Embed Size (px)
Citation preview
For Peer Review
Case Report: DETECTION OF ROTAVIRUS RNA IN THE
CEREBROSPINAL FLUID OF A CHILD WITH ROTAVIRUS
GASTROENTERITIS AND MENINGISM
Journal: Journal of Medical Virology
Manuscript ID: JMV-10-2287.R2
Wiley - Manuscript type: Research Article
Date Submitted by the Author:
11-May-2011
Complete List of Authors: Medici, Maria Cristina; University of Parma School of Medicine,
Department of Pathology and Laboratory Medicine, Section of Microbiology Abelli, Laura Anna; University of Parma School of Medicine, Department of Pathology and Laboratory Medicine, Section of Microbiology Guerra, Paola; University of Parma School of Medicine, Department of Pathology and Laboratory Medicine, Section of Microbiology Dodi, Icilio; University Hospital of Parma, Maternal-Infantile Department, Unit of Paediatrics and Oncohematology Dettori, Giuseppe; University of Parma School of Medicine, Department of Pathology and Laboratory Medicine, Section of
Microbiology Chezzi, Carlo; University of Parma School of Medicine, Department of Pathology and Laboratory Medicine, Section of Microbiology
Keywords: rotavirus, cerebrospinal fluid, central nervous system, extraintestinal spread, pathogenicity
John Wiley & Sons
Journal of Medical Virologype
er-0
0657
580,
ver
sion
1 -
7 Ja
n 20
12Author manuscript, published in "Journal of Medical Virology 83, 9 (2011) 1637"
DOI : 10.1002/jmv.22156
For Peer Review
275x190mm (96 x 96 DPI)
Page 1 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
3
CASE REPORT: DETECTION OF ROTAVIRUS RNA IN THE CEREBROSPINAL 1
FLUID OF A CHILD WITH ROTAVIRUS GASTROENTERITIS AND MENINGISM 2
3
Maria Cristina Medici,*1 Laura Anna Abelli,
1 Paola Guerra,
1 Icilio Dodi,
2 Giuseppe Dettori
1, 4
Carlo Chezzi1. 5
1Section of Microbiology, Department of Pathology and Laboratory Medicine, University of 6
Parma, School of Medicine; 2Unit of Paediatrics and Oncohematology, Maternal-Infantile 7
Department, University Hospital of Parma - Viale Antonio Gramsci, 14, 43126, Parma, Italy. 8
9
Running head: Rotavirus RNA in the cerebrospinal fluid 10
11
12
13
14
15
*Corresponding Author: Prof. Maria Cristina Medici 16
Department of Pathology and Laboratory Medicine, Section of Microbiology, 17
University of Parma School of Medicine, 18
Viale Antonio Gramsci, 14, 43126, Parma, Italy. 19
Phone: ++39 0521903499; Fax: ++39 0521 993620 20
E-mail: [email protected] 21
Page 2 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
4
ABSTRACT 1
Although case reports have described detection of rotavirus (RV) in extraintestinal sites such 2
as the liver, kidney, and central nervous system (CNS) of children with RV gastroenteritis, 3
CNS localization in RV infection seems to be rare. RT-PCR and nucleotide sequencing 4
detected a G1P[8] strain in the stool and cerebrospinal fluid (CSF) samples of a patient with 5
concurrent RV-associated enteritis and CNS signs. Upon sequence analysis, the viruses 6
detected in the CSF was identical to the virus detected in the stools. In the VP7 and VP4 –7
based phylognetic dendograms the strain clustered within the G1-Ic sublineage and the P[8] -8
III lineage. This study supports the hypothesis that RV infection was able to spread from the 9
intestinal tract to the CNS, and likely played a role in the onset of neurological disease. 10
11
12
Key words: rotavirus, cerebrospinal fluid, central nervous system, extraintestinal spread, 13
pathogenicity. 14
15
Page 3 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
5
Rotavirus (RV) infection is localized primarily in the small intestine. Although extra-1
