Embed Size (px)
Citation preview
RESEARCH ARTICLE
Carriage rates and antimicrobial sensitivity of
pneumococci in the upper respiratory tract of
children less than ten years old, in a north
Indian rural community
Sambuddha Kumar1, Debjani Ram PurakayasthaID2, Arti Kapil1, Siddhartha Saha3,
Fatimah S. Dawood3, Bimal Kumar DasID1*, Ritvik Amarchand2, Rakesh Kumar2, Kathryn
E. LafondID3, Seema Jain3, Anand Krishnan2
1 Department of Microbiology, All India Institute of Medical Sciences, New Delhi, India, 2 Center for
Community Medicine, All India Institute of Medical Sciences, New Delhi, India, 3 Centers for Disease Control
and Prevention, Atlanta, Georgia, United States of America
Abstract
Pneumococcal carriage studies are important for vaccine introduction and treatment strate-
gies. Pneumococcal carriage rates estimated in this cohort study among children in a rural
community of northern India. Between August 2012 and August 2014, trained nurses made
weekly home visits to screen enrolled children aged <10 years for acute upper or lower
respiratory infections (AURI/ALRI) in Ballabgarh, Haryana. Nasal swab from infants aged
<1year and throat swab from children aged�1 year were collected. All specimens were cul-
tured for pneumococci; isolates were serotyped and subjected to antimicrobial susceptibility
testing. During the study period, 4348 nasal/throat swabs collected from children with clini-
cal features of ARI (836 ALRI, 2492 AURI) and from 1020 asymptomatic children. Overall
pneumococcal carriage was 5.1%, the highest carriage rate among children <1 year of age
(22.6%). The detection rates were higher among children with ARI (5.6%; 95% CI: 4.8–6.4)
than asymptomatic children (3.3%; 95% CI: 2.3–4.6). Among 220 pneumococcal isolates,
42 diverse serotypes were identified, with 6B/C (8.6%), 19A (7.2%), 19F (6.8%), 23F
(6.4%), 35A/B/C (6.4%), 15B (5%), 14 (4.5%) and 11A/C/D (3.2%) accounting for 50%.
Forty-five percent of the serotypes identified are included in the current formulation of 13-
valent pneumococcal conjugate vaccine. Ninety-six percent of isolates were resistant to co-
trimoxazole, 9% were resistant to erythromycin, and 10% had intermediate resistance to
penicillin with minimum inhibitory concentration ranges (0.125 to 1.5 μg/ml). Pneumococcal
detection was relatively low among children in our study community but demonstrated a
diverse range of serotypes and half of these serotypes would be covered by the current for-
mulation of 13-valent pneumococcal vaccine.
PLOS ONE
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 1 / 10
a1111111111
a1111111111
a1111111111
a1111111111
a1111111111
OPEN ACCESS
Citation: Kumar S, Purakayastha DR, Kapil A, Saha
S, Dawood FS, Das BK, et al. (2021) Carriage rates
and antimicrobial sensitivity of pneumococci in the
upper respiratory tract of children less than ten
years old, in a north Indian rural community. PLoS
ONE 16(2): e0246522. https://doi.org/10.1371/
journal.pone.0246522
Editor: Silvia Ricci, Meyer Children’s University
Hospital - University of Florence, ITALY
Received: August 15, 2020
Accepted: January 20, 2021
Published: February 4, 2021
Peer Review History: PLOS recognizes the
benefits of transparency in the peer review
process; therefore, we enable the publication of
all of the content of peer review and author
responses alongside final, published articles. The
editorial history of this article is available here:
https://doi.org/10.1371/journal.pone.0246522
Copyright: This is an open access article, free of all
copyright, and may be freely reproduced,
distributed, transmitted, modified, built upon, or
otherwise used by anyone for any lawful purpose.
The work is made available under the Creative
Commons CC0 public domain dedication.
Data Availability Statement: All relevant data are
within the paper and its Supporting information
files.
Introduction
According to the World Health Organization (WHO) and Maternal and Child Epidemiology
Estimates Group (MCEE), in 2015, India had the highest number of under-five deaths due to
acute respiratory infection (ARI) in the world [1, 2]. Although pneumococcal disease is vaccine
preventable, Streptococcus pneumoniae remains a major cause of acute lower respiratory infec-
tion (ALRI) in children, causing an estimated 294,000 under-five deaths [3]. Pneumococcal
disease is a major public health problem in India. Almost a quarter of global pneumococcal
cases and deaths occur in India [3, 4].
India introduced pneumococcal vaccine in selected high burden states in 2017 with plans to
roll out across the country to reduce the under-five mortality [5]. Pneumococcal carriage studies
are useful for monitoring circulating serotypes and the proportion that are covered by available
pneumococcal conjugate vaccines (PCV). Pre- and post-PCV introduction nasopharyngeal car-
riage prevalence and serotype distribution are also used as an indirect measure to assess vaccine
impact [6]. The introduction of pneumococcal vaccine is expected to reduce the incidence of
pneumococcal disease by reducing carriage rates of vaccine serotypes. However, in India, data
on pneumococcal carriage are sparse. Few multi-site hospital-based studies from India found
that serotypes 14, 1, 5, 19F and 6B were the most commonly identified serotypes in hospitalized
children aged<5 years with invasive pneumococcal disease and the current PCV13 vaccine may
provide serotype specific immunity against 74% of the serotypes causing invasive disease [7, 8].
