Embed Size (px)
Citation preview

Journal of Clinical Neuroscience 21 (2014) 968–974
Contents lists available at ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Clinical Study
Cavernous sinus hemangioma: A fourteen year single institutionexperience
http://dx.doi.org/10.1016/j.jocn.2013.09.0080967-5868/� 2013 Published by Elsevier Ltd.
⇑ Corresponding author. Tel.: +91 11 2659 3538; fax: +91 11 2658 8559.E-mail address: [email protected] (A. Suri).
Sumit Bansal, Ashish Suri ⇑, Manmohan Singh, Shashank Sharad Kale, Deepak Agarwal,Manish Singh Sharma, Ashok Kumar Mahapatra, Bhawani Shankar SharmaDepartment of Neurosurgery, Neurosciences Center, All India Institute of Medical Sciences, New Delhi 110029, India
a r t i c l e i n f o a b s t r a c t
Article history:Received 21 February 2013Accepted 12 September 2013
Keywords:Cavernous sinusExtradural approachGamma Knife radiosurgeryHemangiomaTranscavernous
Cavernous sinus hemangioma (CSH) is a rare extra-axial vascular neoplasm that accounts for 2% to 3% ofall cavernous sinus tumors. Their location, propensity for profuse bleeding during surgery, and relation-ship to complex neurovascular structures are factors which present difficulty in excising these lesions.The authors describe their experience of 22 patients with CSH over 14 years at a tertiary care center.Patients were managed with microsurgical resection using a purely extradural transcavernous approach(13 patients) and with Gamma Knife radiosurgery (GKRS; Elekta AB, Stockholm, Sweden) (nine patients).Retrospective data analysis found headache and visual impairment were the most common presentingcomplaints, followed by facial hypesthesia and diplopia. All but one patient had complete tumor excisionin the surgical series. Transient ophthalmoparesis (complete resolution in 6–8 weeks) was the most com-mon surgical complication. In the GKRS group, marked tumor shrinkage (>50% tumor volume reduction)was achieved in two patients, slight shrinkage in five and no change in two patients, with symptomimprovement in the majority of patients. To our knowledge, we describe one of the largest series ofCSH managed at a single center. Although microsurgical resection using an extradural transcavernousapproach is considered the treatment of choice in CSH and allows complete excision with minimal mor-tality and long-term morbidity, GKRS is an additional tool for treating residual symptomatic lesions or inpatients with associated comorbidities making surgical resection unsuitable.
� 2013 Published by Elsevier Ltd.
1. Introduction
Cavernous sinus hemangioma (CSH) is a rare extra-axial highlyvascular neoplasm that accounts for 2% to 3% of all cavernous sinus tu-mors [1]. They are benign, well-encapsulated neoplasms arising with-in the confines of the cavernous sinus [1–3]. Hemangiomas most oftenpresent in middle-aged patients and are more common in women [4].
CSH may present with headache or various neurological fea-tures, including visual diminution, diplopia or facial hypesthesia[5]. Although a number of authors have described their extensiveexperience with the surgical treatment of cavernous sinus lesionswith good clinical results [4,6–9], these uncommon lesions remaina challenge for the neurosurgeon, as there are high mortality andmorbidity rates associated with uncontrollable and massive hem-orrhage during surgery. Current treatment modalities includemicrosurgical resection, embolization, fractionated radiation ther-apy and stereotactic radiosurgery (SRS). The optimal management
strategy is still a matter of controversy [10]. Complete resection ofCSH is potentially curative but may be complicated by profuseintra-operative bleeding and new cranial neuropathies [1,11].Gamma Knife radiosurgery (GKRS; Elekta AB, Stockholm, Sweden)has been performed for high-risk or residual CSH. The purpose ofthis study is to report our experience of removal of CSH througha completely extradural transcavernous approach, with use ofGKRS for smaller lesions or medically unfit patients.
2. Patients and methods
We analyzed 22 patients with CSH treated over a period of14 years (from 1999 to 2012), 13 of whom were treated using apurely extradural transcavernous surgical approach, while ninewere given primary GKRS. Interestingly, the majority of patientswere female, with four male patients (three in the surgical andone in the radiosurgery group). The duration of symptoms rangedfrom 6 months to 2 years. Contrast-enhanced CT scans and MRIwere obtained for all patients. All patients had a pre-operativeradiological diagnosis of CSH.

S. Bansal et al. / Journal of Clinical Neuroscience 21 (2014) 968–974 969
In the surgical series, patients were treated using an extraduraltranscavernous approach. The precise access corridor to the tumorin the cavernous sinus depended on the exact location of the tumorand the location of the maximum tumor bulge in the lateral wall ofthe cavernous sinus. Post-operative MRI to determine the extent oftumor removal was obtained for all patients in the surgical series.