intestinal localization of RV has been reported repeatedly [Gilger et al., 1992; Pang et al., 2
1996; Makino et al., 1996; Hongou et al., 1998; Goldwater et al., 2001; Lynch et al., 2001; 3
Nigrovic et al., 2002; Iturriza-Gòmara et al., 2002a; Kehle et al., 2003; Nakagomi T, 4
Nakagomi O, 2005; Dickey et al., 2009; Liu et al., 2009] in children with RV gastroenteritis, 5
localization in the central nervous system (CNS) during RV infection appears to be rather 6
rare. Also, in most cases, sequence information was not obtained on the RVs detected in the 7
cerebrospinal fluid (CSF) of patients with CNS disease. 8
A 27-month-old girl, with no recent history of diseases, was admitted in January 2008 to the 9
Paediatric Emergency Department of the University Hospital of Parma, Italy. Three days 10
before hospital admission, the child developed vomiting, diarrhoea and fever (temperature, 11
37.5 °C). One day before admission, the patient started displaying somnolence and rolling her 12
eyes back. On admission, the patient was depressed, anorexic and apyrexial. Diarrhoea was 13
still present. Also, neurological signs, including stiff neck, photophobia, and vertical 14
nystagmus, were observed. Acute meningoencephalitis was suspected based on the clinical 15
symptoms. At physical examination the heart rate was 150/min and oxygen saturation was 16
99%. No alteration was observed by cranial computed axial tomography. Initial laboratory 17
investigations were as follows: low haemoglobin level (11.7 g/dL) and haematocrit (33.8%); 18
leukocyte count 4.68 x 103 cells/µl (37% neutrophilis, 50.6% lymphocytes, 11.8% 19
monocytes, 0.4% eosinophilis, and 0.2% basophilis); platelet count 244 x 103 cells/ µl; high 20
C-reactive protein level (39.1 mg/L); low urea (7 mg/dL); low creatinine (0.3 mg/dL); high 21
aspartate aminotransferase (92 U/L); high lactate dehydrogenase (505 U/L); with sodium, 22
potassium, calcium, and glucose unremarkable. 23
Intravenous rehydration, treatment with the antibiotic ceftryaxone, and the antiviral acyclovir 24
drug, were administered. Diarrhoea associated with abdominal pain persisted for two days 25
Page 4 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
6
after admission. On the 4th
day after admission, the patient had an episode of transient 1
epistaxis. Lumbar puncture was performed on the 1st day after admission the CSF and was 2
collected and examined. The CSF was clear, slightly raised pressure, and the composition 3
was as follows: protein 19 mg/dL; glucose 61 mg/dL; chlorides 122 mmol/L, 1 leukocyte 4
/mm3, and some red blood cells. Over the subsequent days, the patient’s condition gradually 5
improved, with the stiff neck and vertical nystagmus disappeared. Intravenous therapy was 6
stopped and the patient started eating. 7
Bacteriological investigations and microscopy of the CSF did not reveal any abnormalities. 8
The CFS was negative by PCR/RT-PCR for varicella-zoster virus, (VZV), herpes simplex 9
virus 1-2, (HSV 1-2), parvovirus B19 (B19), cytomegalovirus (CMV), human herpes virus 6, 10
adenovirus, and enterovirus (EV), using commercial assays (Nanogen Advanced Diagnostics, 11
Turin, Italy). 12
Neither bacteria nor respiratory viruses were detected by routine diagnostic laboratory 13
methods from a throat swab. In addition, HSV 1-2, B19, VZV, CMV, and EV were not 14
detected by PCRs/RT-PCRs from the peripheral blood, obtained on the 3rd
day after 15
admission. 16
Rotavirus-like particles were detected by electron microscopy (EM) in the stools collected on 17
the 3rd