Asian countries are unique with culture, society and somehow similar in lifestyle and over-
crowded population of these regions is probably the major reasons for pneumococcal trans-
mission. Pneumococcal distribution from Asian region countries, South Asian Pneumococcal
Alliance (SAPNA) and Asian Strategic Alliance for Pneumococcal Disease Prevention (ASAP)
reported circulating serotypes mostly involving in invasive pneumococcal disease [9]. Among
neighbouring countries Pakistan had started expanded programme of immunization for
PCV10 in 2012, with financial support of the Global Alliance for Vaccines and Immunisation
(GAVI) and after that conjugate vaccine PCV10 included in Bangladesh and PCV13 in Nepal
on 2015 [10].
As a part of the effort to reduce under-five deaths due to pneumonia, frontline health work-
ers in various low- and middle-income countries have been trained to treat pneumonia with
antimicrobials based on symptoms and signs using the Integrated Management of Childhood
Illnesses (IMCI) strategy [11]. However, emergence of antimicrobial resistance (AMR) to com-
monly used antibiotics like co-trimoxazole hampers effective prevention and treatment of
pneumonia [12, 13]. The data on AMR in India, especially for important pathogens such as S.
pneumoniae, are scanty. Data from different regions are needed to guide antibiotic treatment
strategies for children with pneumonia in India.
The present study was carried out to assess the carriage, serotypes and AMR of circulating
pneumococcal isolates among children aged<10 years living in rural northern India, prior to
pneumococcal vaccine introduction. As the concentration of pneumococcal carriage is known
to increase during acute upper respiratory infection (AURI), and acute lower respiratory infec-
tion (ALRI) [14, 15], and also compared carriage rates among children with clinical features
suggestive of AURI, ALRI and asymptomatic children.
Methods
Study population and specimen collection
From August 2012 to August 2014 children aged<10 years surveyed living in four villages of
Ballabgarh block in Faridabad district of the northern state of Haryana, India. This work was
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 2 / 10
Funding: This study was funded under the
cooperative agreement between the All India
Institute of Medical Sciences, New Delhi, India and
Center for Disease Control and Prevention, Atlanta,
USA (U01-IP000492). Sambuddha Kumar, Debjani
Ram Purakayastha, Arti Kapil, Siddhartha Saha,
Fatimah S. Dawood, Bimal Kumar Das, Ritvik
Amarchand, Rakesh Kumar, Kathryn E. Lafond,
Anand Krishnan were all involved in the planning of
the study and development of the study protocols
and tools. Debjani Ram Purakayastha, Rakesh
Kumar, Ritvik Amarchand coordinated community-
based surveillance activities. Sambuddha Kumar,
Bimal Kumar Das and Arti Kapil performed the
bacteriological studies. Sambuddha Kumar,
Rakesh Kumar, Ritvik Amarchand and Siddhartha
Saha analyzed the data. Sambuddha Kumar, Arti
Kapil drafted the manuscript. Siddhartha Saha,
Seema Jain, Kathryn E. Lafond, Fatimah S.
Dawood, Anand Krishnan provided overall
supervision for the project activities. All the authors
have read and reviewed the manuscript.
Competing interests: No competing interest.
part of an ongoing cohort study on acute respiratory tract infections [16]. Briefly, trained
study staff visited all the enrolled children at their homes weekly for the detection of ARI case
defined as onset of at least one of the symptoms of cough, sore throat, rhinorrhea, shortness of
breath or earache/ear discharge in past 7 days. Children with any of these symptoms and signs
of tachypnea, stridor, chest in-drawing, lethargy, convulsions or unconsciousness were classi-
fied as acute lower respiratory infection (ALRI) using the age-appropriate Integrated Manage-
ment of Neonatal and Childhood Illness (IMNCI) [11] and Integrated Management of
Adolescent and Adult Illnesses (IMAI) guidelines [17]. Children with ARI without the signs
and symptoms of ALRI were classified as having acute upper respiratory infection (AURI).
Study nurses collected nasal swabs from infants aged<1year and throat swab from children
aged 1–10 years. Nurses also collected swabs from similar number (ALRI) of conveniently
selected asymptomatic children of similar age +/- 6 months from the same neighborhood with
no respiratory symptoms in past 2 weeks. In addition, also collected specimens from a sample
of AURI cases every day, as testing all samples was not possible because of limited resources.
By rotation, on each workday of the week, one of the project nurses collected specimens from
children with AURI detected in her designated surveillance area. As children were followed
weekly, it is possible that a child may be swabbed more than once during the same episode if it
lasts more than 7 days with worsening from AURI to ALRI. Swabs collected from children
were immediately put into 15 ml falcon tube containing STGG (skimmed milk, tryptone, glu-
cose, and glycerin) transport medium [18] and transported in an icebox per standard protocols
to the bacteriology laboratory [19], at the All India Institute of Medical Sciences (AIIMS), New
Delhi. In addition, separate nasal and throat swabs were also collected from each of these chil-
dren with AURI/ALRI and the asymptomatic children for testing viral pathogens. [16].