In the GKRS series, nine patients were treated using the LeksellGamma Knife. Treatment planning and radiation dosimetry weredone with a goal of conformal and selective coverage of the lesionwith a 50% prescription isodose line using the multi-isocentertechnique. After GKRS, all patients were discharged from hospitalwithin 24 hours. All patients were scheduled for regular clinicaland radiological follow-up every 6 months during the first post-treatment year, and once per year thereafter.
3. Results
Of the 22 patients, 14 presented with headache, eight withvisual impairment, two with facial hypesthesia and seven withdiplopia.
All patients were evaluated pre-operatively with contrast-en-hanced CT scan and MRI. Contrast-enhanced CT scans revealediso- to hyper-dense expansile lesions in the region of the cavernoussinus and middle cranial fossa. There were signs of variable bonyerosion of the anterior clinoid process, sphenoid ridge, or apex ofthe petrous bone. MRI revealed well-demarcated expansile para-sellar lesions, which were hypo- or iso-intense on T1-weightedimages and hyperintense on T2-weighted images, with markedhomogeneous enhancement after intravenous administration ofcontrast in all patients. The tumors had well-defined borders andextended variably into the sella and superior orbital fissure.
3.1. Surgical technique
All 13 surgical patients were approached through a fronto-tem-poral osteoplastic craniotomy with or without orbito-zygomaticosteotomy (Table 1). The sphenoid ridge was removed using ahigh-speed pneumatic drill (Midas Rex; Medtronic, Minneapolis,MN, USA) and the superior orbital fissure was opened. The tentorialduplicature over the base of the anterior clinoid process waspeeled from the bone. The anterior clinoid process was drilledextradurally, the optic canal was deroofed, and the extra-cavern-ous extradural internal carotid artery (ICA) was exposed. The tem-poral base was drilled, the foramen spinosum was opened, and themiddle meningeal artery was coagulated and cut. The meningeallayer of the lateral wall of the cavernous sinus was peeled awayfrom the inner membranous layer using sharp and blunt dissec-tion. The cranial nerves in the lateral wall of the cavernous sinuswere exposed (cranial nerves III and IV, as well as V1, V2, andV3). The tumor was bulging either through the lateral triangle(Parkinson’s triangle, between cranial nerves IV and VI or theanterolateral triangle (Mullan’s triangle, between the V1 and V2nerves). The vascular tumor was removed by rapid decompressionusing an ultrasonic surgical aspirator and dissected along the cra-nial nerves.
The usual feeders from the meningo-hypophyseal trunk of theintra-cavernous ICA were exposed and coagulated early in thecourse of the surgery. Cranial nerve VI was seen in close proximityto the ICA. The medial extension of the lesion into the sella was re-moved. Hemostasis was achieved using gentle packing with gelatin(Spongstan; Johnson & Johnson Medical, New Yorkshire, UK),degraded cellulose (Surgicel; Johnson & Johnson Medical) andhemostatic matrix (Floseal; Baxter Biosurgery, IL, USA), and bloodloss was replaced using a cell saver (Autotranfusion unit; Didecon,Mirandola, Italy). Gross total excision was achieved in all but one
patient who underwent partial resection because of profuse bloodloss.
Post-operative morbidity included transient cranial nerve dys-function for 2 to 3 months in all but three patients. One patientdeveloped permanent VI nerve palsy. Vision improved in allpatients with pre-operative visual diminution, but not in thosewith pre-operative complete vision loss.
Post-operative MRI revealed gross total excision in 12 patients(Fig. 1). Histopathology revealed CSH in all patients. All patientswere evaluated clinically and by imaging 3 months after surgeryand then on an annual basis. Follow-up MRI was compared withthe pre-operative images and tumor dimensions were measuredin the axial, sagittal, and coronal planes. The follow-up period ran-ged from 3–48 months (mean, 21 months).
