Embed Size (px)
Citation preview
BLBS078-CF_A01 BLBS078-Tilley July 23, 2011 2:42
2 Blackwell’s Five-Minute Veterinary Consult
Abortion, Spontaneous (Early Pregnancy Loss)—CatsA
BASICSDEFINITION� Spontaneous abortion—natural expulsionof a fetus or fetuses prior to the point at whichthey can sustain life outside the uterus.� Early pregnancy loss—generalized term forany loss of conceptus including earlyembryonic death and resorption.
PATHOPHYSIOLOGY� Infectious causes result in pregnancy loss bydirectly affecting the embryo, fetus, or fetalmembranes, or indirectly by creatingdebilitating systemic disease in the queen.� Non-infectious causes of pregnancy lossresult from any factor other than infectionthat leads to the death or premature expulsionof the conceptus (e.g., inadequate maternalnutrition, endocrine dysfunction, toxicity,genetic defects).
SYSTEMS AFFECTED� Endocrine � Reproductive � Othersystems—any debilitating illness can result inpregnancy loss.
GENETICSGenetic defects more prevalent in highlyinbred individuals; heritability ofsusceptibility to FIPV very high.
INCIDENCE/PREVALENCEUnknown—pregnancy frequently notconfirmed, owners may not recognize latepregnancy loss if the queen is fastidious; earlyembryonic death is difficult to document;genetic abnormalities account for ∼15% ofpregnancy loss in cats, including abortion.
SIGNALMENTSpeciesCats
Breed PredilectionsPurebred cats—higher incidence ofnon-infectious abortion; in-breeding increasesrisk of genetic disease; abortion is aconsequence of certain forms of heritablediseases (lethal genetic defect, fatalchromosomal error).
Mean Age and RangeInfectious abortion seen in all ages;non-infectious abortion seen more commonlyin young and aged queens.
SIGNSGeneral CommentsEarly embryonic death and resorptionfrequently have no clinical symptoms; anycombination of historical and physicalexamination findings may occur, with somequeens displaying no symptoms.
Historical FindingsFailure to deliver litter at expected time,return to estrus sooner than expected,decrease in abdominal diameter and weight
loss, discovery of fetal material, behaviorchange, anorexia, vomiting, diarrhea.
Physical Examination FindingsPurulent, mucoid, watery, or sanguinousvaginal discharge; dehydration, fever,abdominal straining, abdominal discomfort.
CAUSESInfectious� Bacterial—Salmonella spp., Chlamydia,Brucella; organisms implicated in causingabortion via ascending infection includeEscherichia coli, Staphylococcus spp.,Streptococcus spp., Pasteurella spp., Klebsiellaspp., Pseudomonas spp., Salmonella spp.,Mycoplasma spp., and Ureaplasma spp.� Protozoal—Toxoplasma gondii—uncommon. � Viral—FHV-1; FIV; FIPV;FeLV; FPLV—viruses are the most reportedcause of infectious abortion in the queen.
Non-infectious� Uterine—CEH-pyometra complex, chronicendometritis, mechanical trauma to uterus orfetus. � Ovarian—hypoluteoidism; geneticdefects are more prevalent; early terminationof corpora lutea function causes a decline inserum progesterone concentrations, resultingin early parturition (abortion). � Fetal—chromosomal abnormalities resulting inabnormal or arrested development andembryonic or fetal death. � Systemic—taurinedeficiency; vitamin A deficiency or toxicity;malnutrition; severe non-reproductive illness;exogenous drug administration: estrogens,glucocorticoids, prostaglandin F2α , anddopamine agonists (cabergoline,bromocriptine) will disrupt normal corpusluteum function; fetotoxic or teratogenicdrugs: chemotherapeutic agents, anti-fungalagents (griseofulvin), steroids, someantibiotics (trimethoprim-sulfonamides,quinolones, tetracyclines, gentamicin),antiepileptic medications (phenytoin);modified live vaccines.
RISK FACTORS� Previous history of pregnancy loss� Concurrent systemic disease � Recenttrauma � Purebred cat with high degree ofin-breeding � Very young or old queen� Malnourishment � Overcrowded orunsanitary environment
DIAGNOSISDIFFERENTIAL DIAGNOSIS
� Early pregnancy loss ◦ Failure toconceive ◦ Anovulatory cycle � Vulvardischarge ◦ Pyometra, mucometra, uterinestump pyometra ◦ Vaginitis, metritis,cystitis ◦ Impending parturition or dystocia◦ Neoplasia or trauma of urinary bladder,urethra, vagina, or uterus ◦ Estrus—verylittle discharge typically seen
� Abdominal straining or discomfort
� Urethral obstruction � Intestinal foreignbody, pancreatitis, peritonitis � Trauma� Impending parturition or dystocia
CBC/BIOCHEMISTRY/URINALYSIS� May be normal. � Inflammatory leukogramor stress leukogram depending on systemicdisease response. � Hemoconcentration andazotemia with dehydration.
OTHER LABORATORY TESTSInfectious Causes� Cytology and bacterial culture of vaginaldischarge, fetus, fetal membranes, or uterinecontents (aerobic, anaerobic, andmycoplasma). � FeLV—test for antigens inqueens using ELISA or IFA. � FHV-1—IFAor PCR from corneal or conjunctival swabs,viral isolation from conjunctival, nasal, orpharyngeal swabs. � FIPV—PCR for mRNAof the M gene of feline coronavirus(Molecular Diagnostics, College of VeterinaryMedicine, Auburn University,http://www.vetmed.auburn.edu/feline infectious peritonitis virus2).� FIV—ELISA—confirm positive results withWestern blot. � FPLV—viral isolation fromfetuses submitted for necropsy; documentseroconversion in the queen.
Non-infectious Causes� Hypoluteoidism—serum progesteronelevels; low levels do not indicate a primarycause unless documented prior to theabortion. � To rule out anovulatory cycle,confirm progesterone rise greater than 1.5 ng/ml 1 week following mating. � Behavioralevidence of estrus and vaginal cytology canconfirm estrus; repeatedly obtaining vaginalcytology samples may induce ovulation.
IMAGING� Abdominal ultrasound—confirmpregnancy; screen for evidence of resorption;evaluate health and viability of fetus(es) andassociated fluid and membranes; abnormaluterine fluid accumulation andnon-reproductive disease. � Radiograph—evaluates relative size, number, and position offetal skeletons; can be used to screen for fetalmonsters, fetal malpresentation, andnon-reproductive disease.
DIAGNOSTIC PROCEDURES� Genetic defects—necropsy abortedfetus(es); submit samples from aborted andstillborn fetus to lab for karyotyping.� Nutrition—submit sample of diet fornutritional analysis if concerned about taurineor vitamin A levels in diet, of particularimportance when queen is fed a homemadediet. � Complete history and evaluation ofpedigree to calculate coefficient ofin-breeding. � Evaluate cattery for vaccinationprotocols, feeding regime, general sanitationprocedures, and quarantine procedures forpregnant queens and new arrivals. � Submitreproductive tract (uterus, ovaries, uterinetubes) to reproductive pathologist to evaluatefor anatomical and pathological changes.
COPYRIG
HTED M
ATERIAL
BLBS078-CF_A01 BLBS078-Tilley July 23, 2011 2:42
Canine and Feline, Fifth Edition 3
Abortion, Spontaneous (Early Pregnancy Loss)—Cats A
� Send aborted, stillborn, mummifiedfetus(es) and fetal membranes (fresh,refrigerated, on wet ice) to reproductivepathologist for gross necropsy, histopathology,cultures, and viral isolation; serum from dam;fetal stomach contents and fetal blood useful.
TREATMENTAPPROPRIATE HEALTH CARE� Outpatient management: ◦ Typically nomedical management required fornon-infectious stable queens; queens withinfectious disease should be isolated andtreated appropriately. ◦ Hypoluteoidism—can be managed on an outpatient basis withtocolytics drugs in combination withtocodynamometry if value of queen outweighspotential to perpetuate this possibly heritablecondition. � Inpatient medical management:◦ Required for systemic illness and treatmentwith prostaglandin F2α . � Surgicalmanagement: ◦ OHE for queens with severeillness due to pyometra or metritis.
ACTIVITY� Isolation for queens with suspectedinfectious disease. � No activity restrictionsfor most non-infectious pregnancy losses.� Restrict activity as indicated for pregnancyloss due to trauma.
DIETCorrect diets with inappropriate taurine orvitamin A concentrations.
CLIENT EDUCATION� Infectious diseases—verify client isfollowing good vaccination protocols anddisease surveillance measures and is utilizingquarantine facilities for pregnant queens andnew arrivals. � Breeding management—discuss normal reproductive behavior andgood breeding management; advise clients tokeep detailed records related to reproductiveperformance, pedigree analysis, and socialbehavior of queens within the cattery.� Nutrition—discuss routine dietrecommendations for breeding queens; advisehomemade diets undergo nutritional analysis.� Genetic disease—increases in in-bredindividuals; many reproductive traits areheritable. � Medical management—discussside effects of prostaglandin F2α (PGF2α);medical management should be attempted foryoung to middle-aged queens with valuablereproductive potential. � Discuss risk ofzoonotic disease from Toxoplasma gondii.
MEDICATIONSDRUG(S) OF CHOICE� Will depend on etiology.� Amoxicillin-clavulanic acid 13.75 mg/kgPO q12h or enrofloxacin 5 mg/kg/day PO
depending on bacterial culture results.� Dinoprost tromethamine (PGF2α) 0.05–0.2 mg/kg SC Q 6–12 hours for evacuation ofuterine contents; continue until uterineevacuation complete based onultrasonographic evaluation. � Terbutaline0.08–1.0 mg PO as needed based ontocodynamometry; 0.03 mg/kg PO q8h iftocodynometry not available. � Progesteronein oil—2.0–3.0 mg/kg IM as needed based ontocodynamometry; q72h if tocodynometrynot available.
CONTRAINDICATIONS� PGF2α—intended pregnancy, respiratorycompromise, renal compromise, severeuterine pathology. � Terbutaline—cardiac orrespiratory disease, pyometra, infectiousdisease, hypertension. � Progesterone in oil—diabetes, pyometra, infectious disease, CEH.
PRECAUTIONS� Queens tolerate PGF2α treatment wellcompared to bitches but clients should giveinformed consent prior to instituting therapy;side effects of PGF2α treatment includepanting, salivation, inappetance, urination,diarrhea, vocalization (calling), nesting,tachypnea, vomiting, restlessness, andgrooming. Side effects diminish with repeatedinjections. � Use of tocolytics to maintainpregnancy requires accurate documentation ofbreeding dates to know when treatmentshould be discontinued; tocolytics used mostsuccessfully in combination withtocodynamometry to establish desired dosinginterval based on increasing preterm uterineactivity. � Terbutaline can cause hypertensionleading to increased hemorrhage from theplacental sites during parturition or at thetime of c-section.
POSSIBLE INTERACTIONS� Progesterone administration duringpregnancy is associated with masculinizationof female fetuses; do not administer in thefirst half of pregnancy and use with informedconsent thereafter. � Use of tocolytics tomaintain pregnancy is associated withincreased risk of dystocia, failure of normalplacental separation at parturition, lack ofmammary gland development and milkproduction, and poor maternal behavior forthe first few days post-partum.
ALTERNATIVE DRUG(S)� Altrenogest (Regu-Mate, Hoechst-Roussel)0.088 mg/kg PO q24h—unpredictable abilityto maintain pregnancy in the queen.� Prostaglandin analogues should be avoideddue to their narrow margin for safety and lackof effective dosing information in the cat.
FOLLOW-UPPATIENT MONITORING� Serial ultrasound evaluation q 5 days forqueens treated with prostaglandin F2αα to
determine stopping point. � Serial ultrasoundevaluation q 5–7 days to evaluate fetal viabilityfor queens receiving tocolytics drugs if notmonitored daily with tocodynamometry.
PREVENTION/AVOIDANCE� Institute infectious disease prevention,control, and surveillance plan. � Replaceinfertile queens with more reproductively fitindividuals. � Avoid exposure to abortifacient,teratogenic, or fetotoxic drugs.
POSSIBLE COMPLICATIONS� Depends on etiology. � Metritis,endometritis, uterine rupture, sepsis, shock.� Diabetes, CEH, masculinization of femalefetuses with progesterone treatment.
EXPECTED COURSE AND PROGNOSIS� Infectious disease—normal pregnancy,repeated abortion, or infertility possible withviral disease. � Poor prognosis for normalpregnancy in queens with severe CEH.� Good prognosis for successful pregnancywith treatment for hypoluteoidism; significantmonitoring required for good outcome.� Pregnancy loss due to genetic abnormalitieslikely to recur if queen is bred to tom withsimilar pedigree.
MISCELLANEOUSAGE-RELATED FACTORS� Queens > 6 years old have higher incidenceof infertility. � Pregnancy loss seen mostfrequently in very young and old queens.
ZOONOTIC POTENTIALToxoplasma gondii
SEE ALSO� Breeding, Timing
ABBREVIATIONS� CEH = cystic endometrial hyperplasia� ELISA = enzyme-linked immunosorbentassay � FeLV = feline leukemia virus � FHV-1= feline herpesvirus 1 � FIPV = felineinfectious peritonitis virus � FIV = felineimmunodeficiency virus � FPLV = felinepanleukopenia virus � IFA = indirectfluorescent antibody � OHE =ovariohysterectomy � PGF2α = prostaglandinF2α
INTERNET RESOURCES� www.theriojournal.com� www.whelpwise.comAuthor Milan HessConsulting Editor Sara K. Lyle
Client Education Handoutavailable online
BLBS078-CF_A02 BLBS078-Tilley July 14, 2011 8:49
4 Blackwell’s Five-Minute Veterinary Consult
Abortion, Spontaneous (Early Pregnancy Loss)—DogsA
BASICSDEFINITIONLoss of a fetus because of resorption in earlystages or expulsion in later stages ofpregnancy.
PATHOPHYSIOLOGY� Direct causes—congenital abnormality,infectious disease, trauma. � Indirectcauses—infectious placentitis, abnormalovarian function, abnormal uterineenvironment.
SYSTEMS AFFECTED� Reproductive. � Any dysfunction of a majorbody system can adversely affect pregnancy.
GENETICS� No genetic basis for most causes of abortion.� Lymphocytic hypothyroidism—single-generecessive trait in borzois.
INCIDENCE/PREVALENCE� True incidence unknown. � Resorptionestimated between 11–13%, some estimatesup to 30% of at least one resorption.� Incidence of stillbirth reported as 2.2–4.4%;increases with dystocia up to 22.3%.
SIGNALMENTSpeciesDogs
Breed Predilections� Familial lymphocytic hypothyroidismreported in borzois—prolonged interestrusinterval, poor conception rates, abortionmidgestation, stillbirths. � Many breedsconsidered at risk for familial hypothyroidism(see Hypothyroidism).
Mean Age and Range� Infectious causes, pharmacological agentscausing abortion, fetal defects—seen in allages. � Cystic endometrial hyperplasia—usually > 6 years old.
Predominant SexIntact bitches
SIGNSHistorical Findings� Failure to whelp on time. � Expulsion ofrecognizable fetuses or placental tissues.� Decrease in abdominal size; weight loss.� Anorexia. � Vomiting, diarrhea.� Behavioral changes.
Physical Examination Findings� Sanguineous or purulent vulvar discharge.� Disappearance of vesicles or fetusespreviously documented by palpation,ultrasonography, or radiography. � Abdominalstraining, discomfort. � Depression.� Dehydration. � Fever in some patients.
CAUSESInfectious� Brucella canis. � Canine herpesvirus.� Toxoplasma gondii, Neospora caninum.
� Mycoplasma and Ureaplasma.� Miscellaneous bacteria—E. coli,Streptococcus, Campylobacter, Salmonella.� Miscellaneous viruses—distemper virus,parvovirus, adenovirus.
Uterine� Cystic endometrial hyperplasia andpyometra. � Trauma—acute and chronic.� Neoplasia. � Embryotoxic drugs.� Chemotherapeutic agents. � Estrogens.� Glucocorticoids—high dosages.
Ovarian� Prostaglandins—lysis of corpora lutea.� Dopamine agonists—lysis of corpora luteavia suppression of prolactin; bromocryptine,cabergoline. � Hypoluteoidism—abnormalluteal function in the absence of fetal, uterine,or placental disease: progesteroneconcentrations < 1–2 ng/ml, most often seenat 40–45 days gestation.
Hormonal Dysfunction� Hypothyroidism; new data shows this is lesscommon that previously thought.� Hyperadrenocorticism. � Environmentalfactors—endocrine disrupting contaminantshave been documented in human and wildlifeinstances of fetal loss.
Fetal Defects� Lethal chromosomal abnormality. � Lethalorgan defects.
RISK FACTORS� Exposure of the brood bitch to carrieranimals � Old age � Hereditary factors
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Differentiate infectious from non-infectiouscauses—B. canis of immediate and zoonoticconcern. � Differentiate resorption frominfertility—helped by early diagnosis ofpregnancy. � History of drug use duringpregnancy—particularly during the firsttrimester, or use of drugs (e.g., dexamethasone,prostaglandins, ketoconazole, griseofulvin,doxycycline, tetracycline, dantrolene, amongothers) known to cause fetal death. � Vulvardischarges during diestrus—may mimicabortion; evaluate discharge and origin todifferentiate uterine from distal reproductivetract disease. � Necropsy of aborted fetus,stillborn puppies, and placenta(s)—enhanceschances of a definitive diagnosis, refrigeratebut do not freeze prior to submission.� History of systemic or endocrinedisease—may indicate problems with thematernal environment.
CBC/BIOCHEMISTRY/URINALYSIS� Usually normal. � Systemic disease, uterineinfection, viral infection, or endocrineabnormalities—may produce changes inCBC, biochemistries, or urinalysis.
OTHER LABORATORY TESTS� Serologic testing—B. canis, canineherpesvirus, and Toxoplasma, neospora; collectserum as soon as possible after abortion;repeat testing for raising titers for canineherpesvirus, Toxoplasma, neospora. � Slide testfor B. canis—very sensitive; negative resultsreliable; prevalence of false positives as high as60%; definitive diagnosis made via culture(D-Tec CB, Synbiotics Corp.,800-228-4305). � Tube agglutination test forB. canis—gives titers; titers > 1:200considered positive; titers from 1:50–1:200considered suspicious. � Agar gelimmunodiffusion test for B. canis—effectivelydifferentiates between false positives and truepositives in agglutination tests; detectscytoplasmic and cell surface antigens (CornellUniversity Diagnostic Laboratory,607-253-3900). � Baseline T4 serumconcentration (when no infectious agents areidentified)—hypothyroidism is a commonendocrine disease and has been suggested as acause for fetal wastage; role in pregnancy lossunclear; subnormal T4 concentrationsindicate need for further testing (seeHypothyroidism). � Serum progesteroneconcentration (when no infectious agents areidentified)—hypoluteoidism may cause fetalwastage; dogs depend on ovarian progesteroneproduction throughout gestation (minimumof 2 ng/mL required to maintain pregnancy);collect sample and determine as soon aspossible after abortion; in subsequentpregnancies, start weekly monitoring at week3, which may be before pregnancy can bedocumented with ultrasound; start biweeklysampling around the gestational age ofprevious loss. Pregnancy loss typically occursduring the seventh week of gestation (seePremature Labor). � Vaginal culture—B. caniswith positive serologic test; Mycoplasma,Ureaplasma, other bacterial agents; all exceptB. canis can be normal flora, thereforediagnosis difficult from vaginal cultures alone;Salmonella associated with systemic illness inthe bitch.
IMAGING� Radiography—identifies fetal structuresafter 45 days of gestation; earlier, candetermine uterine enlargement but cannotassess uterine contents.� Ultrasonography—identifies uterine sizeand contents; assesses fluid and itsconsistency; assesses fetal remains or fetalviability by noting heartbeats (normal, > 200bpm; stress, < 150 or > 280 bpm).
DIAGNOSTIC PROCEDURES� Vaginoscopy—identify source of vulvardischarges and vaginal lesions; use a scope ofsufficient length (16–20 cm) to examine theentire length of the vagina. � Cytologicexamination and bacterial culture—vaginamay reveal an inflammatory process (e.g.,uterine infection); technique for culture: use aguarded swab culture instrument to ensure an
BLBS078-CF_A02 BLBS078-Tilley July 14, 2011 8:49
Canine and Feline, Fifth Edition 5
Abortion, Spontaneous (Early Pregnancy Loss)—Dogs A
anterior sample (distal reproductive tract isnormally heavily contaminated with bacteria),or collection of secretions via transcervicalcatheterization.
PATHOLOGIC FINDINGSHistopathologic examination and culture offetal and placental tissue—may revealinfectious organisms; tissue culture,particularly of stomach contents, to identifyinfectious bacterial organisms.
TREATMENTAPPROPRIATE HEALTH CARE� Most bitches should be confined andisolated pending diagnosis. � Hospitalizationof infectious patients preferred. � B. canis—highly infective to dogs; shed in high numbersduring abortion; suspected cases should beisolated. � Outpatient medicalmanagement—medically stable patients withnon-infectious causes of pregnancy loss,endocrinopathies, or endometrial disease.� Partial abortion—may attempt to salvagethe live fetuses; administer antibiotics if abacterial component is identified.
NURSING CAREDehydration—use replacement fluids,supplemented with electrolytes if imbalancesare identified by serum biochemistries.
ACTIVITYPartial abortion—cage rest generallyrecommended, although the positive effect onreducing further abortion is unknown.
DIETNo special dietary considerations foruncomplicated cases
CLIENT EDUCATION� Critical for B. canis—if confirmed,euthanasia recommended due to lack ofsuccessful treatment and to prevent spread ofinfection; may try OHE and long-termantibiotics; discuss surveillance program forkennel situations: monthly serology for allindividuals, culling any positive animals, untilthree consecutive negative tests are obtained;discuss zoonotic potential. � Primary uterinedisease—OHE is indicated in patients withno breeding value; cystic endometrialhyperplasia is an irreversible change.� Infertility or pregnancy loss—may recur insubsequent estrous cycles despite successfulimmediate treatment. � Prostaglandintreatment—discuss side effects (see Abortion,Termination of Pregnancy). � Infectiousdiseases—establish surveillance and controlmeasures.
SURGICAL CONSIDERATIONSOHE—preferred for stable patients with nobreeding value
MEDICATIONSDRUG(S) OF CHOICE� PGF2α (Lutalyse, dinoprosttromethamine)—uterine evacuation afterabortion; 0.05–0.1 mg/kg SC q8–24h;cloporostenol (Estrumate, cloprostenol)—1–5μg/kg SC q24h; not approved for use in dogs,but adequate documentation legitimizes itsuse; use only if all living fetuses have beenexpelled. � Antibiotics—for bacterial disease;initially institute broad-spectrum agent;specific agent depends on culture andsensitivity testing of vaginal tissue or necropsyof fetus. � Progesterone (Regu-Mate) at 0.088mg/kg (1 mL/25 kg PO) or progesterone inoil at 2 mg/kg IM q48–72h—for documentedhypoluteodism only to maintain pregnancy,must have accurate due date to know when todiscontinue therapy—inadvertentlyprolonging gestation will result in fetal death.
CONTRAINDICATIONSProgestogen supplementation—contraindicated in dogs with endometrial ormammary gland disease.
PRECAUTIONSPGF2α—metabolized in the lung; side effectsare related to smooth muscle contraction, aredose-related, and diminish with eachinjection; panting, salivation, vomiting, anddefecation common; dosing critical (LD50 fordinoprost—5 mg/kg).
ALTERNATIVE DRUG(S)Oxytocin—1 U/5 kg SC q6–24h for uterineevacuation; most effective in the first 24–48hours after abortion.
FOLLOW-UPPATIENT MONITORING� Partial abortion—monitor viability ofremaining fetuses with ultrasonography;monitor systemic health of the dam forremainder of pregnancy. � Vulvardischarges—daily; for decreasing amount,odor, and inflammatory component; forconsistency (increasing mucoid content isprognostically good). � PGF2α—continuedfor 5 days or until most of the discharge ceases(3-15 days). � B. canis—monitor afterneutering and antibiotic therapy; yearlyserologic testing to identify recrudescence.� Hypothyroidism—treat appropriately;neutering recommended (hereditary nature);see Hypothyroidism.
PREVENTION/AVOIDANCE� Brucellosis and other infectious agents—surveillance programs to prevent introductionto kennel. � OHE—for bitches with nobreeding value. � Use of modified-live
vaccines (e.g., some distemper, parvovirus,etc., vaccines).
POSSIBLE COMPLICATIONS� Untreated pyometra—septicemia, toxemia,death. � Brucellosis—diskospondylitis,endophthalmitis, recurrent uveitis.
EXPECTED COURSE AND PROGNOSIS� Pyometra—recurrence rate duringsubsequent cycle is high (up to 70%) unlesspregnancy is established. � CEH—recovery offertility unlikely; pyometra commoncomplication. � Hormonal dysfunction—often manageable; familial aspects should beconsidered. � Brucellosis—guarded; extremelydifficult to successfully eliminate infectioneven if combined with neutering.
MISCELLANEOUSAGE-RELATED FACTORSOlder bitches more likely to have CEH
ZOONOTIC POTENTIALB. canis—can be transmitted to humans,especially when handling the aborting bitchand tissues expelled; massive numbers oforganisms expelled during abortion.Pathologists should be warned when B. canisis suspected. People that areimmunocompromised are at greatest risk forinfection.
SEE ALSO� Brucellosis � Hypothyroidism � Infertility,Female—Dogs � Premature Labor � Pyometraand Cystic Endometrial Hyperplasia
ABBREVIATIONS� CEH = cystic endometrial hyperplasia� OHE = ovariohysterectomy � PGF2α =prostaglandin F2α
INTERNET RESOURCESRoot-Kustritz MV. Use of supplementalprogesterone in management of caninepregnancy. In: Concannon PW, England G,Verstegen III J, Linde-Forsberg C, eds.,Recent Advances in Small AnimalReproduction. International VeterinaryInformation Service, Ithaca NY, www.ivis.org,2001; A1220.0401Author Beverly J. PurswellConsulting Editor Sara K. Lyle
Client Education Handoutavailable online
BLBS078-CF_A03 BLBS078-Tilley July 14, 2011 9:3
6 Blackwell’s Five-Minute Veterinary Consult
Abortion, Termination of PregnancyA
BASICSDEFINITIONTermination of an unwanted pregnancy. Maybe accomplished by drugs that alter embryotransport in the oviduct impedingestablishment of a pregnancy, and/or causeluteal regression, terminating an establishedpregnancy. Due to their possible side effects(CEH, aplastic anemia and bone marrowsuppression), drugs that impair embryonictransit through the oviduct (estrogens) are notcommonly used or recommended.
PATHOPHYSIOLOGYAfter fertilization the embryo travels theoviduct in a timely manner before enteringthe uterus. Impaired embryo transportthrough the oviduct leads to embryonicdegeneration and implantation abnormalities.In the dog and cat, pregnancy maintenance isdependent on progesterone production fromthe corpora lutea. In dogs, maintenance of thecorpora lutea during the second half ofgestation is also supported by prolactin.Drugs that cause luteal regression, antagonizePRL, and/or compete with progesteronereceptors will terminate pregnancy.
SYSTEMS AFFECTED� Cardiovascular� Digestive� Neurologic (caused by drugs used fortreatment)� Reproductive� Respiratory
GENETICSN/A
INCIDENCE/PREVALENCEN/A
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsNo breed predilection
Mean Age and RangeN/A
Predominant SexFemale
SIGNS� Depends on stage of gestation
◦ None◦ Vaginal discharge◦ Fetal expulsion
CAUSES� Impaired oviductal transport� Luteal regression� Progesterone receptor antagonism
RISK FACTORSN/A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Ascertain that a breeding took place; a tie inthe bitch and coital “after-reaction” in thequeen.� Determine stage of estrous cycle: vaginalcytology, serum progesterone concentration(see Breeding, Timing).� Presence of sperm cells in vagina cytology;absence of sperm does not rule out a previousbreeding.� Pregnancy diagnosis:
◦ Abdominal palpation (bitch: 31–33 daysafter LH surge; queen: 21–25 days afterbreeding).◦ Transabdominal ultrasound (bitch: > 25days after LH surge; queen: > 16 days afterbreeding).◦ Abdominal radiographs (bitch: > 45 daysafter LH surge; queen: > 38 days afterbreeding).◦ Serum relaxin concentration in the bitch(> 28 days after LH surge) (WitnessRelaxin, Synbiotics Corp.,http://synbiotics.com/index.html).
CBC/BIOCHEMISTRY/URINALYSIS� Within normal limits during first half ofpregnancy in healthy patients.� Decrease in PCV during second half ofpregnancy in bitches and queens is normal.� Recommended as screening test prior totreatment in patients with suspectedunderlying disease.
OTHER LABORATORY TESTS� Vaginal cytologic testing—determines stageof estrous cycle and presence of sperm.� Serum progesterone concentrationdetermines if the female is in diestrus andmonitors luteal regression duringtreatment.
IMAGING� Transabdominal ultrasound (method ofchoice): diagnose pregnancy and monitoruterine evacuation during treatment.� Abdominal radiographs.
PATHOLOGIC FINDINGSN/A
TREATMENTAPPROPRIATE HEALTH CARE� Physical examination before initiation oftreatment.� Monitor 30–60 minutes after treatment forside effects (vomiting, defecation,hypersalivation, hyperpnea, micturition,tachycardia).� Confirmation of pregnancy before initiatingtreatment is recommended; more than 60% ofmismated bitches may not become pregnant.
� Pregnancy status in early diestrus isunknown; ultrasound confirmation ofpregnancy is not possible until 4–5 weeksafter breeding.� Treatment on day 6–10 of diestrus—mayhave reduced efficacy compared tomidgestation but can be less distasteful toclient (less discharge and recognizable fetusesare not passed).� PGF2α and bromocriptine—improvesefficacy of either drug given alone.
NURSING CAREN/A
ACTIVITYNormal
DIETAvoid feeding prior to each treatment and for1–2 hours after treatments (reduces nauseaand vomiting).
CLIENT EDUCATION� Discuss patient’s reproductive future withowner. If no litters are desired, then OHE isthe best option.� Discuss with the client the potential sideeffects of the treatment options; reach amutual agreement on the treatment plan.
SURGICAL CONSIDERATIONSOHE is recommended for patients with noreproductive value or when owners do notdesire future litters.
MEDICATIONSDRUG(S) OF CHOICE� Confirmation of pregnancy beforeinitiating any of the treatment protocolssuggested below is recommended. Lengths oftreatment suggested may vary; treatmentsshould be continued until abortion iscomplete.
◦ PGF2α : causes luteal regression withsubsequent decline in progesteroneconcentration, cervical relaxation, anduterine contractions; bitches: 100 μg/kgSC q8h for 2 days, then 200 μg/kg SC q8huntil pregnancy termination; queens:0.5–1 mg/kg SC q12h every other day >day 40, or 2 mg/cat IM q24h for 5 days >day 33.◦ Cloprostenol (prostaglandin analogue):bitches: 2.5 μg/kg SC q8 or q12h every48 hours until pregnancy termination(∼6 days after start of treatment).◦ Dexamethasone: mode of action isunknown; bitches: 0.2 mg/kg PO q12h for7 days, then decreasing from 0.16 to0.02 mg/kg over the last fiveadministrations; treatment failures notuncommon.◦ Cabergoline (PRL antagonist): causesluteal regression; bitches: 1.65 mg/kg SCq24h for 5 days or 5 mg/kg PO q24h for5 days > day 40; queens: 0.825 mg/kg SC
BLBS078-CF_A03 BLBS078-Tilley July 14, 2011 9:3
Canine and Feline, Fifth Edition 7
(Continued) Abortion, Termination of Pregnancy A
q12h for 5 days > day 30 or 5–15 μg/kgPO q24h for 5 days > day 25.◦ Bromocriptine (PRL antagonist): causesluteal regression; bitches: 62.5 μg/kg POq12h for up to 6 days > day 43.◦ Cloprostenol and cabergolinecombination: bitches: cabergoline 5 μg/kgPO q24h for 10 days plus cloprostenol2.5 μg/kg SC q24h at start of treatment, or1 μg/kg SC q24h at start of treatment andat day 5 of treatment; treatment should beinitiated > 28 days post-LH surge; queen:cabergoline 5 μg/kg PO q24h pluscloprostenol 5 μg/kg SC every 48 hours(> 30 days after breeding) until abortion iscomplete (∼9 days).◦ Cloprostenol and bromocriptinecombination: bitches; bromocriptine30 μg/kg q8h PO of for 10 days pluscloprostenol 2.5 μg/kg SC q24h or1 μg/kg SC at start of treatment and at day5 of treatment; treatment should beinitiated > 28 days post-LH surge.
CONTRAINDICATIONS� PGF2α and analogues: animals withrespiratory disease (bronchoconstriction); donot administer intravenously.� Cabergoline and bromocriptine: animalshypersensitive to ergot alkaloids; these drugsshould be administered with caution inpatients with impaired liver function.� Estrogens—may cause cystic endometrialhyperplasia, pyometra, and bone marrowsuppression leading to pancytopenia.
PRECAUTIONS� PGF2α and analogues: side effects aredose-dependent and include vomiting,defecation, dyspnea, tachycardia, salivation,restlessness, and anxiety; side effects subsidewithin 60 minutes; the severity of effects canbe attenuated with premedication (> 15minutes) with a combination of atropine(0.025 mg/kg); use extreme caution in dogsand cats with preexisting cardiopulmonary,liver, and renal diseases.� Dexamethasone: polydipsia, polyuria, andpolyphagia are reported side effects. Long-term administration has been associated withhyperadrenocorticism.� Cabergoline and bromocriptine: side effectsmay include vomiting and anorexia;prolonged use (> 2 weeks) may cause coatcolor changes.
POSSIBLE INTERACTIONS� PGF2α and analogues: effect may be reducedby concomitant administration of progestins;use may enhance effects of oxytocin.� Cabergoline and bromocriptine: cabergolineeffects may be reduced with concomitanttreatment with dopamine (D2) antagonists;avoid concomitant treatment withhypotensive drugs.
ALTERNATIVE DRUG(S)� The following drugs are recommended foruse in bitches but not available in the UnitedStates:
◦ Mifepristone (RU486; progestin andglucocorticoid receptors antagonist): 2.5mg/kg PO q12h for 4.5 days > day 32 ofpregnancy is recommended; no side effectshave been reported.◦ Aglepristone (progestin andglucocorticoid receptors antagonists): 10mg/kg SC q24h for 2 days > 32 dayspost-LH surge; pregnancy is terminated in4-7 days; no side effects have been reported;mild vaginal discharge may be observed.◦ GnRH antagonists (block GnRHreceptors at the pituitary gland, causing adecline in gonadotropins concentration): asingle treatment with 110–330 μg/kg SC isrecommended; pregnancy is terminatedwithin 6–10 days after treatment;prepartum-like behavior has been observed;abortion may be followed byserosanguineous vaginal discharge for 2–3days.
FOLLOW-UPPATIENT MONITORINGTransabdominal ultrasound examinationsshould be performed to monitor completeevacuation of uterine contents.
PREVENTION/AVOIDANCE� OHE for bitches and queens not intendedfor breeding.� Estrus suppression or confinement ofbitches and queens intended for breedingduring a later cycle to avoid mismating.
POSSIBLE COMPLICATIONSPregnancy termination may not be achievedafter one treatment protocol and continuationor change in treatment protocol may benecessary.
EXPECTED COURSE AND PROGNOSIS� The interestrous interval in bitches treatedwith prostaglandins and PRL inhibitors maybe shortened (∼1 month). Queens mayresume estrous behavior 7–10 days afterpregnancy termination.� Subsequent estrus fertility is not affected.
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMSInduced abortion
SEE ALSOBreeding, Timing
ABBREVIATIONS� CEH = cystic endometrial hyperplasia� GnRH = gonadotropin-releasing hormone� LH = luteinizing hormone� OHE = ovariohysterectomy� PCV = packed cell volume� PGF2α = prostaglandin F2α� PRL = prolactin
INTERNET RESOURCESWanke MM, Romangnoli S, Verstegen J,Concannon PW. Pharmacologic approachesto pregnancy termination in dogs and catsincluding the use of prostaglandins, dopamineagonists, and dexamethasone. In: ConcannonPW, England G, Verstegen III J,Linde-Forsberg C, eds., Recent Advances inSmall Animal Reproduction. InternationalVeterinary Information Service, Ithaca NY,www.ivis.org, 2001.
Suggested ReadingCorrada Y, Klima L, De la Sota RL,
Rodriquez R. Use of prostaglandins andbromocriptine mesylate for pregnancytermination in bitches. JAVMA 2002,220(7):1017–1019.
Eilts BE Pregnancy termination in the bitchand queen. Clin Tech Small Anim Pract2002, 17:116–123.
Fieni F, Dumon C, Tainturier D, Bruyas JF.Clinical protocol for pregnancy terminationin bitches using prostaglandin F2 α . J ReproFert 1997, 51:245–250.
Johnston SD, Root Kustritz MV, Olson PNS.Prevention and termination of caninepregnancy. In: Canine and FelineTheriogenology. Philadelphia: Saunders,2001, pp. 168–192.
Johnston SD, Root Kustritz MV, Olson PNS.Prevention and termination of felinepregnancy. In: Canine and FelineTheriogenology. Philadelphia: Saunders,2001, pp. 447–452.
Author Jose A. LenConsulting Editor Sara K. Lyle
Client Education Handoutavailable online
BLBS078-CF_A04 BLBS078-Tilley March 21, 2011 8:10
8 Blackwell’s Five-Minute Veterinary Consult
AbscessationA
BASICSDEFINITIONAn abscess is a localized collection of purulentexudate contained within a cavity.
PATHOPHYSIOLOGY� Bacteria are often inoculated under the skinvia a puncture wound; the wound surfacethen seals.� When bacteria and/or foreign objects persistin the tissue, purulent exudate forms andcollects.� Accumulation of purulent exudates—if notquickly resorbed or discharged to an externalsurface, stimulates formation of a fibrouscapsule; may eventually lead to abscessrupture.� Prolonged delay of evacuation—formationof a fibrous abscess wall; to heal, the cavitymust be filled with granulation tissue fromwhich the causative agent may not be totallyeliminated; may lead to chronic orintermittent discharge of exudate from adraining sinus tract.
SYSTEMS AFFECTED� Gastrointestinal—pancreas (dogs > cats)� Hepatobiliary—liver parenchyma� Ophthalmic—periorbital tissues� Reproductive—prostate gland (dogs >cats); mammary gland� Skin/Exocrine—percutaneous (cats >dogs); anal sac (dogs > cats)
GENETICSN/A
INCIDENCE/PREVALENCEN/A
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesCats and dogs
Breed PredilectionsN/A
Mean Age and RangeN/A
Predominant SexMammary glands (female); prostate gland(male)
SIGNSGeneral Comments� Determined by organ system and/or tissueaffected.� Associated with a combination ofinflammation (pain, swelling, redness, heat,and loss of function), tissue destruction,and/or organ system dysfunction caused byaccumulation of exudates.
Historical Findings� History of traumatic insult or previousinfection.
� A rapidly appearing painful swelling withor without discharge, if affected area isvisible.
Physical Examination Findings� Determined by the organ system or tissueaffected.� A discrete mass may be detectable.� Inflammation and discharge from a fistuloustract may be visible if the abscess is superficialand has ruptured to an external surface.� A variably sized, painful mass of fluctuant tofirm consistency attached to surroundingtissues may be palpable.� Fever if abscess is not ruptured and draining.� Sepsis occasionally, especially if abscessruptures internally.
CAUSES� Foreign objects.� Pyogenic bacteria—Staphylococcus spp.;Escherichia coli; β-hemolytic Streptococcusspp.; Pseudomonas; Mycoplasma andMycoplasma-like organisms (l-forms);Pasteurella multocida; Corynebacterium;Actinomyces spp.; Nocardia; Bartonella.� Obligate anaerobes—Bacteroides spp.;Clostridium spp.; Peptostreptococcus;Fusobacterium.
RISK FACTORS� Anal sac—impaction; anal sacculitis.� Brain—otitis interna sinusitis oral infection.� Liver—omphalophlebitis sepsis.� Lung—foreign object aspiration bacterialpneumonia.� Mammary gland—mastitis.� Periorbital—dental disease; chewing ofwood or other plant material.� Percutaneous—fighting.� Prostate gland—bacterial prostatitis.� Immunosuppression—FeLV/FIV infection,immunosuppressive chemotherapy, acquiredor inherited immune system dysfunctions,underlying predisposing disease (e.g., diabetesmellitus, chronic renal failure,hyperadrenocorticism).
DIAGNOSISDIFFERENTIAL DIAGNOSISMass Lesions� Cyst—less or only transiently painful;slower growing.� Fibrous scar tissue—firm; non-painful.� Granuloma—less painful; slower growing;generally firmer without fluctuant center.� Hematoma/seroma—variable pain (dependson cause); non-encapsulated; rapid initialgrowth but slow increase once full size isattained; unattached to surrounding tissues;fluctuant and fluid filled initially but morefirm with organization.� Neoplasia—variable growth; consistent;painful.
Draining Tracts� Mycobacterial disease.� Mycetoma—botryomycosis, actinomycoticmycetoma, eumycotic mycetoma.� Neoplasia.� Phaeohyphomycosis.� Sporotrichosis.� Systemic fungal infection—blastomycosis,coccidioidomycosis, cryptococcosis,histoplasmosis, trichosporosis.
CBC/BIOCHEMISTRY/URINALYSIS� CBC—normal or neutrophilia with orwithout regenerative left shift. Neutropeniaand degenerative left shift if sepsis present.� Urinalysis and serum chemistryprofile—depends on system affected.� Prostatic—pyuria.� Liver and/or pancreatic—high liver enzymesand/or total bilirubin.� Pancreatic (dogs)—high amylase/lipase.� Diabetes mellitus—persistenthyperglycemia and glucosuria.
OTHER LABORATORY TESTS� FeLV and FIV—for cats with recurrent orslow-healing abscesses.� CSF evaluation—increase in cellularity andprotein expected with brain abscess.� Adrenal function—evaluate forhyperadrenocorticism.
IMAGING� Radiography—soft-tissue density mass inaffected area; may reveal foreign body.� Ultrasonography—determine if mass isfluid filled or solid; determine organ systemaffected; reveal flocculent-appearing fluidcharacteristic of pus; may reveal foreignobject.� Echocardiography—helpful for diagnosis ofpericardial abscess.� CT or MRI—helpful for diagnosis of brainabscess.
DIAGNOSTIC PROCEDURESAspiration� Reveals a red, white, yellow, or green liquid.� Protein content > 2.5–3.0 g/dL.� Nucleated cell count—3,000–100,000 (ormore) cells/μL; primarily degenerativeneutrophils with lesser numbers ofmacrophages and lymphocytes.� Pyogenic bacteria—may be seen in cells andfree within the fluid.� If the causative agent is not readilyidentified with a Romanowsky-type stain,specimens should be stained with an acid-faststain to detect mycobacteria or Nocardia andPAS stain to detect fungus.
Biopsy� Sample should contain both normal andabnormal tissue in the same specimen.� Impression smears—stained and examined.� Tissue—submit for histopathologicexamination and culture.� Contact the diagnostic laboratory forspecific instructions.
BLBS078-CF_A04 BLBS078-Tilley March 21, 2011 8:10
Canine and Feline, Fifth Edition 9
(Continued) Abscessation A
Culture� Affected tissue and/or exudate—aerobic andanaerobic bacteria and fungus.� Blood and/or urine—isolate bacteriumresponsible for possible sepsis.� Bacterial sensitivity.
PATHOLOGIC FINDINGS� Pus-containing mass lesion accompanied byinflammation.� Palpable—variably firm or fluctuant mass.� Ruptured—may see pus draining directlyfrom the mass or an adjoining tract.� Exudate—large numbers of neutrophils invarious stages of degeneration; otherinflammatory cells; necrotic tissue.� Surrounding tissue—congested; fibrin; largenumber of neutrophils; variable number oflymphocytes; plasma cells; macrophages.� Causative agent variably detectable.
TREATMENTAPPROPRIATE HEALTH CARE� Depends on location of abscess andtreatment required.� Outpatient—bite-induced abscesses.� Inpatient—sepsis; extensive surgicalprocedures; treatment requiring extendedhospitalization.� Establish and maintain adequate drainage.� Surgical removal of nidus of infection orforeign object(s) if necessary.� Institution of appropriate antimicrobialtherapy.
NURSING CARE� Depends on location of abscess.� Apply hot packs to inflamed area as needed.� Use protective bandaging and/orElizabethan collars as needed.� Accumulated exudate—drain abscess;maintain drainage by medical and/or surgicalmeans.� Sepsis or peritonitis—aggressive fluidtherapy and support.
ACTIVITYRestrict until the abscess has resolved andadequate healing of tissues has taken place.
DIET� Sufficient nutritional intake to promote apositive nitrogen balance.� Depends on location of abscess andtreatment required.
CLIENT EDUCATION� Discuss need to correct or prevent riskfactors.� Discuss need for adequate drainage andcontinuation of antimicrobial therapy for anadequate period of time.
SURGICAL CONSIDERATIONS� Appropriate debridement and drainage—may need to leave the wound open to anexternal surface; may need to place surgicaldrains.� Early drainage—to prevent further tissuedamage and formation of abscess wall.� Remove any foreign objects(s), necrotictissue, or nidus of infection.
MEDICATIONSDRUG(S) OF CHOICE� Antimicrobial drugs—effective against theinfectious agent; gain access to site ofinfection.� Broad-spectrum agent—bactericidal andwith both aerobic and anaerobic activity; untilresults of culture and sensitivity are known.Dogs and cats: amoxicillin (11–22 mg/kg POq8–12h); amoxicillin/clavulanic acid (12.5–25 mg/kg PO q12h); clindamycin (5 mg/kgPO q12h); and trimethoprim/sulfadiazine(15 mg/kg PO IM q12h). Cats withMycoplasma and l-forms: doxycycline(3–5 mg/kg PO q12h).� Aggressive antimicrobial therapy—sepsis orperitonitis.
CONTRAINDICATIONSN/A
PRECAUTIONSN/A
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGMonitor for progressive decrease in drainage,resolution of inflammation, and improvementof clinical signs.
PREVENTION/AVOIDANCE� Percutaneous abscesses—prevent fighting.� Anal sac abscesses—prevent impaction;consider anal saculectomy for recurrent cases.� Prostatic abscesses—castration possiblyhelpful.� Mastitis—prevent lactation (spaying).� Periorbital abscesses—do not allow chewingon foreign object(s).
POSSIBLE COMPLICATIONS� Sepsis.� Peritonitis/pleuritis if intra-abdominal orintrathoracic abscess ruptures.
� Compromise of organ function.� Delayed evacuation may lead to chronicallydraining fistulous tracts.
EXPECTED COURSE AND PROGNOSISDepends on organ system involved andamount of tissue destruction.
MISCELLANEOUSASSOCIATED CONDITIONS� FeLV or FIV infection� Immunosuppression
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIAL� Minimal for pyogenic bacteria.� Mycobacteria and systemic fungal infectionscarry some potential.
PREGNANCY/FERTILITY/BREEDINGTeratogenic agents—avoid use in pregnantanimals.
SEE ALSO� Actinomycosis� Anaerobic Infections� Colibacillosis� Mycoplasmosis� Nocardiosis� Sepsis and Bacteremia
ABBREVIATIONS� CSF = cerebrospinal fluid� CT = computed tomography� FeLV = feline leukemia virus� FIV = feline immunodeficiency virus� MRI = magnetic resonance imaging� PAS = periodic acid-Schiff
Suggested ReadingBirchard SJ, Sherding RG, eds., Saunders
Manual of Small Animal Practice.Philadelphia: Saunders, 1994.
DeBoer DJ. Nonhealing cutaneous wounds.In: August JR, ed., Consultations in FelineInternal Medicine. Philadelphia: Saunders,1991, pp. 101–106.
McCaw D. Lumps, bumps, masses, andlymphadenopathy. In: Ettinger SJ, FeldmanEC, eds., Textbook of Veterinary InternalMedicine, 4th ed. Philadelphia: Saunders,1995, pp. 219–222.
Author Johnny D. HoskinsConsulting Editor Stephen C. Barr
Client Education Handoutavailable online
BLBS078-CF_A05 BLBS078-Tilley March 21, 2011 8:13
10 Blackwell’s Five-Minute Veterinary Consult
Acetaminophen ToxicityA
BASICSDEFINITIONResults from owners overdosing the patientwith over-the-counteracetaminophen-containing analgesic andantipyretic medications.
PATHOPHYSIOLOGYWhen the normal biotransformationmechanisms for detoxification(glucuronidation and sulfation) arediminished, cytochrome P450-mediatedoxidation produces a toxic metabolite(N-acetyl benzoquinoneimine) that iselectrophilic, conjugates with glutathione,and toxicologically binds to liver proteins.
Dogs� Receipt of ≥ 150–200 mg/kg—sufficientelectrophilic metabolite generated throughthe cytochrome P450 pathway that RBCglutathione binding producesmethemoglobinemia and damages liverproteins.� Causes hepatotoxicity in a dose-dependentfashion
Cats� Lower ability to glucuronidate; morelimited capacity for acetaminophenelimination than dogs.� Saturate glucuronidation and sulfationbiotransformation routes.� Develop toxic cytochrome P450 metaboliteat much lower doses than dogs.� Poisoned by as little as 50–60 mg/kg (oftenas little as one-half tablet); leads to rapid RBCglutathione depletion that produces rapidlydeveloping methemoglobinemia, because ofthe unique feline hemoglobin molecule witheight sulfhydryl groups sensitive to oxidation.� Slower-developing hepatotoxicosis may notbe fully expressed before development of fatalmethemoglobinemia.
SYSTEMS AFFECTED� Hemic/Lymph/Immune—RBCs aredamaged by glutathione depletion, allowingoxidation of hemoglobin to methemoglobin.� Hepatobiliary—liver necrosis.� Cardiovascular (cats)—edema of the face,paws, and (to a lesser degree) forelimbsthrough an undefined mechanism.
GENETICSCats—genetic deficiency in the glucuronideconjugation pathway makes themvulnerable.
INCIDENCE/PREVALENCE� Most common drug toxicity in cats;considerably less frequent in dogs.� Over-the-counter medications—fourthmost common cause of poison exposures insmall animals.
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesCats more often than dogs
Breed PredilectionsN/A
Mean Age and RangeN/A
Predominant SexN/A
SIGNSGeneral CommentsRelatively common—owing to increasing usein humans
Historical Findings� Depression.� Rapid breathing.� Darkened mucous membranes.� Owner may recall warnings aboutacetaminophen in cats after dosing the pet.
Physical Examination Findings� May develop 1–4 hours after dosing.� Progressive depression.� Salivation.� Vomiting.� Abdominal pain.� Tachypnea and cyanosis—reflectmethemoglobinemia.� Edema—face, paws, and possibly forelimbs;after several hours.� Chocolate-colored urine—hematuria andmethemoglobinuria; especially in cats.� Death.
CAUSESAcetaminophen overdosing
RISK FACTORS� Nutritional deficiencies of glucose and/orsulfate.� Simultaneous administration of otherglutathione-depressing drugs.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Nitrites.� Phenacetin.� Nitrobenzene.� Phenol and cresol compounds.� Sulfites.� History of exposure—important fordifferentiating from methemoglobin-formingdrugs.
CBC/BIOCHEMISTRY/URINALYSIS� Methemoglobinemia and progressivelyrising serum activities of liverenzymes—characteristic.� Heinz bodies (cats)—prominent in RBCs.� Hematuria and/or hemoglobinuria.
OTHER LABORATORY TESTS� Acetaminophen serum concentration—maximally elevated 1–3 hours after ingestion;decay dose-dependent in cats (approximately
one-tenth the plasma elimination rate ofdogs).� Blood glutathione level—low.
IMAGINGN/A
DIAGNOSTIC PROCEDURESN/A
PATHOLOGIC FINDINGS� Methemoglobinemia.� Pulmonary edema.� Liver and kidney congestion.� Dogs—centrilobular necrosis of the liver;icterus in chronic cases.
TREATMENTAPPROPRIATE HEALTH CARE� With methemoglobinemia—must evaluatepromptly.� With dark or bloody colored urine oricterus—inpatient.
NURSING CARE� Gentle handling—imperative for clinicallyaffected patients.� Induced emesis and gastric lavage—usefulwithin 4–6 hours of ingestion.� Anemia, hematuria, or hemoglobinuria—may require whole blood transfusion.� Fluid therapy—maintain hydration andelectrolyte balance.� Drinking water—available at all times.� Food—offered 24 hours after initiation oftreatment.
ACTIVITYRestricted
DIETN/A
CLIENT EDUCATION� Warn client that treatment in clinicallyaffected patients may be prolonged andexpensive.� Inform client that patients with liver injurymay require prolonged and costlymanagement.
SURGICAL CONSIDERATIONSN/A
MEDICATIONSDRUG(S) OF CHOICE� Activated charcoal 2 g/kg PO; immediatelyafter completion of emesis or gastric lavage.� N -acetylcysteine (Mucomyst) 140 mg/kgloading dose PO, IV; then 70 mg/kg PO, IV,q4h for 5–7 treatments.
CONTRAINDICATIONSDrugs that contribute to methemoglobinemiaor hepatotoxicity.
BLBS078-CF_A05 BLBS078-Tilley March 21, 2011 8:13
Canine and Feline, Fifth Edition 11
(Continued) Acetaminophen Toxicity A
PRECAUTIONSDrugs requiring extensive liver metabolism orbiotransformation—use with caution; expecttheir half-lives to be extended.
POSSIBLE INTERACTIONSDrugs requiring activation or metabolism bythe liver have reduced effectiveness.
ALTERNATIVE DRUG(S)� Other sulfur donor drugs—ifN -acetylcysteine not available; sodium sulfate(50 mg 1.6% solution/kg IV q4h for 6treatments); effective use requiresconscientious management.� S-adenosyl-l-methionine (SAMe) as aglutathione donor—a loading dose (40 mg/kgPO) of a stable SAMe salt followed by amaintenance dose (20 mg/kg PO) q24h for 7days; reserved for dogs able to retain oralmedications and with adequate liver functionto metabolize SAMe.� A 1% methylene blue solution—8.8 mg/kgIV q2–3h for 2–3 treatments; combatsmethemoglobinemia without inducing ahemolytic crisis.� Ascorbic acid—125 mg/kg PO q6h for 6treatments; only slowly reducesmethemoglobinemia.
FOLLOW-UPPATIENT MONITORING� Continual clinical monitoring ofmethemoglobinemia—vital for effectivemanagement; laboratory determination ofmethemoglobin percentage every 2–3 hours.� Serum liver enzyme activities (ALT, ALP)—determined every 12 hours; monitor liverdamage.� Blood glutathione level—provide evidenceof the effectiveness of sulfhydryl-replacementtherapy.
PREVENTION/AVOIDANCE� Never give acetaminophen to cats.� Give careful attention to the acetaminophendose in dogs.
POSSIBLE COMPLICATIONSLiver necrosis and resulting fibrosis—maycompromise long-term liver function inrecovered patients.
EXPECTED COURSE AND PROGNOSIS� Rapidly progressive methemoglobinemia—serious sign.� Methemoglobin concentrations ≥ 50%—grave prognosis.� Progressively rising serum liver enzymes12–24 hours after ingestion—serious concern.� Expect clinical signs to persist 12–48 hours;death owing to methemoglobinemia possibleat any time.� Dogs and cats receiving prompt treatmentthat reverses methemoglobinemia andprevents excessive liver necrosis—may recoverfully.� Dogs—death as a result of liver necrosismay occur in a few days.� Cats—death as a result ofmethemoglobinemia occurs 18–36 hours afteringestion.
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSYoung and small dogs and cats—greater riskfrom owner-given single-dose acetaminophenmedications.
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGImposes additional stress and higher risk onexposed animals.
SYNONYMS� Paracetamol� Tylenol
SEE ALSOPoisoning (Intoxication)
ABBREVIATIONS� ALP = alkaline phosphatase� ALT = alanine aminotransferase� RBC = red blood cell
INTERNET RESOURCEShttp://www.aspca.org/pet-care/poison-control/.
Suggested ReadingHjelle JJ, Grauer GF.
Acetaminophen-induced toxicosis in dogsand cats. JAVMA 1986, 188:742–746.
Oehme FW. Aspirin and acetaminophen. In:Kirk, R.W., ed., Current Veterinary TherapyIX: Small Animal Practice. Philadelphia:Saunders, 1986, pp. 188–189.
Rumbeiha WK, Oehme FW. Methylene bluecan be used to treat methemoglobinemia incats without inducing Heinz bodyhemolytic anemia. Vet Hum Toxicol 1992,34:120–122.
Savides MC, Oehme FW, Leipold HW.Effects of various antidotal treatments onacetaminophen toxicosis andbiotransformation in cats. Am J Vet Res1985, 46:1485–1489.
Savides MC, Oehme FW, Nash SL, LeipoldHW. The toxicity and biotransformation ofsingle doses of acetaminophen in dogs andcats. Toxicol Appl Pharmacol 1984,74:26–34.
Wallace KP, Center SA, Hickford FH,Warner KL, Smith S. S-adenosyl-L-methionine (SAMe) for the treatment ofacetaminophen toxicity in a dog. JAAHA2002, 38(3):246–254.
Author Frederick W. OehmeConsulting Editor Gary D. Osweiler
Client Education Handoutavailable online
BLBS078-CF_A06 BLBS078-Tilley March 21, 2011 8:14
12 Blackwell’s Five-Minute Veterinary Consult
Acidosis, MetabolicA
BASICSDEFINITIONDecrease in plasma pH associated with adecrease in bicarbonate concentration(HCO−
3 ) (dogs, < 18 mEq/L; cats, < 16mEq/L) and a compensatory decrease incarbon dioxide tension (PCO2).
PATHOPHYSIOLOGY� Metabolic acidosis may develop secondaryto hyperphosphatemia (hyperphosphatemicacidosis), corrected hyperchloremia(hyperchloremic acidosis), and accumulationof metabolically produced strong anions(strong ion gap or high anion gap acidosis).� Hyperphosphatemic acidosis:
◦ Increase in plasma weak acids (e.g.,inorganic phosphate) is associated withmetabolic acidosis and increased anion gap.At pH of 7.4, a 1 mg/dL increase inphosphate concentration is associated witha 0.58 mEq/L decrease in [HCO−
3 ] and a0.58 mEq/L increase in AG.
� Hyperchloremic acidosis:◦ Hyperchloremic acidosis may be causedby chloride retention (e.g., renal failure,renal tubular acidosis), excessive loss ofsodium relative to chloride (e.g., diarrhea),or by administration of substancescontaining more chloride than sodium ascompared with normal extracellular fluidcomposition (e.g., administration of KCl,0.9% NaCl).◦ Acidemia is usually not severe in patientswith hyperchloremic acidosis.
� High anion gap acidosis:◦ Increase in the concentration of otherstrong anions through addition (e.g.,ethylene glycol toxicity), excessiveproduction (e.g., lactate produced byprolonged anaerobic metabolism), or renalretention (e.g., renal failure) of stronganions other than chloride causes metabolicacidosis without increasing chlorideconcentration (so-called normochloremicor high AG metabolic acidosis).
SYSTEMS AFFECTED� Cardiovascular—a fall in pH results in anincrease in sympathetic discharge butsimultaneously causes a decrease in theresponsiveness of the cardiac myocytes andvascular smooth muscle to the effects ofcatecholamines. In mildly acidemicconditions (pH greater than 7.2), the effectsof increased sympathetic stimulationpredominate and result in a mild increase inheart rate and cardiac output. More severeacidemia (pH below 7.1), especially if acute,may decrease cardiac contractility andpredispose the heart to ventriculararrhythmias and ventricular fibrillation.� Respiratory—increased [H+] stimulatesperipheral and central chemoreceptors toincrease alveolar ventilation; hyperventilation
decreases PCO2, which counters the effects oflow plasma HCO−
3 on pH. In dogs, adecrease of approximately 0.7 mm Hg inPCO2 is expected for each 1 mEq/L decreasein plasma HCO−
3 . Little is known aboutcompensation in cats, but it appears to bealmost non-existent.� Renal/Urologic—the kidneys increase netacid excretion, primarily by increasingexcretion of NH4
+ and chloride. Thiscompensatory mechanism is not very effectivein cats.
SIGNALMENTAny breed, age, or sex of dog and cat
SIGNALMENTHistorical Findings� Chronic disease processes that lead tometabolic acidosis (e.g., renal failure, diabetesmellitus, and hypoadrenocorticism), exposureto toxins (e.g., ethylene glycol, salicylate, andparaldehyde), diarrhea, administration ofcarbonic anhydrase inhibitors (e.g.,acetazolamide and dichlorphenamide).
Physical Examination Findings� Generally relate to the underlying disease.� Depression in severely acidotic patients.� Tachypnea in some patients results fromcompensatory increase in ventilation.� Kussmaul’s respiration, typically seen inhuman beings with metabolic acidosis, is notcommonly observed in dogs and cats.
CAUSESAssociated with Hyperchloremia(Hyperchloremic Metabolic Acidosis)� Diarrhea.� Renal tubular acidosis.� Administration of carbonic anhydraseinhibitors, spironolactone, potassiumchloride, or NH4Cl.� Fluid therapy with chloride-rich fluids (e.g.,0.9% NaCl, fluids supplemented with KCl).� Total parenteral nutrition with fluidscontaining cationic amino acids: lysine,arginine, and histidine.� Rapid correction of hypocapnia (chronicrespiratory alkalosis).
Associated with Normochloremia (HighAnion Gap Metabolic Acidosis)� Uremic acidosis.� Diabetic ketoacidosis.� Lactic acidosis.� Ethylene glycol, salicylate, paraldehyde, andmethanol intoxication.� Hyperphosphatemia.
RISK FACTORS� Patients with chronic renal failure, diabetesmellitus, and hypoadrenocorticism are at highrisk of developing metabolic acidosis as acomplication of the chronic disease process.� Patients with poor tissue perfusion orhypoxia are at risk of developing lacticacidosis.
DIAGNOSISDIFFERENTIAL DIAGNOSISLow plasma HCO−
3 and hyperchloremia mayalso be compensatory in animals with chronicrespiratory alkalosis, in which PCO2 is lowand pH is high or near normal, despitedecreased HCO−
3 and increase in chlorideconcentration. Blood gas determination isrequired to differentiate.
LABORATORY FINDINGSDrugs That May Alter Laboratory Results� Potassium bromide is measured as chloridein most analyzers, so potassium bromideadministration artificially decreases the aniongap.
Disorders That May Alter LaboratoryResults� Too much heparin (> 10% of the sample)decreases HCO−
3 .� Blood samples stored at room temperaturefor more than 20 minutes have low pHbecause of increased PCO2.� Hypoalbuminemia lowers AG; negativecharges of albumin are the main componentof the anion gap.
Valid if Run in Human Laboratory?Yes
CBC/BIOCHEMISTRY/URINALYSIS� Low total CO2—total CO2 in serumsamples handled aerobically closelyapproximates the serum HCO−
3concentration; unfortunately, patients withchronic respiratory alkalosis also have lowtotal CO2, and the distinction cannot bemade without blood gas analysis.� Metabolic acidoses are traditionally dividedinto hyperchloremic and high anion gap bymeans of the anion gap. Anion gap, thedifference between the measured cations andthe measured anions, is calculated as AG =[Na+] − (HCO−
3 + [Cl−]) or AG = ([Na+]+ [K+]) − (HCO−
3 + [Cl−]), depending onthe preference of the clinician or laboratory.Normal values with potassium included in thecalculation are usually 12–24 mEq/L in dogsand 13–27 mEq/L in cats. The negativecharges of albumin are the major contributorsto the normal anion gap; this should be takeninto account when evaluating anion gap inpatients with hypoalbuminemia. At pH 7.4 indogs, a decrease of 1 g/dL in albumin isassociated with a decrease of 4.1 mEq/L in theanion gap.� Normal anion gap (i.e., hyperchloremicmetabolic acidosis)—most common cause isdiarrhea; also, hypoadrenocorticism.� High anion gap (i.e., normochloremicmetabolic acidosis)—most common causesare renal failure, diabetes mellitus, lacticacidosis (caused by tissue hypoperfusion), andhypoadrenocorticism (caused by lacticacidosis). Hyperphosphatemia also raises the
BLBS078-CF_A06 BLBS078-Tilley March 21, 2011 8:14
Canine and Feline, Fifth Edition 13
(Continued) Acidosis, Metabolic A
anion gap. At a pH of 7.4, each 1 mg/dLincrease in phosphate concentration isassociated with a 0.58 mEq/L increase inanion gap.� Hyperglycemia—consider diabetes mellitus.� Azotemia—consider renal failure.� Hyperphosphatemia—consider renalfailure, hypertonic sodium phosphate enematoxicity, and toxicity due to urinary acidifierscontaining phosphate.� High lactate concentration—consider lacticacidosis due to poor tissue perfusion or poormetabolism of lactate (e.g., liver disease andlymphoma).� Hyperkalemia—commonly associated with,but almost never caused by, the acidosis. Onlyacute hyperchloremic acidosis can lead topotassium translocation severe enough tocause hyperkalemia. Otherwise, hyperkalemiaresults from the disease process causing themetabolic acidosis (e.g., renal failure anddiabetes mellitus), not from the acidosis itself.Correction formulas to adjust potassiumconcentration based on pH changes shouldnot be used.
OTHER LABORATORY TESTSBlood gas analysis reveals low HCO−
3 , lowPCO2, and low pH.
IMAGINGNone
DIAGNOSTIC PROCEDURESNone
TREATMENT� Acid-base disturbances are secondaryphenomena; successful resolution depends ondiagnosis and treatment of the underlyingdisease process.� Treat patients with blood pH ≤ 7.1aggressively while pursuing the definitivediagnosis.� Discontinue drugs that may cause metabolicacidosis.� Nursing care—lactated Ringer’s solution isthe fluid of choice for patients with mildmetabolic acidosis and normal liver function.
MEDICATIONSDRUG(S) OF CHOICE� NaHCO3 may help patients withhyperchloremic, hyperhosphatemic, or uremicacidosis, but not patients with lactic acidosisor diabetic ketoacidosis.
◦ Estimation of HCO−3 dose: dogs, 0.3 ×
body weight (kg) × (21 − patientHCO−
3 ); cats, 0.3 × body weight (kg) ×(19 − patient HCO−
3 ). Give half of thisdose slowly IV and reevaluate blood gasesbefore deciding on the need for additionaladministration. An empirical dose of
1–2 mEq/kg followed by reevaluation ofblood gas status is safe in most patients.◦ Potential complications of NaHCO3
administration: volume overload resultingfrom administered sodium, tetany from lowionized calcium concentration, increasedaffinity of hemoglobin for oxygen,paradoxical CNS acidosis, overshootmetabolic alkalosis, and hypokalemia.
� Hyperchloremic acidosis: NaHCO3 iseffective and should be considered wheneverpH < 7.2.� Uremic acidosis: efficacy of NaHCO3 inacute therapy of uremic acidosis is related tothe shift of phosphate inside the cells andconsequent amelioration ofhyperphosphatemic acidosis.� Lactic acidosis: NaHCO3 increases lactateproduction and is of little to no value in lacticacidosis. Therapy should be directed ataugmenting oxygen delivery to the tissues andreestablishing cardiac output. Small titrateddoses of NaHCO3 can be used as atemporizing measure to maintain HCO−
3above 5 mEq/L, if needed.� Diabetic ketoacidosis: NaHCO3 adverselyaffects outcome in humans with diabeticketoacidosis even when pH is below 7.0.� Administration of NaHCO3 to ketoacidoticpatients cannot be recommended at any pH.Therapy should be direct at insulin and fluidadministration. Reestablishing plasma volumeand renal perfusion will allow the kidneys toexcrete ketoanions, replacing them withchloride.
CONTRAINDICATIONS� Avoid NaHCO3 in patients with respiratoryacidosis because it generates CO2.� Patients with respiratory acidosis cannotadequately excrete CO2, and increased PCO2
will further decrease the pH.� Avoid diuretics that act in the distalnephron (e.g., spironolactone).� Avoid carbonic anhydrase inhibitors (e.g.,acetazolamide, dichlorphenamide).
PRECAUTIONSUse NaHCO3 cautiously in patients withcongestive heart failure because the sodiumload may cause decompensation of the heartfailure.
POSSIBLE INTERACTIONSNone
ALTERNATIVE DRUG(S)None
FOLLOW-UPPATIENT MONITORINGRecheck acid-base status; frequency dictatedby the underlying disease and patient responseto treatment.
POSSIBLE COMPLICATIONS� Hyperkalemia in acute hyperchloremicacidosis� Myocardial depression and ventriculararrhythmias
MISCELLANEOUSASSOCIATED CONDITIONS� Hyperkalemia� Hyperchloremia
AGE-RELATED FACTORSNone
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMS� Dilutional acidosis—metabolic acidosisresulting from increased free water in plasma.� Hyperchloremic acidosis—normal aniongap acidosis.� Hyperphosphatemic acidosis—metabolicacidosis resulting from high phosphateconcentration.� Non-respiratory acidosis.� Normochloremic acidosis—high anion gapacidosis.� Organic acidosis—metabolic acidosisresulting from accumulation of organic anions(e.g., ketoacidosis, uremic acidosis, and lacticacidosis).
SEE ALSO� Diabetes Mellitus with Ketoacidosis� Hyperchloremia� Hyperkalemia
ABBREVIATIONS� AG = anion gap� CNS = central nervous system� H+ = hydrogen ion� HCO−
3 = bicarbonate� NaHCO3 = sodium bicarbonate� O2 = oxygen� PCO2 = carbon dioxide tension
Suggested Readingde Morais HA, Constable PD. Strong ion
approach to acid-base disorders. In:DiBartola SP, ed., Fluid, Electrolyte andAcid-Base Disorders, 3rd. ed. Philadelphia:Saunders, 2006, pp. 310–321.
de Morais HA, Leisewitz AL. Mixed acid-basedisorders. In: DiBartola SP, ed., Fluid,Electrolyte and Acid-Base Disorders, 3rd.ed. Philadelphia: Saunders, 2006,pp. 296–309.
DiBartola SP. Metabolic acid-base disorders.In: DiBartola SP, ed., Fluid, Electrolyte andAcid-Base Disorders, 3rd. ed. Philadelphia:Saunders, 2006, pp. 251–283.
Author Helio Autran de MoraisConsulting Editor Carl A. Osborne
BLBS078-CF_A07 BLBS078-Tilley July 23, 2011 2:49
14 Blackwell’s Five-Minute Veterinary Consult
Acne—CatsA
BASICSOVERVIEW� Inflammatory dermatitis affecting the chinand lips� Symptoms may be recurrent or persistent� Precise etiology unknown
SIGNALMENT� Cats� Prevalence for sex, age, or breed not reported
SIGNS� Cats may have a single episode, a lifelongrecurrent problem, or a continual disease.� Frequency and severity of each occurrencevaries with the individual.� Comedones, mild erythematous papules,serous crusts, and dark keratin debris developon the chin and less commonly on the lips.� Swelling of the chin.� Severe cases—nodules, hemorrhagic crusts,pustules, cysts, fistulae, severe erythema,alopecia, and pain.� Pain often associated with bacterialfurunculosis.
CAUSES & RISK FACTORSPrecise etiology unknown; may be a disorderof keratinization, poor grooming, abnormalsebum production, immunosuppression, viralinfection, or stress.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Bacterial folliculitis� Demodicosis� Malassezia Infection� Feline leprosy� Dermatophytosis� Neoplasia of sebaceous or apocrine glands� Eosinophilic granuloma� Contact hypersensitivity
CBC/BIOCHEMISTRY/URINALYSISN/A
OTHER LABORATORY TESTSN/A
IMAGINGN/A
DIAGNOSTIC PROCEDURES� Skin scrapings—demodicosis.� Fungal culture—dermatophytosis.� Cytology—bacteria, Malassezia.� Biopsy—rarely needed; necessary in selectedcases to characterize changes such as cysticfollicles, to differentiate acne from otherdiseases such as demodicosis, infections(bacterial, yeast, or dermatophytes), or todiagnose neoplasia.
PATHOLOGIC FINDINGS� Mild disease—follicular distention withkeratin (comedo), hyperkeratosis, andfollicular plugging.� Severe disease—mild to severe folliculitisand perifolliculitis with follicular pustuleformation.� Follicular rupture releases keratin, hair, andDemodex mites into the dermis; leads tofurunculosis, manifested by neutrophils andnumerous macrophages surrounding keratindebris.� Bacteria and Malassezia in these lesions areconsidered secondary invaders and notcausative agents.� Demodex mites can be primary agents ofthis disease.
TREATMENT� Initial treatment—one or a combination ofthe drugs listed below until all lesions haveresolved.� Discontinue treatment by taperingmedication over a 2- to 3-week period.� Recurrent episodes—once the recurrencerate is determined, an appropriatemaintenance protocol can be designed foreach individual.� Continual episodes—lifelong maintenancetreatment necessary.
MEDICATIONSDRUG(S)� Systemic antibiotics—amoxicillin withclavulanate, a cephalosporin, or afluoroquinolone.� Severe cases may warrant treatment withisotretinoin (Accutane) or cyclosporine,modified (Atopica).� Demodicosis—oral ivermectin 400 ug/kgdaily until mites are cleared.� Shampoo—once or twice weekly withantiseborrheic (sulfur-salicylic acid, benzoylperoxide, or ethyl lactate).� Topical cleansing agents—benzoyl peroxide,salicylic acid, chlorhexidine-phytosphingosine.� Topical antibiotic ointment—mupirocin2%.� Other topicals—clindamycin orerythromycin solution or ointment.� Combination topicals—benzoylperoxide-antibiotic gels (e.g., Benzamycin).� Topical retinoids—Tretinoin (Retin-A0.01% gel).
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Benzoyl peroxide and salicylic acids—can beirritating.� Systemic isotretinoin—use with caution, ifanimal will not allow application of topicalmedications; caution: potential deleteriousside effects in human beings (druginteractions and teratogenicity); containershould be labeled for animal use only andkept separate from human medications toavoid accidental use; currently difficult toobtain for animal patients.
FOLLOW-UP� Monitor for relapses.� Maintenance cleansing programs can beused to reduce relapses.
MISCELLANEOUSPREGNANCY/FERTILITY/BREEDINGSystemic isotretinoin should not be used onbreeding animals.
Suggested ReadingJazic E, Coyner KS, Loeffler DG, Lewis TP.
An evaluation of the clinical, cytological,infectious and histopathological features offeline acne. Vet Dermatol 2006,17(2):134–140.
Rosencrantz WS. The pathogenesis,diagnosis, and management of feline acne.Vet Med 1993, 5:504–512.
Scott DW, Miller WH, Griffin CE.Keratinization defects. In: Muller & Kirk’sSmall Animal Dermatology, 6th ed.Philadelphia: Saunders, 2001, pp.1042–1043.
Werner AH, Power HT. Retinoids inveterinary dermatology. Clin Dermatol1994, 12(4):579–586.
White SD. Feline acne and results oftreatment with mupirocin in an openclinical trial: 25 cases (1994–96). VetDermatol 1997, 8:157.
Author David DuclosConsulting Editor Alexander H. Werner
BLBS078-CF_A08 BLBS078-Tilley March 21, 2011 8:18
Canine and Feline, Fifth Edition 15
Acne—Dogs A
BASICSOVERVIEW� Chronic inflammatory disorder of the chinand lips of young animals.� Characterized by folliculitis andfurunculosis.� Recognized almost exclusively inshort-coated breeds.� Genetic predisposition may play a moreimportant role than hormonal effects.
SIGNALMENT� Dogs.� Predisposed short-coated breeds—boxer,Doberman pinscher, English bulldog, GreatDane, Weimaraner, mastiff, rottweiler, andGerman shorthaired pointer, pit bull terrier.
SIGNS� Ventral chin and lip margins may beminimally to markedly swollen withnumerous erythematous papules and pustules.� Advanced stages—lesions may be exudative,indicating secondary deep bacterialfolliculitis-furunculosis.� Lesions may be painful on palpation; mostare non-painful and non-pruritic.� Chronic resolved lesions may be scarred andlichenified.
CAUSES & RISK FACTORSSome short-coated breeds appear to begenetically predisposed to follicularhyperkeratosis and secondary bacterialinfection.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Dermatophytosis� Demodicosis� Foreign body� Contact dermatitis
CBC/BIOCHEMISTRY/URINALYSISN/A
OTHER LABORATORY TESTSN/A
IMAGINGN/A
DIAGNOSTIC PROCEDURES� Bacterial culture and sensitivity testing—inpatients with suppurative folliculitis andfurunculosis that are non-responsive to initialantibiotic selection.
� Biopsy—histologic confirmation for cases inwhich diagnosis is in question.� Skin scrape—demodicosis.� Dermatophyte culture—dermatophytosis.
PATHOLOGIC FINDINGS� Clinical signs and histopathologic findingsare diagnostic.� Initial lesions—hairless follicular papules;characterized histopathologically by markedfollicular keratosis, plugging, dilatation, andperifolliculitis.� Bacteria—not present and cannot beisolated from lesions in early stages.� As disease progresses, papules enlarge andrupture, promoting a suppurative folliculitisand furunculosis.
TREATMENT� Depends on the severity and chronicity ofthe disease.� Reduce behavioral trauma to the chin (e.g.,rubbing on the carpet, chewing bones thatincrease salivation).� Frequent cleaning with benzoyl peroxideshampoo or gel.� Mupirocin 2% ointment to reduce thebacterial numbers on the surface of the skin.� Instruct owners to avoid expressing thelesions, which may cause internal rupture ofthe papule and massive inflammation.
MEDICATIONSDRUG(S)Topical� Benzoyl peroxide shampoo or gel(antibacterial).� Mupirocin 2% ointment(antibacterial-staphylococcus).� Isotretinoin (Accutane) and tretinoin(Retin-A)—may reduce follicular keratosis.� Corticosteroids—may be necessary toreduce inflammation; limit frequency of useto avoid local and systemic effects.
Systemic� Antibiotics appropriate for deep bacterialinfection—especially cephalosporins(cephalexin, 22 mg/kg PO q8h for 6–8weeks).� May need to perform bacterial culture andsensitivity test.� Oral corticosteroids: tapering dosages ofprednisolone (initial 0.5 mg/kg/day) toreduce significant inflammation; not forcontinued use.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Benzoyl peroxide—may bleach carpets andfabrics; may be irritating.� Mupirocin ointments—greasy.� Topical retinoids—may be drying andirritating.� Topical steroids—may cause adrenalsuppression with repeated use.� Isotretinoin—may causekeratoconjunctivitis sicca, hyperactivity, earpruritus, erythematous mucocutaneousjunction, lethargy with vomiting, abdominaldistension and erythema, anorexia withlethargy, collapse, and swollen tongue; CBCand chemistry screen abnormalities includehigh platelet count, hypertriglyceridemia,hypercholesterolemia, and high alaninetransaminase.
FOLLOW-UPPATIENT MONITORING� Continue until antibiotics until lesions havehealed.� Repeat bacterial culture/sensitivity if lesionsworsen.� Discontinue topical corticosteroids whenpossible.
EXPECTED COURSE AND PROGNOSIS� Long-term topical treatment may berequired.� Chronic scarring may be prevented by earlyand aggressive therapy.
MISCELLANEOUSPREGNANCY/FERTILITY/BREEDINGSynthetic retinoids—teratogens; do not use inpregnant animals, animals intended forreproduction, or intact female animals; shouldnot be handled by women of childbearingage.
Suggested ReadingScott DW, Miller WH, Griffin CE. Bacterial
skin diseases. In: Kirk’s Small AnimalDermatology, 5th ed. Philadelphia:Saunders, 1995, pp. 304–305.
Author Karen Helton RhodesConsulting Editor Alexander H. Werner
BLBS078-CF_A09 BLBS078-Tilley March 21, 2011 8:19
16 Blackwell’s Five-Minute Veterinary Consult
Acral Lick DermatitisA
BASICSOVERVIEWChronic or relapsing skin disease directlycaused by the licking of the extremities. Acycle of obsessive licking and secondarypruritus and infection may develop.
SYSTEMS AFFECTEDSkin/Exocrine
SIGNALMENT� Dogs. � Most common in largebreeds—especially Doberman pinschers,Labrador retrievers, Great Danes, Irish andEnglish setters, golden retrievers, Akitas,Dalmatians, shar-peis, and Weimaraners.� Age at onset—varies with the cause. � Sexpredilection—some sources suggest morecommon in males; others indicate nopreference.
SIGNS� Excessive licking and chewing of theaffected area. � Occasionally a history oftrauma to the affected area. � Alopecic,ulcerative, thickened, and raised firm plaques,usually located on the dorsal aspect of thecarpus, metacarpus, tarsus, or metatarsus.� Lesions often occur singly, although theymay occur in more than one location.
CAUSES & RISK FACTORSAssociated diseases—staphylococcalfurunculosis, allergy, endocrinopathy,demodicosis, dermatophytosis, foreign bodyreaction, neoplasia, arthritis, trauma, andpsychogenic and sensory nerve dysfunction.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Neoplasia � Bacterial furunculosis � Focaldemodicosis � Focal dermatophytosis
CBC/BIOCHEMISTRY/URINALYSISNormal except in cases ofhyperadrenocorticism
OTHER LABORATORY TESTS� Low thyroid levels, elevated TSH—suggestshypothyroidism.� Abnormal ACTH-stimulation test orabnormal LDDST—suggestshyperadrenocorticism.
IMAGINGRadiology—neoplasia; some forms of trauma;radiopaque foreign bodies; bony proliferationmay be seen secondary to the chronicirritation.
DIAGNOSTIC PROCEDURES� Skin scrapings—demodicosis.� Dermatophyte culture—fungal infection.� Epidermal cytology—bacterial infection.
� Bacterial culture and sensitivity—tissueshould be submitted for culture andsensitivity as tissue cultures often differ fromsurface culture. � Food-eliminationdiet—determine food allergy. � Intradermalallergy testing—helpful for atopic animals.� Biopsy—to rule out neoplasia, otherinfections. � Behavioral history.
PATHOLOGIC FINDINGSHistopathology—acanthosis, follicularelongation, lymphoplasmacytic dermalinflammation, folliculitis, furunculosis,perihidradenitis, hidradenitis, and verticalstreaking fibrosis.
TREATMENT� Affected animal should get plenty ofattention and exercise.� Counter-conditioning may be helpful.� Physical restraints—Elizabethan collars andbandaging; short-term use.� Ablation of the lesion with laser therapy hasbeen proposed but no publications evaluatingthe efficacy of this modality are currentlyavailable.� Diet—no modification unless foodhypersensitivity is suspected.� Difficult to treat, especially if no underlyingcause is found; warn owner that patience andtime are necessary.� Surgery—do not consider until all othertherapies have been exhausted; will oftencause increased licking and attention to theaffected area, resulting in poor wound closure;if underlying causes are not addressed,recurrence is likely.
MEDICATIONSDRUG(S)Antibiotics� Based on bacterial culture and sensitivity.� Administer until infection is completelyresolved; often at least 6 weeks.
Systemic� Antihistamines—e.g., hydroxyzine (1–2mg/kg PO q12h); chlorpheniramine (4–8mg/dog PO q12h; maximum of 0.5 mg/kgq12h).� SSRIs: e.g., fluoxetine (1 mg/kg PO q24h);paroxetine (0.5–1 mg/kg PO q24h).� Dopamine antagonists: e.g., naltrexone(2.2 mg/kg PO q12–24h).� Tricyclic antidepressants: e.g., amitriptylineHCl (1.1–2.2 mg/kg PO q12h)—use at thelower dosage for 10 days and if noimprovement, use at the higher dosage for10 days; doxepin (3–5 mg/kg PO q12h;maximum 150 mg q12h); clomipramine(1–3.5 mg/kg PO q12h).
� Combine and/or withdraw administrationof these medications carefully.
Topical� Flunixin meglumine and fluocinolone indimethyl sulfoxide (combined). � Mupirocin.� Topical 5% benzoyl peroxide. � Topicalcapsaicin products. � Intralesionalcorticosteroids have been advocated but arerarely helpful. � Topical medications shouldbe applied with gloves. � Animals should bekept from licking the area for 10–15 minutes.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Doxepin—caution using with monoamineoxidase inhibitors, clonidine, anticonvulsants,oral anticoagulants, steroid hormones,antihistamines, or aspirin.� Antihistamines—caution using more thanone at a time. � Hydroxyzine may decreaseseizure threshold. Avoid in epileptics.� Psychotropic medications should becombined and/or withdrawn carefully.
FOLLOW-UP� Monitor level of licking and chewing closely.� Treat underlying disease to preventrecurrence.� If no underlying disease is detected, suspectpsychogenic causes (compulsive orself-mutilation disorder); prognosis isguarded.� Cardiotoxicity and hepatoxicity have beenreported in rare cases in animals on tricyclicantidepressants. Select and monitor patientswith caution.
MISCELLANEOUSAGE-RELATED FACTORSDogs < 5 years old—strongly consider allergy
ZOONOTIC POTENTIAL� Transmitted to humans only ifdermatophytosis is the underlying cause;exceedingly rare.� Methicillin resistant staphylococcal speciesmay have zoonotic implications.
ABBREVIATIONS� ACTH = adrenocorticotropin hormone� LDDST = low-dose dexamethasone-suppression test� TSH = thyroid stimulating hormone
Suggested ReadingShumaker AK, Angus JC, et al.
Microbiological and histopathologicalfeatures of canine acral lick dermatitis. VetDermatol 2008, 19(5):288–298.
Author Jean S. GreekConsulting Editor Alexander H. Werner
BLBS078-CF_A10 BLBS078-Tilley July 23, 2011 3:4
Canine and Feline, Fifth Edition 17
Acromegaly—Cats A
BASICSOVERVIEW� Syndrome resulting from growth hormone(somatotropin) hypersecretion by tumorousor hyperplastic somatotrophs in the anteriorpituitary. � Clinical signs are due to growthhormone’s direct catabolic/diabetogeniceffects and its indirect anabolic effectsmediated through insulin-like growth factor I,which is secreted by the liver in response togrowth hormone stimulation. � ElevatedIGF1 activity induces excessive soft tissuegrowth, visceral organomegaly, boneremodeling and thickening (especially inbones formed from membranous ossification)resulting in arthropathy, broad facial features,and enlarged “clubbed” paws. � Myocardialhypertrophy occurs in many cats, but heartfailure is uncommon. � The catabolic actionsof GH result from insulin antagonism leadingeventually to pancreatic β cell exhaustion andDM. Between 25 and 33% of diabetic catsmay have acromegaly. � Like most diabeticcats the potential for remission remains if theexcessive GH production can be normalized;likelihood of remission is inversely related tothe duration of DM.
SIGNALMENT� Cats � Median age—11 years (range of6–17 years) � Approximately 80% are males.
SIGNS� Initial signs relate to unregulated DM withthe vast majority of cases presenting withpolyuria, polydipsia, and often profoundpolyphagia accompanied with concurrentweight gain (weight loss has also beenreported). � Many patients gain weight andhave increased body size due to increasedbone and soft tissue mass, not from increasedadipose tissue. Weight gain in an unregulateddiabetic cat strongly suggests acromegaly.� Broadening of facial features, prognathiainferior, and increased paw size reflectlong-standing or severe disease.� Organomegaly—most commonly bilateralrenomegaly and hepatomegaly. � Murmurand/or gallop rhythm occasionally present;signs of heart failure uncommon. � Lamenessmay develop. � Neurological signs referable tointracranial disease through an expandingpituitary mass lesion possible. � Recentreports suggest the majority of acromegaliccats are indistinguishable phenotypically fromnon-acromegalic diabetic cats.
CAUSES & RISK FACTORS� GH hypersecretion. � Progestins do notcause GH secretion and acromegaly in cats asthey do in dogs.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Uncomplicated DM or DM secondary tohyperadrenocorticism � Pituitary-dependenthyperadrenocorticism and acromegaly canboth produce insulin-resistant DM with anassociated pituitary mass lesion.Differentiation may require use of a low-dosedexamethasone suppression test to rule outPDH. � Acromegaly and PDH can occurconcurrently. � Other disorders causingweight loss with polyphagia, polyuria, andpolydipsia such as hyperthyroidism are notusually associated with significant glucoseintolerance. � Insulin-resistant DM (> 2.0 Uof insulin/kg/12h) is to be expected in allacromegalic cats and the dose tends toincrease over time, with doses of 12–50U/cat/12h not uncommon. � Acromegalyshould be suspected in any diabetic catdemonstrating signs of otherwise unexplainedinsulin resistance.
CBC/BIOCHEMISTRY/URINALYSIS� Most abnormalities attributed to poorlycontrolled DM—hyperglycemia, glucosuria,and elevated fructosamine levels are consistentfindings in most acromegalic cats.� Hyperproteinemia. � Traditionallyassociated with renal failure and hypertension,but more recent studies suggest this is not thecase.
OTHER LABORATORY TESTS� IGF1—diabetic cats receiving insulin canhave higher IGF1 levels than normal; hencethere is significant potential for overlapbetween acromegalic and non-acromegalicdiabetic cats; however, dramatically elevatedIGF1 levels (e.g., > 1,000 ng/ml) are stronglysuggestive of the acromegaly. � IGF1 is wellpreserved across the species, so valid assays arecommonly available. � GH—elevated basalserum levels are diagnostic. However, as GHis not well preserved across the species, avalidated fGH assay has limited availability.
IMAGING� Intracranial imaging to demonstrate apituitary mass lesion; MRI is more sensitivethan contrast-enhanced CT, although thedifference is modest and from a cost-benefitperspective CT is generally preferred.� Echocardiographic abnormalities mayinclude left atrial enlargement, asymmetricseptal and left ventricular free-wallthickening, systolic anterior motion of themitral valve, and diastolic dysfunction.� Radiographic changes include increasedoropharyngeal soft tissue, degenerativearthropathy with periarticular osteophytosis,spinal spondylosis deformans, and variableabdominal organomegaly.
TREATMENTRADIOTHERAPY� The only currently available means ofreducing autonomous overproduction of GHfrom the anterior pituitary. Unfortunately,radiotherapy is more suited to reducing thesize of the tumor than achieving clinicallysignificant reductions in GH secretion. � Atotal dose of between 3,500 and 5,500 cGY,administered in variably fractionated doses isoften suggested. Recent reports suggest thatthe greatest success may be achieved with atotal dose of 3,700 cGy administered as anincremental hypofractionated dosage protocolof 10 doses. Using this method, 13 of 14acromegalic cats had markedly improveddiabetic control.HYPOPHYSECTOMY� In people with acromegaly, surgical removalof small, non-invasive pituitary adenomas isfrequently curative; most affected cats havelarge tumors, markedly decreasing the chancefor successful surgical removal; additionally,hypophysectomy in cats has been associatedwith high levels of post-operativecomplications. � Cryohypophysectomy hasbeen described in two cats—one suffered ahypoglycemic crisis and permanent blindness2 months after surgery, while the other had amore successful outcome.
MEDICATIONS� Long-acting somatostatin analogues—uniformly unsuccessful in cats.� Pegvisomant, a GH-receptor antagonist, hasbeen used effectively in people. Efficacy incats has not been assessed. � As medicalcontrol of GH overproduction is not possible,the aim of medical therapy is the managementof insulin-resistant DM to limit the level ofhyperglycemia and prevent ketoacidosis.Twice-daily dosing is essential with doses of3–5 U/kg usual (no upper limit to the doserequired).
FOLLOW-UP� Clinical signs that might be attributed topoor diabetic control (e.g., profoundpolyphagia) will not improve with improveddiabetic control; thus levels of glycatedproteins or blood glucose levels are betterindicators of diabetic control than clinicalsigns. � Serum IGF1 levels are not suitable formonitoring therapy as they do not changeduring or after radiotherapy. � Reportedsurvival times vary enormously—from a fewmonths to many years, and dying from causesunlikely to be related to acromegaly.Author David ChurchConsulting Editor Deborah S. Greco
BLBS078-CF_A11 BLBS078-Tilley June 25, 2011 12:14
18 Blackwell’s Five-Minute Veterinary Consult
ActinomycosisA
BASICSOVERVIEW� An infectious disease caused bygram-positive, branching, pleomorphic,rod-shaped bacteria of the genus Actinomyces.� A. viscosus and A. hodeovulneris—mostcommonly identified isolates (though mostisolates are not identified to the species level);survives in microaerophilic or anaerobicconditions. � Rarely found as the singlebacterial agent in a lesion; more commonly, itis a component of a polymicrobial infection.� There may be synergism betweenActinomyces and other organisms. � Organsystems affected may include: ◦ Skin◦ Respiratory ◦ Cardiovascular◦ Musculoskeletal ◦ Nervous.
SIGNALMENT� Dogs and cats (uncommon). � Mostcommon in young male dogs of sportingbreeds.
SIGNS� Infections—usually localized; may bedisseminated; cervicofacial area commonlyinvolved. � Cutaneous swellings or abscesseswith draining tracts—yellow granules (“sulfurgranules”) may be seen in associated exudates.� Pain, fever, and weight loss. � Exudativepleural or peritoneal effusions; occasionallypericardial effusion noted. � Cough, dyspnea,decreased ventral lung sounds (empyema).� Retroperitonitis—lumbar pain; rear limbparesis or paralysis. � Osteomyelitis ofvertebrae or long bones—probably secondaryto extension of cutaneous infection; lamenessor a swollen extremity may develop. � Motorand sensory deficits—reported with spinalcord compression by granulomas. � Pyothoraxand subcutaneous bite wounds are the mostcommon presenting signs in cats.
CAUSES & RISK FACTORS� Actinomyces spp. normal inhabitants of theoral cavity of dogs and cats. � Loss of normalprotective barriers (mucosa, skin),immunosuppression, or change in thebacterial microenvironment can predispose;thought to occur as an opportunisticinfection. � Specific risk factors—trauma (bitewound), migrating foreign body (grass awnor, in the western United States, a foxtail),and periodontal disease.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Nocardiosis—primary differential diagnosis;Actinomyces not reliably distinguished fromNocardia spp. by gram staining, cytology, orclinical signs. � Other causes of chronic
draining tracts and pleural or peritonealeffusions must be addressed.
CBC/BIOCHEMISTRY/URINALYSIS� Non-specific changes. � Leukocytosis with aleft shift and monocytosis—reported.� Nonregenerative anemia—may develop.� Hypoglycemia and hyperglobulinemia—reported.
IMAGING� Radiographs of infected bone—periostealnew bone production, reactive osteosclerosis,and osteolysis. � Thoracic radiographs—alveolar and interstitial lung patterns withpossible lung consolidation; pleural effusion;pericardial effusion; subcutaneous masses onlateral thorax. � Abdominal radiographs—peritoneal effusion; mass effect in abdomen.� Vertebral column radiographs—periostealnew bone formation, especially T13-L3.
DIAGNOSTIC PROCEDURES� Pus or osteolytic bone fragments submittedin anaerobic specimen containers for culture(see Anaerobic Infections) can provide adefinitive diagnosis; inform the lab to checkfor actinomycosis; advisable to submit aerobicculture, as well. � Fresh smears—gramstaining, cytology, and acid-fast staining;staining does not preclude the need forculture; Actinomyces does not stain acid-fast;Nocardia is variable.
PATHOLOGIC FINDINGSHistopathologic examination—sulfurgranules can be difficult to find so multipletissue sections should be submitted; specialstains may enhance visualization oforganisms; granules are a useful diagnostictool when present; pyogranulomatous orgranulomatous cellulitis with colonies offilamentous bacteria is characteristic.
TREATMENT� Exudative fluid (thorax, abdomen,subcutaneous tissue) should be drained andlavaged. � A chest tube with continuoussuction is needed for cats with pyothorax;dogs are best served with surgical explorationof the chest prior to tube placement in orderto identify and remove any grass awns.� Diseased lung lobes may need to beremoved. � Dogs with solitary massesinvolving the thoracic or abdominal wall mayexperience cure with radical surgical excision.
MEDICATIONSDRUG(S)� Important to distinguish betweenActinomyces and Nocardia for appropriateantimicrobial selection. � Antibiotics—a
retrospective study suggests administration fora minimum of 3–4 months after resolution ofall signs; may need to be directed against otherassociated microbes. � Penicillins—consideredthe drug of choice; in most cases, oral therapycan be initiated and parenteral is not needed;amoxicillin should be administered at 20–22mg/kg q8h PO.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Metronidazole—avoid use; actinomycosisunlikely to respond. � Aminoglycosides—donot use; ineffective against anaerobicinfections. � A. hordeovulneris—cell-walldeficient variant (l-phase); does not usuallyrespond well to penicillin; considerclindamycin, erythromycin, andchloramphenicol.
FOLLOW-UPPATIENT MONITORINGMonitor patients closely for recurrence in themonths after therapy discontinued.
PREVENTION/AVOIDANCEAvoidance of contact with grass awns andprevention of bite wounds.
POSSIBLE COMPLICATIONSConcurrent immune-suppressive disease ortherapy may complicate management.
EXPECTED COURSE AND PROGNOSISRedevelopment of infection at the initial sitemay be expected in about half of all cases.
MISCELLANEOUSAGE-RELATED FACTORSYoung outdoor dogs.
ZOONOTIC POTENTIALThere are no reported cases of actinomycosisbeing transmitted from animals to man;transmission by bite wound may be possibleso appropriate attention should be given tobite wounds.
Suggested ReadingEdwards DF. Actinomycosis and mocardiosis.
In: Greene CE, ed., Infectious Diseases ofthe Dog and Cat, 3rd ed. St. Louis:Saunders Elsevier, 2006, pp. 451–461.
Thomovsky E, Kerl ME. Actinomycosis andnocardiosis. Compend Contin Educ PractVet 2008, 10:4–10.
Author Sharon Fooshee GraceConsulting Editor Stephen C. Barr
BLBS078-CF_A12 BLBS078-Tilley July 15, 2011 1:21
Canine and Feline, Fifth Edition 19
Acute Abdomen A
BASICSDEFINITIONAn emergency condition characterized byhistorical and physical examination findingsof a tense, painful abdomen. May belife-threatening condition.
PATHOPHYSIOLOGY� A patient with an acute abdomen has painassociated with either distention of an organ,inflammation, traction on the mesentery orperitoneum, or ischemia.� The abdominal viscera are sparselyinnervated, and diffuse involvement is oftennecessary to elicit pain; nerve endings alsoexist in the submucosa-muscularis of thebowel wall.� Any process that causes fluid or gaseousdistension (i.e., intestinal obstruction, gastricdilatation-volvulus, ileus) may produce pain.� Inflammation produces abdominal pain byreleasing vasoactive substances that directlystimulate nerve endings.� Many nerves in the peritoneum are sensitiveto a diffuse inflammatory response.
SYSTEMS AFFECTED� Behavioral—trembling, inappetence,vocalizing, lethargy, depression, and abnormalpostural changes such as the praying positionto achieve comfort.� Cardiovascular—severe inflammation,ischemia, and sepsis may lead to acutecirculatory collapse (shock).� Gastrointestinal—vomiting, diarrhea,inappetence, generalized functional ileus;pancreatic inflammation, necrosis, andabscesses may lead to cranial abdominal pain,vomiting, and ileus.� Hepatobiliary—jaundice associated withextrahepatic cholestasis from biliaryobstruction (including pancreatitis) and bileperitonitis.� Renal/Urologic—azotemia can be due toprerenal causes (dehydration, hypovolemia,and shock), renal causes (acute pyelonephritisand acute renal failure), and post-renal causes(urethral obstruction and uroperitoneumfrom bladder rupture).� Respiratory—increased respiratory rate dueto pain or metabolic disturbances.
SIGNALMENT� Dogs and cats.� Dogs more commonly.� Younger animals tend to have a higherincidence of trauma-related problems,intussusceptions, and acquired diet- andinfection-related diseases; old animals have agreater frequency of malignancies.
� Male cats and dogs are at higher risk forurethral obstruction.� Male Dalmatians in particular have a higherrisk of urethral obstruction because of thehigh incidence of urate urinary calculi.� German shepherds with pancreatic atrophyhave a higher risk of mesenteric volvulus.� Patients treated with corticosteroids andnon-steroidal anti-inflammatory drugs are athigher risk for gastrointestinal ulceration andperforation.
SIGNSGeneral CommentsClinical signs vary greatly depending on thetype and severity of the disease leading to anacute abdomen.
Historical Findings� Trembling, reluctance to move,inappetence, vomiting, diarrhea, vocalizing,and abnormal postures (tucked up or prayingposition)—signs that the owner may notice.� Question owner carefully to ascertain whatsystem is affected; for example, hematemesiswith a history of NSAID treatment suggestsGI mucosal disruption.
Physical Examination Findings� Abnormalities include abdominal pain,splinting of the abdominal musculature, gas-or fluid-filled abdominal organs, abdominalmass, ascites, pyrexia or hypothermia,tachycardia, and tachypnea.� Once abdominal pain is confirmed, attemptto localize the pain to cranial, middle, orcaudal abdomen.� Perform a rectal examination to evaluate thecolon, pelvic bones, urethra, and prostate, aswell as the presence of melena.� Rule out extra-abdominal causes of pain bycareful palpation of the kidneys andthoracolumbar vertebrae.� Pain associated with intervertebral diskdisease often causes referred abdominalguarding and is often mistaken for trueabdominal pain. Renal pain can be associatedwith pyelonephritis.
CAUSESGastrointestinal� Stomach—gastritis, ulcers, perforation,foreign bodies, gastric dilatation-volvulus.� Intestine—obstruction (foreign bodies,intussusception, hernias), enteritis, ulcers,perforations.� Rupture after obstruction, ulceration, orblunt or penetrating trauma, or due to tumorgrowth.� Vascular compromise from infarction,mesenteric volvulus, or torsion.
Pancreas� Pain associated with inflammation, abscess,ischemia.� Pancreatic masses or inflammationobstructing the biliary duct/papilla will causejaundice.
Hepatic and Biliary System� Rapid distention of the liver and its capsulecan cause pain.� Gallbladder obstruction, rupture, ornecrosis may lead to bile leakage andperitonitis.� Hepatic abscess.
Spleen� Splenic torsion, splenic masses, splenicthrombus, splenic abscess.
Urinary Tract� Distention is the main cause of pain in theurinary tract.� Lower urinary tract obstruction can be dueto tumors of the trigone area of the bladder orurethra, urinary calculi, or granulomatousurethritis.� Traumatic rupture of the ureters or bladderare associated with blunt trauma andincreased intra-abdominal pressure.� Urethral tears can be associated with pelvicfractures from acute trauma.� Free urine in the peritoneal cavity leads to achemical peritonitis.� Acute pyelonephritis, acute renal failure,nephroliths, and ureteroliths are uncommoncauses of acute abdomen.
Genital Tract� Prostatitis and prostatic abscess, pyometra; aruptured pyometra or prostatic abscess cancause endotoxemia, sepsis, and cardiovascularcollapse.� Infrequent causes include ruptures of thegravid uterus after blunt abdominal trauma,uterine torsion, ovarian tumor or torsion, andintra-abdominal testicular torsion(cryptorchid).
Abdominal Wall/Diaphragm� Umbilical, inguinal, scrotal, abdominal, orperitoneal hernias with strangulated viscera.� Trauma or congenital defects leading toorgan displacement or entrapment in thehernia will lead to abdominal pain if thevascular supply of the organs involvedbecomes impaired or ischemic.
RISK FACTORS� Exposure to NSAIDs or corticosteroidtreatment—gastric, duodenal, or coloniculcers.� Garbage or inappropriate foodingestion—pancreatitis.� Foreign body ingestion—intestinalobstructions.� Abdominal trauma—hollow viscus rupture.� Hernias—intestinal obstruction/strangulation.
BLBS078-CF_A12 BLBS078-Tilley July 15, 2011 1:21
20 Blackwell’s Five-Minute Veterinary Consult
Acute Abdomen (Continued)A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Renal-associated pain, retroperitoneal pain,spinal or paraspinal pain, and disorderscausing diffuse muscle pain may mimicabdominal pain; careful history and physicalexamination are essential in pursuing theappropriate problem.� Parvoviral enteritis can present similarly tointestinal obstructive disease; fecal parvoviralantigen assay and CBC (leukopenia) arehelpful differentiating diagnostic tests.
CBC/BIOCHEMISTRY/URINALYSIS� Inflammation or infection may beassociated with leukocytosis or leukopenia.� Anemia may be seen with blood lossassociated with GI ulceration.� Azotemia is associated with prerenal, renal,and post-renal causes.� Electrolyte abnormalities can help toevaluate GI disease (i.e., hypochloremicmetabolic alkalosis with gastric outflowobstruction) and renal disease (i.e.,hyperkalemia with acute renal failure orpost-renal obstruction).� Hyperbilirubinemia and elevated hepaticenzymes help localize a problem to the liver orbiliary tract.� Urine specific gravity (before fluid therapy)is needed to differentiate prerenal, renal, andpost-renal problems.� Urine sediment may be helpful in acuterenal failure, ethylene glycol intoxication, andpyelonephritis.
OTHER LABORATORY TESTS� Trypsin-like immunoreactivity can be usefulin evaluating feline pancreatitis.� Canine pancreatic lipase immunoreactivityis useful for canine pancreatitis.
IMAGINGAbdominal Radiography� May see abdominal masses or changes inshape or shifting of abdominal organs.� Loss of abdominal detail with abdominalfluid accumulation is an indication for aabdominocentesis.� Free abdominal gas is consistent with aruptured GI viscus or infection withgas-producing bacteria and is an indicationfor emergency surgery.� Use caution when interpreting radiographsfollowing abdominocentesis with an openneedle. Free gas may be introduced with thistechnique.� Use caution when evaluating post-operativeradiographs; free gas is a normalpost-operative finding.� Ileus is a consistent finding with peritonitis.
� Characterize ileus as functional (due tometabolic or infectious causes) or mechanical(due to obstruction).� Foreign bodies may be radiopaque.� Upper GI barium contrast radiographs areuseful in evaluating the GI tract, particularlyfor determination of GI obstruction.� Contrast in the area of the pancreas can belost with pancreatic inflammation.
Abdominal Ultrasound� A sensitive diagnostic tool for the detectionof abdominal masses, abdominal fluid,abscesses, cysts, lymphadenopathy, and biliaryor urinary calculi.
DIAGNOSTIC PROCEDURESAbdominocentesis/Abdominal FluidAnalysis� Perform abdominocentesis on all patientspresenting with acute abdomen. Fluid canoften be obtained for diagnostic evaluationeven when only a small amount of freeabdominal fluid exists, well before detectableradiographic sensitivity. Althoughultrasonography is much more sensitive thanradiography for the detection of fluid, the lackof such detection does not precludeabdominocentesis. Abdominal fluid analysiswith elevated WBC count, degenerateneutrophils, and intracellular bacteria isconsistent with septic peritonitis and is anindication for immediate surgery.� Diagnostic peritoneal lavage can beperformed by introducing sterile saline(10–20 ml/kg) and performingabdominocentesis.� Measurement of glucose concentration inabdominal effusion may aid in the diagnosisof septic abdomen.� Pancreatitis patients may have an abdominaleffusion characterized as a non-septic (sterile)peritonitis.� Creatinine concentration higher inabdominal fluid than in serum indicatesurinary tract leakage.� Similarly, higher bilirubin concentration inabdominal fluid than in serum indicates bileperitonitis.