Laboratory methods
In the laboratory, specimens were vortexed to disperse organisms from the swab tip and cul-
tured on Columbia agar plate with 5% sheep blood (bioMerieux, ™ France), and incubated
overnight in a 5% CO2 incubator at 37˚C. Pneumococcal isolates based on morphological
structure of colony identified by α-hemolytic, microscopic observation, optochin susceptibility
and bile solubility as recommended by the World Health Organization Pneumococcal Car-
riage Working Group [19]. Performed Neufeld’s Quellung reaction for serotyping, using type-
specific omni sera, pool sera, group sera, type sera and factor sera of Statens Serum Institut
(SSI, Copenhagen, Denmark). Non-typeable isolates were further tested by PCR with fresh col-
onies of S. pneumoniae. DNA for PCR was extracted, using the QIAamp1DNA mini kit (Qia-
gen, Germany), according to the manufacturer’s instructions. Molecular confirmation for S.
pneumoniae isolates was performed using polymerase chain reaction (PCR) for the presence of
the conserved sequence for autolysin encoding gene lytA [20]. Oligonucleotide primers used
for 40 pneumococcal serotypes by conventional multiplex PCR method available on the CDC
website (https://www.cdc.gov/streplab/downloads/pcr-oligonucleotide-primers.pdf). The con-
dition for multiplex PCR was, 94˚C for 4 min, followed by 30 amplification cycles of 94˚C for
45 seconds, 54˚C for 45 seconds and 65˚C for 2 minutes and 30 seconds, while the annealing
temperature for individual PCR reaction was at 60˚C [20]. The PCR products were analyzed
by gel electrophoresis on 2% agarose gels.
Antimicrobial susceptibility testing conducted using antibiotic disc (Himedia Laboratories,
Mumbai ™, India), by Kirby-Bauer disc diffusion method, as per the Clinical and Laboratory
Standards Institute (CLSI) guidelines, for ceftriaxone, chloramphenicol, co-trimoxazole, eryth-
romycin, levofloxacin, oxacillin, penicillin, vancomycin [21]. American Type Cell Collection
(ATCC) 49619 of S. pneumoniae was used for a quality control test. Pneumococcal isolates that
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 3 / 10
were not susceptible to penicillin were further tested for minimum inhibitory concentration
(bioMerieux, ™ France) using ETEST1 strips [21].
Data management and analysis
Considered specimens as unit of analysis, collected specimens from a child if s/he had a new
case of ARI or had worsened from AURI to ALRI during the last seven days to detect new
infections. Therefore, the nurses could have collected specimens from same child more than
once; so analyzed the proportion of specimens positive for S. pneumoniae, counting multiple
specimens from the same child as discrete observations. (There was no child whose consecu-
tive weekly specimen tested positive for S. pneumoniae). Used MS Excel™ (Microsoft Office
2010) and Epi Info v3.5 (CDC, Atlanta, GA, USA) for data entry. Laboratory and clinical data-
sets were merged and analyzed using Stata 12SE (Stata Corp, College station, Texas, USA). To
calculate adjusted odds ratios, combined AURI and ALRI cases and used logistic regression to
compare pneumococcal detection in specimens collected from symptomatic (AURI/ALRI)
children compared to asymptomatic children, adjusting for age group, sex, month of detection
and co-detection of any other bacterial and viral pathogens.
Ethical clearance
The study was approved by the Institutional Ethics Committee (IEC) of AIIMS, New Delhi,
India. The institutional review board of the US Centers for Disease Control and Prevention
relied on the review of the IEC of AIIMS. Written informed consent was obtained from all
parents or guardians of enrolled children and assent was obtained from children aged�7
years.
Results
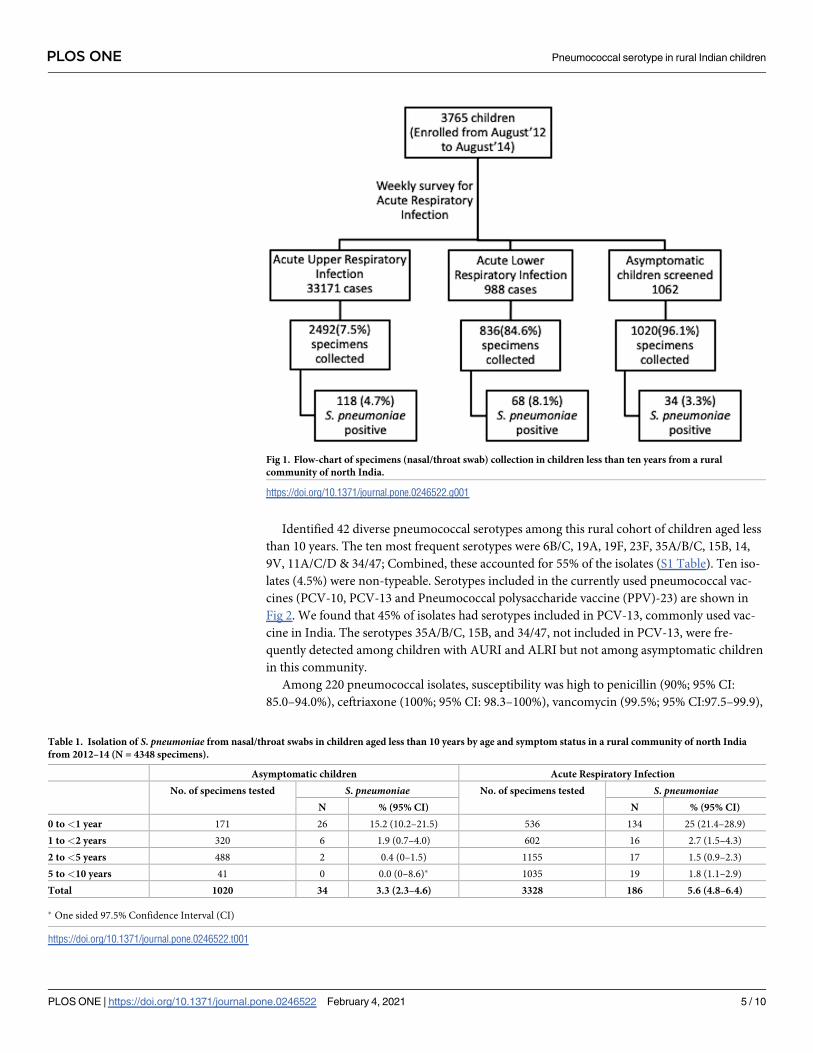
Study followed 3765 children weekly for two years and collected a total of 4348 upper respira-
tory specimens. During the two years, 3328 specimens collected from children with ARI
(including 836 ALRI and 2492 AURI) and 1020 specimen from asymptomatic children (Fig 1).