3.2. Radiosurgical technique
In the nine GKRS patients the Gamma Knife model B was usedup to the year 2010 (n = 6) and the Perfexion model was usedthereafter (n = 3) (Table 2). Three patients were medically unfitfor surgery so GKRS was chosen, while the other six patients wereincluded because of patient preference and small lesion size. Visu-alization of the lesion within the cavernous sinus at the time ofradiosurgery was attained with MRI using axial 1.0 mm slices ofmodified time-of-flight and field echo images with and withoutgadolinium enhancement, as well as coronal 2.0 mm slices of T2-weighted images. Treatment planning and radiation dosimetrywere done with a goal of conformal and selective coverage of thelesion with a 50% prescription isodose line using the multi-isocen-ter technique. The mean marginal dose constituted 16.8 Gy (range12–22.3 Gy). The irradiation dose for the optic pathways was keptbelow 8 Gy. The median number of iso-centers used to formulate aconformal radiosurgery dose plan was seven (range 3–13). Themedian target volume was 6.3 cc (range, 2.3–13.3 cc). After GKRS,all patients were discharged from hospital within 24 hours. All pa-tients were scheduled for regular clinical and radiological follow-up every 6 months during the first post-treatment year, and onceper year thereafter. The mean follow-up period ranged from 6–35 months (mean 17 months). The most recent MRI demonstratedmarked tumor shrinkage (>50% tumor volume reduction) in twopatients, slight shrinkage in five and no change in two patients(Fig. 2). No tumors showed transient enlargement after GKRS. Inthe two tumors in which significant shrinkage was attained, amarked tumor volume decrease had occurred by 10 months inone patient and after 35 months in another patient. At the timeof writing no patient had experienced tumor recurrence.
Headache improved in five patients. Among the five patientswith pre-operative ocular movement disturbances, completeremission of symptoms was obtained in three and no change wasobserved in two patients. Five patients had visual diminution intheir pre-radiosurgery evaluation, and two of these patients expe-rienced improvement in their vision.
4. Discussion
4.1. Patient population and clinical features
CSH are usually diagnosed in middle-aged patients [12–13]. Themajority of reported cases occur in women [4,12]. Similarly, themajority (n = 18) of our patients were women, with four men(three in the surgical and one in the radiosurgery group). The meanage of our patient group was 42 years, with a range from 26 to58 years. Headache, cranial neuropathies (especially cranial nervesIII, IV, V2, V3, and VI), poor vision, diplopia, ptosis, retro-orbitalpain, exophthalmos, endocrinopathy, trigeminal neuralgia, and
Table 1Demographics and characteristics of cavernous sinus hemangioma patients in the surgical group
Patient Age (yr)/sex Side Symptoms Clinical signs Extent ofresection
Complications Follow-upstatus
Follow-up(months)
1 41/F Left Headache: 1 yr; poor vision in L eye:6 mo; L facial hypesthesia: 6 mo
V/a, R: 6/9; L FC: 3ft; Lfacial 10% sensory loss
GTR Transient 3rd and 4thnerve palsy
EOM full 19
2 42/F Left Headache: 1 yr; L ptosis: 8 mo; poorvision, L eye: 2 mo
V/a, R: 6/18; L PL + L 3rdnerve palsy
GTR Transient completeophthalmoplegia
EOM full 12
3 50/F Right Headache: 6 mo; bilateral poor vision:6 mo R PL +
V/a, L: 6/36; R 6th nervepalsy
GTR None EOM full 48
4 36/F Right Diplopia: 6 mo V/a: B/l 6/9; R 6th nervepalsy
STR Permanent 6th nervepalsy
Permanent6th nervepalsy
30
5 38/F Left Headache: 1 yr No deficits GTR Transient completeophthalmoplegia
EOM full 14
6 38/F Right Headache: 2 yr; poor vision R eye anddiplopia: 6 mo; R facial hypoesthesia:6 mo
V/a, R: 6/9; V/a, L: 6/60; RV1 and V2: 25% sensoryloss
GTR Transient 3rd nervepalsy
EOM full 24
7 46/F Left Diplopia: 6 mo R 3rd and 6th nerve palsy GTR Transient 6th nervepalsy
EOM full 19
8 58/F Left Poor vision L eye: 14 mo V/a, L: HMCF GTR Transient L 6th nervepalsy
EOM full,visionimproved
28
9 26/F Left L proptosis: 5 yr; Headache: 3 yr V/a, R: 6/9; V/a, L: 6/18;EOM: full; L proptosis
GTR None Proptosisresolved
24
10 45/M Left Headache: 2 yr; Diplopia: 1 yr V/a, B/L: 6/9; L 6th nervepalsy
GTR Transient completeophthalmoplegia
EOM full 15
11 36/F Right Headache: 3 mo None GTR Transient R 6th nervepalsy
EOM full 15
12 32/M Left Headache: 3 mo None GTR Transient 6th nervepalsy, 20% V2 sensoryloss
EOM full 3
13 50/M Left Vision loss L eye: 1 yr Left PL � GTR Transient completeophthalmoplegia
EOM full 3
B/l = bilateral, EOM = external ocular movements, F = female, FC = finger counting, Ft = feet, GTR = gross total resection, HMCF = hand movement close to face, L = left,M = male, mo = months, PL = perception of light, R = right, STR = subtotal resection, V/a = visual acuity, yr = year, + = present, � = absent.