Sedation and Abdominal Palpation� Because of abdominal splinting associatedwith pain, a thorough abdominal palpation isoften not possible without sedation; this isparticularly useful for detecting intestinalforeign bodies that do not appear on surveyradiographs.
Exploratory Laparotomy� Surgery may be useful diagnostically (as wellas therapeutically) when ultrasonography isnot available or when no definitive cause ofthe acute abdomen has been established withappropriate diagnostics.
TREATMENT� Inpatient management with supportive careuntil decision about whether the problem isto be treated medically or surgically.� Aggressive therapy and promptidentification of the underlying cause is veryimportant.� Many causes of acute abdominal painrequire emergency surgical intervention.
SUPPORTIVE CARE� Keep patient NPO if vomiting, until adefinitive cause is determined and addressed.� Intravenous fluid therapy is usually requiredbecause of the large fluid loss associated withan acute abdomen; the goal is to restore thenormal circulating blood volume.� If severe circulatory compromise (shock)exists, supplement initially with isotoniccrystalloid fluids (90 mL/kg, dogs; 70 mL/kg,cats) over 1–2 hours; hypertonic fluids orcolloids may also be beneficial.� Evaluate hydration and electrolytes (withappropriate treatment adjustments)frequently after commencement of treatment.
SURGICAL CONSIDERATIONS� Many different causes of an acute abdomen(with both medical and surgical treatments)exist; make a definitive diagnosis wheneverpossible prior to surgical intervention.� This can prevent both potentiallyunnecessary and expensive surgical proceduresand associated morbidity and mortality.� It will also allow the surgeon to prepare forthe task and to educate the owner on theprognosis and costs involved.
MEDICATIONSDRUG(S)Analgesics� Pain medication may be indicated forcontrol of abdominal discomfort.� Opioids, such as hydromorphone at0.05–0.1 mg/kg, are often good choices.
Histamine H2 Antagonists� Reduce gastric acid production.� Famotidine 0.1–0.2 mg/kg IV, SC or IMq12h.� Ranitidine 2 mg/kg IV q8h
PPI� Pantoprazole 0.5–1 mg/kg IV as a CRI over24 hours.
Protectants� Sucralfate 0.25–1 g PO q8h.
Antiemetics� Metoclopramide 0.2–0.4 mg/kg IV q6–8h(or 24-hour continuous rate infusion).
BLBS078-CF_A12 BLBS078-Tilley July 15, 2011 1:21
Canine and Feline, Fifth Edition 21
(Continued) Acute Abdomen A
� Maropitant 1 mg/kg SC dogs, 0.5 mg/kgSC cats.� Ondansetron 0.5–1 mg/kg IV slowlyq6–12h.� Dolasetron 1 mg/kg IV q24h.
Antibiotics� Antibiotics may be indicated if signs ofinfection (fever, elevated white blood cellcount, positive culture) are seen.� Broad spectrum for gram positive, gramnegative, and anaerobic bacteria.� Gram stain and cultures prior to treatmentif possible.
CONTRAINDICATIONSDo not use metoclopramide if GI obstructionis suspected.
PRECAUTIONSGentamicin and most NSAIDs can benephrotoxic and should be used with cautionin hypovolemic patients and those with renalimpairment.
FOLLOW-UPPATIENT MONITORINGPatients usually require intensive medical careand frequent evaluation of vital signs andlaboratory parameters.
MISCELLANEOUSSYNONYMSColic
SEE ALSO� Gastric Dilation and Volvulus Syndrome� Gastroduodenal Ulcer Disease� Gastrointestinal Obstruction� Intussusception
� Pancreatitis� Prostatitis and Prostatic Abscess� Urinary Tract Obstruction
ABBREVIATIONS� GI = gastrointestinal� NSAID = nonsteroidal anti-inflammatorydrug
Suggested ReadingBeal MW. Approach to the acute abdomen.
Vet Clin North Am Small Anim Pract 2005,35:375–396.
Heeren V, Edwards L, Mazzaferro EM. Acuteabdomen: Diagnosis. Compend ContinEduc Pract Vet 2004, 26:350–363.
Heeren V, Edwards L, Mazzaferro EM. Acuteabdomen: Treatment. Compend ContinEduc Pract Vet 2004, 26:3566–3673.
Mazzaferro EM. Triage and approach to theacute abdomen. Clin Tech Small AnimPract 2003, 18:1–6.
Author Steven L. MarksConsulting Editor Albert E. Jergens
BLBS078-CF_A13 BLBS078-Tilley May 31, 2011 16:59
22 Blackwell’s Five-Minute Veterinary Consult
Acute Respiratory Distress SyndromeA
BASICSDEFINITIONSyndrome of acute onset of respiratory failuretypified by diffuse bilateral pulmonaryinfiltrates on a dorsoventral thoracicradiograph with no evidence of increasedhydrostatic pressure, cardiogenic pulmonaryedema, or fluid overload. ARDS is due to adiffuse, overwhelming inflammatory reactionof the alveolocapillary membrane in responseto a systemic or pulmonary inflammatoryinsult. It can be divided into two categoriesbased on severity. The less severe form iscalled acute lung injury; ALI is defined as aPaO2/FiO2 ratio of < 300; ARDS is definedas a PaO2/FiO2 < 200.
PATHOPHYSIOLOGY� ARDS is due to a diffuse inflammatoryinsult that causes widespread damage toalveolar epithelial and endothelial cellsresulting in impaired gas exchange. Thisinflammatory insult can be triggered byprimary pulmonary disease or it can be ofnon-pulmonary origin. Mechanisms of injuryinclude neutrophil activation, endothelial celldysfunction, and proinflammatorymediator-triggered cell damage. Damage isthought to be exacerbated byventilator-induced lung injury associated withalveolar over distension and cyclic openingand collapse of atelectatic alveoli. � Earlyexudative phase—initial 12–24 hours istypified by increased alveolar capillarymembrane permeability; protein-rich edemafluid and white blood cells flood into theinterstitium and alveoli. Neutrophilsexacerbate damage by further release ofcytokines and inflammatory mediators.� Type I alveolar epithelial cells die. Alveolarflooding and surfactant dysfunction lead tocollapse and consolidation of alveoli withdevelopment of severe hypoxemia.� Microthrombi in the pulmonaryvasculature, hypoxic pulmonaryvasoconstriction, and release of endogenousvasoconstrictors lead to pulmonary arterialhypertension, which can lead to right-sidedheart failure. � Hyaline membranephase—hyaline membrane formation in thealveolar spaces 3-7 days after initial insult.� Fibroproliferative phase—if the patientsurvives the initial 3-7 days, proliferation oftype 2 alveolar epithelial cells and pulmonaryfibrosis occurs. � An idiopathic form ofARDS associated with acute interstitialpneumonia or idiopathic pulmonary fibrosishas been reported in people and dogs.
SYSTEMS AFFECTED� Respiratory.� Cardiovascular—right-side heart failuresecondary to pulmonary hypertension;hemodynamic compromise may be associatedwith aggressive mechanical ventilator settings.
GENETICSSome people have been found to be moreprone to developing ARDS than others due tospecific gene polymorphisms. This has notbeen investigated in the veterinarypopulation.
INCIDENCE/PREVALENCEUnknown
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsA familial form of ARDS has been reported ina group of related Dalmatian dogs; it isclinically indistinguishable from ARDS.
Mean Age and RangeUnknown
Predominant SexUnknown
SIGNSHistorical Findings� Acute onset of respiratory distress in apatient with a significant underlying disease.� Animal is often hospitalized for its primarydisease when it develops ARDS.
Physical Examination Findings� Severe respiratory distress.� Crackles (if present) heard bilaterally onauscultation.� Fever—depends on underlying disease.� Cyanosis in more severe cases.� Signs relevant to the primary disease process.
CAUSESPrimary Pulmonary Causes� Aspiration pneumonia� Pneumonia� Pulmonary contusion� Near drowning� Smoke inhalation
Non-pulmonary Causes� Severe systemic inflammatory response� Sepsis� Neoplasia� Pancreatitis� Severe trauma and shock� Severe bee sting envenomation
RISK FACTORS� SIRS� Sepsis� Severity of illness� Multiple transfusions� Co-existing disease conditions
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Left-side congestive heart failure� Fluid overload� Diffuse pneumonia� Pulmonary hemorrhage
CBC/BIOCHEMISTRY/URINALYSIS� Leukocytosis or leucopenia.� Other changes dependent on the underlyingdisease process.
OTHER LABORATORY TESTS� Arterial blood gases—low PaO2/FiO2 ratio(where PaO2 is measured in mmHg and FiO2
is 0.21–1.0). Normal PaO2/FiO2 ratio = 500;comparison of this ratio allows evaluation ofseverity of lung disease and allows directcomparison of blood gases taken at differentFiO2. PaCO2 is often low; hypercapnia tendsto be a late (preterminal) development.� Total protein of airway edema fluidcompared with serum total protein—ratio ofedema fluid to serum total protein < 0.5indicates low-protein hydrostatic pressurepulmonary edema (e.g., heart failure); edemafluid/serum total protein ratio > 0.7 indicateshigh-protein, increased permeabilitypulmonary edema such as ARDS andpneumonia.
IMAGINGThoracic Radiographs� Bilateral pulmonary infiltrates.� Severity of radiographic signs may lagbehind clinical disease by 12-24 hours.� Can be difficult to distinguish fromcardiogenic edema. Cardiac silhouette isusually normal in ARDS.
Echocardiography� Attempt to rule out cardiogenic cause forpulmonary edema.� May be able to estimate degree ofpulmonary hypertension.
DIAGNOSTIC PROCEDURESPulmonary artery catheter to measurepulmonary artery occlusion pressure in orderto rule out cardiogenic cause for edema; bydefinition, ALI and ARDS are associated withPAOP ≤ 18 mmHg.
PATHOLOGIC FINDINGSGross PathologyLungs are dark, heavy, and ooze fluid whencut.
Histopathology� Acute phase—pulmonary vascularcongestion with edema fluid andinflammatory cell accumulation in theinterstitium and alveoli; epithelial celldamage, hyaline membrane formation,microthrombi, microatelectasis.� Proliferative phase—hyperplasia of type 2pneumocytes, interstitial mononuclearinfiltration, organization of hyalinemembranes, and fibroproliferation.
TREATMENTAPPROPRIATE HEALTH CARE� There is no specific therapy. General aimsare to maintain tissue oxygenation and to
BLBS078-CF_A13 BLBS078-Tilley May 31, 2011 16:59
Canine and Feline, Fifth Edition 23
(Continued) Acute Respiratory Distress Syndrome A
minimize iatrogenic lung injury while treatingthe underlying disease. � Oxygen therapy—nomore than is required to maintain PaO2 >60–80 mmHg to minimize oxygen toxicity.� Positive-pressure ventilation is essential inthe management of ARDS patients. It isindicated in patients that are hypoxemicdespite oxygen therapy, patients requiringhigh levels of inspired oxygen for prolongedperiods, or patients working so hard tobreathe that they are at risk of exhaustion.Lung-protective strategies of positive-pressureventilation with moderate to high PEEP, lowtidal volumes, and permissive hypercapnia arerecommended to minimize ventilator-inducedlung injury. Tidal volumes of 6 ml/kg havebeen found to increase survival significantly inhuman ARDS patients compared to tidalvolumes of 12 ml/kg. � Recruitmentmaneuvers and high levels of PEEP can bothcause significant hemodynamic compromiseand patients should have constant directarterial blood pressure monitoring.� Intensive supportive care of thecardiovascular system and other organ systemsis vital, as these patients are at high risk fordevelopment of multiple organ dysfunction.
NURSING CARE� Monitor temperature closely, especially ifusing an oxygen cage, as animals withexcessive work of breathing can easily becomehyperthermic. � Ventilator patients requirefrequent position changes and physiotherapy;regular oral care with a dilute chlorhexidinesolution is very important to reduce oralcolonization as a source of sepsis, andfrequent endotracheal tube suctioning isneeded to prevent occlusion. Inflate cuffcarefully and change endotracheal cuffposition regularly to prevent tracheal damage.� Blood pressure monitoring, as septicpatients are prone to hypotension. � Fluidtherapy is important to support thecardiovascular system and to maintainnormovolemia while avoiding fluid overload.
ACTIVITYIf not anesthetized for ventilation, strict cageconfinement.
DIETNutritional support is important butchallenging. Enteral feeding is desired overparenteral nutrition, but must consider highrisk of regurgitation and aspiration in arecumbent patient.
CLIENT EDUCATIONClients need to be aware of the guardedprognosis and high costs of therapy.
SURGICAL CONSIDERATIONSThe underlying disease may require surgery.
MEDICATIONSDRUG(S) OF CHOICE� No specific drug therapy. � Antibiotics forthe underlying disease, if necessary.� Vasoactive drugs to maintain bloodpressure. � Anesthetic drugs to allowpositive-pressure ventilation. � Analgesia asappropriate. � Low-dose corticosteroid—useremains controversial with conflicting reportsof efficacy for low-dose steroids in early or lateARDS.
ALTERNATIVE DRUG(S)Furosemide may produce pulmonary venousdilation and improve lung function, as anintermittent bolus of 1 mg/kg IV q6–12h oras a CRI of 0.2 mg/kg/h IV.
FOLLOW-UPPATIENT MONITORINGArterial blood gases, pulse oximetry, end-tidalcarbon dioxide, thoracic radiographs, arterialblood pressure, ECG, temperature, urineoutput, CBC, coagulation profiles, serumchemistry, blood cultures, monitoring forother organ dysfunction.
PREVENTION/AVOIDANCE� Aggressive therapy of primary diseaseprocesses to reduce the inflammatory insult tothe lung. � Intensive cardiovascularmonitoring and support of critically illanimals to ensure adequate tissue perfusion.� Careful management of recumbent animalsto reduce the chance of aspiration, especiallyif patient has neurologic disease or upperairway disorders that reduce the ability toprotect the airway.
POSSIBLE COMPLICATIONS� Multiorgan dysfunction syndrome—acuterenal failure, DIC, and gastrointestinal diseaseare the more common organ dysfunctionsseen. � Barotrauma—can result inpneumothorax. Incidence is thought to be lesswith lower tidal volume ventilation strategies.� Ventilator-associated pneumonia—patientson PPV have increased risk of pneumoniathat may be difficult to differentiate fromworsening of the initial lung injury. Airwaycultures should be considered in deterioratingpatients. � Oxygen toxicity may beunavoidable due to severity of hypoxemia inspite of PPV. Oxygen toxicity isindistinguishable from ARDS onhistopathology making the incidence of thisproblem impossible to determine.
EXPECTED COURSE AND PROGNOSIS� Mortality in human patients remains at40–60%.� Mortality in veterinary patients likelyapproaches 100%.
MISCELLANEOUSASSOCIATED CONDITIONSSystemic inflammatory response syndrome,multiple organ dysfunction syndrome,sepsis.
SYNONYMS� Acute hypoxemic respiratory failure� Acute interstitial pneumonia� Adult respiratory distress syndrome� High-protein pulmonary edema� Shock lung
SEE ALSO� Dyspnea and Respiratory Distress� Panting and Tachypnea� Pulmonary Edema, Non-cardiogenic� Sepsis and Bacteremia
ABBREVIATIONS� ALI = acute lung injury� ARDS = acute respiratory distresssyndrome� CRI = constant rate infusion� DIC = disseminated intravascularcoagulation� PAOP = pulmonary artery occlusionpressure (formerly pulmonary capillary wedgepressure [PCWP])� PEEP = positive end-expiratory pressure� PPV = positive-pressure ventilation� SIRS = systemic inflammatory responsesyndrome
INTERNET RESOURCEShttp://www.ardsnet.org.
Suggested ReadingMarino PL. Acute respiratory distress
syndrome. In: The ICU Book, 2nd ed.Baltimore: Williams & Wilkins, 1998,pp. 371–387.
Parent C, King LG, Van Winkle TJ, WalkerLM. Respiratory function and treatment indogs with acute respiratory distresssyndrome: 19 cases (1985–1993). JAVMA1996, 208:1428–1433.
Syrja P, Saari S, Rajamaki M, Saario E,Jarvinen A-K. Pulmonary histopathology inDalmatians with familial acute respiratorydistress syndrome (ARDS). J Comp Pathol2009, 141(4):254–259.
Ware LB, Bernard GR. Acute lung injury andacute respiratory distress syndrome. In:Textbook of Critical Care, 5th ed.Philadelphia: Elsevier Saunders, 2005,pp. 571–579.
Ware LB, Matthay MA. The acute respiratorydistress syndrome. N Engl J Med 2000,342:1334–1349.
Author Kate HopperConsulting Editor Lynelle R. Johnson
BLBS078-CF_A14 BLBS078-Tilley June 25, 2011 14:46
24 Blackwell’s Five-Minute Veterinary Consult
Adenocarcinoma, Anal SacA
BASICSOVERVIEW� Uncommon malignant neoplasm derivedfrom apocrine glands of the anal sac. � Locallyinvasive. � High metastatic rate, often tosublumbar lymph nodes. � Frequentlyassociated with hypercalcemia, secondary toparathyroid hormone—related peptidesecretion by tumor cells. � Prognosis guardedto fair.
SIGNALMENT� Older dogs; extremely rare in cats.� Females overrepresented in a few smallstudies, not in larger studies. � May haveincreased risk with neutering (particularlymales). � English cocker spaniels significantlyoverrepresented, springer and Cavalier KingCharles spaniels also overrepresented.
SIGNSHistorical FindingsSigns may be due to primary tumor (rectalmass, tenesmus), local lymph node metastasis(tenesmus, constipation, stranguria), orhypercalcemia (anorexia, polyuria/polydipsia,lethargy).
Physical Examination Findings� Mass associated with anal sac; may be quitesmall despite massive metastatic disease.� Sublumbar lymphadenopathy—on rectal orabdominal palpation.
CAUSES & RISK FACTORSHormonal role hypothesized
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Anal sac abscess � Perianal adenoma/adenocarcinoma � Mast cell tumor� Lymphoma � Squamous cell carcinoma� Perineal hernias
CBC/BIOCHEMISTRY/URINALYSIS� Hypercalcemia—25–50% of cases� Secondary renal failure may develop
OTHER LABORATORY TESTSParathyroid hormone and PTHrPlevels—high PTHrP will help to supportneoplasia as the cause of hypercalcemia.
IMAGING� Abdominal radiography—to evaluatesublumbar lymph nodes and lumbar andpelvic bones. � Thoracic radiography—toevaluate for pulmonary metastasis.� Abdominal ultrasonography—may identifymildly enlarged sublumbar lymph nodes notvisible radiographically, also nodules inliver/spleen.
DIAGNOSTIC PROCEDURES� Fine-needle aspiration of anal sac mass torule out conditions other thanadenocarcinoma; differentiation of benignversus malignant neoplasm of perianal massesis difficult. � Fine-needle aspiration ofenlarged lymph nodes, liver, or splenicnodules to confirm metastasis. � Incisionalbiopsy for histopathology required fordefinitive diagnosis, although excisionalbiopsy may be appropriate if location of massand cytology are supportive of anal glandneoplasia.
TREATMENT� Surgical resection—treatment of choice. � Ifcaught early, cure is possible. � Resection ofprimary tumor and enlarged lymph nodesmay prolong survival. � If mass is large andregionally invasive at diagnosis, surgery oftenpalliative, not curative. � Debulking all diseasepresent may control hypercalcemia untiltumor recurrence. � Saline diuresis (200–300mL/kg/day) preoperatively if hypercalcemia issevere. � Radiation may help delay localrecurrence and control growth of sublumbarmetastases—acute and chronic radiation sideeffects can be moderate to severe.
MEDICATIONSDRUG(S)� Limited reports of partial responses toplatinum compounds in dogs—cisplatin(70 mg/m2 IV with 6-hour salinediuresis—18.3 mL/kg/hour), carboplatin(300 mg/m2 IV as a slow bolus) every 3weeks. � Mitoxantrone (5 mg/m2 IV every 3weeks for five treatments) in combinationwith radiation therapy used in one small caseseries. � Possible role for melphalan afterdebulking surgery (7 mg/m2 PO daily for 5days every 3 weeks).
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Avoid platinum chemotherapeutic agents indogs with renal insufficiency. � Do not usecisplatin in cats.
FOLLOW-UPPATIENT MONITORING� Complete resection—physical examination,thoracic radiography, abdominalultrasonography, and serum biochemistry at1, 3, 6, 9, and 12 months post-operatively.� Incomplete resection—monitor tumor sizeand blood calcium and renal values.
EXPECTED COURSE AND PROGNOSIS� Guarded prognosis with both localprogression and metastasis occurring. � Curesmay occur if tumor is found early and treatedaggressively. � Growth of the tumor may beslow and debulking lymph node metastaticdisease may significantly prolong survival.� Hypercalcemia is variably associated with apoor prognosis. � Four papers (involving 200dogs) showed median survival times of 6 to20 months, depending on stage andtreatment. � A recent report on 16 dogswithout metastasis showed a median survivaltime not met with a follow-up of 33 months.◦ Dogs with lymph node metastasis livedsignificantly longer if the nodes wereextirpated. � Ultimately, dogs that cannothave their tumors excised completelysuccumb to hypercalcemia-relatedcomplications or mass effect from primarytumor or sublumbar nodal metastases.
MISCELLANEOUSASSOCIATED CONDITIONSHypercalcemia as a paraneoplastic syndrome
ABBREVIATIONSPTHrP = parathyroid hormone-related
peptide
Suggested ReadingAnderson CR, McNeil EA, Gillette EL, et al.
Late complications of pelvic irradiation in16 dogs. Vet Radiol Ultrasound 2002,43:187–192.
Emms SG. Anal sac tumours of the dog andtheir response to cytoreductive surgery andchemotherapy. Australian Vet J 2005,83:340–343.
Polton GA, Brearley MJ. Clinical stage,therapy, and prognosis in canine anal sacgland carcinoma. J Vet Intern Med 2007,21:274–280.
Turek MM, Forrest LJ, Adams WM, et al.Postoperative radiotherapy andmitoxantrone for anal sac adenocarcinomain the dog: 15 cases (1991-2001). VetComp Onc 2003, 1:94–104.
Williams LE, Gliatto JM, Dodge RK, et al.Carcinoma of the apocrine glands of theanal sac in dogs: 113 cases (1985–1995).JAVMA 2003, 223:825–831.
Author Laura D. GarrettConsulting Editor Timothy M. Fan
Client Education Handoutavailable online
BLBS078-CF_A15 BLBS078-Tilley March 21, 2011 9:42
Canine and Feline, Fifth Edition 25
Adenocarcinoma, Lung A
BASICSOVERVIEW� Comprises 75% of primary pulmonarytumors in dogs and cats. � Primarypulmonary tumors are rare in dogs and cats.� Strongest predictors of outcome are tumorgrade, node involvement, and clinical signs.� May metastasize. � May be associated withhypertrophic osteopathy.
SIGNALMENTDogs� 1% of all tumors. � Mean age of affectedanimals 10 years, most dogs are older. � Nosex predilection, though more females insome reports. � Boxers or brachycephalicbreeds may be predisposed. � Medium tolarge breeds overrepresented.Cats� More rare than in dogs. � Mean age ofaffected animals 11 years. � No breedpredilection. � Some studies suggest femalesare overrepresented.
SIGNSHistorical FindingsRelated to Presence of a Lung Mass� Non-productive cough (> 50% of dogs).� Dyspnea (may be related to pneumothorax).� Tachypnea. � Weight loss. � Hemoptysis.� Pain—pleural involvement.Paraneoplastic Signs� Lameness—bone metastasis or hypertrophicosteopathy (dogs or cats), weight-bearing lyticdigit metastasis (cats). � Polyuria orpolydipsia—hypercalcemia orhyperadrenocorticism from ectopicproduction of ACTH. � Weakness or musclewasting—polyneuropathy; polymyopathy.Physical Examination Findings� May be asymptomatic. � Tachypnea anddyspnea. � Fever. � Limb swelling. � Pleuraleffusion. � Caval syndrome.
CAUSES & RISK FACTORS� Potential urban environment risk� Potential exposure to passive cigarette smoke
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Granulomatous lesion (fungal, foreign body,parasitic) � Lymphomatoid or eosinophilicgranulomatosis � Pulmonary abscess � Otherprimary lung tumor � Metastatic lung tumor� Pneumonia � Asthma � Pulmonarythromboembolism � Congenital cyst � Lungtorsion or hematoma
CBC/BIOCHEMISTRY/URINALYSISNo specific abnormalities
OTHER LABORATORY TESTS� Arterial blood gas. � Clotting times shouldbe performed prior to aspirate or biopsy.
IMAGING� Thoracic radiography—usuallydemonstrates a focal, solitary,well-circumscribed mass; must be performedin cats presenting with multiple digit tumorsto screen for primary lung tumor (lung-digitsyndrome). � Ultrasonography—may helpwith obtaining an aspirate or biopsy specimen,or to evaluate abdomen. � CT—most accurateassessment for determining surgical feasibility,and identification of lymphadenopathy (93%accuracy) and metastatic disease.
DIAGNOSTIC PROCEDURES� Thoracocentesis with cytologic examination(for pleural effusion).� Cytology—transthoracic fine-needleaspiration (83% agreement withhistopathology); this may be guided byimaging such as CT scan or fluoroscopy, or ifthe tumor is peripherally located against thethoracic wall, then ultrasound may be used.� Percutaneous tissue biopsy—use Tru-Cutinstrument. � Open lung biopsy—specimenvia thoracotomy, or minimally invasivethoracoscopy.
PATHOLOGIC FINDINGS� Adenocarcinoma—classified according tolocation (bronchial, bronchiolar,bronchiolar-alveolar, or alveolar) and degreeof differentiation. � Thyroid transcriptionfactor-1 positivity may distinguish primaryfrom metastatic carcinoma. � Undifferentiatedtumors—more invasive and more likely tometastasize than well-differentiated tumors;sites of metastasis include lymph nodes,bones, pleura, eyes (choroid), and CNS.� Cats tend to have less differentiated tumors,corresponding to more aggressive behavior.
TREATMENT� Surgery—mainstay of treatment; partial orcomplete lobectomy with tracheobronchiallymph node biopsy or removal.� Radiotherapy—reports are anecdotal, butcertain patients may benefit. � Chemotherapyshould be considered following surgery fortumors that are high grade, undifferentiated,and/or have nodal involvement. Select centersmay offer inhalant chemotherapy for higherlocal concentrations with less systemic sideeffects. � Intracavitary chemotherapy can beused to treat pleural effusion.
MEDICATIONSDRUG(S)� Vinorelbine concentrates in lungs andresponses have been seen. � Doxorubicin,cisplatin, carboplatin, mitoxantrone,vinorelbine, and/or vindesine—rationalchoices for palliation.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Doxorubicin—monitor patients withunderlying cardiac disease carefully; considerpretreatment with diphenhydramine andserial echocardiograms and ECGs.� Cisplatin—do not give to cats (fatal); donot use in dogs with preexisting renal disease;never use without appropriate and concurrentdiuresis.
FOLLOW-UPPATIENT MONITORING� Serial thoracic radiographs—consider every3 months; administer a minimum of twocycles of chemotherapy before evaluatingresponse to treatment. � Perform CBC (withany chemotherapy) and renal panel (cisplatin)before each chemotherapy treatment.
POSSIBLE COMPLICATIONSPneumothorax or hemothorax
EXPECTED COURSE AND PROGNOSIS� Metastasis to the tracheobronchial lymphnodes—single best prognostic indicator;median survival without metastasisapproaches 1 year and with metastasis,60 days. � Post-operative survival in dogs (∼1yr) is better than in cats (∼4 months), butaround 2 years in either species if positiveprognostic factors are present. � Otherpatient, tumor, and treatment factorsinfluencing prognosis—complete surgicalexcision; size of the primary tumor (< 5 cmbetter); metastasis (better if none); degree ofcell differentiation (histologic score, better ifwell differentiated), lack of clinical signs priorto surgery.
MISCELLANEOUSPREGNANCY/FERTILITY/BREEDINGChemotherapy is not advised in pregnantanimals
ABBREVIATIONS� ACTH = adrenocorticotropic hormone� CNS = central nervous system � CT =computed tomography � ECG =electrocardiogramSuggested ReadingPaoloni MC, Adams WM, Dubielzig RR, et
al. Comparison of results of computedtomography and radiography withhistopathologic findings in tracheobronchiallymph nodes in dogs with primary lungtumors: 14 cases (1999–2002). JAVMA2006, 228(11):1718–1722.
Rissetto KC, Lucas P, Fan TM. An update ondiagnosing and treating primary lungtumors. Vet Med 2008, 103(3):154.
Author Kim A. SeltingConsulting Editor Timothy M. FanAcknowledgement Renee Al-Saraff
BLBS078-CF_A16 BLBS078-Tilley March 21, 2011 9:45
26 Blackwell’s Five-Minute Veterinary Consult
Adenocarcinoma, NasalA
BASICSOVERVIEW� Represents less than 5% of all tumors indogs and cats. � Progressive local and regionalinvasion of the nasal cavity, paranasal sinuses,and surrounding tissues by neoplasticepithelial and glandular epithelial cells.� Often has progressed to bilateralinvolvement by the time of diagnosis. � Manyarise from the frontal sinuses. � In dogs,adenocarcinoma is more common thansquamous cell carcinoma, chondrosarcoma,and other histologies. � In cats, most commonsinonasal tumor is lymphoma, followed byadenocarcinoma and other histologies.
SIGNALMENT� Dogs and cats. � Median age in dogs is 10years, versus 13 years in cats. � In dogs,medium to large breeds affected morecommonly with a possible overrepresentationof mesocephalic and dolichocephalic breeds.
SIGNSHistorical Findings� Intermittent and progressive history ofunilateral to bilateral epistaxis and/ormucopurulent discharge (median duration, 3months). � Epiphora. � Sneezing andincreased upper respiratory noises.� Open-mouth breathing. � Halitosis.� Anorexia (more frequent in cats). � Seizures(secondary to invasion of cranial vault).
Physical Examination Findings� Nasal discharge (blood, mucopurulent).� Facial deformity, exophthalmia.� Space-occupying orbital mass (eye cannotbe retropulsed). � Pain upon nasal orparanasal sinus palpation or upon opening themouth. � Decreased or absent airflow in thenasal passages (unilateral or bilateral).� Regional lymphadenomegaly. � Abnormalmentation or other neurological findings.
CAUSES & RISK FACTORSDolichocephalic morphology, urbanenvironment, and second-hand smoke may allplay a role.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other sinonasal tumors (e.g., squamous cellcarcinoma, lymphoma, sarcomas). � Viralinfection—cats. � Fungal infections includingaspergillosis (dogs) and cryptococcosis (cats).� Foreign body. � Trauma. � Tooth rootabscess and oronasal fistula. � Coagulopathies.� Parasites (e.g., nasal mites). � Ehrlichiosis,leishmaniasis. � Systemic hypertension.� Bacterial sinusitis—rare.
CBC/BIOCHEMISTRY/URINALYSIS� Usually normal � Occasional blood lossanemia
OTHER LABORATORY TESTS� Cytologic examination: occasionally helpful(e.g., aspirates of the subcutaneous mass iffacial deformity). � Coagulation profile.
IMAGING� Survey skull radiography—may showasymmetrical destruction of turbinatesaccompanied by a soft tissue mass effect; maysee fluid density in the frontal sinusessecondary to outflow obstruction. � Thoracicradiography—evaluate for lung metastasis(uncommon). � CT or MRI best imagingmethod for local staging and observingintegrity of cribriform plate or orbitalinvasion, and also used for therapeuticplanning.
DIAGNOSTIC PROCEDURES� Blood pressure, thorough oral exam underanesthesia. � Rhinoscopy may permit visualobservation of the mass; avoid progressingcaudally into the cribriform plate. Proceduremay not be necessary if mass confirmed viaadvanced imaging or when facial deformity isidentified. � Tissue biopsy necessary fordefinitive diagnosis. Biopsies may beperformed blind, following advancedimaging, using pinch biopsy instrument,cannula (closed suction), or hydropulsiontechniques. � Cytologic evaluation of regionallymph nodes to detect metastatic disease.
TREATMENT� Surgery alone ineffective due to extent andinvasiveness. � Turbinectomy may be donebefore or after irradiation. � Radiationtherapy is standard therapy and provides bestclinical results in dogs and cats.
MEDICATIONSDRUG(S)� Chemotherapy may benefit some patients.Various drugs have been described includingcisplatin (dogs only), carboplatin,doxorubicin, and piroxicam. Consult with anoncologist for more details. � Adequateanalgesic therapy should be employed asneeded in patients suffering from invasivedisease with bone destruction, signs of pain,and painful radiation therapy side effects.� Novel therapies may be considered withcases that are unresponsive to standardtherapy.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSCisplatin—never use in cats
FOLLOW-UPPATIENT MONITORINGSurvey skull radiography or preferablyCT/MRI when clinical signs recur orperiodically.
EXPECTED COURSE AND PROGNOSIS� Untreated—median survival around 3–4months. � Radiation therapy—mediansurvival times around 12–18 months in dogsand 10–18 months in cats; 1-year survival rate20–57% (dogs and cats); 2-year survival rate20–48% (dogs and cats). � Presence of braininvolvement or metastatic disease (advancedstage) are poor prognostic indicators.� Ophthalmic complications of radiationtherapy—more likely in dogs than cats.� Chronic rhinitis is common followingradiation therapy for sinonasal tumors andmay require symptomatic therapy.
MISCELLANEOUSABBREVIATIONS� CT = computed tomography � MRI =magnetic resonance imaging
Suggested ReadingAdams WA, Bjorling DE, McAnulty JF, et al.
Outcome of accelerated radiotherapy aloneor accelerated radiotherapy followed byexenteration of the nasal cavity in dogs withintranasal neoplasia: 53 cases (1990–2002).JAVMA 2005, 227:936–941.
Hahn KA, Knapp DW, Richardson RC,Matlock CL. Clinical response of nasaladenocarcinoma to cisplatin chemotherapyin 11 dogs. JAVMA 1992, 200:355–357.
Henry CJ, Brewer WG, Tyler JW, et al.Survival in dogs with nasal adenocarcinoma:64 cases (1981–1995). J Vet Intern Med1998, 12:436–439.
LaDue TA, Dodge R, Page RL, et al. Factorsinfluencing survival after radiotherapy ofnasal tumors in 130 dogs. Vet RadiolUltrasound 1999, 40:312–317.
Langova V, Mutsaers AJ, Phillips B, Straw R.Treatment of eight dogs with nasal tumourswith alternating doses of carboplatin anddoxorubicin in conjunction with oralpiroxicam. Australian Vet J 2004,82:676–680.
Rassnick KM, Goldkamp CE, Erb HN, et al.Evaluation of factors associated with survivalin dogs with untreated nasal carcinomas:139 cases (1993–2003). JAVMA 2006,229:401–406.
Author Louis-Philippe de LorimierConsulting Editor Timothy M. Fan
BLBS078-CF_A17 BLBS078-Tilley March 21, 2011 9:47
Canine and Feline, Fifth Edition 27
Adenocarcinoma, Pancreas A
BASICSOVERVIEW� Malignant tumor of ductal or acinar originarising from the exocrine pancreas.� Usually metastatic by the time of diagnosis.
SIGNALMENT� Rare in dogs—0.5–1.8% of all tumors� Rare in cats—2.8% of all tumors� Older female dogs and Airedale terriers athigher risk than others� Median age (dogs)—9.2 years
SIGNS� Non-specific—fever; vomiting; weakness;anorexia; icterus; maldigestion; weight loss.� Abdominal pain—variable.� Metastasis to bone and soft tissue common.� Pathologic fractures secondary to metastasisreported.� Abdominal mass.� Paraneoplastic syndromes of epidermalnecrosis, hyperinsulinemia, andhyperglucagonemia may be present.
CAUSES & RISK FACTORSUnknown
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Primary pancreatitis; may be concurrentand complicate or delay early diagnosis.� Pancreatic pseudocyst.� Pancreatic nodular hyperplasia.� Hepatic neoplasia.� Other causes of vomiting and icterus.
CBC/BIOCHEMISTRY/URINALYSIS� Usually non-specific changes (e.g., mildanemia and neutrophilia).� Hyperamylasemia less reliable thanhyperlipasemia.� Lipase concentrations are often markedlyelevated and may be of tumor origin andtherefore can serve as a non-invasivebiochemical marker of neoplasia of thepancreas and liver in dogs.
OTHER LABORATORY TESTSRarely there may be significant metabolicalterations that affect glucagon, insulin, andamino acid concentrations.
IMAGING� Abdominal radiographs may reveal a massor loss of serosal detail associated withconcurrent pancreatitis.� Ultrasonography may reveal a mass orconcurrent pancreatitis (mixed echogenicity,large pancreas, hyperechoic peripancreaticfat). Pancreatic thickening, abdominaleffusion, and single to multiple nodules ofvarying size may be identified. Sonographicfindings may be impossible to distinguishfrom pancreatic nodular hyperplasia. Rarelythe ultrasound of the pancreas may appearnormal except for dilation of the pancreaticduct.
DIAGNOSTIC PROCEDURES� Surgical biopsy—definitive diagnosis� Fine-needle aspirate cytology—supportivediagnosis
TREATMENT� None reported curative.� Palliation of pain and intestinal and biliaryobstruction—surgery, if necessary.� Partial or total pancreatectomy.� Treat concurrent pancreatitis.� Antiemetics and supportive care (hydrationand caloric requirements).
MEDICATIONSDRUG(S)� Gemcitabine is used in humans for thetreatment of pancreatic carcinoma, and whileused in dogs with cancer, it has not beenestablished as the standard of care for dogswith pancreatic adenocarcinoma.� Always consult a veterinary oncologist forupdates in treating this rare neoplasm.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UPPOSSIBLE COMPLICATIONSIntestinal Obstruction� Biliary obstruction� Pancreatic abscess
� Peritonitis� Metastasis
EXPECTED COURSE AND PROGNOSISProgression to death is often rapid given thatthere is no successful curative treatmentavailable.
MISCELLANEOUSASSOCIATED CONDITIONSGastrin-secreting pancreatic carcinoma(gastrinoma) has been reported in dogs andcats. Clinical signs are associated withhypergastrinemia, which results ininappropriate hydrochloric acid secretion bythe stomach, leading to gastroduodenitis.
Suggested ReadingCave T, Evans H, Hargreavest J, et al.
Metabolic epidermal necrosis in a dogassociated with pancreatic adenocarcinoma,hyperglucagonaemia, hyperinsulinaemia,and hypoaminoacidaemia. J Small AnimPract 2007, 48:522–526.
Hecht S, Penninck DG, Keating JH. Imagingfindings in pancreatic neoplasia and nodularhyperplasia in 19 cats. Vet RadiolUltrasound 2006, 48:45–50.
Lurcye JC, Behrend EN. Endocrine tumors.Vet Clin North Am Small Anim Pract 2001,31:1083–1110.
Morrison WB. Primary cancers andcancer-like lesions of the liver, biliaryepithelium, and exocrine pancreas. In:Morrison WB, ed., Cancer in Dogs andCats: Medical and Surgical Management.Jackson, WY: Teton NewMedia, 2002,pp. 535–544.
Newman SJ, Steiner JM, Woosley K, et al.Correlation of age and incidence ofpancreatic exocrine nodular hyperplasia inthe dog. Vet Pathol 2005, 42:510–513.
Quigley KA, Jackson ML, Haines DM.Hyperlipasemia in 6 dogs with pancreatic orhepatic neoplasia: Evidence for tumor lipaseproduction. Vet Clin Pathol 2001,30:114–120.
Author Wallace B. MorrisonConsulting Editor Timothy M. Fan
BLBS078-CF_A18 BLBS078-Tilley March 21, 2011 9:53
28 Blackwell’s Five-Minute Veterinary Consult
Adenocarcinoma, ProstateA
BASICSOVERVIEW� Prostatic adenocarcinoma is a malignanttumor that occurs in both neutered and intactmale dogs.� Although this neoplasm represents < 1% ofall canine malignancies, it is the mostcommon prostatic disorder in neutered maledogs.� Metastases to regional lymph nodes, lungs,and the lumbosacral skeleton are common.
SIGNALMENT� Dogs and rarely cats� Medium- to large-breed intact or neuteredmale dogs� Median age of 9–10 years
SIGNSHistorical Findings� Tenesmus (with the production ofribbon-like stool)� Weight loss� Stranguria and dysuria� Rear limb lameness� Lethargy� Exercise intolerance
Physical Examination Findings� A firm, asymmetrical, and immobileprostate gland.� Prostatomegaly is common, but is notalways present.� Pain may be elicited in response toabdominal or rectal palpation.� Caudal abdominal mass, cachexia, pyrexia,and dyspnea may also be identified.
CAUSES & RISK FACTORSNeutered males are at increased risk forprostatic neoplasia
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other primary neoplasia (i.e., squamous cellcarcinoma, transitional cell carcinoma).� Metastatic or locally invasive neoplasia (i.e.,transitional cell carcinoma).� Acute or chronic prostatitis, benignprostatic hypertrophy, and prostatic cysts arepossible differentials in intact male dogs butare highly unlikely in neutered dogs.
CBC/BIOCHEMISTRY/URINALYSIS� Inflammatory leukogram possible.� Alkaline phosphatase may be high.
� Post-renal azotemia may be present ifurethral obstruction exists.� It is prudent to evaluate urine samples viacystocentesis and free-catch techniques, ashematuria, pyuria, and malignant epithelialcells may be observed in free-catch samplesbut are unusual in samples obtained bycystocentesis.
OTHER LABORATORY TESTSSerum and seminal plasma markers such asacid phosphatase, prostate specific antigen,and canine prostate specific esterase are notelevated in dogs with PAC.
IMAGING� Thoracic radiography—metastases mayappear as pulmonary nodules or increasedinterstitial markings.� Abdominal radiography—sublumbarlymphadenomegaly, mineralization of theprostate, lytic lesions to the lumbar vertebraeor pelvis may be seen.� Abdominal ultrasonography—focal tomultifocal hyperechogenicity with asymmetryand irregular prostatic outline, ± prostaticmineralization.� Contrast cystography may help differentiateprostatic from urinary bladder disease.
DIAGNOSTIC PROCEDURES� Prostatic aspirate (percutaneous ortransrectal).� Prostatic wash.� Prostatic biopsy performed percutaneouslyor surgically.� Percutaneous biopsy has been associatedwith tumor seeding along the biopsy tract.
TREATMENT� Prostatectomy if local disease (success of thisprocedure depends on the skill of the surgeonand extent of disease).� Radiation therapy may palliate signs andprolong survival.� Neutering—however, most tumors are notandrogen responsive.
MEDICATIONSDRUG(S)� Chemotherapy—carboplatin, cisplatin, ordoxorubicin; may offer short-term benefit.
� Pain relief with NSAIDs, morphine-deriveddrugs.� Stool softeners to relieve tenesmus.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UPPATIENT MONITORINGAbility to urinate and defecate, pain secondaryto skeletal metastases, quality of life.
PREVENTION/AVOIDANCEKeeping dogs sexually intact may decreaserisk
POSSIBLE COMPLICATIONS� Urethral obstruction� Metastasis to regional lymph nodes,skeleton, and lungs
EXPECTED COURSE AND PROGNOSISGuarded to poor, survival of 2–6 monthsdepending upon presenting clinicalsymptoms.
MISCELLANEOUSASSOCIATED CONDITIONSNone
AGE-RELATED FACTORSNone
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A
ABBREVIATIONS� NSAID = nonsteroidal anti-inflammatorydrug� PAC = prostatic adenocarcinoma
Suggested ReadingBryan JN, et al. A population study of
neutering status as a risk factor for canineprostate cancer. Prostate 2007,67:1174–1181.
Author Ruthanne ChunConsulting Editor Timothy M. Fan
BLBS078-CF_A19 BLBS078-Tilley March 21, 2011 9:54
Canine and Feline, Fifth Edition 29
Adenocarcinoma, Renal A
BASICSOVERVIEW� Accounts for < 1% of all reportedneoplasms in dogs.� Renal tumors tend to be highly metastatic,locally invasive, and often bilateral.� Renal cystadenocarcinoma, a rare heritablesyndrome with a less aggressive behavior andbetter long-term prognosis than renaladenocarcinoma, has been described inGerman shepherd dogs.
SIGNALMENT� Adenocarcinoma—older (8–9 years) dogs,1.6:1 male-to-female ratio, no breedpredilection.� Cystadenocarcinoma—German shepherddogs, often female.
SIGNS� Adenocarcinoma—insidious, non-specificsigns such as weight loss, inappetance,lethargy, hematuria, and pale mucousmembranes.� Cystadenocarcinoma—may present fornodular dermatofibrosis, a syndrome ofpainless, firm, fibrous lesions of the skin andsubcutaneous tissues.
CAUSES & RISK FACTORS� Adenocarcinoma—unknown.� Cystadenocarcinoma—heritable in Germanshepherd dogs.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other primary neoplasia (i.e., lymphoma,nephroblastoma).� Metastatic neoplasia (i.e.,hemangiosarcoma).� Renal adenoma or cyst.� Pyelonephritis.
CBC/BIOCHEMISTRY/URINALYSIS� CBC may show paraneoplasticpolycythemia or leukocytosis, or anemia.
� Biochemistry may be normal, or may revealazotemia.� Urinalysis may show hematuria,proteinuria, bacteriuria, or casts.
OTHER LABORATORY TESTSUrine culture and sensitivity
IMAGING� Thoracic radiographs—metastatic diseasereported in up to 16% of patients.� Abdominal radiographs—mass visualized in81% of patients.� Abdominal ultrasonography, CT, orcontrast radiography—useful in identifyingand staging the disease.
DIAGNOSTIC PROCEDURESRenal biopsy (ultrasound-guided or surgical)for definitive diagnosis.
TREATMENT� Aggressive surgical excision is the treatmentof choice for unilateral disease.� Successful chemotherapeutic managementof either disease has not been described.� Supportive management for patients inrenal failure may be necessary.
MEDICATIONSDRUG(S)None
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UPPATIENT MONITORING� Renal failure—measure serum urea nitrogenand creatinine; urinalysis.� Quality of life if bilateral or otherwisenon-surgical disease.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONS� Renal failure� Metastatic disease� Invasion of local vital structures (vena cava,aorta)
EXPECTED COURSE AND PROGNOSIS� Adenocarcinoma—median reported survivalof 49 dogs was 16 months (range 0–59).� Cystadenocarcinoma—few large studies ofthis rare disease, reported median survival of12+ months with no definitive therapy.
MISCELLANEOUSASSOCIATED CONDITIONS� The paraneoplastic syndromes ofhypertrophic osteopathy, polycythemia, and aneutrophilic leukocytosis have been reportedin isolated cases.� Renal failure.� Nodular dermatofibrosis and uterineleiomyomas are commonly associated withcystadenocarcinoma.
ABBREVIATIONS� CT = computed tomography
Suggested ReadingBryan JN, et al. Primary renal neoplasia of
dogs. J Vet Intern Med 2006,20:1155–1160.
Knapp DW. Tumors of the urinary system.In: Withrow SJ, Vail DM, eds., SmallAnimal Clinical Oncology, 4th ed.Philadelphia: Saunders, 2007, pp. 649–658.
Author Ruthanne ChunConsulting Editor Timothy M. Fan
BLBS078-CF_A20 BLBS078-Tilley March 21, 2011 9:55
30 Blackwell’s Five-Minute Veterinary Consult
Adenocarcinoma, Salivary GlandA
BASICSOVERVIEW� Tumor arising from major (e.g., parotid,mandibular, sublingual, or zygomatic) orminor salivary glands.� Mandibular or parotid glands constitute80% of cases.� Mandibular gland most frequently affectedin dogs.� Parotid gland most frequently affected incats.� Locally invasive.� Cats typically have more advanced diseasethan dogs at time of diagnosis.� Metastasis—regional lymph node in 39% ofcats and 17% of dogs at diagnosis; distantmetastasis reported in 16% of cats and 8% ofdogs at diagnosis but may be slow to develop.� Other salivary gland neoplasms—carcinoma; squamous cell carcinoma; mixedneoplasia.� Epithelial malignancies—constitute roughly85% of salivary gland tumors.� Fibrosarcomas, lipomas, mast cell tumors,and lymphomas have involved the salivaryglands by direct extension and invasion. Aconcurrent malignant fibrous histiocytoma(giant cell type) and malignant mixed tumor(likely of ductal origin) within the salivarygland has also been described.� Adenomas comprise only 5% of salivarytumors.
SIGNALMENT� Dogs and cats� Mean age, 10–12 years� Siamese cats—may be at relatively higherrisk� Male cats affected twice as often as femalecats� No other breed or sex predilection has beendetermined
SIGNS� Unilateral, firm, painless swelling of theupper neck (mandibular and sublingual), earbase (parotid), upper lip or maxilla(zygomatic), or mucous membrane of lip(accessory or minor salivary tissue).� Other signs may include halitosis, weightloss, anorexia, dysphagia, exophthalmus,Horner’s syndrome, sneezing, and dysphonia.
CAUSES & RISK FACTORSUnknown
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Squamous cell carcinoma.� Mucocele.� Abscess.� Soft tissue sarcoma, e.g., malignant fibroushistiocytoma or fibrosarcoma.� Lymphoma.
CBC/BIOCHEMISTRY/URINALYSISResults often normal
OTHER LABORATORY TESTSN/A
IMAGING� Regional radiographs usually are normal;may see periosteal reaction on adjacentbones or displacement of surroundingstructures.� MRI or CT imaging allows superiordiscrimination of tumor for surgery and/orradiation treatment planning.� Thoracic radiographs indicated to check forlung metastases.
DIAGNOSTIC PROCEDURES� Cytologic examination of aspirate maydifferentiate salivary adenocarcinoma frommucocele and abscess.� Needle core or wedge biopsy forhistopathology—definitive diagnosis.
TREATMENT� Aggressive surgical resection—whenpossible; most are invasive and difficult toexcise completely.� Radiotherapy—good local control andprolonged survival in three reported cases.� Aggressive local resection (usuallyhistologically incomplete) followed byadjuvant radiation can achieve local controland long-term survival, but further studies areneeded to determine the most effectivetreatment, including the possible role forchemotherapy.
MEDICATIONSDRUG(S)Chemotherapy efficacy is largely unreported;however, may be indicated fortreatment/palliation of metastatic disease.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UPPATIENT MONITORINGEvaluations—physical examination andthoracic radiographs every 3 monthsreasonable if aggressive surgery and/orradiation therapy employed.
POSSIBLE COMPLICATIONSTemporary acute side effects (e.g., moistdermatitis and alopecia) expected withradiation therapy.
EXPECTED COURSE AND PROGNOSIS� Improved survival time in dogs withoutevidence of nodal or distant metastasis atdiagnosis; clinical stage not prognostic forcats.� Median survival 550 days for dogs and 516days for cats in retrospective study.� Local control through radiation or multiplesurgeries remains critical.
MISCELLANEOUSABBREVIATIONS� CT = computed tomography� MRI = magnetic resonance imaging
Suggested ReadingHammer A, Getzy D, Ogilvie G, et al.
Salivary gland neoplasia in the dog and cat:Survival times and prognostic factors.JAAHA 2001, 37:478–482.
Author Anthony J. MutsaersConsulting Editor Timothy M. Fan
BLBS078-CF_A21 BLBS078-Tilley March 21, 2011 10:0
Canine and Feline, Fifth Edition 31
Adenocarcinoma, Skin (Sweat Gland, Sebaceous) A
BASICSOVERVIEWMalignant growth originating from sebaceousor apocrine sweat glands of the skin.
SIGNALMENT� Apocrine sweat gland—rare in dogs,uncommon in cats.� Sebaceous gland—rare in both dogs andcats.� Middle-aged to older pets.� Female dogs overrepresented for apocrineadenocarcinoma in one study.
SIGNS� May appear as solid, firm, raised, superficialskin lesions.� May be ulcerated and bleeding andaccompanied by inflammation of thesurrounding tissue.� Apocrine sweat gland—often poorlycircumscribed, ulcerated; very invasive intounderlying tissue; may occur anywhere on thebody, frequently affecting the trunk in dogs.� Sebaceous gland—often ulcerated andinflamed, moderate risk of lymph nodeinvolvement.
CAUSES & RISK FACTORSUnknown
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other more frequent skin tumors� Cutaneous histiocytic diseases� Immune-mediated skin diseases� Bacterial/fungal infections
CBC/BIOCHEMISTRY/URINALYSISNormal
OTHER LABORATORY TESTSN/A
IMAGINGThoracic radiographs recommended at thetime of diagnosis to assess for distantmetastases.
DIAGNOSTIC PROCEDURES� Biopsy for histopathology and definitivediagnosis� Cytologic examination or biopsy of regionallymph nodes
PATHOLOGIC FINDINGS� Apocrine sweat gland carcinomas aretypically invasive into the underlying stromaand blood vessels, and often show poorlydemarcated borders and a high mitotic index.� Sebaceous gland adenocarcinomas oftenreveal lymphatic vessel invasion.
TREATMENT� Aggressive en bloc surgical excision,including resection of draining lymph node,recommended for both types.Histopathologic analysis of lymph nodesassists with determining prognosis andestablishing adjuvant treatment plan.� Margins of entire tissue specimen must beevaluated histologically to assess completenessof resection.� Radiation therapy may be recommended fortreatment of draining lymph nodes site afterresection to prevent recurrence anddevelopment of regional metastasis; treatmentof primary tumor site recommended whenwide and complete resection not possible.
MEDICATIONSDRUG(S)� Multiple chemotherapy drugs have beenused for the treatment of both tumor types, inboth species, with anecdotal benefit(including cisplatin, carboplatin,mitoxantrone, and gemcitabine).� Contact a veterinary oncologist for anyupdated treatments that may be available.� Nonsteroidal anti-inflammatory drugs andother analgesics are recommended, asindicated, for pain control.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSNone
FOLLOW-UP� Sebaceous gland adenocarcinoma—littleknown about the metastatic potential of thismalignancy, but may be rapidly metastatic toregional lymph nodes in some patients;long-term prognosis is anecdotally good withmultimodal therapy combining aggressivesurgery, chemotherapy, and radiation therapy.� Apocrine gland adenocarcinoma—fair togood long-term prognosis; the histologicfinding of vascular invasion a negativeprognostic factor systemic metastases;aggressive surgical resection (local andregional tumor control) followed by adjuvantchemotherapy is recommended to improvesurvival. A study reported a post-excisionalmedian survival time of 30 months in dogs.
MISCELLANEOUSSuggested ReadingCarpenter JL, Andrews LK, Holzworth J.
Tumors and tumor like lesions. In:Holzworth J, ed., Diseases of the Cat:Medicine and Surgery. Philadelphia:Saunders, 1987, pp. 406–596.
Pakhrin B, Kang MS, Bae IH, et al.Retrospective study of canine cutaneoustumors in Korea. J Vet Sci 2007, 8:229–236.
Simko E, Wilcock BP, Yager JA. Aretrospective study of 44 canine apocrinesweat gland adenocarcinomas. Can Vet J2003, 44(1):38–42.
Thomas RC, Fox LE. Tumors of the skin andsubcutis. In: Morrison WB, ed., Cancer inDogs and Cats: Medical and SurgicalManagement. Jackson, WY: TetonNewMedia, 2002, pp. 469–488.
Author Louis-Philippe de LorimierConsulting Editor Timothy M. FanAcknowledgement The author and editorsacknowledge the prior contribution of PhyllisGlawe.
BLBS078-CF_A22 BLBS078-Tilley July 15, 2011 17:53
32 Blackwell’s Five-Minute Veterinary Consult
Adenocarcinoma, Stomach, Small and Large Intestine, RectalA
BASICSOVERVIEW� Uncommon tumor arising from theepithelial lining of the gastrointestinal tract.� Prognosis guarded to poor.
SIGNALMENT� Dogs more commonly affected than cats.� Middle-aged to older (> 6 years) animals;age range 3–13 years.� No breed predisposition.� More common in males than females.
SIGNSHistorical Findings� Signs related to gastrointestinal tract.� Stomach—vomiting, anorexia, weight loss,hematemesis, and melena.� Small intestine—vomiting, weight loss,borborygmus, flatulence, and melena.� Large intestine and rectum—mucous andblood-tinged feces and tenesmus.
Physical Examination Findings� Stomach—non-specific.� Small intestine—may feel midabdominalmass; distended, painful loops of small bowel;melena on rectal exam.� Large intestine and rectum—palpable massper rectum, may form annular ring, ormultiple nodular lesions protruding into thecolon; bright red blood on feces.
CAUSES & RISK FACTORS� Unknown.� Nitrosamines—reported as causative agentin experimental literature.� Possible genetic cause—gastricadenocarcinomas in related Belgian shepherdsand in Dutch Tervueren shepherds.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Foreign body� Inflammatory bowel disease� Lymphoma� Parasites� Leiomyoma� Leiomyosarcoma� Pancreatitis
CBC/BIOCHEMISTRY/URINALYSIS� Stomach and small intestine—may seemicrocytic, hypochromic anemia(iron-deficiency anemia).� Large intestine and rectum—nocharacteristic changes.
OTHER LABORATORY TESTSFecal occult blood may be positive; diet mayaffect results—can recheck to confirm afterfeeding non-meat diet for 3 days.
IMAGING� Ultrasound—may reveal a thickenedstomach or bowel wall; may see mass in thegastrointestinal tract, enlarged lymph nodes.� Positive contrast radiography—filling defect(stomach); intraluminal space-occupying orannular constriction (small bowel); gastricneoplasm most often found in distaltwo-thirds of stomach.� Double contrast radiography—largeintestine and rectum; polypoid or annularspace-occupying masses.
DIAGNOSTIC PROCEDURES� Ultrasound-guided fine-needle aspirate ofbowel mass or enlarged lymph node mayreveal carcinoma cells on cytology, which canbe useful to rule out lymphoma.� Endoscopic biopsy may be non-diagnosticbecause tumors are frequently deep to themucosal surface; thus surgical biopsyfrequently required.
TREATMENT� Surgical resection—treatment of choice;seldom curative.� Gastric—usually non-resectable.� Small intestine—remove by resection andanastomosis; metastasis to regional lymphnodes and the liver common.� Large intestine and rectal—mayoccasionally be resected by a pull-throughsurgical procedure; metastasis common;transcolonic debulking may provide palliationof obstruction.
MEDICATIONSDRUG(S)� Chemotherapy—only anecdotal reports,usually unsuccessful.� Piroxicam 0.3 mg/kg PO q24h can providepalliation for large intestinal and rectaltumors.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSSeek advice before initiating treatment withcytotoxic drugs.
FOLLOW-UPPhysical examination, thoracic radiographs,and abdominal ultrasound—at 1, 3, 6, 9, and12 months post-surgery.
EXPECTED COURSE AND PROGNOSISDogs� Overall poor; pedunculated rectal tumorsdo best; most cases recur locally, developmetastasis, or both rapidly.� Median survival gastric—2 months.� Median survival small intestinal—10months.� Mean survival large intestinal—annular1.6 months versus pedunculated 32 months.
Cats� Guarded.� Few reported cases, but may have prolongedsurvival (> 1 year).
MISCELLANEOUSSuggested ReadingCrawshaw J, Berg J, Sardinas JC, et al.
Prognosis for dogs with nonlymphomatoussmall intestinal tumors treated by surgicalexcision. JAAHA 1998, 34:451–456.
Lubbes D, Mandigers PJ, Heuven HC, et al.[Incidence of gastric carcinoma in DutchTervueren shepherd dogs born between1991 and 2002]. Tijdschr Diergeneeskd2009, 134:606–610.
Morrison WB. Nonlymphomatous cancers ofthe esophagus, stomach, and intestines. In:Morrison WB, ed., Cancer in Dogs andCats: Medical and Surgical. Jackson, WY:Teton NewMedia, 2002, pp. 527–534.
Swann HM, Holt DE. Canine gastricadenocarcinoma and leiomyosarcoma: Aretrospective study of 21 cases (1986–1999)and literature review. JAAHA 2002,38:157–164.
Takiguchi M, Yasuda J, Hashimoto A, et al.Esophageal/gastric adenocarcinoma in adog. JAAHA 1997, 33:42–44.
Author Laura D. GarrettConsulting Editor Timothy M. Fan
BLBS078-CF_A23 BLBS078-Tilley June 16, 2011 10:8
Canine and Feline, Fifth Edition 33
Adenocarcinoma, Thyroid—Dogs A
BASICSDEFINITIONA malignant tumor arising from the follicularor parafollicular cells (medullary/C-cells) ofthe thyroid gland.
PATHOPHYSIOLOGY� About 60% of patients are euthyroid, 30%hypothyroid, and 10% hyperthyroid.� Typically very invasive tumors with high rateof metastasis (lungs, retropharyngeal lymphnodes, liver), with up to 35–40% of dogshaving metastasis at the time of diagnosis.� Animals with bilateral tumors have a sixteentimes greater risk of developing metastaticdisease than animal with unilateral tumors.
SYSTEMS AFFECTED� Cardiovascular—hyperthyroid dogs areusually tachycardic and may have systemichypertension; may see anemia and DIC inadvanced disease.� Endocrine/Metabolic—affected dogs maybe hypothyroid, euthyroid, or hyperthyroid;hypercalcemia may be seen as a paraneoplasticsyndrome or secondary to concurrentparathyroid hyperplasia or parathyroidadenocarcinoma.� Respiratory—dogs may be dyspneic owingto a space-occupying mass adjacent to thetrachea; metastasis to the lungs common.
GENETICSUnknown
INCIDENCE/PREVALENCEAccounts for 1.2–3.8% of all canine tumorsand represents 10–15% of all primary headand neck tumors.
GEOGRAPHIC DISTRIBUTIONMay be more common in iodine-deficientareas
SIGNALMENTSpeciesDogs
Breed PredilectionsBoxers, golden retrievers, and beagles atincreased risk but seen in any breed.
Mean Age and RangeOlder dogs (median 9–11 years; range 4–18years)
Predominant SexNo gender predilection
SIGNSGeneral Comments� Usually not diagnosed until a large mass ispalpable� Approximately 65% are unilateral, 35% arebilateral
Historical Findings� Palpable mass/swelling in cervical neck,coughing, dyspnea, dysphagia, dysphonia,facial edema, neck pain.
� If functional thyroid tumor—may seepolyuria, polydypsia, polyphagia, weight loss,restless behavior, diarrhea.� If hypothyroid—may see poor hair coat,weight gain, lethargy.
Physical Examination Findings� Freely movable or fixed cervical mass,unilateral or bilateral.� Rarely may see Horner’s syndrome, orcranial vena cava syndrome.� If hyperthyroid—cardiac arrhythmias ormurmurs.
CAUSESUnknown
RISK FACTORS� Untreated hypothyroidism has been shownto be a risk factor in a colony of beagles.� Breed predilection.� Iodine deficiency.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other primary neoplasms—lymphoma; softtissue sarcoma; salivary glandadenocarcinoma; parathyroid carcinoma;carotid body tumor.� Secondary tumors—metastatic oralsquamous cell carcinoma; oral melanoma.� Inflammatory—abscess or granuloma.� Salivary mucocele.
CBC/BIOCHEMISTRY/URINALYSIS� Usually normal.� May see non-regenerative normocyticnormochromic anemia of chronic disease,leukocytosis.� Rare—hypercalcemia; isosthenuria; DIC.
OTHER LABORATORY TESTSThyroid hormone (T4 and/or free T4 levels)and endogenous TSH levels.
IMAGING� Thoracic radiography (3 view)—evaluationof lungs and other thoracic structures formetastasis.� Cervical ultrasonography and computedtomography—evaluation of tissue of origin,vascularity, invasion, and cervical lymphnodes.� Technetium-99m scintigraphy to evaluatefor ectopic thyroid tissue or metastatic lesions.� Radioiodine studies—may provideinformation about the tumor’s ability toproduce thyroid hormone.
DIAGNOSTIC PROCEDURESBiopsyTru-Cut not recommended owing to high riskof severe hemorrhage; open biopsy usuallyrequired.
Cytology� Examination of fine-needle aspirate fromtumor and palpable regional lymph nodes.
� Specimen almost always heavilycontaminated with blood owing to highlyvascular nature of tumor.� Homogeneous population of epithelial cells,sometimes with colloid and/ortyrosine-containing granules.� Unable to differentiate malignant frombenign thyroid cells; but almost all thyroidneoplasms in dogs are malignant.
PATHOLOGIC FINDINGSGross� Characterized by high vascularity with areasof hemorrhage and necrosis.� Usually poorly encapsulated; often invadeadjacent tissues (e.g., trachea and esophagus,and surrounding vasculature); may adhere tothe jugular vein, carotid artery, andvagosympathetic trunk.
Histopathology� Three main types—follicular, papillary, andcompact (solid); mixed follicular and solidtumors most common in dogs.� C-cell (e.g., parafollicular, medullary)carcinomas less common.
TREATMENTAPPROPRIATE HEALTH CARE� Definitive treatment is dependent on tumorstage (tumor size, mobility and evidence ofmetastatic disease).� Complete surgical excision recommendedfor freely movable thyroid tumors.� Full course external beam radiation therapyrecommended preoperatively for largetumors, as a sole therapy for non-resectabletumors, or post-operatively for incompletelysurgically removed tumors.� Palliative radiation and/or chemotherapyrecommended for tumors that are metastaticat presentation.� Also can use iodine-131 but doses are verylarge (60–100 mCi) and therefore there arelimited facilities that offer this therapy.
NURSING CAREVaries with signs on examination
ACTIVITYRestrict activity if dyspneic
DIETN/A
CLIENT EDUCATION� Warn owners of the importance ofcontrolling heart rate and rhythm inhyperthyroid patients and of the possibility ofepisodes of collapse.� Warn owners of possible post-operativelaryngeal paralysis and intraoperativehemorrhage.� Warn owners of acute radiation therapytoxicities—moist desquamation, laryngitis,tracheitis, esophagitis.
BLBS078-CF_A23 BLBS078-Tilley June 16, 2011 10:8
34 Blackwell’s Five-Minute Veterinary Consult
Adenocarcinoma, Thyroid—Dogs (Continued)A
SURGICAL CONSIDERATIONSSee “Appropriate Health Care”
Risks� Marked hemorrhage—tumors highlyvascular and invasive into surroundingstructures including vasculature; may needblood transfusion and intensive post-operativecare.� Laryngeal paralysis—owing to trauma torecurrent laryngeal nerve.� Damaged parathyroid glands—may occurduring surgery.
MEDICATIONSDRUG(S) OF CHOICE� Chemotherapeutic agents:
◦ Chemotherapy is recommended as a soletherapy, or in combination with surgeryand/or radiation therapy.◦ Cisplatin (60 mg/m2 every 3 weeks) ordoxorubicin (30 mg/m2 every 3weeks)—reported to effect partialremission in approximately 50% of cases.◦ Cisplatin—nephrotoxic; must use withsaline diuresis (18.3 mL/kg/hour IV over6 hours; give cisplatin after 4 hours).
� Antiemetics for cisplatin therapy:◦ Maropitant 1 mg/kg SC before cisplatin,or◦ Dolasetron 0.6–1 mg/kg IV or PO q24h,or◦ Butorphanol 0.4 mg/kg IM before andafter cisplatin.
� Thyroid management:◦ Thyroxine—maintenance doses todecrease TSH production have beenrecommended; some tumors contain TSHreceptors; value of hormone-replacementtherapy in affected dogs not determined.◦ Methimazole 5 mg PO q8h for mediumto large dogs; may be beneficial forhyperthyroid patients.◦ β-blockers—may be indicated fortachycardia or hypertension inhyperthyroid patients.
CONTRAINDICATIONS� Doxorubicin is cumulatively toxic to cardiacmyocytes causing decreased myocardialfunction. Do not give to animals with poorcardiac function or dilated cardiomyopathy.� Cisplatin is nephrotoxic; do not give toanimals with renal disease.
PRECAUTIONSChemotherapy can cause gastrointestinal,bone marrow, cardiac, and othertoxicities—seek advice from a medicaloncologist if unfamiliar with cytotoxic drugs.
POSSIBLE INTERACTIONSVerapamil—may potentiatedoxorubicin-induced cardiotoxicity
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORING� Serum calcium concentration—if bilateralthyroidectomy was performed; signs ofhypocalcemia (agitation, panting, muscletremors, tetany, and seizures) may beobserved.
◦ Treat with 10% calcium gluconate (1–1.5mL/kg IV over 10–20 minutes).◦ Maintain serum calcium withdihydrotachysterol (vitamin D) orally.
� Thyroid hormone—supplementation withthyroxine may be necessary after bilateralthyroidectomy.� TSH concentration—a goal of thyroxinsupplementation is to downregulate thebody’s secretion of TSH.� Site of primary tumor—physicalexamination and cervical ultrasound; thoracicradiographs every 3 months to detectpulmonary metastasis.
PREVENTION/AVOIDANCEUnknown
POSSIBLE COMPLICATIONS� Tumor—anemia; thrombocytopenia;hypercalcemia; DIC; respiratory distress.� Chemotherapy—dilated cardiomyopathy;renal failure; pancreatitis; sepsis;gastrointestinal upset.� Surgery—hemorrhage; hypothyroidism;hypoparathyroidism leading to hypocalcemia;laryngeal paralysis.� Radiotherapy—acute side effects—moistdesquamation, pharyngeal mucositis;esophagitis; tracheitis; late sideeffects—alopecia, and skin or coat colorchange (at radiation site).
EXPECTED COURSE AND PROGNOSIS� Prognosis—related to stage of disease(tumor size, mobility and evidence ofmetastatic disease) with small, non-attachedunilateral, non-metastatic tumors having bestprognosis.� MST after surgical removal of freelymovable thyroid tumor is > 36 months.� For animals treated with full course externalbeam radiation therapy—progression freesurvival at 1 year—80%, and 72% at 3 yearsin one study and in another study MST24.5 months.
� Palliative radiation therapy in 13dogs—MST 24 months.� 131I therapy in combination withsurgery—MST 34 months, or 131I aloneMST 30 months.� Animals treated with cisplatin alone (13dogs)—overall response rate was 53%, medianprogression free interval for responders was202 days and overall MST was 98 days.
MISCELLANEOUSASSOCIATED CONDITIONS� Non-thyroidal malignancies common� Multiple endocrine neoplasia reported
AGE-RELATED FACTORSNone
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGIt is not recommended to breed animals withcancer. Chemotherapy is teratogenic—do notgive to pregnant animals.
SYNONYMSThyroid carcinoma
ABBREVIATIONS� DIC = disseminated intravascularcoagulation� MST = median survival time� TSH = thyroid stimulating hormone
Suggested ReadingBailey DB, Page RL. Tumors of the endocrine
system. In: Withrow SJ, Vail DM, eds.,Small Animal Clinical Oncology, 4th ed.Philadelphia: Saunders, 2007, pp. 591–596.
Klein MK, Powers BE, Withrow SJ, et al.Treatment of thyroid carcinoma in dogs bysurgical resection alone: 20 cases(1981–1989). JAVMA 1995,206:1007–1009.
Liptak JM. Canine thyroid carcinoma. ClinTech Small Anim Pract 2007, 22(2):75–81.
Pack L, Roberts RE, Davson SD, DookwahHD. Definitive radiation therapy forinfiltrative thyroid carcinoma in dogs. VetRadiol Ultrasound 2001, 42:471–474.
Walers CB, Scott-Moncrieff JCR. Cancer ofendocrine origin. In: Morrison WB, ed.,Cancer in Dogs and Cats: Medical andSurgical Management, 2nd ed. Jackson,WY: Teton NewMedia, 2002, pp. 573–580.
Author Rebecca G. NewmanConsulting Editor Timothy M. FanAcknowledgement The author and editorsacknowledge the prior contribution of LindaS. Fineman.
BLBS078-CF_A25 BLBS078-Tilley July 23, 2011 4:15
Canine and Feline, Fifth Edition 35
Aggression, Fear—Cats A
BASICSOVERVIEWFear-motivated human-directed felineaggression.
SYSTEMS AFFECTED� Behavioral � Gastrointestinal—decreasedappetite � Hemic/Lymphatic/Immune—chronic stress effects on immune function� Ophthalmic—dilated pupils in response toautonomic nervous system stimulation� Skin/Exocrine—may show secondaryproblem behavior such as overgrooming
SIGNALMENTCats of any age, gender, or neuter status
SIGNSEars back, body and tail lowered, piloerection,pupil dilation; may hiss and growl. Avoidanceof person(s) who elicit the aggression. Attackspossible if approached and/or cornered.Extreme cases: expression of anal glands,urination, and/or defecation. Hidingbehavior.
CAUSES & RISK FACTORSPoor socialization with humans and/or feralliving, an aversive event associated with aperson, or people in general.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Pain-motivated aggression � Play-motivatedaggression � Petting intolerance � Redirectedaggression
CBC/BIOCHEMISTRY/URINALYSISUse to rule out contributing medicalconditions. Urinalysis if inappropriateelimination and/or urine marking.
OTHER LABORATORY TESTSSenior cats: a complete thyroid panel
IMAGINGBased on clinical examination and/orsuspected pain component
DIAGNOSTIC PROCEDURESThorough behavioral history including adescription of the cat’s postures duringaggression and injuries inflicted, litter box use,food consumption, and hiding behaviors.
TREATMENTCLIENT EDUCATIONAvoidance of Fear-Inducing Situations� Ongoing exposure to the fear-inducingsituations may worsen signs, cause severestress, and compromise animal welfare.� Exposure to the stimuli only undercontrolled exercises described below.
Behavior Modification ExercisesDesensitization and Counter-Conditioning� Desensitization: exposing cat to thefear-inducing stimulus (scary person) at a lowlevel so the cat does NOT react fearfully oraggressively. Over time, the intensity of thestimulus is increased (i.e., the distancebetween the cat and stimulus is decreased)without causing fearful responses.� Counter-conditioning: rewarding the catwith a special treat, toy, grooming, petting,etc., for relaxation.
CLASSICAL CONDITIONING� Classical conditioning: pairing the stimulus(person threatening to the cat) with a tastytreat, toy, petting. Example: scary person =tuna fish. As cat relaxes in the presence of theperson, relaxation is rewarded.
MEDICATIONSMedication may be necessary to decreaseoverall levels of anxiety and reactivity.
DRUG(S)Azapirones� Buspirone 0.5–1.0 mg/kg q12h. Mostuseful for fearful and withdrawn cats.Decreases anxiety and may increase“self-confidence.” Anecdotal reports of“increase in affection” and possible increase inaggression when given to the aggressor.Response noted in 1–2 weeks.
Selective Serotonin Reuptake Inhibitors� Fluoxetine, paroxetine, sertraline 0.5–1.5mg/kg q24h
Tricyclic Antidepressants� Amitriptyline 0.5–2.0 mg/kg q12–24h� Clomipramine 0.25–1.3 mg/kg q24h� SSRIs and TCAs must be given daily. Maytake 4–8 weeks to reach peak effects.
Benzodiazepines� Alprazolam 0.125–0.25 mg/cat q8–24h� Diazepam 0.1–1.0 mg/kg q12–24h (rarelyused due to potential hepatopathies)� Benzodiazepines can be given “as needed”for specific encounters with people inducingthe fear response and during the DS&CC andclassical conditioning sessions. Thebenzodiazepines can be used in conjunctionwith the azapirones, SSRIs, and TCAs.
Pheromones� Feliway—available in diffuser and spray� Used to help calm the cat during stressfulsituations.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� None of the medications listed are approvedfor use in cats. � All of the medications are tobe administered orally, as they have not beenshown to be effective through transdermaldosing. � Azapirones: side effects areuncommon but occasional excitement isnoted. Should not be given in combination
with monoamine oxidase inhibitors. Avoiduse in the aggressor cat; may increase any“bully” behavior. � Neither SSRIs nor TCAsshould be given with each other, nor incombination with MAOIs. � SSRIs: sideeffects include mild sedation and decreasedappetite, constipation, and urinary retention.Competitive inhibition of cytochrome P450liver enzymes; when administeredconcurrently with medication utilizing theP450 enzymes, elevated plasma levels of themedications may increase, causing toxic levels.� TCAs: side effects include sedation,constipation, diarrhea, urinary retention,appetite changes, ataxia, decreased tearproduction, mydriasis, cardiac arrhythmias,tachycardia, and changes in blood pressure.� Benzodiazepines: side effects includesedation, ataxia, muscle relaxation, increasedappetite, paradoxical excitation, and increasedfriendliness. Idiopathic hepatic necrosis hasbeen reported in cats. � Specificrecommendations for the use of diazepam:baseline physical exam, CBC, and bloodchemistries to confirm good health. Repeatthe blood chemistries at 3–5 days. ElevatedALT or AST, discontinue the medication.
FOLLOW-UPPATIENT MONITORINGWeekly follow-up is recommended, especiallywhen on medication(s). For cats onmedication, follow-up blood workrecommended every 6–12 months.
PREVENTION/AVOIDANCEAvoidance of the fear-inciting stimuli if at allpossible. Early socialization to people andevents may help prevent some occurrences offear-related responses to people.
POSSIBLE COMPLICATIONSPotential human injury—especially if the catis approached or cornered.
EXPECTED COURSE AND PROGNOSISProgress occurs slowly. Relearning is a processand each case is individual. If medications areindicated, begin at a low dose and work up asnecessary. To discontinue taking medication,wait until the new behavior is stable (8–12weeks) and wean off slowly, usually overweeks. If fearful behavior recurs, return to thelast dose that controlled the anxiety andcontinue treatment.
MISCELLANEOUSZOONOTIC POTENTIALPeople injured during a fear-motivated attackshould seek prompt medical attention.Infection by Bartonella henselae can resultfrom a cat scratch or bite.Author Terry Marie CurtisConsulting Editor Debra F. Horwitz
BLBS078-CF_A26 BLBS078-Tilley May 31, 2011 17:32
36 Blackwell’s Five-Minute Veterinary Consult
Aggression, Fear/Defensive—DogsA
BASICSOVERVIEWOccurs when the dog perceives a situation asthreatening. May be within the range ofnormal behavior but excessive fearfulness orphobic behavior is also possible.
SYSTEMS AFFECTED� Behavioral.� Signs of sympathetic stimulation (e.g.,tachypnea, tachycardia).
SIGNALMENT� Dogs.� No gender predilection; not affected byneutering.� Can occur at any age. Signs often develop aspuppies leave the peak period for socialization(approximately 12–16 weeks of age) and againat 6–9 months.
SIGNS� Aggression (growling, lip-lifting, barking,snarling, snapping, lunging, biting)accompanied by fearful or submissive bodypostures/facial expression (head down,crouching, backing away, ears back, tailtucked, looking away, lip licking).� History may include the dog having beenhurt or startled in a similar situation.� Often directed toward unfamiliar people.� May occur when the dog is cornered orcannot escape.� May be more severe on- than off-leash.
CAUSES & RISK FACTORS� May be a normal canine behaviordepending on the circumstances.� Strongly influenced by previous experience(e.g., inadequate early socialization, painfulconditions, rough handling, inappropriatepunishment).� Underlying medical conditions, especiallypain, may increase the level of aggression.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Dominance/social status aggression� Conflict aggression� Others depending on circumstances
CBC/BIOCHEMISTRY/URINALYSISUsually unremarkable. Abnormalities suggestan underlying or contributing medicalcondition.
OTHER LABORATORY TESTSUsually unremarkable.
IMAGINGMRI if CNS disease suspected. Otherimaging as needed to rule out underlyingmedical conditions.
DIAGNOSTIC PROCEDURESN/A
TREATMENTCLIENT EDUCATION� Treatment is aimed at controlling theproblem, not at achieving a “cure.” Successfultreatment, as measured by a decrease inaggressive incidents, depends upon ownerunderstanding of basic canine social behavior,risks involved in living with an aggressive dog,how to follow safety and managementrecommendations, and correct identificationof the fear-eliciting stimuli.� Owners must be aware the only way toprevent all future injuries is euthanasia.� If owners elect not to euthanize, they mustbe aware that their primary responsibility ispreventing human injury by conscientiouslyavoiding situations that may evoke anaggressive reaction, including situations thathave resulted in the dog’s being fearful even ifnot aggressive.� Owners may be more compliant withavoidance recommendations if theyunderstand that in many jurisdictions dogowners are liable for bites and can facecivil/criminal prosecutions should a person beinjured.� Treatment is more likely to be successful if aperiod of preventing exposure tofear-provoking stimuli is instituted prior tobehavior modification.
Safety Recommendations� Confine the dog away from potentialvictims or have the dog be under the directphysical control of a responsible adultwhenever an aggression-provoking situationcould arise (e.g., in any public location, onwalks, when visitors arrive at the house).� Teach the dog to be comfortable wearing ahead halter (e.g., Gentle Leader) and basketmuzzle for easier and safer control.� Due to the current resurgence in popularityof punishment-/dominance-based trainingtechniques, owners must be educated aboutthe etiology (i.e., fear) for their dog’saggression. Use of these techniques may resultin increased aggression, fear, agitation, and/orinjuries.
Behavior Therapy� Affection control: used to increasepredictability of dog’s life and decreaseoccurrence of fear-provoking situations (seeAggression Toward Familiar People—Dogs).� Behavior modification: systematicdesensitization and counter-conditioningto specific fear- and aggression-provokingstimuli (see Aggression Toward FamiliarPeople—Dogs).� Teach the dog to sit and relax on a verbalcommand in neutral locations using foodrewards.
� Gradually expose the dog to a greatlyreduced stimulus so no fearful reaction iselicited.� The non-fearful behavior is rewarded.� Gradually increase the level of stimulationstaying below the threshold that would resultin fear and/or aggression.� Progress is slow, and careful monitoring ofresponses is essential.� Relapses are common, and owners mustalways be vigilant and in control of the dog’sbehavior.
MEDICATIONSDRUG(S)� There are no medications licensed for thetreatment of canine aggression. Owners mustbe aware the use of medication is off-label.Because of liability concerns, note in thepatient’s record that the owners wereinformed of potential risks and side effects. Asigned informed consent form is advisable.� NEVER use medications without behaviormodification.� Before prescribing medication, be sure thatowners understand the risks in owning anaggressive dog, will follow safety procedures,and will not rely on medication to keep otherssafe.� Medication may not be appropriate in somefamily situations, (e.g., those with smallchildren, family members with disabilities, orimmunocompromised individuals).� Research has confirmed there is a strongplacebo effect when using medications to treatcanine aggression. Studies have not shown arobust effect of drug treatment on aggression.
Selective Serotonin Reuptake Inhibitors� Fluoxetine 0.5–2 mg/kg PO q24h (canine)� Paroxetine 0.5–1 mg/kg PO q24h (canine)� Sertraline 1–3 mg/kg PO q24h (canine)� Side effects: sedation, irritability, GITeffects; anorexia is common and usuallytransient.
Tricyclic Antidepressants� Clomipramine 2–4 mg/kg PO q24h ordivided q12h (label-restricted for aggression)(canine)� Side effects: sedation, GIT effects,anticholinergic, possible cardiac conductiondisturbances if predisposed.
Benzodiazepines� Alprazolam 0.05–0.1 mg/kg PO q12h orPRN
PRECAUTIONS� Any psychotropic medication may increaserather than decrease aggression.� Use caution when prescribingbenzodiazepines as disinhibition of aggressionmay result due to a reduction in fear-basedinhibition to biting.
BLBS078-CF_A26 BLBS078-Tilley May 31, 2011 17:32
Canine and Feline, Fifth Edition 37
(Continued) Aggression, Fear/Defensive—Dogs A
� Do not combine SSRIs, TCAs, MAOinhibitors (e.g., amitraz, selegiline), ortramadol—can result in potentially fatalserotonin syndrome.
FOLLOW-UPPATIENT MONITORING� Clients often need ongoing assistance andshould receive at least one follow-up callwithin the first 1–3 weeks after consultation.Provisions for further follow-up should bemade at that time. Ongoing communicationimproves client compliance.
PREVENTION/AVOIDANCE� Treatment recommendations arelifelong—aggression may recur withtreatment lapses and continued exposure tothe fear-producing stimuli. Owners mustalways be vigilant and in control of the dog’sbehavior.� Appropriate early socialization andhabituation may help avoid fear-basedbehaviors later in life. This includes attendingwell-structured, positive reinforcement puppyclasses starting during the peak period forsocialization.
POSSIBLE COMPLICATIONSHuman injuries; euthanasia or relinquishmentof patient
EXPECTED COURSE AND PROGNOSISThere is no cure. Prognosis for improvementis better if aggression is at a low intensity andoccurs only in a few predictable situations.Prognosis is highly dependent on ownercompliance.
MISCELLANEOUSASSOCIATED CONDITIONSMay see other fear- or anxiety-basedconditions (e.g., noise phobias, separationanxiety).
ZOONOTIC POTENTIALHuman injury and bite wounds
PREGNANCY/FERTILITY/BREEDINGDo not breed dogs with extremely fearfulbehavior or fear/aggression.
SEE ALSOAggression Toward Familiar People—Dogs
ABBREVIATIONS� CNS = central nervous system� GIT = gastrointestinal tract� MAO = monoamine oxidase� MRI = magnetic resonance imaging� SSRI = selective serotonin reuptakeinhibitor� TCA = tricyclic antidepressant
Suggested ReadingHerron ME, Shofer SS, Reisner IR. Survey of
the use and outcome of confrontational andnon-confrontational training methods inclient-owned dogs showing undesiredbehaviors. Appl Anim Behav Sci 2009,177:47–54.
Moffat K. Addressing canine and felineaggression in the veterinary clinic. Vet ClinNorth Am Small Anim Pract 2008,38(5):983–1003.
Virga V, Houpt KA, Scarlett JA. Efficacy ofamitriptyline as a pharmacological adjunctto behavioral modification in themanagement of aggressive behaviors in dogs.JAAHA 2001, 37:325–330.
Author Laurie Bergman and Meredith StepitaConsulting Editor Debra F. Horwitz
BLBS078-CF_A27 BLBS078-Tilley July 15, 2011 17:33
38 Blackwell’s Five-Minute Veterinary Consult
Aggression, Food, Possessive, and Territorial—DogsA
BASICSOVERVIEW� Aggressively guarding food (e.g., in foodbowl, rawhides, bones, stolen/found items) orobjects (e.g., toys, stolen objects).� Territorial aggression—aggressivelydefending a territory. Territory may be a fixedlocation (e.g., home, yard, car, bed, or restingarea) and not be evident in other locations. Inother cases, the territory is mobile and is anarea around the dog; aggressive responses mayoccur at any time. Territorial aggression maybe exacerbated if the dog is restrained.� Usually within the range of normalbehavior; learning may contribute to excessiveexpression of aggression.
SYSTEMS AFFECTEDBehavioral
SIGNALMENTNo breed or gender predilections exist forfood/possessive aggression. Territorialaggression is more common in intact malesand initial signs are usually present by age 1.
SIGNS� Food/possessive—aggression (growling,lip-lifting, barking, snarling, snapping,lunging, biting) toward people or otheranimals in the presence of valued food itemsor objects.� Territorial—aggression in defense of alocation or space.
CAUSES & RISK FACTORS� May be part of normal canine behavior.Strongly influenced by previous experiences ofsuccessfully defending food, objects, orterritory through aggression.� Underlying medical conditions andmedications, especially those causingpolyphagia, or calorie-restricted diets mayincrease level of food aggression.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Fear aggression� Social status/dominance or conflictaggression� Others depending on circumstances
CBC/BIOCHEMISTRY/URINALYSISUsually unremarkable. Abnormalities suggestan underlying or contributing medicalcondition.
OTHER LABORATORY TESTSUsually unremarkable.
IMAGINGMRI if CNS disease suspected. Otherimaging as needed to rule out underlyingmedical conditions.
DIAGNOSTIC PROCEDURESN/A
TREATMENTCLIENT EDUCATIONSafety Recommendation� Always confine the dog away from potentialvictims or the dog must be under the directphysical control of a responsible adultwhenever an aggression-provoking situationcould arise.� Feed dogs confined away from people;prevent access to items that may evokeaggression.� Confine territorial dogs in locations wherethey cannot see/hear people approachingterritory before they become aggressivelyaroused.� Teach the dog to be comfortable wearing ahead halter (e.g., Gentle Leader) and basketmuzzle for easier control of potentiallydangerous situations.� The goal of treatment is control of theproblem, not a cure.� Success is measured by a decrease inaggressive incidents.� Success depends on owner understanding ofbasic canine social behavior, risks involved inliving with an aggressive dog, and ability tofollow safety and managementrecommendations.� The only way to absolutely prevent futureinjuries is euthanasia.� If the dog remains in the home, the primaryresponsibility is preventing human injury byconscientiously avoiding situations that mayevoke an aggressive reaction.� To aid in compliance, help ownersunderstand that dog owners are often liablefor bites and can face civil/criminalprosecutions should a person be injured.� A period of preventing exposure toaggression-provoking stimuli prior tobehavior modification may aid in success.� Due to the current resurgence in popularityof punishment/dominance-based trainingtechniques, owners must be educated aboutthe etiology (i.e., fear) of their dog’saggression. Use of these techniques may resultin increased aggression, fear, agitation and/orinjuries.
Behavior Modification� Affection control: used to help increaseowners’ leadership over dogs (see AggressionToward Familiar People—Dogs).� Systematic desensitization andcounter-conditioning to specific
aggression-provoking stimuli. Use pea-sizedpieces of food to reduce the likelihood of afood-aggressive dog becoming aggressiveduring behavior modification (see AggressionToward Familiar People—Dogs).� Teach the dog to perform alternatebehaviors (e.g., a “Quiet” command,relinquishing objects to “Drop,” or get offfurniture with “Off”) on command forrewards. Often referred to as countercommanding or response substitution.
MEDICATIONSDRUG(S)� There are no medications licensed for thetreatment of canine aggression. Owners mustbe aware that the use of medications isoff-label. Because of liability concerns, note inthe patient’s record that the owners wereinformed of potential risks and side effects. Asigned informed consent form is advisable.NEVER use medications without behaviormodification. Before prescribing medication,be sure that owners understand the risks inowning an aggressive dog, will follow safetyprocedures, and will not rely on medication tokeep others safe. Medication may not beappropriate in some family situations (e.g.,those with small children, family memberswith disabilities, or immunocompromisedindividuals).� Research has confirmed there is a strongplacebo effect when using medications to treatcanine aggression. Studies have not shown arobust effect of drug treatment on aggression.
Selective Serotonin Reuptake Inhibitors� Fluoxetine 0.5–2 mg/kg PO q24h (canine)� Paroxetine 0.5–1 mg/kg PO q24h (canine)� Sertraline 1–3 mg/kg PO q24h (canine)� Side effects: sedation, irritability, GITeffects; anorexia is common and usuallytransient.
Tricyclic Antidepressants� Clomipramine 2–4 mg/kg PO q24h ordivided q12h (label restriction for aggression)(canine)� Side effects: sedation, GIT effects,anticholinergic effects, and cardiacconduction disturbances if predisposed.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Any psychotropic medication may increaserather than decrease aggression.� Use caution when prescribingbenzodiazepines, as disinhibition ofaggression may result due to a reduction infear-based inhibition to biting.� Do not combine SSRIs, TCAs, or MAOinhibitors (e.g., amitraz, selegiline) andtramadol—can result in potentially fatalserotonin syndrome.
BLBS078-CF_A27 BLBS078-Tilley July 15, 2011 17:33
Canine and Feline, Fifth Edition 39
Aggression, Food, Possessive, and Territorial—Dogs A
FOLLOW-UPPATIENT MONITORINGClients often need ongoing assistance. Shouldreceive at least one follow-up call within thefirst 1–3 weeks after the consultation.Provisions for further follow-up are made atthat time.
PREVENTION/AVOIDANCETreatment recommendations arelifelong—may see recurrence of aggressionwith treatment lapses and continued exposureto aggressive triggers.
POSSIBLE COMPLICATIONSHuman injuries; euthanasia or relinquishmentof patient
EXPECTED COURSE AND PROGNOSISThere is no cure. Prognosis for improvementis better if aggression is at a low intensity andoccurs in only a few predictable situations.Prognosis is highly dependent on ownercompliance.
MISCELLANEOUSASSOCIATED CONDITIONSFear and dominance/conflict aggression
ZOONOTIC POTENTIALHuman injury and bite wounds
PREGNANCY/FERTILITY/BREEDINGDo not breed dogs with extremeaggression.
SEE ALSO� Aggression, Fear/Defensive—Dogs� Aggression Toward Familiar People—Dogs
ABBREVIATIONS� CNS = central nervous system� GIT = gastrointestinal tract� MAO = monoamine oxidase� MRI = magnetic resonance imaging� SSRI = selective serotonin reuptakeinhibitor� TCA = tricyclic antidepressant
Suggested ReadingdeKeuster T, Jung H. Aggression toward
familiar people and animals. In: HorwitzDF, Mills D, eds., BSAVA Manual ofCanine and Feline Behavioural Medicine,2nd ed. Gloucestershire, UK: BSAVA, 2009,pp. 182–210.
Herron ME, Shofer SS, Reisner IR. Survey ofthe use and outcome of confrontational andnon-confrontational training methods inclient-owned dogs showing undesiredbehaviors. Appl Anim Behav Sci 2009,177:47–54.
Landsberg G, Hunthausen W, Ackerman L.Handbook of Behavior Problems of the Dogand Cat. Oxford: Butterworth-Heinemann,1997.
Mertens PA. Canine aggression. In: HorwitzD, Mills D, Heath S, eds., BSAVA Manualof Canine and Feline Behavioural Medicine.Gloucestershire, UK: BSAVA, 2002,pp. 195–215.
Authors Laurie Bergman and MeredithStepitaConsulting Editor Debra F. Horwitz

BLBS078-CF_A28 BLBS078-Tilley July 15, 2011 17:59
40 Blackwell’s Five-Minute Veterinary Consult
Aggression, Intercat AggressionA
BASICSOVERVIEW� Staring, displacing, vocalizing (growling,yowling, shrieking), spitting, hissing,swatting, lunging, chasing/stalking, and/orbiting other cats. Multiple motivations exist.
SYSTEMS AFFECTED� Behavioral� Hemic/Lymphatic/Immune� Nervous
SIGNALMENT� No age, sex, or breed distribution noted.� Can occur at any age as a chronicmanifestation of redirected aggression orwhen the social environment changes (forinstance, addition of a new cat, return of a catfrom the veterinarian, etc.).� Previously stable cat relationships candisintegrate as cats reach social maturity.
SIGNSAggressor� Covert signs: staring, displacing other cats,stiff body language/movements whileapproaching the other cat.� Overt signs: Growling, yowling, spitting,hissing, swatting, lunging, chasing/stalking,and/or biting other cats, dilated pupils, maybe accompanied by body language of fear(such as the classic Halloween catstance—piloerection, back arched, tail up) ormore offensive body language (stiff muscles,tail head elevated but rest of tail down, backstraight or slightly slanted toward the head,ears forward or to the side), excessive facialmarking, and perhaps urine marking.
Victim� Covert: avoidance of aggressor, hiding,change in grooming and eating habits,hypervigilance, dilated pupils.� Overt: hissing, swatting, running, vocalizing(including growling), Halloween cat stance,may escalate to defensive attack if cornered.
Elimination Outside of the Litter Box� Aggressors may block access to the litter boxarea, forcing victims to choose alternativeelimination locations; secondary substrateand/or location preferences and aversions candevelop.� Both victims and aggressors may urine markeither horizontally or vertically.� Extremely fearful cats may urinate ordefecate in the midst of aggressive events.
Causes & Risk Factors� Resource limitation (not enough verticaland/or horizontal space, lack of appropriatehiding areas, and limited access to food,water, and litter boxes, etc.). � Social andenvironmental instability such as the additionof a new cat, loss of a resident cat, change insmell (return of a cat from the veterinarian orgiving one cat a bath), aging or illness of one
or both cats, one or multiple cats reachingsocial maturity, moving, changing furniture orother resting areas, etc. � Exposure to agitatingstimuli (interloping cats in the yard, visitors,noises, scents, etc.) can cause redirectedaggressive behaviors that can develop intopersistent aggressive interactions. � Lack ofappropriate socialization to other cats as akitten. � Genetically unrelated cats and catsthat have only recently moved in together aremore likely to show aggressive behaviorstoward each other. � Medical problemscausing pain or increased irritability. � Someaggression between cats is normal in cat socialsystems. � Resident cats commonly takeprolonged exposure to new cats before beingwilling to accept them into a group withoutdisplaying defensive or offensive behaviors.
DIAGNOSISDIFFERENTIAL DIAGNOSISBehavioral Differentials� Fear-related aggression, status-relatedaggression, territorial aggression, redirectedaggression, failure of recognition (most likelydue to change in smell of victim), maternalaggression, intermale aggression, sexualaggression, predatory behavior
Medical Differentials� Any illness causing malaise, pain, orincreased irritability (hypertension, arthritis,abscess, dental disease) � Endocrine:hyperthyroidism � Neurologic:space-occupying lesions (meningioma,lymphoma), encephalitis, seizures, felineischemic encephalopathy, trauma, sensory orcognitive decline � Infectious: rabies,toxoplasmosis, aberrant parasitic migrations(such as cuterebriasis), FIV, FeLV� Iatrogenic: administration of medicationsthat can increase irritability or disinhibitaggression (such as mirtazapine,benzodiazepines, buspirone) � Toxins: lead,illicit substance ingestion
CBC/BIOCHEMISTRY/URINALYSIS� Obtain at initial consultation or beforespecialty referral to rule out any contributorymedical problems.� If patient placed on psychotropicmedication: repeat every 6 months to 1 yeardepending on age and general health of pet.
OTHER LABORATORY TESTS� Cats > 6 years should have T4/free T4
measured.� Urine culture and sensitivity should beobtained from cats that are urinating outsideof the box unless there is a clear diagnosis ofurine marking for all urinations out of thebox.
IMAGINGHousesoiling cats should have abdominalradiographs and/or ultrasounds.
DIAGNOSTIC PROCEDURES� Obtain a detailed oral or written history.� Identify: the number, location, and types oflitter boxes, where each of the cats spendsmost of his/her time.� If there are multiple cats within thehousehold, attempt to determine which catsspend time together and which cats avoideach other, the locations of feeding, play, andresting areas, and locations of any housesoiling or marking.� If a house call is not possible, have theclients draw a floor plan with the abovedetails.� Video and still photographs of catsinteracting can be informative.� Note any other changes in demeanor,routine, and eating and grooming habits of allparticipants.
TREATMENT� For chronic, severe cases or for aggressionthat does not respond to treatment, clientsmay elect permanent separation either byrehoming one of the cats or by splitting upthe residence. Be prepared to providerecommendations about this process.� Neuter intact males.
FOR CASES THAT HAVE A LOWFREQUENCY OF INTENSE,INJURIOUS AGGRESSIVEOUTBURSTS� Separate the cats when they cannot bedirectly supervised (create “safe zones”).� Either keep the spaces the same each day inan effort to form a separate core territory foreach cat, or “time share” the spaces betweencats in order to avoid each cat exploiting onlya small area over the long term.� If you elect to keep the safe zones the samefor each cat, give the aggressor the smaller area(keep the aggressor’s core area small).� For multiple cats, separate by stability ofrelationship between cats. Any despotic/bullycats should be confined alone.� Reward the cats with food, play, and/orattention for being in the same room togetherwithout having aggressive events. Cats shouldstay at a distance that allows for calmparticipation.� Engage the cats in daily sessions ofpleasurable activities (play, training, eatingdelectable food treats, etc.) at distances thathave a very low likelihood of creatingaggressive events. Gradually move the funsessions closer to each other.� The goal of management and safetyis to prevent aggressive events from occurring.In an emergency, judicious use of interrupters(such as water gun sprays, blanketstossed on the cats, etc.) can stop eventsin progress but should not be consideredmainstays of treatment. These should be used
BLBS078-CF_A28 BLBS078-Tilley July 15, 2011 17:59
Canine and Feline, Fifth Edition 41
(Continued) Aggression, Intercat Aggression A
as the aggressive behavior is just beginning tobe most effective. If it can be safely done, theaggressor should be placed or lured into his/hersafe zone at the first sign of any threateningbehavior. Use of interrupters and punisherscan increase aggressive behavior in somecats and increase negative associations withother cats, and so must be used cautiously.� Distracters such as laser pointers, tossedtoys, and remote activated toys can be used toredirect aggressors at the beginning of theaggression sequence (staring, tail twitching,and pupil dilation) and do not risk creatingnegative associations between the cats.� Bell the aggressor (using a quick release orsafety collar) so both the owner and the victimcan quickly identify his/her location.� Increase the number of resourcesthroughout the residence.� Increase litter box number to the number ofcats plus one (three boxes for two cats).� Add litter boxes to different locations sothat one cat cannot keep others fromaccessing the boxes; locations with more thanone exit/entry are ideal.� Increase the number and locations of foodand water areas.� Increase the number of hiding places andcomfortable resting areas; especiallyconcentrate on increasing vertical space (i.e.,resting areas on shelves, window sills, etc.).� Increase play and add food-dispensing toys.� No new cats should be added to the house.
FOR CASES WHERE THE CATSCANNOT BE IN THE SAME ROOMWITHOUT IMMEDIATELY BECOMINGAGITATED� Separate cats completely whenunsupervised.� Meet each cat’s needs for play, litter boxes,food, water, and attention.� Set up systematized desensitization andcounter-conditioning sessions daily; initiallyutilize physical and visual barriers.� Teach both cats to tolerate harnesses andleashes so that they can be used duringtraining sessions. This is especially valuablefor the aggressor.� When ready to allow the cats more freedomwith each other, follow the instructions forless severe interact aggression (above).
MEDICATIONSDRUG(S)Azapirone� Buspirone 0.5–1 mg/kg PO q8–24h (felinedose)� Reserved for victims due to potential toincrease social confidence, can potentiallyhelp stop the run-chase cycle, may alsoimprove urine marking.� Need client update q2 weeks. Plan to use forat least 4–6 weeks after resolution of signs.
� Side effects include: may increase intercataggression as victim may now “fight back.”
Benzodiazepines� Lorazepam 0.125 mg–0.25 mg/cat PO upto q12–24h� Oxazepam 0.2 mg–0.5 mg/kg PO q12–24h(feline dose)� For fearfully aggressive cats.� Side effects include increased sociability,decreased hiding, increased appetite, anddisinhibition of aggression, ataxia.� May see clinical effects within 1 hour.� Note: controlled substance, dependence candevelop.� Need client update no more than 48 hoursafter starting medication.
Selective Serotonin Reuptake InhibitorsFluoxetine 0.5–1 mg/kg PO q24h (felinedose)Paroxetine 0.5–1 mg/kg PO q24h (felinedose)For aggression, anxiety, and/or urine marking,may decrease impulsivity.Need client update q2 weeks. Plan to use forat least 4–6 weeks after resolution of signs.Side effects of SSRIs include sedation, urinaryretention, gastrointestinal upset (includingdiarrhea, constipation, vomiting, anorexia),increased agitation/irritability.
Tricyclic Antidepressants� Amitriptyline 0.5–1 mg/kg PO q12–24h(feline dose): for anxious cats with co-morbidrecurrent, severe FIC/FLUTD symptoms� Clomipramine 0.3–0.5 mg/kg PO q24h(feline dose): for anxious and/or aggressivecats, with or without urine markingcomponents� Need client update q2 weeks. Plan to use forat least 4–6 weeks after resolution of signs.� Side effects of TCAs include sedation,increased thirst, urinary retention,constipation, and lowered seizure threshold.Do not use in patients with arrhythmias orcardiopathies.
Pheromones� Feliway and Felifriend (two different felinefacial pheromone fractions) may be helpful incases of intercat aggression when used with amultimodal plan
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� SSRIs and TCAs should be used withcaution in patients with histories of cardiacabnormalities, seizure histories, and/or liverdisease and should not be used together.� Benzodiazepines should be used withcaution in cats due to the potential to causehepatopathies.� Medications that alter serotonin levels canhave important interactions with othermedications (such as selegiline and amitraz).� In the United States, all medications forbehavior problems in cats are off-label at thistime.
FOLLOW-UP� Clinicians should be updated q2 weeks aftertreatment initiation either by phone or inperson. A recheck should be performed nolater than 8 weeks into treatment.� Recheck laboratory work every 6 months to1 year depending on the health and age of thepatients for cats on long-term medication.
PREVENTION/AVOIDANCEProper socialization can help decrease thelikelihood of intercat aggression in some cats.Gradual introduction more closely resemblesthe natural process through which new catsare admitted to an existing group, thereforethis method is preferred when introducingnew cats. Genetically related cats may be lesslikely to have intense intercat aggression. Instable households avoid adding additionalcats.
EXPECTED COURSE AND PROGNOSIS� Recent and mild (low-intensity,low-frequency, rare/mild injuries) cases seemto have better long-term outcomes.� The prognosis is complicated by prolongedduration, high severity, underlying medicalconditions, and incomplete ownercompliance.
ABBREVIATIONS� FeLV = feline leukemia virus� FIC/FLUTD = feline idiopathic cystitis/feline lower urinary tract disease� FIV = feline immunodeficiency virus� SSRI = selective serotonin reuptakeinhibitor� T4 = thyroxine� TCA = tricyclic antidepressant
Suggested ReadingAmat M, et al. Evaluation of inciting causes,
alternative targets, and risk factorsassociated with redirected aggression in cats.JAVMA 2008, 233(4):586–589.
Curtis TM, Knowles RJ, Crowell-Davis SL.Influence of familiarity and relatedness onproximity and allogrooming in domesticcats (Felis catus). Am J Vet Res 2003,64:1151–1154.
Heath S. Feline aggression. In: Horwitz DF,Mills D, Heath, S, eds., BSAVA Manual ofCanine and Feline Behavioral Medicine.Gloucestershire, UK: BSAVA, 2002,pp. 216–228.
Landsberg G, Hunthausen W, Ackerman L.Feline aggression. In: Handbook ofBehavior Problems of the Dog and Cat, 2nded. Philadelphia: Elsevier Saunders, 2003,pp. 427–453.
Author E’Lise Christensen BellConsulting Editor Debra F. Horwitz
BLBS078-CF_A29 BLBS078-Tilley May 31, 2011 18:3
42 Blackwell’s Five-Minute Veterinary Consult
Aggression, Interdog AggressionA
BASICSOVERVIEW� Two basic forms: aggression toward otherdog(s) within a household and aggressiontoward unfamiliar dogs. A variety of differentmotivations exist, including fear, territoriality,and social status. Usually within the range ofnormal behavior, but excessive aggression dueto learning or genetics (dogs bred for fighting)is also possible.
SYSTEMS AFFECTEDBehavioral
SIGNALMENT� Dog.� More common in intact males.� Breed predilection in “fighting breeds” (e.g.,pit bull terriers) and terriers.� Signs usually develop at sexual(approximately 6–9 months of age) or socialmaturity (approximately 18–36 months ofage).
SIGNS� Aggression (growling, lip-lifting, barking,snarling, snapping, lunging, biting) towardother dogs. This may be accompanied byfearful or submissive body postures/facialexpressions (crouching, backing away, earsback, tail tucked, looking away, lip licking) orconfident/dominant body postures (standingstraight up, approaching/direct contact withthe other dog, tail up, ears forward).� History may include the dog having beenthe victim of aggression from other dogs(especially if aggression is toward unfamiliardogs).� When fighting occurs within a household,history prior to the onset of fights may includesubtle signs of social control/dominance (e.g.,staring, lying across doorways to block theother dog’s access to a room) and submission(e.g., turning away from the staring dog ornot entering the same room as the other dog).� Dogs fighting in a household may get alongwell except in specific situations.