day after admission, and a group A RV strain, with long electropherotype (e-type), 18
was identified by polyacrylamide gel electrophoresis [Medici et al., 2004] while cell culture 19
and nRT-PCR for norovirus (Nanogen Advanced Diagnostics) were negative. 20
On the 6th
day after admission, the patient was discharged with a diagnosis of meningism and 21
RV gastroenteritis. 22
Rotavirus RNA was detected using a set of primers amplifying a fragment (380 bp) of the 23
group A RV inner capsid protein VP6 gene [Iturriza-Gòmara et al., 2002b] in a one-step RT-24
PCR (“Superscript One-Step Platinum Taq III”, Invitrogen, California, USA), from the CSF 25
Page 5 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
7
and stools, but not from the plasma. Temperature conditions were as follows: 50°C for 60 1
min, 94°C for 2 min, 35 cycles at 94°C for 1 min, 50°C for 1 min, 68°C for 1 min, and a final 2
extension step of 68°C for 10 min. In order to confirm these unusual findings, the analysis 3
was repeated twice. Also, any possible contamination was ruled out during RNA extraction 4
and RT-PCR as strict procedures (i.e. positive and negative controls and separate extraction 5
of the samples) were adopted. 6
Gel-purified PCR products (Qiaquick Gel Extraction Kit, Qiagen, Hilden, Germany) were 7
sequenced with automated sequencer 3730 DNA Analyzer (Applied Biosystems, Foster City, 8
CA, USA). Sequence data were analyzed using Bioedit software package and phylogenetic 9
analysis was carried out using MEGA version 4.1 [Tamura et al., 2007]. The partial VP6 10
sequence (nucleotide 759 to 1112) generated from the CSF and the stools were 100% 11
identical to each other. In the attempt to characterize the VP7/VP4 genotype specificity of the 12
RV strain, the RNAs extracted from the stools and CSF were tested using several sets of 13
primers able to predict the VP7 and VP4 specificity, as described previously [Medici et al., 14
2007]. In second-round PCRs, genotype P[8]-specific bands were amplified from both the 15
CSF and the stools, while a genotype G1-specific band was obtained only from the patient’s 16
stools. In the first-round PCRs, specific amplicons of the full-length VP7 gene and the VP8* 17
portion of the VP4 gene were generated only from the faecal sample, likely due to the higher 18
viral load present in the faeces. By sequence analysis of the VP4 and VP7 first-round 19
amplicons obtained from the stools, the strain (PR267/08/M) was confirmed to have G1P[8] 20
specificities. The VP4, VP6, and VP7 sequences of strain PR267/08/M have been registered 21
in GenBank under accession numbers HQ694988, HQ694989 and HQ694990, respectively. 22
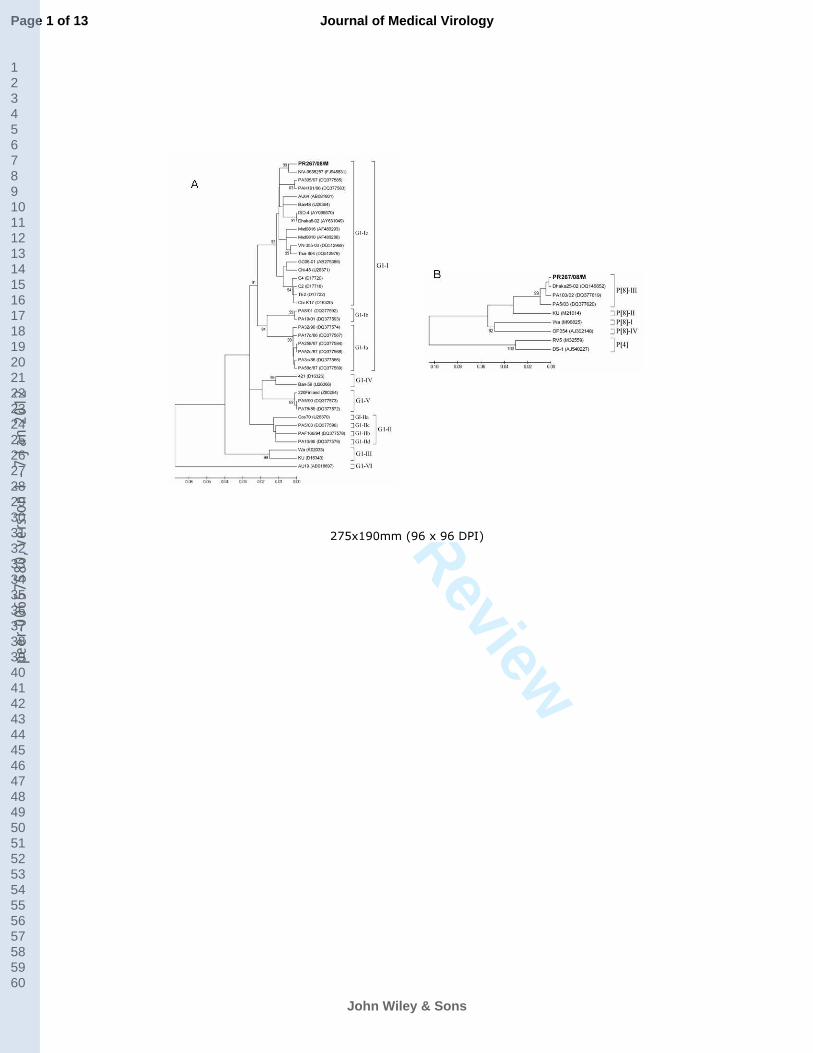
In the VP7 (nt 130 to 995) and VP4 (nt 85 to 1011) -based phylogenetic dendrograms (Fig. 23
1), strain PR267/08/M clustered within the G1 genetic lineage I, sublineage Ic (Fig. 1A), and 24
the P[8] genetic lineage III (Fig. 1B). 25
Page 6 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
8
The tropism of RVs does not seem to be absolutely restricted to enterocytes [Conner, Ramig, 1
1996], as RVs can infect neuronal cells in vitro [Weclewicz et al., 1998] and in vivo [Shaw et 2
al., 1989]. Altered electrolyte balance due to dehydration or inappropriate rehydration could 3
account for the neurological sequelae observed in some reports. However, the detection of 4
RV RNA in CSF, as observed in this study, suggests more direct and unknown RV-mediated 5
mechanisms able to damage the CNS and trigger the neurological signs. 6
In this study, common viral and bacterial infections of the CNS were excluded and only RV 7