970 S. Bansal et al. / Journal of Clinical Neuroscience 21 (2014) 968–974
hemi- or mono-paresis have been reported in CSH patients [1]. Ofthe 22 patients, 14 presented with headache, eight presented withvisual impairment, two presented with facial hypesthesia andseven presented with diplopia. In spite of the vascular nature ofCSH, hemorrhages are extremely unusual during the natural courseof the disease [14].
4.2. Neurological imaging
Lesion growth is typically accompanied by mass effect and canresult in encasement of the adjacent neurovascular structures[5,15]. CSH is the only lesion that is purely intra-cavernous. Thus,even giant lesions remain within the dural confines of the cavern-ous sinus. CSH tend to become quite large before the patient man-ifests signs and symptoms [16].
On CT scans, CSH are isodense or minimally hyperdense, withintense homogenous enhancement with contrast administration.They may show pressure erosion of the petrous bone [15]. OnMRI, these lesions are well demarcated and homogenously hypoin-tense to white matter on T1-weighted images. Characteristically,they are brightly hyperintense on T2-weighted images, althougha few linear septum-like hypointensities may be identified [1,15].They enhance homogenously and intensely after contrast adminis-tration. As the tumors grow in size, they initially displace, and laterencase, the ICA. They are often found to extend toward the sella,inter-cavernous sinus, superior orbital fissure, and Meckel’s cave.On angiography, CSH are usually described as ‘‘occult.’’ However,after prolonged selective contrast injection, a mild tumor blush isvisible in most patients [1,17–18].
Intra-cavernous meningiomas and schwannomas are the mostimportant lesions to be considered in the differential diagnosis.As compared with CSH, meningioma is less hyperintense on T2-
weighted imaging, but syncytial meningiomas are very hyperin-tense on T2-weighted imaging and are difficult to distinguish[19–20]. Schwannomas are hypointense on T1-weighted imagingand hyperintense on T2-weighted imaging, but are more heteroge-neous in appearance [21]. An enlarged foramen ovale favors a diag-nosis of trigeminal schwannoma; similar lesions from cranial nerveIII, IV, or VI are rare.
4.3. Management considerations
Symptomatic CSH can be considered for microsurgical resec-tion, embolization, fractionated radiation therapy or GKRS.
4.3.1. MicrosurgeryLinskey and Sekhar reported use of a combined intra- and extra-
dural approach to treat three patients with CSH and total excisionwas achieved with minimal blood loss and with preservation ofcranial nerve function in two patients [1]. They hypothesized thatthe tumor arises within the cavernous sinus and, when small, takesits blood supply from the intra-cavernous carotid artery. Becausecranial nerve VI is the only cranial nerve truly within the cavernoussinus, it will most often run through the substance of the tumor;cranial nerves III, IV, and V (V1, V2, and V3) will always be foundstretched over the surface of the tumor in the overlying dura. Asthe tumor grows, it can extend medially into the sella turcica orcontralateral cavernous sinus, superiorly into the suprasellar space,or anteriorly into the orbital apex. As the tumor grows laterally, itgradually dissects between the two layers of dura lining the floor ofthe middle fossa so that it comes underneath cranial nerve V2 and,eventually, cranial nerve V3. As it grows into the middle fossa, itpicks up an additional blood supply from the middle meningealand accessory middle meningeal arteries. Because of the presence

Fig. 1. Pre-operative T1-weighted contrast-enhanced (a) axial, (b) sagittal and (c) coronal MRI showing a right cavernous sinus hemangioma and post-operative T1-weightedcontrast-enhanced (d) axial, (e) sagittal and (f) coronal MRI showing complete excision.
S. Bansal et al. / Journal of Clinical Neuroscience 21 (2014) 968–974 971
of the pseudo capsule, there will always be a potential plane be-tween the tumor and the overlying dura and cranial nerves. Thisplane makes it technically easier to preserve cranial nerves III, IV,and V (V1, V2, V3) when removing a hemangioma than whenremoving a cavernous sinus meningioma that arises from the durathat invests these nerves.
Goel et al. described their experience with 13 patients with CSH,seven of whom were operated on using Dolenc’s technique of anentirely extradural approach in 2003 [4]. Of these, 12 patientshad a complete tumor resection. The cranial nerve outcome in theirseries was poor, perhaps because of the large size of the tumors atdiagnosis.
Zhou et al. reported 20 surgically treated cases of CSH, 13 ofwhich were treated using the extradural approach [22]. Complete
tumor removal was achieved in 12 patients, and at a meanfollow-up of 3 years, all patients in this group improved withouttumor recurrence.
Shi et al. retrospectively analyzed 10 patients with CSH [23].Among the 10 patients, total tumor removal was performed in fourpatients, partial removal was performed in two patients, and fourpatients had tumor biopsies. Both patients who underwent partialremoval developed complete opthalmoplegia and diminishedsensation in the distribution of cranial nerve VI after surgery;one patient developed contralateral paralysis.