CAUSES & RISK FACTORS� May be a normal canine behavior; stronglyinfluenced by previous experience (e.g.,inadequate early socialization, aggressiveencounters with other dogs, inappropriatepunishment in the presence of other dogs).� Breed predilections due to selective breedingfor interdog aggression.� Aggression is likely to be more severe towarddogs of the same sex.� In cases of aggression within a household,there may be history of owners interfering innormal canine communication methods,especially when one dog appears to bedenying another dog access to something thatthe owners think they should “share.” Thisshift may actually support one dog in whatwould be considered inappropriate “canine”
behavior and result in escalation of theinterdog aggression. For example, an ownercalling dog “A” into a room when the otherdog “B” has blocked its access even though“A” was willing to remain outside of the roomor the owner punishing dog “B” for blockingdog “A’s” access. Both of these situationsundermine dog “B” in its hierarchal positionwhile it was subtly asserting control that dog“A” was willing to respect.� Underlying medical conditions, especiallypain, may increase the level of aggression.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Play behavior/excited non-aggressive arousal� Others depending on circumstances
CBC/BIOCHEMISTRY/URINALYSISUsually unremarkable. Abnormalities suggestan underlying or contributing medicalcondition.
OTHER LABORATORY TESTSUsually unremarkable.
IMAGINGMRI if CNS disease suspected; as needed torule out underlying medical conditions.
DIAGNOSTIC PROCEDURESN/A
TREATMENTCLIENT EDUCATION� Treatment is aimed at controlling theproblem, not at achieving a “cure.” Successfultreatment, as measured by a decrease inaggressive incidents, depends upon ownerunderstanding of basic canine social behavior,risks involved in living with an aggressivedog(s), and how to follow safety andmanagement recommendations.� Owners must be aware that the only way toabsolutely prevent future injuries is rehoming(if household dog aggression) or euthanasia.� If owners elect not to euthanize, they mustbe aware that their primary responsibility ispreventing human injury by conscientiouslyavoiding situations that may evoke anaggressive reaction, including situations thathave resulted in the dog’s being fearful even ifnot aggressive. Dogs within a household mayneed to be kept separated to prevent contactand fighting.� If needed, owners must be instructed inmethods of safely breaking up dog fights.� Owners may be more compliant withavoidance recommendations if theyunderstand that in many jurisdictions dogowners are liable for bites and can facecivil/criminal prosecutions should a person beinjured.
� Treatment is more likely to be successful if aperiod of preventing exposure toaggression-provoking stimuli is institutedprior to behavior modification.� The dog must be confined away frompotential victims or under the direct physicalcontrol of a responsible adult whenever anaggression-provoking situation could arise(e.g., in any public location, on walks, aroundfood/other valued resources).� Teaching the dog to be comfortable wearinga head halter (e.g., Gentle Leader) and basketmuzzle makes controlling potentiallydangerous situations easier and safer.� For aggression within a household,determine which dog is the more appropriatecontrolling/dominant individual andreinforce that dog by providing him withpriority access to valued resources (e.g., food,toys, resting areas, human attention).� Be aware of “bullies” and that access toresources between household dogs can becontext dependent.
Behavior Therapy� Systematic desensitization andcounter-conditioning to specificaggression-provoking stimuli.� NEVER allow dogs to “fight it out” (seeAggression Toward Familiar People—Dogs).� Affection control: especially for aggressionbetween dogs within a household. To increaseowners’ leadership over dogs andpredictability of dogs’ lives (see AggressionToward Familiar People—Dogs).
MEDICATIONSDRUG(S)� There are no medications licensed for thetreatment of canine aggression. Owners mustbe aware that the use of medication isoff-label. Because of liability concerns, note inthe patient’s record that the owners wereinformed of potential risks and side effects.� A signed informed consent form isadvisable.� NEVER use medications without behaviormodification.� Before prescribing medication, be sure thatowners understand the risks in owning anaggressive dog, will follow safety procedures,and will not rely on medication to keep otherssafe.� Medication may not be appropriate in somefamily situations (e.g., those with smallchildren, family members with disabilities, orimmunocompromised individuals).� Research has confirmed there is a strongplacebo effect when using medications to treatcanine aggression. Studies have not shown arobust effect of drug treatment on aggression.� Medications are most likely to be helpful insituations where there is a strong fear/anxietycomponent, as opposed to situations where
BLBS078-CF_A29 BLBS078-Tilley May 31, 2011 18:3
Canine and Feline, Fifth Edition 43
(Continued) Aggression, Interdog Aggression A
closely ranked dogs use aggression to establishdominance.
Selective Serotonin Reuptake Inhibitors� Fluoxetine 0.5–2 mg/kg PO q24h (canine)� Paroxetine 0.5–1 mg/kg PO q24h (canine)� Sertraline 1–3 mg/kg PO q24h (canine)� Side effects: sedation, irritability, GITeffects; anorexia is common and usuallytransient.
Tricyclic Antidepressants� Clomipramine 2–4 mg/kg PO q24h ordivided q12h (label restriction for aggression)(canine)� Side effects: sedation, GIT effects,anticholinergic effects, and cardiacconduction disturbances if predisposed.
Benzodiazepines� Alprazolam 0.05–0.1 mg/kg PO q12h orPRN
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Any psychotropic medication may increaserather than decrease aggression.� Use caution when prescribingbenzodiazepines as disinhibition of aggressionmay result due to a reduction in fear-basedinhibition to biting.� Do not combine SSRIs, TCAs, MAOinhibitors (e.g., amitraz, selegiline) ortramadol—can result in potentially fatalserotonin syndrome.
FOLLOW-UPPATIENT MONITORINGClients often need ongoing assistance andshould receive at least one follow-up call
within the first 1–3 weeks after theconsultation. Provisions for further follow-upshould be made at that time.
PREVENTION/AVOIDANCETreatment recommendations arelifelong—aggression may recur withtreatment lapses and continued exposure toaggressive triggers.
POSSIBLE COMPLICATIONSInjuries to dogs and humans involved;euthanasia or relinquishment of patient.
EXPECTED COURSE AND PROGNOSISThere is no cure. Prognosis for improvementis better if aggression is at a fairly low intensityand occurs in only a few predictablesituations. Prognosis is highly dependent onowner compliance.
MISCELLANEOUSASSOCIATED CONDITIONSMay see other fear- or anxiety-basedconditions (e.g., noise phobias, separationanxiety); territorial aggression.
ZOONOTIC POTENTIALHuman injury and bite wounds whenseparating fighting dogs.
PREGNANCY/FERTILITY/BREEDINGDo not breed dogs with extreme interdogaggression.
SEE ALSO� Aggression, Fear/Defensive—Dogs� Aggression Toward Familiar People—Dogs
ABBREVIATIONS� CNS = central nervous system� GIT = gastrointestinal tract� MAO = monoamine oxidase� MRI = magnetic resonance imaging� SSRI = selective serotonin reuptakeinhibitor� TCA = tricyclic antidepressant
Suggested ReadingdeKeuster T, Jung H. Aggression toward
familiar people and animals. In: HorwitzDF, Mills D, eds., BSAVA Manual ofCanine and Feline Behavioural Medicine,2nd ed. Gloucestershire, UK: BSAVA, 2009,pp. 182–210.
Herron ME, Shofer SS, Reisner IR. Survey ofthe use and outcome of confrontational andnon-confrontational training methods inclient-owned dogs showing undesiredbehaviors. Appl Anim Behav Sci 2009,177:47–54.
Mertens PA. Canine aggression. In: HorwitzD, Mills D, Heath S, eds., BSAVA Manualof Canine and Feline Behavioural Medicine.Gloucestershire, UK: BSAVA, 2002,pp. 195–215.
Authors Laurie Bergman and MeredithStepitaConsulting Editor Debra F. Horwitz
BLBS078-CF_A30 BLBS078-Tilley July 29, 2011 19:24
44 Blackwell’s Five-Minute Veterinary Consult
Aggression, Overview—CatsA
BASICSDEFINITIONAggression� A behavioral strategy used to manageaversive situations.� May be normal and appropriate in certaincontexts.� May be abnormal with serious deleteriouseffects on the cat’s physical and emotionalwell-being.� Aggressivity: describes both mood andtemperamental traits relating to thepropensity to show aggression whenenvironmental circumstances dictate it mightbe used.
OVERVIEW OF TYPESPlay Aggression (Toward People)� Typically refers to a cat who scratches andbites the owners during play.� Not true aggression but overzealous playwithout proper impulse control due to lack oftraining or proper intraspecific socialfeedback.� The cat’s intent is not to harm the person.� Behavior encouraged and rewarded byowners through rough play with a kitten;when larger and stronger, becomes perceivedas aggression rather than overzealous play.
Predatory Aggression (Toward People orOther Animals)� Cats have an innate drive to “hunt” or showpredation behavior, which includes stalk,hide, and pounce.� Predation is not a direct function of hunger.� Typically stimulated by fast movements andcan progress to the cat hiding and waiting foran animal or person to walk by.� Play is a common way for young cats toperfect predation skills; play aggression andpredatory aggression may overlap.
AGGRESSION
Social interactions
Environment Genetics
physiology
Learning
Learning
Communication
Figure 1.
Redirected Aggression (Toward Peopleor Other Animals)� Cats who see, hear, or smell a trigger anddirect aggressive behavior toward the closestinnocent bystander.� In some cases, one person or animal in thehome becomes the designated victim, and thecat may bypass a nearby individual and lookfor the preferred victim.� Some cats may stay aroused for 24–72 hoursafter a triggered event.� A common trigger inciting redirectedaggression is the cat seeing another cat orwildlife outside.
Fear/Defensive Aggression (TowardPeople or Other Animals)� The cat will show body postures indicativeof fear/anxiety and may use aggression as astrategy to manage that aversive situation.� Typical behaviors shown include acombination of any of the following: hissing,spitting, piloerection, arched back, turningaway, running away, cowering, rolling on itsback and pawing (defensive position, notsubmissive position) if cornered.
Territorial Aggression (Toward People orOther Animals)� Some cats, particularly male cats, showterritorial behaviors in domestic homesettings due to size and the presence of moreresources (e.g., people, food, resting areas,feeding areas, elimination sites, etc.) to defendin a smaller area.� Territorial behaviors include marking withurine, feces, or bunting (the rubbing of thecheeks on surfaces to deposit pheromones)and scratching (also deposits pheromones andleaves visual marker) and may be associatedwith aggression.� In severe cases, the aggressor may seek outthe other individuals and attack.� Body posture with territorial aggression isassertive and confident.
Pain Aggression (Toward People andAnimals)Cats who are in pain may show aggression(hiss, growl, scratch, bite) when they arephysically handled or prior to or aftermovements such as jumping onto or off of apiece of furniture.
Maternal AggressionA female cat may show aggressive behaviorstoward individuals approaching herkittens.
Impulse Control AggressionCats who show intense aggressive responses tomild stimuli without much or any warningmay have a deficiency in serotonin oftencalled an impulse control disorder.
Frustration-Induced Aggression (ToPeople and Other Animals)Some cats have very outgoing, socialpersonalities and exhibit aggression if thecaptive life indoors does not meet theirbehavioral needs.
Contact-Induced/Petting Aggression(Toward People)� Cats will show early signs of aversion whenpeople stroke their cats, with their ears goingback and tail swishing.� If physical contact continues, they typicallybite.� Owners often miss the early warning signs.� When cats groom one another, theytypically limit the grooming to the headregion.� To some cats it may be abnormal andunwanted to be stroked along the dorsum, thecommon method used by owners.
Intercat Aggression within a Home� Fifty percent of cat owners report fighting(scratching and biting) after introducing anew cat to the home.� The number of cats, gender, and age are notsignificant factors in predicting which catswill show aggression.
BLBS078-CF_A30 BLBS078-Tilley July 29, 2011 19:24
Canine and Feline, Fifth Edition 45
(Continued) Aggression, Overview—Cats A
� Any of the above categories of aggression areall possibilities for fights between or amongcats.� Fear/anxiety is the most common cause ofintraspecific aggression.
CONTRIBUTING FACTORS TO THEPATHOPHYSIOLOGYBehavior problems are typically multifactorialin cause, and below is a diagram illustratingsome of the more common components thatneed to be evaluated to accurately diagnoseand treat aggression cases.
SYSTEMS AFFECTED� Behavioral—vary with type of aggression,occur alone or in combination: tailswishing/twitching, ears turned sideways orflattened, stiffening of shoulders/legs,crouching, dilation of pupils, hissing, spitting,growling, piloerection, staring, chasing,stalking, pawing, lunging.� Cardiovascular—signs associated withsympathetic activation and HPA activation.� Endocrine and Metabolic—long-termaggression associated with fear/stress/anxiety,symptoms associated with long-termactivation of the HPA system.� Gastrointestinal—with chronic HPAstimulation may see a cat more prone to GIulcers. With acute fear aggression: evacuationof the bowel and possible diarrhea. IBDpossible in chronic stress.� Hemic/Lymphatic/Immune—decreasedimmune response with chronic HPAstimulation; stress leukogram.� Musckuloskeletal—an outcome of theaggression may result in damage to the skin,muscles from damage by the nails and teeth.� Both the victim and the aggressor maysuffer injuries. With chronic activation of theHPA, may see muscle wasting.� Nervous—increased reactivity for up to72 hours following an aggressive outburst.May see an increase in aggression withdecreased provocation as the synapases in theamygdala become sensitized. Some animalsmay have decreased serotonin, causingaggressive outbursts. Depending on the typeof aggression, may see ritualized motorpatterns, shaking, or trembling.� Ophthalmic—dilated pupils withsympathetic stimulation.� Renal/Urologic—may see associatedspraying or small amounts of urine onhorizontal surfaces. May exhibit signsconsistent with FLUTD with aggression thatis due to stress/anxiety/fear.� Respiratory—tachypnea in acute cases orwhen stressed.� Skin/Exocrine—damage due to fights.Damage due to excessive grooming associatedwith fear-based aggression/anxiety/distress.
SIGNALMENT� There is preliminary evidence thatbehavioral traits in cats vary by breed andgender.
� Males were more likely to show aggressionto cats than females.� Abyssinian, Russian blue, Somali, Siamese,and chinchilla breeds showed more aggression.� Maine coon, ragdoll, and Scottish foldsshowed the least aggressiveness.
SIGNS� May appear at social maturity (2–4 years ofage) except for play-related and should occurin specific social contexts/interactions. If ageof onset occurs in an older cat, medical causesshould be ruled out first.� General comments: most owners are able todetect overt signs of aggression (biting,hissing, growling) but may miss more subtlesigns of aggression that typically occurbetween cats (staring) and the resultinganxious behaviors that can result in aggression(meatloaf position, averting gaze, etc.).Videotapes of intercat interactions allow theclinician to assess the behavior.
CAUSES� Underlying medical issues can causeaggression.� Temperament/behavior is influenced bygenetics, rearing, socialization, environmentin which the cat lives, and types ofinteractions the cat has with people.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� CNS diseases (infections, toxins, tumors,etc.)� Hyperthyroid� Hepatic encephalopathy� Any condition causing pain (arthritis,pancreatitis, dental disease, anal sacculitis, etc.)� Lead poisoning� Rabies� Diabetic neuropathy (pain-inducedaggression when paws touched)
CBC/CHEMISTRY/URINALYSISAll of the above should be done.
OTHER LABORATORY TESTS� Any cat that bites or scratches people shouldhave a Bartonella test.� Thyroid levels.� Urinalysis = /– culture if housesoiling ispart of the aggression issue.� Feline serology (FCV, FeLV, FIV).
TREATMENT� Never use physical correction/punishment;may escalate the aggression.� Never try to physically handle ormanipulate a cat in an aggressive state.� Avoid known triggers.� Identify triggers and desensitize andcounter-condition the cat to the triggers.
� Implement safety measures (soft claws,wearing long pants/long sleeves, keepflattened cardboard boxes around home toplace between yourself and your cat, redirectthe behavior in early arousal phase).� Behavior modifications to redirect the catand reduce arousal (specific plans aredependent upon the specifics of each case).� Train your cat to commands such as “sit,”“go to place,” etc.� Implement environmental enrichment.� Teach owners to identify early signs ofarousal so the cat can be redirected or so theycan avoid the cat.� After a very aggressive outburst, keepaggressor isolated in a room for at least 24hours (if this is a cat who remains arousedafter an attack).� Pheromones.� Medications.
MEDICATIONS� SSRIs: fluoxetine and paroxetine 0.5 mg/kgPO q24h� TCAs: clomipramine 0.5 mg/kg PO q24h� Amitryptiline 0.5–1.0 mg/kg PO q12–24h� Buspirone 0.5–1.0 mg/kg PO q8–24h� Benzodiazepenes: oxazepam 0.2–0.5 mg/kgq12–24h� SAMe: 90 mg PO q24h
CONTRAINDICATIONS� Cats with renal or hepatic disease.� Caution with TCAs and SSRIs in diabetics.� TCAs in patients with cardiac abnormalities.
POSSIBLE INTERACTIONS� TCAs and SSRIs should not be usedtogether.� Certain flea collars.� Certain herbals.� Mirtazapine should not be used incombination with a TCA or SSRI.� Any other medication the cat is on, thepractitioner should look up which liverenzyme system is utilized in metabolism tomaximize safety in combining medications.
FOLLOW-UPPATIENT MONITORING� Call owners once every 1–2 weeks for thefirst 2 months after a treatment plan has beenrecommended. Determine implementation ofsafety recommendations and the behavioralplan.� If medications are involved, the medicationdose should be reevaluated every 3–4 weeks.� Frequency of follow-up will be dictatedby the severity of the case and ownercompliance.� CBC, chemistry, T4 prior to medication.Recheck liver and kidney values 2–3 weeks
BLBS078-CF_A30 BLBS078-Tilley July 29, 2011 19:24
46 Blackwell’s Five-Minute Veterinary Consult
Aggression, Overview—Cats (Continued)A
after starting medication. Recheck bloodworkannually in young healthy patients,semiannually in older patients.� Repeat physical exams in older patientssemiannually, as painful conditions may startto contribute to/exacerbate the pain.
EXPECTED COURSE AND PROGNOSIS� Ultimately depends on the specific kind ofaggression and the compliance of clients withthe suggested treatment plan.� Most cases of aggression need acombination of behavioral modification,environmental modification, training, and,when necessary, medication to maximizechances of improvement.� Some types of aggression can resolve orimprove within a few weeks, whereas othersmay take several months or longer.� Some forms of aggression have a poorprognosis.
MISCELLANEOUSAGE-RELATED FACTORS� Older cats—cognitive decline, CNS disease,arthritis, meningioma, other medicalconditions.
� Age 2–4—social maturity, when cats maystart to show certain kinds of aggression.
ABBREVIATIONS� CNS = central nervous system� FCV = feline calicivirus� FeLV = feline leukemia virus� FIV = feline immunodeficiency virus� FLUTD = feline lower urinary tract disease� GI = gastrointestinal� HPA = hypothalamic-pituitary-adrenal� IBD = inflammatory bowel disease� SAMe = S-adenosyl-L-methionine-tosylatedisulfate� SSRI = selective serotonin reuptakeinhibitor� TCA = tricyclic antidepressant
Suggested ReadingCrowell-Davis SL, Murray T. Veterinary
Psychopharmacology. Ames, IA: Blackwell,2006.
Levine ED. Feline fear and anxiety. Vet ClinNorth Am Small Anim Pract 2008,38:1065–1079.
Levine ED, Perry P, Scarlett J, et al. Intercataggression in households following theintroduction of a new cat. Appl Anim BehavSci 2004, 90:325–336.
Author Emily D. LevineConsulting Editor Debra F. HorwitzAcknowledgement Karen L. Overall
Client Education Handoutavailable online
BLBS078-CF_A31 BLBS078-Tilley July 15, 2011 2:16
Canine and Feline, Fifth Edition 47
Aggression, Overview—Dogs A
BASICSDEFINITION� Action by one dog directed against anotherorganism with the result of harming, limiting,or depriving that organism.� Numerous functional types have beenposited. Here, aggression is classified on thebasis of two categories, offensive or defensive.� Offensive aggression is an unprovokedresponse directed toward an individual inorder to control access to some resource at theexpense of that individual; includes socialstatus/dominance aggression, possessiveaggression, intermale aggression, interfemaleaggression, and predatory aggression.Common targets are familiar individuals.� Defensive aggression is directed toward anindividual perceived as an instigator or threat;includes fear-motivated, territorial, protective,irritable (pain-associated orfrustration-related), and maternal aggression.Common targets are unfamiliar individuals.� Probability of overt aggression may beinfluenced by motivation, arousal, andanxiety. Specific incidents may involve bothoffensive and defensive components.� In all cases, medical explanations (includingpain) must be ruled out.
PATHOPHYSIOLOGY� Aggression is a normal form ofcommunication in dogs.� Some pathologic conditions are associatedwith an increase in aggression because of CNSeffects.� Rage syndrome–impulsive aggression,usually directed toward familiar individuals;abnormalities in the CNS serotoninneurotransmitter system have beenimplicated.� Aggression may have a learned component,leading to an increase in aggression over time.� Except when in actual self-defense,confrontational techniques should not beused to manage aggression. Although widelypromoted, confrontational managementtechniques increase the probability offear-motivated defensive aggression, leadingto an increase in the frequency of aggressionover time.
SYSTEMS AFFECTEDBehavior
GENETICS� Some breed-specific aggressive tendenciesand bite styles have been selected for inbreeding programs, although this cannotpredict the behavior of individual dogs.� One study linked aggressive Englishspringer spaniels to one breeding sire,implicating a heritable component.
INCIDENCE/PREVALENCE� Canine aggression is the most commondiagnostic category seen by board-certifiedveterinary behaviorists in the United States.� According to the Centers for DiseaseControl and Prevention (2009), about4.7 million people are bitten by dogs eachyear in the United States.� Almost one in five of those who are bitten(a total of 885,000) require medical attentionfor dog bite–related injuries.� Among adults and children, males are morelikely than females to be bitten.� The rate of dog bite–related injuries ishighest for children ages 5–9 years.
GEOGRAPHIC DISTRIBUTIONWorldwide
SIGNALMENTSpeciesDogs
Breed Predispositions� Any breed.� Pit bull types and rottweilers are the mostcommon breed types implicated in fatal dogbites in the United States, althoughcomparative rates of aggression based onbreed occurrence are not available.� Selective breeding for behavioral traits maypredispose dogs to specific types of aggression;for example, dogs of breeds bred for dogfighting may be aggressive toward other dogs.� English springer spaniels appear at risk forimpulsive (“rage”) aggression.
Mean Age and Range� Any age.� Aggression commonly becomes moreproblematic at social maturity, 1–2 years ofage.
Predominant SexMales—intact or castrated are mostcommonly implicated in dog bites.
Signs
General Comments� Behavioral warning signs—includeimmobility, growls, snarls, or air snaps.
◦ Offensive—head up, tail up with stiffwag, direct stare, face-on immobility.◦ Defensive—head lowered, tail down,body withdrawn, forepaw lifted.
� History—basis for risk analysis and detailsof treatment program. Important questions:What are the circumstances in whichaggression occurs? Who is the target? Howsevere were the resulting injuries?
Historical FindingsVary according to the situation and thefunctional type of aggression.Offensive� Often directed toward familiar householdmembers.
� Triggers (human directed): reaching for pet,patting on head, approaching or displacingwhen on elevated resting sites, approachingfood, toys, or stolen objects.Defensive� Often directed toward unfamiliar humansor dogs that approach, stand over, or reachfor. Certain familiar people may be exempt.� May be location-specific, as when strangersapproach home, yard, or car.� May be exacerbated if restrained.� As distance from stimulus decreases,response may escalate to agitation, barking,lunging, baring teeth.� Approach/avoidance behavior is common.� Maternal aggression is directed towardindividuals approaching the whelping area orpuppies.
Physical Examination Findings� Usually unremarkable; no specific signsuniversally associated with this condition.� Offensive and defensive aggression may beobserved during the course of theexamination.� Use extreme care when handling aggressivedogs; use muzzles and other restraints toprevent injury.� Abnormalities on the neurologicexamination may suggest an organic diseaseprocess (e.g., rabies).
CAUSES� Part of the normal range of behavior;strongly influenced by breed, sex, earlysocialization, handling, individualtemperament, and other variables.� Manifestation of an organiccondition—possible but rare.� In all cases, rule out medical causes ofaggression.
RISK FACTORS� Male, unneutered.� Inadequate socialization during criticalperiod (3–14 weeks).� Traumatic/negative experience(s).� Predisposing environmentalconditions—associating with other dogs in apack; barrier frustration or tethering; cruelhandling and abuse; and dog baiting andfighting.� Previous aggression/bite history (number ofincidents, target, severity of aggression); legalcitation for biting.� Unpredictability of aggressive incidentswithout warning signals.� Inability of owner to safely confine ormanage the dog in order to prevent futureincidents. Methods include a barrier fence, amuzzle, a collar or head halter, a leash.� Presence of children, elderly people, orother humans or animals at high risk living inor visiting this household.
BLBS078-CF_A31 BLBS078-Tilley July 15, 2011 2:16
48 Blackwell’s Five-Minute Veterinary Consult
Aggression, Overview—Dogs (Continued)A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Identify pathologic conditions associatedwith aggression before a purely behavioraldiagnosis.� A thorough medical evaluation should beconducted on all cases of aggression.� Rule out developmental abnormalities(hydrocephaly, lissencephaly, hepatic shunts),metabolic disorders (hypoglycemia, hepaticencephalopathy, diabetes),neuroendocrinopathies (hypothyroidism,hyperadrenocorticism), dermatopathy,neurologic conditions (intracranial neoplasm,seizures), toxins, inflammatory diseases(encephalitis, rabies), cognitive dysfunction,acute or chronic pain, and iatrogenic causes,such as glucocorticoid administration.
CBC/BIOCHEMISTRY/URINALYSIS� Usually normal.� Abnormalities may suggest underlyingmetabolic, endocrine causes, or other medicalconditions.
OTHER LABORATORY TESTSAs indicated (e.g., thyroid panel,ACTH-stimulation test, other appropriatetests).
IMAGING� May be indicated to identify sources of painor disease.� MRI or CT—particularly if cerebralneoplasia suspected.
DIAGNOSTIC PROCEDURESPostmortem fluorescent antibody test isindicated for any aggressive dog for whichrabies is a differential diagnosis, including anydog not quarantined for 10 days after a biteinjury to a human or other animal.Pathologic FindingsNone, unless an underlying medical etiologyis suspected.
TREATMENTAPPROPRIATE HEALTH CARE� Management success—combination ofmultiple modalities: environmental
Table 1
Drugs and dosages used to manage canine aggression.
Drug Drug Class Oral Dosage in Dog (mg/kg) Dosing Frequency
Fluoxetine SSRI 1–2 mg/kg q24hParoxetine SSRI 1–2 mg/kg q24hSertraline SSRI 2–4 mg/kg q24hClomipramine TCA 1–2 mg/kg q12hAmitriptyline TCA 1–2 mg/kg q12h
control, behavior modification, andpharmacotherapy.� A veterinarian with experience and trainingin aggression management should beconsulted.� Euthanasia should be recommended whenthe risk of injury is high. Noterecommendation in medical record.
NURSING CAREA boarding facility able to safely manage thedog may be used until a safe managementplan can be implemented, or until anoutcome decision made.
ACTIVITYSince frustration and arousal may increase theincidence of aggression, an appropriate andsafe exercise regime should be incorporatedinto the treatment program.
DIETThere is modest evidence that a low-proteindiet may reduce territorial aggression in dogs,an effect that may be enhanced by tryptophansupplementation.
CLIENT EDUCATION� Safe practices should dictate all decisions.These practices include safe confinement,physical barriers, head halters, leash control,muzzle use, and supervision by a competentadult.� The client should be advised to considerpersonal and legal liability risks of keeping thedog. Human injury, bite-related lawsuits, andloss of homeowners insurance can result fromcanine aggression. Such risk assessment mayhelp the client objectively evaluate thesituation.� Situations that have led to aggression in thepast should be listed and a specific plandeveloped to avoid these situations andassociated locations in the future.� Punishment should be avoided, as it hasbeen shown to increase arousal, fear, anddefensive behavior.� Confrontational techniques, such asroll-overs, increase the probability of adefensive aggressive response, may lead tohuman injury, and should be strictly avoided.� Non-confrontational techniques thatmanage resources and teach the dogappropriate responses should be employed.
� The dog should calmly be removed fromaggression-provoking situations.� Euthanasia should be considered if safemanagement cannot be employed, or whenthe risk of injury is high.
SURGICAL CONSIDERATIONSCastration of males
MEDICATIONSDRUG(S) OF CHOICE� None approved by the FDA for thetreatment of aggression.� No drug will eliminate the probability ofaggression.� Use drugs only when a safe managementplan has been implemented.� Inform the client of the experimental natureof medication and risk involved; document inthe medical record, obtain signed informedconsent.� Drugs that increase serotonin may behelpful to reduce anxiety, arousal, andimpulsivity.� Treatment duration: minimum 4 months,maximum: lifetime.� See Table 1 for drugs used to facilitatemanagement of aggression in combinationwith a safe management plan.
CONTRAINDICATIONS� Fluoxetine is contraindicated in cases ofliver disease, seizures.� Clomipramine is contraindicated in cases ofcardiac conduction disturbances or seizures;in one study, no more effective than control incases of owner-directed aggression.� Amitriptyline is contraindicated in patientswith cardiac conduction disturbances,glaucoma, or liver disease.
PRECAUTIONSAvoid the use of benzodiazepines (e.g.,diazepam) in aggressive dogs because of therisk of behavioral disinhibition. Aggressionmay increase when dogs lose their fear of therepercussions of biting.
POSSIBLE INTERACTIONSDo not use SSRIs or TCAs with monoamineoxidase inhibitors, including amitraz andL-deprenyl, or with each other because of therisk of serotonin syndrome.
BLBS078-CF_A31 BLBS078-Tilley July 15, 2011 2:16
Canine and Feline, Fifth Edition 49
(Continued) Aggression, Overview—Dogs A
ALTERNATIVE DRUG(S)� L-Tryptophan 10 mg/kg PO q12h� Megestrol acetate 1 mg/kg PO q24h for2 weeks; then taper to lowest effective dosage;drug of last resort in cases ofdominance-related and intermale aggression;side effects include obesity, blood dyscrasias,pyometra, polyuria/polydipsia, diabetesmellitus, mammary hyperplasia, andmammary carcinoma
FOLLOW-UPPATIENT MONITORING� Weekly to biweekly contact recommendedin the initial phases.� Clients need feedback and assistance withbehavior modification plans and medicationmanagement.
PREVENTION/AVOIDANCE� To prevent aggressive incidents, avoid allsituations that have led to aggression in thepast, using safe confinement, gates, halters,collars, leashes, muzzles.� Reduce the risk of aggression in young dogswith a positive socialization program(3–14 weeks); avoid intimidation techniquesand negative, fear-inducing situations.
POSSIBLE COMPLICATIONS� Injury to humans or animals.� In cases of interdog aggression, although notthe intended target, humans who interfere areoften seriously injured either by accident or byredirected aggression; owners should not reachfor fighting dogs; pull apart with leashes.� Liability to client, veterinarian.
EXPECTED COURSE AND PROGNOSIS� Aggressive dogs weighing over 18.5 kg are atrisk for behavioral euthanasia.� Overtly aggressive dogs are never cured;depending on the situation, they may bemanaged successfully.
� Prognosis is case-dependent due to riskfactors and management features of eachsituation.
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSAdult-onset aggression suggests a medicalcause; carefully evaluate sensory acuity,sources of pain, cognitive function.
ZOONOTIC POTENTIAL� Dog bites are significant public health risk.� Rabies is a potential cause of aggression.
PREGNANCY/FERTILITY/BREEDINGTricyclic antidepressants are contraindicatedin breeding males and pregnant females.
SEE ALSO� Aggression, Fear/Defensive—Dogs� Aggression, Food, Possessive, andTerritorial—Dogs� Aggression, Interdog Aggression� Aggression Toward Familiar People—Dogs
ABBREVIATIONS� ACTH = adrenocorticotropic hormone� CNS = central nervous system� CT = computed tomography� FDA = U.S. Food and DrugAdministration� MRI = magnetic resonance imaging� SSRI = selective serotonin reuptakeinhibitor� TCA = tricyclic antidepressant
INTERNET RESOURCES� American Veterinary Medical AssociationDog Bite Prevention: http://www.avma.org/public health/dogbite/default.asp.
� ASPCA Aggression in Dogs: http://www.aspcabehavior.org/articles/49/Aggression-in-Dogs.aspx.� Centers for Disease Control and PreventionDog Bite Prevention: http://www.cdc.gov/homeandrecreationalsafety/dog-bites/biteprevention.html.� University of California–Davis, CompanionAnimal Behavior Program, Dog Aggression:http://www.vetmed.ucdavis.edu/CCAB/aggression.html.
Suggested ReadingBain M. Aggression toward unfamiliar people
and animals. In: Horwitz DF, Mills D, eds.,BSAVA Manual of Canine and FelineBehavioural Medicine, 2nd ed.Gloucestershire, UK: BSAVA, 2009, pp.211–222.
deKeuster T, Jung H. Aggression towardfamiliar people and animals. In: HorwitzDF, Mills D, eds. BSAVA Manual ofCanine and Feline Behavioural Medicine,2nd ed. Gloucestershire, UK: BSAVA, 2009,182–210.
Herron ME, Shofer FS, Reisner IR. Survey ofthe use and outcome of confrontational andnon-confrontational training methods inclient-owned dogs showing undesiredbehaviors. Appl Anim Behav Sci 2009,117(1–2):47–54.
Luescher AU, Reisner IR. Canine aggressiontoward familiar people: A new look at an oldproblem. Vet Clin North Am Small AnimPract 2008, 38:1107–1130.
Reisner, IR. Differential diagnosis andmanagement of human-directed aggressionin dogs. Vet Clin North Am Small AnimPract 2003, 33:303–320.
Author Barbara L. ShermanConsulting Editor Debra F. Horwitz
Client Education Handoutavailable online
BLBS078-CF_A31a BLBS078-Tilley July 23, 2011 4:26
50 Blackwell’s Five-Minute Veterinary Consult
Aggression toward Familiar People—DogsA
BASICSDEFINITIONAggression (growling, lip-lifting, barking,snarling, snapping, lunging, biting), usuallydirected toward household members or peoplewith an established relationship with the dogin situations involving access to valuedresources. Also referred to as dominanceaggression, status-related aggression, conflictor competitive aggression.
PATHOPHYSIOLOGYHas been thought of as normal canine socialbehavior directed toward people. However,these dogs may show anxiety or be impulsiveand unpredictable.
SYSTEMS AFFECTEDBehavioral
GENETICSBreed predilections exist. Pedigree analyseshave shown increased occurrence in relateddogs. Mode of inheritance is unknown.
INCIDENCE/PREVALENCE20–40% of behavioral referral case loads.
GEOGRAPHIC DISTRIBUTIONRegional breed differences exist.
SIGNALMENTSpeciesDogs
Breed PredilectionsSpaniels (English springer and cocker),terriers, Lhasa apsos, and rottweilers, but maybe exhibited by any breed.
Mean Age and RangeUsually manifested at the onset of socialmaturity (12–36 months of age). May be seenin young dogs.
Predominant SexMales (castrated and intact) more commonlypresented than females.
SIGNSGeneral CommentsCareful history-taking is needed to make adiagnosis, assess the risks to the owners andpublic, and formulate a safe and realistictreatment plan. Owners may not recognize orgive credence to more mild signs of aggressionsuch as staring, growling, baring teeth, orsnapping, which are often present before bitesoccur. Details of early aggressive episodes arevital for establishing the diagnosis andprognosis. Clinicians should be aware that notall owner-directed aggression is motivated bythe desire to control but often is anxiety- orfear-based.
Historical Findings� Aggression around resting areas, food, toys,handling (e.g., petting and reaching toward),and favored possessions, including people.Aggression is directed toward household
members or persons that have an establishedrelationship with the dog. Aggressivebehaviors may be seen in other contexts,including but not limited to defense ofterritory, when dogs are reprimanded ordenied access to items or activities, andtoward unfamiliar people. History-takingshould attempt to establish aggression triggersand frequency/severity of aggressive episodes.� Aggression may not occur every time thedog is in a certain situation and may not bedirected uniformly toward each person withinthe household. � Stiff body posture, staring,head up, ears up and forward, or tail upusually accompanies aggressive behavior.Owners may report a combination of thesepostures with more submissive postures (e.g.,tail is up but ears are tucked, eyes averted),which may represent an element of conflict,anxiety, or fear in the dog’s motivation.� Owners often describe these dogs as“moody” and may be able to judge when thedog is likely to be aggressive. In early episodesthe dog may show fear through eye aversion,tail tucking, and avoidance that may diminishas the dog becomes more confident thataggression will change the outcome. � Anxietymay be noted in pet-owner interactions andother situations such as owner departure ornovel situations. Some dogs control theirenvironment using aggression only because itis effective, but they are anxious about everyencounter, while other dogs appear confidentand secure.
Physical Examination Findings� Usually unremarkable. � Medicalconditions, especially pain, may contribute tothe expression of aggression. These dogs maynot show aggression toward a confident butnon-threatening examiner. However, extremecaution should be taken when examiningdogs that show aggression, including the useof muzzles or other humane restraint devices.
CAUSES� May be part of a normal canine socialbehavioral repertoire, but its expression isinfluenced by environment, learning, andgenetics. � The manifestation of aggressionmay be influenced by underlying medicalconditions, early experiences (learning thataggression works to control situations), andinconsistent or lack of clear rules and routineswithin the household and within human-petinteractions. � Aggression is rarely a symptomof medical conditions; however, concurrentdisease must be ruled out, since illness and/orpain may influence the tendency foraggressive behaviors.
RISK FACTORSInconsistent or inappropriate physicalpunishment and inconsistent ownerinteractions may contribute to thedevelopment of conflicted and/or aggressivebehavior.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Fear-based aggression � Anxiety conditions� Pathological disease conditions associatedwith aggression (e.g., painful conditions,endocrinopathies)
CBC/BIOCHEMISTRY/URINALYSISUsually unremarkable. Abnormalities mayindicate an underlying or contributingmedical condition.
OTHER LABORATORY TESTSAs indicated to rule out underlying diseases.
IMAGINGMRI if CNS disease is suspected; as needed torule out underlying medical conditions; maybe useful to rule out sources of pain.
TREATMENTAPPROPRIATE HEALTH CAREOutpatient behavior modification; medicalmanagement as needed.
ACTIVITYAppropriate physical activity may helpdecrease incidences of aggression.
DIETLow-protein/high-tryptophan diets may helpreduce aggression but are unlikely to make asignificant difference without behaviormodification.
CLIENT EDUCATIONGeneral Comments� Successful treatment, resulting in a decreasein aggressive incidents, depends upon ownerunderstanding of basic canine social behavior,risks involved in living with an aggressive dog,and how to implement safety andmanagement recommendations. � Treatmentis aimed at controlling the problem, not atachieving a “cure.” � Owners must be awarethat the only way to prevent future injuries iseuthanasia. � It is very important that ownersare educated about the risks of using physicalpunishment and training techniques that relyon owners learning to “dominate” their dogs.In recent years, there has been a resurgence ofthese training techniques. The improper andinappropriate use of physical punishments/dominance techniques ranging fromcorrections with choke chains to so-calledalpha rolls to setting up situations to provokeand then correct aggression can lead tohuman injury, increased aggression, anincrease in anxiety, and a disruption of thehuman-animal bond.
Safety Recommendations� If owners elect not to euthanize, they mustbe aware that their primary responsibility ispreventing human injury by conscientiously

BLBS078-CF_A31a BLBS078-Tilley July 23, 2011 4:26
Canine and Feline, Fifth Edition 51
(Continued) Aggression toward Familiar People—Dogs A
avoiding situations that may evoke anaggressive reaction, including situations thathave resulted in the dog’s being fearful even ifnot aggressive. Use information from thepatient’s history to help owners identifyspecific situations to avoid. Do not allow thedog on furniture. Do not give valuable treatsor toys (e.g., rawhides). Pick up toys and haveowners control playtime and activity. Limitphysical contact with the dog, includingpetting. Do not physically punish orreprimand the dog. � Treatment is more likelyto be successful if a period of preventingexposure to aggression-provoking stimuli isinstituted prior to behavior modification.� Teaching the dog to be comfortable wearinga head halter (e.g., Gentle Leader) with alightweight 8- to 10-foot leash attached andbasket muzzle whenever in contact withpeople makes controlling potentiallydangerous situations easier and safer. � Usethe long leash to safely remove the dog fromsituations that may elicit aggression; do notreach for the dog directly.
Behavioral Therapy� Behavior modification—usenon-confrontational methods to teach the dogto view people as leaders and reward-basedtraining techniques to teach the dog to obeycommands from people without experiencingconflict or becoming aggressive. � Affectioncontrol—require the dog to follow acommand before receiving anything it desiresfrom people (also known as “Nothing in life isfree” or “Learn to earn”). For example, the dogmust sit or lie down before feeding, petting,play, or going for a walk. For the initial 2- to3-week period, owners should give the dogattention only during brief, structured (e.g.,command-response-reward) periods. At othertimes, they must ignore the dog, especially ifit is soliciting attention. The owner initiatesinteraction by giving a command andterminates interaction. � Use positivereinforcement (e.g., food, toys, play, petting)to teach behaviors that are incompatible tothose that have resulted in aggression. Forexample, teach an “Off” command to moveoff furniture or “Drop it” command to releasetoys. Also referred to as counter commandingor response substitution. � Desensitizationand counter-conditioning—techniqueused to decrease reactivity to situations thathave resulted in aggression in the past. Amuzzle may be needed for safety. Do notbegin until the owner has assumed a greaterlevel of control over the dog through affectioncontrol and reward-based training. The dog isfirst taught to sit and relax on a verbalcommand in neutral locations using foodrewards. Gradual exposure of the dog to agreatly reduced stimulus is attempted so nofearful and/or aggressive reaction is elicited.The non-fearful and non-aggressive behavioris rewarded. The level of stimulation isincreased gradually, staying below the
threshold that would result in fear and/oraggression. Progress is slow and careful.Monitoring of responses is essential.
SURGICAL CONSIDERATIONS� Neuter intact males. � Females that start toshow dominance aggression at less than 6months of age may be less aggressive whenmature if not spayed.
MEDICATIONSDRUG(S) OF CHOICE� There are no medications licensed for thetreatment of canine aggression. Owners mustbe aware that the use of medications isoff-label. Due to liability concerns, note inthe patient’s record that owners wereinformed of potential risks and side effects. Asigned informed consent form is advisable.NEVER use medications without behaviormodification. Before prescribing medication,be sure that owners understand the risks inowning an aggressive dog, will follow safetyprocedures, and will not rely on medication tokeep others safe. Medication may not beappropriate in some family situations (e.g.,those with small children, family memberswith disabilities, or immunocompromisedindividuals). � Medication studies, includinga double-blind placebo-controlled study ofmedication for dominance aggression, haveshown a strong placebo effect and nodifference between placebo and medication inreducing aggressive behaviors.
Selective Serotonin Reuptake Inhibitors� Fluoxetine 0.5–2 mg/kg PO q24h (canine)� Paroxetine 0.5–1 mg/kg PO q24h (canine)� Sertraline 1–3 mg/kg PO q24h (canine)� Side effects: sedation, irritability, GITeffects; anorexia is common and usuallytransient.
Tricyclic Antidepressants� Clomipramine 2–4 mg/kg PO q24h ordivided q12h (label restriction for aggression)(canine) � Side effects: sedation, GIT effects,anticholinergic effects, and cardiacconduction disturbances if predisposed.
CONTRAINDICATIONSUse caution when prescribingbenzodiazepines, as disinhibition ofaggression may result due to a reduction infear-based inhibition to biting.
PRECAUTIONSAny psychotropic medication may increaserather than decrease aggression.Corticosteroids are contraindicated infood-aggressive dogs; polyphagia can lead toincreased frequency/intensity ofaggression.
POSSIBLE INTERACTIONSDo not combine SSRIs, TCAs, or MAOinhibitors (e.g., amitraz, selegiline) and
tramadol—can result in potentially fatalserotonin syndrome.
FOLLOW-UPPATIENT MONITORINGClients often need ongoing assistance withbehavior cases, especially aggression. At leastone follow-up call within the first 1–3 weeksafter consultation is advisable. Provisions forfurther follow-up either by phone or inperson should be made at that time.
PREVENTION/AVOIDANCETreatment recommendations arelifelong—may see recurrence of aggressionwith treatment lapses. Continued avoidanceof aggression triggers may be necessary.
POSSIBLE COMPLICATIONSHuman injuries; euthanasia or relinquishmentof patient.
EXPECTED COURSE AND PROGNOSISThere is no cure. Prognosis for improvementis better if aggression is at a low intensity andoccurs in relatively few predictable situations.Prognosis is highly dependent on ownercompliance.
MISCELLANEOUSASSOCIATED CONDITIONSOther forms of aggression, especiallyterritorial and interdog aggression. Aggressivedogs often have underlying anxiety.
AGE-RELATED FACTORSBitches showing dominance aggression whenless than 6 months old may show a reductionin the level of aggression if not spayed.
ZOONOTIC POTENTIALHuman injury from bite wounds.
PREGNANCY/FERTILITY/BREEDINGDo not breed aggressive dogs.
SYNONYMS� Competitive aggression � Conflictaggression � Dominance-related aggression� Rage syndrome � Status-related aggression
ABBREVIATIONS� CNS = central nervous system � GIT =gastrointestinal tract � MAO = monoamineoxidase � MRI = magnetic resonance imaging� SSRI = selective serotonin reuptakeinhibitor � TCA = tricyclic antidepressantAuthor Laurie Bergman and Meredith StepitaConsulting Editor Debra F. Horwitz
Client Education Handoutavailable online
BLBS078-CF_A32 BLBS078-Tilley March 21, 2011 20:15
52 Blackwell’s Five-Minute Veterinary Consult
Alkalosis, MetabolicA
BASICSDEFINITIONIncrease in pH associated with an increase inplasma bicarbonate concentration (HCO3
−)(dogs, > 24 mEq/L; cats, > 22 mEq/L) and acompensatory increase in carbon dioxidetension (PCO2).
PATHOPHYSIOLOGY� Metabolic alkalosis may develop secondaryto corrected hypochloremia (hypochloremicalkalosis) or hypoalbuminemia(hypoalbuminemic alkalosis).� Hypochloremic alkalosis:
◦ Loss of chloride—fluid rich in chlorideand hydrogen ion may be lost via thealimentary tract or kidneys. Loss ofchloride and H+ is associated with anincrease in plasma HCO3
− concentration.With chloride loss and volume depletion,the kidneys reabsorb sodium with HCO3
−
instead of chloride, perpetuating themetabolic alkalosis.◦ Chronic administration of alkali (fluidswith high sodium and poor chlorideconcentration)—also may result intransient metabolic alkalosis. Renalexcretion of exogenously administeredalkali is effective, and it is difficult to createmetabolic alkalosis by increasing HCO3
−
intake unless the patient has renaldysfunction.
� Hypoalbuminemic alkalosis:◦ Decrease in plasma weak acids—loss ofalbumin, a weak acid, is associated withmetabolic alkalosis.
SYSTEMS AFFECTED� Nervous—muscle twitching and seizuresoccur rarely in dogs. Metabolic alkalosis andassociated hypokalemia may precipitatehepatic encephalopathy in patients with liverfailure.� Renal/Urologic—the kidneys rapidly andeffectively excrete excessive alkali. In patientswith chloride deficiency (and less importantly,volume depletion), the kidneys cannot excretethe excessive alkali and metabolic alkalosis ismaintained. In these patients, chlorideadministration is required for renalcompensation to occur, whereas volumeexpansion will hasten compensation. Patients
with mineralocorticoid excess have excessivechloride loss and chloride administration doesnot lead to hyperchloremia and correction ofmetabolic alkalosis (so-calledchloride-resistant metabolic alkalosis).� Respiratory—low [H+] reduces alveolarventilation. Hypoventilation increases PCO2
and helps offset the effects of high plasmaHCO3
− on pH. In dogs, an increase ofapproximately 0.7 mm Hg in PCO2 can beexpected for each 1 mEq/L increase in plasmaHCO3
−. Limited data is available for cats,but the degree of respiratory compensationappears to be similar.
SIGNALMENTAny breed, age, or sex of dog and cat
SIGNSHistorical Findings� Administration of loop diuretics (e.g.,furosemide) or thiazides.� Vomiting.
Physical Examination Findings� Signs related to the underlying disease oraccompanying potassium depletion (e.g.,weakness, cardiac arrhythmias, and ileus).� Muscle twitching caused by low ionizedcalcium concentration.� Dehydration in volume-depleted patients.� Muscle twitching and seizures in patientswith neurologic involvement (rare).
CAUSES� Chloride-responsive—diureticadministration, vomiting of stomachcontents, and rapid correction of chronichypercapnia (respiratory acidosis).� Chloride-resistant—hyperadrenocorticismand primary hyperaldosteronism.� Oral administration ofalkali—administration of sodium bicarbonateor other organic anions with sodium (e.g.,lactate, acetate, gluconate); administration ofcation-exchange resin with non-absorbablealkali (e.g., phosphorus binders).� Hypoalbuminemia.
RISK FACTORS� Administration of loop or thiazide diuretics.� Vomiting.� Stomach drainage.� Diseases associated with hypoalbuminemia(e.g., nephritic syndrome, liver failure).
DIAGNOSISDIFFERENTIAL DIAGNOSISHigh plasma HCO3
− and hypochloremia inanimals can also be compensating for chronicrespiratory acidosis, in which PCO2 is highand pH is low despite high HCO3
− and lowchloride concentration; blood gasdetermination required to differentiate.
LABORATORY FINDINGSDrugs That May Alter Laboratory ResultsNone
Disorders That May Alter LaboratoryResults� Too much heparin (> 10% of the sample)decreases HCO3
−.� Blood samples stored at room temperaturefor more than 20 minutes have low pHbecause of increased PCO2.
Valid if Run in Human Laboratory?Yes
CBC/BIOCHEMISTRY/URINALYSIS� High total CO2 (total CO2 in sampleshandled aerobically closely approximatesHCO3
−).� Low blood ionized calcium concentration.� Serum electrolyte abnormalities vary withunderlying cause.� Hypochloremia—consider hypochloremicmetabolic alkalosis, the most common reasonfor metabolic alkalosis in dogs and cats, whichusually results from diuretic administration orvomiting of stomach contents.� High sodium but normal chlorideconcentration—consider chloride-resistantmetabolic alkalosis (e.g.,hyperadrenocorticism or primaryhyperaldosteronism) or administration ofalkali.� Hypoalbuminemia—considerhypoalbuminemic metabolic alkalosis (e.g.,liver failure, protein-losing enteropathy, andprotein-losing nephropathy). In vitro, a 1g/dL decrease in albumin concentration isassociated with an increase in pH of 0.093 incats and 0.047 in dogs.� Hypokalemia—hypokalemia likely resultsfrom metabolic alkalosis or the underlyingproblem (e.g., vomiting of stomach contentsor loop diuretic administration);hypokalemia-induced metabolic alkalosis doesnot occur in dogs and cats.
BLBS078-CF_A32 BLBS078-Tilley March 21, 2011 20:15
Canine and Feline, Fifth Edition 53
(Continued) Alkalosis, Metabolic A
OTHER LABORATORY TESTSBlood gas analysis reveals high HCO3
−, highPCO2, and high pH.
IMAGINGNone
DIAGNOSTIC PROCEDURESNone
TREATMENT� Acid-base disturbances are secondaryphenomena. Diagnosis and treatment of theunderlying disease process is integral to thesuccessful resolution of acid-base disorders.� Severe alkalemia is uncommon, but may belife-threatening. Patients with chronicrespiratory disease and respiratory alkalosis areat risk of developing severe alkalemia if theystart vomiting or receive diuretics.� Discontinue drugs that may cause metabolicalkalosis.
NURSING CAREThe fluids of choice contain chloride; givepatients with volume depletion an intravenousinfusion of 0.9% NaCl supplemented withKCl; patients with hypokalemia may requirelarge doses of KCl (see Hypokalemia).
MEDICATIONSDRUG(S) OF CHOICEHypochloremic Alkalosis� If there is evidence of volume depletion, thedeficit should be repaired with achloride-containing fluid (e.g., 0.9% NaCl).� If the underlying cause cannot be corrected(e.g., chronic heart failure patients receivingdiuretics), oral compounds containingchloride without sodium (e.g., KCl, NH4Cl)can be tried; also consider simultaneous use ofdistal tubule blocking agents (e.g.,spironolactone).� H2-blocking agents such as ranitidine orfamotidine reduce gastric acid secretion andmay be considered as adjunctive therapy ifgastric losses are ongoing.� Chloride-resistant metabolic alkalosis canonly be corrected by resolution of theunderlying disease; metabolic alkalosis isusually mild in these patients.
� If the metabolic alkalosis is associated withhypokalemia and total body potassiumdeficits, correcting the deficit with KCl is aparticularly effective way to reverse thealkalosis.
Hypoalbuminemic AlkalosisTreatment for hypoalbuminemic alkalosisshould be directed at the underlying cause andthe decreased colloid oncotic pressure.
CONTRAINDICATIONS� Avoid chloride-free fluids—they maycorrect volume depletion but will not correcthypochloremic alkalosis.� Avoid using salts of potassium withoutchloride (e.g., potassiumphosphate)—potassium will be excreted inthe urine and will correct neither the alkalosisnor the potassium deficit.
PRECAUTIONSDo not use distal blocking agents (e.g.,spironolactone) in volume-depleted patients.
POSSIBLE INTERACTIONSNone
ALTERNATIVE DRUG(S)None
FOLLOW-UPPATIENT MONITORINGAcid-base status—frequency dictated by theunderlying disease and patient response totreatment.
POSSIBLE COMPLICATIONS� Hypokalemia� Neurologic signs
MISCELLANEOUSASSOCIATED CONDITIONS� Hypokalemia� Hypochloremia
AGE-RELATED FACTORSNone
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMS� Non-respiratory alkalosis.� Chloride-responsive metabolicalkalosis—metabolic alkalosis that respondsto chloride administration.� Chloride-resistant alkalosis—metabolicalkalosis secondary to increasedmineralocorticoid activity that does notrespond to chloride administration.� Hypochloremic alkalosis—metabolicalkalosis caused by low chlorideconcentration.� Hypoalbuminemic alkalosis—metabolicalkalosis caused by low albuminconcentration.� Concentration alkalosis—metabolicalkalosis resulting from decreased free water inplasma.� Contraction alkalosis—metabolic alkalosisformerly attributed to volume contraction,but now known to be caused by chloridedepletion. Volume depletion is a common butnot essential feature.
SEE ALSO� Hypochloremia� Hypokalemia
ABBREVIATIONS� H+ = hydrogen ion� HCO3
− = bicarbonate� PCO2 = carbon dioxide tension
Suggested Readingde Morais HA. Chloride ion in small animal
practice: The forgotten ion. J Vet EmergCrit Care 1992, 2:11–24.
de Morais HA, Constable PD. Strong ionapproach to acid-base disorders. In:DiBartola SP, ed., Fluid, Electrolyte andAcid-Base Disorders, 3rd. ed. Philadelphia:Saunders, 2006, pp. 310–321.
de Morais HA, Leisewitz AL. Mixed acid-basedisorders. In: DiBartola SP, ed., Fluid,Electrolyte and Acid-Base Disorders, 3rd.ed. Philadelphia: Saunders, 2006, pp.296–309.
DiBartola SP. Metabolic acid-base disorders.In: DiBartola SP, ed., Fluid, Electrolyte andAcid-Base Disorders, 3rd. ed. Philadelphia:Saunders, 2006, pp. 251–283.
Robinson EP, Hardy RM. Clinical signs,diagnosis, and treatment of alkalemia indogs: 20 cases (1982–1984). JAVMA 1988,192:943–949.
Author Helio Autran de Morais and StephenP. DiBartolaConsulting Editor Carl A. Osborne
BLBS078-CF_A33 BLBS078-Tilley July 15, 2011 2:40
54 Blackwell’s Five-Minute Veterinary Consult
Alopecia—CatsA
BASICSDEFINITION� Common problem� Pattern of hair loss—varied or symmetrical� Causes—multifactorial
PATHOPHYSIOLOGYSpecific and unique for each cause
SYSTEMS AFFECTED� Endocrine/Metabolic� Hemic/Lymphatic/Immune� Skin/Exocrine
SIGNALMENT� No specific age, breed, or sex predilection.� Neoplastic and paraneoplastic associatedalopecias—generally recognized in older cats.
SIGNSDepends on specific diagnosis
CAUSES� Neurologic/behavioral—compulsivedisorder.� Endocrine—sex hormone alopecia,hyperthyroidism, hyperadrenocorticism,diabetes mellitus.� Immunologic—allergic dermatitis, alopeciaareata, alopecia mucinosa, lymphocytic muralfolliculitis, pseudopelade.� Parasitic—demodicosis, cheyletiellosis.� Infections—dermatophytosis.� Physiologic/metabolic—sebaceous adenitis.� Neoplastic—paraneoplastic dermatitis,squamous cell carcinoma in situ,epitheliotropic lymphoma, thymoma withexfoliative dermatitis.� Idiopathic/inherited—alopecia universalis,hypotrichosis, spontaneous pinnal alopecia,anagen and telogen defluxion.� Injection site reaction.� Medication effect—corticosteroids.� Viral—FeLV- and FIV-associated disease(giant cell dermatosis).
RISK FACTORSFeLV/FIV—for demodicosis
DIAGNOSISDIFFERENTIAL DIAGNOSISEndocrine Alopecia/Sex Hormone� Rarely a hormonal abnormality.� Hormonal causes—primarily castratedmales; alopecia along the caudal aspect of thehind limbs, which may extend along theperineum.� Excessive corticosteroid administration.� Megestrol acetate—may produce lesionssimilar to/associated with diabetes mellitus orhyperadrenocorticism.
Compulsive Disorder� Uncommon as sole source of symptoms.
� Often misdiagnosed in cases of allergicdermatitis.� Often misdiagnosed as endocrine alopecia.� The pattern of alopecia is frequentlysymmetrical without associated inflammation.
Allergic Dermatitis� Varies from mild partial alopecia with littleinflammation to severe excoriation andulceration.� Barbering of the hair coat often occursclandestinely leading to a misdiagnosis ofendocrine alopecia.� Distribution—varied; often the head andneck region are most severely affected.� Food allergy, atopy/contact atopy, andectoparasite hypersensitivity.
Hyperthyroidism� Partial to complete alopecia fromself-barbering.� Varied pattern.� Middle-aged to old cats.� Often misdiagnosed in cases of allergicdermatoses, compulsive disorder, or otherendocrine alopecia.
Diabetes Mellitus� Partial alopecia with an unkempt hair coatand excessive scaling.� Poor wound healing.� Increased susceptibility to infections.� Cutaneous xanthomatosis secondary tohyperlipidemia (nodular to linear, yellow-pinkalopecic plaques that tend to ulcerate).
Hyperadrenocorticism� Rare; characterized by alopecia and fragilityof the skin.� Truncal alopecia, with or without a rattailand a curling of the pinnal tips.� Extreme skin fragility noted inapproximately 70%.� Occurs secondary to pituitary or adrenaltumors.� Iatrogenic form less common in cats than indogs.
Paraneoplastic Alopecia� Most cases associated with pancreaticexocrine adenocarcinomas, bile ductcarcinomas, exfoliative dermatitis withthymoma.� Middle-aged to old cats (9–16 years).� Pancreatic carcinoma/bile duct carcinoma:acute onset, progress rapidly, bilaterallysymmetrical, ventrally distributed (alsolocated along the bridge of the nose andperiocular), hair epilates easily, rare pruritus,erythema with dry fissuring footpads,glistening appearance to alopecic skin, skin isoften thin and hypotonic, rapid weight loss.� Thymoma with exfoliative dermatitis:non-pruritic scaling dermatitis that starts atthe head and neck.
Sebaceous Adenitis� Slowly progressive partial alopecia associatedwith scaling along the dorsum of the bodyand the extremities.
� Sebaceous glands are selectively destroyedby toxic intermediate metabolites orimmunologic mechanisms.� Possible dramatic pigment accumulationalong the eyelid margins.� Questionable association with systemicdisease (e.g., inflammatory bowel disease,lupus-like syndromes, upper respiratory tractinfections).
Squamous Cell Carcinoma In Situ� Multicentric premalignant dermatosis in oldcats.� Associated with papilloma virus; Bowenoidin situ carcinoma.� Slightly elevated, often pigmented,plaque-like or papillated lesions with scalingand partially alopecic surfaces.� Often misdiagnosed as seborrhea beforedistinct lesions develop.� About 25% may convert to squamous cellcarcinoma with in situ lesions along theborders (histologically).
Epitheliotropic Lymphoma� Early stages—varying degrees of alopeciaassociated with scaling and erythema.� Later stages—plaques and nodules.� Old cats.
AlopeciaAreata/Pseudopelade/LymphocyticMural Folliculitis� This group of differentials is oftenconsidered preneoplastic with animmunologic inciting cause.� Alopecia areata—rare; complete alopecia ina patchy distribution with no inflammation;head, neck, ears; histologic lymphocyticaccumulation around the hair bulb.� Lymphocytic mural folliculitis—diffusealopecia of the face, eyelids, muzzle; skin has athick waxy feel; histologic lymphocyticinvasion of the follicular outer root sheathand epidermis.� Pseudopelade—well-circumscribednon-pruritic alopecia that often starts on theface; nails may slough.
Alopecia Universalis (Sphynx Cat)� Hereditary.� Complete absence of primary hairs;decreased secondary hairs.� Thickened epidermis; normal dermis.� Sebaceous and apocrine ducts open directlyonto the skin surface; oily feel to skin.� Wrinkled foreheads; gold eyes; no whiskers;downy fur on paws, tip of tail, and scrotum.� Comedones with or without secondaryfolliculitis.
Feline Hypotrichosis� Siamese and Devon Rex cats (autosomalrecessive alopecia).� Poorly developed primary telogen hairfollicles.� Born with a normal coat; becomes thin andsparse as young adult.
Spontaneous Pinnal Alopecia� Siamese cats predisposed.
BLBS078-CF_A33 BLBS078-Tilley July 15, 2011 2:40
Canine and Feline, Fifth Edition 55
(Continued) Alopecia—Cats A
� May represent a form of alopecia areata orpattern baldness.
Anagen and Telogen Defluxion� Acute loss of hair due to interference withthe growth cycle.� Causes—stress, infection, endocrinedisorder, metabolic disorder, fever, surgery,anesthesia, pregnancy, drug therapy.
Demodicosis� Rare.� Partial to complete multifocal alopecia ofthe eyelids, periocular region, head, and neck.� Variable pruritus with erythema, scale, andcrust, and ceruminous otitis externa.� Demodex cati (elongated shape) oftenassociated with metabolic disease (e.g., FIV,systemic lupus erythematosus, diabetesmellitus).� Short/blunted D. gatoi mite is rarely amarker for metabolic disease; this form maybe transferable from cat to cat and has beenassociated with pruritus.
Cheyletiellosis� Variable pruritus with scaling.� Not all animals in the household may beaffected.
Dermatophytosis� Numerous clinical manifestations; alwaysassociated with alopecia.
CBC/BIOCHEMISTRY/URINALYSISAbnormalities may be noted with diabetesmellitus, hyperadrenocorticism, andhyperthyroidism.
OTHER LABORATORY TESTS� FeLV and FIV—risk factors for demodicosis.� Thyroid hormones—documenthyperthyroidism.� ANA titer—look for systemic lupuserythematosus.� ACTH-response test, LDDST, andHDDST—diagnose hyperadrenocorticism.
IMAGING� Abdominal ultrasound—assess adrenals inhyperadrenocorticism and look for cancer inanimals with paraneoplastic syndrome.� CT scan—look for pituitary tumors inanimals with hyperadrenocorticism.
DIAGNOSTIC PROCEDURES� Skin biopsy� Skin scrapes� Dermatophyte culture� Shirts/collar to prove self-trauma� Food elimination trials� Intradermal allergy test
TREATMENT� Therapy is limited for many of thesedisorders.� Behavioral modification or protecting haircoat with a shirt may prevent self-barbering.
� Removal of an offending dietary item mayalleviate the symptoms of food allergy.� If the pet is compliant, shampoo and topicaltherapy may relieve secondary problems, suchas hyperkeratosis in sebaceous adenitis,crusting in demodicosis, secondary bacterialinfection, and malodor for greasy dermatoses.
MEDICATIONSDRUG(S)� Compulsive disorder—amitriptyline (10mg/cat/day) as well as otherbehavior-modifying medications.� Endocrine alopecia (males)—testosteronesupplementation.� Allergic dermatitis—antihistamines,restricted-ingredient diet, corticosteroids,allergen-specific immunotherapy, ectoparasitecontrol.� Hyperthyroidism—oral medications such asmethimazole (tapazole) or radioactive iodinetherapy.� Diabetes mellitus—regulation of glucoselevels (insulin).� Hyperadrenocorticism—surgery; no knowneffective medical therapy.� Paraneoplastic alopecia—no therapy; oftenfatal.� Epitheliotropic lymphoma—retinoids(isotretinoin), corticosteroids, interferon,cyclosporine, lomustine.� Sebaceous adenitis—retinoids,corticosteroids, cyclosporine.� Squamous cell carcinoma in situ—surgicalexcision, retinoids (topical and oral), topicalimiquimod cream.� Alopecia areata—no therapy; possiblycounterirritants.� Demodicosis—lime sulfur dips at weeklyintervals for four to six dips.� Cheyletiellosis—topical antiparasiticidesand environmental control.� Dermatophytosis—griseofulvin (caution:idiosyncratic toxicity), itraconazole,terbinafine.
PRECAUTIONSToxicity with griseofulvin and itraconazole(see Dermatophytosis)
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGDetermined by specific diagnosis
PREVENTION/AVOIDANCEDetermined by specific diagnosis
POSSIBLE COMPLICATIONSDetermined by specific diagnosis
EXPECTED COURSE AND PROGNOSISDetermined by specific diagnosis
MISCELLANEOUSZOONOTIC POTENTIALDermatophytosis—can cause skin lesions inhumans.� Cheyletiellosis—can cause irritation inhumans.
PREGNANCY/FERTILITY/BREEDINGRetinoids and griseofulvin should not beadministered to pregnant animals.
SEE ALSO� Cheyletiellosis� Demodicosis� Dermatophytosis� Diabetes Mellitus without Complication,Cats� Feline Paraneoplastic Alopecia� Hyperthyroidism� Sebaceous Adenitis, Granulomatous
ABBREVIATIONS� ACTH = adrenocorticotropic hormone� ANA = antinuclear antibody� CT = computed tomagraphy� FeLV = feline leukemia virus� FIV = feline immunodeficiency virus� HDDST = high-dosedexamethasone-suppression test� LDDST = low-dosedexamethasone-suppression test
Suggested ReadingBaer KE, Helton KA. Multicentric squamous
cell carcinoma in situ resembling Bowens’disease in cats. Vet Pathol 1993,30:535–543.
Helton Rhodes KA, Wallace M, Baer KE.Cutaneous manifestations of felinehyperadrenocorticism. In: Ihrke PJ, MasonIS, White SD. Advances in VeterinaryDermatology. New York: Pergamon, 1993.
Scott DW, Griffin CE, Miller BH. Acquiredalopecia. In: Muller & Kirk’s Small AnimalDermatology, 5th ed. Philadelphia:Saunders, 1995, pp. 720–735.
Scott DW, Griffin CE, Miller BH. Congenitaland hereditary defects. In: Muller & Kirk’sSmall Animal Dermatology, 5th ed.Philadelphia: Saunders, 1995, pp. 736–805.
Scott DW, Griffin CE, Miller BH. Endocrineand metabolic diseases. In: Muller & Kirk’sSmall Animal Dermatology, 5th ed.Philadelphia: Saunders, 1995, pp. 627–719.
Author Karen Helton RhodesConsulting Editor Alexander H. Werner
Client Education Handoutavailable online
BLBS078-CF_A34 BLBS078-Tilley June 16, 2011 10:41
56 Blackwell’s Five-Minute Veterinary Consult
Alopecia—DogsA
BASICSDEFINITION� Common disorder.� Characterized by a complete or partial lackof hair in areas where it is normally present.� May be associated with multiple causes, bethe primary problem, or be secondary to anunderlying cause.
PATHOPHYSIOLOGY� Multiple causes.� Represents a disruption in the growth of thehair from infection, trauma, immunologicattack, mechanical “plugging,” endocrineabnormalities, neoplasia, and/or blockage ofthe receptor sites for stimulation of the hairgrowth cycle.
SYSTEMS AFFECTED� Endocrine/Metabolic� Hemic/Lymphatic/Immune� Skin/Exocrine
SIGNALMENTBreed predilection listed below
SIGNS� May be acute in onset or slowly progressive.� Multifocal patches of circularalopecia—most frequently associated withfolliculitis from bacterial infection anddemodicosis.� Large, more diffuse areas of alopecia—mayindicate a follicular dysplasia or metaboliccomponent.� The pattern and degree of hair loss areimportant for establishing a differentialdiagnosis.
CAUSESMultifocal� Localized demodicosis—partial to completealopecia with erythema and mild scaling;lesions may become inflamed and crusted.� Dermatophytosis—partial to completealopecia with scaling; with or withouterythema; not always ring-like.� Staphylococcal folliculitis—circular patternsof alopecia with epidermal collarettes,erythema, crusting, and hyperpigmentedmacules.� Injection reactions—inflammation withalopecia and/or cutaneous atrophy fromscarring.
� Rabies vaccine vasculitis—well-demarcatedpatch of alopecia observed 2–3 monthspost-vaccination.� Localized scleroderma—well-demarcated,shiny, smooth, alopecic, thickened plaque.� Alopecia areata—non-inflammatory areas ofcomplete alopecia.� Sebaceous adenitis (short-coatedbreeds)—annular to polycyclic areas ofalopecia and scaling.
Symmetrical� Hyperadrenocorticism—truncal alopeciaassociated with atrophic skin, comedones, andpyoderma.� Hypothyroidism—alopecia is anuncommon presentation.� Non-inflammatory alopecia (alopeciaX)—symmetrical truncal alopecia associatedwith hyperpigmentation; alopecia often startsalong the collar area of the neck; Pomeranian,chow chow, Akita, Samoyed, Keeshonden,Alaskan malamute, and Siberian husky.� Hyperestrogenism (females)—symmetricalalopecia of the flanks and perineal andinguinal regions with enlarged vulva andmammary glands.� Hypogonadism in intact females—perineal,flank, and truncal alopecia.� Testosterone-responsive dermatosis incastrated males—slowly progressive truncalalopecia.� Male feminization from Sertoli celltumor—alopecia of the perineum and genitalregion with gynecomastia.� Castration-responsive dermatosis—hair lossin the collar area, rump, perineum, and flanks.� Estrogen-responsive dermatosis in spayedfemale dogs—alopecia of the perineum andgenital regions.� Seasonal flank alopecia/cyclic flankalopecia—serpiginous flank alopecia withhyperpigmentation; boxer, English bulldog,Airedale terrier.
Patchy to Diffuse� Demodicosis—often associated witherythema, folliculitis, and hyperpigmentation.� Bacterial folliculitis—multifocal area ofcircular alopecia to coalescing large areas ofhair loss; epidermal collarettes.� Dermatophytosis—often accompanied byscale.� Sebaceous adenitis—alopecia with a thickadherent scale; predominantly on the dorsumof the body, including the head andextremities.
� Color mutant/ dilution alopecia—thinningof the hair coat with secondary folliculitis.� Follicular dysplasia—slowly progressivealopecia.� Anagen defluxion and telogendefluxion—acute onset of alopecia.� Hypothyroidism—diffuse thinning of thehair coat.� Hyperadrenocorticism—truncal alopeciawith thin skin and formation of comedones.� Epitheliotropic lymphoma—diffuse,generalized truncal alopecia with scaling anderythema, later nodule and plaque formation.� Pemphigus foliaceus—hair loss associatedwith scale and crust formation.� Keratinization disorders—alopeciaassociated with excessive scale and greasysurface texture.
Specific Locations� Pinnal alopecia/patternbaldness—miniaturization of hairs andprogressive alopecia; dachshund, greyhound,American water spaniel, Portuguese waterspaniel, Boston terrier, Manchester terrier,whippet, Italian greyhound, Chihuahua.� Traction alopecia—hair loss on the top andlateral aspect of the cranium secondary tohaving barrettes or rubber bands applied tothe hair.� Post-clipping alopecia—failure to regrowafter clipping; may be associated with hairgrowth cycle disruption.� Melanoderma (alopecia of Yorkshireterriers)—symmetrical alopecia of the pinnae,bridge of the nose, tail, and feet.� Seasonal flank alopecia/cyclic flankalopecia—serpiginous flank alopecia withhyperpigmentation; boxer, English bulldog,Airedale terrier.� Black hair follicular dysplasia—alopecia ofthe black-haired areas only.� Dermatomyositis—alopecia of the face, tipof ears, tail, and digits; associated with scalecrusting and scarring.
Breed-Related Alopecia� Alopecic breeds: Chinese crested, Mexicanhairless, Inca hairless, Peruvian Inca Orchid,American hairless terrier (often associatedwith comedones, folliculitis, andfurunculosis).� Congenital hypotrichosis: cocker spaniel,Belgian shepherd, poodle, whippet, beagle,French bulldog, Yorkshire terrier, Labradorretriever, bichon frise, Lhasa apso, bassethound.
BLBS078-CF_A34 BLBS078-Tilley June 16, 2011 10:41
Canine and Feline, Fifth Edition 57
(Continued) Alopecia—Dogs A
� Color dilution alopecia: blue or fawnDoberman pinscher, silver Labrador, creamchow chow, blond Irish setter, blue pit bullterrier, other breeds with dilute coat colors.� Melanoderma with alopecia in Yorkshireterrier.� Seasonal flank alopecia/cyclic flankalopecia—serpiginous flank alopecia withhyperpigmentation; boxer, English bulldog,Airedale terrier.� Pinnal alopecia/patternbaldness—miniaturization of hairs andprogressive alopecia; dachshund, greyhound,American water spaniel, Portuguese waterspaniel, Boston terrier, Manchester terrier,whippet, Italian greyhound, Chihuahua.� Non-inflammatory alopecia (alopeciaX)—symmetrical truncal alopecia associatedwith hyperpigmentation; alopecia often startsalong the collar area of the neck; Pomeranian,chow chow, Akita, Samoyed, Keeshonden,Alaskan malamute, and Siberian husky.
RISK FACTORSN/A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Pattern and degree—important features forformulating a differential diagnosis.� Inflammation, scale, crust, and epidermalcollarettes—important for determiningdiagnosis.
CBC/BIOCHEMISTRY/URINALYSISRule out metabolic causes such ashyperadrenocorticism
OTHER LABORATORY TESTS� Thyroid testing—diagnose hypothyroidism.� ACTH-response test, LDDST, andHDDST—evaluate for hyperadrenocorticism.� Sex hormone profiles (questionablevalidity).
IMAGINGUltrasonography—evaluate adrenal glands forevidence of hyperadrenocorticism.
DIAGNOSTIC PROCEDURES� Response to therapy as a trial� Fungal culture� Skin scraping� Cytology� Skin biopsy
TREATMENT� Demodicosis—amitraz, ivermectin,milbemycin.� Dermatophytosis—griseofulvin,ketoconazole, itraconazole, lime sulfur dips,terbinafine.� Staphylococcal folliculitis—shampoo andantibiotic therapy.� Sebaceous adenitis—keratolytic shampoo,essential fatty acid supplementation,retinoids, cyclosporine.� Keratinization disorders—shampoos,retinoids, vitamin D, cyclosporine.� Endocrine—ovariohysterectomy, castration,Lysodren, trilostane, adrenalectomy.
MEDICATIONSDRUG(S) OF CHOICEVaries with specific cause; see “Treatment”
CONTRAINDICATIONSN/A
PRECAUTIONSToxicity with griseofulvin, retinoids,ivermectin, trilostane, lysodren, cyclosporine.
POSSIBLE INTERACTIONSNone
ALTERNATIVE DRUG(S)None
FOLLOW-UPPATIENT MONITORINGDetermined by cause
POSSIBLE COMPLICATIONSN/A
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALDermatophytosis can cause skin lesions inpeople.
PREGNANCY/FERTILITY/BREEDINGAvoid retinoids and griseofulvin in pregnantanimals.
SEE ALSO� Alopecia, Non-inflammatory—Dogs� Demodicosis� Dermatomyositis� Dermatophytosis� Hyperadrenocorticism (Cushing’sSyndrome)—Dogs� Hypothyroidism� Pemphigus� Sebaceous Adenitis, Granulomatous� Sertoli Cell Tumor
ABBREVIATIONS� ACTH = adrenocorticotropic hormone� HDDST = high-dosedexamethasone-suppression test� LDDST = low-dosedexamethasone-suppression test
Suggested ReadingHelton-Rhodes KA. Cutaneous
manifestations of canine and felineendocrinopathies. Probl Vet Med 1990,12:617–627.
Schmeitzel LP. Growth hormone responsivealopecia and sex hormone associateddermatoses. In: Birchard SJ, Sherding RG,eds., Saunders Manual of Small AnimalPractice. Philadelphia: Saunders, 1994,pp. 326–330.
Scott DW, Griffin CE, Miller BH. Acquiredalopecia. In: Muller & Kirk’s Small AnimalDermatology, 5th ed. Philadelphia:Saunders, 1995, pp. 720–735.
Scott DW, Griffin CE, Miller BH. Endocrineand metabolic diseases. In: Muller & Kirk’sSmall Animal Dermatology, 5th ed.Philadelphia: Saunders, 1995, pp. 627–719.
Scott DW, Griffin CE, Miller BH.Keratinization defects. In: Muller & Kirk’sSmall Animal Dermatology, 5th ed.Philadelphia: Saunders, 1995, pp. 736–805.
Author Karen Helton RhodesConsulting Editor Alexander H. Werner
Client Education Handoutavailable online
BLBS078-CF_A34a BLBS078-Tilley June 16, 2011 10:43
58 Blackwell’s Five-Minute Veterinary Consult
Alopecia, Non-inflammatory—DogsA
BASICSDEFINITION� Uncommon alopecic disorders that areassociated with abnormal hair follicle cycling.� Both endocrine and non-endocrine diseasescan be associated with alopecia.� Definitive diagnosis often requires rulingout the more common endocrine alopecias.� Alopecia X has also been called growthhormone-responsive alopecia,castration-responsive alopecia, adrenalhyperplasia-like syndrome, among others.
PATHOPHYSIOLOGY� There are many factors that affect the haircycle, both hormonal and non-hormonal.� Increased sex hormones can affect the haircycle. Estrogen is a known inhibitor ofanagen, the growth phase of the hair follicle.� The mechanism by which alopecia Xinfluences the hair cycle is not known.
SYSTEMS AFFECTED� Behavioral� Endocrine/Metabolic� Hemic/Lymphatic/Immune� Skin/Exocrine
GENETICSBreed predispositions exist for alopecia X;however, the mode of inheritance isunknown.
INCIDENCE/PREVALENCE� Hyperestrogenism and hyperandrogenismare uncommon to rare causes of alopecia.� Alopecia X is relatively common inpredisposed breeds.
GEOGRAPHIC DISTRIBUTIONNone
SIGNALMENTSpeciesDogs
Breed Predilections� Hyperestrogenism andhyperandrogenism—no breed predilections.� Alopecia X—miniature poodle andplush-coated breeds such as Pomeranian,chow chow, Akita, Samoyed, Keeshonden,Alaskan malamute, and Siberian husky.
Mean Age and Range� Hyperestrogenism andhyperandrogenism—middle-aged to oldintact dogs.� Alopecia X—1–5 years of age; however,older dogs may develop the condition.
Predominant Sex� Hyperandrogenism, primarily intact males.� Hyperestrogenism, primarily intact femalesor males� Alopecia X, neutered or intact dogs of eithersex.
SIGNSHistorical Findings� Overall change in the hair coat—dry orbleached because the hairs are not beingreplaced; lack of normal shed.� Males with hyperestrogenism may attractother male dogs.
Physical Examination Findings� Alopecia—usually diffuse and bilaterallysymmetrical truncal alopecia sparing the headand distal extremities. Uncommon withhyperandrogenism.� Hair coat—may be dry or bleached.� Secondary seborrhea, pruritus, pyoderma,comedones, ceruminous otitis externa, andhyperpigmentation—variable.� Enlargement of nipples, mammary glands,vulva, prepuce—may be associated withhyperestrogenism.� Macular melanosis and linear preputialdermatitis—may be associated withhyperestrogenism.� Abnormal-sized testicles—may be associatedwith hyperestrogenism or hyperandrogenism.� Testicles may also appear normal in size.� Tail gland hyperplasia and perianal glandhyperplasia—usually associated withhyperandrogenism.� Systemic signs (PU/PD/polyphagia) areusually NOT present.
CAUSESHyperestrogenism—Females� Estrogen excess associated with cysticovaries, ovarian tumors (rare), or exogenousestrogen supplementation.� Animals with normal serum estrogenconcentrations may have increased numbersof estrogen receptors in the skin(undocumented).
Hyperestrogenism—Males� Estrogen excess due to Sertoli cell tumor(most common), seminoma, or interstitial celltumor (rare).� Associated with malepseudohermaphrodism in miniatureschnauzers.
Hyperandrogenism—MalesAndrogen-producing testicular tumors(especially interstitial cell tumors).
Alopecia XHairs fail to cycle but an underlyingendocrine cause has not been identified.
RISK FACTORS� Intact male and female dogs are at increasedrisk for developing testicular tumors andovarian cysts/tumors, respectively.� Cryptorchid males are at increased risk fordeveloping testicular tumors.� Exogenous estrogen supplementation.� There are no known risk factors for alopeciaX other than breed predisposition.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Inflammatory causes of alopecia (pyoderma,demodicosis, and dermatophytosis)—shouldbe ruled out; these diseases usually cause apatchy rather than diffuse pattern of alopecia.� Hypothyroidism andhyperadrenocorticism—critical to rule out asthese diseases may cause a very similar patternof diffuse alopecia associated with lack of hairfollicle cycling.� Follicular dysplasias including color-dilutionalopecia and black hair folliculardysplasia—alopecia should be color-restricted.� Patterned alopecia of various breeds(dachshund, Boston terrier, greyhound, waterspaniel, and others)—breed-specific alopeciasof unknown cause.� Cyclic flank alopecia—alopecia of the flankand dorsum, often bizarre patterns withhyperpigmentation, more often inshort-coated breeds (boxer, English bulldog,Airedale) and may recur seasonally.� Post-clipping alopecia—hair fails to regrowfollowing clipping; however, hair regrowthoccurs within a year.� Telogen defluxion—alopecia occurs 1–2months following an illness or severe stressfulepisode and is usually more sudden in onsetwith relative ease of epilation.
CBC/BIOCHEMISTRY/URINALYSIS� Usually unremarkable.� Anemia and/or bone marrow hypoplasia oraplasia can be associated withhyperestrogenism.
OTHER LABORATORY TESTS� Serum sex hormone concentrations—oftennormal, treat according to suspected diagnosisbased on clinical signs and ruling out otherdisorders.� Serum estradiol concentrations—sometimeselevated in male dogs with testicular tumorsor female dogs with cystic ovaries; however,normal fluctuation of estradiol occursthroughout the day, making interpretation ofestradiol concentrations difficult.
IMAGINGRadiography, ultrasonography, andlaparoscopy—identify cystic ovaries, ovariantumors, testicular tumors (scrotal orabdominal), sublumbar lymphadenopathy,and possible thoracic metastases of malignanttumors.
DIAGNOSTIC PROCEDURES� Preputial cytology—may demonstratecornification of cells in males withhyperestrogenism (similar to a bitch in estrus).� Skin biopsy.
BLBS078-CF_A34a BLBS078-Tilley June 16, 2011 10:43
Canine and Feline, Fifth Edition 59
(Continued) Alopecia, Non-inflammatory—Dogs A
PATHOLOGIC FINDINGSHistologic changes associated with endocrinedermatoses (telogen hairs, follicular keratoses,hyperkeratosis, excess trichilemmalkeratinization [flame follicles], thin epidermisand thin dermis) may also be seen withnon-inflammatory alopecias includinghyperestrogenism and alopecia X.Histopathology will help rule outinflammatory causes of alopecia and some ofthe other differentials listed above.
TREATMENTAPPROPRIATE HEALTH CAREN/A
NURSING CAREN/A
ACTIVITYNone
DIETNone
Client EducationAlopecia X is a cosmetic condition resultingin coat loss only and there is not a definitivecure for the hair loss. The risk of treatmentshould be weighed with these facts. Hairregrowth will only occur in a portion of dogsregardless of treatment chosen and hair lossmay recur months to years later in spite ofcontinued treatment.
SURGICAL CONSIDERATIONSHyperestrogenism/Hyperandrogenism� Castration—scrotal testicular tumors.� Exploratory laparotomy—diagnosis andsurgical removal (ovariohysterectomy andcastration) for ovarian cysts and tumors andabdominal testicular tumors.
Alopecia XNeuter intact animals—a certain number willregrow hair following neutering. Hairregrowth can take up to 3 months to becomeevident.
MEDICATIONSDRUG(S) OF CHOICEGeneral Treatments� Topical antiseborrheic shampoos—forcomedones and seborrhea associated withalopecia.� Antibiotics—for secondary skin infectionsassociated with alopecia.
Alopecia XMelatonin—3 mg q12h for small breeds and6–12 mg q12h for large breeds; hair regrowthcan take up to 3 months to become evident.This treatment works in approximately 40%of cases. Because this treatment is the mostbenign, it is considered the treatment ofchoice following neutering. Once hairregrowth has occurred, discontinue treatment.
CONTRAINDICATIONSNone
PRECAUTIONSMelatonin at high doses can cause insulinresistance; therefore, use caution in treatingdogs with diabetes mellitus.
POSSIBLE INTERACTIONSNone
ALTERNATIVE DRUG(S)� Mitotane—15–25 mg/kg—one daily asinduction for 5–7 days, followed by twiceweekly maintenance; hair regrowth occurs ina portion of dogs treated and can take up to3 months to become evident. Use of this drugcan result in an Addisonian crisis and otherside effects as for treatment of Cushing’ssyndrome. Electrolytes and cortisol withACTH stimulation testing should bemonitored regularly.� Trilostane—dosages as described fortreatment of Cushing’s syndrome; hairregrowth occurs in a portion of dogs treatedand can take up to 3 months to becomeevident. Use of this drug can result in anAddisonian crisis and other side effects as fortreatment of Cushing’s syndrome. Electrolytesand cortisol with ACTH stimulation testingshould be monitored regularly.� Growth hormone administration andmethyltestosterone may result in hairregrowth. Growth hormone can causediabetes mellitus. Methyltestosterone canresult in increased aggression,cholangiohepatitis, and seborrhea oleosa.Therefore, these drugs are not recommended.
FOLLOW-UPPATIENT MONITORING� Mitotane—electrolytes and cortisol withACTH stimulation testing regularly.� Trilostane—electrolytes and cortisol withACTH stimulation testing regularly.
PREVENTION/AVOIDANCENone
POSSIBLE COMPLICATIONSNone
EXPECTED COURSE AND PROGNOSIS� Female hyperestrogenism—improvementshould occur within 3–6 months afterovariohysterectomy.� Estrogen- and androgen-secretingtumors—resolution of signs should occurwithin 3–6 months after castration.� Alopecia X—hair regrowth will only occurin a portion of dogs regardless of treatmentchosen and hair loss may recur in spite ofcontinued treatment. Therefore, if hairregrowth occurs, discontinue treatment topreserve treatment for future recurrence of thealopecia. Risk of treatment should be weighedwith the fact that this is a cosmetic disease.
MISCELLANEOUSASSOCIATED CONDITIONS� Pyoderma, seborrhea, comedones may beassociated with the alopecia.� Behavioral—changes associated withhyperestrogenism or hyperandrogenism.
AGE-RELATED FACTORSNone
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A—neutering is usually recommended formanaging these conditions.
SYNONYMSAlopecia X—growth hormone-responsivealopecia, castration-responsive alopecia,adrenal hyperplasia-like syndrome, amongothers.
ABBREVIATIONS� ACTH = adrenocorticotropic hormone� PU/PD = polyuria/polydipsia
INTERNET RESOURCEShttp://www.vet.utk.edu/hairloss/.
Suggested ReadingFrank LA. Sex hormone and endocrine
look-alike dermatoses. In: Birchard SJ,Sherding RG, eds., Saunders Manual ofSmall Animal Practice, 3rd ed. Philadelphia:Saunders, 2006, p. 517.
Author Linda A. FrankConsulting Editor Alexander H. Werner
Client Education Handoutavailable online
BLBS078-CF_A35 BLBS078-Tilley July 15, 2011 20:0
60 Blackwell’s Five-Minute Veterinary Consult
AmebiasisA
BASICSOVERVIEW� Facultative parasitic amoeba that infectspeople and non-human primates, includingdogs and cats.� Found primarily in tropical areasthroughout the world, including NorthAmerica.
SIGNALMENT� Dogs and cats.� Mainly young and/or immunosuppressedanimals are infected.
SIGNSDogs� Entamoeba histolytica infections are usuallyasymptomatic.� Severe infections—result in ulcerative colitisto cause dysentery (may be fatal).� Hematogenous spread—results in failurestates of the organs (invariably fatal).� Granulomatous amoebicmeningoencephalitis (caused byAcanthamoeba spp.)—causes signs similar todistemper (anorexia, fever, lethargy,oculonasal discharge, respiratory distress, anddiffuse neurologic abnormalities).� Syndrome of inappropriate secretion ofantidiuretic hormone has been reported in ayoung dog with acanthamoebisis causinggranulomatous meningoencephalitis withinvasion of the hypothalamus.
Cats� Colitis—causing chronic intractablediarrhea (as per dogs).� Systemic amebiasis or Acanthamoeba—notreported in cats.
CAUSES & RISK FACTORS� Entamoeba histolytic—infection occurs byingesting cysts from human feces.� Encystment of trophozoites seldom occursin dogs or cats so they are not a source ofinfection. � One of the few organismstransmitted from man to pets but rarely frompets to man. � Trophozoites (the pathogenicstage)—inhabit the colonic lumen ascommensals or invade the colonic wall butcan disseminate to other organs (rare)including lungs, liver, brain, and skin.� Trophozoites damage intestinal epithelialcells by secreting enzymes that lyse cells anddisrupt intercellular connections. � Certainbacteria and a diet deficient in proteinincrease the virulence of the amoeba. � Thehost’s immune response to invasionexacerbates pathology. � Colonic ulcerationresults when trophozoites in the submucosaundermine the mucosa. � Acanthamoebacastellani and A. culbertsoni—free-living species found in freshwater,saltwater, soil, and sewage; can infect dogs.� Acanthamoeba spp.—infection thought tobe by inhalation of organisms from
contaminated water or colonization of theskin or cornea; hematogenous spread or directspread from the nasal cavity through thecribiform plate to the central nervous systemmay occur, resulting in a granulomatousamoebic meningoencephalitis.
DIAGNOSISDIFFERENTIAL DIAGNOSISDogs� Causes of bloody diarrhea or tenesmus,including constipation; food intolerance/allergy; parasitism (whip worms,leishmaniasis, balantidiasis); HGE; foreignbody; irritable bowel syndrome; inflammatorybowel disease; diverticula; infectious(parvovirus, clostridial enteritis, bacterialovergrowth and other bacterial causes, fungalsuch as histoplasmosis or blastomycosis);neoplasia; ulcerative colitis; endocrinopathy(Addison’s disease); toxic (lead, fungal, orplant); occasionally major organ diseasecausing colonic ulceration such as renalfailure.� Other causes of diffuse neurologic disease inyoung animals, including infectious(distemper, fungal such as Cryptococcus,Blastomyces, Histoplasma, bacteria, protozoasuch as Toxoplasma and Neospora); toxic(lead, organophosphate); trauma; GME;extracranial (hypoglycemia; hepaticencephalopathy); inherited epilepsy;neoplasia.
Cats� Other causes of diarrhea, including foodintolerance/allergy; inflammatory boweldisease; parasitism (giardiasis, parasites such ashookworms, roundworms, tritrichomonas);infectious (panleukopenia, FIV, FeLVproducing panleukopenia-like syndrome,bacterial including Salmonella, rarelyCampylobacter); drug (acetaminophen);neoplasia; pancreatitis; and major organdysfunction.
CBC/BIOCHEMISTRY/URINALYSISNormal; can reflect severe diarrhea.
OTHER LABORATORY TESTS� Microscopic examination—colonic biopsies(H&E) obtained via endoscopy is the mostreliable method.� Trophozoites in feces—very difficult todetect; methylene blue staining improveschances.� Trichrome and iron-hematoxyline—theideal fecal stains but require a referencelaboratory to perform.� Fecal concentration techniques—no help.� CSF—elevated WBC count (70%mononuclear cells), protein andxanthochromia in dogs with granulomatousamebic meningoencephalitis due toAcanthamoeba.
IMAGINGMRI—shows brain granulomas.
DIAGNOSTIC PROCEDURESBrain biopsy—required to definitivelydiagnose neurologic forms antemortem.
TREATMENT� Colitis (caused by E. histolytica)—respondsto metronidazole, although dogs continue toshed organisms.� Systemic forms (particularly neurologicdisease)—invariably fatal despite treatment.
MEDICATIONSDRUG(S)� Tinidazole (44 mg/kg PO q24h for 6 days)in dogs—found to be more effective thanmetronidazole in treating amebiasis in people.� Metronidazole (20 mg/kg PO q12h for 7days).
CONTRAINDICATIONS/POSSIBLEINTERACTIONSHigh doses of metronidazole (usually> 30 mg/kg) for extended periods may causeneurologic signs in dogs.
FOLLOW-UPPets usually acquire infections from the samesource as their owners; veterinarians mustwarn owners of possible risk.
MISCELLANEOUSABBREVIATIONS� CSF = cerebrospinal fluid� FeLV = feline leukemia virus� FIV = feline immunodeficiency virus� GME = granulomatousmeningoencephalopathy� H&E = hematoxylin and eosin� HGE = hemorrhagic gastroenteritis� MRI = magnetic resonance imaging� WBC = white blood cell
Suggested ReadingBrofman PJ, Knostman KAB, Dibartola SP.
Granulomatous amebicmeningoenchephalitis causing the syndromeof inappropriate secretion of antidiuretichormone in a dog. J Vet Intern Med 2003,17:230–234.
Fung HB, Doan TL. Tinidazole: Anitroimidazole antiprotozoal agent. ClinTher 2005, 27:1859–1884.
Author Stephen C. BarrConsulting Editor Stephen C. Barr
BLBS078-CF_A36 BLBS078-Tilley July 15, 2011 20:13
Canine and Feline, Fifth Edition 61
Ameloblastoma A
BASICSOVERVIEW� Common oral tumor of odontogenic (toothstructure) ectoderm origin.� Biologically these tumors are benignhistologically but possess locally invasiveproperties.� A rare malignant (highly invasive) form hasbeen described.� Tumors may arise anywhere within thedental arcade.� Several histologic subtypes exist and all havesimilar invasive behavior.
SIGNALMENT� Middle-aged and old dogs� Rare in cats
SIGNSDogs may present with a smooth, firm,gingival mass that is usually non-ulcerated.
CAUSES & RISK FACTORSN/A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Epulis� Malignant oral tumor� Gingival hyperplasia
� Other tumors related to the odontogenicapparatus
CBC/BIOCHEMISTRY/URINALYSISUnaffected
OTHER LABORATORY TESTSN/A
IMAGING� Radiographs of skull often show bone lysisdeep to the superficial mass.� Regional and distant metastasis has notbeen described.� Computed tomography may be helpful forplanning surgery or radiation therapy.
DIAGNOSTIC PROCEDURESDeep tissue biopsies are necessary andrecommended for definitive diagnosis.
TREATMENT� Radical surgical excision such asmandibulectomy or maxillectomy with atleast 1–2-cm margins is recommended toensure complete excision.� Radiation therapy may be curative withoutdisfigurement associated with surgery.
MEDICATIONSDRUG(S)N/A
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UPCareful oral examination at 1, 3, 6, 9, and 12months after definitive treatment isrecommended to monitor treatmentoutcomes.
MISCELLANEOUSSuggested ReadingGelberg HB. Alimentary system. In: McGavin
MD, Carlton WW, Zachary JF, eds.,Thompson’s Special Veterinary Pathology.St. Louis: Mosby, 2001, pp. 1–79.
Morrison WB. Cancers of the head and neck.In: Morrison WB, ed., Cancer in Dogs andCats: Medical and Surgical Management.Jackson, WY: Teton NewMedia, 2002,pp. 489–496.
Walsh KM, Denholm LJ, Cooper BJ.Epithelial odontogenic tumors in domesticanimals. J Comp Pathol 1987, 97:503–521.
Author Wallace B. MorrisonConsulting Editor Timothy M. Fan
BLBS078-CF_A37 BLBS078-Tilley July 23, 2011 4:31
62 Blackwell’s Five-Minute Veterinary Consult
Amitraz ToxicosisA
BASICSOVERVIEW� Amitraz—formamidine acaricide; appliedtopically to control ticks, mites, and lice.� Amitraz-containing products (fordogs)—formulated as a 19.9% emulsifiableconcentrate in 10.6-mL bottles for dilutionand sponge-on; as a 9% impregnated 25-inch27.5-g collar and an 18-inch 18.5-g collar; asa 14.34% component of a 0.023 fl. oz., 0.045fl. oz., 0.113 fl. oz., 0.180 fl. oz., or 0.225 fl.oz. spot-on.� Systems affected—nervous; endocrine/metabolic (β cells of the pancreas);gastrointestinal.� Clinical signs—most associated withα2-adrenoreceptor agonist.� After high-dose oral administration(dogs)—peak plasma concentration reachedat approximately 6 hours; elimination half-lifeas long as 24 hours; metabolites excreted inthe urine.� Ingestion of sustained-release- impregnatedcollars—constant release and continuedsystemic exposure until collar segments havepassed in the stool.� Toxicosis—generally occurs whenimpregnated collars are ingested, whenimproperly diluted solutions are appliedtopically, or when solutions are taken orally orapplied to the wrong size animal.� Idiosyncratic reactions may occur.
SIGNALMENT� Thorough history—usually identifies usetopically or as a collar.� Dogs—common, owing to more commonuse.� Cats—more sensitive than dogs althoughcats are less likely involved.� Predilection for old and toy breed animals.
SIGNSHistorical FindingsDevelop acutely after exposure (topical ororal)
Physical Examination Findings� Minor to severe depression� Ataxia� Bradycardia� Vomiting� Hyperthermia/hypothermia� Hyperglycemia� Hypotension� Polyuria� Gastrointestinal stasis� Mydriasis� Death (prognosis is typically good withtreatment)
CAUSES & RISK FACTORS� Ingestion of impregnated collar or pieces ofcollar.� Inappropriate direct dermal application.� Ingestion of undiluted product.� After application of properly diluted andapplied solutions—less common.� Elderly, sick, toy breed, or debilitatedanimals—may be predisposed.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Recreational and prescriptiondrugs—marijuana; opioids; barbiturates;benzodiazepines; phenothiazines;antihypertensive medications; skeletal musclerelaxants; antidepressants (tricyclic, SSRIs),and other depressant drugs or chemicals.� Ivermectins, avermectins, milbemycins—generally very high dose or exceptionallysensitive breed.� Alcohols—ethanol; ethylene glycol(antifreeze); methanol (windshield washerfluid); isopropyl alcohol (rubbing alcohol).� Tick paralysis, botulism, cranial trauma,diabetes, hyperadrenocorticism,hypothyroidism, severe anemia, cardiacfailure, and anaphylactic shock—markeddepression or weakness.� Depends on clinical signs, history ofexposure, or evidence of exposure andelimination of other causes.
CBC/BIOCHEMISTRY/URINALYSIS� Hyperglycemia—common, related toinsulin inhibition� Elevated liver enzymes— uncommon
IMAGINGAbdominal radiography—may reveal a collarbuckle in the gastrointestinal tract.
DIAGNOSTIC PROCEDURESIdentify amitraz on hair or in gastrointestinalcontents—analytical methods described;useful only to prove exposure; no dataavailable correlating concentration withclinical signs.
PATHOLOGIC FINDINGSHigh-dose, prolonged exposure—increasedliver weight; slight enlargement ofhepatocytes; thinning of the zonae fasciculataand reticularis; slight hyperplasia of the zonaglomerulosa of the adrenal glands.
TREATMENT� Inpatient—severely affected patients.� Mild sedation after correctly appliedsponge-on solutions—often transient; mayrequire no treatment.� Mild signs after topicalapplication—wearing gloves, scrub with ahand dishwashing detergent; rinse withcopious amounts of warm water; institutenon-specific supportive therapy (e.g.,intravenous fluids, maintenance of normalbody temperature, and nutritional support);monitor 1–2 days until improvement is noted.� Ingestion of collar possible—endoscopicretrieval of the collar—removal of largesegments from the stomach may be beneficial;usually numerous small pieces are locatedthroughout the gastrointestinal tract, makingremoval unrealistic.
MEDICATIONSDRUG(S)Collar Ingestion, Asymptomatic Patient� Emetic—3% USP hydrogen peroxide(2.2 mL/kg PO; maximum 45 mL afterfeeding a moist meal); apomorphine andespecially xylazine not recommended.� Activated charcoal has not been shown to beeffective.� Bulk diet (whole wheat bread, lactulose,pumpkin).� Warm tap water enema (5–10 ml/kg); willstimulate GI motility and help pass pieces ofcollar through the GI tract.
Marked Depression� May require pharmacologic reversal of theα2-adrenergic effects.� Yohimbine (Yobine) 0.11 mg/kg IV,administered slowly; reverses depression andbradycardia within minutes; improves GImotility; objective is to keep the patient in astate of low-level depression with normalheart rate, blood pressure, body temperature,and blood glucose concentrations.� Collar ingestion—monitor for recurrence ofsymptoms; may need additional yohimbineuntil collar segments appear in the stool.� Atipamezole (Antisedan) 0.05 mg/kg IM;reported to reverse clinical signs withinminutes; repeat as needed; an alternativewhen yohimbine is unavailable.
BLBS078-CF_A37 BLBS078-Tilley July 23, 2011 4:31
Canine and Feline, Fifth Edition 63
(Continued) Amitraz Toxicosis A
� Yohimbine and atipamezole—may requirerepeated administration (as needed) possiblyevery 4–8 hours, because half-life in dogs isshort and elimination half-life of amitraz islonger.� Do not use atropine to reverse bradycardia;use is contraindicated because of potentiationof GI stasis.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSYohimbine and atipamezole—excessiveadministration may result in apprehension,CNS stimulation, and rarely seizures.
FOLLOW-UP� Body temperature, blood pressure, serumglucose, and heart rate—importantparameters.� Close observation for recurrence of clinicalsigns—required for 24–72 hours.� Yohimbine and atipamezole—requiresreadministration in severe cases, becausereversal effects subside before collar segmentshave passed or before amitraz has beeneliminated from the body.� No long-term adverse effects expected.
AGE-RELATED FACTORSElderly, sick, or debilitated animals may takelonger to fully recover.
ABBREVIATIONS� CNS = central nervous system� GI = gastrointestinal� SSRI = selective serotonin reuptakeinhibitor
INTERNET RESOURCEShttp://www.aspcapro.org/animal-poison-control-center-articles.php.
Suggested ReadingGrossman MR. Amitraz toxicosis associated
with ingestion of an acaricide collar in adog. JAVMA 1993, 203:55–57.
Hugnet C, Buronfosse F, Pineau X, et al.Toxicity and kinetics of amitraz in dogs. AmJ Vet Res 1996, 57:1506–1510.
Author Steven R. HansenConsulting Editor Gary D. Osweiler
BLBS078-CF_A37a BLBS078-Tilley June 16, 2011 10:46
64 Blackwell’s Five-Minute Veterinary Consult
Amphetamine ToxicosisA
BASICSDEFINITIONAcute gastrointestinal, neurological,neuromuscular, and cardiac toxicosis as theresult of excessive consumption ofamphetamine or a derivative.
PATHOPHYSIOLOGY� Amphetamine and its derivatives belong tothe CNS stimulant class phenylethylamines.Various substitutions of the basicphenylethylamine structure account for manypharmaceutical and illicit compounds foundtoday.� Amphetamine is a sympathomimetic that isstructurally related to norepinephrine.
◦ Centrally—stimulates cortical centersincluding cerebral cortex, medullaryrespiratory center, and reticular activatingsystems.◦ Peripherally—directly stimulates alphaand beta receptors and stimulates therelease of norepinephrine from stores inadrenergic nerve terminals.◦ Amphetamine may slow downcatecholamine metabolism by inhibition ofmonoamine oxidase.
� Amphetamines are well absorbed orally andreach peak plasma levels in 1–3 hours.� The half-life, which varies from 7–34 hours,and rate of excretion of unchangedamphetamine in the urine are both dependentupon urine pH, with shorter half-lives beingassociated with more acidic urine.� Oral LD50 of amphetamine sulfate in dogsis 20–27 mg/kg, and for methamphetaminesulfate it is 9–11 mg/kg.� Clinical signs may be seen at doses below 1mg/kg.� Amphetamine and its derivatives are used inhumans to treat ADD/ADHD, narcolepsy,and obesity.� Illicit use of amphetamines in humans isalso prevalent.
SYSTEMS AFFECTED� Cardiovascular—stimulation mostcommon: tachycardia and hypertension.� Gastrointestinal—anorexia, vomiting,diarrhea.� Nervous—stimulation most common,depression uncommon.� Neuromuscular—stimulation: muscletremors and seizures.� Ophthalmic—mydriasis.� Respiratory—stimulation: tachypnea.
GENETICSN/A
INCIDENCE/PREVALENCEN/A
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats, although more prevalent indogs; other species
Breed PredilectionsN/A
Mean Age and RangeN/A
Predominant SexN/A
SIGNSHistorical Findings� Abnormal behavior—usually hyperactivity,anxiety or pacing, anorexia, fast heart rate,panting; observed or evidence of exposure byowner/caretaker.� Onset of signs typically begins within 30minutes to 6 hours post-ingestion.
Physical Examination Findings� Nervous—hyperactivity, agitation,restlessness, head bobbing, pacing, circling,vocalization, disorientation, hyperesthesia,ataxia, lethargy or depression (less common).� Cardiovascular—tachycardia or bradycardia(less common, may be reflexive),hypertension.� Neuromuscular—muscle fasciculation ortremors, seizures.� Gastrointestinal—vomiting, diarrhea,anorexia, excessive salivation.� Respiratory—tachypnea.� Ophthalmic—mydriasis with possibly poorto unresponsive pupillary light response.� Other—hyperthermia.
CAUSESAccidental ingestion or administration,malicious poisoning.
RISK FACTORSHouseholds with children or adults currentlytaking prescription or illicit amphetamine orderivative.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Strychnine� Organochlorine insecticides� Methylxanthine� 4 aminopyridine� Metaldehyde� Phenylpropanolamine� Albuterol� Nicotine� Tremorgenic mycotoxins� Hypernatremia� Pseudoephredrine, phenylephrine� 5 fluorouracil� Ma huang, guarana, or ephedra
CBC/BIOCHEMISTRY/URINALYSIS� CBC—disseminated intravascularcoagulopathy secondary to severehyperthermia (rare).
