture treatment (please choose one only)?
▢ Fortnightly (1)
▢ Weekly (2)
▢ Twice weekly (3)
▢ Every second day (4)
▢ Daily (5)
End of Block: CM Treatment Preferences
Start of Block: Demographics
Q44 What is your gender?
o Male (1)
o Female (2)
o Other (3)
Q45 What is your ethnicity?
▼ Please choose your ethnicity (1) ... Other (8)
Aboriginal / Torres Strait Islander

352
Caucasian
Asian
Middle Eastern
Pacific Islander
African
Other
Skip To: Q45 other If What is your Ethnicity? = Other
Q45 Other If you have chosen “other” please specify:
________________________________________________________________
Q46 What is your age?
▼ Please choose your age (1) ... 50+ (9)
15–19
20–24
25–30
31–35
36–40
41–45
46–50
50+
353
Q47 How long have you had acne?
▼ Please choose one (1) ... 10+ years (9)
Less than 3 months
3–6 months
6–9 months
Less than 1 year
1–2 years
3–4 years
5–9 years
10+ years
Q48 Do you think your acne is:
▼ Please choose one (1) ... Severe (4)
Mild
Moderate
Severe

354
Q49 Have you previously sought medical advice for acne?
o Yes (1)
o No (2)
Q50 What medications have you taken for your acne? (Check all that apply)
▢ Topical antibiotics and benzoyl peroxide (such as Duac Once Daily Gel) (1)
▢ Oral antibiotics (2)
▢ Topical antibiotics and benzoyl peroxide (3)
▢ Isotretinoin (such as Roaccutane) (4)
▢ Benzoyl peroxide alone (such as bentonite) (5)
▢ Topical adapalene (such as Differin topical gel or cream) (6)
▢ Topical retinoids (such as Stieva A cream, Re-Trieve cream) (7)
▢ Topical retinoids and benzoyl peroxide (8)
▢ None of the above (9)
▢ Other (10)
355
Skip To: Q50 other If What medications have you taken for your acne? (Check all that apply) = Other
Q50 Other If you have chosen “other” please specify:
________________________________________________________________
Q51 What over-the-counter products have you used for your acne? (check all that apply)
▢ Benzoyl peroxide lotions and creams (such as Proactive or Clearasil) (1)
▢ Azelaic acid preparation (such as Dermatologica or Ego Azclear) (2)
▢ Glycolic acid preparations (such as Glycolix) (3)
▢ Salicyclic acid lotions and creams (such as Clearasil) (4)
▢ None of the above (5)
▢ Other (6)
Skip To: Q51 Other If What over the counter products have you used for your acne? (Check all that apply) = Other
Q51 Other If you have chosen “other” please specify:
________________________________________________________________
End of Block: Demographics

356
Start of Block: Pilot Questions
Q52 How long did it take you to fill out the questions?
________________________________________________________________
Q53 Were there any questions you didn’t understand or make sense to you?
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
End of Block: Pilot Questions
357
Appendix 5 Advertising details for survey
Acne QoL Survey
Go to Facebook:
AcneQoLSurvey
Web link: https://rmit.au1.
qualtrics.com/ jfe/form/SV_
d6Jh5I7kjEwIPGJ
Acne QoL Survey
Go to Facebook:
AcneQoLSurvey
Web link: https://rmit.au1.
qualtrics.com/ jfe/form/SV_
d6Jh5I7kjEwIPGJ
Acne QoL Survey
Go to Facebook:
AcneQoLSurvey
Web link: https://rmit.au1.
qualtrics.com/ jfe/form/SV_
d6Jh5I7kjEwIPGJ
Acne QoL Survey
Go to Facebook:
AcneQoLSurvey
Web link: https://rmit.au1.
qualtrics.com/ jfe/form/SV_
d6Jh5I7kjEwIPGJ
Acne QoL Survey
Go to Facebook:
AcneQoLSurvey
Web link: https://rmit.au1.
qualtrics.com/ jfe/form/SV_
d6Jh5I7kjEwIPGJ
Acne QoL Survey
Go to Facebook:
AcneQoLSurvey
Web link: https://rmit.au1.
qualtrics.com/ jfe/form/SV_
d6Jh5I7kjEwIPGJ
Survey closes 31 August 2018
358
Appendix 6 Permissions for the use of the Acne-QoL survey
An agreement which is private and confidential was signed but is excluded from the thesis. Permission
emails have been included in the following pages.

From: Suzi Mansu Sent: Thursday, 10 August 2017 9:28 AM To: Robbins, Tara Subject: Re: Permission to use the Acne‐QoL for research purposes Hi Tara, Thank you for the instrument and the instructions cheers, Suzi
On 10 August 2017 at 01:28, Robbins, Tara wrote: Dear Suzi, Thank you for the signed UA. Attached you will find the ACNE QOL measure you requested in English. Kind Regards, Tara Robbins Administrative Assistant Economic and Data Sciences (EDS) Center for Observational and Real‐World Evidence (CORE)
From: Suzi Mansu Sent: Monday, August 07, 2017 8:12 PM To: Robbins, Tara Subject: Re: Permission to use the Acne-QoL for research purposes Dear Tara, Thank you very much for following this up for me. Please find attached the signed agreement. cheers, Suzi

On 8 August 2017 at 06:45, Robbins, Tara wrote: Dear Suzi, Enclosed is a brief User Agreement that details the conditions of use for the Acne‐QoL. Please review the agreement and if the terms of the agreement are acceptable to you, please sing and date the agreement an return to me a clean copy (pdf) via email. Kind Regards, Tara Robbins Administrative Assistant Economic and Data Sciences (EDS) Center for Observational and Real‐World Evidence (CORE) From: Suzi Mansu Sent: Thursday, August 03, 2017 9:42 PM To: Robbins, Tara Subject: Permission to use the Acne-QoL for research purposes Dear Tara, Would you be able to follow up on this request sent last month? I am hoping for Dr Martin's permission to get ethics approval for my project. Thanking you in advance. cheers, Suzi
On 14 July 2017 at 07:29, Robbins, Tara wrote: Hi Suzi, Sorry about that, our computer systems were out of service until last week. They are slowly coming back up. I have forwarded this for approval. Thank you, Tara Robbins Administrative Assistant Economic and Data Sciences (EDS) Center for Observational and Real‐World Evidence (CORE)
From: Suzi Mansu Sent: Tuesday, July 04, 2017 1:25 AM To: Robbins, Tara Subject: Fwd: Permission to use the Acne-QoL for research purposes Dear Ms Robbins, I sent an email last week and got a bounce back from your company stating Dr Martin-Nguyen was not reachable. Do you have the authority or someone in your company have the authority to approve my application for the use of Acne-QoL? Or is there a forwarding email address for Dr Martin-Nguyen? Thanking you in advance for your assistance. yours sincerely, Suzi Mansu ---------- Forwarded message ---------- From: Suzi Mansu Date: 30 June 2017 at 11:41 Subject: Permission to use the Acne-QoL for research purposes To: "Martin Nguyen, Allison" Cc: Meaghan Coyle, "Robbins, Tara" Dear Dr. Nguyen, Please find attached my application for permissions to use the Acne-QoL instrument. I am conducting a survey to assess people with acne vulgaris' health related quality of life in Australia. I have come across your validated tool Acne-QoL questionnaire for the assessment of patient health related quality of life across a number of journal articles and would like to request permission to use the questionnaire. A health related quality of life survey has not been conducted in Australia since 1995 and using your health related quality of life tool would further the understanding of the burden of this condition in adolescents and young adults in Australia. We would acknowledge your permission to use the questionnaire in resulting publications. Please also let me know if there is a cost involved for the use of the questionnaire. Thank you for your consideration. yours sincerely, Suzi Mansu

362
Appendix 7 Permissions for the use of the CAM Questionnaire for Young Adults survey
------------------------------------------------------------------------------------------------------
On 2 July 2017 at 21:02, Christine Patterson wrote:
Hello: You can use the tool. All the best in your research.
------------------------------------------------------------------------------------------------------
On Thu, Jun 29, 2017 at 10:55 PM -0400, "Suzi Mansu" wrote:
Dear Dr. Patterson My name is Suzi Mansu, I'm a PhD candidate at RMIT University, Melbourne. As part of my PhD studies, I am conducting a survey to assess health related quality of life among people in Australia with acne vulgaris and to examine their beliefs and usage of CAM.
I have come across your validated tool Complementary Alternative Medicine Questionnaire for Young Adults for the assessment of adolescent usage and decisions to use CAM across a number of journal articles and would like to request permission to use the questionnaire. A CAM beliefs survey has not been conducted in Australia since 2004 which was on pharmacy students. Using your questionnaire would further the understanding of the belief and attitudes in adolescents and young people in Australia, and would inform trial design of a CAM intervention for acne vulgaris.
The findings from this research will be published in peer-reviewed journals, and we would acknowledge your permission to use the questionnaire. Please also let me know if there is a cost involved.
Thank you for your consideration. Yours sincerely, Suzi Mansu

364
Appendix 8 CHEAN ethics approval for survey

College Human Ethics Advisory Network (CHEAN) College of Science, Engineering and Health Email: [email protected] Phone: [61 3] 9925 4620 Building 91, Level 2, City Campus/Building 215, Level 2, Bundoora West Campus
21 August 2017 Dr Meaghan Coyle School of Health and Biomedical Sciences RMIT University Dear Dr Coyle SEHAPP 55-17 Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine Thank you for submitting your amended application for review. I am pleased to inform you that the CHEAN has approved your application for a period of 3 Months from the date of this letter to 30 November 2017 and your research may now proceed. Conditions to approval:
1. School permissions will be provided to the CHEAN upon receipt by researchers 2. The CHEAN will be alerted to any changes to survey questions
The CHEAN would like to remind you that: All data should be stored on University Network systems. These systems provide high levels of manageable security and data integrity, can provide secure remote access, are backed up on a regular basis and can provide Disaster Recover processes should a large scale incident occur. The use of portable devices such as CDs and memory sticks is valid for archiving; data transport where necessary and for some works in progress. The authoritative copy of all current data should reside on appropriate network systems; and the Principal Investigator is responsible for the retention and storage of the original data pertaining to the project for a minimum period of five years.

Page 2 of 2
Please Note: Annual reports are due on the anniversary of the commencement date for all research projects that have been approved by the CHEAN. Ongoing approval is conditional upon the submission of annual reports failure to provide an annual report may result in Ethics approval being withdrawn.
Final reports are due within six months of the project expiring or as soon as possible after your research project has concluded.
The annual/final reports forms can be found at: www.rmit.edu.au/staff/research/human-research-ethics
Yours faithfully,
Associate Professor Barbara Polus Chair, Science Engineering & Health College Human Ethics Advisory Network
Cc Student Investigator/s: Other Investigator/s:
Mrs Suzi Mansu, School of Health & Biomedical Sciences A/Prof Anthony Zhang, School of Health & Biomedical Sciences Prof Charlie Xue, School of Health & Biomedical Sciences

367
Appendix 9 CHEAN ethics approval for survey amendment 1
College Human Ethics Advisory Network (CHEAN) College of Science, Engineering and Health
Email: [email protected] Phone: [61 3] 9925 4620 Building 91, Level 2, City Campus/Building 215, Level 2, Bundoora West Campus
15 September 2017
Dr Meaghan Coyle School of Health and Biomedical Sciences RMIT University
Dear Dr Coyle
SEHAPP 55-17 Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine
Thank you for requesting an amendment and extension to your Human Research Ethics project titled: Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine, which was originally approved by Science Engineering and Health CHEAN in 2017 for a period of 3 months.
I am pleased to inform you that the CHEAN has approved your amendment as outlined in your request and has been extended to 30 May 2018.
The CHEAN notes and thanks you for providing all documentation that incorporates these amendments. This documentation will be appended to your file for future reference and your research may now continue.
The committee would like to remind you that:
All data should be stored on University Network systems. These systems provide high levels of manageable security and data integrity, can provide secure remote access, are backed up on a regular basis and can provide Disaster Recover processes should a large scale incident occur. The use of portable devices such as CDs and memory sticks is valid for archiving; data transport where necessary and for some works in progress; The authoritative copy of all current data should reside on appropriate network systems; and the Principal Investigator is responsible for the retention and storage of the original data pertaining to the project for a minimum period of five years.
Please Note: Annual reports are due on the anniversary of the commencement date for all research projects that have been approved by the CHEAN. Ongoing approval is conditional upon the submission of annual reports failure to provide an annual report may result in Ethics approval being withdrawn.

Page 2 of 2
Final reports are due within six months of the project expiring or as soon as possible after your research project has concluded.
The annual/final reports forms can be found at: www.rmit.edu.au/staff/research/human-research-ethics
Yours faithfully,
Associate Professor Barbara Polus Chair, Science Engineering & Health College Human Ethics Advisory Network
Cc Student Investigator/s: Other Investigator/s:
Mrs Suzi Mansu, School of Health & Biomedical Sciences A/Prof Anthony Zhang, School of Health & Biomedical Sciences Prof Charlie Xue, School of Health & Biomedical Sciences

370
Appendix 10 CHEAN ethics approval for survey amendment 2
College Human Ethics Advisory Network (CHEAN) College of Science, Engineering and Health
Email: [email protected] Phone: [61 3] 9925 4620 Building 91, Level 2, City Campus/Building 215, Level 2, Bundoora West Campus
13 November 2017
Dr Meaghan Coyle School of Health and Biomedical Sciences RMIT University
Dear Dr Coyle
SEHAPP 55-17 Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine
Thank you for requesting an amendment and extension to your Human Research Ethics project titled: Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine, which was originally approved by Science Engineering and Health CHEAN in 2017 for a period of 3 months.
I am pleased to inform you that the CHEAN has approved your amendment as outlined in your request.
The CHEAN notes and thanks you for providing all documentation that incorporates these amendments. This documentation will be appended to your file for future reference and your research may now continue.
The committee would like to remind you that:
All data should be stored on University Network systems. These systems provide high levels of manageable security and data integrity, can provide secure remote access, are backed up on a regular basis and can provide Disaster Recover processes should a large scale incident occur. The use of portable devices such as CDs and memory sticks is valid for archiving; data transport where necessary and for some works in progress; The authoritative copy of all current data should reside on appropriate network systems; and the Principal Investigator is responsible for the retention and storage of the original data pertaining to the project for a minimum period of five years.

Page 2 of 2
Please Note: Annual reports are due on the anniversary of the commencement date for all research projects that have been approved by the CHEAN. Ongoing approval is conditional upon the submission of annual reports failure to provide an annual report may result in Ethics approval being withdrawn.
Final reports are due within six months of the project expiring or as soon as possible after your research project has concluded.
The annual/final reports forms can be found at: www.rmit.edu.au/staff/research/human-research-ethics
Yours faithfully,
Associate Professor Barbara Polus Chair, Science Engineering & Health College Human Ethics Advisory Network
Cc Student Investigator/s: Other Investigator/s:
Mrs Suzi Mansu, School of Health & Biomedical Sciences A/Prof Anthony Zhang, School of Health & Biomedical Sciences Prof Charlie Xue, School of Health & Biomedical Sciences

373
Appendix 11 CHEAN ethics approval for survey amendment 3

College Human Ethics Advisory Network (CHEAN) College of Science, Engineering and Health
Email: [email protected] Phone: [61 3] 9925 4620 Building 91, Level 2, City Campus/Building 215, Level 2, Bundoora West Campus
20 June 2018
Dr Meaghan Coyle School of Health and Biomedical Sciences RMIT University
Dear Dr Coyle
SEHAPP 55-17 Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine
Thank you for requesting an amendment and extension to your Human Research Ethics project titled: Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine, which was originally approved by Science Engineering and Health CHEAN in 2017 for a period of 3 months.
I am pleased to inform you that the CHEAN has approved your amendment as outlined in your request.
The CHEAN notes and thanks you for providing all documentation that incorporates these amendments. This documentation will be appended to your file for future reference and your research may now continue.
The committee would like to remind you that:
All data should be stored on University Network systems. These systems provide high levels of manageable security and data integrity, can provide secure remote access, are backed up on a regular basis and can provide Disaster Recover processes should a large scale incident occur. The use of portable devices such as CDs and memory sticks is valid for archiving; data transport where necessary and for some works in progress; The authoritative copy of all current data should reside on appropriate network systems; and the Principal Investigator is responsible for the retention and storage of the original data pertaining to the project for a minimum period of five years.
Page 2 of 2
Please Note: Annual reports are due on the anniversary of the commencement date for all research projects that have been approved by the CHEAN. Ongoing approval is conditional upon the submission of annual reports failure to provide an annual report may result in Ethics approval being withdrawn.
Final reports are due within six months of the project expiring or as soon as possible after your research project has concluded.
The annual/final reports forms can be found at: www.rmit.edu.au/staff/research/human-research-ethics
Yours faithfully,
Associate Professor Barbara Polus Chair, Science Engineering & Health College Human Ethics Advisory Network
Cc Student Investigator/s: Other Investigator/s:
Mrs Suzi Mansu, School of Health & Biomedical Sciences A/Prof Anthony Zhang, School of Health & Biomedical Sciences Prof Charlie Xue, School of Health & Biomedical Sciences

376
Appendix 12 CHEAN ethics approval for survey amendment 4
College Human Ethics Advisory Network (CHEAN) College of Science, Engineering and Health
Email: [email protected] Phone: [61 3] 9925 4620 Building 91, Level 2, City Campus/Building 215, Level 2, Bundoora West Campus
21 March 2018
Dr Meaghan Coyle School of Health and Biomedical Sciences RMIT University
Dear Dr Coyle
SEHAPP 55-17 Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine
Thank you for requesting an amendment and extension to your Human Research Ethics project titled: Acne in adolescents, young people and adults: impact on quality of life and attitudes to Chinese medicine, which was originally approved by Science Engineering and Health CHEAN in 2017 for a period of 3 months.
I am pleased to inform you that the CHEAN has approved your amendment as outlined in your request and has been extended to 31 December 2018.
The CHEAN notes and thanks you for providing all documentation that incorporates these amendments. This documentation will be appended to your file for future reference and your research may now continue.
The committee would like to remind you that:
All data should be stored on University Network systems. These systems provide high levels of manageable security and data integrity, can provide secure remote access, are backed up on a regular basis and can provide Disaster Recover processes should a large scale incident occur. The use of portable devices such as CDs and memory sticks is valid for archiving; data transport where necessary and for some works in progress; The authoritative copy of all current data should reside on appropriate network systems; and the Principal Investigator is responsible for the retention and storage of the original data pertaining to the project for a minimum period of five years.
Please Note: Annual reports are due on the anniversary of the commencement date for all research projects that have been approved by the CHEAN. Ongoing approval is conditional upon the submission of annual reports failure to provide an annual report may result in Ethics approval being withdrawn.

Page 2 of 2
Final reports are due within six months of the project expiring or as soon as possible after your research project has concluded.
The annual/final reports forms can be found at: www.rmit.edu.au/staff/research/human-research-ethics
Yours faithfully,
Associate Professor Barbara Polus Chair, Science Engineering & Health College Human Ethics Advisory Network
Cc Student Investigator/s: Other Investigator/s:
Mrs Suzi Mansu, School of Health & Biomedical Sciences A/Prof Anthony Zhang, School of Health & Biomedical Sciences Prof Charlie Xue, School of Health & Biomedical Sciences
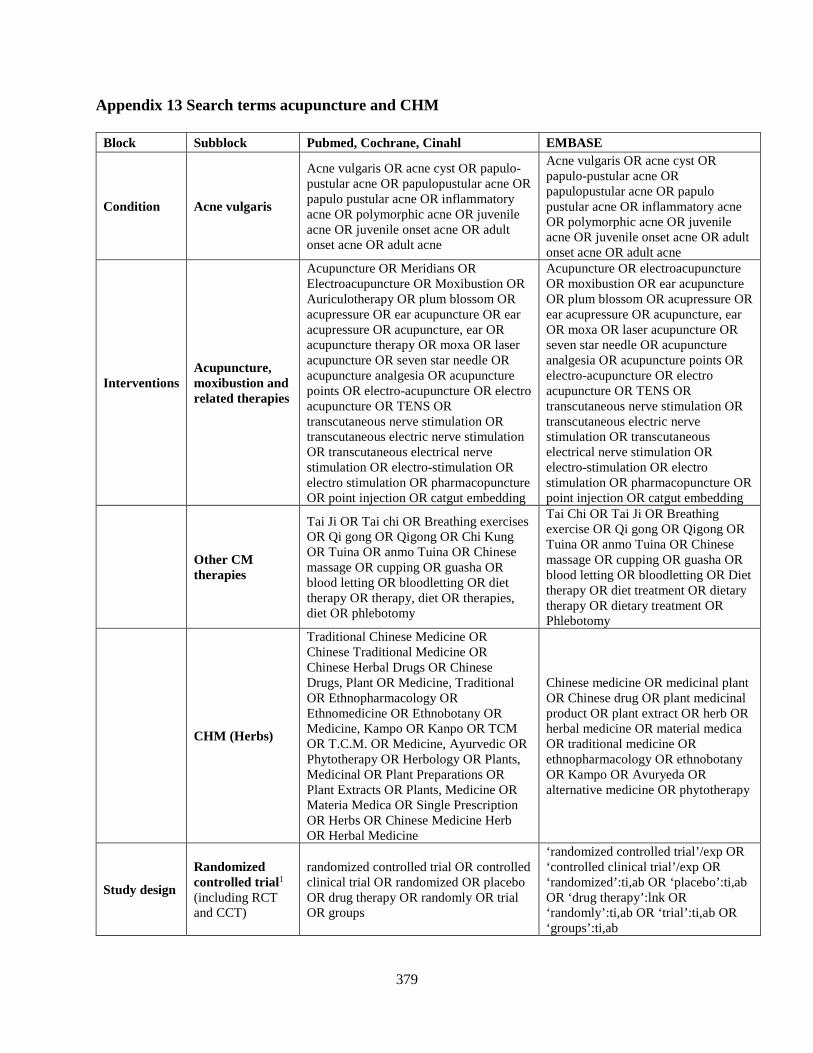
379
Appendix 13 Search terms acupuncture and CHM
Block Subblock Pubmed, Cochrane, Cinahl EMBASE
Condition Acne vulgaris
Acne vulgaris OR acne cyst OR papulo-pustular acne OR papulopustular acne OR papulo pustular acne OR inflammatory acne OR polymorphic acne OR juvenile acne OR juvenile onset acne OR adult onset acne OR adult acne
Acne vulgaris OR acne cyst OR papulo-pustular acne OR papulopustular acne OR papulo pustular acne OR inflammatory acne OR polymorphic acne OR juvenile acne OR juvenile onset acne OR adult onset acne OR adult acne
Interventions Acupuncture, moxibustion and related therapies
Acupuncture OR Meridians OR Electroacupuncture OR Moxibustion OR Auriculotherapy OR plum blossom OR acupressure OR ear acupuncture OR ear acupressure OR acupuncture, ear OR acupuncture therapy OR moxa OR laser acupuncture OR seven star needle OR acupuncture analgesia OR acupuncture points OR electro-acupuncture OR electro acupuncture OR TENS OR transcutaneous nerve stimulation OR transcutaneous electric nerve stimulation OR transcutaneous electrical nerve stimulation OR electro-stimulation OR electro stimulation OR pharmacopuncture OR point injection OR catgut embedding
Acupuncture OR electroacupuncture OR moxibustion OR ear acupuncture OR plum blossom OR acupressure OR ear acupressure OR acupuncture, ear OR moxa OR laser acupuncture OR seven star needle OR acupuncture analgesia OR acupuncture points OR electro-acupuncture OR electro acupuncture OR TENS OR transcutaneous nerve stimulation OR transcutaneous electric nerve stimulation OR transcutaneous electrical nerve stimulation OR electro-stimulation OR electro stimulation OR pharmacopuncture OR point injection OR catgut embedding
Other CM therapies
Tai Ji OR Tai chi OR Breathing exercises OR Qi gong OR Qigong OR Chi Kung OR Tuina OR anmo Tuina OR Chinese massage OR cupping OR guasha OR blood letting OR bloodletting OR diet therapy OR therapy, diet OR therapies, diet OR phlebotomy
Tai Chi OR Tai Ji OR Breathing exercise OR Qi gong OR Qigong OR Tuina OR anmo Tuina OR Chinese massage OR cupping OR guasha OR blood letting OR bloodletting OR Diet therapy OR diet treatment OR dietary therapy OR dietary treatment OR Phlebotomy
CHM (Herbs)
Traditional Chinese Medicine OR Chinese Traditional Medicine OR Chinese Herbal Drugs OR Chinese Drugs, Plant OR Medicine, Traditional OR Ethnopharmacology OR Ethnomedicine OR Ethnobotany OR Medicine, Kampo OR Kanpo OR TCM OR T.C.M. OR Medicine, Ayurvedic OR Phytotherapy OR Herbology OR Plants, Medicinal OR Plant Preparations OR Plant Extracts OR Plants, Medicine OR Materia Medica OR Single Prescription OR Herbs OR Chinese Medicine Herb OR Herbal Medicine
Chinese medicine OR medicinal plant OR Chinese drug OR plant medicinal product OR plant extract OR herb OR herbal medicine OR material medica OR traditional medicine OR ethnopharmacology OR ethnobotany OR Kampo OR Avuryeda OR alternative medicine OR phytotherapy
Study design
Randomized controlled trial1 (including RCT and CCT)
randomized controlled trial OR controlled clinical trial OR randomized OR placebo OR drug therapy OR randomly OR trial OR groups
‘randomized controlled trial’/exp OR ‘controlled clinical trial’/exp OR ‘randomized’:ti,ab OR ‘placebo’:ti,ab OR ‘drug therapy’:lnk OR ‘randomly’:ti,ab OR ‘trial’:ti,ab OR ‘groups’:ti,ab
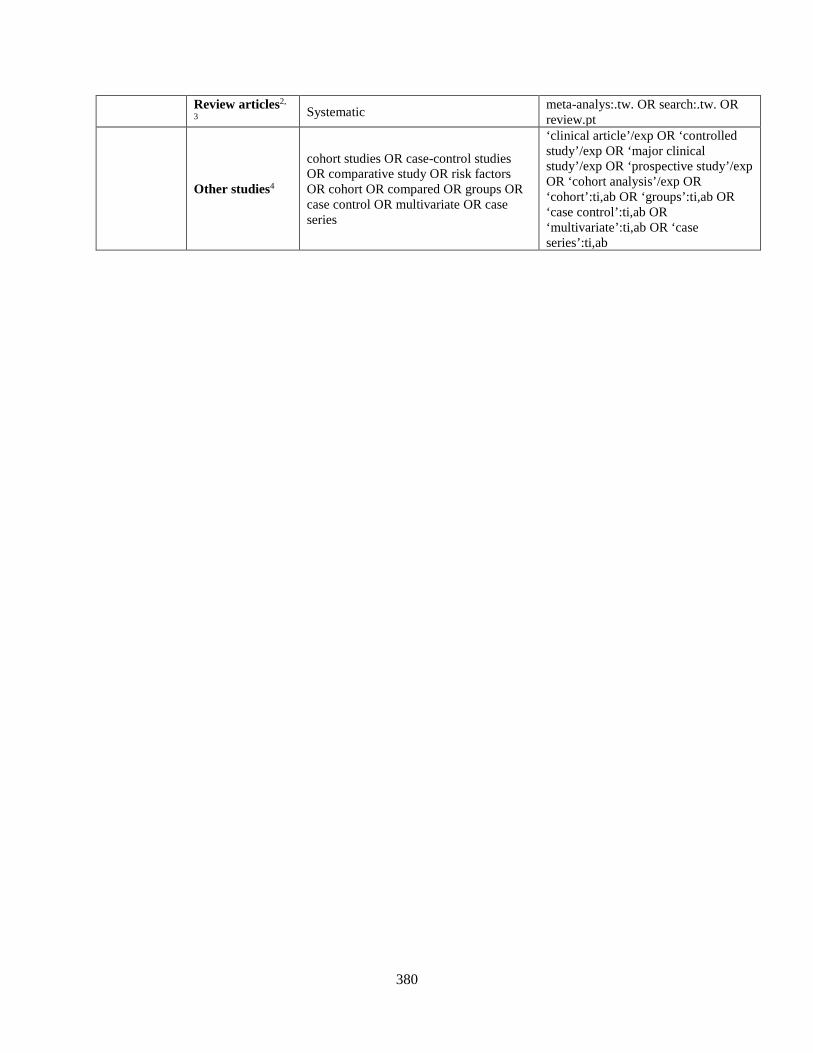
380
Review articles2,
3 Systematic meta-analys:.tw. OR search:.tw. OR review.pt
Other studies4
cohort studies OR case-control studies OR comparative study OR risk factors OR cohort OR compared OR groups OR case control OR multivariate OR case series
‘clinical article’/exp OR ‘controlled study’/exp OR ‘major clinical study’/exp OR ‘prospective study’/exp OR ‘cohort analysis’/exp OR ‘cohort’:ti,ab OR ‘groups’:ti,ab OR ‘case control’:ti,ab OR ‘multivariate’:ti,ab OR ‘case series’:ti,ab