A previous series with seven patients by the senior author (A.S.)in 2007 detailed their technique and recommended rapid decom-pression of the tumor rather than en bloc resection to minimizeretraction on the cranial nerves in the lateral wall of the cavernous

Table 2Demographics and clinical characteristics of cavernous sinus hemangioma patients in the radiosurgery group
Patient Age(yr)/sex
Associatedcomorbidity
Pre-radiosurgery signs andsymptoms
Previous procedures Tumorvolume(cc)
Radiationdose (Gy)
Follow-upperiod(mo)
Imagingresponse
Clinicalresponse
1 46/F None L ptosis: 1 yr; Left 3rd nervepalsy
None 2.9 15 12 Decreasedsize
Same
2 40/F None V/a R: HMCF; V/a L: 6/36; Lophthalmoplegia
Craniotomy and partialexcision
13 15 12 Decreasedsize
Same
3 50/F Hypertension Headache: 2 mo; Poor visionR eye: 2 mo; V/a R: 6/36; V/aL: 6/18
None 3.3 15 35 Significantlydecreasedsize
Headacheimproved;vision improved
4 27/F None Headache: 2 mo; R ptosisand diplopia: 1 mo; V/a R: 6/9; V/a L: 6/6; R 3rd nervepalsy
None 2.3 15 35 Decreasedsize
Headacheimproved; R 3rdnerve palsyimproved
5 38/F None Headache: 1 yr; V/a R: 6/18;V/a L: 6/12
None 13.3 12 20 Decreasedsize (30%)
Headacheimproved
6 42/F None Headache: 1 yr None 5.93 16.9 12 Same size Headacheimproved
7 50/M None Headache: 8 mo None 5.82 22.3 11 Decreasedsize
Headacheimproved
8 46/F Hypertension;hypothyroidism
Diplopia and R ptosis: 2 yr; R3rd nerve palsy
Craniotomy done at othercentre but procedureabandoned because of heavybleeding
3.89 21.3 10 Significantlydecreasedsize
Diplopiaimproved
9 48/F Hypertension;R MCA stroke(on aspirin)
Poor vision and restriction ofR eye movements; V/a R: 6/60; V/a L: 6/18
None 7.39 19.4 6 Same size Eye movementsimproved;vision improved
F = female, HMCF = hand movement close to face, L = left, M = male, MCA = middle cerebral artery, mo = months, R = right, V/a = visual acuity, yr = year.
972 S. Bansal et al. / Journal of Clinical Neuroscience 21 (2014) 968–974
sinus [24]. The authors also stress the importance of early access tothe arterial feeders from the meningo-hypophyseal trunk of the in-ter-cavernous ICA because early coagulation of the vessels reducestumor vascularity and blood loss. The other important pointsinclude maximum exposure of the cranial base for access to thecavernous sinus, dissection of the meningeal layer of the cavernoussinus lateral wall from the inner membranous layer, and minimiz-ing the handling of the oculomotor nerve. The authors also identi-fied two gross pathological subtypes, which differed in surgicaldifficulty; which were the soft type with abundant vasculature,and the solid type with abundant interstitial tissue, for whichbleeding control was easier. In the present surgical series, gross to-tal excision was achieved in all but one patient who underwentpartial resection because of profuse blood loss.
The ideal treatment is total tumor removal with the preserva-tion of neurological function. However the surgery is difficultbecause of the complex structures of the cavernous sinus, encasedcranial nerves and ICA, and potential for severe intra-operativebleeding [3,11,17,18,25,26]. As a result, surgical mortality andmorbidity rates as high as 36% to 38% have been reported in olderseries [11,27]. In the present series, post-operative morbidityincluded transient cranial nerve dysfunction for 2 to 3 months inall but three patients. One patient developed permanent VI nervepalsy. Vision improved in all patients with pre-operative visualdiminution but not in those with pre-operative complete visionloss.
Rapid decompression of the tumor and early control of tumorvascularity on its medial side are keys to the successful removalof giant tumors [2]. Some surgeons have used hypothermia, vascu-lar occlusion, and intra-operative hypotension during surgery [28].The surrounding compressed cavernous sinus and a feeder fromthe meningo-hypophyseal trunk of the intra-cavernous ICA, whichis exposed and coagulated early during the course of surgery, sup-ply the CSH. Intra-operative controlled normotensive anesthesia(mean arterial blood pressure 70–80 mmHg) was used.
Although these tumors are well demarcated by a fibrouspseudocapsule, the peri-operative mortality rate is high as a result
of poorly controlled bleeding. It has been reported to be as high as12.5% in recent articles [29] but older series reported up to 36%.