RNA was detected in the CSF and stools of the patient. A possible contamination of the CSF 8
sample due to the overlying skin having come into contact with faecal material is a possibility 9
even if it is unlikely because the CSF was obtained under sterile conditions. The RV strain 10
detected in the CSF and in the stools were found to be identical by molecular characterization 11
and sequence analysis, thus suggesting that the RV strain was able to spread from the 12
intestinal tract to the CNS. As RV RNA was not detected in the patient’s plasma on the 3rd
13
day after admission, it is difficult to understand how the virus was able to reach the CNS. A 14
possible explanation is that viremia occurred very early and only for a limited time or at low 15
levels, below the limit of detection of the molecular assays. Indeed, it is not possible to 16
correlate virus load in the stools with the virus load in the serum [Ray et al., 2006]. 17
It is unclear whether the detection of RV RNA in the CSF of the patient was a serendipitous 18
event or the neurological signs were actually caused by RV localization in the CNS. Also, in 19
this study, some aspects of the investigations were difficult to interpret. For instance, it was 20
not possible to amplify the VP7 gene from the CSF. This was likely due to the low viral load, 21
below the RT-PCR detection limit, as observed by Ushijima et al. [1994]. Similar technical 22
constraints have been reported during genotyping of RV strains [Nigrovic et al., 2002; Lynch 23
et al., 2002] in RV-positive CSF samples. 24
Page 7 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
9
The RV strain detected in the patient (PR267/08/M) was a common G1P[8] genotype. Other 1
studies reviewing the role of RV in cases of gastroenteritis associated with CNS symptoms 2
[Dickey et al., 2009; Liu et al., 2009] have observed that G1 was the most commonly 3
identified G type [Dickey et al. 2009]. As G1P[8] RVs are largely predominant worldwide 4
[Gentsch et al., 2005], this was not unexpected. 5
In the VP7 strain PR267/08/M clustered in the phylogenetic sub-lineage G1-Ic. This lineage 6
contains an additional three strains detected in CSF samples (C2, C4, and TE2 strains) and 7
one strain (GC06-01) detected in the stools from children with CNS disease, even if in a 8
different sub-cluster [Ushijima et al., 1994; Shiihara et al., 2007]. This observation might be a 9
coincidence, but is noteworthy. 10
Sequencing RV strains associated with neurological disease is important, since this could 11
generate information useful for identifying genetic hallmarks of neurotropism in RV strains, 12
or, in contrast, this information could demonstrate that no specific genetic make up or 13
mutation is required for RVs to invade occasionally the CNS. Several genes have been 14
suspected to be implicated in the spread of RVs from the gut to the CNS, including the NSP4, 15
the VP3, the VP4 and VP7. The NSP4, a non-structural protein with enterotoxic activity, is 16
believed to interact with the enteric nervous system and this might be a route of RV 17
dissemination [Ramig, 2004], The VP4 and VP7, the main RV antigenic determinants, are the 18
sites of virus-cell interactions [Kapikian et al., 2001], while the NSP3 has been suggested as 19
the genetic determinant for RV extra-intestinal spread in the mouse model [Mossel and 20
Ramig, 2002]. 21
In conclusion, the increasing number of reports on CNS disease in association with RV 22
gastroenteritis, along with the present report, suggests that RV should be included in the 23