381
Appendix 14 Published review “Herbal medicine Eriobotrya japonica formula for acne
vulgaris: a systematic review”

Contents lists available at ScienceDirect
Journal of Herbal Medicine
journal homepage: www.elsevier.com/locate/hermed
Review article
Herbal medicine Eriobotrya japonica formula for acne vulgaris: A systematicreview
Suzi Shu Yi Mansua, Meaghan Coyleb, Kaiyi Wanga, Brian Mayb, Anthony Lin Zhangb,⁎,Charlie Chang Li Xueb,c
a Discipline of Chinese Medicine, School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC, Australiab China-Australia International Research Centre for Chinese Medicine, School of Health Sciences, RMIT University, Bundoora, Melbourne, VIC, Australiac Guangdong Provincial Academy of Chinese Medical Sciences, Guangzhou 510120, China
A R T I C L E I N F O
Keywords:Acne vulgarisEriobotrya japonicaChinese traditional medicineSystematic review
A B S T R A C T
Acne vulgaris is a common inflammatory skin condition characterized by comedones. Current pharma-cotherapies are effective but are associated with adverse events (AEs) such as mood disorders and antibioticresistance. The Eriobotrya japonica Formula (EJF) contains six herbs commonly used in traditional Chinesemedicine clinical practice. This paper evaluates the experimental evidence and clinical efficacy of EJF for acnevulgaris.
Searches of 11 English and Chinese databases were conducted to identify eligible randomized controlled trials(RCTs). PubMed was searched for experimental evidence of herbs included in EJF. Meta-analyses were per-formed to analyse the clinical effects of EJF compared to pharmacotherapies.
Ingredients in EJF were reported to have an effect on inhibiting TNF-α, PPAR-γ and IL-6 cytokines. Some alsoinhibited P. acnes and had anti-androgenic and anti-lipogenic effects. There were 15 RCTs included in the clinicalreview. The number of people achieving a clinical improvement based on lesion count was higher with EJF thanpharmacotherapies. The effective rate of EJF was greater than antibiotics and benzoyl peroxide (2 studies, RR:1.47 [1.23, 1.77], I2= 0%), and antibiotics with topical supplements (2 studies, RR: 1.77 [1.18, 2.67], I2= 0%).There were 107 mild AEs reported in 7 trials, 33 in the intervention groups and 74 in the control groups. Noserious AEs were reported.
There is some evidence that EJF can decrease inflammatory lesions in acne vulgaris with fewer AEs in theshort-term. However, due to methodological limitations of the included trials, results on clinical efficacy shouldbe interpreted with caution.
1. Introduction
Acne vulgaris is a common inflammatory condition of the pilose-baceous glands of the skin that begins at adolescence and can affectadults up to 50 years old. The prevalence of acne is higher in westerncountries (Cordain et al., 2002) with around 20% of adolescents suf-fering moderate to severe acne, but acne may persist in 64% of adults intheir 20 s and 43% in their 30 s (Bhate and Williams, 2014). The burdenof the disease is high, with anxiety, depression, body image concerns,poor self-esteem, and suicidal tendencies and attempts reported in anumber of studies (Bowe et al., 2011; Halvorsen et al., 2011; Hull andD'Arcy, 2005).
Comedones and inflammatory nodules are characteristic lesions inacne vulgaris that result from multifactorial pathogeneses. Infectionfrom Proprionibacterium acnes (P. acnes) and mites (Demodex
folliculorum) (Bhate and Williams, 2014; Ren et al., 1997; Vos et al.,2012) stimulate innate and acquired immune responses and triggerinflammation (Dreno et al., 2015). The initiation of inflammation maybe due to androgens such as testosterone and α-dihydrotestosteronewith subsequent increase in sebum, enlargement of sebaceous glandsand hyperkeratinization (Bialecka et al., 2005; Eichenfield et al., 2015).Genetics (Bhate and Williams, 2014), diet (Adebamowo et al., 2006,2008; Smith et al., 2007) and neuroendocrine regulatory mechanisms(Lynn et al., 2016) can also contribute to occurrence and the severity ofacne vulgaris.
Hyperkeratinization is caused by altered sebum and lipid content insebocytes and keratinocytes (Zouboulis et al., 2014). Peroxisome pro-liferator-activated receptors (PPARs) increase human sebum production(Trivedi et al., 2006), and an innate immune response to pathogenssuch as P. acnes activates adaptive immune responses from T- and B-
http://dx.doi.org/10.1016/j.hermed.2017.09.001Received 29 September 2016; Received in revised form 15 May 2017; Accepted 7 September 2017
⁎ Corresponding author at: Discipline of Chinese Medicine, School of Health Sciences, RMIT University PO Box 71, Bundoora, VIC, 3083, Australia.E-mail address: [email protected] (A.L. Zhang).
Journal of Herbal Medicine 11 (2018) 12–23
Available online 09 September 20172210-8033/ © 2017 Elsevier GmbH. All rights reserved.
T

cells (Dreno et al., 2015). P. acnes stimulate keratinocytes that producecytokines causing ductal rupture (Dreno et al., 2015). They activatetoll-like receptor (TLR)-2 and TLR-4 cytokines. IL-6 cytokine productioncaused by lipoxygenase is associated with sebaceous glands, which alsoincreases concomitant PPAR-α and PPAR-γ (Zouboulis et al., 2014).Pro-inflammatory cytokines such as tumour necrosis factor (TNF)-α,interleukin (IL)-1, IL-8 and IL-12 are produced with P. acnes infections(Dreno et al., 2015).
Treatment guidelines recommend four approaches to treatment in-cluding decreasing hyperkeratinization, microbial colonization of P.acnes and sebum production, and inhibiting inflammation (Zaengleinet al., 2016). Treatment of mild acne includes education about skinhygiene and debunking myths (Cook et al., 2010; Eichenfield et al.,2013). Topical and oral retinoids are prescribed for moderate to severeacne and topical benzoyl peroxide is combined with topical antibioticsto decrease antibiotic resistance with long-term use (Vos et al., 2012).Current conventional treatment therapies are effective but can haveside effects. Retinoids are teratogenic and oral use is associated withmood changes, depression and suicidal thoughts (Costa Caroline et al.,2011). Topical retinoids and benzoyl peroxide can leave the skin dryand cause skin irritation (Eichenfield et al., 2013). The effectiveness oftopical and oral antibiotics can decrease over time and increase the riskof antibiotic resistance (Vos et al., 2012).
Many people use complementary and alternative medicine for skinconditions (Fuhrmann et al., 2010; Neamsuvan et al., 2015). A recentsystematic review on botanical and phytochemical treatments for acnevulgaris evaluated 23 clinical trials (Fisk et al., 2014), three of whichevaluated Kampo/Chinese herbal medicine (CHM) formulations. TheCHM preparations showed improvement for mild to moderate acne.Limitations of these clinical trials included lack of acne gradingmethods, and lack of a control or placebo group.
Eriobotrya Japonica Formula (EJF) known as Pi Pa Qing Fei Yin is acommon CHM formula which has been used clinically to treat mild tomoderate inflammatory comedones in acne vulgaris (Shen et al., 1995;Xu, 2004). This formula contains six herbs that have anti-inflammatory,anti-lipogenic and antibacterial effects on P. acnes (Nam et al., 2003;Yang et al., 2014). There are no reviews on CHM for acne vulgaris todate. This review evaluates the efficacy and safety of CHM formula EJFalone or in combination with other CHM in the treatment of acnevulgaris.
1.1. Objectives
This systematic review aims to 1) describe the experimental evi-dence of the six EJF ingredients in reference to the current pharma-ceutical treatment targets for acne including effects on P. acnes andinflammation as well as effects on hyperkeratinization, androgen andsebum production; 2) conduct a systematic review and meta-analysis toevaluate the clinical efficacy and safety of EJF for acne. The systematicreview will include randomized controlled trials (RCTs) of people withacne, which compare EJF with no treatment, placebo or conventionalpharmacotherapy and which report on clinically relevant outcomes.
2. Methods
2.1. Experimental evidence
A search of electronic database PubMed was performed from in-ception to August 2016. The six ingredients of EJF were used as keywords. The pharmaceutical; species; English and pin yin names forEriobotrya japonica Thunb. Lindl. leaf (pi pa ye); Morus alba L. root bark(sang bai pi); Coptis chinensis Franch. or Coptis teeta Wall. or Coptis del-toidea C.Y. Cheng & Hsiao stem; (huang lian); Phellodendron amurenseRupr. or Phllodendron chinense Schneid. cortex (huang bai); Panax gin-seng C.A. Mey. root (ren shen) and Glycyrrhiza glabra L. P. or Glycyrrhizauralensis Fisch. or Glycyrrhiza inflata BAT. stem (gan cao) were used as
search terms. These terms were combined with terms P. acnes; anti-inflammatory; sebum; androgen and hyperkeratinization. Articles werelimited to English.
2.2. Clinical evidence
An electronic search of five English (PubMed, Embase, Allied andComplementary Medicine Database, the Cumulative Index to Nursingand Allied Health Literature and Cochrane Library) and six Chineselanguage databases (Chinese National Knowledge Infrastructure,Chongqing VIP Information Company, Wanfang Data, ChineseBiomedical Literature Database, China's Conference Papers Databaseand China Dissertation database) was conducted from inception to May2013 (and updated in February 2015) to identify RCTs of EJF. Therewere no language restrictions. Search terms were categorized accordingto intervention (CHM, traditional Chinese herbs, Chinese drugs andvariants), condition (acne vulgaris, acne and variants) and trial design(RCT and variants) (see Supplementary file 1).
The title and abstracts were assessed to identify potential RCTs. Fulltext was retrieved for eligible studies and when eligibility could not bedetermined from the title and abstract. RCTs in people with acne vul-garis using EJF formula alone or combined with other CHM (oral ortopical) compared with no treatment, placebo, or conventional phar-macotherapy were included in the review. Modified EJF formula wasdefined as using the original formula with addition, removal or re-placement of one or more herbs. No age, gender or ethnicity limitationswere applied. Trials that used other Chinese medicine techniques suchas acupuncture or CHM as controls were excluded.
The primary outcomes for this review included change in the lesioncount (measured with the Pillsbury scale (Pillsbury, 1956), In-vestigator’s Global Assessment or Global Acne Grading System (Doshiet al., 1997), overall grading (physician’s assessment or self-reporting),length of time between recurrence of symptoms, and the effective ratedefined in guidelines. There is no published consensus guideline onwestern medicine outcome measures for acne although there are cur-rent efforts to standardize them (Tan et al., 2012). Chinese clinicalpractice guidelines (Zheng, 2002) recommend reporting the effectiverate based on lesion count alone or a combination of lesion count,impacted areas, symptoms and laboratory tests (named as “compre-hensive outcome evaluation”). In this guideline, clinical effectiveness isconsidered to be an improvement of at least 50%. For analysis, wefollowed the Chinese guideline and considered a 50% or greater im-provement to be clinically effective. Where it was not possible to de-termine how many participants achieved at least 50% improvement,data were excluded from the analysis. For example, if the study re-ported the number of people achieving 30–60% improvement and≥60% improvement, only the data for those who achieved ≥60% wereanalysed. Secondary outcomes included recurrence, acne severitymeasured with Leeds Revised Acne Grading System (Burke andCunliffe, 1984), quality of life improvements such as Cardiff AcneDisability Index (Motley and Finlay, 1992), Acne Disability Index(Gupta et al., 1998), Acne-Specific Quality of Life (Fehnel et al., 2002)and Skindex (Chren et al., 1996), and adverse events (AEs) reports.
Data was extracted into a predefined file including participantcharacteristics, details of the intervention and comparator, outcomemeasures and results. If there was missing data, the reviewer attemptedto contact the authors to try to obtain the data. Verification of data wasconducted by an independent researcher (IZ).
Methodological quality was assessed independently by two re-searchers (SM and KW) using the Cochrane Collaboration’s Risk of BiasTool (Higgins and Green, 2011). Trials were judged as either low, un-clear or high risk of bias for the domains of sequence generation, al-location concealment, blinding of participants, blinding of personneland outcome assessors, incomplete outcome data, selective reportingand other forms of bias such as conflicts of interest. A third assessor wasconsulted if disagreement existed that could not be resolved through
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
13

discussion (AZ).Statistical analyses were performed using Revman 5.2.4 (The
Cochrane Collaboration, 2012). Dichotomous data were presented asrisk ratios (RR) and continuous data as mean difference, with 95%confidence interval (CI). Data were analysed for available cases and fordichotomous data, additional analysis was performed using the numberrandomized to account for missing data. A random effects model wasused. Substantial heterogeneity was defined as I2 greater than 50%. Theauthors planned to explore publication bias if more than ten studieswere included in a meta-analysis and to perform a subgroup analysisaccording to intervention (EJF alone or in combination with otherCHM). We also planned to perform sensitivity analysis with studiesassessed as low risk of bias for sequence generation. Due to the numberof trials included and methodological quality, not all planned analysescould be performed.
3. Results
3.1. Experimental evidence
Sebocytes and keratinocytes are both important components of thepilosebaceous glands that react to infection with P. acnes and stimulateinflammation (Kurokawa et al., 2009). Androgens testosterone and 5α-dihydrotestosterone stimulate sebocytes and increase lipid droplets byincreasing lipogenesis (Kurokawa et al., 2009). Follicular keratinocytesare under androgen control (Gollnick, 2015). A combination of thesefactors cause hyperkeratinization of cells, contributing to the produc-tion of comedones and pustules seen in acne vulgaris. Relevant to thepathogenesis of acne vulgaris, the six botanicals in EJF were found tohave anti-inflammatory, anti-androgenic, antibacterial to P. acnes andanti-adipogenic and anti-lipogenic effects. Key experimental evidenceof herbs identified from the PubMed search is categorized based on thekey pathogenesis described in the American Academy of Dermatology2016 (Zaenglein et al., 2016) and is presented below.
3.1.1. Microbial colonization with P. acnesThree of the ingredients have antimicrobial actions. Glycyrrhiza
glabra, Glycyrrhiza uralensis, Phellodendron amurense and Coptis chinensishave been found to have anti-microbial actions. The whole herb extractof Glycyrrhiza glabra and Glycyrrhiza uralensis had greater antibacterialpotency than erythromycin with no resistance issues (Nam et al., 2003).Berberine, a compound common to Phellodendron amurense and Coptischinensis, inhibited P. acnes (Higaki et al., 1996). The whole root extractof Panax ginseng prevented P. acnes adhesion to host human and mousecell lines (Lee et al., 2009).
3.1.2. InflammationAll six ingredients of EJF have anti-inflammatory effects. The whole
herb extract of Eriobotrya japonica decreased inducible nitric oxidesynthase (iNOS) and cyclooxygenase-2 (COX-2) in LPS stimulatedRAW.264 cells (Uto et al., 2010). The whole leaf extract of Eriobotryajaponica inhibited LPS-induced IL-8, TNF-α and IL-1β in human lungepithelial cells (Lee et al., 2008), and regulated the production of TNF-α, IL-6 and IL-8 in mast cells by inhibiting nuclear factor (NF)-κB, p38mitogen activated protein kinase and extracellular signal-regulated ki-nase (ERK) (Kim and Shin, 2009). Tormentic acid from Eriobotrya ja-ponica decreased iNOS and COX-2 in the oedematous paw by increasingthe activities of catalase, superoxide dismutase and glutathione perox-idase in the liver of male ICR mice (Chang et al., 2011).
Ginsenosides from Panax ginseng inhibited the expression and pro-duction of inflammatory cytokine TNF-α (Gao et al., 2013). Ginsenosideactivated PPAR-γ nuclear receptor by directly increasing expressions ofPPAR-γ2 and its targeting genes. In addition, ginsenoside sensitizedinsulin action and promoted the uptake and disposal of glucose byadipocytes (Gao et al., 2013; Wang et al., 2013a). Glabridin from Gly-cyrrhiza glabra activated PPAR-γ and binds to it. It also regulated the
PPAR-γ gene expression in hepatoma cells (Rebhun et al., 2015). Ber-berine from Phellodendron amurense inhibited LPS-induced PPAR-γoverexpression and phosphorylation (Feng et al., 2012).
Glycyrrhizin from Glycyrrhizae radix suppressed the production ofcytokines through the inhibition of lipid raft accumulation and LPS-induced TLR-4 signalling, as well as suppressing LPS-induced NF-kBand IRF3 activation (Fu et al., 2014). Glycyrrhizic acid and 18β-gly-cyrrhizic acid have an anti-inflammatory effect. They can inhibit theproduction of nitrous oxide (NO), prostaglandin E2 (PGE2), TNF-α, IL-6, IL-1β and reactive oxygen species (ROS). They reduced expression ofpro-inflammatory genes (iNOS and COX-2) and significantly blockedtranscription factors NF-kB and phosphoinositide-3-kinase, p110δ andp110γ (Wang et al., 2011).
Liquiritigenin from Glycyrrhizae radix blocked the induction of iNOSprotein and its mRNA at the transcriptional level and significantly in-hibited LPS-induced TNF-α, IL-1β and IL-6 secretions (Kim et al., 2008).In this study, inhibition effect was greater on TNF-α, a secondary cy-tokine (Kim et al., 2008). Liquiritigenin inhibited NF-kB activation inmacrophages, due to its inhibition of IkBα phosphorylation (Kim et al.,2008). Whole herb extract of Glycyrrhiza glabra inhibited LPS-inducedNO and ROS production and expression of cytokines, iNOS, COX-2,TNF-α, IL-1β and IL-6; and protected macrophages from cell deathcaused by NO and TNF-α (Li et al., 2015).
Berberine chloride, found in Phellodendron amurense and Coptischinensis, decreased inflammation by inhibiting IL-6 and IL-8 but notTNF-α (Allijn et al., 2016). However, the whole herb extract of Coptischinensis inhibited TNF-α in human keratinocytes (Enk et al., 2007).The whole herb extract of Phellodendron amurense significantly sup-pressed the expression of iNOS and COX-2 (Choi et al., 2014; Jeonget al., 2009; Park et al., 2007) and decreased nuclear NF-κB andphosphorylated IκBα levels (Choi et al., 2014). In addition, the wholeherb extract inhibited IL-6, IL-1β and MCP-1 in vitro and in vivo (Choiet al., 2014; Jeong et al., 2009 Jeong et al., 2009). Berberine may alsodown-regulate the cell-mediated inflammatory response by directlyinhibiting T-cell activation (Park et al., 2007). Berberine inhibited LPS-induced PPAR-γ overexpression and phosphorylation (Feng et al.,2012). It reduces pro-inflammatory cytokines such as TNF-α, IL-6, C-reactive protein (CRP) and haptoglobin (HP); and reducing the ex-pression of LPL (lipoprotein lipase) can be induced by berberine fromPhellodendron amurense (Choi et al., 2006).
The whole herb extract of Morus alba inhibited NO production inLPS-activated RAW264.7 macrophages, decreased the production ofTNF-α (Choi and Hwang, 2005) and inhibited NF-κB and ERK1/2 ac-tivation (Eo et al., 2014).
3.1.3. Follicular hyperkeratinizationThree ingredients have an effect on adipogenesis, lipogenesis and
decreasing serum testosterone levels. Glycyrrhiza glabra, Glycyrrhizauralensis and Phellodendron amurense have been found to have anti-adipogenic and lipolytic actions. Glycyrrhizic acid from Glycyrrhizaglabra and Glycyrrhiza uralensis produced short-term decreases in totalserum testosterone and 5α-dihydrotestosterone in human studies(Armanini et al., 2004). 18β-Glycyrrhetinic acid decreases fat mass byaffecting adipogenesis in maturing preadipocytes and lipolysis in ma-tured adipocyte in 3Te-L1 cells (Moon et al., 2012). Berberine, an al-kaloid of Phellodendron amurense and Coptis chinensis reduced secretionof leptin and glycerol in 3T3-L1 adipocytes and may reduce the mRNAexpression of adipocyte-secreted inflammatory molecules (Choi et al.,2006).
3.1.4. Sebum production, anti-lipogenic and anti-adipogenic effectsTwo of the ingredients have an effect on sebum. Coptis chinensis and
Eriobotrya japonica have anti-lipogenic and anti-adipogenic effects.Coptis chinensis whole herb extract had a greater effect on lipogenesissuppression than 0.01% retinoic acid in hamster skin (Nam et al.,2003). Eriobotrya japonica inhibited lipid accumulation and adipocyte
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
14
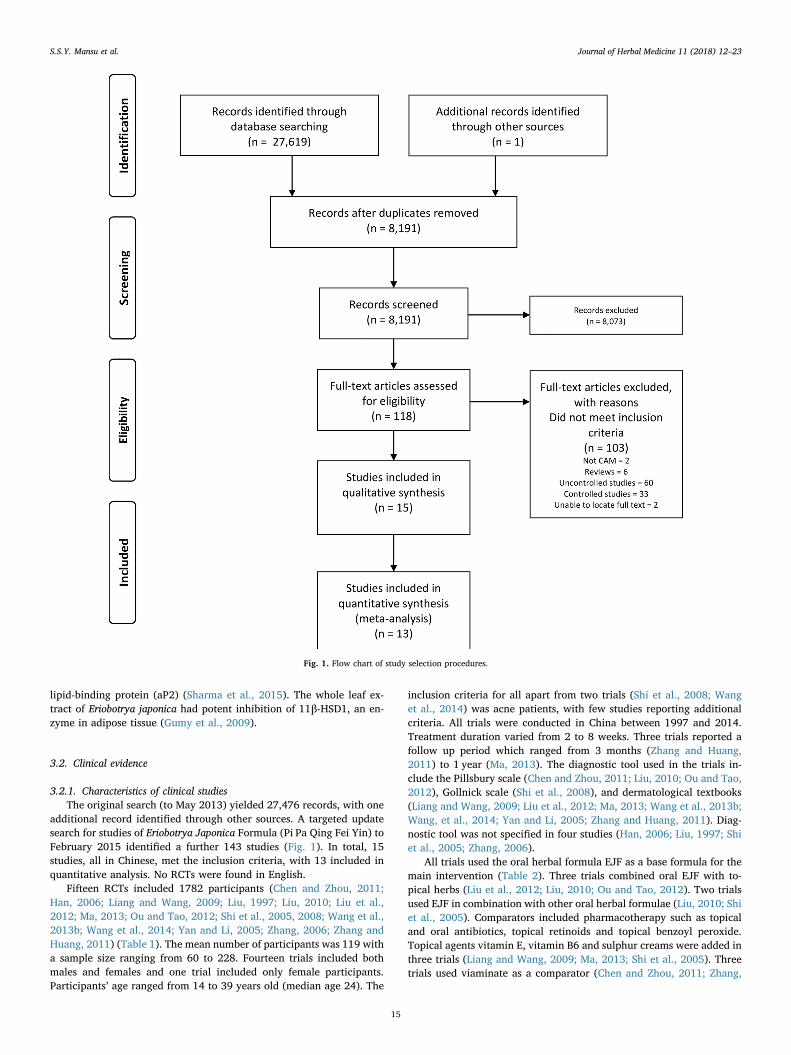
lipid-binding protein (aP2) (Sharma et al., 2015). The whole leaf ex-tract of Eriobotrya japonica had potent inhibition of 11β-HSD1, an en-zyme in adipose tissue (Gumy et al., 2009).
3.2. Clinical evidence
3.2.1. Characteristics of clinical studiesThe original search (to May 2013) yielded 27,476 records, with one
additional record identified through other sources. A targeted updatesearch for studies of Eriobotrya Japonica Formula (Pi Pa Qing Fei Yin) toFebruary 2015 identified a further 143 studies (Fig. 1). In total, 15studies, all in Chinese, met the inclusion criteria, with 13 included inquantitative analysis. No RCTs were found in English.
Fifteen RCTs included 1782 participants (Chen and Zhou, 2011;Han, 2006; Liang and Wang, 2009; Liu, 1997; Liu, 2010; Liu et al.,2012; Ma, 2013; Ou and Tao, 2012; Shi et al., 2005, 2008; Wang et al.,2013b; Wang et al., 2014; Yan and Li, 2005; Zhang, 2006; Zhang andHuang, 2011) (Table 1). The mean number of participants was 119 witha sample size ranging from 60 to 228. Fourteen trials included bothmales and females and one trial included only female participants.Participants’ age ranged from 14 to 39 years old (median age 24). The
inclusion criteria for all apart from two trials (Shi et al., 2008; Wanget al., 2014) was acne patients, with few studies reporting additionalcriteria. All trials were conducted in China between 1997 and 2014.Treatment duration varied from 2 to 8 weeks. Three trials reported afollow up period which ranged from 3 months (Zhang and Huang,2011) to 1 year (Ma, 2013). The diagnostic tool used in the trials in-clude the Pillsbury scale (Chen and Zhou, 2011; Liu, 2010; Ou and Tao,2012), Gollnick scale (Shi et al., 2008), and dermatological textbooks(Liang and Wang, 2009; Liu et al., 2012; Ma, 2013; Wang et al., 2013b;Wang, et al., 2014; Yan and Li, 2005; Zhang and Huang, 2011). Diag-nostic tool was not specified in four studies (Han, 2006; Liu, 1997; Shiet al., 2005; Zhang, 2006).
All trials used the oral herbal formula EJF as a base formula for themain intervention (Table 2). Three trials combined oral EJF with to-pical herbs (Liu et al., 2012; Liu, 2010; Ou and Tao, 2012). Two trialsused EJF in combination with other oral herbal formulae (Liu, 2010; Shiet al., 2005). Comparators included pharmacotherapy such as topicaland oral antibiotics, topical retinoids and topical benzoyl peroxide.Topical agents vitamin E, vitamin B6 and sulphur creams were added inthree trials (Liang and Wang, 2009; Ma, 2013; Shi et al., 2005). Threetrials used viaminate as a comparator (Chen and Zhou, 2011; Zhang,
Fig. 1. Flow chart of study selection procedures.
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
15