There were 162 specimens from 131 children which were collected within 14 days of last sam-
ple collection. Overall, of the 4348 specimens tested, and detected S. pneumoniae in 220 (5.1%,
95% CI: 4.4–5.8) specimens, including 186 (5.6%, 95% CI: 4.8–6.4) of 3328 specimens from
ARI cases (n = 3328) as shown in Table 1. Of these detections among ARI specimens, 118
(63.4%) were from AURI and 68 (36.6%) from ALRI. S. pneumoniae was detected more fre-
quently among children <1 year of age compared to older children, both among symptomatic
children (25.0%; 95% CI: 21.4–28.9�1 year, versus 1.9%; 95% CI 1.4–2.4 >1 year) and asymp-
tomatic children (15.2%; 95% CI: 10.2–21.5�1 year, versus 0.9%, 95% CI 0.4–1.8 >1 year).
Further, of 160 detections among infants aged<1 year, 51 (41 with ARI and 10 asymptomatic)
were among infants aged <6 months; the youngest age of carriage was 36 days which was in
an asymptomatic infant. There was no significant difference in S. pneumoniae detection
between boys and girls (S2 Table).
Among the children with S. pneumoniae detections, also detected Haemophilus influenzaetype b (17, 7.7%), and respiratory viruses including rhinovirus (30, 13.6%), RSV (10, 4.5%),
influenza (5, 2.3%), parainfluenza viruses (3, 1.4%), and metapneumovirus (1, 0.5%).
Using asymptomatic children as the reference group, found statistically significant associa-
tion between S. pneumoniae detection among children with AURI (adjusted OR: 2.6; 95%CI:
1.5–4.4; p = 0.000), and ALRI (adjusted OR: 2.0; 95% CI: 1.1–3.5; p = 0.116), when adjusted for
age groups, sex, co-detection of other bacterial or respiratory viral pathogen and month of
detection (S2 Table).
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 4 / 10
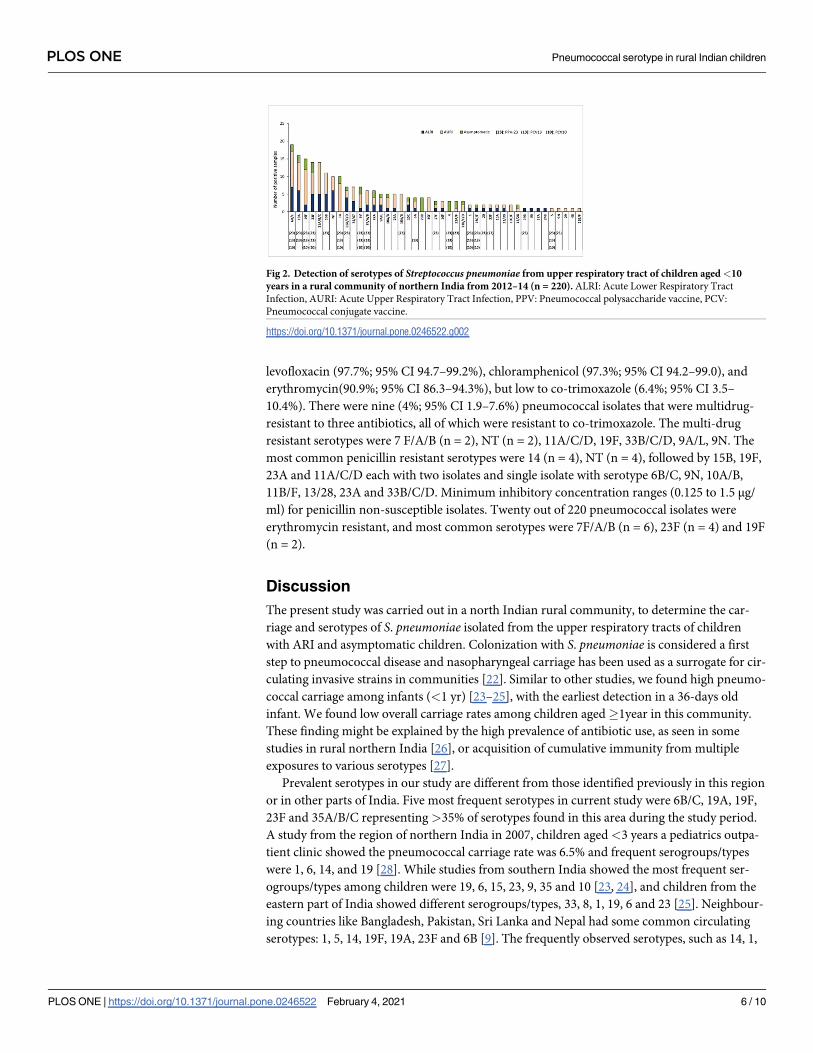
Identified 42 diverse pneumococcal serotypes among this rural cohort of children aged less
than 10 years. The ten most frequent serotypes were 6B/C, 19A, 19F, 23F, 35A/B/C, 15B, 14,
9V, 11A/C/D & 34/47; Combined, these accounted for 55% of the isolates (S1 Table). Ten iso-
lates (4.5%) were non-typeable. Serotypes included in the currently used pneumococcal vac-
cines (PCV-10, PCV-13 and Pneumococcal polysaccharide vaccine (PPV)-23) are shown in
Fig 2. We found that 45% of isolates had serotypes included in PCV-13, commonly used vac-
cine in India. The serotypes 35A/B/C, 15B, and 34/47, not included in PCV-13, were fre-
quently detected among children with AURI and ALRI but not among asymptomatic children
in this community.