4.3.2. RadiosurgeryRadiosurgery is a useful adjunctive treatment for non-operable
CSH or for residual neoplasm after initial attempts at microsurgicalresection, although it is not considered suitable for lesions near theoptic pathways [14,21,22,30]. Several authors reported the efficacyof fractionated radiotherapy for intracranial hemangiomas [31–35].
Nakamura et al. reported three patients with CSH. The mean tu-mor volume was 2.3 mL and the mean margin dose was 13.3 Gy(range 12–14 Gy) [13]. Follow-up MRI after 3 months showed areduction of the tumor volume and improvement in the neurolog-ical symptoms.
Seo et al. reported a patient with a CSH who underwent GKRS[36]. The tumor volume was 8.5 mL, and the dose delivered tothe margin was 15 Gy with a 50% isodose. The dose to the opticapparatus was less than 9 Gy. This investigation reported tumorregression on serial imaging over 2 years. Ivanov et al. reportedthree patients with CSH treated with low-dose (10–12 Gy) GKRS[37]. All the patients demonstrated tumor volume reduction ofmore than 60% after 12 months of follow-up. The mechanism pro-posed is that radiation induces endothelial proliferation, vesselwall hyalinization, and subsequent vessel obliteration in additionto direct cyto-toxicity to the tumor cells [38]. If a tumor showsclear neuroimaging characteristics of CSH and the lesion is small,and without features of either meningioma or schwannoma, GKRScan be performed as the primary treatment procedure.
In the present series, all nine patients underwent periodic MRIfollow-up after GKRS. The mean follow-up period after GKRS was17 months, (range 6–35 months). The most recent MRI demon-strated marked tumor shrinkage (>50% tumor volume reduction)in two patients, slight shrinkage in five and no change in twopatients. No tumors showed transient enlargement after GKRS. Inthe two tumors in which significant shrinkage was attained, amarked tumor volume decrease had occurred by 10 months in
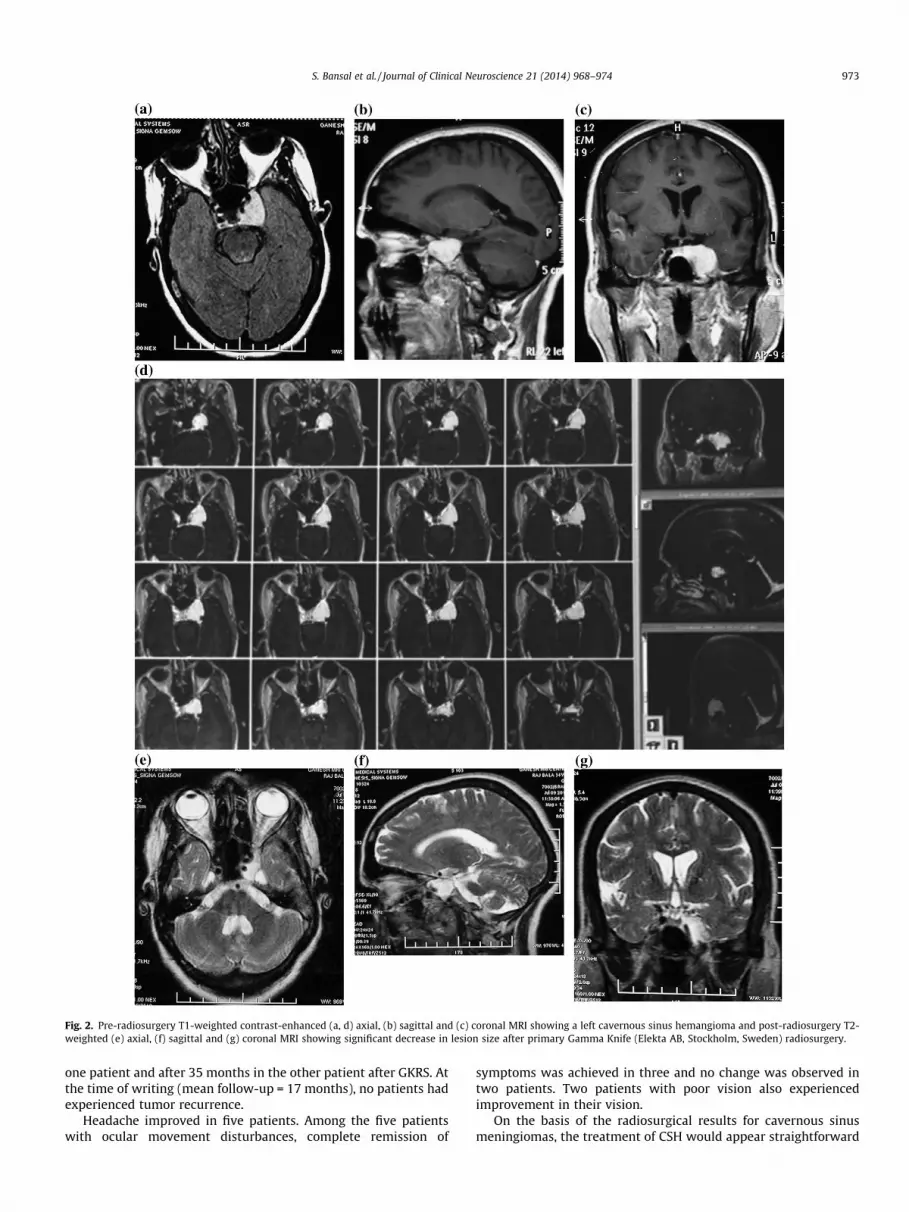
Fig. 2. Pre-radiosurgery T1-weighted contrast-enhanced (a, d) axial, (b) sagittal and (c) coronal MRI showing a left cavernous sinus hemangioma and post-radiosurgery T2-weighted (e) axial, (f) sagittal and (g) coronal MRI showing significant decrease in lesion size after primary Gamma Knife (Elekta AB, Stockholm, Sweden) radiosurgery.