Table1
Cha
racteristics
ofclinical
stud
ies.
Firstau
thor,
publicationye
ar,
coun
try,
setting
Stud
yde
sign
,blinding
,num
ber
ofarms
Eligibility
Criteria
Treatm
entdu
ration
,follo
w-updu
ration
Stag
e,seve
rity
and
duration
ofco
ndition
No.
ofpa
rticipan
tsrand
omized
/assessed
Age
(mean(SD)or
rang
e);g
ende
r(M
/F)
Interven
tion
Che
nLJ
,201
1,China
,Out
patien
tsRCTno
n-blinde
d2arms
Acn
epa
tien
ts,Dec
2008
−Dec
2009
4weeks,0weeks
NS,
Pillsbu
ry:I–IV,
PiPa
QingFe
iYin
JiaJian
(oral)
I:2(1.44)
years
I:53
/53
I:24
(3.3),27
/26
C:2
1.2ye
ars
C:4
7/47
C:25(2.0),24
/23
Han
SX,2
006,
China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
evu
lgaris
patien
ts15
days,0
weeks
NS
I:52
/52
I:NS,
NS
PiPa
QingFe
iYin
(oral)+
Mask
(top
ical)
C:3
8/38
C:N
S,NS
Lian
gXS,
2009
,China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
ts30
days,0
weeks
NS,
NS,
1week-
6ye
ars
I:32
/32
I:24
.5(N
S),2
1/11
PiPa
QingFe
iYin
JiaWei
(oral)
C:2
8/28
C:2
4.5(N
S),1
8/10
LiuH,1
997,
China
,ho
spital,N
SRCT,
non-
blinde
d3arms
Patien
tswithacne
vulgaris
2weeks,0weeks
NS,
NS,
2weeks
−3
years
I1:6
0/60
I1:2
2.5(N
S),N
SI2:6
0/60
I2:2
2.5(N
S),N
SI1:J
iawei
PiPa
QingFe
iYin
(oral)
C:6
0/60
C:2
2.5(N
S),N
SI2:P
iPa
QingFe
iYin
LiuHS,
2012
,China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
tsMar
2005
−Mar
2007
4weeks,0weeks
NS,
Lesion
:I–III,3
mon
ths−
5ye
ars
I:40
/40
I:17
–32,
17/2
3Pi
PaQingFe
iYin
JiaJian
(oral)
+DianDao
San(top
ical)
C:4
0/40
C:1
9–31
,18/
22LiuY,2
010,
China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
ts,Dec
2008
−Dec
2010
4weeks,0weeks
NS,
Pillsbu
ry:slight,
mod
erate,
seve
reI:58
/58
I:22
.2(3.6),30
/28
PiPa
QingFe
iYin
+WuWei
XiaoDuYin
JiaJian
(oral&
topical)
I:1mon
th−
5ye
ars
C:3
0/30
C:2
1.2(2.4),18
/12
C:2
mon
ths−
5ye
ars
MaTL
,201
3,China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
ts,20
02−
2012
NS,
1ye
arNS,
NS,
7da
ys−
5ye
ars
I:42
/42
I:24
.84(N
S),2
9/13
PiPa
QingFe
iYin
JiaJian
(oral)
C:4
2/42
C:2
4.84
(NS),27
/15
OuHB,
2012
,China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
ts3weeks,0weeks
NS,
Pillsbu
ry:I–IV,2
(1.5)ye
ars
I:40
/40
I:28
.73(3.59),1
8/22
PiPa
QingFe
iYin
JiaJian
(oral)
+DianDao
San(top
ical)
C:4
0/40
C:2
9.12
(3.48),
19/2
1Sh
iXB,
2005
,China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
ts2weeks,0weeks
NS,
Mod
erate
−seve
re(Lesion:
II–III),NS
I:82
/79
I:23
.34(9.54),3
2/50
PiPa
QingFe
iYin
(oral)+
Bian
Hua
Fang
C:8
0/78
C:2
0.87
(8.67),
34/4
6Sh
iXB,
2008
,China
,Out
patien
tsRCT,
non-
blinde
d2arms
Stud
ents
aged
12–3
0diag
nosedwithacne
vulgaris;a
nda)
GollnickI–IIifno
tpreviou
streatm
ent,or
b)synd
rome
unde
rco
ntrolifprev
iously
treatedwithviam
inatean
d1%
clinda
mycin
phosph
atege
l,or
c)GollnickI–IIafter
treatm
entwithtanshino
nean
d1%
tretinoincream;M
ar20
05to
Oct
2007
;Gollnickstag
eI−
II(
8weeks,0weeks
NS,
Gollnick:
I–II,
NS
I:39
/39(alldrop
outs
are
includ
edas
“no
improv
emen
t”)
I:12–
30,N
SPi
PaQingFe
iYin
JiaJian
(oral)
C:3
5/35
C:12–
30,N
S
Wan
gS,
2013
,China
,NS
RCT,
non-
blinde
d2arms
Femaleacne
patien
ts1mon
th,0weeks
NS,
slight-sev
ere,
NS
I:61
/61
I:NS,
0/61
PiPa
QingFe
iYin
(oral)
C:6
0/60
C:N
S,0/
60Wan
gX,2
014,
China
,Out
patien
tsRCT,
non-
blinde
d3arms
Acn
epa
tien
tsin
outpatientsde
partmen
t;15
-45
yo;n
otopicaltreatm
ents
inthepa
st7da
ys;n
oacne
oral
med
icationin
thepa
st30
days;
1mon
th,0weeks
NS
I1:6
0/60
15–2
5;NS
PiPa
QingFe
iYin
(oral)
I2:6
0/60
C:6
0/60
Yan
LY,2
005,
China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
ts3weeks,6mon
ths
NS,
light-sev
ere,
560da
ysI:11
4/11
4I:17
.6(N
S),4
9/65
BaiDiSh
eXiJi+
Cuo
Chu
ang
Ling
+Pi
PaQingFe
iYin
Jia
Jian
(oral)
C:1
14/1
14C:1
7.6(N
S),4
9/65
Zhan
gLL
,200
6,China
,Out
patien
tsRCT,
non-
blinde
d2arms
Acn
epa
tien
tswithCM
diag
nosis(dam
p-he
atin
Lung
andStom
ach)
4weeks,0weeks
NS,
NS,
I:2mon
ths
−7ye
ars
I:60
/60
I:22
(2.12),2
6/34
PiPa
QingFe
iYin
JiaJian
(oral)
C:5
mon
ths−
6ye
ars
C:6
0/60
C:2
4(2.34),3
1/29
(con
tinuedon
next
page)
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
16

2006; Zhang and Huang, 2011). Viaminate is a non-conventional oralretinoid derivative that is approved in China for clinical treatment ofacne. One trial used a combination of viaminate and an antibiotic (Shiet al., 2005) which is not a common prescribing practice outside ofChina. None of the trials used placebo control.
Eight trials reported effective rate based on lesion count (Liu, 1997;Liu et al., 2012; Shi et al., 2005, 2008; Wang et al., 2013b; Wang et al.,2014; Zhang, 2006; Zhang and Huang, 2011), six reported effective ratebased on both lesion count and severity (Chen and Zhou, 2011; Liangand Wang, 2009; Liu, 2010; Ma, 2013; Ou and Tao, 2012; Yan and Li,2005) and one study did not report details on how the effective rate wascalculated (Han, 2006). Four trials (Liu et al., 2012; Ma, 2013; Shiet al., 2008; Yan and Li, 2005) reported on recurrence rate. None of thetrials reported on the length of time between recurrences or acne se-verity and only one paper (Wang et al., 2014) reported on the health-related quality of life (HRQoL) measure Dermatology Life Quality Index(DLQI).
3.2.2. Risk of biasOverall, methodological quality of included trials was low to mod-
erate (Fig. 2). Two trials (Ou and Tao, 2012; Zhang, 2006) were as-sessed to have low risk of bias in sequence generation as they usedrandom number generators. Two trials (Chen and Zhou, 2011; Wanget al., 2014) were assessed as high risk, as Chen and Zhou used hospitalrecord numbers (2011) and Wang et al. used sequence of visit order(2014). There was insufficient information reported on blinding ofparticipants in 14 papers and these were assessed as unclear. One paper(Wang et al., 2014) was assessed to have high risk in blinding of par-ticipants based on the inclusion of a subjective quality of life (DLQI)outcome measure. As there was insufficient information reported onallocation concealment and blinding of personnel and outcome asses-sors, all studies were assessed as unclear risk for these domains. Alltrials were assessed as low risk for incomplete outcome data and se-lective reporting. One paper was assessed as high risk for other biasesdue to baseline imbalance of participants (Zhang and Huang, 2011)with no explanation provided. No other biases such as large differencesin sample size between groups, or potential conflict of interests wereobserved in the other 14 trials.
3.2.3. Effective rateTwo studies (Han, 2006; Zhang, 2006) were excluded from the
meta-analysis as they did not report the standard effective rate of 50%as outlined in Zheng (2002). The quality of the evidence was low (seeSupplementary file 2). The effective rate was higher in those who re-ceived EJF compared to pharmacotherapy (13 studies, RR: 1.30 [1.13,1.49], I2= 70%) although substantial heterogeneity was detected(Fig. 3). Analysis to account for missing data did not alter this result (13studies, RR: 1.30 [1.13, 1.49], I2= 70%). Sensitivity analysis excludingtwo studies assessed as high risk of bias for sequence generation re-duced the statistical heterogeneity to 0% (11 studies, RR: 1.38 [1.21,1.58]).
Heterogeneity was explored through subgroup analysis by inter-ventions and comparators. When EJF was used alone the effective ratewas greater compared to pharmacotherapy (8 studies, RR: 1.32 [1.05,1.65], I2= 70%) with considerable heterogeneity, although no benefitwas seen when EJF was combined with oral herbal medicines (2 stu-dies, RR: 1.26 [0.88, 1.80], I2= 89%), or topical herbal medicines (3studies, RR: 1.30 [0.98, 1.73], I2= 69%) (Fig. 3). Again, statisticalheterogeneity was detected. When studies using viaminate or viaminatecombined with other comparators were excluded, the effect size wassimilar to the overall pool (10 studies, RR: 1.31 [1.10, 1.55], I2= 75%),but statistical heterogeneity remained considerable.
Studies were grouped according to comparator type for furtheranalysis. The effective rate of EJF plus topical CHM was greater thanantibiotics and benzoyl peroxide (2 studies, RR: 1.47 [1.23, 1.77],I2= 0%). EJF alone compared to antibiotics with topical supplementsTa
ble1(con
tinued)
Firstau
thor,
publicationye
ar,
coun
try,
setting
Stud
yde
sign
,blinding
,num
ber
ofarms
Eligibility
Criteria
Treatm
entdu
ration
,follo
w-updu
ration
Stag
e,seve
rity
and
duration
ofco
ndition
No.
ofpa
rticipan
tsrand
omized
/assessed
Age
(mean(SD)or
rang
e);g
ende
r(M
/F)
Interven
tion
Zhan
gY,2
011,
China
,NS
RCT,
non-
blinde
d2arms
Patien
tswithAcn
evu
lgaris
4weeks,3mon
ths
NS,
NS,
1.5−
6ye
ars
I:85
/85
I:14
–38,
27/5
8Pi
PaQingFe
iYin
JiaJian
(oral)
C:5
0/50
C:1
5–39
,20/
30
C:c
ompa
rator;
I:interven
tion
;NS:
notspecified
;RCT:
rand
omized
controlle
dtrial;Vit:v
itam
in.
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
17
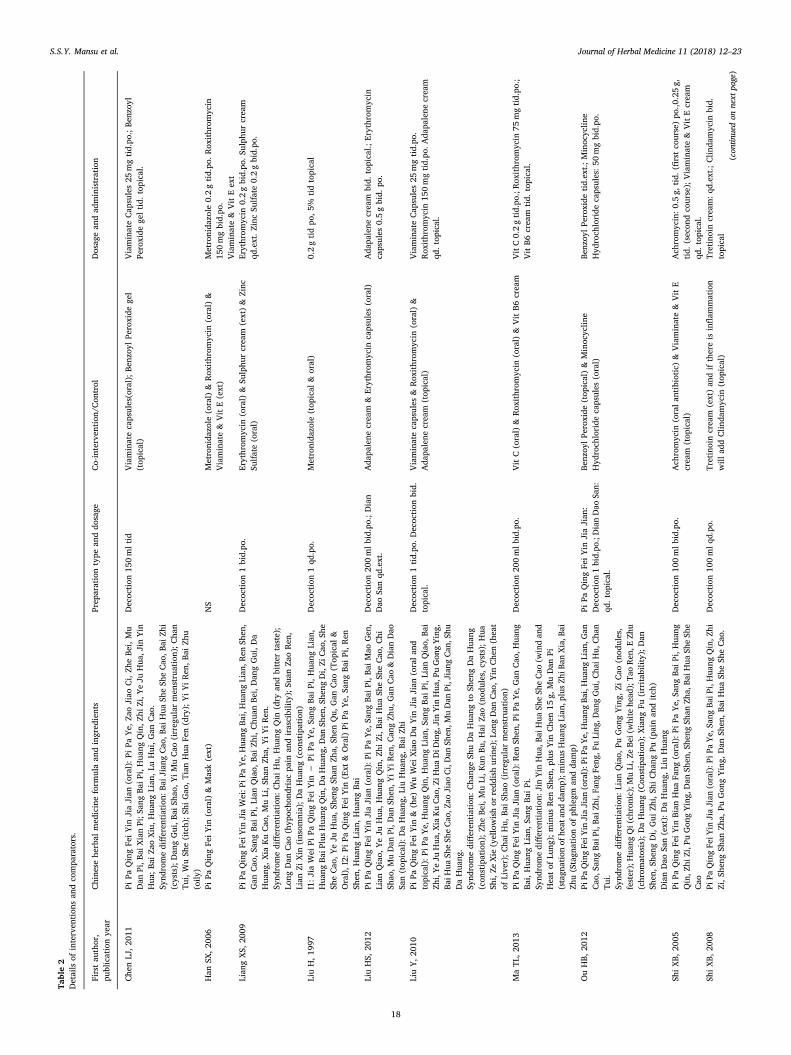
Table2
Details
ofinterven
tion
san
dco
mpa
rators.
Firstau
thor,
publicationye
arChine
sehe
rbal
med
icineform
ulaan
dingred
ients
Prep
arationtype
anddo
sage
Co-interven
tion
/Con
trol
Dosag
ean
dad
ministration
Che
nLJ
,201
1Pi
PaQingFe
iYin
JiaJian
(oral):P
iPa
Ye,
ZaoJiao
Ci,Zh
eBe
i,Mu
Dan
Pi,B
aiXianPi;S
angBa
iPi,Hua
ngQin,Z
hiZi,Y
eJu
Hua
,Jin
Yin
Hua
;Bai
ZaoXiu,Hua
ngLian
,LuHui,G
anCao
.
Decoc
tion
150mltid
Viaminatecapsules(oral);B
enzo
ylPe
roxide
gel
(top
ical)
ViaminateCap
sules25
mgtid.po
.;Be
nzoy
lPe
roxide
geltid.
topical.
Synd
romedifferen
tiation:
BaiJ
iang
Cao
,Bai
Hua
SheSh
eCao
,Bai
Zhi
(cysts);Dan
gGui,B
aiSh
ao,Y
iMuCao
(irreg
ular
men
struation);C
han
Tui,WuSh
e(itch);S
hiGao
,TianHua
Fen(dry);YiYiRen
,Bai
Zhu
(oily
)Han
SX,2
006
PiPa
QingFe
iYin
(oral)
&Mask(ext)
NS
Metronida
zole
(oral)
&Rox
ithrom
ycin
(oral)
&Viaminate&
VitE(ext)
Metronida
zole
0.2gtid.po
.Rox
ithrom
ycin
150mgbid.po
.Viaminate&
VitEext
Lian
gXS,
2009
PiPa
QingFe
iYin
JiaWei:P
iPaYe,
Hua
ngBa
i,Hua
ngLian
,Ren
Shen
,Gan
Cao
,San
gBa
iPi,L
ianQiao,
BaiZh
i,Chu
anBe
i,Dan
gGui,D
aHua
ng,Xia
KuCao
,MuLi,S
hanZh
a,YiYiRen
.
Decoc
tion
1bid.po
.Erythrom
ycin
(oral)
&Su
lphu
rcream
(ext)&
Zinc
Sulfate(oral)
Erythrom
ycin
0.2gbid.po
.Sulph
urcream
qd.ext.Z
incSu
lfate0.2gbid.po
.
Synd
romedifferen
tiation:
Cha
iHu,
Hua
ngQin
(dry
andbitter
taste);
Long
Dan
Cao
(hyp
ocho
ndriac
pain
andirascibility);S
uanZa
oRen
,Lian
ZiXin
(insom
nia);D
aHua
ng(con
stipation)
LiuH,1
997
I1:J
iaWei
PiPa
QingFe
iYin
−Pi
PaYe,
Sang
BaiPi,H
uang
Lian
,Hua
ngBa
iPlusHua
ngQin,D
aHua
ng,D
anSh
en,S
heng
Di,Zi
Cao
,She
SheCao
,YeJu
Hua
,She
ngSh
anZh
a,Sh
enQu,
Gan
Cao
(Top
ical
&Oral),I2:
PiPa
QingFe
iYin
(Ext
&Oral)
PiPa
Ye,
Sang
BaiPi,Ren
Shen
,Hua
ngLian
,Hua
ngBa
i
Decoc
tion
1qd
.po.
Metronida
zole
(top
ical
&oral)
0.2gtidpo
,5%
tidtopical
LiuHS,
2012
PiPa
QingFe
iYin
JiaJian
(oral):P
iPa
Ye,
Sang
BaiPi,B
aiMao
Gen
,Lian
Qiao,
YeJu
Hua
,Hua
ngQin,Z
hiZi,B
aiHua
SheSh
eCao
,Chi
Shao
,MuDan
Pi,D
anSh
en,Y
iYiR
en,C
angZh
u,Gan
Cao
&DianDao
San(top
ical):DaHua
ng,LiuHua
ng,B
aiZh
i
Decoc
tion
200mlbid.po
.;Dian
Dao
Sanqd
.ext.
Ada
palene
cream
&Erythrom
ycin
capsules
(oral)
Ada
palene
cream
bid.
topical.;
Erythrom
ycin
capsules
0.5gbid.
po.
LiuY,2
010
PiPa
QingFe
iYin
&(he)
WuWei
XiaoDuYin
JiaJian
(oralan
dtopical):P
iPaYe,
Hua
ngQin,H
uang
Lian
,San
gBa
iPi,Lian
Qiao,
Bai
Zhi,YeJu
Hua
,Xia
KuCao
,ZiH
uaDiD
ing,
JinYin
Hua
,PuGon
gYing,
BaiH
uaSh
eSh
eCao
,Zao
Jiao
Ci,Dan
Shen
,MuDan
Pi,J
iang
Can
,Shu
DaHua
ng.
Decoc
tion
1tid.po
.Decoc
tion
bid.
topical.
Viaminatecapsules
&Rox
ithrom
ycin
(oral)
&Ada
palene
cream
(top
ical)
ViaminateCap
sules25
mgtid.po
.Rox
ithrom
ycin
150mgtid.po
.Ada
palene
cream
qd.top
ical.
Synd
romedifferen
tiation:
Cha
ngeSh
uDaHua
ngto
Shen
gDaHua
ng(con
stipation);Zh
eBe
i,MuLi,K
unBu
,Hai
Zao(nod
ules,cysts);H
uaSh
i,Ze
Xie
(yellowishor
redd
ishurine);L
ongDan
Cao
,Yin
Che
n(heat
ofLive
r);C
haiHu,
BaiSh
ao(irreg
ular
men
struation)
MaTL
,201
3Pi
PaQingFe
iYin
JiaJian
(oral):R
enSh
en,P
iPaYe,
Gan
Cao
,Hua
ngBa
i,Hua
ngLian
,San
gBa
iPi.
Decoc
tion
200mlbid.po
.VitC(oral)
&Rox
ithrom
ycin
(oral)
&VitB6
cream
VitC0.2gtid.po
.;Rox
ithrom
ycin
75mgtid.po
.;VitB6
cream
tid.
topical.
Synd
romedifferen
tiation:
JinYin
Hua
,Bai
Hua
SheSh
eCao
(windan
dHeatof
Lung
);minus
Ren
Shen
,plusYin
Che
n15
g,MuDan
Pi(stagn
ationof
heat
andda
mp);m
inus
Hua
ngLian
,plusZh
iBan
Xia,B
aiZh
u(Stagn
ationof
phlegm
andda
mp)
OuHB,
2012
PiPa
QingFe
iYin
JiaJian
(oral):P
iPaYe,
Hua
ngBa
i,Hua
ngLian
,Gan
Cao
,San
gBa
iPi,Ba
iZhi,F
angFe
ng,F
uLing
,Dan
gGui,C
haiH
u,Cha
nTu
i.
PiPa
QingFe
iYin
JiaJian
:Decoc
tion
1bid.po
.;DianDao
San:
qd.top
ical.
Benz
oylPe
roxide
(top
ical)&
Minoc
yclin
eHyd
roch
loride
capsules
(oral)
Benz
oylPe
roxide
tid.ext.;
Minoc
yclin
eHyd
roch
loride
capsules:50
mgbid.po
.
Synd
romedifferen
tiation:
Lian
Qiao,
PuGon
gYing,
ZiCao
(nod
ules,
fester);Hua
ngQi(ch
ronic);M
uLi,Z
eBe
i(white
head
);Ta
oRen
,EZh
u(chrom
atosis);
DaHua
ng(C
onstipation);X
iang
Fu(irritab
ility);Dan
Shen
,She
ngDi,Gui
Zhi,Sh
iCha
ngPu
(painan
ditch
)DianDao
San(ext):DaHua
ng,LiuHua
ngSh
iXB,
2005
PiPa
QingFe
iYin
Bian
Hua
Fang
(oral):P
iPaYe,
Sang
BaiP
i,Hua
ngQin,Z
hiZi,P
uGon
gYing,
Dan
Shen
,She
ngSh
anZh
a,Ba
iHua
SheSh
eCao
Decoc
tion
100mlbid.po
.Ach
romycin
(oralan
tibiotic)&
Viaminate&
VitE
cream
(top
ical)
Ach
romycin:0
.5g,
tid.
(firstco
urse)po
.,0.25g,
tid.
(secon
dco
urse);Viaminate&
VitEcream
qd.top
ical.
ShiXB,
2008
PiPa
QingFe
iYin
JiaJian
(oral):P
iPaYe,
Sang
BaiP
i,Hua
ngQin,Z
hiZi,S
heng
Shan
Zha,
PuGon
gYing,
Dan
Shen
,Bai
Hua
SheSh
eCao
.Decoc
tion
100mlqd
.po.
Tretinoincream
(ext)an
difthereis
inflam
mation
will
addClin
damycin
(top
ical)
Tretinoincream:q
d.ext.;
Clin
damycin
bid.
topical
(con
tinuedon
next
page)
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
18
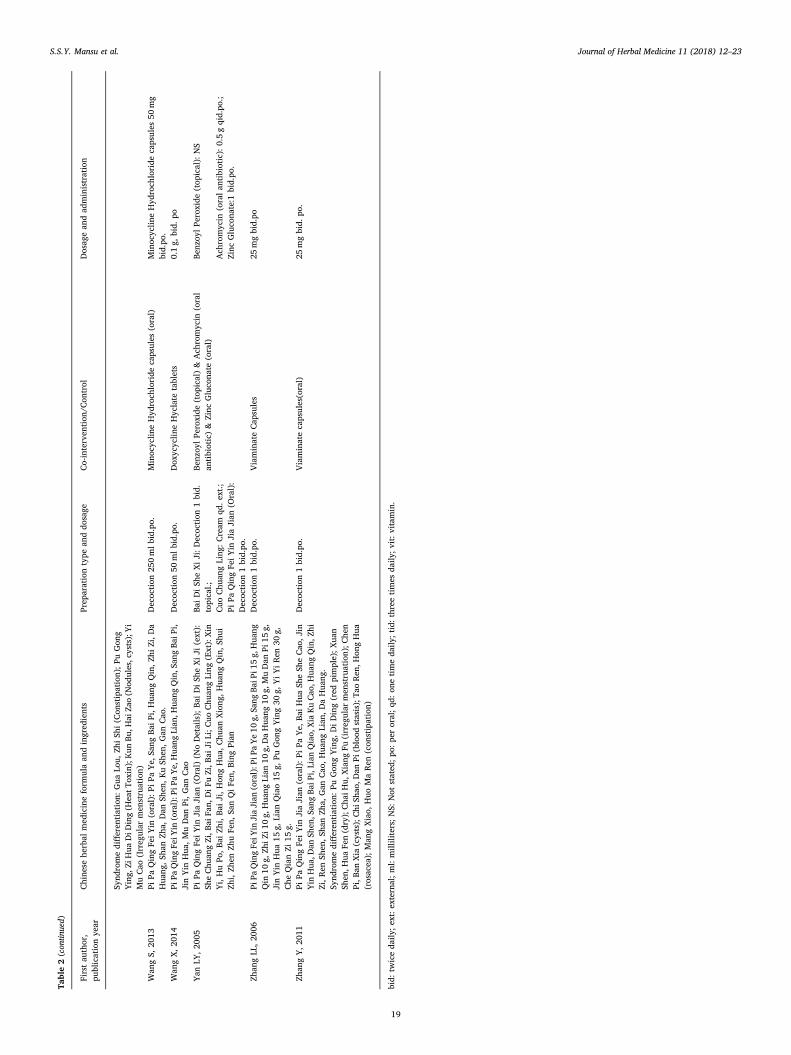
Table2(con
tinued)
Firstau
thor,
publicationye
arChine
sehe
rbal
med
icineform
ulaan
dingred
ients
Prep
arationtype
anddo
sage
Co-interven
tion
/Con
trol
Dosag
ean
dad
ministration
Synd
romedifferen
tiation:
Gua
Lou,
ZhiSh
i(C
onstipation);P
uGon
gYing,
ZiHua
DiD
ing(H
eatT
oxin);Kun
Bu,H
aiZa
o(N
odules,c
ysts);Yi
MuCao
(Irreg
ular
men
struation)
Wan
gS,
2013
PiPa
QingFe
iYin
(oral):P
iPaYe,
Sang
BaiP
i,Hua
ngQin,Z
hiZi,D
aHua
ng,Sh
anZh
a,Dan
Shen
,KuSh
en,G
anCao
.Decoc
tion
250mlbid.po
.Minoc
yclin
eHyd
roch
loride
capsules
(oral)
Minoc
yclin
eHyd
roch
loride
capsules
50mg
bid.po
.Wan
gX,2
014
PiPa
QingFe
iYin
(oral):P
iPaYe,
Hua
ngLian
,Hua
ngQin,S
angBa
iPi,
JinYin
Hua
,MuDan
Pi,G
anCao
Decoc
tion
50mlbid.po
.Dox
ycyclin
eHyclate
tablets
0.1g,
bid.
po
Yan
LY,2
005
PiPa
QingFe
iYin
JiaJian
(Oral)
(NoDetails);Ba
iDiSh
eXiJi
(ext):
SheChu
angZi,B
aiFa
n,DiF
uZi,B
aiJi
Li;C
uoChu
angLing
(Ext):Xin
Yi,HuPo
,Bai
Zhi,Ba
iJi,H
ongHua
,Chu
anXiong
,Hua
ngQin,S
hui
Zhi,Zh
enZh
uFe
n,Sa
nQiFe
n,Bing
Pian
BaiDiSh
eXiJi:D
ecoc
tion
1bid.
topical.;
Benz
oylPe
roxide
(top
ical)&
Ach
romycin
(oral
antibiotic)&
Zinc
Gluco
nate
(oral)
Benz
oylPe
roxide
(top
ical):NS
Cuo
Chu
angLing
:Cream
qd.e
xt.;
Ach
romycin
(oralan
tibiotic):0.5gqid.po
.;Pi
PaQingFe
iYin
JiaJian
(Oral):
Decoc
tion
1bid.po
.Zinc
Gluco
nate:1
bid.po
.
Zhan
gLL
,200
6Pi
PaQingFe
iYin
JiaJian
(oral):P
iPaYe10
g,Sa
ngBa
iPi1
5g,
Hua
ngQin
10g,
ZhiZ
i10g,
Hua
ngLian
10g,DaHua
ng10
g,MuDan
Pi15
g,JinYin
Hua
15g,
Lian
Qiao15
g,Pu
Gon
gYing30
g,YiYiRen
30g,
Che
QianZi
15g.
Decoc
tion
1bid.po
.ViaminateCap
sules
25mgbid.po
Zhan
gY,2
011
PiPa
QingFe
iYin
JiaJian
(oral):P
iPa
Ye,
BaiHua
SheSh
eCao
,Jin
Yin
Hua
,Dan
Shen
,San
gBa
iPi,Lian
Qiao,
Xia
KuCao
,Hua
ngQin,Z
hiZi,R
enSh
en,S
hanZh
a,Gan
Cao
,Hua
ngLian
,DaHua
ng.
Decoc
tion
1bid.po
.Viaminatecapsules(oral)
25mgbid.
po.
Synd
romedifferen
tiation:
PuGon
gYing,
DiDing(red
pimple);X
uan
Shen
,Hua
Fen(dry);Cha
iHu,
Xiang
Fu(irreg
ular
men
struation);C
hen
Pi,B
anXia
(cysts);Chi
Shao
,Dan
Pi(blood
stasis);Ta
oRen
,Hon
gHua
(rosacea);
Man
gXiao,
Huo
MaRen
(con
stipation)
bid:
twiceda
ily;e
xt:e
xterna
l;ml:milliliters;N
S:Not
stated
;po:
peroral;q
d:on
etimeda
ily;tid:three
times
daily
;vit:v
itam
in.
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
19