� Chemistry—◦ Azotemia: prerenal—secondary todehydration; renal—secondary torhabdomylosis and myoglobinuria (rare).◦ High liver enzymes—secondary toseizures and/or hyperthermia (rare).◦ Hypoglycemia.
� Urinalysis—evidence of myoglobinuria,urine specific gravity (high—prerenalazotemia; isosthenuria—renal failure).
OTHER LABORATORY TESTS� Electrolytes—imbalances secondary togastrointestinal signs.� Acid-base status—acidosis may occur.� Over-the-counter urine drugscreens—watch for false positives or negatives.Check the user handbook for furtherinformation.� Amphetamines are present in blood, urine,and saliva; check with local veterinarydiagnostic lab or human hospital foravailability and proper sample submission.
IMAGINGN/A
DIAGNOSTIC PROCEDURES� Electrocardiogram for presence of anytachyarrhythmia or less commonlybradyarrhythmia.� Blood pressure—identification ofhypertension.
PATHOLOGIC FINDINGSOn necropsy presence of amphetamines maybe found in the gastric contents, urine,plasma, liver, kidney, or muscle.
TREATMENTAPPROPRIATE HEALTH CAREMajority of cases require emergency inpatientintensive care management.
NURSING CARE� Intravenous fluid therapy to correctdehydration and electrolyte imbalances as wellas help support renal function and promoteexcretion of amphetamines. Use bloodpressure to help guide fluid rate.� Cool intravenous fluids, fans, cool waterbaths for hyperthermia.
ACTIVITYMinimize activity and stimuli
DIETWithhold food if moderately to severelyaffected. Bland diet for a few dayspost-exposure if significant gastrointestinalsigns were noted.
CLIENT EDUCATIONIn case of an exposure, owner should contactlocal veterinarian or veterinary poison centerimmediately.
SURGICAL CONSIDERATIONSN/A
BLBS078-CF_A37a BLBS078-Tilley June 16, 2011 10:46
Canine and Feline, Fifth Edition 65
(Continued) Amphetamine Toxicosis A
MEDICATIONSDRUG(S) OF CHOICEDecontamination� Induce emesis—if a recent exposure and petis not already symptomatic.
◦ Apomorphine—0.04 mg/kg IV,subconjuctival.◦ Hydrogen peroxide 3%—2.2 ml/kg,maximum dose 45 mls.
� Gastric lavage if extremely large ingestion orpatient is already symptomatic.� Activated charcoal with a cathartic.
CNS Signs of Stimulation� Acepromazine 0.05–1.0 mg/kg IV or IM� Chlorpromazine 10–18 mg/kg IV� Cyproheptadine (serotonin antagonist):dogs, 1.1 mg/kg orally or rectally; cats, 2–4mg/cat
Cardiovascular Signs� Tachyarrhythmia—beta blockers such aspropranolol 0.02–0.04 mg/kg IV ormetoprolol.� Ventricular prematurecontractions—lidocaine: dogs at 2–4 mg/kgIV (to maximum of 8 mg/kg over a10-minute period). Cats—start with 0.1–0.4mg/kg and increase cautiously to 0.25–0.75mg/kg IV slowly if no response. Cats arereportedly very sensitive to lidocaine, somonitor carefully if used.
Promote EliminationAscorbic acid or ammonium chloride—forurinary acidification to promote elimination;however, only use if can measure acid-basestatus.
CONTRAINDICATIONS� While diazepam has been successfully usedto treat amphetamine exposures, there isevidence that benzodiazepines may intensifyneurological signs.� Urinary acidification if unable to monitoracid-base status or if myoglobinuria is present.� Inducing emesis in a symptomatic patient.
PRECAUTIONSN/A
POSSIBLE INTERACTIONS� Amphetamines inhibit the metabolism ofadrenergic blockers (doxazosin,phenoxybenzamine, prazosin, terazosin),Phenobarbital, and phenytoin.
� Amphetamines potentiate the metabolismof coumarin anticoagulants, monoamineoxidase inhibitors, opioid analgesics, andtricyclic antidepressants.
ALTERNATIVE DRUG(S)Phenobarbital, pentobarbital, and propofolfor CNS stimulatory signs.
FOLLOW-UPPATIENT MONITORING� Monitor in hospital until resolution ofclinical signs.� If severely affected, monitor liver andkidney values every 24 hours for 72 hours oruntil resolution.
PREVENTION/AVOIDANCEAll medications and illicit drugs should bekept out of pets’ reach at all times.
POSSIBLE COMPLICATIONSAcute renal failure secondary tomyoglobinuria or DIC (rare).
EXPECTED COURSE AND PROGNOSIS� Expected course of clinical signs is 12–72hours, depending on dose, effectiveness ofdecontamination and treatment, and rate ofelimination.� Prognosis—most patients do well withprompt and appropriate veterinary care.Seizures or severe hyperthermia may be a poorprognostic indicator.
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALPets exposed to human waste products fromthose taking amphetamines or derivativescould become symptomatic.
PREGNANCY/FERTILITY/BREEDINGAmphetamines are a known teratogen inhumans. They have been found to cross theplacenta in animals and may also be found inmilk.
SYNONYMS� Common brand names of prescriptionamphetamine drugs and their activeingredient: Adderall (amphetamine anddextroamphetamine); Ritalin, Metadate,Concerta (methylphenidate); Daytrana(methylphenidate transdermal patch); Focalin(dexmethylphenidate); Vyvanse(lisdexamfetamine), Cylert (pemoline),Adipex-P (phentermine), Dexedrine(Dextroamphetamine).� Illicit drug street names: ice, glass, crank,speed, uppers, ecstasy, meth, and many others.
SEE ALSO� Antidepressants—SSRI Toxicosis� Antidepressants—Tricyclic Toxicosis� Pseudoephredrine Toxicosis� Strychnine Poisoning
ABBREVIATIONS� ADD = attention deficit disorder� ADHD = attention deficit hyperactivitydisorder� CNS = central nervous system� DIC = disseminated intravascularcoagulation
INTERNET RESOURCEShttp://www.aspcapro.org/animal-poison-control-center-articles.php.
Suggested ReadingCudia SP, Poppenga RH, Birdsall WJ.
Pemoline toxicosis in a dog. JAVMA 1998,212(1):74–76.
Mckinney PE, Palmer RB. Amphetaminesand derivatives. In: Brent J, et al., eds.,Critical Care Toxicology. Philadelphia:Elsevier, 2005, pp. 761–775.
Teitler JB. Evaluation of a human on-siteurine multi drug test for emergency use withdogs. JAAHA 2009, 45(2):59–66.
Volmer PA. “Recreational” drugs. In: PetersonME, Talcott PA, eds., Small AnimalToxicology. St. Louis: Elsevier, 2006,pp. 276–280.
Volmer PA. Human drugs of abuse. In:Bonagua JD, Twedt DC, eds., CurrentVeterinary Therapy XIV. St. Louis: Elsevier,2009,pp. 144–145.
Author Kirsten E. WaratukeConsulting Editor Gary D. Osweiler
BLBS078-CF_A38 BLBS078-Tilley July 23, 2011 4:35
66 Blackwell’s Five-Minute Veterinary Consult
AmyloidosisA
BASICSDEFINITIONA group of conditions of diverse cause inwhich extracellular deposition of insolublefibrillar proteins (amyloid) in various organsand tissues compromises their normal function.
PATHOPHYSIOLOGY� Patients usually affected by systemic reactiveamyloidosis; tissue deposits contain AA,which is a fragment of an acute-phase reactantprotein called SAA. � Phases of amyloiddeposition: ◦ Predeposition phase: SAAconcentration is high but without amyloiddeposits; colchicine administration duringthis phase may prevent development of thedisease. ◦ Deposition phase (rapid portion):amyloid deposits increase rapidly; colchicineadministration delays but does not preventtissue deposition of amyloid; DMSO maypromote resolution of amyloid deposits and apersistent decrease in SAA concentration.◦ Deposition phase (plateau portion): netdeposition of amyloid changes little; neitherDMSO or colchicine is beneficial. � Clinicalsigns in dogs and cats usually are associatedwith amyloid deposition in the kidneys.� Dogs—amyloid deposits usually found inthe glomeruli leading to proteinuria andnephrotic syndrome. � Cats—amyloiddeposits usually found in the medullaryinterstitium but may occur in glomeruli.� Some Chinese shar-pei dogs with familialamyloidosis have medullary amyloidosiswithout glomerular involvement. � Siameseand Oriental shorthair cats with familialamyloidosis have hepatic amyloidosis. � Adifferent type amyloid, pancreatic isletamyloid polypeptide, or amylin, deposits inthe pancreas of old cats. Amylin is a hormonesecreted along with insulin by the pancreaticbeta cells. Chronic increased stimulus forsecretion of amylin by beta cells (e.g., states ofinsulin resistance) lead to pancreatic islet cellamyloidosis.
SYSTEMS AFFECTEDRenal/Urologic—predilection for renal AAdeposition; liver, spleen, adrenal glands,pancreas, tracheobronchial tree, andgastrointestinal tract also may be affected.
GENETICSNo genetic involvement is clearly established;familial amyloidosis occurs in Chineseshar-pei, English foxhound, and beagle dogs,and in Abyssinian, Oriental shorthair, andSiamese cats.
INCIDENCE/PREVALENCEUncommon occurs mostly in dogs; rare incats, except Abyssinians.
SIGNALMENTSpeciesDogs and cats
Breed Predilections� Dogs—Chinese shar-pei, beagle, collie,pointer, English foxhound, and walkerhound; German shepherd dog and mixedbreeds are at lower risk. � Cats: Abyssinian,Oriental shorthair, and Siamese.
Mean Age and Range� Most affected dogs and cats are more than5 years old. � Dogs—mean age at diagnosis is9 years; range, 1–15 years. � Cats—mean ageat diagnosis 7 years; range, 1–17 years.� Prevalence increases with age. � Abyssiniancats—range < 1–17 years. � Chinese shar-peidogs—usually < 6 years of age when signs ofrenal failure develop; range, 1.5–6 years.� Siamese cats with familial amyloidosis of theliver and thyroid gland usually develop signsof liver disease when 1–4 years old.
Predominant SexDogs and Abyssinian cats—females appear tobe at a slightly higher risk (< 2 : 1).Female-to-male ratio is higher in Chineseshar-pei dogs (∼2.5 : 1).
SIGNSGeneral Comments� Depend on the organs affected, the amountof amyloid, and the reaction of the affectedorgans to amyloid deposits. � Usually causedby renal involvement; occasionally, hepaticinvolvement may cause signs in Chineseshar-pei dogs and Oriental shorthair andSiamese cats.
Historical Findings� No clear history of a predisposing disorderin most (∼75%) cases. � Anorexia, lethargy,polyuria and polydipsia, weight loss,vomiting, and diarrhea (uncommon).� Ascites and peripheral edema in animalswith nephrotic syndrome. � Chinese shar-peidogs may have a history of previous episodicjoint swelling and high fever that resolvesspontaneously within a few days. � Beagledogs with juvenile polyarteritis may have ahistory of fever and neck pain that persist for3–7 days. � Oriental shorthair and Siamesecats may present with spontaneous hepatichemorrhage leading to acute collapse andhemoabdomen.
Physical Examination Findings� Related to renal failure—oral ulceration,emaciation, vomiting, and dehydration;kidneys usually small, firm, and irregular inaffected cats; they may be small, normal-sized,or slightly enlarged in affected dogs. � Signsof nephrotic syndrome (e.g., ascites,subcutaneous edema). � Related to theprimary inflammatory or neoplastic diseaseprocess. � Thromboembolic phenomena—may occur in up to 40% of affected dogs;signs vary with the location of the thrombus;patients may develop pulmonarythromboembolism (e.g., dyspnea) or iliac orfemoral artery thromboembolism (e.g., caudalparesis). � Chinese shar-pei dogs and Orientalshorthair and Siamese cats may have signs of
hepatic disease (e.g., jaundice, cachexia, andspontaneous hepatic rupture withintraperitoneal bleeding).
CAUSES� Neoplasia and chronic infectious andnon-infectious inflammatory conditions canbe found in 30–50% of dogs with reactiveamyloidosis. � Chronic inflammation—systemic mycoses (e.g., blastomycosis,coccidioidomycosis), chronic bacterialinfections (e.g., osteomyelitis,bronchopneumonia, pleuritis, steatitis,pyometra, pyelonephritis, chronic suppurativedermatitis, chronic suppurative arthritis,chronic peritonitis, nocardiosis, chronicstomatitis), parasitic infections (e.g.,dirofilariasis, leishmaniasis, hepatozoonosis),and immune-mediated diseases (e.g., systemiclupus erythematosus). � Neoplasia (e.g.,lymphoma, plasmacytoma, multiplemyeloma, mammary tumors, testiculartumors). � Familial (e.g., Chinese shar-pei,English foxhound, and beagle dogs;Abyssinian, Siamese, and Oriental shorthaircats). � Others—cyclic hematopoiesis in graycollies; juvenile polyarteritis in beagles.
RISK FACTORS� Chronic inflammation or neoplasia� Family history in certain breeds
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Dogs—glomerulonephritis; proteinuriatends to be more severe in dogs withglomerular amyloidosis than those withglomerulonephritis but there is great overlap.� Cats and Chinese shar-pei dogs withmedullary amyloidosis—consider other causesof medullary renal disease (e.g.,pyelonephritis, chronic interstitial disease).
CBC/BIOCHEMISTRY/URINALYSIS� Nonregenerative anemia is found in somedogs and cats with amyloid-induced renalfailure. � Dogs—may seehypercholesterolemia (> 85%), azotemia(> 70%), hypoalbuminemia (70%),hyperphosphatemia (> 60%), hypocalcemia(50%), and metabolic acidosis.� Hypercholesterolemia—common finding incats with renal disorders (> 70% of cats withrenal disease in one study) but does notreliably predict glomerular disease.� Hypoproteinemia—more common thanhyperproteinemia (24 vs. 8.5%) in dogs withamyloidosis; hyperglobulinemia common incats. � Proteinuria—with an inactivesediment common in dogs; mild or absent inanimals with medullary amyloidosis withoutglomerular involvement (most mixed-breedcats, at least 25% of Abyssinian cats, and atleast 33% of Chinese shar-pei dogs).� Isosthenuria, and hyaline, granular, andwaxy casts in some patients.
BLBS078-CF_A38 BLBS078-Tilley July 23, 2011 4:35
Canine and Feline, Fifth Edition 67
(Continued) Amyloidosis A
OTHER LABORATORY TESTSProteinuria—urinary protein:creatinine ratioto estimate severity.
IMAGINGAbdominal Radiographic Findings� Kidneys usually small in affected cats.� Kidneys small, normal-sized, or large inaffected dogs.
Abdominal Ultrasonographic Findings� Kidneys usually hyperechoic and small inaffected cats; may be small, normal-sized, orlarge in affected dogs.
DIAGNOSTIC PROCEDURESRenal biopsy needed to differentiateamyloidosis from glomerulonephritis. In dogsother than Chinese shar-pei, amyloidosis isprimarily a glomerular disease; diagnose byrenal cortical biopsy. In most domestic cats,some Abyssinian cats, and some Chineseshar-pei dogs, medullary amyloidosis canoccur without glomerular involvement;diagnose by renal medullary biopsy.
PATHOLOGIC FINDINGS� Small kidneys in cats; small, normal, orlarge kidneys in dogs. � Amyloid depositsappear homogeneous and eosinophilic whenstained by hematoxylin and eosin and viewedby conventional light microscopy. Theydemonstrate green birefringence after Congored staining when viewed under polarizedlight. Evaluation of Congo red—stainedsections before and after permanganateoxidation permits presumptive diagnosis ofAA amyloidosis (vs. other types) because AAamyloidosis loses its Congo red affinity afterpermanganate oxidation. � The liver is veryfriable and usually contains extensive amyloiddeposits in cats presented with acute hepatichemorrhage.
TREATMENTAPPROPRIATE HEALTH CARE� Hospitalize patients with chronic renalfailure and dehydration for initial medicalmanagement. � Can manage stable patientsand those with asymptomatic proteinuria asoutpatients.
NURSING CARECorrect dehydration with 0.9% NaClsolution or lactated Ringer’s solution; patientswith severe metabolic acidosis may benefitfrom bicarbonate supplementation (seeAcidosis, Metabolic).
ACTIVITYNormal
DIET� Patients with chronic renal failure—restrictphosphorus and moderately restrict protein.� Patients with hypertension—restrictsodium.
CLIENT EDUCATION� Discuss progression of the disease. � Discussfamilial predisposition in susceptible breeds.� Discuss potential complications (e.g.,hypertension, thromboembolism).
MEDICATIONSDRUG(S) OF CHOICE� Identify underlying inflammatory andneoplastic processes and treat if possible.� Manage renal failure according to theprinciples of conservative medical treatment(see Renal Failure, Acute, and Renal Failure,Chronic). � Normalize blood pressure inpatients with hypertension (see Hypertension,Systemic). � Patients with thromboembolicsyndrome and nephrotic syndrome caused byglomerular amyloidosis usually have a lowplasma concentration of antithrombin; thusheparin is relatively ineffective. Aspirin (0.5mg/kg PO q12h) has been suggested for dogswith glomerular disease; this low dosage is aseffective in preventing platelet aggregation asis 10 mg/kg PO q24h. � DMSO—may helppatients by solubilizing amyloid fibrils,reducing serum concentration of SAA, andreducing interstitial inflammation and fibrosisin the affected kidneys; may cause lensopacification in dogs. Perivascularinflammation and local thrombosis may occurif undiluted DMSO is administeredintravenously. Subcutaneous administrationof undiluted DMSO may be painful. Theauthors have used 90% DMSO diluted 1 : 4with sterile water subcutaneously at a dosageof 90 mg/kg three times per week in dogs.Whether or not DMSO treatment benefitsrenal amyloidosis in dogs remainscontroversial. � Methylsulfonylmethane is anactive metabolite of DMSO that can be givenorally and lacks the smell of DMSO. It hasbeen used empirically in dogs withamyloidosis, but there is no evidence that itbenefits dogs with renal amyloidosis.� Colchicine—impairs release of SAA fromhepatocytes; prevents development ofamyloidosis in humans with familialMediterranean fever (a familial amyloidosis)and stabilizes renal function in patients withnephrotic syndrome but without overt renalfailure; no evidence of benefit once the patientdevelops renal failure; may cause vomiting,diarrhea, and idiosyncratic neutropenia indogs. Colchicine (0.01–0.04 mg/kg POq24h) is used particularly in shar-pei dogswith episodic fever or polyarthritis beforedevelopment of renal failure.
CONTRAINDICATIONSAvoid use of nephrotoxic drugs
PRECAUTIONS� Dosage of drugs excreted by the kidneysmay need adjustment in patients with renalfailure. � Use nonsteroidal anti-inflammatory
drugs cautiously in patients with medullaryamyloidosis; they can decrease renal bloodflow in dehydrated patients.
FOLLOW-UPPATIENT MONITORING� Appetite and activity level daily by theowner; body weight weekly. � Serumalbumin, creatinine, and BUN concentrationsevery 2–6 months in stable patients. � Canassess degree of proteinuria serially by urineprotein:creatinine ratios.
PREVENTION/AVOIDANCEDo not breed affected animals
POSSIBLE COMPLICATIONS� Renal failure � Nephrotic syndrome� Systemic hypertension � Hepatic rupturecausing intraperitoneal hemorrhage� Thromboembolic disease
EXPECTED COURSE AND PROGNOSISDisease is progressive and usually advanced atthe time of diagnosis. Prognosis improves ifan underlying immune, inflammatory, orneoplastic disease is detected and successfullytreated. Survival for dogs with glomerularamyloidosis varied from 3 to 20 months in 1study; some dogs may occasionally live longer.Cats with renal failure because of amyloidosisusually survive < 1 year. Mildly affected catsmay not develop renal failure and have analmost normal life expectancy.
MISCELLANEOUSASSOCIATED CONDITIONS� Urinary tract infection � Polyarthritis inChinese shar-pei dogs � Polyarteritis in beagledogs
PREGNANCY/FERTILITY/BREEDINGHigh risk in affected animals
SEE ALSO� Glomerulonephritis � Nephrotic Syndrome� Proteinuria � Renal Failure, Acute � RenalFailure, Chronic
ABBREVIATIONS� AA = amyloid A protein � DMSO =dimethylsulfoxide � SAA = serum amyloid Aprotein
Suggested ReadingDiBartola SP. Renal amyloidosis. In: Osborne
CA, Low D, Finco DR, eds., Canine andFeline Urology, 2nd ed. Philadelphia:Saunders, 1995, pp. 400–415.
Authors Helio Autran de Morais and StephenP. DiBartolaConsulting Editor Carl A. Osborne
Client Education Handoutavailable online
BLBS078-CF_A39 BLBS078-Tilley March 21, 2011 21:12
68 Blackwell’s Five-Minute Veterinary Consult
Anaerobic InfectionsA
BASICSOVERVIEW� Anaerobic bacteria (i.e., bacteria requiringlow oxygen tension) comprise a large portionof the normal flora, especially on mucosalsurfaces. � May be gram-positive orgram-negative cocci or rods. � Most commongenera—Bacteroides, Fusobacterium,Actinomyces, Propionibacterium,Peptostreptococcus (enteric Streptococcus),Porphyromonas, and Clostridium. � Mostanaerobic infections are polymicrobial andcontain at least two different anaerobe speciesadmixed with facultative anaerobes or aerobicbacteria (especially E. coli). � Individualorganisms vary in potential to withstandoxygen exposure. � Injurious toxins andenzymes may be elaborated by the organisms,leading to extension of the infection intoadjacent, healthy tissue. � All body systemsare at potential risk for anaerobic infection.
SIGNALMENTDogs and cats
SIGNSGeneral Comments� Determined by the body system involved.� Certain areas more commonly associatedwith anaerobic infection (mucous membraneproximity). � It is possible to overlookanaerobes in an infectious process, leading toconfusion in interpreting culture results andselection of antimicrobials.
Physical Examination Findings� A foul odor associated with a wound orexudative discharge. � Gas in the tissue orassociated exudates. � Discolored tissue,especially when black. � Peritonitis,pyothorax, or pyometra. � Severe dentaldisease. � Wounds or deep abscesses that donot heal as anticipated.
CAUSES & RISK FACTORS� Usually caused by normal flora of the body;a break in protective barriers allows bacterialinvasion. � Infection in the proximity of amucous membrane should raise one’s index ofsuspicion for anaerobe involvement.� Predisposing factors—immunosuppression,bite wounds, dental disease, open fractures,abdominal surgery, and foreign bodies.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Wounds that fail to respond to appropriatemedical therapy—if aerobic cultures arenegative, suspect anaerobic organisms. � Catswith non-healing wounds—test for FeLV andFIV. � Middle-aged and old animals—tumorinvasion (e.g., in the gastrointestinal tract).
CBC/BIOCHEMISTRY/URINALYSIS� Neutrophilic leukocytosis and monocytosiscommon. � Biochemical abnormalitiesdepend on specific organ involvement.� Systemic spread of infection suggested byleukocytosis, hypoglycemia, increased ALP,and hypoalbuminemia.
OTHER LABORATORY TESTS� Culture of anaerobic bacteria is oftenunrewarding because of their fastidious natureand errors in sample handling andsubmission. � Appropriate media andcontainers should be on-hand prior to samplecollection; diagnostic laboratories can provideguidance. � Samples should not berefrigerated prior to submission. � Suitablesamples for culture may include fluid (e.g.,pleural, peritoneal, etc.) or tissue.
IMAGINGAs required for the circumstances of theindividual patient (e.g., suspected boneinfection, peritonitis, etc.).
DIAGNOSTIC PROCEDURES� Cytologic inspection reveals abundantdegenerate neutrophils with morphologicallydiverse forms of intracellular and extracellularbacteria; presence of large filamentousbacteria is suggestive. � If not performedin-house, gram staining should be requestedwhen the sample is submitted.
MEDICATIONS� Thoracic drainage—important withpyothorax (see specific chapter). � Hyperbaricoxygen—some potential use; limited inavailability.
SURGERY� Should not be delayed when anaerobes aresuspected. � Combined with systemicantimicrobial therapy—the best chance of apositive outcome. � Usually indicated whenanaerobic organisms complicate pyometra,osteomyelitis, and peritonitis. � Cleanse thewound of toxins and devitalized tissue.� Enhance drainage of pus. � Improve localblood flow. � Increase oxygen tension.
DRUG(S)� Antimicrobial therapy alone—unlikely to besuccessful; poor drug penetration intoexudates. � Antibiotic selection—largelyempiric, owing to the difficulty of isolatinganaerobes and the delay in return of cultureresults. � Because most anaerobic infectionsare polymicrobial, therapy targeted againstboth anaerobes and any aerobic componentsoffers the greatest chance of success.� Amoxicillin with clavulanate—in manycases, considered the antibiotic of choice;convenient and accessible; clavulanateimproves activity against Bacteroides.� Imipenem—beta lactam with significantactivity against serious, resistant infections.
� Cefoxitin—a cephalosporin with reliableactivity against anaerobes.� Clindamycin—may be especially useful forrespiratory tract infections; concentratedwithin leukocytes. � Chloramphenicol—goodtissue penetration but bacteriostatic andassociated with adverse effects, especially incats; concern for human exposure also limitsuse. � Metronidazole—useful against allclinically significant anaerobes (exceptActinomyces). � Aminoglycosides—uniformlyineffective. � Trimethoprim-sulfacombinations—ineffective; poor penetrationinto exudates. � Quinolones—routinelyineffective, although newerexpanded-spectrum quinolones do haveactivity against anaerobes (e.g.,pradofloxacin).
FOLLOW-UPPATIENT MONITORINGMonitoring parameters will vary with thecircumstances of each patient.
POSSIBLE COMPLICATIONSLocalized infection may progress to systemicinfection if not appropriately identified andtreated.
EXPECTED COURSE AND PROGNOSISDependent upon identification and resolutionof the underlying cause; long-term antibiotictherapy may be required.
MISCELLANEOUSASSOCIATED CONDITIONSSee “Causes & Risk Factors”
ABBREVIATIONS� ALP = alkaline phosphtase � FeLV = felineleukemia virus � FIV = felineimmunodeficiency virus
Suggested ReadingHirsh DC, Jang SS. Anaerobic infections. In:
Greene CE, ed., Infectious Diseases of theDog and Cat, 3rd ed. St. Louis: SaundersElsevier, 2006, pp. 381–388.
Author Sharon Fooshee GraceConsulting Editor Stephen C. Barr
BLBS078-CF_A40 BLBS078-Tilley July 15, 2011 5:20
Canine and Feline, Fifth Edition 69
Anal Sac Disorders A
BASICSOVERVIEW� Anal sacs are reservoirs for secretionsnormally evacuated during fecal excretion.� Disorders include impaction, infection(sacculitis), and neoplasia.� Treatment options include manualexpression, flushing, antibiotics, and surgicalexcision.
SIGNALMENT� Dogs and cats (rarely).� Breeds predisposed:
◦ Impaction—miniature and toy poodle,American cocker and English springerspaniel, Chihuahua.◦ Neoplasia (adenocarcinoma)—Germanshepherd dog, golden retriever, Americancocker and English springer spaniel.
� No age or sex predispositions.
SIGNS� Anal pruritus—often manifested by“scooting”� Perianal pruritus� Hesitancy to defecate� Tenesmus� Tail chasing� Foul-smelling, non-fecal matter analdischarge� Refusal to sit and/or lift tail
CAUSES & RISK FACTORS� Possible predisposing factors—soft feces ordiarrhea, excessive glandular secretions, anddermatologic disorders that alter thecharacteristics (cellularity and organismcolonization) of anal sac secretions.� Retained secretions may lead to infectionand abscess formation.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Adverse food reaction or foodhypersensitivity.� Flea bite hypersensitivity.� Atopic dermatitis.� Tapeworm infestation.� Tail fold bacterial folliculitis.� Malassezia dermatitis.� Compulsive disorder (anal licking).
� Colitis or other intestinal disorder.� Keratinization disorder.� Anal sac neoplasia (includingadenocarcinoma, squamous cell carcinoma).� Perianal adenoma.� Perianal adenocarcinoma.� Perianal fistulae.
CBC/BIOCHEMISTRY/URINALYSIS� Usually normal� Hypercalcemia—anal sac adenocarcinoma
OTHER LABORATORY TESTSNone unless indicated by an underlyingcause
IMAGINGNone unless indicated by an underlyingcause
DIAGNOSTIC PROCEDURES� Digital palpation of the anal sacs—normalanal sacs are not palpable externally.� Normal anal sac contents vary widely ingross appearance and microscopiccharacteristics; usually thin or watery, withminimal cellularity and primarily extracellularorganisms.� Impaction—generally more thick, pastybrown secretion; higher numbers ofMalassezia and intracellular bacteria.� Anal sacculitis and abscessation—purulent,often blood-tinged, foul-smelling discharge.� Cytology of anal sac secretions—increasednumber of neutrophils, Malassezia, andintracellular bacteria indicate infection;reports vary but gram-positive cocci morecommon in normal secretions.� Bacterial culture and sensitivity—normalsecretions may contain Proteus mirabilis,Streptococcus spp., Escherichia coli, Bacillusspp., Clostridium perfringens, and Pseudomonasaeruginosa.
TREATMENT� Gentle manual expression of contents forimpaction and sacculitis.� Sedation may be necessary to flush severelyimpacted or painful anal sacs.� Infusion of antibiotic and/or corticosteroidmedications directly into the anal sacs.� Drainage of abscesses.� Use of appropriate oral antibiotics and/orantiyeast medication.
� Anal sac excision with chronic disease.� Surgical excision and staging of anal sacneoplasia; combine with chemotherapy.� Identification of underlying causes ofpredisposing disease.� Feeding high-fiber diets may help naturalexpression of anal sacs.
MEDICATIONSDRUG(S)� Infection—use of appropriate antibiotics:cephalexin (22 mg/kg q12h), amoxicillintrihydrate-clavulanate potassium (10–15mg/kg q12h), clindamycin (11 mg/kgq12–24h), trimethoprim-sulfamethoxasole(15 mg/kg q12h); metronidazole (15 mg/kgq12h); enrofloxacin(10–20 mg/kg q12h dogs;cats 5 mg/kg/day), and orbifloxacin (5 mg/kgq24h).� Chronic disease associated with perianalfistulae; cyclosporine (5 mg/kg q24h) and/ortopical tacrolimus.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UP� Reassess patients weekly initially; then asnecessary to monitor healing.� Manually express anal sac contents and/orflush contents until sacs empty withoutintervention.
MISCELLANEOUSSEE ALSO� Adenocarcinoma, Anal Sac� Perianal Fistula
Suggested ReadingMuse R. Diseases of the anal sac. In:
Bonagura JD, Twedt DC, eds., Kirk’sCurrent Veterinary Therapy, 14th ed. St.Louis: Saunders, 2009, pp. 465–468.
Zoran DL. Rectoanal disease. In: Ettinger SJ,ed., Textbook of Veterinary InternalMedicine, 6th ed. Philadelphia: Saunders,2005, pp. 1408–1420.
Author Alexander H. WernerConsulting Editor Alexander H. Werner
BLBS078-CF_A41 BLBS078-Tilley March 21, 2011 21:23
70 Blackwell’s Five-Minute Veterinary Consult
AnaphylaxisA
BASICSDEFINITION� Acute manifestation of a Type Ihypersensitivity reaction mediated throughthe rapid introduction of an antigen into ahost having antigen-specific antibodies of theIgE subclass.� The binding of antigen to mast cellssensitized with IgE results in the release ofpreformed and newly synthesized chemicalmediators.� Anaphylactic reactions may be localized(atopy) or systemic (anaphylactic shock).� Anaphylaxis not mediated by IgE isdesignated an anaphylactoid reaction and willnot be discussed.
PATHOPHYSIOLOGY� First exposure of the patient to a particularantigen (allergen) causes a humoral responseand results in production of IgE, which bindsto the surface of mast cells; the patient is thenconsidered to be sensitized to that antigen.� Second exposure to the antigen results incross-linking of two or more IgE molecules onthe cell surface, resulting in mast celldegranulation and activation; release of mastcell granules initiates an anaphylactic reaction.� Major mast cell-derived mediators includehistamine, eosinophilic chemotactic factor,arachidonic acid, metabolites (e.g.,prostaglandins, leukotrienes, andthromboxanes), platelet-activating factor, andproteases, which cause an inflammatoryresponse of increased vascular permeability,smooth muscle contraction, inflammatory cellinflux, and tissue damage.� Clinical manifestations depend on the routeof antigen exposure, the dose of antigen, andthe level of the IgE response.
SYSTEMS AFFECTED� Gastrointestinal—salivation, vomiting, anddiarrhea� Hepatobiliary (dogs)—because of portalhypertension and vasoconstriction� Respiratory (cats)—dyspnea and cyanosis� Skin/Exocrine—pruritus, urticaria, andedema
GENETICSFamilial basis reported for Type Ihypersensitivity reaction in dogs.
INCIDENCE/PREVALENCE� Localized Type I hypersensitivity reactionsnot uncommon.� Systemic Type I hypersensitivity reactionsrare.
GEOGRAPHIC DISTRIBUTIONNone
SIGNALMENTSpeciesDogs and cats
Breed Predilections� Dogs—numerous breeds documented ashaving a predilection for developing atopy.� Cats—no breeds documented as havingpredilection for atopy.
Mean Age and Range� Dogs—age of clinical onset ranges from 3months to several years of age; most affectedanimals 1–3 years old.� Cats—age of clinical onset ranges from 6months to 2 years.
Predominant Sex� Dogs—atopy more common in females.� Cats—no reported sex predilection.
SIGNSGeneral Comments� Initial clinical signs vary depending on theroute of exposure to the inciting antigen(allergen).� Shock—end result of a severe anaphylacticreaction.� Shock organ—dogs, liver; cats, respiratoryand gastrointestinal systems.� May be localized to the site of exposure butmay progress to a systemic reaction.
Historical Findings� Onset of signs immediate (usually withinminutes).� Dogs—pruritus, urticaria, vomiting,defecation, and urination.� Cats—intense pruritus about the head,dyspnea, salivation, and vomiting.
Physical Examination Findings� Localized cutaneous edema at the site ofexposure.� Hepatomegaly in some dogs.� Hyperexcitability possible in early stages.� Depression and collapse terminally.
CAUSESVirtually any agent; those commonly reportedinclude venoms, blood-based products,vaccines, foods, and drugs.
RISK FACTORSPrevious exposure (sensitization) increasesthe chance of the animal developing areaction.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other types of shock.� Trauma.� Depends on the major organ systeminvolved or if reaction is localized; diagnosis
can be made largely on the basis of historyand clinical signs.
CBC/BIOCHEMISTRY/URINALYSISBecause of the acute onset of disease, no testsavailable that reliably predict individualsusceptibility.
OTHER LABORATORY TESTS� Intradermal skin testing to identifyallergens.� Radioallergosorbent test to quantify theconcentration of serum IgE specific for aparticular antigen.
IMAGINGN/A
DIAGNOSTIC PROCEDURESLimited because a severely allergic animal candevelop an anaphylactic reaction whenexposed to even small quantities of antigen.PATHOLOGIC FINDINGS� Lesions vary, depending on severity ofreaction, from localized cutaneous edema tosevere pulmonary edema (in cats) and visceralpooling of blood (in dogs).� Other non-specific findings vary and arecharacteristic of shock.� Non-specific characteristics of localizedreactions include edema, vasculitis, andthromboembolism.
TREATMENTAPPROPRIATE HEALTH CAREIn an acutely affected animal, the reaction isconsidered a medical emergency requiringhospitalization.
NURSING CAREElimination of inciting antigen, if possible.
Systemic Anaphylaxis� Goal—emergency life support through themaintenance of an open airway, preventingcirculatory collapse, and reestablishingphysiologic parameters.� Administer fluids intravenously at shockdosages to counteract hypotension.
Localized AnaphylaxisGoal—limit the reaction and preventprogression to a systemic reaction.
ACTIVITYN/A
DIETIf a food-based allergen is suspected(uncommon), avoid foods associated withhypersensitivity reaction.
CLIENT EDUCATION� Discuss the unpredictable nature of thedisease.
BLBS078-CF_A41 BLBS078-Tilley March 21, 2011 21:23
Canine and Feline, Fifth Edition 71
(Continued) Anaphylaxis A
� Discuss the need to recognize that theanimal has an allergic condition that mayrequire immediate medical care.
SURGICAL CONSIDERATIONSNone
MEDICATIONSDRUG(S) OF CHOICESystemic Anaphylaxis� Epinephrine hydrochloride parenterally(1 : 1,000; 0.01 mL/kg) for shock.� Corticosteroids for shock—prednisolonesodium succinate (2 mg/kg IV q8h) ordexamethasone sodium phosphate (0.25mg/kg IV q12h).� Atropine sulfate (0.04 mg/kg IM) tocounteract bradycardia and hypotension.� Aminophylline (10 mg/kg IM or slowly IV)in severely dyspneic patients.
Localized Anaphylaxis� Diphenhydramine hydrochloride (1-2mg/kg IV or IM).� Prednisolone (2 mg/kg PO).� Epinephrine hydrochloride (0.15 ml SC atsite of initiation).� If shock develops, initiate treatment for asystemic anaphylaxis.
CONTRAINDICATIONSNone
PRECAUTIONSLocalized reaction can develop into systemicreaction.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGClosely monitor hospitalized patients for24–48 hours.
PREVENTION/AVOIDANCEIf inciting antigen (allergen) can be identified,eliminate or reduce exposure.
POSSIBLE COMPLICATIONSNone
EXPECTED COURSE AND PROGNOSIS� If localized reaction is treated early,prognosis is good.� If the animal is in shock on examination,prognosis is guarded to poor.
MISCELLANEOUSASSOCIATED CONDITIONSNone
AGE-RELATED FACTORSNone
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A
SEE ALSO� Shock, Cardiogenic
INTERNET RESOURCESMerck Veterinary Manual:www.merckvetmanual.com.
Suggested ReadingMueller DL, Noxon JO. Anaphylaxis:
Pathophysiology and treatment. CompendContin Educ Pract Vet 1990, 12:157–170.
Author Paul W. SnyderConsulting Editor A.H. Rebar
Client Education Handoutavailable online
BLBS078-CF_A42 BLBS078-Tilley March 21, 2011 21:25
72 Blackwell’s Five-Minute Veterinary Consult
Anemia of Chronic Kidney DiseaseA
BASICSDEFINITIONProgressive decreases in PCV, RBC count,and hemoglobin and hypoplasia of erythroidelements of the bone marrow are predictablefeatures of progressive CKD. Anemia isnormocytic, normochromic, nonregenerative,and proportional to the stage of CKD.Principal cause is bone marrow failuresecondary to inadequate production oferythropoietin by the kidneys. ShortenedRBC lifespan, uremic inhibitors oferythropoiesis, blood loss, nutritionaldeficiencies, and marrow fibrosis maycontribute.
SIGNALMENTMiddle-aged to old dogs and cats mostlyaffected; seen in young animals with heritable,congenital, or acquired CKD.
SIGNS� Anemia contributes to development ofanorexia, weight loss, fatigue, lethargy,depression, weakness, apathy, coldintolerance, and behavior and personalitychanges characterizing CKD.� Pallor of the mucous membranes.� Tachypnea.� Tachycardia.� Systolic murmur.� Syncope and seizures (rare).
CAUSES & RISK FACTORS� All inherited, congenital, and acquiredforms of CKD (e.g., pyelonephritis,glomerulonephritis, amyloidosis, polycystickidney disease, and lymphoma).� Exacerbated by iron deficiency,inflammatory or neoplastic disease,gastrointestinal blood loss, hemolysis, andmyeloproliferative disorders.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Anemia of chronic infectious, inflammatory,or neoplastic disease; myeloproliferativedisease; chronic blood loss; aplastic anemia;endocrine disease; drug reaction; and chronicimmune-mediated, toxic, viral, rickettsial, orparasitic anemia; hemodilution.� Regenerative anemia excludes diagnosis ofanemia of CKD.� Generally masked until advanced CKD.
CBC/BIOCHEMISTRY/URINALYSIS� Normocytic, normochromic,hypoproliferative anemia (progressive; anemiamay be masked by dehydration).� Reticulocytes—low corrected indices andabsolute counts (≤ 10,000/ul).� Moderate to advanced CKD—elevatedBUN, creatinine, and phosphorus; variably
high calcium; variably low bicarbonate andpotassium.� High BUN:creatinine ratio may predictconcurrent gastrointestinal blood loss.� Impaired urine-concentrating ability, mildto moderate proteinuria, and variably activesediment.
OTHER LABORATORY TESTS� Serum iron—normal or variably low.� Transferrin saturation—normal or variablylow (< 20%).� FeLV and FIV or haemobartonella testing(cats) or rickettsial titers or PCR (dogs) toexclude agent-induced myelodyscrasia.� Serum erythropoietin—normal(inappropriately) or low.
IMAGING� Small, irregular kidneys with loss ordisruption of renal architecture detected byradiography or ultrasonography.� Enlarged, polycystic, hydronephrotic,infiltrative.
DIAGNOSTIC PROCEDURESCytologic examination of bonemarrow—erythroid hypoplasia;myeloid:erythroid ratio normal or high;stainable iron normal or variably low.
TREATMENT� Increase RBC mass if patient issymptomatic for anemia (dogs, PCV ≤ 25%;cats, PCV ≤ 23).� Stabilize azotemia in patients in uremiccrisis.� Establish appropriate nitrogen, caloric,phosphate, vitamin, and iron intake to reduceuremic inhibitors and bleeding tendency andlengthen life span of RBCs.� Ensure that iron is not deficient.� Correct gastrointestinal ulceration andblood loss by administrating famotidine,ranitidine, omeprazole, or sucralfate.� Correct systemic hypertension.
MEDICATIONSDRUG(S) AND FLUIDSErythropoietin Replacement� Epoetin alfa (r-HuEPO)—original syntheticerythropoiesis stimulating protein, replica ofhuman erythropoietin (Epogen and Procrit);provides consistent, rapid, and long-termcorrection of anemia in dogs and cats withCKD; potential for anti-r-HuEPO antibodyproduction and pure red cell aplasia.� Darbepoetin alfa (Aranesp), a newhyperglycolylated analogue of r-HuEPO withprolonged half-life and sustained effects;appears to be equipotent to r-HuEPO and,with current experience, little tendency for
antibody induction; should be usedpreferentially to epoetin alfa.� Target PCV—dogs, 37–45%; cats, 30–40%.� Initial dosage: darbepoetin alfa—0.45–0.6mcg/kg (for cats and small dogs 2.5–5 mcg)SC once weekly until PCV reaches low end oftarget, then decrease to q2 weeks. Epoetinalfa—50–100 U/kg SC thrice weekly untillow end of target, then decrease to twiceweekly. If converting from epoetin alfa todarbepoetin—divide weekly units by 400 toestablish mcg to give once weekly.� Maintenance dosage: darbepoetinalfa—2.5–5 mcg q2–3 weeks. Epoetinalfa—50–100 U/kg SC once or twice weeklyto maintain target PCV. Individualize to eachpatient; life-long treatment required. If givingepoetin alfa once weekly, give darbepoetinevery 2 weeks with conversion.� If PCV exceeds target, discontinue untilupper target range is achieved, then decreaseprevious dosage by 25–50% or increasedosage interval.� Serum iron and transferrin saturationshould be normalized before initiating andduring treatment. Injectable iron (50 mg/kgIM q4–8 weeks) is preferable and bettertolerated than oral preparations.� Species-specific erythropoietins for dogs andcats and alternative erythropoietin stimulatingtreatments are under development asalternatives for erythropoiesis stimulatingproteins.
Blood Transfusion� Short-term or rapid correction (PCV ≤20%)—give compatible whole blood orpacked RBCs.� Target PCV is 25–30%.� May be given intermittently for prolongedmanagement.
Anabolic Steroids� Little or no efficacy or indication for use.
FOLLOW-UPPATIENT MONITORING� PCV—weekly to semimonthly for 3months, then monthly to bimonthly.� Blood pressure—semimonthly to monthly.� Iron and transferrin saturation—at 1, 3, and6 months, then semiannually.� Discontinue erythropoietin if patientdevelops evidence of erythrocythemia, local orsystemic sensitivity, anti-r-HuEPO antibodyformation, pure red cell aplasia, or refractoryhypertension.
POSSIBLE COMPLICATIONSErythropoietin-Related� Development of erythrocythemia, seizures,hypertension, iron depletion, injection pain,and mucocutaneous reactions.� Development of a pure red cell aplasiaduring the course of epoetin alfa treatmentsuggests formation of anti-r-HuEPO
BLBS078-CF_A42 BLBS078-Tilley March 21, 2011 21:25
Canine and Feline, Fifth Edition 73
(Continued) Anemia of Chronic Kidney Disease A
antibodies, which neutralize r-HuEPO andnative erythropoietin, causing severe anemiain 20–30% of animals; often reversible withcessation of treatment.� Signs associated with production ofanti-r-HuEPO antibodies while the patient isreceiving epoetin alfa include decreasing PCV,erythroid hypoplasia, absolute reticulocytecounts approaching zero, andmyeloid:erythroid ratio ≥ 8. These signs alsoshould be monitored with darbepoetin alfatreatment.� Erythropoietin replacements should be usedcautiously or withheld if hypertension or irondeficiency develop; treatment can bereinstituted once hypertension and irondeficiency are corrected.
Transfusion-Related� Incompatibility reaction� Circulatory or iron overload� Systemic hypertension� Transmissible infection
EXPECTED COURSE AND PROGNOSIS� Correction of anemia increases appetite,activity, grooming, affection and playfulness,weight gain, and cold tolerance, and decreasessleeping.� Use of erythropoietin replacement in dogsand cats requires careful assessment of therisks and benefits for individual patients.� Short-term prognosis depends on theseverity of the renal failure. Long-termprognosis is guarded to poor because of theunderlying chronic renal failure.
MISCELLANEOUSABBREVIATIONS� CKD = chronic kidney disease� FeLV = feline leukemia virus� FIV = feline immunodeficiency virus� PCR = polymerase chain reaction� PCV = packed cell volume� RBC = red blood cell� r-HuEPO = recombinant humanerythropoietin
Suggested ReadingCowgill LD, et al. Use of recombinant human
erythropoietin for management of anemiain dogs and cats with renal failure. JAVMA1998, 212:521–528.
Author Larry D. CowgillConsulting Editor Carl A. Osborne
BLBS078-CF_A43 BLBS078-Tilley May 31, 2011 18:56
74 Blackwell’s Five-Minute Veterinary Consult
Anemia, AplasticA
BASICSOVERVIEW� A disorder of hematopoietic precursor cellscharacterized by replacement of normal bonemarrow with adipose tissue. There isdecreased production of granulocytes,erythrocytes, and platelets, resulting inpancytopenia in the peripheral blood. Thedisease is sometimes also referred to as aplasticpancytopenia.� In the acute form, neutropenia andthrombocytopenia predominate because ofthe shorter life spans of these cells; in thechronic form, nonregenerative anemia alsooccurs. In both forms, the bone marrowexhibits variable degrees of panhypoplasia.� There are many precipitating causes ofdeficient hematopoiesis, including infectiousdiseases, drug administration, starvation andtoxin exposure; immune-mediatedmechanisms are often suspected.� Hemic/lymphatic/immune systems affected.
SIGNALMENTDogs and cats, no apparent breed or sexpredilection. In one study, the mean age ofnine affected dogs was 3 years.
SIGNS� Acute form: fever, petechial hemorrhages,epistaxis, hematuria, melena; i.e., signs due toneutropenia and thrombocytopenia.� Chronic form: pale mucous membranes,weakness, lethargy; i.e., signs due to anemia,in addition to signs observed in acute forms.
CAUSES & RISK FACTORSOften not identified
Infectious Agents� FeLV, FIV� Canine and feline parvovirus� Rickettsial organisms (e.g., Ehrlichia spp.)
Drugs and Chemicals� Estrogen (exogenous administration, Sertoliand interstitial cell tumors).� Methimazole (cats).� Chemotherapeutic drugs, includingazathioprine, cyclophosphamide, cytosinearabinoside, doxorubicin, vinblastine, andhydroxyurea.� Antibiotics, includingtrimethoprim-sulfadiazine, cephalosporins,and chloramphenicol.� Griseofulvin.� NSAIDs, including phenylbutazone andmeclofenamic acid.� Fenbendazole, albendazole.� Captopril.� Quinidine.
� Thiacetarsamide.� Ionizing radiation.� Mycotoxins (cats).
DIAGNOSISDIFFERENTIAL DIAGNOSISCauses of pancytopenia with normal toincreased bone marrow cellularity (e.g.,myelodysplastic disorders, leukemia,myelofibrosis).
CBC/BIOCHEMISTRY/URINALYSIS� Leukopenia characterized by neutropeniawith or without lymphopenia.� Normocytic, normochromic,nonregenerative anemia.� Thrombocytopenia.
OTHER LABORATORY TESTS� Immunologic tests for infectious diseases(e.g., serologic titers, ELISA, IFA).� PCR for infectious agents.� Serologic test for antierythrocyte antibodies(Coombs’ test).
IMAGINGN/A
DIAGNOSTIC PROCEDURES� Bone marrow aspiration—frequently aninadequate or fatty sample is obtained becauseof decreased hemopoietic tissue andreplacement by lipocytes.� Bone marrow core biopsy—allows anevaluation of architecture and revealshypoplasia of cell lines and replacement byadipose tissue.
TREATMENTSupportive treatment, antibiotics, bloodcomponent therapy, as dictated by clinicalcondition.
MEDICATIONSDRUG(S) OF CHOICE� Cyclosporine A—10–25 mg/kg PO q12h(dogs), 4-5 mg/kg PO q12h (cats).� Recombinant hematopoietic growth factors(e.g., rhG-CSF: 5 μg/kg/day SC).� Androgen and corticosteroid administrationhave been largely unsuccessful.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
OTHER DRUGS� Antibiotics to treat secondary infections iffever and neutropenia present.� Whole or component blood transfusion ifindicated.
FOLLOW-UPPATIENT MONITORING� Daily physical examination.� CBC every 3-5 days to weekly.� Repeat bone marrow evaluation if necessary.
PREVENTION/AVOIDANCE� Castration of cryptorchid males.� Vaccination for infectious diseases.� Frequent monitoring of CBC in cancerpatients receiving chemotherapy or radiation.
POSSIBLE COMPLICATIONS� Sepsis� Hemorrhage
EXPECTED COURSE AND PROGNOSIS� Guarded to poor.� Recovery of hematopoiesis may take weeksto months, if it occurs at all.� Spontaneous recovery occasionally occurs,especially in young animals.
MISCELLANEOUSSEE ALSOPancytopenia
ABBREVIATIONS� ELISA = enzyme-linked immunosorbentassay� FeLV = feline leukemia virus� FIV = feline immunodeficiency virus� IFA = immunofluorescent antibody (test)� NSAID = nonsteroidal anti-inflammatorydrug� PCR = polymerase chain reaction� rhG-CSF = recombinant humangranulocyte colony-stimulating factor
Suggested ReadingBrazzell JL, Weiss DJ. A retrospective study of
aplastic pancytopenia in the dog: 9 cases(1996–2003). Vet Clin Path 2006,35:413–417.
Weiss DJ. Aplastic anemia. In: Weiss DJ,Wardrop KJ, eds., Schalm’s VeterinaryHematology, 6th ed. Ames, IA: BlackwellPublishing Ltd., 2010, pp. 256–260.
Author Darren WoodConsulting Editor A.H. Rebar
BLBS078-CF_A44 BLBS078-Tilley May 31, 2011 19:0
Canine and Feline, Fifth Edition 75
Anemia, Heinz Body A
BASICSOVERVIEW� Heinz bodies cause hemolytic anemia andindicate oxidative damage to RBCs. � Heinzbodies form when oxidants overwhelmprotective reductive pathways in RBCs andcause irreversible denaturation of hemoglobin(sulfhydryl groups and/or hemichromes),precipitation and attachment of alteredhemoglobin to the cell membrane, clusteringof band 3, and alteration of surface antigens.� The RBCS are less deformable, targeted forremoval by macrophages in the spleen, andmay undergo intravascular lysis. � The pittingfunction of the spleen may remove Heinzbodies, resulting in spherocytes. � Heinzbodies are usually caused by exposure tochemical or dietary oxidants. � Cats areparticularly susceptible to Heinz bodyformation because their hemoglobin is rich insulfhydryl groups and the feline spleen isnon-sinusoidal with limited pitting function.� Healthy cats may have Heinz bodies with noanemia. � Heinz bodies are frequently foundin cats with hyperthyroidism, lymphoma, anddiabetes mellitus (particularly if ketoacidotic),possibly due to increased endogenousoxidants (e.g., β-hydroxybutyrate). Anemiamay or may not be present. � Heinz bodiesmay be accompanied by methemoglobinemia(hemoglobin containing Fe3+) and/oreccentrocytes (oxidative damage to RBCmembranes with hemoglobin displaced to oneside). The factors that control which type(s)of oxidative damage occurs are not clear.
SIGNALMENT� Dogs and cats. � No sex, breed, or agedisposition.
SIGNSHistorical Findings� Exposure to oxidant. � Sudden onset ofweakness, lethargy, or anorexia. � Reddish-brown urine (hemoglobinuria) if severeintravascular hemolysis. � Signs related tounderlying disease in cats with systemicdisease and Heinz bodies.
Physical Examination Findings� Pale or icteric mucous membranes. � Darkor chocolate-colored blood withmethemoglobinemia. � Tachypnea,tachycardia.
CAUSES & RISK FACTORS� Dietary: onions (raw, cooked, dehydrated,and powdered), garlic (dogs), propylene glycol(cats), Chinese chives (dog). � Drugs:acetaminophen, phenacetin (cats),phenazopyridine (cats), methylene blue,vitamin K1 or K3 (dogs), DL-methionine(cats), benzocaine (topical), phenylhydrazine(dog), propofol (cats). � Miscellaneous: zinc(nuts, bolts, pennies, dermatologic creams),
naphthalene (moth ball ingestion in dogs),skunk musk exposure (dogs).
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other causes of regenerative, hemolyticanemia (e.g., immune mediated,hemoparasites). � Heinz bodies may be foundin healthy or ill cats without anemia.Diagnosis of a Heinz body anemia requiresdocumentation of a regenerative anemia,supporting evidence of a hemolytic process(e.g. hyperbilirubinemia), identification ofHeinz bodies on a smear, and elimination ofother causes of hemolysis or blood loss.
CBC/BIOCHEMISTRY/URINALYSIS� Regenerative anemia (decreased HCT,polychromasia, nucleated RBCs) is expected ifthere has been sufficient time for a bonemarrow response; the severity of anemiadepends on dose of oxidant and duration ofexposure. � Hemoglobin concentration andMCHC may be falsely increased due to Heinzbody interference. � Heinz bodies are visibleon a routine blood smear as small, pale red,round inclusions that may protrude fromRBC surface. They may be difficult to identifyif there is marked poikilocytosis. � Single,small (< 0.5 μm) Heinz bodies may be foundin RBCs of cats without anemia. � Largeand/or multiple Heinz bodies in an anemiccat suggest a Heinz body hemolytic anemia.� Dogs may have concurrent eccentrocytes ona blood smear. � Hyperbilirubinemia andbilirubinuria are possible. � Hemoglobinemiaand hemoglobinuria are uncommon butoccur with severe intravascular hemolysis.� Neutrophilia and monocytosis may occur.
OTHER LABORATORY TESTS� New methylene blue stains Heinz bodiesblue, making them easy to identify andquantify, even with marked poikilocytosis.� Methemoglobin test if blood is dark orchocolate colored. � Serum zincconcentration if indicated.
IMAGINGAbdominal radiographs may revealgastrointestinal metal objects in zinc toxicity.
TREATMENT� Immediate identification and removal ofoxidant may be sufficient, though it may takeseveral days for the severity of anemia to reachnadir. � Supportive care depends on theseverity of the hemolytic crisis and includesIV fluids, RBC transfusions, oxygen, andrestricted activity. � Endoscopy or surgery toremove metallic items in gastrointestinal tract.
MEDICATIONSDRUG(S) OF CHOICE� Severe methemoglobinemia—single slow IVinjection of methylene blue (0.2 mg/kg).� Acetaminophen toxicity in cats—N-acetylcysteine (140 mg/kg PO or IV, followedby seven additional treatments of 70 mg/kgevery 8 hours).
CONTRAINDICATIONS/POSSIBLEINTERACTIONSMethylene blue may aggravateoxidant-induced hemolysis.
ALTERNATIVE DRUG(S)The use of dietary antioxidants (vitamin C,vitamin E, bioflavonoids) is controversial butmay help prevent further formation of Heinzbodies.
FOLLOW-UPPATIENT MONITORINGSerial CBCs and review of blood smears arerecommended to assess RBC regeneration anddisappearance of Heinz bodies.
PREVENTION/AVOIDANCECounsel clients about preventing exposure tooxidants.
POSSIBLE COMPLICATIONSN/A
EXPECTED COURSE AND PROGNOSISPrognosis is good with removal of oxidant andsupportive care once the hemolytic crisis isover.
MISCELLANEOUSSEE ALSO� Acetaminophen Toxicity � Anemia,Regenerative � Methemoglobinemia � ZincToxicity
ABBREVIATIONS� HCT = hematocrit � MCHC = meancorpuscular hemoglobin concentration� RBC = red blood cell
Suggested ReadingAndrews D. Disorders of red blood cells. In:
Handbook of Small Animal Practice, 5th ed.St. Louis: Saunders, 2008, pp. 632–635.
Stockham SL, Scott MA. Erythrocytes. In:Fundamentals of Veterinary ClinicalPathology, 2nd ed. Ames, IA: Blackwell,2008, pp. 186–187.
Author Jennifer S. ThomasConsulting Editor A.H. Rebar
BLBS078-CF_A45 BLBS078-Tilley June 17, 2011 7:3
76 Blackwell’s Five-Minute Veterinary Consult
Anemia, Immune-MediatedA
BASICSDEFINITIONAccelerated destruction or removal of RBCsdue to a Type II hypersensitivity reaction.
PATHOPHYSIOLOGY� Anti-RBC antibodies form againstendogenous unaltered surface antigens(primary IMHA) or altered RBC membraneantigens (secondary IMHA).� Infectious organisms, drugs, exposure ofpreviously unexposed antigens, or adsorptionof preformed antigen—antibody complexes tothe RBC membrane can alter RBC membraneantigens.� Immunoglobulin (IgG or IgM, with orwithout complement) deposits on the RBCmembrane, causing either direct intravascularhemolysis or accelerated removal by themonocyte/macrophage system (extravascularhemolysis).� Intravascular hemolysis occurs whenadsorbed antibodies (usually IgG) activatecomplement.� In vivo agglutination of RBCs occurs whenIgM or high titers of IgG molecules causebridging of RBCs.� Extravascular removal of RBCs occurs in thespleen, liver, bone marrow, or other site ofmacrophage activity.� Nonregenerative IMHA is believed to becaused by immune-mediated destruction ofRBC precursors in the bone marrow.� Rarely cold-acting antibodies cause in vivohemolysis and erythrocyte agglutination inperipheral vasculature.
SYSTEMS AFFECTED� Cardiovascular—hypoxia leads totachycardia; low blood viscosity and turbulentblood flow may cause a low-grade heartmurmur.� Hemic/Lymphatic/Immune—immune-mediated destruction of RBCs, elaboration ofproinflammatory mediators (e.g., cytokines,endothelial-derived substances), DIC.� Hepatobiliary—hemolysis leads tohyperbilirubinemia and icterus as well asbilirubinuria when hepatic function isoverwhelmed; hypoxia may causecentrilobular necrosis.� Respiratory—hypoxia causes tachypnea.Pulmonary thromboembolism may resultfrom a hypercoagulable state due to increasedactivity procoagulant factors, presence of freehemoglobin, decreased concentration offibrinolytic and anticoagulant factors,vasculitis, and increased platelet reactivity.� Skin—rarely cold-type IMHA may causenecrosis of extremities and ear tips because ofRBC agglutination in peripheral vessels.
GENETICSCocker spaniels are at increased risk. Absenceof dog erythrocyte antigen 7 is associated withincreased risk in this breed.
GEOGRAPHIC DISTRIBUTIONSecondary IMHA may have a higherprevalence in areas where associated infectiousdiseases are endemic.
SIGNALMENTSpeciesDogs and cats
Breed Predilections� Cocker spaniel is the breed at highest risk.Other commonly affected breeds includeminiature poodle, Irish setter, Englishspringer spaniel, Old English sheepdog,Doberman pinscher, collie, bichon frise,miniature pinscher, and Finnish spitz.� Domestic shorthair cats.
Mean Age and Range� In dogs, mean age 5–6 years with reportedrange of 1–13 years.� In cats, mean age 2 years with reportedrange of 0.5–9 years.
Predominant Sex� Females may have a higher risk in dogs.� Male cats are overrepresented.
SIGNSHistorical Findings� Lethargy/weakness/collapse� Anorexia� Exercise intolerance/dyspnea� Tachypnea� Vomiting and/or diarrhea� Dark red urine� Pica (cats)
Physical Examination Findings� Pale mucous membranes, tachycardia, andtachypnea.� Splenomegaly and hepatomegaly.� Icterus and pigmenturia (hemoglobin orbilirubin).� Fever and lymphadenomegaly.� Systolic murmur.� Petechiae, ecchymoses, or melena in animalswith concurrent thrombocytopenia or DIC.� Other physical examination findingspossible (e.g., joint pain andglomerulonephritis) when IMHA is acomponent of SLE.� Necrosis of extremities and ear tips incold-type IMHA (rare).
CAUSESPrimary IMHAAutoimmune (idiopathic) hemolytic anemiadue to poorly characterized immunedysregulation.
Secondary IMHA� Infectious causes (hemotrophic Mycoplasmaspp., Ehrlichia canis, Anaplasma
phagocytophilum, Babesia spp., Leishmaniasis,Dirofilaria immitis, Ehrlichia, FeLV, FIP,chronic bacterial infection).� Neoplasia (lymphoma, lymphoid leukemia,hemangiosarcoma, hemophagic histiocyticsarcoma).� Drugs (e.g., beta lactam antibiotics,propylthiouracil, methimazole, sulfonamides).
MISCELLANEOUS CAUSES� SLE� Neonatal isoerythrolysis� Hemolysis due to DEA incompatible bloodtransfusion
RISK FACTORSExposure to infectious agents, vaccination,chemicals or drugs, surgery, hormonal change,or other stressful event is hypothesized as apotential trigger for IMHA.
DIAGNOSISDIFFERENTIAL DIAGNOSISDogs� Pyruvate kinase deficiency.� Phosphofructokinase deficiency.� Toxicity (zinc, onions, garlic, broccoli,copper, naphthalene, skunk musk).� Snake/spider evenomation (coral snakes,recluse spiders).� Severe hypophosphatemia.� Anemia due to hemorrhage(immune-mediated thrombocytopenia,rodenticide toxicosis).� Microangiopathic anemia due to splenicneoplasia, DIC, splenic torsion.
Cats� Toxicity (acetaminophen zinc, onions,garlic).� Severe hypophosphatemia.� Congenital feline porphyria.� Increased osmotic fragility (Abyssinian,Somali).
CBC/BIOCHEMISTRY/URINALYSIS� CBC—anemia, high MCV (3–5 dayspost-hemolytic episode), spherocytes,anisocytosis, polychromasia, nucleated RBCs,increased RBC distribution width, markedleukocytosis with neutrophilia and a left shift.Anemia is nonregenerative in 30% of dogsand 50% of cats.� Serum biochemistry—hyperbilirubinemia,hemoglobinemia, high ALT.� Urinalysis—hemoglobinuria, bilirubinuria.
OTHER LABORATORY TESTS� Spontaneous saline agglutinationtest—before and after washing of red bloodcells.� Positive direct antiglobulin test (Coombs’test)—positive in up to 75% of animals withIMHA.
BLBS078-CF_A45 BLBS078-Tilley June 17, 2011 7:3
Canine and Feline, Fifth Edition 77
(Continued) Anemia, Immune-Mediated A
� Flow cytometric detection ofmembrane-bound immunoglobulin andcomplement.� Reticulocytosis—absolute count> 60,000/μl in dogs and > 50,000/μl in catsin regenerative IMHA.� Thrombocytopenia in 60% of dogs.Thrombocytopenia may be severe in animalswith Evans syndrome and DIC.� Prolonged APTT and PT, increased fibrindegradation products, d-dimer, and decreasedantithrombin in animals with DIC.� Increased fibrinogen concentration.� Positive ANA titer and LE cell test inanimals with SLE.� Positive serologic titers or PCR in secondaryIMHA due to infectious causes.� Evidence of hematologic parasites in bloodsmears of capillary blood in secondary IMHAdue to infectious causes.� Increased RBC osmotic fragility.
IMAGING� Radiographic findings—hepatomegaly andsplenomegaly; thorax usually within normallimits; may see evidence of pulmonarythromboembolism in dogs with IMHA(patchy alveolar pattern, interstitial pattern,pleural fluid), but dogs with pulmonaryembolism may have normal thoracicradiographs.� Ultrasonographic findings—hepatomegalyand splenomegaly; liver and spleen can bemottled and hyperechoic or hypoechoic.
DIAGNOSTIC PROCEDURES� Examination of bone marrow aspirateusually reveals erythroid hyperplasia.� In animals with nonregenerative IMHA,maturation arrest or erythroid hypoplasia maybe evident.� In animals with chronic IMHA,myelofibrosis may be present.
PATHOLOGIC FINDINGS� Hepatosplenomegaly, centrilobular hepaticnecrosis� Splenic and hepatic extramedullaryhematopoiesis� Reactive lymphadenomegaly� Pulmonary thromboembolism and DIC
TREATMENTAPPROPRIATE HEALTH CARE� Inpatient during the acute hemolytic crisis;outpatient when PCV has stabilized, ongoinghemolysis has been controlled, and clinicalsigns of anemia have resolved.� Inpatient if animal has complications suchas DIC, pulmonary thromboembolism,thrombocytopenia, gastrointestinal bleeding,or a need for multiple transfusions.� Chronic low-grade extravascular hemolysiscan be treated on an outpatient basis if thepatient is not exhibiting clinical signssecondary to anemia.
NURSING CARE� Fluid therapy to maintain vascular volumeand correct dehydration.� Careful monitoring for complications suchas pulmonary thromboembolism, bleeding(especially gastrointestinal), disseminatedintravascular coagulation, infection.� Cage rest.
CLIENT EDUCATION� IMHA and its complications (e.g., DIC andpulmonary thromboembolism) can be fatal.� Lifelong treatment may be needed, and thedisease may recur.� Side effects of treatment may be severe.
SURGICAL CONSIDERATIONS� Splenectomy can be considered if medicalmanagement fails to control the disease.� Consider blood product administrationpreoperatively.
MEDICATIONSDRUG(S) OF CHOICE� Packed RBCs typed or cross-matched fornaive recipient. Blood should becross-matched for recipients that havereceived prior transfusions.� Transfusion volume = recipient weight (kg)× 85 (dog) or 50 (cat) × desired PCV-currentPCV/donor PCV.� Transfusion rate 0.25 ml/kg/hour for first30 minutes then 5–10 ml/kg/hour.� Corticosteroids—prednisone 1–2mg/kg/day q12h for 2–4 weeks.� Once the hematocrit increases above 30%,decrease dose to 1 mg/kg q12h.� Subsequently the dose is tapered by amaximum rate of 25–50% per month over a3- to 6-month period, depending upon thehematocrit and severity of side effects. If after6 months the prednisone dose has beentapered to a low every-other-day dose and thedisease is in remission, discontinuation ofmedication should be attempted.� Add azathioprine (dogs) if there is a poorresponse to prednisone after 5–7 days or ifpoor prognostic indicators (e.g., intravascularhemolysis, serum bilirubin > 8–10 mg/dl,persistent autoagglutination, Evanssyndrome).� Azathioprine dose 2 mg/kg/day, candecrease to 2 mg/kg every other day if bonemarrow suppression. Monitor forimmunosuppresson, hepatotoxicosis,pancreatitis.� For prevention of thromboembolism (dogs)consider unfractionated heparin 300 U/kg SCq6–8h (with does adjusted based on APTTprolongation) or ultralow-dose aspirin0.5–1.0 mg/kg/day or enoxaparin(low-molecular-weight heparin) 0.8 mg/kgq6h or 1.5 mg/kg q12h.� Address underlying cause (e.g., infectionand drugs) if secondary IMHA.
CONTRAINDICATIONS� Do not use heparin, enoxaparin, or aspirinin dogs with severe thrombocytopenia(< 80,000/μl).� Do not use multiple cytotoxic drugsconcurrently.
PRECAUTIONS� Do not administer azathioprine to catsbecause of risk of bone marrow toxicity.� Prednisone can cause signs of Cushingsyndrome and potentially increase risk ofpulmonary thromboembolism, pancreatitis,secondary infection, and gastric ulcers(consider gastric protectants).� Cytotoxic drugs can cause bone marrowsuppression, secondary infection, pancreatitis(azathioprine), cystitis (cyclophosphamide),and infertility.
POSSIBLE INTERACTIONSAzathioprine and prednisone have both beenassociated with development of pancreatitis.
ALTERNATIVE DRUG(S)� Dexamethasone (0.25–0.5 mg/kg/dayIV)—can be used instead of prednisone inanimals that do not tolerate oral drugs, untiloral intake is possible.� Chlorambucil—for cats, 0.1–0.2 mg/kg POq24h initially, then q48h.� Cyclosporine—microemulsion, e.g.,Atopica—dogs, 5–10 mg/kg/day PO dividedtwice daily; cats, 0.5–3 mg/kg q12h.� Cyclophosphamide—dogs, 50 mg/M2/dayPO for 4 out of 7 days or 200 mg/M2 IV oncea week (only in dogs that do not tolerateazathioprine or cyclosporine); cats, 2.5mg/kg/day PO for 4 out of 7 days or 7 mg/kgIV once a week.� Human γ -globulin—0.5–1.5 g/kg over12h, single IV infusion.
FOLLOW-UPPATIENT MONITORING� Monitor heart rate, respiratory rate, andtemperature frequently during hospitalization.� Monitor for adverse reactions to treatment(e.g., transfusion reactions andoverhydration).� If pulmonary thromboembolism issuspected, monitor thoracic radiographs andarterial blood gases frequently.� During the first month of treatment, checkthe PCV weekly until stable and then every2 weeks for 2 months; if still stable, recheckPCV monthly for 6 months and then 2–4times per year; rechecks may need to be morefrequent if patient is on long-termmedication.� A CBC and reticulocyte count should berechecked at least monthly during treatment,especially if cytotoxic drugs are used; if theneutrophil count falls < 3,000 cells/μL,
BLBS078-CF_A45 BLBS078-Tilley June 17, 2011 7:3
78 Blackwell’s Five-Minute Veterinary Consult
Anemia, Immune-Mediated (Continued)A
discontinue cytotoxic drugs until the countrecovers; reinstitute at a lower dosage.� Coombs’ test can be monitored to assist indrug tapering.
PREVENTION/AVOIDANCEConsider need for vaccination on acase-by-case basis in dogs in which IMHAdeveloped after vaccination.
POSSIBLE COMPLICATIONS� Pulmonary and multiorganthromboembolism (up to 80% of all cases atnecropsy).� Disseminated intravascular coagulation.� Centrilobular hepatic necrosis, and renaltubular necrosis secondary to hypoxia.� Secondary infection secondary toimmunosuppressive therapy.� Gastrointestinal ulceration due to high-doseglucocorticoids.� Iatrogenic hyperadrenocorticism.
EXPECTED COURSE AND PROGNOSIS� Mortality ranges from 30 to 80% in dogs,25% in cats.� Causes of death include thromboembolism,infection due to immunosuppression, DIC,persistent anemia.� Hyperbilirubinemia > 5 mg/dL,autoagglutination, intravascular hemolysis,severe thrombocytopenia, hypoalbuminemiaare associated with a poorer prognosis.
� Response to treatment may take weeks tomonths; nonregenerative IMHA may have amore gradual onset than typical IMHA andmay be slower to respond to treatment.� IMHA may recur despite previous orcurrent therapy.
MISCELLANEOUSSYNONYMS� Autoimmune hemolytic anemia� Immune-mediated anemia
SEE ALSO� Anemia, Regenerative� Chapters on causes of secondary IMHA� Cold Agglutinin Disease� Disseminated Intravascular Coagulation
ABBREVIATIONS� ALT = alanine aminotransferase� ANA = antinuclear antibody� APTT = activated partial thromboplastintime� DEA = dog erythrocyte antigen� DIC = disseminated intravascularcoagulation� FeLV = feline leukemia virus� FIV = feline immunodeficiency virus
� IMHA = immune-mediated hemolyticanemia� LE = lupus erythematosus� MCV = mean cell volume� PCR = polymerase chain reaction� PCV = packed cell volume� PT = prothrombin time� RBC = red blood cell� SLE = systemic lupus erythematosus
Suggested ReadingKohn B, Weingart C, Eckmann V, et al.
Primary immune-mediated hemolyticanemia in 19 cats: Diagnosis, therapy, andoutcome (1998–2004). J Vet Intern Med2006, 20:159–166.
Piek CJ, Dekker JA, Slappendel RJ, Teske E.Idiopathic immune-mediated hemolyticanemia: Treatment outcome and prognosticfactors in 149 dogs. J Vet Intern Med 2008,22:366–373.
Authors J. Catharine Scott-Moncrieff andRose E. RaskinConsulting Editor A.H. Rebar
Client Education Handoutavailable online
BLBS078-CF_A46 BLBS078-Tilley March 21, 2011 21:34
Canine and Feline, Fifth Edition 79
Anemia, Iron-Deficiency A
BASICSOVERVIEW� Adults—caused by chronic externalhemorrhage.� Develops when erythrocytes are producedunder the condition of limited ironavailability.� Characteristic changes include erythrocytemicrocytosis, hypochromic appearance causedby thin cell geometry, and keratocyte andschistocyte formation.� Important to recognize—leads clinician tothe underlying disease problem, which ischronic external blood loss.
SIGNALMENT� Fairly common in adult dogs.� Rare in adult cats.� Transient, neonatal iron-deficiency anemiaoccurs at 5–10 weeks of age in about 50% ofkittens.
SIGNS� Signs of anemia (e.g., lethargy, depression,weakness, anorexia, and tachypnea) andunderlying disease.� Intermittent melena with gastrointestinalblood loss.� Possible heavy bloodsucking parasite load(e.g., fleas and hookworms).
CAUSES & RISK FACTORS� Any form of chronic external blood loss.� Blood loss most often occurs through thegastrointestinal tract.� Common causes—GI lymphoma,hookworm infestation, stomach or intestinalneoplasia.� Less common sites—skin (e.g., severe fleainfestation) and urinary tract.� Overuse of blood donors.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Any cause of anemia, especially hemorrhage.� Microcytic anemia in portosystemic shuntdisease may or may not be due to irondeficiency.� Anemia of chronic inflammatory disease.
CBC/BIOCHEMISTRY/URINALYSIS� PCV usually but not always decreased,generally 10–40% in dogs.� Anemia may be either regenerative ornonregenerative.� Microcytosis—indicated by low normal orlow MCV, often accompanied by increasedheterogeneity, detected by erythrocytehistogram widening or increased red celldistribution width (RDW) value.� Newer erythrocyte indices, meanreticulocyte volume (MCVr) and reticulocytehemoglobin content (CHr), are sensitive for
detecting iron-deficient erythropoiesis;currently only available on one centrallaboratory hematology system: see Steinbergand Olver and Fry and Kirk.� Changes in erythrocytes may be seen on theblood film—hypochromia (indicated bymarked central pallor), oxidative lesions (e.g.,keratocytes), fragmentation.� Decreased MCHC is neither sensitive norspecific for iron deficiency.� Thrombocytosis may occur.� Hypoproteinemia—consistent finding onlyif the blood loss is sustained; both albuminand globulin fractions are low normal or low.
OTHER LABORATORY TESTS� Hypoferremia (serum iron < 70 μg/dL)and low transferrin saturation (< 15%)support the diagnosis.� Serum iron values may be normal, even inanimals with hematologic features of irondeficiency, if blood loss has ceased and theanimal is undergoing iron repletion.� Fecal flotation to rule out clinicallysuspected hookworm disease.� Fecal examination for occult blood or grossmelena to detect gastrointestinal bleeding.
IMAGINGImaging studies—gastrointestinal disease thataccounts for blood loss.
DIAGNOSTIC PROCEDURESComplete hemogram and iron measurementsas detailed above.
TREATMENT� Identify and correct cause of chronicexternal blood loss.� Administer iron until hematologic featuresof iron deficiency resolve.� If unusually severe (i.e., PCV < 15%),transfusion may be required to treatlife-threatening condition; administer wholeblood (10–20 mL/kg IV) or packed red bloodcells.
MEDICATIONSDRUG(S)Iron SupplementationParenteral Iron Supplementation� Iron replacement therapy should beinitiated with injectable iron.� Iron dextran—a slowly released form ofinjectable iron; one injection (10–20 mg/kgIM) followed by oral supplementation.Oral Iron Supplementation� Animals with severe iron deficiency haveimpaired intestinal absorption of iron,making oral supplementation of little valueuntil partial iron repletion has occurred.� Follow parenterally injected iron with oraliron supplementation for 1–2 months, or
until features of iron deficiency have resolved.� Kittens undergo spontaneous recovery andiron repletion beginning at 5–6 weeks of age,coinciding with intake of solid food.Oral Iron Supplements� Ferrous sulfate powder—place in food ordrinking water (100–300 mg PO q24h).� Ferrous gluconate—one (325 mg) tablet POq24h.� Iron and vitamins—any suitable iron withmultiple vitamin supplement; asrecommended or once daily.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSOral iron supplementation is associated withunexplained death in kittens and should beavoided.
FOLLOW-UP� Monitor CBC every 1–4 weeks; if theanemia is severe, monitor more frequently tofollow the animal through recovery from alife-threatening illness.� Effective treatment associated with anincrease in MCV and reticulocyte volume.� Erythrocyte histogram—effective treatmentassociated with movement to the right as new,normal cells are produced; subpopulation ofmicrocytes produced under conditions of irondeficiency slowly disappear, as these cellscomplete their survival time; may take a fewmonths in some animals to establish a normalhistogram.
MISCELLANEOUSABBREVIATIONS� Chr = reticulocyte hemoglobin content� GI = gastrointestinal� MCHC = mean cell hemoglobinconcentration� MCV = mean cell volume� MCVr = mean reticulocyte volume� PCV = packed cell volume� RDW = red cell distribution width
Suggested ReadingFry MM, Kirk CA. Reticulocyte indices in a
canine model of nutritional iron deficiency.Vet Clin Path 2006, 35:172–181.
Steinberg JD, Olver CS. Hematologic andbiochemical abnormalities indicating irondeficiency are associated with decreasedreticulocyte hemoglobin content (CHr) andreticulocyte volume (rMCV) in dogs. VetClin Path 2005,34:23–27.
Thrall MA. Regenerative anemias. In: ThrallMA, et al., Veterinary Hematology andClinical Chemistry. Baltimore: LippincottWilliams & Wilkins, 2004, pp. 95–98.
Author Glade WeiserConsulting Editor A.H. Rebar
BLBS078-CF_A47 BLBS078-Tilley March 21, 2011 21:38
80 Blackwell’s Five-Minute Veterinary Consult
Anemia, Metabolic (Anemias with Spiculated Red Cells)A
BASICSOVERVIEW� Sometimes occurs concomitantly withdiffuse diseases of the liver, kidney, and, rarely,spleen.� In most animals with liver disease,spiculated cells have 2–10 elongated, blunt,finger-like projections from their surfaces andare classified as acanthocytes.� Acanthocytic anemias can be associatedwith renal disease; anemias of renal diseasemore often have oval red cells with irregularor ruffled membranes (burr cells).� Rarely, acanthocytic anemias can be seen inassociation with splenic disease alone.� Pathogenesis not entirely clear; abnormallipid metabolism with free cholesterol loadingof RBC membranes is most frequentlyimplicated as cause.� Dogs with disseminated abdominalhemangiosarcoma with liver involvementoften have acanthocytes.
SIGNALMENTDogs and cats (infrequently)
SIGNS� None in most animals (usually mild tomoderate condition).� Detection of spiculated RBCs on peripheralblood film can be first marker for liver,kidney, or splenic disease.� In large-breed dogs with vague signs or largespleen, suggests possibility of splenic orhepatic hemangiosarcoma.
CAUSES & RISK FACTORS� Any disease of the liver, kidneys, or possiblyspleen.� The likelihood of RBC morphologicabnormalities parallels the severity of organinvolvement.� Hemangiosarcoma involving the liver is afrequent cause.� Observed in cats with fatty liver syndrome.
DIAGNOSISDIFFERENTIAL DIAGNOSISDetermination of renal or hepatic causesbased on results of biochemistry profile andurinalysis.
CBC/BIOCHEMISTRY/URINALYSIS� Mild to moderately low PCV, RBC count,and hemoglobin.
� Normal mean corpuscular volume andmean corpuscular hemoglobin concentrationin most animals.� Normocytic, normochromic, andnonregenerative.� Polychromasia on blood films only withaccompanying blood loss (as with hepatichemangiosarcoma).� WBC changes variable, based on underlyingcause of hepatic or renal pathology.� Inflammatory conditions likely to beaccompanied by inflammatory leukogram.� Variable findings in liver and kidneyfunction tests (serum biochemistry andurinalysis).
Hepatic Diseases� High ALT, ALP, and γ -glutamyl transferase.� High bile acids, serum ammonia.� Possibly low albumin and serum ureanitrogen.� Bilirubinuria, bilirubin crystals in urine.
Renal Diseases� High serum urea nitrogen, creatinine, andphosphorus.� Highly variable urinalysis findings,including isosthenuria (urine specific gravity1.008–1.025 in dogs; 1.008–1.035 in cats).� Tubular and/or protein casts.� Pyuria.� Proteinuria.� Hematuria.
OTHER LABORATORY TESTSNone
IMAGINGAbdominal radiographs and ultrasound—evaluate hepatic, renal, and splenicstructure.
DIAGNOSTIC PROCEDURESLiver or kidney biopsy if indicated.
TREATMENTFocus treatment on diagnosis and treatmentof underlying hepatic, renal, or splenicdisease.
MEDICATIONSDRUG(S)Variable according to underlying cause.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSVariable according to underlying cause.
FOLLOW-UPMonitor CBC periodically while treating theunderlying condition.
MISCELLANEOUSSEE ALSO� Anemia of Chronic Kidney Disease� Hemangiosarcoma, Spleen and Liver
ABBREVIATIONS� ALP = alkaline phosphatase� ALT = alanine aminotransferase� PCV = packed cell volume� RBC = red blood cell� WBC = white blood cell
Suggested ReadingHarvey JW. Atlas of Veterinary Hematology,
Blood and Bone Marrow of DomesticAnimals. Philadelphia: Saunders, 2001,p. 29.
Rebar AH. Hemogram Interpretation forDogs and Cats. Wilmington, DE: GloydGroup for Ralston Purina Co., 1998,pp. 22–23.
Rebar AH, Lewis HB, DeNicola DB,Halliwell WH, Boon GD. Red blood cellfragmentation in the dog: An editorialreview. Vet Pathol 1981, 18:415–426.
Rebar AH, MacWilliams PS, Feldman BF,Metzger FL, Pollock RVH, Roche J. AGuide to Hematology in Dogs and Cats.Jackson, WY: Teton NewMedia, 2002,p. 36.
Thrall MA, Campbell TW, DeNicola D,Fettman MJ, Lassen ED, Rebar A, WeiserG. Veterinary Hematology and ClinicalChemistry. Baltimore: Lippincott Williams& Wilkins, 2004, p. 96.
Weiser EG. Erythrocyte responses anddisorders. In: Ettinger SJ, Feldman EC, eds.Textbook of Veterinary Internal Medicine,4th ed. Philadelphia: Saunders, 1995,pp. 1864–1891.
Author Alan H. RebarConsulting Editor A.H. Rebar
BLBS078-CF_A48 BLBS078-Tilley July 15, 2011 5:23
Canine and Feline, Fifth Edition 81
Anemia, Nonregenerative A
BASICSDEFINITIONLow RBC mass without evidence of aregenerative response (increasedpolychromasia or reticulocytosis) in theperipheral blood.
PATHOPHYSIOLOGY� Key feature is low or inadequate erythroidproduction or release. � Onset of anemia andits related signs insidious unless RBC survivalis concurrently shortened by hemorrhage orhemolysis. � May be caused by selectivealteration in erythropoiesis or generalizedbone marrow injury affecting leukocytes andplatelets as well. � Mechanisms for selectivelyaltered erythropoiesis include deficienthormonal stimulation, nutritional deficiency,cytokine-mediated sequestration of iron, anddisturbed metabolism in or destruction ofprecursors; generalized bone marrow injuryusually caused by a toxin, infection, orinfiltrative process.
SYSTEMS AFFECTED� Cardiovascular—heart murmur associatedwith low blood viscosity. � Hemic/Lymph/Immune. � Hepatobiliary—centrilobulardegeneration associated with hypoxic injury.
SIGNALMENT� Varies with primary cause. � Giantschnauzers, border collies, beagles—congenital cobalamin malabsorption.
SIGNSGeneral Comments� Usually a secondary condition. � Signsassociated with the primary disease oftenprecede signs attributable to anemia.
Historical Findings� Lack of energy, exercise intolerance,inappetence, and cold intolerance. � Otherfindings reflect the primary condition, such aspolyuria and polydipsia (e.g., CRF), paintexposure from remodeling old houses (e.g.,lead poisoning), living in multicat households(e.g., FeLV), and treating female dogs formismating or urinary incontinence andfeminization in male dogs (e.g.,hyperestrogenism).
Physical Examination Findings� Pallor, heart murmur (severe anemia), andpossibly tachycardia or polypnea. � Signsreflecting the primary condition includeuremic breath and oral ulcerations (e.g.,CRF), cachexia (e.g., cancer),lymphadenopathy and/or splenomegaly (e.g.,lymphoma), gastrointestinal or CNS signs(e.g., lead poisoning), symmetrical alopecia(e.g., hypothyroidism and hyperestrogenism).
CAUSESNonregenerative Anemia without OtherCytopenias� Anemia of inflammatory disease
(AID)—most common cause of mildnonregenerative anemia; anemia can be seenwithin 3–10 days of infection, inflammation,tissue injury, immune-mediated processes,and local or disseminated neoplasia; increasedliver production of hepcidin along withrelease of IL-1, interferon, and TNF fromT-lymphocytes and macrophages lead tosequestration of iron within tissuemacrophages, decreased intestinal ironabsorption; low serum iron and transferrin,increased concentration of macrophage (andserum) ferritin, decreased erythropoietinproduction, impaired marrow response toanemia and shortened RBC lifespan.� Chronic renal failure—kidneys fail toproduce adequate amount of erythropoietin;uremic toxins shorten RBC lifespan andimpair the response to erythropoietin.� Chronic liver disease—RBC morphologicchanges (target cells and acanthocytes) andshortened RBC survival caused by changes inRBC membrane lipids; decreased transferrinsynthesis and impaired mobilization ofhepatic iron contribute to functional irondeficiency. � Endocrine disease—thyroidhormones and cortisol stimulateerythropoiesis and facilitate the effect oferythropoietin; mild anemia is commonlyassociated with hypothyroidism and canoccasionally be seen in patients withhypoadrenocorticism and hypopituitarism.� Immune-mediated destruction ofprecursors–pure red cell aplasia. � Infectiousdestruction of precursors (although usually >one cell line is involved), e.g., FeLV andehrlichiosis, Cytauxzoon felis.
Nutritional or Mineral Deficiency� Iron deficiency—usually caused by chronicexternal blood loss; initially regenerative, butas severity increases, anemia becomesnonregenerative. � Cobalamin (vitamin B12)and/or folate deficiency—rare in dogs andcats but can be caused by dietary insufficiency,malabsorption, or chronic drugadministration (e.g., sulfas, methotrexate, andanticonvulsants) that inhibits folate;congenital defect in cobalamin absorptionreported in giant schnauzers, border collies,and beagles; can occasionally causenormocytic or macrocytic anemia;megaloblastic changes may be seen in themarrow. � Disruption of precursormetabolism—chronic lead toxicity andpossibly high concentrations of aluminumand cadmium inhibit heme synthesis;cadmium also reported to cause renal toxicityand impaired erythropoietin production.
Nonregenerative Anemia with OtherCytopenias� Toxicities—drugs or chemicals (e.g., cancerchemotherapeutics, chloramphenicol,phenylbutazone, trimethoprim-sulfadiazinezonisamide, phenobarbital, griseofulvin,methimazole, fenbendazole, albendazole, andbenzene), hormones (e.g., estrogen toxicity
secondary to abortifacient therapy and Sertolicell tumor). � Infections—FeLV, FIV,ehrlichiosis, babesiosis, and parvoviralinfection (although recovery usually precedesdevelopment of anemia). � Infiltrativeprocesses— myelodysplasia,myeloproliferative disease,lymphoproliferative disease, metastaticneoplasia, myelofibrosis, and osteosclerosis.
RISK FACTORS� Renal failure � Inflammatory or chronicdisease process � Liver failure � Sertoli celltumor � Cancer � Chronic blood loss � Catsfrom multicat households (FeLV) � Leadexposure—chronic
DIAGNOSISDIFFERENTIAL DIAGNOSISRegenerative anemia may initially appearnonregenerative; sudden onset of signs moreconsistent with regenerative thannonregenerative anemia; however, the lattermay appear to have an acute onset ifassociated with a sudden exacerbation of achronic primary condition.
LABORATORY FINDINGSDisorders That May Alter LaboratoryResults� Factors causing turbidity (lipemia) canfalsely elevate hemoglobin and MCHCvalues. � With lead toxicity, increased NRBCmay falsely elevate the WBC count.Valid If Run in Human Laboratory?� Dogs—yes. � Cats—yes, if lab’s hematologyinstrument uses species-specific parameters;instruments designed strictly for analysis ofhuman specimens may under-count smallfeline RBCs.
CBC/BIOCHEMISTRY/URINALYSISCBC and Blood Smear� PCV, RBC count, and hemoglobin low.� Anemia usually normocytic,normochromic, with normal MCV andMCHC. � Macrocytosis (highMCV)—without polychromasia suggests anuclear maturation defect (cells skip adivision); seen in cats with FeLV; occasionallycaused by vitamin B12 or folate deficiency.� Microcytosis (low MCV)—suggests acytoplasmic maturation defect (cells undergoan extra division); iron deficiency the mostcommon cause; in late stages, concurrenthypochromasia (low MCHC) common indogs but not in cats; also seen inapproximately one-third of patients withhepatic insufficiency or vascular shunting.� Specific RBC morphologies-schistocytescommon with iron deficiency; acanthocytesassociated with cholestatic liver disease; targetcells associated with iron deficiency, liverdisease, and hypothyroidism. � Aninflammatory leukogram supports AID.� Thrombocytosis often accompanies iron

BLBS078-CF_A48 BLBS078-Tilley July 15, 2011 5:23
82 Blackwell’s Five-Minute Veterinary Consult
Anemia, Nonregenerative (Continued)A
deficiency. � A high number of NRBCswithout polychromasia or disproportionate tothe degree of anemia and polychromasia seenin animals with lead toxicity, extramedullaryhematopoiesis, heat stroke, and injury to bonemarrow stroma by endotoxemia or hypoxia.� RBC or WBC precursors in the peripheralblood without orderly progression to moremature forms suggest myelodysplasia ormyeloproliferative disease (leukemia).� Concurrent cytopenia in other cell lineswithout evidence of marrow responsiveness(e.g., band neutrophils and macroplatelets)suggests generalized bone marrow injury.
Serum Biochemistry and Urinalysis� High BUN and creatinine with inadequateurine concentration (dogs, < 1.030; cats,< 1.035) support anemia of CRF. � HighALT, total bilirubin suggest liver disease.� High serum cholesterol (> 500 mg/dL)strongly suggests hypothyroidism. � Na/K <23, lymphocytosis, and eosinophilia in illdogs suggest hypoadrenocorticism.
OTHER LABORATORY TESTS� Reticulocyte count—value of < 60,000/μLin dogs or < 50,000/μL in cats accompaniedby a low PCV confirms nonregenerativeanemia. � Direct antiglobulin test(Coombs’)—immune-mediated destructionof erythroid precursors can lead to anemiawithout reticulocytosis; spherocytosis,autoagglutination, or positive Coombs’ testprovides support for immune-mediatedanemia. � Serum iron profile—indicated forpatients with microcytic anemia; in patientswith iron deficiency, serum iron is low, totaliron-binding capacity varies, and serumferritin is low; in patients with AID, serumiron is low but serum ferritin is high (MCVand MCHC usually normal). � Bile acidsmeasurement—may be indicated forevaluation of microcytic anemia andconfirmation of hepatic insufficiency orvascular shunting. � Serum leadmeasurement—indicated when NRBCs arepresent, especially when the patient hasconcurrent gastrointestinal or CNS signs; avalue > 30 μL/dL (0.3 ppm) stronglysupports lead intoxication. � Serologictesting—FeLV test in any cat withnonregenerative anemia; Ehrlichia canis,Anaplasma phagocytophilia (E. equi), andBabesia titers or PCR assays may be indicatedin dogs with unexplained anemia, especiallywhen concurrent with thrombocytopenia orhyperglobulinemia. � Endocrinetesting—indicated when clinical signs andlaboratory tests suggest a possible endocrinedisorder; thyroid: T4, free T4, and TSHconcentrations; adrenal: low-dosedexamethasone suppression test andACTH-stimulation test.
DIAGNOSTIC PROCEDURESCytologic Examination of Bone Marrowand Core Biopsy� Cytologic examination of an aspirateindicated in all patients unless the primarycause is readily apparent (e.g., AID and CRF).� Bone marrow biopsy—useful in evaluationof bone marrow architecture and overallcellularity; important for diagnosis of aplasticmarrow or myelofibrosis. � Erythroidhypoplasia or aplasia confirms the problem,although history and other tests, as indicatedabove, may be needed to determine theunderlying etiology. � Myeloid hyperplasiaand high iron stores support AID. � Absenceof canine (but not feline) bone marrow ironstores, which occurs before microcytosis,supports iron deficiency; classically, irondeficiency associated with an expandederythron and high numbers ofmetarubricytes. � Increasederythrophagocytosis suggests injury to cells(e.g., immune-mediated and toxic causes).� An incomplete maturation sequencesuggests injury to a specific maturation stage(e.g., immune-mediated and toxic causes) orpossibly incomplete recovery from a previousinjury (recheck in 3–5 days). � A disorderlymaturation sequence and atypical cellularmorphology suggest myelodysplasticsyndrome. � A hypercellular marrow with ahigh number of blast cells (> 20% ofnucleated cells) indicates hematopoieticneoplasia; immunophenotyping andcytochemical stains used to identify theaffected cell line(s); circulating neoplastic cellsmay or may not be seen. � Non-marrow cellsindicate metastatic neoplasia.
TREATMENT� Nonregenerative anemia usually resolveswith resolution of the underlying disease.� Conditions associated with severe anemia orpancytopenia often carry a guarded-to-poorprognosis and may involve long-termtreatment without complete resolution.� Metabolic compensation occurs with slowlydeveloping nonregenerative anemia; thus mildto moderately severe anemia (PCV > 15%)generally requires no supportive intervention.� For patients with severe anemia (PCV <10–15%), the degree of hypoxia will probablyrequire restricted exercise, transfusions, orboth. � If blood volume and tissue perfusionare compromised by concurrent blood loss orshock, administer lactated Ringer’s solution orcolloids.
MEDICATIONSDRUG(S)� Erythropoietin in patients with anemia of
CRF (see Anemia of Chronic KidneyDisease). � Iron supplementation in patientswith iron deficiency anemia (see Anemia,Iron-Deficiency). � May supplement withfolic acid at a rate of 4–10 mg/kg/day. � Maysupplement with cobalamin (vitamin B12) at arate of 100–200 mg/day PO (dogs) or50–100 mg/day PO (cats); parenteraladministration (0.5–1 mg IM weekly to onceevery few months) needed in giantschnauzers, beagles, or border collies withinherited cobalamin malabsorption.
PRECAUTIONSMonitor for transfusion reactions in patientsreceiving multiple transfusions.
FOLLOW-UPPATIENT MONITORING� In patients with severe anemia, PCV andblood smear examination every 1–2 days. � Instabilized animals with chronic or slowlyimproving disease course, reevaluation every1–2 weeks.
MISCELLANEOUSPREGNANCY/FERTILITY/BREEDINGSome pregnant animals have a mildly lowPCV, caused by an expanded blood volume.
SYNONYMSNon-responsive anemia
ABBREVIATIONS� ACTH = adrenocorticotropic hormone� AID = anemia of inflammatory disease� ALT = alanine aminotransferase � CNS =central nervous system � CRF = chronic renalfailure � FeLV = feline leukemia virus � FIV= feline immunodeficiency virus � IL-1 =interleukin-1 � MCHC = mean corpuscularhemoglobin concentration � MCV = meancell volume � NRBC = nucleated red bloodcells � PCR = polymerase chain reaction� TNF = tumor necrosis factor � TSH =thyroid stimulating hormone
INTERNET RESOURCESErythrocytes: Overview, Morphology,Quantity; A.H. Rebar, P.S. MacWilliams, B.F.Feldman, et. al.: http://www.ivis.org/advances/Rebar/Chap4/chapter.asp?LA = 1
Suggested ReadingFeldman BF. Nonregenerative anemia. In:
Ettinger SJ, Feldman EC, eds., Textbook ofVeterinary Internal Medicine: Diseases ofthe Dog and Cat, 6th ed. Philadelphia:Elsevier Saunders, 2005, pp. 1908–1917.
Author Joyce S. KnollConsulting Editor A.H. Rebar
BLBS078-CF_A49 BLBS078-Tilley July 15, 2011 5:29
Canine and Feline, Fifth Edition 83
Anemia, Nuclear Maturation Defects (Anemia, Megaloblastic) A
BASICSOVERVIEW� Nonregenerative anemia characterized byarrested development of the nuclei of RBCprecursors (as a result of interference withDNA synthesis) while the cytoplasm developsnormally (nuclear-cytoplasmic asynchrony).� Affected RBC precursors fail to dividenormally and thus are larger thancorresponding normal precursors with thesame degree of cytoplasmic maturity(hemoglobinization); because their nuclei aredeficient in chromatin (DNA), they have adistinctive open and stippled appearance;these giant precursors with atypical, immaturenuclei are known as megaloblasts.� Although these asynchronous changes aremost prominent in RBC precursors, WBCand platelet precursors are similarly affected.
SIGNALMENT� Dogs and cats.� Spontaneous, clinically unimportantoccurrence in toy poodles (occasional).� Breed predilection: giant schnauzers withinherited cobalamin malabsorption.� Defect usually acquired.
SIGNS� In dogs, generally mild, usually notclinically important.� In cats with FeLV-associated nuclearmaturation anemia, FeLV-related signs can beanticipated. Anemia may be mild to severe.
CAUSES & RISK FACTORS� Infectious—FeLV; retroviral infection themost common cause of megaloblastic anemiain cats.� Nutritional—folic acid and vitamin B12
deficiencies.� Toxic—phenytoin (Dilantin) toxicity andmethotrexate toxicity (folate antagonist).� Congenital—toy poodles.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� In dogs, all other mild to moderatenonregenerative anemias, including anemia ofinflammatory disease, renal disease, and leadpoisoning.� Differentiation based on the distinctiveCBC and bone marrow findings listed.� In cats, FeLV infection is the primarydifferential.
CBC/BIOCHEMISTRY/URINALYSIS� In dogs, mild to moderate anemia (PCV:30–40%).
� In cats, anemia can be mild to severe.� Anemia classically macrocytic (high meancorpuscular volume) and normochromic(normal mean corpuscular hemoglobinconcentration).� Large, fully hemoglobinized RBC;occasional to numerous megaloblasts,particularly at the feather edge; minimal to nopolychromasia.� In cats with FeLV, anemia may occur inassociation with a myelodysplastic syndromeor in conjunction with leukemia of a differentcell line.
OTHER LABORATORY TESTSFeLV
IMAGINGN/A
OTHER DIAGNOSTIC PROCEDURESBone Marrow Biopsy� In dogs, usually hyperplastic, often in all celllines.� In cats, marrow findings are highly variableand may be hyper- to hypocellular.� Maturation arrest with nuclear andcytoplasmic asynchrony in all cell lines.� Many megaloblastic RBC precursors may beobserved.� Macrophagic hyperplasia with activephagocytosis of nucleated RBCs andmegaloblasts (common).
TREATMENT� Treat by targeting the underlying cause ifpossible.� Except for that occurring with FeLV in cats,megaloblastic anemia is a relatively mildcondition.� Treat most patients on an outpatient basis.
MEDICATIONSDRUG(S)� In animals with drug toxicity, discontinuethe offending drug.� In all animals, consider supplementationwith folic acid (4–10 mg/kg/day) or vitaminB12 (dogs, 100–200 mg/day PO; cats,50–100 mg/day PO).� Giant schnauzers with inherited cobalaminmalabsorption require parenteral treatmentwith vitamin B12 (0.5–1 mg IM weekly toevery few months).
CONTRAINDICATIONS/POSSIBLEINTERACTIONSDrugs known to cause megaloblastic anemia(e.g., methotrexate and phenytoin) should be
avoided in patients whose condition resultsfrom other causes.
FOLLOW-UP� Monitor response to treatment by CBC(weekly) and occasional bone marrowcollection and evaluation.� Closely monitor FeLV-positive cats forevidence of onset of other signs ofhematopoietic dyscrasia in the peripheralblood and bone marrow.� Prognosis—depends on underlying cause; inFeLV-positive cats, prognosis guarded; inanimals with drug-associated anemia,prognosis good when use of offending drug isinterrupted.
MISCELLANEOUSSEE ALSO� Anemia, Nonregenerative� Feline Leukemia Virus Infection
ABBREVIATIONS� FeLV = feline leukemia virus� PCV = packed cell volume� RBC = red blood cell� WBC = white blood cell
Suggested ReadingHarvey JW. Atlas of Veterinary Hematology,
Blood and Bone Marrow of DomesticAnimals. Philadelphia: Saunders, 2001,pp. 135–137.
Rebar AH. Hemogram Interpretation forDogs and Cats. Wilmington, DE: GloydGroup for Ralston Purina Co., 1998,p. 23.
Rebar AH, MacWilliams PS, Feldman BF,Metzger FL, Pollock RVH, Roche J. AGuide to Hematology in Dogs and Cats.Jackson, WY: Teton NewMedia, 2002,pp. 57–58.
Thrall MA, Campbell TW, DeNicola D,Fettman MJ, Lassen ED, Rebar A, WeiserG. Veterinary Hematology and ClinicalChemistry. Baltimore: Lippincott Williams& Wilkins, 2004, pp. 161–162.
Weiser EG. Erythrocyte responses anddisorders. In: Ettinger SJ, Feldman EC, eds.Textbook of Veterinary Internal Medicine,4th ed. Philadelphia: Saunders, 1995,pp. 1864–1891.
Author Alan H. RebarConsulting Editor A.H. Rebar

BLBS078-CF_A50 BLBS078-Tilley July 23, 2011 4:43
84 Blackwell’s Five-Minute Veterinary Consult
Anemia, RegenerativeA
BASICSDEFINITIONCharacterized by a decreased circulating RBCmass (as indicated by low PCV, hemoglobin,and total RBC count) accompanied byappropriate, compensatory increase in RBCproduction by the bone marrow (e.g.,reticulocytosis in the peripheral blood andRBC hyperplasia in the bone marrow).
PATHOPHYSIOLOGY� Regenerative anemia caused by blood loss orhemolysis. � Hemolysis—caused by intrinsicRBC defects (e.g., congenital RBC membranedefects or enzyme deficiencies) or extrinsicfactors such as RBC parasites, oxidativeinjury, hemolysins, osmotic changes,immune-mediated RBC destruction, heatstroke, and severe hypophosphatemia.� Intravascular hemolysis may lead to DICand hemoglobinuria. � Hemolytic anemiausually more regenerative than blood lossanemia; external blood loss depletes body ofboth cells and iron; hemolysis conserves iron,which is readily available for reuse in RBCproduction, making hemolytic anemiagenerally more responsive.
SYSTEMS AFFECTED� Cardiovascular—murmurs with markedanemia; tachycardia with severe rapid-onsetanemia. � Hemic/Lymph/Immune—markedRBC hyperplasia in the bone marrow; EMHin the spleen; splenomegaly due to EMH andhistiocytic hyperplasia can be a feature ofextravascular hemolytic anemia. � Hepatic—anoxia causes centrilobular degeneration ofthe liver. � Renal—severe intravascularhemolysis can (rarely) lead to renal tubularnecrosis and acute renal failure.
SIGNALMENT� No breed, age, or sex predilections for thebroad category of regenerative anemia.� Pyruvate kinase deficiency—basenjis,beagles, cairn terriers, Chihuahuas,dachshunds, miniature poodles, pugs, WestHighland white terriers, and AmericanEskimo; and Somali, Abyssinian, anddomestic shorthair cats.� Phosphofructokinase deficiency—Englishspringer spaniels, American cocker spaniels,and mixed breed dogs with spaniel parentage.� Spectrin deficiency has been reported ingolden retrievers. � Marked RBC osmoticfragility—English springer spaniels andAbyssinian, Somali, Siamese, and domesticshorthair cats. � Feline congenitalporphyria—Siamese and domestic shorthaircats. � Some breeds of dogs have a geneticpredisposition for heritable coagulopathiessuch as factor VIII deficiency and vonWillebrand disease. � Middle-aged femaledogs, especially American cocker spaniels,English springer spaniels, Irish setters, Old
English sheepdogs, poodles, and Shetlandsheepdogs, have a predisposition toimmune-mediated syndromes, such as SLEand immune-mediated hemolytic anemia.
SIGNS� Pallor. � Weakness, exercise intolerance.� Anorexia. � Possible heart murmur,tachycardia, bounding pulses. � Possiblejaundice and hemoglobinuria. � Petechiae,epistaxis, melena suggest blood loss due tovasculitis or a platelet problem. � Hematomasor cavity bleeds suggest a coagulopathy.� Clinical signs depend on the degree ofanemia and rapidity of onset. � Rapid loss of15–25% of blood volume or acute hemolysisresults in shock and possible death. � Withchronic anemia, compensatory increases inheart rate, and eventually heart size, lessensthe RBC circulation time; hemoglobin candrop to as low as 50% of the minimumnormal value without overt signs of hypoxia.