diagnostic algorithms of CNS disease. 24
Page 8 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
10
ACKNOWLEDGEMENTS 1
Potential conflict of interest. The authors hereby state and declare that they have no 2
association which might represent a conflict of interest. 3
Financial support. This study was supported by the grant "Epidemiologia molecolare di 4
rotavirus in età pediatrica in Italia. Creazione di una rete di sorveglianza per monitorare la 5
diffusione e l’evoluzione di genotipi virali in previsione della vaccinazione" - CCM 06-07 6
program - from the Italian Ministry of Health and by the grants “FIL 2008” and partially “FIL 7
2009” from the University of Parma, Italy. 8
9
Page 9 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
11
REFERENCES 1
Conner M, Ramig R. 1996. Viral enteric diseases. In: Nathanson N, et al. eds. Viral 2
Pathogenesis. Philadelphia: Lippincott-Raven. 713-743. 3
Dickey M, Jamison l, Michaud L, Care M, Bernstein DI, Staat MA. 2009. Rotavirus 4
meningoencephalitis in a previously healthy child and a review of the literature. Pediatr Infect 5
Dis J 28:318-321. 6
Gentsch JR, Laird AR, Bielfelt B, Griffin DD, Banyai K, Ramachandran M, Jain V, Cunliffe 7
NA, Nakagomi O, Kirkwood CD, Fischer TK, Parashar UD, Bresee JS, Jiang B, Glass RI. 8
2005. Serotype diversity and reassortment between human and animal rotavirus strains: 9
implication for rotavirus vaccine programs. J Infect Dis. 192:S146-S159. 10
Gilger MA, Matson DO, Conner ME,Rosenblatt HM, Finegold MJ, Estes MK. 1992. 11
Extraintestinal rotavirus infections in children with immunodeficiency. J Pediatr. 120:912-12
917. 13
Goldwater PN, Rowland K, Thesinger M, Abbott K, Grieve A, Palombo EA, Masendycz PJ, 14
Wilkinson I. 2001. Rotavirus encephalopathy: pathogenesis reviewed. J Paediatr Child 15
Health. 37:206-209. 16
Hongou K, Konishi T, Yagi S, Araki K, Miyawaki T. 1998. Rotavirus encephalitis 17
mimicking afebrile benign convulsions in infants. Pediatr Neurol. 18:354-357. 18
Iturriza-Gómara M, Auchterlonie IA, Zaw W, Molyneaux P, Desselberger U, Gray J. 2002a. 19
Rotavirus gastroenteritis and central nervous system (CNS) infection: characterization of the 20
VP7 and VP4 genes of rotavirus strains isolated from paired fecal and cerebrospinal fluid 21
samples from a child with CNS disease. J Clin Microbiol. 40:4797-4799. 22
Iturriza-Gómara M, Wong C, Blome S, Desselberger U, Gray J. 2002b. Molecular 23
characterization of VP6 genes of human rotavirus isolates: correlation of genogroups with 24
subgroups and evidence of independent segregation. J Virol. 76:6596-6601. 25
Page 10 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
12
Kapikian A, Hoshino Y, Chanock R. 2001. Rotaviruses. In. Knipe DM, Howley PM, eds. 1
Fields Virology. 4th ed. Philadelphia: Lippincott Williams & Wilkins. 1787-1834 p. 2
Kehle J, Metzger-Boddien C, Tewald F, Wald M, Schüürmann J, Enders G. 2003. First case 3
of confirmed rotavirus meningoencephalitis in Germany. Pediatr Infect Dis J. 22:468-470. 4
Liu B, Fujita Y, Arakawa C, Kohira R, Fuchigami T, Mugishima H, Kuzuya M. 2009. 5
Detection of rotavirus RNA and antigens in serum and cerebrospinal fluid samples from 6
diarrheic children with seizures. Jpn J Infect Dis. 62:279-283. 7
Lynch M, Lee B, Azimi P, Gentsch J, Glasser C, Gilliam S, Chang HG, Ward R, Glass RI . 8
2001. Rotavirus and central nervous system symptoms: cause or contaminant? Case reports 9
and review. Clin Infect Dis. 33:932-938. 10
Makino M, Tanabe Y, Shinozaki K, Matsuno S, Furuya T. 1996. Haemorragic shock and 11