resulted in a greater effective rate (2 studies, RR: 1.77 [1.18, 2.67],I2= 0%). No benefit was seen when EJF alone was compared to anti-biotics alone (3 studies, RR: 1.27 [0.82, 1.99], I2= 89%) and withviaminate alone (2 studies, RR: 1.09 [0.59, 2.01], I2= 70%). Resultsfrom single studies showed EJF alone produced a higher effective ratethan retinoids (RR: 1.35 [1.01, 1.79]) and when combined with oralCHM produced a greater effective rate than antibiotics, viaminate andsupplements (RR: 1.47 [1.21, 1.79]).
3.2.4. Recurrence rateFour studies reported on recurrence rate (Liu et al., 2012; Ma, 2013;
Shi et al., 2008; Yan and Li, 2005). Two specified the time point at
which recurrence rate was assessed (Ma, 2013; Yan and Li, 2005) whiletwo did not (Liu et al., 2012; Shi et al., 2008). Results from singlestudies showed lower recurrence rate with EJF (RR: 1.37 [1.18, 1.59](Yan and Li, 2005), RR: 1.63 [1.23, 2.14] (Ma, 2013)) while twoshowed no statistical significant benefit (RR: 1.19 [1.00, 1.41] (Liuet al., 2012), RR: 1.19 [0.99, 1.42] (Shi et al., 2008)).
3.2.5. Quality of lifeOnly one study reported on HRQoL, using DLQI (Wang et al., 2014).
The quality of evidence was moderate (see Supplementary file 2). DLQIscores after 1 month of treatment with EJF were higher, indicatingpoorer HRQoL, than with doxycycline (MD: 3.07 [2.42, 3.72]).
3.2.6. Adverse eventsThere were 107 mild AEs reported in seven of the 15 trials (Liang
and Wang, 2009; Liu, 1997; Liu et al., 2012; Ou and Tao, 2012; Shiet al., 2005, 2008; Yan and Li, 2005) with 33 events in the interventiongroups and 74 in the control groups. There were no serious AEs re-ported in the trials. In the intervention group, AEs included nausea,vomiting or stomach discomfort (29 cases), itch (2), diarrhoea (1) andburning sensation (1). In the control group, AEs included nausea orstomach discomfort (28), scaling (11), dry mouth (10), itching (9),burning sensation (8), erythema (7), nausea or vertigo (3) and er-ythema, itching or scaling (3).
4. Discussion
The experimental evidence showed that all ingredients in EJF ex-hibited at least one mechanism of action relevant to acne pathogenesiswith the majority showing evidence of decreasing inflammation. Inclinical studies, EJF used alone produced greater improvement insymptoms compared with pharmacotherapies. The clinical findingsshould be considered in light of low to moderate methodologicalquality.
EJF is a common CHM formula recommended clinically for acnevulgaris in textbooks (Shen et al., 1995; Xu, 2004). All six ingredients ofEJF may have an effect in decreasing inflammation, sebum productionand hyperkeratinization. They may also have an inhibitory effect on P.acnes as well as preventing P. acnes from adhering to host cells. Panaxginseng and glycyrrhizic acid from Glycyrrhiza glabra and Glycyrrhizauralensis decrease serum testosterone (Armanini et al., 2004) and en-courage lipolysis in mature adipocytes (Moon et al., 2012). Glycyrrhizaglabra, Panax ginseng, Phellodendron amurense and Coptis chinensis allinhibit P. acnes growth (Higaki et al., 1996; Nam et al., 2003; Wanget al., 2013a).
Four of the six ingredients Glycyrrhiza glabra, Coptis coptidis,Eriobotrya japonica and Panax ginseng inhibit PPAR-γ. Phellodendronamurense, Eriobotrya japonica, Panax ginseng, liquiritigenin fromGlycyrrhiza glabra and the whole herb extract of Coptis chinensis all in-hibit TNF-α. NF-κB is activated in comedones and strongly expresses IL-1α which increases hyperkeratinization (Zouboulis et al., 2014). Threeof the ingredients, Phellodendron amurense, Morus alba and Eriobotryajaponica, inhibit NF-κB cytokines. Three of the ingredients, Glycyrrhizaglabra, Phellodendron amurense and Eriobotrya japonica, inhibited IL-1βnot IL-1α (Choi et al., 2014; Lee et al., 2008; Wang et al., 2011).
The clinical evidence showed that the results of the pooled studiesof EJF was more effective in reducing lesion count, and the effect of theintervention was greatest when EJF was used alone compared topharmacotherapy though there was considerable heterogeneity. Theeffect of EJF varied according to the comparator type, with the highesteffect seen when compared with antibiotics plus topical supplements.There were conflicting findings when EJF was compared with anti-biotics alone and in combination with other medications. The reasonsfor this are unclear. Each of the studies varied the ingredients in theirstudies. Future research should use identical herbs to evaluate the effecton acne.
Fig. 2. Risk of bias assessment.
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
20
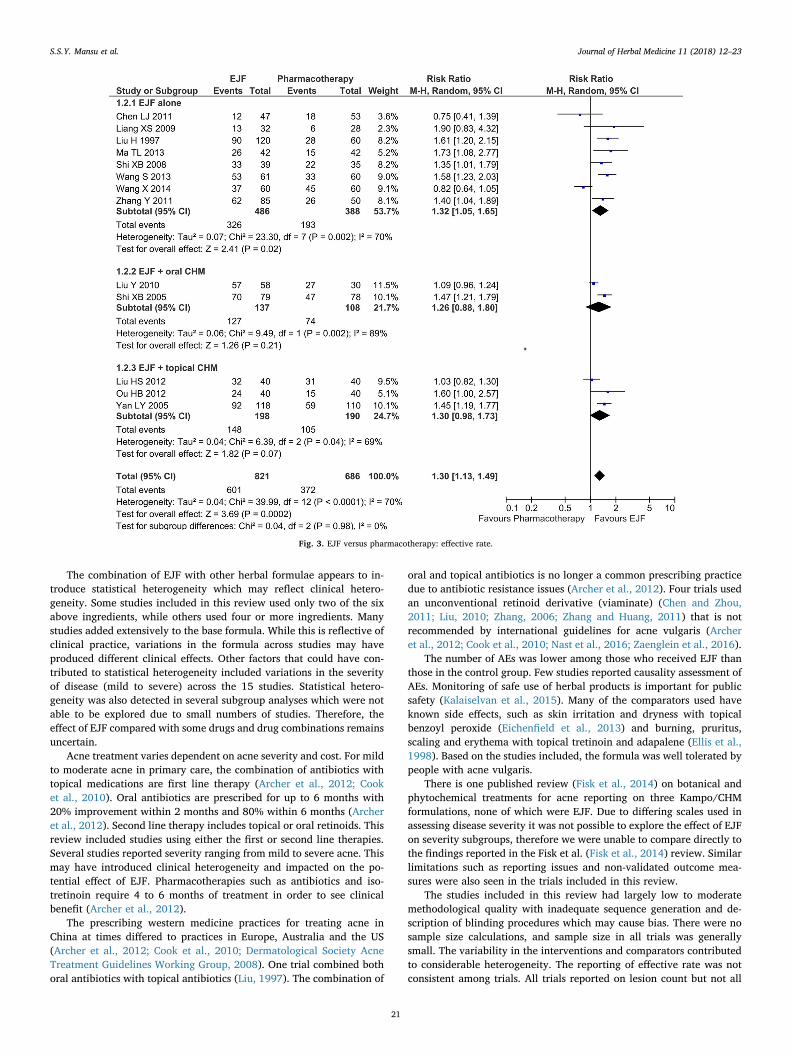
The combination of EJF with other herbal formulae appears to in-troduce statistical heterogeneity which may reflect clinical hetero-geneity. Some studies included in this review used only two of the sixabove ingredients, while others used four or more ingredients. Manystudies added extensively to the base formula. While this is reflective ofclinical practice, variations in the formula across studies may haveproduced different clinical effects. Other factors that could have con-tributed to statistical heterogeneity included variations in the severityof disease (mild to severe) across the 15 studies. Statistical hetero-geneity was also detected in several subgroup analyses which were notable to be explored due to small numbers of studies. Therefore, theeffect of EJF compared with some drugs and drug combinations remainsuncertain.
Acne treatment varies dependent on acne severity and cost. For mildto moderate acne in primary care, the combination of antibiotics withtopical medications are first line therapy (Archer et al., 2012; Cooket al., 2010). Oral antibiotics are prescribed for up to 6 months with20% improvement within 2 months and 80% within 6 months (Archeret al., 2012). Second line therapy includes topical or oral retinoids. Thisreview included studies using either the first or second line therapies.Several studies reported severity ranging from mild to severe acne. Thismay have introduced clinical heterogeneity and impacted on the po-tential effect of EJF. Pharmacotherapies such as antibiotics and iso-tretinoin require 4 to 6 months of treatment in order to see clinicalbenefit (Archer et al., 2012).
The prescribing western medicine practices for treating acne inChina at times differed to practices in Europe, Australia and the US(Archer et al., 2012; Cook et al., 2010; Dermatological Society AcneTreatment Guidelines Working Group, 2008). One trial combined bothoral antibiotics with topical antibiotics (Liu, 1997). The combination of
oral and topical antibiotics is no longer a common prescribing practicedue to antibiotic resistance issues (Archer et al., 2012). Four trials usedan unconventional retinoid derivative (viaminate) (Chen and Zhou,2011; Liu, 2010; Zhang, 2006; Zhang and Huang, 2011) that is notrecommended by international guidelines for acne vulgaris (Archeret al., 2012; Cook et al., 2010; Nast et al., 2016; Zaenglein et al., 2016).
The number of AEs was lower among those who received EJF thanthose in the control group. Few studies reported causality assessment ofAEs. Monitoring of safe use of herbal products is important for publicsafety (Kalaiselvan et al., 2015). Many of the comparators used haveknown side effects, such as skin irritation and dryness with topicalbenzoyl peroxide (Eichenfield et al., 2013) and burning, pruritus,scaling and erythema with topical tretinoin and adapalene (Ellis et al.,1998). Based on the studies included, the formula was well tolerated bypeople with acne vulgaris.
There is one published review (Fisk et al., 2014) on botanical andphytochemical treatments for acne reporting on three Kampo/CHMformulations, none of which were EJF. Due to differing scales used inassessing disease severity it was not possible to explore the effect of EJFon severity subgroups, therefore we were unable to compare directly tothe findings reported in the Fisk et al. (Fisk et al., 2014) review. Similarlimitations such as reporting issues and non-validated outcome mea-sures were also seen in the trials included in this review.
The studies included in this review had largely low to moderatemethodological quality with inadequate sequence generation and de-scription of blinding procedures which may cause bias. There were nosample size calculations, and sample size in all trials was generallysmall. The variability in the interventions and comparators contributedto considerable heterogeneity. The reporting of effective rate was notconsistent among trials. All trials reported on lesion count but not all
Fig. 3. EJF versus pharmacotherapy: effective rate.
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
21

reported on severity of lesions. Although not a validated outcome, re-porting of lesion count and severity is widely used (Barratt et al., 2009).There is a need to establish the criteria for assessing lesion count.
Few studies reported on recurrence rate and follow up, with a lackof descriptions of withdrawals and drop-outs. None of the studies re-ported using intention-to-treat analyses to account for missing data.There was also large variability in comparators and the use of un-conventional retinoid derivatives introduced considerable statisticalheterogeneity in this review. Considering the low to moderate metho-dological quality in study design for most of the trials included in thisreview, the results should be interpreted with caution.
5. Conclusions
The six ingredients of EJF have anti-inflammatory, antibacterial,anti-lipogenic, anti-adipogenic and anti-androgenic effects. These ac-tions may contribute to the effects seen in clinical studies. The numberof people achieving a reduction in lesion count was higher with EJFcompared with various pharmacotherapies, although statistical het-erogeneity was detected in several meta-analyses. No serious AEs werereported in clinical trials, suggesting that EJF was well-tolerated bypeople with acne. Rigorously designed studies that describe originalformula ingredients, grade the severity of acne and report on clinicallyrelevant outcomes such as HRQoL are needed.
Contributions of authors
SM and KW performed searches of English (SM) and Chinese (KW)databases. KW performed data extraction. SM and KW drafted themanuscript. MC, BM and AZ contributed to the interpretation of resultsand reviewed the manuscript for critical contents. CX provided criticalcomments and revised the manuscript. All authors read and approvedthe final version.
Conflict of interest
None.
Acknowledgements
The project is jointly supported by the China-Australia InternationalResearch Centre for Chinese Medicine (CAIRCCM) − a joint initiativeof RMIT University, Australia and the Guangdong Provincial Academyof Chinese Medical Sciences, China. We also thank Dr. Wenyu (Iris)Zhou for data validation and assistance with data extraction.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in theonline version, at http://dx.doi.org/10.1016/j.hermed.2017.09.001.
References
Adebamowo, C.A., Spiegelman, D., Berkey, C.S., Danby, F.W., Rockett, H.H., Colditz,G.A., Willett, W.C., Holmes, M.D., 2006. Milk consumption and acne in adolescentgirls. Dermatol. Online J. 12 (4), 1.
Adebamowo, C.A., Spiegelman, D., Berkey, C.S., Danby, F.W., Rockett, H.H., Colditz,G.A., Willett, W.C., Holmes, M.D., 2008. Milk consumption and acne in teenagedboys. J. Am. Acad. Dermatol. 58 (5), 787–793.
Allijn, I.E., Vaessen, S.F., Quarles van Ufford, L.C., Beukelman, K.J., de Winther, M.P.,Storm, G., Schiffelers, R.M., 2016. Head-to-Head comparison of anti-inflammatoryperformance of known natural products In vitro. PLoS One 11 (5), e0155325.
Archer, C.B., Cohen, S.N., Baron, S.E., 2012. Guidance on the diagnosis and clinicalmanagement of acne. Clin. Exp. Dermatol. 37 (Suppl. 1), 1–6.
Armanini, D., Mattarello, M.J., Fiore, C., Bonanni, G., Scaroni, C., Sartorato, P., Palermo,M., 2004. Licorice reduces serum testosterone in healthy women. Steroids 69(11–12), 763–766.
Barratt, H., Hamilton, F., Car, J., Lyons, C., Layton, A., Majeed, A., 2009. Outcomemeasures in acne vulgaris: systematic review. Br. J. Dermatol. 160 (1), 132–136.
Bhate, K., Williams, H.C., 2014. What's new in acne? an analysis of systematic reviewspublished in 2011–2012. Clin. Exp. Dermatol. 39 (3), 273–277 (quiz 277–278).
Bialecka, A., Mak, M., Biedron, R., Bobek, M., Kasprowicz, A., Marcinkiewicz, J., 2005.Different pro-inflammatory and immunogenic potentials of Propionibacterium acnesand Staphylococcus epidermidis: implications for chronic inflammatory acne. Arch.Immunol. Ther. Exp. (Warsz) 53 (1), 79–85.
Bowe, W.P., Doyle, A.K., Crerand, C.E., Margolis, D.J., Shalita, A.R., 2011. Body imagedisturbance in patients with acne vulgaris. J. Clin. Aesthet. Dermatol. 4 (7), 35–41.
Burke, B.M., Cunliffe, W.J., 1984. The assessment of acne vulgaris–the Leeds technique.Br. J. Dermatol. 111 (1), 83–92.
Chang, C.T., Huang, S.S., Lin, S.S., Amagaya, S., Ho, H.Y., Hou, W.C., Shie, P.H., Wu, J.B.,Huang, G.J., 2011. Anti-inflammatory activities of tormentic acid from suspensioncells of Eriobotrya Japonicaex vivo and in vivo. Food Chem. 127 (3), 1131–1137.
Chen, L.J., Zhou, J.G., 2011. Clinical observation of Chinese Medicine Fomular Pi Pa JingFei Yin for acne vulgaris patients. Asia Pac. Traditional Med. 7 (4), 48–49.
Choi, E.M., Hwang, J.K., 2005. Effects of Morus alba leaf extract on the production ofnitric oxide, prostaglandin E2 and cytokines in RAW264.7 macrophages. Fitoterapia76 (7–8), 608–613.
Choi, B.H., Ahn, I.S., Kim, Y.H., Park, J.W., Lee, S.Y., Hyun, C.K., Do, M.S., 2006.Berberine reduces the expression of adipogenic enzymes and inflammatory moleculesof 3T3-L1 adipocyte. Exp. Mol. Med. 38 (6), 599–605.
Choi, Y.Y., Kim, M.H., Han, J.M., Hong, J., Lee, T.H., Kim, S.H., Yang, W.M., 2014. Theanti-inflammatory potential of Cortex Phellodendron in vivo and in vitro: down-regulation of NO and iNOS through suppression of NF-kappaB and MAPK activation.Int. Immunopharmacol. 19 (2), 214–220.
Chren, M.M., Lasek, R.J., Quinn, L.M., Mostow, E.N., Zyzanski, S.J., 1996. Skindex, aquality-of-life measure for patients with skin disease: reliability, validity, and re-sponsiveness. J. Invest. Dermatol. 107 (5), 707–713.
The Cochrane Collaboration, 2012. Review Manager (RevMan) Version 5.2. The NordicCochrane Centre, The Cochrane Collaboration, Copenhagen.
Cook, D., Krassas, G., Huang, T., 2010. Acne − best practice management. Aust. Fam.Physician 39 (9), 656–660.
Cordain, L., Lindeberg, S., Hurtado, M., Hill, K., Eaton, S.B., Brand-Miller, J., 2002. Acnevulgaris: a disease of Western civilization. Arch. Dermatol. 138 (12), 1584–1590.
Costa, C.S., Bagatin, E., da Silva, E.M.K., Lúcio, M.M., Magin, P., Riera, R., 2011. Oralisotretinoin for acne, Cochrane Database of Systematic Reviews. John Wiley Sons,Ltd.
Dermatological Society Acne Treatment Guidelines Working Group, C.M.D.A., 2008.China acne treatment guidelines (Draft). J. Clin. Dermatol. 37 (5), 339–342.
Doshi, A., Zaheer, A., Stiller, M.J., 1997. A comparison of current acne grading systemsand proposal of a novel system. Int. J. Dermatol. 36 (6), 416–418.
Dreno, B., Gollnick, H.P., Kang, S., Thiboutot, D., Bettoli, V., Torres, V., Leyden, J., 2015.Understanding innate immunity and inflammation in acne: implications for man-agement. J. Eur. Acad. Dermatol. Venereol. 29 (Suppl. 4), 3–11.
Eichenfield, L.F., Krakowski, A.C., Piggott, C., Del Rosso, J., Baldwin, H., Friedlander,S.F., Levy, M., Lucky, A., Mancini, A.J., Orlow, S.J., Yan, A.C., Vaux, K.K., Webster,G., Zaenglein, A.L., Thiboutot, D.M., 2013. Evidence-based recommendations for thediagnosis and treatment of pediatric acne. Pediatrics 131 (Suppl. 3), S163–186.
Eichenfield, L.F., Del Rosso, J.Q., Mancini, A.J., Cook-Bolden, F., Stein Gold, L., Desai, S.,Weiss, J., Pariser, D., Zeichner, J., Bhatia, N., Kircik, L., 2015. Evolving perspectiveson the etiology and pathogenesis of acne vulgaris. J. Drugs Dermatol. 14 (3),263–272.
Ellis, C.N., Millikan, L.E., Smith, E.B., Chalker, D.M., Swinyer, L.J., Katz, I.H., Berger, R.S.,Mills Jr., O.H., Baker, M., Verschoore, M., Loesche, C., 1998. Comparison of adapa-lene 0.1% solution and tretinoin 0.025% gel in the topical treatment of acne vulgaris.Br. J. Dermatol. 139 (Suppl. 52), 41–47.
Enk, R., Ehehalt, R., Graham, J.E., Bierhaus, A., Remppis, A., Greten, H.J., 2007.Differential effect of Rhizoma coptidis and its main alkaloid compound berberine onTNF-alpha induced NFkappaB translocation in human keratinocytes. J.Ethnopharmacol. 109 (1), 170–175.
Eo, H.J., Park, J.H., Park, G.H., Lee, M.H., Lee, J.R., Koo, J.S., Jeong, J.B., 2014. Anti-inflammatory and anti-cancer activity of mulberry (Morus alba L.) root bark. BMCComplement. Altern. Med. 14, 200.
Fehnel, S.E., McLeod, L.D., Brandman, J., Arbit, D.I., McLaughlin-Miley, C.J., Coombs,J.H., Martin, A.R., Girman, C.J., 2002. Responsiveness of the Acne-Specific Quality ofLife Questionnaire (Acne-QoL) to treatment for acne vulgaris in placebo-controlledclinical trials. Qual. Life Res. 11 (8), 809–816.
Feng, A.W., Gao, W., Zhou, G.R., Yu, R., Li, N., Huang, X.L., Li, Q.R., Li, J.S., 2012.Berberine ameliorates COX-2 expression in rat small intestinal mucosa partiallythrough PPARgamma pathway during acute endotoxemia. Int. Immunopharmacol.12 (1), 182–188.
Fisk, W.A., Lev-Tov, H.A., Sivamani, R.K., 2014. Botanical and phytochemical therapy ofacne: a systematic review. Phytother. Res. 28 (8), 1137–1152.
Fu, Y., Zhou, E., Wei, Z., Song, X., Liu, Z., Wang, T., Wang, W., Zhang, N., Liu, G., Yang,Z., 2014. Glycyrrhizin inhibits lipopolysaccharide-induced inflammatory response byreducing TLR4 recruitment into lipid rafts in RAW264.7 cells. Biochim. Biophys. Acta1840 (6), 1755–1764.
Fuhrmann, T., Smith, N., Tausk, F., 2010. Use of complementary and alternative medicineamong adults with skin disease: updated results from a national survey. J. Am. Acad.Dermatol. 63 (6), 1000–1005.
Gao, Y., Yang, M.F., Su, Y.P., Jiang, H.M., You, X.J., Yang, Y.J., Zhang, H.L., 2013.Ginsenoside Re reduces insulin resistance through activation of PPAR-gammapathway and inhibition of TNF-alpha production. J. Ethnopharmacol. 147 (2),509–516.
Gollnick, H.P., 2015. From new findings in acne pathogenesis to new approaches intreatment. J. Eur. Acad. Dermatol. Venereol. 29 (Suppl. 5), 1–7.
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
22
Gumy, C., Thurnbichler, C., Aubry, E.M., Balazs, Z., Pfisterer, P., Baumgartner, L.,Stuppner, H., Odermatt, A., Rollinger, J.M., 2009. Inhibition of 11beta-hydro-xysteroid dehydrogenase type 1 by plant extracts used as traditional antidiabeticmedicines. Fitoterapia 80 (3), 200–205.
Gupta, M.A., Johnson, A.M., Gupta, A.K., 1998. The development of an Acne Quality ofLife scale: reliability, validity, and relation to subjective acne severity in mild tomoderate acne vulgaris. Acta Derm. Venereol. 78 (6), 451–456.
Halvorsen, J.A., Stern, R.S., Dalgard, F., Thoresen, M., Bjertness, E., Lien, L., 2011.Suicidal ideation, mental health problems, and social impairment are increased inadolescents with acne: a population-based study. J. Invest. Dermatol. 131 (2),363–370 (Epub 2010 Sep 2016).
Han, S.X., 2006. Pi Pa Qing Fei Yin Combines with Chinese Medicine Mask to Treat AcneVulgaris in 90 Patients. pp. 266.
Higaki, S., Nakamura, M., Morohashi, M., Hasegawa, Y., Yamagishi, T., 1996. Activity ofeleven kampo formulations and eight kampo crude drugs against Propionibacteriumacnes isolated from acne patients: retrospective evaluation in 1990 and 1995. J.Dermatol. 23 (12), 871–875.
Higgins, J., Green, S., 2011. In: Higgins JPT, G.S. (Ed.), Cochrane Handbook forSystematic Reviews of Interventions Version 5.1.0 [updated March 2011]. TheCochrane Collaboration 2011.
Hull, P.R., D'Arcy, C., 2005. Acne, depression, and suicide. Dermatol. Clin. 23 (4),665–674.
Jeong, H.W., Hsu, K.C., Lee, J.W., Ham, M., Huh, J.Y., Shin, H.J., Kim, W.S., Kim, J.B.,2009. Berberine suppresses proinflammatory responses through AMPK activation inmacrophages. Am. J. Physiol. Endocrinol. Metab. 296 (4), E955–964.
Kalaiselvan, V., Saurabh, A., Kumar, R., Singh, G.N., 2015. Adverse reactions to herbalproducts: an analysis of spontaneous reports in the database of thePharmacovigilance Programme of India. J. Herb. Med. 5 (1), 48–54.
Kim, S.H., Shin, T.Y., 2009. Anti-inflammatory effect of leaves of Eriobotrya japonicacorrelating with attenuation of p38 MAPK, ERK, and NF-kappaB activation in mastcells. Toxicol. In Vitro 23 (7), 1215–1219.
Kim, J.Y., Park, S.J., Yun, K.J., Cho, Y.W., Park, H.J., Lee, K.T., 2008. Isoliquiritigeninisolated from the roots of Glycyrrhiza uralensis inhibits LPS-induced iNOS and COX-2expression via the attenuation of NF-kappaB in RAW 264.7 macrophages. Eur. J.Pharmacol. 584 (1), 175–184.
Kurokawa, I., Danby, F.W., Ju, Q., Wang, X., Xiang, L.F., Xia, L., Chen, W., Nagy, I.,Picardo, M., Suh, D.H., Ganceviciene, R., Schagen, S., Tsatsou, F., Zouboulis, C.C.,2009. New developments in our understanding of acne pathogenesis and treatment.Exp. Dermatol. 18 (10), 821–832.
Lee, C.H., Wu, S.L., Chen, J.C., Li, C.C., Lo, H.Y., Cheng, W.Y., Lin, J.G., Chang, Y.H.,Hsiang, C.Y., Ho, T.Y., 2008. Eriobotrya japonica leaf and its triterpenes inhibitedlipopolysaccharide-induced cytokines and inducible enzyme production via the nu-clear factor-kappaB signaling pathway in lung epithelial cells. Am. J. Chin. Med. 36(6), 1185–1198.
Lee, J.H., Shim, J.S., Chung, M.S., Lim, S.T., Kim, K.H., 2009. Inhibition of pathogenadhesion to host cells by polysaccharides from Panax ginseng. Biosci. Biotechnol.Biochem. 73 (1), 209–212.
Li, C., Eom, T., Jeong, Y., 2015. Glycyrrhiza glabra L. extract inhibits LPS-induced in-flammation in RAW macrophages. J. Nutr. Sci. Vitaminol. (Tokyo) 61 (5), 375–381.
Liang, X.S., Wang, W.P., 2009. Modified Pi Pa Qing Fei Yin for 32 acne vulgaris patients.J. New Chin. Med. 41 (11), 87.
Liu, S.H., Zhang, W.J., Zhuang, M., Wu, R., Gen, J., 2012. clinical observation on treat-ment of acne with modified Pipa Qingfei Yin and supplemented Diandan San. AnhuiMed. Pharm. J. 16 (1), 108–109.
Liu, H., 1997. Clinical observation of modified Pi Pa Qing Fei Yin for acne vulgaris pa-tients. J. Mod. Med. Doctors 2 (5), 55.
Liu, Y., 2010. Modified Pi Pa Qing Fei Yin combines with Wu Wei Xiao Du Yin for 58 acnevulgaris patients. J. Pract. Traditional Chin. Med. 26 (5), 305–306.
Lynn, D.D., Umari, T., Dunnick, C.A., Dellavalle, R.P., 2016. The epidemiology of acnevulgaris in late adolescence. Adolesc. Health Med. Ther. 7, 13–25.
Ma, T.L., 2013. Modified Pi Pa Qing Fei Yin for 32 acne vulgaris patients. Menggu Chin.Med. J. 2013 (8), 12–13.
Moon, M.H., Jeong, J.K., Lee, Y.J., Seol, J.W., Ahn, D.C., Kim, I.S., Park, S.Y., 2012.18beta-Glycyrrhetinic acid inhibits adipogenic differentiation and stimulates lipo-lysis. Biochem. Biophys. Res. Commun. 420 (4), 805–810.
Motley, R.J., Finlay, A.Y., 1992. Practical use of a disability index in the routine man-agement of acne. Clin. Exp. Dermatol. 17 (1), 1–3.
Nam, C., Kim, S., Sim, Y., Chang, I., 2003. Anti-acne effects of oriental herb extracts: anovel screening method to select anti-acne agents. Skin Pharmacol. Appl. SkinPhysiol. 16 (2), 84–90.
Nast, A., Dreno, B., Bettoli, V., Bukvic Mokos, Z., Degitz, K., Dressler, C., Finlay, A.Y.,Haedersdal, M., Lambert, J., Layton, A., Lomholt, H.B., Lopez-Estebaranz, J.L.,Ochsendorf, F., Oprica, C., Rosumeck, S., Simonart, T., Werner, R.N., Gollnick, H.,2016. European evidence-based (S3) guideline for the treatment of acne − update2016 − short version. J. Eur. Acad. Dermatol. Venereol. 30 (8), 1261–1268.
Neamsuvan, O., Kama, A., Salaemae, A., Leesen, S., Waedueramae, N., 2015. A survey ofherbal formulas for skin diseases from Thailand’s three southern border provinces. J.
Herb. Med. 5 (4), 190–198.Ou, H.B., Tao, X.Y., 2012. Modified Pi Pa Qing Fei Yin combined with topical treatment of
Dian Dao San for 80 acne vulgaris patients. J. Liaoning Chin. Med. 39 (7),1313–1314.
Park, E.K., Rhee, H.I., Jung, H.S., Ju, S.M., Lee, Y.A., Lee, S.H., Hong, S.J., Yang, H.I., Yoo,M.C., Kim, K.S., 2007. Antiinflammatory effects of a combined herbal preparation(RAH13) of Phellodendron amurense and Coptis chinensis in animal models of in-flammation. Phytother. Res. 21 (8), 746–750.
Pillsbury, D.M., 1956. Dermatology. Saunders, Philadelphia.Rebhun, J.F., Glynn, K.M., Missler, S.R., 2015. Identification of glabridin as a bioactive
compound in licorice (Glycyrrhiza glabra L.) extract that activates human peroxisomeproliferator-activated receptor gamma (PPARgamma). Fitoterapia 106, 55–61.
Ren, X., Zhou, S., Zhou, J., 1997. Demodex infection in university and middle schoolstudents. Hunan Yi Ke Da Xue Xue Bao 22 (3), 281.
Sharma, B.R., Oh, J., Kim, H.A., Kim, Y.J., Jeong, K.S., Rhyu, D.Y., 2015. Anti-obesityeffects of the mixture of eriobotrya japonica and nelumbo nucifera in adipocytes andhigh-fat diet-induced obese mice. Am. J. Chin. Med. 43 (4), 681–694.
Shen, D., Wu, X., Wang, N., 1995. Manual of Dermatology in Chinese Medicine. EastlandPress, Seattle.
Shi, X.B., Zhou, R.E., Zhao, Y.D., 2005. Clinical observation of modified Pi Pa Qing Fei Yinfor moderate and servere acne vulgaris. Jilin Chin. Med. J. 25 (8), 24–25.
Shi, X.B., Zhou, R.E., Zhao, Y.D., 2008. Effects of loquat qingfei decoction treatment andprevention relapes of acne vulgaris. Chin. J. Dem. Venereal. 22 (6), 375–376.
Smith, R.N., Mann, N.J., Braue, A., Makelainen, H., Varigos, G.A., 2007. A low-glycemic-load diet improves symptoms in acne vulgaris patients: a randomized controlled trial.Am. J. Clin. Nutr. 86 (1), 107–115.
Tan, J., Wolfe, B., Weiss, J., Stein-Gold, L., Bikowski, J., Del Rosso, J., Webster, G.F.,Lucky, A., Thiboutot, D., Wilkin, J., Leyden, J., Chren, M.M., 2012. Acne severitygrading: determining essential clinical components and features using a Delphiconsensus. J. Am. Acad. Dermatol. 67 (2), 187–193.
Trivedi, N.R., Cong, Z., Nelson, A.M., Albert, A.J., Rosamilia, L.L., Sivarajah, S., Gilliland,K.L., Liu, W., Mauger, D.T., Gabbay, R.A., Thiboutot, D.M., 2006. Peroxisome pro-liferator-activated receptors increase human sebum production. J. Invest. Dermatol.126 (9), 2002–2009.
Uto, T., Suangkaew, N., Morinaga, O., Kariyazono, H., Oiso, S., Shoyama, Y., 2010.Eriobotryae folium extract suppresses LPS-induced iNOS and COX-2 expression byinhibition of NF-kappaB and MAPK activation in murine macrophages. Am. J. Chin.Med. 38 (5), 985–994.
Vos, T., Flaxman, A.D., Naghavi, M., Lozano, R., Michaud, C., et al., 2012. Years livedwith disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: asystematic analysis for the Global Burden of Disease Study 2010. Lancet 380 (9859),2163–2196.
Wang, C.Y., Kao, T.C., Lo, W.H., Yen, G.C., 2011. Glycyrrhizic acid and 18beta-glycyr-rhetinic acid modulate lipopolysaccharide-induced inflammatory response by sup-pression of NF-kappaB through PI3K p110delta and p110 gamma inhibitions. J.Agric. Food Chem. 59 (14), 7726–7733.
Wang, L., Yang, X., Yu, X., Yao, Y., Ren, G., 2013a. Evaluation of antibacterial and anti-inflammatory activities of less polar ginsenosides produced from polar ginsenosidesby heat-transformation. J. Agric. Food Chem. 61 (50), 12274–12282.
Wang, S., Wu, B.L., Zhu, J.T., 2013b. The influence of Pi Pa Qing Fei Yin on androgenlevel in female acne vulgaris patients. J. Shandong Univ. Chin.Medicine 37 (3),230–231.
Wang, X., Chen, J.H., Yao, J.H., Lin, Q.F., 2014. Influence of modified pipa qingfei de-coction combined with bloodletting in ear on curative effect and quality of life ofpatients with acne. China Mod. Med. 21 (19), 93–94.
Xu, Y., 2004. Dermatology in Traditional Chinese Medicine. Donica Publishing Ltd, StAlbans.
Yan, L.Y., Li, J.Z., 2005. Clinical Observation on Bai Di She Lotion Combined with ChuoZhuang Ling for Acne Vulgaris. J. Chin. Med. External Treat. 14 (1), 17.
Yang, Y., Yang, X., Xu, B., Zeng, G., Tan, J., He, X., Hu, C., Zhou, Y., 2014. Chemicalconstituents of Morus alba L. and their inhibitory effect on 3T3-L1 preadipocyteproliferation and differentiation. Fitoterapia 98, 222–227.
Zaenglein, A.L., Pathy, A.L., Schlosser, B.J., Alikhan, A., Baldwin, H.E., Berson, D.S.,Bowe, W.P., Graber, E.M., Harper, J.C., Kang, S., Keri, J.E., Leyden, J.J., Reynolds,R.V., Silverberg, N.B., Stein Gold, L.F., Tollefson, M.M., Weiss, J.S., Dolan, N.C.,Sagan, A.A., Stern, M., Boyer, K.M., Bhushan, R., 2016. Guidelines of care for themanagement of acne vulgaris. J. Am. Acad. Dermatol. 74 (5), 945–973 e933.
Zhang, Y., Huang, Y., 2011. Effect observation of Loquat Qingfeiyin with Modification fortreating 135 cases of acne vulgaris. Mod. Med. 27 (3), 334–335.
Zhang, L.L., 2006. Clinical observation on modified Pi Pa Qing Fei Yin for acne vulgarispatients with Chinese medicine syndrome of damp-heat in lung and stomach. J. Pract.Integr. Traditional West. Med. 6 (3).
Zheng, X.Y., 2002. Guideline for New Chinese Herbal Medicine in Clinical Practice andResearch. Chinese Medical Science and Technology Publishing House.
Zouboulis, C.C., Jourdan, E., Picardo, M., 2014. Acne is an inflammatory disease andalterations of sebum composition initiate acne lesions. J. Eur. Acad. Dermatol.Venereol. 28 (5), 527–532.
S.S.Y. Mansu et al. Journal of Herbal Medicine 11 (2018) 12–23
23