CAUSESImmune Mediated� Antibodies, immune complexes, and/orcomplement on the RBC surface shortenRBC lifespan. Antibodies may target RBCmembrane components or may be directedagainst tumor antigens, infectious agents,vaccines, or drugs (e.g., sulfonamides,penicillins, cephalosporins, methimazole,amiodarone) that are either directly adherentto RBC surface or part of immune complexesadherent to RBCs. � Hemolysis may be eitherintravascular or extravascular. IgG-coatedRBCs are typically engulfed by splenicmacrophages. IgM-coated RBCs are oftendestroyed through activation of complement.� Hemolytic antibodies are generally reactiveat body temperature; rarely cold-actingantibodies cause in vivo hemolysis and/orRBC agglutination in cooler, peripheralvasculature. � Transfusion of a blood type Bcat with type A blood can result in rapid,severe, intravascular hemolysis; neonatalisoerythrolysis seen in kittens born to a bloodtype B queen mated to a blood type A tom.� Canine blood type DEA 1.1 can causehemolysis in a DEA 1.1-negative dog,although a single incompatible transfusioncan be tolerated. � The newly identified bloodtypes Mik (cats) and Dal (dogs) can causesignificant hemolytic transfusion reactions inanimals lacking these common RBC antigens.Oxidant Injury� Oxidants can cause Heinz body formation(aggregates of oxidized hemoglobin),eccentrocytes (oxidation of RBC membranes),and methemoglobinemia. � Damaged RBCsare prematurely removed from the circulation(extravascular hemolysis). Destabilization ofRBC membranes causes intravascularhemolysis. � Oxidants include onions andgarlic, acetaminophen (especially in cats), zinc(from pennies minted after 1982, zinc oxideointment, and zinc bolts), acute coppertoxicosis, benzocaine, vitamin K3 (dogs),
propofol, dl-methionine (cats), phenoliccompounds (moth balls), andphenazopyridine (cats). � In cats, somesystemic diseases (e.g, diabetes mellitus,hyperthyroidism, and lymphoma) enhanceHeinz body formation but do not necessarilycause anemia.
Erythrocyte Parasites� Mycoplasma haemofelis (formerlyHaemobartonella felis), M. haemominutum,M. turicensis, and M. haematoparvum (cats).� Mycoplasma haemocanis (formerly H. canis;dogs). � Babesia canis and B. gibsoni (dogs).� Cytauxzoon felis (domestic shorthair andbobcats).
Mechanical RBC Fragmentation� Thromboembolic disease (e.g., DIC).� Heartworm disease. � Vasculitis. � Liver,kidney or heart disease. � Neoplasia (e.g.,hemangiosarcoma). � Splenic torsion.� Hemolytic-uremic syndrome.
Inherited RBC Abnormalities� Pyruvate kinase deficiency—impaired RBCglucose use and ATP formation, leading topremature destruction of RBCs; autosomalrecessive trait. � Phosphofructokinasedeficiency—marked alkaline fragility causedby impaired synthesis of2,3-diphosphoglycerate; hemolytic episodestriggered by hyperventilation-inducedalkalemia such as occurs after vigorousexercise. � Increased RBC osmotic fragilityleads to recurrent severe anemia andsplenomegaly. The responsible RBC defecthas not been identified. � Spectrin deficiencyleads to destabilization of RBC membranes,leading to increased RBC osmotic fragility;autosomal dominant trait; unclear if thisresults in hemolytic anemia. � Felinecongential porphyria—deficiency inuroporphyrinogen III cosynthetase in Siamesecats causes an inability to produce normalamounts of hemoglobin; coproporphyrin anduroporphyrin accumulate, causing brown-reddiscoloration of teeth and bones,photosensitivity, and severe hemolytic anemia;a second, less severe autosomal dominant traitin domestic shorthair cats causes tissuediscoloration without anemia orphotosensitivity.
Blood Loss� Trauma. � Bleeding neoplasms (e.g.,hemangiosarcoma, intestinaladenocarcinoma). � Coagulopathies (e.g.,warfarin poisoning, hemophilia, andthrombocytopenia). � Bloodsucking parasites(e.g., fleas, ticks, and Ancylostoma).� Gastrointestinal ulcers.
DIAGNOSISDIFFERENTIAL DIAGNOSISDifferentiated from nonregenerative anemiaby high reticulocyte count.
BLBS078-CF_A50 BLBS078-Tilley July 23, 2011 4:43
Canine and Feline, Fifth Edition 85
(Continued) Anemia, Regenerative A
LABORATORY FINDINGSDisorders That May Alter LaboratoryResults� Lipemia can cause mild in vitro hemolysis,without appreciable anemia, and may falselyelevate MCHC. � Autoagglutination mayfalsely decrease the RBC count.
Valid If Run in Human Laboratory?� Dogs—yes. � Cats—yes, if lab’s hematologyinstrument uses species-specific parameters;instruments designed for analysis of humanspecimens may under-count small felineRBCs. � Human labs, unfamiliar with felinepunctuate reticulocytes, may include them inthe reticulocyte count, overestimating theregenerative response.
CBC/BIOCHEMISTRY/URINALYSIS� PCV, RBC count, and hemoglobin low.� Total protein is often low with blood lossanemia and may be the only sign ofhemorrhage in dogs with acute blood loss;normal PCV may be maintained throughtransient splenic contraction. � The severityof acute blood loss may be underestimateduntil the plasma volume has been restored byfluid administration and/or internal fluidshifts. � RBC indices vary depending on thecause of anemia and degree of regenerativeresponse—MCV, normal to high; MCHC,normal to low in most patients; MCHC,artificially high with intravascular hemolysisand hemoglobinemia. � With iron deficiencyowing to chronic blood loss, dogs may have alow MCV, MCH, and MCHC; cats have alow MCV but normal MCH and MCHC.� Specific RBC morphologies may suggest acause of hemolysis: marked spherocytosissuggests immune-mediated disease; Heinzbodies or eccentrocytes suggest oxidantinjury; and numerous schistocytes suggestmicroangiopathy. � Spherocytes, formedthrough incomplete RBC phagocytosis,cannot be as easily detected in cats becauseRBCs generally lack central pallor.� Agglutinated RBCs indicate anemia isimmune mediated; autoagglutination must bedistinguished from rouleaux by generoussample dilution with saline. � Hemolysis maycause an inflammatory leukogram(neutrophilia with a left shift andmonocytosis). Acute blood loss may beassociated with a stress leukogram (mildneutrophilia and lymphopenia). � Blood lossmay be accompanied by eitherthrombocytopenia or reboundthrombocytosis; iron deficiency is oftenaccompanied by thrombocytosis.� Hyperbilirubinemia and bilirubinuriaaccompany marked hemolysis;hemoglobinemia and hemoglobinuria seenwith intravascular hemolysis.
OTHER LABORATORY TESTS� In an anemic animal, an absolutereticulocyte count (RBC count ×reticulocyte%) > 50,000/μL (cats) or >
60,000/μL (dogs) suggests regenerativeanemia. � The reticulocyte% should becorrected for the degree of anemia; formula =reticulocyte% × (PCV/normal PCV); normalPCV: cat 37, dog 45; corrected reticulocyte%> 1% suggests a regenerative response. � Ittakes 3–5 days for the bone marrow to mounta peak regenerative response to anemia, soreticulocytosis may initially be absent withacute blood loss or hemolysis. � Directantiglobulin test (Coombs’ test) indicatedwhen immune-mediated hemolytic anemiasuspected; a positive test and evidence ofspherocytosis and polychromasia in theperipheral blood is confirmatory; both falsenegatives and false positives are possible, sothe test must be interpreted cautiously.
DIAGNOSTIC PROCEDURES� Bone marrow aspirate—needed only whenthere is no evidence of RBC responsiveness inthe peripheral blood (i.e., no reticulocytosis);RBC hyperplasia confirms a regenerativeresponse; absence of RBC hyperplasia meansthat the anemia is nonregenerative. � Bonemarrow biopsy—useful in evaluation of bonemarrow architecture and overall cellularity;important for confirmation of anonregenerative process.
TREATMENT� Emergency if anemia is severe and developsrapidly. � Massive hemorrhage leads tohypovolemic shock and anoxia; acutehemolysis leads to anoxia. � Cage rest andcareful observation indicated, depending onseverity of clinical signs.
BLOOD LOSS ANEMIAS� With major traumatic blood loss leading toshock, crystalloid fluids can rapidly correcthypovolemia and restore circulation. Colloidsolutions (e.g., dextran 70) can produce aslightly greater volume expansion. � RBCreplacement (packed RBCs or whole blood) isindicated if PCV is < 15–20% and signs ofhypoxia are severe (i.e., extremely palemucous membranes, weakness, tachycardia,and tachypnea), or oxyhemoglobin (30mL/kg at rate of 10 mL/kg/hr; OPK Biotech,Cambridge, MA) can provide both oncoticpressure and an oxygen transporter. � Animalswith chronic blood loss are normovolemicwith increased cardiac output, thereforetransfusion volumes and rates should beconservative to avoid cardiac failure. Cats areprone to volume overload.
HEMOLYTIC ANEMIASBlood transfusion or oxyhemoglobin may beindicated; in patients with animmune-mediated process, RBCs probablysurvive similarly to the patient’s own RBCs,so transfusion should not be withheld ifmarked signs of anemia are present.
MEDICATIONSDRUG(S)� Blood-loss anemias—administration of ironmay benefit animals with chronic blood-lossanemia (see Anemia, Iron-Deficiency).� Hemolytic anemias—varies with cause ofhemolysis.
FOLLOW-UPPATIENT MONITORING� Initially, measurement of RBC mass (e.g.,PCV, RBC count, and hemoglobin) andmorphologic features on a blood film (i.e.,polychromasia) every 24 hours to monitoreffectiveness of treatment and bone marrowresponsiveness. � As regeneration becomesapparent (rising RBC values andpolychromasia), recheck patients every 3–5days; return to normal values should occurabout 14 days after acute hemorrhage butmay take longer with an immune-mediatedprocess.
MISCELLANEOUSSEE ALSO� Anemia, Heinz Body � Anemia,Immune-Mediated � Anemia,Iron-Deficiency � Babesiosis � Bartonellosis� Cytauxzoonosis � Lupus Erythematosus,Systemic � Zinc Toxicity
ABBREVIATIONS� ATP = adenosine triphosphate � DIC =disseminated intravascular coagulation� EMH = extramedullary hematopoiesis� MCH = mean corpuscular hemoglobin� MCHC = mean corpuscular hemoglobinconcentration � MCV = mean cell volume� PCV = packed cell volume � RBC = redblood cell � SLE = systemic lupuserythematosus
INTERNET RESOURCESErythrocytes: Overview, Morphology,Quantity; A.H. Rebar, P.S. MacWilliams,B.F. Feldman, et al.: http://www.ivis.org/advances/Rebar/Chap4/chapter.asp?LA = 1.
Suggested ReadingGiger U. Regenerative anemias caused by
blood loss or hemolysis. In: Ettinger SJ,Feldman EC, eds., Textbook of VeterinaryInternal Medicine: Diseases of the Dog andCat, 6th ed. Philadelphia: Elsevier Saunders,2005, pp. 1886–1907.
Author Joyce S. KnollConsulting Editor A.H. Rebar
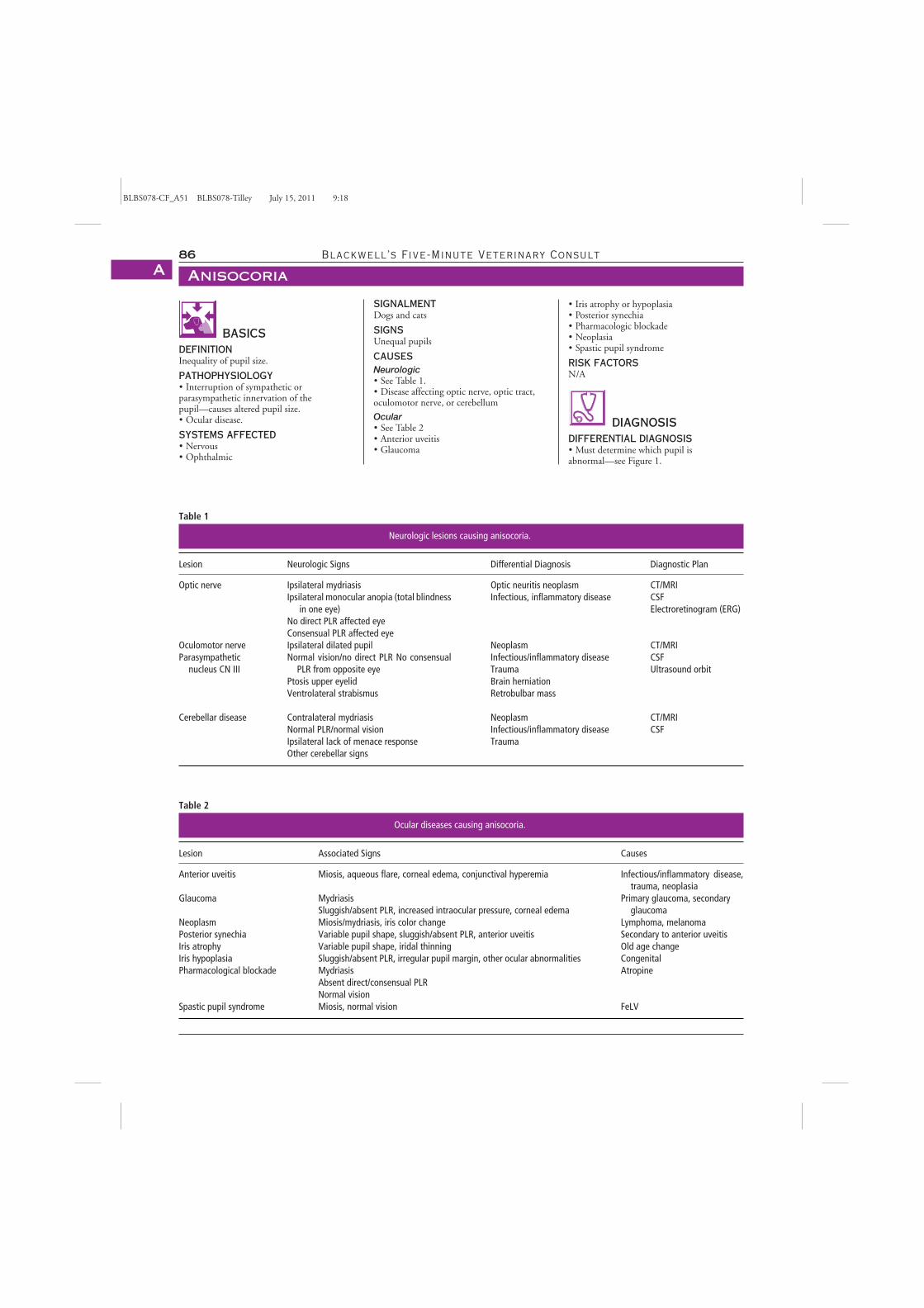
BLBS078-CF_A51 BLBS078-Tilley July 15, 2011 9:18
86 Blackwell’s Five-Minute Veterinary Consult
AnisocoriaA
BASICSDEFINITIONInequality of pupil size.
PATHOPHYSIOLOGY� Interruption of sympathetic orparasympathetic innervation of thepupil—causes altered pupil size.� Ocular disease.
SYSTEMS AFFECTED� Nervous� Ophthalmic
Table 1
Neurologic lesions causing anisocoria.
Lesion Neurologic Signs Differential Diagnosis Diagnostic Plan
Optic nerve Ipsilateral mydriasisIpsilateral monocular anopia (total blindness
in one eye)No direct PLR affected eyeConsensual PLR affected eye
Optic neuritis neoplasmInfectious, inflammatory disease
CT/MRICSFElectroretinogram (ERG)
Oculomotor nerve Ipsilateral dilated pupil Neoplasm CT/MRIParasympathetic
nucleus CN IIINormal vision/no direct PLR No consensual
PLR from opposite eyePtosis upper eyelidVentrolateral strabismus
Infectious/inflammatory diseaseTraumaBrain herniationRetrobulbar mass
CSFUltrasound orbit
Cerebellar disease Contralateral mydriasisNormal PLR/normal visionIpsilateral lack of menace responseOther cerebellar signs
NeoplasmInfectious/inflammatory diseaseTrauma
CT/MRICSF
Table 2
Ocular diseases causing anisocoria.
Lesion Associated Signs Causes
Anterior uveitis Miosis, aqueous flare, corneal edema, conjunctival hyperemia Infectious/inflammatory disease,trauma, neoplasia
Glaucoma MydriasisSluggish/absent PLR, increased intraocular pressure, corneal edema
Primary glaucoma, secondaryglaucoma
Neoplasm Miosis/mydriasis, iris color change Lymphoma, melanomaPosterior synechia Variable pupil shape, sluggish/absent PLR, anterior uveitis Secondary to anterior uveitisIris atrophy Variable pupil shape, iridal thinning Old age changeIris hypoplasia Sluggish/absent PLR, irregular pupil margin, other ocular abnormalities CongenitalPharmacological blockade Mydriasis
Absent direct/consensual PLRNormal vision
Atropine
Spastic pupil syndrome Miosis, normal vision FeLV
SIGNALMENTDogs and cats
SIGNSUnequal pupils
CAUSESNeurologic� See Table 1.� Disease affecting optic nerve, optic tract,oculomotor nerve, or cerebellum
Ocular� See Table 2� Anterior uveitis� Glaucoma
� Iris atrophy or hypoplasia� Posterior synechia� Pharmacologic blockade� Neoplasia� Spastic pupil syndrome
RISK FACTORSN/A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Must determine which pupil isabnormal—see Figure 1.
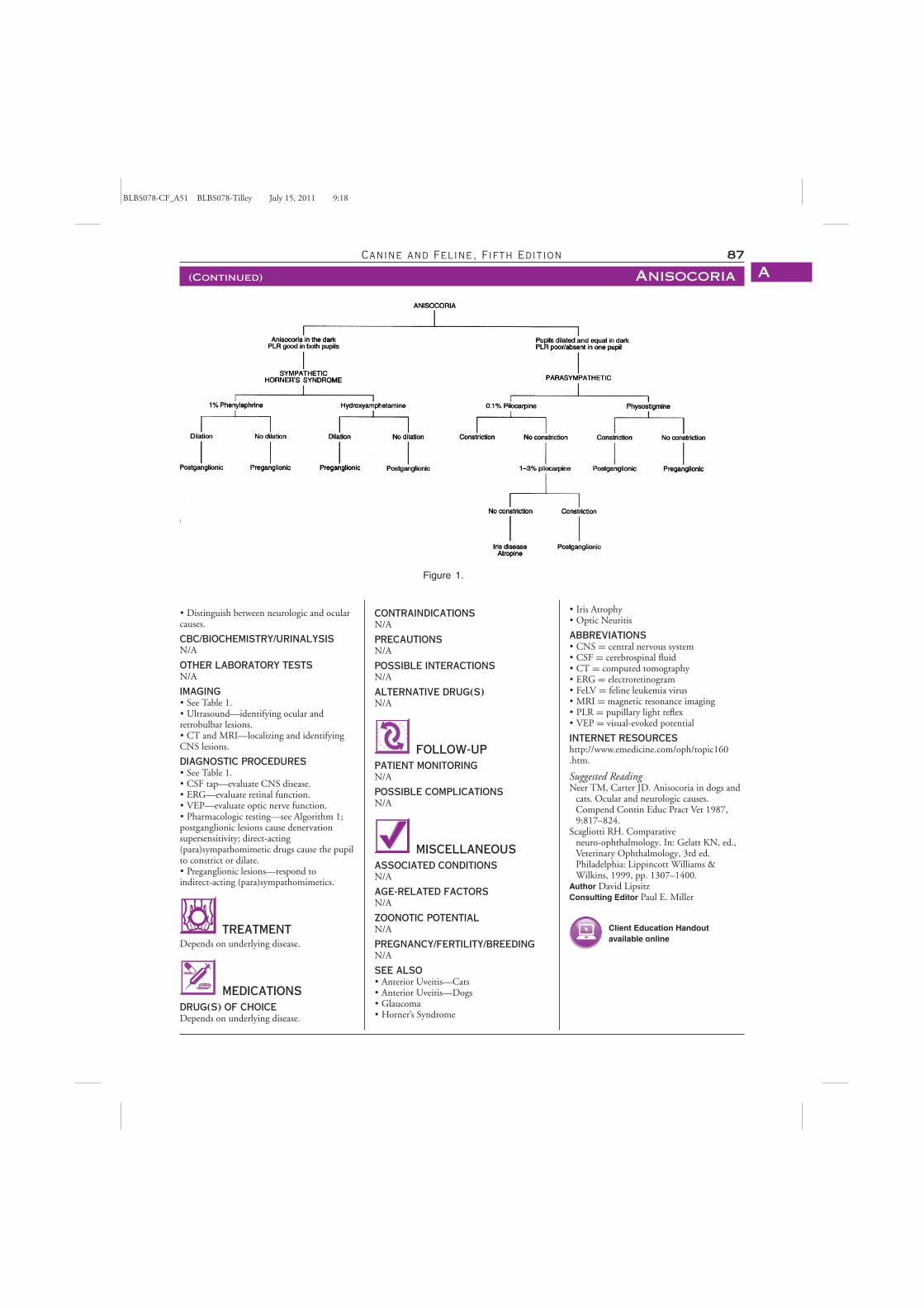
BLBS078-CF_A51 BLBS078-Tilley July 15, 2011 9:18
Canine and Feline, Fifth Edition 87
(Continued) Anisocoria A
Figure 1.
� Distinguish between neurologic and ocularcauses.
CBC/BIOCHEMISTRY/URINALYSISN/A
OTHER LABORATORY TESTSN/A
IMAGING� See Table 1.� Ultrasound—identifying ocular andretrobulbar lesions.� CT and MRI—localizing and identifyingCNS lesions.
DIAGNOSTIC PROCEDURES� See Table 1.� CSF tap—evaluate CNS disease.� ERG—evaluate retinal function.� VEP—evaluate optic nerve function.� Pharmacologic testing—see Algorithm 1;postganglionic lesions cause denervationsupersensitivity; direct-acting(para)sympathomimetic drugs cause the pupilto constrict or dilate.� Preganglionic lesions—respond toindirect-acting (para)sympathomimetics.
TREATMENTDepends on underlying disease.
MEDICATIONSDRUG(S) OF CHOICEDepends on underlying disease.
CONTRAINDICATIONSN/A
PRECAUTIONSN/A
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGN/A
POSSIBLE COMPLICATIONSN/A
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SEE ALSO� Anterior Uveitis—Cats� Anterior Uveitis—Dogs� Glaucoma� Horner’s Syndrome
� Iris Atrophy� Optic Neuritis
ABBREVIATIONS� CNS = central nervous system� CSF = cerebrospinal fluid� CT = computed tomography� ERG = electroretinogram� FeLV = feline leukemia virus� MRI = magnetic resonance imaging� PLR = pupillary light reflex� VEP = visual-evoked potential
INTERNET RESOURCEShttp://www.emedicine.com/oph/topic160.htm.
Suggested ReadingNeer TM, Carter JD. Anisocoria in dogs and
cats. Ocular and neurologic causes.Compend Contin Educ Pract Vet 1987,9:817–824.
Scagliotti RH. Comparativeneuro-ophthalmology. In: Gelatt KN, ed.,Veterinary Ophthalmology, 3rd ed.Philadelphia: Lippincott Williams &Wilkins, 1999, pp. 1307–1400.
Author David LipsitzConsulting Editor Paul E. Miller
Client Education Handoutavailable online

BLBS078-CF_A52 BLBS078-Tilley March 21, 2011 22:1
88 Blackwell’s Five-Minute Veterinary Consult
AnorexiaA
BASICSDEFINITIONThe lack or loss of appetite for food; appetiteis psychological and its existence in animals isassumed. Hunger is physiologically arousedby the body’s need for food. Anorexia may bepartial or complete. Anorexia results indecreased food intake, which then leads toweight loss. Pseudoanorexia is associated withthe inability to prehend or swallow foodrather than actual loss of appetite.
PATHOPHYSIOLOGY� The control of appetite is a complexinteraction between the central nervoussystem and the periphery.� The hypothalamus and brainstem containpeptidergic feeding-regulatory neurons thatact as input stations for hormonal andgastrointestinal information. These cellpopulations project to several brain regionsand interconnect extensively.� Peripheral signals that affect appetiteinclude the palatability, texture, and quantityof recently consumed food.� Satiety is influenced by gastric and duodenaldistention in addition to the presence ofnutrients in the gastrointestinal tract.� Hunger is affected by plasma concentrationsof glucose and fatty acids, by interacting withnutrient-specific receptors in the liver andgastrointestinal tract.� Decreased and increased oxidativemetabolism by the liver leads to hunger andsatiety, respectively.� Learned behavior and circadian rhythmsmodulate appetite and may override othersignals for satiety and hunger.� Leptin is primarily produced by adipocytesand acts on specific hypothalamic receptors todecrease metabolism and decrease appetite.� Neuropeptide Y released from thegastrointestinal tract induces hunger andhyperphagia, and decreases energyexpenditure after food restriction.� Cholecystokinin and bombesin releasedfrom the gastrointestinal tract decreaseappetite.� Ghrelin produced by the stomach is aprokinetic and decreases leptin and increasesneuropeptide Y production.� Serotonin is an important and perhaps finalmediator centrally via a serotonergic tract thatpasses near the ventromedial hypothalamus.� Dopaminergic tracts in the hypothalamushelp regulate food intake and are closelyassociated with the lateral hypothalamus(classical feeding center).� Appetite is stimulated by aldosterone andcorticosterone and suppressed by glucagonsand somatostatin.� Inflammatory and neoplastic disease cancause anorexia by releasing proinflammatorycytokines such as interleukin-1, tumor
necrosis factor, and interferon.� The expected upregulation of dietary intakein response to elevated energy expenditure isfrequently lost in cancer patients.� Decreased appetite associated with aging,the so-called anorexia of aging, predisposesolder patients to protein-energy malnutritionand is probably mediated by CCK and anenhanced satiating effect of small intestinalcarbohydrates.� Exogenous and endogenous toxins (e.g.,renal and liver failure) cause anorexia.� Any disorder that decreases cerebral arousalwill potentially decrease food intake.� Gastroparesis associated with neoplasia,metabolic disorders, and primarygastrointestinal disease is associated withdecreased appetite.� Fear, pain, and stress may decrease appetite.
SYSTEMS AFFECTEDAll body systems
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsN/A
Mean Age and RangeN/A
Predominant SexN/A
SIGNSHistorical Findings� Refusal to eat is a common complaintpresented by pet owners because poor appetiteis strongly associated with illness.� Patients with disorders causing dysfunctionor pain of the face, neck, oropharynx, andesophagus may display an interest in food butcannot eat. These patients are referred to asbeing pseudoanorectic.� Animals lacking a sense of smell (anosmia)often show no sniffing behavior.� Weight loss may be noted.
Physical Examination Findings� Clinical signs in anorexia vary depending onthe underlying cause but include fever, pallor,icterus, pain, changes in organ size, ocularchanges, abdominal distention, dyspnea,muffled heart and lung sounds, adventitiouslung sounds, cardiac murmurs, and masses.� Pseudoanorectic patients commonly displayweight loss, halitosis, excessive drooling,difficulty in prehending and masticating food,and odynophagia (painful swallowing).
CAUSESAnorexia� Almost any systemic disease process cancause anorexia.� Psychological—unpalatable diet, foodaversion, stress, alterations in routine andenvironment.� Acid-base disorders.� Cardiac failure.
� Toxicities and drugs.� Pain.� Endocrine and metabolic disease.� Neoplasia.� Infectious disease.� Immune mediated disease.� Respiratory disease.� Gastrointestinal disease.� Musculoskeletal disease.� Neurologic disease.� Anorexia of aging.� Miscellaneous (e.g., motion sickness, highenvironmental temperature).
Pseudoanorexia� Any disease causing painful or dysfunctionalprehension, mastication, and swallowing.� Stomatitis, glossitis, gingivitis, pharyngitis,and esophagitis (e.g., physical agents, caustics,bacterial or viral infections, foreign bodies,immune-mediated diseases, uremia).� Retropharyngeal disorders (e.g.,lymphadenopathy, abscess, hematoma,sialocele).� Dental disease or periodontal disease.� Retrobulbar abscess.� Oral, glossal, pharyngeal, or esophagealneoplasia.� Neurologic disorders (e.g., rabies;neuropathies of cranial nerves V, VII, IX, X,XII; and central nervous system lesions).� Musculoskeletal lesions (e.g., masticatorymyositis, temporomandibular joint disease,fractures, craniomandibular osteopathy,myasthenia gravis, botulism, andcricopharyngeal achalasia).� Salivary gland neoplasia or inflammation.
RISK FACTORSN/A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Question owners about the patient’s interestin food and ability to prehend, masticate, andswallow food.� Perform a thorough ophthalmic, dental,oropharyngeal, facial, and cervicalexamination (sedation or anesthesia may berequired) in addition to observing the patienteating to rule out pseudoanorexia.� Elicit a thorough history regarding thepatient’s environment, diet, changes inroutine, people, or other pets to help identifypotential psychological etiologies.� A complete physical examination isrequired to determine the presence ofsystemic disease.� A database including a complete bloodcount, serum biochemistry panel, urinalysis,heartworm serology, retrovirus serology,abdominal and thoracic imaging studies,endoscopy, and histologic/cytologicexamination of tissue/cell samples are oftenrequired make a definitive diagnosis.
BLBS078-CF_A52 BLBS078-Tilley March 21, 2011 22:1
Canine and Feline, Fifth Edition 89
(Continued) Anorexia A
� Only if the history, physical examination,and database strongly suggest psychologicanorexia should further diagnostic work-up beforgone; in such cases, daily contact with thepet owner is essential until the anorexia hasresolved.
CBC/BIOCHEMISTRY/URINALYSIS� Abnormalities vary with differentunderlying diseases and causes ofpseudoanorexia and anorexia.� Can be normal in patients with medical aswell as psychologic causes of anorexia.
OTHER LABORATORY TESTSSpecial diagnostic tests may be necessary torule out specific diseases suggested by history,physical examination, and preliminary tests.
IMAGING� Thoracic and abdominal imaging(radiographic and ultrasound) studies areoften included in the minimum database todetect anatomic abnormalities.� Fluoroscopy may be indicated to specificallyevaluate pharyngeal and esophageal function.
DIAGNOSTIC PROCEDURES� Vary with underlying condition suspected.� Endoscopy may be useful for visualizationof the pharyngeal and esophageal structures.
TREATMENT� The mainstay of treatment is aimed atidentifying and correcting the underlyingdisease.� Symptomatic therapy includes attention tofluid and electrolyte derangements, reductionin environmental stressors, and modificationof the diet to improve palatability.� Palatability can be improved by addingflavored toppings such as chicken and beefbroth, seasoning with condiments such asgarlic powder, increasing the fat or proteincontent of the food, and heating the food tobody temperature.� As a general rule, dogs and cats withdebilitating disease should not go withoutfood for longer than 3–5 days before enteralor parenteral feeding is used.� The decision to institute enteral orparenteral feeding can be influenced byseveral factors. In animals that have ≥ 10%body weight loss, hypoalbuminemia,lymphopenia, lower body condition score,and chronic disease processes, supplementalnutrition should be considered.� Techniques for providing enteral nutritioninclude forced feeding and placement of anasoesophageal, esophagostomy, gastrostomy,or jejunostomy tube.
MEDICATIONSDRUG(S) OF CHOICE� Diazepam is a short-acting appetitestimulant with sedative properties dosed at 0.1mg/kg IV daily or 1 mg PO once daily in cats.� Oxazepam (2 mg/cat PO q12h) is ashort-acting appetite stimulant and sedative.� Cyproheptadine, an antihistamine withantiserotonergic properties, has been used asan appetite stimulant with mixed success at adose range of 0.2–0.4 mg/kg PO 10–20minutes prior to feeding.� Analgesics may promote appetite in painfulconditions.� Metoclopramide (0.2–0.4 mg/kg SC orPO), ranitidine (2 mg/kg SC, IV, or PO), orerythromycin (0.5–1 mg/kg PO) are useful ifanorexia is associated with gastroparesis orileus.� Antiemetics such as prochlorperazine(0.1–0.5 mg/kg PO) or metoclopramide areuseful to decrease nausea-associated anorexia.
CONTRAINDICATIONS� Avoid antiemetics if gastrointestinalobstruction is present or suspected.� Drugs with sedative properties should beused with caution in severely debilitatedanimals.
PRECAUTIONSN/A
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORING� Body weight, body condition scoreassessment, and hydration determination.� Return of appetite.
PREVENTION/AVOIDANCEFeed highly palatable diet
POSSIBLE COMPLICATIONS� Dehydration, malnutrition, and cachexiaare most likely; these exacerbate theunderlying disease.� A loss of more than 25–30% of bodyprotein compromises the immune system andmuscle strength, and death results frominfection and/or pulmonary failure.� Feline hepatic lipidosis is a possiblecomplication of anorexia in obese cats.� Breakdown of the intestinal mucosal barrieris a concern in debilitated patients.
EXPECTED COURSE AND PROGNOSISVaries with underlying cause
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSNutritional support and/orglucose-containing fluids may be necessary totreat or prevent hypoglycemia in anorecticpuppies and kittens.
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMSN/A
SEE ALSOSee “Causes”
ABBREVIATIONS� CCK = cholecystokinin
Suggested ReadingGuilford WG. Nutritional management of
gastrointestinal diseases. In: Guilford WG,Center SA, Strombeck DR, et al., eds.,Strombeck’s Small AnimalGastroenterology, 3rd ed. Philadelphia:Saunders, 1996, pp. 889–910.
Hoover JP, Monroe WE. Anorexia. In:Ettinger SJ, Feldman EC, eds., VeterinaryInternal Medicine, 6th ed. Philadelphia:Elsevier Saunders, 2005, pp. 117–119.
Monroe WE. Anorexia and polyphagia. In:Ettinger SJ, Feldman EC, eds., VeterinaryInternal Medicine, 5th ed. Philadelphia:Saunders, 2000, pp. 102–104.
Remillard RL, Armstrong PJ, et al. Assistedfeeding in hospitalized patients: Enteral andparenteral nutrition. In: Hand MS,Thatcher CD, Remillard RL, et al., eds.,Small Animal Clinical Nutrition, 4th ed.Topeka, KS: Mark Morris Institute, 2000,pp. 351–399.
Author Elizabeth M. StreeterConsulting Editor Albert E. Jergens
Client Education Handoutavailable online
BLBS078-CF_A53 BLBS078-Tilley March 21, 2011 22:2
90 Blackwell’s Five-Minute Veterinary Consult
Antebrachial Growth DeformitiesA
BASICSDEFINITIONAbnormally shaped forelimbs and/ormalalignments of the elbow or antebrachialcarpal joints that result from maldevelopmentof the radius or ulna in the growing animal.
PATHOPHYSIOLOGY� Antebrachium—predisposed to deformitiesresulting from continual growth of one boneafter premature growth cessation or decreasedgrowth rate of the paired bone.� Decreased rate of elongation in one bonebehaves as a retarding strap; the growingpaired bone must twist and bow away fromthe short bone or overgrow at the elbow orcarpus; causes joint malalignment.� Normal growth—bones elongate throughthe process of endochondral ossification,which occurs in the physis; physis closureoccurs when the germinal cell layer stopsproducing new cartilage and the existingcartilage hypertrophies, ossifies, and isremodeled into bone.� Hereditary—premature closure of distalulnar physis reported as recessive trait in Skyeterriers; may be a component of commonelbow joint malalignment in manychondrodysplastic breeds (basset hounds andLhasa apsos).� Osteochondrosis or dietaryoversupplementation—possibly associatedwith retardation of endochondral ossification(retained cartilaginous cores) in giant-breeddogs.� Hypertrophic osteodystrophy—juvenilegrowth syndrome with physeal and periostealinflammation that may impede physealgrowth.� Trauma—most common cause; ifchondroproliferative layer of the physis iscrushed (Salter V fracture), new cartilageproduction and bone elongation are stopped.
SYSTEMS AFFECTEDMusculoskeletal
GENETICS� Skye terriers—reported as a recessiveinheritable trait.� Chondrodysplastic breeds(dogs)—predisposed to elbow malalignment.
INCIDENCE/PREVALENCE� Traumatic—may occur after forelimbinjuries in up to 10% of actively growinganimals; uncommon in cats.� Elbow malalignment syndrome ± angulardeformity (chondrodysplastic dogbreeds)—fairly common and can be bilateral.� Nutritionally induced—incidencedecreasing as nutritional standards areimproved.� Congenital agenesis of the radius (cats andrarely dogs)—occasionally seen; results in
severely bowed antebrachium and carpalsubluxation.
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats
Breed Predilections� Skye terriers—recessive inheritable form.� Chondrodysplastic and toy breeds(especially basset hounds, dachshunds, Lhasaapsos, Pekingese, Jack Russell terriers)—maybe predisposed to elbow malalignments.� Giant breeds (e.g., Great Danes,wolfhounds)—may be induced by rapidgrowth owing to excessive or unbalancednutrition, OCD, HOD.
Mean Age and Range� Traumatic—anytime during the activegrowth phase.� Elbow malarticulations—during growth;may not be recognized until secondaryarthritic changes become severe, occasionallyat several years of age.
Predominant SexN/A
SIGNSGeneral Comments� Longer-limbed dogs—angular deformitiesgenerally more common.� Shorter-limbed dogs—tend to develop moresevere joint malalignments.� Age at the time of prematureclosure—affects relative degree of deformityand joint malarticulation; perhaps because ofthe variation in stiffness of bone with age andthe duration of altered growth until maturity.
Historical Findings� Traumatic—progressive limb angulation orlameness 3–4 weeks after injury; owner maynot be aware of causative event.� Developmental elbowmalalignments—insidious onset of lamenessin one or both forelimbs; most apparent afterexercise.
Physical Examination FindingsPremature Distal Ulnar Closure� Three deformities of the distalradius—lateral deviation (valgus), cranialbowing (curvus), and external rotation(supination).� Relative shortening of limb lengthcompared to the contralateral normallygrowing limb.� Caudolateral subluxation of the radial carpaljoint and malarticulation of the elbowjoint—may occur; causes lameness andpainful joint restriction.Premature Radial Physeal Closure� Affected limb—significantly shorter thanthe normal contralateral.� Severity of lameness—depends on degree ofjoint malarticulation.
� Complete symmetrical closure of distalphysis—may note straight limb with awidened radial carpal joint space; may notecaudal bow to radius and ulna.� Asymmetrical closure of medial distalphysis—varus angular deformity; occasionallyinward rotation.� Closure of lateral distal physis—valgusangular deformity; external rotation.� Closure of proximal radial physis withcontinued ulnar growth—malarticulation ofthe elbow joint; widened radial to humeralspace and humeral to anconeal space.
CAUSES� Trauma� Developmental basis� Nutritional basis
RISK FACTORS� Forelimb trauma� Excessive dietary supplementation
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Elbow dysplasia� Fragmented medial coronoid process� Un-united anconeal process� Panosteitis� Flexor tendon contracture� Hypertrophic osteodystrophy
CBC/BIOCHEMISTRY/URINALYSISN/A
OTHER LABORATORY TESTSN/A
IMAGING� Damage to growth potential of thephysis—commonly cannot be seen at the timeof trauma; usually 2–4 weeks beforeradiographically apparent.� Standard craniocaudal and mediolateralradiographic views—include entire elbowjoint; from mid-humerus proximally extendto digits distally; take same series forcomparison to normal contralateral limb.� Degree of angular deformities and relativeshortening—determined by comparingrelative lengths of radius and ulna within thedeformed pair to the normal contralateral pair.� Degree of rotationaldeformity—determined by comparingrotational position of the elbow and carpus onsame view, i.e., lateral of elbow and 45-degreeoblique of carpus documents rotatorydeformity.� Elbow and carpal joints—evaluate formalalignment (treated surgically) and arthritis(e.g., osteophytes; influences prognosis).� Elbow joint—evaluate for associatedun-united anconeal process and fragmentedmedial coronoid process.
DIAGNOSTIC PROCEDURESN/A
BLBS078-CF_A53 BLBS078-Tilley March 21, 2011 22:2
Canine and Feline, Fifth Edition 91
(Continued) Antebrachial Growth Deformities A
PATHOLOGIC FINDINGSCartilage of prematurely closed physisreplaced with bone
TREATMENTAPPROPRIATE HEALTH CARE� Genetic predisposition—do not breed.� Traumatic physeal damage—not seen attime of injury; revealed 2–4 weeks later.� Surgical treatment is recommended as soonas possible following diagnosis.
NURSING CAREN/A
ACTIVITYExercise restriction—reduces jointmalalignment damage; slows arthriticprogression.
DIET� Decrease nutritional supplementation ingiant-breed dogs—slows rapid growth; mayreduce incidence.� Avoid excess weight—helps control arthriticpain resulting from joint malalignment andoveruse.
CLIENT EDUCATION� Discuss heritability in Skye terriers andpossibly chondrodysplastic breeds.� Explain that damage to physeal growthpotential is not apparent at time of forelimbtrauma and that the diagnosis is often made2–4 weeks following an injury.� Discuss the importance of jointmalalignment and resultant arthritis asprimary causes of lameness.� Emphasize that early surgical treatmentleads to a better prognosis.
SURGICAL CONSIDERATIONS� Premature distal ulnar physeal closure in apatient < 5–6 months of age (significantamount of radial growth potentialremaining)—treated with a segmental ulnarostectomy, valgus deformities ≤ 25◦: mayspontaneously correct and may not requireadditional surgery; patients and those withmore severe deformities: often require asecond definitive correction after maturity.� Radial or ulnar physeal closure in a maturepatient (limited or no growth potential)requires deformity correction, jointrealignment, or both.� Deformity correction—may beaccomplished with a variety of osteotomytechniques; may be stabilized with severaldifferent fixation devices; must correct bothrotational and angular deformities; performedat the point of greatest curvature.� Joint malalignment (particularlyelbow)—must correct to minimize arthriticdevelopment (primary cause of lameness);obtain optimal joint alignment via dynamicproximal ulnar osteotomy (use triceps muscletraction and joint pressure) or shortening
longer bone (radial or ulnar ostectomy asindicated).� Significant limb lengthdiscrepancies—distraction osteogenesis;osteotomy of the shortened bone isprogressively distracted at the rate of 1mm/day with an external fixator system tocreate new bone length.
MEDICATIONSDRUG(S) OF CHOICEAnti-inflammatory drugs—symptomatictreatment of arthritis
CONTRAINDICATIONSCorticosteroids—do not use owing topotential systemic side effects and cartilagedamage seen with long-term use.
PRECAUTIONSWarn client of possible gastrointestinal upsetassociated with chronic anti-inflammatorytherapy.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)Neutraceuticals (e.g., glycosamines)—mayhelp minimize cartilage damage and arthritisdevelopment; may be anti-inflammatory andanalgesic.
FOLLOW-UPPATIENT MONITORING� Post-operative—depends on surgicaltreatment.� Periodic checkups—evaluate arthritic statusand anti-inflammatory therapy.
PREVENTION/AVOIDANCE� Selective breeding of susceptible breeds.� Avoid dietary oversupplementation inrapidly growing giant-breed dogs.
POSSIBLE COMPLICATIONSRoutinely seen with various osteotomyfixation techniques (e.g., infection, non-unionof osteotomy, fixator pin tract inflammation).
EXPECTED COURSE AND PROGNOSIS� Generally, best results seen with earlydiagnosis and surgical treatment—minimizesarthritis.� Premature ulnar closure—tends to be easierto manage; yields better results.� Limb lengthening by distractionosteogenesis—requires extensivepost-operative management by theveterinarian and owner; high rate ofcomplications.
MISCELLANEOUSASSOCIATED CONDITIONS� Osteochondrosis� HOD� UAP
AGE-RELATED FACTORSThe younger the age at the time oftraumatically induced physeal closure, themore severe the deformity andmalarticulation.
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMSRadius curvus
ABBREVIATIONS� HOD = hypertrophic osteodystrophy� OCD = osteochondrodysplasia� UAP = un-united anconeal process
Suggested ReadingBalfour RJ, Boudrieau RJ, Gores BR. T-plate
fixation of distal radial closing wedgeosteotomies for treatment of angular limbdeformities in 18 dogs. Vet Surg 2000,29:207–217.
Dismukes DI, Fox DB, Tomlinson JL,Essman SC. Use of radiographic measuresand three-dimensional computedtomographic imaging in surgical correctionof an antebrachial deformity in a dog.JAVMA 2008, 232(1):68–73.
Fox DB, Tomlinson JL, Cook JL, BreshearsLM. Principles of uniapical and biapicalradial deformity correction using domeosteotomies and the center of rotation ofangulation methodology in dogs. Vet Surg2006, 35(1):67–77.
Henney LH, Gambardella PC. Prematureclosure of the ulnar physis in the dog: Aretrospective clinical study. JAAHA 1989,25:573–581.
Meola SD, Wheeler JL, Rist CL. Validation ofa technique to assess radial torsion in thepresence of procurvatum and valgusdeformity using computed tomography: Acadaveric study. Vet Surg 2008,37(6):525–529.
Quinn MK, Erhart N, Johnson AL, SchaefferDJ. Realignment of the radius in canineantebrachial growth deformities treated withcorrective osteotomy and bilateral (Type II)external fixation. Vet Surg 2000,29:558–563.
Author Peter K. ShiresConsulting Editor Peter K. Shires
Client Education Handoutavailable online

BLBS078-CF_A54 BLBS078-Tilley July 15, 2011 9:21
92 Blackwell’s Five-Minute Veterinary Consult
Anterior Uveitis—CatsA
BASICSDEFINITION� Inflammation of the anterior uveal tissues,including iris (iritis), ciliary body (cyclitis), orboth (iridocyclitis). � May be associated withconcurrent posterior uveal and retinalinflammation (choroiditis; chorioretinitis).� May be unilateral or bilateral.
PATHOPHYSIOLOGY� Increased permeability of the blood-aqueousbarrier related to infectious,immune-mediated, neoplastic, traumatic, orother causes; allows entrance of plasmaproteins and blood cellular components intoaqueous humor. � Disruption ofblood-aqueous barrier is initiated andmaintained by numerous chemical mediators,including histamine, prostaglandins,leukotrienes, serotonin, kinins, andcomplement.
SYSTEMS AFFECTED� Ophthalmic. � Other systems may also beaffected by underlying disease process.
INCIDENCE/PREVALENCE� Relatively common condition. � Trueincidence/prevalence unknown.
GEOGRAPHIC DISTRIBUTIONGeographic location may affect incidence ofcertain infectious causes of uveitis.
SIGNALMENTSpeciesCats
Mean Age and Range� Mean age—7–9 years. � Any age may beaffected.
Predominant SexMales/neutered males more commonlyaffected than females.
SIGNSHistorical Findings� Cloudy eye—due to corneal edema, aqueousflare, hypopyon, etc. � Painful eye—manifestby blepharospasm, photophobia, or rubbingeye; usually less pronounced than in dogs.� Red eye—due to conjunctival hyperemiaand ciliary flush; less pronounced than indogs in most cases. � Vision loss—variable.
Physical Examination FindingsImportance of a thorough physicalexamination in cats presenting with uveitiscannot be overstated.Ophthalmic Findings� Ocular discomfort—manifest byblepharospasm and photophobia � Oculardischarge—usually serous; sometimes mucoidto mucopurulent. � Conjunctivalhyperemia—bulbar and palpebral conjunctivaboth usually affected. � Cornealedema—diffuse; mild to severe. � Keraticprecipitates—multifocal aggregates of
inflammatory cells adherent to cornealendothelium; most notable ventrally.� Aqueous flare and cells—cloudiness ofaqueous humor due to increased proteincontent and suspended cellular debris; bestvisualized with a bright, narrow beam of lightshined through anterior chamber. � Ciliaryflush—injection of deep perilimbal anteriorciliary vessels. � Deep cornealvascularization—circumcorneal distribution(brush border). � Miosis and/or resistance topharmacologic dilation. � Iridalswelling—may be generalized or nodular.� Reduced IOP is consistent with anterioruveitis but is not a uniform finding.� Posterior synechia—adhesions betweenposterior iris and anterior lens surface.� Fibrin in anterior chamber. � Hypopyon orhyphema—accumulations of white bloodcells or red blood cells, respectively, in theanterior chamber; usually settles horizontallyin ventral aspect of chamber but may bediffuse. � Chronic changes may includerubeosis iridis, iridal hyperpigmentation,secondary cataract, lens luxation, pupillaryseclusion, iris bombe, secondary glaucoma,and phthisis bulbi.
CAUSES� Infectious—mycotic (Blastomyces spp.,Cryptococcus neoformans; Coccidiodes immitis;Histoplasma capsulatum); protozoal(Toxoplasma gondii); bacterial (Bartonella spp.,Mycobacterium spp. or any bacterialsepticemia); viral (FIV, FeLV, felinecoronavirus; FHV-1); parasitic(ophthalmomyiasis; ocular larval migrans).� Idiopathic—lymphocytic-plasmacyticuveitis. � Immune-mediated—reaction to lensproteins (due to cataract or lens trauma).� Neoplastic—primary ocular tumors (esp.diffuse iris melanoma, ocular sarcoma);metastasis to uveal tract (esp. lymphoma).� Metabolic—hyperlipidemia; hyperviscosity;systemic hypertension.� Miscellaneous—trauma; ulcerative keratitis;corneal stromal abscess; toxemia of any cause.
RISK FACTORSNone specific; immune suppression andgeographic location may increase incidence ofcertain infectious causes of uveitis.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Conjunctivitis—redness limited toconjunctival hyperemia (i.e., no ciliary flush);ocular discharge usually thicker and morecopious than in uveitis; discomfort may bealleviated by topical anesthetic.� Glaucoma—elevated IOP is most consistentdistinguishing feature of this disease; othersmay include dilated pupil, Haab’s striae, andbuphthalmos. � Ulcerative keratitis—cornealfluorescein staining will detect ulcers; corneal
edema associated with ulcers is either localizedto, or most severe at, site of ulcer; oculardischarge often thicker and more copiousthan with uveitis; discomfort may bealleviated by topical anesthetic. � Horner’ssyndrome—miosis, enophthalmos, andnictitans protrusion are similar in bothconditions, but Horner’s is non-painful withno ocular discharge; ptosis with Horner’s isdistinguished from blepharospasm, as thelatter is an active process; minor conjunctivalhyperemia may be noted with Horner’s, butcornea and anterior chamber are clear; clinicalsigns of Horner’s syndrome resolve followingtopical application of ophthalmic 1–10%phenylephrine.
CBC/BIOCHEMISTRY/URINALYSIS� CBC—often normal; changes may bepresent related to underlying disease.� Biochemistry—often normal; mostcommon abnormality in cats with uveitis iselevated serum proteins (usually due topolyclonal gammopathy). � Urinalysis—oftennormal; changes may be present related tounderlying disease.
OTHER LABORATORY TESTS� FeLV serum titers. � FIV serum titers.� Coronavirus titers—not specific for FIP butmay influence the index of suspicion for thisdisease. � Toxoplasma gondii IgM and IgGtiters performed on serum and/or aqueoushumor. � Bartonella spp. serology, PCR(serum or aqueous humor) and/or bloodculture.
IMAGING� Thoracic radiography—may show evidenceof causative disease process (e.g., infiltratesrelated to infectious disease; evidence ofmetastatic neoplastic disease). � Ocularultrasound—indicated if opacity of ocularmedia precludes direct examination; mayreveal intraocular neoplasm or retinaldetachment.
DIAGNOSTIC PROCEDURES� Tonometry—low IOP consistent withuveitis; elevated IOP indicates glaucoma(primary disease or secondary to uveitis).� Ocular centesis—if retinal detachment ispresent, cytology of subretinal aspirate mayreveal causative agents; anterior chambercentesis may be performed for Toxoplasmagondii or Bartonella IgM and IgG titers onaqueous humor.
PATHOLOGIC FINDINGS� Gross—see physical examination findings.� Histopathologic—corneal edema;peripheral corneal deep stromalvascularization; keratic precipitates; preiridalfibrovascular membrane; peripheral anteriorsynechia; posterior synechia; entropion orectropion uveae; leukocyte accumulation iniris, ciliary body, sclera, choroid(lymphocytic-plasmacytic, suppurative, orgranulomatous infiltrates, depending onetiology); secondary cataract; with posterior
BLBS078-CF_A54 BLBS078-Tilley July 15, 2011 9:21
Canine and Feline, Fifth Edition 93
(Continued) Anterior Uveitis—Cats A
segment involvement in inflammatoryprocess, cyclitic membrane; vitreal tractionbands and retinal detachment may be present.� Lymphoplasmacytic infiltrate of iris andciliary body (either diffuse or nodular) is mostcommon histopathologic finding.
TREATMENTAPPROPRIATE HEALTH CAREOutpatient medical management generallysufficient.
ACTIVITYNo changes indicated in most cases.
DIETNo changes indicated.
CLIENT EDUCATION� Inform of potential systemic diseasescausing ophthalmic signs and emphasizeimportance of appropriate diagnostic testing.� In addition to symptomatic uveitistreatment, treatment of underlying disease(when possible) is paramount to a positiveoutcome. � Inform of potential complicationsand emphasize compliance with treatmentand follow-up recommendations that willreduce the likelihood of complications.
SURGICAL CONSIDERATIONS� None in most cases. � Specific instancesrequiring surgical intervention includeremoval of ruptured lenses and surgicalmanagement of secondary glaucoma.� Chronic uveitis leading to secondaryglaucoma commonly necessitates enucleationof affected globes. � Enucleation isrecommended in cats with uveitis related todiffuse iris melanoma or other primaryintraocular tumors.
MEDICATIONSDRUG(S)CorticosteroidsTopical� Prednisolone acetate 1%—apply 2–8 timesdaily, depending on severity of disease; tapermedication as condition resolves.� Dexamethasone 0.1%—apply 2–8 timesdaily, depending on severity of disease; tapermedication as condition resolves. � Othertopical corticosteroids (e.g., betamethasone,hydrocortisone) are considerably less effectivein the treatment of intraocular inflammation.� Taper treatment frequency as conditionimproves; stopping topical corticosteroidsabruptly may result in rebound of ocularinflammation.Subconjunctival� Triamcinolone acetonide 4 mg bysubconjunctival injection.� Methylprednisolone 4 mg by
subconjunctival injection. � Often notrequired. � Indicated only in severe cases asone-time injection, followed by topical and/orsystemic anti-inflammatories.Systemic� Prednisone 1–3 mg/kg/day initially; taperdose after 7–10 days. � Use only if systemicinfectious causes of uveitis have been ruledout.
Nonsteroidal Anti-inflammatory DrugsTopical� Flurbiprofen—apply 2–4 times daily,depending on severity of disease.� Diclofenac—apply 2–4 times daily,depending on severity of disease.Systemic� Meloxicam 0.2 mg/kg IV, SC, PO once,then 0.05 mg/kg IV, SC, PO q24h x 2 days,then 0.025 mg/kg q24–48h. Due to potentialrenal effects, limit duration of use to 4–6 days.Topical Mydriatic/Cycloplegic� Atropine sulfate 1%—apply 1–4 timesdaily, depending on severity of disease. Uselowest frequency adequate to maintain dilatedpupil and ocular comfort; taper medication ascondition resolves. Ointment is preferred oversolution in cats as it causes less salivation.
CONTRAINDICATIONS� Avoid the use of miotic medications (e.g.,pilocarpine), including topical prostaglandins(e.g., latanoprost), in the presence of uveitis.� Topical and subconjunctival corticosteroidsare absolutely contraindicated in the presenceof ulcerative keratitis. � Corticosteroids(especially systemic) should be avoided in catswith systemic hypertension. Avoid systemicNSAIDS in cats with renal disease.
PRECAUTIONSOwing to concern for secondary glaucoma,topical atropine should be used judiciouslyand IOP should be monitored periodically.
POSSIBLE INTERACTIONSSystemic corticosteroids and nonsteroidalanti-inflammatory drugs should not be usedconcurrently.
FOLLOW-UPPATIENT MONITORINGRecheck in 3–7 days, depending on severity ofdisease. IOP should be monitored at recheckto detect secondary glaucoma. Frequency ofsubsequent rechecks dictated by severity ofdisease and response to treatment.
POSSIBLE COMPLICATIONSSystemic ComplicationsOccur as a result of the systemic etiology ofthe uveitis.
Ophthalmic Complications� Secondary glaucoma—commoncomplication of chronic uveitis in cats.� Secondary cataract. � Lens luxation.� Retinal detachment. � Phthisis bulbi.
EXPECTED COURSE AND PROGNOSIS� Guarded prognosis for affected eyes.Depends on underlying disease and responseto treatment. � Cats with treatable underlyingdisease (e.g., toxoplasmosis) are more likely tohave a favorable ophthalmic outcome thanthose with idiopathic lymphocytic-plasmacytic uveitis or untreatable underlyingcondition (e.g., FIP, FIV).
MISCELLANEOUSAGE-RELATED FACTORS� Younger cats more likely to be diagnosedwith infectious etiology. � Older cats at higherrisk of idiopathic lymphocytic-plasmacyticuveitis and intraocular neoplastic causes.
ZOONOTIC POTENTIAL� None in most cases. � Some forms ofsystemic infection causing uveitis may pose aslight risk to immunocompromised owners.
PREGNANCY/FERTILITY/BREEDINGAvoid systemic corticosteroids. Because ofsystemic absorption, topical corticosteroidsmay also pose a risk, especially with frequentapplication.
SYNONYMIridocyclitis
SEE ALSO� Horner’s Syndrome � Red Eye
ABBREVIATIONS� FeLV = feline leukemia virus � FHV-1 =feline herpsevirus � FIP = feline infectiousperitonitis � FIV = feline immunodeficiencyvirus � IOP = intraocular pressure
Suggested ReadingColitz CM. Feline uveitis: Diagnosis and
treatment. Clin Tech Small Anim Pract2005, 20:117–120.
Cullen C, Webb A. Ocular manifestations ofsystemic diseases. Part 2: The cat. In: GelattKN, ed., Veterinary Ophthalmology, 4th ed.Ames, IA: Blackwell, 2007, pp. 1538–1587.
Miller P. Uvea. In: Maggs DJ, Miller PE, OfriR, Slatter’s Fundamentals of VeterinaryOphthalmology, 4th ed. St. Louis:Saunders, 2008, pp. 203–229.
Stiles J, Townsend WM. Felineophthalmology. In: Gelatt KN, ed.,Veterinary Ophthalmology, 4th ed. Ames,IA: Blackwell, 2007, pp. 1095–1164.
Author Ian P. HerringConsulting Editor Paul E. Miller
Client Education Handoutavailable online
BLBS078-CF_A55 BLBS078-Tilley June 16, 2011 10:55
94 Blackwell’s Five-Minute Veterinary Consult
Anterior Uveitis—DogsA
BASICSDEFINITION� Inflammation of the anterior uveal tissues,including iris (iritis), ciliary body (cyclitis), orboth (iridocyclitis). � May be associated withconcurrent posterior uveal and retinalinflammation (choroiditis; chorioretinitis).� May be unilateral or bilateral.
PATHOPHYSIOLOGY� Increased permeability of the blood-aqueousbarrier related to infectious,immune-mediated, traumatic, or other causesallows entrance of plasma proteins and bloodcellular components into aqueous humor.� Disruption of blood-aqueous barrier isinitiated and maintained by numerouschemical mediators, including histamine,prostaglandins, leukotrienes, serotonin,kinins, and complement.
SYSTEMS AFFECTED� Ophthalmic. � Other systems may also beaffected by underlying disease process.
INCIDENCE/PREVALENCE� Relatively common condition. � Trueincidence/prevalence unknown.
GEOGRAPHIC DISTRIBUTIONGeographic location may affect incidence ofcertain infectious causes of uveitis.
SIGNALMENTSpeciesDogs
Breed Predilections� None for most causes. � Uveitis associatedwith iridociliary cysts in golden retriever(a.k.a. golden retriever uveitis). � Increasedincidence of uveodermatologic syndrome inSiberian husky, Akita, Samoyed, and Shetlandsheepdog.
Mean Age and Range� Any age may be affected. � Mean age inuveodermatologic syndrome—2.8 years.� Mean age in golden retriever uveitis—8.6 years.
SIGNSHistorical Findings� Red eye—due to conjunctival hyperemiaand ciliary flush. � Cloudy eye—due tocorneal edema, aqueous flare, hypopyon, etc.� Painful eye—manifest by blepharospasm,photophobia, or rubbing eye. � Visionloss—variable.
Physical Examination FindingsThe importance of a thorough physicalexamination in dogs presenting with uveitiscannot be overstated.Ophthalmic Findings� Ocular discomfort—manifest byblepharospasm, photophobia, and rubbingeye. � Ocular discharge—usually serous;sometimes mucoid to mucopurulent.
� Conjunctival hyperemia—bulbar andpalpebral conjunctiva both usually affected.� Corneal edema—diffuse; mild to severe.� Keratic precipitates—multifocal aggregatesof inflammatory cells adherent to cornealendothelium; most notable ventrally.� Aqueous flare and cells—cloudiness ofaqueous humor due to increased proteincontent and suspended cellular debris; bestvisualized with a bright, narrow beam of lightshined through anterior chamber. � Ciliaryflush—injection of deep perilimbal anteriorciliary vessels. � Deep cornealvascularization—circumcorneal distribution(brush border). � Miosis and/or resistance topharmacologic dilation. � Iridal swelling.� Reduced IOP is consistent with uveitis butis not a uniform finding. � Posteriorsynechia—adhesions between posterior irisand anterior lens surface. � Fibrin in anteriorchamber. � Hypopyon orhyphema—accumulations of white bloodcells or red blood cells, respectively, in theanterior chamber; usually settles horizontallyin ventral aspect of chamber but may bediffuse. � Chronic changes may includerubeosis iridis, iridal hyperpigmentation,secondary cataract, lens luxation, pupillaryseclusion, iris bombe, secondary glaucoma,and phthisis bulbi.
CAUSES� Infectious—mycotic (Blastomycesdermatitidis, Cryptococcus neoformans,Coccidiodes immitis, Histoplasma capsulatum);protozoal (Toxoplasma gondii, Neosporacaninum, Leishmania donovani); rickettsial(Ehrlichia canis, Rickettsia rickettsii); bacterial(Leptospira spp., Bartonella spp., Brucellacanis, Borrelia burgdorferi, any bacterialsepticemia); algal (Prototheca spp.); viral(adenovirus, distemper, rabies, herpes);parasitic (ocular filariasis, ocular larvalmigrans). � Immune-mediated—reaction tolens proteins (due to cataract or lens trauma);uveodermatologic syndrome; post-vaccinalreaction to canine adenovirus vaccine;vasculitis. � Neoplastic—primary oculartumors (especially uveal melanoma,iridociliary adenoma/adenocarcinoma);metastasis to uveal tract (lymphosarcoma mostcommon). � Metabolic—hyperlipidemia;hyperviscosity; systemic hypertension.� Miscellaneous—idiopathic; trauma; goldenretriever uveitis; ulcerative keratitis; cornealstromal abscess; scleritis; lensinstability/luxation; dental/periodontaldisease; toxemia of any cause.
RISK FACTORSNone specific; immune suppression andgeographic location may increase incidence ofcertain infectious causes of uveitis; breedpredispositions, as listed above, should beconsidered.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Conjunctivitis—redness limited toconjunctival hyperemia (i.e., no ciliary flush);ocular discharge usually thicker and morecopious than in uveitis; discomfort may bealleviated with application of topicalanesthetic. � Glaucoma—elevated IOP ismost consistent feature of this disease; othersmay include dilated pupil, Haab’s striae, andbuphthalmos. � Lens luxation—cornealedema may be localized to site of lens contactwith endothelium or may be diffuse as a resultof associated uveitis and/or glaucoma; lensluxation is highly breed associated.� Ulcerative keratitis—corneal fluoresceinstaining will detect ulcers; corneal edemaassociated with ulcers is either localized to, ormost severe at, site of ulcer; ocular dischargeoften thicker and more copious than withuveitis; discomfort may be partially alleviatedby topical anesthetic. � Corneal endothelialdystrophy or degeneration—diffuse cornealedema is present, but IOP is normal;conjunctival hyperemia and signs of oculardiscomfort are generally absent. � Horner’ssyndrome—miosis, enophthalmos, andnictitans protrusion are similar in bothconditions, but Horner’s is non-painful withno ocular discharge; ptosis with Horner’s isdistinguished from blepharospasm as thelatter is an active process; minor conjunctivalhyperemia may be noted with Horner’s, butcornea and anterior chamber are clear; clinicalsigns of Horner’s syndrome resolve followingtopical application of 1–10% phenylephrine.
CBC/BIOCHEMISTRY/URINALYSISOften normal; changes related to underlyingdisease may be present.
OTHER LABORATORY TESTS� Serology for infectious diseases listed under“Causes” may be appropriate, depending onindex of suspicion for infectious etiology.� Clinical signs raising the suspicion ofsystemic disease including lethargy, pyrexia,weight loss, coughing, lymphadenopathy, etc.,warrant serology for infectious diseases.
IMAGING� Thoracic radiography may show evidence ofcausative disease process (e.g., systemicmycoses; metastatic neoplasia). � Abdominalultrasound may be warranted if suspicion formetastatic neoplastic disease is high. � Ocularultrasound is indicated if opacity of ocularmedia precludes direct examination; mayreveal intraocular neoplasm or retinaldetachment.
DIAGNOSTIC PROCEDURES� Tonometry—low IOP consistent withuveitis; elevated IOP indicates glaucoma(primary disease or secondary to uveitis).
BLBS078-CF_A55 BLBS078-Tilley June 16, 2011 10:55
Canine and Feline, Fifth Edition 95
(Continued) Anterior Uveitis—Dogs A
� Lymph node aspirates—if enlarged nodesare palpable, aspiration for cytology isindicated. � Ocular centesis—if retinaldetachment is present, cytology of subretinalaspirate may reveal causative agents; anteriorchamber centesis is generally unrewarding.
PATHOLOGIC FINDINGS� Gross—see physical examination findings.� Histopathologic—corneal edema;peripheral corneal deep stromalvascularization; keratic precipitates; preiridalfibrovascular membrane; peripheral anteriorsynechia; posterior synechia; entropion orectropion uveae; leukocyte accumulation iniris, ciliary body, sclera, choroid (lymphocytic,plasmacytic, suppurative, or granulomatousinfiltrates, depending on etiology); secondarycataract; with posterior segment involvementin inflammatory process, cyclitic membrane;vitreal traction bands and retinal detachmentmay be present.
TREATMENTAPPROPRIATE HEALTH CAREOutpatient medical management is generallysufficient.
NURSING CARENone
ACTIVITY� No changes indicated in most cases.� Reduced exposure to bright light mayalleviate discomfort.
DIETNo changes indicated.
CLIENT EDUCATION� Inform of potential systemic diseasescausing ophthalmic signs and emphasizeimportance of appropriate diagnostic testing.� In addition to symptomatic uveitistreatment, treatment of underlying disease(when possible) is paramount to a positiveoutcome. � Inform of potential complicationsand emphasize compliance with treatmentand follow-up recommendations that willreduce the likelihood of complications.
SURGICAL CONSIDERATIONSNone in most cases. Specific instancesrequiring surgical intervention includeremoval of ruptured lenses, removal ofcataracts causing uveitis (if prognosis forsuccessful surgery is otherwise favorable), andsurgical management of secondary glaucoma.
MEDICATIONSDRUG(S) OF CHOICECorticosteroidsTopical� Prednisolone acetate 1%—apply 2–8 times
daily, depending on severity of disease; tapermedication as condition resolves.� Dexamethasone 0.1%—apply 2–8 timesdaily, depending on severity of disease; tapermedication as condition resolves. � Othertopical corticosteroids (e.g., betamethasone,hydrocortisone) are considerably less effectivein the treatment of intraocular inflammation.� Taper treatment frequency over severalweeks as condition improves; stopping topicalcorticosteroids abruptly may result inrebound of ocular inflammation.Subconjunctival� Triamcinolone acetonide 4–6 mg bysubconjunctival injection.� Methylprednisolone 3–10 mg bysubconjunctival injection. � Often notrequired. � Indicated only in severe cases asone-time injection followed by topical and/orsystemic anti-inflammatories.Systemic� Prednisone 0.5–2.2 mg/kg/day initially;taper dose after 7–10 days. � Use only ifsystemic infectious causes of uveitis have beenruled out.
Nonsteroidal Anti-inflammatory DrugsTopical� Less effective than topical corticosteroids.� Flurbiprofen—apply 2–4 times daily,depending on severity of disease.� Diclofenac—apply 2–4 times daily,depending on severity of disease.Systemic� Do not use concurrently with systemiccorticosteroids; avoid in the presence ofhyphema. � Aspirin 10–25 mg/kg PO q12h� Carprofen 2.2 mg/kg PO q12h or4.4 mg/kg PO q24h � Tepoxalin 10 mg/kgPO q24h � Meloxicam 0.2 mg/kg PO q24hTopical Mydriatic/Cycloplegic� Atropine sulfate 1%—apply 1–4 timesdaily, depending on severity of disease. Uselowest frequency adequate to maintain dilatedpupil and ocular comfort; taper medication ascondition resolves.
CONTRAINDICATIONS� Avoid the use of miotic medications (e.g.,pilocarpine, demecarium bromide), includingtopical prostaglandins (e.g., latanoprost), inthe presence of uveitis. � Topical andsubconjunctival corticosteroids are absolutelycontraindicated in the presence of ulcerativekeratitis. � Avoid systemic corticosteroids indogs with systemic hypertension or systemicinfections.
PRECAUTIONSOut of concern for secondary glaucoma,topical atropine should be used judiciouslyand IOP should be monitored periodically.
POSSIBLE INTERACTIONSSystemic corticosteroids and NSAIDS shouldnot be used concurrently.
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGRecheck in 3–7 days, depending on severity ofdisease. IOP should be monitored at recheckto detect secondary glaucoma. Frequency ofsubsequent rechecks dictated by severity ofdisease and response to treatment.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONS� Many systemic complications, includingdeath, may occur due to systemic etiology ofuveitis. � Ophthalmic complications includesecondary cataract, secondary glaucoma, lensluxation, retinal detachment, phthisis bulbi.
EXPECTED COURSE AND PROGNOSISExtremely variable; depends on underlyingdisease and response to treatment.
MISCELLANEOUSZOONOTIC POTENTIALNone in most cases. Some forms of systemicinfection causing uveitis may pose a slight riskto immune-compromised owners.
PREGNANCY/FERTILITY/BREEDINGAvoid systemic corticosteroids. Because ofpossibility of systemic absorption, topicalcorticosteroids may also pose risk, especiallywith frequent application in small dogs.
SYNONYMSIridocyclitis
SEE ALSORed Eye
ABBREVIATIONS� IOP = intraocular pressure � NSAID =nonsteroidal anti-inflammatory drug
Suggested ReadingCullen C, Webb A. Ocular manifestations of
systemic diseases. Part 1: The dog. In: GelattKN, ed., Veterinary Ophthalmology, 4th ed.Ames, IA: Blackwell, 2007, pp. 1470–1537.
Hendrix D. Diseases and surgery of thecanine anterior uvea. In: Gelatt KN, ed.,Veterinary Ophthalmology, 4th ed. Ames,IA: Blackwell, 2007, pp. 812–858.
Miller P. Uvea. In: Maggs DJ, Miller PE, OfriR, Slatter’s Fundamentals of VeterinaryOphthalmology, 4th ed. St. Louis:Saunders, 2008, pp. 203–229.
Author Ian P. HerringConsulting Editor Paul E. Miller
Client Education Handoutavailable online
BLBS078-CF_A56 BLBS078-Tilley July 23, 2011 9:4
96 Blackwell’s Five-Minute Veterinary Consult
Anticoagulant Rodenticide PoisoningA
BASICSDEFINITIONCoagulopathy caused by reduced circulatingvitamin K1–dependent clotting factors afterexposure to anticoagulant rodenticides.
PATHOPHYSIOLOGY� Inhibits vitamin K1 epoxide reductase, DTdiaphorase, and possibly other enzymesinvolved in the reduction of vitaminK1–epoxide to vitamin K1. � VitaminK1—required for carboxylation of clottingfactors II, VI, IX, and X; uncarboxylatedclotting factors do not bind calciumsufficiently to participate in clot formation.
SYSTEMS AFFECTEDHemic/Lymphatic/Immune
INCIDENCE/PREVALENCECommon—many baits are soldover-the-counter and widely used in homes.
SIGNALMENT� Dogs and cats. � No breed or genderpredilections; younger animals may ingest baitmore readily.
SIGNSGeneral CommentsMay be slightly more prevalent in the springand fall when rodenticide products are used.
Historical Findings� Use of anticoagulant rodenticides� Dyspnea—exercise intolerance � Bleeding
Physical Examination Findings� Hematomas—often ventral and atvenipuncture sites � Muffled heart or lungsounds � Pale mucous membranes � Lethargy
CAUSES� Exposure to anticoagulant rodenticide� First-generation coumarin anticoagulants(e.g., warfarin, pindone)— largely replaced bymore potent second-generation products.� Second-generation anticoagulants (e.g.,brodifacoum, bromadiolone, diphacinone,and chlorophacinone)—generally more toxicand some persist longer before excretion thanfirst-generation agents. � Difenthialone(D-Cease)—less toxic to dogs (LD50 4mg/kg) than are brodifacoum (LD50 0.25–2.5mg/kg), bromadiolone (LD50 11–20 mg/kg),chlorophacinone (LD50 50–100 mg/kg), andwarfarin (LD50 20–50 mg/kg); similar todiphacinone (LD50 3–7.5 mg/kg); cats, LD50
> 16 mg/kg; concentration in baits lower(0.0025%; 25 ppm) than that of othersecond-generation rodenticide baits (0.005%;50 ppm), so dogs and cats may tolerate higherintakes.
RISK FACTORS� Small doses over several days moredangerous than a single large dose; either typeof exposure may cause toxicosis. � Secondary
toxicosis by consumption of poisonedrodents—unlikely.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� DIC � Congenital clotting factor deficiencies
CBC/BIOCHEMISTRY/URINALYSISAnemia—with marked hemorrhage
OTHER LABORATORY TESTS� ACT > 150 sec—supports coagulopathy.� Prolonged PT and PTT—support exposureto rodenticide; PT affected earlier than isPTT. � Analysis of blood or liver—confirmexposure to a specific product.
IMAGINGThoracic radiography—may detecthemothorax or hemopericardium.
DIAGNOSTIC PROCEDURESThoracentesis—may confirm hemothorax.
PATHOLOGIC FINDINGS� Free blood in the thoracic cavity, lungs, andabdominal cavity—common. � Hemorrhageinto the cranial vault, gastrointestinal tract,and urinary tract—less common; may occurboth subcutaneously and intramuscularly.
TREATMENTAPPROPRIATE HEALTH CARE� Inpatient—acute crisis� Outpatient—consider once thecoagulopathy is stabilized
NURSING CAREFresh whole blood or plasma transfusion—may be required with hemorrhaging;provides immediate access to vitaminK–dependent clotting factors; whole bloodmay be preferred with severe anemia.
ACTIVITYConfine patient during the early stages;activity enhances blood loss.
DIETNo recognized effect
CLIENT EDUCATIONWarn client that reexposure could be a seriousproblem.
SURGICAL CONSIDERATIONS� Thoracentesis—may be important forremoving free thoracic blood, which causesdyspnea and respiratory failure. � Mustcorrect coagulopathy before surgery.
MEDICATIONSDRUG(S) OF CHOICE� Vitamin K1 2.5–5.0 mg/kg PO q24h for5 days–6 weeks (depending on the specific
product); bioavailability enhanced by theconcurrent feeding of a small amount of fat,such as canned dog food. � Vitamin K1
administration—continued for 3–4 weekswith suspected second-generationanticoagulant toxicosis.
CONTRAINDICATIONS� Vitamin K3—not efficacious in thetreatment of anticoagulant rodenticidetoxicosis; contraindicated. � Intravenousvitamin K1—reported anaphylactic reactions;avoid this route of administration.
PRECAUTIONS� Avoid unnecessary surgical procedures andparenteral injections. � Use the smallestpossible needle when giving an injection orcollecting samples.
POSSIBLE INTERACTIONSSulfonamides and phenylbutazone—maydisplace anticoagulant rodenticides fromplasma binding sites, leading to more freetoxicant and toxicosis.
FOLLOW-UPPATIENT MONITORINGACT and PT—assess efficacy of therapy;monitoring continued 3–5 days afterdiscontinuation of treatment.
PREVENTION/AVOIDANCEPrevent access to anticoagulant rodenticides.
POSSIBLE COMPLICATIONS� May note secondary bacterial pneumonia,after intrapulmonary hemorrhage.� Intracranial, intra-articular hemorrhage.
EXPECTED COURSE AND PROGNOSISIf the patient survives the first 48 hours ofacute coagulopathy—the prognosis improves.
MISCELLANEOUSPREGNANCY/FERTILITY/BREEDINGWarfarin and diphacinone, perhaps others—may pass into amniotic fluid and on to thefetuses of an exposed pregnant bitch; similarconcerns for feeding affected milk to pups.
ABBREVIATIONS� ACT = activated clotting time � DIC =disseminated intravascular coagulation � PT= prothrombin time � PTT = partialthromboplastin time
INTERNET RESOURCEShttp://www.aspcapro.org/animal-poison-control-center-articles.php.Author Michael J. MurphyConsulting Editor Gary D. Osweiler
Client Education Handoutavailable online
BLBS078-CF_A56a BLBS078-Tilley July 23, 2011 5:11
Canine and Feline, Fifth Edition 97
Antidepressants—SSRI Toxicosis A
BASICSDEFINITION� Toxicity secondary to the overdose of anSSRI or co-ingestion of two types ofserotonergic drugs. � SSRIs includecitalopram (Celexa), escitalopram (Lexapro),fluoxetine (Prozac), fluvoxamine (Luvox),paroxetine (Paxil), sertraline (Zoloft).
PATHOPHYSIOLOGY� SSRIs are a class of antidepressants thatinhibit reuptake of serotonin, aneurotransmitter involved in aggression,anxiety, appetite, depression, migraine, pain,and sleep. � Excessive stimulation of serotoninreceptors can occur by enhanced serotoninsynthesis, increased presynaptic serotoninrelease, inhibition of serotonin uptake intothe presynaptic neuron, inhibition ofserotonin metabolism, or serotonin agonism.Serotonin syndrome is characterized inhumans as a combination of symptoms thatinclude at least three of the following:myoclonus, mental aberration, agitation,hyperreflexia, tremors, diarrhea, ataxia, orhyperthermia. � Toxic dosage varies widelyamong commonly available SSRIs and are notwell defined in veterinary medicine.
SYSTEMS AFFECTED� Cardiovascular—decreased vascular tone(hypotension), increased heart rate and strokevolume (tachycardia). � Gastrointestinal—increased smooth muscle contractility(vomiting, diarrhea). � Nervous—stimulation(agitation, restlessness, seizures) and alteredmental status (vocalization, disorientation).� Neuromuscular—autonomic dysfunction(hyperactivity) and neuromuscularhyperactivity (hyperreflexia, myoclonus,tremors). � Ophthalmic—increasedautonomic function (mydriasis).� Respiratory—increased bronchial smoothmuscle contraction (dypsnea).
INCIDENCE/PREVALENCEIncreasing in incidence due to increasing useof serotonergic drugs.
SIGNALMENTSpeciesDogs and cats
Mean Age and RangeAny age can be affected.
SIGNSHistorical Findings� Agitation or lethargy � Dilated pupils� Vomiting � Tremors � Hypersalivation� Diarrhea � Seizures � Nystagmus
Physical Examination Findings� Agitation � Ataxia � Mydriasis � Tremors� Vomiting � Disorientation � Hyperthermia� Vocalization � Depression � Tachycardia� Hypotension � Diarrhea � Blindness� Seizures � Hypersalivation � Death
CAUSES� SSRI overdose—accidental exposure,inappropriate administration, or therapeuticuse. � Ingestion of an SSRI along withanother class of medications that increasesserotonin (TCAs, SNRIs, MAOIs, novelantidepressants, tramadol, fentanyl,meperidine, amphetamines, cocaine,dextromethorphan, 5-HTP, buspirone,bupropion, triptans, LSD).
RISK FACTORS� Animals on a serotonergic drug� Underlying liver or kidney disease
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Toxicologic: TCAs, SNRIs MAOIs,metaldehyde, lead, ethylene glycol, hops,anticholinergics, antihistamines.� Non-toxicologic: meningitis e.g., (rabies,canine distemper), neoplasia, heat stroke,malignant hyperthermia.
CBC/BIOCHEMISTRY/URINALYSIS� CBC/biochemistry: no changes areexpected. � Urinalysis: myoglobinuriasecondary to rhabdomyolsis may be seen.
OTHER LABORATORY TESTS� Blood gas: metabolic acidosis may be seen.� Testing for SSRIs can be performed, but thetests are not clinically useful.
DIAGNOSTIC PROCEDURESThere are no diagnostic tests to confirmserotonin syndrome
TREATMENTAPPROPRIATE HEALTH CARE� Emesis (if asymptomatic and recentingestion) or gastric lavage (if large number ofpills ingested). � Activated charcoal withcathartics (may need to repeat due to longhalf-life of most of these medications).
NURSING CAREIV fluids to help maintain blood pressure andbody temperature, and to protect kidneysfrom myoglobinuria.
CLIENT EDUCATIONIf animal appears blind, sight should return
MEDICATIONSDRUG(S) OF CHOICE� Agitation: ◦ Phenothiazines (acepromazine0.025–0.05 mg/kg IV, titrate up as needed).◦ Cyproheptadine (dog, 1.1 mg/kg; cat, 2–4mg PO q4–6h or can be given rectally ifvomiting). ◦ Benzodiazepines (diazepam0.5–2 mg/kg IV) (see “Precautions”).
� Tremors: methocarbamol (50–150 mg/kgIV, titrate up but do not exceed330 mg/kg/day).
CONTRAINDICATIONS� High risk of serotonin syndrome: otherSSRIs, MAOIs, TCAs, amphetamines,5-HTP, clarithromycin, dextromethorphan,lithium, St. John’s wort. � Low risk ofserotonin syndrome: tramadol, fentanyl,amantadine, bupropion, carbamazepine,codeine.
PRECAUTIONS� Benzodiazepines (e.g., diazepam) arereported by some sources to exacerbateserotonin syndrome and their use for SSRItoxicosis is not universally recommended.
POSSIBLE INTERACTIONS� Decreased metabolism of SSRIs: cimetidine,diuretics, quinidine, lithium. � Increasedlevels of medications (decreased metabolism):theophylline, coumadin, digoxin.
FOLLOW-UPPATIENT MONITORINGBlood pressure, heart rate, urine color:monitor hourly, then less frequently as theanimal remains stable.
PREVENTION/AVOIDANCE� Keep medications out of the reach ofanimals. � Follow label directions when givingserotonergic drugs to animals.
POSSIBLE COMPLICATIONSRenal failure secondary to myoglobinuriafrom rhabdomyolysis. DIC secondary tohyperthermia.
EXPECTED COURSE AND PROGNOSIS� Prognosis is good in most cases, withrecovery in 12–24 hours. � Patients thatpresent in status epilepticus or with severehyperthermia have a guarded prognosis.
MISCELLANEOUSAGE-RELATED FACTORSYoung and elderly animals are more at risk fordeveloping serious toxicosis.
PREGNANCY/FERTILITY/BREEDINGSSRIs can cause increased litter mortality andpossible birth defects.
ABBREVIATIONS� 5-HTP = 5-hydroxytryptophan � MAOI= monoamine oxidase inhibitor � SNRI =serotonin and norepinephrine reuptakeinhibitor � SSRI = selective serotoninreuptake inhibitor � TCA = tricyclicantidepressantAuthor Tina WismerConsulting Editor Gary D. Osweiler
BLBS078-CF_A56b BLBS078-Tilley July 23, 2011 5:15
98 Blackwell’s Five-Minute Veterinary Consult
Antidepressants—Tricyclic ToxicosisA
BASICSDEFINITION� Toxicity secondary to the acute or chronicingestion of a tricyclic antidepressant.� TCA medications include amitriptyline,amozapine, clomipramine, despiramine,doxepin, imipramine, maprotiline (tetracyclicantidepressant), nortriptyline, protriptyline,and trimipramine.
PATHOPHYSIOLOGY� TCAs block the reuptake of norepinephrine,dopamine, and serotonin at the neuronalmembrane. They also have anticholinergicactivity and are thought to have membranestabilizing effects on the myocardium(particularly inhibiting fast sodium channelsin the ventricular myocardium). They canalso have slight alpha-adrenergic blockingactivity and antihistaminic effects.� TCAs are rapidly and well absorbed acrossthe digestive tract. They can decrease GImotility and delay gastric emptying, resultingin delayed drug absorption.� They are lipophilic, protein bound, and welldistributed across all tissues.� They are metabolized by the liver andundergo enterohepatic recirculation. Theinactive metabolites are eliminated in theurine.
SYSTEMS AFFECTED� Cardiovascular—anticholinergic effects andinhibition of norepinephrine reuptakecontribute to tachycardia; alpha adrenergicblockade, cardiac membrane stabilization, anddecreased cardiac contractility contribute tohypotension and arrhythmias.� Gastrointestinal—anticholinergic effectsmay cause ileus and delayed gastric emptying.� Nervous—increased dopamine, serotonin,and norepinephrine levels in the CNScontribute to CNS signs.� Ophthalmic—anticholinergic effects cancause pupillary dilation.� Renal/Urologic—anticholinergic effectsmay cause urinary retention.
GENETICSSpecies and individual differences inabsorption, metabolism, and elimination canbe significant.
INCIDENCE/PREVALENCEIncidence is unknown
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsNone
Mean Age and RangeNone
Predominant SexNone
SIGNSGeneral Comments� Signs can be seen at therapeutic doses.� Signs of toxicity can be seen within 30–60minutes or delayed by several hours.
Historical Findings� Evidence of accidental consumption of theowner’s or another pet’s medication.� CNS depression (lethargy, ataxia).� Vocalization.� Vomiting or hypersalivation.� Panting.� Agitation or restlessness.� Tachypnea or dyspnea.� Tremors.� Seizures.
Physical Examination Findings� CNS depression or stimulation.� Tachycardia.� Mydriasis.� Hypothermia.� Hypertension.� Pallor.� Cyanosis.� Hyperthermia.� Arrhythmias.� Hypotension.� Urinary retention.� Constipation.
CAUSESAccidental exposure, inappropriateadministration, or therapeutic use.
RISK FACTORS� Concurrent use of other antipsychoticmedication� Preexisting cardiac disease
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Toxicity caused by other antipsychoticmedication, stimulant substances (e.g.,amphetamines, cocaine, methylxanthines, orpseudoephedrine) or substances capable ofcausing cardiac arrhythmias (e.g., quinidine,propranolol, albuterol, digoxin).� Non-toxicologic differentials includehyperkalemia, cardiac ischemia,cardiomyopathy, and other diseases of cardiacconduction.
CBC/BIOCHEMISTRY/URINALYSISExpected to be normal
OTHER LABORATORY TESTS� Blood gases—metabolic acidosis may benoted.� OTC urine drug screen for TCAs—can beused to determine if exposure has occurred.� Serum TCA levels—can be used todetermine if exposure has occurred; not usefulin determining degree of toxicity.
IMAGINGN/A
DIAGNOSTIC PROCEDURES� ECG to monitor for arrhythmias� Blood pressure monitoring
PATHOLOGIC FINDINGSNo specific lesions expected
TREATMENTAPPROPRIATE HEALTH CARE� Outpatient—not recommended forsymptomatic patients, patients with cardiacdisease, or patients ingesting greater than atherapeutic dose of TCAs.� Inpatient—asymptomatic:
◦ Decontamination with emesis (less than15 minutes of exposure time), gastric lavagein large exposures, and activated charcoal.◦ Monitor at a clinic for a minimum of6 hours after exposure.
� Inpatient—symptomatic—stabilize thecardiovascular and CNS systems and providesupportive care.
NURSING CARE� Fluid therapy—restore hydration due tovomiting, regulate blood pressure whenhypotension is noted.� Thermoregulation as needed.� Enema with warm water if not defecatingwithin 6–12 hours.
ACTIVITYN/A
DIETNPO if vomiting
CLIENT EDUCATION� With a prescribed TCA, instruct client tomonitor for adverse or idiosyncratic effects,and to stop the medication and contact theclinic if they occur.� Prevent exposure to non-prescribedmedication.
SURGICAL CONSIDERATIONSN/A
MEDICATIONSDRUG(S) OF CHOICEDecontamination� Emesis within 15 minutes of ingestion onlyif asymptomatic; induce emesis with eitherhydrogen peroxide or apomorphine.� Gastric lavage under anesthesia may beconsidered with large exposures.� After emesis (or if > 15 minutes ofexposure), administer activated charcoal(1–2 g/kg PO) with a cathartic such assorbitol (70% sorbitol at 3 ml/kg) or sodiumsulfate (0.25 tsp/5 kg) if no diarrhea.
BLBS078-CF_A56b BLBS078-Tilley July 23, 2011 5:15
Canine and Feline, Fifth Edition 99
(Continued) Antidepressants—Tricyclic Toxicosis A
� Repeat one-half dose of activated charcoalin 4–6 hours if patient is still symptomatic.
Other� Cyproheptadine: dogs, 1.1 mg/kg q6h POor rectally; cats, 2–4 mg/cat q6h PO orrectally; used for treatment of serotoninsyndrome.� Sodium bicarbonate—used to maintainblood pH at 7.55; if not monitoring acid-basestatus, start with 2–3 mEq/kg IV over 15–30minutes in a symptomatic patient.� Diazepam 0.5–1 mg/kg IV, repeat ifnecessary; for agitation or seizures.� Acepromazine 0.02 mg/kg IV, repeat ifnecessary; for agitation or mild hypertension.� Phenobarbital—as needed for seizurecontrol.
CONTRAINDICATIONS� Atropine should not be used because TCAshave anticholinergic effects that areexacerbated by atropine.� Magnesium sulfate should not be used as acathartic. Ileus or reduced GI motility willenhance absorption of magnesium and mayresult in magnesium toxicity.� Beta-blockers (e.g., propranolol, atenolol)should not be used for tachycardia because oftheir potential to exacerbate hypotension.� Do not induce emesis in a patient alreadyshowing clinical signs.
PRECAUTIONSN/A
POSSIBLE INTERACTIONS� TCAs increase risk of hyperthermia,seizures, and death with use of MAOIs.� Sympathomimetic and anticholinergicmedications increase the risk for arrhythmiasor cardiac effects from TCAs.� Levothyroxine increases the risk forarrhythmias when used with TCAs.
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORING� Acid-base status—monitor for acidosis andif implementing sodium bicarbonate therapy.� Blood pressure—monitor untilasymptomatic.� ECG—monitor until asymptomatic.
PREVENTION/AVOIDANCEKeep medications out of reach of pets.
POSSIBLE COMPLICATIONSPulmonary edema can occur secondary toaggressive fluid therapy.
EXPECTED COURSE AND PROGNOSIS� Due to the variable half-lives of the differentTCAs, signs can last 24 hours or longer.� The prognosis is generally good in patientsexhibiting mild to moderate signs.� The prognosis is guarded in patientsexhibiting severe signs such as seizures,arrhythmias, or hypotension that are poorlyresponsive to therapy.
MISCELLANEOUSASSOCIATED CONDITIONSSerotonin syndrome may occur as a result ofTCA ingestion.
AGE-RELATED FACTORSNone
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGTCAs cross the placenta and can be found inbreast milk; the significance of this is notknown at this time.
SEE ALSO� Antidepressants—SSRI Toxicosis� Poisoning (Intoxication)
ABBREVIATIONS� CNS = central nervous system� ECG = electrocardiogram� GI = gastrointestinal� MAOI = monoamine oxidase inhibitor� OTC = over-the-counter� TCA-tricyclic antidepressant
INTERNET RESOURCEShttp://www.aspcapro.org/animal-poison-control-center-articles.php.
Suggested ReadingGwaltney-Brant S. Antidepressants: Tricyclic
antidepressants. In: Plumlee KH, ed.,Clinical Veterinary Toxicology. St. Louis:Mosby, 2004, pp. 286–288.
Johnson LR. Tricyclic antidepressanttoxicosis. Vet Clin North Am Small AnimPract 1990, 20:393–403.
Volmer PA. “Recreational” drugs: Tricyclicantidepressants. In: Peterson ME, TalcottPA, eds., Small Animal Toxicology, 2nd ed.St. Louis: Saunders Elsevier, 2006,pp. 303–306.
Wismer TA. Antidepressant drug overdoses indogs. Vet Med 2000, 95:520–525.
Author Cristine L. HayesConsulting Editor Gary D. Osweiler
BLBS078-CF_A57 BLBS078-Tilley July 15, 2011 8:22
100 Blackwell’s Five-Minute Veterinary Consult
Aortic StenosisA
BASICSDEFINITIONNarrowing of the left ventricular outflowtract, most commonly seen as a congenital orperinatal disease that worsens over the firstyear of life. Defect can be valvular, subvalvular(most common in dogs), or supravalvular(most common in cats). As a congenitalanomaly in dogs, the obstruction is usuallycaused by fibrous tissue proximal to the valve,and the disease is referred to as subaorticstenosis. Less commonly, mitral valvedysplasia may cause SAS by tethering themitral valve to the interventricular septum.
PATHOPHYSIOLOGYMarked aortic obstruction requires an increasein intraventricular pressure to maintainforward blood flow and systemic bloodpressure. Pressure overload leads to myocytehypertrophy and subsequent thickening of theheart walls. Coronary artery disease, relativecardiac ischemia, arrhythmias, aortic or mitralregurgitation, left-sided congestive heartfailure, and diminished systemic blood flowmay result. The mechanism of sudden deathis poorly understood.
SYSTEMS AFFECTED� Cardiovascular—pressure overload of theleft ventricle. � Pulmonary—if pulmonaryedema develops. � Multisystemic signs maydevelop secondary to CHF or low cardiacoutput. Multisystemic signs with bacterialendocarditis.
GENETICSInherited trait in Newfoundland dogs.Polygenic transmission exhibitingpseudodominance; a major dominant genewith modifiers may be involved. Other breedsmay exhibit similar inheritance characteristics.
INCIDENCE/PREVALENCEApproximately 1.5–2/1,000 dogs admitted toveterinary teaching institutions; SAS isprobably the second most common congenitalheart defect in dogs and the most common inlarge breeds. Approximately 0.2/1,000 catsadmitted to veterinary teaching institutions.In one study, aortic stenosis accounted for 6%of congenital cardiac defects in cats.
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsSAS is most common in Newfoundlands,German shepherds, golden retrievers, Bouvierdes Flanders, rottweilers, and boxers.Samoyeds, English bulldogs, and Great Danesalso at higher risk than other breeds; bullterriers predisposed to valvular aortic stenosis,typically with concurrent mitral valvedysplasia. Boxers exhibit a narrower outflowtract than other similarly sized breeds;
differentiation of mild SAS from this breedvariation is problematic.
Mean Age and RangeSAS develops post-natally over the first weeksto months of life; phenotypic development iscomplete by 1 year of age. Onset of clinicalsigns can occur at any age depending on theseverity of obstruction. Signs may be seen onphysical examination without any historicalevidence of disease.
SIGNSHistorical Findings� Related to the severity of obstruction; rangefrom none to CHF, syncope, and suddendeath. � Genetic history of affected littersfrom same sire or bitch.
Physical Examination Findings� Systolic ejection murmur loudest near theleft, fourth intercostal space at the heart baseto costochondral junction, which may radiateto the thoracic inlet, carotid arteries, and, ifvery loud, even to the cranium. Radiation tothe left apex and right cranial thorax iscommon. Murmur intensity is roughlycorrelated with the severity of disease.Murmur may not be present in puppies lessthan 2 months old, becoming moreprominent during the first 6 months of age.� Thrill at the left heart base to costochondraljunction in some animals. � Diastolicmurmur may be heard at the left apex, ifaortic regurgitation develops. � Holosystolicmurmur at the left apex may be present, ifmitral regurgitation develops. � Dyspnea,tachypnea, and crackles with the onset ofleft-sided CHF. � Femoral pulses typicallyweak and late rising (pulsus tardus) withdisease severe enough to affect hemodynamics.� A left ventricular “heave” in animals withleft ventricular hypertrophy. � Arrhythmias.
CAUSES� Congenital or perinatal disease. � Secondaryto bacterial endocarditis of the aortic valve insome dogs. � In cats with hypertrophiccardiomyopathy, functional stenosis (e.g.,muscular or subvalvular) is common butsignificance unknown. � “Dynamic” subaorticstenosis reported in dogs in which muscularhypertrophy can contribute to narrowing ofthe aortic outflow tract. � As a complicationor variant of mitral valve dysplasia.
RISK FACTORS� Familial history of subaortic stenosis.� Aortic endocarditis is predisposed byimmunosuppression, systemic infection,bacteremia, and abnormal intracardiac bloodflow, including congenital SAS.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� A systolic ejection murmur may representan innocent murmur in a young animal,
anemia, pain, fever, excitement. Systolicmurmurs on the left thorax are commonlycaused by patent ductus arteriosus (usually acontinuous murmur, but diastolic componentmay be localized), pulmonic stenosis, mitralregurgitation, ventricular septal defect, atrialseptal defect, or tetralogy of Fallot in dogs.Some of these conditions may coexist withSAS. � Weak pulses may occur with othercardiac conditions that reduce stroke volume(e.g., pulmonic stenosis and cardiomyopathy)or in animals with aortic obstruction distal tothe outflow tract (e.g., aortic coarctation,aortic interruption, and aorticthromboembolism).
CBC/BIOCHEMISTRY/URINALYSISTypically normal
IMAGINGThoracic Radiographic Findings� May be subtle because myocardialhypertrophy from pressure overload may notincrease the size of the cardiac silhouette(concentric hypertrophy). � Left-sided heartenlargement. � Normal lung fields unlessCHF develops, causing pulmonary venousdistention and interstitial or alveolarpulmonary infiltrates. � Mediastinum may bewidened and cranial waist of the cardiacsilhouette filled as a result of post-stenoticdilation of the aorta.
Echocardiographic Findings� Spectrum of findings depending on theseverity of disease; abnormalities may besubtle. � Thickening of the left ventricularwall and interventricular septum. � Echogenicridge and/or gross narrowing of the leftventricular outflow tract may be visibleproximal to the aortic valve in SAS. � Valvularthickening and increased echogenicity forvalvular subaortic stenosis, vegetative lesionswith endocarditis. � The anterior mitral valveleaflet may also be thickened and echogenic.� Post-stenotic dilation of the aorta in someanimals. � Increased echogenicity of themyocardium in some animals, particularly thesubendocardial zone and papillary muscles.� “Premature closure” of the aortic valve oftenseen on M-mode echocardiography.
Doppler Echocardiographic Findings� Elevated peak ejection velocity (i.e., > 2.25m/s), which may be delayed to a later time inejection if severely affected; flow accelerationproximal to the obstruction, and a jet ofturbulent blood flow distal to the valve.� Transvalvular pressure gradient can beestimated from the flow velocity (pressuregradient = 4 × flow velocity squared) withvariable accuracy. Color-flow Doppler allowsdirect visualization of the turbulent jet distalto the obstruction and “flow convergence”proximal. � Effective orifice area is decreased.
Angiocardiographic Findings/CardiacCatheterization� Contrast radiography may show thickeningof the left ventricular wall and septum,
BLBS078-CF_A57 BLBS078-Tilley July 15, 2011 8:22
Canine and Feline, Fifth Edition 101
(Continued) Aortic Stenosis A
narrowing of the left ventricular outflow tractor valve orifice, and post-stenotic dilation ofthe aorta. � Cardiac catheterization allowsdetermination of the transvalvular pressuregradient. Pressure gradient categories of mild(< 50 mm Hg), moderate (50–l75 mm Hg),severe (75–100 mm Hg), and very severe(> 100 mm Hg) are somewhat arbitrary andloosely related to clinical course. Pressuregradients (by catheterization or Dopplerechocardiography) are greater with increasedejection volume and, therefore, must beinterpreted in light of other aspects of cardiacfunction. Anesthesia (cardiac catheterization)may affect gradients. � Elevated leftventricular diastolic pressure may accompanyloss of ventricular compliance, impending orovert CHF. � Angiocardiography and cardiaccatheterization allow characterization ofuncommon types of stenosis includingvalvular, supravalvular, and “tunnel outflowtract” and evaluation of concurrent defects.
DIAGNOSTIC PROCEDURESElectrocardiographic Findings� ECG may show signs of left ventricularhypertrophy (e.g., tall R waves, wide QRScomplexes, and shift in mean electrical axis tothe left). � Slurring of ST segment consistentwith left ventricular hypertrophy or ischemia;ST-segment deviation after mild exercisestrongly suggests coronary insufficiency.� Ventricular tachyarrhythmias may occur inseverely affected cases and are a potential causefor clinical signs and sudden death. Holter24-hour ECG monitoring is appropriate insymptomatic or significantly affected animals.
TREATMENTAPPROPRIATE HEALTH CAREManagement recommendations arecontroversial and vary among experts.Inpatient management appropriate forcomplications including arrhythmias,syncope, and CHF.
ACTIVITYRestrict in animals with more than milddisease. Syncope, collapse, or sudden deathmay be brought on by exertion in animalswith severe disease.
CLIENT EDUCATION� Affected animals should be neutered orotherwise not permitted to breed. � Evaluateclosely related dogs for evidence of clinicaldisease. � Alert owners to potentialcomplications (e.g., sudden death and CHF)in severely affected animals and increased riskfor endocarditis and anesthetic complications.
SURGICAL CONSIDERATIONS� Definitive treatment requires open heartsurgery to resect, repair (valvuloplasty), orreplace (valve replacement) the obstructivelesion. The risk-to-benefit ratio for open
resection of SAS in dogs does not currentlysupport recommendation, and dogs still maydie suddenly after the procedure. � Balloondilation of the outflow tract during cardiaccatheterization results in acute reduction oftransvalvular gradients and improvement ofclinical signs in some symptomatic dogs.However, despite reduction in valve gradient,a small clinical trial failed to demonstratesurvival advantage of this procedure forseverely affected dogs, compared withbeta-blocker (atenolol) therapy alone.
MEDICATIONSDRUG(S) OF CHOICE� Medical management is palliative andempirical; no placebo controlled clinical trialshave been published supporting a specifictreatment. � Beta adrenergic blockers havebeen advocated for dogs with subaorticstenosis with a history of syncope or collapse,a transvalvular pressure gradient > 75 mmHg, or when ventricular arrhythmias orST-segment changes are evident on apost-exercise ECG. Potential benefits includelimitation of myocardial oxygen requirements,protection from ventricular arrhythmias, andslowing of the heart rate. Beta-blockers aregiven to effect. Therapy should be initiatedwith caution at low dosages and titratedupward over days to weeks. Atenolol (dogs,0.5–1.5 mg/kg PO q12h; cats, 6.25 mg/catPO q12–q24h). � Specific treatment forventricular arrhythmias, atrial fibrillation, orleft-sided CHF may also be required.� Affected animals are at risk of developingbacterial endocarditis. Meticulous treatmentof infections is recommended as ischemoprophylaxis for dental or genitourinaryprocedures. � Treatment of dynamic stenosisin cats with hypertrophic cardiomyopathy iscontroversial.
CONTRAINDICATIONSBeta-blockers are contraindicated in animalswith bronchoconstrictive disorders.Continued use in patients with overt CHF iscontroversial.
PRECAUTIONS� Beta-blockers limit the ability of thedysfunctional heart to increase cardiac output.These drugs should be initiated at a lowdosage and gradually titrated upward to avoidiatrogenic complications. � Overzealous useof diuretics or venodilators may cause aprecipitous drop in cardiac output. � Markedreduction of systemic blood pressure by ACEinhibitors, calcium channel blockers, orarteriolar dilators may worsen outflowobstruction or coronary insufficiency.� Digitalis glycosides and positive inotropessuch as pimobendan may exacerbate outflowobstruction or ventricular arrhythmias.� Anesthetic agents and sedatives with marked
hypotensive, arrhythmogenic, or cardiacdepressant side effects should be avoided. Anarcotic (e.g., butorphanol or oxymorphone)with diazepam for sedation can be combinedwith low inspired concentrations of isofluranefor anesthesia if necessary.
ALTERNATIVE DRUG(S)� Metoprolol tartrate (0.5–1 mg/kg POq8–12h for dogs; 2–15 mg/cat PO q8h),cardvedilol (0.5–1.5 mg/kg PO q12h fordogs) are among alternative beta-blockers.� Diltiazem (dogs, 0.5–2 mg/kg PO q8h; cats,7.5–15 mg/cat PO q8h) may have similartheoretical benefits in this disease.
FOLLOW-UPPATIENT MONITORINGMonitor by ECG, thoracic radiography, and2-dimensional and Dopplerechocardiography. Treatment of complications(e.g., CHF and arrhythmias) necessitatescareful monitoring to detect renal/ electrolyte,proarrhythmic, negative inotropic, andhypotensive side effects of drugs.
POSSIBLE COMPLICATIONSCHF, arrhythmias, myocardial infarction,aortic regurgitation, mitral regurgitation,sudden death, bacterial endocarditis.
EXPECTED COURSE AND PROGNOSIS� Mildly affected dogs may live a normallifespan without treatment. � Severe diseasetypically limits longevity due to CHF orsudden death. � CHF, collapse, or syncopesuggests severe disease and an ominousprognosis.
MISCELLANEOUSAGE-RELATED FACTORSMurmur typically not present at birth in SAS;develops in the first weeks to monthspost-natally along with development ofstenotic lesion.
PREGNANCY/FERTILITY/BREEDINGContraindicated
SEE ALSO� Cardiomyopathy, Hypertrophic—Cats� Cardiomyopathy, Hypertrophic—Dogs� Congestive Heart Failure, Left-Sided� Endocarditis, Infective
ABBREVIATIONS� CHF = congestive heart failure � ECG =electrocardiogram � SAS = subaortic stenosisAuthor Donald J. BrownConsulting Editor Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
BLBS078-CF_A58 BLBS078-Tilley July 15, 2011 8:31
102 Blackwell’s Five-Minute Veterinary Consult
Aortic ThromboembolismA
BASICSDEFINITIONAortic thromboembolism results from athrombus or blood clot that is dislodgedwithin the aorta, causing severe ischemia tothe tissues served by that segment of aorta.
PATHOPHYSIOLOGY� ATE is most commonly associated withmyocardial disease in cats, most commonlyhypertrophic cardiomyopathy. It is theorizedthat abnormal blood flow (stasis) and ahypercoagulable state contribute to theformation of a thrombus within the leftatrium. The blood clot is then embolizeddistally to the aorta. The most common siteof embolization is the caudal aortictrifurcation (hind legs). Other less commonsites include the front leg, kidneys,gastrointestinal tract, or cerebrum.� ATE in dogs typically is associated withneoplasia, sepsis, infectious endocarditis,Cushing’s disease, protein-losing nephropathy,or other hypercoagulable states.
SYSTEMS AFFECTED� Cardiovascular—the majority of affectedcats have advanced heart disease and left heartfailure.� Nervous/Musculoskeletal—severe ischemiato the muscles and nerves served by thesegment of occluded aorta causes variable painand paresis. Gait abnormalities or paralysisresults in the leg or legs involved.
GENETICSHypertrophic cardiomyopathy, a commonassociated disease, is likely heritable.Additionally, a family of domestic shorthaircats with remodeled hypertrophiccardiomyopathy who all died of ATE has beenreported.
INCIDENCE/PREVALENCE� Prevalence is not known in the generalpopulation of cats. In two large studies of catswith hypertrophic cardiomyopathy, 12–16%presented with signs of ATE. In tworetrospective studies of cats with ATE,11–25% of cats had previous evidence ofheart disease.� Rare in dogs.
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesCats, rarely dogs
Breed PredilectionsMixed-breed cats are most commonlyaffected. Abyssian, Birman, and ragdollpurebred cats were overrepresented in onestudy.
Mean Age and RangeAge distribution is 1–20 years. The mean ageis approximately 8 years.