Among 220 pneumococcal isolates, susceptibility was high to penicillin (90%; 95% CI:
85.0–94.0%), ceftriaxone (100%; 95% CI: 98.3–100%), vancomycin (99.5%; 95% CI:97.5–99.9),
Fig 1. Flow-chart of specimens (nasal/throat swab) collection in children less than ten years from a rural
community of north India.
https://doi.org/10.1371/journal.pone.0246522.g001
Table 1. Isolation of S. pneumoniae from nasal/throat swabs in children aged less than 10 years by age and symptom status in a rural community of north India
from 2012–14 (N = 4348 specimens).
Asymptomatic children Acute Respiratory Infection
No. of specimens tested S. pneumoniae No. of specimens tested S. pneumoniaeN % (95% CI) N % (95% CI)
0 to <1 year 171 26 15.2 (10.2–21.5) 536 134 25 (21.4–28.9)
1 to <2 years 320 6 1.9 (0.7–4.0) 602 16 2.7 (1.5–4.3)
2 to <5 years 488 2 0.4 (0–1.5) 1155 17 1.5 (0.9–2.3)
5 to <10 years 41 0 0.0 (0–8.6)� 1035 19 1.8 (1.1–2.9)
Total 1020 34 3.3 (2.3–4.6) 3328 186 5.6 (4.8–6.4)
� One sided 97.5% Confidence Interval (CI)
https://doi.org/10.1371/journal.pone.0246522.t001
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 5 / 10
levofloxacin (97.7%; 95% CI 94.7–99.2%), chloramphenicol (97.3%; 95% CI 94.2–99.0), and
erythromycin(90.9%; 95% CI 86.3–94.3%), but low to co-trimoxazole (6.4%; 95% CI 3.5–
10.4%). There were nine (4%; 95% CI 1.9–7.6%) pneumococcal isolates that were multidrug-
resistant to three antibiotics, all of which were resistant to co-trimoxazole. The multi-drug
resistant serotypes were 7 F/A/B (n = 2), NT (n = 2), 11A/C/D, 19F, 33B/C/D, 9A/L, 9N. The
most common penicillin resistant serotypes were 14 (n = 4), NT (n = 4), followed by 15B, 19F,
23A and 11A/C/D each with two isolates and single isolate with serotype 6B/C, 9N, 10A/B,
11B/F, 13/28, 23A and 33B/C/D. Minimum inhibitory concentration ranges (0.125 to 1.5 μg/
ml) for penicillin non-susceptible isolates. Twenty out of 220 pneumococcal isolates were
erythromycin resistant, and most common serotypes were 7F/A/B (n = 6), 23F (n = 4) and 19F
(n = 2).
Discussion
The present study was carried out in a north Indian rural community, to determine the car-
riage and serotypes of S. pneumoniae isolated from the upper respiratory tracts of children
with ARI and asymptomatic children. Colonization with S. pneumoniae is considered a first
step to pneumococcal disease and nasopharyngeal carriage has been used as a surrogate for cir-
culating invasive strains in communities [22]. Similar to other studies, we found high pneumo-
coccal carriage among infants (<1 yr) [23–25], with the earliest detection in a 36-days old
infant. We found low overall carriage rates among children aged�1year in this community.
These finding might be explained by the high prevalence of antibiotic use, as seen in some
studies in rural northern India [26], or acquisition of cumulative immunity from multiple
exposures to various serotypes [27].
Prevalent serotypes in our study are different from those identified previously in this region
or in other parts of India. Five most frequent serotypes in current study were 6B/C, 19A, 19F,
23F and 35A/B/C representing >35% of serotypes found in this area during the study period.
A study from the region of northern India in 2007, children aged<3 years a pediatrics outpa-
tient clinic showed the pneumococcal carriage rate was 6.5% and frequent serogroups/types
were 1, 6, 14, and 19 [28]. While studies from southern India showed the most frequent ser-
ogroups/types among children were 19, 6, 15, 23, 9, 35 and 10 [23, 24], and children from the
eastern part of India showed different serogroups/types, 33, 8, 1, 19, 6 and 23 [25]. Neighbour-
ing countries like Bangladesh, Pakistan, Sri Lanka and Nepal had some common circulating
serotypes: 1, 5, 14, 19F, 19A, 23F and 6B [9]. The frequently observed serotypes, such as 14, 1,
Fig 2. Detection of serotypes of Streptococcus pneumoniae from upper respiratory tract of children aged<10
years in a rural community of northern India from 2012–14 (n = 220). ALRI: Acute Lower Respiratory Tract
Infection, AURI: Acute Upper Respiratory Tract Infection, PPV: Pneumococcal polysaccharide vaccine, PCV:
Pneumococcal conjugate vaccine.
https://doi.org/10.1371/journal.pone.0246522.g002
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 6 / 10
5, 19F and 6B in some of the recent studies from India on invasive pneumococcal disease
among children <5 years old, were also detected in our study [7–9].