394
Appendix 15 published review “Evidenced-based complementary and alternative medicine”

Review ArticleAcupuncture for Acne Vulgaris: A SystematicReview and Meta-Analysis
Suzi S. Y. Mansu ,1 Haiying Liang ,2 Shefton Parker,1
Meaghan E. Coyle ,1 Kaiyi Wang,1 Anthony L. Zhang ,1 Xinfeng Guo ,2
Chuanjian Lu ,2 and Charlie C. L. Xue 1,2
1China-Australia International Research Centre for Chinese Medicine, School of Health and Biomedical Sciences,RMIT University, P.O. Box 71, Bundoora, VIC 3083, Australia2Guangdong Provincial Hospital of Chinese Medicine, Guangdong Provincial Academy of Chinese Medical Sciences andThe Second Clinical College, Guangzhou University of Chinese Medicine, Guangzhou, China
Correspondence should be addressed to Chuanjian Lu; [email protected] Charlie C. L. Xue; [email protected]
Received 15 September 2017; Accepted 21 January 2018; Published 12 March 2018
Academic Editor: Dawn M. Bellanti
Copyright © 2018 Suzi S. Y. Mansu et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Purpose. To conduct a systematic review and meta-analysis to determine the current best available evidence of the efficacy andsafety of acupuncture and related therapies for acne vulgaris. Methods. Eleven English and Chinese databases were searched toidentify randomized controlled trials (RCTs) of acne vulgaris compared to pharmacotherapies, no treatment, and sham or placeboacupuncture. Methodological quality was assessed using Cochrane Collaboration’s risk of bias tool. Meta-analysis was conductedusing RevMan software. Results. Twelve RCTs were included in the qualitative review and 10 RCTs were included in meta-analysis.Methodological quality of trials was generally low. The chance of achieving ≥30% change in lesion count in the acupuncture groupwas no different to the pharmacotherapy group (RR: 1.07 [95% CI 0.98, 1.17]; 𝐼2 = 8%) and ≥50% change in lesion count inthe acupuncture group was not statistically different to the pharmacotherapy group (RR: 1.07 [95% CI 0.98, 1.17]; 𝐼2 = 50%).Conclusions. While caution should be exercised due to quality of the included studies, acupuncture and auricular acupressure werenot statistically different to guideline recommended treatments but were with fewer side effects and may be a treatment option.Future trials should address the methodological weaknesses and meet standard reporting requirements stipulated in STRICTA.
1. Introduction
Acne vulgaris (acne) is a chronic and self-limiting conditionthat begins in adolescence and can last over 10 years [1]. Acneis characterized by inflamed and noninflamed comedones,oily skin, and cysts [2]. The mechanisms for the initialdevelopment of comedones are not fully understood [3].Four factors have been identified which contribute to acnelesions and are the main targets of treatment. These factorsinclude follicular keratinization, sebum production, Propi-onibacterium acnes (P. acnes), and inflammatory mediatorrelease [4]. Acne lesions may involve cellular inflammationcausing hyperkeratinization of follicular ducts [5]. P. acnescan induce keratinocytes to produce cytokines which ruptureducts, causing comedones [3]. Genetics [6] and androgen
imbalances [7] can influence sebaceous gland lipid synthesis.Exacerbation can result from single or multiple factors suchas P. acnes, menstruation, occupation, personal sweating,diet, or stress [2, 8].
Treatment of acne includes topical benzoyl peroxide andtopical retinoids or antibiotics for mild to moderate acneand oral antibiotics combined with either topical benzoylperoxide or topical or oral retinoids for severe acne [4].Acupuncture is an umbrella term for traditional Chinesemedicine techniques that stimulate acupuncture points.Techniques include acupuncture (insertion of fine needlesat specific loci typically for a period of 20 to 30 minutes),auricular acupuncture (insertion of needles in specific lociof the auricle), auricular acupressure (placement of bluntinstruments such as small metallic ball bearings at specific
HindawiEvidence-Based Complementary and Alternative MedicineVolume 2018, Article ID 4806734, 12 pageshttps://doi.org/10.1155/2018/4806734

2 Evidence-Based Complementary and Alternative Medicine
loci of the auricle), electroacupuncture (mild electric stimu-lation of acupuncture needles) [9], and moxibustion (burningof Artemisia argyi Levl. et Vant or Artemisia vulgaris leafin a processed form) [10]. Several studies have suggested apotential role of acupuncture techniques in acne. Auricularacupressure and surrounding needle (where two to fourneedles are inserted superficially around the acne lesion)have been shown to reduce serum excretion rate (SER) andtestosterone [11]. When acupuncture was combined withbenzoyl peroxide, SER in women was reduced comparedto benzoyl peroxide alone [12]. In animal studies, auricularacupuncture, auricular electroacupuncture, body acupunc-ture, and electro-acupuncture have been shown to decreaseinflammation [13–16]. Auricular acupuncture may reduceacne inflammation through peripheral muscarinic receptors[13] and innate and adaptive immune responses [14, 17, 18],thereby possibly reducing acne inflammation.
Several reviews have examined the potential benefitsof acupuncture techniques in clinical studies. A Cochranereview on complementary therapies for acne [19] evaluatedefficacy of herbal medicine, acupuncture, cupping therapy,dietary modifications, purified bee venom, and tea tree oil.The review found there was a lack of evidence to supportthe use of herbal medicine and acupuncture. Two system-atic reviews of acupuncture for acne have been published,one in English [20] and one in Chinese [21]. Cao et al.[20] included trials which used acupuncture, cupping, andother herbal medicines. While the number of “cured” casesincreased when acupuncture was combined with cupping,or oral or topical herbal medicines, no benefit was foundwhen acupuncture was compared with pharmacotherapy. Thereviewers described the methodological quality of the papersas poor. Li et al. [21] included trials of manual acupuncturecompared to routine conventional medicine (isotretinoinand antibiotics) or multiple Chinese medicine therapies. Theauthors were unable to provide conclusions due to the poorquality of the included trials.
These reviews included herbal medicines and techniquesnot commonly used outside of China. Acupuncture is com-monly used in clinical practice for skin conditions, yet a gapexists in the evaluation of efficacy and safety of acupuncturefor acne vulgaris. This review will analyze acupuncturecompared to pharmacotherapies, no treatment, and sham orplacebo acupuncture to evaluate the efficacy and safety ofacupuncture and acupressure for acne vulgaris.
2. Methods
Eleven databases were searched from inception to May 2013,with an update in May 2016. Five English (PubMed, Embase,Allied and Complementary Medicine Database (AMED),the Cumulative Index to Nursing and Allied Health Liter-ature (CINAHL), and Cochrane Central Register of Con-trolled Trials (CENTRAL)) and six Chinese databases (Chi-nese National Knowledge Infrastructure (CNKI), ChongqingVIP Information Company (CQVIP), Wanfang Data, Chi-nese Biomedical Literature Database (CBM)) as well asChina’s Conference Papers Database and China Dissertationdatabase were searched. There were no language restrictions.
Search terms included acne vulgaris, papulo-pustular acne,acupuncture, acupressure, moxibustion, auricular acupunc-ture and auricular acupressure, electro-acupuncture, electrostimulation, and variants. Moxibustion and acupressure wereincluded as they are commonly used techniques to directlystimulate acupuncture points. Moxibustion in particular iscommonly combined with acupuncture, and the Chineseterm for acupuncture “zhen jiu” literally means acupunctureand moxibustion. Search terms for study design includedrandomized controlled trials, controlled clinical trials, drugtherapy, placebo, and variants.
Titles and abstracts of identified citations were scannedto identify potentially eligible randomized controlled trials(RCTs). Full text was retrieved when eligibility could not beascertained from the title and abstract. RCTs of acupuncture,acupressure, auricular acupuncture, moxibustion, and elec-troacupuncture compared to no treatment, sham acupunc-ture, placebo, or conventional pharmacotherapy for acne vul-garis were included in the review. No age, gender, ethnicity,or language limitations were applied. Trials that includedother modalities, as cointervention, such as pharmacotherapyor Chinese medicine techniques other than those specifiedabove were excluded.
The primary outcome was the change in lesion countmeasured by therapeutic effective rate (TER). Chinesemedicine guidelines recommend reporting the TER ≥50%based on lesion count alone or a combination of lesion countand severity [22]. Many of the studies used a TER of ≥30%as an improvement based on Chinese medicine guidelinesfrom 1994 [23]. The criteria for therapeutic effective ratefrom the 1994 guideline were based on a change in lesioncount and associated symptoms. For analysis, we includeddata for people who achieved 30% or greater on lesion count,irrespective of the minimum threshold used by the study foreffectiveness. Secondary outcomes included severity grading,physician’s overall grading (physician’s assessment or self-reporting), photographic grading, quality of life instruments,and adverse events (AE) reports.
Data extracted included patient demographics, samplesize, dropout rate, details of the intervention and comparator,outcome measures, results, and adverse events. Authors werecontacted if there was missing data. Verification of data wasconducted by an independent researcher (IZ).
Two researchers (KW, IZ) independently assessedmethodological quality using Cochrane Collaboration’srisk of bias tool [24]. Trials were judged as low, unclear, orhigh risk of bias for the domains of sequence generation,allocation concealment, blinding of participants, blindingof outcome assessors, incomplete outcome data, selectivereporting, and other forms of bias such as conflicts ofinterest. For acupuncture studies, it is not feasible to blindpersonnel (practitioner) [25]. Disagreements in judgmentswere resolved by consulting another reviewer (TZ).
Statistical analyses were performed using Review Man-ager 5.3.5 [26]. Dichotomous data are presented as risk ratio(RR) and continuous data as mean difference, with 95% confi-dence intervals (CIs). Data were analyzed for available cases.A random effects model was used. Statistical heterogeneity