Predominant SexMales > females (2:1)
SIGNSHistorical Findings� Acute onset paralysis and pain are the mostcommon complaints.� Lameness or a gait abnormality.� Tachypnea or respiratory distress iscommon.� Vocalization and anxiety are common.� About 15% of cats may vomit prior to ATE.
Physical Examination Findings� Usually paraparesis or paralysis of the rearlegs with signs of lower motor neuron injury.Less commonly, monoparesis of a front leg.� Pain upon palpation of the legs.� Gastrocnemius muscle often becomes firmseveral hours after embolization.� Absent or diminished femoral pulses.� Cyanotic or pale nail beds and foot pads.� Tachypnea or dyspnea.� Hypothermia is common.� Cardiac murmur, arrhythmias, or gallopsound (not always present).
CAUSES� Cardiomyopathy (all types)� Hyperthyroidism� Neoplasia� Sepsis (dogs)� Hyperadrenocorticism (dogs)� Protein-losing nephropathy (dogs)
RISK FACTORSIt is theorized that a markedly enlarged leftatrium, spontaneous echocardiographiccontrast (smoke), or an intracardiac thrombusobserved on an echocardiogram may be riskfactors.
DIAGNOSISDIFFERENTIAL DIAGNOSISHind limb paresis secondary to other causessuch as spinal neoplasia, trauma, myelitis,fibrocartilaginous infarction, or intervertebraldisk protrusion. These conditions resulting inspinal cord injury present with signs of uppermotor neuron disease, whereas ATE patientspresent with signs of lower motor neurondisease.
CBC/BIOCHEMISTRY/URINALYSIS� High creatine kinase as a result of muscleinjury.� High aspartate aminotransferase and alanineaminotransferase as a result of muscle andliver injury.� Hyperglycemia secondary to stress.� Mild increases in blood urea nitrogen andcreatinine due to low cardiac output andpossible renal emboli.
� Electrolyte derangements, due to low outputand muscle damage, such as hypocalcemia,hyponatremia, hyperphosphatemia andhyperkalemia are not uncommon.� CBC and urinalysis changes arenon-specific.
OTHER LABORATORY TESTSRoutinely available coagulation profilestypically do not reveal significantabnormalities because the hypercoagulabilityresults from hyperaggregable platelets.
IMAGINGRadiographic Findings� Cardiomegaly is common in cats.� Pulmonary edema and/or pleural effusion inapproximately 50% of cats.� Rarely, a mass is seen in the lungs,suggestive of neoplasia.
Echocardiographic Findings� Changes consistent with cardiomyopathy.Hypertrophic cardiomyopathy is mostcommon, followed by restrictive orunclassified cardiomyopathy and then dilatedcardiomyopathy.� Most cases (> 50%) have severe left atrialenlargement (i.e., left atrial to aortic ratio of≥2).� A left atrial thrombus or spontaneousechocardiographic contrast (smoke) may beseen.
Abdominal Ultrasonographic Findings� May be able to identify the thrombus in thecaudal aorta.� Typically not necessary to reach a diagnosis.
Angiographic Findings� Non-selective angiography should identify anegative filling defect in the caudal aortarepresenting the thrombus.� Typically not necessary to reach a diagnosis.
DIAGNOSTIC PROCEDURESElectrocardiography� Sinus rhythm and sinus tachycardia mostcommon. Less common rhythms includeatrial fibrillation, ventricular arrhythmias,supraventricular arrhythmias, and sinusbradycardia.� Left ventricular enlargement pattern and leftventricular conduction disturbances (leftanterior fascicular block) are common.
PATHOLOGIC FINDINGS� Thrombus typically is identified at thecaudal aortic trifurcation.� Occasionally, a left atrial thrombus is seen.� Emboli of the kidneys, gastrointestinal tract,cerebrum, and other organs also may be seen.
TREATMENTAPPROPRIATE HEALTH CAREInitially, cats with ATE should be treated asinpatients because many have concurrentcongestive heart failure and require injectable
BLBS078-CF_A58 BLBS078-Tilley July 15, 2011 8:31
Canine and Feline, Fifth Edition 103
(Continued) Aortic Thromboembolism A
drugs, in addition to being in considerablepain and distress.
NURSING CARE� Fluid therapy is cautiously used as most catshave advanced myocardial disease. If incongestive heart failure, IV fluid therapy maynot be necessary.� Supplemental oxygen therapy orthoracocentesis may be beneficial if incongestive heart failure.� Initially, minimally handle the affected legs.However, as reperfusion occurs, physicaltherapy (passive extension and flexion of thelegs) may speed full recovery.� Do not perform venipuncture on theaffected legs.� These cats may have difficulty posturing tourinate and may need to have their bladdersexpressed to prevent overdistention or urinescald.
ACTIVITYRestrict activity and stress
DIETInitially, most cats are anorexic. Tempt thesecats with any type of diet to keep them eatingand avoid hepatic lipidosis.
CLIENT EDUCATION� Short- and long-term prognosis is poor.� Most cats will reembolize. Most cats thatsurvive an initial episode will be on some typeof anticoagulant therapy that may requirefrequent reevaluations and an indoor lifestyle.� Most cats that survive an initial episode willrecover complete function to the legs;however, if ischemia was severe andprolonged, sloughing of parts of the distalextremities or persistent neurological deficitsmay result. In one study, approximately 15%of cats had permanent neuromucscularabnormalities after surviving the initialembolic event.
SURGICAL CONSIDERATIONS� Surgical embolectomy typically is notrecommended because these patients are highrisk for surgery because of severe heart disease.� Rheolytic thrombectomy has been usedwith limited success in a small number of catswith ATE.
MEDICATIONSDRUG(S) OF CHOICE� Thrombolytic therapy such as streptokinase,urokinase, and tissue plasminogen activator isused extensively in humans and infrequentlyin cats. These drugs are expensive and carry asignificant risk for bleeding complications;they have not demonstrated improvedtreatment efficacy and thus are rarely used ingeneral practice.� Unfractionated heparin is the preferred drugin general practice. It has no effect on theestablished clot; however, it prevents further
activation of the coagulation cascade. Give aninitial dose of 100–200 units/kg IV and then200–300 units/kg SC q8h. Alternatively,heparin can be administered as a CRI, if thereis concern about adequate bioavailability viathe SC route, at a dose of 25–35units/kg/hour. Titrate the dose to prolong theactivated partial thromboplastin timeapproximately two-fold.� Aspirin is theoretically beneficial during andafter an episode of thromboembolism becauseof its antiplatelet effects. The dose in cats is an81-mg tablet PO q48–72h. Vomiting anddiarrhea are not uncommon. Some specialistsadvocate a mini dose of 5 mg/cat q72h.Antithrombotic dose recommendations fordogs range from 0.5–2 mg/kg q24h. Alwaysgive aspirin with food.� Clopidogrel is an antiplatelet aggregationdrug. Cat dose is 18.75 mg/cat (one-fourth of75 mg tablet) PO q24h. Dog dose isapproximately 1 mg/kg q24h. Clopidogrelcan be used either in combination or insteadof aspirin.� Buprenorphine is used for analgesia andsedation at a dose of 0.005–0.02 mg/kg IV,SC, or PO q6–8h. For stronger analgesia, usefentanyl or hydromorphone.� Acepromazine may be cautiously used for itssedative and vasodilatory properties at a doseof 0.01–0.02 mg SC q8–12h.� Warfarin, a vitamin K antagonist, is theanticoagulant most widely used in humansand has been proposed for prevention ofreembolization in cats surviving an initialepisode. The initial dose is 0.25–0.5 mg/catPO q24h. Overlap with heparin therapy for3 days. The dose is then adjusted to prolongthe prothrombin time approximately twotimes its baseline value or to attain aninternational normalized ratio of 2 to 4.Long-term management with warfarin can bechallenging because of frequent monitoringand dose adjustments in addition to bleedingcomplications.� Low molecular weight heparin has recentlybeen proposed for the long-term preventionof feline ATE. LMWH has a more predictablerelationship between dose and response thanwarfarin and does not need monitoring ordose adjustments. It also has a lower risk ofbleeding complication. The maindisadvantage of LMWH is high drug cost andthe injectable route of administration. Thetwo LMWHs that have been used in felineATE are: dalteparin (100 units/kg SCq12–24h) and enoxaparin (1 mg/kg SCq12–24h). Best dose unknown. LMWHusually started q24h due to cost. Some studiessuggest q6h dosing necessary for stable bloodlevels, but may increase bleeding risk.
CONTRAINDICATIONSN/A
PRECAUTIONS� Anticoagulant therapy with heparin,warfarin, or the thrombolytic drugs may causebleeding complications.� Avoid a non-selective beta-blocker such aspropranolol as it may enhance peripheralvasoconstriction.
POSSIBLE INTERACTIONSWarfarin may interact with other drugs, whichmay enhance its anticoagulant effects.
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORING� ECG monitoring while the cat is in hospitalis helpful to detect reperfusion injury andhyperkalemia related ECG changes.� Monitoring electrolytes and renalparameters periodically may be helpful tooptimize management of the cardiac disease.� Examine the legs frequently to assess clinicalresponse. Initially, APTT should beperformed once daily to titrate the heparindose.� If warfarin is used, PT or INR is measuredapproximately 3 days after initiation oftherapy and then weekly until the desiredanticoagulant effect is reached. Thereafter,measure three to four times yearly or whendrug regimen is altered.
PREVENTION/AVOIDANCEBecause of the high rate of reembolization,prevention with either aspirin, clopidogrel,warfarin, or LMWH is stronglyrecommended.
POSSIBLE COMPLICATIONS� Bleeding with the anticoagulant therapy.� Permanent neurological deficits or muscularabnormalities in the hind limbs may arisewith prolonged ischemia.� Recurrent congestive heart failure or suddendeath.� Reperfusion injury and death usuallyassociated with hyperkalemic arrhythmias.
EXPECTED COURSE AND PROGNOSIS� Expected course is days to weeks for fullrecovery of function to the legs.� Prognosis in general is poor. In two largestudies, ∼60% of cats were euthanized ordied during the initial thromboembolicepisode. Long-term prognosis varies between2 months to several years; however, theaverage is a few months with treatment.Predictors of poorer prognosis includehypothermia (< 99◦F) and congestive heartfailure. One study demonstrated a mediansurvival time of 77 days in cats withcongestive heart failure and 223 days in catswithout congestive heart failure.
BLBS078-CF_A58 BLBS078-Tilley July 15, 2011 8:31
104 Blackwell’s Five-Minute Veterinary Consult
Aortic Thromboembolism (Continued)A
� Predictors of better prognosis includenormothermia, single leg affected, andpresence of motor function on initial exam.� Recurrence of ATE is common.
MISCELLANEOUSASSOCIATED CONDITIONSSee “Causes” and “Risk Factors”
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMS� Saddle thromboembolism� Systemic thromboembolism
SEE ALSO� Cardiomyopathy, Dilated—Cats� Cardiomyopathy, Hypertrophic—Cats� Cardiomyopathy, Restrictive—Cats
ABBREVIATIONS� APTT = activated partial thromboplastintime� ATE = aortic thromboembolism� CRI = constant rate infusion� ECG = electrocardiogram� INR = international normalized ratio� LMWH = low molecular weight heparin� PT = prothrombin time
Suggested ReadingCole SG, Drobatz KJ. Emergency
management and critical care. In: Tilley LP,Smith FWK, Oyama MA, Sleeper MM,eds., Manual of Canine and FelineCardiology, 4th ed. St. Louis: SaundersElsevier, 2008, pp. 342–355.
Laste NJ, Harpster NK. A retrospective studyof 100 cats with feline distal aorticthromboembolism: 1977–1993. JAAHA1995, 31:492–500.
Smith CE, et al. Use of low molecular weightheparin in cats: 57 cases (1999–2003).JAVMA 2004, 225:1237–1241.
Smith SA. Feline arterial thromboembolism:An update. Vet Clin North Am Small AnimPract 2004, 34:1245–1271.
Smith SA. Arterial thromboembolism in cats:Acute crisis in 127 cases (1992–2001) andlong-term management with low doseaspirin in 24 cases. J Vet Intern Med 2003,17:73–83.
Author Teresa C. DeFrancescoConsulting Editor Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
BLBS078-CF_A59 BLBS078-Tilley March 22, 2011 7:27
Canine and Feline, Fifth Edition 105
Apudoma A
BASICSOVERVIEW� Tumors of endocrine cells that are capableof amine precursor uptake anddecarboxylation and secretion of peptidehormones; the tumors are named after thehormone they secrete.� APUD cells are generally found in thegastrointestinal tract and CNS.� Gastrin- and pancreaticpolypeptide-secreting tumors are discussedhere; insulinoma and glucagonoma arediscussed separately.� Hypergastrinemia from gastrin-secretingtumors causes gastritis and duodenalhyperacidity, which can cause gastriculceration, esophageal dysfunction fromchronic reflux, and intestinal villous atrophy.� High concentration of pancreaticpolypeptide also causes gastric hyperacidityand its consequences.
SIGNALMENT� Gastrinoma—rare in dogs and cats; agerange 3–12 years, mean 7.5 years (dogs).� Pancreatic polypeptide—extremely rare indogs.
SIGNS� Vomiting� Weight loss� Anorexia� Diarrhea� Lethargy, depression� Polydipsia� Melena� Abdominal pain� Hematemesis� Hematochezia� Fever
CAUSES & RISK FACTORSUnknown
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other conditions associated withhypergastrinemia, gastric hyperacidity, andgastrointestinal ulceration.� Uremia.� Hepatic failure,� Drug-induced ulceration (e.g., NSAIDs orsteroids).� Inflammatory gastritis.� Stress-induced ulceration.� Mast cell disease.
CBC/BIOCHEMISTRY/URINALYSIS� Normal or reflect the chronic effects ofgeneral disease.
� Iron-deficiency anemia secondary togastrointestinal bleeding.� Increased BUN secondary togastrointestinal bleeding.� Hypoproteinemia.� Electrolyte abnormalities with chronicvomiting.
OTHER LABORATORY TESTS� Serum gastrin concentration normal orhigh-normal in patients with gastrinoma.� Provocative test of gastrinsecretion—increased gastrin concentrationafter intravenous calcium gluconate or secretinadministration suggests gastrinoma; seeAppendix II for protocol and interpretation.
IMAGINGAbdominal ultrasound sometimesdemonstrates a pancreatic mass but is usuallynormal.
DIAGNOSTIC PROCEDURES� Endoscopy with gastric and duodenalbiopsy.� Aspirate any detectable masses because ofsuspicion of mast cell disease.� If no detectable masses exist, examine abuffy coat smear for mast cells.
PATHOLOGIC FINDINGS� Endoscopic biopsy reveals gastrointestinalulceration.� Histopathologic examination of pancreatictumors reveals findings consistent with isletcell tumor but not specific for hormone type.� Immunocytochemical staining can aid inthe specific diagnosis.� Histopathologic examination also can revealmetastasis to liver and regional lymph nodes.
TREATMENT� Tell owner that most APUDomas aremalignant and have metastasized by the timeof diagnosis and that long-term control isoften difficult.� Aggressive medical management cansometimes palliate signs for months to years.� Surgical exploration and excisional biopsy ofa pancreatic mass are important bothdiagnostically and therapeutically.� Medical management is useful for gastrichyperacidity.
MEDICATIONSDRUG(S)� Histamine H2-receptorantagonists—cimetidine, ranitidine, andfamotidine; decrease acid secretion by gastricparietal cells.
� Omeprazole—a proton pump inhibitor; themost potent inhibitor of gastric acid secretionavailable; highly effective and expensive.� Sucralfate—adheres to ulcerated gastricmucosa and protects it from acid; promoteshealing by binding pepsin and bile acids andstimulating local prostaglandins.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSBecause sucralfate may be less effective in analkaline environment, and may reduce theabsorption of other drugs, it should be given1–2 hours prior to antacid drugs.
FOLLOW-UPPATIENT MONITORING� Physical examination and clinical signs arethe most useful measures of treatmenteffectiveness and disease progression.� Gastroscopy can monitor progression ofgastritis but is not necessary.� Abdominal radiography or ultrasound maydetect development of abdominal masses.
EXPECTED COURSE AND PROGNOSIS� Difficult to predict� Patients with gastrinoma have beencontrolled on medical management formonths to years.� No cure available.
MISCELLANEOUSSEE ALSOGastroduodenal Ulcer Disease
ABBREVIATIONS� APUD = amine precursor uptake anddecarboxylation� CNS = central nervous system� NSAID = nonsteroidal anti-inflammatorydrug
Suggested ReadingLurye JC, Behrend EN. Endocrine tumors.
Vet Clin North Am Small Anim Pract 2001,31(5):1083–1110, ix–x.
Zerbe CA. Islet cell tumors secreting insulin,pancreatic polypeptide, gastrin, or glucagon.In: Kirk RW, Bonagura JD, eds., CurrentVeterinary Therapy XI. Philadelphia:Saunders, 1992, pp. 368–375.
Author Thomas K. GravesConsulting Editor Deborah S. Greco
BLBS078-CF_A60 BLBS078-Tilley March 22, 2011 7:28
106 Blackwell’s Five-Minute Veterinary Consult
Arsenic PoisoningA
BASICSOVERVIEW� Caused by herbicides, insecticides, woodpreservatives, and treatments for bloodparasites.� Leads to disruption of many importantmetabolic reactions.� Exposure—oral most common;percutaneous exposure may cause systemictoxicosis.
SIGNALMENT� Cats and dogs� Any breed, age, or sex
SIGNSAcute Exposure� Abdominal pain� Vomiting� Weakness� Diarrhea� Hematochezia� Rapid weak pulse� Prostration� Subnormal temperature� Collapse� Death
Subchronic to Chronic Oral Exposure� Anorexia� Weight loss
CAUSES & RISK FACTORS� Oral, percutaneous, or therapeutic exposureto arsenic-containing compounds.� Toxicity varies greatly.� Weak and debilitated animals moresusceptible.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Heavy metal toxicosis� Ingestion of caustic agents� Ingestion of irritating plants� Canine or feline parvovirus
CBC/BIOCHEMISTRY/URINALYSISSerum biochemical analysis—evidence of liverand renal damage.
OTHER LABORATORY TESTSArsenic concentration—test urine, vomitus,or stomach contents (acute poisoning),kidney, liver (subacute), hair (chronic);decreases dramatically in urine, kidney, andliver 1–2 days after exposure; unreliable inblood.
IMAGINGN/A
DIAGNOSTIC PROCEDURESN/A
PATHOLOGIC FINDINGS� Peracute poisoning—death without lesions.� Gastrointestinal tract lesions—common andsevere; reddening of the gastric mucosa andproximal small intestine; waterygastrointestinal content; blood and sloughedmucosa in feces.� Liver—soft, yellow liver.� Lungs—congested; edematous.� Skin lesions (cutaneousexposure)—blistering; edema; cracking;bleeding; secondary infections.
TREATMENT� Remove arsenic source.� Emetics followed by gastric lavage—ifvomiting has not occurred.� Promote excretion.� Dialysis in cases of renal failure.� Appropriate fluid therapy.� Kaolin-pectin soothes gastrointestinal tract.� Keep patient warm and comfortable.
DIETWhen patient is able to keep food down,provide small amounts of high-quality food;increase as tolerated.
MEDICATIONSDRUG(S)Dimercaprol(BAL)� Give 2.5–5 mg/kg in oil by deep IMinjection q4h for 2 days; q8h on day 3; q12hfor up to 10 days; 5 mg/kg in only acutelyaffected patients on day 1.
� Signs of toxicosis (pain at injection site,vomiting, tremors, convulsions) subside asBAL is excreted over 3–4 hours.� Releases arsenic, which may worsen signs;give additional BAL.
Other DrugsDMSA (succimer)—less toxic than BAL;effective oral treatment for lead poisoning insmall animals. Potentially useful for arsenicpoisoning but controlled studies for treatmentof arsenic-poisoned dogs and cats not foundin the literature.
FOLLOW-UP� Prognosis is grave with high-dose exposure,unless the diagnosis is made and treatment isstarted early.� Monitor closely for signs of BAL toxicosis.
MISCELLANEOUSSEE ALSOPoisoning (Intoxication)
ABBREVIATIONS� BAL = British anti-Lewisite� DMSA = 2,3-dimercaptosuccinic acid
Suggested ReadingGarland T. Arsenic. In: Gupta RC, ed.,
Veterinary Toxicology: Basic and ClinicalPrinciples. New York: Academic Press,2007, pp. 418–421.
National Research Council. Arsenic. In:Mineral Tolerance of Animals, 2nd ed.Washington, DC: National AcademiesPress, 2005, pp. 31–45.
Neiger RD. Arsenic. In: Peterson ME, TalcottPA, eds., Small Animal Toxicology, 2nd ed.Philadelphia: Saunders, 2006, pp. 592–602.
Author Regg D. NeigerConsulting Editor Gary D. Osweiler
BLBS078-CF_A61 BLBS078-Tilley March 22, 2011 7:29
Canine and Feline, Fifth Edition 107
Arteriovenous Fistula A
BASICSOVERVIEWAn abnormal, low-resistance connectionbetween an artery and vein. A largearteriovenous fistula allows a significantfraction of the total cardiac output to bypassthe capillary bed. The resulting increase incardiac output may lead to (high-output)congestive heart failure. Location ofarteriovenous fistula varies. Reported sitesinclude the head, neck, ear, tongue, limbs,flank, spinal cord, cerebrum, lung, liver, venacava, and gastrointestinal tract. Usually seenas an acquired lesion.
SIGNALMENT� Dogs and cats (rare in both)� No specific age, breed, or sex predilectionsknown
SIGNSHistorical Findings� Animals with acquired disease often have ahistory of trauma to the affected area.� Owner may notice a warm, non-painfulswelling at the site.� History consistent with impending or overtCHF is possible depending on shunt size andduration.� Other historical findings depend on thelocation of the lesion.� The shunt may cause local organdysfunction.
Physical Examination Findings� Vary and depend on location of thearteriovenous fistula.� Signs of CHF (e.g., coughing, dyspnea,tachypnea, and exercise intolerance) maydevelop in animals with long-standing diseaseand high blood flow.� Bounding pulses are present in someanimals because of high ejection volume andrapid runoff through the arteriovenous fistula.� Continuous murmur (bruit) at the sitecaused by blood flow through the lesion.� Cautious compression of the arteryproximal to the lesion abolishes the bruit.When blood flow is high, this compressionmay also elicit an immediate reflex decrease inheart rate (Branham’s sign).� Edema, ischemia, and congestion of organsand tissues caused by high venous pressure inthe proximity of the lesion.� If the lesion is on a limb, pitting edema,lameness, ulceration, scabbing, and gangrenemay result.� Lesion near vital organs may cause signsassociated with organ failure such as ascites
(liver), seizures (brain), paresis (spinal cord),and dyspnea (lung).
CAUSES & RISK FACTORS� Rarely, a congenital lesion.� Acquired arteriovenous fistula typicallyresults from local damage to vasculaturesecondary to trauma, surgery, venipuncture,perivascular injection (e.g., barbiturates), ortumor.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� The lesion may look like an aneurysm orfalse aneurysm.� Bizarre clinical findings, depending onlocation of arteriovenous fistula, may suggestother disease processes; arteriovenous fistulamay be a late diagnostic consideration.
CBC/BIOCHEMISTRY/URINALYSISMay reflect damage to systems in the vicinityof the lesion, i.e., biochemical abnormalitiessuggesting hepatic, renal, or other organdysfunction are possible.
OTHER LABORATORY TESTSN/A
IMAGINGThoracic Radiographic Findings� Cardiac enlargement and pulmonaryovercirculation in some animals withhemodynamically significant arteriovenousfistula.
Echocardiographic Findings� May allow imaging of the arteriovenousfistula depicting its cavernous nature.� Doppler ultrasound may demonstratehigh-velocity, turbulent flow within the lesion.
Angiography� Selective angiography outlines the lesion,may be necessary for definitive diagnosis, andis highly desirable for presurgical evaluation.Placement of the catheter close to the lesionand rapid injection is necessary; high-volumeblood flow dilutes the contrast mediumquickly.
DIAGNOSTIC PROCEDURESN/A
TREATMENT� Historically definitive treatment hasrequired surgery to divide and removeabnormal vascular connections. Definitivetreatment is recommended in animals with
clinical signs related to the arteriovenousfistula, since lesions may increase in size.� Surgery can be difficult and labor-intensiveand may require blood transfusion;delineation of lesion before surgery byangiography is advised.� Although surgery is often successful,arteriovenous fistula may recur. In someanimals, amputation of the affected part maybe necessary.� Transcatheter embolization withvaso-occlusive coils is a newer treatmentoption. Potential advantages include relativelynon-invasive treatment and intravascularaccess to remote lesions.
MEDICATIONSDRUG(S)� Concurrent medical treatment depends onthe site of the arteriovenous fistula andsecondary clinical features.� Medical treatment for congestive heartfailure may be required before surgery.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSAvoid excessive fluid administration; animalswith arteriovenous fistula are volumeoverloaded.
FOLLOW-UPPost-operative reevaluation is needed todetermine whether arteriovenous fistularecurred.
MISCELLANEOUSSEE ALSOCongestive Heart Failure, Left-Sided
ABBREVIATIONSCHF = congestive heart failure
Suggested ReadingFox PR, Petrie J-P, Hohenhaus AE. Peripheral
vascular disease. In: Ettinger SJ, FeldmanEC, eds., Textbook of Veterinary InternalMedicine, 6th ed. St. Louis: Elsevier, 2005.
Author Donald J. BrownConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
BLBS078-CF_A62 BLBS078-Tilley March 22, 2011 7:31
108 Blackwell’s Five-Minute Veterinary Consult
Arteriovenous Malformation of the LiverA
BASICSOVERVIEW� Intrahepatic arteriovenous fistulae arecommunications between proper hepaticarteries and intrahepatic portal veins thatimpose hepatofugal splanchnic circulation.� Blood flows from the hepatic artery to theportal system retrograde into the vena cavathrough multiple APSS.� AV fistulae are uncommon, usuallycongenital, but may be acquired (surgicalinjury, trauma, neoplasia).
SIGNALMENT� Dogs, less common in cats� Age-related presentation (congenital):< 2 yrs� No sex or breed predilection
SIGNSGeneral Comments� Vague or acute illness; present for signs ofportal hypertension and APSS: ascites, HE.
Historical Findings� Dogs may have a normal transition togrowth foods, unlike PSVA that demonstrateHE.� Acute onset of ascites or HE.� Lethargy, anorexia, vomiting, diarrhea,weight loss, polydipsia, dementia, abdominaldistention.
Physical Examination Findings� Lethargic, poor body condition, ascites;enlarged liver segment containing AVfistula(e) rarely palpated.� Hepatic bruit rarely auscultated.
CAUSES & RISK FACTORS� Usually reflect congenital vascularmalformations (single or multiple vessels)reflecting failed differentiation of commonembryologic anlage.� Rarely secondary to abdominal trauma,inflammation, neoplasia, surgicalinterventions, or diagnostic procedures (e.g.,liver biopsy).� Portal hypertension establishes APSS.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� CNS signs—infectious disorders (e.g.,distemper); toxicity (e.g., lead);hydrocephalus; idiopathic epilepsy; metabolicdisorders (e.g., hypoglycemia,hypo-/hyperkalemia); HE (e.g., acquired liverdisease or PSVA).
� Abdominal effusion—pure transudate(ascites; protein-losing nephropathy,protein-losing enteropathy, liver disease);modified transudate (congenital cardiacmalformations, right-sided heart failure,pericardial tamponade, supradiaphragmaticvena caval obstruction, neoplasia, portal veinthrombosis); hemorrhage.� Portal hypertension—chronic hepaticdisease, juvenile fibrosing liver disease,non-cirrhotic or idiopathic portalhypertension, cirrhosis, portal thrombi.
CBC/BIOCHEMISTRY/URINALYSIS� Erythrocyte microcytosis (APSS), targetcells.� Hypoalbuminemia, serum globulin normalor low; ALP and ALT activity normal ormoderately increased; variable low BUN andhypocholesterolemia.� Hyposthenuria or isosthenuria.� Ammonium biurate crystalluria.
OTHER LABORATORY TESTS� Coagulation tests—variable abnormalitiesbut may be normal; low protein C.� Peritoneal fluid—pure transudate (totalprotein < 2.5 g/dL) or modified transudate.� Total serum bile acids—fasting valuesusually high; post-prandial values always high;shunting pattern.� Plasma ammonia—usually high.
IMAGINGRadiography� Abdominal effusion.� Microhepatica or normal size due to largeliver lobe associated with AV fistulae.� Renomegaly.
Abdominal Ultrasonography� Abdominal effusion.� Liver lobe with AV fistula—large comparedto most other lobes that are atrophied due toportal hypoperfusion.� Tortuous anechoic tubular structures (AVfistulae) with unidirectional pulsating orturbulent flow with color-flow Doppler.� Hepatic artery and/or portal vein branchesmay appear tortuous.� Hepatofugal portal flow through APSS.� Renomegaly.� Calculi or sand-like uroliths: urinarybladder or renal pelvis.� Rule out portal thrombosis.
Radiographic Contrast Angiography� Not indicated in most cases.� Venous portography—confirms APSS.� Hepatic arteriography—required todemonstrate AV communication (celiac trunkor anterior mesenteric artery contrastinjection).
Multi-Sector CT� Non-invasive contrast imaging of hepaticvasculature; 3-dimensional reconstructionillustrates malformation.
Echocardiography� Rule out right-sided heart disease,pericardial disease, and vena caval occlusion.
DIAGNOSTIC PROCEDURES� Exploratory laparotomy for lobectomy/AVfistula resection.� Liver biopsy—collect samples from affectedand unaffected liver lobes; “normal” liveroften has severe vascular arterialization (moresevere than associated with PSVA ornon-cirrhotic portal hypertension).
TREATMENTAPPROPRIATE HEALTH CAREInpatient for HE and treatment of ascitesprior to surgical AV fistula resection orpercutaneous selective embolization.
NURSING CARE� Diet—restrict nitrogen intake to ameliorateHE and hyperammonemia; restrict sodium(ascites).� HE—resolve endoparasitism and electrolyteand hydration disturbances, treat infections,initiate treatments to alter enteric uptake andformation of HE toxins (see HepaticEncephalopathy).� Ascites—mobilize by restricting activity andsodium intake; abdominocentesis for tenseascites impairing ventilation or nutrition; andcombined use of furosemide andspironolactone (see Hypertension, Portal andbelow).
SURGICAL CONSIDERATIONS� Resection of liver lobe containing AV fistulais complicated by other vascular malformationwithin the liver; recurrent illness may occur;percutaneous selective acrylamide vascularembolization may result inthromboembolism, improvement (may betemporary), or continued clinical signs.� Multiple microscopic vascularmalformations continue portal hypertensionand APSS.� Do not ligate APSS nor band the vena cava.
MEDICATIONSDRUG(S)Hepatic EncephalopathySee Hepatic Encephalopathy
BLBS078-CF_A62 BLBS078-Tilley March 22, 2011 7:31
Canine and Feline, Fifth Edition 109
(Continued) Arteriovenous Malformation of the Liver A
Ascites� Furosemide (0.5–2 mg/kg PO IM or IVq12–24h)—best used combined withspironolactone.� Spironolactone (0.5–2 mg/kg POq12h)—initiate double dose as loading doseone time.� Chronic diuretic therapy individualized toresponse, 4- to 7-day intervals.� Diuretic resistant ascites may requiretherapeutic abdominocentesis to initiatediuresis or use of vasopressin V2 receptorantagonist.
Bleeding TendenciesSee Coagulopathy of Liver Disease
Gastrointestinal Hemorrhage� Histamine type-2 receptor antagonists(famotidine 0.5 mg/kg PO, IV, or SCq12–24h); give indefinitely, GI bleeding andulceration are common, long-term problems.� Gastroprotectant—sucralfate 0.25-0.5 g/10 kg PO q8–12h.� Eliminate endoparasitism.
CONTRAINDICATIONSAvoid drugs that rely on hepaticbiotransformation and drugs that react withGABA-benzodiazepine receptors.
FOLLOW-UPPATIENT MONITORINGBiochemistry—initially bimonthly tomonthly until stabilized, thereafter quarterly;monitor for hypoalbuminemia, infection, andoptimal management of HE.
EXPECTED COURSE AND PROGNOSIS� Prognosis fair if patient survives surgicalresection of AV fistula.� Most patients require indefinite nutritionaland medical management (HE, ascites)because of co-existing microscopic vascularlesions (all liver lobes); APSS persistsrequiring continued management of HE.
MISCELLANEOUSSEE ALSO� Ascites� Hepatic Encephalopathy� Hypertension, Portal� Portosystemic Shunting, Acquired� Portosystemic Vascular Anomaly,Congenital
ABBREVIATIONS� ALP = alkaline phosphatase� ALT = alanine aminotransferase� APSS = acquired portosystemic shunt� AV = atrioventricular� CNS = central nervous system� CT = computed tomography� GABA = gamma-aminobutyric acid� GI = gastrointestinal� HE = hepatic encephalopathy� PSVA = portosystemic vascular anomaliesAuthor Sharon A. CenterConsulting Editor Sharon A. Center
BLBS078-CF_A63 BLBS078-Tilley March 22, 2011 7:32
110 Blackwell’s Five-Minute Veterinary Consult
Arthritis (Osteoarthritis)A
BASICSDEFINITIONOsteoarthritis or degenerative joint disease isthe progressive and permanent deteriorationof the articular cartilage of diarthrodial(synovial) joints due to primary (idiopathic)and secondary causes.
PATHOPHYSIOLOGY� DJD is initiated by mechanicalstress—traumatic injury, instability, abnormalconformation, abnormal activity, etc.� Metalloproteinases, serine proteases, andcysteine protease enzymes are released fromdamaged chondrocytes, causing collagendegradation and loss of collagen cross-linkingin cartilage. � Collagen synthesis is altered,resulting in decreased collagen/proteoglycaninteraction and reduced hydrophyllic matrixproperties. � Cartilage matrix is furthercompromised by increased breakdown ofPGAs and manufacture of poorer-qualityPGAs. � Nitric oxide is released, whichmediates cartilage breakdown and supportschronic inflammation. Chondrocyteapoptosis is facilitated by cyclooxygenase-2enzymes. � Synovial membrane inflammationresults in decreased viscosity of the synovialfluid, reducing lubrication. � Poorer-qualitysynovial fluid reduces oxygen and nutrientsupply to the chondrocytes. � Subchondralbone becomes sclerotic, worsening loadingqualities of the bone and overlying cartilage.� Pain of DJD results from stimulation ofpain receptors in the tendons, ligament,subchondral bone, and joint capsule. � Theresult of these processes is progressive cartilagedegradation ranging from fibrillation to deepfissuring of cartilage. Full-thickness cartilageloss can eventually occur. � Peri-articularfibrosis occurs to reduce joint motion (andpain), leading to poorer vascularity of thesynovial membrane. � Osteophytes andenthesiophytes develop around and within thejoint to increase the load-bearing surface area.� These changes reduce functionality andeventually lead to ankylosis.
SYSTEMS AFFECTEDMusculoskeletal—diarthrodial joints
GENETICS� Primary DJD is rare—once associated witha colony of beagles. � Dogs—causes ofsecondary DJD are varied, including hip andelbow dysplasias, osteochondrosis dissecans,patellar luxations, congenital shoulderluxation, Legg-Perthes, and cranial cruciateligament rupture. � Cats—causes ofsecondary DJD are patellar luxation, hipdysplasia, and arthropathy.
INCIDENCE/PREVALENCE� Dogs—very common; 20% of dogs olderthan 1 year have some degree of DJD.� Cats—90% of cats over 12 years of age had
evidence of DJD on radiographs. � Clinicalproblems are more prevalent in larger,overweight, and very active animals.� Primary DJD is rare.
SIGNALMENTSpeciesDogs and cats
Mean Age and Range� Secondary DJD due to congenital disorders(OCD, hip dysplasia) seen in immatureanimals; some present with DJD signs whenolder (hip and elbow dysplasia). � Secondaryto trauma—any age.
SIGNSHistorical Findings� Dogs—decreased activity level, unwilling toperform certain tasks; intermittent lamenessor stiff gait that slowly progresses; possiblehistory of joint trauma, OCD, ordevelopmental disorders; may be exacerbatedby exercise, long periods of recumbency, andcold weather. � Cats—overt lameness may notbe seen. May have difficulty grooming,jumping onto furniture, or accessing the litterbox; increased irritability.
Physical Examination Findings� Stiff-legged or altered gait (e.g., bunnyhopping in hip dysplasia) or non-use of leg.� Decreased range of motion. � Crepitus.� Joint swelling (effusion and/or thickening ofthe joint capsule). � Joint pain. � Jointinstability. � Gross joint deformity.
CAUSES� Primary—no known cause.� Secondary—results from an initiatingcause: abnormal wear on normal cartilage(e.g., joint instability, joint incongruity,trauma to cartilage or supporting soft tissues)or normal wear on abnormal cartilage (e.g.,osteochondral defects).
RISK FACTORS� Working, athletic, and obese dogs placemore stress on their joints. � Dogs withdisorders that affect collagen or cartilage(Cushing’s disease, diabetes mellitus,hypothyroidism, hyperlaxity, prolonged,steroids).
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Neoplastic (synovial cell sarcoma; rarely,chondrosarcoma; osteosarcoma). � Septicarthritis (caused by bacteria; spirochetes; Lforms in cats; Mycoplasma; Rickettsia;Ehrlichia; viruses, such as feline calicivirus;fungi, and protozoa). � Immune-mediatedarthritis (erosive vs. non-erosive).
OTHER LABORATORY TESTS� Coombs’ test, ANA, and rheumatoid factormay help to rule out immune-mediatedarthritis. � Serum titers for Borrelia, Ehrlichia,
and Rickettsia to evaluate for infectiousarthritis.
IMAGING� Radiographic changes—include jointcapsular distention, osteophytosis,enthesiophytosis, soft-tissue thickening, andnarrowed joint spaces; in severely affectedpatients: subchondral sclerosis, subchondralbone cysts, attrition of subchondral bone,mineralization of joint soft tissues, andintra-articular calcified bodies (joint mice).� Radiographic severity often does notcorrelate with clinical severity. � Stressradiography may identify underlyinginstability and accentuate joint incongruity(e.g., distraction index, passive hip laxity ofthe coxofemoral joint is predictive of hipDJD). � Bone nuclear scintigraphy can assistin localizing subtle DJD.
DIAGNOSTIC PROCEDURES� Arthrocentesis and synovial fluidanalysis—cell counts are normal or slightlyincreased (< 2,000–5,000 cells/mL)predominantly mononuclear (macrophages)and occasional synovial lining cells.� Bacterial culture of synovial fluid—negative.� Biopsy of synovial tissue to rule outneoplasia or immune-mediated arthridites(lymphocytic plasmacytic synovitis, SLE).� Force plate analysis or static load bearingallows quantification of reduced limb loading.
PATHOLOGIC FINDINGS� Fibrillation or erosion of articular cartilage.� Eburnation and sclerosis of subchondralbone. � Thickening and fibrosis of the jointcapsule. � Synovial fluid can be grosslynormal to thin and watery, usually increasedvolume. � Synovial villous hypertrophy andhyperplasia. � Osteophytes andenthesiophytes at joint capsule attachmentsand adjacent to the joint.� Neovascularization or pannus in severe casesover joint surfaces.
TREATMENTAPPROPRIATE HEALTH CARE� Medical—usually tried initially. � Surgicaloptions—to improve joint geometry orremove bone-on-bone contact areas.
NURSING CARE� Physical therapy—very beneficial.� Maintaining or increasing jointmotion—passive range of motion exercises,massage, cavaletti, swimming. � Painmanagement—cold and heat therapy.� Muscle tone/strengthening—swimming(aerobic exercise with minimal weightbearing); controlled leash walks up hills or onsoft surfaces, such as sand or dry orunderwater treadmill.
BLBS078-CF_A63 BLBS078-Tilley March 22, 2011 7:32
Canine and Feline, Fifth Edition 111
(Continued) Arthritis (Osteoarthritis) A
ACTIVITYLimited to a level that minimizes aggravationof clinical signs
DIET� Weight reduction for obesepatients—decreases stress placed on arthriticjoints. � Omega n-6 and n-3 fatty acidsdecrease the production of certainprostaglandins and modulate inflammation.
CLIENT EDUCATION� Medical therapy is palliative and thecondition is likely to progress. � Discusstreatment options, activity level, and diet.
SURGICAL CONSIDERATIONS� Arthrotomy—used to remove aggravatingcauses (e.g., fragmented coronoid process,un-united anconeal process, osteochondralflaps). � Arthroscopy—used to diagnose andremove aggravating causes; flushing the jointmay be beneficial. � Reconstructiveprocedures—used to eliminate jointinstability and correct anatomic problems(patella luxation, angular deformity). � Jointremoval—femoral head and neck ostectomy,temperomandibular joint arthroplasty. � Jointreplacement—total hip replacement is widelyused, total elbow replacement stillexperimental. � Joint fusion (arthrodesis)—inselected chronic cases and for joint instability,complete or partial; carpus: generally excellentoutcome; shoulder, elbow, stifle, hock: lesspredictable outcome.
MEDICATIONSDRUG(S) OF CHOICENSAIDs� Inhibit prostaglandin synthesis throughcyclooxygenase enzymes. � Deracoxib (3–4mg/kg PO q24h, chewable). � Carprofen (2.2mg/kg PO q12h or q24h). � Etodolac (10–15mg/kg PO q24h). � Meloxicam (load 0.2mg/kg PO, then 0.1 mg/kg PO q24h: liquid).� Tepoxalin (load 20 mg/kg, then 10 mg/kgPO q24h). � Cats—meloxicam (0.1 mg/kgPO q24h: liquid).
Chondroprotective/RegenerativeSupplements� Supply PSGAG molecules to repair andregenerate cartilage. � Host of products, manywith little production oversight so effects varywidely. � Glucosamine and chondroitinsulphate—injectable Adequan, oral Cosequin,oral MSM, mixtures (Glycoflex II, SynFlex,etc.). � Adequan—clinical study in dogs withhip dysplasiam; 4.4 mg/kg IM every 3–5 daysfor 8 injections had a positive, temporaryeffect. � Cosequin—trials showed positiveeffects.
CONTRAINDICATIONS� NSAIDs must not be given with steroids� Acetaminophen must not be given to cats
PRECAUTIONS� NSAIDs—may cause gastric ulceration.� COX-2 selective drugs may interfere withliver function. � When switchingNSAIDs—wait 3 days for washout beforestarting new drug.
POSSIBLE INTERACTIONSSteroids and NSAIDS
ALTERNATIVE DRUG(S)� Free-radical scavengers.� Glucocorticoids—inhibit inflammatorymediators and cytokines; however, chronicuse delays healing and initiates damage toarticular cartilage; potential systemic sideeffects documented; goal is low-dose (dogs,0.5–2 mg/kg; cats, 2–4 mg/kg), alternate-daytherapy. � Prednisone—initial dose 1–2mg/kg PO q24h for dogs and 4 mg/kg POq24h for cats. � Triamcinolonehexacetonide—intra-articular injection of5 mg in dogs showed a protective andtherapeutic effect in one model.
FOLLOW-UPPATIENT MONITORINGClinical deterioration—indicates need tochange drug selection or dosage; may indicateneed for surgical intervention.
PREVENTION/AVOIDANCEEarly identification of predisposing causes andprompt treatment to help reduce progressionof secondary conditions, e.g., surgical removalof osteochondral lesions.
EXPECTED COURSE AND PROGNOSIS� Slow progression of disease likely. � Someform of medical or surgical treatment usuallyallows a good quality of life.
MISCELLANEOUSSYNONYMS� Degenerative arthritis � Degenerative jointdisease � Osteoarthritis � Osteoarthrosis
ABBREVIATIONS� ANA = antinuclear antibody � COX-2 =cyclooxygenase-2 � DJD = degenerative jointdisease � OCD = osteochondrodysplasia� PGA = proteoglycan � PSGAGs =polysulfated glycosaminoglycans � NSAID =nonsteroidal anti-inflammatory drug � SLE =systemic lupus erythematosus
Suggested ReadingAragon CL, Hofmeister EH, Budsberg SC.
Systematic review of clinical trials oftreatments for osteoarthritis in dogs.JAVMA 2007, 230(4):514–521.
Baime MJ. Glucosamine and chondroitinsulphate did not improve pain inosteoarthritis of the knee. Evid Based Med2006, 11(4):115.
Beale BS, Goring RL. Degenerative jointdisease. In: Bojrab MJ, ed., DiseaseMechanisms in Small Animal Surgery.Philadelphia: Febiger, 1993, pp. 727–736.
Budsberg SC, Bartges JW. Nutrition andosteoarthritis in dogs: Does it help? VetClin North Am Small Anim Pract 2006,36(6):1307–1323.
Glass GG. Osteoarthritis. Dis Mon 2006,52(9):343–362 (human review).
Hampton T. Efficacy still uncertain for widelyused supplements for arthritis. JAMA 2007297(4):351–352.
Herrero-Beaumont G, Ivorra JA, et al.Glucosamine sulfate in the treatment ofknee osteoarthritis symptoms: Arandomized, double-blind,placebo-controlled study usingacetaminophen as a side comparator.Arthritis Rheum 2007, 56(2):555–567.
Johnston SJ. Osteoarthritis joint anatomy,physiology and pathobiology. Vet ClinNorth Am 1997, 27:699–723.
Mlacnik E, Bockstahler BA, Muller M,Tetrick MA, Nap RC, Zentek J. Effects ofcaloric restriction and a moderate or intensephysiotherapy program for treatment oflameness in overweight dogs withosteoarthritis. JAVMA 2006,229(11):1756–1760.
Pederson NC. Joint diseases of dogs and cats.In: Ettinger SJ, ed., Textbook of VeterinaryInternal Medicine, 5th ed. Philadelphia:Saunders, 2000, pp. 1862–1886.
Van Der Kraan PM, Van Den Berg WB.Osteophytes: Relevance and biology.Osteoarthritis Cartilage 2007,15(3):237–244.
Author Peter K. ShiresConsulting Editors Peter K. ShiresAcknowledgement The author and editorsacknowledge the contributions of Brian S.Beale and Jennifer J. Warnock in an earlieredition.
Client Education Handoutavailable online
BLBS078-CF_A64 BLBS078-Tilley July 15, 2011 9:33
112 Blackwell’s Five-Minute Veterinary Consult
Arthritis, SepticA
BASICSDEFINITIONPathogenic microorganisms within the closedspace of one or more synovial joints.
PATHOPHYSIOLOGY� Usually caused by contamination associatedwith traumatic injury (e.g., a directpenetrating injury such as a bite, gunshotwound, or foreign object); a sequela tosurgery, arthrocentesis, or joint injection;hematogenous spread of microorganismsfrom a distant septic focus; or the extension ofprimary osteomyelitis.� Primary sources of hematogenousinfection—urogenital, integumentary(including ears and anal sacs), respiratory,cardiac, and gastrointestinal systems.
SYSTEMS AFFECTEDMusculoskeletal—usually affects one joint
GENETICSN/A
INCIDENCE/PREVALENCERelatively uncommon cause of monoarticulararthritis in dogs and cats.
GEOGRAPHIC DISTRIBUTIONMay be an increased incidence in Lymedisease-endemic areas.
SIGNALMENTSpecies� Most common in dogs� Rare in cats
Breed PredilectionsMedium to large breeds—most commonlyGerman shepherd dogs, Dobermans, andLabrador retrievers.
Mean Age and RangeAny age; usually between 4 and 7 years
Predominant SexMale
SIGNSGeneral CommentsAlways consider the diagnosis in patients withmonoarticular lameness associated with softtissue swelling, heat, and pain.
Historical Findings� Lameness—acute onset most common, butcan present as chronic lameness.� Lethargy� Anorexia� May report previous trauma—dog bite,penetrating injury, prior surgery or otherinvasive procedure of the joint.
Physical Examination Findings� Monoarticular lameness, rarelypauciarticular (four or fewer joints) orpolyarticular (five or more joints)involvement.� Joint pain and swelling—commonly carpus,stifle, hock, shoulder, or cubital joint.
� Localized joint heat� Decreased range of motion� Fever
CAUSES� Aerobic bacterial organisms—mostcommon: staphylococci, streptococci,coliforms, and Pasteurella� Anaerobic organisms—most common:Propionibacterium, Peptostreptococcus,Fusobacterium, and Bacteroides� Spirochete—Borrelia burgdorferi� Mycoplasma� Fungal agents—Blastomyces, Cryptococcus,and Coccidioides� Ehrlichia� Leishmania� Feline calicivirus
RISK FACTORS� Predisposing factors for hematogenousinfection—diabetes mellitus;hypoadrenocorticism (Addison’s disease);immunosuppression.� Penetrating trauma to the joint includingsurgery.� Existing osteoarthritis or other jointdamage.� Intra-articular injection, particularly ifsteroid injected.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Osteoarthritis� Trauma� Immune-mediated arthropathy� Post-vaccinal transient polyarthritis� Greyhound polyarthritis� Feline progressive polyarthritis� Crystal-induced joint disease� Synovial cell sarcoma
CBC/BIOCHEMISTRY/URINALYSIS� Hemogram—inflammatory left shift insome cases� Other results normal
OTHER LABORATORY TESTSSerologic testing for specific pathogens
IMAGINGRadiography� Early disease—may reveal thickened anddense periarticular tissues; may see evidence ofjoint effusion. Often difficult to diagnoseearly disease radiographically.� Late disease—reveals bone destruction,osteolysis, irregular joint space, discreteerosions, and periarticular osteophytosis.
DIAGNOSTIC PROCEDURESSynovial Fluid Analysis� Increased volume.� Turbid fluid.� Decreased viscosity.� Decreased mucin clot reaction.
� Make slides immediately; if additional fluidis obtained, place in EDTA tube.� Elevated WBC count— > 80% neutrophilswith > 40,000/mm3 (normal joint fluid <10% neutrophils and < 3,000/mm3).� Neutrophils in synovial fluid may showdegenerative changes (chromatolysis,vacuolation, nuclear swelling, loss ofsegmentation). However, toxic neutrophils arenot necessary for diagnosis.� Definitive diagnosis—neutrophils withphagocytosed bacteria (observed inapproximately half of cases) or bacteria in thesynovial fluid.
Synovial Fluid Culture� Positive culture is definitive but notnecessary for diagnosis.� Must be collected aseptically; requires heavysedation or general anesthesia.� Place fluid sample in aerobic and anaerobicculturettes and in blood culture medium.� Use 1:9 dilution of synovial fluid to bloodculture media.� Culturette samples—cultured immediatelyupon arrival to the laboratory.� Blood culture medium—reculturing after24 hours of incubation increases accuracy by50% and is the preferred method.� Mycoplasma, bacterial L-forms, and protozoarequire specific culture procedures—contactlaboratory prior to sample collection.
Other� Synovial biopsy—to rule outimmune-mediated joint disease; no moreeffective than incubated blood culturemedium for growing bacterial organisms.� Blood and urine cultures if hematogenoussource is suspected.
PATHOLOGIC FINDINGS� Synovium—thickened; discolored; oftenvery proliferative.� Histology—evidence of hyperplasticsynoviocytes.� Increased numbers of neutrophils,macrophages, and fibrinous debris.� Cartilage—loss of proteoglycan, destructionof articular surface, pannus formation.
TREATMENTAPPROPRIATE HEALTH CARE� Inpatient—initial stabilization; initiatesystemic antibiotic therapy as soon as fluid isobtained for bacterial culture; consider jointdrainage/lavage as soon as possible tominimize intra-articular injury.� Identify and treat source if hematogenousspread is suspected.� Outpatient—long-term management.
NURSING CARE� Alternating heat and coldpacking—beneficial in promoting increasedblood flow and decreased swelling.
BLBS078-CF_A64 BLBS078-Tilley July 15, 2011 9:33
Canine and Feline, Fifth Edition 113
(Continued) Arthritis, Septic A
� Joint immobilization may enhance patientcomfort but should not be prolonged due torisk of worsening cartilage damage.
ACTIVITYRestricted until resolution of symptoms
DIETN/A
CLIENT EDUCATION� Discuss probable cause.� Warn client about the need for long-termantibiotics and the likelihood of residualdegenerative joint disease.
SURGICAL CONSIDERATIONS� Acute disease with minimal radiographicchanges—general recommendation for initialjoint decompression via arthrocentesis, andpossibly joint lavage via needle arthrocentesis,arthroscopic lavage, or arthrotomy. Anirrigation catheter (ingress/egress) can beplaced in larger joints. Considerable debateexists regarding superiority of repeated needlearthrocentesis, arthroscopic lavage, or openlavage.� Chronic disease—may require arthroscopyor arthrotomy with debridement of thesynovium and copious lavage; if appropriate,an irrigation catheter (ingress/egress) may beplaced to lavage the joint post-operatively.� Lavage—use warmed physiologic saline orlactated Ringer’s solution (2–4 ml/kg q8h)until effluent is clear. Do not addpovidone/iodine or chlorhexidine to lavagefluid.� Effluent fluid—cytologically monitoreddaily for existence and character of bacteriaand neutrophils.� Removal of catheters—when effluent fluidhas no bacteria and the neutrophils arecytologically healthy.� Arthroscopy allows for visual assessment ofarticular cartilage, lavage, and biopsy, and is aless-invasive method of thorough joint lavagethan arthrotomy.� Recent reports suggest there may be nodifference between combined medical andsurgical management and medicalmanagement alone.
MEDICATIONSDRUG(S) OF CHOICE� Pending culture susceptibilitydata—bactericidal antibiotics, such asfirst-generation cephalosporin oramoxicillin-clavulanic acid, preferred.� Choice of antimicrobial drugs—primarilydepends on in vitro determination ofsusceptibility of microorganisms; toxicity,frequency, route of administration, andexpense also considered; most penetrate thesynovium well; need to be given for aminimum of 4–8 weeks.
� NSAIDs and other analgesics—may helpdecrease pain and inflammation.
CONTRAINDICATIONSAvoid fluorinated quinolones in pediatricpatients; they induce cartilage lesionsexperimentally.
PRECAUTIONSFailure to respond to conventional antibiotictherapy—may indicate anaerobic disease orother unusual cause (fungal, spirochete).
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORING� Observation for clinical signs of joint painand swelling.� Repeated synovial fluid cytology to assessresponse to treatment.� Duration of antibiotic therapy—2 weeksfollowing resolution of clinical signs. Totaltreatment may be 4–8 weeks or longerdepending on clinical signs and pathogenicorganism.� Persistent synovial inflammation withoutviable bacterial organisms (dogs)—may becaused by antigenic bacterial fragments orantigen antibody deposition.� Physical therapy—may be needed toprevent muscle contracture, maintain cartilagehealth, and maximize normal joint dynamics.
PREVENTION/AVOIDANCEIf clinical signs recur, early (within24–48 hours) treatment provides the greatestbenefit.
POSSIBLE COMPLICATIONS� Chronic disease—severe degenerative jointdisease� Recurrence of infection� Limited joint range of motion� Generalized sepsis� Osteomyelitis
EXPECTED COURSE AND PROGNOSIS� Acutely diagnosed disease (within24–48 hours) responds well to antibiotictherapy.� Delayed diagnosis or resistant or highlyvirulent organisms—guarded to poorprognosis.
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMS� Infectious arthritis� Joint ill
SEE ALSO� Osteomyelitis� Polyarthritis, Erosive, Immune-Mediated� Polyarthritis, Non-erosive,Immune-Mediated
ABBREVIATIONS� EDTA = ethylene diamine tetra-acetate� NSAID = nonsteroidal anti-inflammatorydrug� WBC = white blood cell
Suggested ReadingBennett D, Taylor DJ. Bacterial infective
arthritis in the dog. J Small Anim Pract1988, 29:207–230.
Benzioni H, Shahar R, Yudelevitch S,Milgram J. Bacterial infective arthritis of thecoxofemoral joint in dogs with hipdysplasia. Vet Comp Orthop Traumatol2008, 21:262–266.
Clements DN, Owen MR, Mosely JR, et al.Retrospective study of bacterial infectivearthritis in 31 dogs. J Small Anim Pract2005, 46:171–176.
Ellison RS. The cytologic examination ofsynovial fluid. Semin Vet Med Surg SmallAnim 1988, 3:133–139.
Fitch RB, Hogan TC, Kudnig ST.Hematogenous septic arthritis in the dog:Results of five patients treated nonsurgicallywith antibiotics. JAAHA 2003,39:563–566.
Hodgin EC, Michaelson F, Howerth EW.Anaerobic bacterial infections causingosteomyelitis/arthritis in a dog. JAVMA1992, 201:886–888.
Luther JF, Cook JL, Stoll MR. Arthroscopicexploration and biopsy for diagnosis ofseptic arthritis and osteomyelitis of thecoxofemoral joint in a dog. Vet CompOrthop Traumatol 2005, 18:47–51.
Machevsky AM, Read RA. Bacterial septicarthritis in 19 dogs. Australian Vet J 1999,77:233–237.
MacWilliams PS, Friedrichs KR. Laboratoryevaluation and interpretation of synovialfluid. Vet Clin North Am Small Anim Pract2003, 33:153–178.
Author Sherisse A. Sakals and Spencer A.JohnstonConsulting Editors Peter K. Shires
Client Education Handoutavailable online
BLBS078-CF_A65 BLBS078-Tilley March 22, 2011 7:38
114 Blackwell’s Five-Minute Veterinary Consult
AscitesA
BASICSDEFINITIONThe escape of fluid, either transudate orexudate, into the abdominal cavity betweenthe parietal and visceral peritoneum.
PATHOPHYSIOLOGY� Ascites can be caused by the following:
◦ CHF and associated interference invenous return◦ Depletion of plasma proteins associatedwith inappropriate loss of protein fromrenal or gastrointestinal disease—protein-losing nephropathy or enteropathy,respectively◦ Obstruction of the vena cava or portalvein, or lymphatic drainage due toneoplastic occlusion◦ Overt neoplastic effusion◦ Peritonitis—infective or inflammatory◦ Electrolyte imbalance, especiallyhypernatremia◦ Liver cirrhosis.
SYSTEMS AFFECTED� Cardiovascular� Gastrointestinal� Hemic/Lymph/Immune� Renal/Urologic
SIGNALMENT� Dogs and cats� No species or breed predisposition
SIGNS� Episodic weakness� Lethargy� Abdominal fullness� Abdominal discomfort when palpated� Dyspnea from abdominal distension orassociated pleural effusion� Anorexia� Vomiting� Weight gain� Scrotal or penile edema� Groaning when lying down
CAUSES� Nephrotic syndrome� Cirrhosis of liver� Right-sided CHF� Hypoproteinemia� Ruptured bladder� Peritonitis� Abdominal neoplasia� Abdominal hemorrhage
RISK FACTORSN/A
DIAGNOSISDIFFERENTIAL DIAGNOSISDifferentiating Abdominal Distensionwithout Effusion� Organomegaly—hepatomegaly,splenomegaly, renomegaly, and hydrometra.� Abdominal neoplasia.� Pregnancy.� Bladder distension.� Obesity.� Gastric dilatation.
Differentiating Diseases� Transudate—nephrotic syndrome, cirrhosisof liver, right-sided CHF, hypoproteinemia,and ruptured bladder.� Exudate—peritonitis, abdominal neoplasia,and hemorrhage.
CBC/BIOCHEMISTRY/URINALYSIS� Neutrophilic leukocytosis occurs in patientswith systemic infection.� Albumin is low in patients with impairedliver synthesis, gastrointestinal loss, or renalloss.� Cholesterol is low in patients with impairedliver synthesis.
Liver Enzymes� Low to normal in patients with impairedliver synthesis.� High in patients with liver inflammation,hyperadrenocorticism, gallbladderobstruction, and chronic passive congestion.
Total and Direct Bilirubin� Low to normal in patients with impairedliver synthesis.� High in patients with biliary obstructioncaused by tumor, gallbladder distension, orobstruction.
BUN and Creatinine� High in patients with renal failure.� BUN low in patients with impaired liversynthesis or hyperadrenocorticism.
Glucose� Low in patients with impaired liversynthesis.
OTHER LABORATORY TESTS� To detect hypoproteinemia—proteinelectrophoresis and immune profile.� To detect proteinuria—urinaryprotein:creatinine ratio (normal < 0.5:1).
IMAGING� Thoracic and abdominal radiography issometimes helpful.
� Ultrasonography of the liver, spleen,pancreas, kidney, bladder, and abdomen canoften determine cause.� Stages of ascites:
◦ Stage I: minimal ascites. Detected byultrasound only.◦ Stage II: moderate ascites. Abdominaldistention visible and/or noted onballottement.◦ Stage III: significant ascites. Markedabdominal distention. Patientuncomfortable, possibly with laboredbreathing.
DIAGNOSTIC PROCEDURESAscitic Fluid EvaluationExfoliative cytologic examination andbacterial culture and antibioticsensitivity—remove approximately 3–5 mL ofabdominal fluid via aseptic technique.
Transudate� Clear and colorless.� Protein < 2.5 g/dL.� Specific gravity < 1.018.� Cells < 1,000/mm3—neutrophils andmesothelial cells.
Modified Transudate� Red or pink; may be slightly cloudy.� Protein 2.5–5 g/dL.� Specific gravity > 1.018.� Cells < 5,000/mm3—neutrophils,mesothelial cells, erythrocytes, andlymphocytes.
Exudate (Non-septic)� Pink or white; cloudy.� Protein 2.5–5 g/dL.� Specific gravity > 1.018.� Cells 5,000–50,000/mm3—neutrophils,mesothelial cells, macrophages, erythrocytes,and lymphocytes.
Exudate (Septic)� Red, white, or yellow; cloudy.� Protein > 4.0 g/dL.� Specific gravity > 1.018.� Cells 5,000–100,000/mm3—neutrophils,mesothelial cells, macrophages, erythrocytes,lymphocytes, and bacteria.
Hemorrhage� Red; spun supernatant clear and sedimentred.� Protein > 5.5 g/dL.� Specific gravity 1.007–1.027.� Cells consistent with peripheral blood.� Does not clot.
Chyle� Pink, straw, or white.� Protein 2.5–7 g/dL.
BLBS078-CF_A65 BLBS078-Tilley March 22, 2011 7:38
Canine and Feline, Fifth Edition 115
(Continued) Ascites A
� Specific gravity 1.007–> 1.040.� Cells < 10,000/mm3—neutrophils,mesothelial cells, and large population ofsmall lymphocytes.� Other—fluid in tube separates intocream-like layer when refrigerated; fatdroplets stain with Sudan III.
Pseudochyle� White.� Protein > 2.5 g/dL.� Specific gravity 1.007–1.040.� Cells < 10,000/mm3—neutrophils,mesothelial cells, and small lymphocytes.� Other—fluid in tube does not separate intocream-like layer when refrigerated; does notstain with Sudan III.
Urine� Clear to pale yellow.� Protein > 2.5 g/dL.� Specific gravity 1–> 1.040.� Cells 5,000–50,000/mm3—neutrophils,erythrocytes, lymphocytes, and macrophages.� Other—if the urinary bladder ruptured< 12 hours before, urinary glucose andprotein could be negative; if bladder ruptured> 12 hours before, urine becomes a dialysismedium with ultrafiltrate of plasma, andurine contains glucose and protein.
Bile� Slightly cloudy and yellow.� Protein > 2.5 g/dL.� Specific gravity > 1.018.� Cells 5,000–750,000/mm3—neutrophils,erythrocytes, macrophages, and lymphocytes.� Other—bilirubin confirmed by urinedipstick; non-icteric patient may havegallbladder rupture, biliary tree leakage, orrupture in the proximal bowel.
TREATMENT� Can design treatment on an outpatientbasis, with follow-up or inpatient care,depending on physical condition andunderlying cause.� If patients are markedly uncomfortablewhen lying down or become more dyspneicwith stress, consider removing enough ascitesto reverse these signs.� Dietary salt restriction may help controltransudate fluid accumulation due to CHF,cirrhosis, or hypoproteinemia.
� For exudate ascites control, address theunderlying cause; corrective surgery is oftenindicated, followed by specific therapeuticmanagement (e.g., patient with splenictumor: tumor removed, abdominal bleedingcontrolled, blood transfusion administered).
LARGE-VOLUME PARACENTESIS� Stage III treatment.� Pretreat patient with hetastarch (6%) @1–2 ml/kg for 2 hours.� Abdominal tap (paracentesis), until drainageslows.� Post-treat patient with hetastarch (6%) @1–2 ml/kg for 4 hours.
MEDICATIONSDRUG(S) OF CHOICE� Patients with liver insufficiency orCHF—restrict sodium and give a diureticcombination of hydrochlorothiazide(2–4 mg/kg q12h PO) and spironolactone(1–2 mg/kg q12h PO); if control isinadequate, furosemide (1–2 mg/kg q8h PO)can be substituted for the thiazide withspironolactone continued; must monitorserum potassium concentration to preventpotassium imbalances.� Patients with hypoproteinemia, nephroticsyndrome, and associated ascitic fluidaccumulation—can treat as above with theaddition of hetastarch (6% hetastarch in 0.9%NaCl); administer an IV bolus (dogs,20 mL/kg; cats, 10–15 mL/kg) slowly over∼1 hour; hetastarch increases plasma oncoticpressure and pulls fluid into the intravascularspace for up to 24–48 hours.� Systemic antibiotic therapy is dictated bybacterial identification and sensitivity testingin patients with septic exudate ascites.
CONTRAINDICATIONSN/A
FOLLOW-UPPATIENT MONITORING� Varies with the underlying cause.� Check sodium, potassium, BUN, creatinine,and weight fluctuations periodically if thepatient is maintained on a diuretic.
POSSIBLE COMPLICATIONSAggressive diuretic administration may causehypokalemia, which could predispose tometabolic alkalosis and exacerbation ofhepatic encephalopathy in patients withunderlying liver disease; alkalosis causes a shiftfrom NH4 to NH3.
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMSAbdominal effusion
SEE ALSO� Cirrhosis and Fibrosis of the Liver� Congestive Heart Failure, Right-Sided� Hypoalbuminema� Nephrotic Syndrome
ABBREVIATIONSCHF = congestive heart failure
Suggested ReadingKramer RE, Sokol RJ, Yerushalmi B, Liu E,
MacKenzie T, Hoffenberg EJ, NarkewiczMR. Large-volume paracentesis in themanagement of ascites in children. J PedGastro Nutr 2001; 33:245–249.
Lewis LD, Morris ML Jr,, Hand MS. SmallAnimal Clinical Nutrition, 3rd ed. Topeka,KS: Mark Morris Associates, 1987.
Li MK. Management of ascites. Hong KongMed Di 2009, 14:27–29.
Runyon BA. Management of adult patientswith ascites due to cirrhosis. Hepatol 2004,39:1–16.
Author Jerry A. ThornhillConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
BLBS078-CF_A66 BLBS078-Tilley June 16, 2011 11:0
116 Blackwell’s Five-Minute Veterinary Consult
Aspergillosis—DisseminatedA
BASICSOVERVIEW� Opportunistic fungal infection caused byAspergillus spp., common molds that areubiquitous in the environment, formingnumerous spores in dust, straw, grassclippings, and hay.� Disseminated disease does not appear to berelated to the nasal form of the disease,although one report of a dog developingfungal osteomyelitis 6 months after treatmentfor nasal aspergillosis raises the possibility.� Disseminated disease—usually A. terreus;A. deflectus and A. fumigatus also associated;portal of entry not definitively established butpossibly through the respiratory tract orgastrointestinal tract, with subsequenthematogenous spread.
SIGNALMENTDogs� More common in dogs than in cats.� German shepherds overrepresented butreported sporadically in many breeds; averageage 3 years (range of 1–9 years); slight biastoward females.
Cats� Persians—marginally increased incidence.� Disseminated cases mostly affect the lungsand/or gastrointestinal tract.
SIGNSDogs� May develop acutely or slowly over a periodof several months.� Often associated with spinal pain (fungaldiskospondylitis) or lameness (fungalosteomyelitis).� Neurologic—spinal cord damage.� CNS—vestibular signs, seizures,hemiparesis, mental dullness, ataxia,paraparesis, vision impairment, circling.� Polyuria/polydipsia and hematuria—renalinvolvement.� Uveitis—ocular involvement.� Non-specific—fever, weight loss, vomiting,lymphadenopathy, and anorexia.
Cats� Usually non-specific signs (e.g., lethargy,depression, vomiting, and diarrhea).� Ocular—exophthalmos.
CAUSES & RISK FACTORS� Caused by Aspergillus species, mostcommonly A. terreus, A. deflectus and lesscommonly A. fumigatus, A. niger, A. flavipes.� German shepherds at higher risk.� Immune deficiency—may play a factorbecause the organism is widespread but thedisease is uncommon; breed-related immunedefect proposed in German shepherds andtheir crosses.
� Geographic/environmentalconditions—may be a factor, as some regionshave a higher incidence (e.g., California,Louisiana, Michigan, Georgia, Florida, andVirginia in the United States; westernAustralia; Barcelona; and Milan).� Cats—associated with FIP, FePLV, FeLV,diabetes mellitus, and chronic corticosteroidor antibiotic administration.
DIAGNOSISDIFFERENTIAL DIAGNOSISBacterial osteomyelitis/diskospondylitis;spinal neoplasia; intervertebral disk disease;skeletal neoplasia; bacterial pyelonephritis;bacterial pneumonia; other causes ofvestibular signs/seizures; other causes ofuveitis (see Anterior Uveitis—Cats, AnteriorUveites—Dogs).
CBC/BIOCHEMISTRY/URINALYSIS� Non-specific.� Dogs—often have mature neutrophilicleukocytosis and lymphopenia.� Cats—may have nonregenerative anemiaand leucopenia.� Biochemistry—may see high globulins,creatinine, phosphate, BUN and calcium.� Urinalysis—may see isosthenuria,hematuria, pyuria, and possible fungal hyphaein the sediment; detection of the fungalhyphae can be improved by allowing thesample to incubate at room temperature for24–48 hours; sediment samples may beexamined unstained as wet preparations ormay be air dried and stained with Diff-Quick(the hyphae that branch at 45◦ stain purple).
OTHER LABORATORY TESTS� Positive fungal serology (agar gel doublediffusion, counterimmunoelectrophoresis,and ELISA) support the diagnosis; falsenegatives with agar gel immunodiffusionreported; false positives and cross-reactivitywith Penicillium spp. reported.� Interpret serology in conjunction with otherdiagnostic tests.� Cats—test for FeLV and FIV because theyaffect prognosis.� Positive fungal culture from normally sterilebody fluids and tissues, e.g., urine, bone, CSF,blood, lymph node, pleural effusions,intervertebral disc aspirates, kidney, spleen.
IMAGINGRadiographic Findings� Spinal views may show end-plate lysis,attempted bony intervertebral bridging, andlysis of vertebral bodies consistent withdiskospondylitis; productive and destructivelesions of the vertebral bodies.� Bony proliferation and lysis and periostealreaction typical of osteomyelitis of thediaphyseal region of long bones.
� Pulmonary involvement rare, mixedinterstitial/alveolar pattern, enlarged sternaland/or tracheobronchial lymph nodes, pleuraleffusion; productive and destructive lesions ofsternebrae.
Ultrasonographic Findings� Kidneys—commonest site to detectchanges; changes seen include renal pelvisdilation ± echogenic debris within pelvis; lossof corticomedullary distinction; renaldistortion and mottled appearance of theparenchyma; dilation of proximal ureter;renalomegaly; nodules or masses;hydronephrosis.� Spleen—hypoechoic, lacy, sharplydemarcated areas with no doppler signalsuggestive of infarct are most significantfinding in spleen; other findings includenodules/masses, mottled parenchyma, splenicvenous thrombosis.� Other—abdominal lymphadenomegaly;diffuse hepatic hypoechogenicity.
MRI FindingsUseful for further defining brain lesions inanimals with CNS signs; changes similar toother infectious and non-infectiousinflammatory brain diseases.
DIAGNOSTIC PROCEDURESChoice of diagnostic procedure as indicatedby clinical presentation but may include CSFtap, joint aspirates, intervertebral disc spaceaspirates, abdominocentesis/thoracocentesis,aspirate of various organs (spleen, liver, renal).
PATHOLOGIC FINDINGSHistopathology—most likely to render adefinitive diagnosis; special stains may berequired; granulomas and multiple organinfarcts noted with disseminated disease(kidneys, liver, spleen, and vertebrae).
TREATMENTDOGS� Treatment rarely curative; may haltprogression of clinical signs.� Fluid therapy—indicated by the degree ofrenal compromise and azotemia.
CATSDisseminated—likely difficult to treat; dataare limited.
MEDICATIONSDRUG(S)� Itraconazole 5–10 mg/kg PO q24h (can bedivided)—drug of choice; dogs; unlikely to becurative, though the disease may be containedwith continued use.
BLBS078-CF_A66 BLBS078-Tilley June 16, 2011 11:0
Canine and Feline, Fifth Edition 117
(Continued) Aspergillosis—Disseminated A
� Other drug combinations reported butnone have ultimately resulted in reported cureof disease. Some of the combinations reportedinclude
◦ Lipid complex amphotericin B (dogs,2–3 mg/kg IV 3 days per week for a total of9–12 treatments, to cumulative dose of24–27 mg/kg) + itraconazole 5 mg/kg POq24h.◦ Itraconazole (5 mg/kg PO q24h) +terbinafine (5–10 mg/kg PO q24h).◦ New triazoles, voriconazole (5 mg/kgPOq12h) and posaconazole (5 mg/kg POq24h), are potential alternatives to casespoorly responsive to itraconazole. Reportedused in combination with lipid complexamphotericin B.◦ β-glucan synthase inhibitors caspofungin,micafungin, anidulafungin—may proveuseful but very limited clinical information.◦ Combination therapy with flucytosine(25–50 mg/kg PO q6—dogs) andamphotericin B may prove successful, butno published reports.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Amphotericin B—contraindicated in dogswith preexisting renal compromise or failure;amphotericin B lipid complex significantlyreduced nephrotoxicity.
� Oral azoles—nausea, intermittent anorexia,liver enzyme elevation.� Combination of flucytosine andamphotericin B—cutaneous drug eruptionsin dogs.� Avoid midazolam and cisapride withazoles—fatal drug reactions noted in humans.� High dose (10 mg/kg) itraconazoleassociated with ulcerative dermatitis in5–10% dogs—recognize early anddiscontinue, then reinstitute at a reduceddosed, or severe cutaneous and subcutaneoussloughing can occur.
FOLLOW-UPDisseminated—monitor serial radiographsevery 1–2 months, renal function, and urinecultures; prognosis poor, especially in Germanshepherds.
MISCELLANEOUSZOONOTIC POTENTIALNone
ABBREVIATIONS� CNS = central nervous system� CSF = cerebrospinal fluid� ELISA = enzyme-linked immunosorbentassay� FeLV = feline leukemia virus� FePLV = feline panleukopenia virus� FIP = feline infectious peritonitis� FIV = feline immunodeficiency virus� MRI = magnetic resonance imaging
Suggested ReadingMaddison JE, Page SW, Church DB. Small
Animal Clinical Pharmacology, 2nd ed.Edinburgh: Saunders, 2008, pp. 186–197.
Schultz RM, Johnson EG, Wisner ER, BrownNA, Byrne BA, Sykes JE. Clinicopathologicand diagnostic imaging characteristics ofsystemic aspergillosis in 30 Dogs. J VetIntern Med 2008, 22:851–859.
Author Tania N. DaveyConsulting Editors Stephen C. Barr
Client Education Handoutavailable online
BLBS078-CF_A66a BLBS078-Tilley June 1, 2011 12:41
118 Blackwell’s Five-Minute Veterinary Consult
Aspergillosis, NasalA
BASICSDEFINITION� Nasal disease caused by Aspergillus spp.,primarily A. fumigatus.� Saprophytic fungus that is ubiquitous in theenvironment.� Opportunistic pathogen.
PATHOPHYSIOLOGY� Inhalation of fungus leads to disease in thenasal cavity with destruction of turbinates andoverproduction of mucus causing clinicalsigns of nasal disease.� Rarely may be associated with underlyingforeign body or previous trauma.� Causes a locally aggressive and invasivedisease but does not result in systemicmycosis.� Confined to nasal cavity and frontalsinus—sinonasal form (most common indogs).� May also extend to the orbit in cats andrarely in dogs—sino-orbital form.
SYSTEMS AFFECTEDRespiratory—nasal cavity, sinus, orbit (cats,rare in dogs)
GENETICSUnknown
INCIDENCE/PREVALENCEUnknown, but a common diagnosis in dogswith nasal discharge in many locations.
GEOGRAPHIC DISTRIBUTIONWorldwide
SIGNALMENTSpeciesDogs and cats (less common)
Breed Predilections� Dogs—dolichocephalic and mesocephalicbreeds� Cats—brachycephalic breeds may beoverrepresented
Mean Age and Range� Dogs—predominantly young tomiddle-aged� Cats—no predilection
Predominant SexNone identified
SIGNSHistorical Findings� Unilateral or bilateral nasaldischarge—typically mucoid, mucopurulent,or serosanguinous but may be primarilyepistaxis.� Sneezing.� Typically chronic signs—several months.� Many patients will have been treated withantibiotics for a possible bacterial infectionbefore presentation with variable response.
Physical Examination Findings� Unilateral or bilateral nasal discharge.� Increased nasal airflow on the affected side.� Depigmentation with ulceration of the nasalplanum—∼40% of dogs.� Facial pain.� Ipsilateral mandibular lymphadenopathy.� Stertor, exophthalmos, hard palateulceration, loss of nasal airflow—cats.
CAUSES� No underlying cause identified, althoughpreexisting foreign body or trauma isoccasionally implicated.� Likely due to inhalation of a large bolus offungus that is ubiqutous in the environment.� Species—most commonly A. fumigatus;others—A. niger, A. flavus.
RISK FACTORSUnknown
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Foreign body.� Oronasal fistula.� Lymphoplasmacytic rhinitis.� Neoplasia.� Nasopharyngeal polyp, nasal tumor, orcryptococcus—cats only.
CBC/BIOCHEMISTRY/URINALYSIS� Often normal� Possible inflammatory leukogram
OTHER LABORATORY TESTSSerology� Detects fungi-specific serum antibodies.� AGID—commercially available; 98%specificity, 67% sensitivity in dogs; serialserology does not appear to correlate withclinical status.� ELISA—88% sensitivity, 96.8% specificity.� Counter-immunoelectrophoresis—85%specificity in dogs.� Serum galactomannan—shown to beunreliable.
Culture� Tissue fungal culture of affected area;visualized biopsy sample taken from a regionof suspected fungal growth showed 100%specificity, 81% sensitivity.� Culture of nasal discharge is less specific andinsensitive.
IMAGINGComputed Tomography� Imaging method of choice.� Cavitated turbinate lysis.� Thickening of the mucosa along the nasalturbinates.� Frontal sinus proliferative mass effect.� Soft tissue mass in the choana ornasopharynx—cats.� Necessary for evaluation of the cribriformplate before topical antifungal treatment.
Skull Radiography� Intraoral dorsoventral radiograph of thenasal cavity shows turbinate lysis.� Rostrocaudal or skyline frontal sinus viewmay show increased soft tissue density in thefrontal sinus.� Cannot evaluate cribriform plate.
DIAGNOSTIC PROCEDURESRhinoscopy� Flexible rhinoscopy in dogs allowsexamination of the nasopharynx and possiblythe frontal sinus if the opening of thenasofrontal duct is destroyed by fungalinfection.� Rigid rhinoscopy—examination of the nasalcavity alone; good visualization is possible dueto large airspaces caused by turbinate lysis;excessive mucus and bleeding can make fullexamination difficult.� Visualization of fungal plaques (white,yellow, black, or light-green) on the mucosa ofthe nasal cavity and/or frontal sinus confirmsfungal infection.
PATHOLOGIC FINDINGS� Biopsies obtained of affected area underdirect rhinoscopic visualization using cupbiopsy instruments.� Samples immersion-fixed in buffered 10%formalin, routinely processed.� Evidence supportive of a diagnosis ofaspergillosis—identification of septate,branching hyphae and conidia onhistopathology. Surrounding inflammation iscommonly neutrophilic orlymphoplasmacytic, rarely eosinophilic.� Blind biopsies in an unaffected area of thenasal cavity may result in a false diagnosis ofinflammation.
TREATMENTAPPROPRIATE HEALTH CAREOvernight hospitalization required aftertopical treatment or surgery.
NURSING CAREMaintain the nares free of nasal discharge
ACTIVITYRestriction of activity is not required
DIETN/A
CLIENT EDUCATION� Dogs—inform client that multiple topicaltreatments are usually necessary to cure thedisease; follow-up with rhinoscopy is highlyrecommended to ensure resolution.� No established protocols for treatment incats.
SURGICAL CONSIDERATIONSTrephination of the Frontal Sinus� Recommended for dogs with frontal sinusinvolvement.
BLBS078-CF_A66a BLBS078-Tilley June 1, 2011 12:41
Canine and Feline, Fifth Edition 119
(Continued) Aspergillosis, Nasal A
� Performed using a Jacob’s chuck andintramedullary pin.� Allows direct visualization of the frontalsinus with a rigid rhinoscope and localdebridement of fungal plaques.� Allows for lavage and topical treatment ofthe area using a red rubber catheter.
Surgical Debridement and Exenteration� Used in some cats with sino-orbital disease.
Endoscopic Debridement� Extensive curettage and removal of fungalmaterial from the nose and frontal sinus areessential to allow efficacy of topicalmedication.
MEDICATIONSDRUG(S) OF CHOICETopical Clotrimazole or EnilconazoleTherapy� 1-hour infusion into nasal cavity underanesthesia.� Treatment is usually performed during thesame anesthesia as diagnostics.� Treatment of choice in dogs; reportedefficacy 85–89% with multiple treatments.� Foley catheters are used to occlude the naresand nasopharynx.� Dose—Clotrimazole: 1 gram of in 100 mlof polyethylene glycol 200 (1% solution)evenly divided between two 60-ml syringesslowly infused over 1 hour into each side forlarge dogs; if trephination is used, divide theamount between the nasal cavity and sinus onthe same side; less volume in smaller dogs.Enilconazole: 100 mls of 1%, 2%, or 5%solution.� Dog is placed in dorsal recumbency withhead turned to each side every 15 minutesduring the infusion.� Dog is placed in sternal recumbency withhead down at the end of the procedure toallow all of the medication to drain.� Has been used in cats without orbitalinvolvement in combination with oralantifungal therapy with varying success.
Systemic Therapy� Antifungal triazole drugs should beconsidered if the cribriform plate is not intact;also used as primary therapy in some cats.� Can also be used in combination withtopical therapy.� May be cost-prohibitive.� Itraconazole 5 mg/kg PO q12h in dogs witha reported efficacy of 60–70%; 10 mg/kg POq24h in cats.� Voriconazole 5 mg/kg PO q12h; efficacy assole therapy has not been established.� Posaconazole 5 mg/kg PO q24h; efficacy assole therapy has not been established.� Amphotericin B (deoxycholate) 0.8 mg/kgSC in 400 ml of warmed 2.5%dextrose/0.45% saline q 3–4 days; cumulativedose 10–14 mg/kg in combination with
triazole drugs.� Fluconazole is not recommended due toresistance.
CONTRAINDICATIONS� Breach in the cribriform plate can allowcontact of antifungal medication with brainresulting in neurologic signs and possibledeath.� Sino-orbital disease necessitates the use ofsystemic therapy.
PRECAUTIONS� Topical clotrimazole and enilconazole arecaustic to all mucosal surfaces—protectivegear (gloves, goggles) should be worn by allstaff that are in close contact.� Enilconazole can be associated with tissueswelling and upper airway obstruction.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)Enilconazole� Also active in the vapor phase.
Combined Clotrimazole Irrigation andDepot Therapy� Clotrimazole (1%) is flushed through atrephine hole in the frontal sinus over 5minutes; 50 ml in each side in dogs > 10 kg;25 ml in each side in dogs <10 kg.� Clotrimazole cream (1%) is then introducedinto the front sinuses; 20 g in each side in dogs> 10 kg, 10 g in each side in dogs < 10 kg.� Reported efficacy similar to topicalClotrimazole or Enilconazole alone (86%).
FOLLOW-UPPATIENT MONITORINGDogs� Monitor clinical signs, although reductionof clinical signs does not establish resolutionof disease.� Follow-up rhinoscopy is recommended inall cases to establish response to treatment,regardless of clinical signs—histopathologyand culture can help establish response.� Serial serology (AGID) appears not tocorrelate with clinical status.� Repeat CT scan should be considered forreassessment of the cribriform plate beforerepeat topical treatment if a worsening clinicalsigns are seen.� Monitor liver enzymes in animals ontriazole therapy.
Cats� Monitor clinical signs for improvement orresolution.� Monitor liver enzymes in animals ontriazole therapy.� Monitor renal parameters in animals onAmphotericin B.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONS� Topical therapy—monitor after treatmentfor any complications such as swelling oforopharynx, neurologic signs,infection/swelling of trephine site.� Triazoles can cause anorexia and can behepatoxic.� Amphotericin B can be nephrotoxic.
EXPECTED COURSE AND PROGNOSIS� Studies have shown an 87% response rate totopical therapy in dogs after one to threetreatments.� A newer study showed that recurrence orreinfection is more common than previouslythought and can occur years after supposedlysuccessful therapy.� The prognosis for cats with sinonasalaspergillosis is better than with thesino-orbital form.
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALThere are no documented cases of humaninfection from an affected dog or cat.
PREGNANCY/FERTILITY/BREEDINGN/A
ABBREVIATIONS� AGID = agar gel immunodiffusion� CT = computed tomography� ELISA = enzyme-linked immunosorbentassay
Suggested ReadingBarrs VR. Feline sino-orbital aspergillosis: An
emerging clinical syndrome. ACVIMForum Proceedings 2009, pp. 395–397.
Friend E, Anderson DM, White RAS.Combined clotrimazole irrigation and depottherapy for canine nasal aspergillosis. J SmallAnim Pract 2006, 47(6):312–315.
Mathews KG, Davidson AP, Koblik PD, et al.Comparison of topical administration ofclotrimazole through surgically placed versusnonsurgically placed catheters for treatmentof nasal aspergillosis in dogs: 60 cases(1990–1996). JAVMA 1998, 213:501–506.
McLellan GJ, Aquino SM, Mason DR, MyersRK. Use of posaconazole in themanagement of invasive orbital aspergillosisin a cat. JAAHA 2006, 42:302–307.
Pomrantz JS, Johnson LR, Nelson RW,Wisner ER. Comparison of serologicevaluation via agar gel immunodiffusionand fungal culture of tissue for diagnosis ofnasal aspergillosis in dog. JAVMA 2007,230:1319–1323.
Author Jill S. PomrantzConsulting Editors Lynelle R. Johnson
BLBS078-CF_A67 BLBS078-Tilley March 22, 2011 7:45
120 Blackwell’s Five-Minute Veterinary Consult
Aspirin ToxicityA
BASICSOVERVIEW� Given by owners to relieve minor pain anddiscomfort; now less commonly used owingto increasing popularity of otherover-the-counter pain-relieving drugs.� Gastric irritation and hemorrhage occur in10–20% of cases.� Repeated doses may producegastrointestinal ulceration and perforation.� Toxic hepatitis, suppression of bone marrowactivity, and anemia may occur, especially incats.
SIGNALMENTCats and less commonly dogs
SIGNS� Depression� Vomiting—vomitus may be blood-tinged� Tachypnea� Fever� Muscular weakness and ataxia� Coma and death in 1 or more days
CAUSES & RISK FACTORS� Owners employing human dosageguidelines to medicate cats—most common.� Deficiency in glucuronide conjugationcapability (cats).� Biological half-life—cats, 44.6 hours; dogs,7.5 hours; responsible for higher risk in cats.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Clinical signs—uncharacteristic.� History of aspirin ingestion ormedication—important; within 5 days ofsigns should raise concern.
� Preexisting painful condition—questionowner about aspirin administration.
CBC/BIOCHEMISTRY/URINALYSIS� Cats—prone to Heinz body formation� Hyponatremia and hypokalemia
OTHER LABORATORY TESTS� Initial respiratory alkalosis followed bymetabolic acidosis.� Salicylic acid concentrations in serum orurine.� High ketones and pyruvic, lactic, and aminoacid levels.� Decreased sulfuric and phosphoric acidrenal clearance.
IMAGINGN/A
DIAGNOSTIC PROCEDURESN/A
TREATMENT� Inpatient—following general principles ofpoisoning management.� Correction of acid-basebalance—continuous intravenous fluids.� Induced gastric emptying—gastric lavage orinduced emesis.� Peritoneal or hemodialysis orhemoperfusion—heroic procedures.
MEDICATIONSDRUG(S)� No specific antidote available� Activated charcoal—2 g/kg POdecontaminates gut
� Sodium bicarbonate 1 mEq/kg IValkalinizes urine
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UP� Maintaining renal function and acid-basebalance is vital.� Severe acid-base disturbances, severedehydration, toxic hepatitis, bone marrowdepression, and coma are poor prognosticindicators.
MISCELLANEOUSBe sure that history of “aspirin” medicationdoes not refer to other available painmedications.
Suggested ReadingOehme FW. Aspirin and acetaminophen. In:
Kirk RW, ed., Current Veterinary TherapyIX: Small Animal Practice. Philadelphia:Saunders, 1986, pp. 188–189.
Author Frederick W. OehmeConsulting Editors Gary D. Osweiler
BLBS078-CF_A68 BLBS078-Tilley March 22, 2011 7:46
Canine and Feline, Fifth Edition 121
Asthma, Bronchitis—Cats A
BASICSDEFINITION� Chronic bronchitis—inflammation in theairways (bronchi and bronchioles); chronicdaily cough of greater than 2 months induration. � Asthma—acute or chronic airwayinflammation associated with increasedairway responsiveness to various stimuli,airway narrowing due to smooth musclehypertrophy or constriction, reversibility ofairway constriction, and presence ofeosinophils, lymphocytes, and mast cellswithin the airways. � Feline bronchitis orbronchopulmonary disease is used to describethe clinical syndrome of acute or chroniccoughing and/or wheezing due to lowerairway inflammation.
PATHOPHYSIOLOGY� Noxious or allergic stimuli initiateinflammation within the lower airways.� Bronchiolar smooth muscle constriction—reversible spontaneously or with treatment.� Smooth muscle hypertrophy implieschronicity—usually not reversible. � Increasein mucosal goblet cells, mucus production,and edema of bronchial wall. � Excessivemucus can cause bronchiolar obstruction,atelectasis, or bronchiectasis. � Chronicinflammation may lead to fibrosis.
SYSTEMS AFFECTED� Respiratory � Cardiac—pulmonaryhypertension rarely
GEOGRAPHIC DISTRIBUTIONWorldwide. Parasitic causes more common insouthern and midwest U.S. states.Paragonimus kellicotti found in Great Lakesarea. Heartworm disease more prevalent insouthern United States.
SIGNALMENTSpeciesCats
Breed PredilectionsSiamese overrepresentedMean Age and RangeAny age; more common between 2 and 8yearsPredominant SexOne study shows females overrepresented
SIGNSHistorical Findings� Coughing (80%), sneezing (60%), laboredbreathing or wheezing (40%). � Signs aretypically episodic and can be acute or chronic.Physical Examination Findings� Severely affected cats present with open-mouth breathing, tachypnea, and cyanosis.� Increased tracheal sensitivity is common.� Chest auscultation may reveal cracklesand/or expiratory wheezes, or may be normal.� Labored breathing with an abdominal pushon expiration, increase in expiratory effort.
CAUSESTriggers of airway inflammation unknown
RISK FACTORS� Cigarette smoke, dusty cat litter, hair sprays,and air fresheners may exacerbate disease.� Parasitic lung infections are more commonin outdoor cats in certain geographiclocations. � Use of potassiumbromide—implicated in causing signs ofbronchitis/asthma in some cats.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Rule out infectious pneumonia(Mycoplasma, Toxoplasma, bacterial or fungalpneumonia), Dirofilaria immitis and primarylung parasites (Aelurostrongylus abstrusus,Capillaria aerophilia, Paragonimus kellicotti).� Primary or metastatic neoplasia can havesimilar clinical and radiographic appearance.� Idiopathic pulmonary fibrosis may appearsimilar to feline bronchitis.
CBC/BIOCHEMISTRY/URINALYSISFrequently normal, ∼40% of cats withbronchial disease have peripheraleosinophilia.
OTHER LABORATORY TESTS� Fecal exams—flotation for Capillaria,sedimentation for Paragonimus, Baermann forAelurostrongylus. False-negative tests common.� Heartworm antigen and antibody testing.� Radioallergosorbent testing or intradermalskin testing—no correlation between skin andrespiratory allergies currently documented.
IMAGINGRadiography� Classically, diffuse bronchial wallthickening; interstitial or patchy alveolarpatterns possible. � Severity of radiographicchanges may not correlate with clinicalseverity or duration. � Hyperinflation of lungfields—flattened and caudally displaceddiaphragm, increased distance between theheart and diaphragm, extension of lungs tothe first lumbar vertebrae. � Collapse of rightmiddle lung lobe reported in 11% of cases.� Pulmonary lobar arterial enlargement issuspicious for heartworm disease.
EchocardiographyUseful to document heartworm disease orsecondary pulmonary hypertension.
DIAGNOSTIC PROCEDURESTransoral Tracheal Wash� Use a sterile endotracheal tube andpolypropylene catheter to collect airway fluidsat the level of the carina.
Bronchoscopy/Bronchoalveolar Lavage� Allows visualization of trachea and bronchi.Excessive amounts of thick mucus arecommon with bronchitis. Mucosa of theairways is typically hyperemic and edematous.
� BAL performed to collect airway fluids frommost severely affected areas.
Cytology� Eosinophils and neutrophils are mostprominent cell types. A mixed cell populationoccurs in about 21% of cats. � Up to 20%eosinophils on BAL cytology can be found innormal cats.
Bacterial Cultures� Quantitated cultures recommended;bacterial colony counts > 100–300 cfu/mluncommon. � Specific Mycoplasma culturemay be needed.
Biopsy� Keyhole biopsy—can differentiate betweenidiopathic pulmonary fibrosis and bronchitis.
PATHOLOGIC FINDINGSHyperplasia/hypertrophy of goblet cells,hypertrophy of airway smooth muscle,epithelial erosion, and inflammatoryinfiltrates.
TREATMENTAPPROPRIATE HEALTH CARE� Remove patient from inciting environment� Hospitalize for acute respiratory distress
NURSING CAREOxygen therapy and sedatives in an acutecrisis. Minimize manipulation in order tolessen stress and oxygen needs of theanimal.
ACTIVITYUsually self-limited by patient
DIETCalorie restriction for obese cats
CLIENT EDUCATION� Most causes are chronic and progressive.� Do not discontinue medical therapy whenclinical signs have resolved—subclinicalinflammation is common and can lead toprogression of disease. Lifelong medicationand environmental changes usuallynecessary. � Some clients can be taught to giveterbutaline subcutaneously and corticosteroidinjections at home for a crisis situation.
MEDICATIONSDRUG(S) OF CHOICEEmergency Treatment� Oxygen and a parenteral bronchodilator.Injectable terbutaline (0.01 mg/kg IV or SC);repeat if no clinical improvement (decrease inrespiratory rate or effort) in 20–30 minutes.� A sedative can aid in decreasing anxiety(butorphanol tartrate at 0.2–0.4 mg/kg IV orIM, buprenorphine at 0.01 mg/kg IV or IM,or acepromazine at 0.01–0.05 mg/kg SC). � Ashort-acting parenteral corticosteroid may also
BLBS078-CF_A68 BLBS078-Tilley March 22, 2011 7:46
122 Blackwell’s Five-Minute Veterinary Consult
Asthma, Bronchitis—Cats (Continued)A
be required. Dexamethasone sodiumphosphate (0.25–0.5 mg/kg, IV or SC). Canrepeat if no improvement noted within 20–30minutes. Prednisolone sodium succinate(Solu-Delta-Cortef ) can also be used (50–100mg IV).
Long-Term ManagementCorticosteroids� Decrease inflammation. � Oral treatment ispreferred over injectable for closer monitoringof dose and duration. � Prednisolone: 0.5–1mg/kg PO q12h. Begin to taper dose (50%each week) after 1–2 weeks if clinical signshave improved. Maintenance therapy =0.5–1 mg/kg PO q24–48h. � Longer-actingparenteral steroids (Vetalog or Depomedrol)should be reserved only for situations whereowners are unable to administer oralmedication on a routine basis.
Inhaled Corticosteroids� Requires a form-fitting facemask, spacer,and metered-dose inhaler. Veterinary brandsinclude Aerokat (Trudell medical) or Nebulair(DVM pharmaceuticals). � The mostcommon corticosteroid used as an MDI isfluticasone propionate (Flovent). 220-μg or110-μg Flovent MDI is recommended (1–2actuations, 7–10 breaths q12h) along withbronchodilators and oral corticosteroids,depending on the severity of clinical signs. Inone study, use of 44-μg Flovent decreasedBAL eosinophil counts in experimental cats.� Flovent is used for long-term control ofairway inflammation. Takes 10–14 days toreach peak effect; use oral steroidsconcurrently. � Results in some suppression ofthe hypothalamic-pituitary axis but systemicside effects appear to be reduced.Bronchodilators� Methylxanthines: sustained-releasetheophylline formulations recommended, andpharmacokinetics can vary greatly. Onlygeneric currently available. Dose at10–20 mg/kg PO once daily in the evening.� Beta-2 agonists (terbutaline, albuterol)—inhibit smooth muscle constriction. Oralterbutaline dose is 1/4 of a 2.5 mg tabletq12h. Initial albuterol dose is 20 μg/kg POq12h; can increase to 50 μg/kg PO q8h.
Inhaled Bronchodilators� Albuterol—preferred inhalantbronchodilator, effect lasts less than 4 hours.Long-term use of traditional racemic form ofinhaled albuterol (R and S-enantiomers) hasbeen associated with worsened airwayinflammation. Enantiomer specificR-albuterol should be used if the drug isneeded in moderately to severely affected cats(q12–24h) or during respiratory distress.� Ipratropium bromide: inhaledanticholinergic; can provide bronchodilationand may act synergistically with albuterol toprovide maximal bronchodilation.Anthelminthics� Empirical therapy is indicated for cats withclinical signs of FBD and eosinophilic airway
cytology in an appropriate geographiclocation. � Consider fenbendazole,ivermectin, or praziquantel.Antibiotics� Use based on a positive quantitative cultureand susceptibility testing.
CONTRAINDICATIONSBeta-2 antagonists (e.g., propranolol) arecontraindicated because of their ability toblock sympathetically mediatedbronchodilation.
PRECAUTIONS� Long-term use of steroids increases risk ofdevelopment of diabetes mellitus andpredisposes to immunosuppression. � Use ofcorticosteroids in cats may precipitatecongestive heart failure. � Bronchodilatorsmay exacerbate underlying cardiac disease.
POSSIBLE INTERACTIONSFluoroquinolones decrease metabolism ofmethylxanthines in dogs; effect has not beeninvestigated in cats.
ALTERNATIVE DRUG(S)CyproheptadineSerotonin antagonist. Inhibits airway smoothmuscle constriction in vitro, unknown effectsin cats with asthma/bronchitis.
Cyclosporine (Neoral or Gengraf)Give 2.5–5.0 mg/kg PO q12h—monitorcyclosporine levels. May be helpful in patientsrefractory to bronchodilator andcorticosteroid therapy.
Leukotriene Inhibitors or ReceptorBlockersNo evidence to support use.
FOLLOW-UPPATIENT MONITORING� Owners should report any increase incoughing, sneezing, wheezing, or respiratorydistress. Medications should be increasedappropriately if clinical signs worsen.� Follow-up radiographs may be helpful toevaluate response to medical therapy. � Ownershould watch for signs of PU/PD that couldindicate diabetes mellitus or renal disease.Monitor blood glucose and urine cultures.
PREVENTION/AVOIDANCEEliminate any environmental factors that maytrigger a crisis situation (see “Risk Factors”).Change furnace and air-conditioner filters ona regular basis. Consider dust-free litters.
POSSIBLE COMPLICATIONS� Acute episodes can be life-threatening.� Right-sided heart disease may develop as aresult of long-term bronchitis.
EXPECTED COURSE AND PROGNOSIS� Long-term therapy should be expected.� Most cats do well if recurrence of clinicalsigns is carefully monitored and medical
therapy appropriately adjusted. � A few catswill be refractory to treatment; these carry amuch worse prognosis.
MISCELLANEOUSASSOCIATED CONDITIONSCor pulmonale can be a sequela to chroniclower airway disease.
PREGNANCY/FERTILITY/BREEDINGGlucocorticoids are contraindicated in thepregnant animal. Bronchodilators should beused with caution.
SYNONYMSAllergic bronchitis, chronic obstructivepulmonary disease, asthmatic bronchitis,feline lower airway disease, extrinsic asthma,eosinophilic bronchitis, immune-mediatedairway disease.
SEE ALSO� Heartworm Disease—Cats � RespiratoryParasites
ABBREVIATIONS� BAL = bronchoscopy/bronchoalveolarlavage � FBD = feline bronchopulmonarydisease � MDI = metered-dose inhaler� PU/PD = polyuria/polydipsia
INTERNET RESOURCES� www.Aerokat.com: for ordering facemasksand spacers for inhalant therapy.� www.fritzthebrave.com: source for clients toresearch use of inhaled medications.
Suggested ReadingCohn LA, DeClue AE, Cohen RL, Reinero
CR. Effects of fluticasone propionate dosagein an experimental model of feline asthma.J Feline Med Surg 2010, 12(2):91–96.
Dye JA, McKiernan BC, Rozanski EA, et al.Bronchopulmonary disease in the cat:Historical, physical, radiographic,clinicopathologic, and pulmonaryfunctional evaluation of 24 affected and15 healthy cats. J Vet Intern Med 1996,10:385–399.
Kirschvink J, Leemans J, Delvaux F, et al.Inhaled fluticasone reduces bronchialresponsiveness and airway inflammation incats with mild chronic bronchitis. J FelineMed Surg 2006, 8(1):45–54.
Reinero CR, Delgado C, Spinka C, DeClueAE, Dhand R. Enantiomer-specific effectsof albuterol on airway inflammation inhealthy and asthmatic cats. Int Arch AllergyImmunol 2009, 150(1):43–50.
Author Carrie J. MillerConsulting Editors Lynelle R. Johnson
Client Education Handoutavailable online
BLBS078-CF_A69 BLBS078-Tilley June 16, 2011 11:3
Canine and Feline, Fifth Edition 123
Astrocytoma A
BASICSOVERVIEW� Categorized as a glial cell neoplasm, whichmost commonly affects the brain but rarelythe spinal cord. � Neoplastic cells are ofastrocyte origin. � This tumor is the mostcommon intra-axial (situated inside of thebrain parenchyma) intracranial neoplasm ofdogs but is rarely diagnosed in cats. � Tumorsare often located in the pyriform area of thetemporal lobe, the cerebral hemispheres, thethalamus, hypothalamus, or midbrain.� Biologic behavior of this tumor is dictatedby the degree of anaplasia (graded I–IV, frombest to worst prognosis). � Tumors typicallydo not penetrate the ventricular system ormetastasize outside of the cranial vault.
SIGNALMENT� Dogs—often brachycephalic breeds> 5 years of age; no sex predilection reported.� Cats—usually old (> 9 years); no sex orbreed predilection reported.
SIGNS� Location and growth kinetic dependent� Seizures � Behavioral changes� Disorientation � Loss of consciousproprioception � Cranial nerve abnormalities� Upper motor neuron tetraparesis
CAUSES & RISK FACTORSUnknown
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other primary tumors arising from tissuesof the central nervous system. � Metastaticneoplasia with brain tropism.� Granulomatous meningoencephalitis.� Trauma. � Cerebrovascular infarction.� Meningitis.
CBC/BIOCHEMISTRY/URINALYSISUsually normal
OTHER LABORATORY TESTSCSF analysis may show albuminocytologicdissociation (high protein with few cells).Analysis should include the characterizationof the fluid including color, turbidity, proteinconcentration, total nucleated cell count,cytologic evaluation, and titers for antibodiesagainst infectious agents; and culturing.
IMAGING� MRI of brain is ideal for mass lesionconfirmation. Unlike CT scanning,beam-hardening artifacts originating fromthick compact bone do not occur with MRI,and therefore MRI is superior for detectinglesions in the middle and caudal fossae.Additionally, MRI is more sensitive than CTfor the detection of subtle changes in soft
tissue chemical properties so infarcts andedema can be detected in an earlier stage.� CT of brain with and without contrast canbe useful for lesion confirmation but is not assensitive for soft tissue lesion imagingcompared to MRI.
DIAGNOSTIC PROCEDURES� Neurologic exam. � Ophthalmic exam.� Advanced imaging such as MRI or CT.� CSF analysis. � Brain biopsy is rarely donebecause of procedural induced morbidity;however, may provide a definitive diagnosisand aid in treatment planning and prognosis.
TREATMENT� Surgery. � Chemotherapy. � Radiationtherapy can be very effective in some cases,and consultation with a veterinary radiationoncologist is recommended.
MEDICATIONSDRUG(S)Seizure Control� Status epilepticus—diazepam (0.5–1 mg/kgIV given up to three times to achieve effect); ifno response to diazepam, use pentobarbital(5–15 mg/kg IV slowly to effect).� Long-term management—phenobarbital(1–4 mg/kg PO q12h) with or withoutadjuvant potassium bromide (20 mg/kg POq24h).
Tumor Control� Radiation therapy may be effective, andconsultation with a radiation oncologist isrecommended. Stereotactic radiosurgery orintensity modulated radiation therapy shouldbe considered first-line treatment options.� Chemotherapy may be effective for treatingdogs. Potential drugs that may exertmeasurable anticancer effects includelomustine (70 mg/m2 PO every 3 weeks) orcarmustine (50 mg/m2 IV every 6 weeks).� Prednisone (0.5–1 mg/kg q24h), althoughnot cytotoxic to cancer cells, may be effectivein controlling peri-tumoral edema andimproving clinical signs.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Prednisone and phenobarbital may causepolyphagia, polydipsia, and polyuria.� Phenobarbital may cause sedation for up to2 weeks after initiation of treatment, and maycause increase in hepatic enzymes on serumbiochemical panel. � CBC and platelet countis recommended 7–10 days afterchemotherapy and immediately before eachdose of chemotherapy to monitormyelosuppression. � Carmustine has thepotential of causing pulmonary toxicity atcumulative doses of 1,400 mg/m2.
� Chemotherapy may be toxic, and seekingadvice from a veterinary oncologist beforeinitiating treatment is recommended.
FOLLOW-UPPATIENT MONITORING� Blood phenobarbital concentration shouldbe assessed after 7–10 days of treatment, withmodifications to dosages for achieving targetplasma concentrations. � Serial CT or MRImaybe considered for documenting responseif clinically indicated and economicallyfeasible. � Serial CBC and platelet countsshould be performed to documentmyelotoxicity associated with chemotherapy.
EXPECTED COURSE AND PROGNOSIS� Long-term prognosis—guarded. � Survivaltime with no treatment is variable anddependent upon tumor and host factors.� Median survival after chemotherapy plusmedical management may be up to 7 months.� Median survival after radiation therapy hasbeen reported to be as high as 12 months.