The antimicrobial susceptibility pattern of S. pneumoniae isolated in this cohort is similar
to that found in previous studies from India and elsewhere [29]. Antimicrobial resistance was
most common against co-trimoxazole, similar to the findings in previous studies from India
[13, 24, 25]. Asian Network for Surveillance of Resistant Pathogens (ANSORP) multi-coun-
tries collaborative work reported that pneumococcal isolation from India had the lowest resis-
tant to penicillin. A recent study [7] showed slightly increase in the number of penicillin non-
susceptible S. pneumoniae with 8% (n = 29). Our study showed high susceptibility to penicillin,
as found elsewhere in India [25], and unlike the high penicillin resistance observed in other
Asian countries like Thailand, Singapore, Hong-Kong had high resistance to penicillin 68%,
44% and 49%, respectively [9, 30]. In a global review, high rates of resistance against both peni-
cillin and erythromycin were reported in 6B, 6A, 9V, 14, 15A, 19F, 19A, and 23F [31]; how-
ever, in current study serotype 19F showed resistance against both the antibiotics. Two non-
vaccine serotypes 35A/B/C and 11A/C/D, found in this rural community and previously have
been shown to be associated with biofilm formation [32], which may be responsible for the
development of antibiotic resistance.
In this study, 45% of isolates were vaccine serotypes, while the remaining isolates were
either non-typable (10%) or non-vaccine type. The Government of India approved the intro-
duction of pneumococcal vaccine into the universal immunization programme (UIP) in 2017,
starting with high-burden states [5]. Our study area is not considered a high-burden area and
pneumococcal vaccine was not available in the area during this study. Therefore, our study
documents baseline rates of pneumococcal detection and circulating serotypes that can be
used to monitor the impact of pneumococcal vaccine introduction in the future. In other set-
tings, the introduction of mass immunizations has resulted in replacement of non-vaccine
serotypes in the community and reduction in the prevalence of drug resistant serotypes [31].
However, it is still unclear whether the replacement of serotypes is associated with invasive
pneumococcal disease.
One of the limitations of this study was collection of only upper respiratory tract specimens
for detection of S. pneumoniae, which makes it difficult to attribute any etiological role in
ARIs. This study was not originally designed to assess pneumococcal carriage. It leveraged a
community-based surveillance platform for viral pathogens among children [16]. Despite
these limitations, this study is one of few community-based pneumococcal carriage studies
among children in India and provides insights into the dynamics of circulating pneumococcal
serotypes in children 10 years of age and younger in rural India prior to the introduction of
pneumococcal vaccine.
Findings of current study can inform the national guidelines on antimicrobial use for pneu-
mococcal disease and provide critical information about baseline rates of S. pneumoniae car-
riage and circulating serotypes that can be used to measure the impact of vaccine introduction
if the national vaccination program is expanded. The difference in circulating serotypes seen
between our study and previous carriage studies suggests that such community-based carriage
studies can be used to better understand the prevalence of different pneumococcal serotypes in
India and the impact of vaccination.
Supporting information
S1 Data.
(XLSX)
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 7 / 10
S1 Table. Pneumococcal serotypes distribution among 220 isolates from children in rural
northern India, 2012–2014.
(PDF)
S2 Table. Multi-variate analysis of factors associated with detection of pneumococcus in
the upper respiratory specimens collected from children aged<10 years in rural north
India. AURI: Acute upper respiratory infection, ALRI: Acute lower respiratory infection, RSV:
Respiratory syncytial virus, HRV: Human rhinovirus, HMPV: Human metapneumovirus, PIV:
Parainfluenza virus, Hib: Haemophilus influenzae type b.
(PDF)
Acknowledgments
We are indebted to the villagers of the study area for their support and patience despite
repeated visits during the study. We are thankful to the study participants and the project staff
for their cooperation and support for this study. We express our profound gratitude to Dr
Renu Lal and Marc-Alain Widdowson from CDC, and Prof Shobha Broor from AIIMS, who
conceptualized this surveillance platform used for this study. We would like to express our spe-
cial thanks to Dr Srinivas Acharya Nanduri from Division of Bacterial Diseases, CDC for his
comments and suggestions for the manuscript.
Disclaimer: The findings and conclusions in this report are those of the authors and do not
necessarily represent the official position of CDC.
Conferences, where this study has been presented:
1stIMRP (International meeting on respiratory pathogens), 2–4 September 2015, Singapore
(Abstract no.-ASN0-211)
9th International symposium on pneumococci and pneumococcal diseases (ISPPD), 9–13
March 2014, Hyderabad, India (Abstract no. -ISPPD-0268)
Author Contributions
Conceptualization: Sambuddha Kumar, Arti Kapil, Siddhartha Saha, Bimal Kumar Das,
Seema Jain, Anand Krishnan.
Data curation: Sambuddha Kumar, Debjani Ram Purakayastha, Arti Kapil, Siddhartha Saha,
Ritvik Amarchand, Rakesh Kumar.
Formal analysis: Sambuddha Kumar, Siddhartha Saha, Ritvik Amarchand, Rakesh Kumar.
Funding acquisition: Siddhartha Saha, Kathryn E. Lafond, Seema Jain, Anand Krishnan.
Investigation: Sambuddha Kumar, Debjani Ram Purakayastha, Arti Kapil, Bimal Kumar Das,
Ritvik Amarchand, Rakesh Kumar, Anand Krishnan.
Methodology: Sambuddha Kumar, Debjani Ram Purakayastha, Arti Kapil.
Project administration: Debjani Ram Purakayastha, Arti Kapil, Siddhartha Saha, Fatimah S.
Dawood, Bimal Kumar Das, Ritvik Amarchand, Kathryn E. Lafond, Seema Jain, Anand
Krishnan.
Resources: Debjani Ram Purakayastha, Arti Kapil, Bimal Kumar Das, Ritvik Amarchand,
Rakesh Kumar, Anand Krishnan.
Software: Rakesh Kumar.
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 8 / 10
Supervision: Arti Kapil, Siddhartha Saha, Fatimah S. Dawood, Bimal Kumar Das, Kathryn E.