encephalopathy associated with rotavirus infection. Acta Paediatr. 85:632-634. 12
Medici MC, Martinelli M, Arcangeletti MC, Pinardi F, De Conto F, Dodi I, Virdis R, Abelli 13
LA, Aloisi A, Zerbini L, Valcavi P, Calderaro A, Bernasconi S, Izzi GC, Chezzi C, Dettori G. 14
2004. Epidemiological aspects of human rotavirus infection in children hospitalized with 15
acute gastroenteritis in an area of northern Italy. Acta Biomed. 75:100-106. 16
Medici MC, Abelli LA, Martella V, Dettori G, Chezzi C. 2007. Characterization of inter-17
genogroup reassortant rotavirus strains detected in hospitalised children in Italy. J Med 18
Virol.79:1406-12. 19
Mossel EC, Ramig RF. 2002. Rotavirus genome segment 7 (NSP3) is a determinant of 20
extraintestinal spread in the neonatal mouse. J Virol. 76:6502-6650. 21
Nakagomi T, Nakagomi O. 2005. Rotavirus antigenemia in children with encephalopathy 22
accompanied by rotavirus gastroenteritis. Arch Virol. 150:1927-1931. 23
Nigrovic LE, Lumeng C, Landrigan C, Chiang VW. 2002. Rotavirus cerebellitis? Clin Infect 24
Dis. 34:130. 25
Page 11 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
13
Pang XL, Joensuu J, Vesikari T. 1996. Detection of RVRNA in cerebrospinal fluid in a case 1
of rotavirus gastroenteritis with febrile seizures. Pediatr Infect Dis J. 15:543-545. 2
Ramig R.F. 2004. Pathogenesis of intestinal and systemic rotavirus infection. J Virol. 3
78:10213-10220. 4
Ray P, Fenaux M, Sharma S, Malik J, Subodh S, Bhatnagar S, Greenberg H, Glass RI, 5
Gentsch J, Bhan MK. 2006. Quantitative evaluation of rotaviral antigenemia in children with 6
acute rotaviral diarrhea. J Infect Dis.194:588-593. 7
Shaw DP, Morehouse LG, Solorzano RF. 1989. Rotavirus replication in colostrum-fed and 8
colostrum-deprived pigs. Am J Vet Res. 50:1966-1970. 9
Shiihara T, Watanabe M, Honma A, Kato M, Morita Y, Ichiyama T, Maruyama K. 2007. 10
Rotavirus associated acute encephalitis/encephalopathy and concurrent cerebellitis: report of 11
two cases. Brain Dev. 29:670-673. 12
Tamura K, Dudley J, Nei M, Kumar S. 2007. MEGA4: Molecular Evolutionary Genetics 13
Analysis (MEGA) software version 4.0. Mol Biol Evol. 24:1596-1599. 14
Ushijima H, Xin K-Q, Nishimura S, Morikawa S, Abe T. 1994. Detection and sequencing of 15
rotavirus VP7 gene from human materials (stools, sera, cerebrospinal fluids, and throat 16
swabs) by reverse transcription and PCR. J Clin Microbiol. 32:2893-2897. 17
Weclewicz K, Svensson L, Kristensson K. 1998. Targeting of endoplasmic reticulum-18
associated proteins to axons and dendrites in rotavirus-infected neurons. Brain Res Bull. 19
46:353-360. 20
Page 12 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012
For Peer Review
14
FIGURE 1. Neighbour-joining phylogenetic trees (Kimura-2-parameter model) based on 1
partial nucleotide sequences of VP7 (nt 130 to 995) (A) and VP4 (nt 85 to 1011) (B) genes of 2
the rotavirus strain PR267/08/M (in boldface) obtained from the stool of a child hospitalised 3
with gastroenteritis and meningism at Parma, Italy. The trees illustrate the genetic 4
relationships of the PR267/08/M strain with reference strains and other established human 5
strains available in GenBank (accession numbers are shown in parenthesis). The numbers 6
adjacent to the nodes represent the percentage of bootstrap support (of 1,000 replicates). 7
Bootstrap values lower than 80% are not shown. 8
9
Page 13 of 13
John Wiley & Sons
Journal of Medical Virology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
peer
-006
5758
0, v
ersi
on 1
- 7
Jan
2012





