S. Bansal et al. / Journal of Clinical Neuroscience 21 (2014) 968–974 973
one patient and after 35 months in the other patient after GKRS. Atthe time of writing (mean follow-up = 17 months), no patients hadexperienced tumor recurrence.
Headache improved in five patients. Among the five patientswith ocular movement disturbances, complete remission of
symptoms was achieved in three and no change was observed intwo patients. Two patients with poor vision also experiencedimprovement in their vision.
On the basis of the radiosurgical results for cavernous sinusmeningiomas, the treatment of CSH would appear straightforward

974 S. Bansal et al. / Journal of Clinical Neuroscience 21 (2014) 968–974
to most neurosurgeons with experience in radiosurgery. In ourstudy, compared with the results of open surgery for these tumors,radiosurgery appears to have significantly less morbidity but it istoo early to conclude that radiosurgery is better than microsurgicalresection, in view of our early results. Further long term follow-upis required to validate radiosurgery as a primary treatment in allpatients with CSH.
5. Conclusions
Although microsurgical resection using an extradural transcav-ernous approach is considered the treatment of choice in CSH andallows complete excision with minimal mortality or long termmorbidity in patients, GKRS is an additional tool for treating resid-ual symptomatic lesions or patients with associated comorbiditiesmaking surgical resection unsuitable.
Conflicts of interest/disclosures
The authors declare that they have no financial or other con-flicts of interest in relation to this research and its publication.
References
[1] Linskey ME, Sekhar LN. Cavernous sinus hemangiomas: a series, a review, andan hypothesis. Neurosurgery 1992;30:101–8.
[2] Goel A, Muzumdar D, Sharma P. Extradural approach for cavernoushemangioma of the cavernous sinus: experience with 13 cases. Neurol MedChir (Tokyo) 2003;43:112–9.
[3] Sepehrnia A, Tatagiba M, Brandis A, et al. Cavernous angioma of the cavernoussinus: case report. Neurosurgery 1990;27:151–5.
[4] Goel A. The extradural approach to lesions involving the cavernous sinus. Br JNeurosurg 1997;11:134–8.
[5] Hashimoto M, Yokota A, Ohta H, et al. Intratumoral injection of plasticadhesive material for removal of cavernous sinus hemangioma. J Neurosurg2000;93:1078–81.
[6] Al-Mefty O, Smith RR. Surgery of tumors invading the cavernous sinus. SurgNeurol 1988;30:370–81.
[7] Dolenc VV. Transcranial epidural approach to pituitary tumors extendingbeyond the sella. Neurosurgery 1997;41:542–52.
[8] Dolenc VV. Extradural approach to intracavernous ICA aneurysms. ActaNeurochir Suppl 1999;72:99–106.
[9] Eisenberg MB, Al-Mefty O, DeMonte F, et al. Benign nonmeningeal tumors ofthe cavernous sinus. Neurosurgery 1999;44:949–55.
[10] Gonzalez LF, Lekovic GP, Eschbacher J, et al. Are cavernous sinus hemangiomasand cavernous malformations different entities? Neurosurg Focus 2006;21:E6.
[11] Namba S. Extracerebral cavernous hemangioma of the middle cranial fossa.Surg Neurol 1983;19:379–88.
[12] Suzuki Y, Shibuya M, Baskaya MK, et al. Extracerebral cavernous angiomas ofthe cavernous sinus in the middle fossa. Surg Neurol 1996;45:123–32.
[13] Nakamura N, Shin M, Tago M, et al. Gamma knife radiosurgery for cavernoushemangiomas in the cavernous sinus: report of three cases. J Neurosurg2002;97:477–80.