Evidence-Based Complementary and Alternative Medicine 3
Records identified throughdatabase searching
(n = 15,306)
Scre
enin
gIn
clude
dEl
igib
ility
Iden
tifica
tion Additional records identified
through other sources(n = 1)
Records after duplicates removal(n = 10,158)
Records screened(n = 10,158)
Records excluded(n = 7,673)
Full-text articles assessedfor eligibility
(n = 2,485)
Studies included inqualitative synthesis
(n = 12)
Studies included inquantitative synthesis(meta-analysis)
(n = 10)
Full-text articles excluded,with reasons (n = 2,473)
Not acne vulgaris = 97Not acupuncture = 566Not a clinical study = 25Not meeting inclusioncriteria = 1,733Not usable data = 17Duplicates = 23Reviews = 10Unable to locate full text = 2
Figure 1: Study selection flow chart.
was considered substantial when the 𝐼2 statistic was greaterthan 50%. We planned to perform sensitivity analysis withstudies assessed as low risk of bias for sequence generation.Subgroup analyses were also conducted on ≥50% and ≥30%TER. Exploration of publication bias was planned if morethan ten studies were included in any meta-analysis. Due tothe number of included trials and methodological quality, notall planned analyses could be performed.
3. Results
3.1. Search Results. A total of 15,306 records with oneadditional record sourced elsewhere were identified from
database searches. After removal of duplicates, screening oftitles and abstracts excluded 7,673 papers, and 2,485 full textswere reviewed (Figure 1).
3.2. Characteristics of Studies. Twelve RCTs involving 1,026participants met the inclusion criteria [27–38]. Ten RCTswith 975 participants were included in the meta-analysis.The data presented from two trials could not be reanalyzeddue to data not being available for individual groups; thesewere excluded from quantitative analysis [37, 38]. The authorswere contacted for additional information; however this wasunsuccessful. All trials recruited male and female participantsexcept K. S. Kim and Y.-B. Kim [37] who recruited only male
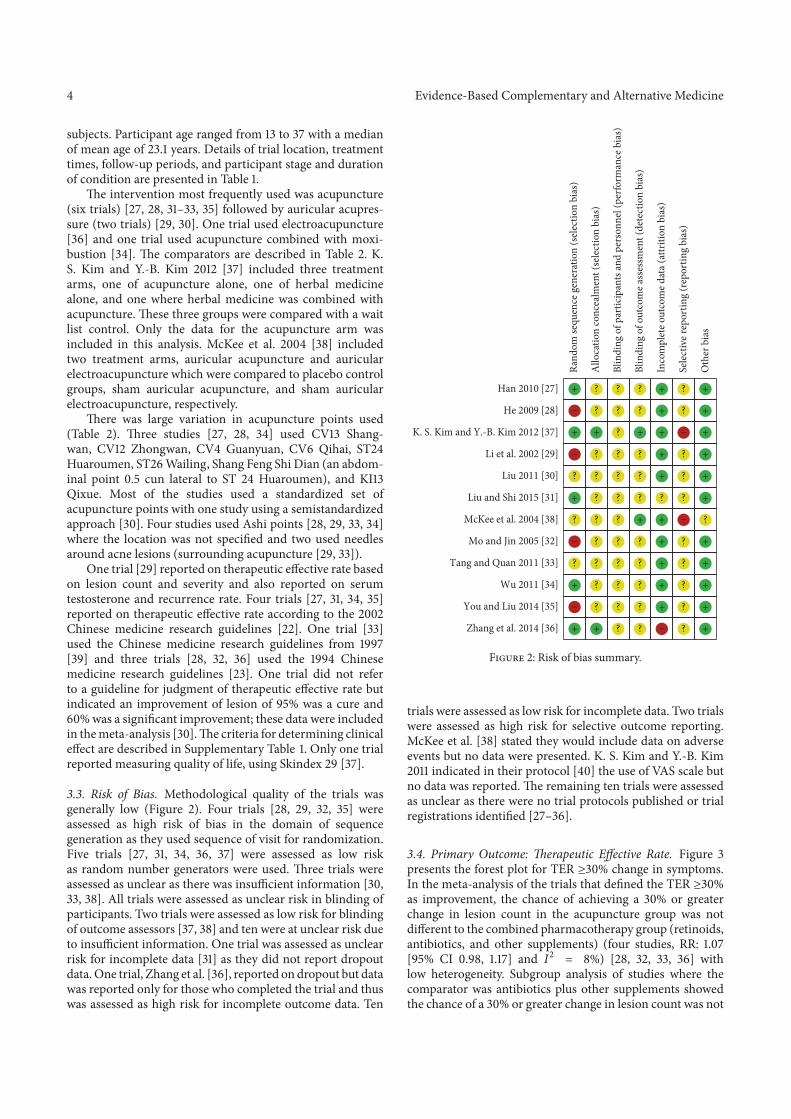
4 Evidence-Based Complementary and Alternative Medicine
subjects. Participant age ranged from 13 to 37 with a medianof mean age of 23.1 years. Details of trial location, treatmenttimes, follow-up periods, and participant stage and durationof condition are presented in Table 1.
The intervention most frequently used was acupuncture(six trials) [27, 28, 31–33, 35] followed by auricular acupres-sure (two trials) [29, 30]. One trial used electroacupuncture[36] and one trial used acupuncture combined with moxi-bustion [34]. The comparators are described in Table 2. K.S. Kim and Y.-B. Kim 2012 [37] included three treatmentarms, one of acupuncture alone, one of herbal medicinealone, and one where herbal medicine was combined withacupuncture. These three groups were compared with a waitlist control. Only the data for the acupuncture arm wasincluded in this analysis. McKee et al. 2004 [38] includedtwo treatment arms, auricular acupuncture and auricularelectroacupuncture which were compared to placebo controlgroups, sham auricular acupuncture, and sham auricularelectroacupuncture, respectively.
There was large variation in acupuncture points used(Table 2). Three studies [27, 28, 34] used CV13 Shang-wan, CV12 Zhongwan, CV4 Guanyuan, CV6 Qihai, ST24Huaroumen, ST26 Wailing, Shang Feng Shi Dian (an abdom-inal point 0.5 cun lateral to ST 24 Huaroumen), and KI13Qixue. Most of the studies used a standardized set ofacupuncture points with one study using a semistandardizedapproach [30]. Four studies used Ashi points [28, 29, 33, 34]where the location was not specified and two used needlesaround acne lesions (surrounding acupuncture [29, 33]).
One trial [29] reported on therapeutic effective rate basedon lesion count and severity and also reported on serumtestosterone and recurrence rate. Four trials [27, 31, 34, 35]reported on therapeutic effective rate according to the 2002Chinese medicine research guidelines [22]. One trial [33]used the Chinese medicine research guidelines from 1997[39] and three trials [28, 32, 36] used the 1994 Chinesemedicine research guidelines [23]. One trial did not referto a guideline for judgment of therapeutic effective rate butindicated an improvement of lesion of 95% was a cure and60% was a significant improvement; these data were includedin the meta-analysis [30]. The criteria for determining clinicaleffect are described in Supplementary Table 1. Only one trialreported measuring quality of life, using Skindex 29 [37].
3.3. Risk of Bias. Methodological quality of the trials wasgenerally low (Figure 2). Four trials [28, 29, 32, 35] wereassessed as high risk of bias in the domain of sequencegeneration as they used sequence of visit for randomization.Five trials [27, 31, 34, 36, 37] were assessed as low riskas random number generators were used. Three trials wereassessed as unclear as there was insufficient information [30,33, 38]. All trials were assessed as unclear risk in blinding ofparticipants. Two trials were assessed as low risk for blindingof outcome assessors [37, 38] and ten were at unclear risk dueto insufficient information. One trial was assessed as unclearrisk for incomplete data [31] as they did not report dropoutdata. One trial, Zhang et al. [36], reported on dropout but datawas reported only for those who completed the trial and thuswas assessed as high risk for incomplete outcome data. Ten
+
−
+
−
?
+
?
−
?
+
−
+
?
?
+
?
?
?
?
?
?
?
?
+
?
?
?
?
?
?
?
?
?
?
?
?
?
?
+
?
?
?
+
?
?
?
?
?
+
+
+
+
+
?
+
+
+
+
+
−
?
?
−
?
?
?
−
?
?
?
?
?
+
+
+
+
+
+
?
+
+
+
+
+
Han 2010 [27]
He 2009 [28]
K. S. Kim and Y.-B. Kim 2012 [37]
Li et al. 2002 [29]
Liu 2011 [30]
Liu and Shi 2015 [31]
McKee et al. 2004 [38]
Mo and Jin 2005 [32]
Tang and Quan 2011 [33]
Wu 2011 [34]
You and Liu 2014 [35]
Zhang et al. 2014 [36]
Rand
om se
quen
ce g
ener
atio
n (s
elec
tion
bias
)
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
Blin
ding
of p
artic
ipan
ts an
d pe
rson
nel (
perfo
rman
ce b
ias)
Blin
ding
of o
utco
me a
sses
smen
t (de
tect
ion
bias
)
Inco
mpl
ete o
utco
me d
ata (
attr
ition
bia
s)
Sele
ctiv
e rep
ortin
g (r
epor
ting
bias
)
Oth
er b
ias
Figure 2: Risk of bias summary.
trials were assessed as low risk for incomplete data. Two trialswere assessed as high risk for selective outcome reporting.McKee et al. [38] stated they would include data on adverseevents but no data were presented. K. S. Kim and Y.-B. Kim2011 indicated in their protocol [40] the use of VAS scale butno data was reported. The remaining ten trials were assessedas unclear as there were no trial protocols published or trialregistrations identified [27–36].
3.4. Primary Outcome: Therapeutic Effective Rate. Figure 3presents the forest plot for TER ≥30% change in symptoms.In the meta-analysis of the trials that defined the TER ≥30%as improvement, the chance of achieving a 30% or greaterchange in lesion count in the acupuncture group was notdifferent to the combined pharmacotherapy group (retinoids,antibiotics, and other supplements) (four studies, RR: 1.07[95% CI 0.98, 1.17] and 𝐼2 = 8%) [28, 32, 33, 36] withlow heterogeneity. Subgroup analysis of studies where thecomparator was antibiotics plus other supplements showedthe chance of a 30% or greater change in lesion count was not
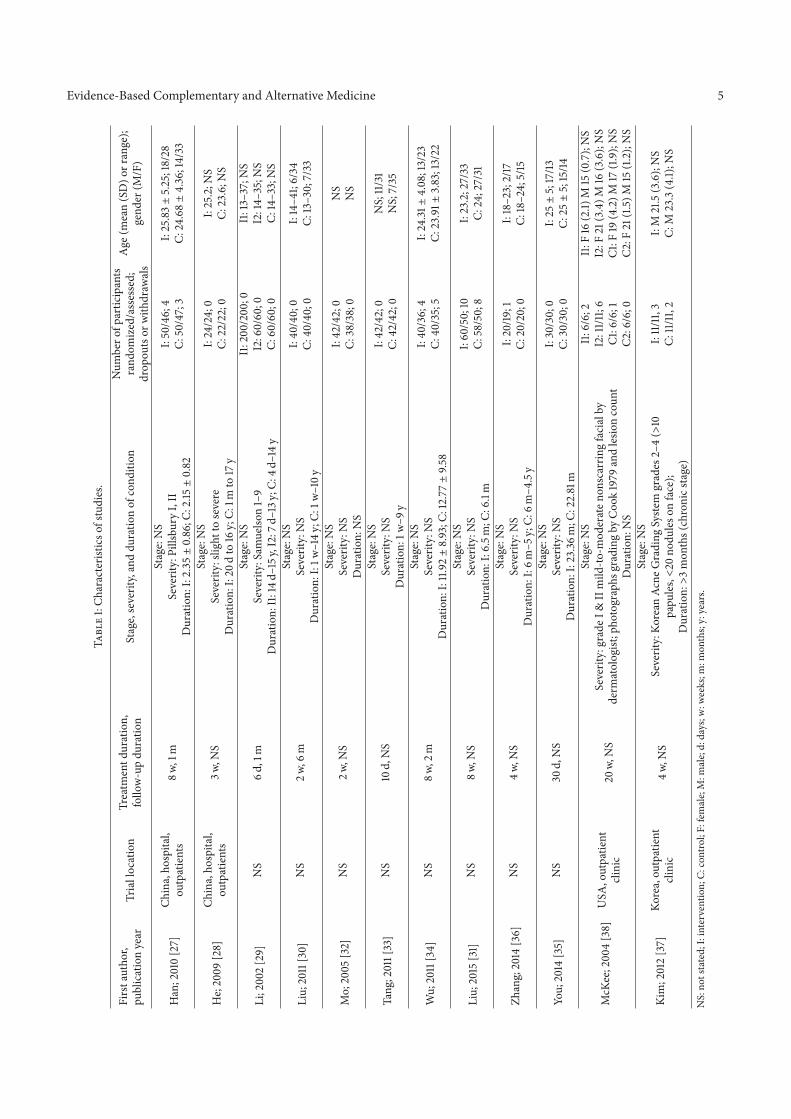
Evidence-Based Complementary and Alternative Medicine 5Ta
ble
1:Ch
arac
teris
ticso
fstu
dies
.
Firs
taut
hor,
publ
icat
ion
year
Tria
lloc
atio
nTr
eatm
entd
urat
ion,
follo
w-u
pdu
ratio
nSt
age,
seve
rity,
and
dura
tion
ofco
nditi
onN
umbe
rofp
artic
ipan
tsra
ndom
ized
/ass
esse
d;dr
opou
tsor
with
draw
als
Age
(mea
n(S
D)o
rran
ge);
gend
er(M
/F)
Han
;201
0[2
7]Ch
ina,
hosp
ital,
outp
atie
nts
8w,1
mSt
age:
NS
I:50
/46;
4C:
50/4
7;3
I:25
.83±
5.25
;18/
28C:
24.6
8±
4.36
;14/
33Se
verit
y:Pi
llsbu
ryI,
IID
urat
ion:
I:2.35±0.86
;C:2
.15±
0.82
He;
2009
[28]
Chin
a,ho
spita
l,ou
tpat
ient
s3w
,NS
Stag
e:N
SI:
24/2
4;0
C:22
/22;
0I:
25.2
;NS
C:23
.6;N
SSe
verit
y:sli
ghtt
ose
vere
Dur
atio
n:I:
20d
to16
y;C:
1mto
17y
Li;2
002
[29]
NS
6d,1
mSt
age:
NS
I1:2
00/2
00;0
I2:6
0/60
;0C:
60/6
0;0
I1:1
3–37
;NS
I2:1
4–35
;NS
C:14
–33;
NS
Seve
rity:
Sam
uelso
n1–
9D
urat
ion:
I1:1
4d–1
5y,I
2:7d
–13y
;C:4
d–14
y
Liu;
2011
[30]
NS
2w,6
mSt
age:
NS
I:40
/40;
0C:
40/4
0;0
I:14
–41;
6/34
C:13
–30;
7/33
Seve
rity:
NS
Dur
atio
n:I:
1w–1
4y;C
:1w
–10y
Mo;
2005
[32]
NS
2w,N
SSt
age:
NS
I:42
/42;
0C:
38/3
8;0
NS
NS
Seve
rity:
NS
Dur
atio
n:N
S
Tang
;201
1[33
]N
S10
d,N
SSt
age:
NS
I:42
/42;
0C:
42/4
2;0
NS;
11/3
1N
S;7/
35Se
verit
y:N
SD
urat
ion:
1w–9
y
Wu;
2011
[34]
NS
8w,2
mSt
age:
NS
I:40
/36;
4C:
40/3
5;5
I:24
.31±
4.08
;13/
23C:
23.9
1±3.
83;1
3/22
Seve
rity:
NS
Dur
atio
n:I:
11.9
2±
8.93
;C:1
2.77±
9.58
Liu;
2015
[31]
NS
8w,N
SSt
age:
NS
I:60
/50;
10C:
58/5
0;8
I:23
.2;2
7/33
C:24
;27/
31Se
verit
y:N
SD
urat
ion:
I:6.
5m;C
:6.1
m
Zhan
g;20
14[3
6]N
S4w
,NS
Stag
e:N
SI:
20/19
;1C:
20/2
0;0
I:18
–23;
2/17
C:18
–24;
5/15
Seve
rity:
NS
Dur
atio
n:I:
6m–5
y;C:
6m–4
.5y
You;
2014
[35]
NS
30d,
NS
Stag
e:N
SI:
30/3
0;0
C:30
/30;
0I:
25±
5;17
/13C:
25±
5;15
/14Se
verit
y:N
SD
urat
ion:
I:23
.36m
;C:2
2.81
m
McK
ee;2
004
[38]
USA
,out
patie
ntcli
nic
20w,
NS
Stag
e:N
SI1
:6/6
;2I2
:11/1
1;6
C1:6
/6;1
C2:6
/6;0
I1:F
16(2
.1)M
15(0
.7);
NS
I2:F
21(3
.4)M
16(3
.6);
NS
C1:F
19(4
.2)M
17(1
.9);
NS
C2:F
21(1
.5)M
15(1
.2);
NS
Seve
rity:
grad
eI&
IIm
ild-to
-mod
erat
enon
scar
ring
faci
alby
derm
atol
ogist
;pho
togr
aphs
grad
ing
byC
ook
1979
and
lesio
nco
unt
Dur
atio
n:N
S
Kim
;201
2[3
7]Ko
rea,
outp
atie
ntcli
nic
4w,N
S
Stag
e:N
SI:
11/11
,3C:
11/11
,2I:
M21
.5(3
.6);
NS
C:M
23.3
(4.1)
;NS
Seve
rity:
Kore
anAc
neG
radi
ngSy
stem
grad
es2–
4(>
10pa
pule
s,<
20no
dule
son
face
);D
urat
ion:>
3m
onth
s(ch
roni
csta
ge)
NS:
nots
tate
d;I:
inte
rven
tion;
C:co
ntro
l;F:
fem
ale;
M:m
ale;
d:da
ys;w
:wee
ks;m
:mon
ths;
y:ye
ars.
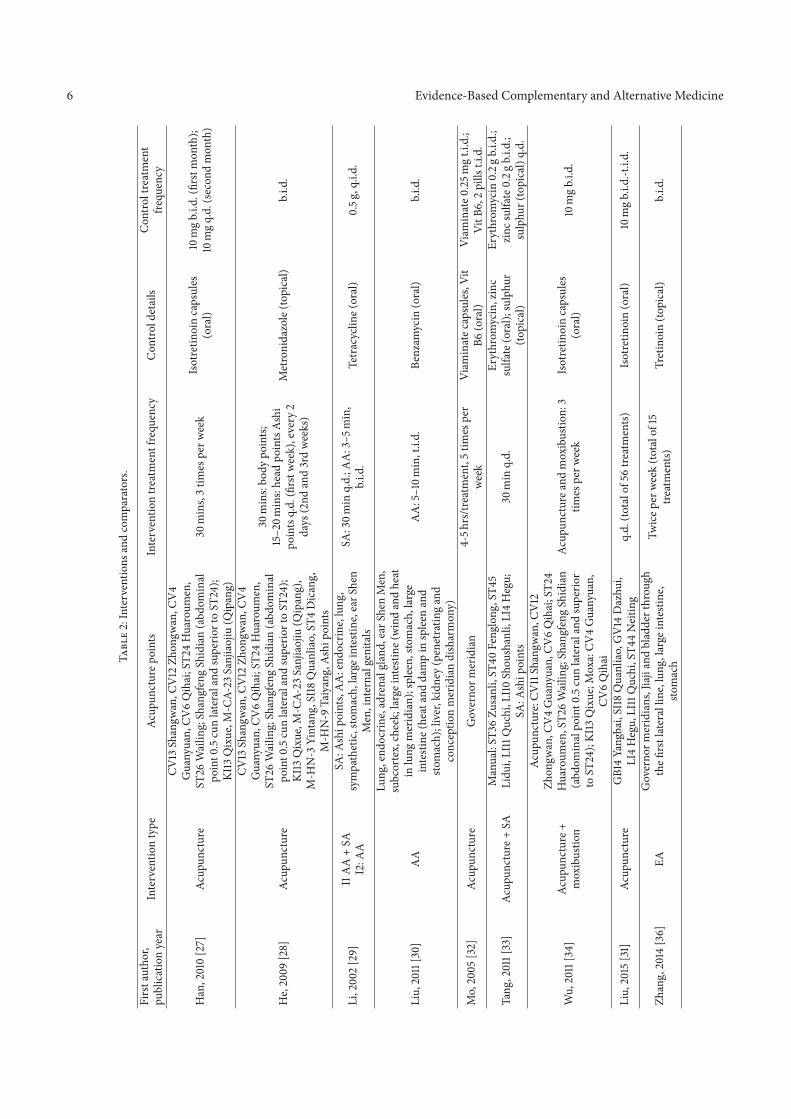
6 Evidence-Based Complementary and Alternative Medicine
Tabl
e2:
Inte
rven
tions
and
com
para
tors
.
Firs
taut
hor,
publ
icat
ion
year
Inte
rven
tion
type
Acup
unct
urep
oint
sIn
terv
entio
ntre
atm
entf
requ
ency
Con
trold
etai
lsC
ontro
ltre
atm
ent
frequ
ency
Han
,201
0[2
7]Ac
upun
ctur
e
CV13
Shan
gwan
,CV
12Zh
ongw
an,C
V4
Gua
nyua
n,CV
6Q
ihai
;ST2
4H
uaro
umen
,ST
26W
ailin
g;Sh
angf
eng
Shid
ian
(abd
omin
alpo
int0
.5cu
nla
tera
land
supe
riort
oST
24);
KI13
Qix
ue,M
-CA-
23Sa
njia
ojiu
(Qip
ang)
30m
ins,
3tim
espe
rwee
kIs
otre
tinoi
nca
psul
es(o
ral)
10m
gb.
i.d.(
first
mon
th);
10m
gq.
d.(s
econ
dm
onth
)
He,
2009
[28]
Acup
unct
ure
CV13
Shan
gwan
,CV
12Zh
ongw
an,C
V4
Gua
nyua
n,CV
6Q
ihai
;ST2
4H
uaro
umen
,ST
26W
ailin
g;Sh
angf
eng
Shid
ian
(abd
omin
alpo
int0
.5cu
nla
tera
land
supe
riort
oST
24);
KI13
Qix
ue,M
-CA-
23Sa
njia
ojiu
(Qip
ang)
,M
-HN
-3Yi
ntan
g,SI
18Q
uanl
iao,
ST4
Dic
ang,
M-H
N-9
Taiy
ang,
Ashi
poin
ts
30m
ins:
body
poin
ts;15
–20m
ins:
head
poin
tsAs
hipo
ints
q.d.
(firs
twee
k),e
very
2da
ys(2
ndan
d3r
dw
eeks
)
Met
roni
dazo
le(to
pica
l)b.
i.d.
Li,2
002
[29]
I1A
A+
SAI2
:AA
SA:A
ship
oint
s,A
A:e
ndoc
rine,
lung
,sy
mpa
thet
ic,s
tom
ach,
larg
eint
estin
e,ea
rShe
nM
en,i
nter
nalg
enita
ls
SA:3
0min
q.d.
;AA
:3–5
min
,b.
i.d.
Tetr
acyc
line(
oral
)0.
5g,q
.i.d.
Liu,
2011
[30]
AA
Lung
,end
ocrin
e,ad
rena
lgla
nd,e
arSh
enM
en,
subc
orte
x,ch
eek;
larg
eint
estin
e(w
ind
and
heat
inlu
ngm
erid
ian)
;spl
een,
stom
ach,
larg
ein
test
ine(
heat
and
dam
pin
splee
nan
dsto
mac
h);l
iver
,kid
ney
(pen
etra
ting
and
conc
eptio
nm
erid
ian
dish
arm
ony)
AA
:5–1
0min
,t.i.
d.Be
nzam
ycin
(ora
l)b.
i.d.
Mo,
2005
[32]
Acup
unct
ure
Gov
erno
rmer
idia
n4-
5hrs
/trea
tmen
t,5
times
per
wee
kVi
amin
atec
apsu
les,
Vit
B6(o
ral)
Viam
inat
e0.2
5mg
t.i.d
.;Vi
tB6,
2pi
llst.i
.d.
Tang
,201
1[33
]Ac
upun
ctur
e+SA
Man
ual:
ST36
Zusa
nli,
ST40
Feng
long
,ST4
5Li
dui,
LI11
Quc
hi,L
I10
Shou
shan
li,LI
4H
egu;
SA:A
ship
oint
s30
min
q.d.
Eryt
hrom
ycin
,zin
csu
lfate
(ora
l);su
lphu
r(to
pica
l)
Eryt
hrom
ycin
0.2g
b.i.d
.;zi
ncsu
lfate
0.2g
b.i.d
.;su
lphu
r(to
pica
l)q.
d.
Wu,
2011
[34]
Acup
unct
ure+
mox
ibus
tion
Acup
unct
ure:
CV11
Shan
gwan
,CV
12Zh
ongw
an,C
V4
Gua
nyua
n,CV
6Q
ihai
;ST2
4H
uaro
umen
,ST2
6W
ailin
g;Sh
angf
eng
Shid
ian
(abd
omin
alpo
int0
.5cu
nla
tera
land
supe
rior
toST
24);
KI13
Qix
ue;M
oxa:
CV4
Gua
nyua
n,CV
6Q
ihai
Acup
unct
urea
ndm
oxib
ustio
n:3
times
perw
eek
Isot
retin
oin
caps
ules
(ora
l)10
mg
b.i.d
.
Liu,
2015
[31]
Acup
unct
ure
GB1
4Ya
ngba
i,SI
18Q
uanl
iao,
GV
14D
azhu
i,LI
4H
egu,
LI11
Quc
hi,S
T44
Nei
ting
q.d.
(tota
lof5
6tre
atm
ents
)Is
otre
tinoi
n(o
ral)
10m
gb.
i.d.-t
.i.d.
Zhan
g,20
14[3
6]EA
Gov
erno
rmer
idia
ns,J
iaji
and
blad
dert
hrou
ghth
efirs
tlat
eral
line,
lung
,lar
gein
testi
ne,
stom
ach
Twic
eper
wee
k(to
talo
f15
treat
men
ts)Tr
etin
oin
(topi
cal)
b.i.d
.
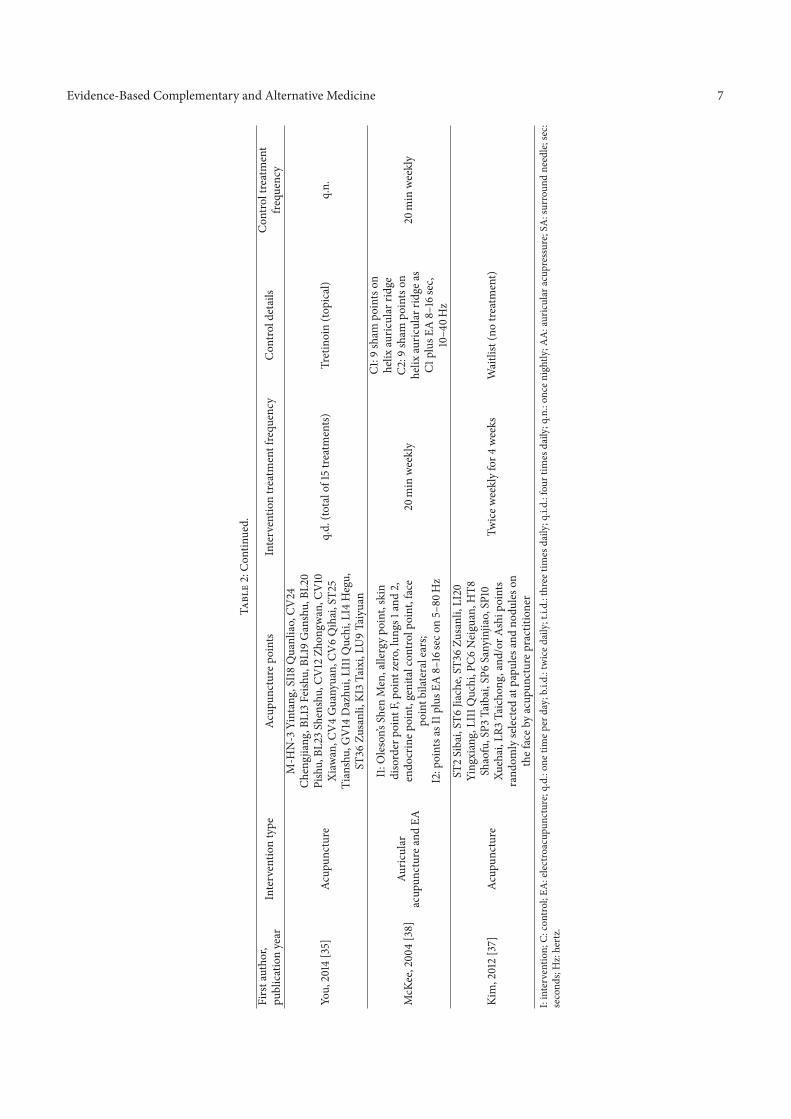
Evidence-Based Complementary and Alternative Medicine 7
Tabl
e2:
Con
tinue
d.Fi
rsta
utho
r,pu
blic
atio
nye
arIn
terv
entio
nty
peAc
upun
ctur
epoi
nts
Inte
rven
tion
treat
men
tfre
quen
cyC
ontro
ldet
ails
Con
trolt
reat
men
tfre
quen
cy
You,
2014
[35]
Acup
unct
ure
M-H
N-3
Yint
ang,
SI18
Qua
nlia
o,CV
24Ch
engj
iang
,BL1
3Fe
ishu,
BL19
Gan
shu,
BL20
Pish
u,BL
23Sh
ensh
u,CV
12Zh
ongw
an,C
V10
Xiaw
an,C
V4
Gua
nyua
n,CV
6Q
ihai
,ST2
5Ti
ansh
u,G
V14
Daz
hui,
LI11
Quc
hi,L
I4H
egu,
ST36
Zusa
nli,
KI3
Taix
i,LU
9Ta
iyua
n
q.d.
(tota
lof1
5tre
atm
ents)
Tret
inoi
n(to
pica
l)q.
n.
McK
ee,2
004
[38]
Auric
ular
acup
unct
urea
ndEA
I1:O
leso
n’sSh
enM
en,a
llerg
ypo
int,
skin
diso
rder
poin
tF,p
oint
zero
,lun
gs1a
nd2,
endo
crin
epoi
nt,g
enita
lcon
trolp
oint
,fac
epo
intb
ilate
rale
ars;
I2:p
oint
sasI
1plu
sEA
8–16
seco
n5–
80H
z
20m
inw
eekl
y
C1:9
sham
poin
tson
helix
auric
ular
ridge
C2:9
sham
poin
tson
helix
auric
ular
ridge
asC1
plus
EA8–
16se
c,10
–40H
z
20m
inw
eekl
y
Kim
,201
2[3
7]Ac
upun
ctur
e
ST2
Siba
i,ST
6Jia
che,
ST36
Zusa
nli,
LI20
Ying
xian
g,LI
11Q
uchi
,PC6
Nei
guan
,HT8
Shao
fu,S
P3Ta
ibai
,SP6
Sany
injia
o,SP
10Xu
ehai
,LR3
Taic
hong
,and
/orA
ship
oint
sra
ndom
lyse
lect
edat
papu
lesan
dno
dules
onth
efac
eby
acup
unct
urep
ract
ition
er
Twic
ewee
kly
for4
wee
ksW
aitli
st(n
otre
atm
ent)
I:in
terv
entio
n;C:
cont
rol;
EA:e
lect
roac
upun
ctur
e;q.
d.:o
netim
eper
day;
b.i.d
.:tw
iced
aily
;t.i.
d.:t
hree
times
daily
;q.i.
d.:f
ourt
imes
daily
;q.n
.:on
ceni
ghtly
;AA
:aur
icul
arac
upre
ssur
e;SA
:sur
roun
dne
edle
;sec
:se
cond
s;H
z:he
rtz.
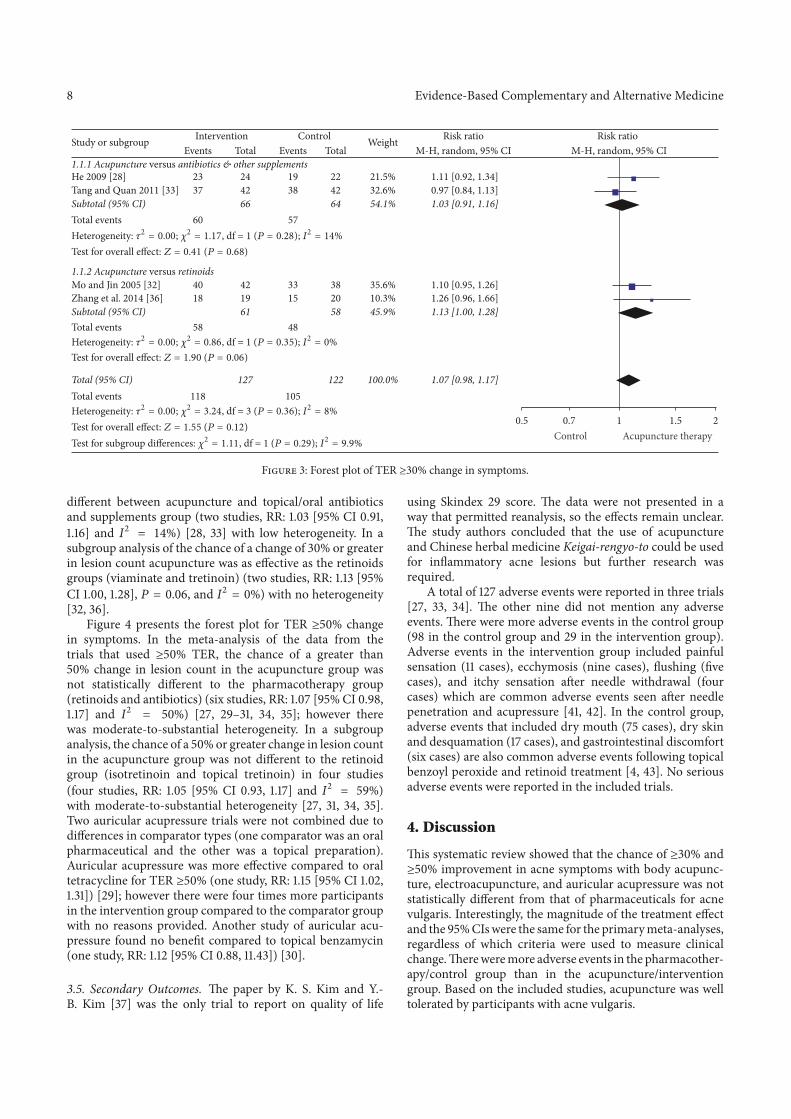
8 Evidence-Based Complementary and Alternative Medicine
Study or subgroup InterventionEvents EventsTotal
ControlTotal
Weight Risk ratioM-H, random, 95% CI
Risk ratioM-H, random, 95% CI
1.1.1 Acupuncture versus antibiotics & other supplements
Total events 60 57
Total events 58 48
23 24 19He 2009 [28] 22 21.5% 1.11 [0.92, 1.34]37 42 38Tang and Quan 2011 [33] 42 32.6% 0.97 [0.84, 1.13]
Subtotal (95% CI) 66 64 54.1% 1.03 [0.91, 1.16]
40 42Mo and Jin 2005 [32] 33 38 35.6% 1.10 [0.95, 1.26]18 19Zhang et al. 2014 [36] 15 20 10.3% 1.26 [0.96, 1.66]
Subtotal (95% CI) 61 58 45.9% 1.13 [1.00, 1.28]
Total (95% CI) 127 122 100.0% 1.07 [0.98, 1.17]Total events 118 105
0.5 0.7 1.51 2Control Acupuncture therapy
1.1.2 Acupuncture versus retinoids
Heterogeneity: 2 = 0.00; 2 = 1.17, df = 1 (P = 0.28); I2 = 14%
Test for overall effect: Z = 0.41 (P = 0.68)
Heterogeneity: 2 = 0.00; 2 = 0.86, df = 1 (P = 0.35); I2 = 0%
Test for overall effect: Z = 1.90 (P = 0.06)
Heterogeneity: 2 = 0.00; 2 = 3.24, df = 3 (P = 0.36); I2 = 8%
Test for overall effect: Z = 1.55 (P = 0.12)Test for subgroup differences: 2 = 1.11, df = 1 (P = 0.29); I2 = 9.9%
Figure 3: Forest plot of TER ≥30% change in symptoms.
different between acupuncture and topical/oral antibioticsand supplements group (two studies, RR: 1.03 [95% CI 0.91,1.16] and 𝐼2 = 14%) [28, 33] with low heterogeneity. In asubgroup analysis of the chance of a change of 30% or greaterin lesion count acupuncture was as effective as the retinoidsgroups (viaminate and tretinoin) (two studies, RR: 1.13 [95%CI 1.00, 1.28], 𝑃 = 0.06, and 𝐼2 = 0%) with no heterogeneity[32, 36].
Figure 4 presents the forest plot for TER ≥50% changein symptoms. In the meta-analysis of the data from thetrials that used ≥50% TER, the chance of a greater than50% change in lesion count in the acupuncture group wasnot statistically different to the pharmacotherapy group(retinoids and antibiotics) (six studies, RR: 1.07 [95% CI 0.98,1.17] and 𝐼2 = 50%) [27, 29–31, 34, 35]; however therewas moderate-to-substantial heterogeneity. In a subgroupanalysis, the chance of a 50% or greater change in lesion countin the acupuncture group was not different to the retinoidgroup (isotretinoin and topical tretinoin) in four studies(four studies, RR: 1.05 [95% CI 0.93, 1.17] and 𝐼2 = 59%)with moderate-to-substantial heterogeneity [27, 31, 34, 35].Two auricular acupressure trials were not combined due todifferences in comparator types (one comparator was an oralpharmaceutical and the other was a topical preparation).Auricular acupressure was more effective compared to oraltetracycline for TER ≥50% (one study, RR: 1.15 [95% CI 1.02,1.31]) [29]; however there were four times more participantsin the intervention group compared to the comparator groupwith no reasons provided. Another study of auricular acu-pressure found no benefit compared to topical benzamycin(one study, RR: 1.12 [95% CI 0.88, 11.43]) [30].
3.5. Secondary Outcomes. The paper by K. S. Kim and Y.-B. Kim [37] was the only trial to report on quality of life
using Skindex 29 score. The data were not presented in away that permitted reanalysis, so the effects remain unclear.The study authors concluded that the use of acupunctureand Chinese herbal medicine Keigai-rengyo-to could be usedfor inflammatory acne lesions but further research wasrequired.
A total of 127 adverse events were reported in three trials[27, 33, 34]. The other nine did not mention any adverseevents. There were more adverse events in the control group(98 in the control group and 29 in the intervention group).Adverse events in the intervention group included painfulsensation (11 cases), ecchymosis (nine cases), flushing (fivecases), and itchy sensation after needle withdrawal (fourcases) which are common adverse events seen after needlepenetration and acupressure [41, 42]. In the control group,adverse events that included dry mouth (75 cases), dry skinand desquamation (17 cases), and gastrointestinal discomfort(six cases) are also common adverse events following topicalbenzoyl peroxide and retinoid treatment [4, 43]. No seriousadverse events were reported in the included trials.
4. Discussion
This systematic review showed that the chance of ≥30% and≥50% improvement in acne symptoms with body acupunc-ture, electroacupuncture, and auricular acupressure was notstatistically different from that of pharmaceuticals for acnevulgaris. Interestingly, the magnitude of the treatment effectand the 95% CIs were the same for the primary meta-analyses,regardless of which criteria were used to measure clinicalchange. There were more adverse events in the pharmacother-apy/control group than in the acupuncture/interventiongroup. Based on the included studies, acupuncture was welltolerated by participants with acne vulgaris.
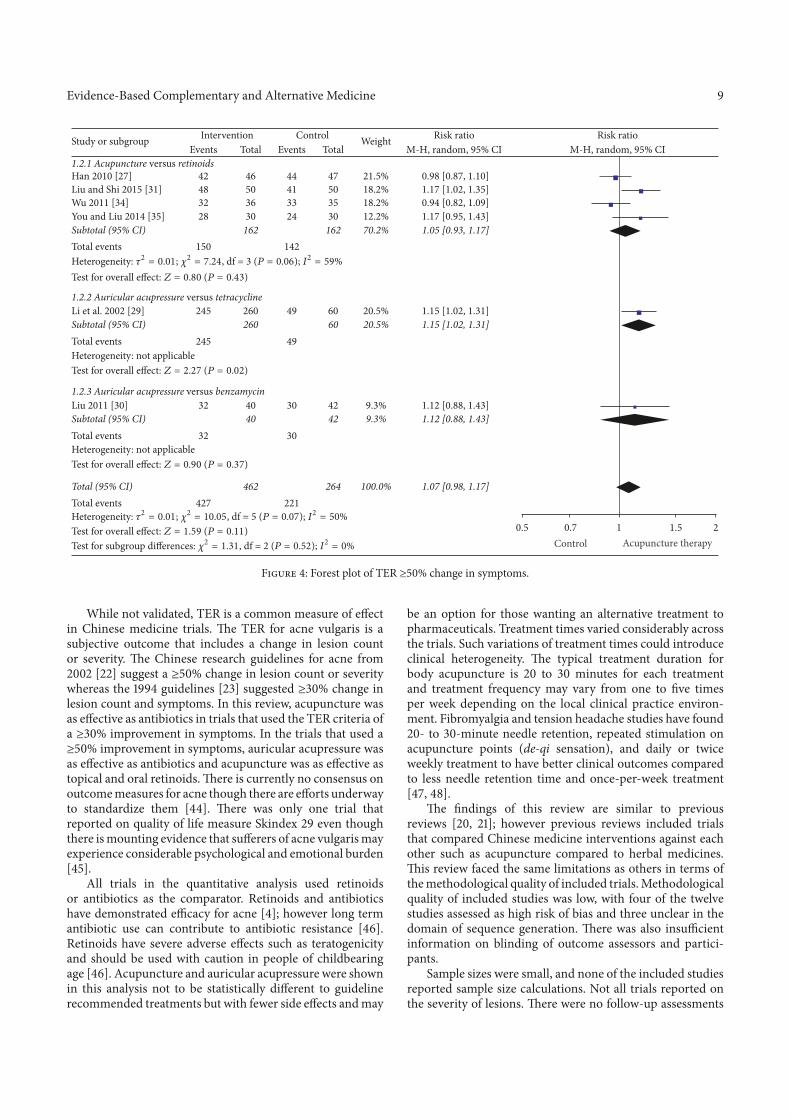
Evidence-Based Complementary and Alternative Medicine 9
1.2.1 Acupuncture versus retinoids
Total events 150 142
49Total events 245Heterogeneity: not applicable
1.2.3 Auricular acupressure versus benzamycin
30Total events 32Heterogeneity: not applicable
Total events 427 221
Han 2010 [27] 42 46 44 47 21.5% 0.98 [0.87, 1.10]48 50 41Liu and Shi 2015 [31] 50 18.2% 1.17 [1.02, 1.35]32 36 33Wu 2011 [34] 35 18.2% 0.94 [0.82, 1.09]
You and Liu 2014 [35] 28 30 24 30 12.2% 1.17 [0.95, 1.43]Subtotal (95% CI) 162 162 70.2% 1.05 [0.93, 1.17]
245 260 49Li et al. 2002 [29] 60 20.5% 1.15 [1.02, 1.31]Subtotal (95% CI) 260 60 20.5% 1.15 [1.02, 1.31]
32 40 30Liu 2011 [30] 42 9.3% 1.12 [0.88, 1.43]Subtotal (95% CI) 40 42 9.3% 1.12 [0.88, 1.43]
Total (95% CI) 462 264 100.0% 1.07 [0.98, 1.17]
0.5 0.7 1.51 2Control Acupuncture therapy
Study or subgroup InterventionEvents EventsTotal
ControlTotal
Weight Risk ratioM-H, random, 95% CI
Risk ratioM-H, random, 95% CI
1.2.2 Auricular acupressure versus tetracycline
Heterogeneity: 2 = 0.01; 2 = 7.24, df = 3 (P = 0.06); I2 = 59%
Test for overall effect: Z = 0.80 (P = 0.43)
Test for overall effect: Z = 2.27 (P = 0.02)
Test for overall effect: Z = 0.90 (P = 0.37)
Test for overall effect: Z = 1.59 (P = 0.11)Test for subgroup differences: 2 = 1.31, df = 2 (P = 0.52); I2 = 0%
Heterogeneity: 2 = 0.01; 2 = 10.05, df = 5 (P = 0.07); I2 = 50%
Figure 4: Forest plot of TER ≥50% change in symptoms.
While not validated, TER is a common measure of effectin Chinese medicine trials. The TER for acne vulgaris is asubjective outcome that includes a change in lesion countor severity. The Chinese research guidelines for acne from2002 [22] suggest a ≥50% change in lesion count or severitywhereas the 1994 guidelines [23] suggested ≥30% change inlesion count and symptoms. In this review, acupuncture wasas effective as antibiotics in trials that used the TER criteria ofa ≥30% improvement in symptoms. In the trials that used a≥50% improvement in symptoms, auricular acupressure wasas effective as antibiotics and acupuncture was as effective astopical and oral retinoids. There is currently no consensus onoutcome measures for acne though there are efforts underwayto standardize them [44]. There was only one trial thatreported on quality of life measure Skindex 29 even thoughthere is mounting evidence that sufferers of acne vulgaris mayexperience considerable psychological and emotional burden[45].
All trials in the quantitative analysis used retinoidsor antibiotics as the comparator. Retinoids and antibioticshave demonstrated efficacy for acne [4]; however long termantibiotic use can contribute to antibiotic resistance [46].Retinoids have severe adverse effects such as teratogenicityand should be used with caution in people of childbearingage [46]. Acupuncture and auricular acupressure were shownin this analysis not to be statistically different to guidelinerecommended treatments but with fewer side effects and may
be an option for those wanting an alternative treatment topharmaceuticals. Treatment times varied considerably acrossthe trials. Such variations of treatment times could introduceclinical heterogeneity. The typical treatment duration forbody acupuncture is 20 to 30 minutes for each treatmentand treatment frequency may vary from one to five timesper week depending on the local clinical practice environ-ment. Fibromyalgia and tension headache studies have found20- to 30-minute needle retention, repeated stimulation onacupuncture points (de-qi sensation), and daily or twiceweekly treatment to have better clinical outcomes comparedto less needle retention time and once-per-week treatment[47, 48].
The findings of this review are similar to previousreviews [20, 21]; however previous reviews included trialsthat compared Chinese medicine interventions against eachother such as acupuncture compared to herbal medicines.This review faced the same limitations as others in terms ofthe methodological quality of included trials. Methodologicalquality of included studies was low, with four of the twelvestudies assessed as high risk of bias and three unclear in thedomain of sequence generation. There was also insufficientinformation on blinding of outcome assessors and partici-pants.
Sample sizes were small, and none of the included studiesreported sample size calculations. Not all trials reported onthe severity of lesions. There were no follow-up assessments