MISCELLANEOUSPREGNANCY/FERTILITY/BREEDINGDo not breed animals undergoingchemotherapy
SEE ALSO� Seizures (Convulsions, StatusEpilepticus)—Cats � Seizures (Convulsions,Status Epilepticus)—Dogs
ABBREVIATIONS� CSF = cerebrospinal fluid � CT =computed tomography � MRI = magneticresonance imaging
Suggested ReadingBley CR, Sumova A, Roos M, Kaser-Hotz B.
Irradiation of brain tumors in dogs withneurologic disease. J Vet Intern Med 2005,19:849–854.
Meyerholz DG, Haynes JS. Solitary retinalastrocytoma in a dog. Vet Pathol 2004,41:177–178.
Morrison WB. Cancer affecting the nervoussystem. In: Morrison WB, ed., Cancer inDogs and Cats: Medical and SurgicalManagement. Jackson, WY: TetonNewMedia, 2002, pp. 631–640.
Snyder JM, Shofer FS, Van Winkle TJ, et al.Canine intracranial primary neoplasia: 173cases (1986-2003). J Vet Intern Med 2006,20:669–675.
Troxel MT, Vite CH, Van Winkle TJ, et al.Feline intracranial neoplasia: Retrospectivereview of 160 cases (1985-2001). J VetIntern Med 2003, 17:850–859.
Author Wallace B. MorrisonConsulting Editors Timothy M. Fan
BLBS078-CF_A70 BLBS078-Tilley June 1, 2011 12:47
124 Blackwell’s Five-Minute Veterinary Consult
Astrovirus InfectionA
BASICSOVERVIEWAn uncommon intestinal viral infectioncharacterized by enteritis and diarrhea.
SIGNALMENT� Cats� No known breed, sex, or age predilection
SIGNS� Small bowel diarrhea often green andwatery.� Kittens show more severe signs.� May be severe and acute enough to causedehydration and anorexia.
CAUSES & RISK FACTORS� A small, non-enveloped, RNA virus of thegenus Astrovirus.� Details of the incidence, prevalence, andpredisposing factors unknown.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Many causes of gastroenteritis.� Food allergy.� Toxin ingestion.� Inflammatory bowel disease.� Neoplasia.� Intestinal parasites.� Viral infections—panleukopenia, rotavirus,enteric coronavirus, enteric calicivirus.� Bacterial infections—salmonellosis,coliforms.� Protozoal infections—Giardia,cryptosporidiosis.
CBC/BIOCHEMISTRY/URINALYSISN/A
OTHER LABORATORY TESTS� Electron microscopy of feces—identifyastrovirus particles.� Difficult to isolate in the laboratory.
IMAGINGN/A
DIAGNOSTIC PROCEDURESNone
PATHOLOGIC FINDINGSNone described; similar to mildenteritis, rotavirus, or coronavirus enteritis.
TREATMENT� Control diarrhea.� Reestablish fluid and electrolyte balance.
MEDICATIONSDRUG(S)No specific antiviral drugs.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSNone
FOLLOW-UPPATIENT MONITORINGMonitor fluid and electrolytes.
PREVENTION/AVOIDANCEIsolate infected cats during acute disease.
POSSIBLE COMPLICATIONSSecondary intestinal viral and bacterialinfections.
EXPECTED COURSE AND PROGNOSIS� Illness usually < 1 week.� Mortality—appears low.� Prognosis—good.� If diarrhea persists, investigate other causes.
MISCELLANEOUSZOONOTIC POTENTIALSequence analysis of human and animalastroviruses suggests human-to-animaltransmission does not occur.
Suggested ReadingBarr MC, Olsen CW, Scott FW. Feline viral
diseases. In: Ettinger SJ, Feldman EC, eds.,Veterinary Internal Medicine. Philadelphia:Saunders, 1995, pp. 409–439.
Lukashov VV, Goudsmit J. Evolutionaryrelationships among Astroviridae. J GenVirol 2002, 83:1397–1405.
Author Fred W. ScottConsulting Editor Stephen C. Barr
BLBS078-CF_A71 BLBS078-Tilley March 22, 2011 11:20
Canine and Feline, Fifth Edition 125
Ataxia A
BASICSDEFINITION� A sign of sensory dysfunction that producesincoordination of the limbs, head, and/ortrunk.� Three clinical types—sensory(proprioceptive), vestibular, and cerebellar; allproduce changes in limb coordination, butvestibular and cerebellar ataxia also producechanges in head and neck movement.
PATHOPHYSIOLOGYSensory (Proprioceptive)� Proprioceptive pathways in the spinal cord(i.e., fasciculus gracilis, fasciculus cuneatus,and spinocerebellar tracts) relay limb andtrunk position to the brain.� When the spinal cord is slowly compressed,proprioceptive deficits are usually the firstsigns observed, because these pathways arelocated more superficially in the white matterand their larger sized axons are moresusceptible to compression than are othertracts.� Generally accompanied by weakness owingto early concomitant upper motor neuroninvolvement; weakness not always obviousearly in the course of the disease.� Ataxia can occur with spinal cord,brainstem, and cerebral lesions; mild withunilateral brainstem lesions, and subtle toabsent with unilateral cerebrallesion.
Vestibular� Changes in head and neck position arerelayed through the vestibulo-cochlear nerveto the brainstem.� Vestibular receptors or the nerve in theinner ear are considered part of the peripheralnervous system, whereas nuclei in thebrainstem are part of the central nervoussystem.� Localize the vestibular signs to peripheral orcentral vestibular nervous system becauseprognosis and rule-outs differ for these twolocations.� Both locations of vestibular disease causevarious degrees of disequilibrium withensuing vestibular ataxia.� Affected animal leans, tips, falls, or evenrolls toward the side of the lesion;accompanied by head tilt.� Central vestibular signs usually havechanging types of nystagmus or verticalnystagmus; somnolence, stupor, or coma (dueto involvement of the nearby reticularactivating system); multiple cranial nervesigns; proprioceptive deficits andquadriparesis or hemiparesis.� Peripheral vestibular signs do not includechanges in mental status, vertical nystagmus,proprioceptive deficits, quadriparesis orhemiparesis.
Cerebellar� The cerebellum regulates, coordinates, andmodulates motor activity.� Proprioception is normal because theascending proprioceptive pathways to thecortex are intact; weakness does not occurbecause the upper motor neurons are intact.� Inadequacy in the performance of motoractivity; strength preservation; noproprioceptive deficits.� Affected animal shows uncoordinatedmotor activity of limbs, head, and neck;hypermetria; dysmetria; head tremors;intention tremors; and truncal sway.
SYSTEMS AFFECTEDNervous—spinal cord (and brainstem andcortex), cerebellum, vestibular system.
SIGNALMENTAny age, breed, or sex
SIGNS� Important to define the type of ataxia tolocalize the problem.� Only one limb involved—consider alameness problem.� Only hind limbs affected—likely a spinalcord disorder affecting the spinocerebellartracts.� All or both ipsilateral limbsaffected—cerebellar.� Head tilt—vestibular.
CAUSESNeurologicCerebellar� Degenerative—abiotrophy (Kerry blueterriers, Gordon setters, rough-coated collies,Australian kelpies, Airedales, Bernesemountain dogs, Finnish harriers, Brittanyspaniels, border collies, beagles, Samoyeds,wirehaired fox terriers, Labrador retrievers,Great Danes, chow chows, Rhodesianridgebacks, domestic shorthair cats); storagediseases often have cerebellomedullaryinvolvement.� Anomalous—hypoplasia secondary toperinatal infection with panleukopenia virus(cats); malformed cerebellum due toherpesvirus infection (newborn puppies);arachnoid or epidermoid cyst located nearfourth ventricle.� Neoplastic—any CNS tumor (primary orsecondary) localized to the cerebellum.� Infectious—canine distemper virus; FIP;and any other CNS infection affecting thecerebellum.� Inflammatory, idiopathic,immune-mediated—granulomatousmeningoencephalomyelitis.� Toxic—metronidazole.Vestibular—Central Nervous System� Infectious—FIP; canine distemper virus;rickettsial diseases.� Inflammatory, idiopathic,immune-mediated—granulomatousmeningoencephalomyelitis.� Nutritional—thiamine deficiency.
� Toxic—metronidazole.Vestibular—Peripheral Nervous System� Infectious—otitis media interna;Cryptococcus granuloma (cats).� Idiopathic—geriatric vestibular disease(dogs); idiopathic vestibular syndrome (cats);nasopharyngeal (middle ear) polyps (cats).� Metabolic—hypothyroidism.� Neoplastic—squamous cell carcinoma, bonetumors.� Traumatic.Spinal Cord� Degenerative—degenerative myelopathy(old German shepherds, Welsh corgis).� Vascular—fibrocartilaginous embolicmyelopathy.� Anomalous—hemivertebrae; denshypoplasia with atlantoaxialsubluxation-luxation; Chiari-likemalformation; other spinal cord and vertebralmalformation; spinal arachnoid cyst.� Neoplastic—primary bone tumors; multiplemyeloma and metastatic tumors that infiltratethe vertebral body; meningioma;others.� Infectious—diskospondylitis; myelitis.� Traumatic—intervertebral disk herniation;fracture or luxation; cervicalspondylomyelopathy; atlantoaxialsubluxation-luxation.
Metabolic� Anemia.� Polycythemia.� Electrolyte disturbances—especiallyhypokalemia, hypocalcemia, andhypoglycemia.
Miscellaneous� Drugs—acepromazine; antihistamines;antiepileptic drugs.� Respiratory compromise.� Cardiac compromise—reverse PDA, aorticthromboembolism.
RISK FACTORS� Intervertebral disk disease—dachshunds,poodles, cocker spaniels, and beagles.� Cervical spondylomyelopathy—Dobermanpinschers and Great Danes.� Fibrocartilaginous embolism—young,large-breed dogs and miniature schnauzers.� Dens hypoplasia and atlantoaxialluxation—small-breed dogs, poodles.� Chiari-like malformation—Cavalier KingCharles spaniels, small-breed dogs.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Differentiate the types of ataxia.� Differentiate from other disease processesthat can affect gait—musculoskeletal,metabolic, cardiovascular, respiratory.� Musculoskeletal disorders—typicallyproduce lameness, pain, and a reluctance tomove; degenerative joint disease often
BLBS078-CF_A71 BLBS078-Tilley March 22, 2011 11:20
126 Blackwell’s Five-Minute Veterinary Consult
Ataxia (Continued)A
improves with increased movements.� Systemic illness and endocrine,cardiovascular, and metabolic disorders—cancause intermittent ataxia, especially of thepelvic limbs; with fever, weight loss,murmurs, arrhythmias, hair loss, or collapsewith exercise, suspect a non-neurologic cause;obtain minimum data from hemogram,biochemistry, and urinalysis.� Head tilt or nystagmus—likely vestibular.� Intention tremors of the head orhypermetria—likely cerebellar.� All four limbs affected: lesion is in thecervical area or is multifocal to diffuse; onlypelvic limbs affected: lesion is anywhere belowthe second thoracic vertebra.
CBC/BIOCHEMISTRY/URINALYSISNormal unless metabolic cause (e.g.,hypoglycemia, electrolyte imbalance, anemia,polycythemia).
OTHER LABORATORY TESTS� Hypoglycemia—determine serum insulinconcentration on the same sample (rule outinsulinoma).� Anemia—differentiate as nonregenerative orregenerative on the basis of the reticulocytecount.� Electrolyte imbalance—correct theproblem; see if ataxia resolves.� Antiepileptic drugs—if being administered,evaluate serum concentration for toxicity.
IMAGING� Spinal radiography, myelography, CT orMRI—if spinal cord dysfunction suspected.� Bullae radiography—if peripheral vestibulardisease suspected; CT or MRI superior; forinner ear disease, MRI superior to CT.� Thoracic radiography—for older patientsand patients suspected to have neoplasia orsystemic fungal infection.
� CT or MRI—if cerebellar disease suspected;evaluate potential brain disease. MRI superiorto CT.� Abdominal ultrasonography—if hepatic,renal, adrenal, or pancreatic dysfunctionsuspected.
DIAGNOSTIC PROCEDURESCerebrospinal fluid—helps confirm nervoussystem etiology.
TREATMENT� Usually outpatient, depending on severityand acuteness of clinical signs.� Exercise—decrease or restrict if spinal corddisease.� Client should monitor gait for increasingdysfunction or weakness; if paresis worsens orparalysis develops, other testing is warranted.� Avoid drugs that could contribute to theproblem; may not be possible in patients onantiepileptic drugs for seizures.
MEDICATIONSDRUG(S) OF CHOICENot recommended until the source or causeof the problem is identified.
FOLLOW-UPPATIENT MONITORINGPeriodic neurologic examinations to assesscondition.
POSSIBLE COMPLICATIONS� Spinal cord—progression to weakness andpossibly paralysis.
� Hypoglycemia—seizures.� Cerebellar disease—head tremors andbobbing.� Brainstem disease—stupor, coma, death.
MISCELLANEOUSAGE-RELATED FACTORSN/A
SEE ALSO� See specific causes� Cerebellar Degeneration� Head Tilt� Paralysis
ABBREVIATIONS� CNS = central nervous system� CT = computed tomography� FIP = feline infectious peritonitis� MRI = magnetic resonance imaging
INTERNET RESOURCESIVIS: www.ivis.org
Suggested ReadingDavies C, Shell L. Neurological problems. In:
Common Small Animal Medical Diagnoses:An Algorithmic Approach. Philadelphia:Saunders, 2002, pp. 36–59.
Lorenz MD, Kornegay JN. Handbook ofVeterinary Neurology, 4th ed. Philadelphia:Saunders, 2004, pp. 219–244.
Thomas WB. Vestibular dysfunction. VetClin North Am Small Anim Pract 2000,30:227–249.
Author Linda G. ShellConsulting Editor Joane M. Parent
Client Education Handoutavailable online
BLBS078-CF_A72 BLBS078-Tilley June 24, 2011 13:9
Canine and Feline, Fifth Edition 127
Atherosclerosis A
BASICSOVERVIEWThickening of the inner arterial wall inassociation with lipid deposits. Chronicarterial change characterized by loss ofelasticity, luminal narrowing, andproliferating and degenerative lesions of theintima and media.
SIGNALMENT� Rare in dogs.� Not described in cats.� Higher prevalence in miniature schnauzer,Doberman pinscher, poodle, and Labradorretriever.� Geriatric patients (> 9 years).
SIGNSHistorical Findings� None in some animals� Lethargy� Anorexia� Weakness� Dyspnea� Collapse� Vomiting� Diarrhea
Physical Examination Findings� Dyspnea� Irregular rhythm� Heart failure� Disorientation� Blindness� Circling� Coma� Episodic lameness
CAUSES & RISK FACTORS� Severe hypothyroidism� Increasing age� Hyperlipidemia in miniature schnauzers� Male gender (male dogs may havepredisposition)� High total cholesterol� Diabetes� Glomerulonephritis
DIAGNOSISDIFFERENTIAL DIAGNOSISArteriosclerosis
CBC/BIOCHEMISTRY/URINALYSIS� Hypercholesterolemia� Hyperlipidemia� High BUN and creatinine� High liver enzymes
OTHER LABORATORY TESTS� Low T3 and T4.� High values for alpha-2 and beta fractionson protein electrophoresis.
IMAGINGRadiographyThoracic and abdominal radiographs mayreveal cardiomegaly and hepatomegaly.
DIAGNOSTIC PROCEDURESElectrocardiography� Conduction abnormalities and notchedQRS complexes.� Atrial fibrillation.� ST segment elevation or depression withmyocardial infarction.
TREATMENT� Treat the underlying disorder and clinicalsigns (e.g., dyspnea if congestive heart failuredevelops).� Diet—low-fat diet, weight loss program,and high soluble fiber intake to controlhyperlipidemia.
MEDICATIONSDRUG(S)� Treat conduction disturbances andarrhythmias if clinically indicated.� Thyroid replacement if hypothyroidism isconfirmed.� Antihypertensive therapy if hypertension isdocumented.� Blood cholesterol-reducing medications ifhyperlipidemic.� Treat diabetes.
CONTRAINDICATIONS/POSSIBLEINTERACTIONSN/A
FOLLOW-UP� Monitor T4 concentration 4–6 hourspost-administration after the first 6 weeks oftreatment and adjust dosage accordingly.� Monitor blood triglyceride and cholesterollevels.� Monitor ECG for conduction disturbancesand ST segment changes.
MISCELLANEOUSASSOCIATED CONDITIONS� Hypothyroidism� Diabetes� Mitral valve disease (myxomatous)� Glomerulonephritis
AGE-RELATED FACTORSGeriatric patients (> 9 years)
SEE ALSOMyocardial Infarction
INTERNET RESOURCESwww.vetgo.com/cardio
Suggested ReadingDrost WT, Bahr RJ, Henay GA, Campbell
GA. Aortoiliac thrombus secondary to amineralized arteriosclerotic lesion. VetRadiol Ultrasound 1999, 40:262–266.
Hamlen HJ. Sinoatrial node arteriosclerosis intwo young dogs. JAVMA 1994, 204:751.
Hess RS, Kass PH, Van Winkle JV.Association between diabetes mellitus,hypothyroidism or hyperadrenocorticismand atherosclerosis in dogs. J Vet InternMed 2003, 17:489–494.
Kidd L, Stepien RL, Amrheiw DP. Clinicalfindings and coronary artery disease in dogsand cats with acute and subacute myocardialnecrosis: 28 cases. JAAHA 2000,36:199–208.
Liu SK, Tilley LP, Tappe JP, Fox PR. Clinicaland pathologic findings in dogs withatherosclerosis: 21 cases (1970–1983).JAVMA 1986, 189:227–232.
Author Larry P. TilleyConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
BLBS078-CF_A73 BLBS078-Tilley June 26, 2011 8:34
128 Blackwell’s Five-Minute Veterinary Consult
Atlantoaxial InstabilityA
BASICSOVERVIEW� Results from malformation or disruption ofthe articulation between the first and secondcervical vertebrae (atlas and axis, respectively);causes spinal cord compression.� AA instability can result in spinal cordtrauma or compression at the junctionbetween the atlas and axis—may cause neckpain and/or varying degrees of generalproprioceptive (GP) ataxia /upper motorneuron (UMN) tetraparesis, tetraplegia (withor without nociception), and death fromrespiratory arrest.
Etiology� Congenital: anomaly of the dens (aplasia,hypoplasia, or malformation [dorsalangulation] of the dens) and its ligamentousattachments.� Acquired: may be a consequence oftraumatic injury.
SIGNALMENT� Congenital—toy-breed dogs (Yorkshireterriers, miniature or toy poodles,Chihuahuas, Pekingese, and Pomeranians).� Age at onset—usually before 12 months ofage.� Uncommon in larger-breed dogs, dogs > 1year old, and cats.� No sex predilection.
SIGNS� Intermittent or progressive ambulatorytetraparesis, usually with neck pain—mostcommon.� Signs vary from mild to moderateGP/UMN ambulatory tetraparesis tonon-ambulatory GP/UMN tetraparesis, ortetraplegia depending on degree of spinal cordcompression and secondary pathology (i.e.,edema, hemorrhage, or gliosis).� Neck pain without concurrent neurologicdeficits.� Episodes of collapse secondary to weakness.� Spinal reflexes are normal to exaggeratedwith normal to increased muscle tone in allfour limbs.� Acute death may occur when accompaniedby trauma and respiratory arrest(uncommon).
CAUSES & RISK FACTORS� Usually caused by abnormal development ofthe dens or ligamentous support structures,resulting in subluxation of the atlantoaxialjoint.� Fracture of the axis.� Clinical signs often occur as a result of mildor insignificant trauma (e.g., jumping orplaying).� Clinical signs may be exacerbated by activitysuch as flexion of the neck.� Toy-breed dogs—at risk for congenitalmalformation of the dens.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Differential diagnoses are consistent withvarious causes of cervical myelopathies,including:
◦ Other congenital malformation.◦ Trauma.◦ Meningitis or meningomyelitis (i.e.,infectious or non-infectious(granulomatousmeningoencephalomyelitis).◦ Fibrocartilaginous embolic myelopathy.◦ Disk herniation.◦ Neoplasia.
CBC/BIOCHEMISTRY/URINALYSISNormal
IMAGING� Plain radiography of the cervical vertebralcolumn:
◦ Lateral view—caudal and dorsaldisplacement of the axis in relationship tothe atlas, resulting in an increased distancebetween vertebrae.◦ Ventral dorsal or oblique view—mayreveal absence, hypoplasia, or malformation(dorsal angulation) of the dens.
� Cross-sectional imaging:◦ MRI.◦ Imaging modality of choice.◦ Diagnosis based on observation of caudaland dorsal displacement of the axis inrelationship to the atlas as evidenced by thefollowing features of the atlantoaxialarticulation:
� Dorsal: displacement of the spinousprocess of the axis.� Ventral: increased size of theoccipito-atlas-axis joint cavity.
◦ Allows identification of spinal cordcompression.◦ Allows recognition of secondary spinalcord pathology such as edema,hemorrhage, or gliosis, which may impactprognosis.
� Computed tomography:◦ May provide detailed visualization ofbony structures, which allows for thecreation of three-dimensional reconstructedimage to help surgical planning.
� Precautions:◦ Proper positioning may require sedationor general anesthesia.
� Sedation or general anesthesia carriessignificant risk for iatrogenictrauma.� Care needs to be exercised whenpositioning animals.� AVOID FLEXION OF THE NECK.� Flexion may exacerbate compression,which may worsen clinical signs or causedeath due to spinal cord trauma.� To protect against neck flexion duringrecovery, affected animals should be
closely monitored until they are capableof maintaining normal head and neckcarriage.
TREATMENT� Prior to treatment, consultation with aboard-certified neurologist or surgeon shouldbe pursued.� Improper treatment can lead to irreversibledeterioration in neurologic function.
MEDICAL� Neck brace (splint) to stabilize the cervicalvertebral column in extension.
◦ Fiberglass cast material is positionedventrally from the rostral aspect ofmandible to the xiphoid and incorporatedinto bandage material, which immobilizesthe head and neck.◦ Strict exercise restriction (cageconfinement) for a minimum of 8 weeks.◦ Frequent bandage/splint changes areneeded.
� Adjunctive medication (see below).
Overall Prognosis� Successful outcome observed in 62.5% ofdogs.� Improved prognosis was associated with anacute onset and short duration of clinicalsigns (< 30 days).� Surgery is recommended to treat animalsthat fail to improve or experience recurrenceof signs following medical treatment.
SURGERY� Treatment of choice in the majority of cases.� Surgical approach; ventral method ispreferred.
◦ Ventral approach—variety of methods:� Transarticular pinning or lag screwtechnique; ventral tips of the pinsincorporated in polymethylmethacrylateto prevent pin migration.� Transarticular pinning and ventralcortical screws or K-wires in the bodiesof the atlas and axis +/− K-wiresapplied longitundinally and wired to thescrews; screw heads and K-wires areincorporated in polymethylmethacrylateto provide fixation.� Dorsal approach—use wire orsynthetic suture material to fix thespinous process of the axis to the dorsalarch of the atlas; provides less rigidfixation and may be associated withgreater implant failure.
� Strict exercise restriction is required for thefirst month post-operatively, followed by agradual return to activity over an additionalmonth.� Adjunctive medication (see below).� Overall prognosis ranges from 63% to 91%success: improved prognosis was associatedwith young (< 24 months) dogs, duration of
BLBS078-CF_A73 BLBS078-Tilley June 26, 2011 8:34
Canine and Feline, Fifth Edition 129
(Continued) Atlantoaxial Instability A
clinical signs < 10 months, and mildneurologic deficits.� Complications:
◦ Failure to improve/worsening ofneurological deficits.◦ Implant failure/infection.◦ Respiratory—dyspnea, cough, andaspiration pneumonia.◦ Death.
MEDICATIONSDRUG(S)� Anti-inflammatory medication:
◦ Corticosteroids: prednisone 0.5–1.0mg/kg PO divided twice daily for 2 weeks,followed by a tapering regime. Suggestedprotocol following initial dose: 0.5 mg/kgPO daily for 5 days, followed by 0.5 mg/kgPO every other day for 5 days.◦ NSAID: 1- to 4-week course.
� Analgesia:◦ Tramadol 2.0–4.0 mg/kg PO q6–8h.◦ Gabapentin 10–20 mg/kg PO q6–8h.
CONTRAINDICATIONS/POSSIBLEINTERACTIONS� Corticosteroid—use caution when given inconjunction with medical treatment; mayreduce pain, resulting in increased activity andspinal cord trauma.� Avoid NSAIDs in combination withcorticosteroids in all patients—increases riskof life-threatening gastrointestinalhemorrhage.
FOLLOW-UP� Dogs treated medically require frequent(weekly) bandage changes for associated softtissue trauma.
� All dogs should be reevaluated at 1 and 3months (post-operatively or after neck braceremoval) and monthly until neurologicaldeficits resolve or remain static over 2–3months.� More frequent rechecks may be needed fordogs experiencing complications or recurrenceof signs.� Untreated animals may experiencedeterioration in neurologic function,catastrophic acute spinal cord trauma,respiratory arrest, and death.
MISCELLANEOUS� Rehabilitation may play a significant role inthe ultimate neurologic functional level of thepatient.� Rehabilitation should only be considered indogs > 30 days post-operatively or after neckbrace (splint) removal.
ABBREVIATIONS� GP = general proprioceptive� MRI = magnetic resonance imaging� NSAID = nonsteroidal anti-inflammatorydrug� UMN = upper motor neuron
INTERNET RESOURCEShttp://www.acvs.org/AnimalOwners/HealthConditions/SmallAnimalTopics/AtlantoaxialInstability/.
Suggested ReadingBeaver DP, Ellison GW, Lewis DD. Risk
factors affecting the outcome of surgery foratlantoaxial subluxation in dogs: 46 cases(1978–1998). JAVMA 2000,216(7):1104–1109.
Fossum TW, Hedlund CS, Johnson AL, et al.Small Animal Surgery. St. Louis:Mosby-Year Book, 1997.
Havig ME, Cornell KK, Hawthorne JC,McDonnell JJ, Selcer BA. Evaluation ofnonsurgical treatment of atlantoaxialsubluxation in dogs: 19 cases (1992–2001).JAVMA 2005, 227(2):257–262.
McCarthy RJ, Lewis DD, Hosgood G.Atlantoaxial subluxation in dogs. CompendContin Educ Pract Vet 1995, 17:215–226
Platt SR, Chambers JN, Cross A. A modifiedventral fixation for surgical management ofatlantoaxial subluxation in 19 dogs. VetSurg 2004, 33(4):349–354.
Sanders SG, Bagley RS, Silver GM, Moore M,Tucker RL. Outcomes and complicationsassociated with ventral screws, pins, andpolymethyl methacrylate for atlantoaxialinstability in 12 dogs. JAAHA 2004,40:204–210.
Schulz KS, Waldron DR, Fahie M.Application of ventral pins andpolymethylmethacrylate for themanagement of atlantoaxial instability:Results in nine dogs. Vet Surg 1997,26(4):317–325.
Shires PK. Atlantoaxial instability. In: SlatterD, ed., Textbook of Small Animal Surgery,3rd ed. Philadelphia: Saunders, 2003.
Tomlinson J. Surgical conditions of thecervical spine. Semin Vet Med Surg SmallAnim 1996, 11(4):225–234.
Authors Mathieu M. Glassman and MarcKentConsulting Editor Peter K. Shires
BLBS078-CF_A74 BLBS078-Tilley July 23, 2011 5:20
130 Blackwell’s Five-Minute Veterinary Consult
Atopic DermatitisA
BASICSDEFINITION� Hypersensitivity reaction to normallyinnocuous substances, such as pollens(grasses, weeds, and trees), molds, house dustmites, epithelial allergens, and otherenvironmental allergens. � Manifests as aninflammatory, chronically relapsing,non-contagious and pruritic skin disease.
PATHOPHYSIOLOGY� Susceptible animals become sensitized toenvironmental allergens by producingallergen-specific IgE (mediated throughLangerhans cells). � Allergen-specific IgEbinds to receptor sites on cutaneous mastcells. � Allergen reexposure, primarily bypercutaneous absorption, causes mast celldegranulation (type I immediatehypersensitivity reaction) and results in therelease of histamine, proteolytic enzymes,cytokines, chemokines, and many otherchemical mediators. � Th2-type cytokineresponse predominates in the acute phase.� In chronic (intrinsic) atopic dermatitis, aTh1-type cytokine response predominates.Bacterial superantigens, auto-antigens releasedvia keratinocyte damage, and Malassezia mayplay a role in perpetuating the inflammation.
SYSTEMS AFFECTED� Ophthalmic � Respiratory � Skin/Exocrine
GENETICS� Dogs—inherited predisposition; mode ofinheritance is unknown and environmentalinfluences are important. � Cats—unclear.
INCIDENCE/PREVALENCE� Canine—true prevalence is unknown;estimated at 3–15% of the canine population;reported to be the second most commonallergic skin disease in the past; however, withthe availability of effective flea controlmeasures, atopic dermatitis may now be moreprevalent. � Feline—unknown; generallybelieved to be much lower than that for dogs.
GEOGRAPHIC DISTRIBUTIONCanine—recognized worldwide; localenvironmental factors (temperature,humidity, and flora) influence the seasonality,severity, and duration of signs.
SIGNALMENTSpeciesDogs and cats
Breed Predilections� Canine—any breed, including mongrels;recognized more frequently in certain breedsor families (can vary geographically). � UnitedStates—Boston terrier, cairn terrier,Dalmatian, English bulldog, English setter,Irish setter, Lhasa apso, miniature schnauzer,pug, Sealyham terrier, Scottish terrier, West
Highland white terrier, wirehaired fox terrier,and golden retriever. � Feline—none reported.
Mean Age and RangeCanine—mean age at onset 1–3 years; range3 months–6 years; signs may be mild the firstyear but usually progress and becomeclinically apparent before 3 years of age.
Predominant SexNone reported
SIGNSGeneral Comments� Pruritus—itching, scratching, rubbing,licking. � Most cutaneous changes caused byself-induced trauma; primary lesions usuallyunrecognized.
Historical Findings� Facial, pedal, or axillary pruritus � Early ageof onset � History in related individuals� May be initially seasonal � Recurring skin orear infection � Temporary response toglucocorticosteroids � Symptomsprogressively worsen with time
Physical Examination Findings� Areas most commonly affected—interdigitalspaces, carpal and tarsal areas, muzzle,periocular region, axillae, groin, and pinnae.� Lesions—vary from none to broken hairs orsalivary discoloration to erythema, papularreactions, crusts, alopecia,hyperpigmentation, lichenification,excessively oily or dry seborrhea, andhyperhidrosis (apocrine sweating).� Secondary bacterial and yeast skin infections(common). � Chronic relapsing otitis externa.� Conjunctivitis may occur.
CAUSES� Pollens (grasses, weeds, and trees) � Moldspores (indoor and outdoor) � Malassezia� House dust mite � Animal dander � Insects(controversial) � Cytokine dysregulation
RISK FACTORS� Temperate environments with long allergyseasons and high pollen and mold spore levels.� Concurrent pruritic dermatoses, such as fleabite hypersensitivity and adverse food reaction(summation effect).
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Adverse food reaction—may cause identicallesion distribution and physical examinationfindings but should be non-seasonal; mayoccur concurrently with atopic dermatitis;differentiation is made by noting response tohypoallergenic diet. � Flea bitehypersensitivity—most common cause ofseasonal pruritus in appropriate geographicalregions; may occur concurrently with atopicdermatitis; differentiation is made by notinglesion distribution, response to flea control,
and elimination of other causes. � Sarcopticmange—often occurs in young or stray dogs;causes severe pruritus of the ventral chest,lateral elbows, lateral hocks, and pinnalmargins; differentiation by multiple skinscrapings and/or complete response to a trialof miticidal therapy. � Secondarypyoderma—usually caused by Staphylococcuspseudintermedius; characterized by follicularpapules, pustules, crusts, and epidermalcollarettes. � Secondary yeastinfections—caused by Malasseziapachydermatis; characterized by erythematous,scaly, crusty, greasy, and very malodorousbody folds and intertriginous areas;differentiation by demonstration of numerousbudding yeast organisms by skin cytology andobtaining a favorable response to antifungaltherapy. � Contact dermatitis (allergic orirritant)—may cause severe erythema andpruritus of the feet and thinly haired areas ofthe ventrum.
CBC/BIOCHEMISTRY/URINALYSISEosinophilia—rare in dogs withoutconcurrent flea infestations; common incats.
OTHER LABORATORY TESTSSerologic Allergy Tests� Tests to measure the amount ofallergen-specific IgE antibody in the patient’sserum are commercially available.� Advantages over IDT—availability; largeareas of hair do not have to be shaved;sedation is not required.� Disadvantages—frequent false-positive orfalse-negative reactions; limited number ofallergens tested; inconsistent assay validation,quality control, and reliability (may vary withthe laboratory used).
DIAGNOSTIC PROCEDURESIntradermal Test (Preferred)� Diagnosis of atopy is made by the history,physical examination, and ruling out ofdifferential diagnoses. � Intradermal testing isused to formulate an immunotherapyprescription. � Small amounts of test allergenare injected intradermally; wheal formation ismeasured and evaluated subjectively. � Resultsmore difficult to interpret in cats owing to therelatively small wheals produced. � Falsepositive and false negative reactions mayoccur.
PATHOLOGIC FINDINGS� Gross lesions—see “Physical ExaminationFindings.” � Skin biopsy—may help rule outother differential diagnoses; results are usuallynot pathognomonic.� Dermatohistopathologicchanges—acanthosis, mixed mononuclearsuperficial perivascular dermatitis, sebaceousgland metaplasia, with secondary superficialbacterial folliculitis.
BLBS078-CF_A74 BLBS078-Tilley July 23, 2011 5:20
Canine and Feline, Fifth Edition 131
(Continued) Atopic Dermatitis A
TREATMENTAPPROPRIATE HEALTH CAREOutpatient
ACTIVITYAvoid offending allergens when possible
DIETDiets rich in essential fatty acids may bebeneficial
CLIENT EDUCATION� Explain the progressive nature of thecondition. � Inform client that it rarely goesinto remission and cannot be cured. � Informclient that some form of therapy may benecessary to maintain quality of life.
MEDICATIONSDRUG(S) OF CHOICEImmunotherapy (Hyposensitization)� Administration of subcutaneous injectionsof gradually increasing doses of the causativeallergens to reduce sensitivity. � Allergenselection—based on allergy test results,patient history, and/or knowledge of localexposure. � Immunotherapy formulationprocedures and administration protocols arenot standardized and vary widely betweenclinicians. � Indicated when it is desirable toavoid or reduce the amount of corticosteroidsrequired to control signs, when signs lastlonger than 4–6 months per year, or whennon-steroid forms of therapy are ineffective.� Successfully reduces pruritus in 60–80% ofdogs and cats. � Response is usually slow,often requiring 3–6 months and up to 1 year,for full effect.
Cyclosporine� Cyclosporine (Atopica 5 mg/kg/day)effective in controlling pruritus associatedwith chronic atopic dermatitis. � Response issimilar to that of glucocorticosteroids.� Onset of activity is slower (1–4 weeks istypical). � Many patients can be adequatelycontrolled long term with less frequent dosing(every 2–4 days). � Frequent patientmonitoring is recommended.
Corticosteroids� May be given for short-term relief and tobreak the itch-scratch cycle. � Should betapered to the lowest dosage that adequatelycontrols pruritus. � Prednisolone ormethylprednisolone tablets (0.2–0.5 mg/kgPO q48h). � Cats—infrequentmethylprednisolone acetate by injection(4 mg/kg).
Antihistamines� Less effective than are corticosteroids.� Evidence of efficacy is poor.� Dogs—hydroxyzine (1–2 mg/kg PO q12h),chlorpheniramine (0.2–0.4 mg/kg PO q12h),diphenhydramine (2.2 mg/kg PO q12h), andclemastine (0.04–0.10 mg/kg PO q12h).� Cats—chlorpheniramine (0.5 mg/kg POq12h); efficacy estimated at 10–50%.
PRECAUTIONS� Corticosteroids—use judiciously in dogs toavoid iatrogenic hyperglucocorticism andassociated problems, aggravation ofpyoderma, and induction of demodicosis.� Antihistamines—can produce drowsiness,anorexia, vomiting, diarrhea, and evenincreased pruritus; use with caution inpatients with cardiac arrhythmias.
POSSIBLE INTERACTIONSConcurrent use of cyclosporine andketoconazole requires a dose reduction ofcyclosporine.
ALTERNATIVE DRUG(S)� Frequent bathing in cool water withantipruritic shampoos is very beneficial.� Diets rich in fatty acids may benefit pruriticpatients; some studies have indicated that ω-3(eicosapentaenoic acid 66 mg/kg/day) may bemore effective than ω-6 (linoleic acid 130mg/kg/day) fatty acids. � Tricyclicantidepressants (doxepin 1–2 mg/kg POq12h; or amitriptyline 1–2 mg/kg PO q12h)have been given to dogs as antipruritics buttheir overall effectiveness and mode of actionis unclear; not extensively studied in the cat.� Topical triamcinolone spray .015% (GenesisVirbac) can be used over large body surfacesto control pruritus with minimal side effects.
FOLLOW-UPPATIENT MONITORING� Examine patient every 2–8 weeks when anew course of therapy is started. � Monitorpruritus, self-trauma, development ofbacterial folliculitis, and possible adverse drugreactions. � Once an acceptable level ofcontrol is achieved, examine patient every3–12 months. � CBC, serum chemistryprofile, and urinalysis—recommended every3–12 months for patients on chroniccorticosteroid or cyclosporine therapy.
PREVENTION/AVOIDANCE� If the offending allergens have beenidentified through allergy testing, the ownershould undertake to reduce the animal’sexposure as much as possible; seldom makes a
significant impact on the level ofpruritus. � Minimizing other sources ofpruritus (e.g., flea infestation, adverse foodreaction, and secondary skin infection) mayreduce the level of pruritus.
POSSIBLE COMPLICATIONS� Secondary bacterial folliculitis or Malasseziadermatitis. � Concurrent flea bitehypersensitivity and/or adverse food reaction.
EXPECTED COURSE AND PROGNOSIS� Not life-threatening unless intractablepruritus results in euthanasia. � Untreated,the degree of pruritus worsens and theduration of signs last longer eachyear. � Some cases spontaneously resolve.
MISCELLANEOUSASSOCIATED CONDITIONS� Flea bite hypersensitivity � Adverse foodreaction/ food hypersensitivity � Bacterialfolliculitis � Malassezia dermatitis � Otitisexterna
AGE-RELATED FACTORSSeverity worsens with age
PREGNANCY/FERTILITY/BREEDING� Corticosteroids—contraindicated duringpregnancy � Affected animals should not beused for breeding
SYNONYMS� Atopy � Canine atopic disease
SEE ALSO� Flea Bite Hypersensitivity and Flea Control� Food Reactions, Dermatologic � OtitisExterna and Media � Pyoderma
ABBREVIATIONS� IDT = intradermal test
Suggested ReadingReedy LM, Miller WH, Willemse T. Allergic
Skin Diseases of Dogs and Cats, 2nd ed.Philadelphia: Saunders, 1997.
Author Alexander H. WernerConsulting Editor Alexander H. Werner
Client Education Handoutavailable online
BLBS078-CF_A75 BLBS078-Tilley March 22, 2011 12:7
132 Blackwell’s Five-Minute Veterinary Consult
Atrial Fibrillation and Atrial FlutterA
BASICSDEFINITION� Atrial fibrillation—rapid, irregularlyirregular supraventricular rhythm. Two formsrecognized: primary atrial fibrillation, anuncommon disease that occurs mostly in largedogs with no underlying cardiac disease, andsecondary atrial fibrillation, which occurs indogs and cats secondary to underlying cardiacdisease.� Atrial flutter is similar to atrial fibrillation,but the atrial rate is generally slower and ischaracterized by saw-toothed flutter waves inthe baseline of the ECG. The ventricularresponse is generally rapid but may be regularor irregular.
ECG FEATURESAtrial Flutter� Atrial rhythm usually regular; rateapproximately 300–400 bpm.� P waves usually discerned as either discreteP waves or a “saw-toothed” baseline.� Ventricular rhythm and rate generallydepend on the atrial rate and AV nodalconduction, but are generally regular orregularly irregular and rapid.� Conduction pattern to the ventricles isvariable—in some cases every other atrialdepolarization produces a ventriculardepolarization (2:1 conduction ratio), giving aregular ventricular rhythm; other times theconduction pattern appears random, givingan irregular ventricular rhythm that canmimic atrial fibrillation.
Secondary Atrial Fibrillation� No P waves present—baseline may be flat ormay have small irregular undulations(“f” waves); some undulations may look like Pwaves.� Ventricular rate high—usually 180–240bpm in dogs and > 220 bpm in cats.� Interval between QRS complexes isirregularly irregular; QRS complexes usuallyappear normal.
Primary Atrial FibrillationSimilar to secondary atrial fibrillation exceptventricular rate usually in the normal range.
PATHOPHYSIOLOGY� Atrial fibrillation—caused by numeroussmall reentrant pathways creating a rapid(> 500 depolarizations/minute) anddisorganized depolarization pattern in theatria that results in cessation of atrialcontraction. Depolarizations continuouslybombard the AV nodal tissue, which acts as afilter and does not allow all depolarizations toconduct to the ventricles. Many atrialdepolarizations activate only a part of the atriabecause the rapid rate renders portions of theatria refractory, and thus they cannot reach theAV junction. Other atrial impulses penetrate
into the AV junctional tissue but are notrobust enough to penetrate the entire length.Blocked impulses affect the conductionproperties of the AV junctional tissue andalter conduction of subsequent electricalimpulses; electrical impulses are conductedthrough the AV junction irregularly,producing an irregular ventricular rhythm.� Atrial flutter—probably originates fromone site of reentry that moves continuouslythroughout the atrial myocardiumand frequently and regularly stimulatesthe AV node. When the atrial rate becomessufficiently fast, the refractory period of the AVnode exceeds the cycle length (P to P interval)of the SVT, and some atrial depolarizationsare blocked from traversing the AVnode (functional second-degree AV block).
SYSTEMS AFFECTEDCardiovascularLoss of atrial contraction may result indecreased stroke volume and cardiac outputdepending on heart rate; high heart rate mayresult in deterioration in myocardial function(tachycardia-induced myocardial failure).
GENETICSNo breeding studies available
INCIDENCE/PREVALENCEN/A
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsLarge- and giant-breed dogs are more proneto primary atrial fibrillation.
Mean Age and RangeN/A
Predominant SexN/A
SIGNSGeneral Comments� Generally relate to the underlying diseaseprocess and/or CHF rather than thearrhythmia itself, but previously stableanimals may decompensate.� Patients with primary atrial fibrillation aregenerally asymptomatic but may demonstratemild exercise intolerance.
Historical Findings� Coughing/dyspnea/tachypnea.� Exercise intolerance.� Rarely syncope.� Dogs with primary atrial fibrillation aretypically asymptomatic.
Physical Examination Findings� On auscultation, patients with atrialfibrillation have an erratic heart rhythm thatsounds like “tennis shoes in a dryer.”� First heart sound intensity in atrialfibrillation is variable; second heart sound
only heard on beats with effective ejection,not on every beat.� Third heart sounds (gallop sounds) may bepresent.� Patients with atrial fibrillation have pulsedeficits and variable pulse quality.� Signs of CHF often present (e.g., cough,dyspnea, cyanosis).
CAUSES� Chronic valvular disease� Cardiomyopathy� Congenital heart disease� Digoxin toxicity� Idiopathic� Ventricular preexcitation (atrial flutter)
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Frequent atrial (supraventricular) prematuredepolarizations� Supraventricular tachycardia with AV block
CBC/BIOCHEMISTRY/URINALYSISN/A
OTHER LABORATORY TESTSN/A
IMAGING� Echocardiography and radiography maycharacterize type and severity of theunderlying cardiac disease; moderate to severeleft atrial enlargement common.� Typically normal in patients with primaryatrial fibrillation, although mild left atrialenlargement may accompany thehemodynamic alterations imposed by thearrhythmia.
DIAGNOSTIC PROCEDURESN/A
PATHOLOGIC FINDINGSN/A
TREATMENTAPPROPRIATE HEALTH CARE� Patients with fast (secondary) atrialfibrillation are treated medically to slow theventricular rate. Converting the atrialfibrillation to sinus rhythm would be ideal,but such attempts in patients with severeunderlying heart disease or left atrialenlargement are generally futile because of alow success rate and high rate of recurrence.Consider quinidine or electrical cardioversionto sinus rhythm for a dog with primary atrialfibrillation.� Patients with primary atrial fibrillation maybe converted back to normal sinus rhythm.The success rate depends on chronicity.Patients that have been in atrial fibrillationfor > 4 months generally have a lower success
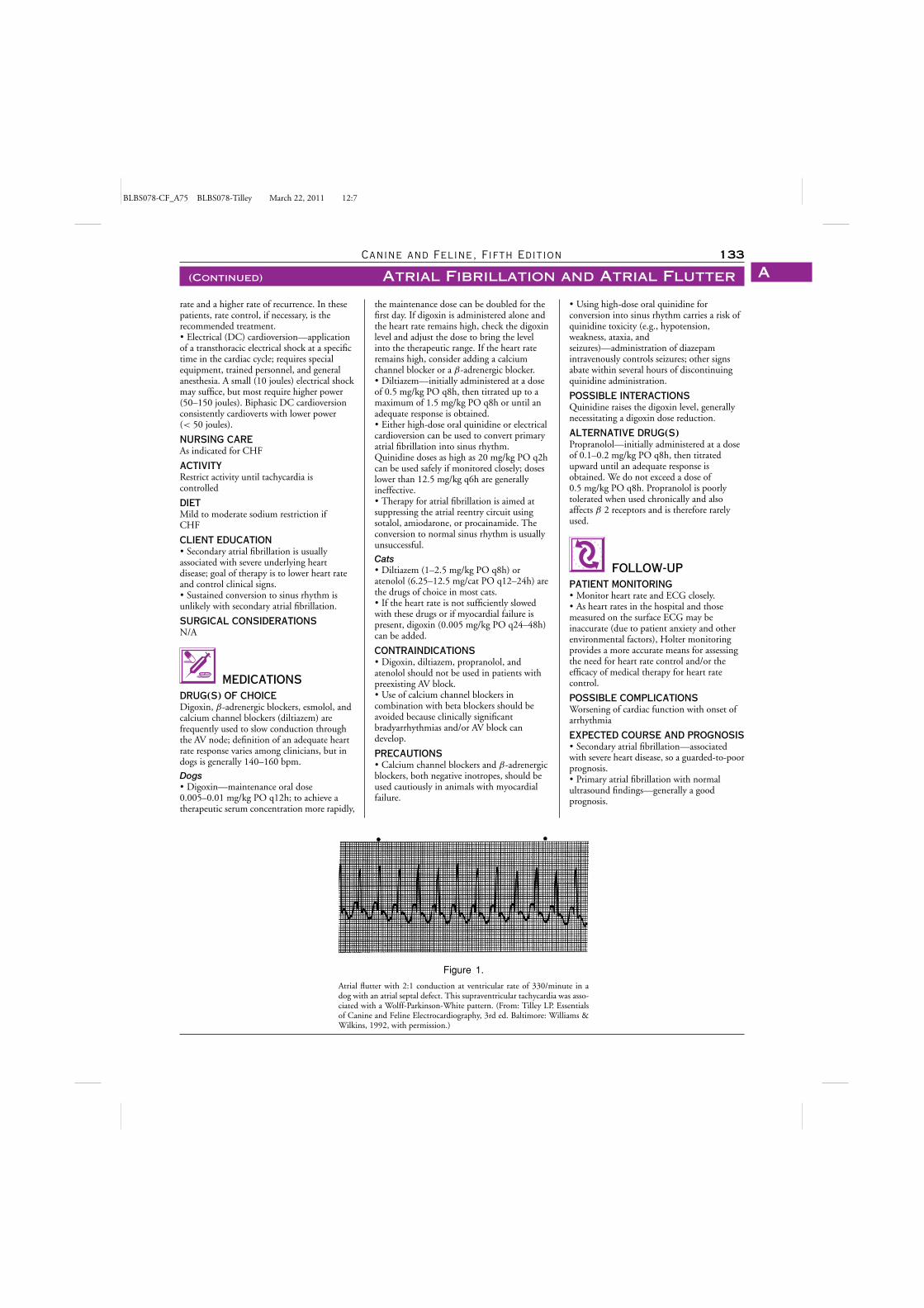
BLBS078-CF_A75 BLBS078-Tilley March 22, 2011 12:7
Canine and Feline, Fifth Edition 133
(Continued) Atrial Fibrillation and Atrial Flutter A
rate and a higher rate of recurrence. In thesepatients, rate control, if necessary, is therecommended treatment.� Electrical (DC) cardioversion—applicationof a transthoracic electrical shock at a specifictime in the cardiac cycle; requires specialequipment, trained personnel, and generalanesthesia. A small (10 joules) electrical shockmay suffice, but most require higher power(50–150 joules). Biphasic DC cardioversionconsistently cardioverts with lower power(< 50 joules).
NURSING CAREAs indicated for CHF
ACTIVITYRestrict activity until tachycardia iscontrolled
DIETMild to moderate sodium restriction ifCHF
CLIENT EDUCATION� Secondary atrial fibrillation is usuallyassociated with severe underlying heartdisease; goal of therapy is to lower heart rateand control clinical signs.� Sustained conversion to sinus rhythm isunlikely with secondary atrial fibrillation.
SURGICAL CONSIDERATIONSN/A
MEDICATIONSDRUG(S) OF CHOICEDigoxin, β-adrenergic blockers, esmolol, andcalcium channel blockers (diltiazem) arefrequently used to slow conduction throughthe AV node; definition of an adequate heartrate response varies among clinicians, but indogs is generally 140–160 bpm.
Dogs� Digoxin—maintenance oral dose0.005–0.01 mg/kg PO q12h; to achieve atherapeutic serum concentration more rapidly,
Figure 1.
Atrial flutter with 2:1 conduction at ventricular rate of 330/minute in adog with an atrial septal defect. This supraventricular tachycardia was asso-ciated with a Wolff-Parkinson-White pattern. (From: Tilley LP. Essentialsof Canine and Feline Electrocardiography, 3rd ed. Baltimore: Williams &Wilkins, 1992, with permission.)
the maintenance dose can be doubled for thefirst day. If digoxin is administered alone andthe heart rate remains high, check the digoxinlevel and adjust the dose to bring the levelinto the therapeutic range. If the heart rateremains high, consider adding a calciumchannel blocker or a β-adrenergic blocker.� Diltiazem—initially administered at a doseof 0.5 mg/kg PO q8h, then titrated up to amaximum of 1.5 mg/kg PO q8h or until anadequate response is obtained.� Either high-dose oral quinidine or electricalcardioversion can be used to convert primaryatrial fibrillation into sinus rhythm.Quinidine doses as high as 20 mg/kg PO q2hcan be used safely if monitored closely; doseslower than 12.5 mg/kg q6h are generallyineffective.� Therapy for atrial fibrillation is aimed atsuppressing the atrial reentry circuit usingsotalol, amiodarone, or procainamide. Theconversion to normal sinus rhythm is usuallyunsuccessful.
Cats� Diltiazem (1–2.5 mg/kg PO q8h) oratenolol (6.25–12.5 mg/cat PO q12–24h) arethe drugs of choice in most cats.� If the heart rate is not sufficiently slowedwith these drugs or if myocardial failure ispresent, digoxin (0.005 mg/kg PO q24–48h)can be added.
CONTRAINDICATIONS� Digoxin, diltiazem, propranolol, andatenolol should not be used in patients withpreexisting AV block.� Use of calcium channel blockers incombination with beta blockers should beavoided because clinically significantbradyarrhythmias and/or AV block candevelop.
PRECAUTIONS� Calcium channel blockers and β-adrenergicblockers, both negative inotropes, should beused cautiously in animals with myocardialfailure.
� Using high-dose oral quinidine forconversion into sinus rhythm carries a risk ofquinidine toxicity (e.g., hypotension,weakness, ataxia, andseizures)—administration of diazepamintravenously controls seizures; other signsabate within several hours of discontinuingquinidine administration.
POSSIBLE INTERACTIONSQuinidine raises the digoxin level, generallynecessitating a digoxin dose reduction.
ALTERNATIVE DRUG(S)Propranolol—initially administered at a doseof 0.1–0.2 mg/kg PO q8h, then titratedupward until an adequate response isobtained. We do not exceed a dose of0.5 mg/kg PO q8h. Propranolol is poorlytolerated when used chronically and alsoaffects β 2 receptors and is therefore rarelyused.
FOLLOW-UPPATIENT MONITORING� Monitor heart rate and ECG closely.� As heart rates in the hospital and thosemeasured on the surface ECG may beinaccurate (due to patient anxiety and otherenvironmental factors), Holter monitoringprovides a more accurate means for assessingthe need for heart rate control and/or theefficacy of medical therapy for heart ratecontrol.
POSSIBLE COMPLICATIONSWorsening of cardiac function with onset ofarrhythmia
EXPECTED COURSE AND PROGNOSIS� Secondary atrial fibrillation—associatedwith severe heart disease, so a guarded-to-poorprognosis.� Primary atrial fibrillation with normalultrasound findings—generally a goodprognosis.
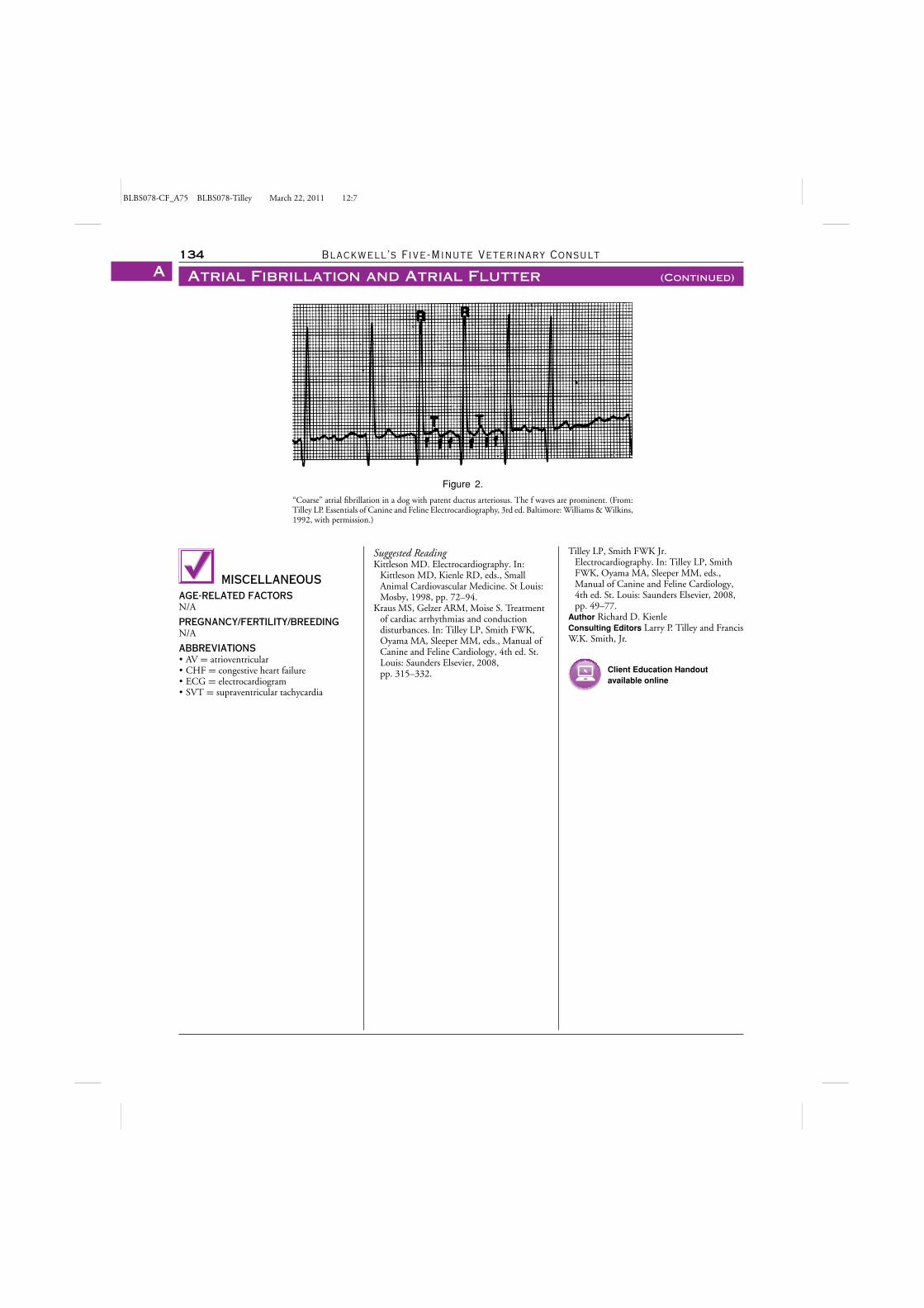
BLBS078-CF_A75 BLBS078-Tilley March 22, 2011 12:7
134 Blackwell’s Five-Minute Veterinary Consult
Atrial Fibrillation and Atrial Flutter (Continued)A
Figure 2.
“Coarse” atrial fibrillation in a dog with patent ductus arteriosus. The f waves are prominent. (From:Tilley LP. Essentials of Canine and Feline Electrocardiography, 3rd ed. Baltimore: Williams & Wilkins,1992, with permission.)
MISCELLANEOUSAGE-RELATED FACTORSN/A
PREGNANCY/FERTILITY/BREEDINGN/A
ABBREVIATIONS� AV = atrioventricular� CHF = congestive heart failure� ECG = electrocardiogram� SVT = supraventricular tachycardia
Suggested ReadingKittleson MD. Electrocardiography. In:
Kittleson MD, Kienle RD, eds., SmallAnimal Cardiovascular Medicine. St Louis:Mosby, 1998, pp. 72–94.
Kraus MS, Gelzer ARM, Moise S. Treatmentof cardiac arrhythmias and conductiondisturbances. In: Tilley LP, Smith FWK,Oyama MA, Sleeper MM, eds., Manual ofCanine and Feline Cardiology, 4th ed. St.Louis: Saunders Elsevier, 2008,pp. 315–332.
Tilley LP, Smith FWK Jr.Electrocardiography. In: Tilley LP, SmithFWK, Oyama MA, Sleeper MM, eds.,Manual of Canine and Feline Cardiology,4th ed. St. Louis: Saunders Elsevier, 2008,pp. 49–77.
Author Richard D. KienleConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
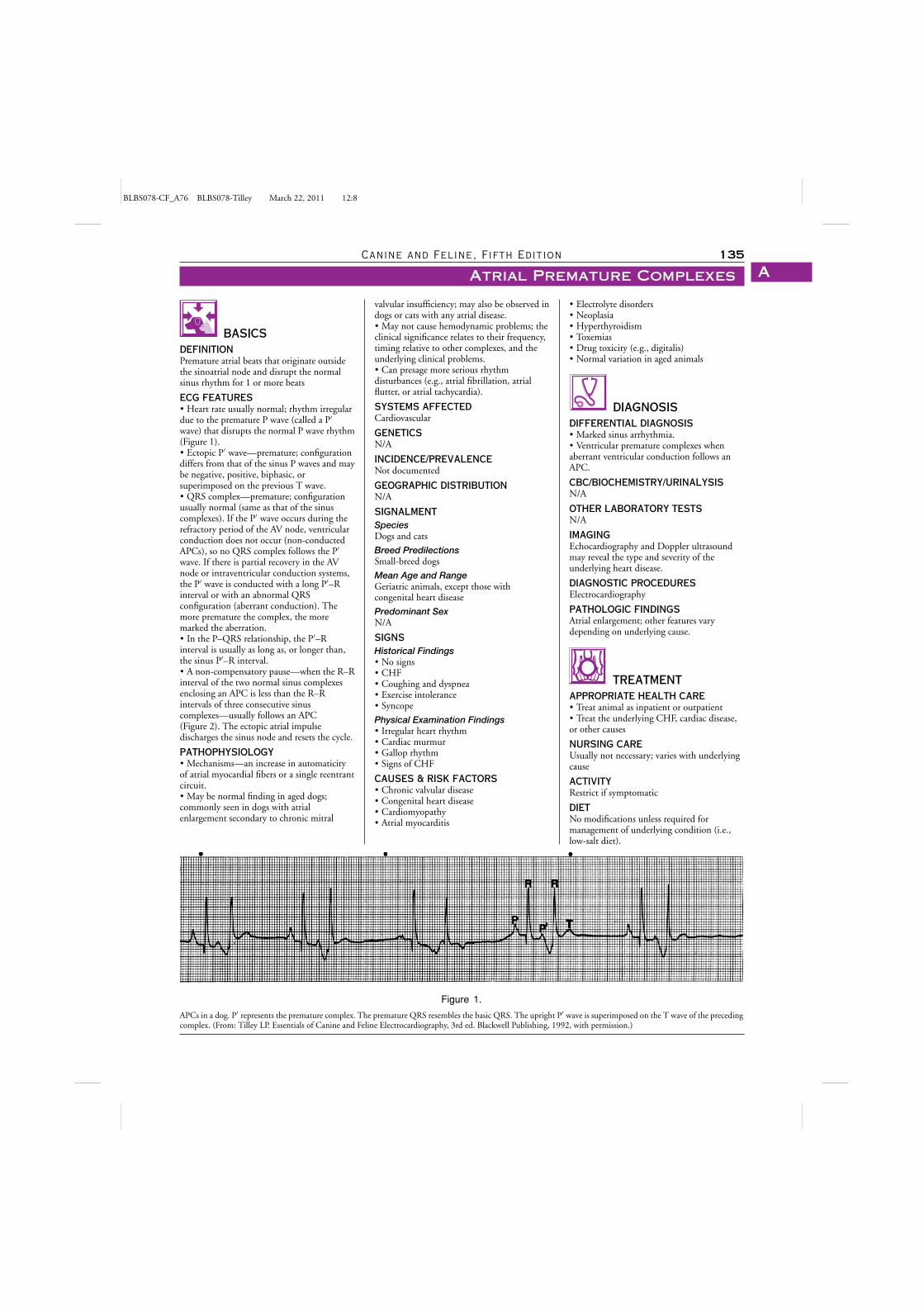
BLBS078-CF_A76 BLBS078-Tilley March 22, 2011 12:8
Canine and Feline, Fifth Edition 135
Atrial Premature Complexes A
BASICSDEFINITIONPremature atrial beats that originate outsidethe sinoatrial node and disrupt the normalsinus rhythm for 1 or more beats
ECG FEATURES� Heart rate usually normal; rhythm irregulardue to the premature P wave (called a P′
wave) that disrupts the normal P wave rhythm(Figure 1).� Ectopic P′ wave—premature; configurationdiffers from that of the sinus P waves and maybe negative, positive, biphasic, orsuperimposed on the previous T wave.� QRS complex—premature; configurationusually normal (same as that of the sinuscomplexes). If the P′ wave occurs during therefractory period of the AV node, ventricularconduction does not occur (non-conductedAPCs), so no QRS complex follows the P′
wave. If there is partial recovery in the AVnode or intraventricular conduction systems,the P′ wave is conducted with a long P′–Rinterval or with an abnormal QRSconfiguration (aberrant conduction). Themore premature the complex, the moremarked the aberration.� In the P–QRS relationship, the P′–Rinterval is usually as long as, or longer than,the sinus P′–R interval.� A non-compensatory pause—when the R–Rinterval of the two normal sinus complexesenclosing an APC is less than the R–Rintervals of three consecutive sinuscomplexes—usually follows an APC(Figure 2). The ectopic atrial impulsedischarges the sinus node and resets the cycle.
PATHOPHYSIOLOGY� Mechanisms—an increase in automaticityof atrial myocardial fibers or a single reentrantcircuit.� May be normal finding in aged dogs;commonly seen in dogs with atrialenlargement secondary to chronic mitral
Figure 1.
APCs in a dog. P′ represents the premature complex. The premature QRS resembles the basic QRS. The upright P′ wave is superimposed on the T wave of the precedingcomplex. (From: Tilley LP. Essentials of Canine and Feline Electrocardiography, 3rd ed. Blackwell Publishing, 1992, with permission.)
valvular insufficiency; may also be observed indogs or cats with any atrial disease.� May not cause hemodynamic problems; theclinical significance relates to their frequency,timing relative to other complexes, and theunderlying clinical problems.� Can presage more serious rhythmdisturbances (e.g., atrial fibrillation, atrialflutter, or atrial tachycardia).
SYSTEMS AFFECTEDCardiovascular
GENETICSN/A
INCIDENCE/PREVALENCENot documented
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsSmall-breed dogs
Mean Age and RangeGeriatric animals, except those withcongenital heart disease
Predominant SexN/A
SIGNSHistorical Findings� No signs� CHF� Coughing and dyspnea� Exercise intolerance� Syncope
Physical Examination Findings� Irregular heart rhythm� Cardiac murmur� Gallop rhythm� Signs of CHF
CAUSES & RISK FACTORS� Chronic valvular disease� Congenital heart disease� Cardiomyopathy� Atrial myocarditis
� Electrolyte disorders� Neoplasia� Hyperthyroidism� Toxemias� Drug toxicity (e.g., digitalis)� Normal variation in aged animals
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Marked sinus arrhythmia.� Ventricular premature complexes whenaberrant ventricular conduction follows anAPC.
CBC/BIOCHEMISTRY/URINALYSISN/A
OTHER LABORATORY TESTSN/A
IMAGINGEchocardiography and Doppler ultrasoundmay reveal the type and severity of theunderlying heart disease.
DIAGNOSTIC PROCEDURESElectrocardiography
PATHOLOGIC FINDINGSAtrial enlargement; other features varydepending on underlying cause.
TREATMENTAPPROPRIATE HEALTH CARE� Treat animal as inpatient or outpatient� Treat the underlying CHF, cardiac disease,or other causes
NURSING CAREUsually not necessary; varies with underlyingcause
ACTIVITYRestrict if symptomatic
DIETNo modifications unless required formanagement of underlying condition (i.e.,low-salt diet).
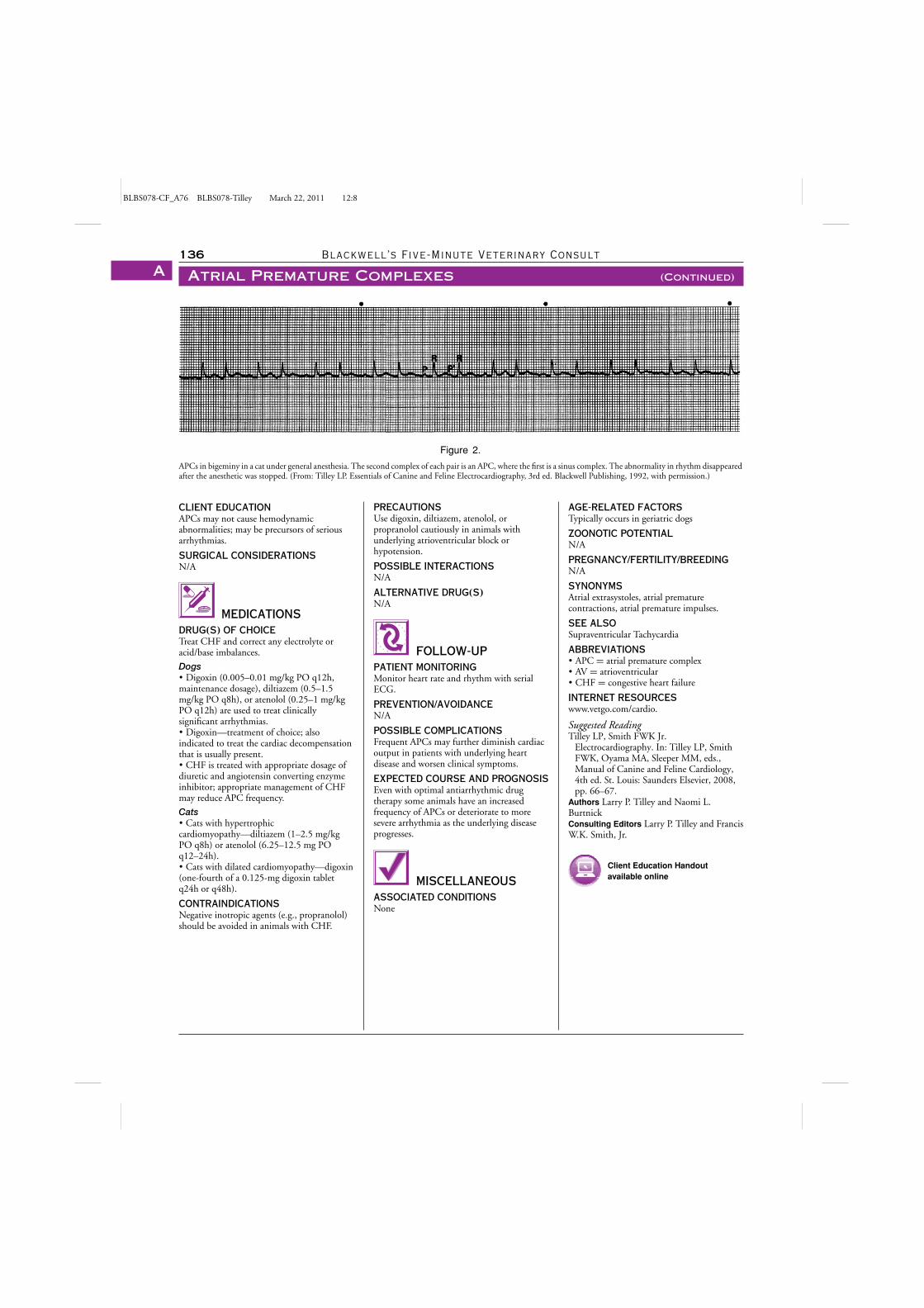
BLBS078-CF_A76 BLBS078-Tilley March 22, 2011 12:8
136 Blackwell’s Five-Minute Veterinary Consult
Atrial Premature Complexes (Continued)A
Figure 2.
APCs in bigeminy in a cat under general anesthesia. The second complex of each pair is an APC, where the first is a sinus complex. The abnormality in rhythm disappearedafter the anesthetic was stopped. (From: Tilley LP. Essentials of Canine and Feline Electrocardiography, 3rd ed. Blackwell Publishing, 1992, with permission.)
CLIENT EDUCATIONAPCs may not cause hemodynamicabnormalities; may be precursors of seriousarrhythmias.
SURGICAL CONSIDERATIONSN/A
MEDICATIONSDRUG(S) OF CHOICETreat CHF and correct any electrolyte oracid/base imbalances.
Dogs� Digoxin (0.005–0.01 mg/kg PO q12h,maintenance dosage), diltiazem (0.5–1.5mg/kg PO q8h), or atenolol (0.25–1 mg/kgPO q12h) are used to treat clinicallysignificant arrhythmias.� Digoxin—treatment of choice; alsoindicated to treat the cardiac decompensationthat is usually present.� CHF is treated with appropriate dosage ofdiuretic and angiotensin converting enzymeinhibitor; appropriate management of CHFmay reduce APC frequency.
Cats� Cats with hypertrophiccardiomyopathy—diltiazem (1–2.5 mg/kgPO q8h) or atenolol (6.25–12.5 mg POq12–24h).� Cats with dilated cardiomyopathy—digoxin(one-fourth of a 0.125-mg digoxin tabletq24h or q48h).
CONTRAINDICATIONSNegative inotropic agents (e.g., propranolol)should be avoided in animals with CHF.
PRECAUTIONSUse digoxin, diltiazem, atenolol, orpropranolol cautiously in animals withunderlying atrioventricular block orhypotension.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGMonitor heart rate and rhythm with serialECG.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONSFrequent APCs may further diminish cardiacoutput in patients with underlying heartdisease and worsen clinical symptoms.
EXPECTED COURSE AND PROGNOSISEven with optimal antiarrhythmic drugtherapy some animals have an increasedfrequency of APCs or deteriorate to moresevere arrhythmia as the underlying diseaseprogresses.
MISCELLANEOUSASSOCIATED CONDITIONSNone
AGE-RELATED FACTORSTypically occurs in geriatric dogs
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMSAtrial extrasystoles, atrial prematurecontractions, atrial premature impulses.
SEE ALSOSupraventricular Tachycardia
ABBREVIATIONS� APC = atrial premature complex� AV = atrioventricular� CHF = congestive heart failure
INTERNET RESOURCESwww.vetgo.com/cardio.
Suggested ReadingTilley LP, Smith FWK Jr.
Electrocardiography. In: Tilley LP, SmithFWK, Oyama MA, Sleeper MM, eds.,Manual of Canine and Feline Cardiology,4th ed. St. Louis: Saunders Elsevier, 2008,pp. 66–67.
Authors Larry P. Tilley and Naomi L.BurtnickConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
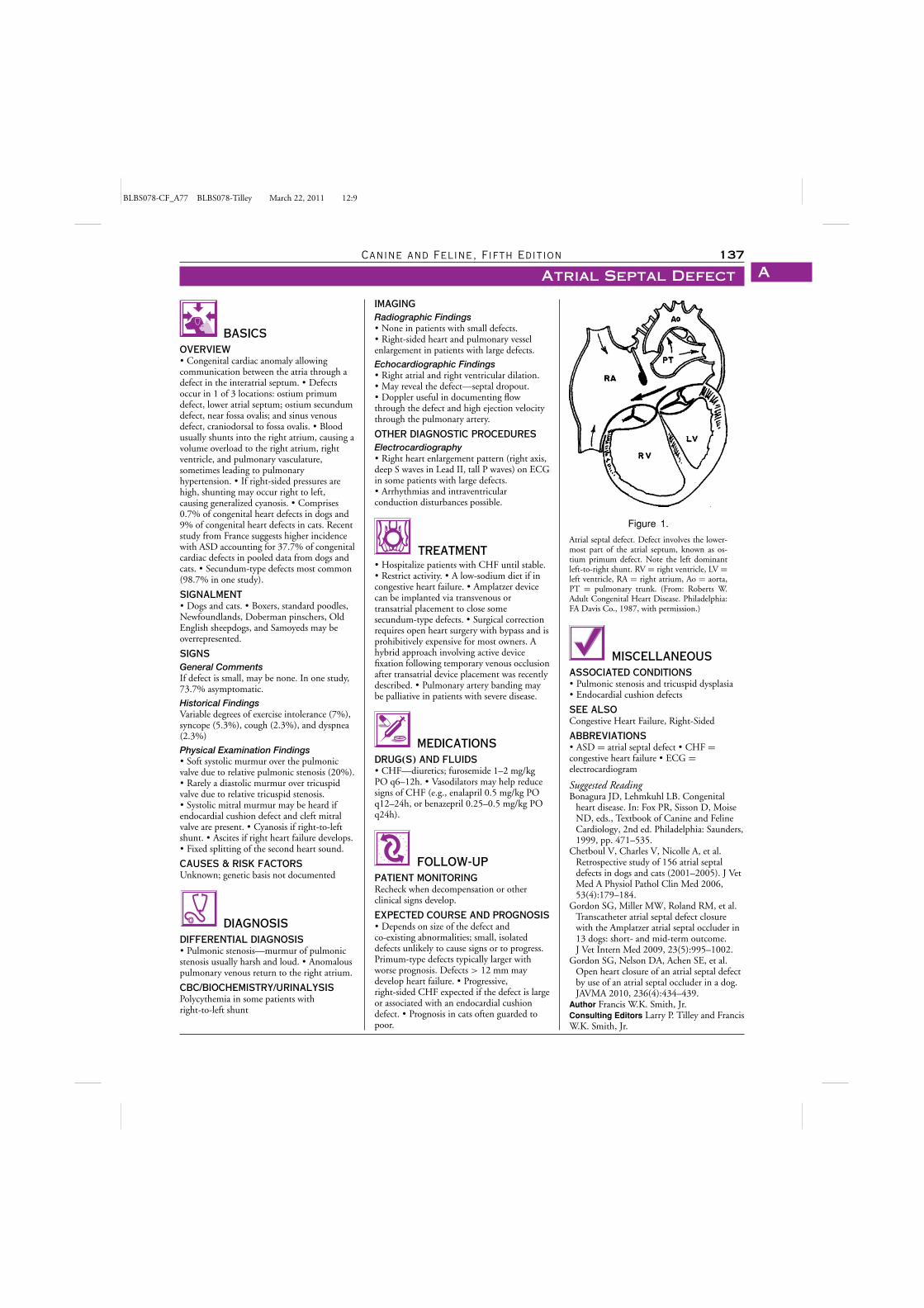
BLBS078-CF_A77 BLBS078-Tilley March 22, 2011 12:9
Canine and Feline, Fifth Edition 137
Atrial Septal Defect A
BASICSOVERVIEW� Congenital cardiac anomaly allowingcommunication between the atria through adefect in the interatrial septum. � Defectsoccur in 1 of 3 locations: ostium primumdefect, lower atrial septum; ostium secundumdefect, near fossa ovalis; and sinus venousdefect, craniodorsal to fossa ovalis. � Bloodusually shunts into the right atrium, causing avolume overload to the right atrium, rightventricle, and pulmonary vasculature,sometimes leading to pulmonaryhypertension. � If right-sided pressures arehigh, shunting may occur right to left,causing generalized cyanosis. � Comprises0.7% of congenital heart defects in dogs and9% of congenital heart defects in cats. Recentstudy from France suggests higher incidencewith ASD accounting for 37.7% of congenitalcardiac defects in pooled data from dogs andcats. � Secundum-type defects most common(98.7% in one study).
SIGNALMENT� Dogs and cats. � Boxers, standard poodles,Newfoundlands, Doberman pinschers, OldEnglish sheepdogs, and Samoyeds may beoverrepresented.
SIGNSGeneral CommentsIf defect is small, may be none. In one study,73.7% asymptomatic.
Historical FindingsVariable degrees of exercise intolerance (7%),syncope (5.3%), cough (2.3%), and dyspnea(2.3%)
Physical Examination Findings� Soft systolic murmur over the pulmonicvalve due to relative pulmonic stenosis (20%).� Rarely a diastolic murmur over tricuspidvalve due to relative tricuspid stenosis.� Systolic mitral murmur may be heard ifendocardial cushion defect and cleft mitralvalve are present. � Cyanosis if right-to-leftshunt. � Ascites if right heart failure develops.� Fixed splitting of the second heart sound.
CAUSES & RISK FACTORSUnknown; genetic basis not documented
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Pulmonic stenosis—murmur of pulmonicstenosis usually harsh and loud. � Anomalouspulmonary venous return to the right atrium.
CBC/BIOCHEMISTRY/URINALYSISPolycythemia in some patients withright-to-left shunt
IMAGINGRadiographic Findings� None in patients with small defects.� Right-sided heart and pulmonary vesselenlargement in patients with large defects.
Echocardiographic Findings� Right atrial and right ventricular dilation.� May reveal the defect—septal dropout.� Doppler useful in documenting flowthrough the defect and high ejection velocitythrough the pulmonary artery.
OTHER DIAGNOSTIC PROCEDURESElectrocardiography� Right heart enlargement pattern (right axis,deep S waves in Lead II, tall P waves) on ECGin some patients with large defects.� Arrhythmias and intraventricularconduction disturbances possible.
TREATMENT� Hospitalize patients with CHF until stable.� Restrict activity. � A low-sodium diet if incongestive heart failure. � Amplatzer devicecan be implanted via transvenous ortransatrial placement to close somesecundum-type defects. � Surgical correctionrequires open heart surgery with bypass and isprohibitively expensive for most owners. Ahybrid approach involving active devicefixation following temporary venous occlusionafter transatrial device placement was recentlydescribed. � Pulmonary artery banding maybe palliative in patients with severe disease.
MEDICATIONSDRUG(S) AND FLUIDS� CHF—diuretics; furosemide 1–2 mg/kgPO q6–12h. � Vasodilators may help reducesigns of CHF (e.g., enalapril 0.5 mg/kg POq12–24h, or benazepril 0.25–0.5 mg/kg POq24h).
FOLLOW-UPPATIENT MONITORINGRecheck when decompensation or otherclinical signs develop.
EXPECTED COURSE AND PROGNOSIS� Depends on size of the defect andco-existing abnormalities; small, isolateddefects unlikely to cause signs or to progress.Primum-type defects typically larger withworse prognosis. Defects > 12 mm maydevelop heart failure. � Progressive,right-sided CHF expected if the defect is largeor associated with an endocardial cushiondefect. � Prognosis in cats often guarded topoor.
Figure 1.
Atrial septal defect. Defect involves the lower-most part of the atrial septum, known as os-tium primum defect. Note the left dominantleft-to-right shunt. RV = right ventricle, LV =left ventricle, RA = right atrium, Ao = aorta,PT = pulmonary trunk. (From: Roberts W.Adult Congenital Heart Disease. Philadelphia:FA Davis Co., 1987, with permission.)
MISCELLANEOUSASSOCIATED CONDITIONS� Pulmonic stenosis and tricuspid dysplasia� Endocardial cushion defects
SEE ALSOCongestive Heart Failure, Right-Sided
ABBREVIATIONS� ASD = atrial septal defect � CHF =congestive heart failure � ECG =electrocardiogram
Suggested ReadingBonagura JD, Lehmkuhl LB. Congenital
heart disease. In: Fox PR, Sisson D, MoiseND, eds., Textbook of Canine and FelineCardiology, 2nd ed. Philadelphia: Saunders,1999, pp. 471–535.
Chetboul V, Charles V, Nicolle A, et al.Retrospective study of 156 atrial septaldefects in dogs and cats (2001–2005). J VetMed A Physiol Pathol Clin Med 2006,53(4):179–184.
Gordon SG, Miller MW, Roland RM, et al.Transcatheter atrial septal defect closurewith the Amplatzer atrial septal occluder in13 dogs: short- and mid-term outcome.J Vet Intern Med 2009, 23(5):995–1002.
Gordon SG, Nelson DA, Achen SE, et al.Open heart closure of an atrial septal defectby use of an atrial septal occluder in a dog.JAVMA 2010, 236(4):434–439.
Author Francis W.K. Smith, Jr.Consulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
BLBS078-CF_A78 BLBS078-Tilley July 15, 2011 8:57
138 Blackwell’s Five-Minute Veterinary Consult
Atrial StandstillA
BASICSDEFINITIONECG rhythm characterized by absence of Pwaves; condition can be temporary (e.g.,associated with hyperkalemia ordrug-induced), terminal (e.g., associated withsevere hyperkalemia or dying heart), orpersistent.
ECG FeaturesPersistent Atrial Standstill� P waves absent.� Heart rate usually slow (< 60 bpm).� Rhythm regular with supraventricular typeQRS complexes.� Heart rate does not increase with atropineadministration.Hyperkalemic Atrial Standstill� Heart rate normal or slow.� Rhythm regular or irregular.� QRS complexes tend to be wide andbecome wider as the potassium level rises;with severe hyperkalemia (potassium > 10mEq/L), the QRS complexes are replaced by asmooth biphasic curve.� Heart rate may increase slightly withatropine.
PATHOPHYSIOLOGYPersistent Atrial StandstillCaused by an atrial muscular dystrophy;skeletal muscle involvement common.
Hyperkalemic Atrial StandstillGenerally occurs with serum potassium levels> 8.5 mEq/L; value influenced by serumsodium and calcium levels and acid-basestatus. Hyperkalemic patients with atrialstandstill have sinus node function, butimpulses do not activate atrial myocytes; thus,the associated rhythm is termed asinoventricular rhythm. Since the sinus nodeis functional, an irregular rhythm may be dueto sinus arrhythmia.
SYSTEMS AFFECTEDCardiovascular
GENETICSNone
INCIDENCE/PREVALENCERare rhythm disturbance
GEOGRAPHIC DISTRIBUTIONNone
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsPersistent atrial standstill—most common inEnglish springer spaniels; other breedsoccasionally affected.
Mean Age and RangeMost animals with persistent atrial standstillare young; animals with hypoadrenocorticismare usually young to middle-aged.
Predominant SexHypoadrenocorticism more common infemales (69%).
SIGNSHistorical Findings� Vary with underlying cause.� Lethargy common; syncope may occur.� Patients with persistent atrial standstill mayshow signs of congestive heart failure.
Physical Examination Findings� Vary with underlying cause.� Bradycardia common.� Patients with persistent atrial standstill mayhave skeletal muscle wasting of theantebrachium and scapula.
CAUSES� Hyperkalemia.� Atrial disease, often associated with atrialdistension (e.g., cats with cardiomyopathy).� Atrial myopathy (persistent atrial standstill).
RISK FACTORSHyperkalemic Atrial Standstill� Hypoadrenocorticism.� Conditions leading to obstruction orrupture of the urinary tract.� Oliguric or anuric renal failure.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Slow atrial fibrillation� Sinus bradycardia with small P waves lost inthe baseline
CBC/BIOCHEMISTRY/URINALYSISPersistent Atrial Standstill� Normal.
Hyperkalemic Atrial Standstill� Hyperkalemia.� Hyponatremia and sodium:potassium ratio< 27 if atrial standstill secondary tohypoadrenocorticism.� Azotemia and hyperphosphatemia withhypoadrenocorticism, renal failure, andrupture or obstruction of the urinary tract.
OTHER LABORATORY TESTSACTH stimulation test ifhypoadrenocorticism suspected
IMAGINGEchocardiogram and electromyography ifpersistent atrial standstillsuspected—cardiomegaly and depressedcontractility may be seen.
DIAGNOSTIC PROCEDURESSkeletal muscle biopsy in animals withpersistent atrial standstill.
PATHOLOGIC FINDINGSPersistent Atrial Standstill� Greatly enlarged and paper-thin atria;usually biatrial involvement, although one
case of only left atrial involvement wasreported.� Severe scapular and brachial muscle wastingin some dogs.� Marked fibrosis, fibroelastosis, chronicmononuclear cell inflammation, and steatosisthroughout the atria and interatrial septum.
TREATMENTAPPROPRIATE HEALTH CAREPersistent Atrial StandstillNot life-threatening condition; animal can betreated as an outpatient.
Hyperkalemic Atrial StandstillPotentially life-threatening; often requiresaggressive treatment.
NURSING CAREAggressive fluid therapy with 0.9% salineoften required to correct hypovolemia andlower serum potassium levels (seeHyperkalemia) in patients with hyperkalemicatrial standstill.
ACTIVITYRestrict activity in patients with persistentatrial standstill and signs of CHF orsyncope.
DIETN/A
CLIENT EDUCATIONPersistent Atrial StandstillClinical signs generally improve afterpacemaker implantation; signs of CHF maydevelop, and weakness and lethargy maypersist even after heart rate and rhythm arecorrected with the pacemaker.
SURGICAL CONSIDERATIONSPersistent Atrial StandstillImplant permanent ventricular pacemaker toregulate rate and rhythm.
Hyperkalemic Atrial StandstillHyperkalemia secondary to urinary tractobstruction or rupture may require surgery.
MEDICATIONSDRUG(S) OF CHOICEPersistent Atrial StandstillTreat with diuretics and ACE inhibitor (e.g.,enalapril or benazepril) if CHF develops.
Hyperkalemic Atrial Standstill� Treat the underlying cause (e.g., oliguricrenal failure, hypoadrenocorticism).� Aggressive fluid therapy with 0.9% salineand possibly sodium bicarbonate or insulinwith dextrose as discussed underHyperkalemia.
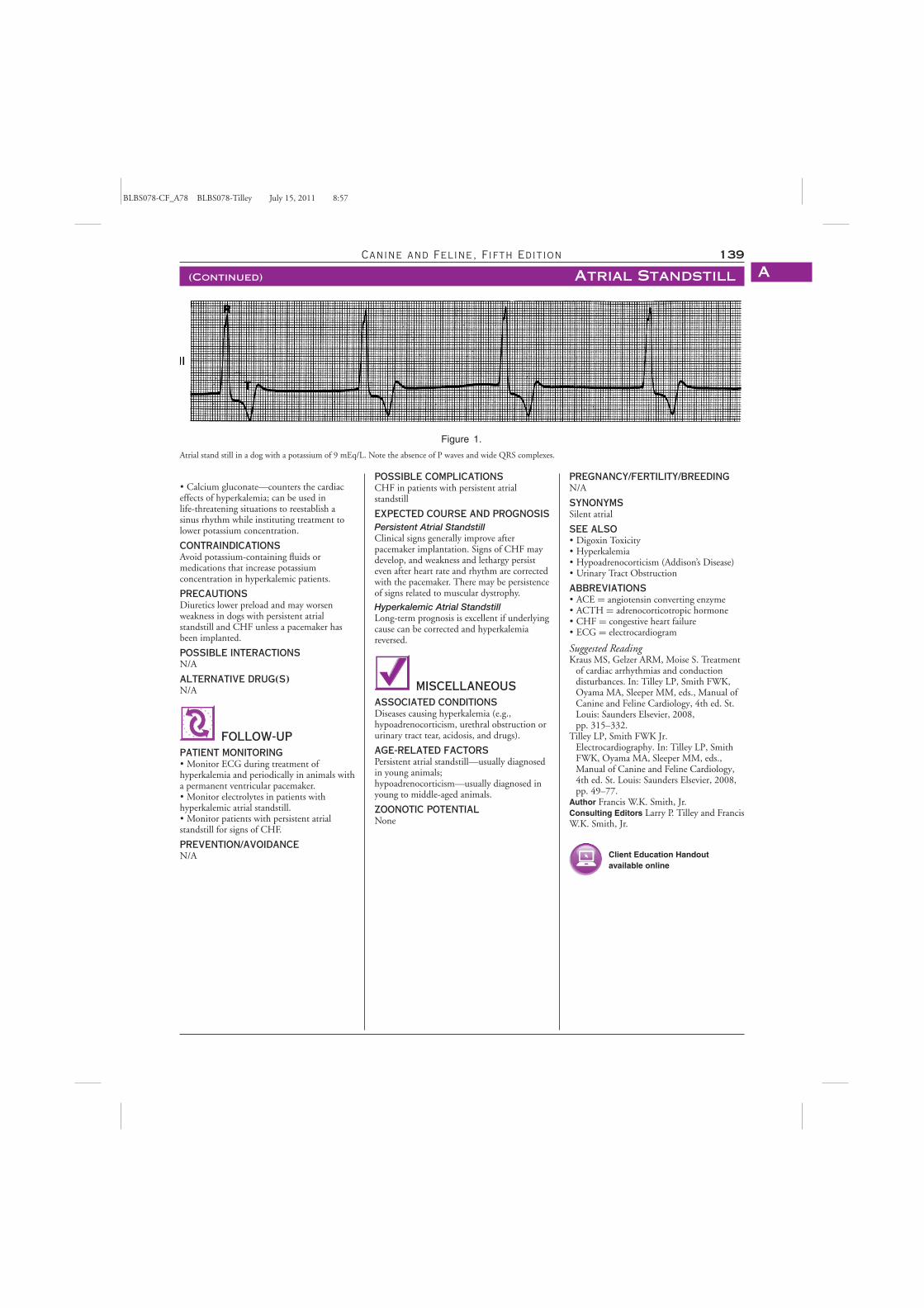
BLBS078-CF_A78 BLBS078-Tilley July 15, 2011 8:57
Canine and Feline, Fifth Edition 139
(Continued) Atrial Standstill A
Figure 1.
Atrial stand still in a dog with a potassium of 9 mEq/L. Note the absence of P waves and wide QRS complexes.
� Calcium gluconate—counters the cardiaceffects of hyperkalemia; can be used inlife-threatening situations to reestablish asinus rhythm while instituting treatment tolower potassium concentration.
CONTRAINDICATIONSAvoid potassium-containing fluids ormedications that increase potassiumconcentration in hyperkalemic patients.
PRECAUTIONSDiuretics lower preload and may worsenweakness in dogs with persistent atrialstandstill and CHF unless a pacemaker hasbeen implanted.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORING� Monitor ECG during treatment ofhyperkalemia and periodically in animals witha permanent ventricular pacemaker.� Monitor electrolytes in patients withhyperkalemic atrial standstill.� Monitor patients with persistent atrialstandstill for signs of CHF.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONSCHF in patients with persistent atrialstandstill
EXPECTED COURSE AND PROGNOSISPersistent Atrial StandstillClinical signs generally improve afterpacemaker implantation. Signs of CHF maydevelop, and weakness and lethargy persisteven after heart rate and rhythm are correctedwith the pacemaker. There may be persistenceof signs related to muscular dystrophy.
Hyperkalemic Atrial StandstillLong-term prognosis is excellent if underlyingcause can be corrected and hyperkalemiareversed.
MISCELLANEOUSASSOCIATED CONDITIONSDiseases causing hyperkalemia (e.g.,hypoadrenocorticism, urethral obstruction orurinary tract tear, acidosis, and drugs).
AGE-RELATED FACTORSPersistent atrial standstill—usually diagnosedin young animals;hypoadrenocorticism—usually diagnosed inyoung to middle-aged animals.
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMSSilent atrial
SEE ALSO� Digoxin Toxicity� Hyperkalemia� Hypoadrenocorticism (Addison’s Disease)� Urinary Tract Obstruction
ABBREVIATIONS� ACE = angiotensin converting enzyme� ACTH = adrenocorticotropic hormone� CHF = congestive heart failure� ECG = electrocardiogram
Suggested ReadingKraus MS, Gelzer ARM, Moise S. Treatment
of cardiac arrhythmias and conductiondisturbances. In: Tilley LP, Smith FWK,Oyama MA, Sleeper MM, eds., Manual ofCanine and Feline Cardiology, 4th ed. St.Louis: Saunders Elsevier, 2008,pp. 315–332.
Tilley LP, Smith FWK Jr.Electrocardiography. In: Tilley LP, SmithFWK, Oyama MA, Sleeper MM, eds.,Manual of Canine and Feline Cardiology,4th ed. St. Louis: Saunders Elsevier, 2008,pp. 49–77.
Author Francis W.K. Smith, Jr.Consulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online

BLBS078-CF_A79 BLBS078-Tilley June 16, 2011 11:8
140 Blackwell’s Five-Minute Veterinary Consult
Atrial Wall TearA
BASICSDEFINITION� Endocardial splitting is a linear defectlimited to the endocardial layer of the atrium(typically the left atrium) resulting fromdistension of the atrial wall beyond its elasticlimits. � An atrial tear may result if the splitextends through the myocardium andepicardium, resulting in a full thickness defectin the atrial wall and hemorrhage into thepericardial space.
PATHOPHYSIOLOGY� Endocardial splitting typically results fromincreased left atrial pressure secondary tosevere mitral regurgitation; endocardialdegeneration may also play a role. � If thesplit is incomplete, fibrin may seal the defecttemporarily; this either heals as a lineardepression in the endocardial surface orsubsequently extends through themyocardium resulting in a complete left atrialtear. � A left atrial tear results in peracutebleeding into the pericardial sac and severe,life-threatening hemodynamic compromisesecondary to acute cardiac tamponade . � If atear occurs in the interatrial septum, anacquired atrial septal defect may form.� Tearing of either atria may also rarely occursecondary to blunt trauma.
SYSTEMS AFFECTED� Cardiovascular � Respiratory
GENETICSPredisposition to endocardiosis has beenshown to have a heritable component in somebreeds.
INCIDENCE/PREVALENCEAtrial tear is a rare cause of hemorrhagicpericardial effusion in the dog encompassingapproximately 2% of pericardial effusioncases.
SIGNALMENTSpeciesDogs; uncommon in cats
Breed Predilections� Same as endocardiosis breeds; morecommon in small- to medium-sized dogs.� Poodles, dachshunds, cocker spaniels, andShetland sheepdogs may be overrepresented.� If trauma is the cause, any breed may berepresented.
Mean Age and RangeMiddle-aged to older dogs are predisposed.
Predominant SexA higher incidence of both endocardiosis andleft atrial tear is noted in male dogs.
SIGNSHistorical Findings� Acute onset of weakness and collapse thatmay progress quickly to respiratory or
cardiopulmonary arrest; episode may follow aperiod of increased excitement or activity.� History of long-standing cardiac diseasewith signs of CHF described in most patients.� Acute worsening of cough or dyspnea arecommonly observed. � Possible history ofblunt trauma.
Physical Examination Findings� Collapse. � Tachycardia. � Weak arterialpulses or pulsus paradoxus. � Pale, muddy, orashen mucous membranes; prolonged CRT.� Other signs of significant cardiac disease(e.g., murmur, gallop rhythm, arrhythmia,cough, or dyspnea) are typically present.� Signs of right heart failure (e.g., ascites andjugular venous distension) may also be seen insome patients. � Heart sounds may bemuffled, or if a murmur was heard before theatrial wall tear occurred, it may be reduced inintensity.
CAUSES� Mitral valve endocardiosis—chronicvalvular heart disease. � Dilatedcardiomyopathy. � Patent ductus arteriosus.� Cardiac neoplasia, most commonlyhemangiosarcoma. � Chest trauma. � Cardiaccatheterization.
RISK FACTORS� Severe mitral regurgitation, left atrialenlargement. � May be precipitated by anepisode of excitement, stress, or activity.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Other causes of acute cardiovascularcollapse. � Pericardial effusion from othercauses (e.g., neoplastic and idiopathic).� Heart failure. � Severe cardiac arrhythmias.� Myocardial infarction. � Pulmonarythromboembolism. � Other causes ofhypotension.
CBC/BIOCHEMISTRY/URINALYSIS� Anemia is uncommon unlesspericardiocentesis is performed since volumeof blood loss is relatively small. � Elevations inserum lactate, metabolic acidosis. � IncreasedALT, AST in some patients. � Prerenalazotemia; hyponatremia or other electrolytederangements may be seen.
OTHER LABORATORY TESTSNT-proBNP and TnI levels may be elevated
IMAGINGRadiographic Findings� Moderate to severe left atrial enlargement isexpected. � Comparison with previousthoracic radiographs may show rounding andfurther enlargement of cardiac silhouette;characteristic globoid cardiac silhouetteassociated with pericardial effusion may bemore obvious on the DV view. � Interstitial to
alveolar pulmonary infiltrates if concomitantleft-sided CHF is present. � Small volumepleural effusion, ascites, hepatomegaly, andlarge caudal vena cava may be seen due toright-sided CHF.
Echocardiographic Findings� Pericardial effusion is evidenced by ahypoechoic space between the heart andpericardial sac; the volume of pericardialeffusion identified may be relatively small asthe pericardium remains inelastic due to theacute nature of the bleed; a characteristiclinear, hyperechoic blood clot may be seenwithin the pericardial sac. � The actual tear isoften not identified though an associatedthrombus is occasionally visualized within theleft atrium. � Cardiac tamponade is evidencedby diastolic collapse of the right atrium and/orventricle. � Signs of advanced mitralendocardiosis, including mitral valvethickening and prolapse, moderate to severemitral regurgitation, moderate to severe leftatrial enlargement and often one or moreruptured chordae tendineae.
DIAGNOSTIC PROCEDURESElectrocardiographic Findings� Sinus tachycardia � Atrial or ventriculararrhythmias � Dampened QRS complexes� Electrical alternans � ST-segmentabnormalities � Possible left ventricular or leftatrial enlargement pattern
PATHOLOGIC FINDINGS� Endocardial splitting is noted grossly as apale or white linear depression in the atrialendocardium. � Atrial wall tears appear as fullthickness defects extending through the atrialendocardium, myocardium and epicardium;an associated thrombus may or may not bepresent. The caudolateral aspect of the leftatrium is most commonly affected, with manytears occurring at the atrio-auricularjunction. � Hemorrhagic pericardial effusionor pericardial thrombus is seen with acutetears. � Mitral endocardiosis characterized bythickened mitral valve leaflets with rollededges; chordae tendinae rupture may be seen;atrial jet lesions are possible. � Cardiomegalywith severe left atrial enlargement expected.
TREATMENTAPPROPRIATE HEALTH CARE� If a left atrial tear is strongly suspected,perform pericardiocentesis only if the effusionis causing symptomatic, life-threateningcardiac tamponade, since further hemorrhageinto the pericardial sac or exsanguination mayoccur once pericardial fluid is removed. � Ifpericardiocentesis is performed, remove onlyenough fluid to improve clinical signs.� Pericardiocentesis will likely be difficultgiven the small volume of effusion typicallyidentified, severe cardiac enlargement, and thesmall size of most dogs with left atrial rupture;
BLBS078-CF_A79 BLBS078-Tilley June 16, 2011 11:8
Canine and Feline, Fifth Edition 141
(Continued) Atrial Wall Tear A
ultrasound guidance and continuous ECGmonitoring are highly recommended. � Bestpractices for management of left atrial tearshave not been clearly established; however,aggressive medical management to lower leftatrial pressure using afterload and preloadreducers is recommended based on theauthor’s clinical experience. � If a fibrin clotforms over the defect, the patient maystabilize and recover.
NURSING CARE� Administer oxygen to dogs with dyspnea orsigns of hemodynamic instability.� Administer IV fluids or blood products onlyif evidence of hypovolemia is present; mostdogs remain in a volume overloaded state andfurther intravascular volume expansion willincrease left atrial pressure and potentiallyworsen tamponade.
ACTIVITYStrict cage rest in the acute period should befollowed by chronic exercise restriction.
CLIENT EDUCATIONLeft atrial tear typically accompaniesadvanced cardiac disease and chronic medicaltherapy will be necessary; though theprognosis is guarded for surviving the acuteevent some dogs with left atrial tear have livedmore than a year after the incident.
SURGICAL CONSIDERATIONS� Exploratory thoracotomy may beconsidered if hemorrhage persists or recursbut should be undertaken cautiously given theadvanced state of cardiac disease typicallypresent. � Transcatheter septal puncture andballoon tear of the fossa ovalis may also beconsidered to decompress the left atrium;however, right heart failure or hypoxemia dueto right-to-left shunting may result.
MEDICATIONSDRUG(S) OF CHOICE� Atrial tears occur secondary to elevated leftatrial pressure; thus medical therapy should befocused on lowering of left atrial pressures inorder to reduce continued hemorrhage intothe pericardial space and permit fibrin clotformation at the site of the tear; this may beaccomplished with preload (e.g., diuretics,nitroglycerin paste) and/or afterload reducers(arterial vasodilators). � Preload and afterloadreduction must be undertaken cautiously toavoid worsening of hemodynamiccompromise. � Afterload reduction may beachieved by conservative doses of sodiumnitroprusside; a low starting CRI dose of0.5–1 ug/kg/min is recommended to achievea decrease in LA pressure withoutprecipitating significant hypotension; blood
pressure monitoring is recommended and thedose may be uptitrated as necessary every15–30 minutes up to a maximum of 10ug/kg/min to achieve an improvement inclinical signs and/or a reduction in bloodpressure of 10–15 mm Hg. � Alternatively,amlodipine may be started at 0.1–0.2 mg/kgPO q24h; chronic amlodipine therapy may beimplemented in normotensive or hypertensiveanimals to reduce regurgitant fraction andlower left atrial pressure. � Diuretics shouldbe used cautiously if needed to treat dyspneaassociated with concomitant congestive heartfailure (e.g., 1–2 mg/kg of furosemide IV asneeded); signs of left-sided congestive heartfailure may worsen as cardiac tamponaderesolves due to augmentation of preload; moreaggressive diuretic therapy may then berequired. � Pimobendan (0.2–0.3 mg/kg POq12h) may result in a further reduction in leftatrial pressure though studies have notspecifically examined its use in the setting ofleft atrial rupture. � Once the patient is stable,ACE inhibitors (e.g., enalapril 0.5 mg/kgq12–24h) should be implemented for chronicmanagement of accompanying heart failure.
PRECAUTIONS� Aggressive fluid therapy is not warranted inthese patients; further volume expansion mayincrease left atrial pressure, worsen cardiactamponade, and contribute to hemodynamiccompromise. � Best practices for managementof left atrial tear have not been clearlyestablished; the choice of whether to performpericardiocentesis, and whether to administerpreload and/or afterload reducers should bemade based on assessment of the volumestatus, blood pressure and clinical stability ofthe patient.
POSSIBLE INTERACTIONSSodium nitroprusside should never beadministered concurrently withphosphodiesterase-V inhibitors (e.g., sildenafilor tadalafil) due to the potential forlife-threatening systemic hypotension.
FOLLOW-UPPATIENT MONITORING� Recommend close monitoring of respiratoryrate and effort, mucous membrane color andCRT, pulse quality, and heart rate; bloodpressure monitoring is recommended ifarterial vasodilators are implemented.� Follow-up examination withechocardiography helps determine resolutionof pericardial effusion and resorption of anatrial or pericardial clot. � Close follow-upevery 2–3 months thereafter is recommendedfor repeat pericardial fluid checks andmedication adjustments as deemedappropriate.
PREVENTION/AVOIDANCERecommend avoidance of strenuous physicalactivity and excitement.
POSSIBLE COMPLICATIONS� Even if the tear seals, the patient is prone tofurther tears because of underlying cardiacdisease. � Most dogs have or will developconcurrent CHF.
EXPECTED COURSE AND PROGNOSISPrognosis for survival is guarded to poor;however, some animals can do well for severalmonths or longer with close monitoring,exercise restriction and optimal medicalmanagement of cardiac disease.
MISCELLANEOUSASSOCIATED CONDITIONS� CHF � Mainstem bronchial compression� Pulmonary hypertension
SYNONYMS� Atrial rupture � Atrial splitting
SEE ALSO� Chapters on CHF � Pericardial Effusion
ABBREVIATIONS� ACE = angiotensin converting enzyme� ALT = alanine aminotransferase � AST =aspartate aminotransferase � CHF=Congestive heart failure
INTERNET RESOURCESJames Buchanan Cardiology Library:http://www.vin.com/MEMBERS/CMS/Misc/Default.aspx?id=7703.
Suggested ReadingFox PR, Sisson D, Moise S. Textbook of
Canine and Feline Cardiology. Philadelphia:Saunders, 1999.
Reineke EL, Burkett DE, Drobatz KJ. Leftatrial rupture in dogs: 14 cases(1990–2005). J Vet Emerg Crit Care 2008,18:158–164.
Rush JR. Chronic valvular disease in dogs. In:Bonagura JD, Twedt DC, eds., Kirk’sCurrent Veterinary Therapy XIV. St. Louis:Saunders Elsevier, 2009, pp. 780–786.
Sadanaga KK, MacDonald MJ, BuchananJW. Echocardiography and surgery in a dogwith left atrial rupture andhemopericardium. J Vet Intern Med 1990,4:216–221.