[14] Kida Y, Kobayashi T, Mori Y. Radiosurgery of cavernous hemangiomas in thecavernous sinus. Surg Neurol 2001;56:117–23.
[15] Sohn CH, Kim SP, Kim IM, et al. Characteristic MR imaging findings ofcavernous hemangiomas in the cavernous sinus. AJNR Am J Neuroradiol2003;24:1148–51.
[16] Zabramski JM, Awasthi D. Extraaxial cavernous malformations. In: Awad IA,Barrow DL, editors. Cavernous malformations. Park Ridge III: AANS; 1993. p.133–144.
[17] Mori K, Handa H, Gi H, et al. Cavernomas in the middle fossa. Surg Neurol1980;14:21–31.
[18] Numaguchi Y, Kishikawa T, Fukui M, et al. Prolonged injection angiography fordiagnosing intracranial cavernous hemangiomas. Radiology 1979;131:137–8.
[19] Bradac GB, Riva A, Schorner W, et al. Cavernous sinus meningiomas: an MRIstudy. Neuroradiology 1987;29:578–81.
[20] Elster AD, Challa VR, Gilbert TH, et al. Meningiomas: MR and histopathologicfeatures. Radiology 1989;170:857–62.
[21] Peker S, Kilic T, Sengoz M, et al. Radiosurgical treatment of cavernous sinuscavernous haemangiomas. Acta Neurochir (Wien) 2004;146:337–41.
[22] Zhou LF, Mao Y, Chen L. Diagnosis and surgical treatment of cavernous sinushemangiomas: an experience of 20 cases. Surg Neurol 2003;60:31–7.
[23] Shi J, Hang C, Pan Y, et al. Cavernous hemangiomas in the cavernous sinus.Neurosurgery 1999;45:1308–18.
[24] Suri A, Ahmad FU, Mahapatra AK. Extradural transcavernous approach tocavernous sinus hemangiomas. Neurosurgery 2007;60:483–8.
[25] Dolenc VV. Cavernous angioma of the cavernous sinus: case report.Neurosurgery 1990; 27:155 (comment).
[26] Laws ER Jr. Cavernous angioma of the cavernous sinus: case report.Neurosurgery 1990; 27:155 (comment).
[27] Kudo T, Ueki S, Kobayashi H, et al. Experience with the ultrasonic surgicalaspirator in a cavernous hemangioma of the cavernous sinus. Neurosurgery1989;24:628–31.
[28] Goel A, Nadkarni TD. Cavernous haemangioma in the cavernous sinus. Br JNeurosurg 1995;9:77–80.
[29] Ohata K, El-Naggar A, Takami T, et al. Efficacy of induced hypotension in thesurgical treatment of the large cavernous sinus cavernoma. J Neurosurg1999;90:702–8.
[30] Aversa do Souto A, Marcondes J, Reis da Silva M, et al. Sclerosing cavernoushemangioma in the cavernous sinus: case report. Skull Base 2003;13:93–9.
[31] Grosu AL, Nieder C. Stereotactic fractionated radiotherapy for recurrentcapillary hemangioma of the cavernous sinus. Strahlenther Onkol 2006;182:179–82.
[32] Maruishi M, Shima T, Okada Y, et al. Cavernous sinus cavernoma treated withradiation therapy – case report. Neurol Med Chir 1994;34:773–7.
[33] Miserocchi G, Vaiani S, Migliore MM, et al. Cavernous hemangioma of thecavernous sinus. Complete disappearance of the neoplasm after subtotalexcision and radiation therapy. Case report. J Neurosurg Sci 1997;41:203–7.
[34] Rigamonti D, Drayer BP, Johnson PC, et al. The MRI appearance of cavernousmalformations (angiomas). J Neurosurg 1987;67:518–24.
[35] Shibata S, Mori K. Effect of radiation therapy on extracerebral cavernoushemangioma in the middle fossa. Report of three cases. J Neurosurg 1987;67:919–22.
[36] Seo Y, Fukuoka S, Sasaki T, et al. Cavernous sinus hemangioma treated withgamma knife radiosurgery: usefulness of SPECT for diagnosis – case report.Neurol Med Chir (Tokyo) 2000;40:575–80.
[37] Ivanov P, Chernov M, Hayashi M, et al. Low-dose gamma knife radiosurgery forcavernous sinus hemangioma: report of 3 cases and literature review. MinimInvasive Neurosurg 2008;51:140–6.
[38] Schneider BF, Eberhard DA, Steiner LE. Histopathology of arteriovenousmalformations after gamma knife radiosurgery. J Neurosurg 1997;87:352–7.





