Lafond, Seema Jain, Anand Krishnan.
Validation: Ritvik Amarchand, Anand Krishnan.
Visualization: Arti Kapil, Bimal Kumar Das, Kathryn E. Lafond, Seema Jain, Anand
Krishnan.
Writing – original draft: Sambuddha Kumar, Arti Kapil, Bimal Kumar Das.
Writing – review & editing: Sambuddha Kumar, Debjani Ram Purakayastha, Arti Kapil, Sid-
dhartha Saha, Fatimah S. Dawood, Bimal Kumar Das, Ritvik Amarchand, Rakesh Kumar,
Kathryn E. Lafond, Seema Jain, Anand Krishnan.
References1. Million Death Study C, Bassani DG, Kumar R, Awasthi S, Morris SK, Paul VK, et al. Causes of neonatal
and child mortality in India: a nationally representative mortality survey. Lancet. 2010. 376
(9755):1853–60. https://doi.org/10.1016/S0140-6736(10)61461-4 PMID: 21075444.
2. Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child
mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis.
Lancet. 2015. 385(9966):430–40. https://doi.org/10.1016/S0140-6736(14)61698-6 PMID: 25280870
3. Wahl B, O’Brien KL, Greenbaum A, Majumder A, Liu L, Chu Y, et al. Burden of Streptococcus pneumo-
niae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: global,
regional, and national estimates for 2000–15. Lancet Glob Health. 2018. 6 (7):e744–e57. https://doi.
org/10.1016/S2214-109X(18)30247-X PMID: 29903376.
4. Mathew JL, Singhi S, Ray P, Hagel E, Saghafian-Hedengren S, Bansal A, et al. Etiology of commu-
nity acquired pneumonia among children in India: prospective, cohort study. J Glob Health. 2015.
5(2):050418. https://doi.org/10.7189/jogh.05.020418 PMID: 26528392.
5. Sachdeva A. Pneumococcal Conjugate Vaccine Introduction in India’s Universal Immunization Pro-
gram. Indian Pediatrics. 2017. 54:445–6. https://doi.org/10.1007/s13312-017-1044-z PMID: 28667711
6. Murdoch DR. Assessing the Impact of Pneumococcal Conjugate Vaccines. Clin Infect Dis. 2020. 10;
70(8):1589–1590. https://doi.org/10.1093/cid/ciz484 PMID: 31175809.
7. Manoharan A, Manchanda V, Balasubramanian S, Lalwani S, Modak M, Bai S, et al. Alliance for Sur-
veillance of Invasive Pneumococci (ASIP) Study Group. Invasive pneumococcal disease in children
aged younger than 5 years in India: a surveillance study. Lancet Infect Dis. 2017. 17(3):305–12. https://
doi.org/10.1016/S1473-3099(16)30466-2 PMID: 27956163.
8. Balaji V, Jayaraman R, Verghese VP, Baliga PR, Kurien T. Pneumococcal serotypes associated with
invasive disease in under five children in India & implications for vaccine policy. Indian J Med Res.
2015. 142(3):286–92. https://doi.org/10.4103/0971-5916.166588 PMID: 26458344.
9. Bravo LC, Asian Strategic Alliance for Pneumococcal Disease Prevention (ASAP) Working Group.
Overview of the disease burden of invasive pneumococcal disease in Asia. Vaccine. 2009 Dec 9; 27
(52):7282–91. https://doi.org/10.1016/j.vaccine.2009.04.046 PMID: 19393708.
10. Kumar R, Arora N, Santosham M. South Asia symposium on pneumococcal disease and the promise of
vaccines–Meeting report. Vaccine. 2016 May 17; 34(23): 2622–2626. https://doi.org/10.1016/j.
vaccine.2016.03.071 PMID: 27026150.
11. World Health Organization, Ministry of Health and Family Welfare, Government of India. Integrated
Management of Neonatal and Childhood Illness (IMNCI) 2003. [http://nrhm.gov.in/nrhm-components/
rmnch-a/child-healthimmunization/child-health/guidelines.html8.
12. Rodrigues CMC. Challenges of Empirical Antibiotic Therapy for Community-Acquired Pneumonia in
Children. Curr Ther Res Clin Exp. 2017. 84:e7–e11. https://doi.org/10.1016/j.curtheres.2017.01.002
PMID: 28761583.
13. Kumar KL, Ashok V, Ganaie F, Ramesh AC. Nasopharyngeal carriage, antibiogram & serotype distri-
bution of Streptococcus pneumoniae among healthy under five children. Indian J Med Res. 2014.
140(2):216–20. PMID: 25297353.
14. Morpeth SC, Munywoki P, Hammitt LL, Bett A, Bottomley C, Onyango CO, et al. Impact of viral upper
respiratory tract infection on the concentration of nasopharyngeal pneumococcal carriage among Ken-
yan children. Sci Rep. 2018. 8(1):11030. https://doi.org/10.1038/s41598-018-29119-w PMID:
30038420.
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 9 / 10
15. Chochua S, D’Acremont V, Hanke C, Alfa D, Shak J, Kilowoko M, et al. Increased Nasopharyngeal Den-
sity and Concurrent Carriage of Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella
catarrhalis Are Associated with Pneumonia in Febrile Children. PLoS One. 2016. 11(12):e0167725.
https://doi.org/10.1371/journal.pone.0167725 PMID: 27907156.
16. Krishnan A, Amarchand R, Gupta V, Lafond KE, Suliankatchi RA, Saha S, et al. Epidemiology of acute
respiratory infections in children—preliminary results of a cohort in a rural north Indian community. BMC
Infect Dis. 2015. 15:462. https://doi.org/10.1186/s12879-015-1188-1 PMID: 26502931.