Author Suzanne M. CunninghamConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
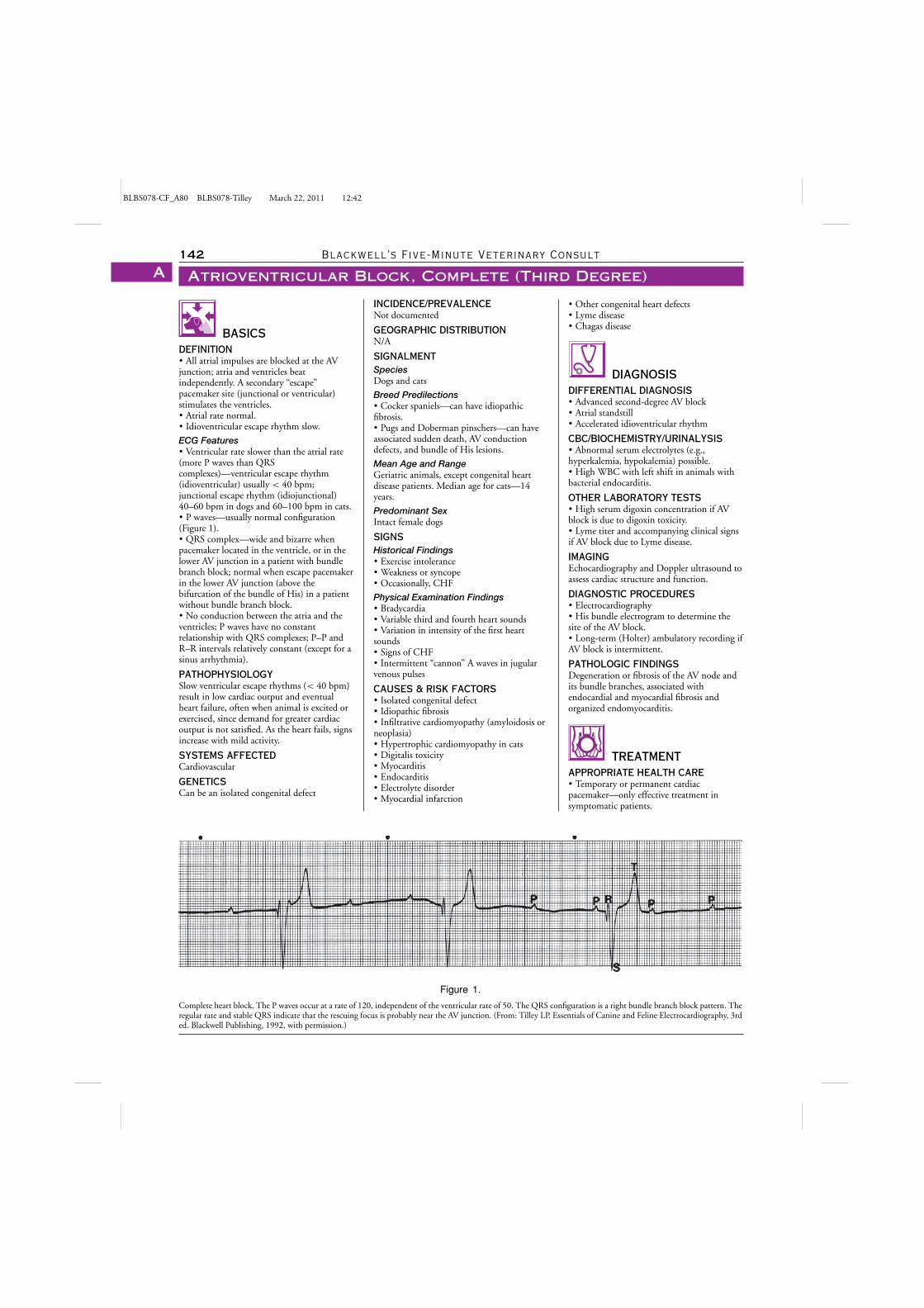
BLBS078-CF_A80 BLBS078-Tilley March 22, 2011 12:42
142 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Block, Complete (Third Degree)A
BASICSDEFINITION� All atrial impulses are blocked at the AVjunction; atria and ventricles beatindependently. A secondary “escape”pacemaker site (junctional or ventricular)stimulates the ventricles.� Atrial rate normal.� Idioventricular escape rhythm slow.
ECG Features� Ventricular rate slower than the atrial rate(more P waves than QRScomplexes)—ventricular escape rhythm(idioventricular) usually < 40 bpm;junctional escape rhythm (idiojunctional)40–60 bpm in dogs and 60–100 bpm in cats.� P waves—usually normal configuration(Figure 1).� QRS complex—wide and bizarre whenpacemaker located in the ventricle, or in thelower AV junction in a patient with bundlebranch block; normal when escape pacemakerin the lower AV junction (above thebifurcation of the bundle of His) in a patientwithout bundle branch block.� No conduction between the atria and theventricles; P waves have no constantrelationship with QRS complexes; P–P andR–R intervals relatively constant (except for asinus arrhythmia).
PATHOPHYSIOLOGYSlow ventricular escape rhythms (< 40 bpm)result in low cardiac output and eventualheart failure, often when animal is excited orexercised, since demand for greater cardiacoutput is not satisfied. As the heart fails, signsincrease with mild activity.
SYSTEMS AFFECTEDCardiovascular
GENETICSCan be an isolated congenital defect
Figure 1.
Complete heart block. The P waves occur at a rate of 120, independent of the ventricular rate of 50. The QRS configuration is a right bundle branch block pattern. Theregular rate and stable QRS indicate that the rescuing focus is probably near the AV junction. (From: Tilley LP. Essentials of Canine and Feline Electrocardiography, 3rded. Blackwell Publishing, 1992, with permission.)
INCIDENCE/PREVALENCENot documented
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats
Breed Predilections� Cocker spaniels—can have idiopathicfibrosis.� Pugs and Doberman pinschers—can haveassociated sudden death, AV conductiondefects, and bundle of His lesions.
Mean Age and RangeGeriatric animals, except congenital heartdisease patients. Median age for cats—14years.
Predominant SexIntact female dogs
SIGNSHistorical Findings� Exercise intolerance� Weakness or syncope� Occasionally, CHF
Physical Examination Findings� Bradycardia� Variable third and fourth heart sounds� Variation in intensity of the first heartsounds� Signs of CHF� Intermittent “cannon” A waves in jugularvenous pulses
CAUSES & RISK FACTORS� Isolated congenital defect� Idiopathic fibrosis� Infiltrative cardiomyopathy (amyloidosis orneoplasia)� Hypertrophic cardiomyopathy in cats� Digitalis toxicity� Myocarditis� Endocarditis� Electrolyte disorder� Myocardial infarction
� Other congenital heart defects� Lyme disease� Chagas disease
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Advanced second-degree AV block� Atrial standstill� Accelerated idioventricular rhythm
CBC/BIOCHEMISTRY/URINALYSIS� Abnormal serum electrolytes (e.g.,hyperkalemia, hypokalemia) possible.� High WBC with left shift in animals withbacterial endocarditis.
OTHER LABORATORY TESTS� High serum digoxin concentration if AVblock is due to digoxin toxicity.� Lyme titer and accompanying clinical signsif AV block due to Lyme disease.
IMAGINGEchocardiography and Doppler ultrasound toassess cardiac structure and function.
DIAGNOSTIC PROCEDURES� Electrocardiography� His bundle electrogram to determine thesite of the AV block.� Long-term (Holter) ambulatory recording ifAV block is intermittent.
PATHOLOGIC FINDINGSDegeneration or fibrosis of the AV node andits bundle branches, associated withendocardial and myocardial fibrosis andorganized endomyocarditis.
TREATMENTAPPROPRIATE HEALTH CARE� Temporary or permanent cardiacpacemaker—only effective treatment insymptomatic patients.
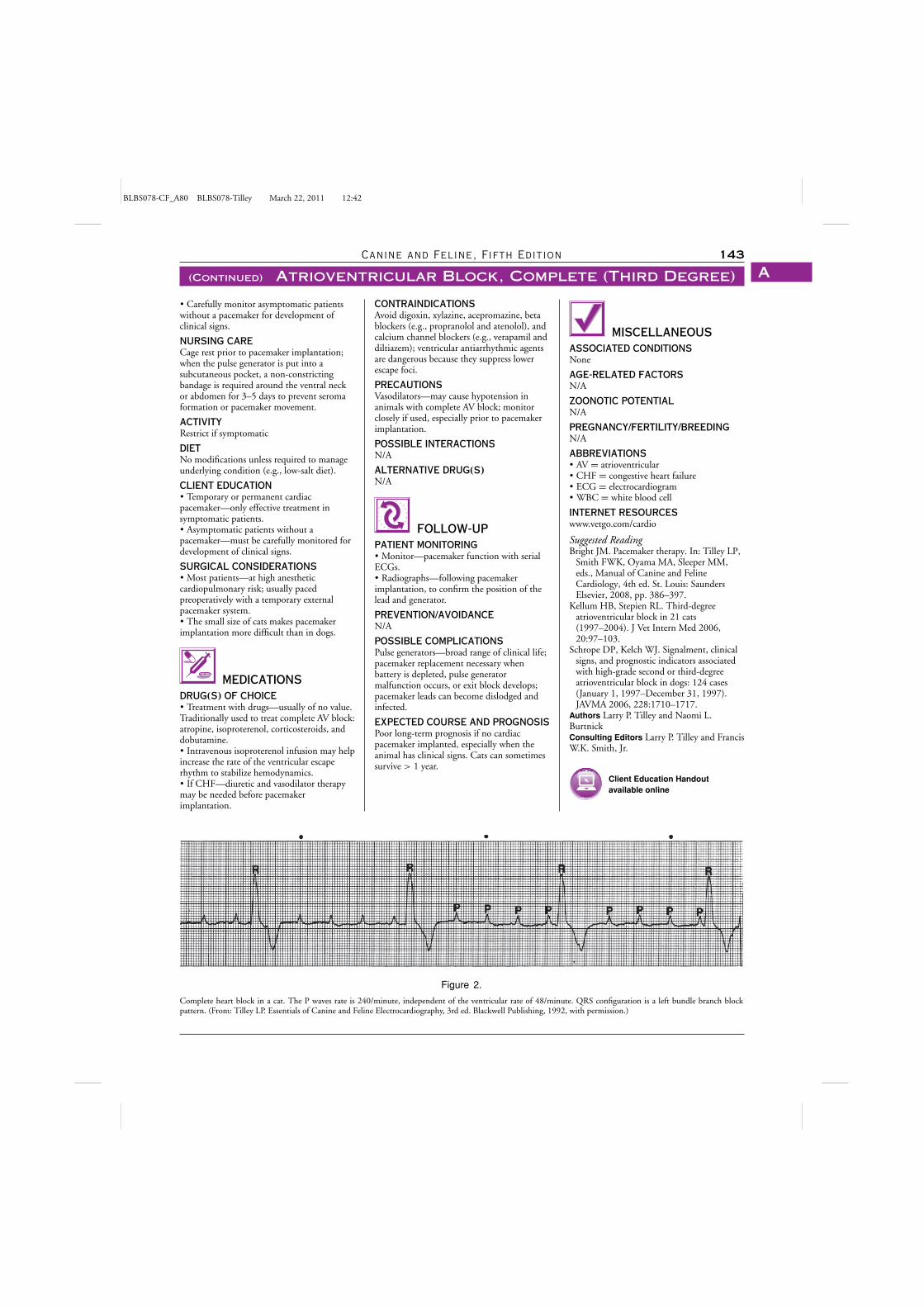
BLBS078-CF_A80 BLBS078-Tilley March 22, 2011 12:42
Canine and Feline, Fifth Edition 143
(Continued) Atrioventricular Block, Complete (Third Degree) A
� Carefully monitor asymptomatic patientswithout a pacemaker for development ofclinical signs.
NURSING CARECage rest prior to pacemaker implantation;when the pulse generator is put into asubcutaneous pocket, a non-constrictingbandage is required around the ventral neckor abdomen for 3–5 days to prevent seromaformation or pacemaker movement.
ACTIVITYRestrict if symptomatic
DIETNo modifications unless required to manageunderlying condition (e.g., low-salt diet).
CLIENT EDUCATION� Temporary or permanent cardiacpacemaker—only effective treatment insymptomatic patients.� Asymptomatic patients without apacemaker—must be carefully monitored fordevelopment of clinical signs.
SURGICAL CONSIDERATIONS� Most patients—at high anestheticcardiopulmonary risk; usually pacedpreoperatively with a temporary externalpacemaker system.� The small size of cats makes pacemakerimplantation more difficult than in dogs.
MEDICATIONSDRUG(S) OF CHOICE� Treatment with drugs—usually of no value.Traditionally used to treat complete AV block:atropine, isoproterenol, corticosteroids, anddobutamine.� Intravenous isoproterenol infusion may helpincrease the rate of the ventricular escaperhythm to stabilize hemodynamics.� If CHF—diuretic and vasodilator therapymay be needed before pacemakerimplantation.
Figure 2.
Complete heart block in a cat. The P waves rate is 240/minute, independent of the ventricular rate of 48/minute. QRS configuration is a left bundle branch blockpattern. (From: Tilley LP. Essentials of Canine and Feline Electrocardiography, 3rd ed. Blackwell Publishing, 1992, with permission.)
CONTRAINDICATIONSAvoid digoxin, xylazine, acepromazine, betablockers (e.g., propranolol and atenolol), andcalcium channel blockers (e.g., verapamil anddiltiazem); ventricular antiarrhythmic agentsare dangerous because they suppress lowerescape foci.
PRECAUTIONSVasodilators—may cause hypotension inanimals with complete AV block; monitorclosely if used, especially prior to pacemakerimplantation.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORING� Monitor—pacemaker function with serialECGs.� Radiographs—following pacemakerimplantation, to confirm the position of thelead and generator.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONSPulse generators—broad range of clinical life;pacemaker replacement necessary whenbattery is depleted, pulse generatormalfunction occurs, or exit block develops;pacemaker leads can become dislodged andinfected.
EXPECTED COURSE AND PROGNOSISPoor long-term prognosis if no cardiacpacemaker implanted, especially when theanimal has clinical signs. Cats can sometimessurvive > 1 year.
MISCELLANEOUSASSOCIATED CONDITIONSNone
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
ABBREVIATIONS� AV = atrioventricular� CHF = congestive heart failure� ECG = electrocardiogram� WBC = white blood cell
INTERNET RESOURCESwww.vetgo.com/cardio
Suggested ReadingBright JM. Pacemaker therapy. In: Tilley LP,
Smith FWK, Oyama MA, Sleeper MM,eds., Manual of Canine and FelineCardiology, 4th ed. St. Louis: SaundersElsevier, 2008, pp. 386–397.
Kellum HB, Stepien RL. Third-degreeatrioventricular block in 21 cats(1997–2004). J Vet Intern Med 2006,20:97–103.
Schrope DP, Kelch WJ. Signalment, clinicalsigns, and prognostic indicators associatedwith high-grade second or third-degreeatrioventricular block in dogs: 124 cases(January 1, 1997–December 31, 1997).JAVMA 2006, 228:1710–1717.
Authors Larry P. Tilley and Naomi L.BurtnickConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
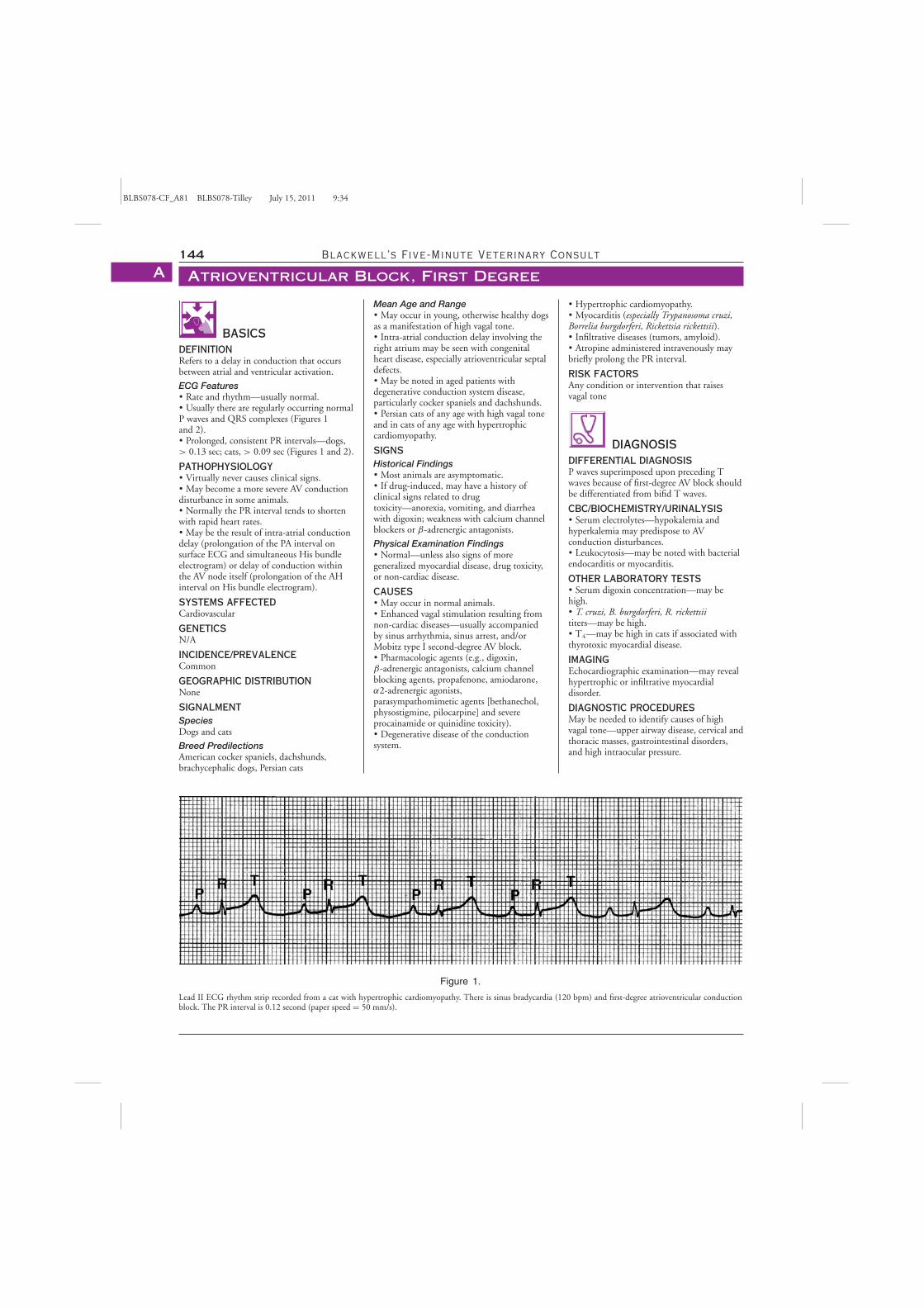
BLBS078-CF_A81 BLBS078-Tilley July 15, 2011 9:34
144 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Block, First DegreeA
BASICSDEFINITIONRefers to a delay in conduction that occursbetween atrial and ventricular activation.
ECG Features� Rate and rhythm—usually normal.� Usually there are regularly occurring normalP waves and QRS complexes (Figures 1and 2).� Prolonged, consistent PR intervals—dogs,> 0.13 sec; cats, > 0.09 sec (Figures 1 and 2).
PATHOPHYSIOLOGY� Virtually never causes clinical signs.� May become a more severe AV conductiondisturbance in some animals.� Normally the PR interval tends to shortenwith rapid heart rates.� May be the result of intra-atrial conductiondelay (prolongation of the PA interval onsurface ECG and simultaneous His bundleelectrogram) or delay of conduction withinthe AV node itself (prolongation of the AHinterval on His bundle electrogram).
SYSTEMS AFFECTEDCardiovascular
GENETICSN/A
INCIDENCE/PREVALENCECommon
GEOGRAPHIC DISTRIBUTIONNone
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsAmerican cocker spaniels, dachshunds,brachycephalic dogs, Persian cats
Figure 1.
Lead II ECG rhythm strip recorded from a cat with hypertrophic cardiomyopathy. There is sinus bradycardia (120 bpm) and first-degree atrioventricular conductionblock. The PR interval is 0.12 second (paper speed = 50 mm/s).
Mean Age and Range� May occur in young, otherwise healthy dogsas a manifestation of high vagal tone.� Intra-atrial conduction delay involving theright atrium may be seen with congenitalheart disease, especially atrioventricular septaldefects.� May be noted in aged patients withdegenerative conduction system disease,particularly cocker spaniels and dachshunds.� Persian cats of any age with high vagal toneand in cats of any age with hypertrophiccardiomyopathy.
SIGNSHistorical Findings� Most animals are asymptomatic.� If drug-induced, may have a history ofclinical signs related to drugtoxicity—anorexia, vomiting, and diarrheawith digoxin; weakness with calcium channelblockers or β-adrenergic antagonists.
Physical Examination Findings� Normal—unless also signs of moregeneralized myocardial disease, drug toxicity,or non-cardiac disease.
CAUSES� May occur in normal animals.� Enhanced vagal stimulation resulting fromnon-cardiac diseases—usually accompaniedby sinus arrhythmia, sinus arrest, and/orMobitz type I second-degree AV block.� Pharmacologic agents (e.g., digoxin,β-adrenergic antagonists, calcium channelblocking agents, propafenone, amiodarone,α2-adrenergic agonists,parasympathomimetic agents [bethanechol,physostigmine, pilocarpine] and severeprocainamide or quinidine toxicity).� Degenerative disease of the conductionsystem.
� Hypertrophic cardiomyopathy.� Myocarditis (especially Trypanosoma cruzi,Borrelia burgdorferi, Rickettsia rickettsii).� Infiltrative diseases (tumors, amyloid).� Atropine administered intravenously maybriefly prolong the PR interval.
RISK FACTORSAny condition or intervention that raisesvagal tone
DIAGNOSISDIFFERENTIAL DIAGNOSISP waves superimposed upon preceding Twaves because of first-degree AV block shouldbe differentiated from bifid T waves.
CBC/BIOCHEMISTRY/URINALYSIS� Serum electrolytes—hypokalemia andhyperkalemia may predispose to AVconduction disturbances.� Leukocytosis—may be noted with bacterialendocarditis or myocarditis.
OTHER LABORATORY TESTS� Serum digoxin concentration—may behigh.� T. cruzi, B. burgdorferi, R. rickettsiititers—may be high.� T4—may be high in cats if associated withthyrotoxic myocardial disease.
IMAGINGEchocardiographic examination—may revealhypertrophic or infiltrative myocardialdisorder.
DIAGNOSTIC PROCEDURESMay be needed to identify causes of highvagal tone—upper airway disease, cervical andthoracic masses, gastrointestinal disorders,and high intraocular pressure.
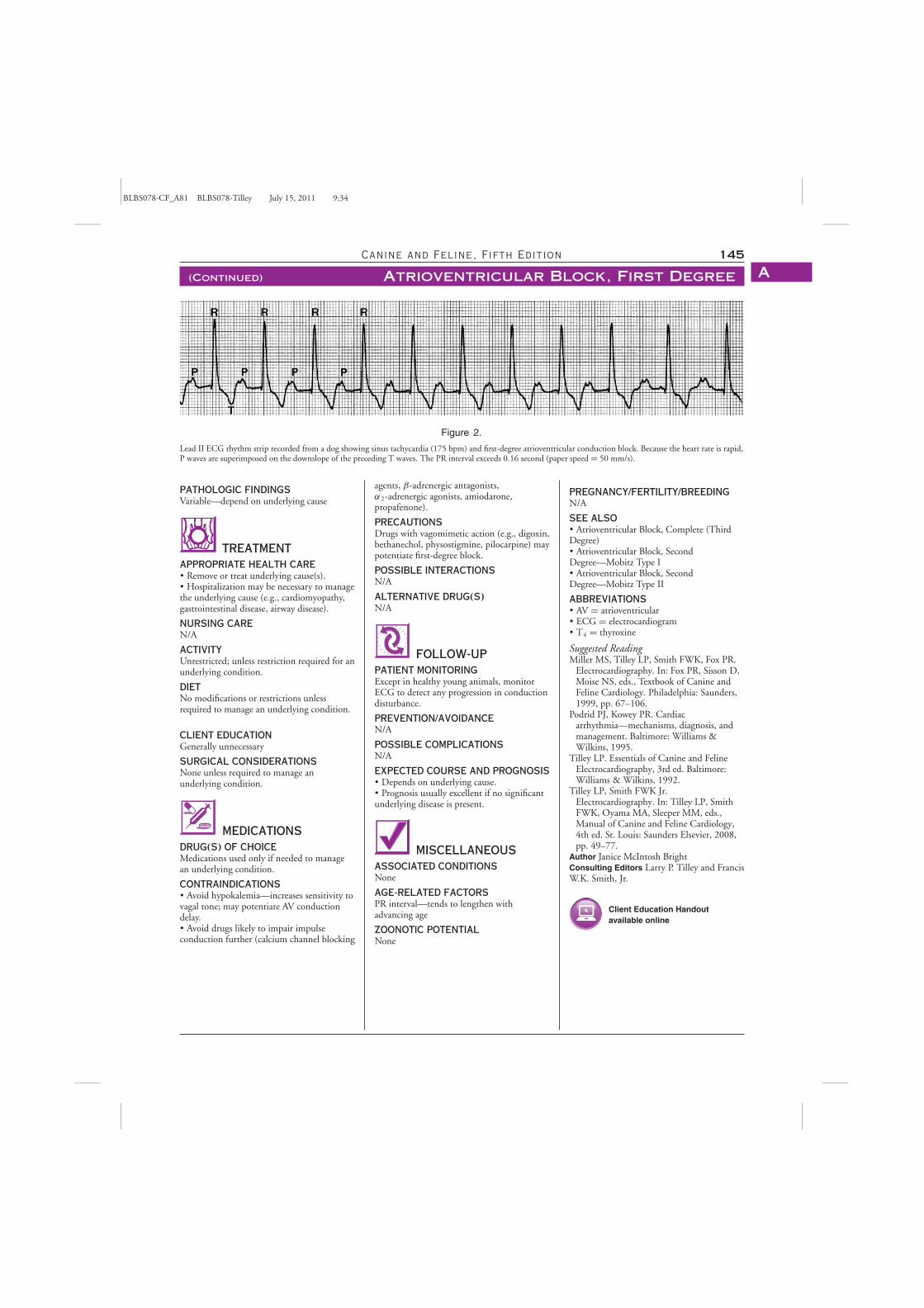
BLBS078-CF_A81 BLBS078-Tilley July 15, 2011 9:34
Canine and Feline, Fifth Edition 145
(Continued) Atrioventricular Block, First Degree A
Figure 2.
Lead II ECG rhythm strip recorded from a dog showing sinus tachycardia (175 bpm) and first-degree atrioventricular conduction block. Because the heart rate is rapid,P waves are superimposed on the downslope of the preceding T waves. The PR interval exceeds 0.16 second (paper speed = 50 mm/s).
PATHOLOGIC FINDINGSVariable—depend on underlying cause
TREATMENTAPPROPRIATE HEALTH CARE� Remove or treat underlying cause(s).� Hospitalization may be necessary to managethe underlying cause (e.g., cardiomyopathy,gastrointestinal disease, airway disease).
NURSING CAREN/A
ACTIVITYUnrestricted; unless restriction required for anunderlying condition.
DIETNo modifications or restrictions unlessrequired to manage an underlying condition.
CLIENT EDUCATIONGenerally unnecessary
SURGICAL CONSIDERATIONSNone unless required to manage anunderlying condition.
MEDICATIONSDRUG(S) OF CHOICEMedications used only if needed to managean underlying condition.
CONTRAINDICATIONS� Avoid hypokalemia—increases sensitivity tovagal tone; may potentiate AV conductiondelay.� Avoid drugs likely to impair impulseconduction further (calcium channel blocking
agents, β-adrenergic antagonists,α2-adrenergic agonists, amiodarone,propafenone).
PRECAUTIONSDrugs with vagomimetic action (e.g., digoxin,bethanechol, physostigmine, pilocarpine) maypotentiate first-degree block.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGExcept in healthy young animals, monitorECG to detect any progression in conductiondisturbance.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONSN/A
EXPECTED COURSE AND PROGNOSIS� Depends on underlying cause.� Prognosis usually excellent if no significantunderlying disease is present.
MISCELLANEOUSASSOCIATED CONDITIONSNone
AGE-RELATED FACTORSPR interval—tends to lengthen withadvancing age
ZOONOTIC POTENTIALNone
PREGNANCY/FERTILITY/BREEDINGN/A
SEE ALSO� Atrioventricular Block, Complete (ThirdDegree)� Atrioventricular Block, SecondDegree—Mobitz Type I� Atrioventricular Block, SecondDegree—Mobitz Type II
ABBREVIATIONS� AV = atrioventricular� ECG = electrocardiogram� T4 = thyroxine
Suggested ReadingMiller MS, Tilley LP, Smith FWK, Fox PR.
Electrocardiography. In: Fox PR, Sisson D,Moise NS, eds., Textbook of Canine andFeline Cardiology. Philadelphia: Saunders,1999, pp. 67–106.
Podrid PJ, Kowey PR. Cardiacarrhythmia—mechanisms, diagnosis, andmanagement. Baltimore: Williams &Wilkins, 1995.
Tilley LP. Essentials of Canine and FelineElectrocardiography, 3rd ed. Baltimore:Williams & Wilkins, 1992.
Tilley LP, Smith FWK Jr.Electrocardiography. In: Tilley LP, SmithFWK, Oyama MA, Sleeper MM, eds.,Manual of Canine and Feline Cardiology,4th ed. St. Louis: Saunders Elsevier, 2008,pp. 49–77.
Author Janice McIntosh BrightConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
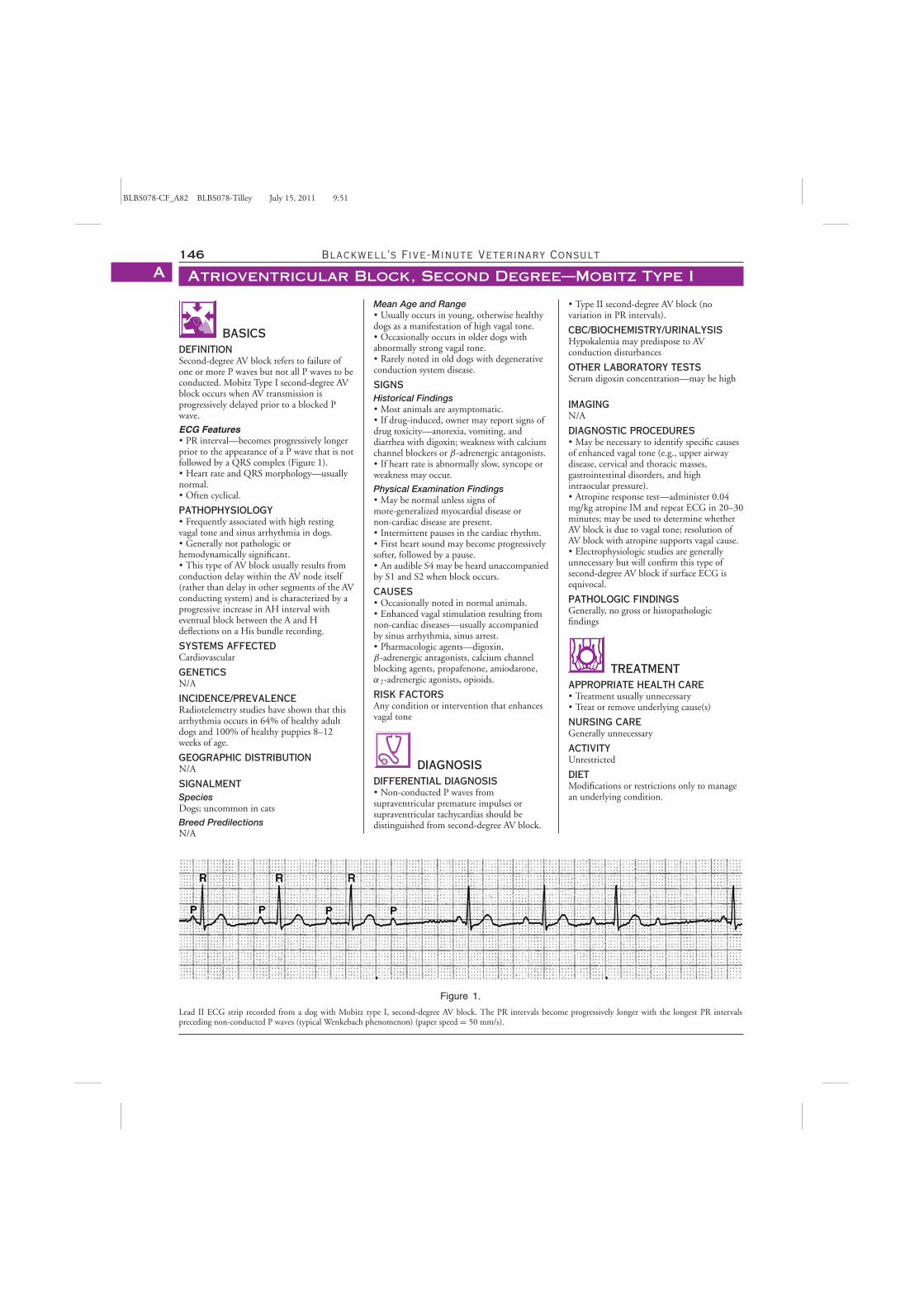
BLBS078-CF_A82 BLBS078-Tilley July 15, 2011 9:51
146 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Block, Second Degree—Mobitz Type IA
BASICSDEFINITIONSecond-degree AV block refers to failure ofone or more P waves but not all P waves to beconducted. Mobitz Type I second-degree AVblock occurs when AV transmission isprogressively delayed prior to a blocked Pwave.
ECG Features� PR interval—becomes progressively longerprior to the appearance of a P wave that is notfollowed by a QRS complex (Figure 1).� Heart rate and QRS morphology—usuallynormal.� Often cyclical.
PATHOPHYSIOLOGY� Frequently associated with high restingvagal tone and sinus arrhythmia in dogs.� Generally not pathologic orhemodynamically significant.� This type of AV block usually results fromconduction delay within the AV node itself(rather than delay in other segments of the AVconducting system) and is characterized by aprogressive increase in AH interval witheventual block between the A and Hdeflections on a His bundle recording.
SYSTEMS AFFECTEDCardiovascular
GENETICSN/A
INCIDENCE/PREVALENCERadiotelemetry studies have shown that thisarrhythmia occurs in 64% of healthy adultdogs and 100% of healthy puppies 8–12weeks of age.
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs; uncommon in cats
Breed PredilectionsN/A
Figure 1.
Lead II ECG strip recorded from a dog with Mobitz type I, second-degree AV block. The PR intervals become progressively longer with the longest PR intervalspreceding non-conducted P waves (typical Wenkebach phenomenon) (paper speed = 50 mm/s).
Mean Age and Range� Usually occurs in young, otherwise healthydogs as a manifestation of high vagal tone.� Occasionally occurs in older dogs withabnormally strong vagal tone.� Rarely noted in old dogs with degenerativeconduction system disease.
SIGNSHistorical Findings� Most animals are asymptomatic.� If drug-induced, owner may report signs ofdrug toxicity—anorexia, vomiting, anddiarrhea with digoxin; weakness with calciumchannel blockers or β-adrenergic antagonists.� If heart rate is abnormally slow, syncope orweakness may occur.
Physical Examination Findings� May be normal unless signs ofmore-generalized myocardial disease ornon-cardiac disease are present.� Intermittent pauses in the cardiac rhythm.� First heart sound may become progressivelysofter, followed by a pause.� An audible S4 may be heard unaccompaniedby S1 and S2 when block occurs.
CAUSES� Occasionally noted in normal animals.� Enhanced vagal stimulation resulting fromnon-cardiac diseases—usually accompaniedby sinus arrhythmia, sinus arrest.� Pharmacologic agents—digoxin,β-adrenergic antagonists, calcium channelblocking agents, propafenone, amiodarone,α2-adrenergic agonists, opioids.
RISK FACTORSAny condition or intervention that enhancesvagal tone
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Non-conducted P waves fromsupraventricular premature impulses orsupraventricular tachycardias should bedistinguished from second-degree AV block.
� Type II second-degree AV block (novariation in PR intervals).
CBC/BIOCHEMISTRY/URINALYSISHypokalemia may predispose to AVconduction disturbances
OTHER LABORATORY TESTSSerum digoxin concentration—may be high
IMAGINGN/A
DIAGNOSTIC PROCEDURES� May be necessary to identify specific causesof enhanced vagal tone (e.g., upper airwaydisease, cervical and thoracic masses,gastrointestinal disorders, and highintraocular pressure).� Atropine response test—administer 0.04mg/kg atropine IM and repeat ECG in 20–30minutes; may be used to determine whetherAV block is due to vagal tone; resolution ofAV block with atropine supports vagal cause.� Electrophysiologic studies are generallyunnecessary but will confirm this type ofsecond-degree AV block if surface ECG isequivocal.
PATHOLOGIC FINDINGSGenerally, no gross or histopathologicfindings
TREATMENTAPPROPRIATE HEALTH CARE� Treatment usually unnecessary� Treat or remove underlying cause(s)
NURSING CAREGenerally unnecessary
ACTIVITYUnrestricted
DIETModifications or restrictions only to managean underlying condition.
BLBS078-CF_A82 BLBS078-Tilley July 15, 2011 9:51
Canine and Feline, Fifth Edition 147
Atrioventricular Block, Second Degree—Mobitz Type I A
CLIENT EDUCATIONExplain that any treatment is directed towardreversing or eliminating an underlying cause.
SURGICAL CONSIDERATIONSN/A except to manage an underlyingcondition
MEDICATIONSDRUG(S)Only as needed to manage an underlyingcondition
CONTRAINDICATIONSDrugs with vagomimetic action (e.g., digoxin,bethanechol, physostigmine, pilocarpine) maypotentiate block.
PRECAUTIONSHypokalemia increases the sensitivity to vagaltone and may potentiate AV conductiondelay.
POSSIBLE INTERACTIONSN/A
FOLLOW-UPPATIENT MONITORINGTypically not necessary
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONSN/A
MISCELLANEOUSASSOCIATED CONDITIONSN/A
AGE-RELATED FACTORSN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SYNONYMS� Wenckebach periodicity� Wenckebach phenomenon
SEE ALSO� Atrioventricular Block, Complete (ThirdDegree)� Atrioventricular Block, First Degree� Atrioventricular Block, SecondDegree—Mobitz Type II
ABBREVIATIONS� AV = atrioventricular� ECG = electrocardiogram
Suggested ReadingBranch CE, Robertson BT, Williams JC.
Frequency of second-degree atrioventricularheart block in dogs. Am J Vet Res 1975,36:925–929.
Mangrum JM, DiMarco JP. The evaluationand management of bradycardia. N Engl JMed 2000, 342:703–709.
Podrid PJ, Kowey PR. CardiacArrhythmia—Mechanisms, Diagnosis, andManagement. Baltimore: Williams &Wilkins, 1995.
Tilley LP, Smith FWK Jr.Electrocardiography. In: Tilley LP, SmithFWK, Oyama MA, Sleeper MM, eds.,Manual of Canine and Feline Cardiology,4th ed. St. Louis: Saunders Elsevier, 2008,pp. 49–77.
Tilley LP. Essentials of Canine and FelineElectrocardiography, 3rd ed. Baltimore:Williams & Wilkins, 1992.
Author Janice McIntosh BrightConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
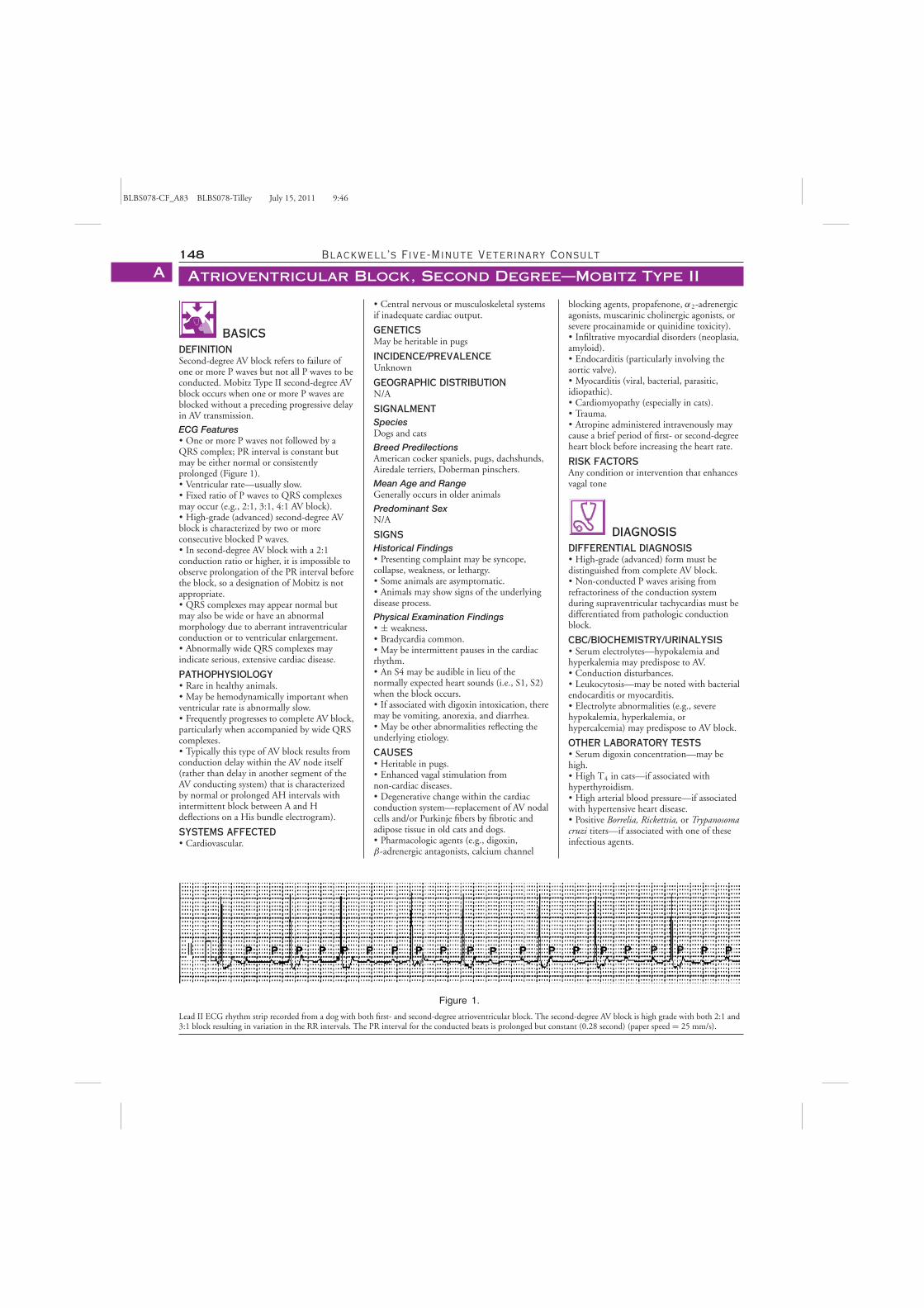
BLBS078-CF_A83 BLBS078-Tilley July 15, 2011 9:46
148 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Block, Second Degree—Mobitz Type IIA
BASICSDEFINITIONSecond-degree AV block refers to failure ofone or more P waves but not all P waves to beconducted. Mobitz Type II second-degree AVblock occurs when one or more P waves areblocked without a preceding progressive delayin AV transmission.
ECG Features� One or more P waves not followed by aQRS complex; PR interval is constant butmay be either normal or consistentlyprolonged (Figure 1).� Ventricular rate—usually slow.� Fixed ratio of P waves to QRS complexesmay occur (e.g., 2:1, 3:1, 4:1 AV block).� High-grade (advanced) second-degree AVblock is characterized by two or moreconsecutive blocked P waves.� In second-degree AV block with a 2:1conduction ratio or higher, it is impossible toobserve prolongation of the PR interval beforethe block, so a designation of Mobitz is notappropriate.� QRS complexes may appear normal butmay also be wide or have an abnormalmorphology due to aberrant intraventricularconduction or to ventricular enlargement.� Abnormally wide QRS complexes mayindicate serious, extensive cardiac disease.
PATHOPHYSIOLOGY� Rare in healthy animals.� May be hemodynamically important whenventricular rate is abnormally slow.� Frequently progresses to complete AV block,particularly when accompanied by wide QRScomplexes.� Typically this type of AV block results fromconduction delay within the AV node itself(rather than delay in another segment of theAV conducting system) that is characterizedby normal or prolonged AH intervals withintermittent block between A and Hdeflections on a His bundle electrogram).
SYSTEMS AFFECTED� Cardiovascular.
Figure 1.
Lead II ECG rhythm strip recorded from a dog with both first- and second-degree atrioventricular block. The second-degree AV block is high grade with both 2:1 and3:1 block resulting in variation in the RR intervals. The PR interval for the conducted beats is prolonged but constant (0.28 second) (paper speed = 25 mm/s).
� Central nervous or musculoskeletal systemsif inadequate cardiac output.
GENETICSMay be heritable in pugs
INCIDENCE/PREVALENCEUnknown
GEOGRAPHIC DISTRIBUTIONN/A
SIGNALMENTSpeciesDogs and cats
Breed PredilectionsAmerican cocker spaniels, pugs, dachshunds,Airedale terriers, Doberman pinschers.
Mean Age and RangeGenerally occurs in older animals
Predominant SexN/A
SIGNSHistorical Findings� Presenting complaint may be syncope,collapse, weakness, or lethargy.� Some animals are asymptomatic.� Animals may show signs of the underlyingdisease process.
Physical Examination Findings� ± weakness.� Bradycardia common.� May be intermittent pauses in the cardiacrhythm.� An S4 may be audible in lieu of thenormally expected heart sounds (i.e., S1, S2)when the block occurs.� If associated with digoxin intoxication, theremay be vomiting, anorexia, and diarrhea.� May be other abnormalities reflecting theunderlying etiology.
CAUSES� Heritable in pugs.� Enhanced vagal stimulation fromnon-cardiac diseases.� Degenerative change within the cardiacconduction system—replacement of AV nodalcells and/or Purkinje fibers by fibrotic andadipose tissue in old cats and dogs.� Pharmacologic agents (e.g., digoxin,β-adrenergic antagonists, calcium channel
blocking agents, propafenone, α2-adrenergicagonists, muscarinic cholinergic agonists, orsevere procainamide or quinidine toxicity).� Infiltrative myocardial disorders (neoplasia,amyloid).� Endocarditis (particularly involving theaortic valve).� Myocarditis (viral, bacterial, parasitic,idiopathic).� Cardiomyopathy (especially in cats).� Trauma.� Atropine administered intravenously maycause a brief period of first- or second-degreeheart block before increasing the heart rate.
RISK FACTORSAny condition or intervention that enhancesvagal tone
DIAGNOSISDIFFERENTIAL DIAGNOSIS� High-grade (advanced) form must bedistinguished from complete AV block.� Non-conducted P waves arising fromrefractoriness of the conduction systemduring supraventricular tachycardias must bedifferentiated from pathologic conductionblock.
CBC/BIOCHEMISTRY/URINALYSIS� Serum electrolytes—hypokalemia andhyperkalemia may predispose to AV.� Conduction disturbances.� Leukocytosis—may be noted with bacterialendocarditis or myocarditis.� Electrolyte abnormalities (e.g., severehypokalemia, hyperkalemia, orhypercalcemia) may predispose to AV block.
OTHER LABORATORY TESTS� Serum digoxin concentration—may behigh.� High T4 in cats—if associated withhyperthyroidism.� High arterial blood pressure—if associatedwith hypertensive heart disease.� Positive Borrelia, Rickettsia, or Trypanosomacruzi titers—if associated with one of theseinfectious agents.
BLBS078-CF_A83 BLBS078-Tilley July 15, 2011 9:46
Canine and Feline, Fifth Edition 149
Atrioventricular Block, Second Degree—Mobitz Type II A
� Blood cultures may be positive in patientswith vegetative endocarditis.
IMAGINGEchocardiographic examination may revealstructural heart disease (e.g., endocarditis,neoplasia, or cardiomyopathy).
DIAGNOSTIC PROCEDURES� Atropine response test—administer0.04 mg/kg atropine IM and repeat ECG in20–30 minutes; may be used to determinewhether AV block is due to high vagal tone.� Electrophysiologic testing is generallyunnecessary but can be done to confirm thistype of AV block if surface ECG findings areequivocal.
PATHOLOGIC FINDINGS� Variable—depend on underlying cause.� Old animals with degenerative change ofthe conduction system may have focalmineralization of the interventricular septalcrest visible grossly; chondroid metaplasia ofthe central fibrous body and increased fibrousconnective tissue in the AV bundle is notedhistopathologically.
TREATMENTAPPROPRIATE HEALTH CARE� Treatment—may be unnecessary if heartrate maintains adequate cardiac output.� Positive dromotropic interventions areindicated for symptomatic patients.� Treat or remove underlying cause(s).
NURSING CAREGenerally unnecessary
ACTIVITYCage rest advised for symptomatic patients
DIETModifications or restrictions only to managean underlying condition.
CLIENT EDUCATION� Need to seek and specifically treatunderlying cause.� Pharmacologic agents may not be effectivelong term.
SURGICAL CONSIDERATIONSPermanent pacemaker may be required forlong-term management of symptomaticpatients.
MEDICATIONSDRUG(S) OF CHOICE� Atropine (0.02–0.04 mg/kg IV, IM) orglycopyrrolate (0.005–0.01 mg/kg IV, IM)may be used short term if positive atropineresponse.� Chronic anticholinergic therapy(propantheline 0.5–2 mg/kg PO q8–12h orhyoscyamine 0.003–0.006 mg/kgq8h)—indicated for symptomatic patients ifimproved AV conduction with atropineresponse test.� Isoproterenol (0.04–0.09 μg/kg/minute IVto effect) or dopamine (2–5 μg/kg/minute IVto effect) may be administered in acute,life-threatening situations to enhance AVconduction and/or accelerate an escape focus.
CONTRAINDICATIONS� Drugs with vagomimetic action (e.g.,digoxin, bethanechol, physostigmine,pilocarpine) may potentiate block.� Avoid drugs likely to impair impulseconduction further or depress a ventricularescape focus (e.g., procainamide, quinidine,lidocaine, calcium channel blocking agents,β-adrenergic blocking agents).
PRECAUTIONSHypokalemia—increases sensitivity to vagaltone and may potentiate AV conductiondelay.
POSSIBLE INTERACTIONSN/A
ALTERNATIVE DRUG(S)N/A
FOLLOW-UPPATIENT MONITORINGFrequent ECG because often progresses tocomplete (third-degree) AV block.
PREVENTION/AVOIDANCEN/A
POSSIBLE COMPLICATIONSProlonged bradycardia may cause secondarycongestive heart failure or inadequate renalperfusion.
EXPECTED COURSE AND PROGNOSISVariable—depends on cause.If degenerative disease of the cardiacconduction system, often progresses tocomplete (third-degree) AV block.
MISCELLANEOUSASSOCIATED CONDITIONSMay be noted in cats with primary orsecondary myocardial disease.
AGE-RELATED FACTORSN/A
ZOONOTIC POTENTIALN/A
PREGNANCY/FERTILITY/BREEDINGN/A
SEE ALSO� Atrioventricular Block, Complete (ThirdDegree)� Atrioventricular Block, SecondDegree—Mobitz Type I
ABBREVIATIONS� AV = atrioventricular� ECG = electrocardiogram� T4 = thyroxine
Suggested ReadingKittleson MD. Electrocardiography. In:
Kittleson MD, Kienle RD, eds., SmallAnimal Cardiovascular Medicine. St. Louis:Mosby, 1998, pp. 72–94.
Mangrum JM, DiMarco JP. The evaluationand management of bradycardia. N Engl JMed 2000, 342:703–709.
Podrid PJ, Kowey PR. CardiacArrhythmia—Mechanisms, Diagnosis, andManagement. Baltimore: Williams &Wilkins, 1995.
Tilley LP, Smith FWK Jr.Electrocardiography. In: Tilley LP, SmithFWK, Oyama MA, Sleeper MM, eds.,Manual of Canine and Feline Cardiology,4th ed. St. Louis: Saunders Elsevier, 2008,pp. 49–77.
Tilley LP. Essentials of Canine and FelineElectrocardiography, 3rd ed. Baltimore:Williams & Wilkins, 1992.
Author Janice McIntosh BrightConsulting Editors Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
BLBS078-CF_A84 BLBS078-Tilley July 15, 2011 9:55
150 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Valve DysplasiaA
BASICSDEFINITIONA congenital malformation of the mitral ortricuspid valve apparatus.
PATHOPHYSIOLOGY� Atrioventricular valve dysplasia can result invalvular insufficiency, valvular stenosis, ordynamic outflow tract obstruction, dependingon the anatomic abnormality. AVVD mayoccur alone or in association withabnormalities of the ipsilateral outflow tract(e.g., valvular or subvalvular aortic orpulmonic stenosis). It is not uncommon formitral and tricuspid valve dysplasia to occurtogether in the same patient. � Valvularinsufficiency results in dilation of theipsilateral atrium, eccentric hypertrophy ofthe associated ventricle, and, if sufficientlysevere, signs of CHF. Cardiomyopathy ofchronic volume overload and elevated atrialpressures are the end result culminating inpulmonary congestion if the mitral valve isaffected and systemic congestion if thetricuspid valve is affected. � Valvular stenosisresults in atrial dilation and hypertrophy and,when severe, hypoplasia of the receivingventricle. Tricuspid valve stenosis results inelevated right atrial pressure and systemiccongestion if pressures exceed 15–20 mm Hg.Right-to-left shunting may occur if there is anatrial septal defect or patent foramen ovale.Mitral valve stenosis results in elevatedpulmonary capillary pressure and pulmonaryedema if pressures exceed 25–30 mm Hg.Pulmonary hypertension is a commoncomplicating condition in animals with mitralvalve stenosis. � Outflow tract obstructionmay develop from defects that translocate theanterior leaflet to a position closer to theinterventricular septum. Concentric leftventricular hypertrophy develops inproportion to the severity of the obstruction.
SYSTEMS AFFECTED� Cardiovascular—inflow obstruction due tovalvular stenosis and chronic volume overloadfrom valvular insufficiency result in elevatedpulmonary (left AV valve) or systemic (rightAV valve) venous pressures. Signs of lowcardiac output develop if the lesion issufficiently severe. Concentric left ventricularhypertrophy develops secondary to dynamicoutflow obstruction.� Respiratory—pulmonary edema maydevelop secondary to mitral stenosis or mitralvalve insufficiency. Pulmonary hypertension isa common complication in animals withmitral stenosis. � Neurologic—collapse andloss of consciousness, most often duringphysical exertion, may occur with severedisease due to low cardiac output andhypotension. Collapse in animals withdynamic outflow obstruction is most oftendue to ventricular arrhythmia.
GENETICSTricuspid valve dysplasia is inherited as anautosomal recessive trait in Labradorretrievers. Heritability and pattern ofinheritance not established in other breeds.
INCIDENCE/PREVALENCEThese are common congenital cardiacanomalies in cats (17% of reported congenitalcardiac defects in one study). Less frequentlydiagnosed in dogs.
SIGNALMENTSpeciesDogs and cats
Breed Predilections� Tricuspid valve dysplasia—increased risk forLabrador retrievers, German shepherd dogs,Great Pyrenees, possibly Old Englishsheepdogs. Also common in cats. � Mitralvalve dysplasia—increased risk in bull terriers,Newfoundlands, Labrador retrievers, GreatDanes, golden retrievers, Dalmatians, andSiamese cats. Perhaps the most commoncongenital heart defects of cats. Mitral valvemalformations often are noted in cats withhypertrophic cardiomyopathy.
Mean Age and RangeVariable; signs are most often manifest withinthe first few years after birth.
Predominant SexMales are more likely to evidence heartfailure.
SIGNSHistorical Findings� Exercise intolerance is the most commonproblem in dogs and cats with AV valvedysplasia. � Abdominal distention, weightloss, and stunting may be observed withsevere tricuspid valve dysplasia. � Laboredrespiration is common in dogs or cats withmitral valve dysplasia. � Syncope and collapseif critical mitral or tricuspid valve stenosis,severe outflow tract obstruction, an associatedarrhythmia, or heart failure from AV valvularinsufficiency.
Physical Examination FindingsMitral Valve Dysplasia� A holosystolic murmur is heard over thecardiac apex on the left. With severe diseasethe murmur is accompanied by a thrill orgallop heart sounds. A soft diastolic murmurmay be present in the same location inanimals with mitral stenosis but manyaffected animals have no audible murmur. Asystolic ejection murmur that intensifies withexercise or excitement is audible in animalswith dynamic outflow tract obstructions.� Evidence of left heart failure—tachypnea,increased respiratory efforts, pulmonarycrackles, and cyanosis in animals with severedefects.Tricuspid Valve Dysplasia� A holosystolic murmur is heard over thecardiac apex on the right. With severe diseasethe murmur is accompanied by a thrill or
gallop heart sounds. Silent tricuspidregurgitation is well documented in cats andis attributable to a large regurgitant orificeand laminar regurgitant flow. Distention andpulsation of the external jugular veins may beevident. � Evidence of right heartfailure—ascites and, more rarely, peripheraledema with severe malformations.
DIAGNOSISDIFFERENTIAL DIAGNOSIS� With the noted exception of the age ofonset, congenital AV valvular insufficiencyresembles acquired degenerative AV valveinsufficiency with respect to historicalfindings, physical examination abnormalities,and clinical sequelae. � The right-sidedmurmur of tricuspid insufficiency issometimes confused with the right-sidedmurmur of a ventricular septal defect.� Ascites caused by silent tricuspidregurgitation or tricuspid valve stenosis isoften attributed to pericardial effusion,hepatic disease, or obstruction of the caudalvena cava. � Dogs and cats with cortriatriatum share many of the clinical featuresof AV valve stenosis. � There is no certain wayto distinguish mitral valve dysplasiaproducing outflow tract obstruction and theobstructive form of cardiomyopathy. If theobstruction can be abolished with a betablocker and left ventricular hypertrophyresolves, it is likely that the primaryabnormality was mitral valve dysplasia.
CBC/BIOCHEMISTRY/URINALYSISUsually normal
IMAGINGRadiographic FindingsMitral Valve Dysplasia� Left atrial and left ventricular enlargementwith valvular insufficiency. Isolated left atrialenlargement with valvular stenosis. Mild leftatrial enlargement with dynamic outflowobstruction. � Evidence of left heartfailure—distended pulmonary veins,interstitial or alveolar edema in severe cases.Tricuspid Valve Dysplasia� Right atrial and right ventricularenlargement with valvular insufficiency.Cardiac silhouette may appear globoid withpronounced enlargement. Isolated right atrialenlargement with valvular stenosis.� Evidence of right heart failure—dilatedcaudal vena cava, hepatosplenomegaly, orascites in severe cases.
EchocardiographyMitral Valve Dysplasia� Valvular insufficiency results in left atrialdilation and eccentric hypertrophy of the leftventricle. The papillary muscles are typicallyflattened and displaced dorsally. Chordaetendineae are often short and thickened.Doppler echocardiography demonstrates a
BLBS078-CF_A84 BLBS078-Tilley July 15, 2011 9:55
Canine and Feline, Fifth Edition 151
(Continued) Atrioventricular Valve Dysplasia A
high velocity retrograde systolic transmitral jetand modestly increased transmitral inflowvelocities. � Mitral stenosis results in left atrialdilation while the left ventricular dimensionsare normal or small. The valve leaflets areoften thickened, relatively immobile, andoften fused. Doppler echocardiographydemonstrates a high velocity transmitraldiastolic jet with a reduced EF slope. Theremay also be evidence of concurrent mitralinsufficiency and/or secondary pulmonaryhypertension. Exclude the possibility of cortriatriatum sinister. � Dynamic left ventricularoutflow obstruction is characterized bysystolic motion of the anterior mitral valveleaflet toward the interventricular septum,increased LV outflow tract velocities, andconcentric left ventricular hypertrophy.Tricuspid Valve Dysplasia� Valvular insufficiency results in right atrialdilation and eccentric hypertrophy of theright ventricle. The papillary muscles andchordae tendineae may be fused, creating acurtain-like appearance of the tricuspid valve.Doppler echocardiography demonstrates ahigh velocity retrograde systolic trans-tricuspid jet and modestly increasedtrans-tricuspid inflow velocities. � Tricuspidstenosis results in right atrial dilation withnormal or small right ventricular dimensions.The valve leaflets do not open completely.Doppler echocardiography demonstrates ahigh velocity diastolic trans-tricuspid jet witha reduced EF slope. There may be evidence ofconcurrent tricuspid valve insufficiencyand/or right-to-left shunting across a patentforamen ovale or associated atrial septaldefect. Exclude the possibility of cortriatriatum dexter.
Cardiac Catheterization� Indicated only in those cases in which thediagnosis cannot be confirmed byechocardiography or if surgical correction isanticipated. � Mitral dysplasia—hemodynamic measurements should includeleft ventricular pressures, pulmonary capillarywedge pressure or direct measurement of LApressure, pulmonary artery pressures, and, incases of dynamic obstruction, simultaneousrecording of aortic and left ventricularpressures with medical provocation. Contraststudies are best accomplished with a leftventricular injection in cases of valvularinsufficiency, and direct left atrial injection viatrans-septal catheterization in cases of valvularstenosis. � Tricuspid dysplasia—hemodynamic measurements should includeright ventricular and right atrial pressures.Contrast studies are best accomplished with aright ventricular injection in cases of valvularinsufficiency, and right atrial injection in casesof valvular stenosis.
DIAGNOSTIC PROCEDURESElectrocardiographic FindingsUsually reflect pattern of chamberenlargement.
Severe defects may be accompanied by avariety of arrhythmias, particularly atrialpremature beats, supraventricular tachycardia,or atrial fibrillation.
TREATMENTAPPROPRIATE HEALTH CAREInpatient treatment required for CHF.
CLIENT EDUCATIONOwners should be informed of heritabilityand advised against breeding.
ACTIVITYRestricted in accordance with severity.
DIETSodium-restricted if overt or pending CHF.
SURGICAL CONSIDERATIONS� Valve repair or replacement is available in afew centers. � Balloon valvuloplasty issometimes effective for valvular stenosis.
MEDICATIONSDRUG(S) OF CHOICE� Mitral or tricuspid dysplasia withinsufficiency—diuretics, angiotensinconverting enzyme inhibitors, andpimobendan (0.3 mg/kg q12h) for patientswith imminent or overt congestive heartfailure. Furosemide (2–4 mg/kg q12–24h),enalapril (0.5 mg/kg q12h) are used to controlcongestion. Digoxin (0.002–0.004 mg/kgq12h) is used to control supraventriculartachyarrhythmias. � Mitral or tricuspidstenosis—diuretics to control edema.Furosemide (2–4 mg/kg q12–24h) doseadjusted to resolve congestion. Heart rateshould be maintained near 150 bpm usingdigoxin (0.002–0.004 mg/kg q12h), acalcium channel blocker such as diltiazem(1–1.5 mg/kg q8h), or a beta-receptorblocking drug, such as atenolol (0.5–1.5mg/kg q12–24h). � Dynamic outflow tractobstruction—titrate a beta-receptor blockingdrug, such as atenolol (0.5–1.5 mg/kgq12–24h), to abolish or diminish severity ofoutflow obstruction.
PRECAUTIONSStandard patient monitoring for cardiacmedication side effects (e.g., digitalis toxicity,azotemia).
FOLLOW-UPPATIENT MONITORING� Recheck yearly if no signs of heart failure.� Recheck at a minimum of every 3 months ifsigns of CHF (thoracic radiographs, ECG,and echocardiography advisable).
PREVENTION/AVOIDANCEDo not breed affected animals.
POSSIBLE COMPLICATIONS� Congestive heart failure—left-sided withmitral valve dysplasia; right-sided withtricuspid valve dysplasia. � Collapse orsyncope with exercise. � Paroxysmalsupraventricular tachycardia or atrialfibrillation with severe disease.
EXPECTED COURSE AND PROGNOSIS� Depends on severity of underlying defect� Guarded to poor with serious defects
MISCELLANEOUSASSOCIATED CONDITIONS� Mitral valve dysplasia commonlyaccompanies valvular or subvalvular aorticstenosis as well as TVD. � Tricuspid valvedysplasia commonly accompanies pulmonicstenosis as well as MVD.
PREGNANCY/FERTILITY/BREEDINGShould be avoided—heritable defect andpossibility of causing decompensated orworsening heart failure.
SEE ALSO� Congestive Heart Failure, Left-Sided� Congestive Heart Failure, Right-Sided
ABBREVIATIONS� AV = atrioventricular � AVVD =atrioventricular valve dysplasia � CHF =congestive heart failure � ECG =electrocardiogram � MVD = mitral valvedysplasia � TVD = tricuspid valve dysplasia
Suggested ReadingBonagura JD, Lehmkuhl LB. Congenital
heart disease. In: Fox PR, Sisson D, MoiseNS. Textbook of Canine and FelineCardiology: Principles and Clinical Practice,2nd ed. Philadelphia: Saunders, 1999, pp.520–526.
Oyama MA, Sisson DD, Thomas WP,Bonagura JD. Congenital heart disease. In:Ettinger SJ, Feldman EC, eds., Textbook ofVeterinary Internal Medicine, 6th ed. St.Louis: Elsevier, 2005.
Strickland KN. Congenital heart disease. In:Tilley LP, Smith FWK, Oyama MA, SleeperMM, eds., Manual of Canine and FelineCardiology, 4th ed. St. Louis: SaundersElsevier, 2008, pp. 215–239.
Author David SissonConsulting Editor Larry P. Tilley and FrancisW.K. Smith, Jr.
Client Education Handoutavailable online
BLBS078-CF_A85 BLBS078-Tilley July 15, 2011 9:57
152 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Valve EndocardiosisA
BASICSDEFINITIONA chronic degenerative disease affecting themitral and tricuspid valves, leading to valvularinsufficiency and heart failure.
PATHOPHYSIOLOGY� Proliferation and deposition ofmucopolysaccharide within thesubendothelial spongiosa layer leads tothickening, distortion, and stiffening of theAV valves; initially, swellings are nodular, butcoalescence occurs until the entire valve andoften the attached chordae are involved.� AV valve incompetence causes regurgitation,high atrial pressure, reduced cardiac output,activation of compensatory mechanisms(sympathetic nervous system,renin-angiotensin-aldosterone system, andnatriuretic peptides), and CHF.� Volume overload leads to progressiveventricular dilation, advancing ventricularstiffness, and impaired ventricular function;congestive and low-output (forward) failureresult.� With atrial tear, acute cardiac tamponademay result.� Degenerative changes in the chordaetendineae lead to distortion, weakening, andrupture, causing valvular instability andincreased regurgitation.
SYSTEMS AFFECTED� Cardiovascular—both AV valves areaffected, but 1 study found the distribution innecropsy specimens to be mitral alone, 62%;tricuspid alone, 1%; and both, 33%.� Hepatobiliary—passive congestion.� Renal/Urologic—prerenal azotemia.� Respiratory—if edema develops.
GENETICSSome breeds (Cavalier King Charles spaniels,dachshunds) appear to have an inheritedcomponent to their disease.
INCIDENCE/PREVALENCEChronic valvular disease increases from about5% in middle-aged dogs (5–7 years) to >35% in old dogs (12 years).
SIGNALMENTSpeciesMainly dogs, but may be seen in old cats
Breed Predilections� Typically small breeds (< 20 kg but seenless frequently in larger dogs).� Highest prevalence—Cavalier King Charlesspaniels, Chihuahuas, miniature schnauzers,Maltese, Pomeranians, cocker spaniels,Pekingese, fox terriers, Boston terriers,miniature poodles, toy poodles, miniaturepinschers, and whippets.
Mean Age and RangeHeart failure onset at 10–12 years, althoughmay detect a murmur several years earlier;
Cavalier King Charles spaniels typicallyaffected much earlier (6–8 years).
Predominant SexMales—male: female ratio, 1.5:1
SIGNSSigns depend on the stage of disease. Variousgrading schemes have been developed tocategorize patients based on the severity oftheir disease and the signs they are showing.These grades are then used to facilitatetherapeutic decision making. The descriptionshere align with the grading system describedin the ACVIM consensus statement on valvedisease and the modified NYHA classificationscheme.
Asymptomatic Valve Disease� Systolic murmur is heard best at the leftfifth intercostal space (mitral) or right fourthintercostal space (tricuspid).� Murmurs may vary from a low-frequency,holosystolic, band shaped sound to a shorter,high-frequency, midsystolic murmur;occasionally only a midsystolic click isdetected.� As the disease progresses, the murmurtypically gets louder and radiates more widely;with severe disease, the volume ofregurgitation becomes so large that themurmur may decrease in frequency andloudness.� Initially patients will have no obviousradiographic or echocardiographic evidence of“remodeling” (changes in cardiac chambers ormuscular components) (ACVIM stage 2a). Asthe disease progresses, evidence ofcardiomegaly will be seen, often beforeobvious clinical signs of heart failure arerecognized (ACVIM stage 2b). Any animalwith signs of heart failure (regardless ofseverity) is ACVIM stage C, but varies in itsNYHA class depending on severity.
Mild Heart Failure (NYHA Class II)� Coughing, exercise intolerance and dyspneawith strenuous exercise; occasionally, syncopemay be the only owner complaint.
Moderate Heart Failure (NYHA Class III)� Coughing, exercise intolerance and dyspneamost of the time.
Severe Heart Failure (RequiresHospitalization—NYHA Class 4)� Severe dyspnea, profound weakness,abdominal distention, productive coughing(i.e., pink, frothy fluid), orthopnea, cyanosis,and syncope.
Refractory Heart Failure� Clinical signs that persist despiteconventional therapeutic management.
CAUSESIdiopathic, although the role of a number ofinflammatory modulators is beinginvestigated in either the onset or propagationof the disease.
RISK FACTORSN/A
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Dilated cardiomyopathy� Congenital heart disease� Chronic airway or interstitial lung disease� Pneumonia� Pulmonary embolism� Pulmonary neoplasia� Heartworm disease
CBC/BIOCHEMISTRY/URINALYSIS� Prerenal azotemia secondary to impairedrenal perfusion; urinary specific gravity is highunless complicated by underlying renaldisease or previous diuretic administration.� High liver enzyme activity in many patientswith passive congestion.� A “stress leukogram” may be seen.
OTHER LABORATORY TESTSElevation in N-Terminal Pro BNP has beendocumented in patients with both disease andfailure. Studies show levels correlate withseverity of disease, the presence of heartfailure as a cause for clinical signs and apossible decrease in response to therapy.Elevations in NTproBNP may also helppredict which asymptomatic patients arelikely to progress to heart failure, and assessprognosis in those that do.
IMAGINGRadiographic Findings� Heart size ranges from normal to left-sidedor generalized cardiomegaly.� Left atrial enlargement in the lateralprojection exhibits elevation of the distalfourth of the trachea and splitting of themainstem bronchi; dorsoventral projectionshows accentuation of the angle between themainstem bronchi, a double shadow at the sixo’clock position, where the caudal edge of theatrium extends beyond the left ventricle, andbulging of the left atrial appendage in the oneto three o’clock position.� Left-sided heart failure—the pulmonaryvein is larger than the associated pulmonaryartery; an increased interstial pattern ± airbronchograms are typical of, but notpathognomonic for, cardiogenic pulmonaryedema; initially, congestion and edema areperihilar, with all lung fields eventuallyshowing changes. The right lung may beaffected before the left.
Echocardiographic Findings� Thickening and distortion of the mitralvalve; septal leaflet is most severely affected.� Elongation and rupture of the chordaetendineae, causing mitral valve prolapse.� Large left atrium.� The left ventricle may be distended and ishyperdynamic if the regurgitant flow is highand myocardial function intact; as theventricle becomes more grossly distended, it
BLBS078-CF_A85 BLBS078-Tilley July 15, 2011 9:57
Canine and Feline, Fifth Edition 153
(Continued) Atrioventricular Valve Endocardiosis A
may become hypodynamic because ofmyocardial failure.� Pericardial effusion in some patients.� Doppler studies document a jet ofregurgitation into the left atrium and the areaof the regurgitant jet on color flow.� Doppler indices, including regurgitantfraction, are used to assess severity.� Doppler evaluation for the presence ofpulmonary hypertension should be a routinecomponent of any echocardiographicevaluation in patients with chronic valvedisease.
DIAGNOSTIC PROCEDURES� Abdominocentesis/pleurocentesis—amodified transudate is characteristic of CHF.� Arterial/venous blood gases have been usedto quantify hypoxemia and monitor treatmentresponse.� Systemic blood pressure should be evaluatedto check for concurrent systemic hypertensionin all patients with chronic valve disease.
Electrocardiographic Findings� Sinus tachycardia is common in animalswith CHF.� May show evidence of left atrialenlargement (P mitrale) or left ventricularenlargement (tall and wide R waves).� Atrioventricular arrhythmias may develop.
PATHOLOGIC FINDINGS� Gross valvular changes are divided into fourtypes—type I shows only a few discretenodules at the line of closure; type IV showsgross distortion of the valve by gray-whitenodules and plaques causing contraction ofthe cusps and rolling of the free edge; thechordae are irregularly thickened, withregions of tapering and rupture.� Jet lesions—irregular thickening andopacity of the atrial endocardium.� Recent and healed left atrium splits or tearsin some patients; full-thickness tears lead tohemopericardium (free wall) or acquired atrialseptal defect (septum).� Left atrium and left ventricle dilation inmany patients.� The degree of left ventricular hypertrophymay be apparent only on weighing the heart.� Small thrombi in the left atrium rare indogs—more common and extensive in cats.
TREATMENTAPPROPRIATE HEALTH CARETreat patients that need oxygen support asinpatients; if stable, patients may be lessstressed at home.
NURSING CAREOxygen therapy as needed for hypoxemia.
ACTIVITY� Absolute exercise restriction forsymptomatic patients.
� Stable patients receiving medicaltreatment—restrict exercise to leash walking;avoid sudden, explosive exercise.
DIET� Preventing cardiac cachexia by ensuringadequate calorie intake should be the primaryobjective in the dietary management ofpatients with chronic valve disease.� A salt-restricted diet is recommended, iftolerated, for a patient in heart failure;monitor sodium concentration closely.� Hyponatremia may develop as CHFprogresses and in patients fed severelysodium-restricted diets in conjunction withloop diuretics and angiotensin convertingenzyme inhibitors.� If hyponatremia develops, switch to a lesssodium-restricted diet (e.g., renal or geriatricdiet).
CLIENT EDUCATION� Discuss the progressive nature of the disease.� Emphasize the importance of consistentdosing of all medications and exercisemanagement.� Emphasize the importance of avoidingcardiac cachexia by paying close attention toappetite and using the appropriate diet.� Highlight the signs of digoxin toxicity, andadvise the owner to stop treatment and notifythe veterinarian immediately should anydevelop.� Education of owners in simple techniques,like monitoring the patient’s respiratory rate,or heart rate at rest, helps engage them in theirpet’s care and may detect increases suggestiveof developing or recurring congestive failure.
SURGICAL CONSIDERATIONSSurgical valve replacement and purse-stringsuture techniques to reduce the area of themitral valve orifice have been used; experiencewith these techniques is limited, but surgicalrepair may be an option when access to acardiovascular surgeon and cardiopulmonarybypass are available.
MEDICATIONSDRUG(S) OF CHOICERecommended treatment depends on thestage of the disease; these recommendationsfollow the guidelines set by the consensusstatement developed by the ACVIM.
Asymptomatic Patients� If no cardiac enlargement, no treatment isrecommended.� Administering ACE inhibitors toasymptomatic patients showing progressivecardiomegaly is advocated in patients withsignificant left sided cardiomegaly by somecardiologists. Administration of pimobendanto asymptomatic patients is of unknown valueat this time but studies are ongoing toevaluate this.
Chronic Congestive Heart Failure(Typically Treated as an Outpatient)� Diuretics—furosemide (1–2 mg/kgq8–12h).� ACE inhibitors enalapril (0.5 mg/kgq12–24h), benazepril (0.25–0.5 mg/kg q24h).� Pimobendan, an inodilator, has a rapidonset of action (30–60 minutes) and isrecommended for the management of heartfailure.� Spironolactone, while typically used for itsdiuretic effect in combination with otherdiuretics, has been shown to have a positiveinfluence on deleterious remodeling thatoccurs as heart disease progresses. It is usedinitially at 0.5–1 mg/kg PO q24h. The dosecan be raised to 1–2 mg/kg PO q12h forrefractory heart failure.� Nitroglycerin—2% percutaneous ointment(0.125–1 inch q6h until patient is stable).� Digoxin—especially if supraventriculararrhythmias, including atrial fibrillation, aredocumented (0.005 mg/kg or 0.22 mg/m2
PO q12h).� Sodium restriction if tolerated.� Antiarrhythmics—as needed.� Calcium channel blockers—to treat atrialarrhythmias.� Beta blockers—to treat atrial and ventriculararrhythmias. Some cardiologists advocate theuse of beta blockers in patients with intactmyocardial function to negate the negativeeffects of excessive beta receptor stimulation.� Class 1 antiarrhythmics—procainamide,mexiletine, and tocainide; to treat clinicallyimportant ventricular arrhythmias.� Class III antiarrhythmics—sotalol,amiodarone for intractable arrhythmias.� PDE 5 inhibitors (sildenafil) should beconsidered if pulmonary hypertension ispresent.
Acute Congestive Heart Failure (OftenTreated as an Inpatient)� Oxygen—40% in O2 cage (can go as highas 100%) up to 24 hours; use nasal O2 inlarge-breed dogs, 50–100 mL/kg/minutethrough humidifier.� Diuretics—furosemide (2–4 mg/kg IVq4–8h).
Vasodilators� Benazepril (0.25–0.5 mg/kg q24h).� Enalapril (0.5 mg/kg q12h–24h).� Pimobendan (0.25 mg/kg PO q12h) usedalone or in combination with othervasodilators and/or digoxin.� Hydralazine (0.5 mg/kg q12h titrated up to2 mg/kg if necessary)—used in acute stages todecrease afterload rapidly; may causehypotension.� Nitroglycerin—ointment (one-fourthinch/5 kg up to 2 inches percutaneously) orinjectable (1–5 μg/kg/minute CRI).� Sodium nitroprusside (1–10 μg/kg/minute)—monitor blood pressure.� Pulmonary arterial vasdilators such assildenafil (PDE 5 inhibitors) should be
BLBS078-CF_A85 BLBS078-Tilley July 15, 2011 9:57
154 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Valve Endocardiosis (Continued)A
considered in patients with pulmonaryhypertension.
Positive Inotropes� Pimobendan (0.25 mg/kg PO q12h).� Digoxin (0.005 mg/kg or 0.22 mg/m2 POq12h).� Dobutamine (dogs, 1–10 μg/kg/minute;cats, 1–5 μg/kg/minute)—may cause seizures.� Dopamine (1–10 μg/kg/minute).� Agents with β-blocking properties (e.g.,carvedilol) are being investigated for theirability to upregulate β-receptors in patientswith severe myocardial dysfunction.Carvedilol (0.1–0.4 mg/kg PO q12h) is analpha- and beta blocker with antioxidantactivity. Start at the low end of the dose rangeand gradually raise dose if tolerated.
PRECAUTIONS� Use digoxin, diuretics, and ACE inhibitorswith caution in patients with renal disease.� Nitrate tolerance may develop if appropriate12-hour nitrate-free intervals are omittedfrom the dosing schedule.� Beta blockers are negative inotropes andmay have an acute adverse effect onmyocardial function, although their long-termuse may improve myocardial function.
POSSIBLE INTERACTIONSMonitor digoxin concentration in patientsreceiving concurrent calcium channel blockersor quinidine.
ALTERNATIVE DRUG(S)� Diuretics—add thiazide and potassiumsparing diuretic (e.g., spironolactone) inrefractory animals.� Bumetanide is an alternative to furosemide.� Vasodilators—other ACE inhibitors includelisinopril; isosorbide dinitrate can be used in
place of nitroglycerin ointment in patientsrequiring long-term nitrate administration.
FOLLOW-UPPATIENT MONITORING� Take a baseline radiograph when a murmuris first detected and every 6–12 monthsthereafter to document progressivecardiomegaly.� Evidence suggests that NTproBNP may beused in a similar way. A baseline is taken whenthe murmur is first heard, and then the test isrun serially to assess for significant change.� After an episode of CHF, check patientsweekly during the first month of treatment;may repeat thoracic radiographs and an ECGat the first weekly checkup and on subsequentvisits if any changes are seen on physicalexamination.� Monitor BUN and creatinine whendiuretics and ACE inhibitors are used incombination. Monitor serum potassium levelswhen spironolactone and ACE inhibitors areused concurrently, especially when combinedwith digoxin.
POSSIBLE COMPLICATIONSEndocarditis because of bacterial colonizationof the diseased mitral valve has been suggestedalthough the evidence remains controversial.
EXPECTED COURSE AND PROGNOSISProgressive degeneration of both valvechanges and myocardial function occurs,necessitating increasing drug dosages;long-term prognosis depends on response totreatment and stage of heart failure.
MISCELLANEOUSSYNONYMS� Acquired valvular insufficiency� Chronic valve disease� Degenerative valve disease� Valve fibrosis
SEE ALSO� Atrial Wall Tear� Congestive Heart Failure, Left-Sided� Congestive Heart Failure, Right-Sided
ABBREVIATIONS� ACE = angiotensin converting enzyme� AV = atrioventricular� CHF = congestive heart failure
Suggested ReadingAbbott JA. Acquired valvular disease. In:
Tilley LP, Smith FWK, Oyama MA, SleeperMM, eds., Manual of Canine and FelineCardiology, 4th ed. St. Louis: SaundersElsevier, 2008, pp. 2110–2138.
Atkins C, et al. Guidelines for the diagnosisand treatment of canine chronic valvularheart disease. J Vet Intern Med 2009,23:1142–1150.
Kvart C, Haggstrom J, Pedersen HD, et al.Efficacy of enalapril for prevention ofcongestive heart failure in dogs withmyxomatous valve disease andasymptomatic mitral regurgitation. J VetIntern Med 2002, 16(1):80–88.
Author Andrew BeardowConsulting Editors Larry P. Tilley andFrancis WK. Smith, Jr.
Client Education Handoutavailable online
BLBS078-CF_A86 BLBS078-Tilley July 23, 2011 5:25
Canine and Feline, Fifth Edition 155
Atrioventricular Valvular Stenosis A
BASICSDEFINITIONAtrioventricular valvular stenosis is apathologic narrowing of the mitral ortricuspid valve orifice.
PATHOPHYSIOLOGY� Ventricular filling in clinically significantdisease requires a persistent diastolic pressuregradient between atrium and ventricle.� Concomitant valvular regurgitation iscommon.� The increased atrial pressure can lead toatrial dilation, venous congestion, and CHF.Pulmonary edema occurs with mitral stenosis;ascites, pleural effusion and chylothorax candevelop in cases of severe tricuspid stenosis.� The foramen ovale may remain patent(PFO) in patients with tricuspid stenosis,allowing right-to-left shunting with signs ofcyanotic heart disease.� Cardiac output and exercise capacity arelimited with atrioventricular valvular stenosis.� Mitral stenosis can lead to exertionaldyspnea from transient pulmonary edema.� Pulmonary hypertension can developconsequent to MS, leading to exerciseintolerance and right ventricular hypertrophy.This can be severe, especially in cats withmitral stenosis.
SYSTEMS AFFECTED� Respiratory—with MS—bronchialcompression from enlarged left atrium,pulmonary edema; pleural effusion withatelectesis in tricuspid stenosis.� Hepatobiliary—with TS—hepaticcongestion, ascites.
GENETICSUncertain
INCIDENCE/PREVALENCERare
GEOGRAPHIC DISTRIBUTIONWorldwide
SIGNALMENTSpeciesDogs and cats
Breed Predilections� MS is overrepresented in bull terriers andNewfoundlands, and possibly Siamese cats.� TS has been reported most often in OldEnglish sheepdogs and Labrador retrievers.
Mean Age and RangeMost patients are presented at a young age,though exceptions occur, especially in cats.
Predominant SexN/A
SIGNSHistorical Findings� Exercise intolerance
� Syncope� Exertional dyspnea or tachypnea� Cough—MS� Cyanosis� Abdominal distention—TS� Acute posterior paresis—cats with MS� Stunted growth� Hemoptysis from rupture ofintrapulmonary vessels—MS
Physical Examination Findings� Soft diastolic murmur with point ofmaximal intensity over the left apex (MS) orright hemithorax (TS).� Holosystolic murmur of mitral or tricuspidregurgitation is common.� Crackles, tachypnea, dyspnea with MS.� Jugular distention, jugular pulses, ascites,hepatomegaly with TS.� Cyanosis from right to left shunt with TS.
CAUSES� Usually due to congenital dysplasia of themitral or tricuspid valve.� Supravalvular obstructing rings of tissuehave been associated with atrioventricularstenosis� Infective endocarditis, intracardiacneoplasia, hypertrophic cardiomyopathy incats are potential causes of acquired stenosis.� Tricuspid stenosis has been observed withfibrous scarring of the tricuspid valve in dogswith transvenous pacing leads.
RISK FACTORSSee “Risk Factors” for Endocarditis, Infective;permanent transvenous pacing.
DIAGNOSISDIFFERENTIAL DIAGNOSISAtrioventricular valvular stenosis must bedifferentiated from the more common causesof mitral and tricuspid regurgitation in theabsence of stenosis. These include bothcongenital and acquired lesions of theatrioventricular valves and supportapparatus.
CBC/BIOCHEMISTRY/URINALYSISMay be normal or reflect changes related toCHF or drug therapy for CHF.
IMAGINGThoracic Radiography� Atrial enlargement is the most consistentand outstanding feature; may see generalizedcardiomegaly.� MS—may see pulmonary venouscongestion and pulmonary edema;intrapulmonary hemorrhage can bemisinterpreted as pneumonia or anotherparenchymal disease.� TS—may see hepatomegaly; increaseddiameter of caudal vena cava.
Echocardiography� Diagnostic test of choice.
� Two-dimensional echocardiography revealsa markedly dilated atrium and attenuatedvalve excursion during diastole, often withthickened, irregular AV valve leaflets; valveleaflets may appear to “dome” during diastole.A supravalvular obstructing ring also may beevident as well as other lesions (see “Causes”above).� M-mode studies show an enlarged atriumand concordant motion of the AV valveleaflets indicating commissural fusion; theE-to-F slope is decreased.� Color-flow imaging reveals a turbulentdiastolic jet that originates at the stenotic valveand projects toward the apex of the ventricle;AV valve regurgitation is often present.� Spectral Doppler studies show increaseddiastolic transvalvular flow velocities;prolonged calculated pressure half-time is ahallmark feature; E-wave/A-wave amplitudereversal may be seen in cases still in normalsinus rhythm.� Right-sided chamber enlargements in MSwith pulmonary hypertension.
Angiography� Right atrium: injection demonstrates amarkedly dilated atrium; with TS and usuallya PFO or an ASD; opacification of the leftatrium may be observed following right atrialinjection.� May visualize thickened, irregular valveleaflets or a stenotic valve funnel.� Ventricular injection typically revealsvalvular regurgitation.� There may be delayed opacification of theventricle and great vessels.
Cardiac Catheterization� A diastolic pressure gradient is identifiedbetween the atrium and ventricle. A large “A”wave is common if atrial function is preserved.� High left atrial, pulmonary capillary wedge,and pulmonary artery pressures occur in MS.� High right atrial and central venouspressures are present in TS.� Ventricular pressure may be normal in theabsence of concurrent defects.
DIAGNOSTIC PROCEDURESElectrocardiography� There may be variable enlargement patterns.� Ectopic rhythms, especially of atrial origin,are often observed. Atrial fibrillation is themost important rhythm disturbance as atrialcontribution to filling is lost.
PATHOLOGIC FINDINGS� The atrioventricular valve is abnormal, withthickened leaflets and fused commissures.Other lesions may be identified such as asupra-mitral ring (see “Causes”).� Many cases also have abnormal chordaetendineae and papillary muscles.� Atrial dilation and hypertrophy arecommon.
BLBS078-CF_A86 BLBS078-Tilley July 23, 2011 5:25
156 Blackwell’s Five-Minute Veterinary Consult
Atrioventricular Valvular Stenosis (Continued)A
TREATMENTAPPROPRIATE HEALTH CAREPatients in overt CHF should be treated withinpatient medical management. Surgical orcatheter-based interventions may beconsidered once heart failure has beenstabilized. Control of heart rhythmdisturbances, especially AF, is also important.These patients are typically complicated andconsultation with a cardiologist isrecommended.
NURSING CAREOxygen therapy should be administered tothe patient with dyspnea or hypoxemia fromleft-sided congestive heart failure. Fluidtherapy is typically contraindicated in thepatient with overt CHF except in cases ofconcurrent moderate to severe azotemia, renalcompromise, or severe dehydration.Therapeutic paracentesis may be consideredin the patient with pleural effusions ortympanic ascites. Sedation with butorphanolis appropriate for dyspneic patients.
ACTIVITYExercise restriction is recommended for anyanimal with this condition. Cage rest is idealfor patients with CHF.
DIETFeed a low-sodium diet to patients in CHF.
CLIENT EDUCATIONThe client must be advised of symptomsassociated with CHF and the urgency oftreatment, particularly with left-sided CHF.The likelihood of recurrent bouts of CHFshould also be discussed.
SURGICAL CONSIDERATIONS� Surgical valve replacement or repair requirescardiopulmonary bypass or hypothermia; costand availability are greatly limiting factors.� Balloon valvuloplasty is an alternativereferral treatment and has been usedsuccessfully for managing AV stenosis.
MEDICATIONSDRUG(S) OF CHOICECHF� Furosemide—dogs, 2–6 mg/kg IV, IM, SC,PO q8–24h; cats, 1–4 mg/kg IV, IM, SC, POq8–24h. � Enalapril—dogs, 0.25–0.5 mg/kgPO q12h; cats, 0.25–0.5 mg/kg POq12–24h; see below under “Follow-Up” forpatient monitoring. � Nitroglycerin paste(1/4–1 inch topically q12h) to reducepulmonary venous pressures, but this has notbeen evaluated critically.
Atrial Tachyarrhythmias� Digoxin—dogs, 0.003–0.005 mg/kg POq12h; cats, one-fourth of a 0.125-mg tablet
PO q24–48h; adjust dosage based on serumconcentrations. � Beta-blockers such asatenolol or the calcium channel blockerdiltiazem for suppression of frequent atrialpremature complexes and for heart ratecontrol in atrial tachyarrhythmias such asatrial tachycardia/flutter/fibrillation. Beware:using these drugs in uncontrolled CHF.� Typical atenolol dosages: dogs, 0.25–1.0mg/kg q12h; cats, 6.25–12.5 mg/catq12–24h; start low and titrate to effect.� Diltiazem dosages: dogs, 2–6 mg/kg daily intwo (long-acting diltiazem) or three divideddosages; start low and titate to effect); cats,7.5 mg diltiazem HCl PO q8h, 15–30 mgDilacor XR q12–24h, or 10 mg/kg CardizemCD q24h. � Sotalol for intractablearrhythmias—dogs, 1–2 mg/kg PO q12h;cats, 10–20 mg/cat q12h. � Dogs can bereferred for electrocardioversion to convert AFto sinus rhythm (with follow-up therapy withsotalol or amiodarone); however, reversionback to AF is common owing to marked atrialdilatation.
Pulmonary Hypertension� Sildenafil—dogs, 0.5–3 mg/kg PO q8–12hours.
PRECAUTIONS� As a general rule pimobendan should not beused with pure valvular stenosis; however,some dogs and cats with advanced CHF havebeen treated with this drug with apparentsuccess, especially when there is combinedstenosis/regurgitation of the valve. � Use ACEinhibitors or other vasodilators judiciously inpatients with CHF; cardiac output is limitedand vasodilation may induce hypotension.Monitor arterial blood pressure and renalfunction.
POSSIBLE INTERACTIONS� Furosemide and ACE inhibitors can affectkidney function, alter blood electrolytes, andreduce blood pressure; these parametersshouldbe monitored.� Sildenafil can also reduce systemic bloodpressure and should not be used withnitroglycerin paste or another nitrate.
ALTERNATIVE DRUG(S)Spironolactone (2 mg/kg PO q12–24h) maybe considered as an ancillary diuretic and forits antifibrotic benefit (as an aldosteroneantagonist).
FOLLOW-UPPATIENT MONITORING� Thoracic radiographs for pulmonary edemaor pleural effusion. � Echocardiography withDoppler studies—to estimate pulmonarypressures and subjectively assess right heartfunction if on sildenafil. � Digoxinlevel—check 7–10 days following institutionof therapy; 8- to 12-hour trough should be
0.8–1.5 ng/mL. � Renal function, electrolytestatus, and arterial blood pressure when ondiuretic and/or ACE inhibitor. � Standardrhythm ECG or Holter (ambulatory ECG) ifarrhythmias are present.
POSSIBLE COMPLICATIONS� CHF � Atrial fibrillation � Syncope� Arterial thromboembolism—cats� Pulmonary hemorrhage with MS
EXPECTED COURSE AND PROGNOSIS� Morbidity is high; except for mild cases,prognosis is generally poor. However, someanimals will live for 6–8 years even withrelatively severe stenosis of the mitral valve.� Surgical intervention or balloonvalvuloplasty may alter course of disease, butdata are limited.
MISCELLANEOUSASSOCIATED CONDITIONSConcurrent congenital defects are common(e.g., subaortic stenosis in MS, PFO in TS).
PREGNANCY/FERTILITY/BREEDINGThe possibility that this may be a heritabledefect must be considered in assessingsuitability of the animal for breeding,particularly in breeds with a predilection forthis defect. The additional hemodynamicburden of gestation may be poorly toleratedby an already compromised heart.
SYNONYMSAtrioventricular valve dysplasia with stenosis
SEE ALSO� Atrioventricular Valve Dysplasia� Endocarditis, Infective
ABBREVIATIONS� ACE = angiotensin converting enzyme� AF = atrial fibrillation� AV = atrioventricular� CHF = congestive heart failure� ECG = electrocardiogram� MS = mitral stenosis� PFO = patent foramen ovale� TS = tricuspid stenosis
Suggested ReadingBrown WA, Thomas WP. Balloon
valvuloplasty of tricuspid stenosis in aLabrador Retriever. J Vet Intern Med 1995,9:419–424.
Lehmkuhl LB, Ware WA, Bonagura JD.Mitral stenosis in 15 dogs. J Vet Intern Med1994, 8:2–17.
Stamoulis ME, Fox PR. Mitral valve stenosisin three cats. J Small Anim Pract 1993,34:452–456.
Authors Lora S. Hitchcock andJohn D. BonaguraConsulting Editors Larry P. Tilley andFrancis W.K. Smith, Jr.

BLBS078-CF_A87 BLBS078-Tilley July 15, 2011 21:2
Canine and Feline, Fifth Edition 157
Azotemia and Uremia A
BASICSDEFINITION� Azotemia is an excess of urea, creatinine, orother non-protein nitrogenous substances inblood, plasma, or serum. � Uremia is thepolysystemic toxic syndrome that results frommarked loss in kidney functions. Uremiaoccurs simultaneously in animals withincreased quantities of urine constituents inblood.
PATHOPHYSIOLOGY� Azotemia can be caused by (1) increasedproduction of non-protein nitrogenoussubstances, (2) decreased glomerular filtrationrate, or (3) reabsorption of urine that hasescaped from the urinary tract into thebloodstream. High production of non-proteinnitrogenous waste substances may result fromhigh intake of protein (diet or gastrointestinalbleeding) or accelerated catabolism ofendogenous proteins. Glomerular filtrationrate may decline because of reduced renalperfusion (prerenal azotemia), acute orchronic kidney disease (renal azotemia), orurinary obstruction (post-renal azotemia).Reabsorption of urine into the systemiccirculation may result from leakage of urinefrom the excretory pathways (also a form ofpost-renal azotemia). � Pathophysiology ofuremia—incompletely understood; may berelated to (1) metabolic and toxic systemiceffects of waste products retained because ofrenal excretory failure, (2) deranged renalregulation of fluids, electrolytes, and acid-basebalance, and (3) impaired renal productionand degradation of hormones and othersubstances (e.g., erythropoietin and1,25-dihydroxycholecalciferol).
SYSTEMS AFFECTED� Uremia affects virtually every body system.� Cardiovascular—arterial hypertension, leftventricular hypertrophy, heart murmur,cardiomegaly, cardiac rhythm disturbances.� Endocrine/Metabolic—renal secondaryhyperparathyroidism, inadequate productionof 1,25-dihydroxycholecalciferol anderythropoietin, hypergastrinemia, weight loss.� Gastrointestinal—anorexia, nausea,vomiting, diarrhea, uremic stomatitis,xerostomia, uremic breath, constipation.� Hemic/Lymph/Immune—anemia andimmunodeficiency. � Neuromuscular—dullness, drowsiness, lethargy, fatigue,irritability, tremors, gait imbalance, flaccidmuscle weakness, myoclonus, behavioralchanges, dementia, isolated cranial nervedeficits, seizures, stupor, coma, impairedthermoregulation. � Ophthalmic—scleral andconjunctival injection, retinopathy,acute-onset blindness. � Respiratory—dyspnea. � Skin/Exocrine— pallor, bruising,increased shedding, unkempt appearance, lossof normal sheen to coat.
SIGNALMENTDogs and cats
SIGNSGeneral CommentsAzotemia may not be associated withhistorical or physical abnormalities. Unlesspatient has uremia, clinical findings arelimited to the disease responsible forazotemia. Findings described here are thoseof uremia.
Historical Findings� Weight loss � Declining appetite or anorexia� Reduced activity � Depression � Fatigue� Weakness � Vomiting � Diarrhea � Halitosis� Constipation � Changes in urine volume(increase or decrease) � Poor haircoat orunkempt appearance
Physical Examination Findings� Muscle wasting: cachexia � Mentaldepression � Dehydration � Weakness � Pallor� Petechiae and ecchymoses � Dull andunkempt haircoat � Uremic breath � Uremicstomatitis � Scleral and conjunctival injection� Relative hypothermia
CAUSESPrerenal Azotemia� Reduced renal perfusion due to low bloodvolume or low blood pressure. � Acceleratedproduction of nitrogenous waste productsbecause of enhanced catabolism of tissues inassociation with infection, fever, trauma,corticosteroid excess, or burns. � Increasedgastrointestinal digestion and absorption ofprotein sources (diet or gastrointestinalhemorrhage).
Renal Azotemia� Acute or chronic kidney diseases (primarykidney disease affecting glomeruli, renaltubules, renal interstitium, or renalvasculature) that impair at least 75% ofkidney function.
Post-renal Azotemia� Urinary obstruction; rupture of theexcretory pathway.
RISK FACTORS� Medical conditions—kidney disease,hypoadrenocorticism, low cardiac output,hypotension, fever, sepsis, polyuria, liverdisease, pyometra, hypoalbuminemia,dehydration, acidosis, exposure tonephrotoxic chemicals, gastrointestinalhemorrhage, urolithiasis, urethral plugs incats, urethral trauma, and neoplasia.� Advanced age may be a risk factor.� Drugs—potentially nephrotoxic drugs,nonsteroidal anti-inflammatory drugs,diuretics, antihypertensive medications;failure to adjust dosage of drugs primarilyeliminated by the kidneys to correspond withdecline in renal function. � Toxins—ethyleneglycol, grapes (dogs), lilies (cats).
DIAGNOSISDIFFERENTIAL DIAGNOSIS� Dehydration, poor peripheral perfusion,low cardiac output, history of recent fluidloss, high protein diet, or black, tarry stools—rule out prerenal azotemia. � Recent onset ofaltered urine output (high or low), clinicalsigns consistent with uremia, exposure topossible nephrotoxicants or ischemic renalinjury, or kidney size normal or enlarged—rule out acute renal failure. � Progressiveweight loss, polyuria, polydipsia, smallkidneys, pallor, and signs of uremia that havedeveloped over several weeks to months—ruleout chronic renal failure. � Abrupt decline inurine output and onset of signs of uremia;occasionally dysuria, stranguria, andhematuria; large urinary bladder or fluid-filledabdomen—rule out post-renal azotemia.
CBC/BIOCHEMISTRY/URINALYSISCBC� Nonregenerative anemia (normocytic,normochromic)—often present with chronicrenal failure. � Hemoconcentration—oftenpresent with prerenal azotemia; can also beseen with acute renal failure and post-renalazotemia.
Biochemistry� Serial determinations of serum ureanitrogen and creatinine concentrations mayhelp differentiate the cause of azotemia.Appropriate therapy to restore renal perfusiontypically yields a dramatic reduction inazotemia in patients with prerenal azotemia(typically within 24–48 hours). Correctingobstruction to urine flow or a rent in theexcretory pathway typically is followed by arapid reduction in the magnitude of azotemia.� Concurrent hyperkalemia may be consistentwith post-renal azotemia, primary renalazotemia due to oliguric renal failure, orprerenal azotemia associated withhypoadrenocorticism. � Increased serumalbumin and globulin concentration suggestprerenal azotemia or a prerenal component.
Urinalysis� A urine specific gravity value ≥ 1.030 indogs and ≥ 1.035 in cats supports a diagnosisof prerenal azotemia. Administration of fluidtherapy before urine collection may interferewith interpretation of low specific gravityvalues. � Azotemic patients that have not beentreated with fluids and have urine specificgravity < 1.030 in dogs and < 1.035 in catstypically have primary renal azotemia. Anotable exception to this rule is dogs and catswith glomerular disease. Glomerulopathy issometimes characterized by glomerulotubularimbalance in which adequate urine-concentrating ability may persist despitesufficient renal glomerular damage to causeprimary renal azotemia; these patients arerecognized by moderate to marked
BLBS078-CF_A87 BLBS078-Tilley July 15, 2011 21:2
158 Blackwell’s Five-Minute Veterinary Consult
Azotemia and Uremia (Continued)A
proteinuria in the absence of hematuria andpyuria. � Urine specific gravity is not useful inidentifying post-renal azotemia.
OTHER LABORATORY TESTSEndogenous or exogenous creatinine, iohexol,or inulin clearance tests or other specific testsof glomerular filtration rate may be used toconfirm that azotemia is caused by reducedglomerular filtration rate.
IMAGING� Abdominal radiographs—used to determinekidney size (small kidneys consistent withchronic kidney disease; mild-to-moderateenlargement of kidneys may be consistentwith acute renal failure or urinary obstruction)and to rule out urinary obstruction (markeddilation of the urinary bladder or mineraldensities within the excretory pathway).� Ultrasonography—may detect changes inechogenicity of the renal parenchyma and sizeand shape of kidneys that support a diagnosisof primary renal azotemia; useful to rule outpost-renal azotemia characterized bydistension of the excretory pathway anduroliths or masses within or impinging on theexcretory pathway and intra-abdominal fluidaccumulation (with rupture of the excretorypathway). � Excretory urography,pyelography, or cystourethrography—mayhelp establish the diagnosis of post-renalazotemia due to urinary obstruction orrupture of the excretory pathway.
DIAGNOSTIC PROCEDURESRenal biopsy can be used to confirm thediagnosis of primary kidney disease, todifferentiate acute from chronic kidneydisease, and to attempt to establish theunderlying disease process responsible forprimary kidney disease.
TREATMENT� Prerenal azotemia caused by impaired renalperfusion—correct the underlying cause ofrenal hypoperfusion; aggressiveness oftreatment depends on the severity of theunderlying condition and the probability thatpersistent renal hypoperfusion will lead toprimary renal injury or failure. � Primaryrenal azotemia and associated uremia—(1)specific therapy directed at halting orreversing the primary disease process affectingthe kidneys, and (2) symptomatic, supportive,and palliative therapies that ameliorate clinicalsigns of uremia; minimize the clinical impactof deficits and excesses in fluid, electrolyte,acid-base balances; minimize the effects ofinadequate renal biosynthesis of hormonesand other substances, and maintain adequatenutrition. � Post-renal azotemia—eliminateurinary obstruction or repair rents in theexcretory pathway; supplemental fluidadministration is often required to preventdehydration that may develop during the
solute diuresis that follows correction ofpost-renal azotemia. � Fluid therapy—indicated for most azotemic patients;preferred fluids include 0.9% saline orlactated Ringer’s solution. Determine fluidvolume to administer on the basis of severityof dehydration or volume depletion. If noclinical dehydration is evident, cautiouslyassume that the patient is less than 5%dehydrated and administer a correspondingvolume of fluid. Generally provide 50 to 75%of volume replacement over 2–6 hours, exceptin patients with overt or suspected cardiacfailure. � Mannitol (0.5–1 g/kg IV q8h or0.25–0.5 mg/kg/hr as CRI) may be used inpolyuric patients to promote diuresis andenhance elimination of nitrogenous waste.� Treat patients in shock appropriately.� Consider feeding diets formulated forkidney disease to reduce the magnitude ofazotemia, hyperphosphatemia, and acidosis.
MEDICATIONSDRUG(S) OF CHOICE� Symptomatic therapy may be indicated foruremia in patients with kidney disease.� Famotidine (0.5–1.0 mg/kg PO, SC, IM, IVq12–24h) or other H2-receptor antagonistsmay be used to reduce gastric hyperacidityand nausea. � Antiemetics such as maropitant(1 mg/kg q24h PO or SC × 5 days).
CONTRAINDICATIONSAdministration of nephrotoxic drugs
PRECAUTIONS� Use caution when administering drugsrequiring renal excretion. Consult appropriatereferences concerning dose-reductionschedules or adjustments of maintenanceintervals. � Use caution in administeringfluids to patients that are oliguric or anuric.Monitor urine production rates and bodyweight during fluid therapy to minimize thelikelihood of inducing overhydration. � Usecaution in administering drugs that maypromote hypovolemia or hypotension (e.g.,diuretics); carefully monitor the response tosuch drugs by assessing hydration status,peripheral perfusion, and blood pressure, withserial evaluation of renal function tests.� Corticosteroids may worsen azotemia byincreasing catabolism of endogenous proteins.
ALTERNATIVE DRUG(S)Azodyl, a probiotic, may enhancegastrointestinal excretion of nitrogenouswastes, thereby reducing the magnitude ofazotemia and possibly ameliorating someuremic signs.
FOLLOW-UPPATIENT MONITORINGSerum urea nitrogen and creatinine
concentrations 24 hours after initiating fluidadministration; also urine production, bodyweight, and hydration status.
POSSIBLE COMPLICATIONS� Failure to correct prerenal azotemia causedby renal hypoperfusion rapidly could result inischemic primary kidney disease. � Primaryrenal azotemia can progress to uremia.� Failure to restore normal urine flow inpatients with post-renal azotemia can result inprogressive renal damage or death due tohyperkalemia and uremia.
MISCELLANEOUSASSOCIATED CONDITIONSAn association may exist betweenhypokalemia and azotemia in cats.Preliminary findings suggest thathypokalemia may be associated withfunctional or structural renal changes leadingto azotemia.
AGE-RELATED FACTORSPrimary renal failure may occur in animals ofany age, but geriatric dogs and cats appear tobe at substantially higher risk for both acuteand chronic kidney disease. However, do notassume that azotemia in geriatric dogs andcats indicates primary kidney disease; thesepatients are also at higher risk for prerenal andpost-renal causes for azotemia.
ZOONOTIC POTENTIALLeptospirosis
PREGNANCY/FERTILITY/BREEDING� Data on azotemia and pregnancy in dogsand cats are very limited. Humans maytolerate minimal renal disease well duringpregnancy; however, ability to sustain a viablepregnancy declines as renal function declines.� Pregnant azotemic animals—pharmacologicagents excreted by non-renal pathways arepreferred.
SEE ALSO� Chapters on acute and chronic kidneydisease � Urinary Tract Obstruction
INTERNET RESOURCESInternational Renal Interest Society (IRIS):www.iris-kidney.com.
Suggested ReadingPolzin D. Chronic kidney disease. In: Ettinger
SJ, Feldman EC, eds., Textbook ofVeterinary Internal Medicine, 7th ed.Philadelphia: Saunders, 2010,pp. 2036–2067.
Ross L. Acute renal failure. In: Bonagura JD,Twedt DC, Kirk’s Veterinary Therapy XIV.Philadelphia: Saunders, 2009, pp. 879–882.
Author David J. PolzinConsulting Editor Carl A. Osborne





