10 Evidence-Based Complementary and Alternative Medicine
in the included trials. Statistical heterogeneity was alsodetected in several subgroup analyses which were not ableto be explored due to small numbers of studies. Detailedreporting of trial information was lacking; none of the trialsaddressed all items from Consolidated Standard of ReportingTrials (CONSORT) [49] or Standards for Reporting Inter-ventions in Clinical Trials of Acupuncture (STRICTA) [50]standard reporting conventions. The STRICTA guidelines areimportant to improve transparency of intervention reportingin acupuncture clinical trials. For studies included in thisreview, several items were reported well in all trials: thetype of acupuncture used, standard acupuncture name and/orlocations of acupuncture points, the number and durationof treatment sessions, and the precise descriptions of thecontrols or comparators (Supplementary Table 2). The trialsconducted in China did not provide information about prac-titioners, the setting and context of treatment, instructionsto practitioners, and information and explanations to thepatients. This can pose an issue with reproducibility of studiesand may be a source of bias. Reporting of such detailswould enhance accurate analysis and interpretation of dataand improve research reliability in acupuncture interventions[51].
5. Conclusions
There was no statistical difference in the efficacy of acupunc-ture compared to pharmacotherapies for acne vulgaris; how-ever acupuncture interventions reported less adverse effects.Poor methodological quality of trial design and lack ofconsistent reporting of outcome measures from some trialswere found in this review; therefore results should be inter-preted with caution. Future trials should include rigorousmethodological design and reporting should follow standardreporting conventions such as CONSORT and STRICTA.Quality of life measures and further understanding of themechanisms of acupuncture on acne should also be consid-ered for future studies.
Conflicts of Interest
The authors report no conflicts of interest.
Acknowledgments
This project is jointly supported by the China-AustraliaInternational Research Centre for Chinese Medicine (CAIR-CCM), a joint initiative of RMIT University, Australia,the Guangdong Provincial Academy of Chinese MedicalSciences, China, and Chinese Government’s State Admin-istration of Traditional Chinese Medicine, with additionalfunding support from the Ministry of Science & Technol-ogy of China (International Cooperation Project, Grant no.2012DFA31760). The authors also thank Dr. Wenyu (Iris)Zhou for performing risk of bias analysis and data validation.
Supplementary Materials
Supplementary Table 1: therapeutic effective rate criteria andsecondary outcomes. Supplementary Table 2: assessment ofreporting of STRICTA items. (Supplementary Materials)
References
[1] H. P. M. Gollnick, A. Y. Finlay, and N. Shear, “Can we define acneas a chronic disease? If so, how and when?” American Journal ofClinical Dermatology, vol. 9, no. 5, pp. 279–284, 2008.
[2] H. C. Williams, R. P. Dellavalle, and S. Garner, “Acne vulgaris,”The Lancet, vol. 379, no. 9813, pp. 361–372, 2012.
[3] B. Dreno, H. P. M. Gollnick, S. Kang et al., “Understandinginnate immunity and inflammation in acne: Implications formanagement,” Journal of the European Academy of Dermatologyand Venereology, vol. 29, no. 4, pp. 3–11, 2015.
[4] A. L. Zaenglein, A. L. Pathy, B. J. Schlosser et al., “Guidelinesof care for the management of acne vulgaris,” Journal of theAmerican Academy of Dermatology, vol. 74, no. 5, pp. 945–973e933, 2016.
[5] L. F. Eichenfield, J. Q. Del Rosso, A. J. Mancini et al., “Evolvingperspectives on the etiology and pathogenesis of acne vulgaris,”Journal ofDrugs inDermatology, vol. 14, no. 3, pp. 263–272, 2015.
[6] K. Bhate and H. C. Williams, “Epidemiology of acne vulgaris.,”British Journal of Dermatology, vol. 168, no. 3, pp. 474–485, 2013.
[7] C. C. Zouboulis, E. Jourdan, and M. Picardo, “Acne is aninflammatory disease and alterations of sebum compositioninitiate acne lesions,” Journal of the European Academy ofDermatology and Venereology, vol. 28, no. 5, pp. 527–532, 2014.
[8] D. H. Suh and H. H. Kwon, “What’s new in the physiopathologyof acne?”British Journal of Dermatology, vol. 172, no. 1, pp. 13–19,2015.
[9] R. Bertschinger, M. Qiu, L. Y. Li, and S. C. Zang, Chineseacupuncture and moxibustion, Churchill Livingstone, Edin-burgh, 1993.
[10] D. Bensky, S. Clavey, and E. Stoger, Chinese herbal medicine.Materia medica, Eastland Press, Seattle, Wa, USA, 3rd edition,2015.
[11] F. Li, H. Wu, X. Wang, Y. Bao, and R. Zou, “The effectof acupuncture combined with auricular acupoint - pressingtherapy on the main morbidity factors of acne vulgaris,” JournalChinese Acupuncture, vol. 3, pp. 161–164, 2002.
[12] Y. Xie, K. Gu, B. Deng, and Y. Dai, “Effects of acupuncturecombined with benzoyl peroxide on sebum secretion rate,”Journal of Hainan Medical University, vol. 11, pp. 1470–1472,2010.
[13] W. Y. Chung, H. Q. Zhang, and S. P. Zhang, “Peripheralmuscarinic receptors mediate the anti-inflammatory effects ofauricular acupuncture,” Chinese Medicine, vol. 6, article 3, 2011.
[14] J. Q. Fang, J. F. Fang, Y. Liang, and J. Y. Du, “Electroacupuncturemediates extracellular signal-regulated kinase 1/2 pathwaysin the spinal cord of rats with inflammatory pain,” BMCComplementary&AlternativeMedicine, vol. 14, no. 1, article 285,2014.
[15] F. Liu, J. Fang, X. Shao, Y. Liang, Y. Wu, and Y. Jin, “Elec-troacupuncture exerts an anti-inflammatory effect in a rat tissuechamber model of inflammation via suppression of NF-𝜅Bactivation,”Acupuncture inMedicine, vol. 32, no. 4, pp. 340–345,2014.
Evidence-Based Complementary and Alternative Medicine 11
[16] Q. Song, S. Hu, H. Wang et al., “Electroacupuncturing at Zusanlipoint (ST36) attenuates pro-inflammatory cytokine release andorgan dysfunction by activating cholinergic anti-inflammatorypathway in rat with endotoxin challenge,” African Journal ofTraditional, Complementary and Alternative medicines, vol. 11,no. 2, pp. 469–474, 2014.
[17] J.-Y. Du, J.-Q. Fang, Y. Liang, and J.-F. Fang, “Electroacupunc-ture attenuates mechanical allodynia by suppressing the spinalJNK1/2 pathway in a rat model of inflammatory pain,” BrainResearch Bulletin, vol. 108, pp. 27–36, 2014.
[18] Z. Wang, T. Chen, M. Long et al., “Electro-acupuncture at Acu-point ST36 Ameliorates Inflammation and Regulates Th1/Th2Balance in Delayed-Type Hypersensitivity,” Inflammation, vol.40, no. 2, pp. 422–434, 2017.
[19] H. Cao, G. Yang, Y. Wang et al., “Complementary therapies foracne vulgaris,” Cochrane Database of Systematic Reviews, vol. 1,Article ID CD009436, 2015.
[20] H.-J. Cao, G.-Y. Yang, Y.-Y. Wang, and J.-P. Liu, “Acupoint stim-ulation for acne: A systematic review of randomized controlledtrials,” Medical Acupuncture, vol. 25, no. 3, pp. 173–194, 2013.
[21] B. Li, H. Chai, Y.-H. Du, L. Xiao, and J. Xiong, “Evaluationof therapeutic effect and safety for clinical randomized andcontrolled trials of treatment of acne with acupuncture andmoxibustion,” Zhongguo Zhen Jiu, vol. 29, no. 3, pp. 247–251,2009.
[22] X. Y. Zheng, Guideline for New Chinese Herbal Medicine inClinical Practice and Research, Chinese Medical Science andTechnology Publishing House, 2002.
[23] State Administration of TCM,Guideline for NewChinese HerbalMedicine in Clinical Practice and Research, Guideline for NewChinese Herbal Medicine, 1994.
[24] J. Higgins and S. Green, “Cochrane Handbook for SystematicReviews of Interventions Version 5.1.0,” The Cochrane Collabo-ration, 2011.
[25] L. Vase, S. Baram, N. Takakura et al., “Can acupuncturetreatment be double-blinded? An evaluation of double-blindacupuncture treatment of postoperative pain,” PLoS ONE, vol.10, no. 3, Article ID e0119612, 2015.
[26] The Cochrane Collaboration, “Review Manager (RevMan) Ver-sion 5.3,” 2012, Copenhagen: The Nordic Cochrane Centre, TheCochrane Collaboration.
[27] B. Han, A clinical study on abdominal acupuncture for acneby conditioning Liver and Kidney, Guangzhou University ofChinese Medicine, 2010.
[28] X. He, “24 cases of treating facial acne with abdominal andfacial acupuncture,” InnerMongol Journal of Traditional ChineseMedicine, vol. 28, no. 15, p. 33, 2009.
[29] F. Li, H. Wu, X. Wang, Y. Bao, and R. Zou, “Effect of surroundneedling combined with auricular point sticking on mainpathogenetic factors of acne vulgaris,” Zhongguo Zhen Jiu, vol.22, no. 3, pp. 161–163, 2002.
[30] L. Liu, “[Clinical observation on treatment of acne vulgaris withauricular point taping and pressing],” Zhongguo Zhen Jiu, vol.21, no. 10, p. 601, 2011.
[31] S. Liu and B. Shi, “Effect of acupuncture therapy on immunefunction in patients with acne,” Chinese Journal of Acupunctureand Moxibustion, vol. 4, no. 2, pp. 1–3, 2015.
[32] X. Mo and J. Jin, “42 cases of treating acne vulgaris with Cu zhenshen zhu tou ling tai method,” Journal of Traditional ChineseMedical Sciences, vol. 13, no. 5, p. 14, 2005.
[33] P. Tang and Y. Quan, “The clinical effect of treating acnevulgaris with manual acupuncture on Yangming meridian andsurrounding acupuncture,” Shanghai Journal of Acupunctureand Moxibustion, vol. 30, no. 2, p. 127, 2011.
[34] Y. Wu, “The clinical research on treating acne of Spleendeficiency combined with Phlegm and Damp with abdominalacupuncture,” in Proceedings of the 12th Academic Conferenceof Acupuncture Association of Guangdong Province, pp. 213–217,Guangdong, China, 2011.
[35] M. You and G. Liu, “Therapeutic observation of bu xu tongluo needling method for facial acne,” Shanghai Journal ofAcupuncture and Moxibustion, vol. 33, no. 9, pp. 836-837, 2014.
[36] L. Zhang, F. Wu, L. Xue, and H. Zhao, “A controlled study oftreating acne vulgaris with electro plum blossom acupuncturetreatment,” Lishizhen Medicine and Materia Medica Research,vol. 25, no. 11, pp. 2817-2818, 2014.
[37] K. S. Kim and Y.-B. Kim, “Anti-inflammatory effect of Keigai-rengyo-to extract and acupuncture in male patients with acnevulgaris: a randomized controlled pilot trial,” The Journal ofAlternative and ComplementaryMedicine, vol. 18, no. 5, pp. 501–508, 2012.
[38] D. McKee, K. Oring, I. Aban, M. Lu, K. Peele, and B. Scott,“Treating facial acne in adolescents and young adults withauriculoacupuncture and auriculotherapy: A Pilot Study,” Med-ical Acupuncture, vol. 16, no. 1, 2004, Article no. 6.
[39] State Administration of TCM,Guideline for NewChinese HerbalMedicine in Clinical Practice and Research, Chinese MedicalScience and Technology Publishing House, 1997.
[40] K. S. Kim and Y.-B. Kim, “Interaction and efficacy of Keigai-rengyo-to extract and acupuncture in male patients with acnevulgaris: A study protocol for a randomized controlled pilottrial,” Trials, vol. 12, article no. 82, 2011.
[41] S. Birch, T. Alraek, and A. J. Norheim, “Acupuncture adverseevents in China: A glimpse of historical and contextual aspects,”The Journal of Alternative and Complementary Medicine, vol. 19,no. 10, pp. 845–850, 2013.
[42] W. He, X. Zhao, Y. Li, Q. Xi, and Y. Guo, “Adverse eventsfollowing acupuncture: a systematic review of the chineseliterature for the years 1956–2010,”The Journal of Alternative andComplementary Medicine, vol. 18, no. 10, pp. 892–901, 2012.
[43] R. C. Blasiak, C. R. Stamey, C. N. Burkhart, A. Lugo-Somolinos,and D. S. Morrell, “High-dose isotretinoin treatment and therate of retrial, relapse, and adverse effects in patients with acnevulgaris,” JAMA Dermatology, vol. 149, no. 12, pp. 1392–1398,2013.
[44] J. Tan, B. Wolfe, J. Weiss et al., “Acne severity grading: Determin-ing essential clinical components and features using a Delphiconsensus,” Journal of the American Academy of Dermatology,vol. 67, no. 2, pp. 187–193, 2012.
[45] E. A. Tanghetti, A. K. Kawata, S. R. Daniels, K. Yeomans, C. T.Burk, and V. D. Callender, “Understanding the burden of adultfemale acne,” The Journal of Clinical and Aesthetic Dermatology,vol. 7, no. 2, pp. 22–30, 2014.
[46] L. F. Eichenfield, A. C. Krakowski, C. Piggott et al., “Evidence-based recommendations for the diagnosis and treatment ofpediatric acne,” Pediatrics, vol. 131, no. 3, pp. S163–S186, 2013.
[47] X. Hao, C. C. Xue, L. Dong, and Z. Zheng, “Factors associatedwith conflicting findings on acupuncture for tension-typeheadache: Qualitative and quantitative analyses,” The Journal ofAlternative andComplementaryMedicine, vol. 19, no. 4, pp. 285–297, 2013.