17. World Health Organization. Acute Care: Integrated Management of Adolescent and Adult Illness.
Geneva 2004. [http://apps.who.int/iris/bitstream/10665/68535/1/WHO_CDS_IMAI_2004.1.pdf.
18. O’Brien KL, Bronsdon MA, Dagan R, Yagupsky P, Janco J, Elliott J, et al. Evaluation of a medium
(STGG) for transport and optimal recovery of Streptococcus pneumoniae from nasopharyngeal secre-
tions collected during field studies. J Clin Microbiol. 2001; 39(3):1021–4. https://doi.org/10.1128/JCM.
39.3.1021-1024.2001 PMID: 11230421.
19. Satzke C, Turner P, Virolainen-Julkunen A, Adrian PV, Antonio M, Hare KM, et al. Standard method for
detecting upper respiratory carriage of Streptococcus pneumoniae: updated recommendations from
the World Health Organization Pneumococcal Carriage Working Group. Vaccine. 2013. 17; 32(1):165–
79. https://doi.org/10.1016/j.vaccine.2013.08.062 PMID: 24331112.
20. Pai R, Gertz RE, Beall B. Sequential multiplex PCR approach for determining capsular serotypes of
Streptococcus pneumoniae isolates. J Clin Microbiol. 2006. 44(1):124–31. https://doi.org/10.1128/
JCM.44.1.124-131.2006 PMID: 16390959.
21. Clinical and Laboratory Standard Institute. Performance standards for antimicrobial susceptibility test-
ing; Twenty-fourth informational supplement, Document M100–S24. 2014. CLSI, Wayne, PA.
22. Simell B, Auranen K, Kayhty H, Goldblatt D, Dagan R, O’Brien KL; Pneumococcal Carriage Group. The
fundamental link between pneumococcal carriage and disease. Expert Rev Vaccines. 2012. 11
(7):841–55. https://doi.org/10.1586/erv.12.53 PMID: 22913260.
23. Jebaraj R, Cherian T, Raghupathy P, Brahmadathan KN, Lalitha MK, Thomas K, et al. Nasopharyngeal
colonization of infants in southern India with Streptococcus pneumoniae. Epidemiol Infect. 1999. 123
(3):383–8. https://doi.org/10.1017/s0950268899003131 PMID: 10694148.
24. Coles CL, Kanungo R, Rahmathullah L, Thulasiraj RD, Katz J, Santosham M, et al. Pneumococcal
nasopharyngeal colonization in young South Indian infants. J. Pediatr Infect Dis. 2001. 20(3):289–95.
https://doi.org/10.1097/00006454-200103000-00014 PMID: 11303832.
25. Devi U, Ayyagari A, Devi KR, Narain K, Patgiri DK, Sharma A, et al. Serotype distribution & sensitivity
pattern of nasopharyngeal colonizing Streptococcus pneumoniae among rural children of eastern India.
Indian J Med Res. 2012. 136(3):495–8. PMID: 23041746.
26. Tripathy JP, Bahuguna P, Prinja S. Drug prescription behavior: A cross-sectional study in public health
facilities in two states of North India. Perspect Clin Res. 2018. 9(2):76–82. https://doi.org/10.4103/picr.
PICR_75_17 PMID: 29862200.
27. Weinberger DM, Dagan R, Givon-Lavi N, Regev-Yochay G, Malley R, Lipsitch M. Epidemiologic evi-
dence for serotype-specific acquired immunity to pneumococcal carriage. J Infect Dis. 2008. 197
(11):1511–8. https://doi.org/10.1086/587941 PMID: 18471062.
28. Wattal C, Oberoi JK, Pruthi PK, Gupta S. Nasopharyngeal carriage of Streptococcus pneumoniae.
Indian J Pediatr. 2007. 74(10):905–7. https://doi.org/10.1007/s12098-007-0166-z PMID: 17978447.
29. Jain A, Kumar P, Awasthi S. High nasopharyngeal carriage of drug resistant Streptococcus pneumoniae
and Haemophilus influenzae in North Indian school children. Trop Med Int Health. 2005. 10(3):234–9.
https://doi.org/10.1111/j.1365-3156.2004.01379.x PMID: 15730507.
30. Batuwanthudawe R, Karunarathne K, Dassanayake M, de Silva S, Lalitha MK, Thomas K, et al. Surveil-
lance of invasive pneumococcal disease in Colombo, Sri Lanka. Clin Infect Dis. 2009. 48 Suppl 2:
S136–40. https://doi.org/10.1086/596492 PMID: 19191609.
31. Linares J, Ardanuy C, Pallares R, Fenoll A. Changes in antimicrobial resistance, serotypes and geno-
types in Streptococcus pneumoniae over a 30-year period. Clin Microbiol Infect. 2010. 16(5):402–10.
https://doi.org/10.1111/j.1469-0691.2010.03182.x PMID: 20132251.
32. Domenech M, Damian D, Ardanuy C, Linares J, Fenoll A, Garcia E. Emerging, Non-PCV13 Serotypes
11A and 35B of Streptococcus pneumoniae Show High Potential for Biofilm Formation In Vitro. PLoS
One. 2015. 10(4):e0125636. https://doi.org/10.1371/journal.pone.0125636 PMID: 25927917.
PLOS ONE Pneumococcal serotype in rural Indian children
PLOS ONE | https://doi.org/10.1371/journal.pone.0246522 February 4, 2021 10 / 10





