12 Evidence-Based Complementary and Alternative Medicine
[48] R. E. Harris, X. Tian, D. A. Williams et al., “Treatment offibromyalgia with formula acupuncture: investigation of needleplacement, needle stimulation, and treatment frequency,” TheJournal of Alternative and Complementary Medicine, vol. 11, no.4, pp. 663–671, 2005.
[49] K. F. Schulz, D. G. Altman, and D. Moher, “CONSORT 2010statement: updated guidelines for reporting parallel grouprandomized trials,” Annals of Internal Medicine, vol. 152, no. 11,pp. 726–732, 2010.
[50] H. MacPherson, D. G. Altman, R. Hammerschlag et al.,“Revised standards for reporting interventions in clinical trialsof acupuncture (STRICTA): extending the CONSORT state-ment,” The Journal of Alternative and Complementary Medicine,vol. 16, no. 10, pp. ST1–ST14, 2010.
[51] L. Liu, M. Skinner, S. M. McDonough, P. Kannan, and D. G.Baxter, “STRICTA: Is it time to do more?”BMCComplementaryand Alternative Medicine, vol. 15, no. 1, article no. 190, 2015.
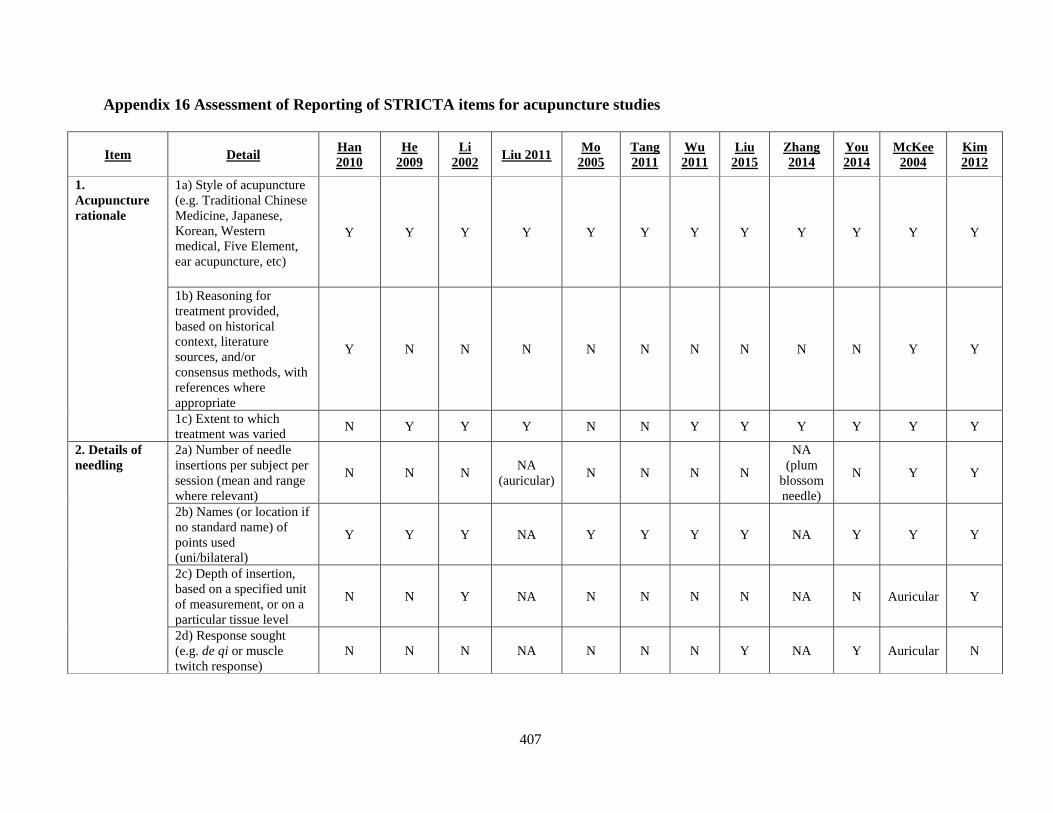
407
Appendix 16 Assessment of Reporting of STRICTA items for acupuncture studies
Item Detail Han 2010
He 2009
Li 2002 Liu 2011 Mo
2005 Tang 2011
Wu 2011
Liu 2015
Zhang 2014
You 2014
McKee 2004
Kim 2012
1. Acupuncture rationale
1a) Style of acupuncture (e.g. Traditional Chinese Medicine, Japanese, Korean, Western medical, Five Element, ear acupuncture, etc)
Y Y Y Y Y Y Y Y Y Y Y Y
1b) Reasoning for treatment provided, based on historical context, literature sources, and/or consensus methods, with references where appropriate
Y N N N N N N N N N Y Y
1c) Extent to which treatment was varied N Y Y Y N N Y Y Y Y Y Y
2. Details of needling
2a) Number of needle insertions per subject per session (mean and range where relevant)
N N N NA (auricular) N N N N
NA (plum
blossom needle)
N Y Y
2b) Names (or location if no standard name) of points used (uni/bilateral)
Y Y Y NA Y Y Y Y NA Y Y Y
2c) Depth of insertion, based on a specified unit of measurement, or on a particular tissue level
N N Y NA N N N N NA N Auricular Y
2d) Response sought (e.g. de qi or muscle twitch response)
N N N NA N N N Y NA Y Auricular N
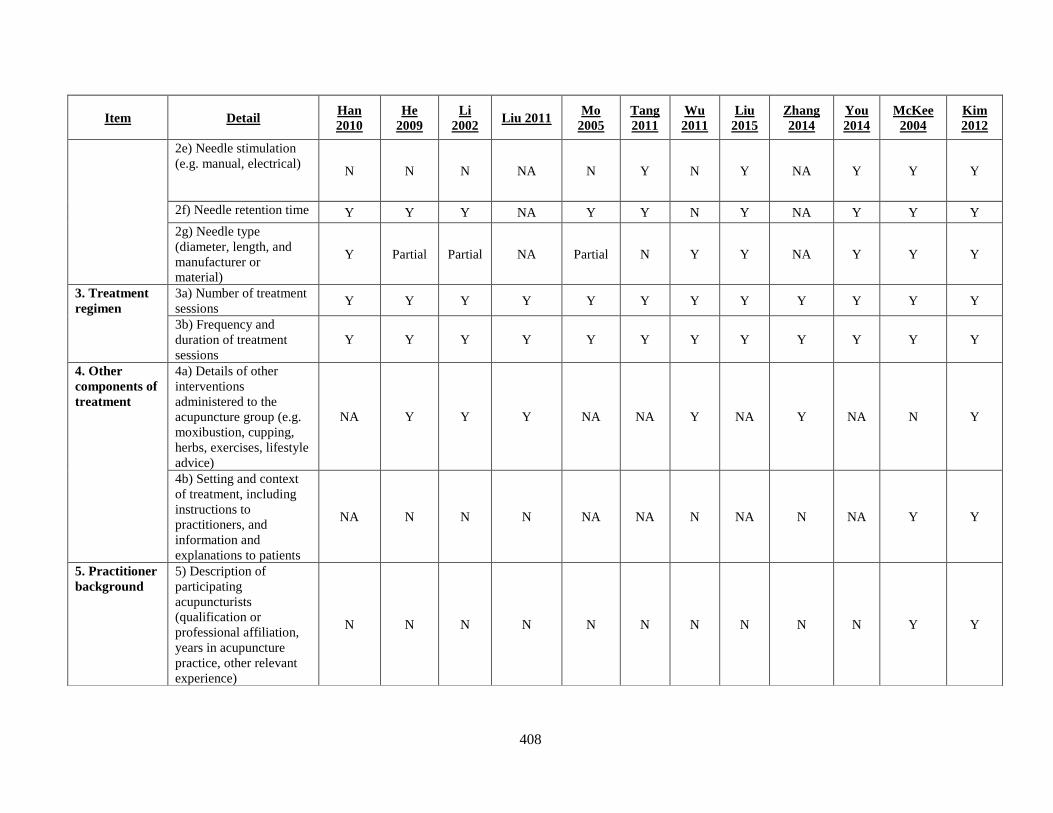
408
Item Detail Han 2010
He 2009
Li 2002 Liu 2011 Mo
2005 Tang 2011
Wu 2011
Liu 2015
Zhang 2014
You 2014
McKee 2004
Kim 2012
2e) Needle stimulation (e.g. manual, electrical) N N N NA N Y N Y NA Y Y Y
2f) Needle retention time Y Y Y NA Y Y N Y NA Y Y Y 2g) Needle type (diameter, length, and manufacturer or material)
Y Partial Partial NA Partial N Y Y NA Y Y Y
3. Treatment regimen
3a) Number of treatment sessions Y Y Y Y Y Y Y Y Y Y Y Y
3b) Frequency and duration of treatment sessions
Y Y Y Y Y Y Y Y Y Y Y Y
4. Other components of treatment
4a) Details of other interventions administered to the acupuncture group (e.g. moxibustion, cupping, herbs, exercises, lifestyle advice)
NA Y Y Y NA NA Y NA Y NA N Y
4b) Setting and context of treatment, including instructions to practitioners, and information and explanations to patients
NA N N N NA NA N NA N NA Y Y
5. Practitioner background
5) Description of participating acupuncturists (qualification or professional affiliation, years in acupuncture practice, other relevant experience)
N N N N N N N N N N Y Y
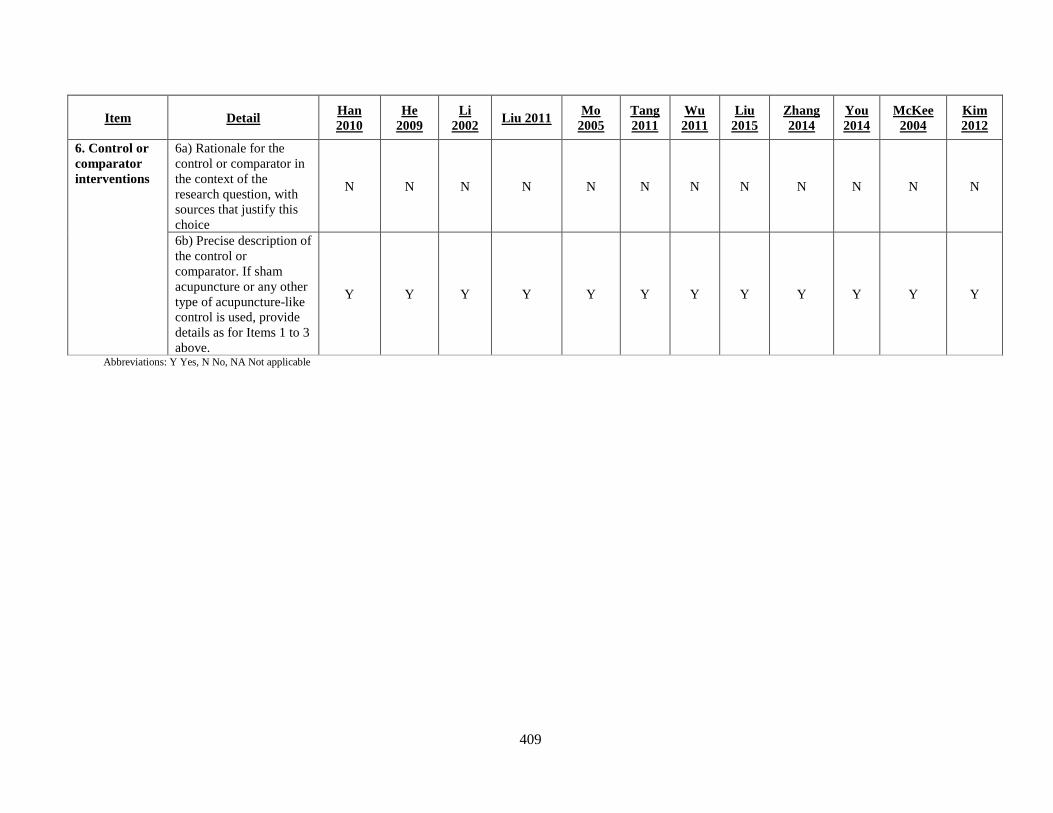
409
Item Detail Han 2010
He 2009
Li 2002 Liu 2011 Mo
2005 Tang 2011
Wu 2011
Liu 2015
Zhang 2014
You 2014
McKee 2004
Kim 2012
6. Control or comparator interventions
6a) Rationale for the control or comparator in the context of the research question, with sources that justify this choice
N N N N N N N N N N N N
6b) Precise description of the control or comparator. If sham acupuncture or any other type of acupuncture-like control is used, provide details as for Items 1 to 3 above.
Y Y Y Y Y Y Y Y Y Y Y Y
Abbreviations: Y Yes, N No, NA Not applicable
410
Appendix 17 Assessment of P. acnes
Specify location (location must be the same each visit)
Count at baseline (week 0)
Count at end of treatment (week 8)
Count at follow-up (week 12)

411
Appendix 18 SPIRIT statement
SPIRIT 2013 Checklist: Recommended items to address in a clinical trial protocol and related documents* Section/item Ite
m No
Description Addressed on page number
Administrative information
Title 1 Descriptive title identifying the study design, population, interventions, and, if applicable, trial acronym
N/A
Trial registration
2a Trial identifier and registry name. If not yet registered, name of intended registry
N/A
2b All items from the World Health Organization Trial Registration Data Set N/A
Protocol version
3 Date and version identifier N/A
Funding 4 Sources and types of financial, material, and other support N/A
Roles and responsibilities
5a Names, affiliations, and roles of protocol contributors N/A
5b Name and contact information for the trial sponsor N/A
5c Role of study sponsor and funders, if any, in study design; collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication, including whether they will have ultimate authority over any of these activities
N/A
5d Composition, roles, and responsibilities of the coordinating centre, steering committee, endpoint adjudication committee, data management team, and other individuals or groups overseeing the trial, if applicable (see Item 21a for data monitoring committee)
N/A
Introduction
Background and rationale
6a Description of research question and justification for undertaking the trial, including summary of relevant studies (published and unpublished) examining benefits and harms for each intervention
228-239
6b Explanation for choice of comparators 237-239
Objectives 7 Specific objectives or hypotheses 215
Trial design 8 Description of trial design including type of trial (eg, parallel group, crossover, factorial, single group), allocation ratio, and framework (eg, superiority, equivalence, noninferiority, exploratory)
228
Methods: Participants, interventions, and outcomes
Study setting 9 Description of study settings (eg, community clinic, academic hospital) and list of countries where data will be collected. Reference to where list of study sites can be obtained
N/A
Eligibility criteria
10 Inclusion and exclusion criteria for participants. If applicable, eligibility criteria for study centres and individuals who will perform the interventions (eg, surgeons, psychotherapists)
229-232, 258
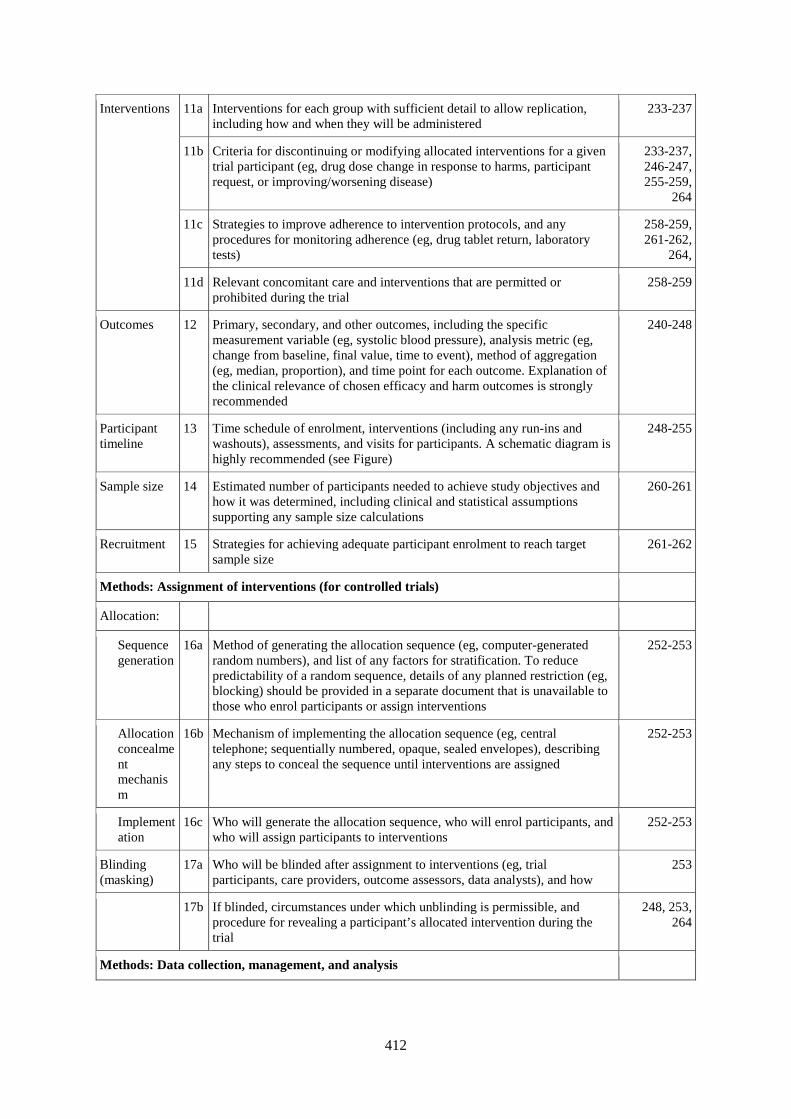
412
Interventions 11a Interventions for each group with sufficient detail to allow replication, including how and when they will be administered
233-237
11b Criteria for discontinuing or modifying allocated interventions for a given trial participant (eg, drug dose change in response to harms, participant request, or improving/worsening disease)
233-237, 246-247, 255-259,
264
11c Strategies to improve adherence to intervention protocols, and any procedures for monitoring adherence (eg, drug tablet return, laboratory tests)
258-259, 261-262,
264,
11d Relevant concomitant care and interventions that are permitted or prohibited during the trial
258-259
Outcomes 12 Primary, secondary, and other outcomes, including the specific measurement variable (eg, systolic blood pressure), analysis metric (eg, change from baseline, final value, time to event), method of aggregation (eg, median, proportion), and time point for each outcome. Explanation of the clinical relevance of chosen efficacy and harm outcomes is strongly recommended
240-248
Participant timeline
13 Time schedule of enrolment, interventions (including any run-ins and washouts), assessments, and visits for participants. A schematic diagram is highly recommended (see Figure)
248-255
Sample size 14 Estimated number of participants needed to achieve study objectives and how it was determined, including clinical and statistical assumptions supporting any sample size calculations
260-261
Recruitment 15 Strategies for achieving adequate participant enrolment to reach target sample size
261-262
Methods: Assignment of interventions (for controlled trials)
Allocation:
Sequence generation
16a Method of generating the allocation sequence (eg, computer-generated random numbers), and list of any factors for stratification. To reduce predictability of a random sequence, details of any planned restriction (eg, blocking) should be provided in a separate document that is unavailable to those who enrol participants or assign interventions
252-253
Allocation concealment mechanism
16b Mechanism of implementing the allocation sequence (eg, central telephone; sequentially numbered, opaque, sealed envelopes), describing any steps to conceal the sequence until interventions are assigned
252-253
Implementation
16c Who will generate the allocation sequence, who will enrol participants, and who will assign participants to interventions
252-253
Blinding (masking)
17a Who will be blinded after assignment to interventions (eg, trial participants, care providers, outcome assessors, data analysts), and how
253
17b If blinded, circumstances under which unblinding is permissible, and procedure for revealing a participant’s allocated intervention during the trial
248, 253, 264
Methods: Data collection, management, and analysis
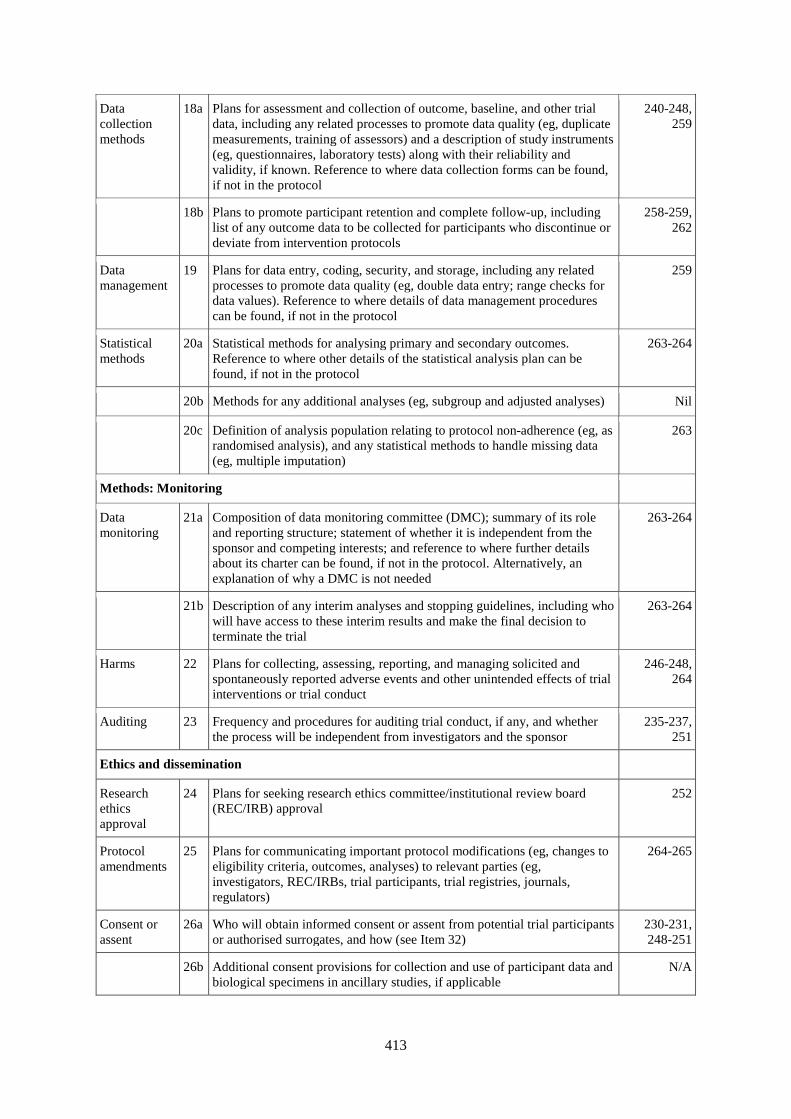
413
Data collection methods
18a Plans for assessment and collection of outcome, baseline, and other trial data, including any related processes to promote data quality (eg, duplicate measurements, training of assessors) and a description of study instruments (eg, questionnaires, laboratory tests) along with their reliability and validity, if known. Reference to where data collection forms can be found, if not in the protocol
240-248, 259
18b Plans to promote participant retention and complete follow-up, including list of any outcome data to be collected for participants who discontinue or deviate from intervention protocols
258-259, 262
Data management
19 Plans for data entry, coding, security, and storage, including any related processes to promote data quality (eg, double data entry; range checks for data values). Reference to where details of data management procedures can be found, if not in the protocol
259
Statistical methods
20a Statistical methods for analysing primary and secondary outcomes. Reference to where other details of the statistical analysis plan can be found, if not in the protocol
263-264
20b Methods for any additional analyses (eg, subgroup and adjusted analyses) Nil
20c Definition of analysis population relating to protocol non-adherence (eg, as randomised analysis), and any statistical methods to handle missing data (eg, multiple imputation)
263
Methods: Monitoring
Data monitoring
21a Composition of data monitoring committee (DMC); summary of its role and reporting structure; statement of whether it is independent from the sponsor and competing interests; and reference to where further details about its charter can be found, if not in the protocol. Alternatively, an explanation of why a DMC is not needed
263-264
21b Description of any interim analyses and stopping guidelines, including who will have access to these interim results and make the final decision to terminate the trial
263-264
Harms 22 Plans for collecting, assessing, reporting, and managing solicited and spontaneously reported adverse events and other unintended effects of trial interventions or trial conduct
246-248, 264
Auditing 23 Frequency and procedures for auditing trial conduct, if any, and whether the process will be independent from investigators and the sponsor
235-237, 251
Ethics and dissemination
Research ethics approval
24 Plans for seeking research ethics committee/institutional review board (REC/IRB) approval
252
Protocol amendments
25 Plans for communicating important protocol modifications (eg, changes to eligibility criteria, outcomes, analyses) to relevant parties (eg, investigators, REC/IRBs, trial participants, trial registries, journals, regulators)
264-265
Consent or assent
26a Who will obtain informed consent or assent from potential trial participants or authorised surrogates, and how (see Item 32)
230-231, 248-251
26b Additional consent provisions for collection and use of participant data and biological specimens in ancillary studies, if applicable
N/A

414
Confidentiality
27 How personal information about potential and enrolled participants will be collected, shared, and maintained in order to protect confidentiality before, during, and after the trial
259
Declaration of interests
28 Financial and other competing interests for principal investigators for the overall trial and each study site
N/A
Access to data
29 Statement of who will have access to the final trial dataset, and disclosure of contractual agreements that limit such access for investigators
259
Ancillary and post-trial care
30 Provisions, if any, for ancillary and post-trial care, and for compensation to those who suffer harm from trial participation
246-248, 264
Dissemination policy
31a Plans for investigators and sponsor to communicate trial results to participants, healthcare professionals, the public, and other relevant groups (eg, via publication, reporting in results databases, or other data sharing arrangements), including any publication restrictions
264
31b Authorship eligibility guidelines and any intended use of professional writers
N/A
31c Plans, if any, for granting public access to the full protocol, participant-level dataset, and statistical code
N/A
Appendices
Informed consent materials
32 Model consent form and other related documentation given to participants and authorised surrogates
N/A
Biological specimens
33 Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in the current trial and for future use in ancillary studies, if applicable
244-248, 250-251
* It is strongly recommended that this checklist be read in conjunction with the SPIRIT 2013 Explanation & Elaboration for important clarification on the items. Amendments to the protocol should be tracked and dated. The SPIRIT checklist is copyrighted by the SPIRIT Group under the Creative Commons “Attribution-NonCommercial-NoDerivs 3.0 Unported“ license.





























